antenatal fetal monitoring
TRANSCRIPT



Prof Mahmoud Zakherah

Intrapartum assessment of fetal well-being
• Many antepartum deaths occur in women at risk for uteroplacental insufficiency.
• Ideal test: allows intervention before fetal death or damage from asphyxia.

ILOS
• Different methods of intra partum assessment of fetal wellbeing
• MAS diagnosis and management• What is normal?• What is abnormal ?• Results and management

Methods
• Assessment of uterine growth( SFH )• Fetal movement counting• Antepartum fetal heart rate testing NST (health) CST( Uteroplacental)• Biophysical profile and Modified • Doppler velocimetry • Pubs

Assessment of uterine growth( SFH )

Fetal movement counting
FETAL MOVEMENT ASSESSMENT
• Fetal “kicks” count • Perception of 10 distinct movements in a
period of up to 2 hours is considered reassuring
• Decreased placental perfusion and fetal acidemia and acidosis are associated with decreased fetal movements

FETAL MOVEMENT ASSESSMENT
• Maternal perception of a decrease in fetal movements may be a sign of impending fetal death
. • It costs nothing.

FETAL MOVEMENT ASSESSMENT

Antepartum fetal heart rate testing
1-CST( Uteroplacental)2-NST (health)

CONTRACTION STRESS TEST
• Response of the fetal heart rate to uterine contractions

CONTRACTION STRESS TEST
Methods• Oxytocin challenge test (OCT)• Breast (nipple) stimulation• Goal: three contractions in ten minutes.

Oxytocin Challenge Test

Early decelerations: The nadir occurs with the peak of a contraction. Head compression

Late decelerations:The nadir occurs after the peak of a contraction. Hypoxia

Management• Administer O2 by tight face mask • Discontinue oxytocin. • Correct any hypotension • IV hydration. • If hyperstimulation is present consider terbutaline 0.25
mg SC • If late decelerations persist for more than 30 minutes
despite the above maneuvers, fetal scalp pH is indicated.
• Scalp pH > 7.25 is reassuring, pH 7.2-7.25 may be repeated in 30 minutes.
• Deliver for pH < 7.2 or minimal baseline variability with late or prolonged decelerations and inability to obtain fetal scalp pH
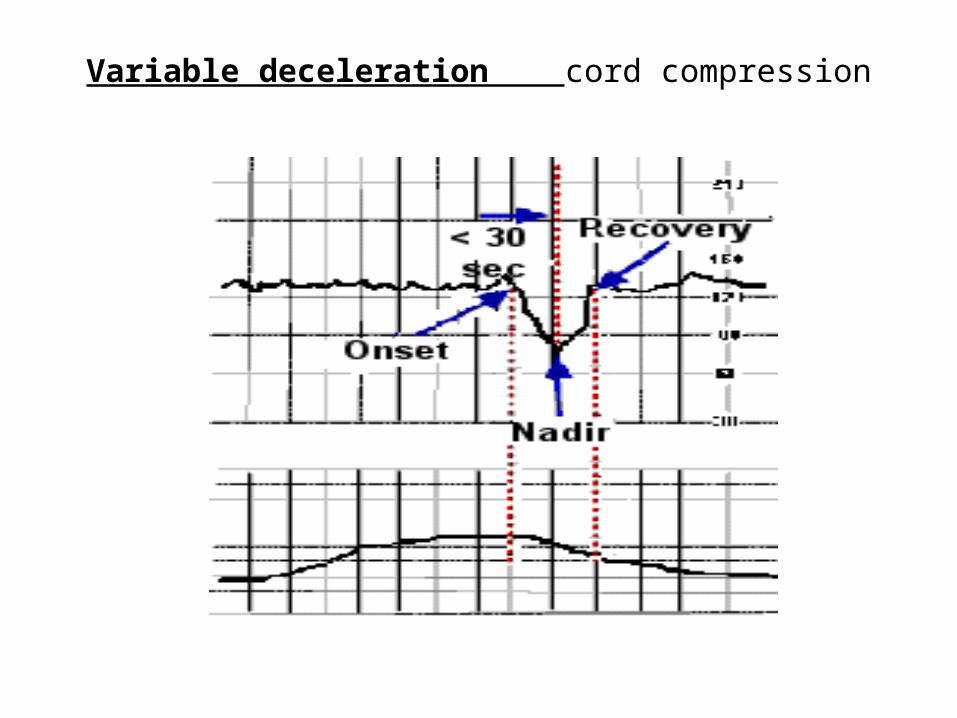
Variable deceleration cord compression

Interpretation of the CST
• Negative: no late decelerations and adequate FHR recording
• Positive: Late decelerations present with the majority of contractions (without excessive uterine activity)
• Equivocal : Suspicious, hyperstimulation, unsatisfactory.

Contraindications to CST
• PROM • Previous classical cesarean delivery • Placenta previa • Incompetent cervix • History of premature labor in this pregnancy • Multiple gestation

Electronic monitor

Electronic monitor
Pressure Transducer
Ultrasound Probe


• Baseline• Variability short term long term• Acceleration• Deceleration

NONSTRESS TEST
• Accelerate with fetal movement• Fetal sleep cycle• Central nervous system depression• Reactive : two or more fetal heart rate
accelerations within a 20-minute period• Nonreactive: lacks sufficient fetal heart rate
accelerations over a 40-minute period.

Baseline Fetal Heart Rate
Two Minutes

Reactive NST

Non Reactive NST



Components of the Biophysical Profile Score
Component Definition
Non-stress test
Two or more fetal heart rate accelerations peak (but do notnecessarily remain) at least 15 beats per minute above thebaseline and last 15 seconds from baseline to baseline withina 20-minute period with or without fetal movement discernibleby the woman.
Amniotic fluid volume
A single 2 cm x 2 cm pocket is considered adequate or AFIgreater than 5.0 cm .
Fetal breathing movements
One or more episodes of rhythmic fetal breathing movementsof 30 seconds or more within 30 minutes.Hiccups are considered breathing activity.
Fetal movementsAt least three discrete body or limb movements. Episodes of continuous movement are considered as a singlemovement.
Fetal tone One or more episodes of extension of a fetal extremity ortrunk with return to flexion, or opening or closing of a hand

MODIFIED BIOPHYSICAL PROFILE
Non-stress test amniotic fluid index (5-24)The modified biophysical profile is considered normal if thenonstress test is reactive and the amniotic fluid index is greater than 5 cm
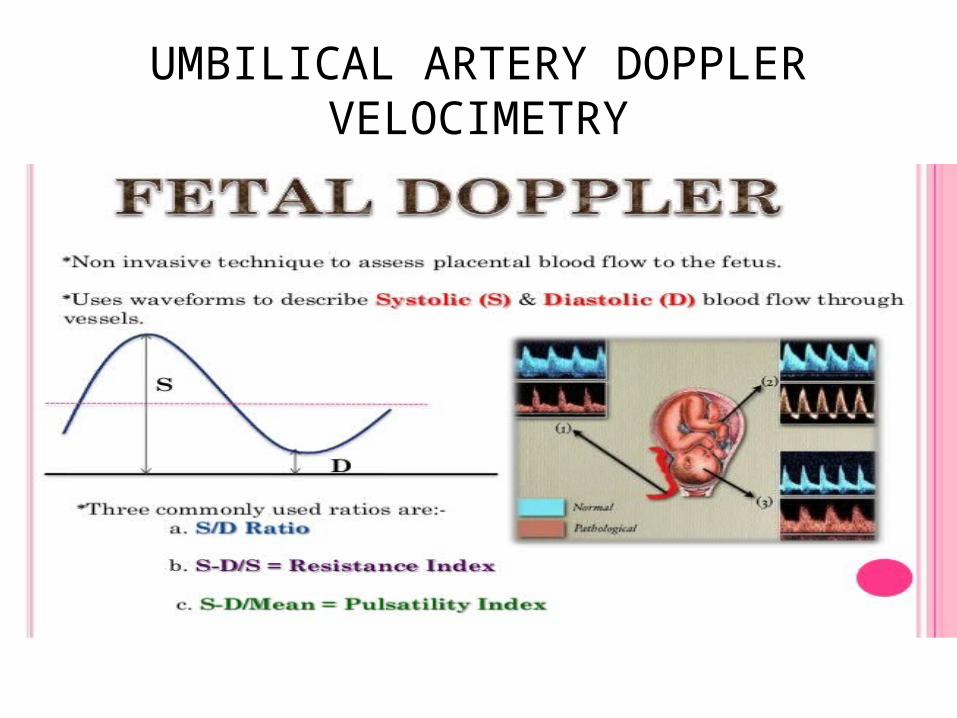
UMBILICAL ARTERY DOPPLER VELOCIMETRY



Indications for Antepartum Fetal Surveillance
• Maternal Conditions: – Diabetes Mellitus – Chronic Renal Failure – Congenital Heart Disease – Rheumatic Heart Disease – Thyroid Diseases – Hemoglobinopathies (hemoglobin SS, SC,
Thalassemia) – Hypertensive disorders

• Pregnancy-related Conditions: – Pregnancy-induced hypertension – Decreased fetal movement – Oligohydramnios – Polyhydramnios – Intrauterine growth restriction – Post-term Pregnancy – Isoimmunization – Previous fetal demise

Meconium Aspiration syndrome
• Definition
• Diagnosis
• Management

Meconium Aspiration syndrome
• The first intestinal discharge from newborns is meconium,
• Meconium-stained amniotic fluid may be aspirated before or during labor and delivery
• In utero meconium passage results from neural stimulation of a maturing GI tract and usually results from fetal hypoxic stress

Meconium Aspiration syndrome
• increasing the risk of perinatal bacterial infection.
• meconium is irritating to fetal skin, thus increasing the incidence of erythema toxicum.

Aspiration induces hypoxia via four major pulmonary effects
• Airway obstruction Complete obstruction of the airways by
meconium results in atelectasis
• Surfactant dysfunctionMeconium deactivates surfactant and may also
inhibit surfactant synthesis

• Chemical pneumonitis
• Persistent pulmonary hypertension of the newborn

Causes of MAS
• Placental insufficiency• Maternal hypertension• Preeclampsia• Oligohydramnios• Maternal infection/chorioamnionitis• Fetal hypoxia

Diagnosis
HistoryPresence of meconium in amniotic fluidThe presence of thick particulate meconium in
the amniotic fluid increases the likelihood of prenatal aspiration.
the presence of meconium stained amniotic fluid or neonatal respiratory distress, and characteristic radiographic abnormalities.

Diagnosis
Physical• Severe respiratory distress may be present• Cyanosis grunting• Intercostal retractions Tachypnea• Barrel chest (increased anteroposterior
diameter) due to the presence of air trapping• Yellow-green staining of fingernails, umbilical
cord, and skin may be observed.

Laboratory Studies
• Acid-base status• Serum electrolyte• CBC count

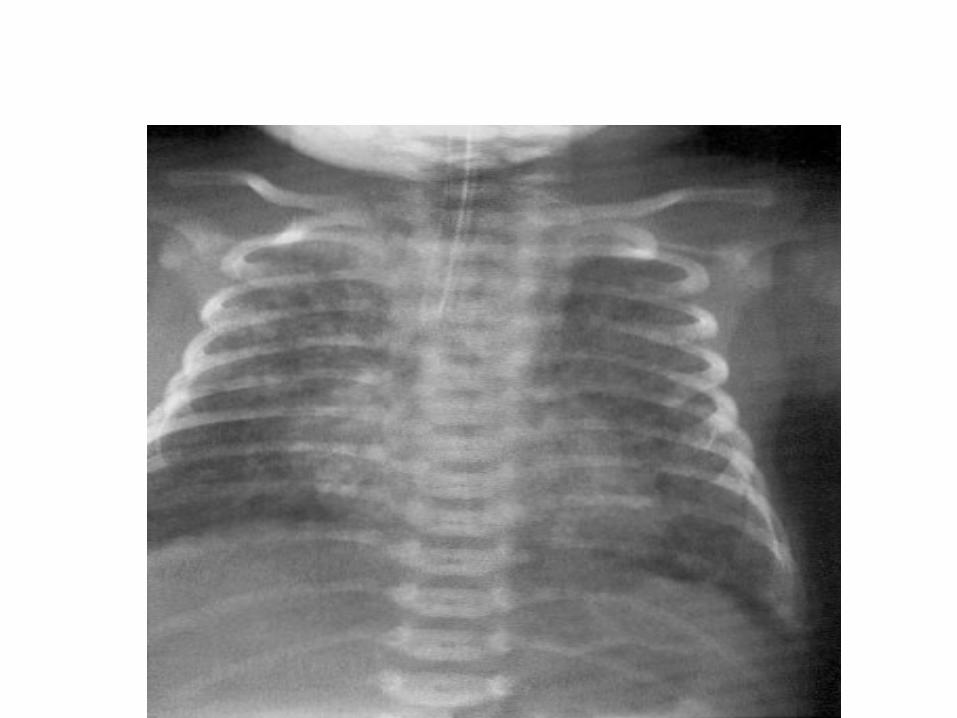
Imaging Studies
• Chest radiography • Identify areas of atelectasis and air block
syndromes • Ensure appropriate positioning of the
endotracheal tube and umbilical catheters

• Echocardiography is necessary to ensure normal cardiac structure and assess cardiac function, as well as determine the severity of pulmonary hypertension and right-to-left shunting.

Differential Diagnoses
• Aspiration Syndromes• Congenital Diaphragmatic Hernia• Pneumonia• Pulmonary Hypertension, Idiopathic• Pulmonary Hypertension, Persistent-Newborn• Sepsis• Transient Tachypnea of the Newborn• Transposition of the Great Arteries

Prevention of meconium aspiration syndrome (MAS)
• Obstetricians should closely monitor fetal status in an attempt to identify fetal distress
• When meconium is detected, amnioinfusion

Management
When aspiration occurs• intubation and immediate suctioning of the
airway can remove much of the aspirated meconium.
• neonatal ICU (NICU)
