antimicrobial prescribing guidelines - … antimicrobial prescribing... · antimicrobial...
TRANSCRIPT
Document Title:
Antimicrobial Prescribing Guidelines for Adult Patients
Document Number (must be entered by Folder Holder)
CG 232
Version Number 3
Name and date and version number of previous document (if applicable):
Antimicrobial Prescribing Guidelines for Adult Patients 2012 Antibiotic Prescribing Guidelines for Adult Patients 2007
Staff involved in development
Dr Rohinton Mulla, Consultant Microbiologist Dr Abraham Teferi, Consultant Microbiologist Nisha Patel, Antimicrobial Specialist Pharmacist
Staff with overall responsibility for development, implementation and review:
Dr Rohinton Mulla, Consultant Microbiologist Nisha Patel, Antimicrobial Specialist Pharmacist
Development / this review period:
January 2015– Dec 2015
Date approved by Clinical Guidelines Committee
27th January 2016
Signed by the Chair Clinical Guidelines Committee:
Malcolm Griffiths
Date for next review:
May 2018
Date document was Equality Impact Assessed:
June 2012
Target Audience:
Trust medical staff, pharmacist, nurses
Key Words: Antimicrobials, antibiotics, infection, prophylaxis Associated Trust Documents:
The management of neutropenic sepsis in adult oncology/haematology patients Management of Clostridium difficile Management of deep seated fungal infections

Antimicrobial Prescribing Guidelines for Adult Patients
CONTENTS Link to guidelines on website Treatment
Bacterial Infections Parasitic infections Viral infections Fungal infections
Prophylaxis
Introduction Glossary and Abbreviations Contact details for advice General Information Antibiotic resistance levels tables Serum monitoring Antimicrobials available at the L & D
Prevention of infection post-splenectomy Endoscopic procedures: prophylaxis in
neutropenic patients Surgical procedures Surgical procedures in MRSA positive
patients
References
Appendix

INTRODUCTION
The aim of these guidelines is to provide appropriate advice for the rational and effective prescribing of antibiotics in order to preserve their therapeutic value.
Inappropriate prescribing may be harmful to patients, leads to the emergence of resistant strains of bacteria and is costly.
The recommendations that follow are for initial antibacterial therapy in adult patients with normal renal function. It may be necessary to review therapy once
microbiology results are available.
These guidelines have been updated to take account of emerging evidence, national guidance and local resistance patterns. Prescribers are encouraged to
follow these empirical guidelines to ensure that patients receive therapy in line with current recommendations.
These guidelines will be reviewed regularly.
FORMAT FOR RANKING EVIDENCE SUPPORTING GUIDELINES FOR ANTIBIOTCS: Level A: data derived from multiple randomised clinical trials or meta-analyses
Level B: data derived from a single randomised trial or nonrandomised studies
Level C: expert consensus opinion, case studies, or standard of care.
Please note, we have tried to produce a ranking for the level of evidence but it is not based on any standard method e.g. NICE.
I would like to thank all those who have contributed in the production of these guidelines particularly Dr Abraham Teferi, the Antimicrobial pharmacist Nisha Patel
and her pharmacy colleagues.
Rohinton Mulla

GLOSSARY AND ABBREVIATIONS IV intravenous
IM intramuscular
PR per rectum
MRSA Meticillin Resistant Staphylococcus aureus
VRE Vancomycin Resistant Enterococci
PCP Pneumocystis (jerovicii) pneumonia
HIV Human Immunodeficiency Virus
NG nasogastric
NJ naso-jejunal
PEG percutaneous enterogastrostomy
g gram
mg milligram
kg kilogram
min minute
ft foot/feet
ml millilitre
GUM Genito-Urinary Medicine
BTS British Thoracic Society
BNF British National Formulary
ESBL Extended Spectrum Beta Lactamase
CRE Carbapenamase Resistant Enterobacteriaceae
CONTACT NUMBERS FOR ADVICE
Consultant Microbiologists
Monday – Friday 9am – 5pm extension 7337/7338
Out of hours On-call via switchboard
Antimicrobial Pharmacist
Monday – Friday 9am – 5pm bleep 287
Medicines Information
Monday – Friday 9am – 5pm extension 7114 or bleep 200

GENERAL INFORMATION
Basic principles Guidance on individual drugs
Selecting a suitable oral antimicrobial formulation
Duration of use
Recommended oral alternatives to common IV antibiotics
Penicillin allergy

BASIC PRINCIPLES Microbiology samples Bacteriological samples should be taken before starting therapy wherever possible. However antibiotic therapy should never be delayed in an emergency.
Samples should be good specimens e.g. a sample of pus rather than a swab. Relevant clinical details should be given when submitting samples e.g. clinical
presentation, details of current and recent antibiotics, date of onset (important for serology). Samples should reach the laboratory as soon as possible.
Choice of Antibiotic Knowledge of the common causative pathogens is essential to choose the most appropriate antibiotic. When a bacterial pathogen is isolated from a clinical
specimen and sensitivities are known, treatment should be adjusted to use the narrowest-spectrum antibiotic. This will reduce the likelihood of Clostridium difficile
selection and of emerging bacterial resistance and other adverse effects.
Route of Administration For a significant proportion of patients, the oral route of administration will be appropriate either on initiation or after 2 to 3 days of intravenous therapy. Certain
infections e.g. severe sepsis, bacterial meningitis and neutropenic sepsis require intravenous antibiotics for the full period of treatment.
All intravenous therapy should be reviewed at 48 hours (ideally daily). A switch from IV to oral therapy should be considered as soon as it is clinically appropriate
with the exception of patients with osteomyelitis, necrotising fasciitis, septic arthritis and infections mentioned above. Refer to relevant tables for further
information.

SELECTING A SUITABLE ORAL ANTIMICROBIAL FORMULATION (START SMART THEN FOCUS) Initially when the infecting organism or the source of infection is unknown, 'broad-spectrum' antibiotics are appropriate. Once clarified (laboratory results), therapy
should be altered to a 'narrow spectrum' agent to help minimise the risk of development of antimicrobial resistance. This is based on the patient’s clinical
condition, referral to the Antimicrobial Prescribing Guidelines and Microbiology advice.
When considering a switch from the IV to oral route: Confirm that the oral route is suitable for the condition being treated.
Ensure that the oral dose is at the upper end of the oral dose range to help maximise tissue antimicrobial concentrations.
Ensure that the patient is able to swallow.
Where NG, NJ or PEG feeding is employed ensure the oral antibiotic is compatible with the feed and administration route.
This is a table illustrating the recommended oral alternatives to commonly used IV antibiotic agents. In the event of queries or special circumstances, seek advice
from the microbiologist.
Prescribers should note that the antibacterial spectrum of the orally active first generation cephalosporins cefalexin and cefradine is generally too narrow to make them appropriate oral alternatives to commonly used second generation cephalosporins used intravenously. Their use in this situation
should be avoided unless sensitivity has been established and /or they have been recommended by microbiology.

ORAL ALTERNATIVES TO IV ANTIBIOTICS
IV drug Adult dose range Oral drug Adult dose range
Amoxicillin 500mg – 1g 8 hourly Amoxicillin 500mg 8 hourly
Benzylpenicillin 1.2g 4-6 hourly Amoxicillin 500mg 8 hourly
Ceftazidime 1-2g 8 hourly Ciprofloxacin 500mg 12 hourly
Ceftriaxone 1-2g 24 hourly Seek micro advice
Cefuroxime 750mg – 1.5g 8 hourly Co-amoxiclav 625mg 8 hourly
Ciprofloxacin 400mg 12 hourly Ciprofloxacin 250 – 750mg 12 hourly
Clarithromycin 500mg 12 hourly Clarithromycin 250-500mg 12 hourly
Clindamycin 300 – 600mg 6 hourly Clindamycin 300 – 450mg 6 hourly
Co-amoxiclav 1.2g 8 hourly Co-amoxiclav 625mg 8 hourly
Erythromycin 500mg – 1g 6 hourly Erythromycin 500mg 6 hourly
Flucloxacillin 500mg – 2g 6 hourly Flucloxacillin 500mg – 1g 6 hourly
Fluconazole 200 – 400mg 24 hourly Fluconazole 200 – 400mg 24 hourly
Gentamicin 7mg/kg (max 560mg) Seek micro advice
Levofloxacin 500mg 12 – 24 hourly Levofloxacin 500mg 12 – 24 hourly
Linezolid 600mg 12 hourly Linezolid 600mg 12 hourly
Meropenem 500mg 8 hourly Seek micro advice
Metronidazole 500mg 8 hourly Metronidazole 400mg 8 hourly
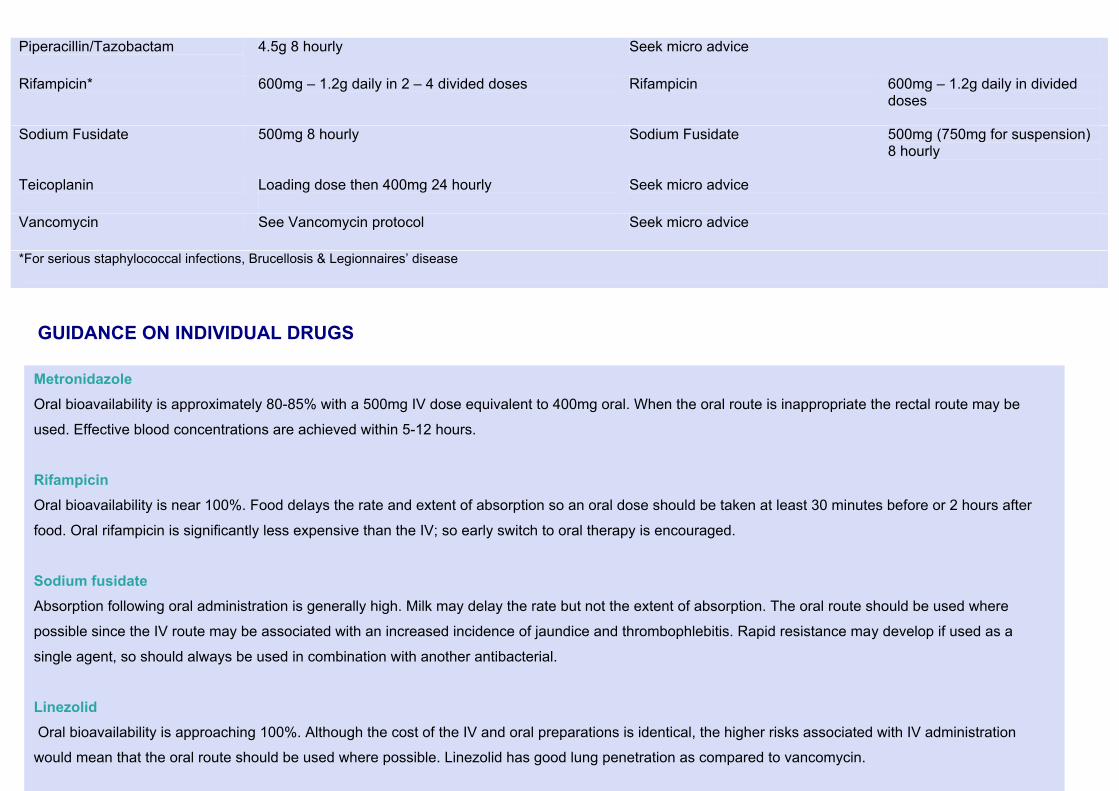
Piperacillin/Tazobactam
4.5g 8 hourly Seek micro advice
Rifampicin* 600mg – 1.2g daily in 2 – 4 divided doses Rifampicin 600mg – 1.2g daily in divided doses
Sodium Fusidate 500mg 8 hourly Sodium Fusidate 500mg (750mg for suspension) 8 hourly
Teicoplanin Loading dose then 400mg 24 hourly
Seek micro advice
Vancomycin See Vancomycin protocol Seek micro advice
*For serious staphylococcal infections, Brucellosis & Legionnaires’ disease
GUIDANCE ON INDIVIDUAL DRUGS
Metronidazole Oral bioavailability is approximately 80-85% with a 500mg IV dose equivalent to 400mg oral. When the oral route is inappropriate the rectal route may be
used. Effective blood concentrations are achieved within 5-12 hours.
Rifampicin Oral bioavailability is near 100%. Food delays the rate and extent of absorption so an oral dose should be taken at least 30 minutes before or 2 hours after
food. Oral rifampicin is significantly less expensive than the IV; so early switch to oral therapy is encouraged.
Sodium fusidate Absorption following oral administration is generally high. Milk may delay the rate but not the extent of absorption. The oral route should be used where
possible since the IV route may be associated with an increased incidence of jaundice and thrombophlebitis. Rapid resistance may develop if used as a
single agent, so should always be used in combination with another antibacterial.
Linezolid Oral bioavailability is approaching 100%. Although the cost of the IV and oral preparations is identical, the higher risks associated with IV administration
would mean that the oral route should be used where possible. Linezolid has good lung penetration as compared to vancomycin.

Amoxicillin / co-amoxiclav (amoxicillin + clavulanic acid) Amoxicillin has good oral bioavailability (unlike ampicillin). The switch from IV to oral amoxicillin should take place as soon as a patient’s clinical condition
improves. Clavulanic acid also has good oral bioavailability so co-amoxiclav should be switched from IV to oral early.
Ciprofloxacin Oral bioavailability of ciprofloxacin is approximately 70%. For treatment of gram negative sepsis recommended IV dose is 400 mg 12 hourly. Food delays the
rate but not the extent of absorption. Early switch to oral therapy is encouraged
Clindamycin Oral bioavailability of clindamycin is approximately 90%. Food delays the rate but not the extent of absorption. Early switch to oral therapy is encouraged.
Erythromycin Erythromycin should be given orally if possible to help avoid adverse reactions associated with the rate of IV infusion.
Flucloxacillin Oral bioavailability of flucloxacillin is approximately 80%. Absorption of oral Flucloxacillin is reduced in the presence of food & should be administered half to
one hour before food.
Fluconazole There is rapid absorption and widespread distribution after both oral and parenteral administration, with identical serum concentrations attained.
Vancomycin Vancomycin does not have significant absorption following oral administration; consequently the IV formulation must always be used to treat systemic
infection.

DURATION OF USE It is good clinical practice to review antibiotic prescriptions regularly. The stop date must be indicated on the prescription chart e.g. ‘5 days’ added to the drug line
on ePMA. In general therapeutic courses should be limited to 5-7 days. Inappropriately prolonged treatment is a contributing factor for the emergence of bacterial
resistance.
Unless duration is clearly identified on the prescription chart, pharmacy will suspend and leave a note for r/v after 5 days.
Prolonged treatment courses may however be needed in certain infections e.g. infective endocarditis, osteomyelitis, septic arthritis and tuberculosis, in which
case the prescriber must add an indication to the drug line on ePMA.
It is mandatory for all antibiotics prescribed to have an indication note attached to them unless an ‘ABX protocol’ has been used to prescribe the antibiotics on ePMA.

PENICILLIN ALLERGY
Diagnosis of ‘penicillin allergy’ is often accepted without obtaining a detailed history of the reaction. It has been reported that a significant
percentage of patients labelled as ‘penicillin allergic’ are not truly allergic to the drug. As a result, penicillins are unnecessarily withheld from these
patients, which may subsequently affect their clinical outcomes.
Penicillin hypersensitivity reactions (e.g. rash) occur in between 1 and 10% of exposed patients but true anaphylactic reactions (which can be fatal)
occur in less than 0.05% of treated patients.
Patients who have a vague history of symptoms or gastro-intestinal intolerance are probably not truly allergic to penicillins.
Individuals with a history of Type I allergy clinically recognisable by features of urticaria, laryngeal oedema, bronchospasm, hypotension or local
swelling within 72 hours of administration, or development of a pruritic rash (even after 72 hours) should NOT receive a penicillin.
Studies suggest that the incidence of cross-reactivity to cephalosporins in penicillin-allergic patients is around 10% but this is thought to be an
overestimate. The true incidence of cross-sensitivity is uncertain. Second and third generation cephalosporins are less likely to be associated with
cross reactivity.
Patients with no evidence of Type I allergy to penicillin may be treated with any cephalosporin or beta lactam antibiotic.
Patients with symptoms suggestive of a Type I allergy should avoid cephalosporins and other beta-lactam antibiotics.
In life threatening infections, when use of a non-cephalosporin antibiotic would be sub-optimal, consider giving, under observation, a
second or third generation cephalosporin (e.g. cefuroxime, ceftriaxone, ceftazidime). Discuss with Consultant Microbiologist.
The following are safe to use in penicillin allergic patients:
Tetracyclines (e.g. doxycycline)
Quinolones (e.g. ciprofloxacin)
Macrolides (e.g. clarithromycin)
Aminoglycosides (e.g. gentamicin)
Glycopeptides (e.g. vancomycin)
Trimethoprim
Metronidazole
Nitrofurantoin
Daptomycin (Consultant Authorisation only)
Linezolid (Consultant Authorisation only)
Tigecycline (Consultant Authorisation only)
Always identify and document the nature of the reported allergy and drug name on the medicine chart (ePMA) and in the medical notes. The
prescriber has the primary responsibility for ensuring that the allergy/sensitivity details are completed on ePMA and medical notes.

ANTIBIOTIC RESISTANCE LEVELS TABLES
Antibiotic resistance levels from urine cultures at L&D Hospital Jan – Jun 2015 inpatient samples
E. coli Enterococcus sp.
Proteus sp.
Klebsiella sp.
Pseudomonas sp.
Amoxicillin 60.6% 12.5% 40% 100% - -
Co-amoxiclav 21% - 6.2% 33.3% -
Ciprofloxacin 13.8% - 6.25% 11.9% 0%
Gentamicin 10.7% - 10.3% 12.9% 0%
Trimethoprim 39.8% - 36.3% 28.2% -
Cefalexin 12.4% 100% 9.3% 29.4% 100%
Nitrofurantoin
8.5% 12.7% - 66% -
Phosphomycin 8.1% - 22% 27.5% -

Antibiotic resistance levels from urine cultures at L&D Hospital Jan-Jun 2015 Out-patient & GP samples
E. coli Enterococcus sp.
Proteus sp.
Klebsiella sp.
Pseudomonas sp.
Amoxicillin 52% 2.8% 20% 100% - -
Co-amoxiclav 16.3% - 5.4% 15.9% -
Ciprofloxacin 8.6% - 2.4% 4.2% 2.9%
Gentamicin 6.8% - 5.4% 4.9% 1.9%
Trimethoprim 33.9% - 42% 29.8% -
Cefalexin 8.2% 100% 4.26% 13.7% 100%
Nitrofurantoin
5.6% 7.0% 100% 57% -
Phosphomycin 5.9% - 24% 22.8% -

Antibiotic resistance levels of common gram negative isolates from blood cultures at L&D Hospital during Jan-Jun 2014
E.coli (98)
E. coli ESBL (14)
P. aeruginosa (8)
K. pneumoniae (20)
P. mirabilis (7)
Amoxicillin 63.2% 100% 100% 95% 28.5%
Co-amoxiclav 19.3% 80% 100% 30.0% 0.0%
Ciprofloxacin 15.5% 92.8% 0.0% 15% 0.0%
Gentamicin 7.1% 28.5% 37.5% 10% 0.0%
Piperacillin + tazobactam
11.2% - 0.0% 20% 0.0%
Meropenem
0% 0% 25% 0% 0.0%
Cefuroxime
7.1% 100% N/A 30.0% 0.0%

Antibiotic resistance levels from other specimens at L&D Hospital Jan-Jun 2014
H. influenzae S. pneumoniae S. pyogenes S. aureus (MSSA)
S. aureus (MRSA)
Amoxicillin 32.2% - - - -
Co-amoxiclav 5.9% - - - -
Erythromycin 100% 10.2% 5.2% 14% 67%
Gentamicin - - - 0.6% 9.6
Penicillin - 2.4(R) 7.2%(I) 0.0% 68.2% -
Tetracycline - - 6.8%
Sodium Fusidate - - - 17.7% 24.7
Vancomycin N/A 0.0% 0.0% 0.0% 0.0%
- - - -
R = resistant I = intermediate MSSA = meticillin sensitive Staphylococcus aureus MRSA = meticillin resistant Staphylococcus aureus
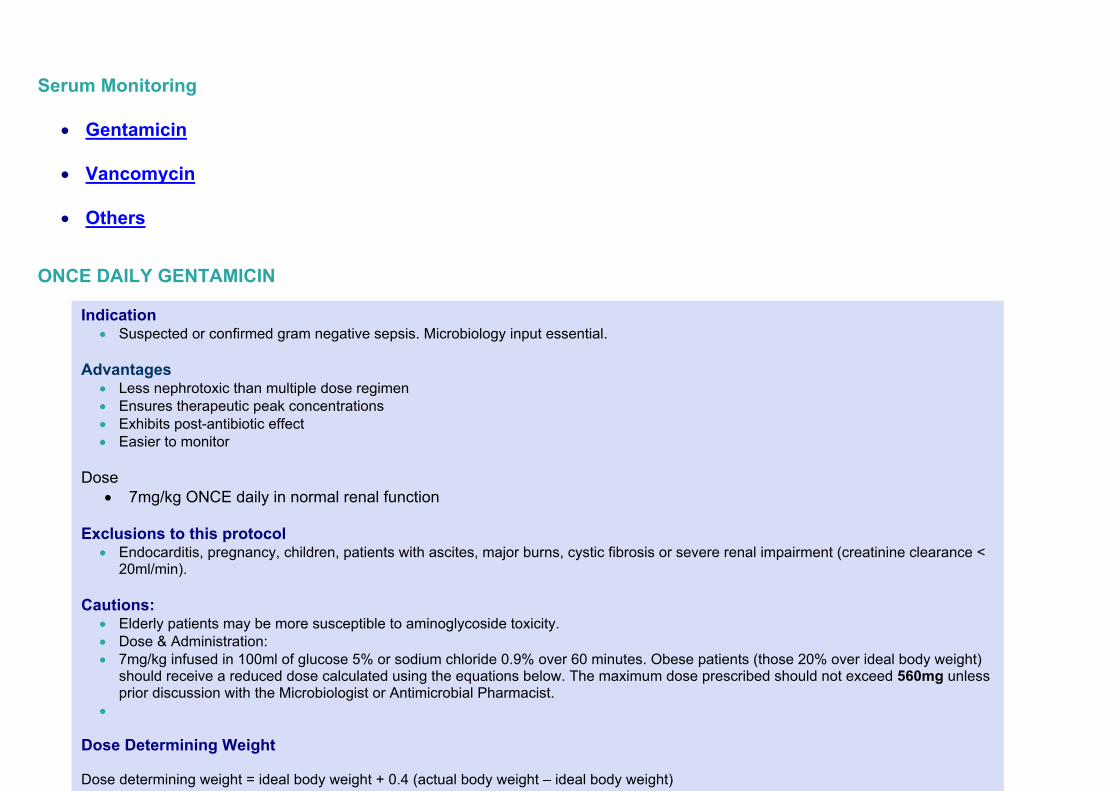
Serum Monitoring
Gentamicin Vancomycin Others
ONCE DAILY GENTAMICIN
Indication Suspected or confirmed gram negative sepsis. Microbiology input essential.
Advantages
Less nephrotoxic than multiple dose regimen Ensures therapeutic peak concentrations Exhibits post-antibiotic effect Easier to monitor
Dose
7mg/kg ONCE daily in normal renal function Exclusions to this protocol
Endocarditis, pregnancy, children, patients with ascites, major burns, cystic fibrosis or severe renal impairment (creatinine clearance < 20ml/min).
Cautions:
Elderly patients may be more susceptible to aminoglycoside toxicity. Dose & Administration: 7mg/kg infused in 100ml of glucose 5% or sodium chloride 0.9% over 60 minutes. Obese patients (those 20% over ideal body weight)
should receive a reduced dose calculated using the equations below. The maximum dose prescribed should not exceed 560mg unless prior discussion with the Microbiologist or Antimicrobial Pharmacist.
Dose Determining Weight Dose determining weight = ideal body weight + 0.4 (actual body weight – ideal body weight)

Creatinine Clearance (CrCl) CrCl = N x (140 – age) x weight (Kg) N=1.23 for males Serum creatinine (micromol./l) N=1.04 for females CrCl (ml/min)
Estimated dosing interval
>60 40-59 20-39 <20
24 hours 36 hours 48 hours Avoid once daily gentamicin
Duration of treatment Treatment must be reviewed after 5 days and discuss with the microbiologist if continuation is considered necessary. THE HARTFORD NOMOGRAM 1. If the level falls into the area designated Q24h, Q36h or Q48h, the interval should be every 24, 36 or 48 hours respectively. If the point falls on the line, choose the longer interval. 2. If the level is off the nomogram at the given time, stop scheduled therapy and obtain serial levels to determine the appropriate time of the next dose (<1mg/litre). Consider using a lower dose.
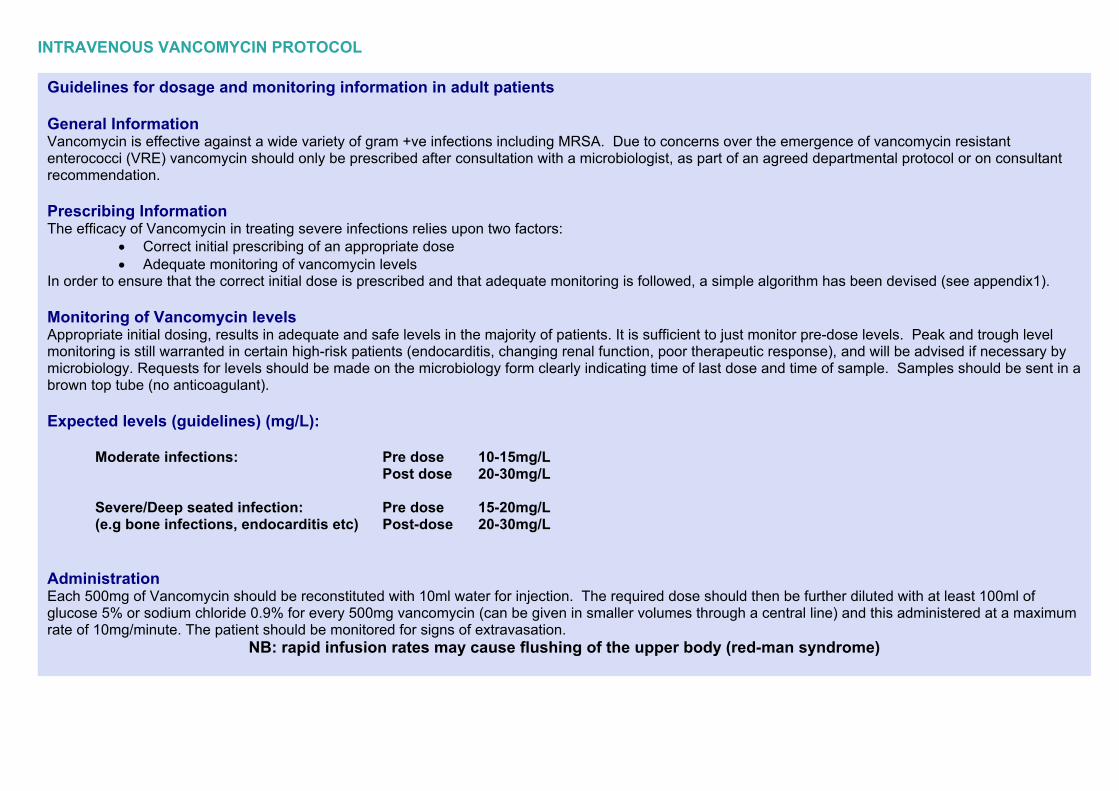
INTRAVENOUS VANCOMYCIN PROTOCOL
Guidelines for dosage and monitoring information in adult patients General Information Vancomycin is effective against a wide variety of gram +ve infections including MRSA. Due to concerns over the emergence of vancomycin resistant enterococci (VRE) vancomycin should only be prescribed after consultation with a microbiologist, as part of an agreed departmental protocol or on consultant recommendation. Prescribing Information The efficacy of Vancomycin in treating severe infections relies upon two factors:
Correct initial prescribing of an appropriate dose Adequate monitoring of vancomycin levels
In order to ensure that the correct initial dose is prescribed and that adequate monitoring is followed, a simple algorithm has been devised (see appendix1). Monitoring of Vancomycin levels Appropriate initial dosing, results in adequate and safe levels in the majority of patients. It is sufficient to just monitor pre-dose levels. Peak and trough level monitoring is still warranted in certain high-risk patients (endocarditis, changing renal function, poor therapeutic response), and will be advised if necessary by microbiology. Requests for levels should be made on the microbiology form clearly indicating time of last dose and time of sample. Samples should be sent in a brown top tube (no anticoagulant). Expected levels (guidelines) (mg/L):
Moderate infections: Pre dose 10-15mg/L Post dose 20-30mg/L Severe/Deep seated infection: Pre dose 15-20mg/L (e.g bone infections, endocarditis etc) Post-dose 20-30mg/L Administration Each 500mg of Vancomycin should be reconstituted with 10ml water for injection. The required dose should then be further diluted with at least 100ml of glucose 5% or sodium chloride 0.9% for every 500mg vancomycin (can be given in smaller volumes through a central line) and this administered at a maximum rate of 10mg/minute. The patient should be monitored for signs of extravasation.
NB: rapid infusion rates may cause flushing of the upper body (red-man syndrome)

SERUM LEVELS OF SOME OTHER ANTIBIOTICS
ANTIBIOTIC DOSE PRE-DOSE LEVEL ONE HOUR POST-DOSE LEVEL
Amikacin Once daily regime <5mg/L >50mg/L (every 6-8 days providing normal renal function)
Teicoplanin
400 mg 12 hourly 3 doses, then 400 mg
OD If over 70kg then
6mg/kg
>15 mg/L <60 mg/L
*Reference: Antimicrobial Reference Laboratory, Guidelines for users, 12th edition, 2006, Bristol.
NOTE: Levels for other antimicrobials may occasionally be required. These samples may need to be sent to other laboratories. Please contact the microbiology
department in this instance.

ANTIMICROBIALS AVAILABLE AT THE L & D A restricted antimicrobial policy is necessary in order to slow the development of resistance or because a less toxic or less expensive antibiotic is available. ANTIBACTERIAL DRUGS PENICILLINS BENZYLPENICILLIN AND PHENOXYMETHYLPENICILLIN Benzylpenicillin (Penicillin G) Phenoxymethylpenicillin (Penicillin V) PENICILLINASE-RESISTANT PENICILLINS Flucloxacillin Temocillin BROAD-SPECTRUM PENICILLINS Amoxicillin Co-amoxiclav ANTIPSEUDOMONAL PENICILLINS Piperacillin/ Tazobactam (Consultant authorisation only, or Consultant Microbiologist) CEPHALOSPORINS Due to the high association with Clostridium difficile infection these must only be prescribed in accordance with the approved indications for use listed in this anti-microbial guideline or by recommendation from the Microbiologist. Cefalexin (for UTI in pregnancy only) Ceftazidime (Consultant authorisation only, or Consultant Microbiologist for antibiotics) Ceftriaxone (must be prescribed only in accordance with the Antimicrobial guideline or after authorisation from the Consultant Microbiologist) OTHER BETA-LACTAMS Meropenem (Consultant authorisation only, or Consultant Microbiologist) Aztreonam (Consultant Microbiologist approval only) Ertapenam (Consultant Microbiologist approval only) TETRACYCLINES Demeclocycline Doxycycline Oxytetracycline Tigecycline (Consultant authorisation only, or Consultant Microbiologist)

AMINOGLYCOSIDES Amikacin (Consultant authorisation only, or Consultant Microbiologist) Gentamicin Neomycin (only topical use) Tobramycin (Consultant authorisation only, or Consultant Microbiologist) MACROLIDES Azithromycin (Consultant authorisation only, or Consultant Microbiologist) Clarithromycin Erythromycin LINCOSAMIDES Clindamycin SULPHONAMIDES & TRIMETHOPRIM Trimethoprim Trimethoprim and sulfamethoxazole (high dose used for treatment of PCP pneumonia in HIV) NITROIMIDAZOLES Metronidazole QUINOLONES These must only be prescribed in accordance with the approved indications for use listed in this antimicrobial guideline or by recommendation from the Consultant Microbiologist. Ciprofloxacin Levofloxacin URINARY ANTI-SEPTICS Nitrofurantoin Fosfomycin OTHER ANTIBACTERIALS Chloramphenicol (Consultant authorisation only, or Consultant Microbiologist) Colistin (Consultant authorisation only, or Consultant Microbiologist) Linezolid (Consultant authorisation only, or Consultant Microbiologist) Sodium fusidate Teicoplanin (Consultant authorisation only, or Consultant Microbiologist) Vancomycin Daptomycin

ANTIMYCOBACTERIAL DRUGS ANTITUBERCULOUS DRUGS Ethambutol (Consultant authorisation only, or Consultant Microbiologist) Isoniazid (Consultant authorisation only, or Consultant Microbiologist) (liquid unlicensed) Pyrazinamide (Consultant authorisation only, or Consultant Microbiologist (unlicensed) Rifampicin (Consultant authorisation only, or Consultant Microbiologist) ”Rifinah” (Consultant authorisation only, or Consultant Microbiologist) “Rifater” (Consultant authorisation only, or Consultant Microbiologist) Streptomycin (Consultant authorisation only, or Consultant Microbiologist) ANTILEPROTIC DRUGS Dapsone ANTIFUNGAL DRUGS Liposomal Amphotericin (Consultant authorisation only, or Consultant Microbiologist) Fluconazole Flucytosine (Consultant authorisation only, or Consultant Microbiologist) Griseofulvin Itraconazole (Consultant authorisation only, or Consultant) Nystatin (suspension) Terbinafine Voriconazole (Consultant authorisation only, or Consultant Microbiologist) Caspofungin (Microbiology recommendation only) Micafungin (Microbiology recommendation only) ANTIVIRAL DRUGS HERPES SIMPLEX AND VARICELLA-ZOSTER INFECTION Aciclovir Famciclovir and Valciclovir – more expensive alternatives to Aciclovir. CYTOMEGALOVIRUS INFECTIONS Foscarnet sodium (Consultant authorisation only, or Consultant Microbiologist) Ganciclovir (Consultant authorisation only, or Consultant Microbiologist) INFLUENZA Oseltamivir (NICE) (Consultant microbiologist authorisation only)

RESPIRATORY SYNCYTIAL VIRUS Palivizumab (Consultant authorisation only, or Consultant Microbiologist) Tribavirin (Consultant authorisation only, or Consultant Microbiologist) ANTIPROTOZOAL DRUGS ANTIMALARIALS Chloroquine sulphate ”Fansidar” Mefloquine Primaquine Proguanil Quinine sulphate AMOEBICIDES Metronidazole TRICHOMONACIDES Metronidazole ANTIGIARDIAL DRUGS Metronidazole DRUGS FOR PNEUMOCYSTIS PNEUMONIA Co-trimoxazole – high dose (Consultant authorisation only, or Consultant Microbiologist) Pentamidine (Consultant authorisation only, or Consultant Microbiologist) ANTHELMINTICS DRUGS FOR THREADWORMS Mebendazole Piperazine (”Pripsen”) ASCARICIDES Mebendazole Piperazine (”Pripsen”) DRUGS FOR TAPEWORM INFECTIONS

Niclosamide (unlicensed) DRUGS FOR HOOKWORMS Mebendazole SCHISTOSOMICIDES Praziquantel (unlicensed) (Consultant authorisation only, or Consultant Microbiologist) FILARICIDES All unlicensed (Consultant authorisation only, or Consultant Microbiologist) – contact Pharmacy DRUGS FOR STRONGYLOIDIASIS All unlicensed (Consultant authorisation only, or Consultant Microbiologist) – contact Pharmacy
Bacterial Infections
Skin & soft tissue
Infections in diabetic feet
Bone & joint
Central nervous system

Cardiovascular Endocarditis
Sepsis
Respiratory tract Upper
Lower
Gastrointestinal
Genital Infections & Sexually
Transmitted Diseases

Urinary tract
Miscellaneous febrile disease

SKIN AND SOFT TISSUE Infection Antibacterial therapy References, level of
evidence CELLULITIS Usually caused by group A streptococci, or Staphylococcus aureus. N.B. Spreading cellulitis requires high dose IV treatment.
Mild: Penicillin V oral 500mg 6 hourly OR Amoxicillin oral 500mg 8 hourly PLUS
Flucloxacillin oral 500mg 6hourly For 10 days Moderate to severe:
Benzyl penicillin IV 1.2 to 2.4g 4-6 hourly PLUS
Flucloxacillin IV 500mg – 1g 4-6 hourly For 10 – 14 days In penicillin allergy:
Clarithromycin IV 500mg 12 hourly If oral appropriate
Clarithromycin oral 500mg 12 hourly OR
Clindamycin IV 300-450mg 6 hourly High risk of C. difficile infection Discuss with Consultant Microbiologist For patients going home via OPAT only Teicoplanin 6mg/kg 24 hourly (consultant approval only)
SS1, SS3, SS7 A

ORBITAL CELLULITIS Seek expert advice immediately. May be caused by Staphylococcus aureus, group A streptococci, Streptococcus pneumoniae +/- anaerobes.
3rd generation cephalosporins e.g.
Cefotaxime IV 1g 8 hourly or ceftriaxone 2g 24 hourly for 7 days PLUS
Flucloxacillin IV 1 – 2g 4 hourly for 7 days PLUS
Metronidazole IV 500mg 8 hourly for 7 days In penicillin allergy:
Clindamycin IV 300-450mg 6hourly for 7 days PLUS
Ciprofloxacin IV 400mg 12 hourly for 7 days Discuss with Consultant Microbiologist
SS2, SS3, A
ERYSIPELAS Usually caused by Group A Streptococci
Initially,
Benzyl penicillin IV 1.2g 6 hourly Followed by
Amoxicillin oral 500mg 8 hourly In penicillin allergy:
Clarithromycin IV 500mg 12hourly Followed by oral clarithromycin 500mg 12 hourly
C

NECROTISING FASCIITIS A polymicrobial infection including haemolytic streptococci and anaerobes. First line for community acquired: NB/ If high suspicion of Group A strep add clindamycin 900mg – 1.2g 6 hourly First line in hospital acquired:
Seek urgent surgical opinion and Microbiology advice.
Amoxicillin IV 500mg 8 hourly PLUS
Metronidazole IV 500mg 8 hourly PLUS
Gentamicin IV 7mg/kg/day (max 560mg)
Gent dose calculator
In penicillin allergy: Clindamycin IV 900mg - 1.2g 6 hourly PLUS
Ciprofloxacin IV 400mg 12 hourly Discuss with Consultant Microbiologist
Meropenem IV 500mg 6 hourly or 1g 8 hourly PLUS
Clindamycin IV 1.2g 6 hourly
+/- Gentamicin IV 7mg/kg/day (max 560mg)
Gent dose calculator
SS3
A

ANIMAL & HUMAN BITES Usually polymicrobial, often including anaerobes. Surgical toilet is most important. Assess tetanus and rabies risk. Prophylactic antibiotics are recommended for penetrating wounds of the hands, feet, face or wounds involving joints, bone or ligaments. Also for patients at risk of serious wound infection complications e.g. diabetics, immunosuppressed patients. N.B. Extensive infected lesions may require broad-spectrum intravenous antibiotics and hospitalisation. Review human bite wounds after 24 and 48 hours.
Co-amoxiclav oral 625mg 8 hourly for 7 days In penicillin allergy:
Metronidazole oral 400mg 8hourly for 7 days PLUS
Doxycycline oral 200mg stat then 100mg daily for 7 days
SS3, SS4 A
POST-OPERATIVE WOUND INFECTION Usually caused by Staphylococcus aureus. Post operative wound collections and abscesses should be surgically drained and usually do not need antibiotics.
Flucloxacillin oral 500 – 1g 6 hourly If severe:
Flucloxacillin IV 1-2g 6 hourly In penicillin allergy:
Clarithromycin oral 500mg 12 hourly If severe give:
Clarithromycin IV 500mg – 1g 12 hourly
SS3, SS5 C

In perineal or abdominal wounds with faecal contamination:
Amoxicillin IV 500mg 8 hourly PLUS
Metronidazole IV 500mg 8 hourly PLUS
Gentamicin IV 7mg/kg/day (max 560mg)
Gent dose calculator
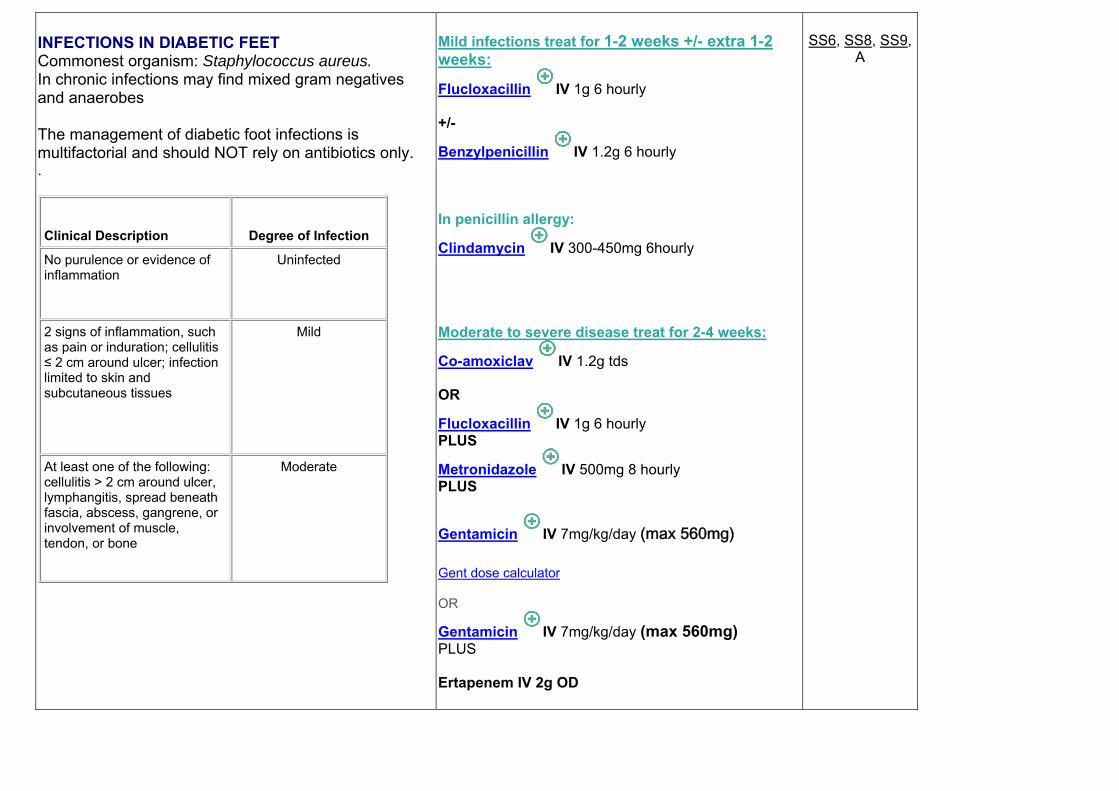
INFECTIONS IN DIABETIC FEET Commonest organism: Staphylococcus aureus. In chronic infections may find mixed gram negatives and anaerobes The management of diabetic foot infections is multifactorial and should NOT rely on antibiotics only. .
Clinical Description Degree of Infection
No purulence or evidence of inflammation
Uninfected
2 signs of inflammation, such as pain or induration; cellulitis ≤ 2 cm around ulcer; infection limited to skin and subcutaneous tissues
Mild
At least one of the following: cellulitis > 2 cm around ulcer, lymphangitis, spread beneath fascia, abscess, gangrene, or involvement of muscle, tendon, or bone
Moderate
Mild infections treat for 1-2 weeks +/- extra 1-2 weeks:
Flucloxacillin IV 1g 6 hourly +/-
Benzylpenicillin IV 1.2g 6 hourly In penicillin allergy:
Clindamycin IV 300-450mg 6hourly Moderate to severe disease treat for 2-4 weeks:
Co-amoxiclav IV 1.2g tds OR
Flucloxacillin IV 1g 6 hourly PLUS
Metronidazole IV 500mg 8 hourly PLUS
Gentamicin IV 7mg/kg/day (max 560mg)
Gent dose calculator OR
Gentamicin IV 7mg/kg/day (max 560mg) PLUS Ertapenem IV 2g OD
SS6, SS8, SS9,
A

Evidence of local infection as well as systemic toxicity, such as fever, hypotension, leukocytosis, or renal dysfunction
Severe
In renal failure patients: Meropenem (for renal dosing consult latest BNF or ward pharmacist for guidance) Osteomyelitis: duration from 5 days to >6 weeks (depending upon residual infected tissue / bone found after amputation) :
Flucloxacillin IV 500mg-1g 6 hourly PLUS
Sodium fusidate ORAL 500mg 8 hourly PLUS
Metronidazole IV 500mg 8 hourly If no improvement:
Flucloxacillin IV 500mg-1g 6 hourly PLUS
Sodium fusidate ORAL 500mg 8 hourly PLUS
Ciprofloxacin IV 400mg 12 hourly Discuss with Consultant Microbiologist Review treatment once culture/sensitivity results available. If patient known to be MRSA positive: Or if penicillin allergic: Vancomycin or Teicoplanin instead of Flucloxacillin. Linezolid is an alternative gram positive antibiotic with the added advantage of good oral bio-availability.

BONE AND JOINT
Infection Antibacterial therapy References,
level of evidence
ACUTE OSTEOMYELITIS Always discuss with Microbiologist Commonest causative organism in adults is Staphylococcus aureus. Treatment duration should be 4 – 6 weeks but change to oral when appropriate (at least 2 weeks of intravenous therapy is needed).
Flucloxacillin IV 1-2g 6 hourly PLUS
Sodium fusidate oral 500mg 8- hourly Penicillin allergy:
Vancomycin IV or Teicoplanin IV (discuss with Consultant microbiologist)
BJ1, BJ2, BJ3, BJ4, BJ5 A
SEPTIC ARTHRITIS Adults No risk factors for atypical organisms:
Flucloxacillin IV 1-2 g 6 hourly In Penicillin allergy:
Vancomycin IV or Teicoplanin IV Discuss with Consultant Microbiologist
If Neisseria gonorrhoea or Neisseria meningitides is suspected
Ceftriaxone IV 1-2g once daily

Infections in prosthetic joints can be caused by a variety of organisms among which Coagulase negative staphylococci are common Once sensitivities are confirmed deescalate antibiotics to narrow spectrum
Vancomycin IV or Teicoplanin IV PLUS
Ciprofloxacin Discuss with Consultant Microbiologist
High risk of Gram negative sepsis: (Elderly, frail, recurrent UTI, and recent abdominal surgery)
Flucloxacillin IV 1-2 g 6 hourly PLUS
Ciprofloxacin IV 400mg 12 hourly In Penicillin allergy:
Teicoplanin IV PLUS
Ciprofloxacin IV 400mg 12 hourly
MRSA risk (known MRSA, recent inpatient, nursing home resident, leg ulcers or catheters, or other risk factors determined locally)
Vancomycin IV (see vancomycin protocol) PLUS
Rifampicin IV 600mg-1.2g in 2 divided doses.
IV drug users
Discuss with Consultant Microbiologist
ITU patients, known colonisation of other organs (i.e. cystic fibrosis)
Discuss with Consultant Microbiologist

CENTRAL NERVOUS SYSTEM INFECTIONS
Infection Antibacterial therapy References, level of evidence
CNS SHUNT INFECTIONS
Expert advice needed. Contact microbiologist and neurosurgical specialist.
ENCEPHALITIS Seek specialist advise Common causative organisms:
Herpes simplex
Aciclovir IV 10mg/kg 8 hourly 3 weeks Use IBW to calculate dose for obese patients Varicella zoster
Aciclovir IV 10mg/kg 8 hourly 3 weeks Use IBW to calculate dose for obese patients Cytomegalovirus in immunocompromised patients Discuss with Consultant Microbiologist
Ganciclovir IV 5mg/kg 12 hourly 14-21 days PLUS
Foscarnet IV 40-60 mg/kg 8 hourly 2-3 weeks
CNS2, A CNS7, A CNS8, A CNS9, A

MENINGITIS Neisseria meningitidis is the most common pathogen causing bacterial meningitis. Streptococcus pneumoniae is common at extremes of age. Meningitis due to H. influenzae is very uncommon in developed countries after the introduction of Hib vaccine Review treatment once sensitivities known. If resistance to penicillin or cephalosporin antibiotics is expected i.e. history of recent travel to certain foreign countries (e.g. Spain, South Africa) initial treatment should include a cephalosporin + vancomycin + rifampicin. Modify treatment once sensitivities are available.
Notify CCDC
Ceftriaxone IV 2g 12 hourly Duration: Meningococcal: 7 days Pneumococcal: 14 days If penicillin resistant Streptococcus pneumoniae is suspected
Ceftriaxone IV 2g 12 hourly PLUS
Vancomycin IV 1 to 1.5 g 12 hourly PLUS
Rifampicin IV/PO 0.6-1.2g daily in 2-4 divided doses In penicillin allergy:
Chloramphenicol IV 50-100mg/kg daily in 4 divided doses
CNS3, B CNS4, A CNS5, A CNS8, A CNS 10, A
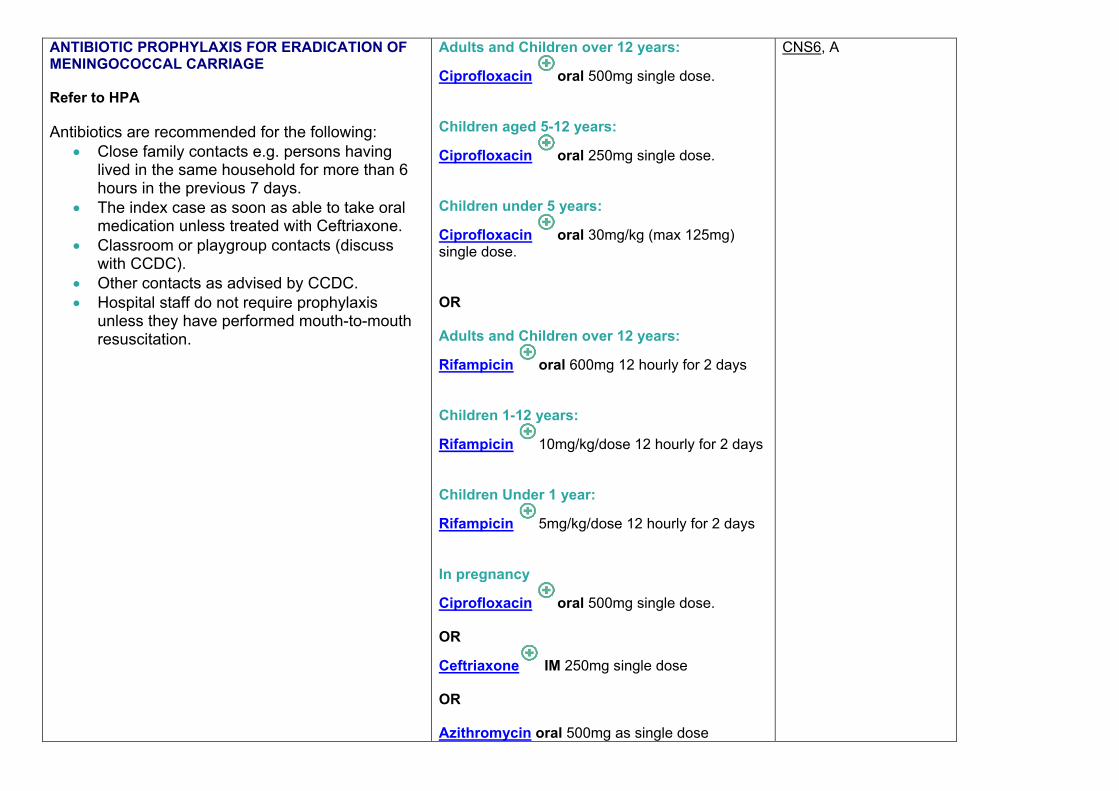
ANTIBIOTIC PROPHYLAXIS FOR ERADICATION OF MENINGOCOCCAL CARRIAGE Refer to HPA Antibiotics are recommended for the following:
Close family contacts e.g. persons having lived in the same household for more than 6 hours in the previous 7 days.
The index case as soon as able to take oral medication unless treated with Ceftriaxone.
Classroom or playgroup contacts (discuss with CCDC).
Other contacts as advised by CCDC. Hospital staff do not require prophylaxis
unless they have performed mouth-to-mouth resuscitation.
Adults and Children over 12 years:
Ciprofloxacin oral 500mg single dose. Children aged 5-12 years:
Ciprofloxacin oral 250mg single dose. Children under 5 years:
Ciprofloxacin oral 30mg/kg (max 125mg) single dose. OR Adults and Children over 12 years:
Rifampicin oral 600mg 12 hourly for 2 days Children 1-12 years:
Rifampicin 10mg/kg/dose 12 hourly for 2 days Children Under 1 year:
Rifampicin 5mg/kg/dose 12 hourly for 2 days In pregnancy
Ciprofloxacin oral 500mg single dose. OR
Ceftriaxone IM 250mg single dose OR Azithromycin oral 500mg as single dose
CNS6, A
CARDIOVASCULAR INFECTIONS - endocarditis ALL PATIENTS MUST BE DISCUSSED WITH CONSULTANT MICROBIOLOGIST AND CARDIOLOGY CONSULTANT Infective endocarditis may present as an acute rapidly progressing infection or as a sub-acute or chronic disease with low-grade fever. In acutely unwell patients with suspected infective endocarditis, two sets of blood cultures should be taken at different times within 1 hour of commencing empirical antimicrobial therapy. For the purposes of these guidelines, treatment recommendations has been split into those for initial empirical treatment and for when the causative organism has been identified. This has been further split into native valve endocarditis (NVE) and for prosthetic valve endocarditis (PVE). PVE includes all prosthetic valves, annuloplasty rings, intracardiac patches and shunts. Fungal endocarditis is a specialist area and where suspected must be discussed with the Consultant Microbiologist. The following summary for the treatment of endocarditis is based on the British Society for Antimicrobial Chemotherapy guidelines. Prescribers may use the following summary for guidance but are advised to read the BSAC guidelines for more detailed information. The BSAC guidelines are: Gould F K et al. Guidelines for the antibiotic treatment of endocarditis in adults: report of the Working Party of the British Society for Antimicrobial Chemotherapy. J. Antimicrobial Chemotherapy 2012; 67: 269-289 Available at: http://jac.oxfordjournals.org/content/early/2011/11/14/jac.dkr450.full.pdf+html
Empirical Treatment Native Valve Prosthetic Valve
Causative organism known Native Valve Prosthetic Valve

CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
evidence EMPIRICAL TREATMENT (before causative organism known) Native Valve Endocarditis Initial Antibacterial therapy
Acute presentation
Vancomycin IV 1g 12 hourly PLUS
Gentamicin IV 1mg/kg 12 hourly Acute presentation with risk factors for multiresistant enterobacteriaceae, Pseudomonas etc…
Vancomycin IV 1g 12 hourly PLUS
Meropenem IV 2g 8 hourly Long onset (indolent)
Amoxicillin IV 2g 4 hourly PLUS
Gentamicin IV 1mg/kg 8 hourly If allergic to penicillin
Vancomycin IV 1g 12 hourly PLUS
Gentamicin IV 1mg/kg 12 hourly
CV1, CV2, CV3, A

CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
evidence EMPIRICAL TREATMENT (before causative organism known) Prosthetic Valve Endocarditis Initial Antibacterial therapy Regardless of <1 year or >1 year after surgery
Vancomycin IV 1g 12 hourly PLUS Gentamicin IV 1mg/kg 12 hourly PLUS Rifampicin oral/IV 300-600mg 12 hourly
CV1, CV2, CV3, A
CARDIOVASCULAR INFECTIONS - endocarditis Native Valve Endocarditis
Causative organism known Staphylococcal Streptococcal Enterococcal HACEK organism: - Haemophilus species - Acintobacillus species - Cardiobacterium species - Eikenella species - Kingella species

CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
evidence STAPHYLOCOCCI (S.AUREUS AND COAG NEGATIVE STAPH Native Valve Endocarditis
Staphylococcal species: Flucloxacillin IV 2g 4-6 hourly for at least 4 weeks (if < 85kg body weight: use 2g 6 hourly) (if > 85kg body weight: use 2g 4 hourly) If allergic to penicillin Vancomycin IV 1g 12 hourly for at least 4 weeks PLUS Rifampicin oral/IV 300-600mg 12 hourly for at least 4 weeks MRSA (Vanc sensitive) Vancomycin IV 1g 12 hourly for at least 4 weeks PLUS Rifampicin oral/IV 300-600mg 12 hourly for at least 4 weeks MRSA (Vanc resistant) Daptomycin IV 6mg/kg for at least 4 weeks PLUS Rifampicin oral/IV 300-600mg 12 hourly for at least 4 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 4 weeks
CV1, A

CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
evidence STREPTOCOCCI Native Valve Endocarditis
Streptococcal species (fully penicillin sensitive, MIC < 0.125mg/L): Benzylpenicillin IV 1.2g 4 hourly for 4-6 weeks OR Ceftriaxone IV 2g OD IV/IM for 4-6 weeks (High C. Diff risk) OR Benzylpenicillin IV 1.2g 4 hourly for 2 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 2 weeks OR Ceftriaxone IV 2g OD IV/IM for 2 weeks (High C. Diff risk) PLUS Gentamicin IV 1mg/kg 12 hourly for 2 weeks Streptococcal species (intermediate penicillin sensitivity, MIC >0.125 - ≤0.5mg/L): Benzylpenicillin IV 2.4g 4 hourly for 4-6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 2 weeks Abiotrophia and Granulicatella species: Benzylpenicillin IV 2.4g 4 hourly for 4-6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 4-6 weeks
CV1, A
Streptococcal species (penicillin resistant) Or if allergic to penicillin: Vancomycin IV 1g 12 hourly for at least 4-6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 2 weeks OR Teicoplanin IV 10mg/kg BD for 2 doses then OD for 4-6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 2 weeks

CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
evidence ENTEROCOCCI Native Valve Endocarditis
Enterococcal species (penicillin sensitive): Amoxicillin IV 2g 4 hourly for 4-6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 4-6 weeks OR If Streptococcus bovis: Benzylpenicillin IV 2.4g 4 hourly for 4-6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 4-6 weeks Enterococcal species (penicillin sensitive but gentamicin resistant): Amoxicillin IV 2g 4 hourly for ≥6 weeks Enterococcal species (penicillin resistant) Or if allergic to penicillin: Vancomycin IV 1g 12 hourly for at least 4-6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 4-6 weeks OR Teicoplanin IV 10mg/kg BD for 2 doses then OD for 4-6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 4-6 weeks
CV1, A

CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
evidence HACEK Native Valve Endocarditis Haemophilus species Acintobacillus species Cardiobacterium species Eikenella species Kingella species
Amoxicillin IV 2g 4 hourly for 4 weeks OR Ceftriaxone IV 2g OD IV/IM for 4 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 2 weeks OR Ciprofloxacin IV 400mg 12 hourly for 4 weeks
CV1, A

CARDIOVASCULAR INFECTIONS - endocarditis Prosthetic Valve Endocarditis
Causative organism known Staphylococcal Streptococcal Enterococcal HACEK organism: - Haemophilus species - Acintobacillus species - Cardiobacterium species - Eikenella species - Kingella species
CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
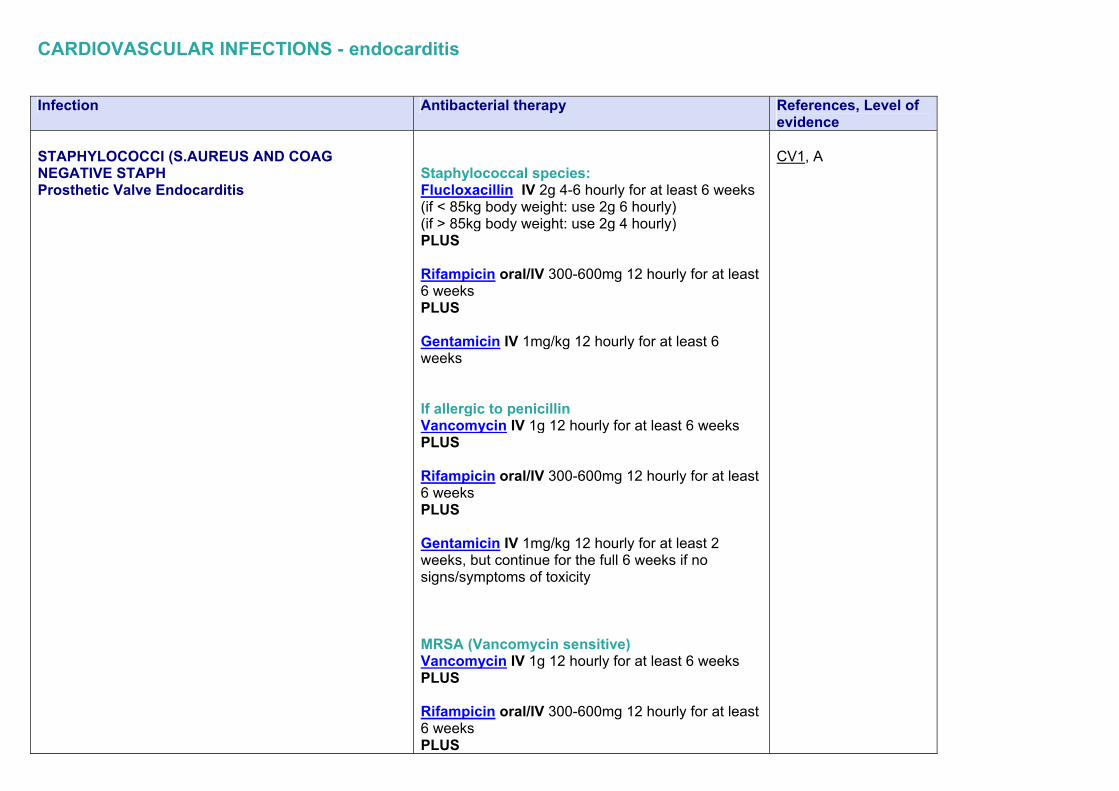
evidence STAPHYLOCOCCI (S.AUREUS AND COAG NEGATIVE STAPH Prosthetic Valve Endocarditis
Staphylococcal species: Flucloxacillin IV 2g 4-6 hourly for at least 6 weeks (if < 85kg body weight: use 2g 6 hourly) (if > 85kg body weight: use 2g 4 hourly) PLUS Rifampicin oral/IV 300-600mg 12 hourly for at least 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 6 weeks If allergic to penicillin Vancomycin IV 1g 12 hourly for at least 6 weeks PLUS Rifampicin oral/IV 300-600mg 12 hourly for at least 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 2 weeks, but continue for the full 6 weeks if no signs/symptoms of toxicity MRSA (Vancomycin sensitive) Vancomycin IV 1g 12 hourly for at least 6 weeks PLUS Rifampicin oral/IV 300-600mg 12 hourly for at least 6 weeks PLUS
CV1, A

Gentamicin IV 1mg/kg 12 hourly for at least 2 weeks, but continue for the full 6 weeks if no signs/symptoms of toxicity MRSA (Vancomycin resistant) Daptomycin IV 6mg/kg for at least 6 weeks PLUS Rifampicin oral/IV 300-600mg 12 hourly for at least 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 2 weeks, but continue for the full 6 weeks if no signs/symptoms of toxicity

CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
evidence STREPTOCOCCI Prosthetic Valve Endocarditis
Streptococcal species (fully penicillin sensitive, MIC < 0.125mg/L): Benzylpenicillin IV 1.2g 4 hourly for 6 weeks OR Ceftriaxone IV 2g OD IV/IM for 6 weeks (High C. Diff risk) Streptococcal species (intermediate penicillin sensitivity, MIC >0.125 - ≤0.5mg/L): Benzylpenicillin IV 2.4g 4 hourly for 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 2 weeks Abiotrophia and Granulicatella species: Benzylpenicillin IV 2.4g 4 hourly for 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 6 weeks Streptococcal species (penicillin resistant) Or if allergic to penicillin: Vancomycin IV 1g 12 hourly for at least 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 2 weeks
CV1, A

OR Teicoplanin IV 10mg/kg BD for 2 doses then OD for 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 2 weeks
CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
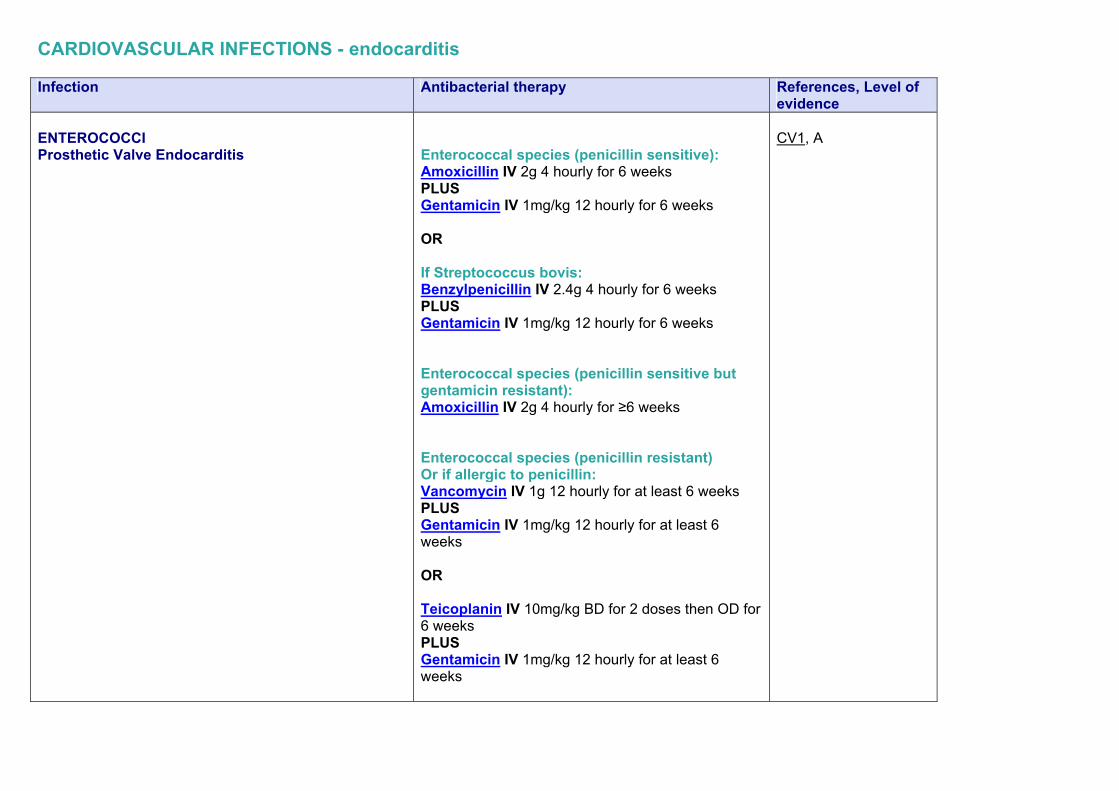
evidence ENTEROCOCCI Prosthetic Valve Endocarditis
Enterococcal species (penicillin sensitive): Amoxicillin IV 2g 4 hourly for 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 6 weeks OR If Streptococcus bovis: Benzylpenicillin IV 2.4g 4 hourly for 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 6 weeks Enterococcal species (penicillin sensitive but gentamicin resistant): Amoxicillin IV 2g 4 hourly for ≥6 weeks Enterococcal species (penicillin resistant) Or if allergic to penicillin: Vancomycin IV 1g 12 hourly for at least 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 6 weeks OR Teicoplanin IV 10mg/kg BD for 2 doses then OD for 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for at least 6 weeks
CV1, A

CARDIOVASCULAR INFECTIONS - endocarditis Infection Antibacterial therapy References, Level of
evidence HACEK Prosthetic Valve Endocarditis Haemophilus species Acintobacillus species Cardiobacterium species Eikenella species Kingella species
Amoxicillin IV 2g 4 hourly for 6 weeks OR Ceftriaxone IV 2g OD IV/IM for 6 weeks PLUS Gentamicin IV 1mg/kg 12 hourly for 2 weeks OR Ciprofloxacin IV 400mg 12 hourly for 6 weeks
CV1, A

SEPSIS The successful treatment of severe infections depends upon early recognition of sepsis, rapid laboratory investigations, and early goal directed therapy. Antibiotics play an important role in a symphony of actions, which if performed in a timely fashion can improve survival. Very often the source of the infection may be unclear. Even when the physician has a good idea regarding the source a major confounder is the type of organisms and their antibiotic sensitivity. Empirical treatment choice:
Should be “broad spectrum” May include a combination of 2 or more agents Should be commenced within 1 hour of initial assessment
When deciding on choice of agents please consider
The patient’s recent microbiology results if available Colonisation status: Any multi-resistant organisms like MRSA, GRE or ESBL producing E.coli and Klebsiella spp History of travel
As soon as results of blood cultures, urines, CSF and wound swabs etc. are available (usually 48-72 hours) antibiotic treatment should be modified.

Infection Antibacterial therapy References, level of evidence
Treat according to the source of sepsis. In severe infection or penicillin allergy Discuss with Consultant Microbiologist UNKNOWN ORIGIN OR ASSOCIATED WITH ALIMENTARY TRACT, BILIARY TRACTS OR THE PELVIS:
Piperacillin/tazobactam IV 4.5g 8 hourly PLUS
Gentamicin IV 7mg/kg/day (max 560mg)
Gent dose calculator PLUS
Metronidazole IV 500mg 8 hourly
C

SOFT TISSUE / SKIN:
Benzyl penicillin IV 2.4g 4-6 hourly PLUS
Flucloxacillin IV 2g 6 hourly If MRSA is suspected:
Vancomycin IV 1g 12 hourly OR
Linezolid IV 600mg 12 hourly OR
Tigecycline IV 100mg initially then 50mg IV once daily
URINARY TRACT:
Co-amoxiclav IV 1.2g 8 hourly PLUS
Gentamicin IV 7mg/kg/day (max 560mg)
Gent dose calculator
IMMUNOCOMPROMISED PATIENTS: (NEUTROPENIC SEPSIS)
Refer to ‘Guidelines for the Management of Emergency Admission for the Immunocompromised Patient

RESPIRATORY TRACT – UPPER Infection Antibacterial therapy References, level of
evidence
ACUTE PHARYNGITIS Most cases are viral. β-haemolytic streptococci of the Lancefield group A are responsible for the majority of bacterial infections.
Penicillin V oral 500mg 6hourly 7-10 days In penicillin allergy:
Clarithromycin oral 500mg 12 hourly 5-10 days or 250mg 6hourly 5-10 days
RT5, RT6 A
ACUTE EPIGLOTTITIS Medical emergency with a HIGH risk of morbidity and mortality. In adults, the most common organisms that cause acute epiglottitis are Haemophilus influenzae (25%), followed by H parainfluenzae, Streptococcus pneumoniae, and group A streptococci. Less common infectious etiologies include other bacteria (eg, Staphylococcus aureus, mycobacteria, Bacteroides melaninogenicus, Enterobacter cloacae, Escherichia coli, Fusobacterium necrophorum, Klebsiella pneumoniae, Neisseria meningitidis, Pasteurella multocida), herpes simplex virus (HSV), other viruses, infectious mononucleosis, Candida (in immunocompromised patients), and Aspergillus (in immunocompromised patients).
Ceftriaxone IV 2g once daily for 7 days In penicillin allergy:
Chloramphenicol IV 12.5mg/kg every 6 hours for 7 days
RT1, RT13 A

ACUTE OTITIS MEDIA Often viral and resolves without treatment. Common bacterial pathogens are S.pneumoniae, H.influenzae and M.catarrhalis.
First line:
Amoxicillin oral 500mg 8 hourly 5days Second line:
Co-amoxiclav oral 625mg 8 hourly 5 days In penicillin allergy:
Clarithromycin oral 500mg 12 hourly 5 days
RT2, RT6 B
OTITIS EXTERNA If infection is present this is usually treated topically. In severe cases systemic treatment may be required. Treat according to result of microbiological investigations
Gentamicin 0.3% ear drops Apply 2-3 drops 3 – 4 times daily and at night For Pseudomonas aeruginosa:
Ciprofloxacin oral 500mg 12 hourly 7 days For Staphylococcus aureus:
Flucloxacillin oral 500mg 6 hourly 7 days Or
Clarithromycin oral 500mg 12 hourly for 7 days For Streptococcus pyogenes:
Amoxicillin oral 500mg 8 hourly 7 days
RT1, RT12 A

ACUTE SINUSITIS Often viral and may not require antibiotics and will usually improve without antibiotics within 2 weeks..Treat if nasal pus and severe symptoms persists 10 days or worse at 7 days. Causative organisms include: S.pneumoniae, H.influenzae and M.catarrhalis.
First line:
Amoxicillin oral 500mg 8 hourly 7 days OR
Doxycycline oral 200mg stat, followed by 100mg OD for a total of 7 days Second line: (commence if no improvement after 48 hours)
Co-amoxiclav oral 625mg 8 hourly 7 days In penicillin allergy:
Clarithromycin oral 500mg 12 hourly 7 days OR
Doxycycline oral 200mg stat, followed by 100mg OD for a total of 7
RT3, RT4, RT6 A

RESPIRATORY TRACT – LOWER Infection Antibacterial therapy References, level of
evidence ACUTE EXACERBATION OF COPD Most common pathogens are H.influenzae, S.pneumoniae and M.catarrhalis.
First line:
Amoxicillin oral 500mg 8 hourly 7-14 days Second line & penicillin allergy
Doxycycline oral 200mg stat then 100mg daily for a total of 7 days OR Levofloxacin oral 500mg 12 hourly for 7 days SEVERE disease:
Co-amoxiclav IV 1.2g 8 hourly for 7 days PLUS
Clarithromycin IV 500mg 12 hourly for 7 days
RT11, C
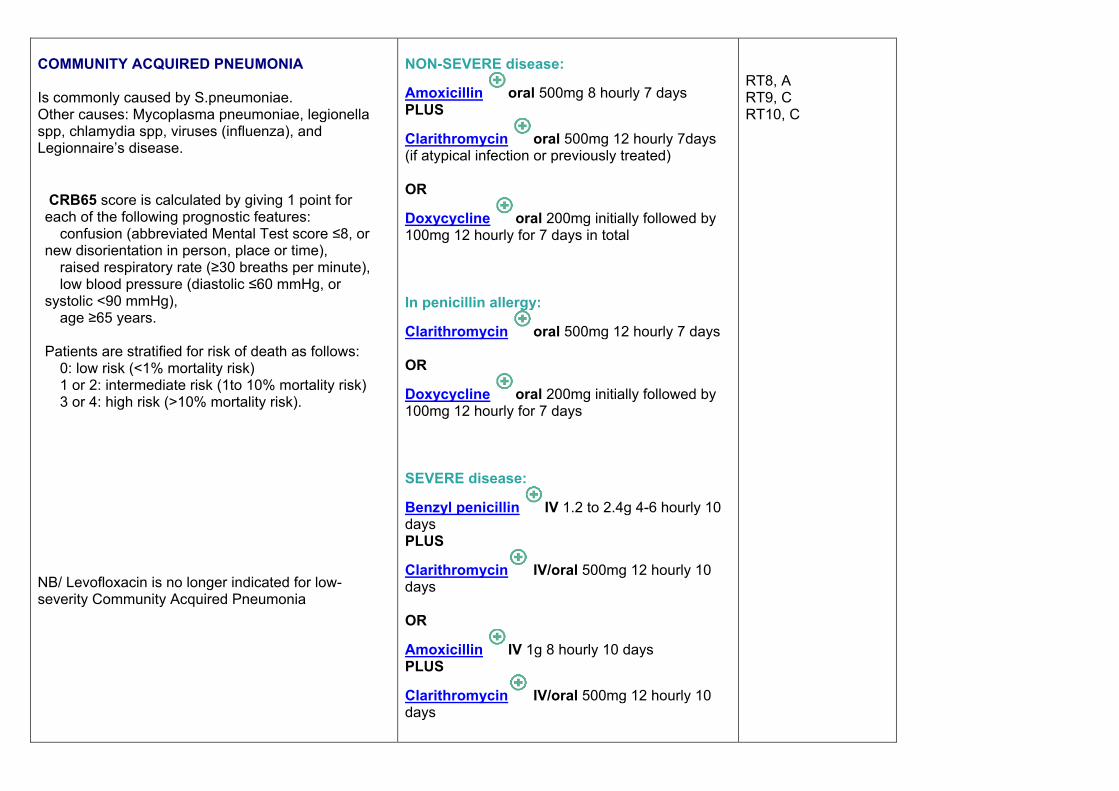
COMMUNITY ACQUIRED PNEUMONIA Is commonly caused by S.pneumoniae. Other causes: Mycoplasma pneumoniae, legionella spp, chlamydia spp, viruses (influenza), and Legionnaire’s disease. CRB65 score is calculated by giving 1 point for each of the following prognostic features: � confusion (abbreviated Mental Test score ≤8, or new disorientation in person, place or time), � raised respiratory rate (≥30 breaths per minute), � low blood pressure (diastolic ≤60 mmHg, or systolic <90 mmHg), � age ≥65 years. Patients are stratified for risk of death as follows: � 0: low risk (<1% mortality risk) � 1 or 2: intermediate risk (1to 10% mortality risk) � 3 or 4: high risk (>10% mortality risk).
NB/ Levofloxacin is no longer indicated for low- severity Community Acquired Pneumonia
NON-SEVERE disease:
Amoxicillin oral 500mg 8 hourly 7 days PLUS
Clarithromycin oral 500mg 12 hourly 7days (if atypical infection or previously treated) OR
Doxycycline oral 200mg initially followed by 100mg 12 hourly for 7 days in total In penicillin allergy:
Clarithromycin oral 500mg 12 hourly 7 days OR
Doxycycline oral 200mg initially followed by 100mg 12 hourly for 7 days SEVERE disease:
Benzyl penicillin IV 1.2 to 2.4g 4-6 hourly 10 days PLUS
Clarithromycin IV/oral 500mg 12 hourly 10 days OR
Amoxicillin IV 1g 8 hourly 10 days PLUS
Clarithromycin IV/oral 500mg 12 hourly 10 days
RT8, A RT9, C RT10, C
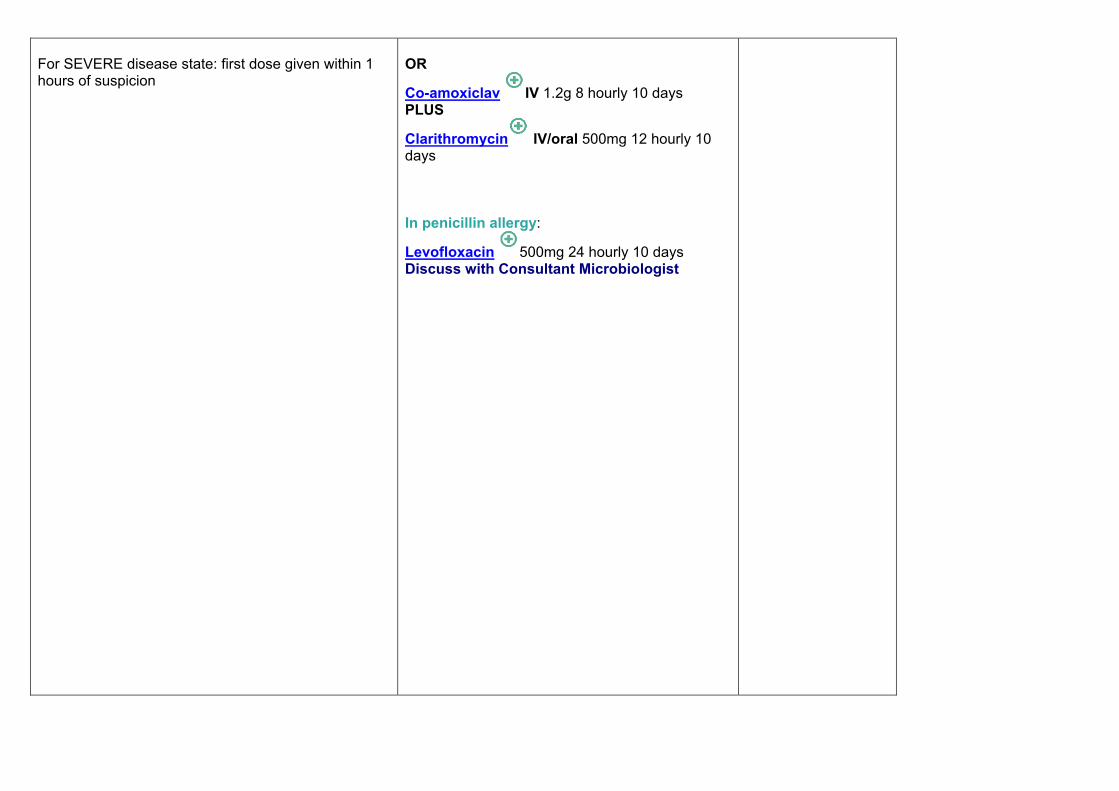
For SEVERE disease state: first dose given within 1 hours of suspicion
OR
Co-amoxiclav IV 1.2g 8 hourly 10 days PLUS
Clarithromycin IV/oral 500mg 12 hourly 10 days In penicillin allergy:
Levofloxacin 500mg 24 hourly 10 days Discuss with Consultant Microbiologist

Severe disease may be caused by S.aureus especially during influenza epidemics or in IV drug abusers. Refer to Appendix 2 to assess severity N.B. Treatment duration: for ‘atypical’ pathogens including legionellosis or staphylococcal infections treat for 14 days or 21 days if severe.
If suspect S. aureus ADD:
Flucloxacillin IV 1g 6 hourly 7 days
If HIV suspected:
Inform Microbiologist + GUM specialist

HOSPITAL ACQUIRED PNEUMONIA i.e. patients have been hospitalised for > 5 days Often caused by gram-negative bacilli. Neutropenic patients and intensive care patients need cover for pseudomonal infection. If HIGH risk of ESBL producing organisms AVOID cephalosporins Adjust treatment when microbiology results available. CURB65 score is calculated by giving 1 point for each of the following prognostic features: � confusion (abbreviated Mental Test score ≤8, or new disorientation in person, place or time), � raised blood urea nitrogen (>7 mmol/litre), � raised respiratory rate (≥30 breaths per minute), � low blood pressure (diastolic ≤60 mmHg, or systolic <90 mmHg), � age ≥65 years. Patients are stratified for risk of death as follows: � 0 or 1: low risk (<3% mortality risk) � 2: intermediate risk (3 to15% mortality risk) � 3 to 5: high risk (>15% mortality risk).
In penicillin allergy (anaphylaxis, urticaria) or allergy to cephalosporins:
Piperacillin/tazobactam IV 4.5g 6-8 hourly 10 days If SEVERE add:
Ciprofloxacin IV 400mg 12 hourly Discuss with Consultant Microbiologist VENTILATED patients:
Piperacillin/tazobactam IV 4.5g 6-8 hourly OR
Meropenem IV 500mg 6 hourly (first line if patient has had a previous course of antibiotics during current episode) OR Discuss with Consultant Microbiologist
RT9, C RT13, RT14, RT15 A
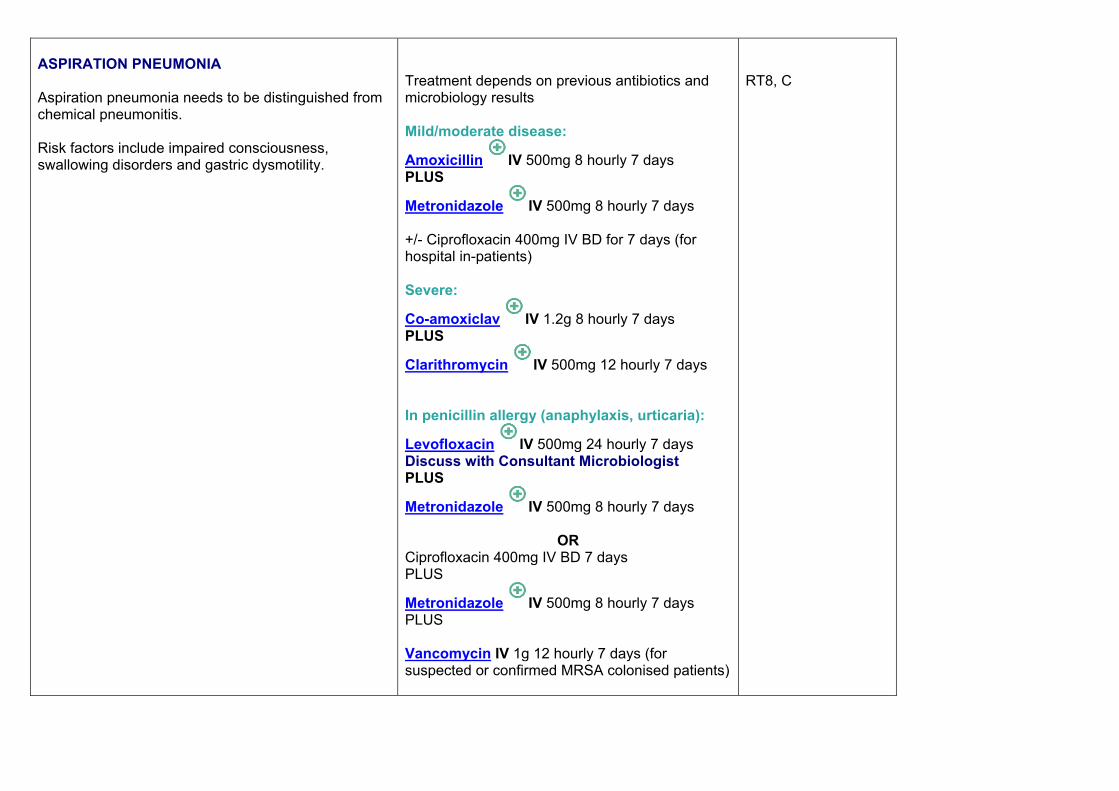
ASPIRATION PNEUMONIA Aspiration pneumonia needs to be distinguished from chemical pneumonitis. Risk factors include impaired consciousness, swallowing disorders and gastric dysmotility.
Treatment depends on previous antibiotics and microbiology results Mild/moderate disease:
Amoxicillin IV 500mg 8 hourly 7 days PLUS
Metronidazole IV 500mg 8 hourly 7 days +/- Ciprofloxacin 400mg IV BD for 7 days (for hospital in-patients) Severe:
Co-amoxiclav IV 1.2g 8 hourly 7 days PLUS
Clarithromycin IV 500mg 12 hourly 7 days In penicillin allergy (anaphylaxis, urticaria):
Levofloxacin IV 500mg 24 hourly 7 days Discuss with Consultant Microbiologist PLUS
Metronidazole IV 500mg 8 hourly 7 days
OR Ciprofloxacin 400mg IV BD 7 days PLUS
Metronidazole IV 500mg 8 hourly 7 days PLUS Vancomycin IV 1g 12 hourly 7 days (for suspected or confirmed MRSA colonised patients)
RT8, C
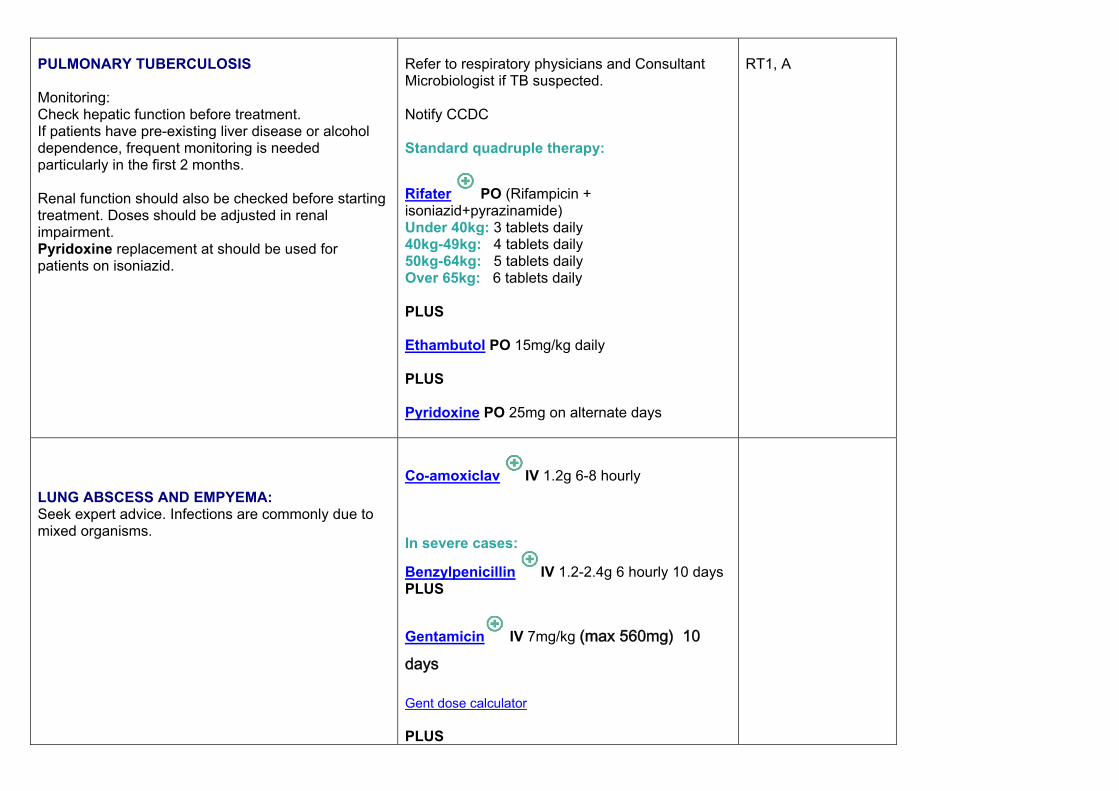
PULMONARY TUBERCULOSIS Monitoring: Check hepatic function before treatment. If patients have pre-existing liver disease or alcohol dependence, frequent monitoring is needed particularly in the first 2 months. Renal function should also be checked before starting treatment. Doses should be adjusted in renal impairment. Pyridoxine replacement at should be used for patients on isoniazid.
Refer to respiratory physicians and Consultant Microbiologist if TB suspected. Notify CCDC Standard quadruple therapy:
Rifater PO (Rifampicin + isoniazid+pyrazinamide) Under 40kg: 3 tablets daily 40kg-49kg: 4 tablets daily 50kg-64kg: 5 tablets daily Over 65kg: 6 tablets daily PLUS Ethambutol PO 15mg/kg daily PLUS Pyridoxine PO 25mg on alternate days
RT1, A
LUNG ABSCESS AND EMPYEMA: Seek expert advice. Infections are commonly due to mixed organisms.
Co-amoxiclav IV 1.2g 6-8 hourly In severe cases:
Benzylpenicillin IV 1.2-2.4g 6 hourly 10 days PLUS
Gentamicin IV 7mg/kg (max 560mg) 10 days
Gent dose calculator PLUS
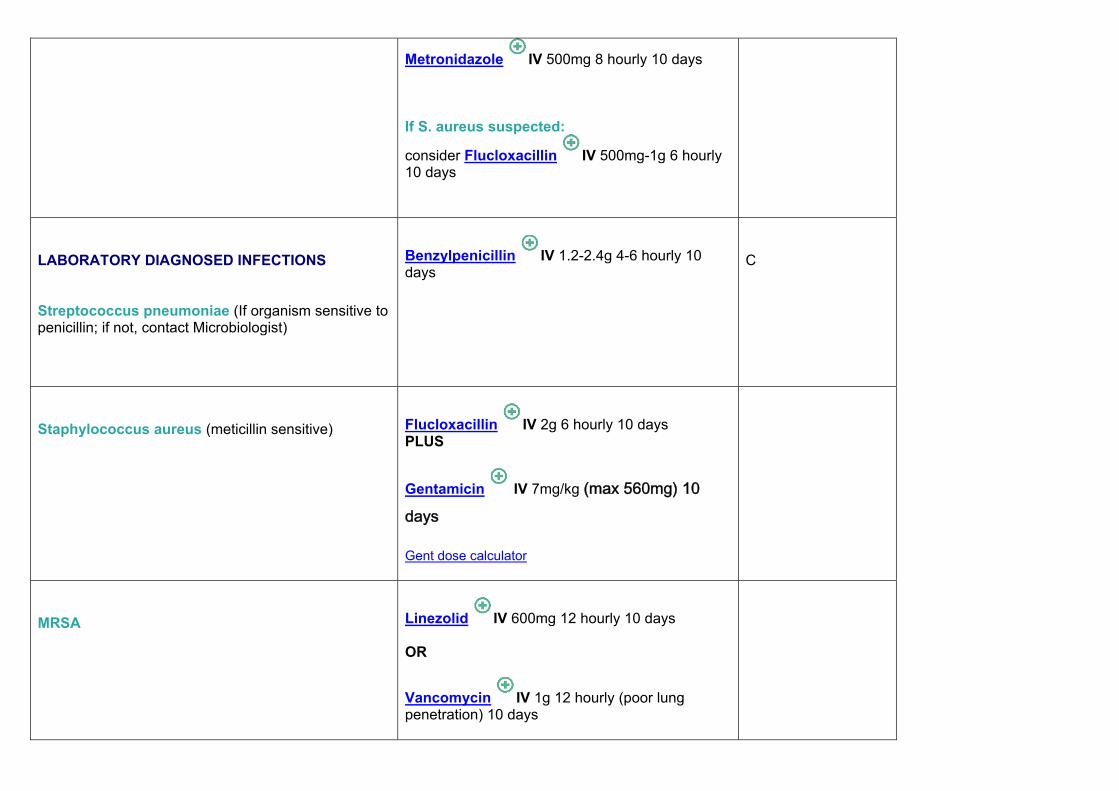
Metronidazole IV 500mg 8 hourly 10 days If S. aureus suspected:
consider Flucloxacillin IV 500mg-1g 6 hourly 10 days
LABORATORY DIAGNOSED INFECTIONS Streptococcus pneumoniae (If organism sensitive to penicillin; if not, contact Microbiologist)
Benzylpenicillin IV 1.2-2.4g 4-6 hourly 10 days
C
Staphylococcus aureus (meticillin sensitive)
Flucloxacillin IV 2g 6 hourly 10 days PLUS
Gentamicin IV 7mg/kg (max 560mg) 10 days
Gent dose calculator
MRSA
Linezolid IV 600mg 12 hourly 10 days OR
Vancomycin IV 1g 12 hourly (poor lung penetration) 10 days

Legionella spp. SEEK EXPERT ADVISE BEFORE TREATMENT
Azithromycin IV 500mg once daily for 10 days OR
Levofloxacin IV 500mg once daily for10 days OR
Clarithromycin IV 500mg bd 10 days
+/- Rifampicin (in mild disease)
Mycoplasma pneumoniae
Clarithromycin oral 500mg 12 hourly 7-14 days OR
Doxycycline oral 100mg 12 hourly for 7-14 days
C
Chlamydia psittaci
Doxycycline oral 100mg 12 hourly 21 days
Coxiella burnetii
Seek expert advice

GASTROINTESTINAL INFECTIONS Infection Antibacterial therapy References, level of
evidence ANTIBIOTIC ASSOCIATED DIARRHOEA Positive for Clostridium difficile. Often self-limiting and may not require treatment.
1. Stop other broad spectrum antibiotic treatment if possible.
2. If symptoms mild, observe. 3. If symptoms severe or antibiotics cannot be
stopped treat with metronidazole. 4. If relapse or no response, if severe or
immunocompromised patient discuss with Consultant Microbiologist
Metronidazole oral 400mg 8 hourly 7-14 days OR
Vancomycin oral 125mg – 500mg 6 hourly 7-14 days If severe disease suspected:
Vancomycin oral 500mg 6 hourly 10-14 days OR
Fidaxomicin oral 200mg 12 hourly 10-14 days (Consultant Microbiologist approval only) Can also add in: VSL sachet oral ONE sachet to continue until 2 weeks after diarrhoea subsides
GI1, A GI2, A GI15, A
CHOLANGITIS & ACUTE CHOLECYSTITIS Antibiotics should be started empirically if the patient has systemic signs or if no improvement is seen after 12-24 hours. Treat for 5 – 7 days then review.
Amoxicillin IV 500mg tds PLUS
Gentamicin IV 7 mg/kg/day (max 560mg)
Gent dose calculator

PLUS
Metronidazole IV 500mg 8 hourly
For 5 -7 days In SEVERE disease:
Piperacillin/Tazobactam IV 4.5g 8 hourly 5 days OR
Meropenem IV 500mg 8 hourly
GI3, B GI4, B GI16, A
ENTERIC FEVER Caused by Salmonella typhi or Salmonella paratyphi. The incidence of quinolone resistance in Salmonella infections is increasing. Please ensure laboratory sensitivity tests are done. Discuss with Consultant Microbiologist
Notify CCDC Ceftriaxone IV 1-2g 24 hourly If sensitivity to Ciprofloxacin confirmed:
Ciprofloxacin IV 400mg 12 hourly Change to oral as soon as appropriate
Ciprofloxacin oral 500-750mg 12 hourly for 10 days
GI1, GI6, A GI14, B
GASTROENTERITIS Most infections are self-limiting and require only rehydration. An antibiotic may be needed if the patient is systemically unwell and in an at risk group (immunocompromised, extremes of age,
Antibiotic usually not required. Campylobacter spp:
Ciprofloxacin oral 500mg 12 hourly OR
GI1, A GI5, B GI17, A

haematological or cardiovascular abnormalities). Erythromycin oral 500mg 6 hourly E.coli 0157
Antibiotics contraindicated Salmonella or Shigella spp:
Ciprofloxacin oral 500mg 12 hourly OR
Trimethoprim-sulphamethoxazole (co-trimoxazole) oral 960mg 12 hourly
HELICOBACTER PYLORI ERADICATION See BNF for alternative combinations. e.g. recently treated with amoxicillin for another infection.
First-line:
Omeprazole oral 20mg 12 hourly PLUS
Amoxicillin oral 1g 12 hourly PLUS
Clarithromycin oral 500mg 12 hourly all for 7 days
GI1, A
LIVER ABSCESS (bacterial) Frequently polymicrobial with Gram negative aerobic and anaerobic organisms predominating. Surgical drainage is essential in these patients. Duration: Depends on response and number and size of abscesses. Give first 2 weeks IV then oral if needed. May need 4 to 6 weeks of treatment.
Amoxicillin IV1g 8 hourly PLUS
Metronidazole IV 500mg 8 hourly PLUS
Gentamicin IV 7mg/kg (max 560mg)
Gent dose calculator
GI7, B GI16, A
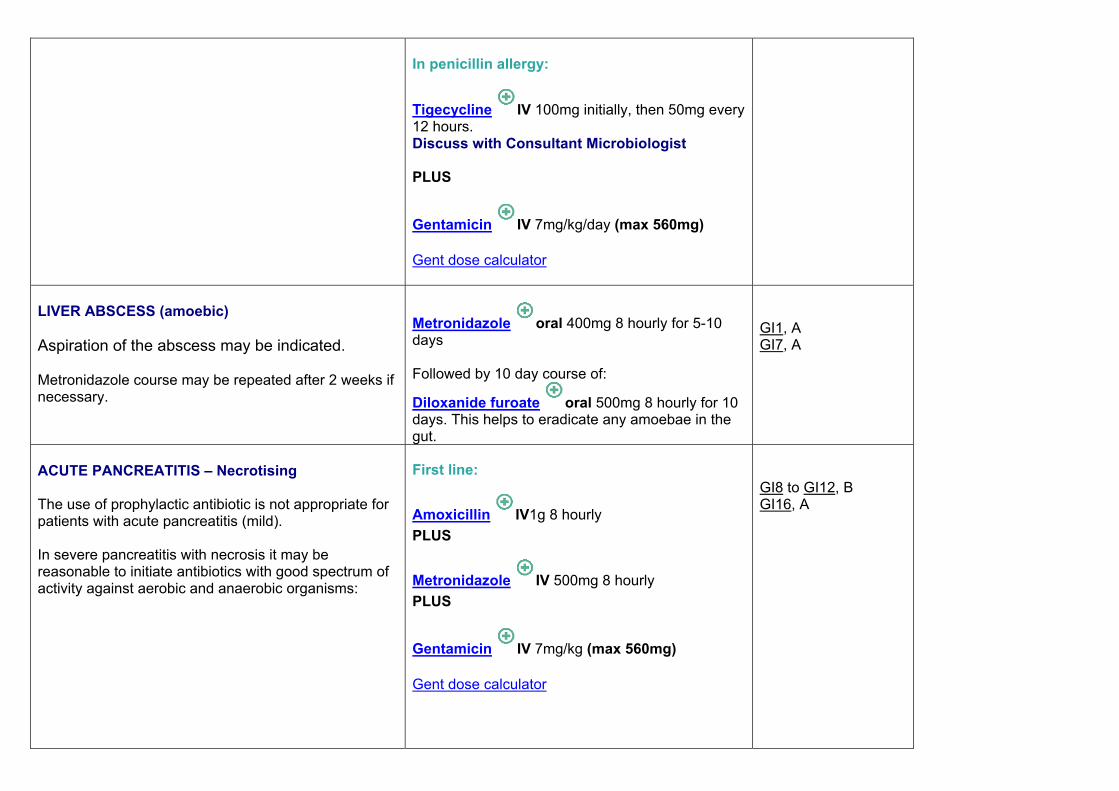
In penicillin allergy:
Tigecycline IV 100mg initially, then 50mg every 12 hours. Discuss with Consultant Microbiologist PLUS
Gentamicin IV 7mg/kg/day (max 560mg)
Gent dose calculator
LIVER ABSCESS (amoebic) Aspiration of the abscess may be indicated. Metronidazole course may be repeated after 2 weeks if necessary.
Metronidazole oral 400mg 8 hourly for 5-10 days Followed by 10 day course of:
Diloxanide furoate oral 500mg 8 hourly for 10 days. This helps to eradicate any amoebae in the gut.
GI1, A GI7, A
ACUTE PANCREATITIS – Necrotising The use of prophylactic antibiotic is not appropriate for patients with acute pancreatitis (mild). In severe pancreatitis with necrosis it may be reasonable to initiate antibiotics with good spectrum of activity against aerobic and anaerobic organisms:
First line:
Amoxicillin IV1g 8 hourly PLUS
Metronidazole IV 500mg 8 hourly PLUS
Gentamicin IV 7mg/kg (max 560mg)
Gent dose calculator
GI8 to GI12, B GI16, A

Discuss with Consultant Microbiologist regarding antifungal therapy.
Second line:
Meropenem IV 500mg 8 hourly
PERITONITIS Primary (Spontaneous Bacterial Peritonitis) Secondary / Surgical Review after 5 days.
Piperacillin/Tazobactam IV 4.5g 8 hourly 5 days OR Cefotaxime 2g IV 8 hourly 5 days
Amoxicillin IV 1g 8 hourly PLUS
Metronidazole IV 500mg 8 hourly PLUS
Gentamicin IV 7mg/kg (max 560mg)
Gent dose calculator all for 5 days
GI1, A GI13, B GI16, A

Selective decontamination of the gut has been shown to decrease the frequency of SBP in patients awaiting liver transplant. Discuss with Consultant Microbiologist
Norfloxacin oral 400mg once daily OR
Trimethoprim-sulphamethoxazole (co-trimoxazole) 960mg once daily for 5 days each week

Genital Infections & Sexually Transmitted Diseases
Infection Antibacterial therapy References, level of
evidence
BACTERIAL VAGINOSIS Usually caused by Gardnerella vaginalis infections.
Metronidazole oral 400mg 12 hourly 7 days OR Metronidazole oral 2g SINGLE DOSE OR Metronidazole 0.75% gel, 5g intravaginally once daily 5 days OR Clindamycin 2% cream, 5g intravaginally nocte 7 days
GU1, A GU5, A
EPIDIDYMO-ORCHITIS
See under URINARY TRACT INFECTIONS
GONORRHOEA Always refer to GU medicine specialist. Resistance is increasing especially to quinolones, therefore empirical treatment with ciprofloxacin / ofloxacin should be avoided. Spectinomycin is unlicensed in the UK. The main wholesalers of non-licensed medicines in the UK are IDIS of Weybridge and Durbin of South Harrow, Middlesex. The drug is available from both as Trobicin® 2g injection.
Uncomplicated disease: Ceftriaxone IM 500mg single dose Co-treatment: Azithromycin 1g (regardless of Chlamydia result) given at the same time as gonorrhoea treatment In cephalosporin allergy: Alternatives include quinolones and spectinomycin. Contact GUM or Microbiology consultant
GU1, A GU2, A GU3, A

PELVIC INFLAMMATORY DISEASE Often a complication of STD. Organisms commonly implicated includes N.gonorrhoeae, Chlamydia trachomatis, anaerobes, streptococci and coliforms. In the presence of increasing resistance in N. gonorrhoea to quinolone antibiotics AVOID empirical use of ciprofloxacin or ofloxacin- use cephalosporin-based regime (as above).
MILD to MODERATE disease: Ceftriaxone IM 500mg single dose PLUS Doxycycline oral 100mg 12 hourly for 14 days PLUS Metronidazole oral 400mg 12 hourly for 14 days
SEVERE disease: In severe disease e.g. pyrexia > 38oC, clinical signs of tubo-ovarian abscess, signs of pelvic peritonitis, initial treatment should be given intravenously. Continue IV therapy until 24 hours after clinical improvement then switch to oral (see outpatient regime). Use a combination of: Ceftriaxone IV 2g 24 hourly PLUS Doxycycline IV/oral 100mg 12 hourly Then: Doxycycline oral 100mg 12 hourly for a total 14 days PLUS Metronidazole oral 400mg 12 hourly for a total of 14 days Penicillin allergy: Clindamycin IV 900mg 8- hourly PLUS Gentamicin IV or IM Single daily dosing 7mg/kg Then: Clindamycin PO 450mg 6- hourly for a total of 14 days OR Doxycycline oral 100mg 12 hourly for a total 14 days PLUS Metronidazole oral 400mg 12 hourly for a total of 14 days
GU1, A GU4, A

SYPHILIS .
Seek advice from microbiology and GU medicine specialist.
CANDIDAL VAGINITIS See BNF for further advice and for advice on recurrent infection.
Clotrimazole vaginal pessary 100mg at night for 6 days OR Clotrimazole vaginal pessary 500mg stat at night OR Fluconazole oral 150mg as a single dose +/- clotrimazole 2% cream apply to anogenital area 2-3 times daily for 7 days
GU1, A GU7, A
TRICHOMONAL VAGINITIS
Metronidazole oral 2g as single dose OR Metronidazole oral 400mg 12- hourly 7 days
GU1, A GU8, A
URETHRITIS (MALE) Mostly caused by Chlamydia or similar organisms:
Doxycycline oral 100mg 12- hourly 7 days OR Azithromycin oral 1g as single dose
GU1, A GU9, A
URINARY TRACT INFECTION Infection Antibacterial therapy References, level of
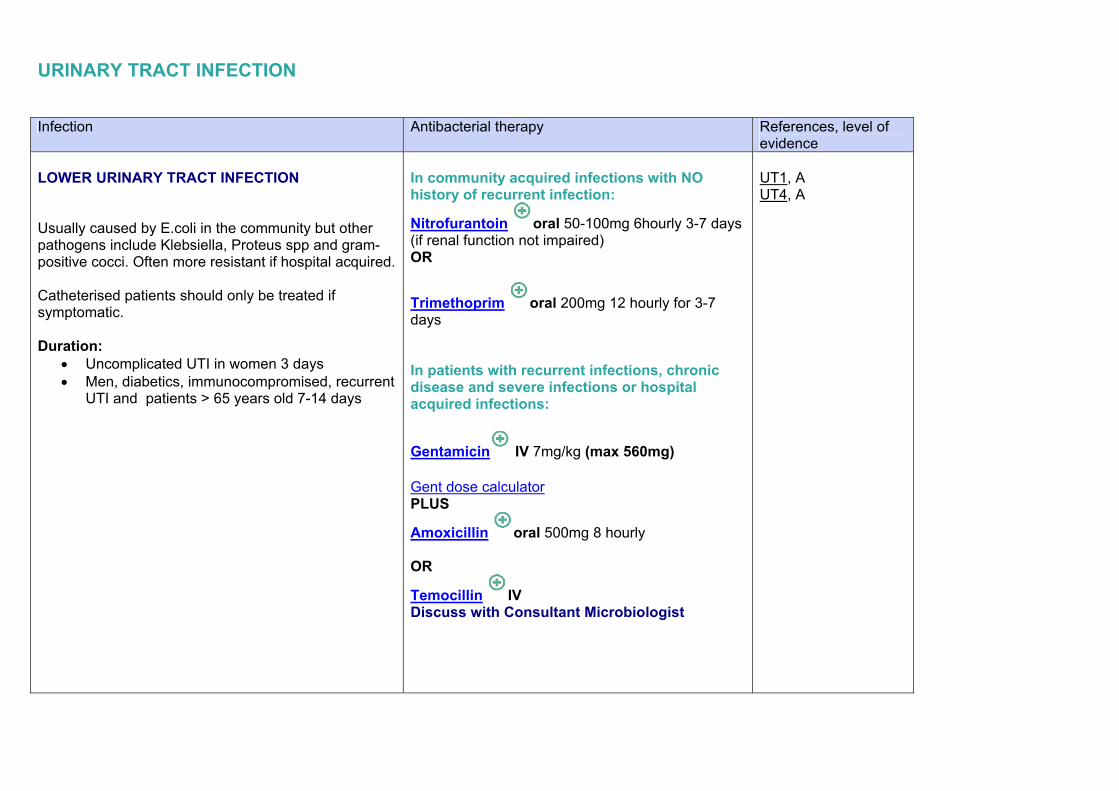
evidence LOWER URINARY TRACT INFECTION Usually caused by E.coli in the community but other pathogens include Klebsiella, Proteus spp and gram-positive cocci. Often more resistant if hospital acquired. Catheterised patients should only be treated if symptomatic. Duration:
Uncomplicated UTI in women 3 days Men, diabetics, immunocompromised, recurrent
UTI and patients > 65 years old 7-14 days
In community acquired infections with NO history of recurrent infection:
Nitrofurantoin oral 50-100mg 6hourly 3-7 days (if renal function not impaired) OR
Trimethoprim oral 200mg 12 hourly for 3-7 days In patients with recurrent infections, chronic disease and severe infections or hospital acquired infections:
Gentamicin IV 7mg/kg (max 560mg)
Gent dose calculator PLUS
Amoxicillin oral 500mg 8 hourly OR
Temocillin IV Discuss with Consultant Microbiologist
UT1, A UT4, A
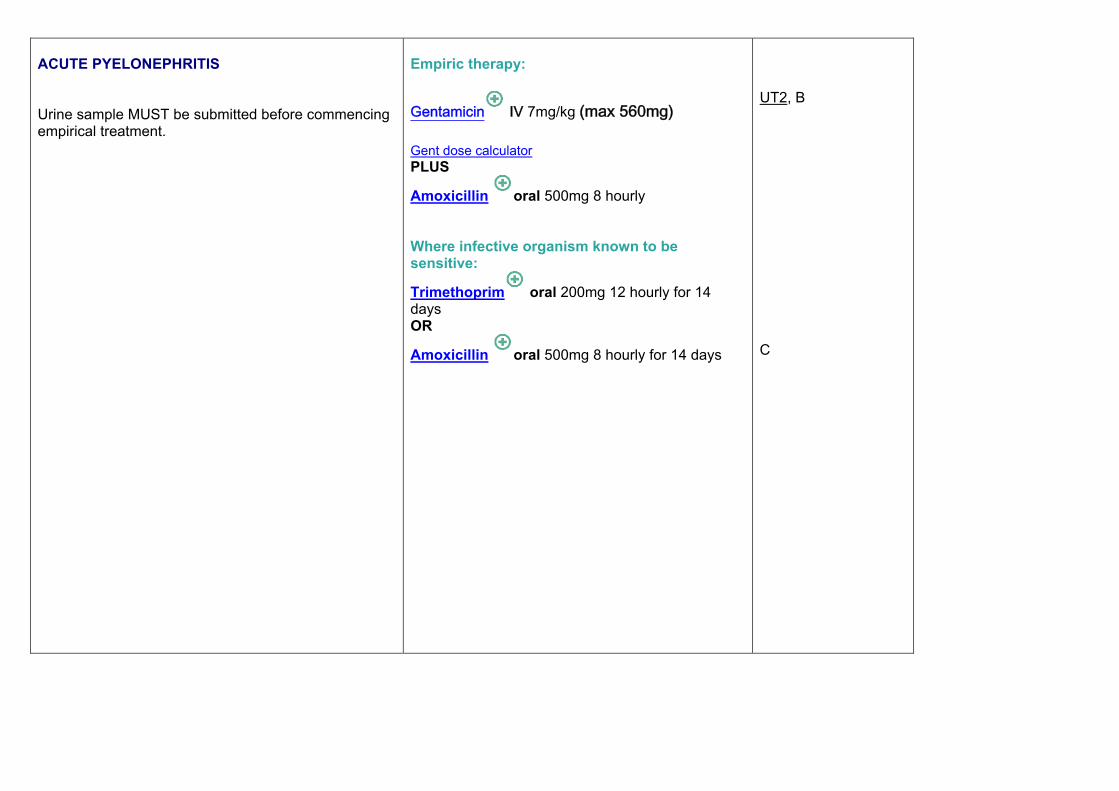
ACUTE PYELONEPHRITIS Urine sample MUST be submitted before commencing empirical treatment.
Empiric therapy:
Gentamicin IV 7mg/kg (max 560mg)
Gent dose calculator PLUS
Amoxicillin oral 500mg 8 hourly Where infective organism known to be sensitive:
Trimethoprim oral 200mg 12 hourly for 14 days OR
Amoxicillin oral 500mg 8 hourly for 14 days
UT2, B C

EPIDIDYMO-ORCHITIS Usually caused by gram-negative bacteria e.g. E.coli, P.aeruginosa, but in young males STD’s need to be considered.
For epididymo-orchitis due to any sexually transmitted organism: Ceftriaxone IM 500g single dose PLUS Doxycycline oral 100mg 12 hourly for 10-14 days For epididymo-orchitis most likely due to enteric organism: Ofloxacin oral 200mg 12 hourly for 14 days OR Ciprofloxacin oral 500mg 12 hourly for 10 days
UT5, A
UT6, C
PROSTATITIS
Ciprofloxacin oral 500mg 12 hourly for 28 days
UT1, A
Extended Spectrum Beta-Lactamse Be aware of Extended Spectrum Beta Lactamase (ESBLS) producing gram negative organisms like E.coli and Klebsiella spp. These organisms are resistant to ALL cephalosporin antibiotics and sometimes exhibit multi-resistant profile to quinolone and aminoglycoside antibiotics. NB/ Fosfomycin should be used as last line treatment. A dose should be repeated after 3 days. Creatinine clearance <80ml/min, including the physiological reduction in the elderly, increases the halflife of fosfomycin therefore repeat after 5 days.
Discuss with Consultant Microbiologist Options include:
Temocillin IV 2g 12 hourly OR
Meropenem IV 500mg 6 hourly OR Fosfomycin PO 3g stat

MISCELLANEOUS FEBRILE DISEASES Infection Antibacterial therapy References, level of
evidence
LEPTOSPIROSIS In severely ill patients: In less severe cases, when oral treatment can be tolerated:
Benzylpenicillin IV 1.2g 6 hourly 5-7 days Doxycycline oral 100mg 12 hourly 7 days OR Amoxicillin oral 500mg 6 hourly 5-7 days
M1, A
LYME DISEASE Causative organism: Borrelia burdorferi
Erythema chronicum migrans Doxycycline oral100mg 12 hourly 21 days OR Amoxicillin oral 500mg 8 hourly 21 days Carditis Ceftriaxone IV 2g once a day for 14-21 days OR Benzylpenicillin IV 2.4g 4-6g- hourly for 28 days (once patient is stabilised consider oral) CNS disease Ceftriaxone IV 2g 24 hourly 14-28 days Arthritis Doxycycline oral 100mg 12 hourly 30-60 days
M1, A

RICKETTSIAL DISEASES
Doxycycline oral 100mg 12 hourly 5-7 days OR Chloramphenicol may be considered in some rickettsial diseases
M1, A
PLAGUE Causative organism: Yersinia pestis
Streptomycin IM. Daily 30mg/kg/day in 2 divided doses for 7 days OR Doxycycline oral 100mg 12 hourly 7-10 days (loading dose 200mg every 12 hours for 1st 24 hours)
M1, A
ANTHRAX Causative organism: Bacillus anthracis
Seek expert advice immediately
M1, A

PARASITIC INFECTIONS
Scabies
Head lice
Pediculosis pubis (Crab lice)
Malaria

Infection Antimicrobial therapy References,
level of evidence
SCABIES Inform infection control nurse and refer to infection control policy. Repeat application after 1 week
First line: Permethrin 5% dermal cream apply 5% preparation over whole body (not head and face) and wash off after 8–12 hours Second line: Malathion 0.5% aqueous liquid apply preparation over whole body, and wash off after 24 hours; if hands are washed with soap within 24 hours, they should be retreated
P1, A P3, A P4, A
For the treatment of Crusted (Norwegian) scabies a single oral dose of Ivermectin will be required. Discuss with the Consultant Microbiologist.
Infection Antimicrobial therapy References, level of evidence
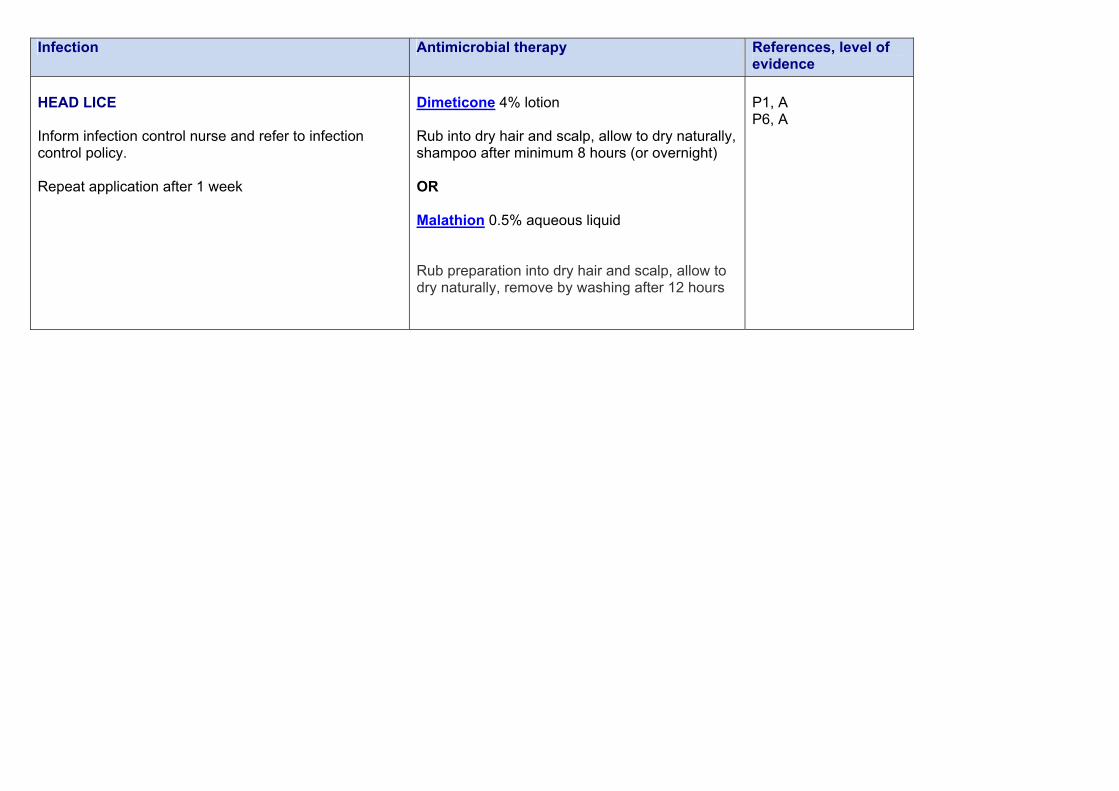
HEAD LICE Inform infection control nurse and refer to infection control policy. Repeat application after 1 week
Dimeticone 4% lotion Rub into dry hair and scalp, allow to dry naturally, shampoo after minimum 8 hours (or overnight) OR Malathion 0.5% aqueous liquid Rub preparation into dry hair and scalp, allow to dry naturally, remove by washing after 12 hours
P1, A P6, A

Infection Antimicrobial therapy References, level of evidence
Pediculosis pubis (Crab lice) Inform infection control nurse and refer to infection control policy.
Permethrin 1% lotion apply to wet hair, wash out after 10 minutes All hairy areas of the body from the neck down should be treated. Any moustache or beard should also be treated if infested. Treatment may be repeated after one week if necessary Malathion 0.5% aqueous liquid apply 0.5% aqueous preparation over whole body, allow to dry naturally, wash off after 12 hours or overnight; repeat application after 7 days
P1, A P2, A P5, A

Infection Antimicrobial therapy References, level of evidence
MALARIA
Advice on specific problems available from: Prophylaxis only: Public Health England (PHE) Malaria Reference Laboratory (020) 7637 0248 (fax) Treatment: London: 0845 155 5000 UCLH guidance: http://www.thehtd.org/Malaria%20guideline_final_June2013.pdf An algorithm for the initial assessment and management in adults can be found at: http://www.gov.uk/government/collections/malaria-reference-laboratory-mrl

Viral Infections
Herpes simplex
Varicella-zoster

Infection Antimicrobial therapy References level of evidence
HERPES SIMPLEX Famciclovir and Valciclovir are analogues of Aciclovir – but more expensive. For use in GU medicine ONLY Longer duration of treatment required if new lesions appear during treatment or healing is incomplete
Immunocompetent patients: First episode. Aciclovir oral 200mg 5 times daily 5 days OR Famciclovir oral 250mg 8hourly for 5 days OR Valaciclovir oral 500mg 12 hourly for 5 days Immunocompromised patients: Aciclovir oral 400mg 5 times daily 7-10 days OR Famciclovir oral 500mg 8 hourly for 7-10 days OR Valaciclovir oral 500mg 12 hourly 7-10 days Prophylaxis in immunocompromised: Aciclovir oral 200 - 400mg 6 hourly Suppression in immunocompetent patients: Aciclovir oral 200mg 6 hourly or 400mg 12 hourly
V1, A V2, A

Infection Antimicrobial therapy References level of evidence
VARICELLA & HERPES ZOSTER Longer duration of treatment required if new lesions appear during treatment or healing is incomplete
Aciclovir oral 800mg 5 times daily 7 days OR Famciclovir oral 500mg 8 hourly 7 days OR Valaciclovir oral 1g 8 hourly 7 days Immunocompromised patients or severe infection: Aciclovir IV 10mg/kg 8 hourly (use IBW in obese patients)
V1, A
FOR HIV TREATMENT PLEASE REFER TO GUM CLINIC
Seek Specialist advise
FUNGAL INFECTIONS Infection Antimicrobial therapy References, level of
evidence
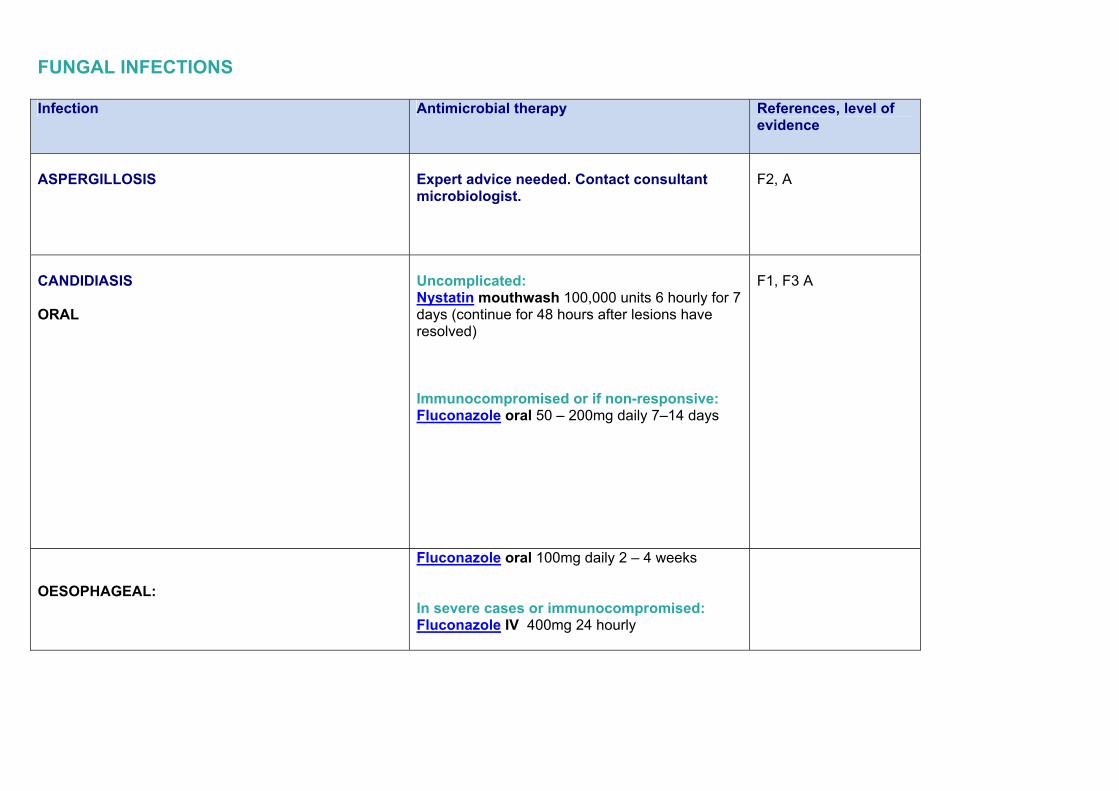
ASPERGILLOSIS
Expert advice needed. Contact consultant microbiologist.
F2, A
CANDIDIASIS ORAL
Uncomplicated: Nystatin mouthwash 100,000 units 6 hourly for 7 days (continue for 48 hours after lesions have resolved) Immunocompromised or if non-responsive: Fluconazole oral 50 – 200mg daily 7–14 days
F1, F3 A
OESOPHAGEAL:
Fluconazole oral 100mg daily 2 – 4 weeks In severe cases or immunocompromised: Fluconazole IV 400mg 24 hourly

VAGINAL: Sexual partners should also be treated if symptomatic. Additional use of a topical cream may be needed to treat vulvitis and other sites of superficial infection.
Clotrimazole vaginal pessary 100mg at night for 6 nights OR Clotrimazole vaginal pessary 500mg stat at nightOR Fluconazole oral 150mg stat Treatment failure or recurrence: Submit vaginal swab for culture and sensitivities and discuss with Microbiologist
CANDIDAEMIA: And disseminated candidiasis
Refer to Systemic Antifungal Guidelines for Adults
CRYPTOCOCCAL INFECTION & OTHER SYSTEMIC MYCOSES
Refer to Systemic Antifungal Guidelines for Adults Expert advice needed. Contact consultant microbiologist.
B
SPLENECTOMY PATIENTS Overwhelming post-splenectomy infection (OPSI) is considered to be a lifelong risk. All causes of absence of splenic function carry this risk. The majority of serious infections are due to Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitidis. IMMUNISATION ANTIBIOTIC PROPHYLAXIS SPLENECTOMY CARD Issue to ALL splenectomised patients on discharge from hospital, and send to their GP. These are available from Public Health England , publications order line or order online. www.gov.uk/government/publications/splenectomy-leaflet-and-card ACUTE INFECTIONS If suspected of developing a serious infection, immediate medical attention is required. Benzyl penicillin should be given (if not allergic) prior to admission to hospital. DOCUMENTATION Patient records must be clearly labelled to indicate the underlying risk of infection. Vaccination and re-vaccination status must be clearly and adequately documented. OTHER ADVICE When travelling abroad, patients should also be warned of their increased risk of severe falciparum malaria and potentially serious infections following animal & tick bites. Travel to malaria-endemic areas should be discouraged. Strict adherence to anti-malarial prophylaxis and protective measures to avoid insect bites are essential.

IMMUNISATIONS Before splenectomy - at least 2 weeks (preferably 4-6 weeks) pre-op, if possible. Or at 2 weeks post-op, because functional pneumococcal antibody responses are better if post-op vaccination is delayed 14 days. If vaccines need to be given by the patient's GP, this should be arranged with the GP prior to discharge and should also be specified in the hospital discharge note Otherwise give prior to discharge from hospital If given after immunosuppressive chemotherapy/ radiotherapy, immunisation should be delayed for at least 3 months
Where possible, vaccination course should ideally be started at least two weeks before surgery or commencement of immunosuppressive treatment. If not possible, see advice in the pneumococcal chapter..Influenza vaccine should be given annually.
For details on immunisation and vaccination schedule follow link below regularly updated and reviewed by Public Health England: https://www.gov.uk/government/publications/immunisation-of-individuals-with-underlying-medical-conditions-the-green-book-chapter-7 PS1, A

Infection Antibacterial therapy References, level of
evidence ANTIBIOTICS Lifelong prophylaxis is strongly recommended for all patients. (immunisations will not protect against all serotypes of pneumococcus or group B meningococcus)
Children up to age 16 Adults up to 2 years post-splenectomy Immunocompromised patients – LIFELONG: Penicillin V Adult and Child >5yrs 250mg 12 hourly Child <5 yrs 125mg 12 hourly Child <1 yr old 62.5mg 12 hourly OR Amoxicillin Adult 500mg 12 hourly Child 12 -18 yrs 500mg 12 hourly Child 5 -12 yrs 250mg 12 hourly 1 month - 5 years old 125mg 12 hourly In penicillin allergy Erythromycin Adult & child > 8 yrs 500mg 12 hourly Child 2 – 8 yrs 250mg 12 hourly Child < 2 yrs 125mg 12 hourly
PS2 A

Procedure Antibacterial prophylaxis References, level of
evidence
ENDOSCOPIC PROCEDURES Prophylaxis for neutropenic patients For all endoscopic procedures (including PEG) give the following at least 30 minutes before procedure:
Metronidazole IV 500mg over 20 minutes PLUS Gentamicin IV 1.5mg/kg (max.160mg) PLUS Amoxicillin IV 1g In penicillin allergy Substitute amoxicillin with a glycopeptide e.g. Teicoplanin or Vancomycin

SURGICAL PROPHYLAXIS Peri-operative antibiotics have been shown to reduce the rate of postoperative infection. Antibiotics are directed towards achieving peak serum concentrations at the time of surgery. This is usually achievable with a single pre-operative dose. A second dose may be indicated if the surgical procedure lasts more than the half-life of the antibiotic used (see Table 1). Antibiotics chosen should cover the most likely organisms contaminating the site of the surgery. It is important to distinguish between prophylaxis and treatment. When there is overt infection, antibiotic should be used for longer period of time. Treatment after the surgical procedure is complete should not be considered prophylaxis.
Gastrointestinal Surgery/Procedure
Gynaecological Surgery/Procedure
Obstetric Surgery/Procedure
Orthopaedic Surgery/Procedure

Vascular Surgery/Procedure
Miscellaneous Surgery/Procedure

GASTROINTESTINAL SURGERY / PROCEDURE PROPHYLAXIS Infection Antibacterial therapy References, level
of evidence
APPENDECTOMY No further doses required, unless peritonitis or an abscess is found during surgery, when treatment should be with:
Single dose prophylaxis with: Metronidazole IV 500mg stat at induction of anaesthesia Amoxicillin IV1g 8 hourly PLUS Metronidazole IV 500mg 8 hourly PLUS
Gentamicin IV 7mg/kg (max 560mg)
Gent dose calculator
SP1, SP4, A SP3, C
COLORECTAL SURGERY For extended duration surgery, further prophylactic doses should be given at the following intervals:
Cefuroxime 4-hourly Metronidazole 6-hourly
Cefuroxime IV (750mg if < 50kg, 1.5g if > 50kg) at induction of anaesthesia PLUS Metronidazole IV 500mg at induction of anaesthesia If over 65 years: Amoxicillin IV1g 8 hourly PLUS Metronidazole IV 500mg 8 hourly PLUS
Gentamicin IV 7mg/kg (max 560mg)
Gent dose calculator
SP1, SP2, A SP3, C

No further doses required, unless peritonitis or an abscess is found during surgery, when treatment should be with:
Amoxicillin IV1g 8 hourly PLUS Metronidazole IV 500mg 8 hourly PLUS
Gentamicin IV 7mg/kg (max 560mg)
Gent dose calculator
ERCP
Ciprofloxacin oral 500mg stat
C
PEG INSERTION MRSA is becoming an increasingly common cause of peristomal infection and consequently patients should be screened for MRSA pre-operatively and managed accordingly
Standard prophylaxis: Cefuroxime IV (750mg if < 50kg, 1.5g if > 50kg) stat OR Co-amoxiclav IV 1.2g stat In penicillin allergy: Teicoplanin IV 400mg stat
C

UPPER GI SURGERY Gastric tumour surgery: Other gastro-duodenal surgery: Small intestine, biliary, hepatic & pancreatic:
Cefuroxime IV (750mg if < 50kg, 1.5g if > 50kg) at induction of anaesthesia PLUS Metronidazole IV 500mg at induction of anaesthesia Cefuroxime IV (750mg if < 50kg, 1.5g if > 50kg) at induction of anaesthesia PLUS Metronidazole IV 500mg at induction of anaesthesia Cefuroxime IV (750mg if < 50kg, 1.5g if > 50kg) at induction of anaesthesia PLUS Metronidazole IV 500mg at induction of anaesthesia
SP1, B SP3, C
VARICEAL HAEMORRHAGE Non cirrhotic patients: Cirrhotic patients:
Antibiotic therapy generally NOT required Ciprofloxacin oral 500mg 12 hourly for 7 days
SP1, A
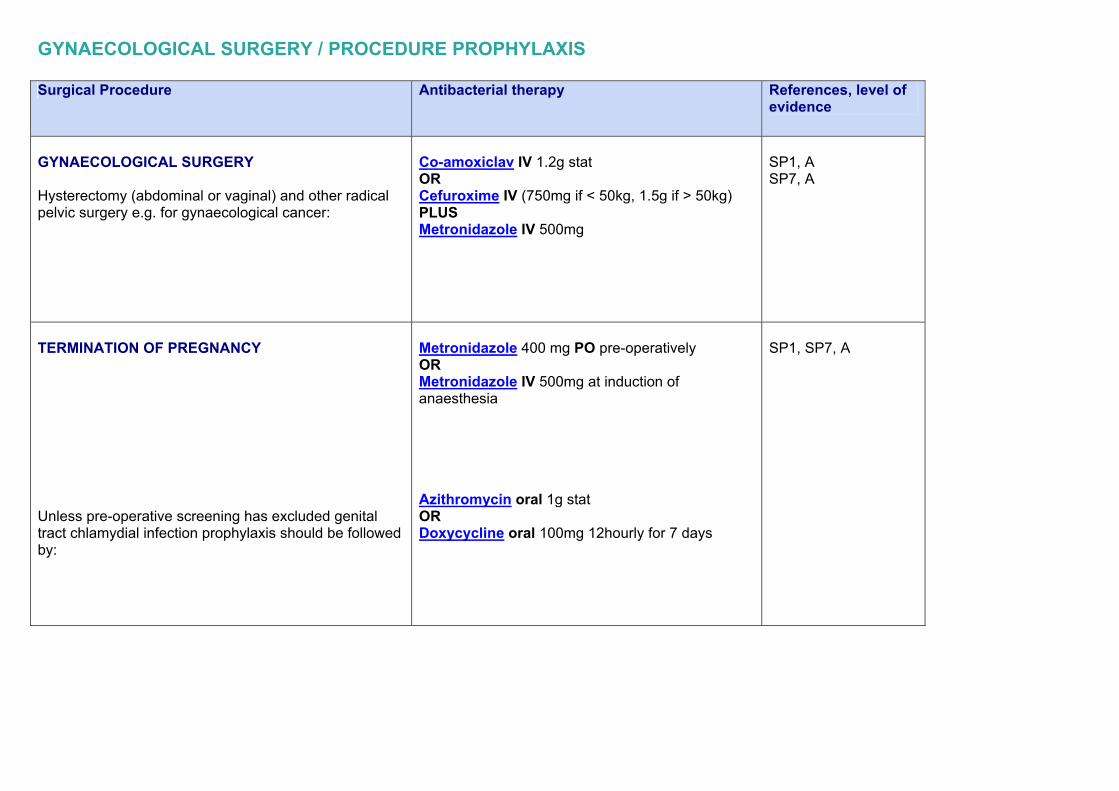
GYNAECOLOGICAL SURGERY / PROCEDURE PROPHYLAXIS Surgical Procedure Antibacterial therapy References, level of
evidence
GYNAECOLOGICAL SURGERY Hysterectomy (abdominal or vaginal) and other radical pelvic surgery e.g. for gynaecological cancer:
Co-amoxiclav IV 1.2g stat OR Cefuroxime IV (750mg if < 50kg, 1.5g if > 50kg) PLUS Metronidazole IV 500mg
SP1, A SP7, A
TERMINATION OF PREGNANCY Unless pre-operative screening has excluded genital tract chlamydial infection prophylaxis should be followed by:
Metronidazole 400 mg PO pre-operatively OR Metronidazole IV 500mg at induction of anaesthesia Azithromycin oral 1g stat OR Doxycycline oral 100mg 12hourly for 7 days
SP1, SP7, A

IUD INSERTION Routine insertion: Patients requiring IUD insertion for emergency contraception who have risk factors for sexually transmitted infection
No prophylaxis required Azithromycin oral 1g stat OR Doxycycline oral 100mg 12 hourly for 7 days
SP1, SP7, A

OBSTETRIC SURGERY / PROCEDURE PROPHYLAXIS Infection Antibacterial therapy References, level of
evidence OBSTETRIC PROCEDURES Caesarean section (planned or emergency): Offer prophylactic antibiotics before skin incision. Inform them that this reduces the risk of maternal infection. This will expose the neonate to the drug but no effect has been demonstrated. Do not use co-amoxiclav before cord clamping.
Before skin incision: Cefuroxime IV 750mg if <50kg ; 1.5g if >50kg After cord clamping: Cefuroxime IV 750mg if <50kg ; 1.5g if >50kg OR Co-amoxiclav IV 1.2g (ask Dr Mulla for advise not mentioned in RCOG guidelines or Trust guidance or BNF)
SP5, SP7, A

ORTHOPAEDIC SURGERY / PROCEDURE PROPHYLAXIS Surgical Procedure Antibacterial therapy References, level of
evidence
ORTHOPAEDIC SURGERY All patients undergoing elective prosthetic surgery should be screened for MRSA pre-operatively and managed accordingly. Prophylaxis is indicated in ALL cases of implants of metal or other prosthetic material and in other cases where probability of infection is high
Teicoplanin IV 400mg stat
SP1, SP6, A

VASCULAR SURGERY / PROCEDURE PROPHYLAXIS Surgical Procedure Antibacterial therapy References, level of
evidence
VASCULAR RECONSTRUCTION Includes all grafts whether vein or prosthetic
Co-amoxiclav IV 1.2g OR Cefuroxime IV 1.5g PLUS Metronidazole IV 500mg If penicillin anaphylaxis/urticaria or allergy to cephalosporin: Teicoplanin IV 400mg as single dose at induction of anaesthesia PLUS Gentamicin IV 3mg/kg as single dose at induction of anaesthesia PLUS Metronidazole IV 500mg at induction or anaesthesia
SP1, A SP9, A
In patients known to be colonised with MRSA
Vancomycin IV 750mg – 1g as single dose at induction of anaesthesia PLUS Cefuroxime IV 1.5g single dose PLUS Metronidazole IV 500mg at induction or anaesthesia followed by 2 doses of metronidazole oral 400mg at 8 hourly intervals

MISCELLANEOUS SURGERY / PROCEDURE PROPHYLAXIS Surgical Procedure Antibacterial therapy References, level of
evidence
CENTRAL LINE INSERTION
No prophylaxis required
OTHER PERCUTANEOUS PROCEDURES e.g. Biopsies
No prophylaxis required
SURGICAL PROPHYLAXIS IN MRSA POSITIVE PATIENTS Patients requiring antibiotic prophylaxis will need to be covered with appropriate antibiotics active against MRSA. VANCOMYCIN IV 750mg-1g as infusion over 100min before surgery is a recommended substitute to cover for gram-positive organisms Additional antibiotics for covering gram negatives and anaerobes should be added where appropriate.

REFERENCES Bone & Joint Infections BJ1. BSR & BHPR, BOA, RCGP and BSAC guidelines for management of the hot swollen joint in adults; Rheumatology 2012; 45:1039-1041 BJ2. National Health Service (UK). Map of Medicine Healthguides. Septic arthritis:2014 BJ3. Concia E, Prandini N, Massari L, Ghisellini F, Consoli V, Menchetti F, Lazzeri E. Osteomyelitis: clinical update for practical guidelines. Nucl Med Commun 2006 Aug; 27(8):645-60 BJ4. Hatzenbuehler J, Pulling T. Diagnosis and management of Osteomyelitis. Am Fam Physician. 2011;84(9):1027-1033 BJ5. Mathews CJ, Kingsley G, Field M, Jones A, Weston VC, Phillips M, Walker D, Coakley G. Management of septic arthritis: a systematic review. Ann Rheum Dis 2007; 66:440-445 CNS Infections CNS2. Mandell, Bennett & Dolin; Principles and practice of infectious diseases; 8th edition CNS3. Drugwatch bulletin no.9 July 2003 L&D Hospital NHS Trust CNS4. British National Formulary (BNF) 2015 CNS5. Prasad K et al. Third generation cephalosporins versus conventional antibiotics for treating acute bacterial meningitis. The Cochrane Database of Systematic Reviews 2011; 2: CD001832. CNS6. Zalmanovici Trestioreanu A, Fraser A, Gafter-Gvili A, Paul M, Leibovici L. Antibiotics for preventing meningococcal infections (Review). The Cochrane Database of Systemic Reviews 2013; 10: CD004785 CNS7. Infectious Diseases Society of America. The Management of Encephalitis: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clinical Infectious Diseases 2008; 47:303–27 CNS8. Infectious Diseases Society of America. Practice Guidelines for the Management of Encephalitis. Clinical Infectious Diseases 2004; 39:1267–84 CNS9. NICE Clinical Guideline. Bacterial meningitis and meningococcal septicaemia in children. June 2010 (revised Sept 2010) CNS10. SIGN National Clinical Guideline 102. Management of invasive meningococcal disease in children and young people. May 2008.

Cardiovascular Infections – Endocarditis CV1. Gould F K et al. Guidelines for the antibiotic treatment of endocarditis in adults: report of the Working Party of the British Society for Antimicrobial Chemotherapy. J. Antimicrobial Chemotherapy 2012; 67: 269-289 CV2. Baddour L M et al. Infective endocarditis, diagnosis, antimicrobial chemotherapy, and management of complications. Circulation 2005, 111:3167-3184 CV3. The Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Guidelines on the prevention, diagnosis, and treatment of infective endocarditis. European Heart Journal (2009) 30, 2369–2413 Gastrointestinal Infections GI1. British National Formulary (BNF) 2015 GI2. Mandell, Bennett & Dolin; Principles and practice of infectious diseases; 8th edition GI3. Indar A., Beckingham I., Acute Cholecystitis. British Medical Journal 2002; 325: 639-643 GI4. Clinical Knowledge Summaries: Acute Cholecystitis 2013. [online] Available at: http://www.cks.nhs.uk/cholecystitis_acute [accessed on 02/04/2015] GI5. Sirinavin S, Garner P. Antibiotics for treating salmonella gut infections. The Cochrane Database of Systematic Reviews 1999(1): CD001167. Updated 2009. GI6. Effa EE, Lassi ZS, Critchley JA, Garner P, Sinclair D, Olliaro PL, Bhutta ZA. Fluoroquinolones for treating typhoid and paratyphoid fever (enteric fever). Cochrane Database of Systematic Reviews 2011, Issue 10. CD004530. GI7. Clinical Immediate Reference: Liver abscess and cysts. 2014. [online] Available at: http://www.patient.co.uk/doctor/Liver-Abscesses-and-Cysts.htm [accessed on 02/04/2015] GI8. O’Reilly & Kingsnorth N. Management of acute pancreatitis. BMJ 2004; 328: 968-9 GI9. Villatori E, Mulla M, Larvin M. Antibiotic therapy for prophylaxis against infection of pancreatic necrosis in acute pancreatitis. The Cochrane Database of Systematic Reviews 2009: CD002941 GI10. Jafri NS, Mahid SS, Idstein SR, Hornung CA, Galandiuk S. Antibiotic prophylaxis is not protective in severe acute pancreatitis: a systematic review and meta-analysis. American Journal of Surgery 2009; 197(6): 806-813 GI11. Wittau M, Mayer B, Scheele J, Henne-Bruns D, Dellinger EP, Isenmann R. Systematic review and meta-analysis of antibiotic prophylaxis in severe acute pancreatitis. Scand J Gastroenterol. 2011; 46(3):261-70 GI12. Beckingham I.J. & Bornman P.C. Acute pancreatitis. BMJ 2014;322: 595-98
GI13. Runyon B. Spontaneous bacterial peritonitis in adults: Treatment and prophylaxis. UpToDate. 2015 [online]. Available at: http://www.uptodate.com/contents/spontaneous-bacterial-peritonitis-in-adults-treatment-and-prophylaxis [accessed on 02/06/15] GI14. Effa EE, Lassi ZS, Critchley JA, Garner P, Sinclair D, Olliaro PL, Bhutta ZA. Fluroquinolones for treating typhoid and paratyphoid fever (enteric fever) (review) 2011; 10: CD004530 GI15. Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, Pepin J, Wilcox MH. Clinical Practice Guidelines for Clostridium difficile Infection in Adults: 2010 Update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). 2010. Infection Control and Hospital Epidemiology, Vol. 31, No. 5 (May 2010), pp. 431-455 GI16. Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJC, Baron EJ, O’Neill PJ, Chow AW, Dellinger EP, Eachempati SR, Gorbach S, Hilfiker M, May AK, Nathens AB, Sawyer RG, Bartlett JG. Diagnosis and Management of Complicated Intra-abdominal Infection in Adults and Children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. 2010. Clinical Infectious Diseases 2010; 50:133–64 GI17. Health Protection Agency. Management of infection guidance for primary care for consultation and local adaptation. 2014. Genital Tract & Sexually Transmitted Diseases GU1. Sexually Transmitted Diseases Treatment Guidelines 2010, Department of Health and Human Services, Centres for Disease Control and Prevention, MMWR, December 17, 2010/ Vol. 59/ No. RR-12. GU2. Bignell C, FitzGerald M. UK national guideline for the management of gonorrhoea in adults, 2011. International Journal of STD & AIDS 2011; 22: 541–547 GU3. Spectinomycin for treatment of Gonorrhoea BASHH CEG statement June 2011 GU4. Ross J, McCarthy G. UK National Guideline for the Management of Pelvic Inflammatory Disease 2011. GU5. British Association for Sexual Health and HIV, Clinical Effectiveness Group. National Guideline For The Management Of Bacterial Vaginosis. 2012. GU6. Kingston M, French P, Goh B, Goold P, Higgins S, Sukthankar A, Stott C, Turner A, Tyler C, Young H. UK National Guidelines on the Management of Syphilis 2008. International Journal of STD & AIDS 2008; 19: 729–740 GU7. British Association for Sexual Health and HIV, Clinical Effectiveness Group. United Kingdom National Guideline on the Management of Vulvovaginal Candidiasis 2007. GU8. British Association for Sexual Health and HIV, Clinical Effectiveness Group. United Kingdom National Guideline on the Management of Trichomonas vaginalis. 2014. GU9. British Association for Sexual Health and HIV, Clinical Effectiveness Group. UK National Guideline on the Management of Nongonococcal Urethritis. Updated Dec 2014

Miscellaneous M1. Mandell, Bennett & Dolin; Principles and practice of infectious diseases; 8th edition Parasitic Infections P1. British National Formulary (BNF) 2015 P2. British Association for Sexual Health and HIV, Clinical Effectiveness Group. United Kingdom National Guideline on the Management of Phthirus pubis infestation. 2007. P3. British Association for Sexual Health and HIV, Clinical Effectiveness Group. United Kingdom National Guideline on the Management of Scabies infestation. 2007. P4. Health Protection Agency North West. The Management of Scabies infection in the Community. 2010 P5. Scott GR, Chosidow O. European Guideline for the Management of Pediculosis pubis. 2010. P6. Clinical Knowledge Summaries: Head Lice 2015 [online].Available at: http://cks.nice.org.uk/head-lice [accessed on 02/06/15] Respiratory Tract Infections – upper & lower RT1. British National Formulary (BNF) 2015 RT2. Clinical Knowledge Summaries: Acute Otitis Media 2009. [online] Available at: http://cks.nice.org.uk/otitis-media-acute [accessed on 02/04/2015] RT3. Clinical Knowledge Summaries: Acute Sinusitis 2013 [online]. Available at: http://cks.nice.org.uk/sinusitis [accessed on 02/06/2015] RT4. Ahovuo-Saloranta A, Rautakorpi UM, Borisenko OV, Liira H, Williams Jr JW, Mäkelä M. Antibiotics for acute maxillary sinusitis. Cochrane Database of Systematic Reviews 2014, Issue 2. Art. No.: CD000243. RT5. Clinical Knowledge Summaries: Sore throat-acute 2012 [online]. Available at: http://cks.nice.org.uk/sore-throat-acute [accessed on 02/06/15] RT6. Health Protection Agency. Management of infection guidance for primary care for consultation and local adaptation. 2014. RT7. Mandell, Bennett & Dolin; Principles and practice of infectious diseases; 8th edition

RT8. British Thoracic Society Community Acquired Pneumonia in Adults Guideline Group. Guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax 2009;64(Suppl III):iii1–iii55 RT9. NICE Clinical Guideline. Pneumonia: Diagnosis and management of community – and hospital-acquired pneumonia in adults. December 2014. RT10. Chalmers JD, Al-Khairalla M, Short PM, Fardon TC, Winter JH. Proposed changes to management of lower respiratory tract infections in response to the Clostridium difficile epidemic. Antimicrob Chemother 2010; 65: 608–618 RT11. NICE Clinical Guidelines. Chronic obstructive pulmonary disease: Management of chronic obstructive pulomary disease in adult in primary and secondary care. July 2014 RT12. Clinical Knowledge Summaries: Chronic Otitis Externa 2015. [online] Available at: http://cks.nice.org.uk/otitis-externa#!scenario:2 [accessed on 02/06/2015] RT13. American Thoracic Society. Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and Healthcare-associated Pneumonia. Am J Respir Crit Care Med Vol 171. pp 388–416, 2005 RT14. File T. Treatment of hospital-acquired, ventilator-associated, and healthcare-associated pneumonia in adults. UpToDate 2014 [online]. Available at http://www.uptodate.com/contents/treatment-of-hospital-acquired-ventilator-associated-and-healthcare-associated-pneumonia-in-adults?source=search_result&search=treatment+of+hospital-acquired%2C+ventilator&selectedTitle=1%7E150 [accessed on 02/06/15] RT15. Masterton RG, Galloway A, French G, Street M, Armstrong J, Brown E, Cleverley J, Dilworth P, Fry C, Gascoigne AD, Knox A, Nathwani D, Spencer R, Wilcox M. Guidelines for the management of hospital-acquired pneumonia in the UK: Report of the Working Party on Hospital-Acquired Pneumonia of the British Society for Antimicrobial Chemotherapy. Journal of Antimicrobial Chemotherapy (2008) 62, 5–34 Skin & Soft Tissue Infections SS1. British National Formulary (BNF) 2015 SS2. Clinical Immediate Reference: Orbital and Preseptal Cellulitis. 2009. [online] Available at: http://www.patient.co.uk/doctor/Orbital-Cellulitis.htm [accessed on 02/04/2012] SS3. Infectious Diseases Society of America. Practice Guidelines for the diagnosis and management of Skin and Soft Tissue Infections. 2014 SS4. Broom J. Management of bite injuries. Australian Prescriber. 2006; 29(1): 6-8 SS5. National Collaborating Centre for Women’s and Children’s Health. Surgical site infection prevention and treatment of surgical site infection. October 2008.

SS6. Lipsky B, Peters J, Sennerville E, Berendt A, Embil, Lavery L, Urbancic-Rovan V, Jeffcoate W. Expert opinion on the management of infections in the diabetic foot. Diabetes Metab Res Rev 2012 ; 28(1) :163-178 SS7. CREST guidelines. Guidelines on the management of cellulitis in adults. June 2005. SS8. National Institute for Health and Clinical Evidence. NICE clinical guideline 119 : Diabetic foot problems Inpatient management of diabetic foot problems. March 2011. SS9. Infectious Diseases Society of America. Clinical Practice Guideline for the Diagnosis and Treatment of Diabetic Foot Infections. 2012 Surgical prophylaxis SP1. Scottish Intercollegiate Guidelines Network. Antibiotic prophylaxis in surgery – a national clinical guideline. SIGN, publication number 104, July 2014. http://www.sign.ac.uk/guidelines/fulltext/45/index.html SP2. Nelson RL, Glenny AM, Song F. Antimicrobial prophylaxis for colorectal surgery (Review). Cochrane Database of Systematic Reviews 2014, Issue 1. Art. No.: CD001181. SP3. Dale W, Bratzler E Dellinger P et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health-Syst Pharm 2013; (70) 195-283 SP4. Ravari H, Jangjoo A, Motamedifar J, Moazzami K. Oral metronidazole as antibiotic prophylaxis for patients with nonperforated appendicitis. Clinical and Experimental Gastroenterology 2011: 4 273-276 SP5. Gyte GML, Dou L, Vazquez JC. Different classes of antibiotics given to women routinely for preventing infection at caesarean section (review). Cochrane Database of Systematic Reviews 2014, Issue 11 Art No: CD008726 SP6. British Association of Plastic, Reconstructive and Aesthetic Surgeons & British Orthopaedic Association. Standards for the management of open fractures of the lower limb. September 2009. SP7. The American College of Obstretricians and Gynecologists. Antibiotic Prophylaxis for Gynecologic Procedures. ACOG Practice Bulletin Vol. 113, No. 5, May 2014. SP8. National Institute for Health and Clinical Excellence. Caesarean section. NICE clinical guideline 132. November 2012 SP9. Stewart A, Eyers PS, Earnshaw JJ. Prevention of infection in arterial reconstruction. Cochrane Database of Systematic Reviews 2006, Issue 3. Art. No.: CD003073. Updated Sept 2010

Urinary Tract Infections UT1. British National Formulary (BNF) 2015 UT2. Clinical Knowledge Summaries: Acute Pyelonephritis 2013. [online] Available at: http://www.cks.nhs.uk/pyelonephritis_acute [accessed on 16/03/2015] UT3. Sexually Transmitted Diseases Treatment Guidelines 2010, Department of Health and Human Services, Centres for Disease Control and Prevention, MMWR, December 17, 2010/ Vol. 59/ No. RR-12. UT4. Scottish Intercollegiate Guidelines Network. Management of suspected bacterial urinary tract infection in adults. August 2012 UT5. Clinical Effectiveness Group, British Association for Sexual Health and HIV. United Kingdom national guideline for the management of epididymo-orchitis. 2010 UT6. European guideline on the management of epididymo-orchitis 2012. Revised August 2013. Viral Infections V1. Mandell, Bennett & Dolin; Principles and practice of infectious diseases; 8th edition V2. British National Formulary (BNF) 2015 Fungal Infections F1. Pappas PG, Kauffman CA, David Andes DA, Benjamin DK, Calandra TF, Edwards JE, Filler SG, Fisher JF, Kullberg B, Ostrosky-Zeichner L, Reboli AC, Rex JH, Walsh TJ, Sobel JD. Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Diseases Society of America. Clinical Infectious Diseases 2009:48 (1 March) 503- 535. F2. Walsh TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP, Marr KA, Morrison VA, Segal BH, Steinbach WJ, Stevens DA, Burik JV, Wingard JR, Patterson TF. Treatment of Aspergillosis. Clinical Practice Guidelines. Infectious Diseases Society of America. 2008: 46 (1st Febuary) 327-360 F3. British National Formulary (BNF) 2015 Splenectomy PS1. Public Health England. Immunisation against infectious disease. P49-56. 2014 PS2. British National Formulary (BNF) 2015