approach to diffuse parenchymal lung diseases
DESCRIPTION
Approach To Diffuse Parenchymal Lung DiseasesTRANSCRIPT


Approach To
Interstitial Lung Diseases
or
Diffuse Parenchymal Lung
Diseases
Gamal Rabie Agmy, MD, FCCP
Professor of Chest Diseases, Assiut university
ERS National Delegate of Egypt

Objectives
• Review the spectrum of ILD or DPLD
• Identify clues on presentation to make the diagnosis
• Review common radiographic findings in ILD
• Come up with an algorithm to make the diagnosis


• Interstitial compartment is the portion of the lung sandwiched between the epithelial and endothelial basement membrane
• Expansion of the interstitial compartment by inflammation with or without fibrosis – Necrosis
– Hyperplasia
– Collapse of basement membrane
– Inflammatory cells
What is the Pulmonary
Interstitium?


The interstitium of the lung is not normally visible radiographic-
ally; it becomes visible only when disease (e.g., edema,
fibrosis, tumor) increases its volume and attenuation.
The interstitial space is defined as continuum of loose
connective tissue throughout the lung composed of three
subdivisions:
(i) the bronchovascular (axial), surrounding the bronchi,
arteries, and veins from the lung root to the level of the
respiratory bronchiole
(ii) the parenchymal (acinar), situated between the alveolar
and capillary basement membranes
(iii) the subpleural, situated beneath the pleura, as well as in
the interlobular septae.
The Lung Interstitium

Secondary pulmonary lobular
anatomy

The terminal bronchiole in the center
divides into respiratory bronchioles with
acini that contain alveoli.
Lymphatics and veins run within the
interlobular septa
Centrilobular area in blue (left)
and perilymphatic area in yellow
(right)

Pulmonary lesions Focal Diffuse

Pulmonary lesions
Focal Diffuse

Clinical Presentation
• Dyspnea on exertion or a persistent non
productive cough
• Abnormal CXR
• Pulmonary symptoms associated with
another disease, such as CVD
• PFT abnormalities

Approach to DPLD
DPLD of known
Cause
Idiopathic Interstitial
Pneumonias
Granulomatous
Lung Diseases
(Sarcoidosis)
Drugs Exposure CVD IPF IIP other than IPF
Desquamative Interstitial
Pneumonia
Non Specific Interstitial
Pneumonia
Respiratory Bronchiolitis-
Interstitial Lung disease
Acute Interstitial
Pneumonia
Cryptogenic Organizing
Pneumonia
Lymphocytic Interstitial
Pneumonia
Hypersensitivity
Pneumonitis Pneumoconiosis
Others
LAM
Histiocytosis X
Malignancy
Radiation Toxic Inhalation
IPF: 47-64%
NSIP: 14 to 36%
RBILD/DIP: 10-17%
COP: 4-12%
AIP: 2%
LIP: 2%

Incident Cases of ILD
Sarcoidosis
8%
Occupation
11% DILD
5% DAH
4%
CTD
9%
Other
11%
Pulmonary Fibrosis
52%
Coultas AJRCCM 1994; 150:967
(Incidence of IPF=26-31 per 100,000)

Adapted from Ryu JH, et al. Mayo Clin Proc. 1998;73:1085-1101.
Adapted from ATS/ERS. Am J Respir Crit Care Med. 2002;165:277-304.
1970 Liebow and Carington
2002 ATS/ERS
UIP
NSIP
DIP-RBILD
AIP
UIP/IPF
NSIP
DIP RB-
ILD
AIP
Cellular
Fibrotic
COP
LIP
Historical Classification of IIP
UIP
DIP
UIP-BO
LIP
Giant cell IP
1997 Katzenstein
Clinical Assessment
• History
• Physical Exam
• Chest Radiograph
• Pulmonary Function Testing
– At Rest
– Exercise
• Serologic Studies
• Tissue examination

History
• Age
• Gender
• Smoking history
• Medications
• Duration of symptoms
• Environmental exposure
• Occupational exposure
• Family history

History: Age and Gender
– LAM
– Tuberous sclerosis
– Pneumoconiosis
Age Gender

History: Smoking
• All of the following
DPLD are associated
with smoking :
a) IPF
b) RBILD
c) DIP
d) Histiocytosis X
e) Syndrome of IPF &
emphysema
• In Goodpasture’s
syndrome
– 100% of smokers vs. 20%
of nonsmokers
experience pulmonary
hemorrhage
• Individuals exposed to
asbestos who smoke are
more likely to develop
asbestosis

www.pneumotox.com
History: Medications
Schwartz, ILD text book, 4th edition

History: Occupational and
Environmental
INORGANIC

ORGANIC: Hypersensitivity Pneumonitis

Occupational ????

2. Subacute Diseases (weeks to months)
• HSP, Sarcoid, Cellular NSIP, Drug,
“Chronic” EP, Bronchiolitis/ SAD __________________________________________________________________________________________________________________
3. Chronic Diseases (months to years)
• UIP, Fibrotic NSIP, Pneumoconioses,
CVD-related, Chronic HSP
Smoking (RBILD and PLCH)
1. Acute Diseases (Days to weeks)
• DAD (AIP), EP, Vasculitis/DPH, Drug, CVD ________________________________________________________________________________________________________________
History: Duration of Illness

Modified Liebow classification of the idiopathic
interstitial pneumonias (Katzenstein)
• Acute
• Acute interstitial pneumonia (AIP)
• Chronic
• Usual interstitial pneumonia (UIP)
• Subacute • Nonspecific interstitial pneumonia (NSIP)
• Lymphocytic Interstitial Pneumonia (LIP)
• Cryptogenic Organizing Pneumonia (COP)
• Desquamative interstitial pneumonia/ (DIP)
Respiratory bronchiolitis-associated
interstitial lung disease (RBILD)

Physical Findings
• Resting Tachypnea
• Shallow breathing
• Dry crackles
• Digital clubbing
• Pulmonary HTN
• Non-pulmonary
findings





Laboratory

ILD: Evaluation
• Rdiographic – CXR
– HRCT
• Physiologic testing – PFT
– Exercise test
• Lung Sampling
– BAL
– Lung biopsy: (TBBx, Surgical)

CXR: LlMITATIONS
• CXR is normal:
– in 10 to 15 % of symptomatic patients with proven infiltrative lung disease
– 30% of those with bronchiectasis
– ~ 60 % of patients with emphysema
• CXR has a sensitivity of 80% and a specificity of 82% percent for detection of DPLD
• CXR can provide a confident diagnosis in ~ 23 % of cases

A normal CXR does not rule
out the presence of DPLD

CXR CLUES
Alveolar Filling
• Air-bronchograms
• Acinar rosettes
• Diffuse consolidation
• Nodule like, poor
boarder definition
• Silhouetting:
obliteration of normal structures
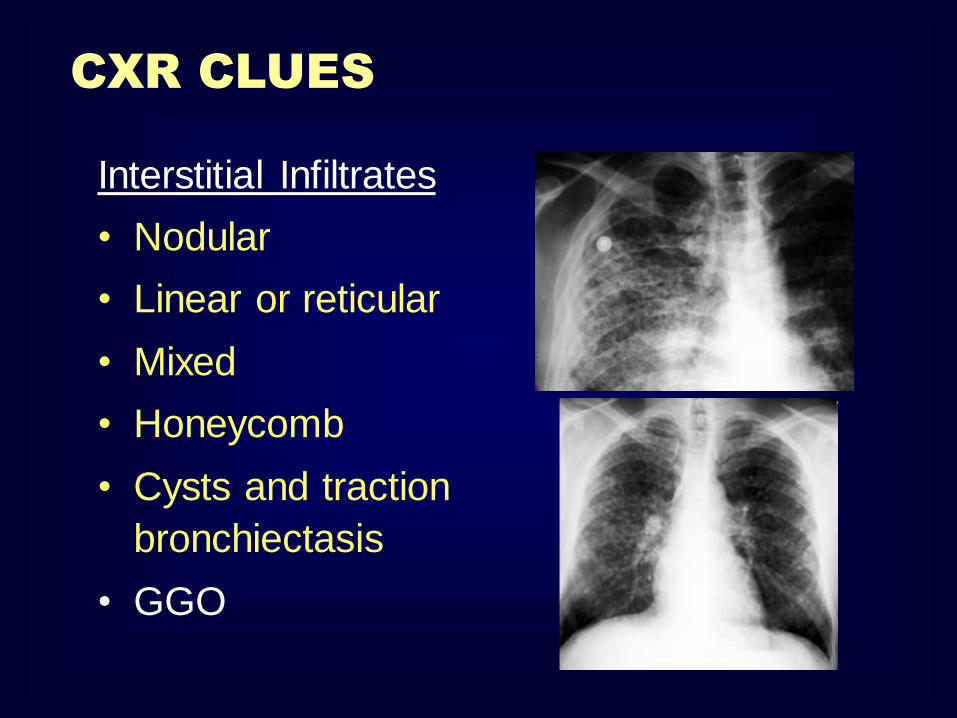
Interstitial Infiltrates
• Nodular
• Linear or reticular
• Mixed
• Honeycomb
• Cysts and traction
bronchiectasis
• GGO
CXR CLUES

Reticular pattern
Ground glass pattern
Nodular pattern
Cystic pattern
4 Radiographic patterns

Ground glass pattern
Alveolar Interstitial

Cystic pattern

Nodular pattern


Reticular pattern
[ Interlacing linear shadows appearing as a mesh or net]
Usual interstitial pneumonia
Desquamative interstitial pneumonia
Acute interstitial pneumonia
Non specific interstitial pneumonia
Interstitial pulmonary edema
Idiopathic pulmonary fibrosis
Collagen vascular diseases
Drug induced lung diseases
Radiation induced lung diseases
Interstitial lung disease

50 Y F, with cough and fever
Interstitial peumonia

Radiological findings Peribronchial cuffing [bronchial wall thickening]
Septal lines [short lines perpendicular to the pleura]
Honeycombing [Cystic abnormalities =multiple peripheral cysts, mm-cm, thick walls]
Traction bronchiectasis

Other findings Spider appearance of the interlobular vessels due to interstitial opacities around the vessels
Thickened interlobar fissures
Sub-pleural lines [curvilinear arc lines parallel to the pleura]
Ground glass density
Interstitial lung disease

Idiopathic pulmonary fibrosis

Interstitial fibrosis

Honeycombing

F 78Y Diabetic and hypertensive presented with severe dyspnea
suspected to pulmonary embolism , treated with anticoagulants with mild
improvement


• Multi system granulomatous disease
• Unknown etiology • 90% of patients with sarcoidosis have
chest changes • Bilateral hilar and mediastinal adopathy
• Interstitial disease lymph nodes
• Alveolar pattern simulating acute inflammatory disease]
• Cavitation, atelectasis, effusion (rare)
Sarcoidosis

Sarcoidosis Nodal and Interstitial patterns

Lymphadenopathy Sarcoidosis
F 45Y
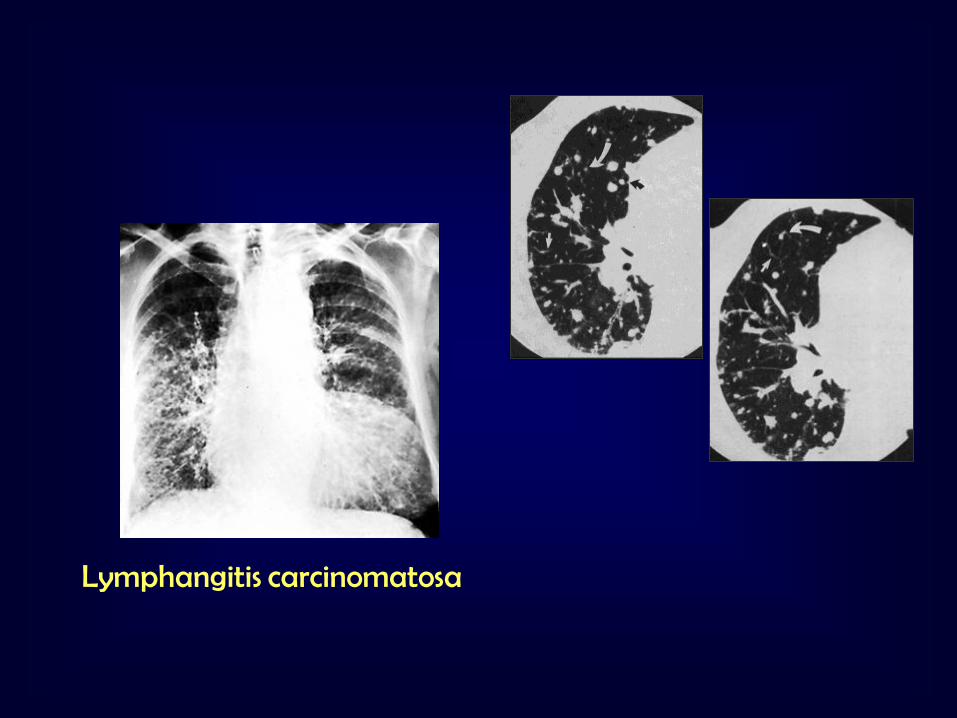
Lymphangitis carcinomatosa

F 59Y, with radical mastectomy
Lymphangitis carinomatosa

• Interstitial pattern similar to interstitial edema
which progresses to alveolar pattern
[busulfan, bleomycin, cytoxan,..]
• Alveolar in filtrates similar to pulmonary
edema [penicillin, sulfonamides,..]
• Pleural and pericardial effusion + basal
infilterates [isonaizid,…]
• Hilar adenopathy [antionvulsant,..]
Drug induced lung diseases Immunologic reaction to drugs
Busulfan interstitial lung disease

Air space filling disease
Replacement of alveolar air by fluid, cells, other material Represents an ongoing potentially treatable lesion
Ground glass density [geographic distribution] morphologic changes below the resolution of CT due to
Ground glass pattern
Alveolar Interstitial

ERS 2008
HISTOLOGIC CORRELATIONS IN
GGO
a) granulomata beyond special resolution
b) thickening of the interstitium (cellular phase OR fibrosis)
c) partial filling of the alveoli (associated with cellular phase
at BAL)
d) increased blood volume
e) combination of all the above

ERS 2008
GROUND GLASS OPACITIES
CT-pathologic correlation
•Partially filled alveoli
•Active interstitial inflammation
•Fine fibrotic process
•Hyperemia
variety of interstitial, alveolar and vascular diseases
below the threshhold of spatial resolution of HRCT
Leung AN, Miller RR, Muller NL. Radiology 1993;188:209 –214
RULE OUT FINE
FIBROSIS:
traction
bronchiectasis
TO FURTHER FOCUS DD
TIMING
CLINICAL SETTING
BAL
Vessel caliber

ERS 2008
DIP
• onset of symptoms : ~ 40 yrs
• dyspnoea and cough
• male predominance: 2>1
• inspiratory crackles : 60%
• digital clubbing :50%
90% of patients with DIP smoked or had smoked cigarettes
-in children DIP it is probably a different disease not related to smoking -DIP also occurs in non-smokers (of 40 cases of Carrington et al: 10%) -association with systemic disorders or infections -DIP element (focal pigmented macrophage accumulation) histologically in all smokers - “DIP-like reaction”
RARE DISEASE Hartman et al Radiology 1993 (n=22 from 5 centers)

ERS 2008
GROUND GLASS: PREVAILING FEATURE
GGO in: Outpatients with Slowly Progressive Dyspnea

ERS 2008
DIP
Typically: subpleural /lower lung zones
Reticulation seen in ~40-50%
Honeycombing NOT significant

ERS 2008
DIP

ERS 2008
EAA
1. Centilobular nodules • Ill defined (unlike
sarcoidosis)
2. Patchy or diffuse GGO
3. Superimposition of (1) and (2)
4. Geographic low
density areas on inspiratory HRCT
5. Regional air trapping on expiratory HRCT
Outpatients with Slowly Progressive Dyspnea

ERS 2008

Ground glass pattern [ Increased attenuation of the lung with preserved broncho vascular marking]
Patients with AIDS, ground glass opacities= P.carinii pneumonia
Patients with lung transplant
ground glass opacities= cytomegalovirus pneumonia or rejection
P.carinii pneumonia in an AIDS patient

Air bronchogram sign Air filled bronchi passing through opaque lung parenchyma
Pulmonary lesion
Alveolar pathology
Consolidation

Bilateral lower lobe pneumonia

Air space filling
TRASEUDATE ALVEOLAR EDEMA *
EXEUDATE PNEUMONIA*
BLOOD HEMORRHAGIC DISORDERS* TUMOR CELLS ALVEOLAR CELL CACINOMA
PROTEINS ALVEOLAR PROTIENOSIS*

Pulmonary edema

Pulmonary edema, 2 cases

Diffuse pulmonary hemorrhage Hemoptysis, anemia and air space opacities
Appear rapidly and clear within few days
Spare the lung apex and peripheral zones
Bilateral, may be asymmetric, air bronchogram
Repeated attacks → pulmonary fibrosis
Pulmonary hemorrhage (normal heart) [3 days, 6 days, one month]

Pulmonary hemorrhage in SLE

Bronchoalveolar carcinoma
6-10% of primary lung cancer
Cough, sputum, weight loss, hemoptysis, bronchorrhea
Radiographic patterns : Single or multiple pulmonary nodules[ Air bronchogram]
Segmental or lobar consolidation. Diffuse air space disease .
CT angiogram (non specific)
Other causes: Lymphoma, pulmonary edema, some types of pneumonia [obstructive, lipoid]
Visualization of
pulmonary vessels
within airless lung

Alveolar cell Carcinoma

Broncho aleveolar carcinoma

Brocho-alveolar cell Carcinoma
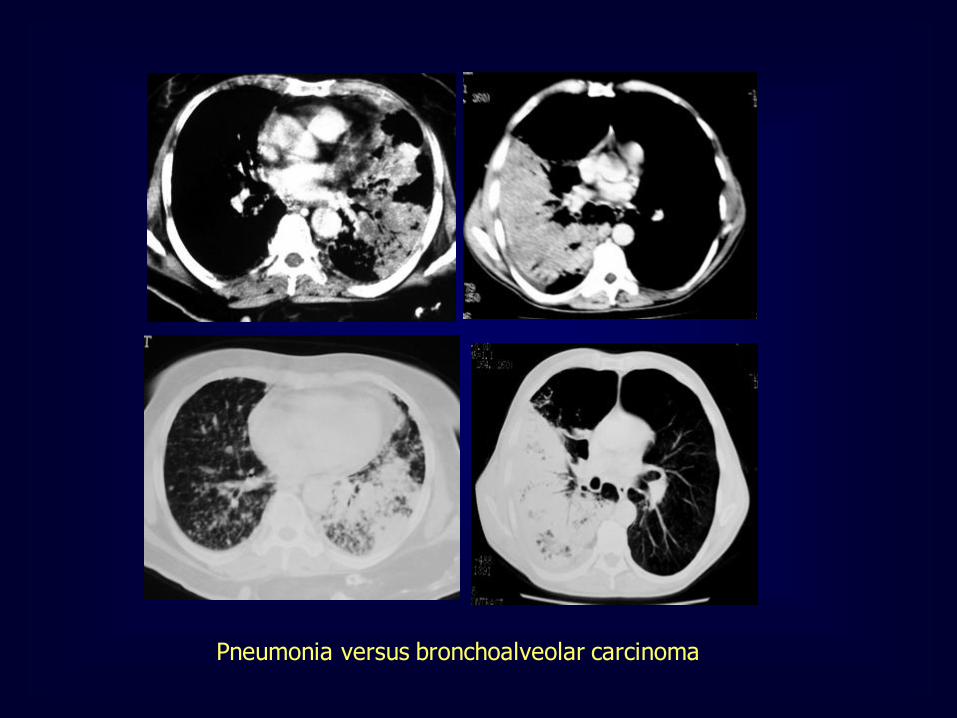
Pneumonia versus bronchoalveolar carcinoma

F 72 Y with chest pain dyspnea and frothy expectoration

Alveolar proteinosis
Alveolar filling by proteinaceous material
Male : female 4:1
Possible causes:
Idiopathic Occupational (silica)
Drug- induced Immune compromise
Geographic distribution of areas of ground glass opacities + thickened interlobular septa
within crazy paving appearance Air bronchogram is uncommon

Photograph of a pavement street in Buenos Aires, Argentina (left), drawings
of the lungs (center) and lung tissue (top right), and close-up high-resolution CT scan (bottom right) show the crazy-paving pattern.

Alveolar proteinosis [crazy- paving]

Nodular pattern [ multiple rounded opacities 1-
10mm] Miliary [1-2mm], the size of millet seeds
TB
Metastases
Pneumoconiosis
Sarcoidosis
Alveolar cell carcinoma
Miliary TB
Hematogenous dissemination
Innumerable fine nodules
Uniform distribution
Mild thickening of
the interstitial lung markings

Miliary TB

Sarcoidosis with miliary nodules and lymph nodes
M 57 Y

Miliary deposits of breast cancer

• Fine interstitial opacities with B Kerley’s lines (early)
• Multiple nodular shadows scattered in the lungs (classic)
• Sparing apex and base
• Calcification may occur
Silicosis Inhalation of high concentrations of silicon dioxide

Progressive massive fibrosis
Nodules enlarge and coalesce to form masses
Bilateral, almost symmetrical
• Almost always in the upper ½ of the lungs
• The more the fibrosis, the less apparent nodules

Silicosis

• Most patients are asymptomatic
• Dense sharply defined nodules
• The density is greatest in the lung bases
• Black pleura sign [unaffected pleura
between lung and ribs]
Pulmonary alveolar microlithiasis Innumerable tiny calcific particles are diffusely distributed in the alveoli

Alveolar microlithiasis

Cystic pattern [ multiple thin walled air containing lesions 1cm or more ] Histeocytosis
Lymphangioleiomyomatosis
Lymphocytic interstitial pneumonia
Emphysema
Cystic bronchiectasis
Tuberous sclerosis


Lung Cysts
Differential Diagnosis
Pulmonary fibrosis (Honeycombing)
Lymphangliomyomatosis
Langerhans cell histiocytosis
Lymphocytic Interstitial Pneumonia (LIP)

Rough Reticular Fine Reticular
Traction
Bronchiectasis
and
Interface
sign
Honey
combing
UIP UIP or NSIP

Usual Interstitial Pneumonia
UIP
HRCT Findings
Reticular opacities, thickened intra- and
interlobular septa
Irregular interfaces
Honey combing and parenchymal distorsion
Ground glass opacities (never prominent)
Basal and subpleural predominance

Basal and subpleural
distribution
UIP

The Many ‘HRCT Faces’ of NSIP
Honeycombing not a
prominent feature
!!!!

Lymphangioleiomyomatosis
(LAM)
HRCT Morphology
Thin-walled cysts (2mm - 5cm)
Uniform in size / rarely confluent
Homogeneous distribution
Chylous pleural effusion
Lymphadenopathy
in young women



Lymphangioleiomyomatosis
(LAM)

Tuberous Sclerosis (young man)

Langerhans Cell Histiocytosis
HRCT Findings
Small peribronchiolar nodules (1-5mm)
Thin-walled cysts (< 1cm),
Bizarre and confluent
Ground glass opacities
Late signs: irreversible / parenchymal fibrosis Honey comb lung, septal thickening,
bronchiectasis

1 year later
Peribronchiolar Nodules Cavitating nodules and cysts
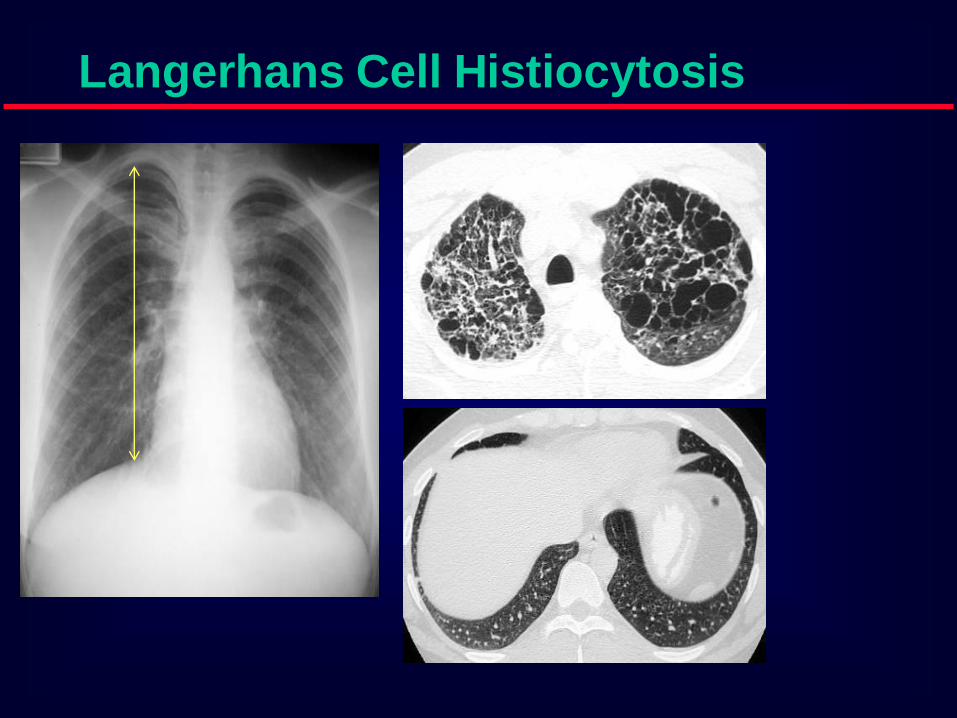
Langerhans Cell Histiocytosis

Langerhans Cell Histiocytosis
Langerhans Cell Histiozytosis
Key Features
Upper lobe predominance
Combination of cysts and noduli
Characteristic stages
Increased Lung volume
Sparing of costophrenic angle
S
M
O
K
I
N
G
Langerhans Cell Histiocytosis

Langerhans Cell Histiocytosis
Differential Diagnosis
Only small nodules Sarcoidosis, Silicosis
Only cysts idiopathic Fibrosis
LAM
Destructive emphysema

A professional diver.............

.......after cessation of smoking

Benign lymphoproliferative
disorder Diffuse interstitial infiltration of
mononuclear cells
Not limited to the air ways as
in follicular Bronchiolitis
LIP = Lymphocytic Interstitial
Pneumonia

Sjögren: LIP

LIP = Lymphocytic Interstitial
Pneumonia
Rarely idiopathic
In association with: Sjögren’s syndrome
Immune deficiency syndromes, AIDS
Primary biliary cirrhosis
Multicentric Castlemean’s disease

Sjoegren disease
Dry eye and dry mouth
Fibrosis, bronchitis and bronchiolitis
LIP
Overlap
Sarcoid, DM/PM, MXCT
SLE, RA (pleural effusion)
Up to 40 x increased risk for lymphoma (mediastinal
adenopathy) and
2 x times increased risk for neoplasma

Young woman Dry mouth Smoker
LAM LIP Histiocytosis

Emphysema Fibrosis (UIP)

Wegener‘s disease

Rheumatoid Arthritis

Outline
Typical HRCT patterns of lung diseases
with cysts
Mosaic pattern and its differential
Emphysema
Atypical HRCT patterns
Quiz

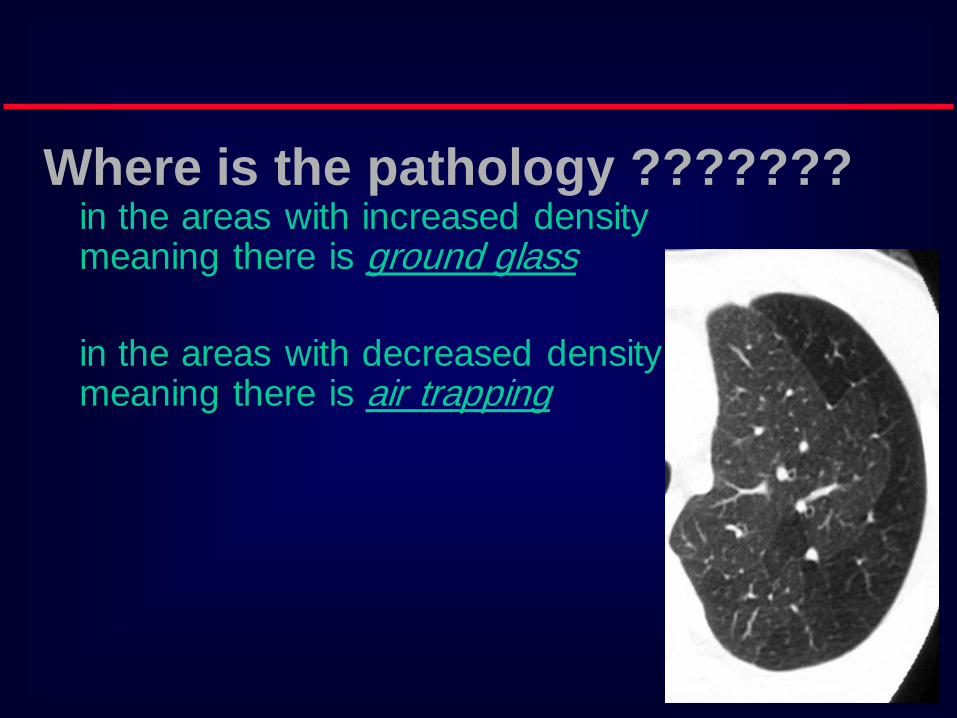
Where is the pathology ???????
in the areas with increased density meaning there is ground glass
in the areas with decreased density meaning there is air trapping

Pathology in black areas
Airtrapping: Airway
Disease
Bronchiolitis obliterans (constrictive bronchiolitis) idiopathic, connective tissue diseases, drug reaction,
after transplantation, after infection
Hypersensitivity pneumonitis granulomatous inflammation of bronchiolar wall
Sarcoidosis granulomatous inflammation of bronchiolar wall
Asthma / Bronchiectasis / Airway diseases

Airway Disease
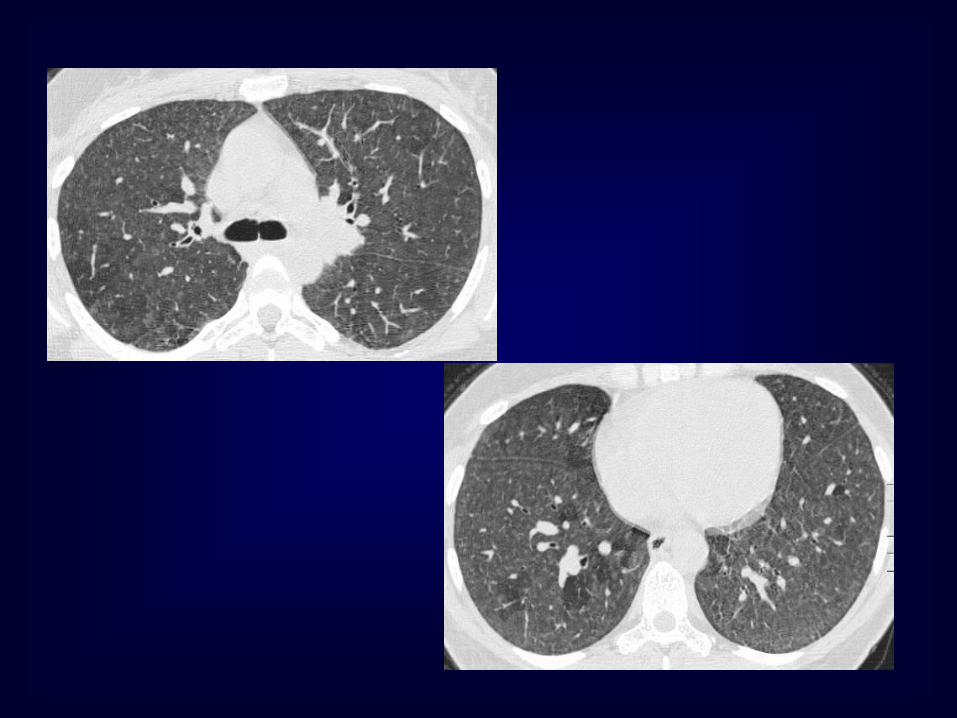
what you see……
In inspiration sharply demarcated areas of seemingly increased
density (normal) and decreased density
demarcation by interlobular septa
In expiration ‘black’ areas remain in volume and density
‘white’ areas decrease in volume and increase in
density
INCREASE IN CONTRAST
DIFFERENCES
AIRTRAPPING

Bronchiolitis
obliterans

Early Sarcoidosis

Chronic EAA

Hypersensitivity pneumonitis
Extr. Allerg. Alveolitis (EAA) HRCT
Morphology
chronic: fibrosis
Intra- / interlobular septal thickening
Irregular interfaces
Traction bronchiectasis
acute - subacute
acinar (centrilobular) unsharp densities
ground glass (patchy - diffuse)


Pathology in white Areas
Alveolitis / Pneumonitis
Ground glass desquamative intertitial pneumoinia (DIP)
nonspecific interstitial pneumonia (NSIP)
organizing pneumonia
In expiration both areas (white and black) decrease in
volume and increase in density
DECREASE IN CONTRAST
DIFFERENCES

DI
P

Cellular
NSIP

Mosaic Perfusion
Chronic pulmonary embolism
LOOK FOR
Pulmonary hypertension
idiopathic, cardiac disease, pulmonary
disease

CTEPH =
Chronic thrombembolic
pulmonary hypertension

Outline
Typical HRCT patterns of lung diseases
with cysts
Mosaic pattern and its differential
Emphysema
Atypical HRCT patterns
Quiz

Emphysema
histopathological definition
…..permanent abnormal enlargement of
airspaces distal to the bronchioles terminales
and
…...destruction of the walls of the involved
airspaces

Centrilobular Emphysema

Panlobular Emphysema

CLE and PLE in one Patient

Fibrosis and Emphysema

CT findings:
• Relatively well-defined, low attenuation areas
with very thin (invisible) walls, surrounded by
normal lung parenchyma.
• As disease progresses:
– Amount of intervening normal lung decreases.
– Number and size of the pulmonary vessels
decrease.
– +/- Abnormal vessel branching angles (>90o), with
vessel bowing around the bullae.

Emphysema
•Curved arrow: area of low attenuation.
•Solid arrow: zones of vascular disruption.
•Open arrow: area of lung destruction.

Emphysematous Bullae
www.ctsnet.org/doc/6761
Quantitative CT:
• Spirometically triggered images at 10% and
90% vital capacity (VC) have been reported
to be able to distinguish patients with chronic
bronchitis from those with emphysema.
– Patients with emphysema had significantly lower
mean lung attenuation at 90% VC than normal
subjects or patients with chronic bronchitis.
– Attenuation was the same for normal subjects and
those with chronic bronchitis.

Asthma:
Marc Gosselin,
MD

HRCT findings:
• Bronchial wall thickening
• Mucoid impaction
• Mosaic lung attenuation with air
trapping
– Findings may be reversible with
pharmacologic treatment.
• Centrilobular thickening
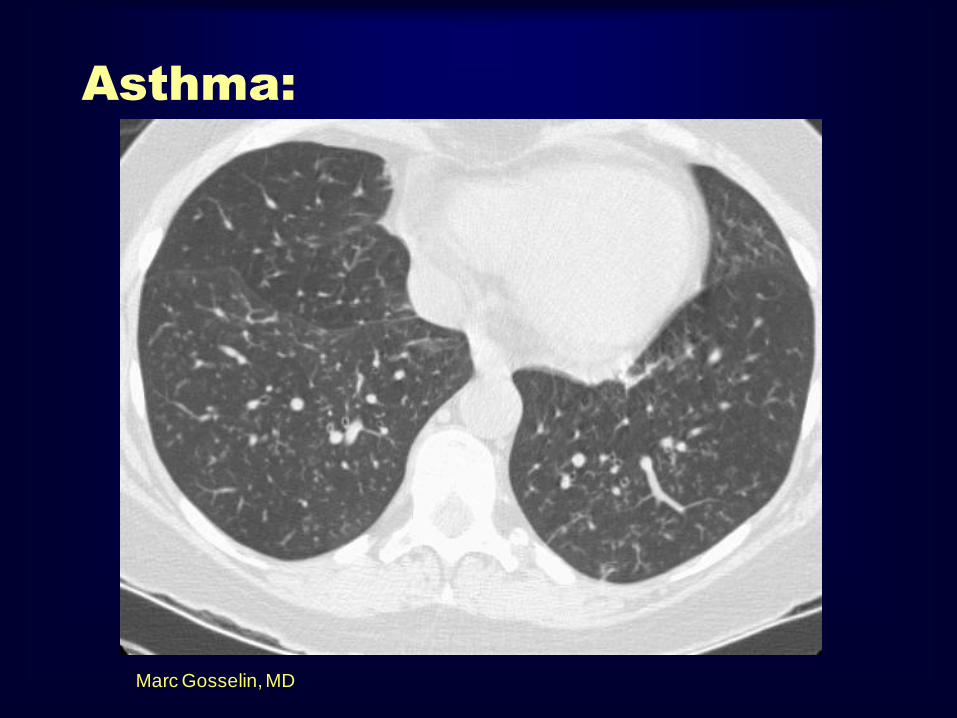
Asthma:
Marc Gosselin, MD

Most frequent CT findings of
bronchiactasis:
• Lack of tapering of the bronchial
lumen
• Bronchial wall thickening
• Bronchial dilatation
• Visualized peripheral bronchi
• Mucus plugging
Most frequent
Less frequent

Bronchiectasis
Radiology 2002; 225: 663-672
Arrows demonstrating various grades of bronchial wall thickening,
with lack of tapering of the bronchial wall lumen.

Cystic Bronchiectasis
www.emedicine.com

Bronchiectasis
Radiology 1999; 212: 67-68
“Signet ring” sign
Signet ring?
“Question Dogma”
…Marc Gosselin, MD
or
Solitaire ring?
What is Your Diagnosis ?
Cystic Changes and Decreased Density
Quiz

LAM Emphysema Fibrosis

LCH Emphysema

Bronchiolitis LCH

…..black holes……
Clues to Diagnosis
Is there a wall ?
What is the shape and size ?
Smoker ?
Other signs
(e.g., bronchiectasis, pulmonary hypertension)


ERS 2008
Reversed Halo Sign on High-Resolution CT of Cryptogenic
Organizing Pneumonia
Kim et al AJR 2003; 180:1251-1254
90% of their pts!
reversed halo signs (central ground-glass opacity and surrounding air-space consolidation of
crescentic and ring shapes)
Voloudaki et al
GGO ring : septal inflammation
cellular debris
organising pneumonia

Uncommon cause of respiratory distress in young males
Patients have history of significant cigarette smoking
Multiple large bullae impair the pulmonary mechanics
Bullous lung disease
Primary bullous disease – Vanishing lung syndrome
50Y M

Reticular pattern
Interstitial lung disease
Usual interstitial pneumonia
Desquamative interstitial pneumonia
Acute interstitial pneumonia
Non specific interstitial pneumonia
Interstitial pulmonary edema
Idiopathic pulmonary fibrosis
Collagen vascular diseases
Drug induced lung diseases
Radiation induced lung diseases

Clinical
HISTORY EXAMINATION
DRUGS
RADIATION
COLLAGEN DISEASE
CARDIAC TROUBLES
MEDIASINAL NODES
SARCOID , LYMPHAGITIS
Interstitial lung disease

AIR SPACE FILLING
• TRASEUDATE ALVEOLAR EDEMA *
• EXEUDATE PNEUMONIA*
• BLOOD HEMORRHAGIC
DISORDERS*
• TUMOR CELLS ALVEOLAR CELL
CACINOMA
• PROTEINS ALVEOLAR
PROTIENOSIS* CLINICAL IMAGING

Nodular pattern
[ multiple rounded opacities 1-10mm]
Milliary [1-2mm], the size of millet seeds
• TB
• Metastases
• Pneumoconiosis
Milliary TB

Clinical
History
DUST EXPOSURE
PRIMARY MALIGNANCY
Imaging
DENSITY & SIZE OF NODULES
SUGGESTIVE FINDINGS
OTHER DEPOSITS [ BONES , LIVER ]
COMPLICATIONS OF PNUMOCONIOSIS

Cystic pattern
[ multiple thin walled air containing lesions 1cm or more ]
Histeocytosis
Lymphangioleiomyomatosis
Lymphocytic interstitial pneumonia
Emphysema
Cystic bronchiectasis
Tuberous sclerosis
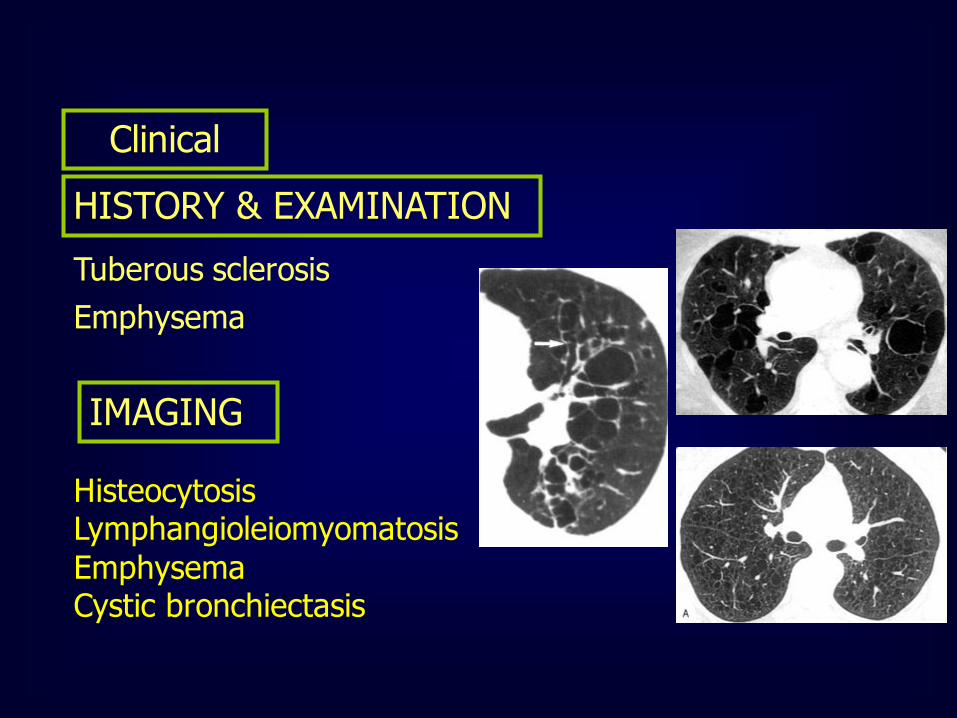
Clinical
HISTORY & EXAMINATION
Tuberous sclerosis
Emphysema
IMAGING
Histeocytosis Lymphangioleiomyomatosis
Emphysema Cystic bronchiectasis

HRCT: Radiographic Pattern

Radiographic Patterns in ILD
Pleural Involvement
Lymphangitic Carcinomatosis
LAM Drug Induced Radiation Pneumonitis
Asbestosis Effusion
Thickening Plaques Mesothelioma
Collagen vascular disease
Kerley B lines
Chronic LV failure
Lymphangitic CA Lymphoma LAM
Veno-occlusive disease Acute Eosinophilic Pneumonia
Adenopathy
Sarcoidosis
Lymphoma Lymphangitic CA LIP
Amyloidosis Berylliosis
Silicosis

PFT: Lung Volumes
Restrictive Disease
TLC
RV
VC
TLC
RV
VC TLC
RV
VC
Normal ILD NM Disease

Probability of Histologic Diagnosis of Diffuse Diseases
Surgical
Biopsy
1. Granulomatous diseases
2. Malignant tumors/lymphangitic
3. DAD (any cause)
4. Certain infections
5. Alveolar proteinosis
6. Eosinophilic pneumonia
7. Vasculitis
8. Amyloidosis
9. EG/HX/PLCH
10. LAM
11. RB/RBILD/DIP
12. UIP/NSIP/LIP COP
13. Small airways disease
14. PHT and PVOD
Often
Sometimes
Never
Transbronchial
Biopsy
Courtesy of Kevin O. Leslie, MD.

Pracical Aproach to
Interstitial Lung Diseases

Patterns of Interstitial
Lung Disease

Linear Pattern
A linear pattern is seen when there is
thickening of the interlobular septa,
producing Kerley lines.
Kerley B lines
Kerley A lines
The interlobular septa contain
pulmonary veins and lymphatics.
The most common cause of interlobular
septal thickening, producing Kerley A
and B lines, is pulmonary edema, as a
result of pulmonary venous
hypertension and distension of the
lymphatics.
Kerley B lines
Kerley A lines

DD of Kerly Lines:
Pulmonary edema is the most common cause
Mitral stenosis
Lymphangitic carcinomatosis
Malignant lymphoma
Congenital lymphangiectasia
Idiopathic pulmonary fibrosis
Pneumoconiosis
Sarcoidosis


b. Reticular Pattern
A reticular pattern results from the summation
or superimposition of irregular linear
opacities.
The term reticular is defined as meshed, or in
the form of a network. Reticular opacities can be
described as fine, medium, or coarse, as the
width of the opacities increases.
A classic reticular pattern is seen with pulmonary fibrosis,
in which multiple curvilinear opacities form small
cystic spaces along the pleural margins and lung
bases (honeycomb lung)

This 50-year-old man presented with end-stage lung fibrosis
PA chest radiograph shows medium to coarse reticular
B: CT scan shows multiple small cysts (honeycombing) involving
predominantly the subpleural peripheral regions of lung. Traction
bronchiectasis, another sign of end-stage lung fibrosis.

c. Nodular pattern
A nodular pattern consists of multiple round opacities,
generally ranging in diameter from 1 mm to 1 cm
Nodular opacities may be described as miliary (1 to 2 mm,
the size of millet seeds), small, medium, or large, as the
diameter of the opacities increases
A nodular pattern, especially with predominant
distribution, suggests a specific differential diagnosis

Disseminated histoplasmosis and nodular ILD.
CT scan shows multiple bilateral round circumscribed
pulmonary nodules.
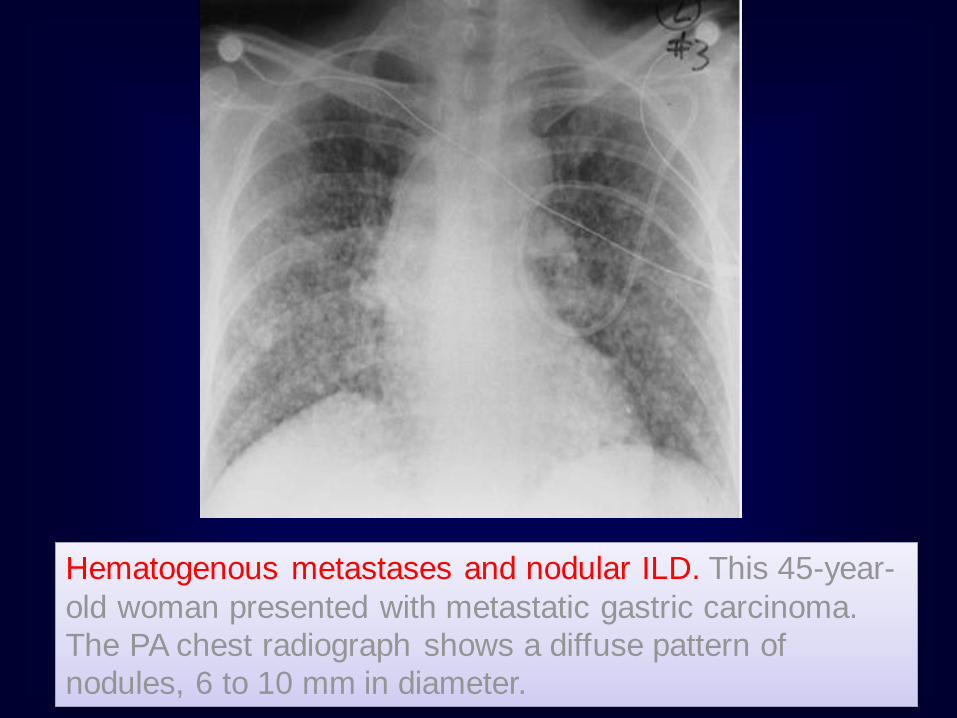
Hematogenous metastases and nodular ILD. This 45-year-
old woman presented with metastatic gastric carcinoma.
The PA chest radiograph shows a diffuse pattern of
nodules, 6 to 10 mm in diameter.
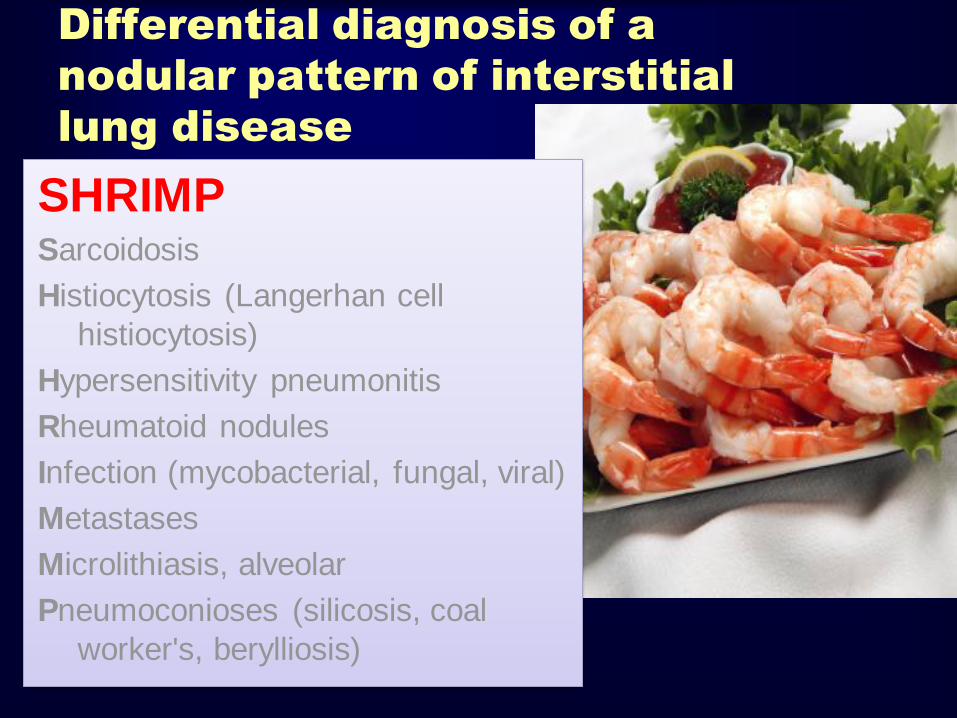
Differential diagnosis of a
nodular pattern of interstitial
lung disease
SHRIMP Sarcoidosis
Histiocytosis (Langerhan cell
histiocytosis)
Hypersensitivity pneumonitis
Rheumatoid nodules
Infection (mycobacterial, fungal, viral)
Metastases
Microlithiasis, alveolar
Pneumoconioses (silicosis, coal
worker's, berylliosis)

d. Reticulonodular pattern results
A reticulonodular pattern results from a combination of reticular and nodular opacities.
This pattern is often difficult to distinguish from a purely reticular or nodular pattern, and in such a case a differential diagnosis should be developed based on the predominant pattern.
If there is no predominant pattern, causes of both nodular and reticular patterns should be considered.

How To Approach
a Practical
Diagnosis?
An acute appearance suggests pulmonary
edema ,miliary TB,DAD or pneumonia
Rule no. 1

Disseminated histoplasmosis and reticulonodular ILD.
A: PA chest radiograph, close-up of right upper lung, shows reticulonodular
ILD.
B: CT scan shows multiple circumscribed round pulmonary nodules, 2 to 3
mm in diameter.

Reticulonodular lower lung predominant
distribution with decreased lung volumes
suggests: (APC)
1. Asbestosis
2. Aspiration (chronic)
3. Pulmonary fibrosis (idiopathic)
4.Collagen vascular disease
Rule no. 2
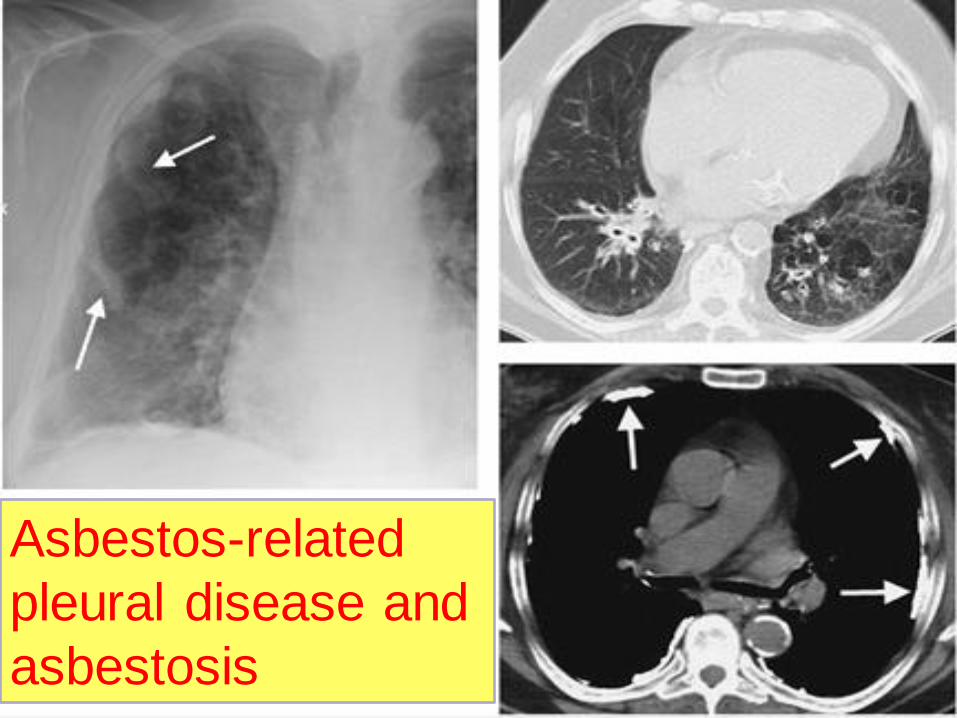
Asbestos-related
pleural disease and
asbestosis

Pulmonary fibrosis and rheumatoid arthritis.

Systemic sclerosis. A: PA chest radiograph shows a bibasilar and subpleural distribution of fine
reticular ILD. The presence of a dilated esophagus (arrows) provides a clue
to the correct diagnosis.
B: CT scan shows peripheral ILD and a dilated esophagus (arrow).

A middle or upper lung predominant distribution
suggests: (Mycobacterium Settle Superiorly in
Lung)
1. Mycobacterial or fungal disease
2. Silicosis
3. Sarcoidosis
4. Langerhans Cell Histiocytosis
Rule no. 3

Complicated silicosis. PA chest radiograph shows multiple
nodules involving the upper and middle lungs, with coalescence
of nodules in the left upper lobe resulting in early progressive
massive fibrosis
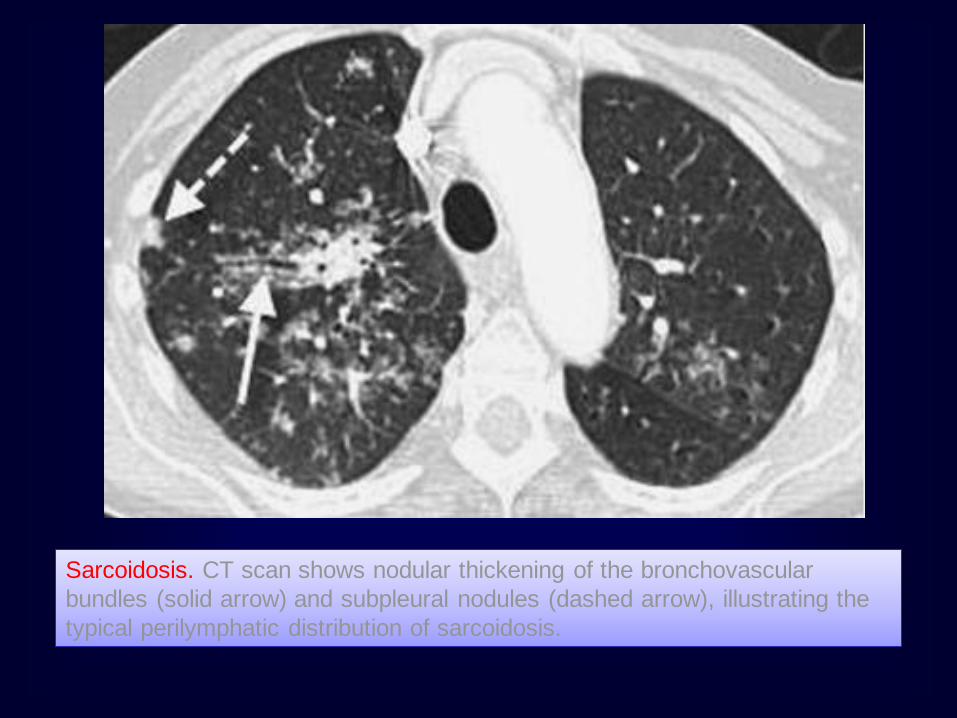
Sarcoidosis. CT scan shows nodular thickening of the bronchovascular
bundles (solid arrow) and subpleural nodules (dashed arrow), illustrating the
typical perilymphatic distribution of sarcoidosis.

Langerhan cell histiocytosis.
This 50-year-old man had a
30 pack-year history of
cigarette smoking.
A: PA chest radiograph
shows hyperinflation of the
lungs and fine bilateral
reticular ILD.
B: CT scan shows multiple
cysts (solid arrow) and
nodules (dashed arrow).

Associated lymphadenopathy suggests :
1.Sarcoidosis
2.neoplasm (lymphangitic carcinomatosis,
lymphoma, metastases)
3. infection (viral, mycobacterial, or fungal)
4. Silicosis
5.Congestive heart failure with congestive
lymphadenopathy.
Rule no. 4

Simple silicosis.
A: CT scan with lung windowing shows numerous
circumscribed pulmonary nodules, 2 to 3 mm in diameter
(arrows).
B: CT scan with mediastinal windowing shows densely
calcified hilar (solid arrows) and subcarinal (dashed arrow)
nodes.

Associated pleural thickening and/or
calcification suggest asbestosis.
Rule no. 5

Associated pleural effusion suggests :
1.pulmonary edema
2.lymphangitic carcinomatosis
3.lymphoma
4.collagen vascular disease
5.LAM
Rule no. 6

Cardiogenic pulmonary edema.
PA chest radiograph shows enlargement of the cardiac
silhouette, bilateral ILD, enlargement of the azygos vein
(solid arrow), and peribronchial cuffing (dashed arrow).

Lymphangitic carcinomatosis. This 53-year-old man
presented with chronic obstructive pulmonary disease and
large-cell bronchogenic carcinoma of the right lung.
CT scan shows unilateral nodular thickening (arrows) and a
malignant right pleural effusion.

Associated pneumothorax suggests
lymphangioleiomyomatosis or LCH.
Rule no. 7

Lymphangioleiomyomatosis
(LAM).
A: PA chest radiograph shows a
right basilar pneumothorax and
two right pleural drainage
catheters. The lung volumes are
increased, which is
characteristic of LAM, and there
is diffuse reticular ILD.
B: CT scan shows bilateral thin-
walled cysts and a loculated
right pneumothorax (P).

Tell me the rules
again?

1. Acute
•P.Edema
•Pneumonia
•.Miliary TB
•.DAD
2. Pleural effusion
•1.pulmonary edema
•2.lymphangitic carcinomatosis
•3.lymphoma
•4.collagen vascular disease
3.Pneumothorax
•lymphangioleiomyomatosis
•LCH
4.Predominantly Below with reduced volume
1.Asbestosis
2. Aspiration (chronic)
3. Pulmonary fibrosis (idiopathic)
4.Collagen vascular disease

5. A middle or upper lung predominant
1. Mycobacterial or fungal disease
2. Silicosis
3. Sarcoidosis
4. Langerhans Cell Histiocytosis
6. Associated lymphadenopathy
1.Sarcoidosis
2.neoplasm (lymphangitic
carcinomatosis, lymphoma,
metastases)
3. infection (viral, mycobacterial, or
fungal)
4. Silicosis 5.CHF
7. Pleural Thickening
and or Calcification
•Asbestosis

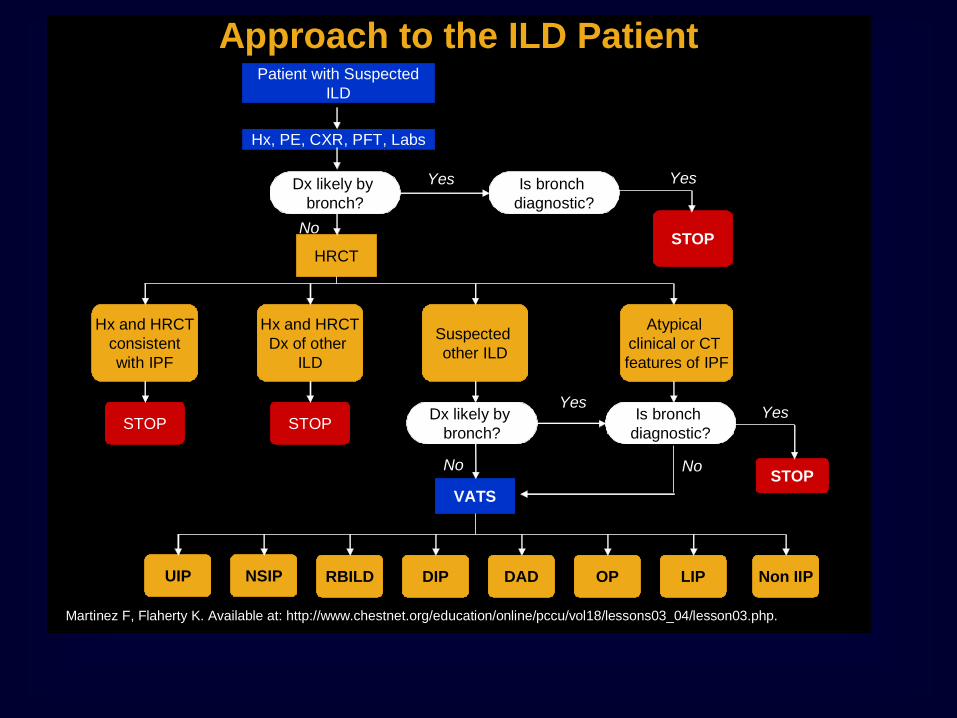
Approach to the ILD Patient
Martinez F, Flaherty K. Available at: http://www.chestnet.org/education/online/pccu/vol18/lessons03_04/lesson03.php.
Patient with Suspected
ILD
Hx, PE, CXR, PFT, Labs
STOPHRCT
Hx and HRCT
consistent
with IPF
Hx and HRCT
Dx of other
ILD
Suspected
other ILD
Atypical
clinical or CT
features of IPF
STOP STOP
STOP
VATS
UIP Non IIPLIPOPDADDIPNSIP RBILD
Yes
No
Yes
No
Dx likely by
bronch?
Is bronch
diagnostic?
Dx likely by
bronch?
Is bronch
diagnostic?
Yes
Yes
No
