antibiotics
DESCRIPTION
Antibiotics. Judith Coombes, University of Queensland. General Principles. Establish the need for antibiotic therapy When not to prescribe Viral or minor bacterial disease Viral diarrhoea Sore throat Sinusitis Common cold Are self limiting Common cold needs common sense campaign. - PowerPoint PPT PresentationTRANSCRIPT
Antibiotics
Judith Coombes, University of Queensland

General Principles
• Establish the need for antibiotic therapy• When not to prescribe
– Viral or minor bacterial disease– Viral diarrhoea– Sore throat– Sinusitis– Common cold
Are self limitingCommon cold needs common sense campaign
Antibiotic treatment can be• Prophylactic antibiotics prevent serious infection in
specific situations (e.g. preventing the spread of meningococcal disease).
• Presumptive antibiotic therapy is indicated in some circumstances (e.g. a human bite to the hand
• Use empirical antibiotic therapy — which is aimed at the likely causative organism — to manage an infection until microbiological culture and susceptibility results are known
• When the cause of an infection is confirmed, directed therapy is aimed at the specific pathogen.
MIND ME
M microbiology guides therapy wherever possibleI indications should be evidence-basedN narrowest spectrum requiredD dosage appropriate to the site and type of
infectionM minimise duration of therapyE ensure monotherapy in most situations
5 Antibiotics• Benzylpenicillin or Amoxycillin
– Streptococcis• Cloxacillin
– Staphylococcis• Vancomycin
– MRSA• Gentamicin
– Pseudomonas• Metronidazole
– anaerobes
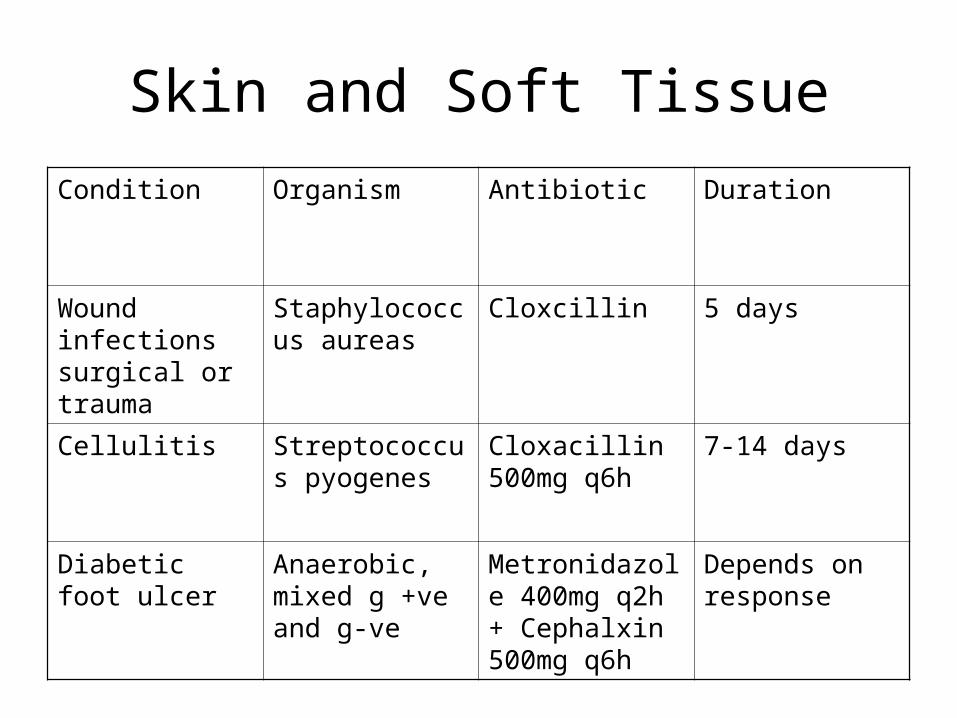
Skin and Soft TissueCondition Organism Antibiotic Duration
Wound infections surgical or trauma
Staphylococcus aureas
Cloxcillin 5 days
Cellulitis Streptococcus pyogenes
Cloxacillin 500mg q6h
7-14 days
Diabetic foot ulcer
Anaerobic, mixed g +ve and g-ve
Metronidazole 400mg q2h + Cephalxin 500mg q6h
Depends on response

UTICondition Organism Antibiotic Duration
Cystitis in men + non pregnant women
E coli, ebsiella, Enterococcus faecalis, proteus mirabilis
Trimethoprim 300mg daily or Amoxycillin/clavulanate 875/125 q12h
W 3 days men 14 daysW 5 days men a4 days
Catheter associated infections
Only treat if symptoms, change catheter
Cystitis in pregnant women
As above Cephalexin 500mg q12h
10-14 days
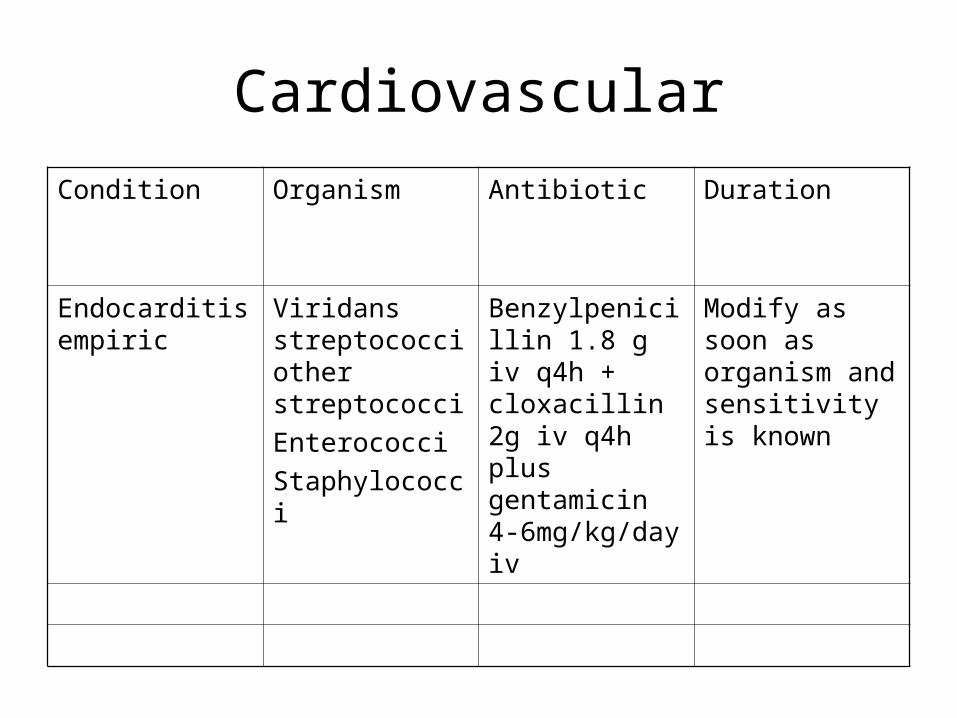
CardiovascularCondition Organism Antibiotic Duration
Endocarditis empiric
Viridans streptococci other streptococciEnterococciStaphylococci
Benzylpenicillin 1.8 g iv q4h + cloxacillin 2g iv q4h plus gentamicin 4-6mg/kg/day iv
Modify as soon as organism and sensitivity is known
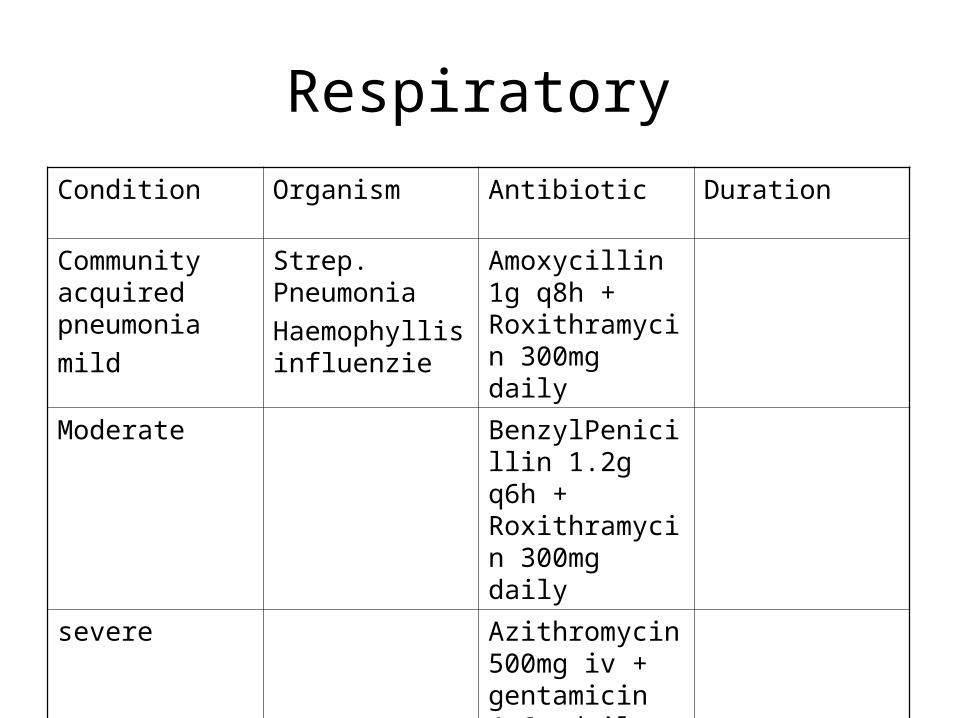
RespiratoryCondition Organism Antibiotic Duration
Community acquired pneumoniamild
Strep. PneumoniaHaemophyllis influenzie
Amoxycillin 1g q8h + Roxithramycin 300mg daily
Moderate BenzylPenicillin 1.2g q6h + Roxithramycin 300mg daily
severe Azithromycin 500mg iv + gentamicin 4-6g daily + Benzylpenicillin 1.2g q6h
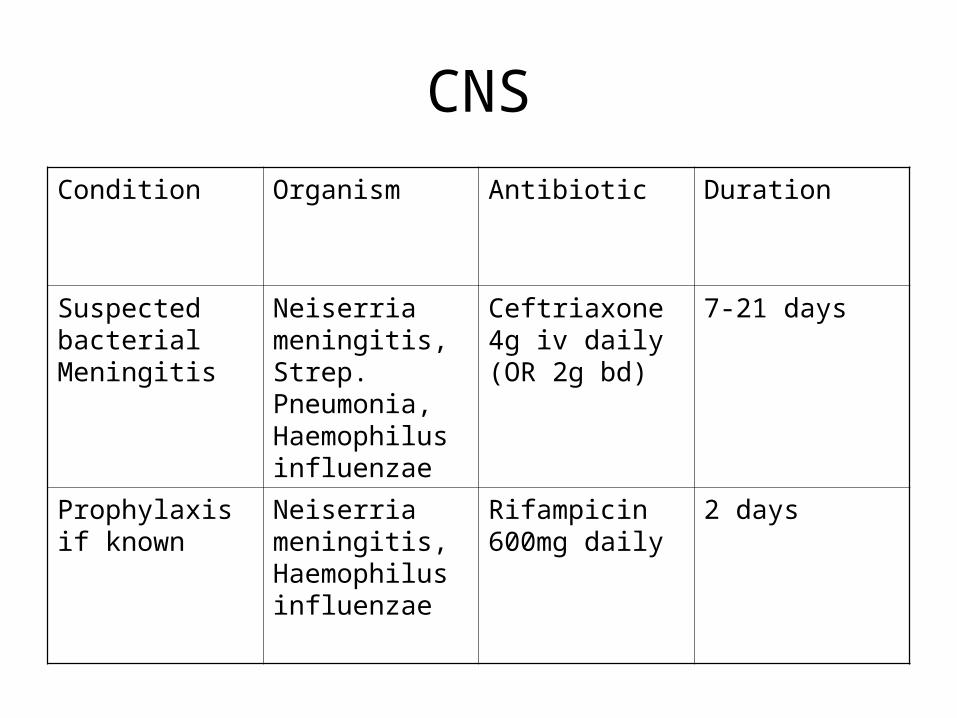
CNSCondition Organism Antibiotic Duration
Suspected bacterial Meningitis
Neiserria meningitis, Strep. Pneumonia, Haemophilus influenzae
Ceftriaxone 4g iv daily (OR 2g bd)
7-21 days
Prophylaxis if known
Neiserria meningitis, Haemophilus influenzae
Rifampicin 600mg daily
2 days
Sepsis- definition
• In adults and older children, severe sepsis is the systemic response to an infection manifested by organ dysfunction, hypoperfusion or hypotension combined with 2 or more of the following: – fever, – tachycardia, – tachypnoea, – elevated white cell count
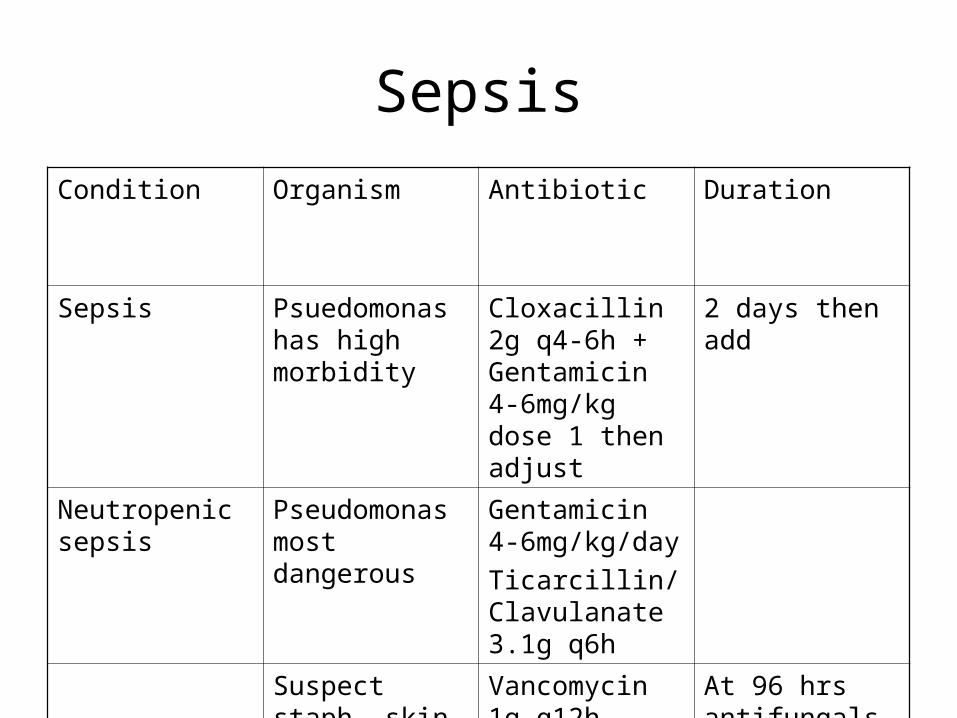
SepsisCondition Organism Antibiotic Duration
Sepsis Psuedomonas has high morbidity
Cloxacillin 2g q4-6h + Gentamicin 4-6mg/kg dose 1 then adjust
2 days then add
Neutropenic sepsis
Pseudomonas most dangerous
Gentamicin 4-6mg/kg/dayTicarcillin/Clavulanate 3.1g q6h
Suspect staph- skin wound or at 48 hrs
Vancomycin 1g q12h
At 96 hrs antifungals

Gentamicin Revision
• Gram negative bactericidal agent• Excellent anti-pseudomonal cover• Once daily dosing benefits vs tds or bd:
- high peak level – excellent distribution- post antibiotic effect (>24-36 hours) - reduced monitoring and administration- reduced nephro and ototoxicity- easier monitoring (10-12 hours post dose)

Severe risks of nephrotoxicity and ototoxicity
• Mrs HR• 78 years, wt 57kg• Admitted to outlying hospital acute exacerbation
COPD• Baseline Cr 80mol/L, Urea 8.5 • Charted gentamicin 160mg daily for 5/7 – no
levels requested • Baseline CrCl = 45ml/min

Date Gent Dose Level Cr Urea3/6 0.08 8.55/6 160mg6/6 160mg 0.11 15.57/6 160mg 6.2 0.138/6 160mg 9.0 0.17 21.99/6 160mg10/6 ceased 16.9 0.22 28.311/612/6 7.8 0.36 35.013/6 0.3914/6 0.41 33.615/6 0.5016/6 0.59 38.917/6 0.65 40.6
Patient progress• 15/6 K+ = 6.7, Acidotic to ICU + haemodialysis
• 21/6 Gent level still 1.4!!!!
• 23/6 complaining of dizziness, unsteady feeling, vestibular symptoms, vomiting
• 1/7 Cr 0.21 recovering
• 14/11 Out patient – permanent Ototoxicity
Local Sri Lankan Hospital
• 75 yr old patient post amputation, septic• Gentamicin iv 80mg tds, Co Amoxyclav iv +
metronidazole iv• Day 7 reviewed by anesthetists – pain control• Noted Urea increased from 7.1 – 15.2• Patient not septic - ? Need for antibiotic• Seen Day 12 post operative, Urea = 26 same
dose gentamicin
Aminoglycoside dosing and Monitoring
Case continued…
Day 3:• Mr AD (67yrs) has now developed sever hospital
acquired pneumonia • Ward round decisions
- start gentamicin once a day dose as per levels each night at 20:00 recall patient weighs 70 kg creatinine has improved (now 140 micro mole/l)
- start Co-Amoxiclav 1.2g IV q8h
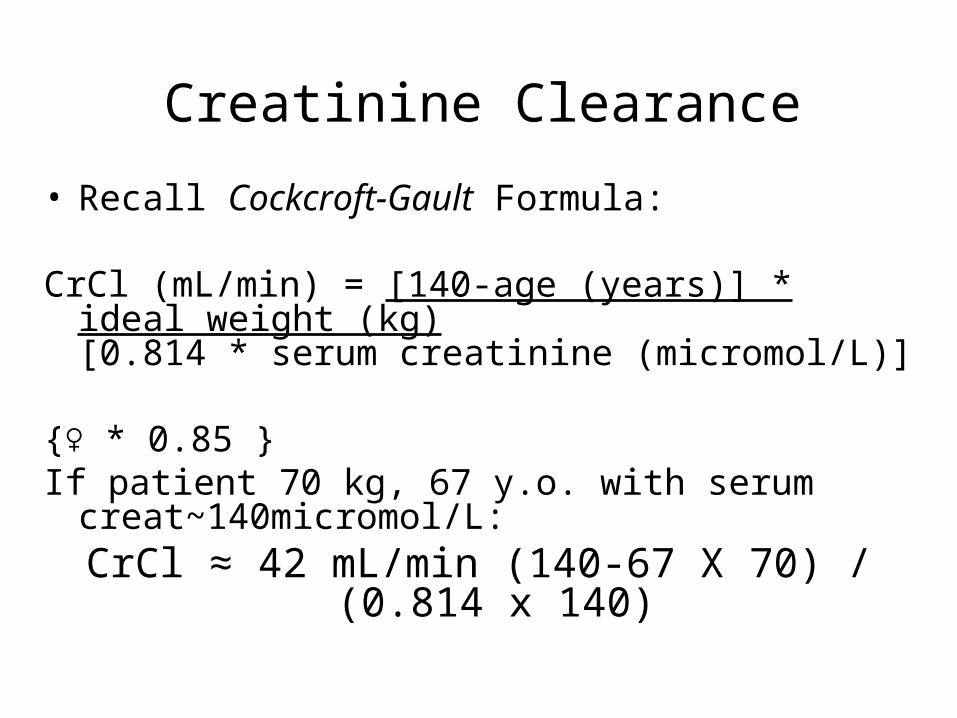
Creatinine Clearance• Recall Cockcroft-Gault Formula:
CrCl (mL/min) = [140-age (years)] * ideal weight (kg) [0.814 * serum creatinine
(micromol/L)]
{♀ * 0.85 }If patient 70 kg, 67 y.o. with serum
creat~140micromol/L:CrCl ≈ 42 mL/min (140-67 X 70) / (0.814 x
140)

Calculating first dose gent

Gentamicin Dose Adjustment
Day 4: gentamicin level = 2.5
(taken 08:00, 12 hrs post dose)• The initial dose given in emergency department was
280mg (4mg/kg x approx 70kg)
Prescribe new gentamicin dose based on level

2.5
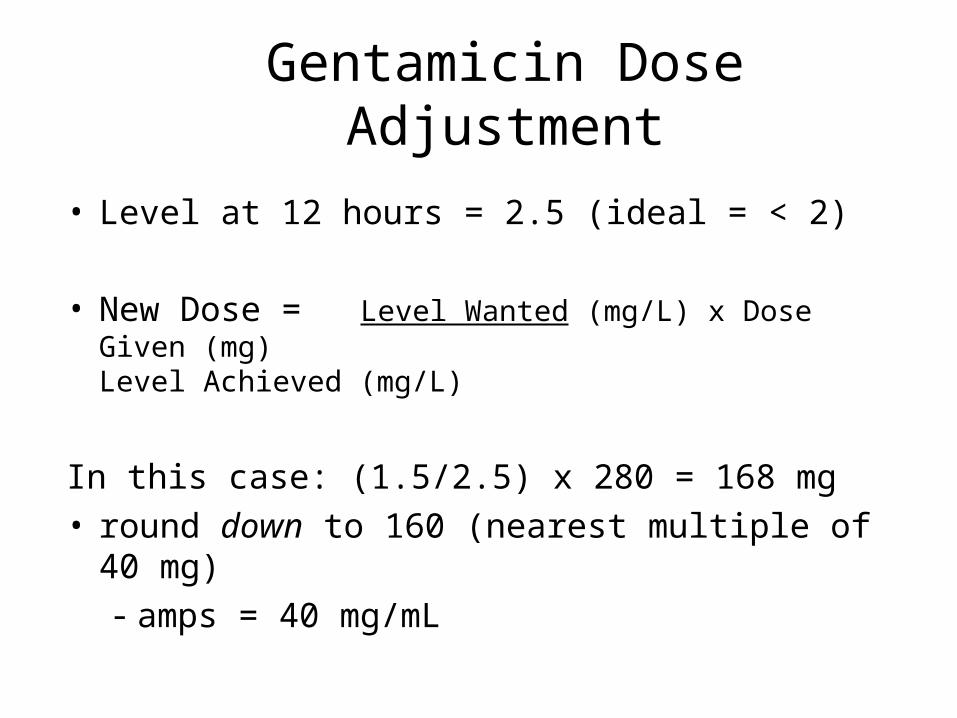
Gentamicin Dose Adjustment
• Level at 12 hours = 2.5 (ideal = < 2)
• New Dose = Level Wanted (mg/L) x Dose Given (mg)
Level Achieved (mg/L)
In this case: (1.5/2.5) x 280 = 168 mg• round down to 160 (nearest multiple of 40 mg)
- amps = 40 mg/mL
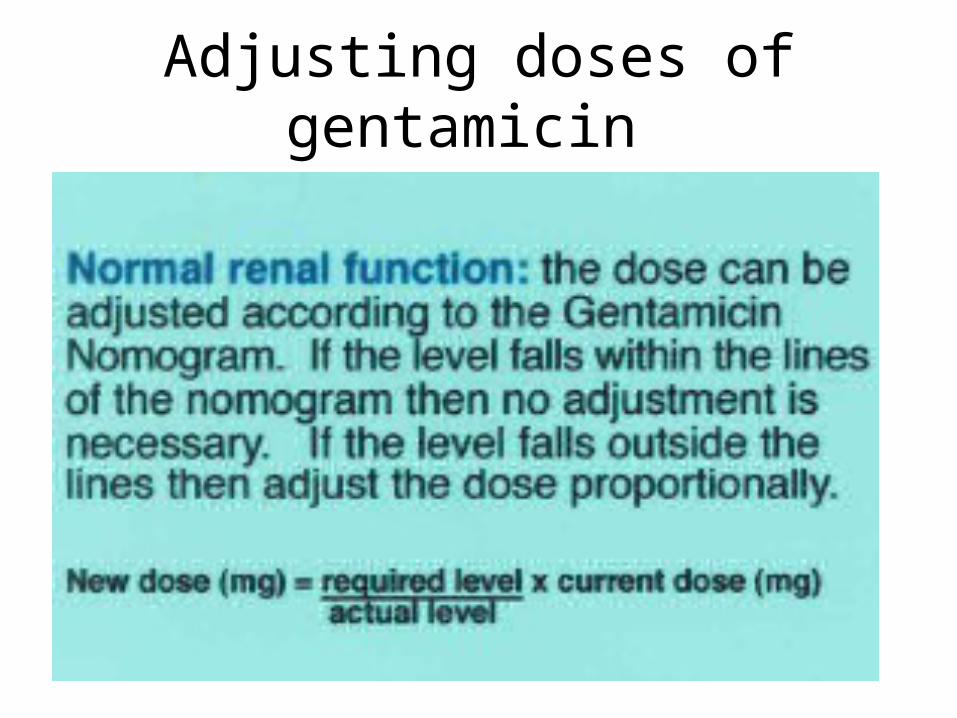
Adjusting doses of gentamicin
When NOT to take levels
• Do not take levels if:• Stat dose • Or• Patient has Normal renal function and is
only receiving 1 or 2 doses ie prophylactic

Variable Dose MedicationDrug Level and Time Taken
Dose Time and Actual Time Given
Use in moderate to severe renal function
• Where ever possible withhold other nephrotoxic drugs and ensure no other altenative
• Ie unavoidable use of gentamicin:• Requires extended dose intervals 36, 48
or 96 hours• Effectively daily levels wait til < 1.0mmol/l
then dose again
