anti-racism in medical education: concrete actions to
TRANSCRIPT

Anti-Racism in Medical Education: Concrete Actions to Further Social Justice and Racial Equity
Rachel Bonnema, MD, Kate Lupton, MD, Sarah Merriam MD, MS and Aditi Puri, MD, MS
Acknowledge: Daniel le Jones, MD, Rani Nandiwada, MD, Laura Snydman, MD, Carla Spagnolett i , MD, MS and Eloho Ufomata, MD, MS
On behalf of the SGIM Education Committee

Ufomata E, Merriam S, Puri A, et al . J Gen Intern Med. 2021.https://doi.org /10.1007/s11606-020-06445-2

By the end of this session, attendees will be able to:
1) Define structural racism
2) Identify historical and current manifestations of structural racism within institutions of medical education
3) Employ a multidimensional strategy to combat systemic racism
4) Advocate at the local level for broader institutional commitment and organizational policy changes to achieve the ultimate goal of social justice and racial equity
Structural racism, defined
The practices, policies, and norms that perpetuate white supremacy
Embedded within the DNA of institutions of medical education

Historical manifestations of structural racism within institutions of medical education
“Color line”- Exclusion of Black Americans from US medical training
1910: Flexner report
1965: exclusion of Black Americans from medical education legally ends

Many manifestations of structural racism persist within institutions of medical education
•Exclusion from the profession and professional development◦ Discrimination in grading and honors/awards impacts access to
medical training1,2
◦ Dearth of Black faculty (2.2% Black women, 1.5% Black men)3
◦ Absence of role models4,5
1. Teherani et al. Acad Med. 20182. Ross et al. PLoS ONE. 20173. 2020 US Medical School Faculty. AAMC4. Bullock et al. Acad Med. 20205. Ackerman-Barger. Acad Med. 2020

Many manifestations of structural racism persist within institutions of medical education
•Exclusion from the profession and professional development
•Curricular biases◦ Lack of equity in use of curricular images6,7
◦ Misrepresentation of race as a biologic factor8-10
◦ Differential outcomes result from social determinants and racism11
◦ Patients of color are underrepresented in “evidence-based” teaching12
6. Brooks KC. JAMA. 20157. Nolen L. NEJM. 20208. Tsai et al. Acad Med. 2016
9. Amutah et al. NEJM. 202110. Vyas et al. NEJM. 2020
11. Hall et al. Amer J Public Health. 201512. Terry M. Biospace. 2020

Many manifestations of structural racism persist within institutions of medical education
•Exclusion from the profession and professional development
•Curricular biases
•Professional◦ No standards for curriculum or competencies on structural racism,
social justice, and social determinants of health

Anti-racism within Medical EducationFormal integration of anti-racism education remains underemphasized
Existing curricula focus on individual-level factors (unconscious bias, cultural competency) instead of systems and structures

Call to Action As medical educators, we must develop a workforce that can best care for diverse patients
We must progress beyond individual-level interventions to directly combat racism and structural oppression
We must acknowledge the structural racism integrated into all levels of training, adopt an actively anti-racist framework, and work together to dismantle discriminatory institutional policies at the organizational level

In the next 60 minutes, 1) Outline organizational strategies within four broad areas of
impact to promote racial justice and equity◦ Furthering Anti-Racist Curricula
◦ Learner Support and Academic Environment
◦ Educational Policy
◦ Professional Culture
2) Identify concrete steps that we as teachers, education researchers, and education program leaders can adopt to support an anti-racist mission

Organizational Actions• Furthering Anti -Racist Curricula
• Learner Support and Academic Environment
• Educational Policy
Aditi Puri, MD, MS
Acknowledge: Laura Snydman, MD

Furthering Anti-Racist CurriculaWhat can organizations do?
1. Create a longitudinal anti-racist thread in medical education
2. Maintain better curricular oversight
3. Provide faculty development
4. New LCME and ACGME core competency
Furthering Anti-Racist Curricula: 1. Longitudinal Anti-Racist Thread in Med Ed• Across all courses
• Infuses content on racism & social determinants of health
• Overarching goal = critically shape students’ interest and competencies in caring for minority populations
• Pay special attention to Racial qualifiers
Description of patent histories, health beliefs and behaviors
• Highlight racism and social determinants of health as sources of chronic stress and disparities in health outcomes

Furthering Anti-Racist Curricula: 2. Maintain Curricular Oversight
Brown University School of Medicine
Conducted an internal review of how race and racialized disparities are presented within all existing curricula
UCSF School of Medicine
Anti-racist liaison program
Provided faculty with resources and support to modify/adapt content with an anti-racist equity lens

Furthering Anti-Racist Curricula: 2. Maintain Curricular Oversight
Curricular oversight lessons
Train educators how to develop, teach, and assess anti-racist curricula
Incorporate and compensate a “consult team” to perform curricular mapping of social justice and racial equity
Use evidence-based tools to examine the portrayal of race and structural inequities within clinical teaching cases
Furthering Anti-Racist Curricula: 2. Maintain Curricular Oversight

Furthering Anti-Racist Curricula:3. Provide Faculty Development
Micro/macroaggressions
Implicit bias
Bystander upstander
Advocacy training for faculty, learners, and staff
Examples:◦ UCSF Diversity Equity, and Inclusion Champion Training
◦ Bias Reduction in Internal Medicine (BRIM) Initiative
UCSF
BRIM

“Mastering the health effects of structural
racism”
Furthering Anti-Racist Curricula:4. Create New Core Competencies
Hardeman RR, Medina EM, Boyd RW. Stolen Breaths. New England Journal of Medicine. 2020;383(3):197-9.
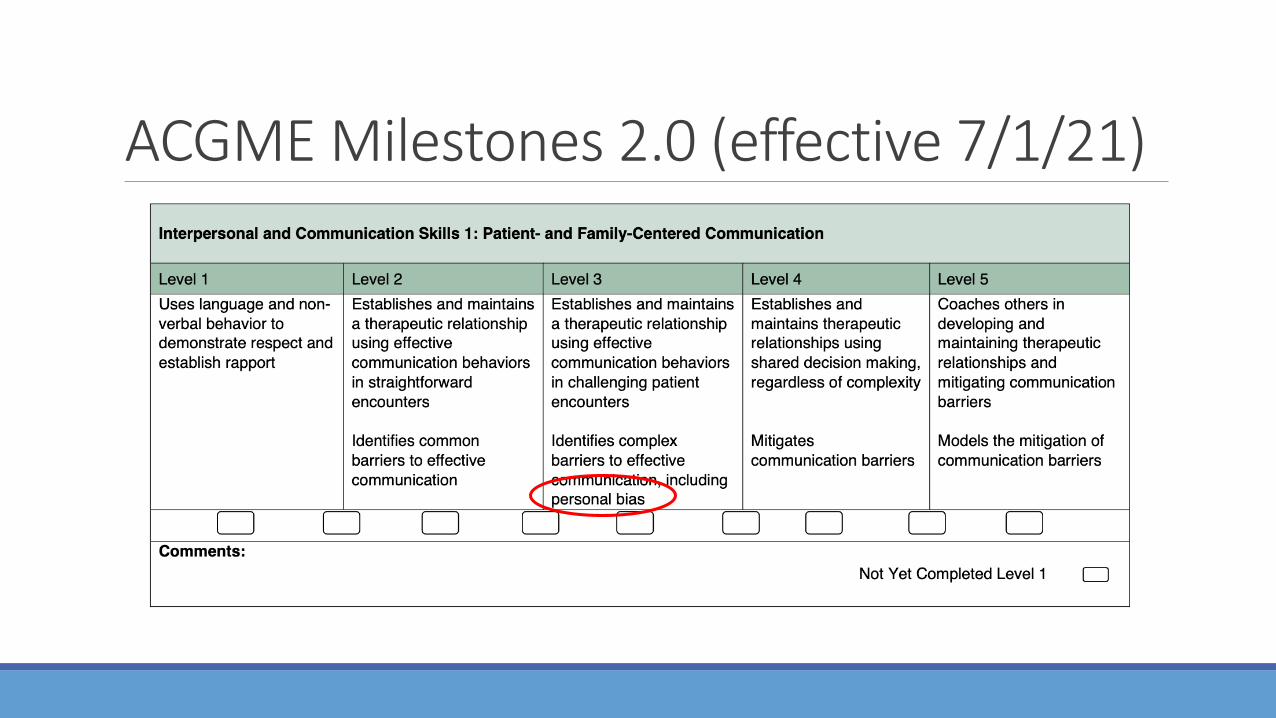
ACGME Milestones 2.0 (effective 7/1/21)
AAMC Competencies under development
https://www.aamc.org/what-we-do/mission-areas/medical-education/cbme/competency

Organizational Actions• Furthering Anti -Racist Curricula
• Learner Support and Academic Environment
• Educational Policy
Rachel Bonnema, MD
Acknowledge: Rani Nandiwada, MD
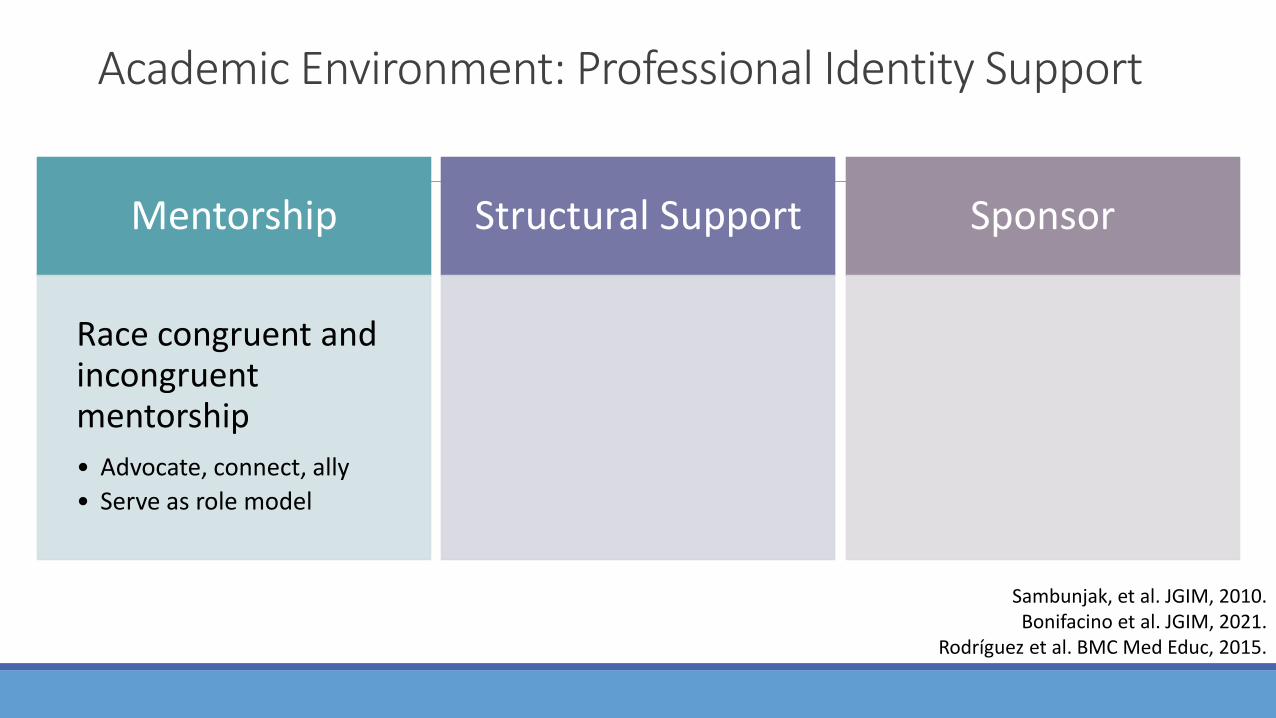
Academic Environment: Professional Identity Support
Mentorship
Race congruent and incongruent mentorship
• Advocate, connect, ally
• Serve as role model
Structural Support
Mentorship and training of new URiM faculty
• Navigating isolation, hypervisibility, stereotype threat, and institutional racism
Sponsor
URiM trainees/faculty for:
• awards
• scholarships
• professional development opportunities
Sambunjak, et al. JGIM, 2010.Bonifacino et al. JGIM, 2021.
Rodríguez et al. BMC Med Educ, 2015.

Academic Environment: Professional Identity Support
Mentorship
Race congruent and incongruent mentorship
• Advocate, connect, ally
• Serve as role model
Structural Support
Mentorship and training of new URiM faculty
• Navigating isolation, hypervisibility, stereotype threat, and institutional racism
Sponsor
URiM trainees/faculty for:
• awards
• scholarships
• professional development opportunities
Sambunjak, et al. JGIM, 2010.Bonifacino et al. JGIM, 2021.
Rodríguez et al. BMC Med Educ, 2015.

Academic Environment: Professional Identity Support
Mentorship
Race congruent and incongruent mentorship
• Advocate, connect, ally
• Serve as role model
Structural Support
Mentorship and training of new URiM faculty
• Navigating isolation, hypervisibility, stereotype threat, and institutional racism
Sponsor
URiM trainees/faculty for:
• awards
• scholarships
• professional development opportunities

Academic Environment: Professional Identity Support
Promote affiliations with and creation of organizations dedicated to URIM belonging and success ◦ Emory Division of GIM Faculty Review
committee◦ Geared toward helping achieve
promotion at earliest rank/time possible
◦ Institution/Chair supported faculty development focused on supporting URiM faculty

Academic Environment: Admissions Adopt a holistic review model for trainee/faculty recruitment • Examine/report existing processes for equity• Reduce reliance on discriminatory metrics (standardized test scores, AOA)• Identify surrogates for standardized tests congruent with mission
Track and report programmatic diversity (including leadership, faculty, and staff)
Set and report pre-defined metrics of success in a transparent and accessible manner

Academic Environment: Bias in Assessment—Learner
“Assessment experiences, particularly during clinical education, play a critical role in shaping learners’ future training and career opportunities, identity, and growth. Efforts to create an inclusive, fair, and equitable clinical training experience must address the development of an equitable assessment system that considers how UIM learners achieve and succeed.
An assessment system that capitalizes on this antideficit framing would avoid comparison to peers, emphasize narrative assessment, focus on patient care and learner growth, train clinical supervisors to minimize bias, and consider learner identity. Nurturing and capitalizing on learner strengths and contributions can create and sustain a diverse and equitable learning environment that optimizes patient care.”
Teherani et al. Acad Med. 2020.
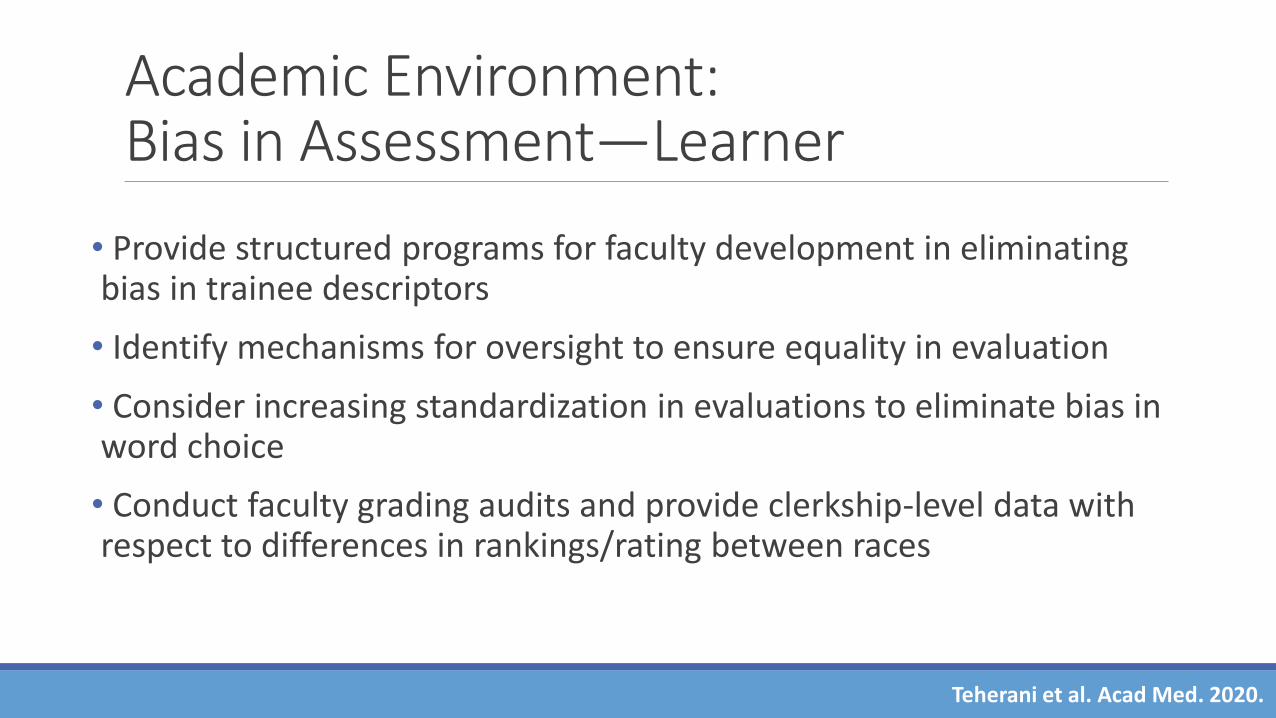
Academic Environment: Bias in Assessment—Learner
• Provide structured programs for faculty development in eliminating bias in trainee descriptors
• Identify mechanisms for oversight to ensure equality in evaluation
• Consider increasing standardization in evaluations to eliminate bias in word choice
• Conduct faculty grading audits and provide clerkship-level data with respect to differences in rankings/rating between races
Teherani et al. Acad Med. 2020.
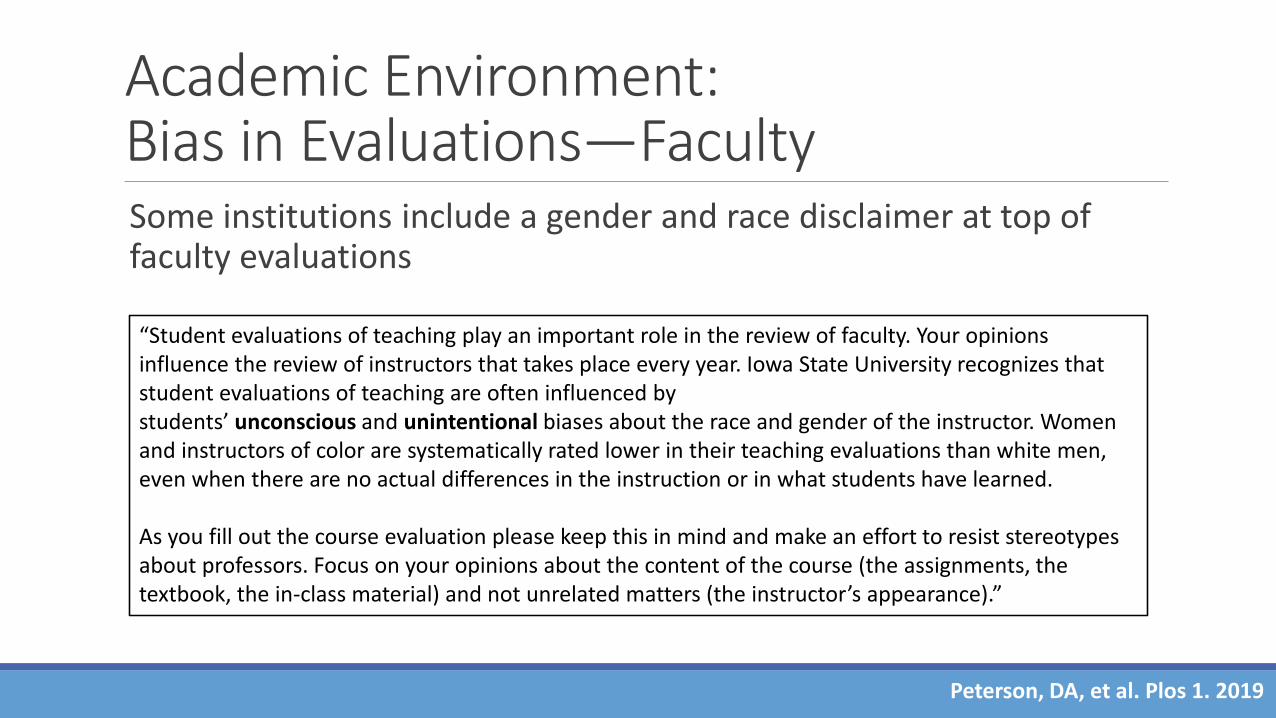
Academic Environment: Bias in Evaluations—Faculty Some institutions include a gender and race disclaimer at top of faculty evaluations
Peterson, DA, et al. Plos 1. 2019
“Student evaluations of teaching play an important role in the review of faculty. Your opinions influence the review of instructors that takes place every year. Iowa State University recognizes that student evaluations of teaching are often influenced by students’ unconscious and unintentional biases about the race and gender of the instructor. Women and instructors of color are systematically rated lower in their teaching evaluations than white men, even when there are no actual differences in the instruction or in what students have learned.
As you fill out the course evaluation please keep this in mind and make an effort to resist stereotypes about professors. Focus on your opinions about the content of the course (the assignments, the textbook, the in-class material) and not unrelated matters (the instructor’s appearance).”

Organizational Actions• Furthering Anti -Racist Curricula
• Learner Support and Academic Environment
• Educational Policy
Sarah Merriam, MD, MS
Acknowledge: Kate Lupton, MD

Educational Policy
Organizations should focus policy efforts that promote equity in the following areas:
1. Professional effort
2. Career advancement
3. Recruitment and retention

Educational Policy: Professional Effort• Ensure that DEI committees are equivalent to other standing committees with respect to support, membership, compensation ◦ Review % budgetary allotments to equity, diversity, inclusion and justice efforts◦ Prioritize funding streams for equity work
• Conduct transparent salary audits to ensure equal compensation for URiMfaculty across standard metrics of education, research, and clinical care
• Identify metrics to capture this “invisible work” for purposes of promotion
De Los Reyes & Uddin. Nature Neuroscience. 2021Butkus et al. Annals of Int Med. 2018

Educational Policy: Professional Effort
Broaden currency of promotion to include equity work
Educational Policy: Career Advancement
• Sponsor URiM students and faculty
• Publicize leadership and professional development opportunities to URiM trainees and faculty
• Leverage, create and augment funding targeted at URiMtrainees and faculty
Bhalla. MBoC. 2019Butkus et al. Annals of Int Med. 2018

Educational Policy: Career Advancement • Ensure URiM representation on award and selection committees
All committees appointed by the Chancellor or members of the Chancellor’s Cabinet shall comprise 50% women and underrepresented minorities (URM), i.e., committees must include both women and URM members, together totaling at least 50% of the membership. Efforts should be made to include other marginalized groups, such as individuals with disabilities, members of the LGBTQ+ community, and veterans.

Educational Policy: Career Advancement
• Conduct periodic advancement audits
• Broadly apply institution-wide anti-racist indicators or benchmarks for all faculty◦ Objective metric for equity work, “Contribution to Diversity”
section on CV
◦ Review as a part of annual performance evaluations
Flaherty. Inside Higher Ed. 2017; De Los Reyes & Uddin. Nature Neuroscience. 2021; Fasiotto et al. Acad Med. 2020

Educational Policy: Recruitment & Retention• Earmark resources to recruit and retain URiM faculty
• UCSF Dean Diversity Fund
• Brigham and Women’s Center for Diversity and Inclusion: Minority Faculty Career Development Award
• MGH Physician Scientist Development Award
• Institutional funding for URiM faculty recruitment packages
• Intentional efforts to ensure faculty positions for promising URiMresidency/fellowship graduates
Griffin in Perna (ed) Higher Education. 2020Bhalla. MBoC. 2019

Educational Policy: Recruitment & Retention• Ensure job postings/position requirements are unbiased
• Standardize anti-bias processes for hiring committees
• Faculty applicants must supply a statement of contribution to diversity
• Transparent, easily accessible division/department hiring audits
• Emphasize retention strategies
Bhalla. MBoC. 2019Flaherty. Inside Higher Ed. 2017

Building an Anti-Racist Professional Identity and Culture Kate Lupton, MD
Acknowledge: Danielle Jones, MD and Eloho Ufomata, MD, MS

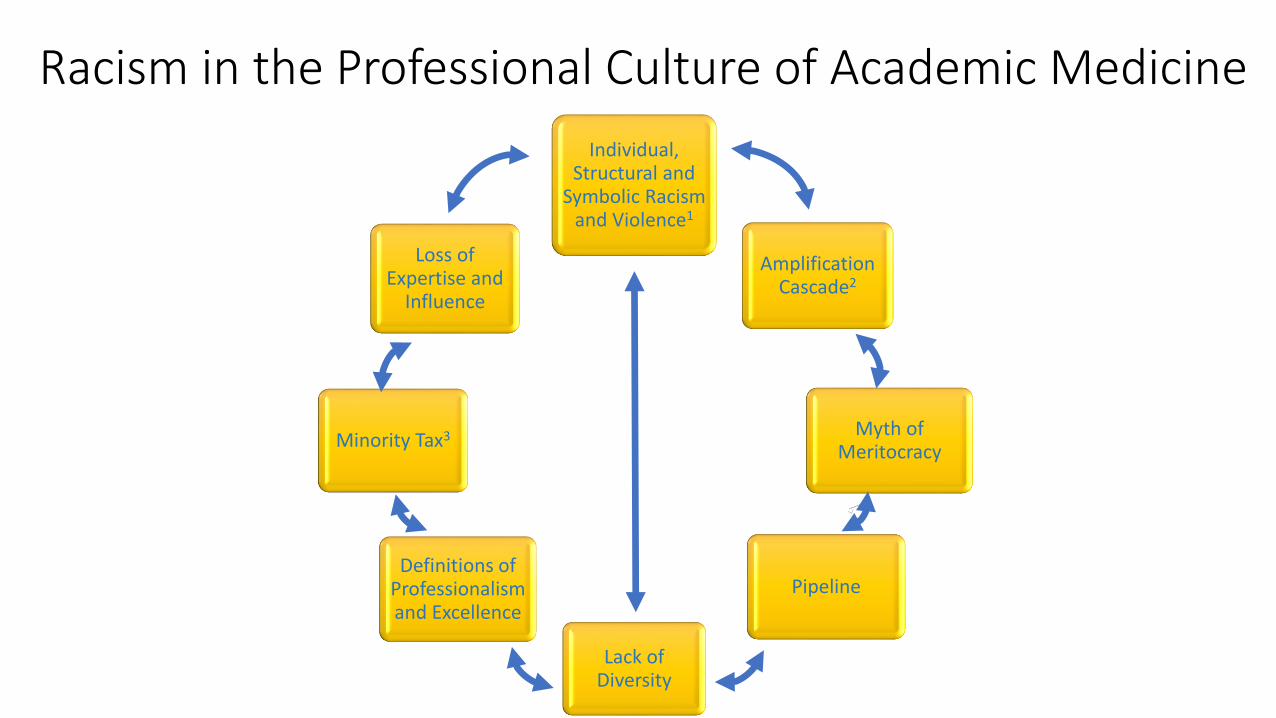
Racism in the Professional Culture of Academic Medicine
Individual, Structural and
Symbolic Racismand Violence1
Amplification Cascade2
Myth of Meritocracy
Pipeline
Lack of Diversity
Definitions of Professionalism and Excellence
Minority Tax3
Loss of Expertise and
Influence
Individual, Structural and
Symbolic Racismand Violence1
Amplification Cascade2
Myth of Meritocracy
Pipeline
Lack of Diversity
Definitions of Professionalism and Excellence
Minority Tax3
Loss of Expertise and
Influence

Setting the Stage
PROFESSIONAL IDENTITY
The attitudes, values, knowledge, beliefs and skills shared with others within a professional group
PROFESSIONAL CULTURE
The proper way to behave within an organization or group
and
Attitudes that contribute to the emotional and relational environment of your workplace

• Intangible assets◦ Internal locus of control
◦ Self-esteem
◦ Sense of purpose
◦ Ability to self actualize
◦ Critical thinking abilities
Assertion of Professional Identity -Identity capital
• Tangible assets◦ Social class
◦ Gender
◦ Prior degrees
◦ Membership of “clubs”
•What happens if you lack identity capital?
Goldie. Medical Teacher, 2012.

Professional Identity Formation• Socialization
• Hidden curriculum
• What happens when professional culture influences professional identity?
Jenkins, Social Identity, 2008de Montigny, Knowledge, Experience and Ruling Relations, 1995

Microaggressions and Stereotype ThreatIn medical education, microaggressions can trigger “stereotype threat”
Burgess et al. Stereotype Threat and Health Disparities: What Medical Educators and Future Physicians Need to Know. JGIM 2010
Burgess, JGIM 2010
“Pet to Threat” Phenomenon• Coined by Dr. Kecia M. Thomas PhD in early 2010’s
• Initially treated like a “pet” – beloved, cared for, treated in child-like fashion• Pets often experience feelings of tokenism, invisibility, pressure to assimilate,
mistreatment, and being overprotected by colleagues• Might uncover unrecognized racism and become a reporter on racist acts (canary in
the coalmine)
• Attempts to assert oneself are viewed as threatening especially at times of opportunity for promotion or leadership

Professional Culture – Lessons from the Business World
• Leaders are instrumental in creating and changing an organization’s culture
• Culture determines what types of people are hired what types are left out
• Onboarding is an organizational socialization process
• Organizational culture is an organism that protects itself

Professional Culture of Academic Medicine
•Eurocentric norms
Racism in the Professional Culture of Academic Medicine
Individual, Structural and
Symbolic Racismand Violence1
Amplification Cascade2
Myth of Meritocracy
Pipeline
Lack of Diversity
Definitions of Professionalism and Excellence
Minority Tax3
Loss of Expertise and
Influence

Professional Culture of Academic Medicine• Eurocentric norms
• Forces “Code Switching”
• The duality of isolation and hypervisibility
Doll, NEJM 2020Roberts, HBR 2018

Shifting the Paradigm from Inclusion to Belonging• Diversity is the measure; inclusion is the mechanism
• Inclusion is a dynamic state of operating in which diversity is leveraged to create a fair, healthy, and high performing organization or community which ensures equitable access to resources and opportunities for all
• Belonging means full membership
Diversity, Equity, Inclusion and Belonging Toolkit (Harvard)

Organizational Actions• Redefine professionalism in medicine to incorporate cultural diversity
• Reimagine the criteria for entrance into the academy
• Restructure promotion criteria
• Embrace anti-racism as a core tenet of their organizational mission
• Assert organizations antiracist viewpoint while onboarding
• Provide continuous quality improvement and education on anti-racism

To conclude… KATE LUPTON, MD

The road ahead is not easy, nor the endpoint short-termWe must: •Adopt an actively anti-racist framework
• Shift the paradigm from fostering diversity to dismantling a system that fosters exclusion
• Rebuild a system that enables all within it to thrive
• This will require a multidimensional strategy
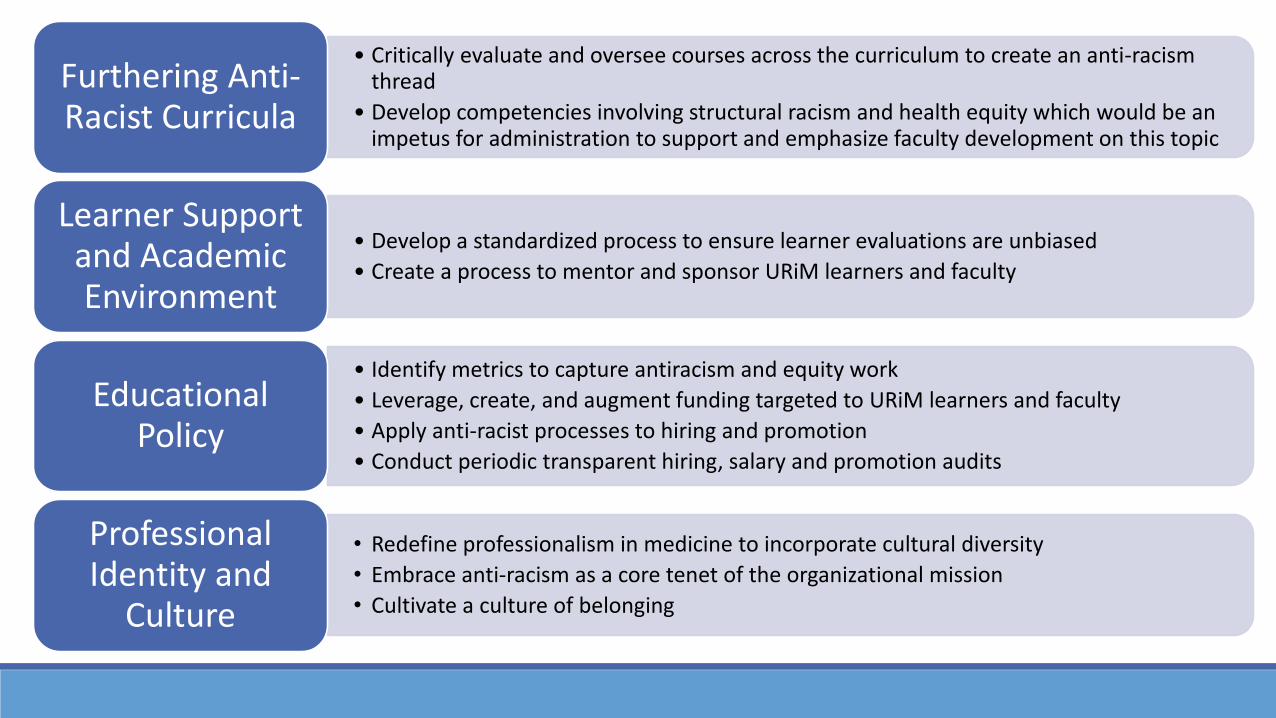
• Critically evaluate and oversee courses across the curriculum to create an anti-racism thread
• Develop competencies involving structural racism and health equity which would be an impetus for administration to support and emphasize faculty development on this topic
Furthering Anti-Racist Curricula
• Develop a standardized process to ensure learner evaluations are unbiased
• Create a process to mentor and sponsor URiM learners and faculty
Learner Support and Academic Environment
• Identify metrics to capture antiracism and equity work
• Leverage, create, and augment funding targeted to URiM learners and faculty
• Apply anti-racist processes to hiring and promotion
• Conduct periodic transparent hiring, salary and promotion audits
Educational Policy
• Redefine professionalism in medicine to incorporate cultural diversity
• Embrace anti-racism as a core tenet of the organizational mission
• Cultivate a culture of belonging
Professional Identity and
Culture

It’s time to commit: Which of these actions will you advocate for within your division, department, or school?
Questions ?