an update on evidence-based practices to improve infant
TRANSCRIPT

Mountain State MilestonesAn Update on Evidence-Based
Practices to Improve Infant Outcomes
Funding for this project provided by ASTHO
Association of State and Territorial Health Officersand
West Virginia Department of Health and Human Resources/Office of Maternal, Child and Family Health
Physcian Faculty :
IBCLC Faculty:Charlita Atha, RN, IBCLC
Tammy Foley, RN, BSN, IBCLC
Course Facilitators:Charlita Atha, RN, IBCLC
Cynthia M. Kittle, MS Christine T. Compton, MPH Candidate, CLS
Anne Banfield, MD, FACOGEmily Nease, MD, FAAP

Disclosure Statement We hereby declare that the program
authors have prepared this information for educational purposes only and will not
promote any company’s products directly or indirectly. Furthermore, we declare that this
program is free of commercial influence or bias.

Objectives• Review Mountain State Milestones program• Review each step in The Ten Steps to Successful
Breastfeeding and the Baby-Friendly Hospital Initiative
• Overview of mPINC scores (Maternity Practices in Infant Nutrition and Care survey)
• Discuss implementation of each step/Milestone• Discuss most recent evidence to support each
step• Discuss developing a team for success• Provide resources for implementation

• An initiative of the WV Breastfeeding Alliance to encourage implementation of The Ten Steps to Successful Breastfeeding in WV maternity facilities
• Provides recognition to facilities as they select and achieve Milestones based on the Ten Steps

The Ten Steps to Successful Breastfeeding
1. Have a written breastfeeding policy that is routinely communicated to all heath care staff.
2. Train all health care staff in the skills necessary to implement this policy.
3. Inform all pregnant women about the benefits and management of breastfeeding.
4. Help mothers initiate breastfeeding within one hour of birth.
5. Show mothers how to breastfeed and how to maintain lactation, even if they are separated from their infants.

6. Give infants no food or drink other than breast-milk, unless medically indicated.
7. Practice rooming in – allow mothers and infants to remain together 24 hours a day.
8. Encourage breastfeeding on demand.9. Give no pacifiers or artificial nipples to
breastfeeding infants.10.Foster the establishment of breastfeeding
support groups and refer mothers to them on discharge from the hospital or birth center.
The Ten Steps to Successful Breastfeeding
http://www.babyfriendlyusa.org/about-us/baby-friendly-hospital-initiative/the-ten-steps

Maternity Care Practices in Infant Nutrition and Care : mPINC
• Nationwide survey administered by the CDC in 2007, 2009, 2011, 2013 then every 2 years
• All maternity facilities in US were invited to participate • To be completed by person most knowledgeable about the
issues• 89% of the 28 eligible hospitals and birth centers in WV
responded• Each of those received their facility-specific benchmarks• State composite scores for mPINC are available at:
http://www.cdc.gov/breastfeeding/data/mpinc/reports.htmhttp://www.cdc.gov/breastfeeding/pdf/mpinc/states/2013/westvirginiampinc13_508tagged.pdf

Summary WV composite scores are improving!
2007 : 53 2009: 582011: 602013 : 69WV Rank: 45 (out of 53)
WV 2013 mPINC Score69/100

World Health OrganizationCode
In recognition of the devastating effect of formula and bottle marketing, the World Health Organization and UNICEF adopted the “WHO-CODE” in 1981. The “WHO-CODE” is short for the World Health Organization’s
International Code of the Marketing of Breastmilk Substitutes.• No advertising of breast milk substitutes to families. • No free samples or supplies in the health care system.• No promotion of products through health care facilities, including no free or low-cost formula.• No contact between marketing personnel and mothers.• No gifts or personal samples to health workers.• No words or pictures idealizing artificial feeding, including pictures of infants, on the labels or the
product.• Information to health workers should be scientific and factual only.• All information on artificial feeding, including labels, should explain the benefits
of breastfeeding and the costs and hazards associated with artificial feeding.• Unsuitable products should not be promoted for babies.• All products should be of high quality and take account of the climate and
storage conditions of the country where they are used.
http://www.bestforbabes.org/what-is-the-who-code/

Formula Advertising is Everywhere…
Free formula samples, coupons and gift bags given by many hospitals and healthcare provider offices can greatly influence parental choice of infant feeding methods.

Commercial Samples of Breastmilk Substitutes
• Elimination of formula samples:– Increases a mothers’ breastfeeding
duration over first 10 weeks postpartumRosenberg KD, Eastham CA, Kasehagen LJ, Sandoval AP. Marketing Infant formula through hospitals: the impact of commercial hospital discharge packs on breastfeeding. Am J Public Health. 2008;198(2);290-295.
–Significantly more likely to breastfeed exclusively for 6 months Sadacharan R, Grossman X, Matlak S, Merewood A. Hospital discharge bags and breastfeeding at 6 months; data from the Infant Feeding Practices Study II. J Hum Lact. 2014;30(1):73-79.

Ban the Bags
• Register online at: www.banthebags.org
Number of Bag Free US Hospitalsand Birth Centers registered: 891
WV: 13
What it Means to Ban the Bags
• Banning the bags does not mean you have to start paying for your infant formula and other products
• You can ban the bags tomorrow at no cost
• Increase your mPINC score by 7 points

1. Have a written policy that is routinely
communicated to all health care staff.

Importance of Policy1. Safety: A well-researched and reviewed policy establishes clear guidance about those practices that are most effective at reducing and managing risk.2. Effectiveness: Developing policy through a process of thorough review of the current body of scientific knowledge ensures that policy is evidence-based and that the most effective strategies are consistently implemented. Establishing and communicating this type of written policy provides a framework for a sanctioned course of action that all staff should be expected to follow. The standards laid out in the policy provide a “road map” for carrying out and evaluating best practices in patient care.3. Patient-centeredness: Implementation of an evidence-based policy establishes a framework for providing coordinated, respectful, responsive care that can be tailored to individual patient preferences, values and needs.4. Timeliness: A consistently communicated policy assures that appropriate support will be delivered throughout the patient’s stay and that continuity of care will be maximized.5. Efficiency: When all staff are trained in and consistently adhere to the same evidence-based standards of care, cross-purpose efforts are avoided, reducing waste on many levels.6. Equity: Establishment and clear communication of policy sets an explicit standard for consistent delivery of care. When the Ten Steps are consistently implemented, disparities in outcomes are reduced.
Source: http://texastenstep.org/

Step One ResourcesHave a written policy that is routinely communicated to all health care staff.
Academy of Breastfeeding Medicine’s Clinical Protocol #7: Model Hospital Policy
• Create a breastfeeding policy that promotes patient-centered care• Policy must require staff to implement the Ten Steps and the Code• Train staff on the policy within six months of hire and provide ongoing
continuing education on the principles of the policy. See also Step 2• Display the policy and/or a printed patient guide in all patient care areas
where pregnant women, mothers, babies and children are served• Through regular auditing, ensure that all staff adhere to the policy

2. Train all health care staff in the skills necessary to implement this policy.

Breastfeeding Rates Increase When:
• Breastfeeding education includes evidence based practice regardless of personal attitudes and experiences
• New employees receive breastfeeding education
• Nurses updated in breastfeeding education yearly

Step Two ResourcesTrain all health care staff in the skills necessary
to implement this policy.
• Incorporate training into staff new hire orientation • Maintain regular staff competencies
Becoming Baby-Friendly: Practical Solutions Toolkit. Mass.gov website.http://www.mass.gov/eohhs/docs/dph/wic/staff-competency-assessment.pdfAccessed 7/10/15.

3. Inform all pregnant women about the benefits
and management of breastfeeding.

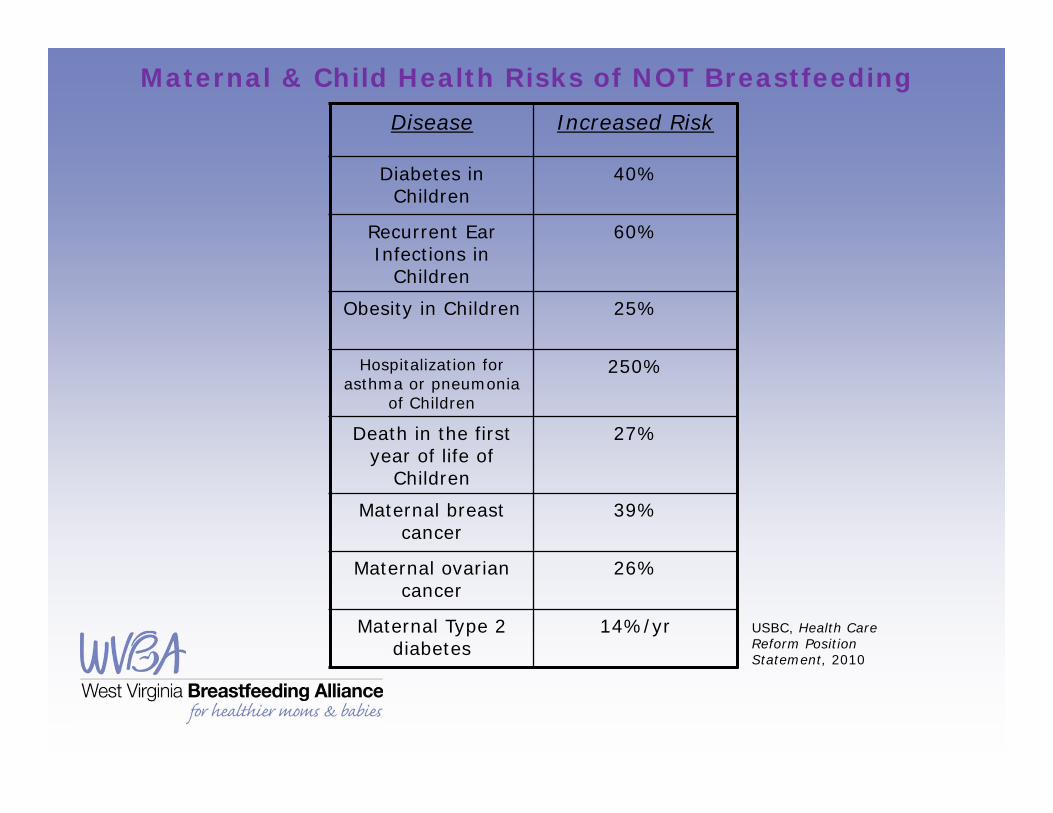
Maternal & Child Health Risks of NOT BreastfeedingDisease Increased Risk
Diabetes in Children
40%
Recurrent Ear Infections in
Children
60%
Obesity in Children 25%
Hospitalization for asthma or pneumonia
of Children
250%
Death in the first year of life of
Children
27%
Maternal breast cancer
39%
Maternal ovarian cancer
26%
Maternal Type 2 diabetes
14%/yr USBC, Health Care Reform Position Statement, 2010

Duration Increases Benefits
Breastfeeding status
>12months
none
Hypertension 38.6% 42.1%Diabetes 4.3% 5.3%Hyperlipidemia 12.3% 14.8%Cardiovasculardisease
9.1% 9.9%
Comparison of percentage of population affected by condition for postmenopausal parous women who breastfed for more than 12
months versus those who did not breastfeed
Schwarz EB, Ray RM, Stuebe AM, et al. Duration of Lactation and Risk Factors for Maternal Cardiovascular Disease. Obstetrics & Gynecology. 2009; 113(5): 974-982.
Policy Statements• AAP: "The American Academy of Pediatrics reaffirms its
recommendation of exclusive breastfeeding for about 6 months, followed by continued breastfeeding as complementary foods are introduced, with continuation of breastfeeding for 1 year or longer as mutually desired by mother and infant“
American Academy of Pediatrics. Breastfeeding and the use of human milk. Pediatrics website http://pediatrics.aappublications.org/content/129/3/e827.full#content-blockUpdated February 27, 2012. Accessed July 10, 2015.
• WHO: Breastfeeding for first 2 years of life– Exclusive breastfeeding for the first 6 months
Infant and young child feeding. World Health Organization Website http://www.who.int/mediacentre/factsheets/fs342/en/ Updated February 2014. Accessed July 10, 2015.

Women who were encouraged to breastfeed were four times more likely to initiate breastfeeding than those that were not encouraged.
Lu MC (2001, Feb.). Provider encouragement of breast-feeding: evidence from a national survey. NCBI PubMed. http://www.ncbi.nlm.nih.gov/pubmed/11165597. Accessed July 7, 2015.
Management of Breastfeeding
• Educate parent(s) before and after birth– Initiation rates increased from 41% to 74%
when expectant fathers attended breastfeeding promotion class
Wolfberg AJ, Michels KB, Shields W, et al. Dad as breastfeeding advocates: Results from a randomized controlled trial of an educational intervention. AJOG. 2004; 191: 708-712.

Step Three ResourcesInform all pregnant women about the benefits and
management of breastfeeding.
Incorporate breastfeeding education prenatally with:• Prenatal Classes• Flyers for Expectant Families• Primary Care Providers Promotion Prenatally
Academy of Breastfeeding Medicine Protocol #19:Breastfeeding Promotion in the Prenatal Setting (American
Academy of Pediatrics, American College of Obstetrics and Gynecology, American Academy of Family Practitioners, American College of Nurse-Midwives)

4. Help mothers initiate breastfeeding within one
hour of birth.

89.1% of women breastfed more than 6 weeks compared to 80.5% who did not have initiation in 1st hour (study population intended to breastfeed > 2 months)
0%
10%
20%
30%
40%
0 steps 1 step 2 steps 3 steps 4 steps 5 steps 6 steps
Breastfeeding discontinuation < 6wks
Series 1
Dose-related response to number of steps experienced
DiGirolamo AM, Grummer-Straw LM, Fein SB. Effect of Maternity-Care Practices on Breastfeeding. Peds. 2008; 122: S43-S49

Step Four ResourcesHelp mothers initiate breastfeeding within one hour of birth.
• Consistent use of skin-to-skin for all eligible mothers and babies, regardless of feeding intention
• Skin-to-skin as the standard of care • Infant remains skin-to-skin with mother until first
feed is established• To learn more about WV’s Kangaroo Care project,
contact: www.wvperinatalpartnership.org

5. Show mothers how to breastfeed and how to
maintain lactation, even if they are separated from their
infants.
Gina Bodnar and baby Stephen

Proper Support MattersInappropriate feeding restrictions, unresolved positioning and latch issues, and inconsistent breastfeeding counseling are factors in failure to establish sufficient milk supply.Woolridge MW. Problems of establishing lactation. Food Nutr Bull. 1996;17(4): 316–23
“Formal evaluation of breastfeeding, including observation of position, latch and milk transfer, should be undertaken by trained caregivers at least twice daily and fully documented in the record during each day in the hospital after birth.”
American Academy of Pediatrics. Breastfeeding and the use of human milk. Pediatrics website http://pediatrics.aappublications.org/content/129/3/e827.full#content-blockUpdated February 27, 2012. Accessed July 10, 2015.

Getting it RightChoose a standardized breastfeeding assessment tool. For consistent and accurate communication of lactation acuity, train and assess staff in the use of the tool.
thepassionatemom.wordpress.com
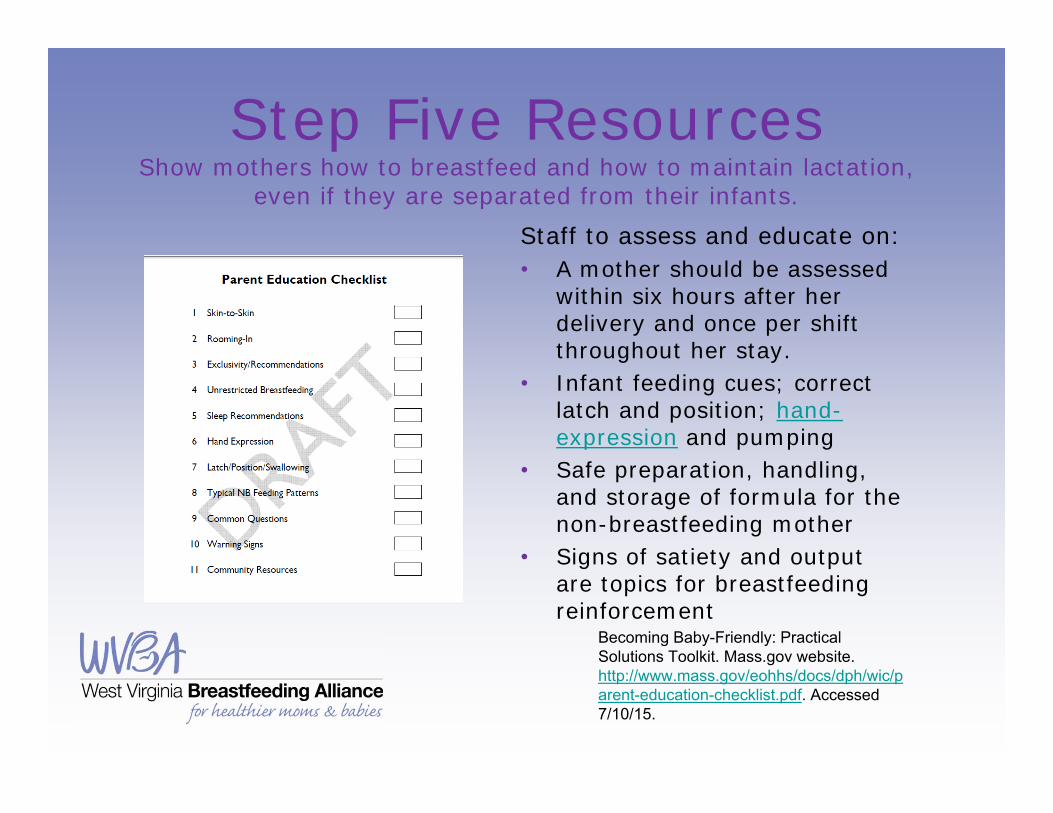
Step Five ResourcesShow mothers how to breastfeed and how to maintain lactation,
even if they are separated from their infants.Staff to assess and educate on:• A mother should be assessed
within six hours after her delivery and once per shift throughout her stay.
• Infant feeding cues; correct latch and position; hand-expression and pumping
• Safe preparation, handling, and storage of formula for the non-breastfeeding mother
• Signs of satiety and output are topics for breastfeeding reinforcement
Becoming Baby-Friendly: Practical Solutions Toolkit. Mass.gov website. http://www.mass.gov/eohhs/docs/dph/wic/parent-education-checklist.pdf. Accessed 7/10/15.

6. Give newborn infants no food or drink other than
breastmilk, unless medically indicated.
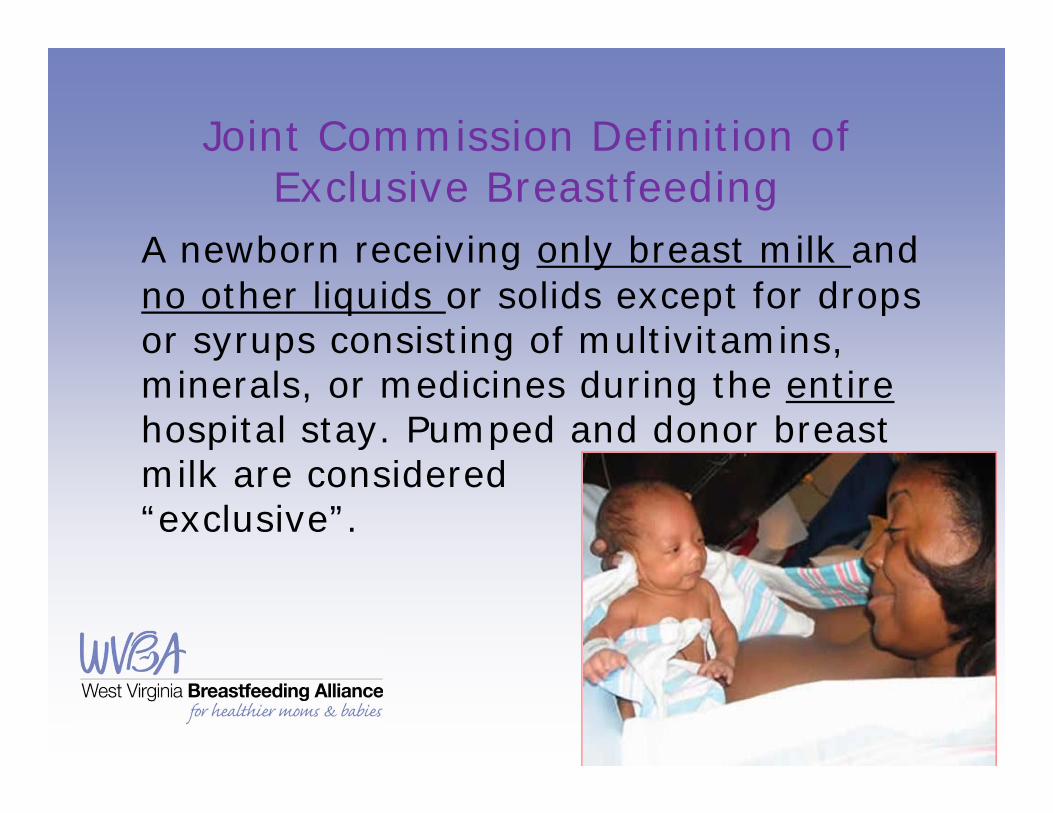
Joint Commission Definition of Exclusive Breastfeeding
A newborn receiving only breast milk and no other liquids or solids except for drops or syrups consisting of multivitamins, minerals, or medicines during the entirehospital stay. Pumped and donor breast milk are considered “exclusive”.

Why Healthcare Workers Give Supplements/Prelacteal Feeds*
• Survey. Europe 2002– Nurses: perceived breastmilk insufficiency– Doctors: dehydration, hypoglycemia, and
neonatal jaundice– Non-medical staff: prepare GI tract and
quench infant thirst*fluids given before lactation is established
Akuse RM, Obinva EA. Why healthcare workers give prelacteal feeds. Eu J Clin Nutr. 2002 Aug;56(8):729-34.

Supplements/ Prelacteal feeds*
• C- section deliveries more likely to receive formula supplement/PLF
• Formula as PLF = inverse association to breastfeeding
• PLF associated with cessation of breastfeeding before 6 months
• Antenatal counseling and support from hospital staff shown to decrease PLF
Raheem RA, Binns CW, Chih HJ, Sauer K. Determinants of the introduction of prelacteal feeds in the Maldives. Breastfeed Med. 2014 Nov;9(9):473-8. doi: 10.1089/bfm.2014.0028.

Step Six ResourcesGive newborn infants no food or drink other than
breastmilk unless medically indicated.
Staff Training once again the key. Policies and training must first be in place to adequately support breastfeeding, thereby reducing reliance on and need for supplemental feedings.
WHO/UNICEF Acceptable Medical Reasons for Use of Breastmilk Substitutes and the Academy of Breastfeeding Medicine’s Clinical Protocol #3: Academy of Breastfeeding Medicine Clinical Protocol Number 3—Hospital Guidelines for the Use of Supplementary Feedings in the Healthy Term Breastfed Neonate.
http://www.bfmed.org/Resources/Protocols.aspx

7. Practice rooming-in –allow mothers and infants
to remain together –24 hours a day.
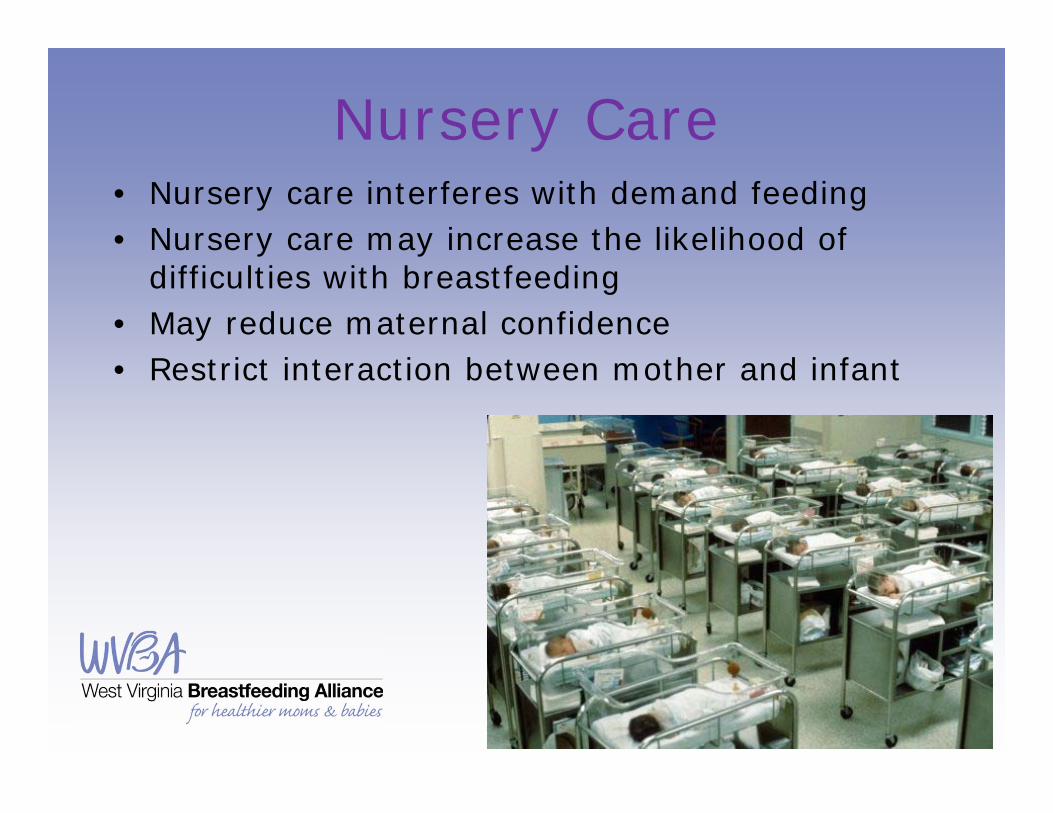
Nursery Care• Nursery care interferes with demand feeding• Nursery care may increase the likelihood of
difficulties with breastfeeding• May reduce maternal confidence• Restrict interaction between mother and infant

Step Seven ResourcesPractice rooming-in – allow mothers and infants to
remain together 24 hours a day.
• Care for baby in mom’s room – bath, nursing and pediatrician assessments, vital signs, weights, hearing screening
• Train staff first and provide ideas for scripted responses
• Newborns to remain with parents 23 out of 24 hours
8. Encourage breastfeeding on demand

Pitfalls of Scheduled Feedings
Outcomes of Scheduled Feeds:• Less intake of nutrient-rich
and immunity-rich colostrum• Higher rates of jaundice• Delayed and reduced weight
gain• Increased introduction of
formula and other supplements
• Early weaning from the breast• Increased lifetime health risks
associated with non-exclusive breastfeeding
Scheduled: Frequency of feeds predetermined and usually time restricted
Texas Ten Step. Star Achiever Toolkit. Texas Ten Step Modules website.http://texastenstep.org/starachiever-texastenstep/Star_Achiever_Ten_Step_Modules/ Updated 2010. Accessed July 10, 2015.

Breastfeed on Demand On Demand: no restrictions placed on the frequency or length of feeds
Outcomes of On Demand Feeds:• Improved nutritional homeostasis• Lower weight loss and increased weight gain• Earlier passage of meconium• Lower level of serum bilirubin• Decreased incidence of hyperbilirubinemia• Stabilized neonatal serum glucose levels
Texas Ten Step. Star Achiever Toolkit. Texas Ten Step Modules website.http://texastenstep.org/starachiever-texastenstep/Star_Achiever_Ten_Step_Modules/ Updated 2010. Accessed July 10, 2015.

Step Eight ResourcesEncourage breastfeeding on demand.
Mothers and their families should be educated about infant feeding cues and normal infant transitional behavior. They should be supported and provided unlimited
opportunities to respond to infant feeding cues.
Breastfeeding Crib Cards for boys and girls can be downloaded for print from the Centers for Disease Control and Prevention: http://www.cdc.gov/breastfeeding/promotion/healthcare.htm
9. Give no artificial nipples or pacifiers to breastfeeding
infants

Risks of Early Pacifier Use• Interfere with demand feeding• Reduce time suckling at the breast• Alter oral dynamics• May lead to “nipple confusion”• May indicate a breastfeeding problem
The AAP has clarified its position on giving pacifiers to breastfeeding infants, stating that it:“does not support a categorical ban on pacifiers…[but] pacifier use in the hospital in the neonatal period should be limited to specific medical indications…Mothers of healthy term breastfed infants should be instructed to delay pacifier use until breastfeeding is well-established, usually about 3 to 4 weeks after birth.”

Breastfeeding and Pacifier Use
• Pacifier use in first 2 weeks postpartum=increased risks for stopping exclusive breastfeeding
• No increased problems noted with pacifier use after the first 2 weeks postpartum
(Lindau et al 2014)

Step Nine ResourcesGive no artificial nipples or pacifiers to breastfeeding infants.
Use pacifiers for painful procedures only then discard before return to parents.
Academy of Breastfeeding Medicine Clinical Protocol #3: Hospital Guidelines for the Use of Supplementary Feedings in the Healthy Term Breastfed Neonate, Revised 2009
http://www.bfmed.org/Resources/Protocols.aspx
Becoming Baby-Friendly: Practical Solutions Toolkit. Mass.gov website. http://www.mass.gov/eohhs/docs/dph/wic/pacifier-notification-families.pdf . Accessed 7/10/15.

10. Foster the establishment of breastfeeding support groups and refer mothers to them on discharge from the hospital or clinic.

Access to Professional Support
• Randomized control trial N=722• Primiparous, uncomplicated full term • Follow up at 1, 2, and 3 months postpartum• Rates of any and exclusive breastfeeding higher
among those with in hospital support sessions and telephone support post dischargeFu IC, Fong FY Heys M, Lee IL, Sham A, Tarrant M. Professional breastfeeding support for first-time mothers: a multicentre cluster randomised control trial. BJOG. 2014 Dec;121(13): 1673-83

Access to Professional Support“All infants should be seen by their provider within 48–72 hours after discharge; infants discharged before 48 hours of age should be seen within 24–48 hours after discharge.”
Academy of Breastfeeding Medicine 2014

Technology/Social Media Support for Moms
• Nested Intervention study within longitudinal cohort
• N=414. Australia• Intervention= Internet support web site• Intervention group more likely to
exclusively breastfeed at 6 months• Positive effect on long term exclusive
breastfeeding Giglia R, Cox K, Zhao Y, Binns, CW. Exclusive breastfeeding increased by an internet intervention. Breastfeed Med 2015. Jan-Feb:10:20-5.
Online Resources for Families
• Text 4 Baby• KellyMom.com• Womenshealth.gov
It is important to guide families towards credible resources.
Be mindful that many online sites are backed by formula companies and can actually impede success.

Step Ten ResourcesRefer to breastfeeding support on discharge.
Primary Goals of Step 10:• Foster development and success of infant feeding
support resources• Identify and maintain an active directory of
recommended resources• Refer mothers and their families to support
resources• Follow up with families after discharge to ensure
continuity of care
Baby-Friendly Hospital Initiative
• The Baby-Friendly Hospital Initiative (BFHI) was launched by the World Health Organization (WHO) and United Nations Children's Fund (UNICEF) in 1991 to ensure that all birthing hospitals and centers become "centers of breastfeeding support."
• In order to receive a Baby-Friendly designation, birthing facilities must implement the Ten Steps to Successful Breastfeeding and comply with the International Code of Marketing of Breast-Milk Substitutes.
• To date, more than 20,000 maternity facilities in 150 countries around the world have earned the Baby-Friendly designation.
Baby-Friendly Hospital Initiative. Baby-Friendly USA website. https://www.babyfriendlyusa.org/about-us/baby-friendly-hospital-initiative Accessed July 10, 2015.

Organizational Support for the Ten Steps To Successful
Breastfeeding• American Academy of Family Physicians• American Academy of Nurses• American Academy of Pediatrics• American College of Nurse-Midwives• Academy of Breastfeeding Medicine• Academy of Nutrition and Dietetics• Association of Women's Health, Obstetric and Neonatal Nurses (AWHONN)• Centers for Disease Control and Prevention (CDC)• National WIC Association• U.S. Breastfeeding Committee (USBC)• U.S. Preventive Services Task Force• U.S. Surgeon General• National Collaborative for Advancing the Ten Steps (NCATS)

Public recognition of your efforts towards becoming breastfeeding friendlyIncreasing satisfaction with maternity care services in your facilityFree marketing to the public about your effortsImproving the health of the mother-baby dyad by providing evidence-based standard of care Contributing to the improvement of breastfeeding initiation, duration and exclusivity in West Virginia
Why Participate?

Form a Team for Positive Change• Use mPINC data to guide decision making• Include lactation staff, staff nurse champions
from multiple shifts, administration and physicians
• Pick which step/steps to work on first and form a plan

Resources• WHO • Baby-Friendly USA • Texas Ten Step Program• Ten Steps YouTube• Baby Friendly Initiative Ontario • North Carolina Breastfeeding Friendly Promotion & Support

Resources• DiGirolamo AM, Grummer-Straw LM, Fein SB. Effect of Maternity-Care Practices on Breastfeeding. Peds. 2008;
122: S43-S49. • Kramer MS, Chalmers B, Hodnett ED, et al. Promotion of Breastfeeding Intervention Trial (PROBIT), A
Randomized Trial in the Republic of Belarus. JAMA. 2001; 285(4): 413-420.• Committee on Health Care for Underserved Women, Committee on Obstetric Practice. Breastfeeding: Maternal
and Infant Aspects. In: ACOG Clinical Review. 2007; 1: 1S-16S.• Stuebe AM, Schwarz EB, Grewen K, et al. Duration of Lactation and Incidence of Maternal Hypertension: A
Longitudinal Cohort Study. Am J Epidemiol. 2011; 174(10): 1147-1158.• Schwarz EB, Ray RM, Stuebe AM, et al. Duration of Lactation and Risk Factors for Maternal Cardiovascular
Disease. Obstetrics & Gynecology. 2009; 113(5): 974-982. • Wolfberg AJ, Michels KB, Shields W, et al. Dad as breastfeeding advocates: Results from a randomized
controlled trial of an educational intervention. AJOG. 2004; 191: 708-712. • American Academy of Pediatrics. Breastfeeding and the Use of Human Milk. In: Pediatrics, Official Journal of the
American Academy of Pediatrics. 2005; 115: 496- 506.• Harder T, Bergmann R, Kallischnigg G, Plagemann A. Duration of Breasfeeding and Risk of Overweight: A Meta-
Analysis. Am J Epidemiol. 2005; 162: 397-403.• Baker JL, Gamborg M, Heitmann BL, Lissner L, Sorensen TIA, Rasmussen KM. Breastfeeding reduces
postpartum weight retention. Am J Clin Nutr. 2008; 88: 1543-1551.• Stuebe AM, Rich-Edwards JW, Willett WC, Manson JE, Michels KB. Duration of Lactation and Incidence of Type
2 Diabetes. JAMA. 2005; 294(20): 2601-2610.• Kozhimannil KB, Jou J, Attanasio LB, Joarnt LK, McGovern P. Medically Complex Pregnancies and Early
Breastfeeding Behaviors: A Retrospective Analysis. PLoS ONE. 2014; 9(8): e104820

Resources• Baby Friendly USA. The Baby Friendly Hospital Initiative. The Ten Steps to Successful
Breastfeeding. http://www.babyfriendlyusa.org/about-us/baby-friendly-hospital-initiative/the-ten-steps. Accessed May 21, 2015.
• American Academy of Pediatrics Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics. 2012;129(3):e827-e841.
• World Health Organization. Infant and young child feeding. Fact Sheet 342. http://www.who.int/mediacentre/factsheets/fs342/en/. Updated February 2014. Accessed November 10, 2014.
• Akuse RM, Obinva EA. Why healthcare workers give prelacteal feeds. Eu J Clin Nutr. 2002 Aug;56(8):729-34.
• Raheem RA, Binns CW, Chih HJ, Sauer K. Determinants of the introduction of prelacteal feeds in the Maldives. Breastfeed Med. 2014 Nov;9(9):473-8. doi: 10.1089/bfm.2014.0028.
• Perez-Escamilla R, Segura-Millan S, Canahuati J, Allen, H. Prelacteal feeds are negatively associated with breast-feeding outcomes in Honduras. J. Nutr. 1996 Nov;126(11);2765-73.
• Chantry CJ Dewey KG, Peerson JM, Wagner EA, Nommsen-Rivers LA. In-hospital formula use increases early breastfeeding cessation among first time mothers intending to exclusively BF. J Pediatrics 2014;164(6): 1339. E5-1345.e5
• Mattsson E, Funkquist EL, Wickström M, Nyqvist KH, Volgsten H. Healthy late preterm infants and supplementary artificial milk feeds: Effects on breast feeding and associated clinical parameters. Midwifery. 2014 Dec 31.
• Academy of Breastfeeding Medicine Protocol Committee. ABM clinical protocol #3: hospital guidelines for the use of supplementary feedings in a healthy term breastfed neonate, revised 2009. Breastfeed Med. 2009;4(3):175-182.

Resources• World Health Organization. Evidence for the ten steps to successful breastfeeding. Geneva,
Switzerland; World Health Organization 1998. • World Health Organization. International Code of Marketing of Breast-milk Substitutes. Geneva,
Switzerland; World Health Organization; 1981. http://www.who.int/nutririon/publicationscode_english.pdf. Accessed February10, 2015.
• Rosenberg KD, Eastham CA, Kasehagen LJ, Sandoval AP. Marketing Infant formula through hospitals: the impact of commercial hospital discharge packs on breastfeeding. Am J Public Health. 2008;198(2);290-295.
• Sadacharan R, Grossman X, Matlak S, Merewood A. Hospital discharge bags and breastfeeding at 6 months; data from the Infant Feeding Practices Study II. J Hum Lact. 2014;30(1):73-79.
• Koskinen KS, Aho AL, Hannula L, Kaunonen M. Maternity hospital practices and breast feeding self-efficacy in Finnish primiparous and multiparous women during the immediate postpartum period.Midwifery. 2014 Apr;30(4):464-70.
• Howie PW, Houston MJ, Cook A, Smart L, McArdle T, McNeilly AS. How long should a breastfeed last? Early Hum Dev. 1981 Feb;5(1):71-7.
• De Carvalho M, Robertson S, Friedman A, Klaus M. Effect of frequent breastfeeding on early milk production and infant weight gain. Pediatrics. 1983 Sep;72(3):307-11.
• De Carvalho M, Robertson S, Merkatz R, Kaus M. Milk intake and frequency of feeding in breastfed infants. Early Human Development 1982:7:155-63.

Resources• Blomquist HK, Jonsbo F, Serenius F, Persson LA. Supplementary feeding in the maternity ward
shortens the duration of breast feeding. Acta Paediatr. 1994 Nov;83(11):1122-6.• Lindau JF, Mastroeni S, Gaddini A, Di Lallo D, Nastro PF, Patanè M, Girardi P, Fortes C.
Determinants of exclusive breastfeeding cessation: identifying an "at risk population" for special support. Eur J Pediatr. 2014 Oct 14. [Epub ahead of print]
• O’Connor, R, Tanabe KO, Siadaty MS, Hauk FR. Pacifiers and Breastfeeding. A systematic review. Arch Pediatr Adolesc med. 163(4)378-382.
• Jenik AG, Vain NE, Gorestein AN, Jacobi NE; Pacifier and Breastfeeding Trial Group. Does the recommendation to use a pacifier influence the prevalence of breastfeeding? J Pediatr. 2009 Sep;155(3):350-4.e1
• Kramer MS, Barr RG, Dagenais S, Yang H, Jones P, Ciofani L, Jané F. Pacifier use, early weaning, and cry/fuss behavior: a randomized controlled trial. JAMA. 2001 Jul 18;286(3):322-6.
• American Academy of Pediatrics. Task Force on Sudden Infant Death Syndrome. Policy Statement SIDS and Other Sleep-Related Infant Deaths: Expansion of Recommendations for a Safe Infant Sleeping Environment. Pediatrics128(5)1030 -1039.
• Fu IC, Fong FY Heys M, Lee IL, Sham A, Tarrant M. Professional breastfeeding support for first-time mothers: a multicentre cluster randomised control trial. BJOG. 2014 Dec;121(13): 1673-83
• Jolly K, Ingram L , Khan KS, Deeks JJ, Freemantle N, MacArthur C. Systematic review of peer support for breastfeeding continuation: metaregression analysis of the effect of setting, intensity ,and timing. BMJ. 2012 Jan 25;344:d8287
• Haroon S, Das JK, Salam RA, Imdad A, Bhutta ZA. Breastfeeding promotion interventions and breastfeeding practices: a systematic review. BMC Public Health. 2013; 13 Suppl 3:S20.

Resources• Spatz DL, Kim GS, Froh EB. Outcomes of a hospital-based employee lactation program. Breastfeed
Med. 2014 Dec;9 (10):510-4• Di Manno L, Macdonald JA, Knight T. The intergenerational Continuity of Breastfeeding intention,
initiation and duration: a systematic review. Birth. 2015. Jan 21. • Abbass_Dick, Stern SB, Nelson LE, Watson W, Dennis CL. Coparenting breastfeeding support and
exclusive breastfeeding: a randomized control trial. Pediatrics. 2015 Jan; 135 (1):102-10.• Giglia R, Cox K, Zhao Y, Binns, CW. Exclusive breastfeeding incrased by an internet intervention.
Breastfeed Med 2015. Jan-Feb:10:20-5. • DiGirolamo AM, Grummer-Straw LM, Fein SB. Effect of Maternity-Care Practices on Breastfeeding.
Peds. 2008; 122: S43-S49.• Schwarz EB, Ray RM, Stuebe AM, et al. Duration of Lactation and Risk Factors for Maternal
Cardiovascular Disease. Obstetrics & Gynecology. 2009; 113(5): 974-982.• Wolfberg AJ, Michels KB, Shields W, et al. Dad as breastfeeding advocates: Results from a
randomized controlled trial of an educational intervention. AJOG. 2004; 191: 708-712

Conclusion• Thank you for joining us for this
e-learning session• To receive continuing education credit for
this course, please complete the survey found at: www.wvbfa.com