anteriorly displaced transverse fracture of the sacrum with fracture-dislocation at the l4–l5...
TRANSCRIPT

354 Injury (1985) 16,354-357 Printed in Great Britain
Anteriorly displaced transverse fracture of the sacrum with fracture-dislocation at the LAL5 lumbar level
George Sapkas, Theodoros Pantazopoulos and Panos Efstathiou
Orthopaedic Department of the Medical School, K.A. T. Hospital, Athens, Greece
INTRODUCTION WE present an unusual case of fracture-dislocation of the spine at two levels. A transverse fracture of the sacrum, combined with fracture-dislocation at the L4-L.5 lumbar level, is rare.
CASE REPORT A 24-year-old married woman attempted suicide by jumping from a fourth floor and landed on the road. She sustained multiple injuries, including brief concussion. On admission to the hospital, she was found to have paraparesis below the fourth lumbar segment with loss of bladder and sphincter control due to severe injury at the lumbosacral level of the spine.
Plain radiographs revealed the following injuries at the lumbosacral area of the spine (Figs. 14):
1.
2. 3.
4. 5. 6. 7.
Fracture-dislocation at L4-L5 level due to a flexion- distraction injury. Sagittal fracture of the body of L5. Displacement of bone fragments from body of L5 into the spinal canal. Fractures of the transverse processes of L5. Anteriorly displaced fracture-subluxation of S3 on S4. Sagittal fracture in the upper part of the sacrum. Fracture of the upper part of the sacrum at the region of the right sacral crest, parallel to the median fracture of the sacrum and the right sacroiliac joint. The upper part of the sacrum was rotated to the right.
Radiographs also revealed a wedge compression fracture of T12, fracture at the midshaft of the left humerus, fractured left ribs, fractures of both ankles and of the left OS calcis, and a slightly displaced fracture of the left ischiopubic rami.
Fig. 1. Anteroposterior radiograph of the lumbosacral spine. There is a clear rotation of the sacrum to the right. Both sacroiliac joints remain undisturbed.
Fig. 2. Lateral radiograph of the lumbosacral spine showing the flexion-distraction injury at the L4-L5 lumbar level and the anterior displacement of the upper part of the sacrum in relation to its lower part, at the S3-S4 sacral segment.

Sapkas et al.: Fracture-dislocation of the spine
Fig. 3. Anteroposterior tomogram of the lumbosacral spi It is quite clear that there has been great distortion of lumbosacral area of the spine, and the vertical fractures of fifth lumbar vertebra and sacrum are well shown.
ine. the the
The patient was treated conservatively in the General Hospital and 2 days later was transferred to our hospital. Initially her general condition was poor because of post- traumatic anaemia and a right haemothorax. She developed high fever and blood cultures grew Klebsiella. She was treated with gentamicin (Garamycin).
Three weeks after the accident there was improvement in her neurological condition and electromyographic examina- tion of the lower limbs demonstrated lesions of all the nerve roots below the fourth lumbar level. Two days later she underwent an operation on her spine. Through a posterior median approach the spine was exposed from the second lumbar vertebra to the level of the transverse fracture of the sacrum. The sacro-spinalis muscles were lifted off their insertions to permit better exposure of the spine.
There were fractures of the laminae and transverse processes of the fifth lumbar vertebra, disruption of the zygapophyseal joint capsules and of the interspinous ligament at the L4-L5 level with fracture-dislocation of the facet joints, and the previously described vertical and transverse fractures of the sacrum. The laminae on both sides of the fourth and fifth lumbar vertebrae, and partly of the first sacral segment were removed to allow wide exposure of the spinal canal. The meninges were disrupted extensively and all the nerve roots below the fourth lumbar level had been severely damaged. Few of them had been separated in bundles, many of which had been completely divided. Two big fragments from the body of the fifth lumbar vertebra were protruding into the spinal canal, compressing the nerve roots; they were re- moved. The remaining intact nerve roots and bundles were released from any pressure on them.
Reduction of the anteriorly displaced transverse fracture of the sacrum was not possible. We failed also to reduce the dislocation at the L4-L5 level, probably because of the long time that had elapsed since the accident and the technical difficulties arising from the use of short Harrington distrac- tion rods that allow bending.
The operation was completed by stabilizing the lumbosac- ral spine with two Harrington distraction rods and spondy- lodesis. To avoid insertion of the lower hooks into the fractured upper segment of the sacrum, a Harrington sacral bar was passed through the posterior iliac crests and the two Harrington distraction rods were fitted between the laminae of the third lumbar vertebra and the special adaptation sockets (sacral rod eyelet) of the sacral bar. The laminae of the third lumbar vertebra were chosen in order to reduce the length of spondylodesis, preserving as much motion as possible from the remaining undisturbed upper levels of the lumbar spine. However, this obliged us to use the shortest length of Harrington rods, which do not permit bending of the rod in order to preserve the normal lumbar lordosis; therefore the forward tilt of the lumbar spine remained uninfluenced (Figs. 5 and 6). For spondylodesis, we used freeze-dried allografts from preserved femoral heads. Finally, the meninges and the nerve roots were covered by auto- genous fat.
The postoperative course was uneventful apart from fever of unknown aetiology that appeared on the 8th postoperative day and lasted for 5 days. The patient remained in an ordinary bed throughout. Two weeks later she started sitting wearing a protective brace for the spine. Eight weeks later she attended the gymnasium of the physiotherapy depart- ment, walking with support and wearing orthopaedic devices for the legs; this delay in walking was due to the bilateral fractures of ankle joints. Three months after the operation the patient obtained complete control of her bladder and bowels.
Fig. 4. Lateral tomogram of the lumbosacral spine. demonstrates the anteriorly displaced fracture of the sacs at the S3-S4 sacral level, as well as the flexion-distrac injury at the L4-L.5 lumbar level.
It _um tion Fracture-dislocations of the sacrum are rare injuries.
Even more rare is the combination of such an injury of
DISCUSSION
Injury: the British Journal of Accident Surgery (1985) Vol. 16/No. 5
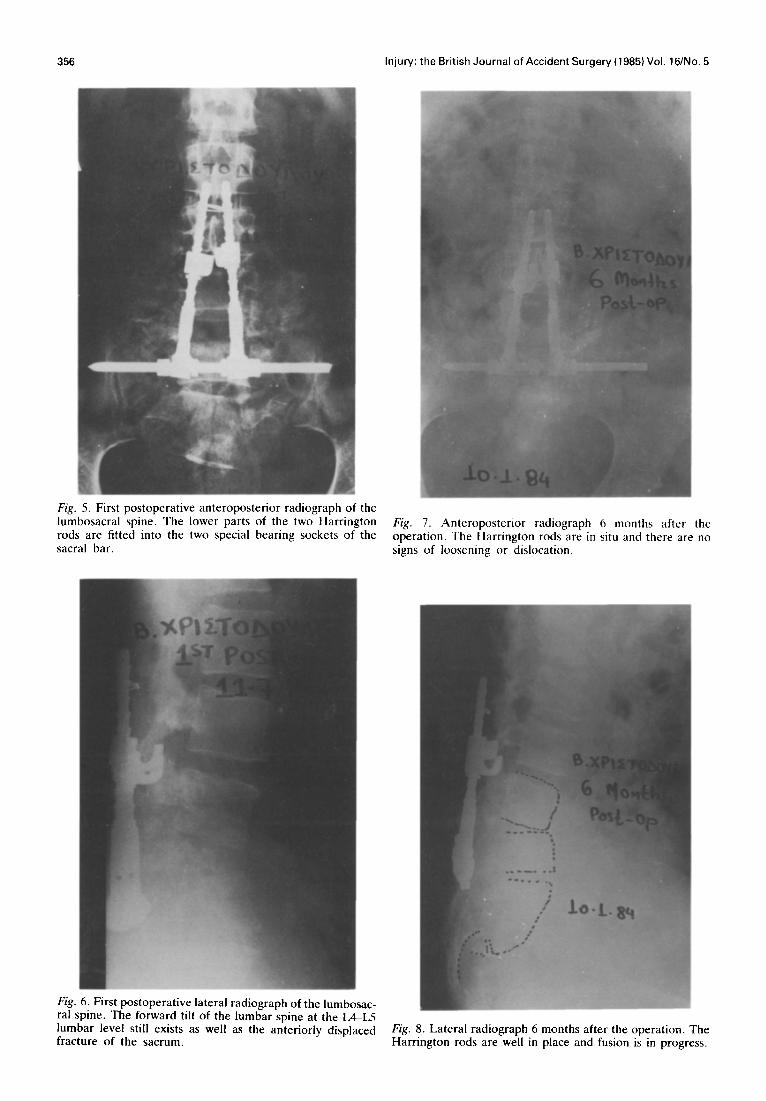
Fig . 5. First postoperative anteroposterior radiograph of the IUIY tbosacral spine. The lower parts of the two Harrington rod s are fitted into the two special bearing sockets of the sac ral bar.
Fig. 7. Anteroposterior radiograph 6 months after operation. The Harrington rods are in situ and there are signs of loosening or dislocation.
the no
Fig ral
:. 6. First postoperative lateral radiograph of the lumbosac- spine. The forward tilt of the lumbar snine at the L4-L5
lumbar level still exists as well as the anteriorly displaced Fig. 8. Lateral radiograph 6 months after the operation. The fracture of the sacrum. Harrington rods are well in place and fusion is in progress.

Sapkas et al.: Fracture-dislocation of the spine
the sacrum with a fracture-dislocation at the L4L5 level.
Reports in the literature (Wakeley, 1929; Furey, 1942; Bonnin, 1945; Burman, 1952; Dunn and Morris, 1968; Purser, 1969; Woodward and Kelly, 1974; Burnes et al., 1977) refer only to injuries of the sacrum with or without associated injuries of the sacroiliac joints, of the transverse processes of the fifth lumbar vertebra and of the pelvis.
Nicoll (1949) described the mechanism of this injury of the sacrum as a violent force in a forward direction applied to the lower part of the lumbar spine while the pelvis is held stable by flexed hips and the knees are locked in extension. We believe that the above mechanism of injury applies to our case. It is interesting that the level of the fracture of the sacrum involves the third over the fourth sacral segment. Bucknill and Blackburne (1976), who reported three cases, and Ferris and Hutton (1983), who reported another two, noticed that the fracture line in these cases passes through the sacrum at the anatomical junction between the first and second segments.
Neurological injury associated with sacral fracture was first reported by Lam (1936). Of the nine patients previously reported with fractures of the sacrum, only one was treated surgically, but no neural improvement resulted. Six patients who had neural involvement improved with conservative treatment, having residual pelvic discomfort, low backache and neurological deficit in varying degrees.
Finally, we believe that the result was good following operative treatment with release of the nerve roots and stabilization of the lumbosacral spine with Harrington
rods and bone grafts, although literature claim good results from ment.
357
reports from the conservative treat-
REFERENCES Bonnin J. G. (1945) Sacral fractures and injuries to the cauda
equina. J. Bone Joint Surg. 27, 112. Bucknill T. M. and Blackburn J. S. (1976) Fracture-
dislocations of the sacrum. J. Bone Joint Surg. 58B, 467. Burman M. (1952) Tear of the sacrospinous and sacrotuber-
ous ligaments. J. Bone Joint Surg. 34A, 331. Burnes D. P., Russo G. L., Ducker T. B. et al. (1977)
Sacrum fractures and neurological damage. Report of two cases. J. Neurosurg. 47, 459.
Dunn A. W. and Morris H. D. (1968) Fractures and dislocations of the pelvis. J. Bone Joint Surg. SOA, 1639.
Ferris B. and Hutton P. (1983) Anteriorly displaced trans- verse fracture of the sacrum at the level of the sacro-iliac joint. J. Bone Joint Surg. 65A, 407.
Furey W. W. (1942) Fractures of the pelvis with special reference to associated fractures of the sacrum. Am. J. Roentgenol. Radium Ther. 47, 89.
Lam C. R. (1936) Nerve injury in fracture of the pelvis. Ann. Surg. 104, 945.
Nicoll E. A. (1949) Fractures of the dorso-lumbar spine. J. Bone Joint Surg. 31B, 376.
Purser D. W. (1%9) Displaced fracture of the sacrum. J. Bone Joint Surg. 51B, 346.
Wakeley C. P. G. (1929) Fractures of the pelvis: an analysis of 100 cases. Br. J. Surg. 17, 22.
Woodward A. N. and Kelly P. J. (1974) An unusual fracture of the sacrum. Minn. Med. 57, 465.
Paper accepted 16 July 1984.
Requests for reprints should be addressed to: Dr George Sapkas, University of Athens, 13 Patriatchou Maximou St., Kefalari, Kifissia, Athens, Greece.