aortic regurgitation in seropositive juvenile...
TRANSCRIPT
Annals of the Rheumatic Diseases, 1981, 40, 229-234
Aortic regurgitation in seropositive juvenile arthritisA. M. LEAK,' M. W. MILLAR-CRAIG,2 AND BARBARA M. ANSELL1
From the 'Juvenile Rheumatism Unit, Canadian Red Cross Memorial Hospital, Taplow, and the 2CardiologyDepartment, Northwick Park Hospital, Harrow, Middlesex
SUMMARY Seropositive juvenile chronic arthritis is a relatively uncommon form of childhoodarthritis, but it often causes severe destruction of joints associated with considerable functionaldisability. During the last 7 years lone aortic regurgitation has been seen to develop in 4 suchpatients and pursue a particularly aggressive course. Sudden deterioration occurred in 2, 1 of whomrequired urgent aortic valve replacement and 1 died while awaiting assessment. Because of this itis important to include regular cardiac appraisal as part of the routine assessment in seropositivejuvenile arthritis.
Seropositive disease accounts for somewhat less than10% of all chronic arthritis beginning under 16 yearsof age. The onset is usually about the age of 10 or11, and girls are affected much more commonlythan boys. A particular feature of this type of dis-ease is the persistence of activity and the very rapiddestruction of joints. Elbow nodules are seen in onlyabout a fifth of the cases, but when they do occurthey have a typical rheumatoid histology.' Thepurpose of this report is to draw attention to the
Accepted for publication I August 1980Correspondence to Dr B. M. Ansell, Juvenile RheumatismUnit, Canadian Red Cross Memorial Hospital, Taplow,Maidenhead, Berks SL6 OHN.
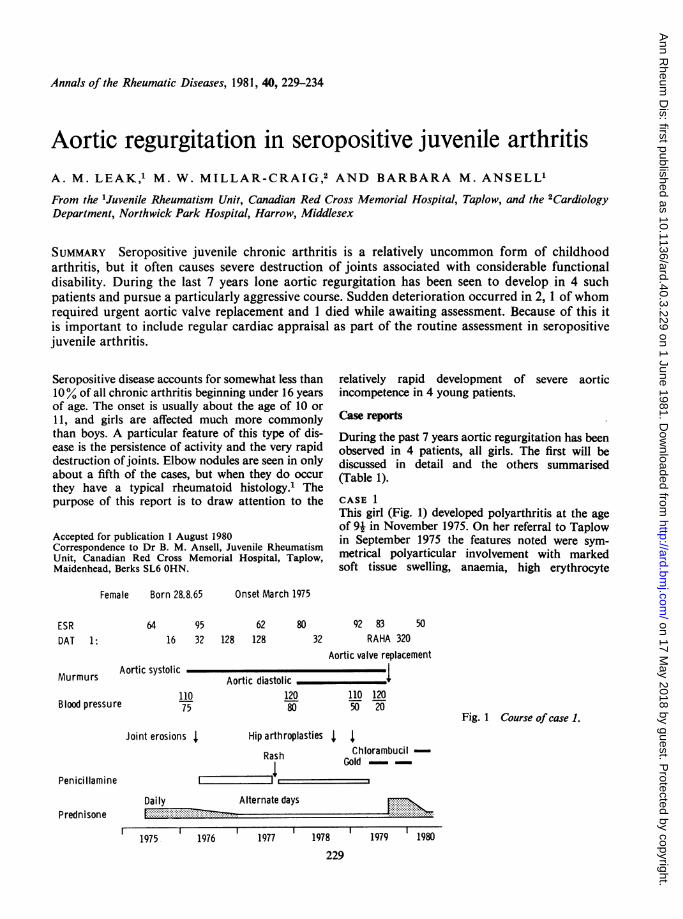
Female Born 28.8.65
ESRDAT 1:
Murmurs
Blood pressure
64 9516 32
Aortic systolic
11075
relatively rapid development of severe aorticincompetence in 4 young patients.
Case reports
During the past 7 years aortic regurgitation has beenobserved in 4 patients, all girls. The first will bediscussed in detail and the others summarised(Table 1).
CASE 1This girl (Fig. 1) developed polyarthritis at the ageof 91 in November 1975. On her referral to Taplowin September 1975 the features noted were sym-metrical polyarticular involvement with markedsoft tissue swelling, anaemia, high erythrocyte
Onset March 1975
62128 128
80 92 8332 RAHA 320
50
Aortic valve replacement
Aortic diastolic - _ _ i,120 110 12080 50 20
Fig. 1 Course of case 1.
Joint erosions X Hip arthroplasties X 4,Rash unioIUI
Gold
Daily
19761975
F. ....... Alternate... das
1977 1978 1979 1980
229
Penicillamine
Prednisone
irambucil-
Alternate days
on 17 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.40.3.229 on 1 June 1981. Dow
nloaded from
230 Leak, Millar-Craig, Ansell
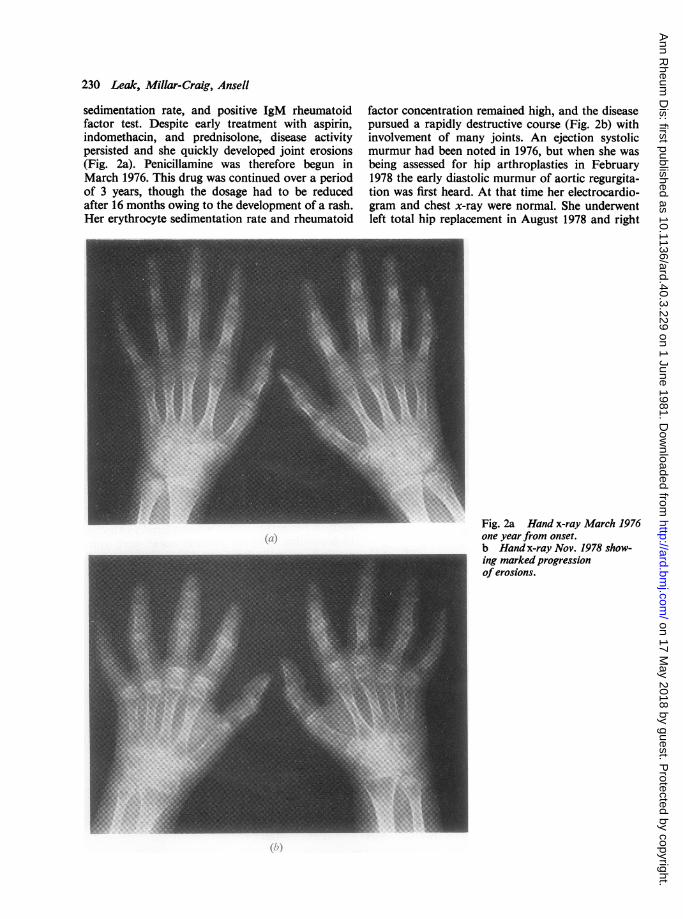
sedimentation rate, and positive IgM rheumatoidfactor test. Despite early treatment with aspirin,indomethacin, and prednisolone, disease activitypersisted and she quickly developed joint erosions(Fig. 2a). Penicillamine was therefore begun inMarch 1976. This drug was continued over a periodof 3 years, though the dosage had to be reducedafter 16 months owing to the development of a rash.Her erythrocyte sedimentation rate and rheumatoid
factor concentration remained high, and the diseasepursued a rapidly destructive course (Fig. 2b) withinvolvement of many joints. An ejection systolicmurmur had been noted in 1976, but when she wasbeing assessed for hip arthroplasties in February1978 the early diastolic murmur of aortic regurgita-tion was first heard. At that time her electrocardio-gram and chest x-ray were normal. She underwentleft total hip replacement in August 1978 and right
Fig. 2a Hand x-ray March 1976one year from onset.b Hand x-ray Nov. 1978 show-
- ~~~~~ingmarked progressionof erosions.
on 17 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.40.3.229 on 1 June 1981. Dow
nloaded from
Aortic regurgitation in seropositive juvenile arthritis 231
total hip replacement in January 1979 withoutcomplication.Two months after the latter operation she had her
first bout of chest pain. Initially a diagnosis of
Table 1 Summary of cases
Case
1 2 3 4
Age at onset ofarthritis (years) 9 10 8 8
Age systolicmurmur heard(years) 10 11 14 17
Age diastolicmurmur heard(years) 12 16 15 18
Worseningsymptoms(months) 4 2 6 Nil
Outcome 1980 Aortic valve Aortic valve Death Moderatereplacement replacement aortic
regurgit-ation
* 9.8.78. V.5.. ~~~~~~~~~~~~......~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
--.:-.......-- .... .<~~~~~~~~~~~~~~~~~~~~~~~~~~~.:.c^._.?~~~~~~~~~~~~~~~~~~~~~~~~~~... ... ... ....
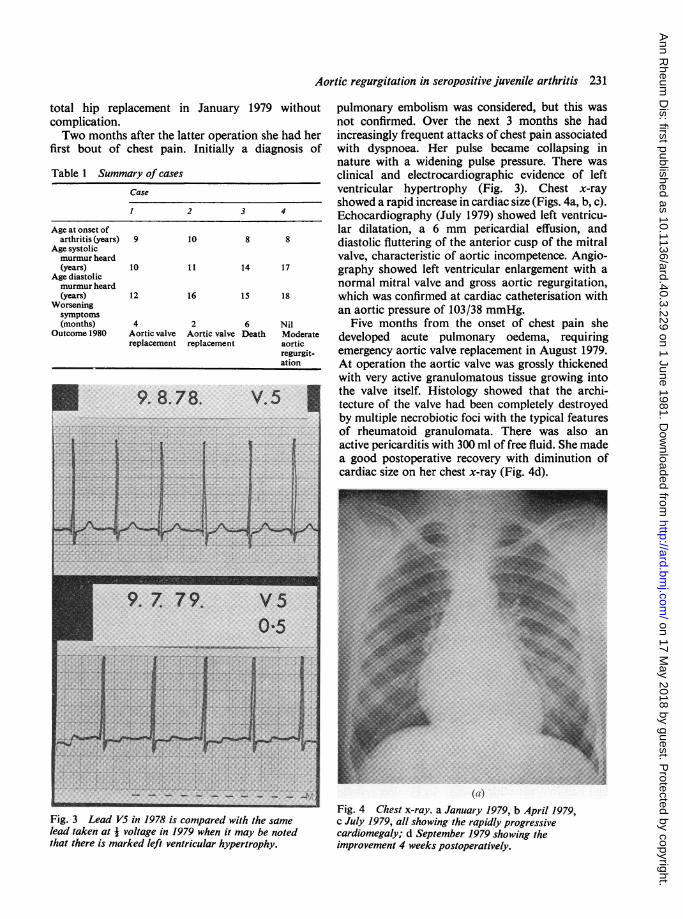
pulmonary embolism was considered, but this wasnot confirmed. Over the next 3 months she hadincreasingly frequent attacks of chest pain associatedwith dyspnoea. Her pulse became collapsing innature with a widening pulse pressure. There wasclinical and electrocardiographic evidence of leftventricular hypertrophy (Fig. 3). Chest x-rayshowed a rapid increase in cardiac size (Figs. 4a, b, c).Echocardiography (July 1979) showed left ventricu-lar dilatation, a 6 mm pericardial effusion, anddiastolic fluttering of the anterior cusp of the mitralvalve, characteristic of aortic incompetence. Angio-graphy showed left ventricular enlargement with anormal mitral valve and gross aortic regurgitation,which was confirmed at cardiac catheterisation withan aortic pressure of 103/38 mmHg.
Five months from the onset of chest pain shedeveloped acute pulmonary oedema, requiringemergency aortic valve replacement in August 1979.At operation the aortic valve was grossly thickenedwith very active granulomatous tissue growing intothe valve itself. Histology showed that the archi-tecture of the valve had been completely destroyedby multiple necrobiotic foci with the typical featuresof rheumatoid granulomata. There was also anactive pericarditis with 300 ml of free fluid. She madea good postoperative recovery with diminution ofcardiac size on her chest x-ray (Fig. 4d).
(a)Fig. 4 Chest x-ray. a January 1979, b April 1979,c July 1979, all showing the rapidly progressivecardiomegaly; d September 1979 showing theimprovement 4 weeks postoperatively.
Fig. 3 Lead V5 in 1978 is compared with the samelead taken at i voltage in 1979 when it may be notedthat there is marked left ventricular hypertrophy.
....:
on 17 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.40.3.229 on 1 June 1981. Dow
nloaded from

232 Leak, Millar-Craig, Ansell
CASE 2
This girl developed polyarticular seropositive dis-ease at the age of 10; it was associated with nodulesand nail-fold vasculitic lesions. An ejection systolicmurmur was first heard at the age of 11 when shehad a bout of chest pain thought to be due topericarditis. Aortic regurgitation was established 5years later and remained mild over the next 4 years,
with only occasional dyspnoea on exertion. Hercondition then deteriorated suddenly over 2 monthswith the development of angina, and cardiaccatheterisation confirmed severe aortic regurgitation.She underwent a successful aortic valve replacementin August 1976.
CASE 3This girl developed polyarticular seropositivearthritis at the age of 8, and despite treatment withsteroids, penicillamine, and later azathioprine, thedisease ran a severe destructive course. Aorticregurgitation was first noted at the age of 15, butshe underwent successful bilateral total hip replace-ment at the age of 17. Two years later she developedsymptoms of angina and dyspnoea, and her con-dition deteriorated over the next 6 months; whilecardiac investigations were being arranged, shecollapsed with acute pulmonary oedema and died.
CASE 4This patient developed polyarticular disease at theage of 8, which was treated with gold for 12 years,but she has had severe joint destruction requiringbilateral hip arthroplasty and a right total kneereplacement during the last year. She has hadasymptomatic aortic regurgitation for 2 years, andechocardiography in July 1979 confirmed moderateaortic regurgitation with early left ventriculardilatation. She is being carefully followed up as anoutpatient, with serial assessment of left ventricularsize using echocardiography and chest radiography.
on 17 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.40.3.229 on 1 June 1981. Dow
nloaded from

Aortic regurgitation in seropositive juvenile artlhritis 233
All these 4 girls persistently had high titres ofIgM rheumatoid factor associated with a severedestructive arthropathy requiring major jointreplacement. Three had subcutaneous nodules, and1 vasculitis, but none had episcleritis. They had allbeen treated with either gold or penicillamine forseveral years, and 3 out of 4 had had long-termsteroid therapy. In each case a systolic murmur washeard for some years before the development ofaortic incompetence. None had had acute rheumaticfever as defined by the Duckett-Jones criteria.2 Allwere assessed cardiologically and 3 of them had fullinvestigations as detailed in case 1; none had anyevidence of mitral valve involvement. Surgicalintervention was required in 2 cases owing to suddendeterioration in left ventricular function. At thistime 2 of the patients had pericarditis as well asaortic valvular disease and there was no aortic rootdilatation. At no time had there been evidence ofinfective endocarditis.
Discussion
The commonest cardiac complication in juvenilearthritis is pericarditis, which may be diagnosedclinically in 7% of all cases,3 but is more frequentlydetected by echocardiography,4 and has been foundin 45% of cases at necropsy.3 It is most common inthose children with systemic illness, who are, ofcourse, negative for IgM rheumatoid factor.Myocarditis has also been reported in this group.5The decline in the incidence of rheumatic fever hasemphasised the importance of considering othercauses of valvular disease in patients with jointsymptoms. In a necropsy study of 400 cases offunctionally severe valvular disease it was concludedthat when aortic incompetence occurs without mitralvalve disease it is not of rheumatic origin.6The concept of rheumatoid heart disease was
postulated in 1960 by Bywaters7 and has graduallyfound acceptance.8 Both specific granulomatousnodules and nonspecific lesions have been found inthe hearts of adults with rheumatoid arthritis.8 In-volvement of the pericardium, myocardium, andendocardium has been well documented,8-" but thelesions have generally been thought to be haemo-dynamically unimportant. However, nodulardeformity of a valve is known to lead to its in-competence,10 and cardiovascular disease accountsfor 25% of all deaths due to rheumatoid disease.8Seropositive juvenile arthritis resembles the adultdisease, and when valvular lesions occur in adultrheumatoid arthritis the aortic valve is the one mostcommonly affected. However, coexistent mitralvalve disease has been found in 63.6% of cases.12Post-rheumatic fever aortic regurgitation usually
remains mild for many years, and even severeregurgitation may be tolerated for a decade or morewithout symptoms.13 This is in sharp contrast tosome recently reported cases of rheumatoid arthritisand aortic regurgitation causing left ventriculardysfunction and requiring aortic valve replacement.8These patients show similarities to our juveniles. In3 of our cases valvular dysfunction lasted less than 4years before sudden deterioration: 2 required aorticvalve replacement and 1 died while awaiting assess-ment. Histology of the 2 removed valves showeddestruction of the normal architecture by rheuma-toid granulation tissue. Therapy with gold andpenicillamine is known to cause dissolution ofnodules. If healing of endocardial granulomataoccurs, retraction of the valve cusps could cause adeterioration in function. While the second of ourpatients was on penicillamine, her elbow nodulesdisappeared at a time when her cardiac functionworsened. However, in the first case active nodularlesions were obviously responsible for the de-struction of her valve, leading to severe incompe-tence. It is suggested that regular cardiac assessmentshould be carried out in such patients to look forthe development of an aortic diastolic murmur. Ifone is found it should be watched closely, since thenatural history of aortic regurgitation in sero-positive juvenile arthritis appears to be particularlyshort.
Repeated noninvasive assessment can be made byechocardiography, with which it has been shownthat measurement of the left ventricular diastolicdimension and fractional shortening are useful inpredicting deterioration and may be helpful whenconsidering the timing of surgery.'4 15 The develop-ment of left ventricular dysfunction is an indicationfor urgent surgical referral, because rapid deteriora-tion with the development of angina in a youngpatient is associated with an increased risk ofsudden death.13
We thank Dr J. Raftery, Northwick Park Hospital, Harrow,and Dr R. C. Radley Smith and Mr M. H. Yacoub, Hare-field Hospital, for their assistance in the investigation andmanagement of these patients.
References
Ansell B M. Heberden Oration, 1977. Chronic arthritis inchildhood. Ann Rheum Dis 1978; 37: 107-20.
2 Stollerman G H, Markowitz M, Taranta A, WannamakerL W, Whittemore R. Report of the Jones criteria (revised)for guidance in the diagnosis of rheumatic fever. Circu-lation 1965; 32: 664-8.
3 Lietman P S, Bywaters E G L. Pericarditis in juvenilerheumatoid arthritis. Pediatrics 1963; 32: 855-60.
4 Bernstein N, Takahashi M, Hanson V. Cardiac involve-ment in juvenile rheumatoid arthritis. J Pediatr 1974; 85:313-7.
on 17 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.40.3.229 on 1 June 1981. Dow
nloaded from

234 Leak, Millar-Craig, Ansell
5 Miller J J, French J W. Myocarditis in juvenile rheumatoidarthritis. Am J Dis Child 1977; 131: 205-209.
6 Roberts W J. Anatomically isolated aortic valvulardisease. The case against its being of rheumatic etiology.AmJ Med 1970; 49: 151-9.Bywaters E G L. The relation between heart and jointdisease. Br Heart J 1950; 12: 101-31.
8 Iveson J M I, Pomerance A. Cardiac involvement inrheumatoid disease. Clin Rheum Dis 1977; 3: 467-500.
9 Clark W S, Bauer W. Cardiac changes in rheumatoidarthritis. Ann Rheum Dis 1948; 7: 39-40.
10 Fassbender H G. In: Loewi G, trans. Pathology of Rheu-matic Diseases. Springer, 1975: 149-57.Prakash R, Atassi A, Poske R, Rosen K M. Prevalence ofpericardial effusion and mitral valve involvement inpatients with rheumatoid arthritis without cardiac
symptoms. An echocardiographic evaluation. N Engl JMed 1973; 289: 597-600.
12 Iveson J M I, Thadani U, Ionescu M, Wright V. Aorticvalve incompetence and replacement in rheumatoidarthritis. Ann Rheum Dis 1975; 34: 312-20.
13 Reichek N, Shelburne J C, Perloff J K. Clinical aspectsof rheumatic valvular disease: aortic regurgitation. ProgCardiovasc Dis 1973; 15: 518-23.
14 Henry W L, Bonow R 0, Borer J A, et al. Observationson the optimum time for operative intervention foraortic regurgitation. 1. Evaluation of the results ofaortic valve replacement in symptomatic patients.Circulation 1980; 61: 471-83.
15 O'Rourke R A, Crawford M H. Editorial: Timing ofvalve replacement in patients with chronic aorticregurgitation. Circulation 1980; 61: 493-5.
on 17 May 2018 by guest. P
rotected by copyright.http://ard.bm
j.com/
Ann R
heum D
is: first published as 10.1136/ard.40.3.229 on 1 June 1981. Dow
nloaded from