anesthesia for-carotid-endarterectomy
TRANSCRIPT

Moderator : Dr. C.V.R.Mohan
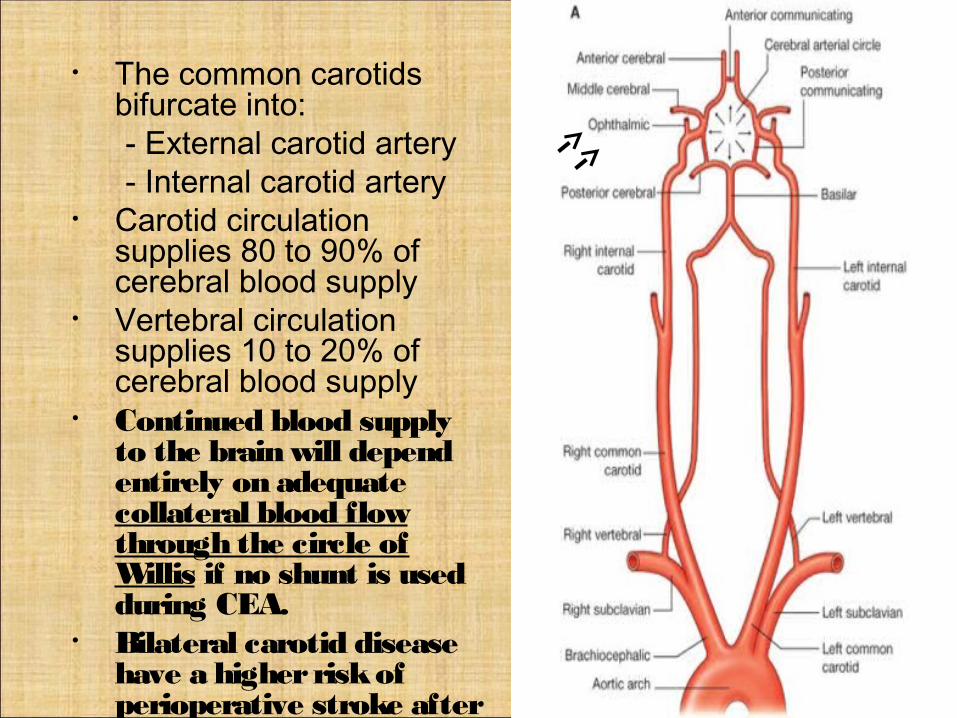
• The common carotids bifurcate into:
- External carotid artery - Internal carotid artery• Carotid circulation
supplies 80 to 90% of cerebral blood supply
• Vertebral circulation supplies 10 to 20% of cerebral blood supply
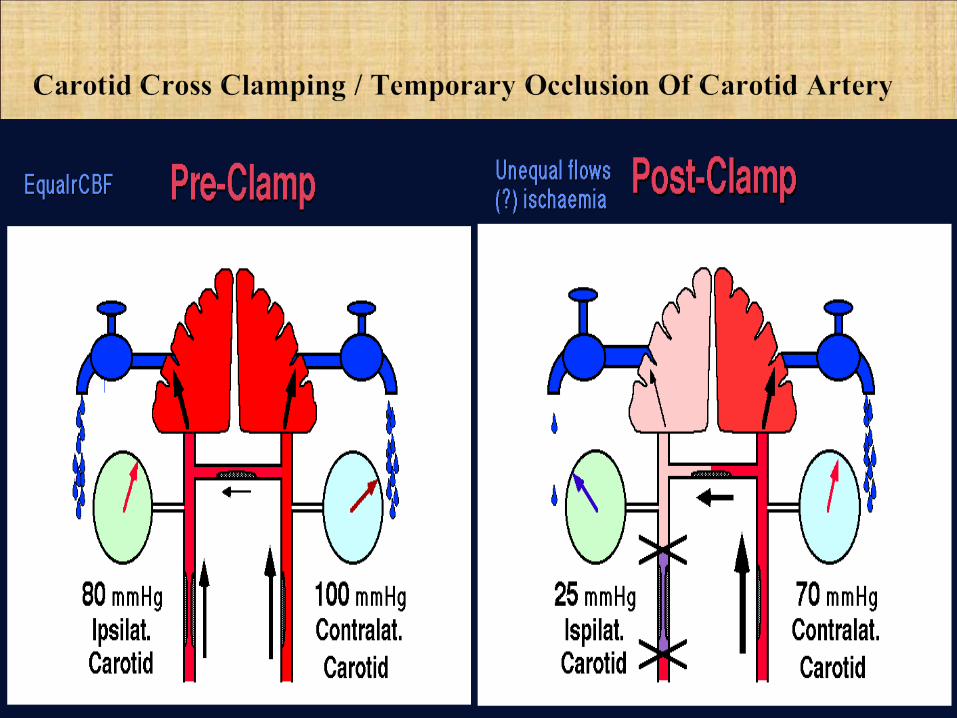
• Continued blood supply to the brain will depend entirely on adequate collateral blood flow through the circle of Willis if no shunt is used during CEA.
• Bilateral carotid disease have a higher risk of perioperative stroke after CEA than patients with unilateral disease only
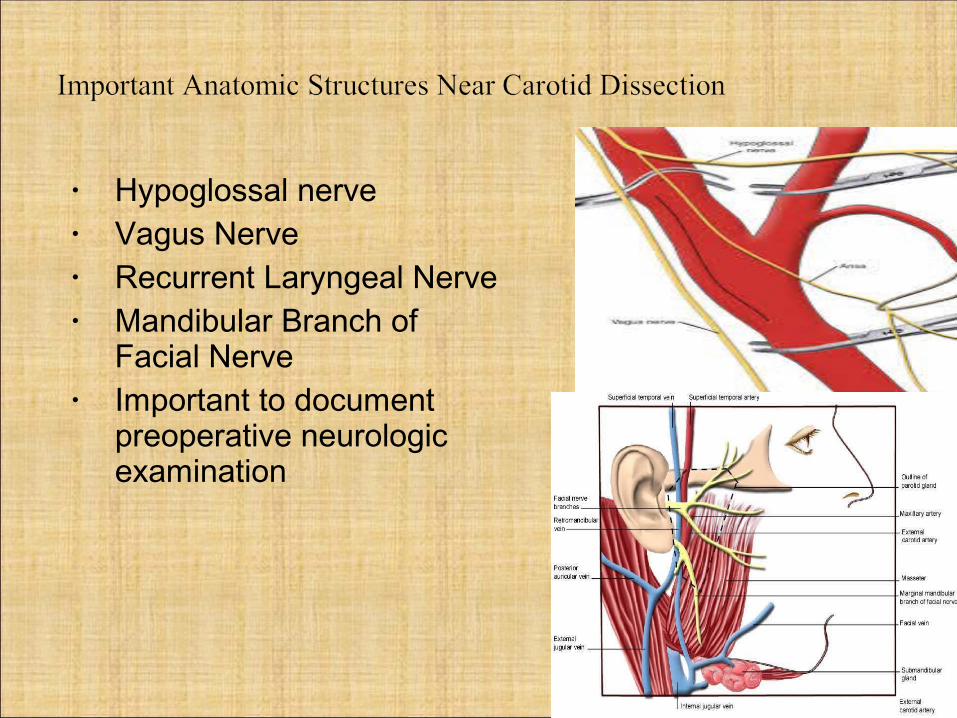
• Hypoglossal nerve• Vagus Nerve• Recurrent Laryngeal Nerve• Mandibular Branch of
Facial Nerve• Important to document
preoperative neurologic examination
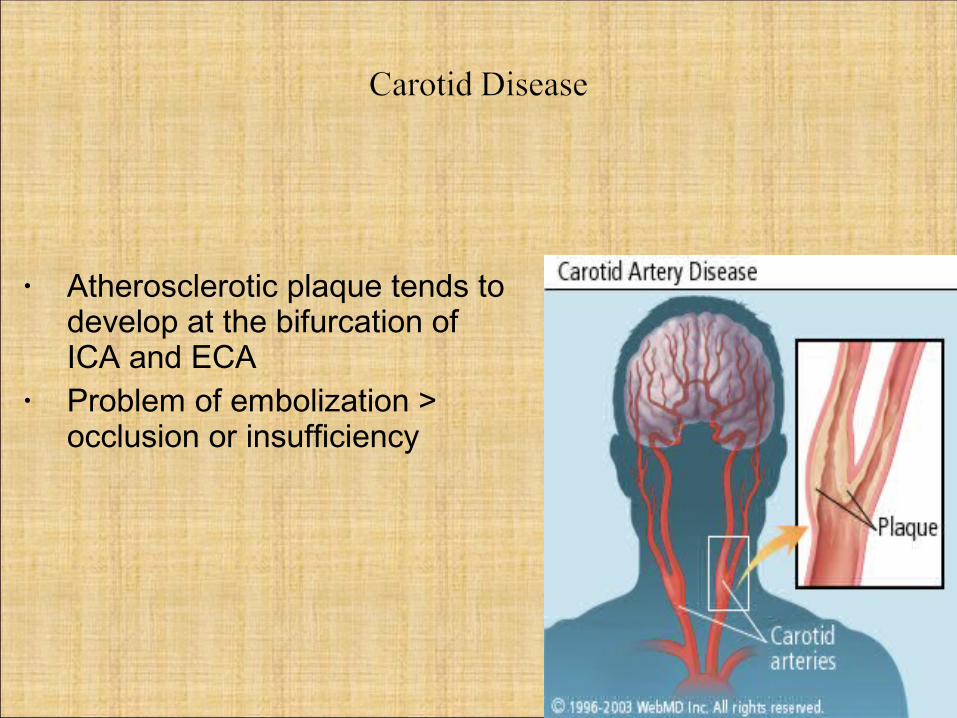
• Atherosclerotic plaque tends to develop at the bifurcation of ICA and ECA
• Problem of embolization > occlusion or insufficiency

• Clinical presentation: Varies by site of stenosis and distal embolization
• Isolated cervical Bruit in asymptomatic pts - high risk of stroke
• Part of a generalized vascular disease• Amaurosis Fugax ( Transient Mono ocular blindness ) -
ophthalmic artery• Transient Ischemic Event (TIA) - Sudden onset of focal
neurologic deficit which resolves within 24 hours• Reversible Ischemic Neurologic Deficit (RIND)
Neurologic dysfunction greater than 24 hours but less than 2 weeks
• Important to differentiate between carotid disease and posterior vertebro-basilar artery disease

• Advanced age• Hypertension• Diabetes• Hyperlipidemia• Hypercoagulable states• Smoking
• Most common Non invasive test - carotid duplex ultrasonography
• Positive tests are followed by confirmatory angiography
Treatment options :• Medical management• Carotid endarterectomy• Percutaneous transluminal Carotid angioplasty &
stenting
Indications for surgery :• TIAs with angiographic evidence of stenosis• RIND with >70% stenosis or ulcerated plaque with
or without stenosis• An unstable neurological status that persists
despite anticoagulation

• Individualized - assessment of stroke risk weighing medical management versus risk of perioperative stroke, death, or cardiac event
• Large multicenter trials - comparing medical versus surgical management ( anti-platelet therapy versus surgery )
• Patients with a minimum of 50% to 70% stenosis are candidates with ipsilateral disease and acceptable surgical risk
• The greater the degree of stenosis, the greater the difference in outcome statistics compared to medical therapy.

• Prophylactic intervention to prevent cerebral infarction and relieve symptoms of carotid atherosclerosis.
• This involves occluding the common,external, and internal carotid arteries, isolating the diseased segment, opening the vessel wall, and removing the plaque.
• The vessel is then closed. • If the remaining intima is
too thin, the vessel is closed with a vein graft or a synthetic (Dacron) patch.
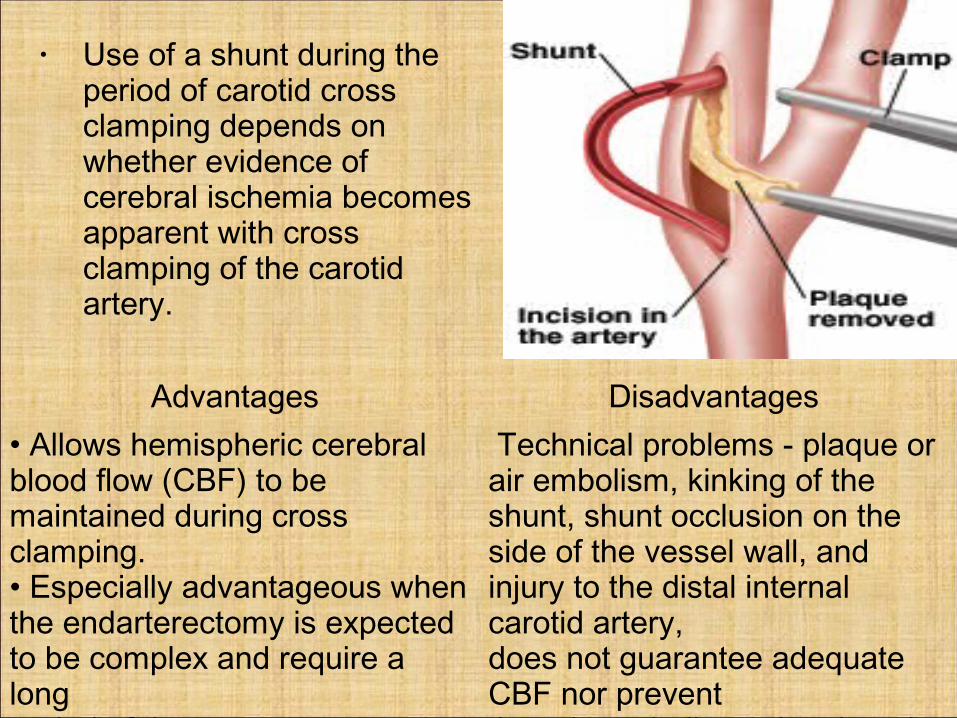
• Use of a shunt during the period of carotid cross clamping depends on whether evidence of cerebral ischemia becomes apparent with cross clamping of the carotid artery.
Advantages Disadvantages • Allows hemispheric cerebral blood flow (CBF) to be maintained during cross clamping.• Especially advantageous when the endarterectomy is expected to be complex and require a longperiod of time.
Technical problems - plaque or air embolism, kinking of the shunt, shunt occlusion on the side of the vessel wall, and injury to the distal internal carotid artery,does not guarantee adequate CBF nor prevent thromboembolic stroke , impairs surgical access & ↑ cross clamping time

Advantages • Avoidance of surgical incision,• Minimal anesthetic requirements, • Avoidance of cranial nerve injury and wound infections, • Shorter duration of induced carotid occlusion by the
balloon catheter than with surgical clamping of the carotid artery
• Lower hospital costs for shorter hospital and intensive care unit (ICU) stays.
Clinical trials comparing CEA with angioplasty have been done.
• Study results - angioplasty & carotid endarterectomy equally effective in preventing stroke.
• Also disabling stroke & death rates were same after surgery & stenting

Other manifestations of generalized arteriosclerosis -• Coronary artery disease, • Hypertension, and • Renal disease renal dysfunction (end - organ
effects)Medical conditions associated with• Obesity,• Diabetes mellitus, and • Pulmonary disease secondary to cigarette smokingThe patient's Neurologic Status and airway will need to be
evaluated.

• 30% to 50% of patients undergoing carotid endarterectomy (CEA) have coronary artery disease.
• Patients should be specifically asked whether they have angina, or have had a myocardial infarction (MI) or congestive heart failure.
• Based on the Cardiac Risk Stratification for noncardiac surgical procedures by the AHA/American College of Cardiology Task force on assessment of therapeutic cardiovascular procedures, CEA is classified as an Intermediate Risk procedure with a reported cardiac risk generally less than 5%.
• Hypertension is present in 55% to 80% of patients with carotid artery disease, and its presence would alter intraoperative blood pressure management.
• A range of acceptable blood pressures, where the patient is free of symptoms of both cardiac and cerebral ischemia should be determined
• To provide acceptable range of perfusion pressures during anaesthesia & surgery.
• Normal autoregulation will be lost in blood vessels in the ishcemic region
• Raising the blood pressure excessively to improve cerebral perfusion may exacerbate myocardial ischemia
• Lowering the blood pressure to reduce the work of the heart may compromise cerebral perfusion, exacerbating cerebral ischemia.

• Aspirin should be continued throughout the perioperative period
• Continuing of other agents must be balanced against the risk of bleeding
• Clopidogrel - stopped 1-5 days before surgery depending on presence, type & type of coronary stenting.
• Preferable to medically optimize the patient with Uncontrolled Hypertension Or Untreated Metabolic Disease, or if possible, delay surgery in the patient with a recent MI
• Presence of crescendo transient ischemia attacks (TIAs) may not allow the delay.
AIRWAY ASSESMENT• For ease of ventilation and intubation. • If it is difficult to establish ventilation pt. may become
hypercarbic during induction adverse effects on regional cerebral blood flow (CBF).
• Range of motion of the patient's neck that is tolerated - Extreme extension and rotation of the neck may occlude the patient's vertebral artery and contribute to postop neurologic deficits.

• # Management of intraoperative ventilation should be aimed at maintaining the patient's normal arterial carbon dioxide level.
• One of the anesthetic goals for CEA under GA is to have a patient who promptly emerges from anesthesia and is able to cooperate with a basic neurologic evaluation.
• Reassuring preoperative visit• Benzodiazepine (e.g., diazepam 5 mg orally, 1 hour
preoperatively or midazolam 1 to 2 mg intravenously) will provide anxiolysis and minimal respiratory depression
• Protecting brain and heart from ischemic injury• Maintaining hemodynamic stability• Ablate stimulatory(pain) and stress response to
surgery• Awake, cooperative patient at end of procedure
allowing clear neurologic evaluation

• Electrocardiogram (ECG) leads II and V5• Noninvasive blood pressure monitor• Pulse oximetry• End-tidal capnometry• Esophageal temperature• An intraarterial catheter should be used to monitor the
patient's blood pressure closely.• CEA is not an operation in which large fluid shifts are
anticipated.• A pulmonary artery catheter/CVP/TEE should not be
required in the patient with normal left ventricular function
• i.v access - one well-secured and well-running, medium-bore, intravenous catheter because major blood loss or fluid shifts during CEA are rare
• Adequate cerebral perfusion• Helps to decide when to place the shunt during carotid
cross clamping• No monitoring modality is as effective as watching an
awake patient• If the patient receives general anesthesia : Electroencephalograph (EEG) - often
used, Somatosensory Evoked Potentials
(SSEP), Transcranial Doppler, Internal Carotid Stump Pressure, And Jugular Venous Oxygen Saturation Cerebral Oximetry Direct Xenon Cerebral Blood Flow
Measurement

• Intraoperative EEG monitoring is the most common choice for CEA
• Continuous, non-invasive, inexpensive and provides direct feedback within seconds after carotid clamping that the brain is adequately perfused and oxygenated.
• Increasing levels of ischemia lead to a decrease in recorded electrical activity
• Its sensitivity in detecting perioperative stroke is limited - most strokes occur following surgery and are likely related to thromboembolic phenomena.
• Rapid changes in anesthetic depth may also complicate interpretation.
• This is particularly relevant where barbiturates or propofol infusions are used to induce EEG suppression in hopes of reducing CMRO2

• Deep brain structures are not monitored by EEG. • In patients with preexisting or fluctuating neurologic
deficits - false negative.• EEG may not be an ischemia-specific monitor - changes that occur with hypothermia,
hypocarbia, hypoxemia, and deep anesthesia mimic electroencephalographic signs of ischemia
# EEG changes secondary to anesthetics or hypothermia
are more likely to be bilateral, whereas hemispheric ischemia is more likely to affect the electrical activity of only one side of the brain.

Transcranial doppler :• Measures ipsilateral middle cerebral artery blood flow
velocities.• Detect and quantify embolic signals, which almost
always arise during dissection and/or angioplasty.• Disadvantage - technically demanding.SSEPs :• Reflects the presence of intact sensory pathways from
a stimulated peripheral nerve to the cortex where electrical activity is monitored.
• Distortion of certain waveforms is associated with ischemia
• May be used when ischemia cannot be detected during barbiturate anesthesia ( isoelectric EEG )
• Relative advantage over the EEG in patients with prior CVAs
Cerebral oximetry / Near Infrared Spectroscopy (NIRS) :• Noninvasive, continuous, and easy to use.• A relative decrease of 20% or greater in regional cerebral
oxygen saturation (rSO₂) suggested cerebral ischemia.• Low positive predictive value and low specificity.• If used exclusively - unnecessary shunting and lead to over-
shunting of patients.Internal carotid stump pressure :• Pressure in the portion of the internal carotid artery
cephalad to the carotid cross-clamp• Used to determine whether cerebral blood flow (CBF)
during cross clamping was adequate to avoid neuronal damage.
• Reflects pressure transmitted through collateral vessels.• Anesthetic agents can alter carotid stump pressure without
changing regional CBF
General anesthesia :
Regional anaesthesia :
Advantages Disadvantages• A still patient• A quiet operative field,• Early control of the airway and ventilation,• Ability to “protect” the brain form ischemia
• Inability to perform repeated neurologic evaluationsduring surgery.• Therefore, patients receiving general anesthesia should have their CBF or function monitored
Advantages Disadvantages•Patient remains awake allowing for repeated neurologic evaluations
•Loss of patient cooperation.•Alteration of mental status with cerebral ischemia , Seizures•Cannot provide brain protection

• Patients present hypertensive despite having taken their morning antihypertensive and antianginal medications.
• Most prone to hypotension after the induction of general anesthesia.
• Propofol / etomidate may be used for induction.• During the induction and intubation sequence, the
patient's blood pressure is kept in normal range by the use of vasopressors - phenylephrine and vasodilators - nitroglycerin or sodium nitroprusside.
• Phenylephrine - α agonist, has no direct effect on the cerebral vasculature; cerebral perfusion is increased by an elevation in the CPP.
• It increases blood pressure, cerebral perfusion pressure, stump pressure, and regional cerebral blood flow (CBF).
• Fluid overload may contribute to postop hypertension.
• Trachea may be sprayed with 100 mg lidocaine to minimize stimulation by the endotracheal tube during surgery.
• LMA ↓ hypertensive & tachycardic episodes• Sudden onset bradycardia & hypotension may be
caused by baroreceptor reflexes with surgical irritation of carotid sinus.
- surgeons may infiltrate the carotid bifurcation with 1% lidocaine to attenuate this response.
- this may result in more postoperative hypertension.
• Relaxant.

• Maintenance of a “light” anesthetic appears to have several advantages over deep anesthesia.
• It allows ischemic patterns on the EEG to be recognized easily.
• Facilitates maintenance of the patient's blood pressure.• Light anesthetic, compared to a deep anesthetic using
phenylephrine to maintain blood pressure, results in a lower incidence of perioperative myocardial infarction (MI).
• Any anesthetic regimen is suitable if it provides hemodynamic stability, does not exacerbate cerebral ischemia, and allows for a prompt emergence from anesthesia at the conclusion of surgery

• Hypercapnia dilates cerebral blood vessels increases cerebral blood flow.
• In CEA, may be detrimental if it dilates vessels in normal areas of the brain while vessels in ischemic brain areas that are already maximally dilated cannot respond “steal phenomenon”
• Hypocarbia vasoconstriction worsens cerebral ischemia
• ‘ maintenance of NORMOCARBIA’• Moderate hyperglycemia may worsen ischemic brain
injury.

• Hypothermia can depress neuronal activity sufficiently to decrease cellular oxygen requirements below the minimum levels normally required for continued cell viability.
• In theory, hypothermia represents the most effective method of cerebral protection.
• Almost all commonly used anesthetic agents reduce cerebral metabolism, thereby decreasing the brain's requirements for oxygen.
• Desflurane & Sevoflurane compared to Isoflurane allow for faster emergence & recovery
• Volatile anaesthetics may provide preconditioning & neuronal protection by inducing nitric oxide synthase.
• Barbiturates - offer a degree of brain protection during
periods of regional ischemia. - Thiopental decreases cerebral metabolic
oxygen requirements to about 50% of baseline. - These maximally achievable reductions in
oxygen requirements correspond to a silent EEG.• Etomidate and Propofol decrease brain electrical
activity and decrease cellular oxygen requirements.• Etomidate preserves cardiovascular stability and
beneficial in a patient population whose cardiac reserves are often limited.
• Propofol allows rapid awakening of pt & neurological assessment at the end of surgery.
• Cerebral autoregulation is impaired by sevoflurane but preserved under propofol-remifentanil anesthesia
• Propofol-remifentanil lower incidence of MI

• A sensory blockade is required in the C2 to C4 dermatomes.
• This can be accomplished with either deep or superficial cervical plexus blocks.
• In performing the blocks, care must be taken not to excessively palpate the neck, because part of the plaque in the carotid artery may dislodge and embolize.
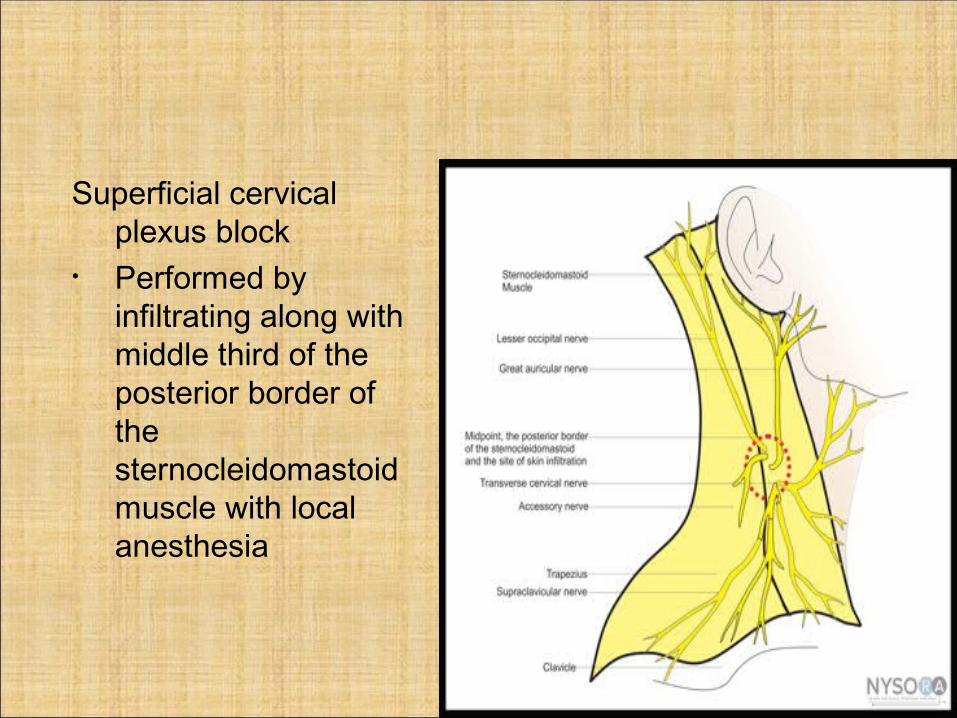
Superficial cervical plexus block
• Performed by infiltrating along with middle third of the posterior border of the sternocleidomastoid muscle with local anesthesia
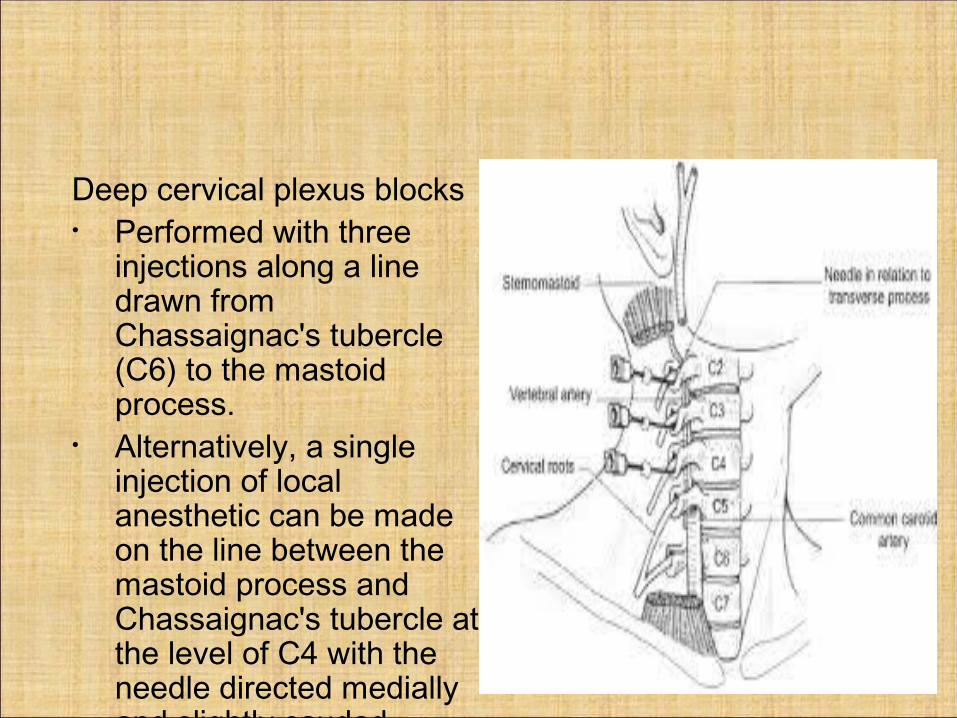
Deep cervical plexus blocks • Performed with three
injections along a line drawn from Chassaignac's tubercle (C6) to the mastoid process.
• Alternatively, a single injection of local anesthetic can be made on the line between the mastoid process and Chassaignac's tubercle at the level of C4 with the needle directed medially and slightly caudad.

• Superficial cervical plexus block may be combined with GA
- reduces postop opioid requirements - reduces PaCO₂ - increases patient satisfaction with analgesia• Deep cervical plexus block - does not increase the patients comfort
during procedure compared to superficial cervical plexus block.
- increases complications from block placement
- rate of conversion to GA is more ( 2% vs. 0.5%)
• α₂ agonists may be used for sedation• Dexmedetomidine reduces ischemic damage after
transient and permanent ischemia .• Dexmedetomidine has been shown to reduce arousal
and decrease CBF• Clonidine @ 1µg/kg/hr suppresses the
hyperadrenergic response to CEA• GA + superficial cervical plexus block + clonidine =
hemodynamic stability• Choice of anesthetic technique should take into
account the preference of the surgeon and the experience and expertise of the anesthesiologist.

• Common problems : - new neurologic dysfunction - hemodynamic instability - respiratory insufficiency• Other problems : - temporary cranial nerve injuries - temporary marginal mandibular nerve
deficits - temporary & permanent post.
Auricular nerve deficits - mild cervical numbness• Hematomas - 1%• Headache , wound infection

• Hyperperfusion syndrome - headache & hypertension• Results from blood flow to the brain that is greatly in
excess of its metabolic needs following CEA.• May not occur until several days after surgery• present with severe ipsilateral headache and can
progress to develop signs of increased cerebral excitability or frank seizures.
• Transcranial Doppler - role in predicting which patients will develop this syndrome.
• Steroids may be used in the treatment of hyperperfusion syndrome.

• Hypertension is more common than hypotension after CEA
• Poorly controlled preoperative hypertension.• Acute tachycardia and hypertension may precipitate
acute myocardial ischemia and failure• It may lead to cerebral edema and/or hemorrhage• Post-CEA hypertension is significantly associated with
adverse events like stroke or death• Exclude and/or treat other causes of hypertension such
as bladder distention, pain, hypoxemia, and hypercarbia.
• Lower the pressures to preop values most often with labetalol in 5-mg increments
• In patients with reactive airways disease / bradycardia - Hydralazine
• Usually, the hypertensive episode has its peak 2 to 3 hours after surgery, but in individual cases it may persist for 24 hours.

• Postoperative hypotension is less common.• Causes : residual effects of anesthesia drugs,
overzealous treatment of hypertension, baroreceptor resetting after increase in the flow
• 12-lead ECG should be obtained in the recovery room in hemodynamically unstable patients because significant hypertension or hypotension can be caused by MI
• Postoperative respiratory insufficiency may be caused by recurrent laryngeal nerve or hypoglossal nerve injury, a massive hematoma, or deficient carotid body function
Hematoma:• small hematomas - venous oozing - treatment : gentle digital
compression / reversing residual heparin with protamine
• Expanding hematoma - tracheal compression - immediate evacuation• More common with patch angioplasty
• Unilateral loss of carotid body - not very significant• Bilateral loss of carotid body - loss of hypoxic drive• Supplemental oxygen to be given routinely• Drugs causing resp. depression should be avoided.

• The patient who awakens with a major new neurologic deficit or who develops a suspected stroke in the immediate postoperative period represents a surgical emergency.
• Inadequate collateral flow, carotid thrombosis may cause postoperative stroke
• Prompt surgical reexploration can produce significant neurologic improvement.
• If the deficit - focal and minor, it is most commonly due to microembolization.
• Noninvasive assessment of internal carotid flow and anticoagulation after exclusion of a hemorrhagic brain lesion is the indicated treatment
• For patients undergoing neck exploration for a wound hematoma following CEA - tracheostomy / cricothyroidotomy tray should be available.
• Management of a difficult airway• Esmolol - control of hyperdynamic cardiovascular
responses during awake intubation• Difficulty in managing airway - wound is opened &
drained externally tracheal intubation before GA is induced
EMERGENCY CAROTIDENDARTERECTOMY :• Patient may have full stomach -- aspiration prophylaxis• Anesthetic technique is similar.

THANK YOU