asperilluspneumonie bei abwehrschwäche Œ die qual der … · caspofungin case-documentation:...
TRANSCRIPT

Asperilluspneumonie bei Abwehrschwäche � die Qual der Wahl
Azole, Echinocandine oder Ampho B
Gudrun Just - Nübling
Zentrum der Inneren Medizin - InfektiologieJohann Wolfgang Goethe-Universität Frankfurt am Main

0
2
4
6
8
10
12
14
1990 1991 1992 1993 1994 1995 1996 1997 1998
Inzidenz invasiver Aspergillosen nach Knochenmarkstransplantation
Marr CID 2002
allogen
autolog
%

Invasive Mykosen durch �seltene Erreger�
0
2
4
6
8
10
12
14
16
1985-1989 1990-1994 1995-1999
Scedosporium
Zygomyzeten
Fusarium
Marr CID 2002
n

Definition invasiver Mykosen
! Sichere invasive Infektion:histopathologischer Nachweis bzw. pos. mikroskopischer Nachweis in sterilen Materialien in Assoziation mit klin. Bild
! Wahrscheinliche invasive Infektion:Wirt + Klinik + Mikrobiologie
! Mögliche invasive Infektion:Wirt + Klinik oder Mikrobiologie
Ascioglu CID 02

V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Invasive pulmonale Aspergillose
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

A.D.H. 1.7.97 A.D.H. 1.7.97
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Mucor Frühinfiltrate
A.D.H. 1.7.97 A.D.H. 1.7.97
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Invasive pulmonale Aspergillose
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Mucor Infiltrate
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt


NocardioseZwei Jahre nach Nieren-Tx

Labor-Diagnostik von Mykosen
! Direkte Mikroskopie von Körperflüssigkeiten
! Histologie! Kultur! Serologie: Antigen-Nachweis! PCR-Methoden

Systemisch wirksame AntimykotikaPolyen Amphotericin B Deoxycholat
Neuere Präparationen� Liposomales Ampho B (Ambisome®)� ABCD (Amphocil®)� ABLC (Abelcet®)
PyrimidinMiconazol (Daktar®)Ketoconazol (Nizoral®)Fluconazol (Diflucan®)Itraconazol (Sempera®)Voriconazol (Vfend®)
Imidazole
Echinocandin Caspofungin (Cancidas®)
5-Fluorocytosin (Ancotil®)
Allylamin Terbinafin (Lamisil®)

Neue Antimykotika
Triazol-Derivate
Echinocandine
Polyen
Posaconazol (Schering)Ravuconazol (BMS)
Micafungin (Fujisava)Anidulafungin (Versicor)
LiposomalesNystatin (Avonex)

In vitro - Wirksamkeit gegenüber Sproß- bzw. Hefepilzen
C. C. albicans ++ ++ ++ ++C. C. glabrataglabrata (+)(+) (+) (+) ++ ++C. C. kruseikrusei ((--)) -- ++ ++C. C. tropicalistropicalis ++ ++ ++ ++C. C. paraspilosisparaspilosis ++ ++ ++ (+)(+)
Erreger Itraconazol Fluconazol Voriconazol Caspofungin
Cryptococcus neof. + + + -
Trichosporon asahii + + + -

In vitro - Wirksamkeit gegenüber Schimmelpilzen
Aspergillus spp. + - + +
Erreger Itraconazol Fluconazol Voriconazol Caspofungin
Zygomyceten (+) - - -
Fusarium - - + -
Scedosporium /Pseudallescheria
(+) - + -

Bisherige Standardtherapie bei
Aspergillus-Mucorpneumonie
Amphotericin B evt. plus Ancotil

Probleme der kAmB-Therapie
! Hohe Rate unerwünschter Wirkungen �vorzeitiges Absetzen oftmals notwendig
! D.W. Bates CID 2001: bei 30% akutes Nierenversagen und 54% Mortalität in dieser Gruppe
! Intensives Monitoring! Zentraler Venenkatheter
! Keine orale Gabe

Liposomales Amphotericin B
! Mehrere offene und kontrollierte Studien
! Trend zur höheren Effektivität im Vergleich zu kAmB
! Empirische Tx: LAmB vs kAmB kein signifikanter Unterschied, weniger Durchbruch-Infekt. unter LAmBWalsh NEJM 2004
! Bessere Verträglichkeit
! Höhere Dosierungen möglich Walsh AAC 2001
! Hohe Therapiekosten
! Wichtige Vergleichssubstanz für neue Antimykotika

Liposomales Amphotericin B! Leenders Brit J Hematol 1998:
Vergleich von kAmB (1mg/kg/d) mit L-AmB (5mg/kg/d) bei neutropenischen Pat. mit nachgewiesenen Mykosen
! 66 pat. Auswertbar (Schimmelp.32/26; Candida 3/7)
! Ansprechen nach Studienende:
kAmB 19/34 (56%) L-AmB 21/32 (66%)
Aspergillus-Pneumonie: 11 (42%) mit L-AmB
6 ( 21%) mit k-AmB

Invasive pulmonale Aspergillosebei immunsuppremierten Patienten
Intravenöses Itraconazol
! 31 Patienten n = 28 Hämatolog. Grunderkrankung(3 allog.BMT, 3 autolog. BMT, 19 Neutropenie)
n = 3 chron. granulomatöse Erkrankung
n = 1 AIDS
! Itra i.v. Tag 1+2 400mg, 12 Tage 200mg
! Anschluss- Tx mit Itra oral 400 mg/Tag 12 Wochen
! 37 Patienten zuvor antimykotische Therapie
Caillot et al. CID, October 2001

Intravenous ItraconazoleTreatment of invasive pulmonary aspergillosis
Clinical Outcome

Invasive AspergilloseVoriconazol
� offene, nicht vergleichende Studie
� 116 immunsupprimierte Patienten
� 41% gesicherter Infektion, 59 % mit Verdacht auf Infektion
� Dosis: i.v. 3 mg/kg/Tag 2x (loading dose 6mg/kg/Tag 2x)
� Dauer: 6-27 Tage oral 200mg/Tag 2x bis zu 24 Wochen
� offene, nicht vergleichende Studie
Ergebnis: CR + PRGesamtansprechrate 48 %Primärtherapie 59 %�Salvage�-Therapie 38 %Pulmonal und Tracheobronch. (n=84) 60 %Cerebral (n=19) 16 %Disseminiert (n=6) 50 %
D. Denning, CID 2002

Voriconazol
� Behandlung von invasiven Mykosen bei Versagen bzw. Unverträglichkeit der Primärtherapie (n=273)
� Gesamtansprechrate 50%
Aspergillose Lunge 40/86 (46,5%)alle Manifestationen 62/142 (43,7%)
Fusariose 5/11 (45,5%)
Scedosporiose 3/10 (30%)
± oral Vori 5 mg / kg / d
� Gute Verträglichkeit, Sehstörungen bei 22,8%!
JR Perfect CID 2003:36,1122-1130

Voriconazole vs. Amphotericin B
Primary TX in invasive Aspergillosis
� Randomized Ampho B 1-1.5 mg / kg daystudy VRC 6 mg / kg (2 doses) """" 4 mg / kg q 12 h
"""" followed by other licensed antifungal drugs
� Underlying diseasesallo BMT: 26 % VRC , 23 % Ampho Bauto BMT / hematological disease: 56 % VRC , 63 % Ampho Bother: 18 % VRC , 14 % Ampho B
� 392 patients were enrolled over 3 years in 92 centersin 19 countries
R.Herbrecht et al. N Engl J Med, August 2002

Herbrecht, NEJM 02


Ansprechen auf antimykotische Therapie
Herbrecht, NEJM 02

Voriconazole vs. Amphotericin BPrimary TX in invasive Aspergillosis
R.Herbrecht et al. N Engl J Med, August 2002
85.4 %Pulmonary IA
VoriconazoleN = 144
88 %
Ampho BN = 133
2.8 %Dissem. IA 0.8 %
3.5 %CNS 3.8 %
52.8 %CR / PR 31.6 %
70.8 %Survival 57.9 %
Clinical outcome week 12



OH
N
NH
HN
OHHNO
NH
OH
O
HN
NH
HO
N
HO
HO
H
HH
H
O
HO
OH
O
O
HO
OH2N
H2N
Caspofungin

Caspofungin in Adults with IA Refractoryor Intolerant to AMB ± Azoles
� Refractory: Progression of disease or failure to improvedespite therapy with at least 7 days of standard antifungaltherapy (AMB, L-AMB, any azole with activity againstAspergillus)
� Intolerant: Doubling of creatinine or creatinine ≥2.5 mg/dl; other significant intolerance to AMB or L-AMB
Maertens J et al, 40th ICAAC, abstr #1103 (2000)

Caspofungin in Adults with IA Refractory orIntolerant to AMB ± Azoles
PatientsPatientsPatientsPatients EnrolledEnrolledEnrolledEnrolled
! n = 81 enrolled, 56 evaluated by external expert panel #### TJ Walsh, DW Denning, TF Patterson
! Proven (39) or probable (17) IA! Pulmonary (40), disseminated (10) or single-organ (6) aspergillosis! Refractory (46): 70% > 14 d, 50% > 21d prior therapy! Intolerant (10): 9/10 < 14 d prior therapy
Maertens J et al, 40th ICAAC, abstr #1103 (2000)

! Response (PR/CR):! overall 41%
➜ Complete response 5.6%! in pts. with >7 days caspofungin (45) 49%! in pts. with AMB/azole refractory IA 34%! in pts. intolerant to AMB/azole 70%! in pts. with pulmonary aspergillosis 46%
� with definite pulmonary aspergillosis (22) 40.9%! in pts. with disseminated aspergillosis 20%
Maertens J et al, 40th ICAAC, abstr #1103 (2000)
Caspofungin in Adults with IA Refractory orIntolerant to AMB ± Azoles
Response (1)Response (1)Response (1)Response (1)

! Response (PR/CR):! in neutropenic pts. (11) 18.2%! in non-neutropenic pts. 46.5%! in pts. with steroids < 20 mg/d (32) 46.9%! in pts. with steroids ≥≥≥≥ 20 mg/d 31.8%! after 4 weeks follow-up (54) 29.6%
Maertens J et al, 40th ICAAC, abstr #1103 (2000)
Caspofungin in Adults with IA Refractory orIntolerant to AMB ± Azoles
Response (2)Response (2)Response (2)Response (2)

! Drug-related clinical AEs were uncommon (13.6%)! fever (3.4%)! phlebitis/thrombophlebitis (3.4%)! nausea/vomiting (3.4%)
! Drug-related laboratory AEs also occurred uncommonly (15.6%)! increased eosinophils (3.4%)
! 47% treated for > 28 days (up to 162 days) without the develop-ment of new drug-related AEs
! 17 pts have received concomitant caspofungin and tacrolimustherapy without the development of drug-related increases in hepatic transaminases
Caspofungin in Adults with IA Refractory orIntolerant to AMB ± Azoles: Safety
Maertens J et al, 40th ICAAC, abstr #1103 (2000)

Caspofungin in Adults with IA Refractory orIntolerant to AMB ± AzolesUpdate Update Update Update ICAAC 2002ICAAC 2002ICAAC 2002ICAAC 2002
! n = 90 enrolled, 83 evaluated! Definite IA 64 %, probable 36 %
Ergebnis: CR + PRPulmonary (N=64) 32 (50.0 %)Disseminated (N=13) 3 (23.0 %) Single Organ (N=6) 2 (33.0 %) Overall (N=83) 37 (44.6%) Tx > 7 days (N=66) 37 (56.1 %)

Durchbruch-Infektion unter Voriconazol
! September 2002 � Juni 2003: 124 SCT! 4 Patienten mit AML, CML (n=2), CMML! Durchbruch-Infektion mit Zygomyceten, median 125 Tage! 3 x Vori-Prophylaxe, 1 x Vori-empirische Therapie! alle Patienten GvHD! Manifestation: NNH: n = 1
Lunge: n = 3Haut: n = 1
! alle Patienten verstorbenMarty F, NEJM, Feb 26, 2004

Durchbruch-Infektion unter Voriconazol
! Bei 4 Patienten nach allogener Stammzell-Transplantation + GVHD Mucor-Infektion unter Vori-ProphylaxeSiwek CID August 04
! �Break -Through� Infektion bei 13 von 139 mit Vori behandelten Patienten n allogener Stammzell-Tx: n=6 Zygomyceten; n=4 C.glabrataImhof CID September 04

Primär für Aspergillus-InfektionenFusarium, Scedosporium, PseudallescheriaFluconazol-resistente schwere Candida-Infektionen
Zulassungs-Bedingungen
VoriconazolVfend ®
Versagen der Primär-Therapie beiAspergillus-InfektionenInvasive Candida-InfektionenEmpirische Therapie
Mk-0991Caspofungin ®

Vor- und Nachteile neuer AntimykotikaVoriconazol
� Breites Wirkungsspektrum, inklusive non-albicans, Aspergillus, Fusarium, Scedosporium, Pseudallescheria
� Oral und i.v.
Vorteile
� Keine ausreichende Aktivität gegenüber Zygomyceten� i.v.-Gabe durch Cyclodextrin limitiert #### Krea > 2mg/dl bzw. Hämodialyse
� Häufiges Auftreten von Sehstörungen bzw. Halluzinationen, potentielle Lebertoxizität
� Interaktionen mit anderen wichtigen Medikamenten
Nachteile

Vor- und Nachteile neuer AntimykotikaCaspofungin
� Breites Wirkungsspektrum, inklusive Aspergillus und non-albicans-Arten� Vergleichsweise geringe Interaktion mit anderen Medikamenten� Bislang gute Verträglichkeit in Studien� 1x tägliche Dosierung
Vorteile
� Keine ausreichende Aktivität gegenüber vielen Zygomyceten-Arten� ungenügende Wirksamkeit gegenüber Cryptococcus� Nur i.v.-Applikation� Dosisanpassung bei Leberinsuffizienz� Kaum ZNS-Penetration
Nachteile
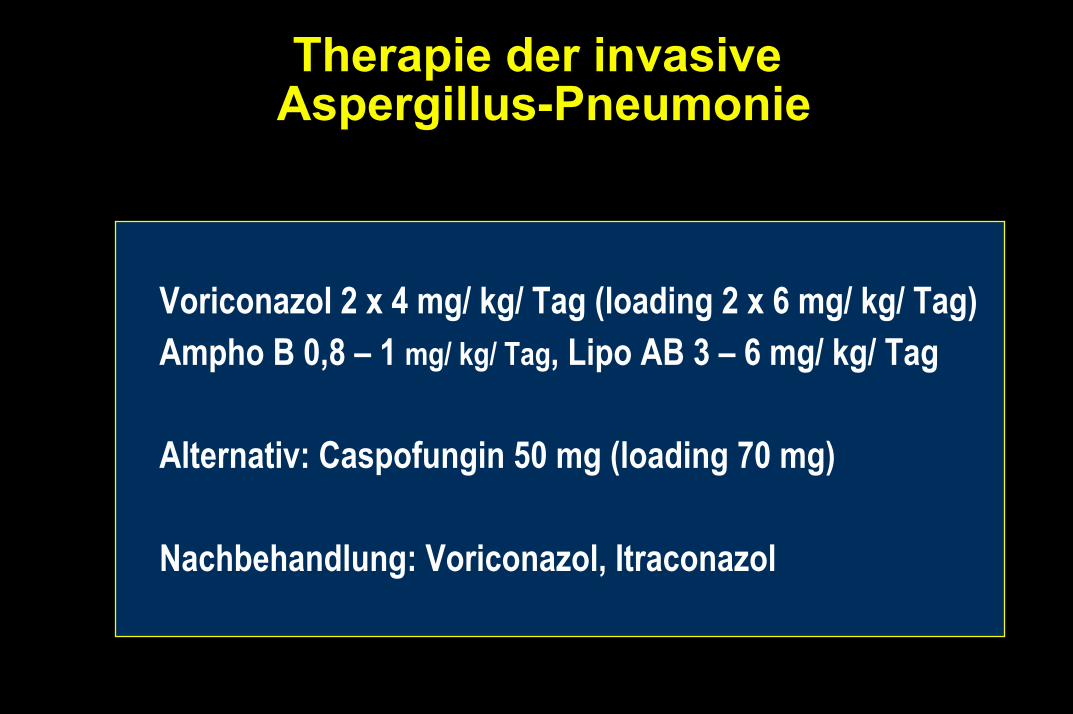
Therapie der invasiveAspergillus-Pneumonie
Voriconazol 2 x 4 mg/ kg/ Tag (loading 2 x 6 mg/ kg/ Tag)Ampho B 0,8 � 1 mg/ kg/ Tag, Lipo AB 3 � 6 mg/ kg/ Tag
Alternativ: Caspofungin 50 mg (loading 70 mg)
Nachbehandlung: Voriconazol, Itraconazol


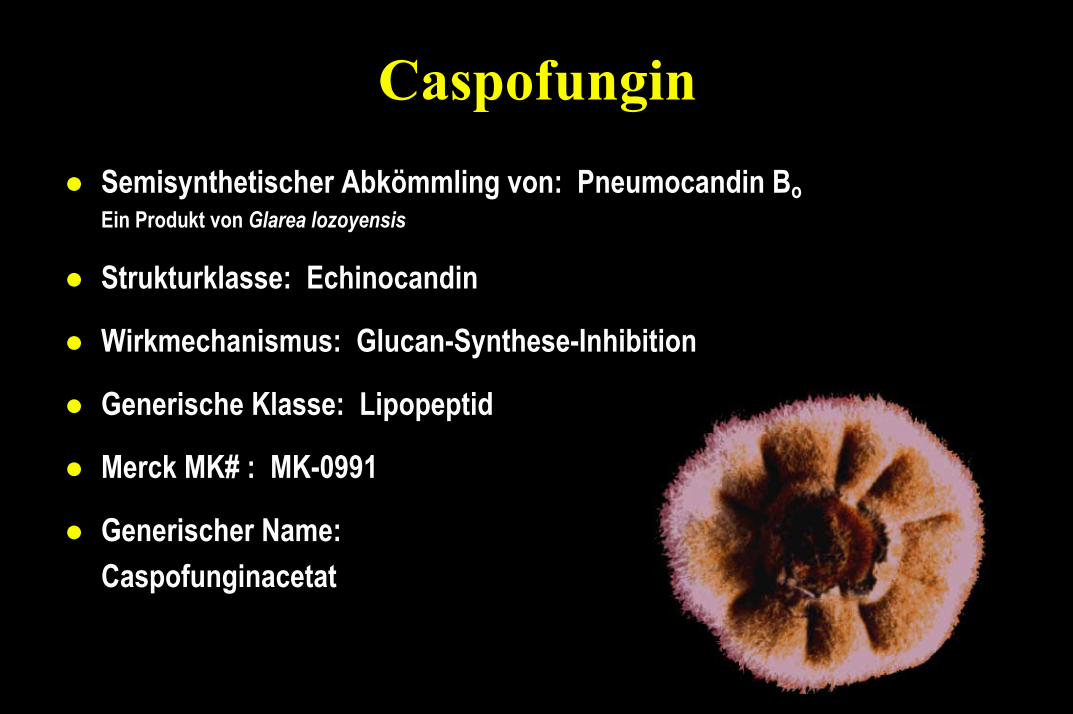
Caspofungin! Semisynthetischer Abkömmling von: Pneumocandin Bo
Ein Produkt von Glarea lozoyensis
! Strukturklasse: Echinocandin
! Wirkmechanismus: Glucan-Synthese-Inhibition
! Generische Klasse: Lipopeptid
! Merck MK# : MK-0991
! Generischer Name: Caspofunginacetat

Therapie invasive Aspergillus-Infektion
! Lunge:Voriconazol 2 x 4 mg/ kg/ Tag (loading 2 x 6 mg/ kg/ Tag)Ampho B 0,8 � 1 mg/ kg/ Tag, lipo AB 3 � 6 mg/ kg/ TagAlternativ: Caspofungin 50 mg (loading 70 mg)Nachbehandlung: Voriconazol, Itraconazol
! CNS:Lipo-AB 3 � 6 mg/ kg/ TagVoriconazol, evtl. Kombination
! NNH: => operative SanierungVoriconazol, Ampho B oder lipo-ABReserve: Caspofungin

SCH 56592! Triazol-Antimykotikum mit breitem Wirkungsspektrum! Aspergillus spec., Rhizopus sp.,Candida spec., insbes. Non-
albicans-Stämme, C. neoformans, Pseudallescheria boydii, Histoplasma, Blastomyces, Dermatophyten.
! orale ( i.v ) Applikation! in vitro Tests:
! Azole:4-8x höhere Wirksamkeit gegen Aspergillus specbis zu 8fach höhere Aktivität gegen Candida
! Ampho B: 4-16 fach höhere Aktivität gegen Aspergillus spec.gleiche Aktivität gegen Rhizopus spec.
! Tiermodell: bessere Wirksamkeit gegen C. neoformans als Fluconazol

Efficacy of caspofungin in neutropenic and non- neutropenic
patients: a case-documentation
On behalf of the group:Axel Glasmacher (Univ. Bonn, Germany)
Gudrun Just-Nübling (Univ. Frankfurt, Germany)

CaspofunginCase-Documentation: Purpose
! To evaluate the clinical use of caspofungin! in any indication in which the drug is clinically used by
decision of the treating physician! without the restrictions of inclusion/exclusion criteria! most cases where treated prior to caspofungin�s
authorisation in Germany! with a comprehensive questionaire focusing on
� the diagnosis of the fungal infection� toxicity and comedication� outcome of the fungal infection
! Not to substitute a clinical trial

Caspofungin plus liposomales Ampho Bbei refraktärer Aspergillus-Pneumonie
� 14 hämatologische Patienten mit Aspergillus-Infektion der Lunge (2 Pat. gesichert 12 Pat. Verdacht)1 Patient gleichzeitig C. tropicalis-Fungämie
� AML n=9 ALL n=2 biphenotypische Leukämie, CLL, MDS je n=1
� Initiale Therapie: Ampho B n=6lipo Ampho B n=8Ampho B + Itra n=5
� Mediane Dauer der initialen Ampho B-Therapie 15 (4-64) Tage
Ergebnis: komplette/partielle Heilung 57 % (8/14)4 Pat. nahezu völlige Remission Mediane Dauer der Kombination 23 (9-48) Tage
Aliff T, et al.: ASH 2001 Abstract 1381
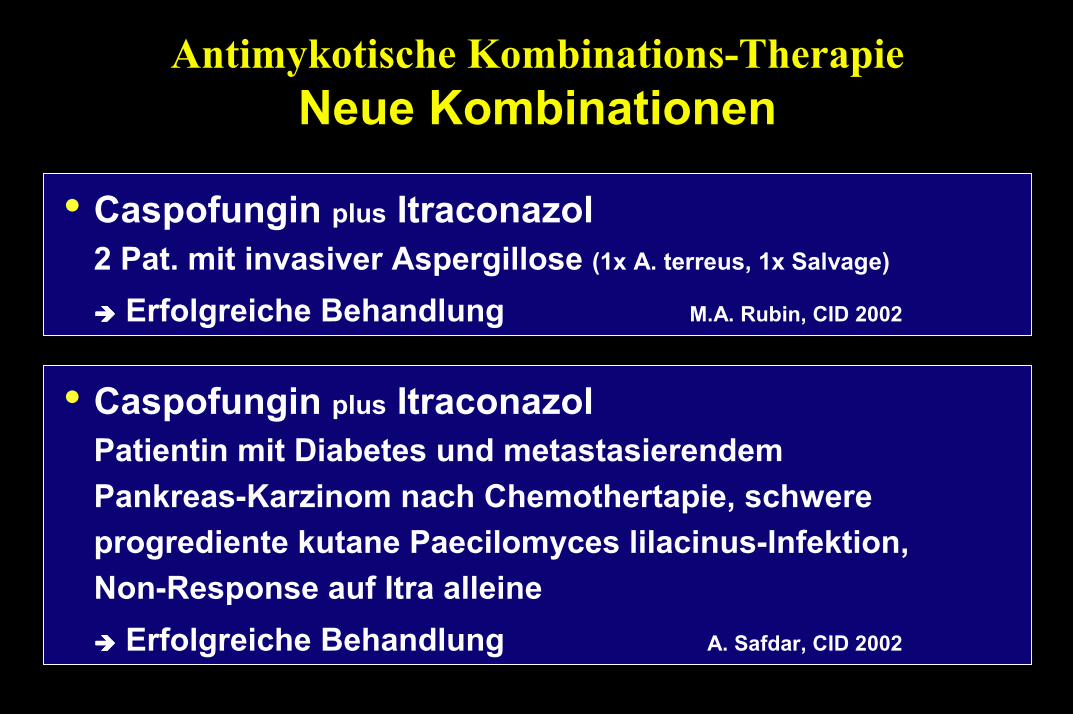
Antimykotische Kombinations-TherapieNeue Kombinationen
� Caspofungin plus Itraconazol2 Pat. mit invasiver Aspergillose (1x A. terreus, 1x Salvage)
#### Erfolgreiche Behandlung M.A. Rubin, CID 2002
� Caspofungin plus ItraconazolPatientin mit Diabetes und metastasierendemPankreas-Karzinom nach Chemothertapie, schwereprogrediente kutane Paecilomyces lilacinus-Infektion,Non-Response auf Itra alleine#### Erfolgreiche Behandlung A. Safdar, CID 2002
Antimykotische Kombinations-TherapieNeue Kombinationen
� Ampho B plus Fluconazol (n=107) versus Fluconazol (n=104) bei
Candidämie, prosp. randomisierte Studie
#### Schnellere Sterilisierung der BK, gleiche Mortalität Rex et al. ICAAC, J-681a
� Ampho B (n=10) versus Ampho B plus Itraconazol (n=11)
bei invasiver Aspergillose, retrospektive Studie
#### höhere Heilungsrate mit Kombination (82%) vs. Mono-Tx (50%)
Popp et al. (1999), Int J Infect Dis

Invasive pulmonale Aspergillose
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Invasive pulmonale Aspergillose
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Mucor Infiltrate
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Wann sollte man an eine Pulmonale Mucormykose
denken?
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Mucor: Infiltratives Wachstum
A.D.H. 1.7.97 A.D.H. 1.7.97A.D.H. 1.7.97
U.K. 25.11.98 U.K. 30.12.98
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Mucor: Tumorähnliches Wachstum
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Mucor Frühinfiltrate: �Nestzeichen�
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Mucor Frühinfiltrate
A.D.H. 1.7.97 A.D.H. 1.7.97
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt

Mucor - Mykose
17.2.97 10.3.97
V. Jacobi Z. Rad Uni FrankfurtV. Jacobi Z. Rad Uni Frankfurt


Voriconazol Pharmakokinetik� Orale Gabe #### schnelle Resorption, Tmax < 2 Stunden
#### Bioverfügbarkeit > 96 %
� Eiweißbindung ca. 58 %
� Wasserlöslichkeit schlecht
� Serumhalbwertzeit 6-12 Stunden
� starke Metabolisierung
� Clearance über Leber, < 5 % unverändert im Urin
� Gute Gewebediffusiuon
� Liquorgängigkeit 40 - 70 %
� Applikation oral und i.v. 2x täglich
� Nichtlineare Pharmakokinetik

Omeprazol halbe Dosierung
Medikament Vorgehen
Interaktionen mit Voriconazol
Rifabutin + Phenytoin Erhöhung der Voriconazol-Dosis#### 5 mg / kg i.v., 400 mg oral / 2x täglich
Tacrolimus 1/3 der initialen Tacrolimus-Dosis#### Bestimmung der Serumkonzentration
Cyclosporin 1/2 der initialen Cyclosporin-Dosis#### Bestimmung der Serumkonzentration
Warfarin PT-Kontrolle

� Terfenadin
� Astemizol
� Cisaprid
� Pimozid
KontraindikationVoriconazol
� Chinidin
� Carbamazepin
� Sirolimus
� Rifampicin
� Phenobarbital
� Ergot-Akaloide

CaspofunginWirkmechanismus
! Inhibition der ββββ-(1,3)-D-Glucan-Synthese! Störung der Zellwandintegrität vieler Pilze
! Kommt in menschlichen Zellen nicht vor
! Candida spp.: ββββ-1,3- (~40-50%) & ββββ-1,6-Glucan
! Aspergillus spp.: Hyphen überwiegend ββββ-1,3-Glucan
! Wirksamkeit korreliert möglicherweise mitdem Gehalt an ββββ-1,3-Glucan

! Gut wasserlöslich, schlechte orale Resorption (<1%)
! t1/2ββββ ca. 9-11 h, Einmal-Dosierung! Hepatischer Metabolismus! Relevante Interaktion nur mit Ciclosporin A! Geringe Interaktion mit Tacrolimus (Cmin$$$$ 26 %)! Dosis-Erhöhung (auf 70 mg / d) bei Kombination mit: Efavirenz,
Nelfinavir, Dexamethason, Rifampicin, Phenytoin, Carbamazepin
! Anreicherung in Leber und Niere, geringe Konzentration in ZNS und Urin
CaspofunginPharmakokinetik

! Aufsättigungsdosis (Tag 1) 70 mg / Tag
CaspofunginDosierung
! Erhaltungsdosis 50 mg / Tagbei > 80 kg KG 70 mg / TagChild-Pugh 7-9 35 mg / Tag
Max. tolerable Dosis noch nicht bekannt

! AUC-Anstieg bei Niereninsuffizienz! Creat.-Clear. 80-50 ml/min: 6% (⇑⇑⇑⇑) (n=7)
49-31 ml/min: 12% (⇑⇑⇑⇑) (n=8)30- 5 ml/min: 61% (⇑⇑⇑⇑) (n=9)HD/HF: 47% (⇑⇑⇑⇑) (n=9)
! Dosisanpassung nicht empfohlen! Nicht dialysierbar
! AUC-Anstieg bei Leberinsuffizienz:! CHILD-Pugh5-6: 43% (⇑⇑⇑⇑), CHILD-Pugh 7-9: 72% (⇑⇑⇑⇑)! Bisher keine Gabe bei Bilirubinerhöhung! Dosisanpassung bei CHILD-Pugh 7-9: 70 mg d1 →→→→ 35 mg/d
SableSable ICAAC 2000ICAAC 2000
CaspofunginPharmakokinetik: klinische Daten

! Keine orale Resorption! Klinisch relevante Halbwertszeit: ca. 10h! Einmaldosierung! Hepatischer Metabolismus
(Cave: Leberinsuffizienz)! Relevante Interaktion nur mit Ciclosporin A! Anreicherung in Leber und Niere, geringe Konzentration
in ZNS und Urin
CaspofunginPharmakokinetik: Zusammenfassung

Voriconazole Combined with Echinocandins! Checker-board technique. 10 A. fumigatus isolates
Drug Combination InteractionMK + AMB SynergisticFK + AMB SynergisticVCZ + FK AdditiveVCZ + MK AdditiveVCZ + AMB Indifferent
! Two drug combinations of an echinocandin with a polyene or an azole may be more effective against A. fumigatus than using them individually.
Manavathu et al. (2001). IDSA, 39th, San Francisco

Voriconazole vs. Amphotericin BPrimary TX in invasive Aspergillosis
R.Herbrecht et al. N Engl J Med, August 2002
85.4 %Pulmonary IA
VoriconazoleN = 144
88 %
Ampho BN = 133
2.8 %Dissem. IA 0.8 %
3.5 %CNS 3.8 %
52.8 %CR / PR 31.6 %
70.8 %Survival 57.9 %
Clinical outcome week 12

Angriffsorte von Antimykotikain der Pilz-Zelle