antidiabetic agent
TRANSCRIPT

ANTIDIABETICAGENTS
By Sara Sami Yuzuncu Yil University
2015
Aims of management
• To achieve near normal glycaemia- Short term- to prevent symptoms of hyper &
hypo- Long term- to prevent complications• Good quality of life, near normal life
expectancy

InsulinHuman Insulin : • Do not contain measurable amounts of
proinsulin or contaminants.• Diminished antibody• Less allergic reactions• Less lipodystrophy• Preferred in gestational diabetes

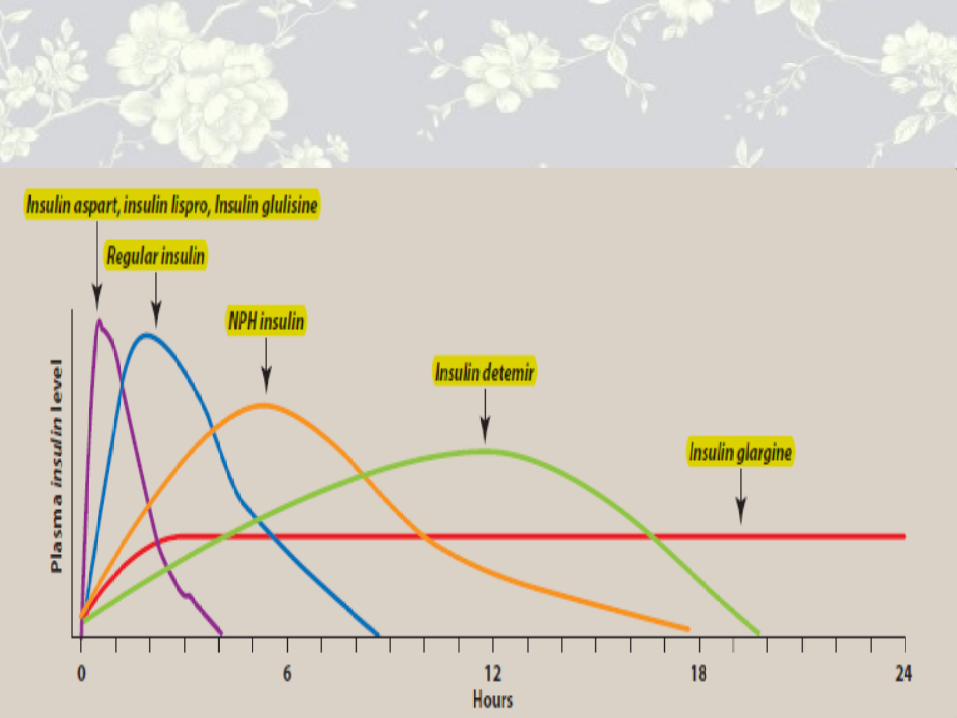
Types of Insulin• Short acting - Soluble / Neutral insulin Insulin aspart Insulin lispro
Insulin glulisin• Intermediate acting – Isophane or NPH• Long acting - Insulin Zinc suspension
new insulin analogue - Glargine Detemir
• Biphasic- mixture of short and intermediate Biphasic lispro Biphasic Isophane

Types of Insulin
Insulin LisproAspart
Neutral/regular
Isophane ultratard Glargine
Onset 10-20′ 30′ 1h 4h 2-4h
Peak 1h 1-3h 4-6h 6-18h peak less
Duration 3-5h 4-8h 8-14h 24h 20-24h

Soluble insulin / neutral /clear
• Names - Human actrapid/ Humulin S• Species- Bovine, porcine, human• Following s/c injection
Onset of action – 30 min Peak- 1-3 hours Duration- 4-8 hours
• Only insulin suitable for intravenous route –plasma half life < 5 min, required continuous infusion
• Used in diabetes Ketoacidosis

Sites of injections - Subcutaneous
• Thighs• Upper buttocks• Abdomen• ArmsImportant to rotate the siteRate of absorption may be significantly different
– faster from arm and abdomen than from thigh and buttock

Routes of Administration
• Subcutaneous for long term regular use• Intravenous infusion in acute conditions- diabetes
Ketoacidosis, Perioperative period, Hyperosmolar Nonketotic state ONLY NEUTRAL/ CLEAR INSULIN CAN BE USED
• Continuous subcutaneous insulin infusion via pump – neutral
• Intraperitoneal – Peritoneal dialysis patients• Inhaled insulin- experimental

Side effect of insulin
• Hypoglycaemia• Weight gain- anabolic hormone• Lipohypertrophy- injection to same site• Insulin oedema• Transient deterioration in retinopathy• Insulin neuritis – actively regenerating
neurone, uncommon• Postural hypotension

Example
injections
Short acting Short acting Short actingIntermediate/long acting
breakfast lunch dinner
breakfast lunch dinner bedtime
bedtimeinjections
Biphasic insulin Biphasic insulin

Rules
qnever stop insulinqmonitor more frequentlyqmaintain your hydrationqCheck for ketonesqKnow when & how to call for help

Different types of Insulin Preparations:Type Appearance Onset (hr) Peak (hr) Duration (hr)
RAPID ACTING
Insulin lispro Clear 0.2-0.3 1-1.5 3-5
Insulin aspart Clear 0.2-0.3 1-1.5 3-5
Insulin Glulisin Clear 0.2-0.4 1-2 3-5
SHORT ACTING
Regular (soluble) insulin
Clear 0.5-1 2-3 6-8
INTERMEDIATE ACTING
Insulin zinc suspension or Lente
Cloudy 1-2 8-10 20-24
NPH or isophane Insulin
Cloudy 1-2 8-10 20-24
LONG ACTING
Insulin Glargine and Insulin detemir
Clear Glargine: 2-4Detemir: 1-4
_ _
Glargine: 24Detemir: 20-24

Oral Medications to Treat Type 2 Diabetes
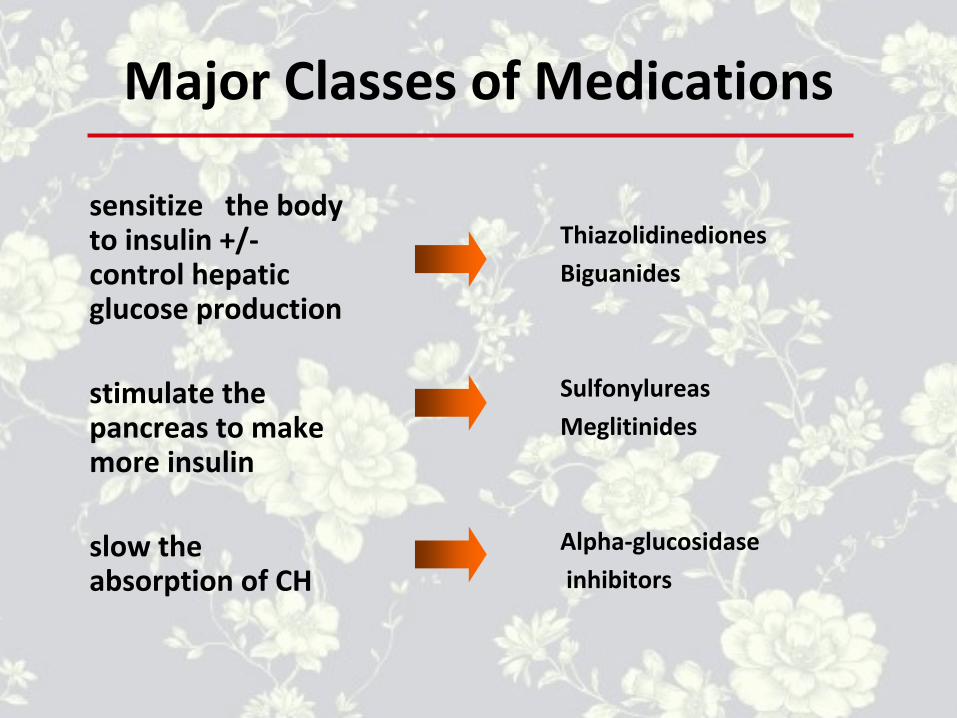
Major Classes of Medications
sensitize the body to insulin +/- control hepatic glucose production
stimulate the pancreas to make more insulin
slow the absorption of CH
ThiazolidinedionesBiguanides
SulfonylureasMeglitinides
Alpha-glucosidase inhibitors

Sites of action of Antidiabetics

Thiazolidinediones• ↓ insulin resistance by making muscle and adipose
cells more sensitive to insulin. They also suppress hepatic glucose production.
• Efficacy• Enhance glucose and lipid metabolism through
action on Peroxisome Proliferator Activated Receptor (PPAR–γ)
• by increasing the GLUT 4 glucose transporters–↓ fasting plasma glucose ~1.9-2.2 mmol/L– 6 weeks for maximum effect

• Other Effects– Weight gain, oedema – Hypoglycemia (if taken with insulin or agents that
stimulate insulin release)– Improves HDL cholesterol and plasma triglycerides ;
usually LDL neutral• Medications in this Class: pioglitazone (Actos),
rosiglitazone (Avandia), troglitazone (Rezulin) - taken off market due to liver toxicity]
Biguanides• Biguanides ↓ hepatic glucose production and increase insulin-
mediated peripheral glucose uptake.• Efficacy
– Decrease fasting plasma glucose 60-70 mg/dl (3.3-3.9 mmol/L)• Other Effects
– Diarrhea and abdominal discomfort– Lactic acidosis if improperly prescribed– Cause small decrease in LDL cholesterol level and triglycerides– No specific effect on blood pressure– No weight gain, with possible modest weight loss– Contraindicated in patients with impaired renal function – Medications in this Class: metformin (Glucophage), metformin
hydrochloride extended release (Glucophage XR)

Metformin (Glucophage) :• It does not cause hypoglycemia.
• It produces a significant ↓ TG and LDL, and ↑HDL.
• There is a serious concern about lactic acidosis especially in patients with kidney disease.

Sulfonylureas• Sulfonylureas increase endogenous insulin secretion• Efficacy
– Decrease fasting plasma glucose 3.3-3.9 mmol/L• Other Effects
– Hypoglycemia– Weight gain – No specific effect on plasma lipids or blood pressure– Generally the least expensive class of medication
• Medications in this Class:– First generation : chlorpropamide , tolazamide, acetohexamide ,
tolbutamide– Second generation : glyburide , glipizide – Third generation : Glimiperide
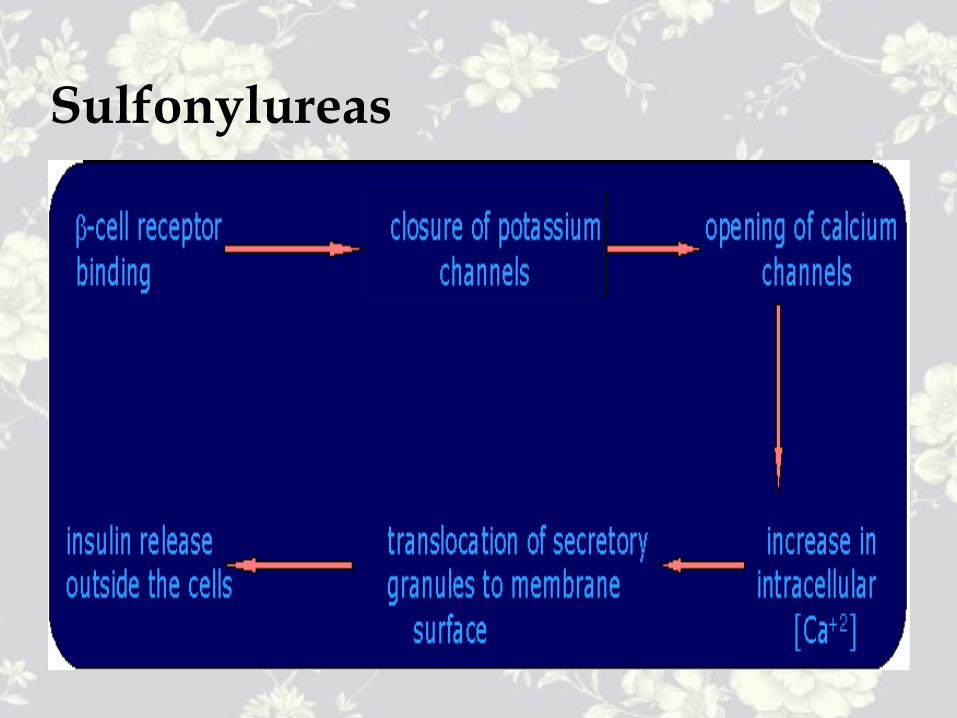
Sulfonylureas

Sulfonylureas Adverse effects :
• Hypoglycemia• Cholestatic jaundice• Weight gain• Cross placenta – fetal hypoglycemia.• Chlorpropamide : It can cause water
retention by ↑ release of ADH (SIADH)• Disulfiram-like reaction with alcohol.

Meglitinides• stimulate insulin secretion (rapidly and for a short duration) in the
presence of glucose.• Efficacy
– ↓ peak postprandial glucose– ↓ plasma glucose 3.3-3.9 mmol/L
• Other Effects– Hypoglycemia (may be less than with sulfonylureas if patient
has a variable eating schedule)– Weight gain – No significant effect on plasma lipid levels– Safe at higher levels of serum Cr than sulfonylureas
• Medications in this Class: repaglinide , nateglinide

Alpha-glucosidase Inhibitors• Alpha-glucosidase inhibitors block the enzymes that digest starches
in the small intestine• It reduces absorption of glucose after meals• Efficacy
– ↓ peak postprandial glucose 2.2-2.8 mmol/L– ↓ fasting plasma glucose 1.4-1.7 mmol/L
• Other Effects– Flatulence or abdominal discomfort – No specific effect on lipids or blood pressure– No weight gain– Contraindicated in patients with inflammatory bowel disease or
cirrhosis• Medications in this Class: acarbose , miglitol

Efficacy of Monotherapy with Oral Diabetes Agents


Anti-diabetic drugsGlucagon like Peptide : GLP-1 analog :
Xenatide : (Byetta) :• GLP is an incretin released from the small
intestine which increase the glucose dependent insulin secretion.
• Xenatide suppress glucagon release and reduce appetite
• It is administered by SC injection.

Anti-diabetic drugsGlucagon like Peptide : GLP-1 analog : Xenatide : (Byetta) :

Anti-diabetic drugs
Dipeptidyl peptidase 4 (DPP-4) inhibitors: SITAGLIPTIN (januvia)
Xenatide (Byetta) inj
Sitagliptin(januvia)

Anti-diabetic drugs• Sitagliptin (Januvia) is an oral anti-
diabetic drug.• It inhibit the dipeptidyl peptidase 4 (DPP-
4), an enzyme which inactivates the incretins GLP-1 and GIP, that are released in response to a meal.
• It potentiates the secretion of insulin and suppress the release of glucagon by the pancreas.

Endocrine pancreasGlucagon :• It has positive inotropic action and
chronotropic action on the heart.• It acts by stimulation of glucagon
receptors and not through beta 1 receptors.
• This is the basis for using glucagon in beta blocker overdose.

Treatment of Type 2 DiabetesDiagnosis
Therapeutic Lifestyle Change
Combination Therapy - Oral Drug with Insulin
Combination Therapy - Oral Drugs Only
Monotherapy

Sulfonylurea + Biguanide Glyburide + Metformin - Glucovance Glipizide + Metformin - Metaglip
Thiazolidinedione + Biguanide Rosiglitazone + Metformin - Avandamet
Fixed Combination Pills
Combination Therapy for Type 2 Diabetes

Combination Therapy for Type 2 Diabetes
Biguanides
Insulin
Sulfonylureas
Alpha-glucosidase Inhibitors
Meglitinide Thiazolidinediones
www.freelivedoctor.com
Special circumstances
• Intercurrent illness• Peri-operative period• Pregnancy• Childhood and adolescents• Others- travelling across time zones
Exercise Alcohol
Driving

THANK YOU FOR WASHING