art advances-into the next decade james hakim mb mmed msc frcp professor of medicine, university of...
TRANSCRIPT

ART Advances-into the Next Decade
James Hakim MB MMed MSc FRCPProfessor of Medicine, University of Zimbabwe
AIDS 2010
Vienna-Austria18-23 July 2010

Antiretroviral Therapy Into the Next Decade
Historical perspectives
Current Status of ART
ART Into the Next Decade

Historical PerspectivesART Milestones
Vancouver Durban
Vancouver1996
Durban2000
Barcelona2002

Key ART Initiatives
UNGASS
WHO
UNAIDS
GFATM
PEPFAR
CHAI
UNITAID
National & Regional Initiatives
NGO & Other Initiatives

When/What is the next Milestone
• ? Universal Access

Status of ART Roll-Out 2009
• 5.2m PLH on ART– Most - MLIC
• Infection outstrips Treatment by 5:2
• 5m more need treatment
• 2010 WHO Guidelines takes this to 10 Mill

Achievements of ART
• Improved survival • Decreased
opportunistic infections
• Improved quality of life
Restores Hope & Dignity
Kim J, Farmer P. NEJM 2006

Mortality RLS vs RRS
• ART-LINC vs ART-CC comparisonsLow-INC High-
INC
Female 51% 25%
CD4 (base)
108 235
CD4 gain (6mths)
106 103
VL (6mths)<500c/ml
76% 77%
Mortality Adjusted HR1-6 mths - 4.3 (95%CI 1.6-11.8)7-12 mths-1.5 (95% CI 0.7-3.0)
Braitstein P. Lancet 2006;367;817

Mortality in RRS
• Resource rich settings– Increasing
importance of non-AIDS illnesses beyond second year
ART-CC CID 2010;50:1387
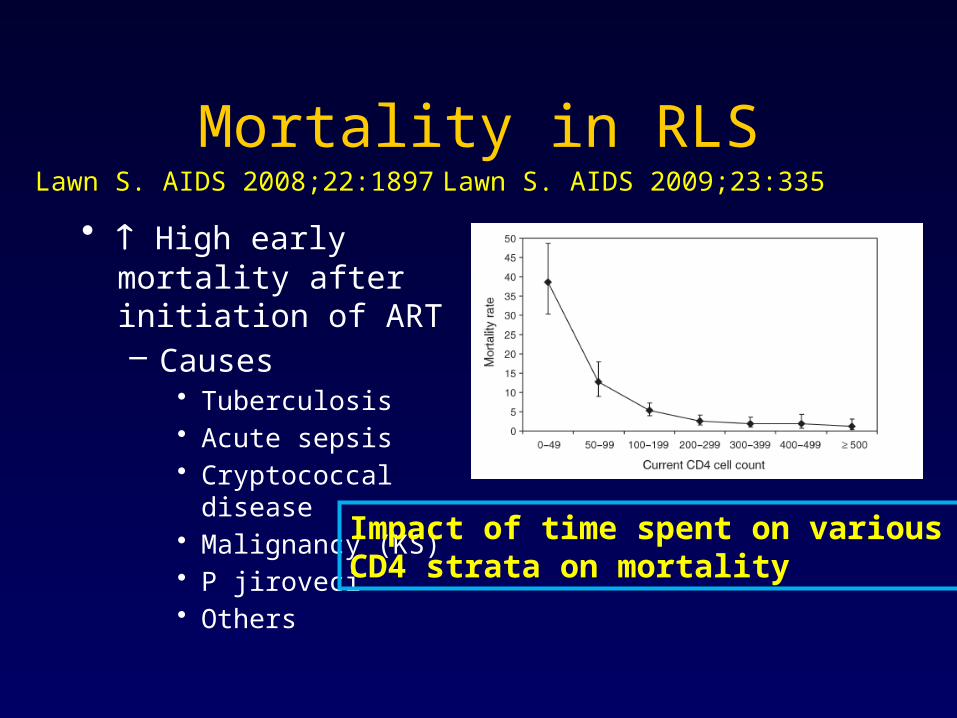
Mortality in RLS
• High early mortality after initiation of ART– Causes
• Tuberculosis• Acute sepsis• Cryptococcal disease• Malignancy (KS)• P jiroveci• Others
Lawn S. AIDS 2008;22:1897 Lawn S. AIDS 2009;23:335
Impact of time spent on various CD4 strata on mortality

Other Achievements of ART
• Impact:– Tuberculosis– Maternal and child mortality
» Hogan M, et al. Lancet 2010;375:1609
– Improves school attendance & workforce» Zivin J, et al. J Publ Econ 2009;93:1008» Thirumurthy H, et al. J Hum Res 2008;43:511
– HIV transmission» Donnell D, et al. Lancet 2010;375:2092

Impact on Tuberculosis
• Ecological analysis• Fall in TB
prevalence in HIV patients
• 1,250 pts in S. Africa
• RCT– Early vs Delayed
ART– 816 participants– TB cases:
• 18 vs 36 p=0.0125
2005 2008 P-value
All 3.2% 1.6% P=0.02
HIV+ve 9.2% 3.6% p=0.003
Rxd TB 4% 2.3% p=0.06
Middelkoop K, et al. IAS C Town 2009; Am J Resp Crit Care 2010; Jun 25
Severe P, et al. NEJM 2010;363:257
Early ART Delayed ART p-value
18 36 P=0.0125

ART in the Developing World
• Implementation has been greatly helped by WHO guidelines– 2002– 2003– 2006– 2010
2010 WHO ART Guidelines for Adults & Adolescents Guidelines

Early Initiation of ART CD4 threshold 350c/mm3
• CIPRA-HT-001– Severe P, et al. NEJM
2010;363:257
– 816 participants– Deaths:
• 6 vs 23 p=0.0011
• Cohort Analysis– Even higher
thresholds– 350-500– >500
– Kitahata MM, et al. NEJM 2009;360:1815

Guidelines-CD4 ThresholdsGuidelines CD4-Asymptomatic Pts
DHHS (2010) <350 (consider 500)
IAS (2010) <500
EACS (2008) <350 (consider >350)
BHIVA (2008 <350 (consider >350)
WHO EURO (2007/8) 200-350
WHO (2006) <200 (consider 200-350)
WHO (2010) <350

Treat Earlier-2010 WHO Guidelines
To start earlier is the right thing to do
“Harmonize treatment guidelines”
CD4<350 c/mm3
Seek and Treat (earlier diagnosis)
Public Health Approach
DART
CIPRAS. Africa
JinjaUganda

IAS July 2009 18
SurvivalSurvival
0.90
0.87
0.08
0.92
0.90
0.18
0.95
0.94
0.55
0 1 2 3 4 5
0.0
0.2
0.4
0.6
0.8
1.0
Pro
port
ion
aliv
e
Years from enrolment
Entebbe Cohort(Uganda):pre-ART 1996-2000, median CD4 75 at enrolment:57.7/100 PY
164 eventsLCM: 2.2/100 PYCDM: 2.9/100 PY
218 events
Survival at 5 yrs: LCM-90%, CDM-87%

Trained Lay Workers-monitoring ART
• Home-based vs Facility based care– End point-Virologic
Failure (RNA >500c/ml)
• 859 participants – (HBC-729 vs FBC-483)
• Rate Ratio:– 1.04 (95%CI 0.78-1.4)
HBC is as effective as FBC
Jaffar S, et al. Lancet 2009;374:2080

CIPRA South Africa
• Nurse monitored vs Doctor monitored– Randomized non-
inferiority trial
• Follow up-120 wks
Doctor monitored n=408
Nurse monitored n=404
Total Failure
179(44%) 192(48%)
Deaths 10 11
Virol Fail 44 39
Toxicity 68 66
LTFU 70 63
Nurse vs Doctor monitoring is non-inferiorHR 1.09 (95% CI 0.89-1.33)
Sanne I, et al. Lancet 2010;376:33

Antiretroviral Drugs
• NRTIs– Zidovudine– Lamuvudine– Stavudine– Didanosine– abacavir– Tenofovir– Emtricitabine
• NNRTIs– Nevirapine– Efavirenz– Etraverine
• Integrase Inhibitors– Raltegravir
• Protease inhibitors– Lopinavir– Atazanvir – Tipranavir– Darunavir– Indinavir– Ritonavir– Nelfinavir– Saquinavir– Amprenavir– Fosamprenavir
• Fusion Inhibitors– Enfuvertide
• CCR5 antagonists– Maraviroc

First-Line ART
• Harmonized to include TB and pregnant women
• ART to all TB and HBV patients• Preferred-NNRTI based regimen• Preferred use of TDF or AZT• d4T withdrawal and elimination
WHO 2010 Guidelines

Second-Line ART
• Boosted PI-based regimens– Poor evidence of efficacy of NRTI
backbone in public health approach– High resistance mutations when failure is
clinically or immunologically diagnosed» Hosseinipour M, et al. AIDS 2009;23:1127
– ? Immediate use of new classes/drugs immediately (RAL, ETV, Darunavir)
Second-Line ART
• Need for studies to provide evidence for public health approach to second line regimens– EDCTP trial-EARNEST (enrolling)– ACTG trial– Other
• The place of PI/r monotherapy

Third-Line ART
• Real need to treat those failing second-line ART
• Can this be addressed with public health approach principles?
– ? Need for resistance testing– WHO 2010 recommends drugs eg DRV,
ETV, RLV– Does this obviate resistance testing?

Monitoring
• Issues – Efficacy tests (CD4, RNA VL)
• Cost• Lab capacity• Impact on pace of roll-out• Need for evidence-based monitoring
– Evidence for RNA VL monitoring is good-but availability to date is limited
• Need for roll-out of low-cost point-of-care tests– CD4, RNA VL, resistance testing

Monitoring
• Toxicity tests– CBC
• Chronic illness, AZT, malignancies, malnutrition, etc
– Renal function test (which? creatinine, urine)• TDF
• Other– Tropism tests, HLAB5701 (ABC)

Into the Next Decade• Pipeline for new
antiretroviral drugs• The pace of
development has slowed in this area

Into the Next Decade
• Current drugs are efficacious with good safety and tolerance– But there is still need for drugs that are:
• More efficacious• Better tolerated (Better adherence)• More safe (Less monitoring)• More forgiving (Less resistance)• Compatible with TB, pregnancy, hepatitis,
malaria, etc...
Treatment 2.0

Into the Next Decade
Address long- term non-AIDScomplications
Cardiovascular
Neuro-congnitive
Hepatic
Renal
SMART. NEJM 2006;355:2283DAD NEJM 2007;356:1723
Bone

Into the Next Decade
• Non-AIDS outcomes– unmitigated HIV replication or ART
• cardiovascular, hepatic, renal, bone, neuro-cognitive effects, cancer
• Aging/senescence
Limited data from RLSMore research required

Into the Next DecadeLaboratory Monitoring
• Accelerate roll-out of Point-of-care technology– CD4 counts– RNA Viral Load– Resistance– Other

HIV Eradication
• A preventive HIV vaccine is an important intermediate step
• The eradication and cure of HIV remains the only victory that we can celebrate
• The science and strategy required to achieve this is of the highest priority
• Granich R. Lancet 2009;373:48• Hütter G. NEJM 2009;360:692• Carter C. Nature Med 2010;16:446

Conclusions-Current
• The last decade has seen a momentous expansion of ART in LMIC
• We continue to see the benefits of ART in improved survival, reduction in disease progression & improved quality of life
• ART impacts non-AIDS conditions in both negative and positive ways. This must continue to be a focus of research

ConclusionsInto the Next Decade
• The quest for more efficacious, better tolerated, safer and more forgiving antiretroviral drugs must continue
• Better delivery modes of ART are needed to improve access to all
• Preventive value of ART has come of age-pMTCT and beyond...
• HIV cure remains the ultimate prize in the response to AIDS

Acknowledgements
• UCSF– Diana Havlir
• ARASA– Michaela Clayton
• Univ of Zimbabwe– Anthony Chisada– Nehemiah Nhando– Wadzanai Samaneka
– Mike Chirenje
• YRG-Care– Kumar Kumarasamy
• University of Denver– Thomas Campbell
• WHO– Marco Vitoria
• Slides & Comments– Many

Thank You