an overview of dengue information management system by punjab informatioon technology board,...
TRANSCRIPT

• Health care systems depended more on IT centric initiatives to gather information. Non availability of
organized historical data of a disease limits the capability of government for early preparedness and
emergency response.
• Same happened in the case of dengue spread in Pakistan where the basic health infrastructure was not
ready to address the issue.
• However the government utilised ICT in health care using emerging Cellular and web technologies
involving smart phones and geo tagging in order to overcome the epidemic of Dengue.
• This practice was initiated within In Lahore, Pakistan’s second-most populous city. There were 21,292
confirmed dengue patients in 2011. At least 350 of them died.

• Dengue, also called break bone fever is an acute self-limiting mosquito borne transmissible viral
infection mainly in the tropics.
• Dengue is transmitted by the bite of a female mosquito Aedes. Aegypti and A. albopictus.
• Symptoms develop in 3-14 days like fever, head ache, muscle and joint pains and in severe cases it
develops life threatening Dengue High Fever, which exhibits severe bleeding. There is no medication
and vaccine available.
• Thus dengue control is dependent on effective vector control and community awareness.

• The first suspected dengue-like epidemics emerged in French West Indies in the year 1635 and common
by 1800s. The first mosquito eradication effort was in 1901 in Cuba. Dengue was first reported in
Pakistan in 1994.
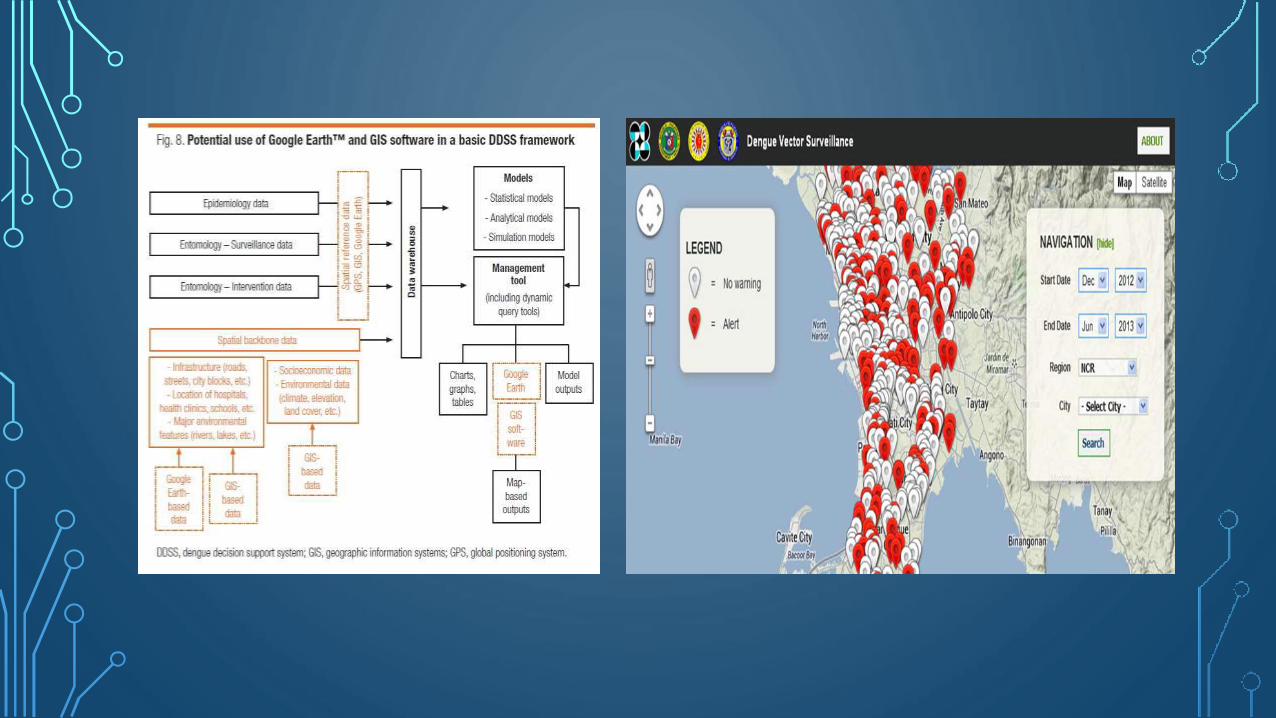
• A Dengue map is like this:

By 2010, around 3.97 billion people are at risk in 128 countries, or more than 40 percent of the world’s population

• Accurate risk analysis and allocation of resources for dengue control depends on disease surveillance.
• Formal Dengue surveillance in usually done by capturing case counts. It has many advantages such as
precise counts of case numbers with a good geographic localization.
• However they have some limitations, including lags or total failure to report cases because of limited
resources in developing countries.
• It is expensive, requires trained personnel, infrastructure and equipment and can lose data at any point
of interaction.
• One such example of a failure of a surveillance systems is dengue transmission in the Texas-Mexico
border due to marked economic disadvantage difference on both sides.

• Informal surveillance systems have been developed to address these drawbacks.
• They are based on unofficial reports of disease, from clinicians or web based health related news media, to report on
disease outbreaks.
• Such systems have proven reliable and got recognized in the 2005 revision of the International Health Regulations as
important sources of epidemic intelligence.
• The rapid and accelerating growth of the Internet has improved the usefulness and sensitivity of these systems.

Use Of Emerging Cellular Web Technology in Health Care
• In the year 2012 in Pakistan, the provincial Punjab government initiated a monitoring mechanism in response to
thousands of cases being reported.
• It was devised to log all field activities related to prevention/eradication of the disease and is still operational and
entomologists and field officers report activities on regular basis.
• It uses a data driven early outbreak detection and surveillance system serving as a policy engine for the health
department.
• It is a joint collaborating by researchers at New York University (NYU), Lahore University of Management Sciences
(LUMS) and Punjab Information Technology Board (PITB).
Dengue Management Information System
This system coordinates the colossal Dengue prevention activities by the Govt. of Punjab.
It provides a central dashboard for all stakeholders to view and dispose of complaints on real-time basis coming in from
the Helpline and Hospitals e-CRS (Electronic Complaint Routing System).
It is an efficient Vector Surveillance System for track/report of field activities. It includes
• Dengue Activity Tracking System
• Geo-Tagged e-Blood Line and Blood / Donor inventory system
• Punjab Health Line
• Disease Surveillance System

DENGUE ACTIVITY TRACKING SYSTEM
• 1854 in London, Doctor John Snow changed epidemiology forever by mapping the cholera outbreak.
• He discovered that the source of contamination was in the water from a pump on Broad Street, not from ‘bad air' as
previously believed. He also pioneered the field of data journalism and data visualizations, now a staple for public
health organizations.

• A similar mechanism was used by the authorities when they used the mapping technology. They used
100 dollar android based smartphones with a revolutionary android app to help them put up a better
fight against the mosquitoes.

• It uses 1500 android smartphones, logged 38718 preventive activities by the Health department over a
period of 5 months and accurately tracked both Aedes larvae clusters and confirmed patients.
• Workers took “before and after” geo-tagged photographs while performing the designated tasks and
uploaded them onto the app.
• The resulting data were then analysed to create a visualisation showing where and when dengue was
infecting people. It was then possible to predict where dengue-infected mosquitoes would buzz up
next, to start fogging and larvae-hunts.
• The use of smartphones also had more subtle effects. Knowing they were being monitored and tracked
in public, municipal workers also applied themselves more assiduously to their tasks. Anyone looking at
the online map could see if the work being done in a particular area was adequate—and complain if it
was not.

• All this seems to have worked. Last year Lahore suffered just 255 dengue cases, and no deaths.
• Because of the tracking system and the efforts of government employees on the ground, we could look
at a map and tell if certain areas were going to develop into an epidemic.
• Fig shows dengue activity tracking on day to day to monthly scale basis for 1 year at a time.

Workers drop tilapia fish into a small pond at a neighborhood park, as an inspector enters the activity into the Clean Lahore app. The fish eat the larvae of mosquitoes that spread dengue fever. Gambusia affinis and Poeciliareticulate.


Geo Tagged e-Blood Line and Blood /Donor Inventory System
• E-Blood line connects the right donor with needful patient at the right time to deal with dengue
epidemic in order to cope with blood shortage.
• Since Dengue fever results in loss of blood platelets and white blood cells, therefore in severe
conditions, patients need fresh blood otherwise this can lead to fatalities
• A distinct feature is that, patient’s family cannot contact donors directly. Call Centre Agents (CCAs)
contact the active donors from that particular area and direct the willing donors to the blood bank
which raised the blood requisition.
• Government data and statistics describes more than 600,000 blood donations per year in Pakistan
by this system.

Punjab Health Line- Call Centre
• DMIS takes logs and records from health line call centre as well.
• Government formulated e-health line (toll free Health Line: 080099000) to take immediate measures.
• This Call Centre was established in a record time of 48 hours for counselling the citizens 24/7 and was
manned by 150 doctors taking calls on a toll free helpline.
The services being provided are:
• Patient counselling
• Briefing on preventive measures to the citizens
• Advise on treatment protocol to health practitioners
• Logging of Fumigation Service requests
• Solid Waste Disposal and sanitation requests
• Complaints (Over charging by laboratories, Private hospitals, Govt. hospitals, etc.)
• Behaviour Change Communication (BCC) as part of health education
• The information received at the Call Centre was further used to bring all stakeholders of anti-dengue campaign on a single platform and send to DIMS (Dengue Information Management System).
Disease Surveillance System
• Procedure to start with, Teaching Hospitals, City Headquarters (THQs) and District Headquarters
(DHQs) are manned with dedicated data entry operators, who are responsible to report cases in
predefined templates.
• The data entry interface is exposed to Government Hospitals via secured usernames and
passwords.
• Health Officers and District In charges, report disease cases via SMS.
• DSS uses Early Aberration Reporting System (EARS) as used by Centre of Disease Control and
Prevention in USA .
• The system connects all stakeholders to respond to any alarming situation in a coordinated
manner to ensure emergency response.

The project features of DSS are:
• Case detection, case registration, case confirmation and case supervision
• Data Analysis and Interpretation
• Representation on G Maps
• Timely escalation indicators
• District/Tehsil and UC wise disease widespread trends
• Dispersion of disease over time, space or space and time
• Time periodic disease surveillance for early detection of disease outbreaks.

The project is live in four hospitals at the moment where results are getting compiled for finalization of implementation strategy throughout Punjab with more than 25 departments involved and 550+ users
reporting.
Strengths of the System
• Data reporting on the go
• Real time submission to the centralized server
• Consolidated dashboard to view departmental activities
• analysis to identify intersecting areas with breeding hotspots and patients reported
• Built in early disease detection/warning system with geographical illustrations

• Early detection of activities and disease with the help of geographically mapping of data. Thus, helps in prevention
and enhance disease management capabilities.
• Centralized dashboard through which management and efficiency of departments are controlled.
• Provide platform for reporting the disease by any healthcare organizations and practitioners.
• It involves both top-down and bottom-up elements. For instance, involves the provincial government activities as
well as by various community to improve the delivery of public services.
• Aware the public and indulge them in the project.
• Growth of specialized indigenous technology and providers as well as.
• Admission of a central database.
Weaknesses
• It is expensive to implement.
• Need trained personnel with larger involvement of manpower.
• Required strong leadership and management to implement the system.
• Lack of standardization.( Problems of quality assurance and quality control and lack of regional sharing
of experiences and skills)
• It requires trained personnel.
• Decisions about financing are about political and inevitably, inadequate or insufficient human and
financial resources were commonly identified as weakness throughout the system.
• Difficult to manage.
• Potential risks of loss of data and irregular entomological surveillance.

Recommendations
• Epidemiological and Entomological monitoring need further refinement and strengthening. (Monitoring, assessment
and evaluation of dengue should be accorded).
• Invest in the technology.
• Plan for project operations and maintenance at a project outset.
• Streamline data collection should be there
• Effective communication system should be focused
• Check the data if it matches with the Google trends to provide a conformity status.

• Each week, millions of users around the world search for health information online, and Google has found a close
relationship between how many people search for dengue-related topics and how many people actually have
dengue symptoms using official dengue estimates.
• Google was able to build a model that offers near real-time estimates of dengue activity based on the popularity of
dengue-related search terms.


• Aileen Y Chang, M. E. P. (2009). Combining Google Earth and GIS mapping technologies in a dengue surveillance system for developing countries. International Journal of Health Geographics, 8(49). doi: doi:10.1186/1476-072X-8-49
• Farra, J. (2007). Editorial: Towards a global dengue research agenda. Tropical Medicine & International Health, 12(695-699). doi: DOI: 10.1111/j.1365-3156.2007.01838.x
• Hales, S. (2002). Potential effect of population and climate changes on global distribution of dengue fever: an empirical model. The Lancet, 360(9336), 830-834. doi: http://dx.doi.org/10.1016/S0140-6736(02)09964-6
• Samir Bhatt, W. G. (2013). The global distribution and burden of dengue. Nature International, 496, 504-507.
• Su MD, C. N. (1994). Framework for application of geographic information system to the monitoring of dengue vectors. Gaoxiong yi xue kexue za zhi = The Kaohsiung Journal of Medical Sciences, 94-101.
• Farra, J. (2007). Editorial: Towards a global dengue research agenda. Tropical Medicine & International Health, 12(695-699). doi: DOI: 10.1111/j.1365-3156.2007.01838.x
• . from http://punjab-idss.org/
• http://www.technologyreview.com/news/506276/pakistan-uses-smartphone-data-to-head-off-dengue-outbreak/
• http://www.economist.com/news/technology-quarterly/21578520-technology-and-government-how-clever-use-mobile-phones-helping-improve
• http://www.npr.org/blogs/health/2013/09/16/223051694/how-smartphones-became-vital-tool-against-dengue-in-pakistan
• http://lums.edu.pk/news-detail/lums-...gy-review-1049
• http://www.smartplanet.com/blog/bulletin/androids-help-prevent-dengue-outbreaks-in-pakistan/
• http://www.fiercemobilehealthcare.com/story/smartphone-monitoring-system-helps-pakistan-control-dengue-outbreaks/2012-11-05
• http://dengue.pchrd.dost.gov.ph/
• http://www.who.int/topics/dengue/en/
• http://www.who.int/tdr/publications/documents/dengue-diagnosis.pdf?ua=1
• http://health.punjab.gov.pk/?q=system/files/SoPs%20for%20Prevention%20and%20Control%20of%20Dengue.pdf
