anaesthesia challenges in organ retrieval
TRANSCRIPT

Krishna Institute of Medical Sciences ( KIMS )
Dr. JAYASHREE PATKI MBBS, MD, PGDHHMSr. ConsultantKrishna Institute of Medical SciencesHyderabad
Transplantation of Human Organs Act, 1994
Aims
Regulate removal, storage and transplantation of human organs for therapeutic purposes
To prevent commercial dealings in organs
Recognise Brain Death
Historical Aspects – Cadaver Transplantation – India
1967 - First successful cadaver Kidney Transplant in India at KEM Hospital, Bombay
1994 - First successful heart transplant done at AIIMS, N.Delhi
1995 - First successful multi-organ transplant done at Apollo Hospital, Chennai
1998 – First Successful Lung transplant, Madras Medical Mission Hospital, Chennai
1999 – First Pancreas Transplant, Ahemdabad


Indian facts –Around 10 lakh ESRD patients
Only 2% (20,000) patients get treated
Only 500 dialysis centers
Only 3000 dialysis machines
Only 80 transplant centers
Only 3000 kidney transplants take place / year
98% are live related transplants
Only 2% are cadaveric transplants
MOHAN FOUNDATION MultiOrganHarvestingAidNetworkFormation1997
Type nongovernment charityPurposeOrganDonation
Headquarters Chennai, India
Founder SunilShroff
Website www.mohanfoundation.org
The anesthesiologist plays a pivotal role in organ procurement from the brain dead patient, as haemodynamics, thermoregulation, volume status, and skeletal muscle paralysis require active management which are vital to the procurement of healthy organs.
In the presence of brain death, spinal cord function is still intact and both somatic and visceral reflexes still remain.
Effective anesthetic management of donor requires an understanding of these effects .
Brain Death :Definition :
Cardiac death:Heartbeat and breathing stop
Brain death:Irreversible cessation of all functions of the entire brain, including the brain stem Irreversible coma and apnoeaLoss of brain stem functions
The declaration of brain death is based on :
The presence of unresponsive coma
The absence of brainstem reflexes
The absence of respiratory drive after CO2 challenge
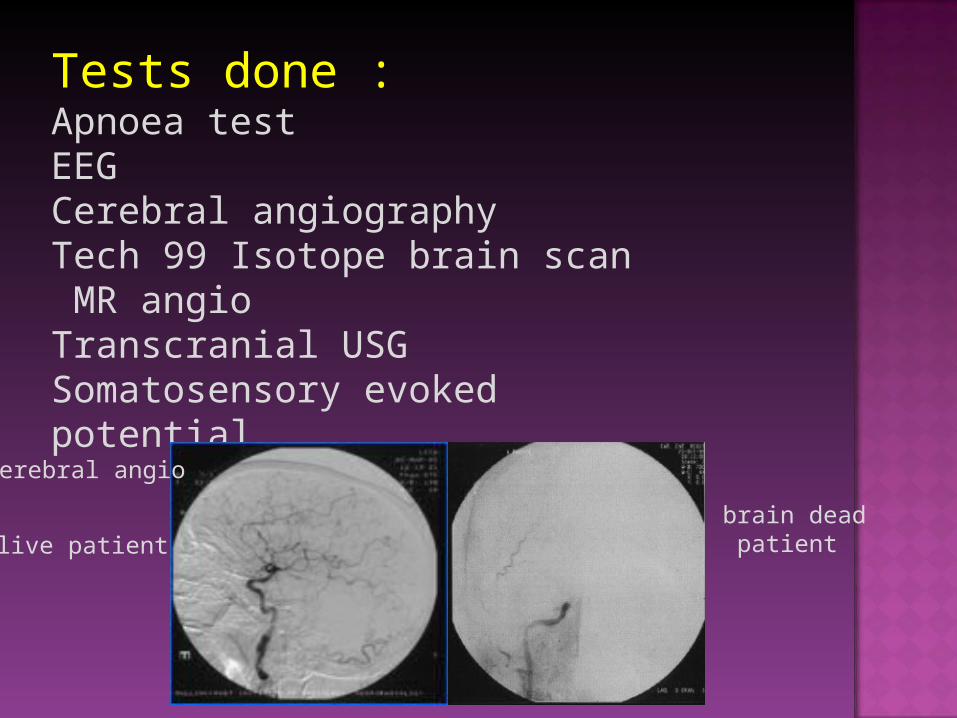
Tests done : Apnoea testEEGCerebral angiographyTech 99 Isotope brain scan MR angioTranscranial USGSomatosensory evoked potential
live patient brain dead patient
Cerebral angio
Management of donor :
Starts in ICU and ends on OT
Continuation of ICU care till the organs are harvested
Main goal shifts from optimizing cerebral perfusion pressure to maintaining hemodynamic stability

Following the diagnosis of Brain Death:
The normal squeals of brain death results in cardiovascular instability & poor organ perfusion.
Anesthetist must focus on:- Providing hemodynamic stabilization.- Support of body homeostasis.- Maintenance of adequate cellular
oxygenation and donor organ perfusion.
Without appropriate intervention brain death is followed by severe injury to most other organ systems. Circulatory collapse will usually occur within 48hrs.

Common Clinical Problems Of Brain Stem Dead Patient :
HypotensionHypothermiaEndocrine DisturbancesElectrolyte ImbalanceArrhythmiasHypoxia
Uncommon Clinical Problems
CoagulopathyNeurogenic Pulmonary Oedema

Pathophysiology :
Loss of brain stem function results in systemic physiologic instability
Loss of vasomotor control leads to hyperdynamic state
Cardiac arrhythmias
Loss of respiratory function
Loss of temperature regulation Hypothrmia
Hormonal imbalence DI, Hypothyriodism
Cardiovascular management :
Rule of 100’s: SBP >100 mm HgU /O >100 ml / hrPaO2 >100 mm Hg Hb >100 gm / L HR > 100RBS = 100CVP = 10
Avoiding lactic acidosis (pH = 7.35 – 7.45) and hypothermia (temperature > 34o C)
Preoprative preperation :Check ----
ConsentMLC Formalities Police enquiryInvestigationsVitalsSupportsAntibioticsLines-CVC, art . LineTransfer to OT Work up of the Receipient
Intraoperative Management :Monitors –Pulse oximetry 5 lead electrocardiogram (ECG) Invasive arterial blood pressure Central venous pressure Urine output Temperature monitoring with nasopharyngeal probe P A Pressure and Cardiac output (in selected cases
having low LVEF )Fluid warmers n body warmersTransport- chance of disconnection of circuit and iv
lines leading to hypotention and hypoxia
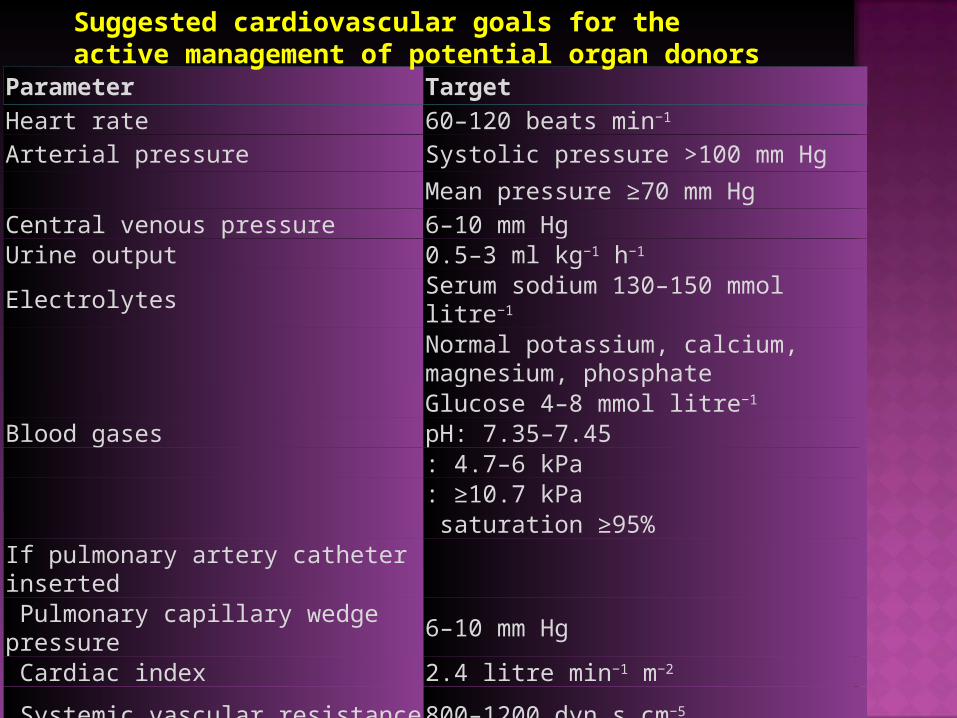
Parameter TargetHeart rate 60–120 beats min−1
Arterial pressure Systolic pressure >100 mm HgMean pressure ≥70 mm Hg
Central venous pressure 6–10 mm HgUrine output 0.5–3 ml kg−1 h−1
Electrolytes Serum sodium 130–150 mmol litre−1
Normal potassium, calcium, magnesium, phosphateGlucose 4–8 mmol litre−1
Blood gases pH: 7.35–7.45: 4.7–6 kPa: ≥10.7 kPa saturation ≥95%
If pulmonary artery catheter inserted Pulmonary capillary wedge pressure 6–10 mm Hg Cardiac index 2.4 litre min−1 m−2
Systemic vascular resistance 800–1200 dyn s cm−5
Suggested cardiovascular goals for the active management of potential organ donors

Anaesthetic Management: Goals
Pt. preservation to organ preservation
Maintain hemodynamic stability
Avoid ischemia
Maintain adequate urine volume
Prevention of hypothermia
Critical care management of potential organ donor is crucial in maximizing the number and the quality of transplanted organs
Goal is to provide adequate oxygen supply and tissue perfusion

Cardiac Myocardial injury Loss of vascular tone Hemodynamic instability Hypovolemia
Pulmonary • Increased pulmonary capillary permeability
• Pulmonary edema
Endocrine • Pituitary infarction may lead to diabetes
insipidus and obliteration of thyroid axis • Hyperglycemia • Hypernatremia
Hematologic • Coagulopathy, which may progress to
disseminated intravascular coagulation
Skeletal muscles
Restore intravascular volume, replacing evaporative and DI urinary losses.
• Use vasopressors as necessary to maintain adequate organ perfusion.
• Maintain SBP > 100 mmHg, MAP > 70, HR 60-120 beats·min−1.
• “Lung-protective” ventilatory strategy: TV 6-8 mL·kg−1 of predicted body weight, PEEP 8-10 cm H2O.
• Judicious intravenous fluid; CVP 4-8 (< 10) mmHg.
• Vasopressin to support hemodynamics and control polyuria. • Insulin infusion to maintain serum glucose < 180 mg·dL−1
• Consider hormone replacement—thyroxine or T3 infusion, corticosteroids
• Transfuse for hemoglobin < 7 or 8 g·dL−1 for optimal oxygen delivery to organs.
• Correct coagulopathy with clotting factors or platelets if evidence of ongoing bleeding.
• Reflex somatic movements mediated by spinal reflexes • Skeletal muscle relaxents

Intraoperative Management :
Faced with the knowledge of the persistence of higher brain and spinal function in some donors,
the inability to test the reticular formation directly
And the dramatic peroperative haemodynamic
changes that occur
--- sedation and analgesia should be given with muscle relaxation for organ donation
Haemodynamic response could be considered to represent an organism in distress and probably occurs at a spinal level, although we are unaware of EEG studies during organ collection to confirm this.
There is as yet no way to know whether these cases indeed have no sensation.
Anaesthetic Agents :
Isoflurane and sevoflurane cause ischemic preconditioning of organs and improve graft organ function by offering protection against cold and warm ischemia .
They may have a beneficial effect by causing peripheral vasodilation.
Neuromuscular blockade required to inhibit spinal motor reflexes.
Brain death may cause hemodynamic response to noxious stimuli like pain which need to be abolished
Muscle relaxants (Vecuronium 0.1mg/kg) are given to allow adequate surgical exposure and suppress the possibility of spinal-reflex-induced patient movement.
Analgesia can be provided with Narcotic analgesic-Fentany1 1-5 µg/kg.
Air and oxygen mixture with inhalation agent can be given
In 2003, Fitzgerald et al19 hypothesized that the administration of
fentanyl could suppress this intraoperative release of catecholamines associated with the hemodynamic changes during the organ procurement surgery.
Fitzgerald RD, Hieber Schweitze E, Luo A, Oczenski W, Lackner -- Eur J Anaesthesiol. 2003;20(12):952-956
Better organ function post transplant and less acute rejection in the recipient
Potential Benefits for Organ Recipients When Inhalational Anesthetic Agents are Administered During Organ Procurement Surgery
De Hert SG, Turani F, Mathur S, Stowe DF. Cardioprotection with volatile anesthetics:
mechanisms and clinical implications. Anesth Analg. 2005;100(6):1584-1593.
Reducing the release of TNF-α and other proinflammatory substances reduces incidence of infiltration into donor organs that can increase probability of acute rejection
Anesthetic preconditioning could reduce ischemia reperfusion injury and resulting organ dysfunction in heart, liver and kidney
Preventing or reducing adrenergic responses could lead to less ischemia reperfusion injury and infiltration of inflammatory substances into transplanted organs
These findings call into question the routine recommendations of the organ procurement agencies that the donors require no anesthesia.
Elliot JM. Brain death. Trauma. 2003;5:23-42.
