an analysis of decisions by european general practitioners to admit
TRANSCRIPT

Thorax 1996;51:1017-1022
An analysis of decisions by European generalpractitioners to admit to hospital patients withlower respiratory tract infections
Tom Schaberg, Giuliana Gialdroni-Grassi, Gerard Huchon, Paul Leophonte, FedericoManresa, Mark Woodhead for the European Study Group of Community AcquiredPneumonia (ESOCAP) of the European Respiratory Society
Pulmonary Section,Chest Clinic ZumHeckeshorn 33,D-14109 Berlin,GermanyT Schaberg
Cattedra diChemioterapia,Universita di Pavia,ItalyG Gialdroni-Grassi
Service dePneumologie, HopitalAmbroise Pare,University de ParisRene Descartes, Paris,FranceG Huchon
Service dePneumologie, HopitalRangueil, Universityde Toulouse, Toulouse,FranceP Leophonte
Servei dePneumologia, Hospitalde Bellvitge,L'Hospitalet deLlobregat, Barcelona,SpainF Manresa
Manchester RoyalInfirmary, Manchester,UKM Woodhead
Correspondence to:Dr T Schaberg.
Received 2 October 1995Returned to authors13 March 1996Revised version received27 March 1996Accepted for publication29 March 1996
AbstractBackground - The purpose of this studywas to identify factors on which Europeangeneral practitioners (GPs) base theirdecisions to admit to hospital patientswith lower respiratory tract infections(LRTI).Methods - A survey was carried out fromDecember 1993 to January 1994 to identifyfactors that affect GPs' decisions to admitto hospital patients with LRTI by collect-ing data on 2056 patients from 605 GPs inFrance, Germany, Italy, Spain, and theUK.Results - Only 93 (4.5%) of the patientsincluded in the study were admitted tohospital. Univariate analysis showed thatage > 60 years, institutionalisation of thepatient, concomitant diseases, cardiacinsufficiency, asthma, a diagnosis ofpneu-monia, and clinical signs such as chestpain, cyanosis, tachypnoea and hypoten-sion significantly (odds ratio (OR) > 2.0,p < 0.002) influenced the decision toadmit to hospital. No influence could beshown for sex, smoking habits, history ofbronchiectasis or chronic bronchitis, thepresence of fever, chills, myalgia, cough orpurulent sputum, and the diagnoses ofacute bronchitis, influenza or exacerba-tion of chronic bronchitis. In the multi-variate analysis only the presence of chestpain (OR 2.3,95% confidence interval (CI)1.5 to 3.5), cyanosis (OR 4.1, 95% CI 2.4 to7.1), dyspnoea (OR 4.9, 95% CI 3.1 to 7.9),and hypotension (OR 2.9, 95% CI 1.6 to5.2), as well as a diagnosis of pneumonia(OR 6.6, 95% CI 4.3 to 10) (all p < 0.00001)remained as factors that significantlyaffected the decision to admit to hospital.Conclusions - Clinical signs of severeinfection and a diagnosis of pneumoniaare the main factors that induce GPs toadmit patients with LRTI to hospital inEurope.(Thorax 1996;51:1017-1022)
Keywords: hospitalisation, community acquired pneu-monia, chronic bronchitis, lower respiratory tract infec-tion.
Infections of the respiratory tract are the mostcommon types of infectious diseases in devel-oped countries. In the USA it has been
estimated that over 200 million episodes of res-piratory tract infections occur each year, corre-sponding to an incidence of nearly oneinfection per inhabitant per year.' In this studythe morbidity of these infections was found toaccount for an estimated 75 million physicianvisits and almost 150 million days lost fromwork per year. The costs of medical care alonewere estimated to amount to more than $10billion each year.' Although exact data on theincidence of respiratory tract infections are notavailable for Europe, an estimate of the trueincidence of lower respiratory tract infections(LRTI) in Europe is available from a study inthe UK where, in 1993, an incidence of 4400cases per 100 000 per year has been foundwhich was age related, ranging between 810cases per 100 000 in the 16-19 age group and12 150 per 100 000 in those aged 70-79years.2Most types of respiratory tract infections are
self-limiting but infections of the lower respira-tory tract such as pneumonia and acuteexacerbations of chronic bronchitis are stillsevere diseases associated with severe morbid-ity and a substantial mortality rate. Moreover,LRTI account for a substantial proportion oftotal public health costs, of which admission tohospital is one of the most important cost fac-tors. In the USA the cost of hospital admissionof patients with community acquired pneumo-nia exceeds 1.5 billion dollars per year,3 soevery effort has to be made to reduce thenumber of hospital admissions for LRTI. Onthe other hand, for some subgroups of patientswith LRTI, admission to hospital will clearlyreduce the risk of death or severe complica-tions.For physicians it is often difficult to differen-
tiate between patients with LRTI who can betreated at home and those for whom admissionto hospital will be life-saving. Previous studieshave shown that there is considerable variabil-ity in hospital admissions of, for example,patients with community acquired pneumo-nia,4 which suggests that there is a need forrecommendations on the decision whether ornot to admit such patients to hospital. Manystudies performed so far on the admission tohospital of patients with LRTI have concen-trated on the evaluation of patient-related ordisease-related risk factors associated with ahigher mortality or a complicated course.These studies have identified a number of riskfactors and strongly suggest hospital based
1017
Schaberg, Gialdroni-Grassi, Huchon, Leophonte, Manresa, Woodhead
Table 1 Demographic characteristics of the study population
Hospitalised patients Non-hospitalised patientsDemographic data (n=93) (n=1963)
Mean (SD) age (years) 61 (16) 50 (20)% male 61 52% employed 26 45% institutionalised 13 4% smokers 23 45% ex-smokers 35 23
Table 2 Concomitant diseases of the study population (Os)
Hospitalised patients Non-hospitalised patientsConcomitant disease (n=93) (n=1963)
Chronic bronchitis 21.5 14.5Cardiac insufficiency 20.4 8.4Asthma 16.1 7.2Diabetes mellitus 4.5 3.0Allergy 2.7 1.5Bronchiectasis 3.2 1.4Upper respiratory tract infection - 1.3Hepatic diseases 1.2Bronchial carcinoma - 0.3Others 6.9 3.6Any concomitant disease 67 43
treatment for those patients who show one ormore of these factors.6'i7 However, most ofthese studies have been performed from a hos-pital perspective and therefore may not beapplicable to general practitioners (GPs).We have therefore carried out a survey of
European GPs with regard to their manage-ment of patients with LRTI and have analysedtheir current practice of admission to hospitalin this patient group."i-19 The main goal of thisstudy was to identify factors that affect GPs'decisions to admit to hospital a patient withLRTI rather than to determine high riskgroups of patients with LRTI who should betreated in hospital.
MethodsData were obtained by interviews of 605 GPsconducted in five European countries (France(F), n = 123; Germany (G), n = 121; Italy (I),n = 120; Spain (S), n = 121 (Manresa, personalcommunication); UK, n = 120) from Decem-ber 1993 to January 1994 as describedpreviously.'0 0 GPs were asked to describe theway they had managed their last four patientswith an LRTI such as bronchopneumonia,pneumonia, acute bronchitis, acute exacerba-tion of chronic bronchitis, or flu or flu-like syn-drome. In this manner, information on 2056patients was obtained (F, 369; G, 484; I, 360;S, 363; UK, 480). The interviews were carriedout by SOFRES (Montrouge, France).
METHODS OF ANALYSISDifferences in variables between patient sub-groups were analysed using the X2 test andFisher's exact test for categorical variables asappropriate. The Student's t test was used forcontinuous variables. A two-tailed p value ofless than 0.01 was considered statisticallysignificant. When appropriate, continuousvariables were analysed as categorical variablesusing clinically defined cut off points. All vari-ables in the database were analysed to comparepatients with an LRTI admitted to hospitalwith those treated on an outpatient basis. Odds
ratios and their 95% confidence intervals werecalculated using a computed statistical analysissystem (GraphPad, San Diego, USA).
All factors which showed a significantassociation with the decision to admit to hospi-tal by univariate analysis (p < 0.01) wereentered into a multivariate analysis performedby multiway frequency tables, measures ofassociation, and the log-linear model using theP4F routines of the BMDP software package(University of California, Berkeley, USA). Thelog-linear model was used because the res-ponse variable was a binomial random variable(admission or no admission to hospital).Partial association tests were used to analysethe significance of deleting a particular effectfrom the model by calculation of the likelihoodratio. X2 and marginal association tests wereused to test the significance of deleting aneffect from the model which contains all effectsafter summing over levels of categorical vari-ables not included in the effect by calculationof the Pearson X2. Because of the multiple testsand the relatively small number of patientsadmitted to hospital, only p values of< 0.00001 were considered significant in themultivariate analysis.
Results
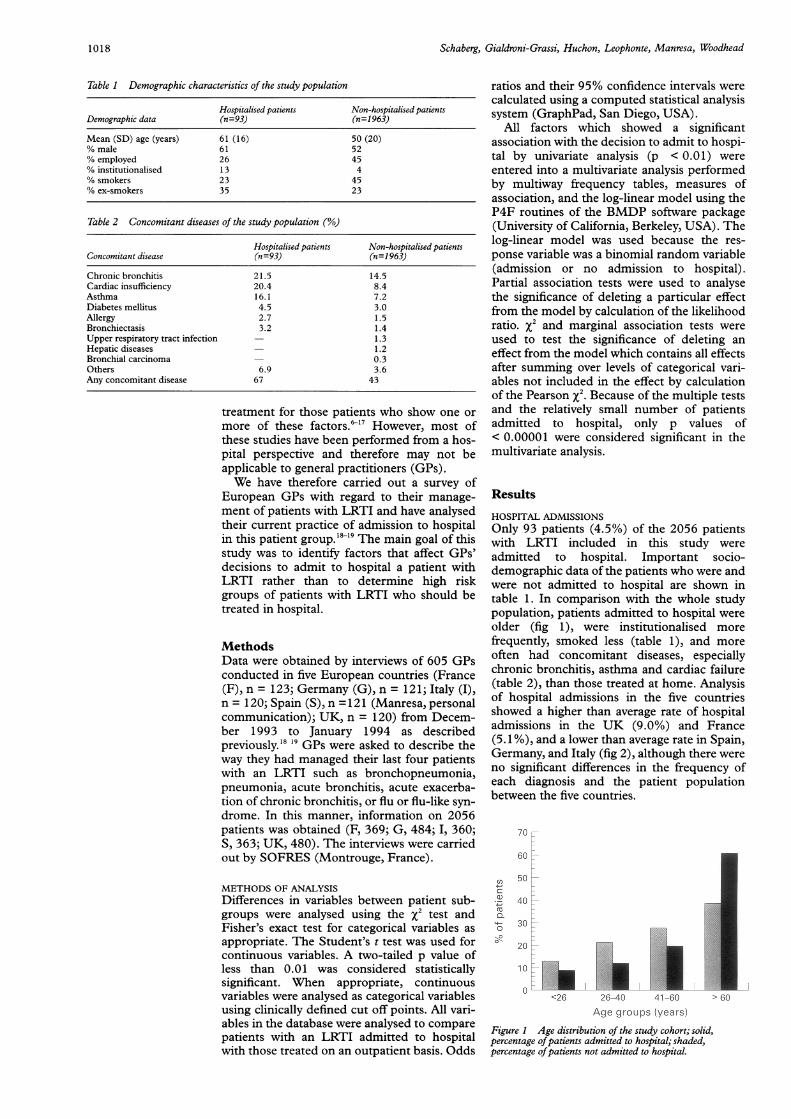
HOSPITAL ADMISSIONSOnly 93 patients (4.5%) of the 2056 patientswith LRTI included in this study wereadmitted to hospital. Important socio-demographic data of the patients who were andwere not admitted to hospital are shown intable 1. In comparison with the whole studypopulation, patients admitted to hospital wereolder (fig 1), were institutionalised morefrequently, smoked less (table 1), and moreoften had concomitant diseases, especiallychronic bronchitis, asthma and cardiac failure(table 2), than those treated at home. Analysisof hospital admissions in the five countriesshowed a higher than average rate of hospitaladmissions in the UK (9.0%) and France(5.1 %), and a lower than average rate in Spain,Germany, and Italy (fig 2), although there wereno significant differences in the frequency ofeach diagnosis and the patient populationbetween the five countries.
70
60
C',
0.
50
40:
30
20:
10
0<26 26-40 41 60 > 60
Age groups (years)
Figure 1 Age distribution of the study cohort; solid,percentage ofpatients admitted to hospital; shaded,percentage ofpatients not admitted to hospital.
1018

Admission to hospital ofpatients with lower respiratory tract infections
109
C. 9U,0°C 80
7
_ 6 ~~~~5.1E 5z.4.5-0
c 3z-2.8 2.7 2.5U,co 20."o 1
UK France Italy Germany Spain Average
Figure 2 Hospital admissions by country.
REASONS FOR ADMISSION TO HOSPITALPresentationSymptoms and signs present at the firstconsultation are shown in fig 3. The most fre-quent symptoms were cough, fever, and expec-toration of purulent sputum. Signs of moresevere infection were only seen in a fewpatients (cyanosis 6.5%, hypotension 6.6%).With the exception of cough (17.9%) and dys-pnoea (12.3%), only a small proportion of allsymptoms had been present before the onset ofthe current LRTI ( < 5%), but no differencescould be observed between patients admittedand not admitted to hospital. In contrast,patients admitted to hospital more oftenshowed signs of more severe types of infectionssuch as chest pain, cyanosis, dyspnoea orhypotension, whereas no differences were seenin the incidence of fever, chills, myalgia, cough,purulent sputum, and focal signs duringauscultation at the time of first presentation(fig 3).
Presumptive diagnosisBased on patient history, symptoms and signs,the .GP made a presumptive clinical diagnosisofLRTI which was attributed to one of the fol-lowing diseases: acute bronchitis (n = 678,33%), flu or flu-like syndrome with lowerrespiratory tract involvement (n = 605,29.4%), acute exacerbation of chronic bron-chitis (n = 397, 19.3%), and bronchopneumo-nia (without focal signs) or pneumonia (withfocal signs) (n = 368, 17.9%). Not surprisingly,
fewer patients with acute bronchitis or flu wereadmitted to hospital than those with pneumo-nia (table 3). The diagnosis of acute exacerba-tion of chronic bronchitis was the same in thewhole study population and in the groupadmitted to hospital. Univariate analysis ofassociation between the clinical diagnosis andthe rate of hospital admission showed a signifi-cant association of acute bronchitis or flu withoutpatient management and of pneumoniawith hospital treatment (table 3).
History of current LRTIAn abrupt onset of the symptoms of thecurrent LRTI was reported by 1342 (65.1%)patients and a more gradual onset by 720(34.8%). The mean time elapsed between theinitial symptoms of LRTI and the first consul-tation was 4.2 (2.7) days, but nearly half of thepatients saw their GPs within two days of theonset of symptoms. The first consultation tookplace at the doctor's surgery in 58.4% of thecases and at home in 41.6%. No significantdifferences were observed between patientswho were and were not admitted to hospital.
ANALYSIS OF ASSOCIATION BETWEENPATIENT-RELATED FACTORS, SYMPTOMS, ANDSIGNS AND ADMISSION TO HOSPITALThe association of 23 patient-related factors,symptoms, and signs with the hospital admis-sion rate was investigated by univariate analy-sis. No association was found for sex, smokinghabits, concomitant bronchiectasis or chronicbronchitis, and the current history of LRTIdevelopment (data not shown). This was basi-cally the same for the symptoms or signs suchas fever, chills, myalgia, cough, purulentsputum production, and auscultation findings(data not shown). In contrast, 10 patient-related factors, symptoms and signs showed asignificant association with the rate of hospitaladmission by univariate analysis (tables 4 and5). However, age >60 years, institutionalisa-tion, any concomitant disease, cardiac insuffi-ciency, and a history of asthma no longershowed a significant association with thehospital admission rate when analysed by multi-variate analysis (table 4). Only a presumptiveclinical diagnosis of pneumonia or broncho-pneumonia and signs of a more severe type ofinfection (chest pain, cyanosis, dyspnoea, andhypotension) were found to show a significantassociation with the hospital admission ratewhen analysed using a multivariate log-linearmodel (table 5).
!nt sputum ,//,/,////////////////>Discussionn_sputum Our findings show that the decision ofChest pain European GPs to admit to hospital patientsDyspnoea with lower respiratory tract infections is mainly
Fever _______________________________________________//////////S influenced by the presence of clinical signs of
Cough ,zZzzzzzZ/z/////////////////////////////////Smore severe infection and the presumptiveCough diagnosis of pneumonia. The overall rate oflIllIlllliiI ll iiI iiiIlIit9ali l |i hospital admission in patients with LRTI is
0 10 20 30 40 50 60 70 80 90 100 therefore low. This finding is encouraging forPercentage of patients all those concerned with the use of health care
3 Clinical symptoms and signs of the study population; solid, patients admitted to resources since costs of hospital admissionsrl (n = 93); shaded, patients not admitted to hospital (n = 1963). account for a considerable proportion of the
Diffuse signs
Hypotension
Cyanosis
Focal signs
Myalgia
Chills
Purule
Figurehospita
1019
666.7=
&"666i"

Schaberg, Gialdroni-Grassi, Huchon, Leophonte, Manresa, Woodhead
Table 3 Univariate analysis of association between clinical diagnosis and admission to hospital
Non-hospitalisedHospitalised patients
Diagnosis patients (n=93) (n=1 963) Odds ratio 95% CI p value
Acute bronchitis 5 (5.4%) 673 (34%) 0.10 0.04 to 0.3 < 0.0001Flu or flu-like syndrome 12 (12.9%) 593 (30%) 0.30 0.2 to 0.6 0.0002Acute exacerbation of chronic bronchitis 24 (25.8%) 373 (19%) 1.48 0.9 to 2.4 NSBronchopneumonia or pneumonia 52 (55.9%) 316 (16%) 6.61 4.3 to 10.1 < 0.0001Not defined - 8 (0.4%) - -
Table 4 Univariate analysis ofpatient relatedfactors, signs and symptoms in relation to admission to hospital
Hospitalised Non-hospitalisedFactors patients patients Odds ratio 95% CI Univariate p values
Age > 60years 57 720 3.0 1.7 to 4.0 < 0.0001Institutionalised 12 70 4.2 2.2 to 8.0 < 0.0001Any chronic disease 62 842 2.7 1.7 to 4.2 < 0.0001Cardiac insuffiency 19 164 2.8 1.6 to 4.8 < 0.0001Asthma 15 133 2.7 1.5 to 4.7 0.001
overall costs of LRTI. Previous studies ofpatients with LRTI showed admission ratesbetween 1% for patients with infections of theairways' up to 42% for those with communityacquired pneumonia." Since our study sum-marised all types of LRTI, our data are in goodaccordance with these findings. The differ-ences in the hospital admission rate betweenthe UK and the other four European countriesare likely to be related to the different types ofhealth care systems.Although there are no established guidelines
in Europe on hospital admission of patientswith LRTI, our results show that appropriateclinical assessment is a strong and usefulinstrument for making this decision. It issurprising to see how closely the practice ofGPs in Europe agrees with the guidelines forthe management of community acquired pneu-monia recently published by the AmericanThoracic Society (ATS). Specific risk factorsidentified by the ATS to increase the risk ofdeath or the risk of a complicated course inpatients with community acquired pneumoniaare age over 65 years, severe concomitantdiseases such as chronic obstructive airway dis-ease or cardiac failure, and physical findings ofsevere infection such as dyspnoea, hypoten-sion, or hypoxaemia. Admission to hospital ofpatients with community acquired pneumoniais strongly recommended when these riskfactors are present, especially if they occur incombination. In our study most ofthese factorsshowed a significant association with the GPs'decision to admit to hospital patients withLRTI, reflecting a wide agreement betweensuch recommendations and current clinicalpractice.The decision to admit patients with LRTI to
hospital is important, both from a clinical point
Table 5 Multivariate analysis ofpatient related factors, signs and symptoms in relation toadmission to hospital
Hospitalised Non-hospitalised Odds MultivariateFactors patients patients ratio 95% CI p values
Diagnosis of pneumonia 52 316 6.6 4.3 to 10.1 < 0.00001Chest pain 58 826 2.3 1.5 to 3.5 < 0.00001Cyanosis 47 87 4.1 2.4 to 7.1 < 0.00001Dyspnoea or tachypnoea 68 715 4.9 3.1 to 7.9 < 0.00001Hypotension 15 121 2.9 1.6 to 5.2 < 0.00001
of view and from a public health perspective.Despite this clinical and economic importance,to our knowledge only two studies have so faraddressed this issue. In a study by Fine andcoworkers22 physicians were asked to give theirreasons for admitting to hospital 63 patientswith community acquired pneumonia and notadmitting a further 87 patients with the samedisease. Their results suggested that physiciansrelied most often on the general clinicalappearance of their patients when making adecision about admission to hospital. Morespecifically, the severity of the current illness, ahigh age, and coexistent diseases were the mostimportant and significant criteria for this deci-sion, while financial considerations or socialfactors had a low ranking. A study by Koivulaand coworkers"3 identified a history of asthma,immunosuppressive therapy, and chronic lungdiseases as factors that significantly influencedthe decision to admit to hospital patients withcommunity acquired pneumonia, whereas ageor institutionalisation of the patient did notincrease the admission rate. The results ofthese two studies are in partial agreement withour findings in patients with communityacquired LRTI. However, when using multi-variate analysis for investigating a number ofsignificant factors that influence the decision toadmit these patients to hospital, we were ableto show that, besides a diagnosis of pneumo-nia, signs of more severe infectious disease aremost important.Our study does have some shortcomings.
Firstly, due to the design of the study it was notpossible to verify the diagnosis given by theGPs to an individual patient. However, we feelthat this is unimportant as it does not matterhow the GP makes the diagnosis, but it is whathe or she thinks with regard to the manage-ment of the patient with LRTI that isimportant. Secondly, since the patients werenot followed up we cannot draw any conclu-sions with regard to the actual necessity ofhospital admission in individual cases.Nevertheless, since the primary aim of ourstudy was to identify the criteria currently usedby European GPs in their decision to admit tohospital patients with LRTI, this does notinfluence our conclusions. However, the crite-
1020

Admission to hospital ofpatients with lower respiratory tract infections
Table 6 Risk factors for mortality andlor complicated course of lower respiratory tractinfections or community aquired pneumonia in seven studies
Type ofRisk factors Odds ratio p value analysis Reference no.
Age 2.8 < 0.05 MV 221.5 < 0.01 MV 16NA < 0.01 WV 6NA < 0.05 WV 12NA < 0.002 UV 10NA < 0.001 UV 15
Concomitant diseases 3.2 < 0.05 MV 222.5 < 0.01 MV 16NA 0.008 UV 10
Institutionalisation 3.2 < 0.0001 MV 169.0 < 0.05 MV 13NA < 0.05 UV 14
Immunosuppression 12.0 < 0.05 MV 2213.5 < 0.05 MV 132.8 < 0.05 MV 16NA < 0.05 UV 15
Arterial hypotension 3.7 0.014 MV 10NA < 0.01 WV 12NA < 0.05 UV 14
Tachypnoea ( > 30/min) 3.2 0.028 MV 101.5 < 0.01 MV 16
NA = not applicable; MV = multivariate; UV = univariate.
ria identified in this study should not be misin-terpreted as risk factors for admitting patientswith LRTI to hospital.
In contrast to the lack of information on thecurrent practice of admission to hospital ofpatients with LRTI, there are a lot of data onthe risk factors associated with death or a com-plicated course in these patients.II722 Most ofthese studies investigated patients with com-munity acquired pneumonia. Table 6 gives anoverview of recent studies on this subject.Sociodemographic factors significantly associ-ated with death or a complicated courseinclude age, concomitant diseases, immuno-suppression, and origin of the patient from aninstitution. Of the wide range of clinical signsand symptoms investigated in the differentstudies, hypotension and tachypnoea seem tobe the most important clinical factors associ-ated with morbidity and mortality. In our studythree of these factors (age, institutionalisation,concomitant diseases) were shown by univari-ate analysis to influence significantly GPs'decisions to admit to hospital, and the twoclinical signs (hypotension, tachypnoea) werealso found to be significant criteria in multi-variate analysis. Thus, the current clinicalpractice revealed in our study agrees, notonly with recent recommendations, but alsowith well documented risk factors that lead tothe admission to hospital of patients withLRTI.Based on the known risk factors for patients
with community acquired pneumonia, severalattempts have been made to develop apneumonia-specific risk score or prognosticindex for deciding when to admit such patientsto hospital.23-25 The most widely used risk fac-tors included in such indices are demographicand clinical parameters. An index based oncomorbidity, pre-existing lung diseases, extentof lung involvement on radiography, possibilityof aspiration, and duration of symptoms wasevaluated by Black and coworkers."4 Theyfound this scoring system to be useful in a rela-tively small number of patients (n = 141), butthis result remains to be validated in larger
trials. A pneumonia prognostic index devel-oped by Fine and coworkers primarily usesclinical data"5 such as age, chest pain, abnor-mality of vital signs, mental status, and highrisk aetiology of the infection. The scoring sys-tem, developed in a prospective study of 346patients admitted to hospital, was validated inmore than 14 000 patients and performed wellin classifying low risk patients but failed toidentify high risk patients. Moreover, scoringsystems using criteria such as high riskaetiology of the infection are of no use to GPssince this information is never available tothem.With regard to the currently used decision
criteria of GPs identified in our study, we feelthat future recommendations should lay em-phasis on the careful assessment of patient-related risk factors and on the physicalexamination instead of using scoring systems.Our finding that the criteria on whichEuropean GPs currently base their decisionto admit to hospital a patient with LRTIagree with both recent international recom-mendations and significant risk factors formortality or a complicated course of LRTIis encouraging and reflects good clinicalpractice.
This study was supported by grants from Rhone DPC Europeand Association pour l'Etude de la Respiration et del'Environement.
1 Garibaldi RA. Epidemiology of community-acquired respi-ratory tract infections in adults: incidence, etiology, andimpact. Am J Med 1985; 78: 32-7S.
2 Macfarlane JT, Colville A, Guion A, Macfarlane RM, RoseDH. Prospective study of aetiology and outcome of adultlower respiratory tract infections in the community. Lancet1993;341:511-4.
3 LaForce FM. Community-acquired lower respiratory tractinfections. Am J Med 1985;78(Suppl 6B):52-7.
4 Weinberg JE, McPhearson K, Caper P. Will payment basedon diagnosis-related groups control hospital costs? N EnglJMed 1984;311:295-300.
5 Fine MJ. Pneumonia in the elderly: the hospital admissionand discharge decision. Sem Respir Infect 1990;5:303-14.
6 Woodhead MA, Macfarlane JT, McCracken JS, Rose DH,Finch RG. Prospective study of the aetiology and outcome ofpneumonia in the community. Lancet 1987;i:671-4.
7 Research Committee of the British Thoracic Society and thePublic Health Laboratory Service. Community-acquiredpneumonia in adults in British hospitals in 1982-1983: asurvey of aetiology, mortality, prognostic factors andoutcome. QJ7Med 1987;239:195-220.
8 Macfarlane JT, Finch RG, Ward MJ, Macrae AD. Hospitalstudy of adult community-acquired pneumonia. Lancet1982;ii:255-61.
9 Sullivan RJ, Dowdle WR, Marine WM, Hierholzer JC.Adult pneumonia in a general hospital: etiology and hostrisk factors. Arch Intern Med 1972;129:935-42.
10 Farr BM, Sloman AJ, Fisch MJ. Predicting death in patientshospitalized for community-acquired pneumonia. AnnIntern Med 1991;115:428-36.
11 Feldman C, Kallenbach JM, Levy H, Reinach SG, HurwitzMD, Thorburn JR, et al. Community-acquired pneumoniaof diverse aetiology: prognostic features in patients admit-ted to an intensive care unit and a "severity of illnessscore". Intensive Care Med 1989;15:302-7.
12 Dahmash NS, Chowdhury MN. Re-evaluation of pneumo-nia requiring admission to an intensive care unit: aprospective study. Thorax 1994;49:71-6.
13 Koivula I, Sten M, Makela PH. Risk factors for pneumoniain the elderly. Am JtMed 1994;96:313-20.
14 Venkatesan P, Gladman J, Macfarlane JT, Barer D, BermanP, Kinnear W, et al. A hospital study of community-acquired pneumonia in the elderly. Thorax 1990;45:254-8.
15 Ortqvist A, Sterner G, Nilsson JA. Severe communityacquired pneumonia: factors influencing need of intensivecare treatment and prognosis. Scand Jf Infect Dis 1985;17:377-86.
16 Marrie TJ, Durant H, Yates L. Community acquired pneu-monia requiring hospitalization: a 5 year prospective study.Rev Infect Dis 1989;11:586-99.
17 Marrie TJ, Haldane EV, Faulkner R, Durant H, Kwan C.Community-acquired pneumonia requiringhospitalization - is it different in the elderly? JAm GeriatrSoc 1985;33:671-80.
1021

Schaberg, Gialdroni-Grassi, Huchon, Leophonte, Manresa, Woodhead
18 Huchon G, Gialdroni-Grassi G, Leophonte P, Manresa F,Schaberg T, Woodhead M. Initial antibiotic therapy forlower respiratory tract infection in the community: aEuropean survey. Eur RespirJ 1996 (in press).
19 Woodhead M, Huchon G, Gialdroni-Grassi G, LeophonteP, Manresa F, Schaberg T. Investigations of lower respira-tory tract infection in the community: a European survey.Eur RespirJ 1996 (in press).
20 Jokinen C, Heiskanen L, Juvonen H. Incidence ofcommunity-acquired pneumonia in the population of fourmunicipalities in Eastern Finland. Am Epidemiol1993;137:977-88.
21 American Thoracic Society. Guidelines for the initialmanagement of adults with community-acquired pneumo-nia: diagnosis, assessment of severity, and initial antimicro-bial therapy. Am Rev Respir Dis 1993;148:1418-26.
22 Fine MJ, Smith DN, Singer DE. Hospitalization decision inpatients with community-acquired pneumonia: a prospec-tive cohort study. Am Med 1990;89:713-21.
23 Karalus NC, Cursons RT, Leng RA, Mahood CB, RothwellRP, Hancock B, et al. Community acquired pneumonia:aetiology and prognostic index evaluation. Thorax 1991;46:413-8.
24 Black ER, Mushlin AI, Griner PF, Suchman AL, James RIJr, Schoch DR. Predicting the need for hospitalization ofambulatory patients with pneumonia. Gen Intern Med199 1;6:394-400.
25 Fine MJ, Singer DE, Hanusa BH, Lave JR, Kapoor WN.Validation of a pneumonia prognostic index using theMedis Group's Comparative Hospital Database. AmMed 1993;94:153-9.
1022