application of positron emission tomography ( pet ) in colorectal cancer dr chan wai keung...
TRANSCRIPT

Application of PositronEmission Tomography ( PET ) in Colorectal Cancer
Dr Chan Wai KeungDepartment of SurgeryRuttonjee and Tang Shiu Kin Hospitals

• What is PET
• Liver metastasis
• Extrahepatic metastasis
• Elevated CEA
• Local recurrence
• Monitor resposnse to therapy

PET - Background
• Positron emission tomography ( PET ) in use for 20 years
• Initially for research purposes
• Clinical application since 90s
• Wide clinical uses: carcinomas, melanoma, lymphoma,
epilepsy, dementia, cerebrovascular disease, coronary
artery disease and others




PET - Basic Principles
• A PET tracer is administered and takes part in physiological processes
• Different concentrations at different locations
• The PET scanner detects signals
• The resulting images showed functional information

Anhilation
PET - Basic Principles
• Metabolically active cells can take up the tracer
• Enhanced activity seen in brain, skeletal muscle, bowel, myocardium, genitourinary tract, thyroid and others
• “Functional imaging”help detection at earlier stage than cross sectional imaging

18 Fluoro-2-deoxy-D-glucose ( 18FDG )
• A glucose analogue developed in 1970s
• Tumor cells have increased metabolism and glucolysis and hence increased uptake of 18FDG
• Uptake not exclusive to tumor cells
• Good accumulation in tumor cells, long half-life, ease of availability

Glucose

18FDG
a

18FDG

Standard Uptake Value ( SUV )
• The most common parameter
• Related to the injected dose per body mass
• Correct emission scan with an attenuation scan
• Higher in tumor


• Sensitivity : TP / ( TP + FN )
• Specificity : TN / ( FP + TN )
• Positive predictive value : TP / ( TP + FP )
• Negative predictive value : TN / ( TN + FN )

Pre-operative Diagnosis
• A study of 48 patients with established or suspicious
diagnoses of colorectal cancer
• PET scan detected all lesions
• Positive and negative predective values of 90% and 100%
Abdel-Nabi H., Radiology, 1998

Lymph Node Detection
• CT scan and MRI - sensitivity of 22 to 48%, accuracy of 40 to 65% for colonic cancer
• For rectal cancer, sensitivity of 73% and accuracy of 70%
Thoeni R.F., Radiol Clin North Am, 1997
• Sensitivity of lymph node detection by PET of 29%
Abdel-Nabi H., Radiology, 1998

Colorectal Liver Metastasis
• 25% have liver metastasis at diagnosis
• Another 20% will have liver metastasis
• 30 to 40% have 5-years survival after hepatectomy
• Patient selection - anatomical resectability and no extra-
hepatic involvement

PET in Liver Metastasis
• Superiority of PET over CT in detecting liver metastasis
not eastablished
• No adequate spatial information about metastases
• The main role into detect extrahepatic involvement

Arulampalam T.H.A., 2003

a
Para-caval LNPara-aortic LNLiver

Extrahepatic Disease in Liver Metastasis
• 51 patients analyzed for resection for colorectal liver
metastasis
• PET result in 20% change of management because of
unexpected extrahepatic involvement
Ruers T.J., J Clin Oncol, 2002
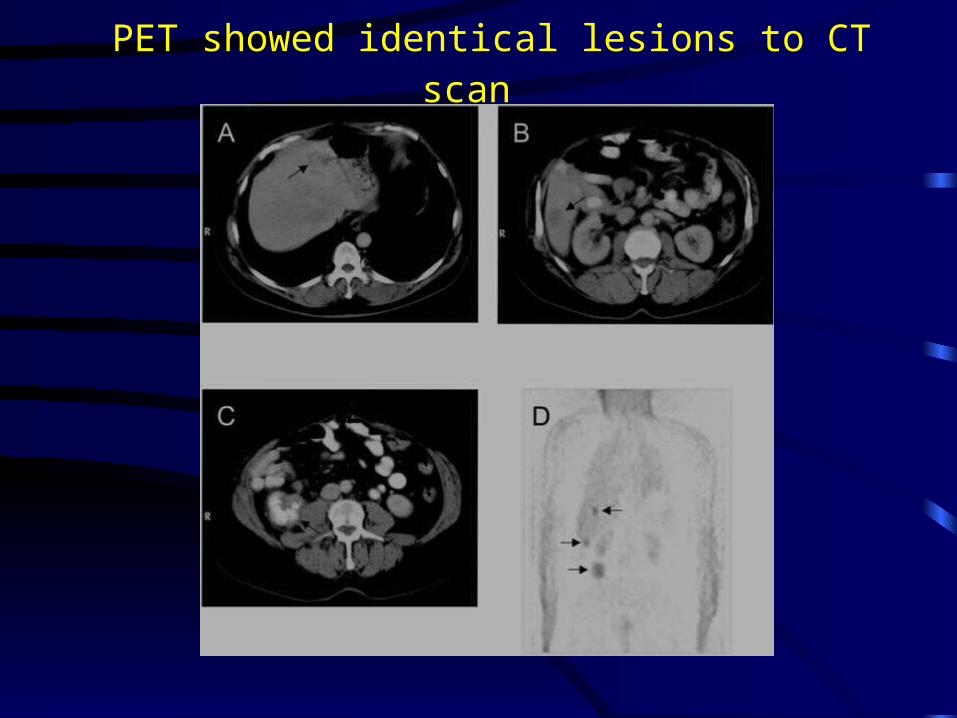
PET showed identical lesions to CT scan

Spinal metastasis
• Spinal metastasis detected by PET but not by CT
• Spinal cord compression 3 months after hepatectomy

Hepatic and Extrahepatic Lesions

PET and Liver Resectability
• 43 patients for hepatectomy for liver metastasis
• 6 patients spared of surgery due to extrahepatic disease
• Hepatectomy in 35 out of 37 patients
• 95% resectability rate of hepatic metastasis with PET in
addition to other imaging techniques
• At 3 years 77% overall and 40% disease free survival
Strasberg S.M., Ann Surg, 2000

Overall Survival

Disease Free Survival

Elevated CEA
• Investigated by conventional imaging modalities and colonoscopy - still some have negative imaging
• CEA directed laparotomy: low resectability rate of 44 to 58% because of unexpected presence of extensive disease
Minton J.P., Cancer, 1985
Martin E.W.Jr., Am J Surg, 1979

Elevated CEA
• PET for 32 patients with elevated CEA
• Histological diagnosis, serial CT and clinical follow-up as standards
• Sensitivity - 90%, specificity 92%
• Positive predicitive value 95%
• Negative predicitive value 85%
Valk P.E., Arch Surg, 1999


Elevated CEA with Normal Imaging
• 22 patients with elevated CEA and normal conventional imaging
• 17 recurrent lesions found - histological confirmation in 7, recurrence on follow up in 8, false positive in 2
• No recurrence in those with negative PET
Flanagan F.L., Ann Surg,
1999

Metastatic Disease - PET vs CT
• 41 patients had laparotomy for metastatic colorectal cancer
• All have pre-op PET and CT
• Sensitivity : liver ( 100% vs 69% ), extraheaptic ( 90% vs 52% ), abdomen ( 87% vs 61%), pelvis ( 87% vs 61%)
Johnson K., Dis Colon Rectum,
2001


Local Recurrent Disease - PET vs CT
• 70 patients with suspected locally recurrent colorectal cancer
• PET compared with CT / Colonoscopy
• Sensitivity : 90% vs 71%
• PPV and NPV: PET - 88% and 92%
CT - 79% and 79%
Whiteford M.H., Dis Colon Rectum, 2000

Arulampalam T.H.A., 2003

Monitoring Therapy of Colorectal Cancer
• Response to chemotherapy and regional therapy
monitored by PET
• FDG uptake decreased in responding lesions
• To separate responsders from non-responders
• Residual uptake help to guide further therapy

Pre Chemotherapy

Post Chemotherapy

Limitation of PET
• Detectability depends on size and degree of uptake
• False -ve in small lesion and necrotic lesions
• Low sensitivity in mucinous adenocarcinoma
• False +ve in inflammed tissue
• Usual FDG activity at gastrointestinal tract

Impact on Management
• Early detection of abnormal tissue metabolism
• Detection of tumor at usual and unexpected sites
• Avoid unnecessary surgery
• Allow earlier treatment by diagnosing recurrence earlier
• Monitor treatment response
• PET is a power imaging modality but its use needs to be refined

Conclusion
• PET is a functional imaging technique
• It detects hepatic and extrahepatic lesions, and help to
avoid unnecessay surgery by detecting extrahepatic
disease
• It detects recurrent disease in patients with elevated CEA
and negative imaging
• Its helps to monitor treatment and guide further treatment
Thank You !