applying the evidence for clinical pharmacy services to pharmacy practice provided by: michael g....
Post on 20-Dec-2015
227 views
TRANSCRIPT

Applying the Evidence for Clinical Pharmacy Services to Pharmacy Practice
Provided by:Michael G. Liebl, BS, PharmD, BCPSClinical Manager, Pharmacy ServicesThe Methodist HospitalHouston, TX 77030Pager: 281-735-5815Phone: 713-441-6973Email: [email protected]

Program Learning Objectives
At the completion of this program, the participant will be able to:
1. Review the pharmacy and medical literature that evaluates clinical pharmacy services.
2. Identify key clinical pharmacy services demonstrated to improve morbidity and mortality outcomes.
3. Estimate the relative pharmacoeconomic benefit of certain clinical pharmacy services.
4. Relate the findings from the pharmacy and medical literature to an institution's provision of clinical pharmacy services.

Disclosures:• No financial interest in any entity or individual cited in the presentation
• Regarding disclosures for non-commercial content and conclusions within:
• Active memberships in ACCP, ASHP, TSHP, GCSHSP & SCCM
• My primary position: Manager, clinical pharmacy services
• Previous role: Clinical pharmacist MICU & CVICU
• Conducted and involved in clinical pharmacy research studies that evaluating the value of clinical pharmacy services
• I have a significant (and financial) relationship with a clinical pharmacist

A timeline of our clinical pharmacy ancestry in the words of leaders of the movement
W. Arthur Purdum
...within the new minimum standard lies the key to our first objective: improving and extending the usefulness of the hospital pharmacist.
…Today we are still recognized as a complementary service department and we must continue our efforts until pharmacy is regarded as essential.
1950

• Is there an essential, established need for advanced clinical pharmacy services?
• If yes, how great is the need? Is there a cost for not providing them?
• What type of clinical services make the greatest difference?
• What training is required to provide these services?
• How many providers for a given institution?
• Can the value of these services be measured?
• Is the difference realized significant to stakeholders?• Patients• Administrators• Quality / regulatory agencies• Others
• Has the call for advanced clinical pharmacy services been endorsed by: our profession, administrators, quality / regulatory agencies & patients?
Fast Forward to 2008 and ask the tough questions…

So, where to begin…
Is there an essential, established need for advanced clinical pharmacy service?
...what is the problem or the void in healthcare?

Medications:Medications:Estimated as the #4 Killer AnnuallyEstimated as the #4 Killer Annually
Heart disease 743,460 dead
Cancer 529,904 dead
Stroke 150,108 dead
MedicationsMedications 137,000 dead137,000 dead
Pulmonary disease 101,077 dead
Accidents 90,523 dead
Pneumonia 75,719 dead
Lazarou, et al. JAMA 1998;279:1200-5

42% with moderate to severe adverse event potential
% of meds with error pre: 62%
% of meds with error post: 39%
Weiner B, Venarske JL, Yu M & Mathis K. Spine 2008;
38% with moderate to severe adverse event potential
% of Patients with error: 53%Cornish P. Arch Int Med 2005; 165: 424-429. – Admission
Mortality 2%, LOS 2 days at a cost of $2,000/event
2.4%Classen DC.JAMA. 1997; 277: 301-6
LOS 6.6 days; ~70% type ”A” Events
23.1%
10% severe
Bowman L. Can J of Hosp Pharm 1994; 5: 209-216. (Wishard, IN)
7.9% Hospital readmissions due to medication events
NRForester A. Ann Intern Med 2003; 138: 161-167.
1.9% of ADRs attributed to increased morbidity
4.9%NRChaudhry S, Olofinboba K, J Gen Intern Med 2003; 18: 595-600.
LOS 15.3 days6%7.5Holdsworth M. Arch Pediatr Adolesc Med 2003; 157: 60-65.
NRNR9.7Cullen D. CCM 1997; 25: 1289-97.
LOS 3.9 days9.2%NRVargas E. CCM 2003; 31: 694-98.
Estimated as the 4th - 6th leading cause of death
6.7% (total)
0.32% (fatal)
NRLazarou J. JAMA 1998; 279: 1200.
(Meta-analysis of ADRs)
LOS 8.5 days; 7.6% of all hosp days
NR5.6Moore N. Br J Clin Pharmacol 1998; 3: 301-8.
CommentsComments% of % of
Patients with Patients with ADRsADRs
# of Events # of Events
(1000 pt days)(1000 pt days)How common are ADRs & How common are ADRs & ADEs?ADEs?

Could these be the most dangerous Could these be the most dangerous (and expensive) medical devices?(and expensive) medical devices?

How Hazardous Is Health Care?How Hazardous Is Health Care?
1
10
100
1,000
10,000
100,000
1 10 100 1,000 10,000 100,000 1,000,000 10,000,000
Number of encounters for each fatality
REGULATEDANGEROUS(>1/1000)
ULTRA-SAFE(<1/100K)
HealthCare
Mountain Climbing
Bungee Jumping
Driving
Chemical Manufacturing
Chartered Flights
Scheduled Airlines
European Railroads
Nuclear Power
Ann
ual C
ost:
Liv
es L
ost
Source: Roger Resar, MD (Mayo Clinic) IHI Symposium 2001
Neil M. Davis
“…After studying the Institute of Medicine’s To Err Is Human, a suggestion for
improving might be that there should be a person who has expert knowledge
about drugs and drug therapy to review the entire drug selection and
monitoring aspects of patient care. In a world where there were no such
people as pharmacists, they would have to be invented. Perhaps, on that
planet, they would be called “medicationists”.
Well, our world does have drug experts. They are
called pharmacists, so there is no need to create
a new professional to fill that void.”
2000

Clinical Pharmacy Services That Impact Patient Care Outcomes
• Specifics on individual services rendered
• Admitting Pharmacist Services
• Pharmacist Rounding
• ICU
• Acute Care
• Anticoagulation Services
• Pharmacokinetic Services
• High-risk populations
• Transplant
• Oncology

Admitting Pharmacy Services:Addressing Medication Errors From the Start
• Consistent finding of error rates
• Consistent estimation of harm potential
• Consistent finding of a meaningful improvement (reduction in error rate) with
pharmacist involvement in the process
*Two phases reported for this evaluation: Pre-intervention & post-intervention
Cornish P. Cornish P. Arch Int Med 2005Arch Int Med 2005
N = 523N = 523
Gleason K. Gleason K. AJHP 2004AJHP 2004
N = 204N = 204
Weiner, Venarske, Yu Weiner, Venarske, Yu
& Mathis; Spine 2008& Mathis; Spine 2008**N = 82 & 87N = 82 & 87
Medication Error Rate 53.6% 54.6% 64%, 38%
Most Common Error Type – Omission
46.4% 42.3% 22%, 40.4%
Harm Potential:
Moderate to High
38.6% 45% 40%, 22%

Study (Population)Study (Population) Control Control
Group / PeriodGroup / Period
Pharmacist Pharmacist Group / PeriodGroup / Period
RRR / ARR / NNTRRR / ARR / NNT
(Defined Below)(Defined Below)
Herfindal E. Drug Intel & Clin Pharm. 1985 (CVICU)
Trend toward decreased LOS in pharmacy periodTrend toward decreased drug costsSignificant decrease in ABTX use
White CM. Hospital Pharmacy 1998 (CVICU)
Evaluated 14 days of services in a 12 bed ICU: 6.14 interventions /day.
Costs reduced and clinical benefits from interventions demonstrated
Montazeri M & Cook D. Crit Care Med 1994
54 working days activities chronicled and analyzed
$67,000 annually in drug cost reduction estimated if 7 days per week.
Leap L. JAMA 1999
(CCU & MICU)
Serious ADRs: 10.4% 3.5% 66% / 7% / 14.2 pts
Lee A. Hospital Pharmacy 2007
(ICU)
Errors Identified: 54
Omitted Drug: 9%
256
41%
No difference in LOS
Kucukarslan S. Arch Int Med 2003 (IM Acute Care)
Serious ADRs:10% 2.5% 78% / 7.5% / 13.3 pts
Boyko WL. AJHP 1997
(IM Acute Care)
LOS – 5.5 Days
Hosp cost/pt – 6,155
Pharm cost/pt – 782
4.2
4,501
481
23% RRR
26% RRR
38% RRR
RRR: Relative Risk Reduction
ARR: Absolute Risk Reduction
NNT: Number needed to treat = [(1/ARR)x100]
Clinical Pharmacist Impact: Inpatient Rounds
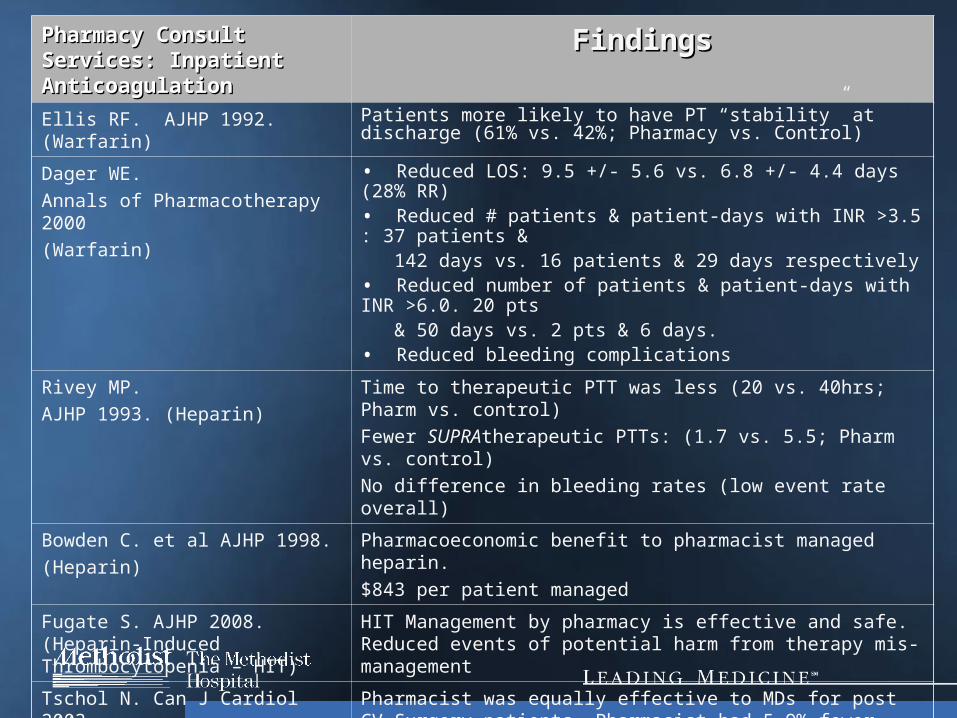
Pharmacy Consult Services: Pharmacy Consult Services: Inpatient AnticoagulationInpatient Anticoagulation
FindingsFindings
Ellis RF. AJHP 1992. (Warfarin) Patients more likely to have PT “stability” at discharge (61% vs. 42%; Pharmacy vs. Control)
Dager WE.
Annals of Pharmacotherapy 2000
(Warfarin)
• Reduced LOS: 9.5 +/- 5.6 vs. 6.8 +/- 4.4 days (28% RR)• Reduced # patients & patient-days with INR >3.5 : 37 patients & 142 days vs. 16 patients & 29 days respectively• Reduced number of patients & patient-days with INR >6.0. 20 pts & 50 days vs. 2 pts & 6 days. • Reduced bleeding complications
Rivey MP.
AJHP 1993. (Heparin)
Time to therapeutic PTT was less (20 vs. 40hrs; Pharm vs. control)
Fewer SUPRAtherapeutic PTTs: (1.7 vs. 5.5; Pharm vs. control)
No difference in bleeding rates (low event rate overall)
Bowden C. et al AJHP 1998.
(Heparin)
Pharmacoeconomic benefit to pharmacist managed heparin.
$843 per patient managed
Fugate S. AJHP 2008. (Heparin-Induced Thrombocytopenia – HIT)
HIT Management by pharmacy is effective and safe. Reduced events of potential harm from therapy mis-management
Tschol N. Can J Cardiol 2003 Pharmacist was equally effective to MDs for post CV Surgery patients. Pharmacist had 5.9% fewer days with INR > 4.
Bond CA. Pharmacotherapy 2004.* (Warfarin & Heparin)
Reduction in transfusions, morbidity (bleeding complications), patient charges and mortality for both heparin and warfarin services
*Only 20% & 11% of hospitals have heparin & warfarin consult services respectively

Published Studies on Pharmacy Published Studies on Pharmacy Consult Services: Consult Services: Pharmacokinetic ServicesPharmacokinetic Services
FindingsFindings
Hospitals with the service vs. Hospitals with the service vs.
Hospitals without the serviceHospitals without the serviceBond CA. AJHP 2005.
(Vancomycin & Aminoglycosides)Death rate was 1% less
LOS: 1.4 days less
Renal complications: 11% less
Drug, Lab & Total hospital charges were less


ADE Frequency: Outpatient SettingADE Frequency: Outpatient Setting FindingsFindingsGandhi TK.
Adverse Drug Events in Ambulatory Care
NEJM 2003
• ADEs affected 25% of patients. 13% serious (of these,
13% ameliorable and 11% preventable)
• ADEs increased 10% for each medication taken
• Number of medications per patient: •No ADE: 1.45(0.04, 0-5) •With ADE: 1.85 (0.09, 0-6)
Budnitz. National surveillance of ED visits for OP ADEs. JAMA 2006
• 2.7% of ED admits were 2* to ADE
• 6.7% of hospital admissions were ADE related
Samoy LJ. Drug-related hospitalization in a Tertiary Care IM Service of a Canadian Hospital: A Prospective Study. Pharmacotherapy 2006
• 25% of admissions were ADE related
• 72.1% of these were considered preventable
• 7% severe and 0.7% were fatal


Published Studies on Pharmacy Consult Services: Discharge CounselingPublished Studies on Pharmacy Consult Services: Discharge Counseling
StudyStudy InterventionsInterventions FindingsFindings
Schnipper J. Role of Pharmacist Counseling in Preventing Adverse Drug Events after Hospitalization.
Arch Int Med 2006.
• Randomized patients to receive discharge counseling by a pharmacist and a re- education phone call within 5- 7 days
• ADE Rate at 28 days
• Preventable ADEs reduced: 10% (11% vs. 1%) NNT = 10
• Adverse Medication Related ED Admissions Reduced: 7% (8% vs. 1%; NNT=14.2)
Delate T. Clinical Outcomes of a Home-Based Medication Reconciliation Program After Discharge from a Skilled Nursing Facility.
Pharmacotherapy 2008
• Quasi experimental prospective, controlled study
• Pharmacist reconciled discharge medications and counseled patients as needed
• Review and intervention session lasted on average 45 – 60 minutes
• Patients assessed for a death at 60-days after discharge from SNF
• All Cause Mortality: 5.9 vs. 2.7% (NS)
• Adjusted HR: 0.22 (0.06 – 0.88)

How many clinical pharmacists does one need?
• How few is too few?
• Opportunity loss costs?
• When are there too many?
• Diminishing marginal return?
• Where does one prioritize service?
Neil M. Davis
…The time needed for clinical activities can be gained from better utilization of
pharmacy technicians, bar coding, automation and a well-designed, fully integrated
CPOE. For some facilities, all of this will still not be enough to substantially reduce
the error problem and more pharmacists will have to be hired.
…Institutions will have to attract and retain pharmacists…
Junior high and high school students must be exposed to the
benefits of pharmacy as a career choice to ensure that there
is an adequate pool of bright and motivated students.
2000

Inpatient pharmacy staffing relationship to outcomes:Mortality Rates

Donald E. Franke
...We see today that there are stirrings of a more objective approach towards sound drug therapy and…the pharmacist plays an increasingly important role.
…It seems to me that this trend which is gaining momentum constantly, offers great opportunities for pharmacists to increase our professional responsibilities through cooperative efforts with colleagues in the medical profession, we can increase our value as professionals benefiting not only to pharmacy but also to medicine, our hospital and patients. These are indeed goals to which we should strive.
1952
…I am confident that the hospital pharmacist will…occupy an increasingly important position not only in the selection and procurement of pharmaceuticals but also as a valued consultant to the physician.

Sister Mary John
…We are beginning a new era…more medical cases will increase the
volume of drugs dispensed and paid for by a third party who will
want prices to reflect costs. Hospital revenue must equal
expenditures…so unnecessary expenditures must be curtailed.
...It is the pharmacist’s major duty to maintain rational therapeutics in
his hospital. He must keep himself well informed about drugs so
that he can withstand the flood of unsubstantiated claims often
made for new products.
1957
…To challenge scientifically, one needs an
equality of knowledge. The doctor, so skilled in
the basic sciences, is still vulnerable to the
high pressured salesmanship of even
nonpharmacists.
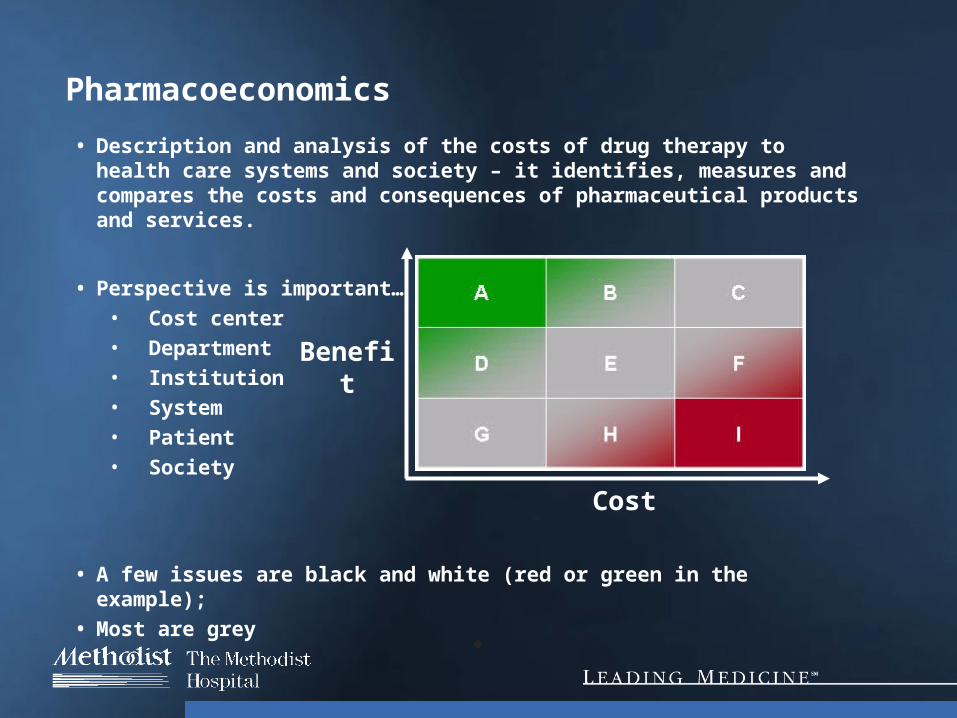
Pharmacoeconomics
• Description and analysis of the costs of drug therapy to health care systems and society – it identifies, measures and compares the costs and consequences of pharmaceutical products and services.
• Perspective is important…• Cost center• Department• Institution• System• Patient• Society
• A few issues are black and white (red or green in the example);
• Most are grey
Cost
Benefit

Recent Cost of Adverse Events Data (ICU)
• Setting – 10 bed MICU and a 10 bed CCU at Brigham & Women’s Hospital & Harvard Medical School
• Authors cited existing patient safety parameters already in place:
• CPOE
• Pharmacist on rounds
• Nursing coverage nearly 1:1
• Just culture
• Intensivist physician staffing in place




• Finding: Costs of the pharmacist were NOT overcome by savings from identifiable drug costs
• Setting:• 480 bed Community Teaching Hospital• 12 bed MICU, 11 Bed Surgical ICU
• Study Concerns:• Part time position – 2 hrs per day • Rotated days of the week • Rotated hours of the day (intentionally)• Excluded protocol management (intentionally)• No interventions to add new drugs for untreated diseases• TDM• No interactions with MDs on rounds
Am J Hosp Pharm. 1991 Oct;48(10):2154-7

Pharmacy Staffing Associations and total costs of care in US Hospitals
Services Associated With Reduced Hospital Costs
Drug Evaluation Services (DUE / MUE)
Drug Information
Medical Rounds Participation
ADR Reporting
Drug Protocol Management
Admission Drug Histories
# of Dispensing Pharmacist / 100 Occupied Beds
# of Pharmacy Admin. / 100 Occupied Beds
# of Clinical Pharmacist / 100 Occupied Beds

Please write down a number
ROI or Cost to Benefit Ratio for Clinical Pharmacy Services
What Should Be Expected?

Endorsements of Clinical Pharmacy Services:(Not a comprehensive list...)
• ASHP & ACCP
• SCCM – Standards for pharmacy services in the ICU that include various levels of clinical pharmacy activities: Fundamental, Desirable & Optimal
• AHRQ – Several chapters (5, 7,8, & 9) on the benefit to quality and cost for hospitals in areas such as ADE reduction, Medication error reduction, Anticoagulation.
• Society for Hospital Medicine (SHM) & ASHP Joint Position Paper
• Infectious Diseases Society of America
• The Joint Commission
• UNOS
• Leapfrog Group

Where will the clinical pharmacists of tomorrow come from?
• What experience or training is required?
• Who will train them?

Joe Smith
…Let me summarize this recommendation for an entry level residency program in hospital pharmacy. 1st training in clinical (general) practice becomes the focus of the program. 2nd a Pharm.D. degree should be a prerequisite for entry into the program. 3rd the training program should provide meaningful experience in the other important services and in the overall management of the department. 4th this generalist entry-level residency should be a prerequisite for advanced specialized residency programs. It is this level of training that we should set our sights on for all pharmacists who are preparing for a future in hospital pharmacy practice.
…Beyond this entry-level training program, there is a growing need for highly specialized clinical training programs. I believe that there is now a much greater demand for highly specialized clinicians than we can supply, and the demand will likely increase.
1988
…The leaders of a clinical profession must be committed to, almost obsessed with, the idea of clinical practice. And, most important, they will need to project that idea into images that create excitement in other people about that activity.

ACCP White Paper
Estimated Needs:
Increase to 7,500 residency slots up from 1,250 offered today in mostly general practice (PGY-1)
PGY2 offerings should increase similarly

An Institutional, Case-Based Application
• Setting:• 1,300-bed Tertiary Care, Private Teaching Hospital
• Adult medical / surgical population with oncology, transplant, psychiatry, women’s health and advanced heart failure populations
• Teaching Affiliations• Medical, Nursing & Pharmacy Schools
• Patient Payor Mix• Medicare / Medicaid: ~52%
• Private pay: ~45%

Pharmacy Department Overview:
• Highly automated: Robotics, automated dispensing cabinets, CPOE,
electronic medication tracking system, and knowledge based
medication administration pending
• Technician driven order entry
• Clinical pharmacy specialists in all major inpatient servicelines, nearly
all with PGY1 and/or PGY2 training and several with board certification
• Intensity of coverage M-F; 7AM – 5PM. Basic service commitments on
the weekends
• Code blue team response: 24/7
• On-site Drug information Center & formulary management
• PGY1 and PGY2 Pharmacy Residency Provider
• Active Doctor of Pharmacy externship program
• Active pharmacy and medical research initiatives
• ACPE Provider

Clinical Pharmacist - Resource Distribution
*Ratio: Less 4.5 FTE for Weekend, Holiday & Vacation Coverage
90% 95% 90% 95%
Neurology 82 74 2 0 74 78 37 39 36.9
Cardiology 172 155 5 1 155 163 26 27 25.8
Heme/Onc 43 39 1 1 39 41 19 20 19.4
IM 346 311 10 1 311 329 28 30 28.3
Transplant 30 27 1 1 27 29 14 14 13.5
General Sx 120 108 2 2 108 114 27 29 27.0
ICUs 111 100 5 0 100 105 20 21 20.0
0 1
Total 904 814 26 7 25.4 26.8 25.4
33 28.5 30.1 29.6
ServicelineAvailable
Patient BedsBudgeted
ADC
Clin Spec
1
Clin Spec
2
No. of Patients with Daily Census
ONCOLOGY Infusion center: 25-35 Patients Managed Daily. Breast Cancer Center Service
Pending
Total Clinical Pharmacists Involved in Daily Patient Care
90% 95% 90% 95%
Neurology 82 74 2 0 74 78 37 39 36.9
Cardiology 172 155 5 1 155 163 26 27 25.8
Heme/Onc 43 39 1 1 39 41 19 20 19.4
IM 346 311 10 1 311 329 28 30 28.3
Transplant 30 27 1 1 27 29 14 14 13.5
General Sx 120 108 2 2 108 114 27 29 27.0
ICUs 111 100 5 0 100 105 20 21 20.0
0 1
Total 904 814 26 7 25.4 26.8 25.4
33 28.5 30.1 29.6
Clinical Pharmacist: Patient Ratio
*
FTE
Drug Information CS2 0
Medication Safety CS2 1
Investigational Drugs CS2 1
Project Specialist* CS2 0.3
1
1
*Supports Direct Patient Care 20% TOTAL 2.3
Non-direct Patient Care Clin Specss & Support Staff
Clinical Pharmacy Research Coordinator
Secretary III - Clinical Pharmacy Section Focus
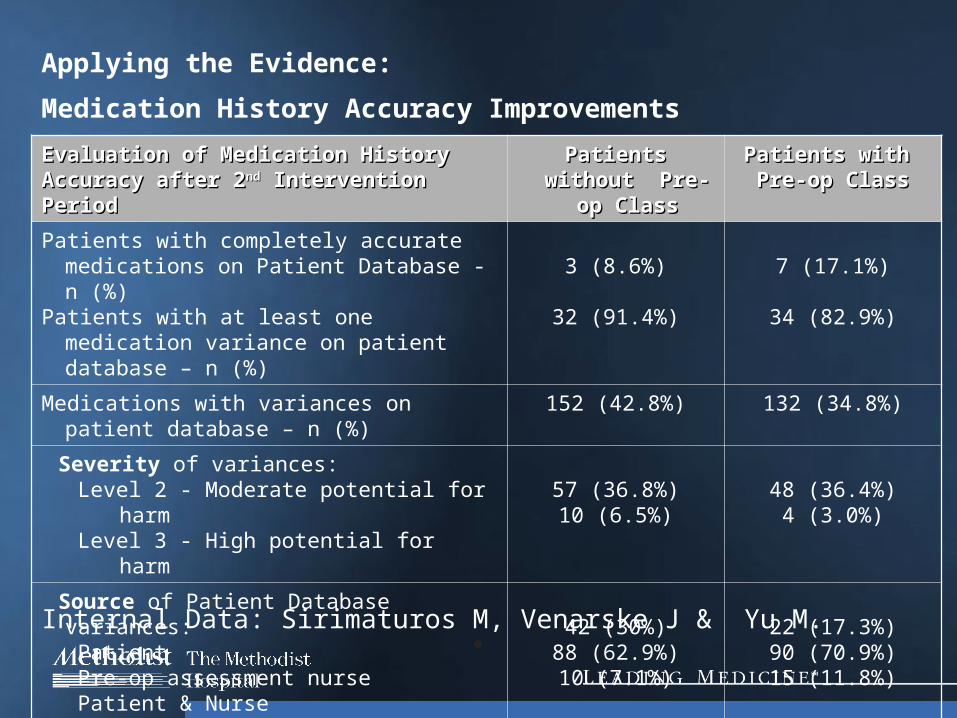
Evaluation of Medication History Accuracy Evaluation of Medication History Accuracy after 2after 2ndnd Intervention Period Intervention Period
Patients without Patients without Pre-op ClassPre-op Class
Patients with Patients with Pre-op ClassPre-op Class
Patients with completely accurate medications on Patient Database - n (%)
Patients with at least one medication variance on patient database – n (%)
3 (8.6%)
32 (91.4%)
7 (17.1%)
34 (82.9%)
Medications with variances on patient database – n (%)
152 (42.8%) 132 (34.8%)
Severity of variances:Level 2 - Moderate potential for harmLevel 3 - High potential for harm
57 (36.8%)10 (6.5%)
48 (36.4%)4 (3.0%)
Source of Patient Database variances:Patient Pre-op assessment nursePatient & Nurse
42 (30%)88 (62.9%)10 (7.1%)
22 (17.3%)90 (70.9%)15 (11.8%)
Internal Data: Sirimaturos M, Venarske J & Yu M.
Applying the Evidence:
Medication History Accuracy Improvements
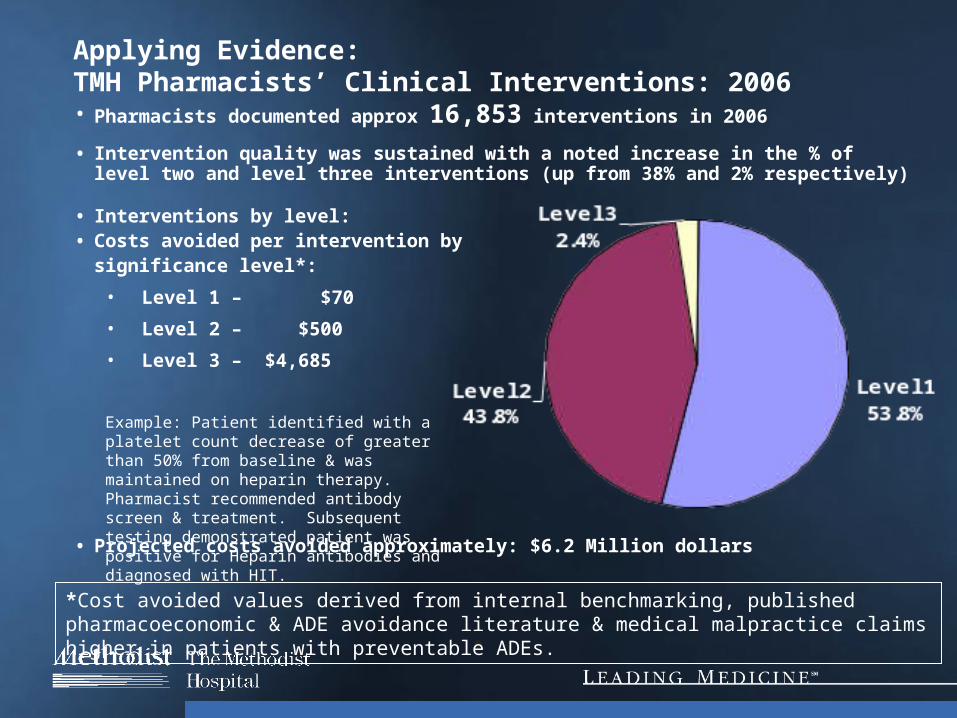
Applying Evidence: TMH Pharmacists’ Clinical Interventions: 2006• Pharmacists documented approx 16,853 interventions in 2006
• Intervention quality was sustained with a noted increase in the % of level two and level three interventions (up from 38% and 2% respectively)
• Interventions by level:• Costs avoided per intervention by significance level*:
• Level 1 – $70
• Level 2 – $500
• Level 3 – $4,685
• Projected costs avoided approximately: $6.2 Million dollars
Example: Patient identified with a platelet count decrease of greater than 50% from baseline & was maintained on heparin therapy. Pharmacist recommended antibody screen & treatment. Subsequent testing demonstrated patient was positive for Heparin antibodies and diagnosed with HIT.
*Cost avoided values derived from internal benchmarking, published pharmacoeconomic & ADE avoidance literature & medical malpractice claims higher in patients with preventable ADEs.

Estimated Clinical Pharmacy Consultation Services Provided*• Anticoagulation
• Warfarin – 150 pts
• Heparin – 130 pts
• Falls Prevention – 60 pts
• Polypharmacy – 30 pts
• Discharge counseling – 200 pts
• Pharmacokinetic – 2 pts
• TPN – 25 pts
• Renal dosing – 38 pts
• Severe Sepsis – 20 pts
• Other – 10 pts
*Based Upon Consult Orders Received per Month

A Pharmacoeconomic Estimation of Clinical Pharmacy Services:
ROI Range Estimate: 2.5 – 4
Clinical Service DomainEstimated Annual Financial Return Comments and Notes
$3,122,330
$4,621,130
$316,781
$112,271
$0
$0
$338,000
$8,510,512
Standardized protocol development and management services
Direct patient care services
Medication use education & informational services
Regulatory compliance & Medication safety initiatives
Medication formulary maintenance and drug use evaluation services
Professional leadership and training programs
Continuous quality improvement initiatives of existing protocols ?
?

• Is there an essential, established need for advanced clinical pharmacy services?
• If yes, how great is the need? Is there a cost for not providing them?
• What types of clinical services make the greatest difference?
• Can the value of these services be measured?
• Is the difference realized significant to stakeholders?• Patients, Administrators, Quality / regulatory agencies• Others
• Has the call for advanced clinical pharmacy services been endorsed by: our profession, administrators, quality / regulatory agencies & patients?
• What training is required to provide these services?
• How many providers for a given institution?
In closing, have we answered the questions?

R. David Anderson
…pharmacists who are not in constant face-to-face contact with physicians, nurses & particularly patients where they are being treated & who are unable to see exactly how drugs work…are destined to know little more than a myriad of unorganized details.
…The pattern most idealized of a professional pharmacist would be one who has a close association with patients; a comprehensive awareness of previous medication habits; knows allergies, sensitivities, & idiosyncrasies; extracts information about them from charts, laboratory, x-ray, and other data; has access to drug-oriented information; is able to correlate that information with knowledge about the patient’s physiology & disease; & recommends to physicians, nurses, & others the proper course to follow where drugs are indicated. He emphasizes and insures safety and effectiveness of drugs.
1976
…The hypothetical professional pharmacist would serve as a counselor, advisor, teacher… & patient care team member
…The model which comes closest to conformance with this professional ideal is the clinical pharmacist.

Questions & Discussion