anesthesia for laparoscopic surgery garrett peterson dnp, rn, crna association of veterans affairs...
TRANSCRIPT

Anesthesia for Laparoscopic Surgery
Garrett Peterson DNP, RN, CRNAAssociation of Veterans Affairs
Nurse AnesthetistsAnnual Education Meeting May 2012
Objectives
• Discuss the technique used to create a pneumoperitoneum
• Describe the complications of laparoscopic surgery• Recognize the physiologic effects of
pneumoperitoneum• Select the appropriate anesthetic management
techniques used for laparoscopic surgery• Identify the postoperative considerations for
laparoscopic surgery

Introduction
• Laparoscopy– Greek words• Laparo- meaning flank• Skopein – meaning to examine
– Definition: process of examining the contents of the abdominal cavity using a specially designed endoscope
– Use of laparoscopy has been expanded by different surgical specialities over the decades

Common surgical applications of laparoscopy
• General Surgery– Diagnosis– Evaluation of abdominal
trauma– Lysis of adhesions– Cholecystectomy– Appendectomy– Inguinal hernia repair– Bowel resection– Esophageal reflux surgery– Splenectomy– Adrenalectomy
• Gynecologic Surgery– Diagnosis– Lysis of adhesions– Fallopian-tube surgery– Fulgration of endometrrosis– Ovarian cyst surgery– Laparoscopic-assisted
hysterectomy
• Urologic Surgery– Nephrectomy
Advantages of laparoscopic surgery
• Incisions are small• Earlier postoperative mobility • Shorter hospital stays
Creation of a Pneumoperitoneum
• Pneumoperitoneum– Air within the peritoneal cavity
– Essential to perform the surgery– Clears the view of the operative site allowing room to
move instruments
– Causes physical stress to the body and has residual effects that can increase morbidity
– Highest risk to patient is during creation of the pneumoperitoneum
Creation of a Pneumoperitoneum
• Creation of pneumoperitoneum– Two techniques
• “open or closed”
• Closed technique (older of the two)– Spring loaded needle (Veress
needle) used to pierce the abdominal wall at the thinnest point the infraumbilical region
– Position confirmed by injection of 10 ml of saline
– If unable to aspirate saline, placement is correct
– Carbon dioxide (CO2) is placed through the needle to create a space between abdominal wall and organs

Creation of a Pneumoperitoneum
• The “open” or Hasson technique– Small incision (1.5-3 cm)
inferior to the umbilicus– Peritoneum is directly
incised – Trocar (Hasson cannula)
is placed– Abdomen is insufflated
and the catheter is sutured in place

Creation of a Pneumoperitoneum
• Research– Visceral injuries less frequent with open technique
(not statistically significant)– Major vascular injuries were less when Hasson
technique was used compared to the Veress needle
Complications of Laparoscopic Surgery
• Potential for injury– Structures close to puncture site• IVC, aorta, iliac arteries and veins, bladder, bowel, and
uterus– Obesity, thin habitus, adhesions, masses (tumors)
– Additional injuries • Trauma to major vascular structures
– 0.02-0.9% of cases• Gas embolism• Injury to abdominal or pelvic organs• Migration of gas to extraperitoneal spaces
Complications of Laparoscopic Surgery
• Gas embolism– Rare risk of cardiac arrest– Reported incidence 1 in 77,604 cases– Likely to occur during insufflation• Wrong placement of needle into vessel or organ
– Gas bubbles enter circulation• Pulmonary hypertension• Right ventricular failure• Pulmonary edema• Large bubble can cause a “gas lock” phenomenon
which can obstruct right ventricular outflow
Complications of Laparoscopic Surgery
• Gas embolism–Signs/symptoms•Hypotension•Dysrhythmia• “mill wheel” murmur (churning
sound)•Cyanosis •Pulmonary edema
Complications of Laparoscopic Surgery
• Gas embolism–Management• Stop gas insufflation• Shut off nitrous if being used• 100% O2 administration• Release pneumoperitoneum• Place patient in left lateral decubitus
position• Aspirate gas through a central venous
catheter

Complications of Laparoscopic Surgery
• Visceral Injuries– Occurring when closed technique is used• 0.1 – 0.4%
– Trocar insertion• Gastrointestinal tract perforation• Hepatic and spleen tears
– Reduction of risk of trauma• Decompression with NG for stomach• Emptying of bladder with foley catheter

Complications of Laparoscopic Surgery
• Visceral lesions–Not recognized right away–Most in postoperative period when
symptoms arise• Sepsis• Fistulas• Peritonitis• Abscesses
Complications of Laparoscopic Surgery
• Pneumothorax (serious but rare)– A review of 968 cases revealed the incidence of
pneumothorax or pneumomediastinum in 1.9% of patients
– Higher risk for those undergoing surgery for esophageal reflux disease
– Occurs by two mechanisms• Gas entering weak points in esophagus or aorta• Barotrauma secondary to increased airway pressures and
decreased pulmonary compliance– Ruptured bleb
Complications of Laparoscopic Surgery
• Subcutaneous emphysema (minor complication)–Trocar or Veress needle misplacement
in subcutaneous tissue–Manifested by crepitus

Complications of Laparoscopic Surgery
• Gas used– Most common is CO2– Readily available and inexpensive– Does not support combustion– Rapidly absorbed from the vascular space– Easily excreted
– Can cause hypercarbia– Peritoneal and diaphragmatic irritation
• Leading to shoulder pain

Physiologic Effects of Pneumoperitoneum
• Degree of intraabdominal pressure (impede diaphragmatic expansion)
• Presence of preexisting cardiac disease (increased catecholamine release)• Intravascular volume depletion (decrease
cardiac output)• Duration of the surgery (hypercarbia)

Physiologic Effects of Pneumoperitoneum
• Three mechanisms of how pneumoperitoneum affects the body– Direct mechanical effect– Presence of neurohumoral responses– Effects of absorbed CO2
• Pneumoperitoneum-induced physiological changes – Ventilatory techniques– Intraoperative positioning– Surgical conditions (presence of retractors and packing in)
Physiologic Effects of Pneumoperitoneum
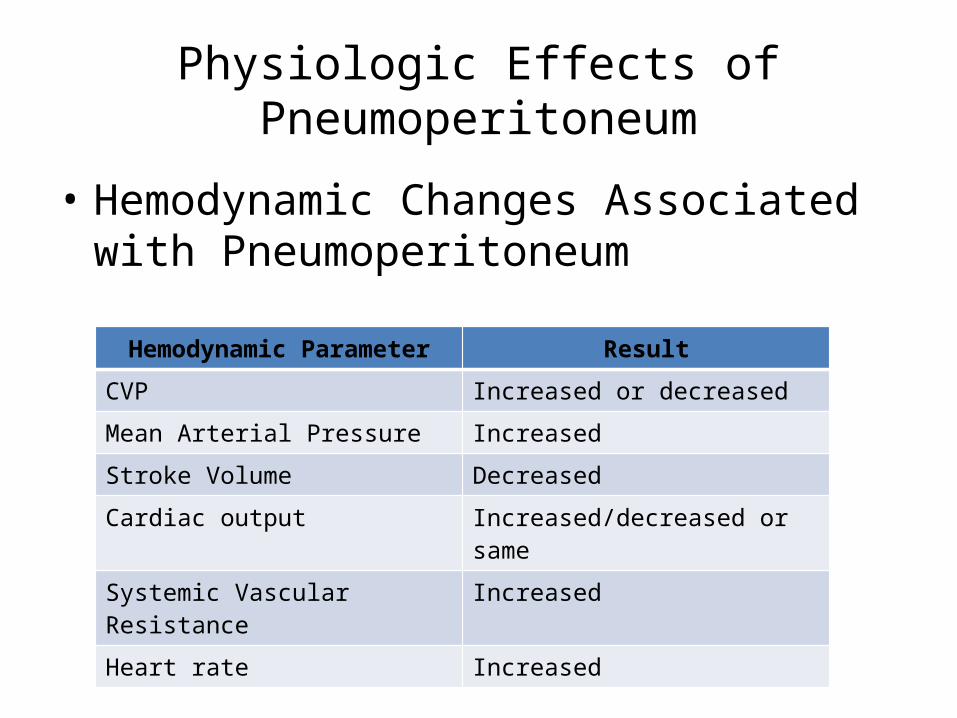
• Hemodynamic Changes Associated with Pneumoperitoneum
Hemodynamic Parameter Result
CVP Increased or decreased
Mean Arterial Pressure Increased
Stroke Volume Decreased
Cardiac output Increased/decreased or same
Systemic Vascular Resistance Increased
Heart rate Increased

Physiologic Effects of Pneumoperitoneum
• SVR increased– Documented in laparoscopy patients• At intraabdominal pressures of 14 mmHg• Increases in SVR as high as 65%
– Mechanism• Increased compression of abdominal arteries and
humoral factor release (vasopressin, renin) have caused increased afterload
Physiologic Effects of Pneumoperitoneum
• CVP filling pressures– Mixed opinions• Patients with increased intrabdominal pressures in
range of 14 to 20 mmHg had increased CVP• Patients with increased intraabdominal pressures > 20
mmHg had a decrease in CVP
– Mechanisms• Vasodilation actions of anesthetics• Intraoperative positioning
Physiologic Effects of Pneumoperitoneum
• Stroke Volume– Reduction• Decreases seen when intraabdominal pressure was in
range of 14 to 15 mmHg
– Interventions to attenuate the decrease in SV• Trendelenburg position• Adequate hydration• Compression of the lower extremities

Physiologic Effects of Pneumoperitoneum
• Cardiac Output/Cardiac Index– Typically decreased
• Up to 50% reduction in CO has been seen• Noticed with intraabdominal pressures of 8 to 12 mmHg, with
significant reduction at 16 mmHg• 5 to 10 minutes after initial decrease, it will partially reverse and
increase back to baseline• Increase in heart rate occurs in laparoscopy patients
– Interventions• Wrapping of legs • Optimize intravascular volume
Physiologic Effects of Pneumoperitoneum
• Arterial Blood Pressure– Increased• At intraabdominal pressures as low as 14 mmHg• Up to 35% increase in MAP
– Mechanism• Increased afterload caused from pneumoperitoneum

Physiologic Effects of Pneumoperitoneum
• Humoral factors– Increased afterload in patients with CO2
pneumoperitoneum• Increased dopamine, vasopressin, epinephrine,
norepinephrine, renin, and cortisol• Vasopressin is the most significant mediator• Catecholamine level increase secondary to stress
response
Physiologic Effects of Pneumoperitoneum
• Cardiovascular effect of pneumoperitoneum– Distention of the vagus nerve during insufflation– Bradycardia is sometimes observed
• Increased intraabdominal pressure can reduce lower extremity blood flow velocity

Physiologic Effects of Pneumoperitoneum
• Patients who are ASA Class III or IV are significantly more prone to the effects of pneumoperitoneum especially if they suffer from altered hemodynamics
Physiologic Effects of Pneumoperitoneum
• CO2 pneumoperitoneum– Increases in partial pressure of arterial CO2 (PaCO2) and
end-tidal CO2 with or without acidosis
• Caused by absorption of gas on peritoneal surface• No increase in O2 consumption during insufflation
• Maximum absorption rate of CO2 is noted with intraabdominal pressure of 10 mmHg
• PaCO2 levels reach a plateau approximately after 40 minutes of induction of the peritoneum

Physiologic Effects of Pneumoperitoneum
• Mild hypercapnia (45 to 50 mmHg) not clinically significant
• Hypercapnia (50 to 70 mmHg) can cause increased physiologic effects– Increased CBF– Peripheral vasodilation– Pulmonary vasoconstriction– Increase risk of cardiac dysrhythmias

Physiologic Effects of Pneumoperitoneum
• Pulmonary Function Changes Associated with Pneumoperitoneum
Pulmonary Change Result
Positive inspiratory pressure (PIP) Increased
Pulmonary compliance Decreased
Vital capacity Decreased
Functional residual capacity Decreased
Intrathroacic pressure Increased

Physiologic Effects of Pneumoperitoneum
• Controlled ventilation– Increase of 20 to 30 % in minute ventilation will
help to decrease the hypercapnia that occurs during pneumoperitoneum
– Careful with respiratory compromised patients • May have CO2 retention leading to decreases in arterial
pH• With very high ETCO2, a direct measurement of PaCO2
may be warranted because ETCO2 may underestimate PaCO2
Physiologic Effects of Pneumoperitoneum
• Endobronchial intubation–Cephalad displacement of the
diaphragm from the increased intraabdominal pressure• One study 50 patients with IAP 15 mmHg• Patients in reverse Trendelenburg
position–6% had right mainstem intubation

Physiologic Effects of Pneumoperitoneum
• Kidneys– Oliguria• Compression of kidneys• Compression of inferior vena cava• Increase in levels of antidiuretic hormone
– Significant reduction in renal blood flow• Intraabdominal pressure around 24 mmHg
– Humoral factors• Vasopressin, renin, aldosterone
Physiologic Effects of Pneumoperitoneum
• Hepatic/Spleen– One study, Intraabdominal pressure around 16 mmHg and
elevated head of bed caused a 68% decrease in hepatic blood flow
– Another study, IAP of 12 mmHg increased hepatic perfusion
– Splanchnic blood flow not disrupted with IAP of 11 to 13 mmHg
Anesthetic Management
• General, regional and local have been used• Local– Minor GYN procedures• Diagnostic laparoscopy or sterilization• Only one hole is created and scope is very small• Shorter hospital stay and reduction in anesthetic costs• 5.5% converted to general• Surgical exposure was limited
Anesthetic Management
• General, regional and local have been used• Regional– Limited to minor GYN surgical procedures– Shoulder and chest discomfort result from
pneumoperitoneum is not well managed with the regional technique

Anesthetic Management
• General, regional and local have been used• General– Most practical– Manages patient discomfort– Controlled ventilation– Use of muscle relaxation
Anesthetic Management
• Use of LMA– Controversial– Increased intraabdominal and intrathoracic pressures
• Increase risk of gastroesophageal reflux and pulmonary aspiration
– Study with 1469 GYN laps concluded that use of an LMA “appears safe”
– Study using fiberoptic examination of the laryngopharynx of 91 pts with an LMA failed to show any regurgitation

Anesthetic Management
• Guidelines for Use of the Laryngeal Mask Airway During Laparoscopy– Ensure clinician is an experienced LMA user– Select patients carefully (e.g., fasted, not obese)– Use correct size of LMA– Make surgeon aware of the use of the LMA– Use total IV anesthetic technique or volatile agent– Adhere to “15” rule: <15 degrees tilt; < 15 cm H2O intraabdominal
pressure; <15 min duration– Avoid inadequate anesthesia during surgery– Avoid disturbance of the patient during emergence
– Maltby JR et al. LMA-Classic and LMA-ProSeal are effective alternatives to endotracheal intubation for gynecological laparoscopy. Can J Anaesth. 2003; 50:71-77.

Postoperative Considerations
• N&V – Common after laparoscopy surgery– Some research shows 50-62% incidence
• Pain– Usually visceral quality on day of surgery
• Abdominal distension – Traction on the nerves and trauma to blood vessels
– Shoulder pain on first day post-op• CO2 induced intraperitoneal acidosis irritates the phrenic
nerve, leading to the shoulder pain

Postoperative Considerations
• Post-op pain– Managed with multimodal approach• NSAIDS, local anesthetics, and opioids
– Research shows the use of NSAIDS in combination with opioids result in a synergism leading to decreased opioid consumption
– Research on port-site infiltration showed value but short lived
Future of Laparoscopic Surgery
• Overcomes some of the limitations imposed by standard laparoscope technology– Robotic surgery– Robotic-assisted surgery– daVinci surgical system
• Surgeon can be 100’s of miles away• 3-d imaging
– Robot assisted radical prostatectomy requires steep Trendelenburg tile (30 to 45 degrees) which increases laryngeal edema and brachial plexus injury
References
• Nagelhout, John J. & Plaus, Karen L. Nurse Anesthesia, W.B. Saunders Company, 4th ed., 2010;32:771-779.
• Sandhu, T., Yamada, S, et al. (2008). Surgical Endoscopy