analysing data for risk-based regulation in nursing & midwifery and other health professions
TRANSCRIPT

Analysing Data for Risk-Based RegulationIn Nursing & Midwifery and other Health Professions.

Introduction
• Who we are• Opportunities for new approaches• What we needed to learn• What we have put in place• How we apply it• What’s next?• Some advice…
Who we are

Australia
• 23 million people• Federal system of government• 9.3% of GDP on health • Joint government funders• 70% public – 30% private mix• Good health status overall• Major gap for indigenous health• Mal-distribution of heath workforce• Significant international workforce

Major Consolidation• Eight State & Territory
based arrangements
• More than 95 health profession boards
• 75 Acts of Parliament
• 38 regulatory operations
• 1.5 million data items from 94 sources
• One national scheme
• 14 health profession boards
• Nationally consistent legislation (largely)
• One national organisation (AHPRA)
• National on-line registers

What we doAHPRA works with the 14 National
Health Practitioner Boards to:• Set professional standards • Register practitioners
Maintain national registers• Manage notifications • Accreditation

Objectives of legislation
• Protection of the public• Workforce mobility within Australia • High quality education and training• Rigorous and responsive assessment of overseas
trained practitioners• Facilitate access to services in accordance with
the public interest• Enable a flexible, responsive and sustainable
health workforce and enable innovation

Harmonising Registration Standards
• Criminal history • English language requirements • Professional Indemnity
Insurance arrangements• Continuing Professional
Development • Recency of Practice
Codes and Guidelines• Advertising• Mandatory reporting• Conduct

The diverse nature of the professions
Profession Registrants (2014-15)
Proportion of total
registrants
Notifications (2014-15)
Proportion of total notifications
Medical 103,133 16% 4,541 54%
Nursing and Midwifery
370,303 58% 1,807 22%
Psychology 32,766 5% 432 5%
Pharmacy 29,014 5% 490 6%
Dentistry 21,209 3% 766 9%
- Other Boards 80,793 12% 390 4%
Patient safety and workforce: driving reform of
regulation

Opportunities for new approaches
Lessons from the UK Professional Standards
Authority
Harry Cayton, CEO UK Professional Standards Authority
• Be clear on the problem
• Quantify the risk
• Pay attention to unintended consequences
• Keep it simple

What we needed to learn

What would Malcolm say?
Prof Malcolm Sparrow
• Detect patterns• Understand the
problems• Develop regulatory
solutions• Implement solutions• Measure effectiveness• Tell people about it
Collect information on harm in a systematic manner,
and then identify hotspots of risk
that are amenable to a regulatory response.

Reducing rule-breaking vs Reducing harm
Compliance based
Harm based
The value of harm information
“Conclusion: Systematic reviews compound the poor reporting of harms data in primary studies by failing to report on harms or doing so inadequately.”
Liliane Zorzela, ‘Quality of reporting in systematic reviews of adverse events: a systematic review’ BMJ, 8 January 2014
“[Health] …complaints have considerable sentinel value: for every adverse event complained of, dozens more lie below the waterline.”
Marie M Bismark, David M Studdert, ‘Realising the research power of complaints data’, New Zealand Medical Journal, 2010
17
What we have put in place
AHPRA’s Regulatory Principles
While we balance all the objectives of the National Registration and Accreditation Scheme, our primary consideration is to protect the public.
In all areas of our work we: • identify the risks that we are obliged to respond to • assess the likelihood and possible consequences of the risks, and • respond in ways that are proportionate and manage risks so we can
adequately protect the public
When we take action about practitioners, we use the minimum regulatory force to manage the risk posed by their practice, to protect the public. Our actions are designed to protect the public and not to punish practitioners.

NRAS Risk-based Regulation Unit
To reduce harm to the public and facilitate safe workforce reform by increasing the use
of data and research to inform policy and regulatory decision-making.
Moving from a reporting system to a learning system.
20

Using analysis to inform risk-based regulation
1. Quantitative analysis to detect patterns
2. Semi-quantitative analysis
to identify issues and themes
3. Case reviews & qualitative methods to understand the problems

Which of the following should be the greatest influence on the regulatory actions of a risk-based regulator?a) The characteristics of high-risk practitioners?
b) The patients who are most at risk of harm?
c) Which health care settings create the greatest risk?
d) Which procedures create the greatest risk?
How we apply it

Key QuestionsDescriptive Can we create clear, comprehensive,
accurate and timely risk profiles for each health profession?
Consistent Are our regulatory responses consistent across jurisdictions, years and professions?
Predictive Can we predict which practitioners and situations are more likely to cause harm?
Responsive What are the best right touch responses to the hot spots of risks that we identify?
Effective Are our regulatory responses effective in reducing harm to the public?

Medical Radiation Practitioner
Midwife
Occupational Therapist
Nurse
Physiotherapist
Osteopath
Chinese Medicine Practitioner
Optometrist
Psychologist
Podiatrist
Pharmacist
ATSIH
Chiropractor
Medical Practitioner
Dental Practitioner
0 10 20 30 40 50 60
Notification Rates (2010-2014)(enquiries, formal notifications and offences)
Notifications per year per 1000 practitioners
Under 24
25 to 34
35 to 44
45 to 54
55 to 64
Over 65
Female
Male
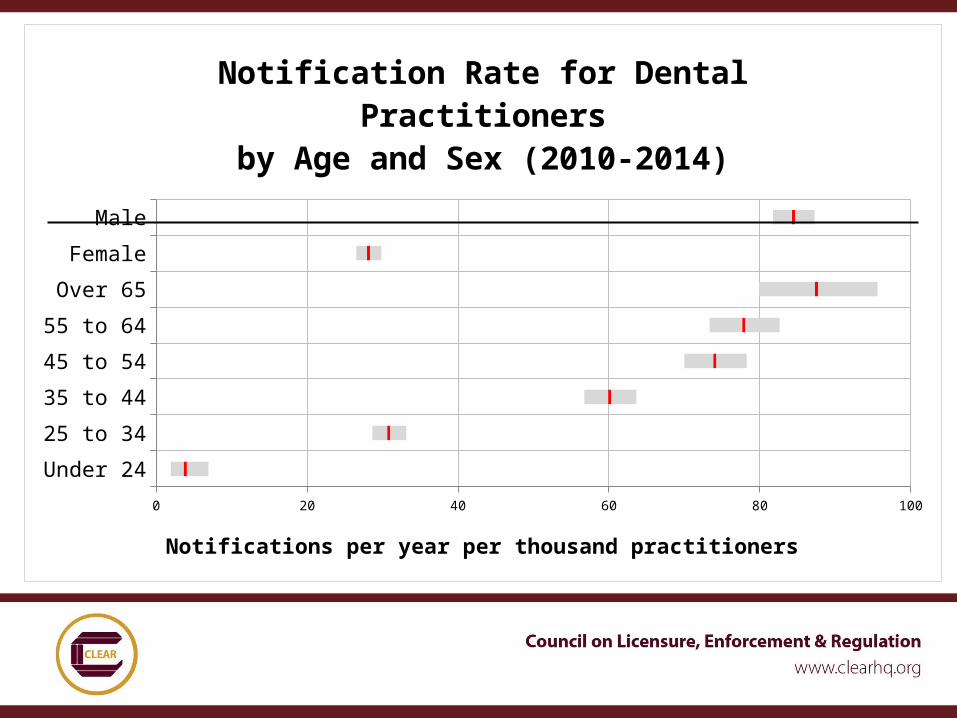
0 20 40 60 80 100
Notification Rate for Dental Practi-tioners
by Age and Sex (2010-2014)
Notifications per year per thousand practitioners

Predicting Risk
0 1 2 3 4 5+0%
20%
40%
60%
80%
100%
Probability of practitioner receiving another noti-fication
in next 12 months
Number of Notifications Practitioner Received in prior 12 months
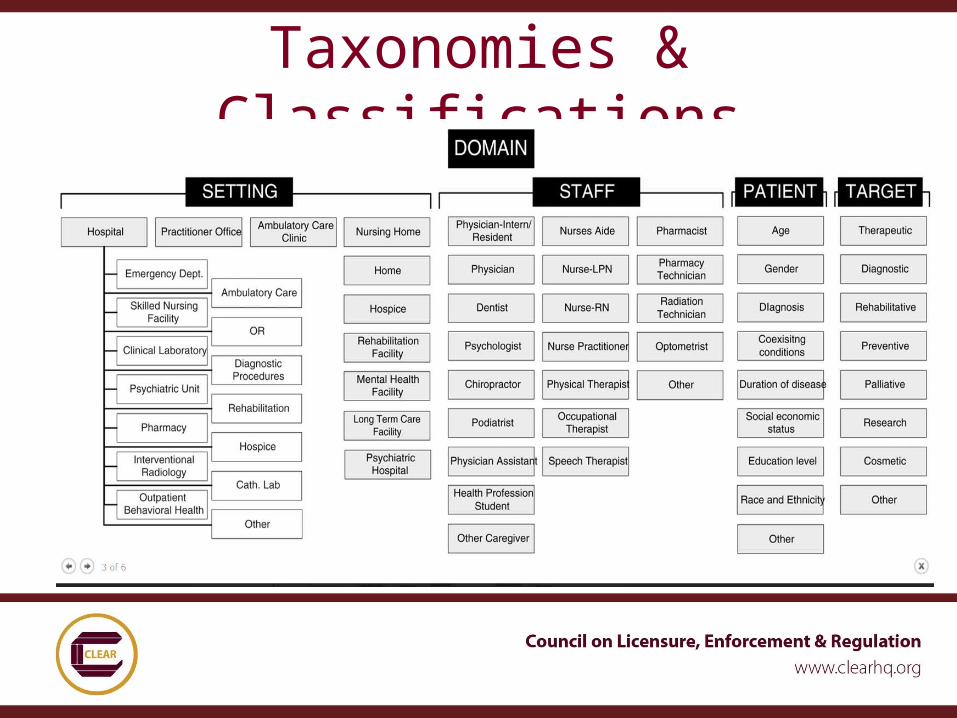
Taxonomies & Classifications
Examples from risk analysis• The proportion of nursing notifications
relating to Health Impairment is 4.9 times higher than for all other professions combined.
• Approximately 10% of all notifications about nurses and midwives result in immediate action.
• The likelihood of a practitioner originated notification resulting in a caution or reprimand is 1.5 times higher than for a patient initiated notification.

Qualitative analysis on boundaries
• Professional boundaries fall along a spectrum from under-involvement and neglect to over-involvement all the way to sexual assault.
• Our data systems seem to be better at capturing the over-involvement end, and these are easier to deal with.
• An analysis of ‘under-involvement’ cases suggests concerning potential for risk of harm to patients
• In some cases the regulator only became aware after a pattern of behaviour not dealt with in the workplace
• In some cases, regulatory action can be an effective tool to change behaviour
30
What’s next?

Future Core Focus
• Frequently reported practitioners• Increased risk of notifications with
age• Identification of factors most
associated with patient harm • Risk associated with overseas trained
practitioners• Evaluating impact of practice
restrictions

Regulatory topics for NMBA• National Health Impairment: Referral, treatment &
rehabilitation services for health professionals• How continuing competence is/can be defined &
assessed• Exploring factors related to nursing & midwifery
medication management & prescribing• Review of code of conduct and guidelines on
professional boundaries• Development of new model of IQNM assessment• The role of accreditation in risk based regulation
http://ecommerce.dent.unimelb.edu.au/product.asp?pID=91&cID=36

Some advice…
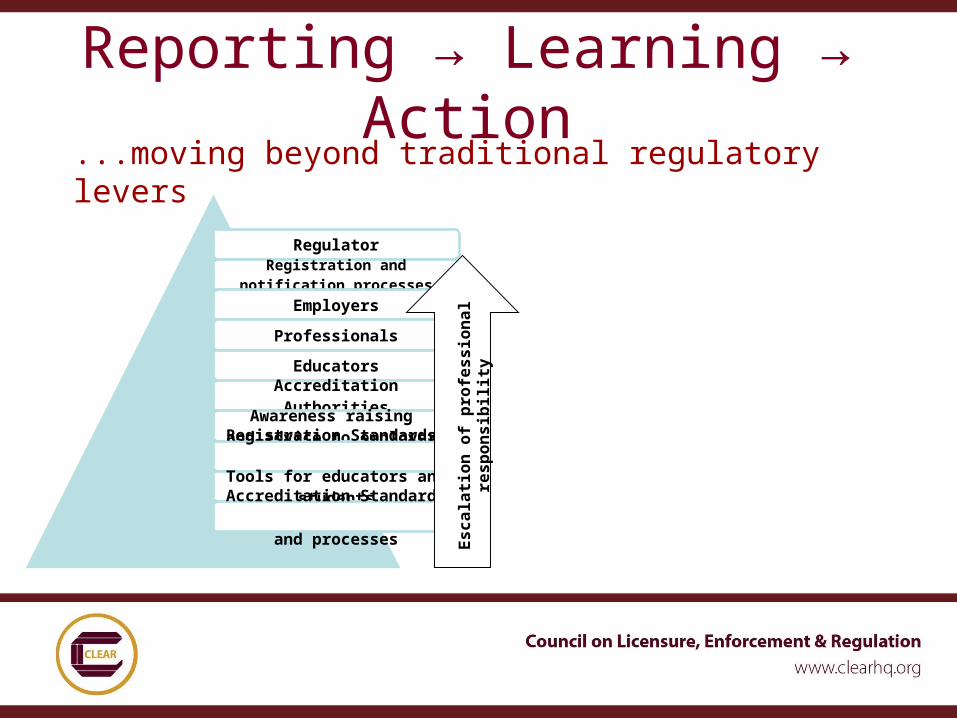
Reporting → Learning → Action
...moving beyond traditional regulatory levers
RegulatorRegistration and
notification processes
Employers
Professionals
EducatorsAccreditation Authorities
Awareness raising and advice to employersRegistration Standards,
codes and guidelinesTools for educators and
studentsAccreditation Standards
and processes
Esca
latio
n of
pro
fess
iona
l res
pons
ibili
ty

Lessons Learnt• Be clear: are you a risk-based
regulator?• Set realistic expectations• Requires new/different skills• Partner with external researchers• Data classifications and taxonomy
essential• Will always need subjective, qualitative • Close the loop – response system is
more important than the reporting system

Contact Information
Australian Health Practitioner Regulation Agency
• Martin Fletcher, Chief Executive Officer• Michelle Thomas, Executive officer – dental
www.ahpra.gov.auNursing and Midwifery Board of Australia• Veronica Casey, Practitioner MemberDental Board of Australia• Dr John Lockwood (AM), Chair