annual report - healogics, inc. · this is the annual report for the period ... 4.1 lymphoedema...
TRANSCRIPT

Page 1 of 39
ANNUAL REPORT Author Associate Clinical Director
Associate Clinical Operations Director Regional Director (South East)
14/03/2016
Approval Senior Management Team
2015
Julie Stanton/Fiona Collins [email protected] [email protected]
Abstract This is the annual report for the period of 01January – 31December 2015 for Healogics Limited

Page 2 of 39
Contents Page(s) 1. About Healogics Limited 3
2. Our Mission and Vision 3
3. Our Staff 3
4. Principle activities and achievements 2015 4
4.1 Activity 4
4.2 Clinical outcomes 4
4.3 Performance against Key patient targets 4
4.4 Patient experience 5-7
4.5 Complaints and compliments 8-9
4.6 Safety and quality 9-11
4.7 Staff performance 11-14
5. Care Quality Commission Regulation 14
6. Infection Control and Prevention 14
7. Information Governance 14-15
8. Priorities and Plans for 2016 15-16
Appendices Appendix 1 Key performance indicators 17-19 Appendix 2 Patient experience, quality of life and 20-22 expectation survey Appendix 3 Audit schedule 23 Appendix 4 Adult Safeguarding report and audit 24-34 Appendix 5 Care Quality Commission compliance 35-39

Page 3 of 39
1. About Healogics Limited Healogics are a provider of wound healing services to the NHS in England. In 2013 Healogics
opened its first Wound Healing Centre in the UK in Eastbourne followed by the opening of six
subsequent Wound Healing Centres across Crawley, Horsham and Mid Sussex. Healogics
employ an evidence based systematic approach to wound healing led by nurses in the UK;
underpinned by a collaborative approach to working with partner agencies.
2. Our Mission and Vision 2.1 Mission: Our Mission is as an organisation we are committed to advancing wound healing by creating and sharing our wound care expertise: everywhere we can, for every patient who would benefit, by the best means available. 2.2 Vision: We are the wound healing expert; driving wound science, healing and prevention forward to help heal more wounds and change more lives. 2.3 Nursing Mission Statement The Clinicians at Healogics Ltd strive to support the organisational mission by consistently providing holistic, personalised, quality clinical and nursing care through a spirit of excellence.
3. Our Staff Number of staff employed = 26
Male 5 Female 21
Registered Nurses 10 Podiatrists 2
Administration staff 8 Health care support workers 6
4. Principle activities and achievements 2015 4.1 Lymphoedema Services - Healogics currently provides lymphoedema services to four
CCG’s, each of which has a slightly different service provision, as detailed below. We have a
total of 4 qualified lymphoedema specialists. The staff group work across one or two CCG’s,
depending on location and size of contract:
Eastbourne, Hailsham and Seaford (EHS) CCG: Healogics provides both a specialist tissue
viability service for this CCG and a separate lymphoedema service, for patients who have
lymphoedema, chronic oedema and lipoedema of the lower limb. We undertake initial
assessments, provide intensive treatment where necessary and provide ongoing personalised
maintenance plans, including hosiery measurement and selection. Provision can be either
clinic based or domiciliary based depending on patient need. (N.B. The CCG has a separate
provider for lymphoedema related to Cancer and end of life).
Hastings and Rother CCG:
Healogics provides a lymphoedema service, for patients who have lymphoedema, chronic
oedema and lipoedema of the lower limb. We undertake initial assessments, provide intensive
treatment where necessary and provide ongoing personalised maintenance plans, including

Page 4 of 39
0%
20%
40%
60%
80%
100%
10 wks 20 wks 30 wks 40 wks 50 wks
Venous Leg Ulcers Healing Rates
NHS usual care NHS systematic care Healogics US Healogics UK
hosiery measurement and selection. Whilst we do not provide specialist tissue viability
services to this CCG, where patients have wounds on the lower limb we are contracted to treat
these in conjunction with our lymphoedema treatment to ensure best outcomes. Provision can
be either clinic based or domiciliary based depending on patient need. (N.B. The CCG has a
separate provider for lymphoedema related to Cancer and end of life).
High Weald Lewes Havens CCG
Healogics is currently contracted to provide a lymphoedema service, for patients who have lymphoedema, chronic oedema and lipoedema of the lower limb. We undertake initial assessments, provide intensive treatment where necessary and provide ongoing personalised maintenance plans, including hosiery measurement and selection. Whilst we do not provide specialist tissue viability services to this CCG, where patients have wounds on the lower limb we are contracted to treat these in conjunction with our lymphoedema treatment to ensure best outcomes. Provision is entirely clinic based.
Western Sussex NHS Trust
Healogics is currently contracted to provide a lymphoedema service, for patients who have lymphoedema, chronic oedema and lipoedema of the lower limb and cancer related lymphoedema. We primarily undertake initial assessments and where authorised, provide intensive treatment, hosiery and garments. We are not contracted to provide maintenance for patients. 4.1.2 Any Qualified Provider - Venous Leg Ulcer pathway. This service is undertaken for Crawley, Horsham and Mid Sussex CCG, we offer clinic based assessment and treatment for venous leg ulcers which has now been extended to all wounds excluding diabetic foot ulcers and domiciliary pressure ulcers. The healing rates for this service have exceeded the Key Performance targets outlined in the AQP document of 70% at 12 weeks for the simple pathway and 70% at 18 weeks for the complex pathway respectively. The current healing rate is 93% at 12 weeks and 87% at 18 weeks (see table 1) Table 1. 4.2 Clinical outcomes Improving Clinical Practice
Development of guidance for staff around the use of the formulary and compression therapy to support Healogics policies.
Development of a competency workbook for staff to promote good practice in assessment and management of wounds.
Page 5 of 39
Review of the competency framework for all clinical staff and increased the number of mandatory competencies.
Introduction of lymphoedema guidelines, training and policy.
All clinical staff have undertaken mandatory 5 and 3 day Tissue Viability training courses and compulsory examination of which they have to achieve an 85% pass rate.
Increasing the number of trained lymphoedema specialist nurses who can undertake manual lymphatic drainage techniques.
Development of clinical procedure manuals for wound care and infection control.
4.3 Key Performance Indicators Healogics has met the Key Performance Indicators of both its commissioning contracts (see appendix 1). 4.4 Patient experience Healogics provides person centred care tailored to the patient needs and preferences were possible. Healogics undertakes a combined Patient Quality of Life and Expectation Survey on all patients on admission to their care, at 4 weeks and on discharge. The Quality of Life questionnaire allows Healogics to monitor the patient’s response to treatment and to alter care plans if required. The patient expectation survey is used in order to ascertain what they require of the service and what their expectations are of their treatment. The results of the surveys are shown in Appendix 2. The surveys have shown that in relation to quality of life and improvements in activities of daily living the service has improved the lives of the patients. Patients are also asked to complete an anonymous patient experience survey. 78% had an excellent experience, 20% good and only 1% had a fair experience. The results are from a random selection of 150 patient questionnaires completed in 2015; 50 completed upon the patient’s initial visit to the clinic, 50 upon review, and 50 upon discharge. The patient’s experience and expectations surveys were good overall but the feedback from the patients were that the forms were too long and they did not like filling too many forms. Therefore the forms have now been shortened to 9 questions as opposed to 20 and the survey in relation to quality of life will now be undertaken for two monthly periods a year to obtain continuity of patient data. NB: The questionnaire underwent a number of changes during 2015. This version of the questionnaire was introduced in quarter 3 of 2015. Where we did complete a review questionnaire every four weeks that a patient was being treated, this is now only completed at 4 weeks and at discharge.
4.5 Complaints and compliments
Complaints, PALs enquiries and Compliments comparative figures (see table 2) Table 2
2014 2015.
PALS enquiries 0 0
Compliments data (cards and letters 78 95
Complaints 0 0
Patient comments: “Having suffered since June with no help from my surgery nurse and having to improvise with dressings, this clinic has been fantastic. After only 3 weeks there was improvement and I am extremely grateful to them.”

Page 6 of 39
“Excellent service from all staff”. “They met all my expectations” “So pleased with everything, restored my confidence and made me comfortable. My sincere thanks.” “The Nurses are a great team, I get on with all of them” “We can only say the service you have given my husband is excellent. Thank you so much It has been most excellent and I am so pleased I was referred here” “Everything was perfect. Many thanks for excellent treatment” “All the staff are so friendly and professional. Thank you” . “An excellent service provided by great staff. Thank you” Healogics continues to work and support Clinical Teams in responding to issues or concerns. We are currently in the process of updating our complaints procedure which will also be included on our television presentation in our reception area.
4.6 Safety and quality
4.6.1 Risk assessments Healogics undertake risk assessments to ensure patient health and safety during any care or treatment and make sure our staff have the qualifications, competence, skills and experience to keep patients safe. A quarterly and annual thematic review of all serious incidents takes place and actions are identified to support further improvements in patient safety. There have been no SUI’s reported. 4.6.2 Clinical and operational audits Healogics developed effective governance and systems to check on the quality and safety of care. For 2015, Healogics set a number of priorities for improving clinical effectiveness. This is outlined below along with details how we performed in meeting this priority, along with progress in the implementation of NICE guidance. (See appendix 3 for audit schedule) Clinical Audits:
Record keeping audit
NICE standards audit
Infection control and prevention audits - Hand hygiene, waste management and environment and cleaning audits
Safeguarding standards audit Operational Audits:
Health and safety
Water safety
Fire safety
Training and competency
Appraisal and staff performance

Page 7 of 39
Staff survey
Action Plans from Audits As a result of the Safeguarding audit numerous changes to practice have been made. These include redesign of the Safeguarding tracker, to ensure that outcomes are captured, integration of Safeguarding in all HR policies, job descriptions and contracts. We have forged links with CCG Safeguarding teams and, based on their advice, made changes to referral forms and consent in relation to mental capacity. The infection control audit identified that the sinks currently installed in each clinic were unsuitable for clinical use. These have all been removed and replaced by appropriate models. The Health and Safety audit determined a need for a designated member of staff to undergo appropriate training. Kathleen McLean agreed to undertake this as part of her Facilities role. Since then, a number of Health and Safety risk assessments have been developed (some in association with HR policies) and these are currently being worked through. Results of Health and Safety audits are shown in table 3. Table 3
Record Keeping Audit A record keeping audit was undertaken at the beginning of the year and the results showed an improvement in key areas, overall on all areas we achieved a standard of 73% which is below the required standard of 85%. However there have been improvements in many keys areas such leg ulcer assessment and wound assessment and treatment charts which the service has been achieving almost 100% and the staff should be congratulated on this improvement. There now needs to be a concentrated effort to improve the poor scoring areas highlighted in the report and with the introduction of the simplified forms this should be made easier to achieve. All areas such as consent to treatment, treatment plans, legibility, signed, dated and contemporaneous were 100% achieved. NICE Guidance Implementation We have continued to strengthen our process around the implementation of NICE guidance within the organisation, the following NICE-related audit was completed during the year:
ITEMFREQUENCY
REQUIRED
FREQUENCY
OCCURRED
FREQUENCY
PERCENTAGE
FREQUENCY
OCCURRED
FREQUENCY
PERCENTAGE
Water Temperature Checks Daily 113 92% 85 66%
Locking Up Checks Daily 98 87% 126 100%
Cleaning Daily Daily 80 98% 127 100%
Cleaning Weekly Weekly 17 100% 26 100%
Fire Warden Weekly Safety Check Weekly 15 58% 20 73%
1st Aid boxes & accident book - monthly check Monthly 6 100% 6 100%
Asbestos monthly check (started July) Monthly 3 100% 5 83
Emergency Lighting- Internal (started June) Monthly 4 100% 7 100
Bi-annual Deep Clean of the clinic Bi Annual 1 100% 1 100%

Page 8 of 39
Leg ulceration Standards We have achieved 84% compliance with the standard. This just fell below the required standard of 85%, the areas that were missed were the following:
The majority of patients had not had a documented health education section ticked
Exercise information was not given
Referral at 6 weeks if non-healing was not undertaken in many cases Therefore we need to improve the documentation in relation to health education given to the patient and exercise regimes need to be routinely supplied to patients. NICE implementation has a key role in the delivery of quality and clinically effective services. It is therefore essential that we are able to demonstrate compliance with NICE guidance as a health and social care provider. Key priorities for 2016 are listed below:
To continue to establish strong links between implementation of NICE Guidance and to develop protocols and Standard Operating Procedures (SoP) on best practice based on NICE Guidance and other national clinical guidance and standards of practice.
Identify NICE Guidance that have explicit recommendations around staffing, and ensure that this is linked with the organisations training programme and staff competencies
Infection control and prevention audits Both EHS and CHMS (at Horsham) conducted quarterly Infection Control Audits throughout 2015. The compliance score ratings are explained as follows:
Compliant (>85%): An excellent standard has been achieved.
Partial Compliance (70 - 85%): Some good practice but there is room for improvement.
Non-compliant, (<70%): Problems were identified on the audit. Complete the action plan as soon as possible and review on a monthly basis. Recommend re-audit in 6 months
Both clinics achieved full compliance at each audit. The clinics also achieved full compliance in relation to hand hygiene, waste management and environment cleanliness. (See table 4) Table 4.
0%
20%
40%
60%
80%
100%
Jan-15 Apr-15 Jul-15 Oct-15
Per
cen
tage
Co
mp
lian
ce S
core
Jan-15 Apr-15 Jul-15 Oct-15
CHMS 98% 98% 98% 98%
EHS 85% 85% 94% 94%
Infection Control Audit Results 2015

Page 9 of 39
(For full report see Infection Control and Prevention annual report 2015)
4.6.3 Safeguarding
The organisation is committed to ensuring that the organisation and its staff have due regard to the need to safeguard and promote the welfare of children and adults. We continue to work closely with local partners to monitor and develop our safeguarding arrangements, and to provide a co-ordinated response to vulnerable children and adults. There have been 35 safeguarding referrals made by the service to the Adult Social Care team in relation to poor standards of care within Nursing Homes. There have been no safeguarding referrals or concerns made to social services about Healogics care and services. (See safeguarding report 2015 – appendix 4a) Safeguarding standards audit In order to check the compliance of the organisation with both National and Local standards for safeguarding the organisation undertook a standards audit, utilising the local safeguarding standards supplied by Sussex CCG. (See appendix 4b for results). The audit showed a number of areas that required additional training of staff and internal processes to improve the reporting mechanism of outcomes. Each standard was RAG rated and action plans produced.
4.7 Staff performance
4.7.1 High quality workforce It is evident that high quality patient care strongly links to a highly skilled and motivated workforce. Workforce performance reporting is a monthly process and includes sickness absence, temporary staffing, appraisal, training and induction information, and HR management. This informs the organisation on our level of performance in relation to quality and what actions may need to be taken. Healogics sickness levels are well below NHS levels and national sickness rates. (See table 5) Table 5
2014/2015 2015 Staff sickness 1.83% - End 2014 1.23% - End 2015
Temporary/agency staff 0 3
% Staff having annual appraisals 100% 100%
% staff undergoing induction training 1.83% - End 2014 1.23% - End 2015
% clinical staff achieving mandatory competency assessments N/A 100%
Number of disciplinary or poor staff performance 4 1
Feedback from staff is mainly via monthly staff meetings however the organisation has plans to introduce an annual staff survey. This information will be analysed and appropriate action plans are to be put in place to improve identified areas. Healogics has robust workforce policies in place to ensure staff are safely recruited, inducted, supervised and appraised and provide a minimum standard. The policies are monitored to ensure managers and staff are compliant with these standards. Mandatory Training compliance is monitored on a monthly basis and a dashboard produced which is reported centrally to the SMT to demonstrate compliance. Healogics is in the process of developing a workforce establishment review which will review current usage of staff, against funded establishment to ensure appropriate staffing levels and skill mix and competencies are in place. A robust recruitment procedure is in place to ensure new staff are safe to work and this complies with all the national recruitment standards which include appropriate pre-

Page 10 of 39
employment checks. All staff are fully inducted corporately and locally when they commence. This includes ensuring they complete the appropriate mandatory training to ensure they are safe to practice. Robust monitoring is in place to ensure our compliance. Checks have been undertaken to ensure appropriate DBS are in place and professional registrations are up to date. 4.7.2 Planning and Developing the Workforce All staff receive annual and bi annual performance and development appraisals. This ensures that any training and development needs are identified and addressed were possible. Also areas of development such as Lymphoedema have been recognised and external training courses sourced to ensure continued provision of safe and effective care. Additional courses provided by external sources (see table 6) Table 6
Course Number of staff attending
Lymphoedema 4
PREVENT 1
Safeguarding Adults enquiry officer training 1
Safer recruiting 2
Sharp debridement 4
Institute of Occupational Safety and Health course. 1
4.7.3 Staff Engagement Regular communications are provided to staff via monthly staff meetings and direct emails from the Regional Director and Clinical Director. Staff have opportunities to directly feedback to the Regional Director in a monthly management meeting and all questions and comments are responded to. We are also developing a Moodle intranet communication and training tool to be launched in the New Year to assist with communication and training issues. 4.7.4 Staff Training Healogics maintain a staff training, education and competency assessment tracker. Healogics has a comprehensive training programme in order to equip its staff to provide highly specialised wound care your care. There has been the development of 4 core competencies and 3 additional competencies to ensure all staff are suitably qualified to provide the essential care required. The staff are managed and supervised by highly skilled Nurse Consultants. (See table 7a &7b)
Wound assessment and management (core)
Leg ulcer assessment and management (core)
Aseptic non-touch technique and infection control (core)
Pressure ulcer prevention and management (core)
Larvae Therapy
Negative pressure wound therapy
Assessment, prevention and management of diabetic foot disease (core-podiatry only)
Health Care Support Workers complete all four of these core competencies:
Wound assessment and management
Leg ulcer assessment and management
Aseptic non-touch technique and infection control

Page 11 of 39
Pressure ulcer prevention and management
Table 7a
Table 7b
5. Care Quality Commission Regulation
5.1 Care Quality Commission (CQC) Registration The Care Quality Commission is the independent regulator of all health and social care services in England. Its role is to ensure that healthcare providers meet government standards of quality and safety. The CQC carry out inspections of healthcare providers to ensure that they meet these standards. There has not been an assessment since 2011 so the organisation has not been able to supply a rating as yet. However, as an organisation we have been ensuring that we can achieve the regulations required by improving our practices and governance procedures. (See appendix 5 for core regulation compliance and action plans).
6. Infection Control and Prevention
Healogics comply with the Standards for Better Health and The Health Act 2006 and have “systems to ensure that the risk of health care acquired infection to patients is reduced, with particular emphasis on high standards of hygiene and cleanliness”.
There have been 11 reported episodes of MRSA patients attending clinics on admission to our care; 8 in the CHMS clinics and 3 at Eastbourne. These patients are triaged to attend
100% 100% 100% 100% 100%78%
100% 100%
0%
25%
50%
75%
100%
EHS Clinical Training Completion Data - Dec 2015
100% 100% 100% 100% 100%90%
100% 100%
10%
35%
60%
85%
CHMS Clinical Training Completion Data - Dec 2015

Page 12 of 39
clinics at the end of the clinic day and the clinical room is then deep cleaned by the domestic staff.
There have been no reported MRSA bacteraemia in 2015.
There have been no outbreaks of infection. The organisation monitor all wound infections that present on assessment at clinic and provide data to the CCG’s as to where there are potential risks of cross infection from referrers may be arising.
7. Information Governance
7.1 Data Quality and Information Governance 7.1 Background Information Governance (IG) allows organisations and individuals to ensure that personal information is handled legally, securely, efficiently and effectively, in order to deliver the best possible care. It additionally enables organisations to put in place procedures and processes for their corporate information that support the efficient location and retrieval of corporate records where and when needed, in particular to meet requests for information and assist compliance with Corporate Governance standards. The Information Governance Framework brings together all of the requirements, standards and best practice that apply to the handling of information allowing implementation of central advice and guidance; compliance with the law; and year on year improvement plans. Information Governance plays a key role in supporting all areas of governance (clinical, financial and corporate), service planning and performance management. Healogics Ltd recognises the importance of reliable information, both in terms of care management of individual service users and the efficient management of services and resources. 7.2 Information Governance Toolkit Return
The submission of the annual Information Governance Toolkit gives assurances to Healogics
Ltd, other organisations and to individuals that personal information is dealt with legally,
securely, efficiently and effectively.
The Information Governance Toolkit is divided into six main areas:
Information Governance Management
Confidentiality/Data Protection
Information Security
Clinical Information
Secondary Use Information
Corporate Information
Healogics Ltd first Information Governance Toolkit Return March 2015 achieved 66%
Satisfactory, Level 2 which is the required standard for an AQP.
Attainment achieved in the second Information Governance Toolkit Return for March 2016:
There are 34 Controls, 3 are Not Applicable to the organisation. Of the 31, 23 are Level 2, 8
are Level 3 compliant:

Page 13 of 39
Grade Key
Not Satisfactory
Not evidenced Attainment Level 2 or above on all requirements (Version 8 or after)
Satisfactory with Improvement Plan
Not evidenced Attainment Level 2 or above on all requirements but improvement actions
provided (Version 8 or after)
Satisfactory
Evidenced Attainment Level 2 or above on all requirements (Version 8 or after)
This year Healogics Ltd has improved its overall score to 75% 'Satisfactory'.
As part of the Information Governance Toolkit submission Healogics Ltd confirmed the IG
Statement of Compliance. (IGSoC). The IGSoC is the agreement between NHS Connecting
for Health (CFH) and Approved Service Recipients on the terms and conditions of access to
NHS CFH systems and services including N3 network.
7.3 Data Quality/Information Assurance
During the year Healogics Ltd has undertaken a security check of its premises and the contents
in order to ensure that the company has adequate provision to safeguard and protect
members of staff, patients, the building and other physical assets including sensitive and
personal information. Action plans have been raised to address any gaps or weaknesses in
provision.
External Auditors undertook a care record keeping audit. The audit is based on the Principles
of Good Record Keeping which is part of the Records Management Framework. The results
Version 13 (Latest) Breakdown by Attainment Level
Level 0
Level 1
Level 2
Level 3
Not Relevant
Page 14 of 39
of these audits were presented to the Information Governance Steering Group. Audits
continue to be carried out on paper care records and these audits are presented to the
Information Governance Steering Group to ensure year on year improvement.
Healogics Ltd is working with Healogics US to develop and implement an Electronic Patient
Record.
7.4 Information Governance Training
Information Governance Training is mandatory for all staff to attend at induction and on an
annual basis. The training is offered either through facilitated sessions or through E-learning.
Information Governance training is supported through raising awareness on particular issues
through team meetings, staff bulletins, Managers Meetings etc.
7.5 Information Governance Incident Reporting
Information governance issues are recorded through the Incident Reporting System. I incident
was reported in the last year involving crypto locker virus, this was reported via the Information
Governance website and recorded as Cyber SIRI Level 1, incident investigated and action
plan put in place to mitigate risk.
7.6 Caldicott Guardian Report
Since the Caldicott Report was published in 1997 by Dame Fiona Caldicott, there have been
significant changes to both Legislation and Codes of Practice which govern access to and use
of patient identifiable information. Implementation of the Caldicott Report recommendations
and a programme of continuous improvement of the organisation’s status against the Caldicott
Principles is reported on to the Information Governance Steering Group quarterly.
7.7 Information Governance Work Plan
An Information Governance work plan as outlined below will be monitored by the Information
Group Steering Group:
a) All outstanding issues from 2014-15 version of the Information Governance Toolkit including
areas where we aspire to a higher score;
b) Any new issues from the Information Governance Toolkit version 14
c) Roll out mandatory update training to achieve 95% of staff trained by March 2016
d) Implement a Document Management System to support maintenance of corporate records
e) Continue to develop the Information Asset Register and ensure that Asset owners
understand their roles and responsibilities
f) Ensure paper records have appropriate procedures in place for tracking, reporting missing
files, etc.
k) Undertake compliance checks to ensure that requests for information are being handled
appropriately, in particular subject access requests and gain customer feedback on the
process;
g) Carry out regular audits to gain an understanding of information governance knowledge of
staff and support the development of action plans to improve information governance in these
areas as required.

Page 15 of 39
8. Priorities and Plans for 2016/2017
8.1 Patient Experience Priorities 2016/17 Priority 1 To improve the routine patient feedback mechanisms across all care pathways. Priority 2 To continue to maintain Cleanliness and reducing Healthcare Associated Infections (HCAI).The organisation remains committed to ensuring patients receive care in clean and safe environments. During the year we will continue to build on the measures put in place in order to support good practice and reduce the risk of infection. Infection Prevention and Control training - To develop an e-learning training programme which runs alongside the face-to-face training helps to ensure that staff maintain knowledge and skills in the control and prevention of infection. To develop a link nurse system within each clinic. Priority 3- To encourage patient forums to develop. Priority 4 –To improve the health education information given to patients. 8.2 Clinical Priorities Healogics will further strengthen the links between clinical audit and the CQC standards to support Healogics objectives and continue with our focus on the quality, clinical effectiveness and patient safety. Key priorities around clinical audit are listed below.
Improve communication strategy for clinical audit to promote staff engagement in the audit process and support the development of services.
Improve the process around the development, implementation and monitoring of action plans to ensure that clinical audit continues to support quality and service improvement
Review and improve the engagement of service users in clinical audit.
To improve the data collection and accuracy of the quality of life and patient expectation surveys.
Key priorities around clinical practice are listed below:
Improve healing outcomes from 110 days to 100 days.
Continue to improve patient education and involvement in their plan of care.
Improve formulary usage and expenditure in order to promote clinical effectiveness.
In addition to the above actions, a number of improvements in the quality of our services have been made as a result of local audits during 2015/16, examples include:
Development of Infection control lead and information governance leads across each clinical area to support teams and clinicians.
Development of guidance for staff for the management of Lymphoedema.
Provision of ongoing training and education on all aspects of tissue viability including updates on relevant NICE guidance around Pressure ulcers , surgical wounds, diabetic foot ulcers and leg ulceration.
Pilot of a new electronic record system (EPR).
Review and revision of the Clinical Record Keeping audit tool.

Page 16 of 39
NICE standards audit tool developed for leg ulceration and diabetic foot ulcers.
8.3 Organisation and operational priorities
1. Implementation of the Electronic records system to improve efficiency.
2. Expansion of current premises to ensure capacity issues and growth are maintained.
3. Completion and implementation of a new staff appraisal system.
4. To continue to maintain high standards and achieve key performance targets.
8.4 Future developments
We will take forward our vision over the next three years through six strategic objectives:- 1. To provide safe and effective care and an excellent patient experience 2. To provide services through empowered staff who have the right skills, attitudes and behaviours 3. To provide an estate and IT infrastructure that is safe, modern and fit for purpose 4. To ensure financial sustainability 5. To develop a culture of personal accountability and earned autonomy 6. To develop a reputation as a good organisation to do business with.

Page 17 of 39
Appendix 1 Key performance Indicators
EHS CCG:
Audit/standards Data Requirements: Reporting Data/Performance
1. Reporting details: “PRIORITY STATUS” required for each referral : HIGH, MEDIUM OR LOW
Very Urgent: 97
Urgent: 203
Non Urgent: 146
Undefined by Referrer: 116
Total: 562
2. Number of 6 week referrals received 256
3. Number of remote care plans produced: Number of remote care plans proceeded as a result of 6 week referrals:
22
4. Number re-referred at 12 weeks for ongoing assessment and treatment Referrals with joint care plan that are re-referred for further treatment at 12 weeks
2
5. Length of time between accepted onto caseload and referral back into practice. Split by healing or ongoing maintenance categorised as type showing weekly bands : 0-4, 4-8, 8-12
0-4 Remote Care Plan 29 RIP 14 Declined treatment 12 Healed 10 Ongoing 9 Discharge, status unknown 7 Assessment Only 2 Other (please state) 24 4-8 Healed 8 Discharge, status unknown 6 Declined treatment 2 Other (please state) 2 Ongoing 1 Remote Care Plan 1 8-12 Discharge, status unknown 17 Healed 8 Other (please state) 5 Ongoing 2 Declined treatment 1 Remote Care Plan 1 RIP 1
Waiting times – receipt of referral to : Average 2 days
6b. production of joint care plans
6c. or assessment at 12 weeks 0
7. Types of wounds - % and numerical split of wound types
· Venous leg ulcer 17% - 116
· Arterial leg ulcer 3% - 20
· Diabetic ulcer 1% - 10
· Other acute wound (surgical and trauma) 4% - 30
. Lymphoedema 7% - 51
· Decubitus (pressure) ulcer 22% - 154
· Other Chronic wound 10% - 71
Page 18 of 39
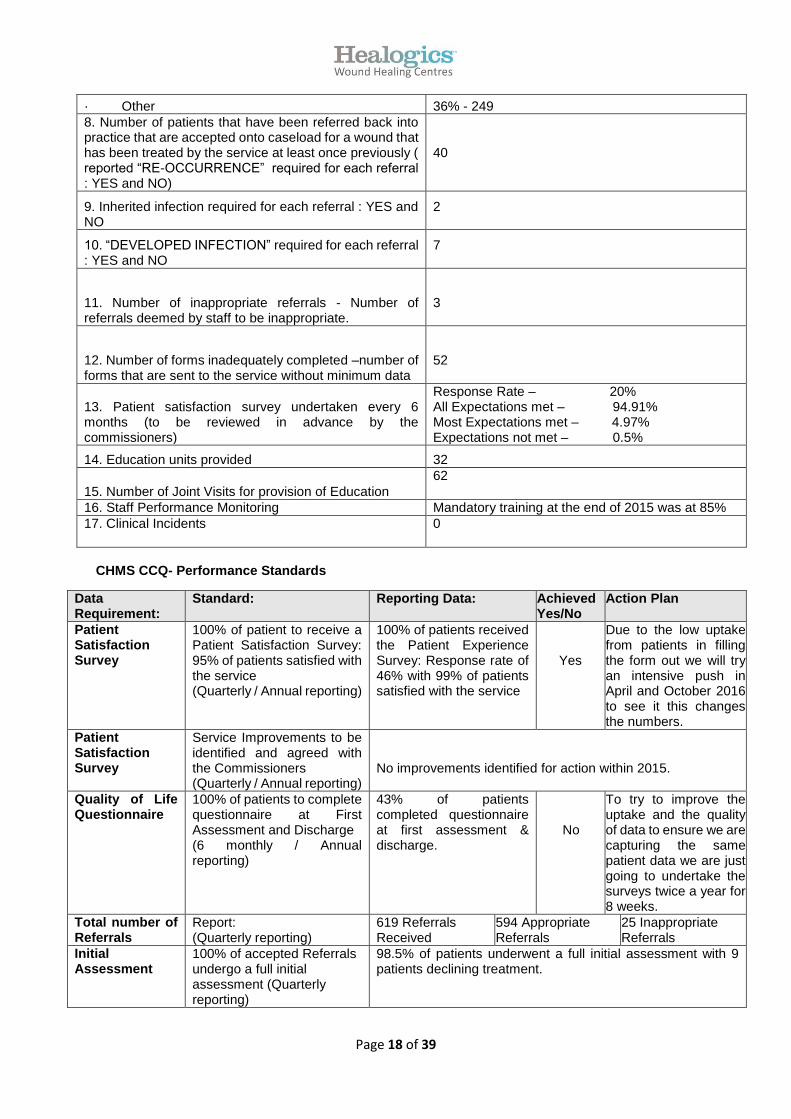
· Other 36% - 249
8. Number of patients that have been referred back into practice that are accepted onto caseload for a wound that has been treated by the service at least once previously ( reported “RE-OCCURRENCE” required for each referral : YES and NO)
40
9. Inherited infection required for each referral : YES and NO
2
10. “DEVELOPED INFECTION” required for each referral : YES and NO
7
11. Number of inappropriate referrals - Number of referrals deemed by staff to be inappropriate.
3
12. Number of forms inadequately completed –number of forms that are sent to the service without minimum data
52
13. Patient satisfaction survey undertaken every 6 months (to be reviewed in advance by the commissioners)
Response Rate – 20% All Expectations met – 94.91% Most Expectations met – 4.97% Expectations not met – 0.5%
14. Education units provided 32
15. Number of Joint Visits for provision of Education
62
16. Staff Performance Monitoring Mandatory training at the end of 2015 was at 85%
17. Clinical Incidents 0
CHMS CCQ- Performance Standards
Data Requirement:
Standard: Reporting Data: Achieved Yes/No
Action Plan
Patient Satisfaction Survey
100% of patient to receive a Patient Satisfaction Survey: 95% of patients satisfied with the service (Quarterly / Annual reporting)
100% of patients received the Patient Experience Survey: Response rate of 46% with 99% of patients satisfied with the service
Yes
Due to the low uptake from patients in filling the form out we will try an intensive push in April and October 2016 to see it this changes the numbers.
Patient Satisfaction Survey
Service Improvements to be identified and agreed with the Commissioners (Quarterly / Annual reporting)
No improvements identified for action within 2015.
Quality of Life Questionnaire
100% of patients to complete questionnaire at First Assessment and Discharge (6 monthly / Annual reporting)
43% of patients completed questionnaire at first assessment & discharge.
No
To try to improve the uptake and the quality of data to ensure we are capturing the same patient data we are just going to undertake the surveys twice a year for 8 weeks.
Total number of Referrals
Report: (Quarterly reporting)
619 Referrals Received
594 Appropriate Referrals
25 Inappropriate Referrals
Initial Assessment
100% of accepted Referrals undergo a full initial assessment (Quarterly reporting)
98.5% of patients underwent a full initial assessment with 9 patients declining treatment.

Page 19 of 39
Onward Referral to Secondary Care
Report: (Quarterly reporting)
52 patients where referred on to Secondary Care.
Total number of patients assigned to Care Pathway 1
Report figures citing rationale for assignment
60 patients met the criteria for Care Pathway 1.
Total number of patients assigned to Care Pathway 2
Report figures citing rationale for assignment
205 patients met the criteria for Care Pathway 2.
Unusual Referral or Activity Trend
Report: (Quarterly reporting)
No unusual Referral or Activity Trends to report.
Assess Concordance at 4 weeks
Report Concordance Levels There were 12 cases of non-concordance in 2015.
Infection Rates Report: (Monthly/Quarterly/Annual Reporting)
There were no cases of MRSA bactereamia.
Information Sharing
Correspondence sent within 5 working days of initial assessment and follow up appointments in 95% of cases
Level of information sharing as agreed with Commissioners.
Support Service Information to patient
Report % of patients who received data on support services (Quarterly reporting)
100% of patients received appropriate literature.
Bounce back Report Bounce back: 1st Referral – Accept 2nd Referral – Accept and Report 3rd Referral – Report and Request a Case Conference (Quarterly reporting)
Identified 12 Bounce backs, who were re referred back to the service.
Personalised Care Planning
100% (Quarterly/Annual reporting)
100%
Patient Healing Rates Care Pathway 1
70% of patients to be healed at discharge (Monthly/Quarterly reporting)
93% of patients discharged from Care Pathway 1 were healed at discharge.
Patient Healing Rates Care Pathway 2
70% of patients to be healed at discharge (Monthly/Quarterly reporting)
87% of patients discharged from Care Pathway 2 were healed at discharge.
Complaints and Litigation Claims
Report (Monthly/Quarterly/Annual reporting)
0
Never Events Report 0
PALS Enquiries Report (Quarterly reporting)
0 0
Peer Satisfaction Survey
Report (Annual reporting)
Annual Peer Satisfaction Survey sent out to GP’s in January 2016. Awaiting results.
RIDDOR Report 0

Page 20 of 39
Appendix Two: Patient Quality of Life and Expectation Survey and Experience survey Numbers shown in the graphs below indicate patient’s positive responses to questions. 1. What problems do you experience in relation to daily living at present relating to your wound?
The patient’s that were questioned had improved in all areas of their activities of daily living of
life.
2. What problems do you experience in relation to your feeling of well-being?
The problems found with survey is that we were not able to catch the original patients and the
consecutive data at 4 weeks and then at discharge. So the patient’s data that we collected
initially was not necessarily the same patients at 4 weeks then at discharge so this is not
comparative data. Therefore we are currently working on a new data collection method to
ensure that this is valid and comparable data.
3. What physical wound related problems are you experiencing?
1511
15
711
25
128
118
1116
6 5 5 37
12
05
1015202530
Difficultywearingnormalclothes
DifficultySleeping
Difficultymaintaining
hygeine
Unable to goshopping
Difficultyundertakinghousework
Difficultywalking
Problems you experience in daily living relating to your wound.
Initial
Review
Discharge
2
20
512 8
23
17
5 6 3 1515
8 8 83
0102030
PoorAppetite
UndertakingUsual
Activities
SocialIsolation
Anxiety /Low Mood
Depression MaintainingRelationships
Problems you experience in relation to your feeling of well being
Initial
Review
Discharge
16
3
13 14
21
2
19
69
16
1 0
11
0 2 30 0
05
10152025
Pain Odour / Smell Pain /Irritation
from dressing
Leakage Swelling Other (Pleasestate)
Physical wound-related problems are you experiencing
Initial
Review
Discharge

Page 21 of 39
4. We would like to know how good or bad your health is today on a scale of 1 - 100
The problems found with this survey is that we were not able to catch the original patients and
the consecutive data at 4 weeks and then at discharge. So the patient’s data that we collected
initially was not necessarily the same patients at 4 weeks then at discharge so this is not
comparative data.
5. What are you expecting the service to achieve in relation to your wound? (Initial)
4.4 (b) Patient Expectation Survey
The Healogics Patient Experience Survey asks 20 questions to measure patient experience
and satisfaction and to identify potential areas for improvement.
As above, the results shown are from a random selection of 150 patient questionnaires
completed in 2015; 50 completed upon the patient’s initial visit to the clinic, 50 upon review,
and 50 upon discharge.
NB: The questionnaire underwent a number of changes during 2015. This version of the
questionnaire was introduced in Quarter 3 of 2015. Where we did complete a review
questionnaire every four weeks that a patient was attending Healogics, this is now only
completed at 4 weeks and at discharge.
1 Level of satisfaction with the manner in which you were treated
69% 69% 71%
0%
50%
100%
Initial Review Discharge
How is your health today?
Patient self-score out of100
Linear (Patient self-score out of 100)
39
164 12 20 20
313 7 4 3 4 4 25 2 2 1 3 4 0
Healing Control of pain Control ofodour / smell
Control ofleakage
Reduceswelling
Improvequality of life
Reduce socialisolation
What are your expectations? (Initial) /Have these been achieved? (Review, Discharge)
Initial Review Discharge
78%
20%
1% 0% 1%0%
50%
100%
Excellent Good Fair Poor N/A% P
ate
int
Re
spo
nse
s
Level of satisfaction with how you were treated

Page 22 of 39
2 Level of satisfaction with the amount of information provided
3 How would you rate the overall satisfaction with the service provided
Total 2015
The following graph is based on responses to all 20 questions from the sample of 150
questionnaires.
.
79%
18%1% 0% 0%
0%
50%
100%
Excellent Good Fair Poor N/A
% P
atie
nt
Re
spo
nse
s
Level of satisfaction with the amount of information provided
74%
23%
1% 1% 1%0%
20%
40%
60%
80%
Excellent Good Fair Poor N/A% P
atie
nt
Re
spo
nse
s
Level of overall satisfaction with the service provided
75.4%
20.2%
1.7% 0.6% 2.1%
0.0%
20.0%
40.0%
60.0%
80.0%
Excellent Good Fair Poor N/A
% P
atie
nt
Re
spo
nse
s
Totals 2015

Page 23 of 39
Appendix 3: Audit Schedule
Audit
Responsible
person January February March April May June July August September October November December
CLINICAL
Records/
documentation
DR/nominated
admin- results to Bi annual Bi annual
Waste
management HCA Quarterly Quarterly Quarterly Quarterly
Hand hygiene HCA Quarterly Quarterly Quarterly Quarterly
Patient
expectation ongoing ongoing ongoing Quarterly ongoing ongoing Quarterly ongoing ongoing Quarterly ongoing ongoing
Patient
experience ongoing ongoing ongoing Quarterly ongoing ongoing Quarterly ongoing ongoing Quarterly ongoing ongoing
Leg ulcer
standards(NICE) Bi annual Bi annual
Diabetic foot
ulcer standard Bi annual Bi annual
Cleaning HCA
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual Annual
Infection control RD/NC Quarterly Quarterly Quarterly Quarterly
OPERATIONAL
Health and
safety Annual
Fire safety
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
weekly check/ bi
annual check/ annual
Training and
competency Annual
Appraisal/perfor
mance Bi annual Bi annual
Staff survey Annual
CQC by RD Bi annual Bi annual
Healogics Audit schedule

Page 24 of 39
Appendix 4a: – Safeguarding Report 2015
Authors: Fiona Collins, Caoimhe Ntuli
Contents:
Safeguarding Annual Report
1. CHMS Safeguarding Alerts 2015 2. EHS Safeguarding Alerts 2015 3. Input Requested EHS 2015 4. Other Relevant Information 5. Safeguarding Training 6. Key actions/conclusion
1. CHMS Safeguarding Alerts 2015
CHMS Clinicians raised one safeguarding alert during 2015. In November, a patient attending
Horsham clinic tripped and fell. The TVN Consultant at CHMS became concerned at the
apparent lack of concern or support from the patient’s wife and reported the incident to West
Sussex Safeguarding. Upon reporting the incident, she was advised that the Safeguarding
team were already aware of the patient. A representative of the West Sussex Safeguarding
team requested that, at the patient’s next appointment, Healogics staff ask if the patient would
like a call bell for his home. Healogics offered this and wrote to the patient’s GP to advise that
this was done.
2. EHS Safeguarding Alerts 2015
EHS Clinicians identified thirty four safeguarding incidents throughout 2015. A breakdown of
these issues is shown below.
The majority of these incidents, 26 (73%), were reports of pressure damage. Please see below
for a further breakdown of these reports.
3%6%
6% 3%
3%
76%
3%
Breakdown of EHS Safeguarding Incidents Reported 2015
Deterioration of wound: Concernabout Quality of Care
Concern/Suspicion ofAbuse/Neglect
Concern about patient's capacityto make decisions
Patient Reported Domestic Abuse
Photographs received to Healogicsunsecured email
Pressure Damage
Suspected deep tissue injurycaused by inappropriate bandaging

Page 25 of 39
There were thirteen cases of unstageable Pressure Damage reported in 2015. In five cases,
the incident was reported by Healogics, in three cases the incident was reported by the
Nursing Home where the patients were resident.
In two of these cases, a safeguarding was not raised. Both patients were non-compliant with
pressure relieving equipment. It was decided that although neither patient was compliant, both
had the capacity to make decisions about her care.
There were four incidents of Grade 4 Pressure Damage reported. In each of the incidents,
Adult Social Care was informed. In one case the CQC were already aware of the incident.
There were five cases of Grade 3 Pressure Damage reported. In all five cases, the incident
was reported. In two of the cases this was done by Healogics, in another two cases, the
Nursing Home where the patients were resident reported the incidents and in the remaining
case, Healogics prepared a Care Plan for the District Nurses and requested that they report
the incident as part of this plan.
One incident related to a Grade 2 pressure ulcer. The Healogics clinician found that this patient
was also suffering with a suspected deep tissue injury. The incident was reported to the East
Sussex Safeguarding Team.
Two of these incidents related to the discovery of more than one pressure sore at different
stages. The first of these incidents was reported in March when a patient was discovered to
have ungradeable pressure ulcers to both heels and a Grade 4 sacral pressure sore. The
second was reported in November, the patient had developed a Grade 4 pressure ulcer on
his foot and a Grade 2 pressure ulcer to his sacrum.
One incident in October was reported as a “possible pressure ulcer” to the patient’s foot. This
patient is diabetic. In this case a remote care plan was prepared and off-loading advice was
given. The Safeguarding team for East Sussex were informed.
13
45
10
1 1 1
Incidents of Pressure Damage 2015

Page 26 of 39
Non-Pressure Damage Safeguarding Incidents EHS 2015
The remaining eight safeguarding incidents are broken down as follows:
Two of these reported incidents, one in May and another in June, related to concerns about a
patient’s capacity to make decisions. In May, a Healogics clinician visited a patient at an
Eastbourne nursing home. The clinician reported deterioration to an existing wound to sacrum
and also reported that the patient had lost a significant amount of weight since the last visit in
April. The clinician was concerned about the patient’s mental state and the response of the
staff at the nursing home, so the incident was reported to Adult Social Care.
In June, a patient attending Eastbourne Clinic refused bandages. The treating clinician felt
that the patient lacked the insight to make an informed decision about his care and observed
that the patient demonstrated a short term memory and disorientation – he was unable to
remember how he had arrived at the clinic and was not able to confirm the date. The clinician
reported the incident to Social Services and to the patient’s GP.
Two of these incidents were reported out of concerns about abuse or neglect of a vulnerable
adult. The first patient visited Eastbourne clinic for an appointment in May. The attending
clinician was concerned about the patient’s appearance and the way in which her daughter,
who is her main carer, interacted with the patient and Healogics staff during her appointment.
The clinician contacted the patient’s support worker and reported his concerns.
The second patient visited Eastbourne clinic in June and reported that her hair had caught
alight earlier that morning. Her hair was singed to the scalp and she had a superficial burn to
top of head. The accounts of the incident from the patient and her carer differed, so Social
Services contacted and the incident was reported.
In one of these cases, in April, a patient reported domestic abuse to a Healogics clinician
during her appointment. The nurse attending the patient and Associate Clinical Director, Julie
Stanton, who was also attending the patient, advised that they must contact and inform Adult
Social Care and the patient’s GP. The incident was reported to social services on the same
day.
In one case in June there was concern about a suspected deep tissue injury caused to a
patient by inappropriate bandaging carried out by staff at the nursing home where he lived.
1
2
2
1
1
1
0 1 2
Deterioration of wound: Concern about Quality of Care
Concern/Suspicion of Abuse/Neglect
Concern about patient's capacity to make decisions
Patient Reported Domestic Abuse
Photographs received to Healogics unsecured email
Suspected deep tissue injury caused by inappropriatebandaging
Non-Pressure Damage Safeguarding Incidents 2015

Page 27 of 39
Healogics informed Adult Social Care, and further discussed their concerns with the
Registered Nurse and the Manager of the nursing home. Upon follow up, our clinician was
advised that training in compression bandaging techniques was delivered by the CQC at the
home to avoid a reoccurrence of the issue.
In June and into July there was concern over the quality of care delivered to another patient
at the same home. Because compression bandaging was suspended until the training was
complete, another patient who required compression bandaging did not have this delivered to
her. Two Healogics clinicians advised on alternative dressing regimes and alternative
bandaging. The wound deteriorated and the patient also showed signs of infection and an
episode of varicose eczema during this period. Healogics continued home visits, took swabs
and tracings, provided care plans and a course of topical steroids. Adult Social Care was
informed of the incident.
In the final case, in September, photographs of patient were sent from a Nursing Home to an
unsecured Healogics email. The email did not contain any other patient information, but the
photographs were personal in nature. The incident was reported to Julie Stanton, who advised
contacting the CQC. They in turn advised Healogics to raise an Adult Protection against the
Nursing Home.
3. Input Requested EHS 2015
In October, Healogics, along with members of the Community Nursing team, members of the
East Sussex Safeguarding team and a CQC inspector, were copied in correspondence from
the interim manager at a Care Home in Polegate to the GP of a Healogics patient. The
manager raised concerns about the apparent deterioration of the leg ulcers of this patient and
drew attention to what he described as “disharmony” in the arrangement of collaborative
meetings between District Nurses and Healogics clinicians, a factor which he feared had
contributed to the patient’s worsening condition.
The manager requested that a Multi-Disciplinary Team meeting be arranged to discuss the
patient’s future treatment and agree a collaborative approach. He advised that the matter had
been mentioned in a Safeguarding meeting and that he had completed a notification to the
CQC concerning the issue. Following this letter, a joint visit was arranged with the District
Nursing Manager and a Healogics clinician. During this visit the clinician also consulted with
the Home manager and the patient’s wife. The clinician reported the meeting as an opportunity
to clarify some of the misunderstandings which occurred and further underlined Healogics full
availability to collaborate with all involved parties for the patient’s best interest, as is the usual
practice for Healogics. A new care plan was prepared and a new schedule for collaborative
visits was arranged.
In 2015, while Healogics captured data on Safeguarding referrals made to the Care Quality
Commission and Adult Social Care services, it did not capture incidents when input from
Healogics was requested as part of other Safeguarding investigations or enquiries. To remedy
this, a new page has been created for the 2016 Safeguarding Tracker which will capture this
data using the following fields.
Date Received
Patient ID
Nature of Request (Report/Meeting/Discussion)
Requested by: (Organisation/Role)
Action Taken
Date/By Whom (Clinician Initials)

Page 28 of 39
Outcome
Updated Outcome
Further Comments
No Response from ASC, update after 6 Weeks
4. Other Relevant Information
From November 2015, two new fields of data capture have been added to the Clinical
Governance Exception Report section in the Monthly Clinical Reports prepared for EHS and
CHMS, reflecting our obligations under PREVENT and Female Genital Mutilation (FGM)
Safeguarding reporting.
In December 2015, a meeting was held to discuss current methods of reporting Safeguarding
incidents at EHS.
5. Safeguarding Training
Both EHS and CHMS Clinicians have achieved 100% compliance in Child Safeguarding
Training. CHMS Clinicians have also achieved 100% compliance in Safeguarding Vulnerable
Adult Training. EHS Clinicians have achieved 67% compliance, with two members of staff due
to completed their Annual Update Training by the end of February, and one new staff member
due to undertake this training within one week.
6. Key Actions/conclusion
The organisation is committed to ensuring that the organisation and its staff have due regard
to the need to safeguard and promote the welfare of children and adults. We continue to work
closely with local partners to monitor and develop our safeguarding arrangements, and to
provide a co-ordinated response to vulnerable children and adults.
There have been no safeguarding referrals or concerns made to social services about
Healogics care and services.
In order to check the compliance of the organisation with both National and Local standards
for safeguarding the organisation undertook a standards audit, utilising the local safeguarding
standards supplied by Sussex CCG. The audit showed a number of areas that required
additional training of staff and internal processes to improve the reporting mechanism of
outcomes. Each standard was RAG rated and action plans produced.

Page 29 of 39
Appendix 4b: Safeguarding Standards Audit Name Of Organisation: Healogics
Address: 43 Gildredge Road, Eastbourne, East Sussex BN21
Name of Lead Person and Job Title: Richard Vaux –Managing Director
Name of Person completing this
Audit/Job Title
Julie Stanton- Associate Clinical Director
Fiona Collins – Regional Director – South East
Tel No: 07 E-Mail:[email protected]
Briefly describe the nature of the work that your organisation does with Children/Adults:
Healogics comes into contact with children and / or vulnerable adults through the following activities:
Wound care clinics
Domiciliary Visits for tissue viability assessment and treatment
Residential and Care Homes with nursing visits for tissue viability assessment and treatment The types of contact with children and / or vulnerable adults will be regulated contact dependent on their or their relatives wound care needs.
Standard-Strategic Leadership Yes No N/A Action Plan Person responsible
Action by: RAG rating
1.1, 1.3 The Safeguarding policy is adopted at senior level and there is a lead director responsible for dissemination.
Section added to SMT meetings to include safeguarding , to ensure Richard is kept up to date of developments
Julie Stanton September 2015
1.2 and 1.10 The safeguarding policy is promoted and disseminated within the organisation
1.4.The organisation has a PREVENT lead who implements the policy within the organisation
The PREVENT lead has now been identified and will commence training ASAP. PREVENT policy in the process of being developed and then disseminated.
Fiona Collins Julie Stanton
Dec 2015 October 2015
1.5, 1.9 Links and collaborative working have been made with local and regional safeguarding networks ,committees and other services, teams
Fiona Collin to investigate with commissioners whether this is a mandatory requirement or whether the organisation can receive minutes and ensure dissemination amongst staff via monthly clinical meetings.
Fiona Collins December 2015

Page 30 of 39
Standard-1. Strategic Leadership Yes No N/A Action Plan Person responsible
Action by: RAG rating
1.6, 1.7 .Safeguarding is included in training plans and strategy and is an organisational KPI
Update planned for the staff Policy and guideline memory sticks for January 2016
Sue D’Ancey January 2016
1.8 Lead operational role for child safeguarding with clear responsibilities
Do not need a lead Julie Stanton
1.11 Effective systems to monitor and respond to issues with shortfalls in capacity leading to safeguarding risks
There needs to be an agreed policy for capacity and demand, activity versus staff ratio to be worked on
Sue D’Ancey and Fiona Collins
December 2015
1.12 Organisation to inform of any CQC inspection relating to safeguarding and outcomes
No CQC inspections related to safeguarding Two additional columns are to be added to the SUI tracker to include date of safeguarding referral and outcome of referral
Sue D’Ancey October 2015
1.13,1.14. Annual safe guarding report to the SMT
Safeguarding report to be produced Fiona Collins and Sue D’ Ancey
December 2015
Standard- 2. Lead effectively to reduce the potential of abuse
Yes No N/A Action Plan Person responsible
Action by: RAG rating
2.1 Staff are aware of the whistleblowing policy and now how to implement the policy
This needs to be better publicised for all staff and updated into separate policy from the staff handbook- Liaison with HR consultant to update
Fiona Collins November 2015
2.2 Staff understand their obligations under the equality Act 2010.
Quick guides to be developed for work stations Julie Stanton December 2015
2.3 Well publicised zero tolerance of abuse policy
There has been an added section to the safeguarding guidelines but this needs to be developed further with the HR consultant
Fiona Collins December 2015
2.4 Safeguarding information etc.,, dissemination
Any outcomes of new information is disseminated via the monthly team meetings
Fiona Collins December 2015

Page 31 of 39
Standard- 2. Lead effectively to reduce the potential of abuse
Yes No N/A Action Plan Person responsible
Action by: RAG rating
2.5 Staff understand diversity, beliefs and values which may influence safeguarding
Quick guides to be developed for work stations Julie Stanton December 2015
2.6 Complaints procedure –well publicised, external bodies and advocacy and advisory services
Need to review information available in reception areas. PALS leaflets, CAB etc.
Fiona Collins October 2015
2.7 People who use the service understand the safeguarding process
Need to review information available to patients in reception areas.
Julie Stanton October 2015
Standard 3 – Responding effectively to allegations of abuse
Yes No N/A Action Plan Person responsible
Action by : RAG rating
3.1 ,3.2,3.3 Staff respond immediately and effectively to ensure children and adults are protected as per organisation/regional/national safeguarding policy /guidance
3.4, 3.5 Written policy for managing allegations against staff which is compliant with regional safeguarding procedures- including reporting to local authority.
This needs to be produced in conjunction with the HR consultant
Fiona Collins December 2015
3.6 Systems to respond to investigations SUI’s, case reviews etc... and collaborative working with other agencies
Two additional columns are to be added to the SUI tracker to include date of safeguarding referral and outcome of referral
Sue D’Ancey October 2015
3.7 Nominated people trained to handle complaints and allegations against staff
Standard 3 – Responding effectively to allegations of abuse
Yes No N/A Action Plan Person responsible
Action by : RAG rating
3.8 Access to safeguarding advice and support following an incident
Counselling service available to staff, introduction of staff debrief session following referral, and team meeting discussion at monthly meeting to be added to the agenda of monthly meeting
Sue D’Ancy October 2015

Page 32 of 39
3.9 People who are users who are abused or suspected are supported and kept informed.
Standard 4 –Safeguarding practice and procedures
Yes No N/A Action Plan Person responsible
Action by : RAG rating
4.1 Safeguarding procedures are followed, monitored and reviewed
Currently updated Sep 2015
4.2 , 4.3 PREVENT policy and referrals Prevent policy now completed awaiting ratification Section to be added to the exception report on PREVENT referrals
Julie Stanton Sue D’Ancey
October 2015
4.4 Assessment process includes wishes and feelings of children/young adults
4.5 Written guidance to staff on record keeping, information sharing and governance compatible with multi agency policy and procedures
4.6 Restraint policy Do not use restraint within the organisation
4.7 Understanding of legal requirement of mental capacity act – consent to examination and treatment
Quick guides to be developed for work stations
4.8 Deprivation of liberty (DOL,s) policy and understanding
Quick guides to be developed for work stations
4.9 Access to Local multi agency safeguarding policy
Via hyperlink – need to have a printed copy in each centre due to potential IT issues
Fiona Collins October 2015
Standard 4 –Safeguarding practice and procedures
Yes No N/A Action Plan Person responsible
Action by : RAG rating
4.10, 4.11 up to date contact details and guidelines /policy on safeguarding and evidence of dissemination
Require contact names and numbers to local safeguarding leads etc...
Fiona Collins October 2015
4.12, 4.13 Actions plans developed to address areas of noncompliance and risk and process to document actions taken
Inclusion into monthly clinical and SMT meetings- safeguarding sections and annual report
David Gray and Richard Vaux
January 2016
Standard 5 –Staff competence Yes No N/A Action Plan Person responsible
Action by : RAG rating
5.1, 5.2, 5.3 Staff understand and recognise the signs of abuse, how to

Page 33 of 39
refer, liaise with social services and understand multi agency procedures
5.4 Staff access comprehensive training, awareness training is mandatory and staff are trained at appropriate levels,
5.5 Staff receive Prevent awareness training based on NHS England competencies
This has now been placed on the online training Moodle platform and will be undertaken by all staff within the next 3 months
Jane Powell and Sue D’Ancey
December 2015
5.6, 5.7 Staff understand their duty to share information , even without consent in line with local multi agency policies and understand their roles and that of other agencies
Quick guides to be developed for work stations Julie Stanton December 2015
5.8.Supervision polices which also inform practice improvements
5.9 All staff have statements in their JD,s and Person specs which are reviewed in their PDRs
All statements have now been added to the JD,s and Person specs PDR process to be reviewed to include safeguarding process
Fiona Collins December 2015
Standard 5 –Staff competence Yes No N/A Action Plan Person responsible
Action by : RAG rating
5.10 Staff surveys should seek staff views on sharing of information, lessons learnt, recommendation and staff needs in relation to fulfilling their safeguarding responsibilities.
These needs to be added to the staff survey Fiona Collins December 2015
5.11 Lead professionals for safeguarding require supervision
Standard 6 Safer recruitment Yes No N/A Action Plan Person responsible
Action by : RAG rating
6.1 6.2 6.3 Adhere to statutory requirements of the DBS and undertake regular 3 yearly checks
DBS tracker to be updated to include 3 yearly checks
Sue D’Ancey December 2015
6.4 Referral policy for any member of staff suspected of abuse
This needs to be produced in conjunction with the HR consultant
Fiona Collins December 2015
6.5 All appointing staff adhere to safer recruitment guidance and staff access to training in safer recruitment
Appointing staff to attend update training Fiona Collins December 2015

Page 34 of 39
6.6 Induction- new employees are made aware of policies and procedures and training needs are identified
6.7. Demonstrate commitment to safe guarding through recruitment process in advertising or information sent to prospective candidates
This can be improved by adding additional information in advertisements and information sent to prospective candidates
Fiona Collins December 2015
Standard 7 –Learning from incidents Yes No N/A Action Plan Person responsible
Action by : RAG rating
7.1 All safe guarding incident’s and SUI,s and complaints are reported , assessment of risks
Two additional columns are to be added to the SUI tracker to include date of safeguarding referral and outcome of referral
Sue D’Ancey October 2015
Standard 7 –Learning from incidents Yes No N/A Action Plan Person responsible
Action by : RAG rating
7.2,7.3,7.4 Process in place to disseminate serious case review, SUI,s, changes to practice , from lessons learnt and monitoring of compliance to recommendations and action plans
Two additional columns are to be added to the SUI tracker to include date of safeguarding referral and outcome of referral Agenda item to be added to monthly team meetings and SMT and clinical reports and meetings
Sue D’Ancey Julie Stanton
October 2015
7.5 ,7.6 and 7.7 Themes , trends and incidents and complaints will be monitored and actions plans developed, staff encouraged to discuss and debrief and have access to training
Two additional columns are to be added to the SUI tracker to include date of safeguarding referral and outcome of referral Agenda item to be added to monthly team meetings and SMT and clinical reports and meetings
Sue D’Ancey Julie Stanton
October 2015
Standard 8 –Commissioning Yes No N/A Action Plan Person responsible
Action by : RAG rating
8.1, 8.2 SLA,s contracts include safeguarding process
Standard 9 –Safeguarding data requested by the DOH , LSCB
Yes No N/A Action Plan Person responsible
Action by : RAG rating
9.1 , 9.2 Data collection on female genital mutilation and report and training
Column to be added to exception report for FGM Training to be added on identification of FGM
Sue D’Ancey Jane Powell
October 2015
9.3 Information leaflet on support available for women who have undergone FGM
Leaflet to be provided Julie Stanton October 2015
9.4 Prevent referrals to CCG Section to be added to the exception report on PREVENT referrals
Sue D’Ancey October 2015

Page 35 of 39
Appendix 5: CQC regulations and compliance – Action Plans
CQC regulation
Performance requirement
Method of monitoring Outcome Action Plan
Care and welfare of service users
1. To ensure that Infection control procedures are adhered to 2. Health and safety procedures are robust 3. Staff capacity is maintained 4. Staff are appropriately trained
-Hand hygiene audit -Waste audit -Environment audit -Legionella assessment -Fire safety assessment Staff sickness figures % of clinics in month with temporary staff % of staff completing mandatory training 100 % of staff completing Tissue viability course 100 % of staff completing mandatory competency assessments
-Hand Hygiene Audit completed monthly. Incidents of failure in Jan, Jul, Sep & Oct. All other months achieved >95% compliance -Waste Audit completed quarterly, 100% compliance achieved at each audit. - Environment Audit completed monthly, CHMS achieved full compliance. EHS failed the audit by 3% in July, but otherwise achieved full compliance. Both the Legionella & Fire safety assessments had no actions required. Staff sickness figures1.83 % 100% of staff have completed clinical mandatory training in tissue viability 100% of clinical staff completed mandatory competency checks
All staff identified as failing have had additional training and supervision and have now passed the audit. Environment audit –taps replaced Competency updates planned for 2016
Person centred care
1. All patients are given appropriate education and information about their treatment 2.Patients are satisfied with the service they receive and would
Record keeping audit –Bi-annually Patient experience survey 80% (complete) Patient quality of life audit 80% (complete)
100% of patients received the appropriate education & information relating to their treatment. EHS & CHMS struggled to reach the 80% completion standards for the surveys with 20% & 46% reached respectively. Both services combined recorded satisfaction results of 98%. 90% of patients would refer to family and friends
The forms have now been changed and discussion are taking place to get the surveys onto a tablet based system and to undertake the audits bi annually to achieve 100% uptake over the 8 weeks

Page 36 of 39
recommend to family and friends 3. Patients are included in the development of their plan of care. 4. Patients Are treated with dignity and respect and their confidentiality maintained
Patient expectation audit 80% (complete) 2.90% excellent to good 90% refer to friends and family 3. 85% involvement in plan of care and information provided 4. 95% treated with dignity and respect 90% level of Patient Confidentiality.
Patient expectation audit results 90% met 80% concordance rate with treatment 85% of patients involved in their plan of care 100% of patients were treated with dignity & respect.
Need to investigate why the other 15% did not engage? Capacity of lack of understanding.
Dignity and respect
1. all patients are treated with respect and dignity 2. All staff are appropriately trained
95% treated with dignity and respect 100 % of Staff Competency assessments completed 100% of staff trained on Dignity and respect and equality and diversity mandatory training on induction and 3 yearly-
100% of patients were treated with dignity & respect. 100% of staff completed their competency assessments.
Need for consent
1. All patients are given detailed information and are asked to consent prior to treatment and assessment.
Bi annual record audit- 100% compliance 95% Staff competency assessments- annually
100% of patients are given detailed information and are asked to consent prior to treatment and assessment.
Safe care and treatment
1. All serious untoward incidents occurring in Healogics care are recorded and action plans developed and monitored
1. SUI tracker- Monthly clinical governance report to CMT and SMT - % of serious incidents reported to CQC within 3 working days - % of serious incidents completed within 45 working days
1. 0 SUI’s were reported.

Page 37 of 39
2. All registered staff receive a specialist tissue viability 5 day course 3. All Health care support staff are trained on 3 day course 4. All staff receive Mandatory training 5. All clinical staff receive mandatory Competency assessments. 6. All staff are to have annual staff performance appraisals and staff development interviews
- % incidents signed off by managers within 10 working days and action plans produced 2.. 100 % of staff trained 3. 100% of staff are trained 4. 84% of staff completing mandatory training 5.100% of clinical staff undertaking mandatory competency assessments 6.100 % of staff receiving IPR and development reviews
2. 100% of staff are trained. 3. All HCA’s are fully trained. 4. 84% of staff have completed non-clinical mandatory training. 5. 100% of clinical staff have undertaken the mandatory competency assessments. 6. 100% of staff have received an annual appraisal.
Safeguarding service users form abuse
1. All safeguarding referrals are recorded and monitored
1. The number of referrals to adult/child safeguarding teams made by Healogics staff- (Safeguarding tracker) 2. The number of adult/child safeguarding referrals made against Healogics staff
1. There were 34 EHS referrals to adult/child safeguarding teams & 1 for CHMS. 2. None

Page 38 of 39
3. Action plans and outcome reports monitored at monthly clinical management meetings
3. There are no outcome reports but this has been highlighted & will commence in 2016.
Cleanliness, safety and maintenance of equipment and premises
1. To ensure that all equipment and premises are cleaned to National standards 2. All equipment is maintained as per manufacturers instruction and safety requirements
1. Weekly Environment audit % target 95% 2. Equipment maintenance tracker
1. 100% achieved in both EHS & CHMS apart from July when EHS failed by 3%. Action taken & resolved. 2. There is a tracker in place to make sure all equipment is of the correct standard.
Receiving and acting on complaints
1. Number of complaints against the service and staff and response times
1. % of complaints 2. % of Complaints responded to within 3 days 3. % of complaints investigated within 30 days
There were no complaints recorded.
Good governance
1.Healogics has a robust clinical audit programme 2. Information governance audit 3. Safeguarding standards audit
1. Infection control and prevention audit results 95% target –hand hygiene 95% target –environment 95% target – waste management -. NICE standards audit- Leg ulcers and Diabetic foot ulcers Bi annually 85% target - Record keeping audit 85% target
-Hand Hygiene Audit completed monthly. Incidents of failure in Jan, Jul, Sep & Oct. All other months achieved >95% compliance - Environment Audit completed monthly, CHMS achieved full compliance. EHS failed the audit by 3% in July, but otherwise achieved full compliance. The results of the record keeping audits showed a standard of 76% some essential standards have achieved 100% NICE Leg ulcer standards 84% failed by 1% all essential standards met
Ongoing audit plan and link nurse implementation programme to commence to increase awareness around infection control and prevention Nurse consultants to address the shortfalls in the record keeping audit by implementation of training programme and monthly mini record keeping audits.
Fit and proper persons employed
1. All staff receive DBS checks prior to employment and every three years.
% of staff with up to date DBS checks.
100% of staff up to date

Page 39 of 39
Duty of candour
1. Healogics ensures that it admits to patients when mistakes are made and formally apologises and investigates the mistake and ensures lessons are learnt.
1. Number of mistakes in care provision (SUI tracker) 2. Number of apologises given. 3. Reports to SMT and action plans produced
None None required None required