anxiety and depression management in primary...
TRANSCRIPT

Anxiety and Depression Management in Primary Care
=Supported by the Ohio Colleges of Medicine Government Resource Center with
funding from the Ohio Department of Health and the Ohio Department of Medicaid

CME Disclosure
• We have no financial relationships to disclosure
• We will be discussing off label use of Sertraline for the treatment of Generalized Anxiety Disorder

Objectives
1. Understand the formal recommendations for the evaluation and management of anxiety and depression in primary care.
2. Develop a plan to address psychiatric emergencies that may arise in primary care.
3. Implement first line strategies to address symptoms of anxiety and depression in primary care.

Depression…why and how

High prevalence http://www.nimh.nih.gov/health/statistics/prevalence/major-depression-among-adolescents.shtml
2.6 million youth ages 12-17 with an episode
of major depressive disorder in the last year
High morbidity and mortality
• Risk factor for • School problems
• Negative health outcomes
• Relational difficulties
• Substance use
• Suicide
Lewandowski. Pediatrics. 2013.
http://www.techtimes.com/articles/23794/20141230/north-carolina-teenage-girl-commits-suicide-after-posting-heartbreaking-status-on-
facebook-victim-of-bullying.htm
http://healthshire.com/93-depression-quotes/

Good practice
Youth depression screening is endorsed by several national organizations
At health supervision visits annually for ages 11-21y
In youth ages 12-18y when adequate systems are in place for diagnosis, treatment, and monitoring.
% of patients ≥12y screened for depression and if positive, with appropriate follow up

Stein. Academic Pediatrics. 2015.
Opportunities for improvement

http://www.samhsa.gov/data/sites/default/files/NSDUHmhfr2013/NSDUHmhfr2013.pdf

Ashley is a 14 year old who presents for a health supervision visit. Her mother is concerned that she’s been spending less time with friends and
family. She wonders if that’s just normal for teens. Ashley is worried that her mother might
mention her decreasing grades or tell the doctor that she thinks she’s depressed. You start
Ashley’s visit 20 minutes behind. You notice that Ashley looks nervous. Her mother pulls out a
long list of questions as you sit down…
What if your practice had implemented universal depression screening for all teens?


Ashley’s PHQ-9 score is 9
http://glad-pc.org/

Assessment
• Low, sad mood or irritability
• Loss of interest
• Thoughts about dying
• Pessimism or hopelessness
• Changes in thoughts about oneself
• Loss of self confidence
• Guilt or low-self worth, over-focus on past errors
APA. DSM-5. 2013.

Assessment • Somatic changes
• Disturbed sleep
• Disturbed appetite
• Fatigue or loss of energy
• Agitation or slowing of movement or speech
• Cognitive changes
• Trouble with memory/concentration
APA. DSM-5. 2013.

Assessment
• How long have you been feeling like this?
• Other stressors? And supports?
• Appetite and sleep?
• Drugs and alcohol?
• Thoughts of self harm or harm to others?

“Making” the diagnosis
Major depressive disorder
• 5 or more symptoms present ≥ 2 weeks (≥ 1 being low mood or decreased pleasure)
• Screeners can help identify teens at risk and clarify diagnosis
Presentations in primary care more likely to be subclinical and/or shorter in duration
APA. DSM-5. 2013.

Questions to ask • Have you ever felt so sad that you didn’t
want to be here anymore? Or wanted to die?
• Have you ever felt that you or your family would be better off if you were dead?
• Have you ever had a plan to hurt yourself?
• Have you ever hurt yourself?
• Are you thinking of hurting yourself now?
Suicide risk assessment

Increasing risk with
• Access to lethal means
• Substance use
• Family history
• Recent trauma or stress
Suicide risk assessment

Assess level of risk and respond accordingly
• Implement pre-determined office plan for mental health emergencies
• Review safety planning
• Assist with linkage to services
• Provide resources
• Make a plan to follow up with the family
Suicide risk assessment

Process Title: Mental Health Crisis Plan
Purpose: Procedure for a child who is from our office that expresses thoughts of harm to self or harm to others. Procedure Steps: PRESENT and IN OUR OFFICE: 1. The provider is to evaluate, document and make a
determination if the child is in acute mental health emergency (i.e. expressing harm to self or harm to others).
2. Referral to PIRC (Psychiatric Intake Response Center) 3. Security to be called XXX-XXXX to escort the child in a
wheelchair to the ER. 4. The provider calls the ER – Comm Center XXX-XXXX 5. Clinical staff to talk or walk down to share information with the
ER triage nurse.
BUCKEYE STATE PRIMARY CARE
Revised 1/12/2015

When to refer
• Longer duration or recurrent episodes
• Lack of response to first line treatment
• Significant impairment
• Environmental stressors
• Increasing number of comorbidities
• Use of drugs and alcohol

Cheung. Pediatrics. 2007.

Intervention Description
Psychoeducation Depression is common; often occurs in families; is treatable; is associated with physical symptoms
Problem-solving skills How can we lighten the load? consider both short term and long term goals; list and prioritize
Behavioral activation Practice healthy habits; set goals that increase enjoyment or confidence
Behavioral rehearsal What triggers mood problems? Practice new responses
Cognitive/coping skills Recognize Automatic Negative Thoughts (ANTS); practice positive self-talk; use relaxation techniques
Brief supportive counseling

Handouts • Stopping ANTS
• Family support action plan
• Self care success
• Suicide: what I should know
• Tools to manage stress (child and adolescent)
• Problem Solving
• Guided Imagery
• Progressive Muscle Relaxation
24
Depression Toolkit

Stopping Automatic Negative Thoughts(ANTS)
Put your automatic negative thoughts into your egg and forget about them. ANT species:
1. Mind reading - predicting you know that another person is thinking something negative about you without them telling you. "A negative look from someone else may mean nothing more than he or she is constipated. You don't know. You can't read minds. “
2. Fortune telling -- predicting a bad outcome to a situation before it has occurred. Your mind makes happen what
it sees. Unconsciously, predicting failure will often cause failure. For example, if you say, "I know I will fail the test," then you will likely not study hard enough and fail the test.
3. Always or never thinking - this is where you think in words like always, never, every time, or everyone. These
thoughts are overgeneralizations which can alter behavior. For example, I no a teen who asked out an attractive girl. She turned him down. He told himself that no one will ever go out with him again. This ANT prevented him from asking out anyone else for over nine months.
4. Guilt beatings - being overrun by thoughts of "I should have done... I'm bad because…. I must do better at… I
have to…). Guilt is powerful at making us feel bad. It is a lousy motivator of behavior.

Activities
Healthy Habits
Education
Relationships
Adherence

Considerations for medication
• Significant impairment or distress
• Recurrent or persistent symptoms
• Inability to access psychosocial interventions

Selective Serotonin Reuptake Inhibitors (SSRIs)
US Food and Drug Administration Indications
• Depression
– Fluoxetine: age ≥8
– Escitalopram: age ≥12
• Anxiety disorders
– Sertraline: age ≥6 for obsessive-compulsive disorder (OCD)
– Fluoxetine: age ≥7 for OCD

SSRI Starting Dose, mg
Increments, mg
Effective Dose, mg
Maximum Dose, mg
Fluoxetine 10 10-20 20 60
Sertraline 12.5-25 12.5-25 50 200
Escitalopram 5 5 10 20
Adapted from Cheung AH, Zuckerbrot RA, Jensen PS, et al. Guidelines for Adolescent Depression in Primary Care (GLAD-PC): II. Treatment and ongoing management.
Pediatrics. 2007;120(5):e1313–1326.

Medication or counseling?
TADS Team. Archives of General Psychiatry. 2007.
Com>Med>CBT
Com=Med=CBT

Anxiety…why and how

High prevalence http://www.nimh.nih.gov/health/statistics/prevalence/any-anxiety-disorder-among-children.shtml

Stein. Academic Pediatrics. 2015.
Opportunities for improvement

Excessive worry with behavioral
changes
Panic Disorder
Selective Mutism
Panic Disorder
Separation Anxiety Disorder Generalized
Anxiety Disorder
Obsessive Compulsive
Disorder
Social Anxiety Disorder
APA. DSM-5. 2013.

Miguel is a 10 year old boy who presents for a well child care visit. His mother
completes the SDQ as part of the visit. You are running behind, and your MA scores the SDQ and notices that the emotional
problems scale is elevated. She asks Miguel and his mother to complete the SCARED while they are waiting. The results are available to you as you begin the visit.


Scoring Instructions Scale Items Cut Off* Miguel’s score
Emotional problems
3, 8, 16, 24 ≥5-6 6
Conduct problems
5, 7, 12, 18, 22 ≥4-5 1
Hyperactivity 2, 10, 15, 21, 25 ≥8 4
Peer problems
6, 11, 14, 19, 23 ≥4 0
Prosocial 1, 4, 9, 17, 20 ≤6 10
Total Difficulties
Sum of all items except prosocial group
≥17-19 11
*high


Scoring Instructions
Items Score Suggestive Of
All ≥ 25 Any anxiety disorder
1, 6, 9, 12, 15, 18, 19, 22, 24, 27, 30, 34, 38
≥ 7 Panic disorder
5, 7, 14, 21, 23, 28, 33, 35, 37 ≥ 9 Generalized Anxiety Disorder
4, 8, 13, 16, 20, 25, 29, 31 ≥ 5 Separation Anxiety Disorder
3, 10, 26, 32, 39, 40, 41 ≥ 8 Social Anxiety Disorder
2, 11, 17, 36 ≥ 3 Significant School Avoidance

Miguel’s Results
Score Cut Off Suggestive Of
30 ≥ 25 Any anxiety disorder
3 ≥ 7 Panic disorder
15 ≥ 9 Generalized Anxiety Disorder
4 ≥ 5 Separation Anxiety Disorder
5 ≥ 8 Social Anxiety Disorder
1 ≥ 3 Significant School Avoidance
Assessment
• How long have you been feeling like this?
• Other stressors? And supports?
• Appetite and sleep?
• Drugs and alcohol?
• Thoughts of self harm or harm to others?

“Making” the diagnosis
Presentations in primary care more likely to be subclinical and/or shorter in duration
Generalized Anxiety Disorder • Excessive anxiety and worry that is
difficult to control and causes significant impairment or distress for >6 months
• Screeners can help identify teens at risk and clarify diagnosis

• CAMS Intervention Description
Psychoeducation Anxiety is common; often occurs in families; is treatable; is associated with physical symptoms
Problem-solving skills
How can we lighten the load? Consider both short term and long term goals; list and prioritize
Cognitive/coping skills
Recognize Automatic Negative Thoughts (ANTS); practice positive self-talk, progressive relaxation, guided imagery, deep breathing, and graded exposure
Brief supportive counseling


Worksheets
• Stopping ANTS
• Tools to manage stress (children and adolescent)
• My Fears
• My Worry Box
• Problem Solving
• Guided Imagery
• Progressive Muscle Relaxation
45
Anxiety Tool Kit
http://ohioaap.org/BMWeLearning
Anxiety Treatment in Primary Care
Online module available at:

46
• Keep a pad of paper, pencil and a box near your bed.
• At bedtime, talk about your worry with someone you love.
• Write down your worries. • Put them in your box where they can’t
bother you. • Keep your worry box in a safe place
The Worry Box

When to refer
• Longer duration or recurrent episodes
• Lack of response to first line treatment
• Significant impairment
• Environmental stressors
• Increasing number of comorbidities
• Use of drugs and alcohol

Considerations for medication
• Significant impairment or distress
• Recurrent or persistent symptoms
• Inability to access psychosocial interventions

Selective Serotonin Reuptake Inhibitors (SSRIs)
US Food and Drug Administration Indications
• Depression
– Fluoxetine (Prozac®): age ≥8
– Escitalopram (Lexapro®): age ≥12
• Anxiety disorders
– Sertraline (Zoloft®): age ≥6 for obsessive-compulsive disorder (OCD)
– Fluoxetine (Prozac®): age ≥7 for OCD
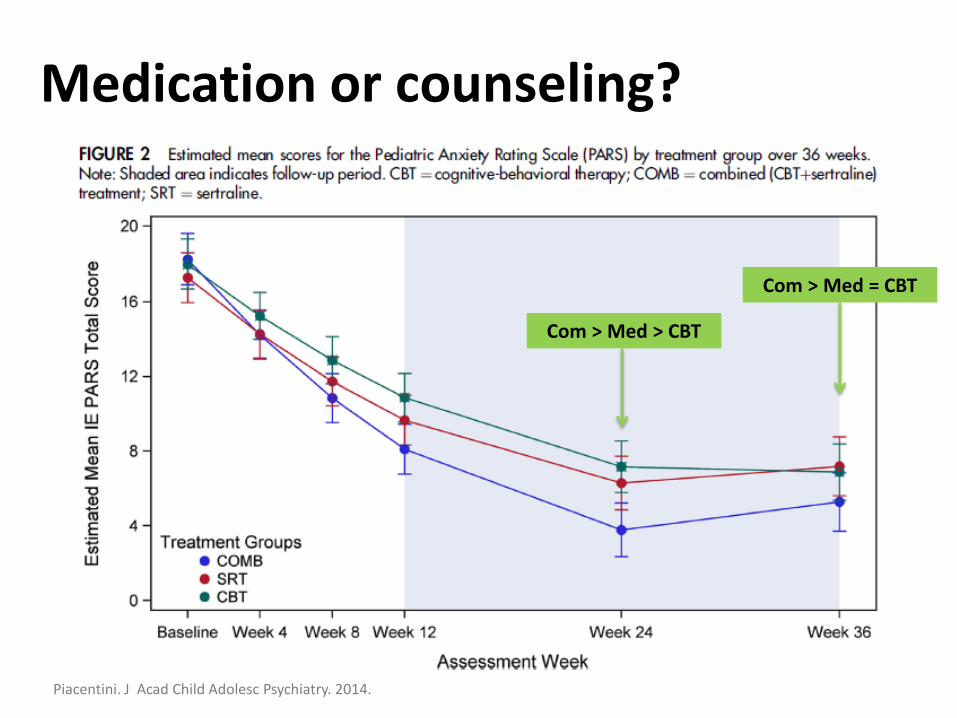
Medication or counseling?
Piacentini. J Acad Child Adolesc Psychiatry. 2014.
Com > Med = CBT
Com > Med > CBT

After obtaining additional history, you diagnose Miguel with Generalized Anxiety Disorder.
Based on the level of impairment, you refer him for counseling and decide to begin Sertraline 12.5mg daily for one week, then increasing to 25mg. You review the Anxiety Action Plan and Worry Box handouts. You make a plan to see Miguel back in 4 weeks and ask your nurse to
call the family in 2 weeks.

Summary
1. Improvements are needed regarding the care for children with anxiety and depression.
2. Straightforward and effective strategies are available to improve identification and management of anxiety and depression in primary care.