annual slide seminar june 21-23 2007 bratislava slovakia b. fredrik petersson md, phd department of...
TRANSCRIPT
ANNUAL SLIDE SEMINAR
June 21-23 2007
Bratislava Slovakia
B. Fredrik Petersson MD, PhD
Department of Pathology,
Karolinska University Hospital
Stockholm Sweden

2 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
CASE 1:
Male, age 48 years.
Previously healthy. A slowly growing
(some year) tumor, left cheek, 1 cm - excision.

3 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
Case 1: Macroscopy
Excision measuring 25x25x15 mm with a central 10 mm large non-ulcerated flesh-
coloured nodule.

4 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
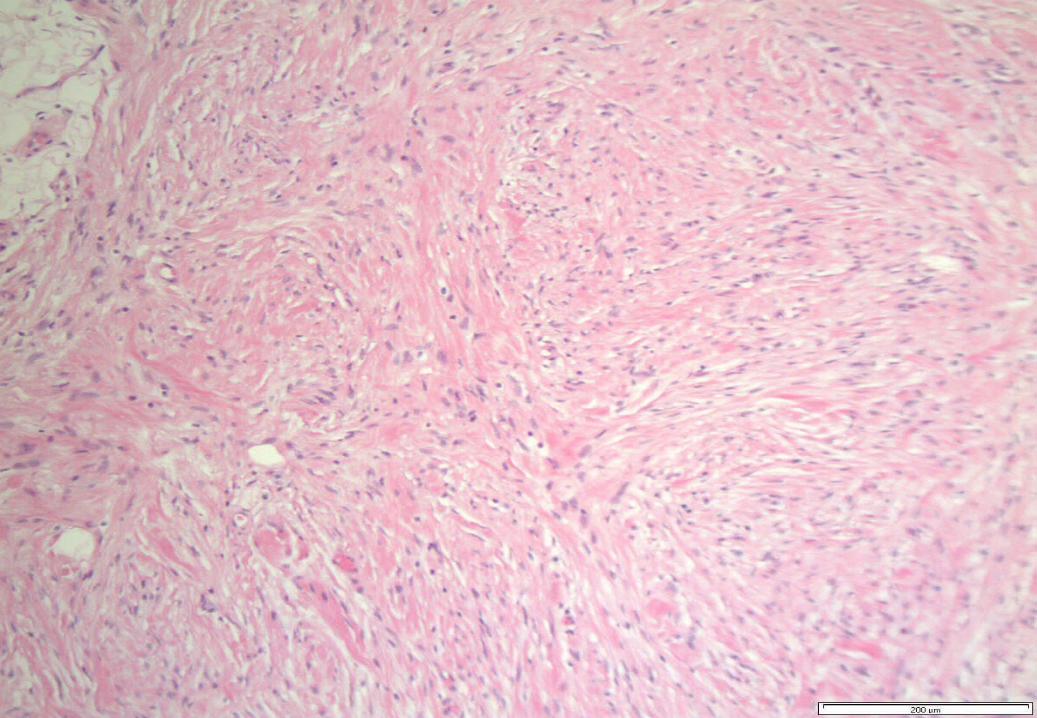
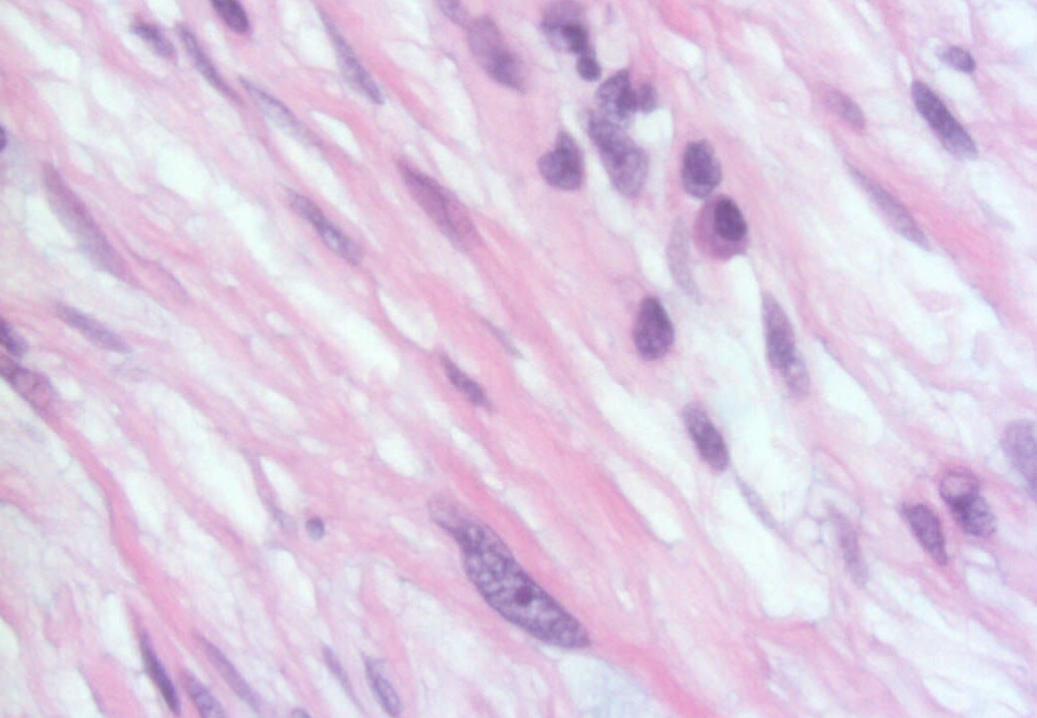
Case 1: Histology
- Dermal, poorly demarcated, spindle cell lesion with low to moderate cellularity growing into the subcutis.
- Mostly monomorphic spindle cells with wavy nuclei in fascicular arrangements and scattered cells with large atypical, hyperchromatic nuclei. Abundant relatively loose collagenous matrix.
- Intra- and perilesional small lymfoid nodules.
- Focally atypical cells -intraepidermally and in the superficial dermis.

5 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
6 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

7 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
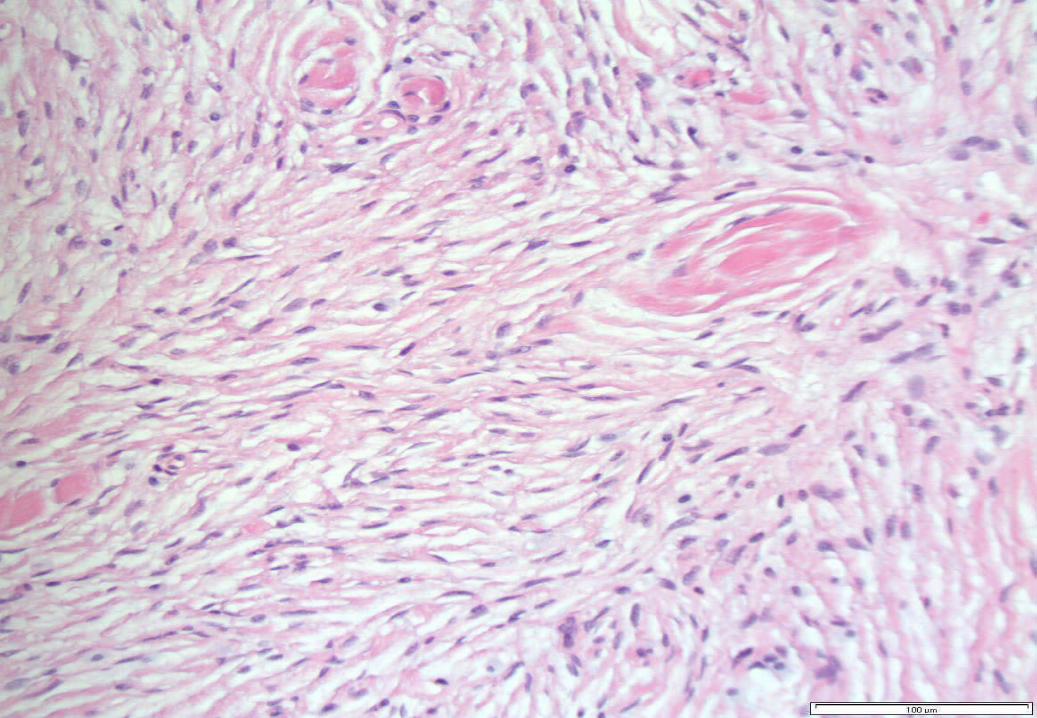
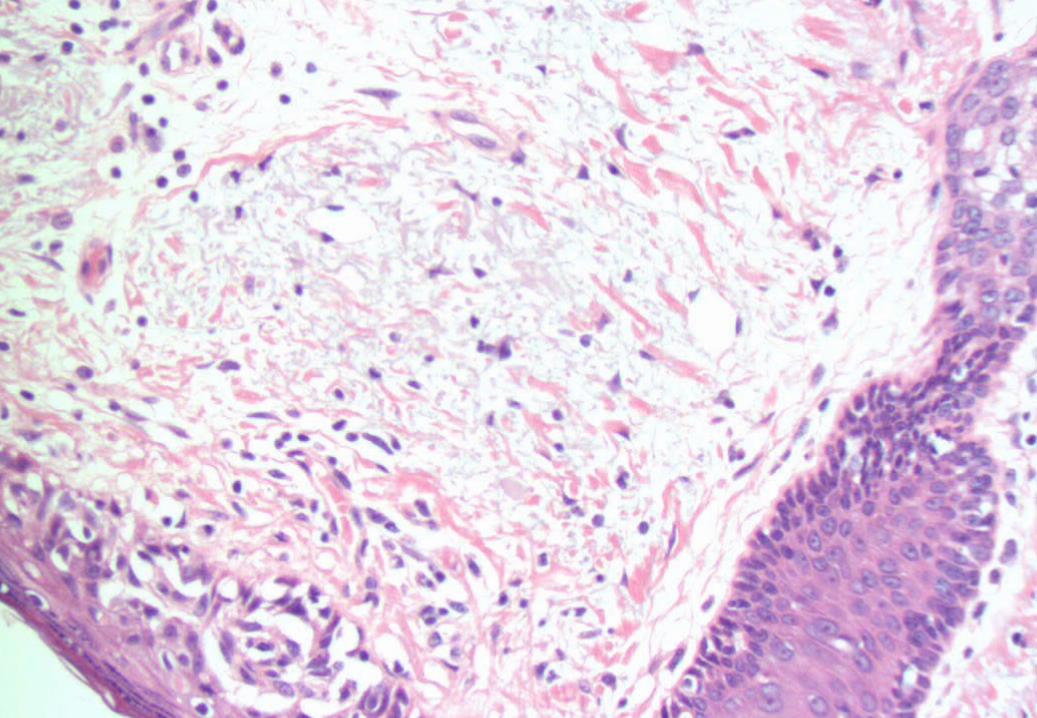
Case 1: Histology
- Dermal, poorly demarcated, spindle cell lesion with low to moderate cellularity growing into the subcutis.
- Mostly monomorphic spindle cells with wavy nuclei in fascicular arrangements and scattered cells with large atypical, hyperchromatic nuclei. Abundant relatively loose collagenous matrix.
- Intra- and perilesional small lymfoid nodules.
- Focally atypical cells intraepidermally and in the superficial dermis.
8 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

9 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
10 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

11 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
12 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

13 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
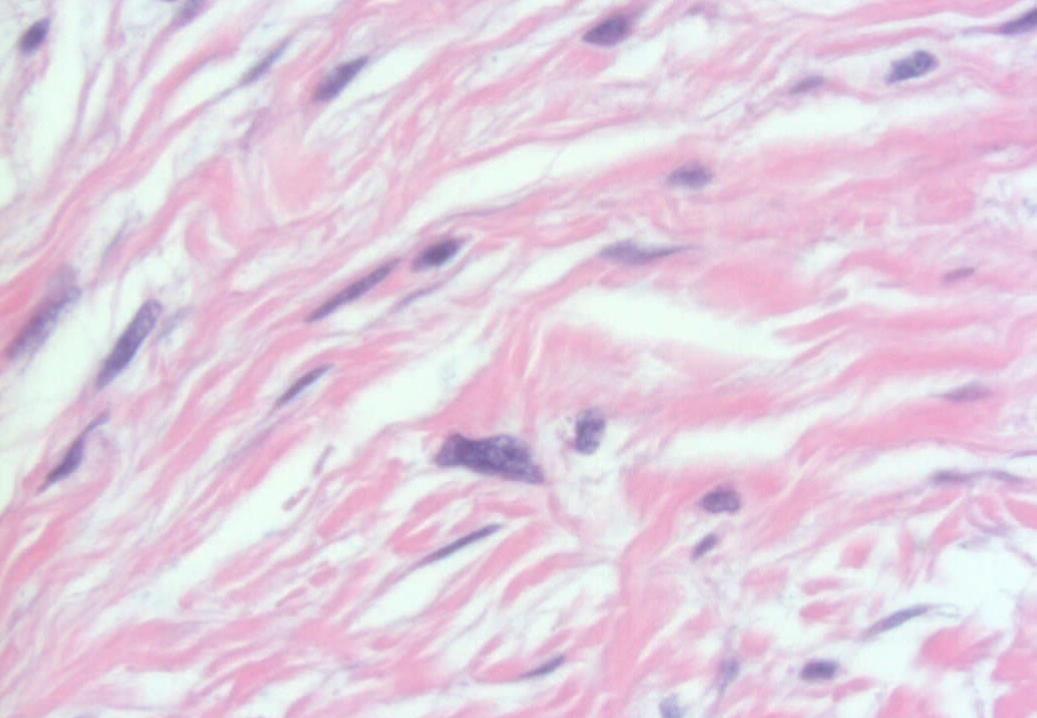
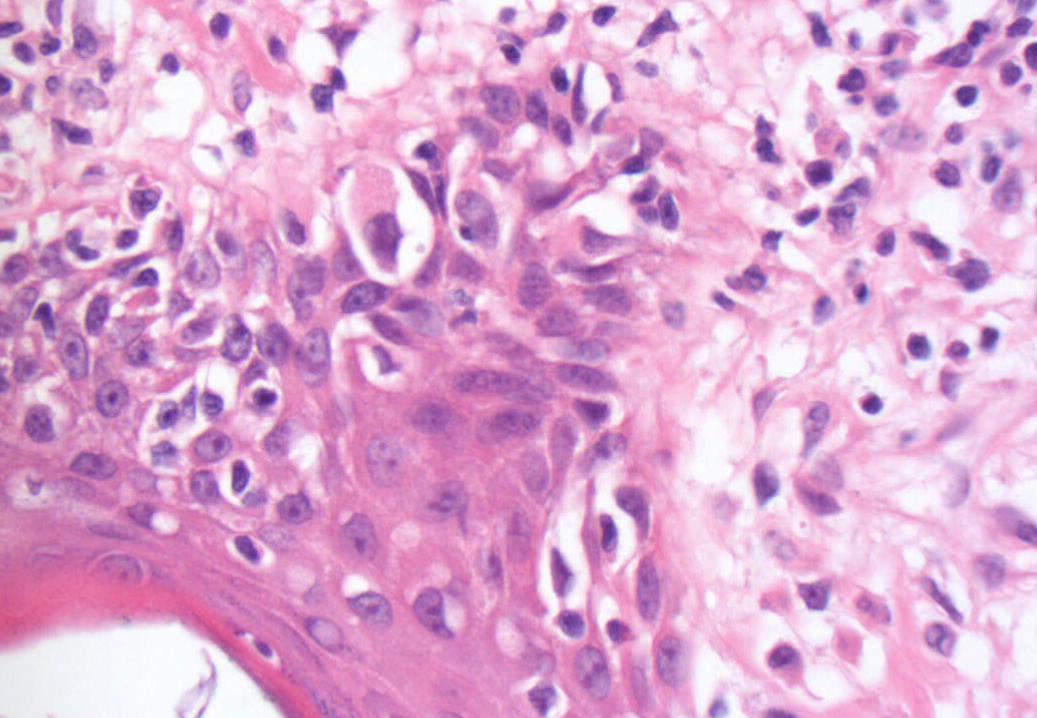
Case 1: Histology
- Dermal, poorly demarcated, spindle cell lesion with low to moderate cellularity growing into the subcutis.
- Mostly monomorphic spindle cells with wavy nuclei in fascicular arrangements and scattered cells with large atypical, hyperchromatic nuclei. Abundant relatively loose collagenous matrix.
- Intra- and perilesional small lymfoid nodules.
- Focally atypical cells intraepidermally and in the superficial dermis.

14 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

15 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

16 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
Case 1: Histology
- Dermal, poorly demarcated, spindle cell lesion with low to moderate cellularity growing into the subcutis.
- Mostly monomorphic spindle cells with wavy nuclei in fascicular arrangements and scattered cells with large atypical, hyperchromatic nuclei. Abundant relatively loose collagenous matrix.
- Intra- and perilesional small lymfoid nodules.
- Focally atypical cells intraepidermally and in the superficial dermis.
17 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
18 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

19 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

20 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

21 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

22 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1

23 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
24 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
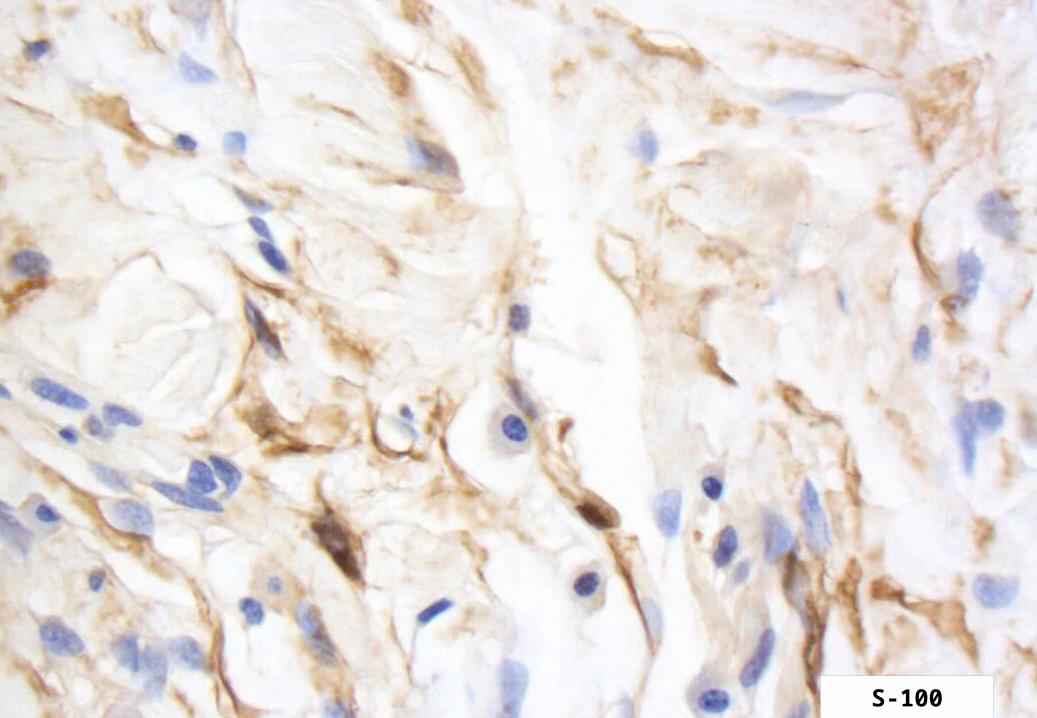
Case 1. Immunohistochemistry
Cytokeratin (MNF116) –
Actin SM –
Actin SR –
HMB-45 -
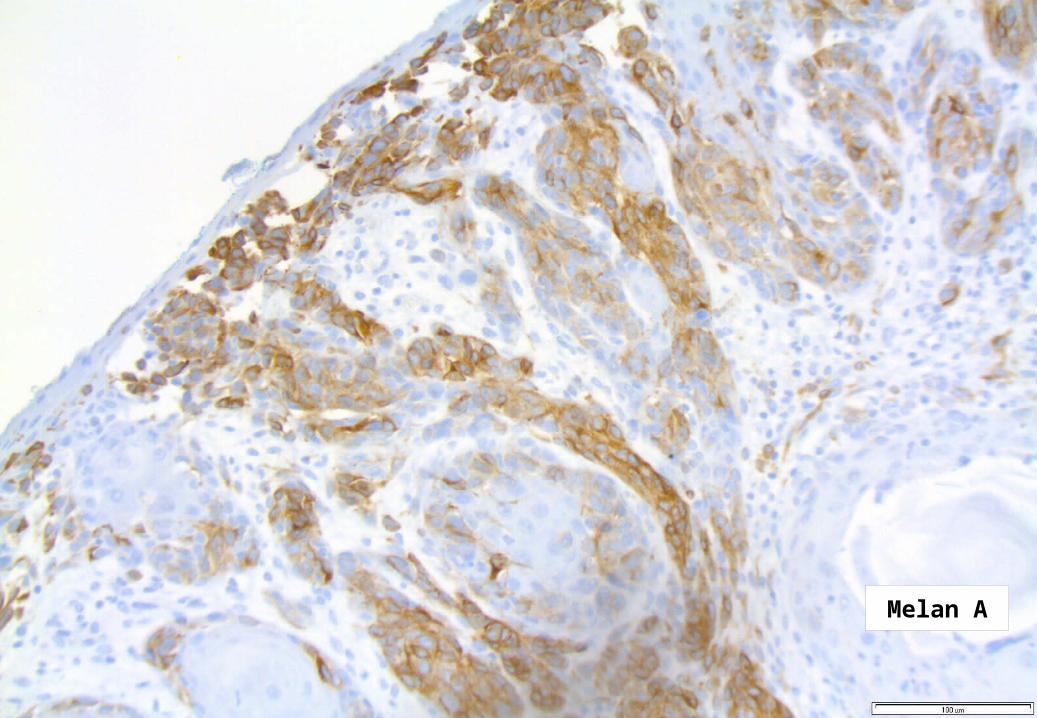
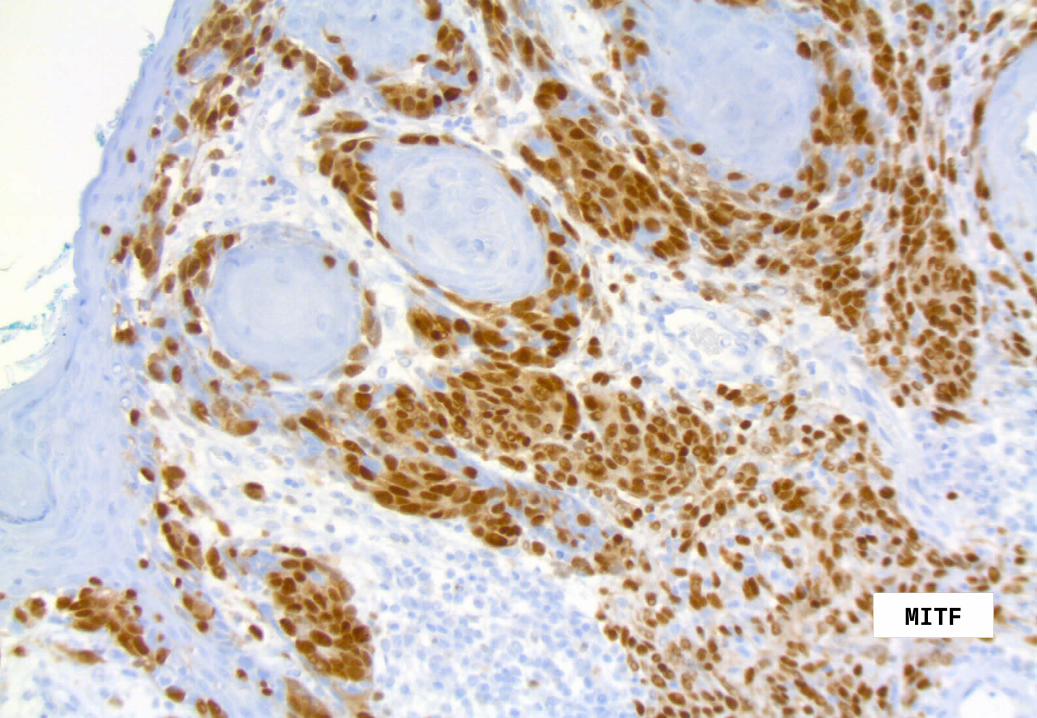
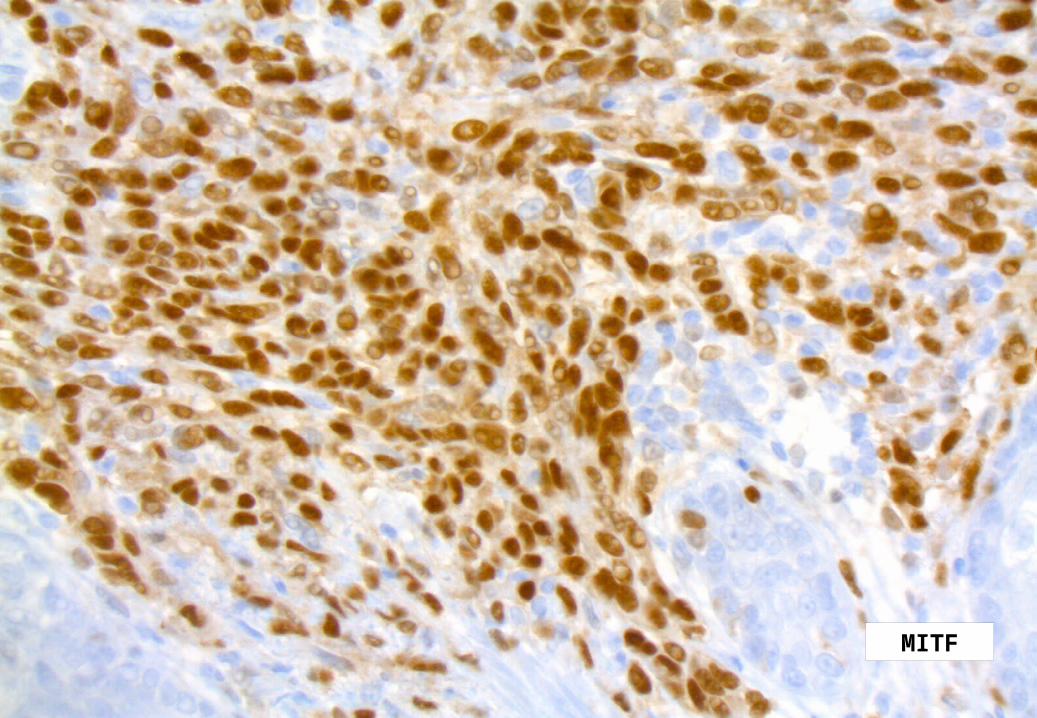
S-100, Melan-A, MITF, Ki-67 as follows:

25 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1S-100
26 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1S-100

27 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1 S-100
28 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
Melan A

29 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
Melan A

30 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
Melan A
31 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
MITF
32 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
MITF

33 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
MITF
34 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
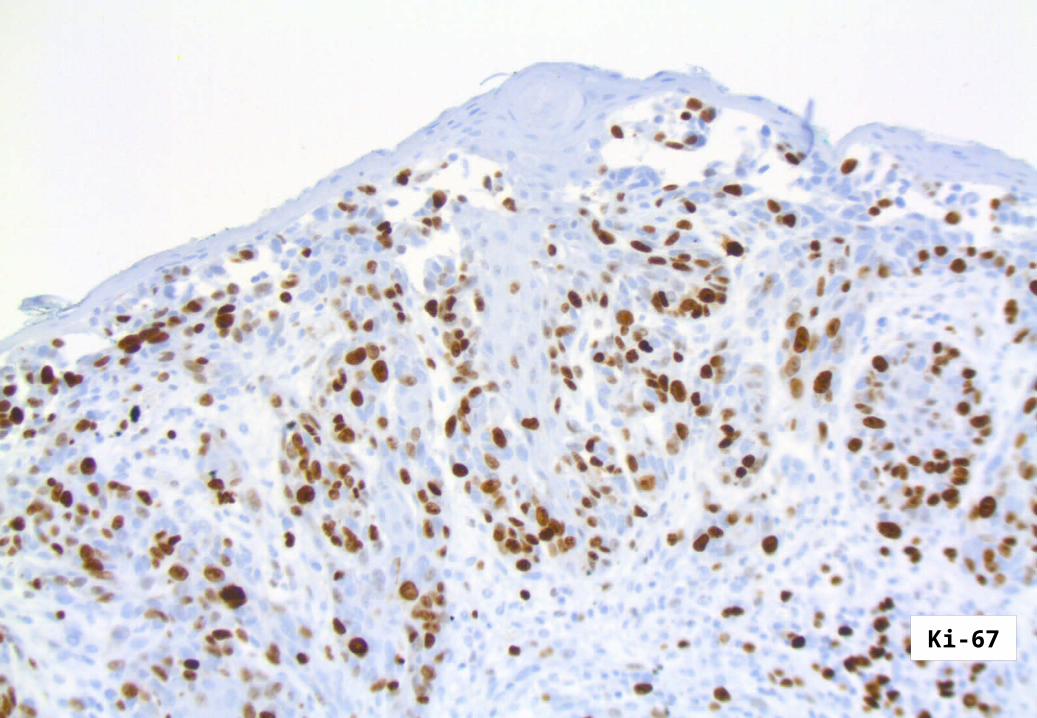
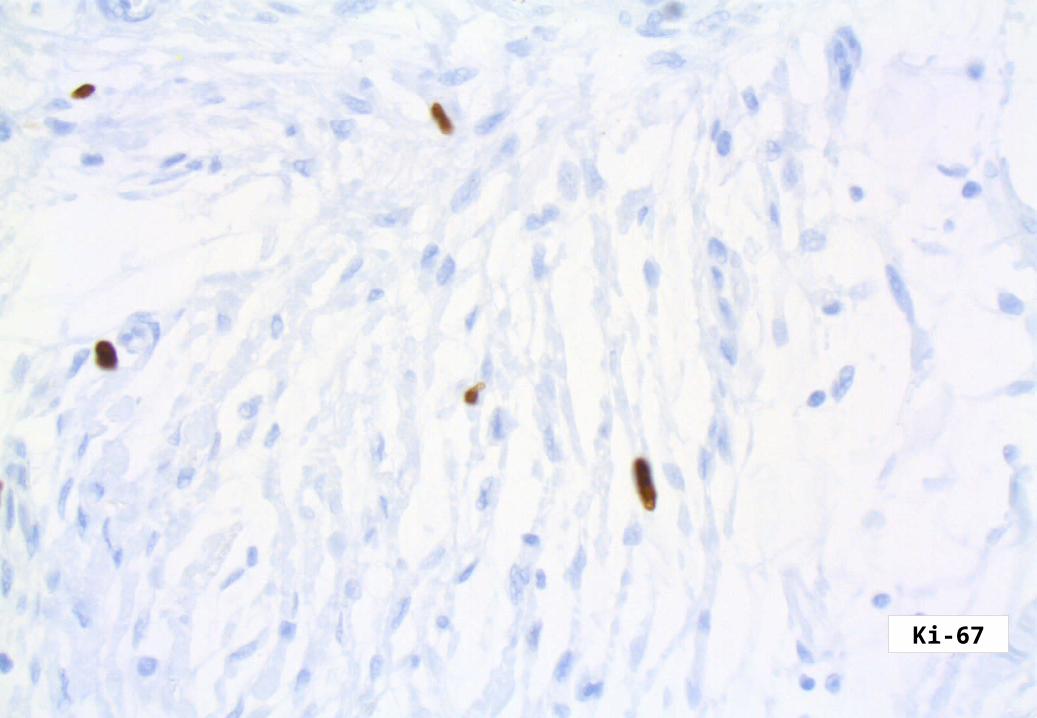
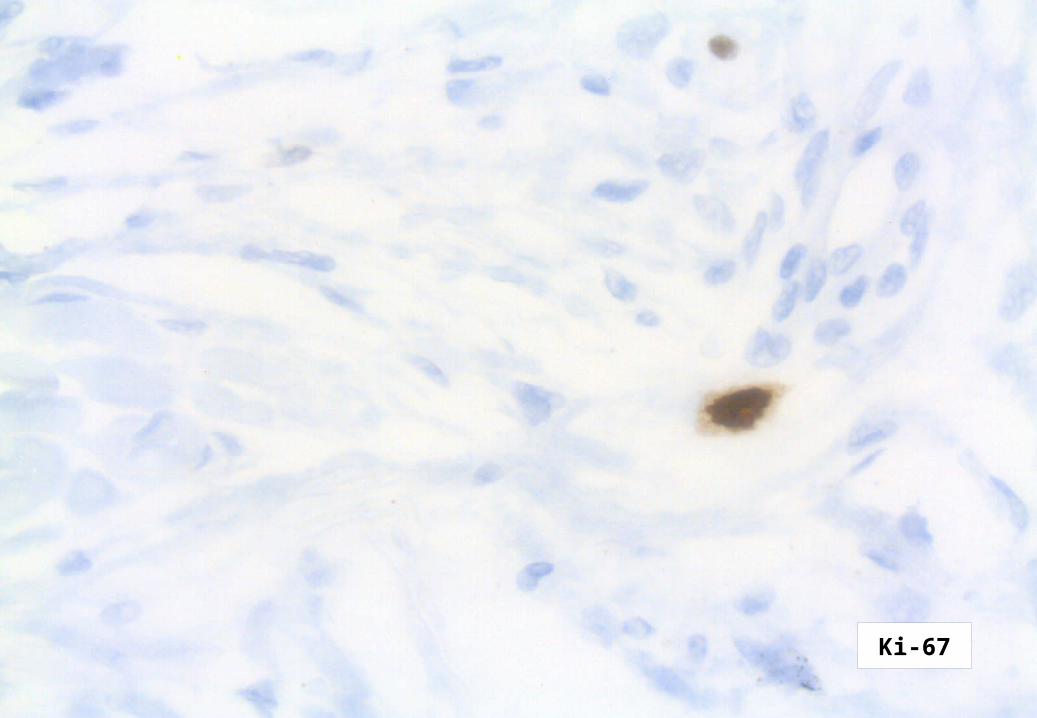
Ki-67
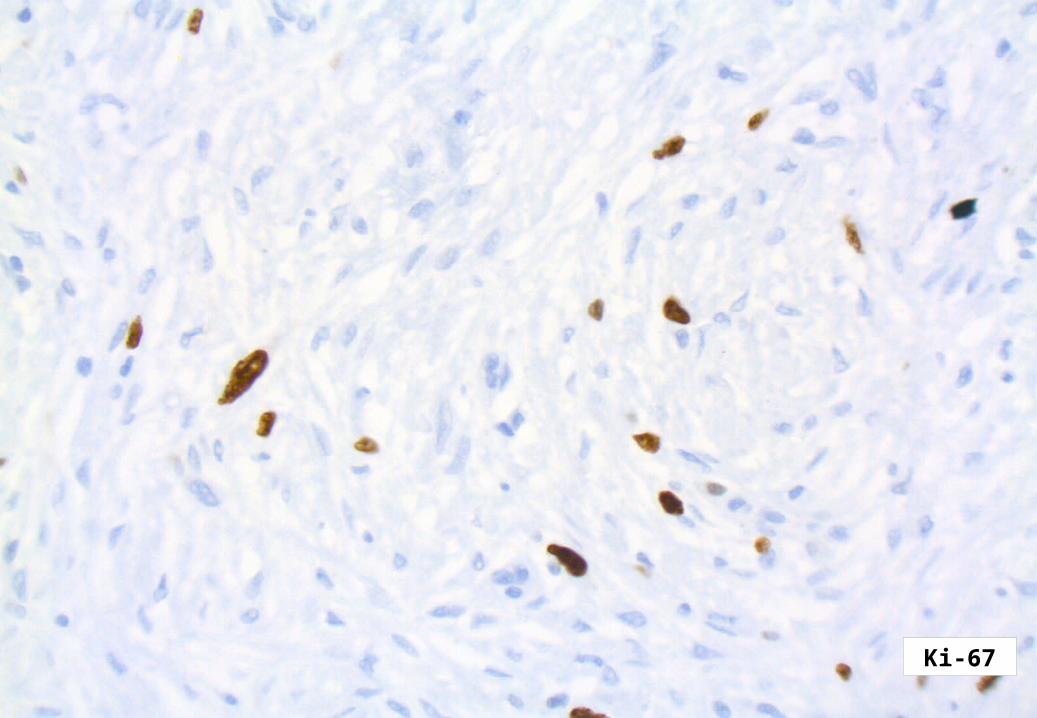
35 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1Ki-67
36 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
Ki-67
37 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
Ki-67
DIAGNOSIS:
DESMOPLASTIC MELANOMA

39 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA
First described by Conley J et al. Cancer, 1971.
Reed and Leonard; Neurotropic melanoma, a variant of DM showing neurotropism or neural differentiation. Am J Surg Pathol, 1979.

40 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA
Clinical appearance highly variable. May be mistaken for scar, fibroma, BC, sarcoma etc.
Sometimes pronounced mucin deposition. Wharton JM et al. Hum Pathol, 1999.
Tend to occur in the head and neck area (75% Carlson et al. Cancer, 1995) and upper back, but are also described in the vulva, gingiva and in acral locations.
Occur typically in older patients, mean ages in the larger published studies, 6th-8th decade.
41 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMAThere is a spectrum of morphological appearances, at one end the paucicellular scar-like variant with fairly bland cytology, scattered atypical nuclei and at the other end a high-grade sarcoma-like, pleomorphic lesion with only partial desmoplasia/collagenization and in between a neural-type-morphology with sometimes abundant myxoid matrix.
This variation in morphology most probably relates to clinical behaviour and have prognostic and therapeutic implications.

42 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Immunohistochemistry
Strong and homogenous staining (nuclear and cytoplasmic) for S-100, (as opposed to MPNST). Longacre TA et al. Am J Surg Pathol, 1996.
The majority of DMs are negative for the melanocyte differentiation markers HMB-45, Melan-A/Mart-1, tyrosinase, microphtalmia transcription factor.
However, focal staining may be present. Busam KJ et al. Am J Surg Patholm, 2001.
On occasion DM may show immuno-reactivity for SMA, desmin, factor XIIIa.
43 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Why desmoplasia?
The source of collagen is debated
- Myo-fibroblastic, reactive origin?
- Neoplastic cells with acquired collagen synthesis capacity?
- Or both?

44 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Differential diagnosis
Clinical : Almost anything! High index of suspicion; age, location, focal pigmentation.
Hisopathological : A plethora of cutaneous both benign and malignant tumors.
Scar, LMS, DFSP, neurofibroma, sclerosing blue nevus, desmoplastic Spitz nevus, MPNST, neurothekeoma, dermatofibroma, fibrosarcoma, spindle cell squamous cell carcinoma, pleomorphic fibroma, AFX, fibromatosis, leiomyosarcoma.
45 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Definitions
There is no consensus as to the extent of the paucicellular fibrosing neoplastic component in order to qualify for as DM.

46 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Definitions
Data from memorial Sloan-Kettering highlighting the importance of strict definitions. Pure (>90%) desmoplastic morphology is associated with longer disease-free survival. Busam KJ et al. Am J Surg Pathol, 2004.
The exact cut-off is not known.
One study suggesting that myxoid DM is associated with poorer prognosis than the classic fibrous paucicellular pattern. Payne WG et al. Am J Surg Pathol, 2001.

47 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Definitions
The term neurotropic melanoma bears some confusion and groups of NM in the literature most likely consist of different lesions, for example;
DM and non-desmoplastic MM with more or less extensive perineural involvement,
DM with Schwannian-/neurofibro(sarcomatous) morphology, so called ”neural transformation” (Arbiser ZK et al. Am J Clin pathol, 2001),
Intra-neural DM mimicking a primary peripheral nerve sheath tumor, ”nerve-centered DM” (Arbiser ZK et al. Am J Clin pathol, 2001).

48 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMAIs associated with a lesser risk for metastatic disease than conventional melanomas of similar depth. Tsao H et al Semin Cutan Med Surg 1997.
Infiltration around nerves (”hypercellular endoneurium”) may be found at significant distance from the main tumor mass.
Mitotic index usually low, average 2/10 HPF. In one series 10/28 cases no mitoses. Carlson et al. Cancer, 1997.
Usually non- or scarcely pigmented, however cases with heavy melaninization have been published. Brujin JA et al. Histopathol, 1992
Myxoid stroma may be excessive.
Osteoid and bone fromation may be seen, particularly in subungual DM. Moreno A et al. J Cutan Pathol, 1986.

49 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA
Mostly non-pigmented (60%) and if there is a usual-type MM, the most common type is LMM. Carlson et al. Cancer, 1995.
Local recurrence is common (30%) Malignant cranial neuropathy occurred in 4/58 patients. Smithers BM et al. World J Surg, 1992.
Neurotropism (i.e. perineural spread) strongly increases the likelihood of local recurrence. Large material, 280 patients. Quinn MJ et al. Cancer, 1998.

50 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Clinical features
Lens MB et al.; Large Meta-analysis, Br J of Dermatol, 2005.
All studies with 10 or more cases of DM; 17 papers; 856 patients.

51 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA
Follow-up for 15 studies.
Overall survival: 67-100%
Disease-free survival: 52-100%
Incidence of regional lymph node metastasis: 7% (no correlation with Breslow thickness.)
Incidence of local recurrence: 27%

52 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA
Incidence of local recurrence: Correlates with;
Breslow thickness < 4 mm: 19.5%
Breslow thickness > 4 mm: 40%
53 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Prognosis
Initially, based on Conley´s and Egbert at al´s series DM was thought of as ”highly malignant, stubbornly recurring and often metastasizing” (Conley).
Neither of these papers provided information on tumor thickness (or other prognostic parameters).
This concept began to change in 1988 (Walsh N et al. Arch Pathol Lab Med) and was substantiated by two papers in 1995. (Carlson JA et al. Cancer, Skelton HG et al. J Am Acad of Dermatol). Better prognosis compared to conventional MM of same Breslow thickness.
Further supported by Spatz A et al. Histopathol, 1998 and Jaroswewski DE et al. Am J Surg, 2001.
54 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Metastatic beaviour
DM with a component of conventional vertical growth phase MM have:
1. worse prognosis,
2. substantially increased frequency of regional lymph-node metastasis (10% vs 1%).
Disease specific 5-year mortality 11% for pure DM and 31% for those with hybrid morphology. Hawkins WG et al. Ann Surg Oncol, 2005.

55 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Lymph node metastasis
- 0/59 patients had positive regional metastatic disease (SLN biopsy or elective dissection) at the Mayo-Clinic Scottsdale and Rochester. Jarosewski DE et al Am J Surg pathol, 2001.
- 0/27 had positive SLN in the material from MSKCC. Gyorki DE et al. Ann Surg Oncol, 2003.
-Similar observations from University of Calif, San Francisco. Thelmo et al. J Am Acad dermatol, 2001.

56 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Distant metastasis
Most common first site of distant metastasis is the lung.
Incidence of systemic metastatic disease: 7-44%
Correlates with
1. local recurrences,
2. depth of initial lesion and with
3. non-desmoplastic melanoma component.
57 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
DESMOPLASTIC MELANOMA Morphology of metastasis
The morphology of mets do rarely show desmoplastic features, supporting the concept that it is preferentially the non-desmoplastic component that determines the risk for metastatic behavior.

58 B.F. Petersson MD PhD, Annual Slide Seminar, Bratislava June 21-23, 2007. Case 1
Thank you for the attention.