an exploration of the efficacy of ... - king's college london · dr emma ream, senior lecturer...
TRANSCRIPT
Dr Emma Ream, Senior LecturerKing’s College London
Ms Catherine Oakley, Lead Cancer Nurse,Princess Royal University Hospital
Ms Jibby Medina, Research Associate.King’s College London
Professor Alison Richardson, Professor of Cancer &Palliative Nursing Care. King’s College London
AN EXPLORATION OF THE EFFICACYOF ARM MASSAGE IN FACILITATINGINTRAVENOUS CANNULATION FORADMINISTRATION OF CYTOTOXICCHEMOTHERAPY
Final Report November 2004

Exploration of the Efficacy of Arm massage 1
Acknowledgements
This study was supported by a European Oncology Nursing Society (EONS) – Roche
Research Award.
We thank the nurses, massage therapists and patients that took part in this study for their
contribution. Without their invaluable collaboration this research project would not have
been performed. In particular the research team would like to recognise the contributions
made by Dee Bryan, Bettina Donkin and Helen Hannon in the conduct of this work.
This report should be referenced as: Ream E, Oakley C, Medina J, Richardson A (2004)
An exploration of the efficacy of arm massage in facilitating intravenous cannulation for
administration of cytotoxic chemotherapy. King’s College London

Exploration of the Efficacy of Arm massage 2

Exploration of the Efficacy of Arm massage 3
Abstract
Purpose: The purpose of this exploratory study was to examine the outcomes of providing
massage to patients on a Chemotherapy Day Unit, prior to administration of
chemotherapy.
Multi-method design: Prospective, randomised controlled trial, interviews, focus group
Setting: Chemotherapy Day Unit within a cancer unit in South East England
Samples:
• 52 patients; 68% female. Aged 24-79 years (mean = 59yrs) with breast (50%),
colorectal (30%), haematological (12%) or lung (8%) cancer. All provided
questionnaire data: 28 (54%) patients in the arm massage group (15 of whom were
also interviewed) and 24 (46%) in the control group.
• 9 nurses; all female. Aged 24-49 years (mean = 34yrs). All provided questionnaire
data; 2 were interviewed.
• 7 massage therapists; all female. Aged 33-59 years (mean = 46yrs). All participated
in the focus group.
• 3 service stakeholders; all female. Aged 38-49 years (mean = 45yrs). All were
interviewed.
Methods: A multi-method study was conducted to determine the benefits of providing arm
massage prior to intravenous cannulation. Primarily this comprised a randomised
controlled trial (RCT), which investigated the impact of massage on the cannulation
process and patients’ experiences of it. Patients were randomised to either the arm
massage (experimental) group or the control (standard care) group. Data were collected
from patients on up to 6 cannulation episodes. Investigator-designed questionnaires were
completed by both patients and nurses on these occasions. These questionnaires
gathered data on pain and anxiety – both expected and experienced – and time taken to
cannulate. Semi-structured interviews were carried out with patients and service
stakeholders, along with a focus group conducted with the massage therapists, to further
inform understanding of the benefits of massage and the impact of its provision on the
chemotherapy service. Resulting quantitative and qualitative data were analysed and
triangulated to gain detailed understanding of its outcomes.

Exploration of the Efficacy of Arm massage 4
Results: Statistical modelling through backwards stepwise regression, suggested that
massage had a statistically significant effect on anxiety and pain, when combined with
other factors such as a patients’ age, gender, or drug regime. When analysed on its own,
its benefits appeared marginal.
In both study groups 25% of cannulations were unsuccessful on first attempt. In order to
understand this, factors other than massage – including the patients’ gender, age and the
drug regime they having – were analysed. These factors did impact significantly on the
outcome variables of anxiety, pain and time taken to cannulate. Female patients, younger
patients, and those on vesicant drug regimes, were significantly more likely to anticipate
and experience high levels of procedural pain. Further, they were more likely to feel
anxious, and typically took longer to cannulate.
Implications: Although massage, on its own, did not impact significantly on the main
outcomes of the study – pain, anxiety, and time taken to cannulate – the patient and
stakeholder interviews did highlight general positive effects and benefits of massage.
These were neither sought nor captured by the questionnaire tools utilised in this study.
Patients that did benefit were typically young and female. The qualitative data that were
collected suggest that massage made attendance for chemotherapy less stressful and
more palatable, and may have helped in making veins easier to see and palpate.
Many positive feelings and emotions were mentioned in the patient interviews with regards
to experiences of arm massage. Patients felt ‘privileged’ to receive the treatment, which
was ‘relaxing’ and perceived as a ‘treat’. Likewise, those providing it referred to being
‘privileged’ in being able to do so. Massage enhanced the experience of care for patients
having chemotherapy and had a positive impact on the environment in which they received
it.

Exploration of the Efficacy of Arm massage 5
Contents
Section Page
1 Introduction and Aims ................................................................................................ 11
1.1 Introduction ......................................................................................................... 11
1.2 Aims.................................................................................................................... 12
2 Literature Review ....................................................................................................... 13
2.1 Complementary therapies................................................................................... 13
2.1.1 General massage ........................................................................................ 14
2.1.2 Aromatherapy massage............................................................................... 16
2.2 The experience of chemotherapy........................................................................ 17
2.3 Cannulation for chemotherapy............................................................................ 18
2.4 CAM in the NHS.................................................................................................. 20
3 Method ....................................................................................................................... 23
3.1 Introduction ......................................................................................................... 23
3.2 Study aims .......................................................................................................... 23
3.3 Research questions ............................................................................................ 23
3.4 Massage treatment ............................................................................................. 24
3.5 Research design ................................................................................................. 24
3.6 Sampling............................................................................................................. 25
3.6.1 Patients........................................................................................................ 25
3.6.2 Nurses ......................................................................................................... 27
3.6.3 Stakeholders................................................................................................ 27
3.6.4 Massage therapists...................................................................................... 27
3.7 Access arrangements ......................................................................................... 28
3.7.1 Patient sample ............................................................................................. 28
3.7.2 Nurse sample............................................................................................... 28
3.7.3 Therapist sample ......................................................................................... 29
3.8 Instruments ......................................................................................................... 29
3.8.1 Questionnaires............................................................................................. 29
3.8.2 Patient telephone interview schedule .......................................................... 31
3.9 Stakeholder interview schedule .......................................................................... 31

Exploration of the Efficacy of Arm massage 6
3.10 Therapist focus group ......................................................................................... 32
3.11 Pilot work ............................................................................................................ 32
3.12 Data analysis ...................................................................................................... 32
3.12.1 Questionnaire data ...................................................................................... 32
3.12.2 Interview and focus group data.................................................................... 33
3.13 Ethics .................................................................................................................. 33
4 Results ....................................................................................................................... 35
4.1 Introduction ......................................................................................................... 35
4.2 Sample accrual and attrition ............................................................................... 35
4.2.1 Patient sample ............................................................................................. 35
4.2.2 Therapist sample ......................................................................................... 36
4.3 Demography of patient sample ........................................................................... 37
4.3.1 Demography of patients interviewed............................................................ 38
4.4 Demography of nurse sample............................................................................. 39
4.5 Demography of therapist sample ........................................................................ 40
4.6 Demography of stakeholders .............................................................................. 41
4.7 Patients’ cannulation experiences....................................................................... 41
4.7.1 Experience of pain ....................................................................................... 42
4.7.2 Anxiety......................................................................................................... 44
4.7.3 Time taken to cannulate .............................................................................. 46
4.7.4 Cannulation on first attempt ......................................................................... 48
4.8 Attitudes towards, and perceptions of, massage................................................. 48
4.9 Factors affecting cannulation .............................................................................. 52
4.9.1 Variable factors............................................................................................ 52
4.9.2 Demographic factors affecting cannulation.................................................. 62
4.9.3 Experience of first treatment ........................................................................ 73
4.10 Models explaining factors impacting on cannulation ........................................... 74
4.10.1 Model explaining anxiety prior to cannulation .............................................. 75
4.10.2 Model explaining anxiety following cannulation ........................................... 76
4.10.3 Model explaining anticipated pain prior to cannulation ................................ 77
4.10.4 Model explaining procedural pain ................................................................ 78
4.10.5 Model explaining time taken to cannulate.................................................... 78
4.11 Impact of massage service on delivery of chemotherapy day care..................... 79
4.12 Impact of massage service on cancer services................................................... 80
4.13 Summary of results ............................................................................................. 82

Exploration of the Efficacy of Arm massage 7
5 Discussion.................................................................................................................. 83
5.1 Introduction ......................................................................................................... 83
5.2 Massage and cannulation ................................................................................... 83
5.2.1 Massage and time taken to cannulate ......................................................... 84
5.2.2 Massage and cannula usage....................................................................... 85
5.2.3 Massage and procedural pain...................................................................... 86
5.2.4 Massage and feelings of anxiety.................................................................. 87
5.3 Massage and well being ..................................................................................... 88
5.4 Factors affecting cannulation .............................................................................. 89
5.5 Study limitations.................................................................................................. 90
5.6 Recommendations for practice ........................................................................... 91
5.7 Recommendations for future research................................................................ 92
6 References................................................................................................................. 95
7 Appendices ................................................................................................................ 99
Appendix 1: Arm massage protocol ............................................................................. 100
Appendix 2: Patient information sheet ......................................................................... 102
Appendix 3: Patient Consent form ............................................................................... 108
Appendix 4: Therapist information sheet ..................................................................... 109
Appendix 5: Patient Questionnaire .............................................................................. 115
Appendix 6: Nurse Questionnaire................................................................................ 120
Appendix 7: Patient Interview schedule....................................................................... 123
Appendix 8: Stakeholder interview schedule ............................................................... 124
Appendix 9: Focus group guide ................................................................................... 126
Appendix 10: Model explaining anxiety prior to cannulation (SPSS output) ................ 128
Appendix 11: Model explaining anxiety following cannulation (SPSS output).............. 129
Appendix 12: Model explaining anticipation of pain prior to cannulation (SPSS output)
.................................................................................................................................... 132
Appendix 13: Model explaining procedural pain (SPSS output) .................................. 134
Appendix 14: Model explaining time taken to cannulate (SPSS output) ...................... 135

Exploration of the Efficacy of Arm massage 8
Figures
Figure 3.1 Research design .............................................................................................. 24
Figure 3.2 Sequence of data collection ............................................................................. 25
Figure 4.1 Flow diagram of patient accrual and attrition.................................................... 36
Figure 4.2 Massage therapist accrual and attrition............................................................ 37
Figure 4.3 Time taken to cannulate according to gender .................................................. 63

Exploration of the Efficacy of Arm massage 9
TABLES
Table 2.1. Models of CAM provision ................................................................................. 21
Table 4.1 Patient demographics........................................................................................ 38
Table 4.2 Demographics of patients that were interviewed............................................... 39
Table 4.3 Nurse demographics ......................................................................................... 40
Table 4.4 Demography of therapists that participated in focus group ............................... 40
Table 4.5 Anticipated pain................................................................................................. 42
Table 4.6 Procedural pain following cannulation ............................................................... 43
Table 4.7 Anxiety prior to cannulation ............................................................................... 45
Table 4.8 Anxiety after treatment administration ............................................................... 46
Table 4.9 Time taken to cannulate (minutes) .................................................................... 47
Table 4.10 Association between massage and vein palpability/visibility prior to cannulation
.......................................................................................................................................... 47
Table 4.11 Feelings when massaged................................................................................ 50
Table 4.12 Feelings generated by massage according to gender..................................... 51
Table 4.13 Effect of ease of cannulation on time taken..................................................... 53
Table 4.14 Effect of ease of cannulation on procedural pain............................................. 54
Table 4.15 Effect of ease of cannulation on anxiety following cannulation........................ 54
Table 4.16 Effect of ease of cannulation on time taken to cannulate ................................ 55
Table 4.17 Impact of vein visibility/palpability on procedural pain ..................................... 55
Table 4.18 Impact of vein visibility/palpability on anxiety .................................................. 56
Table 4.19 Impact of vein visibility/palpability on time taken to cannulate......................... 56
Table 4.20 Association between vein palpability/visibility and cannulation on first attempt
.......................................................................................................................................... 57
Table 4.21 Time taken to cannulate according to the nurse that cannulated .................... 58
Table 4.22 Procedural pain according to the nurse that cannulated ................................. 59
Table 4.23 Anxiety following cannulation according to the nurse that cannulated............. 59
Table 4.24 Failed cannulation according to the nurse that cannulated ............................. 60
Table 4.25 Effect of cannula size on anxiety ..................................................................... 61
Table 4.26 Effect of cannula size on procedural pain........................................................ 61
Table 4.27 Association between gender and insertion of cannula on first attempt............ 62
Table 4.28 Time taken to cannulate (in mins) according to gender................................... 63

Exploration of the Efficacy of Arm massage 10
Table 4.29 Association between gender and vein palpability/visibility prior to cannulation ...
.......................................................................................................................................... 64
Table 4.30 Procedural pain following cannulation experienced according to gender ........ 64
Table 4.31 Association between gender and level of pain following cannulation .............. 65
Table 4.32 Anxiety following cannulation experienced according to gender ..................... 66
Table 4.33 Association between gender and anxiety following cannulation...................... 66
Table 4.34 Procedural pain following cannulation experienced according to age ............. 67
Table 4.35 Association between age and level of pain following cannulation ................... 68
Table 4.36 Anxiety experienced after cannulation according to age ................................. 68
Table 4.37 Association between age and anxiety experience after cannulation ............... 68
Table 4.38 Time taken to cannulate according to age....................................................... 69
Table 4.39 Association between age and time taken to cannulate.................................... 69
Table 4.40 Chemotherapy regime classifications.............................................................. 70
Table 4.41 Association between nature of regime and insertion of cannula on first attempt
.......................................................................................................................................... 70
Table 4.42 Time taken to cannulate (in mins) with vesicant and other regimes ................ 71
Table 4.43 Association between nature of regime and ease of cannulation ..................... 71
Table 4.44 Procedural pain following cannulation experienced with vesicant and other
regimes ............................................................................................................................. 72
Table 4.45 Association between nature of regime and level of pain following cannulation ...
.......................................................................................................................................... 72
Table 4.46 Anxiety following cannulation experienced with vesicant and other regimes... 73
Table 4.47 Association between nature of regime and anxiety following cannulation ....... 73
Table 4.48 Trends in anxiety and anticipated pain over time ............................................ 74
Table 4.49 Model of factors impacting on anxiety prior to cannulation.............................. 75
Table 4.50 Model of factors impacting on anxiety following cannulation ........................... 76
Table 4.51 Model of factors impacting on anticipated pain prior to cannulation ................ 77
Table 4.52 Model of factors affecting patients’ pain following cannulation ........................ 78
Table 4.53 Model of factors affecting time taken to cannulate patients............................. 79

Exploration of the Efficacy of Arm massage 11
1 Introduction and Aims
1.1 Introduction
Cancer is a life threatening disease. More than 270,000 new cases were diagnosed in
2000 in the UK (1). Of the one in three people who are diagnosed with cancer throughout
their lives (2), approximately 60% will receive chemotherapy during their treatment (3).
Chemotherapy is often a source of distress and discomfort for patients not least because
of its side effects. Further, the physical experience of cannulation can be for some
individuals a traumatic and painful experience (4).
It is widely recognised that the experience of having chemotherapy can be a dreaded one
for patients (4-7); the prospect of cannulation and the treatment process itself causes
stress and discomfort. This is often accompanied by anxiety and fear of pain and their
illness itself. Others report feeling distressed because of their lack of knowledge about
chemotherapy (4, 6); these feelings can impact negatively on the process (8). Attempts to
improve the manner in which patients are cannulated and the treatments given are likely to
enhance the process and outcome of treatment.
Therapies that fall under the umbrella of complementary and alternative medicine (CAM)
are increasingly being accessed by patients with cancer as a means to treat their
symptoms and enhance feelings of well being (9, 10). CAM has been found to have a
positive effect on nausea (11, 12) and pain perception (10, 12, 13), and significantly
reduces anxiety (10-14).
The Chemotherapy Day Unit, where the study was conducted, has been offering a
complementary therapy service to outpatients since August 2001. Tailor-made treatments
have been offered to patients. Patients have been having massage to the head, neck,
shoulders, arms, legs and feet; these treatments have been administered to enhance
wellbeing and alleviate psychological symptoms such as stress and anxiety.
Chemotherapy patients have received gentle effleurage arm massage while waiting for
treatment and it was suggested this might reduce anxiety and contribute to less traumatic
cannulation. It was also speculated that this might result in fewer cannulation attempts.

Exploration of the Efficacy of Arm massage 12
To investigate whether the massage was impacting on the experience of cannulation, a
multi-method study was undertaken.
1.2 Aims
The study aimed to determine:
1. The value of providing arm massage prior to intravenous cannulation
2. The potential impact of this therapy on the chemotherapy service
In order to explore these aims fully the following research questions were developed:
Does a 10-minute gentle effleurage arm massage with basic carrier oil prior to intravenous
cannulation for administration of chemotherapy:
1. Reduce time taken for successful cannulation
2. Reduce number of cannulas used
3. Reduce pain associated with the procedure
4. Reduce feelings of stress and distress in patients and health professionals
5. Enhance patients’ wellbeing
Further, the research was designed to address the following:
6. How does integration of a massage service impact on chemotherapy day care
services?
The report that follows provides an account of the study conducted to explore these
research questions. Chapter 3 outlines the relevant literature and provides the background
and context to the study. This is followed by a description of the methods used to execute
the study. Chapter 5 provides an account of the results derived from both the quantitative
and qualitative data analysis. Finally, in Chapter 6, a discussion of the main findings,
limitations of the study and recommendations for future research are presented.

Exploration of the Efficacy of Arm massage 13
2 Literature Review
2.1 Complementary therapies
Complementary therapies and alternative medicine (CAM) are increasingly being
accessed by cancer patients. Appraisals of CAM, such as those carried out by Rees et al
(9) and Buckley (15), have documented its popularity (16). Typically its provision is
enthusiastically received by patients; especially for emotional and psychological support.
Most commonly they are used alongside orthodox medical treatment, rather than as a
replacement.
Moreover, there has been increased integration of aspects of CAM into NHS cancer
services. Integration of complementary therapy approaches with orthodox cancer care
has been influenced by patients accessing (or seeking to access) CAM – surveyed to be
between 9% and 30% of patients with cancer – and by growing evidence of the value of
CAM in achieving positive patient outcomes.
The therapies shown by surveys to be the most widely used by cancer patients are the
touch ones, such as massage and aromatherapy (17), along with mind-body therapies,
such as relaxation (18). Although the evidence base for complementary therapies is still
limited, it does not imply that they are ineffective. Rather, it is a reflection of the limited
resources that have been devoted to research in the past, and that many of the trials have
been of poor methodological quality (15), and yielded inconsistent findings (14). The
therapy that appears to have the ‘best’ scientific evidence – as far as cancer care is
concerned – is acupuncture for chemotherapy and radiotherapy-induced nausea. Few
formal trials have been conducted into touch therapies such as aromatherapy, massage
and reflexology (18).
This project evaluates massage as preparation for cannulation prior to patients receiving
intravenous chemotherapy. In order to provide some context to the study a brief review of
the application of massage within cancer care will follow. Subsequent to this, studies

Exploration of the Efficacy of Arm massage 14
investigating patients’ experience of chemotherapy, and in particular aspects of the
experience that provoke anxiety and discomfort, will be reviewed. Finally, the current
provision of CAM within the context of the NHS will be outlined.
2.1.1 General massage
As stated above, some of the most popular complementary therapies accessed by patients
are the massage therapies; with aromatherapy massage being a popular choice.
Massage is used mainly for the relief of musculo-skeletal pain, including that caused by
tension. It has been suggested that a further benefit of massage is the relief of other kinds
of pain – such as cancer pain – by inducing a state of relaxation (18). Unfortunately
methods used to evaluate the benefits of massage for cancer patients vary greatly and
have yielded inconclusive evidence of its effect (18).
Massage has been examined in terms of its effect on a range of symptoms and specific
populations. Massage ranging from full-body massage (19) to localised massage of the
feet (20), has been administered to populations ranging from a sample of mixed cancer
patients (20), to solely female (9, 21) or male patients (10), or those undergoing
autologous bone marrow transplantation (ABMT) (11). Contexts have included the
palliative (22, 23), hospice (19) and inpatient oncology setting (24, 25). Samples have
ranged from 87 patients (20) to 8 single case studies (21). These studies have aimed to
assess massages’ ‘general effects’ (22, 23); its impact on symptom distress (10, 24, 26);
and its effect on specific symptoms such as nausea (20). Qualitative (15, 21, 22) and
quantitative (10, 20) evaluations have been carried out. Outcome measures used in
quantitative evaluations have included a number of measures such as the State-Trait
inventory to measure anxiety (11), Visual-Analogue Scales (VAS) to measure pain
perception (25), and the Hospital Anxiety and Depression Scale (HADS) (14, 26). These
studies and service evaluations have shown massage to have a range of effects from
being generally beneficial (14, 21, 23), to having an ability to reduce specific symptoms
such as nausea (11) and anxiety (10, 13). Studies prominent in the literature on cancer
care are outlined below.
Studies have found that general massage not only significantly reduces anxiety levels in
cancer patients (14), it has also been described as being “universally beneficial by
Exploration of the Efficacy of Arm massage 15
patients, it assisted relaxation and reduced physical and emotional symptoms” (p.67) (14).
In addition, therapeutic massage - of the feet, back, neck & shoulders - has also been
found to be a beneficial intervention for cancer patients, not only reducing anxiety levels,
but also promoting relaxation and alleviating pain perceptions (10).
Furthermore, therapeutic massage was found to reduce the perception of pain and reduce
anxiety (13) in radiotherapy and chemotherapy patients. Smith et al (13) found that –
following a therapeutic massage nursing intervention – patients’ symptom distress was
reduced, and subjective quality of sleep improved slightly (whereas sleep deteriorated
significantly in the control group).
In a study by Ahles et al (11), specifically with patients undergoing (ABMT), general
massage therapy was found to have immediate effects. Following receipt of their first
session of Swedish/Esalen shoulder, neck, face and scalp massage, patients’ distress,
fatigue, nausea, and anxiety were significantly reduced as compared to the control group.
Mid-treatment - patients had up to 9 sessions - anxiety was significantly reduced in both
the intervention and control groups (but this reduction did not differ significantly between
the groups). And at the pre-discharge assessment stage of the study, fatigue was found to
have significantly reduced in the massage group (it also significantly reduced in the control
group; consequently the 2 groups did not differ significantly).
Using a phenomenological qualitative approach Billhult & Dahlberg (21) evaluated the
experience of 10 consecutive days of massage of the hand/forearm, or foot/lower part of
the leg, in eight female patients on an oncology ward. Participants were interviewed and it
was found that the essential meaning of receiving massage as part of daily care was
described as “getting a meaningful relief from suffering” (p.180) (21). Furthermore, from
the qualitative data gathered through interview, Billhult & Dahlberg (21) found that the
massage provided relief from suffering because patients:
• Experienced being “special”
• Found it beneficial to have the opportunity to develop a positive relationship with the
‘therapist’
• Experienced a sense of feeling strong
• Experienced more of a balance between autonomy and dependence
• Found and reported that it just “feels good’’

Exploration of the Efficacy of Arm massage 16
Of significance is that such physical and emotional benefits were gained in a relatively
short period of massage.
Grealish et al (20) looked at the effect of foot massage on symptoms suffered by patients
hospitalised with cancer. On the occasions where the patients had massage (on 2 out of 3
evenings), a significant immediate effect on patients’ perceptions of pain and nausea was
found; massage additionally had a significant effect on the sensation of relaxation. These
authors recommended the use of foot massage as a complementary means of helping
patients to manage the symptoms of pain and nausea.
A further study examining the effects of massage on patients with cancer was carried out
by Wilkie et al (19). This study focused specifically on full-body massage (where this was
possible) as a potential non-pharmacologic therapy to relieve cancer pain. When
compared with a control group (routine hospice care), quantitative data analysis revealed
that, immediately after the massage, pain intensity, pulse rate, and respiratory rate were
significantly reduced. This led them to conclude that the massage intervention produced
immediate relaxation and pain relief.
2.1.2 Aromatherapy massage
Aromatherapy massage differs from other forms of massage in that essential oils are used
with the aim of improving both the emotional and physical well being of an individual; the
benefits of these oils is gained through touch and inhalation, whereas massage is solely a
touch therapy. In relation to cancer patients, aromatherapy is thought to enhance symptom
control and reduce psychological distress (27).
Hadfield (26), in working with a group of patients with malignant brain tumours, found that
aromatherapy massage (of the foot, hand or neck/shoulder) affected the autonomic
nervous system, inducing relaxation. Hadfield (26) concluded that an aromatherapeutic
massage intervention appeared to be a good way of offering support, and of improving the
quality of life in this particular population, who are often faced with restricted treatment
options and poor prognosis (26).

Exploration of the Efficacy of Arm massage 17
Focusing on symptom control, Evans (22) carried out an audit into the physiological and
psychological effects of aromatherapy massage (usually to the face and/or extremities) on
cancer patients receiving palliative and terminal care. Both the qualitative and descriptive
ststistical data indicated that most participants found it soothing and/or relaxing, and that
they felt ‘better’ afterwards. The massage was described as: “beneficial”, making patients
“feel much better”, and an “excellent supplement to the medical care provided” and
“good…for pain” (p.240) (22).
A recent Cochrane review (12) examined the evidence on the effectiveness of the use of
aromatherapy and massage on symptom relief and physical and psychological wellbeing.
It concluded that the impact of massage / aromatherapy in cancer patients was as follows:
• Its impact on depression was variable
• Three studies found a reduction in pain following the intervention
• Two studies found a reduction in nausea
• Individual trials measured reduction in other symptoms such as fatigue, anger,
hostility, and digestive problems, and improved communication, but none of these
findings were replicated
• Interventions were consistently found to have an effect on reducing anxiety
Despite the variable findings highlighted by this review, it has been suggested that stress
relieving techniques that have been found to enhance well being, such as massage,
should be made available to patients “to augment and ease the experience of cancer
treatment and recovery” (p.362) (28).
2.2 The experience of chemotherapy
Chemotherapy is something that many patients with cancer dread. Apart from the prospect
of the side effects of chemotherapy, there are number of psychological issues that arise as
result of receiving treatment (6). For some patients the very thought of going in for their
treatment is often a distressing component of the whole process; another major concern
for patients stems from contemplating a needle being inserted (usually in their arm) for the
administration of their chemotherapy treatments (4). In fact, it is non-physical symptoms
such as these that account for 54% of the 15 most severe side effects experienced by
patients receiving cancer chemotherapy, as rated in a survey by Coates et al (4).

Exploration of the Efficacy of Arm massage 18
Studies such as those carried out by Rhodes et al (6), McDaniel & Rhodes (7), and Ream
et al (8) have further confirmed the fact that patients often dread chemotherapy, with the
experience often dominated by the sensory aspect of insertion of a needle for the
Intravenous (IV) line. Furthermore, patients are known to be unhappy when difficulties
arise with IV access and needles (5); these difficulties are a key source of stress and
discomfort to patients (4). Concerns linked to the procedural element of receiving
chemotherapy are often accompanied by psychological responses; some patients express
uncertainty, fear, anxiety, and distress due to lack of knowledge of chemotherapy, and
cancer in general (6).
In reality, distress, anxiety and fear of pain are common reactions to a cancer diagnosis
and even the prospect of chemotherapy (8). It is because of these reactions and their
effects on the process of cannulation that it is viewed as important to attempt to not only
improve ease of cannulation but also reduce patients’ anxiety during drug administration.
2.3 Cannulation for chemotherapy
Chemotherapy is one of the most frequently administered treatments in patients with
cancer. In many instances this treatment is administered via peripherally-sited IV
cannulas. Insertion of these portals is usually technically easy - following training and with
experience - but can be problematic and time consuming in patients requiring repeated
cycles of chemotherapy (29), due to the toxic effects of the chemotherapy and the damage
caused to the veins by repeated cannulation.
Furthermore, patients often find cannulation painful (8). For some individuals the pain and
associated stress and distress results in their increasing needle phobia with each cycle of
treatment. Cannulation is often more difficult when individuals are afraid of needles or
fearful because previous attempts have been painful or unsuccessful (29). With these
facts in mind, Lenhardt et al (29) looked at the effect of local warming on the insertion of
peripheral venous cannulas for the administration of chemotherapy. Neurosurgical
patients’ hands and forearms were covered with a mitt for 15 minutes (passive warming),
and leukaemia patients’ hands and forearms were covered for 10mins with a carbon fibre
heating mitt (active warming). This was carried out to determine whether ‘active’ local

Exploration of the Efficacy of Arm massage 19
warming facilitated peripheral venous cannulation. It was found that it took significantly
less time, with fewer failed attempts, to insert a cannula in the active warming group.
These findings lead to the conclusion that active warming of the limb significantly facilitates
insertion of peripheral venous cannulas; reducing time and number of attempts.
Wendler (30) studied the effects of Tellington Touch (TT) – a form of touch therapy
entailing gentle physical touch (originally developed for the calming of horses) – on
patterns of mean blood pressure, heart rate, state anxiety, and procedural pain
(anticipated versus perceived pain) in a sample of healthy individuals awaiting
venipuncture. Participants were randomly assigned to the intervention (TT) or control
group (who received a social visit). The 5-minute intervention was delivered by a nurse -
trained in the TT procedure - to the upper back, upper arms and shoulders. Data collection
determined that those in the intervention group experienced decreases in mean blood
pressure and heart rate, which were both statistically and clinically significant (although
this change was transient).
Anxiety provoked by cannulation, and the anticipation of receiving chemotherapy, often
results in vasoconstriction rendering the procedure more difficult (29). As a result,
intravenous cannulation can have many associated costs. It can be costly in terms of the
health professionals’ time and the cannulas wasted in the process. It can also increase
treatment time and anxiety for patients.
In some instances, poor venous access and needle phobia necessitate insertion of central
venous catheters like Hickman catheters, or peripherally inserted central venous catheters
(PICCs) for administration of chemotherapy (31). Although these provide long-term
venous access in patients undergoing chemotherapy, there are greater associated costs;
the cost of insertion, whether surgically or angiographically are greater. Also the risk of
systemic sepsis is greater. For many patients it would appear advantageous if the
cannulation process could be enhanced through complementary, inexpensive and non-
invasive methods such as massage.

Exploration of the Efficacy of Arm massage 20
2.4 CAM in the NHS
Approximately half the hospices and oncology departments within the UK offer a form of
complementary therapy to patients, and over 50% of those that offer CAM are reported to
offer more than five different therapies (Kohn (In press) cited in NICE Guidance (32)).
Wilkes (17) carried out a survey, which included gathering information on provision of
complementary therapies in palliative care settings. He reported that of the 108 hospices
surveyed 70% of them offered massage, 68% offered aromatherapy, and 66% offered the
mind-body therapy of relaxation.
Later, Rees et al (9) evaluated the use of complementary therapies in cancer patients.
Based on data gathered from 714 women diagnosed with breast cancer in the South
Thames region, it was found that massage/ aromatherapy was the most commonly
received therapy (22% of the sample). Therapists were mostly visited to treat symptoms of
cancer rather than to cure it or slow it down. It was recorded that 70% of NHS hospital
oncology departments in England and Wales claimed to be using some form of CAM to
benefit cancer patients. Massage was reported to be offered in just over a third of these
NHS hospitals, and relaxation and aromatherapy were available in almost half the
departments. This study was the first in the UK to provide precise estimates for the use of
complementary medicine among this group of patients (9).
A national survey was carried out by Kohn (18) examining cancer patients’ use of
complementary therapies throughout the UK. As a result she has outlined five key discrete
models for the provision of CAM in cancer care (See Table 3.1).

Exploration of the Efficacy of Arm massage 21
Table 2.1. Models of CAM provision
MODEL PROVISION
1: Hospital based individuals
Provided within a hospital setting by professionals who
themselves practice complementary therapies; such as
nurses, doctors, physiotherapists and radiographers
2: Provision within a multi-disciplinary
setting
Provided within a multi-disciplinary setting (such as hospice or
information and support centre), and planned and managed as
a discrete service e.g. Richard Dimbleby Cancer Information
and Support Service at Guys and St Thomas' Hospital
3: Patient groups within a healthcare
setting
Whereby certain patients are offered access to therapeutic or
supportive techniques, within a healthcare setting. These
techniques or therapies are psychological treatments intended
to alter negative perceptions of cancer, and promote positive
attitudes, decreasing stress and potentially influencing survival
e.g. Behavioural Oncology Unit, Aberdeen Royal Infirmary.
4: Independent approaches within the
NHS
Whereby they are 'external' (that is independently organized to
cancer services), but still provided within context of NHS e.g.
NHS homeopathic hospitals
5: Independent organizations
Whereby organisations offer services for patients with cancer
independent of the NHS. Often aspects of the work carried
out by these organizations has subsequently been adapted for
use within the NHS e.g. Bristol Cancer Help Centre
Source: Kohn (18)
These models of delivery of CAM in cancer care have scope to overlap. For example,
cancer care within a given service could be delivered by adopting aspects of Models 1 and
3. These models are key to planning integration of CAM with orthodox cancer care,
whether they are provided within NHS facilities or commissioned by the NHS. Kohn (18)
considered that provision of CAM, in line with one or more of these models, will most likely
be determined by current patterns of prioritisation within services’ budgets; and will be
guided by current standards outlined by organisations such as NICE.

Exploration of the Efficacy of Arm massage 22
NICE recently published a guidance document (32) on improving supportive and palliative
care for adults with cancer. The recommendations emphasise collaboration between
stakeholders and service users in order to make decisions regarding:
• The range of complementary therapies to be provided within the context of the NHS
• The regulation of practice and training standards
• The nature of information to be provided on CAM to patients with cancer
The NICE guidelines are complemented by the National Council for Hospice and Specialist
Palliative Care Services (NCHSPC) guidelines (33) for the use of complementary
therapies in supportive and palliative care. These provide broad advice in relation to CAM
and on how to meet requirements of clinical governance. Together, these documents aim
to inform those responsible for developing CAM in the statutory and voluntary sectors; and
they emphasise the importance of integration of CAM within the NHS.
A complementary therapy service has been established within the Chemotherapy Day Unit
in the acute NHS Trust, in which the study was carried out, since August 2001. This has
provided patients waiting for intravenous chemotherapy with gentle effleurage arm
massage. Patients, nurses and therapists have reported that this has reduced patients’
anxiety, enabled less traumatic cannulation and can result in fewer cannulation attempts.
This study aimed to determine, primarily through conduct of a randomised controlled trial
(RCT) the benefits of providing arm massage prior to intravenous cannulation. However
qualitative data were also collected to further inform understanding potential impact of this
therapy on the chemotherapy service.
This study will provide new evidence on the impact and potential of this relatively easy-to-
use and non-invasive intervention. It will help to determine which individuals, if any,
benefit most from this approach and will reflect on barriers and facilitators to the process.
It will provide understanding, hitherto lacking, of the outcomes of arm massage for
cannulation in patients undergoing chemotherapy.

Exploration of the Efficacy of Arm massage 23
3 Method
3.1 Introduction
This chapter is organised to provide a description of the methods employed in the
investigation.
3.2 Study aims
The study aimed to investigate the impact of arm massage prior to chemotherapy.
Principally through the conduct of a randomised controlled trial (RCT) it sought to
determine:
1. The value of arm massage prior to intravenous chemotherapy
2. The potential impact of this therapy for the chemotherapy service
Patients, nurses and therapists provided data through completion of questionnaires, or
participation in interviews or a focus group. These three different elements, outlined in this
chapter, provided complementary and detailed data on the efficacy, suitability and
popularity of using gentle arm massage to assist cannulation for administration of
chemotherapy.
3.3 Research questions
This study addressed the following research questions:
Does a 10 minute gentle effleurage arm massage with basic carrier oil prior to intravenous
cannulation for administration of chemotherapy:
1. Reduce time taken for successful cannulation?
2. Reduce number of cannulas used?
3. Reduce pain associated with the procedure?
4. Reduce feelings of stress and distress in patients and health professionals?
5. Enhance patients’ wellbeing?
Exploration of the Efficacy of Arm massage 24
3.4 Massage treatment
The massage intervention was a standard procedure, guided by a detailed protocol
(Appendix 1). Each therapist received additional training in the procedure to ensure the
same treatment was administered to those in the experimental group. All therapists
followed operational policy that had been agreed by the Trust.
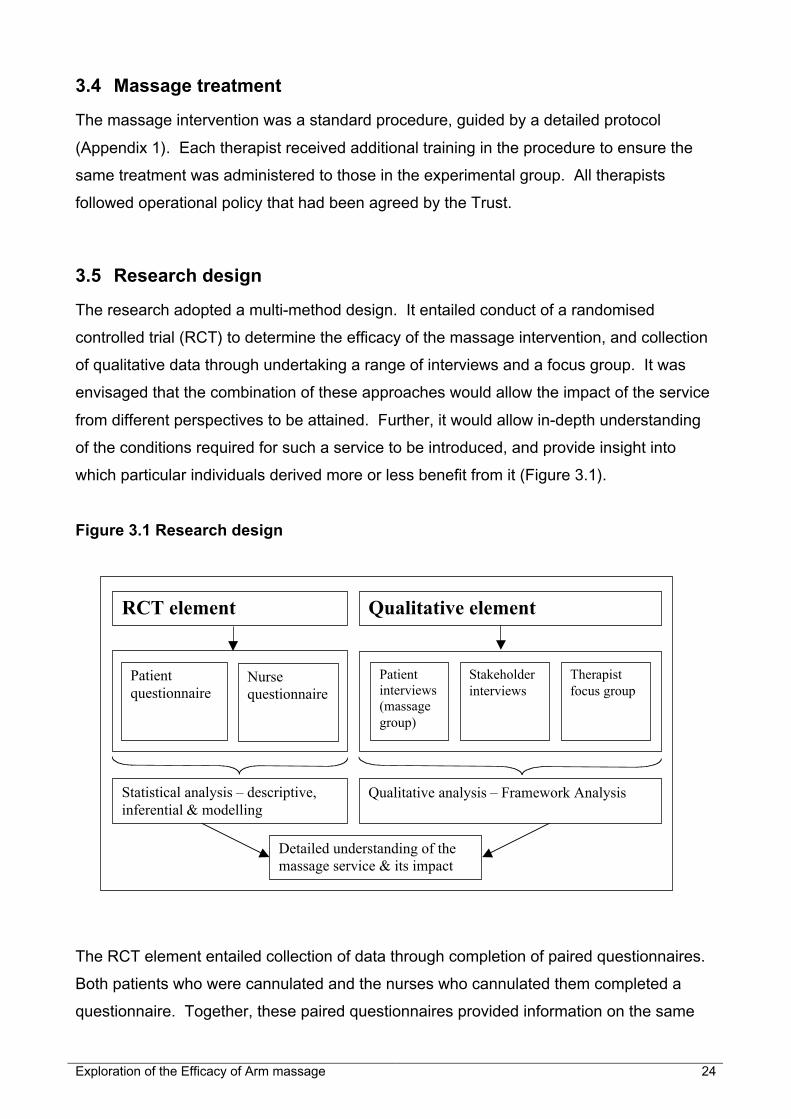
3.5 Research design
The research adopted a multi-method design. It entailed conduct of a randomised
controlled trial (RCT) to determine the efficacy of the massage intervention, and collection
of qualitative data through undertaking a range of interviews and a focus group. It was
envisaged that the combination of these approaches would allow the impact of the service
from different perspectives to be attained. Further, it would allow in-depth understanding
of the conditions required for such a service to be introduced, and provide insight into
which particular individuals derived more or less benefit from it (Figure 3.1).
Figure 3.1 Research design
The RCT element entailed collection of data through completion of paired questionnaires.
Both patients who were cannulated and the nurses who cannulated them completed a
questionnaire. Together, these paired questionnaires provided information on the same
Patient questionnaire
Nurse questionnaire
RCT element Qualitative element
Patient interviews (massage group)
Stakeholder interviews
Therapist focus group
Statistical analysis – descriptive, inferential & modelling
Qualitative analysis – Framework Analysis
Detailed understanding of the massage service & its impact

Exploration of the Efficacy of Arm massage 25
cannulation episode. They recorded time taken to cannulate, the ease with which the
cannula was placed and the number of attempts this required. Levels of pain and anxiety
experienced by the patient throughout were also recorded. Further details of the
questionnaires are given in section 3.8. These questionnaire data were collected from
individuals in both the intervention and control groups on their first ever cannulation for
chemotherapy and on subsequent cannulations for treatment, up to a maximum of 6
occasions. On completion of this element of the study, a random sample of patients were
invited to participate in a telephone interview to explore their experiences further.
Patients’, and the other samples’, involvement in the study is presented diagrammatically
below (Figure 3.2). The stakeholder interviews and therapist focus group were conducted
at the end of the study.
Figure 3.2 Sequence of data collection
3.6 Sampling
3.6.1 Patients
The study sought inclusion of 50 patients that had not previously received chemotherapy.
A convenience sample was drawn, thus the first 52 individuals that met the inclusion
criteria, and were willing to take part, were recruited to the study.
Control group
Experimental group
Questionnaires completed when cannulated (2-6 times)
Questionnaires completed when cannulated (2-6 times)
Interview when questionnaire element finished
Nurses Questionnaires completed after cannulating
Stakeholder Interviews at end of study
Therapists Focus group at end of study

Exploration of the Efficacy of Arm massage 26
To be eligible patients were:
• 18 years of age, or older
• due to commence first course of intravenous chemotherapy for treatment of breast,
lung, colorectal or haematological cancer
• able physically and emotionally to cope with the research protocol
• able to speak and write in English
Patients were excluded if they:
• had previously had intravenous chemotherapy
• were having chemotherapy via a peripherally inserted central catheter (PICC) or
Hickman line
• had signs of bilateral lymphoedema
The size of the study was not determined through conduct of power calculations as there
were limited data from previous studies on which to base this. Instead, the research
hers opted for a sample size that would allow data to be collected on 100 cannulation
episodes over the planned period when data would be collected. Retrospective review of
chemotherapy administered at the study site where data were collected had determined
that it was feasible to collect data on 100 cannulation episodes - 50 in the experimental
group and 50 in the control- over a 6 month period. It was also anticipated that this
number of cannulation episodes would be sufficient to determine between-group
differences, and allow statistical modelling of the factors impacting on cannulation to be
undertaken.
3.6.1.1 Randomisation of patients
Patients were randomised at the outset to either the experimental or control groups. Once
randomised to a study arm, they remained within that arm for the duration of the study.
Thus, those randomised to the massage arm had massage each time they attended for
chemotherapy, prior to placement of the cannula, and vice versa.
Patients were randomised through selection of a card detailing the group they were to be
allocated to. One hundred identical envelopes were filled detailing the group patient
participants were to be allocated to. These envelopes were sealed and placed in a secure
box. There were equal numbers (n=50) of envelopes with ‘Experimental group’ cards as
there were ‘Control group’ cards. On consenting to take part in the study an envelope was

Exploration of the Efficacy of Arm massage 27
selected from the shuffled envelopes in the box by the recruiting nurse. Thus, each patient
had an equal chance of being allocated to either of the two groups.
3.6.2 Nurses
All nurses that cannulated the sample of patients participating in the study were invited to
take part in the study. This included permanent members of nursing staff and those on 6-
month secondment as part of an educational Rotation Programme for inexperienced
cancer and palliative care nurses.
3.6.3 Stakeholders
A purposive sample of three stakeholders was invited to take part in an interview in which
to explore the running, impact and potential of the massage service. To gain a wide
perspective it was decided to involve the Lead Nurse for Cancer Services, the Manager of
the Volunteer Therapists and the Nurse managing the Chemotherapy Day Unit.
3.6.4 Massage therapists
In addition to attaining the patients’, nurses’ and stakeholders’ views, it was decided to
provide opportunity for the therapists to share their experiences of providing massage to
patients prior to chemotherapy and to understand the challenges and benefits of providing
such a service from their perspective.
Literature on the conduct of focus groups suggests that groups of between 4 to 12
members are recommended. The basis for this recommendation is that groups larger than
this can become unwieldy and inhibit all members sharing their insights. Conversely,
small groups can provide an insufficient range of perceptions. It was decided for this study
to conduct only one group and to invite all those providing massage on completion of the
study to attend. If all had attended this would have resulted in a group of nine therapists;
in the event a convenience sample of seven people could be present at the time the group
was scheduled, and all took part.

Exploration of the Efficacy of Arm massage 28
3.7 Access arrangements
3.7.1 Patient sample
As per usual care, patients met with their doctor in the outpatient clinic to discuss and
determine their treatment plan. When a decision was made for chemotherapy, the doctor
and clinical nurse specialist assessed whether the individual met the eligibility criteria for
this study. If they did, the clinical staff issued them with the Patient Information Sheet
concerning the study (Appendix 2). A verbal explanation of the study was given at this
time by the clinical staff, and patients were encouraged to read the sheet prior to their next
planned meeting with the oncology team prior to their treatment. They next met with the
chemotherapy team when they attended the treatment suite in the Day Unit for their ‘Work-
Up’ (usually a minimum of 24 hours later). This meeting provided patients with the
opportunity to discuss their treatment with a chemotherapy nurse. At this meeting
individuals were given further verbal explanation of the aims of the study, and their
potential role in it, by the chemotherapy nurse. Individuals willing to take part then signed
the consent form (Appendix 3).
In addition to providing written consent to take part, participants checked a box to indicate
whether or not they were happy to be interviewed over the telephone on completion of the
study. A sample of 15 was randomly selected from those that checked the box, and were
in receipt of massage. These patients were contacted by the nurses on the Day Unit to
check that they remained happy to be interviewed and for their names and contact details
to be forwarded to the research team. One of the researchers then telephoned them at
home and arranged a time when they could call back to interview them over the telephone.
3.7.2 Nurse sample
The nurses cannulating patients on the Day Unit were provided details of the study by
members of the research team who provided oral and written information regarding it. The
data collection process was discussed and considered in detail prior to the study
commencing. All nurses that agreed to take part (in the event all that worked on the unit)
provided written consent before the study commenced.

Exploration of the Efficacy of Arm massage 29
3.7.3 Therapist sample
The therapists met regularly with their manager, and at one such meeting the latter
provided them with details of the study and gave out information sheets (Appendix 4)
explaining plans for the conduct of the therapist focus group. The manager provided them
with the scheduled meeting date and time and gathered names of those willing and able to
attend. Willing participants signed their consent form prior to attending the focus group,
and returned them to the research team at the focus group.
3.8 Instruments
3.8.1 Questionnaires
Two brief self-report questionnaires were designed by the research team, one for
completion by patients on the occasions they were cannulated, and the other by the
nurses that performed the procedure. This pair of questionnaires was designed with the
study aims in mind; the study aimed to determine whether gentle effleurage arm massage
reduced pain associated with cannulation, reduced feelings of anxiety before and during
the procedure, and enhanced feelings of wellbeing. They were informed by work
conducted by Lenhardt (29) and Wilkinson et al. (23).
3.8.1.1 Patient Questionnaire
The questionnaire filled in by patients (Appendix 5) was made up of 3 sections and
completed by them in 2 stages.
Stage 1 - Prior to the cannula being placed: All the patients completed Section 1 detailing
their feelings of anxiety, and their perceptions of how uncomfortable they anticipated the
placement of the cannula would be. Patients did this by means of two separate 11-point
numeric rating scales ranging from 0 to 10 (i.e. one for pre-anxiety and one for pre-pain).
Stage 2 - After the patients had had their intravenous treatment: All the patients completed
Section 2 by recording how anxious they were following cannulation and the pain they
actually experienced during the procedure. Once again, patients did this by means of two

Exploration of the Efficacy of Arm massage 30
separate 11-point numeric rating scales ranging from 0 to 10 (i.e. one for post-anxiety and
one for post-pain).The patients further recorded the amount of time they spent in the unit.
Section 3 was completed solely by those in the massage group. This extra section detailed
their perceptions of massage on that occasion. They stated their expectation of the arm
massage, their level of satisfaction with it, and the level of pleasantness they experienced
from the process through fixed choice questionnaire items. They also recorded the feelings
that accompanied receiving the arm massage through fixed choice. Next, patients
responded to statements describing their thoughts and feelings - before, during and after
their massage - through the use of 4-point forced choice Likert scales. Finally, patients
stated their desire to repeat the arm massage experience prior to chemotherapy, and to
recommend it to a fellow patient, through fixed choice questionnaire items. Following these
items there was a space left available for additional comments to be made, regarding arm
and hand massage.
Through patients completing questions immediately before, and directly following, the
procedure, retrospective recall and associated difficulty recounting the experience were
minimised.
3.8.1.2 Nurse Questionnaire
Completion of the nurses’ questionnaire (Appendix 6) mirrored that of the patients; it was
made up of 3 sections and completed in two stages.
Stage 1 - Prior to the cannula being placed: Section 1 asked nurses to rate the condition of
patients’ veins immediately prior to attempting to cannulate. Nurses did this by means of
one fixed choice questionnaire item, made up of varying descriptions of vein visibility and
palpability.
Stage 2 - After the patients had had their intravenous treatment: In Section 2 nurses
detailed the amount of time taken to insert the cannula, the size of the cannula used and
the number of failed attempts at cannulation. This was followed by them rating the degree
of difficulty encountered when cannulating on a 5-point scale. They further recorded the
use of other measures used to achieve a successful cannulation; 5 options were available
including an “other” option, accompanied by the opportunity to specify the “other” option

Exploration of the Efficacy of Arm massage 31
used. They then completed a fixed choice questionnaire item, which recorded the
presence or absence of additional factors that might impinge on cannulation, accompanied
by an opportunity to specify as to the factor(s).
Section 3 required the nurse to record treatment and patient demographics. These
included the patients’ chemotherapy programme, their cycle of treatment (at the point of
completing the questionnaire), and their age, gender and type of cancer.
These questionnaire data allowed differences in ease of cannulation between the
experimental and control groups to be determined and described statistically.
3.8.2 Patient telephone interview schedule
Telephone interviews had previously been utilised by the research team to explore
sensory feelings experienced whilst chemotherapy was given (8). Experience gained from
these informed the development of a telephone interview schedule that was brief
(maximum half an hour) (Appendix 7), but encouraged disclosure and detail regarding their
experience of being cannulated, and of receiving massage. These interviews were tape
recorded and then transcribed verbatim for analysis.
The interviews centred on:
• Experience of receiving chemotherapy & of being cannulated
• Influential factors impacting on the process
• Experience and views of massage
• Potential for massage service in future
3.9 Stakeholder interview schedule
Face-to-face interviews were conducted with the three selected stakeholders and recorded
on audio tape. As with the patient interview schedule it was intended to keep interviews
under half an hour in duration but allow detailed and comprehensive discussion about the
massage service, its potential and factors that both impeded and facilitated the process.
To this end a semi-structured interview schedule was developed (Appendix 8) which
guided and prompted discussion. Key themes covered in these interviews were:
• Value of massage for patients
• Impact of massage on Day Unit/Cancer services/Hospital Trust

Exploration of the Efficacy of Arm massage 32
• Challenges affecting setting up/running of service
• Potential for massage service in future
3.10 Therapist focus group
The massage therapists took part in a one-off focus group. It was anticipated that this
group would last approximately 1 hour, and it was facilitated and recorded by two
members of the research team. Both the focus group facilitators were from outside the
institution where data were collected in the hope that conversation generated would be
frank, and in the main uninhibited.
They were invited to discuss their perceptions of how patients responded to the
intervention treatment, and to reflect on factors that both impeded and facilitated the
process. They were also encouraged to consider patient characteristics that influenced
outcomes of the massage treatment. Conversation was also directed towards considering
the potential of the service and discussing the manner in which therapists themselves and
the service would need to be supported in future. The focus group guide that acted as an
aide-memoir during the group can be seen in the appendix (Appendix 9). It centred on:
• Process of providing massage
• Impact of massage
• Factors affecting its effects
• Potential for massage service in future
3.11 Pilot work
The questionnaires and patient telephone interview schedule were piloted prior to the main
study. 23 patient and nurse questionnaires were piloted, and the interview schedule was
piloted twice. Minimal changes were required to wording within each. Both the
questionnaire and the telephone interviews took in the main under half an hour to
complete, which had been the aim.
3.12 Data analysis
3.12.1 Questionnaire data
Following descriptive tests, the quantitative data attained from the investigator-designed
patient and nurse questionnaires were subject to inferential analysis to determine the

Exploration of the Efficacy of Arm massage 33
relative efficacy of arm massage in facilitating cannulation. The data were largely of
ordinal level, and hence nonparametric tests were principally employed. On occasion
interval/ratio data were recoded into grouped data in order to carry out alternative or more
complex statistical tests. For example, pain and anxiety, rated on the 11-point numeric
scales ranging from 0-10 were recoded into low (scores 0-3), medium (scores of 4-6) and
high (scores of 7-10) pain/anxiety in order to be crosstabulated with categorical data (e.g.
massage group). A series of models were tested using backwards stepwise regression to
determine factors, including demographic ones, impacting on the cannulation process.
3.12.2 Interview and focus group data
The data attained from the telephone interviews with selected patients, and from the
therapists’ focus group, were transcribed verbatim and subject to Framework Analysis.
This allowed commonly held views and discrepancies in opinion to be described. In
combination, the analysis outlined above gave rise to complementary and insightful
findings relating to factors affecting cannulation and the impact of arm massage.
3.13 Ethics
The research proposal was submitted to, and a favourable opinion given by, the Local
Research Ethics Committee and associated Research and Development Committee.
They required no amendments to be made.
As with all research, care had to be taken during the study to ensure participants’
(patients’, nurses’ and therapists’) responses were anonymous. To this end, patients
completing questionnaires were allocated a study number; their name did not appear on
any documentation other than the consent form, which was stored away from the data that
were generated. All data were stored in accordance with the Data Protection Act (1998).
In presentation of qualitative data, all participants are allocated a pseudonym. In this way
comments are not attributable to any particular individual.
The conduct and progress of the study was monitored and guided by a Steering Group
which entailed representation of health professionals, massage therapists, a service user
(patient that had received treatment on the Day Unit) and members of the research team.
The group met regularly throughout the study.

Exploration of the Efficacy of Arm massage 34

Exploration of the Efficacy of Arm massage 35
4 Results
4.1 Introduction
The results chapter is organised to provide a description of the impact of the massage
service on patients being cannulated for chemotherapy, on the chemotherapy Day Unit
service and on the hospital more generally. It also presents outcomes of analysis
conducted to determine factors other than massage that influenced the cannulation
process. Before these findings are presented the chapter commences with an overview of
the sample accrual and attrition, and provides a description of the demography of the
different samples that provided data during the study.
4.2 Sample accrual and attrition
4.2.1 Patient sample
Sixty-eight eligible patients received treatment over the period that data were collected
(from the 2nd week of September 2003 to the of end June 2004). Fifty-four of these
individuals were recruited to the study over this 9-month period. They were randomly
allocated between the experimental group (n=28) and the control (n=24). Two people
withdrew from the study after consent but before data collection; one patient withdrew from
the experimental group due to being admitted to hospital and the other withdrew from the
control group because they had a PICC line inserted. In total data were collected on 266
cannulation episodes, 138 of these came from people within the intervention group and
128 from those in the control. Study participants provided data on between 2-6 occasions
when cannulated for treatment. The median number of episodes on which data were
collected was 5 occasions in the experimental arm and 6 occasions in the control (Figure
4.1).

Exploration of the Efficacy of Arm massage 36
Figure 4.1 Flow diagram of patient accrual and attrition
4.2.2 Therapist sample
The intention was to recruit 10 part-time massage therapists to work on the Day Unit to
provide arm massage to those in the intervention group. Initial recruitment resulted in 8
therapists commencing work on the Day Unit in July 2003 (2 months before data collection
commenced) (Figure 4.2). Over time, four of these left the service due to personal
reasons, notably their need for paid employment. As a consequence, a second
recruitment drive was required. This occurred in February 2004 and 5 further therapists
were recruited. As the study drew to a close, a further three therapists left the Day Unit
for reasons similar to those given by the therapists that left the service previously.
Identified as eligible (n=68)
Excluded (n=14)• Missed (n=2)• Refused (n=12)
Randomised n=54
Allocated to intervention (n=29)
Allocated to control (n=25)
Lost to follow up (n= 1)
• Withdrew (n=0)
• Decline in health (n=1)
Lost to follow up (n=1)
• Withdrew (n=1)
• Decline in health (n=0)
Available for analysis (n=28)
Data on 138 cannulations
Available for analysis (n=24)
Data on 128 cannulations
Identified as eligible (n=68)
Excluded (n=14)• Missed (n=2)• Refused (n=12)
Randomised n=54
Allocated to intervention (n=29)
Allocated to control (n=25)
Lost to follow up (n= 1)
• Withdrew (n=0)
• Decline in health (n=1)
Lost to follow up (n=1)
• Withdrew (n=1)
• Decline in health (n=0)
Available for analysis (n=28)
Data on 138 cannulations
Available for analysis (n=24)
Data on 128 cannulations

Exploration of the Efficacy of Arm massage 37
Figure 4.2 Massage therapist accrual and attrition
4.3 Demography of patient sample
Demographic data were collected on the 52 patients recruited to the study. Twenty-eight
of these participants were randomised to receive massage prior to cannulation, and 24
were allocated to the control. The majority were receiving treatment for breast cancer
(50%) and consequently the sample comprised more women than men. Eight different
treatment regimes were administered to the study participants, and all were chemotherapy
naïve on recruitment. The mean age of participants was 59 years (SD 14) (see Table 4.1).
It was decided that cannulation data would be collected from participants on a minimum of
two and maximum of six occasions. The median number of occasions was 6 (Range 2-6).
Comparison between the two study groups confirmed that there were no statistically
significant differences between the two study groups’ demography.
Recruited in July 2003 N = 8
Left for personal / financial reasons N = 4
By February 2004 N = 4
Recruited in March 2004 N = 5
From March 2004 N = 9
At the end of data collection - June 2004
Left for personal / financial reasons N = 3
From July 2004
N = 6
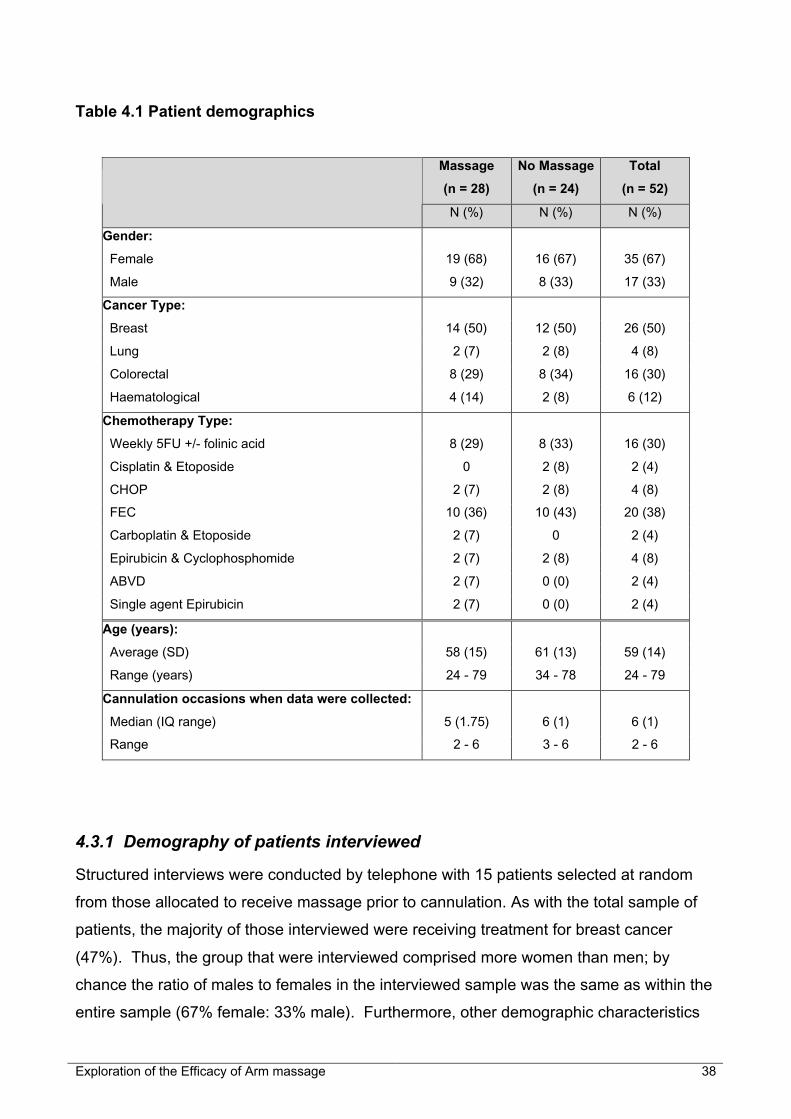
Exploration of the Efficacy of Arm massage 38
Table 4.1 Patient demographics
Massage
(n = 28)
No Massage
(n = 24)
Total
(n = 52)
N (%) N (%) N (%)
Gender:
Female 19 (68) 16 (67) 35 (67)
Male 9 (32) 8 (33) 17 (33)
Cancer Type:
Breast 14 (50) 12 (50) 26 (50)
Lung 2 (7) 2 (8) 4 (8)
Colorectal 8 (29) 8 (34) 16 (30)
Haematological 4 (14) 2 (8) 6 (12)
Chemotherapy Type:
Weekly 5FU +/- folinic acid 8 (29) 8 (33) 16 (30)
Cisplatin & Etoposide 0 2 (8) 2 (4)
CHOP 2 (7) 2 (8) 4 (8)
FEC 10 (36) 10 (43) 20 (38)
Carboplatin & Etoposide 2 (7) 0 2 (4)
Epirubicin & Cyclophosphomide 2 (7) 2 (8) 4 (8)
ABVD 2 (7) 0 (0) 2 (4)
Single agent Epirubicin 2 (7) 0 (0) 2 (4)
Age (years):
Average (SD) 58 (15) 61 (13) 59 (14)
Range (years) 24 - 79 34 - 78 24 - 79
Cannulation occasions when data were collected:
Median (IQ range) 5 (1.75) 6 (1) 6 (1)
Range 2 - 6 3 - 6 2 - 6
4.3.1 Demography of patients interviewed
Structured interviews were conducted by telephone with 15 patients selected at random
from those allocated to receive massage prior to cannulation. As with the total sample of
patients, the majority of those interviewed were receiving treatment for breast cancer
(47%). Thus, the group that were interviewed comprised more women than men; by
chance the ratio of males to females in the interviewed sample was the same as within the
entire sample (67% female: 33% male). Furthermore, other demographic characteristics

Exploration of the Efficacy of Arm massage 39
of those interviewed were akin to the entire sample (see Tables 4.1 & 4.2), except for the
age of the group. The mean age of the interviewed participants was 52years (SD 15); 7
years younger than the entire sample’s mean age.
Table 4.2 Demographics of patients that were interviewed
N
(n = 15) %
Gender:
Female 10 67
Male 5 33
Cancer Type:
Breast 7 47
Lung 1 7
Colorectal 5 33
Haematological 2 13
Chemotherapy Type:
Weekly 5FU +/- folinic acid 5 33
Cisplatin & Etoposide 0 -
CHOP 1 7
FEC 5 33
Carboplatin & Etoposide 1 7
Epirubicin & Cyclophosphomide 1 7
ABVD 1 7
Single agent Epirubicin 1 7
Age (years):
Average (SD)
Range (years)
52 (15)
24-79
Cannulation occasions when data were collected:
Median (IQ range)
Range
5 (1)
3 – 6
4.4 Demography of nurse sample
Nine nurses worked on the Day Unit and cannulated patients who participated in the study
(Table 4.3). All were female and had been working in oncology on average for 5 years 2
months before commencing on the Day Unit. Some cannulated patients regularly (up to
86 times during the study) whilst others, notably the Lead Nurse for Cancer who helped if

Exploration of the Efficacy of Arm massage 40
required, cannulated infrequently during the study (once). Typically they were experienced
nurses. The average length of time they had been qualified was 9 years 11 months.
Table 4.3 Nurse demographics
Gender: (n = 9) Years qualified:
Female 9 Mean (SD) 9yrs 11mths (7yrs 8mths)
Male - Range 18mths to 24yrs
Age: Cannulations performed during study:
Mean (SD) 34yrs (8.5) Mean (SD) 29.6 (30)
Range 24 to 49 years Range 1 to 86 cannulations
Oncology experience before recruited to Day Unit:
Mean (SD) 5yrs 2mths (6yrs 2mths)
Range 0 to 17yrs
4.5 Demography of therapist sample
Thirteen therapists provided massage to patients randomised to the treatment arm. Of
these, seven participated in the focus group. These individuals were among the nine
working on the Day Unit when the focus group was conducted towards the end of the
study. All were female, and relatively mature. The mean age of the therapists who took
part in the focus group was 46 years. They varied in the length of time that they had been
providing massage to patients in the Day Unit, and in the time they had been involved with
the study. Typically they provided one half-day of massage per week (Table 4.4).
Table 4.4 Demography of therapists that participated in focus group
Gender: (n = 7) Years qualified:
Female 7 Mean (SD) 3yrs (2yrs 7mths)
Male - Range 1 to 8 years
Age: Sessions provided per week (1/2 day):
Mean (SD) 46yrs (8.5) Mean (SD) 1 session per week (0.19)
Range 33 to 59 years Range 1 to 1.5 sessions
Time providing massage on Day Unit:
Mean (SD) 9.9 months (6.6 months)
Range 2 to 23 months

Exploration of the Efficacy of Arm massage 41
4.6 Demography of stakeholders
Three stakeholders were interviewed; the Lead Nurse for Cancer Services, the manager of
the volunteer therapists and the nurse managing the Chemotherapy Day Unit.
The Lead Nurse for Cancer Services was a 38-year-old female who had been qualified
and working in oncology for 17 years and 3 months. She had cared for patients receiving
chemotherapy for 15 years. Her qualifications included a Diploma in Nursing, a BSc in
Cancer Nursing, and post registration courses in oncology and chemotherapy.
The manager of the volunteer therapists was a 48-year-old female who had been a
qualified therapist for 6 years, held a number of therapeutic and massage qualifications.
She had provided massage therapy on the Chemotherapy Day Unit for 2 years and 10
months, providing 4 half-day sessions at the unit per week.
The nurse managing the Chemotherapy Day Unit was a 49-year-old female who had been
qualified for 12 years and working in oncology for over 5 of these. She had cared for
patients receiving chemotherapy for over 5 years. Her qualifications included being a
registered general nurse (RGN) and she held a Care of Patients Requiring Chemotherapy
(N59) qualification.
4.7 Patients’ cannulation experiences
The study was conducted to evaluate the efficacy of arm massage in facilitating
cannulation and decreasing levels of anxiety and pain associated with the procedure. It
investigated whether a 10-minute gentle effleurage arm massage with basic carrier oil prior
to intravenous cannulation for administration of chemotherapy:
1. Reduced the time taken for successful cannulation?
2. Reduced the number of cannulas used?
3. Reduced the pain associated with the procedure?
4. Reduced feelings of stress and distress in patients?
5. Enhanced patients’ wellbeing?
It was hypothesised that the intervention would have a positive outcome and result in
quicker cannulation with fewer failed attempts (questions 1 and 2). It was also
hypothesised that massage would result in cannulation evoking less anxiety and being
less painful (questions 3 and 4). These hypotheses were tested through the conduct of
nonparametric statistical tests for comparison of two independent groups (Mann-Whitney

Exploration of the Efficacy of Arm massage 42
tests). Other tests were also conducted, notably the Chi-square which was utilised to
determine associations within the data. The results of this statistical testing are presented
in sections 4.7.1- 4.7.4. Section 4.8 considers the impact of massage on patients’
wellbeing more generally (answers the 5th research question). Factors other than
massage impacting on cannulation are presented in section 4.9.
4.7.1 Experience of pain
Data were collected both prior to, and following, cannulation to attain information on both
anticipated pain prior to the procedure and procedural pain arising as a result of it.
4.7.1.1 Anticipated pain
Participants scored ‘how much hurt’ they anticipated placement of the needle would cause,
prior to the procedure taking place, on a scale of 0 (no hurt) to 10 (worst possible hurt).
Although there was considerable variation, there was no statistically significant difference
between the two study groups (p > 0.05).
Non-parametric independent samples t-test (Mann Whitney) = z = -0.14, p = 0.45 (ns)
Typically, patients anticipated little pain prior to cannulation (mean 2.3, SD 2.2) (Table
4.5).
Table 4.5 Anticipated pain
Study group Anticipated pain
Mean (SD)
Range z-value p-value
Massage 2.3 (2.1) 0-9
Control 2.3 (2.3) 0-9
-0.14 0.45 (ns)
Patients’ in the massage group when asked about experiences of pain stated that they had
not known what to expect prior to having treatment for the first time. As one lady phrased
it: ‘The unknown…you don’t know what to expect, so you, you think the worst’ (022). In
the event it tended to be viewed as ‘acceptable’ and ‘bearable’. It became almost routine
to some. One gentleman expressed: ‘I suppose I gradually got more confident…in the fact
that it wasn’t going to hurt…before I knew what was involved, then I didn’t know whether

Exploration of the Efficacy of Arm massage 43
there’d be pain or not…But, soon, having experienced it, I realised that there wasn’t any
particular pain at all’ (003).
4.7.1.2 Procedural pain
In addition to anticipated pain, participants recorded the procedural pain associated with
cannulation. The same numeric rating scale was used, where 0 represented ‘no hurt’ and
10 ‘worst possible hurt’. As with anticipated pain, there was no difference between the two
study groups’ procedural pain following cannulation (p > 0.05).
Non-parametric independent samples t-test (Mann Whitney) = z = -1.39, p = 0.08 (ns)
These procedural pain scores were typically low (Table 4.6), although some individuals did
report feeling extreme pain (i.e. maximum value).
Table 4.6 Procedural pain following cannulation
Study group Pain following cannulation
Mean (SD)
Range z-value p-value
Massage 2.2 (2.1) 0-9
Control 2.0 (2.2) 0-10
-1.39 0.08
(ns)
During interviews conducted with those in the massage group it became clear that
experience of pain was very variable. On one end of the scale, three people spoke of it as
only an uncomfortable ‘prick’ (010, 029, 031). A number of patients matched the pain to
previous experiences, such as that experienced when donating blood. One third of
patients expressed that in general they did not find cannulation particularly painful.
Nevertheless, these same people did recall and detail the ‘one time’ it went wrong. They
used words including ‘prodding’ (024), ‘ploughing’ and ‘poking’ (029) to describe what
occurred when a nurse had to ‘have several goes’ (023). One gentleman described how
on a couple of occasions the needle bent in his arm, but went on to express that he felt he
was ‘quite a strong bloke’ (038), suggesting that he had not been overly distressed by this.
Other patients expressed a clear dislike of needles, and explained that they always found
them uncomfortable and painful. One such lady described herself as being ‘a bit of a
coward when it comes to needles and things’ (046). For some patients the cannulation
process became more difficult with time, often requiring at least two attempts before the

Exploration of the Efficacy of Arm massage 44
cannula was successfully placed. One lady to whom this applied revealed: ‘it (the
cannulation process) did get worse (with time) …I didn’t really know how the chemo
worked but it just, it didn’t help - my veins were not really that good, so, it did cause me a
lot of pain’ (021). In all, seven of those interviewed reported having veins that were difficult
to cannulate and told of the discomfort associated with positioning the cannula. All of
these were female.
It was interesting to note that a small number of patients (27%) suggested that the level of
pain they felt varied according to the ‘experience’ of the nurse who cannulated.
The statistical analysis of the questionnaire data suggested that there was no difference in
the pain that was experienced following cannulation by those in the experimental and
control groups. This can be better understood when the interview data are reviewed.
Those in the intervention group explained that although the massage was pleasant, it did
not necessarily affect how painful the ensuing cannulation was. One lady summarised the
feelings of many of those interviewed: ‘I think no amount of massaging makes up for the
fact if the nurse isn’t skilful… (I) think that any human being would screw themselves
up…and, and wait for the needle…But as, as time, as I found the ones that were good at
it…the massaging helped and it didn’t go away. I didn’t screw myself up because I knew
she’d get it and that, it didn’t destroy the massaging’ (029).
4.7.2 Anxiety
Anxiety was measured on two occasions during the time patients were in the Day Unit for
treatment – before cannulation and immediately afterwards. These data were analysed
independently and results are presented in the following sections.
4.7.2.1 Before cannulation
Participants were requested to record their feelings of anxiety immediately prior to
cannulation. Thus, for those that had had massage this referred to their anxiety levels
once massage had been given. It was anticipated that massage would reduce anxiety;
and this reduction did near significance (p > 0.05).
Non-parametric independent samples t-test (Mann Whitney) = z = -1.57, p = 0.059 (ns)

Exploration of the Efficacy of Arm massage 45
Those in the massage group appeared to record lower anxiety levels prior to cannulation
(Table 4.7).
Table 4.7 Anxiety prior to cannulation
Study
group
Anxiety before cannulation
Mean (SD)
Range z-value p-value
Massage 2.1 (2.5) 0-10
Control 2.5 (2.6) 0-10
-1.57 0.059 (ns)
The benefit afforded by massage in this situation was explored during the telephone
interviews. Some participants explained how pre-treatment, they were often just generally
stressed, ‘nervous anyway’ (023) and feeling ‘daunted’ (038) about what was to come.
However, they spoke of how massage often allowed them to settle and feel ready for
cannulation and treatment. Other patients similarly stated that they believed they benefited
greatly from arm massage (021, 028, 029, 031, 046, 048) because it helped them feel
positive and relaxed. This was especially true on the first visit to the Day Unit for treatment
(031 & 046). Reference was made by patients during the interviews to the way in which
massage helped to warm up the arm and veins, making them more visible (021, 028, 029,
031). It was also felt by two interviewees to help with cannulation (028, 046). One lady’s
views expressed those of many. She said: ‘It was very nice and relaxing...I really did enjoy
it.... it was a nice part to start with the chemotherapy I think… I had a chat and you
unwound before you had the treatment... and she (the therapist) always done both arms…
she always covered it up (arm she would have treatment in) to make sure that, you know, I
had plenty of veins that were good for taking blood, you know, for the needle to go in... I
mean I just found it quite a nice experience... It’s quite calming before um the other
treatment started” (048).
4.7.2.2 Following cannulation
Participants recorded their anxiety levels after chemotherapy had been administered. This
enabled the research team to determine whether massage prior to cannulation impacted
on their feelings of well-being after treatment was administered. Analysis of these data
revealed that there was little difference between the groups (p > 0.05).

Exploration of the Efficacy of Arm massage 46
Non-parametric independent samples t-test (Mann Whitney) = z = -1.25, p = 0.105 (ns)
Both groups did have reduced anxiety following administration of their treatment, and the
massage group scored marginally higher at this time (Table 4.8).
Table 4.8 Anxiety after treatment administration
Study
group
Anxiety after treatment
Mean (SD)
Range z-value p-value
Massage 1.6 (1.9) 0-9
Control 1.4 (1.8) 0-8
-1.25 0.105 (ns)
Thus, the limited benefit afforded by massage appeared not to be sustained following
cannulation. Patients explained in the interviews that massage was delivered identically
during the study. It did not vary from one time to the next. But for some, massage
consistently afforded them little benefit during or after the procedure. These people
determined that this was because they were neither anxious nor uncomfortable about the
needle beforehand. Others felt that the massage, although it had been pleasant, was
unable to distract them from procedural pain and discomfort. Nonetheless, it was never felt
to have been negative. It could still make them feel ‘that little bit more comfortable’ (003).
One gentleman illustrated this well, he said: ‘It was nice. It was pleasing. I don’t think it
made one iota difference as regards to whether I felt the needle any more or less. It might
make a difference to someone who is frightened of needles. But, needles don’t in general
frighten me… Yep, it felt nice, calm, it felt like someone did care. Like you had been
personally taken care of. So that was very nice... I wouldn’t say it’s a waste of time, no”
(024).
4.7.3 Time taken to cannulate
Nurses cannulating the sample recorded how long the process took. Typically the process
was quick (mean 3.7 minutes, SD 5.1). On 44% of occasions it reportedly took less than
one minute, and on 64% of occasions cannulation was successfully accomplished in under
2 minutes. Analysis of the data revealed that the time taken to cannulate was not impacted
by massage (p > 0.05).
Non-parametric independent samples t-test (Mann Whitney) = z = -0.67, p = 0.25 (ns)
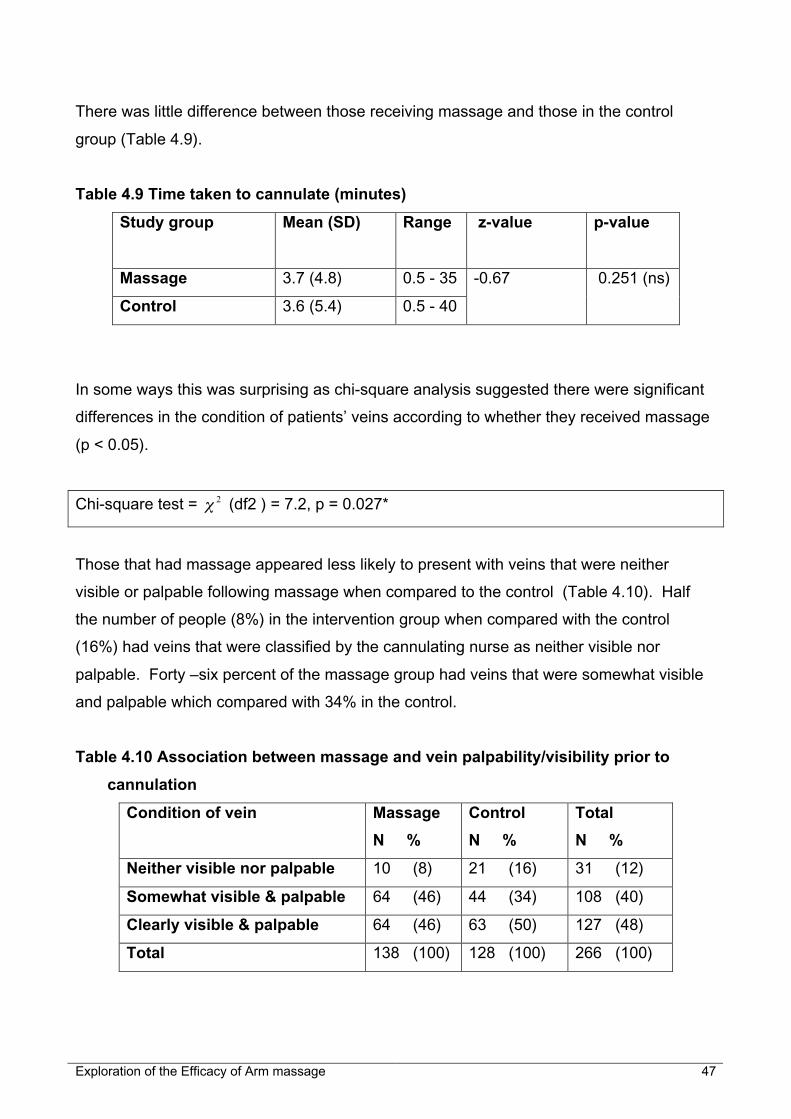
Exploration of the Efficacy of Arm massage 47
There was little difference between those receiving massage and those in the control
group (Table 4.9).
Table 4.9 Time taken to cannulate (minutes)
Study group Mean (SD) Range z-value p-value
Massage 3.7 (4.8) 0.5 - 35
Control 3.6 (5.4) 0.5 - 40
-0.67 0.251 (ns)
In some ways this was surprising as chi-square analysis suggested there were significant
differences in the condition of patients’ veins according to whether they received massage
(p < 0.05).
Chi-square test = 2χ (df2 ) = 7.2, p = 0.027*
Those that had massage appeared less likely to present with veins that were neither
visible or palpable following massage when compared to the control (Table 4.10). Half
the number of people (8%) in the intervention group when compared with the control
(16%) had veins that were classified by the cannulating nurse as neither visible nor
palpable. Forty –six percent of the massage group had veins that were somewhat visible
and palpable which compared with 34% in the control.
Table 4.10 Association between massage and vein palpability/visibility prior to
cannulation
Condition of vein Massage
N %
Control
N %
Total
N %
Neither visible nor palpable 10 (8) 21 (16) 31 (12)
Somewhat visible & palpable 64 (46) 44 (34) 108 (40)
Clearly visible & palpable 64 (46) 63 (50) 127 (48)
Total 138 (100) 128 (100) 266 (100)

Exploration of the Efficacy of Arm massage 48
4.7.4 Cannulation on first attempt
Although it appeared from the data that it generally took little time to cannulate, there were
occasions when the process was lengthy. Undoubtedly, it became lengthy when the
cannula was not successfully inserted on first attempt. On 25% of occasions cannulation
failed on first attempt, and one in every ten required three or more attempts. On one
occasion it took 7 attempts to place the cannula.
The number of failed attempts to cannulate appeared to differ little between the massage
and control groups. Individuals in both groups recorded on average two failed attempts
during the period they provided data. However, there was great variability. In the control
group there was an individual that reported 11 failed attempts to cannulate them over the 6
cycles they provided data. This compared with a maximum of 6 failed attempts across an
individual’s 6 treatment cycles in the massage group. Although there was some variability
in the number of unsuccessful cannulations between the massage and control groups,
these were not statistically significant.
On the 41 (18%) occasions when cannulation proved difficult, the nurses did use other
measures in attempt to dilate veins. In all but four of these they used warm water to
increase blood flow, and lumen volume.
Inability to cannulate on first attempt clearly has cost implications. Costs can be
considered in terms of patients’ pain and anxiety, nursing time as well as the tangible cost
of discarded cannulas. To determine whether factors, other than massage, impacted on
the cannulation process and thereby contributed to such costs, further statistical analyses
were undertaken. These are presented in section 4.9.
4.8 Attitudes towards, and perceptions of, massage
Data were collected on the 138 occasions when patients had massage to determine their
attitudes towards it. Responses recorded to questions regarding the intervention were
very positive. Almost all responses stated satisfaction with arm massage (95%); the other
5% of answers recorded feeling neutral about it.

Exploration of the Efficacy of Arm massage 49
On 93% of occasions, patients reported that massage had met their expectations,
although 7% of responses stated they had not known what to expect. This was referred to
in the interviews with stakeholders, where it emerged that for many people, massage
during the study had been their first experience of touch or other complementary
therapies.
From the interviews, it was gathered that whether or not patients believed massage aided
cannulation or relaxed them prior to it, they often looked forward to it and perceived it as a
‘positive’ aspect of the chemotherapy experience. All bar one of the interviewees spoke of
massage as being in some way comforting or relaxing. Massage was described as
‘luxurious’ (058), ‘pampering’ (022), and a ‘nice little treat!’ (021) that was ‘soothing’ (029).
One individual considered themselves ‘lucky’ through feeling ‘relaxed’ and ‘cared for’
through massage and reported that they ‘would recommend it (029)’to others. Another
had found it ‘relaxing’ and ‘reassuring’ (046). A further person found it a way of ‘passing
the time in a pleasant manner’ while waiting for treatment (003). Of the seven women that
repeatedly found cannulation problematic and painful, three specifically mentioned
massage as helping the process (007, 028, 031). Two further women suggested that it
might possibly have aided the process (010, 021).
Many interviewees found that not only was the massage positive but that the therapists
themselves made a very positive contribution. Familiarity was a key issue that arose.
Individuals enjoyed the familiarity, continuity and rapport they developed with the
therapist(s) they came into contact with (007, 010, 022, 038). It was viewed as ‘lovely to
have the same person’ (007, 023, 029, 031). One person explained, ‘you found yourself
sort of having a one-to-one conversation (with)…you were being looked after (by),
cosseted’ (029).
On 89% of occasions massage was perceived as a ‘very pleasant’ experience.
Descriptors commonly selected to describe feelings evoked by it included feeling relaxed
(98%), warm (62%), calm (61%) and sleepy (18%). Few negative responses were given
(Table 4.11)

Exploration of the Efficacy of Arm massage 50
Table 4.11 Feelings when massaged
(n = 133) Frequency %
Relaxed 131 98
Warm 83 62
Calm 81 61
Sleepy 24 18
Worried 2 2
Tickly 2 2
On most occasions, participants reported feeling very relaxed before massage
commenced (91%). However on almost 10% of occasions, participants felt some, or quite
a lot of, anxiety. They reported that they were not sceptical of the value of massage (98%
of occasions), and generally felt comforted during the process (81% of occasions), and
reported that it conveyed the feeling that they were being ‘treated as an individual’ (87% of
times) by ‘someone that had time to care’ (88% of times). After the massage they reported
feeling relaxed (89% of times), calm (87% of times) and reported on 75% of occasions that
it helped them cope with cannulation. This relatively low figure, when compared with other
feelings associated with massage, was explained during the interviews. Some individuals
articulated that whilst it was enjoyable, it did not make cannulation any less painful or
unpleasant. As one lady expressed: ‘The arm massage was lovely...And it was nice to
feel, you know that…being pampered a little bit…but, it didn’t really help...it didn’t take
away, the fear, you know...you’re going in and you’re going to have it’ (022). On 95% of
occasions individuals reported that, based on their experiences that day, they would
choose to have arm massage again if they had to have chemotherapy in future; 96%
would recommend it to others.
To determine whether there was any difference in perceptions of massage according to
gender or age, a series of chi-square tests were undertaken. These revealed no
difference according to age, but did identify differences associated with gender. It
appeared women were significantly more apprehensive than men before massage
commenced and responded more favourably to the process; they reported feeling
significantly more comforted, nurtured, relaxed, and calm. They also stated they felt
treated as an individual by someone with time to care significantly more than men (Table

Exploration of the Efficacy of Arm massage 51
4.12). However, they did not perceive that it helped them cope any better with cannulation
when compared with the men in the study.
Table 4.12 Feelings generated by massage according to gender
Feeling/perception Men
N %
Women
N %
2χ statistic p-value
Apprehension
before massage
Little/None
Some/much
44 (100)
0
77 (88)
11 (12)
6 0.016*
Comforted Little/None
Some/much
14 (35)
26 (65)
10 (11)
78 (89)
10.1 0.003**
Nurtured Little/None
Some/much
16 (44)
20 (56)
10 (11)
77 (89)
16.6 0.000**
Relaxed Little/None
Some/much
9 (20)
35 (80)
6 (7)
83 (93)
5.5 0.037*
Calm Little/None
Some/much
9 (23)
30 (77)
8 (9)
81 (91)
4.7 0.046*
Treated as
individual
Little/None
Some/much
12 (32)
25 (68)
4 (5)
84 (95)
18.1 0.000**
Someone had time
to care
Little/None
Some/much
12 (28)
31 (72)
4 (4)
85 (96)
14.9 0.000**
Helped to cope Little/None
Some/much
14 (33)
29 (67)
20 (22)
69 (78)
1.5 0.29
The findings presented above are exemplified by quotes attained during the telephone
interviews, where a difference in views towards the benefit of massage became evident.
The five males that were interviewed did not express specific anxiety prior to cannulation,
but found the massage to be pleasant. One man viewed it as ‘another aspect of it,
passing the time in a pleasant manner…I was fairly relaxed beforehand. But it was a
pleasant experience, rather than anything else’ (003). In general, the men tended to
suggest that others would benefit more from it than they had. One gentleman commented
‘I should imagine they’ll (massage therapists) be tremendous help to people that are
shaking…like are really quivering…and really down and wondering what’s going to happen
to their lives and that, and so I would think it would be very good for them indeed’ (058).
Thus, in general the men interviewed could see that massage may benefit others although
it had proved to offer them personally relatively little.

Exploration of the Efficacy of Arm massage 52
Conversely, females expressed stronger feelings about the effects of massage during
interviews. One lady brought together feelings expressed by other women that had found
cannulation problematic when she explained that massage was ‘very helpful because … it
puts you, especially the first time when you don’t know what, what, what’s going to
happen…the lady sort of does your arm … chats to you… puts (you in a) nice relaxed
mood, you know… brought the veins to, to the surface a bit more…it warms your
arm…and that brings your veins to the surface’.
4.9 Factors affecting cannulation
Initial analysis of the data revealed that although 25% of attempts to cannulate were
unsuccessful, these did not seem to be impacted by massage. Thus, further analysis was
undertaken in attempt to determine factors impacting on the cannulation process. These
are divided into factors that could vary on each visit such as the ease of the process or the
nurse that cannulated, and fixed demographic variables.
4.9.1 Variable factors
The variable independent factors that were investigated included the ease of cannulation,
the condition of patients’ veins, the nurse that cannulated and the cannula size. Each was
examined to determine whether they affected the time cannulation took, the pain
associated with the procedure and anxiety felt by individuals after cannulation.
4.9.1.1 Ease of cannulation
As would be expected it took less time to cannulate when it was perceived an easy
process (Table 5.13). On average (mean) it took 1.7 minutes (SD 1.4) to cannulate when
the process was straightforward and easy. When it was considered neither easy nor
difficult, time taken rose to 2.4 minutes (SD 1.9), and increased to 6.6 (SD 7.2) when
considered difficult. A Kruskal-Wallis test (a non-parametric one-way ANOVA) determined
these differences to be highly significant (p < 0.001).
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df2 ) = 70.7, p = 0.000***

Exploration of the Efficacy of Arm massage 53
A Tukey’s post hoc test pointed out that it took significantly longer to cannulate when it
was ‘difficult’, than when it was felt to be neutral or easy. It is interesting to note that the
nurses recorded almost as many difficult cannulation episodes (n=98) as easy ones
(n=110) (Table 4.13).
Table 4.13 Effect of ease of cannulation on time taken
Ease of cannulation Number Mean time (mins) SD
Easy 110 1.7 1.4
Neutral 52 2.4 1.9
Difficult 98 6.6 7.2
The stakeholder interview that was conducted with the manager of the Day Unit provided
opportunity to discuss a view put forward by them that some individuals had ‘good veins’
that could be cannulated with ease, and in a timely fashion. This individual questioned
whether massage assisted cannulation and noted instead that in their experience the vein
palpability/visibility was an important factor. They elaborated: ‘I’m not sure if it (massage)
actually helps the, the nurses to cannulate…I think that where we ought to have had
difficulties we were still, we’ve still had them. So from a physical point of view…I can’t see
that it’s been, it hasn’t slapped me in the face to say: “Gosh, that vein has really come
up”…if you’re going to get very awkward hard veins to find, then they have remained so.
And I think, some of the times, we’ve had to go underneath hot water and all those things’.
The view above was supported by one patient who explained: ‘every single time it was
difficult to get a vein…I had the aromatherapy but I had to stand under hot water as well’
(007). Another lady revealed: ‘I had a hot water bottle, I used to take a hot water bottle with
me…and that helped as well…right from before they started anything…the nurse
suggested that and that helped as well. So the whole area was nice and warm. With the
massage it was even better to get the veins up.’ (029)
As would be expected, cannulation was felt by patients to be less painful when it was
perceived as an easy process (Table 4.14). On average (mean) pain was given a score of
1.3 (SD 1.5), on a 0-10 scale, when the process was straightforward and easy. When it
was considered neither easy nor difficult average pain scores rose to 2 (SD 1.9), and
increased to 3.03 (SD 2.5) when considered difficult. A Krukal-Wallis test determined
these differences to be highly significant (p < 0.001).

Exploration of the Efficacy of Arm massage 54
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df2 )= 28.7, p = 0.000**
A Tukey’s post hoc test pointed out that cannulation was felt to be significantly more
painful when the process was ‘difficult’, than when it was felt to be ‘neutral’ or ‘easy’ (Table
4.14).
Table 4.14 Effect of ease of cannulation on procedural pain
Ease of cannulation Number Mean pain scores SD
Easy 106 1.3 1.5
Neutral 47 2.0 1.9
Difficult 96 3.03 2.5
Cannulation caused patients less anxiety when it was perceived as an ‘easy’ process
(Table 4.15). On average (mean) anxiety was given a score of 1.1 (SD 1.8), on a 0-10
scale, when the process was straightforward and easy. When it was considered neither
easy nor difficult average anxiety scores rose to 1.5 (SD 1.6), and increased to 1.9 (SD
2.02) when considered difficult. A Krukal-Wallis test determined these differences to be
highly significant (p < 0.01).
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df2 ) = 11.7, p = 0.003**
A Tukey’s post hoc test pointed out that cannulation caused significantly more anxiety
when it was ‘difficult’, than when it was felt to be ‘easy’ (Table 5.15).
Table 4.15 Effect of ease of cannulation on anxiety following cannulation
Ease of cannulation Number Mean anxiety scores SD
Easy 104 1.1 1.8
Neutral 51 1.5 1.6
Difficult 99 1.9 2.02
Cannulation was quicker when it was perceived as an easy process (Table 4.16). On
average (mean) it took 1.7 (SD 1.4) minutes to cannulate when the process was
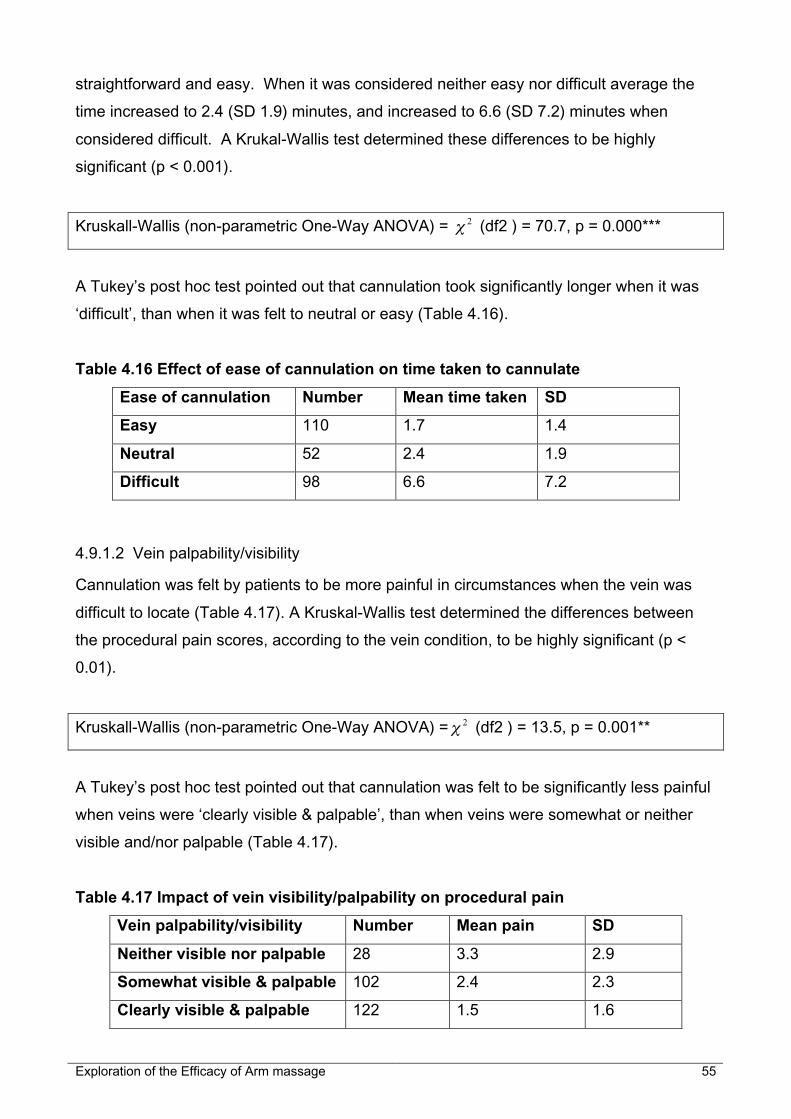
Exploration of the Efficacy of Arm massage 55
straightforward and easy. When it was considered neither easy nor difficult average the
time increased to 2.4 (SD 1.9) minutes, and increased to 6.6 (SD 7.2) minutes when
considered difficult. A Krukal-Wallis test determined these differences to be highly
significant (p < 0.001).
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df2 ) = 70.7, p = 0.000***
A Tukey’s post hoc test pointed out that cannulation took significantly longer when it was
‘difficult’, than when it was felt to neutral or easy (Table 4.16).
Table 4.16 Effect of ease of cannulation on time taken to cannulate
Ease of cannulation Number Mean time taken SD
Easy 110 1.7 1.4
Neutral 52 2.4 1.9
Difficult 98 6.6 7.2
4.9.1.2 Vein palpability/visibility
Cannulation was felt by patients to be more painful in circumstances when the vein was
difficult to locate (Table 4.17). A Kruskal-Wallis test determined the differences between
the procedural pain scores, according to the vein condition, to be highly significant (p <
0.01).
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df2 ) = 13.5, p = 0.001**
A Tukey’s post hoc test pointed out that cannulation was felt to be significantly less painful
when veins were ‘clearly visible & palpable’, than when veins were somewhat or neither
visible and/nor palpable (Table 4.17).
Table 4.17 Impact of vein visibility/palpability on procedural pain
Vein palpability/visibility Number Mean pain SD
Neither visible nor palpable 28 3.3 2.9
Somewhat visible & palpable 102 2.4 2.3
Clearly visible & palpable 122 1.5 1.6

Exploration of the Efficacy of Arm massage 56
Cannulation was associated with more anxiety in circumstances when the vein was difficult
to locate (Table 4.18). A Kruskal-Wallis test determined the differences between the
anxiety experienced, according to the vein condition, to be statistically significant (p <
0.05).
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df2 ) = 6.7, p = 0.035*
A Tukey’s post hoc test identified that cannulation was associated with significantly less
anxiety when veins were ‘clearly visible & palpable’, than when veins were ‘neither visible
nor palpable’ (Table 4.18).
Table 4.18 Impact of vein visibility/palpability on anxiety
Vein palpability/visibility Number Mean anxiety SD
Neither visible nor palpable 30 2.2 2.5
Somewhat visible & palpable 105 1.6 1.7
Clearly visible & palpable 122 1.2 1.7
As would be expected, it took longer to cannulate in circumstances when the vein was
difficult to locate (Table 4.19). A Kruskal-Wallis test determined the differences between
the times taken to cannulate, according to the vein condition, to be highly significant (p <
0.001).
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df2 ) = 41.2, p = 0.000***
A Tukey’s post hoc test pointed out that it took significantly longer time to cannulate when
veins were ‘neither visible nor palpable’, than when somewhat or clearly visible and
palpable (Table 4.19).
Table 4.19 Impact of vein visibility/palpability on time taken to cannulate
Vein palpability/visibility Number Mean (time) SD
Neither visible nor palpable 30 8.4 9.5
Somewhat visible & palpable 106 4.1 4.9
Clearly visible & palpable 127 2.2 2.3

Exploration of the Efficacy of Arm massage 57
However, it is interesting to note that although massage appeared to make veins easier to
locate (section 4.7.3 – Table 4.10), this did not translate into those in the massage group
being easier to cannulate, or experiencing less pain (section 4.7.1.2 – Table 4.6) or anxiety
(section 4.7.2.2 – Table 4.8).
Once again, as would be expected, there were more successful cannulations on first
attempt when the vein was easy to locate (Table 4.20). A Chi-square test showed a
significant association between the ease with which a vein was located and the successful
placing of a cannula on first attempt (p < 0.001).
Chi-square test = 2χ (df2 ) = 16.7, p = 0.000***
71% of failures to cannulate on first attempt occurred when the vein was ‘somewhat’
difficult to locate or ‘neither visible nor palpable’ (Table 4.20).
Table 4.20 Association between vein palpability/visibility and cannulation on first
attempt
Vein palpability/visibility Didn’t Fail
N (%)
Failed attempt (s)
N (%)
Total
N (%)
Neither visible nor palpable 16 (9) 15 (23) 31 (12)
Somewhat visible & palpable 76 (38) 32 (48) 108 (41)
Clearly visible & palpable 106 (53) 19 (29) 125 (47)
Total 198 (100) 66 (100) 264 (100)
4.9.1.3 Nurse cannulating
The nurse cannulating appeared to be an important factor with respect to the time taken to
cannulate, and with regards to successful placing of cannulae on first attempt. This was
revealed when data from all cannulations performed by the individual nurses were
aggregated. Data were combined for those nurses that had performed less than 19
cannulations over the study period (Tables 4.21 to 4.24). Analysis of variance through
conduct of a Kruskal-Wallis test confirmed the differences between the nurses cannulating
were statistically significant (p < 0.001).

Exploration of the Efficacy of Arm massage 58
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df5 ) = 52.6, p = 0.000***
Table 4.21 confirms that some nurses took half as long as others to cannulate. There was
great variation in speed between the different nurses.
Table 4.21 Time taken to cannulate according to the nurse that cannulated
Nurse ID No. cannulations
performed
Mean time
(mins)
SD Range
(mins)
A 84 3.9 6.9 0.5 – 40
B 57 2.7 3.1 0.5 –15
C 54 2.4 3.9 0.5 – 25
D 29 6.5 3.6 1 – 15
E 19 3.6 5.2 0.5 – 23
Others: F, G, H & I 20 4.6 3.3 1 –15
A Tukey’s post hoc test identified that nurses B and C were significantly quicker at
cannulating when compared to the other nurses, while nurse D was significantly less swift
than the others.
Further chi-square analysis determined that there was a statistically significant difference
between the different nurses’ and their ability to cannulate successfully on first attempt (p <
0.05).
Chi-square test = 2χ (df5 ) = 13.8, p = 0.017*
Analysis of variance through conduct of a Kruskal-Wallis test found no statistically
significant difference between the nurse cannulating and the pain experienced by patients
following cannulation (p > 0.05).
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df5 ) = 1.9, p = 0 .9 (ns)
Pain scores did not differ greatly according to the nurse cannulating (Table 4.22)

Exploration of the Efficacy of Arm massage 59
Table 4.22 Procedural pain according to the nurse that cannulated
Nurse ID No. cannulations
performed
Mean pain SD
A 86 2.1 2.2
B 54 2.02 2.1
C 52 2.2 2.3
D 27 2.1 2.2
E 18 2.3 1.8
Others: F, G, H & I 15 1.7 2.3
Analysis of variance through conduct of a Kruskal-Wallis test found no statistically
significant difference between the nurse cannulating and the anxiety experienced by
patients following cannulation (p > 0.05).
Kruskall-Wallis (non-parametric One-Way ANOVA) = 2χ (df5 ) = 2.3, p = 0.8 (ns)
Anxiety scores did not differ greatly according to the nurse cannulating (Table 4.23)
Table 4.23 Anxiety following cannulation according to the nurse that cannulated
Nurse ID No. cannulations
performed
Mean anxiety SD
A 85 1.5 1.9
B 52 1.5 1.7
C 54 1.7 2.2
D 29 1.2 1.8
E 18 1.3 1.3
Others: F, G, H & I 19 1.3 1.9
Table 4.24 below suggests that the nurses had differing levels of skill – unless particular
nurses always cannulated patients with difficult veins, and thus the findings reflect this
factor rather than the nurses’ skills.

Exploration of the Efficacy of Arm massage 60
Table 4.24 Failed cannulation according to the nurse that cannulated
Nurse ID No failed attempt
N (%)
Failed attempt(s)
N (%)
Total
N (%)
A 58 (67) 28 (33) 86 (100)
B 45 (79) 12 (21) 57 (100)
C 49 (92) 4 (8) 53 (100)
D 19 (66) 10 (34) 29 (100)
E 13 (68) 6 (32) 19 (100)
Others: F, G, H & I 14 (70) 6 (30) 20 (100)
Evidence in Tables 4.21 and 4.24 demonstrate that nurses referred to as Nurses B and C
were both more rapid and successful in their attempts to cannulate than others
undertaking this task. Findings from analysis of the stakeholder and patient interview data
suggest that nurses’ differing skill is an important factor. Both the patients themselves and
the nurse in charge of the Day Unit explained the importance of skill and experience.
The nurse in charge of the Day Unit was clear in outlining factors that aid successful
cannulation, and these included “definitely the experience of the nurse, her confidence.
Getting to know the patient, there’s definitely an aspect of that…you do get to know their
veins…So it’s the experience of the nurses, their confidence”.
When patients reported experiencing pain following cannulation, they often blamed it on
their veins and removed blame from the person cannulating. Nevertheless, 27% of those
interviewed commented that the level of pain they felt varied depending on the
‘experience’ of the nurse who cannulated: ‘some are absolutely brilliant, some, you know,
need a bit more practice basically. I mean, there’s nothing you can do about it. There’s no
substitute for experience’ (024). ‘Some people seem to do it…might do it easier that
others, and others have a problem with it…I think it’s more (problematic) when it’s the
experienced, inexperienced ones, but then they’ve got to learn, haven’t they?’ (010).
4.9.1.4 Cannula size
A Mann Whitney test found a statistically significant difference between the size of the
cannula used and the anxiety experienced by patients following cannulation (p < 0.05).

Exploration of the Efficacy of Arm massage 61
Non-parametric independent samples t-test (Mann Whitney) = z = -2.15, p = 0.032*
Typically, being cannulated with a 22 cannula was associated with more anxiety (Table
4.25).
Table 4.25 Effect of cannula size on anxiety
Study group Anxiety after cannulation
Mean (SD)
Range z-value p-value
22 cannula 1.6 (1.8) 0-9
24 cannula 1.2 (1.9) 0-9
-2.15 0.032*
Furthermore, conduct of a Mann Whitney test found a statistically significant difference
between the size of cannula used and procedural pain experienced by patients following
cannulation (p < 0.001).
Non-parametric independent samples t-test (Mann Whitney) = z = -4.69, p = 0.000***
Typically, being cannulated with a 22 cannula was associated with more procedural pain
(Table 4.26).
Table 4.26 Effect of cannula size on procedural pain
Study group Procedural Pain
Mean (SD)
Range z-value p-value
22 cannula 2.4 (2.1) 0-10
24 cannula 1.4 (2.1) 0-9
-4.69 0.000***
The fact that patients were more anxious and experienced more pain when cannulated
with a smaller needle is counterintuitive. In the main, women (78%) we cannulated using a
size 22 cannula. Therefore, it is possible that the anxiety and pain reported relates to the
fact that those cannulated with the smaller sized cannulas they were predominantly female
(See section 4.9.2.1).

Exploration of the Efficacy of Arm massage 62
Nevertheless, cannula size did not have an effect on the process itself, as neither he time
taken to cannulate was not impacted significantly by the size of cannula (Mann-Whitney
test, 2-tailed, p = 0.48), nor was failure to cannulate (Chi-square, p = 0.19).
4.9.2 Demographic factors affecting cannulation
The impact of specific demographic factors that were constant over time (including gender,
age and treatment regime) on the cannulation process was determined.
The following features of cannulation were included in the analysis: time taken to
cannulate, pain associated with the procedure, and anxiety following cannulation.
4.9.2.1 Gender
It was decided to look at the impact of gender in recognition that men and women may
react to stressful situations and medical procedures, including cannulation for
chemotherapy, differently.
Analysis of data relating to successful insertion of cannula at first attempt identified that
there were differences between men and women (p < 0.05).
Fisher exact test (Chi-square analysis) = 2χ (df1 ) = 5.82, p = 0.016*
Females failed to be cannulated on first attempt on 30% of occasions, while this failure
occurred on only 16% of occasions for males (Table 4.27).
Table 4.27 Association between gender and insertion of cannula on first attempt
Number of failed
attempts
Male
N %
Female
N %
2χ statistic p-value
None
One or more
74 (84)
14 (16)
124 (70)
52 (30)5.8 0.016*
Likewise, analysis of data relating to the time taken to cannulate men and women in the
sample identified that there did appear to be a gender difference (p < 0.001)

Exploration of the Efficacy of Arm massage 63
Non-parametric independent samples t-test (Mann Whitney) = z = -3.8, p=0.000***
Women took significantly longer to cannulate than men (Table 4.28)
Table 4.28 Time taken to cannulate (in mins) according to gender
Gender Mean (SD) Range z-value p-value
Male 2.3 (2.4) 0.5 – 14
Female 4.3 (5.9) 0.5 – 40
-3.8 0.000**
The relationship between gender and time taken to cannulate is further exemplified in
figure 4.3:
Figure 4.3 Time taken to cannulate according to gender
Time to cannulate
Above 5 minutes
2 to 5 minutes
1 to 2 minutes
1min and under
Cou
nt
70
60
50
40
30
20
10
0
Gender of patient
Male
Female

Exploration of the Efficacy of Arm massage 64
Data were then analysed to see whether the condition of men and women’s veins prior to
cannulation differed. This suggested that they did significantly (p < 0.001)
Chi-square test = 2χ (df2 ) = 60.4, p = 0.000***
Outcome of this analysis suggested that women had veins that were significantly more
difficult to locate prior to the procedure than men (Table 4.29).
Table 4.29 Association between gender and vein palpability/visibility prior to
cannulation
Vein palpability/visibility Male
N %
Female
N %
2χ statistic p-value
Neither visible nor palpable
Somewhat visible & palpable
Clearly visible & palpable
1 (1)
16 (18)
72 (81)
30 (17)
92 (52)
55 (31)
60.4 0.000
The apparently greater difficulty with cannulating women was reflected in data relating to
pain following cannulation (p < 0.001)
Non-parametric independent samples t-test (Mann Whitney) = z = -6.75, p = 0.000***
However, women not only reported significantly greater pain than men, they also
experienced a greater range of pain (0-10) than men. Men reported relatively low levels of
pain associated with the procedure (0-3) (Table 4.30).
Table 4.30 Procedural pain following cannulation experienced according to gender
Study group P a i n f o l l o w i n g
cannulation
Mean (SD)
Range z-value p-value
Male 0.86 (0.96) 0 – 3
Female 2.7 (2.3) 0 – 10
-6.75 0.000

Exploration of the Efficacy of Arm massage 65
Chi-square analyses were conducted on the data recording pain following cannulation.
These data were recoded to provide three classifications of pain (low, medium and high –
See section 3.12.1) (Table 4.31). These tests confirmed the statistically significant
association between gender and pain experienced following cannulation (p < 0.001).
Chi-square test = 2χ (df2 ) = 33.6, p = 0.000**
There was a clear difference between the groups with 1/3 of women reporting medium or
high levels of pain following cannulation. None of the men at any stage registered more
than a low level of pain (Table 4.31)
Table 4.31 Association between gender and level of pain following cannulation
Pain fo l lowing
cannulation
Men
N ( %)
Women
N (%)
2χ statistic p-value
Low pain
Medium pain
High pain
84 (100)
0 -
0 -
115 (68)
36 (21)
17 (11)
33.6 0.000
As previously reported, 70% of women interviewed reported having veins that were
problematic to cannulate, resulting in pain. One lady expressed during her interview: ‘They
had terrible problems trying to find my veins as well, which had added to the grief’ (021).
This differed markedly to the explanations provided by the men that were interviewed.
They revealed that in general they did not find cannulation painful. They appeared to
adapt to the cannulation process and associated discomfort – to them it became routine.
As one gentleman said, it was ‘not painful so I would cry out “ouch” or anything like
that...No, I mean, it’s mildly discomfortable. Uncomfortable. But I wouldn’t put it any higher
than that’ (003).
The apparently greater difficulty with cannulating women was further reflected in data
relating to anxiety after cannulation (p < 0.001).
Non-parametric independent samples t-test (Mann Whitney) = z = -6.6, p = 0.000***

Exploration of the Efficacy of Arm massage 66
Women not only reported significantly greater anxiety than men, they also experienced a
greater range of anxiety (0-9) than men. Men reported relatively low levels of anxiety
associated with the procedure (0-3) (Table 4.32).
Table 4.32 Anxiety following cannulation experienced according to gender
Study
group
Anxiety following cannulation
Mean (SD)
Range z-value p-value
Male 0.5 (0.8) 0 – 3
Female 1.9 (2.01) 0 – 9
-6.6 0.000***
Chi-square analyses were conducted on the data recording anxiety following cannulation.
These data were recoded to provide three classifications of anxiety (low, medium and high
– See Table 5.31). These tests confirmed the statistically significant association between
gender and anxiety experienced following cannulation (p < 0.001).
Chi-square test = 2χ (df2 ) = 19.4, p = 0.000***
There was a clear difference between the groups with 20% of women reporting medium or
high levels of anxiety following cannulation. None of the men at any stage registered over
low levels of anxiety (Table 4.33).
Table 4.33 Association between gender and anxiety following cannulation
Anxiety following
cannulation
Men
N ( %)
Women
N (%)
2χ statistic p-value
Low pain
Medium pain
High pain
85 (100)
0 -
0 -
138 (80)
27 (16)
7 (4)
19.4 0.000

Exploration of the Efficacy of Arm massage 67
4.9.2.2 Age
To determine whether age was a factor that impacted on the cannulation process, the age
data were coded into those under or over the age of 56. Analyses were then undertaken to
determine whether there were differences according to age with regards to time taken to
cannulate, successful cannulation on first attempt and on anxiety and pain associated with
the procedure.
Initial analysis was undertaken through conduct of Mann-Whitney and Chi-Square tests to
determine any differences between the two age groups with regards to time taken to
cannulate, or the success/failure rate in placing cannula on first attempt. These revealed
no statistically significant differences between age and successful insertion of cannula on
first attempt (p = 0.248), or between age and time taken to cannulate (p = 0.076).
The levels of pain reported by the sample were then analysed to determine whether there
were differences according to participants’ age. This was ascertained through conduct of
a Mann-Whitney test; a statistically significant difference was confirmed (p < 0.001).
Non-parametric independent samples t-test (Mann Whitney) = z = -7.51, p=0.000***
This analysis suggested that younger patients reported significantly greater pain following
cannulation than older patients (p < 0.001) (Table 4.34).
Table 4.34 Procedural pain following cannulation experienced according to age
Study group Pain following cannulation
Mean (SD)
Range z-value p-value
24-55 yrs 3.5 (2.2) 0 – 8
56-79 yrs 1.5 (1.8) 0 – 10
-7.51 0.000***
When further chi-square analysis was undertaken this association became more evident (p
< 0.001).
Chi-square test = 2χ (df2 ) = 28.4, p = 0.000***
It appears that only 12% of individuals aged 56 years and over experienced medium or
high levels of pain in comparison with over 40% of those in the younger age group (Table
4.35).

Exploration of the Efficacy of Arm massage 68
Table 4.35 Association between age and level of pain following cannulation
Pain following
cannulation
24-55 yrs
N %
56-79 yrs
N %
2χ statistic p-value
Low pain
Medium pain
High pain
45 (58)
21 (27)
11 (15)
154 (88)
15 (9)
6 (3)
28.4 0.000***
Similar tests were conducted on data recording patients’ levels of anxiety. This analysis
determined that younger patients also reported significantly greater anxiety following
cannulation than older patients (p < 0.001) (Table 4.36).
Table 4.36 Anxiety experienced after cannulation according to age
Study group Anxiety following cannulation
Mean (SD)
Range z-value p-value
24-55 yrs 2.84 (2.1) 0 – 9
56-79 yrs 0.86 (1.3) 0 – 8
-8.05 0.000
Once again, chi-square analysis clarified the association between patients’ age and
anxiety experienced following cannulation (p < 0.001).
Chi-square test = 2χ (df2 ) = 37.7, p = 0.000***
Nearly all those in the older age group reported low anxiety after the procedure (96%)
whereas 32% of younger patients reported feeling medium or high levels of anxiety
afterwards (Table 4.37).
Table 4.37 Association between age and anxiety experience after cannulation
Anxiety following
cannulation
24-55 yrs
N %
56-79 yrs
N %
2χ statistic p-value
Low anxiety
Medium anxiety
High anxiety
54 (68%)
21 (26%)
5 (6%)
169 (96%)
6 (3%)
2 (1%)
37.7 0.000***

Exploration of the Efficacy of Arm massage 69
Tests were also conducted on data recording the time taken to cannulate patients. This
analysis determined that there was not a statistically significant difference between the
time taken to cannulate younger patients when compared to older patients (p > 0.05)
(Table 4.38). However, the difference between the time taken to cannulate and age did
approach significance; older patients appeared to be cannulated quicker on average.
Table 4.38 Time taken to cannulate according to age
Study group Time to cannulate
Mean (SD)
Range
(mins)
z-value p-value
24-55 yrs 4.3 (5.2) 0.5 – 30
56-79 yrs 3.4 (5.01) 0.5 – 40
-1.8 0.08 (ns)
Chi-square analysis showed a lack of clear association between patients’ age and the time
taken to cannulate them (p > 0.05).
Chi-square test = 2χ (df3 )= 5.9, p = 0.1 (ns)
It is of interest to note that almost half of those in the older age group were cannulated in
under a minute (48%), when compared to the younger group (37%). Furthermore, _ of the
younger patients took more than 5 minutes to cannulate (Table 4.39).
Table 4.39 Association between age and time taken to cannulate
Time to cannulate 24-55 yrs
N %
56-79 yrs
N %
2χ statistic p-value
1 min and under
1 to 2 minutes
2 to 5 minutes
Above 5 minutes
30 (37%)
19 (23%)
12 (15%)
20 (25%)
87 (48%)
33 (18%)
35 (19%)
27 (15%)
5.9 0.1 (ns)
4.9.2.3 Nature of regime
The impact of treatment type on the cannulation process was investigated. This was
undertaken in realisation that the vesicant nature of chemotherapeutic agents often makes

Exploration of the Efficacy of Arm massage 70
repeated cannulation for the administration of treatment difficult. To do this, regimes were
classified as either vesicants or as irritants/non vesicants (Table 4.40).
Table 4.40 Chemotherapy regime classifications
Vesicants Irritants/Non vesicants
Cisplatin & Etoposide
CHOP
FEC
Epirubicin + Cyclophosphomide
ABVD
Single Epirubicin
Weekly 5FU +/- folinic acid
Carboplatin & Etoposide
Analysis was then undertaken to determine the impact of treatment classification on time
taken to cannulate, number of failed attempts when cannulating and on pain and anxiety
associated with the procedure.
Conduct of Chi-square tests determined that vesicant regimes were significantly
associated with failed cannulation attempts (p < 0.01) (Table 4.41).
Chi-square test = 2χ (df1 ) = 8.99, p = 0.003**
Failure to cannulated occurred when the treatment was a vesicant drug regime in 29% of
cases, while failure only occurred in 15% of cases when the treatment was non-vesicant or
an irritant (Table 4.41)
Table 4.41 Association between nature of regime and insertion of cannula on first
attempt
Number of failed
attempts
Vesicant
N %
Other
N %
2χ statistic p-value
None
One or more
122 (71)
51 (29)
86 (85)
15 (15)
8.99 0.003**
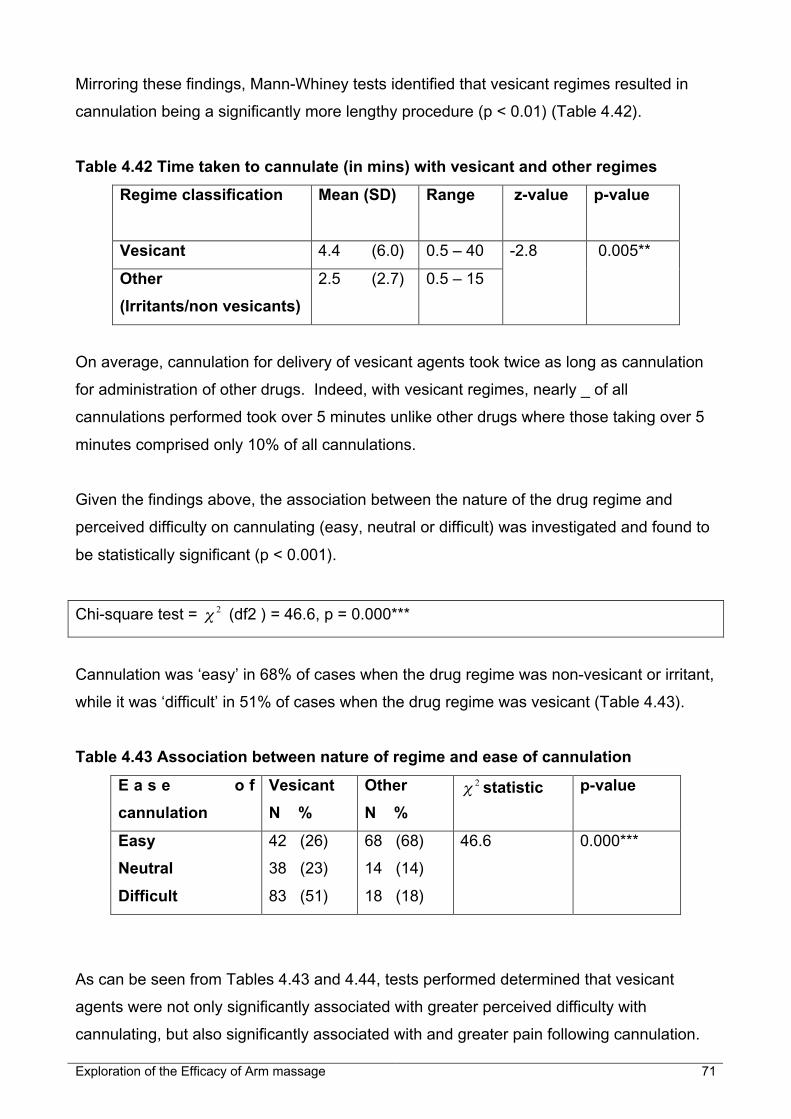
Exploration of the Efficacy of Arm massage 71
Mirroring these findings, Mann-Whiney tests identified that vesicant regimes resulted in
cannulation being a significantly more lengthy procedure (p < 0.01) (Table 4.42).
Table 4.42 Time taken to cannulate (in mins) with vesicant and other regimes
Regime classification Mean (SD) Range z-value p-value
Vesicant 4.4 (6.0) 0.5 – 40
Other
(Irritants/non vesicants)
2.5 (2.7) 0.5 – 15
-2.8 0.005**
On average, cannulation for delivery of vesicant agents took twice as long as cannulation
for administration of other drugs. Indeed, with vesicant regimes, nearly _ of all
cannulations performed took over 5 minutes unlike other drugs where those taking over 5
minutes comprised only 10% of all cannulations.
Given the findings above, the association between the nature of the drug regime and
perceived difficulty on cannulating (easy, neutral or difficult) was investigated and found to
be statistically significant (p < 0.001).
Chi-square test = 2χ (df2 ) = 46.6, p = 0.000***
Cannulation was ‘easy’ in 68% of cases when the drug regime was non-vesicant or irritant,
while it was ‘difficult’ in 51% of cases when the drug regime was vesicant (Table 4.43).
Table 4.43 Association between nature of regime and ease of cannulation
E a s e o f
cannulation
Vesicant
N %
Other
N %
2χ statistic p-value
Easy
Neutral
Difficult
42 (26)
38 (23)
83 (51)
68 (68)
14 (14)
18 (18)
46.6 0.000***
As can be seen from Tables 4.43 and 4.44, tests performed determined that vesicant
agents were not only significantly associated with greater perceived difficulty with
cannulating, but also significantly associated with and greater pain following cannulation.

Exploration of the Efficacy of Arm massage 72
Table 4.44 Procedural pain following cannulation experienced with vesicant and
other regimes
Study group Pain following cannulation
Mean (SD)
Range z-value p-value
Vesicant 2.8 (2.3) 0-10
Other 0.9 (0.3) 0-9
-7.4 0.000**
When level of pain was classified into low, medium and high and crosstabulated by nature
of regime, this association between regime and pain following cannulation was highly
significant (p <0.001).
Chi-square test = 2χ (df2 ) = 28.7, p = 0.000***
Nearly all those in receipt of non-vesicant drugs reported low pain following cannulation
whereas 1/3 of those prescribed vesicant ones reported medium or high pain (Table 4.45).
Table 4.45 Association between nature of regime and level of pain following
cannulation
E a s e o f
cannulation
Vesicant
N %
Other
N %
2χ statistic p-value
Low pain
Medium pain
High pain
108 (68)
34 (22)
16 (10)
91 (97)
3 (2)
1 (1)
28.7 0.000***
Tests performed determined that vesicant agents were significantly associated with
greater anxiety following cannulation (p < 0.001) (Table 4.46).

Exploration of the Efficacy of Arm massage 73
Table 4.46 Anxiety following cannulation experienced with vesicant and other
regimes
Study group Anxiety following cannulation
Mean (SD)
Range z-value p-value
Vesicant 1.9 (1.9) 0-9
Other 0.7 (1.3) 0-8
-6.3 0.000***
A chi-square test further reinforced the previous findings; anxiety was classified into low,
medium and high and crosstabulated by nature of regime. This association between
regime and anxiety following cannulation was highly significant (p < 0.01).
Chi-square test = 2χ (df2 ) = 13.7, p = 0.001**
It was found that nearly all those in receipt of non-vesicant or irritant drugs reported low
anxiety following cannulation whereas 19% of those prescribed vesicant ones reported
medium or high anxiety (Table 4.47).
Table 4.47 Association between nature of regime and anxiety following cannulation
Ease of cannulation Vesicant
N %
Other
N %
2χ statistic p-value
Low anxiety
Medium anxiety
High anxiety
130 (81)
25 (15)
6 (4)
93 (97)
2 (2)
1 (1)
13.7 0.001
4.9.3 Experience of first treatment
It was anticipated that patients could find their first ever cannulation for chemotherapy
more difficult and stressful than subsequent ones since they were uncertain of what to
expect, and many had been recently diagnosed. To determine whether this was the case,
the data recorded at first cycle were compared with two subsequent ones (Table 4.48)
through conducting Friedmann’s tests. The five variables analysed in this manner were:
the time taken to cannulate; and both the anticipated and procedural pain experienced by
participants. These determined that feelings recorded immediately prior to cannulation,
i.e. anxiety prior to cannulation and anticipated pain, for first treatment, were significantly

Exploration of the Efficacy of Arm massage 74
higher than those reported on subsequent cycles. This was not the case with procedural
pain, anxiety after cannulation or the time taken to cannulate. There were no statistically
significant differences in the latter variables over time.
Table 4.48 Trends in anxiety and anticipated pain over time
Mean Chi-square
statistic
DF p-value
Anxiety pr ior to 1st
chemotherapy cycle
2.49
Anxiety prior to 2nd
chemotherapy cycle
1.66
Anxiety pr ior to 3rd
chemotherapy cycle
1.85
7.73 2 0.021 *
Pain anticipated prior to 1st
chemotherapy cycle
2.30
Pain anticipated prior to 2nd
chemotherapy cycle
1.66
Pain anticipated prior to 3rd
chemotherapy cycle
2.04
10.9 2 0.004**
4.10 Models explaining factors impacting on cannulation
Regression models were constructed to ascertain factors that impacted on 5 key
dependant variables: Anxiety before and after cannulation, anticipated pain and actual
experienced pain, and time taken to cannulate.
A two-stage process was used to arrive at the models reported in this section:
1) Stage one: Inferential statistical tests (including Mann-Whitney and Chi-square
tests) were carried out involving the 5 dependant variables (presented in previous
sections).
2) Stage two: Various models were constructed to predict each of the 5 dependant
variables. More than one model was constructed to explain each one because the
number of possible contributing factors was too great to place in one model. A high

Exploration of the Efficacy of Arm massage 75
number of factors placed in a model can give rise to a large error value. This can
result in derivation of spurious results.
The modelling process used in step two entailed backwards stepwise elimination of non-
significant (and therefore non-impacting) main effects and 2-way interactions from the
models. Main effects are independent variables that impact on the dependent one. Two-
way interactions comprise the effect on the dependant variable created by two
independent factors interacting together. Main effects were only removed from the model
when all its interactions with other factors had been removed. Therefore in the results
presented within this section of the chapter, the reader will notice that non-significant main
effects remain in a model where they contribute to a significant interaction effect.
(Interaction effects are denoted by a §).
4.10.1 Model explaining anxiety prior to cannulation
In Table 4.49, the reader will note that factors in previous sections that appeared to impact
on anxiety prior to cannulation (age, gender, anticipated pain and massage group) were
incorporated into the model. Through backwards stepwise regression, it became apparent
that factors that did contribute to feelings of anxiety prior to cannulation were anticipated
pain, gender and the intervention group to which participants were allocated.
Table 4.49 Model of factors impacting on anxiety prior to cannulation
Dependant
variable
Factors Resulting factors
Anxiety prior to
cannulation
• Massage group
• Age group
• Gender
• Anticipated pain
(Covariate)
• Massage group (p = 0.02*)
• Gender (p = 0.002**)
• Anticipated pain
(p = 0.000***)
Patients were significantly more anxious prior to cannulation when they did not have
massage, were female, or anticipated experiencing high levels of pain following
cannulation (Appendix 10).

Exploration of the Efficacy of Arm massage 76
4.10.2 Model explaining anxiety following cannulation
Once again, factors identified from previous analyses as impacting on anxiety following
cannulation (age, gender, cannulating nurse, average pain following cannulation) were
incorporated into the model along with the intervention group people were allocated to
(Table 4.50). Through backwards stepwise regression, it became apparent that many
factors contributed to feelings of anxiety following cannulation. Significant main effects
included age, pain typically experienced following cannulation and the intervention group
individuals were randomised to. Furthermore, interactions between gender and massage
group, massage group and average cannulation pain, and the nurse cannulating and
average pain were statistically significant factors.
Table 4.50 Model of factors impacting on anxiety following cannulation
Dependant
Variable
Factors Resulting factors
Anxiety
Following
Cannulation
• Massage group
• Age group
• Gender
• Nurse ID
• Grouped average pain
scores following
cannulation
• Massage group (p = 0.014*)
• Age group (p = 0.000***)
• Gender (p = 0.073) (§)
• Nurse ID (p = 0.083) (§)
• Average pain (p = 0.000***)
• Gender x Massage (p = 0.037*)
• Massage x Average pain
(p = 0.000***)
• Nurse ID x Average pain
(p = 0.039*)
§ No significant main effect but remain in the model as they contribute to a significant interaction with
another factor
From this model it appeared that individuals felt more anxiety after cannulation if they were
younger, typically found cannulation painful, and were not in receipt of massage prior to
the procedure. Furthermore, interaction effects suggested men that did not have massage
were susceptible to feeling anxious after cannulation, as were people that did not have
massage but typically experienced medium ranking (or more) pain. The model also
identified a statistically significant interaction effect between the cannulating nurse and the
pain typically experienced following cannulation. This final interaction effect suggests that
when particular nurses cannulated and the procedure was typically associated with
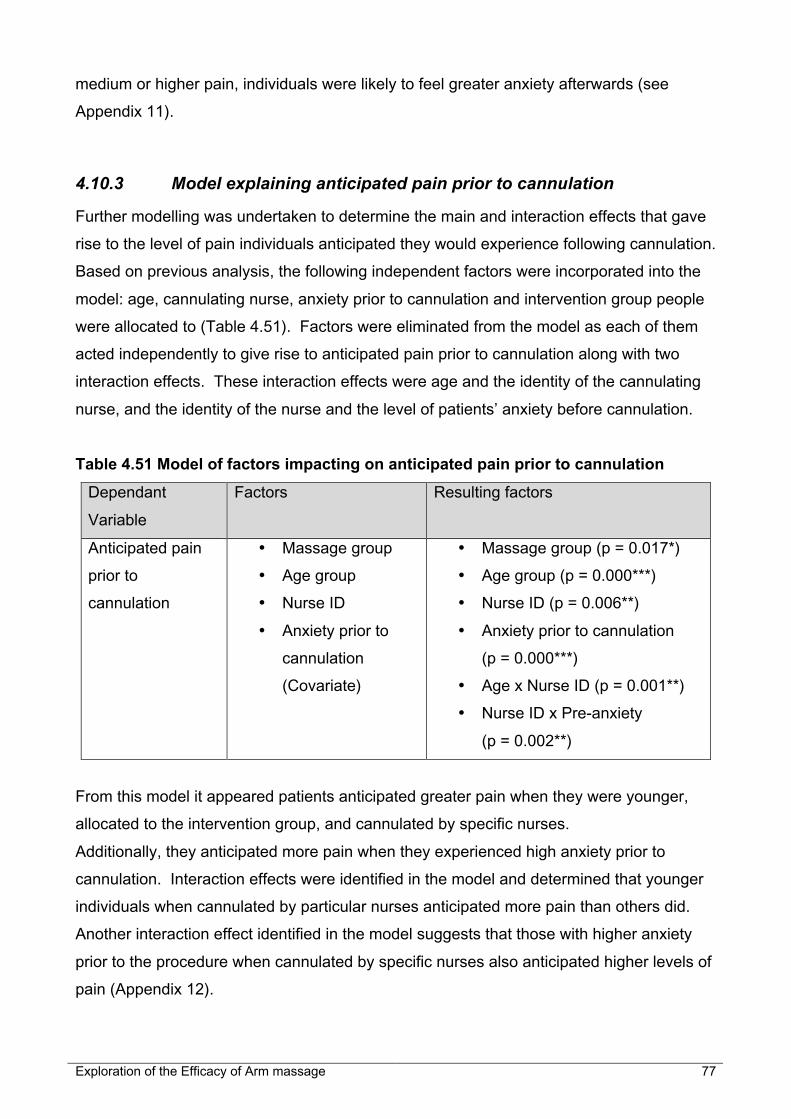
Exploration of the Efficacy of Arm massage 77
medium or higher pain, individuals were likely to feel greater anxiety afterwards (see
Appendix 11).
4.10.3 Model explaining anticipated pain prior to cannulation
Further modelling was undertaken to determine the main and interaction effects that gave
rise to the level of pain individuals anticipated they would experience following cannulation.
Based on previous analysis, the following independent factors were incorporated into the
model: age, cannulating nurse, anxiety prior to cannulation and intervention group people
were allocated to (Table 4.51). Factors were eliminated from the model as each of them
acted independently to give rise to anticipated pain prior to cannulation along with two
interaction effects. These interaction effects were age and the identity of the cannulating
nurse, and the identity of the nurse and the level of patients’ anxiety before cannulation.
Table 4.51 Model of factors impacting on anticipated pain prior to cannulation
Dependant
Variable
Factors Resulting factors
Anticipated pain
prior to
cannulation
• Massage group
• Age group
• Nurse ID
• Anxiety prior to
cannulation
(Covariate)
• Massage group (p = 0.017*)
• Age group (p = 0.000***)
• Nurse ID (p = 0.006**)
• Anxiety prior to cannulation
(p = 0.000***)
• Age x Nurse ID (p = 0.001**)
• Nurse ID x Pre-anxiety
(p = 0.002**)
From this model it appeared patients anticipated greater pain when they were younger,
allocated to the intervention group, and cannulated by specific nurses.
Additionally, they anticipated more pain when they experienced high anxiety prior to
cannulation. Interaction effects were identified in the model and determined that younger
individuals when cannulated by particular nurses anticipated more pain than others did.
Another interaction effect identified in the model suggests that those with higher anxiety
prior to the procedure when cannulated by specific nurses also anticipated higher levels of
pain (Appendix 12).
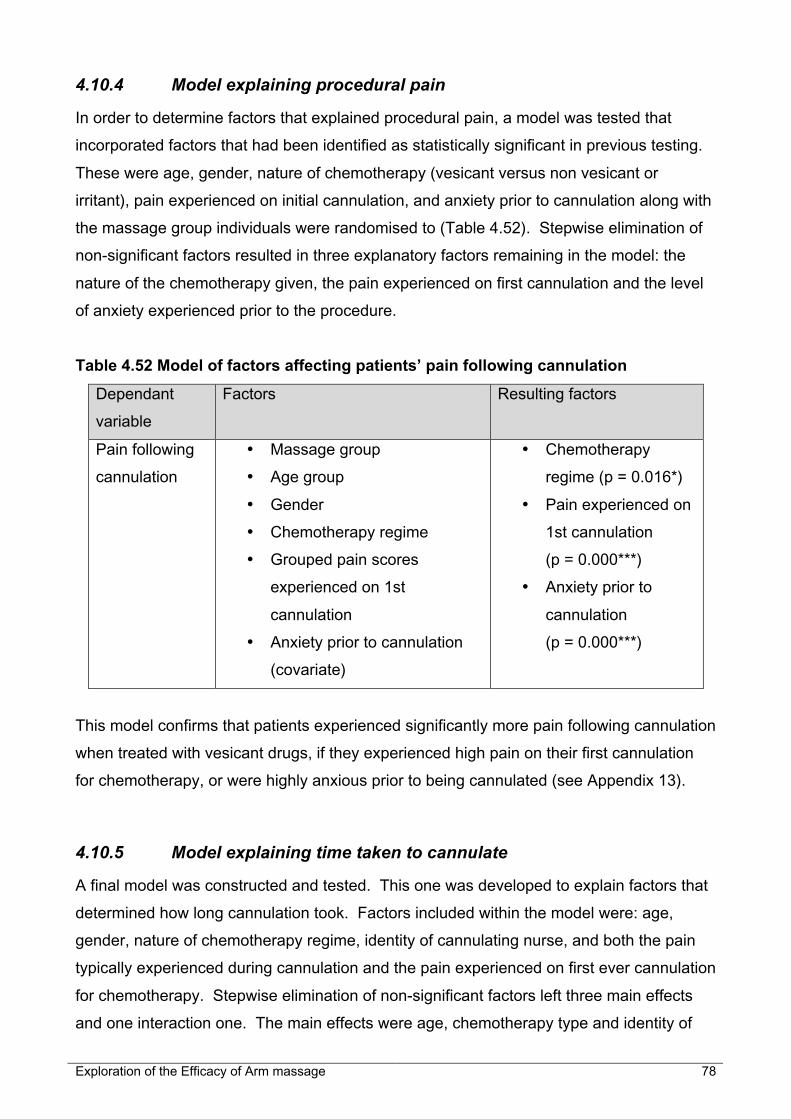
Exploration of the Efficacy of Arm massage 78
4.10.4 Model explaining procedural pain
In order to determine factors that explained procedural pain, a model was tested that
incorporated factors that had been identified as statistically significant in previous testing.
These were age, gender, nature of chemotherapy (vesicant versus non vesicant or
irritant), pain experienced on initial cannulation, and anxiety prior to cannulation along with
the massage group individuals were randomised to (Table 4.52). Stepwise elimination of
non-significant factors resulted in three explanatory factors remaining in the model: the
nature of the chemotherapy given, the pain experienced on first cannulation and the level
of anxiety experienced prior to the procedure.
Table 4.52 Model of factors affecting patients’ pain following cannulation
Dependant
variable
Factors Resulting factors
Pain following
cannulation
• Massage group
• Age group
• Gender
• Chemotherapy regime
• Grouped pain scores
experienced on 1st
cannulation
• Anxiety prior to cannulation
(covariate)
• Chemotherapy
regime (p = 0.016*)
• Pain experienced on
1st cannulation
(p = 0.000***)
• Anxiety prior to
cannulation
(p = 0.000***)
This model confirms that patients experienced significantly more pain following cannulation
when treated with vesicant drugs, if they experienced high pain on their first cannulation
for chemotherapy, or were highly anxious prior to being cannulated (see Appendix 13).
4.10.5 Model explaining time taken to cannulate
A final model was constructed and tested. This one was developed to explain factors that
determined how long cannulation took. Factors included within the model were: age,
gender, nature of chemotherapy regime, identity of cannulating nurse, and both the pain
typically experienced during cannulation and the pain experienced on first ever cannulation
for chemotherapy. Stepwise elimination of non-significant factors left three main effects
and one interaction one. The main effects were age, chemotherapy type and identity of

Exploration of the Efficacy of Arm massage 79
the nurse. The interaction effect that was statistically significant within the model was one
between age and the identity of the nurse performing the procedure (Table 4.53).
Table 4.53 Model of factors affecting time taken to cannulate patients
Dependant
variable
Factors Resulting factors
Time taken to
cannulate
• Age group
• Gender
• Chemotherapy regime
• Nurse ID
• Grouped pain scores
experienced on 1st
cannulation
• Average pain following
cannulation (Covariate)
• Age group (p = 0.032*)
• Chemotherapy regime
(p = 0.025*)
• Nurse ID (p = 0.001**)
• Age x Nurse ID
(p = 0.01**)
This model determines that individuals take longer to cannulate when the procedure is
undertaken by particular nurse(s), and when patients are younger and in receipt of
vesicant treatments. An interaction effect evident in the model determined that when
younger patients were cannulated by specific nurse(s) the procedure took longer than at
other times (Appendix 14).
4.11 Impact of massage service on delivery of chemotherapy day care
Previous sections of this chapter reported on the impact of massage, and other influential
factors, on individual experience. We will now turn to consider the impact of the massage
service on the atmosphere within, and delivery of care by, the Day Unit itself. This was
alluded to particularly in the stakeholder interviews and therapist focus group.
The massage therapists themselves alluded to their contribution to care delivery on the
Day Unit under investigation during the focus group. They recognised that the nursing
staff were usually very busy, and that their perception of this ‘busyness’ distanced them
from those they were providing care to. The therapists perceived that they performed a
very specific role in the treatment suite. The group discussed how they might represent a
link between the staff and patients. They felt very much ‘part of the team’ and explained
‘we’ve all got a place in that team, and we do bridge gaps between the nurses and the

Exploration of the Efficacy of Arm massage 80
medical staff and the family’. The group also hoped that the massage service would help
chemotherapy be ‘a less stressful experience’, reduce anxiety, and have a generally
positive effect through helping patients relax.
The stakeholders spoke of their visions for the massage service before it was instituted.
They explained how they had felt it would be ‘hugely successful’ and ‘very beneficial’,
through providing ‘relaxation and stress release’. They envisaged it would be ‘therapeutic’
and anticipated it would be viewed positively by both patients and staff through providing
an ‘improved’ and ‘nice atmosphere’ within the treatment suite. It was also hoped that it
would facilitate nurses’ cannulation of patients. Although the effect of massage on
cannulation remained unanswered when the stakeholder interviews were conducted, it
became apparent that their other visions had come to fruition. Patients, therapists and
stakeholders alike considered the massage service successful. It was seen as very
beneficial and enhanced the atmosphere within the Unit as a whole.
One stakeholder spoke of a particular benefit for nurses following introduction of the
massage service. They explained ‘it helps the nurses’ and ‘buys them time’ in their
schedule of administering treatment; “I think it helps the nurses. In fact I know it does. I’d
like to see the service maintained and grow with time; grow with patients that we get. I
would hate not to have anything there. And I think we’d miss being able to not being able
to offer something important to us”. Therapists themselves talked of the benefit provided to
nurses through providing ‘more hands and less formality’. They explained in the focus
group that by providing massage they were able to use and fill the time that patients had to
wait before the nurse was ready to administer treatment. The nurses were said to feel a
kind gratitude towards the therapists for their voluntary presence and contribution. One
stakeholder discussed how the therapists adapted as they integrated into the daily
workings of the Day Unit. Clearly initial stages were difficult at times as it can be a
challenge ‘having strange people coming into the treatment suite.’ However, this eased
with time as staff and volunteers got to know and appreciate each other and liaised
increasingly over time.
4.12 Impact of massage service on cancer services
Comments made by patients, stakeholders and therapists referred to the high quality
service provided to patients by the cancer services team. They also referred to the
contribution made to this by the massage service. Patients perceived the massage
initiative as ‘first class’, a ‘luxury’ worthy of recommendation to others.

Exploration of the Efficacy of Arm massage 81
Most patients in the interviews spoke highly of the general environment within the Day
Unit. They expressed the importance of feeling ‘welcome’, ‘relaxed’, ‘calm’, ‘comfortable’
and ‘stress-free’. The received view was that the massage service enhanced this within
the Day Unit.
The therapists discussed a number of ways in which the massage service might expand in
future during the focus group discussion. A few therapists mentioned how positive they
thought it would be to offer massage to carers. The group also felt it would be ‘wonderful
to see it on all the wards…to have a therapist available usually’. In this way they surmised
the service might not ‘just be offered to patients, there are nurses too that could benefit’.
The focus group spent some considerable time discussing whether therapists should be
paid for their services. They stressed that with complementary therapies becoming more
recognised professions ‘especially with college diplomas, courses that are becoming
available now’, and with the cost of training to be a therapist that ‘the way forward…in
some future time…will be paid’ posts. They hoped that posts that were remunerated would
be provided with regular one-to-one supervision and support and a clear method of
appraisal. These were areas that were considered to be lacking somewhat at present.
Further, the group expressed awareness of the need for formalised guidelines. They
articulated that guidelines or protocols were needed to standardise procedures. They also
considered that guidelines might help the issue of ‘confidentiality’. There was discussion
over how therapists should go about passing on important information about the patient
‘for their well-being, for their comfort’ to appropriate staff. Most of the group felt that the
passing on of patient-related information to staff was down to ‘common sense’, although
others did question ‘how can we breach confidentiality when we’re actually within the work
environment?’ when ‘you’re acting in the patients’ best interest’. Members of the focus
group perceived this as a grey area, and one that could do with clarification. Similarly, the
stakeholders echoed concerns and considerations regarding patient confidentiality,
support and supervision of therapists, development and use of guidelines, and the desire
of therapists to have paid posts. Funding was a key factor in considering the expansion of
the service and institution of paid therapist posts.
When looking to the future, the stakeholders talked of four ways they hoped it could be
developed in future. First, they voiced the hope that the service might be expanded to
patients in their homes. They explained that at the present time patients could end up
‘feeling quite upset when they’ve finished treatment…and we just can’t accommodate that’.
Second, they explored the possibility of having paid therapist posts in the evening. This
would allow for additional service cover in future. Another key development would be

Exploration of the Efficacy of Arm massage 82
having dedicated space, ‘facilities’ where complementary therapies could be provided.
One individual explained that ‘it would be very nice to have a proper sort of therapy
area…a proper designated area’. The final aspect that stakeholders wished to improve
was the level of cover provided by therapists. This was variable during the study, and at
times therapists struggled to come into the Day Unit, and cover for other not able to work,
in order to provide arm massage to those in the study. The stakeholders talked of their
desire for the massage service to be available full-time and expanded to cover not only
patients but carers and staff within the hospital, and even patients at home in the
community.
4.13 Summary of results
The data provided by the various approaches to data collection provided an insightful
picture of the massage service and the benefit it afforded. The results from this study
suggest that massage can be beneficial in facilitating cannulation and certainly enhances
the environment in which chemotherapy is administered. It is one factor, along with a
number of others, which can influence the pain and anxiety that accompanies the
procedure. It appears, however, to impact less on the speed at which successful
cannulation is achieved. Rathermore, the skill of the cannulating nurse is fundamental in
this respect. The demographic characteristics of individual patients play an important part
with younger women appearing to find cannulation more problematic, painful and anxiety-
provoking. Further, certain chemotherapy treatments, notably those that are more
vesicant, are more commonly associated with pain. Patients having vesicant drugs
typically prove difficult and time-consuming to cannulate.

Exploration of the Efficacy of Arm massage 83
5 Discussion
5.1 Introduction
This chapter provides a discussion of outcomes associated with introducing a massage
service for patients undergoing cannulation prior to treatment in a Chemotherapy Day Unit.
The previous chapter pointed to the marginal statistically significant benefit afforded by
massage to those in the intervention group. However, it also provided colourful
descriptions from those that had had the massage intervention, suggesting that for some it
could provide a clinically significant effect. This chapter will explore this anomaly and
discuss the role massage may have in future delivery of cancer services. Following this,
the discussion turns to consideration of factors that are associated with difficult
cannulation. The chapter then concludes by detailing the study limitations and
recommendations for future research.
5.2 Massage and cannulation
The study aimed, through adopting a multi-method research approach incorporating an
RCT to determine:
1. The value of arm massage prior to intravenous chemotherapy
2. The potential impact of this therapy for the chemotherapy service
More specifically it sought to answer whether the massage intervention
1. Reduced time taken for successful cannulation?
2. Reduced number of cannulas used?
3. Reduced pain associated with the procedure?
4. Reduced patients’ feelings of anxiety?
Results presented in the previous chapter suggested that massage had not impacted as
hypothesised. Rather, its measurable benefits were limited even though the qualitative
data strongly supported its use. The reasons for this are discussed below.
Exploration of the Efficacy of Arm massage 84
5.2.1 Massage and time taken to cannulate
Data from the Nurse Questionnaire suggested that arm massage was beneficial in
preparing patients’ veins for cannulation. A statistically significant association was
identified between massage and the vain palpabili prior to cannulation. Those massaged
had veins that were easier to locate both visually and on palpation. Twice as many in the
control group, when compared to the treatment group, had veins that the cannulating
nurses classified as ‘neither visible nor palpable’. These statistical findings were echoed in
the qualitative data. Seven women who had received massage reported that nurses found
their veins hard to locate at times. Of these, five alluded to the manner in which massage
benefited the cannulation procedure through making veins easier to access. Given this
finding, one could expect that this would be reflected in the time taken to cannulate. It
would seem logical that it would be quicker to insert a cannula into veins that are easily
located. However, this proved not to be the case in this study.
There are three plausible explanations for the above anomaly. First, it appeared that the
nurses were not accurate in their recording of time taken to cannulate. The intention was
that they recorded this time period on their own watches. However, feedback from the
nurses has indicated that in many instances they were only estimating the time taken and
thus it could be argued that the recorded time should be viewed only as a guide. Given
this, it would appear plausible that small, but important differences, in the time taken to
cannulate may have arisen but were not recorded due to the insensitivity/inaccuracy of
recording. This suggestion is lent support by the study conducted by Lenhardt et al. (29).
They determined that local warming halved cannula insertion time, but this difference
amounted to only around 20-30 seconds. If such a small difference had arisen in this
study also, it would not have been detected through the crude estimates of time that were
reported.
The second explanation for the anomaly relates to the lack of blinding in this study. The
nurses were not blind to the treatment arm patients were in. Due to lack of space, patients
received massage in the treatment suite where nurses were cannulating patients and
giving treatment. Further, there were often traces of oil on the arm that had been
massaged. Thus, it is possible that this realisation biased how they classified the condition
of patients’ veins prior to cannulation. Richardson (34) provides a discussion on the
complexities of using RCTs to evaluate complementary therapies. She, along with other

Exploration of the Efficacy of Arm massage 85
researchers including Anthony (35) suggest that blinding is often difficult to achieve in
studies of complementary therapies, as the therapist is an integral part of the intervention
and thus patients – and often others - will be aware of the group they are randomised to.
Further Richardson suggests that overemphasis on significance testing and inadequate
sample sizes often increase the probability of type 2 error and conclusions being
erroneously drawn that suggest the inefficacy of the intervention. To counteract this,
Kacperek (36) advocates incorporating patients’ views into the evaluation – the approach
used in this study.
Third, it could be argued that although patients’ veins may have been easier to locate in
those that had massage, it is possible that the residue of oil made the arm more slippery
and difficult to cannulate. If this were the case the benefit offered by massage may have
been counterbalanced by the difficulty imposed through the arm being slippery. This factor
was mentioned by one patient in their interview, and was a topic of informal discussion in
one of the steering group meetings. Thus, although this factor is worth bearing in mind, it
was not looked at specifically in this study.
5.2.2 Massage and cannula usage
Data relating to the success rate for insertion of cannulas suggested that 25% of cannulas
were not placed on first attempt. This figure supports the conduct of studies, such as this
one, that attempt to facilitate this process. Failed attempts are costly, embarrassing for the
nurse undertaking the procedure, and painful and anxiety provoking for those undergoing
it.
Analysis of data from the Nurses’ Questionnaire compared the success and failure rates
for cannulation between the two study groups. It had been hypothesised that when
massage was given there would be fewer unsuccessful attempts to cannulate. This was
not borne out in this study. Both groups reported a failure rate of around 25%; there was
failure to cannulate (with one or more attempts made before successful cannulation) in
26% of cannulations carried out within massage group, and 25% of those made within the
control group. This figure is in line with previous ones reporting failure to cannulate on first
attempt. Lenhardt et al. (29) studied the efficacy of local warming in aiding cannulation
and reported 28-30% of cannulas failed to be placed on first attempt in their control
groups. However, they determined that local warmth reduced these rates to 6%. Thus it
would appear from the current study that massage did little to reduce the number of
cannulas used, and proved less effective than local warming.

Exploration of the Efficacy of Arm massage 86
5.2.3 Massage and procedural pain
The third research question that this study sought to answer was whether arm massage
reduced the pain (both anticipated and actual) associated with cannulation. To determine
this, data were attained from the Patient Questionnaire and analysed to allow between-
group differences to be examined. These analyses suggested that both groups
anticipated similarly low pain prior to the procedure and found it relatively painless. There
were no statistically significant differences between the anticipated and procedural pain
experienced by the two study groups. The average anticipated pain (mean for both groups
2.3) was very similar to that actually experienced (mean massage group 2.2 and control
2.0). As may be expected, anticipated pain was highest prior to the first treatment cycle,
when patients had limited understanding of what they would experience, and fell with time.
It also appeared that with experience, patients learned what to expect. Over time their
anticipated and actual levels of pain became congruent.
It is worthy of note that the levels of anticipated and procedural pain reported in this study
were similar to those reported by a control group recruited to a study investigating the
efficacy of Tellington Touch in facilitating venipuncture (30). Whilst venipuncture is
different to cannulation, it is similar in so far as a needle of similar guage is inserted in to
the arm. Tellington Touch is another form of touch therapy entailing 5-minutes of gentle
physical touch. In the study by Wendler (30), a nurse trained in the procedure delivered
Telllington Touch to upper portions of participants’ shoulders, back and arms. The control
group in Wendler’s evaluation reported (on a similar scale of 0-10 with 0 being ‘no hurt’
and 10 ‘the worst possible hurt’) a mean value for anticipated pain prior to the procedure of
2.3 – the same as that reported by both study groups in the current study. As with the
current study, the control group in Wendler’s study (30) also reported low average actual
procedural pain (mean 1.4). Unlike the current study, their investigation reported on a
one-off venipuncture procedure. This might explain the discrepancies between actual and
anticipated pain that were not evident in the current study. Also, similar to the current
study, Tellington Touch appeared to impact little on the anxiety or pain associated with
gaining venous access.
Although the results of this study suggest that massage had little effect on either
anticipated or procedural pain, it is possible that a floor effect occurred with the numeric
rating scale questions. Participants generally recorded low levels of anxiety and pain and
it is possible that this floor in the response range created an instrument bias against

Exploration of the Efficacy of Arm massage 87
recording benefits of massage. If this were to be the case, improvements or benefits of
massage would be difficult to demonstrate given the low recordings typically reported.
However, the findings from the qualitative analysis provide further insight into the apparent
ineffectiveness of massage with regards to experiences of pain. It appeared that for the
relatively few individuals that found cannulation painful and stressful, massage acted as a
welcome distraction, and for some was perceived as a pampering process they looked
forward to. However, it seemed that these feelings and positive emotions were not of
sufficient strength or long lasting to influence the level of pain experienced.
Furthermore, it was apparent from the telephone interviews with patients that many of
them were not overly concerned about cannulation itself. They perceived cannulation as a
means to the end that for some was little more than inconvenient. If this was the case for
the majority of those recruited to the sample, any benefit afforded people that found the
procedure painful and anxiety-provoking would have been masked. Thus it would be
unsurprising that statistically significant results were not forthcoming and the hypotheses
put forward at the outset not supported.
5.2.4 Massage and feelings of anxiety
As with both actual and anticipated pain, patients in the study reported little anxiety in the
main, either before or after cannulation. The procedure was perceived as routine and an
aspect of treatment that they came to accept. Consequently, both study groups reported
low levels of anxiety both prior to, and after, cannulation. However, although anxiety was
low in both groups, it was 16% lower in the massage group prior to cannulation. Although
this difference was not statistically significant, it neared significance (p = 0.059). Certainly,
the comments made during telephone interviews were positive and suggested that it
helped individuals feel less daunted, and better prepared for needle insertion and ensuing
treatment.
Previous research has established that anxiety causes venous constriction. Given this
association, it would seem plausible that reduction of anxiety through whatever means,
including massage, may be reflected in veins becoming easier to access. The data from
this study lend support to this. Not only was there a trend for anxiety to be lower prior to
cannulation in the massage group, the massage group also had veins that were
significantly more visible and palpable.
Unfortunately any trends in relaxation induced by massage were negated on cannulation.
Following the procedure anxiety was similar in the two study groups. What is unclear from
Exploration of the Efficacy of Arm massage 88
this study is whether anxiety would have remained low had massage continued in some
form throughout the procedure. Further, it is unclear whether the benefits with respect to
venous access and pre-cannulation anxiety would have occurred had massage been
delivered to other areas of the body.
5.3 Massage and well being
This study suggests that there is a complex relationship between arm massage and
cannulation outcomes. It appears that for some individuals massage can aid cannulation
and make attendance for chemotherapy less stressful and more palatable. These people
stereotypically are young and female. However, there are many confounding factors other
than age and gender. It appears that the nurse undertaking the procedure and the type of
drug being administered also have a bearing on the experience and individuals’ perceived
wellbeing. Their previous experiences impact on how they anticipate and experience
future cannulation and treatment. Thus, it appears that individuals’ response to having
chemotherapy and to receiving massage is individualistic and highly complex.
Previous research and a systematic review of aromatherapy published in 2000 (37)
support the belief that massage can help to reduce anxiety in the short term, is pleasant
and acts as a mild anxiolytic in stressful situations. However, like this study the findings
do not suggest that the relaxing effects induced are sufficient to recommend that massage
be used to treat anxiety. As recognised by Cooke and Ernst (37), it appears that massage
has no lasting effects, either good or bad.
However, counter arguments would suggest that many studies, including the current one,
were sufficiently flawed to prevent more firm conclusions being drawn. Conducting
methodologically rigorous research in complementary and alternative medicine is difficult
(34, 38). Study designs can be compromised through lack of funding, difficulty in
measuring outcomes of concern to patients (like quality of life or existential meaning), and
inability to maintain blinding (38). Further, studies can be compromised when the required
sample is not attained; for example symptomatically ill patients may be unwilling to
participate in an RCT (38). In the current study, the sampling method precluded
recruitment of only those people that found cannulation stressful.
If methodologically rigorous experimental or quasi-experimental designs are not possible
to implement in evaluation of certain complementary therapies like massage, it would be
logical to propose researchers use other methodological approaches to understand its
holistic process and outcomes. Indeed, a number of qualitative studies have been

Exploration of the Efficacy of Arm massage 89
conducted in an attempt to understand how people respond to massage. In some cases it
appears to help individuals open up, recognise and express emotions, and come to terms
with changed self-image (39). Research by Bredin (39) described how a body-centred
intervention for women following mastectomy, that incorporated massage, helped
participants come to terms with some of their innermost private experiences. Thus, the
therapeutic effects of massage and engagement in open and meaningful dialogue can be
far reaching; it may be difficult to capture such benefits with standard psychometric
measures.
The channel through which massage can allow patients to build a positive and valued
relationship with the masseuse was a theme identified in both the patient interviews and
the therapist focus group. Patients felt privileged to have the treatment and those
providing it likewise referred to being privileged. Billhult and Dahlberg (21) refer to the
relief brought about by massage given to patients with cancer as ‘meaningful relief’ (p.
180); it allows them to ‘get away’ from physical, social and psychological suffering and
enables them to ‘feel good’. Once again, these very personal yet desired feelings and
emotions may be difficult to capture in instruments that tend to deconstruct feelings of
wellbeing and quality of life.
There is some debate over how much of an impact gender may have in response to
massage. The current study suggests that men are more stoical than women, and may
find benefits of massage more elusive. However, previous research conducted by
Weinrich and Weinrich (25) would not support this. In the latter study men with cancer
achieved more relief from pain through massage than women. The affects of gender and
other variables also appear to impact on the cannulation process itself. These are
discussed in the next section.
5.4 Factors affecting cannulation
Previous research has documented that certain individuals are more difficult to cannulate
than others. Infants, children, the obese, and black patients, along with IV drug users,
have been identified as groups in whom gaining venous access through cannulation can
prove difficult (29). However, the sample in this study did not include children or infants,
and included few obese people or patients that were not Caucasian and so we are unable
to comment on this. However, it did suggest that certain groups were more vulnerable
with regards to failed or difficult attempts to cannulate. Women, younger individuals, and
those receiving vesicant drugs were statistically more likely to undergo unsuccessful or

Exploration of the Efficacy of Arm massage 90
problematic cannulation. It is becoming more usual for women with breast cancer to be
given high doses of anthracyclines. These are associated with pain on their administration,
which can persist after the treatment is given. It would appear logical that such people
would be particularly vulnerable to the pain and anxiety that the women in this study
alluded to.
5.5 Study limitations
The findings from any study should be considered in the light of limitations in its design or
conduct. This study utilised a multi-method design in attempt to minimise weakness in the
study design. However, statistical data attained through the RCT element were likely to be
compromised. Blinding is a hallmark of a quality RCT, but this was not achieved in this
study. Some authors would suggest that this shortfall would not undermine the study.
Richardson (34) proposes that it is neither essential nor possible in many trials of
complementary therapies. Either way, it is likely that the current study was compromised
through lack of blinding. This proved unavoidable in so far that insufficient space in the
clinical area and residue of oil on patients’ arms alerted those cannulating to the study
group people were allocated. It is possible that this biased their perceptions and recording
of the cannulation process. Further, patients themselves were aware of the study group to
which they belonged and this may also have influenced their views of the process.
A further limitation relates to the documentation of time. The RCT element required
nurses to time and document the period it took to cannulate patients. This proved to be
inaccurate with nurses documenting an estimate on many occasions. This hampered the
accurate documentation of these data and may have prevented real differences between
the study groups from being identified.
The questionnaires that were used in the study were developed by the research team and
have not been subject to psychometric testing. Thus their validity and reliability cannot be
assured. However, they did follow the same approaches to those used successfully in
previous evaluations of massage and other interventions for cannulation (23, 29, 30).
Furthermore, data from the qualitative elements triangulated with that recorded in the
questionnaires suggesting that the questionnaires were valid and accurately captured the
experiences of both cannulating and cannulation.
Finally, the massage was intended to be a standard intervention but it is possible that
there was some variation in how the treatment was given. Such variation can affect the
efficacy of the approach, and contribute to experimental error. The research team

Exploration of the Efficacy of Arm massage 91
attempted to counteract this through ensuring that all therapists underwent the same
protocol-directed training. The apparent success of this was referred to in data attained
from the interviews with patients and from the therapist focus group. These data
suggested that the massage varied little within or between therapists over time. However,
this cannot be assured.
5.6 Recommendations for practice
The results from this study are not sufficiently favourable to suggest that cancer services
establish an NHS resourced massage service to enhance delivery of chemotherapy.
However, given the way in which it contributed to the general atmosphere in the Day Unit,
making the environment less stressful, and clinical, it is evident that the massage service
was a welcomed and valued initiative within the Unit itself and Acute Trust at large. On
many occasions, patients, therapists and stakeholders talked of feeling privileged at
having the facility. To this end, it should be maintained if possible and it would seem that
this would be achievable if massage is financed through voluntary contribution and fund
raising, or given on a volunteer basis. It could be argued that if provided on a volunteer
basis, this will only work in the long term if volunteers receive some recompense for their
contribution. Recompense can come in the form of gaining valuable training, skills and
experience in working with patients with cancer. The NICE guidance states that those who
work with patients with cancer, including therapists that do so on a voluntary basis, should
receive sufficient training to allow them to be familiar with, and adhere to, Network policies
designed to ensure best practice (32). Further the National Guidelines for the use of
Complementary Therapies in Supportive and Palliative Care suggest that the educational
and training needs of therapists vary according to skills and experience but should be
assessed and planned for (33). It may be that newly qualified therapists could offer to
work within the service before moving on to paid employment. The environment in this
case should be considered a learning one for the therapists, and they would require
guidance, support and supervision to facilitate this. Implementation of action learning sets
where therapists would meet as a group and discuss their challenges, experiences and
ways of working might be valuable in this context.
It is evident from the current study that space was at a premium within the Day Unit. The
therapists lacked space and privacy in which to provide the therapy. This is one area that
needs addressing. A massage service would benefit from having dedicated space.
Without this the service is likely to be compromised. This need not be away from the point

Exploration of the Efficacy of Arm massage 92
where the treatment is delivered. In fact their presence within the Unit was felt to enhance
the atmosphere within it. An alternative approach would be to train nurses in this skill.
However, the advantages and disadvantages of nurses providing massage as oppose to
massage therapists have yet to be explored. Further we don’t know how feasible it is,
given the time pressures that many nurses that give chemotherapy operate under.
However, it could be possible to provide massage whilst assessing the patient prior to
cannulation.
The findings from this study also raise issues about the training of nursing staff to
cannulate. Cannulation is a skill that nurses and patients alike realise varies between
those that perform the procedure. The findings from this study confirm those found
previously (40) which suggests practice enhances skill. However, this may not always be
the case and it is important that attempts are made to accelerate the learning process.
Typically, nurses undergo one-off training in cannulation for chemotherapy. This study
suggests that whilst this provides a basis for their practice, some nurses are more
competent than others. It is possible that ‘top-up’ training could be beneficial. Reference
is made in the literature to different instruction methods to teach theoretical and clinical
cannulation skills, and to enable individuals to gain practise in the procedure (41-43).
Institution of ongoing and innovative approaches to cannulation training, including self-
directed training, could serve to optimise skills in this area of nursing practice. What is
clear from the current findings is that a failure rate of around 25% is not unusual. This
could serve as a benchmark for future audit of practice. In this manner, those that find
cannulation difficult could be identified and supported.
5.7 Recommendations for future research
The findings from this study suggest that cannulation can prove very difficult and stressful
to vulnerable individuals. It would appear that women, and notably young women, are
difficult to cannulate and can find the experience both painful and stressful. Those with
only one arm available for cannulation, most often those having treatment for breast
cancer, may be at particular risk of damage to their veins along with people receiving
vesicant drugs. It remains unanswered from the current study whether these individuals
would benefit from massage prior to cannulation, but it does suggest that this would be a
valuable area to research in future. The sampling criteria in any future research evaluating
the efficacy of massage prior to cannulation for chemotherapy might usefully be refined to

Exploration of the Efficacy of Arm massage 93
focus on patients who are problematic to cannulate and find the process painful and
stressful.
Further research also needs to be undertaken to understand gender differences in both
the giving and receiving of massage. Typically, the men in the study were less effusive
and complimentary about massage. This may be because massage requires a closeness
that may not be welcome by all. Further, in this study all volunteer massage therapists
were women. This may have altered the men’s perception of, and receptiveness to, it.
Unfortunately, the gender of the therapists was not discussed during the telephone
interviews and thus needs further consideration in future. It is also important to note that
there may have been an age effect operating. The men in this study were of an age
(mean age for men was 65years (SD=12), Females: 57 year (SD=13)) where they may
have felt that massage was inappropriate. Future research should try to explore some of
these issues further.
Mention was made in the previous section of different ways that nurses’ competence in
cannulating patients could be enhanced through education and training. However, the
relative efficacy of these different approaches has yet to be determined. This could be a
fruitful area for research that would greatly inform our understanding of ways in which
clinical skill such as these can be taught, enhanced and maintained.
During the interviews and focus groups, mention was made of extending the massage
service to both carers and to patients in their homes. This is an area that has not been
studied before and may be worthy of both service development and subsequent evaluation
in future.
Whatever the group that is massaged in future research, the design adopted for its
evaluation should be considered carefully. Where possible, if an RCT is conducted,
individuals (those both receiving the intervention and documenting outcomes) should be
blind to the treatment. This was not the case in the current study, and this may have
biased the findings. Alternatively, a pre-test post-test design, with or without an equivalent
control, may be a better alternative. Such designs are frequently used when random
selection or assignment is impracticable. However, such quasi-experimental approaches
are less robust than RCTs as extraneous factors are less easy to control.
Further, whilst an RCT is the gold-standard for evaluations, researchers would be wise not
to overly deconstruct the experience of having massage. It is a holistic treatment, and it is
possible that through looking at the minutiae, or small treatment effects such as its impact
on cannulation, its wider benefits may not be addressed. Through adopting a multi-
method approach, these shortcomings may be overcome.

Exploration of the Efficacy of Arm massage 94

Exploration of the Efficacy of Arm massage 95
6 References
1. Cancer Research UK. CancerStats: Incidence - UK. 2004. http://www.cancerresearchuk.org/statistics/ (Accessed 3 September 2004)
2. Department of Health. The NHS Cancer Plan: A plan for investment. A plan for reform. London: HMSO; 2000.
3. Bremnes RM. Experience with and attitudes to chemotherapy among newly employed nurses in oncological and surgical departments: A longitudinal study. Supportive Care in Cancer 1999;7(1):11-16.
4. Coates A, Abraham S, Kaye SB, Sowerbutts T, Frewin C, Fox RM, et al. On the Receiving End- Patient Perception of theSide-effects of Cancer Chemotherapy. European Journal of Cancer and Clinical Oncology 1983;19:209-220.
5. Liu G, Franssen E, Fitch MI, Warner E. Patient Preferences for Oral Versus Intravenous Palliative Chemotherapy. Journal of Clinical Oncology 1997;15(1):110-115.
6. Rhodes VA, McDaniel RW, Hanson B, Markway E, Johnson M. Sensory perception of patients on selected antineoplastic chemotherapy protocols. Cancer Nursing 1994;17(1):45-51.
7. McDaniel RW, Rhodes VA. Development of a preparatory sensory information videotape for women receiving chemotherapy for prest cancer. Cancer Nursing 1998;21(2):143-148.
8. Ream E, Richarson A, Alexandre-Dann C. Patients' sensory experiences before, during and immediately following the administration of intravenous chemotherapy. Journal of Cancer Nursing 1997;1(1):25-31.
9. Rees R, Feigel I, Vickers A, Zollman C, McGurk R, Smith C, et al. Use of complementary therapies by women with breast cancer in the South Thames region: Research Council for Complementary Medicine (RCCM); 1999.
10. Ferrell-Torry AT, Glick OJ. The use of therapeutic massage as a nursing intervention to modify anxiety and the perception of cancer pain. Cancer Nursing 1993;16(2):93-101.
11. Ahles TA, Tope DM, Pinkson B, Walch S, Hann D, Whedon M, et al. Massage Therapy for Patients UndergoingAutologous Bone Marrow Transplantation. Journal of Pain and Symptom Management 1999;18(3):157-163.
12. Fellowes D, Barnes K, Wilkinson S. Aromatherapy and massage for symptom relief in patients with cancer (Cochrane Review). Chichester, UK: John Wiley & Sons, Ltd; 2004.
13. Smith MC, Kemp J, Hemphill L, Vojir CP. Outcomes of therapeutic Massage for Hospitalized Cancer Patients. Journal of Nursing Scholarship 2002;34(3):257-262.
14. Corner J, Cawley N, Hildebrand S. An evaluation of the use of massage and essential oils on the wellbeing of cancer patients. International Journal of Palliative Nursing 1995;1(2):67-73.
15. Buckley J. Massage and aromatherapy massage: Nursing art and science. International Journal of Palliative Nursing 2002;8(6):276-280.
16. Trevelyan J. Complementary Options. Nursing Times 1998 April 1:28-29.17. Wilkes E. Complementary Therapy in Hospice and Palliative Care. Sheffiled: Trent
Palliative Care Centre and the Executive of Help the Hopsices; 1992.

Exploration of the Efficacy of Arm massage 96
18. Kohn M. Complementary Therapies in Cancer Care: Abridged report of a study produced for Macmillan Cancer Relief: Macmillan Cancer Relief; 1999 June 1999.
19. Wilkie DJ, Kampbell J, Cutshall S, Halabisky H, Harmon H, Johnson LP, et al. Effects of massage on pain intensity, analgesics and quality of life in patients with cancer pain: A pilot study of a randomised clinical trial conducted within hospice care delivery. The Hospice Journal 2000;15(3):31-53.
20. Grealish L, Lomasney A, Whiteman B. Foot Massage: A nursing intervention to modify the distressing symptoms of pain and nausea in patients hospitalised with cancer. Cancer Nursing 2000;23(3):237-243.
21. Billhult A, Dahlberg K. A Meaningful Relief From Suffering.Experiences of Massage in Cancer Care. Cancer Nursing 2001;24(3):180-184.
22. Evans B. An audit into the effects of aromatherapy massage and the cancer patient in palliative and terminal care. Complementary Therapies in Medicine 1995;3:239-241.
23. Wilkinson S, Aldridge J, Salmon I, Cain E, Wilson B. An evaluation of aromatherapymassage in palliative care. Palliative Medicine 1999;13(5):409-417.
24. Stephenson NLN, Weinrich SP, Tavakoli AS. The effects of foot reflexology on anxiety and pain in patients with breast and lung cancer. Oncology Nursing Forum 2000;27(1):67-72.
25. Weinrich SP, Weinrich MC. The effect of massage on pain in cancer patients. Applied Nursing Research 1990;3(4):140-145.
26. Hadfield N. The role of aromatherapy massage in reducing anxiety in patients with malignant brain tumours. International Journal of Palliative Nursing 2001;7(6):279-285.
27. Dunwoody L. Cancer patients' experiences and evaluations of aromatherapy massage in palliative care. International Journal of Palliative Nursing 2002;8(10):497-504.
28. Cassileth BR. Evaluating Complementary and AlternativeTherapies for Cancer Patients. Ca: A Cancer Journal for Clinicians 1999;49(6):362-375.
29. Lenhardt R, Seybold T, Kimberger O, Stoiser B, Sessler DI. Local warming and insertion of peripheral venous cannulas: single blinded prospective randomised controlled trial and single blinded crossover trial. British Medical Journal 2002;325(24 August):409-412.
30. Wendler MC. Effects of Tellington Touch in healthy adults awaiting venipuncture. Research in Nursing and Health 2003;26:40-52.
31. Harrington KJ, Kelly SA, Pandha HS, Jackson JE, Hollyer JS, McKenzie CG. An audit of Hickman catheter use in patients with solid tumours. Clinical Oncology 1994;6(5):288-293.
32. NICE. Guidance on Cancer Services: Improving Supportive and Palliative Care for Adults with Cancer. The Manual. London: National Institute for Clinical Excellence; 2004 March 2004.
33. NCHSPCS. National Guidelines for the Use of Complementary Therapies in Supportive and Palliative Care. London: National Council for Hospice and SpecialistPalliative Care Services; 2003.
34. Richardson J. The use of randomized control trials in complementary therapies: exploring the issues. Journal of Advanced Nursing 2000;32(2):398-406.
35. Anthony HM. Clinical research: Questions to ask and the benefits of asking them. In: Lewith GT, Aldridge D, editors. Clinical Research Methodology for Complementary Therapies. London: Hodder & Stoughton; 1993.

Exploration of the Efficacy of Arm massage 97
36. Kacperek L. Patients' views on the factors which influence the use of an aromatherpy massage outpatient service. Complementary Therapies in Nursing & Midwifery 1997;3:51-57.
37. Cooke B, Ernst E. Aromatherapy: a systematic review. British Journal of General Practice 2002;50(455):493-496.
38. Pan CX, Morrison S, Ness J, Fugh-Berman A, Leipzig RM. Complementary and Alternative Medicine in the Management of Pain, Dyspnea, and Nausea and Vomiting Near the End of Life: A Systematic Review. Journal of Pain and Symptom Management 2000;20(5):374-387.
39. Bredin M. Mastectomy, body image and therapeutic massage: a qualitative study of women's experience. Journal of Advanced Nursing 1999;29(5):1113-1120.
40. Ung L, Cook S, Edwards B, Hocking L, Osmond F, Buttergieg H. Peripheral Intravenous Cannulation in Nursing. Journal of Infusion Nursing 2002;25(3):189-200.
41. Hewitt J, Roberts CM. Evaluating the practice outcomes of a venepuncture and intravenous cannulation. Nurse Education in Practice 2003;4(1):77-79.
42. Chang KK-P, Chung JW-Y, Wong TK-S. Learning intravenous cannulation: A comparison of the conventional method and the CathSim Intravenous Training System. Journal of Clinical Nursing 2002;11(1):73-78.
43. Snelling PC. Developing self-directed training for intravenous cannulation. Professional Nurse 2002;18(3):137-139, 141-142.

Exploration of the Efficacy of Arm massage 98

Exploration of the Efficacy of Arm massage 99
7 Appendices
Appendix 1
Appendix 2
Appendix 3
Appendix 4
Appendix 5
Appendix 6
Appendix 7
Appendix 8
Appendix 9
Appendix 10
Appendix 11
Appendix 12
Appendix 13
Appendix 14
Arm massage protocol
Patient information sheet
Patient consent form
Therapist information sheet
Patient questionnaire
Nurse questionnaire
Patient interview schedule
Stakeholder interview schedule
Focus group guide
Model explaining anxiety prior to cannulation (SPSS output)
Model explaining anxiety following cannulation (SPSS output)
Model explaining anticipation of pain prior to cannulation (SPSS output)
Model explaining procedural pain (SPSS output)
Model explaining time taken to cannulate (SPSS output)

Exploration of the Efficacy of Arm massage 100
Appendix 1: Arm massage protocol
PROCEDURE
* Ask patient if they wish to use the toilet facilities prior to commencing the massage,
as cannulation should take place directly following this.
* Ensure patient is comfortable and place a pillow covered with a clean towel on the
patient’s lap.
* Please ask the patient if they have an allergy to sunflower oil before applying this.
* The patient’s sleeves should be rolled up the arms, well away from the potential risk
of staining with carrier oil, and jewellery wherever possible should be removed.
* Establish which arm is likely to be cannulated. This is particularly so in breast
cancer patients. If axillary lymph nodes have been removed - using the arm for
cannulation is generally avoided and especially if lymphoedema is present.
The following technique should last for approximately 10 minutes if possible.
* Place your hands over the patient’s to establish contact, then proceed to apply oil
over the arms and hands using effleurage movements.
* Cover one arm with an edge of the towel to maintain warmth.
* Warm up the arm with effleurage massage.
* Gently petrissage over the top of the forearm, working up and down the arm.
* Effleurage the forearm 2 or 3 times more before moving to the hand.

Exploration of the Efficacy of Arm massage 101
* Lightly pettrisage the top of the hand and fingers, then turn the hand over and
massage the palms.
* Finish with effleurage of the forearm and hand, stroking down the arm to finish.
* Cover this arm and repeat the sequence on the other arm if appropriate.
* To finish, keep the arms covered with the towel to maintain warmth, laying your
hands on the arms or hands to signify the end of treatment to the patient. Inform the staff
nurse and of course offer the patient a drink.
Note
Do not massage the arms if lymphoedema is present, nor over inflammed, hot or tender
areas.

Exploration of the Efficacy of Arm massage 102
Appendix 2: Patient information sheet
PATIENT INFORMATION SHEET
Study title: A study investigating the effects of arm massage prior to chemotherapy
Introduction
You are being invited to take part in a research study. Before you decide whether or not
to, it is important for you to understand why the research is being done and what it will
involve. Please take time to read the following information carefully and discuss it with
others if you wish. Ask us if there is anything that is not clear or if you would like more
information. Take time to decide whether or not you wish to take part.
Thank you for reading this.
Purpose of the study
This study is being conducted over a period of a year. It aims to find out the impact of arm
massage prior to chemotherapy. Arm massage has been used on Chartwell Unit for some
months now. It appears that it may help to relax people and make the nurses’ insertion of
the needle (cannula) required for chemotherapy more easy. Because of this observation,
a team of researchers has decided to formally study its effectiveness. The study will look
at the discomfort associated with the needle (cannula) being placed in the arm before
chemotherapy is given. It will look at the emotions felt prior to, and after, chemotherapy is
given and investigate the views of people about the impact of arm massage .
The researchers will also be asking nurses and the massage therapists for their views of
the massage service.
Through looking at these factors the researchers will find out
1. The value of arm massage prior to intravenous chemotherapy
2. The potential impact of this therapy for the chemotherapy service

Exploration of the Efficacy of Arm massage 103
Why you have been chosen
You are being asked if you would like to take part in this study because you are about to
begin chemotherapy that will be given to you via a form of needle (cannula). All patients
like you, who have not previously had chemotherapy this way, and are being treated on
Chartwell Unit are being invited to take part. We are aiming to involve 50 patients in this
research study.
Do you have to take part?
It is up to you to decide whether or not to take part. If you do decide to take part you will
be given this information sheet to keep and be asked to sign a consent form. If you decide
to take part you are still free to withdraw at any time without giving a reason. This will not
affect the standard of care you receive now or in the future.
What will happen if you take part?
The research tem will be collecting data on Chartwell Unit for a 6-month period.
To find out whether arm massage assists in the giving of chemotherapy, those that take
part
in the study will be divided into 2 groups. The first group will be given the arm massage in
addition to their usual care. The second group will not have the massage but will have the
routine care offered to patients whilst undergoing chemotherapy. Patients will be placed in
the relevant group by chance. You will be informed of the group you will be in by the
nurses caring for you. If allocated to the massage group your chemotherapy treatment will
normally be booked between the hours of 1130 and 1600.
Whichever group you are in (with-massage or without-massage) you will be asked to
complete a booklet of questions immediately before and after each chemotherapy
treatment is given to you. This will ask about the level of pain and anxiety you
experienced on that occasion, and
the time taken for treatment. Those that have the massage will be asked about their
experiences of, and satisfaction with, arm massage. A small number of those in the
massage group (fifteen people) will additionally be asked to take part in a recorded

Exploration of the Efficacy of Arm massage 104
telephone interview that will last around 20 minutes. This will provide an opportunity to
discuss experiences in greater depth. Again, these people will be selected by chance.
The research team will send you a letter at a later date if you are chosen for this part of the
study.
What do I have to do?
Having the arm massage will not have any implications for what you can or cannot do in
your daily life; you will be able to use other types of complementary therapies if you wish.
Through participating in the study you will have to complete a questionnaire each time you
attend the unit for your chemotherapy. You will be required to answer questions
immediately before and after you have had your treatment. A small group of people,
fifteen individuals, will be invited to take part in a short interview to talk about their
experiences of chemotherapy and arm massage once the study is complete. Again, you
will be informed by letter sent by the research team if you are selected to take part in this
aspect of the study.
What is the drug or procedure that is being tested?
What is being tested is a gentle 10-minute arm massage with basic carrier oil.
What are the alternatives for treatment?
Those that do not have the massage treatment will have the usual care provided to
patients prior to cannualtion for chemotherapy.
What are the side effects of any treatment received when taking part?
None are expected.

Exploration of the Efficacy of Arm massage 105
What are the possible disadvantages and risks of taking part?
Gentle arm massage, the treatment being given in attempt to make cannulation easier, is
not physically invasive but does require a physical closeness and type of touch that some
patients may find unpleasant. However, it is anticipated that in general people will find the
treatment relaxing and beneficial to them.
What are the possible benefits of taking part?
We hope that the arm massage will help those who receive it. However, this cannot be
guaranteed. The information we get from this study may help us to understand the
potential of arm massage and indicate how the process of giving chemotherapy may be
improved in future.
Those that do not receive the arm massage may enjoy being part of a study that could
improve the care for patients undergoing chemotherapy in future.
What if new information becomes available?
Sometimes during the course of a research project, new information becomes available
about the treatment that is being studied. If this happens, the research team will tell you
about it and discuss with you whether you want to continue in the study. If you decide to
withdraw, your research doctor will make arrangements for your care to continue. If you
decide to continue in the study you will be asked to sign an updated consent form.
What happens when the research study stops?
In the past, arm massage has been offered to patients treated in Chartwell Unit on an ad
hoc basis. During data collection for this study, it will only be available to those in the
experimental group, or those not taking part in the research. On completion of the study,
and dependant on the results, the massage service will return to being offered on an ad
hoc basis.

Exploration of the Efficacy of Arm massage 106
What if something goes wrong?
The principal investigator is indemnified through the general King’s College London
Liability Insurance, with the principle of ‘No Fault’ compensation in operation for subjects of
clinical research. Liability for damages/compensation claims by human research subjects
for bodily injury from participation in clinical trial or healthy volunteer studies conducted by
King’s. The basis for damages or compensation will be in accordance with ABPI
guidelines irrespective of fault on the College’s part.
Will my taking part in this study be kept confidential?
All responses you give will be anonymous. Any information about you, which leaves the
hospital, will have your name and address removed so that you cannot be recognised from
it. All study information will be stored in accordance with the Data Protection Act (1998) in
a locked filing cabinet to which only the researchers will have access.
Any information you provide during an interview may be presented in quotes in future
research articles or presentations. However, if this is the case you will be given a different
name so you will not be identifiable from your comments.
What will happen to the results of the research study?
The researchers intend to circulate the findings locally, nationally and internationally. The
research team will return to Chartwell Unit and talk through the findings with the staff at a
suitable opportunity. They will also be provided with a written report of the findings. If you
would like such a copy of the findings, please let the staff on Chartwell Unit know.
The principal researcher, Dr Emma Ream, has been invited to present about interim
findings at a symposium during the European Cancer Conference (ECCO 12) to be held in
Copenhagen in September 2003. Furthermore, one of the conditions of accepting the
grant was that the researchers would publish their findings in a European cancer journal.
In this way the findings will reach both a national and international audience.
Exploration of the Efficacy of Arm massage 107
The researchers will also seek opportunities to publish in a journal of complementary
medicine to reach an audience wider than a nursing one.
Who is organising and funding the research?
Nurses on Chartwell Unit are undertaking this study alongside nurse researchers from
King’s College, London University.
The European Oncology nursing Society has provided funding for the study. This covers
the necessary researchers’ expenses.
Who has reviewed the study?
The European Oncology Nursing Society and Bromley Local Research Ethics Committee
have reviewed the study.
Contact for Further Information
Please contact Helen Hannon in the Treatment Suite on Chartwell Unit if you would like to
discuss the study further, phone number 01689 863155
Thank you for taking part in this study.
Please keep this copy of the information sheet alongside your copy of the consent form.
30.04.2003 Patient Information Sheet Version 1

Exploration of the Efficacy of Arm massage 108
Appendix 3: Patient Consent form
Centre Number:Study Number:Patient Identification Number for this trial:
CONSENT FORM FOR PATIENTS
Title of Project: An exploratory trial of the efficacy of arm massage in facilitating intravenous cannulation foradministration of cytotoxic chemotherapy
Name of Researcher: Dr Emma Ream
1. I confirm that I have read and understand the information sheet dated 30.04.2003 (version 1) for the above study and have had the opportunity
to ask questions
2. I understand that my participation is voluntary and that I am free towithdraw at any time, without giving any reason, without mymedical care or legal rights being affected.
3. I understand that sections of any of my medical notes may be looked at byresponsible individuals from the research team or from regulatoryauthorities where it is relevant to my taking part in research. I givepermission for these individuals to have access to my records.
4. I understand that I may be requested to take part in a taped telephoneinterview.
5. I agree to take part in the above study.
________________________ ________________ ____________________Name of Patient Signature Date
_________________________ ________________ _______________Name of Person taking consent Signature Date(if different from researcher)
_________________________ ________________ ____________________Researcher Signature Date
Exploration of the Efficacy of Arm massage 109
Appendix 4: Therapist information sheet
THERAPISTS INFORMATION SHEET
Study title: A study investigating the effects of arm massage prior to chemotherapy
Introduction
You are being invited to take part in a research study. Before you decide whether or not
to, it is important for you to understand why the research is being done and what it will
involve. Please take time to read the following information carefully and discuss it with
others if you wish. Ask us if there is anything that is not clear or if you would like more
information. Take time to decide whether or not you wish to take part.
Thank you for reading this.
Purpose of the study
This study is being conducted over a period of a year. It aims to find out the impact of arm
massage prior to chemotherapy. Arm massage has been used on Chartwell Unit for some
months now. It appears that it may help to relax people and make the nurses’ insertion of
the (needle) cannula required for chemotherapy more easy. Because of this observation,
a team of researchers has decided to formally study its effectiveness. The study will look
at the discomfort associated with the (needle) cannula being placed in the arm before
chemotherapy is given. It will look at the emotions felt prior to, and after, chemotherapy is
given and investigate the views of people about the impact of arm massage.
The researchers will also be asking patients and the nurses placing the needle (cannula)
in the patients arm for their views of the massage service.
Through looking at these factors the researchers will find out
1. The value of arm massage prior to intravenous chemotherapy
2. The potential impact of this therapy for the chemotherapy service

Exploration of the Efficacy of Arm massage 110
Why you have been chosen
You are being asked if you would like to take part in this study because you are regularly
massaging patients arms before their chemotherapy treatment. All patients who have not
previously had chemotherapy and are being treated on Chartwell Unit are being invited to
take part. We are aiming to involve 50 patients in this research study.
Do you have to take part?
It is up to you to decide whether or not to take part. If you do decide to take part you will
be given this information sheet to keep and be asked to sign a consent form. If you decide
to take part you are still free to withdraw at any time without giving a reason.
What will happen if you take part?
The research team will be collecting data on Chartwell Unit for a 6-month period.
Information regarding arm massage prior to cannulation will be gathered from the
therapists performing arm massage, the patients receiving arm massage and the nurses
performing the cannulation.
To find out whether arm massage assists in the giving of chemotherapy, those patients
that take part in the study will be divided into 2 groups. The first group will be given the
arm massage in addition to their usual care. The second group will not have the massage
but will have the routine care offered to patients whilst undergoing chemotherapy. Patients
will be placed in the relevant group by chance. The nurse will inform the patient of the
group they will be in. If allocated to the massage group the patient's chemotherapy
treatment will be booked between the hours of 1130 and 1430.
Whichever group the patient is in (with-massage or without-massage) they will be asked to
complete a booklet of questions immediately before and after each chemotherapy
treatment is given to them. This will ask about the level of pain and anxiety they
experienced on that occasion, and the time taken for treatment. Those that have the
massage will be asked about their experiences of, and satisfaction with, arm massage. A
small number of those in the massage group (fifteen people) will additionally be asked to

Exploration of the Efficacy of Arm massage 111
take part in a recorded telephone interview that will last around 20 minutes. This will
provide an opportunity to discuss experiences in greater depth. Again, these people will
be selected by chance and the nurses looking after them on Chartwell Unit will tell them if
you have been chosen for this part of the study.
The nurses will complete a brief questionnaire for each needle (cannula) they insert on a
patient participating in the study. This will allow data to be collected from nurses
cannulating the patients on the 100 episodes that will be evaluated in this study. It will
allow data to be collected on the state of patients’ veins prior to the procedure, time taken
for successful cannulation, number of cannulation attempts, degree of difficulty
encountered in the process and other methods used to achieve cannulation (e.g.
application of heat). These data will allow differences in ease of cannulation between the
two groups to be determined and described statistically.
What do I have to do?
The study aims to determine whether gentle arm massage:
1. Enhances patients’ wellbeing.
You will be invited on completion of the study to share your views on arm massage during
a one-off focus group anticipated to last approximately 1 hour. It will be facilitated and
recorded by 2 members of the research team (those outside the institution where data will
be collected).
A focus group is an informal discussion between 6-10 people, focusing on a particular
experience which all those taking part can talk about. This focus group is about the
experience of providing arm massage before cannulation. In particular your perceptions on
how patients responded to the massage and to reflect on factors that both impeded and
facilitated the process. You will also be encouraged to consider patient characteristics that
may influence outcomes of the treatment.
What is the drug or procedure that is being tested?
What is being tested is a gentle 10-minute arm massage with basic carrier oil.

Exploration of the Efficacy of Arm massage 112
What are the alternatives for treatment?
Those that do not have the massage treatment will have the usual care provided to
patients prior to cannualtion for chemotherapy.
What are the side effects of any treatment received for the patient taking part?
None are expected.
What are the possible disadvantages and risks of taking part?
Your time is required to attend the focus group
What are the possible benefits of taking part?
We hope that the arm massage will help those who receive it. However, this cannot be
guaranteed. The information we get from this study may help us to understand the
potential or arm massage and indicate how the process of giving chemotherapy may be
improved in future.
Those that do not receive the arm massage may enjoy being part of a study that could
improve the care for patients undergoing chemotherapy in future.
What if new information becomes available?
Sometimes during the course of a research project, new information becomes available
about the treatment that is being studied. If this happens, the research team will tell you
about it and discuss with you whether you want to continue in the study. If you decide to
continue in the study you will be asked to sign an updated consent form.

Exploration of the Efficacy of Arm massage 113
What happens when the research study stops?
In the past, arm massage has been offered to patients treated in Chartwell Unit on an ad
hoc basis. During data collection for this study, it will only be available to those in the
experimental group. On completion of the study, and dependant on the results, the
massage service will return to being offered on an ad hoc basis.
What if something goes wrong?
The principal investigator is indemnified through the general King’s College London
Liability Insurance, with the principle of ‘No Fault’ compensation in operation for subjects of
clinical research. Liability for damages/compensation claims by human research subjects
for bodily injury from participation in clinical trial or healthy volunteer studies conducted by
King’s. The basis for damages or compensation will be in accordance with ABPI
guidelines irrespective of fault on the College’s part.
Will my taking part in this study be kept confidential?
All responses you give will be anonymous. Any information about you, which leaves the
hospital, will have any personal details, such as your name removed so that you cannot be
recognised from it. All study information will be stored in accordance with the Data
Protection Act (1998) in a locked filing cabinet to which only the researchers will have
access.
What will happen to the results of the research study?
The researchers intend to circulate the findings locally, nationally and internationally. The
research team will return to Chartwell Unit and talk through the findings with the staff at a
suitable opportunity. They will also be provided with a written report of the findings. If you
would like such a copy of the findings, please let the Manager of the Chartwell Unit know.

Exploration of the Efficacy of Arm massage 114
The principal researcher, Dr Emma Ream, has been invited to present about interim
findings at a symposium during the European Cancer Conference (ECCO 12) to be held in
Copenhagen in September 2003. Furthermore, one of the conditions of accepting the
grant was that the researchers would publish their findings in a European cancer journal.
In this way the findings will reach both a national and international audience. The
researchers will also seek opportunities to publish in a journal of complementary medicine
to reach an audience wider than a nursing one.
Who is organising and funding the research?
Nurses on Chartwell Unit are undertaking this study alongside nurse researchers from
King’s College, London University.
The European Oncology nursing Society has provided funding for the study. This covers
the necessary researchers’ expenses.
Who has reviewed the study?
The European Oncology Nursing Society and Bromley Local Research Ethics Committee
have reviewed the study.
Contact for Further Information
Please contact Helen Hannon in the Treatment Suite on Chartwell Unit if you would like to
discuss the study further, phone number 01689 863155
Thank you for taking part in this study.
Please keep this copy of the information sheet alongside your copy of the consent form.
30.04.2003 Therapist Information Sheet Version 1

Exploration of the Efficacy of Arm massage 115
Appendix 5: Patient Questionnaire

Exploration of the Efficacy of Arm massage 116
Exploration of the Efficacy of Arm massage 117

Exploration of the Efficacy of Arm massage 118

Exploration of the Efficacy of Arm massage 119
Exploration of the Efficacy of Arm massage 120
Appendix 6: Nurse Questionnaire
Exploration of the Efficacy of Arm massage 121

Exploration of the Efficacy of Arm massage 122
Next…

Exploration of the Efficacy of Arm massage 123
Appendix 7: Patient Interview schedule
PATIENT INTERVIEW GUIDE
1. How did you find the experience of attending the unit for chemotherapy?
2. How had you anticipated it would be before you started the treatment?
3. Did your feelings towards it change over time?
4. In general how anxious did you feel when you attended the unit?
5. What factors affected how you felt?
6. Did anything in particular improve the experience for you?
7. How would you describe any feelings of pain or discomfort that you felt when the
cannula was placed in your arm?
8. In general how bad (intense/severe) would you say that this feeling was?
9. How did you find the arm massage?
10. How many times did you have it?
11. In what ways did the arm massage affect how you felt (for good or bad)?
12. What factors impacted on the process?
a. Environmental
b. Situational
c. Interpersonal
13. On what occasions (if any) was the massage helpful?
14. In what ways was it helpful?
15. On what occasions (if any) was the massage unhelpful?
16. In what ways was it unhelpful?
17. How in your opinion could the massage service be improved?
THANK YOU

Exploration of the Efficacy of Arm massage 124
Appendix 8: Stakeholder interview schedule
NURSE/THERAPIST MANAGER (STAKEHOLDERS) INTERVIEW GUIDE
Service related issues
1. What vision did you have for the service?
a. Role or function?
b. What had you hoped to achieve by it?
2. How successful do you believe it has been?
a. What aspects of the service are working well/not so well?
3. How has it evolved over time?
4. Thinking back to when the service was being set up:
a. What challenges did you encounter in setting up the service?
5. What challenges have impacted on its daily delivery?
a. Administrative
b. Manning
c. Housing – space
6. How did you deal with these?
7. Based on these service-related issues, what is key for its smooth running?
Patient related issues – if either delivered massage or cannulated during process of study
8. What do you see as the benefits (if any) for patients?
9. Did any patients benefit particularly?
a. If so who were they?
b. What was this benefit?
c. Why do you think this was the case?
10. Did any patients seem to find it unhelpful?
a. If so who were they?
b. In what way did it seem unhelpful?
c. Why do you think this was the case?

Exploration of the Efficacy of Arm massage 125
Considering the therapists themselves
11. In your view what are key criteria for therapists recruited to the post?
a. What specific experience should they have if any?
12. What specific attributes/characteristics should they have, if any?
13. What ongoing support/supervision do the therapists need? (Therapy manager only)
14. What training issues, if any, have arisen? (Therapy manager only)
15. How has individual performance been reviewed? (Therapy manager only)
Looking to the future for the massage service
16. How could the service be improved?
a. What potential would you like to see realised in future?
17. What might stop this from happening?
18. How could these challenges be overcome?
Looking to the future as regards successful cannulation for chemotherapy
19. What other than massage would you consider instituting to improve future
chemotherapy/cannulation?
20. What other thoughts comments would you like to add regarding cannulation for
chemotherapy, and the role of massage?
THANK YOU
Exploration of the Efficacy of Arm massage 126
Appendix 9: Focus group guide
FOCUS GROUP GUIDE
1. Welcome
2. Refreshments- whilst waiting for all participants to arrive
3. Ask participants to complete short questionnaire, to collect demographic data
4. Completion of consent forms with Primary Researcher (two copies signed)
Introduction
Welcome participants to group introduce primary and secondary researchers. Open group
discussion by reaffirming confidentiality of group and guidelines/rules, including level of
group confidentiality and right to withdraw at any time.
Questioning Route
Opening Question (ice breaker to each individual & act as voice identifier for transcription)
1. Can you begin by telling us your name and one thing that you are looking forward to this
year?
Introductory Question
2. How do you think patients find attending Chartwell Unit for chemotherapy?
Transition Questions
3. What difference does it make providing patients in places like Chartwell with massage?
4. How do you think it impacted on the people in this study?
5. What do you see as the benefits (if any) for patients?

Exploration of the Efficacy of Arm massage 127
6. What factors impacted on the process?
a. Environmental
b. Situational
c. Interpersonal
7. Did any people seem to derive particular benefit?
a. If so whom were they?
b. What was this benefit?
c. Why do you think this was the case?
8. In what situations, if any, was it less beneficial?
9. Did any people seem to find it unhelpful?
a. If so whom were they?
b. In what way did it seem unhelpful?
c. Why do you think this was the case?
Process questions
10. How did you find the process of providing arm massage for the patients in the study?
11. Was it as you had anticipated?
12. How sufficient was your training to prepare you for the work you have been doing on
Chartwell?
13. Were there any occasions when you were unable to give provide massage?
a. Perhaps due to pain/discomfort/lymphoedema
b. Other reasons
14. What challenges are there with regards to providing massage to patients in a unit like
Chartwell?
15. What concerns do you have about the service?
Concluding questions
16. How could the arm massage service be improved?
17. Anything else to add?
THANK YOU

Exploration of the Efficacy of Arm massage 128
Appendix 10: Model explaining anxiety prior to cannulation (SPSS output)
Tests of Between-Subjects Effects
Dependent Variable: Anxiety prior to cannulation
11.280 1 5.447 .020
20.442 1 9.871 .002
873.812 1 421.958 .000
542.563 262
1705.538 265
SourceMASSAGE
GENDER
ANTHURT
Error
Corrected Total
Type III Sumof Squares df F Sig.
Massage group
Dependent Variable: Anxiety prior to cannulation
1.994a .127 1.743 2.245
2.406a .131 2.148 2.664
Massage groupHad massage
Didn't have massage
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Evaluated at covariates appeared in the model: Anticipated pain = 2.32.a.
Gender of patient
Dependent Variable: Anxiety prior to cannulation
1.884a .160 1.568 2.200
2.516a .111 2.298 2.735
Gender of patientMale
Female
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Evaluated at covariates appeared in the model: Anticipated pain =2.32.
a.
Parameter Estimates
Dependent Variable: Anxiety prior to cannulation
.898 .044 20.542 .000 .812 .984ParameterANTHURT
B Std. Error t Sig. Lower Bound Upper Bound
95% Confidence Interval

Exploration of the Efficacy of Arm massage 129
Appendix 11: Model explaining anxiety following cannulation (SPSS output)
Tests of Between-Subjects Effects
Dependent Variable: Anxiety after cannulation
5.676 1 3.244 .073
10.725 1 6.129 .014
32.847 1 18.771 .000
17.275 5 1.974 .083
131.713 2 37.635 .000
7.722 1 4.413 .037
26.523 1 15.157 .000
26.458 7 2.160 .039
414.719 237
874.086 256
SourceGENDER
MASSAGE
AGE (2 groups)
RNURSEID
RAVACTHR
GENDER * MASSAGE
MASSAGE * RAVACTHR
RNURSEID * RAVACTHR
Error
Corrected Total
Type III Sumof Squares df F Sig.
1. Gender of patient
Dependent Variable: Anxiety after cannulation
2.197a .215 1.773 2.622
2.603a .142 2.324 2.882
Gender of patientMale
Female
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Based on modified population marginal mean.a.
2. Massage group
Dependent Variable: Anxiety after cannulation
2.326a .191 1.950 2.702
2.493a .203 2.094 2.893
Massage groupHad massage
Didn't have massage
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Based on modified population marginal mean.a.
3. Age of patient (2 groups)
Dependent Variable: Anxiety after cannulation
2.868a .203 2.468 3.268
1.933a .169 1.599 2.266
Age of patient (2groups)Aged 24-55
Aged 56-79
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Based on modified population marginal mean.a.
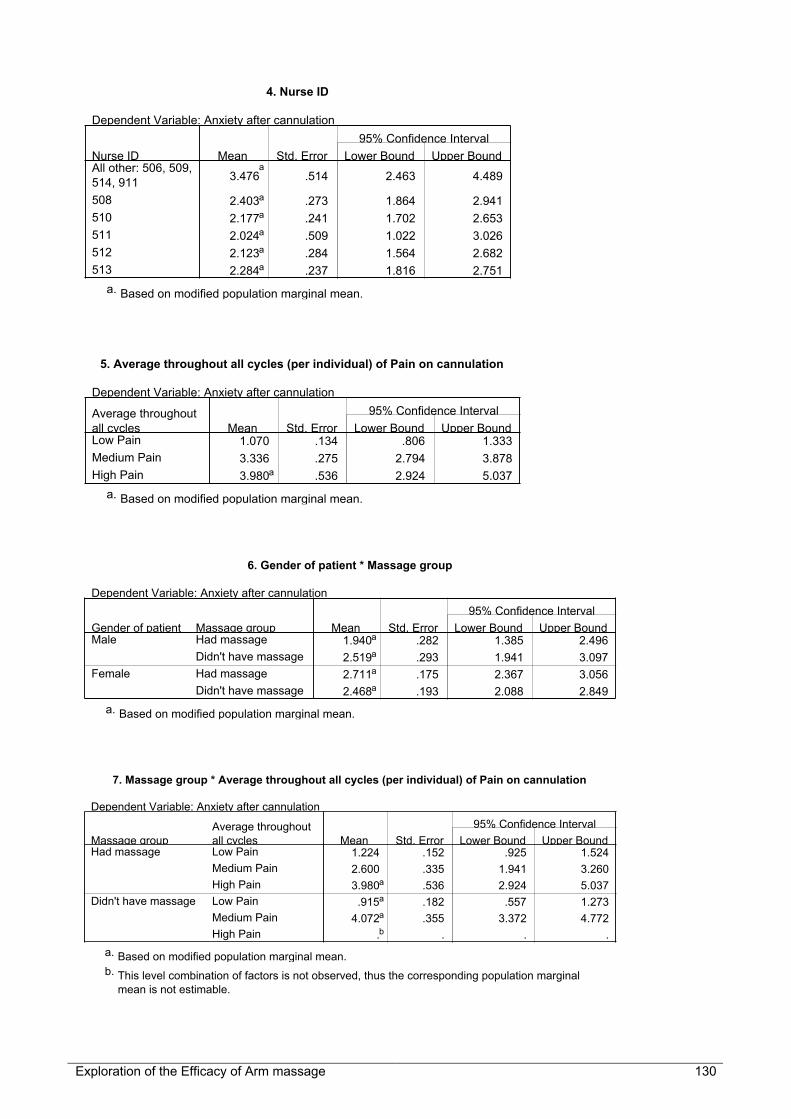
Exploration of the Efficacy of Arm massage 130
4. Nurse ID
Dependent Variable: Anxiety after cannulation
3.476a
.514 2.463 4.489
2.403a .273 1.864 2.941
2.177a .241 1.702 2.653
2.024a .509 1.022 3.026
2.123a .284 1.564 2.682
2.284a .237 1.816 2.751
Nurse IDAll other: 506, 509,514, 911
508
510
511
512
513
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Based on modified population marginal mean.a.
5. Average throughout all cycles (per individual) of Pain on cannulation
Dependent Variable: Anxiety after cannulation
1.070 .134 .806 1.333
3.336 .275 2.794 3.878
3.980a .536 2.924 5.037
Average throughoutall cyclesLow Pain
Medium Pain
High Pain
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Based on modified population marginal mean.a.
6. Gender of patient * Massage group
Dependent Variable: Anxiety after cannulation
1.940a .282 1.385 2.496
2.519a .293 1.941 3.097
2.711a .175 2.367 3.056
2.468a .193 2.088 2.849
Massage groupHad massage
Didn't have massage
Had massage
Didn't have massage
Gender of patientMale
Female
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Based on modified population marginal mean.a.
7. Massage group * Average throughout all cycles (per individual) of Pain on cannulation
Dependent Variable: Anxiety after cannulation
1.224 .152 .925 1.524
2.600 .335 1.941 3.260
3.980a .536 2.924 5.037
.915a .182 .557 1.273
4.072a .355 3.372 4.772
.b . . .
Average throughoutall cyclesLow Pain
Medium Pain
High Pain
Low Pain
Medium Pain
High Pain
Massage groupHad massage
Didn't have massage
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Based on modified population marginal mean.a.
This level combination of factors is not observed, thus the corresponding population marginalmean is not estimable.
b.

Exploration of the Efficacy of Arm massage 131
8. Average throughout all cycles (per individual) of Pain on cannulation * Nurse ID
Dependent Variable: Anxiety after cannulation
1.134 .329 .485 1.783
1.006 .219 .575 1.438
1.237 .225 .794 1.680
1.228 .370 .500 1.956
.794 .302 .198 1.390
1.019 .183 .657 1.380
5.818 .965 3.917 7.719
2.927 .432 2.076 3.778
2.133 .380 1.384 2.882
2.820 .941 .967 4.673
3.452 .480 2.506 4.399
2.867 .303 2.270 3.464
.a
. . .
4.147b .950 2.274 6.019
4.147b .782 2.606 5.688
.a . . .
.a . . .
3.647b .950 1.774 5.519
Nurse IDAll other: 506, 509,514, 911
508
510
511
512
513
All other: 506, 509,514, 911
508
510
511
512
513
All other: 506, 509,514, 911
508
510
511
512
513
Average throughoutall cyclesLow Pain
Medium Pain
High Pain
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
This level combination of factors is not observed, thus the corresponding population marginalmean is not estimable.
a.
Based on modified population marginal mean.b.

Exploration of the Efficacy of Arm massage 132
Appendix 12: Model explaining anticipation of pain prior to cannulation (SPSSoutput)
Tests of Between-Subjects Effects
Dependent Variable: Anticipated pain
7.706 1 5.773 .017
16.676 1 12.493 .000
22.514 5 3.373 .006
315.498 1 236.354 .000
27.763 5 4.160 .001
26.736 5 4.006 .002
329.709 247
1256.195 265
SourceMASSAGE
AGE (2 groups)
RNURSEID
PREANX
AGE (2g)*NURSEID
RNURSEID * PREANX
Error
Corrected Total
Type III Sumof Squares df F Sig.
1. Massage group
Dependent Variable: Anticipated pain
2.744a .155 2.439 3.050
2.374a .161 2.056 2.692
Massage groupHad massage
Didn't have massage
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Evaluated at covariates appeared in the model: Anxiety prior tocannulation = 2.30.
a.
2. Age of patient (2 groups)
Dependent Variable: Anticipated pain
3.050a .260 2.538 3.562
2.069a .096 1.880 2.257
Age of patient (2groups)Aged 24-55
Aged 56-79
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Evaluated at covariates appeared in the model: Anxiety prior tocannulation = 2.30.
a.
3. Nurse ID
Dependent Variable: Anticipated pain
1.831a
.410 1.024 2.638
2.193a .163 1.872 2.515
2.275a .165 1.949 2.601
3.274a .613 2.068 4.481
3.127a .273 2.590 3.664
2.655a .133 2.394 2.917
Nurse IDAll other: 506, 509,514, 911
508
510
511
512
513
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Evaluated at covariates appeared in the model: Anxiety prior tocannulation = 2.30.
a.

Exploration of the Efficacy of Arm massage 133
4. Parameter Estimates - Anxiety prior to cannulation
Dependent Variable: Anticipated pain
.802 .058 13.733 .000 .687 .917ParameterPREANX
B Std. Error t Sig. Lower Bound Upper Bound
95% Confidence Interval
5. Age of patient (2 groups) * Nurse ID
Dependent Variable: Anticipated pain
1.270a
.734 -.175 2.716
2.453a .282 1.897 3.010
2.600a .284 2.039 3.160
4.366a 1.204 1.995 6.736
4.576a .505 3.582 5.571
3.035a .229 2.583 3.486
2.392a
.294 1.814 2.970
1.933a .193 1.553 2.313
1.950a .212 1.532 2.368
2.183a .282 1.628 2.738
1.677a .246 1.192 2.162
2.276a .161 1.958 2.593
Nurse IDAll other: 506, 509,514, 911
508
510
511
512
513
All other: 506, 509,514, 911
508
510
511
512
513
Age of patient (2groups)Aged 24-55
Aged 56-79
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Evaluated at covariates appeared in the model: Anxiety prior to cannulation = 2.30.a.
6. Parameter Estimates - Nurse ID*Anxiety prior to cannulation
Dependent Variable: Anticipated pain
-.231 .159 -1.449 .149 -.544 8.289E-02
-.199 .084 -2.371 .019 -.365 -3.373E-02
-.188 .091 -2.063 .040 -.367 -8.506E-03
-.129 .134 -.960 .338 -.393 .136
-.451 .103 -4.375 .000 -.655 -.248
0a
. . . . .
Parameter[RNURSEID=100] *PREANX
[RNURSEID=508] *PREANX
[RNURSEID=510] *PREANX
[RNURSEID=511] *PREANX
[RNURSEID=512] *PREANX
[RNURSEID=513] *PREANX
B Std. Error t Sig. Lower Bound Upper Bound
95% Confidence Interval
This parameter is set to zero because it is redundant.a.
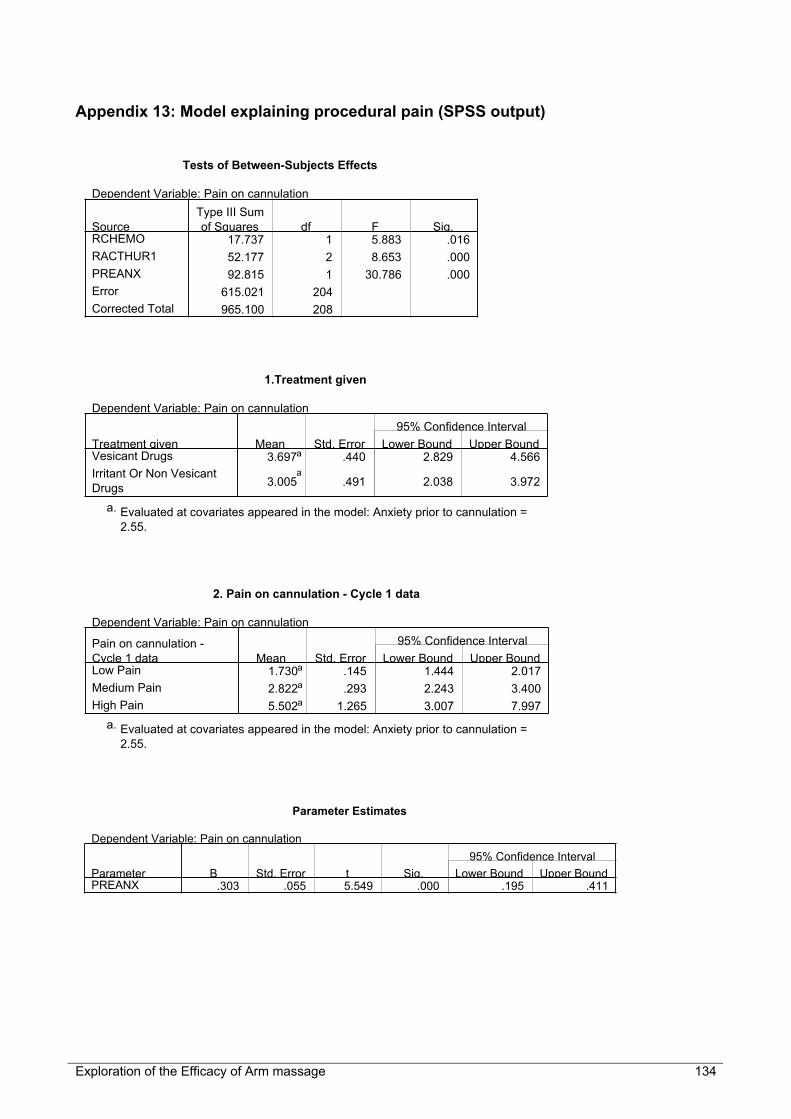
Exploration of the Efficacy of Arm massage 134
Appendix 13: Model explaining procedural pain (SPSS output)
Tests of Between-Subjects Effects
Dependent Variable: Pain on cannulation
17.737 1 5.883 .016
52.177 2 8.653 .000
92.815 1 30.786 .000
615.021 204
965.100 208
SourceRCHEMO
RACTHUR1
PREANX
Error
Corrected Total
Type III Sumof Squares df F Sig.
1.Treatment given
Dependent Variable: Pain on cannulation
3.697a .440 2.829 4.566
3.005a
.491 2.038 3.972
Treatment givenVesicant Drugs
Irritant Or Non VesicantDrugs
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Evaluated at covariates appeared in the model: Anxiety prior to cannulation =2.55.
a.
2. Pain on cannulation - Cycle 1 data
Dependent Variable: Pain on cannulation
1.730a .145 1.444 2.017
2.822a .293 2.243 3.400
5.502a 1.265 3.007 7.997
Pain on cannulation -Cycle 1 dataLow Pain
Medium Pain
High Pain
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Evaluated at covariates appeared in the model: Anxiety prior to cannulation =2.55.
a.
Parameter Estimates
Dependent Variable: Pain on cannulation
.303 .055 5.549 .000 .195 .411ParameterPREANX
B Std. Error t Sig. Lower Bound Upper Bound
95% Confidence Interval

Exploration of the Efficacy of Arm massage 135
Appendix 14: Model explaining time taken to cannulate (SPSS output)
Age of patient (2 groups)
Dependent Variable: Time taken to cannulate
6.564 1.171 4.255 8.873
3.848 .471 2.920 4.777
Age of patient (2groups)Aged 24-55
Aged 56-79
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Tests of Between-Subjects Effects
Dependent Variable: Time taken to cannulate
137.960 1 5.099 .025
126.038 1 4.658 .032
626.345 5 4.630 .001
423.708 5 3.132 .010
5411.290 200
6443.432 212
SourceCHEMO
AGE (2 Groups)
NURSEID
AGE (2g)*NURSEID
Error
Corrected Total
Type III Sumof Squares df F Sig.
Treatment given
Dependent Variable: Time taken to cannulate
6.175 .655 4.885 7.466
4.237 .861 2.539 5.935
Treatment givenVesicant Drugs
Irritant Or Non VesicantDrugs
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval
Nurse ID
Dependent Variable: Time taken to cannulate
3.735 1.637 .506 6.964
2.693 .872 .975 4.412
1.878 .807 .287 3.469
12.015 2.701 6.690 17.341
6.785 1.282 4.256 9.314
4.130 .693 2.763 5.497
Nurse IDAll other: 506, 509,514, 911
508
510
511
512
513
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval

Exploration of the Efficacy of Arm massage 136
Age of patient (2 groups) * Nurse ID
Dependent Variable: Time taken to cannulate
1.677 3.007 -4.252 7.605
2.700 1.424 -.107 5.508
1.715 1.268 -.786 4.216
22.031 5.219 11.739 32.323
6.697 2.166 2.425 10.969
4.563 1.066 2.462 6.665
5.793 1.328 3.175 8.412
2.686 1.001 .712 4.661
2.041 .943 .183 3.900
2.000 1.390 -.741 4.741
6.873 1.346 4.219 9.527
3.697 .832 2.055 5.338
Nurse IDAll other: 506, 509,514, 911
508
510
511
512
513
All other: 506, 509,514, 911
508
510
511
512
513
Age of patient (2groups)Aged 24-55
Aged 56-79
Mean Std. Error Lower Bound Upper Bound
95% Confidence Interval