analysis of the primary presenting symptoms and
TRANSCRIPT
1
Analysis of the primary presenting symptoms and
hematological findings of COVID-19 patients in Bangladesh
Abu Taiub Mohammed Mohiuddin Chowdhury1, Md Rezaul Karim2, H.M. Hamidullah Mehedi3,
Mohammad Shahbaz4, Md Wazed Chowdhury5, Guo Dan1, Shuixiang He1*
1Dept. of Gastroenterology, First affiliated hospital of Xi’an Jiaotong University, Xi’an, China. 1Hubei Key Laboratory of Embryonic Stem Cell Research, Institute of Neuroscience, Hubei
University of Medicine, Shiyan, China. 3Chattagram General Hospital, Chattagram, Bangladesh. 4Chakaria Upazilla Health Complex, Cox’s Bazar, Bangladesh. 5Civil Surgeon’s Office, Chattagram, Bangladesh.
*Correspondence to: Prof. Dr. Shuixiang He, Dept. of Gastroenterology, First affiliated hospital
of Xi’an Jiaotong University, Xi’an, Shaanxi 710061, China. Email: [email protected];
And, Dr. Abu Taiub Mohammed Mohiuddin Chowdhury, Dept. of Gastroenterology, First
affiliated hospital of Xi’an Jiaotong University, Xi’an, Shaanxi 710061, China. Email:
ABSTRACT: Objective: SARS-Cov-2 infection or COVID-19 is a global pandemic. From the
time of identification to till, multiple clinical symptoms and parameters have been identified by
the researchers of various countries and regions regarding the diagnosis and presentations of
COVID-19 disease. In this manuscript, we investigated the primary symptoms and basic
hematological presentations of SARS-CoV-2 infection among the Bangladeshi patients.
Methodology: We have collected the disease history of mild to moderate degree of COVID-19
patients; hematological and biochemical on admission reports of moderate degree COVID-19
patients. All of them were tested positive for SARS-CoV-2 by RT-PCR in different institutes in
Bangladesh. Results: According to this study though COVID-19 patients in Bangladesh
commonly presented with fever, cough, fatigue, shortness of breath, and sore throat, but
symptoms like myalgia, diarrhea, skin rash, headache, Abdominal pain/cramp, nausea, vomiting,
restlessness, and a higher temperature of >1000F have a greater presentation rate and more
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
© 2020 by the author(s). Distributed under a Creative Commons CC BY license.

2
frequent than other published studies. CRP and Prothrombin time was found to increase in all the
patients. Serum ferritin, ESR, SGPT, and D-Dimer were found increased among 53.85%, 80.43,
44%, and 25% patients respectively. 17.39% of the patients had leucocytosis and neutrophilia.
28.26% of patients presented with lymphocytopenia. 62.52% of patients had mild
erythrocytopenia. Conclusion: Despite some similarities, our study has evaluated a different
expression in presenting symptoms in the case of COVID-19 patients in Bangladesh. CRP,
Prothrombin time, serum ferritin, ESR, SGPT, D-Dimer, erythrocytopenia, and lymphocytopenia
can be initial diagnostic hematological findings and assessment for prognosis COVID-19 disease.
Also, gender variations have a different scenario of clinical and laboratory appearance in this
region.
Keywords: SARS-CoV-2; COVID-19; real-time RT-PCR; COVID-19 symptoms; COVID-19
hematological findings; Bangladesh
Introduction
SARS-Cov-2 infection or COVID-19 is a current global pandemic. This is a single-stranded
RNA virus originated from the beta Coronavirus family. [1] The rapid spread of SARS-CoV-2
has led to the declaration of a global pandemic barely three months after emerging [2]. The
disease was first notified in December 2019 in the Hubei province of the Republic of China as a
cluster of 27 cases of pneumonia of an unknown cause. [3] All these patients presented with
Radiological findings like glassy lung opacity along with clinical presentations like fever,
dyspnoea, and dry cough. From the time of identification to till, multiple clinical symptoms and
parameters have been identified by the researchers of various countries and regions regarding the
diagnosis and presentations of COVID-19 disease. In this manuscript, we investigated the
primary symptoms and hematological presentations of SARS-CoV-2 infection among
Bangladeshi patients.
Methodology
For the analysis of the presenting symptoms of SARS-CoV-2 infection, we collected the data of
COVID-19 patients from Chattagram Civil Surgeon’s office, and the Chakoria Upazilla Health
and Family Welfare Officer’s (UH&FPO) office. All the patients were tested positive for SARS-
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
3
CoV-2 by RT-PCR at Bangladesh Institute of Tropical and Infectious Disease (BITID) and
Cox’s Bazar Medical College Hospital and were treated (either as outpatient or as inpatient with
mild to moderate degree of illness) under different COVID-19 dedicated hospitals in Chattagram
district, and Chokoria Upazilla Health complex. A total of 638 patient’s data that were tested
positive from May 5th to June 5th, 2020 were collected. Each of the patients was individually
interviewed to find out the details of the disease symptoms, history, comorbid condition, and
associated complaints.
Patients with severe comorbid conditions like severe Bronchial asthma, COPD exacerbation,
severe ischemic heart disease, severe uncontrolled diabetes mellitus, advanced renal and hepatic
disease, patients with carcinoma, hospitalized and Immuno-compromised patients were not
included in this study. Due to misconception and unreliable statement 127patient's data were
discarded. 138 patients had comorbid conditions that affected the presenting symptoms or had
existing symptoms from before, so these were also excluded. 53 patients did not respond to our
call or unwilling to participate in the study. Following exclusion for symptomatic analysis 320
patients of 13 to 56 years (mean age 35.81 years) of age were included in this study.
To evaluate the hematological changes in the patients we gathered the hematological and
biochemical on admission reports of 89 admitted patients (moderate degree COVID-19 disease)
from May 5th to June 5th, 2020. This included Hemoglobin level, Erythrocyte Sedimentation rate,
total and differential count of WBC, RBC, Platelet, C-Reactive Protein (CRP), SGPT, Serum
Ferritin, Prothrombin time, D-Dimer, and Serum creatinine. According to the clinical
presentation patients with fever were tested for Dengue NS1 antigen, Dengue IgG & IgM
antibody, Salmonella Typhi IgM and IgG antibody, ICT for malaria (Antigen for Plasmodium
Falciparum, Vivax, Malaria, and Ovale) and Widal test to exclude Dengue, Malaria, and Enteric
fever. Patients who had a chronic comorbid condition and any recent history of hematological,
biochemical abnormalities, or chest radiograph abnormality within a period of 30days were not
included in this study. In our observation, all patients with severe diseases had pre-existing
comorbid conditions. Therefore, only the laboratory findings of patients with moderate COVID-
19 disease were collected. Following exclusion criteria (others as described earlier) 39 patients
were excluded from the study. A total of 50 patient’s data were included for the analysis. Male
37 male and 13 female of 31 to 59 years of age (mean 42.8 years).
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
4
Informed consent was obtained in every case. Statistical analysis was done by Graphpad Prism
software.
Results and findings
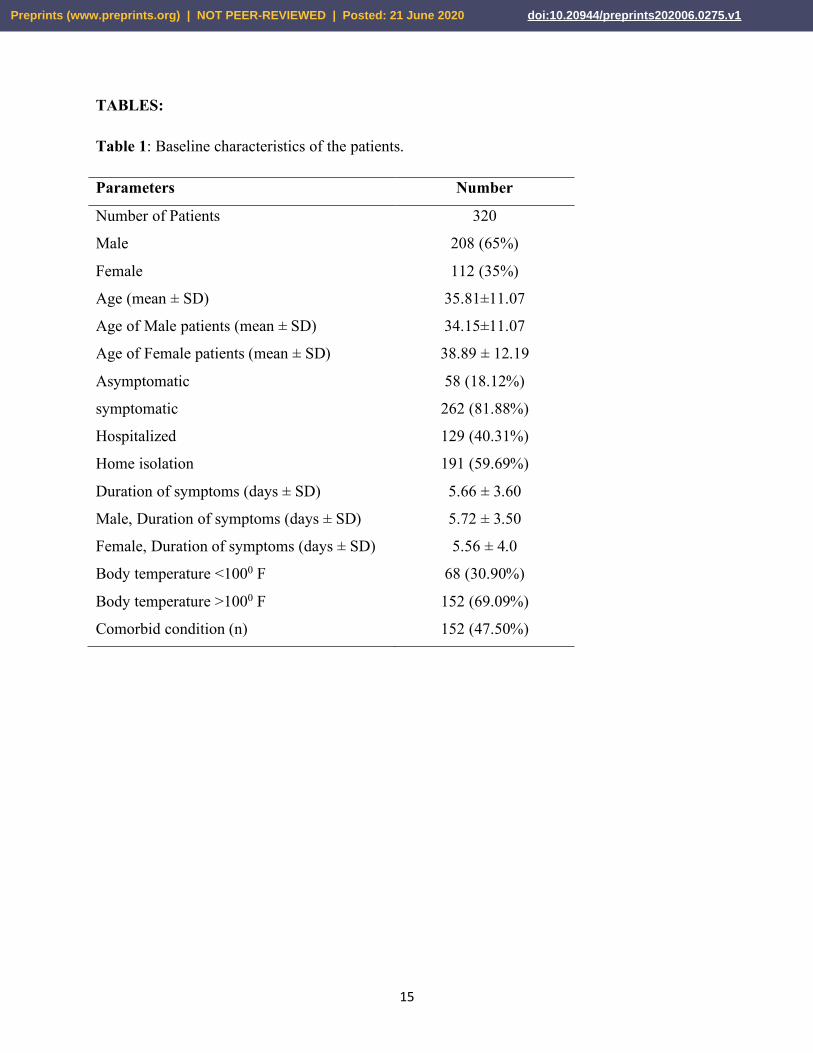
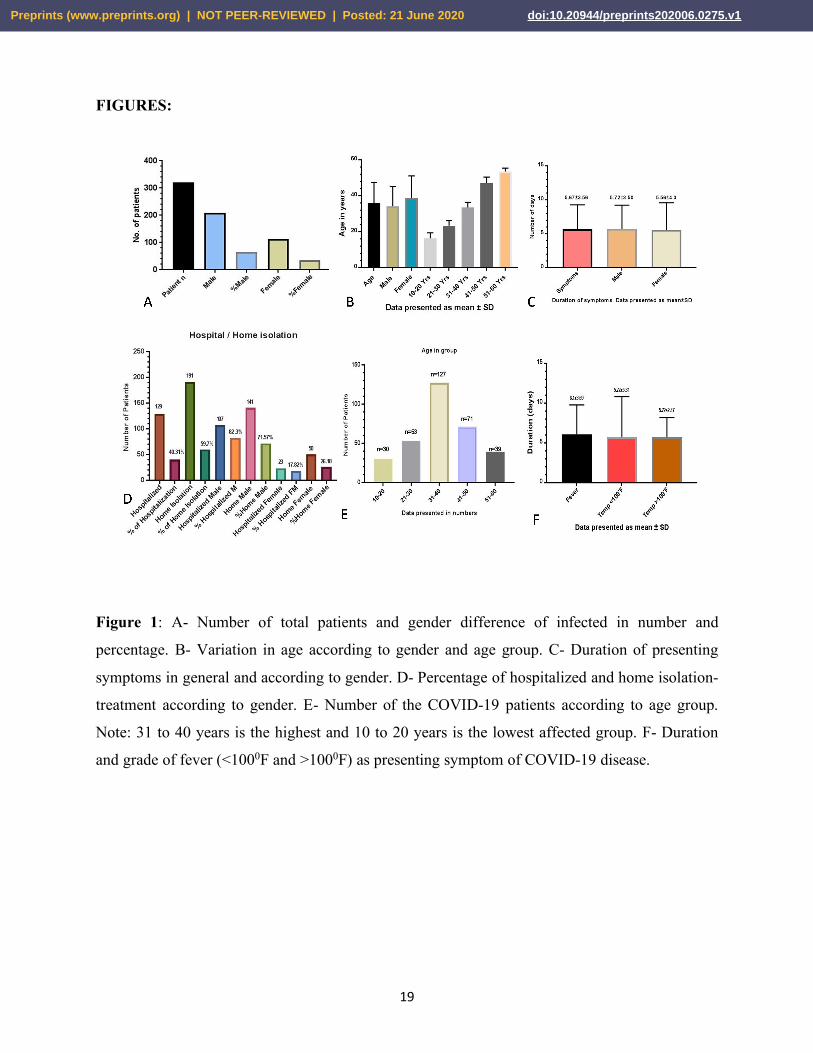
Table 1: A total of 320 patients were included in the study. The patient’s ages were 13 to 56years.
208 (65%) were male and 112 (35%) were female. [Figure 1 A] The Mean age of the patients
was 35.81±11.68 years. The mean age of male and female patients was 34.16±11.08 years and
38.89±12.19 years respectively. [Figure 1 B] 129 (40.31%) patients were under hospital and 191
(59.69%) were under home isolation. Out of 320 patients, 262(81.88%) were symptomatic and
58 (18.13%) were asymptomatic. The age of male and female symptomatic patients was
34.15±11.07 years and 38.89 ± 12.19 years. The duration of symptoms was 5.66 ± 3.60 days in
general. In the case of male patients, this was 5.72 ± 3.50 days and female was 5.56 ± 4.0days.
[Figure 1 C]
Sub-group analysis of hospital/home isolated patients hospitalized patients 107 (82.3%) were
male, 23 (17.82%) were female; in the case of home isolation 141(71.57%) were male and 50
(26.18%) were female. [Figure 1 D] T-test was not significant among the groups. Age group was
as following 10 to 20 years 30patients, 21 to 30 years 53 patients, 31 to 40 years 127 patients, 41
to 50 years 71 patients, and 51 to 60 years 39 patients. [Figure 1 E]
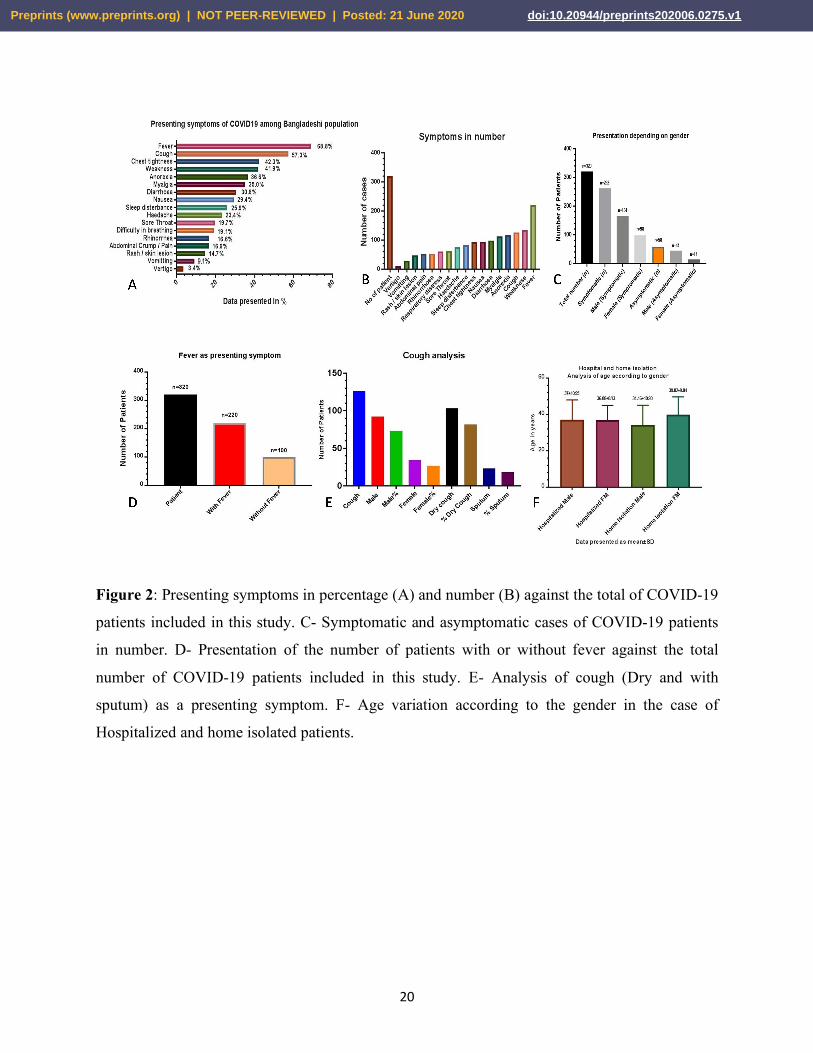
Among all the patients, highest 220 (68.8%) patient presented with fever, weakness 134 (41.9%),
cough 126 (57.3%), anorexia 117 (36.6%), myalgia 112 (35.0%), diarrhea 98 (30.6%), nausea 94
(29.4%), chest tightness 93 (42.3%), sleep disturbance 83 (25.9%), headache 75 (23.4%), sore
throat 63 (19.7%), respiratory distress 61 (19.1%), rhinorrhoea 53 (16.6%), abdominal crump/
pain 53 (16.6%), small localize rash on the body (with or without itching) 47 (14.7%), vomiting
29 (9.1%), and vertigo 11 (3.4%). [Figure 2 A & B]
The maximum temperature was found 1040F. 220 patients had a history of fever and 100 patients
had no fever history. [Figure 2 D] Out of 220 patients presented with fever, 68 patients had
temperatures <1000F and 152 presented with >1000F temp. [Table 1] Febrile patients had a
history of a minimum of 2days and a maximum 14days with a mean of 6.09±3.69 days of fever
history. Patients with <1000F temperature had a history of 5.72 ± 5.13 days (2 to 14 days) and
patients with >1000F temperature had a history of 5.73±2.47 days (2 to 10 days) of febrile history.
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
5
[Figure1 F] Among 126 patients with a history of cough 103 (81.75%) experienced dry cough
and 23 (18%) complained of sputum with cough; among them, males were 93(73%) and female
were 34 (26.95%). [Figure 2 E] Patients had 5.67±3.60 days (2-14 days) of history of symptoms
in general. Male patients have 5.72±3.5 days (2-13 days) and females had 5.56±4.0days (2-
14days) of the history of symptoms. These figures are not significant in the t-test, P=0.998.
Among the hospitalized patients 107 were male patients of 37±10.95years (22 to 54 years), 48
were female of 36.88±8.13 years (22 to 50years). In the case of home isolation, this was
34.16±10.93 years (17 to 54 years) in males and 39.82±9.84 (24 to 56years) in females. [Figure 2
F]
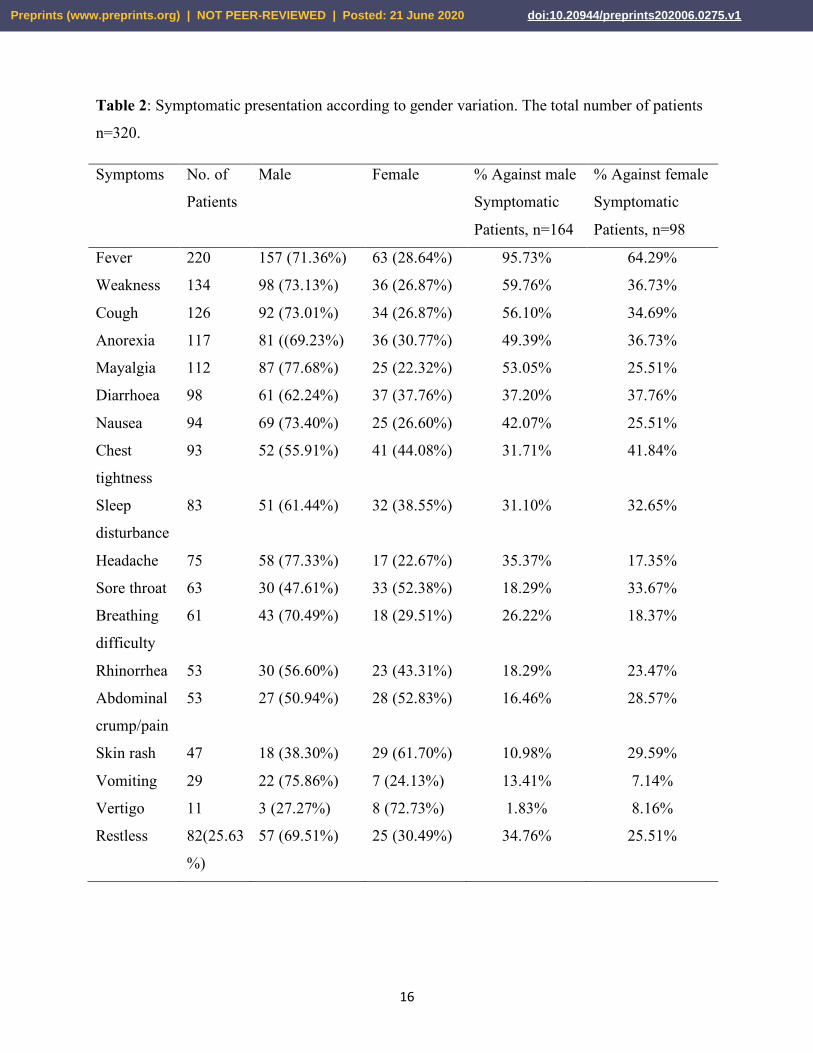
Table 2: Subgroup analysis of patients according to the symptoms. Fever was presented by
220patients, among this male were 157(71.36%) and females were 63(28.64%); this is 95.73%
and 64.29% against total symptomatic male and female patients. Weakness was presented by
134patients, male 98(73.13%), and female 36(26.87%); this is 59.76% and 36.73% against total
symptomatic male and female patients. The cough was presented by 126patients male 92(73.01%)
and female 34 (26.87%); this is 56.10% and 34.69% against total symptomatic male and female
patients. Anorexia was presented by 117patients, male 81(69.23%), and female 36(30.77%); this
is 49.39%% and 36.73% against total symptomatic male and female patients. Generalized
Myalgia was presented by 122 patients, male 87(77.68%), and female 25(22.32%); this is 53.05%
and 25.51% against total symptomatic male and female patients. Diarrhoea was presented by 94
patients, male 61(62.24%), and female 25(26.60%); this is 37.20% and 37.76% against total
symptomatic male and female patients. Nausea was presented by 98 patients, male 61(62.24%),
and female 37(37.76%); this is 42.07% and 25.51% against total symptomatic male and female
patients. Chest tightness was presented by 93 patients, male 52(55.91%), and female 41(44.08%);
this is 31.71% and 41.84% against total symptomatic male and female patients. Sleep
disturbance was presented by 83 patients, male 51(61.44%), and female 32 (38.55%); this is
31.10% and 32.65% against total symptomatic male and female patients. Headache was
presented by 75 patients, male 58(77.33%), and female 17(22.67%); this is 35.37% and 17.35%
against total symptomatic male and female patients. Sore throat was presented by 63 patients,
male 30(47.61%), and female 33 (52.38%); this is 18.29% and 33.67% against total symptomatic
male and female patients. Breathing difficulty was presented by 61 patients, male 43(70.49%),
and female 18(29.51%); this is 26.22% and 18.37% against total symptomatic male and female
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
6
patients. Rhinorrhea was presented by 53 patients, male 30(56.60%), and female 23(43.31%);
this is 18.29% and 23.47% against total symptomatic male and female patients. Abdominal
cramp/pain was presented by 53 patients, male 27(50.94%), and female 28(52.83%); this is 16.46%
and 28.57% against total symptomatic male and female patients. Skin rash was presented by 47
patients, male 18(38.30%), and female 29(61.70%); this is 10.98% and 29.59% against total
symptomatic male and female patients. Vomiting was presented by 29 patients, male 22(75.86%),
and female 7(24.13%); this is 13.41% and 7.14% against total symptomatic male and female
patients. Vertigo was presented by 11patients, male 3(27.27%), and female 8(72.73%); this is
1.83% and 8.16% against total symptomatic male and female patients. Restlessness was
presented by 82patients, male 57(69.51%), and female 25(30.49%); this is 34.76% and 25.51%
against total symptomatic male and female patients. [Figure 3 A & B]
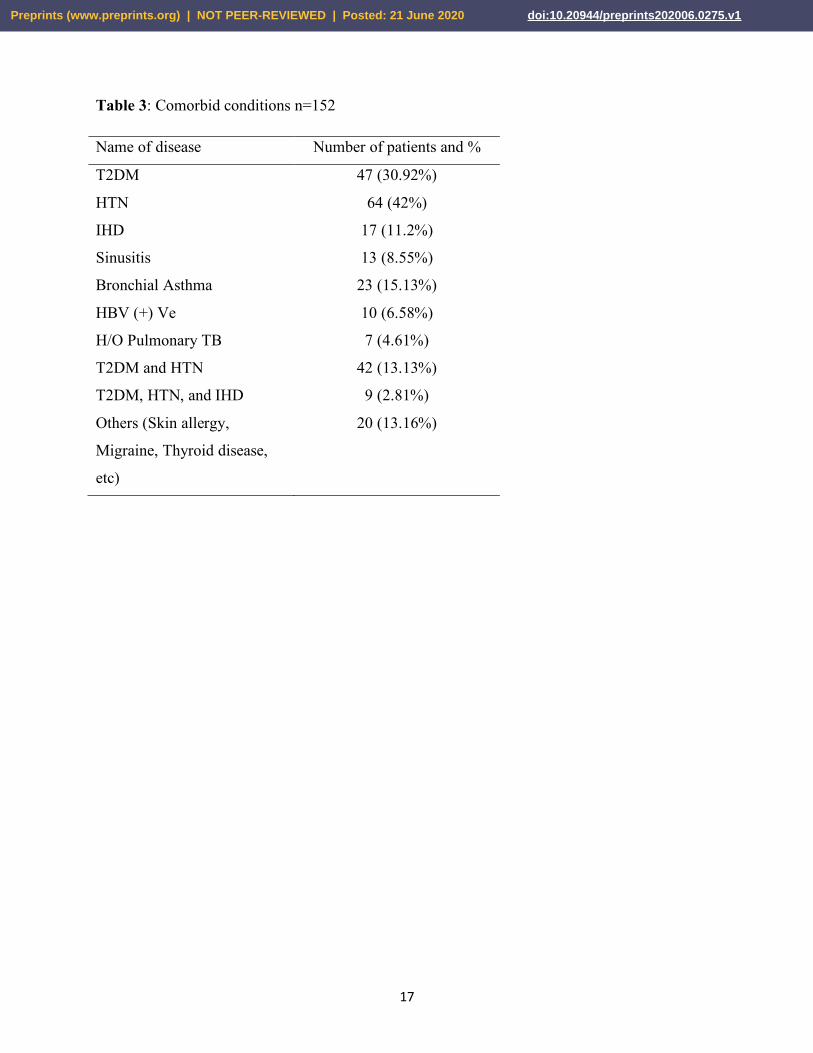
Table 3: 152 (47.50%) patients have a comorbid condition. 47 (30.92%) had T2 DM, 64 (42%)
had HTN, 23 (15.13%) had bronchial asthma, 17 (11.2%) had ischemic heart disease, 13 (8.55%)
has sinusitis, 20 (13.16%) had other manifestations like a fungal infection, hypothyroid, hepatitis
B (+)ve, etc. 42 (13.13%) had DM and HTN and 9 (2.81%) had DM-HTN-Ischemic Heart
Disease.
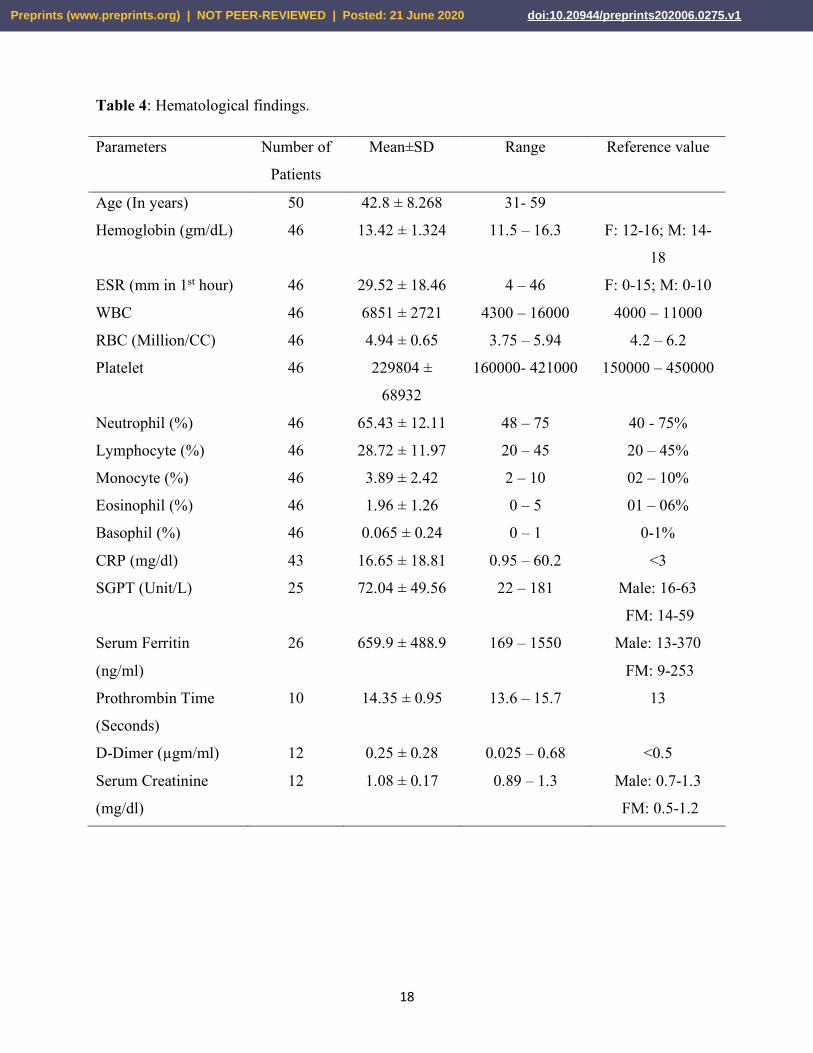
Table 4: Hematological findings, numbers of patients were n=50. Male 37 male and 13 female,
mean age was 42.8 ± 8.268 (31to 59years). Routine blood count was done on 46 patients,
findings with ranges were as following: Hemoglobin 13.42 ± 1.324 gm/dL (11.5 to 16.3 gm/dL);
ESR 29.52 ± 18.46 mm in 1st hour (4 to 46mm in 1st hour), WBC 6851 ± 2721 (4300 to
16000/CC), RBC 4.94 ± 0.65 Million/CC (3.75 to 5.94 Million/CC); Platelet 229804 ± 68932
/CC (160000- 421000/CC), Neutrophil 65.43 ± 12.11% (48 to 85%); Lymphocyte 28.72 ± 11.97 %
(20 to 45%), Monocyte 3.89 ± 2.42% (2 to 10%), Eosinophil 1.96 ± 1.26% (0 to 5%), Basophil
0.065 ± 0.24% (0 to 1%). CRP 16.65 ± 18.81 mg/dl (0.95 to 60.2 mg/dl, number of patients 43);
SGPT 72.04 ± 49.56 Unit/L (22 to 181, number of patients 25); Serum Ferritin 659.9 ± 488.9
ng/ml (169 to 1550, number of patients 26); Prothrombin Time 14.35 ± 0.95 seconds (13.6 to
15.7 seconds, number of patients 10); D-Dimer 0.25 ± 0.28 µgm/ml (0.025 – 0.68 µgm/ml,
number of patients 12), Serum Creatinine 1.08 ± 0.17 mg/dl (0.89 to 1.3 mg/dl, number of
patients 12).
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1

7
Subgroup analysis of the laboratory routine hematological findings based on patients gender
variations are as follows: Hemoglobin level was deceased among 71.42% male and 36.36%
female; ESR was increased in 80%male and 72.73% female; Leucocytosis was found in 17.14%
male and 18.2% female; Neutrophilic leucocytosis was detected in 17.14% male and 18.2%
female; Lymphocytopenia was found among 31.43% male and 18.18% female; Reduce RBC
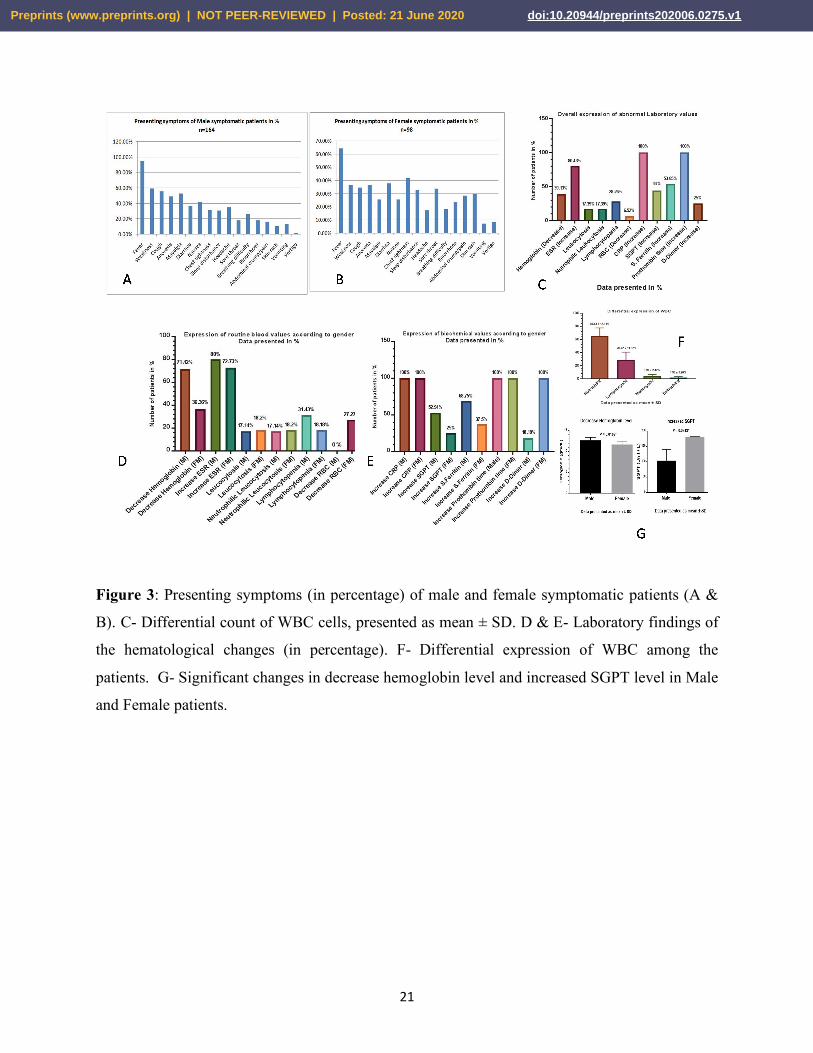
level was noted in 27.27% female this was normal in all male patients. [Figure 3 D]
Subgroup analysis of patients biochemical evaluation depending on patients gender: CRP and
Prothrombin time (PT) was increased in all the male and female patients; increased SGPT level
was found among 52.94% male and 25% female; increased serum ferritin level was seen among
68.75% male and 37.5% female; 18.8% male and 100% of female (1 of 1 female patient) had an
increased level of serum D-Dimer. [Figure 3 F] Difference between the decrease hemoglobin
level (P=0.0243) and increased SGPT (P=0.0108) against male and female in Chi-square test and
t test patients were found significant, others are not. [Figure 3 G]
Discussion
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causing COVID-19 has
rapidly evolved as an epidemic outbreak and infected more than six and a half million
individuals all over the world. Besides this, billions of others are directly affected by the citizens
are affected by measures of social distancing and the socio-economic impact. COVID-19 is a
systemic infection causing a significant impact on the hematopoietic system and hemostasis
mechanism. [3] The incubation period of this virus can be up to 14days following exposure.
According to the center for disease control and prevention (CDC), the individuals with COVID-
19 have had a wide range of symptoms reported ranging from mild to severe illness. These
symptoms may appear from the second day till the incubation period. These symptoms may
include but not limited to cough, fever, chills, muscle pain, the heaviness of chest, shortness of
breath or difficulty breathing, sore throat, and loss of taste or smell. Warning signs of COVID-19
include breathing difficulty, persistent pain or pressure in the chest, inability to wake or stay
awake, sings of central cyanoses like bluish lips or face, and confusion. [4] Multiple studies have
reported presenting symptoms of COVID-19 worldwide among which several symptoms are
common, but due to geographical locations, these symptoms may differ.
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1

8
In this study, we analyzed the COVID-19 cases in multiple centers in Bangladesh to
assess these symptomatic and hematological variations from the rest of the world. Following
exclusion, our study revealed that the primary presenting symptoms of 320 COVID-19 patients
in treated in multiple centers in Bangladesh include fever, cough, chest tightness, weakness,
anorexia, myalgia, diarrhea, nausea, sleep disturbance, headache, sore throat, respiratory distress,
rhinorrhea, abdominal pain, rash or skin lesion, vomiting, vertigo, and restlessness. Among these
primary presenting symptoms, fever and cough were most common, and vomiting and vertigo
were relatively uncommon. Chest tightness and weakness were relatively common in COVID-19
cases but not as much as fever and cough, which was present in the maximum number of cases
affected by SARS-CoV-2 [Figure 2 A & B]. This study can help healthcare professionals in
Bangladesh and others to narrow down the suspected COVID-19 affected cases and perform
testing accordingly. In Bangladesh, unlike developed countries, real-time reverse transcription-
polymerase chain reaction (RT-PCR) is the only available test which is recommended by the
Institute of Epidemiology, Disease Control and Research (IEDCR) for the healthcare settings.
The real-time RT-PCR is of the high value of interest for the detection of COVID-19 disease due
to its simplicity and specificity. [5-7] But unfortunately RT-PCR test has the risk of eliciting
false-negative and false-positive results, as the sensitivity and specificity of the RT-PCR test are
not 100%. [8] However, a chest computed tomography (CT) was reported 98% and 97%
sensitive in two different studies. [9, 10]
One of the early studies regarding clinical characteristics of COVID-19 done on 1099
patients in china revealed that the most common symptoms were fever, cough, and fatigue which
resembles findings of our study (68.8%, 57.3%, and 41.9%). [Figure 2 A & B] A study on the
systematic review focusing on upper airway symptoms revealed that the common symptoms of
COVID-19 were fever, cough, and fatigue. [11] These studies with our study confirm that fever
and cough are the two most common onset symptoms of COVID-19, including in Bangladesh.
Diarrhoea, on the other hand, was uncommon (3.8%) [12] Which is not uncommon in COVID-
19 cases analyzed in our study, 30.6%. Symptoms like Hemoptysis (0.9% Vs 0%) and breathing
difficulty (18.7% Vs 19.1%) show similarity with our findings. But Sore throat 13.9% Vs 19.7%;
Headache 13.6% Vs 23.4%; Nausea & Vomiting 5% Vs 29% & and 9.1%; Myalgia 14.9% Vs 35%
and Skin rash 0.2% Vs 14.7% has revealed a very different trends of presenting symptoms then
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
9
the other reported studies. Our findings of Diarrhoea (30.6%) are similar to Song et al. This
study reported SARS-CoV-2 induced diarrhoea could be the onset symptom in patients with
COVID-19. [13] Up to 30% of patients with the Middle East respiratory syndrome (MERS) and
10.6% of patients with SARS had diarrhoea as the onset symptom. [14] Bao et al. revealed that
vomiting is also associated as the onset symptom in some cases of COVID-19, [15] which was
also present in the COVID-19 cases found in our study (9.1%). A similar result was also found in
the case of rash/skin lesion in this study, which resembles a case study where a young male with
full-body rash was a presenting symptom of COVID-19. [16] 16.6% of the patients in our study
complained of mild to moderate amounts of abdominal cramp or pain. This finding also similar
to a case study reported earlier that the acute abdomen was the early symptom of COVID-19. [17]
During the data collection we have noticed 2 severe cases of COVID-19 with hemoptysis. As all
the severe cases had per existing comorbid conditions, so were not included in his study. We
have also observed three cases presented only with anorexia and two cases of severe myalgia
later were diagnosed as SARS-CoV-2 infection. As an additional finding, restlessness was
complained by 85 (25.63%) of patients this was 34.76% of symptomatic males and 25.51% of
the symptomatic females [Table 2]. Based on our study findings minimally symptomatic patients
or symptoms like abdominal cramp or pain, Myalgia, localize skin lesion or rash, sleep
disturbance, and restlessness are important presenting symptoms for this region of COVID-19
disease besides common other symptoms.
According to our study males have a higher infection rate than females 208 (65%) & 112 (35%).
[Figure 1 A] Also only 18.12% of patients were asymptomatic whereas symptomatic cases were
81.88%. [Figure 2 C] This is due to lack of test availability and also tests were made available
only to the definite symptomatic patients or those who have radiological or laboratory findings
suggestive of SARS-CoV-2 infection. The duration of symptoms had no variation depending on
gender and age. [Figure 1 C, Figure 2 F] Male patient’s home isolation and treatment number are
higher than the female patients. [Figure 1 D] In case of age group 31 to 40 years are the most
affected n= 127/320 and 10 to 20 are the least n=30/320. [Figure 1 E] Cases with or without
fevers were high 68.75% and 31.25% compare to Wei-jie Guan et al. [11] Duration of fever has
no significant difference regarding presenting temperature. [Figure 1 F] But temperature >1000F
was relatively higher then <1000F 47.5% and 21.25% of total patients, this is 152 (69.09%) and
68 (30.90%) [Table 1] of patients with fever and does not correlate with the other study. [11]
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
10
Male patients were more affected with cough than female and dry cough was more common than
sputum. [Figure 2 E] Fever, weakness, anorexia, Myalgia, nausea, headache, breathing difficulty,
vomiting, and restlessness were more prominent in the case of male than female patients. [Table
2, Figure 3 A & B] Chest tightness, sore throat, skin lesion/rash, and vertigo were more common
in female patients. [Table 2, Figure 3 A & B] Other than that diarrhea, sleep disturbance and
rhinorrhoea/nasal congestion have an almost similar presentation in both sexes.
SARS-CoV-2, on the other hand, is a systemic infection with a significant impact on the
hematopoietic system and hemostasis, according to the critical review by Terpos et al. done on
hematological findings of COVID-19. They have found that COVID-19 disease has prominent
manifestations from the hematopoietic system and is often associated with a major blood
hypercoagulability. The study indicated that Lymphopenia might be considered as a cardinal
finding with prognostic potential. On the other hand, Neutrophil/lymphocyte ratio and peak
platelet/lymphocyte ratio may also have prognostic value in determining severe cases.
Furthermore, blood hypercoagulability is common among hospitalized COVID-19 patients.
Elevated D-dimer levels are consistently reported as well. Thus, the study concluded that in
patients with COVID-19 either for hospitalized or not, are at high risk for venous
thromboembolism, and an early and prolonged pharmacological thromboprophylaxis with
LMWH is highly recommended. [18]
We had analyzed the on-admission laboratory values of 50 patients with moderate degree
of COVID-19 disease to assess the overall expression. The study revealed an increased level of
ESR, CRP, SGPT, S. Ferritin, Prothrombin time, and D-Dimer. However, the level of
Hemoglobin and RBC were decreased and also revealed leucocytosis, neutrophilia, and
lymphocytopenia. [Figure 2 C & D] The differential expression of WBC analysis revealed
normal mean Neutrophil, Lymphocyte, Monocyte and Eosinophil count. [Figure 3 F] Analysis of
biochemical values according to gender revealed differences between males and females in a few
parameters. Increased levels of SGPT and S. Ferritin were found among males, and increased
levels of D-Dimer were found among females (One in one patient). [Figure 3 E] There were no
differences in the levels of CRP and prothrombin times between males and females in patients
with COVID-19. [Figure 3 E] Hemoglobin count was decrease in case of male (71.42%) than
female (36.36%), though RBC count was normal in all the males and decreased among 27.27%
of female patients. [Figure 3 D] Difference between the decrease hemoglobin count and
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1

11
increased SGPT against male and female patients were found significant. [Figure 3 G] All these
suggests us to provide more attention towards gender in cease of laboratory findings for COVID-
19 diagnosis and prognosis
One of our important observation was in delay in diagnosis and therefore treatment from the time
of appearance of symptoms, 5.67± 3.56 days. [Figure 1 C] This is probably explained by delay in
publishing test results (2 to 3days from sample collection) unwilling to take tests by patients due
to testing and social hazards, and strict indications followed for the PCR test (Fever, breathing
difficulty, chest discomfort, Chest X ray findings and associated hematological findings) by the
COVID-19 tertiary centre doctors due to limited resources.
Conclusion
According to this study COVID-19 patient in Bangladesh though has similarity with the
presenting symptoms like fever, cough and berating complaints, but symptoms like myalgia,
diarrhea, skin rash, headache, Abdominal pain/cramp, nausea, vomiting, restlessness, and a
higher temperature of >1000F have a greater presentation rate and more frequent even as an
isolated presentation of SARS-CoV-2 infection than other published studies. Hematological
findings like CRP and Prothrombin time were found to increase among all of our study patients.
Besides, an increase in Serum ferritin, ESR, SGPT, and D-Dimer along with erythrocytopenia
and lymphocytopenia can be important supportive diagnostic criteria. Due to differences in
presentations and difficulty in testing, some common symptoms create confusion regarding
diagnosis and mislead a SARS-CoV-2 infection like a common viral flue. This might cause
morbidity and mortality to COVID-19 patients. Moreover, a chest CT is neither affordable for
most of the patients nor available in rural healthcare settings in Bangladesh. So, there is a
possibility of patients affected by SARS-CoV-2 may remain undiagnosed due to a false negative
real-time RT-PCR test or not being sensitive to the real-time RT-PCR test. Thus, if further tests
can’t be done to confirm the diagnosis such as a chest CT in patients having these common
symptoms and hematological manifestations should be treated as COVID-19 patients to narrow
the spread of the COVID-19 and stop the symptomatic patients from developing severe illness
any further. Our study has limitations, namely the small sample size and selection of mild to
moderate cases that may affect the study outcome. But we believe the above findings will help to
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
12
guide physicians and researchers to have a different view and better management of COVID-19
disease during this crisis period.
Conflict of Interests
None to declare.
Ethics Approval and Consent to Participate
The study was approved by the hospital ethics committee, First Affiliated Hospital of Xi’an
Jiaotong University, Xi’an, Shaanxi, China. The purpose of this research was explained to the
participant. Once the verbal consent was understood and agreed, a written consent was then
obtained from the participant. In the case of bellow 16 years old participants written consent was
obtained from a parent or guardian.
Authors’ contributions
ATMMC: concept development, data collection and analysis, statistical analysis, review and
manuscript writing; MRK: review and manuscript writing; MS and MWC: data collection;
HMHM: laboratory data collection; GD: data analysis and interpretation; HS: supervision and
critical review of the manuscript.
Acknowledgment
The authors are thankful for the kind cooperation of the Chattagram Civil surgeon’s office,
Chokoria Upazilla Health Complex, and Chattagram General Hospital.
Declaration
All the authors approved to publish this work.
Funding
Not applicable.
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
13
References
1. Xu, X., et al. "Evolution of the novel coronavirus from the ongoing Wuhan outbreak and
modeling of its spike protein for risk of human transmission." SCIENCE CHINA Life
Sciences, vol. 63, 2020, pp. 457–460, doi: 10.1007/s11427-020-1637-5
2. Thevarajan, I., et al. "Clinical presentation and management of COVID-19." The Medical
Journal of Australia, 8 Apr. 2020. https://www.mja.com.au/system/files/2020-
04/Preprint%20Thevarajan%20%28Cowie%29%208%20April%202020.pdf.Accessed
28 May 2020.
3. Lu, H., et al. "Outbreak of pneumonia of unknown etiology in Wuhan, China: the
mystery and the miracle. " Journal of Medical Virology, vol. 92, 2020, pp. 401–402, doi:
10.1002/jmv.25678
4. Centers for Disease Control and Prevention. "Symptoms of Coronavirus Disease 2019
poster." Centers for Disease Control and Prevention, 20 May 2020,
www.cdc.gov/coronavirus/2019-ncov/downloads/COVID19-symptoms.pdf. Accessed
28 May 2020.
5. Shen, Minzhe, et al. "Recent advances and perspectives of nucleic acid detection for
coronavirus." Journal of Pharmaceutical Analysis, vol. 10, no. 2, 2020, pp. 97-101,
doi:10.1016/j.jpha.2020.02.010.
6. Wan, Zhenzhou, et al. "A Melting Curve-Based Multiplex RT-qPCR Assay for
Simultaneous Detection of Four Human Coronaviruses." International Journal of
Molecular Sciences, vol. 17, no. 11, 2016, p. 1880, doi:10.3390/ijms17111880.
7. Noh, Ji Y., et al. "Simultaneous detection of severe acute respiratory syndrome, Middle
East respiratory syndrome, and related bat coronaviruses by real-time reverse
transcription PCR." Archives of Virology, vol. 162, no. 6, 2017, pp. 1617-1623,
doi:10.1007/s00705-017-3281-9.
8. Tahamtan, Alireza, and Abdollah Ardebili. "Real-time RT-PCR in COVID-19 detection:
issues affecting the results." Expert Review of Molecular Diagnostics, vol. 20,
no. 5, 2020, pp. 453-454, doi:10.1080/14737159.2020.1757437.
9. Fang, Yicheng, et al. "Sensitivity of Chest CT for COVID-19: Comparison to RT-
PCR." Radiology, 2020, p. 200432, doi:10.1148/radiol.2020200432.
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
14
10. Ai, Tao, et al. "Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease
2019 (COVID-19) in China: A Report of 1014 Cases." Radiology, 2020, p. 200642,
doi:10.1148/radiol.2020200642.
11. Lovato, Andrea, and Cosimo De Filippis. "Clinical Presentation of COVID-19: A
Systematic Review Focusing on Upper Airway Symptoms." Ear, Nose & Throat
Journal, 2020, p. 014556132092076, doi:10.1177/0145561320920762.
12. Guan, W. J., et al. "Clinical Characteristics of Coronavirus Disease 2019 in China." The
New England Journal of Medicine, vol. 382, 2020, pp. 1708-1720,
doi:10.1056/NEJMoa2002032.
13. Song, Y., et al. "SARS-CoV-2 induced diarrhoea as onset symptom in patient with
COVID-19." Gut, vol. 69, no. 6, 2020, pp. 1143-1144, doi:10.1136/gutjnl-2020-320891.
14. Chan, Jasper F., et al. "A familial cluster of pneumonia associated with the 2019 novel
coronavirus indicating person-to-person transmission: a study of a family cluster." The
Lancet, vol. 395, no. 10223, 2020, pp. 514-523, doi:10.1016/S0140-6736(20)30154-9.
15. Fu, Bao, et al. "SARS-CoV-2-Induced Vomiting as Onset Symptom in a Patient with
COVID-19." Digestive Diseases and Sciences, vol. 65, no. 6, 2020, pp. 1568-1570,
doi:10.1007/s10620-020-06285-4.
16. Hunt, Madison, and Christian Koziatek. "A Case of COVID-19 Pneumonia in a Young
Male with Full Body Rash as a Presenting Symptom." Clinical Practice and Cases in
Emergency Medicine, vol. 4, no. 2, 2020, pp. 219-221, doi:10.5811/cpcem.2020.3.47349.
17. Sellevoll, H. B., et al. "Acute abdomen as an early symptom of COVID-19." The Journal
of the Norwegian Medical Association, 2020, doi:10.4045/tidsskr.20.0262.
18. Terpos, Evangelos, et al. "Hematological findings and complications of COVID
-19." American Journal of Hematology, 2020, doi:10.1002/ajh.25829.
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
15
TABLES:
Table 1: Baseline characteristics of the patients.
Parameters Number
Number of Patients 320
Male 208 (65%)
Female 112 (35%)
Age (mean ± SD) 35.81±11.07
Age of Male patients (mean ± SD) 34.15±11.07
Age of Female patients (mean ± SD) 38.89 ± 12.19
Asymptomatic 58 (18.12%)
symptomatic 262 (81.88%)
Hospitalized 129 (40.31%)
Home isolation 191 (59.69%)
Duration of symptoms (days ± SD) 5.66 ± 3.60
Male, Duration of symptoms (days ± SD) 5.72 ± 3.50
Female, Duration of symptoms (days ± SD) 5.56 ± 4.0
Body temperature <1000 F 68 (30.90%)
Body temperature >1000 F 152 (69.09%)
Comorbid condition (n) 152 (47.50%)
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
16
Table 2: Symptomatic presentation according to gender variation. The total number of patients
n=320.
Symptoms No. of
Patients
Male Female % Against male
Symptomatic
Patients, n=164
% Against female
Symptomatic
Patients, n=98
Fever 220 157 (71.36%) 63 (28.64%) 95.73% 64.29%
Weakness 134 98 (73.13%) 36 (26.87%) 59.76% 36.73%
Cough 126 92 (73.01%) 34 (26.87%) 56.10% 34.69%
Anorexia 117 81 ((69.23%) 36 (30.77%) 49.39% 36.73%
Mayalgia 112 87 (77.68%) 25 (22.32%) 53.05% 25.51%
Diarrhoea 98 61 (62.24%) 37 (37.76%) 37.20% 37.76%
Nausea 94 69 (73.40%) 25 (26.60%) 42.07% 25.51%
Chest
tightness
93 52 (55.91%) 41 (44.08%) 31.71% 41.84%
Sleep
disturbance
83 51 (61.44%) 32 (38.55%) 31.10% 32.65%
Headache 75 58 (77.33%) 17 (22.67%) 35.37% 17.35%
Sore throat 63 30 (47.61%) 33 (52.38%) 18.29% 33.67%
Breathing
difficulty
61 43 (70.49%) 18 (29.51%) 26.22% 18.37%
Rhinorrhea 53 30 (56.60%) 23 (43.31%) 18.29% 23.47%
Abdominal
crump/pain
53 27 (50.94%) 28 (52.83%) 16.46% 28.57%
Skin rash 47 18 (38.30%) 29 (61.70%) 10.98% 29.59%
Vomiting 29 22 (75.86%) 7 (24.13%) 13.41% 7.14%
Vertigo 11 3 (27.27%) 8 (72.73%) 1.83% 8.16%
Restless 82(25.63
%)
57 (69.51%) 25 (30.49%) 34.76% 25.51%
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
17
Table 3: Comorbid conditions n=152
Name of disease Number of patients and %
T2DM 47 (30.92%)
HTN 64 (42%)
IHD 17 (11.2%)
Sinusitis 13 (8.55%)
Bronchial Asthma 23 (15.13%)
HBV (+) Ve 10 (6.58%)
H/O Pulmonary TB 7 (4.61%)
T2DM and HTN 42 (13.13%)
T2DM, HTN, and IHD 9 (2.81%)
Others (Skin allergy,
Migraine, Thyroid disease,
etc)
20 (13.16%)
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
18
Table 4: Hematological findings.
Parameters Number of
Patients
Mean±SD Range Reference value
Age (In years) 50 42.8 ± 8.268 31- 59
Hemoglobin (gm/dL) 46 13.42 ± 1.324 11.5 – 16.3 F: 12-16; M: 14-
18
ESR (mm in 1st hour) 46 29.52 ± 18.46 4 – 46 F: 0-15; M: 0-10
WBC 46 6851 ± 2721 4300 – 16000 4000 – 11000
RBC (Million/CC) 46 4.94 ± 0.65 3.75 – 5.94 4.2 – 6.2
Platelet 46 229804 ±
68932
160000- 421000 150000 – 450000
Neutrophil (%) 46 65.43 ± 12.11 48 – 75 40 - 75%
Lymphocyte (%) 46 28.72 ± 11.97 20 – 45 20 – 45%
Monocyte (%) 46 3.89 ± 2.42 2 – 10 02 – 10%
Eosinophil (%) 46 1.96 ± 1.26 0 – 5 01 – 06%
Basophil (%) 46 0.065 ± 0.24 0 – 1 0-1%
CRP (mg/dl) 43 16.65 ± 18.81 0.95 – 60.2 <3
SGPT (Unit/L) 25 72.04 ± 49.56 22 – 181 Male: 16-63
FM: 14-59
Serum Ferritin
(ng/ml)
26 659.9 ± 488.9 169 – 1550 Male: 13-370
FM: 9-253
Prothrombin Time
(Seconds)
10 14.35 ± 0.95 13.6 – 15.7 13
D-Dimer (µgm/ml) 12 0.25 ± 0.28 0.025 – 0.68 <0.5
Serum Creatinine
(mg/dl)
12 1.08 ± 0.17 0.89 – 1.3 Male: 0.7-1.3
FM: 0.5-1.2
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
19
FIGURES:
Figure 1: A- Number of total patients and gender difference of infected in number and
percentage. B- Variation in age according to gender and age group. C- Duration of presenting
symptoms in general and according to gender. D- Percentage of hospitalized and home isolation-
treatment according to gender. E- Number of the COVID-19 patients according to age group.
Note: 31 to 40 years is the highest and 10 to 20 years is the lowest affected group. F- Duration
and grade of fever (<1000F and >1000F) as presenting symptom of COVID-19 disease.
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
20
Figure 2: Presenting symptoms in percentage (A) and number (B) against the total of COVID-19
patients included in this study. C- Symptomatic and asymptomatic cases of COVID-19 patients
in number. D- Presentation of the number of patients with or without fever against the total
number of COVID-19 patients included in this study. E- Analysis of cough (Dry and with
sputum) as a presenting symptom. F- Age variation according to the gender in the case of
Hospitalized and home isolated patients.
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1
21
Figure 3: Presenting symptoms (in percentage) of male and female symptomatic patients (A &
B). C- Differential count of WBC cells, presented as mean ± SD. D & E- Laboratory findings of
the hematological changes (in percentage). F- Differential expression of WBC among the
patients. G- Significant changes in decrease hemoglobin level and increased SGPT level in Male
and Female patients.
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 21 June 2020 doi:10.20944/preprints202006.0275.v1