arrhythmias and sudden death in athletes
TRANSCRIPT


THE ECG INACUTE MYOCARDIAL
INFARCTION AND UNSTABLEANGINA

A. Bayés de Luna, F. Furlanello, B.J. Maron and D.P. Zipes (eds.):Arrhythmias and Sudden Death in Athletes. 2000 ISBN: 0-7923-6337-XJ-C. Tardif and M.G. Bourassa (eds): Antioxidants and Cardiovascular Disease.2000. ISBN: 0-7923-7829-6J. Candell-Riera, J. Castell-Conesa, S. Aguadé Bruiz (eds): Myocardium atRisk and Viable Myocardium Evaluation by SPET. 2000.ISBN: 0-7923-6724-3M.H. Ellestad and E. Amsterdam (eds): Exercise Testing: New Concepts for theNew Century. 2001. ISBN: 0-7923-7378-2Douglas L. Mann (ed.): The Role of Inflammatory Mediators in the FailingHeart. 2001 ISBN: 0-7923-7381-2Donald M. Bers (ed.): Excitation-Contraction Coupling and CardiacContractile Force, Second Edition. 2001 ISBN: 0-7923-7157-7Brian D. Hoit, Richard A. Walsh (eds.): Cardiovascular Physiology in theGenetically Engineered Mouse, Second Edition. 2001 ISBN 0-7923-7536-XPieter A. Doevendans, A.A.M. Wilde (eds.): Cardiovascular Genetics for Clinicians2001 ISBN 1-4020-0097-9Stephen M. Factor, Maria A.Lamberti-Abadi, Jacobo Abadi (eds.): Handbook ofPathology and Pathophysiology of Cardiovascular Disease. 2001
ISBN 0-7923-7542-4Liong Bing Liem, Eugene Downar (eds): Progress in Catheter Ablation. 2001
ISBN 1-4020-0147-9Pieter A. Doevendans, Stefan Kääb (eds): Cardiovascular Genomics: NewPathophysiological Concepts. 2002 ISBN 1-4020-7022-5Antonio Pacifico (ed.), Philip D. Henry, Gust H. Bardy, Martin Borggrefe,Francis E. Marchlinski, Andrea Natale, Bruce L. Wilkoff (assoc. eds):Implantable Defibrillator Therapy: A Clinical Guide. 2002
ISBN 1-4020-7143-4Hein J.J. Wellens, Anton P.M. Gorgels, Pieter A. Doevendans (eds.):
The ECG in Acute Myocardial Infarction and Unstable Angina: Diagnosis and RiskStratification. 2002 ISBN 1-4020-7214-7
Previous volumes are still available
Developments in Cardiovascular Medicine
232.
233.
234.
235.
236.
237.
238.
239.
240.
241.
242.
243.
244.

THE ECG INACUTE MYOCARDIAL
INFARCTION AND UNSTABLEANGINA
Diagnosis and Risk Stratification
by
Hein J.J. WellensAnton P.M. Gorgels
Academic Hospital, MaastrichtThe Netherlands
and
Pieter A. Doevendans, MDInteruniversity Cardiology Institute of The Netherlands
Utrecht, The Netherlands
KLUWER ACADEMIC PUBLISHERSNEW YORK, BOSTON, DORDRECHT, LONDON, MOSCOW
eBook ISBN: 0-306-48202-9Print ISBN: 1-4020-7214-7
©2002 Kluwer Academic PublishersNew York, Boston, Dordrecht, London, Moscow
Print ©2003 Kluwer Academic Publishers
All rights reserved
No part of this eBook may be reproduced or transmitted in any form or by any means, electronic,mechanical, recording, or otherwise, without written consent from the Publisher
Created in the United States of America
Visit Kluwer Online at: http://kluweronline.comand Kluwer's eBookstore at: http://ebooks.kluweronline.com
Dordrecht

CONTENTS
Introduction
Determining the size of the area at risk, the severity
of ischemia, and identifying the site of occlusion in
the culprit coronary artery
A. The ST segment deviation score
B. The terminal QRS-ST segment pattern
C. Specific ECG patterns indicating the site of
coronary artery occlusion:
I Infero-posterior myocardial infarction with
or without right ventricular infarction
II Anterior wall myocardial infarction
Conduction disturbances in acute myocardial
infarction
A. The sino-atrial region
B. The AV nodal conduction system
C. The sub-AV nodal conduction system
Myocardial infarction in the presence of abnormal
ventricular activation
A. Left bundle branch block
B. Paced ventricular rhythm
C. Pre-excitation
Chapter 1
Chapter 2
Chapter 3
Chapter 4
1
5
9
11
13
13
24
43
45
49
53
65
68
76
79

Arrhythmias in acute myocardial infarction:
Incidence and prognostic significance
A. Supraventricular arrhythmias
B. Ventricular arrhythmias
The electrocardiographic signs of reperfusion
The electrocardiogram in unstable angina
Recognition of multivessel and left main disease
Recognition of critical narrowing of the left anterior
descending coronary artery
Chapter 5
Chapter 6
Chapter 7
Index 127
117
85
87
91
99

ERRATA
The ECG in Acute Myocardial Infarction and Unstable Angina: Diagnosis andRisk Stratificationby: Hein J.J. Wellens, Anton P.M. Gorgels and Pieter A. DoevendansISBN: 1-4020-7214-7
The publisher regrets that due to a publishing error, the incorrect series numberappears on the series page and the back cover. The correct series number isDICM245. The corrected series page appears below.
Kluwer Academic Publishers
A. Bayés de Luna, F. Furlanello, B.J. Maron and D.P. Zipes (eds.):Arrhythmias and Sudden Death in Athletes. 2000 ISBN: 0-7923-6337-XJ-C. Tardif and M.G. Bourassa (eds): Antioxidants and Cardiovascular Disease.2000. ISBN: 0-7923-7829-6J. Candell-Riera, J. Castell-Conesa, S. Aguadé Bruiz (eds): Myocardium atRisk and Viable Myocardium Evaluation by SPET. 2000.ISBN: 0-7923-6724-3M.H. Ellestad and E. Amsterdam (eds): Exercise Testing: New Concepts for theNew Century. 2001. ISBN: 0-7923-7378-2Douglas L. Mann (ed.): The Role of Inflammatory Mediators in the FailingHeart. 2001 ISBN: 0-7923-7381-2Donald M. Bers (ed.): Excitation-Contraction Coupling and CardiacContractile Force, Second Edition. 2001 ISBN: 0-7923-7157-7Brian D. Hoit, Richard A. Walsh (eds.): Cardiovascular Physiology in theGenetically Engineered Mouse, Second Edition. 2001 ISBN 0-7923-7536-XPieter A. Doevendans, A.A.M. Wilde (eds.): Cardiovascular Genetics for Clinicians2001 ISBN 1-4020-0097-9Stephen M. Factor, Maria A.Lamberti-Abadi, Jacobo Abadi (eds.): Handbook of
Pathology and Pathophysiology of Cardiovascular Disease. 2001ISBN 0-7923-7542-4
Liong Bing Liem, Eugene Downar (eds): Progress in Catheter Ablation. 2001ISBN 1-4020-0147-9
Pieter A. Doevendans, Stefan Kääb (eds): Cardiovascular Genomics: NewPathophysiological Concepts. 2002 ISBN 1-4020-7022-5Daan Kromhout, Alessandro Menotti, Henry Blackburn (eds.): Preventionof Coronary Heart Disease: Diet, Lifestyle and Risk Factors in the SevenCountries Study. 2002 ISBN 1-4020-7123-XAntonio Pacifico (ed.), Philip D. Henry, Gust H. Bardy, Martin Borggrefe,Francis E. Marchlinski, Andrea Natale, Bruce L. Wilkoff (assoc. eds):Implantable Defibrillator Therapy: A Clinical Guide. 2002
ISBN 1-4020-7143-4Hein J.J. Wellens, Anton P.M. Gorgels, Pieter A. Doevendans (eds.):
The ECG in Acute Myocardial Infarction and Unstable Angina: Diagnosis and RiskStratification. 2002 ISBN 1-4020-7214-7
Previous volumes are still available
Developments in Cardiovascular Medicine
232.
233.
234.
235.
236.
237.
238.
239.
240.
241.
242.
243.
244.
245.

Authors
Pieter A. Doevendans, M.D.Associate Professor of Cardiology,Department of CardiologyAcademic Hospital MaastrichtUniversity of Maastricht, the Netherlands
Anton P. Gorgels, M.D.Associate Professor of CardiologyDepartment of CardiologyAcademic Hospital MaastrichtUniversity of Maastricht, the Netherlands
Hein J.J.Wellens, M.D.Professor of CardiologyMedical Director of the Interuniversity Cardiology Institute of the Netherlands(ICIN)Utrecht, the Netherlands

Acknowledgements
Over the years the cardiologists, residents, fellows and nursing staff, working atthe Department of Cardiology of the Academic Hospital of Maastricht, havecarefully collected the electrocardiograms published in this book. We are verymuch indebted to them for their enthusiasm and willingness to donate thosepearls to us!To have the electrocardiograms perfectly reproduced we had the good fortuneto have Adrie van den Dool working for us. She and the medical photographygroup of the hospital did a perfect job, demonstrating again their ability tomake beautiful illustrations.Excellent secretarial assistance was provided by Birgit van den Burg, MiriamHabex, Vivianne Schellings and Willemijn Gagliardi. We greatly appreciatedtheir pleasant, never complaining way of helping us again and again!Manja Helmers played an important role in the final phase by expertlyproducing the layout of the manuscript.
Hein J.J. WellensAnton P.M. GorgelsPieter A. Doevendans

Chapter 1
Introduction

INTRODUCTION
The electrocardiogram (ECG) remains the most accessible and inexpensivediagnostic tool to evaluate the patient presenting with symptoms suggestive ofacute myocardial ischemia. It plays a crucial role in decision making about theaggressiveness of therapy especially in relation to reperfusion therapy, becausesuch therapy has resulted in a considerable reduction in mortality from acutemyocardial infarction.
Several factors play a role in the amount of myocardial tissue that can besalvaged by reperfusion therapy, such as the time interval between onset ofcoronary occlusion and reperfusion, site and size of the jeopardized area, typeof reperfusion attempt (thrombolytic agent or an intracoronary catheterintervention), presence or absence of risk factors for thrombolytic agents, etc.
Most important in decision making on reperfusion therapy and the type ofintervention is to look for markers indicating a higher mortality rate frommyocardial infarction.
The ECG is a reliable, inexpensive, non-invasive instrument to obtain thatinformation. Recently it has become clear that both in anterior and inferiormyocardial infarction, the ECG frequently allows not only to identify theinfarct related coronary artery, but also the site of occlusion in that artery andtherefore the size of the jeopardized area. Obviously, the more proximal theocclusion, the larger the area at risk and the more aggressive the reperfusionattempt. The ECG will also give an indication of the size of the jeopardizedarea by making an ST segment deviation score and tell us about the severityand reversibility of cardiac ischemia by analyzing the pattern of the QRS andthe beginning of ST segment elevation.
It will inform us about other factors of importance for the management andprognosis of the patient such as heart rate, width of the QRS complex, presenceof abnormalities in impulse formation and conduction, and presence or absenceof a prior infarction.
Following reperfusion therapy the ECG can inform us about the result andhelp us to select which patient should receive a rescue angioplasty in case offailure of thrombolytic therapy.
At present, decision making on management of acute myocardialinfarction should be individualized and the purpose of this book is to show thatthe ECG is an indispensable tool to reach that goal.
Often the patient with an acute coronary syndrome presents with differentST-T segment patterns such as ST elevation, ST depression and T waveinversion. In recent years it has become clear that the ECG at presentationallows immediate risk stratification across the whole spectrum of acutecoronary syndromes. For example, we learned that the patient with extensiveST segment depression may have a worse long term prognosis that the patientwith an acute myocardial infarction.
Risk of the patient with acute myocardial ischemia will depend on site andseverity of coronary artery disease. Therefore the identification of the patientwith left main stenosis, severe three vessel disease or proximal narrowing ofthe left anterior descending branch is of obvious importance. Again, also under
3

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
these circumstances the ECG allows us to select those patients who needinvasive diagnostic studies.
4

Chapter 2
Determining the size of the area at risk, the severity of
ischemia, and identifying the site of occlusion in the culprit
coronary artery

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION
ST SEGMENT DEVIATION SCORE
More than 15 mm indicates an area sufficiently large to attemptreperfusion
THE TERMINAL QRS-ST SEGMENT PATTERN
Grade III ischemia indicates poorer short and long term prognosis
SPECIFIC ECG PATTERNS: IDENTIFYING THE SITE OFOCCLUSION IN THE CULPRIT CORONARY ARTERY
I Infero posterior infarction
RCA or CX?
7
A.
B.
C.
RCA
CX
1.2.
1.2.3.
ST elevation in lead III higher than in lead IIST depression in lead I
ST elevation in lead II higher than in lead IIIST iso-electric or elevated in lead IST iso-electric or depressed with negative T wave in lead
Proximal (with right ventricular infarction) or distal RCA?
Proximal RCAST elevation with positive T wave in lead
Distal RCAIso electric ST with positive T wave in lead
Posterior wall involvement?
ST depression in precordial leads

Lateral wall involvement?
ST elevation in leads I, AVL, and
Atrial infarction?
Pta segment elevation in lead II
Anterior wall infarction
LAD occlusion proximal to first septal and first diagonal branch
Acquired right bundle branch blockST elevation lead AVRST elevation > 2mm in leadST depression in leads II, III and AVF
LAD occlusion distal to first septal and proximal to first diagonalbranch
ST depression lead III> Lead IIQ in lead AVL
LAD occlusion distal to first diagonal and proximal to first septalbranch
Signs of occlusion proximal to first septal branchST depression in lead AVL
Distal LAD occlusion
Q waves in leadsAbsence of ST depression in leads II, III and AVF
8 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
II

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION
In acute myocardial infarction (MI) the surface electrocardiogram (ECG)allows risk assessment in the individual patient by estimating the size of thearea involved. This will be of help in selecting those patients most likely toprofit from reperfusion of that area. Risk on admission can be assessed fromseveral variables 1) The total score of ST segment deviation reflecting theseverity of ischemia and global size of the ischemic area (1-3), 2) the heart rate(3-5), 3) QRS width (3), 4) the terminal QRS-ST segment pattern (6,7), and 5),by identifying the leads showing ST segment deviation, because they reflect thesite and size of the ischemic process. As will be shown in this chapter the latterusually allows to identify not only the culprit coronary artery, but also the siteof occlusion in that artery and thereby the area at risk. This is importantbecause coronary arteries differ as far as the size of the ventricular area thatthey perfuse. In general the left anterior descending coronary artery (LAD)supplies 50% of left ventricular mass and the right coronary artery (RCA) andcircumflex coronary artery (CX) each 25%.
The size of a MI may differ between patients because of individualvariations of the coronary artery system and the site of occlusion in the culpritvessel (proximal or distal). Also collateral circulation or multivessel ischemiawill influence the extent of the ischemic area. This may sometimes lead toparadoxical situations: ST segment elevation in the precordial leads can becaused by RCA occlusion and ST segment elevation in the inferior leads byLAD occlusion.
To understand the findings on the ECG, it is helpful to look at the patternof ST segment elevation and depression in the different leads by applying thevectorial concept of electrical forces (8).
A. THE ST SEGMENT DEVIATION SCORE
The number of ECG leads showing ST segment deviation (elevation ordepression) and the ST segment deviation score (using the sum of ST segmentdeviation in all 12 leads) are markers for the extent of the ischemic area inacute coronary syndromes (9).
Soon after the introduction of thrombolytic therapy for treatment of acuteMI, it was shown that the greatest reduction in infarct size could be obtained inpatients showing a large ST segment deviation score (1,10,11). The absoluteST segment deviation score was especially of great value in estimating theextent of posterior ischemia in patients with infero-posterior infarction (12,13).
Hathaway et al (3) using the information from the GUSTO-I study showedthat the sum of absolute ST segment deviation added major information aboutthe area at risk and 30 days mortality of acute MI when included in anomogram for risk stratification on admission. As shown in table 2-1 alsoincluded in their nomogram were data on systolic blood pressure, heart rate,QRS duration, age, height, diabetes, Killip class, prior MI and prior coronaryartery bypass grafting.
9

10 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION
It is important to know that in the very acute phase of ischemia locallymarked ST segment elevation may occur. With ongoing ischemia the amountof ST segment deviation stabilizes after 1 to 4 hours which is the time whenusually the first ECG is made (9).
For practical purposes it is useful to accept a 15mm value of ST segmentdeviation as a figure indicating a large area at risk. As will be discussed later,especially in the precordial leads in anterior wall MI there may be adiscrepancy between the area at risk as determined from the ST segmentdeviation score and ECG findings indicating the site of occlusion in the culpritcoronary artery.
B) THE TERMINAL QRS-ST SEGMENT PATTERN AND THESEVERITY OF CARDIAC ISCHEMIA
As pointed out by Sclarovsky and Birnbaum (6,7) typical patterns of the end ofthe QRS complex and ST segment morphology may be of prognostic signifi-cance in acute myocardial infarction. They divided the ischemic changes afterocclusion of the coronary artery into three grades (figs 2.1 and 2.2). Grade I ischaracterized by tall, peaked, symmetrical T waves without ST segmentelevation. Grade II shows ST segment elevation without changes in theterminal portion of the preceding QRS complex; while in grade III ischemia,apart from ST segment elevation, changes are present in the last part of theQRS complex such as an increase in the amplitude of the R wave anddisappearance of the S wave.
These serial ECG changes following acute coronary occlusion are relatedto severity and size of the ischemic area. However, decision making onnecessity and type of reperfusion therapy is usually based on the admissionECG. Sclarovsky and Birnbaum therefore called attention to two importantsigns indicating distortion of the terminal portion of the QRS in grade IIIischemia: presence of the junction point more than 50% of the height of the Rwave in leads with a qR configuration, and disappearance of the S wave inleads expected to have an RS configuration (6,7).
Several studies looked at the prognostic significance of the three grades ofischemia on presentation (14-17). They indicated that ischemia grading on theadmission ECG correlated with in-hospital mortality, final infarct size, severityof left ventricular dysfunction and late mortality. Grade III ischemia had themost ominous prognosis doubling early and late mortality as compared to gradeII ischemia. It was also shown that early reperfusion therapy (within 2 hoursafter onset of symptoms) resulted in similar beneficial results in grade II andgrade III ischemia. This was no longer the case when such therapy was appliedlater, grade III ischemia patients having a significantly higher in-hospitalmortality (18). This suggests that ischemia grading in relation to time intervalafter onset of complaints can also give an indication of the reversibility ofcardiac ischemia. The same authors also showed a higher incidence ofcomplications in grade III patients during hospital admission such as high
11

12 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION
degree AV block and reinfarction (19). These date suggest that an earlyprimary percutaneous coronary intervention should be considered in patientspresenting with grade III ischemia.
Birnbaum and Sclarovsky discussed why patients with grade III ischemiaon the admission ECG have worse short and long term prognosis and lessbenefit from reperfusion therapy (7). They came to the conclusion that thedifference in infarct size between grade II and Grade III ischemia patients isprobably due to faster progression of necrosis in grade III ischemia possiblyrelated to thickness of the ventricular wall, lack of collaterals and lack ofprotection by ischemic preconditioning (7).
C. SPECIFIC ECG PATTERNS: IDENTIFYING THE SITE OFOCCLUSION IN THE CULPRIT CORONARY ARTERY
In cardiac ischemia the direction and displacement of the ST segment isdetermined by the sum of direction and magnitude of all ST vectors at thatpoint in time. The resulting main vector will point in the direction of the mostpronounced ischemia. This results in ST elevation in that area. The oppositearea will record (reciprocal) ST segment depression. Although no ischemiamay be present in that area, this is not excluded by the reciprocal changes. Thelead perpendicular to the dominant vector will record an iso-electrical STsegment (6). This vectorial concept is particularly useful when analyzing thefrontal plane leads. In the horizontal plane the electrodes may be so close to themyocardium that the local vector overrules the far field electrical forces.
Infarction patterns are usually classified as inferoposterior and anterior. Itwill be shown that additional information from the ECG allows the recognitionof the culprit coronary artery and frequently the location of the occlusion inthat artery.
I Infero-posterior wall infarction
Infero-posterior wall infarction is either caused by the occlusion of the RCA orthe CX and is characterized by ST segment elevation in leads II, III and AVF.Discriminating ECG features between these two coronary arteries are basedupon the specific anatomic location of these vessels.
Coronary patho-anatomyThe perfusion areas of the RCA (1) and the CX are depicted in figure 2.3. TheRCA originates from the right aortic sinus. It passes down the rightatrioventricular groove towards the crux, where it crosses the interventricularseptum and continues to the postero(lateral) area of the left ventricle. Thefollowing side branches are of importance: 2) The conus branch. This branchmay provide blood flow to the basal part of the interventricular septum in caseof a proximal LAD occlusion(20). 3) The sinoatrial branch. This vesseloriginates in 60% from the RCA, and in about 40% from the CX (11 in fig. 2.3)
13

14 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
and rarely from both arteries. Involvement of this vessel may lead to sinus nodeischemia with sinus bradycardia, sino-atrial block and atrial infarction and mayfavor the occurrence of atrial fibrillation. 4) The right ventricular branch, whichperfuses the anterolateral part of the right ventricle. The RCA before the rightventricular branch is called the proximal, thereafter the distal RCA. Occlusionof the proximal RCA leads to right ventricular (RV) infarction, with diminishedfunction of the RV, possibly leading to underfilling of the LV with hypotensionand cardiogenic shock. In proximal RCA occlusion there is also a highincidence of high degree AV nodal conduction disturbances (see chapter 3) 5)The distal RCA has the acute marginal branch perfusing the posterior area ofthe RV. 6) The posterior descending branch which brings blood to theinferobasal septum and the posteromedial papillary muscle. Obstruction of flowleads to septal involvement, and possibly papillary muscle dysfunction andmitral regurgitation. It may also result in block or conduction delay in theposterior fascicle of the left bundle branch, especially when also the proximalLAD is narrowed or occluded. 7) The branch to the AV node. 8) Theposterolateral branch(es). In case of a dominant RCA, occlusion may result inposterior wall infarction, and even left lateral involvement. The CX originatesfrom the main stem of the left coronary artery (9) and runs through the leftatrioventricular groove. The CX usually gives one to three large obtusemarginal branches (12) supplying the free wall of the LV from superior to

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 15
inferior along the lateral border. In case of a dominant CX one or more medialposterobasal branches may arise from this vessel (13 in fig. 2.3).
DominanceThe RCA is dominant in about 70% of cases, passing the interventricularseptum, giving rise to posterolateral branches. In 30% of patients no RCAdominance is present, the CX being dominant in about half of them. In thosecases the CX is large and continues down to the diafragmatic surface of theLV, where it gives rise to the posterolateral branches, reaching the crux, endingin the posterior descending branch with a branch to the AV node. It is veryimportant to recognize which vessel is dominant because this identifies patientsat risk for extensive myocardial damage with complications of heart failure,ventricular arrhythmias and death.
RCA or CX occlusion in acute inferior wall myocardial infarction?Because of the different anatomic structures perfused and the resulting clinicalconsequences in case of ischemia and necrosis, it is important to identify theculprit coronary artery in infero posterior wall infarction. As pointed outbefore, both vessels perfuse the inferior part of the left ventricle, but the RCAmore specifically the medial part including the inferior septum, whereas the CXperfuses the left postero basal and lateral area. This results in a ST segmentvector directed inferior and rightward in case of a RCA occlusion versus aninferior and leftward vector in CX occlusion (figure 2.4). In RCA occlusion theST vector will therefore result in more ST elevation in III than in II leading toST depression in lead I. In case of CX occlusion the vector will point towardslead II, leading to ST elevation or an isoelectric ST segment in lead I. When thevector points towards AW, the ST vector is perpendicular to lead I, resulting
16 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
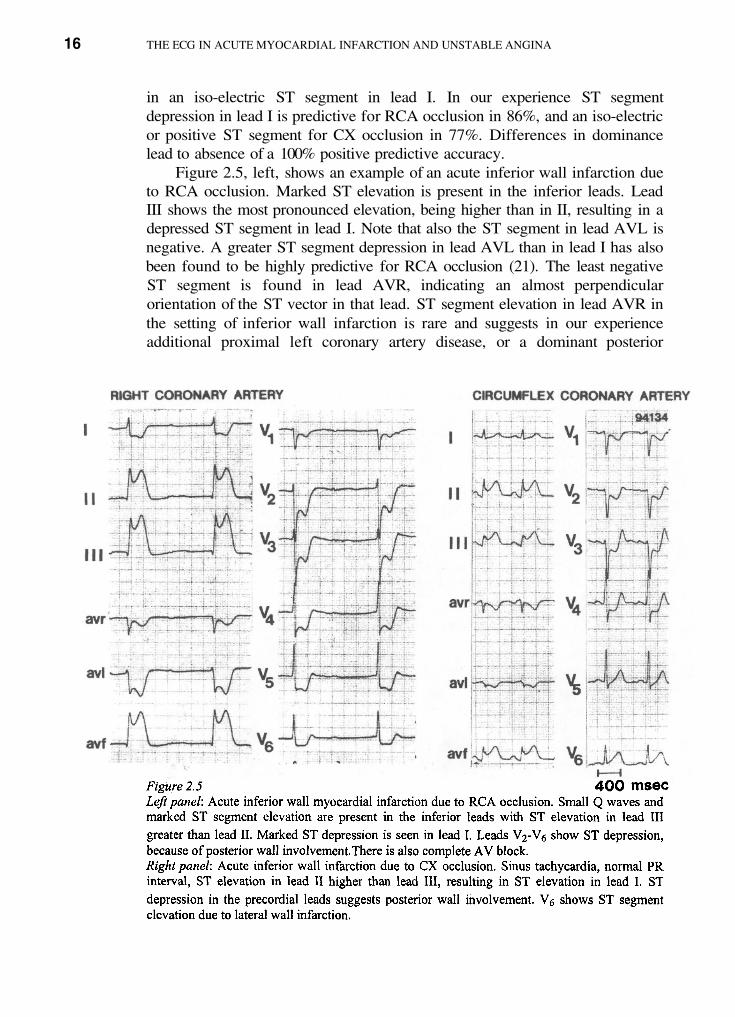
in an iso-electric ST segment in lead I. In our experience ST segmentdepression in lead I is predictive for RCA occlusion in 86%, and an iso-electricor positive ST segment for CX occlusion in 77%. Differences in dominancelead to absence of a 100% positive predictive accuracy.
Figure 2.5, left, shows an example of an acute inferior wall infarction dueto RCA occlusion. Marked ST elevation is present in the inferior leads. LeadIII shows the most pronounced elevation, being higher than in II, resulting in adepressed ST segment in lead I. Note that also the ST segment in lead AVL isnegative. A greater ST segment depression in lead AVL than in lead I has alsobeen found to be highly predictive for RCA occlusion (21). The least negativeST segment is found in lead AVR, indicating an almost perpendicularorientation of the ST vector in that lead. ST segment elevation in lead AVR inthe setting of inferior wall infarction is rare and suggests in our experienceadditional proximal left coronary artery disease, or a dominant posterior

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION
Posterior wall involvementPosterior wall involvement is diagnosed by finding reciprocal ST segmentdepression in the precordial leads. When present in RCA occlusion, it indicatesdominance of this vessel.
In case of CX occlusion posterior wall involvement is almost obligatory.Absence of precordial ST depression in inferior wall infarction is thereforestrongly suggestive of RCA involvement (22). In figure 2.5, left, an example isgiven of posterior wall involvement in RCA occlusion. ST depression ispresent in leads to with deepest negativity in lead In figure 2.5, right,a CX occlusion is shown with ST depression in leads to
Recent data indicate that larger infarctions, more postinfarctioncomplications and a higher mortality rate occur in patients with precordial ST-depression (20-22). As pointed out by Birnbaum et al (23) when the greatestamount of ST depression is seen in leads 3-vessel disease and a low leftventricular ejection fraction should be suspected.
Isolated ST depression in the precordial leads may present the difficulty todifferentiate acute CX occlusion, resulting in true posterior wall infarction,from nonocclusive anterior myocardial ischemia. It has been suggested that inthat situation maximal ST depression in or is predictive for acute CXocclusion (24-26). Also the recording of qR complexes with ST segmentelevation in leads has been recommended to diagnose a CX occlusion(27,28).
Lateral wall involvementLateral wall involvement is reflected by ST segment elevation in leads and
It can be seen in both RCA or CX occlusion, but occurs more frequently inthe latter. Independent of the vessel involved, ST segment elevation in theseleads implies a larger ischemic area and the need for aggressive reperfusiontherapy (29).
Figure 2.6 shows an inferior wall infarction due to RCA occlusion asassessed by the typical changes in the extremity leads and the absence of STdepression in the precordials. ST elevation in and indicates lateralinvolvement and therefore the presence of a dominant RCA.
Figure 2.7 shows an example of a CX occlusion: there is only minor STelevation in the inferior leads, with most ST elevation in lead I, suggesting anon dominant CX. The vector in the frontal plane suggests a more high laterallocalization of the ischemia, consistent with a not very large obtuse marginalbranch. Most ischemia is found in the left posterior wall, due to a prominentposterolateral branch.
17
descending branch perfusing large parts of the septum. Figure 2.5, right, showsinferior wall infarction due to a CX occlusion. Most ST elevation is seen inlead II, resulting in a positive ST segment in lead I. The ST segment in AVR isiso-electric indicating that the ST vector is perpendicular to that lead. Thisresults in a markedly negative ST segment in lead AVL.

18 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
RV infarctionIn RCA occlusion the presence of RV involvement is important because itidentifies a subgroup of patients at high risk (30-42). Clinically the patient maypresent with hypotension, frequently combined with bradycardia, due to sinusbradycardia or high degree AV nodal block. AV-nodal conduction disturbancesand late VT are more frequently encountered in inferior wall MI with RVinvolvement. As also discussed in chapter 3, patients with AV nodalconduction disturbances have a higher mortality than patients without AVnodal conduction disturbances, also in the thrombolytic era (30-33).Diagnosing RV-involvement in inferior wall infarction is difficult from thestandard 12 lead ECG. The reason being that precordial leads overlying the RV
frequently record ST depression due to reciprocal ST segment changesof ischemia of the posterior wall.

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 19
Therefore it is necessary to record the right precordial leads. Figure 2.6(right panel) shows ST elevation in the right precordial leads to
has been found to be especially useful for diagnosing right ventricularinvolvement. ST-elevation of predicts an occlusion proximal to theRV-branch with an accuracy of 90% and ST-segment depression anocclusion of the CX (fig. 2.8) with an accuracy of 100% (43). An isoelectricST-segment predicts distal RCA occlusion (fig. 2.9). It is important to stressthat sufficient ST-segment elevation in the inferior leads of the standard ECG(at least 2mm) is needed to use the right precordial leads for determining thesite of coronary artery occlusion.

20 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
In a minority of cases of RV involvement the precordial lead shows ST-elevation. The sensitivity of ST elevation in lead is 24% but the specificity100%. Figure 2.10 shows an acute inferior wall infarction due to RCAocclusion. In lead the ST segment is elevated, indicating RV involvement.
Even less frequent than ST elevation in only, as the result of RVinvolvement, is the finding of more leftward precordial leads with STelevation. An example is shown in figure 2.11. The extremity leads indicateinferior wall infarction due to RCA occlusion. The precordial leads todisplay ST elevation, most prominent in consistent with RV involvement.Lack of posterior wall ischemia leads to these findings because of ischemia ofthe relatively thin RV anterior wall. This is confirmed by the positive rightprecordial leads (right panel).

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 21

22 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Isolated RV infarctionRarely the ECG shows only minor or no changes in the inferior leads and STelevation is only seen in leads and in the right precordial area. Anexample is given in figure 2.12. This picture reflects a predominant RVinfarction and is related to a non dominant RCA, a collaterally filled RCA or anisolated occlusion of a RV branch (44). It may also be seen after occlusion ofthe RV branch following PTCA or stenting of the right coronary artery (45).

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 23

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Atrial infarctionAtrial infarction may occur when a RCA or CX occlusion is proximal to thesinoatrial branch. An example is given in figure 2.6. It shows slight elevation ofthe baseline following the P wave, best seen in lead II. This Pta segmentelevation reflects the repolarization phase of the P wave. The presence of atrialinfarction not only identifies a proximal RCA or CX occlusion, but isfrequently accompanied by sinus node dysfunction, sino-atrial conductiondisturbances and episodes of atrial fibrillation.
AV nodal blockAV nodal block is common in inferior wall infarction, especially in case of aproximal RCA occlusion. ECG features, prognostic significance andmanagement are discussed in chapter 3.
Difficulties in diagnosing CX occlusionOne of the pitfalls in diagnosing acute MI is the underestimation of the areainvolved in CX infarction. This is due to several causes: 1) The left ventriculararea supplied by the CX is activated in the second half of the QRS complex andtherefore both abnormalities in activation and repolarization may be obscuredby preceding and ongoing activation and repolarization of other areas of theheart. 2) Posterior wall ischemia may only become manifest by ST segmentdepression and therefore unstable angina rather than MI is diagnosed. In thatsetting it has been suggested that presence of maximal ST depression in leads
or is predictive for acute CX occlusion (24-26). Also the use ofadditional leads has been recommended (27,28). A finding in CXocclusion can be delayed activation of the posterolateral wall. This can berecognized as a late positive deflection in lead I, and a late negative deflectionin leads III and AVF indicating that the terminal activation vector points to theleft baso lateral area (fig. 2.5, right).
A clue pointing to an extensive CX infarction is shown in figure 2.13. Itshows an inferior wall infarction with an iso-electric ST segment in lead I,consistent with a CX occlusion. The left and right precordial leads are inaccordance with that diagnosis.
Suggestive of CX dominance is the clearly prolonged PR interval,indicating AV nodal involvement.
II Anterior wall infarction
The left anterior descending branch (LAD) is usually the largest coronaryartery and supplies the anterior, lateral, septal and in 70% of humans the infero-apical segment of the left ventricle (figure 2.14). It also perfuses the bundle ofHis and the proximal part of the bundle branches. The size of the ischemic areaand the prognosis is dependent on the site of occlusion in the LAD. Dependingupon the site of LAD occlusion, apart from ST segment elevation in theprecordial leads, specific changes will occur in the extremity and lateral leads.
24

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 25
Involvement of the distal AV conduction system leads to impaired conduction,varying from intra hissal block to right bundle branch block (RBBB) with orwithout left fascicular block, to complete sub AV nodal block (46). The clinicalpicture may include heart failure and in the subacute phase ventriculartachycardia and fibrillation may occur, leading to increased in-hospital and oneyear mortality (47,48).
Anterior wall infarction is diagnosed by the presence of ST elevation in theprecordial leads to The challenge in anterior wall infarction is torecognize the size of the area at risk and the site of the occlusion in the LAD.This information can be obtained by observing additional changes in the otherprecordial and extremity leads.
The ST segment vector to localize the site of ischemiaThe anteroseptal area of the left ventricle which is perfused by the LAD can bedivided into 3 main parts: 1) The basoseptal part, supplied by the first septalbranch(es), 2) The lateral basal part, perfused by the first diagonal branch(es),or intermediate branch, 3) The inferoapical part, receiving blood from the distalLAD, frequently wrapped around the apex (figure 2.14, left panel).

26 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
As shown in a recent study by Engelen et al (49) occlusions at different sites(figure 2.14, right panel) lead to 4 electrocardiographically different pictures:1. Proximal of the septal and diagonal branches. This results in ischemia of all3 named areas. 2. Distal of the first septal and diagonal branches. This leads toischemia of the inferoapical area only. 3. Occlusion before the first diagonalbut distal of the first septal branch. This leads to ischemia of the baso lateralwall and the infero apical wall but not the basal septum. 4. Proximal before thefirst septal but distal of the first diagonal branch. This leads to ischemia of theseptum and the inferoapical area, whereas the basolateral area remains free. Inthe study by Engelen et al (49) the incidence of these sites of occlusion in theLAD territory were as follows: 40%, 40%, 10% and 10% respectively.Obviously, risk varies with these different sites of occlusion.
LAD occlusion proximal to the first septal and the first diagonal branch.High risk!Typically the ECG shows one or more of the following findings. Acquiredright bundle branch block, ST elevation in AVR, ST elevation of more than2mm in lead and ST depression in the inferior leads and in lead (42-44).An example is given in fig. 2.15. Figure 2.16 depicts the likely mechanism of

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 27
these findings: Global involvement of the left ventricle with contribution to theECG from all ischemic areas. Because of the larger mass of the basal part thevector of the ST segment will point in the superior direction (figure 2.16, leftpanel). In the frontal plane this results in ST elevation in leads AVR and AVLas the consequence of basal septal and lateral ischemia (figure 2.16, rightpanel). The more cranially positioned lead will also record ST elevation.This upward orientation of the ST vector causes reciprocal ST depression in theinferior leads (50) and also sometimes in the lateral leads Frequentlythe ST vector points not only upward but somewhat more to the left than to theright. This results in more ST elevation in AVL than in AVR, and more STdepression in lead III than in lead II. Local conduction delay in the lateral leadsmay lead to widening of the Q wave in lead AVL.Statistical values of criteria to identify a proximal occlusion are listed in table2.2.

28 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Distal LAD occlusion. Low risk.Figure 2.17 shows an example of an acute anterior wall infarction due to adistal LAD occlusion (behind the major proximal septal and diagonalbranches). Typical findings are the presence of Q waves in leads andand the absence of ST depression in the inferior leads (53,54).In this situation there is ischemia in the infero-apical part therefore the STvector will point inferiorly (figure 2.18 left panel).
The ST segment in the inferior leads will become isoelectric or evenpositive (figure 2.18, right panel). The Q waves in the left precordial leads arelikely due to the combination of local conduction delay in that area combinedwith persistence of the regular septal q wave in these leads.

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 29

30 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
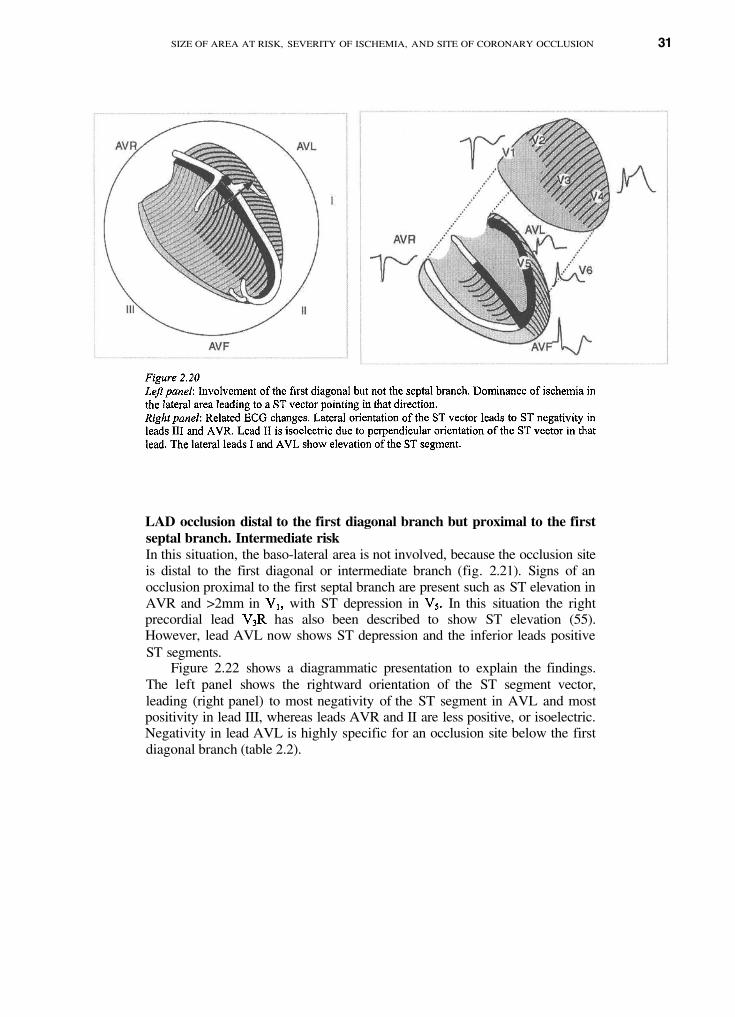
LAD occlusion distal to the first septal branch, but proximal to the firstdiagonal branch. Intermediate risk.Figure 2.19 shows the ECG of an acute anterior wall infarction with anocclusion site distal to the first septal, but proximal to the first diagonal branch.Typical features are: ST elevation in lead AVL and the left lateral leads and STdepression in lead III which is more pronounced than in lead II. Figure 2.20shows a diagram with the distribution of ischemia in that situation, leading tothe ST segment vector pointing in a left lateral direction (left panel). Becauseof that direction of the ST segment vector the difference in ST depressionbetween leads III and II is now much more pronounced than in the LADocclusion proximal to both the first septal and the first diagonal (fig. 2.15).
SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 31
LAD occlusion distal to the first diagonal branch but proximal to the firstseptal branch. Intermediate riskIn this situation, the baso-lateral area is not involved, because the occlusion siteis distal to the first diagonal or intermediate branch (fig. 2.21). Signs of anocclusion proximal to the first septal branch are present such as ST elevation inAVR and >2mm in with ST depression in In this situation the rightprecordial lead has also been described to show ST elevation (55).However, lead AVL now shows ST depression and the inferior leads positiveST segments.
Figure 2.22 shows a diagrammatic presentation to explain the findings.The left panel shows the rightward orientation of the ST segment vector,leading (right panel) to most negativity of the ST segment in AVL and mostpositivity in lead III, whereas leads AVR and II are less positive, or isoelectric.Negativity in lead AVL is highly specific for an occlusion site below the firstdiagonal branch (table 2.2).

32 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 33
Criteria to identify the site of occlusion in anterior wall infarctionTable 2.2 lists the criteria to identify the site of occlusion in anterior wallinfarction. They are especially useful in patients presenting with a first acuteanterior infarction. In contrast to sensitivity, the specificity of these criteria ishigh, indicating that their presence accurately predicts the occlusion site, butthat a specific site is not excluded by their absence.
Right bundle branch block remains, as described in chapter 3, a veryspecific marker of an occlusion before the first septal branch. ST elevation in
has to be more than 2mm to be sufficiently specific for that location. STelevation in AVR is apart from being specific the most sensitive marker forproximal LAD occlusion. ST depression in is not a very frequent, butspecific marker.
Lead AVL is the most useful lead to identify an occlusion site proximal(starting with a Q wave) or distal (showing a negative ST segment) to the firstdiagonal branch.
Left main occlusionFigures 2.23 and 2.24 show the tracings of patients with a left main occlusion.Apart from acquired right bundle branch block and other features of anocclusion proximal to the first septal branch the ECG also shows signs ofsevere posterobasal ischemia. This combination is very suggestive for severe

34 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
ischemia caused by an occlusion proximal to the take off of the LAD and theCX. Recently Yamaji et al (56) reported that left main occlusion should besuspected when ST segment elevation in AVR is higher than ST segmentelevation in lead
ST deviation score and location of the coronary artery occlusionIn our experience there is an acceptable correlation between the ST segmentdeviation score and the location of the occlusion in the culprit coronary artery(fig. 2.25). There are exceptions however (fig. 2.26), especially in anterior wallinfarction where the precordial leads reflect a more local than global area ofischemia of the left ventricle.

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 35

36 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
A new infarction in the presence of an old oneObviously, the occurrence of a new infarction in a coronary vessel territorydifferent from the previous one places the patient in a high risk categorybecause of pre-existent myocardial tissue loss from the old infarction. Such asituation should be recognized on the ECG and an indication for aggressivereperfusion therapy. An example is given in figure 2.27.
LimitationsAlthough the ECG has proven to be very useful to determine the extent andseverity of ischemia and the site of the occlusion in the culprit artery, it may belimited in the individual patient by factors such as: A location in the CX area,the presence of old infarction(s), left ventricular hypertrophy, altered activationas in left bundle branch block, preexcitation or a ventricular paced rhythm (seechapter 5), preexisting ST-T abnormalities, ischemia at a distance because ofocclusion of a coronary artery which was also supplying the territory of anothercoronary artery by collateral circulation, dominance or underdevelopment ofcoronary arteries and a congenital abnormal site of origin of coronary arteries.

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION
Conclusion
Anyone involved in decision making in the patient with acute cardiac ischemiashould be familiar with the electrocardiographic signs that indicate the severityand size of the area at risk. This includes knowledge and understanding of theimportance of the ST segment deviation score; ischemia grading based uponthe behaviour of the terminal portion of the QRS and the beginning of STelevation; and the ECG signs that indicate which coronary artery is occludedand where the occlusion is located.
Such knowledge is essential for optimal decision making in relation to theuse and the type of reperfusion therapy.
37

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
References
Bar FW, Vermeer F, de Zwaan C, et al. Value of admission electrocardiogram in predictingoutcome of thrombolytic therapy in acute myocardial infarction. Am J Cardiol 1987:59:6-13.
Aldrich HR, Wagner NB, Boswick J, et al. Use of the ST segment deviation for predictionof final electrocardiographic size of acute myocardial infarcts. Am J Cardiol 1988,61:749-753.
Hathaway WR, Peterson ED, Wagner GS, et al. Prognostic significance of the initialelectrocardiogram in patients with acute myocardial infarction. JAMA 1998; 279:387-391.
Crimm A, Severance HW Jr, Coffey K. Prognostic significance of isolatedsinustachycardia during first three days of acute myocardial infarction. Am J Med1984;76:983-988.
Zuanetti G, Mantini C, Hernandez-Bernal F, et al. Relevance of heart rate as a prognosticfactor in patients with acute myocardial infarction: Insights from the G1551-2 study. EurHeart J 1998;19 (supplement F):19-26.
Sclarovsky S: Electrocardiography of acute myocardial ischaemic syndromes. London:Martin Duntz Ltd, 1999.
Birnbaum Y, Sclarovsky S. The grades of ischemia on the presenting electrocardiogram ofpatients with ST elevation acute myocardial infarction. J Electrocardiography 2001;34(suppl): 17-26.
Hurst JW. Methods used to interpret the 12-lead electrocardiogram: Pattern memorizationversus the use of vector concepts. Clin. Cardiol. 2000;24:4-13.
Foerster JM, Vera Z, Janzen DA, Foerster SJ, Mason DT. Evaluation of precordialorthogonal vectrorcardiographic lead ST-segment magnitude in the assessment ofmyocardial ischemia injury. Circulation 1977;55:728-735.
Vermeer F, Simoons ML, Bar FW, et al. Which patients benefit most from earlythrombolytic therapy with intra coronary streptokinase? Circulation 1986; 74:1379-1389.
Mauri F, Gasparini M, Barbonaglia L, et al. Prognostic significance of the extent ofmyocardial injury in acute myocardial infarction treated by streptokinase (the GISSI trial).Am J Cardiol 1989;63:1291-1295.
Berland J, Caribier A, Behar P, Letal B. Anterior ST depression in inferior myocardialinfarction: correlation with results of intracoronary thrombolysis. Am Heart J1986;111:481-488.
Peterson ED, Hathaway WR, Zabel KM, et al. Prognostic significance of precordial STdepression during inferior myocardial infarction in the thrombolytic era: results in 16.251patients. J Am Coll Cardiol. 1996; 28:305-312.
Birnbaum Y, Sclarovsky S, Blum A, et al. Prognostic significance of the initialelectrocardiographic pattern in a first acute anterior wall myocardial infarction. Chest1993;103:1681-1687.
38
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.

SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION 39
Birnbaum Y, Kloner R, Sclarovsky S, et al. Distortion of the terminal portion of the QRSon the admission electrocardiogram in acute myocardial infarction and correlation withinfarct size and long term prognosis (Thrombolysis in Myocardial Infarction 4 Trial). Am JCardiol 1996;78:396-403.
Birnbaum Y, Maynard C, Wolfe S, et al. Terminal QRS distortion on admission is betterthan ST segment measurements in predicting final infarct size and assessing the potentialeffect of thrombolytic therapy in anterior wall acute myocardial infarction. Am J Cardiol1999;84:530-539.
Birnbaum Y, Criger DA, Wagner GS, et al. Prediction of the extent and severity of leftventricular dysfunction in anterior acute myocardial infarction by the admissionelectrocardiogram. Am Heart J 2001;141:915-920.
Birnbaum Y, Herz I, Sclarovsky S, et al. Prognostic significance of the admissionelectrocardiogram in acute myocardial infarction. J Am Coll Cardiol 1996;27:1128-1133.
Birnbaum Y, Sclarovsky S, Herz I, et al. Admission clinical and electrocardiographiccharacteristics predicting in-hospital development of high degree atrio ventricular block ininferior wall acute myocardial infarction. Am J Cardiol 1997;80:1134-1139.
Ben-Gal T, Sclarovsky S, Herz I, et al. Importance of the conal branch of the rightcoronary artery in patients with acute anterior wall myocardial infarction:electrocardiographic and angiographic correlation. J Am Coll Cardiol 1997;29:506-511.
Herz I, Assali AR, Adler Y, Solodky A, Sclarovsky S. New electrocardiographic criteriafor predicting either the right or left circumflex artery as the culprit coronary artery ininferior wall acute myocardial infarction. Am J Cardiol 1997;80:1343-1345.
Kontos M, Desai PV, Jesse RL, Ornato JP. Usefulness of the admission electrocardiogramfor identifying the infarct related artery in inferior wall acute myocardial infarction. Am JCardiol 1997;79:182-184.
Birnbaum Y, Herz I, Sclarovsky S, et al. Prognostic significance of precordial ST segmentdepression on admission electrocardiogram in patients with inferior wall myocardialinfarction. J Am Coll Cardiol 1996;28:313-318.
Borgia MC, Gori F, Pellicelli A, Curcio D, Lionetti M, Buccarella PA, Lucidi M. Influenceof thrombolytic therapy on inferior acute myocardial infarction with concomitant anteriorST segment depression. Angiology 1999;50:619-628.
Birnbaum Y, Wagner GS, Barbash GI et al. Correlation of angiographic findings and rightversus left precordial ST-segment depression in inferior wall acute
myocardial infarction. Am J Cardiol 1999;83:143-148.
Shah A, Wagner GS, Green CL, et al. Electrocardiographic differentation of the ST-segment depression of acute myocardial injury due to left circumflex artery occlusion fromthat of myocardial ischemia of nonocclusive etiologies. Am J Cardiol 1997;80:512-513.
Casas R, Marriott HJL, Glancy L. Value of leads in diagnosing posterior wall acute
myocardial infarction and other causes of tall R waves in Am J Cardiol 1997;80:8-9.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Matetzky S, Freimark D, Chouraqui P, et al. Significance of ST segment elevations inposterior chest leads (V7 to V9) in patients with acute inferior myocardial infarction:application for thrombolytic therapy. J Am Coll Cardiol 1998;31:506-511.
Assali A, Sclarovsky S, Herz I, et al. Comparison of patients with inferior wall acutemyocardial infarction with versus without ST-segment elevation in leads V5 and V6. Am JCardiol 1998;81:81-83.
Braat SH, Brugada P, de Zwaan C, Wellens HJJ. Value of electrocardiogram in diagnosingright ventricular involvement in patients with an acute inferior wall myocardial infarction.Br Heart J 1983;49:368-372.
Widdershoven J,Gorgels A, Vermeer F, et al. Changing characteristics and in-hospitaloutcome of patients admitted with acute myocardial infarction. Eur Heart J 1997;18:1073-1080.
Berger PB, Ruocco N, Ryan T, Frederick M, Jacobs A, Faxon D. Incidence and prognosticimplications of heart block complicating acute inferiotr myocardial infarction treated withthrombolytic therapy: results from TIMI II. J Am Coll Cardiol 1992;20:533-540.
Kimura K, Kosuge M, Ishikawa T, et al. Comparison of the results of early reperfusion inpatients with inferior wall acute myocardial infarction with and without completeatrioventricular block. Am J Cardiol 1999;83:731-733.
Klein HO, Trjordman T, Ninio R, et al. The early recognition of right ventricularinfarction: diagnostic accuracy of the electrocardiographic V4R lead. Circulation1983;67:558-565.
Simons GR, Sgarbossa E, Wagner G, Califf RM,Topol EJ,Natale A. Atrioventricular andintraventricular conduction disorders in acute myocardial infarction: a reappraisal in thethrombolytic era. PACE 1992;21:2651-2663.
Berger PB, Ryan TJ. Inferior myocardial infarction: high-risk sub-groups. Circulation1990;81:401-411.
Berger PB, Ruocco NA, Ryan TJ, et al. Frequency and significance of right ventriculardysfunction during inferior wall left ventricular myocardial infarction treated withthrombolytic therapy (results from the Thrombolysis in Myocardial Infarction (TIMI) IItrial. Am J Cardiol 1993;71:1148-52.
Zehender M, Kapere W, Kauder E, et al. Right ventricular infarction as independentpredictor of prognosis after acute myocardial infarction. N Engl J Med 1993;328:981-988.
Zeymer U, Neuhaus KL, Wegscheider K, Tebbe U, Molhoek P, Schroder R, for HIT-4Trial Group. Effects of thrombolytic therapy in acute inferior myocardial infarction with orwithout right ventricular involvement. J Am Coll Cardiol 1998;32:876-881.
Buono H, Lopez-Palop R, Bermejo J, Lopez-Sendon JL, Delcan JL. In-hospital outcome ofelderly patients with acute myocardial infarction and right ventricular involvement.Circulation 1997;96:436-441.
Buono H, Lopez-Palop R, Perez-David E, Garcia-Garcia J, Lopez-Sendon JL, Delcan JL.Combined effect of age and right ventricular involvement on acute inferior myocardialinfarction. Circulation 1998;98:1714-1720.
40
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
SIZE OF AREA AT RISK, SEVERITY OF ISCHEMIA, AND SITE OF CORONARY OCCLUSION
Mehta SR, Eikelboom JW, Natarajan MK, et al. Impact of right ventricular involvement onmortality and morbidity in patients with inferior myocardial infarction. J Am Coll Cardiol2001;37:37-43.
Braat SH, Gorgels APM, Bar FWHM, Wellens HJJ. Value of the ST-T segment in leadV4R in inferior wall acute myocardial infarction to predict the site of coronary arteryocclusion. Am J Cardiol 1998;62:140-142.
Mittal SR. Isolated right ventricular infarction. Int J Cardiol. 1994;46:53-60.
Van der Bolt CLB, Vermeersch PHMJ and Plokker HWM. Isolated acute occlusion of alarge right ventricular branch of the right coronary artery following coronary balloonangioplasty. Eur Heart J 1996;17:247-250.
Li e KI, Wellens HJ, Schuilenburg RM, Becker AE, Durrer D. Factors influencingprognosis of bundle branch block complicating acute anteroseptal infarction: the value ofHis bundle recordings. Circulation 1974;50:935-941.
Lie KI, Wellens HJ,Schuilenburg RM, David GK, Durrer D. Early identification of patientsdeveloping late in-hospital fibrillation after discharge from the CCU. Am J Cardiol1978;41:674-677.
Melgarejo-Moreno A, Galcera-Tomas J, Garcia-Alberola A, et al. Incidence, clinicalcharacteristics, and prognostic significance of right bundle-branch block in acutemyocardial infarction: a study in the thrombolytic era. Circulation 1997;96:1139-1146.
Engelen DJ, Gorgels AP, Cheriex EC, et al. Value of the electrocardiogram in localizingthe occlusion site in the left anterior descending coronary artery in acute anteriormyocardial infarction. J Am Coll Cardiol. 1999;34:389-395
Birnbaum Y, Solodky A, Herz I et al. Implications of inferior ST-segment depression inacute anterior myocardial infarction: electrocardiographic and angiographic correlation.Am Heart J 1994;127:1467-73.
Tamura A, Kataoka H, Mikuriya Y, Nasu M. Inferior ST-segment depression as a usefulmarker for identifying proximal left anterior descending artery occlusion during acuteanterior wall myocardial infarction. Eur Heart J 1995;16:1795-9.
Porter A, Sclarovsky S, Ben-Gal T, Herz I, Solodky A, Sagie A. Value of T wave inversionwith lead III ST-segment depression in acute anterior myocardial infarction:electrocardiographic prediction of a wrapped left anterior descending coronary artery. ClinCardiol 1998;21:562-6.
Sapin PM, Musselman DR, Dehmer GJ, Cascio WE. Implications of inferior ST-segmentelevation accompanying anterior wall acute myocardial infarction for the angiographicmorphology of the left anterior descending coronary artery morphology and site ofocclusion. Am J Cardiol 1992;69:860-865.
Tamura A, Kataoka H, Nagase K, Mikuriya Y, Nasu M. Clinical significance of inferior STelevation during acute myocardial infarction. Br Heart J 1995;74:611-614.
Kataoka H, Tamura A,Yano S,Kanzaki K,Mikuriya Y. ST elevation in the right chest leadsin anterior wall ventricular acute myocardial infarction. J Am Cardiol 1990;66:1146-1147.
41
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Yamaji H, Iwasachi S, Kusachi S, et al. Prediction of acute left main coronary obstructionby 12-lead electrocardiogram:AVR ST-segment elevation with less V, ST-segmentelevation. J Am Coll Cardiol 2001;38:1348-1354.
42
56.

Chapter 3
Conduction disturbances in acute myocardial infarction

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Sinus arrest and sino-atrial block
Low incidenceInfero-posterior infarction with proximal occlusion of RCA or CXTherapy other than reperfusion dictated by hemodynamic and/orarrhythmic consequences
AV nodal conduction disturbances
Common in proximal RCA occlusionWorsens prognosis, stressing necessity of aggressive reperfusiontherapyTemporary pacing in case of pump failure, cardiogenic shock orfrequent ventricular ectopic activity. Permanent pacing rarely needed
Sub-AV nodal conduction disturbances
Differentiate between pre-existent and acquired bundle branch blockAcquired bundle branch block indicates proximal LAD occlusionAcquired bundle branch block worsens prognosis indicating aggressivereperfusion therapyTemporary pacing in case of advanced intra Hissal or sub Hissal blockPermanent pacing rarely needed
44

CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION 45
A. THE SINO-ATRIAL REGION
Blood supply of the sinus node and the atrio-ventricular conduction system
In discussing abnormalities in sinus node behavior, sino-atrial conduction andatrio-ventricular conduction during acute cardiac ischemia, it is essential toknow by which coronary artery these structures receive their blood supply.
Sinus node and sino-atrial regionThe sinus node and the sino-atrial region are in 55% of cases perfused by anatrial branch from the proximal part of the right coronary artery (RCA) and in45% of cases by a proximal branch of the circumflex (CX) coronary artery (1).Therefore, a proximal occlusion of the RCA or CX may lead to ischemia of thesinus node and the surrounding atrium.
The atrio-ventricular (AV) conduction systemAs shown in figure 3.1 the RCA perfuses the AV node and the proximal part ofthe bundle of His. The distal part of the His bundle, the right bundle branch andthe anterior fascicle of the left bundle branch are supplied by the septalbranches of the left anterior descending (LAD) coronary artery. The posteriorfascicle of the left bundle branch is perfused both by the septal branches of theLAD and by the RCA (1).

46 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
This means that AV nodal conduction disturbances in acute myocardialinfarction point to a RCA occlusion and sub AV nodal conductionabnormalities are found in case of impaired perfusion of the upper part of theinterventricular septum caused by an LAD occlusion proximal to the first septalbranch.
Slow rhythms and conduction abnormalities at the sinus nodal and sino-atrial level
ECG findings
Sinus bradycardiaThis is defined as the presence of sinus P waves at a rate of less than 60 beatsper minute (figure 3.2).

CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION 47
Sino atrial block and sinus arrestSino-atrial (SA) conduction abnormalities can become manifest as seconddegree (SA Wenckebach, SA Mobitz-2 block, 2 to 1 block) or complete sino-atrial block. In the absence of electrogram recordings from the sinus nodeitself, it is impossible to know in case of a sinus bradycardia or absence ofsinus P waves whether abnormalities in impulse formation, impulse conductionor both are responsible.
Figure 3.3 is an example of second degree sino-atrial block of the Mobitz-2 type. Figure 3.4 shows complete absence of P waves either because ofcomplete sino-atrial block or absence of impulse formation in the sinus node.
Incidence, mechanisms and prognostic significanceIn 1976 Liem et al. (2) published an incidence of sinus bradycardia of 12,5% in800 consecutive patients with an acute myocardial infarction. It was three timesmore common in infero-posterior than in anterior wall myocardial infarction.They showed that patients with sinus bradycardia had a better prognosis as tomortality and infarct size than patients without sinus bradycardia.

48 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
As indicated in table 1 different mechanisms have been suggested as causefor sinus bradycardia (1,3,4). Especially, in the early stage of myocardialinfarction slow or absent sinus rhythm seems to be caused by activation of theparasympathetic nervous system because of pain, anxiety and the Bezold-Jarisch reflex. In our experience a slow or absent sinus rhythm is much morecommon in proximal than in distal RCA occlusion. Emergence at a later stageof sinus bradycardia and SA block suggests perfusion abnormalities of thesino-atrial area. The ECG finding of atrial infarction supports ischemia as thecause. The effect of atropine can be of help to distinguish between a vagal andan ischemic cause. In the first situation sinus bradycardia or sinus arrest willdisappear. This is not the case when ischemia is responsible for the slow orabsent sinus rhythm. Unfortunately, no information is available on theincidence of sino-atrial conduction abnormalities in acute infero-posteriorinfarction, nor do we have knowledge about their prognostic significance, forexample in relation to the development of the sick sinus syndrome later.
ManagementAbnormalities in impulse formation and conduction in the sinus node regionresult in slow heart rates and may thereby lead to a lower cardiac output,

CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION
increased occurrence of atrial fibrillation and (because of a slow heart rate) toincreased ventricular ectopy.
Differentiation between a vagal and non-vagal origin should be attempted.Reperfusion of the culprit coronary artery is certainly indicated when ECGsigns are present of atrial infarction or advanced sino-atrial block because theyindicate proximal RCA occlusion with right ventricular involvement or aproximal CX occlusion.
In general, sinus bradycardia, because it is vagally induced, indicates asmaller infarction with a good short and long-term prognosis. Atropineadministration or cardiac pacing is seldom indicated.
B. THE AV-NODAL CONDUCTION SYSTEM
Conduction abnormalities at the atrio-ventricular nodal level
ECG findingsIn infero-posterior infarction conduction abnormalities in the AV node are mostcommonly seen in case of an occlusion of the RCA proximal to the rightventricular branch leading to a right ventricular infarction as well (see chapter2). Conduction disturbances in the AV node may become manifest on the ECGas: 1) a prolonged PR interval of more than 200 msec, 2) second degree AVblock (of the Wenckebach type, or 2 to 1 block) and 3) complete AV nodalblock. Examples of a Wenckebach, a 2 to 1 and a complete AV nodal block aregiven in figures 3.5, 3.6 and 3.7. In all 3 examples a proximal RCA occlusionwas responsible and right ventricular involvement was present (lead notshown in figures 3.5 and 3.6). All three cases show atrial infarction (asmanifested by a PTa shift after the P wave).
49

50 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION 51
Typically for AV nodal Wenckebach and 2 to 1 AV nodal block is themarkedly prolonged PR interval of the conducted P wave. This is in contrast toWenckebach conduction or 2 to 1 conduction in the sub AV nodal conductionsystem where smaller PR increments are seen during the Wenckebach sequenceand less PR prolongation of the conducted P wave. In fact, in 2 to 1 block subAV nodally the PR interval of the conducted beat is often not prolonged.
Left bundle branch block in inferior wall myocardial infarctionIn 1974, Lie et al. (5) noted that in patients with inferior wall infarction andhigh degree AV nodal block a bundle branch block pattern was present in beatsterminating a long RR interval. However, in contrast to the right bundle branchblock (RBBB) shaped beats terminating a long RR interval, the LBBB shapedones had a His potential in front of the QRS and represented conducted beats orAV junctional escape beats with phase 4 (bradycardia dependent) block in theleft bundle branch. A typical example is shown in figure 3.8. Therefore, LBBB

52 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
shaped beats occurring after a critical RR interval in patients with high degreeAV nodal block in acute inferior infarction do not indicate infra AV nodalblock, meaning absence of an indication for implantation of a permanentpacemaker!
Incidence, mechanism and prognostic significanceIn the prethrombolytic era, Tans et al. (6) found that 144 out of 843 patients (17%) with an infero-posterior infarction had advanced AV nodal block defined assecond degree AV nodal block or worse. More recently, in the era ofreperfusion, the incidence is similar, varying between 12 and 20% (7,8). Alsoas pointed out by Simons et al. (9) the incidence of third degree AV nodalblock remained similar in the thrombolytic era (around 10%). Increased vagalstimulation because of pain, anxiety and the Bezold Jarisch reflex, and

CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION
ischemia of the AV node have been suggested as mechanisms for AV nodalblock. As with sinus bradycardia and sino-atrial block, the distinction betweenthese two mechanisms can be made by giving atropine. Vagally induced AVnodal block will disappear and ischemic AV nodal block will persist. Also theECG can give a clue as to the most likely mechanism. For example in figure3.6 during 2 to 1 AV nodal block the ECG shows a sinus rate of 150 beats perminute, clearly indicating absence of vagal dominance.
AV nodal block is common in case of a proximal RCA occlusion. Asshown by Braat et al. (10), approximately 45% of these patients have advancedAV nodal block during the acute phase of myocardial infarction. A proximalRCA occlusion means a larger inferior infarct, with right ventricularinvolvement. It is not surprising therefore that AV nodal block is accompaniedby a 2,5 times higher in hospital mortality rate also in the thrombolytic era.
AV nodal block in inferior wall myocardial infarction is typically transientdisappearing after a few days. It may last up to 16 days, as shown by Barold(11) in a careful analysis of 20 studies of patients with second and third degreeAV nodal block after inferior wall myocardial infarction.
ManagementThe occurrence of high degree AV nodal block in inferior wall infarctionusually means a proximal RCA occlusion and a large infero-posterior infarctwith right ventricular involvement. This stresses the necessity of earlyreperfusion of the occluded RCA. This is frequently followed by a return ofnormal AV nodal conduction when reperfusion is accomplished (12), which isin fact an electrocardiographic marker of reperfusion. Temporary ventricular ordual chamber pacing is indicated when pump failure, cardiogenic shock orfrequent ventricular ectopic activity accompany high degree AV nodal block ininferior wall MI. Results of pacing can be disappointing because outcome isprimarily determined by the size of the myocardial infarction and theassociated hemodynamic status. The necessity of permanent pacing in AVnodal block after inferior MI is very rare (11). In fact only when persistentsymptomatic second or third degree AV nodal block is present more than 2weeks after inferior MI.
C. CONDUCTION ABNORMALITIES AT THE SUB-AV NODALLEVEL
ECG findingsAs previously indicated, the bundle of His and the proximal and distal parts ofthe bundle branches are perfused by the septal branches from the LAD. Theposterior fascicle of the left bundle branch is frequently also supplied by theposterior descending coronary artery (which may come from the RCA or CX).Conduction disturbances in the His bundle and the bundle branch systemoccurring in the setting of anterior wall infarction indicate a very proximalocclusion in the LAD. Figures 3.9 and 3.10 are examples of 2 to 1 and
53


CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION 55
Mobitz-2 intrahissal block in a proximal LAD occlusion. The presence ofconduction disturbances in or below His means that a large area of the leftventricle is in jeopardy. Essential in using bundle branch block (BBB) in acutemyocardial infarction as a marker of a large area at risk and the likelihood of apoor prognosis is to know the duration of BBB. Was BBB present beforemyocardial infarction (pre-existent BBB) or is it the consequence (acquiredBBB) of impaired blood supply to the conduction system because of an LADocclusion proximal to the first septal branch? Twenty five years ago, Lie et al.(13) showed that when RBBB was present before infarction and patients werematched for age and sex, hospital mortality was not different from patientswithout RBBB. This was totally different in patients developing bundle branchblock in the setting of their acute myocardial infarction. Acquired BBB istypically seen in anteroseptal myocardial infarction with right (R) BBB with orwithout left fascicular block (figure 3.11). This is much more common thanacquired complete left (L) BBB and has a more ominous prognosis (13).

56 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Occasionally acquired bundle branch block in anterior wall infarction mayoccur in the left anterior fascicle only (figure 3.12). Marked left axis deviationwith increased QRS duration in acute anterior wall myocardial infarctionshould make one suspicious of a proximal LAD occlusion.
The ECG is helpful in distinguishing between acquired and pre-existentRBBB. As shown in figure 3.13 and table 3.2 acquired RBBB is characterizedby a QR complex, while pre-existent RBBB shows an RsR1 configuration inlead Preexistent RBBB is more commonly found in the elderly patient.
When RBBB develops in acute anterior MI it occurs suddenly (figure3.14) and it may or may not be accompanied by a conduction disturbance inone of the fascicles of the left bundle branch (figure 3.14)

CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION 57

58 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Time of onset, duration of RBBB and the additional presence of aconduction problem in one of the fascicles of the left bundle branch all affectprognosis.
Early onset, long duration and additional disturbances in left fascicularconduction all increase the chance of the development of complete AV blockand increase early mortality (13). Lie et al. (14) also showed that in these

CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION 59
patients the HV but not the PR interval was helpful in determining whichpatient with bifascicular block is at high risk for developing complete infra AVnodal block. When complete infra AV nodal block develops (figure 3.15) itusually does so within 3 days after infarction (14).
Complete LBBB secondary to acute anterior wall MI is rare. Already in1976 (13) Lie et al. showed that in acute anterior wall MI acquired RBBB ismuch more common then acquired LBBB. Occasionally, one may observeacquired complete RBBB followed by acquired complete LBBB (fig 3.16).Obviously, this finding indicates the necessity to attempt rapid reperfusion.Figure 3.16 shows the effect of primary PTC A in such a patient.

60 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Incidence, mechanism and prognostic significanceIn the pre-thrombolytic era Lie et al. (13) found an incidence of acquiredRBBB of 26% in patients admitted because of an acute anterior wall MI.Mortality was 3 times higher than in patients with anterior MI without bundlebranch block.
Unfortunately, we have no data on the incidence of acquired BBB in acuteanterior wall MI in the era of reperfusion therapy. Articles have appeared onthe incidence of BBB in patients treated with thrombolytic therapy (15) butpeople have not been divided into those with preexistent and acquired BBB.When all BBB’s (transient and persistent) in all infarct locations were includedNewly et al. (15) found an incidence of 23,6%. Patients with an LAD infarctionhad the highest incidence of BBB. The in hospital mortality rates in patientswith BBB were 2½ times higher as compared to those without BBB. Patientswith persistent BBB had a higher mortality rate than those with transient BBB.When complete AV block develops mortality rate continues to be higher in thethrombolytic era when compared to patients without complete AV block (16).Harpaz et al. (16) also found that while the incidence of complete AV block

CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION
diminished in the thrombolytic era the higher mortality rate was still presentand similar in thrombolysis-treated and non treated patients with complete AVblock.
In that study no information is available on the timing of complete AVblock in relation to thrombolytic therapy. Was it present before or did itdevelop later? The mechanism of RBBB and hemiblock and complete sub AVnodal block is the interruption of blood supply to the proximal part of the sub-AV nodal conduction system. This means an LAD occlusion proximal to thefirst septal branch resulting in a large anterior wall myocardial infarction withclear consequences as to mortality and morbidity. Reperfusion should beattempted as early as possible. Depending upon the rapidity of the interventionprimary PTCA could be more beneficial than thrombolytic therapy in thissituation.
ManagementApart from rapid reperfusion, intravenous beta-blocking therapy andadministration of an ACE-inhibitor, prophylactic insertion of a pacing wireshould be done when in the setting of an acute anterior wall MI RBBBdevelops accompanied by a frontal QRS axis to the left of –60° (indicatingadditional left anterior hemiblock) or to the right of + 90 (suggesting additionalleft posterior hemiblock).
Pacing is indicated in case of: 1) apparent second or third degreeintrahissal block 2) RBBB with prolonged PR (with or without left hemiblock)or advanced (second or third degree) AV block.When pacing is indicated it should preferably be done in a dual chamberfashion.
As pointed out by Hauer et al. (17) chronic pacing is rarely required. Likein inferior wall MI sub-AV nodal conduction disturbances following anteriorwall myocardial infarction rarely result in persistent high degree conductiondisturbances.
The future of the patient with anterior wall MI and AV conductiondisturbances is determined by the degree of impairment in LV function and theoccurrence of life-threatening ventricular arrhythmias.
Conclusions
As indicated in table 3.3 high degree block in the AV node (infero-posteriorMI) and below the AV node (anterior MI) significantly worsens short and long-term outcome. Primarily because of the size of the myocardial infarction and itshemodynamic consequences.Rapidity of reperfusion of the ischemic area is therefore important. Especially,in these high risk patients the possible advantages of primary PTCA overthrombolytic therapy should be evaluated.
61

62 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
CONDUCTION DISTURBANCES IN ACUTE MYOCARDIAL INFARCTION
James TN. The coronary circulation and conduction system in acute myocardial infarction.Progr Cardiovasc Dis 1968; 10:410-428.
Liem KL, Lie KI, Louridtz WJ, Durrer D, Wellens HJJ. Sinusbradycardie bij het acutehartinfarct. Ned T Geneesk 1976;120:604-608.
James TN. Cardiac innervation. Anatomic and pharmacological relations. Bull New YorkAcad Med 1967;43:1041-1050.
Zipes DP. The clinical significance of bradycardiac rhythm in acute myocardial infarction.Am J Cardiol 1969;24:814-819.
Lie KI, Wellens HJ, Schuilenburg RM, Becker AE, Durrer D. Mechanism and significanceof widened QRS complexes during complete AV block in acute inferior myocardialinfarction. Am J Cardiol 1974;33:833-841.
Tans A, Lie KI, Durrer D. Clinical setting and prognostic significance of high degreeatrioventricular block in acute inferior myocardial infarction; a study of 144 patients. AmHeart J 1980;99:4-8.
Berger P, Ruocco N, Ryan T, Frederick M, Jacobs A, Faxon D. Incidence and prognosticimplications of heart block complicating acute inferior myocardial infarction treated withthrombolytic therapy: results from TIMI II. J Am Coll Cardiol 1992;20:533-540.
Kimura K, Kosuge M, Ishikawa T, Shimizu M, Hongo Y, Sugiyama M, Tochikubo O,Umemura S. Comparison of the results of early reperfusion in patients with inferior wallacute myocardial infarction with and without complete atrioventricular block. Am JCardiol 1999;84:731-733.
Simons GR, Sgarbossa E, Wagner G, Califf RM, Topol EJ, Natale A. Atrioventricular andintraventricular conduction disorders in acute myocardial infarction: A reappraisal in thethrombolytic era. PACE 1992;21:2651-2663.
Braat S, de Zwaan C, Brugada P, Coenegracht J, Wellens H. Right ventricular involvementwith acute myocardial infarction identifies high risk of developing atrioventricular nodalconduction disturbances. Am Heart J 1984;107:1183-7.
Barold SS. American College of Cardiology/American Heart Association guidelines forpacemaker implantation after acute myocardial infarction. What is persistent advancedblock at the atrioventricular node? Am J Cardiol 1997; 80:770-774.
Kimura K, Kosuge M, Ishikawa T et al. Comparison of results of early reperfusion inpatients with inferior wall acute myocardial infarction with and without completeatrioventricular block. Am J Cardiol 1999;84:731-733.
Lie KI, Wellens HJ, Schuilenburg RM. Bundle branch block and acute myocardialinfarction. In: The conduction system of the heart, Editors H. Wellens, KI Lie and MJJanse. Philadelphia, Lea and Febiger 1976, pp 663-672.
Lie KI, Wellens HJ, Schuilenburg RM, Becker AE, Durrer D. Factors influencingprognosis of bundle branch block complicating acute anteroseptal infarction: the value ofHis bundle recordings. Circulation 1974;50:935-941.
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
63
10.
11.
12.
13.
14.

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Newby KH, Pisano E, Krucoff MW, Green C, Natale A. Incidence and clinical relevanceof the occurrence of bundle branch block in patients treated with thrombolytic therapy.Circulation 1996;94:2424-2428.
Harpaz D, Behar S, Gotlieb S, Boyko V, Kishon Y, Eldar M. Complete atrioventricularblock complicating acute myocardial infarction in the thrombolytic era. J Am Coll Card1999;34:1721-1728.
Hauer R, Lie KI, Liem KL, Durrer D. Long-term prognosis in patients with bundle branchblock complicating acute anteroseptal infarction. Am J Cardiol 1982;49:1581-1585.
15.
16.
17.
64

Chapter 4
Myocardial infarction in the presence of abnormal
ventricular activation
Left bundle branch block, paced ventricular rhythm,
pre-excitation

66 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Presence of pre-existent left bundle branch block (LBBB) worsensprognosis in acute myocardial infarction.
Abnormal left ventricular activation, as in LBBB, right ventricular pacingand ventricular pre-excitation, results in low sensitivity and specificity ofthe ECG to diagnose site and size of a myocardial infarction.
Serial ECG’s are most helpful to diagnose myocardial infarction in case ofabnormal ventricular activation.
In case of abnormal left ventricular activation the clinical impressionshould determine decision making as to reperfusion therapy.

MYOCARDIAL INFARCTION IN THE PRESENCE OF ABNORMAL VENTRICULAR ACTIVATION 67
The use of the electrocardiogram to identify the area at risk and the culpritcoronary artery during acute myocardial ischemia is based upon spread ofventricular activation during sinus rhythm over an intact bundle branch system.
Locating ischemic or infarcted areas is possible when they are in parts ofthe ventricle that under normal circumstances are activated early in the QRScomplex (1) but is more difficult when the infarcted areas are in parts of theventricle that are activated late in the QRS complex. Damage to myocardium inthe anterior and inferior areas of the left ventricle, which are activated early bythe left anterior and left posterior fascicle respectively, is thus more easilyidentified than is damage in the postero-basal area.
When the sequence of ventricular activation is altered by bundle branchblock, ventricular pacing or ventricular pre-excitation, there will be a change inthe timing of activation in the areas that are normally activated earliest.
In right bundle branch block (RBBB) the diagnosis of ischemia orinfarction is usually not affected. The left ventricle accounts for the largestmass of myocardium and sites of early activation of the left ventricle are ingeneral not altered by RBBB. But depending upon the proximity of the exit ofthe RBB to the inferior portion of the heart a false diagnosis of inferior wallinfarction can be made in the presence of RBBB (figure 4.1). The closer theexit of the RBB to the inferior portion of the heart, the larger the delay ofactivation of the inferior portion. This is of course aggravated in the presenceof additional left posterior hemiblock.

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
However, ventricular activation is markedly different when the sequenceof left ventricular activation is completely changed by left bundle branch block,right ventricular pacing and ventricular pre-excitation.
A. LEFT BUNDLE BRANCH BLOCK (LBBB)
In LBBB the left ventricle is activated by radial spread from the point oftermination of the RBBB. Therefore areas of the left ventricle that are normallyactivated early, are activated much later in the QRS complex making it difficultto recognize ischemia or infarction in those areas.
This problem is not new; it has puzzled experienced electrocardiographersfor more than 50 years (2). It is also known for a long time that the patient withLBBB and acute MI has a much worse prognosis than a patient with infarctionand normal intraventricular conduction (3). As shown by Lie et al. (4) this istrue both for patients who already have LBBB before infarction (frequentlypatients with hypertensive heart disease) and for those in whom LBBBdevelops as a result of acute anteroseptal infarction. It is still the case in themodern era of thrombolytic therapy (5-7). The unfortunate problem is thatbecause of the difficulties in making the diagnosis of acute myocardialischemia in the presence of LBBB these patients are often not receiving therapyto reperfuse the ischemic area (8).
Twenty years ago Wackers et al. (9) reviewed the variouselectrocardiographic criteria that were reported to be of value in making thediagnosis of acute myocardial infarction in the presence of complete LBBB.This was done by reviewing ECG findings in patients with LBBB in whominfarct diagnosis and localization was based upon the outcome of thallium -201scintigraphy. The conclusion of that study was that the electrocardiographiccriteria suggested to be helpful in diagnosing acute myocardial infarction inLBBB were relatively insensitive and not specific for a particular location ofinfarction. ST segment elevation (the amount not specified!) had a sensitivityfor myocardial infarction of 52 %, and abnormal Q waves a 31 % sensitivity.Initial positivity in lead and a Q wave in lead and a 20 % sensitivity,but a 100 % specificity for anteroseptal infarction (figures 4.2 and 4.3).
The most valuable finding was serial electrocardiographic changes havinga 67 % sensitivity for acute myocardial infarction. These serial changesoccurred mainly during the early phase (24-48 hours) of infarction andfrequently disappeared after 4-5 days.
More recently Sgarbossa et al. (10) reported on a retrospective study of131 patients with LBBB who were among the 26.003 patients enrolled in theGUSTO-I trial of thrombolytic therapy in patients with acute myocardialinfarction. They were compared with asymptomatic patients with LBBB. ThreeECG findings were found to have independent value in the diagnosis of acuteinfarction in the presence of LBBB: 1/ ST segment elevation equal to a greaterthan 1 mm in the presence of a positive QRS complex (figure 4.4); 2/ STsegment depression equal to or greater than 1 mm in lead V1, V2 or V3
68

MYOCARDIAL INFARCTION IN THE PRESENCE OF ABNORMAL VENTRICULAR ACTIVATION 69
(figure 4.5); 3/ ST segment elevation equal to or greater than 5 mm in thepresence of a negative QRS complex (fig 4.6). They also constructed an indexscore using these three criteria (see table 4.1)

70 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

MYOCARDIAL INFARCTION IN THE PRESENCE OF ABNORMAL VENTRICULAR ACTIVATION 71

72 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
These findings were recently criticized by Shlipak et al. (11). Theyperformed a retrospective cohort study in 83 patients with LBBB whopresented 103 times with symptoms suggestive of myocardial infarction. Theycould not find an ECG pattern which distinguished the 30 % of patients withmyocardial infarction from those with other diagnoses. They could not confirmthe value of the algorithm proposed by Sgarbossa et al. (10). Similar findingswere reported in abstract form by Kontos et al. (12) and by Eriksson (13).Obviously a prospective study is needed to evaluate the true value of theSgarbossa algorithm.
Information from intermittent LBBBAs discussed in chapter 3 in acute infero-posterior infarction intermittent,frequently bradycardia-related, phase-4 LBBB may occur. This gives theopportunity to compare the QRS-T complex during normal intraventricularconduction and LBBB in the same patient. As shown in figures 4.7 to 4.9, ininferior wall myocardial infarction, ST segment elevation persists duringLBBB in the inferior leads II,III and AVF. This is even more outspoken whenleft axis deviation is present during LBBB (figures 4.8 and 4.9). As also shownin figures 4.7 to 4.9 wide and notched QS-complexes are frequently present ininferior leads in infero-posterior infarction.

MYOCARDIAL INFARCTION IN THE PRESENCE OF ABNORMAL VENTRICULAR ACTIVATION 73

74 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
The importance of serial ECG’sAlready 20 years ago Wackers et al. (9) pointed out the importance ofrecording serial ECG’s in patients with LBBB admitted with chest pain.Examples are given in figures 4.10 and 4.11. Note widening of the QRS, axisshift and ST-T segment changes during chest pain. Serial ECG’s also allow todocument reperfusion of the culprit coronary artery (figure 4.12).
Practical approachAlthough as indicated above ECG clues may be present indicating myocardialischemia or infarction in the presence of LBBB, the ECG is frequently not areliable source of information. Possibly, as suggested by Eriksson et al. (14)dynamic vector cardiography might be a better tool. In the mean time we (15)strongly support the guidelines of the American College of Cardiology /American Heart Association (16) which recommend acute reperfusion therapyfor patients with LBBB and a clinical presentation suggestive of acutemyocardial infarction.
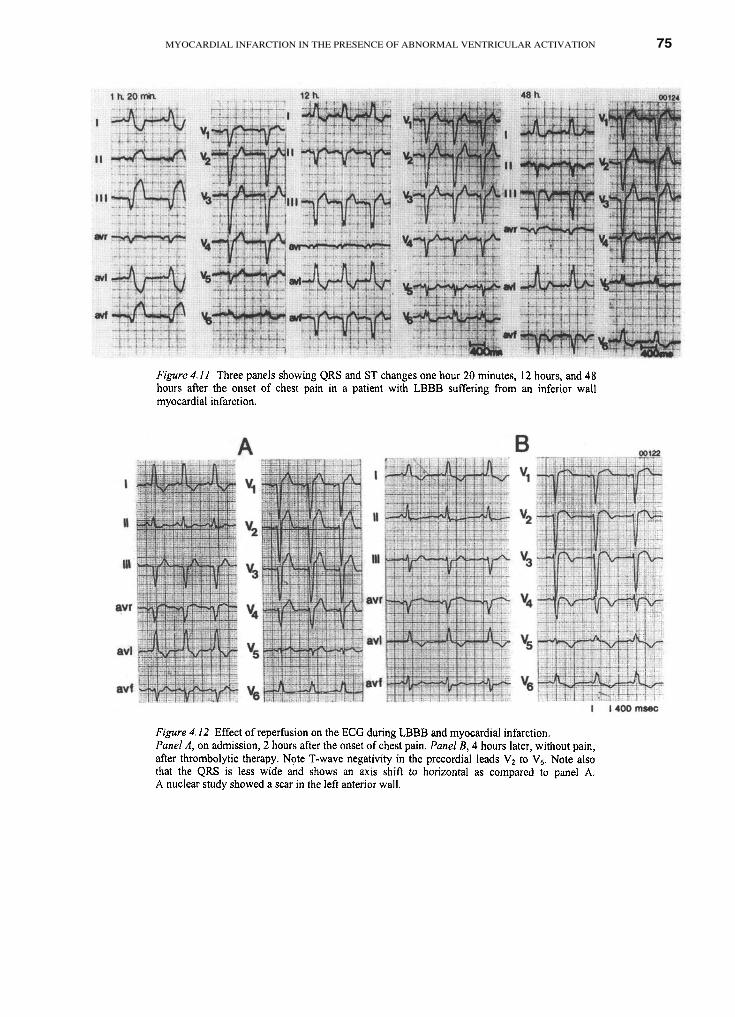
MYOCARDIAL INFARCTION IN THE PRESENCE OF ABNORMAL VENTRICULAR ACTIVATION 75

76 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
B. PACED VENTRICULAR RHYTHM
At present, when ventricular pacing is indicated, the pacing electrode is usuallyplaced in the right ventricle. This will lead to sequential activation of first theright ventricle which is followed by the left ventricle, similar to LBBB. Theconsequences in diagnosing myocardial infarction were pointed out by Baroldet al. (17) and Dodinot et al. (18) more than 20 years ago.
Figure 4.13 gives an example in a patient with a circumflex occlusion.Note the widening and notching of the QRS in the precordial leadsaccompanied by marked ST segment depression. Barold (17) and Dodinot (18)also showed the importance of examining the 12 lead ECG without pacingwhich in the older type pacemakers might require chest wall stimulation (figure4.14 and 4.15). Occasionally, alternation of the paced QRS may be observed(fig 4.16).

MYOCARDIAL INFARCTION IN THE PRESENCE OF ABNORMAL VENTRICULAR ACTIVATION 77

78 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Two important points have to be mentioned when discussingmyocardial infarction in paced ventricular rhythms. First, as pointed out byChatterjee et al. (19) in hearts without ischemia abnormal ventriculardepolarization by ventricular pacing may lead to T-wave negativity whennormal intraventricular conduction returns. This can be observed when pacingis intermittent or suppressed. Characteristically, the T-wave negativity ispresent in leads showing a negative or predominantly negative QRS complexduring ventricular pacing (figure 4.17). Second, as pointed out by Dodinot et al.(18), in myocardial infarction there may be an increase in the interval betweenthe pacing stimulus and the onset of the QRS complex (so-called latency). Thiscan be the result of pacing in the infarcted area.

MYOCARDIAL INFARCTION IN THE PRESENCE OF ABNORMAL VENTRICULAR ACTIVATION 79
C. VENTRICULAR PRE-EXCITATION
During ventricular pre-excitation part or the whole of the ventricle is activatedby way of an accessory atrio-ventricular pathway. This will result in abnormalventricular activation. As in LBBB and ventricular pacing this will hamper thediagnosis of myocardial infarction. It may also lead to pseudo-infarct patternsbecause early activation of for example the inferior portion of the heart by wayof an infero-postero septal accessory pathway may result in initial QRSnegativity (because of the delta wave) in the inferior leads (figure 4.18). Theability to mask myocardial infarction by ventricular pre-excitation dependsupon the location of the accessory pathway. A pathway inserting in theposterior wall of the left ventricle may make the diagnosis of anterior wallmyocardial infarction more difficult (figure 4.19). On the other hand inferiorinfarction in the presence of a posteroseptal accessory pathway can still bediagnosed (figure 4.20). In general if the location of the infarction iscontralateral to the accessory pathway it will mask infarction, while anipsilateral location will allow recognition of ischemia or infarction.

80 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

MYOCARDIAL INFARCTION IN THE PRESENCE OF ABNORMAL VENTRICULAR ACTIVATION 81
Conclusion
Abnormal left ventricular activation may hamper or impair the diagnosis ofmyocardial infarction. This means that decision making as to a myocardialreperfusion attempt should be based upon the clinical impression rather thanthe electrocardiogram.

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Durrer D, van Dam RTH, Freud GE et al. Total excitation of the isolated human heart.Circulation 1970;41:899-912.
Wilson FN, Rosenbaum FF, Johnston F, Barker PS. The electrocardiographic diagnosis ofmyocardial infarction complicated by bundle branch block. Arch Inst Cardiol Mex1945; 14:201-212.
Col JJ, Weinberg SL. The incidence and mortality of intraventricular conduction defects inacute myocardial infraction. Am J Cardiol 1972;29:344-350.
Lie KJ, Wellens HJJ, Schuilenburg RM. Bundle branch block and acute myocardialinfarction. In: Wellens HJJ, Lie KJ, Janse MJ, eds. The conduction system of the heart.Philadelphia: Lea and Febiger 1976: 662-672.
Fibrinolytic Therapy Trialists’ (FTT) Collaborative Group. Indications for fibrinolytictherapy in suspected acute myocardial infarction: Collaborative overview of early mortalityand major morbidity results from all randomized trials of more than 1000 patients. Lancet1994;343:311-322.
Sgarbossa EB, Pinski SL, Topol EJ et al., for the GUSTO-I investigators. Acute myocardialinfarction and complete bundle branch block at hospital admission. Clinical characteristicsand outcome in the thrombolytic era. J Am Coll Cardiol 1998;31:105-110.
Go AS, Barron HV, Rundle AC, Ornato JP, Avins AL, for the National Registry ofmyocardial infarction 2 Investigators. Bundle branch block and in-hospital mortality inacute myocardial infarction. Ann Int Med 1998; 129: 690-697.
Barron HV, Bowlby BJ, Breen T et al. Use of reperfusion therapy for acute MyocardialInfarction in the United States. Data from the National Registry of Myocardial Infarction.Circulation 1998;97:1150-1156.
Wackers FJT, Lie KJ, David G, Koster RM, Wellens HJJ, Assessment of the value ofelectrocardiographic signs for myocardial infarction in left bundle branch block. In: WellensHJJ, Kulbertus HE, eds. What’s new in electrocardiography? The Hague, The Netherlands:Martinus Nijhoff, 1981:37-57.
Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diagnosis of evolvingacute myocardial infarction in the presence of left bundle branch block. N Engl J Med1996;334: 481-487.
Shlipak MS, Lyons WL, Go AS et al. Should the electrocardiogam be used to guide therapyfor patients with left bundle branch block and suspected myocardial infarction. JAMA1999;281:714-719.
Kontos MC, Mc Green RJ, Jesse R, Tatum J, Omato J. Can the ECG diagnose acutemyocardial infarction in emergency department patients with chest pain and left bundlebranch block (abstract). J Am Coll Cardiol 1999;33:347A.
Eriksson P, 1998, personal communication.
Eriksson P, Gunnarson G, Dellborg M. Diagnosis of acute myocardial infarction in patientswith chronic left bundle branch block. Standard 12-lead ECG compared to dynamicvectorcardiography. Scand Cardiovasc J 1999;33:17-22.
References
82
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.

MYOCARDIAL INFARCTION IN THE PRESENCE OF ABNORMAL VENTRICULAR ACTIVATION 83
Wellens HJJ. Acute myocardial infarction and left bundle branch block. Can we lift theveil? N Engl J Med 1996;334:528-529.
Ryan TJ, Anderson JL, Antman EM et al. ACC / AHA guidelines for the management ofpatients with acute myocardial infarction: executive summary: a report of the AmericanCollege of Cardiology / American Heart Association task force on Practice Guidelines(Committee on Management of Acute Myocardial Infarction). Circulation 1996;94:2341-2350.
Barold SS, Ong LS, Heinle RA. Electrocardiographic diagnosis of myocardial infarction inpatients with transvenous pacemakers. J Electrocardiol 1976;9:99-111.
Dodinot B, Kubler L, Godemir JP. Electrocardiographic diagnosis of myocardial infarctionin pacemaker patients. In Wellens HJJ, Kulbertus HE, eds. What’s new inelectrocardiographs? The Hague, The Netherlands, Martinus Nijhoff, 1981:79-90.
Chatterjee K, Harris A, Davies S, Leatham A. Electrocardiographic changes subsequent toartificial ventricular depolarization. Br Heart J 1969;31:770-779.
15.
16.
17.
18.
19.

Chapter 5
Arrhythmias in acute myocardial infarction
Incidence and prognostic significance

86 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Sinus tachycardia in acute MI indicates poor prognosis and urges a carefulsearch for the cause.
Atrial fibrillation developing after onset of MI worsens prognosis.
Sustained ventricular tachycardia in acute MI is rare. When present itusually indicates a closed coronary artery or a scar from a previous MI.
Prognostic significance of successfully resuscitated VF in acute MI isunclear, probably because its occurrence is not related to the size of thearea at risk and extent of coronary artery disease.

ARRHYTHMIAS IN ACUTE MYOCARDIAL INFARCTION
Cardiac arrhythmias, ranging from a premature beat to sustained tachycardias,are common in acute myocardial infarction. They may be transient, occurringonly during the acute ischemic phase like primary ventricular fibrillation, orlonger lasting because of structural changes or hemodynamic consequences ofmyocardial infarction. Their significance may vary from innocent to lifethreatening. As will be pointed out in this chapter, correct identification ofarrhythmias is not only of importance for decision making as to treatment, butalso for the short and long term prognosis of the patient.
A. SUPRAVENTRICULAR ARRHYTHMIAS
Sinus tachycardiaShortly after the introduction of the coronary care unit, it was realized that thefinding of sinustachycardia after a myocardial infarction was of importantprognostic significance (1). This was confirmed by several subsequent studiesboth in the pre- and post thrombolytic era (2-8). Both Hathaway et al. (7) andZuanetti and coworkers (8) found in the thrombolytic era that in a large seriesof patients from respectively the GUSTO-I and the GISSI-2 study earlymortality increased when sinus heart rate on admission was above 80 beats perminute with mortality increasing threefold at sinus rates above 100 beats perminute. Zuanetti et al. (8) also noted that sinus tachycardia at the time ofdischarge from hospital indicated a marked increase in mortality at 6 months.
When sinus tachycardia is present in the patient with an acute myocardialinfarction, the patient should be carefully examined for additional and possiblycorrectable abnormalities. Those may or may not be related to myocardialinfarction.
As shown in table 5.1, related complications include (impending)myocardial rupture; heart failure because of infarct size, presence of a previousinfarction, mechanical damage from papillary muscle dysfunction or rupture(figure 5.1); ventricular septal rupture; and ischemia at a distance because theculprit coronary artery supplies other vessel territories by collateral circulation.
87

88 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Complications not related to the myocardial infarction itself include anemia,fever, pulmonary embolism, infection, etc. The important message is that sinustachycardia should always be a stimulus for a careful search for the cause!
Atrial fibrillationAtrial fibrillation is a common complication of acute myocardial infarction.Depending upon the age of the patient, the incidence may be as high as 20% (9,10). Approximately half of the patients with atrial fibrillation have thearrhythmia on admission while in the other half it develops during admission(10). Interestingly, the prognostic significance of atrial fibrillation varies

ARRHYTHMIAS IN ACUTE MYOCARDIAL INFARCTION 89
between different studies. Some found no effect of atrial fibrillation (9, 11-14)while others reported increased in-hospital and long term mortality (10, 15-18).Small sample size, enrollment in different centers, short follow-up and patientselection may have played a role in these differences.
Twenty five years ago, Liem et al. (19) showed in a consecutive series of1000 patients admitted to hospital because of a myocardial infarction that 8%developed atrial fibrillation after admission. If atrial fibrillation occurred inpatients without heart failure, the arrhythmia did not affect in-hospital cardiacmortality. Also when severe heart failure was present, occurrence of atrialfibrillation did not change the high in-hospital mortality. Interestingly, in caseof mild heart failure, the development of atrial fibrillation was accompanied bya 2,5 times higher in-hospital mortality rate. Atrial fibrillation may occurduring the initial phase of acute inferior infarction as an expression of (pain andanxiety induced) increased vagal tone and is than accompanied by high degreeAV nodal block (fig. 5.2). When atrial fibrillation develops in acute anteriorwall myocardial infarction, it is frequently a marker of manifest or impendingpump failure (fig. 5.3).

90 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Recently, Rathore et al. (10) reported on 106.780 Medicare patientsyears who were included in the Cooperative Cardiovascular Project and treatedfor acute myocardial infarction. They found that 10,5% of those patientspresented with atrial fibrillation on admission, while 11,6% developed thearrhythmia later. Particularly when atrial fibrillation develops duringhospitalization, the prognosis becomes worse as reflected by higher in-hospital,30 days and 1-4 year mortality.
These data indicate that loss of atrial contribution to ventricular filling andan inappropriate ventricular rate during atrial fibrillation often result in a worseoutcome. Unfortunately, no studies are available showing that in acutemyocardial infarction pharmacological or non-pharmacological attempts toconvert atrial fibrillation to sinus rhythm is rewarded by a better prognosis.That question has to be answered by prospective studies.

ARRHYTHMIAS IN ACUTE MYOCARDIAL INFARCTION 91
B. VENTRICULAR ARRHYTHMIAS
Ventricular premature beatsShortly after the introduction of the coronary care unit for the management ofacute myocardial infarction, attention was focussed on certain characteristics ofectopic ventricular beats that qualified them as malignant (so-called warningarrhythmias) because of their ability to initiate life-threatening ventriculararrhythmias. Early occurrence, close to the summit of the T wave of thepreviously conducted sinus beat, frequent occurrence, multiform configurationand runs of ventricular premature beats were all suggested as pointing to amalignant character and an indication to treat the patient with lidocaine (20).However, a few years later, several investigators (21-24) indicated that earlypremature ventricular beats showing the R (of the premature ventricular beat)on T (of the preceding conducted sinus beat) phenomenon were just ascommon in patients developing ventricular fibrillation as in patients notdeveloping that arrhythmia.
Examples are shown in figure 5.4. Panel A in figure 5.4 shows veryfrequent, early occurring ventricular premature beats in the setting of an acuteinferior myocardial infarction. As shown in panel B and C from the samepatient, ventricular fibrillation could be initiated both by an early or a lateventricular premature beat.
THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Chiladakis et al. (24) recently showed that also in the thrombolytic era R-on-T ventricular premature beats and R-on-T ventricular tachycardias are rarefeatures in acute myocardial infarction, and that R-on-T ventricular prematurebeats do not serve as triggers for severe ventricular tachyarrhythmias.Because of the inability to predict which ventricular premature beat (early orlate) would initiate ventricular fibrillation, Lie et al. (25) made a plea to treatthe patient with an acute myocardial infarction with prophylactic lidocaine.Over the years, the enthusiasm to give lidocaine prophylactically hasdecreased, primarily because of the side effects of lidocaine and the fact thatboth in the out-of-hospital advanced life support situation and in the coronarycare unit, personnel is available which is well trained in the recognition andtreatment of ventricular fibrillation. Antman and Berlin (26), in reviewing allthe randomized studies on prophylactic lidocaine use in acute myocardialinfarction, came to the conclusion that lidocaine should not be usedprophylactically because of the declining incidence of VF after a myocardialinfarction and the reported trend towards excess mortality in lidocaine treatedpatients. Another factor decreasing the use of lidocaine is the routineadministration of a beta-blocking agent to patients with acute myocardialinfarction.
Ventricular tachycardiaSustained monomorphic ventricular tachycardia (VT) defined as a tachycardiawith identical wide, QRS complexes at a rate of at least 130 beats per minute,is rare in acute myocardial infarction (27) because a stable re-entry circuit isrequired. This is usually not the case in acute myocardial infarction. VT eitherstops spontaneously after a limited number of beats (non-sustained VT) ordegenerates into VF. In our experience, sustained VT in acute MI either occursduring reinfarction in the same coronary artery territory as the previousinfarction (fig. 5.5), or in a scar from a previous infarction in another location.
Typically, therefore the patient with sustained monomorphic VT in theacute phase of MI is older, and has a diminished left ventricular ejectionfraction because of a previous MI. In the GUSTO-I study (28) 2423/40895(5,7%) patients were reported as having sustained VT during the acute phase ofMI. Unfortunately, no information is given about time of occurrence (before,during or after thrombolytic therapy) and on the rate and configurationalcharacteristics of the arrhythmia. It is therefore likely that long episodes ofaccelerated idioventricular rhythm (AIVR) were classified as monomorphicsustained VT. Outcome of patients with VT was worse as compared to no VTin the GUSTO-I study (28). This was the case in early and late (more than 2days after infarction) VT patients. The poor prognosis of patients developingsustained monomorphic VT during the late phase of hospital admission foracute MI has been reported before (29), because these patients have larger(usually anterior) infarcts. Heidbüchel et al. (30) found that in acute MI patientswith VT after thrombolytic therapy, the culprit coronary artery was usuallyoccluded in contrast to VF patients. They suggested that presence of a
92

ARRHYTHMIAS IN ACUTE MYOCARDIAL INFARCTION 93
sustained VT should be a reason to perform coronary angiography to assess thepatency status of the coronary artery and to perform a reperfusion procedurewhen needed. As discussed more extensively in chapter 6, acceleratedidioventricular rhythm (AIVR) is also a ventricular arrhythmia (monomorphic,rate 60-120/min) occurring in acute myocardial infarction during reperfusion. Itwas initially thought to be a benign arrhythmia, but as indicated by Gorgels etal (31) always accompanied by myocardial muscle loss. Recently, work byEngelen et al. (32) indicated that incidence and duration of AIVR is related toleft ventricular wall motion abnormalities late after MI. This may explain theoutcome of the GUSTO-I study that indicated a poorer short and long termprognosis of patients with ventricular tachycardias after MI (28).
Ventricular fibrillationSeveral studies have addressed the question whether occurrence of ventricularfibrillation (VF) in the acute phase of myocardial infarction has prognosticsignificance after the arrhythmia has been treated successfully (33-38).

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Volpi et al. (33) reported that primary VF worsened in-hospital mortalitybut not long term prognosis. Similar findings were described by Behar et al.(34) In contrast, Tofler et al.(35) found no difference in hospital mortality inpatients with primary VF.
Chiriboga et al. (36) found in a community-wide observational study thatneither the incidence (around 5 % of patients developed VF) nor the prognosisassociated with primary VF in acute myocardial infarction changed over aperiod of 15 years (1975-1990).
Berger and coworkers (37) looked at the significance of primary VF in thethrombolysis era. They found that VT and VF are not markers for reperfusion.These arrhythmias were associated with occlusion, not patency of the infarctrelated coronary artery. Early mortality, but not long term mortality wasincreased in VT/VF patients even in the absence of heart failure andhypotension.
Brezins et al. (38) found that in hospital primary VF was rare in non Qwave myocardial infarction. Most cases of primary VF occurred out-of-hospitalor in the emergency room. Smoking, atrial fibrillation, left bundle branch blockand hypokalemia were found more often in the primary VF patients.Thrombolytic therapy reduced the incidence of primary VF.Recently, Gheeraert et al. (39) looked at coronary angiographic findings inpatients with out-of-hospital VF in patients with acute myocardial infarction.They found that patients with an occlusion of the left anterior descending orcircumflex coronary artery had a greater risk for out-of-hospital VF thanpatients with an occlusion of the right coronary artery. Interestingly, thelocation (proximal or distal in the vessel) of the occlusion, the amount ofmyocardium at risk for necrosis and the extent of coronary artery disease werenot related to out-of-hospital VF. These findings are important because theyindicate that many patients suffering from cardiac arrest outside hospital havehearts too good to die.
Early ischemia related, so-called primary VF has to be distinguished fromsecondary VF occurring in the presence of hypotension or heart failure. Thishappens in patients with large (usually anteriorly located with acquired rightbundle branch block) infarcts having pump failure. Such episodes occur lateafter the acute phase of a myocardial infarction usually in the second or thirdweek (40). The poor prognosis of these patients is not so much related to VF, iftreated appropriately, but to the degree of left ventricular muscle loss.
Conclusion
Cardiac arrhythmias are common in acute myocardial infarction, varying frombenign to life threatening. Proper identification should be followed byunderstanding their significance and be the basis for decisions about treatment.
94

ARRHYTHMIAS IN ACUTE MYOCARDIAL INFARCTION
De Sanctis RW, Block P, Hutter AM. Tachyarrhythmias in myocardial infarction.Circulation 1972;65:681-688.
Crimm A, Severance HW Jr, Coffey K. Prognostic signifiance of isolated sinus tachycardiaduring the first three days of acute myocardial infarction. Am J Med 1984;76:983-988.
Madsen EB, Gilpin E, Henning H, et al. Prediction of late mortality after myocardialinfarction from variables measured at different times during hospitalization. Am J Cardiol1984;53:47-54.
Willems JL, Pardaens J, De Geest H. Early risk stratification using clinical findings inpatients with acute myocardial infarction. Eur Heart J 1984;5:130-139.
Hillis LD, Forman S, Braunwald E, and the Thrombolysis in Myocardial Infarction (TIMI)Phase II Co-investigators. Risk stratification before thrombolytic therapy in patients withacute myocardial infarction. J Am Coll Cardiol 1990;16:313-315.
Lee KL, Woodlief LH, Topol EJ, et al., for the GUSTO-1 Investigators. Predictors of 30-day mortality in the era of reperfusion for acute myocardial infarction. Results from aninternational trial of 41021 patients. Circulation 1995;91:1659-1668.
Hathaway WR, Peterson ED, Wagner GS, et al, for the GUSTO-I Investigators. Prognosticsignificance of the initial electrocardiogram in patients with acute myocardial infarction.JAMA 1998;279:387-391.
Zuanetti G, Mantini L, Hernandez-Bernal F, et al. Relevance of heart rate as a prognosticfactor in patients with acute myocardial infarction: insights from the GISSI-2 study. EurHeart J 1998;19(suppl. F):19-26.
Goldberg RJ, Seeley D, Becker RC. Impact of atrial fibrillation on the in-hospital and longterm survival of patients with acute myocardial infarction: a community wide perspective.Am Heart J 1990;114:996-1003.
Rathore SS, Berger AK, Weinfurt KP et al. Acute myocardial infarction complicated byatrial fibrillation in the elderly. Prevalence and outcomes. Circulation 2000; 101:969-974.
Madias JE, Patel DC, Singh D. Atrial fibrillation in acute myocardial infarction: aprospective study based on data from a consecutive series of patients admitted to thecoronary care unit. Clin Cardiol 1996;19:180-186.
Vaage-Nilsen M, Hansen JF, Mellemgaard K, Hagerup L, Sigurd B, Steinmetz E, for theDAVIT II Study Group. Short- and long-term prognostic implications of in-hospitalpostinfarction arrhythmias. Cardiology 1995:86:49-55.
Sugiura T, Iwasaka T, Ogawa A, Shiroyama Y, Tsuji H, Onoyama H, Inada M. Atrialfibrillation in acute myocardial infarction. Am J Cardiol 1985;56:27-29.
Serrano CV, Ramiers JAF, Mansur AP, Pileggi F. Importance of the time of onset ofsupraventricular tachyarrhythmias on prognosis of patients with acute myocardialinfarction. Clin Cardiol 1995;18:84-90.
95
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Behar S, Zahavi Z, Goldbourt U, Reicher-Reiss H, for the SPRINT-study group. Long-termprognosis of patients with paroxysmal atrial fibrillation complicating acute myocardialinfarction. Eur Heart J 1992;13:45-50.
Eldar M, Canetti M, Rotstein Z, Boyko V, Gottlieb S, Kaplinsky E, Behar S, for theSPRINT and Thrombolytic Survey groups. Significance of paroxysmal atrial fibrillationcomplicating acute myocardial infarction in the thrombolytic era. Circulation 1998;97:965-970.
Crenshaw BS, Ward SR, Granger CB, Stebbins AL, Topol EJ, Califf RM, for the GUSTO-I Trial Investigators. Atrial fibrillation in the setting of acute myocardial infarction; theGUSTO-I experience. J Am Coll Cardiol 1997;30:406-413.
Sakata K, Kurihara H, Iwamori K, et al. Clinical and prognostic significance of atrialfibrillation in acute myocardial infarction. Am J Cardiol 1997;80:1522-1527.
Liem KL, Lie KI, Durrer D, Wellens HJJ. Clinical setting and prognostic significance ofatrial fibrillation complicating acute myocardial infarction. Eur J Cardiol 1976;4:59-62.
Lown B, Fakhro AM, Hood WB, et al. The coronary care unit: new perspectives anddirections. JAMA 1967;119:188-198.
Lawrie DM, Higgins MR, Godman MJ, et al. Ventricular fibrillation complicating acutemyocardial infarction. Lancet 1968;2:523-528.
Dhurandar RW, MacMillan RL, Brown KWG. Primary ventricular fibrillationcomplicating acute myocardial infarction. Am J Cardiol 1971;27:347-351.
Lie KI, Wellens HJJ, Durrer D. Characteristics and predictability of primary ventricularfibrillation. Eur J Cardiol 1974;1:379-384.
Chiladakis JA, Karapanos G, Davlouros P, Aggelopoulos G, Alexopoulos D, Manolis AS.Significance of R-on-T phenomenon in early ventricular tachyarrhythmia susceptibilityafter acute myocardial infarction in the thrombolytic era. Am J Cardiol 2000;85:289-293.
Lie KI, Wellens HJJ, Van Capelle FJ, Durrer D. Lidocaine in the prevention of primaryventricular fibrillation. New Engl J Med 1974;291:1324-1326.
Antman EM, Berlin JA. Declining incidence of ventricular fibrillation in myocardialinfarction. Implications for the prophylactic use of lidocaime. Circulation 1992; 86: 764-773.
Wellens HJJ, Lie KI, Durrer D. Further observations on ventricular tachycardia as studiedby electrical stimulation of the heart. Chronic recurrent ventricular tachycardia andventricular tachycardia during acute myocardial infarction. Circulation 1974;49:647-653.
Newby KH, Thompson T, Stebbins A, Topol EJ, Califf RM, Natale A; for the GUSTOinvestigators. Sustained ventricular arrhythmias in patients receiving thrombolytic therapy.Incidence and outcomes. Circulation 1998;98:2567-2573.
Wellens HJJ, Bär FW, Vanagt EJ, Brugada P. Medical treatment of ventricular tachycardia.Considerations in the selection of patients for surgical treatment. Am J Cardiol1982;49:186-193.
96
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.

ARRHYTHMIAS IN ACUTE MYOCARDIAL INFARCTION
Heidbuchel H, Tack J, Vanneste L, Ballet A, Ector H, Van de Werf F. Significance ofarrhythmias during the first 24 hours of acute myocardial infarction treated with alteplaseand effect of early administration of beta-blocker or a bradycardiac agent on theirincidence. Circulation 1994;89:1051-1059.
Gorgels AP, Vos MA, Letsch JS, et al. Usefulness of the accelerated idioventricular rhythmas a marker for myocardial necrosis and reperfusion during thrombolytic therapy in acutemyocardial infarction. Am J Cardiol 1988;61:231-235.
Engelen DJ, Gressin V, Theuns DA, et al. Incidence and duration of reperfusionarrhythmias predict left ventricular wall motion abnormalities in reperfused anterior wallmyocardial infarction. Submitted.
Volpi A, Maggioni A, Franzosi MJ, Pampallona S, Mauri F, Tognoni G. In hospitalprognosis of patients with acute ventricular infarction complicated by primary ventricularfibrillation. N Engl J Med 1987; 317:257-261.
Behar S, Goldbourt U, Reicher-Reiss H, Kaplinsky E, and the principal investigators of theSPRINT-study. Prognosis of acute myocardial infarction complicated by primaryventricular fibrillation. Am J Cardiol 1990;66:1208-1211.
Tofler GH, Stone PH, Muller JE, et al. Prognosis after cardiac arrest due to ventriculartachycardia or ventricular fibrillation associated with acute myocardial infarction (the Milisstudy). Am J Cardiol 1987;60:755-761.
Chiriboga D, Yarzebski J, Goldberg RJ, Gore JM, Alpert JS. Temporal trends (1975through 1990) in the incidence and case fatality rates of primary ventricular fibrillationcomplicating acute myocardial infarction. Circulation 1994; 89: 998-1003.
Berger PB, Ruocco NA, Ryan TJ, Frederick MM, Podrid PJ, and the TIMI investigators.Incidence and significance of ventricular tachycardia and fibrillation in the absence ofhypotension or heart failure in acute myocardial infarction treated with recombinant tissue-type plaminogen activator: results from the thrombolysis in myocardial infarction (TIMI)phase II trial. J Am Coll Cardiol 1993; 22: 1773-1779.
Brezins M, Elyassov S, Elimelech I, Roguin N. Comparison of patients with acutemyocardial infarction with and without ventricular fibrillation. Am J Cardiol 1996;78:948-950.
Gheeraert PJ, Henriques JPS, de Buyzere ML, et al. Out-of-hospital ventricular fibrillationin patients with acute myocardial infarction. J Am Coll Cardiol 2000; 35: 144-150.
Lie KI, Liem KL, Schuilenburg RM, David GK, Durrer D. Early identification of patientsdeveloping late in-hospital ventricular fibrillation after discharge from the CCU. Am JCardiol 1978;41:674-677.
97
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.

Chapter 6
The electrocardiographs signs of reperfusion

100 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Resolution of ST segment deviation of more than 70% within one hourafter thrombolytic therapy strongly suggests patency of the infarct relatedcoronary artery.
Patients with anterior infarction may show less ST segment resolution onreperfusion than patients with inferior infarction.
An accelerated idioventricular rhythm is more common after reperfusionby thrombolytic therapy than by coronary angioplasty.
Severity and duration of an accelerated idioventricular rhythm correlateswith left ventricular wall motion abnormalities late after myocardialinfarction
Non-invasive ECG parameters are helpful to determine the presence ofreperfusion, but do not distinguish between TIMI II or TIMI III flow.

THE ELECTROCARDIOGRAPHIC SIGNS OF REPERFUSION
As pointed out in chapter 2, the surface ECG is of great value in acutemyocardial infarction, to decide whether an aggressive approach to regaincoronary artery patency is required or conservative treatment is the preferredtreatment modality. Once the decision is made that the area at risk is such thatreperfusion should be attempted different strategies are possible, such asthrombolytic therapy, primary percutaneous transluminal coronary angioplasty(PTCA) with or without stenting, or when thrombolytic therapy fails,secondary (rescue) PTCA. The choice of treatment depends on local facilitiesand experience, the recognition of site and size of an acute myocardialinfarction and the time elapsed from the onset of symptoms.
Assessment of reperfusion of the myocardial tissue at risk is important toguide treatment in the acute phase of the infarction, with in addition prognosticconsequences for the future (1). Furthermore, new treatments are beingdeveloped to limit myocardial damage during the process of reopening of theinfarct-related vessel. To analyze efficacy of these new treatments to limitreperfusion damage, the ECG may provide useful information. To recognizereperfusion non-invasively most attention has been given towards ST-Tsegment behavior (1) and the occurrence of brady-and tachyarrhythmias.
ST-T segment behavior
ST segment changesMonitoring the 12 lead electrocardiogram during the treatment of patientssuffering from an acute myocardial infarction is an inexpensive and reliabletool to determine vessel patency. It is crucial to realize that in the absence ofreperfusion during the first hours after occlusion of the coronary artery onlyminor (<25%) changes in the amount of ST segment deviation occur. Duringrecovery of blood flow different patterns of ST segment behavior can berecognized. The most important change being normalization of the ST segment(2) (fig. 6.1). For practical purposes Zeymer et al. (3) recently indicated that amore than 70% ST resolution is an excellent marker for reperfusion followingthrombolysis. However, the absence of ST resolution does not accuratelypredict an occluded culprit coronary artery. Approximately 50% of patientswith no (<30%) ST resolution have a patent culprit coronary artery.
In about half of the patients receiving thrombolytic therapy, the initialchange is an increase in ST segment elevation at the time of reperfusion (fig.6.2) (4,5) followed by a significant decrease of ST segment deviation. It is ofinterest that the initial ST segment elevation on reperfusion less frequentlyoccurs in patients undergoing primary PTCA compared with thrombolytictherapy (10 % versus 50% respectively)(6).
One should realize that important differences may exist between anteriorand inferior MI with regard to ST segment resolution. On restoration ofepicardial blood flow patients with anterior infarction frequently developsignificantly less ST resolution than those with inferior infarction (7). This ledde Lemos et al. (8) to the suggestion that resolution of ST deviation by > 70%
101

102 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

THE ELECTROCARDIOGRAPHIC SIGNS OF REPERFUSION
is the optimal threshold for patients with inferior MI but > 50% may be optimalfor anterior MI.
Normalization of the ST segment can be explained by recovery ofmyocardial blood flow. The mechanism of the initial increase in ST segmentdeviation, which is often accompanied by a marked increase in chest pain, isless clear. Possible explanations include peripheral embolization of thromboticmaterial, increased microvascular resistance and reperfusion damage.Preliminary data suggest that reperfusion damage may occur in the humanheart (9). From experimental models we know that damage to the myocardiumis inflicted by reperfusion. Reperfusion injury occurs in two stages, acute dueto the formation of oxygen derived free radicals and calcium overload indamaged myocytes and later by activation of neutrophils (10,11). Thesechanges may lead to apoptotic cell death (9). Whether pharmacologicalinterventions during reperfusion can reduce infarct size has yet to be proven inman.
The normalization of the ST segment has important prognosticsignificance. Van ‘t Hof et al., analyzed mortality in patients after primaryPTCA and reported an increased relative risk of 8.7 in the absence of STsegment normalization and of 3.6 when ST segment recovery was incompleteafter one hour of reperfusion (12). Also, increased mortality rates have beenreported in patients with persisting ST segment elevation in the setting ofanterior MI (15% versus 2%). (13).
The absence of ST segment resolution following PTCA worsens prognosisas indicated by increased in-hospital and long term mortality. In addition,impaired left ventricular function and congestive heart failure were more oftenfound in patients with persistent ST segment elevation after return to thecoronary care unit following reopening of the vessel (14).
In patients with large infarcts treated with thrombolytics absence of STresolution should be an indication for a percutaneous coronary intervention.Although, as indicated above, the vessel may be open one has to be certain inview of the prognostic consequences of an occluded coronary artery.
Several groups have shown that continuous ST segment monitoring is thebest way to document flow in the infarct related coronary artery (15-21).Recently Johanson et al (22) indicated that even small variations in ST segmentshift during the first 4 hours of acute myocardial infarction predict worseoutcome. Continuous ST segment monitoring allows early recognition ofreocclusion making optimal management possible.
T wave changesT wave inversion occurring within the first two hours after the start ofthrombolytic therapy indicates reperfusion (fig. 6.3). In anterior wall MI adecrease in the ST segment elevation is found together with the development ofterminal T-wave negativity in the precordial leads. A similar phenomenon canbe observed in leads II, III and AVF in inferior MI. In posterior MI, indicated
103

104 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
by ST segment depression in the precordial leads, the reverse pattern can befound as the terminal part of the T-wave becomes positive.
The recognition of terminal T-wave inversion development duringthrombolytic therapy is important as it indicates successful reperfusion. Whenterminal T-wave inversion is already present on the admission ECG in thesetting of an acute MI, it gives no information with respect to artery patency.Late T wave inversion > 4 hours is not an indicator of reperfusion as it is afeature of the ST segment behavior after acute myocardial infarction. Changesin T-wave polarity can be a sign of unstable angina (see chapter 7).
Incidence, mechanism and prognostic implicationsThe development of early T-wave inversion during thrombolytic therapy ishighly specific for reperfusion (>90%). However, T-wave inversion occurs inonly approximately 60% of the recordings (5,6). Therefore, the absence ofterminal T-wave inversion can not be considered indicative of failedthrombolysis. When the blood supply to the ischemic and partially necroticmyocardium is restored, many changes occur at the cellular level. Areas whereelectrical activation and conduction were absent are gradually recovering. Thisprocess of recovery is responsible for segments with delayed repolarization

THE ELECTROCARDIOGRAPHIC SIGNS OF REPERFUSION 105
(23). Recovery occurs more rapidly in the epicardial than in the midmyocardialand endocardial layers. This dispersion in the duration of repolarization in theinfarcted area relative to the normal myocardium increases during reperfusion.When in anterior MI the restored repolarization current lasts longer in the endo-than the epicardium, the terminal portion of the T-wave becomes negative inthe precordial leads.
Ectopic activity
ECG findingsThe moment patency of an occluded infarct artery is restored, arrhythmias canoccur. Most often premature ventricular beats are seen and sometimesventricular tachycardias or ventricular fibrillation.
The value of these arrhythmic events for decision making as to thereopening of the coronary vessel, depends upon their specificity or positivepredictive value. Rarely, supraventricular arrhythmias mark reopening of thevessel and in the setting of an inferior wall myocardial infarction, bradycardiacan be observed. To compare the relevance of these findings in differentstudies the definitions used are essential (table 6.1). Special attention must bedirected to Accelerated Idiopathic Ventricular Rhythms (AIVR) as they arevery specific and are observed from the moment of the start of reperfusion (24).AIVR is defined by the rate (60-120 beats/min.), and the mechanism ofinitiation and termination. In general, the arrhythmia starts with a long couplinginterval to the preceding sinus beat and stops when sinus rhythm recaptures theventricles (24) (see fig. 6.4).

106
VPB and AIVR
Incidence, mechanism and prognostic implicationsAIVR is a very specific reperfusion arrhythmia, and only occurring in thesetting of myocardial damage (figure 6.5). The specificity of AIVR forreperfusion has been reported to be >80% with a positive predictive value of>90%. (25,26). The characteristics of the QRS complex during AIVR dependupon the site of occlusion, and can be helpful to determine which vessel causedthe myocardial infarction (table 6.2).
The width of the QRS complex is smaller in anterior wall MI because theAIVR arises close to the midline (fig. 6.6) resulting in more symmetricalactivation of the ventricles. In reperfusion of an RCA occlusion the electricalaxis is always superior, and in CX lesions RBBB patterns have been reportedexclusively (25). Interestingly, the site of AIVR origin may shift down thecoronary artery, when reperfusion occurs (fig. 6.7). An increase in the numberof VPBs often marks the reperfusion event. In many patients this will befollowed by AIVRs. The value of the number of VPBs per time interval (for
THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

THE ELECTROCARDIOGRAPHIC SIGNS OF REPERFUSION 107

108 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

THE ELECTROCARDIOGRAPHIC SIGNS OF REPERFUSION
example 5 min.) is less specific and has lower positive predictive value forreperfusion (approximately 70 and 80% respectively). The mechanism of VPBsand AIVR is possibly related to calcium overload in the survivingcardiomyocytes in the border of the myocardial infarction. The calciumoverload is secondary to an increased influx of sodium into the vulnerablemyocytes. The increased calcium load and calcium cycling through thesarcoplasmatic reticulum upon restoration of energy supplies (ATP) provokesdelayed after depolarizations and induces triggered arrhythmias (27). AIVRscan be prevented or blocked by treatment with dipyridamole and reducedcellular adenosine uptake (28).
AIVR is probably caused by reperfusion damage. The arrhythmia in itselfhas no major acute hemodynamic consequences, and is no precursor of moremalignant tachycardias. A reduction in frequency and duration of AIVR couldtherefore be indicative for a reduction in reperfusion damage and be beneficial(23). Following primary PTCA less AIVR was found compared withreperfusion after thrombolytic treatment (6,29). AIVR is a transient, self-terminating arrhythmia that does not need treatment. In general, it should beconsidered a positive sign of reperfusion in an acute myocardial infarction.Future studies should be performed to confirm that AIVR indicates reperfusiondamage and that interventions resulting in less AIVR indicate improvedsalvage of myocardial tissue.
The analysis of reperfusion arrhythmias in general, may therefore be ofhelp in comparing different reperfusion strategies and pharmacologicalinterventions aimed at reducing reperfusion damage and cell death aftermyocardial infarction.
NSVT and VF
Incidence, mechanism and prognostic implicationsSustained monomorphic ventricular tachycardia is not a reperfusionarrhythmia. When it occurs in the setting of an acute myocardial infarction, ascar from a previous myocardial infarction is usually present (30). Duringreperfusion non-sustained ventricular tachycardias (NSVT) have been reported(fig. 6.8). However, NSVTs are also frequently seen in the absence ofreperfusion. Therefore the clinical importance of this arrhythmia as an indicatorof reperfusion is limited. Polymorphic ventricular tachycardia and ventricularfibrillation are common reperfusion arrhythmias in experimental models ofischemia and reperfusion and do occur but rarely during reopening of theinfarct-related vessel in man. However, in a large randomized trial, assessingthe safety of thrombolytic therapy at home the incidence of VF was higher inpatients receiving thrombolytics compared with placebo (2.5 vs. 1.6%)indicating that VF can be a reperfusion arrhythmia (31). No information isavailable on the short-term prognostic importance of NSVT and VF occurringduring reperfusion. As discussed in chapter 5 the effect of primary VF on longterm prognosis of patients with MI is not clear (32).
109

110 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Supraventricular arrhythmias
ECG findingsAtrial tachycardia and atrial fibrillation (fig. 6.9) have been observed in thesetting of reperfusion. Ectopic atrial activity is seen predominantly in thesetting of an inferior wall myocardial infarction based on a proximal occlusionof the RCA. In most cases a short lasting (<1 min.) episode of ectopic atrialactivity is observed.
Incidence, mechanism and prognostic implicationsBoth atrial tachycardia and atrial fibrillation are rare during reperfusionoccurring in 10, respectively 5% of all cases (5,6). There is no definiteexplanation for the occurrence of these arrhythmias. However, the relationbetween atrial damage and reperfusion suggests a similar mechanism asdescribed above for ventricular reperfusion arrhythmias involving calciumoverload and triggered activity.
The significance of these arrhythmias in patients treated for an acute MI isnot clear. Although the arrhythmias can indicate successful reopening of thevessel, also complications of the MI could initiate ectopic atrial activity andatrial fibrillation.
Therefore, the interpretation of these events depends on other concomitantchanges on the ECG and the clinical condition of the patient.
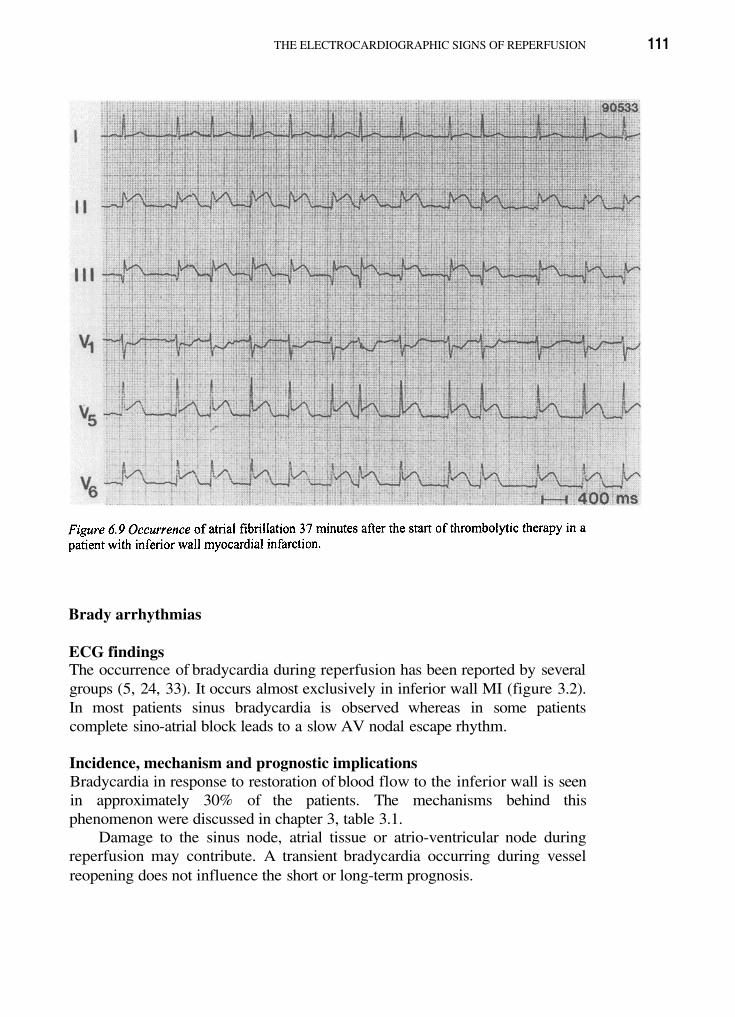
THE ELECTROCARDIOGRAPHIC SIGNS OF REPERFUSION 111
Brady arrhythmias
ECG findingsThe occurrence of bradycardia during reperfusion has been reported by severalgroups (5, 24, 33). It occurs almost exclusively in inferior wall MI (figure 3.2).In most patients sinus bradycardia is observed whereas in some patientscomplete sino-atrial block leads to a slow AV nodal escape rhythm.
Incidence, mechanism and prognostic implicationsBradycardia in response to restoration of blood flow to the inferior wall is seenin approximately 30% of the patients. The mechanisms behind thisphenomenon were discussed in chapter 3, table 3.1.
Damage to the sinus node, atrial tissue or atrio-ventricular node duringreperfusion may contribute. A transient bradycardia occurring during vesselreopening does not influence the short or long-term prognosis.

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
ManagementReperfusion brady- and tachyarrhythmias require treatment only when theyaffect the hemodynamic condition or, as in reperfusion induced VF, threatenthe life of a patient.
Conclusion
The described ECG changes are of help to document reperfusion non-invasively and are of value to determine the need of other strategies to obtainreperfusion. One should keep in mind however that we do not have ECGcriteria to distinguish reliably between TIMI II and TIMI III flow (34).
112

THE ELECTROCARDIOGRAPHIC SIGNS OF REPERFUSION
de Lemos JA, Braunwald E, ST segment resolution as a tool for assessing the efficacy ofreperfusion therapy. J Am Coll Cardiol 2001 ;38:1283-1294.
Ganz W, Buchbinder N, Marcus A, et al. Intracoronary thrombolysis in acute myocardialinfarction. Am Heart J 1981; 101 -4-13.
Zeymer U, Schroder R, Tebbe U, Molhoek GP, Wegscheider K, Neuhaus KL. Noninvasive detection of early infarct vessel patency by resolution of ST-segment elevation inpatients with thrombolysis for acute myocardial infarction. Eur Heart J 2001;22:769-775.
Arstall MA, Stewart S, Haste MA, Horowitz JD. Streptokinase-induced transientaggravation of myocardial injury. Int J Cardiol 1995; 50:107-116.
Doevendans PA, Gorgels AP, van der Zee R, Partouns J, Bar FW, Wellens HJ.Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acutemyocardial infarction. Am J Cardiol 1995;75:1206-1210.
Wehrens XH, Doevendans PA, Oude Ophuis TJ, Wellens HJ. A comparison ofelectrocardiographic changes during reperfusion of acute myocardial infarction bythrombolysis or PTCA. Am Heart J 2000; 139:430-436.
Buszman P, Szafranek A, Kalarus Z, Gasior M. Use of changes in ST segment elevationfor prediction of infarct artery recanalization in acute myocardial infarction. Eur Heart J1995;16:1207-1214.
de Lemos JA, Antman EM, McCabe CH, et al. ST segment resolution and infarct relatedartery patency and flow after thrombolytic therapy. Am J Cardiol 2000;85:299-304.
Hofstra L, Liem IH, Dumont EA, et al. Visualization of cell death in vivo in patients withacute myocardial infarction. Lancet 2000;356:209-212.
Jordan JE, Zhoa ZQ, Vinten-Johansen J. The role of neutrophils in myocardial ischemiareperfusion injury. Cardiovasc Res 1999;43:860-878.
McCord JM. Oxygen-derived free radicals in postischemic tissue injury. N Engl J Med1985;312:159-163.
‘t Hof AW van, Liem A, de Boer MJ, Zijlstra F. Clinical value of the 12-leadelectrocardiogram after succesful reperfusion therapy for acute myocardial infarction.Zwolle Myocardial Infarction Study Group. Lancet 1997;350:615-619.
Clays MJ, Bosnians J, Veenstra L, et al. Determinants and prognostic implications ofpersistent ST-segment elevation after primary angioplasty for acute myocardial infacrtion:importance of microvascular reperfusion injury on clinical outcome. Ciculation1999;99:1972-1977.
Matetzky, Novikov M, Gruberg L, et al. The significance of persistent ST elevation versusearly resolution of ST segment elevation after primary PTCA. J Am Coll Cardiol1999;1932-1938.
Krucoff MW, Green CE, Satler LF, et al. Noninvasive detection of coronary artery patencyusing continuous ST-segment monitoring. Am J Cardiol 1986;57:916-22.
113
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.

THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Klootwijk P, Langer A, Meij S, et al. Non-invasive prediction of reperfusion and coronaryartery patency by continuous ST segment monitoring in the GUSTO-I trial. Eur Heart J1996;17:689-98.
Schroder R, Wegscheider K, Schroder K, Dissmann R, Meyer-Sabellek W. Extent of earlyST segment elevation resolution: a strong predictor of outcome in patients with acutemyocardial infarction and a sensitive measure to compare thrombolytic regimens. Asubstudy of the International Joint Efficacy Comparison of Thrombolytics (INJECT) trial.J Am Coll Cardiol 1995;26:1657-64.
Langer A, Krucoff MW, Klootwijk, et al. Prognostic significance of ST segment shift earlyafter resolution of ST elevation in patients with myocardial infarction treated withthrombolytic therapy: the GUSTO-I ST Segment Monitoring Substudy. J Am Coll Cardiol1998; 31:783-9.
Carlsson J, Kamp U, Hartel D, et al. Resolution of ST-segment elevation in acutemyocardial infarction—early prognostic significance after thrombolytic therapy. Resultsfrom the COBALT trial. Herz 1999;24:440-7.
Shah A, Wagner GS, Granger CB, et al. Prognostic implications of TIMI flow grade in theinfarct related artery compared with continuous 12-lead ST-segment resolution analysis.Reexamining the “gold standard” for myocardial reperfusion assessment. J Am CollCardiol 2000;35:666-72.
Holmvang L, Andersen K, Dellborg M, et al. Relative contributions of a single admission12-lead electrocardiogram and early 24-hour continuous electrocardiographic monitoringfor early risk stratification in patients with unstable coronary artery disease. Am J Cardiol1999;667-74.
Johanson P, Svensson AM, Dellborg M. Clinical implications of early ST-segmentvariability. A report from the ASSENT 2 ST-monitoring substudy. Cor Art Dis2001; 12:277-283.
Gottwald E, Gottwald M, Dhein S. Enhanced dispersion of epicardial activation recovery atsites of histological inhomogenity during regional cardiac ischemia and reperfusion. Heart1998;474-480.
Goldberg S, Greenspon AJ, Urban PL, et al. Reperfusion arrhythmia: a marker ofrestoration of antegrade flow during intracoronary thrombolysis for acute myocardialinfarction. Am Heart J 1983; 105:26-32.
Gorgels AP, Vos MA, Letsch IS, et al. Usefulness of the accelerated idioventricular rhythmas a marker for myocardial necrosis and reperfusion during thrombolytic therapy in acutemyocardial infarction. Am J Cardiol 1988;61:231-235.
Gressin V, Louvard Y, Pezzano M, Lardoux H. Holter recording of ventricular arrhythmiasduring intravenous thrombolysis for acute myocardial infarction. Am J Cardiol1992;69:152-159.
Piper HM, Garcia-Dorado D. Prime causes of rapid cardiomyocyte death duringreperfusion. Ann Thorac Surg 1999;68:1913-1919.
Yoshida Y, Hirai M, Yamada T, et al. Antiarrhythmic efficacy of dipyridamole intreatment of reperfusion arrhythmias : evidence for cAMP-mediated triggered activity as amechanism responsible for reperfusion arrhythmias. Circulation 2000; 101:624-630.
114
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.

THE ELECTROCARDIOGRAPHIC SIGNS OF REPERFUSION
Engelen DJ, Gressin V, Krucoff MW, et al. Reperfusion arrhythmias in acute anteriormyocardial infarction are related to the mode of reperfusion and predict worsening of leftventricular function after the acute phase. In press.
Wellens HJ, Lie KI, Durrer D. Further observations on ventricular tachycardia as studiedby electrical stimulation of the heart. Chronic recurrent ventricular tachycardia andventricular tachycardia during acute myocardial infarction. Circulation 1974; 49: 647-653.
Boissel JP, Castaigne A, Mercier C, Lion L, Leizorovicz A. Ventricular fibrillationfollowing administration of thrombolytic treatment. The EMIP experience. EuropeanMyocardial Infarction Project. Eur Heart J 1996; 17:213-221.
Doevendans PA, Cheriex E, van der Zee R, et al. Risk stratification in the thrombolytic era:results of a prospective study. Cardiologie 1996; 3:319-323.
Hohnloser SH, Zabel M, Kasper W, Meinertz T, Just H. Assesment of coronary arterypatency after thrombolytic therapy: accurate prediction utilizing the combined analysis ofthree non-invasive markers. J Am Coll Cardiol 1991; 18:44-49.
Chesebro JH, Knatterud G, Roberts R, et al. Thrombolysis in Myocardial Infarction (TIMI)Trial, Phase I: A comparison between intravenous tissue plasminogen activator andintravenous streptokinase. Clinical findings through hospital discharge. Circulation 1987;76:142-154.
115
29.
30.
31.
32.
33.
34.

Chapter 7
The electrocardiogram in unstable angina

118 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
ST segment depression on admission identifies a high risk group of patientswith unstable coronary artery disease
Magnitude and distribution of ST segment depression should determineinvasive versus conservative management strategy
In patients with acute myocardial ischemia continuous 12 lead ECG orserial ECG’s recordings may be needed to diagnose unstable angina or nonST-segment elevation myocardial infarction
Determine troponin level to document recent loss of myocardial tissue
In left main or 3 vessel disease ST segment changes in 8 or more ECGleads develop during chest pain
In critical LAD narrowing precordial T wave negativity develops afterchest pain has subsided

THE ELECTROCARDIOGRAM IN UNSTABLE ANGINA 119
An unstable plaque in a coronary artery may lead to critical narrowing orcomplete occlusion resulting in acute ischemia and/or necrosis of themyocardium. The resulting clinical entities are called acute coronarysyndromes and include unstable angina and acute myocardial infarction.Initially it may not be clear which of the two is present, and the determinationof biochemical cardiac markers such as troponin requires time and may have alow sensitivity in the early phase of myocardial ischemia.
The importance of ST segment depressionIn unstable angina and non-ST-segment elevation myocardial infarction, the 12lead surface electrocardiogram (ECG) on admission can give importantinformation about the site and the extent of ischemia. Antman et al (1) showedthat in those patients the number of leads showing ST depression and theamount of ST depression indicate size and severity of the ischemic area. Thiswas recently confirmed by Kaul et al (2). It was also shown that patients withST segment depression may have a poorer long-term prognosis than patientswith an acute myocardial infarction (3,4). Magnitude and distribution of STdepression should determine which patient will profit from an invasive versus aconservative management strategy (5). Recent data from the FRISC II studyindicate that the presence of ST depression on admission is already sufficientevidence to propose early invasive treatment to the patient (6).
The ECG also allows identification of high-risk syndromes such asunstable angina due to a lesion proximal in the left anterior descending (LAD)branch of the left coronary artery or due to either 3 vessel disease or left mainstem stenosis. Recognizing these entities is important in the decision making tore-open the culprit artery, either pharmacologically or invasively using apercutaneous coronary intervention or bypass surgery. These strategies haveled to a marked improved in-hospital and post discharge prognosis of unstableangina during the last decade (7).
The value of serial ECG’sDiagnosing unstable angina and also non-ST-segment elevation myocardialinfarction can be particularly difficult both in relation to the presence orabsence of chest pain and the changes on the ECG. At the time of recording theECG the chest pain may have already subsided. In that situation it is veryimportant to look for the development of postischemic T wave changes.
They may occur within a few hours. Ideally they should be picked up by acontinuous recording of the 12-lead ECG (8). The importance of this wasrecently shown by Akkerhuis et al. (9) who used continuous multilead ST-Tsegment monitoring to identify patients with acute coronary syndromes at highrisk of adverse cardiac events. They especially recommended this approach inpatients not showing on admission either clear ST elevation pointing to acuteMI or definite ST segment depression. In those patients diagnostic ST-Tsegment changes may occur during continuous multilead ECG monitoring andcan be helpful to identify patients that will profit from an early invasive

120 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
intervention. When continuous ECG monitoring is not possible, it isrecommended to keep the patient in the emergency room, to wait for thetroponin value and to record at least one more ECG before deciding to send thepatient home.
Occasionally the ECG findings are not specific even during chest pain,especially in case of a circumflex coronary artery narrowing or occlusion. Alsoin that situation it is very helpful to record sequential ECG’s during theobservation period, to demonstrate ischemia. Keep in mind that a single normalECG in a patient with a typical syndrome of chest pain is insufficient toexclude myocardial ischemia.
The ECG in 3 vessel or left main stem diseaseUnstable angina, such as angina at rest carries an increased risk for myocardialinfarction or sudden death. It is important to record the ECG during chest pain,not only to document the ischemic nature of the complaints, but also to assessthe site and the extent of ischemia. Typically, high-risk situations are proximalLAD involvement (10,11) 3-vessel disease and left main stem stenosis (12)(fig. 7.1). The latter 2 conditions result in a typical ECG pattern during chestpain (figure 7.2) with generalized, often marked ST-segment depressioncombined with ST-segment elevation in lead AVR and frequently in In astudy of 120 patients with rest angina we found that the larger the number ofleads with and the greater the amount of ST segment depression, the higher therisk of 3-vessel disease or main stem stenosis: A 75% positive predictiveaccuracy of 3 vessel disease or a left main stenosis was present when 8 leads ormore showed ST-segment changes during chest pain (11), with leads AVR and
showing ST-elevation!These ECG findings are also valid for determining the extent of ischemia
when they are observed during exercise (figure 7.3). The unstable nature of thesyndrome is confirmed by the persistence of changes during the recovery phase(figure 7.3C)
The proximal LAD syndrome
During chest pain: Peaked T-waves in the precordial leadsChanges in the ST segment and the T-wave are important to diagnose bothacute and subacute ischemia. During acute ischemia predominant T-wavechanges can be found, without marked changes in the ST-segment. Typically,the T-waves become peaked, more symmetric and shorter in duration (figure7.4). These changes reflect ischemia rather than injury and are probablyexplained by shortening of the subendocardial repolarization phase with intactduration of repolarization in the subepicardial layers (13). The coronaryperfusion is not completely blocked either because there is a subtotal stenosisor a complete occlusion but with collateral circulation.

THE ELECTROCARDIOGRAM IN UNSTABLE ANGINA 121

122 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA

THE ELECTROCARDIOGRAM IN UNSTABLE ANGINA 123
After chest pain: T wave negativity in the precordial leadsRecording the development of negative T waves in at least the precordial leads
to following the episode of chest pain has been very useful to identify asubgroup of patients with unstable angina having an increased risk ofsubsequent MI or sudden cardiac death (figure 7.5). Coronary angiographiccorrelations invariably showed severe proximal stenosis in the left anteriordescending (LAD) branch or total LAD occlusion in the presence of collateralcirculation (10,14,15). LAD obstruction will lead to MI of the anterior wall asshown in fig. 7.5, which was recorded before the advent of thrombolytictherapy. Recognition of the ECG pattern of a critical LAD stenosis is importantbecause vessel occlusion will lead to a large anterior wall myocardial infarctionand early death may occur due to pump failure or high degree sub-AV nodalblock. Ventricular tachycardia may appear later during the subacute and thechronic phase and can be prevented by prompt measures to restore flow (16).
After an acute coronary syndrome in the anterior wall occasionally giant Twave negativity can be observed (figure 7.6). This latter phenomenon hasrecently been described to predict good prognosis, as evidenced by recovery ofR-waves and preservation of left ventricular function (17).

124 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Recovery of T wave abnormalities following ischemiaIn patients having unstable angina because of a proximal LAD stenosis andsurviving for at least 6 months after the ischemic event, our group foundnormalization of the ST-T-segment within 6 weeks in half of the population,and in 80% within 6 months (16). Similar findings were reported in anotherstudy after balloon angioplasty, revealing normalization of the T wave in 90%of patients after 28 weeks (14). A more recent study also confirmed the rapidresolution of postischemic T wave inversion (within 3-21 days of presentationin 75% of cases). Persistence of T wave inversion was related to a worseoutcome: More new events were found during follow-up of these patients,when compared with an unstable angina group without postischemic T waveabnormalities (14).
Conclusion
While Troponin determination will document loss of myocardial tissue inunstable angina the standard 12 lead ECG gives important information aboutthe site and extent of ischemia. It is possible to identify high risk situationssuch as unstable angina due to a proximal LAD lesion or caused by either 3vessel disease or left main stem stenosis. Recognizing these entities isimportant for decision making to restore adequate patency in the culpritvessel(s).

THE ELECTROCARDIOGRAM IN UNSTABLE ANGINA 125
References
Antman EM, Cohen M, Bernink PJ et al. The TIMI risk score for unstable angina from STelevation MI: a method for prognosticitation and therapeutic decision making. JAMA 2000;284:835-842.
Kaul P, Fu Y, Shang WC, et al. Prognostic value of ST segment depression in acutecoronary syndromes : insights from PARAGON-A applied to GUSTO-II b. J Am CollCardiol 2001;38:64-71.
Savonitto S, Ardissino D, Granger CB, et al. Prognostic value of the admissionelectrocardiogram in acute coronary syndromes. JAMA 1999;281:707-713.
Hyde TA, French JK, Wong CK, et al. Four-year survival of patients with acute coronarysyndromes without ST-segment elevation and prognostic significance of 0,5 mm ST-segment depression. Am J Cardiol 1999;84:379-385.
Solomon DH, Stone PH, Glynn RJ, et al. Use of risk stratification to identify patients withunstable angina likeliest to benefit from an invasive versus conservative managementstrategy. J Am Coll Cardiol 2001;38:969-976.
Didenholm E, Andren B, Frostfeldt G, et al. ST depression in ECG at entry indicates severecoronary lesions and large benefits of an early invasive treatment strategy in unstablecoronary artery disease. Eur Heart J 2002;23:41-49.
Widdershoven JW, Gorgels AP, Vermeer F, et al. Changing characteristics and in-hospitaloutcome of patients admitted with acute myocardial infarction. Observations from 1982-1994. Eur Heart J 1997;1073-1080.
Klootwijk P, Mey S, Van Es GA, et al. Comparison of usefulness of computer-assistedcontinuous hour 3-lead with 12-lead ECG-ischemia monitoring for detection andquantification of ischemia in patients with unstable angina. Eur Heart J 1997; 18: 931-940.
Akkerhuis KM, Klootwijk PAJ, Lindeboom W, et al. Recurrent ischemia during continuousmultilead ST-segment monitoring identifies patients with acute coronary syndromes at highrisk of adverse cardiac events. Eur Heart J 2001; 22:1997-2006.
De Zwaan C, Bar FW, Wellens HJ. Characteristic electrocardiographic pattern indicating acritical stenosis high in left anterior descending coronary artery in patients admitted becauseof impending myocardial infarction. Am Heart J 1982;103:730-735.
De Zwaan C, Bar FW, Gorgels AP, Wellens HJ. Unstable angina: are we able to recognizehigh-risk patients? Chest 1997;112:224-50.
Gorgels APM, Vos MA, Mulleneers R, de Zwaan C, Bar FW, Wellens HJ. Value of theelectrocardiogram in diagnosing the number of severely narrowed coronary arteries in restangina pectoris. Am J Cardiol 1993;72:999-1003.
Fozzard HA, Makielski JC.The electrophysiology of acute myocardial ischemia. Annualreview of medicine 1985;36:275-280.
Simon K, Hackett D, Szelier A, et al. The natural history of postischemic T wave inversion:a predictor of poor short-term prognosis? Coronary Artery Disease 1994;5:937-942.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.

126 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
Shawl FA, Velasco CE, Goldbaum TS, Forman BM. Effect of coronary angioplasty onelectrocardiographic changes in patients with unstable angina secondary to left anteriordescending coronary artery disease. J Am Coll Cardiol 1990;16:325-331.
De Zwaan C, Bar FW, Janssen JH, et al. Angiographic and clinical characteristics ofpatients with unstable angina showing an ECG pattern indicating critical narrowing of theproximal LAD coronary artery. Am Heart J. 1989;117:657-666.
Agetsuma H, Hirai M, Hirayama H, et al. Transient giant negative T-wave in acute anteriorwall infarction predicts R-wave recovery and preservation of left ventricular dysfunction.Heart 1996;75:229-234.
15.
16.
17.
Index
AAbnormal ventricular activation, myocardial
infarction with, 65–83left bundle branch block, 68–75
intermittent, 72–73practical approach, 74–75serial ECG’s, 74
paced ventricular rhythm, 76–79ventricular pre-excitation, 79–81
Accelerated idiopathic ventricular rhythm,106–109
Acute myocardial infarctionarrhythmias in, 85–98AV-nodal conduction system, 49–53
atrio-ventricular nodal levelECG findings, 49–51incidence, 52–53left bundle branch block, inferior
wall myocardial infarction,51–52
conduction abnormalities,atrio-ventricular nodal level, 49–53
management, 53conduction abnormalities, sub-AV-nodal
level, 53–63ECG findings, 53–59incidence, 60–61management, 61–62
conduction disturbances, 43–64sino-atrial region, 45–49
atrio-ventricular conduction system,45–46
blood supply of sinus node,atrio-ventricular conductionsystem, 45
ECG findings, 46incidence, 47management, 48–49sino atrial block, sinus arrest, 47–48sinus bradycardia, 46sinus node, sino-atrial region, 45slow rhythms, conduction
abnormalities, sinus nodal,sino-atrial level, 46
sinus arrest, sino-atrial block, 44
sub-AV nodal conduction disturbances, 44supraventricular arrhythmias, 87–90
atrial fibrillation, 88–90sinus tachycardia, 87–88
ventricular arrhythmias, 91–94ventricular fibrillation, 93–94ventricular premature beats, 91–92ventricular tachycardia, 92–93
Angina, unstable, ECG in, 117–126chest pain
peaked T-waves in precordial leads,120–122
T wave negativity in precordial leads, 123ischemia, recovery of T wave abnormalities
following, 124left main stem disease, 120proximal LAD syndrome, 120–124serial ECG’s, 119–120ST segment depression, 119
Anterior wall infarction, coronary arteryocclusion, 24–37
distal LAD occlusion, 28–29LAD occlusion
distal to first diagonal branch, proximal tofirst septal branch, 31–32
distal to first septal branch, proximal to firstdiagonal branch, 30
proximal to first septal, first diagonalbranch high risk, 26–28
left main occlusion, 33–34new infarction in presence of old one, 36site of occlusion in, criteria to identify, 33ST deviation score, location, coronary artery
occlusion, 34–36ST segment vector, to localize site of
ischemia, 25–26Anterior wall myocardial infarction, coronary
artery occlusion, grades of ischemia, 12Arrhythmias in acute myocardial infarction,
85–98supraventricular arrhythmias, 87–90
atrial fibrillation, 88–90sinus tachycardia, 87–88
ventricular arrhythmias, 91–94ventricular fibrillation, 93–94

128 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
ventricular premature beats, 91–92ventricular tachycardia, 92–93
Atrial fibrillation, 88–90Atrial tachycardia, 106Atrio-ventricular conduction system
acute myocardial infarction, 45conduction disturbances, 45
acute myocardial infarction, sino-atrialregion, 45–46
sino-atrial region, 45sinus node, blood supply of, 45
Atrio-ventricular nodal levelacute myocardial infarction, ECG
findings, 49–51AV-nodal conduction system, conduction
disturbances, 49–51AV nodal conduction disturbances,
conduction disturbances, acutemyocardial infarction, 44
AV-nodal conduction system, conductiondisturbances, acute myocardialinfarction, 49–53
atrio-ventricular nodal levelECG findings, 49–51incidence, 52–53left bundle branch block, inferior wall
myocardial infarction, 51–52conduction abnormalities,
atrio-ventricular nodal level, 49–53management, 53
BBlood supply of sinus node, 45Brady arrhythmias, 111–112
ECG findings, 111incidence, 111mechanism, 111prognosis, 111
CChest pain
peaked T-waves in precordial leads,120–122
T wave negativity in precordial leads, 123Conduction abnormalities
acute myocardial infarction,sub-AV-nodal level, 53–63
ECG findings, 53–59incidence, 60–61management, 61–62
AV-nodal conduction system, acutemyocardial infarction,atrio-ventricular nodal level, 49–53
Conduction disturbances, acute myocardialinfarction, 43–64
AV-nodal conduction system, 49–53atrio-ventricular nodal level
ECG findings, 49–51incidence, 52–53left bundle branch block, inferior wall
myocardial infarction, 51–52mechanism, 52–53prognostic significance, 52–53
conduction abnormalities, atrio-ventricularnodal level, 49–53
management, 53conduction abnormalities, sub-AV-nodal level,
53–63ECG findings, 53–59incidence, 60–61management, 61–62mechanism, 60–61prognostic significance, 60–61
sino-atrial region, 45–49atrio-ventricular conduction system, 45–46blood supply of sinus node,
atrio-ventricular conduction system, 45ECG findings, 46incidence, 47management, 48-49mechanisms, 47prognostic significance, 47sino atrial block, sinus arrest, 47–48sinus bradycardia, 46sinus node, sino-atrial region, 45slow rhythms, conduction abnormalities,
sinus nodal, sino-atrial level, 46sinus arrest, sino-atrial block, 44sub-AV nodal conduction disturbances, 44
Coronary arteryanterior wall infarction, 24–37
distal LAD occlusion, 28–29LAD occlusion
distal to first diagonal branch, proximalto first septal branch, 31–32
distal to first septal branch, proximal tofirst diagonal branch, 30
proximal to first septal, first diagonalbranch high risk, 26–28
left main occlusion, 33–34new infarction in presence of old one, 36site of occlusion in, criteria to identify, 33ST deviation score, location of coronary
artery occlusion, 34–36ST segment vector, to localize site of
ischemia, 25–26anterior wall myocardial infarction, grades of
ischemia, 12

INDEX 129
coronary artery, infero-posterior wallinfarction, 13–24
identification of, 5–42anterior wall infarction, 8–9
distal LAD occlusion, 8–9LAD occlusion
distal to first diagonal, proximal tofirst septal branch, 8
distal to first septal, proximal tofirst diagonal branch, 8
proximal to first septal, firstdiagonal branch, 8
ECG patterns, 7–9infero posterior infarction, 7–8
atrial infarction, 8lateral wall involvement, 8posterior wall involvement, 7
ST depression in precordial leads,7
proximal, distal RCA, 7RCA, CX, 7
infero posterior myocardial infarction,grades of ischemia, 12
infero-posterior wall infarctionatrial infarction, 24AV nodal block, 24coronary patho-anatomy, 13–15CX occlusion, diagnosing, difficulties
in, 24dominance, 15inferior wall myocardial infarction,
RCA, CX occlusion in, 15–17isolated RV infarction, 22–23lateral wall involvement, 17posterior wall involvement, 17RV infarction, 18–21
mortality, clinical, ECG variables, 10severity of ischemia, 5–42site of occlusion, coronary artery, ECG
patterns, 13–37size of area at risk, 5–42ST segment deviation score, 7, 9–11terminal QRS-ST segment pattern, 7
severity of cardiac ischemia, 11–13Coronary artery occlusion, severity of
ischemia, 5–42
EEctopic activity, 105
ECG findings, 105
FFibrillation
atrial, 88–90ventricular, 93–94
IInferior wall myocardial infarction, left bundle
branch block, atrio-ventricular nodal level,51–52
Infero posterior myocardial infarction, coronaryartery occlusion, grades of ischemia, 12
Infero-posterior wall infarction, coronary arteryocclusion
atrial infarction, 24AV nodal block, 24coronary patho-anatomy, 13–15CX occlusion, diagnosing, difficulties in, 24dominance, 15inferior wall myocardial infarction, RCA, CX
occlusion in, 15–17isolated RV infarction, 22–23lateral wall involvement, 17posterior wall involvement, 17RV infarction, 18–21
LLeft bundle branch block, 68–75
acute myocardial infarction, 51–52AV-nodal conduction system, conduction
disturbances, 51–52inferior wall myocardial infarction,
atrio-ventricular nodal level, 51–52intermittent, 72–73practical approach, 74–75serial ECG’s, 74
Left main stem disease, 120
MMyocardial infarction, with abnormal ventricular
activation, 65–83left bundle branch block, 68–75
intermittent, 72–73practical approach, 74–75serial ECG’s, 74
paced ventricular rhythm, 76–79ventricular pre-excitation, 79–81
NNon-sustained ventricular tachycardia, 106, 109
OOcclusion, coronary artery
130 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
anterior wall infarction, 24–37distal LAD occlusion, 28–29LAD occlusion
distal to first diagonal branch,proximal to first septal branch,31–32
distal to first septal branch, proximalto first diagonal branch, 30
proximal to first septal, first diagonalbranch high risk, 26–28
left main occlusion, 33–34new infarction in presence of old one,
36site of occlusion in, criteria to identify,
33ST deviation score, location of
coronary artery occlusion, 34–36ST segment vector, to localize site of
ischemia, 25–26anterior wall myocardial infarction,
grades of ischemia, 12infero posterior myocardial infarction,
grades of ischemia, 12infero-posterior wall infarction
atrial infarction, 24AV nodal block, 24coronary patho-anatomy, 13–15CX occlusion, diagnosing, difficulties
in, 24dominance, 15inferior wall myocardial infarction,
RCA, CX occlusion in, 15–17isolated RV infarction, 22–23lateral wall involvement, 17posterior wall involvement, 17RV infarction, 18–21
mortality, clinical, ECG variables, 10site of, identification, 5–42site of occlusion
coronary arteryECG patterns, 13–37infero-posterior wall infarction,
13–24identification of
anterior wall infarction, 8–9distal LAD occlusion, 8–9LAD occlusion
distal to first diagonal, proximalto first septal branch, 8
distal to first septal, proximal tofirst diagonal branch, 8
proximal to first septal, firstdiagonal branch, 8
ECG patterns, 7–9infero posterior infarction, 7–8
atrial infarction, 8lateral wall involvement, 8posterior wall involvement, 7
ST depression in precordial leads, 7proximal, distal RCA, 7RCA, CX, 7
size of area at risk, 5–42ST segment deviation score, 7, 9–11terminal QRS-ST segment pattern, 7
severity of cardiac ischemia, 11–13
PPre-excitation, ventricular, 79–81Premature beats, ventricular, 91–92
RReperfusion, ECG signs of, 99–116
accelerated idiopathic ventricular rhythm, 106atrial tachycardia, 106brady arrhythmias, 111–112
ECG findings, 111incidence, 111
ectopic activity, 105ECG findings, 105
non-sustained ventricular tachycardia, 106,109
reperfusion arrhythmias, defined, 106sinus bradycardia, 106ST-T segment behavior, 101–105
incidence, 104–105ST segment changes, 101–103T wave changes, 103–104
supraventricular arrhythmias, 110ECG findings, 110incidence, 110
ventricular premature beats, 106–109increase in, 106
Reperfusion arrhythmias, defined, 106
SSino-atrial block
conduction disturbances, acute myocardialinfarction, sinus arrest, 44
sino-atrial region, conduction disturbances,acute myocardial infarction, sinus arrest,47–48
Sino-atrial regionconduction disturbances, acute myocardial
infarction, 45–49atrio-ventricular conduction system, 45–46blood supply of sinus node,
atrio-ventricular conduction system, 45

INDEX 131
ECG findings, 46incidence, 47management, 48–49sino atrial block, sinus arrest, 47–48sinus bradycardia, 46sinus node, sino-atrial region, 45slow rhythms, conduction
abnormalities, sinus nodal,sino-atrial level, 46
sinus node, conduction disturbances,acute myocardial infarction,sino-atrial region, 45
Sinus arrestsino atrial block, sino-atrial region,
conduction disturbances, acutemyocardial infarction, 47–48
sino-atrial block, conduction disturbances,acute myocardial infarction, 44
Sinus bradycardia, 106sino-atrial region, conduction
disturbances, acute myocardialinfarction, 46
Sinus nodeblood supply of, atrio-ventricular
conduction system, conductiondisturbances, acute myocardialinfarction, sino-atrial region, 45
sino-atrial region, conductiondisturbances, acute myocardialinfarction, sino-atrial region, 45
Sinus tachycardia, 87–88Site of occlusion
coronary arterycoronary artery occlusion
ECG patterns, 13–37infero-posterior wall infarction,
13–24identification of, 5–42
identification of, coronary artery occlusionanterior wall infarction, 8–9
distal LAD occlusion, 8–9LAD occlusion, 8
proximal to first septal, firstdiagonal branch, 8
ECG patterns, 7–9infero posterior infarction, 7–8
atrial infarction, 8lateral wall involvement, 8posterior wall involvement, 7
ST depression in precordial leads,7
proximal, distal RCA, 7RCA, CX, 7
Size of area at risk, coronary arteryocclusion, 5–42
Slow rhythmsconduction disturbances, acute myocardial
infarction, sino-atrial region, conductionabnormalities, sinus nodal, sino-atriallevel, 46
sinus nodal, sino-atrial level, conductiondisturbances, acute myocardialinfarction, sino-atrial region, 46
ST segment deviation score, coronary arteryocclusion, 7, 9–11
ST-T segment behavior, 101–105incidence, 104–105mechanism, 104–105prognastic implications, 104–105ST segment changes, 101–103T wave changes, 103–104
Sub-AV nodal conduction disturbances,conduction disturbances, acute myocardialinfarction, 44
Supraventricular arrhythmias, 87–90, 110atrial fibrillation, 88–90ECG findings, 110incidence, 110mechanism, 110prognosis, 110sinus tachycardia, 87–88
TTachycardia
sinus, 87–88ventricular, 92–93
Terminal QRS-ST segment patterncoronary artery occlusion, 7severity of cardiac ischemia, coronary artery
occlusion, 11–13
UUnstable angina, ECG in, 117–26
chest painpeaked T-waves in precordial leads,
120–122T wave negativity in precordial leads, 123
ischemia, recovery of T wave abnormalitiesfollowing, 124
left main stem disease, 120proximal LAD syndrome, 120–124serial ECG’s, 119–120ST segment depression, 119
VVentricular activation, abnormal, myocardial
infarction with, 65–83

132 THE ECG IN ACUTE MYOCARDIAL INFARCTION AND UNSTABLE ANGINA
left bundle branch block, 68–75intermittent, 72–73practical approach, 74–75serial ECG’s, 74
paced ventricular rhythm, 76–79ventricular pre-excitation, 79–81
Ventricular arrhythmias, 91–94
ventricular premature beats, 91–92ventricular tachycardia, 92–93
Ventricular fibrillation, 93–94, 109Ventricular pre-excitation, 79–81Ventricular premature beats, 91–92, 106–109
increase in, 106Ventricular tachycardia, 92–93