andrew walby - st vincent’s hospital melbourne
TRANSCRIPT
The Emergency Department A Laboratory for Error
Dr Andrew Walby
Director of Emergency Medicine
St Vincent’s Hospital Melbourne
Summary
• Why doctors “mess up” in the ED
• The role of cognitive and affective bias in medical error
• Why patients “screw up” in the ED
• The important role of EBM (experience-based medicine)
The emergency department is a natural laboratory for the study of error
Pat Croskerry
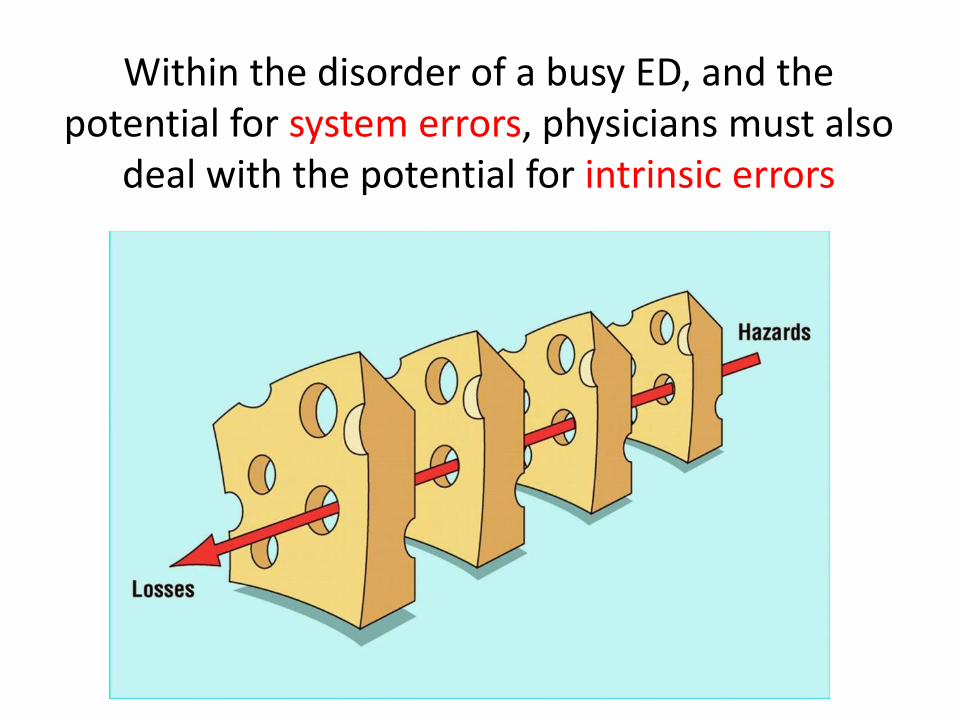
Within the disorder of a busy ED, and the potential for system errors, physicians must also
deal with the potential for intrinsic errors
High levels of diagnostic uncertainty
1849 – 1919
symptom A + sign B = diagnosis C
treatment = cure D
1984
common things occur commonly
and
uncommon things occur in exams
symptom A + sign B = diagnosis C
treatment = cure D
2017
common things occur at medical school
and
uncommon things occur in the ED
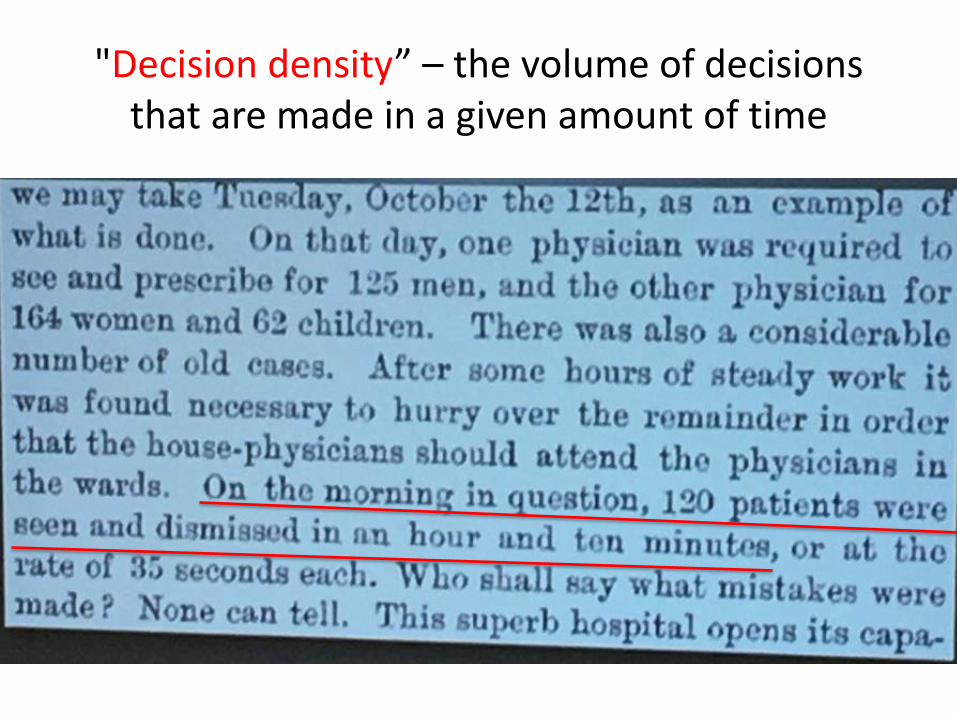
"Decision density” – the volume of decisions that are made in a given amount of time
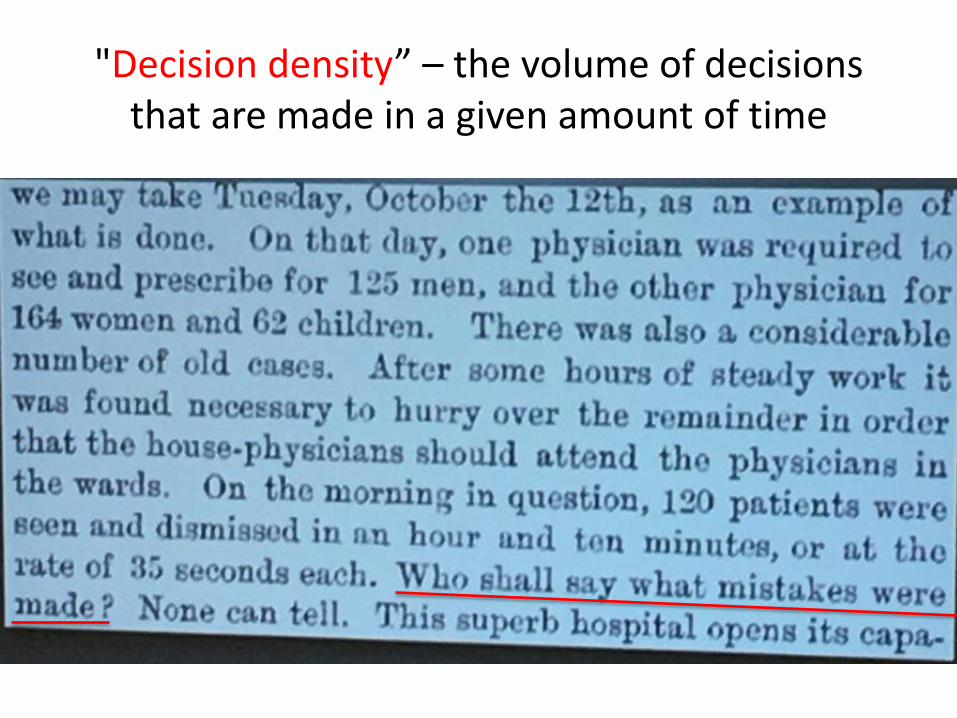
"Decision density” – the volume of decisions that are made in a given amount of time
A high amount of cognitive load needed to process a large volume of data
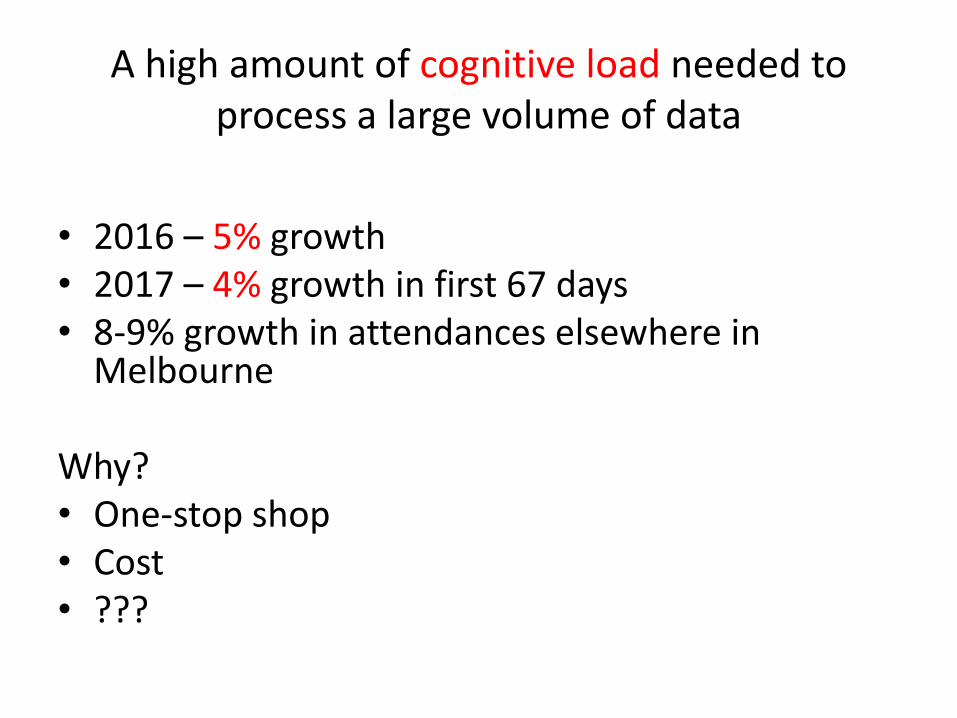
A high amount of cognitive load needed to process a large volume of data
• 2016 – 5% growth • 2017 – 4% growth in first 67 days • 8-9% growth in attendances elsewhere in
Melbourne Why? • One-stop shop • Cost • ???

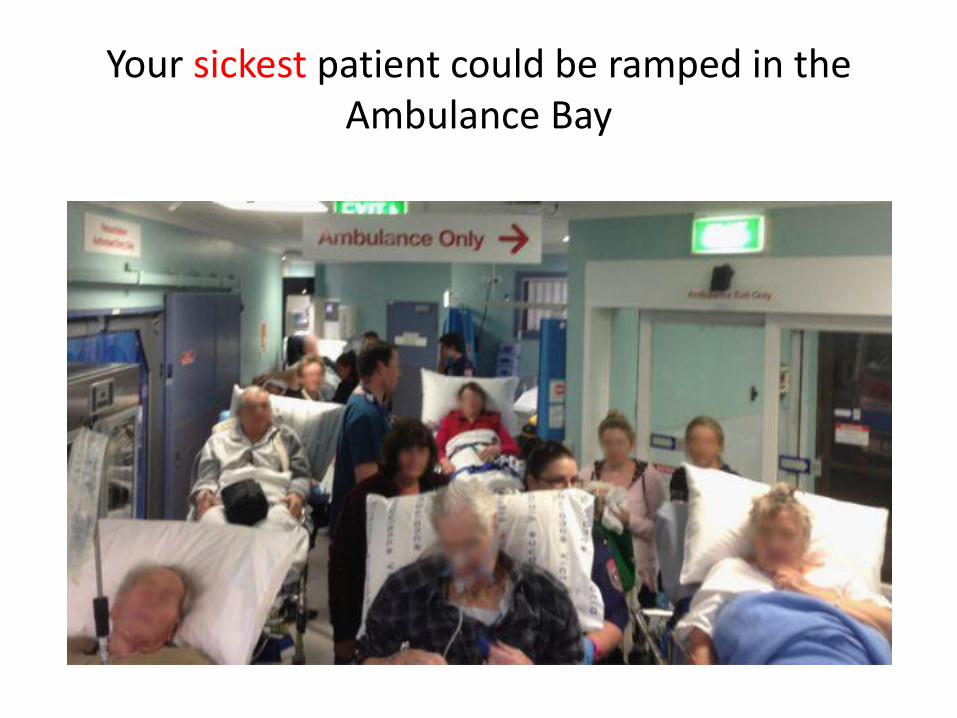
Your sickest patient could be ramped in the Ambulance Bay
Your sickest patient could be sitting in your Waiting Room
Narrow time windows for patient assessment
Multiple care transitions for any given patient
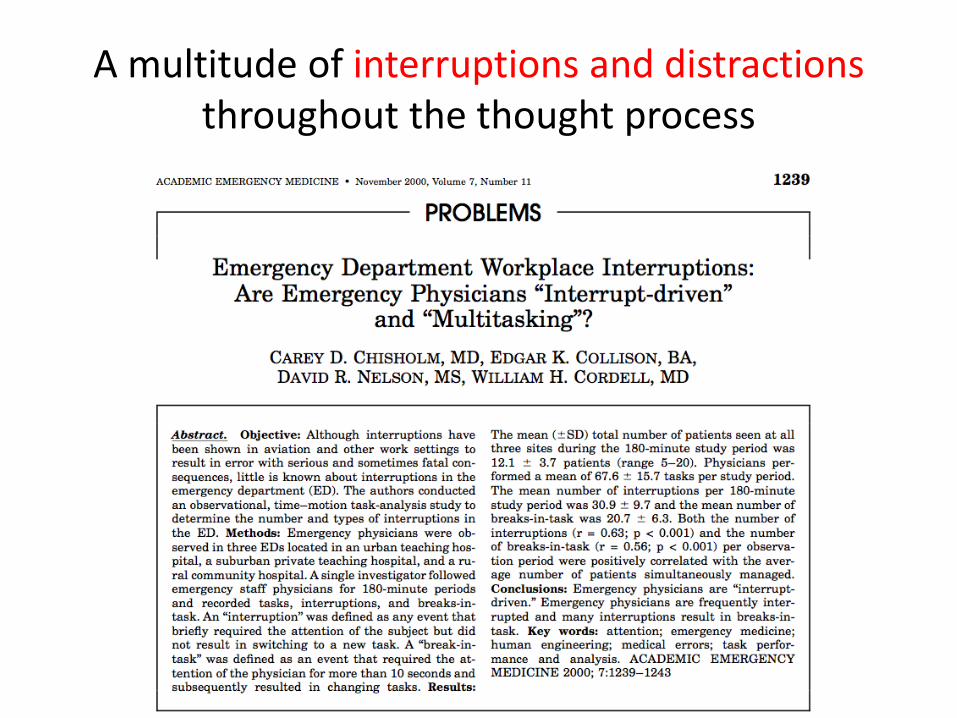
A multitude of interruptions and distractions throughout the thought process
A multitude of interruptions and distractions throughout the thought process
Westbrook – The impact of interruptions on clinical task completion (2010)
• Interruptions occurred 6.6x per hour (every 9 minutes)
• 11% of tasks were interrupted (with 3.3% disrupted > 2 times)
• Physicians did not revisit tasks 18.5% of the time after an interruption
• The most frequently occurring interruptions were during documentation; 47% came while documenting discharge
Westbrook – The impact of interruptions on clinical task completion (2010)
• An average 12.8% of physician time was spent multi-tasking
• Professionals in all categories multi-tasked almost equally (physicians 14.4%; registrars 13.2%; residents 12.3%; interns 9.4%)
• The average time on task declined as physician seniority increased in these categories: direct care, indirect care, and documentation; seniority made no difference during professional communication
Cognitive and Affective Bias
• Aggregate bias
• Ambiguity effect
• Anchoring
• Ascertainment bias
• Attentional bias
• Availability
• Bandwagon effect
• Base-rate neglect
• Belief bias
• Blind spot bias
• Commission bias
• Confirmation bias
• Congruence bias
• Contrast effect
• Diagnosis momentum
• Ego bias
Cognitive and Affective Bias
• Expectation bias
• Feedback sanction
• Framing effect
• Fundamental attribution error
• Gambler’s fallacy
• Gender bias
• Hawthorne effect
• Hindsight bias
• Illusory correlation
• Information bias
• Multiple alternatives bias
• Mere exposure effect (familiarity principle)
• Need for closure
• Omission bias
• Order effects
• Outcome bias
Cognitive and Affective Bias
• Overconfidence bias
• Playing the odds
• Posterior probability error
• Premature closure
• Psych-out error
• Reactance bias
• Representativeness restraint
• Search satisficing
• Self-serving bias
• Semmelweis reflex
• Sutton’s slip
• Sunk costs
• Triage cueing
• Unpacking principle
• Vertical line failure
• Visceral bias
• Yin-yang out
• Zebra retreat
Anchoring
• Over-reliance on the first piece of information you hear.
• During history taking, it was established that he had in fact taken the following prescription medications at approximately 1800 hours: 10 x 50mg tramadol; 10 x 5mg diazepam; 2 x Panadeine Forte.
Availability bias
• Recent experience with a disease may inflate the likelihood of it being diagnosed.
Availability bias
• I saw a zebra last week…I think I may have seen another
Diagnosis momentum
• Once diagnostic labels are attached to patients they tend to become stickier and stickier – accepting a previous diagnosis without sufficient skepticism
Psych-out error
• Medical conditions are overlooked or minimized in mental health patients
Triage cueing
• Many biases are initiated at Triage: geography is destiny
• I need a Gynae consult because she is a female with pain (thereby ignoring other organ systems or causes of pain)
“We do not make good decisions when our viscera are aroused”
Pat Croskerry
“I want my daughter to have a CT scan of the brain”
Lawyer to Triage Nurse
(and his brother-in-law is a Paediatrician…)
Amygdala Hijack
• emotional responses from people which are immediate and overwhelming, and out of measure with the actual stimulus because it has triggered a much more significant emotional threat
Why patients “screw up” in the ED
• You’re not clear why it's an EMERGENCY • You don’t disclose all of your medical problems • You don’t know what medication you take • You’re looking for a third or fourth opinion • You treat it like a primary care visit • You lie or hide the truth • You beat around the bush • You text, or are constantly on the phone • You don’t share when you're frustrated • You have consulted Dr Google and already know what
is wrong
You’re not clear why it’s an EMERGENCY You treat it like a primary care visit
• One person’s emergency may be another person’s runny nose
You don’t disclose all of your medical problems You lie or hide the truth You beat around the bush
You don’t know what medication you take You haven’t been taking them as prescribed
You’re looking for a third or fourth opinion
You text, or are constantly on the phone
You have consulted Dr Google and know what is wrong
You have consulted Dr Google and know what is wrong
You have consulted Mr Google LLB…
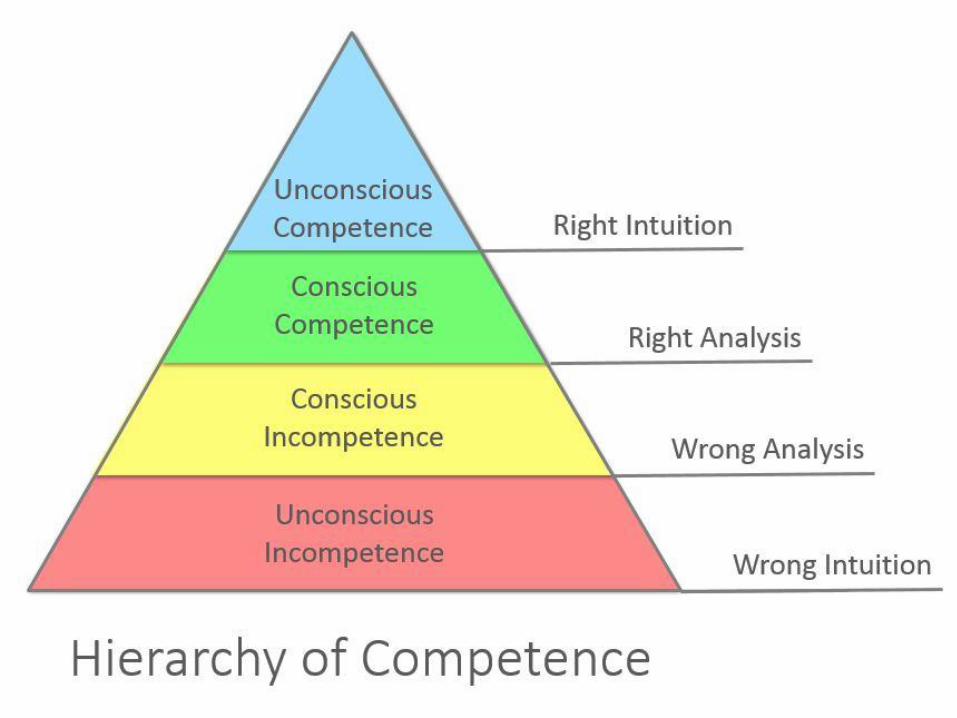
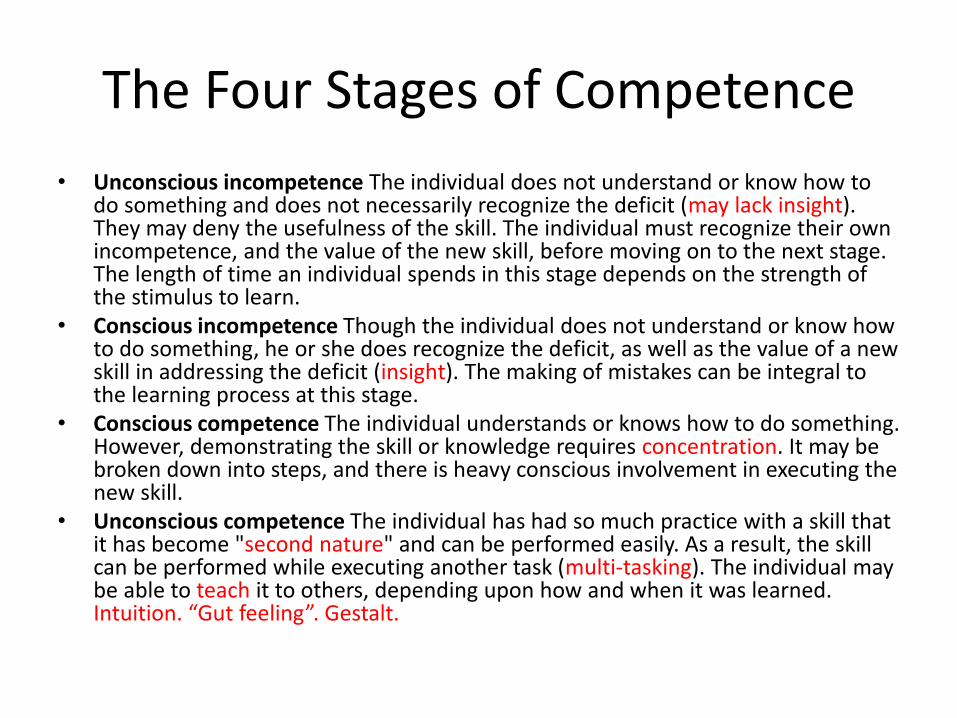
The Four Stages of Competence
• Unconscious incompetence The individual does not understand or know how to do something and does not necessarily recognize the deficit (may lack insight). They may deny the usefulness of the skill. The individual must recognize their own incompetence, and the value of the new skill, before moving on to the next stage. The length of time an individual spends in this stage depends on the strength of the stimulus to learn.
• Conscious incompetence Though the individual does not understand or know how to do something, he or she does recognize the deficit, as well as the value of a new skill in addressing the deficit (insight). The making of mistakes can be integral to the learning process at this stage.
• Conscious competence The individual understands or knows how to do something. However, demonstrating the skill or knowledge requires concentration. It may be broken down into steps, and there is heavy conscious involvement in executing the new skill.
• Unconscious competence The individual has had so much practice with a skill that it has become "second nature" and can be performed easily. As a result, the skill can be performed while executing another task (multi-tasking). The individual may be able to teach it to others, depending upon how and when it was learned. Intuition. “Gut feeling”. Gestalt.
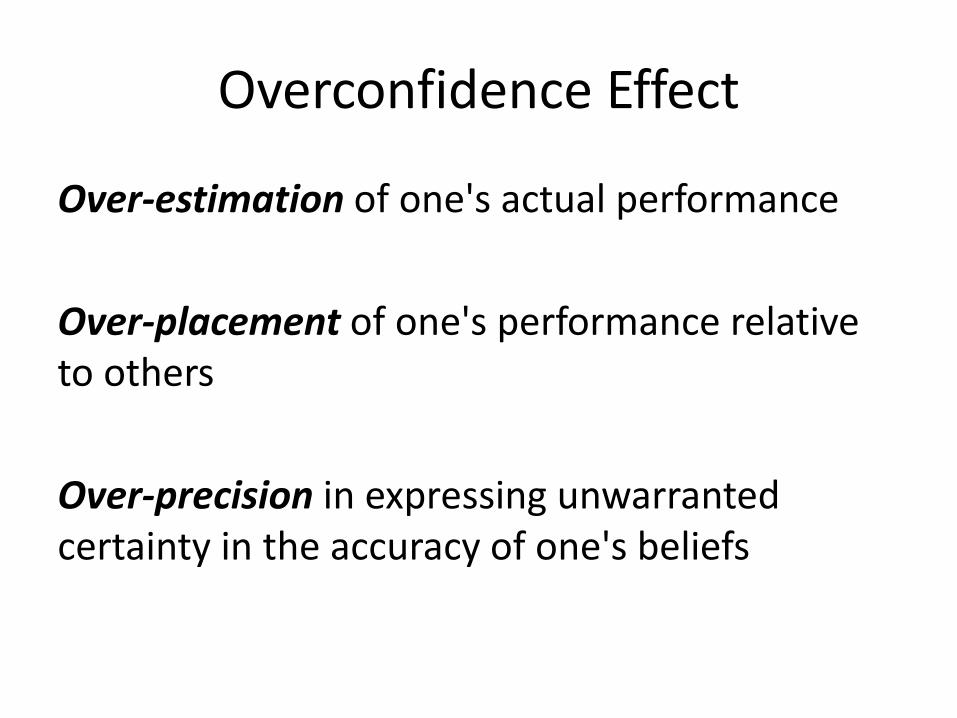
Overconfidence Effect
Over-estimation of one's actual performance
Over-placement of one's performance relative to others
Over-precision in expressing unwarranted certainty in the accuracy of one's beliefs
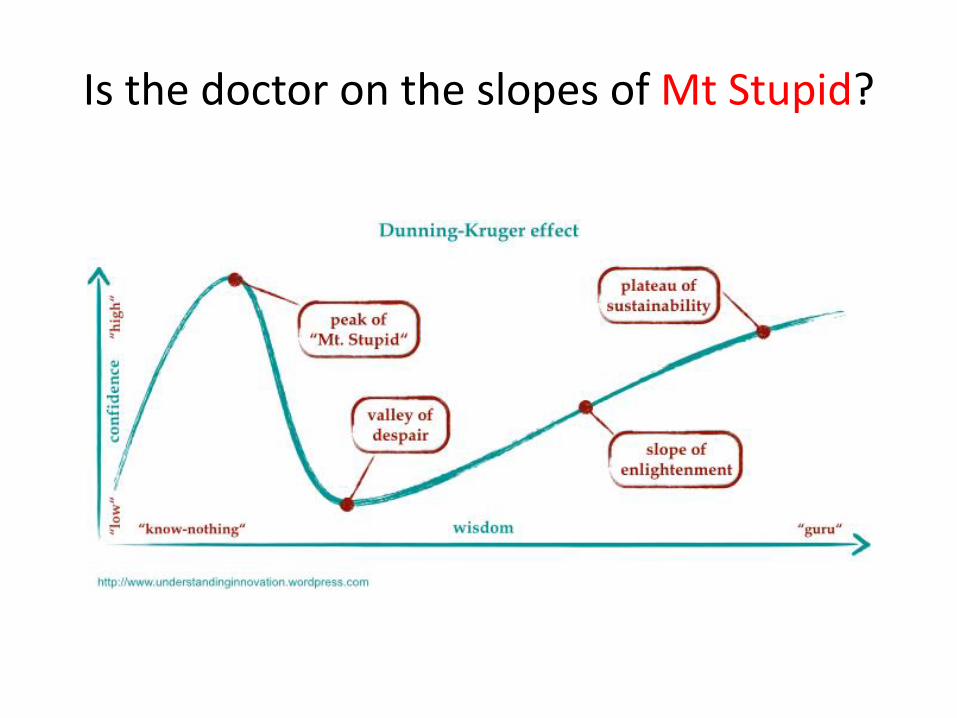
Is the doctor on the slopes of Mt Stupid?
Types of Medicine
• Evidence-based (EBM)
• Anecdotal-based (narrative-based) (ABM)
• Experience-based (EBM)
What makes a good doctor?
Sadly there will always be doctors like these…
What makes a good patient?
• Only come if it is a real emergency • Speak the same language as me • Have an acceptable level of (health) literacy and
intelligence • Listen to my questions and answer them
comprehensively (and promptly) • Arrive in an orderly and even-spaced fashion • See your GP (if appropriate), have some investigations
and bring a comprehensive (and legible) letter (and all your medications & x-rays)
• Don’t arrive with pre-conceived ideas about why they are there, what I can provide, what their diagnosis is
• Don’t arrive affected by alcohol and other drugs