applied physiology camp at colorado state …
TRANSCRIPT

Applied Physiology Camp is a hands-on academic day camp for high school sophomores, juniors, and seniors
who have a strong interest in science and are considering pursuing a career in a health-related field such as
medicine, physical or occupational therapy, health and exercise science, or in scientific research. The camp blends
exciting concepts in physiology and neuroscience and gives students the opportunity to uniquely explore how
our bodies experience, process, and react to different environments. Lessons and interactive demos throughout
the week culminate in a sensory and physical challenge at CSU’s Mountain Campus ropes course. Topics covered
during the week include sensory systems, neuroanatomy, neuronal signaling, and experimental physiology.
PROGRAM INCLUDES:• Handling and dissecting real neuroanatomy specimens
• Human physiology in response to high altitude, space, and diving environments
• Taste and visual sensory demonstrations
• Guided sensory experiences
• An overnight adventure and ropes course experience at CSU’s Mountain Campus
$950. SPACE IS LIMITED.
REGISTRATION: appliedphysiologycamp.colostate.edu CONTACT: [email protected] | (970) 491-3982
APPLIED PHYSIOLOGY CAMPA T C O L O R A D O S T A T E U N I V E R S I T Y
JULY 22-27
2019

Updated 2/2019
2019 Applied Physiology Day Camp
APPLICATION MATERIALS CHECKLIST Please use this form as a checklist for your summer registration materials. Obtain all required parent or guardian signatures. Any forms with missing signatures will be returned to you and your registration will be considered incomplete. These forms are required for your participation in the program, and you will not be considered fully registered or allowed to participate in camp activities until all forms have been completed.
Student Name: _________________________________________________
ALL SIGNED FORMS MUST BE POSTMARKED BY JULY 1, 2019 AND RECEIVED, PROCESSED, AND COMPLETE BEFORE CAMP COMENCES
Form Signature(s) Included Forms rec’d/complete
(office use only) Student Contract Camper Information Questionnaire Camper Health History Form (Form 1) Recommendations for Licensed Medical Personnel Form (Form 2) *must be reviewed and signed by a physician
Emergency Contact Information Form Release from Liability and Risk Waiver Photography Consent/Media Release Form Roommate Request Form Challenge Course Health Information Form Challenge Course Release from Responsibility, Assumption of Risk and Waiver
Please Return All Completed Forms and this Checklist to:
Mail Electronic
Applied Physiology Camp c/o Brittany Runyan
Colorado State University 1680 Campus Delivery
Fort Collins, CO 80523-1680 (970) 491-3982
e-mail: [email protected]
Fax: (970) 491-7569
*Please include cover sheet and give notice of fax

Updated 2/2019
2019 Applied Physiology Day Camp
STUDENT CONTRACT
A high degree of responsibility and maturity is expected of our students. It is important for reasons of safety and program effectiveness that certain standards of behavior be followed by all students. Your signature on this form indicates that you have read, understand, and agree to follow all of the rules listed below. Violation of any of the rules may be cause for expulsion from the program or for other appropriate disciplinary action to be determined by staff. Expectations:
1. All students must attend all classes and activities. Absence or tardiness is unacceptable except for excused medical emergencies or when arrangements cannot be made outside of class time. Students must inform the Camp Directors in advance in order for the excuse to be considered valid.
*Note: Excused absence must be arranged on an individual basis, and must be
specifically authorized by the Camp Directors.
2. The use or possession of drugs, alcohol, or weapons while in the Applied Physiology Day Camp at Colorado State University is not permitted under any circumstances, and will be cause for immediate expulsion. This includes being in the company of another person who is using or is in possession of drugs, alcohol, or weapons. CSU Police department will be contacted to handle any such occurrences.
3. Curfew at Colorado State Mountain Campus: In-room at 10:30 p.m.
4. No student may ride in or drive any personal vehicle during the camp, unless
arrangements are made in advance with the Camp Directors
5. Students are not allowed to leave campus alone at any time unless accompanied by a staff member or parent/guardian with prior approval.
6. Students are expected to behave in a respectful, responsible, and non-
disruptive fashion at all times, and are expected to exercise sound judgment regarding behavior. Any questions about particular situations should be addressed to camp staff in advance.
7. Students are not to engage in any verbal, physical or sexual harassment of
other participants, counselors, leaders, or any other people, and will be cause for immediate expulsion. This includes harassing or intimidating others via

Updated 2/2019
text, electronic mail, newsgroups or web pages while using CSU’s Computing and Network Resources.
8. Students must follow all rules of anatomy and dissection labs without
question, or will be cause for immediate expulsion (see separate document for rules).
9. Students must follow all rules and terms of dormitories and student
recreation center, including:
a. I understand that I am liable as an individual or as part of the Applied Physiology Day Camp group for any damage that I, or we, as a group may cause in and around the residence hall, classroom or visited facility and agree to pay for the replacement or restoration of the property.
b. I understand that I am responsible for my room key and, if lost, I will
be charged $65.00 for the replacement of the lock and key.
c. I understand that UNDER NO CIRCUMSTANCES may any screen be removed from any window. If a screen is tampered with, damaged, or removed, I will be charged $50.00.
10. All students will have access to CSU’s computer networks. In consideration of
being allowed to use the University's central computer and network services, students agree to refrain from any illegal activity or for any activity prohibited by CSU’s Acceptable Use Policy for Computing and Networking Resources. If you have questions regarding illegal activity, inappropriate or destructive actions pertaining to computing resources, you may view CSU’s complete policy at: http://housing.colostate.edu/acceptable-use-policy.
Consequences Violation of the camp rules will result in incident-appropriate disciplinary action as determined by camp staff and camp directors. Campers may be removed from individual activities, removed from dormitories, or expelled from camp at the expense of the parents. Please read and sign the following statement: I, (student printed name) _______________________________________________, have read the rules of the Applied Physiology Day Camp at Colorado State and I understand the consequences for breaking the aforementioned rules of the camp.

Updated 2/2019
Student Signature: ______________________________________DATE__________________ Parent/Guardian (printed name): ____________________________DATE_________________ Parent/Guardian (signature): ________________________________DATE________________

2019 Applied Physiology Day Camp INFORMATION FOR STUDENTS
Expectations of Campers While at Camp
• Attend every class and program activity and arrive on time • Be an active participant in all lectures, labs, and discussions • Work together as a team • Positively participate in the activities • Communicate with instructors when further clarity and explanation on material is needed • Demonstrate respect for all classmates, faculty and instructors • Follow established classroom/activity expectations and policies • Respect classrooms, CSU campus, visited facilities and yourself at all times • Turn off cell phones and electronic devices during presentations and any scheduled activities • Learn, be present, be engaged and have fun!
Health Awareness Altitude sickness is something that visitors to Colorado commonly experience, and it can affect a traveler's sense of well-being quite profoundly. In addition to making one feel dizzy or full of nausea, the lack of moisture in the air can cause your hair, skin and eyes to become uncomfortably dry, and may even cause nosebleeds. A feeling of breathlessness, especially when exercising, is also commonly reported. However, these symptoms may or may not be medically classified as altitude sickness, or AMS. The official diagnosis of AMS is made when a headache, with any one or more of the following symptoms, is present after a recent ascent above 8,000 feet:
• Loss of appetite, nausea, or vomiting • Fatigue or weakness • Dizziness or light-headedness • Difficulty sleeping
Fort Collins is at a comfortable 5,003 ft, so this kind of reaction to altitude is extremely rare. However, if you feel any symptoms of altitude sickness during your stay on campus, please alert camp staff immediately. The weather in Colorado in July is typically very hot and dry, but can change very quickly with afternoon thunderstorms. Please plan to drink plenty of water. You will probably walk up to 3 miles a day around campus during our daily activities so please bring comfortable shoes and a refillable water bottle. CSU is proud to be an environmentally responsible campus by using resources and non- wasteful ways of keeping our campus beautiful. Water used to sprinkle the grass on campus is untreated lake water, which means you should not drink it, or get it in your eyes, mouth, or open wounds. As tempting as it is on a hot summer day, please DO NOT run through sprinklers.

Altitude Chamber Laboratory Activity During the week, campers will be learning about effects of high altitude and the physiological response associated with changes in pressure. The Colorado State University altitude chamber simulates ascent to higher altitude by reducing the air pressure inside the chamber via a vacuum pump and offers the opportunity for students to gain an appreciation for the overall effects of barometric pressure change on human physiology. The laboratory activity will simulate a slow ascent to 12,000 feet (the summit of Pikes Peak is 14,110 feet) and the total time at 12,000 feet will be limited to approximately 10 minutes. During the activity, campers will measure and record their oxygen saturation and pulse through non-invasive use of a pulsoximeter (just like at the doctor’s office). They will then compare that data to information that is provided during the classroom lectures. Discussions will include why supplemental oxygen is necessary for aircrew, as well as for climbers ascending Mount Everest. Campers that choose to participate will be under the supervision of the Director, Hypo-Hyperbaric Chamber Facility at all times. Any camper who does not want to participate in the activity directly will be able to observe from the outside and participate in all discussions and related activities. While many tourists to Colorado make the drive to the top of Pikes Peak (14,110 feet) and Mt. Evans (14, 265 feet), as well as to many of the ski resorts throughout the state, ascent to high altitudes is not without some risk for many visitors. The most common is the development of altitude sickness as discussed earlier under Health Awareness. Participation in the altitude chamber activity to a simulated altitude of 12,000 feet carries the same risk as driving to these high-altitude areas in Colorado. If at any time a participant feels unwell, they will be removed from the chamber and returned to ground level. Challenge Course at Mountain Campus Located at an elevation of 9,000 feet, the Colorado State University Mountain Campus Challenge Course is designed to enhance team building and personal growth. Risk taking, group problem solving, and leadership skills also are common focal points. Low elements of the course emphasize teamwork and effective communication, while high elements provide an opportunity for personal challenges and growth. Appropriate Clothing for participating in the Challenge Course include:
• Loose fitting pants or long shorts • Sneakers or light hiking boots (no open toe sandals) • Layered clothing and rain coat (weather is unpredictable at 9,000 ft.) • Hat with a sun visor • Sunglasses and sunscreen • Safety strap for glasses • Please leave jewelry and valuables at home
Smoking is not permitted on or near the Challenge Course.

Please bring a full quart water bottle; there is minimal water available at the course. Recommended Camper Packing List for Mountain Campus Toiletries:
• Toothpaste and toothbrush • Deodorant • Hairbrush/ comb • Shampoo/conditioner • Soap (with case) • Bug spray/ Insect repellent • Sunscreen • Chap stick • Refillable water bottle (suggested 1 Liter) • Hat
Clothing:
• Casual summer clothes (please keep it school appropriate) • Clothes you are comfortable hiking in • Fleece Jacket and long pants or jeans (nights are cool in Colorado) • Rain jacket (Colorado is known to have rainy summers)
All items on this list are highly recommended but may not be all inclusive. Please use your personal discretion to bring any other items necessary for your week at camp!

Updated 2/2019
Dear Campers: We want to get to know you! Please answer the following prompts and include this sheet with your registration packet:
1. How would your friends describe you?
2. Why do you want to attend the Applied Physiology Day Camp?
3. What activities are you most excited about and/or worried about at camp?
4. What are some things you want your camp staff and counselors to know about you?
5. What are your personal goals for the week and how can your counselors help you achieve them?
6. Anything else you want us to know?

Updated 2/2019
2019 Applied Physiology Day Camp INFORMATION FOR PARENTS
Camp Contact Information: If you need to contact the camp directors for any reason, please call Brittany Runyan at 970-491-3982. If you can’t get a hold of anyone at this number, you can also call the main office number: 970-491-3259. We will also have an emergency cell phone, which will be activated just prior to the start of camp. We will send you the number to that phone when we send you more details about arrival at camp. Accommodations: As a day camp, no overnight accommodations are available or provided on Colorado State University. The only exception to this if for those campers that will be participating in the over-night stay at the Colorado State University Mountain Campus on Friday night. During the stay at the Mountain Campus, lodging, linens, and meals will be provided. Camp Counselors will be present in the dorm facilities to ensure camper safety and adherence to camp rules. Camp staff will assign roommates based on common interests. Please have your child take time and consideration when filling out the roommate request form. Transportation to the Colorado State University Mountain Campus: Transportation will be provided by CSU Motor Pool. All campers are required to meet at the regular classroom on Friday morning and will then be transported to the Mountain Campus as a group. Dining: Campers will be dining at Ram’s Horn at Academic Village for lunch Monday through Thursday. Our showcase facility, Ram’s Horn dining center features 8 different food venues including a Mongolian Grill, Tex-Mex station, pasta, deli, salad bar, and more. Lunch and dinner will be provided at the CSU Mountain Campus on Friday, as will breakfast on Saturday before campers return to the CSU Main Campus. Expectations of Campers While at Camp
1. Attend every class and program activity and arrive on time 2. Be an active participant in all lectures, labs, and discussions 3. Work together as a team 4. Positively participate in the activities 5. Communicate with instructors when further clarity and explanation on material is
needed 6. Demonstrate respect for all classmates, faculty and instructors
Updated 2/2019
7. Follow established classroom/activity expectations and policies 8. Respect classrooms, CSU campus, visited facilities and yourself at all times 9. Turn off cell phones and electronic devices during presentations and any
scheduled activities 10. Learn, be present, be engaged and have fun!
Health Awareness Altitude sickness is something that visitors to Colorado commonly experience, and it can affect a traveler's sense of well-being quite profoundly. In addition to making one feel dizzy or full of nausea, the lack of moisture in the air can cause your hair, skin and eyes to become uncomfortably dry, and may even cause nosebleeds. A feeling of breathlessness, especially when exercising, is also commonly reported. However, these symptoms may or may not be medically classified as altitude sickness, or AMS. The official diagnosis of AMS is made when a headache, with any one or more of the following symptoms is present after a recent ascent above 8,000 feet:
Loss of Appetite, nausea or vomiting Fatigue or weakness Dizziness or lightheadedness Difficulty sleeping
Fort Collins is at a comfortable 5,003 ft, so this kind of reaction to altitude is extremely rare. However, if you feel any symptoms of altitude sickness during your stay on campus, please alert camp staff immediately. The weather in Colorado in July is typically very hot and dry, but can change very quickly with afternoon thunderstorms. Remind your student to drink plenty of water. They will probably walk up to 3 miles a day around campus during our daily activities so be sure they bring comfortable shoes and a refillable water bottle. CSU is proud to be an environmentally responsible campus by using resources and non- wasteful ways of keeping our campus beautiful. Water used to sprinkle the grass on campus is untreated lake water, which means you should not drink it, or get it in your eyes, mouth, or open wounds. As tempting as it is on a hot summer day, please DO NOT run through sprinklers.
Lab Activities: During the course of the week, campers will have the opportunity to participate in many hands-on activities. Examples of activities may include, sheep brain dissection, cow eyeball dissection, sensory demonstrations: visual/touch/taste, surface electrode gentle muscle stimulation, spatial disorientation demonstration in Bárány chair, and participation in an altitude chamber
Updated 2/2019
ride to 12,000 feet (information below). The camp culminates in an overnight stay at the Colorado State University Mountain Campus where campers will have the opportunity to participate in the Challenge Course (information below), hiking, and other activities under the supervision of Camp Counselors. Participation in all activities is voluntary.
Altitude Chamber Laboratory Activity During the week, campers will be learning about effects of high altitude and the physiological response associated with changes in pressure. The Colorado State University altitude chamber simulates ascent to higher altitude by reducing the air pressure inside the chamber via a vacuum pump and offers the opportunity for students to gain an appreciation for the overall effects of barometric pressure change on human physiology. The laboratory activity will simulate a slow ascent to 12,000 feet (the summit of Pikes Peak is 14,110 feet) and the total time at 12,000 feet will be limited to approximately 10 minutes. During the activity, campers will measure and record their oxygen saturation and pulse through non-invasive use of a pulsoximeter (just like at the doctor’s office). They will then compare that data to information that is provided during the classroom lectures. Discussions will include why supplemental oxygen is necessary for aircrew, as well as for climbers ascending Mount Everest. Campers that choose to participate will be under the supervision of the Director, Hypo-Hyperbaric Chamber Facility at all times. Any camper who does not want to participate in the activity directly will be able to observe from the outside and participate in all discussions and related activities. While many tourists to Colorado make the drive to the top of Pikes Peak (14,110 feet) and Mt. Evans (14,265 feet), as well as to many of the ski resorts throughout the state, ascent to high altitudes is not without some risk for many visitors. The most common is the development of altitude sickness as discussed earlier under Health Awareness. Participation in the altitude chamber activity to a simulated altitude of 12,000 feet carries the same risk as driving to these high-altitude areas in Colorado. If at any time a participant feels unwell, they will be removed from the chamber and returned to ground level. Mountain Campus Challenge Course Information Nestled in a beautiful, secluded mountain valley at an elevation of 9,000 ft (2,743 m) lies Colorado State University's 1,600-acre Mountain Campus. As a site for student learning, conferences, workshops, meetings, and retreats, the Mountain Campus offers a unique opportunity to leave the hectic pace of urban life behind and be immersed in the natural world of the Rocky Mountains. The Mountain Campus Challenge Course is designed to enhance team building and personal growth. Risk taking, group problem solving, and leadership skills also are common focal points. Low elements emphasize teamwork and effective communication, while high elements provide an opportunity for personal challenges and growth.
Updated 2/2019
In order to participate in the Challenge Course at the Mountain Campus, campers must complete and return the following forms with their Applied Physiology Day Camp registration forms (these forms are included in the registration package):
• Participant Health Form • Release/Assumption of Risk Waiver
If you have questions or concerns about the Challenge Course, please call our Main Campus office at 970-491-4747 or the Mountain Campus office at 970-881-2150.

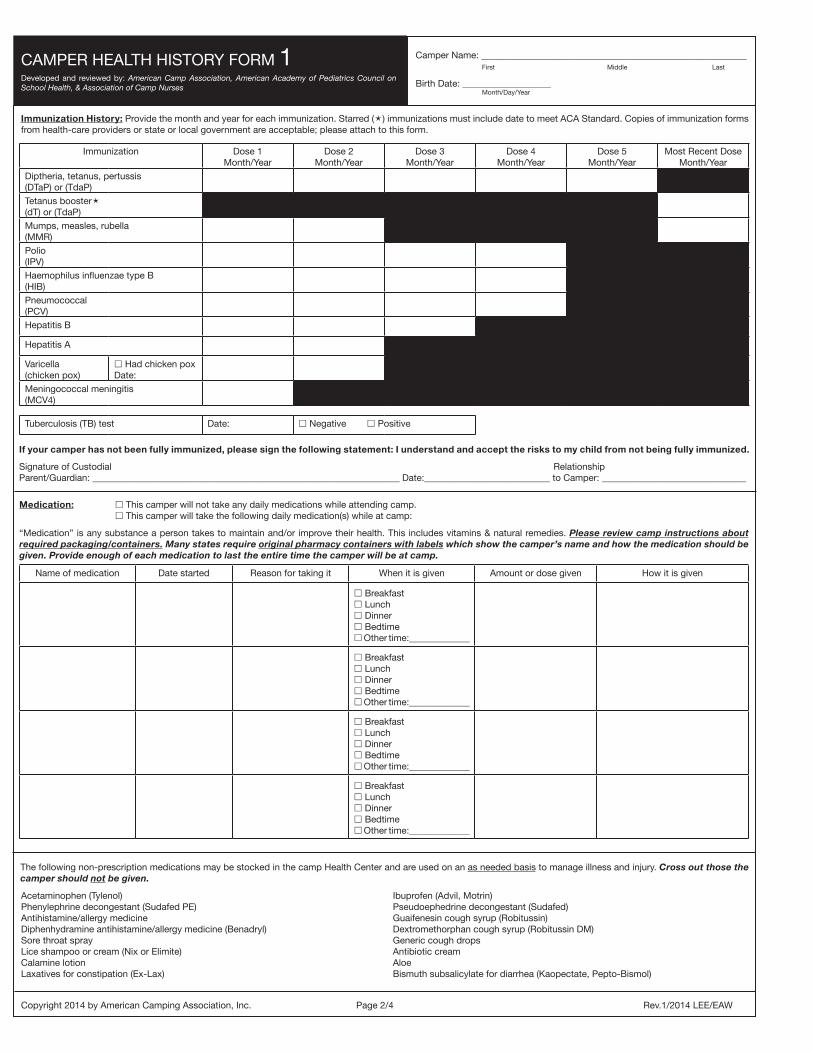
CAMPER HEALTHHISTORY FORM1
Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
Mail this form to the address below by (date)
Camper Home Address: _____________________________________________________________________________________________________________________________________ Street Address City State Zip Code
Parent/guardian with legal custody to be contacted in case of illness or injury: RelationshipName: _________________________________________ to Camper: _______________________________ Preferred Phones: (______) ________________(______)_________________
Email: __________________________________________________________
Home Address: ____________________________________________________________________________________________________________________________________________(If different from above) Street Address City State Zip Code
Second parent/guardian or other emergency contact:
RelationshipName:_________________________________________ to Camper: _______________________________ Preferred Phones: (______) ________________(______)_________________
Email: __________________________________________________________
Additional contact in event parent(s)/guardian(s) can not be reached: RelationshipName: _________________________________________ to Camper: _______________________________ Preferred Phones: (______) ________________(______)_________________
Allergies: No known allergies. This camper is allergic to: Food Medicine The environment (insect stings, hay fever, etc.) Other (Please describe below what the camper is allergic to and the reaction seen.)
Diet, Nutrition: This camper eats a regular diet. This camper eats a regular vegetarian diet. This camper is lactose intolerant. This camper is gluten intolerant. Other, please explain in space.
Restrictions: I have reviewed the program and activities of the camp and feel the camper can participate without restrictions.
I have reviewed the program and activities of the camp and feel the camper can participate with the following restrictions or adaptations. (Please describe below.)
Medical Insurance Information:
This camper is covered by family medical/hospital insurance Yes No
Include a copy of your insurance card if appropriate; copy both sides of the card so information is readable.
Insurance Company____________________________________________ Policy Number______________________________________________
Subscriber____________________________________________________ InsuranceCompany Phone Number (______)_______________________
Parent/Guardian Authorization for Health Care:
This health history is correct and accurately reflects the health status of the camper to whom it pertains. The person described has permission to participate in all camp activities except as noted by me and/or an examining physician. I give permission to the physician selected by the camp to order x-rays, routine tests, and treatment related to the health of my child for both routine health care and in emergency situations. If I cannot be reached in an emergency, I give my permission to the physician to hospitalize, secure proper treatment for, and order injection, anesthesia, or surgery for this child. I understand the information on this form will be shared on a “need to know” basis with camp staff. I give permission to photocopy this form. In addition, the camp has permission to obtain a copy of my child’s health record from providers who treat my child and these providers may talk with the program’s staff about my child’s health status.
Signature of Custodial RelationshipParent/Guardian __________________________________________________________________Date: _____________________________ to Camper: _________________________
If for religious or other reasons you cannot sign this, contact the camp for a legal waiver which must be signed for attendance. Page 1/4
To Parent(s)/Guardian(s): Please follow the instructions below. Attach additional information if needed.
1) Complete pages 1, 2 and 3 of this form (FORM 1) and make a copy.
2) Send the original, signed FORM 1 to camp by the requested date.
3) Complete the top of FORM 2 (CAMPER HEALTH-CARE RECOMMENDATIONS) and provide the copy of FORM 1 with FORM 2 to your child’s health-care provider for review and completion.
4) After it has been completed and signed by your child’s health-care provider, return FORM 2 to camp by the requested date.
Cam
per N
ame _________________________________________________________________________________________ (For C
amp
Use) C
abin or G
roup_____________________________ (For C
amp
Use) S
ession Cod
e(s): _______________
First
Mid
dle
Last
Dates will attend camp: from _______________________to___________________ Month/Day/Year Month/Day/Year
Camper Name: _____________________________________________________________________________________ First Middle Last
Male Female Birth Date ________________ Age on arrival at camp: ________ Month/Day/Year
CAMPER HEALTH HISTORY FORM 1Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
Immunization Dose 1Month/Year
Dose 2Month/Year
Dose 3Month/Year
Dose 4Month/Year
Dose 5Month/Year
Most Recent DoseMonth/Year
Diptheria, tetanus, pertussis(DTaP) or (TdaP)
Tetanus booster(dT) or (TdaP)
Mumps, measles, rubella(MMR)
Polio(IPV)
Haemophilus influenzae type B(HIB)
Pneumococcal(PCV)
Hepatitis B
Hepatitis A
Varicella(chicken pox)
Had chicken poxDate:
Meningococcal meningitis(MCV4)
Tuberculosis (TB) test Date: Negative Positive
If your camper has not been fully immunized, please sign the following statement: I understand and accept the risks to my child from not being fully immunized.
Signature of Custodial RelationshipParent/Guardian: __________________________________________________________________ Date:___________________________ to Camper: _______________________________
Medication: This camper will not take any daily medications while attending camp. This camper will take the following daily medication(s) while at camp:
“Medication” is any substance a person takes to maintain and/or improve their health. This includes vitamins & natural remedies. Please review camp instructions about required packaging/containers. Many states require original pharmacy containers with labels which show the camper’s name and how the medication should be given. Provide enough of each medication to last the entire time the camper will be at camp.
Name of medication Date started Reason for taking it When it is given Amount or dose given How it is given
Breakfast Lunch Dinner Bedtime Other time:_____________
Breakfast Lunch Dinner Bedtime Other time:_____________
Breakfast Lunch Dinner Bedtime Other time:_____________
Breakfast Lunch Dinner Bedtime Other time:_____________
The following non-prescription medications may be stocked in the camp Health Center and are used on an as needed basis to manage illness and injury. Cross out those the camper should not be given.
Immunization History: Provide the month and year for each immunization. Starred () immunizations must include date to meet ACA Standard. Copies of immunization forms from health-care providers or state or local government are acceptable; please attach to this form.
Camper Name: _________________________________________________________ First Middle Last
Birth Date: ___________________ Month/Day/Year
Acetaminophen (Tylenol) Phenylephrine decongestant (Sudafed PE) Antihistamine/allergy medicineDiphenhydramine antihistamine/allergy medicine (Benadryl) Sore throat sprayLice shampoo or cream (Nix or Elimite) Calamine lotion Laxatives for constipation (Ex-Lax)
Ibuprofen (Advil, Motrin)Pseudoephedrine decongestant (Sudafed)Guaifenesin cough syrup (Robitussin)Dextromethorphan cough syrup (Robitussin DM)Generic cough dropsAntibiotic creamAloeBismuth subsalicylate for diarrhea (Kaopectate, Pepto-Bismol)
Copyright 2014 by American Camping Association, Inc. Page 2/4 Rev.1/2014 LEE/EAW

CAMPER HEALTH HISTORY FORM 1Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
General Health History: Check “Yes” or “No” for each statement. Explain “Yes” answers below.
Has/does the camper:
Mental, Emotional, and Social Health: Check “Yes” or “No” for each statement.
Has the camper:
1. Ever been treated for attention deficit disorder (ADD) or attention deficit/hyperactivity disorder (AD/HD)? ……………………….................................................. Yes No
2. Ever been treated for emotional or behavioral difficulties or an eating disorder?……..................................................................................................................... Yes No
3. During the past 12 months, seen a professional to address mental/emotional health concerns?……….…………………………………........................................ Yes No
4. Had a significant life event that continues to affect the camper’s life?............................................................................................................................................ Yes No(History of abuse, death of a loved one, family change, adoption, foster care, new sibling, survived a disaster, others)
Please explain “Yes” answers in the space below, noting the number of the questions. The camp may contact you for additional information.
Camper Name: _________________________________________________________ First Middle Last
Birth Date: ___________________ Month/Day/Year
Health-Care Providers:
Name of camper’s primary doctor(s): _____________________________________________________________________ Phone: (________) _______________________
Name of dentist(s):_____________________________________________________________________________________ Phone: (________) _______________________
Name of orthodontist(s):_________________________________________________________________________________ Phone: (________) _______________________
Copyright 2014 by American Camping Association, Inc. Page 3/4 Rev.1/2014 LEE/EAW
1. Ever been hospitalized? …………………………........ Yes No 11. Had fainting or dizziness? .......................................................... Yes No
2. Ever had surgery? ..............................…………........ Yes No 12. Passed out/had chest pain during exercise? ….……………...... Yes No
3. Have recurrent/chronic illnesses? .......……….…..... Yes No 13. Had mononucleosis (“mono”) during the past 12 months?........ Yes No
4. Had a recent infectious disease? .......…………....... Yes No 14. If female, have problems with periods/menstruation?.……........ Yes No
5. Had a recent injury? ...........................…………....... Yes No 15. Have problems with falling asleep/sleepwalking? ...................... Yes No
6. Had asthma/wheezing/shortness of breath?........... Yes No 16. Ever had back/joint problems?…….………...……………........... Yes No
7. Have diabetes? ..................................…………...... Yes No 17. Have a history of bedwetting?………………….……………........ Yes No
8. Had seizures? ......................................................... Yes No 18. Have problems with diarrhea/constipation?………………......... Yes No
9. Had headaches? …………………………………...... Yes No 19. Have any skin problems?……………………............................... Yes No
10. Wear glasses, contacts, or protective eyewear? Yes No 20. Traveled outside the country in the past 9 months?................... Yes No
Please explain “Yes” answers in the space below, noting the number of the questions. For travel outside the country, please name countries visited and dates of travel.
What Have We Forgotten to Ask? Please provide in the space below any additional information about the camper’s health that you think important or that may affect the camper’s ability to fully participate in the camp program. Attach additional information if needed.
Parents/Guardians: STOP here. The rest of this is form is completed when the camper arrives at camp. Keep a copy for your records.

CAMPER HEALTH HISTORY FORM 1Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
Individual Health Record (For Camp Use Only)
Camper Name: _________________________________________________________ First Middle Last
Birth Date: ___________________ Month/Day/Year
Copyright 2014 by American Camping Association, Inc. Page 4/4 Rev.1/2014 LEE/EAW
Initial Screening Date/Time: _________ Initials: ____________
Screening has been conducted according to camp protocol and significant findings noted as follows:
A. Any signs/symptoms of illness or injury upon arrival?........................ No Yes as noted below
B. History of exposure to communicable disease?.................................. No Yes as noted below
C. Additions or corrections to information on this health history?............ No Yes as noted below
D. Medication given to health-care staff?.................................................. No Yes as noted below
E. Any signs/symptoms of head lice?...................................................... No Yes as noted below
Provider notes: (date/time/initial all entries) _________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
Exit Note: Check one of the following:
Left camp this day with no reported illness or injury symptoms.
Left camp this day with the following problem/concern:
_____________________________________________________________________________________________________________________________________________________
_____________________________________________________________________________________________________________________________________________________
This person was told about the problem and instructed about follow-up as noted above: ______________________________________________________________________
Date/Time: _________________________ Initials: ____________________________

Recommendations for Licensed Medical Personnel
FORM 2Developed and reviewed by: American Camp Association, American Academy of Pediatrics Council on School Health, & Association of Camp Nurses
Mail this form to the address below by (date)
The following non-prescription medications are commonly stocked in camp Health Centers and are used on an as needed basis to manage illness and injury. Medical personnel: Cross out those items the camper should not be given.
Diet, Nutrition: Eats a regular diet. Has a medically prescribed meal plan or dietary restrictions:(describe below)
The camper is undergoing treatment at this time for the following conditions: (describe below) None.
Medication: No daily medications. Will take the following prescribed medication(s) while at camp: (name, dose, frequency—describe below)
Other treatments/therapies to be continued at camp: (describe below) None needed.
Do you feel that the camper will require limitations or restrictions to activity while at camp? No Yes
If you answered “Yes” to the question above, what do you recommend? (describe below—attach additional information if needed)
“I have reviewed the CAMPER HEALTH HISTORY FORM (FORM 1), and have discussed the camp program with the camper’s parent(s)/guardian(s). It is my opinion that the camper is physically and emotionally fit to participate in an active camp program (except as noted above.)
Name of licensed provider (please print): _____________________________________________________Signature: _________________________________Title: _________________
Office Address_____________________________________________________________________________________________________________________________________________ Street City State Zip Code
Telephone: (________)_____________________ Date:_______________________
Copyright 2014 by American Camping Association, Inc. Rev. 1/14 LEE/EAW
To Parent(s)/Guardian(s): Complete this section and give this form (FORM 2) and a copy of yourcompleted CAMPER HEALTH HISTORY FORM (FORM 1) to your child’s health-care provider for review.Dates will attend camp: from ______________to_____________ Month/Day/Year Month/Day/Year
Camper Name: _____________________________________________________________________________________ First Middle Last
Male Female Birth Date __________________ Age on arrival at camp ________________ Month/Day/Year
Camper home address: ______________________________________________________________________________
____________________________________________________________________________________________________City State Zip Code
Custodial parent(s)/guardian(s) phone: (_______)________________________ (_______)_________________________Parent(s)/guardian(s) stop here. Rest of form to be completed by medical personnel.
Physical exam done today: Yes No (If “No,” date of last physical: ____________________) Month/Day/YearACA accreditation standards specify physical exam within the last 12 months.
Medical Personnel: Please review the CAMPER HEALTH HISTORY FORM (FORM 1) and complete all remaining sections of this form (FORM 2). Attach additional information if needed.
Weight: _______ lbs Height: _____ft_____in Blood Pressure_______/_______
Allergies: No Known Allergies
To foods (list):
To medications: (list):
To the environment (insect stings, hay fever, etc.– list):
Other allergies: (list):
Describe previous reactions:
Cam
per Nam
e _________________________________________________________________________________________ (For Cam
p Use) C
abin or Group_____________________________ (For C
amp U
se) Session Code(s): ________________
First
M
iddle
Last
Acetaminophen (Tylenol)Ibuprofen (Advil, Motrin)Phenylephrine (Sudafed PE)Pseudoephedrine (Sudafed)Chlorpheneramine maleateGuaifenesinDextromethorphanDiphenhydramine (Benadryl)Generic cough dropsChloraseptic (Sore throat spray)Lice shampoo or scabies cream
(Nix or Elimite)
Calamine lotionBismuth subsalicylate (Pepto-Bismol)Laxatives for constipation (Ex-Lax)Hydrocortisone 1% creamTopical antibiotic creamCalamine lotionAloe

Updated 2/2019
2019 Applied Physiology Day Camp
Emergency Contact Information
Student’s Name: ________________________________________ Date of Birth: _________________Gender:_____________ Parent’s/Guardian’s Name:_______________________________ Parent’s/Guardian’s Name:_________________________
Home Phone:______________ Alt Phone: __________________ Home Phone:_______________ Alt Phone:_____________ Address: _____________________________________________ Address: ________________________________________ City/State/Zip:_________________________________________ City/State/Zip:____________________________________
Primary Emergency Contact: _______________________________ Secondary Emergency Contact:______________________ Home Phone:______________ Alt Phone: ____________________ Home Phone:_______________ Alt Phone:_____________ Address: ______________________________________________ Address: ________________________________________ City/State/Zip:__________________________________________ City/State/Zip:____________________________________
Physician’s Name:_______________________________________ Phone:__________________________________________ Insurance Company:_____________________________________ Policy Number:___________________________________ Allergies/Special Health Concerns:____________________________________________________________________________ ________________________________________________________________________________________________________ I authorize all medical and surgical treatment, X-ray, laboratory, anesthesia, and other medical and/or hospital procedures as may be prescribed by the attending physician and/or paramedics for my child, and waive my right to informed consent of treatment. This waiver only applies in the event that neither parent/guardian can be reached in the case of an emergency. _____________________________________________________________________________________________________ Parent/Guardian Signature Date ______________________________________________________________________________________________________ Witness Signature Date
Emergency Contact and Information for a Student
Alternative Emergency Contacts
Medical Information

Updated 2/2019
2019 Applied Physiology Day Camp
RELEASE OF LIABILITY AND RISK WAIVER
READ THIS DOCUMENT COMPLETELY BEFORE SIGNING. ITS EFFECT IS TO RELEASE THE UNIVERSITY FROM ANY LIABILITY RESULTING FROM YOUR CHILD’S VOLUNTARY PARTICIPATION IN THE ABOVE-NAMED ACTIVITIES AND WAIVES ALL CLAIMS FOR DAMAGES OR LOSSES AGAINST THE UNIVERSITY.
Name of Participant/s:______________________________________________________________
RELEASE FROM RESPONSIBILITY, ASSUMPTION OF RISK, AND WAIVER
In consideration of my child being permitted by Applied Physiology Day Camp at Colorado State University to participate in the following activities:
• Brain and Eye Dissections • Muscle stimulation using surface electrodes • Sensory experiences: taste, visual and touch demonstrations • Altitude chamber ride to an altitude no higher than 12,000 ft (information below) • Staying in on-campus dormitory at the CSU Mountain Campus • Hiking at Colorado State University Mountain Campus (including transportation to and from) • Colorado State University Mountain Campus Challenge Course (including transportation to
and from) (information below) • On-campus Team Games and Activities
I, the undersigned parent/legal guardian of (printed name) _________________________, exercising my own free choice given my consent for my child to participate voluntarily in the above-named activities, hereby release and discharge, indemnify and hold harmless The State of Colorado, the Board of Governors of the Colorado State University System, Colorado State University, and their members, officers, agents, employees, and any other persons or entities acting on their behalf, and the successors and assigns for any and all of the afore-mentioned persons and entities, against all claims, demands, and causes of action whatsoever, either in law or in equity, relating to injury, disability, death or other harm, to person or property or both, arising from my child’s participation in and/or presence at the above listed activities. I acknowledge that I have been informed of hazards and risks which may be associated with my child’s participation in the above-named activities; I understand, accept, and assume those hazards and risks, and waive all claims against The Board of Governors of the Colorado State University System, and Colorado State University, and other entities or persons set forth above. I understand that I am solely responsible for any costs arising out of any bodily injury or property damage sustained through my child’s participation in normal or unusual acts associated with the above-named activities.

Updated 2/2019
I have had sufficient time to review and seek explanation of the provisions contained above, have carefully read them, understand them fully, and agree to be bound by them. After careful deliberation, I voluntarily give my consent and agree to this Release from Responsibility, Assumption of Risk, and Waiver. Read and acknowledged this________ day of______________, 20_____. I, (printed name) _________________________________, am the parent or legal guardian of the participant/s (insert name/s here) _____________________________. I have read and understand the provisions of this document, I consent to my child participating in the activities described above, and I fully enter into and agree to the above Release from Responsibility, Assumption of Risk, and Waiver. ______________________________________________________________________________ Signature of Parent or Legal Guardian Date

Updated 2/2019
2019 Applied Physiology Day Camp Photography Consent / Media Release Form
RELEASE FOR MINOR CHILDREN (Under 18)
I, (print name) ___________________________________, parent / legal guardian of (child’s name) ________________________________ hereby grant permission to Colorado State University, its employees or representatives to take and use (check all that apply):
__ Photographs/ digital images __ Videotape __ Audio recording or quoted remarks
Of my child for use in promotional or educational materials as follows:
__ Printed publications or presentations __ Web sites
I agree that my child’s name and identity ___ may / ___ may not be revealed (select one) in descriptive text or commentary in connection with the image(s). I agree that the media __ may/ __ may not (select one) contact my family to speak with my child regarding his / her involvement with Colorado State University Applied Physiology Day Camp activities. I authorize the use of this materials indefinitely without compensation to me. All negatives, positives, prints, digital reproductions and video or audio recordings shall be the property of Colorado State University. Signature of parent/guardian: ______________________Date:________________ Address: ___________________________________________________________ City, State, Zip: ______________________________________________________

Updated 2/2019
2019 Applied Physiology Day Camp ROOMATE REQUEST FORM
Overnight at Colorado State University Mountain Campus
Personal Contact Information Name:___________________________________________________________________ E-mail:___________________________________________________________________ Phone: Cell:______________________________ Home:___________________________ What state do you currently live in? ___________________________________________ Personal Compatibility Information Gender/Identity:___________________________________________________________ Year in School (Fall 2019):____________________________________________________ Where do you attend school?_________________________________________________ I have the following roommate(s) in mind:_______________________________________ Personal Attributes (please give accurate representation. This information is confidential and is used to make your housing experience the best it can be, thus making you happier) On a scale of 1 to 5, where 1 is ‘do not agree at all’ and 5 is ‘highly agree’, how much do you agree with the following statements?
I am very neat 1 2 3 4 5 I am very outgoing 1 2 3 4 5 I like to stay up late 1 2 3 4 5 I like to be very social and chatty 1 2 3 4 5 I am a morning person 1 2 3 4 5

Updated 2/2019
Describe your hobbies, interest, clubs/organizations, other considerations or special requests: List 3 traits/characteristics you look for in a roommate: 1._______________________________________________________________________ 2._______________________________________________________________________ 3._______________________________________________________________________
MOUNTAIN CAMPUS CHALLENGE COURSE INFORMATION SHEET Welcome to the Mountain Campus Challenge Course! Please help us by sharing the following information with all your group members. Please make copies of the waiver/health information sheet and be certain each member of your group brings signed copies of these on the day of the course. 1. All Challenge Course participants must bring a signed:
• Participant Health Form
• Release/Assumption of Risk Waiver 2. Appropriate Clothing:
• Loose fitting pants or long shorts
• Sneakers or light hiking boots (no open toe sandals)
• Layered clothing and rain coat (weather is unpredictable at 9,000 ft.)
• Hat with a sun visor
• Sunglasses and sunscreen
• Safety strap for glasses
• Please leave jewelry and valuables at home 3. Smoking is not permitted on or near the Challenge Course. 4. Please bring a full quart water bottle; there is minimal water available at the course.
If you have questions, concerns or would like weather related information, please call our Main Campus office at 970-491-4747 or the Mountain Campus office at 970-881-2150.

MOUNTAIN CAMPUS CHALLENGE COURSE PARTICIPANT HEALTH INFORMATION The information provided on this form is confidential. Participant Name: Phone: Address: Emergency Contact: Phone: Name of Doctor: Phone (if you know it): MEDICAL INFORMATION Age: Approx. Height: Approx. Weight: Are you taking any medication? Describe: Are you allergic to anything? Describe: Do you or anyone in your family have a history of heart problems? Describe: Do you have a history of respiratory problems/asthma? Describe: Do you have any pre-existing conditions we should know about? Describe: Note: Research has demonstrated that challenge course activities can raise heart and respiration rates in participants. People with a history of heart and respiratory problems can be placed at extreme risk. If you have any heart or respiratory history, you must consult your physician prior to participating on the Challenge Course. My signature below indicates that I understand that: 1. The Challenge Course involves physically and mentally demanding activities at 9,000 ft. 2. Participation has certain risks including but not limited to: elevated heart rates, bruises, scrapes, sunburn. 3. I will be called upon to support others both physically and emotionally. 4. Elements of the course take place 10’ - 35' in the air. 5. I believe that I (my child/ward) am in good health, and I affirm that my (child's/ward's) participation in the
Challenge Course activities will in no way aggravate any condition(s) present. If in doubt, I will seek and follow medical advice.
6. The information I have provided on this form is current, factual and complete.
SIGNATURE: DATE: Parent/Guardian, if you are under 18: In the event of a non-life threatening injury to my child, you have my permission to medically treat him/her without my being present. Signature of parent or guardian: Date:

COLORADO STATE UNIVERSITY MOUNTAIN CAMPUS CHALLENGE COURSE
RELEASE FROM RESPONSIBILITY, ASSUMPTION OF RISK, WAIVER
PLEASE READ THIS DOCUMENT COMPLETELY BEFORE SIGNING. ITS EFFECT IS TO RELEASE THE UNIVERSITY, COLLEGE, AND/OR DEPARTMENT FROM ANY LIABILITY RESULTING FROM YOUR PARTICIPATION IN THE CSU MOUNTAIN CAMPUS CHALLENGE COURSE AND WAIVES ALL CLAIMS FOR DAMAGES OR LOSSES AGAINST THE UNIVERSITY, COLLEGE, AND/OR DEPARTMENT.
I, ________________________________________, intend to participate on the Mountain Campus Challenge Course of Colorado State University, on________________________(date of activity). In consideration of Colorado State University making arrangements for and permitting and assisting me in participating on the Challenge Course, I exercise my own free choice to participate voluntarily in activities on the Challenge Course, and promise to take due care during such participation. I hereby release and discharge, indemnify and hold harmless, the University Board of Governors and Colorado State University, Mountain Campus, and their members, officers, agents, employees, and any other persons or entities acting on their behalf, and the successors and assigns for any and all of the aforementioned persons and entities, against all claims, demands, and causes of action whatsoever, either in law or in equity, relating to injury, disability, death or other harm, to person or property or both, arising from my participation in and/or presence at the Mountain Campus Challenge Course. Furthermore, I am aware that the CSU Mountain Campus is located at an elevation of 9,000 ft. (2743m) and understand the potential hazards of inclement weather and physical stress on cardiopulmonary function, including tachycardia (rapid heart rate) and possible sudden cardiac arrest. I am also aware that the Challenge Course in which I intend to participate may include other occurrences beyond human control, creating hazards, which could place me in perilous situations. Although rare, these hazards can include cable and rope burns, sprained joints, muscle pulls, twisted knees, back strains, shoulder and finger dislocations, neck injuries, skin abrasions, broken fingernails, sunburn and splinters, psychological trauma, as well as other hazards and perils not specifically named herein. I acknowledge that I have been informed of the hazards and risks which may be associated with my participation on the Challenge Course; I understand, accept, and assume those hazards and risks, and waive all claims against the University Board of Governors and Colorado State University, and other persons as set forth above. I understand that I am solely responsible for any costs arising out of any bodily injury or property damage sustained through my participation in normal or unusual acts associated with the CSU Mountain Campus Challenge Course. I have had sufficient time to review and seek explanation of the provisions contained above, have carefully read them, understand them fully, and agree to be bound by them. After careful deliberation, I voluntarily give my consent and agree to this Release, Assumption of Risk, and Waiver.
Today’s Date:
Signature of Participant: If Participant is under the age of 18, her/his parents or legal guardians must also sign: I/We (printed name)___________________________________________ are the legal guardians of the participant who has signed above. I/We have read and understand the provisions of this document. I/We consent to the student or non-student participating in the activity described above, and I/We enter into and agree to the above Release of Responsibility, Assumption of Risk and Waiver. _______________________________________________________________________________ SIGNATURE OF PARENT (S)/LEGAL GUARDIAN (S) DATE