anti-depressant medications
DESCRIPTION
Anti-Depressant Medications. Brian Ladds, M.D. Outline. Earliest meds: MAOI TCA Neurotransmitter emphasized: NOR More recent meds: SSRI Neurotransmitter emphasized: SE. Discovery of Anti-Depressants. Historical Serendipity: An early anti-TB medication was noted incidentally to have: - PowerPoint PPT PresentationTRANSCRIPT

Anti-Depressant Medications
Brian Ladds, M.D.

Outline
• Earliest meds:– MAOI– TCA
• Neurotransmitter emphasized: NOR
• More recent meds:– SSRI
• Neurotransmitter emphasized: SE
Discovery of Anti-Depressants• Historical Serendipity:
– An early anti-TB medication was noted incidentally to have:
• anti-depressant effects• and was found to inhibit MAO enzyme as one of its
properties
– Since making more monoamines available alleviated depression, perhaps the basis of depression is a deficiency of one or another monoamine in the brain

Monoamines and Depression
• For many decades the principal monoamine thought to be most relevant in depression was norepinephrine.
• In the last decade, the role of another monoamine, serotonin, has also been emphasized.

Neurotransmitters
• 3 principal types of neurotransmitters – monoamine neurotransmitters (MA)– amino acid neurotransmitters– neuropeptide neurotransmitters

Monoamine Neurotransmitters• Catecholamines
– dopamine– norepinephrine
• tyrosine hydroxylase enzyme– synthesizes l-dopa from tyrosine
– rate-limiting step (usually saturated )
• Serotonin• Acetylcholine• (Histamine)

Monoamine Neurotransmitters
• Monoamine neurotransmitters comprise only a small percentage of neurons (vs. amino acid neurotransmitters), but:
• Monoamines may regulate the balance of:– the excitatory actions of glutamate and the inhibitory
actions of GABA
• The receptor sites for the monoamine neurotransmitters are involved in many psychiatric disorders

Monoamine Neurotransmitters
• The neurons that produce monoamines originate in nuclei of the brainstem (or basal forebrain) and project widely to the cortex, where they release the neurotransmitters.


Norepinephrine Pathways
• Locus coeruleus in pons
• -> inervation to the forebrain

Life Cycle of the Monoamine Neurotransmitters
• Synthesis:– from simple precursors (tyrosine, tryptophan,
choline)
• Storage:– stored in terminal pre-synaptic vesicles
• Release:– into synaptic cleft
• Site of Action:– act on post-synaptic receptors and elsewhere
• Inactivation

Monoamine Neurotransmitters: Inactivation
• Inactivation: – primarily via re-uptake back into the pre-
synaptic nerve terminal and then recycled– distinct “re-uptake transporters” (trans-
membrane proteins) for:• dopamine vs. norepinephrine vs. serotonin
– and also by degradation by intra-cellular (and extra-cellular) enzymes

Monoamine Oxidase Enzyme
• Monoamine oxidase (MAO) enzyme – on external membrane of mitochondria– catabolizes (or degrades) monoamines in the
nerve terminal cytosol (unprotected by vesicles)
• MAOA breaks down serotonin and norepi
• MAOB breaks down dopamine

MAO Inhibitors (MAOI)
• Examples: phenelzine (Nardil) or tranylcypromine (Parnate)
• Irreversibly inhibit MAO enzyme– Therefore takes 2 weeks after stopping the
MAOI to replenish new MAO enzyme
• Increase the availability of monoamines – such as norepinephrine and serotonin, which
are thought to be decreased in depression

MAOI: Side Effects
• Tyramine Hypertensive Crises
– tyramine: contained in aged cheese, smoked meats, certain wines
– is sympathomimetic and causes release of norepi from sympathetic terminals, which in the presence of MAOI can cause acute hypertensive crises and stroke

MAOI: Side Effects
• Medication Interactions– hypertensive crises with sympathomimetic
medications (as with tyramine)– hyperthermia, e.g. with meperidine (Demerol)
(as in the case of Libby Zion)
• Other side effects– as with TCA’s

Tri-cyclic Anti-depressants
• Tri-cyclic anti-depressants (TCA):
• Block re-uptake of monoamines, especially NE (and some block to a lesser extent SE)– the therapeutic mechanism of action

Anti-Depressants: Efficacy
• 2/3 respond
• Not a euphoriant or stimulant among people who are not depressed

Anti-Depressants: Time Course
• Time course: 2-4 weeks delay of therapeutic effect.
• Possibly due in part to:– gene expression and the synthesis of new
structures & synapses– down-regulation

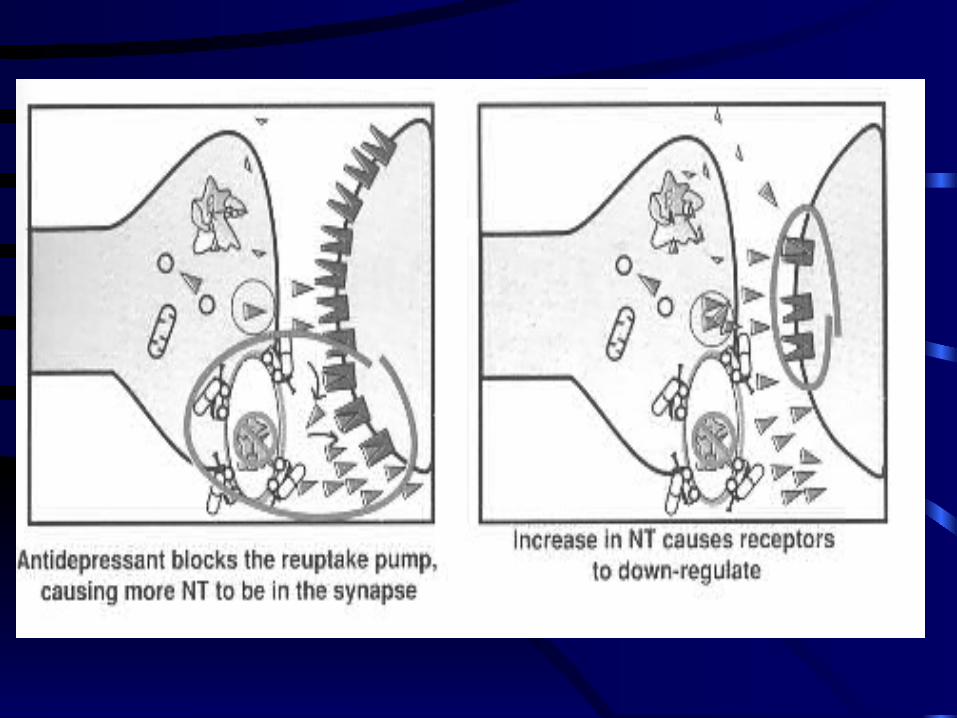
A Theory of Down-Regulation
MAOI and TCA are thought to bring about an anti-depressant effect by:
• making more norepinephrine available in the synaptic cleft,
• thereby leading to the down-regulation of the post-synaptic adrenergic receptors
• restoring them to their normal number and function.


Tri-cyclic Anti-depressants: Side Effects
TCA also block post-synaptic:
• Histamine receptors – causing sedation, weight gain
• Adrenergic receptors – causing hypotension, dizziness
• Ach receptors – causing anti-cholinergic side effects

Anti-cholinergic Side Effects
• Blurred vision
• Urinary retention
• Constipation
• Dry mouth
• (Confusion)

TCA and Risk of Overdose
• Can be fatal in overdose

Tri-cyclic Anti-depressants
• Some TCA’s and their side effect profile:– Imipramine: one of the earliest, highly effective
but many side effects– Desipramine: a metabolite of IMI, only blocks
re-uptake of NE (not SE); it is the least anti-cholinergic TCA
– Nortriptyline: least likely TCA to cause blood pressure changes
– Others: amitriptyline, doxepin, amoxapine

Serotonin

Serotonin
• 5-HT (Hydroxy-tryptamine) = Serotonin• synthesized from essential amino acid
tryptophan• the rate-limiting enzyme not usually
saturated – therefore increased levels of precursors cause
increased synthesis of serotonin• (but dietary supplements of tryptophan not very
effective AD and have had contaminants)
Serotonin Pathways
• Serotonin– several nuclei in the dorsal raphe in the mid-
brain – projects to striatum, hypothalamus, and neo-
cortex


Inactivation of Serotonin
• Inactivation via pre-synaptic re-uptake
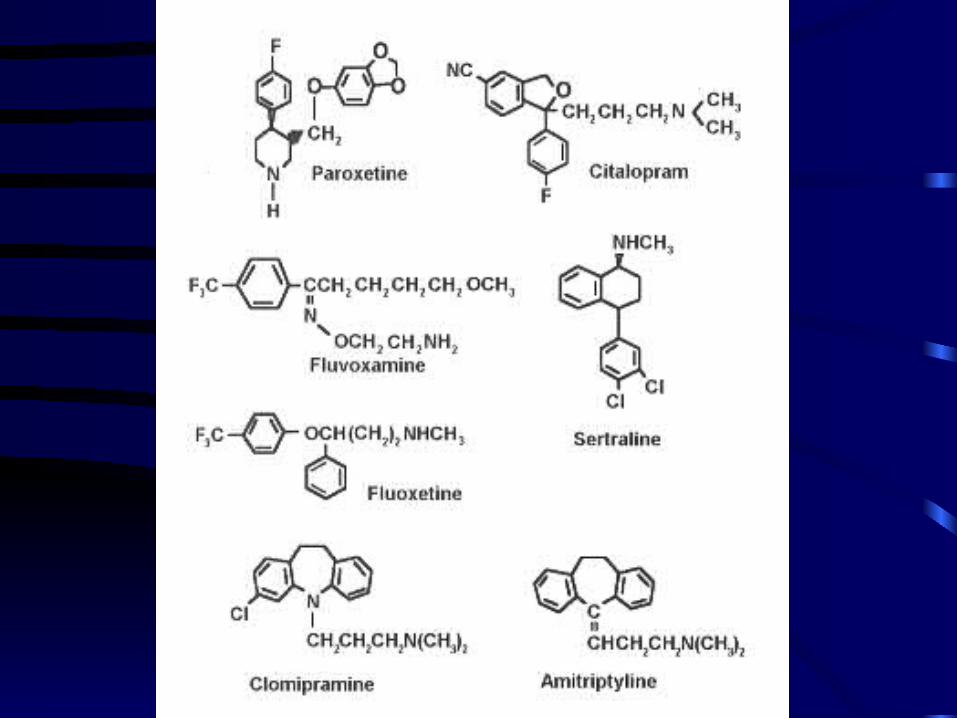
• This re-uptake transport process is inhibited by some anti-depressants – TCA: imipramine (non-selective)– SSRI: fluoxetine (Prozac), paroxetine (Paxil),
sertraline (Zoloft), citalopram (Celexa)

SSRI
• “Selective Serotonin Re-uptake Inhibitors”– probably as effective as TCA in most sub-types
of depression• most are structurally unrelated to TCA’s
– minimal anti-cholinergic or cardio-vascular side effects
– safe in overdose

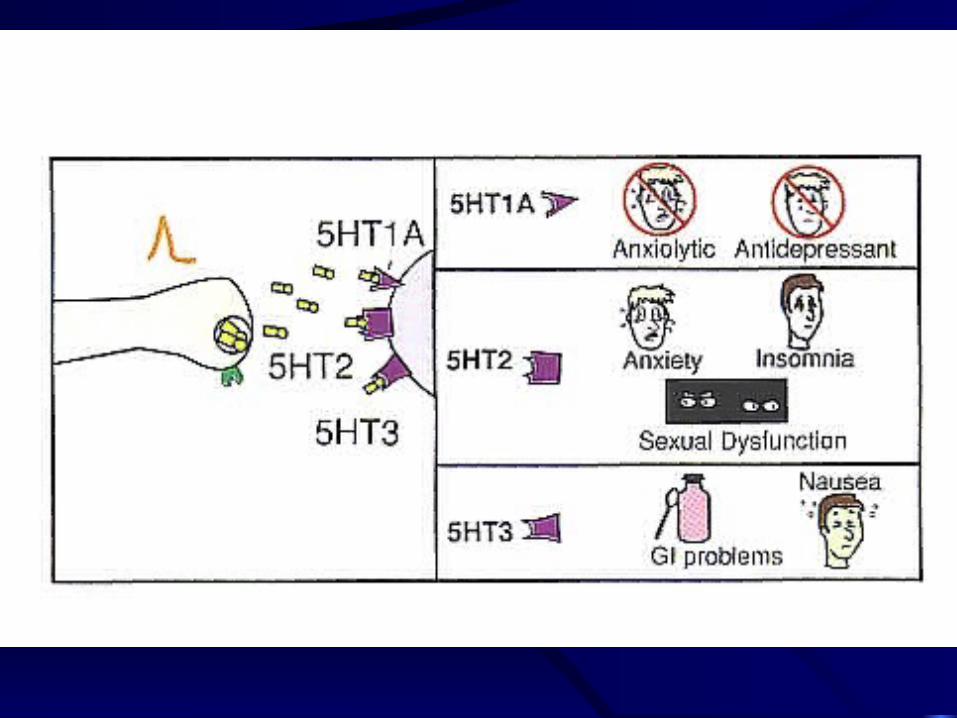
Serotonin Receptors
• Serotonin receptors (~ 13) – 5HT-1– 5HT-2– 5HT-3

SSRI: Side Effects
• GI upset
• weight loss
• insomnia, jitteriness
• sexual dysfunction (less libido, ED)

Other Anti-Depressants
• There are many other anti-depressants, some with different mechanism of actions, or combinations of receptor effects and side effect profiles– mirtazapine (Remeron)
• alpha-2 antagonist; also with 5HT-2, 5HT-3 and histamine antagonist properties
– buproprion (Wellbutrin)• NE and DA reuptake inhibitor

Uses of Anti-Depressants
• Depression– Dysthymia ?
• Anxiety Disorders– Panic Disorder– OCD
• Eating disorders• Pain• PTSD