anthroposophical basis for understanding autoimmune diseases · anthroposophical basis for...
TRANSCRIPT

F i n t e l m a n n | u n d e r s ta n d i n g a u t o i m m u n e d i s e a s e s | D e r M e r k u r s ta bE n g l i s h I s s u e 2 0 0 5 1
The issue
In the medicine based on modern science, a number oftheories and hypotheses have been developed on thecauses of autoimmune disorders. (1, 2) Examples are
the release of inflammation mediators and cytotoxiccells by antibodies, production of antigen-antibody im-munocomplexes which are deposited in the organism,or sensitized T cells attacking structures in the organism.‘Genetic and other factors’ are said to be the causes. (3)Generally a disruption of normal immunotolerance pro-cesses is postulated, and again a number of hypothesesfor this are under discussion. (4) All in all we have here aremarkable lack of knowledge, despite the fact that au-toimmune disorders have become common over the last30 or 40 years and major scientific advances have beenmade in the field of immunology.
Can more light be thrown on the matter by conside-ring the phenomena and their non-physical backgroundin the anthroposophical science of the spirit?
In the invitation to the Anthroposophical Medical As-sociation’s Conference on 22 and 23 November 2003 inKassel it said:“Autoimmune disorders on the other handreflect disruption in the human organism’s self-recogni-tion and self-regulation. Internal organs become foreignelements in the body.” This would therefore also affectthe immunotolerance which functions in health, i.e. theimmune system attacks tissue belonging to the organand to the body as though it were foreign. Quite naivelyone might ask: “Has the organism gone mad?” (seeingthat it is senselessly destroying itself).
A basic law in anthroposophical medicine is that alarge part of disorders are due to auto- rather than he-terogenic factors. These take effect in the wrong place,at the wrong time, or show excessive or inadequate in-tensity in the site where they normally take effect: (5)
Disorders reflect bodily processes which take effectin the wrong place, at the wrong time and/or act withthe wrong intensity (too powerful/too weak).
Does this basic law also apply to autoimmune disor-ders? This is what we want to explore in what follows.
Polarity of I and bodyA first area for our consideration derives from anot-
her basic fact in anthroposophy. It is that the differentia-
Anthroposophical basis for understanding autoimmune diseasesVo l k e r F i n t e l m a n n
Translation of “Menschenkundliche Grundlagen zum Verständnis der Autoimmunkrankheiten”by Volker Fintelmann. Der Merkurstab 2004; 57/5:336-40. English by A. R. Meuss, FCIL, MTA.
Anthroposophical basis for understandingautoimmune diseasesn AbstractIn modern scientific medicine, questions concerningthe aetio-logy of autoimmune diseases do not take us beyondestablishing a number of hypotheses with a theore-tical basis. Findings made in anthroposophical spiri-tual investigation by Rudolf Steiner can help us tosee autoimmune diseases as an attempt to makeuntransformed (not individualized) remnants of theinherited body one’s own at a later time in the bio-graphy, i.e. create an individual body that accordswith the I or self also in this organic site. Inflamma-tory and digestive processes to destroy matter andthen give a new configuration are pathophysiologi-cal in the case. Suppressing them with anti-inflam-matory drugs or immunosuppressants is counterpro-ductive, for the self is impeded in its efforts to healitself. World substances such as Phosphorus, Quartzor mistletoe treat the causes by guiding and suppor-ting I-activity. Reconciliation with the world of theancestors from whom the body primarily comes isanother element in causal treatment.n KeywordsAetiologyAutoaggression Inherited body Individual bodyRemnants of inherited body

ted body (“organism”) is seen as the instrument or toolof the real human being who is wholly spiritual by na-ture. Rudolf Steiner called it the “I”.With the help of hig-her (“hierarchic”) spirits, this I creates instruments for it-self in soul and body so that the intentions it had in thespirit before birth (plan for life) may be brought to reali-zation in existence between conception, birth and death.The body must be seen as polar opposite to the I, withthe soul active between the opposite poles (matter andspirit), always mediating and maintaining balance. Aspecial aspect is that the body is pre-formed and gene-tically determined by the parents, which makes it prima-rily foreign and not self. It only becomes self in long sta-ges of development taking 20 to 30 years.This will be animportant aspect when it comes to understanding au-toimmune disorders.
Let us first consider the opposite nature of body andI (spirit). Rudolf Steiner spoke of a fact which his investi-gations had shown and I want to quote him here.“Whe-rever the spirit enters directly into physical matter wehave a destructive process. A subtle death process co-ming from the senses thus spreads along the nervetracts in the human organism.”(6) This relates to the “vi-sible” human being, i.e. once again the body whichthroughout life has an invisible human being everywhe-re within it. Essentially all constructive processes origi-nate in this. The body of physical matter, also known as“physical body”, is destroyed under the direct influenceof the I, or subject to destructive processes.This leads toa first hypothesis for a possible cause of autoimmunedisorders:
Autoimmune disorders reflect an excessively power-ful, destructive influence of the I on the organism.(“The spirit burns up the body.”)
Anticipating slightly, let us note that this manifests ininflammatory processes, above all those that result inpurulence and liquefaction. Inflammation plays a majorrole in autoimmune disorders and also determines es-sential aspects of modern treatment. It is, however, scar-cely of the kind discussed above but rather involves chro-nic destruction of tissue. The image one might have ismore that of a smouldering fire.
The organ which has turned foreignThe second area for our consideration is that of an or-
gan or tissue turning foreign. The most characteristicexample are viral diseases where incorporation of the vi-ruses in cells of the organs will, in the sight of the immu-ne system, cause such alienation. The immune systemattacks the material affected by the viruses, often in aviolent, acutely destructive way. A typical example is ful-minant hepatitis with hepatitis B virus infection, for-merly also known as acute hepatic dystrophy. Essential-ly, however, inflammatory changes with virus hepatiti-des reflect an immune reaction on the part of the organ-ism and therefore attempts to heal and not sickness. Fordecades, acute virus hepatitis was treated with anti-in-flammatory drugs such as glucocorticoids. Later, when
the immunological process was understood and onecould see why such treatment was largely ineffectiveand did actually in many cases lead to protracted chro-nic evolutions.
Autoimmune processes connected with virus-asso-ciated disorders continue to be seen, and for a time itwas therefore also thought that autoimmune disordersmight be viral in origin, with research taken in this di-rection.The second hypothesis for a possible cause of au-toimmune disorders therefore is the following.
Autoimmune diseases indicate that an organ hasbeen alienated under external influences. (“The or-gan becomes outside world.”)
This hypothesis is more likely to help us find an ans-wer to our question concerning the causes of autoim-mune disorders. Viruses or other pathogens clearly can-not be the only external factors to be considered. A vastfield has to be opened up for research to investigate thisand look for answers. There can be no question but thatthe human organism is today exposed to many differentenvironmental pollutants in material form or also inform of different kinds of radiation. We need only thinkof the indeterminable number of food additives, pestici-de or heavy metal pollution, and both natural and artifi-cially produced radiation of many different kinds. Fromthe point of view of anthroposophy, where existence insoul and spirit is something very real, one must also con-sider if external influences of a non-material kind maynot also cause an organ to become foreign. Think of the“indigestible”flood of images and information providedby the media, but also the actions, feeling and thoughtsof others and the effect these can have on us. Any kindof childhood abuse must also be mentioned as a primeexample.
Organic focus of destruction within usA third area for our consideration is again created on
the basis of Rudolf Steiner’s investigations. He describedhow in every human organism there is an organic andtherefore unconscious area where an intensive form ofdestruction arises which is directed towards the organ-ism”s physical matter: “Matter is never completely de-stroyed in the outside world. In more recent times, phi-losophers and scientists for the external world have the-refore spoken of the conservation of matter. This law ofthe conservation of matter applies only in the outsideworld, however. In the inner human being, matter iscompletely transformed back into nothingness. Matteris there destroyed completely in its essence. Our humannature actually bases on the fact that we are able tothrow matter back into chaos, destroy matter complete-ly at a level deeper than the mirroring of memory.”(7)
He then referred to the way pupils were taught in ear-lier mystery centres, mainly in Ireland and the West alto-gether, though originating from the Orient: “Beneaththe capacity for memory, you bear something in you asa human being which is out to destroy; without this in-side you, you would not have been able to develop your
2 D e r M e r k u r s ta b | F i n t e l m a n n | u n d e r s ta n d i n g a u t o i m m u n e d i s e a s e s E n g l i s h I s s u e 2 0 0 5

ability to think, for you must develop your thinking inthat powers of thought penetrate the ether body. Anether body filled with powers of thought will, however,have the effect on the physical body of throwing its mat-ter back into chaos, destroying it.”(8) Later he introducedtwo further important concepts, speaking of a focus ofdestruction and a destructive frenzy.
These spiritual facts are profound and may well awa-ken defensive or negative reactions in someone follo-wing the line of thought.The known facts of research in-to digestion show, however, that such powers do indeedexist in us. Destruction or degradation of matter in theprocess we call “digestion” involves powerful, aggressi-ve forces located in the different digestive organs, withcorresponding digestive enzymes acting as mediators.Our organs of mastication, acid production in the sto-mach and bile acids also come under this heading.We al-so find this destructive frenzy in the rejection of organtransplants, a process with an immunological basis. Ma-ny readers may perhaps for the first time become awa-re here of a situation which is experienced and describedall over the world, a phenomenon of our time that al-most seems beyond comprehension. This is the enor-mous increase in a (seemingly?) incomprehensible de-structive frenzy as an expression of uncontrolled aggres-siveness which culminates in terrorism. Do we not beco-me aware of a need here for research in medicine as tohow far such aggressiveness discharging itself in an out-ward direction does not also reflect digestive activitynot adequately put to use, i.e. digestive powers “stray-ing” into the soul sphere? And should not our attentionturn to causal phenomena in nutrition, fast foods beingbut one form of expression? Reference must also be ma-de to the highly successful commercialized world offilms which profit from showing such extreme forms ofmaterial destruction, their “material” also including thehuman being.
These questions concerning the phenomena of ourtime will not, however, help us to understand autoim-mune disorders. Here the destructive frenzy woiuld ha-ve to be directed towards parts of the organism itself,which is also an important aspect of self. Suddenly theearlier term “autoaggression” gains fresh new signifi-cance. Permit me to refer to an image from the world offolk tales. In Rumpelstiltskin we find an accurate pictu-re of autoaggression of the kind which at the level of or-gans we see in the extreme situation of pancreatitis, forinstance, a situation where an organ digests itself. Weare thus able to formulate a third hypothesis for under-standing the cause of autoimmune disorders.
Autoimmune disorders reflect an (organ-related) de-structive frenzy directed against oneself. (Rumpel-stiltskin type of autoaggression)
Acute pancreatitis is not an autoimmune disorder,though the triggering factors do in many cases remainunknown. But it is striking how often extreme psycholo-gical stress is seen in conjunction with this disease, of-ten having persisted for a long time and finally finding
an outlet.This is the field of psychosomatics, interactionbetween body and body-related soul. Scientists ack-nowledge that psychological factors can become soma-tic, connecting with it the idea of a pathophysiologicalprocess. This may well play much more of an aetiologi-cal and pathophysiological role in the development ofautoimmune disorders than modern scientists haverealized so far. And no careful observer can fail to seehow intensively the symptoms of autoimmune disor-ders also involve the psyche.
Untransformed elements of the inherited bodyThe fourth area to be considered takes us deep down
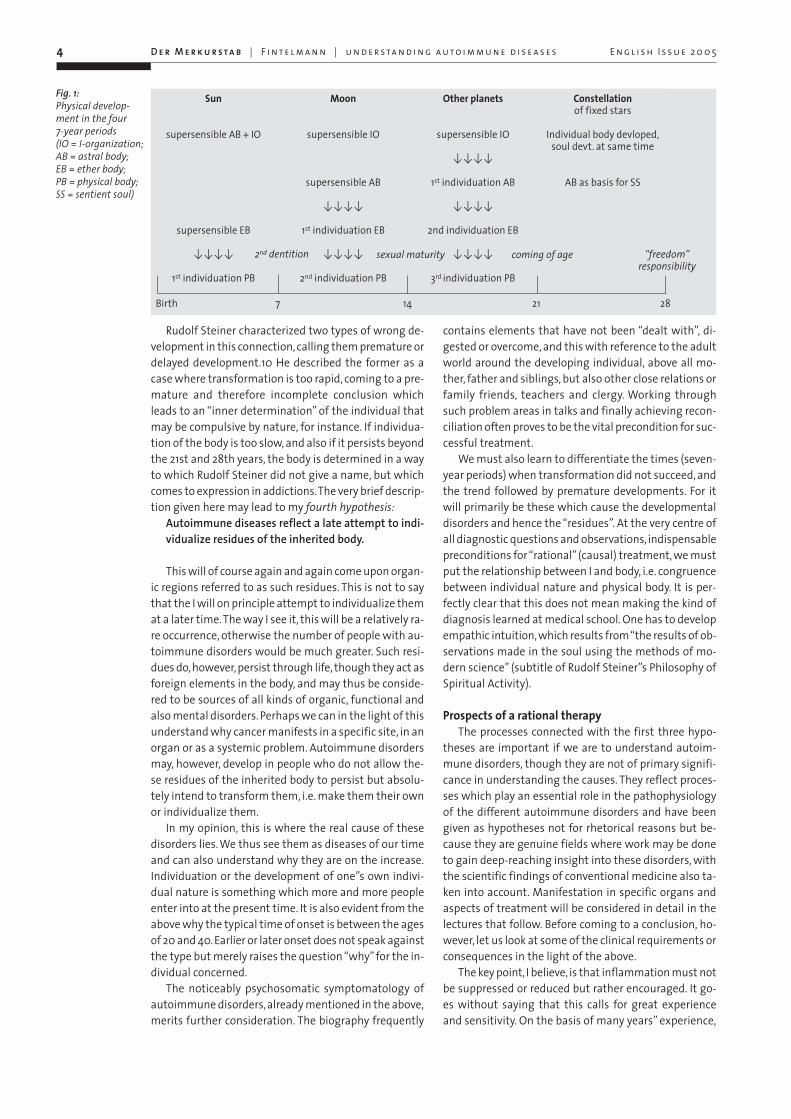
into the true causes of autoimmune disorders. It presup-poses the situation mentioned earlier, which is that theindividual human spirit, the I, can only incarnate if pa-rents create the necessary living body. In every case andwith utter logic this is foreign to the I. Rudolf Steinerwould frequently mention in his collected works thatthe time needed for human infancy and childhood deve-lopment until maturation is reached is extremely longcompared to the whole animal world and can only beunderstood if we consider that the I needs this time totransform the inherited body, also called a “model”, intoan individual body, which has to happen at all levels ofphysical matter, life, sentience and soul and ultimatelyalso of the spirit. This happens in developmental stagesof 7 years each. Initially the material consistency of theinherited body is transformed and replaced, as is clearlyevident in the changing of the teeth, though it also ap-plies to all tissues and organs in the organism.
More work is done on transforming physical matterin the second seven-year period, but the emphasis isnow on the sphere of life, most evident in all functionalprocesses in the organism. These, too, must becomehighly individual to serve the unique (individual) natureof the I as ideal tools for future life. These individuationprocesses come from the above-mentioned invisible orsupersensible human being who is not embodied but in-fluences the body by different routes.(9) It is always thenext higher member of the supersesible organizationwhich works on this individuation, always guided by theI which on its part has the help of spiritual (hierarchic)entities of planetary origin (Fig 1).
After 3 times 7 years, i.e. around the 21st year of life,individuation of the body is complete, the individual has“come of age”.The I then works to develop the three soulelements (sentient, rational and spiritual soul) out ofthe body which also need to be given wholly individualcharacter. In our time this reaches its culmination inabout the 28th year, when ideally the human being is atrue individual and takes personal responsibility concer-ning self and world.This is the ideal form of an indepen-dent individual nature. All kinds of problems, resistanceand obstacles do, of course, arise, so that the work willscarcely be wholly successful. “Bodily residues” left in-complete will persist, with hereditary body elements re-maining in them.
F i n t e l m a n n | u n d e r s ta n d i n g a u t o i m m u n e d i s e a s e s | D e r M e r k u r s ta bE n g l i s h I s s u e 2 0 0 5 3
4 D e r M e r k u r s ta b | F i n t e l m a n n | u n d e r s ta n d i n g a u t o i m m u n e d i s e a s e s E n g l i s h I s s u e 2 0 0 5
Rudolf Steiner characterized two types of wrong de-velopment in this connection, calling them premature ordelayed development.10 He described the former as acase where transformation is too rapid, coming to a pre-mature and therefore incomplete conclusion whichleads to an “inner determination” of the individual thatmay be compulsive by nature, for instance. If individua-tion of the body is too slow, and also if it persists beyondthe 21st and 28th years, the body is determined in a wayto which Rudolf Steiner did not give a name, but whichcomes to expression in addictions.The very brief descrip-tion given here may lead to my fourth hypothesis:
Autoimmune diseases reflect a late attempt to indi-vidualize residues of the inherited body.
This will of course again and again come upon organ-ic regions referred to as such residues. This is not to saythat the I will on principle attempt to individualize themat a later time.The way I see it, this will be a relatively ra-re occurrence, otherwise the number of people with au-toimmune disorders would be much greater. Such resi-dues do, however, persist through life, though they act asforeign elements in the body, and may thus be conside-red to be sources of all kinds of organic, functional andalso mental disorders. Perhaps we can in the light of thisunderstand why cancer manifests in a specific site, in anorgan or as a systemic problem. Autoimmune disordersmay, however, develop in people who do not allow the-se residues of the inherited body to persist but absolu-tely intend to transform them, i.e. make them their ownor individualize them.
In my opinion, this is where the real cause of thesedisorders lies. We thus see them as diseases of our timeand can also understand why they are on the increase.Individuation or the development of one”s own indivi-dual nature is something which more and more peopleenter into at the present time. It is also evident from theabove why the typical time of onset is between the agesof 20 and 40. Earlier or later onset does not speak againstthe type but merely raises the question “why” for the in-dividual concerned.
The noticeably psychosomatic symptomatology ofautoimmune disorders, already mentioned in the above,merits further consideration. The biography frequently
contains elements that have not been “dealt with”, di-gested or overcome, and this with reference to the adultworld around the developing individual, above all mo-ther, father and siblings, but also other close relations orfamily friends, teachers and clergy. Working throughsuch problem areas in talks and finally achieving recon-ciliation often proves to be the vital precondition for suc-cessful treatment.
We must also learn to differentiate the times (seven-year periods) when transformation did not succeed, andthe trend followed by premature developments. For itwill primarily be these which cause the developmentaldisorders and hence the “residues”. At the very centre ofall diagnostic questions and observations, indispensablepreconditions for “rational” (causal) treatment, we mustput the relationship between I and body, i.e. congruencebetween individual nature and physical body. It is per-fectly clear that this does not mean making the kind ofdiagnosis learned at medical school. One has to developempathic intuition, which results from “the results of ob-servations made in the soul using the methods of mo-dern science” (subtitle of Rudolf Steiner”s Philosophy ofSpiritual Activity).
Prospects of a rational therapyThe processes connected with the first three hypo-
theses are important if we are to understand autoim-mune disorders, though they are not of primary signifi-cance in understanding the causes. They reflect proces-ses which play an essential role in the pathophysiologyof the different autoimmune disorders and have beengiven as hypotheses not for rhetorical reasons but be-cause they are genuine fields where work may be doneto gain deep-reaching insight into these disorders, withthe scientific findings of conventional medicine also ta-ken into account. Manifestation in specific organs andaspects of treatment will be considered in detail in thelectures that follow. Before coming to a conclusion, ho-wever, let us look at some of the clinical requirements orconsequences in the light of the above.
The key point, I believe, is that inflammation must notbe suppressed or reduced but rather encouraged. It go-es without saying that this calls for great experienceand sensitivity. On the basis of many years” experience,
Fig. 1:Physical develop-ment in the four 7-year periods (IO = I-organization;AB = astral body;EB = ether body;PB = physical body;SS = sentient soul)
Sun
supersensible AB + IO
supersensible EB
[[[[
1st individuation PB
Moon
supersensible IO
supersensible AB
[[[[
1st individuation EB
[[[[
2nd individuation PB
Other planets
supersensible IO
[[[[
1st individuation AB
[[[[
2nd individuation EB
[[[[
3rd individuation PB
Constellation of fixed stars
Individual body devloped,soul devt. at same time
AB as basis for SS
2nd dentition sexual maturity coming of age “freedom”responsibility
Birth 7 14 21 28

F i n t e l m a n n | u n d e r s ta n d i n g a u t o i m m u n e d i s e a s e s | D e r M e r k u r s ta bE n g l i s h I s s u e 2 0 0 5 5
Phosphorus and potentized mistletoe preparations arean elementary help in this. Secondly there is need tohelp the I to perceive both the inner and the outer boun-daries of the body and also achieve them, i.e. actively setboundaries. Quartz has causal activity in this respect.
Finally spheres of life must be worked through in thebiography that have created obstacles or trauma in theperiod of development and must be seen as connectedwith the disease. Reconciliation with these situations,and often also with oneself, is an important element inovercoming the disease or bring one’s bodily develop-ment to a good conclusion.
Prof. Volker FintelmannCarl Gustav Carus AcademyRissener Landstr. 193D-22559 Hamburg
References1 Classen M, Diehl V, KochsieckK. Innere Medizin. Urban &Schwarzenberg 1993, 402-4062 Johnson AG. Immunologieauf 70 Seiten. Thieme 2001,58-593 Classen M, Diehl V, KochsieckK. Innere Medizin. Urban &Schwarzenberg 1993, 402-4064 Johnson AG. Immunologieauf 70 Seiten. Thieme 2001,58-595 Fintelmann V. Intuitive Medi-zin. Einführung in eine anthro-posophisch ergänzte Medizin.Hippokrates, 4. Auflage 2000,66-736 Steiner R. The Invisible Manwithin Us. tr. A. Wulsin, G. Kar-now. Spring Valley: MercuryPress 1987.7 Steiner R. Cosmosophy vol. 1.Lecture of 23 Sept. 1921. Tr. A.Wulsin. Steiner Books.8 Steiner R. Loc. cit.9 Steiner R. As ref. 6.10 Steiner R. Pastoral Medicine.Lecture of 11 Sept. 1924. Tr. G.Hahn. Steiner Books 1987.

6 D e r M e r k u r s t a b | S o l d n e r · S o m m e r | A u to i m m u n e d i s o r d e r s o f t h e Ty r o i d E n g l i s h I s s u e 2 0 0 5
1) Case recordsMrs M, age 33, hyperthyroidism
A slender young woman brought her 8-month-oldinfant for treatment. The child had been born with amarked premature cranial suture synostosis and is alrea-dy showing definite psychomotor retardation—unableto turn round, communication not possible in the wayappropriate to the age. Mental disability had to be con-sidered. The indication for surgical correction, not wit-hout risk to life and prognosis, had to be established.Theintervention was due to be done at about 12 months.Currently the decision had to be made as to which sur-geon would do the operation. The patient came for aroutine check on the child before going on holiday.
The child presented with a mild upper respiratorytract infection; the mother seemed exhausted. As atten-tion turns to her, one sees the eye signs of stare and lidretraction, she seems rushed, never taking time for her-self. Asked if there was something wrong she said thatshe had felt weak and exhausted for the last 2 months,‘something not right’. Further questions elicited that shehad lost 3 or 4 kg in weight, and has palpitations nowand then.The pulse was 110 – 120/min, BP 130/75 mmHg,pulsating goitre size 2. Clinically, Graves’ disease was su-spected, the holiday trip cancelled, blood taken, andthen an injection given of
- Glandula Thyroidea D30 amp. Wala- Cuprum met. prep. D30 amp. Weleda i.v.,on the assumption of a florid inflammatory autoag-
gressive disorder of the thyroid (for this a relatively highpotency of the homologous organ was recommended)and also because experience had shown that mothers ofchildren with serious, life-threatening conditions gainimmediate relief and relaxation with Cuprum met. prep.D30.
Laboratory findings. TSH depressed, T3 19.6 pg/ml(normal < 4.2 pg/ml), T4 7.74 ng/dl (normal < 1.75 ng/dl),TRAB 12.4 (normal < 1 U/L), TAK (thyreogl. AB) 64 U/ml(normal < 60 U/ml), anti-TPO 283 U/ml (normal up to 60U/ml), zinc borderline, reduced to 624 µg/l (normal 630– 1180 µg/l), transaminases incr. to about twice normal,sonography showing thyroid enlarged to 31 ml (normalup to 18 ml), diffusely reduced echo, structure of paren-chyma coarse with no nodules, technetium uptakegreatly increased at 11.4 %.
Autoimmune thyroid diseases and problems in psychological maturationG e o r g S o l d n e r , M a r k u s S o m m e r
n AbstractIn the biography of many patients with autoimmunethyroid diseases characteristic problems are identi-fied at the age of 9 to 15 years, a phase which may beseen as the time of awakening in mind and spirit.The pathogenetic background and possible consequen-ces for therapy are discussed.n KeywordsAutoimmune diseases of the thyroidProblems with psychological maturity2nd 7-year period in lifeHyperthyroidismHashimoto thyroiditis
Abridged version of a lecture given at a conference of the Anthroposophical Medical Association in Germany (Kassel, November 2003)Translation of “Autoimmunerkrankungen der Schilddrüse und Störungen der seelischen Reifung“ by Georg Soldner, Markus Sommer.Der Merkurstab 2004; 57/5:341-9. English by A. R. Meuss, FCIL, MTA.

Treatment. Immediately following the clinical diagnosis,anthroposophic treatment with
- Colchicum Rh D3 Weleda per os, t.d.s.(varying no. of drops)- Glandula Thyroidea D30, 3 times a week s.c. 1 ml,later D12- Cuprite D20 trit. Weleda per os, a pinch once dailyThyreostasis once laboratory findings were known and following discussion with the patient, with- carbimazole 10 mg dailyand arrangements for a full biographical consultati-
on, with the patient making her own written record (thisis an important part of the treatment):
“I had a good, protected childhood and youth until mymother started a new relationship, confronting me,then 14 or 15, fully with the situation after a very shorttime. I was torn apart between my parents and couldnot understand why my mother discussed her pro-blems with her daughter, for these intense problemsaffected me greatly, causing great stress. My fatherdid not help much, for I could not talk to him aboutthis; even later on, when he knew about it, he couldnot talk. Achievement counted, feelings did not—atleast he could not and cannot show his feelings. Inspite of this I appreciate and respect my father,though I no longer respect my mother. When my fat-her asked my mother to move out I was on the onehand relieved to have matters clarified, but it is al-ways painful when parents separate. I stayed with myfather and took on all the housekeeping, which I en-joyed, for I was given a free hand.”
The patient then trained for her work and after initi-al problems she and her husband established an inde-pendent firm where both worked 7 days a week until thechild was born, with just a few days holiday now andthen.
“Initially there were massive problems with my mo-ther-in-law. Then, after a difficult time for me and abrief separation, my husband decided to run the busi-ness without his mother and with me instead.The re-lationship between son and mother and mother andme was extremely fraught—we had had no contactuntil the wedding. From then on the relationship hasbeen friendly, contact relatively infrequent. The rela-tionship with my own mother is wonderful in her ey-es, catastrophic in mine. She is jealous, pessimistic,dissatisfied with everything, upset about everythingfor days, unpopular, gradually losing her friends ...My thyroid disorder developed because of psycholo-gical and other stress. I am convinced that mydaughter’s illness has much to do with it.”
The patient felt that the biographical talk helped agreat deal.
Two more followed. Consequences for her daily rou-tine were worked out, e.g. that she now takes the babyout in her pram herself and does not leave this to thenanny (a phenomenon which is not uncommon with
mothers running their own businesses). Among otherthings she then looked consciously at the natural world,took in light, breathed consciously, and switched off thetelephone for hours, playing with her child free frompressure.
Painting therapy was also started.
Evolution.• After one month, her mood was balanced, the volumeof the goitre regressing.• After four months, the patient was pregnant again, T3was wholly normal at this time (4.27 pg/ml, TRAB 4.6U/l). After five months the first child’s operation wentwell, without complications.• After seven months,TSH above 1,TRAB negative,TAB be-low 20, anti-TPO 184 U/ml. Carbimazole 5 mg continuedin reducing dosage, to be discontinued after ten months.She gave birth to a healthy second child after 13 months.• Two years later, TSH 0.92 mU/ml, T3 2.96 pg/ml, T4 1.35ng/dl, anti-TPO elevated, TRAB negative. No treatment.Clinically n.a.d.
The first child had normal thyroid parameters for thewhole period. It was only during the mother’s illnessthat the following information became available, whichso far had not received any attention.“Newborn infantswith congenital hyperthyroidism ... (not applicable here)As a rule the indicator is maternal Graves’disease. If not,the diagnosis is often made very late, at a time whencomplications such as premature sutural synostosis ha-ve become established...” (1)
This means that every premature sutural synostosismay point to a thyroid disorder of mother or child, whichneeds to be clarified – something which no one, inclu-ding the author, had done so far.
The first child had caught up on all delayed develop-ment within two years of the corrective operation.Todayhis motor functions are just on normal for his age, psy-chosocial behaviour is normal, nor are there cognitivedeficits. As with all children with premature sutural sy-nostosis, treatment by a qualified osteopath was of ma-jor importance. The second child has no appreciabledisease.
The above case record shows important motifs whichare frequently seen in the life history of patients with au-toimmune hyperthyroidism:
- mostly affects women- relationship to mother plays specific role- mainly in 2nd 7-year period,“loss of maternal mant-le” comes like a shock, not by the child initiating theprocess as the soul matures, but because it is takenaway from outside.- stresses due to being a refugee, siblings needing ca-re (as well) and so on may also cause the protectivespace necessary for inner development to be lost- This loss causes “emergency” inner maturing inchildhood, and at the same time more or less sup-pressed aggressive feelings which cannot be adequa-tely expressed to the parents
S o l d n e r · S o m m e r | A u to i m m u n e d i s o r d e r s o f t h e Ty r o i d | D e r M e r k u r s t a b 7E n g l i s h I s s u e 2 0 0 5
- Not infrequently the role of provider changes ab-ruptly, with the growing child becoming the mater-nal provider, e.g. for siblings, father or mother- As a rule, “reminder” of traumatizing childhood ex-periences will come with renewed loss of security,(threatened or real) loss of a child, or too much beingasked again in a maternal role- The disease will usually only develop in this stress si-tuation.
We might speak of a premature birth at the level ofthe psyche, premature labour pains, or the waters brea-king early.The space for buoyancy for childhood soul de-velopment (corresponding to the buoyancy provided byamniotic fluid) is lost too soon.
This aetiological model appears to be of particular re-levance to Graves’ disease, but terms such as “Graves’disease” and “Hashimoto’s thyroiditis“ merely mark theextremes in a range of autoimmune thyroid diseases.The case records given below are an attempt to showcharacteristic backgrounds to the disease process in eit-her direction and are therefore largely limited to the bio-graphical aspect.
Mrs B, aged 60, Graves’ diseaseHer father’s first wife died of cervical cancer 18
months before the patient was born; her father was 54when she was born, the second wife, a new partner wit-hin a fairly short time, was 38. When the patient was 12,her mother was diagnosed as having breast cancer. Inthe 2 years that followed the patient increasingly tookon the nursing care for her mother whose death was aheavy blow to her. It was noted at the time that the pa-tient seemed “more serious, and older” than other girlsof her age.
At 17, the patient entered into a partnership with aman who “was strong, making me feel safe and secure”.At 22, birth of her first child. At 23, birth her of secondchild, a premature infant. Two days after returninghome, the infant died of sudden infant death syndrome.The patient said she was “as if frozen”after this, and wasnot able to talk about it to anyone.
At age 50, the patient saw a man in the street whowas very upset, suddenly poured petrol over himself andset himself on fire. Shortly after this she developedGraves’ disease. Treatment with carbimazole resulted inremission. (Victor von Weizsaecker said that in his view,onset of Graves’ disease frequently followed incendiarybomb attacks and the mental stress they induced. Hesaw the disease as a reflex shock effect and a kind of“self-cremation”by an abnormal metabolism.) When thepatient was 55, her daughter gave birth to her first child;at the same time partnership problems caused uncer-tainty. She suddenly developed great anxieties and withthis a compulsive need to check again and again that hergrandchild was still alive. Recurrence of her Graves’disease. Relatively low doses of carbimazole, Cuprite D8(amp., Weleda) and Glandula thyreoides Gl D15 (amp.,Weleda) quickly brought remission.
Four years later the patient needed to deal quicklywith a mountain of “paper stuff” to avoid financial pro-blems posing an existential threat. She had by then se-parated from her husband. She felt exhausted after this.Again Cuprite (now D8 trit.) helped. When hyperthyroi-dism was again confirmed, as feared, it was decided totreat the goitre with radioiodine. This resulted in euthy-roidism. The patient still felt frozen in her soul, however,and that her vitality was reduced. Anthroposophicalpainting therapy proved a great help to her.
Mrs A., aged 66, autoimmune thyroiditisHer father had been an engineer. She said that she
only rarely saw him but felt much connected. Psycholo-gically he was anacastic and hostile to the flesh. “I didnot relate to my mother at all.” The patient was the el-dest of four children. “They are all cracked. I really cameoff best.”
Her mother developed neurodermatitis whilst preg-nant with her. The patient says her mother tended to bedepressed and frequently suicidal, so that the patientwas often afraid for her. She had been brought up strict-ly and pietistically and was always her mother’s confi-dante.
They had to flee from Silesia when she was seven—she had to push her siblings’ pram. “I was so afraid; Icouldn’t breathe from the effort.“ From the age of 11 shepractically took sole care of her siblings. “I had to begrown-up so early.” The others would still say to hertoday:“You were our mother.”
At 38 she had four children. She was also fostering aboy at the time.“After bitter disappointments I was qui-te beside myself; it was not the way I had perceived it tobe.” Since then recurrent periods of depression and fre-quently changing hyper- and hypo-thyroid phases, Initi-ally only TPO antibodies elevated, later also TRAB. – Dis-orders of thyroid function are among the most impor-tant differential psychiatric diagnoses when there arepsychosis-like problems with perception and drive.
Medical treatment proved particularly helpful with- Colchicum Rh D3 dil. Weleda- combined injections ofAmnion Gl D10 amp. WeledaStibium met. prep. D6 amp. WeledaSolum inject. amp. Wala
Mrs S. age 54, Hashimoto’s thyroiditis with hypothyroidism
Well-rounded female form, in menopause. The pa-tient developed manifest hypothyroidism, with labora-tory findings typical of Hashimoto’s thyroiditis.
Massive cervical tension (as if she could only hold upher head and keep her eyes open with an effort), alope-cia, tiredness, moderate degree of arterial hypertension.
Her story: “I grew up in the GDR. My parents escapedseparately, first my father, and we then followed (mo-ther, patient and three siblings) via Berlin before the Wallwas built (the patient remembers every detail of that es-cape). Her father, village teacher in Lower Saxony, develo-ped Alzheimer’s early. No support was available in the vil-
8 D e r M e r k u r s t a b | S o l d n e r · S o m m e r | A u to i m m u n e d i s o r d e r s o f t h e Ty r o i d E n g l i s h I s s u e 2 0 0 5

lage. Her mother gave her children little care and only didthe most necessary things for the father, being involvedin catching up on her university studies.The children feltvery much left alone with a father who had changed somuch. It was too much for them. They had little psycho-logical support from their mother. Following their fat-her’s early death, her mother continued her medical stu-dies, developed breast cancer and continued to work onher doctorate to the very end, even on her sickbed.
The patient left home at 17, much like her siblings. Fol-lowing a first marriage in France with a man who beca-me an alcoholic she returned to Germany. In her secondpartnership, which is still continuing, she had two chil-dren; neither partner felt like getting married, the finan-cial situation remained precarious, with the patient li-ving largely on social payments and later part-timework, her partner’s income being very irregular.The part-nership clearly did not develop fully as regards inner ful-filment, though it did develop more at an academic andcultural level as time went on, yet there would be repea-ted serious crises.
The disease developed when her first daughter had apuberty crisis, presenting both parents with major pro-blems.
In this case and those that follow thyroid hormonereplacement was necessary in conjunction with anthro-posophical treatment.
Mrs G. age 46, rheumatoid arthritis and Hashimoto’sthyroiditis with hypothyroidism
The patient first came on account of chronic recur-rent sinusitis. She is Danish, slim, blonde and alwaysfeels cold in the lower body, a chilly feeling which is dif-ficult to deal with. Happily married, with two children.Soon after first admission, it became evident that shewas developing massive rheumatoid arthritis, with hu-moral inflammatory parameters (CRP, IgM and IgG RF,and so on). In the course of establishing the diagnosis,she was found to be hypothyroid (TSH 21.7 µl U/ml) withelevated anti TPO antibody titres as with Hashimoto’sthyroiditis.
The biographic history was as follows: Father an inde-pendent businessman. When the patient was 15, he suf-fered from severe depression. The family’s financial si-tuation was precarious for some time. The patient wasgreatly worried about maintaining the family and herfather’s recovery at the time, being much attached tohim. About a year ago, she said, her father, now 70, hadagain suffered from depression. She was worried abouthim – generally rather reserved and under control, thepatient started to cry at this point – and about how hermother would be able to cope. She goes to Denmarkwhenever she has some free days. Another point is thatin recent years the family have always gone to their pa-rents or in-laws for their holidays.
This patient, too, felt greatly relieved once she hadput her inner problems in words and also worked onthem in painting therapy. On the other hand she stop-ped her painting therapy when the emotional problem
situation of being so closely attached to her parents be-came evident. It took years before the subject could beproperly discussed; in the meantime her father has diedand the relationship to her mother has been harmonio-usly resolved. L. Simon is treating her rheumatoid arthri-tis using an anthroposophical approach, with no basictherapy or steroids, and the evolution is very satisfacto-ry, with no progression to joint destruction evident in theX-rays.
The sensation of coldness and chronic susceptibilityto infection only responded finally to mistletoe therapywith Iscusin salicis, with strengths E and F given by in-jection two or three times a week, initially increasing thedose slowly over years (starting with strength A, 0.5 mlonce a week).
Mrs C, age 74, Hashimoto’s thyroiditis with hypothyroidism
The patient grew up in Königsberg. Her father “wasalways drunk”, often beating her mother. In her 10th to14th years, she first experienced time spent in air-raidshelters, then the devastating bombing attacks on thecity, seeing dead bodies and smelling them afterwards.When she was 14, she and her mother fled to the west,all the time afraid of being strafed or raped. The shipthey tried to reach left before they got on board. She sawpeople fall in the water and drowning. As they continu-ed in their flight, her mother collapsed unconscious and,terribly afraid, the patient had to get help from enemysoldiers. To her surprise she and her mother were welltreated, ending up in a camp and then on a farm whereshe had to work hard.
Later in life the patient went to Brazil, where shecould only get poorly-paid work. Then she cared for hermother who had had a number of strokes, continuing towork for financial reasons. Panic attacks at work first de-veloped when she was 64. Hashimoto’s thyroiditis withhypothyroidism was diagnosed. The patient is still wor-king as a secretary at 74, has she does not have adequa-te pension rights.
The biographical conversation, when she was for thefirst time able to speak about the difficulties in her lifeclearly brought relief. Following exhibition of AconitumC30 (which has proved its value in the treatment ofshock sequels) she felt altogether very much better.WithThyreoidea comp. (Wala), 7 pilules t.d.s. and 12.5 µg thy-roxin per day she is feeling well, with TSH back to normal(2.57 µlU/ml, normal range 0.27 – 42). On one occasionshe faced up to a noisy man on the underground whothen followed her for miles and spit in her face. She de-veloped fear of persecution for a time, but following adose of Aconitum 30c this ceased within a few days. Formore than a year now she has felt very well indeed.
2) Phenomenology of hyper- and hypothyroidism
Making a deliberate comparison between hypo- andhyperthyroidism, we note that waking up has differentqualities.
S o l d n e r · S o m m e r | A u to i m m u n e d i s o r d e r s o f t h e Ty r o i d | D e r M e r k u r s t a b 9E n g l i s h I s s u e 2 0 0 5

Hypothyroidism HyperthyroidismEyes look Eyes looksleepy, dull, tired wide-awake, fixed, wide
with fear, when seen, the individual feels taken hold of by a powerful inner energy
Palpebral fissure narrow, Palpebral fissure widelatent prosis
Shoulders and back of neck may tense when trying hard to say awake and keep eyes open
Voice rough, low, with Voice bright, rich in timbre,little psychic modulation. over-tense (like Mozart’sPatients says little. “Queen of the Night”)
Increased need for sleep Reduced need for sleep
Reduced drive Restless in action, in spite of growing muscular weakness
Pulse slowed down Pulse accelerated
Patient feels chilly Characteristic feature – rather warm, slightly sweaty handshake
Hair thick and dull, Hair thin and glossy, soft,sticking out, combing style won’t holddoes not help
In both cases, emotional rangey is limited, the state ofconsciousness altered, subtly or markedly, depending onthe case.
3) Biographical aspects of Graves’ disease andHashimoto’s thyroiditis
In the authors’ view, the biographical aspects in rela-tion to these polar features of an autoimmune thyroidi-tis may be contrasted as follows.
Hashimoto’s thyroiditis• Always worried, loss of support (family, native land)
and the feeling of too much being asked all the time maydescribe the situation of the parents in the patient’schildhood but then also affect the child growing into ayoung person in the second seven-year period in life.This triggers the process of premature maturing and pa-rentification, as described. At the same time the need formaternal warmth is not adequately met. The loosing ofbonds which happens physiologically at this develop-mental stage is
• handicapped by their growing need for care andthis impedes the child’s developing independence.
• Triggering elements in later life are situations remi-niscent of earlier ones, above all of having too much as-ked of one once again, esp. in form of social responsibili-ties as mother, or concerning one’s own mother or pa-rents, generally combined with a feeling of lack of sup-
port (e.g. no partner, partner absent for work reasons orpartner unable to cope).
∑ Therapeutic measures are seen to be meaningfulwhen when the situation is addressed and the biogra-phical context clarified, with targeted relief of stress,drawing on available support, and above all also art the-rapy which offers the experience of free expression andalso a protected space.
Graves’ disease• The quality of sudden loss of security, like an assault,
is a dominant feature, the shock of having to awaken inthe soul suddenly, above all between 9 and 15 years ofage. This concerns above all the bonding with motherand father, at that time still the inner relationships nee-ded to sustain the child.
• Reversal of the maternal relationship appears to bea particularly significant factor, with the child forced in-to a maternal care provider role in the family (as in thefirst cases described), or having to care for the mother,with the child’s own need for maternal care is split offand suppressed (rather than gradually reduced). The ex-perience of “having to be mother” gets inwardly boundup with an ambivalence concerning the maternal; thismay break out again at any time and “poison” the situa-tion of being a mother (or becoming a mother, a wo-man). Biographically it is the element less of deficiencybut rather of being “toxic” which is dominant in Graves’disease, the traumatic reversal of the maternal relations-hip. Mozart’s “Queen of the Night”embodies a maternalfigure whose daughter has deeply ambivalent feelingsabout her; her voice is excessively young (with a hyper-thyroid quality).
• The triggering situations later in life also tend to beacutely dramatic with Graves’ disease—death of one’schild, a man setting fire to himself in front of the pa-tient’s eyes, the child facing a life-threatening operation,etc. Here it is not a question of wanting simply to shutone’s eyes, which it is above. No, it is a matter of gettingwholly caught up in the situation.The eye wide with ter-ror becomes a signature of Graves’ disease.
• As to treatment, the aim is first of all to convey a fee-ling of security and being protected to the patient, brea-king through compulsive actions, and stabilizing her insoul and body. Intervention to establish a new metabo-lic balance is necessary not only to prevent organic da-mage but also to enable her suddenly to have adequatemeans again of experience and conscious awareness.On this basis it is then possible to clarify biographicalbackground situations and aim to relieve mental stressand allow for a late maturing. It is particularly importantto identify traumatic events in youth and work throughthem, and to clarify ambivalent bonding situations. Arttherapy, especially painting, is again very helpful.
• Girls and women differ from boys and men in theirneed and capacity for bonding, the depth and degree ofdifferentiation in inwardly perceiving their referencepersons, and in their resonance in soul and body to thequality of relationships. The difference is demonstrable
10 D e r M e r k u r s t a b | S o l d n e r · S o m m e r | A u to i m m u n e d i s o r d e r s o f t h e Ty r o i d E n g l i s h I s s u e 2 0 0 5

from birth; it unfolds fully with puberty in the second se-ven-year period of life. A well-known though pathogene-tically little understood phenomenon is that the inci-dence of autoimmune thyroid disorders is much higheramong women than men—after puberty by a factor ofabout 10 (2). No pathophysiological reason for this has sofar been established in medical science.The pathogene-tic connection shown here would, on the other hand,make us expect a higher incidence among women. It al-so gives the reasons why the period from the 9th to the15th year of life has particular significance in this re-spect.
4) Phylogenetic aspects of the thyroidIn simple chordates (e.g. Amphioxus) the thyroid de-
velops close to the gills at the entrance to the digestivetract. The localization of this organ between respiratoryand digestive organs, in a site which will later differentia-te into the cervical region, is thus of primary significan-ce.The original Glandula thyroidea, e.g. in Amphioxus, isidentifiable from the iodine-containing secretion whichin this chordate animal still passes into the digestivetract (to be absorbed with the food). The thyroid can beidentified ab initio as an iodine-absorbing organ whichorganizes (“potentizes” (3)) iodine in a form effective forthe organism. This originally exocrine secretion into thedigestive tract can help us to understand why thyroxinetaken by mouth retains its action on the internal organ-ism (4). Functionally one assumes the secretion to act on(katabolic) metabolism, growth and sexual maturation.
The thyroid became an endocrine organ in the fishes,which at the same time developed a mobile internal ske-leton differentiated into vertebrae and the ability notonly to develop bone but also to break it down and re-build bone tissue (as distinct from the molluscs, for in-stance). This process brings the skeleton itself into theanimal’s ensouled movement. Thyroid function plays amajor part in this and all the way to maturation of thehuman skeleton.
The thyroid plays a key role in amphibian metamor-phosis which enables these vertebrates to leave the wa-ter and go on land as they mature, leaving the sphere ofbirth and childhood and growing independent.
- The development and maturation of the lungs and- the development of the limbs (7)are made possible through thyroid activity. In an ex-
periment done in the carefree way of childhood, one ofthe authors saw how when thyroxine was added to thewater in the aquarium, tadpoles developed into dwarffrogs and came on land prematurely—a picture of pre-mature maturation under exogenic influence. Converse-ly, pharmacological blocking of thyroid hormone cansuppress tadpole metamorphosis.
It is worth noting that the greatest accumulation ofiodine occurs in the vegetative zone of coastal regionsaround the world’s oceans (you can smell the iodine inthe ozone in those regions), e.g. in bladder-wrack (Fucusvesiculosus) and related plants. The plants concentrateiodine by a factor of 10,000 – 100,000 (from 50 mg of io-
dine/t of seawater to up to 19 kg/t of plant). It is not cle-ar what this means for the plant (whereas the signifi-cance of the iodine organization for ensouled, animal or-ganism is all the more evident). Note, however, the sitewhere this accumulation occurs—the seashore wherevertebrates originally came on land. It is a site where po-lar opposite qualities come together (continent and oce-an) and relate to one another (which also applies in theregion of the human neck).
The element iodine was first produced from seaweedash in 1811. Industrial production was for a long time ba-sed on these plants as living “iodine deposits”. With thehalogens bromine and chlorine, the metals gold, copperand caesium and the non-metal sulphur, it is one of theseven coloured elements occurring in nature; the name“iodine” derives from the Greek adjective for “violet”.(5)At room temperature, iodine gradually sublimates to thegaseous state (a signature telling us of a strong con-nection with the air organism, the soul sphere, the astralbody). Kolisko (6) repeatedly characterized the connecti-on between lung and limbs.
Coming on land, actively overcoming gravity, increa-singly developing internal warmth as respiratory andmetabolic activity gains in importance, the soul princi-ple incarnates more and more in the animal organism.This evolution culminated in the achievement of homo-thermia, a stable internal temperature which permits in-dependent movement and waking consciousness in va-riable external temperatures. This step came with thebirds; taking it to extremes they are able to move fromground to air.Their physiological body temperature is upto 40 ºC with a correspondingly high basal metabolismwhich in turn correlates with the level of circulating thy-roid hormone and intensive respiratory activity. The re-spiratory organs extend into the bones, resulting in a“physiological osteoporosis”. Tachycardia, rapid move-ments which in the head region appear jerky, the sharp,wide-awake eye, even the liquid stools remind of hyper-thyroidism.(15)
This evolution reached its “goal”, a balanced uprightwalk, in human beings. The birth of a child is anotherway of “coming on land” and depends on thyroid activi-ty, especially with regard to the maturing of lungs; up tothe time of birth, however, maternal thyroid hormonecan compensate fully if fetal thyroxine is lacking. It is on-ly from birth that a child has to depend on its own thy-roxine production. In addition to the above, maturationof the nervous system, and above all its myelinization,depend on thyroid function. If the thyroid does notfunction adequately, the child cannot develop full cons-cious awareness.
Again it is worth noting that the thyroid is located inthe throat region, beside the larynx, the organ which inspeech enables the singular “birth” of the soul principlein producing the meaningful world. Humanity owe thepotential for speech to the fact that the larynx moveddown; at the same time an unstable crossing-over aro-se of air and food passages (in the dimensions of abo-ve/below and posterior/anterior). Compared to the ani-
S o l d n e r · S o m m e r | A u to i m m u n e d i s o r d e r s o f t h e Ty r o i d | D e r M e r k u r s t a b 11E n g l i s h I s s u e 2 0 0 5

mals, human beings are at a high risk of aspiration, espe-cially when consciousness fades. The human throat andneck region thus proves unusually dramatic.(8) A furthercross-over in the craniocervical transition area lies in thesphere of the nervous system (in the left/right dimensi-on). The neck mediates between the fundamental pola-rities of the head on one hand and the trunk and limbson the other, with opposite developmental principlesand different embryonic tissue origin.(9)
Rudolf Steiner described from supersensible observa-tion and in agreement with many other investigatorsworking at this level(10) that it is exactly in this location,at the level of the larynx (and thyroid) that spiritual in-vestigators perceive a particular “chakra”(wheel) as an or-gan primarily at the astral and soul level. Suitable trainingcan develop this into an organ for perceiving the “natureof the thoughts of other ensouled beings”. Chakras or-ganize and orientate the intervention of etheric powersin the physical organism. They may be called organs inthe human soul organism. M. Girke developed a thera-peutic approach for patients with thyroid disorders fromthe exercises which R. Steiner gave for the unfolding ofthis chakra.(11)
It is only at this level that one finds the organizingpowers which in the course of evolution brought aboutthe development of the relevant organs and faculties inthe physical body. To the extent to which the evolutionand health of the individual depend more and more onhis own conscious awareness and actions, it will be pos-sible for human beings to make progress in perceiving,taking note of and developing soul and spirit as organi-zing reality.
5) Age-relationship of disorders and pathological dispositions affecting the thyroid
It will be evident from the above that hypothyroidismindicates that the soul organization primarily involved inrespiration is not intervening strongly enough, or lessand less. Hyperthyroidism is a condition where the soulprinciple exerts too much of its catabolic potential in theliving body. This is reflected in the age distribution. Con-genital hypothyroidism, incidence 1 : 4,000 newborn in-fants, is the most frequent endocrine disase. Hyperthy-roidism on the other hand is reatively rare up to the 18thyear (1 : 50,000 – 1 : 100,000). Graves’ disease, which in-volves hyperthyroidism, most frequently develops inmid-life, between the 20th and 40th years, when body-bound soul activity is most intensive. Hashimoto’s thy-roiditis most frequently manifests between the 30thand 60th years; up to 10 % of all women aged 60 are af-fected (12), with 85% showing subclinical to manifesthypothyroid metabolic status at diagnosis. Withdrawalof the soul principle from the living body shows itself.
In the second seven-year period, the thyroid developsa different volume corresponding to the developing se-xual characteristics. The female thyroid generally has avolume of 18 ml compared to the male at 25 ml (ratio of2 : 3). Physiologically this may be said to relate to the re-
lative muscular development, depth of breathing andphysical strength, but it does also show how much thedevelopment of this endocrine organ is determined bythe differentiation into genders.This quantitative aspectmay be considered a further indication that it mattershow the soul develops in a phase in life which is sensiti-ve to thyroid maturation, and how the young person isable to identify with this. This includes the metamor-phosis of bonds with the same-sex and the other-sex pa-rent. Diseases involving autoaggression later in life mayalso be considered to indicate that identification in souland spirit with physical maturation and the responsibi-lities that come with this has been incomplete or distur-bed.
Between the 9th and 15th years, iodine requirementsare particularly high (also in pregnancy), and dependingon the availability of iodine, the thyroid also developsdispositions for potential diseases that have far-rea-ching significance for the whole of life. A diet low in io-dine, and also one rich in “goitrogens”(e.g. soya) will mo-re frequently lead to the development of (iodine defi-ciency goitre); later in life the risk of autonomous adeno-ma and multifocal autonomy is distinctly higher, and ifcancer develops, follicular and undifferentiated tumoursare more frequent.
A diet rich in iodine, on the other hand (originallyconnected with living near the sea, but nowadays, withchemical substitution possible, depending primarily oncultural factors) significantly increases the risk of auto-immune thyroid disorders but reduces the risk of goitreand adenoma; any thyroid cancer would be more likelyto be papillary. It appears that the disposition for cancerdevelops early—by the 14th year—and 80 % of papilla-ry carcinomata develop before the 40th year (in areaswhere iodine supply is adequate); the ratio for female :male gender is again around 2 or 3 : 1.(16)
6) Consequences for medical practiceRegarding the history, include biographical questi-
ons:- what happened between the 9th and 15th year?- what is the relationship to each of the parents?- in how far was there a feeling of security and warmth?- how did personal autonomy relative to parents and siblings develop?
In the authors’ experience these questions are parti-cularly important with autoimmune thyroid disorders.They provide a possible starting point for anthroposo-phical biography research.
With regard to diagnosis, it is important to identifytriggers for the presenting condition and clarify howthey relate to earlier stresses (v.s.)—is it an instance ofre-living something?
As to treatment, possible methods have been descri-bed above. Medically, treating earlier shocks may be im-portant as a first stage, especially with Graves’ disease,for instance giving Aconitum in relatively high dosage. Abroadly stabilizing effect on autoimmune thyroiditis
12 D e r M e r k u r s t a b | S o l d n e r · S o m m e r | A u to i m m u n e d i s o r d e r s o f t h e Ty r o i d E n g l i s h I s s u e 2 0 0 5
may be achieved, especially at the beginning of treat-ment, with
- Amnion D30 amp. Walaand- Cuprum met. prep. D30 amp. Weledaas a combined injection.Good results have been seen with both Graves’disea-
se and Hashimoto’s thyroiditis—including a measurableand in individual cases even remarkable reduction in au-to antibodies—with the organ preparation
- Glandula Thyroidea D30 amp. Wala(per os or s.c., 2 or 3 times a week)
Painting is particularly suitable for art therapy in thebeginning; later speech therapy can above all addressthe I for a positive effect on its role in stabilizing theastral body, the soul organization. This may also beachieved with eurythmy therapy exercises done daily.This also provides better conditions for entering on innerdevelopment (13, 14) in terms of the “eightfold path”, forthis has a specific relationship to the configuration ofsoul powers in the region of the thyroid.
Georg Soldner, paediatricianMarkus Sommer, physicianJosef Retzer Str. 36D-81241 Munich
S o l d n e r · S o m m e r | A u to i m m u n e d i s o r d e r s o f t h e Ty r o i d | D e r M e r k u r s t a b 13E n g l i s h I s s u e 2 0 0 5
References1 Schulte, Spranger. Pädiatrie 2.Aufl. Springer 2003:S.5142 Remmele W. Pathologie Bd. 4.2.Aufl. Springer 1997:584/5883 von Laue B. Kalzium als Sub-stanz und als Prozess im Men-schen. Der Merkurstab 57 2004:78-954 Romer AS, Parsons TS. Verglei-chende Anatomie der Wirbeltie-re, 5.Aufl., Hamburg/Berlin 1991:5365 Trueb L. Die chemischen Ele-mente. S. Hirzel, Stuttgart 1996.S. 3476 Kolisko E. Auf der Suche nachneuen Wahrheiten, Verlag amGoetheanum, Dornach 1989:1387/8 Husemann A. The Harmonyof the Human Body. Tr. C. v. Ar-nim. Ednburgh: Floris Books2002.9 Rohen, Lütjen-Drecoll. Funk-tionelle Embryologie. 2. Aufl.Schattauer Stuttgart 2004:111-14910 Steiner R. Knowledge of theHigher Worlds / How to KnowHigher Worlds.11 Girke M. Die Schilddrüse. DerMerkurstab (48) 1995:404-416,564 -58312 Dietel M, Dudenhausen J,Suttorp N (Hrsg.). Harrisons In-nere Medizin. ABW-Verlag Berlin15. Aufl. 2003:226013 Girke M. Die Schilddrüse. DerMerkurstab (48) 1995: 404-416,564-58314 Bittlestone A. Das Lebenmeistern. Zur Praxis des acht-gliedrigen Pfades. Verlag FreiesGeistesleben, 2. Aufl. Stuttgart200215 Husemann F. Das Belladon-nagift und seine Wirkprinzipien.Beitr. z. Erw. d. Heilkunst (32)1979:198-20616 Reiner C, Stuschke M, DralleH, Schmidt HJ. Schilddrüsenkar-zinom. In: Schmoll HJ, Höfken K,Possinger K. Kompendium inter-nistische Onkologie. Bd. 2 Sprin-ger Berlin, Heidelberg New York1999:668-710

14 D e r M e r k u r s t a b | G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s E n g l i s h I s s u e 2 0 0 5
The thyroid and its disorders are closely connectedwith the nature of the human soul and spirit. Inthis sense, thyroid status may offer a differentia-
ted picture of astral-body activity and also the relations-hip between astral body and I-organization. If thechanges in the activities of the four bodies which aredescribed below develop, an organ becomes ‘foreign’andbegins to drop out of the comprehensive integrity of theorganism.The human organism responds to any foreignquality with inflammation. Inflammatory changes in thethyroid are rarely acute but tend to be subacute, like deQuervain’s thyroiditis, and the frequently seen chroniclymphocytic thyroiditides.The atrophic evolution of Has-himoto’s thyroiditis, with the development of initially la-tent and later manifest hypothyroidism, is the oppositeof Graves’ disease, where hyperthyroidism tends to bemarked. A polarity does, of course, also always point toan inner relationship. This makes it possible to considerthe spectrum of thyroid disorders, polar in composition,in the aspect of metamorphosis.
Graves’ diseaseGraves’ disease belongs to the group of immunoge-
nic thyroid disorders which will be considered in moredetail below. With these conditions, too, one cannotoverlook the significance of the human psyche. ThusGraves’ disease may manifest after sometimes severemental shocks. Major strokes of destiny and separationfrom people to whom one has been close can, if the phy-sical constitution goes in this direction, provide the ba-sis for psychic dynamics which the individual is unableto cope with. Here the age at which Graves’ diseasetends to manifest is telling. From the fourth seven-yearperiod onwards, the I-organization changes soul life, dif-ferentiating it into sentient soul, rational soul and spiri-tual (or consciousness) soul. With the seventh seven-ye-ar period, i.e. in the early forties, it generally begins to un-fold the next important step in development, which isthe spirit self. Similar to the way in which diffuse goitrereflects inadequate astral activity, Graves’ disease pre-sents as the pathology of unfolding, “being born” of in-dividual character, starting from the fourth seven-yearperiod. The transformation of the astral body into thequalities of the spiritual self in the “knighthood” periodof human life, approximately between the 42nd and
Polar opposites in autoimmune diseases of the thyroidM at t h i a s G i r k e
Translation of “Die Polarität in den autoimmunen Schilddrüsenerkrankungen” by Matthias Girke.Der Merkurstab 2004; 57/7: 350-65. English by A. R. Meuss, FCIL, MTA.
AbstractGraves’ disease and the atrophic form of Hashimo-to’s thyroiditis are in several respects polar opposi-tes. Thus the pathological process may lead to in-creased blood supply in conjunction with the inflam-mation in Graves’ disease, and sclerosis with autoim-mune atrophic thyroiditis. The clinical syndromewith developing hyperthyroidism on one hand andhypothyroidism on the other also points to the pola-rity. Behind this is the characteristic function of thedifferent human bodies, which leads to therapeuticapproaches in anthroposophical medicine aiming tobroaden the approach using suppression or substitu-tion of the organ’s function. Eurythmy therapy is animportant element next to medical treatment. Thesethyroid conditions also present an inner challengewhich patients may take up.KeywordsGraves’ diseaseHashimoto’s thyroiditisAutoimmune atrophic thyroiditisMultiple endocrine adenomatosisPolyglandular autoimmune syndromeMyxoedemaHypothyroidismHyperthyroidismColchicumCupriteChalcosineLevicoBryophyllumLycopusIodumThyreoidea
G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s | D e r M e r k u r s t a b 15E n g l i s h I s s u e 2 0 0 5
49th years, is a special characteristic of the relationshipbetween astral body and I-organization which pertainswith Graves’disease. It is worth mentioning at this pointthat the condition evidently does not occur in the animalworld.
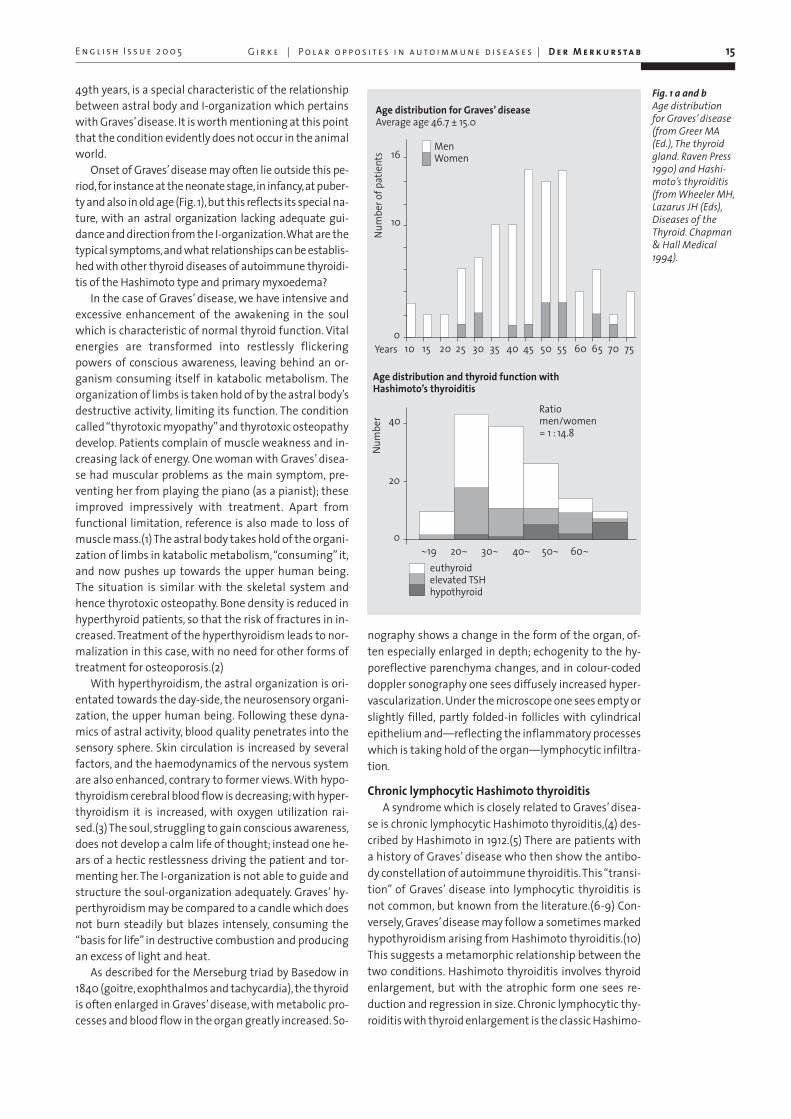
Onset of Graves’ disease may often lie outside this pe-riod,for instance at the neonate stage,in infancy,at puber-ty and also in old age (Fig. 1),but this reflects its special na-ture, with an astral organization lacking adequate gui-dance and direction from the I-organization.What are thetypical symptoms,and what relationships can be establis-hed with other thyroid diseases of autoimmune thyroidi-tis of the Hashimoto type and primary myxoedema?
In the case of Graves’ disease, we have intensive andexcessive enhancement of the awakening in the soulwhich is characteristic of normal thyroid function. Vitalenergies are transformed into restlessly flickeringpowers of conscious awareness, leaving behind an or-ganism consuming itself in katabolic metabolism. Theorganization of limbs is taken hold of by the astral body’sdestructive activity, limiting its function. The conditioncalled “thyrotoxic myopathy”and thyrotoxic osteopathydevelop. Patients complain of muscle weakness and in-creasing lack of energy. One woman with Graves’ disea-se had muscular problems as the main symptom, pre-venting her from playing the piano (as a pianist); theseimproved impressively with treatment. Apart fromfunctional limitation, reference is also made to loss ofmuscle mass.(1) The astral body takes hold of the organi-zation of limbs in katabolic metabolism,“consuming” it,and now pushes up towards the upper human being.The situation is similar with the skeletal system andhence thyrotoxic osteopathy. Bone density is reduced inhyperthyroid patients, so that the risk of fractures in in-creased. Treatment of the hyperthyroidism leads to nor-malization in this case, with no need for other forms oftreatment for osteoporosis.(2)
With hyperthyroidism, the astral organization is ori-entated towards the day-side, the neurosensory organi-zation, the upper human being. Following these dyna-mics of astral activity, blood quality penetrates into thesensory sphere. Skin circulation is increased by severalfactors, and the haemodynamics of the nervous systemare also enhanced, contrary to former views. With hypo-thyroidism cerebral blood flow is decreasing; with hyper-thyroidism it is increased, with oxygen utilization rai-sed.(3) The soul, struggling to gain conscious awareness,does not develop a calm life of thought; instead one he-ars of a hectic restlessness driving the patient and tor-menting her. The I-organization is not able to guide andstructure the soul-organization adequately. Graves’ hy-perthyroidism may be compared to a candle which doesnot burn steadily but blazes intensely, consuming the“basis for life” in destructive combustion and producingan excess of light and heat.
As described for the Merseburg triad by Basedow in1840 (goitre, exophthalmos and tachycardia), the thyroidis often enlarged in Graves’ disease, with metabolic pro-cesses and blood flow in the organ greatly increased. So-
nography shows a change in the form of the organ, of-ten especially enlarged in depth; echogenity to the hy-poreflective parenchyma changes, and in colour-codeddoppler sonography one sees diffusely increased hyper-vascularization. Under the microscope one sees empty orslightly filled, partly folded-in follicles with cylindricalepithelium and—reflecting the inflammatory processeswhich is taking hold of the organ—lymphocytic infiltra-tion.
Chronic lymphocytic Hashimoto thyroiditisA syndrome which is closely related to Graves’ disea-
se is chronic lymphocytic Hashimoto thyroiditis,(4) des-cribed by Hashimoto in 1912.(5) There are patients witha history of Graves’ disease who then show the antibo-dy constellation of autoimmune thyroiditis.This “transi-tion” of Graves’ disease into lymphocytic thyroiditis isnot common, but known from the literature.(6-9) Con-versely, Graves’disease may follow a sometimes markedhypothyroidism arising from Hashimoto thyroiditis.(10)This suggests a metamorphic relationship between thetwo conditions. Hashimoto thyroiditis involves thyroidenlargement, but with the atrophic form one sees re-duction and regression in size. Chronic lymphocytic thy-roiditis with thyroid enlargement is the classic Hashimo-
Fig. 1 a and bAge distributionfor Graves’ disease(from Greer MA(Ed.), The thyroidgland. Raven Press1990) and Hashi-moto’s thyroiditis(from Wheeler MH,Lazarus JH (Eds),Diseases of theThyroid. Chapman& Hall Medical1994).
Age distribution for Graves’ diseaseAverage age 46.7 ± 15.0
Age distribution and thyroid function with Hashimoto’s thyroiditis
MenWomen
Num
bero
fpat
ient
s
Years
Ratiomen/women= 1 : 14.8
Num
ber
euthyroidelevated TSHhypothyroid

to thyroiditis.The atrophic form, occasionally also calledprimary myxoedema with reference to the untreated cli-nical picture, seems to be the other end of the spectrum.It is certainly justifiable with the present state ofknowledge and in contradistinction to the view that wasformerly taken of the different disease entities, to referto an immunogenic thyroiditis with different forms ofevolution which may involve goitre or also atrophy of thegland.
The spectrum beginning with Graves’ disease, inwhich we are looking for connections with autoimmu-ne thyroiditis, thus appears to extend as far as the atro-phic form of thyroiditis.
If we first of all consider the morbid processuality, wehave excessive increase in metabolism with Graves’disease, and a massive increase in blood flow in the or-gan, as demonstrable by doppler sonography. This is theabove-mentioned emphasis on the metabolic system,also evident in the thrill frequently noted over the glandon auscultation in the past. With Hashimoto’s thyroidi-tis, on the other hand, the disease has a different orien-tation even at this point. It is a chronic lymphocytic thy-roiditis with progressively increasing connective tissueinvolvement and marked fibrosis in parts of the organ.In advanced stages, normal parenchyma has largely dis-appeared.(11) Similar changes may ultimately characte-rize the atrophic form of thyroiditis. Instead of the em-phasis on the metabolic system one sees with floridGraves’ hyperthyroidism, there is progressive sclerosisas the disease spectrum evolves, with the neurosensorysystem functioning in a way which here is not physiolo-gical.
These changes in the activities of the different bodiescan be seen in the symptoms and signs of Hashimoto’sthyroiditis in the threefold organism. In the organizati-on of limbs, the astral organization separates itself fromits physiological movement function. Contraction andrelaxation slow down in the course of hypothyroidism.A feeling of stiffness may develop and it is not too un-common for patients to report this. Myalgiform symp-toms may develop when the astral body, normally co-ming into its own in movement, separates itself in thisway. Occasionally one also hears of muscle fasciculationsbeing a problem, in one woman with Hashimoto’s thy-roiditis this escalated into a clinically visible “fascicula-tion storm” of striated muscles. Symptoms indicative ofchanges in the activities of the bodies are also found inthe articular system. Various problems with joints andarthralgia (often of the MCP and PIP in the hands) mayoccasionally also involve swelling. An inflammatory “re-sponse” to changes in the activities of the higher bodiesmay lead to Hashimoto’s thyroiditis associating withrheumatoid arthritis.(12) Here a sclerotic condition ma-nifests in the articular system not only at the functionallevel, as with the muscular symptoms, for instance, butalso physically. Other sclerotic changes which may deve-lop in the locomotor system in connection with hypothy-roidism and this autoimmune thyroid disease indicatechanges in astral organization activity going in the same
direction. This applies to Dupuytren’s contracture andcarpal tunnel syndrome.(13)
Apart from these manifestations in the system oflimbs, all due to changes in astral body activity, corres-ponding processes are evident in the metabolic system,starting with autoimmune diseases of the liver (autoim-mune hepatitis). Approximately 20 % of patients withprimary biliary cirrhosis (PBC) are said to have or deve-lop hypothyroidism.(14)
Another involvement of the glandular system in theupper human being must also be mentioned. This isSjoegren’s syndrome,(15) or sicca syndrome, which initi-ally affects the salivary and lachrymal glands. Patientscomplain of dry eyes, sometimes also a developing xe-rostomia, an indication that astral activity has with-drawn from glandular function. Tiredness is a generalsymptom mentioned in some cases, again pointing towithdrawal of the astral body. Sjoegren’s syndrome is as-sociated with autoimmune liver diseases and may alsoinvolve arthralgia and even non-erosive arthritis. Gas-trointestinal motility disorders may occur, again due toastral body withdrawal.These have also been seen in hy-pothyroidism without Sjoegren’s syndrome.
The associated coeliac disease also comes in thesphere of the metabolic organization. These patientsshow an increased incidence of autoimmune thyroidconditions; as one would expect with a syndrome whe-re the higher bodies do not sufficiently intervene in themetabolic organization, hypothyroidism is more fre-quent than hyperthyroidism.(16) Mention must also bemade here of the association between autoimmune thy-roid diseases and autoimmune (metaplastic) atrophicgastritis, where atrophy of the glandular organizationpoints to withdrawal of the astral body.(17)
Effects of the sclerotic process are also apparent inthe middle human being and the rhythmical system.With subclinical hypothyroidism, only a discrete changeinitially involving endothelial dysfunction has been no-ted.(18) The constrictive and hardening qualities of theupper human being impose form principles on the vas-cular system. The relaxant gesture of dilatation con-nected with processes remote from conscious aware-ness in the lower human being can then no longer beadequate. Hypothyroidism is connected with a decreasein myocardial contractility and a reduction in ventriculardiastolic relaxation. It appears that with subclinical hy-pothyroidism a limitation of diastolic relaxation also de-velops,(19) a finding which typologically corresponds toendothelial dysfunction. A connection exists also bet-ween hypothyroidism and artherosclerosis (20) and co-ronary disease, frequently marked, and reduced HDL-cholesterol levels. At this point we may also go beyondthe above phenomena leading to sclerosis and harde-ning and refer to possible changes in blood coagulation.This has its place in the polarity of hardening coagulati-on processes belonging to the upper human being andthe dissolving fibrinolysis processes relating to the lowerhuman being. The blood is in the field of tension bet-ween these polar opposite activities. It seems that in
16 D e r M e r k u r s t a b | G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s E n g l i s h I s s u e 2 0 0 5

connection with (also subclinical) hypothyroidism a hy-pofibrinolytic and hypercoagulant constellation may de-velop, reflecting the sclerotic process.(21)
A revealing connection also exists between autoim-mune thyroiditis and pernicious anaemia, with a largeproportion of these thyroid patients being positive forparietal cell antibodies. The symptoms of the anaemiaalso reflect a withdrawal of the upper bodies from or-ganic activity, as in the picture of autoimmune thyroidi-tis which was presented above.
With hyperthyroidism, excessive activity on the partof the astral body goes hand in hand with increased bo-dy temperature and intolerance of heat. Conversely, hy-pothyroidism involves cooling—patients easily feel chil-ly and do not tolerate cold well.
Finally with regard to the nervous system, attentionmust be drawn to the extremely rare (steroid-sensitive)Hashimoto’s encephalitis. A connection with the thyroi-ditis may exist and needs to be investigated.
With hyperthyroidism one sees increased cerebralhaemodynamics; with Hashimoto’s thyroiditis, bloodflow appears to be diminished. Comparing euthyroid pa-tients with a group of healthy controls, cerebral perfusi-on was found to be reduced. Anxiety and depressionscores showed significant differences between the twogroups, though these did not relate to the changes inperfusion.(22)
It is interesting that there have been occasional re-ports of reduced hearing which is said to have returnedto normal following exhibition of thyroid hormone.Where a patient with Graves’ disease develops the cha-racteristic eye symptoms, hypothyroidism means thathearing and speech (myxoedema voice) are affected. Ru-dolf Steiner characterized the polarity of the eye, whichis turned towards the outside world, and the ear with itsorientation, which is directed towards inner essence;this is evident with these thyroid disorders.
The sclerotic process can also be shown with otherconditions associated with autoimmune thyroiditis. Aconnection exists between sclerosis and diabetes melli-tus, for instance. Every 5th type-1 diabetic is said to de-velop autoimmune thyroiditis as well.(23) The connecti-ons Hashimoto’s thyroiditis has especially with the adre-nal gland (Schmidt syndrome) or beyond this, with dia-betes (Carpenter syndrome) as part of an autoimmunepolyglandular syndrome, point to pathological astral bo-dy activity behind these individual phenomena. RudolfSteiner referred to this in his Pastoral Medicine Course.“Now the I-organization and the astral body are morebound to each other, and the two together are not ente-ring into the physical and the ether body the way theyshould.” There follows the suggestion “that one seesmarked abnormalities in the more subtle glands andhormone production, in the glands we refer to as adre-nals and in the small glands that lie hidden in the thy-roid here in the neck region.” Reference is also made toother glands (pituitary and pineal body), as well aschanges in the sensory and the nervous systems.(24)The psychic phenomenology of fading sensory percepti-
ons and the tendency to “giddy dream states” arising inthis context are also described which arise because theastral body and the I-organization are not adequatelyconnecting with the sensory organization.
The polar opposite to polyglandular autoimmunesyndrome, which points to withdrawal of the astral or-ganization, is multiple endocrine neoplasia, MEN I and II,which points to autonomous endocrine function that isno longer subject to the guiding power of the I-organi-zation and therefore drops out of the regulatory systemof the organism as a whole. Medullary carcinoma of thethyroid, which comes under this heading, is an impor-tant thyroid-related disease.
Another important point is that above all lymphomasof the thyroid and also papillary carcinoma of the thy-roid are said to show a higher incidence with lymphocy-tic thyroiditis.(25) It is no doubt premature to see the lat-ter as a precancerous change, but the relationship bet-ween chronic inflammation and malignancy, referred toon several occasions, may come into this. It is interestingto note that patients with differentiated carcinoma andthyroiditis are said to have a better prognosis than pa-tients with differentiated carcinoma and no inflamma-tory changes.(26) The qualities of both the acute andchronic forms of inflammation may be seen in these fin-dings.
Hashimoto’s thyroiditis shows the above-mentionedpolarity of being associated with goitre or atrophic evo-lution. Constitutionally one also sees a polar sympto-matology. Thus one has a “hysterical” constitution withinner excitability and restlessness, sometimes also rapidspeech and sequence of thoughts, and on the otherhand the neurasthenic typology with signs of astheniaand weakness.
Autoimmune disease processes of the thyroidagainst the background of threefoldness
At the level of morbid processuality, we have the po-larity between a syndrome with the emphasis on meta-bolism and increased blood flow on the one hand and athyroid condition involving progressive connective-tis-sue sclerosis on the other. In the one case, the system ofmetabolism and limbs is dominant, in the other the neu-rosensory system.
If we consider the functionality of thyroid metabo-lism, the hyperthyroidism of Graves’ diseases is the op-posite of atrophic autoimmune thyroiditis in the se-quence of thyroid diseases given above. The middle po-sition is again held by autoimmune thyroiditis, whichfrequently starts with an initially hyperthyroid metabo-lism and may later develop a latent hypothyroidism.
What then are the characteristics of the psyche withthese syndromes, ascending from morbid processualityto the organization of the psyche?
In connection with autoimmune thyroiditis one oftensees a lively, agitated inner life, on occasion with restless-ness, reminding of Graves’disease.The elevated TSH-ba-sal which suggests a latent hypothyroidism is in markedcontrast to subjective and objective findings. Unlike
G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s | D e r M e r k u r s t a b 17E n g l i s h I s s u e 2 0 0 5

18 D e r M e r k u r s t a b | G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s E n g l i s h I s s u e 2 0 0 5
Graves’disease, the metabolic changes characteristic forhyperthyroidism are absent, however. It is an inner lifethat often seems to have little guidance from the I-or-ganization but does not take hold of metabolism inten-sively—as in the case of the initially frequent hyperthy-roidism and Graves’ disease. The astral body turns morefrom metabolic activity to influencing the consciousmind, here appearing as wide-awake and restless innerlife.
With the soul-organization’s metabolic activity part-ly withdrawn, metamorphosis of vital energies intopowers of conscious awareness finally can only be ina-dequate. The clinical picture of hypothyroidism evolves.Initially the patient’s increased need for sleep suggeststhat conscious awareness will be limited to a level com-parable to sleep. The recuperative, anabolic side of sleepdoes, however, have a very different quality and must notbe confused with the hypothyroidism which develops inthis case as a circumscribed type of disease frequentlytending towards sclerosis. Rudolf Steiner spoke of theopposing qualities of sleep, how it gives health and alsosickness.(27) Hyperthyroid people show a dull, apatheticwaking state which is growing rigid, with interest in theenvironment progressively lost. In connection with hy-perthyroidism and hypothyroidism, which manifests atthe opposite pole, we thus find two opposite gestures inthe soul (Fig. 2).
Dynamic and sclerosing inner lifeContrasting the two different forms of immunogenic
thyreopathy, we see the different ways in which theastral organization is active.With Graves’disease we ha-ve extreme activation of metabolism in terms of a life-consuming catabolism, with powers of conscious awa-reness evolving.With Hashimoto’s thyroiditis this is lessso. It is quite often that one still sees an agitated innerlife, with activity not so strongly directed to metabo-lism, and this may ultimately change into hypothyroiddimming of consciousness.
Considering the evolving contrast it is important tolook at the fundamental factors that constitute our wa-king consciousness. An important description of howour world of thoughts arises was given by Rudolf Steiner:“Never would our thoughts flash through the soul if I
and astral body did not work together, and this is re-flected in the way blood and nervous system work toget-her. Scientists of the future will feel that it was a stran-ge thing for scientists today to look only in the nervoussystem for the source of thought. The source and originof thought does not lie in the nerves alone.We must ac-cept that it is the interplay between blood and nervoussystem which allows thoughts to arise.”(28)
He then evolved the macrocosmic image which liesbehind the development of thoughts:“When the blood,our inner fire, and the nervous system, our inner air, worktogether in this way, the thought flashes through thesoul. And the genesis of the thought in the inner soulcorresponds to the roar of thunder in the macrocosm.When the fire of lightning ignites in the masses of air,when fire and air come together to create thunder, thisis the same macrocosmic event in the big world; the cor-responding process develops when the fire of the bloodand the play of the nervous system discharge in innerthunder, which, however, sounds out in thoughts, doingso gently and quietly in a way imperceptible to the out-side world.”
Powers of thought, powers of conscious awarenessemerge from the organization in the process of katabo-lic metabolism which is part of every unfolding of cons-ciousness and presents as enveloped in the warmth andquantitatively especially emphasized circulation of thehead organization. “Pre-conscious” powers, they thenshine out against the structural quality of the nervoussystem as conscious thoughts.
With hypothyroidism, the “blood pole” of thinkingappears to be progressively receding, the element whichin hyperthyroidism pushes overwhelmingly into theconscious state falls progressively silent.
We can find this aspect in Rudolf Steiner’s words:“Reading medical books today, it is described as if the hu-man being loses his rationality with disease or absenceof the thyroid. No, he merely loses interest, involvement,grows dull and does not use his rational mind.The ratio-nal mind remains intact when you lose interest.What islost is the lively interest one takes in things, wanting todirect attention to things. Someone who does not takean interest does not turn his attention to anything be-cause he lacks the tool for this.We do not give him ratio-
Fig. 2.Graves’ disease –
autoimmune thyroiditis – atro-phic thyroiditis in
relation to thethreefold nature
of the human organism.
Type of disease Thyroid function Psychic phenomenology
N E U R O S E N S O R Y S Y S T E M
Sclerosis and fibrosis of thyroidAutoimmune atrophic Hypothyroidism Psyche growing rigid,
thyroiditis apathetic, dull
autoimmune (Latent) hypothyroidismthyroiditis initially frequently hyperthyroidHashimoto
Graves’ disease Hyperthyroidism Restless, excited psyche
increased blood flow and metabolic activity
M E T A B O L I C S Y S T E M

nal understanding with the thyroid but a tool which en-ables him to take a lively interest in the things of theworld.”(29)
This is unequivocal reference in connection with thethyroid to the active, will-related side of the inner worldin soul and spirit, developing active interest and attenti-veness and involving oneself in the things of the world.
Starting from this characterization, important light iscast on the dimming of consciousness with hypothyroi-dism, and beyond this also with some forms of demen-tia. One will often see an apathetic, frozen inner livewhich nevertheless is awake, having lost the inner-lifedynamics connected with the blood. Apart from reducedattentiveness to things in their surroundings, patientswith manifest hypothyroidism often show reducedspeech activity(30) and a slowing-down in their thin-king. A hardening quality has arisen; in many of the phe-nomena described above it also shows itself to be a formof sclerosis.
To sum up, the above-mentioned diseases of the thy-roid lie within the polarity of neurosensory system andthe system of limbs and metabolism.Via a description ofthe morbid processuality one comes to perceive a corres-ponding differentiation in inner-life activities.
Influence of the different bodies in hyper- and hypothyroidism
In hyperthyroid patients, astral activity takes hold ofthe organism dynamically in katabolic, warmth-genera-ting metabolic processes and pushes restlessly towardsthe upper human being. The “hectic spots” describedand also increased blood flow in the nervous system ac-company the inner experience of unrest evolving fromthe organism and point to relevant astral-body activity.This—compared in the above to a fire evolving light andheat as a metaphor—increasingly consumes its organicbase and orientates itself centrifugally towards the up-per human being.
A wholly different gesture develops with hypothyroi-dism. Here the astral body does not adequately take holdof the living body but remains in the periphery—as in anunphysiological sleep. The organism, neither adequate-ly taken hold of nor still bearing soul and warmth, thenbecomes subject to progressive rigidity and sclerosis.
Where hyperthyroidism presents as excessive wake-fulness, a pathological daytime aspect, manifest hypo-thyroidism has to do with a tendency to pathologicalsleep, a predominantly night-time aspect. With hyper-thyroidism, the bodies consume life as they develop to-wards the upper human being and hence the wakingstate; with hypothyroidism, they seek the periphery—asin sleep. Rudolf Steiner’s characterization of the differentbodies is relevant to these day and night constellationswhich arise morbidly.
“We thus have the difference between waking andsleep state characterized in that we are able to say: OurI and our astral body act in all directions from the insidein the waking state. Our I and our astral body act back onus from outside with the spiritual powers of the cosmosin the sleep state.”(31) (Fig. 3)
To sum up, we see polar changes for the four bodiesin hypothyroidism and hyperthyroidism. At the physicallevel we have the contrast between the emaciated-loo-king figure of someone with long-term hyperthyroidismand the sometimes oedematous changes in the body ofsomeone with manifest hypothyroidism. The etheric or-ganization shows a corresponding contrast.With hyper-thyroidism, powers of life metamorphose into powers ofconscious awareness; metabolism has been observed tobe accelerated and more katabolic. With hypothyroi-dism, vita processes slow down, the fluid principle dropsout of the etheric body, with fluid accumulating and oe-dema developing.The influence of the astral body is dif-ferent, as evident from pathological waking and slee-ping. The I finally seems to have become remote in a hy-pothyroid individual. The tired look in the eye is not fil-led with the power of the I and often noticeably “emp-ty”. With hyperthyroidism, astral dynamics goes beyondthe inadequate guiding powers of the I-organization.
Subclinical hypothyroidism and hyperthyroidismThe so-called subclinical functional disorders of the
thyroid fit in with the described activities of the four bo-dies.They also deserve mention here because their clini-cal significance is often underestimated. The sclerosingprocess which has been described appears to exist evenwith subclinical hypothyroidism, i.e. elevated basal TSHand peripheral (free) thyroid hormones at normal levels.
G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s | D e r M e r k u r s t a b 19
Fig. 3.Centrifugal (ar-rows) and periphe-ral (ellipse) astral-body activity withhyperthyroidism(Graves’ disease)and hypothyroi-dism.
E n g l i s h I s s u e 2 0 0 5

In Hak’s Rotterdam study,(32) women with subclinicalhypothyroidism were found to face c. twice the risk ofdeveloping atherosclerosis or myocardial infarction thaneuthyroid women. At the astral level of this disorder, anumber of investigations have found a psychic sympto-matology which agrees with the activities of the four bo-dies described above. We may characterize them asmood changes, e.g. depression, disorders affecting at-tention, feelings of weakness and a slowing-down of co-gnitive functions.(33)
Conversely, subclinical or latent hyperthyroidism in-volves excitation of astral activity, often connected withanxiety and emotional irritability. Overlaps may occurwith the symptoms seen in latent hypothyroidism. Stu-dies on the subclinical thyroid disorders are noticeablyfew considering the frequency and intensity of symp-toms reported by patients.With regard to other manifes-tations, there are indications for excitation of the astralbody affecting e.g. the rhythmical system. Biondi etal.(34) thus conclude that subclinical hyperthyroidisminvolves elevated pulse rate, atrial fibrillation, increasedleft ventricular mass with marginally concentric remo-delling, abnormal ventricular relaxation, reduced perfor-mance and increased risk of cardiovascular death.
Therapeutic aspectsThe described pathology of thyroid diseases may be
developed further into an approach to treatment whichis to be given in outline below.This alone gives them realsignificance for medical action.
With regard to medical treatment, every human ill-ness presents a multilayered task with different empha-sis. In the first place we have the physical manifestationof the disease, usually dealt with by suppression, thyros-tasis, in the case of hyperthyroidism, and substitution ofthyroxine in the case of hypothyroid metabolic changes.The other areas of thyroid disease continue to be total-ly disregarded. What possibilities are there of treatingthe disease process which, for instance, is found in thespectrum of inflammation-related or sclerosing morbidprocesses? How do we approach the characteristicchanges in the psyche? What is the individual inner taskwhich may bring a new step in the development of thehuman being?
Medical treatment—copper and ironImportant pointers can be gained from considering
the two functional gestures characterizing the hyper-thyroid and hypothyroid metabolic states. It will, of cour-se, be necessary first to establish status. Working withthyroid conditions for many years, insight into their na-ture has led to a number of therapeutic approaches.Thisfirst step of gaining a concept has been followed by ap-plication in practice in the case of patients who had beengiven the relevant information and wished to have an-throposophical treatment. The case studies, some im-pressive, have led to consolidation in various areas, andthis must be followed by validation.
As an introduction, let us recall the metamorphosisdescribed for thyroid activity. Water-bound gill-breat-
hing changed to breathing air, leading to the sensesbeing able to breathe in light. If we look not so much atlarval metamorphosis but the spheres of life with the li-fe-forms belonging to them, a telling polarity may showitself. Marine molluscs, shellfish and snails, and alsofreshwater and even land snails, crabs and octopusesbreathe with the aid of a pigment which is known tocontain copper (haemocyanine). They do not have theirown inherent temperature. Enveloped in a dim, voicelessinner life they develop a soft body, excreting the harde-ning element to the outside in shells, carapaces, etc.When air-filled space is conquered, a different metalquality gains significance—iron. Its main function maybe evident from the way in which levels of life in spiritand soul are brought into the living organism. Indepen-dent warmth, air-breathing and a soul presenting itselfto the outside in sound can develop. Any iron deficiencyanaemia with its inner adynamics of soul can make ussee a clear picture in contrast of iron quality bringing inspirit and soul. In the neurosensory system with itsabundance of arterial blood, phylogenetically develo-ping early with arterialization of the circulation, iron hasthe dynamic qualities of conscious life. In the rhythms ofthe blood it addresses itself to respiratory processuality.In the system of metabolism and limbs it finds its placein energy and warmth processes. In the metabolic pro-cesses of the respiratory chain with its surprisingly greatamount of free warmth produced, it is one of the essen-tial metals, here seeking to relate to phosphorus.
In the language of the phenomenology here conside-red, we thus see a polarity of substances. With copper itpoints to the night-sphere of the inner life, and with ironactivity it develops the unfolding endowment with soul.
The following phenomenology is taken from the ex-tensive body of knowledge available on copper and iron.It directs our attention to the pathological processes.
Among the vital processes of acute inflammation,those of heating up and secretion are very evident. Theextensive vital process of respiration in incorporated in-to them, as apparent from the steep increase in oxygenuptake called a “respiratory burst”.(35) Oxygen consump-tion is a key element in inflammatory processuality, withdependence on the microbicidal activity of oxygen. Theactivated oxygen metabolites are also important. Oxy-gen’s relationship to iron demonstrates the significanceof the metal in acute inflammatory processes. We willconcentrate on this here, leaving aside the other aspectof iron activity as it may be evolved for the healing pha-se of inflammation.
The destructive aspect of acute inflammation is metwith a number of limiting metabolic processes with dif-ferent enzymatic processes which protect cells from thedestructive metabolism of activated oxygen com-pounds. One is superoxide dysmutase (SOD): “In themammalian extra cellular environment extra cellularSOD (ECSOD) and ceruloplasmin serve as antoxidant en-zymes.”(36)
Ceruloplasmin is the serum protein with copper con-tent; SOD also contains copper. Iron and copper are op-
20 D e r M e r k u r s t a b | G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s E n g l i s h I s s u e 2 0 0 5

G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s | D e r M e r k u r s t a b 21E n g l i s h I s s u e 2 0 0 5
posites in this, with iron relating to the acute inflamma-tory processes whereas copper does more act to limitthe katabolic metabolism of oxygen radicals, guiding theinflammation-geared metabolism towards the healingand constructive phase of its night-side. This compareswith the polarity of the metals. It is important to notethat this is merely one aspect of specific characteristicsin the comprehensive picture of the essential nature ofthese metals.
The aim has been to show how these two metal qua-lities can be related to one another for an awakening in-ner life that takes hold of the organism on the one hand,and an inner life that goes to sleep, calming down, on theother. Iron and copper thus are of major importance inthe treatment of hypothyroid and hyperthyroid diseases.
Fundamental aspects of medical treatment for hyperthyroid individuals
Rudolf Steiner spoke of chalcosine (chalcosite, copperglance) and cuprite as important medicinal agents totreat Graves’ disease hyperthyroidism. Chalcosine, acompound of copper and sulphur, shows metallic lustrein fresh surfaces, otherwise it is opaque, its colour a darkleaden grey, usually tarnished black. Beautiful chalcosi-ne crystals can sometimes be seen, their structure rhom-bic or pseudo-hexagonal. Cuprite on the other hand is adeep red, flame coloration green. The crystals are octa-hedral, dodecahedral and more rarely cubic. With thiscompound of copper and oxygen, the ordering, formedcrystal principle confronts the effervescent inner life ofthe hyperthyroid patient. Its form-giving powers streng-then the I-organization so that it may act to heal. Con-cerning chalcosine, Rudolf Steiner wrote: “I have shownyou the influence which chalcosine has on the I-organi-zation. I have shown you what we have to consider withGraves’disease, so that one is able to say: If one is in a po-sition to look on the human being on the one hand, howthere physical, etheric and astral body and I are in inter-play and interaction, and how this grows abnormal inthe morbid state, and if one also gains insight into theprinciple found in nature, then one sees the following,for instance: There the I-organization is too weak inGraves’ disease. Out there I have chalcosine. Brought to-gether with the I-organization, this copper compoundwill greatly strengthen it.”(37)
In 1933 Dr Norbert Glas compiled a unique (and to myknowledge so far the only) list of seven patients withGraves’ disease, on the whole diagnosed clinically, andtheir treatment which included chalcosine.(38) The fol-lowing case record comes from this.
“Case V. Nurse aged 30, Graves’ disease from her ear-ly 20s. Recently difficult night duties and in consequen-ce unfit for work because of heart problems, restless-ness, weakness. On admission, marked tachycardia, exo-phthalmos, particularly noticeable vasomotor excitabi-lity, poor quality sleep. The patient had always been le-an, always keen to work, and in spite of her illness verysensible. Clinical symptoms worse than her experienceof them.
“Treatment. Chalcosine (copper glance) 3x twice dai-ly; 2 or 3 times a week s.c. injection of chalcosine 8x. Car-diodoron. In the mornings she was for a short time givena hot fomentation with a decoction of Berberis, in theevenings 0.1% silver ointment in the bladder region. Shereturned to work after five weeks.The significant impro-vement persisted.”
The excited inner life of a hyperthyroid individual canbe calmed by giving phosphorus.Three kinds of use refer-red to by Rudolf Steiner may be considered. Oral exhibiti-on addresses metabolic activity; subcutaneous injectionserves if there is marked excitation of the rhythmical sys-tem (tachycardia, tachypnoea),and occasionally externalapplication in a full bath will be indicated for a will-o’-the-wisp, restless thought life with flight of ideas.
Excitation of astral-body activity, getting “frozen” inthe orientation of its conscious awareness and notachieving the opposite pendulum swing to its night-ti-me constellation, can be regulated using iodine in highpotencies. Iodine in the low-potency algal preparationprepares the way for astral-body intervention; given in ahigher potency it can reduce its excessive activity. Com-bination with an organ preparation of the thyroid incomparable potency (Glandula thyreoidea D20 amp.Wa-la) has proved effective. At this potency, the material le-vel has been left well behind. With the organ preparati-on, the structuring principle belonging to the thyroidprepares the way for the other therapeutic approaches.This is a special quality in anthroposophical medicine,not only looking for a medicinal agent from the naturalsurroundings but also considering how it can reach the“site”of its medicinal action.Thus the healing answer tothe process of sclerosis lies in the essential nature oflead. Its quality as substance must, however, metamor-phose before it can be the medicinal agent needed, forinstance in the form of Scleron.
Another important medicament which can be almostseen to have astral activity connected with its vital or-ganization is Colchicum. Both Graves’ hyperthyroidismand circumscribed, multifocal or disseminated autono-my involve intensive metabolic processes. Doppler sono-graphy can be used to demonstrate these as increasedblood flow, scintigraphy as increased uptake. These en-hanced metabolic processes, in Graves’ disease also evi-dent in inflammation-related lymphocytic infiltration ofthe organ, can be regulated with low potencies of Colchi-cum. For the significance of Colchicum as an importantmedicament in anthroposophical thyrology, see previo-us publications.(39) First prospective studies (observati-on following exhibition) of Colchicum actions with la-tent hyperthyroidism and goitre have been completedand will be published shortly.
Bryophyllum may be used to support guidance of theastral body.
Lycopus virginicus or—as a native plant—Lycopus eu-ropaeus, a labiate, is another important medicinal plant.Labiates show intense relation to warmth in numerousvariations.(40) In hot sunny climes, preferably Mediter-ranean, they take warmth into their organization in the

substance-language of volatile oils. Closeness to soulquality is impressive in the sphere of warmth, experi-enced when walking through a field of flowering laven-der with its rich hum of bees, for instance. In Lycopus, vo-latile oil production is reduced, however.The plant growsin the vicinity of damp grasslands, ditches and bodies ofwater, needing a connection to the watery element.Thisgesture appears to define the medicinal quality whichconsists in subduing excited astral activity when meta-bolism is hyperthyroid. In accord with the image we ha-ve gained, the time for harvesting the aerial parts of theplant is just before flowering.
The above medicinal agents provide the therapeuticqualities desired: strengthening activity of the I-organi-zation, reducing excessive astral activity and guiding itback from overweening orientation towards consciousawareness to the physiological level.
From these points of view, additional light may bethrown on conventional antithyroid medication withthiourea derivatives.These agents were developed follo-wing discovery of the goitre-producing effect of a dietconsisting largely of cabbage in wartime. Thiocyanateions are believed to compete with iodide for uptake intothe thyroid resulting in competitive inhibition of iodideuptake. Rhodanide (thiocyanate) ions are obtained bysplitting mustard oil glycosides.The mustard oils in cab-bage may also yield vinyl thio-oxazolidines (goitrins)with thyrostatic activity. Neither principle is used as athyrostatic, but goitrins show structural similarity to car-bimazole.(41) Cabbage (Brassica oleracea(42)) is full of vi-tality. A water content of c. 90 % indicates tremendousetheric development. Established use as a poultice totreat leg ulcers or decubitus demonstrates its power tostimulate regeneration. Vigorous development of theetheric sphere of life will in the case of hyperthyroidismset limits to an astral organization which is restlesslypushing for conscious awareness.
Apart from aiming for a euthyroid state, an importantquestion will be in how far the anthroposophical ap-proach to treatment will guide evolution to achieve re-mission with Graves’ disease. It is largely unknownwhich factors lead to autoimmune thyroiditis. Manyquestions require further consideration, among themthe possible significance of Rudolf Steiner’s reference tochalcosine to treat the pathological process which hasbeen described.
After normalization of metabolism and the influen-ce, not so far examined, of the time form of the disease,the next level touches on the typical sentient configura-tion of someone with thyroid disease. It does not usual-ly correlate with the laboratory findings. Patients some-times continue to complain of “hyperthyroid symptoms”even if the metabolism is well “balanced”. Others stillfeel hyperthyroid although latent hypothyroidism hasalready developed with autoimmune thyroiditis. Pa-tients who need thyrostatic treatment also benefit fromthe anthroposophical medication given above. Euryth-my therapy is particularly effective. It appears that posi-tive steps in inner development can help to make treat-
ment successful. A connection between emotionalstrain going beyond the I’s powers to cope and onset ofautoimmune hyperthyroidism has been established, al-so with regard to the prognosis. In a prospective cohortstudy, patients with Graves’ disease with euthyroid me-tabolism were subjected to a range of psychologicaltests 2 – 5 years after completing treatment. Comparedto people with no thyroid disease, significant correlati-on was found between stress score,TRAB and/or thyroidvolume. The group of patients who had had a recurren-ce showed a greater frequency of hypochondriac, de-pressive, paranoid and asthenic “personality structures”than patients in stable remission. Compared to patientsin remission, patients with a recurrence of Graves’disea-se did in addition have a significantly higher score forproblems.(43) These findings make it very clear that wemust go beyond medical treatment, establish the innertasks and find ways in which patients may be supportedin this respect.
Fundamental aspects of medical treatment for hy-pothyroid patients
Treatment is the opposite for hypothyroid metabo-lism. Support is needed for an organization of soul andspirit which is not fully effective. Here iron is an majormedicinal agent. An important observation is that irondeficiency with or without anaemia can influence thy-roid metabolism. Animals with iron deficiency are said tohave significantly lower T3 and T4 levels compared toanimals which are not anaemic. Similar phenomena areknown with humans. Thyroid peroxidase (TPO) activityseems to correlate with the degree of iron deficiencyanaemia.(44) Iron thus also relates to thyroid hormonemetabolism and hence the incarnation of the higher bo-dies.
For clinical use we may think of Levico Water with itscomplex composition (among the medical consultati-ons he gave, Rudolf Steiner once recommended Levicofor a woman with goitre “to stimulate astral body acti-vity”).(45) It is exactly through iron quality that the soul-and-spirit level of being can gain the orientation in thedescribed way to take hold of the organism. The arsenicin Levico water is also important.The essential nature ofthe arsenic here corresponds to the waking-up processin human beings.(46) The thyroid is reported to be par-ticularly rich in arsenic.(47) Through the substance-language of iron and arsenic, therefore, this medicamentrecommended by Rudolf Steiner is a convincingly effecti-ve means of energizing the astral body. Levico Water hasa very low pH.This acidity can with clinical use guide theastral body to connect with the organism. Levico Wateralso contains phosphorus and this guides the I-organi-zation, its activity changed to be sleep-like with hypothy-roidism, to take hold of the living body. The copper con-tained in this uniquely medicinal water appears to pre-pare a receptive gesture towards the higher bodies asthey are once again incarnating more strongly. (Table 1)
Scorodite, natural iron arsenate, may be consideredanalogous to Levico Water. As an oil-producing medici-
22 D e r M e r k u r s t a b | G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s E n g l i s h I s s u e 2 0 0 5
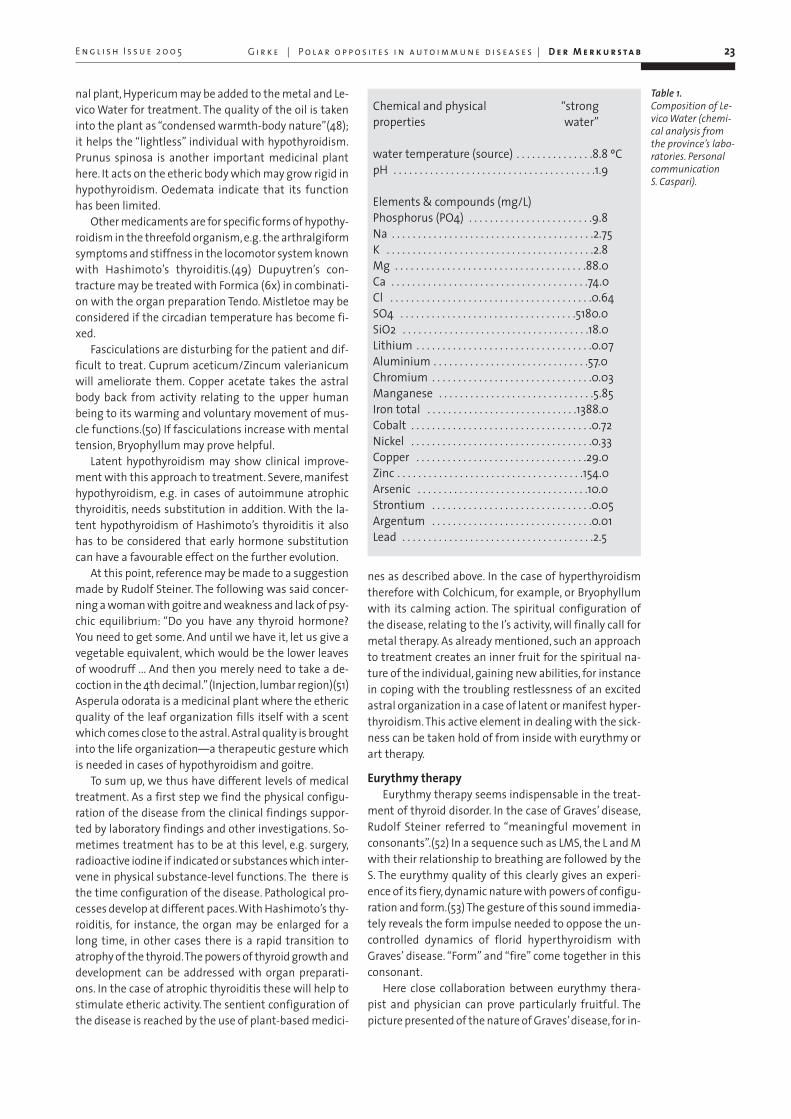
nal plant, Hypericum may be added to the metal and Le-vico Water for treatment. The quality of the oil is takeninto the plant as “condensed warmth-body nature”(48);it helps the “lightless” individual with hypothyroidism.Prunus spinosa is another important medicinal planthere. It acts on the etheric body which may grow rigid inhypothyroidism. Oedemata indicate that its functionhas been limited.
Other medicaments are for specific forms of hypothy-roidism in the threefold organism, e.g. the arthralgiformsymptoms and stiffness in the locomotor system knownwith Hashimoto’s thyroiditis.(49) Dupuytren’s con-tracture may be treated with Formica (6x) in combinati-on with the organ preparation Tendo. Mistletoe may beconsidered if the circadian temperature has become fi-xed.
Fasciculations are disturbing for the patient and dif-ficult to treat. Cuprum aceticum/Zincum valerianicumwill ameliorate them. Copper acetate takes the astralbody back from activity relating to the upper humanbeing to its warming and voluntary movement of mus-cle functions.(50) If fasciculations increase with mentaltension, Bryophyllum may prove helpful.
Latent hypothyroidism may show clinical improve-ment with this approach to treatment. Severe, manifesthypothyroidism, e.g. in cases of autoimmune atrophicthyroiditis, needs substitution in addition. With the la-tent hypothyroidism of Hashimoto’s thyroiditis it alsohas to be considered that early hormone substitutioncan have a favourable effect on the further evolution.
At this point, reference may be made to a suggestionmade by Rudolf Steiner. The following was said concer-ning a woman with goitre and weakness and lack of psy-chic equilibrium: “Do you have any thyroid hormone?You need to get some. And until we have it, let us give avegetable equivalent, which would be the lower leavesof woodruff ... And then you merely need to take a de-coction in the 4th decimal.”(Injection, lumbar region)(51)Asperula odorata is a medicinal plant where the ethericquality of the leaf organization fills itself with a scentwhich comes close to the astral. Astral quality is broughtinto the life organization—a therapeutic gesture whichis needed in cases of hypothyroidism and goitre.
To sum up, we thus have different levels of medicaltreatment. As a first step we find the physical configu-ration of the disease from the clinical findings suppor-ted by laboratory findings and other investigations. So-metimes treatment has to be at this level, e.g. surgery,radioactive iodine if indicated or substances which inter-vene in physical substance-level functions. The there isthe time configuration of the disease. Pathological pro-cesses develop at different paces.With Hashimoto’s thy-roiditis, for instance, the organ may be enlarged for along time, in other cases there is a rapid transition toatrophy of the thyroid.The powers of thyroid growth anddevelopment can be addressed with organ preparati-ons. In the case of atrophic thyroiditis these will help tostimulate etheric activity. The sentient configuration ofthe disease is reached by the use of plant-based medici-
nes as described above. In the case of hyperthyroidismtherefore with Colchicum, for example, or Bryophyllumwith its calming action. The spiritual configuration ofthe disease, relating to the I’s activity, will finally call formetal therapy. As already mentioned, such an approachto treatment creates an inner fruit for the spiritual na-ture of the individual, gaining new abilities, for instancein coping with the troubling restlessness of an excitedastral organization in a case of latent or manifest hyper-thyroidism. This active element in dealing with the sick-ness can be taken hold of from inside with eurythmy orart therapy.
Eurythmy therapyEurythmy therapy seems indispensable in the treat-
ment of thyroid disorder. In the case of Graves’ disease,Rudolf Steiner referred to “meaningful movement inconsonants”.(52) In a sequence such as LMS, the L and Mwith their relationship to breathing are followed by theS. The eurythmy quality of this clearly gives an experi-ence of its fiery, dynamic nature with powers of configu-ration and form.(53) The gesture of this sound immedia-tely reveals the form impulse needed to oppose the un-controlled dynamics of florid hyperthyroidism withGraves’ disease. “Form” and “fire” come together in thisconsonant.
Here close collaboration between eurythmy thera-pist and physician can prove particularly fruitful. Thepicture presented of the nature of Graves’disease, for in-
G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s | D e r M e r k u r s t a b 23
Table 1.Composition of Le-vico Water (chemi-cal analysis fromthe province’s labo-ratories. Personalcommunication S. Caspari).
E n g l i s h I s s u e 2 0 0 5
Chemical and physical “strong properties water”
water temperature (source) . . . . . . . . . . . . . . .8.8 ºCpH . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1.9
Elements & compounds (mg/L)Phosphorus (PO4) . . . . . . . . . . . . . . . . . . . . . . . .9.8Na . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.75K . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.8Mg . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .88.0Ca . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .74.0Cl . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .0.64SO4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5180.0SiO2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18.0Lithium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .0.07Aluminium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .57.0Chromium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .0.03Manganese . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5.85Iron total . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1388.0Cobalt . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .0.72Nickel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .0.33Copper . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29.0Zinc . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .154.0Arsenic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10.0Strontium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .0.05Argentum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .0.01Lead . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2.5

stance, leads directly to the indications for treatment, inthe form-giving quality in the substance-language ofchalcosine, for example, just as much as in the move-ment for the consonant “S” in eurythmy therapy.
The dual nature of the “S” can take us to eurythmytherapy for hypothyroidism. An organism which is gro-wing rigid, tending towards sclerosis and abandoned bywarmth, can be set in motion with the “fire quality” ofthe “S”. If the form given to its dynamics is close toGraves’ disease, the “fire quality” appears to develop therelationship to hypothyroidism.
The metamorphotically related disease spectrumranging from Graves’ disease hyperthyroidism to mani-fest hypothyroidism based on autoimmune thyroiditiscomes together, as it were, in this one element of euryth-my therapy in the “form” and “fire” of the consonant “S”.Here one can see why prescribing the same sequence,again with the “S”, as SMIA was suggested for hyper- aswell as hypofunction of the thyroid.(54) The “I” in this se-quence points to the I-organization’s guiding power, the“A” is the sound belonging to copper quality and can ad-dress astral activity.“Repeated practice with the “A””cau-ses the upper light aspect of the soul to be taken hold ofand given strength in I-quality. This strength flowsthrough the organic part of the astral body. ...”(55)
Inner workPowers of soul which restlessly push for conscious
awareness in hyperthyroid patients call for form andconfiguration to be given by the individual character. Itwill, of course, at first be mainly necessary to use medi-cal treatment to get the I-organization to be sufficient-ly active. This can then be effectively supported by eu-rythmy therapy, where practising consonants takes upthe form-giving principle, analogous to the crystallinechalcosine. It is beyond doubt that such an illness ask forinner work to be done by the patient, so that individualnature may be the charioteer who masters the dynamicsof horses gone out of control. At the inmost level, whol-ly within the individual’s own activity, we then see forthe third time the need for a guiding, configuring prin-ciple. Individual nature must hold its own within theheightened dynamics of the psyche. This also relates tothe biography and events in life which the individualwas unable to work through so that they would have ashock-like effect. Patients with Graves’ disease show anincreased incidence of life crises prior to onset, and in acomprehensive approach to treatment, these need to beinwardly worked through.The same applies to the prog-nosis and frequency of recurrences with this disease.
When the inner life has grown progressively moreapathetic, lacking drive, with hypothyroidism, it is alsonecessary to rediscover the inner tasks and encouragethe patient to take an active part in the recovery process.Thus the warmth and will power of the individual flowinto a psyche in danger of growing rigid.
Thyroid disorders reveal areas of inner work wherethe patient should become active. New abilities may de-velop as the inner fruit of the illness.The eight exercises
given below are not placed at random but form a who-le.They let abilities arise which come together to form akind of organ. The spiritual-scientific view is that this islocated near the larynx. It is also called the 16-petalledlotus flower.
Another organism of exercises, the “six accessoryqualities”or “accessory exercises”, create an organ whichmay develop from the “germ layers” of thinking, feelingand will. Rudolf Steiner characterized this as the 12-pe-talled lotus flower near the heart organization. Apartfrom its significance for every individual’s inner develop-ment, it can provide healing powers for a morbid heartorganization. Healing and development on the road toinner insight are closely connected here, for the moreprofound aim with any recovery process is not to repaira faulty function but for the human being to developnew abilities.
In a similar way, developing the eight qualities belon-ging to the 16-petalled lotus flower(56) can be the innerwork to be done by someone with a thyroid disorder. Itshould be possible to find these inner tasks in anthropo-sophical psychotherapy. Here the eight exercises belon-ging to this immaterial organ may gain specific signifi-cance in bringing healing for someone with thyroiddisease (Table 2).
The first exercise refers to cultivation of the life ofthought and ideas (I in Table 2). The thoughts of the hy-perthyroid individual, often hectic and restless, need itsguidance if they are to be a “true mirror of the outsideworld”. A first step in development, often immediatelygiven in many situations involving sickness.
The second exercise already points to training thewill, and this is taken up again in many of the exerciseswhich follow.
Every act of will which is not to be involuntary, drivenas it so often is in hyperthyroid individuals, but guidedby the I, calls for a well-thought-out way of doing things.The conscious decision, conscious motivation, is the se-cond goal in development (II in Table 2).
The mode of speech often changes with hyperthyroi-dism. Instead of talking calmly and thoughtfully one hasrapid, hasty communication. The relationship betweencontent and manner of speech has gone awry. The thirdaim is to “speak rightly”. Things which are significantneed to be said.The individual spirit’s powers of guidan-ce in speaking develop (III in Table 2).
Many thyroid patients act quickly and precipitatelyand may be out of step with others around them (IV inTable 2). Here attention must be taken out of the rushand pressure of everyday activity and directed towardsother people.
Finally the fifth exercise (V in Table 2) concerning thebalance between excessive activity and indolence appe-ars to be a particular challenge.Thoughtfulness must bebrought to one’s doing.
The sixth exercise (VI in Table 2) is the endeavour notto be a cogwheel in life, without thought, but to knowone’s tasks and look beyond the everyday level.(57) Acti-vity loaded with stress, often blind to many things and
24 D e r M e r k u r s t a b | G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s E n g l i s h I s s u e 2 0 0 5

“like a hamster in its wheel”, must change. The exerciserelates to the “driven” state of some thyroid patients. Itis also necessary to be thoughtful in one’s doing, not un-dertaking things that lie outside one’s limits of compe-tence, nor neglecting those which lie within them.
This sixth exercise demands a seventh, which is to le-arn from life (VII in Table 2). This calls for calm thought-fulness in one’s doing, the only way of developing newdegrees of perfection. This quality, too, proves a challen-ge in connection with thyroid disorders.
The last exercise (VIII in Table 2) finally is given cha-racteristic relevance for thyroid disorders. The psyche istoo much directed to the outside. Exophthalmos is like aphysical illustration of an inner orientation which is di-rected too much to the outside.The eighth exercise callsfor a reversal of this—the individual must look inwardand examine his principles, responsibilities and goals.
No thyroid patient will show all these specific charac-teristics, some actually have none. Patients who havehad the disease for some time may already have gainednew qualities. With every patient one meets, it is there-fore important to consider the individual configurationof the disease and work with the patient to establish thetasks which are set by considering the given biographi-cal and destiny situation. Talking to patients about theexercises we must not forget that they are being askedto develop abilities which everyone needs to develop, butthat their illness does so in particularly definite terms.
MeditationWith some patients, the question of meditation co-
mes up. Here a fundamental distinction must be madebetween abstract, comparatively intellectual develop-ment of the mind, and meditation as an activity.The for-mer metamorphoses vital energies into powers of mind,thus opposing rather than helping the healing principle.Meditation does not lead to destructive processes, forone begins to develop a spiritual activity which separa-tes from the bodily instrument. We are in no way refer-ring to “meditative” practice supported by listening tocassettes. It is an inner spiritual activity developed by theindividual, with external stimuli deliberately excluded.
The development of the eight exercises and hence a hy-gienic development of the psyche may be considered tobe a healing impulse for thyroid disorders. Meditationcan support the supersensible organ which develops inthe process.
The thyroid has a special relationship to the humanability to speak. No other organ is filled in the same waywith sound development and speech. In speech, a furt-her quality is added to the conceptual and idea-relatedelement of thinking. When different words are used forone and the same concept in different languages (e.g.“head”, “Kopf”, “téte”, “caput”) it is evident that in addi-tion to the translatable meaning there is also an emoti-ve element which is difficult to translate. You feel some-thing different with “Kopf”,“téte”or “caput”.“Speech andlanguage are produced when we fully imbue ourthoughts with inner feeling, inner sentience.”(58) Withmeditation, the quality has to be found which linksthoughts with feeling, sentience, without losing clarity.“To give thinking warmth as well as clarity” (59) may beconsidered to characterize this. When an idea becomesideal, this warmth, this fire added to the idea-content,and indeed born out of it, can clearly be experienced.
Rudolf gave the example of a meditation (“Wisdomlives in the light”) to describe a first stage where the sen-tence is wholly taken into active thinking. This elementof light in meditation can be linked to feeling. Warmthis added to light. As it continues, the meditation can betaken into inner activity of the will in thinking as the in-dividual feels his own inner nature to be connected withthe radiant power of light.These three stages have an in-fluence on the immaterial human being. The develop-ment of the 16-petalled lotus flower is connected withthe second. “Someone who through meditation has de-veloped thoughts that are filled with feelings will thanksto this power which he has developed, which otherwisewould have been speech, become aware of the “16-petal-led lotus flower” in the region of the larynx.”(60) Here apower which is otherwise active in speech relates to thepower which corresponds to it in active meditation.
G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s | D e r M e r k u r s t a b 25E n g l i s h I s s u e 2 0 0 5
Table 2.Eight exercises to develop the 16-petalled lotusflower (eightfoldpath) (Steiner R.Knowledge of theHigher Worlds)
I Gaining ideas . . . . . . . . . . . . . . . .Conceptual life as true mirror of the outside worldII Reasoned actions . . . . . . . . . . . . .Decide on even the simplest thing only for well-founded reasonsIII Speech . . . . . . . . . . . . . . . . . . . . . .Only words that have meaning and significance to be spokenIV Outward actions . . . . . . . . . . . . . .Make sure your actions fit in with those of others and events in the
world around you.V Life in balance where work . . . .Excessive activity and indolence are equally avoided.
is concernedVI Endeavour . . . . . . . . . . . . . . . . . . .Not to do anything beyond your powers, nor fail to do anything which
is within them. Goals related to a human being’s ideals and sublime responsibilities.
VII Learning from life . . . . . . . . . . . . .Anything not perfectly done is opportunity for perfection.Gathering a treasure of experience.
VIII Looking inward . . . . . . . . . . . . . . .Developing and testing principles for life. Go through knowledge in your mind, weigh and consider responsibilities, reflecting on the meaning of life.

The path to higher insight has an inner connectionwith healing. If patients ask about it, these and otheraspects may come into the conversation with the physi-cian.
We thus have an approach at many levels, includingphysical intervention if indicated, medication, eurythmyand art therapy and also the question of one’s innertasks. It can yield a significant fruit of the illness, an im-portant step in the individual’s human development.The shadow side of the illness begins to let its light-fil-led side emerge.
Matthias Girke, MDHavelhöhe Community HospitalKladower Damm 221D-14089 Berlin
26 D e r M e r k u r s t a b | G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s E n g l i s h I s s u e 2 0 0 5
Literatur1 Norrelund H, Hove KY, Brems-Dalgaard E, Grethe Jurik A, Niel-sen LP, Nielsen S, Lunde Jorgen-sen JO , Weeke J, Moller N. Mus-cle mass and function in thyro-toxic patients before and duringtreatment. Clin Endocrinol 1999;51 (6): 693-6992 Vestergaard P, Mosekilde L.Hyperthyroidism, bone mineral,and fracture risk – a meta-analy-sis. Thyroid 2003; 13: 585-5933 Adams RD, DeLong GR. Theneuromuscular system andbrain (Hyperthyreosis). 885 –894. In: Ingbar S.H., BravermanL.E.: Werner´s The Thyroid.J.B.Lippincott Company Philadel-phia 1986 4 Volpé R. Pathogenesis of au-toimmune thyroid diesease; 747– 767. In: Ingbar S. H. BravermannL.E.: Werner´s The Thyroid. J.B.Lippincott Company Philadel-phia 19865 Hashimoto H. Zur Kenntnisder lymphomatösen Verände-rung der Schilddrüse (Strumalymphomatosa). Arch Klin Chir1912; 97: 219ff6 Tamai H, Kasagi K, Takaichi Yet al. Development of spontane-ous hypothyroidism in patientswith Graves´disease treatedwith anti thyrroidal drugs: clini-cal, immunological, and histolo-gical findings in 26 patients. JClin Endocrinol Metab 1989;69:49;7 Oertel JE, LiVosi VA. Pathologyof thyroid gland. 651-686. In:Ingbar S. H. ,Bravermann L.E.:Werner´s The Thyroid. J.B. Lippin-cott Company Philadelphia 19868 Volpé R. Pathogenesis of au-toimmune thyroid disease; 747 –767. In: Ingbar S. H. BravermannL.E.: Werner´s The Thyroid. J.B.Lippincott Company Philadel-phia 19869 Ibido.10 Takasu N, Yamada T, Sato A etal. Graves’ disease following hy-pothyreoidism due to hashimo-to´s disease: studies of eight ca-ses. Clin Endocrinol 1990; 33:687ff11 Oertel JE, LiVolsi VA. Patholo-gy of thyroid gland, 651 – 686. In:Ingbar S. H., Bravermann, L.E.:Werner´s The Thyroid. J.B. Lippin-cott Company Philadelphia 198612 Gärtner R. EntzündlicheSchilddrüsenerkrankungen. In-ternist 2002;43:635-653
13 Cakir M, Samanci N, Balci MK.Musculoskeletal manifestationsin patients with thyroid disease.Clin Endocrinol (Oxf) 2003; 59(2): 162-16714 Elta GH, Sepersky RA, Gold-berg MJ. Increased incidence ofhypothyroidism in primary bilia-ry cirrhosis. Dig Dis Sci 1983; 28:971ff15 Volpé R. Pathogenesis of au-toimmune thyroid disease. 747-767. In: Ingbar SH, BravermannLE. Werner´s The Thyroid. JB. Lip-pincott Company Philadelphia198616 Counsell CE, Taha A, RuddelWS. Coeliac disease and autoim-mune thyroid disease. Gut 1994;35:844ff17 Centanni M, Marignani M,Gargano L et al. Atrophic bodygastritis in patients with auto-immune thyroid disease. An un-derdiagnosed association. ArchIntern Med 1999; 159:1726ff18 Taddei S, Caraccio N, Virdis A,Dardano A, Versari D, Ghiadoni L,Salvetti AE, Ferrannini A, Monza-ni F. Impaired endothelium-de-pendent vasodilatation in sub-clinical hypothroidism: benefici-al effect of levothyroxine thera-py. J Endocrinol Metab 2003 Aug;88(8): 3731-373719 Brenta G,. Mutti LA, Schnitt-mann M , Fretes O, Perrone A ,.Matute ML. Assessment of leftventricular diastolic function byradionuclide ventriculography atrest and exercise in subclinicalhypothyroidism, and its respon-se to L-thyroxine therapy.Am J Cardiol 2003; 91: 1327-1330 20 Hak AE, Pols HAP, Visser TJ,Drexhage HA, Hofman A, Witte-man, JCM. Subclinical Hypothy-reoidism is an independent riscfactor for atherosklerosis andmyocardial infarction in elderlywomen. Ann Intern Med 2000;132: 270-27821 Cantürk Z, Cetinarslan B, Tar-kun I, Cantürk NZ, Özden M, Du-man C. Hemostatic system as arisk factor for cardiovasculardisease in woman with subclini-cal hypothyreoidism. Thyroid2003. 13: 971-977 22 Zettinig G, Asenbaum S, Fue-ger BJ, Hofmann A, Diemlimg M,Mittleboeck M, Dudczak R. In-creased prevalance of subclinicalbrain perfusion abnormalities inpatients with autoimmune thy-roiditis: evidence of hashimoto´sencephalitis? Clin Endocrinol 59,2003: 637ff
G i r k e | P o l a r o p p o s i t e s i n a u t o i m m u n e d i s e a s e s | D e r M e r k u r s t a b 27E n g l i s h I s s u e 2 0 0 5
23 Gärtner R. EntzündlicheSchilddrüsenerkrankungen. In-ternist 2002.43:635-65324 Steiner R. Pastoral Medicine.2nd lecture. Tr. G Hahn. Hudson:Anthroposophic Press 1987.25 Matovinovic J. Thyroid carci-noma-general pathogenesis, 768– 801. In: Ingbar, S. H. Braver-mann, L.E.: Werner´s The Thyroid.J.B. Lippincott Company Philadel-phia 198626 Souza SL et al. Impact of pre-vious thyroid autoimmunediseases on prognosis of pa-tients with well-differentiatedthyroid cancer. Thyroid 2003; 13:491-495 27 Steiner R. The Healing Pro-cess. Lectures of 16 Nov. 1923 &29 Aug. 1924. Tr. C. E. Creeger.Hudson: Anthroposophic Press2000.28 Steiner R. Rosicrucian Esoteri-cism. Lecture of 10 Apr. 1909. Tr.D. S Osmond. New York: Anthro-posophic Press 1978.29 Steiner R. Die Mission derneuen Geistesoffenbarung (GA127). Lecture of 26 Feb. 1911. Nottranslated into English.30 Adams RD. The neuromuscu-lar system and brain (Hypothy-reosis). In: Ingbar S. H. Braver-mann L.E.: Werner’s The Thyroid.J.B. Lippincott Company Philadel-phia 198631 Steiner R. As ref. 27. Lecture of28 Aug. 1924.32 Hak AE, Pols AP, Visser TJ. et al.Subclinical hypothyreoidism isan independant risk factor foratherosklerosis and myocardialinfarction in elderly women: theRotterdam study. 2002. Ann. In-tern. Med. 132 : 270-27833 Haggerty JJ, Stern RA., MasonGA. et al. Subclinical hypothyroi-dism: a modifiable riskfactor fordepression? Am J.Psychiatry1993;150: 508-510 34 Biondi B, Palmieri EA, Lombar-di G, Fazio S. Effects of subclinicalthyroid dysfunction on the he-art. Ann. Intern. Med. 2002;7:904- 914 35 Winyard PG, Perret D, HarrisG, Blake DR. The role of toxic oxy-gen species in inflammationwith spcial reference to DNA da-mage. In: Wicher J.T., Evans S.W.:Biochemistry of inflammation.1992, Kluver Academic PublishersS. 109-129.36 Ibido.37 Ibido. Lectures of 16 Nov. 1923& 29 Aug. 1924.
38 Glas N. Behandlung bei Mor-bus Basedowii. Hippokrates:Zeitschrift für praktische Heil-kunde. Organ für die Einheitsbe-strebungen in der Medizin. Au-gust 1933; Heft 8: 267-27039 Girke M, Kröz M. Colchicumautumnale in der Therapie derlatenten und manifesten Hyper-thyreose. Der Merkurstab2001(54)4:244-24940 Pelikan W. Healing Plants. Pa-ge 51. Tr. A. R. Meuss. Spring Val-ley: Mercury Press 1997.41 Weiss RF. Herbal Medicine.Page 279. Tr. A. R. Meuss. Bea-consfield: Beaconsfield 1988.42 Hegi G. Illustrierte Flora vonMitteleuropa. Band IV. Teil I. Ver-lag Paul Paray Berlin, Hamburg198643 Fukao A. Takamatsu J., Mura-kami Y., Sakane S., Miyauchi, A.,Kuma K., Hayashi S., Hanafusa T.The relationship of psychologicalfactors to the prognosis of hy-perthyroidism in antithyroiddrug-treated patients withGraves’ disease. Clin Endocrinol2003; 58: 550-55544 Zimmermann M.B., Köhrle J.The Impact of Iron and SeleniumDeficiencies on Iodine and Thy-roid Metabolism: Biochemistryand Relevance to public Health.Thyroid 2002; 12: 867-87845 Heilmittelangaben RudolfSteiners. Blatt Arsenicum46 Steiner R. AnthroposophicalSpiritual Science and MedicalTherapy. Tr. rev. G. F. Karnow.Spring Valley: Mercury Press 1991.47 Vogel H.-H. Beiträge zu einermedizinischen Menschenkunde.Band 1,Teil 1 S. 152 Karl F. HaugVerlag Heidelberg 198448 Pelikan W. Healing Plants. Pa-ge 295. Tr. A. R. Meuss. Spring Val-ley: Mercury Press 1997.49 Simon L. Ein anthroposophi-sches Therapiekonzept für ent-zündlich-rheumatische Erkran-kungen. Ergebnisse einer zwei-jährigen Pilotstudie. Der Merkur-stab 2001;54 (3): Sonderheft:Rheumatologie: 60-70
50 Sommer M. Potenziertes Kup-fer bei Alpträumen von Verstor-benen – Wirksamkeitsbeleg anEinzelfällen. Der Merkurstab2001; 54 (3):146-15251 Heilmittelangaben RudolfSteiners. Blatt Asperula odorata52 Steiner R. As ref. 46.53 Kirchner-Bockholt M.: Grund-elemente der Heileurythmie.Philosophisch-Anthroposophi-scher Verlag. Goethenaum. Dor-nach/Schweiz. 3. Aufl. 198154 Ibido.55 Ibido.56 Steiner R. Knowledge of theHigher Worlds. Tr. G. Metaxa.London: Rudolf Steiner Press1963.57 Ibido.58 Steiner R. Self Transformati-on. Lecture of 1 May 1913. London:Rudolf Steiner Press.59 Steiner R. Calendar of theSoul.60 Steiner R. As ref. 58.

28 D e r M e r k u r s t a b | H u b e r | D i e t a r y a s p e c t s E n g l i s h I s s u e 2 0 0 5
With autoimmune diseases (AI), the immune sys-tem reacts to and attacks the body’s ownstructures as if they were foreign. These are
acquired disorders manifesting in the course of life. It isnot uncommon for them to develop after or during in-fectious diseases, e.g. as post streptococcal glomerulo-nephritis or post infectious thrombopenia, panarteritisnodosa with chronic hepatitis B, etc. Quite differentdrugs (oestrogens, methotrexate, penicillamine, etc.)and radioactive radiation may also cause AI or a conditi-on similar to AI, e.g. pneumonitis following prophylacticirradiation of breast cancer. Apart from such influenceson the physical body, the history of patients with AI fre-quently includes psychic shocks and difficult events in li-fe which the patients themselves also consider to befactors in the genesis of the condition. One woman whohad been in good health until her 25th year told how shehad become mentally completely dependent on a reli-gious sect.The strict rules and celibacy went against herfeelings and a need she felt for love and partnership. La-cking the strength to evade the moral pressure exertedby her teacher she felt her life to be determined fromoutside and ultimately could see no way out. Then shefell in love again. At that time she noticed that her fin-gers had turned white and her abdomen brown andhard. It was the onset of severe scleroderma. She died ofthis seven years later although all possible therapeuticmeans had been used.
With many AI patients no direct connection with ex-ternal or inner situations is, of course, discernible. In spi-te of this, the “trauma hypothesis” can be helpful in un-derstanding AI from the anthroposophical point of view.
A common aspect of physical and mental traumata isthat powers of soul directed towards the body can nolonger effect integration. These powers, normally provi-ding for a healthy measure of degradation in the organ-ism, can no longer maintain themselves in the physicalbody and come free in a way.They then address themsel-ves to the structures that have grown foreign and so setthe AI process in motion. In addition, the physical andetheric body is no longer properly penetrated and there-fore more open to foreign antigens and forces. In con-ventional medicine, the current view also is that with so-me AIs such as reactive arthritis, sacroiliitis and the ar-
Dietary aspects to the treatment of autoimmune diseasesR o m a n H u b e r
Translation of „Diätetische Aspekte in der Behandlung von Autoimmunerkrankungen“ by Roman Huber.Der Merkurstab 2004; 57/5:366-9. English by A. R. Meuss, FCIL, MTA.
n SummaryFrom the viewpoint of anthroposophy, qualitativeaspects as the kind of cultivation and the content ofetheric forces play a major role in nutrition. Ethericforces can be separated according to their relation tolife, sound, light and warmth. Because these ethericforces act also in the human being and can there bestimulated from forces in food, the rationale for adifferentiated dietary intervention is given. Patientswith autoimmune diseases often have reducedetheric forces. In clinical studies, food containinghigh amounts of polyunsaturated fatty acids and sti-mulates etheric forces related to the warmth fromthe viewpoint of anthroposophy, seems to have posi-tive effects in some autoimmune diseases. Foodfrom animals, which particularly stimulates ethericforces related to life can however aggravate the in-flammatory activity in patients with e.g. rheumatoidarthritis. The nutrition of patients with autoimmunediseases should be adjusted to the nutritional per-formance and constitutional factors.n KeywordsEtheric forcesVegetablesMeatConstitution
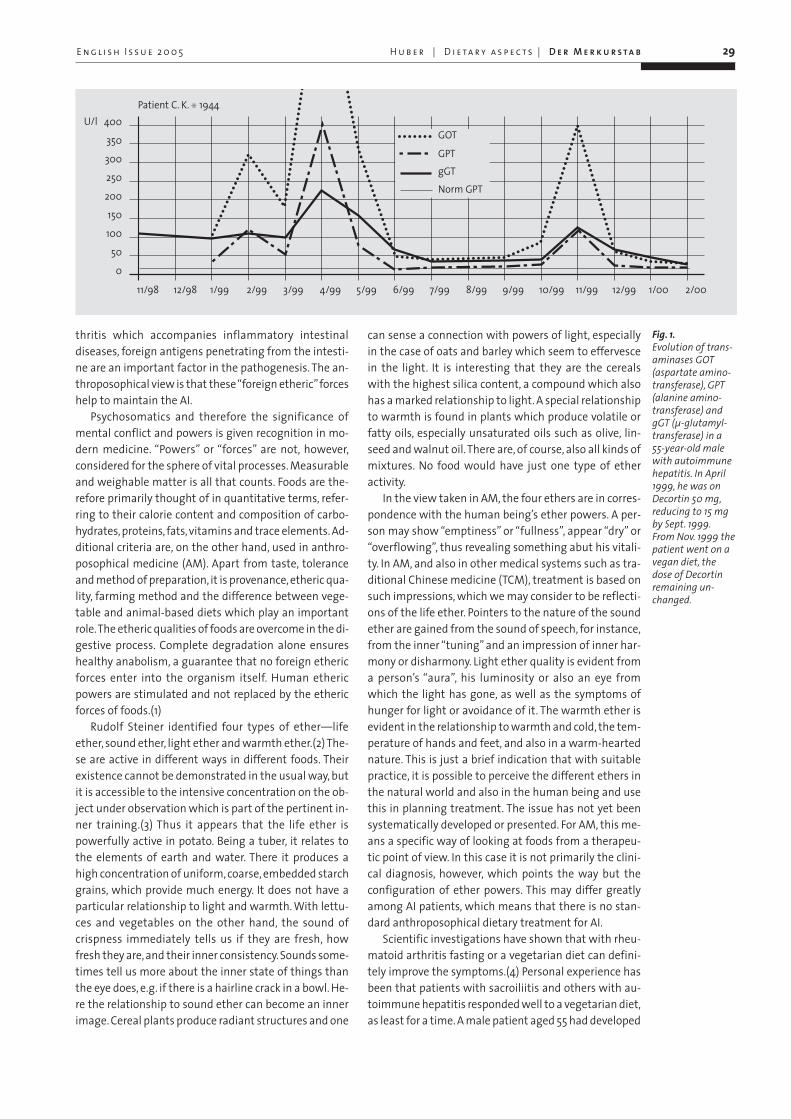
thritis which accompanies inflammatory intestinaldiseases, foreign antigens penetrating from the intesti-ne are an important factor in the pathogenesis. The an-throposophical view is that these “foreign etheric”forceshelp to maintain the AI.
Psychosomatics and therefore the significance ofmental conflict and powers is given recognition in mo-dern medicine. “Powers” or “forces” are not, however,considered for the sphere of vital processes. Measurableand weighable matter is all that counts. Foods are the-refore primarily thought of in quantitative terms, refer-ring to their calorie content and composition of carbo-hydrates, proteins, fats, vitamins and trace elements. Ad-ditional criteria are, on the other hand, used in anthro-posophical medicine (AM). Apart from taste, toleranceand method of preparation, it is provenance, etheric qua-lity, farming method and the difference between vege-table and animal-based diets which play an importantrole.The etheric qualities of foods are overcome in the di-gestive process. Complete degradation alone ensureshealthy anabolism, a guarantee that no foreign ethericforces enter into the organism itself. Human ethericpowers are stimulated and not replaced by the ethericforces of foods.(1)
Rudolf Steiner identified four types of ether—lifeether, sound ether, light ether and warmth ether.(2) The-se are active in different ways in different foods. Theirexistence cannot be demonstrated in the usual way, butit is accessible to the intensive concentration on the ob-ject under observation which is part of the pertinent in-ner training.(3) Thus it appears that the life ether ispowerfully active in potato. Being a tuber, it relates tothe elements of earth and water. There it produces ahigh concentration of uniform, coarse, embedded starchgrains, which provide much energy. It does not have aparticular relationship to light and warmth. With lettu-ces and vegetables on the other hand, the sound ofcrispness immediately tells us if they are fresh, howfresh they are, and their inner consistency. Sounds some-times tell us more about the inner state of things thanthe eye does, e.g. if there is a hairline crack in a bowl. He-re the relationship to sound ether can become an innerimage. Cereal plants produce radiant structures and one
can sense a connection with powers of light, especiallyin the case of oats and barley which seem to effervescein the light. It is interesting that they are the cerealswith the highest silica content, a compound which alsohas a marked relationship to light. A special relationshipto warmth is found in plants which produce volatile orfatty oils, especially unsaturated oils such as olive, lin-seed and walnut oil.There are, of course, also all kinds ofmixtures. No food would have just one type of etheractivity.
In the view taken in AM, the four ethers are in corres-pondence with the human being’s ether powers. A per-son may show “emptiness” or “fullness”, appear “dry” or“overflowing”, thus revealing something abut his vitali-ty. In AM, and also in other medical systems such as tra-ditional Chinese medicine (TCM), treatment is based onsuch impressions, which we may consider to be reflecti-ons of the life ether. Pointers to the nature of the soundether are gained from the sound of speech, for instance,from the inner “tuning” and an impression of inner har-mony or disharmony. Light ether quality is evident froma person’s “aura”, his luminosity or also an eye fromwhich the light has gone, as well as the symptoms ofhunger for light or avoidance of it. The warmth ether isevident in the relationship to warmth and cold, the tem-perature of hands and feet, and also in a warm-heartednature. This is just a brief indication that with suitablepractice, it is possible to perceive the different ethers inthe natural world and also in the human being and usethis in planning treatment. The issue has not yet beensystematically developed or presented. For AM, this me-ans a specific way of looking at foods from a therapeu-tic point of view. In this case it is not primarily the clini-cal diagnosis, however, which points the way but theconfiguration of ether powers. This may differ greatlyamong AI patients, which means that there is no stan-dard anthroposophical dietary treatment for AI.
Scientific investigations have shown that with rheu-matoid arthritis fasting or a vegetarian diet can defini-tely improve the symptoms.(4) Personal experience hasbeen that patients with sacroiliitis and others with au-toimmune hepatitis responded well to a vegetarian diet,as least for a time. A male patient aged 55 had developed
H u b e r | D i e t a r y a s p e c t s | D e r M e r k u r s t a b 29
Fig. 1.Evolution of trans-aminases GOT (aspartate amino-transferase), GPT(alanine amino-transferase) andgGT (µ-glutamyl-transferase) in a55-year-old malewith autoimmunehepatitis. In April1999, he was onDecortin 50 mg,reducing to 15 mgby Sept. 1999.From Nov. 1999 thepatient went on avegan diet, the dose of Decortinremaining un-changed.
E n g l i s h I s s u e 2 0 0 5
400
350
300
250
200
150
100
50
0
11/98 12/98 1/99 2/99 3/99 4/99 5/99 6/99 7/99 8/99 9/99 10/99 11/99 12/99 1/00 2/00
Patient C. K. S 1944U/l
gGT
GOT
GPT
Norm GPT

autoimmune hepatitis, probably in connection with in-take of a lipid-lowering drug (Fig. 1). Steroids essentiallynormalized the elevated transaminase levels, but a re-duction in dosage resulted in a further rise in transami-nase levels. He therefore came to see us. He was evi-dently stout, a plethora syndrome (overweight, distal ex-tremities very warm, red-faced, etc.), and we advised himto try a vegan diet. This excludes all animal products, in-cluding dairy foods. An adequate supply of purely vege-table fats and protein is no problem for adults given pro-per information. Children and pregnant women shouldnot use this diet, however, as serious deficiencies arepossible with it. In this case, transaminase levels retur-ned to normal on a vegan diet, with no changes made inmedication. We consider this to indicate efficacy. Fromthe AM point of view, animal foods demand less effort todigest, being more closely related to the human sub-stance, but contain impulses arising from the animal’svital energies and are therefore more likely than vegeta-ble foods to retain their ether forces as a foreign elementin the human organism. A vegan diet on the other handwill bind unintegrated destructive psychic powers morein digestion, and this prevents their being active in theinflammatory process. It also stimulates the light andwarmth ethers more than an animal-food diet does,which is evident at the substance level in higher vitaminand antoxidant levels, and it contains less foreign ether-ic potential.
Scientific investigations have shown that a majorpart of the positive effects of a vegan diet is due to a re-duction in arachidonic acid levels, an acid found solely inanimal fats.(5) Arachidonic acid does among otherthings encourage the production of pro-inflammatoryeicosanoids (prostaglandins, thromboxan, leucotrines,etc.) which can help to maintain inflammatory AI. It hasalso been found that multi unsaturated omega-3 andomega-6 fatty acids—from the anthroposophical pointof view particularly connected with the warmth ether—antagonize the actions of arachidonic acid. This led tothe interesting idea of using multi unsaturated acids inthe treatment of AI. Apart from a number of vegetableoils which above all contain the omega-3 fatty acid alphalinolenic acid (linseed, walnut and rape oil), therapeuticexpectations focus on the omega-3 fatty acids of cold-water fish (salmon, mackerel, herring, tuna). Trials doneprovide first indications of positive results with rheuma-toid arthritis, and also IgA nephritis, for instance.(5, 6)Rheumatoid arthritis is more common in northern lati-tudes, frequently with aggravation from cold and wetconditions. Light and warmth ameliorate the symptoms,indicating the ether qualities which these patients need.Algae in the cold waters of those regions have a good al-pha linolenic acid content which relates very much tothe warmth ether and are like a counter agent. Fish fee-ding on the algae are able to increase the degree ofwarmth and hence also the number of double bonds intheir metabolism, thus producing substances that havetherapeutic significance for rheumatic “diseases of cold-ness”.
All in all, therefore, important approaches to treatingAI come from the field of nutrition.Treatment should onprinciple always be based on the given situation. A vegandiet can be continued for some time if a patient with thesymptoms of plethora benefits, though unfortunatelythese symptoms are rare with AI. Patients of this typeusually also tolerate a raw-food diet well. Others who areweak, underweight and pale, their vitality reduced, willnot usually tolerate raw foods well, and these may in-deed be harmful, as they increase the weakness. Thesepatients need hot meals and a diet rich in warmth-ether-ic quality. They should certainly take dairy produce, fish,and perhaps even meat, as these stimulate the life ether.As with all medicine, it is thus important to be guided bythe patient’s condition in giving dietary advice—particu-larly as there are so many dogmas and different beliefsin the field of nutrition—and supporting the needs ofthe individual patient.
Roman Huber, MDFreiburg University HospitalNatural Medicine UnitBreisacher Str. 60D-79106 Freiburg
30 D e r M e r k u r s t a b | H u b e r | D i e t a r y a s p e c t s E n g l i s h I s s u e 2 0 0 5
Literatur1 1 Steiner R, Wegman I. Exten-ding Practical Medicine, chap-ters 9, 10 and 12. Tr. A. R. Meuss.London: Rudolf Steiner Press1996.2 Anthroposophical SpiritualScience and Medical Therapy,lecture of 12 April 1921. rev. G.Karnow. Spring Valley: MercuryPress 1991.3 SSteiner R. Knowledge of theHigher Worlds or How to KnowHigher Worlds.4 Kjeldsen-Kragh J, Haugen M,Borchgrevink CF, Laerum E, EekM, Mowinkel P, Hovi K, Forre O.Controlled trial of fasting andone-year vegetarian diet inrheumatoid arthritis.Lancet. 1991;338:899-902.5 Adam O, Beringer C, Kless T,Lemmen C, Adam A, Wiseman M,Adam P, Klimmek R, Forth W. An-ti-inflammatory effects of a lowarachidonic acid diet and fish oilin patients with rheumatoid ar-thritis. Rheumatol Int.2003;23(1):27-36.6 Donadio JV Use of fish oil totreat patients with immunoglo-bulin a nephropathy. Am J ClinNutr. 2000 71(1 Suppl):373S-5S.