an anesthesia handbook for residents - harvard … · this includes an introduction to the ......
TRANSCRIPT

An Anesthesia Handbook for Residents

Name:Phone:Pager:

3
Dear colleague:
Welcome to the BIDMC anesthesia residency program. This booklet was written by several classes of residents to try and ease the transition from your internship into our anesthesia residency program. As you will see over the next few months, this is a big change. The first few months are the most challenging, so allow yourself four to six months to adjust to your new environment. All of us in the department will do everything possible to make this transition as seamless and painless as possible and the first year of residency a favorable experience.
This orientation booklet summarizes most of the pertinent information that you will need to help you during your day-to-day work. This includes an introduction to the first year of residency as well as a list of relevant phone numbers, and finally a list of drugs that you will be using in your daily work. We hope you find this book useful and that your residency will be educational as well as enjoyable. As you become more familiar with your new settings, we would appreciate any feedback and sugges-tions you may have.
Good luck.
Chief Residents2009-2010: Brian Hashim, Stephen Ratcliff, and Susie Wang

4
Table of Contents
I. Introduction Table of Contents ................................................. 1 Map ...................................................................... 6 “First Few Months” .............................................. 6 Calling Your Attending ...................................... 4 Setting Up for the Day……………….. ............... 7 Narcotic Kit .................................................. 8 Getting to Know the OR ............................... 9 Machine Check ............................................. 9 Room Set-Up ............................................... 10 OB Primer Week .............................................. 14 First Year Rotations ......................................... 15 End of the Day………… .................................. 17II. General Information for Residents ...................... 18 Lectures and Education ................................... 18 Pre-operative Evaluations ................................ 18 Post-operative Follow-up ................................. 21 Calls ................................................................ 22 OB Calls ...................................................... 23 West Calls…………………… ...................... 24 Codes……………… .................................... 29 Last East Calls ............................................. 30 Sick Calls .................................................... 31 Procedure for Calling in Sick ....................... 31 Float Week .................................................. 32 Call Requests and Red Book ....................... 32
5
III. Room Set-Ups and Checklists ............................. 33 Basic Room Set-Up .......................................... 33 Trauma Room Set-Up ...................................... 35 OB Call and Room Set-Up ............................... 37IV. Helpful Odds and Ends ....................................... 40 Lockers ............................................................ 40 Door Codes…………….. ................................. 40 Breaks………………………. ............................ 40 ACGME Case Log……………….. ................... 40 New Innovations………………. ....................... 41 Printing the Schedule………. ........................... 42IV. Phone Numbers and Contact Information .......... 43 Radiology Phone Numbers .............................. 43 Helpful Phone Numbers……………… ............. 45 Contact Information……………… .................. 49V. Commonly Used Anesthetic Medications….. ...... 51

6
Wes
t C
amp
us

7
East
Cam
pu
s

8
The first few months…
Welcome to residency!! We are sure that you will en-joy this time very much. In a few months you will be comfortable in your new environment and increasingly confident as an anesthesiologist. However, the transition period can be a little overwhelming. To help you in the first few weeks, you will be assigned to three attendings with which you will conduct most of your cases. This will provide a stable setting for you to learn the basics of an-esthesia. Other than 1-2 late calls observing the call team, you will not be taking any overnight calls in July. And as always, if you run into any problems or have any ques-tions…just ask any of the senior residents or chiefs.
Calling Your Attending
Usually, the new residents start on the East campus in the ambulatory setting with healthier patients and simpler cases. This will provide you with more opportunities to practice intubations, start IVs, etc. Throughout your residency, you will be expected to call your attending each night to discuss the next’s days cases. This will help you formulate an anesthetic plan for your patients. To add to the courtesy, please call your attending before 9 pm, while this can be intimidating initially, all the attendings know that you are starting out and are more than happy to help you formulate a plan for the next day.

9
Take a few minutes to think about what you would like to discuss with your attending prior to your call. Here are a few things to consider mentioning: 1. OR assignment and surgeon2. Patient basics (age, ht, wt, medical conditions)3. Airway concerns (airway exam, prior views on intuba-
tion, extra equipment needed)4. Anesthesia concerns (liver failure, renal failure, aller-
gies, PONV, motion sickness, etc.)5. Anything else that you might be worried or curious
about6. This is also a good time to bring up any topic you
would like to discuss or any procedure you would like to try for the next day
Setting Up For The Day
In the first few weeks, plan to arrive around 6:00-6:15 to set up your room. As you become more experienced with this, you may choose to arrive later. In any case, you should have set up your room and have started seeing your patient by 7:00. This will give you 30 minutes to conduct a preoperative assessment and start an IV. All pa-tients are to be in the OR by 7:30 and handed over to the surgeon by 7:45 (after induction). Please note: the East campus is very busy with a high turnover of cases. Being prepared and organized is key and will help your day run smoothly.

10
Narcotic Kit
When working on the East campus, you will receive a narcotic kit for the whole day. Once you sign out a narcotic kit you are RESPONSIBLE for all the narcs! Don’t be shy and count your narcotics before leaving the pharmacy window! Each OR has a box where you can lock your narcotics with two keys -- don’t lose the keys. On the East, when you get your kit they will also give you a key for the lock box in that OR. Be sure to either lock your narcs or keep them with you AT ALL TIMES! DO NOT leave any narcs in the room unattended.
If you leave the floor, please hand your narcs to your attending. Do not leave the building with narcs – this is especially important for Wednesday morning grand rounds. If transferring a kit to an attending or fellow resi-dent, make sure he/she signs his/her name on the narcotic sheet. The pharmacy is open from 6:45 am to 5:00 pm on the East Campus and 6:00 am to 6:00 pm on the West. If you’ve completed your cases by then, return your narcs (and key on the East) to the pharmacy. Otherwise, sign the narcotic sheet, seal the bag and then drop it in the safe next to the pharmacy on the East.
On the West Campus, you have to sign out a narcotic kit for each case (as opposed to the whole day as on the East) and you MUST keep your narcs with you at all times!! (If you would like to use the lock box on the West, make sure you ask the pharmacy for the key in the morning.)

11
The West Campus narcotics night drop safe is next to the double doors that lead to the Trauma ICU directly adja-cent to the pharmacy.
Getting to Know the OR
Knowing where to find your equipment will make you feel more comfortable in the OR environment. Try to be proactive and orient yourself with the blue bell cart, the OR, and the anesthetic workrooms.
You will be much more at ease on your West campus overnight calls if you know where to find some key equip-ment. It is very likely that you may have never seen some of the “gadgets” that we routinely use. Try to learn where to find them how to operate them (i.e. LMA’s, intubating LMA’s, light wand etc.) You can learn a lot about airway management by talking to the attendings and senior resi-dents that you work with.
Machine Check
It is important to make sure all of your equipment is set-up and working everyday. While it’s a good idea to read through the following procedure, do not worry if it sounds overwhelming. Your assigned attending can help you go though a proper machine check. And there will also be a formal session to go over the procedure that offers an opportunity to try everything out and ask ques-tions.
12
Room Set-Up
Policy Statement: The following inspection guidelines should be conducted in preparation for anesthesia. These guidelines will vary according to differences in equipment design and variations in clinical practice. Modification is necessary for non-circle breathing systems. The user should refer to the operator’s manual for special proce-dures or precautions.
Asterisk (*) indicates steps REQUIRING repeating, if same machine/successive cases/same anesthetist (after initial check out)
Procedure:1. Inspect anesthesia machine for: a) machine control number (note on anesthesia record) b) undamaged flowmeters, vaporizers, gauges, and
supply hoses c) complete, undamaged breathing system with ad-
equate CO2 absorbent d) correct mounting of cylinders in yokes; presence of
cylinder wrench2. Inspect and turn on electrical equipment requiring
warm-up; expose O2 Sensor to air (21% O2) a) Before plugging in Anesthesia machine into AC out-
let, turn main power switch to test electrical discon-nect alarm.
b) Check electrical outlets on the back of the anesthesia machine (if present).
13
1. Only the anesthesia ventilator, vaporizer, gas monitor, and/or devices that live on the machine should be plugged into these outlets.
2. Make sure all devices (from 1.) are receiving power.
c) Check electrical outlets. Make sure anesthesia machine and monitoring system are plugged into an independent AC power circuit; avoid using outlets in common with ESU’s (“Bovie”), blood warmers, OR tables, etc.
3. Connect waste gas scavenging system and adjust vacuum as required.
4. Check initial status, as follows: a) flow control valves are off. b) vaporizers are off, filled, and caps are sealed/tight-
ened5. Activate Fabius by pressing any button or turning on
the Oxygen flow.6. Check oxygen cylinder supplies. a) Disconnect oxygen pipeline supply and return
cylinder and pipeline pressure gauges to zero with oxygen flush valve.
b) Open one oxygen cylinder and check pressure (at least 600 psig). Close cylinder and observe gauge for evidence of high pressure leak.
c) With the oxygen flush valve, flush to empty piping. d) Open second oxygen cylinder (if present) and check
as in (b) and (c) above. e) Insure that at least one oxygen cylinder is full.
14
f) Open less full oxygen cylinder. g) Verify levels of other cylinders, if present, such as
Heliox or N2O; then close them.7. Test flowmeters, proportioning, and oxygen pressure
failure system. a) Connect N2O hose to pipeline (if necessary), verify
operation of all flowmeters throughout full range. b) Test Proportioning system by attempting to create a
hypoxic oxygen/N2O mixture. c) Set oxygen and other gas flows to mid-range. d) Close oxygen cylinder supply and flush system to
release oxygen pressure. e) Verify that all flows fall to zero and oxygen failure
alarm sounds; N2O & air should fall before oxygen. f) CLOSE FLOW-CONTROL VALVES8. Test central pipeline gas supplies. a) Inspect supply hoses (should not be cracked or
worn). b) Connect supply hoses, verify correct color-coding. c) Adjust all flows to at least mid-range. d) Verify that supply pressures hold (45-55 psig). e) CLOSE FLOW-CONTROL VALVES9. Ensure machine is in Standby mode (Fabius only) Run
System Checks and Calibrations. a) Press Run System Test and observe that the Fabius
passes all self-tests. b) Perform Flow Calibration as directed on screen. c) Perform calibration of oxygen monitor as directed
on screen.

15
d) Test low alarm; set alarm for next case. e) Verify additional gas monitor (i.e. Datex), if present,
at 21% and 100% oxygen. *f) Perform Leak/Compliance test as directed on screen
(first open circuit to expected length for next proce-dure)
10. Test manual and automatic ventilation systems and unidirectional valves.
a) Place the breathing bag (simulated lung) on Y-piece. b) Set appropriate ventilator parameters for next pa-
tient. c) Set O2 flow to 250 ml/min, other gas flows to zero. d) Switch to Ventilation mode (choose Volume or Pres-
sure controlled). e) Turn ventilator on and fill fresh gas decoupling bag
(on bag arm) and test lung with O2 flush. f) VERIFY that: -during inhalation, the breathing bag compresses ap-
propriately and test lung expands -during exhalation, the breathing bag refills and the
test lung contracts -volume monitor reading and pressure waveform are
consistent with ventilator settings g) Check for proper operation of unidirectional valves. h) Exercise breathing circuit accessories to ensure
proper function; test ventilator alarms. i) Turn ventilator OFF and switch to Manual/Sponta-
neous mode; remove and store test lung in bottom drawer.

16
*11. Check for appropriate level of patient suction.12. Connect and verify function/calibration of all other
monitors and accessories: such as Temperature, Air-way Pressure, ECG, CO2, SaO2, Blood Pressure, and Gas/Agent.
*13. Verify final settings of all controls: vaporizers off, all flowmeters off, set to Manual/Spontaneous mode, APL valve open.
14. Set and enable appropriate alarm systems on the anes-thesia machine and on other equipment to be used.
Room Set-Up – Please see the Basic Room Set-Up Section
OB Primer Week
Starting in August, each resident will spend a week in Labor and Delivery (L&D) learning the basics of OB anesthesia and how to place epidurals and spinals - AKA crash epidural course. Everyday, you should be on L&D promptly at 6:45AM to start setting up for the day and getting ready for check-out. By the end of this week you should be more comfortable with these procedures. Your OB week ends with a Friday/Sunday OB call. On Friday, there will be another CA-1 (already OB-trained) on call with you to help you out. Then, on Sunday you will take a regular junior OB call. From that point on, you will be taking both OB and West calls.

17
First Year Rotations
The majority of the first year is dedicated to providing anesthesia for “regular” OR cases on the East and West campuses. West campus cases tend to be more complex with a sicker patient population. In addition to these “regular” OR months, your will be doing a few subspeci-ality rotations
You will do rotations on OB, PAT, PACU, neuro, cardiac and vascular:
OB Month: During the OB month (not to be confused with the OB primer week,) you will learn about OB an-esthesia and become even more experienced taking care of laboring women. You will also become more experi-enced with handling routine and emergency C-sections. CA-1’s should always be on L&D by 6:45am.
PAT: There are a total of four weeks scheduled in the pre-op clinic. This four week period will be divided into two-week blocks in combination with two-weeks of PACU and two weeks of OR. This is a great time to learn about what is important in assessing patients before surgery.
PACU: You will also spend two weeks in the Post An-esthesia Care Unit (PACU) taking care of patients. This is a great opportunity to see how patients do after you take care of them in the OR. It can offer a lot of insight

18
into how you may want to manage your anesthetic intra-operatively and how it can affect the patient post-operatively.
Neuro Month: For neuro, you can be doing anything from craniotomies to carotid repairs to cerebral angio-grams to spine cases. These are great learning cases and often require a-lines and occasionally central lines.
Cardiac Month: There is also a full month in the Cardiac room. Once again, you are not expected to know everything, so don’t stress out! The idea here is to expose you to cardiac patients and the cardiac room. Usually you will do a few cases with a senior resident or a fellow in the room.
Vascular Month: Finally, during your vascular month you will learn to care for some of the sickest patients in the hospital – the vasculopaths. The neuro, cardiac and vascular months are good months to practice plac-ing A-lines, CVPs and PA catheters. Even though these months are demanding, they can be fun with a lot of hands-on work.
Float Week: Everyone also spends at least one week a year as the Float Resident, where you help the call team by giving dinner breaks, taking care of pre-ops, and lending a helping hand wherever it’s needed. Your
19
Float Week is discussed in further detail in the Calls Section.
End of the Day
When you finish your last scheduled case for the day, check with the floor manager before you take off for the day or head over to lecture. The floor manager may need you to start a new case, take over one, or do a preop. On a good day, he/she may just need you to go home!
20
II. General Information for Residents
Lectures and Education
One of the top strengths and priorities of this program is education. To meet this need, there are great resident lectures and books provided throughout your residency. Also, the staff is very knowledgeable and is always inter-ested in resident education. But ultimately, your education is your responsibility. If there are topics that you are inter-ested in – please take advantage of the resources available to you. Pick topics to discuss with your attending or ask them to help you learn about all the equipment you have available to you.
Resident Lecture: takes place three times a week at 4:30pm (usually in the following locations):
Monday 4:30pm West 4th Floor Conference Room (CC-439)
Tuesday 4:30pm West 4th Floor Conference Room (CC-439)
Thursday 4:30pm East Campus Simulator
These lectures vary from formal attending lectures to case presentations, resident presentations, to Evidence Based Medicine (EBM), mock orals, and more. Attendance is mandatory!! You will get relieved from the OR to attend the lecture most days.
21
Every once in a while the schedule will be very busy and you may not get relieved for lecture. If you are not relieved, email Stacey Chiacchio and the chief residents so that you can be excused from lecture. Please remember that attending lecture is a privilege, not a chore. There will be a sign in sheet in the conference room. Do not forget to sign it. On call residents do not attend lectures.
In addition to the 4:30 pm lectures, there are the 3:30 pm lectures for the CA-1’s in July. This is part of you core lec-ture series which will orient you to the theoretical aspects of anesthesia. The lectures are based on the baby Miller that was given to you by the department.
Once a month, we have an Evidence Based Medicine (EBM) conference, aka Journal Club. In these conferenc-es, 4 residents present papers from journals. The idea is to learn about the evidence behind our practice of anesthe-sia. Each resident presents once or twice each year. When asked to present a paper, please choose a paper from a “major” journal (i.e. Anesthesiology, Anesthesia & An-algesia, NEJM, Critical Care, JAMA or other prestigious journals). In addition, try to pick up a paper that is recent and relevant to our practice of anesthesia. These presenta-tions should be on power point.
Grand Rounds: begin at 7:00 am sharp on Wednesday mornings, followed by M&M conference at 8:00.
Wed 7:00am East Campus Sherman Auditorium

22
Attendance is mandatory unless you are on call. If you enter the main East campus entrance, you can ask about Sherman auditorium at the information desk. Please make sure that you set up your room before coming to grand rounds
Occasionally, you will be asked to prepare a M&M pre-sentation. When preparing a M&M presentation, please make a power point presentation and include any perti-nent parts of the OR anesthesia record and post operative documents. Electronic summary forms must be completed and emailed to Donna Johnson at [email protected] by the Monday prior to your presentation. In your presentation include pertinent references, which should be emailed to the department clinical staff (do not send it to the administrative staff) prior to your presenta-tion. All power point presentations MUST be loaded on the computer prior to the 7:00am lecture. Anesthesia Intranet: This is a great resource for residents. The Anesthesia Intranet can be accessed from any com-puter through the BIDMC homepage (http://home.care-group.org/) via “My Portal”. Information regarding call schedules, lecture schedules, ADEL (with rotation details), Red Book (see below), and attending contact info can all be accessed from the Anesthesia Intranet.

23
Pre-Operative Evaluations
Pre-operative evaluations are your responsibility. This is not only important for your learning and for calling your attending the night prior, but it is essential for patient safety.
In many cases, patients who were seen in the PAT clinic will have a pre-op done on our online system. If a patient does not have a pre-op, you can always look at the chart in the holding areas and get an idea about the patient’s medical history. This can be supplemented by the online record under CareWeb/OMR.
In addition, if you have an inpatient posted by 6pm, he/she MUST BE SEEN and have a preop done and con-sent signed the day BEFORE the procedure. This is your responsibility unless otherwise notified.
Post-Operative Follow-Ups
Post op checks (and notes) are MANDATORY for all inpatients and same day admit (SDA) patients within 24 - 48 hours after the surgery.
You are required to see your patients after surgery (if they are admitted to the hospital) and make sure that there were no anesthesia-related complications. This should also be documented in the patient’s chart (a short 3-4 sentences note should suffice). Notes should include

24
things like pain control, PONV, sore throat, recall, line/procedure complications, etc. Any complication related to anesthesia should be discussed with the attending anesthe-siologist.
Calls
As mentioned earlier, during the month of July you will not take any overnight calls. Instead, you will be assigned to 1-2 “late calls” on the West Campus to observe the call team. This is your month to absorb as much as you can, orient yourself to the hospital, the ORs and the depart-ment. You are not expected to know everything in the beginning, but that will change as time goes by, so keep up with your reading!!
There are several different types of OR call you will be taking during your residency: West call, OB call, late east, float, sick call, heart call and transplant call. As a CA-1, only the first five will apply to you. West and OB calls are overnight calls. With the late east calls, you will stay until the last cases of the day on the East are finished (generally 7-9pm). If you are there past 9pm, let the floor manager and the senior on overnight call know so that he/she can find someone to help you with starting cases the next day.
As the volume of cases continues to increase at BIDMC, our calls have been getting progressively busier. You may
25
even have a few nights when you do not see your call room. However, overnight calls can be very high-yield. This is when you get to participate in big cases that you may not see during the day.
1. OB Calls
When you have an OB call you may occasionally be scheduled to work in OB during the day. However, you usually have a regular day in the OR and then get relieved to your OB call at 4 pm. Therefore, you need to check your schedule the day before an OB call to find out if you are in the OR before your call. In fact, you should check your schedule every day because there may be mistakes that you can catch.
As a CA-1, you take a 24-hour call for OB. Senior resi-dents start their OB calls at 2 pm. There are two residents (junior and senior) and one attending on OB call. Your responsibilities include managing all the labor epidurals and any overnight C-sections.
When on call, make sure to carry the code beeper with you at all times. Please refer to the Codes Section for a more detailed description of responsibilities. Tips to surviving OB calls:
1. Make sure that the OR’s are ALWAYS set up for a stat c-section! See OB Set-Up Section for more details
26
2. Always make sure there are enough local anesthetic bolus syringes as well as CPC ready for stat c-sections
3. Don’t be shy – if you have questions, ask your senior resident or attending at any time!
4. Make sure you send a courtesy page to your attending before placing an epidural.
5. As in any other ward in the hospital, nurses are valu-able resources so be open to their advice and sugges-tions. However, never feel pressured to do something you are not comfortable with or do not feel is appro-priate. If in doubt, never hesitate to call your senior resident or attending for help/support.
2. West Calls
During your call on the West Campus you will take care of very sick patients. On weekdays, you will start your day by doing your own cases and then taking over cases until all the scheduled surgeries are done. During the day and overnight there will be add-on cases (typically urgent or emergent cases from the floors, ICU or ED). These add-on’s will be done by the call team as well.
On weekends and holidays the call team – residents and attending – need to show up at the OR board, in scrubs, ready to go, no later than 6:45AM. The previous night call team, in coordination with nursing, will plan the order of next day’s cases. It is the responsibility of the previous night call team, to have the OR room(s) set up,

27
the patient(s) preoped and lined up, so that case(s) can be started by 7:30AM.
A Tuesday night call ends about 8:45 AM on Wednesday (to allow for the new call team to attend grand rounds/M&M). Any other weekday call ends at approximately 7am.
Our designated trauma room is 15. Please make sure to set up this room as soon as you have time. This is impor-tant because a trauma case can come at anytime. If the room is not set up correctly, patient care may be com-promised. Please refer to the Trauma Room Section for correct set up.
When there are no anesthesia techs (generally: weekdays– after 10 pm, Saturdays – after 2 pm, Sundays – before 3pm) you are expected to turn over your room. A clean tray with clean ETT and Mac 3 blade can be found in the work-room. The dirty tray with the dirty blade should be placed in the cleaning room next to room 15. Also, please change the circuit and wipe down the anesthesia machine and blue bell cart with anti-septic solution. Also return the standard box and all other left over drugs (other than narcotics) to the omnicell.
We know that the last thing you want to do at 3 AM is clean your machine, but please think of your colleagues who will be using the machine next. We want to maintain

28
a clean workplace not only for our patients, but also for each other. We do this so that the teams in the morning can start their day smoothly. If you do not turn over your room it may cause delays in the morning and more impor-tantly, it may annoy your fellow colleagues.
The pharmacy closes at 6 pm. If you need medications after that, go to the omnicell between rooms 3 and 5. During weekdays, 5% albumin is the only medication you will be removing from the omnicell while the pharmacy is still open.
These are the abbreviations for the omnicell that will get you what you need for a case:• Standard=standardanesthesiabox.ItdoesNOT
contain your emergency drugs so you’ll have to take them separately.
• Major=Majornarcotickit• Syringepack=emergencydrugkitwithsmallphe-
nylephrine, atropine and succinylcholine syringes. You may want to get a couple extra phenylephrine syringes, especially if the patient is sick (a common theme during call…)
• You’llneedtopickupaninductionagentifyouplanon using something other than propofol (etomidate, ketamine, etc). Once again, if you have a sick patient it is not a bad idea to bring etomidate with you to the room.
• Inadditiontoalloftheaboveyoumaytakeantiemet-

29
ic medication and antibiotics as needed (the standard antibiotic is cefazolin 2 gm. For abdominal surgery you can pick up levaquin and flagyl, or ask the sur-geon when setting up your room). You may need to bring other medications like beta-blockers, pressors, etc. (depending on the patient’s medical condition). If you are not sure, ask your senior resident or attend-ing.
• Donottakeanythingfromanopenomnicellcom-partment other than what you have checked out. This is the only way pharmacy knows when to refill it!!
• Intraop,donothesitatetoaskthecirculatingnursefor help (getting you medications, for example) when on call. It is part of their responsibility as a circulator to get you meds and such. This is especially true on call when your attending and senior may be busy do-ing other cases.
After all the cases are done, you and your senior resident will split the pre-ops that need to be done for the next day’s add-on cases that have not already been seen by the float resident. All next day patients posted by 6:30am MUST be seen, H&P taken and consent signed prior to start of the next day. If there is a liver transplant, cardiac case, or any other major case scheduled to be done the next day, you MUST see them (regardless of the posted time). Communicate any outstanding issues to your at-tending or the floor manager before you leave.

30
If there is a cardiac case that is booked after 6 PM, the call team should pre-op the patient and call/text page the resident assigned to the case and fill them in. If, however, you are swamped in the OR, call the cardiac resident and let them know you will not be able to see their patient by a reasonable hour. They will have to come in from home and do their own pre-op.
The PACU is covered 24 hours by our department. During the day, it is covered by the PACU resident and attending. When the resident goes home (officially at 8 pm, but sometimes earlier), the resident signs out the patients to the float and overnight team. Sometimes, there are ICU boarders in the PACU (overflow patients). These patients are covered by the ICU team. All other patients are covered by us. It is a good practice to get to know the patients before going to sleep since you may be called by the nurses with questions/issues during the night. Nurses will be calling you for sign-outs as patients are ready to leave the PACU. In the morning, any non-ICU patient needs a short note describing the overnight events and the patient condition. It is the CA-1’s responsibility to sign-out patients and to write the morning notes unless you are in the OR. The PACU patients should then be signed out to the next day’s team or floor manager.
And finally, before going home after a long, hard call – be sure to hand your code beeper to the CA-1 on call that day and let the floor manager know that you are leaving. It is important to update the next day’s floor manager on

31
any issues with pre-ops, PACU patients, etc. before leav-ing post call. And just imagine going home and realizing you still have the code pager!
3. Codes
The anesthesia teams cover “code blue” and “anesthesia stat” on both campuses 24/7. When on call, make sure your code pager is on and that the battery is not dying. (There are extra batteries in Laura’s office on the West and Margaret’s office on the East.) You will get your pager from the overnight team. The overnight CA-1 CANNOT leave the hospital without handing over the code pager to the morning on call CA-1!!
The West campus is the “busier” campus as far as codes. When the code pager goes off, please go to the code loca-tion immediately. If you get there before your attending, try to get as much information about the patient.
Even if the patient is “crashing” and needs immediate intubation, according to hospital policy, you DO NOT attempt to intubate without your attending!! Bag mask the patient until your attending arrives, at which time you will formulate a plan with your attending and execute it together. While you are waiting, you should also let the nurses and respiratory therapists know what medications and equipment you might need.

32
Once you are done with the intubation you are required to write a note in the chart describing the events and the procedure. In addition, take the patient’s label to the anes-thesia office and fill out the blue form (ask your attending or senior the first time) for billing purposes.
Sometimes your attending will be giving either you or the senior resident a break during cases. If the code pager goes off, immediately return to your OR room to relieve your attending.
4. Late East Calls
In addition to overnight calls, we have a late call where three late residents (late 1, 2, and 3) and the float resident stay on the East campus to finish all the cases of the day. The float resident is relieved first to go to the West side. Late 1 finishes before late 2. Typically, this call ends any-where from 6 pm to 9 pm, but residents will stay to finish the cases for as long as needed.
The next day is a regular day. On weekdays, the late 1 resident acts as the sick call back-up, so please have your pager on you after you leave the hospital. On Fridays, the late 1 resident is also the sick call resident for the weekend and should keep their pager on for the whole weekend. As per duty hour requirements, residents are provided with 10 hours off between shifts. This means if you are at the hospital after 10 PM you may not return until 8 AM the next day. The late resident should then notify the senior

33
resident on call who can make arrangements and notify the AM floor manager. If it is not too late, it is also nice to let your attending for the next day know that you will not be starting the case the next morning because of the 10 hour rule.
5. Sick Calls
Sick calls are designed as back up in case a resident becomes sick. On weekdays, the late 1 resident is the sick call backup and should have their pager on even after leaving the hospital. The weekend “sick call” resident is late 1 on Friday. You must have your pager on you both Saturday and Sunday in case someone calls in sick.
6. Procedure for Calling in Sick
If you are unexpectedly unable to make it to work for any reason, and it is after hours, please speak with the Over-night West Attending. He or she is the only person who has the schedule in front of them and who has the ability to arrange for the appropriate coverage as well as prepare the room and patient as necessary. As a courtesy, it is ap-propriate to page your individual attending if it is before 9PM and let them know you will not be in the next day, but please do not page your attending late at night.
Please note: all unscheduled absences must be made-up from your vacation time – email the chief resident in charge of the vacation schedule to let them know of the unscheduled absence.

34
7. Float Week
This is a pretty long week. As float, you are expected to be at the hospital from noon to midnight. Make sure you eat lunch before arriving to the East Campus. As soon as you arrive, page the East Campus floor manager. Duties will include lunches and afternoon breaks, preops, and the occasional remote or add-on case. At 4:15 pm, you will be assigned to relieve a non-call resident on East for lecture. When East Campus goes down to 3 rooms the Float Resident will report to the West Campus floor man-ager. Duties on West include dinner breaks, pre-ops, and general assistance. It is not expected that the float resident will cover an additional (third) OR except in case of emer-gency. At 8:00 pm the float resident will assume coverage of the PACU after rounding with the PACU resident and attending.
The float resident is relieved when the pre-ops are done or by midnight, whichever comes first. Always check in with the West overnight attending before you leave for the night.
8. Call requests and Red Book
Specific call requests will be solicited by email by the scheduler a month or two ahead of time. Please check the draft copy of the schedule as it comes out for any con-flicts.

35
The Red Book is an electronic request book located on the anesthesia intranet. If you have a specific request, for example a committee meeting you need to attend, please make this request via the red book. Medical and dental appointments should be scheduled for post call days as much as possible.
III. Room Set-Ups and Checklists
Again, as a general room you should plan to arrive around 6:00-6:15 to set up your room (especially during your first few weeks). As you become more experienced with this, you may choose to arrive later. For most cases, you should have set up your room and have started seeing your patient by 7:00. But some cases will require more extensive room set-ups and patient preparations. If you have a big case, it is your responsibility to manage your time so that you will have the room and patient ready to go by your 7:30 start time. For the room, this can include setting up triple tranducers, ultrasound, fiberoptic carts, etc. For the patient, this may include several large IV’s, a-lines, epidurals, or blocks.
1. Basic Room Set-up – A commonly used pneumonic is MSMAIDS
a. MACHINE - Complete your machine checkb. SUCTION – i. Check that suction is on MAX ii. Make sure that canister is upright with appropri

36
ate tubing iii. Attach your Yankauer tipc. MONITORS – Make sure that all of your monitors are
working appropriately and the necessary equipment is available (including pulse ox, CO2 monitor, BP cuff, ECG, temp probe, invasive monitoring if needed, etc)
d. AIRWAYS – i. Check the laryngoscope handles and attach appropri-
ate blades ii. Set-up ETT (with stylette if needed) with cuff checked
and syringe attached iii. Oral airway with tongue blades iv. Make sure that there are LMAs, boogies, lube, nasal
airways, OGTs, temp probes, and bite block availablee. IV – i. For pre-op 1. IV catheters 2. Alcohol swabs 3. Gauze 4. Tourniquet 5. Lidocaine in skin needle 6. Tegaderm and tape ii. For the OR, in addition to all the pre-op things you
also want to make sure you have 1. LR/NS available 2. IV tubing with stopcocks 3. Fluid warmer and blood tubing available if neededf. DRUGS – Label and date all syringes. You may want to
keep all vials until the case is concluded

37
i. Induction 1. Lidocaine 2. Propofol and/or Etomidate 3. Paralytic (Sux/Vec/Roc/Cis) ii. Controlled 1. Midazolam 2. Narcotic (Usually fentanyl for induction and pos-
sibly morphine or dilaudid for the case) iii. Emergency 1. Sux 2. Atropine 3. Phenylephrine 4. Ephedrine 5.Available in blue bell a. Bicarb, epi, calcium, etc.g. SPECIAL STUFF – i. Ambu Bag ii. Eye tape iii. ETT tape iv. And everything that you may need for your cases
(including a chair or stool)
2. Trauma Room Set-Up
a. Set up and check the anesthesia machine b. Have 7.0 and 7.5 ETT’s ready with stylettes and sy-
ringes for the cuffsc. Have syringes labeled (but no meds drawn up!)d. Have at least 2 syringe pumps (Baxter pumps) con-
nected to the AC cord

38
e. Med box in the blue bell cart (leave narcs in PYXIS until you need them)
f. ECG, pulse ox, BP cuff all checked and ready to gog. Have two LR IV bags hanging (but don’t spike them
open!). Tape Y-piece IV tubing (blood tubing) to each bag (so all you need is to spike them thus ready to go…)
h. Have a-line equipment (20g iv, guide wire, armboard etc) ready
i. Hang pressurized heparin bag, transducers (3-in-one), but not spiked. You can connect the transducers to the cables, tape the tubing to the heparin bag and organize everything in such a way that you only need to spike the bag at the beginning of a case (basically connect everything but don’t spike the bag. When trauma comes in, all you need to do is spike the bag and zero the transducers).
j. In addition to the regular blue cart, bring the trauma cart in (is behind OR 15 and has lines etc.)
k. Have the LEVEL ONE with lines in room (once again, don’t spike the bags)
l. Make sure you have at least one fluid warmer with tub-ing. If possible, have two fluid warmers ready to go
m. Make sure you have a forced air unit (Bair Hugger)in the room and upper as well as lower body blankets
n. Make sure things are generally where they should belong and that you have enough supplies. Get yourself familiar with the room once you set it up. This will help you find things that you need when you start a hectic case.

39
o. The reason why we don’t want to open meds/IV bags is that we will throw things away if not used. Also, there have been problems with outdated meds (for example Neo/Nitro sticks). Therefore get everything in the room, but don’t open up unless you hear about a case that might go.
3. OB Call and Room Set-Up
a. Check OR A, B, and C so that you are ready for a c-section at any time.
i. Do the usual set-up and machine check used for any OR case. Pay special attention to having a variety of ETT sizes and blades. Make sure the suction is working
ii. Make sure there is pitocin available in the bluebell iii. Check the refrigerator for ephedrine, phenyleph-
rine, hemabate, cytotec, and methergine (pay attention to the expiration dates)
iv. Have the fluid warmer ready to go with extension tubing
v. Make sure there is a new Med box in the blue bell cart
vi. ECG, pulse ox, BP cuff all checked and ready to go
vii. Have a-line equipment (20g iv, guide wire, arm-board etc) ready
b. Draw medications for the day in the morning and twelve hours later. This should always be done with

40
two people so that one can witness the other. Make sure all syringes are labeled clearly with medication, date, time, and both people’s initials. Check the dates and times on the previous days medications and throw out anything that is older than 12 hours.
i Lidocaine: mix Lidocaine 2% (19 ml) + bicarbon-ate (1 ml) in a 20 ml syringe x2
ii. CPC: mix CPC 3% (19 ml) + bicarbonate (1 ml) in a 20 ml syringe x2
iii. Bupivicaine bolus: mix Bupivicaine ¼% (30 ml) + NS (30 ml) in a 60 ml syringe. Divide the solution into 8ml increments into 10 ml syringes x7
c. Epidurals/CSE/Spinals i. Stock epidural cart with all the things you might
need 1. Kit (epidural kit, spinal kit, or CSE kit depend-
ing on the procedure) 2. Iodine cleaning solution 3. Epidural pump tubing 4. Arrow catheter ii. Remove medications from the pyxis
1. Labor a. CSE - Bicitra/ BF bag/ Bupivicaine 2mg &
Fentanyl 12.5 syringe b. Epidural – Bicitra/ BF bag2. Scheduled C-section a. Spinal – Bicitra/Fentanyl 25 mcg (0.5ml)/
Astromorph 0.25 mg (0.5ml) /Bupivicaine PF 0.75%/11.25mg (1.5ml)

41
b. CSE – same medications. May need Lido-caine syringe if you need a longer block.
3. STAT C-sections with an epidural a. Fentanyl 100 mcg x2/Astromorph 10 mg
x1/Ancef 2 g x1/Zofran 4mg/CPC syringe/Lidocaine syringe
d. Unplanned C-sections with an Epidural i. Dose up the epidural for C-section 1. Give Fentanyl 100 mcg via epidural 2. If emergent: give CPC 10 ml in the room. Be
very careful to watch the BP once you are in the OR. Have Lidocaine available for a longer act-ing block.
3. If urgent: give Lidocaine 5 ml at a time. Redose every 10-15 minutes while checking the patient’s level.
4. Give astromorph 3mg after the baby is out ii. Place monitors on the pt prior to dosing up the
epidural if possible iii. Keep left uterine displacement with the wedge iv. Connect the fluid warmer v. Give O2 via face mask until the baby is delivered vi. Start Antibiotics vii. Once uterine incision has been made 1. Get ready to lower the bed 2. Warn the pt that there will be a lot of pressure
with delivery viii. When the baby has been delivered. 1. Remove the wedge

42
2. Mix the pitocin into your fluid (about 10 units per 500 ml of LR). The pt can get nausea with the pitocin-so have Zofran ready
3. Give astromorph (if appropriate) via epidural 4. Remove face mask
IV. Helpful ODDS and ENDS
1. Lockers
Each resident should have a locker on the East and West campus. Please let us know if you have a problem getting a locker.
2. Door Codes
CC-439 Library/Conference room: access swipe cardWest campus residents lounge: 13112Call rooms: access swipe card
3. Breaks
Morning and afternoon breaks are 15 minutes, lunch is 30 minutes.
4. ACGME Case Logs
After getting your ACGME login name and password, you should log in your cases on the ACGME web site – www.acgme.org. This is a self-explanatory site, but you may want to ask a senior resident to show you how to do
43
it the first time. You must log all cases/procedures even during non OR months such as ICU and Pain. Please note: in the top section marked “A1 region” any region of the body that is not specified by one of the tabs should be marked as “other.” As the ACGME has changed the training requirements, it is imperative that you update your case logs monthly or more frequently to ensure that you have accurate records of your cases.
It’s easiest to log in your cases at the end of each day, but the AIMS system can help you keep track of all your pro-cedures and cases (except the OB cases and pain consults/procedures). For OB, make sure you record all of the epidurals, spinals, and c-sections that you are involved in. CSE’s can be logged as BOTH an epidural and a spinal. 5. New Innovations
The Graduate Medical Office has changed to a web based evaluation program called New Innovations which all GME programs use. Copies of the power point presenta-tion on how to use this program will be given to you. The program also has an extensive “Help” section. You are required to complete confidential evaluations of all your rotations and attendings upon completion of your monthly rotations. Make sure you keep up with your evaluations, they can really add up. You may view your own evaluations at any time on this program.

44
Twice a year, you will also use New Innovations to com-plete you duty hour audit. This helps the department en-sure that we are within the 80 hour work week guidelines.
6. Checking and Printing Your Schedule
Around 2-3 pm each day the schedule becomes avail-able online. To check and print your schedule, go to the CareWeb home page (upper left of Caregroup home page, www.home.caregroup.org/). Then:
1. click on perioperative information management system
2. enter outlook username and password3. click on OR schedule display option4. click on OR schedule view5. select date and all suites6. find and select your name under the anesthesiologists
list7. click continue8. sort by anesthesiologist
This should yield your schedule for the day, you may view and print your schedule from home. Additionally, a copy of the schedule is posted in the East and West anesthesia offices. It’s a good idea to check the posted schedule in the morning, as rooms and cases can occasionally be changed overnight

45
V. BIDMC Phone Numbers:
All numbers are listed as x4#### (617.774.####) or x7#### (617.667.####)
Helpful Radiology Phone Numbers
Location Phone #Listening line 4-8583Body CT East Campus (includes CT-guided) 7-2745Body CT West Campus (includes CT-guided) 4-2603
4-2534Body MRI 7-9453Chest X-ray 7-5691
4-2537Chest CT 4-2537
7-5691Emergency roomPager
4-230637045
Fluoro East 7-2745Fluoro West 4-2745
4-2671Interventional Radiology 4-2552Musculoskeletal (x-ray and MRI) 7-9451
7-94557-9406
Neuro (CT and MRI) 7-1100Nuclear Medicine East 7-5242

46
Nuclear Medicine West 4-2640Ultrasound East Campus (includes U/S-guided)
7-2745
Ultrasound East Campus (includes U/S-guided)
4-2628
Ultrasound Outpatients (Shapiro) 7-8391
On weekdays after hours (5 PM-9AM) and weekends:
For West Campus cases: 4-2306 or page 37045For East Campus Cases: PAGE 3XRAY (39729)

47
East ORs Nursing Anesthesia
Feldberg 1 77601 78601
Feldberg 2 77602 78602
Feldberg 3 77603 78603
Feldberg 4 77604 78604
Feldberg 5 77605 78605
Feldberg 6 77606 78606
Feldberg 7 77607 78607
Feldberg 8 77608 78608
Feldberg 9 77609 78609
Feldberg 10 77610 78610
Feldberg 11 77611 78611
Shapiro 1 67101 67201
Shapiro 2 67102 67202
Shapiro 3 67103 67203
Shapiro 4 67104 67204
Shapiro 5 67105 67205
Shapiro 6 67106 67206
Shapiro 7 67107 67207
Shapiro 8 67108 67208
Cysto 77624 77626
Lithotripsy 78618
Anes L&D 73077
Pain Clinic 73334
Helpful Phone Numbers

48
West ORs Nursing Anesthesia
1 43061 43081
2 43062 43082
3 43063 43083
4 43064 43084
5 43065 43085
6 43066 43086
7 43067 43087
8 43068 43088
9 43069 43089
10 43070 43090
11 43071 43091
12 43072 43092
12A 43073 43093
14 43074 43094
15 43075 43095
16 43076 43096
17 43077 43097
Anes. Admin Phone Fax
Laura McLean 42675 754-2677
Margaret W. 73112 754-2735
Mary Jane Cahill 42733 754-2735
Stacey Chiacchio 42713 754-2735
Marcia Rich 42670 754-2735
Joanne Grzybinski 75042 667-5013

49
West Floors Phone
CC6 43150
CC7 43200
Farr 2 27272
Farr 3 27171
Farr 5 27550
Farr 6 27660
Farr 7 28710
Farr 8 28447
Farr 9/VICU 28738
Farr 10/Tx 28731
SICU 43250
T/SICU 43130
MICU A 43270
MICU B 43180
CCU 27600
CSRU 42900
ECT 28355
PACU Phone
Shapiro Phase I 70300
Shapiro Phase II 74790
Feldberg 73905
West 42800
Holding Area Phone
Shapiro 70200
Feldberg 75663/4
West 43100

50
Work Room Phone
Feldberg 74481
Shapiro 73432
West 43098
Call Rooms Phone
West senior 42737
West junior 43060
East junior 73084
East attending 75548
Pharmacy Phone
West (OR’s) 42870
East 74049
OR Main Desks Phone
West 43000
Feldberg 72411
Fish Bowl Phone
Window Tel 42852
Far side Tel 42851
Anes Lounge Phone
East 72970
West 42752
Anesthesia Tech Pager
East 31044
West 31043
Anes Lounge Phone
East 72970
West 42752
Others Phone
P.A.T. 43360
Neurointervention 42691
Blood Bank Phone
East 74480
West 43300
Stat Lab Phone
East 75227
West 43230
Cath Lab Phone
Room 6 27476
Room 7 27477
Holding area 27447

51
Staff 90623 Airen, Anshul (315) 372-305138116 Akhouri, Vimal (617) 243-096132820 Aner, Moris (857) 654-400033141 Bajwa, Zahid (617) 909-502133467 Barnett, Sheila (617) 965-608032329 Bose, Ruma (617) 734-734732340 Cohen, Bob (508) 847-545831725 Cohen, Stephen (781) 652-848431991 Cronin, Mary (617) 566-488132032 Desilva, Don (617) 965-079232495 Feinstein, David (781) 449-566290622 Fisher, Lauren (617) 803-613231239 Garry, Brendan (617) 243-036037189 Glidden, Randy (508) 653-762438469 Gulati, Patrick (781) 729-765438806 Hendricks, Cale (617) 276-793134467 Hess, Phil (781) 274-663491986 Jachna, Bo (617) 566-772932852 Jankun, Jeffrey (617) 451-183692491 Jones, Stephanie (774) 270-046833784 Karthik, Swaminathan (617) 959-138839042 Kindred, Amy (617) 320-770131035 Koch, Bill (781) 862-238235857 Kunze, Lisa (617) 987-017038809 Kveraga, Riki (508) 361-065231670 Leckie, Rob (617) 731-521839578 Leng, Kenny (917) 584-602030765 Leng, Shirie (617) 990-443632758 Lerner, Adam (978) 352-497338124 Li, Yunping (617) 969-6958

52
32181 Lisbon, Alan (508) 785-162831283 Long, Selina (508) 660-861236964 Mahmood, Feroze (781) 793-995936198 Matyal, Robina (781) 793-995932327 Mitchell, John (617) 519-391835874 Nagda, Jyotsna (617) 552-505331717 Oren-Grinberg, Achikam (617) 990-609031371 Panzica, Peter (978) 356-132631150 Pawlowski, John (781) 674-280835504 Peeters-Asdourian, Christine (617) 227-554131377 Pratt, Steve (617) 277-439931680 Ratnaraj, Joyson (617) 323-299831183 Reynolds, Deborah (617) 244-960039848 Sandrock, Norma (617) 916-203936204 Sarge, Todd (978) 769-553332056 Shahul, Sajid (773) 398-295633387 Shapiro, Fred (617) 720-373331156 Shnider, Marc (978) 526-754835304 Simopoulos, Tom (508) 460-382539579 Spiegel, Joan (617) 935-350035124 Steinbrook, Rick (781) 639-270833382 Subramaniam, Bala (781) 863-054238341 Sundar, Eswar (617) 264-918032966 Sundar, Sugantha (617) 264-918032178 Talmor, Daniel (617) 277-179938348 Vann, Maryann (508) 359-750232840 Vasudevan, Anu (617) 823-511293970 Wakakuwa, Jason (508) 655-387032004 Warfield, Carol (617) 416-173933777 Zapson, Dan (617) 244-748533112 Wilkerson, Margaret (617) 325-3706

53
Analgesics/NarcoticsFentanyl 25-100 mcg (0.7-2 mcg/kg). gtt: 0.3-3 mcg/kg/h
RemifentanilInduction: 1 mcg/kg/min. Maint: 0.25-0.4 mcg/kg/min
SufentanilInduction: 2-10 mcg/kg. gtt: 0.1-0.5 mcg/kg/h
Morphine 2.5-10mg (peds: 0.05-0.1 mg/kg) q 1-4 h
Hydromorphone 0.2-2 mg ( 0.01-0.04 mg/kg) q 4-6 h
Ketorolac 15-30 mg (0.5 mg/kg) q 6-8 h
Meperidine25-100 mg (0.5-2.0 mg/kg) SLOW IV. IM/SC: 50-150 (1-3 mg/kg)
Anesthetics/Sedatives
MidazolamSedation: 0.5-4 mg. Seizure: 2-5 mg (0.5-0.1 mg/kg)
DiazepamSedation: 2-10 mg SLOW IV. Seizure: 5-10 mg q 10-15 min
PropofolInduction: 2-2.5 mg/kg. gtt: 20-150 mcg/kg/min
Thiopental Induction: 3-5 mg/kg. Seizure: 0.5-2 mg/kg as needed
EtomidateInduction: 0.1-0.4 mg/kg. gtt: 0.25-1 mg/min (5-20 mcg/kg/min)
KetamineInduction: 1-2.5 mg/kg. Sedation: 0.5-1 mg/kg
DexmedetomidineInduction: 0.5-1 mcg/kg over >10 min. Then gtt: 0.2-0.7 mcg/kg/h
Methohexital Induction: 1.5-2.5 mg/kg. Sedation: 0.25-1 mg/kg
VI. Commonly Used Anesthetic Medications
Note: fellow residents prepared this chart for your refer-ence. For complete drug index and dosing instructions please refer to appropriate resources.

54
Muscle RelaxantsSuccinylcholine 0.7-1.0 mg/kg IV. IM: 2.5-4 mg/kg. Max 5 mg/kg
Vecuronium Intubating: 0.08-0.1 mg/kg. Maint: 0.01-0.05 mg/kg
Pancuronium Intubating: 0.04-0.1 mg/kg. Maint: 0.01-0.05 mg/kg
Cisatracurium Intubating: 0.15-0.2 mg/kg. Maint: 0.02-0.1 mg/kg
Rocuronium Intubating: 0.6-1.2 mg/kg. Maint: 0.06-0.6 mg/kg
Emergency/CardiacAtropine 20-40 mcg/kg. Asystole: 1 mg IV push
Adenosine 6 mg rpid push. Repaeat with 12 mg rapid push
AmiodaronePulsles VF/VT: 300 mg in 30 cc NS push. May repeat with
150 mg push. Max dose 2.2 g/d then 1 mg/min x 6 h,
then 0.5 mg/min
Supravent tachy: 300 mg IV over 1 h, then 20 mg/kg over 24 h
Dantrolene1-2 mg/kg q 5-10 min. Max 10 mg/kg or until MH symptoms resolve
Reversal AgentsNaloxone 40-80 mcg IV. Repeat every 2-3 min as needed
Flumazenil0.2 mg IV @ rate of 0.2 mg/min. Titrate to effect. Max dose 3 mg
Neostigmine0.05-0.07 mg/kg. Max dose 5 mg. Use with glycopyr-rolate (one dose)
Edrophonium0.5-1 mg/kg slow IV. Max 40 mg. Use with atropine (one dose)
Unless specified otherwise, most medications may be repeated to achieve a desired effect.
55
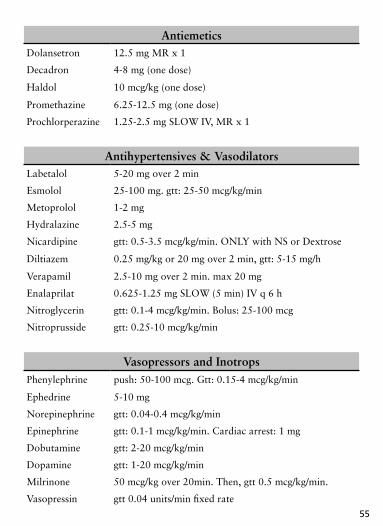
Verapamil 2.5-10 mg over 2 min. max 20 mg
Enalaprilat 0.625-1.25 mg SLOW (5 min) IV q 6 h
Nitroglycerin gtt: 0.1-4 mcg/kg/min. Bolus: 25-100 mcg
Nitroprusside gtt: 0.25-10 mcg/kg/min
Vasopressors and InotropsPhenylephrine push: 50-100 mcg. Gtt: 0.15-4 mcg/kg/min
Ephedrine 5-10 mg
Norepinephrine gtt: 0.04-0.4 mcg/kg/min
Epinephrine gtt: 0.1-1 mcg/kg/min. Cardiac arrest: 1 mg
Dobutamine gtt: 2-20 mcg/kg/min
Dopamine gtt: 1-20 mcg/kg/min
Milrinone 50 mcg/kg over 20min. Then, gtt 0.5 mcg/kg/min.
Vasopressin gtt 0.04 units/min fixed rate
AntiemeticsDolansetron 12.5 mg MR x 1
Decadron 4-8 mg (one dose)
Haldol 10 mcg/kg (one dose)
Promethazine 6.25-12.5 mg (one dose)
Prochlorperazine 1.25-2.5 mg SLOW IV, MR x 1
Antihypertensives & VasodilatorsLabetalol 5-20 mg over 2 min
Esmolol 25-100 mg. gtt: 25-50 mcg/kg/min
Metoprolol 1-2 mg
Hydralazine 2.5-5 mg
Nicardipine gtt: 0.5-3.5 mcg/kg/min. ONLY with NS or Dextrose
Diltiazem 0.25 mg/kg or 20 mg over 2 min, gtt: 5-15 mg/h

56

330 Brookline Avenue Boston, MA 02215 www.bidmc.harvard.edu
Affiliated with Joslin Clinic
A research partner of Dana-Farber/Harvard Cancer Center
Official hospital of the Boston Red Sox
Revised 6/09