annual report pakistan initiative for mothers and newborns...
TRANSCRIPT

0
Annual Report
Pakistan Initiative for Mothers and Newborns (PAIMAN) Cooperative Agreement No. 391-A-00-05-01037-00
October 2008 to September 2009

1
TABLE OF CONTENTS
Acronyms 2 Message From the Chief of Party 5 Executive Summary 8 Summary of Targets and Results 12 INTRODUCTION 21 PAIMAN’s Vision of Success 22 PAIMAN’s Goal 22 PAIMAN’s Project Strategy 22 1. ACTIVITIES AND ACCOMPLISHMENTS 25 Strategic Objective 1: Increase Awareness and Promotion of Positive Maternal and Neonatal Health Behaviors 25
Strategic Objective 2: Increase Access and Community Involvement in Maternal and Neonatal Health Services 33
Strategic Objective 3: Improve Service Quality in the Public and Private Sectors, Particularly Related to Management of Obstetrical Care and Neonatal Complications 39
Strategic Objective 4: Increase Capacity of MNH Managers and Health Care Providers 44 Strategic Objective 5: Improve Management and Integration of Services at All Levels 46 2. GRANTS MANAGEMENT 48 3. MONITORING 51 4. EVALUATION AND RESEARCH ACTIVITIES 55 5. OPERATION RESEARCH 56 6. KNOWLEDGE MANAGEMENT 59 7. ADMINISTRATION 59 8. FINANCE 61 9. CHALLENGES AND CONSTRAINTS 64 ANNEXES: 65 Annex 1: JSI PAIMAN Staff 65 Annex 2: Status of Civil Works/Renovations 69 Annex 3: Reports and Documents 74 Annex 4: PAIMAN Organizational Chart 75

2
Acronyms ADHO Assistant District Health Officer AIOU Allama Iqbal Open University AKMCCC Aga Khan Maternal and Child Care Center AJK Azad Jammu and Kashmir AKU Aga Khan University ANC Antenatal care AMHS Assistant Manager Health Services AMTSL Active Management of Third Stage of Labor BCC Behavior Change Communication BHUs Basic Health Units BLS Basic Life Support CAI Child Advocacy International CAM Communication, Advocacy and Mobilization CBA Child Bearing Age CBOs Community-based Organizations CCA Client Centered Approach CCP Center for Communication Programs CDKs Clean Delivery Kits CEmONC Comprehensive Emergency Obstetric and Newborn Care CEO Chief Executive Officer CH Civil Hospital CMW Community Midwife CMWRA Currently-Married Women of Reproductive Age COP Chief of Party CS Clinic Sahoolats DAOP District Annual Operation Plans DCO District Coordination Officer DDOH Deputy District Officer Health DG Director General DHDC District Health Development Center DHMT District Health Management Teams DHQ District Headquarter DHQH District Headquarter Hospital DHSS District Health System Strengthening DHIS District Health Information System DMIS District Management Information System DNIT Draft Notice Inviting Tender DPC District Program Coordinator DPWO District Population Welfare Officer DOH Department of Health DSA Decision Space Analysis DSAS District Supervisory Assessment System EDHI EDHI EDO Executive District Officer EDOH Executive District Officer Health EmONC Emergency Obstetric and Neonatal Care

3
EMNC Essential Maternal and Newborn Care EPI Expanded Program on Immunization FATA Federally Administered Tribal Areas FOM Field Operations Manager FMTs Female Medical Technicians FP Family Planning (Birth spacing) GL GoodLife GMMMC Ghulam Muhammad Mahar Medical College GOP Government of Pakistan HCPs Health Care Providers HCWM Hospital Care Waste Management HIS Health Information System HIV/AIDS Acquired Immuno Deficiency Syndrome HMIS Health Management Information Systems HQ Headquarter HSO Health Services Officer HWMS Hospital Waste Management System IDP Internally Displaced Persons IEC Information, Education and Communication IP&C Infection Prevention and Control IPC Interpersonal Communications ITA Idara-e-Taraqi-o-Agahee JHU Johns Hopkins University JSI JSI Research and Training Institute, Inc. LHS Lady Health Supervisor LHVs Lady Health Visitors LHWs Lady Health Workers LQAS Lot Quality Assessment Surveys MCH Maternal and Child Health MIS Management Information System MNH Maternal Newborn Health MNCH Maternal, Newborn and Child Health MO Medical Officer MOH Ministry of Health MOIC Medical Officer In-Charge MOPW Ministry of Population Welfare MOU Memorandum of Understanding M/T Medical Technician M/w Midwife NATPOW National Trust For Population Welfare NGOs Non-governmental organizations NWFP North West Frontier Province OB/Gyn Obstetrics/Gynecology ORS Oral Rehydration Salts PAIMAN Pakistan Initiative for Mothers and Newborns PAVHNA Pakistan Voluntary Health and Nutrition Association PC Population Council PC - 1 Planning Commission - 1

4
PDQ Partnership Defined Quality PDHS Pakistan Demographic Health Survey PHSA Provincial Health Services Academy PHDC Provincial Health Development Center PHNS Public Health Nursing School PIMS Pakistan Institute of Medical Sciences PNC Pakistan Nursing Council PNC Postnatal Care PRISM Performance of Routine Information System Management PTV Pakistan Television Pvt. Private PWD Population Welfare Department PY Project Year QA Quality Assurance QI Quality Improvement RHC Rural Health Centers RMOI Routine Monitoring of Output Indicators SBA Skilled Birth Attendance SCUS Save the Children US SON School of Nursing SG Support Groups TAG Technical Advisory Group TBA Traditional Birth Attendant THQ Tehsil Headquarters THQH Tehsil Headquarter Hospital TOR Terms of Reference ToT Training of Trainer TT Tetanus Toxoid TVC Television Commercials UC Union Councils UNICEF United Nations Children’s Fund UNFPA United Nations Population Fund USAID United States Agency for International Development WHO World Health Organization WMO Women Medical Officers

5
Message from Chief of Party Improvement in maternal and child health continues to be a challenge for Pakistan. According to the Pakistan Demographic and Health Survey (PDHS) 2006-07, one in 89 women in Pakistan die of maternal causes. Although skilled birth attendance (SBA) has increased from 19% to 39% still 61% women do not have access to SBAs. While infant mortality has decreased by 32% in last three decades the progress is extremely slow, neonatal mortality has virtually remained constant over last four decades. The current estimate for Neonatal Morality Rates in Pakistan is 54 deaths for every 1,000 live births. The unmet need for family planning (FP) is 30%. Government of Pakistan has taken several steps to address these issues, however, the scale of challenge merits extra ordinary efforts to deal with the gigantic task of improving MNCH/FP situation in Pakistan. Pakistan Initiative for Mothers and Newborns- PAIMAN funded by USAID received generous support from people of the USA for the people of Pakistan during this year and became a truly integrated MNCH/FP project. The PAIMAN Project started with focus on maternal and newborn care in 2004, after four years of Project life child health and family planning was added to the scope of work and scale increased to 24 districts along with two FATA Agencies and two Frontier Regions. The total population increased from 13 million to 34 million. The year 2008-2009 was the most challenging year for PAIMAN. Project implementation continued in the initial districts whereas in additional districts the PAIMAN was introduced, strategic planning meetings were held we were in the process of hiring new staff as well as introducing child health and FP in all districts. The security situation in Swat worsened and in no time the residents of Swat, Upper Dir and Buner became IDPs. Project activities continued as we changed our strategy and hired local staff and worked through local NGOs. The IDP crisis changed the way the business was being run in NWFP. The sub-grantee NGOs working in Swat, Mardan and Charsadda who in one way were IDPs themselves worked day and night to run birthing centers in the camps. Skilled birth attendants were providing obstetric services and student CMWs/LHWs enrolled by USAID/PAIMAN joined hands and delivered babies, carried out antenatal and postnatal checkups. Fourteen NGOs covered 18 union councils with a plan of 64 mobile health camps a month. The geographic coverage was expanded to 49 union councils in July in consultation with EDO-H Mardan. From May 25 to August 16, 2009, PAIMAN sub-grantee NGOs organized 222 health camps and operated four birthing centers. Through these interventions 53,307 IDPs received basic health services, 76 babies were delivered, 1,209 pregnant women received TT immunizations, and 785 children were immunized. Additionally, 3,007 women were given antenatal care, 2,434 postnatal care and 942 received contraceptives. The situation improved in August and the sub-grantee NGOs along with IDPs from Swat went back. The 78 local NGOs are working as partners in areas which are not covered by LHWs. These NGOs provide support in community mobilization for TT immunization, orientation of 2,150 TBAs, holding joint health and population camps, etc. In the fifth year of PAIMAN we reached 4.96 million beneficiaries out of 5.4 million through inter-personal communication and 10 million people through mass media interventions. The 11,000 LHWs acquired communication and counseling skills to disseminate key MNCH/FP messages to the women in their catchment area. National Program for FP&PHC has decided to introduce Support Group counseling in their PC-1 revision so that this intervention is scaled up through out Pakistan. The communication strategy for MOH was designed and finalized which

6
includes all elements of PAIMAN’s Communication, Advocacy and Mobilization strategy. This is acknowledgement of the effectiveness of the strategy and guarantees sustainability of PAIMAN efforts. The 1,623 Community Midwives are enrolled out of which 446 graduated after 18 months of training in different provinces. It was a moment of great joy and happiness to witness the graduation ceremony of young women who have now established Midwife Homes in their community. Equipment was handed over to them in a simple ceremony along with guidelines to run their business and establish linkages with their nearest health facility. The early results of this intervention are encouraging and will surely help reduce the unacceptably high maternal and newborn mortality in Pakistan. Acknowledging the quality of CMWs training by USAID/PAIMAN, MOH and provincial health departments requested to train 226 master tutors. This support was beyond the PAIMAN district focus. Besides introducing a range of in-service training programs for public sector doctors and paramedics the skills and competencies of 22,318 HCPs have been enhanced according to their job description and 2,503 master trainers trained which is an indigenous resource established to continue MNCH in-service training programs. The trainings are reflected in the MNCH National Program and have been institutionalized through Provincial Health Development Center (PHDCs) and District Health Development Centers (DHDCs. The 89 selected health facilities have started functioning round the clock and have shown impressive improvements in performance. The human resource issues were dealt through a variety of ways: advocacy with district health government, post-graduate student rotation and placement, hiring on contract basis, and holding camps in collaboration with a teaching hospital in that district/province. In the draft Health Policy, the Pakistan Human Resource Strategy takes a prominent place with the hope to have the required number of female health care providers especially gynecologists and obstetricians. The 76 ambulances procured for handling maternal, newborn and child mortality have been handed over to the provinces to improve access to health services and minimize the time lapse in reaching the appropriate health facility. The 158 ORT corners, 86 Well Baby Clinics and 14 Baby Friendly Hospital Initiative are efforts to improve child health care. Child health indicators in the recent PDHS revealed that progress was static in the last decade. The capacity building of 90% of health facility (1,100) and community (650) staff is accomplished along with provision of protocols for management. This effort is being complemented in Punjab by organizing Maternal and Child Health Weeks twice a year. The integration of Health and Population Welfare activities were scaled up from one district pilot in a previous year to five districts. PAIMAN is tracking the progress on various selected health indicators through Routine Monitoring of Output Indicators (RMOI). Health services performance data collection is established in all 24 PAIMAN districts. Analysis of RMOI data shows 10% increase in deliveries, 41% increase in admissions of serious/life threatening obstetric complications, and a 2% increase in number of emergency C-sections performed at upgraded health facilities in Project Year 5 compared to Year 4. It also shows, at the district level, a 21% increase in pregnant women receiving two doses of tetanus toxoid (TT) immunization and 12% increase in mothers receiving pre-natal care in Year 6 compared to Year 4. The private sector initiatives and innovations to address the inherent systemic issues like enrolling 162 young women with Allama Iqal Open University (AIOU) and Idara-e-taraqi-o-taleem-o-agahee (ITA), Birthing Centers in non-functional BHUs as public private partnership will go a long way in addressing the diversity and specific issues that have hampered progress

7
in the past. The objective of PAIMAN is to show how we can address the issues of access and service delivery in challenging situations. In 2008-2009 PAIMAN has initiated operations research in consultation with MOH to understand the impact of interventions and provide evidence before scaling-up. The PAIMAN Technical Advisory Group (TAG) Meeting was held in Dubai due to security reasons. We got encouraging feedback from the TAG members like: to scale up Best Practices, make efforts undertaken by PAIMAN sustainable, and publish Project results. The “Best Practices Scaling- up National Policy Seminar” was organized in collaboration with White Ribbon Alliance Pakistan. The outcome of the meeting was buy in from MOH, MOPW, Provincial Health and Population Departments and Karachi Declaration was signed. This is a unique achievement which requires follow-up through provincial consultations to prepare operational plans. What makes the above achievements and progress impressive is working in an environment where security is a huge challenge, law and order situation is not optimal, uncertainty is looming all over. The staff motivation and support of public sector partners and communities has made it all possible. The lesson learnt is if program strategies are flexible and adjust according to the changing environment we can achieve program goals. As we enter the last year of PAIMAN project implementation the focus is on consolidation, integration, documentation and dissemination of what worked and where we still need extra efforts. With the hope that situation in Pakistan will improve and the PAIMAN efforts will bear fruit and help in improving the lives of women and children in Pakistan we feel huge responsibility and look forward to work as a TEAM as Together We Achieve More. Chief of Party PAIMAN Nabeela Ali

8
Executive Summary The Pakistan Initiative for Mothers and Newborns (PAIMAN) is a six-year project funded by USAID. PAIMAN is implemented through a consortium led by JSI Research & Training Institute, Inc. (JSI), in close partnership with a number of local and international organizations. PAIMAN’s initial mandate was to assist the Government of Pakistan to improve the status of maternal and newborn health in ten districts. In 2007 two Agencies of FATA, two Frontier Regions, and District Swat were added. In September 2008, USAID awarded the consortium an expansion of the Project, adding 13 more districts and increasing the scope of work to include child health and child spacing. PAIMAN is now an integrated maternal, newborn, child health and family planning project. The end-of-project date is September 30, 2010, and the budget US$ 92,900,064. In view of its programmatic and geographical expansion PAIMAN’s communication, advocacy, and Mobilization (CAM) strategy was revised to accommodate the expanded scope of work. Based on the theme, A healthy mother means a healthy family, this strategy promotes positive maternal, newborn, and child health behaviors. Expanding contraceptive choice and introduction of healthy timing and spacing of pregnancy are also included. In Year 5 PAIMAN organized 21 meetings for sharing and finalizing district-specific CAM action plans, one in each district. PAIMAN’s CAM strategy identifies ulama as an important communication channel for conveying MNCH messages to local communities. The National Research and Development Foundation, in collaboration with PAIMAN, implemented the third phase of the project, entitled Health of Mothers and Newborns-The Involvement of Ulama, in 12 districts of Punjab and NWFP. Ulama were identified around catchment areas of health facilities being upgraded by PAIMAN and rural areas with low LHW coverage. Individual consultation meetings were held with these ulama in four districts. The 13-episode drama serial Paiman, successfully aired during prime time on Pakistan Television and was preceded by an extensive marketing campaign. For international viewership, Paiman was subtitled in English. One dubbed in Pashto was aired on regional cable station KVT. ATV showed Paiman free of cost as a re-telecast. Clean delivery kits (CDKs) make at-home delivery cleaner and safer. PAIMAN partner, Greenstar marketed CDKs under the brand Clean Start. During Year 5, in PAIMAN districts, 76,748 CDKs were sold and 15,847 were distributed to TBAs as samples and incentive for detecting early warning signs and making timely referrals. Clinic sahoolat is a free consultation day performed by health care providers of the Greenstar GoodLife network. From 231 Clinic Sahoolats, 5,223 women benefited this year. In 2006, PAIMAN supported the MOH in training a core group of 44 master CMW trainers. Building on this core, PAIMAN trained an additional 12 CMW tutors this year. These master trainers trained 182 CMW midwifery tutors. PAIMAN enrolled 1,150 CMW students in Project Year 4, an additional 473 were enrolled in Year 5. Enrolled in March 2009, these CMW students hailed from the additional 14 PAIMAN

9
districts, mostly from existing midwifery schools. PAIMAN provided textbooks to 1,623 CMW students and initiated a three-month CMW practical training attachment at peripheral health facilities, enabling CMW students to become familiar with the environment in which they will be working after graduation. On January 12, 2009 PAIMAN held a National Consultative Meeting of the MNCH Program to discuss field deployment of newly-graduated CMWs. Placement guidelines were finalized; provincial meetings were organized for CMW deployment; equipment delivery and facilitation for midwifery homes were discussed. District-level handing-over ceremonies of PAIMAN-procured equipment to 150 new CMWs from eight districts were attended by provincial, district, and MNCH Program representatives. After receiving equipment, instruments, and furniture to establish midwife homes, CMWs began delivering MNCH services. PAIMAN community mobilization partners and sub-grantee NGOs introduced CMWs during events, themed Welcome, Midwife. Events focused on introducing to and building CMWs’ community image. TBAs oriented on clean delivery practices were introduced to CMWs. PAIMAN, MNCH Program, and other stakeholders are reviewing and finalizing midwifery practice monitoring and reporting tools developed by UNICEF. A 24/7 functional health facility is a key back-up support to community-level HCPs. By upgrading 32 selected health facilities in its first 10 districts, PAIMAN made them functional 24/7. In its new districts, PAIMAN is upgrading 55 more health facilities. Lack of essential staff is the largest hurdle for 24/7 operation of health facilities. Through PAIMAN advocacy efforts, the Government began placing essential staff at health facilities. To administer 24/7 services, MNCH Program’s PC-1 provides for one WMO and one LHV at RHCs. PAIMAN is supporting district health departments to deal with staffing by testing easy-to-scale-up, sustainable innovations, like the post-graduate trainee rotation program initiated in September 2009. PAIMAN and UNICEF signed a MOU to build HCP managers’ infection prevention and control (IP&C) capacity. Lady Aitcheson Hospital, Lahore was selected as a model hospital and training center for IP&C trainings. Two sets of trainings were designed, a three-day and a six-day. Year 5 saw 96 staff from upgraded health facilities in PAIMAN districts trained. During training, an IP&C plan for each facility was developed. To expand functional integration of services between Health and Population Welfare Departments to four additional districts, a consultative meeting was held. Secretaries of the Ministries of Health and Population Welfare, and representatives of the four selected provinces were present. Through field visits, data analyses, district- and provincial-level consultation, situational analysis reports were completed for the four districts. The reports were discussed through visits to the districts. Recommendations were finalized and implementation work plans prepared. In one national and four provincial and AJK TOTs, 122 community IMNCI master trainers were trained. Forty-seven extra were trained per National Program recommendation. In 195 batches 3,963 LHWs were trained on community IMNCI.

10
After sharing the district health management team concept with district authorities, DHMTs were successfully implemented in 14 new districts. As a health system strengthening intervention, individual meetings and two workshops with high provincial and district officials were held. Improved DHMT performance in all districts led to legislated adoption of DHMT models by six districts. After seeking agreements from national, provincial/regional, and district stakeholders, a full district health information system (DHIS) package was launched. It included trainings, supply of data collection instruments, and software support. A total of 2,405 health care providers from 15 districts of Sindh, Balochistan, AJK, and NWFP were trained in 100 district-level workshops.
A comprehensive community emergency ambulance services strategy was developed and procurement of 50 Suzuki Bolan vans to be converted to ambulances begun. Sub-agreements were signed with implementing NGO’s. Monitoring tools were developed and clustering/mapping of union councils completed. To improve access to MNCH services sub-grantee NGOs conducted 132 rounds of TT vaccination to vaccinate 243,974 pregnant mothers. To identify EPI defaulters 1,011 meetings were held. Defaulters were reached and motivated to be vaccinated. During the year 224 community-level medical health camps benefited 78,443 patients. Health camps provided services for basic ailments and, through Population Welfare Department representatives, family planning services were made available. In addition, health camps provided TT and EPI vaccinations. In response to the internally displaced persons (IDP) humanitarian crisis PAIMAN joined Ministry of Health, NWFP and various humanitarian agencies to provide immediate life-saving assistance. PAIMAN repositioned its 14 NWFP NGOs to provide health care to Mardan and Charsadda IDPs. PAIMAN NGOs worked in close collaboration with EDOsH on a two pronged strategy to provide essential health care to IDPs; 1) mobile health camps for IDPs living with host families and; 2) birthing centers for IDP families in camps. Eleven PAIMAN operations research projects, from simple field visits to carefully designed observation studies, were ongoing at the end of Year 5. These cover a broad range of activities designed to test new approaches, evaluate outputs and impact. In Year 5, Project expenditures were US$24.9 million with total Years 1 through 5 expenditures of US$58.4 million. As of September 30, 2009, there were additional US$2.4 million in accruals.

11
Challenges and Constraints Finding competent public health professionals for program implementation in remote, conservative districts was difficult. Compliance to USAID procurement regulations--the market research, approval of waivers, and international shipping took significantly longer than anticipated. CMW students identified from the 14 additional districts missed the PNC training cycle that began March 2009. They will not complete their 18 months training until September 2010. In the absence of a concrete plan for deployment and supervision of CMWs once in the field, about 100 were lost, as they either entered a lucrative job in their district, were hired by PPHI, or were married and moved out of their district. The security situation in NWFP in particular and Pakistan in general slowed pace of Project activities. Although other than Swat, Buner, and Upper Dir, no field office was closed, frequent threats and incidents forced a slowdown Project implementation.

12
Summary of Targets and Results Year 5 (October 2008-September 2009)
Cooperative Agreement 391-A-00-05-01037
Annual Target and Result by Quarter Year 5 (2008-2009) Life of Project Targets and Results by Year (2004-2010)
Result by Quarter Result by Project Year Remarks
Activity Target
QI QII QIII QIV Total PY5
Target
PY1 PY2 PY3 PY4 PY5 PY6 Total PYs1-5
SO 1: Increase Awareness and Promote Positive Maternal and Neonatal Health Behaviors
Communication Planning and Evaluation Training for Managers
Federal/provincial/district managers 34 0 0 0 0 0 160 0 39 26 28 0 93
Due to security situation lead facilitator could not visit Pakistan, this activity moved to PY6
Training of Journalists/ Ulama
Journalists 85 30 25 0 0 55 254 0 0 141 28 55 224 Activity carried forwarded to Year 6
Ulama trained/oriented 350 104 0 234 112 450 735 0 0 100 285 450 835 Life of project target achieved
Mass Media
Produce TV drama serial/series on MNCH issues (no. of episodes) 14 0 0 0 0 0 27 0 0 7 6 0 13
In consultation with the partners and with USAID approval, activity dropped and replaced with feature film
Produce and air district level talk show 13 0 0 0 0 0 35 0 0 12 0 0 12
Poor security in NWFP and Balochistan districts and government reorganization resulted in this activity begin dropped

13
Summary of Targets and Results Year 5 (October 2008-September 2009) Cooperative Agreement 391-A-00-05-01037
Annual Target and Result by Quarter Year 5 (2008-2009) Life of Project Targets and Results by Year (2004-2010)
Result by Quarter Result by Project Year Remarks
Activity Target
QI QII QIII QIV Total PY5
Target
PY1 PY2 PY3 PY4 PY5 PY6 Total PYs1-5
Produce and air radio talk shows 39 0 0 39 0 39 39 0 0 0 0 39 39 Life of project target achieved
Prepare, print and distribute district-specific PAIMAN brochures
14 0 0 9 5 14 24 0 5 5 0 14 24 Life of project target achieved
Produce and air MNCH music video 1 0 0 0 0 0 2 0 0 0 1 0 1
Music video is in production and will be released in Year 6
Develop concept for and produce MNCH/FP TV magazine show 7 0 0 0 0 0 13 0 0 0 0 0 0 Carried forward to
Year 6 Theater Performance
Community theater groups/performances 22 6 7 5 4 22 75 8 5 16 24 22 75 Life of project target
achieved
Stage plays at federal/provincial headquarters 2 0 0 0 0 0 7 0 0 2 1 0 3 Carried forward to
Year 6
Putlee Tamashas conducted in PAIMAN districts' rural communities
200 0 0 150 50 200 662 0 0 112 350 200 662 Life of project target achieved
Appoint goodwill ambassadors and support their activities 1 0 0 1 1 Life of project target
achieved Sensitization
Support village fairs 36 3 7 26 36 Life of project target achieved
Organize district assembly briefings on MNCH 14 1 2 4 3 10 34 2 5 7 7 10 31
Sensitize local line departments 516 4 387 125 516 Life of project target achieved
Sensitize CBOs and NGOs 362 9 212 141 362 Life of project target achieved
Sensitize village elders/opinion leaders (hujra/chopal meetings) 647 6 399 242 647 Life of project target
achieved
Sensitize parliamentarians, nazims, and DCOs 30 0 0 0 0 0 115 0 85 0 0 0 85
Due to security situation lead facilitator could not visit Pakistan, this activity carried forward to Year 6

14
Summary of Targets and Results Year 5 (October 2008-September 2009) Cooperative Agreement 391-A-00-05-01037
Annual Target and Result by Quarter Year 5 (2008-2009) Life of Project Targets and Results by Year (2004-2010)
Result by Quarter Result by Project Year Remarks
Activity Target
QI QII QIII QIV Total PY5
Target
PY1 PY2 PY3 PY4 PY5 PY6 Total PYs1-5
Sensitization meetings with local nazims and elected representatives 357 4 259 94 357 Life of project target
achieved Events for Community Mobilization (CM) Partners
Local MNCH CAM events organized 61 13 17 15 16 61 431 30 103 143 94 61 431 Life of project target
achieved
MNCH issue mega events organized 39 1 8 3 19 31 81 0 2 14 8 31 55
Due to security concerns eight mega events could not be organized and are carried forward to Year 6
CM - medical camps 11 2 3 3 3 11 50 0 0 6 33 11 50 Life of project target achieved
Support Group (Group Counseling)
Support groups (SG) organized 15,080 2,725 2,628 3,780 7,185 16,318 45,231 - -
9,792 20,359 16,318 46,469
SG meetings held 158,487 33,164 34,115 40,680 45,949 153,908 454,786 - 645
16,454 80,804 153,908 251,811
SG beneficiaries reached 1,584,870 315,942 425,492 467,771 504,299 1,713,504 4,770,226 - 6,450
267,760 927,186 1,713,504 2,914,900
Committee Meetings
Organize and support facility-based health committees (BHU, RHC,THQ)
209 8 53 79 22 162
Conduct facility-based health committee meetings (# of meetings)
368 8 53 75 90 226
Activities judged not cost effective and stopped after Year 4
Products
Market and sale of CDKs-samples 23,085 1,703 12,332 1,607 205 15,847 45,605 - 700
4,905 16,915 15,847 38,367
Market and sale of CDKs-commercial 62,600
8,553 33,236 27,118 7,841 76,748 124,395 - 4,300 22,895 34,600 76,748
138,543
Life of project target achieved
Interpersonal Communication (IPC)
IPC meetings 12,243 4,240 7,049 954 - 12,243 173,834 - 2,000
61,734 97,857 12,243 173,834
Life of project target achieved

15
Summary of Targets and Results Year 5 (October 2008-September 2009) Cooperative Agreement 391-A-00-05-01037
Annual Target and Result by Quarter Year 5 (2008-2009) Life of Project Targets and Results by Year (2004-2010)
Result by Quarter Result by Project Year Remarks
Activity Target
QI QII QIII QIV Total PY5
Target
PY1 PY2 PY3 PY4 PY5 PY6 Total PYs1-5
Beneficiaries 24,486 8,480 14,098 1,908 - 24,486 350,203 - 3,200
126,377 196,140 24,486 350,203
Services (Clinic Sahoolat)
Clinic Sahoolat provider outlets 231 80 133 18 - 231 3,022 - 40
904 1,847 231 3,022
Beneficiaries 5,082 1,840 3,059 324 - 5,223 67,871 - 200
19,800 42,789 5,223 68,012
Life of project target achieved
SO 2: Increase Access to and Community Involvement in MNCH Services
Improve Access to Health Facilities
GoodLife surgical clinics established 50 0 0 41 9 0 50 Life of project target
achieved Establish GoodLife non-surgical clinics 550 0 50 430 89 0 569 Life of project target
achieved Orient TBAs on clean delivery practices
Facilitators trained 22 22 0 0 0 22 50 0 0 28 0 22 50 Life of project target achieved
TBAs oriented by JSI 350 0 20 0 210 230 1850 0 0 1082 437 230 1,749
TBAs oriented by Greenstar 400 0 0 369 22 391 Life of project target achieved (JSI to train nine Upper Dir TBAs)
Emergency Transport
Ambulances for community-managed emergency transport system (RESAI)
50 0 0 0 0 0 50 0 0 0 0 0 0
Procurement started ambulances available first quarter Year 6
SO 3: Improve Service Quality in Both Public and Private Sectors
Up gradation Selected Health Facilities
DHQ Hospitals 100.0% 98.3% 98.7% 98.7% 98.6% 98.7% 100.0% 0.0% 0.0% 90.0% 98.2% 98.6% 98.6%
THQ Hospitals 100.0% 96.6% 97.4% 98.1% 98.1% 98.1% 100.0% 0.0% 0.0% 89.0% 96.4% 98.1% 98.1%
RHC/ BHU 100.0% 98.5% 97.7% 98.0% 97.9% 98.0% 100.0% 0.0% 0.0% 89.0% 98.3% 97.9% 97.9%
31 Health Facilities of the existing 10 districts

16
Summary of Targets and Results Year 5 (October 2008-September 2009) Cooperative Agreement 391-A-00-05-01037
Annual Target and Result by Quarter Year 5 (2008-2009) Life of Project Targets and Results by Year (2004-2010)
Result by Quarter Result by Project Year Remarks
Activity Target
QI QII QIII QIV Total PY5
Target
PY1 PY2 PY3 PY4 PY5 PY6 Total PYs1-5
Hospital Waste Management
Conventional incinerators provided 8 0 2 4 2 8 11 0 0 0 2 8 10
Swat incinerator could not be installed due to security situation
SO 4: Increase Capacity of MNCH Managers and Health Care Providers
Essential Maternal and Newborn Care (EMNC)
Master trainers trained (6 days) 75 0 51 19 0 70 145 0 70 0 0 70 140 Life of project target achieved
Health care providers trained (6 days) 507 30 22 186 245 483 2,201 0 440 652 587 483
2,162
Sibi training carried forward to year 6, unavailability of participants in planned month (Ramadan)
Health care providers who received refresher training (4 days) 122 500 0 0 17 356 122 495 Life of project target
achieved Training of EMNC monitors (1 day) 75 0 15 64 0 79 138 0 63 0 0 79 142 Life of project target
achieved
Comprehensive EmONC Trainings
HCPs who received CEmONC (2 weeks) 75 0 0 47 27 74 Life of project target
achieved
Specialist advance skill training 30 0 0 0 16 16 60 0 0 0 0 16 16 One training for 14 pediatricians carried forward to Year 6
Training of LHWs on SG Methodology
National/provincial level master trainers trained 45 0 50 0 0 50 82 0 0 37 0 50 87 Life of project target
achieved District level trainers trained 560
23 97 - 78 198 1,603 - - 741 302 198
1,241
LHWs trained 3,770 873 117 - 1,415 2,405 11,022 - -
3,419 3,833 2,405 9,657

17
Summary of Targets and Results Year 5 (October 2008-September 2009) Cooperative Agreement 391-A-00-05-01037
Annual Target and Result by Quarter Year 5 (2008-2009) Life of Project Targets and Results by Year (2004-2010)
Result by Quarter Result by Project Year Remarks
Activity Target
QI QII QIII QIV Total PY5
Target
PY1 PY2 PY3 PY4 PY5 PY6 Total PYs1-5
Community Midwifery Training
Master trainers trained for regular midwifery training new curriculum (4 weeks)
44 0 44 44 Life of project target achieved
Tutors trained for regular midwifery training new curriculum (4 weeks)
100 0 22 41 0 63 219 0 85 20 14 63 182
Tutors trained for refresher midwifery training (2 weeks) 22 0 22 0 0 0 22 Target for the life of
the project achieved HCPs receiving refresher midwifery training 233 36 55 0 126 217 730 0 80 417 0 217 714
Students enrollment CMW 18 month midwifery training-new curriculum
475 25 448 0 0 473 1,624 0 0 775 375 473 1,623 Life of project target
achieved Women supported for 8th grade education to become eligible to be LHWs
200 0 0 0 82 82 200 0 0 0 0 82 82
Women supported under matric (10th. grade) certificate to become eligible for CMW enrollment
80 0 0 0 80 80 80 0 0 0 0 80 80 Life of project target achieved
Training of Private Providers
Trained on essential maternal and newborn care 550 0 50 430 89 0 569 Life of project target
achieved Trained on advanced maternal and newborn care 50 0 0 41 9 0 50 Life of project target
achieved
Implementation of IMNCI trainings

18
Summary of Targets and Results Year 5 (October 2008-September 2009) Cooperative Agreement 391-A-00-05-01037
Annual Target and Result by Quarter Year 5 (2008-2009) Life of Project Targets and Results by Year (2004-2010)
Result by Quarter Result by Project Year Remarks
Activity Target
QI QII QIII QIV Total PY5
Target
PY1 PY2 PY3 PY4 PY5 PY6 Total PYs1-5
Trainers at provincial community IMNCI TOTs 75 0 0 20 102 122 75 0 0 0 0 122 122
Life of project target achieved. 47 extra trained on the advice of NP to have 2-3 trainers in each district. 20 provincial trainers trained during National TOT previous quarter
Participants district community IMNCI TOT 640 0 0 23 615 638 640 0 0 0 0 638 638
LHWs trained on community IMNCI 5,555 0 0 0 3,965 3,965 6,570 0 0 0 0 3,965
3,965
Trained at facility-based IMNCI trainings 1,100
39 111 253 421 824 1,100 0 0 0 0 824 824
Trained on IYCF 350 51 94 61 70 276 350 0 0 0 0 276 276
Client Centered Approach (CCA) for Delivering RH Services Training
District trainers receiving CCA TOT 27 27 0 0 0 27 27 0 0 0 0 27 27 Life of project target
achieved Doctors and paramedics receiving CCA training 400 0 82 155 125 362 400 0 0 0 0 362 362
Clinical Training Health Care Providers on CS Procedures non-FALAH districts
HCPs trained on IUCD insertion 116 0 0 54 66 120 116 0 0 0 0 120 120 HCPs trained on minilap 32 0 0 0 29 29 32 0 0 0 0 29 29 HCPs trained on vasectomy 32 0 0 0 28 28 32 0 0 0 0 28 28 Other Trainings

19
Summary of Targets and Results Year 5 (October 2008-September 2009) Cooperative Agreement 391-A-00-05-01037
Annual Target and Result by Quarter Year 5 (2008-2009) Life of Project Targets and Results by Year (2004-2010)
Result by Quarter Result by Project Year Remarks
Activity Target
QI QII QIII QIV Total PY5
Target
PY1 PY2 PY3 PY4 PY5 PY6 Total PYs1-5
HCPs trained on AMTSL and partograph use 370 0 79 62 93 234 618 0 0 0 268 234 502
Due to security situation in NWFP and Balochistan training could not be organized, other districts life of project targets achieved
HCPs trained on infection prevention 250 58 53 79 50 240 370 0 0 0 120 240 360
HCPs trained on essential surgical skills (MNCH/FP) 200 0 0 87 0 87 320 0 0 120 0 87 207
Ambulance staff (drivers and paramedics) trained in basic life support
100 0 0 69 0 69 220 0 0 0 122 69 191
Remaining targets are mainly from NWFP and Balochistan, therefore due to security situation these trainings could not be organized
District management staff trained in leadership skills 60 18 0 0 17 35 169 0 17 72 0 35 124
SO 5: Improve Management and Integration of Services at all Levels
Capacity Building of District Health Managers
Trained on strategic and annual operational planning 120 0 74 12 0 86 240 0 60 60 0 86 206
Trained in strategic annual operational plan preparation 57 0 0 0 57 57 Life of project target
achieved
Trained in logistical systems 46 0 0 32 14 46 Life of project target achieved
Trained in financial management 120 0 0 0 61 61 218 0 0 60 38 61 159
Trained in supportive supervisory 120 0 28 46 9 83 205 0 0 0 85 83 168 Non-availability of participants from district Peshawar due to IDPs
Trained/briefed district managers/planners on performance target setting
46 0 42 0 0 ` 46 0 0 0 0 ` 0

20
Summary of Targets and Results Year 5 (October 2008-September 2009) Cooperative Agreement 391-A-00-05-01037
Annual Target and Result by Quarter Year 5 (2008-2009) Life of Project Targets and Results by Year (2004-2010)
Result by Quarter Result by Project Year Remarks
Activity Target
QI QII QIII QIV Total PY5
Target
PY1 PY2 PY3 PY4 PY5 PY6 Total PYs1-5
Health Management Information System (HMIS)
District managers trained on evidence based decision making 157
78 79 157
Life of project target achieved
Trained on HMIS data collection tools and methods 1,240 0 1,240
1,240 Life of project target achieved
Received refresher DHIS data collection tools and methods training
4,095 0 0 1,223 1,010 2,233 4,059 0 0 0 0 2,233 2,233
Target is annual to be achieved by 2nd quarter. It could not be due to delay in finalization of manuals. Trainings for three NWFP districts could not be started due to security issues and in Punjab to delay in determining number of HCPs
Trainers receiving DHIS TOT 69 0 0 85 0 85 69 0 0 0 0 85 85 Life of project target achieved
Computer personnel trained DHIS software use 80 0 0 0 0 0 80 0 0 0 0 0 0
Delayed due to issues regarding DHIS software

21
Introduction to PAIMAN The Pakistan Initiative for Mothers and Newborns (PAIMAN) is a six-year project (2004–2010) funded by the United States Agency for International Development (USAID) as a Cooperative Agreement. PAIMAN is implemented through a consortium led by JSI Research & Training Institute, Inc. (JSI), a US-based public health organization, in close partnership with a number of local and international organizations. Partners include Aga Khan University (AKU), Contech International, Greenstar Social Marketing, Johns Hopkins University Center for Communication Programs, Pakistan Voluntary Health and Nutrition Association (PAVHNA), The Population Council, and Save the Children US. In addition, the National Commission for Maternal and Neonatal Health (NCMNH), the Midwifery Association of Pakistan (MAP), and Mercy Corps assist with specific Project areas. Partners and other collaborating organizations have extensive experience implementing maternal, newborn, and child health (MNCH) projects in Pakistan and globally, and together form an ideal team to implement this ambitious project. PAIMAN’s initial mandate was to assist the Government of Pakistan (GOP) to improve the status of maternal and newborn health (MNH) in ten districts of Pakistan through viable and demonstrable initiatives. In 2007 two Agencies of FATA, two Frontier Regions, and District Swat were added to the initial ten districts. In September 2008, USAID/Pakistan, through a modification of the Cooperative Agreement, awarded the JSI consortium an expansion of the Project, adding 13 more districts and increasing the scope of work to include child health and child spacing. Therefore, PAIMAN is now an integrated maternal, newborn, child health and family planning project (MNCH/FP). The end-of-project date for the expanded PAIMAN is now September 30, 2010, and the budget has been increased from US$ 49,943,857 to US$ 92,900,064. In the beginning of PAIMAN, a baseline survey and various formative research activities were carried out in the ten districts, studying issues such as access to health care, availability of services, and behavioral determinants of health-seeking behavior. The baseline survey findings proved useful in designing strategies around health care access, as the ten districts are extremely diverse in regards to culture, socioeconomic status, and geographic profile. Yet the designed strategy was not only tailored to the unique characteristics of PAIMAN districts, but also took into careful account issues such as sustainability, equity, quality, empowerment, and partnerships. The obvious choice in almost all districts was to work with both public and private sectors, with an emphasis on rural communities, as 67% of population resides there. Having just completed Project Year 5, JSI and its consortium partners have gone a long way towards addressing MNCH gaps and behavioral determinants. The range of innovative and diverse interventions used include designing a comprehensive communication strategy to reach a population of 14 million; working with lady health workers (LHWs) in rural areas and with local NGOs in areas where there were no LHWs; initiatives to reach private providers in urban centers; enabling young women to attend classes in order to qualify as community midwives; supporting civil works projects to improve health facilities; and working to improve district data health information systems. These efforts have been highly successful and well-received, and a number of assessments have indeed shown an increase in knowledge and skill levels and in positive health-seeking behaviors.

22
PAIMAN’s Vision of Success PAIMAN fully endorses the vision in the National Maternal, Child, and Neonatal Health Strategic Framework: “The Government of Pakistan recognizes and acknowledges the access to essential health care as a basic human right. The Government’s vision in MNCH is of a society where women and children enjoy the highest attainable levels of health and no family suffers the loss of precious life. Pakistan henceforth pledges to ensure availability of high-quality MNCH services to all, especially for the poor and the disadvantaged.” Islamabad Declaration in National Maternal and Child Health Policy and Strategic Framework (2005-2015), Ministry of Health, April 2005. PAIMAN’s Goal The PAIMAN Project will directly contribute to reducing maternal, newborn and child mortality in Pakistan through viable and demonstrable initiatives. These include the capacity building of existing programs and structures within Pakistan’s health systems and communities to ensure improvements and supportive linkages in the continuum of health care for women from home to hospital. PAIMAN’s Project Strategy Effective MNCH care consists of a continuum of interventions, beginning before pregnancy and covering the prenatal, delivery, and post-partum periods, and addressing the individual health of women and children. In the Pakistani context, in order to have an immediate effect on mortality rates, the focus must be on the labor, delivery, and immediate postpartum period—from the onset of labor through day seven. PAIMAN therefore promotes skilled attendance as the long-term goal for all deliveries in Pakistan. The MNCH literature speaks of the "three delays" which contribute to maternal and newborn death. The first is delay in seeking care, which may occur because the woman must wait for permission from the family decision-maker because she knows the family can’t afford the costs or she doesn't recognize that her pregnancy is in trouble. The second delay regards transportation, which may be unavailable or take too long. The third delay is in receiving care—a woman might arrive at a facility only to find no staff, inadequate equipment, and no blood for a transfusion. PAIMAN opts for a multi-pronged strategy, with attention to all three delays. MNCH outcomes are influenced by factors other than health care alone. The public health evidence base clearly shows maternal, newborn and child survival depends upon a range of socio-cultural, economic, and geographic determinants, all of which must be considered within the Pakistani context. Determinants must be addressed in order to develop comprehensive and sustainable solutions to address maternal, newborn and child mortality. PAIMAN supports an integrated, evidence-based, and multi-pronged approach combining individual health care with public health and community-based interventions. This approach is summarized in the “The Pathway to Care and Survival,” which outlines the steps necessary to increase the likelihood of maternal, newborn and child survival in the event of a complication or illness.

23
PAIMAN Pathway to Care and Survival
Goal: Healthy Mothers and Children in Pakistan
The Pathway to Care and Survival
Increased
Awareness/BCCIncreased Access
Strengthen
Quality
Improved
Management &
Service Integration
•Communitybased Obstetricalcare
•Communityinvolvement
•Barriers to healthcare for women
•Reduce transportcosts and time
•Involve privatesector providers
•Introduce client-focused services
•Standard protocolsand guidelines
•Referral systemsand quality control
• Infection control
• Improve facilitiesand equipment
•Curriculum design
•Conduct mastertraining
•Training of CMW
• Training of TBAsand LHWs
• Training of careproviders
•Pre-servicetraining
•BCC campaigndevelopment
•Research formessagedevelopment
•Use allcommunicationchannels
•Create supportiveenvironment
• Policy environmentand strengthenmanagement systems
•Increasingaccountability to thecommunity
•Use health informationsystem and evidence-based management
•Logistic systems
•Supportive supervision
•Private/PublicPartnerships
•Integrated health systems
GuidingPrinciples:
•Involvementof allstakeholders
•Buildingintegratedsystems
•Developmentof scale-upactivities
•Addressinggenderinequalities
•Building onlessons learned
Increased
Capacity
Step 1: Recognition of Problem
Step 2: Decision
to seek care
Step 3: Transport to
health care setting
Step 4: Get timely and
quality careSURVIVAL
Step 4: Get timely and
quality care
The PAIMAN Project’s strategic objectives are to:
• Increase awareness and promote positive maternal and neonatal health behaviors. • Increase access to and community involvement in maternal and neonatal health services. • Improve service quality focusing on management of obstetrical, neonatal, and child
health complications. • Increase the capacity of district maternal, newborn, and child care providers and
managers. • Improve management and integration of health services at all levels.
After the initial phase of putting in place the required support systems and undertaking a program of massive institutional and individual capacity building, PAIMAN is now seeing positive results of these efforts. As discussed in the monitoring and evaluation section of this report, PAIMAN has made substantial progress, as translated in its main output indicators such as prenatal care, tetanus-toxoid (TT), and postnatal care coverage. One exception is with the skilled birth attendance indicator, which has not increased significantly. To address SBA, two main strategies are being implemented: (1) the community midwife (CMW) initiative and (2) the up-gradation of referral facilities providing 24/7 MNCH services. Both require substantial investment of time. As explained in detail under sections 2 and 3 of this report, setting up and providing an 18-month CMW training program, in addition to

24
renovating and equipping 89 health facilities, are time-consuming. It is therefore anticipated that substantial results in SBA attendance will be seen only after Project Year 5. The following sections provide a summary of activities undertaken and the input, process, and output results for each.

25
I. ACTIVITIES AND ACCOMPLISHMENTS 1. Increased Awareness and Promote Positive Maternal and Neonatal Health Behaviors Communication approaches such as behavior change communications and social marketing represent systematic attempts to influence the health of populations. There goal is to bring improvements in health through awareness raising and the promotion of positive behaviors. PAIMAN communication and advocacy activities include mass media campaigns, interpersonal communications, and events to raise the public’s awareness of key issues.
1.1 Formative Research After the extension in PAIMAN’s scope of work, there was a need to conduct research on the new areas. Johns Hopkins Center for Communication Programs (CCP) designed a formative research based on behavioral issues surrounding child health. Questions pertain to knowledge, attitudes, self-efficacy, cultural norms, malnutrition, diarrhea/dehydration, acute respiratory infections, and routine immunization of children under 5 years of age. As answers were not found during extensive literature review of latest available research on child health, CCP launched a Request for Assistance to prospective research agencies for conducting formative research. Research is planned in Year 6 for Districts Charsadda and Sibi of NWFP and Balochistan Provinces, respectively. It is anticipated research will measure existing knowledge and attitudes and explore perceptions regarding key child health practices. Barriers and facilitating factors regarding positive health practices pertaining to child health will also be highlighted.
1.2 Review and Revise CAM Strategy In view of its programmatic and geographical expansion, CCP revised the Communication, Advocacy, and Mobilization (CAM) strategy to accommodate the expanded scope of work and feedback from ongoing community-based activities. Based on the theme, A healthy mother means a healthy family, this strategy promotes maternal, newborn, and child health behaviors revolving around birth preparedness; recognition of danger signs during pregnancy, delivery, and post-partum period; exclusive breastfeeding; home-based neonatal care; recognition of acute respiratory infection; danger signs in infants and children under 5 years of age; and use of ORS for diarrhea. Expanding contraceptive choice and introduction of healthy timing and spacing of pregnancy are also included in the revisions. The CAM strategy addresses a number of cross-cutting themes to support these core behaviors.

26
1.3 Communication, Advocacy, and Mobilization Action Plans PAIMAN district-based teams organized 21 meetings for sharing and finalizing district-specific CAM action plans, one in each district. Meetings were attended by LHW Program district coordinators, assistant district health officers, medical superintendents, JSI field operations managers (FOM) and/or district program coordinators (DPC), and sub-grantee NGO and Government line department representatives. District-specific maternal and newborn health status and a matrix of PAIMAN CAM activities for the year were shared. 1.4 Develop and Implement a National CAM Strategy CCP continued providing strategic support to the National Program for Family Planning and Primary Health Care. CCP technical assistance was instrumental in establishing and strengthening the Program’s Research and Publication Cell, which it supported to design, conduct, and analyze formative research to modify the existing behavior change communication (BCC) strategy. Ten focus group discussions were conducted with 105 LHWs and their supervisors in five districts of four provinces and Azad Jammu and Kashmir (AJK). CCP also provided input to the evaluation of maternal-focused psycho-educational approach to promote exclusive breastfeeding, an approach tested in a cluster-randomized controlled trial in NWFP Project districts. Revised Planning Commission (PC)-1 on communication strategy for the second five years included recommendations from these researches. CCP worked with the National Program to develop the Urdu newsletter, Raabta , which provides LHWs with the latest information on health care issues with community-level remedies and care. CCP editorial support to the three issues printed so far were effective as educational resources and motivation for the 110,000 LHWs and their supervisors. Raabta was also translated, printed, and distributed in Sindhi. With CCP support, the National Program also developed a quarterly advocacy publication, Integrated Primary Health Care Communiqué, for national and international partners. 1.5 Information, Education and Communication Materials for Households and Communities District Brochures. CCP revised the district-based brochures for the first ten Project districts to include family planning and child health issues and latest updates on maternal and newborn health. District brochures for 14 new Project districts were also prepared, printed, and distributed to all district-based partners.
District‐based brochure of Sibi District‐based brochure of Vehari
CCP developed an advocacy kit, PAIMAN – After the Promise. Its 19 one-pagers were each devoted to a specific intervention and arranged according to the Project’s five strategic objectives. This kit was shared with national and international partners at the 4th PAIMAN Technical Advisory Group meeting. The second edition included more initiatives under PAIMAN, especially women support groups, knowledge management and leadership, and client-centered services. This kit was distributed at the 36th Annual Conference of the Global Health

27
Council in Washington, D.C. It is an excellent repository of various innovative PAIMAN interventions over the last five years. To celebrate Breastfeeding Week, CCP designed a brochure with messages about the importance of breastfeeding. Also developed were eye catching banners with breastfeeding messages. LHWs distributed brochures to target audiences. Banners and streamers captured attention of people in Project districts. Flyers to build community awareness. Using extensive civil works, PAIMAN renovated or reconstructed maternity wards, labor rooms, operation theaters, and nurseries at selected health facilities in the first ten Project districts. This tremendously improved service provision for obstetrical emergencies. To assure target populations were aware of these upgraded health facilities and services, one-page flyers for each facility, highlighting its full range of available services and timings were designed, printed and distributed. MNCH Messages for All. CCP established a network of 700 ulama who promote MNCH through interactions with their disciples and general public. To support these efforts, a pamphlet with key MNCH message was designed and distributed for ulama to use to supplement their verbal messages. Because human figures are not appreciated by the vast majority of ulama, special hand drawings using symbols depicted content. These handouts serve as reminders to Friday sermon audiences and for other messages delivered by ulama. 1.6 Communication Interventions through Mass/Traditional Media Campaigns. The 13-episode drama serial Paiman, successfully aired during prime time on Pakistan Television and was preceded with an extensive marketing campaign using leaflets, posters, branded vehicles, and street announcements. For each episode, more than 150 callers participated in the quiz competition. At the end of the series, prizes were awarded to lucky winners. For international viewership, Paiman was subtitled in English. One dubbed in Pashto aired on regional cable station KVT. The leading Urdu satellite channel, ATV, showed Paiman free of cost as a re-telecast, assuring wider coverage. A set of five television commercials (TVCs) with a range of maternal and newborn health messages were produced. They were aired in two rounds on terrestrial and various national and regional cable channels, including PTV Home, ATV, Khyber TV, KTN, AAJ TV, Sindh TV, and Hum TV. To reach a wider audience, these TVCs were dubbed in Pushto and Sindhi languages. Radio adaptations were also produced and broadcast over the leading FM and MW channels across the country. As a sequence to the previously-produced TVCs, PAIMAN commissioned a renowned media agency to produce two new TVC, which will highlight importance of exclusive breastfeeding and management of diarrhea in children. Focusing on child health issues, CCP developed a music video. It is being directed by an award-winning director of Pakistan and will feature the country’s leading music and show business talent.

28
CCP developed a television magazine show that focuses on MNCH issues. In this 13-episode show, notable celebrities were invited to share stories related to MNCH and high- ranking senior officials from relevant ministries and organizations shared opinions. Each show featured a documentary based on true MNCH stories from the field. Pre-production was completed and production is underway. In July 2009, PAIMAN launched production of a feature film to highlight the importance of family planning for individual and household health and wellbeing. After elaborate discussions, the project was cleared by all stakeholders and production began. First showing is planned for July 11, 2010, World Population Day. Video-on-Wheels. Provision of electricity in rural and far-flung areas of Pakistan is limited. When available, power outrages are common. Television signals cover less than 100% of Pakistan and TV ownership is less than 60%. These conditions make any electronic media intervention limited in scope and confined to those who have electricity and TVs. To overcome these constraints, PAIMAN experimented with an innovative intervention. Video-on-Wheels shows selected episodes of drama series Paiman, its music video, and TVCs. Video-on-Wheel uses big screens in specially-designed tents for men and women in far-flung and remote Project areas. The pilot test, conducted in Sukkur, will be extended to additional districts in Sindh and Punjab Provinces. Urdu episodes were shown during the pilot, but in subsequent shows, dramas dubbed in local languages were shown for greater audience response. Through the elaborate marketing and mobilization efforts of PAIMAN partners, each show was enjoyed by 300 to 500 men and women who sat separately under the same tent. Putlee tamasha (puppet shows), the indigenous form of community media, are used by PAIMAN to disseminate maternal and child health messages. With child health and family planning added to PAIMAN’s scope of work, story lines were also changed to include the new interventions. Use of puppets as MNCH messengers added another medium of communication while maintaining traditional richness. More than 200 putlee tamasha were performed in rural areas in Project districts of Punjab and Sindh Provinces. Theater group performances organized at Punjab, Sindh and Balochistan health facilities were attended by 7,771 participants (3,721 men and 4,050 women). Health managers from provinces and districts participated. 1.7 CAM Advocacy Campaigns In connection with Father’s Day, a television talk show on the Role of Men in Promoting MNCH was produced by Adetude and aired free of cost. Hosted by Ms. Samina Pirzada, a popular media personality, participants included Dr. Aitzaz Ahsan, a well known politician, and Mr. Mushtaq Minhas, the host of a famous talk show Bolta Pakistan. Support to White Ribbon Alliance-Pakistan (WRA-P) an independent, non-profit, non-political professional organization established to advocate for MNCH in Pakistan was supported by PAIMAN. It is affiliated with the Global White Ribbon Alliance for Safe Motherhood based in Washington, D.C., which has the mission to save women’s and newborns’ lives. PAIMAN has been assisting WRA-P in becoming a viable and effective advocacy forum. PAIMAN supported WRA-P to consolidate selected high-impact best practices for improving MNCH and family planning and developing advocacy material. CCP also helped WRA-P secure funding for various projects.

29
Ulama Project. PAIMAN’s CAM strategy identifies ulama as an important communication channel for conveying MNCH messages to local communities. The National Research and Development Foundation, in collaboration with CCP, implemented the third phase of the project, entitled Health of Mothers and Newborns-The Involvement of Ulama, in 12 districts of Punjab and NWFP. Ulama were identified around catchment areas of health facilities being upgraded by PAIMAN and rural areas with low LHW coverage. Individual consultation meetings were held with these ulama in four districts. Due to security alerts and threats, DI Khan meetings had to be delayed. In the third phase of the Ulama Project, the Senior Ulama Central Advisory Committee was reconstituted to become more vibrant and effective, with across-the-board ulama representation. Ulama intervention continued with the same zeal despite challenging security situations. The special phase of the Project for District Swat was completed under extremely difficult conditions. The Project sensitized ulama on MNCH issues and motivated them to spread MNCH messages through their sermons and lectures. The booklet, Role of Ulama in Ensuring Mother and Child Health in Pakistan, was revised. Its second edition contains endorsements from several influential Pakistani religious personalities as well as information on MNCH issues. It is used as a primary resource during ulama consultations and group meetings. CCP asked ulama to suggest improvements; these will be incorporated in the third edition. Sensitized ulama effectively disseminate MNCH messages during Friday sermons and daross (sermons for ladies only). Follow-up visits to ulama continued with the objective to reinforce the importance of MNCH and role of ulama in social issues

30
Commitment to Enhance Coordinated Efforts for Improving Maternal, Newborn, Child Health and Family Planning in Pakistan
Pakistan has sustained efforts over the years to improve maternal health and family planning services, but the progress has been slow for want of holistic approach and lack of evidence based policy input. It continues to have one of the highest maternal mortality rates with estimates varying from 276 to750 deaths per 100, 000 births. The situation for newborns is similar, with a child mortality rate of 94 per thousand life births. There is a need to accelerate efforts to improve maternal and newborn health. A 32 member Pakistan Country Team with representatives from MOH, MOPW, national and international organizations, and development partners participated in a technical meeting on MNCH-FP Best Practices in Bangkok in September 2007. At the meeting more than 400 participants shared their experiences and best practices. The Pakistan team presented high-impact MNCH/FP best practices that could be scaled up in Pakistan.
PAIMAN steered efforts for scaling up MNCH/FP Best Practices through a series of meetings the last two years by the Pakistan Country Team. In September 2009 White Ribbon Alliances-Pakistan, at the request of PAIMAN, organized a policy level seminar. This event, held in Karachi, brought together health and population welfare stakeholders to reach an agreement, the historic Karachi Declaration on Scaling up MNCH-FP Best Practices in Pakistan, through the federal, provincial and district level operational interventions. The progress made in advancing a common MNCH approach is an important milestone to harness desired results within the shortest possible time. The next crucial step is to convert the recommendations of the seminar into implementable action points. It is hoped that through further persuasion/assurance/support and collective reviews birth spacing goals required to ensure improvement in MNCH health in Pakistan can be achieved

31
Journalist Intervention. Assisted by implementing partner Intermedia, CCP organized the Second National MNCH Award ceremony. Chief Guest, Mir Aijaz Hussain Jakhrani, Federal Minister for Health, conferred awards to winning electronic and print journalists. This event coincided with an alumni meeting of PAIMAN-trained journalists from various areas of Pakistan and Project districts. A draft manual was developed for journalist training on methodology and techniques for reporting on MNCH issues. Articles on maternal health by renowned journalists, most of who were sensitized by PAIMAN, were published in the country’s leading newspapers. PAIMAN Video Presentation. Comparing the present with the pre-Project situation and based on successes and innovations in each strategic objective, CCP developed a comprehensive PAIMAN video presentation, PAIMAN-After the Promise. Containing clips of various interventions, mass-media products, community interventions, and capacity building/trainings, it was first shown at the PAIMAN TAG meeting. Interviews of beneficiaries highlighting impact, animated slides of impact statistics, and visuals of intervention areas and localities present PAIMAN’s success story to national and international forums. Updated to include detailed Project activities, the modified version was shown by the JSI-PAIMAN COP at the Global Health Council Conference. It concludes with highlights of future courses of action to improve lives of mothers and children in Pakistan. 1.8 Mobilizing Communities PAIMAN launched ceremonies at provincial and district levels to induct new Project districts. Each ceremony was preceded with provincial/district consultative meetings, attended by Provincial Health Secretaries, DG Health, National Program provincial coordinators, and MNCH Program and EPI managers. EDO Health/District Health officers from the new districts also participated. The health facilities for up-gradation were agreed on by consensus. A number of community mobilization activities, such as mega-events, local events, and theater performances, were conducted across PAIMAN districts. A total of 47 local events for 9,565 men and women, 31 mega events for 26,305 men and women, and 22 theater performances for 7,771 men and women were conducted in Year 5. Activities raised community awareness regarding positive reproductive health behaviors, increased coordination between facility staff and community, and encouraged community members to utilize available services. PAIMAN employed creative activities and presentations to generate interest needed to effectively deliver MNCH messages, including healthy baby shows, stage performances, youth gatherings, quiz competitions, and stalls by PAIMAN partners and sub-grantee NGOs, local NGOs/CBOs, and line departments. PAIMAN district teams in Punjab actively participated in Child Health Week. Activities included de-worming of 350,000 children 2-5 years of age and routine vaccination of 0- to 2-year-olds. Pregnant ladies were provided antenatal care and TT vaccinations. LHW support groups conducted more than 37,000 health education sessions. To increase MNCH awareness, printed materials were distributed in communities. In collaboration with Health Departments, PAIMAN organized 11 melas (health camps) for 3,635 women and children. Gynecologists, pediatricians, and other physicians provided free preventive and curative medical services to remote communities, which face difficulty in accessing the services.

32
1.9 Monitoring CAM Activities At the PAIMAN CAM Thematic Group meeting, CCP presented Impact Evaluation Report of Media Products. The report focused on selected media activities, including the 13-episode TV drama series, TVCs, and PAIMAN music video. Data from content analysis of drama scripts, viewer group discussions, and a population-based quantitative survey were from Districts Rawalpindi, Sukkur, and Jafarabad. Nearly 41 percent of currently-married women of reproductive age (CMWRA) demonstrated behavior change towards positive maternal outcomes that resulted from exposure to the drama series and TV spots. More than 71% reinforced their learning from the TV dramas by advising others in their social networks to take specific actions promoted by the dramas. To assess effectiveness of the Ulama Project, an evaluation was done in Districts DG Khan and Khanewal. Comprised of secondary and primary data collection, information was generated on qualitative and quantitative aspects. Focus remained primarily on how effective Friday sermons are for communicating health-related messages. Findings affirm ulama are open to development issues and can be effective in BCC campaigns. Level of knowledge of respondents exposed to health messages is 25% higher than those not exposed. 1.10 Advocacy and Coordination Campaigns Health care providers (HCPs), including newly-inducted CMWs, in Project districts were trained in active management of the third stage of labor (AMTSL) and use of partographs. PAIMAN encouraged Health Department and health facility (HF) staff to keep records of AMTSL practice and partograph use in labor rooms. Regular monitoring by MNCH Program district coordinators and PAIMAN FOMs reported increased use of partograph and AMTSL in HFs across the districts. To ensure coordination of all PAIMAN activities, 52 meetings with local sub-grantee NGOs and PAIMAN partners were held this year, with 508 staff members participating. During these quarterly meetings, participants shared quarterly and bi-monthly progress reports and work plans, identified challenges, and proposed solutions. A key PAIMAN activity involves working with the LHW Program to support and counsel women on MNCH and family planning. By working with the LHW Program, 15,812 support groups were organized through trained LHWs and 153,908 support group meetings provided 1,713,504 women with information and support. PAIMAN staff monitored 5,046 support group meetings and 1,090 health committees meetings. 1.13 Social Marketing for Health Clean delivery kits (CDKs) make at-home delivery cleaner and safer by providing the health attendant with all necessary equipment in one convenient package. Each package contains a plastic sheet, cord clip, gloves, razor, soap, and instructions. CDKs have proved particularly useful in low-income areas lacking hospital facilities. Main clients are traditional birth attendants. Greenstar marketed CDKs under the brand Clean Start. During Year 5, in PAIMAN districts, 76,748 CDKs were sold and 15,847 were distributed to TBAs as samples and incentive for detecting early warning signs and making timely referrals. Greenstar promoted the GoodLife network by using community and mass media. GoodLife network symbolizes quality services by qualified and trained HCPs to mothers and children. TV commercials’ theme highlighted the importance of health care for the whole family and the role

33
of family males. GoodLife advertisements were shown on local cable networks and GoodLife hoardings were displayed at 14 locations in five districts. Greenstar interpersonal communication (IPC) interventions are based on CCP’s latest formative research, with strategies outlined in the CAM strategy. IPC increases informed demand for availability of low-cost or free MNCH GoodLife provider services and increases awareness among low-income populations of required preventive behaviors to improve obstetric outcomes. During visits, the IPC teams share MNCH messages using brochures and counseling cards. Clinic sahoolat is a free consultation day performed by HCPs of GoodLife networks. To prepare, outreach workers visited HCP catchment areas and invite target groups to visit the clinic for care. These clinics provide free consultation and are a tool for HCP quality assurance. Effective IPC generated supportive community response and increased number of women and children participants in Clinic Sahoolat. From 231 Clinic Sahoolats, 5,223 women benefited this year. Greenstar reached out to 24,486 beneficiaries during 12,243 interpersonal communication meetings, during which MNCH messages were given and birth preparedness docu-dramas were shown on portable DVD players. 2. Community-Based Obstetric Care Services: Community Midwives Skilled attendance at all births is considered the single most critical intervention for ensuring safe motherhood. Skilled birth attendance ensures timely delivery of emergency obstetric and newborn care when life-threatening complications arise. It denotes not only the presence of community midwives, but also the enabling environment they need to perform capably. Considering Pakistan’s high maternal, infant, and child mortality rates and that SBA is the most important intervention for their reduction PAIMAN is supporting the Ministry of Health in training 2,354 CMWs. PAIMAN trained a core group of 44 master trainers, developed training material for training of midwifery tutors, trained 182 midwifery tutors, and developed training material and lesson plans for rollout CMW training. PAIMAN provided textbooks to 1,623 CMW students in public and private schools and developed and distributed quality assurance and monitoring tools for CMW training to all development partners and the National MNCH Program. PAIMAN initiated a three-month CMW practical training attachment at peripheral health facilities, enabling CMW students to become familiar with the environment in which they will be working after graduation and to obtain first-hand community experience. 2.1 Selection and Enrollment of CMW Students PAIMAN enrolled 1,150 CMW students in Project Year 4. To achieve life-of-Project (LOP) target of 1,624, an additional 473 were enrolled in Year 5 (LOP total 1,623) . Enrolled in March 2009, these CMW students hailed from the additional 14 PAIMAN districts, mostly from existing midwifery schools. New schools selected to achieve target were:
• Public Health School Abottabad • School of Nursing (SON) DI Khan • SON Vehari • SON Khairpur • Public Health School Quetta • Public Health School Sibi • Public Health School Chitar Pari Mirpur, AJK

34
Midwifery tutors of new schools were trained at Pakistan Institute of Medical Sciences (PIMS), Islamabad during the January-March quarter. These new schools were also provided logistics support before classes began. CMW student selection, strictly adhering to Pakistan Nursing Council (PNC) criteria, is made by the district selection committee chaired by the EDO Health. A PAIMAN representative also sits as a member. Rural union councils, where CMW students were required to be enrolled, were identified and their details provided to the selection committee. In December 2008, subject union councils advertised in national and local newspapers for candidates. After scrutiny of applications and short listing per PNC criteria, candidates were interviewed. The Lady Health Worker Program provided spot verification of those selected. Students joined respective schools in March 2009.
PAIMAN-Supported CMW Schools and Students (December 2006-March 2009)
School Batch 1 (12/06)
Batch 2 (03/07)
Batch 3 (06/08)
Batch 4 (03/09)
Punjab
SON Holy Family Hospital, Rawalpindi 34 34
SON DHQ Hospital, Rawalpindi 33
SON RGH, Rawalpindi 36 28
PHNS, Jhelum 35 34
Paramedical School, Jhelum 40 15
SON Lady Wellington Hospital, Lahore 43 33
SON Lady Aitcheson Hospital, Lahore 40 25
SON UCH, Lahore 42
PHNS, DG Khan 35 36 38
PHNS, Bahawalpur 37 31
SON DHQ Hospital, Khanewal 36 35
PHNS, Multan 35 34 55
SON, Vehari 50
Sindh
CMW students attending practical training session, SON, Sindh Qatar Hospital, Karachi

35
PAIMAN-Supported CMW Schools and Students (December 2006-March 2009)
School Batch 1 (12/06)
Batch 2 (03/07)
Batch 3 (06/08)
Batch 4 (03/09)
Sindh Qatar Hospital, Karachi 14
PHS, Karachi 43 15
PHS (HANDS), Karachi 20
AKHSP Midwifery School, Karachi 50 29 18
PHS, Hyderabad 46 19
AKMCC, Hyderabad 24 17
Midwifery School (HANDS), Hala 20
PHS, Sukkur 21 15
SON, Khairpur 45
Balochistan
PHNS, Quetta 24
PHNS, Sibi 8 NWFP
PHNS Nishterabad, Peshawar 30 16 PHNS Hayatabad, Peshawar 23 30
PHNS, Mardan 26 40 PHNS, Swat 22 24
PHNS, Abottabad 24 PHNS, DI Khan 45
AJK PHNS, Chitar Pari Mirpur 20
190 585 399 449
TOTAL 1,623
2.2 Training Midwifery Tutors In 2006, PAIMAN supported the MOH in training a core group of 44 master CMW trainers through the International Confederation of Midwives and World Education. Using this core, PAIMAN continued supporting training of CMW tutors. During Year 5, 12 CMW tutors, three each from Districts DI Khan and Khairpur, two each from Abottabad and Mardan, and one each from Vehari and Peshawar, trained at Training Center, PIMS, Islamabad. Two more sessions were organized at MCH Center, PIMS, March 31-April 25 for 19 participants and May 19-June 13 for 22 from NWFP, Balochistan, and AJK. Most tutors were from the seven new CMW training schools. Also trained this year were women medical officer (WMO) and lady health visitor clinical tutors involved in CMW practical training
Midwifery tutor attending clinical training session, delivery room PIMS Islamabad

36
attachment at peripheral health facilities. Tutors were provided guidelines for practical and community training. A contract for post-training assessment of trained midwifery tutors’ knowledge and skills was awarded to the School of Nursing, Aga Khan University, Karachi. Assessment tools were developed and finalized. Field work will begin November 2009. 2.3 Supervision, Monitoring, Quality Assurance of Midwifery Training PAIMAN-developed monitoring and quality assurance tools for the CMW training program are used by all PAIMAN FOMs and program staff during routine field visits. To improve training quality, they discussed issues and problems with principals, tutors, and CMW students. Hands-on trainings at peripheral health facilities were also monitored and meetings held with health facility in-charges and focal training persons. In joint visits with MNCH Program Coordinator to PHNS, Multan; Lady Wellington Hospital,
Lahore; and SON, Khanewal to assess training quality, PAIMAN-supported schools were found well equipped and feedback from school staff and students very encouraging. During every visit, use of partograph and AMTSL were observed and discussed. During FOM visits, tutors and clinical staff jointly met to resolve clinical coordination and hands-on practice issues. For health managers such as MS, EDO Health, Director MCH, PC National MNCH Program, and Director General (DG) Health, PAIMAN prepared simple, user-friendly monitoring tools. Conducting supervisory visits to CMW training programs alone or with PAIMAN support, health managers monitor training quality and administrative and logistic aspects, especially students’ labor room and gynecology, obstetrics, and pediatrics wards’ duty rosters. Visits help ensure staffs’ day and night presence to supervise training. On June 15, 2009, the third batch of PAIMAN-sponsored CMW students from Punjab and Sindh began community-based practical training at peripheral facilities in respective districts. A one-day training/orientation for clinical staff from these health facilities was conducted before students’ placement. To help clinical staff understand their role and responsibilities, practical training guidelines were discussed. 2.4 CMW Graduation In January 2009, 446 CMWs from Punjab, Sindh, and Balochistan schools graduated. The PAIMAN-organized first graduation ceremony at Nishtar Medical College, Multan on February 7, 2009 was attended by Secretary Health, Punjab, who was Chief Guest.
CMW class Sindh Qatar Hospital. Karachi
Punjab, Secretary Health addressing CMW graduation, Multan

37
The second for Sindh CMWs occurred on May 5, 2009, the International Day of the Midwife, in collaboration with National MNCH Program, Sindh. Approximately 700 participants included Chief Guest, Health Minister Dr. Sagheer Ahmed; Sindh Assembly members; Ms. Humera Alwani, Secretary Health; Mr. Muhammad Hussain Syed, Special Secretary Health; Dr. Capt. Abdul Majid, DG Health-Sindh; Dr. Abdul Sattar Korai, PD National MNCH Program-Sindh; and PAIMAN COP, Dr. Nabeela Ali. For 100% graduation, PAIMAN awarded computers with printers to PHS, Karachi; HANDS School, Hala; and Aga Khan MW School, Kharadar. PAIMAN awarded Certificates of Appreciation to the four best CMW tutors and five top CMW students. The third PAIMAN-organized graduation ceremony was on June 11, 2009 at Serena Hotel Quetta for 38 CMW students from Jafarabad and Lasbella. Mr. Qayum Nazar Chagazi, Secretary Health-Balochistan was Chief Guest. More than 450 guests included DG Health, other senior Health and PWD officials and COP PAIMAN. 2.5 Field Deployment of CMWs On January 12, 2009 at its Islamabad office, PAIMAN held a National Consultative Meeting of the MNCH Program to discuss field deployment of newly-graduated CMWs. Chaired by National Coordinator, National MNCH Program, the meeting included Population Council, MNCH Program, PAIMAN, and UNICEF representatives. Placement guidelines were finalized. Provincial meetings were organized for CMW deployment. Equipment delivery and facilitation for midwifery homes (MWH) were discussed. Deployed in Districts Rawalpindi, Jhelum, Khanewal, DG Khan, Dadu, Sukkur, Lasbella, and Jafarabad during July-September 2009 were 150 new graduates. District-level handing-over ceremonies of PAIMAN-procured equipment to new CMWs were attended by DG Health, DCO, EDO-Health, and provincial and district MNCH Program representatives. After receiving equipment, instruments, and furniture to establish midwife homes, CMWs began delivering MNCH services. On the day they received MWH equipment, CMWs were oriented on procedures for communicating with the nearest health facility able to provide essential emergency obstetric and neonatal care (EmONC) services. For emergency referrals, contact numbers of transporters and
CMWs taking oath during graduation ceremony, Quetta
Midwife Home equipment before handover, EDO Health Office, Sukkur

38
referral facilities are displayed at MWHs. Nearly all CMWs have access to a mobile phone and were requested to maintain close communication with referral facilities in case of emergencies. Local sub-grantee NGOs aid CMWs with their community placement. TBAs oriented on clean delivery practices through local NGOs were introduced to CMWs. Through its community mobilization partners and sub-grantee NGOs, PAIMAN created CMW, LHW, TBA, and local health facilities linkages. Community mobilization partners and sub-grantee NGOs introduced CMWs during events, themed Welcome, Midwife. Events and mega events focus on introducing to and building CMWs’ image. PAIMAN, MNCH Program, and other stakeholders are reviewing and finalizing midwifery practice monitoring and reporting tools developed by UNICEF. A mechanism for communicating, reporting, and supporting was pre-tested by UNICEF at MWHs.
For Year 5, PAIMAN planned a study tour to Indonesia for policy makers and health managers. As several years ago, Indonesia started a similar CMW model, the tour aim was to learn issues and challenges Indonesia faced in scaling up and lessons learned. The tour is now planned for January 2010. Population Council began operations research for CMW supervisory model and placement. Two models proposed are franchise and MNCH Program, in which CMWs work under the National MNCH Program. 2.6 Women’s Accelerated Educational Program In partnership with National MNCH Program and Idara-e-Taleem-o-Aagahi, a local NGO working on education, PAIMAN began educational support that enables graduates to enroll in CMW training after matriculation. A pilot Grade 10 matriculation course was designed to meet pre-requisites for induction into CMW training. The course is for 80 female students from NWFP (Buner, Charsadda, DI Khan, Upper Dir) and Balochistan (Sibi, Zhob, Jafarabad, Gwadar). After JSI signed a cost reimbursement agreement with ITA, students were enrolled and the educational training commenced in preparation for matriculation exams to be held in March 2010.
Training of teachers for accelerated educational program in Balochistan
Dr. Nabeela Ali, COP PAIMAN, with Dr. Zahid Larak (L), NC MNCH Program, speaking with CMWs during equipment handing over ceremony at EDO-H office, Rawalpindi on
September 2, 2009

39
MOU signing ceremony with AIOU
A memorandum of understanding (MOU) signed with Allama Iqbal Open University (AIOU), Islamabad provides educational support so young women can upgrade their education through Grade 8. They then can be selected as LHWs. This initiative is conducted in NWFP (Upper Dir, Peshawar, Buner, DI Khan, Swat, Mardan, Charsadda) and Balochistan (Lasbella, Gwadar, Jafarabad, Sibi, Zhob, Quetta). AIOU training of Balochistan teachers on the condensed course was completed. Study sites were selected and student training will start the first week of October 2009. 3. Facility-based Obstetric Care Services: Back-up Support for Community-based Health Care Providers 3.1 Health Facilities Functioning 24/7 A 24/7 functional health facility is a key back-up support to community-level HCPs. Without it, community-level interventions can not succeed. By upgrading 32 selected health facilities in its first 10 districts, PAIMAN made them functional 24/7. In its new districts, PAIMAN is upgrading 55 more health facilities. PAIMAN regularly advocates providing support to district Health Departments to make all selected health facilities functional 24/7. Duty
rosters are regularly displayed, emergency medicines are available, ambulances are ready to transport emergency cases, and essential equipment is present. Routine Monitoring of Output Indicators data show that because health facilities are functional 24/7, patient turnover increased. Lack of essential staff is the largest hurdle for 24/7 operation of health facilities. Through PAIMAN advocacy efforts, the Government began placing essential staff at health facilities. At district-level, NWFP Provincial Health Department deployed nurses, resulting in the new, functioning Gynecology and Obstetrics Unit at DHQ Hospital, Upper Dir, previously non-existent due to staff shortage. Provincial MNCH Programs are pursued to help place rural health center (RHC) staff. To ensure 24/7 RHC services, EDOs Health-Upper Dir and Buner placed LHVs and nurses on general duty. To administer 24/7 services, MNCH Program’s PC-1 provides for one WMO and one LHV at RHCs. WMOs are now available at RHC Kandhra, Sukkur and THQ Hospital KN Shah, Dadu.
PAIMAN-renovated and equipped pediatric nursery, DGQ Hospital Daggar, Buner

40
EDO Health-Jhelum sent a senior WMO from THQ Hospital Sohawa, Jhelum for training at DHQ Hospital, Jhelum to enable her to perform C-sections at the THQ Hospital. In Punjab, most WMO, LHV, and nurse positions were filled through the provincial MNCH Program, improving health facility functioning. Using a scoring matrix, PAIMAN quarterly tracks health facilities’ 24/7 functioning. In the first 10 PAIMAN districts, with completion of civil works and supply of about 90% of equipment, 95-99% of selected health facilities are functional 24/7. Frequent HCP transfer and posting at these health facilities is a major challenge. As provision of necessary staff is one area requiring innovation, PAIMAN approached teaching hospitals for attachment of post-graduate trainees at selected hospitals. Specialist doctor and private sector specialist visits were also explored. Scoring of the 31 functioning health facilities operating 24/7 during 2008-2009 follows. DHQ Hospitals
Balochistan Sindh NWFP Punjab
DHQ Uthal DHQ Dera Allah Yar
DHQ Dadu
DHQ Sukkur
DHQ Daggar
DHQ Dir Khas
DHQ Khanewal
DHQ DG Khan
DHQ Jhelum
97% 97% 99% 100% 99% 98% 99% 99% 100% THQ Hospitals
Balochistan Sindh Punjab
THQ Hub
THQ Usta Mohd.
THQ KN Shah
THQ Rohri
THQ Mian Channu
THQ Tounsa Sharif
THQ Murree
THQ Gujar Khan
THQ Sohawa
98% 95% 93% 99% 99% 99% 100% 100% 100% RHC and BHU
Balochistan Sindh NWFP RHC Bella
RHC Rohjan Jamali
RHC Sita Road
RHC Kandhra
RHC Barawal
RHC Jawar
RHC Wari
RHC Chamla
99% 97% 100% 100% 94% 96% 96% 95%
Punjab RHC Kacha Khu RHC Choti Zarin RHC Mandra RHC Domeli BHU Kali Matti
99% 99% 100% 100% 100% 3.2 Innovations to Meet Human Resource Issues Post-graduate Trainee Rotation and Training of Hospital Technical Staff PAIMAN is supporting district health departments to deal with staffing by testing easy-to-scale-up, sustainable innovations. A post-graduate trainee rotation program was initiated in September 2009 at THQ Hospital Shujabad in collaboration with Nishtar Hospital, Multan. A second post-graduate rotation at DHQ Hospital Uthal and THQ Hospital Hub, District Lasbella through collaboration with Sindh Qatar Government Hospital, Karachi is ongoing.
Prof. Sher Shah performing vaginal hysterectomy at THQ Hospital Rohri District Sukkur on May
27, 2009

41
The post-graduate trainees program initiated in 2008 at THQ Hospital Murree in collaboration with Holy Family Hospital, Rawalpindi was extended to July 2009. Patient turnover and ANC, C-section, and normal vaginal delivery services increased tremendously. Three or four post-graduate gynecology and obstetrics trainees and an anesthetist residing at these hospitals on monthly rotation provide 24-hour basic and comprehensive obstetric care services. Besides an increase in patient turnover, to sustain future service level and quality, EmONC capacity of existing staff is being enhanced. Previously-posted local WMOs regularly assist with C-sections and have performed some under post-graduate and surgeon supervision. Availability of an anesthetist at the Civil Hospital Multan was ensured through a temporary contract. One THQH Shujabad medical officer received three months’ anesthesia training at Nishtar Hospital Multan. In collaboration with Sindh Qatar Government Hospital, Karachi, PAIMAN supported improving skills of two newly-graduated gynecologists at Jafarabad via a six-month contract posting of a gynecologist there. At the request of Medical Superintendent, DHQ Hospital Upper Dir, two anesthesia technicians were trained in spinal anesthesia at Lady Reading Hospital, Peshawar. With PAIMAN support, a private sector anesthetist placed at THQ Hospital Rohri, Sukkur from January 2009 serviced all emergency and elective C-sections. With support of Pakistan Society of Obstetricians and Gynecologists, PAIMAN placed for six months one gynecologist each at THQ Hospital Hub and DHQ Hospital Uthal, District Lasbella. Each trained, and mentored local staff on providing EmONC services. Specialist Health Camps. To build hospitals’ image and attract community utilization, PAIMAN, in collaboration with medical colleges and teaching hospitals, organized specialist medical camps at various hospitals, which coincided with mega community mobilization events. One camp was organized at THQ Hospital Mian Channu February 19-21, 2009. Based on an agreement between PAIMAN and the Principal, Nishtar Medical College, seven
Nishtar Hospital specialists attended. A three-day camp was conducted with the Lady Wellington Hospital, Lahore team at
Post-graduate trainee examining a patient at THQ Shujabad Multan
THQ Murree specialist medical camp inauguration by Mr. Saeed Elahi, Advisor to Chief Minister Punjab, and Mr.
Hanif Abbasi, Member National Assembly

42
THQ Hospital Sohawa, May 21-23, 2009. Before the camp, one WMO and a staff nurse trained on pre-operative care, C-section, and post-operative care at Lady Wellington Hospital, Lahore. In collaboration with the Sindh Qatar Hospital Karachi, PAIMAN organized a specialist medical camp at DHQ Hospital, Uthal, Lasbella, June 15-17, 2009. The 18 surgeries performed included six tubal ligations, utero-vaginal prolapse, abdominal laparotomy, and one C-section. A camp at THQ Hospital Rohri, Sukkur, May 25-27, 2009, saw 1,706 patients. Of them, 1,217 were females, 247 males, and 242 were under 5 years of age. Free medicines from the hospital dispensary were provided and 22 females were registered and admitted for surgeries after screening. Prof. Dr. Sher Shah and team performed 21 operations, including 16 vaginal hysterectomies, two abdominal hysterectomies, two vesico-vaginal fistula repairs, and one ovarian cyst removal. With support of Nishtar Medical College Multan, Rawalpindi Medical College Rawalpindi and Sin-Qatar Hospital Karachi, a free three-day specialist medical camp was arranged at THQ Hospital Murree, THQ Hospital Shujabad, and THQ Hospital Burewala. Gynecologists, pediatricians, and anesthetists from tertiary care hospitals provided free consultations and performed emergency and elective surgery. With the assistance of Population Welfare Departments and SCUS, family planning services and community mobilization sessions were conducted. The resulting community trust in hospital-provided MNCH services increased utilization. PAIMAN also began building the public image of selected health facilities. Brochures prepared for each of 31 upgraded health facilities were distributed during community mobilization events. 3.3 Ensuring Quality MNCH Services Infection Prevention and Control. Hospital-acquired infection is one factor of increased mortality and morbidity rates of hospital patients. Consequently, PAIMAN and UNICEF signed a MOU to build HCP managers’ infection prevention and control (IP&C) capacity. Internationally-accepted practices covered in PAIMAN training employed practical, simple, easy-to-use, low-technology, cost-effective approaches. Lady Aitcheson Hospital, Lahore was selected as a model hospital and training center for IP&C trainings, conducted by UNICEF master trainers. Two sets of trainings were designed. A three-day one includes district managers, EDOs Health, MS of DHQ and THQ hospitals. A standard six-day training is oriented towards WMOs, registrars, gynecologists, OT nurses, OT technicians, and labor room nurses from DHQ and THQ hospitals and RHCs. Year 5 saw 96 from upgraded health facilities in PAIMAN districts trained. During training, an IP&C plan for each facility was developed. In routine monitoring visits, FOMs support plan implementation. Except Swat, where follow up could not be conducted due
Free specialist medical camp at THQ Hospital Shujabad, District Multan

43
to security reasons, all selected health facilities in the first 10 PAIMAN districts showed marked infection rate reduction. Through PAIMAN-trained master trainers, District Jhelum institutionalized IP&C training at the District Health Development Center. In November, it trained its first batch of 15 participants from its peripheral facilities. Hospital Waste Management. After successful completion of hospital waste management pilot testing and learning from RHC Mandra and THQ Hospital Gujar Khan experiences, replicating the model in eight health facilities in Districts Quetta, Vehari, Multan, and Khairpur began. A project proposal was finalized and a consultant hired in January 2009. The consultant immediately began work at DHQ Hospital Vehari and THQ Hospital Burewala. Four Hospital Waste Management trainings for medical staff and waste handlers from DHQ Vehari and THQ Hospital Burewala were completed in March 2009. In April-June, site surveys were completed in the remaining six health facilities, RHC Mardanpur and THQH Shujabad, Lady Wellington Hospital Khairpur, RHC Pir Jo Goth Taluka Kingri District Khairpur, RHC Surang and RHC Panj Pai District Quetta. Two types of trainings were conducted for health facility staff, one for doctors, nurses, and paramedics and another for housekeeping and sanitation staff. Conventional incinerators were constructed and are functional in four District Vehari and Khairpur health facilities. Two more incinerators in Multan will be completed in November 2009. Three awareness posters for health facility staff and one for the general public were designed, printed, and distributed in August 2009. Monitoring visits were completed in all six facilities. Frequent monitoring by FOMs and the consultant ensured waste disposal plants worked and staff maintained them correctly. 3.4 Family Planning Family Planning Training. The year’s target for IUCD Insertion Training was 116, of which 108 from Districts Rawalpindi, Multan, Khanewal, Vehari, Bhimber, Sudhnoti, Khairpur, Khanewal, and DI Khan participated. Eight left from District Peshawar will be trained first quarter Year 6. Of target 32 bilateral tubal ligation trainees, 29 were trained. Lack of eligible participants meant the training could not be conducted in Districts Bhimber and Sidhunati. Of targeted 32 vasectomy trainees, 28 attended. Due to non-availability of participants at Bhimber and Sidhunati, training could not be conducted in the given time period. It was postponed to next year. Functional Integration of Health and Family Planning Services. In 2007-08 in District Rawalpindi, PAIMAN conducted a pilot study on functional integration of services between Health and Population Welfare Departments. Encouraging results led to functional integration in one district in each province. To select the four districts, a consultative meeting was held in Islamabad on April 14, 2009. Secretaries of the Ministries of Health and Population Welfare, and representatives of the four provinces were present. It was decided to extend functional integration to Districts Multan, Khairpur, Quetta, and Peshawar. Through field visits, data analyses, district- and provincial-level consultation, a situational analysis was completed for the four districts. The four reports recommend improvements to the level of functional integration. The reports, sent to the federal government, provinces, and

44
districts, were discussed through visits to the districts. Recommendations were finalized and implementation work plan prepared. Strategic Planning for NATPOW. JSI-PAIMAN and the National Trust for Population Welfare (NATPOW) signed a memorandum of understanding to develop strategies and to assess NATPOW’s needs to make it a viable, sustainable organization. Meetings with the NATPOW CEO and visits to the NATPOW Lahore regional office were conducted. An internal consultation meeting to revise NATPOW’s mission, vision, and objectives was conducted June 26, 2009. 4. Increased Capacity of MNCH Health Care Providers and Managers Year 5 was one of the most productive in terms of trainings of health care providers in 24 PAIMAN districts. All training partners conducted their respective national-, provincial-, and district-level trainings, completing the bulk of Project-life training targets. 4.1 Mother and Newborn Care Training Training on Essential Maternal and Newborn Care (EMNC) was provided to 483 health care providers in new PAIMAN districts. MOs, WMOs, LHVs, nurses, and dispensers were imparted knowledge and skills. From 13 districts 70 district level trainers, predominantly gynecologists and pediatricians were also trained at provincial-level TOTs. Provincial trainers rolled out this training in their respective districts. To ensure quality, all trainings were monitored by external monitors. In four one-day workshops held in all provinces 79 monitors were oriented on quality assurance tools and EMNC trainings. Advanced Skills in Obstetrics course was organized at Department of Gynecology and Obstetrics, Federal Government Services Hospital, Islamabad. Sixteen obstetricians from ten PAIMAN districts received a six-day state-of-the-art training. Focused on building district-level specialists’ capacity on advanced and applied obstetrics and gynecology skills. 4.2 Communication Skill Training During the year 3,805 LHWs were trained in all PAIMAN districts on Support Group Methodology and the Use of IEC Material. Trained LHWs are carrying out support group meetings on a regular basis, using information, education, communication materials in their respective catchment areas. To train these LHWs, 557 facility-level trainers, mostly MOs, WMOs, LHVs, and LHSs, were trained in district TOTs. Fifty provincial-level trainers were trained in four TOTs. Trainings emphasized endowing LHWs with communication, organization, and networking skills to better form and manage community support groups to address basic maternal and newborn health care needs. The training also used local resources and IEC materials to create maternal and child health awareness. 4.3 Community IMNCI Trainings Community IMNCI trainings are aimed at building LHW capacity to adapt an integrated approach in identification, home based management, and referral of children with common illnesses such as diarrhea and pneumonia and issues such as nutrition. With the support of AKU for module design, PAIMAN implemented these trainings. In 195 batches, 3,963 LHWs were trained on community IMNCI versus targeted 5,555. The remaining were carried forward to Year 6. Rollout trainings were imparted by 615 facility-based

45
trainers trained through 31 district TOTs in 23 districts. The planned District Rawalpindi TOT was carried forward to Year 6. In one national and Punjab, Sindh, Balochistan, NWFP, and AJK provincial TOTs, 122 community IMNCI master trainers were trained. Forty-seven extra were trained per National Program recommendation to have at least four trainers for each district TOT. Training was a blend of lectures, group discussions, and hands-on hospital work. In communities, trainers used customized cards and wall charts LHWs will routinely utilize for identification, management, and referral of common childhood illnesses. 4.4 Management Skills Trainings During Project Year 5, PAIMAN organized trainings for district health management teams (DHMT) of new districts in three management areas--planning, financial management, and supervision. A three-day District Annual Operational Planning (DAOP) training trained 86 district managers. Participants were introduced to the district health planning process, rationale, and steps to DAOP preparation with special focus on MNCH. Hands-on training HealthPlan® software was also imparted. PAIMAN completed three-day trainings on Financial Management for Budget Rules 2003 for new districts. A total of 61 staff trained included managers (EDOH, MS DHQH), accountants, and computer operators. Participants were oriented on local government budgeting laws and regulations. Hands-on training on Finsoft® software was also imparted. Two-day supportive supervision trainings were conducted for 83 district supervisors from 11 PAIMAN districts. Capacity was enhanced for supervision planning, conduction of supervisory visits, development and usage of supervisory checklists, feedback, and development of district-level supervision related policy framework. Training in District Peshawar could not be conducted due to engagement of health officials with IDPs. PAIMAN arranged two Lot Quality Assurance Sampling (LQAS) training workshops for district health managers from 14 PAIMAN districts. Fifty were trained including EDOHs, DOHs, DDOHs, district coordinators for LHW Program, and HMIS and EPI demographers and statisticians. During Year 5, a nine-day TOT workshop was organized to build capacity of district health department trainers to train service providers in Client-Centered Approach (CCA) for Delivering RH Services. Three each from Districts Peshawar, Mardan, Swat, DI Khan, Quetta, Sibi, Khanewal, Rawalpindi, and Bhimber were trained. Remaining PAIMAN districts were covered through the FALAH Project. These trainers rolled out the training in their respective districts. Each training was five days. Training was conducted for 320 participants. Two batches will be conducted next project year. The first batches of district level CCA trainings were supervised by Population Council master trainers. Having supervised the training process for the full five days, master trainers gave feedback to district trainers to strengthen their CCA training skills. A CCA Supervisory Guide was used to conduct the supervision. A DPC or FOM monitored all district-level training. During Year 5, two seven-day Strengthening District Health Systems through Leadership and the Client Centered Services workshops were held. Thirty-five district managers from eight PAIMAN districts were trained, including EDOs (Health, Finance and Planning, and Community

46
PAIMAN INSTITUTIONALIZES DHMT WITH LEGAL COVER
The original district health management team (DHMT) concept was an administrative, multi-disciplinary, non-elected body that utilizes available resources to manage all district health-related matters. A major challenge to a functional DHMT was lack of district ownership. To resolve this, PAIMAN proposed legislation for district assembly approval, with main components being composition and defined responsibilities, such as preparation of annual health department plans and budgets, approval of development schemes, and monitoring of health plan implementation. District Swat was first to pass DHMT legislation, followed by District Gwadar. It is expected that, with this legal cover, respective DHMTs will respond effectively and efficiently to decentralization challenges and that each DHMT will emerge as the most appropriate institutional support for evidence-based collective decision making and district health system streamlining.
Development), deputy district officers health (DDOH), district population welfare officers (DPWOs), medical superintendents, community coordinator/social organizers, district coordinators (MNCH, HMIS, and LHW Program), program director DHDC, deputy demographer, nazims, and chairmen-zila health committee. The Provincial Coordinator National Program for Family Planning and Primary Health Care and Provincial EPI Program Manager from AJK were also trained. 5. Improve Management and Integration of Services at All Levels One of PAIMAN’s key strategic objectives is to strengthen the overall district health system. The main focus areas of health system strengthening are: 1) the district health management team; 2) the health management information system; 3) public-private partnerships; and 4) monitoring and evaluation. 5.1 District Health Management Teams After sharing the district health management team concept with district authorities, DHMTs were successfully implemented in 14 new districts. To maintain regularity and performance, districts were continuously encouraged to schedule quarterly DHMT meetings. As a result, 60 of 72 (excluding Buner and Swat) planned meetings were held.
As a health system strengthening intervention, individual meetings and two workshops with high provincial and district officials were held, proving useful in motivating these officials. Improved DHMT performance in all districts led to legislated adoption of DHMT models by six districts.
Experience sharing visits provided an excellent opportunity for new districts to learn best practices for district health system strengthening. A total of seven visits for 13 districts were conducted. Target Setting and Annual Operation Plan Preparation. In a one-day training on target setting for district health staff from all districts, 42 of planned 46 health personnel were trained. Training focused on the concept of targets and indicators, steps to target setting, and linking them with action plans. Trainings proved useful for districts in setting targets for district annual operation plan (DAOP) preparation and performing self-reviews. With PAIMAN technical assistance, all districts produced DAOPs for 2009-10.

47
5.2 District Health Information System After seeking agreements from national, provincial/regional, and district stakeholders, a full district health information system (DHIS) package was launched. It included trainings, supply of data collection instruments, and software support. A total of 2,405 health care providers from 15 districts of Sindh, Balochistan, AJK, and NWFP were trained in 100 district-level workshops.
DHIS software installation and training began. Software was presented to National Health Information and Resource Center, which consented to implement it in PAIMAN districts. Districts were continuously assisted in compiling and presenting routine health information system (HIS) reports from LHW-MIS, EPI-MIS, HMIS/DHIS, and DPWO data. They were also assisted in applying LQAS to assess routine HIS and other management areas.
To provide DHMTs and consortium implementation partners baseline information, 13 district health profiles were prepared for new PAIMAN districts. These helped design interventions to address MNCH. 5.3 Public Private Partnerships Establishment of Community Emergency Ambulance Services. A comprehensive working strategy was developed and procurement of 50 Suzuki Bolan vans to be converted to ambulances begun. Contech completed mapping and clustering of target union councils. Sub-agreements were signed with implementing NGO’s. Monitoring tools were developed and clustering/mapping of the union councils completed. Workshops for capacity building of five selected NGO’s were arranged by Contech. GoodLife Providers. In a meeting with the Greenstar Chief Executive Officer and the National Manager-PAIMAN, transfer of data and smooth transition of the GoodLife providers and the Vouchers for Health scheme to JSI-PAIMAN was discussed. Physical verification of GoodLife providers in all districts was completed. JSI sent partnership offer letters to all providers to continue their involvement with PAIMAN after their partnership with Greenstar ended on September 30, 2009. A performance-based incentive package designed for these providers is in procurement stage. Agreement signing ceremonies early in Year 6 are planned for the official start of the partnerships. Medical Helpline. For the PAIMAN Helpline, begun March 1, 2009, a list of district health facilities was prepared and consents from doctors and specialists obtained. A tool was designed to monitor performance. Due to the limited number of calls in the first four months, the Helpline was given two months, starting July 1, to improve. After two months, an evaluation showed no improvement, rather a deteriorating trend. Helpline was closed September 30, 2009. Private Health Care Providers. JSI signed agreements with 49 private health care providers from 12 districts. All have been regularly reporting. An incentive performance package encourages and supports the initiative. Health care providers will be judged on performance markers and given incentives in the form of small medical equipment. They will also participate in capacity building trainings and events. Blood Bank THQ Hospital Mian Channu This initiative a partnership of Health Department Punjab, Greenstar and a local NGO, Welfare Association for Altruism, supported a blood bank at THQ Hospital Mian Channu. Lack of blood bank resulted in no surgeries at the THQH despite presence of an obstetrician and a surgeon. In view of the September 30th end of Greenstar’s PAIMAN sub-agreement a meeting was held with

48
Secretary Health Punjab for support and to request filling the Blood Bank Officer and supporting staff posts. This and a request for blood bags and screening kits were honored. The initiative has been handed over to the Provincial Health Department Punjab, effective September 30, 2009. II. GRANTS MANAGEMENT This Project year saw significant grant management activity. With the addition of 14 districts, new sub-grantee NGOs were added and scopes of work of many were expanded to include child health and family planning components. Five capacity building exercises were organized to orient new sub-grantee NGOs. At year end JSI is managing 78 sub-grants in 23 PAIMAN districts (no District Bhimber NGO qualified). Extension and Expansion. Applications from NGOs in new districts were initiated during the first quarter followed by short listing and pre-award assessment. After receiving USAID approval, agreements were signed with 44 new local NGOs, additionally agreements with 11 Swat sub-grantees were signed during the first quarter, although they were selected during Quarters 3 and 4 of Year 4. With revised scopes of work, 23 previous NGOs were extended for 12 months. Activities. Using CAM activities NGOs delivered MNCH messages to 88,283 male and female beneficiaries. To improve access to MNCH services sub-grantee NGOs conducted 132 rounds of TT vaccination to vaccinate 243,974 pregnant mothers. To identify EPI defaulters 1,011 meetings were held. Defaulters were reached and motivated to be vaccinated. Community-level medical health camps improved access to health services. During the year, 224 benefited 78,443 patients. Health camps provided services for basic ailments and, through Population Welfare Department representatives, family planning services were made available. In addition, through collaboration with Department of Health, health camps provided TT and EPI vaccinations. Training of TBAs on clean delivery practices remained an essential NGO activity. Previously trained TBAs were provided three-day refresher training. To maintain quality of training, Population Council trained 22 trainers, followed by rollout refresher trainings. NGO staff followed up with trained TBAs and reviewed their referral slips. In new districts, 255 TBAs received clean delivery practices and timely referrals orientations. To conduct the eight-day TBA orientation, 26 trainers were first trained by master trainers. NGOs established seven birthing centers in new Project districts in consultation with Departments’ of Health recommendations. During the year, 26,445 patients received general OPD, ANC, PNC, deliveries, TT, and referrals through these centers. Out of 15 birthing centers established to date, three have been handed over, two, including one-each in Wahi Pandi, Dadu and Baghtal, Jafarabad have been handed over to People’s Primary Health Care Initiative under the Ministry of Establishment and one at, CD- Mossani, Lasbella, to Department of Health. Internally Displaced Persons. In May 2009 an estimated 2.5 million persons primarily from Districts Swat and Buner fled their homes following the start of military operations against the Taliban. These internally displaced persons (IDPs) found shelter in official camps (20%) and with local host families, rented houses, and schools converted to camps (80%). Mardan and

49
Charsadda, both PAIMAN districts, hosted the majority, about 1.6 million in Mardan and 200,000 in Charsadda. In response to the IDP humanitarian crisis JSI-PAIMAN joined Ministry of Health, NWFP and various humanitarian agencies to provide immediate life-saving assistance. PAIMAN repositioned its Swat and Buner partner NGOs to provide health care to Mardan and Charsadda IDPs. Fourteen NGOs -nine Swat, one Buner, one Charsadda and three Mardan- served IDPs in Mardan and Charsadda. PAIMAN NGOs worked in close collaboration with EDOsH on a two pronged strategy to provide essential health care to IDPs; 1) mobile health camps for IDPs living with host families and; 2) birthing centers for IDP families in camps. PAIMAN’s response began the last week of May. As a first step, PAIMAN NGOs made quick visits to IDP communities and gathered information about health needs and identified diseases common in each area and the required medicines. Many females and children had not received required vaccinations when they were in Swat, as the extremists banned female and children vaccinations. In order to meet IDP pregnant women’s needs four birthing centers were established one each in RHC Toru, RHC Shahbaz Gari, RHC Gambat, and Charsadda Sugar Mill IDP camps. Utilizing RHCs helped strengthen the health system. Each birthing center was staffed by LHVs and TBAs and provided 24/7 service. Fourteen NGOs covered 18 union councils with 64 mobile health camps a month. The geographic coverage was expanded to 49 union councils in July in consultation with EDO-H Mardan. Camps were staffed by female and male doctors, nurses, EPI technician and health technicians. Camps were female-friendly as the female doctor provided specialized services to women. Drugs were obtained from the EDOH. The camps provided health check-ups to all, antenatal care, postnatal and delivery service. Basic immunizations for children and TT vaccination and contraceptives for women were available.
From May 25 to August 16, 2009, PAIMAN sub-grantee NGOs organized 222 health camps and operated four birthing centers. Through these interventions 53,307 IDPs received basic health services, 76 babies were delivered, 1,209 pregnant women received TT immunizations, and 785

50
children were immunized. Additionally, 3,007 women were given antenatal care, 2,434 postnatal care, and 942 received contraceptives. Major health problems facing IDPs were watery diarrhea, fever, gastritis, anemia, eye infections, scabies and other minor diseases. Many women reported urinary track infections, and anemia.
Health Services Provided by PAIMAN NGOs to IDPs May 25-August 16, 2009
Service provided Health Camp Birthing Center Total
Health camps 222 - 222
Patients 48,122 5,185 53,307 Antenatal care 2,099 908 3,007
Birth delivery - 76 76
Pregnant vaccinated with TT 957 252 1,209
Postnatal care 2,335 99 2,434
Referrals 748 101 849
Children vaccinated 785 - 785
Women provided contraceptives 778 164 942
The military operation in Buner and Swat destroyed power and water supply to the district hospitals. At the request of the DGs Health and EDOsH PAIMAN provided Rs.70,000 per month each for diesel for generators at DHQ Hospital Daggar, Buner and Saidu Sharif Hospital, Swat. The Project also provided a 30 KVA generator along with Rs.40,000 fuel support per month to RHC Shahbaz Gari. With electricity the DHQ hospitals were functional and could handle medical emergencies and water was pumped. PAIMAN also provide diesel assistance to Swat; a 30 KVA generator along with Rs.40,000 per month for fuel to RHC Shahbaz Gari. Two air conditioners for delivery room and patient examination room each were provided to RHC Toro and RHC Shahbaz Gari. On June 24 Dr. Nabeela, COP, JSI-PAIMAN led a high profile PAIMAN team to IDP camps and birthing centers in Mardan and Charsadda. She visited IDPs living in camps and met with women and children to get a better idea about the problems they faced. The team learned postpartum mothers and newborns did not have adequate clothes, sanitary pads and so on. In response, PAIMAN provided 300 newborn health and garment kits for postpartum mother and newborns. PAIMAN also provided 100 cotton mattresses and 100 mattresses under laid to pregnant ladies living in Sugar Mills, Charsadda IDP camp. From July 15, the Government initiated repatriation starting with IDPs living in camps, then in schools and finally living with host families. It is estimated that over 1.6 million of estimated 2.6

51
IDPS have returned to their homes in Buner and Swat. On August 6 PAIMAN convened a meeting of sub-grantee NGOs and jointly worked out a plan for return of the Swat and Buner based sub-grantee NGOs to their respective places of origin. Project sub-grantee NGOs are now serving IDP returnees in Swat and Buner through their regular project activities. III. MONITORING As initial Project emphasis was getting PAIMAN up and running, the Project monitoring system primarily focused on monitoring inputs and processes of individual interventions. As PAIMAN progressed, emphasis shifted to monitoring and results in addition to inputs and processes. PAIMAN Monitoring and Evaluation Plan clearly defines specific performance-measuring indicators. Government service data from districts, upgraded public hospitals, and franchised private providers are used to monitor PAIMAN performance in achieving objectives. Unfortunately, there are HMIS gaps. The government sector does not capture data from hospital in-patient departments and private health providers and facilities have no formal recordkeeping and reporting system. The Ministry of Health, through a JICA-funded study, supported district health information system (DHIS), an improved HMIS. Implementation, however, is still in initial stages. Pending countrywide DHIS implementation, PAIMAN deemed it necessary to establish a system of routine collection of relevant intermediate output/outcome data from upgraded/franchised health facilities in addition to utilizing relevant data from districts’ routine HIS, HMIS, LHW-MIS, and EPI-MIS. In early 2007, PAIMAN operationalized RMOI. Using an MS Access-based data entry and analysis program, data from upgraded public health facilities are entered and reports generated. Using a simple format, FOMs collect data monthly through corresponding hospital authorities. PAIMAN partner Contech collects and enters HMIS/LHW-, MIS/EPI-, and MIS/DPWO-based data into an MS Excel-based database. Monitoring Performance of Upgraded Health Facilities. In its districts, PAIMAN upgraded selected health facilities to enable emergency obstetric and neonatal care (EmONC) services. Upgraded health facilities now accept normal and obstetric deliveries, treat obstetric complications, and perform lifesaving C-sections. Upgraded health facilities include DHQHs, THQHs, some RHCs, and four civil hospitals. All report births and obstetric services data to PAIMAN monthly. Data entered into the PAIMAN database are used for analysis, feedback, and reporting. As illustrated below, all three services improved. In Year 5, births increased 10%, treatment of obstetric complications 41%, and C-sections 2% compared with Year 4, clearly showing
Table : Upgraded Health Facilities in PAIMAN’s 24 Districts (September 30, 2009)
Facility
Original 10 Districts
Additional 14 Districts Total
DHQH 9 11 24 THQH 10 7 33 RHC 11 28 28 BHU 1 - 85 Civil hospital - 4 4 Total 31 50 85

52
upgraded health facilities are progressing well in handling these services to save mothers’ and neonates’ lives.
Reported Births and Obstetric Care in Upgraded Health Facilities PAIMAN Districts in Year 4 and Year 5
0
5000
10000
15000
20000
25000
Y04(Oct'07-Sep'08)
Y05(Oct'08-Sep'09)
Y04(Oct'07-Sep'08)
Y05(Oct'08-Sep'09)
Y04(Oct'07-Sep'08)
Y05(Oct'08-Sep'09)
Births in HF Obs Complications Admitted Emergency C-sectionsChange:Number of births increased by 10%Number obstetric complications treated increased by 41%Number of C-sections performed increased by 2%
Num
ber
In Year 5 RMOI data was collected from the 14 additional PAIMAN districts. The table below shows January-September 2009 services provided by upgraded health facilities in 10 original and 14 new districts. In the first nine months of 2009, in 24 districts, 34,127 births occurred in upgraded health facilities, 87% of which used AMTSL and 31% partograph. Rates in 10 original districts are higher than in the new 14. AMTSL in original districts is 89% compared with 85% in new. Partograph use is 50% in original districts versus 14% in new. Interventions in new districts began only recently. Year 5 reports showed AMTSL use at 99% and partograph 70%. Figures were based on the January-March 2009 quarter data for original districts, excluding some NWFP districts due to late receipt that reflected lower AMTSL and partograph use.
Table : Key Obstetric Care in Health Facilities (January-September 2009) Districts Obstetric Care Original 10 New 14 Total Total Births 16,169 17,958 34,127 Births using AMTSL (%) 89.1 84.6 86.7 Births using partograph (%) 49.6 14.2 31

53
Monitoring Public Sector Health Performance in Original Project Districts. Key maternal health services include antenatal, TT2, and postnatal services. The chart shows Year 4 and Year 5 data from nine original PAIMAN districts. Buner is excluded; due to armed conflict. Included data are from government health sector HMIS, EPI-MIS, and LHW-MIS. PAIMAN districts made significant progress. Pregnant women attending health facilities for first ANC increased 12% over previous year. TT2 immunization increased 21%. The EPI program in Pakistan recommends at least two TT immunization doses for every pregnant woman to protect newborns from tetanus toxoid. Postnatal visits by LHWs remained the same. These community-based health workers are informed about all pregnant women, deliveries, etc. They visit mothers who have given birth within three days to provide care and educational support. Because there are insufficient LHWs to cover Pakistan’s entire population, coverage is low. With additional Project mandates of child health and reproductive health beginning October 2008, key child health and family planning data were collected. Indicators are: 1) number of children under 5 years of age treated for diarrhea, 2) number of children under 5 years of age treated for pneumonia, 3) number children under 12 months of age who received DPT3, and 4) contraceptive years protection (CYP). Data is from HMIS, LHW-MIS, and EPI-MIS. The table below summarizes October 2008-September 2009 services provided in PAIMAN original 10 districts. September data from most district health offices were not available but are expected in November. Diarrhea treatment data are from all health facilities and LHW reports. As shown, 630,687 children under 5 years of age were treated for diarrhea, about 130,000 for pneumonia, and about 325,000 received third dose of DPT vaccination.
Table : Child Health and Family Planning Services Nine PAIMAN Original Districts (October 2008-September 2009*)
Service Patients Under-5 children treated for diarrhea (HMIS, LHW-MIS) 630,687 Under-5 children treated for pneumonia (HMIS) 129,136 Children less than 12 months of age who received DPT3 (EPI-MIS) 325,050 Pills (cycles) dispensed 66,850 Condoms dispensed 54,594 IUCDs performed 428,064 Injectibles given 29,239 Male sterilizations performed 11,150 Female sterilizations performed 140,410 CYP-Total 730,308
*September 2009 data incomplete
Maternal Health Services in 9 PAIMAN orginal districts
-50
100150200250300
Pregnant women newlyregistered (HMIS)
TT2 Immunization (EPIMIS)
Postnatal visit byLHWs(LHW-MIS)
Thou
sand
sChange:Prenatal care increased by 12%TT2 immunization increased by 21%
Sep 07 to Aug 08Sep 08 to Aug09

54
The above table shows CYP by method. HMIS-, DPW-, and LHW-MIS-provided oral contraceptives, condoms, injectibles, IUCDs, and male and female sterilizations data are calculated into CYP by multiplying or dividing by a standard factor. About 730,000 CYP were provided. IUCD is the most popular, followed by female sterilization via pills and condoms. Male sterilization is least popular. The table below portrays data from new Project districts. September data is incomplete, data from several district health offices will be submitted by November. Receipt depends on ongoing security problems. Data are from HMIS, EPI-MIS, LHW-MIS, and DPWO. The October 2008-September 2009 summary shows about 285,000 pregnant ladies received two TT vaccination doses, about 128,000 attended antenatal care, and LHWs visited about 120,000 postpartum mothers for newborn care and counseling. Child health services show close to 900,000 children received treatment for diarrhea and little more than 500,000 for pneumonia. About 370,000 infants received third DPT dose.
Table : Child Health and Family Planning Services in New Project Districts (October 2008-September 2009*)
Indicator Total Maternal Health
TT immunization of pregnant women (EPI-MIS) 285,965
ANC registration at HFs (HMIS) 128,965
Postnatal visit by LHWs (LHW-MIS) 119,600
Child Health
Under-5 children treated for diarrhea (HMIS, LHW-MIS) 897,268
Under-5 children treated for pneumonia (HMIS) 538,552
Children less than 12 months of age who received DPT3 (EPI-MIS) 369,647
Family Planning
Pills (cycles) dispensed 124,656
Condoms dispensed 44,661
IUCDs performed 356,066
Injectibles given 39,982
Male sterilizations performed 3,880
Female sterilizations performed 137,400
CYP-Total 706,645 *September 2009 data incomplete
Data shows more than 706,000 CYPs were provided during the year. IUCD, followed by female sterilization were most popular, then pills, condoms, and injectibles. Male sterilization was least favored. PAIMAN Technical Advisory Group. At Project inception, PAIMAN constituted a Technical Advisory Group to provide guidance on overall Project implementation strategies and to share national and international experiences and best practices. Bringing together professionals well-known in their area of expertise, the annual TAG meeting is an important Project planning and review function. Membership consists of international and national experts in various PAIMAN-specific thematic areas.

55
TAG meetings were held in 2005, 2006, 2008, and 2009. The most recent, held March 13-14, 2009 in Dubai, for security reasons, was significant because of PAIMAN’s recent programmatic and geographic expansion and one-year extension. More than 100 delegates from all major stakeholders, including USAID and Ministries of Health and Population Welfare, actively participated. A highlight was the comprehensive video presented by PAIMAN Chief of Party that eloquently projected all Project strategic objectives. Based on successes of each strategic objective, it compared the present with Project inception. IV. EVALUATION AND RESEARCH ACTIVITIES Baseline Survey. During Year 5, Population Council completed baseline household surveys for Districts Multan, Vehari, Khairpur, Mardan, Zhob, Bhimber, and Sidhunati. Baseline household survey for District Charsadda was completed through the FALAH Project, since the District overlaps both projects. The remaining NWFP and Balochistan districts were excluded due to their volatile security situation. Draft reports were developed. GIS Mapping. Population Council completed GIS mapping of health facilities for Districts Khairpur, Vehari and Khanewal. Draft reports were prepared and plans to conduct GIS mapping in District Multan were finalized. Digitalization of maps of Khairpur, Vehari, and Khanewal started this year. GIS mapping of 12 PAIMAN districts was conducted under the FALAH Project; reports were published and disseminated. Community Mobilization Process Evaluation. The evaluation focused on three areas: support group (SG) meetings, male health committees, and facility-based health committees (FBHCs). Findings suggest that SG meetings were promptly implemented compared with male health committees and FBHCs. The process of implementing SG meetings is through three major phases: training of LHWs (SG facilitators) in SG methodology, establishment of support groups in communities, and conduction of SG meetings by LHWs. The process was accomplished in all PAIMAN districts evaluated. LHWs were trained in SG methodology and most LHW training protocols were followed. The majority of LHWs followed SG meeting protocols, but some gaps were identified in organizing meetings and low participation by SG members. The process evaluation revealed that antenatal, newborn, and delivery care were usually discussed during SG meetings but family planning and postnatal care were not. Several messages related to these MNH areas were given during SG meetings. However, few important messages, such as danger signs of pregnancy, arrangements for SBA, use of iron folic acid tablets, arrangement for transport and delivery, and money for delivery were not. Only a fifth of the SG meetings were supervised by LHSs or other supervisors, but LHSs who supervised meetings supported the LHWs.
Analysis of male health committees showed that a quarter of LHWs had never formed or revitalized a male health committee. Of those who formed a committee, half were facilitating meetings themselves. The remaining facilitated through the LHW’s husband or her male relative. Generally, there was low frequency of male health committee meetings but when held, sufficient members attended. Duration of a third of the meetings was less than 30 minutes.
Assessment of facility-based health committees revealed several gaps in the implementation process, demanding a close review of the strategy and execution. Coverage was low; a quarter of FBHC members had never attended a meeting, probably due to gaps in the member selection process. Although a majority of FBHC members had a positive attitude and considered it a

56
potentially positive platform, important issues such as regular, frequent meetings, setting the agenda and distributing minutes prior to meetings, and inclusion of a broader representation of the community need to be addressed. Findings were shared with PAIMAN partners and National Program for Family Planning and Primary Health Care.
Private Sector Activities Process Evaluation. Greenstar Social Marketing established a health care private provider’s network (GoodLife Clinics), primarily in urban areas of the first 10 PAIMAN districts. This network provides MNCH and RH/FP services and products. Greenstar undertook several other community-level initiatives to improve and expand MNCH and RH/FP services: GoodLife Clinics, GoodLife Clinic Sahoolat (free consultation), community interpersonal communication activities, TBA involvement in MNCH services, clean delivery kit marketing, birth preparedness and complication readiness, public-private partnership, Vouchers for Health, and health care provider training.
During Year 5, in five randomly selected districts, a process evaluation for these private sector activities was conducted. The evaluation report was finalized. Formal dissemination in Year 6 will be held after consultation with JSI and Greenstar. V. OPERATIONS RESEARCH PAIMAN uses operations research to test new approaches, evaluate outputs and impacts. Operations research under PAIMAN is a broad range of activities designed to improve understanding of what works, from simple field visits to carefully designed observation studies. Some studies are relatively large, some small. Assessing the Feasibility of Home Administration of Misoprostol in the Prevention of PPH in Rural Pakistan (Population Council) Efficacy of misoprostol has been widely assessed in preventing postpartum hemorrhage (PPH) at national and international levels. Postpartum hemorrhage is one of the leading causes of maternal death in many developing countries, including Pakistan. Because in Pakistan, access to health facilities is limited, about 61% of deliveries are conducted by unskilled birth attendants within home settings. Misoprostol’s ease of administration, low cost, and heat stability make it the drug of choice where home delivery is the norm. To help prevent PPH in women of rural areas and delivering at home, PAIMAN conducted an operations research with the following objectives: • To document feasibility of misoprostol administration at home by CMWs or next of kin. • To assess the acceptability and use of misoprostol by pregnant women for the prevention of
PPH when administered at home. • To identify misoprostol’s common side-effects and the demand for referral for reducing PPH
in Pakistan, where the standard, active management of third stage of labor is not commonly practiced.
Study sample size was 1,600 women in both intervention and comparison areas in Districts Khanewal and Dadu. Each pregnant woman was administered a set of five questionnaires. A technical advisory group was formed, two TAG meetings conducted and the study design approved. Briefings on the Project activities were provided to Ministry of Health (MNCH

57
Program). EDOs Health of both districts were briefed. Social scientists, logistics supervisors, and district supervisors were identified. The first phase of training of social scientists for the two districts was completed. Training materials and pictorials for health care providers and study participants were developed. The study will be completed in Year 6. Assessing the Acceptability of a New Cadre of CMWs for Pregnancy and Delivery Related Care in Rural Pakistan (Population Council) This study is to guide the Ministry of Health regarding response of communities to placement of CMWs in rural areas. The study was in three phases: Phase I (Baseline): Qualitative research and interviews with CMWs were completed. A report is available. Data from CMW interviews was edited and analyzed and a report written. A household survey was conducted in CMW catchment areas in Districts Rawalpindi, Jhelum, Khanewal, DG Khan, Dadu, and Sukkur. This survey began in Year 5. Phase II: Six months after the baseline survey, interviews were conducted with LHVs who supervise CMWs, one LHW, and one TBA working in the CMW catchment area. Phase-III: Two main activities planned for this phase, to occur one year post-intervention are: 1) interviews with CMWs to obtain information regarding their experience in the field and any problems they faced and 2) endline household survey on the same lines as the baseline. The household survey of Phase I commenced. Report on qualitative data is available for three districts. Findings from the qualitative research were utilized in developing the household questionnaire. Evaluation of the Effectiveness of Application of 4% Chlorhexidine Solution on Umbilical Cord Stump as Part of a Neonatal Postpartum Care Package in Rural Pakistan-Dadu (Aga Khan University) This study concluded this year. Formative qualitative research through focus group discussions and key informant interviews were conducted. Based on an early Year 6 meeting with PAIMAN and USAID, follow-up visits to assess potential impact beyond the neonatal period will be undertaken. Evaluation of the Effectiveness of Vitamin A Supplementation as Part of a Neonatal Postpartum Care Package in Rural Pakistan (Aga Khan University) The study sample size was achieved in July 2009. On-going follow-up of recruited newborns will be completed by the end of January 2010. Of 12,191 reported births, 11,124 newborns were supplemented and enrolled in the study. Mortalities in enrolled infants were reported to be 179. Verbal autopsies were conducted for those children (i.e. from birth up to age 6 months) who died during the study period. Out of 179 mortalities, 109 verbal autopsies were conducted. Year 6 plans that include follow-up of recruited children will continue until recruited children achieve six months of age. Hence, the last follow-up will be the end of January 2010. Verbal autopsies of all children who die within the study period will continue. Postpartum Maternal and Neonatal Intervention Package; A Cluster Randomized Control Trial in District Sukkur, Pakistan (Aga Khan University) Complete mapping of health care providers in control and interventions clusters was completed. Two refresher trainings on post-partum maternal and neonatal care refresher trainings were
58
completed. In January, post-partum visit forms to be filled by LHWs were introduced in the intervention area. Independent data collection through Project CHWs was conducted in intervention and control areas. So far, 408 post-partum visit forms were collected from intervention clusters. Improved Recognition of and Response to Prolonged Labor and Birth Asphyxia; An Observational Study in Districts Matiari and Sukkur (Aga Khan University) Task 1: Ninety semi-structured interviews with women of reproductive age, TBAs, and older women were completed. Data entry and report writing are completed. Task 2: This phase was based on 120 structured interviews which included all previous 90 respondents. Ten more women of reproductive age (focal female) were included from each field site. The questionnaire was based on the findings of Phase I. Data gathering, entry, and analysis is complete. Task 3: Group interviews will be completed in October- December 2009. A Community-based Introduction and Evaluation of the Impact of Social Marketing of a Diarrhea Management Pack (Comprising Low-Osmolality ORS, Zinc Tablets, Water Purification Tablets and Pictorial Chart) on Childhood Diarrhea, Districts Khairpur and Jhelum (Aga Khan University) Identification of supervisory staff, ethical review committee clearance, finalization, pre-testing, and printing of instruments were completed this year. Hiring and training staff for baseline census and conducting the census were completed. Data entry and analysis is ongoing. Preparation of social marketing plan, development of material for social mobilization (posters, booklet, and banners), development of diarrhea pack, and hiring staff for social mobilization and staff for routine data collection were completed. Community-based Management of Severe Acute Malnutrition-Dadu (Aga Khan University) Hiring of staff, acquisition of vehicles, printing of questionnaires for rollout of study were completed and field office is fully operational. Baseline census was conducted July 5, 2009 to September 6, 2009. Preliminary report from the baseline census shows that rate of moderate wasting is between 16 to 30% and that of severe is 5 to 13% in different clusters. Recruitment of malnourished children started and will continue per plan. First progress report is expected in January 2010.
Vitamin D Study (Aga Khan University) Proposal writing completed, field site selected, data instruments developed, operating plan completed, recruitment of staff and office completed, and required commodity on the way.
Evaluation of the Effectiveness of Short Duration IMNCI Training versus Standard Duration IMNCI Training (Aga Khan University) Staff was recruited and training material arranged for an 11-day training scheduled for November 2009 and seven-day training late November-December 2009. Training assessments will be finalized six months after training completion. Pre- and post-test tools to assess knowledge and video assessment tool for clinical assessment were developed and pilot tested. Evaluation of Integrated Maternal and Newborn Care Package (Aga Khan University) Planned, but not started during Year 5. Mortality Survey (Aga Khan University) Planned, but not started during Year 5.

59
VI. KNOWLEDGE MANAGEMENT Four issues of PAIMAN News Roundup in English and Urdu versions were published and circulated to partners and stakeholders. PAIMAN profile information was updated on the PAIMAN homepage website. The website was been updated with the following:
1. Issues 5-8 of PAIMAN NewsRoundup 2. Weekly Highlights 3. Brochures
a. Pakistan Initiative for Mothers and Newborns revised (2009) brochure b. District-specific PAIMAN MNCH brochures c. PAIMAN-After the Promise d. Health facility image building brochures e. PAIMAN Behavior Change Communication: Matching Diversity with Variety
4. News and alerts 5. Photographs 6. Music Video 7. TV drama series 8. TV Commercials 9. Radio Magazine Show 10. Documentary on Puppet Shows
Uploading Project-related resources onto PAIMAN Intranet and its public website was a regular practice throughout the year. VII ADMINISTRATION
Over the five years, since the start date of November 15, 2004, PAIMAN has continuously assessed staff required to efficiently carry out Project objectives. Since 2004 the Project has expanded significantly, with a significant staff increase when the number of PAIMAN districts increased from 10 to 24 in October 2008. All JSI positions are filled following established recruitment, review and selection policies. To meet staff needs for the 14 additional districts, 59 staff were hired between December 2008 and February 2009. On February 16-18, 2009, orientation was held for new and old JSI-PAIMAN staff. Covered were programmatic, administrative, and finance activities.

60
This year, 18 interns served an average of four months each. The PAIMAN intern program has been beneficial to both interns, who had the opportunity to learn from PAIMAN, and to the Project which gains assistance from bright energetic interns. Interns are selected based on Project needs. Some who performed well were given fixed-term contracts. International Travel. Administration supported 89 international trips this year more than 50% were for Technical Advisory Group Meeting in Dubai. Events Management. During Year 6, Administration supported 177 events, including the Dubai TAG meeting. This meeting, initially scheduled for Pakistan, it was shifted to Dubai, due to security concerns. Administration successfully organized the event and arranged travel of the large number of Pakistan participants. Printing and Publications. Administration arranged printing of material in bulk quantities for different program activities. Printing included office stationery, training material, and printing publications. During the year, 94 printing jobs were completed, including 792,980 copies of brochures (TT vaccination, PAIMAN district-specific brochures, PAIMAN Helpline, etc.), 237,000 forms (IMNCI, Private Health Care Providers, RMOI forms, partographs, etc.) and 47,476 manuals/books (Sehat Ki Dastak, Family Booklet, Advocacy Kits, AMST Training Material, Midwifery Manuals, LHW Manuals, IMNCI Modules, PAIMAN-After the Promise). Safety and Security. To address the current unstable security in Pakistan and in many PAIMAN districts, USAID in February approved a security enhancement plan for JSI offices. Security enhancements included, among others: erecting iron grills on boundary walls and anti-shatter film on glass windows, hiring additional armed guards, improved office access control, and installed CCTV cameras. Procurement. With additions of FATA and Swat and later Project expansion to 14 additional districts, the procurement team remained very busy. A needs assessment of selected health facilities in the new districts was conducted by Contech. A procurement plan worth US$7.65 million was prepared and approved by USAID. The plan included laboratory equipment, electro-medical equipment, medical and office furniture, exam room furnishings and supplies, stainless steel surgical instruments, ambulances, power generators, IT equipment, training electronic equipment, office equipment, and training models. A source and origin waiver for procurement of 48 Toyota purpose-built ambulances was obtained from USAID and order placed. USAID source and origin waiver for 50 Suzuki ambulances for RESAI was obtained and contract issued for procurement. Both types of ambulances will be delivered early in Year 6. Waivers were received, procurement initiated and completed, and five Toyota purpose-built ambulances handed over to the Health Department, Government of NWFP for use in Districts Charsaddah, Mardan, and Buner. Establishment in three phases of 1,100 midwives homes,
PAIMAN International Travel Year 5 Trips
Pak-USA-Pak 6
Ethiopia-Pak-Ethiopia 1
Ethiopia-USA 1
Pak-Switzerland-Pak 1
Ethiopia-Pak 1
Pak-Dubai-Pak 62
USA-Dubai-USA 6
Pak-Cairo-Pak 2
Pak-Bkk-Pak 3
Nepal-Pak 1
USA-Pak-USA 5
Total 89

61
entailing huge procurement will be completed by December 2009. JSI awarded contracts for 27 essential equipment and supplies worth $678,675 for the homes. PAIMAN provided equipment for 150 midwifery homes during the last quarter of Year 6. The balance will be supplied in Year 6. A huge amount of off-shore equipment arrived in Pakistan this year. All laboratory and medical equipment, supplies, furniture, and ambulances for 32 selected health facilities in the 10 districts were been provided, except for stainless steel surgical instruments. Civil Works/Renovation of Health Facilities. A Needs Assessment Survey for civil works/renovation in 55 health facilities in the 14 expansion districts was conducted this year. Contracts for renovation work in nine District Multan health facilities were awarded and work begun in Year 5. Work will commence in the remaining health facilities in November/December 2009, with completion scheduled July 2010. To accommodate 86 well baby clinics, renovations are required at each selected health facility. Contracts were awarded to two firms for the work, which will be completed early in Year 6. Due to the adverse security situation in Swat, construction of dormitory for community midwifery students was shifted from Swat to Mardan. Mardan Health Department issued a No Objection Certificate, a USAID environmental assessment was conducted and all architectural and structural drawings were prepared and submitted to USAID for approval. Construction will begin in Year 6 after receipt of USAID approval. VIII. FINANCE In Year 5, JSI expanded from four provincial to 19 provincial and district field offices. Field offices’ financial operations were closely monitored as the number of offices, financial transactions, and rupee volume of disbursements increased significantly. The JSI Finance Section continued to maintain and track disbursement/expenditure trends and monitor cash flow requirements and Project expenditures. Accruals were tracked and accounted for in expenditure trends and projections. Significant activities of the financial management section in Year 5 were:
• Participating in sub-grantee proposal writing workshops and sub-grantee capacity-building initiatives.
• Facilitating budget reviews and assisting with development of CMW training budgets. • Reviewing, processing, and disbursing quarterly advances to 78 sub-grantees and
tracking advances versus expenditures. • Supporting, assisting, guiding, and building the capacity of JSI field offices’ financial
management operations. • Tracking and reporting cost share for JSI, partners, and sub-grantees. • Reviewing and processing 2,844 disbursement vouchers worth approximately US$16
million.

62
This year, disbursements increased significantly, resulting in greatly-accelerated Project burn rate. This increase is reflective of the accelerated level of Project implementation.
Annual Expenditures - Trend
$0
$5
$10
$15
$20
$25
$30
Year‐1 Year‐2 Year‐3 Year‐4 Year‐5
Mill
ions
In Year 1, expenditures were low as staff were recruited, offices opened, and work plans were developed and approved. In Year 2, Project activities and, therefore, expenditures started to pick up momentum. In Years 3, 4, and 5, activities were fully active, with significant purchases of medical equipment, furniture and ambulances. In Year 5, expenditures totaled US$24.9 million with total Years 1 through 5 expenditures of US$58.4 million. As of September 30, 2009, there were additional US$2.4 million in accruals.
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
Millions
FY05 FY06 FY07 FY08 FY09
Quarterly Expenditures Comparasion1st Qtr2nd Qtr3rd Qtr4th Qtr
The upward trend represents the addition of 14 districts, increased staff and significant purchases of medical equipment, including ambulances. Quarterly expenditures in the last two quarters, compared with the first two increased by almost two and half times. Based on current and planned expenditures, the Project is well poised to achieve its objectives in terms of disbursements.

63
Project Consortium Partners’ Budget Allocation. Of the total Cooperative Agreement amount of US$92.9 million, 60% is for direct JSI expenditure with the balance for subcontracts with consortium partners. Of the 40% for partners, 60% is allocated to three US-based partners and the remaining 40% to four Pakistan-based partners. Greenstar and PAVHNA, two of the four Pakistan-based partners, agreements concluded on September 30, 2009.
PAIMAN Budget Distribution with Partners
JSIAKUContechGreenstarPAVHNASCUSPCJHU
Cost Share: Cooperative Agreement Modification 12 set the approved cost share at US$4,094,684.
Total Cost Share vs. Reported Cost Share ApprovedReported
As of September 30, 2009, cost share of US$1,634,228 was reported. JSI is confident the remaining cost share will be reported in Year 6. The Finance Section strengthened its systems through random checks and reviews and maintained internal controls to ensure transparency and accountability. Sub-grantee finance management required extensive coordination and liaison with the Project’s Program Section to ensure timely provision of resources to sub-grantees. Regular financial review assisted and helped greatly in building the sub-grantee financial management capacity.

64
Overall, during the reporting year, the Finance Section was able to positively respond to Project implementation requirements, complimenting and contributing positively to the effective implementation of Project activities at the field level. IX. CHALLENGES AND CONSTRAINTS PAIMAN faced challenges in implementation of Project activities outside its control. After the addition of child health and FP to its existing scope of work and geographic expansion, the quantum of work increased several fold. Challenges and constraints were as follows: Administrative Finding competent public health professionals for program implementation in remote, conservative districts was difficult. It required a quarter to complete the recruitment process. Compliance to USAID procurement regulations--the market research, approval of waivers, and international shipping took significantly longer than anticipated. Programmatic To start IMNCI trainings at facility and community levels, curriculum required go-ahead from MOH. It was only after a couple of months that PAIMAN was formally allowed to start the trainings. CMW students identified from the 14 additional districts missed the PNC training cycle that began March 2009. They will not complete their 18 months training until September 2010. In the absence of a concrete plan for deployment and supervision of CMWs once in the field, about 100 were lost, as they either entered a lucrative job in their district, were hired by PPHI, or were married and moved out of their district. The operations research on CMWs was delayed due in examinations and announcement of results and procurement of equipment for Midwifery Homes. Operations research will be completed in September 2010 and analysis and report writing will take a month. Receipt of approval to produce the feature film on population issues was delayed beyond the startup date reflected in the 2008-2009 work plan. The IDPs from Swat, Upper Dir, and Buner were in camps for four months. Project programmatic activities in NWFP could not be accomplished in time as the entir strategy changed when Government notified the Project no staff could attend any training because they were deployed in the camps.
Security The security situation in NWFP in particular and Pakistan in general slowed pace of Project activities. Although other than Swat, Buner, and Upper Dir, no field office was closed, frequent threats and incidents forced a slowdown Project implementation.
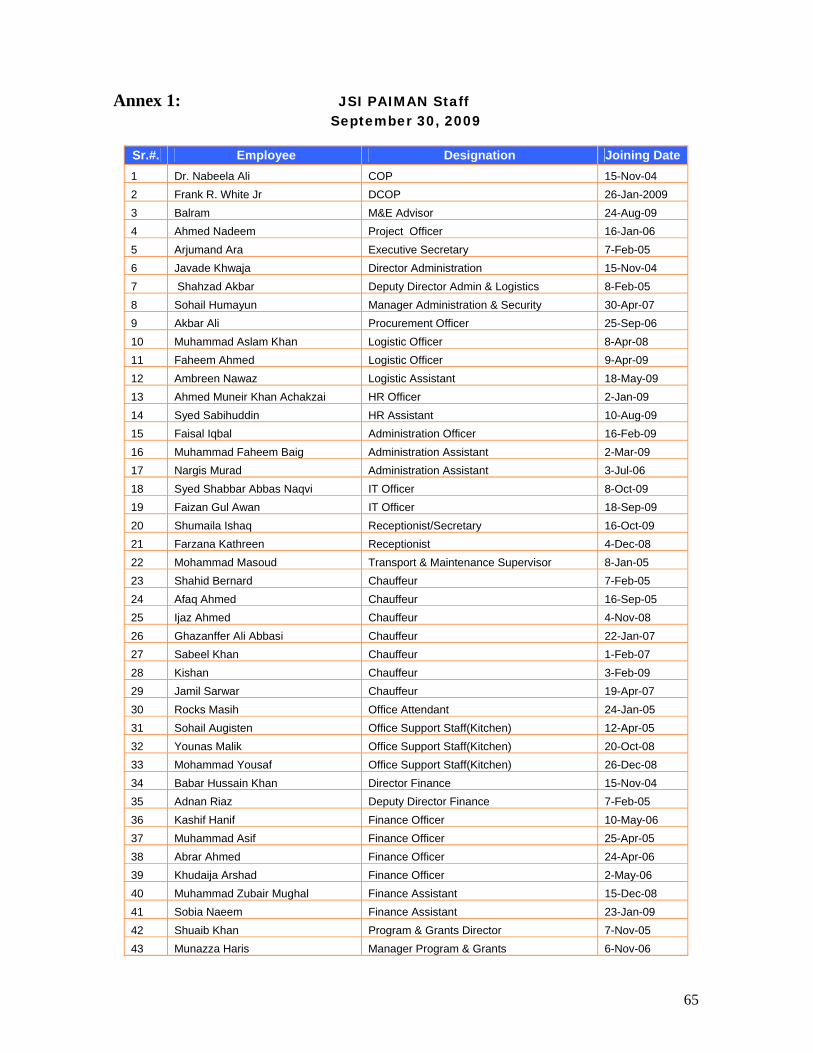
65
Annex 1: JSI PAIMAN Staff September 30, 2009
Sr.#. Employee Designation Joining Date 1 Dr. Nabeela Ali COP 15-Nov-04 2 Frank R. White Jr DCOP 26-Jan-2009 3 Balram M&E Advisor 24-Aug-09 4 Ahmed Nadeem Project Officer 16-Jan-06 5 Arjumand Ara Executive Secretary 7-Feb-05 6 Javade Khwaja Director Administration 15-Nov-04 7 Shahzad Akbar Deputy Director Admin & Logistics 8-Feb-05 8 Sohail Humayun Manager Administration & Security 30-Apr-07 9 Akbar Ali Procurement Officer 25-Sep-06 10 Muhammad Aslam Khan Logistic Officer 8-Apr-08 11 Faheem Ahmed Logistic Officer 9-Apr-09 12 Ambreen Nawaz Logistic Assistant 18-May-09 13 Ahmed Muneir Khan Achakzai HR Officer 2-Jan-09 14 Syed Sabihuddin HR Assistant 10-Aug-09 15 Faisal Iqbal Administration Officer 16-Feb-09 16 Muhammad Faheem Baig Administration Assistant 2-Mar-09 17 Nargis Murad Administration Assistant 3-Jul-06 18 Syed Shabbar Abbas Naqvi IT Officer 8-Oct-09 19 Faizan Gul Awan IT Officer 18-Sep-09 20 Shumaila Ishaq Receptionist/Secretary 16-Oct-09 21 Farzana Kathreen Receptionist 4-Dec-08 22 Mohammad Masoud Transport & Maintenance Supervisor 8-Jan-05 23 Shahid Bernard Chauffeur 7-Feb-05 24 Afaq Ahmed Chauffeur 16-Sep-05 25 Ijaz Ahmed Chauffeur 4-Nov-08 26 Ghazanffer Ali Abbasi Chauffeur 22-Jan-07 27 Sabeel Khan Chauffeur 1-Feb-07 28 Kishan Chauffeur 3-Feb-09 29 Jamil Sarwar Chauffeur 19-Apr-07 30 Rocks Masih Office Attendant 24-Jan-05 31 Sohail Augisten Office Support Staff(Kitchen) 12-Apr-05 32 Younas Malik Office Support Staff(Kitchen) 20-Oct-08 33 Mohammad Yousaf Office Support Staff(Kitchen) 26-Dec-08 34 Babar Hussain Khan Director Finance 15-Nov-04 35 Adnan Riaz Deputy Director Finance 7-Feb-05 36 Kashif Hanif Finance Officer 10-May-06 37 Muhammad Asif Finance Officer 25-Apr-05 38 Abrar Ahmed Finance Officer 24-Apr-06 39 Khudaija Arshad Finance Officer 2-May-06 40 Muhammad Zubair Mughal Finance Assistant 15-Dec-08 41 Sobia Naeem Finance Assistant 23-Jan-09 42 Shuaib Khan Program & Grants Director 7-Nov-05 43 Munazza Haris Manager Program & Grants 6-Nov-06

66
44 Tahseen Ahmad Program & Grants Assistant 17-Sep-07 45 Zareef Uddin Khan National Manager Child Health 17-Oct-08 46 Nasir Idrees National Manager Public Private Partnership 16-Oct-08 NWFP 47 Nadeem Hassan National Manager Child Spacing 2-Feb-09 48 Fazle Jamal Afridi Field Operations Manager 1-Mar-07 49 Nadeem Akhtar Field Operations Manager 15-Dec-08 50 Bilal Alam Program Coordination Officer 8-Jan-08 51 Muhammad Ikram District Program Coordinator 12-Feb-09 52 Sardar Ahmad District Program Coordinator 2-Jan-09 53 Farrukh Jamil District Program Coordinator 2-Jan-09 54 Rafiullah Khan District Program Coordinator 20-Aug-08 55 Samia Irshad Grants Coordinator 27-Aug-09 56 Hasan Sajid Finance Officer 3-Mar-06 57 Faheem Ullah Admin & Finance Assistant 22-Apr-08 58 Muhammed Ayaz Khan District Finance Assistant 2-Feb-09 59 Zahid Rauf District Finance Assistant 2-Feb-09 60 Sohail Khan District Finance Assistant 9-Feb-09 61 Taimur Orakzai District Finance Assistant 2-Feb-09 62 Syed Ajmal Shah District Finance Assistant 2-Feb-09 63 Zia ur Rehman Receptionist/Admin Assistant 10-Apr-09 64 Asmat Ullah Chauffeur 2-Feb-09 65 Amanatullah Chauffeur 11-Sep-06 66 Abdul Hadi Chauffeur 25-Nov-08 67 Jamshed Ahmed Chauffeur 2-Feb-09 68 Mir Azam Chauffeur 2-Feb-09 PUNJAB 69 Fazal Mahmood Khan Field Operations Manager 15-Dec-06 70 Nazia Saeed District Program Coordinator 2-Jun-09 71 Nasir Dilshad District Program Coordinator 2-Feb-09 72 Zeeshan Lodhi Admin & Finance Assistant 25-Sep-06 73 Zameer Haider Program & Admin Assistant 16-Sep-08 74 Hafiz Munawar Hussain District Finance Assistant 2-Feb-09 75 Malik Amir Iqbal District Finance Assistant 26-Aug-09 76 Muhammad Ashraf Chauffeur 26-Feb-08 77 Muhammad Shuaib Chauffeur 20-Feb-09 78 Abdul Sattar Chauffeur 26-Aug-09 SINDH 79 Iftikhar Ahmed Field Operations Manager 20-Jun-05 80 Syed Hasan Mehdi Zaidi Field Operations Manager 1-Jul-05 81 Rohina Rizvi District Program Coordinator 12-Jan-09 82 Muhammed Faisal Saeed Admin & Finance Assistant 28-May-07 83 Sheeba Cecelia David Admin & Finance Assistant 7-Dec-07 84 Fazal Rehman Chauffeur 13-Nov-06 85 Aitbar Khan Chauffeur 2-Mar-09 86 Habibullah Baloch Chauffeur 9-Feb-09 BALOCHISTAN

67
87 Majed Latif Field Operations Manager 2-Jan-09 88 Mir Dad Kakar District Program Coordinator 2-Jan-09 89 Abdul Qadir District Program Coordinator 16-Feb-09 90 Aziz Ullah District Program Coordinator 2-Feb-09 91 Kamalan Gichki District Program Coordinator 5-Jan-09 92 Umar Shah District Finance Assistant 16-Feb-09 93 Irfan Ahmed District Finance Assistant 2-Feb-09 94 Zubair Ahmed District Finance Assistant 26-Jan-09 95 Kamal Khan District Finance Assistant 15-Jan-09 96 Nosheen Rais Admin & Finance Assistant 16-Feb-09 97 Hidayatullah Chauffeur 13-Nov-06 98 Hussain Khan Kakar Chauffeur 26-Jan-09 99 Muhammed Ismail Chauffeur 27-Jan-09 100 Muhammed Yunus Chauffeur 15-Jan-09 101 Muhammad Ismail Chauffeur 6-Apr-09 AJK 102 Fida Hussain Field Operations Manager May 22,2009 103 Faisal Rehman District Program Coordinator 9-Mar-09 104 Riffat Hayat District Program Coordinator 19-Mar-09 105 Khwaja Nasir Abbas Admin & Finance Assistant 9-Feb-09 106 Muhammed Khushnood Khan Chauffeur 16-Feb-09 107 Sheraz Sadique District Finance Assistant 13-Feb-09 108 Azhar Mehmood Shah District Finance Assistant 9-Feb-09 109 Muhammad Azim Chauffeur 23-Feb-09 110 Arshad Hussain Shah Chauffeur 16-Feb-09
FIXED-TERM STAFF IN YEAR 5
S. No Name Status Location
1 Robina Azmat Fixed term Islamabad 2 Dr. Syed Gohar Sajjad Fixed term Islamabad 3 Shiraz Ali Fixed term Islamabad 4 Babar Aziz Fixed term Islamabad 5 Faiza Farooq Fixed term Islamabad 6 Fiza Iftikhar Fixed term Islamabad

68
INTERNS IN YEAR 5
S. No Name Status Location
1 Shiraz Ali Intern Islamabad 2 Faiza Farooq Intern Islamabad 3 Babar Aziz Intern Islamabad 4 Fiza Iftikhar Intern Islamabad 5 Sana Benish Abbas Khan Intern Islamabad 6 Sumbal Sarfaraz Intern Islamabad 7 Fawaz Yazdani Intern Islamabad 8 Mansoor Mumtaz Intern Islamabad 9 Saima Sarfraz Intern Islamabad 10 Syed Mohsin Mazhar Intern Islamabad 11 Hira Naeem Sadique Intern Islamabad 12 Syed Armaghan Hussain Intern Islamabad 13 Saira Butt Intern Islamabad 14 Mansoor Mumtaz Intern Islamabad 15 Fatima Shahryar Intern Islamabad 16 Basit Jamil Intern Quetta 17 Faisal Usman Malik Intern Lahore 18 Syed Rameez Hussain Intern Peshawar
RESIGNED IN YEAR 5
S. No Name Designation Date of Leaving Location 1 Tariq Mehmood Field Operations Manager 04-May-2009 AJK 2 Dr. Imran Munir DPC 10-Feb- 2009 Balochistan 3 Muhammed Zubair Rana Logistics Assistant 07-May-2009 Islamabad 4 Dr. Tassadaq Farooq National Program coordinator 25-May-2009 Islamabad 5 Sana Benish Abbas Khan HR Assistant 17-Jul-2009 Islamabad 6 Toqeer Syed Ali IT Officer 25-Aug-2009 Islamabad 7 Tariq Azeem M&E Advisor 31-Aug-09 Islamabad 8 Dr. Nuzhat Rafique FOM 05-Sep-2009 Lahore 9 Dr. Hameed Ullah DPC 27-Feb-2009 NWFP 10 Muhammed Safder Ali Rajput District Finance Assistant 22-Apr-2009 Sindh 11 Imran Raza Malik IT Specialist 05-Oct-2009 Islamabad

69
Annex 2: Pakistan Initiative for Mothers and Newborns
Status of Civil Works/Renovations Selected Health Facilities 24 Districts
September 30, 2009
Project Province Sr. # District Sr. # Health Facility Status
1 DHQ Hospital, Upper Dir Completed
2 THQH, Warri Completed 1 Upper Dir
3 RHC, Barawal Completed
4 DHQ Hospital, Daggar Completed
5 THQH, Chamla Completed
NWFP
2 Buner
6 RHC, Jower Completed
7 THQ Hospital, Gujjar Khan Completed
8 THQ Hospital, Murree Completed
9 RHC, Mandra Completed 3 Rawalpindi
10 BHU, Kali Mitti Completed
11 DHQH Completed
12 THQ, Sohawa Completed 4 Jhelum
13 RHC, Domeli Completed
14 DHQ Hospital, KhanewaL Completed
15 THQ Hospital, Mian Channu Completed 5 Khanewal
16 RHC Kacha Khu Completed
17 DHQ Hospital DG Khan Completed
18 THQ Hospital Tounsa Completed
PUNJAB
6 D.G. Khan
19 RHC Choti Zarin Completed
20 DHQ Hospital, Uthal Completed
21 THQ Hospital, Hub Completed 7 Lasbella
22 RHC, Bela Completed
23 DHQ Hospital, Dera Allah Yar Completed
P A
I M
A N
O
R I
G I
N A
L
BALOCHISTAN
8 Jafarabad
24 THQ Hospital, Usta Muhammad Completed

70
Pakistan Initiative for Mothers and Newborns
Status of Civil Works/Renovations Selected Health Facilities 24 Districts
September 30, 2009
Project Province Sr. # District Sr. # Health Facility Status
25 RHC, Rohjan Jamali Completed
26 DHQ Hospital, Sukkur Completed
27 THQ Hospital, Rohri Completed 9 Sukkur
28 RHC, Kandra Completed
29 DHQ Hospital, Dadu Completed
30 THQ Hospital, KN Shah Completed
31 RHC, Sita Road Completed
SINDH
10 Dadu
32 BHU, Wahi Pandi Completed
1 DHQ Hospital (Govt. Maternity Hospital)
Work to be started in first quarter of
year 6
2 THQ Hospital (Govt. Infectious Diseases Children Hospital)
Work to be started in first quarter of
year 6 1 Peshawar
3 RHC Gari Tajik Work to be started in first quarter of
year 6
4 DHQ Hospital - Pediatrics Unit Work to be started in first quarter of
year 6
5 THQ Hospital Katlung Work to be started in first quarter of
year 6
6 RHC Sher Garh Work to be started in first quarter of
year 6
7 RHC Toro Work to be started in first quarter of
year 6
2 Mardan
8 RHC Shahbaz Gari Work to be started in first quarter of
year 6
9 DHQ Hospital Work to be started in first quarter of
year 6
10 RHC Jamal Abad Work to be started in first quarter of
year 6
P A
I M
A N
E
X P
A N
S I
O N
.
NWFP
3 Charsadda
11 RHC Battagram Work to be started in first quarter of
year 6

71
Pakistan Initiative for Mothers and Newborns
Status of Civil Works/Renovations Selected Health Facilities 24 Districts
September 30, 2009
Project Province Sr. # District Sr. # Health Facility Status
12 DHQH Hospital (Zanana Hospital) Work to be started in first quarter of
year 6
13 THQ Hospital Kolachi Work to be started in first quarter of
year 6
14 RHC Paharpur Work to be started in first quarter of
year 6
4 DI Khan
15 RHC Panyala Work to be started in first quarter of
year 6
16 DHQ Hospital Work to be started in first quarter of
year 6
17 THQ Hospital Burewala Work to be started in first quarter of
year 6 5 Vehari
18 RHC Luddon Work to be started in first quarter of
year 6
19 DHQ Hospital (Fatima Jinnah WomenHospital, Multan) Work Started
20 THQ Hospital Shujabad Work to be started in first quarter of
year 6
21 RHC Mardan Pur Bosan Work Started
22 BHU Qasim Bela Work Started
23 BHU Muzafar Abad Work Started
24 BHU Binda Sandila Work Started
25 BHU Buch Khusrooabad Work Started
26 BHU Lutaf Abad Work Started
27 BHU Jahangir Abad Work Started
Punjab
6 Multan
28 BHU Jhoke Vaince Work Started
Sindh 7 Khairpur 29 DHQ Hospital (Lady Willington Hospital)
Work to be started in first quarter of
year 6

72
Pakistan Initiative for Mothers and Newborns
Status of Civil Works/Renovations Selected Health Facilities 24 Districts
September 30, 2009
Project Province Sr. # District Sr. # Health Facility Status
30 RHC Pir Jo Goth Work to be started in first quarter of
year 6
31 RHC Gari Mori Work to be started in first quarter of
year 6
32 RHC Kot Deiji Work to be started in first quarter of
year 6
33 RHC Panj Pai Work to be started in first quarter of
year 6
34 RHC Kachlak Work to be started in first quarter of
year 6 8 Quetta
35 RHC Sor Range Work to be started in first quarter of
year 6
36 DHQ Hospital Work to be started in first quarter of
year 6
37 RHC Jiwani Work to be started in first quarter of
year 6
38 RHC Pasni Work to be started in first quarter of
year 6
9 Gwadar
39 RHC Ormara Work to be started in first quarter of
year 6
40 DHQ Hospital Work to be started in first quarter of
year 6
41 RHC Lehri Work to be started in first quarter of
year 6
42 RHC Talli Work to be started in first quarter of
year 6
10 SIBI
43 RHC Luni Work to be started in first quarter of
year 6
44 DHQ Hospital Work to be started in first quarter of
year 6
45 RHC Meena Bazar Work to be started in first quarter of
year 6
Balochistan
11 Zhob
46 RHC Omzha Work to be started in first quarter of
year 6

73
Pakistan Initiative for Mothers and Newborns
Status of Civil Works/Renovations Selected Health Facilities 24 Districts
September 30, 2009
Project Province Sr. # District Sr. # Health Facility Status
47 RHC Qamardin Karez Work to be started in first quarter of
year 6
48 DHQ Hospital Work to be started in first quarter of
year 6
49 THQ Hospital Samahni Work to be started in first quarter of
year 6
50 RHC Barnala Work to be started in first quarter of
year 6
12 Bhimber
51 RHC Panjari Work to be started in first quarter of
year 6
52 DHQ Hospital Work to be started in first quarter of
year 6
53 THQ Hospital Tararkhel Work to be started in first quarter of
year 6
54 RHC Mang Work to be started in first quarter of
year 6
AJK
13 Sadhunati
55 RHC Baluch Work to be started in first quarter of
year 6
Swat CMW Dormitory 56 CMW Schools Mardan (shifted for security reasons)
Work to be started in first quarter of
year 6

74
Annex 3:
Reports and Documents
• PRISM Assessment, Contech International • Supervisory Report of Rollout Client-Centered Approach Training in Rawalpindi,
Bhimber and Khanewal, Population Council • Supervisory Report of Rollout TBA Refresher Training- Districts Rawalpindi, Jhelum,
Sukkur, Dadu, Lasbella, Khanewal and D.G. Khan, Population Council • Decision Space Analysis, Contech International • District Supervisory Assessment System, Contech International
• Performance Assessment of DHMTs, Contech International • Maa Aur Bachay Ki Sehet Kay Tahaffuz Mai Ulama-e-Din Ka Kirdar (Book for Ulama
on MNCH), Johns Hopkins University –Center for Communication Programs
• PAIMAN-After the Promise, Johns Hopkins University –Center for Communication Programs
• National MNCH Brochure, Johns Hopkins University –Center for Communication
Programs
• District -Based MNCH Brochures (23), Johns Hopkins University –Center for Communication Programs
• Breastfeeding Brochure, Johns Hopkins University –Center for Communication Programs
• Health Facility Image Building Brochures (31), Johns Hopkins University –Center for Communication Programs
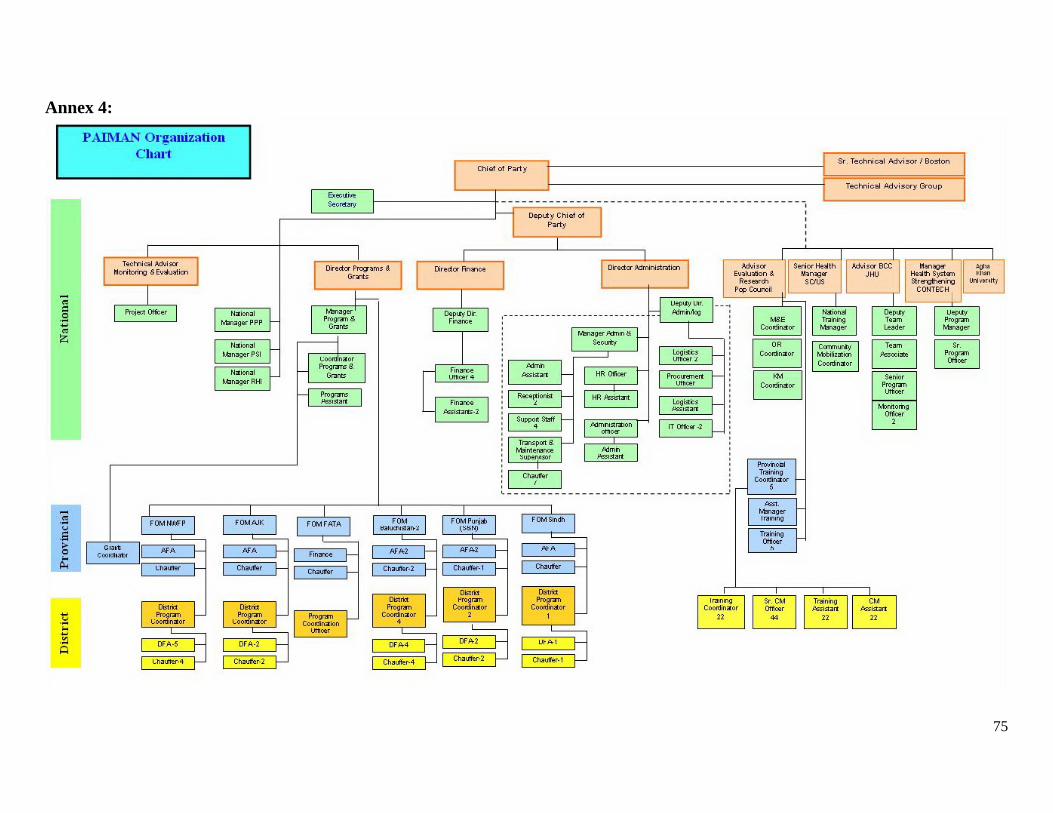
75
Annex 4:
76
CA # 391-A-00-05-01037-00 project is funded by the United States Agency for
International Development and implemented by JSI Research & Training Institute, inc. in conjunction with Aga Khan University, Contech International, Greenstar Social Marketing, JHU/CCP, PAVHNA, Population Council, Save the Children USA