application of real time rt-pcr to detect avian influenza ... of... · application of real time...
TRANSCRIPT
Application of Real Time RT-PCR to Detect Avian Influenza Virus
David L. Suarez D.V.M., Ph.D.Research Leader Exotic and
Emerging Avian Viral Disease Research Unit
Agricultural Research ServiceUnited States Department of
Agriculture

Diagnosis of Avian Influenza Virus
• Clinical signs– Low pathogenic avian influenza– Highly Pathogenic avian influenza
• Diagnostic Tests– Antibody detection
• AGID, HI• ELISA
– Virus detection• Virus isolation• Directigen• Realtime RT-PCR (RRT-PCR)• Traditional RT-PCR• NASBA
– Other Diagnostic Tests
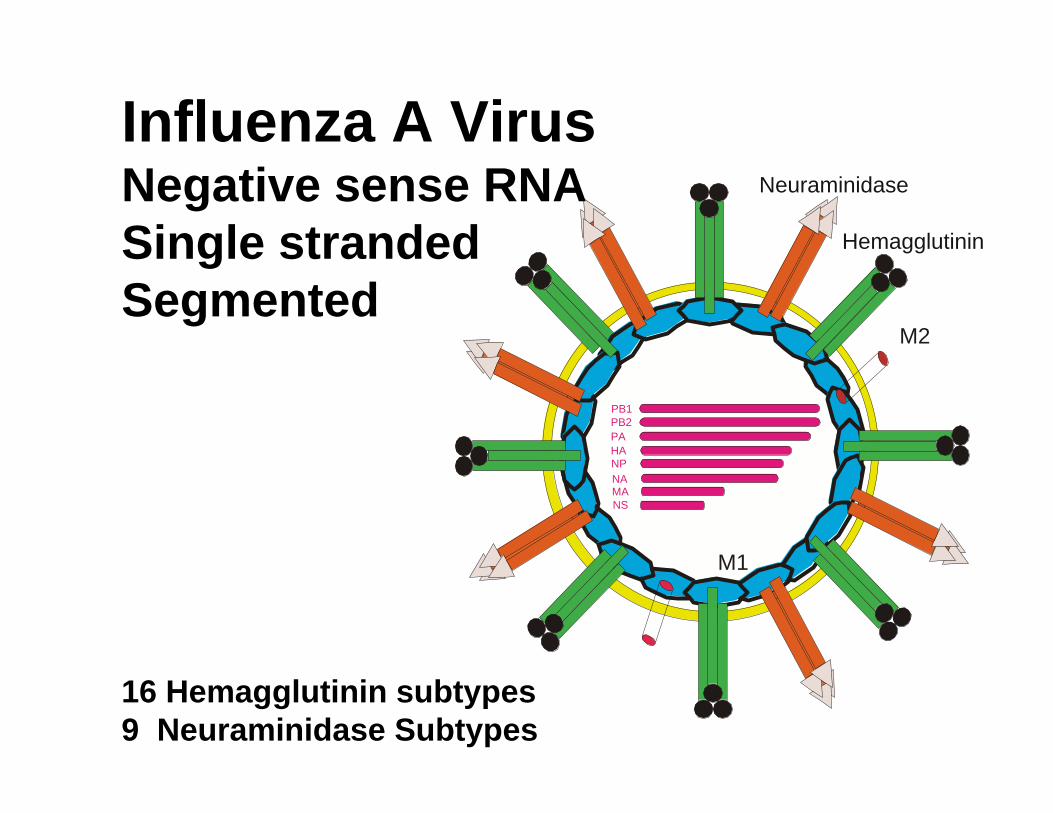
HA
PB1PB2PA
NPNAMANS
M2
Hemagglutinin
Neuraminidase
M1
Influenza A VirusNegative sense RNA Single strandedSegmented
16 Hemagglutinin subtypes9 Neuraminidase Subtypes

Clinical Signs• Highly Pathogenic Avian Influenza
– Symptoms depend on species– Systemic lesions with high mortality
• Low Pathogenic Avian Influenza– Can be subclinical– Increased daily mortality– Respiratory disease symptoms– Drops in egg production– Increased condemnation at slaughter– Other symptoms can be strain dependant

Serology• Detection of type and subtype specific
antibodies to previous influenza infection (AGID, ELISA, and HI)
• Typically have antibody response 7-10 days after bird is infected
• Birds stop shedding virus soon after antibodies are detectable
• Widely used for routine surveillance for LPAI viruses because of cost and birds stay seropositive for months
• Serology less valuable for HPAI

Direct Detection of Virus“Critical Component of Outbreak
Control”• Virus Isolation• Real-time RT-PCR • Traditional RT-PCR• NASBA• Antigen Capture Elisa tests• Other tests

Virus Isolation in SPF embryonated chicken eggs
• Sensitive• Necessary for viral characterization• Embryonated chicken eggs are
perishable and supply may be limited• Requires days to weeks for results• Concerns about cross contamination• Requires high levels of biosecurity


Real-time RT-PCR (RRT-PCR)• One-Step RT-PCR test was developed for
typing and subtyping of influenza viruses using fluorescent Taqman probes
• Sensitivity similar to virus isolation• The test doesn’t require running the PCR
product on a gel and the probe confirms specificity
• The complete test, including the RNA isolation step, can be completed in less than three hours
• Requires expensive equipment, but can be done faster and cheaper than conventional

Positive
Negative

Traditional RT-PCR
• Perform RT-PCR in a one-step or two-step format
• Analyze DNA product on an ethidium bromide stained agarose gel
• Sensitivity can be similar to virus isolation • Working with large amounts of amplified DNA
creates a cross contamination risk!• Numerous recommendations to reduce
contamination• Requires less expensive equipment, but
greater manpower to perform test

NASBA Technology
• Nucleic acid sequence based amplification (NASBA)
• Isothermal amplification with several enzymes
• NASBA-ECL similar sensitivity to virus isolation
• Commercial kit-requires additional equipment• Not quantitative• Expensive

Antigen Capture ELISA Tests• Antigen capture test-most produced for human
use only• Type A test only- does not subtype• Lower sensitivity than virus isolation or RRT-PCR• Low level of false positives from clean samples• Test is easy to use and requires no additional
equipment• Not always available in large quantities• Directigen most commonly used in U.S. ($15-
20/test)


Why RRT-PCR for AIV?• Advantages
– Rapid test results (3 hours for rush samples)
– Reduced cross contamination– Reagent Cost
• RNA extraction $2-4• RRT-PCR $4
– Scalable- large numbers of samples may be processed
– Can type and subtype AIVs– Viable virus not necessary

Development and Evaluation of an RRT-PCR Test for AIV
• Test Design• Bench Validation• Field Validation• Transfer of technology to other
laboratories• Proficiency testing• Performance during an outbreak• Future goals

Critical Control Points For Successful RRT-PCR
• RNA extraction procedure– Efficient and reproducible extraction procedure– Works with a variety of samples– High throughput and cost are issues
• RT-PCR Amplification reagents– Commercial kits preferred– Sensitivity, cost and ease of use are issues
• PCR primers and probes– Provides specificity– Affects sensitivity

Real-time PCR chemistries
• Sequence specific– Taqman/ Dual-labeled probe/ Hydrolysis probe– Fluorescence resonance energy transfer (FRET)– Molecular Beacons– Lux primers– Scorpion probes
• Non-sequence specific– dsDNA binding dyes (SYBR green)

Hydrolysis/Taqman probes
Taq
Taq
Reporter
Reporter
Quencher
Quencher
Primer 1
Primer 2

RRT-PCR for Avian InfluenzaA Two Test Procedure
• Type A influenza Test– Detects any Type A
influenza virus – Detects conserved
Matrix gene– Works with samples
from any species– Used as screening
test– Sensitivity similar to
virus isolation
• Subtype specific Test– Different test for
every subtype– Provides
confirmation of Matrix (MA) test
– Less sensitive than MA
– Available H5, H6, H7 and H9 tests
– More affected by strain variation
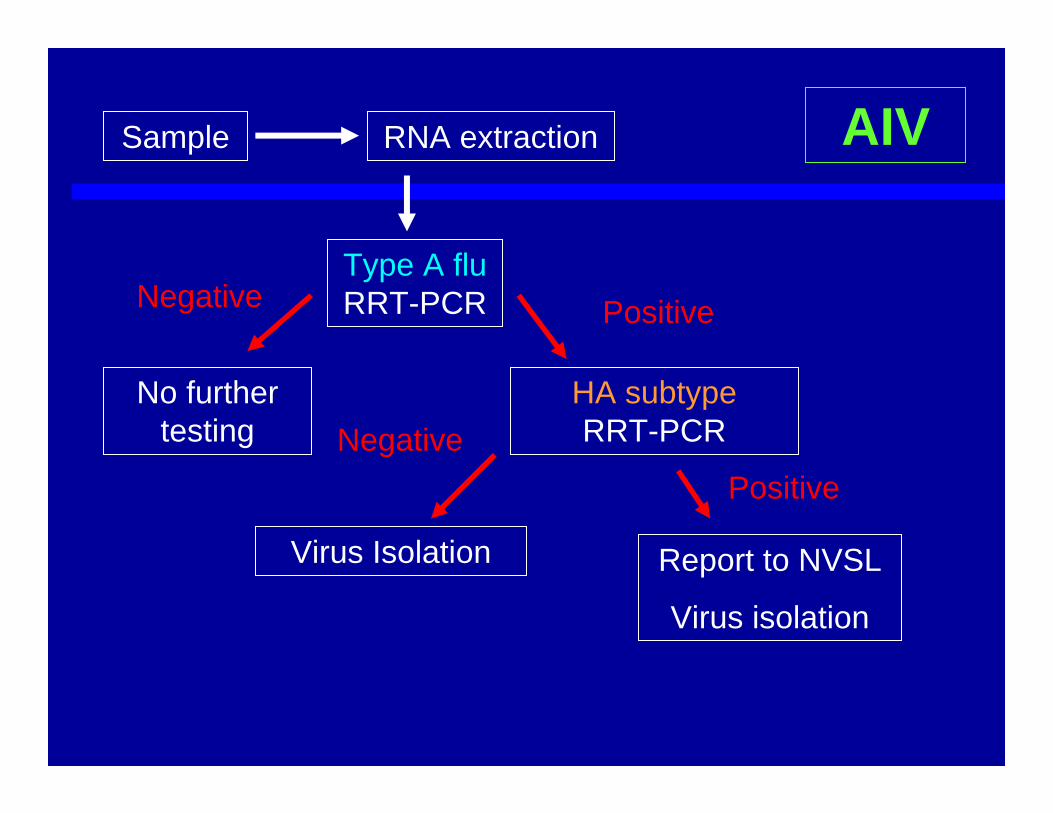
Sample RNA extraction
Type A fluRRT-PCR
HA subtype RRT-PCR
Positive
No further testing
Negative
NegativePositive
Virus Isolation Report to NVSL
Virus isolation
AIV

Bench Validation Procedures
• Develop specific primers and probes for pathogen based on available sequence
• Optimize for Mg, cycling parameters, probe/primer concentrations
• Determine sensitivity and limit of detection on laboratory samples
• Determine specificity with a panel of characterized viruses
• Compare samples from experimentally infected animals to performance standard
Real-time RT-PCR for AIV Sensitivity
• Compared to Egg Infectious Dose– Type A influenza – 10-1 EID50– H5 and H7 subtype- 101 EID50
• Determined with in vitro transcribed RNA– Type A influenza - 103 copies– H5 and H7 subtypes– 104 copies

Specificity Panel Isolate Subtype Matrix H5 H7
Chicken/Netherlands/03 + - -
Turkey/Ontario/6118/67 H8N4 + - -
Chicken/NJ/1220/97 H9N2 + - -
Chicken/Korea/96006/96 H9N2 + - -
Chicken/Germany/N/49 H10N7 + - -
Turkey/VA/31409/91 H10N7 + - -
Chicken/NJ/15906-6/96 H11N1 + - -
Duck/England/56 H11N1 + - -
Duck/LA/188B/87 H12N5 + - -
Gull/MD/704/77 H13N6 + - -
Mallard/Gurjev/263/82 H14N5 + - -
Shearwater/W.Australia/2576/79 H15N6 + - -
Aichi/68 H3N2 + - -
Equine/KY/211/87 H3N8 + - -
Swine/MN/9088/99 H3N2 + - -
Swine/IN/1726/89 H1N1 + - -
Isolate Subtype Matrix H5 H7
Duck/NJ/7717-70/95 H1N1 + - -
Mallard/NY/6750/78 H2N2 + - -
Env/NY/19019-6-98 H3N8 + - -
Duck/Victoria/9211-18-1400/92 H3N8 + - -
Duck/Alberta/286/78 H4N8 + - -
Chicken/Puebla/8629-602/94 H5N2 + + -
Chicken/MA/11801/86 H5N2 + + -
Avian/NY/31588-2/00 H5N2 + + -
Chicken/NJ/17169/93 H5N2 + + -
Chicken/Hong Kong/220/97 H5N1 + + -
Duck/Malaysia/97 H5N3 + + -
Chicken/NY/14677-13/98 H6N2 + - -
Turkey/PA/7975/97 H7N2 + - +
Chicken/PA/13552-1/98 H7N2 + - +
Quail/AR/16309/94 H7N3 + - +
Chicken/NY/8030-2/96 H7N2 + - +

Initial Comparison of Tests• Virus isolation and RRT-PCR were
compared during the summer of 2001 on 1550 samples from the LBMs of NY and NJ
• H7N2 was commonly isolated from birds in the markets
• Good correlation of tests at market level• Virus isolation appeared to be more
sensitive than RRT-PCR although both tests appeared to miss positive samples

Field Validation of Diagnostic Tests
• Literature on validation primarily targeted to serologic tests
• Goal of 1000 negative samples and 300 positive samples
• Compare diagnostic sensitivity (Dsn) and diagnostic specificity (Dsp) with performance (“Gold”) standard
• Ideally compare 3 different geographic regions

H7 Low Pathogenic Outbreak in Virginia, USA
• March 2002, a low pathogenic H7N2 was diagnosed in turkeys in Virginia
• Outbreak quickly spread and eventually 197 infected flocks were identified
• Control was by eradication (stamping out)• 4.5 million turkeys and chickens were destroyed• Direct government costs for eradication was 65
million dollars and total cost was over 160 million dollars
• First time a real-time RT-PCR test was used significantly in an animal disease outbreak

Results of VA Study• >3,600 samples tested between 4/30 – 5/15
– Directigen – Harrisonburg, VA– VI – NVSL (DVL)– RRT-PCR – NVSL (CVB-L)
• USDA-ARS, SEPRL, Athens, GA (6), DVL (1), CVB-L (1)
• Samples included dead bird surveillance and suspect samples
• Evaluated at specimen and submission level

ResultsBy Specimen
InterpretationDirectigen VI
+
+
+
+
–
–
–
+
+
–
–
+
+
–
PCR*
+
–
+
–
+
–
+
Total agreement (48/95 = 50.5%)
VI missed (4/95 = 4.2%)
D missed (19/95 = 20.0%)
D & VI missed (13/95 = 13.7%)
PCR missed (3/95 = 3.2%)
D false positive (2/95 = 2.1%)
PCR and D missed (6/95 = 6.3%)
*MA+ and H7+ only

Statistical AnalysisBy Specimen
Paired ComparisonsPCR/VI
88/80
1.88
0.170
Dir/VI
60/80
10.45
0.002
PCR/Dir
88/60
18.27
0.001
Tests
# of Positive Specimens
Chi-Square Statistic
p-value

Statistical AnalysisBy Specimen
Sensitivity 88.2 67.1
Specificity 99.5 99.8
PCR/VI Dir/VI
Total agreement on all samples (+, – ) = 98.7%n = 3,628

Conclusions• RRT-PCR was equal to or more sensitive than
VI– Could replace VI without adversely affecting control
program• Directigen test was valuable because of rapid
detection• Virus isolation used to confirm RRT-PCR and
Directigen positives and characterize isolates• RRT-PCR was eventually used in the VA state
lab to provide faster diagnosis

Conclusions:Sensitivity, Speed, and Cost
Sensitivity Speed Cost
Virus Isolation Best Worst Intermediate
Directigen Worst Best Worst
RRT-PCR Best Intermediate Best
All 3 types of tests have a role in future disease outbreaks

Real-time PCR platforms• Many real-time PCR platforms
available• Some optimization of test
required• Platforms have different
characteristics– Speed– Capacity– Optical channels (multiplex)– Cost

Lab Equipment Logistics
• Bio-safety cabinet space– Ideally 3 cabinets
• 1. RNA extraction (full exhaust if Trizol is used)
• 2. RNA Transfer to reaction tubes• 3. Clean reagents, master mix preparation
(Cell culture hood)– Two cabinets (more realistic)
• 1. RNA extraction• 2. RNA transfer/ master mix preparation
Between uses hoods need to be wiped out with disinfectant and gloves should be changed.

RNA extraction
• Methods– Silica binding columns (ex. RNeasy, Qiagen)– Magnetic beads (ex. MagMax, Ambion) – Organic solvents (ex. Trizol, Invitrogen)
• Formats– Individual samples/ centrifuge– Vacuum manifolds– 96 well plates– Robots/automated (96, 48, 32 sample)

Sample types and processing methods
RRT-PCR can detect inactivated virus, so may be inappropriate
Virus isolation to detect live virus
(Swab)Environmental samples
For HPAI viruses high levels of virus may be in tissues.
Macerate with glass beads in trizoland then Magnetic beads
Tissue samplesAny species
Virus primarily replicates in the intestinal tract. RNA extraction method must be modified for cloacal samples
Ambion Magnetic Bead RNA extraction then RRT-PCR
Cloacal SwabWaterfowl-ducks
Virus primarily replicates in the respiratory tract (LPAI)
RNeasy or Ambion Magnetic bead RNA extraction, then RRT-PCR
Tracheal or oropharyngealswab
Gallinaceous Poultry (chickens, turkeys, quail)
NotesProcessing Method
Recommended Specimen
Species/ Sample Type

National Animal Health Laboratory Network (NAHLN)
• NAHLN laboratories are veterinary diagnostic laboratories (state, veterinary school, private) throughout the U.S. capable of testing for Foreign Animal Diseases
• Goal was to provide NAHLN labs a validated RRT-PCR test for AIV, NDV, FMD and other select agents
• Provide a rapid diagnostic response during an outbreak
• Increase surge capacity• Continued federal (USDA/APHIS) oversight


Authorized Testing Laboratories
• Person, not the laboratory, is authorized to perform the test
• Person has to go through RRT-PCR training or have suitable experience
• Must pass, on a yearly basis, a proficiency panel
• Must provide data to USDA/APHIS to receive reimbursement for testing as part of surveillance programs

Proficiency Testing• Panel of 10-14 samples • Samples are whole virus inactivated by a
phenol disinfectant • Includes negatives, strong and weak
positives• Includes different HA subtypes• Successful tests require RNA extraction
and amplification • Testing started by SEPRL, but
transferred to NVSL/APHIS for AIV

Proficiency Panel ResultsReal-time PCR
InstrumentNumberof labs
Samples (data sets)
SD CVCorrect
sample ID’s (%)
SmartCycler 9 336 (24) 1.34 5.19 325 (96.7)
Light Cycler without BSA
1§ 56 (4) ND* ND 49 (87.5)
Light Cycler with BSA 1 56 (4) ND ND 56 (100)
iCycler 1 28 (2) ND ND 28 (100)
ABI 7900 1 14 (1) ND ND 14 (100)
Total 12 490 (35) ND ND 472 (96.3)

Delmarva Outbreak 2004• 1st flock identified by passive surveillance (clinical
disease) in Harrington, DE on Feb 5th, 2004• Presumptive diagnosis the following day by RRT-
PCR for H7 AI• Quarantines on farm and 2 mile buffer zone
established per MOU the same day• Agreement in place to cover indemnification,
depopulation, C+D, carcass disposal, etc.• Extensive surveillance in 2 mile quarantine and 6
mile buffer zone (11,728 samples in 10 weeks)• 2nd and 3rd infected flocks identified and depopulated
quickly

H5N2 in Texas• Feb. 16 – increased mortality in a non-commercial
broiler flock in Gonzales, Texas • Feb. 17 – diagnostic samples tested positive for H5
AIV at Texas Veterinary Medical Diagnostic Laboratory
• Texas state officials arrived Feb. 17, placed flock under Hold Order, began to trace & test epidemiologic links
• Two LBMs in Houston tested AI positive by RRT-PCR• Baseline testing began on all flocks within 8K and
16K-radius around the index farm• All flocks within 8K of index placed under Hold Order• Feb. 20 – NVSL confirmed virus as H5N2 • Feb. 21 – Index farm depopulated (6,608 birds)

Texas Outbreak Continued• Feb. 23 – NVSL determined H5N2 virus had amino
acid sequence compatible with HPAI• Infected LBMs and their holding facilities were
depopulated on Feb. 23• All other Houston LBMs (3) depopulated as
dangerous contacts • C&D of LBMs completed Feb. 29• March 1 – NVSL reported results of chicken/embryo
innoculation tests – no illness or deaths (pathogenicity index=0)
• Surveillance-Over 2000 RRT-PCR tests and 3000 serologic tests performed in first month.

HPAI H5N2 – Gonzales, Texas
5-mile “infected zone”39 non-commercial5 commercial
10-mile “surveillance zone”178 non-commercial35 commercial

Keys to Rapid Control
• Availability of sensitive and specific diagnostic test at a local or regional laboratory
• Once a positive sample is identified initiate quarantine and confirm sample identity (virus isolation required)
• Plans for control, including indemnity, carcass disposal, and movement controls, must be in place before outbreak occurs

Maintenance of Test
• Sequence variation can cause test failure
• Monitoring of new outbreaks to assure test performance is necessary
• New commercial reagents should be evaluated for improved performance
• Issues of application need to be evaluated

Evaluation of H5 Subtype RRT-PCR Test for Asian H5N1
• H5 test was originally designed primarily for North American isolates
• Could identify Asian H5N1 viruses with lower sensitivity
• Sequence analysis of Asian isolates showed good conservation with reverse primer and probe, but 4 mismatches with forward primer
• Redesigned H5 test to include forward primers optimized for both Asian and North American viruses– NA H5F TGACTATCCACAATACTCA– EA H5F TGACTACCCGCAGTATTCA

Future Developments
• Dried down reagent beads– Includes Primer, probes, buffers, and
internal control– Internal control should prevent false
negatives– Multiplex test (requires multiple channels)– Longer shelf-life– Better reagent consistency among labs
and tests– Simpler protocol

Acknowledgements
Suzanne DeBlois
Thank you