assessing maternal, environmental and individual …
TRANSCRIPT

Assessing Maternal, Environmental and Individual RiskIndicators for Dental Caries in a Population of Children fromQueensland, Australia
Author
Fernando, Surani
Published
2017-08
Thesis Type
Thesis (PhD Doctorate)
School
School of Dentistry&Oral Hlth
DOI
https://doi.org/10.25904/1912/859
Copyright Statement
The author owns the copyright in this thesis, unless stated otherwise.
Downloaded from
http://hdl.handle.net/10072/371955
Griffith Research Online
https://research-repository.griffith.edu.au

i
ASSESSING MATERNAL, ENVIRONMENTAL AND
INDIVIDUAL RISK INDICATORS FOR DENTAL CARIES IN
A POPULATION OF CHILDREN FROM QUEENSLAND,
AUSTRALIA
Surani Fernando
BDS, MSc, MD
School of Dentistry and Oral Health
Menzies Health Institute Queensland
Griffith University
Submitted in fulfillment of the requirements for the degree of Doctor of
Philosophy
August 2017

ii
STATEMENT OF ORIGINALITY
This work has not previously been submitted for a degree or diploma in any
University. To the best of my knowledge and belief, the thesis contains no
material previously published or written by another person except where due
reference is made in the thesis itself.
Surani Fernando
25.08.2017

iii
ACKNOWLEDGEMENTS
This doctoral thesis was carried out under the primary supervision of Professor Newell Johnson
and Professor Paul Scuffham with the assistance of, Professor Rodney Lea and Dr. David
Speicher as associate supervisors. I acknowledge their co-operation, time, and contributions,
which have helped to bring this work to its current form. I am thankful for their constant
motivation and encouragement when I needed it. I am grateful to each one of them for helping
me to sharpen my skills in scientific writing and critical thinking.
Particularly, I am indebted to Professor Newell Johnson and Professor Paul Scuffham for many
aspects of the oral health arm of the Environments for Healthy Living Study. I wish to thank
Professor Paul Scuffham for his kind and generous support during the stressful phase of
merging oral health data with the main EFHL data base and data analysis. I thank Professor
Rodney Lea for his continuous encouragement and support throughout the Epigenome–Wide
Association Study. I also acknowledge the advice and training given by Dr. David Speicher
during laboratory work.
A special thank you goes to Mr. Gabor Mihala, for all the advice and support given throughout
data management and analysis. I am thankful for the contributions of the EFHL Project
Manager, Rani Scott, and the current and past Database Managers. I thank Dr. Miles Benton
for helping with DNA sequencing and methylation assays and Dr. Ping Zhang for her advice
on bioinformatics analysis. I would also like to acknowledge the contribution of Professor Shu
Kay Ng and Dr. Santhosh Kumar for their statistical support. I am grateful for the help I have
received from Dr. Mahmoud Bakr during clinical data collection.

iv
I acknowledge the support of the Head of School, Dentistry and Oral Health, management of
Griffith Health Clinics and its team of Dental Assistants and Receptionists with the clinical
work.
Professional editor, Dr. John McAndrew, provided copyediting and proofreading services,
according to the guidelines laid out in the university-endorsed national Guidelines for Editing
Research Theses.
This study would not be possible without the co-operation of the mothers and children who
participated. I especially appreciate the mothers who were willing to spare their time to bring
their children for oral examinations at the Griffith Dental clinics. They agreed to participate
and they were kind enough to complete the questionnaires and patiently sit through the clinical
examination during late afternoons.
Although words cannot merely explain my gratefulness, I am thankful to my wonderful
husband, Shaun who lovingly and without complaining helped me with the housework and
children. He has been my constant support and pillar of strength throughout this journey. Thank
you, my lovely daughters, Kiyashi, Amaya, Emalshi, and Tiasha, for sacrificing many cuddles,
late-nights, weekends, and school holidays, so that I could remain focused on my work. I would
not have been able to complete this thesis without my family’s support and understanding.
I will be failing in my duties if I do not express my gratitude to my parents, Dawson and Dulcey,
for their sacrifices, support, love, and prayers without which I could not have come this far.

v
I am very grateful to Griffith University for scholarships and support. Lastly, I would like to
acknowledge and thank my examiners for the time and effort they have dedicated to reading
this thesis and providing valuable feedback to improve my work as a researcher.

vi
ABSTRACT
Oral diseases affect 3.9 billion people worldwide, and dental caries is the most prevalent oral
condition. Untreated caries in permanent and deciduous dentitions were reported among
approximately 35% and 9% of the world population, respectively, in 2010. Moreover, it is the
fourth-most expensive chronic disease to treat according to the World Health Organization.
The importance of various social, environmental, familial, and behavioural factors on
childhood caries has been identified by earlier researchers. In the past, epidemiological
research on caries has mainly focused on describing biological and dietary determinants of the
disease. During the past few decades, there has been an effort to explore children’s oral health
outcomes using a broader framework, incorporating behavioural, social, and environmental
predictors with biological and genetic factors. Despite the fact that these characteristics have
been found to be significantly associated with childhood caries experience in different
population groups, there has been scarce research exploring the whole range of putative risk
factors, and their associated risk indicators, and their possible interactions, simultaneously, in
a single child cohort. In particular, the impact of the epigenome and of the in utero environment
on susceptibility to dental caries has not been reported in children from a typical Western
industrialised country. Hence, this thesis explored a wide range of factors: environmental,
socio-economic, behavioural, maternal (including throughout pregnancy), children’s
individual factors (including well-established risks associated with diet and hygiene practices),
and a screen for epigenetic modifications, as indicators of risk for childhood caries.
Participants were 174, six- to seven-year-old children and their mothers from South East
Queensland, who were originally enrolled in the Environments for Healthy Living (EFHL)
Griffith University birth cohort study. Participants for the oral health sub-study were volunteers

vii
obtained from the EFHL database who were willing to come for an oral examination at Griffith
dental clinics.
Mothers completed a questionnaire on oral health knowledge and behaviours at the dental clinic
followed by anthropometric measurements. Trained and calibrated examiners conducted
detailed head and neck, and oral examinations, and recorded participant’s salivary
characteristics and dental caries scores. Total DNA was extracted from each participant’s saliva
for sequencing and methylation arrays to detect epigenetic changes. Descriptive statistics,
negative binomial regression, and path analyses were performed to evaluate the associations
between risk indicators and the lifetime dental caries experience of each child.
Maternal risk indicators included mother’s age at examination, her lifetime caries experience,
oral health knowledge and practices, body mass index, saliva characteristics of clinical oral
hydration, stimulated flow rate, pH, buffering capacity, and load of salivary mutans
Streptococci and Lactobacilli.
Results indicated that low annual household income was a risk indicator for dental caries
experience in this child population. Maternal behaviours: initiating child’s tooth brushing later
than six months of age and a high frequency of giving carbonated drinks to the child were
associated with increased caries experience in their children. In addition, high loads of maternal
oral Lactobacilli were related to the children’s increased risk of caries. Moreover, children’s
past caries experience, and increased levels of salivary mutans Streptococci were recognised
to be significant risk indicators for their dental caries experience. Children whose mothers took
iron supplements during pregnancy had low levels of caries (past and current) compared to
their counterparts.

viii
One highlight of the thesis has been the cutting-edge evidence of an association between
epigenetic modifications and caries experience of individuals. There were significant
differences in differentially methylated regions between persons with high and low caries
experience on chromosomes 1, 2, 5, 7, 12, 20 and 22. Chromosome 12, in particular, showed
the highest average methylation difference between the two groups. Further, functional
annotations of related genes revealed that there are two gene clusters related to zinc (Zn)
metabolism and membrane protein functions, which could indirectly be related to the caries
process.
In summary, the study found maternal, environmental, and children’s characteristics that were
risk indicators for caries experience in this child population. It was observed that low maternal
income and poor oral health behaviours had positive associations with children’s caries
experience. Also, bad oral health of the mother, expressed as maternal caries experience, placed
their children at risk of dental caries. Similarly, children with poor oral health with past caries
and high counts of cariogenic bacteria, along with reported low maternal iron supplements
during pregnancy were more at risk of continuing to develop dental caries than their
counterparts. The latter could reflect inadequate iron during pregnancy and consequent sub-
optimal development of foetal tissues and immune responses. The pilot study of 12 mother
child dyads to explore associations between epigenetic changes and lifetime caries experience
suggests that epigenetic modifications might, indeed, predispose individuals to dental caries.
However, with such a small sample size, this cannot be a firm conclusion. Nevertheless it leads
to the generation of hypotheses which can be tested in further studies.”
This thesis adds new knowledge to the current literature on local, systemic and environmental
factors influencing susceptibility and resistance to the process of childhood caries. The results
also offer new avenues for health promotion using a common risk factor approach to improve

ix
maternal behaviours and nutrition, which would eventually enhance the clinical caries
outcomes in children.

x
TABLE OF CONTENTS
STATEMENT OF ORIGINALITY ........................................................................................... ii
ACKNOWLEDGEMENTS ..................................................................................................... iii
ABSTRACT .............................................................................................................................. vi
TABLE OF CONTENTS ........................................................................................................... x
LIST OF TABLES ................................................................................................................... xv
LIST OF FIGURES ............................................................................................................... xvii
LIST OF APPENDICES ...................................................................................................... xviii
STATEMENT OF ETHICS APPROVAL.............................................................................. xix
LIST OF PUBLISHED AND SUBMITTED PAPERS FROM THE THESIS ....................... xx
ACKNOWLEDGEMNET OF PUBLICATIONS INCLUDED IN THE THESIS ............... xxii
Chapter 1: Introduction .............................................................................................................. 1
1.1 Background ...................................................................................................................... 1
1.2 Rationale for conducting the research in South East Queensland .................................... 5
1.3 Research questions and objectives ................................................................................... 7
1.4 Contribution of the study.................................................................................................. 9
1.5 The structure of the thesis .............................................................................................. 10
Chapter 2: Review of literature ................................................................................................ 12
2.1 Introduction .................................................................................................................... 12
2.2. The burden of dental caries in children ......................................................................... 13
2.3 Proposed Conceptual frameworks describing the process of dental caries .................... 15
2.4 Determinants of dental caries ......................................................................................... 19
2.4.1 Maternal and environmental determinants .............................................................. 20
2.4.1.1 Socio-economic status .......................................................................................... 20
2.4.1.2 Family structure and environment ........................................................................ 21
2.4.1.3 Maternal level of education, oral health knowledge and behaviours ................... 22
2.4.1.4 Maternal body mass index .................................................................................... 23
2.4.1.5 Maternal caries ..................................................................................................... 24
2.4.1.6 Maternal cariogenic bacteria ................................................................................ 25
2.4.1.7 Maternal salivary physiology ............................................................................... 26
2.4.2 Influence of children’s individual factors ................................................................ 28

xi
2.4.2.1 Intrauterine environment of child and birth weight .............................................. 28
2.4.2.2 Age and gender ..................................................................................................... 29
2.4.2.3 Past dental caries .................................................................................................. 30
2.4.2.4 Physicochemical properties of saliva ................................................................... 31
2.4.2.5 Oral cariogenic bacteria ........................................................................................ 32
2.5 Concluding remarks ....................................................................................................... 42
Chapter 3: Protocol for assessing maternal, environmental and epigenetic risk indicators for
dental caries in a population of Queensland children .............................................................. 43
3.1 Abstract .......................................................................................................................... 44
3.1.1Background ............................................................................................................... 44
3.1.2 Methods ................................................................................................................... 44
3.1.3 Discussion ................................................................................................................ 45
3.2 Background .................................................................................................................... 45
3.3 Methods .......................................................................................................................... 50
3.3.1 Study population ...................................................................................................... 50
3.3.2 Sample recruitment and examination ...................................................................... 51
3.3.3 Primary outcome variable ........................................................................................ 53
3.3.4 Main explanatory variables ..................................................................................... 53
3.3.5 Oral health knowledge and practices ....................................................................... 53
3.3.6 Anthropometric measurements ................................................................................ 54
3.3.7 Saliva characteristics ............................................................................................... 54
3.3.8 Periodontal status ..................................................................................................... 54
3.3.9 Demographic and environmental data ..................................................................... 55
3.3.10 Genetic and epigenetic markers ............................................................................. 55
3.4 Analysis .......................................................................................................................... 56
3.5 Discussion ...................................................................................................................... 59
Chapter 4: Maternal caries experience, household income, carbonated drinks and age at
commencement of tooth-brushing are associated with caries experience among 6- to 7-year-
old children in Australia........................................................................................................... 60
4.1 Abstract .......................................................................................................................... 61
4.2 Introduction .................................................................................................................... 62
4.3 Materials and methods ................................................................................................... 64
4.3.1 Study population ...................................................................................................... 65
4.3.2 Data collection ......................................................................................................... 65
xii
4.3.3 Outcome and risk indicators .................................................................................... 66
4.3.4 Statistical analyses ................................................................................................... 67
4.4 Results ............................................................................................................................ 68
4.5 Discussion ...................................................................................................................... 72
Chapter 5: Mothers who report taking iron supplements during pregnancy and child’s oral
carriage of mutans Streptococci are associated with a child’s lower and higher lifetime dental
caries experience, respectively................................................................................................. 78
5.1 Abstract .......................................................................................................................... 79
5.1.1 Objective .................................................................................................................. 79
5.1.2 Methods ................................................................................................................... 79
5.1.3 Results ..................................................................................................................... 79
5.1.4 Conclusions ............................................................................................................. 80
5.2 Introduction .................................................................................................................... 80
5.3 Methods .......................................................................................................................... 82
5.4 Results ............................................................................................................................ 87
5.5 Discussion ...................................................................................................................... 90
5.6 Conclusions .................................................................................................................... 93
Chapter 6: Influence of genes on the process of dental caries and what lies beyond .............. 94
6.1 Introduction .................................................................................................................... 94
6.2 Evidence that the host genome influences the natural history of dental caries .............. 95
6.3 Types of molecular genetic studies ................................................................................ 96
6.3.1 Genome-wide Studies .............................................................................................. 96
6.3.1.1 Genome-wide linkage studies ............................................................................. 96
6.3.1.2 Genome-wide association studies ....................................................................... 97
6.3.2 Candidate gene studies .......................................................................................... 101
6.3.2.1 Enamel formation genes ................................................................................... 105
6.3.2.2 Immune response genes .................................................................................... 107
6.3.2.3 Genes related to taste sensation ........................................................................ 110
6.3.2.4 Genes related to saliva ...................................................................................... 112
6.4 Genes, caries and environment..................................................................................... 114
6.4.1 Evidence from twin studies ................................................................................. 115
6.5 Epigenetics ................................................................................................................... 116
Mechanisms of Epigenetic modification ............................................................................ 117
6.6.1 DNA methylation .................................................................................................. 117

xiii
6.6.2 Histone modification ............................................................................................. 118
6.6.3 Non-coding RNA ................................................................................................... 119
6.7 Environmental stimuli which may result in epigenetic changes which could influence the
process of dental caries ...................................................................................................... 119
6.7.1 Diet and nutrition ................................................................................................... 120
6.7.2 Tobacco ................................................................................................................. 121
6.7.3 Bacteria and inflammation..................................................................................... 121
6.8 Future research ............................................................................................................. 122
Chapter 7: An Epigenome- Wide Association Study of mother-child dyads discordant for
dental caries: A pilot study .................................................................................................... 124
7.1 Abstract ........................................................................................................................ 125
7.1.1 Background ............................................................................................................ 125
7.1.2. Objective ............................................................................................................... 125
7.1.3 Methods ................................................................................................................. 125
7.1.4 Results ................................................................................................................... 126
7.1.5 Conclusion ............................................................................................................. 126
7.2 Introduction .................................................................................................................. 126
7.3 Methods ........................................................................................................................ 128
7.3.1 Study Population.................................................................................................... 128
7.3.2 Dental caries assessment ....................................................................................... 129
7.3.3 Sample Collection and Epigenetic analysis ........................................................... 129
7.4 Results .......................................................................................................................... 135
7.4.1 Methylation differences on chromosomes ............................................................. 136
7.4.2 Functions of identified genes ................................................................................. 136
7.5 Discussion, conclusion and limitations ........................................................................ 138
7.5.1 Discussion .............................................................................................................. 138
7.5.2 Conclusion ............................................................................................................. 141
7.5.3 Limitations ............................................................................................................. 141
Chapter 8: General Discussion............................................................................................... 143
8.1 Introduction .................................................................................................................. 143
8.2 Overview of the study .................................................................................................. 143
8.2.1 Background and research objectives ..................................................................... 143
8.3 Main empirical findings ............................................................................................... 145
8.3.1 Dental caries experience in the sample of children and their mothers .................. 145

xiv
8.3.2 Oral health knowledge and behaviours of mothers ............................................... 147
8.3.3 Maternal and environmental factors that influence the caries experience of children
........................................................................................................................................ 148
8.3.4 Children’s individual factors: prenatal environment, birth weight, and intra oral
characteristics as risk indicators for caries experience ................................................... 149
8.3.5 Epigenome-Wide Association Study of individuals discordant for dental caries: The
pilot study ....................................................................................................................... 151
8.4 Limitations ................................................................................................................... 154
8.5 Discussion and recommendations for future studies .................................................... 155
8.5.1Strengths of the study ............................................................................................. 155
8.5.2 Future research directions ...................................................................................... 156
8.6 Conclusions .................................................................................................................. 159
References .............................................................................................................................. 161
Appendix A : Oral Health Questionnaire............................................................................... 188
Appendix B: Kappa statistics for dental caries examination ................................................. 194
Appendix C: Search strategy used in litrrature search ........................................................... 196
Appendix D: Supplementary tables for differentially methylated CpG sites on chromosome 12
between cases and controls .................................................................................................... 199
Appendix E: Results of further pyrosequencing done on an extended sample of individuals
discordant for dental caries .................................................................................................... 201
Appendix E 1. Rationale .................................................................................................... 201
Appendix E 2. Results ........................................................................................................ 202
Appendix E 3. Future directions ........................................................................................ 205

xv
LIST OF TABLES
Table No: Title Page/s
Table 2.1 A summary of maternal, environmental and individual
determinants of childhood dental caries
34-41
Table 3.1 Percentage and of 6-7 year old children with caries experience in
Australia in 2011 ( 95% Confidence Interval )
46
Table 4.1 Frequency distribution of children’s and mothers’ socio
demographic and clinical characteristics.
70
Table 4.2 Frequency distribution of mother’s oral health related knowledge
and behaviours
71
Table 4.3 Risk indicators for children with and without dental caries using
logistic regression
71
Table 4.4 Risk indicators for childhood dental caries using negative binomial
regression
72
Table 5.1 Children’s individual characteristics explored as risk indicators for
dental caries experience and current activity
85
Table 5.2 Potential subject-based risk indicators for dental caries in children
analysed by structural equation modelling
86
Table 6.1 A summary of Genome-wide linkage and Genome-wide
association studies for human dental caries
99-100
Table 6.2 A summary of candidate genes studies for human dental caries 102-104
Table 7.1 Caries experience of controls and cases 132
Table 7. 2 Demographic and socio economic characteristics of controls and
cases
133
Table 7.3 Annotated data for the 16 identified Differentially Methylated
Regions between controls and cases
134
Table 7.4 Functions of gene clusters derived from DAVID 135
Table 7.5 Summary of Differentially Methylated Regions (with only one
CpG site) related to a gene promoter region.
137
Appendix B
Table 1
Calibration of examiner 1 for ICDAS criteria against a gold
standard
194

xvi
Appendix B
Table 2
Calibration of examiner 2 for ICDAS criteria against a gold
standard
195
Appendix C
Table 1
Search strategy used in PubMed 196
Appendix C
Table 2
Search strategy used in Scopus 197
Appendix C
Table 3
Search strategy used in Google Scholar 198
Appendix D
Table 1
Comparison of mean Differentially Methylated Regions on
chromosome 12 between controls and cases amongst children
199
Appendix D
Table 2
Comparison of mean Differentially Methylated Regions on
chromosome 12 between controls and cases amongst mothers.
200
Appendix E
Table 1
Percentage methylation analysis of CpG sites; Chr12:11700151,
Chr12:11700148 and Chr12:11700124 between individuals with
high and low caries experience
203
Appendix E
Table 2
Comparison of differential methylation of Chr12:11700151,
Chr12:11700148 and Chr12:11700124 between individuals with
high and low caries experience
204
Appendix E
Table 3
Correlation between individuals with high and low caries
experience and percentage methylation of CpGs;
Chr12:11700151, Chr12:11700148 and Chr12:11700124
204

xvii
LIST OF FIGURES
Figure Title Page
Figure 1.1 Community, maternal, child and epigenetic influences on
dental caries of children.
7
Figure 2.1 Child, family and community influences on oral health
outcome of children.
18
Figure 3.1 Conceptual framework for the possible interaction of risk
indicators under investigation.
48
Figure 3.2 Flowchart showing the process of data collection 52
Figure 5.1 Path analysis model with estimate of association between
dependant and independent variables
89
Figure 6.1 Environmental factors effecting epigenetic modification 115
Figure 6.2 A CpG island in relation to a gene promoter region 117
Figure 6.3 DNA methylation at CpG sites. 118

xviii
LIST OF APPENDICES
Appendix Title Page
Appendix A Oral Health Questionnaire 188
Appendix B Kappa statistics for dental caries examination 194
Appendix C: Search strategy used in literature search 197
Appendix D Supplementary tables for differentially methylated CpG sites
on chromosome 12 between cases and controls
199
Appendix E Results of further pyrosequencing done on an extended
sample of individuals discordant for dental caries
203

xix
STATEMENT OF ETHICS APPROVAL
I confirm that ethical clearance for this research was granted by the Griffith University Human
Research Ethics Committee, Australia (GU Ref No: DOH/20/12/HREC and GU Ref No:
OTH/25/13/HREC). I confirm that research was conducted in accordance with the approved
protocol.
Surani Fernando
Supervisor: Professor Newell Johnson Supervisor: Professor Paul Scuffham
xx
LIST OF PUBLISHED AND SUBMITTED PAPERS FROM
THE THESIS
Published papers
1. Fernando S, Speicher DJ, Bakr MM, Benton MC, Lea RA, Scuffham PA et al. (2015).
Protocol for assessing maternal, environmental and epigenetic risk indicators for dental
caries in children. BMC Oral Health 15(1):167. DOI.org/10.1186/s12903-015-0143-2
(29 December 2015).
Submitted papers
1 Surani Fernando, Gabor Mihala, Mahmoud Bakr, Shu-Kay Ng, Rodney Lea, Paul A
Scuffham, Newell W Johnson. Maternal caries experience, household income,
carbonated drinks and age at commencement of tooth-brushing are associated with
caries experience among 6-7 year old children in Australia. (Submitted to “Caries
Research” and under review- manuscript ID 201705020 )
2 Surani Fernando, Santosh Kumar, Mahmoud Bakr, David Speicher, Rodney Lea, Paul
A Scuffham, Newell W Johnson. Mothers who report taking iron supplements during
pregnancy and child’s oral carriage of mutans Streptococci are associated with a child’s
lower and higher lifetime dental caries experience, respectively (Submitted to “Journal
of Public Health Dentistry” and under review- manuscript JPHD-OA-08-17-0226).
xxi
3 Surani Fernando, Miles Benton, David Jeremiah Speicher, Mahmoud Bakr, Ping
Zhang, Rodney Lea, Paul A Scuffham, Newell Walter Johnson. An Epigenome Wide
Association Study of mother child dyads discordant for dental caries: A Pilot Study.
(Submitted to “BMC Oral Health” and under review-manuscript ID OHEA-D-17-
00215)

xxii
ACKNOWLEDGEMNET OF PUBLICATIONS INCLUDED IN
THE THESIS
The publications (published and submitted) included in this thesis are co-authored with other
researchers. These publications are in accordance with Section 9.1 of the Griffith University
Code for the Responsible Conduct of Research (“Criteria for Authorship”), Section 5 of the
Australian Code for the Responsible Conduct of Research, and Section 9.3 of the Griffith
University Code (“Responsibilities of Researchers”).
My contribution to each co-authored paper is outlined at the front of the relevant chapter.
Appropriate acknowledgments of those who contributed to the research but did not qualify as
authors are included in the thesis acknowledgments.
Surani Fernando
Supervisor: Professor Newell Johnson Supervisor: Professor Paul Scuffham

1
Chapter 1: Introduction
1.1 Background
Dental caries remains the most prevalent disease worldwide, burdening billions of people,
especially children, with pain and subsequently poor quality of life and general health
(Schwendicke et al., 2015; Kassebaum et al., 2015). According to the FDI World Dental
Federation, in 2010 44% of the world’s population was affected by tooth decay (Kieu et al.,
2017). Untreated dental caries is a major public health problem affecting 621 million children
worldwide (Kassebaum et al., 2015). Despite progress made in caries control by the protective
effects of fluoride, increased interventions in oral health promotion, widespread health
education, and advanced treatment options, dental caries still persists as a disease that places
a significant financial burden on both individuals and health care systems (Splieth et al., 2016).
The basics of the caries process are simple: acids derived from the fermentation of carbohydrate
foods dissolve enamel, and later dentine, if oral hygiene is poor and large volumes of microbial
biofilm remain on tooth surfaces. This means that, fundamentally, prevention of this disease is
simple and within the means of most ordinary members of society through self-care: restrict
the intake of readily fermentable carbohydrate and brush teeth thoroughly once or twice a day
with a fluoridated toothpaste (Cohen et al., 2017). Nevertheless, in real life, most people fail to
maintain their own oral health, and the predisposing susceptibility and resistance factors are
highly complex. In that sense, dental caries is a multifactorial disease, complexly modified by
genetic, behavioural, social, and environmental factors (Ditmyer et al., 2010; Splieth et al.,
2016). Historically, research was focused more on biological and dietary influences on the
disease. Recent years have seen interest growing in exploring a broader framework,
2
incorporating psychosocial and environmental influences, along with biological measures.
There remain many gaps in knowledge as to how these wider risk indicators, and possible risk
factors, interrelate, and why some children suffer a greater burden of disease than others.
It has been well researched that maternal education and income have a significant impact on a
child’s oral health. Socio-economic circumstances, mainly income (Schwendicke et al., 2015),
maternal level of education (Kumar et al., 2014), employment status (Tanaka et al., 2013), and
age (Niji et al., 2010), influence children’s susceptibility to, and experience of, dental caries,
as higher income is said to promote improved living conditions and reception of health care
(Capurro et al., 2015; Jepsen et al., 2017). Despite changing roles and responsibilities within
the family (Poutanen et al., 2007), the mother is still recognised as the key influencer of a
child’s eating and oral hygiene habits, and thus caries status, more than others (Saied-Moallemi
et al., 2008). Consequently, maternal oral health-related knowledge, beliefs, and attitudes
influence the oral health behaviour of their children (Poutanen et al., 2007; Saied-Moallemi et
al.; 2008, Szatko et al., 2004). Arguably, family circumstances reflect their socio-economic
status (SES); families provide support and role modelling to children so that their oral health
is influenced by their caregivers’ behaviours and perceptions. For example, single parent
families tend to be stressed, including financially, so that the principal role model may not be
setting a good example regarding health behaviours, with impact on the dental caries status of
the children (Hooley et al., 2012; Östberg et al., 2016; dos Santos Pinto et al., 2016). Given
that dental caries is a lifestyle disease and shares risk indicators with several other chronic
conditions like obesity, maternal body mass index could be expected to predict dental caries of
children to some degree (Wigen and Wang, 2011), especially because of the influence mothers
have on their children’s eating habits (Wigen and Wang, 2014). Thus, high levels of untreated
caries in mothers increased the odds of their children having untreated caries (Ersin et al., 2005;

3
Warren et al., 2016; Birungi et al., 2016) and were associated with more severe disease in the
children (Weintraub et al., 2010). Poor maternal oral health was a predictor of their children’s
caries experience both in childhood and adulthood (Shearer et al., 2011). Additionally,
mother’s oral carriage of cariogenic bacteria, mutans Streptococci (MS) and Lactobacilli (LB),
are associated with early oral colonisation of their children with these microorganisms and has
been used as a predictor of increased childhood caries occurrence (Chaffee et al., 2014). As
mentioned above, an individual’s risk for initiation of a carious lesion lies in an acidic
environment at tooth surfaces, (Kianoush et al., 2014, Varma et al., 2008), perhaps with low
flow rates of saliva (Diaz de Guillory et al., 2014), which may have poor buffering capacity
(Gao et al., 2016), and be reflected in low hydration of the mouth (Varma et al., 2008). The
homoeostasis of the oral environment is thus critical, and little attempt has been made to
explore maternal saliva characteristics and any association they might have with their child’s
oral environment and levels of dental disease. That is not to imply a direct effect on the child:
rather if the mother’s markers of caries risk in her saliva are high, it is likely that some of the
conditions which have produced this situation will also apply to her child.
It is evident that the prenatal circumstances of a child, which is strongly influenced by maternal
health and nutrition, will affect the development of children’s teeth because the deciduous
dentition is formed throughout most of the foetal period (Billings et al., 2004). Especially,
maternal intake of calcium, iron, folate, multivitamins, vitamin D, vitamin C, and fluoride
affect the development and mineralisation of their baby’s dentition (Tanaka et al., 2015;
Takahashi et al., 2015; Schroth et al., 2014). Vitamin and mineral deficiencies during
pregnancy are frequently accompanied by recurrent infections and have an adverse effect on
the daily functioning and well-being of both mother and foetus (De-Regil et al., 2016). It is of
interest, therefore, to understand the intra-uterine environment and to explore if any

4
abnormalities therein are related in any way to the caries experience of their offspring.
Moreover, low birth weight is a marker of foetal growth and has been linked to a variety of
chronic diseases in later life (Barker et al., 2002; Barker and Thornburg, 2013). Likewise,
compromised foetal nutrition and growth may affect the development of deciduous teeth, which
starts in utero. Low birth weight has especially been linked with enamel hypoplasia (Nelson et
al., 2013) and thereby with increased levels of caries (Bernabé et al., 2017).
As a child ages, he/she is exposed to many risk conditions. The mores of the wider community
and family influence the risk of developing caries, and risks will be reflected in intra-oral
conditions which play a direct role in the disease process. The physicochemical properties of a
child’s saliva, pH, buffering capacity, and flow rate play a major role in determining the levels
of MS and LB in saliva (Ramamurthy et al., 2014) and therefore in the susceptibility to caries
(Preethi et al., 2010). However, baseline (past) caries was the strongest single predictor of
accumulated carious lesions in children throughout the first one or two decades of their lives,
post-partum (Attaran et al., 2016). Thus caries experience in the deciduous dentition has been
found to predict caries experience in the permanent dentition (Casanova-Rosado et al., 2005).
Despite growing, detailed knowledge of the biochemical and biophysical mechanisms of the
caries process, and increasing attention paid to behavioural, social, and wider environmental
factors, dental caries persists as the main chronic disease among children worldwide
(Kassebaum et al., 2015). To this effect, The National Institute of Health Consensus
Development Program (USA) released a statement in 2001, specifying that there is a great
need for studies to identify genetic drivers, or at least genetic markers, which could be related
to diagnosis, prognosis, and therapy for dental caries
(http://consensus.nih.gov/2001/2001DentalCaries115html.htm). Even though the impact of

5
the human genome on dental caries has been researched for decades through twin (Boraas et
al., 1988), family (Bretz et al., 2005), genome-wide sssociation studies (GWAS; Vieira et al.,
2008), and candidate gene studies (Vieira et al., 2014), no potent effect variants have been
identified, indicating that factors other than the genome itself may have an impact on the
development of the disease: the epigenome may be one such. The epigenetic code, which is a
subject’s genome modified by environmental stimuli, determines when and where in the body
genes are expressed. Along with many other diseases, understanding the epigenome is
increasingly relevant to research in cariology (Williams et al., 2014; Seo et al., 2015).
1.2 Rationale for conducting the research in South East Queensland
Levels of dental caries in children have risen in Australia in recent years. From 1977 to 1995,
data from school dental services suggested that there was a drop in dental decay in deciduous
teeth (AIHW, 2014). However, by the year 2002, just over 47% of 5- to 6-year-old children
had one or more teeth with carious cavities measured with dmft index and, of these lesions,
80% were untreated. Out of all states and territories, Queensland (QLD) children aged six years
had the second highest caries scores (dmft 2.28) (Armfield et al., 2007). Moreover, by 2010,
55% of 6-year-old Australian children had experienced decay in their deciduous teeth
(Chrisopoulos et al., 2016). In 2010, out of the children who visited school dental services,
48% of 5-year-olds with caries had a mean decayed, missing or filled teeth index of 2.32
(AIHW, 2014). Oral health surveillance data from 2004-2006 revealed that there is a substantial
variation in children’s oral health across Australian states and territories (ARCPOH, 2009,
2014). With New South Wales as the reference state, QLD children who were 6-7 years old
had the highest caries experience (dmft 2.17) (Lucas et al., 2011,; Plonka et al., 2013). Mean
dmft scores of children varied between geographical regions in QLD: Among 5- to 6-year-olds,

6
it was 1.9 in Brisbane, 2.0 in the wider South-East, 2.4 in Northern Queensland, but only 1.4
in Townsville, which has had fluoridation of public water supplies since 1965, the only town
to receive this benefit in the State. Dental caries statistics in children, especially in the state of
QLD, show that this disease is a serious public health problem (Wong et al., 2012; Do and
Spencer, 2016).
Further, it has been highlighted that over a period of three years (from January 2008 to August
2010), the majority of emergency cases in children below 18 years who presented at community
dental clinics in Logan Beaudesert region were caries related, compared to other dental
emergencies (trauma and orthodontic related) (Wong et al., 2012). When compared with other
areas of QLD, the South East region has a higher proportion of children living in low-income
households (Do and Spencer, 2014). It was reported that the prevalence of untreated decay in
children from low-income areas such as Logan District (36.9%), was more than that of children
from medium-income areas (27.7%) and high-income areas (19.3%) (Do and Spencer, 2014).
Predictive and precise caries risk assessment allows the clinician to identify problems early
for effective preventive therapies and appropriate treatment planning, according to an
individual child’s level of risk. The literature on predictors of dental caries in children is
overwhelming, with numerous systematic reviews identifying socio-demographic, dietary,
and family-level as important risk indicators of childhood dental caries in different child
populations. Although the importance of understanding risk indicators of the process of dental
caries among Western industrialised countries is widely acknowledged, little attempt has been
made to explore the association between caries and a multitude of factors simultaneously
among the same population of children. Given this research gap, this thesis aims to gain
insights into associations between wider socio-economic, environmental, and family

7
variables, especially related to mothers of the children under study, and their child’s caries
history and current activity. We consider the intra-uterine environment of the child from
information on mothers during pregnancy. We then study the general health and oral
physiology of the children and search for epigenetic modifications which might be related to
the cariogenic process (Figure 1.1).
Figure 1.1: Community, maternal, child, and epigenetic influences on dental caries in children
1.3 Research questions and objectives
Based on the research gap identified in the literature on associations between children’s dental
caries and risk indicators, the main research theme of this thesis is centred on three main
research questions.
Wider socio-economic environment
Dental caries
Children’s in-utero environment
Epigenetic modifications
Maternal factors
Children’s intra oral Environment

8
1. Is there a relationship between maternal and environmental risk indicators, SES, mother’s
body mass index, intra oral characteristics, oral health knowledge, behaviours, and the caries
experience of their children?
2. What are the associations between children’s past dental caries experience, salivary
characteristics, prenatal conditions, birth weight, and both lifetime experience of dental caries
and current active dental caries?
3. Are there any differences in epigenetic modifications between individuals discordant for
lifetime, cumulative caries experience?
Answering these questions based on the caries status of a population of mother-child dyads in
South East Queensland (SEQ) is expected to fill the research gap identified. Specific objectives
of the thesis are to:
measure the level of dental caries in a sample of 6- to 7-year-old children and their mothers;
assess the oral health knowledge and behaviours of mothers of 6- to 7-year-old children in
the study sample;
develop risk factor models based on a proposed conceptual framework for dental caries in
a sample of 6- to 7-year-old children inclusive of maternal, environmental and children’s
individual characteristics as markers of risk; and
conduct a pilot study to screen for epigenetic modifications which might, conceivably, have
effects on cariogenesis.

9
1.4 Contribution of the study
The thesis makes two significant contributions to the literature around dental caries in general,
and childhood dental caries in SEQ in particular.
First, the thesis endeavours to narrow the gap in the existing literature on risk markers for
childhood dental caries in a typical Western industrialised population. Although there are
plenty of studies which document possible risk indicators for dental caries among children of
such populations, the amount of research which seeks to identify and quantify such a wide
range of risk factors, including epigenetic influences, is limited. This research explores the
impact of maternal, environmental, and children’s factors as potential risk indicators for
childhood dental caries. Possible interactions between variables were analysed to arrive at the
most significant correlations, and from these to fit hypothetical models of risk indicators. The
salient feature of these models is that they allow researchers to infer the findings in clinically
and biologically meaningful ways.
Second, the thesis adds new empirical findings to the literature on epigenetics and dental caries.
It examines the associations of epigenetic modifications, measured as differential methylations
in DNA, and lifetime experience of dental caries. In addition, new techniques are used to
sequence DNA with bisulfite treated DNA for methylation analysis on the SeqCap Epi 4 M
CpGIANT enrichment platform (Roche NimbleGen, USA). It examines, on a limited number
of dyads, as a pilot experiment, the differentially methylated CpG sites between individuals
with high and low caries experience. At the date of submission, this study may be the first of
its kind to assess epigenetic variations with regards to dental caries experience. Preliminary
10
experiments on deep sequencing of putative genetic loci associated with caries susceptibility
are described.
1.5 The structure of the thesis
The remainder of the thesis is organised into eight chapters. Chapter 2 provides an overview
of current understanding of the aetiopathogenesis of dental caries in otherwise healthy children,
on current Australian and global epidemiology, and on quantification of risk indicators for
dental caries in children. This chapter lays the foundation for the thesis and highlights the main
focus of the thesis.
Chapter 3 is presented as a published paper entitled, “Protocol for assessing maternal,
environmental and epigenetic risk indicators for dental caries in children”. It describes the
study design and methodological approach. Sample selection, sample size calculation, data
collection methods and proposed analyses are described in detail.
Chapter 4 is a results chapter and is presented as a submitted paper entitled, “Maternal caries
experience, household income, carbonated drinks and age at commencement of tooth-brushing
are associated with caries experience among 6- to 7-year-old children in Australia”. This
chapter gives the findings on risk indicators for dental caries in children concerning children’s
socio-economic environment and maternal characteristics, including behavioural and intra oral
attributes, and oral health knowledge.
Chapter 5 is a results chapter and is presented as a submitted paper entitled, “Mothers who
report taking iron supplements during pregnancy and child’s oral carriage of mutans

11
Streptococci are associated with a child’s lower and higher lifetime dental caries experience,
respectively.” The chapter explores the risk markers for children’s current caries experience,
measured with International Caries Detection and Assessment System (ICDAS > 0 at time of
examination), focusing on the child as an individual. Child’s prenatal environment and birth
weight, saliva physiology, and past caries experience (measured by the number of tooth
surfaces with restorations) are considered.
Chapter 6 provides an overview of the genetic predisposition to dental caries and explores what
lies beyond the current knowledge on genetics. It discusses the possible relationships between
caries and epigenetics, and it highlights the lack of empirical research in the area. Further, the
chapter provides the foundation for the next results chapter.
Chapter 7 is a results chapter presented as a submitted paper entitled, “An epigenome wide
association study of mother-child dyads discordant for dental caries: A Pilot Study”. It presents
the findings of a pilot study exploring epigenetic changes, detected in differential methylations
in DNA, between mother-child dyads with high and with low lifetime caries experience.
Chapter 8 is a regular thesis chapter. It concludes the study with an overview of the research,
focusing on research questions and objectives. The main findings regarding risk markers for
dental caries in a population of SEQ children are then discussed. Following this, the chapter
highlights the limitations of the study, future research directions and concluding remarks.

12
Chapter 2: Review of literature
2.1 Introduction
The purpose of this chapter is to examine the literature on current understanding of the
aetiopathogenesis of dental caries in children. The chapter also presents a brief description of
conceptual frameworks that have been proposed as means of understanding the risk indicators
for the process of childhood dental caries.
For this narrative review, PubMed via Medline and Google Scholar were used as data bases.
Key words used were children, caries, dental caries, risk, susceptibility, influence, maternal,
environmental, familial, individual, gender and caries history. Additional Boolean commands
were used to narrow down the search. Further the search was limited to full text journal articles
published between 1912/01/01 and 2017/08/01 on humans. Mesh terms for keywords were
used during the literature search in PubMed.
The chapter organisation is as follows. Section 2.2 outlines the burden of dental caries among
children over the last few decades. Section 2.3 briefly discusses the conceptual frameworks
proposed by researchers to identify risk indicators for dental caries. Section 2.4 reviews the
literature on determinants of dental caries in children from community level influences to
family level and child-level influences. Section 2.5 summarises the chapter with concluding
remarks.

13
2.2. The burden of dental caries in children
Since oral health is merely a part of the general wellbeing of individuals, compartmentalisation
of the mouth and the rest of the body regarding health conditions is not justified. Oral health
affects children’s general health by causing pain, suffering, and changing their dietary habits,
speech and quality of life (Sanders et al., 2009). Dental caries manifests as a continuum of
disease states of increasing severity and tooth destruction, ranging from subclinical changes to
lesions with dentinal involvement (Kidd and Fejerskov, 2004), and it is the fourth-most
expensive chronic disease to treat according to the World Health Organization (WHO)
(Petersen, 2008). If left untreated, caries augments oral infection (Selwitz et al., 2007) and
affect children’s school attendance and performance (Jackson et al., 2011). In 2010, untreated
caries in deciduous teeth was the 10th most prevalent condition affecting 9% of the global child
population (Kassebaum et al., 2015). In Asia Pacific high-income countries, the prevalence of
deciduous caries declined slightly from 10.8% in 1990 to 9.6% in 2010 (Kassebaum et al.,
2015). In Australasia, the decrease was from 5.5% to 4.9%, whereas in Europe (Central,
Eastern, and Western) the prevalence did not show a marked difference from 1990 to 2010
(Kassebaum et al., 2015). These data show that, worldwide, dental caries in the deciduous
dentition is not under control, in spite of our detailed knowledge of aetiopathogenesis. We
know how to prevent most caries in most individuals, but fail to apply these approaches at a
population level.
Decay of deciduous teeth (measured with decayed, missing, and filled teeth index; dmft, with
decay recorded at the level of cavitation) in children aged 6 attending school dental services in
Australia decreased from a mean dmft of 3.19 in 1978 to 1.45 in 1996, followed by a gradual
increase to a mean of 2.58 in 2010. According to National Child Oral Health Study in Australia

14
(2012-2014), one in every four children aged 5-to 10-years at that time had untreated decay in
their deciduous teeth (Do and Spencer, 2016). In 2013, approximately two-thirds (64.4%) of
children aged 5 and over had made a dental visit. Almost 4 in 5 (78.8%) children aged 5-14
had made a dental visit in the previous 12 months, with 90.6% having visited within the past
two years, although the nature of the visits were not explained (Chrisopoulos et al. 2016).
Furthermore, Chrisopoulos et al. (2016) report that mean dmft of Australian children in the
year 2015 was 1.83 for 5-year-olds, 1.74 for 6-year-olds and 2.63 for 8-year-olds (Chrisopoulos
et al., 2016). However, oral health surveillance data indicate significant variations in children’s
oral health and dental service attendance across Australian states and territories (ARCPOH,
2009; AIWH, 2014). In 2007, 5- to 6-year-old QLD children had the highest caries mean dmft
of 1.72 (Ha et al., 2011). Lucas et al. (2011) made the same observation in 2011 and report that
caries experience of 6- to 7-year-old children in QLD was the highest: mean dmft score 2.17,
followed by 1.68 in Northern Territory, and 1.53 in Western Australia. Dental caries is clearly
a serious public health problem, especially in QLD (Wong et al., 2012). Even within the state,
areas of high social disadvantage such as the Logan-Beaudesert district have the highest caries
prevalence among children (Plonka et al., 2013). In SEQ, dental caries was the number one
reason among children for attending hospital emergencies: in 2009 it accounted for 75% of all
emergency attendances and in 2010, 74% (Wong et al., 2012). In 2009, restoration of carious
teeth represented 26% of all treatment provided per month, and 20% in 2010. There was an
overall rise in the number of paediatric emergency visits in SEQ from 2008 to 2010, and the
most common cause was caries-related, for instance, dental pain and abscesses (Wong et al.,
2012). These observations show considerable geographical variations in population oral health,
which exist from a young age.
15
During the past few decades research into population oral health has focused on describing
biological and dietary determinants of disease. In more recent years there has been a growing
interest in exploring children’s oral health outcomes using a broader framework, incorporating
psychosocial, and environmental influences, together with biological (Crall et al., 1990) and
genetic (Boraas et al., 1988) variables. The effort towards a more comprehensive approach
stems partly from the recent shift in thinking about population health, in which academic
reports have proposed increasingly complex conceptualizations of oral health determinants.
Studies assessing risk factors for dental caries in children have reported different results, due
to variations in study designs, analytical methods, subjects’ ages, and definitions of risk factors
and caries phenotypes (Chankanka et al., 2011).
From a public health perspective, exploring consistent caries-related factors would be essential
for the prevention of the disease. However, the values of generalising such indicators among
different populations is debatable due to the ever present population diversities. Investigations
that look into associations of these varied characteristics and childhood caries are needed to
understand the disease trajectory, and thereby to reduce the disease burden.
2.3 Proposed Conceptual frameworks describing the process of dental caries
The common risk factor approach (CRFA) for oral diseases has been widely accepted and
endorsed globally by dental researchers and promoters of oral health, prompted to some extent
by policy recommendations from the WHO in the 1980s (Petersen and Kwan, 2010). This
concept was further developed and applied to oral health with an emphasis on directing action
at shared risk factors for chronic diseases including dental caries. Sheiham and Watt in 2000
proposed a conceptual framework addressing the broader shared social determinants of chronic

16
diseases, highlighting that a behavioural preventive approach alone would only widen the oral
health inequalities across populations (Sheiham and Watt, 2000). They placed a key emphasis
on socio-economic and political contexts which generate and maintain educational systems,
labour markets, welfare, and health systems leading to the maintenance of an individual’s
socio-economic position. They argued that this, in turn, would result in changes in behavioural,
biological factors, psychosocial, and health care utilisation leading to oral health inequalities.
However, they do not discuss possible interactions between the different levels, and the
proposed conceptual framework is unidirectional.
A more comprehensive CRFA approach was taken by Petersen in 2005, based on the risk factor
model in the promotion of oral health suggested by the WHO (Petersen, 2003). The design
incorporates evidence available on potential socio-behavioural risks of dental caries and some
widely used outcome measures. Interrelated health system and oral health services,
sociocultural factors, and environmental risk indicators are explained as dynamics that
influence the use of oral health services and risk behaviours of individuals, families, or
populations. The outcome; prevalence, and severity of dental caries, is described as a result of
these proximal factors (Petersen, 2005). Moreover, the model is based on empirical evidence
from both developed and developing countries. However, biological and physiological
characteristics have not been included in the model.
A unifying conceptual model proposed by Seow (2012) addresses broader social,
environmental, maternal, and child factors that are commonly associated with childhood dental
caries. This model is centred on the mother, coming from a socially disadvantaged background,
low SES, and a relatively low-level of education. The author describes in detail how the
external environment could affect maternal economic stress, dysfunctional parenting, health

17
beliefs, and behaviours which eventually lead children to a high risk of caries (Kim Seow,
2012). It also highlights possible interactions between the wider environment and the mother’s
characteristics. However, the model lacks a multi-level approach as child’s characteristics,
biological, and physiological risk factors have not been considered. According to the
conceptual framework proposed by Johnson in the early 1990s, dental caries is described as a
disease process that depends on a continually changing balance between external stimuli and
the host’s biological response to such stimuli. These stimuli act in an environment conditioned
by a range of local and general predisposing factors, and a range of local and general resistance
factors. The initiation of dental caries itself, as outlined in the model, is a relatively simple
series of physicochemical interactions at the tooth surface (Johnson, 1991). The balance
between demineralisation and remineralisation, which varies over time, is determined by
interactions amongst this wide range of predisposing and resistance factors.
A comprehensive model of children’s oral health, considering the wider social environment,
immediate family environment, children’s characteristics, and their possible interactions was
proposed by Fisher-owens, in 2007 (Figure 2.1) (Fisher-Owens et al., 2007). This conceptual
model of oral health is based on a solid foundation of social science and epidemiologic studies
of population health. The particular factors chosen to be included in the model were based on
research identifying key influences on children’s oral health, including genetic and biological,
social and physical environment, support system, health behaviours, and dental and medical
care. This conceptual model includes a broad range of genetic, social, and environmental risk
factors and appropriate multiple levels of influences, including a time or developmental
dimension.

18
Figure 2.1. Child, family and community influences on oral health outcome of children (Source: Fisher-Owens et al., 2007; Copy rights license
Number 4204590201918 https://s100.copyright.com/CustomerAdmin/PLF.jsp?ref=05f7487f-ec06-4b22-a903-9511ee5d81b5 )
19
A conceptual model directs researchers towards recognising risk indicators for disease and the
model’s greatest value would be when it can be used empirically, even though the relative
importance of each influence will vary between different populations. With the evolution of
social contexts and human behaviours, new risk markers and risk indicators evolve. Hence,
researchers need to be constantly aware of emerging trends. New analytical approaches guided
by the conceptual models are needed to reach the next stage of public health policy in order to
combat still high levels of dental caries.
2.4 Determinants of dental caries
The answer to the question ‘What causes dental caries in children?’ is an important, and
complex one. It concerns those in both developed and developing countries where many
children experience the adverse consequences of the disease. Understanding the aetiology and
pathogenesis of the disease would have a direct influence on the most appropriate preventive
and treatment interventions. They may include past caries experience, information about socio-
demography, socio-economy, oral hygiene, dietary habits, oral bacteria, and saliva
characteristics (Table 2.1). These comparatively objective parameters are often accompanied
by a subjective assessment of risk level. Children are especially vulnerable since they are
exposed to risk indicators for dental caries, notably high sugar-containing foods and treats,
provided by well-meaning adults and poor oral hygiene practices (Seow et al., 2009).
According to the conceptual frameworks described, dental caries is a social, cultural, and
behavioural condition that has a genetic interplay within the individual.

20
2.4.1 Maternal and environmental determinants
2.4.1.1 Socio-economic status
Socio-economic circumstances early in life help determine future health outcomes such as
dental caries. Low SES and neighbourhood poverty are significantly associated with a greater
risk of caries, unmet dental care needs, and poor oral health-related quality of life (OHRQOL)
(da Fonseca and Avenetti 2017). According to Vargas (1998), SES is a complex construct that
is operationally defined in many ways (Vargas, 1998). Most of the dental studies use parents’
education, income, and occupation as associated factors of SES (Nicolau et al., 2005). In
general, there is an inverse relationship between caries and SES: a high prevalence of childhood
caries has been shown to be related to low family income (dos Santos Junior et al., 2014).
Higher income promotes healthy living, better access to dental health care, and improved
conditions of life, although the reverse is often seen in developing countries (Fisher-Owens et
al., 2007). Aida et al., (2017) from their longitudinal survey of “Babies in the 21st Century”,
reported that in Japanese preschool children the rate of caries treatment at the age of
approximately 3 years was <10% for all SES groups and this increased to more than 30% at
around age 6. Children from lower SES received more frequent caries treatment compared to
their affluent counterparts (Aida et al., 2017). Similar observations were made in the USA
among children from low-income families (Ismail et al., 2008). Nevertheless, in rural settings
of developing countries, where traditional diets have low cariogenicity, it is the wealthier
classes, often urban, who have access to high sugar diets and hence higher caries experience
among children (Petersen, 2005). Not all studies agree: Chaffee et al. reports that dental caries
associated lower oral health-related-quality-of-life scores were similar across all social groups
among a population of Brazilian children (Chaffee et al., 2017). Moreover, Carvalho et al.,

21
(2014) did not find a significant association between caries development and household
monthly income in Brazil (Carvalho et al., 2014).
2.4.1.2 Family structure and environment
Family structure and stability are paramount for children to develop well and for the
establishment of healthy oral habits. Children in a family that experiences instability, for
instance, loss of resources, frequent moves, violence, child support issues, divorce,
incarceration, or maternal depression tends to have poor health behaviours (da Fonseca and
Avenetti, 2017; Piva et al., 2017). Parents play a pivotal role in the establishment of oral health
promoting behaviours that prevent the development of childhood dental caries (Hooley et al.,
2012). Mattila et al. (2000) reported that children in single-parent households are more likely
to have advanced levels of caries and have more periodic use of dental services (Mattila et al.,
2000), probably due to the lack of resources and social support being distributed among all
family members. Family structure and household crowding also have a significant impact on
children’s caries status, with single children showing a lower caries experience and a lower
impact of oral health on their quality of life (Kumar et al., 2016; Moimaz et al., 2014). Further,
lack of help in raising children is considered as a risk indicator for dental caries in children
since it can be a barrier for seeking oral health care for working mothers (Kim Seow, 2012).
Children from poorer functioning families on the dimensions responsiveness, communication,
organisation, and social network had higher levels of dental decay than children from normal
functioning families. Furthermore, they were also more likely to engage in less favourable oral
hygiene behaviours (Duijster et al., 2014). Reynolds et al. (2015) however, disagree that family
composition was not significantly associated with the oral health status of children. They report
that neighbourhood social capital plays a more prominent role in childhood dental caries than

22
the individual family structure (Reynolds et al., 2015). Nevertheless, studies linking the broader
home environment and family functioning to childhood dental caries are limited.
2.4.1.3 Maternal level of education, oral health knowledge and behaviours
When it comes to child rearing, the mother still plays the major role (Kavanaugh et al., 2006).
A systematic review reported that more studies are demonstrating a significant effect with a
child’s dental caries and mother’s level of education than that of the father’s (Hooley et al.,
2012). Maternal education level is an important indicator that reflects knowledge and skills for
making healthy behaviour choices (Laaksonen et al., 2005) For example, highly educated
mothers report more positive attitudes and stronger intentions to control children’s sugar intake
than low-educated mothers (Warren et al., 2016). In populations where the majority of people
have a low level of education, caries risk behaviours like frequent consumption of fermentable
carbohydrates and sweetened low pH beverages, and poor oral hygiene habits are more
common (Ashkanani and Al-Sane, 2012). Sweet food intake has a clear causal relationship
with dental caries, and maternal education has been reported as a risk indicator that affects
sweet food intake of children (Ju et al., 2016). Despite mothers’ high-level oral health
knowledge, perceptions of self and child oral health would ultimately determine the oral health
status of the offspring (Heaton et al., 2017). Research evidence suggests that the mother's
positive attitudes towards good oral health have an influence on her children's brushing habits,
diet, and oral diseases (Saied-Moallemi et al., 2008). Nevertheless, a study conducted in
Kuwait reported that maternal oral health knowledge was weakly correlated with practice,
suggesting that changing oral health-related behaviours takes more than just improving
knowledge (Ashkanani and Al-Sane, 2012). An added factor could probably be a child’s
temperament and the self-efficacy of the mother. A study on a population of Hispanic mothers
and children revealed that child’s resistance towards tooth brushing and lack of time in

23
supervising the children during brushing were some reasons for poor oral hygiene for the
children (Tiwari et al., 2017). It also has been revealed that negative child temperaments can
exacerbate parental stress and worsen parental feeding and oral health practices (Tiwari et al.,
2017). It also has been reported that negative child temperaments can exacerbate parental stress
and worsen parental feeding and oral health practices (Tiwari et al., 2017).
2.4.1.4 Maternal body mass index
Maternal body mass index (BMI) is an indication of health and lifestyle habits, such as diet,
physical activity, and attitudes to health and well-being, which ultimately influence the children
and the establishment of their oral health behaviours (Wigen and Wang, 2011). Children’s
dietary intake has been shown to be strongly associated with their mothers’ dietary intake, and
the children’s dietary habits are developed early in life (Oliveria et al., 1992). When exploring
the association between maternal diet and caries development in children, the results showed
that having a mother who consumed more sugar and fat than recommended, was associated
with caries development in children. Moreover, a mother with BMI classified as obese was
associated with caries development in their children before 5 years of age (Wigen and Wang,
2014). The association of BMI with dental caries is not necessarily causal and is complicated
by many intervening variables (Silva et al., 2013). For instance, dietary habits and income are
considered important factors for both dental caries and obesity. Dietary habits related to obesity
may provide a higher quantity and frequency of sucrose intake, which are important factors in
caries aetiology (Carvalho Sales-Peres et al., 2010). However, a study done in India reports
that maternal BMI is not significantly associated with dental caries in children as the
associations of BMI with dental caries varied across SES categories (Kumar et al., 2017).

24
2.4.1.5 Maternal caries
As far back as 1946, it was found that there can be a significant increase in dental caries among
children whose parents had untreated caries (Klein, 1946). The relationship between maternal
caries levels and children's caries experience has been found to be stronger than that of their
fathers (Weintraub et al., 2010). Mothers caries status has been related to preschool children’s
caries in Turkey (Ersin et al., 2005), Thailand (Thitasomakul et al., 2009), and the USA (Smith
et al., 2002). However, in a Japanese population of pre-schoolers, maternal caries experience
was not a risk indicator (Kawashita et al., 2009). Nevertheless, Moyer (2014) proposed that as
a prevention strategy for dental caries in American children, mothers caries levels should be
assessed as a risk factor (Moyer, 2014). Proença et al. (2015) reported that Brazilian children
who had mothers with increased levels of dental caries were more at risk of developing the
disease themselves, and that the family environment and maternal attitudes exert a significant
influence on the child and can affect children’s behaviour, thus reflecting on oral health
(Proença et al., 2015). Since mothers play a vital role in rearing children, certain maternal
characteristics expose the child to adverse environmental conditions that encourage caries
development and progression in children. For instance, frequency of dental visit, maternal
sugar consumption, oral hygiene practices, maternal attitudes towards oral health (Kumar et
al., 2016), and genetic predisposition (Boraas et al., 1988). This is evident by the conceptual
framework proposed by Fisher-Owens, as dental caries being a multi-level, multifactorial
disease having interactions within the oral cavity to include child, mother, and community-
level influences that vary over time (Fisher-Owens et al., 2007).

25
2.4.1.6 Maternal cariogenic bacteria
Other than the impact of unhealthy practices of caregivers, maternal-child transmission of oral
bacteria is one such potential mechanism, given the essential, albeit not sufficient, role of oral
infection in caries development. Despite conflicting evidence that has challenged the accepted
concept of vertical transmission as the mode of initial colonisation with MS, the mother as a
source is logical, due to closest contact when initial colonisation occurs (Douglass et al., 2008).
During and shortly after birth, the epithelial surfaces in the oral cavity of infants become
colonised by numerous bacterial species. This cross-establishment is usually from mother to
child, particularly when the mother has active caries and high levels of cariogenic bacteria in
their mouths (Hooley et al., 2012). Childers et al. (2017) report that the fidelity of MS genotype
between mother and child through vertical transmission was 58%, where, 40 out of 69 African
American mother-child dyads who participated in the study shared the same MS genotype
(Childers et al., 2017). Moreover, significant reductions in the incidence of MS carriage and
caries experience were observed in children whose mothers received preventive and restorative
interventions aimed at reducing the count of these organisms in their mouths before and shortly
after the birth of a child (Brambilla et al., 1998; Köhler and Andreen, 1994). Nonetheless, MS
(i.e., MS and Streptococcus sobrinus) have been implicated as the principal etiologic agent
involved in the initiation of human dental caries (Gross et al., 2010) and LB species as primary
late colonizers that are associated with advanced cavitation (Dige et al., 2014), both of which
could be taken as risk indicators for childhood dental caries.

26
2.4.1.7 Maternal salivary physiology
The interplay between microorganisms, diet, and host susceptibility determines whether dental
caries will occur. As teeth are constantly bathed in saliva, the constituents and properties of
this oral fluid play an essential role in the occurrence and progression of dental caries. Saliva
is believed to be one of the most important host factors and a key mediator controlling the
speed and direction of the cariogenic pathway (Fejerskov and Kidd, 2008). Saliva may protect
teeth through several mechanisms, such as clearance of food debris and sugar, aggregation and
elimination of microorganisms, buffering actions to neutralise acid, and maintaining
supersaturation on tooth mineral (Dawes, 2008). Salivary flow rate is the most important caries
preventive function of saliva for its “flushing/oral clearance” capacity by some researchers
(Lagerlöf, 1994), and the higher the flow rate, the faster the clearance and the more protection
for teeth from dental caries (Lagerlöf, 1994). However, low salivary flow rates (< 0.8 – 1.0
ml/min stimulated whole saliva) are found in pathological conditions and have reduced
sensitivity as a predictor for caries (Lenander-Lumikari and Loimaranta, 2000; Leone and
Oppenheim, 2001). Nevertheless, some research evidence suggests that there is no correlation
with caries process and salivary flow rate (Russell et al., 1991; Varma et al., 2008) while others
site salivary flow rate as a potential risk marker for dental caries (Gao et al., 2016). These
results cannot be generalised as dental caries phenotypes and methods used to measure flow
rate may vary within studies.
The carbonic acid/bicarbonate buffer is the primary buffer in stimulated saliva, with
bicarbonate acting mainly to neutralise acids produced by bacteria when they digest sugars in
the mouth or acids from the stomach (Lenander-Lumikari and Loimaranta, 2000). The pH of
the oral cavity is maintained at 6.3 to ensure the maintenance of the integrity of the tooth
structure with the acid neutralising capacity of the salivary bicarbonate buffering system
27
(Bardow et al., 2000). However, a recent study done in the USA among individuals with cystic
fibrosis gave conflicting results. It was observed that there was no significant association
between salivary flow rate or buffering capacity and caries prevalence among the participants.
However, the results cannot be generalised to the general population as the sample size was
small with n = 83 cystic fibrosis patients (Alkhateeb et al., 2017).
The pH of saliva is modulated by salivary bicarbonates, phosphates, and urea (Humphrey and
Williamson, 2001) maintaining the saliva pH between 6 and 7. The pH of saliva measured
directly from the ducts of individual salivary glands varies between 5.3 at low flow rates to 7.8
at maximum flow rates (Bardow et al., 2004; Humphrey and Williamson, 2001). A drop in pH
below 5.5 means that such acidic saliva has harmful effects on enamel and dentine (Aframian
et al., 2006; Bardow et al., 2004). There is sparse literature on the association between the pH
of resting saliva and dental caries (Varma et al., 2008), for it is plaque pH that contributes most
for the demineralization of the tooth surface and ultimately to the development of dental caries
(Lenander-Lumikari and Loimaranta, 2000). A dissimilar result was observed by Dos Santos
et al. in 2015 in a group of children with sialorrhea. Onabotulinum toxin given to control
sialorrhea reduces the salivary flow rate and alters salivary pH. The level of acidity, measured
by mean pH, among the group remained within neutrality range, and had not caused
demineralization of enamel surface. However, they observed a significant and positive
association with caries, stating that poor oral hygiene and cariogenic diet could have
contributed to an increase in caries activity even though the saliva pH remained neutral (Ferraz
dos Santos et al., 2016).

28
There is no published literature that explores the association of buffering capacity of saliva in
mothers, pH, and flow rate as risk indicators for children’s dental caries; hence, an investigation
is timely and would address the existing research gap.
2.4.2 Influence of children’s individual factors
2.4.2.1 Intrauterine environment of child and birth weight
The foetal environment is considered as a crucial indicator in the causality of diseases later in
life (Barker and Thornburg, 2013). Many studies are supporting the hypothesis that adult life
can be ‘modelled’ during intrauterine life, implying that intrauterine nutritional deficiencies
could be associated with adult diseases such as hypertension, diabetes, and obesity (De Boo
and Harding, 2006). Intrauterine growth is taken as an independent predictor of diseases in
childhood and throughout life (Barker, 1998; Cameron et al., 2012). Likewise, deciduous tooth
formation and mineralisation start during the foetal period. Hence the intrauterine environment,
which is affected by factors such as smoking and maternal nutrition during pregnancy, might
influence the development, formation, and mineralisation of children’s teeth (Winter, 1976).
Reported maternal intake of prenatal supplements by mothers has been associated with foetal
nutrition, lack of which linking to the development of conditions like autism (Schmidt et al.,
2011). Therefore, supplementation use is usually recommended during pregnancy to meet the
nutrition needs of both mother and foetus (Scholl, 2005). Maternal vitamin D deficiency in
pregnancy is reported to predispose children to developmental dental defects (specifically
hypermineralized enamel) since during prenatal development, vitamin D reaches the fetus only
through the placenta (Riggs et al., 2016). Reed et al. (2017) reported that children whose
mothers did not take vitamin D supplements during pregnancy were more at risk of developing
enamel hypoplasia (Reed et al., 2017). Hypoplastic enamel is more susceptible to colonisation
by cariogenic bacteria and is often hypersensitive, making adequate oral hygiene difficult and

29
hence increasing the risk of the child developing caries (Reed et al., 2017). Moreover, Bergel
et al., in 2010 showed that children whose mothers received calcium supplementation when
pregnant showed a significant reduction in dental caries compared to their corresponding
counterparts (Bergel et al., 2010). Research done with animal models have shown that vitamin
A deficiency during foetal life would result in failure of ameloblastic activity, which may lead
to enamel agenesis and hypoplasia (Armstrong, 1948). There is a dearth of literature on humans
that investigates the association between reported maternal prenatal supplement intake and
dental caries status of the mother’s offspring, hence the need to further investigations.
With, recently, attention shifting to early life factors for dental caries, the role of birth weight
is far from settled. Low birth weight, a marker of foetal growth, has been linked to a variety of
chronic diseases in later life (Barker and Thornburg, 2013). Even though birthweight was not
associated with baseline dental caries experience in a population of Scottish children, low birth
weight put them on a trajectory of increased dental caries over a period of 4 years (Bernabé et
al., 2017). There is evidence suggesting that infants with very low birth weight have an
increased risk for enamel hypoplasia and hence are placed at high risk of developing dental
caries (Nelson et al., 2013). These findings support the view that the prenatal and postnatal
environments are important for children’s dental status and also underscore the advantages of
focusing on accumulation of disease over time
2.4.2.2 Age and gender
One of the factors that are currently associated with dental caries in children is the lifetime of
dentition. Older aged children were more likely to have caries than their younger counterparts.
This difference is liable to be because caries experience measures the cumulative effects of
dental caries in the life time of a dentition (Mwakayoka et al., 2017). In a population of Nigerian

30
children, the proportion of children with caries increased significantly with increasing age up
to the age of 4 years, although there were other social and oral hygiene determinants associated
with the age (Folayan et al., 2015). A study conducted in China revealed that the prevalence of
caries in three age groups (36-47 months, 48-59 months, and 60-70 months) showed significant
differences, with the oldest group having the highest mean dmft of 5.54 (Li et al., 2011). These
observations are as expected because as age increases children have more teeth, they are
exposed to more cariogenic food and beverages, and if coupled with poor oral hygiene
behaviours are more predisposed to dental caries (Mwakayoka et al., 2017).
Though there are few studies undertaken specifically in children on the association of dental
caries and gender, the existing ones give contrasting evidence. Pecharki et al. (2016) showed
that caries was negatively associated with being male (Pecharki et al., 2016), whereas Declerck
et al. reported that boys were more at risk of developing caries than girls (Declerck et al., 2008).
Moreover, in a Chinese population of children aged 6 to 71 months, females were less likely
to have childhood caries (Li et al., 2011). Nevertheless, a study undertaken among a group of
Indian adolescents reported that females significantly made up most of the high caries cluster
(Warren et al., 2017). In Brazilian children who were aged 9 years, no significant association
could be observed with gender and dental caries experience (Casanova-Rosado et al., 2005).
This observation was also made by Chankanka et al., (2011) in a group of 5-year-old children
in the USA (Chankanka et al., 2011), and by Aida et al., (2008) in Japanese toddlers (Aida et
al., 2008).
2.4.2.3 Past dental caries
According to Attaran et al., (2016) baseline caries was shown as the strongest single predictor
of future caries in children (Attaran et al., 2016). Dental caries is diagnosed typically at the
31
tooth surface level, where both the shape and the depth of any potential lesions are scored on
an ordinal scale representing the stages of the disease process, ranging from sound (no lesion)
to lesions into the dental pulp. These observations enable epidemiological and clinical studies
to describe the intraoral susceptibility of dental caries and predict future risk through Bayesian
latent variable models (Zhang et al., 2011). Based on that, Pak et al. (2015) developed a
Bayesian approach to predict future transition probabilities of dental caries, given a child’s
observed caries life history data. The established model could predict future development of
caries not only for individual teeth but also at the mouth level (Pak et al., 2017). Whilst the
most reliable evidence comes from empirical research, although different population groups
may show unique predictive values (Attaran et al., 2016). Survival analysis revealed that
children without past caries experience in deciduous teeth at baseline remained caries free in
permanent teeth for a longer period than children with previous caries experience at baseline
(Cortellazzi et al., 2013). Piva et al. (2017) reported that dental caries progression in a cohort
of Brazilian pre-schoolers was directly associated with baseline caries (Piva et al., 2017). After
two years follow-up, the severity of baseline caries which included dentine lesions (ICDAS 4,
5 and 6) had almost doubled (Piva et al., 2017). According to Parisotto et al. (2012) even past
non-cavitated lesions (ICDAS 1 and 2) at baseline increased the risk of developing new caries
in a population of 3- to 4-year-old preschool children in Brazil (Parisotto et al., 2012),
indicating the importance of early screening for detection of dental caries.
2.4.2.4 Physicochemical properties of saliva
The saliva circulating in the mouth at any given time is termed as the whole saliva, and it
comprises a mixture of secretions from the major and minor salivary glands and traces from
the gingival crevicular fluid. Evaluating the causative factors in saliva of individual’s at risk to
dental caries can pay the way to make recommendations that will cater specifically to children’s

32
individual needs (Gopinath and Arzreanne, 2006). Salivary buffering capacity and pH have an
inverse relationship as buffering mechanisms in saliva (bicarbonate, phosphate, and protein)
act to neutralise salivary pH (Lenander-Lumikari and Loimaranta, 2000). A study undertaken
among 7- to 14-year-old children from India showed that salivary pH and buffering capacity
were low in a caries group compared to a caries free group (Preethi et al., 2010). However, the
associations were not significant, probably due to factors like microflora, diet and retention of
food might have dominated the buffering capacity and pH to initiate caries. Tulunoglu et al.
(2006) observed contradictory results in their study between caries free and caries active
groups. Salivary pH values were higher in the 7- to 10-year-old girls, in the caries free group
than in the caries-active group, whereas in the 11- to 15-year-old group, pH values were
significantly higher in caries active girls. They stated that individual and environmental
variations could be a major cause of the results. For instance, different foods containing varied
levels of dietary proteins and carbohydrates, can affect the salivary buffering capacity and
hence the observed differences in the sample of children (Tulunoglu et al., 2006). Nevertheless,
there is evidence that larger quantities and faster rates of acid production are present in caries
active children than that in caries-free children (El-kwatehy and Youssef, 2016). Even though
the evidence regarding salivary pH and buffering as a risk marker for dental caries is
inconclusive, it is still considered as a non-invasive and reliable risk assessment method for
caries in children (El-kwatehy and Youssef, 2016; Preethi et al., 2010).
2.4.2.5 Oral cariogenic bacteria
Even though dental caries is multifactorial, the crucial role of microorganisms is well
established in childhood dental caries (Palmer et al., 2010). According to Tanzer et al. (2001),
dental caries is a dieto-bacterial disease resulting from interactions between a susceptible host,
cariogenic bacteria, and cariogenic diets (Tanzer et al., 2001). The primary infection is by MS

33
and LB are found to play a role in the progression of caries (Samaranayake, 2012), and are part
of normal oral flora (Samaranayake, 2012) transmitted from parents or caregivers (Childers et
al., 2017). In an Indian child population (aged 3-5), a significant positive association was found
between salivary MS levels and caries experience and also between LB counts and caries
experience, where salivary loads of MS was the predominant bacterial species in the oral
microbiota (Ramamurthy et al., 2014). El-kwatehy and Youssef (2017) demonstrated that the
number of 6- to 12-year-old Egyptian children with MS or LB ≥ 105 colony forming units/ml
of saliva was significantly higher in caries affected children compared to caries free children
(El-kwatehy and Youssef, 2016). Even though MS and LB have been identified as the main
cariogenic bacteria, there are much more undetected genera in the oral cavity (Wade, 2013).
ElSalhy et al. (2016) demonstrated that there were more than 98 bacterial species in their
sample of 11- to 12-year-old children with carious lesions in Kuwait. Surprisingly, in their
sample of children, microbiota of the caries-affected vs. caries-free children was similar
(ElSalhy et al., 2013). Instead of MS and LB, they have found that the microbiota of the caries-
affected children was associated with higher levels of A. defective, A. meyeri, and A.
odontolyticus compared with caries-free children, and the levels also significantly correlated
with caries severity and the number of lesions (ElSalhy et al., 2013). A possible reason for this
observation could be that all children were initially selected for the study based on high MS
and LB levels in either plaque or saliva. Thus, an association might not have been detected.
Nevertheless, compared to other oral bacteria, MS possess an extraordinary ability to infect and
colonise teeth and promote the development of cariogenic biofilms in the presence of sucrose
(Leme et al., 2006). Early acquisition and colonization of MS (before 3 years of age) has
resulted in higher levels of oral MS and Decayed–Missing–Filed (DMF) index at the age of 19
years (Köhler and Andréen, 2012), indicating the importance of controlling infection by these
bacteria in the oral cavity of young children (Hajishengallis et al., 2017)

34
Table 2.1: A summary of maternal, environmental and individual determinants of childhood dental caries
Author/s Study setting Type of
study
Risk indicators investigated Outcome variable Significant risk indicators
Maternal and environmental determinates
Nicolau et al. 2005 13 year old
Brazilian school
children (n=764)
Cross
sectional
Mother’s level of education, Father’s level of
education, Family income
Area of residence, Family structure, Paternal
levels of punishment, Birth order, Tooth
brushing frequency
Sugar consumption, Pattern of dental
attendance, Use of fluoride mouth rinse,
Height
DMFT Being second or later child (p=0.008),
Children from rural areas(OR = 2.74, 95% CI
=1.56–4.82), Mothers with lower levels of
education (OR = 2.10, 95% CI=1.03–4.27),
High levels of paternal punishment(OR
=1.60, 95% CI = 1.02–2.52)
Ismail et al. 2008 1021 African
American
caregiver-child (5-
year - old) dyads
Annual household income, Highest
education level, Caregivers’ relationship to
children, Frequencies of moving, Types of
insurance, Religiosity, Children’s
consumption of sugary foods, Depressive
symptoms of care givers, Parenting stress,
Perceived discrimination
dmfs Intake of soda beverages by children
(p=0.04), Caregivers’ fatalistic oral health
beliefs ( p=0.01) ), Religiosity ( p=0.02)
Carvalho et al.
2014
2,511 Brazilian 1-
to–5-year-olds
Cross
sectional
Mother’s education, Mother’s age, Monthly
family income, Parental practices to child’s
oral health,
Bottle-feeding the child during the night on
demand (p=0.0001), Not assisting the child in
tooth brushing (p=0.0001), Ensuring visit to
the dentist in case of troubles with teeth only
(p = 0.0001), Intake of sugary products 2–4
times daily at nursery (p = 0.026)
dos Santos Junior
et al. 2014
320 Brazilian
preschool children
Cross
sectional
Family income, Adolescent pregnancy
Birth weight, Gestational age, Nutritional
Risk
dmft Family income (p = 0.009), Birth weight (p <
0.001), Nutritional Risk (p < 0.001)
Aida et al. 2017 Japanese children
from 2.5 – years- to
-5.5 -years
(n=35260)
Longitudinal
(3-year
follow up)
SES measured by parental level of education Slope index of
inequality (SII) and
relative index of
inequality (RII) for
caries treatment
SII increased for ages 2.5 and 5.5 (95%
CI=3.16-5.09 and 13.68-17.32) respectively.
RII decreased for two age groups (95% CI,
1.59- 2.11 and 1.46- 1.61 respectively)

35
Author/s Study setting Type of
study
Risk indicators investigated Outcome variable Significant risk indicators
Family structure
Mattila et al. 2000 1443 Finnish
mother-child (5 –
year- old) dyads
Longitudinal
(5-year
follow up)
Mother’s tooth brushing, Father’s caries
history, Marital status, Place of dwelling,
Mother’s age at child birth, Sugar
consumption at 18 months of age, Headache
episodes of child
dmft Mother's irregular tooth brushing (OR 2.2;
95% CI 1.4-3.5), Annual occurrence of
several carious teeth in the father (OR 2.6;
95% CI 1.9-3.6), Daily sugar consumption at
the age of 18 months (OR =2.4, 95% Cl=1.4-
4.1), Occurrence of child's headaches (OR
3.7; 95% CI 1.5-8.8), Parents' cohabitation
(OR 3.3; 95% CI 1.5-7.6), Rural domicile
(OR 2.4; 95% CI 1.2-4.5), Mother's young
age (OR 5.0; 95% CI 1.3-19.8).
Duijster et al. 2014 5- to- 6-year-old
Netherlands
children (n=630)
Cross
sectional
Location of dental clinic, Education level of
mother, Family functioning dimensions
Ethnicity, Relationship status of caregiver,
Birth order of the child, Oral hygiene
behaviours,
dmft Sociodemographic characteristics (p <
0.001), Oral hygiene behaviours (p < 0.001),
Family functioning dimensions (P < 0.05)
Moimaz et al.
2014
272 Brazilian
mother-child (1-to -
5 -year -old) dyads
Cross
sectional
Marital status, Number of children,
Education level, Employment, Income,
Frequency of visits to a dentist
Need for dental
treatment (NDT=
decayed teeth)
Maternal education (p<0.0001), Household
income (p<0.0001), Frequency of visits to a
dental professional (p<0.0018), Number of
children in the household (p<0.0001)
Maternal level of education, oral health knowledge and behaviours
Ju et al. 2016 1720 Australian
indigenous mother–
child (3- to -5 –
year- old) dyads
Longitudinal
(5-year
follow up)
Mother’s education level Maternal report of
child’s decay, or
extracted teeth due
to decay
0–9 years (β=1.21, 95% CI=1.05-1.39) , 10
years (β=1.06, 95% CI= 0.94–1.19) and 11–
12 years (β=1.06, 95% CI= 0.95–1.19
compared to > 12 years of education

36
Author/s Study setting Type of
study
Risk indicators investigated Outcome variable Significant risk indicators
Maternal body mass index (BMI)
Wigen and Wang
2014
5 year old
Norwegian children
(n=1348)
Longitudinal
(5-year
follow up)
Oral health behaviour at 1.5 year of age,
Sugary drinks, Sugary drinks at night,
Maternal health and lifestyle, Maternal
dietary fat, Maternal BMI, Maternal
education, Parental origin, Family status
from pregnancy to age 5
dmft Having mother with non-western background
(β=5.4, 95% CI= 2.8–10.6), Having mother
with low education (β=1.5, 95% CI= 1.1–
2.3), A change in family situation from two
to one parent family (β=2.0, 95% CI= 1.1–
3.4), Having mother who consumed more
sugar and fat than recommended (β=1.6, 95%
CI= 1.1–2.5), Having mother with BMI
classified as obese (β=2.3, 95% CI= 1.3–4.1),
Low tooth brushing frequency at 1.5 year of
age (β=2.3, 95% CI= 1.4–3.7) , frequent
consumption of sugary drinks at 1.5 year of
age (β=1.7, 95% CI= 1.1–2.8)
Maternal caries
Smith et al. 2002 60 mother-child (3-
to- 5- year- old)
dyads from the
USA
Cross
sectional
Maternal high mutans Sreptococci level,
Maternal caries experience, reported sugar
consumption and demographic variables of
mother,
dmft Maternal high mutans Sreptococci levels (p <
0.001), Sugar consumption (p= 0.01),
Maternal active decay (p=0.004),
Ersin et al. 2005 101 Turkish
mother-child (15-
to- 36 months)
dyads
Cross
sectional
Maternal caries experience, Maternal
education, Breast feeding duration, Maternal
sharing of utensils, Child’s caregiver type,
First primary teeth eruption, Using a pacifier
dfs High maternal DMFS scores (OR=1.074;
95%
CI=1.0-1.15)
Kawashita et al.
2009
369 Japanese
mother-child (3 –
year- old) dyads
Cross
sectional
Residential area, Health insurance, Age of
the mother, Drinking alcohol, Smoking
habit, Knowledge of dental terminology,
Frequency of tooth brushing a day,
Frequency of eating between meals a day,
Maternal caries, Sex of child, Birth order,
Habit of feeding in bed, Frequency of eating
between meals a day, Frequency of
consuming sports drinks, Preventive dental
care
dmft Birth order of child (p=0.05), Habit of
feeding in bed (p=0.02), Higher frequency of
eating between meals a day (p<0.001),
Higher frequency of consuming increased
amounts of sports drinks (p=0.001),
Preventive dental care (p=0.002)

37
Author/s Study setting Type of
study
Risk indicators investigated Outcome variable Significant risk indicators
Thitasomakul et al.
2009
406 Thailand
mother-child dyads
Longitudinal
(9 – to -18
months
follow up)
Maternal caries experience, Maternal
Educational level, Annual Income, Mother’s
decayed teeth, Calcium supplement during
pregnancy, Drinking milk during pregnancy,
Infant’s birthweight, Type of milk feeding,
Having commercial cereal at 3 months,
Having rice at 3 months, Mother started
sweetening food, Child start having snacks,
Child started having vegetables, Child
started having fish, Child started having
sugary snacks at 9 months, Child started
having local traditional dessert at 9 months,
Child started having soft drinks at 9 months,
Mother brushed the child’s teeth at 9 months
dmft Mother’s decayed teeth ≥ 10 (p ≤ 0.05), No
calcium supplement during pregnancy (p ≤
0.05), Mixed breast- and bottle-feeding (p ≤
0.001), No rice at 3 months (p ≤ 0.05), No
commercial cereal at 3 months (p ≤
0.001),Mother start sweetening food at ≤ 5
months (p ≤ 0.001),Child started snacking at
≤ 5 months (p ≤ 0.01), Child started having
sugary snacks at 9 months (p ≤ 0.05), Child
started having soft drinks at 9 months (p ≤
0.01), No daily tooth brushing at 9 months (p
≤ 0.001).
Weintraub et al.
2010
179 Hispanic
mothers and their <
18 year old children
(n=387) in the USA
Cross
sectional
Maternal untreated caries ds and DFS Maternal untreated caries (OR = 1.85, 95%
CI =1.12, 3.07)
Proença et al. 2015 77 Brazilian mother
child (1 - to-3 -
years) dyads
Cross
sectional
Children’s eating habits, Children’s oral
hygiene habits, Oral health conditions of
mother (dental caries, gingival bleeding and
plaque index), Oral health conditions of child
(caries, visible plaque, bleeding gums)
dmft High maternal caries experience (P < 0.001),
Maternal gingival bleeding (P < 0.001)
Maternal cariogenic bacteria
Chaffee et al. 2014 361 Hispanic
mother-child dyads
Cross
sectional
Maternal sociodemographic measures, Child
feeding and care practices, Maternal oral
health status,
Child’s relative
caries
incidence
feeding and care practices, and maternal
dental status, higher maternal salivary
challenge of both MS (p=0.01) and LB
(p=0.03) over the study period predicted
nearly double the child caries incidence
versus lower MS and LB

38
Author/s Study setting Type of
study
Risk indicators investigated Outcome variable Significant risk indicators
Childers et al.
2017
69 African
American mother-
child (1-to -3- year
- old) dyads
Longitudinal
(3-year
follow up)
S mutans genotypes (GT) of mothers and
children.
dmfs Mother-child pair with S mutans GT match
(p=0.014), S mutans in children at age
18 months (>500 CFU/ml) (p=0.002), S
mutans in children at age 18 months (>500
CFU/ml) (p=0.014)
Intrauterine environment of child and birthweight
Bergel et al. 2010 12-year-old
Argentina children
and their mothers
(n=195)
Cross
sectional
Calcium supplementation during pregnancy dmft/DMFT Children whose mother received calcium
during pregnancy had a 27% reduction
in the risk of developing at least one
DMFT/dmft (RR: 0.73, CI 95%=0.62-0.87)
Nelson et al. 2013 Infant-mother
dyads from the
USA
Longitudinal
(2-year
follow up)
Child’s birth weight (normal, low, very low) ICDAS ≥ 2 -
Bernabé et al.
2017
1102 Scottish
children from birth
up to 4 years
Longitudinal
(4-year
follow up)
Child’s early life factors: Age, Gender, Birth
order, Birth weight, Maternal age at birth,
Maternal education, Breastfeeding duration,
Marital status, Maternal smoking, Parental
employment, Area deprivation, Child’s tooth
brushing frequency
dmfs Predicted mean difference in dmfs = 1.86
(95% CI= 0.03 - 3.74) between children with
low and normal birth weight, Predicted mean
difference in dmfs= 1.66 (95% CI=0.57 -
2.75) between children of smoking and non-
smoking mothers.
Child’s age and gender
Casanova-Rosado
et al. 2005
1,644 Brazilian
children aged 6–13
years
Cross
sectional
Social, Economic, Behavioural,
Demographic variables
DMFT,
dmft, SiC
Mother’s schooling (OR=0.95, 95% CI=
0.90-0.97), Caries experience in the primary
dentition (OR= 6.31, 95% CI=4.57-8.72)

39
Author/s Study setting Type of
study
Risk indicators investigated Outcome variable Significant risk indicators
Declerck et al.
2008
3-year-old
(n=1250) and 1283
5-year-old
(n=1283) pre-
school children
from Belgium
Cross
sectional
Oral hygiene levels, Reported oral health
behaviours, Socio-demographic factors.
dmft In 3-year-olds,
Caries experience with presence of dental
plaque (OR = 7.93; 95% CI= 2.56–24.55),
Reported consumption of sugared drinks at
night (OR = 7.96; 95% CI=1.57–40.51),
In 5-year-olds,
Age (OR = 7.79; 95% CI= 2.38–25.43),
Gender (OR = 0.37 with 95% CI= 0.19–0.71
for girls), presence of visible dental plaque
(OR = 3.36; 95% CI= 1.64–6.89) Reported
habit of having sugar containing drinks in
between meals (OR = 2.60 with 95% CI=
1.16–5.84 and OR = 3.18 with 95% CI=
1.39–7.28, respectively for 1·/day and >
1·/day
Versus not every day).
Li et al. 2011 1523 Chinese
children aged < 71
months.
Cross
sectional
Age, Gender, Eating habits, Family status,
Childcare provider, Oral intervention
dmft/dmfs Rural residency (β= 0.78, AOR=2.2, 95%
CI=1.25-3.82, p=0.006), Private child care
facility (β = 0.73, AOR=2.1, 95% CI=1.34-
3.20, p=0.001), High frequency of carbonated
drinks (β = 0.52, AOR=1.6, 95% CI=1.02-
2.29, p=0.001), Using dairy products every
day (β = -0.53, AOR=0.59, 95% CI=0.35-
0.98, p=0.04), Bedtime eating (β = 0.88,
AOR=2.4, 95% CI=1.33-4.40, p=0.003), Age
(β = -0.92, AOR=0.40, 95% CI=0.24-0.65,
p=0.000)
Folayan et al. 2015 497 Nigerian
children aged 6
months- to – 6 -
years
Cross
sectional
Children’s ages, Sex, Socioeconomic status,
Tooth brushing habits, Sugary snacks
consumption, Use of fluoridated toothpaste,
Birth rank, Infant-feeding practices,
Breastfeeding practices, Maternal age at
childbirth, Maternal knowledge of oral
health
dmft Consumption of sugary snacks in between
meals more than three times a day (PR=0.05,
95% CI= 0.003 – 0.01, p = 0.04) , Child’s
oral hygiene status (PR: 0.05, 95 % CI=
0.005–0.10, p = 0.03)Child’s gender/female
(PR=−0.06, 95% CI=−0.10- -0.01, p= 0.02),
Mothers’ knowledge of oral health
(PR=−0.06, 95% CI=−0.11- -0.008,p= 0.02)

40
Author/s Study setting Type of
study
Risk indicators investigated Outcome variable Significant risk indicators
Pecharki et al.
2016
687 Brazilian
students aged 12-
years-old
Cross
sectional
Individual level, School level, District level DMFT Female (OR=0.51, p=0.33-0.79).
Mwakayoka et al.
2017
525 Tanzanian
children
aged 2-4 - years
and their
parents/caregivers
Cross
sectional
Children’s demographic variables (location,
gender, age, parent/care giver education,
parent occupation), Children’s dietary
behaviours
dmft Older age (OR =2.722 p< 0.001), frequent
consumption of factory made sugary
foods/snacks at age 1-2 years (OR=3.061,
p=0.021).
Warren et al. 2017 396 children aged
5-to-17-years from
the Iowa Fluoride
Study (IFS) cohort
Longitudinal
(17-year
follow up)
Fluoride and demographic/behavioural data
from 9-to-17-years
DFS at age 13 and
age 17
The high caries cluster was associated with
lower maternal education level (p<0.001 ),
lower 100% juice consumption (p<0.01),
lower brushing frequency (p=0.02) and being
female (p=0.01).
Child’s past dental caries
Parisotto et al.
2012
179, 3-and-4-year-
old pre-schoolers
from Brazil
Longitudinal
(1-year
follow up)
Dental caries experience at baseline and at 1
year follow up
dmft Children with caries activity at baseline were
at a higher risk of developing new lesions
than caries-free children (OR=17.3 for early
caries lesion
development, OR=24.5 for
cavitations/fillings, p<0.001)
Cortellazzi et al.
2013
5-year-old Brazilian
preschool children
(n=427)
Longitudinal
(3-year
follow up)
Caries experience at baseline and after 3
years, Gingivitis, Gender, Monthly family
income, Number of people living in the
household, Father’s educational level,
Mother’s educational level, Home
ownership, Fluorosis, Car ownership
dmft Past caries experience (p=0.0004)
Piva et al. 2017 3-to-4-year-old
Brazilian children
(n=119)
Longitudinal
(2-year
follow up)
Socioeconomic variables, Caries at baseline,
Presence of Streptococcus mutans, and
Lactobacillus, with the progression of caries
lesions after
two years of follow-up
ICDAS=0, ICDAS
1, 2, 3 and ICDAS
4, 5, 6
Marital status (RR= 0.73, p=0.04),
MS(RR=0.71, p=0.03), Non-cavitated lesions
(RR=0.48, p <0.001)

41
Author/s Study setting Type of
study
Risk indicators investigated Outcome variable Significant risk indicators
Child’s oral cariogenic bacteria
Tulunoglu et al.
2006
80 children aged 7–
15 years from
Turkey.
Cross
sectional
Unstimulated salivary flowrates, pH,
Buffering, Calcium, Total proteins, Total
antioxidants
DMFS=0 (caries
free) and DMFS>0
(caries active)
Salivary pH (p<0.000), Calcium
concentrations (p<0.000) between 11-to-15-
year-old caries active and caries free girls
Preethi et al. 2010 120 Indian children
in 7-10 and 11-14
year age groups
Cross
sectional
Salivary pH, Buffering capacity, Total
protein, Calcium, Total antioxidant capacity
dmfs/DMFS Significant differences between caries free
and caries active groups; Total antioxidant
Capacity in 7-10-year-old girls (p<0.001),
Total protein (p<0.01), Total calcium
(p<0.05) and Total antioxidant capacity (
p<0.05) in -10-year-old boys, Buffering
capacity (p<0.05), Total protein (p<0.05),
Total calcium (p<0.05) and Total antioxidant
capacity (p<0.01) in 11-to-14-year old girls,
Total protein (p<0.01), Total calcium
(p<0.01), Total antioxidant capacity (p<0.05).
Köhler and
Andréen 2012
Children of mothers
with high salivary
MS levels followed
up at 3, 4, 7, 11, 15
and 19-years-of-age
Longitudinal
(19-year
follow up)
Salivary MS, MS in plaque from 12 selected
proximal surfaces.
Lesion prevalence
(DFS)
Early-colonised children (≤ 3 year olds who
had mothers with high MS levels) had higher
DFS at 19 years of age than those who were
non-MS-colonised at 3 years (p=0.003)
ElSalhy et al. 2013 122 children aged
11-to-12 yeas from
Kuwait
Cross
sectional
Saliva and plaque MS counts, Daily
brushing, Beverage consumption, Sweet
consumption, Rinsing and flossing frequency
ICDAS, CI (CI),
DMFT and dmft
Correlation between plaque MS and ICDAS
CI (p < 0.05). Children who brushed once a
day or more had significantly lower ICDAS
CI (p < 0.01). Children who consumed sweets
or drank soft drinks more than once a day had
significantly higher ICDAS CI (p < 0.05).
El-kwatehy and
Youssef 2016
80 Egyptian
children aged 6-to-
12-years
Cross
sectional
Saliva flow rate, pH, Total protein
concentration, Total antioxidant, Cariogenic
microorganisms.
DMFT and DMFS Saliva pH (p<0.000) and α-defensin (p=0.04)
between caries active and caries free children
Ramamurthy et al.
2014
50 children aged 2–
5-
years from India
Cross
sectional
Salivary MS and LB dmft/dmfs Correlation between salivary MS dmft
(r=0.34, p=0.02) and between MS and dmfs
(r=0.37, p=0.01). Correlation between
salivary LB and dmft (r=0.30, p=0.03).
Presence of MS and LB between caries free
and children with caries (p=0.004).
DMFT-Decayed Missing Filled Teeth index (for permanent teeth)/ dmfs-decayed missing filled surfaces index (for deciduous teeth)/ dmft- decayed missing filled
teeth index (for deciduous teeth/, dfs-decayed filled surfaces (for deciduous teeth)/ ds-decayed surfaces (for deciduous teeth)/ DFS-Decayed Filled Surfaces (for
permanent teeth)/ ICDAS-International Caries Detection and Assessment System/ SiC-Significant Caries index/ CI- Caries Index

42
2.5 Concluding remarks
This chapter provided an overview of the conceptual models used to determine risk factors for
dental caries and how they have evolved over the years with ever-changing sociobehavioural
and environmental characteristics. In particular, the chapter discussed the determinants of the
development and progression of dental caries in children, and conflicting results observed in
different populations. As evident by this overview, although a multitude of risk indicators for
caries exist, and empirical research has been done in various population groups with different
age limits, some results are contrasting, indicating that sets of unique risk indicators act upon
each population. The conceptual model proposed by Fisher-Owens (2006) describes the
interaction within and between factors which ultimately result in dental caries development.
This thesis will use the model suggested by Fisher-Owens as a guide to build a conceptual
framework in assessing risk indicators for childhood dental caries in a population of SEQ
children.

43
Chapter 3: Protocol for assessing maternal, environmental and
epigenetic risk indicators for dental caries in a population of
Queensland children
This chapter is a published paper (paper 1). The bibliographic details of the paper, including
all authors, are as follows:
Fernando S, Speicher DJ, Bakr MM, Benton MC, Lea RA, Scuffham PA, Mihala G Johnson
NW (2015). Protocol for assessing maternal, environmental and epigenetic risk indicators for
dental caries in children. BMC Oral Health 15(1):167. DOI.org/10.1186/s12903-015-0143-2
(29 December 2015).
My contribution to the paper involved the conception and design of the study, exploring data
collection and statistical analysis methods and drafting the article.
The journal in which this article has been published is an open access peer-reviewed journal
with an international readership. Permission has been provided by the publisher, Biomed
Central, under their open access policy, which states that “As an author of an article published
in BMC Oral Health, you retain the copyright of your article and you are free to reproduce and
disseminate your work”.
Surani Fernando
Corresponding author: Newell Johnson
Supervisor: Professor Newell Johnson Supervisor: Professor Paul Scuffham

44
3.1 Abstract
3.1.1Background
Expenditure on dental and oral health services in Australia is AUD $3.4 billion annually. This
is the sixth highest health cost and accounts for 7% of total national health expenditure.
Approximately 49% of Australian children aged 6 years have caries experience in their
deciduous teeth, and this is rising. The aetiology of dental caries involves a complex interplay
of individual, behavioural, social, economic, political, and environmental conditions, and there
is increasing interest in genetic predisposition and epigenetic modification.
3.1.2 Methods
The Oral Health Sub-study, a cross-sectional study of a birth cohort, began in November 2012
by examining mothers and their children who were six years old at the time of the initiation of
the study, which is ongoing. Data from detailed questionnaires of families from birth onwards
and data on mothers’ knowledge, attitudes, and practices towards oral health collected at the
time of clinical examination are used. Subjects’ height, weight and mid-waist circumference
are taken and BMI computed, using an electronic bioimpedance balance. Dental caries
experience is scored using the ICDAS. Saliva is collected for physiological measures. Salivary
DNA is extracted for genetic studies including epigenetics using the SeqCap Epi Enrichment
Kit. Targets of interest are being confirmed by pyrosequencing to identify potential epigenetic
markers of caries risk.

45
3.1.3 Discussion
This study will examine a wide range of potential determinants for childhood dental caries and
evaluate inter-relationships amongst them. The findings will provide an evidence base to plan
and implement improved preventive strategies.
Keywords Dental Caries, Children, Risk, Environment, Genetic, Epigenetic
3.2 Background
Dental caries affects children and adults alike all over the world. It is a disease of the poor as
well as of the rich. Largely preventable, it remains the most prevalent chronic disease among
children with a significant impact on individuals, families and society. It has recently been
reported that 2.4 billion people globally have untreated dental caries (Kassebaum et al., 2015).
More than 40% of preschool and primary school children in Western industrialised countries
and other middle-income countries, including children in the United States of America (Ismail
et al., 2008b), Sweden (Wendt et al., 1996), Brazil (Oliveira et al., 2008) and Australia (Seow
et al., 2009) experience a high prevalence of dental caries. Despite progress made in caries
control over the years by the protective effects of fluoride, increased efforts in oral health
promotion, widespread health education, and remarkable advances in treatment options, dental
caries remains the most common chronic childhood disease (Kassebaum et al., 2015). Among
Australian children aged 6 to 7 years the prevalence of dental caries (treated and untreated
combined) was 32.4% in 2011(Lucas et al., 2011). This figure varies by state from 26.5% in
New South Wales to 43.8%, in Queensland (Table 1) (Lucas et al., 2011). According to the
Queensland Child Oral Health Survey in 2012, 49.5% of children aged 5-10 had experienced
dental caries (Center, 2014). More alarmingly, among South East Queensland children this

46
figure was just over 50% (ARCPOH, 2014). The mean decayed missing and filled teeth index
(dmft) for the same child population was 2.0 with 0.8 teeth being untreated (ARCPOH, 2014).
This worsening situation is despite substantial resources being allocated for the prevention and
treatment of oral diseases (AIHW, 2014).
Table 3.1: Percentage of 6- to 7-year-old children with caries experience in Australia in
2011 (95% confidence Interval)
State Caries prevalence of
6- to 7- year-old children (95% CI)
Australian Capital Territory 32.4% (21.8-43.1)
South Australia 29.8 %(24.6-35.0)
Western Australia 35.5% (31.1-40.0)
Victoria 30.0% (27.3-32.7)
New South Wales 26.5% (28.2-46.3)
Tasmania 37.3% (40.6-47.1)
Queensland 43.8% (40.6-47.1)
Northern Territory 37.8% (15.7-42.1)
All States 32.4% (31.0-33.8)
Source Lucas et al. 2011
Oral health is determined by many factors: socio-economic (Vargas et al., 1998),
environmental (Van De Mheen et al., 1997), political (Petersen et al., 2005), availability of oral
health care facilities (Lave et al., 2002), and their level of utilization (Kim and Telleen, 2004).
Furthermore an individual’s health related behaviours (Petersen, 2005; Rossow, 1992), as well
as oral health knowledge (Ashkanani and Al-Sane, 2012), attitudes (Schultz et al., 2001) and
practices (Ashkanani and Al-Sane, 2012), and biological factors (Nicolau et al., 2005)
including the intrauterine environment (Smith et al., 2002) and genes (Harris et al., 2004) have
an impact on his/her oral health. Additionally, maternal factors like the mother’s level of caries
(Harris et al., 2004; Shearer et al., 2011), her oral health knowledge (Ashkanani and Al-Sane,
2012; Kim Seow, 2012; Saied-Moallemi et al., 2008; Shearer et al., 2011; Smith et al., 2002;

47
Traebert et al., 2011), salivary loads of cariogenic bacteria (Li et al., 2005; Ramamurthy et al.,
2014; Van Houte, 1993), salivary characteristics including pH, flow rate and buffering capacity
(Bardow et al., 2000; Bardow et al., 2004) as well as maternal genetics (Harris et al., 2004) are
significant risk indicators to be considered for childhood dental caries. Furthermore, an holistic
approach in identifying risk indicators for dental caries is required as oral health is but a part
of general health (Fisher-Owens et al., 2007). Investigating newly emerging risk factors and
risk indicators for dental caries is crucial, and these can be discovered by studying the natural
history of disease and by using modern molecular-based approaches (Johnson, 1991). A
conceptual model of how we envision that these factors might interact is presented in figure
3.1.

48
Figure 3.1 Conceptual framework for the possible interaction of risk indicators under
investigation (Permission has been provided by the publisher, Biomed Central, under their open
access policy, which states that “As an author of an article published in BMC Oral Health, you
retain the copyright of your article and you are free to reproduce and disseminate your work)
49
The importance of inherited factors in susceptibility to dental caries has been recognized for
decades (Klein and Palmer, 1940; Klein, 1946). Heritability is the proportion of phenotype
variation explained by genetic factors. These have been estimated to account for 30-60% (p ≤
0.01) of the variation in caries scores for the permanent dentition and 54-70% (p ≤ 0.01) for
deciduous caries scores (Wang et al., 2010). According to Shaffer et al. (2015), there is direct
evidence for a genetic component in the aetio-pathogenesis of dental caries (Shaffer et al.,
2015) but very little is known about the specific casual mechanisms (Olszowski et al., 2012).
There are many genes related to the composition and structure of dental enamel, inherited
alterations in sugar metabolism, and genetic regulation of salivary gland function.
Unsurprisingly, no single host gene that directly regulates dental caries initiation or progression
has been identified (Shaffer et al., 2012a). Epigenetics, however, may provide the missing link
to these unanswered questions (Barros and Offenbacher, 2009). Epigenetics investigates the
molecular mechanisms that link genetic and environmental cofactors to disease outcomes
(Williams et al., 2014). There are many complex mechanisms underlying epigenetic alterations,
such as DNA methylation, histone modification and gene regulation by non-coding RNA, of
which DNA methylation is the most common (Seo et al., 2015). Such changes may be heritable
or could be environmentally modulated. DNA methylation seems to be the primary mechanism
to suppress retro-transposable elements which are responsible for creating genetic variation
and, on occasion, disease-causing mutations within the human genome. Because these elements
remain partially methylated in sperm, there may be a prolonged period of transposition lasting
a few generations before gene expression (Tang et al., 2015). Possible epigenetic contributions
are currently being investigated in many diseases, but such studies are relatively novel in the
dental field (Seo et al., 2015) and are needed to fully understand DNA-based factors important
for development of oral diseases (Fisher-Owens et al., 2007).

50
3.3 Methods
3.3.1 Study population
The research described in this paper is the oral health arm of the main “Environments for
Healthy Living – the Griffith Birth Cohort Study” (EFHL), which, beginning in 2006, has
recruited some 3,000 families from South East Queensland. EFHL is a prospective, multi-year
longitudinal birth cohort study, collecting information during pregnancy through infancy and
adulthood (Cameron et al., 2012b). The EFHL study population includes all births from three
geographically defined adjoining Health Districts in Queensland (Logan, Beaudesert, and the
Gold Coast) and Northern Rivers/Tweed in NSW from 2006 to 2011. These four areas cover
30% of Queensland’s population. Women waiting for antenatal clinic appointments from the
three public maternity hospitals (Logan, Gold Coast, and Tweed) in the participating districts
were contacted by research-trained midwives, provided with a detailed explanation of the study
aims, and invited to participate (Cameron et al., 2012a). Written informed consent was obtained
from participants to access their information from hospital databases, to complete a maternal
baseline survey and for individual follow-up (Cameron et al., 2012b). The initiators of the
EFHL study expected to incorporate future sub-studies including research on dental and oral
health (Cameron et al., 2012a). The population for the oral health sub-study, which began in
2012, is a subset of 6- to 7-year-old EFHL children and their mothers who accepted our
invitation to participate.
Ethics approval to initiate the oral health sub-study was obtained from the Griffith University
Human Research Ethics Committee on 26.12.2012, based on a full National Ethics Approval
Form process, with N.W. Johnson as responsible Principal Investigator. A Variation to archive
and analyse DNA was approved on 17.07.2014 (GU Ref No: OTH/25/13/HREC). The ethics

51
approvals and informed consents obtained cover the clinical examination of mothers and their
child/children and parental consent for full participation for their child/children in all aspects
of the study.
3.3.2 Sample recruitment and examination
In 2012, mothers of the first cohort of children, who were 6 years old at the time, were sent
letters alerting them to the oral health study, followed by a telephone call to assess their level
of interest. Since then we went on to recruit participants from 2007 to 2009 cohorts and the
recruitments are still taking place. Participants who find it difficult to travel far, who have
serious illness and who are not willing to undergo a detailed oral examination are excluded
from the study. Those who agree to attend the dental clinic at Griffith Dental School are given
appointments for a free dental examination of the mother and child by two qualified dental
surgeons, which includes offer of free treatment for the child if required. Both mother and child
are asked not to brush their teeth 2-3 hours prior to examination, not to consume sweet food or
beverages, smoke, or use a mouthwash as per oral examination criteria. Mothers who are
pregnant or who are wearing cardiac pace makers are excluded from weighing on the
bioimpedance scale. Detailed medical histories are taken when subjects arrive at chair side
(Figure 3.2).

52
Figure 3.2: Flow chart showing the process of data collection (Permission has been provided
by the publisher, Biomed Central, under their open access policy, which states that “As an
author of an article published in BMC Oral Health, you retain the copyright of your article and
you are free to reproduce and disseminate your work)
A careful examination of the head and neck, visually and by palpation, is performed. Each
participant is then examined for salivary physiology, for the health of the oral soft tissues, for
dental status, and for experience of dental caries. Periodontal disease requirement (n = 147
dyads) was initially guided by the one-sample correlation test to determine whether a
correlation coefficient differs from zero, set at a low correlation level of r=0.4 (2-tailed alpha
=0.05, power=0.80), calculated using the “power one correlation” command of STATA v 13.1
data analysis statistical software (STATACorp, United States) (VanVoorhis and Morgan,

53
2007). In this study the sample size is limited by pragmatic factors (budget, time, and available
sample population).
3.3.3 Primary outcome variable
Each child’s dental caries experience is assessed using the International Caries Detection and
Scoring system (ICDAS) (CICDAS, 2005). The dentition is examined in detail, and every
surface of every tooth scored after drying. Lesions of dental caries on both smooth surfaces
and in pits and fissures, are scored from a range of 0 to 6 depending on severity. These scores
cover a range from non-cavitated “white spot” and “brown spot” lesions to overt cavities. A
special feature of ICDAS is the additional information it gives on the presence of, and type of,
any restorations on every surface which would be counted as past caries experience. Overall
caries experience per individual is calculated as a percentage of surfaces affected out of all
surfaces examined, and this can be set at any level of caries severity.
3.3.4 Main explanatory variables
Mother and child related variables are collected using questionnaires, clinical examinations and
laboratory testings.
3.3.5 Oral health knowledge and practices
After informed consent, a detailed questionnaire with 43 questions in total (developed for the
study) related to oral health is administered to mothers before the clinical examinations, to
collect data on knowledge, attitudes and practices towards oral health (Appendix A). Mothers
are questioned on their knowledge on oral diseases, the causes of dental caries in children and
adults and available oral health care services. With closed-ended questions, their dietary

54
practices, oral hygiene methods and frequency, use of oral health care services, and infant
feeding practices are assessed. A Likert scale measures the attitudes toward oral health, and the
importance mothers place on child’s oral health and deciduous teeth.
3.3.6 Anthropometric measurements
Height, waist circumference, and stride length of mother and child are measured. Participants
are weighed with an electronic bioimpedance balance, which gives measurements of body fat,
body water composition and BMI for adults and only weight for children. Mothers who are
pregnant or who have a cardiac pacemaker implanted are excluded from weighing on the
bioimpedance balance.
3.3.7 Saliva characteristics
We evaluate oral hydration and salivary viscosity (sticky/frothy, frothy/bubbly, or watery) by
visual observation. Simulated saliva is collected over a period of 5 minutes by chewing on
paraffin wax, and dribbling into a sterile cup. The expectorated volume is recorded. The pH
and buffering capacity of stimulated saliva are measured using Saliva-check BUFFER kits
(GC, United States of America) (Kitasako et al., 2008; Varma et al., 2008). Further, Caries
Risk Test (CRT) kits (Ivoclar Vivadent, Australia) are used to assess saliva buffering and
salivary counts of MS and LB (Kitasako et al., 2008).
3.3.8 Periodontal status
Mothers are examined for periodontal status using Periodontal Screening and Recording (PSR)
index measures, which measure the depth of periodontal pockets from the free gingival margin
to the bottom of the gingival sulcus (Khocht et al., 1995; Polk et al., 2012). Both upper and

55
lower teeth are divided in to sextants. Each and every tooth in the oral cavity is examined and
the highest score in each sextant is recorded. The scores vary from 0, denoting healthy
periodontium to 4, representing severe periodontitis (Landry and Jean, 2002).
3.3.9 Demographic and environmental data
Demographic, social, and environmental data were collected using detailed questionnaires
during recruitment and follow-up phases of the EFHL study from 2006 to 2011. All selected
factors are hypothesized predictors of the primary outcome. The present study will use the data
on each family’s socio-economic and demographic information of the mother, maternal age,
mother’s highest level of education, employment status, and total annual family income. The
child’s intrauterine environment will be assessed by maternal prenatal nutrition, mother’s
smoking habits, prescribed and illicit drug use, and alcohol. Data on breastfeeding and weaning
practices, types of food and beverages consumed, infant supplementary food, and bottle feeding
practices, will be used as covariates to include in the risk factor model. Oral and other health
care received by the child will be assessed from data on dental and medical check-ups (GP
visits), emergency department attendances, and availability of a medical insurance (health care
card).
3.3.10 Genetic and epigenetic markers
To identify genetic and epigenetic markers associated with dental caries, we will target host
genomic DNA obtained from saliva samples and use next-generation sequencing technology
to measure DNA-based variants on a genome-wide scale.

56
Specifically, stimulated saliva will be collected in 2 ml tubes and stored at -80 degrees C until
DNA is extracted with the High Pure PCR Template Preparation Kit (Roche Diagnostics,
Australia) using a method which was extensively modified in order to significantly increase
the DNA yield to a concentration needed for next-generation sequencing (unpublished
protocols). The extracted DNA will be sent to the Centre for Clinical Genomics at University
of Queensland to perform sequencing of bisulphite treated DNA for methylation analysis. This
approach will allow us to gain information on DNA sequences, variance, and CpG methylation
at ~ 450000 CpG sites spanning the human genome. These assays will be performed using the
SeqCap Epi 4 M CpGIANT Enrichment kit (Roache NimbleGen, Australia) and the HiSeq
2500 sequencer in (Illumina, United States) (Duhaime-Ross, 2014). A manuscript by Allum et
al., provides a detailed description of the assay protocols (Allum et al., 2015).
To date we have conducted a pilot study with 12 mother-child dyads; six with high caries
experience (average caries experience, 27.1% of surfaces affected in mothers and 12.4% in
children); and six with low caries experience (average caries experience, 11.2% in mothers,
2.5% in children), which was initiated using data collected within the oral health sub study of
EFHL. As a result of this pilot study, we have been able to establish the DNA extraction,
purification and sequencing protocols (in our hands) and have also established the necessary
bio informatics and statistical analysis methods for identifying target genes for dental caries.
3.4 Analysis
Observations will be stored as de-identified data, using a unique identifier for each participant.
The dataset for the analysis will be prepared in SPSS in a wide data format (one row per

57
participant). Data cleaning will be performed. Outliers will be investigated and corrected or
replaced with missing values if necessary. The pattern of missing values will be investigated,
and variables will not be used for further analysis if < 30% of values are found missing; missing
data will not be imputed.
The dependant variable (dental caries experience of children) is expected to be a ratio type
continuous variable, right-skewed with a mode of zero and which could be modelled using a
generalized linear model (GLM) with log-link and gamma family. The number of independent
variables will be reduced where possible (e.g. oral health knowledge and practices, periodontal
status) by using aggregate values. Independent variables without a known or hypothesized
association with the dependant variable will not be used in regression analysis. The
independent variable (covariates) will be prepared as follows: (a) dichotomous variables: coded
as 0/1, the zero category with the higher frequency, presented as number and proportion (%),
ignored for GLM if rare (frequency < 20); (b) categorical variables: coded as 0/1/2/ etc., sorted
by frequency in descending order, presented as number and proportion, for GLM the smaller
categories will be collapsed to form categories with frequency < 20, dummy coded for GLM;
(c) ordinal variables: coded as 0/1/2/ etc., sorted in a meaningful way, presented as number and
proportion, for GLM neighbouring categories will be collapsed to form categories with n <20;
and (d) continuous variables: re-scaled where necessary to ensure a change of a value of 1 can
be interpreted in a meaningful way, centred over mean where necessary (e.g. for age), presented
as mean and standard deviations (symmetrical distributions) or median and 25th / 75th
percentiles.
Descriptive statistics of participant characteristics (of values before re-categorization or
transformation) will be presented. Unadjusted associations between dependant variables and

58
covariates will be explored with bivariate GLMs. The covariates of interest for a multivariate
model will be shortlisted at p > 0.02. Correlations between the shortlisted covariates will be
investigated (using Pearson or Spearmen correlation and scatter plots), and covariates will not
be used together in a multivariate model if statistically significant correlation is found at |r| >
0.4. Scatter plots will be drawn to investigate the relationships between the dependant variables
and the covariates. Interaction terms will be created where necessary. The multivariate GLM
will be built by manually adding covariates one-by-one (forward method; sorted by descending
univariate p-values), whilst observing changes to the coefficients and errors for variables
already in the model. Covariates will be dropped from the multivariate model at p > 0.05.
Collinearity between covariates will be checked with the variance inflation factor. Model
building will be repeated using a backward method to check the final model. The number of
covariates in the model will be limited to avoid overfitting, as discussed in the sample size
section. Assumptions of GLM will be checked and the model adjusted if necessary.
Coefficients will be presented with the 95% confidence intervals, and evaluated considering
clinical significance. Intervals will be evaluated considering clinical significance. Statistical
significance will be declared at p > 0.05; the effect of multiple comparisons on overall error
rates will be considered during discussion of the results.
For epigenetic variation analysis, site-specific methylation levels will be defined as a
percentage methylation, with values ranging between 0 and 1. Each identified differentially
methylated site will be attributed a percentage methylation that will be included in the
regression modelling approach. Pyrosequencing on selected differentially methylated sites will
be done to validate the SeQCap Epi data.

59
3.5 Discussion
This cross-sectional study to assess maternal, environmental and individual risk indicators for
childhood dental caries will examine a wide range of determinants. It will evaluate the
interrelationship among independent variables and their relative effects on dental caries of
children. Furthermore, this research will pioneer research in epigenetic variation for dental
caries in children. The study will also potentially provide evidence on the interrelationship of
epigenetic variations with other social and environmental predictors for dental caries in the
participating child population. It is hoped that the evidence generated by the current study will
enable a more effective “risk factor modification approach” to overcome the problem of this
chronic disease that commences in childhood and continues throughout life. The data generated
in this thesis may possibly be extrapolated to similar populations worldwide, but further testing
on a much larger and more varied sample will be required. From thereon, we expect that
appropriate interventions will be recognized and implemented to tackle dental caries in children
and improve oral health and quality of life of the affected. However, we note that due to time
and logistic constraints, obtaining a larger sample size is one limitation of the study.

60
Chapter 4: Maternal caries experience, household income,
carbonated drinks and age at commencement of tooth-brushing
are associated with caries experience among 6- to 7-year-old
children in Australia.
This chapter is a submitted paper (paper 2). The bibliographic details of the paper, including
all authors, are as follows:
Surani Fernando, Gabor Mihala, Mahmoud Bakr, Shu-Kay Ng, Rodney Lea, Paul A Scuffham,
Newell W Johnson. Maternal caries experience, household income, carbonated drinks and age
at commencement of tooth brushing are associated with caries experience among 6- to 7-year-
old children in Australia.
My contribution to the paper involved the conception and design of the study, data collection,
statistical analysis, and drafting of the article.
The paper is submitted and under review with the journal Caries Research, which is a peer
reviewed journal (Manuscript ID 201705020).
Surani Fernando
Corresponding author: Surani Fernando
Supervisor: Professor Newell Johnson Supervisor: Professor Paul Scuffham

61
4.1 Abstract
Dental caries in children is a major public health problem worldwide, and research has shown
that there are a multitude of risk indicators acting upon children to different degrees in different
communities. The objective of this study was to determine the maternal and environmental
indicators which are associated with dental caries activity in a population of 6- to 7-year-old
children in SEQ, Australia. Maternal education, employment status, annual household income,
and marital status were used as proxies for environmental indicators; whereas maternal risk
markers included mother’s age at examination, lifetime caries experience, oral health
knowledge and practices, and BMI. Data were collected on mother’s saliva characteristics of
clinical oral hydration, stimulated flow rate, pH, buffering capacity, viscosity, and colony
forming units per ml of salivary MS and LB, which were included as covariates. These data
were analysed as follows: (i) using binary logistic regression with child’s lifetime cumulative
caries experience as the dependent variable; and (ii) using negative binomial regression with
child’s number of tooth surfaces affected with caries as dependent variable. Results indicated
that delayed child’s age when brushing started (p = 0.05), low annual household income (p
=0.03), child’s daily consumption of carbonated drinks (p = 0.02), and mother’s high caries
experience (p = 0.01) were directly associated with children’s caries experience. However,
maternal saliva LB levels were inversely associated with dental caries in children (p =0.01).
These data support the evidence of associations between maternal and environmental indicators
and caries in children in a typical western industrialised country.
Key words – Risk, Dental, Caries, Children, Mothers, Environment, Tooth-brushing,
Carbonated, Income

62
4.2 Introduction
Untreated caries in permanent teeth was the most prevalent disease condition worldwide in
2010, affecting 2.4 billion people. Untreated caries in deciduous teeth was the tenth most
prevalent condition, affecting 621 million children worldwide (Kassebaum et al., 2015) and
nearly 30% of 5- to 10-year-old Australian children (Do and Spencer, 2016). Dental caries
experience in children aged 5 to 6 years in Australia has varied over the last four decades: there
was a decline in prevalence during the 1970s and 1980s followed by an increase, captured by
both the Child Dental Health Survey 2014 and the National Oral Health Survey of Australia
1987–88 (Mejia et al., 2014). The prevalence of untreated dental caries [defined as decayed,
missing or filled surfaces (dmfs) more than zero] among 5- to 10-year-old children had
increased from 35% to 42% over two decades between 1988 and 2014 (Do and Spencer, 2016;
Slade and Spencer, 1998). Moreover, the Child Dental Health Survey 2014 reported that the
mean dmfs of deciduous teeth among the same age group of children was 3.1, of which 6% of
children had teeth missing due to caries, and 26% had filled tooth surfaces (Do and Spencer,
2016). Current caries prevalence in the deciduous dentition was higher among Queensland
children (50.2%) (Do and Spencer, 2016), compared to 1988 (48%) (Slade and Spencer, 1998).
It might be expected that with improvements in large-scale oral health promotion efforts,
increased exposure to fluoride from all sources, opportunities for better nutrition, and improved
treatment options, the incidence of caries would have declined in Australia in recent decades
(Do et al., 2017). However, individuals and populations are exposed all their lives to multiple
risk factors for dental diseases at different magnitudes (Johnson, 1991). Identifying the balance
or mix of factors affecting particular population groups and individuals is important for

63
prevention and management of the disease. No risk occurs in isolation, and many of these
happen in a complex series of events (Petersen, 2005).
Children from socially disadvantaged populations such as low socio-economic groups,
indigenous communities, and ethnic minorities have the highest risk for dental caries across
the globe (Seow et al., 2009; Tanaka et al., 2013; Zander et al., 2013). Since mothers play a
major role in rearing children, the maternal level of education (Kumar et al., 2014),
employment status (Kumar et al., 2014; Tanaka et al., 2013), oral health knowledge (Lee et al.,
2014), and behaviours (Nourijelyani et al., 2014) as well as maternal age (Ju et al., 2016;
Warren et al., 2016) are known to contribute to the health of her offspring. Because dental
caries is a lifestyle disease, chronic conditions such as obesity and diabetes share common risk
indicators with dental decay. Having mothers who consumed more than the daily recommended
sugar, fat and carbohydrate intake was found to be associated with caries development in young
Norwegian children (Wigen and Wang, 2014): children with obese mothers had more than
twice the risk of developing dental caries than the children of mothers who had a normal body
mass index BMI (Wigen and Wang, 2011). We hypothesise that caries experience in a
population of 6- to 7-year-old children living in SEQ is associated with maternal socio-
economic, demographic and behavioural factors.
Relationships between parental and children’s oral health status have been studied for decades
(Klein, 1946), and mothers’ caries status has been recognized as a stronger influence on caries
experience of children compared to fathers’ (Birungi et al., 2016; Mattila et al., 2000;
Weintraub et al., 2010). This is because certain parent-caregiver characteristics expose the child
to adverse environmental conditions that are conducive for caries development and
progression. Other than imitating unhealthy practices of caregivers, children are thought to be

64
at risk of acquiring cariogenic bacteria from their mothers. Maternal and child strains of MS
have been found to be similar, and higher salivary counts in mothers were associated with early
colonization of these organisms in children (Li et al., 2005). Mothers’ salivary MS (Warren et
al., 2009) and LB (Chaffee et al., 2014) levels have been able to predict children’s dental decay.
Putatively cariogenic bacteria thrive in environments such as low salivary flow rates (Diaz de
Guillory et al., 2014), low buffering capacity of saliva (Gao et al., 2016; Varma et al., 2008),
and low pH levels produced by cariogenic bacteria from dietary carbohydrates (Burne and
Marquis, 2000; Kianoush et al., 2014), increasing the risk of enamel and dentine
demineralization (Melo et al., 2016). Assuming that mothers associate more closely with their
children, we hypothesize that physiological features of maternal saliva could be taken as
predictors of the child’s dental caries experience.
From an epidemiological point of view, it is important to identify prominent indicators
contributing to dental caries development among children in each individual community.
Identifying risk indicators may substantially advance appropriate preventive and restorative
care. Hence, the objectives of the current study were to establish the prevalence of dental caries
in a population of children in SEQ, Australia, and to estimate associations of maternal and
environmental factors with dental caries experience in children.
4.3 Materials and methods
A protocol for the study was published in BMC Oral Health (2015) (Fernando et al., 2015).

65
4.3.1 Study population
The population for this cross-sectional study was 6- to 7-year-old children and their mothers
from three districts of SEQ (Logan, Beaudesert and Gold Coast), enrolled in the Griffith
University EFHL birth cohort study (Cameron et al., 2012b). According to Cameron et al the
EFHL cohort was compared with the rest of the SEQ and Australian demographics (Cameron
et al., 2012b). Participants of the oral health sub study was hence a representative sample of
SEQ. Recruiting participants for the oral health sub-study started in November 2012 from the
first cohort of children (2006), who were 6 years of age at the time, followed by participants
from 2007, 2009 and 2010 cohorts. It is a possibility that families which accepted our invitation
were better motivated towards health and were grateful for the opportunity to receive an oral
health examination and seized an opportunity for treatment. Data collection was completed in
April 2016 with a total sample of 174 mother-child dyads. However, data on oral health
knowledge and practices, salivary physiochemical characteristics and dental caries experience
was missing for one mother, hence the sample of 173 mother-child dyads.
4.3.2 Data collection
A questionnaire specifically developed for the oral health sub-study (non-validated) was
administered to mothers before clinical examinations. Data were collected on knowledge,
attitudes and practices related to oral health.
Mothers who were not pregnant or who did not have a cardiac pacemaker were weighed with
an electronic bioimpedance balance (Tanita, Australia), which gives measurements of body fat,
body water composition and BMI.

66
Oral examinations were carried out by trained and calibrated examiners at Griffith University
Dental clinics. Weighted Kappa values for two examiners against a gold standard were .810
(SE = 0.102, 95% CI = 0.414-0.813) and 0.928 (SE =0.093, 95% CI =0.628-0.992) (Appendix
B; Table 1 and 2). Dental caries experience was measured using the ICDAS (CICDAS, 2005),
with scores ranging from 0 (no disease) to 6 (overt caries) on each tooth surface. Presence of
restorations was considered as past caries experience. Saliva hydration was evaluated by visual
observation, and stimulated saliva was collected over 5 minutes whilst chewing on a piece of
paraffin wax and the volume measured. Saliva pH and buffering capacity were measured on
the expectorated sample with Saliva-check BUFFER kits (GC, Australia) and Caries Risk Test
kits (Ivoclar Vivadent, Australia). MS and LB colony forming units were measured according
to manufacturers’ instructions after 48 hours incubation at 370 C.
Demographic, socio-economic and environmental data were collected using detailed
questionnaires at recruitment for the EFHL study (Cameron et al., 2012a). In depth data of
participants and their families were merged with the oral health clinical data for analysis.
4.3.3 Outcome and risk indicators
The primary outcome variable was children’s dental caries experience, expressed as number of
tooth surfaces affected by dental caries (at the time of examination) including initial enamel
white spot lesions (ICDAS 1, 2 and 3) and dentinal caries (ICDAS 3, 4 5 and 6). The reason
being that the majority of children (61%) were caries free and the rest of the sample needed to
be included in the analysis for meaningful outcomes. This outcome was used as follows: (i) a
dichotomized variable: children with caries (ICDAS > 0) and children without caries (ICDAS
= 0); and (ii) as a continuous variable: total number of surfaces affected with caries (counts).

67
There were very few teeth extracted due to dental caries it was not considered for analysis,
since the influence would have been negligible.
Based on the questionnaire a total score (out of 100) for each participating mother was given
to evaluate their oral health knowledge attitudes and behaviours. Questions related to oral
hygiene practices, use of dental care services, feeding practices and consumption of cariogenic
food/beverages from the questionnaire were selected separately, to estimate mothers’ oral
health practices.
Moreover, mothers’ saliva hydration (normal, low), buffering capacity, pH, MS colony
forming units/ml of saliva (<105 = low, >105 = high), and LB colony forming units/ml of saliva
(<105 = low, >105 = high) were taken as saliva characteristics that could possibly be associated
with their children’s dental caries experience. Other explanatory variables included maternal
age, level of education, employment status, and annual household income.
4.3.4 Statistical analyses
Data were analysed using SPSS-21 (IBM, Chicago, IL). Measures of central tendency for
continuous variables, and frequency and percentages for categorical variables, were computed.
Categorical variables were recoded to ensure the frequency was at least 20 in each category.
Based on our research hypothesis, logistic regression was performed in GLM to explore
indicators that might have an impact on caries experience of children. Explanatory variables
were systematically tested in simple regression analyses, and shortlisted at p < 0.10 (Mota-
Veloso et al., 2016; Peres et al., 2005). Shortlisted explanatory variables were tested in
multivariable regression models with the significance level set at p < 0.05 and variables that
were insignificant were dropped to arrive at the final models. Final models were determined

68
by the significance levels of Omnibus test X2 (p ≤ .05) and clinically meaningful significant
associations between explanatory and outcome variables. The risk indicators for caries in
children were expressed with Adjusted Odds Ratios (AOR), Adjusted Rate Ratios (ARR) and
95% Confidence Intervals (CI).
4.4 Results
Of the 173 children, 88 (50.6%) were girls. Mean age for children without caries (n = 106) was
6.5 years (SD = 0.65) and 6.1 years (SD = 1.02) for children with caries (n = 67). Mean caries
experience (measured with the mean number of tooth surfaces affected with caries) was 8.8
(SD = 10.1) among children with caries. Mean maternal caries experience was 22.6 (SD =
13.13) within the caries free group and 25.29 (SD = 19.16) among the caries group. Mean
overall age for mothers on the day of clinical examination was 37.3 years (SD = 5.46). Other
maternal sociodemographic and clinical characteristics explored are given in Table 4.1.
Variables on maternal oral health knowledge, behaviour, and environment, explored as risk
indicators for childhood caries, are listed in Table 4.2.
Table 4.3 shows the variables in the multivariable binomial logistic regression model. Only
“age when child started brushing” was significantly associated with child’s caries experience
(p = 0.05). Children whose mothers initiated their children’s brushing after 6 months of age
were two times more at risk than their counterparts who initiated brushing at six months or
earlier (AOR = 2.23, 95% CI = 1.01-4.95). Initial frequency distribution showed that the
outcome variable was skewed with more children free of dental caries (61%), hence analytical
methods had to be improved according to the distribution.

69
As the total number of surfaces affected with caries were over dispersed (mean = 5.39, variance
= 80.2), negative binomial regression was used to assess risk indicators for dental caries.
Amongst all maternal independent variables entered into the model (listed in Tables 4.1 and
4.2), high levels of maternal LB was associated with low dental caries experience in children
(ARR = 0.61, 95% CI = 0.40-0.87, p = 0.01), whereas mother’s higher caries experience was
a risk marker for children’s caries (ARR = 1.02, 95% CI = 1.01-1.03, p = 0 .01). Low household
income (ARR = 0.67, 95% CI = 0.47-0.96, p = 0.03) and child’s consumption of carbonated
drinks once a day compared to never having such drinks (ARR = 2.03, 95% CI = 1.32-3.57, p
= 0.02) were significantly associated with high caries experience in our child population (Table
4.4).

70
Table 4.1: Frequency distribution of children’s and mother’s socio demographic and
clinical characteristics
Variable Children without
caries (n=106)
Children with
caries (n=67)
Mean SD Mean SD
Child age (years) 6.5 0.65 6.1 1.02
Child caries experience as number of tooth
surfaces affected with caries¥
0 0 8.8 10.10
Mother age 37.4 5.62 37.1 5.24
Mother saliva pH 7.0 0.41 7.1 0.53
Mother saliva buffering (GC*) 8.70 3.54 8.57 3.16
Mother caries experience as a percentage of
affected surfaces
22.6 13.1
3
25.29 19.16
Mother saliva volume in 5 minutes 5.21 2.30 4.87 3.36
N % N %
Child gender
Female 51 48 38 56
Male 55 52 29 44
Mother saliva hydration
Low 15 14 7 10
Normal 91 86 60 90
Mother saliva buffering capacity
(CRT**)
Low 20 19 16 23
High 86 81 51 77
Mother saliva mutans Streptococci
Low 33 31 27 40
High 73 69 40 60
Mother saliva Lactobacilli
Low 51 48 32 48
High 55 52 35 52
Mother level of education
Completed primary education 14 13 10 14
Completed high school 32 30 17 26
Completed tertiary education 60 57 40 60
Mother employment status
Unemployed 49 46 31 46
Employed 57 54 36 54
Mother marital status
Single 12 11 6 9
With partner/husband 94 89 61 91
Annual household income
Low (<$59999) 56 53 31 46
High (>$59999) 50 48 36 54 ¥ Caries experience was for both deciduous and permanent dentition in children, *Saliva-check BUFFER
kits (GC, United States of America), ** Caries Risk Test kits (Ivoclar Vivaden)t, Australia).

71
Table 4.2: Frequency distribution of mothers’ oral health related knowledge and
behaviours
Variable Children without
caries(n=106)
Children with
caries (n=67)
Mean SD Mean SD
Mothers oral health knowledge 72.6 9.65 72.6 10.8
N % N %
Mothers visits to dentist during pregnancy
Yes 72 68 48 72
No 34 32 19 28
Child’s age when brushing started
Six months 30 28 13 19
More than six months 76 72 54 81
Child’s dental visits since birth
Yes 75 74 48 72
No 25 26 19 28
Use of fluoridated tooth paste
Yes 63 59 33 49
No 43 41 34 51
Frequency of giving carbonated drinks per day
Never 65 61 49 73
Once a day 20 19 5 7
More than once a day 21 20 13 20
Mother BMI at beginning of pregnancy
Normal 62 58 38 57
Over weight 21 20 12 18
Obese 23 22 17 25
Main language spoken at home
English 93 88 61 91
Other 14 12 6 9
Table 4.3: Risk indicators for children with and without dental caries using logistic
regression
Omnibus test X2 for the model = 11.44, p=0.04, * Reference variables, AOR= Adjusted Odds Ratio, CI=
Confidence Interval, MS=mutans Streptococci
Variable AOR (95% CI) P value
Mother saliva MS levels 0.68 (0.34-1.36) 0.28
Mother caries experience 0.98 (0.96-1.00) 0.07
Use of fluoridated toothpaste at home (Yes*/No) 1.25 (0.88-1.77) 0.21
Age when child started brushing (6 months*/> 6 months) 2.23 (1.01-4.95) 0.05
Main language spoken at home (English*/non-English) 0.48 (0.16-1.37) 0.17

72
Table 4.4: Risk indicators for childhood dental caries using negative binomial regression
Variable Adjusted ARR (95% CI) P
value
Mothers’ levels of saliva LB
(Low*/High)
0.61 (0.40- 0.87) 0.01
Mothers’ saliva buffering capacity
(GC)
0.96 (0.91-1.01) 0.11
Mothers’ saliva pH 1.14 (0.75-1.73) 0.55
Mothers’ caries experience 1.02 (1.01-1.03) 0.01
Mothers’ annual income
(Low* /High) 0.67 (0.47-0.96) 0.03
Frequency of giving carbonated
drinks
Never*
Once a day 2.03 (1.32-3.57) 0.02
>Once a
day
1.06 (0.66-1.68) 0.82
Variance of outcome variable =80.25, Mean of outcome variable=5.39, Kolmogorov–Smirnov
statistic=1.075(p=0.198), Omnibus test X2 for the model=40.56, p=0.001, Dispersion parameter=2.57, ARR=
Adjusted Rate Ratio, CI= Confidence Interval, *Reference variables.
4.5 Discussion
The present study is based on our findings of caries prevalence and severity in a sample of 173
mother-child dyads in SEQ. We found that 34% boys and 42% of girls between 6 and 7 years
of age had active caries as per ICDAS criteria, whereas the Australian National Oral Health
survey 2012-2014 found it to be 30% for boys and 27% for girls in the same age group (Do
and Spencer, 2016). The higher rates in the current study could be due to the fact that volunteers
who presented at our clinics had a self-assessed treatment need. This is logical because
participants’ own perception of treatment need has been found to correlate significantly with
examiner ratings in a study conducted in Sweden with 1000 individuals aged 20-89 years
(Petersson et al., 2016). In the USA, around 37% of children aged 2 to 8 years had caries in
their deciduous teeth (Dye et al., 2015), and in Spain the prevalence of caries in 6-year-olds
was 30% (Almerich Silla et al., 2014). Bosnian 6-year-old children had a mean dmft of 6.7 (SD
±3.9) with decayed teeth contributing to 88.8% of the index (Markovic et al., 2013). A

73
longitudinal study in UK, to investigate caries progression through childhood to adolescence,
found that the mean caries prevalence of 7- to 9-year-olds’ was 16.7% which increased with
age (Hall-Scullin et al., 2017). These observations indicate that caries experience in the same
age group varies considerably in different communities, presumably because of differing
mixtures of risk indicators.
Evidence suggests that preventive interventions such as initiation of oral hygiene habits before
the age of 12 months are important to prevent the development of dental caries (Lee et al.,
2006). Children who started brushing at an early age were at comparatively low risk for
developing dental caries in a multicentre study from paediatric dentistry departments in the
Netherlands and Turkey (Özen et al., 2016). Moreover, caries prevalence was found to be
significantly higher (p = 0.04) in a population of Myanmar preschool children who did not start
brushing until after 2 years of age (Thwin et al., 2016). Similar results were observed by Huong
et al., (2017) in their study of Vietnamese pre-schoolers. Children who started brushing at the
eruption of their first deciduous tooth had less decayed surfaces than children who started
brushing later (p = 0.009) (Ngoc et al., 2017), and lack of tooth brushing past the age of 2 years
was a strong risk factor for dental caries in 6-year-old Cambodian children (Turton et al., 2016).
These findings are underlined by the results of the present study where we found that children
who started brushing at a later age were more likely to acquire caries than children who initiated
brushing earlier.
Socio-economic disparities in oral health are considered as a valid measure of progress or
deterioration of overall health status, and provide key information for health policies (Capurro
et al., 2015). Annual household income is an absolute measure of SES (Bernabe et al., 2009).
Children with one or more carious lesions were associated with lower family income, and our

74
findings are in line with others (Jepsen et al., 2017; Schwendicke et al., 2015). We report that
in our study population, children who had families with an annual income of more than AUD
59,999 were 33% less likely to develop dental decay than their lower income counterparts
(Table 4.4). In the USA, income-related inequalities were observed in untreated dental caries
among 2- to 12-year-old children in National Health and Nutrition Examination Surveys done
over three decades. It was found that children from low income families were three to five
times more likely to have untreated decay than children from high income families (Macek,
2016). Children from ethnic minorities with low income levels were reported to be more at risk
of dental caries than native children (van der Tas et al., 2016). For instance, an indigenous
population in Brazil exhibited that high income was a “protective factor” for dental caries,
whereas children from low income ethnic minority groups were more than twice as likely to
develop dental decay (Arantes and Frazão, 2016).
Alarmingly, in a review paper published a decade ago, it was reported that in many countries
22% of 1- and 2-year-old children consume high sugar carbonated beverages at an average of
1 cup/day, and this increases through childhood to adulthood (Tahmassebi et al., 2006). In
addition, these levels are likely to have risen since such drinks have become more accessible
(Lee and Giannobile, 2016). Findings in different studies are diverse, due to variations in study
designs, techniques of statistical analysis, and phenotype definitions. For instance, among 6-
year-old Korean children (n = 1214), “mild decay” had no significant association with
consuming carbonated drinks, whereas consuming soda drinks once a day was a risk factor for
“severe decay” (Han et al., 2014). Juices, frizzy drinks and smoothies were reportedly
associated with children’s past caries history (p = 0.04), and the number of “early” carious
lesions (p = 0.04) in 6- to 15-year-old Spanish children (Llena et al., 2015). López-Gómez et
al., (2016), reported that loss of deciduous teeth increased with high consumption of soft drinks

75
(OR = 1.89, 95% CI = 1.13–3.16): the variable was dichotomized into “≤ 1 times/day and >1
times/day”, and similar to our study, questionnaires were administered to mothers of 6- to 7-
year-old Mexican children (n = 833) to retrieve the information (López-Gómez et al., 2016).
Other authors have reported that consumption of 100% juices were associated with lower caries
incidence (Ghazal et al., 2015). Our observation that children who consumed carbonated drinks
more than once a day did not have greater caries could in part be due to participating mothers
having given their children 100% juice instead of carbonated drinks, and/or coupling fizzy
drink consumption with frequent tooth brushing (Asif et al., 2015). According to a dissimilar
observation by Cheng and Campbell (2016), in a sample of rural Ugandan children aged 8-10
years (n = 84), a relationship between cariogenic beverages (soft drinks and sweetened tea) and
dental caries could not be discovered (Cheng and Campbell, 2016). In their study, the frequency
of cariogenic beverages was taken on a weekly consumption, and there was a greater chance
of recall bias in children which might have influenced the findings.
The current study reports that this sample of SEQ children, whose mothers had high caries
experience, were only 2% more at risk of developing decay than children with mothers with
low caries experience, an overall weak association (Table 4.4). Similar results were found in a
study of American Indian children (OR = 1.04, 95% CI = 1.02-1.07); however, the children
were 3-year-olds and the environmental context was very different (Warren et al., 2016).
Nevertheless, Ersin et al., (2016), in their study of Turkish children, reported a much stronger
association: children of mothers with high DMFS scores had almost double the caries
experience of those whose mothers had low caries experience (Ersin et al., 2005). Another
study reported that caries prevalence was 22.5 times higher in children whose mothers had
severely decayed teeth than children whose mothers had low caries experience (PR = 22.5,
95% CI = 3.2-156.6) (Proença et al., 2015). In Cambodia, where caries prevalence is very high

76
among preschool children, maternal caries was found to be a strong predictor (Turton et al.,
2015). Correspondingly, higher maternal DMFS could predict child caries in a population of
Hispanic and African-American children (OR = 3.9, 95% CI = 1.1-14.6) (Smith et al., 2002).
Moreover, a five year follow up study among Ugandan mother child dyads provided further
evidence that caretaker’s caries experience was positively associated with childhood caries
(IRR = 2.0, 95% CI = 1.3-3.0) (Birungi et al., 2016). Kawashita et al., (2009), however,
reported contrasting findings as maternal caries was not found to be a predictor in a population
of Japanese children, probably due to higher socio-economic factors and level of education of
mothers (Kawashita et al., 2009).
Interestingly, we found that children who had mothers with high LB levels were 39% less likely
to get caries compared to mothers with low LB levels (Table 4.4). At a superficial level this
association is counter-intuitive, given the oft reported positive association with an individual’s
number of carious lesions and high counts of lactobacilli in saliva (Ahirwar et al., 2017) relating
to the acidogenic, and especially to the aciduric, properties of LB in general (Samaranayake,
2012). It has been established that children acquire cariogenic bacteria predominantly from
their mothers, and bacterial transmission from mothers with tooth decay to their infants takes
place earlier than in families where mothers have healthier mouths (Li et al., 2005). According
to Mattsson et al., (2007), naturally occurring oral LB inhibits the growth of autologous MS,
and the observation was more marked in caries-free subjects who harboured LB that suppressed
the growth of host’s oral MS (Simark‐Mattsson et al., 2007). Furthermore, LB species have
been recognized as later invaders of cavity formation, and infrequent colonizers of enamel and
early caries lesions (Guo and Shi, 2013; Samaranayake, 2012). In other words, invasion of LB
was seen only at advanced stages of dental caries which involve cavity formation and
destruction of dentine (Dige et al., 2014). In our study, 61% of the children were caries-free,

77
and a further 16% had carious lesions limited to enamel. There is evidence that MS species
play a significant role in the initiation of caries on smooth surfaces, fissures of crowns and on
root surfaces, and the role of LB in inducing caries is not well supported (Samaranayake, 2012).
Taking into account the evidence from previous studies, our finding is rational; nevertheless,
the significant association we observed needs to be explored in depth in similar populations
with larger sample size.
Limitations of this study are the modest sample size, which was compromised by practical
factors like budget, time limits, and number of volunteers willing to attend the dental clinics
for oral examinations (Fernando et al., 2015).
In conclusion, amongst the maternal and environmental factors explored in our study, low
income levels of mothers and giving carbonated drinks significantly increased the risk of their
6- to 7-year-old children developing dental caries, while maternal caries had a weakly positive
association with children’s caries experience. Maternal income presumably is related to
education, to attitudes to oral hygiene behaviours, and to dietary practices that ultimately
influence caries experience. Maternal saliva LB levels were inversely related to caries
experience in this child population; hence that cannot be taken as a risk marker for children’s
caries experience.

78
Chapter 5: Mothers who report taking iron supplements during
pregnancy and child’s oral carriage of mutans Streptococci are
associated with a child’s lower and higher lifetime dental caries
experience, respectively.
This chapter is a submitted paper (paper 3). The bibliographic details of the paper, including
all authors, are as follows:
Surani Fernando, Santosh Kumar, Mahmoud Bakr, David Speicher1, Rodney Lea, Paul A
Scuffham, Newell W Johnson. Mothers who report taking iron supplements during pregnancy
and child’s oral carriage of mutans Streptococci are associated with a child’s lower and higher
lifetime dental caries experience, respectively.
My contribution to the paper involved the conception and designing of the study, data
collection, statistical analysis and drafting the article.
The manuscript was submitted to the Journal of Public Health Dentistry, and is under review.
Manuscript ID is JPHD-OA-08-17-0226.
Surani Fernando
Corresponding author: Surani Fernando
Supervisor: Professor Newell Johnson Supervisor: Professor Paul Scuffham
79
5.1 Abstract
5.1.1 Objective
This study explored the association of children’s salivary characteristics, birth weight, and
reported maternal prenatal vitamin and mineral supplementation with the dental caries
experience of the child.
5.1.2 Methods
This cross-sectional study, a sub-study of Griffith University Environments for Healthy Living
birth cohort study, was conducted on 174 mother-child dyads. Mother’s prenatal usage of
vitamin and mineral supplements; child’s birthweight; salivary pH, buffering capacity, and
levels of salivary MS and LB were explored as risk indicators. Dental caries experience was
assessed using International Caries Detection and Assessment System criteria. Path analysis
was conducted to evaluate the association of risk indicators with children’s current and past
dental caries experience.
5.1.3 Results
Children’s past caries experience (β = 0.332, p = 0.018), and salivary MS counts (β = 0.215, p
= 0.032) were positively associated with current caries experience. With a trend towards
significance, children whose mothers had reported taking iron supplements during pregnancy
experienced lower levels of past (β = -0.137, p = 0.068) and current dental caries (β = -0.046,
p = 0.051).

80
5.1.4 Conclusions
This study confirms that a child’s current dental caries status is positively associated with their
past caries, and that it correlates with current levels of salivary MS. Children of mothers who
reported to have taken iron supplements during pregnancy experienced less caries throughout
their lives. These observations confirm the importance to offspring of monitoring maternal
health throughout pregnancy and of early monitoring of children’s oral health in preventing
future dental disease.
Key words: Birth weight, Caries, Children, Past caries, Prenatal supplements, Saliva
5.2 Introduction
Dental caries is the most common oral disease in Australian children, and understanding the
risk indicators of cariogenesis ultimately assists with improved early-life prevention.
According to the Australian National Child Oral Health study (2012-2014), 27% of children
aged 5-10 years had untreated caries in their deciduous dentition (Do and Spencer 2016). Dental
caries progresses very rapidly in deciduous teeth as they have relatively thin enamel, and
dentine and pulp involvement can occur quickly (dos Santos Junior et al. 2014). For a child,
treatment of caries is a stressful and often painful experience which frequently requires multiple
visits, extensive restorations, and extractions. It is also expensive for parents, and an added
burden on health expenditure for many countries. Identification of the factors which influence
dental caries in children allows the family, perhaps with advice from a clinician, to practice a
healthy life style and, where indicated, for a clinician to institute preventive interventions such
as topical fluorides. The literature surrounding dental caries in children is overwhelming, with

81
numerous systematic reviews identifying socio-demographic, dietary and family circumstances
and behaviours being important predictors of disease. However, the association of children’s
individual characteristics, particularly in terms of their foetal well-being, (dos Santos Junior et
al. 2014) and features of their own oral physiology, have not been studied simultaneously (Do
and Spencer 2016).
Since tooth formation starts during the foetal period, the intrauterine environment, which is
affected by maternal nutrition and supplement intake during pregnancy, influences the
development of children's teeth (Tanaka et al. 2015). Studies have shown that nutritional
supplements during pregnancy, like vitamin D (Tanaka et al. 2015), calcium, and iron,
influences tooth formation in children (Bergel et al. 2010). Low birth weight, a marker of sub-
optimal foetal nutrition and growth, is indicative of an increased risk for ill health throughout
life (Barker and Thornburg 2013), including the development of dental caries (Bernabé et al.
2017). On the other hand, it has long been established that low salivary pH and poor buffering
capacity, and a comparatively high load of salivary MS) and LB (Samaranayake 2012), help
drive cariogenesis in the child (Lenander-Lumikari and Loimaranta 2000). Age in general, is a
risk indicator for dental caries (Hunter 1988) as the teeth of older children have been at risk for
a longer period (Al-Shalan et al. 1997). Previous studies have been inconsistent in their findings
on the relation between caries and gender, with no consistent pattern favouring higher caries
propensity in one gender (Chankanka et al. 2011). Importantly, past dental caries experience is
widely recognised as the strongest single predictor of future dental caries (Attaran et al. 2016).
This study explored the association of children’s salivary characteristics, birth weight, and
maternal prenatal vitamin and mineral supplementation with the dental caries experience of the
child.
82
5.3 Methods
This study followed a previously published detailed protocol regarding sample size, participant
recruitment, and data collection (Fernando et al. 2015). In brief, the study cohort consisted of
174 children aged 6-7 years and their mothers from Logan, Beaudesert, and Gold Coast in SEQ,
Australia, who were enrolled in the Griffith University EFHL birth cohort study (Cameron et
al. 2012). Participant enrollment for the present oral health sub-study started in November 2012
with children who were 6 years of age at the time, followed by participants from 2007, 2009
and 2010 cohorts. Data collection was concluded in April 2016.
The primary outcome variable was each child’s dental caries level at the time of examination
expressed as the number of tooth surfaces affected by caries, including initial white spot
lesions, according to the ICDAS criteria (CICDAS, 2005; Fernando et al. 2015). Past caries
experience was measured by the number of tooth surfaces that had restorations (Fernando et
al. 2015). Explanatory variables included reported maternal intake of nutritional supplements
(iron, Zn folate, and multivitamins) during pregnancy. Prenatal nutrition was evaluated by
reported maternal intake of supplements, which is considered to be a valid and an
uncomplicated method of obtaining such data (Schmidt et al., 2011). Although information
related to substance use (tobacco, alcohol, and illicit drugs) and calcium supplemets were
collected through the EFHL study, these variables could not be considered in the analysis as
most of the mothers participating in the oral health substudy had not answered the relevant
questions. Child’s salivary pH, buffering capacity, counts of MS and LB, past dental
experience, age, and gender were other independent variables under study. Salivary buffering
capacity was assessed using Saliva-check BUFFER kits (GC, Australia), salivary MS and LB
levels as measured with Caries Risk Test kits (Ivoclar Vivadent, Australia). Salivary data of

83
the children were collected during the oral health substudy (Fernando et al. 2015). Data on
maternal, iron, Zn, folate and multivitamin supplementation during pregnancy, and child’s
birth weight were collated from the main EFHL birth cohort database, and merged with the
oral health data (Cameron et al. 2012).
Mean salivary pH and buffering capacity, mean birth weight and past caries experience were
compared between children with no current or past caries (ICDAS = 0) and those with any
caries experience (ICDAS > 0). Moreover, the percentage of mothers who have reported to
taking nutritional supplements during pregnancy, proportions of children with low and high
salivary bacterial levels, were compared between the two groups of children.
Data analysis was performed using SPSS-21 (IBM, Chicago, IL) and AMOS (IBM SPSS
AMOS 22.0, Meadville, PA). Measures of central tendency for continuous variables and
frequency and percentages for categorical variables were computed. Normality of the data was
assessed using the Shapiro-Wilk test. As the data were not normally distributed, non-parametric
tests were used for univariate analysis. Mann-Whitney U test was used to compare the mean
age, past caries experience, and salivary pH between children with caries and those with no
caries. For comparison of proportions, Fisher’s Exact and Chi-square tests were used according
to the type of data. Based on the research hypothesis, path analysis, which describes the directed
dependencies among a set of variables, was used as it facilitated simultaneous assessment of
associations between several independent and dependent variables (Kumar et al. 2017). In the
path analysis, whether or not mothers took the particular nutritional supplements and birth
weight of the particular child, were hypothesised to have a direct relationship to the child’s
cumulative past dental caries experience and both direct and an indirect association to current
caries experience. Moreover, while a child’s current salivary characteristics, age, and gender

84
were hypothesised to have direct association with current caries levels (figure 5.1). In addition,
past dental caries experience was hypothesised to have a relationship to current dental caries
experience. All the variables related to maternal intake of supplements and child’s salivary
characteristics were allowed to covary in the path analysis. The model has 2 endogenous
(dependent) and 11 exogenous (independent) variables. The minimum required sample size for
the path model, as determined by N > 50 + 8m where N is the number of participants and m is
the number of predictor variables, with 12 predictors, was 146 children. As two variables (past
and present caries experience) deviated significantly from normality, Bollen-Stine
bootstrapping was used to estimate the fit indices (Kim and Millsap 2014). Further,
bootstrapping and bias-corrected confidence intervals were used to analyse direct and mediated
parameter estimates, and the bootstrapping sample was set to the generally accepted value of
250 (Nevitt and Hancock 1998). The model was considered to have a good fit if Root Mean
Square Error of Approximation (RMSEA) and Standardized Root Mean Square
Residual (SRMR) were < 0.08, and Comparative Fit Index (CFI) and Tucker Lewis Index
(TLI) were ≥ 0.9 (Hoyle and Panter 1995).

85
Table 5.1: Children’s individual characteristics explored as risk indicators for dental
caries experience and current activity
Variable Cases (n = 67) Controls (n = 107) Significance
Mean (SD) Mean (SD) t (p value)
Age at examination 6.07(1.02) 6.49(0.65) 2.6 (0.09)
Saliva pH 7.17(0.45) 7.26 (0.49) 1.3 (0.19)
Saliva buffering capacity (*GC) 8.26(3.85) 9.41(3.15) 1.4 (0.16)
Child’s birthweight (g) 3438 (438.82) 3487(481.85) 0.8 (0.42)
Past caries experience (number
of surfaces with restorations)
2.10 (5.52) 0.21 (0.86) 4.1 (0.0001)
Current caries experience
(number of surfaces with caries)
8.26 (9.96) 0 8.9 (0.0001)
N (%) N (%) X2 (p value)
Gender 2.75 (0.25)
Female 37(55) 51 (48)
Male 30(45) 56 (52)
Saliva �MS levels 8.33 (0.004)
<105 CFU/ml of saliva 52 (78) 60 (56)
>105 CFU/ml of saliva 15 (22) 47 (44)
Saliva ∞LB levels 0.14 (0.71)
<105 CFU/ml of saliva 37 (55) 56 (52)
>105 CFU/ml of saliva 30 (45) 51 (48)
Maternal Folate
supplementation during
pregnancy
0.27 (0.61)
No 17 (25) 31 (29)
Yes 50 (75) 76 (71)
Maternal Iron
supplementation during
pregnancy
0.001 (0.97)
No 28 (42) 45 (42)
Yes 39 (58) 62 (58)
Maternal Multi Vitamin
supplementation during
pregnancy
3.8 (0.05)
No 23 (34) 53 (49)
Yes 44 (66) 54 (51)
Maternal Zn intake during
pregnancy
0.32 (0.57)
No 46 (69) 69 (64)
Yes 21 (31) 38 (36)
*Saliva-check BUFFER kits (GC, Australia), � mutans Streptococci, ∞Lactobacilli

86
Table 5.2: Standardised boot strapped estimates with 95% confidence intervals of the
path model with past and current dental caries experiences as the endogenous variables
Effect β Bias corrected
95% CI
P
DIRECT EFFECTS
Predicting past dental caries
Maternal Zn supplementation during
pregnancy 0.132 -0.066 - 0.298 0.210
Maternal Folate supplementation during
pregnancy 0.042 -0.089 - 0.140 0.582
Maternal Iron supplementation during
pregnancy -0.137 -0.241- 0.018 0.068
Maternal Multi vitamin supplementation
during pregnancy 0.076 -0.076- 0.234 0.339
Child’s birth weight -0.048 -0.151-0.058 0.303
Predicting current caries
Age 0.006 -0.167-0.141 0.95
Gender 0.036 -0.11-0.181 0.566
Maternal Zn intake during pregnancy 0 -0.175-0.211 0.977
Maternal Folate intake during pregnancy 0.026 -0.231-0.208 0.911
Maternal Iron intake during pregnancy 0.013 -0.164-0.26 0.882
Maternal Multi vitamin intake during
pregnancy -0.054 -0.219-0.107 0.585
Child’s birth weight -0.005 -0.178- 0.145 0.839
Child’s past caries 0.332 0.131- 0.503 0.018
Child’s Salivary pH 0.086 -0.008-0.19 0.06
Child’s Salivary MS 0.215 0.02-0.382 0.032
Child’s Salivary LB 0.097 -0.067-0.224 0.254
Child’s Buffering capacity (*GC) -0.034 -0.219-0.131 0.722
INDIRECT EFFECTS
Predicting current caries
Iron -0.046 -0.1 – 0.001 0.051
Quantified influence not mediated by other variables in the model, Chi-square = 83.730, p = 0.348, TLI – 0.954,
CFI – 0.969, RMSEA – 0.028 and SRMR = 0.0592, *Saliva-check BUFFER kits (GC, Australia)

87
5.4 Results
Of the children enrolled, 88/174 (51%) were girls. The mean age for children with caries was
6.1 years (SD = 1.02) and for children without caries was 6.5 years (SD = 0.65). At time of
examination, 67/174 (38%) children had caries, of which 37/67 (55%) were girls. Mean number
of tooth surfaces affected with caries in the total sample of children at the time of examination
was 5.44 (SD = 8.95), and mean number of tooth surfaces with past caries was 1.37 (SD =
4.45). In the subset with caries the mean was 8.26 (SD = 9.96). Children with at least one
carious tooth surface currently, had significantly greater caries experience in the past (Mean:
2.1, SD = 5.52, p = 0.0001) than those who were completely caries free (Mean: 0.21, SD =
0.86, p = 0.0001) at the time of examination (Table 5.1). Salivary loads of MS (p = 0.005) and
reported maternal multivitamin intake during pregnancy (p = 0.05) were significantly different
between caries and caries free groups in univariate analysis, even though reported multivitamin
intake during pregnancy was not associated with caries experience of children in the path
analysis. Our hypothesised model, which provides estimates of the magnitude and the
significance of association between explanatory and the outcome variables, demonstrated a
good fit with the data (Chi-square = 83.730, p = 0.348, TLI = 0.954, CFI = 0.969, RMSEA
=0.028 and SRMR = 0.0592) and shows a relationship and degree of association between
dependant and independent variables (figure 5.1). Table 5.2 gives the 95% CI and the level of
significance (p) against the β values (associations between independent and dependant
variables) obtained and indicated in figure 5.2 There was a significant association between the
past and current dental caries experience (β = 0.332, p = 0.018), with children who had more
carious tooth surfaces in the past tending to have a greater number of new carious surfaces at
the time of examination (Table 5.2). A positive association was also observed in path analysis
between child’s salivary MS levels and current dental caries experience (β = 0.215, p = 0.032).
88
Although only approaching statistical significance, children whose mothers reported to have
taken prenatal iron supplements had fewer tooth surfaces affected with caries in the past (β = -
0.137, p = 0.068). Maternal intake of iron supplements during pregnancy was indirectly
associated with current dental caries experience with marginal significance (β = -0.046, p =
0.051), while there was no association between reported intake of Zn, and folate supplements
during pregnancy and dental caries experience. Loads of LB in saliva and other salivary
characteristics were not associated with current dental caries experience in this child
population.

89
Figure 5.1. Path analysis with standardised bootstrapped estimates (β) of the associations
between maternal intake of nutritional supplements during pregnancy, salivary characteristics,
age, and gender with dental caries experience of children. (Significant standardised estimates
(*p ≤ 0.05) are in bold font. Error terms and covariances between exogenous variables are not
presented for ease of understanding. Β values of the associations are written on the connected
line arrows.
Maternal Multi-vitamin intake in Pregnancy
Maternal Folate intake in Pregnancy Age at examination
Maternal Zn intake in Pregnancy
Maternal Iron intake in Pregnancy
Gender
Saliva pH
Saliva MS
levels
Saliva buffering capacity
-0.05
Saliva LB
levels
Birth weight
Past caries experience Current caries experience
0.04
-0.05
-0.005
0.33*
-0.03 0.10
0.22*
0.09
0.006
0.04
0.03
0
0.01
0.08 -0.14
0.13
90
5.5 Discussion
The present study confirms that children with a history of dental caries are more at risk of
developing future caries. This is consistent with much of the published literature. A recent
systematic review reports that baseline caries was the strongest predictor for future dental caries
in very high human development countries (Attaran et al. 2016). Similarly, progression of
carious lesions was positively associated with baseline caries among a population of Brazilian
children (Piva et al. 2017). Furthermore, according to Brennan and Spencer, greater caries
experience at age 13 was associated with more missing or filled teeth at 30 years of age among
Australians (Brennan and Spencer 2014). These findings emphasise the importance of early
and regular screening for caries and associated risk indicators in families so that appropriate
preventive approaches to control future disease can be put in place. This is best achieved by
educating families in oral hygiene and healthy eating habits, although occasional referral to a
clinician for preventive interventions such as topical fluorides and/or fissure sealants may be
necessary.
Both longitudinal and cross-sectional studies have shown that their oral MS levels are
positively associated with caries experience in children (Piva et al. 2017). In accordance, we
found that children who had high salivary MS counts (> 105 cfu/ml saliva), were more likely
to have greater caries experience than children who harboured lower MS counts (< 105 cfu/ml
of saliva). Levels of MS in saliva were identified as a useful and a quick method to evaluate
caries risk among a small sample of children from India, where mean MS scores for children
with caries were significantly higher than for children without caries (p ≤ 0.001) (Nanda et al.
2015). From a cohort of American 6-year-old children, Edelstein et al. reported that even within
families with high-income and who were accessing preventive care, the most useful predictor

91
of current caries was salivary MS count (Edelstein et al. 2016). Contrastingly, Widita et al.
found that the predictive value of MS counts for scores of dental caries among Indonesian pre-
schoolers was high only when combined with other predictive factors like cavitated teeth,
unhealthy feeding practices, and poor oral hygiene, demonstrating the importance of
identifying risk indicators within individual families and communities for effective public
health initiatives (Widita et al. 2017).
We have observed that the children of mothers who took iron supplements during pregnancy
had comparatively low levels of dental caries at age approximately 6 years. Supplementation
with iron is generally recommended during pregnancy to meet the iron needs of both mother
and foetus (Scholl 2005); there can be depletion of iron stores during pregnancy and oral
supplements can prevent maternal iron stores from reaching deficient levels (Fenton et al.
1977) although there was no way of knowing whether nutritional supplements taken by any
individual pregnant mother were prescribed because of a measured deficiency, as routine
treatment or were self-administered. Early iron supplementation, even during foetal period and
in breastfed human infants, is feasible and increases iron status which is carried into early
childhood (Lima et al. 2006). A possible mechanism supporting our observation was proposed
by Alves et al, where they demonstrated in an in vitro study that higher concentrations of Iron
reduced the demineralization of enamel (Alves et al. 2011). Martinhon et al, reported similar
findings in bovine enamel. Their results showed that ferrous sulphate reduced the
demineralization of enamel blocks and altered the ionic composition of the dental biofilm
formed in situ (Martinhon et al. 2006). A recent randomized control study investigating the
effect of ferrous sulphate on deciduous teeth have found that ferrous sulphate indeed reduces
the demineralization of enamel and has a cariostatic effect (De Gauw et al. 2017).

92
Moreover, iron supplementation could be a proxy or marker for a wider set of psychosocial
and health behavioural variables which are associated with childhood caries. For instance,
serum haemoglobin levels, mean corpuscular volume and packed cell volume (Haematocrit)
have been shown to be significantly low in children with caries compared to caries free children
in studies from India, with a low socio economic background (Bansal et al. 2016) and in a
similar background in Egypt (Abed et al. 2014). Tang et al. (2013) reported that severe early
childhood caries was strongly associated with anaemia of the child, which could be because of
significant illness of the child or, again, be a result of poor diet and related to economic status
(Tang et al. 2013)
Our univariate analysis showed that, reported maternal multivitamin intake during pregnancy
showed a significant difference between children with and without caries, though a significant
association could not be found in path analysis. Even though this is worth investigating further
we cannot overlook the fact of ambiguity in the data. Perhaps some of this variable is correlated
strongly with other variables that are in the final model and have been masked by other
variables. For example reported intake of other supplements. This is hardly surprising as the
types of vitamins included in the multivitamin “pill” or “capsule” were not asked in the
questionnaire.
Our study has some limitations. Participants were volunteers and may not be representative of
the general population. Further, information on prenatal supplements is as reported by
participants themselves, and serum levels were unavailable. The study was cross-sectional,
hence the associations found cannot be presumed as causal. Moreover, past caries experience
was assessed based on the number of surfaces with restorations at examination; thus, the
periods of life during which a child had active caries is not known, and may not be comparable.
93
5.6 Conclusions
This study confirms that a child’s current activity of dental caries is positively associated their
past caries experience, and both are likely to relate to future caries unless there is improved
behaviour and/or preventive interventions. It also confirms that current levels of salivary MS
are associated with both past and present levels of caries, and likely also future disease. Mothers
who have reported to taking nutritional supplements throughout pregnancy could be associated
with lower caries experience in their 6-year-old child, consistent with the Barker hypothesis,
in that a healthy foetus predisposes to a healthy child, and vice versa. This study is the first to
explore associations between mothers’ reported intake of nutritional supplements during
pregnancy and their dental caries experience in a path model adjusting for the effects of salivary
and demographic variables. Further longitudinal studies are required to explore if these
associations have true predictive value and if any of the attributes studied might be regarded as
part of the causal chain of disease, and can be regarded as true risk factors.
These findings may be typical of Western industrialised countries and indicate the importance
of promoting good family health throughout the lifespan, including pregnant mothers.

94
Chapter 6: Influence of genes on the process of dental caries and
what lies beyond
6.1 Introduction
The purpose of this chapter is to review the literature on the influence of genetic and epigenetic
contributions to susceptibility to dental caries
The organization is as follows. Section 6.2 outlines the evidence reported over the last few
decades on the genetic influences on dental caries; particular attention is paid to research
conducted with humans irrespective of age, gender, and other population characteristics.
Section 6.3 briefly discusses the types of molecular genetic studies conducted and their
outcome in relation to susceptibility to dental caries, paying attention to possible biological
pathways that promote or prevent progression of the disease. Section 6.4 briefly describes
possible reasons why a dominant genetic influence could not be observed with dental caries
and describes the landmark twin studies. Section 6.5 briefly reviews the field of epigenetics
with an emphasis on mechanisms of DNA modification. Section 6.6 focuses on potential
environmental stimuli that might initiate or inhibit DNA modifications and eventually
influence dental caries. Section 6.7 describes the importance of future research on epigenetics
in relation to dental caries, acknowledging the dearth of empirical research in the area.

95
6.2 Evidence that the host genome influences the natural history of dental
caries
Following completion of the Human Genome Project in 2003 (www.genome.gov), interest
grew to understand the underlying genetic mechanisms influencing susceptibility to dental
caries. The high prevalence of caries among certain ethnic groups and observations that
fluoride exposure is not protective for all individuals motivated research seeking possible
genetic contributors (Slade et al., 2013; Vieira et al., 2014). Whilst genome-wide and candidate
gene studies have delivered some successes, they have also exposed challenges, such as the
need for robust phenotype definitions and sample sizes that allow enough statistical power to
detect modest genetic effects.
In 1988, Borass et al. showed evidence of a genetic contribution to caries susceptibility by
studying twins raised together and apart (Boraas et al., 1988). More recent studies involving
both monozygotic (MZ) and dizygotic (DZ) twins (Bretz et al., 2005; Bretz et al., 2006), and
family studies (Shaffer et al., 2015; Wang et al., 2010), estimated the heritability component
(proportion of phenotype variation due to genetic factors) for caries experience, measured by
decayed, missing, and filled teeth/surfaces index (dmft/s, DMFT/S) as ranging from 45%-64%
in the deciduous dentition, and an apparently lower heritability of 35%-55% in the permanent
dentition. However, heritability studies alone cannot fully quantify a genetic component in a
disease because shared behaviour and environmental factors contribute to covariance within
families and populations.
There are also important methodological considerations. On the one hand it is currently
unknown which methods of quantifying dental caries best reflect underlying genetic risk, so

96
research to identify phenotypes associated with specific genetic information is important
(Shaffer et al., 2013; Wang et al., 2010). On the other hand, better understanding of the structure
and function of DNA has generated a new era in genetics, namely the field of epigenetics. This
is now emerging as a significant platform in searching for answers to questions that were left
blank with earlier genetic studies (Seo et al., 2015). Electronic databases Medline via PubMed,
Scopus and Google scholar were used to search literature on genetic and epigenetic influences
on caries. The search strategy applied is described in Appendix C Table 1. The following is a
review of the cariology literature involving molecular genetic studies, and it emphasises how
epigenetics, through environmental modifications of the host genome, might ultimately be
important in determining risk and in preventing dental caries.
6.3 Types of molecular genetic studies
There are two main types of molecular genetic studies: genome-wide studies and candidate
gene studies (Vieira et al., 2014).
6.3.1 Genome-wide Studies
6.3.1.1 Genome-wide linkage studies
Genome-wide linkage studies constitute a powerful tool to investigate the genetic construction
of complex diseases (Hardy and Singleton, 2009; Manolio et al., 2009) and are based on
exploring for segregation of alleles within a recorded pedigree, investigating the transmission
to offspring of alleles that are physically close or linked to each other in relation to disease
traits within families (Kemper et al., 2012). In respect to the caries process, published literature
has shown three gene loci (5q13.3, 14q11.2, and Xq27.1) associated with low caries experience

97
(DMFT 1 and 2) implying a degree of resistance, and two loci (at 13q31.1 and 14q24.3)
associated with high caries experience (DMFT 3 and 4), implying susceptibility in such
individuals (Riley et al., 2007; Vieira et al., 2008; Wang et al., 2013a). The former loci
appeared to be associated with the functional properties of a psycho-stimulant; the latter pair
with taste and flavour (Vieira et al., 2008), attributes which, intuitively, would influence diet,
especially the intake of sugars (Table 6.1). However, a strong and statistically significant
association with dental caries experience was not found, perhaps because the separation of the
disease groups was not marked.
6.3.1.2 Genome-wide association studies
Genome-wide association studies (GWAS) search for associations between genetic variants
and phenotypic differences within a population and analyse genome-wide structural variations,
which are detected by screening the whole genome (Kemper et al., 2012). Several GWAS have
been performed on dental caries (Table 6.1). In 2012, Shaffer et al. reported a GWAS screening
study related to caries experience in the deciduous dentition of 3- to 12-year-old children in the
USA. That study found several genomic regions suggestive of association, although no specific
loci were statistically significant (Shaffer et al., 2011). Vieira et al. subsequently found loci not
previously described which did have a significant association with disease history in the
deciduous dentition (Vieira et al., 2014). In 2012, Wang et al. published a GWAS in relation
to experience of dental caries in the permanent dentition, and although, again, no statistically
significant associations were found, several “statistically suggestive” loci were identified
(Wang et al., 2012a). With adults, advancing age increases the influence of behavioural
(including diet and oral hygiene) and environmental influences, and confounding diseases such
as diabetes, perhaps operating over decades, will all have cumulative effects which may
overshadow genuine genetic effects (Wang et al., 2012b). As is evident from the results

98
presented by Shaffer et al. (2012), where the heritability of caries scores in the permanent
dentition was 35%-55% (p < 0.01) compared to 70% in deciduous dentition (Shaffer et al.,
2012a). However it is possible that different caries phenotypic definitions might have given the
observed variations in results as indices like DMFT might not be sensitive enough to precisely
detect these effects. Moreover, the different biological samples (blood, mouthwash, buccal
swab, saliva) used to obtain DNA, and various genotyping techniques used might have given
dissimilar study findings.

99
Table 6.1 A summary of genome-wide linkage and genome-wide association studies for human dental caries
Reference Study design and study
population
Phenotype Results
Suggestive loci (gene) Significant loci (gene)
Genome-wide linkage studies
Vieira et al. , 2008 Cross sectional
642 Philippine individuals
from 46 families
Decayed Missing Filled Teeth
index (DMFT), permanent
dentition
For low caries experience:
5q13.3, 14q11.2,
Xq27.1
For high caries experience:
13q31.1, 14q24.3
-
-
Genome-wide association studies
Shaffer et al., 2011 Cross sectional
1305 US children aged 3-12
years
decayed missing filled teeth
index (dmft), primary dentition
1q42–q43 (ACTN2, MTR,
EDARADD), 11p13
(MPPED2), 17q23.1 (LPO)
-
Wang et al., 2012a Cross sectional
7443 adults from US
DMFT, permanent dentition 1q42.11–q42.3
(RHOU), 4q13.3
(ADAMTS3), 8p21.1
(PTK2B)
4q32 (TLR2), 5q11.1 (ISL1), 6q27
(RP56KA2), 7q21 (FZD1), 14q22
(CDKN3, CNIH, GMFB,
CGRRF1, BMP4)
Shaffer et al., 2013
Cross sectional
920 US adults aged 17-75
years
Decayed Missing Filled
Surface index (DMFS) scores
1-5, permanent dentition
DMFS2: 4q31.22 (EDNRA)
DMFS5:
1p36 (SPSB1),
2p24 (TRIB2),
4p15 (PROM1), 4q22
(ABCG2, PKD2,
SCPP), 4q31.22
(EDNRA), 7q22
(ATXN7), 17q11
(WSB1)
DMFS2: 10p11.23 (LYZL2)
DMFS5: 1p36 (AJAP1)

100
Reference Study design and study
population
Phenotype Results
Suggestive loci (gene) Significant loci (gene)
Zeng et al., 2013 Cross sectional
1017 US adults aged 14-56
years
DMFS scores-pit and fissure
and smooth surface caries in
permanent dentition
For pit and fissure:
7p15 – 13 (INHBA), 8q21.3,
Xp11.4 (BCOR)
For smooth surface:
2q35 (CXCR1,
CXCR2), Xq26.1
(BCORL1)
Smooth surface: 8q21.3 (no gene)
Zeng et al., 2014 Cross sectional
1006 US children aged 3-12
years
dfs scores-pit and fissure and
smooth surface caries in
deciduous dentition
For pit and fissure:
11p14.1 (MPPED2)
For smooth surface:
1p36 (AJAP1),
6q27 (RP56KA2),
16p11.2 (ITGAL),
20q11.21 (PLUNC)
Pit and fissure: 3q26.1 (KPNA4)
Genome-wide association with gene set enrichment Gene sets Gene sets for;
Wang et al., 2013b Cross sectional
1142 US children aged 3-12
years
dfs scores in deciduous
dentition
Several suggestive gene sets,
refer Wang et al, 2013 (61).
I. cytokine secretion (18, including
INS)
II. ligase activity forming carbon
nitrogen bonds (68, including
WWP2, RNF217)
III. ubiquitin protein ligase activity (49)
IV. protein secretion (32)
V. regulation of protein secretion (22)
VI. regulation of cytokine secretion (16)
VII. regulation of axonogenesis (10)
VIII. regulation of neurogenesis (14,
including ROBO2, SLIT2)
IX. central nervous system
development (122)
X. small conjugating protein ligase
activity (51)
XI. glycoprotein catabolic process (12)
XII. axonogenesis (43)
XIII. cell matrix junction (16; includes
ACTN2)
GWAS on dental caries can be accessed at https://www.ebi.ac.uk/gwas/search?query=dental%20caries

101
6.3.2 Candidate gene studies
Selection of candidate genes is based on extant knowledge of the biology of the caries process,
and are, therefore, limited to genes that have already been identified and characterised. There
are several advantages to this approach as these studies may provide adequate power to detect
relative low risk for dental caries (Daly and Day, 2001). As most candidate gene studies focus
directly on a single gene and frequently look directly at functionally significant
polymorphisms, concerns about the extent of linkage disequilibrium and the adequacy of SNP
markers to detect associations are not relevant (Daly and Day, 2001). Different expressions of
dental caries phenotypes between candidate gene studies and the diversity of populations
studied, however, make it difficult to generalize the findings.
Major candidate gene categories reported to date in relation to the process of dental caries
include genes involved in enamel formation, immune response genes, genes related to salivary
function, and genes related to taste (Kutsch et al., 2013; Opal et al., 2015; Vieira et al., 2014)
(Table 6.2). Since these candidate genes are associated with the process of dental caries,
researchers have shown interest in investigating several of these gene loci simultaneously in
their respective studies. However most of these associations have not been replicated in each
independent study, perhaps due to population differences, contrasting case definitions, or issues
with sample size and statistical power.

102
Table 6.2 A summary of candidate genes studies for human dental caries
Gene Gene Function Results References
Enamel formation genes
Tuftelin (TUFT1) Expressed in the developing and
mineralized tooth and non-
mineralizing soft tissues
Associated with higher caries experience;
this association can be dependent of the
presence of Streptococcus mutans
Slayton et al., 2005, Deeley et al. 2008,
Patir et al., 2008, Shimizu et al., 2012
Amelogenin (AMELX) Involved in the mineralization
during tooth enamel development
Associated with higher caries experience Deeley et al., 2008, Patir et al., 2008,
Kang et al., 2011, Shimizu et al., 2012,
Slayton et al., 2005, Olszowski et al.,
2012
Enamelin (ENAM) Involved in the mineralization and
structural organization of the
enamel
Associated with higher caries experience Patir et al., 2008, Shimizu et al., 2012,
Slayton et al., 2005, Olszowski et al.,
2012
Tuftelin-interacting
protein 11 (TFIP11)
Interact with tuftelin and can play
a role in spliceosome disassembly
in Cajal bodies
Associated with initiation of carious lesions
and higher
caries experience
Shimizu et al., 2012 , Slayton et al., 2005,
Deeley et al., 2008, Patir et al., 2008,
Shimizu et al., 2012
Ameloblastin (AMBN) Involved in enamel matrix
formation and mineralization
Associated with higher caries experience Patir et al., 2008, Shimizu et al., 2012,
Slayton et al., 2005, Deeley et al., 2008
Matrix metalloproteinase
20 (MMP20)
Degrades amelogenin Associated with higher caries experience in
Whites with poor oral health habits
Tannure et al., 2012b
Matrix metalloproteinase
13 (MMP13)
Involved in endochondral
ossification and bone remodelling
Associated with lower caries experience Tannure et al., 2012a

103
Gene Gene Function Results References
Immune response genes
CD14 molecule (CD14) Mediates innate immune response
to bacterial lipopolysaccharide
Absent in the saliva of individuals with
active carious lesions
Bergandi et al., 2007
Human leukocyte antigen;
major histocompatibility
complex, class II, DR beta
1 (HLA-DRB1) and DQ
beta 1 (HLA-DQB1)
Presents peptides derived from
extracellular proteins
Frequency of allele 4 of DRB1 is increased
in children with early childhood caries; also
allele 2 of DQB1 is increased in adolescents
affected by caries; DRB1 allele 1 and DQB1
allele 3 frequencies are increased in the
presence of Streptococcus mutans
Altun et al., 2008, Bagherian et al., 2008,
Valarini et al., 2012, Wallengren et al.,
1997
Beta defensin 1 (DEFB1) Implicated in the resistance of
epithelial surface to microbial
colonization
Distinct DEFB1 haplotypes are associated
with low and high caries experience
Ozturk et al., 2010, Krasone et al., 2014
Lactotransferrin (LTF) Major iron-binding protein in milk
and body secretions with
antimicrobial activity
Associated with lower caries experience
Azevedo et al., 2010
Mucin 7 (MUC7) Facilitates the clearance of
bacteria in the oral cavity
Associated with higher caries experience
with poor oral hygiene
Pol, 2010
Mannose-binding lectin
(protein C) 2, soluble
(MBL2)
Recognizes mannose and N-
acetylglucosamine on many
microorganisms
Associated with higher caries experience
Olszowski et al., 2012
Genes related to saliva composition and function
Carbonic anhydrase VI
(CA6)
Maintains pH homeostasis in body
tissues
No association with caries but positive
association with buffer capacity
Peres et al., 2010
Proline-rich protein
HaeIII subfamily 1 (PRH1)
Involved in oral biofilm formation,
tissue
Homeostasis and immunological
investigation
Associated with higher caries experience
and
colonization by Streptococcus mutans
Zakhary et al., 2007
Cysteine rich glycoprotein
(gp-340 I)
Adhesion of MSto the dental bio
film
Associated with high caries experience Jonasson et al., 2007

104
Gene Gene Function Results References
Basic proline rich proteins
(PRB1 and PRB2)
Regulates plaque pH Associated with low caries experience Ayad et al., 2000
TIMP metallopeptidase
inhibitor 2 (TIM2)
Important to the maintenance of
tissue homeostasis by suppressing
the proliferation of quiescent
tissues in response to angiogenic
factors, and inhibit protease
activity in tissues undergoing
remodelling of the extracellular
matrix.
No evidence of association
Tannure et al., 2012a
Genes related to taste sensation
Taste receptor, type 2,
member 38 (TAS2R38)
Controls the ability to taste
glucosinolates
Associated with lower caries experience Wendell et al., 2010, Pidamale et al.,
2012
Taste receptor, type 1,
member 2 (TAS1R2)
Sweet taste receptor Associated with both lower and higher caries
experience
Wendell et al., 2010, Kulkarni et al., 2013
Guanine nucleotidebinding
protein, alpha
transducing 3 (GNAT3)
Involved in dietary preferences
No evidence of association
Wendell et al., 2010
Solute carrier family 2
(facilitated glucose
transporter), member 2
(SLC2A2)
Mediates bidirectional glucose
transport
Associated with higher caries experience
Kulkarni et al., 2013
Taste receptors TAS1R2 and
TAS1R3
Sweet taste receptors Associated with high caries experience Fushan et al., 2009

105
6.3.2.1 Enamel formation genes
Calcium phosphate hydroxyapatite crystals form the bulk of enamel. Enamel formation is
regulated through the interaction of a number of organic matrix molecules including
amelogenin, enamelin, ameloblastin and tuftelin. The amelogenin gene (AMELX) is located
on the p arm of the X chromosome, at Xp22.31-p22.1 and promotes the formation of a scaffold
for enamel crystallites and controls their growth (Patir et al., 2008; Rauth et al., 2009). The
ameloblastin gene (AMBN), which controls the functions of ameloblastin, is nested in
chromosome 4q21 between D4S409 (4q13) and D4S400 (4q21) (MacDougall et al., 1997).
Ameloblastin is a vital adhesion molecule for enamel formation, while playing an important
role in binding and maintaining the secretory ameloblasts (Sasaki et al., 2008). Tuftelin plays
a vital role during the development and mineralization of enamel, facilitating the initial stages
of enamel mineralisation (Deutsch et al., 2002). Functions of this phosphorylated glycoprotein
are regulated by TUFTI gene and an over expression of the gene will cause imperfections in
both enamel prisms and crystallite structure (Luo et al., 2004), making the enamel vulnerable
to acid challenges causing demineralisation (Cai et al., 2007). However, Shimizu et al. (2012)
reported that variations in TUFT1 were associated with the ability of the enamel surface to
uptake fluoride in very low concentrations, thus lowering the individual susceptibility to
demineralization at subclinical levels (Shimizu et al., 2012). A systematic removal of the
organic matrix and replacement with mineral is fundamental to generate an enamel layer that
is harder and unstained by retained enamel protein. Matrix metalloprotease 20 (regulated by
MMP-20) and kalikrien 4, (regulated by KLK4 gene), synchronize this process, making the
enamel layer harder, less porous, and unblemished by retained enamel proteins (Lu et al.,
2008). Hence, defects of these genes can result in the fabrication of abnormal proteins or reduce
the amount of MMP-20 and KLK 4 in developing teeth. Defective mineralisation caused by

106
these malformations could influence both bacterial adherence and resistance of enamel to acid,
increasing the susceptibility of tooth surfaces to dental caries (Opal et al., 2015).
Shimizu et al. (2012) showed that variations in AMELX, TUFT1, AMBN, and ENAM have
associations with caries experience by studying microhardness changes under simulated
cariogenic challenges (Shimizu et al., 2012). They found that the frequency of T allele of
AMELX rs946252 and C allele of AMBN rs4694075 was significantly higher in a group of
Filipino families with high caries experience. Comparable results were observed in a Korean
population, where two SNPs of AMELX; rs5933871 (p = 0.02) and rs5934997 (p = 0.02) were
significantly associated with increased dental caries experience in individuals living/lived in
fluoridation areas (Kang et al., 2011). Genotype of the tuftelin rs3790506 marker was reported
to be overrepresented in cases with higher dmft scores especially in the presence of MS (Patir
et al., 2008). Similarly, Slayton et al. (2005) observed that tuftelin, a gene involved in enamel
mineralization, when combined with high levels of MS increased the susceptibility of dental
caries significantly (R2 = 0.268) and they were able to explain 27% of the variation in the dmfs
scores by this interaction (Slayton et al., 2005). Deeley et al. (2008), on the other hand, reported
an association between the tuftelin-1 rs2337360 marker and high caries experience only when
individuals with DMFT≤ 2 were compared with DMFT ≥ 3 (p = 0.03), ≥4 (p = 0.02), ≥ 5 (p
= 0.042), and ≥ 6 (p = 0.049) (Deeley et al., 2008). Further, polymorphism in MMP-13 (OR =
0.538, 95% CI = 0.313-0.926) revealed a significantly reduced caries risk, and the result
remained significant even after adjusting for other candidate genes, type of dentition, and
dietary factors in a population of children and adolescents 3- to 21-years-old (Tannure et al.,
2012b). In addition, Shaffer et al. showed that, candidate genes have an effect on enamel
according to the surface features of teeth, such as smooth surface or pits and fissures (Shaffer
et al., 2012b). They observed that heritability score for caries in pit and fissure (h 2 = 19–53%;
107
p < 0.001) and smooth surface caries (h 2 = 17–42%; p < 0.001) in deciduous teeth was more
than for their permanent counterparts. A suggestive association was observed on chromosome
Xq26.1 (gene BCORL1) with smooth surface caries and BCOR with pit and fissure caries
(Zeng et al., 2013). Both are x-linked genes with sequence similarity, providing evidence for
the hypothesis proposed by Vieira et al. (2008) that x-linked genetic variants may partly explain
gender differences in dental caries susceptibility (Vieira et al., 2008; Zeng et al., 2013; Zeng et
al., 2014).
These studies report the role of specific genes in increasing susceptibility to caries, as well as
differential effects on the two dentitions and on specific surfaces. However, the complexity in
dental caries is further complicated by genetic phenotypes, which manifest differently in
different populations, races, dentition, or surfaces being studied. Most studies have compared
individuals who are caries free to individuals with one or more tooth surfaces affected, meaning
that extremes of disease experience, and thus presumptively of disease susceptibility, would be
difficult to detect. Further research is needed to identify the interactions of different phenotypes
and other environmental factors.
6.3.2.2 Immune response genes
Genes control the immune response, as all bodily development and function. Hitherto, CD14,
Human leukocyte antigen (HLA), Beta defensin (DEFB), Lactotransferrin (LTF), Mucin
(MUC), Mannose-binding lectin (MBL), and Manna-binding lectin serine peptidase (MASP)
have been studied extensively as genes that have the potential to make the host susceptible to
dental caries (Vieira et al., 2014). These genes operate by maintaining the immune system in
promoting or inhibiting oral cariogenic bacteria. The innate immune system relies on the
recognition of pathogen-associated molecules, such as bacterial cell wall components. CD14,

108
a 55-kD membrane glycoprotein, is expressed predominantly on the surface of monocytes,
macrophages, and neutrophils. They play a crucial role in the recognition of several microbial
products, such as lipopolysaccharide (LPS, endotoxin) and peptidoglycan, which are major
components of gram-negative and gram-positive bacterial surfaces (Lien and Ingalls, 2002).
CD14 is a multifunctional protein and has been suggested to reduce endotoxin-induced
activities of salivary pathogens.
The presence of salivary soluble CD14 has been found to reveal an inverse relationship with
the carious lesions; that is, CD14 was completely absent in the saliva of patients affected by
two to eight carious lesions (Bergandi et al., 2007). Moreover, HLA and major
histocompatibility complex (MHC) molecules have important roles in immune responsiveness.
Polymorphisms in the molecules may cause some variations in immune responses against oral
colonization levels and may influence an individual’s susceptibility to caries (Opal et al., 2015).
For instance, being positive for HLA-DRB1FNx0104 gene was reported to increase the risk of
developing caries by ten times (p = 0.03) in a group of 1- to 6-year-old children from Iran
(Bagherian et al., 2008). According to Altun et al. (2008), an increased frequency in HLA-
DRB1*01(p = 0.02) and HLA-DQB1*O3 (p = 0.009) were significantly associated with the
salivary MS among a group of children, though no association could be observed with caries
experience (Altun et al., 2008). Nevertheless, a population of adolescents in Brazil who were
positive for HLA-DQ2 allele were less likely to have dental caries than their counterparts who
were negative for this allele (OR = 0.33, CI = 0.16–0.66) (Valarini et al., 2012). A similar trend
was found towards a relationship between the presence of HLA-DR4 and high levels of MS;
however, the results were not statistically significant, probably due to the small number (28)
of subjects involved (Wallengren et al., 1997). DEFB 1 on the other hand is an oral anti-
microbial peptide, which provides the first line of defence against a wide spectrum of pathogens
109
(Krasone et al., 2014). Two haplotypes in the DEFB 1 promoter were linked with high and low
caries experience: a high-caries-experience haplotype (GCA), which were associated with
DMFT scores 2-folds higher, and a low-caries-experience haplotype (ACG), with DMFT
scores 2-folds lower (Ozturk et al., 2010). Variation in the promoter region of DEFB 1 plays a
role in the aetiology of caries since it has been proven that carrying a copy of the variant allele
of the DEFB 1 marker rs11362 (G-20A) was associated with a more than 5-folds higher DMFT
and DMFS scores (Krasone et al., 2014). Azevedo et al. (2010) observed that LTF, a major
iron-binding protein in milk and body secretions with antimicrobial activity, was associated
with lower caries experience in a population of 12-year-old Brazilian children (Azevedo et al.,
2010).
MBL (protein) is a lectin that is instrumental in innate immunity in humans as the protein
recognises mannose and N-acetylglucosamines on oral microorganisms. MBL is capable of
binding to carbohydrate moieties predominantly present on the surfaces of bacteria (Eddie Ip
et al., 2009). High serum levels and high activity of MBL, regulated by MBL2 gene, have been
associated with inflammatory diseases, transplant rejection, and diabetic nephropathy. Further,
MBL2 polymorphisms have been linked with bacterial infections such as Pseudomonas
aeruginosa and mycobacteria (Bouwman et al., 2006). According to Olszowski et al. (2012),
MBL2 gene polymorphism was significantly associated with increased caries experience in
Polish children. However, the direction of the association was found to be opposite in
deciduous and permanent dentition (Olszowski et al., 2012). Defensins are small cysteine-
rich cationic proteins localized in oral cavities and are an important component of the innate
immune system. Most defensins function by binding to the microbial cell membrane, and once
embedded, form pore-like membrane defects that allow efflux of essential ions and nutrients
(Fellermann and Stange, 2001). Ozturk et al. (2010) investigated three promoter

110
polymorphisms of the beta defensin 1 gene (DEFB1) and found that the presence of G-20A
(DEFB1 marker rs11362) variant were associated with DMFT and DMFS scores 5-folds
higher, while the G-52A (DEFB1 marker rs179946) variant was associated with lower DMFT
scores (Ozturk et al., 2010). This observation is most probably due to defensins playing a
greater or lesser role in bacterial aggregation, after which they will be swallowed, as first line
of defence, and on colonisation of tooth surfaces.
6.3.2.3 Genes related to taste sensation
It has been hypothesized that food preferences of children are learned although the desire to
select one food over another is more closely linked to taste and other sensory properties of
foods (Pidamale et al., 2012). Given the influence of dietary habits on dental caries, it can be
theorized that taste pathway genes, such as genes for taste preference, might influence caries
risk. Although taste preferences based on chemical tastants have been proven useful for the
assessment of dietary habits, studies have demonstrated the importance of dietary habits, and
nutritional status coupled with genetically determined taste sensitivity with respect to caries
risk (Bretz et al., 2006; Wendell et al., 2010). Inappropriate intakes of fermentable
carbohydrates, particularly sucrose, are well established as dominant factors in the
pathogenesis of caries. The cariogenic flora can metabolise sucrose moieties in the oral
environment in a unique manner, synthesising extracellular polysaccharides which help form
oral biofilms, and producing acids that can demineralize the tooth structure (Loesche, 1986).
Human sweet taste perception is mediated by the heterodimeric G protein-coupled receptor
encoded by the TAS1R2 and TAS1R3 genes (Fushan et al., 2009). Fushan et al. found that two
C/T SNPs located at positions 21572 (rs307355) and 21266 (rs35744813) upstream of the
TAS1R3 coding sequence strongly correlate with human taste sensitivity to sucrose (Fushan et

111
al., 2009). Further, they suggested that there were strong deviations from evolutionary neutral
genetic drift for variation in the coding regions of TAS1R2 and, to a lesser extent, TAS1R3,
which could contribute to sensitivity to sweet compounds. People who carried T alleles
displayed decreased sucrose sensitivity scores (using quantitative stimuli of sucrose solutions
with different concentrations) compared to those who carried C alleles (Fushan et al., 2009).
Kulkarni et al. (2013) observed similar outcomes in a group of Caucasians aged 21-32 years
by studying polymorphisms in the sweet taste receptor (TAS1R2) and glucose transporter
(GLUT2). They found that subjects with GLUT2 and TAS1R2 genotypes, both individually
and in combination, were associated with caries risk. A higher DMFT score was observed
(mean DMFT 4.3 vs 6.1, p = 0.04) among carriers of the Ile allele for GLUT2 (regarded as a
high/higher risk group), whereas carriers of the Val allele for TAS1R2 showed lower DMFT
scores (mean DMFT 4.1 vs 5.8, p = 0.05) and were regarded as a resistant group (Kulkarni et
al., 2013). Pidamale et al. (2012) demonstrated that the sensitivity to bitter taste, which is
mediated by the TAS2R38 gene, was associated with dental caries. Children aged 36-71
months who carried TAS2R38 gene could taste bitter sensation more and had less affinity
towards sweet sensation and had low dmft scores compared to non-tasters (Pidamale et al.,
2012). By hypothesizing that genetic variation in taste pathway genes may be associated with
dental caries, Wendell et al. investigated TAS2R38, TAS1R2 and GNAT3 genes in families
recruited by the Centre for Oral Health Research in Appalachia. Results revealed that
TAS2R38 and TAS1R2 are associated with experience of, and presumptively with
susceptibility to, dental caries, while the taste gene TAS2R38 (bitter taste receptors) appears to
be “protective” in the primary dentition: certain alleles of taste genes TAS1R2 (sweet taste
receptors) were associated with caries risk in the mixed dentition group (Wendell et al., 2010).
When the concern is taste genes and dental caries, it is logical to accept the fact that genetic

112
variations contribute to differences in dietary habits which in turn influence the caries process,
rather than having a direct relationship with caries.
6.3.2.4 Genes related to saliva
Numerous studies bear evidence that individuals who lack the ability to produce adequate
saliva volumes to maintain equilibrium in pH and buffering capacity suffer from several
diseases. It has long been understood that saliva has important properties that protect the
dentition: volume and flow which can dilute acids and flush food debris and microorganisms
from the mouth, a pH which can neutralise acids, and a significant buffering ability (Lenander-
Lumikari and Loimaranta, 2000). Although these properties of saliva are known to modify the
caries process, the role of genetic polymorphism remains relatively unexplored. There is hardly
any literature that shows an association between genetic variations in salivary physiology and
dental caries (Opal et al., 2015). Peres et al. in 2009 investigated the allele and genotype
distribution of three polymorphisms in the coding sequence of the Carbonic anhydrase VI
(CA6) gene and checked possible associations with saliva buffering capacity, plaque pH,
plaque index, and dental caries experience (Peres et al., 2010). They observed that among the
245 children studied there was a positive association between buffer capacity and the CA6 gene
rs2274327 (C/T) polymorphism. The allele T (p = 0.023) and genotype TT (p = 0.045) were
less frequent in children with higher buffer capacity. Since the association between CA6 gene
polymorphism and caries experience was not found to be statistically significant (Peres et al.,
2010), it is probable that the effects are overshadowed by other genetic variables, diet, and oral
hygiene practices.
The acidic proline-rich proteins (PRPs) account for 25%-30% of all proteins in saliva, and these
influence the attachment of cariogenic bacteria to tooth surfaces (Lenander-Lumikari and

113
Loimaranta, 2000). Human PRPs are encoded by six closely linked genes on chromosome
12p13.2 (Kim et al., 1990). Zakhary et al. (2007) studied one of the three acidic PRP alleles of
PRH1 locus (Db) to determine its association with dental caries (Zakhary et al., 2007). Results
revealed that in Caucasians, the Db gene frequency was 14%, similar to Db protein from parotid
saliva, and in African-Americans the similarity was 37%. All Caucasians, when compared to
African-Americans had significantly high caries experience along with greater MScounts. They
concluded that racial differences in caries experience, and by implication caries susceptibility,
might be explained in part by the differences in Db alleles (Zakhary et al., 2007). Similarly, the
salivary scavenger receptor cysteine-rich glycoprotein gp-340, which facilitates adhesion of
Streptococcus mutans, shelters three major size variants, designated gp-340 I, II and III, each
specific to an individual’s saliva. The gp-340 I was found to correlate positively with caries
experience in a group of 12-year-old Swedish children (Jonasson et al., 2007). Moreover, the
allelic acid PRP protein variant Db positively correlated with high caries experience, and the
gp-340 I protein was more common among Db+ subjects than among Db- subjects. Hence, the
phenotypes positive for both gp-340 I and Db experienced more caries than those negative for
both proteins (Jonasson et al., 2007). Similar findings were reported by Ayad et al. (2000),
where the phenotype of PRPs, PS1 encoded by PRB1 and con1 encoded by PRB2, were
significantly higher in caries free individuals (Ayad et al., 2000).
Owing to the fact that caries is a disease modified by a multitude of factors in different
population groups the variation of which cannot be explained by genetic endowment alone.
Genetic polymorphisms in a large number of genes have been shown to quantitatively and
qualitatively affect dental caries, with effects on susceptibility and severity of diverse
communities. Yet the human genome is diverse and when looked at individually, important
variations such as different SNPs and haplotypes can be observed. Multiple scans for these

114
variations across the genome have pointed to genes involved in behavioural traits as well as to
those that may predict deferred disease liability. Stimuli and mechanisms that influence these
inter-individual differences may help in explaining personal susceptibility to dental caries.
6.4 Genes, caries and environment
Although genetic studies have indicated some associations of DNA variants to dental caries
phenotypes, there have been no truly "potent" effect variants identified with causal biological
relevance. This could be due to the influence of environmental factors having a long-term
influence on genetic modifications; in other words, epigenetic modifications could have an
effect on gene expression leading to altered dental caries phenotypes (figure 6.1). Williams et
al. (2014) emphasized this following the difficulty to establish causal relationships between
specific genes and a number of complex diseases, many of which manifest later in life (Eichler
et al., 2010; Williams et al., 2014).
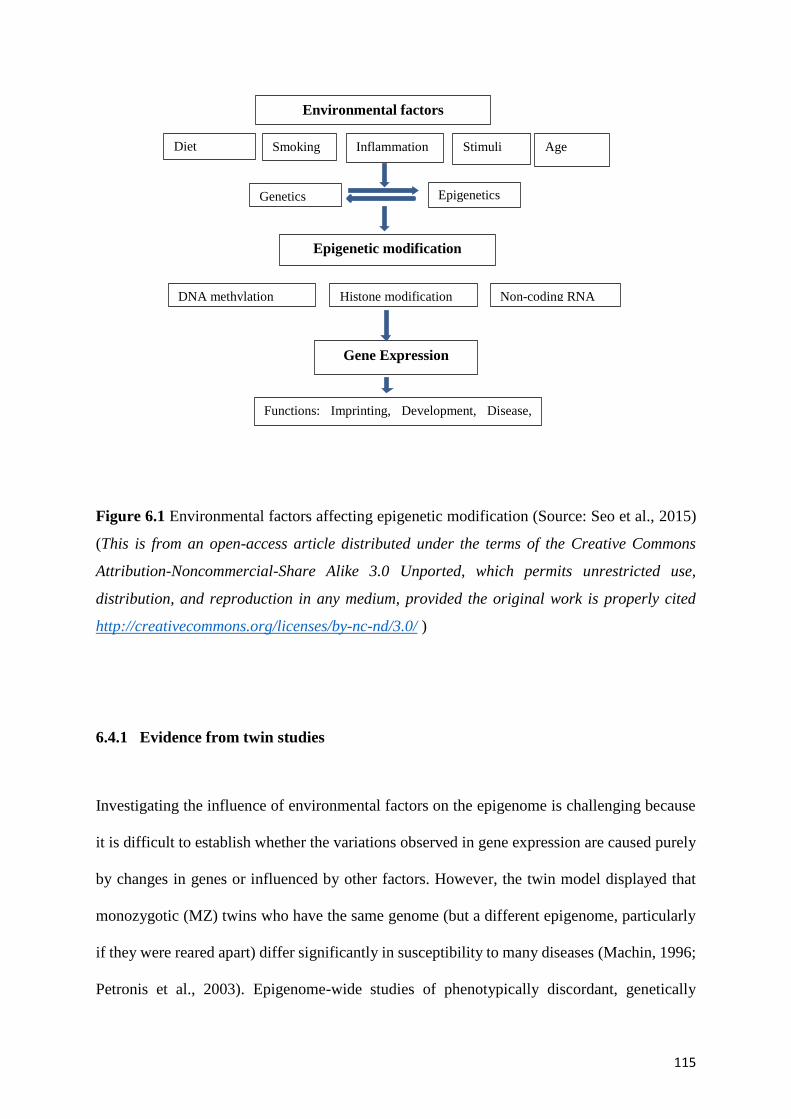
115
Figure 6.1 Environmental factors affecting epigenetic modification (Source: Seo et al., 2015)
(This is from an open-access article distributed under the terms of the Creative Commons
Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use,
distribution, and reproduction in any medium, provided the original work is properly cited
http://creativecommons.org/licenses/by-nc-nd/3.0/ )
6.4.1 Evidence from twin studies
Investigating the influence of environmental factors on the epigenome is challenging because
it is difficult to establish whether the variations observed in gene expression are caused purely
by changes in genes or influenced by other factors. However, the twin model displayed that
monozygotic (MZ) twins who have the same genome (but a different epigenome, particularly
if they were reared apart) differ significantly in susceptibility to many diseases (Machin, 1996;
Petronis et al., 2003). Epigenome-wide studies of phenotypically discordant, genetically
Environmental factors
Diet Smoking Inflammation Stimuli Age
Genetics Epigenetics
Epigenetic modification
DNA methylation Non-coding RNA Histone modification
Gene Expression
Functions: Imprinting, Development, Disease,
Cancer

116
‘identical’ MZ twins have provided information about gene-environment interaction and
variable penetrance; however, the study lacked balanced MZ and DZ comparison groups
(Boraas et al., 1988). In 2005, Fraga et al. demonstrated that MZ twins could differ significantly
in patterns of both methylation and histone modification of their genomes, with these
differences increasing with age (Fraga et al., 2005). Twins who had spent less of their lifetime
together (i.e. different environmental exposures) showed the greatest differences in histone
modification (Fraga et al., 2005). These epigenetic modifications were associated with, or
caused by, environmental factors like smoking, diet, age, and lifestyle factors, for example,
unhealthy BMI (Fraga et al., 2005; Seddon et al., 2011). Such findings support the current
hypothesis that epigenetic changes increase with age and that epigenetic biomarkers can predict
disease long before clinical onset (Craig, 2013; Fernando et al., 2015). Hence, the need for
investigations in the field of oral diseases especially in the area of dental caries is further
emphasised; we have not detected any publications to date on the epigenetics of cariogenesis.
6.5 Epigenetics
Epigenetics is the study of alterations in gene regulation that are not necessarily caused by
changes in the DNA sequence (Seo et al., 2015). Historically “epigenetics” was used to
describe inherited influences that could not be described solely by genetic principles (Goldberg
et al., 2007). These include chemical and environmental alterations in the DNA and associated
proteins, with remodelling of the chromatin and dysregulation of specific gene function, thus
influencing pathogenesis (Gomez et al., 2009; Su et al., 2011; Wilson, 2008).

117
Mechanisms of Epigenetic modification
6.6.1 DNA methylation
DNA methylation is the most studied epigenetic alteration of DNA in humans (Barros and
Offenbacher, 2009; Leenen et al., 2016) and the most characteristic type of chromatin
modification (Seo et al., 2015). The process of DNA methylation is by the covalent transfer of
a methyl group from S-adenosyl methionine (SAM) to a cytosine present in CpG dinucleotides
of the DNA chain (Williams et al., 2014). In the normal cell, gene promoter-associated CpG
islands are predominantly unmethylated, whereas CpG sites within gene bodies are generally
methylated (Patterson et al., 2011) (figure 6.2).
Figure 6.2 A CpG island in relation to a gene promoter region (Source: Patterson et al., 2011).
(This is from an open-access article distributed under the terms of the Creative Commons
Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use,
distribution, and reproduction in any medium, provided the original work is properly cited
http://creativecommons.org/licenses/by-nc-nd/3.0/ )
Promoter-associated
CpG Island

118
Hypermethylation of CpG inlands causes inhibition of gene transcription in the area and
hypomethylation results in activation of these genes, both of which have been implicated in the
development and progression of diseases such as cancer (Mani and Herceg, 2011) (figure 6.3).
Figure 6.3. DNA methylation at CPG sites (Source: Seo et al., 2015). (This is from an open-
access article distributed under the terms of the Creative Commons Attribution-
Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is properly cited
http://creativecommons.org/licenses/by-nc-nd/3.0/ )
6.6.2 Histone modification
The nucleosome is the fundamental subunit of chromatin. Each nucleosome is composed of
less than two turns of DNA wrapped around a set of eight proteins called “histones” (Seo et
al., 2015). The structure of histones determines how the DNA is condensed, ultimately
affecting gene expression (Önder et al., 2015; Williams et al., 2014). The commonest form of
histone modification is through acetylation of its eight sub-units (Seo et al., 2015). Hyper- and
hypo-acetylation can affect chromatin condensation either allowing or preventing gene
transcription respectively (Williams et al., 2014). Differences in gene expression associated
with differential acetylation will affect disease outcomes.
CPG Gene
CPG Gene
Unmethylated Transcription Activation
Methylated Transcription Inactivation

119
6.6.3 Non-coding RNA
RNA makes up coding units which produce proteins. RNAs are broadly categorized into coding
RNA, RNAs with an open reading frame (ORF) which are translated to proteins; and non-
coding RNA without an ORF, which do not produce proteins, though they are active
themselves (Williams et al., 2014). Non-coding RNA includes important RNAs like tRNA
(transfer RNA), rRNA (ribosome RNA), miRNA (mitochondrial RNA) and siRNA (small
interfering RNA), which can regulate gene expression without altering DNA sequence
(Goldberg et al., 2007; Seo et al., 2015). These non-coding RNAs have the ability to control
epigenetic mechanisms like gene silencing (Goldberg et al., 2007) and have been shown to
contribute significantly to the progression of oral mucosal lesions through a combination of
oral RNA molecules (oral transcriptome) derived from oral premalignant lesions (Perez et al.,
2014).
6.7 Environmental stimuli which may result in epigenetic changes which
could influence the process of dental caries
Dental caries is known to be a disease with many risk modifiers, both environmental and
intrinsic, to an individual’s biological make up. Environmental stressors, including an
unbalanced diet, microbial exposures which cause a shift from a healthy ecology to a
potentially pathogenic ecology, tobacco smoking, and high alcohol intake can change
epigenetic patterns and thereby effect changes in gene activation and cell phenotypes and
functions (figure 6.1). However, confounders like age, sex, and ethnicity might mask the real
effect. As epigenetic changes are frequently retained following cell division, altered patterns

120
in tissues can accumulate over time and lead to variations phenotypes, reflecting a molecular
consequence of gene-environment interaction, which can then be inherited by following
generations.
6.7.1 Diet and nutrition
Alterations in DNA methylation due to environmental stimuli begin even before birth.
Methylation of foetal DNA in utero due to low dietary levels of folate, methionine, and/or
selenium can change epigenetic programming, and this can persist into adulthood (Zaina et al.,
2005). However, established epigenetic patterns during the foetal period can become altered in
adulthood by environmental factors (Su et al., 2011). Folate is a critical methyl donor for S-
Adenosyl Methionine (SAM), which is used by the enzyme DNA methyltransferase (DNMT)
to methylate CpG residues selectively during embryonic development (Razin and Shemer,
1995). Hence, a decreased folate intake by the mother during pregnancy would cause a
subsequent decrease in DNA methylation in the foetus (Okano et al., 1999), although the level
“decreased” is subjective. Furthermore, nutritional components like vitamin D, betaine and
methionine can also cause epigenetic changes and consequently lead to disease not only at the
time of ingestion but even during intrauterine life (Seddon et al., 2011). Low intake of folate
and high alcohol consumption has been associated with altered methylation patterns in global
DNA, presenting an increased risk for colon cancer (Seddon et al., 2011). Studies like these
need to be interpreted with caution as there can always be recall bias. Nevertheless, high
consumption of alcohol was found to be associated with changes in methylation patterns of
squamous cells in the colon, promoting colon cancer (Schernhammer et al., 2010). This was
further emphasized by Sue et al., who elaborated that a wide range of dietary factors including
both macro-nutrients and micro nutrients have the potential to alter methylation of DNA.
Through diet an individual can be exposed not only to the nutritional components but also to
121
toxins that can cause hypomethylation of cancer cells and embryonic stem cells, for example,
arsenic, cadmium, mercury, and nickel (Davis and Uthus, 2004; Su et al., 2011); however, these
are rare.
6.7.2 Tobacco
Tobacco use is another cause for differential methylation of DNA. Tobacco smoke induces a
reduction in monoamine oxidase B (MAOB) promoter methylation and has long-lasting effects
on MAOB transcription (Launay et al., 2009). According to Launay et al. smoking causes long-
term hypo- and hyper-methylation changes in platelet and peripheral blood mononuclear cells
of smokers. These changes are present not only in current smokers but also in former smokers
(Belinsky et al., 2002; Launay et al., 2009). Hillemacher et al. reported that smoking has long
term effect on global DNA methylation across multiple tissues, and these changes are
demonstrable in leukocytes of offspring if parents smoked (Hillemacher et al., 2008).
6.7.3 Bacteria and inflammation
The human microbiomes, including the oral microbiota, comprise another set of influences on
the human genome, with potential to generate significant epigenetic changes. Complex
interactions between oral bacteria and host genome are the basis of susceptibility to
periodontitis (Pihlstrom et al., 2005). For example, specific polymorphisms of the serum
Interleukin-6 gene have been shown in patients with severe forms of destructive periodontitis
and correlate with the presence of Aggregatibacter actinomycetemcomitans and
Porphyromonas gingivalis (Nibali et al., 2008). A similar result was observed by Wu et al.,
where loss of function of the adenine methyltransferase (DAM) gene via DNA methylation by
reduced production of leokotoxins (Wu et al., 2006). In the cariology literature, Cardoso et al.,

122
in 2010, reported that differential methylation of the promoter region of the IFN-ɤ gene was
associated with human pulpal tissue affected with pulpitis. Either partial methylation or un-
methylation was observed in 93.75% of samples of inflamed pulp tissue (Cardoso et al., 2010).
6.8 Future research
Many studies have shown the importance of epigenetics in oral health. This has been shown in
relation to periodontal diseases (Zhang et al., 2010), oral squamous cell carcinoma (Sandoval
and Asteller, 2012), malocclusion (Carlson, 2005; Dave Singh and Callister, 2013), and cleft
lip/palate (Beaty et al., 2011; Marazita, 2012). However, there is little information related to
the pathogenesis of dental caries. Epigenetics, the potential conduit between phenotype and
genotype, has much promise in becoming increasingly relevant to cariology because of its role
in gene expression. Dental caries has been studied for decades as a multifactorial disease but
is still among the ten most common chronic diseases among children (Fisher-Owens et al.,
2007; Kassebaum et al., 2015). In this context, the notion that gene-environment interactions
(i.e. epigenetics) are important in caries pathogenesis is appealing as it could prove to be the
missing link to understanding of the role of genetics in caries initiation and progression.
Future studies utilizing epigenetics are important to the individual as well as for society, as
findings regarding the interplay of environmental and genetic factors can be used in
identification of individuals and groups at high risk of developing dental caries. This can help
to identify new preventive strategies and treatment approaches. As epigenetic patterns and
modifications are found to be reversible, it may also be possible to use this knowledge to devise
approaches to reduce risk (Azad et al., 2013). Combined clinical and longitudinal

123
epidemiological studies are needed to quantify the extent to which environmental factors may
influence epigenetic changes that can predispose to dental caries.

124
Chapter 7: An Epigenome- Wide Association Study of mother-
child dyads discordant for dental caries: A pilot study
This chapter is the fourth paper in this thesis. The bibliographic details of the paper, including
all authors, are as follows:
Surani Fernando, Miles Benton, David Jeremiah Speicher, Mahmoud Bakr, Ping Zhang,
Rodney Lea, Paul A Scuffham, Newell Walter Johnson. An epigenome wide association study
of mother child dyads discordant for dental caries: A pilot study.
My contribution to the paper involved the conception and designing of the study, clinical data
collection, DNA extraction and sample preparation, statistical analysis and drafting the article.
The manuscript has been submitted to the journal BMC Oral Health, which is a peer reviewed
journal. Manuscript ID is OHEA-D-17-00215.
Surani Fernando
Corresponding author: Surani Fernando
Supervisor: Professor Newell Johnson Supervisor: Professor Paul Scuffham

125
7.1 Abstract
7.1.1 Background
Dental caries is a major public health problem affecting millions of children worldwide. GWAS
have examined the gene structure associated with dental caries, but few have investigated
environmental effects on the epigenome. Whilst the environment can significantly impact the
epigenome, there are currently no published epigenome-wide association studies (EWAS) on
dental caries.
7.1.2. Objective
To conduct a pilot study to identify potential differentially methylated regions associated with
dental caries experience in a cohort of mother-child dyads.
7.1.3 Methods
For this pilot study, 12 mother-child dyads from SEQ, Australia were selected from within the
Griffith University EFHL birth cohort study based on high (6 dyads) and low (6 dyads) caries
experience according to ICDAS. Epigenetic screening was conducted on total DNA extracted
from saliva using the SeqCap Epi 4M CpGIANT Enrichment Kit and HiSeq2500 Sequencer.
CpG counts were analysed using the methylKit package in R. The statistical significance
threshold was set using Bonferroni correction based on testing 435508 CpG sites (p = 1.1E10-
7).
126
7.1.4 Results
Differentially methylated regions (DMR) between cases and controls were found on
chromosomes 1, 2, 5, 7, 12, 20 and 22. Chromosome 12 showed the highest average
methylation difference (41%) between case and control groups (p < 2.17E-103). DAVID gene
function analysis of all DMR showed two clusters related to Zn metabolism and membrane
protein functions.
7.1.5 Conclusion
This pilot EWAS identified significantly differentially methylated sites discordant for dental
caries on chromosome 12 closely related to a gene promoter region responsible for cell
membrane function and Zn metabolism. Further work is required to understand the mechanisms
by which these epigenetically modified sites might influence susceptibility to dental caries.
Key words Dental caries, Epigenomics, Methylation, CpG, EWAS
7.2 Introduction
Dental caries remains a major public health problem in most low and middle income countries,
affecting more than 621 million children and 2.4 billion adults worldwide (Kassebaum et al.,
2015). It is an almost ubiquitous disease throughout the life course, with peak prevalence at
ages 6, 25 and 70 years. The burden of untreated dental caries is greatest in developing low-
middle income countries, particularly in Africa (Kassebaum et al., 2015), but is a problem in
some population groups within all countries. It is unsurprising that dental scientists are turning

127
their attention to the role of epigenetic changes, most commonly through gene methylation, in
susceptibility to, and the pathogenesis of, oral diseases (Hughes et al., 2013; Seo et al., 2015).
Recently, GWAS have explored associations between the structure and function of particular
genes and the presence or absence of many diseases, whilst EWAS have revealed genetic
changes associated with environmental factors and disease. DNA methylation, characterized
by covalent transfer of a methyl group from SAM in cytosine located in CpG islands, is the
most studied epigenetic modification and the most distinctive category of chromatin changes
(Barros and Offenbacher, 2009; Schübeler, 2015; Williams et al., 2014). DNA methyl-
transferases mediate DNA methylation and stabilise the transmission of differential
methylation changes during cell division (Bestor, 2000; Okano et al., 1999). In a normal cell,
CpG sites associated with gene promoters are usually unmethylated, whereas CpG sites within
genes are generally methylated (Patterson et al., 2011). Hyper-methylation of CpG sites inhibits
gene transcription, whereas hypomethylation results in gene activation (Mani and Herceg,
2011). Availability of high-throughput genotyping methods and high-density reference panels
of the human methylome have made it feasible to conduct EWAS at population levels (Sun,
2014). Seo et al. (2015) argued that DNA methylation patterns associated with inflammatory
and immune responses potentially affect the pathogenesis of oral diseases.
Emerging evidence highlights the importance of epigenetic regulatory mechanisms in
controlling the inflammatory response in inflamed dental pulps of carious teeth. Recently,
Cardoso et al., reported that 93.75% of inflamed pulps showed unmethylation in the promoter
regions of the IFN-ɤ gene (Cardoso et al., 2010), whereas hypomethylated TLR2 and CD14
genes were a regular characteristic of healthy dental pulps (Cardoso et al., 2014). An in-vitro
study of human dental pulp cells showed that, even though no direct association with dental

128
caries could be found, the DNA methyltransferase inhibitor 5-Aza_CdR could inhibit
proliferation and heighten odontogenic differentiation of cells (Zhang et al., 2015). This
suggests that methylome status could influence the production of reparative dentine in response
to a carious lesion or other injury. During amelogenesis, pre-ameloblasts express high levels
of DNAMT1, a regulator of DNA methylation, whilst in their undifferentiated state (Yoshioka
et al., 2015). If hypermethylation were to occur, amelogenesis could be damaged through
expression of DNMT1, producing hypomineralisation of the enamel. In this pilot study, we
conducted an EWAS of 12 mother-child dyads with high and low experience of dental caries
to detect associations of differentially methylated regions (DMR) with dental caries experience.
Given the expensive nature of the techniques involved, the study was designed to identify
potential sites for further investigation in a larger population.
7.3 Methods
7.3.1 Study Population
Six- to eight-year-old children and their mothers who were enrolled in the Griffith University
EFHL (Cameron et al., 2012a) were recruited for the oral health sub study of EFHL following
ethical approval (Griffith University: OTH/25/13/HREC). A protocol for the main oral health
sub study was published in BMC Oral Health (2015), which describes enrolment of subjects
and data collection in detail (Fernando et al., 2015). For this pilot study 12 mother-child dyads
discordant for dental caries were enlisted to screen for changes in the epigenome which were
associated with low or high caries experience.

129
7.3.2 Dental caries assessment
The severity and extent of dental caries were measured using ICDAS criteria, where all surfaces
of all teeth of participating individuals were recorded by trained examiners (CICDAS, 2005).
Past caries experience (surfaces of teeth missing due to caries and restored tooth surfaces) and
current caries was recorded as diseased surfaces ranging from demineralisation without
cavitation (Score 1) to overt cavities (Score 6). Teeth that were not erupted and extracted for
reasons other than caries were excluded from the calculation. Cases and controls were
determined according to the caries experience of both mother and child: controls, low caries
experience of both; and cases, high caries experience of both. The criteria used here for
classification of caries experience took the percentage of surfaces affected with caries and age
into consideration, since it is expected that caries experience will increase in the general
population with age, and also because our pilot study sample lacked totally caries-free mother-
child dyads (Küchler et al., 2014). Hence average caries experience for both mothers and
children were calculated; children who had positive caries scores of more than 6% of their tooth
surfaces and mothers with caries in more than 20% of their tooth surfaces were cases and the
rest controls (Table 7.1).
7.3.3 Sample Collection and Epigenetic analysis
Saliva is an effective, efficient and non-invasive source of host DNA (Kaczor-Urbanowicz et
al., 2017), which may be especially relevant to studies of the epigenetics of oral diseases as it
bathes the tissues of interest. Hence saliva was collected from the 12 mother-child dyads and
stored at -80oC (Fernando et al., 2015). Genomic DNA was extracted from saliva using the
High Pure PCR Template Preparation Kit (Roche Diagnostics, Australia). Total DNA was

130
quantified on the NanoDrop® ND-1000 Spectrophotometer (ThermoFisher Scientific,
Australia). DNA was considered pure if optical density at 260/280 was 1.70–2.00.
DNA sequencing was performed with bisulfite treated DNA for methylation analysis. Assays
were performed using the SeqCap Epi 4 M CpGIANT Enrichment Kit (Roche NimbleGen,
USA) and the HiSeq2500 Sequencer (Illumina®, USA) at the University of Queensland Centre
for Clinical Genomics (UQCCG) (Brisbane, Australia). This approach obtained both DNA
sequence variants and CpG methylation simultaneously at ~450,000 CpG sites across the whole
genome.
Initial read quality assessment was performed using FastQC (Andrews, 2010) while adapter
trimming was implemented using the Trimmomatic software
(http://www.usadellab.org/cms/?page=trimmomatic). Due to the bisulfite treatment, reads
were required to be aligned to an in-silico bisulfite converted reference genome. This was
achieved by performing an in-silico conversion of hg19 using bowtie2 (http://bowtie-
bio.sourceforge.net/bowtie2/index.shtml). Read alignment was then carried out using Bismark,
a software suite specifically designed for bisulfite sequence mapping
(www.bioinformatics.bbsrc.ac.uk/projects/bismark/). After alignment, all bam files for each
individual were merged using bamtools (https://github.com/pezmaster31/bamtools).
Deduplication of reads was conducted using the ‘MarkDuplicates’ function within Picard
Tools (http://broadinstitute.github.io/picard/command-line-overview.html#MarkDuplicates). Finally,
the software PileOMeth (https://github.com/dpryan79/PileOMeth) was used to extract all CpG
sites and read counts formatted for the R analysis package methylkit
(http://code.google.com/p/methylkit).

131
Site specific methylation levels were defined as β values, which is the ratio of methylated probe
signal over methylated plus unmethylated probe signals. Each identified differentially
methylated site was attributed a percentage methylation that was included in the statistical
analyses. A DMR was defined as a genomic region that contained ≥ 3 directly adjacent
differentially methylated CpGs.
General statistical analysis was performed using SPSS Statistics V21.0 (IBM, USA).
Parametric tests were used as the data were normally distributed and where relevant chi-square
tests were used to compare the two groups. To evaluate the differences between cases and
controls with respect to DMR changes in CpGs on Chr12, t-tests were performed.
Analysis of CpG counts was performed in R using the methylKit package (Team, 2013). Data
were imported and treated as a case/control setup. CpG sites were filtered out if they exhibited
read count coverage lower than 10. Differential analysis was performed using the methylkit
‘calculateDiff’ function, which calculates differential methylation statistics between two
groups of samples using logistic regression. A custom R script was written to identify DMR.
Briefly, this method uses a sliding window to identify CpG sites showing significant
differential methylation in a similar direction within a defined region. An overall DMR p-value
is assigned by assessing all individual p-values of CpG sites contained within a DMR,
combining these using a modified version of Fisher's approach (Zaykin, 2011). All CpG and
DMR objects were annotated using Granges and R tracklayer, based on hg19 annotation data
available from Bioconductor (http://www.bioconductor.org). Statistical significance (i.e. alpha
level) was set based on Bonferroni correction for the number of CpGs tested. In this study, we
observed and tested 435508 CpG sites and thus set the empirical alpha-level to
0.05/435508=1.1E10-7. Annotation and functional analysis of the list of genes that are

132
associated with DMR or selected CpGs were identified through the DAVID bioinformatics
functional annotation tool (Huang et al., 2009a; b).
Table 7.1: Caries experience of controls and cases
Child #ID Child’s caries
*experience
Mother ID Mother’s caries
*experience
Controls Controls
FAM1C 0 FAM1M 7.69
FAM2C 0 FAM2M 4.29
FAM3C 2.61 FAM3M 10.00
FAM4C 3.00 FAM4M 0
FAM5C 3.33 FAM5M 19.85
FAM6C 6.00 FAM6M 15.71
Cases Cases
FAM7C 6.50 FAM7M 24.29
FAM8C 9.00 FAM8M 26.43
FAM9C 11.00 FAM9M 39.49
FAM10C 13.33 FAM10M 22.14
FAM11C 16.00 FAM11M 33.79
FAM12C 19.00 FAM12M 25.00 # Identity, *Caries experience was measured as a percentage of tooth surfaces affected with dental caries
(including early enamel caries)
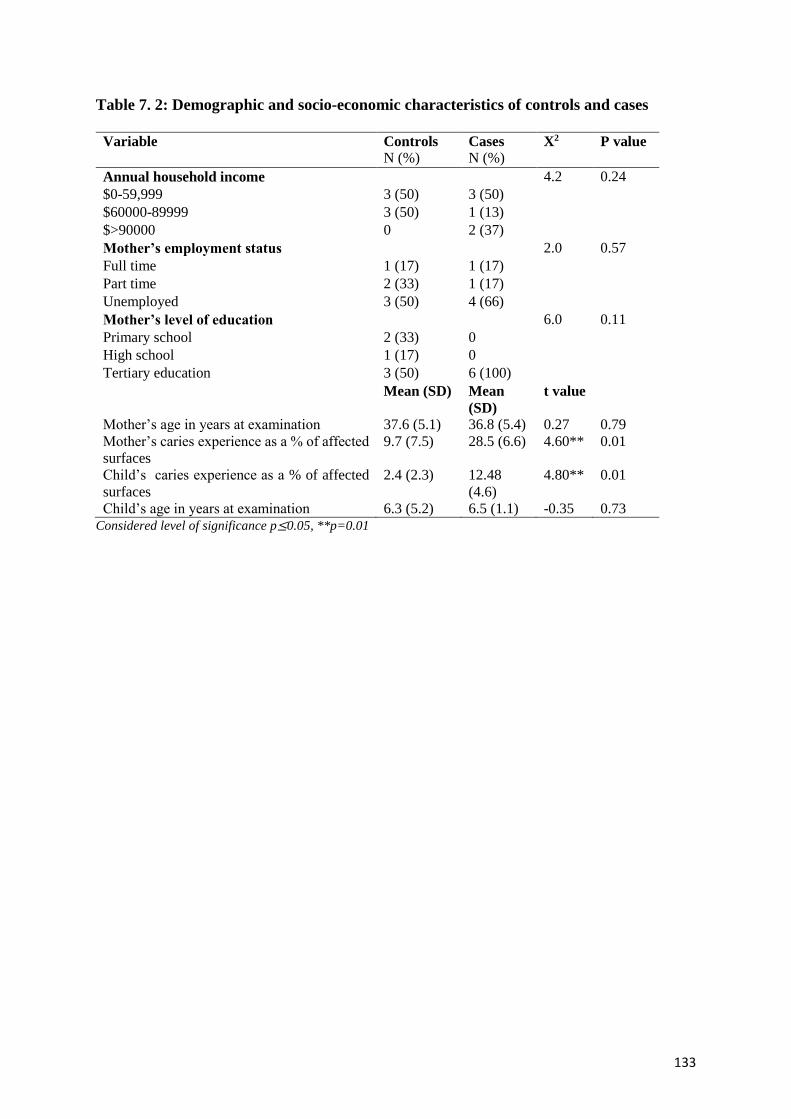
133
Table 7. 2: Demographic and socio-economic characteristics of controls and cases
Variable Controls Cases X2 P value
N (%) N (%)
Annual household income 4.2 0.24
$0-59,999 3 (50) 3 (50) $60000-89999 3 (50) 1 (13) $>90000 0 2 (37) Mother’s employment status 2.0 0.57
Full time 1 (17) 1 (17) Part time 2 (33) 1 (17) Unemployed 3 (50) 4 (66) Mother’s level of education 6.0 0.11
Primary school 2 (33) 0 High school 1 (17) 0 Tertiary education 3 (50) 6 (100) Mean (SD) Mean
(SD)
t value
Mother’s age in years at examination 37.6 (5.1) 36.8 (5.4) 0.27 0.79
Mother’s caries experience as a % of affected
surfaces
9.7 (7.5) 28.5 (6.6) 4.60** 0.01
Child’s caries experience as a % of affected
surfaces
2.4 (2.3) 12.48
(4.6)
4.80** 0.01
Child’s age in years at examination 6.3 (5.2) 6.5 (1.1) -0.35 0.73 Considered level of significance p≤0.05, **p=0.01

134
Table 7.3: Annotated data for the 16 identified Differentially Methylated Regions between controls and cases
¥Chr Number of §CpG
Start End ɤDMR
length
ɤDMR
P value
Average
different
methylation
Entrez ID Gene
Symbol
Promoter
chr1 14 1.47E+08 1.47E+08 6798 2.38E-107 16.31 644861 NBPF13P FALSE
chr2 3 88802707 88802733 26 4.53E-11 17.89 200523 TEX37 FALSE
chr2 3 1.28E+08 1.28E+08 25 1.38E-17 15.57 84826 SFT2D3 FALSE
chr2 4 2.32E+08 2.32E+08 121 1.96E-15 19.757 348761 SPATA3-AS1 FALSE
chr5 3 23951427 23951496 69 1.12E-13 -20.60* 56979 PRDM9 FALSE
chr5 20 28928022 28928448 426 6.44E-266 -32.58* 729862 LSP1P3 FALSE
chr5 7 1.77E+08 1.77E+08 62 1.26E-75 20.58 10636 RGS14 FALSE
chr5 3 1.78E+08 1.78E+08 46 1.10E-13 -18.08* 6940 ZNF354A FALSE
chr5 3 1.8E+08 1.8E+08 75 6.89E-08 17.81 255426 RASGEF1C FALSE
chr5 3 1.8E+08 1.8E+08 191 1.77E-09 19.58 9945 GFPT2 FALSE
chr7 3 120449 120480 31 2.99E-11 -16.11* 56975 FAM20C FALSE
chr7 3 1.55E+08 1.55E+08 55 5.98E-13 -18.26* 3638 INSIG1 FALSE
chr12 8 11700085 11700343 258 2.17E-103 -41.17* 338817 LINC01252 TRUE
chr20 4 61590651 61591049 398 3.72E-15 -16.22* 63910 SLC17A9 FALSE
chr22 4 32600622 32601130 508 8.11E-15 19.56 10739 RFPL2 TRUE
chr22 3 45832692 45832871 179 3.38E-13 -18.60* 26150 RIBC2 FALSE ¥Chr – Chromosome, *A negative average different methylation indicates that cases have lower methylation on average compared to controls, §CpG - Cytosine
Guanine sites, ɤDMR - Differentially Methylated Regions

135
Table 7.4: Functions of gene clusters derived from DAVID
Term Gene symbols Function
Cluster1
*GO:0008270~Zn ion
binding
ZNF354A, RFPL2,
PRDM9
Interacting selectively and non-covalently with Zn
ions. GO:0046872~metal ion
binding
FAM20C, ZNF354A,
RFPL2, PRDM9
Interacting selectively and non-covalently with Zn
and any metal ion
GO:0043169~cation
binding
FAM20C, ZNF354A,
RFPL2, PRDM9
Interacting selectively and non-covalently with Zn
ad other cations, charged atoms or groups of atoms
with a net positive charge
GO:0043167~ion
binding
FAM20C, ZNF354A,
RFPL2, PRDM9
Interacting selectively and non-covalently with
ions, charged atoms or groups of atoms
Zn binding ZNF354A, RFPL2,
PRDM9
Protein which binds at least one Zn atom or protein
whose function is Zn dependent.
Cluster2
GO:0016021~integral
to membrane
INSIG1, SFT2D3,
SLC17A9
The component of a membrane consisting of the
gene products and protein complexes having at
least some part of their peptide sequence embedded
in the hydrophobic region of the membrane.
GO:0031224~intrinsic
to membrane
INSIG1, SFT2D3,
SLC17A9
The component of a membrane consisting of the
gene products having some covalently attached
portion, for example part of a peptide sequence or
some other covalently attached group such as a GPI
anchor, which spans or is embedded in one or both
leaflets of the membrane.
Transmembrane INSIG1, SFT2D3,
SLC17A9
Protein with at least one transmembrane domain, a
membrane-spanning helical or beta-stranded
domain embedded in a membrane. *GO– Gene Ontology
7.4 Results
The six dyads with low caries experience and six dyads with high caries experience were
similar with respect to their demographic and socio-economic characteristics (Table 7.2).
Children had mean ages of 6.3 years (SD = 1.1) and 6.5 years (SD = 5.2) in controls and cases
respectively. In the control group, the mean ICDAS scores of the mothers and children were
9.7 (SD = 7.5; p ≤ 0.01) and 2.4 (SD = 2.3; p ≤ 0.01), respectively. In the case group, the mean
ICDAS scores of the mothers and children were 28.5 (SD = 6.6; p ≤ 0 .01) 12.48 (SD = 4.6; p
136
≤ 0.01), respectively. Mean total DNA concentration for controls was 132.26 ng/μL (range:
76.95 ng/μL – 224.66 ng/μL) and it was 178.58 ng/μL (range: 77.58 ng/μL – 370.32 ng/μL)
and for cases.
7.4.1 Methylation differences on chromosomes
Epigenetic analysis identified 435508 CpG sites with methylation that differed significantly
between controls and cases in DMR on chromosomes 1, 2, 5, 7, 12, 20 and 22 (p < 1.1E10-7;
Table 7.2). Chr12 had the highest average methylation difference (41%) between the two
groups for one CpG site (28928022 to 28928448) with eight differentially methylated CpGs in
relation to the promoter region of LINCO1252 (p = 2.17E-103). DMRs between cases and
controls on Chr12 were analysed separately for children (Appendix D, Table 1) and mothers
(Appendix D, Table 2).
7.4.2 Functions of identified genes
Analysis via DAVID showed that only the DMR on Chr12 (LINC01252, p = 2.17E-103) and
on Chr22 (RFPL2, p = 8.11E-15) were related to a gene promoter region (Table 7. 3). Chr12
showed the highest average methylation difference between control and case groups and thus
had the highest possibility of being linked with dental caries. Associated genes on Chr12 fell
into two functional clusters: (1) Zn or other metal ion binding; and (2) proteins of cell
membranes (Table 7.4). Moreover, chromosomes that had a single CpG cite differentially
methylated and associated with a gene promoter region were also explored through DAVID
gene function classification: BTNL8 on Chr 5, PFKFB3 on Chr10, ENOSF1 on Chr18, and
RFPL2 on Chr 22 could be related to possible functions related to dental caries (Table 7.5).

137
Table 7.5: Summary of Differentially Methylated Regions (with only one CpG site) related to a gene promoter region.
* A negative average different methylation indicates that cases have lower methylation on average compared to controls
Chromosome Start End Transcript Entrez ID Gene Symbol PROMOTER P-value Q value Methylation
difference
chr1 25292420 25292420 uc009vrl.1 864 RUNX3 TRUE 4.10572E-06 0.001587897 -15.08*
chr1 95556966 95556966 uc021oqe.1 148534 TMEM56 TRUE 9.81552E-08 7.95521E-05 19.17
chr1 101003634 101003634 uc001dth.3 54112 GPR88 TRUE 1.22669E-08 1.34245E-05 -16.53*
chr1 110254662 110254662 uc010ovu.1 2949 GSTM5 TRUE 2.66108E-09 3.56719E-06 22.56
chr1 182922582 182922582 uc001gpu.3 81626 SHCBP1L TRUE 5.00135E-05 0.009360155 -16.75*
chr1 182922588 182922588 uc001gpu.3 81626 SHCBP1L TRUE 1.32452E-06 0.000669004 -19.29*
chr1 223887895 223887895 uc010puy.2 824 CAPN2 TRUE 0 0 42.13
chr2 139538610 139538610 uc002tvi.3 11249 NXPH2 TRUE 3.06171E-10 5.31894E-07 -16.26*
chr2 139538640 139538640 uc002tvi.3 11249 NXPH2 TRUE 2.0518E-07 0.0001472 -16.51*
chr3 101658926 101658926 uc003dvr.1 152225 LOC152225 TRUE 1.86141E-08 1.94372E-05 -15.78*
chr5 6447161 6447161 uc003jdp.4 134111 UBE2QL1 TRUE 1.82771E-07 0.000134358 -16.83*
chr5 135418248 135418248 uc021ydy.1 100126299 VTRNA2-1 TRUE 0 0 -16.02*
chr5 180324777 180324777 uc003mmp.3 79908 BTNL8 TRUE 2.79604E-09 3.73517E-06 -15.40*
chr6 168198215 168198215 uc003sic.3 26238 C6orf123 TRUE 3.18527E-05 0.007035302 16.16
chr7 103849116 103849116 uc003vcb.3 5001 ORC5 TRUE 7.36078E-14 2.45828E-10 -21.03*
chr8 74007003 74007003 uc003xzf.3 157869 SBSPON TRUE 0.000000014 1.51094E-05 -20.19*
chr10 4868202 4868202 uc010qam.2 83592 AKR1E2 TRUE 2.02326E-06 0.000932887 21.52
chr10 6185422 6185422 uc001ijd.3 5209 PFKFB3 TRUE 8.36163E-06 0.002745206 -16.80*
chr10 82296143 82296143 uc001kck.1 387694 SH2D4B TRUE 2.50535E-06 0.001094318 20.68
chr11 300286 300286 uc001low.2 387733 IFITM5 TRUE 5.96865E-10 9.2863E-07 -15.90*
chr11 65327098 65327098 uc010rok.1 4054 LTBP3 TRUE 0.000000211 0.000150287 -15.39*
chr11 124439829 124439829 uc010san.2 390275 OR8A1 TRUE 0 0 -37.99*
chr15 89155014 89155014 uc010upm.2 407044 MIR7-2 TRUE 1.66276E-11 3.72348E-08 -19.64*
chr17 5674423 5674423 uc002gcm.3 339166 LOC339166 TRUE 6.28094E-06 0.002210056 -16.33*
chr17 16593135 16593135 uc002gqk.1 9720 CCDC144A TRUE 0.000013245 0.003834968 15.85
chr17 16593243 16593243 uc002gqk.1 9720 CCDC144A TRUE 5.74144E-06 0.002069085 18.14
chr18 713049 713049 uc002kkt.4 55556 ENOSF1 TRUE 1.34432E-06 0.000678121 15.51
chr19 36800807 36800807 uc021utf.1 100134317 LOC100134317 TRUE 8.93061E-08 0.000074244 15.89
chr19 36800819 36800819 uc021utf.1 100134317 LOC100134317 TRUE 1.32736E-10 2.53314E-07 17.38
chr22 22874959 22874959 uc002zwe.3 129025 ZNF280A TRUE 3.66237E-07 0.000236866 15.28
chr22 32601130 32601130 uc003amh.3 10739 RFPL2 TRUE 1.60469E-07 0.000120245 17.07
chr22 37256261 37256261 uc003apy.4 4689 NCF4 TRUE 1.32181E-05 0.003831219 19.21
138
7.5 Discussion, conclusion and limitations
7.5.1 Discussion
Though epigenetic examination of dental caries is in its infancy, it is increasingly understood
that environmental, physiological, and pathological events can affect the methylation status of
genes and thus regulate gene expression. This pilot EWAS explored the epigenome of
individuals discordant for dental caries in 12 mother-child dyads, and identified significantly
differentially methylated regions on chromosomes 1, 2, 5, 7, 12, 20 and 22 between cases and
controls. DAVID gene function analysis identified two clusters of genes related to DMR.
Genes identified in cluster 1 (ZNF354A, RFPL2, PRDM9 and FAM20C) mainly interact with
Zn and other metal ions at the cellular level. Zn fingers are clustered into more than 20 classes
of physically different components and are known to interact with a variety of proteins, lipids,
and nucleic acids (Lupo et al., 2013), whilst playing a significant role in metabolism of enzymes
and other proteins (Fatima et al., 2016). None of the genes identified in our study could be
directly functionally linked with the process of dental caries, though Zn is an important
component in health and disease, including in relation to oral diseases.
Zn is an essential co-enzyme in mineral metabolism that has long been recognized as an
element that influences all aspects of tooth development and repair, such as the
demineralisation/remineralisation equilibrium of dental hard tissues. Zn oxide is widely
recognized as a substance that inhibits dentine demineralization (Takatsuka et al., 2005). Zn, a
divalent cation (Zn+2), is electronically attracted to negatively charged oral hard tissues. In this
scenario, cariogenic bacteria like MS may have difficulty attaching to enamel surfaces, and as
a result have difficulty in acquiring nutrients essential for their survival (Burguera-Pascu et al.,
2007).

139
Zn favours the precipitation of calcium phosphate and is important in both the development of
enamel and its remineralisation after damage during cariogenesis (Lynch, 2011). The in-vitro
caries-simulating model of Mohammed et al. (2014), demonstrates significant reductions in
calcium release from enamel after exposure to Zn. Nevertheless, the adsorption of Zn and
formation of Zn phosphate depends on Zn concentration and the available surface area for solid
liquid interactions (Mohammed et al., 2014). Zn is an essential co-enzyme for matrix MMP,
which are fundamental to the progression of the caries process in dentine, notably in destroying
organic matrix after demineralisation by bacterial acids (Chaussain-Miller et al., 2006).
However, some studies have shown that metals including Zn can inhibit MMPs, thereby
reducing MMP-mediated collagen degradation in carious dentine (Henn et al., 2012; Santos et
al., 2004). Toledano et al., found that when Zn was added to dentine beams made from
extracted non-carious molars, which were then demineralised in phosphoric acid, degradation
in demineralised dentine was strongly reduced, as Zn served as an effective inhibitor of MMP-
mediated collagen degradation (Toledano et al., 2012). An in-vitro study investigating the local
environment of Zn atoms in dentine has reported that treatment with Zn compounds made
dentin more acid resistant (Takatsuka et al., 2005).
Abnormalities of Zn availability and metabolism may thus influence susceptibility to dental
caries, justifying further investigation with a larger sample size and specific phenotype
definitions for cases and controls of disease.
The cluster 2 genes, INSIG1, SFT2D3 and SLC17A9, predominantly code for proteins that are
embedded in membranes. Integral (intrinsic) and transmembrane proteins are permanently
attached to cell membranes by interactions between their hydrophobic dimer units and the
phospholipids of the membrane and play vital roles in cellular functions (Mishra et al., 2014).
The passage of solutes such as ions and small molecules through biological membranes are
140
mediated by these proteins, which are also called membrane transport proteins (Mishra et al.,
2014). As far as we are aware, direct associations of this group of genes with dental tissues or
with dental caries have not been reported in the literature. Nevertheless, genes identified in our
study code for proteins that have general functions, such as transportation of small vesicles,
vesicular uptake, storage and secretion of ATP, and fusion of transport vesicles with the Golgi
complex. Whilst there is no published evidence of a direct association with cariogenesis,
general protein functions coded by this group of genes might be involved in the caries process
as proper membrane function is fundamental to the formation and repair of all tissues, and the
secretion of enamel matrix through the ruffled border of ameloblasts could be compromised.
Amongst the genes that had only “one CpG site differentially methylated” between cases and
controls (Table 7.5) and were closer to a gene promoter, two genes, PFKFB3 and ENOSF1,
are part of fructose and mannose metabolism pathways respectively (Ogata et al., 1999). These
pathways are involved in the synthesis, utilization and/or degradation of these sugars (Musen
et al., 2012; Whetzel et al., 2011). Another two genes from this list, BTNL8 and RFPL2, are
associated with PRY and butyrophylin-like domains as defined by SMART (simple modular
architecture research tool) (Schultz et al., 1998). Whist the function of PRY is unknown, its
distant homologues are protein domains (a sealed part of a given protein sequence that can
change, function, and exist independently of the rest of the protein chain) in butyrophilin, the
major protein associated with fat droplets in the milk, and pyrin, a neutrophil protein (Finn et
al., 2017). Interestingly, a group of proteins identified by the PRY domain contain a ring-finger
domain that binds two atoms of Zn (Doerks et al., 2002; Schultz et al., 1998). Several proteins
in the butyrophylin-like domain also contain RING fingers and a well-conserved 40-residue
cysteine-rich domain termed a B-box Zn finger (Borden, 1998).

141
7.5.2 Conclusion
To the best of our knowledge, this is the first EWAS study performed on the human genome
in relation to dental caries. The aim was to identify specific areas differentially methylated
among individuals with high and low dental caries experience. Our research provides evidence
for an association between epigenetic changes and dental caries evaluated through DMR. The
two sets of genes that were identified associated with the DMR between high-caries and low--
caries dyads are of high interest and warrant further investigation of the biological mechanisms
mediated through Zn and membrane proteins. Findings of our pilot study highlight a further
need for investigations on larger and diverse populations to clarify the role of epigenetic factors
in cariogenesis, the mechanisms involved, and how these might be manipulated in caries
prevention on an individual and population level.
Further pyrosequencing on an extended sample of 38 mother-child dyads was conducted in
order to validate the region of interest on chromosome 12 (chromosome region between
11700080 and 11700350). However, there were technical difficulties and the proposed region
could not be replicated. Hence, three different CpG sites within the discovery region were
pyrosequenced. The observed results, however, did not show any significant association
between individual with high and low lifetime cumulative caries experience (Appendix E).
7.5.3 Limitations
The study was unfunded, and hence a larger number of subjects could not be recruited for this
pilot EWAS. Because caries experience in our population was a continuous variable, trait
definitions for cases and controls had to be based on extremes of burden of disease, precluding

142
a standard case-control study design. A very large and expensive study would be necessary to
analyse epigenomic differences across a full range of caries experience.

143
Chapter 8: General Discussion
8.1 Introduction
The purpose of this final chapter is to fulfil three main tasks. First, it summarises the research
background and objectives (Section 8.2). Second, it discusses the findings of the study and the
implications for the prevention of dental caries in children (Section 8.3). Section 8.4 briefly
discusses the limitations of the study. Finally, it discusses strengths and recommendations for
future studies in Section 8.5 and gives concluding remarks in Section 8.6.
8.2 Overview of the study
8.2.1 Background and research objectives
Despite marked improvements over the past century, especially in industrialised countries, poor
oral health is still a significant problem, not least among children (Kassebaum et al., 2015).
Caries is the commonest chronic disease of childhood; nevertheless, oral health researchers
primarily examine influences on the disease process from within the oral cavity, with
consideration of limited individual-level factors to identify risks for the disease (Fisher-Owens
et al., 2007). Individuals are exposed to a multitude of risk indicators throughout their life,
placing them at varying magnitudes of risk. Different communities with their unique
behaviours and practices face different risk conditions; especially this variation is more marked
between industrialised and non-industrialised countries (Attaran et al., 2016). Conceptual
models have been proposed to help in understanding these inequalities, though many do not

144
incorporate individual, family, and community level factors with a multilevel approach which
considers possible interactions among the variables. In the methodology of the thesis we have
proposed a conceptual framework based on genetic and biological factors, the social
environment, health behaviours, and dental and medical care utilisation and their possible
interactions (Figure 3.1) (Fernando et al., 2015). As yet, not many studies reported in the
literature have focused on empirically investigating this concept by recognising the presence
of a complex interplay of causal factors. Therefore, this study was conducted with the objective
of filling this knowledge gap by testing the proposed conceptual framework and identifying
risk indicators in connection to childhood dental caries in a typical industrialised country.
The main objective of this thesis was to identify relationships between maternal,
environmental, and individual-level parameters and the severity and extent of dental caries in
children. This included exploring pathways and interactions of these parameters within a
broader framework containing mothers’ socio-economic situation, oral health status,
knowledge, attitudes and behaviours towards their own and their families’ oral and general
health, children’s intraoral pathophysiology, in utero circumstances, birth weight, and possible
epigenetic modifications.
The study has specifically answered three central research questions:
1. Are there relationships between maternal and environmental risk indicators, SES, BMI,
salivary characteristics, dental caries experience, oral health knowledge and behaviours, and
the caries experience of their children?
2. What are the associations between children’s past dental caries experience, salivary
characteristics, prenatal environment, birth weight, and current experience of dental caries?
145
3. Are there any differences in epigenetic modifications between individuals discordant for
lifetime, cumulative, experience of dental caries?
In the process of addressing these research questions, the study expected to discover a range of
risk indicators, which may or may not be risk factors that influence the process of dental caries
in children, and to quantify this effect in a clinically and epidemiologically meaningful way.
Negative Binomial Regression Modelling (Mota-Veloso et al., 2016) and Structural Equation
Modelling (SEM) (Jeon, 2015) were used to test these associations, as they allow simultaneous
assessment of direct and mediating effects between dependent as well as between independent
variables.
8.3 Main empirical findings
The series of results chapters contain the specific research findings related to the research
questions covering the research gap identified in Chapters 1 and 6. A summary of these results
is presented next.
8.3.1 Dental caries experience in the sample of children and their mothers
The sample of children was aged between 6 to 7 years, (mean 6.3, SD = 0.83) years, and just
over half (51%) were girls. Caries experience was measured using ICDAS criteria. Hence it
was possible to report cumulative caries experience from initial white spot lesions to pulp-
exposed extended cavities. The assumption was made – as is often the case in the literature,
but is not entirely valid – that “white spot” lesions represented “initial” or “early” lesions, and
might thus represent current caries activity. Of the 174 children, 61% were caries-free, and

146
16% had carious lesions limited to enamel (ICDAS = 1 and ICDAS = 2). As the majority of
the children were caries free, exploring risk markers for caries in this population was
challenging. Mean cumulative caries experience, the percentage of surfaces affected by past
and current caries, was 6.5 (SD = 11.07) in the total sample. Mean current caries experience,
the number of surfaces affected with caries (ICDAS > 0) at the time of examination, was 5.39
(SD = 8.90). Mean past caries experience (the number of surfaces with restorations), was 1.29
(SD =4.52) in the population. Out of all children who had caries, 56% were girls. Do and
Spencer (2016) reported that 27% of girls in the same age group in Australia were experiencing
the disease in 2014, and just over 27% of children had untreated caries in their deciduous
dentition (Do and Spencer, 2016). This thesis reports much higher caries prevalence (38%) in
the same age group; however, the prevalence is for deciduous and permanent teeth combined.
It was observed that the mean caries experience of mothers, measured with ICDAS (both
current and past) was 23.64 (SD = 28.28) in the total sample. Mean caries experience of mothers
with children who had caries was 25.29 (SD = 19.16) whereas mothers of children who were
caries free had lower lifetime experience of the disease: 22.60 (SD = 13.13). A similar
observation was made by Do et al. (2017), where 52% of the females aged 35 to 44 years had
experienced caries and mean DMFS was 24.8 (SD = 76.74) (Do et al., 2017). However, the
study was done to evaluate the effectiveness of water fluoridation in the prevention of dental
caries in adults and comparisons between maternal and childhood caries were not reported.
There is no recent information from Australia comparing maternal and children’s caries
experience; hence, findings from this thesis fill this gap in the literature.
147
8.3.2 Oral health knowledge and behaviours of mothers
In the sample investigated, the mean oral health knowledge, attitudes and practice (KAP) score
of mothers was 72.64 (SD =10.10). Surprisingly, mothers’ mean KAP score in both groups,
children with and without caries, was the same (72.6). This is a reasonably high score (Ahmed,
2015), yet the caries experience of the cohort of children was higher than the Australian average
for the same age group. It is acknowledged that the questionnaire used for the study was a self-
administered one and participating mothers had the freedom to answer as they wish. Hence it
can be assumed that even though they did not practice optimal oral hygiene habits, they would
still gave socially acceptable answers to indicate that they practiced good oral hygiene (Ju et
al., 2017).
It is understood that good oral health can be achieved and enjoyed by all through the application
of known preventive regimens and following good dietary and oral health practices.
Nevertheless, the theoretical model that reinforces oral health knowledge and its role in oral
health outcomes are that without functional, applied, and contextual understanding of both oral
health behaviours and oral health services, optimal oral health cannot be reached (Baur et al.,
2005). However, it is questionable if oral health services are designed to establish health since
dentists are paid and evaluated according to the number of treatment procedures performed.
Arguably, dentists can worsen oral health conditions, especially diseases like caries, whereas
early establishment of good diet and good hygiene practices can easily prevent, and even
reverse non-cavitated lesions, through good home care. This concept was advocated in the La
Cascada Declaration, which argues that most individuals are well able to care for their own
oral health, perhaps supported by a cadre of primary health care professionals who would
integrate health promotion, health education, and necessary interventions like vaccination and

148
perhaps provide topical fluoride applications, throughout particular communities. This could
be integrated with other primary health services such as mother and child services, and
vaccination (Cohen et al., 2017). Even though it is a good concept, a policy for integrating oral
health as a part of general health would take time, because health professionals need to be
educated and empowered with the notion to care for the individual without compartmentalising.
8.3.3 Maternal and environmental factors that influence the caries experience of children
One of the objectives of this thesis was to evaluate the effects of maternal and environmental
factors on dental caries experience of children. Based on the literature, maternal SES, measured
with annual household income (Zander et al., 2013), mother’s level of education (Kumar et al.,
2014) and employment status (Kumar et al., 2014), have negative associations with children’s
caries experience. Moreover, marital status (Piva et al., 2017), mother’s poor oral health
knowledge (Lee et al., 2014), practices (Nourijelyani et al., 2014), and age (Warren et al., 2016)
were significant indicators of children’s poor oral health. Maternal BMI, which is a reflection
of personal and lifestyle behaviours such as dietary and health promotion activities has been
associated with dental caries in children in an indirect pathway, through the common risk factor
approach (Wigen and Wang, 2014). Also, mothers who harbour increased levels of oral
cariogenic bacteria have been found to be associated with increased levels of the same bacterial
species (Li et al., 2005) and higher levels of dental caries in their children’s oral cavities
(Chaffee et al., 2014). Furthermore, mothers’ caries status was recognised as one of the main
risk indicators for dental caries in their children (Birungi et al., 2016). Even though there is no
literature available on the association between maternal salivary characteristics (pH, buffering,
and stimulated saliva flow rate) and children’s caries experience, it was assumed that since
mothers associate closely with their children, these features would reflect their children’s caries
levels. Hence it was hypothesised that caries experience in a child population of a typical

149
Western industrialised country is associated with maternal socio-economic, behavioural, and
demographic and intra oral indicators.
Our negative binomial regression model demonstrated that low maternal levels of salivary LB
(ARR = 0.61, p = 0.01), high caries experience (ARR = 1.02, p = 0.01), low annual income
(ARR = 0.67, p = 0.03), and high frequency of giving carbonated drinks to children (ARR =
2.03, p = 0.02) were associated with high caries experience in their children. Observed results
were in line with current literature with regards to high maternal caries experience (Birungi et
al., 2016), low income (Jepsen et al., 2017), high frequency of giving carbonated drinks
(López-Gómez et al., 2016), and initiation of tooth brushing practices (Ngoc et al., 2017). One
possible reason for all selected variables not being significantly associated with childhood
caries could be because only 67 out of 174 children had dental caries, and that number might
not have been adequate to provide enough statistical power. This was a limitation of using an
existing cohort. Moreover, it could be that other mediating factors which were not included in
the models have an impact on childhood dental caries. For example, parenting style (Kumar et
al., 2017), maternal stress, coping strategies (Wendt et al., 1995), and child temperament (Kim
Seow, 2012) have been reported to be risk indicators of caries in children. These data were not
included in the risk factor model because over 50% of participating mothers had not answered
the relevant questions.
8.3.4 Children’s individual factors: prenatal environment, birth weight, and intra oral
characteristics as risk indicators for caries experience
Literature reveals that children’s prenatal environment determined by maternal nutrition and
supplement intake during pregnancy impacts tooth development for the children. For instance,
lack of vitamin D, calcium, and iron during foetal life caused hypoplastic teeth in offspring

150
(Bergel et al., 2010). Moreover, birth weight, an indicator of foetal growth and nutrition, has
been associated with dental caries, where children with low birth weight were more at risk of
developing the disease (Bernabé et al., 2017). As children get older, they are exposed to
environmental risk indicators, and if coupled with poor oral hygiene practices, are more
predisposed to caries (Plaka et al., 2017). Progression of caries is synergized with increased
loads of oral cariogenic bacteria, like MS and LB (Samaranayake, 2012). In addition, it has
been long established that intra oral salivary characteristics, like low pH and low buffering
capacity, create a caries inducing environment (Lenander-Lumikari and Loimaranta, 2000).
Literature is inconsistent with evidence for an association between gender and dental caries
(Chankanka et al., 2011). However, past caries experience has been identified as the strongest
single predictor of current and future caries in children (Attaran et al., 2016). Therefore, to
assess these effects on dental caries experience a pathway model was constructed by
hypothesising that these individual factors: maternal supplement intake during pregnancy (as a
surrogate for prenatal environment), birth weight of the child, salivary buffering, pH, and past
caries experience would influence current dental caries status.
It was observed that children’s previous dental caries experience was significantly associated
with current dental caries experience (β = 0.332, p = 0.018), reinforcing the literature (Attaran
et al., 2016). Moreover, a positive association was also detected between child’s salivary MS
levels and current dental caries experience (β = 0.215, p = 0.032). Edelstein et al. (2017)
reported similar findings in a group of 6-year-old American children: they observed that even
within high SES groups, the most useful predictor of current caries was high salivary MS count
(Edelstein et al., 2016). Interestingly, in our study population, children whose mothers had
reported to have taken iron supplements during pregnancy had lower past caries experience,
which was a direct effect in the path model (β = -0.137, p = 0.068), although the results were

151
not statistically significant. In addition, it was observed that reported maternal intake of iron
supplement during pregnancy was indirectly associated with higher current dental caries
experience of their offspring (β = -0.046, p = 0.051). Mothers of the EFHL study answered
questions during the initial recruitment about prenatal supplement intake (including iron), and
the information was used as an indicator of intra uterine growth and foetal environment
(Cameron et al., 2012). Schmidt et al. followed the same method of data collection during
preconception and prenatal periods to evaluate the maternal nutrition status during gestation
(Schmidt et al., 2011). Supplementation with iron is generally recommended during pregnancy
to meet the iron needs of both mother and foetus (Scholl, 2005) because there is a decrease in
maternal iron stores during pregnancy (Fenton et al., 1977), and oral iron supplements have
been observed to prevents the stores from reaching deficient levels in mothers and thereby in
the foetus (Fenton et al., 1977). To the best of the knowledge of the investigators, there are no
previous studies that have found a link between the reported prenatal maternal intake of iron
and dental caries in their offspring. The observed results in the thesis should be interpreted with
caution, since serum iron levels were not measured in participating mothers and it is not proven
in humans that foetal iron deficiency is carried into the childhood. However, researchers have
linked iron deficiency anaemia to children with caries experience (Abed et al., 2014; Bansal et
al., 2016; Tang et al., 2013).
8.3.5 Epigenome-Wide Association Study of individuals discordant for dental caries: The
pilot study
Another focus of the thesis was to investigate associations between epigenetic changes and
dental caries experience. Despite decades of preventive and curative interventions and
researchers identifying various risk indicators, dental caries continues to remain a public health
problem globally (Kassebaum et al., 2015), and this has motivated investigators to search for

152
possible genetic contributors to the disease (Vieira et al., 2014). In 1988, Borass et al. showed
evidence of a genetic contribution to caries susceptibility by studying monozygotic twins who
were raised apart, showing that there was a significant resemblance to monozygotic twins
raised together with regards to lifetime caries experience. He thereby suggested a genetic
influence on susceptibility to dental caries (Boraas et al., 1988), which was further tested and
confirmed by other scientists (Bretz et al., 2005; Wang et al.; 2012, Shaffer et al., 2012).
Nevertheless, the association between dental caries and a potent single genotype with causal
biological relevance was not established. Hence, a few investigators became keen on exploring
epigenetic modifications, brought about by influences of environmental factors having a long-
term impact on the epigenome (Seo et al., 2015).
A pilot study was conducted to evaluate the epigenetic changes between individuals with high
and low caries experience. To the best of our knowledge, this was the first ever, EWAS,
conducted on dental caries and the results are very promising. In this study, 435508 CpG sites
were tested epigenome-wide. It was identified that there were significant DMR between
persons – both mothers and their child – with high and low caries experience on chromosomes
1, 2, 5, 7, 12, 20, and 22, out of which Chromosome 12 showed the highest average methylation
difference (41%) between high and low caries experience groups (p < 2.17E-103). There were
8 CpG sites differentially methylated between the region of 11700085 and 11700343 on
chromosome 12 within the promoter region of the gene, Long Intergenic Non-Protein Coding
RNA 1252 (LINC01252), which regulates non-coding RNA in humans
(https://www.ncbi.nlm.nih.gov/gene/?term=LINC01252). Annotation and functional analysis
of DMR related to all genes, which was significantly differentially methylated between high
and low caries experience groups, were investigated through the DAVID bioinformatics
functional annotation tool (Huang et al., 2009a).

153
It was observed that the associated genes fell into two functional clusters regulating (i) Zn or
other metal binding ions and (ii) cell membrane proteins. Zn is an essential co-enzyme in
mineral metabolism that regulates demineralization/remineralization equilibrium of dental hard
tissues. Moreover, it is an element that inhibits dentine demineralization (Takatsuka et al.,
2005). Zn acts as a co-enzyme for MMP, which destroy the organic matrix after
demineralization by bacterial acids (Chaussain-Miller et al., 2006). An opposing evidence was
described by Henn et al. (2012) and Santos et al. (2004), where Zn was reported to inhibit MMP
thereby reducing MMP-mediated collagen degradation in carious dentine (Santos et al., 2004;
Henn et al., 2012). Moreover, Zn enhances calcium phosphate precipitation on and in enamel,
both during tooth development and after an attack of caries (Lynch, 2011; Mohammed et al.,
2014). Also, as a divalent cation, Zn is electronically attracted to negatively charged oral hard
tissue surfaces, causing cariogenic bacteria like MS to detach from enamel (Burguera-Pascu et
al., 2007).
The second cluster of genes identified in the current study predominantly code for membrane
proteins that have general functions, such as transportation of small vesicles, vesicular uptake,
storage, and secretion of ATP, and fusion of transport vesicles with the Golgi complex. Even
though a direct relationship with dental caries could not be established, these intrinsic proteins
play a vital role in cellular functions by mediating the passage of solutes (ions, molecules)
through biological membranes (Mishra et al., 2014).
Among the DMR which showed differential methylation of a single CpG between individuals
discordant for caries, and were within proximity of a gene promoter region, two genes,
PFKFB3 and ENOSF, were found to be part of fructose and mannose metabolism pathways
respectively (Ogata et al., 1999). These pathways are implicit in the synthesis, utilisation, and
154
degradation of these sugars (Musen et al., 2011), which might be of importance to the process
of caries by means of providing a substrate for bacterial growth, though direct evidence for
such is not available.
Further deep pyrosequencing of the significant DMR on chromosome 12, between sites
11700080 and 11700350, was conducted on DNA from saliva of an extended sample (n = 76).
There were 38 mother child dyads: 19 dyads with high caries experience and 19 with low caries
experience. The results, however, did not give conclusive evidence of discovery analysis
(Appendix E, Table 1). The targeted sites were found to be located in a non-specific long
terminal repeat region, hence designing primers for the region failed. Therefore, three substitute
target sites with specific primers were selected (Chr12:11700151, Chr12:11700148, and
Chr12:11700124) for analysis. Nevertheless, there was no significant variation in methylation
between individuals with high and low caries experience on the alternative sites chosen
(Appendix E, Table 2 and Table 3).
8.4 Limitations
There are several limitations to highlight. One of the main limitations is that due to restrictions
of time and logistics, a larger sample of mother-child dyads could not be recruited. Moreover,
the response rate of volunteer participants was low, and to achieve the required sample size
data collection continued for over three years. Further, mothers’ oral health related behaviours
were assessed by a self-administered questionnaire with closed-ended questions. Hence,
practices were not observed directly by the investigator. More variables related to maternal
behaviours would have been reliable and perhaps significantly associated with childhood caries

155
if properly observed and objectively recorded by investigators. These limitations are inherent
when tapping into an existing cohort study where questionnaires have been designed and used
for several years, and substantial volumes of data have been collected. Included with this
limitation is that data on the prenatal environment were also based on answers provided by
participants and serum levels of prenatal supplements were unavailable to support the data.
Many variables related to the prenatal environment could not be included in data analysis as
most of the participating mothers have answered “not relevant” to the use of certain
supplements, alcohol consumption, and smoking during pregnancy. Finally, there were only
12 dyads (24 participants) selected for the pilot study of EWAS, due to lack of funding. Further
research using a larger representative sample is required to validate the discovered findings.
8.5 Discussion and recommendations for future studies
8.5.1Strengths of the study
Despite the limitations, the study explored pathways linking maternal characteristics,
children’s socio-economic and family environment, children’s prenatal environment, birth
weight, and epigenetic changes with childhood caries are the novel contributions of this thesis.
Whilst several associations of maternal, environmental, and child factors with regards to dental
caries in children have already been established (Ersin et al., 2005; Ju et al. 2016; Kim Seow,
2012), this thesis adds to knowledge on risk indicators for dental caries experience in children
and emphasises the possible role of prenatal environment on susceptibility to childhood caries.
The thesis followed the conceptual frame work proposed in chapter three, incorporating
community level, family level, and child level including epigenetic endowment and intra oral

156
characteristics of children (Fernando et al., 2015). The findings are imperative for a population
of children in a Western industrialised country since the study area is culturally and
geographically similar to other states of Australia and to many similar populations across the
globe. Further, the study adds much-needed evidence for an association between epigenetic
changes and dental caries experience. However, the study findings might not be generalizable
to a child population in low- and middle-income countries. Further, it needs to be understood
that the associations extrapolated in this thesis might not be causal owing to the cross-sectional
design of the study.
8.5.2 Future research directions
The findings from the thesis indicate that the effect of maternal oral health related behaviours
on children’s caries levels is persistent throughout infancy and childhood as maternal
perseverance and responsiveness influence oral health-related behaviours of their children
(Tiwari et al., 2017). Therefore, future research needs to consider collecting behavioural data
by naturalistic observation, where the participants’ behaviours are observed in their natural
environment (Jha et al., 2017) or by the direct observational method (Dart et al., 2016), since
these methods provide unbiased information.
Maternal caries status has been found in this thesis to be associated with children’s oral health
status; this effect has been observed to continue into adulthood by others (Shearer et al., 2011).
These pathways of association could be validated by conducting studies that are prospective
and longitudinal that examine multi-level determinants of oral diseases (Cameron et al., 2012).
The best method would be to recruit participants from early pregnancy and follow them through
childhood to adulthood. However, this is clearly a very expensive operation, and one which
cannot be accomplished within a PhD timespan. An alternative would be to use existing data

157
on potential determinants of dental caries (such as records from hospitals with dental outpatient
facilities), and explore associations with current disease status by conducting retrospective
cohort studies (Lai et al., 1997; Sedgwick, 2014).
An interesting finding from the thesis was that reported maternal intake of iron during
pregnancy has an association with their children’s caries experience: these children had
comparatively low levels of caries. Nevertheless, there is a need to use serum levels of these
supplements to reaffirm data obtained via information provided by participants. There is further
evidence for a positive relationship with other supplement use during pregnancy, for example,
vitamin A, vitamin D, and calcium and childhood dental caries (Bergel et al., 2010), indicating
the need to integrate dental and non-dental health care providers to reduce the burden of oral
diseases. However, research shows limited emphasis being placed on oral health by non-dental
professionals in Australia, and hence there is a need for further education and empowering of
general medical practitioners in this area (George et al., 2014). Therefore, there is a requisite
to integrate dentistry with medicine and the health care system as a whole to provide greater
research support for an oral-systemic health connection including paediatricians, pedodontists,
physicians, gynaecologists, nurses, and midwives (Cohen et al., 2017). Furthermore, since
dental caries shares common risk factors with a number of systemic conditions (Williams,
2011), and the interventions for improving prenatal nutrition of mothers have a positive effect
in preventing systemic diseases of the offspring (Roseboom et al., 2001, De Boo and Harding,
2006, Barker et al., 2002), there is a high likelihood that these strategies can also be used in
preventing dental caries. Therefore, it is logical to have a common risk factor approach rather
than oral disease-specific approach, which would be a more effective and cost-effective method
of utilising human and financial resources.

158
A highlight of the thesis was the results observed for associations between epigenetic changes
and caries experience of individuals. However, the pilot study used only 24 individuals for this
discovery. In EWAS, power depends on several factors: study design, sample size, effect size,
and correction for multiple testing. Also the longitudinal stability of the epigenetic markers and
their variance within a biological sample also matter, as epigenetic signals in a biological
sample from one individual represent frequency measures from a population of cells (Tsai and
Bell, 2015). To date EWAS have predominantly focused on DNA methylation, identifying
many differentially methylated positions (DMPs), DMR, and allele-specific methylation
(ASM) regions related to complex diseases (Liu et al., 2013). To achieve an 80% power to
detect DMRs at epigenome-wide significance, at least 100 cases and 100 controls are required
(Tsai and Bell, 2015). Therefore, future research is needed to confirm the findings of the thesis
from a population with similar demographic and geographic backgrounds. However, site-
specific DNA methylation analysis does not provide a global picture of DNA methylation
changes within a genome. Hence future researchers need to focus on global assays that could
study multiple DNA repetitive elements, such as Alu, long interspersed nucleotide elements
(LINE 1) (Yang et al., 2004), or SAT2 (Delgado-Cruzata et al., 2014), as these global assays
cover multiple transposable regions throughout the genome. Moreover, successful genetic
studies require careful measurement of caries phenotypes that define cases and controls. For
example, caries measured by ICDAS criteria to delineate a control as a person who has ICDAS
= 0 on all their tooth surfaces and a case with ICDAS > 0 on one or more of their tooth surfaces.
159
8.6 Conclusions
In conclusion, the findings from this study of SEQ children and their mothers demonstrate that
maternal oral health behaviours, income, and maternal caries experience are significantly
associated with, and probably, directly and/or indirectly, exert a significant influence on caries
susceptibility of their children. Children, in particular, are more at risk of developing caries if
they had high loads of salivary MS, past caries experience, and if their mothers have reported
not to take prenatal iron supplements. One of the main findings of the study was discovering
an association between epigenetic modifications and dental caries experience. The results of
this study are relevant to oral health policy makers in order to make decisions to reduce the
burden of dental caries in children, and especially for health care managers who have to decide
how to use scarce resources in combination with non-dental professionals while maximising
chances of preventing dental caries in children. The findings are also relevant for dental
professionals who seek risk indicators for childhood caries to help them design preventive
interventions. Oral health professionals who wish to reduce the burden of caries in children
need to involve mothers from the prenatal period by providing advice on the importance of
supplement intake and maintaining a healthier lifestyle. The concept of epigenetics in the field
of caries research is in its infancy, and dental professionals are unaware of the epigenetic
endowment on caries progression and the underlying biology. They need to be educated on the
environmental stimuli that impact the epigenome and ultimately influence the development of
dental caries. Hence, proper history taking during clinical procedures and explicit maintenance
of records are critical in identifying high-risk mothers and thereby high-risk children.
Moreover, the whole family need to be engaged in oral health friendly behaviours as the
children’s behaviours are influenced by parents. Clinicians can use the knowledge thus

160
obtained in assessing the family circumstances that would increase the risk of dental caries in
children.

161
References
Abed NT, Aly IA, Deyab SM, Ramoon FM (2014). The relation between early dental caries
and iron-deficiency anaemia in children. Med Res J 13(2):108-114.
Aframian D, Davidowitz T, Benoliel R (2006). The distribution of oral mucosal pH values in
healthy saliva secretors. Oral Dis 12 (4):420-423.
Ahirwar SS, Gupta M, Gupta G, Singh V (2017). Screening, Isolation and Identification of
Lactobacillus Species from Dental Caries of Children. Int J Curr Microbiol App Sci 6(1):497-
503.
Ahmed MS (2015). Oral health knowledge and attitude among primary school teachers of
Madinah, Saudi Arabia. J Contemp Dent Pract 16 (4):275-279.
Aida J, Ando Y, Oosaka M, Niimi K, Morita M (2008). Contributions of social context to
inequality in dental caries: a multilevel analysis of Japanese 3‐ year‐ old children. Community
Dent Oral Epidemiol 36(2):149-156.
Aida J, Matsuyama Y, Tabuchi T, Komazaki Y, Tsuboya T, Kato T et al. (2017). Trajectory of
social inequalities in the treatment of dental caries among preschool children in Japan.
Community Dent Oral Epidemiol DOI: 10.1111/cdo e.12304 (2 April 2017).
[AIHW] Australian Institute of Health and Welfare (2014). Oral health and dental care in
Australia: key facts and figures trends. Canberra. http://www.aihw.gov.au/publication-
detail/?id=60129548265 (Accessed on 10 December 2016)
Alves KMRP, Fancoa KS, Sassaki KT, Rabelo AM, Buzala MAR, DElbem ACB (2011). Effect
of iron on enamel demineralization and remineralization in vitro. Arch Oral Biol 56(11): 1192-
119.
[ARCPOH] Australian Research Centre for Population Oral Health (2009) Geographic
variation in oral health and use of dental services in the Australian population 2004–06. (Dental
Statistics and Research Unit: Adelaide, SA)
http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=6442455420 (Accessed on 25
April 2014).
[ARCPOH] Australian Research Centre for Population Oral Health (2014). The Beginning of
Change- Queensland Child Oral Health Survey 2010-2012.
https://publications.qld.gov.au/storage/f/2014-08-06T03%3A11%3A44.862Z/oral-health-
survey-2010-12.pdf (Accessed on 18 June 2015)
Al-Shalan T, Erickson P, Hardie N (1997). Primary incisor decay before age 4 as a risk factor
for future dental caries. Pediatr Dent 19(1):37-41.
Alkhateeb AA, Mancl LA, Presland RB, Rothen ML, Chi DL (2017). Unstimulated Saliva-
Related Caries Risk Factors in Individuals with Cystic Fibrosis: A Cross-Sectional Analysis of
Unstimulated Salivary Flow, pH, and Buffering Capacity. Caries Res 51(1):1-6.

162
Allum F, Shao X, Guénard F, Simon M-M, Busche S, Caron M et al. (2015). Characterization
of functional methylomes by next-generation capture sequencing identifies novel disease-
associated variants. Nat Commun: DOI: 10.1038/ncomms8211 (29 May 2015).
Almerich Silla JM, Boronat Ferrer M, Iranzo Cortés JE (2014). Caries prevalence in children
from Valencia (Spain) using ICDAS II criteria, 2010. Med Oral Patol Oral Cir Bucal 19
(6):574-580.
Altun C, Guven G, Orkunoglu F, Cehreli ZC, Karaaslan A, Basak F et al. (2008). Human
leukocyte antigen class II alleles and dental caries in a child population. Pediatr Dent
30(2):154-159.
Andrews S (2013). FastQC: A quality control tool for high throughput sequence data. Available
at: http://www.bioinformatics.babraham.ac.uk/projects/fastqc/
Arantes R, Frazão P (2016). Income as a Protective Factor for Dental Caries among Indigenous
People from Central Brazil. J Health Care Poor Underserved 27(1):81-89.
Armstrong WD (1948). An Evaluation of the Role of Vitamins and Minerals in the Control of
Caries. J Dent Res 27(3):376-396.
Ashkanani F, Al-Sane M (2012). Knowledge, attitudes and practices of caregivers in relation
to oral health of preschool children. Med Princ Pract 22(2):167-172.
Asif Z, Raza SM, Rana N, Zafar T, Zehra A (2015). An Assessment of Association between
Carbonated Drink Consumption and Dental Caries Prevalence: A Cross-Sectional Study. J Isl
Int Med Col 10(2):168-172.
Attaran N, Khoshnevisan MH, Ghorbani Z, Pakkhesal M, Dehghanian D (2016). Dental Caries
Predictors in Countries with Different Human Development Index: A Review of Articles. J Int
Oral Health 8(2):182-190.
Ayad M, Van Wuyckhuyse B, Minaguchi K, Raubertas R, Bedi G, Billings R et al. (2000). The
association of basic proline-rich peptides from human parotid gland secretions with caries
experience. J Dent Res 79(4):976-982.
Azad N, Zahnow CA, Rudin CM, Baylin SB (2013). The future of epigenetic therapy in solid
tumours—lessons from the past. Nat Rev Clin Oncol 10(5):256-266.
Azevedo LF, Pecharki GD, Brancher JA, Cordeiro CA, Jr., Medeiros KG, Antunes AA et al.
(2010). Analysis of the association between lactotransferrin (LTF) gene polymorphism and
dental caries. J Appl Oral Sci 18(2):166-170.
Bagherian A, Nematollahi H, Afshari JT, Moheghi N (2008). Comparison of allele frequency
for HLA-DR and HLA-DQ between patients with ECC and caries-free children. J Indian Soc
Pedod Prev Dent 26(1):18-21.
Bansal K, Goyal M, Dhingra R (2016). Association of severe early childhood caries with iron
deficiency anemia. J Indian Soc Pedod Prev Dent 34(1):36.

163
Bardow A, Moe D, Nyvad B, Nauntofte B (2000). The buffer capacity and buffer systems of
human whole saliva measured without loss of CO2. Arch Oral Biol 45(1):1-12.
Bardow A, Pedersen A, Nauntofte B (2004). Saliva. In: MilesTS, NauntofteB, SvenssonP eds.
Clinical Oral Physiology. Quintessence: Copenhagen, pp. 17–18, 30–33.
Barker D, Thornburg K (2013). Placental programming of chronic diseases, cancer and
lifespan: a review. Placenta 34(10):841-845.
Barker DJ, Eriksson JG, Forsén T, Osmond C (2002). Fetal origins of adult disease: strength
of effects and biological basis. Int J Epidemiol 31(6):1235-1239.
Barker DJP (1998). Mothers, babies and health in later life. Churchill Livingstone, Edinburg.
Barros S, Offenbacher S (2009). Epigenetics: connecting environment and genotype to
phenotype and disease. J Dent Res 88(5):400-408.
Baur C, Comings J, Evans C, Garcia R, Horowitz A, Ismail A et al. (2005). The invisible
barrier: literacy and its relationship with oral health. J Public Health Dent 65(3):174-182.
Beaty TH, Ruczinski I, Murray JC, Marazita ML, Munger RG, Hetmanski JB et al. (2011).
Evidence for gene‐ environment interaction in a genome wide study of nonsyndromic cleft
palate. Genet Epidemiol 35(6):469-478.
Belinsky SA, Palmisano WA, Gilliland FD, Crooks LA, Divine KK, Winters SA et al. (2002).
Aberrant promoter methylation in bronchial epithelium and sputum from current and former
smokers. Cancer Res 62(8):2370-2377.
Bergandi L, Defabianis P, Re F, Preti G, Aldieri E, Garetto S et al. (2007). Absence of soluble
CD14 in saliva of young patients with dental caries. Eur J Oral Sci 115(2):93-96.
Bergel E, Gibbons L, Rasines MG, Luetich A, Belizán JM (2010). Maternal calcium
supplementation during pregnancy and dental caries of children at 12 years of age: follow-up
of a randomized controlled trial. Acta Obstet Gynecol Scand 89(11):1396-1402.
Bernabé E, Sheiham A, Sabbah W (2009). Income, income inequality, dental caries and dental
care levels: an ecological study in rich countries. Caries Res 43(4):294-301.
Bernabé E, MacRitchie H, Longbottom C, Pitts N, Sabbah W (2017). Birth weight,
breastfeeding, maternal smoking and caries trajectories. J Dent Res 96(2):171-178.
Bestor TH (2000). The DNA methyltransferases of mammals. Hum Molec Genet 9(16):2395-
2402.
Billings RJ, Berkowitz RJ, Watson G (2004). Teeth. Pediatrics 113(Supplement 3):1120-1127.
Birungi N, Fadnes LT, Nankabirwa V, Tumwine JK, Åstrøm AN (2016). Caretaker’s caries
experience and its association with early childhood caries and children’s oral health-related
quality of life: A prospective two-generation study. Acta Odontol Scand 74(8):605-612.

164
Boraas J, Messer L, Till M (1988). A genetic contribution to dental caries, occlusion, and
morphology as demonstrated by twins reared apart. J Dent Res 67(9):1150-1155.
Borden KL (1998). RING fingers and B-boxes: Zn-binding protein-protein interaction
domains. Biochem Cell Biol 76(2-3):351-358.
Bouwman LH, Roep BO, Roos A (2006). Mannose-binding lectin: clinical implications for
infection, transplantation, and autoimmunity. Hum Immunol 67(4):247-256.
Brambilla E, Felloni A, Gagliani M, Malerba A, Strohmemger D (1998). Caries prevention
during pregnancy. J Am Den Assoc 129(871-877.
Brennan D, Spencer A (2014). Childhood oral health and SES predictors of caries in 30-year-
olds. Caries Res 48(3):237-243.
Bretz WA, Corby PM, Schork NJ, Robinson MT, Coelho M, Costa S et al. (2005). Longitudinal
analysis of heritability for dental caries traits. J Dent Res 84(11):1047-1051.
Bretz WA, Corby PM, Melo MR, Coelho MQ, Costa SM, Robinson M et al. (2006).
Heritability estimates for dental caries and sucrose sweetness preference. Arch Oral Biol
51(12):1156-1160.
Burguera-Pascu M, Rodríguez-Archilla A, Baca P (2007). Substantivity of Zn salts used as
rinsing solutions and their effect on the inhibition of Streptococcus mutans. J Trace Elem Med
Biol 21(2):92-101.
Burne RA, Marquis RE (2000). Alkali production by oral bacteria and protection against dental
caries. FEMS Microbiol Lett 193(1):1-6.
Cai F, Manton D, Shen P, Walker G, Cross K, Yuan Y et al. (2007). Effect of addition of citric
acid and casein phosphopeptide-amorphous calcium phosphate to a sugar-free chewing gum
on enamel remineralization in situ. Caries Res 41(5):377-383.
Cameron CM, Scuffham PA, Shibl R, Ng S, Scott R, Spinks A et al. (2012a). Environments
For Healthy Living (EFHL) Griffith birth cohort study: characteristics of sample and profile of
antenatal exposures. BMC Public Health 12(1):1080. DOI. 10.1186/1471-2458-12-1080 (15
December 2012).
Cameron CM, Scuffham PA, Spinks A, Scott R, Sipe N, Ng S et al. (2012b). Environments for
healthy living (EFHL) griffith birth cohort study: background and methods. Matern Child
Health J 16(9):1896-1905.
Capurro DA, Iafolla T, Kingman A, Chattopadhyay A, Garcia I (2015). Trends in income‐related inequality in untreated caries among children in the United States: findings from
NHANES I, NHANES III, and NHANES 1999–2004. Community Dent Oral Epidemiol
43(6):500-510.
Cardoso FP, Viana MB, Sobrinho APR, Diniz MG, Brito JAR, Gomes CC et al. (2010).
Methylation Pattern of the IFN-γ Gene in Human Dental Pulp. J Endod 36(4):642-646.

165
Cardoso FP, de Faria Amormino SA, Dutra WO, Sobrinho APR, Moreira PR (2014).
Methylation pattern of the CD14 and TLR2 genes in human dental pulp. J Endod 40(3):384-
386.
Carlson DS (2005).Theories of craniofacial growth in the postgenomic era. Semin Orthod
11(4):172-183.
Carvalho JC, Silva EF, Vieira EO, Pollaris A, Guillet A, Mestrinho HD (2014). Oral health
determinants and caries outcome among non-privileged children. Caries Res 48(6):515-523.
Carvalho Sales-Peres SHd, Goya S, Moreira de Freitas Sant'Anna R, Mendes Silva H, Carvalho
Sales-Peres Ad, Pianta Rodrigues da Silva R et al. (2010). Prevalência de sobrepeso e
obesidade e fatores associados em adolescentes na região centro-oeste do estado de São Paulo
(SP, Brasil). Ciência & Saúde Coletiva 15(2):3175-3184.
Casanova-Rosado AJ, Medina-Solís CE, Casanova-Rosado JF, Vallejos-Sánchez AA,
Maupomé G, Ávila-Burgos L (2005). Dental caries and associated factors in Mexican
schoolchildren aged 6–13 years. Acta Odontol Scand 63(4):245-251.
Chaffee B, Gansky S, Weintraub J, Featherstone J, Ramos-Gomez F (2014). Maternal oral
bacterial levels predict early childhood caries development. J Dent Res 93(3):238-244.
Chaffee BW, Rodrigues PH, Kramer PF, Vítolo MR, Feldens CA (2017). Oral health‐ related
quality‐ of‐ life scores differ by socio-economic status and caries experience. Community
Dent Oral Epidemiol 45(3):216-224.
Chankanka O, Cavanaugh JE, Levy SM, Marshall TA, Warren JJ, Broffitt B et al. (2011).
Longitudinal associations between children's dental caries and risk factors. J Public Health
Dent 71(4):289-300.
Chaussain-Miller C, Fioretti F, Goldberg M, Menashi S (2006). The role of matrix
metalloproteinases (MMPs) in human caries. J Dent Res 85(1):22-32.
Cheng J, Campbell K (2016). Caries and dental erosion: are Soroti children and adolescents at
risk from increased soft-drink availability in Uganda? Afr Health Sci 16(4):943-946.
Childers NK, Momeni SS, Whiddon J, Cheon K, Cutter GR, Wiener HW et al. (2017).
Association Between Early Childhood Caries and Colonization with MSGenotypes From
Mothers. Pediatr Dent 39(2):130-135.
Chrisopoulos S, Harford J, Ellershaw A (2016). Oral health and dental care in Australia: key
facts and figures.
https://digital.library.adelaide.edu.au/dspace/bitstream/2440/98160/2/hdl_98160.pdf
(Accessed on 11 November 2016).
Cohen L, Dahlen G, Escobar A, Fejerskov O, Johnson NW, Manji F (2017). La Cascada
Declaration Colombia. Aust Dent J: DOI: 10.1111/adj.12546 (9 August 2017). Available at
https://lacascada.pressbooks.com

166
[CICDAS] Committee International Caries Detection and Assessment System (2005). Criteria
Manual; International Caries Detection and Assessment System (ICDAS II) Baltimore,
Maryland, USA
https://www.icdas.org/uploads/Rationale%20and%20Evidence%20ICDAS%20II%20Septem
ber%2011-1.pdf (Accessed on September 2012).
Cortellazzi KL, da Silva Tagliaferro EP, Pereira SM, Bovi Ambrosano GM, Guerra LM, de
Lima Vazquez F et al. (2013). A cohort study of caries incidence and baseline socio-economic,
clinical and demographic variables: a Kaplan-Meier survival analysis. Oral Health Prev Dent
11(4): 349-358.
Craig JM (2013). Epigenetics in Twin Studies. Medical Epigen 1(1):78-87.
Crall JJ, Edelstein B, Tinanoff N (1990). Relationship of microbiological, social, and
environmental variables to caries status in young children. Pediatr Dent 12(4):233-236.
Da Fonseca MA, Avenetti D (2017). Social Determinants of Pediatric Oral Health. Dent Clin
N Am 61: 519–532.
Daly AK, Day CP (2001). Candidate gene case‐ control association studies: advantages and
potential pitfalls. Br J Clin Pharmacol 52(5):489-499.
Dart EH, Radley KC, Briesch AM, Furlow CM, Cavell HJ (2016). Assessing the Accuracy of
Classwide Direct Observation Methods: Two Analyses Using Simulated and Naturalistic Data.
Behav Disord 41(3):148-160.
Dave Singh G, Callister JD (2013). Effect of a maxillary appliance in an adult with obstructive
sleep apnea: A case report. Cranio 31(3):171-175.
Davis CD, Uthus EO (2004). DNA methylation, cancer susceptibility, and nutrient interactions.
Exp Biol Med (Maywood) 229(10):988-995.
Dawes C (2008). Salivary flow patterns and the health of hard and soft oral tissues. J Am Dent
Assoc 139(supplement 2):18S-24S.
De-Regil LM, Harding KB, Roche ML (2016). Preconceptional Nutrition Interventions for
Adolescent Girls and Adult Women: Global Guidelines and Gaps in Evidence and Policy with
Emphasis on Micronutrients. J Nutr : DOI: 10.3945/jn.115.223487 (8 June 2016).
De Boo HA, Harding JE (2006). The developmental origins of adult disease (Barker)
hypothesis. Aust N Z J Obstet Gynaecol 46(1):4-14.
Declerck D, Leroy R, Martens L, Lesaffre E, Garcia‐ Zattera MJ, Broucke SV et al. (2008).
Factors associated with prevalence and severity of caries experience in preschool children.
Community Dent Oral Epidemiol 36(2):168-178.
Deeley K, Letra A, Rose E, Brandon C, Resick J, Marazita M et al. (2008). Possible association
of amelogenin to high caries experience in a Guatemalan-Mayan population. Caries Res
42(1):8-13.

167
De Gauw JH, Costa LMM ,Silva RN, Santos NB, Tenorio MDH (2017). Evaluation of the
effect of ferrous sulphate on enamel deminaralization of human deceduous teeth : an in vitro
study. Journals Bahiana DOI: 10.17267/2238-2720revbahianaodonto.v8i3.1549( 09/29/2017)
Delgado-Cruzata L, Vin-Raviv N, Tehranifar P, Flom J, Reynolds D, Gonzalez K et al. (2014).
Correlations in global DNA methylation measures in peripheral blood mononuclear cells and
granulocytes. Epigenetics 9(11):1504-1510.
Deutsch D, Leiser Y, Shay B, Fermon E, Taylor A, Rosenfeld E et al. (2002). The human
tuftelin gene and the expression of tuftelin in mineralizing and nonmineralizing tissues.
Connect Tissue Res 43(2-3):425-434.
Diaz de Guillory C, Schoolfield JD, Johnson D, Yeh CK, Chen S, Cappelli DP et al. (2014).
Co‐ Relationships between glandular salivary flow rates and dental caries. Gerodontology
31(3):210-219.
Dige I, Grønkjær L, Nyvad B (2014). Molecular studies of the structural ecology of natural
occlusal caries. Caries Rres 48(5):451-460.
Ditmyer M, Dounis G, Mobley C, Schwarz E (2010). A case-control study of determinants for
high and low dental caries prevalence in Nevada youth. BMC Oral Health 10(1):24.
Do L, Spencer AJ (2014). The Beginning of Change: Queensland Child Oral Health Survey
2010-2012: Australian Research Centre for Population Oral Health, The University of Adelaide
Press.
Do L, Spencer A (2016). Oral health of Australian children. The National Child Oral Health
Study 2012–14 Adelaide (Australia): University of Adelaide Press.
Do L, Ha D, Peres MA, Skinner J, Byun R, Spencer AJ (2017). Effectiveness of water
fluoridation in the prevention of dental caries across adult age groups. Community Dent Oral
Epidemiol 45(3):225-232.
Doerks T, Copley RR, Schultz J, Ponting CP, Bork P (2002). Systematic identification of novel
protein domain families associated with nuclear functions. Genome Res 12(1):47-56.
dos Santos Junior VE, de Sousa RMB, Oliveira MC, de Caldas Junior AF, Rosenblatt A (2014).
Early childhood caries and its relationship with perinatal, socio-economic and nutritional risks:
a cross-sectional study. BMC Oral Health 14(1):47.
dos Santos Pinto G, de Ávila Quevedo L, Britto Correa M, Sousa Azevedo M, Leão Goettems
M, Tavares Pinheiro R et al. (2016). Maternal Depression Increases Childhood Dental Caries:
A Cohort Study in Brazil. Caries Res 51(1):17-25.
Douglass JM, Li Y, Tinanoff N (2008). Association of mutans streptococci between caregivers
and their children. Pediatr Dent 30(5):375-387.
Duhaime-Ross A (2014). Revved-up epigenetic sequencing may foster new diagnostics. Nat
Med 20(1):2-2.

168
Duijster D, Verrips G, Loveren C (2014). The role of family functioning in childhood dental
caries. Community Dent Oral Epidemiol 42(3):193-205.
Dye BA, Thornton-Evans G, Li X, Iafolla TJ (2015). Dental caries and sealant prevalence in
children and adolescents in the United States, 2011-2012: US Department of Health and
Human Services, Centers for Disease Control and Prevention, National Center for Health
Statistics.
Eddie Ip W, Takahashi K, Alan Ezekowitz R, Stuart LM (2009). Mannose‐ binding lectin and
innate immunity. Immunol Rev 230(1):9-21.
Edelstein BL, Ureles SD, Smaldone A (2016). Very High Salivary MSPredicts Caries
Progression in Young Children. Pediatr Dent 38(4):325-330.
Eichler EE, Flint J, Gibson G, Kong A, Leal SM, Moore JH et al. (2010). Missing heritability
and strategies for finding the underlying causes of complex disease. Nat Rev Genet 11(6):446-
450.
El-kwatehy W, Youssef A (2016). Salivary Biomarkers in Caries Affected and Caries Free
Children. Int J Dentistry Oral Sci 3(10):348-352.
ElSalhy M, Honkala S, Söderling E, Varghese A, Honkala E (2013). Relationship between
daily habits,< i> Streptococcus mutans</i>, and caries among schoolboys. J Dent 41(11):1000-
1006.
Ersin NK, Eronat N, Cogulu D, Uzel A, Aksit S (2005). Association of maternal-child
characteristics as a factor in early childhood caries and salivary bacterial counts. J Dent Child
(Chic) 73(2):105-111.
Fatima T, Rahim ZBHA, Lin CW, Qamar Z (2016). Zn: A precious trace element for oral health
care? J Pak Med Assoc 66:1019-1023.
Fejerskov O, Kidd E (2008). Dental caries: the disease and its clinical management. 2nd Edn.
ed. New Jersey: Wiley-Blackwell.
Fellermann K, Stange EF (2001). Defensins–innate immunity at the epithelial frontier. Eur J
Gastroenterol Hepatol 13(7):771-776.
Fenton V, Cavill I, Fisher J (1977). Iron stores in pregnancy. Br J Haematol 37(1):145-149.
Fernando S, Speicher DJ, Bakr MM, Benton MC, Lea RA, Scuffham PA et al. (2015). Protocol
for assessing maternal, environmental and epigenetic risk factors for dental caries in children.
BMC Oral Health 15(1):167. DOI.org/10.1186/s12903-015-0143-2 (29 December 2015).
Ferraz dos Santos B, Dabbagh B, Daniel SJ, Schwartz S (2016). Association of onabotulinum
toxin A treatment with salivary pH and dental caries of neurologically impaired children with
sialorrhea. Int J Paediatr Dent 26(1):45-51.
Finn RD, Attwood TK, Babbitt PC, Bateman A, Bork P, Bridge AJ et al. (2017). InterPro in
2017—beyond protein family and domain annotations. Nucleic Acids Res 45(1):D190-D199.

169
Fisher-Owens SA, Gansky SA, Platt LJ, Weintraub JA, Soobader M-J, Bramlett MD et al.
(2007). Influences on children's oral health: a conceptual model. Pediatrics 120(3):e510-e520.
DOI: 10.1542/peds.2006-3084 (2 March 2007).
https://s100.copyright.com/AppDispatchServlet copyright order link
Folayan MO, Kolawole KA, Oziegbe EO, Oyedele T, Oshomoji OV, Chukwumah NM et al.
(2015). Prevalence, and early childhood caries risk indicators in preschool children in suburban
Nigeria. BMC Oral Health 15(1):72.
Fraga MF, Ballestar E, Paz MF, Ropero S, Setien F, Ballestar ML et al. (2005). Epigenetic
differences arise during the lifetime of monozygotic twins. Proc Natl Acad Sci U S A
102(30):10604-10609.
Fushan AA, Simons CT, Slack JP, Manichaikul A, Drayna D (2009). Allelic polymorphism
within the TAS1R3 promoter is associated with human taste sensitivity to sucrose. Curr Biol
19(15):1288-1293.
Gao X, Jiang S, Koh D, Hsu CYS (2016). Salivary biomarkers for dental caries. Periodontol
2000 70(1):128-141.
Garcia CA, Ahmadian A, Gharizadeh B, Lundeberg J, Ronaghi M, Nyrén P (2000). Mutation
detection by pyrosequencing: sequencing of exons 5–8 of the p53 tumor suppressor gene. Gene
253(2):249-257.
George A, Duff M, Johnson M, Dahlen H, Blinkhorn A, Ellis S et al. (2014). Piloting of an
oral health education programme and knowledge test for midwives. Contemp Nurse 46(2):180-
186.
Ghazal T, Levy SM, Childers NK, Broffitt B, Cutter GR, Wiener HW et al. (2015). Factors
associated with early childhood caries incidence among high caries‐ risk children. Community
Dent Oral Epidemiol 43(4):366-374.
Goldberg AD, Allis CD, Bernstein E (2007). Epigenetics: a landscape takes shape. Cell
128(4):635-638.
Gomez RS, Dutra WO, Moreira PR (2009). Epigenetics and periodontal disease: future
perspectives. Inflammation Res 58(10):625-629.
Gopinath V, Arzreanne A (2006). Saliva as a diagnostic tool for assessment of dental caries.
Arch Orofac Sci 1:57-59.
Gross EL, Leys EJ, Gasparovich SR, Firestone ND, Schwartzbaum JA, Janies DA et al. (2010).
Bacterial 16S sequence analysis of severe caries in young permanent teeth. J Clin Microbiol
48(11):4121-4128.
Guo L, Shi W (2013). Salivary biomarkers for caries risk assessment. J Calif Dent Assoc
41(2):107.

170
Ha D, Roberts-Thomson KF, Armfield JM (2011). The child dental health surveys Australia,
2005 and 2006: Australian Institute of Health and Welfare, Dental Statistics and Research Unit.
http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737420632 (Accessed on 8
February 2014).
Hajishengallis E, Parsaei Y, Klein MI, Koo H (2017). Advances in the microbial etiology and
pathogenesis of early childhood caries. Mol Oral Microbiol 32(1):24-34.
Hall-Scullin E, Whitehead H, Milsom K, Tickle M, Su T-L, Walsh T (2017). Longitudinal
study of caries development from childhood to adolescence. J Dent Res 96(7):762-767.
Han DH, Kim DH, Kim MJ, Kim JB, Jung‐ Choi K, Bae KH (2014). Regular dental checkup
and snack–soda drink consumption of preschool children are associated with early childhood
caries in Korean caregiver/preschool children dyads. Community Dent Oral Epidemiol
42(1):70-78.
Hardy J, Singleton A (2009). Genomewide association studies and human disease. N Engl J
Med 360(17):1759-1768.
Harris R, Nicoll AD, Adair PM, Pine CM (2004). Risk factors for dental caries in young
children: a systematic review of the literature. Community Dent Health 21(1):71-85.
Heaton B, Crawford A, Garcia RI, Henshaw M, Riedy CA, Barker JC et al. (2017). Oral health
beliefs, knowledge, and behaviors in Northern California American Indian and Alaska Native
mothers regarding early childhood caries. J Public Health Dent: DOI: 10.1111/jphd.12217 (27
April 2017).
Henn S, de Carvalho RV, Ogliari FA, de Souza AP, Line SRP, da Silva AF et al. (2012).
Addition of Zn methacrylate in dental polymers: MMP-2 inhibition and ultimate tensile
strength evaluation. Clin Oral Investig 16(2):531-536.
Hillemacher T, Frieling H, Moskau S, Muschler MA, Semmler A, Kornhuber J et al. (2008).
Global DNA methylation is influenced by smoking behaviour. Eur Neuropsychopharmacol
18(4):295-298.
Hooley M, Skouteris H, Boganin C, Satur J, Kilpatrick N (2012). Parental influence and the
development of dental caries in children aged 0–6 years: a systematic review of the literature.
J Dent 40(11):873-885.
Hoyle R, Panter A (1995). Writing about structural equation modeling. In: Structural equation
modeling Concepts issues and application Hoyle RH editor. Thousand Oaks, CA: Sage.
Huang DW, Sherman BT, Lempicki RA (2009a). Systematic and integrative analysis of large
gene lists using DAVID bioinformatics resources. Nat Protoc 4(1):44-57.
Huang DW, Sherman BT, Lempicki RA (2009b). Bioinformatics enrichment tools: paths
toward the comprehensive functional analysis of large gene lists. Nucleic Acids Res 37(1):1-
13.

171
Hughes T, Bockmann M, Mihailidis S, Bennett C, Harris A, Seow WK et al. (2013). Genetic,
epigenetic, and environmental influences on dentofacial structures and oral health: ongoing
studies of Australian twins and their families. Twin Res Hum Genet 16(1):43-51.
Humphrey SP, Williamson RT (2001). A review of saliva: normal composition, flow, and
function. J Prosthet Dent 85(2):162-169.
Hunter PB (1988). Risk factors in dental caries. Int Dent J 38(4):211-217.
Ismail AI, Lim S, Sohn W, Willem JM (2008a). Determinants of early childhood caries in low-
income African American young children. Pediatr Dent 30(4):289-296.
Ismail AI, Sohn W, Tellez M, Willem JM, Betz J, Lepkowski J (2008b). Risk indicators for
dental caries using the International Caries Detection and Assessment System (ICDAS).
Community Dent Oral Epidemiol 36(1):55-68.
Jackson SL, Vann Jr WF, Kotch JB, Pahel BT, Lee JY (2011). Impact of poor oral health on
children's school attendance and performance. Am J Public Health 101(10):1900-1906.
Jeon J (2015). The Strengths and Limitations of the Statistical Modeling of Complex Social
Phenomenon: Focusing on SEM, Path Analysis, or Multiple Regression Models. Int J Soc
Behav Educ Econ Bus Ind Eng 9(1559-1567.
Jepsen S, Blanco J, Buchalla W, Carvalho JC, Dietrich T, Dörfer C et al. (2017). Prevention
and control of dental caries and periodontal diseases at individual and population level:
consensus report of group 3 of joint EFP/ORCA workshop on the boundaries between caries
and periodontal diseases. J Clin Periodontol 44(S18):S85-S93.
Jha A, Tiwari G, Mohan D, Mukherjee S, Banerjee S (2017). Analysis of pedestrian movement
on Delhi roads by using naturalistic observation techniques. Transp Res Rec 2634:95-100.
Johnson NW (1991). Introduction: the nature of the caries process and the need for markers of
risk. In: Risk Markers for oral diseases NW Johnson editor. New York: Cambridge University
press, pp. 1-11.
Jonasson A, Eriksson C, Jenkinson HF, Kallestal C, Johansson I, Stromberg N (2007). Innate
immunity glycoprotein gp-340 variants may modulate human susceptibility to dental caries.
BMC Infect Dis 7:57: DOI:10.1186/1471-2334-7-57 (11 June 2007).
Ju X, Jamieson LM, Mejia GC (2016). Estimating the effects of maternal education on child
dental caries using marginal structural models: The Longitudinal Study of Indigenous
Australian Children. Community Dent Oral Epidemiol 44(6):602-610.
Ju X, Brennan D, Parker E, Mills H, Kapellas K, Jamieson L (2017). Efficacy of an oral health
literacy intervention among Indigenous Australian adults. Community Dent Oral Epidemiol
DOI: 10.1111/cdoe.12305 (19 May 2017).
Kaczor-Urbanowicz KE, Martin Carreras-Presas C, Aro K, Tu M, Garcia-Godoy F, Wong DT
(2017). Saliva diagnostics–Current views and directions. Exp Biol Med (Maywood)
242(5):459-472.

172
Kang S, Yoon I, Lee H, Cho J (2011). Association between AMELX polymorphisms and dental
caries in Koreans. Oral Dis 17(4):399-406.
Kassebaum N, Bernabé E, Dahiya M, Bhandari B, Murray C, Marcenes W (2015). Global
Burden of Untreated Caries A Systematic Review and Meta-regression. J Dent Res 94(5):650-
658.
Kavanaugh M, Halterman JS, Montes G, Epstein M, Hightower AD, Weitzman M (2006).
Maternal depressive symptoms are adversely associated with prevention practices and
parenting behaviors for preschool children. Ambulatory Pediatr 6(1):32-37.
Kawashita Y, Fukuda H, Kawasaki K, Kitamura M, Hayashida H, Furugen R et al. (2009).
Dental Caries in 3‐ Year‐ Old Children is Associated More with Child‐ Rearing Behaviors
than Mother‐ Related Health Behaviors. J Public Health Dent 69(2):104-110.
Kemper KE, Daetwyler HD, Visscher PM, Goddard ME (2012). Comparing linkage and
association analyses in sheep points to a better way of doing GWAS. Genet Res 94(04):191-
203.
Khocht A, Zohn H, Deasy M, Chang K-M (1995). Assessment of periodontal status with PSR
and traditional clinical periodontal examination. J Am Dent Assoc 126(12):1658-1665.
Kianoush N, Adler CJ, Nguyen K-AT, Browne GV, Simonian M, Hunter N (2014). Bacterial
profile of dentine caries and the impact of pH on bacterial population diversity. PLoS One 9(3)
DOI:10.1371/journal.pone.0092940 (27 March 2014).
Kidd E, Fejerskov O (2004). What constitutes dental caries? Histopathology of carious enamel
and dentin related to the action of cariogenic biofilms. J Dent Res 83(1):35-38.
Kieu TQ, Ngo LTQ, Pham TAAV (2017). Dental Caries and Related Factors in Vietnamese
Dental Patients. UIP Health Med 1(1):148-154.
Kim H-S, Smithies O, Maeda N (1990). A physical map of the human salivary proline-rich
protein gene cluster covers over 700 kbp of DNA. Genomics 6(2):260-267.
Kim H, Millsap R (2014). Using the Bollen-Stine Bootstrapping Method for Evaluating
Approximate Fit Indices. Multivariate Behav Res 49(6):581-596.
Kim Seow W (2012). Environmental, maternal, and child factors which contribute to early
childhood caries: a unifying conceptual model. Int J Paediatr Dent 22(3):157-168.
Kim Y, Telleen S (2004). Predictors of the utilization of oral health services by children of
low-income families in the United States: beliefs, cost, or provider? Taehan Kanho Hakhoe
Chi 34(8):1460-1467.
Kitasako Y, Burrow M, Stacey M, Huq L, Reynolds E, Tagami J (2008). Comparative analysis
of three commercial saliva testing kits with a standard saliva buffering test. Aust Dent J
53(2):140-144.Klein H, Palmer CE (1940). Dental caries in brothers and sisters of immune and
susceptible children. Milbank Mem Fund Q 8(1):67-82.

173
Klein H (1946). The family and dental disease; dental disease (DMF) experience in parents and
offspring. J Am Dent Assoc 33(11):735-743.
Köhler B, Andreen I (1994). Influence of caries-preventive measures in mothers on cariogenic
bacteria and caries experience in their children. Arch Oral Biol 39(10):907-911.
Köhler B, Andréen I (2012). Mutans streptococci and caries prevalence in children after early
maternal caries prevention: a follow-up at 19 years of age. Caries Res 46(5):474-480.
Krasone K, Lace B, Akota I, Care R, Deeley K, Kuchler EC et al. (2014). Genetic variation in
the promoter region of beta-defensin 1 (DEFB 1) is associated with high caries experience in
children born with cleft lip and palate. Acta Odontol Scand 72(3):235-240.
Küchler EC, Feng P, Deeley K, Fitzgerald CA, Meyer C, Gorbunov A et al. (2014). Fine
mapping of locus Xq25. 1-27-2 for a low caries experience phenotype. Arch Oral Biol
59(5):479-486.
Kulkarni GV, Chng T, Eny KM, Nielsen D, Wessman C, El-Sohemy A (2013). Association of
GLUT2 and TAS1R2 genotypes with risk for dental caries. Caries Res 47(3):219-225.
Kumar S, Kroon J, Lalloo R (2014). A systematic review of the impact of parental socio-
economic status and home environment characteristics on children’s oral health related quality
of life. Health Qual Life Outcomes 12:41. DOI:10.1186/1477-7525-12-41 (21 March 2014).
Kumar S, Tadakamadla J, Kroon J, Johnson NW (2016). Impact of parent-related factors on
dental caries in the permanent dentition of 6–12-year-old children: A systematic review. J Dent
46:1-11. DOI:10.1016/j.jdent.2015.12.007 (26 December 2015).
Kumar S, Kroon J, Lalloo R, Kulkarni S, Johnson NW (2017a). Relationship between body
mass index and dental caries in children, and the influence of socio‐ economic status. Int Dent
J 67(2):91-97.
Kumar S, Tadakamadla J, Zimmer‐ Gembeck M, Kroon J, Lalloo R, Johnson N (2017b).
Parenting practices and children's dental caries experience: A structural equation modelling
approach. Community Dent Oral Epidemiol DOI: 10.1111/cdoe.12321 (8 June 2017).
Kumar S, Zimmer-Gembeck M, Kroon J, Lalloo R, Johnson N (2017c). The role of parental
rearing practices and family demographics on oral health-related quality of life in children.
Qual Life Res 26(8): 2229–2236.
Kutsch VK, Kois JC, Chaiyabutr Y, Milicich G (2013). Reconsidering remineralization
strategies to include nanoparticle hydroxyapatite. Compend Contin Educ Dent 34(3):2-6.
Laaksonen M, Rahkonen O, Karvonen S, Lahelma E (2005). Socio-economic status and
smoking: analysing inequalities with multiple indicators. Eur J Public Health 15(3):262-269.
Lagerlöf F (1994). Caries-protective factors in saliva. Adv Dent Res 8(2):229-238.
Lai P, Kim Seow W, Tudehope D, Rogers Y (1997). Enamel hypoplasia and dental caries in
very-low birthweight children: a case-controlled, longitudinal study. Pediatr Dent 19:42-49.

174
Landry R, Jean M (2002). Periodontal Screening and Recording (PSR) Index: precursors,
utility and limitations in a clinical setting. Int Dent J 52(1):35-40.
Launay J-M, Del Pino M, Chironi G, Callebert J, Peoc’h K, Mégnien J-L et al. (2009). Smoking
induces long-lasting effects through a monoamine-oxidase epigenetic regulation. PLoS One
4(11): DOI:10.1371/journal.pone.0007959 (23 November 2009).
Lave JR, Keane C, Lin C, Ricci E (2002). The impact of dental benefits on the utilization of
dental services by low-income children in western Pennsylvania. Pediatr Dent 24(3):234-240.
Lee J, Giannobile W (2016). Taxes on sugar-sweetened beverages a strategy to reduce
epidemics of diabetes, obesity, and dental caries? J Dent Res 95(12): 1325–1326.
Lee JY, Bouwens TJ, Savage MF, Vann Jr WF (2006). Examining the cost-effectiveness of
early dental visits. Pediatri Dent 28(2):102-105.
Lee JY, Divaris K, DeWalt DA, Baker AD, Gizlice Z, Rozier RG et al. (2014). Caregivers’
health literacy and gaps in children’s Medicaid enrollment: findings from the Carolina Oral
Health Literacy Study. PLoS One 9(10): DOI:10.1371/journal.pone.0110178 (10 October
2014).
Leenen FA, Muller CP, Turner JD (2016). DNA methylation: conducting the orchestra from
exposure to phenotype? Clin Epigenetics 8:92 DOI 10.1186/s13148-016-0256-8 (6 September
2016).
Leme AP, Koo H, Bellato C, Bedi G, Cury J (2006). The role of sucrose in cariogenic dental
biofilm formation—new insight. J Dent Res 85(10):878-887.
Lenander-Lumikari M, Loimaranta V (2000). Saliva and dental caries. Adv Dent Res 14(1):40-
47.
Leone CW, Oppenheim FG (2001). Physical and chemical aspects of saliva as indicators of
risk for dental caries in humans. J Dent Educ 65(10):1054-1062.
Li Y, Caufield P, Dasanayake A, Wiener H, Vermund S (2005). Mode of delivery and other
maternal factors influence the acquisition of MSin infants. J Dent Res 84(9):806-811.
Li Y, Zhang Y, Yang R, Zhang Q, Zou J, Kang D (2011). Associations of social and
behavioural factors with early childhood caries in Xiamen city in China. Int J Paediatr Dent
21(2):103-111.
Lima AC, Lima MC, Guerra MQ, Romani SA, Eickmann SH, Lira PI (2006). Impact of weekly
treatment with ferrous sulfate on hemoglobin level, morbidity and nutritional status of anemic
infants. J Pediatr 82(6):452-7. DOI: 10.2223/JPED.1568.
Liu Y, Aryee MJ, Padyukov L, Fallin MD, Hesselberg E, Runarsson A et al. (2013).
Epigenome-wide association data implicate DNA methylation as an intermediary of genetic
risk in rheumatoid arthritis. Nat Biotechnol 31(2):142-147.

175
Llena C, Leyda A, Forner L, Garcet S (2015). Association between the number of early carious
lesions and diet in children with a high prevalence of caries. Eur J Paediatr Dent 16(1):7-12.
Loesche WJ (1986). Role of MSin human dental decay. Microbiol Rev 50(4):353-380.
López-Gómez SA, Villalobos-Rodelo JJ, Ávila-Burgos L, Casanova-Rosado JF, Vallejos-
Sánchez AA, Lucas-Rincón SE et al. (2016). Relationship between premature loss of primary
teeth with oral hygiene, consumption of soft drinks, dental care, and previous caries experience.
Sci Rep 6: 21147 DOI: 10.1038/srep21147 (26 February 2016).
Lu Y, Papagerakis P, Yamakoshi Y, Hu JC-C, Bartlett JD, Simmer JP (2008). Functions of
KLK4 and MMP-20 in dental enamel formation. Biol Chem 389(6):695-700.
Lucas N, Neumann A, Kilpatrick N, Nicholson J (2011). State‐ level differences in the oral
health of Australian preschool and early primary school‐ age children. Aust Dent J 56(1):56-
62.
Luo W, Wen X, Wang H-J, MacDougall M, Snead ML, Paine ML (2004). In vivo
overexpression of tuftelin in the enamel organic matrix. Cells Tissues Organs 177(4):212-220.
Lupo A, Cesaro E, Montano G, Zurlo D, Izzo P, Costanzo P (2013). KRAB-Zn finger proteins:
a repressor family displaying multiple biological functions. Curr Genomics 14(4):268-278.
Lynch RJ (2011). Zn in the mouth, its interactions with dental enamel and possible effects on
caries; a review of the literature. Int Dent J 61(3):46-54.
MacDougall M, DuPont BR, Simmons D, Reus B, Krebsbach P, Kärrman C et al. (1997).
Ameloblastin gene (AMBN) maps within the critical region for autosomal dominant
amelogenesis imperfecta at chromosome 4q21. Genomics 41(1):115-118.
Macek MD (2016). Although the Magnitude Varied, Income-Related Inequalities in Untreated
Dental Caries were Consistently Found among Young Children in 3 US Surveys. J Evid Based
Dent Pract 16(2):142-144.
Machin GA (1996). Some causes of genotypic and phenotypic discordance in monozygotic
twin pairs. Am J Med Genet A 61(3):216-228.
Mani S, Herceg Z. DNA methylation changes in cancer. In: Craig JM, Wong NC, eds.
Epigenetics: a reference manual. Norfolk, UK: Caister Academic Press, 2011:195–210.
Manolio TA, Collins FS, Cox NJ, Goldstein DB, Hindorff LA, Hunter DJ et al. (2009). Finding
the missing heritability of complex diseases. Nature 461(7265):747-753.
Marazita ML (2012). The evolution of human genetic studies of cleft lip and cleft palate. Annu
Rev Genomics Hum Genet 13:263-283.
Markovic N, Muratbegovic AA, Kobaslija S, Bajric E, Selimovic-Dragas M, Huseinbegovic A
(2013). Caries prevalence of children and adolescents in Bosnia and Herzegovina. Acta Med
Acad 42(2):108-116.

176
Martinhon CCR, Italiani FM, Padilha PM, Bijella MFTB, Delbem ACB, Buzalaf MAR (2006).
Effect of iron on bovine enamel and on the composition of the dental biofilm formed “in situ”.
Arch Oral Biol 51 (6): 471-475
Mattila M-L, Rautava P, Sillanpää M, Paunio P (2000). Caries in five-year-old children and
associations with family-related factors. J Dent Res 79(3):875-881.
Mejia G, Jamieson L, Ha D, Spencer A (2014). Greater inequalities in dental treatment than in
disease experience. J Dent Res 93(10):966-971.
Melo M, Weir M, Passos V, Powers M, Xu H (2016). pH-activatable nano-amorphous calcium
phosphate to reduce dental enamel demineralization. Dent Mater 32(1):e64
DOI:10.1016/j.dental.2016.08.132 (August 2016).
Mishra NK, Chang J, Zhao PX (2014). Prediction of membrane transport proteins and their
substrate specificities using primary sequence information. PLoS One 9(6):
10.1371/journal.pone.0100278 (26 June 2014).
Mohammed N, Mneimne M, Hill R, Al-Jawad M, Lynch R, Anderson P (2014). Physical
chemical effects of Zn on in vitro enamel demineralization. J Dent 42(9):1096-1104.
Moimaz SAS, Fadel CB, Lolli LF, Garbin CAS, Garbin AJÍ, Saliba NA (2014). Social aspects
of dental caries in the context of mother-child pairs. J Appl Oral Sci 22(1):73-78.
Mota-Veloso I, Soares MEC, Alencar BM, Marques LS, Ramos-Jorge ML, Ramos-Jorge J
(2016). Impact of untreated dental caries and its clinical consequences on the oral health-related
quality of life of schoolchildren aged 8–10 years. Qual Life Res 25(1):193-199.
Moyer VA (2014). Prevention of dental caries in children from birth through age 5 years: US
Preventive Services Task Force recommendation statement. Pediatrics 133(6):1102-1111.
Musen MA, Noy NF, Shah NH, Whetzel PL, Chute CG, Story M-A et al. (2011). The national
center for biomedical ontology. J Am Med Inform Assoc 19(2):190-195.
Musen MA, Noy NF, Shah NH, Whetzel PL, Chute CG, Story M-A et al. (2012). The national
center for biomedical ontology. J Am Med Inform Assoc 19(2):190-195.
Mwakayoka H, Masalu JR, Kikwilu EN (2017). Dental Caries and Associated Factors in
Children Aged 2-4 Years Old in Mbeya City, Tanzania. J Dent 18(2):104-111.
Nanda J, Sachdev V, Sandhu M, Deep-Singh-Nanda K (2015). Correlation between dental
caries experience and mutans streptococci counts using saliva and plaque as microbial risk
indicators in 3-8 year old children. A cross Sectional study. J Clin Exp Dent 7(1): e114 –e118.
Nelson S, Albert J, Geng C, Curtan S, Lang K, Miadich S et al. (2013). Increased enamel
hypoplasia and very low birthweight infants. J Dent Res 92(9):788-794.
177
Nevitt J, Hancock GR (1998). Relative Performance of Rescaling and Resampling Approaches
to Model Chi Square and Parameter Standard Error Estimation in Structural Equation Modeling
http://files.eric.ed.gov/fulltext/ED420711.pdf (Accessed on 28 February 2017).
Ngoc VTN, Chu D-T, Le D-H (2017). Prevalence of early childhood caries and its related risk
factors in preschoolers: Result from a cross sectional study in Vietnam. Pediatr Dent J
27(2):79-84.
Nibali L, Tonetti MS, Ready D, Parkar M, Brett PM, Donos N et al. (2008). Interleukin-6
polymorphisms are associated with pathogenic bacteria in subjects with periodontitis. J
Periodontol 79(4):677-683.
Nicolau B, Marcenes W, Allison P, Sheiham A (2005). The life course approach: explaining
the association between height and dental caries in Brazilian adolescents. Community Dent
Oral Epidemiol 33(2):93-98.
Niji R, Arita K, Abe Y, Lucas ME, Nishino M, Mitome M (2010). Maternal age at birth and
other risk factors in early childhood caries. Pediatr Dent 32(7):493-498.
Nourijelyani K, Yekaninejad MS, Eshraghian MR, Mohammad K, Foroushani AR, Pakpour A
(2014). The influence of mothers’ lifestyle and health behavior on their children: an exploration
for oral health. Iran Red Crescent Med J 16(2): DOI: 10.5812/ircmj.16051 (5 February 2014).
Ogata H, Goto S, Sato K, Fujibuchi W, Bono H, Kanehisa M (1999). KEGG: Kyoto
encyclopedia of genes and genomes. Nucleic Acids Res 27(1):29-34.
Okano M, Bell DW, Haber DA, Li E (1999). DNA methyltransferases Dnmt3a and Dnmt3b
are essential for de novo methylation and mammalian development. Cell 99(3):247-257.
Oliveira LB, Sheiham A, Bönecker M (2008). Exploring the association of dental caries with
social factors and nutritional status in Brazilian preschool children. Eur J Oral Sci 116(1):37-
43.
Oliveria SA, Ellison RC, Moore LL, Gillman MW, Garrahie EJ, Singer MR (1992). Parent-
child relationships in nutrient intake: the Framingham Children's Study. Am J Clin Nutr
56(3):593-598.
Olszowski T, Adler G, Janiszewska-Olszowska J, Safranow K, Kaczmarczyk M (2012).
MBL2, MASP2, AMELX, and ENAM gene polymorphisms and dental caries in Polish
children. Oral Dis 18(4):389-395.
Önder Ö, Sidoli S, Carroll M, Garcia BA (2015). Progress in epigenetic histone modification
analysis by mass spectrometry for clinical investigations. Expert Rev Proteomics 12(5):499-
517.
Opal S, Garg S, Jain J, Walia I (2015). Genetic factors affecting dental caries risk. Aust Dent J
60(1):2-11.

178
Östberg AL, Skeie MS, Skaare AB, Espelid I (2016). Caries increment in young children in
Skaraborg, Sweden: associations with parental sociodemography, health habits, and attitudes.
Int J Paediatr Dent 27(1):47-55.
Özen B, Van Strijp A, Özer L, Olmus H, Genc A, Cehreli SB (2016). Evaluation of possible
associated factors for early childhood caries and severe early childhood caries: a multicenter
cross-sectional survey. J Clin Pediatr Dent 40(2):118-123.
Ozturk A, Famili P, Vieira A (2010). The antimicrobial peptide DEFB1 is associated with
caries. J Dent Res 89(6):631-636.
Pak D, Li C, Todem D, Sohn W (2017). A multistate model for correlated interval‐ censored
life history data in caries research. J R Stat Soc Ser C Appl Stat 66(2):413-423.
Palmer C, Kent Jr R, Loo C, Hughes C, Stutius E, Pradhan N et al. (2010). Diet and caries-
associated bacteria in severe early childhood caries. J Dent Res 89(11):1224-1229.
Parisotto TM, Santos MN, Rodrigues LK, Costa LS (2012). Behavior and progression of early
carious lesions in early childhood: a 1-year follow-up study. J Dent Child (Chic) 79(3):130-
135.
Patir A, Seymen F, Yildirim M, Deeley K, Cooper ME, Marazita ML et al. (2008). Enamel
formation genes are associated with high caries experience in Turkish children. Caries Res
42(5):394-400.
Patterson K, Molloy L, Qu W, Clark S (2011). DNA methylation: bisulphite modification and
analysis. J Vis Exp (56): DOI: 10.3791/3170 (21 October 2011).
Pecharki GD, Brancher JA, Olandoski M, Doetzer AD, Moyses SJ, Trevilatto PC (2016).
Multilevel modeling for dental caries among adolescents in a Brazilian large city. Dent 3000
4(1):43-54.
Peres MA, Latorre MdRDd, Sheiham A, Peres KG, Barros FC, Hernandez PG et al. (2005).
Social and biological early life influences on severity of dental caries in children aged 6 years.
Community Dent Oral Epidemiol 33(1):53-63.
Peres RCR, Camargo G, Mofatto LS, Cortellazzi KL, Santos MCLG, Nobre-dos-Santos M et
al. (2010). Association of polymorphisms in the carbonic anhydrase 6 gene with salivary buffer
capacity, dental plaque pH, and caries index in children aged 7-9 years. Pharmacogenomics J
10(2):114-119.
Perez P, Jang SI, Alevizos I (2014). Emerging landscape of non‐ coding RNAs in oral health
and disease. Oral Dis 20(3):226-235.
Petersen PE (2003). The World Oral Health Report 2003: continuous improvement of oral
health in the 21st century–the approach of the WHO Global Oral Health Programme.
Community Dent Oral Epidemiol 31(s1):3-24.
Petersen PE (2005). Sociobehavioural risk factors in dental caries–international perspectives.
Community Dent Oral Epidemiol 33(4):274-279.

179
Petersen PE, Bourgeois D, Ogawa H, Estupinan-Day S, Ndiaye C (2005). The global burden
of oral diseases and risks to oral health. Bull World Health Organ 83(9):661-669.
Petersen PE (2008). World Health Organization global policy for improvement of oral health‐World Health Assembly 2007. Int Dent J 58(3):115-121.
Petersson GH, Åkerman S, Isberg P-E, Ericson D (2016). Comparison of risk assessment based
on clinical judgement and Cariogram in addition to patient perceived treatment need. BMC
Oral Health 17:13. DOI 10.1186/s12903-016-0238-4 (7 July 2016).
Petronis A, Gottesman II, Kan P, Kennedy JL, Basile VS, Paterson AD et al. (2003).
Monozygotic twins exhibit numerous epigenetic differences: clues to twin discordance?
Schizophr Bull 29(1):169-178.
Pidamale R, Sowmya B, Thomas A, Jose T (2012). Genetic sensitivity to bitter taste of 6-n
Propylthiouracil: A useful diagnostic aid to detect early childhood caries in pre-school children.
Indian J Hum Genet 18(1):101-105.
Pihlstrom BL, Michalowicz BS, Johnson NW (2005). Periodontal diseases. The Lancet
366(9499):1809-1820.
Piva F, Pereira JT, Luz PB, Hashizume LN, Hugo FN, Araujo FBd (2017). A Longitudinal
Study of Early Childhood Caries and Associated Factors in Brazilian Children. Braz Dent J
28(2):241-248.
Plaka K, Ravindra K, Mor S, Gauba K (2017). Risk factors and prevalence of dental fluorosis
and dental caries in school children of North India. Environ Monit Assess 189:40. DOI
10.1007/s10661-016-5684-6 (26 December 2016).
Plonka K, Pukallus M, Holcombe T, Barnett A, Walsh L, Seow W (2013a). Randomized
controlled trial: a randomized controlled clinical trial comparing a remineralizing paste with
an antibacterial gel to prevent early childhood caries. Peadiatr Dent 35(1):e8-e12.
Plonka KA, Pukallus ML, Barnett A, Holcombe TF, Walsh LJ, Seow W (2013b). A controlled,
longitudinal study of home visits compared to telephone contacts to prevent early childhood
caries. Int J Paediatr Dent 23(1):23-31.
Polk DE, Wang X, Feingold E, Shaffer JR, Weeks DE, Weyant RJ et al. (2012). Effects of
smoking and genotype on the PSR index of periodontal disease in adults aged 18–49. Int J
Environ Res Public Health 9(8):2839-2850.
Poutanen R, Lahti S, Seppä L, Tolvanen M, Hausen H (2007). Oral health-related knowledge,
attitudes, behavior, and family characteristics among Finnish schoolchildren with and without
active initial caries lesions. Acta Odontol Scand 65(2):87-96.
Preethi B, Reshma D, Anand P (2010). Evaluation of flow rate, pH, buffering capacity,
calcium, total proteins and total antioxidant capacity levels of saliva in caries free and caries
active children: an in vivo study. Indian J Clin Biochem 25(4):425-428.

180
Proença MAM, Franco MM, Rodrigues VP, Costa JF, Costa EL (2015). Association between
early childhood caries and maternal caries status: A cross-section study in São Luís, Maranhão,
Brazil. Eur J Dent 9(1):122-126.
Ramamurthy P, Swamy H, Bennete F, Rohini M, Nagarathnamma T (2014a). Relationship
between severe-early childhood caries, salivary mutans streptococci, and lactobacilli in
preschool children of low socio-economic status in Bengaluru city. J Indian Soc Pedod Prev
Dent 32(1):44-47.
Rauth RJ, Potter KS, Ngan AY-W, Saad DM, Mehr R, Luong VQ et al. (2009). Dental enamel:
genes define biomechanics. J Calif Dent Assoc 37(12):863-868.
Razin A, Shemer R (1995). DNA methylation in early development. Hum Molec Genet
4(1):1751-1755.
Reed SG, Voronca D, Wingate JS, Murali M, Lawson AB, Hulsey TC et al. (2017). Prenatal
vitamin D and enamel hypoplasia in human primary maxillary central incisors: A pilot study.
Pediatr Dent J 27(1):21-28.
Reynolds JC, Damiano PC, Glanville JL, Oleson J, McQuistan MR (2015). Neighborhood and
family social capital and parent‐ reported oral health of children in Iowa. Community Dent
Oral Epidemiol 43(6):569-577.
Riggs E, Slack-Smith L, Yelland J, Chadwick B, Robertson L, Kilpatrick N (2016).
Interventions with pregnant women andnew mother s for preventing caries in children.
Cochrane Database Syst Rev (4): CD012155. DOI:10.1002/14651858.CD012155 (21 April
2016).
Riley B, Schultz R, Cooper M, Goldstein‐ McHenry T, Daack‐ Hirsch S, Lee K et al. (2007).
A genome‐ wide linkage scan for cleft lip and cleft palate identifies a novel locus on 8p11‐23. Am J Med Genet A 143(8):846-852.
Ronaghi M (2001). Pyrosequencing sheds light on DNA sequencing. Genome Res 11(1):3-11.
Roseboom TJ, van der Meulen JH, van Montfrans GA, Ravelli AC, Osmond C, Barker DJ et
al. (2001). Maternal nutrition during gestation and blood pressure in later life. J Hypertens
19(1):29-34.
Rossow I (1992). Intrafamily influences on health behavior. J Clin Periodontol 19(10):774-
778.
Russell JI, MacFarlane TW, Aitchison TC, Stephen KW, Burchell CK (1991). Prediction of
caries increment in Scottish adolescents. Community Dent Oral Epidemiol 19(2):74-77.
Saied-Moallemi Z, Virtanen J, Ghofranipour F, Murtomaa H (2008). Influence of mothers’ oral
health knowledge and attitudes on their children’s dental health. Eur Arch Paediatr Dent
9(2):79-83.
Samaranayake L (2012). Essential microbiology for dentistry Edinburgh; Fourth ed. New
York: Churchill Livingstone Elsevier Health Sciences.

181
Sanders AE, Slade GD, Lim S, Reisine ST (2009). Impact of oral disease on quality of life in
the US and Australian populations. Community Dent Oral Epidemiol 37(2):171-181.
Sandoval J, Asteller M (2012). Cancer epigenomics: beyond genomics. Curr Opin Genet Dev
22(1):50-55.
Santos M, De Souza A, Gerlach R, Trevilatto P, Scarel‐ Caminaga R, Line S (2004). Inhibition
of human pulpal gelatinases (MMP‐ 2 and MMP‐ 9) by Zn oxide cements. J Oral Rehabil
31(7):660-664.
Sasaki T, Takagi M, Yanagisawat T (2008). Structure and function of secretory. In: Dental
enamel 785:32-50.
Schernhammer ES, Giovannucci E, Kawasaki T, Rosner B, Fuchs CS, Ogino S (2010). Dietary
folate, alcohol and B vitamins in relation to LINE-1 hypomethylation in colon cancer. Gut
59(6):794-799.
Schmidt RJ, Hansen RL, Hartiala J, Allayee H, Schmidt LC, Tancredi DJ et al. (2011). Prenatal
vitamins, one-carbon metabolism gene variants, and risk for autism. Epidemiology 22(4):476.
Scholl TO (2005). Iron status during pregnancy: setting the stage for mother and infant. Am J
Clin Nutr 81(5):1218S-1222S.
Schroth RJ, Lavelle C, Tate R, Bruce S, Billings RJ, Moffatt ME (2014). Prenatal vitamin D
and dental caries in infants. Pediatrics 133(5):e1277-e1284.
Schübeler D (2015). Function and information content of DNA methylation. Nature
517(7534):321-326.
Schultz J, Milpetz F, Bork P, Ponting CP (1998). SMART, a simple modular architecture
research tool: identification of signaling domains. Proc Natl Acad Sci 95(11):5857-5864.
Schultz ST, Shenkin J, Horowitz A (2001). Parental perceptions of unmet dental need and cost
barriers to care for developmentally disabled children. Pediatr Dent 23(4):321-325.
Schwendicke F, Dörfer C, Schlattmann P, Page LF, Thomson W, Paris S (2015). Socio-
economic inequality and caries a systematic review and meta-analysis. J Dent Res 94(1):10-
18.
Seddon JM, Reynolds R, Shah HR, Rosner B (2011). Smoking, dietary betaine, methionine,
and vitamin D in monozygotic twins with discordant macular degeneration: epigenetic
implications. Ophthalmology 118(7):1386-1394.
Sedgwick P (2014). Retrospective cohort studies: advantages and disadvantages. BMJ (Online)
348: DOI: 10.1136/bmj.g1072 (24 January 2014)
Selwitz RH, Ismail AI, Pitts NB (2007). Dental caries. The Lancet 369(9555):51-59.

182
Seo JY, Park YJ, Yi YA, Hwang JY, Lee IB, Cho BH et al. (2015). Epigenetics: general
characteristics and implications for oral health. Restor Dent Endod 40(1):14-22.
Seow W, Clifford H, Battistutta D, Morawska A, Holcombe T (2009). Case-control study of
early childhood caries in Australia. Caries Res 43(1):25-35.
Shaffer J, Wang X, Feingold E, Lee M, Begum F, Weeks D et al. (2011). Genome-wide
association scan for childhood caries implicates novel genes. J Dent Res 90(12):1457-1462.
Shaffer JR, Feingold E, Wang X, Lee M, Tcuenco K, Weeks D et al. (2013). GWAS of dental
caries patterns in the permanent dentition. J Dent Res 92(1):38-44.
Shaffer JR, Feingold E, Wang X, Tcuenco KT, Weeks DE, DeSensi RS et al. (2012a). Heritable
patterns of tooth decay in the permanent dentition: principal components and factor analyses.
BMC Oral Health 12:7. DOI:10.1186/1472-6831-12-7 (9 March 2012).
Shaffer JR, Wang X, Desensi RS, Wendell S, Weyant RJ, Cuenco KT et al. (2012b). Genetic
susceptibility to dental caries on pit and fissure and smooth surfaces. Caries Res 46(1):38-46.
Shaffer JR, Wang X, McNeil DW, Weyant RJ, Crout R, Marazita ML (2015). Genetic
susceptibility to dental caries differs between the sexes: a family-based study. Caries Res
49(2):133-140.
Shearer D, Thomson W, Broadbent J, Poulton R (2011). Maternal oral health predicts their
children’s caries experience in adulthood. J Dent Res 90(5):672-677.
Sheiham A, Watt RG (2000). The common risk factor approach: a rational basis for promoting
oral health. Community Dent Oral Epidemiol 28(6):399-406.
Shimizu T, Ho B, Deeley K, Briseno-Ruiz J, Faraco IM, Jr., Schupack BI et al. (2012). Enamel
formation genes influence enamel microhardness before and after cariogenic challenge. PLoS
One 7(9): DOI:10.1371/journal.pone.0045022 (24 September 2012).
Silva AER, Menezes AMB, Demarco FF, Vargas-Ferreira F, Peres MA (2013). Obesity and
dental caries: systematic review. Rev Saude Publica 47(4):799-812.
Simark‐ Mattsson C, Emilson CG, Håkansson EG, Jacobsson C, Roos K, Holm S (2007).
Lactobacillus‐ mediated interference of mutans streptococci in caries‐ free vs. caries‐ active
subjects. Eur J Oral Sci 115(4):308-314.
Slade G, Sanders A, Do L, Roberts-Thomson K, Spencer A (2013). Effects of fluoridated
drinking water on dental caries in Australian adults. J Dent Res 92(4): 376-382.
Slade G D, Spencer A J (1988). Population estimates, standard errors and hypothesis tests from
the 1987–88 National Oral Health Survey of Australia. AIHW Dental Statistics and Research
Series No. 14. Adelaide: The University of Adelaide.
Slayton RL, Cooper ME, Marazita ML (2005). Tuftelin, mutans streptococci, and dental caries
susceptibility. J Dent Res 84(8):711-714.

183
Smith R, Badner VM, Morse DE, Freeman K (2002). Maternal risk indicators for childhood
caries in an inner city population. Community Dent Oral Epidemiol 30(3):176-181.
Splieth CH, Christiansen J, Foster Page L (2016). Caries Epidemiology and Community
Dentistry: Chances for Future Improvements in Caries Risk Groups. Outcomes of the ORCA
Saturday Afternoon Symposium, Greifswald, 2014. Part 1. Caries Res 50(1):9-16.
Su LJ, Mahabir S, Ellison GL, McGuinn LA, Reid BC (2011). Epigenetic contributions to the
relationship between cancer and dietary intake of nutrients, bioactive food components, and
environmental toxicants. Front Genet 2:91. DOI: 10.3389/fgene.2011.00091 (9 January 2011).
Sun YV (2014). The influences of genetic and environmental factors on methylome-wide
association studies for human diseases. Curr Genet Med Rep 2(4):261-270.
Szatko F, Wierzbicka M, Dybizbanska E, Struzycka I, Iwanicka-Frankowska E (2004). Oral
health of Polish three-year-olds and mothers' oral health-related knowledge. Community Dent
Health 21(2):175-180.
Tabachnick BG, Fidell LS (2007). Using multivariate statistics (5th ed.) Boston: USA: Allyn
& Bacon, Inc.
Tahmassebi J, Duggal M, Malik-Kotru G, Curzon M (2006). Soft drinks and dental health: a
review of the current literature. J Dent 34(1):2-11.
Takahashi R, Ota E, Hoshi K, Naito T, Toyoshima Y, Yuasa H et al. (2015). Fluoride
supplementation in pregnant women for preventing dental caries in the primary teeth of their
children. Cochrane Libr : DOI: 10.1002/14651858.CD011850 (28 August 2015).
Takatsuka T, Hirano J, Matsumoto H, Honma T (2005). X‐ Ray absorption fine structure
analysis of the local environment of Zn in dentine treated with Zn compounds. Eur J Oral Sci
113(2):180-183.
Tanaka K, Miyake Y, Sasaki S, Hirota Y (2013). Socio-economic status and risk of dental
caries in Japanese preschool children: the Osaka Maternal and child health study. J Public
Health Dent 73(3):217-223.
Tanaka K, Hitsumoto S, Miyake Y, Okubo H, Sasaki S, Miyatake N et al. (2015). Higher
vitamin D intake during pregnancy is associated with reduced risk of dental caries in young
Japanese children. Ann Epidemiol 25(8):620-625.
Tang R-S, Huang M-C, Huang S-T (2013). Relationship between dental caries status and
anemia in children with severe early childhood caries. Kaohsiung J Med Sci 29(6):330-336.
Tang WW, Dietmann S, Irie N, Leitch HG, Floros VI, Bradshaw CR et al. (2015). A unique
gene regulatory network resets the human germline epigenome for development. Cell
161(6):1453-1467.
Tannure PN, Kuchler EC, Falagan-Lotsch P, Amorim LMF, Raggio Luiz R, Costa MC et al.
(2012a). MMP13 polymorphism decreases risk for dental caries. Caries Res 46(4):401-407.
184
Tannure PN, Küchler EC, Lips A, Costa MdC, Luiz RR, Granjeiro JM et al. (2012b). Genetic
variation in MMP20 contributes to higher caries experience. J Dent 40(5):381-386.
Tanzer JM, Livingston J, Thompson AM (2001). The microbiology of primary dental caries in
humans. J Dent Educ 65(10):1028-1037.
Team RDC (2013) R: A language and environment for statistical computing. Vienna, Austria:
R Foundation for Statistical Computing. Available: http://www.R-project.org/ ISBN 3-
900051-07-0, Available: http://www.R-project.org/ .
Thitasomakul S, Piwat S, Thearmontree A, Chankanka O, Pithpornchaiyakul W, Madyusoh S
(2009). Risks for early childhood caries analyzed by negative binomial models. J Dent Res
88(2):137-141.
Thwin KM, Zaitsu T, Ueno M, Kawaguchi Y (2016). Early Childhood Caries and Related Risk
Factors among Myanmar Preschool Children. Int J Clin Prev Dent 12(4):229-236.
Tiwari T, Rai N, Colmenero E, Gonzalez H, Castro M (2017). A Community-Based
Participatory Research Approach to Understand Urban Latino Parent’s Oral Health Knowledge
and Beliefs. Int J Dent 2017: DOI:10.1155/2017/9418305 (29 March 2017).
Toledano M, Yamauti M, Osorio E, Osorio R (2012). Zn-inhibited MMP-mediated collagen
degradation after different dentine demineralization procedures. Caries Res 46(3):201-207.
Traebert J, Jinbo Y, de Lacerda JT (2011). Association between maternal schooling and caries
prevalence: a cross-sectional study in southern Brazil. Oral Health Prev Dent 9(1):47-52
Tsai P-C, Bell JT (2015). Power and sample size estimation for epigenome-wide association
scans to detect differential DNA methylation. Int J Epidemiol 44(4):1429-1441.
Tulunoglu Ö, Demirtas S, Tulunoglu I (2006). Total antioxidant levels of saliva in children
related to caries, age, and gender. Int J Paediatr Dent 16(3):186-191.
Turton B, Durward C, Manton D, Bach K, Yos C (2016). Socio-behavioural risk factors for
early childhood caries (ECC) in Cambodian preschool children: a pilot study. Eur Arch
Paediatr Dent 17(2):97-105.
Turton BJ, Durward CS, Manton DJ (2015). Early childhood caries and maternal caries
experience in a convenience sample of Cambodian pre-schoolers. Pediatr Dent J 25(1):14-18.
Valarini N, Maciel S, Moura S, Poli-Frederico R (2012). Association of dental caries with HLA
class II allele in Brazilian adolescents. Caries Res 46(6):530-535.
Van De Mheen H, Stronks K, Van Den Bos J, Mackenbach JP (1997). The contribution of
childhood environment to the explanation of socio-economic inequalities in health in adult life:
a retrospective study. Soc Sci Med 44(1):13-24.
van der Tas JT, Kragt L, Veerkamp JJ, Jaddoe VW, Moll HA, Ongkosuwito EM et al. (2016).
Ethnic disparities in dental caries among six-year-old children in the Netherlands. Caries Res
50(5):489-497.

185
Van Houte J (1993). Microbiological predictors of caries risk. Adv Dent Res 7(2):87-96.
VanVoorhis CRW, Morgan BL (2007). Understanding power and rules of thumb for
determining sample sizes. Tutor Quant Methods Psychol 3(2):43-50.
Vargas CM, Crall JJ, Schneider DA (1998). Sociodemographic distribution of pediatric dental
caries: NHANES III, 1988-1994. J Am Dent Assoc 129(9):1229-1238.
Varma S, Banerjee A, Bartlett D (2008). An in vivo investigation of associations between saliva
properties, caries prevalence and potential lesion activity in an adult UK population. J Dent
36(4):294-299.
Vieira A, Marazita M, Goldstein-McHenry T (2008). Genome-wide scan finds suggestive
caries loci. J Dent Res 87(5):435-439.
Vieira AR, Modesto A, Marazita ML (2014). Caries: review of human genetics research.
Caries Res 48(5):491-506.
Wade WG (2013). The oral microbiome in health and disease. Pharmacol Res 69(1):137-143.
Wallengren ML, Johnson U, Ericson D (1997). HLA-DR4 and number of mutans streptococci
in saliva among dental students and staff. Acta Odontol 55(5):296-298.
Wang Q, Jia P, Cuenco KT, Feingold E, Marazita ML, Wang L et al. (2013a). Multi-
Dimensional Prioritization of Dental Caries Candidate Genes and Its Enriched Dense Network
Modules. PLoS One 8(10): DOI:10.1371/journal.pone.0076666e76666 (11 October 2013).
Wang Q, Jia P, Cuenco KT, Zeng Z, Feingold E, Marazita ML et al. (2013b). Association
signals unveiled by a comprehensive gene set enrichment analysis of dental caries genome-
wide association studies. PLoS One 8(8): DOI:10.1371/journal.pone.007265372653 (14
August 2014).
Wang X, Shaffer J, Weyant R, Cuenco K, DeSensi R, Crout R et al. (2010). Genes and their
effects on dental caries may differ between primary and permanent dentitions. Caries Res
44(3):277-284.
Wang X, Shaffer JR, Zeng Z, Begum F, Vieira AR, Noel J et al. (2012a). Genome-wide
association scan of dental caries in the permanent dentition. BMC Oral Health 12:57.
DOI:10.1186/1472-6831-12-57 (21 December 2012).
Wang X, Willing MC, Marazita ML, Wendell S, Warren JJ, Broffitt B et al. (2012b). Genetic
and environmental factors associated with dental caries in children: the Iowa Fluoride Study.
Caries Res 46(3):177-184.
Warren JJ, Weber‐ Gasparoni K, Marshall TA, Drake DR, Dehkordi‐ Vakil F, Dawson DV et
al. (2009). A longitudinal study of dental caries risk among very young low SES children.
Community Dent Oral Epidemiol 37(2):116-122.
186
Warren JJ, Blanchette D, Dawson DV, Marshall TA, Phipps KR, Starr D et al. (2016). Factors
associated with dental caries in a group of American Indian children at age 36 months.
Community Dent Oral Epidemiol 44(2):154-161.
Warren JJ, Van Buren JM, Levy SM, Marshall TA, Cavanaugh JE, Curtis AM et al. (2017).
Dental caries clusters among adolescents. Community Dent Oral Epidemiol: DOI:
10.1111/cdoe.12317 (3 July 2017).
Watt RG, Sheiham A (2012). Integrating the common risk factor approach into a social
determinants framework. Community Dent Oral Epidemiol 40(4):289-296.
Weintraub J, Prakash P, Shain S, Laccabue M, Gansky S (2010). Mothers’ caries increases
odds of children’s caries. J Dent Res 89(9):954-958.
Wendell S, Wang X, Brown M, Cooper ME, DeSensi RS, Weyant RJ et al. (2010). Taste genes
associated with dental caries. J Dent Res 89(11):1198-1202.
Wendt L-K, Hallonsten A-L, Koch G, Birkhed D (1996). Analysis of caries-related factors in
infants and toddlers living in Sweden. Acta Odontol 54(2):131-137.
Wendt L, Svedin C, Hallonsten A, Larsson I (1995). Mental health, family interaction, and life
events in infants and toddlers with caries. Swed Dent J 19(1-2):17-27.
Whetzel PL, Noy NF, Shah NH, Alexander PR, Nyulas C, Tudorache T et al. (2011). BioPortal:
enhanced functionality via new Web services from the National Center for Biomedical
Ontology to access and use ontologies in software applications. Nucleic Acids Res 39(2):W541-
W545.
Widita E, Pamardiningsih Y, Vega CA (2017). Caries Risk Profiles amongst Preschool Aged
Children Living in the Sleman District of Yogyakarta, Indonesia. J Dent Indon 24(1):1-6.
Wigen TI, Wang NJ (2011). Maternal health and lifestyle, and caries experience in preschool
children. A longitudinal study from pregnancy to age 5 years. Eur J Oral Sci 119(6):463-468.
Wigen TI, Wang NJ (2014). Health behaviors and family characteristics in early childhood
influence caries development. A longitudinal study based on data from MoBa. Nor Epidemiol
24(1-2):91-95.
Williams DM (2011). Global oral health inequalities: The research agenda. J Dent Res
90(5):549-551.
Williams S, Hughes T, Adler C, Brook A, Townsend G (2014). Epigenetics: a new frontier in
dentistry. Aust Dent J 59(1):23-33.
Wilson AG (2008). Epigenetic regulation of gene expression in the inflammatory response and
relevance to common diseases. J Periodontol 79(8):1514-1519.
Winter G (1976). Maternal nutritional requirements in relation to the subsequent development
of teeth in children. J Hum Nutr 30(2):93-99.
187
Wong N, Tran C, Pukallus M, Holcombe T, Seow W (2012). A three‐ year retrospective study
of emergency visits at an oral health clinic in south‐ east Queensland. Aust Dent J 57(2):132-
137.
Wu H, Lippmann J, Oza J, Zeng M, Fives‐ Taylor P, Reich N (2006). Inactivation of DNA
adenine methyltransferase alters virulence factors in Actinobacillus actinomycetemcomitans.
Oral Microbiol Immunol 21(4):238-244.
Yang AS, Estécio MR, Doshi K, Kondo Y, Tajara EH, Issa JPJ (2004). A simple method for
estimating global DNA methylation using bisulfite PCR of repetitive DNA elements. Nucleic
Acids Res 32(3): DOI: 10.1093/nar/gnh032 (21 January 2004).
Yoshioka H, Minamizaki T, Yoshiko Y (2015). The dynamics of DNA methylation and
hydroxymethylation during amelogenesis. Histochem Cell Biol 144(5):471-478.
Yun KH, Lee HS, Nam OH, Moon CY, Lee JH, Choi SC (2017). Analysis of bacterial
community profiles of endodontically infected primary teeth using pyrosequencing. Int J
Paediatr Dent 27(1):56-65.
Zaina S, Lindholm MW, Lund G (2005). Nutrition and aberrant DNA methylation patterns in
atherosclerosis: more than just hyperhomocysteinemia? J Nutr 135(1):5-8.
Zakhary G, Clark R, Bidichandani S, Owen W, Slayton R, Levine M (2007). Acidic proline-
rich protein Db and caries in young children. J Dent Res 86(12):1176-1180.
Zander A, Sivaneswaran S, Skinner J, Byun R, Jalaludin B (2013). Risk factors for dental caries
in small rural and regional Australian communities. Rural Remote Health 13(3):2492.
Zaykin DV (2011). Optimally weighted Z‐ test is a powerful method for combining
probabilities in meta‐ analysis. J Evol Biol 24(8):1836-1841.
Zeng Z, Shaffer JR, Wang X, Feingold E, Weeks DE, Lee M et al. (2013). Genome-wide
association studies of pit-and-fissure- and smooth-surface caries in permanent dentition. J Dent
Res 92(5):432-437.
Zeng Z, Feingold E, Wang X, Weeks DE, Lee M, Cuenco KT et al. (2014). Genome-wide
association study of primary dentition pit-and-fissure and smooth surface caries. Caries Res
48(4):330-338.
Zhang D, Li Q, Rao L, Yi B, Xu Q (2015). Effect of 5-Aza-2′-deoxycytidine on Odontogenic
Differentiation of Human Dental Pulp Cells. J Endod 41(5):640-645.
Zhang S, Barros S, Niculescu M, Moretti A, Preisser J, Offenbacher S (2010). Alteration of
PTGS2 promoter methylation in chronic periodontitis. J Dent Res 89(2):133-137.
Zhang Y, Todem D, Kim K, Lesaffre E (2011). Bayesian latent variable models for spatially
correlated tooth-level binary data in caries research. Stat Modelling 11(1):25-47.

188
Appendix A : Oral Health Questionnaire
STUD Study ID
0
MATERNAL, ENVIRONMENTAL AND EARLY CHILDHOOD INFLUENCES ON DENTAL CARIES
IN CHILDREN
Questionnaire assessing the oral health Knowledge, Attitude and Practices
of mothers giving birth to infants within the EFHL study
Please answer all of the following questions on a scale of 1 to 5 (1=Strongly Agree; 2=Agree;
3=Neutral/Not Sure; 4=Disagree; 5=Strongly Disagree), and place a circle around the
corresponding number.
Strongly
Agree Agree
Neutral /
Not Sure Disagree
Strongly
Disagree
I feel that it is important to acquire
information on oral health care for my child. 1 2 3 4 5
I understand what the term ‘dental decay’
means. 1 2 3 4 5
I believe my oral health could affect my
child’s oral health. 1 2 3 4 5
I believe that baby teeth are important. 1 2 3 4 5
I believe that problems with baby teeth will
affect adult teeth. 1 2 3 4 5
I believe that rotten baby teeth could affect a
child’s health. 1 2 3 4 5
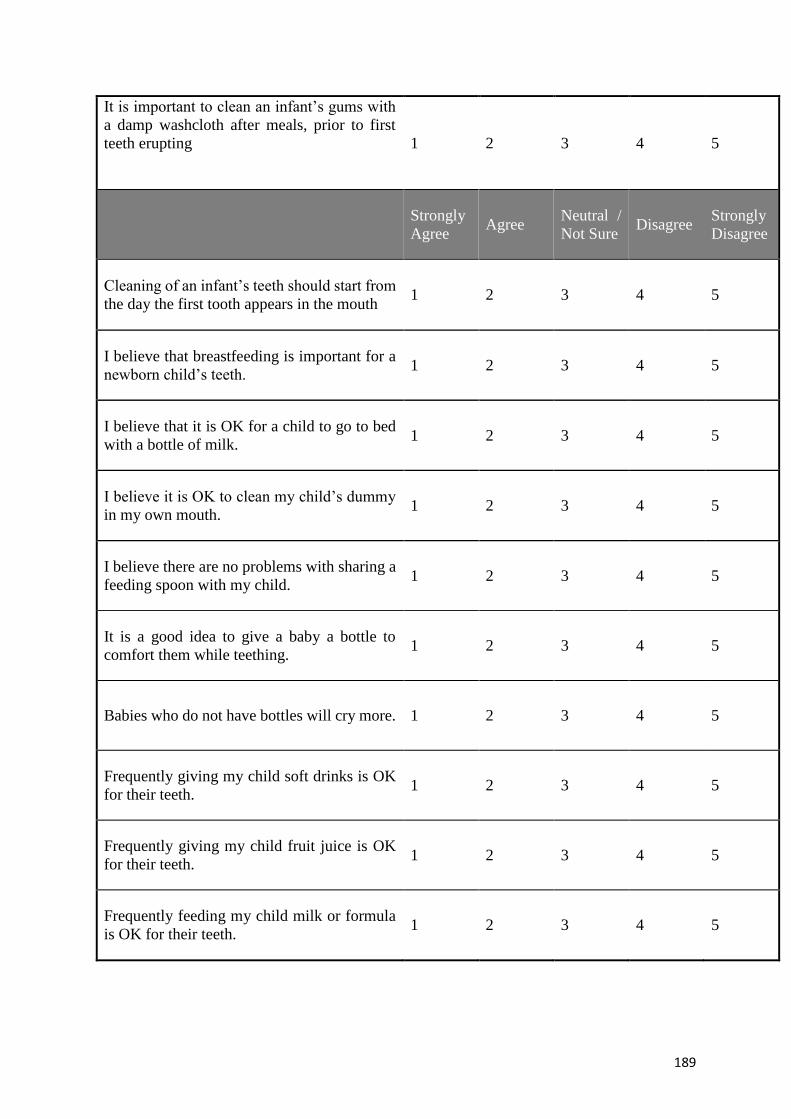
189
It is important to clean an infant’s gums with
a damp washcloth after meals, prior to first
teeth erupting
1 2 3 4 5
Strongly
Agree Agree
Neutral /
Not Sure Disagree
Strongly
Disagree
Cleaning of an infant’s teeth should start from
the day the first tooth appears in the mouth 1 2 3 4 5
I believe that breastfeeding is important for a
newborn child’s teeth. 1 2 3 4 5
I believe that it is OK for a child to go to bed
with a bottle of milk. 1 2 3 4 5
I believe it is OK to clean my child’s dummy
in my own mouth. 1 2 3 4 5
I believe there are no problems with sharing a
feeding spoon with my child. 1 2 3 4 5
It is a good idea to give a baby a bottle to
comfort them while teething. 1 2 3 4 5
Babies who do not have bottles will cry more. 1 2 3 4 5
Frequently giving my child soft drinks is OK
for their teeth. 1 2 3 4 5
Frequently giving my child fruit juice is OK
for their teeth. 1 2 3 4 5
Frequently feeding my child milk or formula
is OK for their teeth. 1 2 3 4 5

190
Using fluoride toothpaste helps to prevent
tooth decay.
1 2 3 4 5
Strongly
Agree Agree
Neutral /
Not Sure Disagree
Strongly
Disagree
I believe it is safe for infants to use fluoride
toothpaste. 1 2 3 4 5
I believe that regular visits to the Dentist will
prevent problems with my baby’s teeth. 1 2 3 4 5
Children should see a Dentist or Dental
Therapist by the time they are 1 year old. 1 2 3 4 5
I believe that maintaining both my and my
infant’s oral health costs too much. 1 2 3 4 5
I believe that keeping baby teeth until they are
due to fall out is not that important. 1 2 3 4 5
I am afraid of going to the Dentist because of
possible pain. 1 2 3 4 5
I believe that good oral health is important to
my overall health and well-being. 1 2 3 4 5
26. Did you visit the Dentist during your pregnancy? (Please tick one response only)
Yes
No
27. Which of the following did you give your new born child?
I practiced exclusive breast feeding up to 6 months for my new born
child
I only bottle-fed my new born child
I both breastfed and bottle-fed my new born child beyond 12 months
of age
28. Prior to my infant’s first teeth erupting, I cleaned my infant’s gums with a damp wash
cloth before bed.

191
Yes
No
29. How often have you taken your child to a Dentist since he/she was born?
Never
Once
Twice
Three times
More than 3 times
30. How old was your child when you started brushing his/her teeth with tooth paste?
Six months
Nine months
One year
After one year
After two years
31. Do you use fluoridated toothpaste for your child?
Always
Sometimes
Never
Don’t know
32. At what age did you leave your child with the responsibility of brushing his/her own
teeth?
33. Does your child brush his teeth on his/her own?
Yes
No
Two years
Three years
Four years
Five years
I still brush my child’s teeth
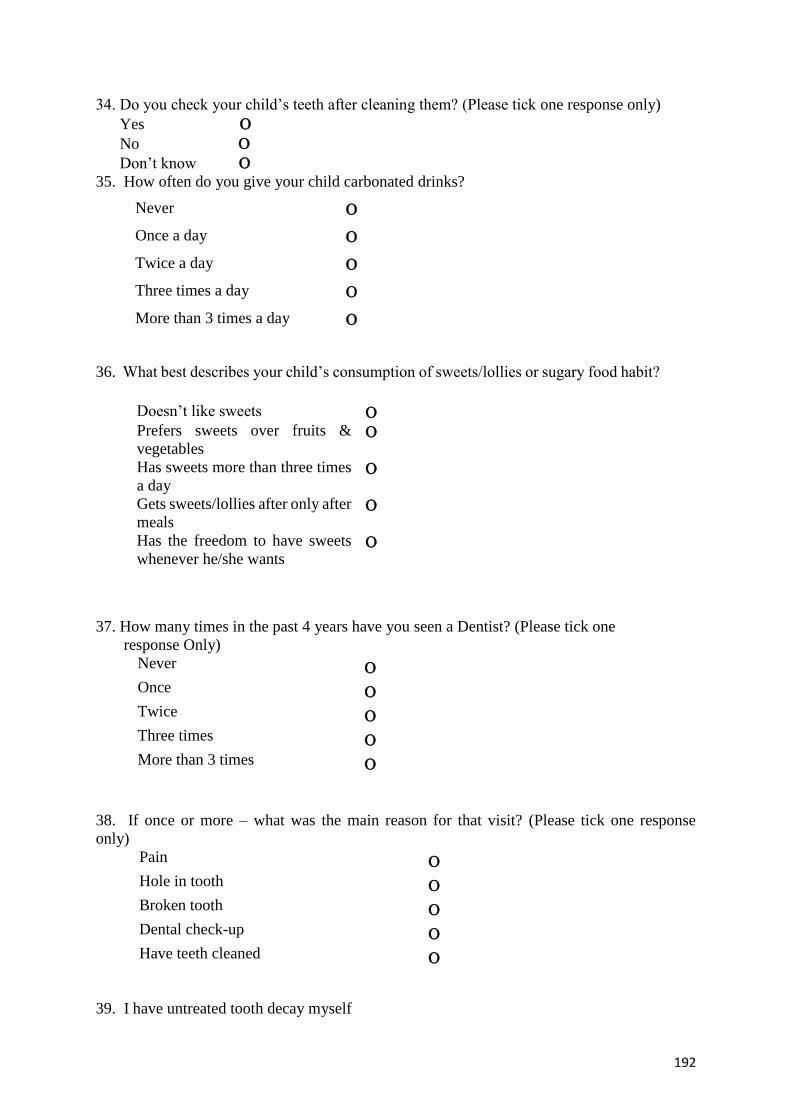
192
34. Do you check your child’s teeth after cleaning them? (Please tick one response only)
Yes
No
Don’t know
35. How often do you give your child carbonated drinks?
Never
Once a day
Twice a day
Three times a day
More than 3 times a day
36. What best describes your child’s consumption of sweets/lollies or sugary food habit?
37. How many times in the past 4 years have you seen a Dentist? (Please tick one
response Only)
Never
Once
Twice
Three times
More than 3 times
38. If once or more – what was the main reason for that visit? (Please tick one response
only)
Pain
Hole in tooth
Broken tooth
Dental check-up
Have teeth cleaned
39. I have untreated tooth decay myself
Doesn’t like sweets
Prefers sweets over fruits &
vegetables
Has sweets more than three times
a day
Gets sweets/lollies after only after
meals
Has the freedom to have sweets
whenever he/she wants

193
Yes
No
40. How often do you brush your teeth? (Please tick one response only)
Once a day
Two or more times a day
Never
Once a week
Other (specify)
41. Which of the following do you use to clean your teeth? (Please tick as many as you use)
Tooth brush
Dental floss
Tooth picks
Interdental brush
Chew sticks
Other (specify)
42. Do you use toothpaste containing fluoride? (Please tick one response only)
Yes
No
Don’t know
43. Cleaning of my infant’s teeth should start from (Please tick one response only)
The day the first tooth appears in the mouth
Once the first 4 teeth appear
Once the first 6 teeth appear
After my child becomes two years old
END

194
Appendix B: Kappa statistics for dental caries examination
Appendix B: Table 1 Calibration of examiner 1 for ICDAS criteria against a gold
standard
Mothers and children were included as participants for the calibration exercise. Table
indicates the number of surfaces examined by each examiner.
Number of observed agreements: 139 (92.67% of the observations)
Number of agreements expected by chance: 121.6 (81.04% of the observations)
Weighted Kappa= 0.810
SE of kappa=0.102
95% CI: From 0.414 to 0.813
Gold standard ICDAS 0 ICDAS 1 ICDAS 2 ICDAS 3 ICDAS 4 ICDAS 5 ICDAS 6 Total
surfaces
Ex
am
iner
1
ICDAS 0 130 0 0 0 0 0 0 130
ICDAS 1 6 2 0 0 0 0 0 8
ICDAS 2 4 0 0 0 0 0 0 4
ICDAS 3 0 0 2 0 0 0 0 2
ICDAS 4 0 0 0 0 1 0 0 1
ICDAS 5 0 0 0 0 0 3 0 3
ICDAS 6 0 0 0 0 1 0 1 2
Total
surfaces
140 2 0 2 2 3 1 150

195
Appendix B: Table 2 Calibration of examiner 2 for ICDAS criteria against a gold
standard
Mothers and children were included as participants for the calibration exercise. Table
indicates the number of surfaces examined by each examiner.
Number of observed agreements: 146 (97.33% of the observations)
Number of agreements expected by chance: 129.0 (85.97% of the observations)
Weighted Kappa= 0.928
SE of kappa = 0.093
95% confidence interval: From 0.628 to 0.992
Gold standard ICDAS 0 ICDAS 1 ICDAS 2 ICDAS 3 ICDAS 4 ICDAS 5 ICDAS 6 Total
surfaces
Ex
am
iner
2
ICDAS 0 137 1 0 0 0 0 0 138
ICDAS 1 2 1 0 0 0 0 0 3
ICDAS 2 1 0 1 0 0 0 0 2
ICDAS 3 0 0 0 2 0 0 0 2
ICDAS 4 0 0 0 0 1 0 0 1
ICDAS 5 0 0 0 0 0 3 0 3
ICDAS 6 0 0 0 0 0 0 1 1
Total
surfaces
140 2 1 2 1 3 1 150

196
Appendix C
Appendix C Table 1: Search strategy used in PubMed
# 1 dental caries [MeSH Terms]
# 2 dental [All Fields] AND caries [All Fields]
#3 dental caries [All Fields]
#4 Susceptibility [All Fields]
# 5 (#1 or #2 or #3 or #4)
# 6 Genetic [MeSH Term]
# 7 Genetic [All fields]
# 8 #7 AND #3
# 9 #5 AND #8
#10 epigenetics [MeSH Terms]
# 11 epigenetics [All Fields]
#12 #3 AND #11
#13 candidate genes [All Fields]
# 14 genome wide [All Fields]
#15 (#3 AND #7 or 11or #13 or #14)
#16 linkage [All Fields]
#17 association [All Fields]
#18 (#13 or #14 or #16 or #17 AND #4 AND #3)
Search limited to Journal Article[ptyp] AND ("1912/01/01"[PDAT] : "2015/12/31"[PDAT])
AND "humans"[MeSH Terms] AND English[lang] AND dental caries [Mesh Terms])

197
Appendix C Table 2: Search strategy used in Scopus
Data base selection
#1 Health
#2 Dentistry
#3 Oral Health
Subject area in Scopus
#4 Health Sciences
Key word search with additional search fields
# 5 dental caries [All Fields]
# 6 dental AND caries [All Fields]
#7 dental caries [All Fields]
#8 Susceptibility [All Fields]
#9 Genetic [All Fields]
# 10 (#5 or #6 or #7 or #8 and#9)
# 11 #5 AND #9
# 12 #10 AND #11
# 13 epigenetics [All Fields]
#14 #5 AND #13
#15 candidate genes [All Fields]
# 16 genome wide [All Fields]
#17 (#5 AND #9 or 13 or #15 or #16)
#18 association [All Fields]
#19(#15 or #16 or #17 or #18 AND #5 AND #8)
Search limited to Journal Article AND ("1912/01/01"[PDAT] : "2015/12/31"[PDAT]) AND
AND English[lang]

198
Appendix C Table 3: Search strategy used in Google Scholar
Key word search with additional search fields
# 1 dental caries
# 2 dental AND caries
#3 Susceptibility
#4 Genetic
# 5 (#1 or #2 or #3 or #1 and#4)
# 6 #1 AND #4
# 7 #5 AND #6
# 8 epigenetics
#9 #1 AND #8
#10 candidate genes
# 11 genome wide
#12 (#1 AND #4 or 8 or #10 or #11)
#13 association
#14 (#10 or #11 or #12 or #13 AND #1 AND #3)
Search limited to Journal Article AND ("1912/01/01"[PDAT] : "2015/12/31"[PDAT]) AND
AND English[lang] AND humans in all subject areas.

199
Appendix D: Supplementary tables for differentially methylated
CpG sites on chromosome 12 between cases and controls
Appendix D Table 1: Comparison of mean Differentially Methylated Regions on
chromosome 12 between controls and cases amongst children.
*DMR Location Controls Cases
Mean SD Mean SD P value
chr12_740087 27.787 26.31351 44.2081 29.1216
chr12_2690385 17.8054 31.74555 46.0709 23.2653
chr12_3333760 3.5088 8.5947 41.1555 22.28168 0.05
chr12_4303130 42.6501 17.17231 23.8803 28.69158
chr12_6929513 80.107 23.86684 59.122 36.98673
chr12_11700085 59.6729 15.06503 35.8385 22.20227
chr12_11700254 76.0531 4.57678 42.3561 36.46868
chr12_11700256 78.3614 2.93485 42.7813 36.24977
chr12_11700258 76.2923 4.99635 41.417 37.31218
chr12_11700277 79.5354 4.61533 45.0658 38.06553
chr12_11700292 80.6821 3.56008 44.5347 37.99269
chr12_11700303 83.743 6.17952 44.8866 38.21628 0.05
chr12_11700343 67.8906 9.03084 43.9098 37.80618
chr12_14974998 75.7742 28.12442 47.7288 19.24457
chr12_18845488 78.5426 13.75798 58.4449 38.35139
chr12_20960555 92.4863 5.89851 51.9749 14.75764 0.001
chr12_22408980 51.3718 8.81698 31.0428 7.8338 0.01
chr12_26351890 20.0206 15.5864 46.651 32.75298
chr12_27622729 68.6844 22.28025 32.7252 23.32907 0.05
inchr12_30309985 75.5484 14.37837 61.5824 19.80425
chr12_31821824 63.3135 30.45111 80.7474 29.0153
chr12_33139261 72.0545 17.1057 49.504 39.61165
chr12_55805945 88.2937 8.54696 64.8014 16.62681 0.05
chr12_64503585 83.0138 7.16783 67.0699 23.15768
chr12_90418121 50.303 30.44237 64.4311 23.76368
chr12_117363165 16.7824 26.26586 33.547 36.76977
chr12_117482887 20.2448 15.75705 37.2619 24.33456
chr12_117482900 21.532 16.36244 32.4161 20.41894
chr12_119594418 64.6671 16.36121 82.2457 12.68901
chr12_121198298 46.5608 20.15452 30.3233 37.48128
chr12_124421877 84.2063 13.21861 64.2233 15.49226 0.05
chr12_125448960 63.3316 35.20476 55.4548 35.54152
chr12_130498324 28.4407 5.41868 48.238 8.59233 0.001
chr12_130604735 69.6955 12.57381 82.0722 12.55787
chr12_131118432 7.6121 9.45917 35.0168 22.99084 0.05
chr12_131606752 20.8859 23.74313 34.5049 39.39545
chr12_132333255 62.1149 20.15986 75.2436 8.07253
chr12_132639381 67.8602 7.46409 85.6348 8.94127 0.01
chr12_133324690 96.3769 4.40792 74.1954 12.43519 0.01
*DMR - Differentially Methylated Regions, Considered level of significance p≤0.05
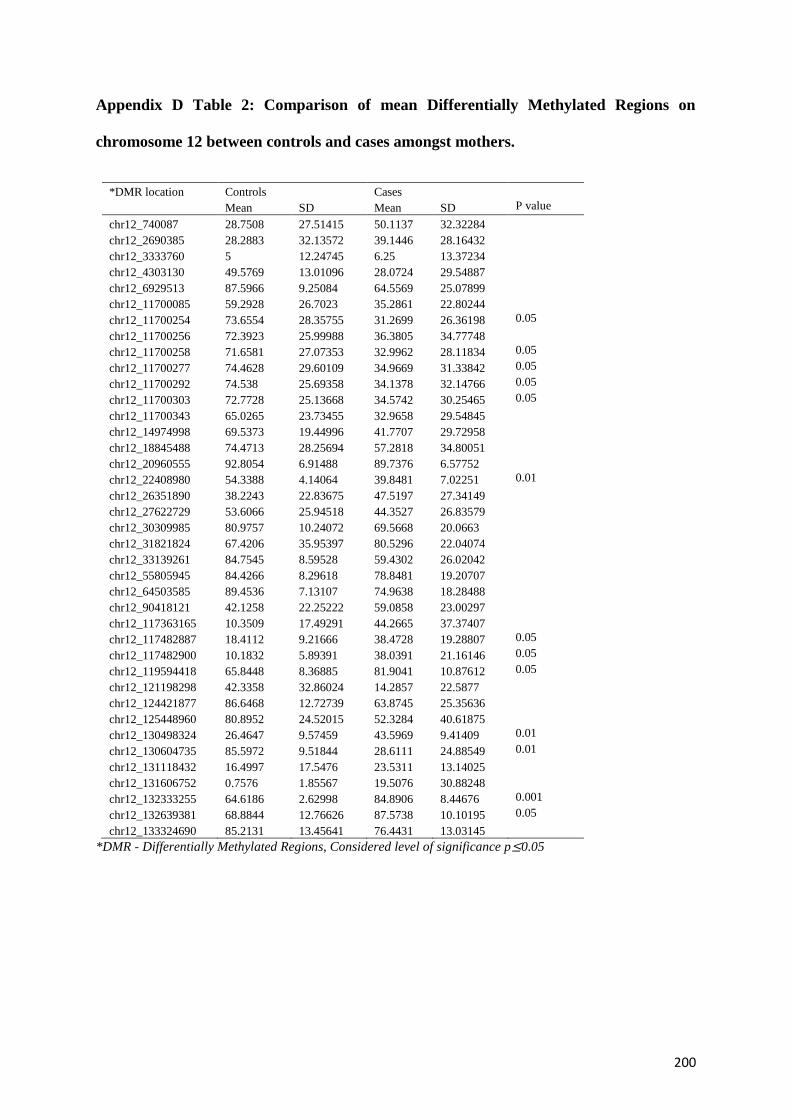
200
Appendix D Table 2: Comparison of mean Differentially Methylated Regions on
chromosome 12 between controls and cases amongst mothers.
*DMR location Controls Cases
Mean SD Mean SD P value
chr12_740087 28.7508 27.51415 50.1137 32.32284
chr12_2690385 28.2883 32.13572 39.1446 28.16432
chr12_3333760 5 12.24745 6.25 13.37234
chr12_4303130 49.5769 13.01096 28.0724 29.54887
chr12_6929513 87.5966 9.25084 64.5569 25.07899
chr12_11700085 59.2928 26.7023 35.2861 22.80244
chr12_11700254 73.6554 28.35755 31.2699 26.36198 0.05
chr12_11700256 72.3923 25.99988 36.3805 34.77748
chr12_11700258 71.6581 27.07353 32.9962 28.11834 0.05
chr12_11700277 74.4628 29.60109 34.9669 31.33842 0.05
chr12_11700292 74.538 25.69358 34.1378 32.14766 0.05
chr12_11700303 72.7728 25.13668 34.5742 30.25465 0.05
chr12_11700343 65.0265 23.73455 32.9658 29.54845
chr12_14974998 69.5373 19.44996 41.7707 29.72958
chr12_18845488 74.4713 28.25694 57.2818 34.80051
chr12_20960555 92.8054 6.91488 89.7376 6.57752
chr12_22408980 54.3388 4.14064 39.8481 7.02251 0.01
chr12_26351890 38.2243 22.83675 47.5197 27.34149
chr12_27622729 53.6066 25.94518 44.3527 26.83579
chr12_30309985 80.9757 10.24072 69.5668 20.0663
chr12_31821824 67.4206 35.95397 80.5296 22.04074
chr12_33139261 84.7545 8.59528 59.4302 26.02042
chr12_55805945 84.4266 8.29618 78.8481 19.20707
chr12_64503585 89.4536 7.13107 74.9638 18.28488
chr12_90418121 42.1258 22.25222 59.0858 23.00297
chr12_117363165 10.3509 17.49291 44.2665 37.37407
chr12_117482887 18.4112 9.21666 38.4728 19.28807 0.05
chr12_117482900 10.1832 5.89391 38.0391 21.16146 0.05
chr12_119594418 65.8448 8.36885 81.9041 10.87612 0.05
chr12_121198298 42.3358 32.86024 14.2857 22.5877
chr12_124421877 86.6468 12.72739 63.8745 25.35636
chr12_125448960 80.8952 24.52015 52.3284 40.61875
chr12_130498324 26.4647 9.57459 43.5969 9.41409 0.01
chr12_130604735 85.5972 9.51844 28.6111 24.88549 0.01
chr12_131118432 16.4997 17.5476 23.5311 13.14025
chr12_131606752 0.7576 1.85567 19.5076 30.88248
chr12_132333255 64.6186 2.62998 84.8906 8.44676 0.001
chr12_132639381 68.8844 12.76626 87.5738 10.10195 0.05
chr12_133324690 85.2131 13.45641 76.4431 13.03145
*DMR - Differentially Methylated Regions, Considered level of significance p≤0.05

201
Appendix E: Results of further pyrosequencing done on an
extended sample of individuals discordant for dental caries
Appendix E 1. Rationale
Based on the results of differentially methylates CpG sites between cases and controls in the
12 mother child dyads, further 26 DNA samples from mother child dyads (52 individual
samples) with high and low dental caries experience, were analysed for epigenetic variations.
It was decided to investigate Chromosome 12 was further, since it gave the highest differential
methylation between individuals with high and low dental caries experience. Eight CpGs
between sites 11700085 and 11700343 showed 41% methylation difference between cases and
controls where on average, cases had significantly lower methylation differences than cases (p
< 2.17E-103) (Table 7.3). Therefore, this particular CpG site on Chr12 was selected for further
pyrosequencing to support and validate the initial discovery results.
High-throughput pyrosequencing technique is a widely applicable, alternative technology for
the detailed characterization of nucleic acids. Pyrosequencing is a DNA sequencing technique
that is based on the detection of released pyrophosphate (PPi) during DNA synthesis
(http://www.biology-pages.info/P/Pyrosequencing.html). Pyrosequencing has the potential
advantages of accuracy, flexibility, parallel processing, and can be easily automated (Yun et
al., 2017). Furthermore, the technique dispenses with the need for labelled primers, labelled
nucleotides, and gel-electrophoresis (Ronaghi, 2001). Pyrosequencing is currently the fastest
method for sequencing a PCR product. Due to the fact that, pyrosequencing generates an
accurate quantification of the mutated nucleotides, the resequencing of PCR-amplified disease
genes for mutation scanning is one of the more interesting applications of the technique

202
(Ronaghi, 2001). Using this technique for resequencing results in longer read length than de
novo sequencing because nucleotide delivery can be specified according to the order of the
sequence (Garcia et al., 2000).
Appendix E 2. Results
Our initial pyrosequencing test runs on the targeted CpG sites indicated that the sites were
located in a highly repetitive region of the chromosome with much non-specific amplifications.
Hence there was a difficulty in designing precise primers with adequate specificity for reliable
results. Therefore, three different CpGs that had good amplification were selected from the
proposed region (Chr 12 between genomic positions 11700080 and 11700350) although they
were not included in our discovery results. It was expected that the three CpG sites might carry
the same association signal by way of being directly adjacent in the DNA sequence for this a
frequent observation for strings of CpGs in a DNA region. The first CpG site
(Chr12:11700151) was very accurate and could be validated with specific primers. The second
CpG site (Chr12:11700148) was polymorphic and not present in all sample types, so the data
for this site were variable. The third CpG site (Chr12:11700124) was downstream of a very
variable region, and the results at this site depended on the particular samples and the sequence
variation was observed in the region (Appendix D Table 1).
However, according to the data there appears to be very little variation among all the samples
tested (Appendix D Table 1). This implies that there was no association signal in the cohort,
which is contrary to our initial results and indicates that our expectation of association-by-
proxy was not realised (Appendix D Table 2).
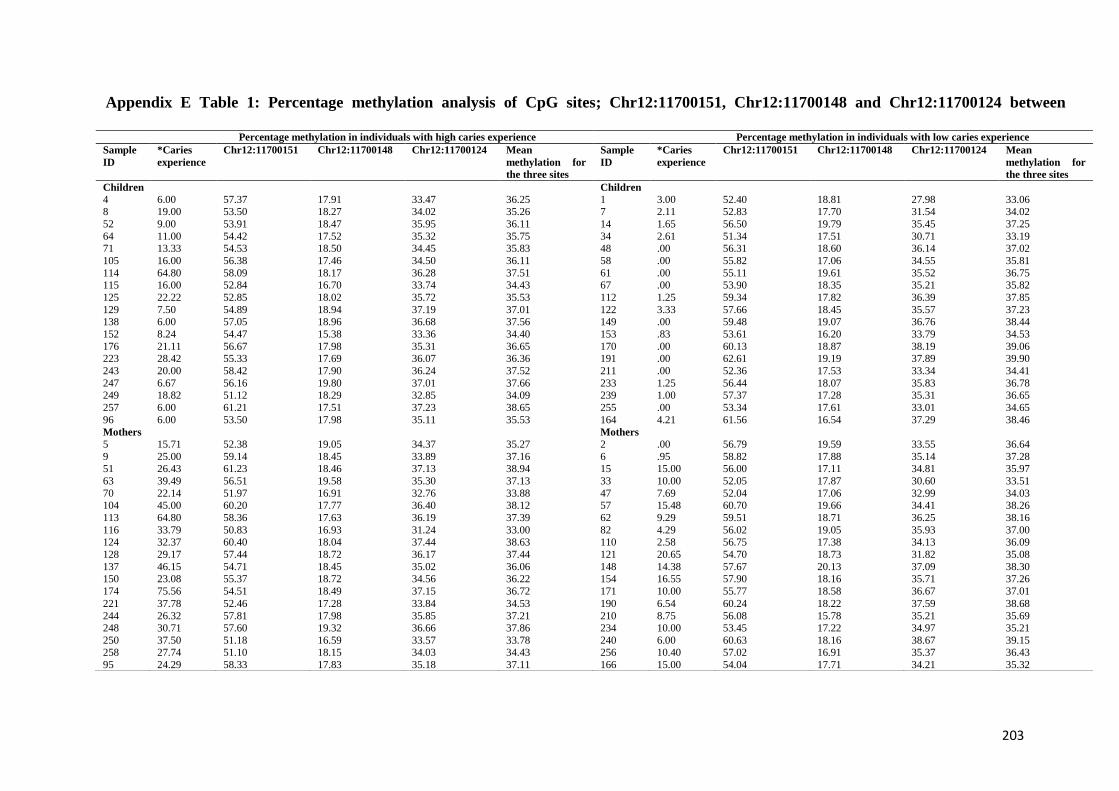
203
Percentage methylation in individuals with high caries experience Percentage methylation in individuals with low caries experience
Sample
ID
*Caries
experience
Chr12:11700151 Chr12:11700148 Chr12:11700124 Mean
methylation for
the three sites
Sample
ID
*Caries
experience
Chr12:11700151 Chr12:11700148 Chr12:11700124 Mean
methylation for
the three sites
Children Children
4 6.00 57.37 17.91 33.47 36.25 1 3.00 52.40 18.81 27.98 33.06 8 19.00 53.50 18.27 34.02 35.26 7 2.11 52.83 17.70 31.54 34.02
52 9.00 53.91 18.47 35.95 36.11 14 1.65 56.50 19.79 35.45 37.25
64 11.00 54.42 17.52 35.32 35.75 34 2.61 51.34 17.51 30.71 33.19 71 13.33 54.53 18.50 34.45 35.83 48 .00 56.31 18.60 36.14 37.02
105 16.00 56.38 17.46 34.50 36.11 58 .00 55.82 17.06 34.55 35.81
114 64.80 58.09 18.17 36.28 37.51 61 .00 55.11 19.61 35.52 36.75 115 16.00 52.84 16.70 33.74 34.43 67 .00 53.90 18.35 35.21 35.82
125 22.22 52.85 18.02 35.72 35.53 112 1.25 59.34 17.82 36.39 37.85
129 7.50 54.89 18.94 37.19 37.01 122 3.33 57.66 18.45 35.57 37.23 138 6.00 57.05 18.96 36.68 37.56 149 .00 59.48 19.07 36.76 38.44
152 8.24 54.47 15.38 33.36 34.40 153 .83 53.61 16.20 33.79 34.53
176 21.11 56.67 17.98 35.31 36.65 170 .00 60.13 18.87 38.19 39.06 223 28.42 55.33 17.69 36.07 36.36 191 .00 62.61 19.19 37.89 39.90
243 20.00 58.42 17.90 36.24 37.52 211 .00 52.36 17.53 33.34 34.41
247 6.67 56.16 19.80 37.01 37.66 233 1.25 56.44 18.07 35.83 36.78 249 18.82 51.12 18.29 32.85 34.09 239 1.00 57.37 17.28 35.31 36.65
257 6.00 61.21 17.51 37.23 38.65 255 .00 53.34 17.61 33.01 34.65
96 6.00 53.50 17.98 35.11 35.53 164 4.21 61.56 16.54 37.29 38.46
Mothers Mothers
5 15.71 52.38 19.05 34.37 35.27 2 .00 56.79 19.59 33.55 36.64
9 25.00 59.14 18.45 33.89 37.16 6 .95 58.82 17.88 35.14 37.28 51 26.43 61.23 18.46 37.13 38.94 15 15.00 56.00 17.11 34.81 35.97
63 39.49 56.51 19.58 35.30 37.13 33 10.00 52.05 17.87 30.60 33.51
70 22.14 51.97 16.91 32.76 33.88 47 7.69 52.04 17.06 32.99 34.03 104 45.00 60.20 17.77 36.40 38.12 57 15.48 60.70 19.66 34.41 38.26
113 64.80 58.36 17.63 36.19 37.39 62 9.29 59.51 18.71 36.25 38.16
116 33.79 50.83 16.93 31.24 33.00 82 4.29 56.02 19.05 35.93 37.00 124 32.37 60.40 18.04 37.44 38.63 110 2.58 56.75 17.38 34.13 36.09
128 29.17 57.44 18.72 36.17 37.44 121 20.65 54.70 18.73 31.82 35.08
137 46.15 54.71 18.45 35.02 36.06 148 14.38 57.67 20.13 37.09 38.30 150 23.08 55.37 18.72 34.56 36.22 154 16.55 57.90 18.16 35.71 37.26
174 75.56 54.51 18.49 37.15 36.72 171 10.00 55.77 18.58 36.67 37.01
221 37.78 52.46 17.28 33.84 34.53 190 6.54 60.24 18.22 37.59 38.68
244 26.32 57.81 17.98 35.85 37.21 210 8.75 56.08 15.78 35.21 35.69 248 30.71 57.60 19.32 36.66 37.86 234 10.00 53.45 17.22 34.97 35.21
250 37.50 51.18 16.59 33.57 33.78 240 6.00 60.63 18.16 38.67 39.15 258 27.74 51.10 18.15 34.03 34.43 256 10.40 57.02 16.91 35.37 36.43
95 24.29 58.33 17.83 35.18 37.11 166 15.00 54.04 17.71 34.21 35.32
Appendix E Table 1: Percentage methylation analysis of CpG sites; Chr12:11700151, Chr12:11700148 and Chr12:11700124 between
individuals with high and low caries experience
*Caries experience was measured as a percentage of tooth surfaces affected with dental caries (including early enamel caries)
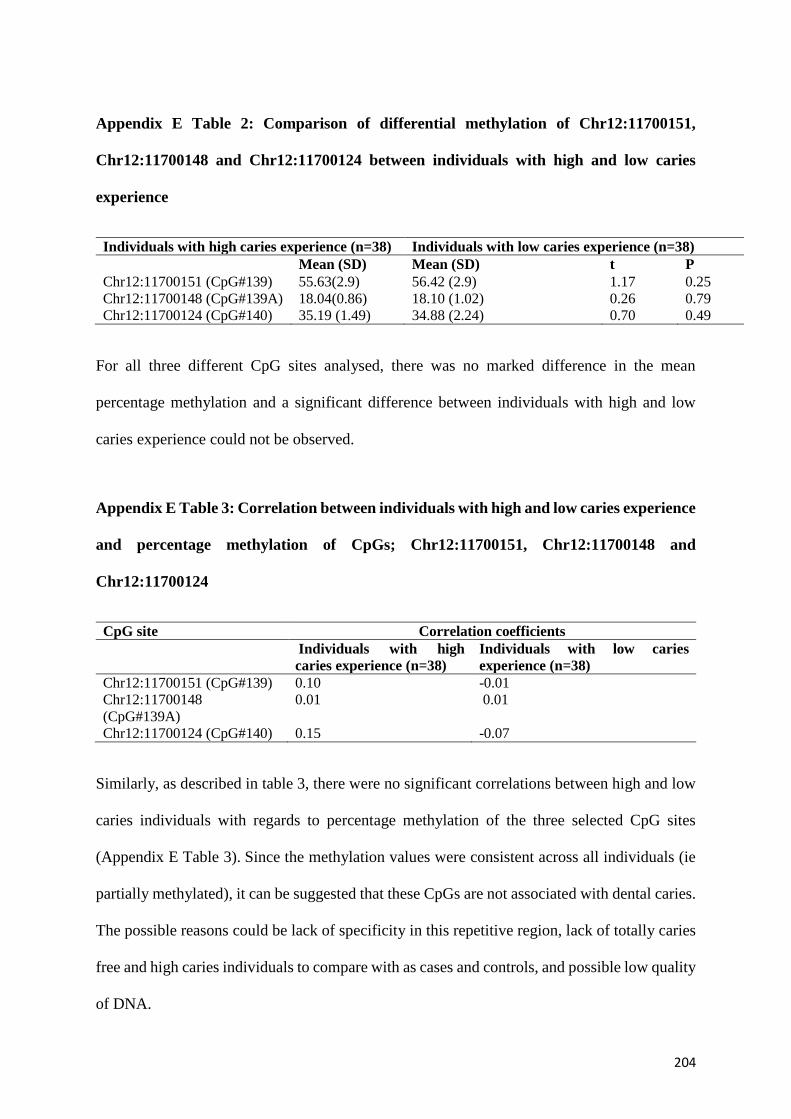
204
Appendix E Table 2: Comparison of differential methylation of Chr12:11700151,
Chr12:11700148 and Chr12:11700124 between individuals with high and low caries
experience
Individuals with high caries experience (n=38) Individuals with low caries experience (n=38)
Mean (SD) Mean (SD) t P
Chr12:11700151 (CpG#139) 55.63(2.9) 56.42 (2.9) 1.17 0.25
Chr12:11700148 (CpG#139A) 18.04(0.86) 18.10 (1.02) 0.26 0.79
Chr12:11700124 (CpG#140) 35.19 (1.49) 34.88 (2.24) 0.70 0.49
For all three different CpG sites analysed, there was no marked difference in the mean
percentage methylation and a significant difference between individuals with high and low
caries experience could not be observed.
Appendix E Table 3: Correlation between individuals with high and low caries experience
and percentage methylation of CpGs; Chr12:11700151, Chr12:11700148 and
Chr12:11700124
CpG site Correlation coefficients
Individuals with high
caries experience (n=38)
Individuals with low caries
experience (n=38)
Chr12:11700151 (CpG#139) 0.10 -0.01
Chr12:11700148
(CpG#139A)
0.01 0.01
Chr12:11700124 (CpG#140) 0.15 -0.07
Similarly, as described in table 3, there were no significant correlations between high and low
caries individuals with regards to percentage methylation of the three selected CpG sites
(Appendix E Table 3). Since the methylation values were consistent across all individuals (ie
partially methylated), it can be suggested that these CpGs are not associated with dental caries.
The possible reasons could be lack of specificity in this repetitive region, lack of totally caries
free and high caries individuals to compare with as cases and controls, and possible low quality
of DNA.

205
Appendix E 3. Future directions
As the initial discovery assay failed due to lack of specificity and high repetitiveness, further
repetitive assays for instance, LINE1, ALU, SAT2, or HERV could be performed, for these are
global assays that cover repetitive regions throughout the genome. Moreover, pyrosequencing
could be performed on the second best target of the discovery analysis, by selecting target
regions which do not belong to a repetitive region.