antibodies trypsin sensitive pancreatic antigen in chronic … · used to detect antibodies against...
TRANSCRIPT

Gut, 1991,32, 1192-1197
Antibodies to a trypsin sensitive pancreatic antigen inchronic inflammatory bowel disease: specific markersfor a subgroup of patients with Crohn's disease
F Seibold, P Weber, H Jenss, K H Wiedmann
AbstractThe presence of antibodies against pancreaticjuice (PAB) in patients with Crohn's diseasehas recently been reported. In our study serafrom 273 patients with inflammatory boweldisease (222 with Crohn's disease, 51 withulcerative colitis) have been examined for PABand also for antibodies against gut tissues bymeans of indirect immunofluorescence. PABwere found in 68 of the 222 patients withCrohn's disease (31%), with titres ranging from1/10 to 1/1280, and in only two patients withulcerative colitis (4%), with titres of 1/20. Nonewere found in 198 patients with various chronicinflammatory diseases and healthy controlsubjects. No differences were found betweenthe PAB positive and negative patients whenthe foliowing parameters were compared:disease activity (Crohn's disease activityindex), involvement of bowel segments,incidence of extraintestinal disease, or treat-ment with anti-inflammatory drugs. Only sevenof the patients with Crohn's disease had ahistory of pancreatic disease and of these, fourhad detectable pancreatic antibodies. Longi-tudinal observations of40 patients with Crohn'sdisease showed a stable pattern for PAB,independent of disease activity and treatment.Partial characterisation of the PAB antigen,isolated from pancreatic juice, showed a trypsinsensitive macromolecular protein ofmore than106 daltons not identical with a panel of definedexocrine pancreatic proteins. By contrast, anti-bodies against goblet celis (GAB) were found in13 of 51 patients with ulcerative colitis (29%)and in none ofthe patients with Crohn's diseaseor control subjects. PAB were found as a highlyspecific serological marker for Crohn's diseaseand GAB for ulcerative colitis, but therelevance ofPAB and GAB in the pathogenesisin Crohn's disease remains unclear.
Department of InternalMedicine I, University ofTubingen, Otfried MiierStrasse 10, D 7400TUbingen, GennanyF SeiboldP WeberH JenssK H WiedmannCorrespondence to:Dr K H Wiedmann,Krankenhaus derbarmherzigen Brider,Priifeninger Str 86, D 8400Regensburg, Germany.Accepted for publication12 November 1990
The aetiology and pathogenesis of chronicinflammatory bowel disease has not yet beenresolved. Recently, many studies have focusedon immunopathogenetic mechanisms. Dis-turbed functions in both the cellular and thehumoral aspects of the immune system havebeen shown. The current thinking favours an
inappropriate immune response to luminal anti-gens, caused by a failure of adequate suppressorT cell function, leading to a chronic immuneactivation of immune cells in the intestinaltract. 2
Unlike in classical autoimmune diseases, thevarious antibodies decribed in both ulcerative
colitis and Crohn's disease are not considered tohave pathogenic and diagnostic importance.2In ulcerative colitis Broberger and Perlmannreported on antibodies against an extract ofcolonmucosa in 1959,3 and later on antibodies againstintestinal goblet cells were reported.45 Morelikely to be important in ulcerative colitis areautoantibodies to colonic mucosa antigens whichhave been found using isolated colon epithelialcells.6
Stocker et al7 recently showed in 39% ofpatients with Crohn's disease specific autoanti-bodies against an antigen in pancreatic juice.These findings seem to be specific for this groupof inflammatory bowel diseases. The clinicalimportance of these antibodies remains unclear.Furthermore, preliminary analysis ofthe antigenshowed a macromolecule in pancreatic juice thatdid not crossreact with amylase, lipase, trypsin,and chymotrypsin, but no further characterisa-tion has been reported.The aim ofour study was therefore to show the
disease specificity and relevance of those anti-bodies in patients with inflammatory boweldisease in respect of the clinical features, such asthe course of the disease, extraintestinal disease,and involvement ofbowel inflammation, in orderto evaluate whether these antibodies describe asubgroup of patients with Crohn's disease. Also,further characterisation of the pancreatic antigenwas performed.
Patients and methodsSera from 273 patients with inflammatory boweldisease were included in this study. In 222patients (107 women, 115 men) a diagnosis ofCrohn's disease was established on endoscopic,histological, and clinical criteria, according tothe European Cooperative Crohn's diseasestudy.8 The ages of these 222 patients rangedfrom 17-74 years, mean age 28 years. The meanduration of disease was nine years (range 4weeks-28 years). Eighty six (39%) of the patientswere being treated with corticosteroids at thetime of blood sampling. In 142 (64%) patientsthe ileum and colon were affected, in 38 (17%)the small bowel, and in 42 (19%) the colon only.In 32 patients the duodenum or stomach, orboth, was also affected. Seven patients had ahistory of pancreatitis. Extraintestinal diseasewas present in 25 (11%) patients at the time ofblood sampling: erythema nodosum (10), irido-cyclitis (four), oligoarthritis (four), sacroiliitis(six), and primary sclerosing cholangitis (one).Fistulas were found in 15 patients. Diseaseactivity was determined using the Crohn's
192
on 13 June 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.32.10.1192 on 1 October 1991. D
ownloaded from

Antibodies to a trypsin sensitive pancreatic antigen in chronic inflammatory bowel disease: specific markersfora subgroup ofpatients with Crohn's disease 1193
disease activity index,9 which was over 150 in 65patients and under 150 in 157 cases at the time ofblood sampling.
In 51 patients (27 women, 24 men) ulcerativecolitis was diagnosed according to the criteria ofTruelove and Witts.'° The mean age was 33years, range 20-73 years. The mean duration ofthe disease was 12 years (range 3 months-32years). Endoscopic investigation showed thatinflammation was limited to the left side ofthe colon in 28 patients and in the remainderinvolved the whole colon. Forty two patientswere in remission, nine had active disease.
Control sera were tested from 198 patients: 12with coeliac disease, 15 acute and chronic pan-creatitis, 10 autoimmune hepatitis, 10 acute andchronic viral hepatitis, eight alcoholic hepatitis,10 primary biliary cirrhosis, six primary scleros-ing cholangitis, 20 colon cancer, 11 lupuserythematosus, 11 rheumatoid arthritis, eightSjogren's disease, 12 thyroiditis, and 65 healthyblood donors.
TISSUES FOR IMMUNOHISTOCHEMISTRYSpecimens of human pancreas from three organdonors (blood group 0) for transplantation wereused to detect antibodies against pancreas(PAB). To test the organ and species specificitytissues from the normal human liver, obstructedliver with bile duct proliferation, stomach, duo-denum, ileum, colon, rectum, parotid gland,and mouse and rat tissues were tested. Humancolon and ileum were used to detect antibodiesagainst intestinal goblet cells. Tissues wereembedded in Tissue-tek (Miles, USA), snapfrozen in 2-methyl-butane cooled with dry ice,and stored at -80°C. Sections 5 [im thick werecut (at a temperature of -16 to -20°C onCryocut E (Reichert-Jung, Germany)), air dried,and fixed in acetone-chloroform (1:1) for 4minutes at 4°C.
IMMUNOFLUORESCENCE AND PEROXIDASETECHNIQUE FOR DETECTION OF PAB AND OTHERANTIBODIESSections of pancreas and control tissues wereincubated for 40 minutes in a moist chamber at20°C with 50 ,tl of serum samples (diluted 1:10with phosphate buffered saline (PBS), pH 7.4).After washing with PBS incubation followedwith polyvalent fluorescein-conjugated sheepantihuman immunoglobulin (Wellcome, diluted1:25 in PBS) for 30 minutes at ambient tempera-ture. Subsequently, after washing the sectionswere embedded in Immuno-Mount (Shandon,UK) and immediately read in a Leitz fluores-cence microscope (HDO 200 W mercurylamp with a filter combination 12, mirror RKP510).
Alternatively, an immunoperoxidase tech-nique was performed after serum incubation,using a peroxidase-conjugated polyvalent anti-human immunoglobulin from sheep (Wellcome,diluted 1:25 in PBS). After a second wash theperoxidase reaction was developed by incubatingsections with 0O1% 3'-3'diamino-benzidine-tetrahydrochloride and 0.003% H202 for 10minutes. Sections were then counterstained with
Mayer's hemalum (Merck, Germany) for 30seconds and mounted in Kaiser's glycerin-gelatine (Merck, Germany).
Antibody positive sera were diluted for recip-rocal titres. Determination of immunoglobulinclasses was done using monovalent antihumanimmunoglobulins (Wellcome).
All slides were read under code by twodifferent investigators. Results for PAB wereconsidered positive if the lumen contents ofpancreatic acini were labelled.
ELISA TESTPAB positive sera tested on a variety of knownpancreatic antigens or partially purified pancreasantigen (see below) using an enzyme linkedimmunosorbent assay (ELISA). The followingcommercially available pancreatic proteins wereused at a concentration of 5 [ig/ml: amylase,lipase, phospholipase A and C, enterokinase,carboxypeptidase A and B, chymotrypsin A andB, chymotrypsinogen, elastase, trypsin, trypsininhibitor (Bohringer, Germany), lactoferrin(Sigma), and kallikrein (Sigma). Microtitreplates were coated with antigens in bicarbonatebuffer for 20 hours at 4°C. After washing, strongPAB positive sera and control sera from patientswith ulcerative colitis, pancreatitis, viral hepa-titis, autoimmune diseases, and healthy subjects(1:80 diluted in PBS) were applied for one hour.After washing, peroxidase conjugated anti-human immunoglobulins (1:500 diluted) (Dako-patts, Denmark) were added and developed withorthophenyldiamine 0.05% and 0-01% H202 incitrate buffer, pH 5.0. Reaction was stoppedafter 20 minutes with H2S04. Analysis was doneby Microelisa Auto Reader, MR 580 (Dynatech,USA) at 520 nm wave length. Tested sera wereconsidered positive when extinction was higherthan double the standard deviation of the meanextinction of 45 sera from healthy subjects.
CHARACTERISATION OF PANCREATIC ANTIGEN
Pancreatic juicePancreatic juice was obtained from five surgicalpatients by draining pancreatic ducts afterpartial pancreas resection and stored at -200C(after adding trypsin inhibitor to some of thesamples).
Absorption studyFour different high titre sera with PAB detectedby immunofluorescence, were absorbed withincreasing amounts of pancreatic juice from twodifferent patients to a final dilution of 1:30 for 30minutes and centrifuged at 15 000 g for 10minutes before testing by immunofluorescence.As antigen control, liver homogenate and bilewere used.
ChromatographyFractionation of pancreatic juice was performedby gel chromatography on a Sephacryl S 300column (Pharmacia, Sweden) with a gel-bed of90x2.5 cm. Fractions were eluted with 0.05
on 13 June 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.32.10.1192 on 1 October 1991. D
ownloaded from

Seibold, Weber, Jenss, Wiedmann
Figure 1: Immunofluorescence pattern ofpancreatic antibodies(PAB) on human pancreas: positive labelling in the lumen ofpancreatic acini.
mol/l Tris/HCl buffer. Antigen activity in thepooled fractions were tested in an ELISA systemwith three different strong positive sera. Forfurther purification the antigen-containing peakof the Sephacryl S 300 run was submitted to ionexchange chromatography on DEAE-Sephacel(Pharmacia). Gradient elution was done by a0-01 mol/l Tris/HCl buffer with increasing NaCIsolution from 0.05 to 0.25 mol/l in five steps.
Detergents, solvents, thermolabilityCryostat sections were exposed to sodiumdodecylsulphate 1% (Serva, Germany), Tritonx100 1% (Serva), Tween 20 1% (Serva) for 30seconds and to ethanol 95% and acetone-chloroform (1:1) for 15 minutes. Thermolabilityof the antigen was measured by exposing tovarious temperatures in a water bath.
EnzymesMicrotitre plates were incubated with 6.5 [tg/mlof partially chromatographically purifiedpancreatic antigen as above. Various enzymessuch as bovine trypsin (Bohringer), nagarsefrom Bacillus subtilis (proteinase, Serva), entero-kinase from swine intestine (Sigma), phospho-lipase A from bovine pancreas and C fromClostridium perfringens (Sigma), mixed glyco-sidase from T corneatus (Seikagaku Kogyo,Japan), neuraminidase from C perfningens type 5(Sigma), hyaluronidase from sheep testes(Bohringer), chondroitinase ABC from Proteusvulgaris (Seikagaku Kogyo), amylase type VIa,elastase type I, and lipase type II from swinepancreas (Sigma), and carboxypeptidase A andB, alpha and beta chymotrypsin from bovine
Min-" f* m_
Figure 2: Immunofluorescence on mouse pancreas: stronglabelling in the lumen ofpancreatic acini.
pancreas (Sigma) were added at a concentrationof 100 ,ug/mg protein in appropriate buffers andtemperatures for 8 hours. After extensive wash-ing the ELISA procedure was continued asshown above.
Alternatively, enzyme treatment was per-formed in Eppendorf tubes. Chromatographic-ally purified pancreatic antigen was incubatedin a time dependent manner with enzymes (100ptg/mg pancreatic antigen) from 10 minutes to 24hours. Enzymes were inactivated by chloroform.The aqueous phase adjusted to 6.5 [ig protein/ml was taken to incubate ELISA plates. Trypsinwas inactivated by trypsin inhibitor (200 [ig/mg). Pancreatic protein treated in an identicalmanner but without added enzymes was used asa control.
Results
IMMUNOCYTOCHEMISTRY PATTERN, ORGANSPECIFICITY, AND ABSORPTION STUDIES OF PABSpecific labelling of PAB positive sera on pan-creatic tissue appeared as a dense aggregation inthe lumen of pancreatic acini (Fig 1). Occasion-ally a weak reaction in the cytoplasm of thehuman acinar cells was observed as well. Thepancreatic islets did not show any labelling. Thesame pattern was obtained using pancreatictissue from three humans or from rats and mice(Fig 2). Human salivary gland, breast, stomach,small and large intestine, liver, adrenal cortex,and kidney showed no fluorescence with PABpositive sera. Specific labelling ofPAB serum onpancreas could be abolished after absorptionwith human pancreatic juice, but not with liverhomogenate and bile control experiments.
1194
on 13 June 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.32.10.1192 on 1 October 1991. D
ownloaded from
Antibodies to a trypsin sensitive pancreatic antigen in chronic inflammatory bowel disease: specific markersfora subgroup ofpatients with Crohn's disease 1195
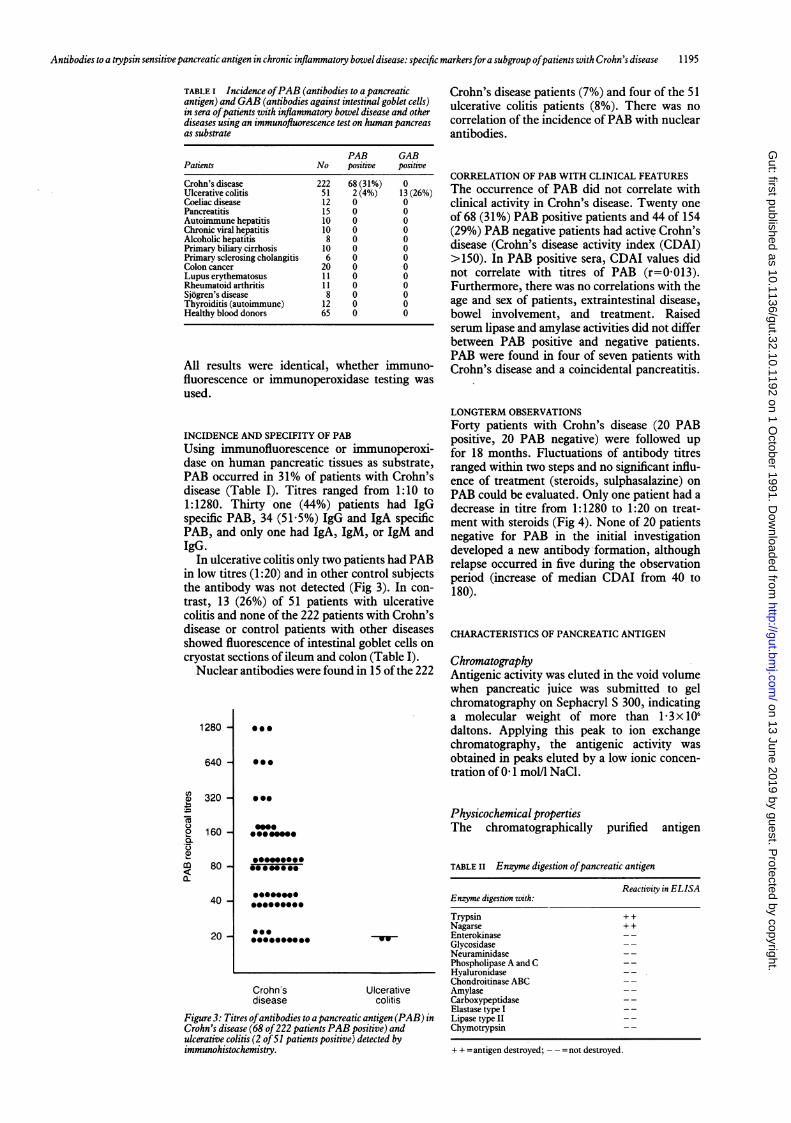
TABLE I Incidence ofPAB (antibodies to a pancreaticantigen) and GAB (antibodies against intestinal goblet cells)in sera ofpatients with inflammatory bowel disease and otherdiseases using an immunofluorescence test on human pancreasas substrate
PAB GABPatients No positive positive
Crohn's disease 222 68 (31%) 0Ulcerative colitis 51 2(4%) 13 (26%)Coeliac disease 12 0 0Pancreatitis 15 0 0Autoimmune hepatitis 10 0 0Chronic viral hepatitis 10 0 0Alcoholic hepatitis 8 0 0Primary biliary cirrhosis 10 0 0Primary sclerosing cholangitis 6 0 0Colon cancer 20 0 0Lupus erythematosus 11 0 0Rheumatoid arthritis 11 0 0Sjogren's disease 8 0 0Thyroiditis (autoimmune) 12 0 0Healthy blood donors 65 0 0
All results were identical, whether immuno-fluorescence or immunoperoxidase testing was
used.
Crohn's disease patients (7%) and four of the 51ulcerative colitis patients (8%). There was nocorrelation of the incidence ofPAB with nuclearantibodies.
CORRELATION OF PAB WITH CLINICAL FEATURESThe occurrence of PAB did not correlate withclinical activity in Crohn's disease. Twenty one
of 68 (3 1%) PAB positive patients and 44 of 154(29%) PAB negative patients had active Crohn'sdisease (Crohn's disease activity index (CDAI)>150). In PAB positive sera, CDAI values didnot correlate with titres of PAB (r=0.013).Furthermore, there was no correlations with theage and sex of patients, extraintestinal disease,bowel involvement, and treatment. Raisedserum lipase and amylase activities did not differbetween PAB positive and negative patients.PAB were found in four of seven patients withCrohn's disease and a coincidental pancreatitis.
INCIDENCE AND SPECIFITY OF PABUsing immunofluorescence or immunoperoxi-dase on human pancreatic tissues as substrate,PAB occurred in 31% of patients with Crohn'sdisease (Table I). Titres ranged from 1:10 to1:1280. Thirty one (44%) patients had IgGspecific PAR, 34 (51.5%) IgG and IgA specificPAB, and only one had IgA, IgM, or IgM andIgG.
In ulcerative colitis only two patients had PABin low titres (1:20) and in other control subjectsthe antibody was not detected (Fig 3). In con-trast, 13 (26%) of 51 patients with ulcerativecolitis and none of the 222 patients with Crohn'sdisease or control patients with other diseasesshowed fluorescence of intestinal goblet cells oncryostat sections of ileum and colon (Table I).
Nuclear antibodies were found in 15 ofthe 222
1280 -
640 -
in
a)00
b..
320 -
160 -
80 -
40 -
20 -
000
@00
LONGTERM OBSERVATIONSForty patients with Crohn's disease (20 PABpositive, 20 PAB negative) were followed upfor 18 months. Fluctuations of antibody titresranged within two steps and no significant influ-ence of treatment (steroids, sulphasalazine) on
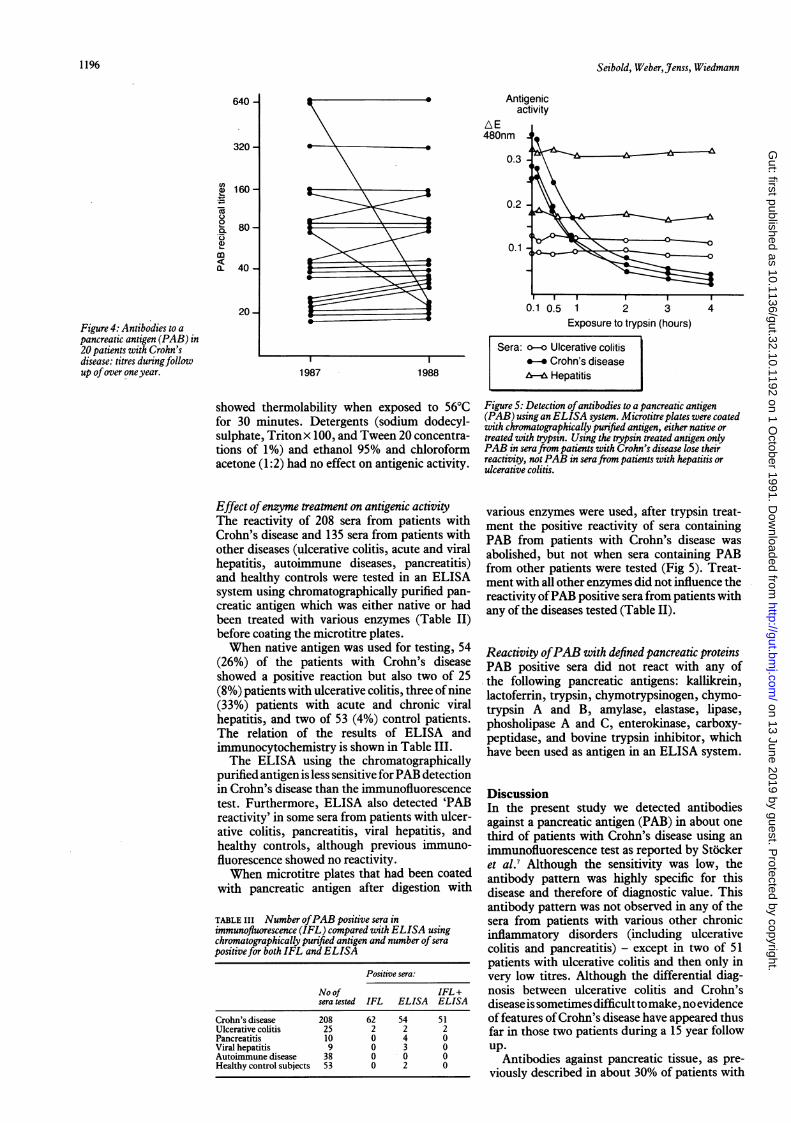
PAB could be evaluated. Only one patient had adecrease in titre from 1:1280 to 1:20 on treat-ment with steroids (Fig 4). None of 20 patientsnegative for PAB in the initial investigationdeveloped a new antibody-formation, althoughrelapse occurred in five during the observationperiod (increase of median CDAI from 40 to180).
CHARACTERISTICS OF PANCREATIC ANTIGEN
ChromatographyAntigenic activity was eluted in the void volumewhen pancreatic juice was submitted to gelchromatography on Sephacryl S 300, indicatinga molecular weight of more than 1 3x 106daltons. Applying this peak to ion exchangechromatography, the antigenic activity was
obtained in peaks eluted by a low ionic concen-
tration of 0-1 mol/l NaCl.
000
Physicochemical propertiesThe chromatographically purified antigen
0a
000
.*..... 0. -'UF-
Crohn's Ulcerativedisease colitis
Figure 3: Titres ofantibodies to a pancreatic antigen (PAB) inCrohn's disease (68 of222 patients PAB positive) andulcerative colitis (2 of51 patients positive) detected byimmunohistochemistry.
TABLE II Enzyme digestion ofpancreatic antigen
Reactivity in ELISAEnzyme digestion with:
Trypsin + +Nagarse + +Enterokinase - -GlycosidaseNeuraminidase - -Phospholipase A and C --Hyaluronidase - -Chondroitinase ABCAmylase - -Carboxypeptidase - -Elastase type I - -Lipase type II --Chymotrypsin - -
+ + =antigen destroyed;destroyed.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
+ + =antigen destroyed; = not destroyed.
on 13 June 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.32.10.1192 on 1 October 1991. D
ownloaded from
Seibold, Weber,Jenss, Wiedmann
640 -
320 -
a 160-
.
0
a 80-.9_0
a)
m(L 40-
20-
Figure 4: Antibodies to apancreatic antigen (PAB) in20 patients with Crohn'sdisease: titres duringfollowup ofover one year. 1987 1988
Antigenicactivity
E480nm
0.3
0.2-
0.1
a
I II0.1 0.5 1 2 3
Exposure to trypsin (hours)
Sera: o-o Ulcerative colitis_-- Crohn's diseaseA-A Hepatitis
showed thermolability when exposed to 56°Cfor 30 minutes. Detergents (sodium dodecyl-sulphate, Tritonx 100, and Tween 20 concentra-tions of 1%) and ethanol 95% and chloroformacetone (1:2) had no effect on antigenic activity.
Effect ofenzyme treatment on antigenic activityThe reactivity of 208 sera from patients withCrohn's disease and 135 sera from patients withother diseases (ulcerative colitis, acute and viralhepatitis, autoimmune diseases, pancreatitis)and healthy controls were tested in an ELISAsystem using chromatographically purified pan-creatic antigen which was either native or hadbeen treated with various enzymes (Table II)before coating the microtitre plates.When native antigen was used for testing, 54
(26%) of the patients with Crohn's diseaseshowed a positive reaction but also two of 25(8%) patients with ulcerative colitis, three ofnine(33%) patients with acute and chronic viralhepatitis, and two of 53 (4%) control patients.The relation of the results of ELISA andimmunocytochemistry is shown in Table III.The ELISA using the chromatographically
purified antigen is less sensitive forPAB detectionin Crohn's disease than the immunofluorescencetest. Furthermore, ELISA also detected 'PABreactivity' in some sera from patients with ulcer-ative colitis, pancreatitis, viral hepatitis, andhealthy controls, although previous immuno-fluorescence showed no reactivity.When microtitre plates that had been coated
with pancreatic antigen after digestion with
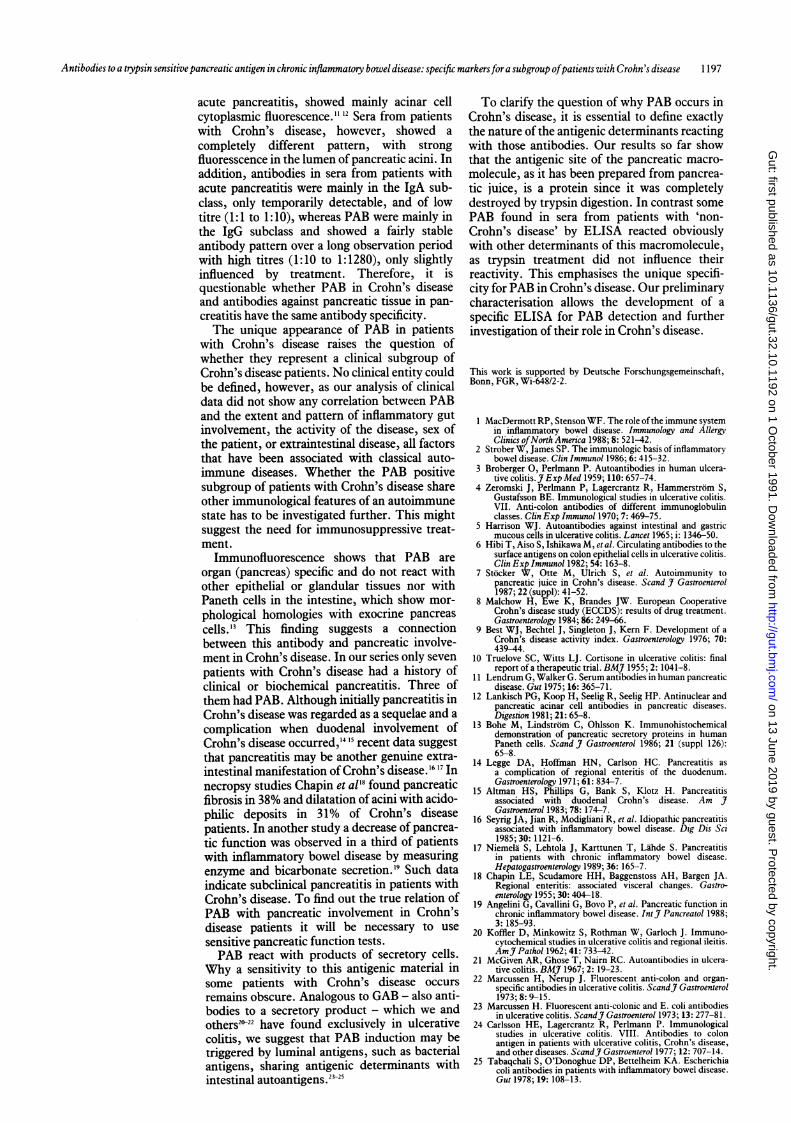
TABLE III Number ofPAB positive sera inimmunofluorescence (IFL) compared with ELISA usingchromatographically purified antigen and number ofserapositive for both IFL and ELISA
Positive sera:
No of IFL+sera tested IFL ELISA ELISA
Crohn's disease 208 62 54 51
Ulcerative colitis 25 2 2 2Pancreatitis 10 0 4 0Viral hepatitis 9 0 3 0Autoimmune disease 38 0 0 0
Healthy control subjects 53 0 2 0
Figure 5: Detection ofantibodies to a pancreatic antigen(PAB) using an ELISA system. Microtitre plates were coatedwith chromatographically purified antigen, either native ortreated with trypsin. Using the trypsin treated antigen onlyPAB in serafrom patients with Crohn's disease lose theirreactivity, not PAB in serafrom patients with hepatitis orulcerative colitis.
various enzymes were used, after trypsin treat-ment the positive reactivity of sera containingPAB from patients with Crohn's disease wasabolished, but not when sera containing PABfrom other patients were tested (Fig 5). Treat-ment with all other enzymes did not influence thereactivity ofPAB positive sera from patients withany of the diseases tested (Table II).
Reactivity ofPAB with defined pancreatic proteinsPAB positive sera did not react with any ofthe following pancreatic antigens: kallikrein,lactoferrin, trypsin, chymotrypsinogen, chymo-trypsin A and B, amylase, elastase, lipase,phosholipase A and C, enterokinase, carboxy-peptidase, and bovine trypsin inhibitor, whichhave been used as antigen in an ELISA system.
DiscussionIn the present study we detected antibodiesagainst a pancreatic antigen (PAB) in about onethird of patients with Crohn's disease using animmunofluorescence test as reported by Stockeret al.7 Although the sensitivity was low, theantibody pattern was highly specific for thisdisease and therefore of diagnostic value. Thisantibody pattern was not observed in any of thesera from patients with various other chronicinflammatory disorders (including ulcerativecolitis and pancreatitis) - except in two of 51patients with ulcerative colitis and then only invery low titres. Although the differential diag-nosis between ulcerative colitis and Crohn'sdisease issometimes difficult tomake, no evidenceof features ofCrohn's disease have appeared thusfar in those two patients during a 15 year followup.
Antibodies against pancreatic tissue, as pre-viously described in about 30% of patients with
1 1
1196
on 13 June 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.32.10.1192 on 1 October 1991. D
ownloaded from
Antibodies to a trypsin sensitive pancreatic antigen in chronic inflammatory bowel disease: specific markersfora subgroup ofpatients with Crohn's disease 1197
acute pancreatitis, showed mainly acinar cellcytoplasmic fluorescence." 12 Sera from patientswith Crohn's disease, however, showed acompletely different pattern, with strongfluoresscence in the lumen of pancreatic acini. Inaddition, antibodies in sera from patients withacute pancreatitis were mainly in the IgA sub-class, only temporarily detectable, and of lowtitre (1:1 to 1:10), whereas PAB were mainly inthe IgG subclass and showed a fairly stableantibody pattern over a long observation periodwith high titres (1:10 to 1:1280), only slightlyinfluenced by treatment. Therefore, it isquestionable whether PAB in Crohn's diseaseand antibodies against pancreatic tissue in pan-creatitis have the same antibody specificity.The unique appearance of PAB in patients
with Crohn's disease raises the question ofwhether they represent a clinical subgroup ofCrohn's disease patients. No clinical entity couldbe defined, however, as our analysis of clinicaldata did not show any correlation between PABand the extent and pattern of inflammatory gutinvolvement, the activity of the disease, sex ofthe patient, or extraintestinal disease, all factorsthat have been associated with classical auto-immune diseases. Whether the PAB positivesubgroup of patients with Crohn's disease shareother immunological features of an autoimmunestate has to be investigated further. This mightsuggest the need for immunosuppressive treat-ment.
Immunofluorescence shows that PAB areorgan (pancreas) specific and do not react withother epithelial or glandular tissues nor withPaneth cells in the intestine, which show mor-phological homologies with exocrine pancreascells.'3 This finding suggests a connectionbetween this antibody and pancreatic involve-ment in Crohn's disease. In our series only sevenpatients with Crohn's disease had a history ofclinical or biochemical pancreatitis. Three ofthem had PAB. Although initially pancreatitis inCrohn's disease was regarded as a sequelae and acomplication when duodenal involvement ofCrohn's disease occurred,'4 '5 recent data suggestthat pancreatitis may be another genuine extra-intestinal manifestation ofCrohn's disease.'6 17 Innecropsy studies Chapin et al'8 found pancreaticfibrosis in 38% and dilatation of acini with acido-philic deposits in 31% of Crohn's diseasepatients. In another study a decrease of pancrea-tic function was observed in a third of patientswith inflammatory bowel disease by measuringenzyme and bicarbonate secretion.'9 Such dataindicate subclinical pancreatitis in patients withCrohn's disease. To find out the true relation ofPAB with pancreatic involvement in Crohn'sdisease patients it will be necessary to usesensitive pancreatic function tests.PAB react with products of secretory cells.
Why a sensitivity to this antigenic material insome patients with Crohn's disease occursremains obscure. Analogous to GAB - also anti-bodies to a secretory product - which we andothers21322 have found exclusively in ulcerativecolitis, we suggest that PAB induction may betriggered by luminal antigens, such as bacterialantigens, sharing antigenic determinants withintestinal autoantigens.23~25
To clarify the question of why PAB occurs inCrohn's disease, it is essential to define exactlythe nature of the antigenic determinants reactingwith those antibodies. Our results so far showthat the antigenic site of the pancreatic macro-molecule, as it has been prepared from pancrea-tic juice, is a protein since it was completelydestroyed by trypsin digestion. In contrast somePAB found in sera from patients with 'non-Crohn's disease' by ELISA reacted obviouslywith other determinants of this macromolecule,as trypsin treatment did not influence theirreactivity. This emphasises the unique specifi-city for PAB in Crohn's disease. Our preliminarycharacterisation allows the development of aspecific ELISA for PAB detection and furtherinvestigation of their role in Crohn's disease.
This work is supported by Deutsche Forschungsgemeinschaft,Bonn, FGR, Wi-648/2-2.
1 MacDermott RP, Stenson WF. The role of the immune systemin inflammatory bowel disease. Immunology and AllergyClinics ofNorth America 1988; 8: 521-42.
2 Strober W, James SP. The immunologic basis of inflammatorvbowel disease. Clin Immunol 1986; 6: 415-32.
3 Broberger 0, Perlmann P. Autoantibodies in human ulcera-tive colitis.J Exp Med 1959; 110: 657-74.
4 Zeromski J, Perlmann P, Lagercrantz R, Hammerstrom S,Gustafsson BE. Immunological studies in ulcerative colitis.VII. Anti-colon antibodies of different immunoglobulinclasses. Clin Exp Immunol 1970; 7: 469-75.
5 Harrison WJ. Autoantibodies against intestinal and gastricmucous cells in ulcerative colitis. Lancet 1965; i: 1346-50.
6 Hibi T, Aiso S, Ishikawa M, et al. Circulating antibodies to thesurface antigens on colon epithelial cells in ulcerative colitis.Clin Exp Immunol 1982; 54: 163-8.
7 Stocker W, Otte M, Ulrich S, et al. Autoimmunity topancreatic juice in Crohn's disease. Scand J Gastroenterol1987; 22 (suppl): 41-52.
8 Malchow H, Ewe K, Brandes JW. European CooperativeCrohn's disease study (ECCDS): results of drug treatment.Gastroenterology 1984; 86: 249-66.
9 Best WJ, Bechtel J, Singleton J, Kern F. Development of aCrohn's disease activity index. Gastroenterology 1976; 70:439-44.
10 Truelove SC, Witts LJ. Cortisone in ulcerative colitis: finalreport of a therapeutic trial. BMJ 1955; 2: 1041-8.
11 Lendrum G, Walker G. Serum antibodies in human pancreaticdisease. Gut 1975; 16: 365-71.
12 Lankisch PG, Koop H, Seelig R, Seelig HP. Antinuclear andpancreatic acinar cell antibodies in pancreatic diseases.Digestion 1981; 21: 65-8.
13 Bohe M, Lindstrom C, Ohlsson K. Immunohistochemicaldemonstration of pancreatic secretory proteins in humanPaneth cells. Scand J Gastroenterol 1986; 21 (suppl 126):65-8.
14 Legge DA, Hoffman HN, Carlson HC. Pancreatitis asa complication of regional enteritis of the duodenum.Gastroenterology 1971; 61: 834-7.
15 Altman HS, Phillips G, Bank S, Klotz H. Pancreatitisassociated with duodenal Crohn's disease. Am JGastroenterol 1983; 78: 174-7.
16 Seyrig JA, Jian R, Modigliani R, et al. Idiopathic pancreatitisassociated with inflammatory bowel disease. Dig Dis Sci1985; 30: 1121-6.
17 Niemela S, Lehtola J, Karttunen T, Lahde S. Pancreatitisin patients with chronic inflammatory bowel disease.Hepatogastroenterology 1989; 36: 165-7.
18 Chapin LE, Scudamore HH, Baggenstoss AH, Bargen JA.Regional enteritis: associated visceral changes. Gastro-enterology 1955; 30: 404-18.
19 Angelini G, Cavallini G, Bovo P, et al. Pancreatic function inchronic inflammatory bowel disease. IntJ7 Pancreatol 1988;3: 185-93.
20 Koffler D, Minkowitz S, Rothman W, Garloch J. Immuno-cytochemical studies in ulcerative colitis and regional ileitis.AmJr Pathol 1962; 41: 733-42.
21 McGiven AR, Ghose T, Nairn RC. Autoantibodies in ulcera-tive colitis. BMJ 1967; 2: 19-23.
22 Marcussen H, Nerup J. Fluorescent anti-colon and organ-specific antibodies in ulcerative colitis. ScandJf Gastroenterol1973; 8: 9-15.
23 Marcussen H. Fluorescent anti-colonic and E. coli antibodiesin ulcerative colitis. ScandJr Gastroenterol 1973; 13: 277-81.
24 Carlsson HE, Lagercrantz R, Perlmann P. Immunologicalstudies in ulcerative colitis. VIII. Antibodies to colonantigen in patients with ulcerative colitis, Crohn's disease,and other diseases. ScandJf Gastroenterol 1977; 12: 707-14.
25 Tabaqchali 5, O'Donoghue DP, Bettelheim KA. Escherichiacoli antibodies in patients with inflammatory bowel disease.Gut 1978; 19: 108-13.
on 13 June 2019 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.32.10.1192 on 1 October 1991. D
ownloaded from