appropriate use and interpretation of cardiac...
TRANSCRIPT

Appropriate Use and Interpretation of Cardiac Biomarkers
Dr. Vikas TandonAssociate Professor, Cardiology
McMaster UniversityNovember 1, 2017
Canadian Society of Internal MedicineAnnual Meeting 2017
Toronto, ON

CSIM Annual Meeting 2017Conflict Disclosures
I have the following conflicts to declare:
Company/Organization Details
Advisory Board or equivalent X X
Speakers bureau member X X
Payment from a commercial organization. (including gifts or other consideration or ‘in kind’ compensation)
X X
Grant(s) or an honorarium X X
Patent for a product referred to or marketed by a commercial organization. X X
Investments in a pharmaceutical organization, medical devices company or communications firm.
X X
Participating or participated in a clinical trial McMaster University Participated in periop research studies
including VISION, POISE-2, MANAGE

CSIM Annual Meeting 2017
The following presentation represents the views of the speakerat the time of the presentation. This information is meant foreducational purposes, and should not replace other sources
of information or your medical judgment.
Learning Objectives:• Develop an approach to managing patients elevated troponins who present with non-coronary presentations • Develop short- and long-term management plans for patients with post-operative troponin elevations • Understand the indications for ordering a BNP in acute medical patients and interpret results

Perioperative Care Congress: Science, Evidence and Practice
Save the date: Perioperative Care Congress 2018
May 11-13, 2018Toronto, Ontario
CANADA
Visit our website http://periopcongress.org/or follow us on twitter @periopcongress
More information to follow!

• Biomarkers are commonly used in medical patients as a means to diagnosis and prognosis
• Biomarkers very sensitive but not necessarily specific for any one particular disease process
• Interpretation can sometimes be challenging thus requiring an organized approach
Scope of problem

• 66 F presents with 8/10 RSCP, diaphoresis, palpitations• Baseline ECG shows rapid atrial fibrillation on admission
• Cardiac RF – DM, HTN, dyslipidemia, remote smoker• Meds: ASA 81 mg, Rosuvastatin 10 mg, Perindopril 8 mg,
Metoprolol 50 mg BID
• O/E – HR 120-140 bpm, BP 130/78; otherwise normal• hs-trop I 620 (peak)
Case 1

12 Lead

1. Normal coronaries
2. Mild atherosclerotic plaque with no significant stenosis
3. Single vessel disease
4. Multivessel disease
This patient has:

• 50 F presents with 2 day history of headaches, chest and back pain lasting hours at a time
• Cardiac RF – HTN, current smoker (30 pack year history)
• O/E – Hypertensive urgency with BP 200/118 on admission, HR 67; symptoms resolved when normotensive in hospital
• hs-trop I 68 (peak)
Case 2

12 Lead

1. Normal coronaries
2. Mild atherosclerotic plaque with no significant stenosis
3. Single vessel disease
4. Multivessel disease
This patient has:

• 58 F presents with bright red blood per rectum, known history of Ulcerative Colitis
• Cardiac RF – HTN, 40 pack year smoking history (recently quit)
• No cardiac symptoms. O/E – HR 110-120, BP 130/78
• hs-trop I 108 (peak), Hb 118 (stable)
Case 3

12 Lead

1. Normal coronaries
2. Mild atherosclerotic plaque with no significant stenosis
3. Single vessel disease
4. Multivessel disease
This patient has:

The cases thus far:Case 1 Case 2 Case 3
66 F w 8/10 RSCPrapid A Fib 120-140
50 F headaches, CP and back pain lasting hoursHTN urgency: BP 200/118
58 F bright red blood per rectum; known UC
DM, HTN, Chol, remote smoker (5 pack yr history)
HTN, current smoker (30 pack year history)
HTN, recent smoker (40 pack year history)
Peak trops = 620 Peak trops = 68 Peak trops = 108

The cases thus far:Case 1 Case 2 Case 3
66 F w 8/10 RSCPrapid A Fib 120-140
50 F headaches, CP and back pain lasting hoursHTN urgency: BP 200/118
58 F bright red blood per rectum; known UC
DM, HTN, Chol, remote smoker (5 pack yr history)
HTN, current smoker (30 pack year history)
HTN, recent smoker (40 pack year history)
Peak trops = 620 Peak trops = 68 Peak trops = 108
Cath: Mild plaque No significant stenosis
Cath: 90% stenosis ostialRCA; mild dz LAD/LCX
Cardiac CT: Normal coronaries
• The size of the troponin elevation does not correlate with extent of coronary disease
But
• The rise of the troponin does indicate poorer outcome in patients compared to normal troponin counterparts
Concept

Ostermann et al. Critical Care 2014


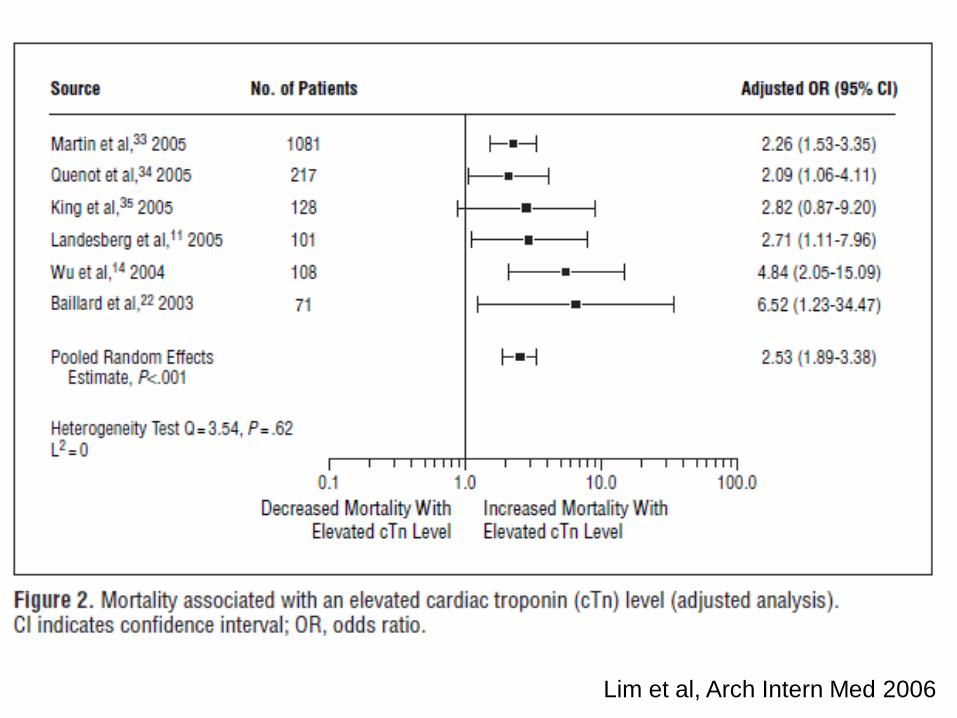
Lim et al, Arch Intern Med 2006

Other Medical Conditions
Condition Hazard Ratio
Critical Illness OR 2.5 for all cause mortality
Chronic Kidney Disease Trop T adjusted HR = 3Trop I adjusted HR = 2.7
Pulmonary Embolism OR 4.8 for all cause mortality

The Importance of Myocardial Injury
Devereaux, JAMA, 2012

Approach• Look for and correct physiological abnormalities
– hypoxia, hypotension, tachycardia (if BP adequate), Hb if <70, sepsis, PE
• If no signs of bleeding initiate ASA 81 mg daily
• Initiate or intensify Statin therapy
• Inpatient vs. outpatient risk stratification and follow up

CASE 4: Postoperative troponin monitoring
• 64 y/o male • Postop day 3 orthopedic surgery• No symptoms, trop 0.15 (0.04 ULN)• EKG: Anterior biphasic T waves • Cath/OCT - 3 days after trop increase

1. Normal coronaries
2. Mild atherosclerotic plaque with no significant stenosis
3. Single vessel disease with plaque rupture/thrombus
4. Single vessel disease but no thrombus/stable plaque
This patient has:

CASE 5: Perioperative Myocardial Infarction
• 83 y/o male • Postop day 5 orthopedic surgery• Sudden chest pain trop 9.85 (0.04 ULN), • EKG: No acute changes • Cath/OCT - 2 days after trop increase

1. Normal coronaries
2. Mild atherosclerotic plaque with no significant stenosis
3. Single vessel disease with plaque rupture/thrombus
4. Single vessel disease but no thrombus/stable plaque
This patient has:

Summary of Cases 4 and 5Case 4 Case 5
64 year old male 83 year old male
POD 3 orthopedic surgery POD 5 orthopedic surgery
No symptoms, trop 0.15 (ULN 0.04) Sudden chest pain, trops 9.85 (ULN 0.04)
Biphasic T waves anterior leads No acute ECG changes

Case 4 Cath Findings

Case 4 OCT findings

PCI with BMS, Dual antiplatelet therapy with ASA and Plavix for 1 year
Uncomplicated course at 1 year

CASE 5: Perioperative Myocardial Infarction
• 83 y/o male • Postop day 5 orthopedic surgery• Sudden chest pain trop 9.85 (0.04 ULN), • EKG: No acute changes • Cath/OCT - 2 days after trop increase
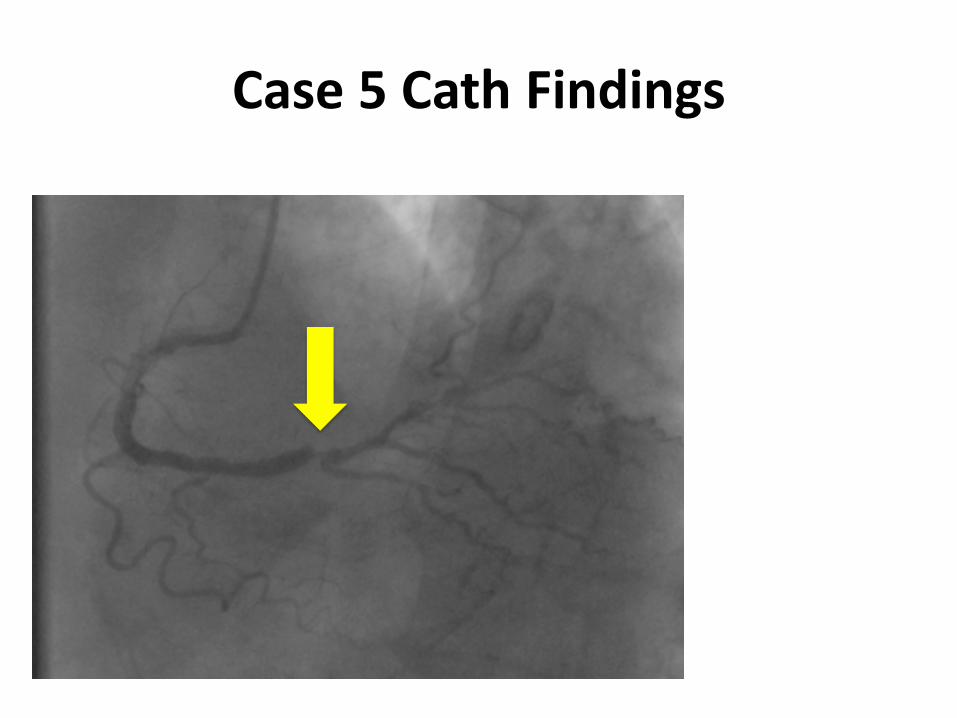
Case 5 Cath Findings
Moderate LAD stenosis Distal LCX stenosis >80% in small vessel
Normal LV function

Case 5 OCT findings

PCI with BMS 3.5 mm
Dual antiplatelet therapy x 12 months
Uncomplicated course at 30 days

Summary of Cases 4 and 5Case 4 Case 5
64 year old male 83 year old male
POD 3 orthopedic surgery POD 5 orthopedic surgery
No symptoms, trop 0.15 (ULN 0.04) Sudden chest pain, trops 9.85 (ULN 0.04)
Biphasic T waves anterior leads No acute ECG changes

Summary of Cases 4 and 5Case 4 Case 5
64 year old male 83 year old male
POD 3 orthopedic surgery POD 5 orthopedic surgery
No symptoms, trop 0.15 (ULN 0.04) Sudden chest pain, trops 9.85 (ULN 0.04)
Biphasic T waves anterior leads No acute ECG changes
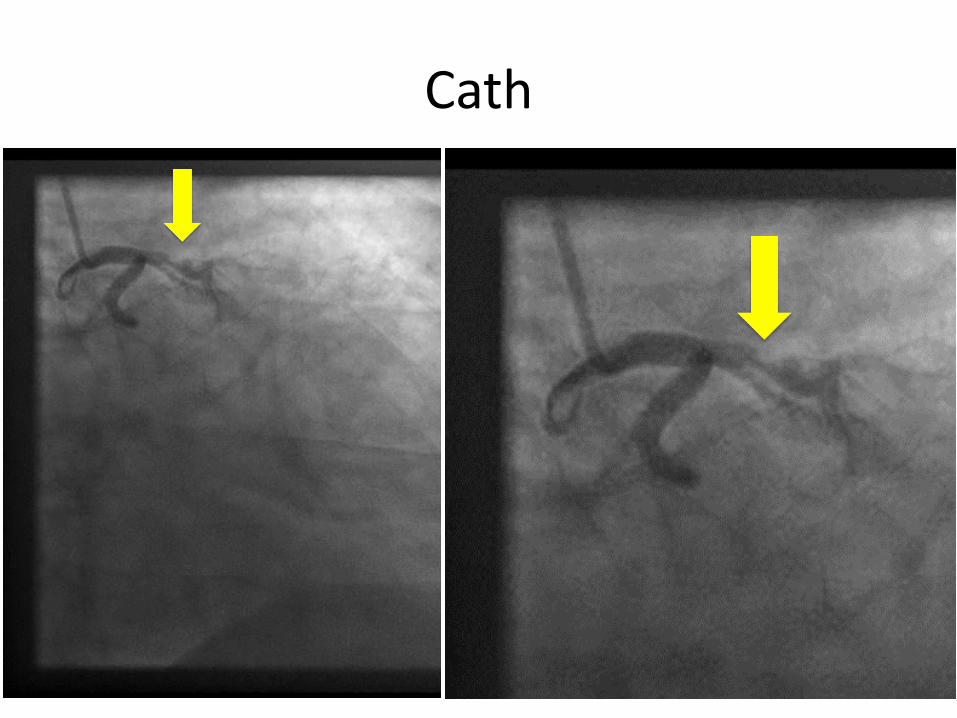
Plaque rupture and thrombus - LAD Significant stenosis RCA but no plaque rupture

• The size of the troponin elevation does not correlate pathophysiology– i.e. cannot distinguish between plaque rupture vs.
supply demand
• Presence or absence of symptoms not helpful in determining pathophysiology– Further, no significant difference in mortality
outcomes
Concept

MINS that probably will go undetected without trop monitoring
• MINS without chest discomfort, other possible symptoms (i.e., arm, neck, or jaw discomfort, shortness of breath), or pulmonary edema
• 84.2%

MINS – High Sensitivity Assay
• Among 3904 patients who had MINS
• 93.1% did not experience an ischemic symptom
• 21.7% fulfilled universal definition of MI – elevated hsTnT with ≥1 ischemic feature
• Thus, troponin screening is the most effective way to screen for cardiac complications

Approach to MINS• Look for and correct physiological
abnormalities – hypoxia, hypotension, tachycardia (if BP adequate),
Hb if <70
• If no signs of bleeding initiate ASA 81 mg daily
• Initiate or intensify Statin therapy

BNP/nt-pro BNP
• Usage in diagnosis of CHF vs. Resp cause
• Usage in prognosis of CHF and acute decomp
• Usage in periop risk stratification

Case 6
• 67 M seen in preop for bariatric surgery• Cardiac RF: DM, HTN, remote smoker• Other PMHX: prev colon ca, OSA, GERD,
migraines• Meds: Rosuvastatin, Ramipril, Metformin,
Empagliflozin• “Asymptomatic” but nt-pro BNP = 219

Nuclear Perfusion StudyNo Persantine ECG changes

Nuclear Perfusion Study

Nuclear Perfusion – PET/CT
Cath

Concept
• For the vast majority of patients pre-op BNP/nt-pro BNP will filter out low risk patients
• Need for a patient centred approach when the nt-pro BNP is abnormal– Symptoms– Urgency of surgery– Awareness of risk involved– Patient preferences

Summary
• Patients with troponin elevation are prognostically at higher risk of death at 180-365 days compared to their normal trop counterparts– Critical care, PE, CKD, Periop literature
• Approach includes treating the underlying medical condition– Initiating basic cardiovascular therapies such as ASA, statins– In/Outpatient risk stratification plan and followup
• While for the vast majority, BNP/NT-proBNP will clear people into lower risk categories– Need a patient centred approach for when abnormal– Patient symptoms, urgency of surgery, risk involved, pt preferences

CSIM Annual Meeting 2017
Special thanks to Dr. PJ Devereaux• Scientific Leader, Perioperative Research
Group, PHRI, McMaster University• VISION, POISE 1, POISE 2• MANAGE, HIP ATTACK, VISION 2, POISE 3
• Co-Chair, CCS Perioperative Guidelines

Questions and Comments