antibiotic medications for infections in athletes: which ... · antibiotic medications for...
TRANSCRIPT

Antibiotic Medications for Infections in Athletes:
which to use or not to use?
Prof Wayne DermanMBChB,BSc (Med)(Hons) PhD, FFIMS

2
3
Clinical questions team physicians encounter
regarding antibiotic treatment
• What are the most common infections
encountered in a team setting?
• What are the other considerations regarding
prescribing antibiotics?
• Clinical recommendations?
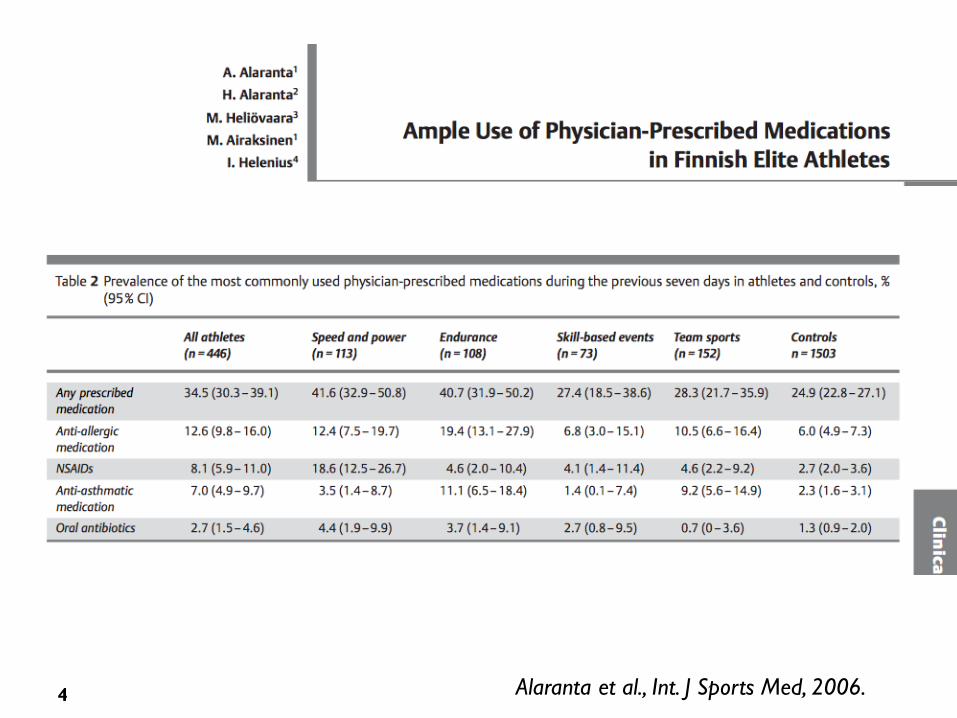
4 Alaranta et al., Int. J Sports Med, 2006.
Factors to take into account when considering
antibiotic therapy
• Most “infections” we
encounter are not bacterial
• Likelihood of specific
causative pathogen
• Susceptibility
• Dosing frequency
• Mode of administration
• Allergies
5

Resp/ENT: Causative Organisms
Viruses (over 200) Bacteria Idiopathic
Rhinovirus Group A Streptococcus *(No organism isolated)*
Corona virus Bordetella Pertussis
Influenza & Parainfluenza virus Corynaebacterium Diphtheria
Respiratory Syncytial Virus
Adenovirus
Enterovirus
Bacterial vs Viral can you tell?
• Moderate indicators:– Typical examination
– Fever higher in bacterial
– Fever gets worse few days in
– Symptoms persist longer than expected (10-14 days)
– Localized (Sinusitis, ear, lung).
– Full blood count
Good indicators:
Swab for MC&S
Specific blood tests: ASO, EBV, H1N1
New tests? CRP? Rapid PCR?


Bacterial vs Viral can you tell?
• Moderate indicators:– Typical examination
– Fever higher in bacterial
– Fever gets worse few days in
– Symptoms persist longer than expected (10-14 days)
– Localized (Sinusitis, ear, lung).
– Full blood count
Good indicators:
Swab for MC&S
Specific blood tests: ASO, EBV, H1N1
New tests? CRP? Rapid PCR?


• The diagnosis of nonspecific upper respiratory tract infection should be used to denote an acute infection in which sinus, pharyngeal, and lower airway symptoms, although frequently present, are not prominent.
• These infections are predominantly viral in origin, and complications are rare.
• Antibiotics should not be used to treat nonspecific upper respiratory tract infections in previously healthy adults.
• Purulent secretions from the nares or throat do not predict bacterial infection or benefit from antibiotic treatment.
• Antibiotic treatment of adults with non-specific upper respiratory tract infections does not enhance illness resolution or prevent complications.
Snow et al., Annals Internal Medicine: 134, 2011

• Toxins: – ETEC (entero-toxic E Coli - principal cause of
traveler’s diarrhea
• Infective:– Viral (norovirus, rotavirus)
– Bacterial (Eschericia Coli, Camplyobacter jejuni, Shigella, Clostridium difficile)
– Parasitic (Giardia lamblia, Entamoebahistolytica)
Infectious “traveller’s” diarrheaMore common pathogens

Simple travellers diarrhea • > 2 lose stools in 24hrs• Other symptoms: nausea, vomiting, mild intermittent abdominal
cramping • No fever or blood in stools
Significant travellers diarrhea • As for simple travellers diarrhea and >1 of the following:• Temperature > 37oC• Blood in stools• Constant or severe abdominal pain• Rebound and/or guarding
Infectious “traveller’s” diarrheaClinical features - classification
Tillett et al, BJSM, 2009, 1045-1048

Infectious “traveller’s” diarrheaPharmacological treatment
Drug Dose Notes
Ciprofloxacin 500mg bd. for 3 days
Risk of tendon injury, rupture (NB: Athletes)
Levofloxacin 500mg qds. for 3 days
Risk of tendon injury, rupture (NB: Athletes)
Azithromycin 1000mg single dose
Nausea, effective against invasive forms (bloody stool and fever), risk of arrthymia (NB: Athletes)
Rifaximin (Xifaxin)
200mg tds. For 3 days
Not effective against invasive forms (bloody stool and fever) ? Athletes
Du Pont, Alim Pharm Ther, 2009, 187-196

15
Tendon injuries
• 2002 – Flouroquinolones most commonly prescribed class of
antibiotic in US adult population.
• Increasing association with Achilles tendon
• 2008 – black box warning of Achilles tendinopathy and rupture
• 3-6x increased risk of tendon problems or rupture
• Absolute risk of 7.74 per 100.000 days at risk and 3.2 /1000 patient
years
• Mechanism free radical & toxin damage to watershed area of the
tendon, remodeling of tendon and matrix disorder
• Association with increased age and corticosteroid use
• Discuss risk, alternate drugs.

• Tendinopathy can be a complication of treatment with
fluoroquinolone antibiotics and usually is linked with 1 or more
synergistic factors.
• Symptoms of fluoroquinolone-related tendinopathy can present
within hours of starting treatment or up to 6 months after ceasing
treatment, and recovery can be slower and require a less
aggressive approach early in rehabilitation than for other types of
tendinopathy.
• Treatment with fluoroquinolones should be discontinued and
treatment with a nonquinolone antibiotic should be considered in
patients who present with tendinopathy.
• Clinicians, athletes, athletic trainers, and medical support teams
should be aware of and alert to the potential adverse effects of
fluoroquinolones.
16

Antibiotic prescription Risk of serious arrhythmia
0
0,5
1
1,5
2
2,5
3
Day 1-5 Day 6-10
Ad
jus
ted
HR
of
all c
au
se
de
ath
Amoxycillin Azithromycin Levofloxacin
Gowtham A, et al Ann Fam Med. 2014;12(2):121-127

Cardiac Arrhythmia
• Macrolides and fluoroquinalones may
be associated with an increased risk
of ventricular arrhythmia and cardiac
arrest
• Small increase number of
cardiovascular related deaths with
azithromycin
• Prolongation of QT interval by
erythromycin, clarythromycin and
moxifloxacin
• Mean increase in the QT interval
with fluoroquinolones is 3-6 ms little
clinical significance in N but might
place extra risk in those with long
QT syndrome
18

Antibiotic- induced diarrhea
• Acutely or up to 3-4 wks after
initiation of antibiotic treatment
• Most common after broad
spectrum, enterobacteriaciae
• Proliferation of C.difficile or
impaired microflora
• Risk factors: duration, repeated
use or combination AB’s
• Minimum exposure, narrow
spectrum, probiotics
• Saccharomyces boulardii &
Lactobacillus rhamnosus
19

20
Photosensitivity
• Photosensitivity : phototoxicity after single does or photoallergic –
an immune mediated response and requires re-exposure
• Tetracyclines – doxycyline (most), minocycline (rare;
hyperpigmentation 2-15%)
• Seen with 2 weeks of onset of treatment, dosage dependent
• Fluoroquinalones also cause photosensitivity (ciplofloxacin 1-4%).
Levofloxacin least
• Sulfonamides also; Stevens-Johnson syndrome
• If athlete is participating in outdoor events avoid photosensitizing
antibiotics or use anti-sun measures

21
Other adverse effects to consider
• Tetracyclines staining teeth skin, sclera conjunctiva and
bone.
• Chelation & is reversible through remodeling.
• Teeth permanent
• Contraindicated in young athletes
• Fatigue and underperformance
• ? Effects of illness or drug
• Tetracycline, ampicillin and trimethoprim-sulfamethoxazole
to placebo over three days showed no effect on VO2max,
muscle strength, [CK], fatigue scores
• Higher fatigue with multiple antibiotics, tetracyclines 1,2%
with doxycycline, 23% with minocycline.
• Know your destination and the risks
• Develop a prevention strategy
• Education of athletes and officials
• Develop a clinical approach to diagnosis
• Develop a management approach
• Get to know 4-5 agents that you can use that work
for you
Prevention of Infections
fosfamycin
Kantrexil
Thank you for your attention!
Prof Wayne DermanMBChB,BSc (Med)(Hons) PhD, FFIMS