amniotic infection syndrome: nosology and reproducibility...
TRANSCRIPT

Amniotic Infection Syndrome: Nosologyand Reproducibility of Placental ReactionPatterns
RAYMOND W. REDLINE,1* ONA FAYE-PETERSEN,2 DEBRA HELLER,3
FAISAL QURESHI,4 VAN SAVELL,5 CAROLE VOGLER,6 AND THE SOCIETY FOR PEDIATRICPATHOLOGY, PERINATAL SECTION, AMNIOTIC FLUID INFECTION NOSOLOGY COMMITTEE1Department of Pathology, University Hospitals of Cleveland and Case Western Reserve University, 11100 EuclidAvenue, Cleveland, OH 44106, USA2Department of Pathology, University of Alabama at Birmingham, Birmingham, AL, USA3Department of Pathology, University of Medicine and Dentistry of New Jersey—New Jersey Medical School,Newark, NJ, USA4Pathology Department, DMC University Laboratories, Hutzel Site and Wayne State University, Detroit, MI, USA5Department of Pathology, Driscoll Children’s Hospital, Corpus Christie, TX, USA6Department of Pathology, St. Louis University School of Medicine, St. Louis, MO, USA
Received July 1, 2002; accepted May 12, 2003; published online September 11, 2003.
ABSTRACTClinically responsive placental examination seeks to pro-vide useful information regarding the etiology, progno-sis, and recurrence risk of pregnancy disorders. Thepurpose of this study was to assemble and validate acomplete set of the placental reaction patterns seen withamniotic fluid infection in the hope that this might pro-vide a standardized diagnostic framework useful forpracticing pathologists. Study cases (14 with amnioticfluid infection, 6 controls) were reviewed blindly by sixpathologists after agreement on a standard set of diag-nostic criteria. After analysis of initial results, criteriawere refined and a second, overlapping set of cases werereviewed. Majority vote served as the gold standard.Grading and staging of maternal and fetal inflammatoryresponses was found to be more reproducible using atwo- versus three-tiered grading system than a three-versus five-tiered staging system (overall agreement81% vs. 71%). Sensitivity, specificity, and efficiency forindividual observations ranged from 67–100% (24/30� 90%). Reproducibility was measured by unweightedkappa values and interpreted as follows: � 0.2, poor;
0.2–0.6, fair/moderate; � 0.6, substantial. Kappa valuesfor the 12 lesions evaluated in 20 cases by the six pathol-ogists were: acute chorioamnionitis/maternal inflamma-tory response (any, 0.93; severe 0.76; advanced stage,0.49); chronic (subacute) chorioamnionitis (0.25); acutechorioamnionitis/fetal inflammatory response (any,0.90; severe, 0.55; advanced stage, 0.52); chorionic vesselthrombi (0.37); peripheral funisitis (0.84); acute villitis(0.90); acute intervillositis/intervillous abscesses (0.65),and decidual plasma cells (0.30). Adoption of this clearlydefined, clinically relevant, and pathologically reproduc-ible terminology could enhance clinicopathologic corre-lation and provide a framework for future clinical re-search.
Key words: amniotic infection syndrome, chorioamnio-nitis, nomenclature, placenta, reproducibility
INTRODUCTIONThe general sequence of pathologic changes ac-companying amniotic fluid infection has been rec-ognized for some time [1, 2]. Other clinically rele-vant histologic patterns have been added to thisbasic framework [3–9]. Despite a fairly extensive*Corresponding author, e-mail: [email protected]
Pediatric and Developmental Pathology 6, 435–448, 2003
DOI: 10.1007/s10024-003-7070-y
© 2003 Society for Pediatric Pathology

literature on this topic, there has been little changein the prevailing diagnostic terminology which hasbasically been “acute chorioamnionitis with orwithout funisitis.” Recent data has suggested a re-lationship between placental inflammation andimportant clinical outcomes such as neurologicimpairment and chronic lung disease [10–12]. Thishas coincided with a more active clinical approachto the management of chorioamnionitis and pre-term labor [13]. These changes have led to the needfor more detailed description, more specific diag-nostic criteria, and greater standardization of di-agnostic terminology in this area.
As in other organ systems, questions havebeen raised regarding the reliability of placentaldiagnosis, i.e., the ability of expert placental pa-thologists to agree with each other and with theirgeneral pathology colleagues [14–16]. With re-newed interest in the clinical significance of pla-cental pathology, the time seems appropriate tointroduce more precision and uniformity in pla-cental diagnosis. With this in mind, the PerinatalSection of the Society for Pediatric Pathology hasundertaken an initiative to review, define, and val-idate diagnostic criteria for a number of differentplacental reaction patterns. The current report pre-sents the results of the Amniotic Fluid InfectionNosology Committee.
METHODSA study set of 20 cases was assembled from the filesof University Hospitals of Cleveland. Three slidesfrom each case (umbilical cord, placental mem-brances, and one full-thickness section of placentalparenchyma) were selected. Gestational age andplacental weight were provided for each case.Fourteen placentas were originally diagnosed byone of the pathologists (R.W.R.) with one or morefindings consistent with amniotic fluid infection.The remaining six placentas had other pathologicdiagnoses, but lacked signs of amniotic fluid infec-tion. Placental reaction patterns relevant to amni-otic fluid infection were chosen for evaluation.These patterns are described below, summarizedin Table 1, and illustrated in Figures 1–3. All caseswere examined in a blinded fashion by the sixmembers of the study group using a previouslyagreed upon set of diagnostic criteria (round 1).Terminology was chosen to correspond as closely
as possible to that proposed by the College ofAmerican Pathologists consensus group on placen-tal diagnosis [17]. Tabulated results from the pre-liminary round (round 1) were circulated and dis-cussed. Representative photomicrographs of eachlesion were reviewed at a meeting of the Society forPediatric Pathology—Perinatal Section. After theinitial review a second revised set of diagnosticcriteria were proposed and agreed upon. Twelve ofthe original cases were retained, eight new caseswere added (five new cases and three new con-trols), and the numerical order was changed. Thissecond overlapping set of 20 cases was then circu-lated for reexamination followed by an analysis ofindividual performance and reproducibility (round2).
The revised diagnostic criteria as agreed uponby the study participants before the final evalua-tion (round 2) were as follows:
Maternal inflammatory responsesStage/progression of disease
Stage 1 (acute subchorionitis/early acute chorion-itis) � patchy-diffuse accumulations of neutro-phils in the subchorionic plate fibrin (Fig. 1a)and/or membranous chorionic trophoblast layer (afew scattered neutrophils in the lower half of cho-rionic plate and/or the membranous chorionicconnective tissue are allowed) (Fig. 1b). Stage 2(acute chorioamnionitis) � more than a few scat-tered neutrophils in the chorionic plate or mem-branous chorionic connective tissue and/or theamnion (Fig. 1c). Stage 3 (necrotizing chorioam-nionitis) � degenerating neutrophils (karyorrhe-xis), thickened eosinophilic amniotic basementmembrane, and at least focal amnionic epithelialdegeneration/sloughage (Fig. 1d).
Grade/intensity
Grade 1 (mild–moderate) � individual or smallclusters of maternal neutrophils diffusely infiltrat-ing amnion, chorionic plate, chorion laevae, and/orsubchorionic fibrin (Fig. 1c). Grade 2 (severe) �
three or more chorionic microabscesses (microab-scess � confluent neutrophils measuring at least10 � 20 cells in extent) between chorion anddecidua in the membranes and/or under the cho-rionic plate (Fig. 1e) or a continuous band ofconfluent chorionic polymorphonuclear leuko-
436 R.W. REDLINE ET AL.

Tab
le1.
Pla
cen
tare
acti
on
pat
tern
sre
late
dto
amn
ioti
cfl
uid
infe
ctio
n:
no
men
clat
ure
and
defi
nit
ion
s
Dia
gno
stic
cate
gori
esS
ugg
este
dd
iagn
ost
icte
rmin
olo
gyD
efin
itio
ns
Mat
ern
alin
flam
mat
ory
resp
onse
Sta
ge 1—E
arly
Acu
tesu
bch
orio
nit
isor
chor
ion
itis
PM
Nin
sub
chor
ion
icfi
bri
nan
d/o
rm
emb
ran
etr
oph
obla
st(F
ig.
1a,b
)
2—In
term
edia
teA
cute
chor
ioam
nio
nit
isD
iffu
se-p
atch
yP
MN
infi
bro
us
chor
ion
and
/or
amn
ion
(Fig
.1c
)
3—A
dva
nce
dN
ecro
tizi
ng
chor
ioam
nio
nit
isP
MN
kary
orrh
exis
,am
nio
cyte
nec
rosi
s,an
d/o
ram
nio
nb
asem
ent
mem
bra
ne
thic
ken
ing/
hyp
ereo
sin
oph
ilia
(Fig
.1d
)
Gra
de 1—
Mil
d–m
oder
ate
No
spec
ial
term
inol
ogy
requ
ired
Not
seve
reas
defi
ned
bel
ow
2—S
ever
eS
ever
eac
ute
chor
ioam
nio
nit
isor
wit
hsu
bch
orio
nic
mic
roab
sces
ses
Con
flu
ent
PM
N(�
10�
20ce
lls
inex
ten
t)b
etw
een
chor
ion
and
dec
idu
a;�
3is
olat
edfo
cior
con
tin
uou
sb
and
(Fig
.1e
)
Oth
erC
hro
nic
(or
sub
acu
te)
chor
ioam
nio
nit
isS
ub
amn
ion
icm
onon
ucl
ear
cell
infi
ltra
tew
ith
occa
sion
alP
MN
(mec
oniu
man
dh
emos
ider
in-l
aden
mac
rop
hag
esex
clu
ded
)(F
ig.
1f)
Fet
alin
flam
mat
ory
resp
onse
Sta
ge 1—E
arly
Wit
hch
orio
nic
vasc
uli
tis
oru
mb
ilic
alp
hle
bit
isIn
tram
ura
lP
MN
-ch
orio
nic
vess
els
and
/or
um
bil
ical
vein
(Fig
.2a
,b)
2—In
term
edia
teW
ith
um
bil
ical
vasc
uli
tis
(on
eor
two
arte
ries
�ve
in)
oru
mb
ilic
alp
anva
scu
liti
s(a
llve
ssel
s)In
tram
ura
lP
MN
-um
bil
ical
arte
ryor
arte
ries
(�u
mb
ilic
alve
in)
(Fig
.2c
)
3—A
dva
nce
dW
ith
(su
bac
ute
)n
ecro
tizi
ng
fun
isit
isor
wit
hco
nce
ntr
icu
mb
ilic
alp
eriv
ascu
liti
sP
MN
�as
soci
ated
deb
ris
inco
nce
ntr
icb
and
s-ri
ngs
-hal
osar
oun
don
eor
mor
eu
mb
ilic
alve
ssel
s(F
ig.
2d)
Gra
de 1—
Mil
d–m
oder
ate
No
spec
ial
term
inol
ogy
requ
ired
Not
seve
reas
defi
ned
bel
ow
2—S
ever
eW
ith
ase
vere
feta
lin
flam
mat
ory
resp
onse
orw
ith
inte
nse
chor
ion
ic(u
mb
ilic
al)
vasc
uli
tis
Nea
rco
nfl
uen
tin
tram
ura
lP
MN
-ch
orio
nic
and
/or
um
bil
ical
vess
els
wit
hat
ten
uat
ion
/deg
ener
atio
nof
VS
MC
(Fig
.2e
,f)
Oth
erW
ith
asso
ciat
edfe
tal
vess
elth
rom
bi
Rec
ent
thro
mb
osis
asso
ciat
edw
ith
intr
amu
ral
PM
N(F
ig.
2f)
Oth
ersp
ecifi
cfe
atu
res
Per
iph
eral
fun
isit
isF
ocal
aggr
egat
esof
PM
Nat
the
um
bil
ical
cord
surf
ace
(Fig
.3a
)
Acu
tevi
llit
isP
MN
invi
llou
sst
rom
a(o
rb
etw
een
trop
hob
last
and
stro
ma)
(Fig
.3b
)
Acu
tein
terv
illo
siti
sw
ith
inte
rvil
lou
sab
sces
ses
Pat
chy-
dif
fuse
PM
Nin
inte
rvil
lou
ssp
ace
(Fig
.3c
)
Dec
idu
alp
lasm
ace
lls
Un
equ
ivoc
alp
lasm
ace
lls
ind
ecid
ua
bas
alis
orca
psu
lari
s(F
ig.
3d)
PM
N,
pol
ymor
ph
onu
clea
rle
uko
cyte
;V
SM
C,
vasc
ula
rsm
ooth
mu
scle
cell
.
AMNIOTIC INFECTION SYNDROME 437

cyte (PMN) more than 10 cells in width occupy-ing more than half of the subchorionic fibrin orone revolution of the membrane role. Chronic(or subacute) chorioamnionitis � more than oc-
casional maternally derived mononuclear cells(usually macrophages) in the chorionic plate(most frequently below the amnion) in caseswithout exogenous pigment deposition (i.e.,
Figure 1. Histologic features of reaction patterns relatedto the maternal inflammatory response to amniotic fluidinfection. a. Acute subchorionitis (maternal stage 1):neutrophils emanating from the intervillous space arediffusely scattered in the subchorionic fibrin. b. Acutechorionitis of chorion laevae (maternal stage 1): a bandof neutrophils emanating from decidual small venulesare gathered at the chorion laevae trophoblast layerwithout spread to the overlying amnion. c. Acute chorio-amnionitis, not otherwise specified (maternal stage 2,grade 1): neutrophils are seen in both chorionic and am-nionic connective tissue in the placental membranes. d.
Necrotizing (maternal stage 3) chorioamnionitis: degen-erating subamnionic neutrophils, thickened amnionicbasement membrane, and desquamation of amnionic epi-thelial cells are seen in placental membranes. e. Severe (ma-ternal grade 2) acute chorioamnionitis: (sub)chorionicmicroabscesses are depicted comprised of confluent ag-gregates of maternal neutrophils, at least 10 � 20 cells inextent. f. Chronic (subacute) chorioamnionitis: patchymaternally derived histiocytic infiltrate of the chorionicplate concentrated immediately below the amnionic sur-face (left). Occasional neutrophils are also present.
438 R.W. REDLINE ET AL.

meconium, hemosiderin). Neutrophils may berare or abundant, but a coexistent acute chorio-amnionitis should be present in at least one sec-tion (Fig. 1f).
Fetal inflammatory responsesStage/progression of diseaseStage 1 (chorionic vasculitis/umbilical phlebitis) �
neutrophils in the wall of any chorionic plate vessel
Figure 2. Histologic features of reaction patterns relatedto the fetal maternal inflammatory response to amnioticfluid infection. a. Acute chorionic vasculitis (fetal stage 1,grade 1): neutrophils are scattered throughout the up-per amnionic aspect of a major chorionic plate vessel. b.Umbilical phlebitis (fetal stage 1): neutrophils are iden-tified between the widely separated smooth muscle fas-cicles of the umbilical vein. c. Umbilical arteritis (fetalstage 2): neutrophils infiltrate the subendothelial cush-ion and tightly packed smooth muscle cells of the umbil-
ical artery. d. Subacute necrotizing funisitis (fetal stage3): an arc of degenerating neutrophils and mineralizedcell debris in Wharton’s jelly surrounds an umbilical ves-sel. e. Intense chorionic vasculitis (fetal grade 2): nearconfluent fetal neutrophils infiltrate the outer (am-nionic) wall of a chorionic vessel. f. Chorionic vasculitiswith adherent fetal vessel thrombus: a recent nonocclu-sive thrombus adheres to the outer (amnionic) wall of anacutely inflamed chorionic vessel.
AMNIOTIC INFECTION SYNDROME 439
(Fig. 2a) or the umbilical vein (Fig. 2b). Extensionof neutrophils into Wharton’s jelly is allowed if notaggregated in a concentric band, ring, or haloaround the umbilical vein. Stage 2 (umbilical vas-culitis) � neutrophils in one or both umbilicalarteries � vein (Fig. 2c). Extension of neutrophilsinto Wharton’s jelly is allowed if not aggregated ina concentric band, ring, or halo around the umbil-ical vessel(s). Stage 3 (necrotizing funisitis or con-centric umbilical perivasculitis) � neutrophils, cel-lular debris, eosinophilic precipitate, and/ormineralization arranged in a concentric band,ring, or halo around one or more umbilical vessels(generally most severe on the side nearest the pe-riphery of the cord) (Fig. 2d).
Grade/intensity
Grade 1 (mild–moderate) � scattered neutrophilicinfiltrate in the subendothelial or intramural por-tions of any chorionic (or umbilical) vessel (Fig.
2a). Grade 2 (severe) � chorionic plate (or umbil-ical) vessels with near confluent neutrophils plusattenuation and/or degeneration of vascularsmooth muscle cells on the side facing the amni-otic cavity (Fig. 2e). Associated fetal vessel thrombi� recent thrombosis of chorionic plate (or umbil-ical) vessel(s) in the context of a fetal inflammatoryresponse (Fig. 2f).
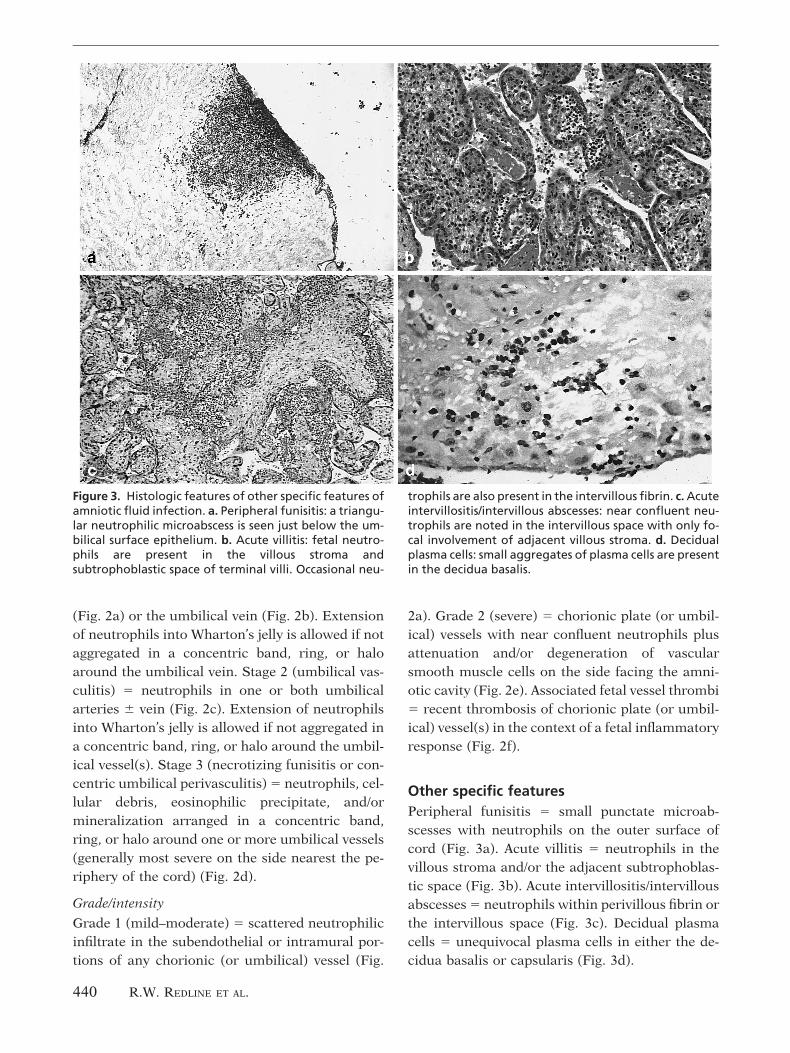
Other specific featuresPeripheral funisitis � small punctate microab-scesses with neutrophils on the outer surface ofcord (Fig. 3a). Acute villitis � neutrophils in thevillous stroma and/or the adjacent subtrophoblas-tic space (Fig. 3b). Acute intervillositis/intervillousabscesses � neutrophils within perivillous fibrin orthe intervillous space (Fig. 3c). Decidual plasmacells � unequivocal plasma cells in either the de-cidua basalis or capsularis (Fig. 3d).
Figure 3. Histologic features of other specific features ofamniotic fluid infection. a. Peripheral funisitis: a triangu-lar neutrophilic microabscess is seen just below the um-bilical surface epithelium. b. Acute villitis: fetal neutro-phils are present in the villous stroma andsubtrophoblastic space of terminal villi. Occasional neu-
trophils are also present in the intervillous fibrin. c. Acuteintervillositis/intervillous abscesses: near confluent neu-trophils are noted in the intervillous space with only fo-cal involvement of adjacent villous stroma. d. Decidualplasma cells: small aggregates of plasma cells are presentin the decidua basalis.
440 R.W. REDLINE ET AL.

Data analysisThe gold standard for the presence or absence of adiagnosis in each case was the group consensus.The diagnosis from the original institution was tobe used as the “tie breaker” in split cases, but wasnot required for any diagnosis in any case. Individ-ual variations from consensus grades and stageswere tabulated for rounds 1 and 2 and the percentagreement was determined. The final analysis(round 2) evaluated the following 12 reaction pat-terns: any maternal of fetal inflammatory response(grade and stage not � 0), severe maternal or fetalinflammatory response (grade 2), advanced stagematernal or fetal inflammatory response (stage 3),and the six other features listed above. Collectiveperformance of the group was assessed by combin-ing the individual diagnoses to derive specificity(true negatives/true negatives plus false positives),sensitivity (true positives/true positives plus falsenegatives), and efficiency (true positives plus truenegatives/total observations) relative to the goldstandard. Interobserver reliability was assessed byunweighted kappa analysis [18]. Kappa analysis isa measurement of agreement between observerson a case to case basis. Kappa values can varyfrom �1 to �1, with �1 indicating perfect in-verse correlation; 0, no correlation; and �1, per-fect positive correlation. Interpretation of kappavalues can vary. We used the following guide-lines: � 0.2, poor agreement; 0.2–0.6, fair/moder-ate agreement; � 0.6 substantial agreement [18].
RESULTSPreliminary analysisThe initial study set of 20 cases, 14 with featuresassociated with amniotic fluid infection and 6 con-trols, was circulated to group members for blindedreview and coding on standardized forms (round1). Analysis of the first round results revealed un-acceptable interobserver variation. A revised andsimplified set of definitions was circulated andagreed upon and a second overlapping set of studycases was circulated for review (round 2). The le-sions, terminology, and definitions used in the finalround are described in the Methods section, sum-marized in Table 1, and illustrated in Figures 1, 2,3.
Grading and stagingAll possible histologic gradations of intensity(grade) and progression of disease (stage) for ma-ternal and fetal inflammatory responses are poten-tially relevant to clinical outcome. However, exces-sive subclassification in the absence ofdocumented clinical significance is one cause ofunacceptable interobserver variability amongst pa-thologists. Table 2 compares the group perfor-mance using two different classification schemes,and shows the results from round 1 using a slightmodification of a previously described classifica-tion system used in research studies correlatingplacental diagnosis with clinical outcome [19].This scheme utilized three-tiered grading and five-tiered staging of both maternal and fetal inflam-matory responses. Overall agreement using thissystem was modest (71%) and particular problemsexisted in separating intermediate and low gradesof inflammation (Table 2). These distinctions areof no documented clinical significance. Most ofdisagreement was the result of minor disagree-ments (� 1) suggesting that a simplified schememight yield better reproducibility without sacrific-ing the clinical significance associated with highgrade and stage. For round 2, the number of gradeswas reduced to two, retaining the high grade cate-gories because of their established clinical signifi-cance (see Discussion). The number of stages wasreduced to three, distinguishing only those caseswith findings suggestive of early and advancedstage infection from those without these character-istics. The results shown in Table 2 showed a sub-stantial improvement in overall agreement (81%).
Final group survey results (round 2)A complete analysis of the group’s performance isshown in Table 3. Twelve reaction patterns wereevaluated: presence of any maternal or fetal in-flammation, presence of severe (grade 2) maternalor fetal inflammation, presence of advanced (stage3) maternal or fetal inflammation, chronic (sub-acute) chorioamnionitis, fetal vessel thrombi, pe-ripheral funisitis, acute villitis, acute intervillositis/intervillous abscesses, and decidual plasma cells.The gold standard for the presence or absence ofeach condition (prevalence) in the 20 study caseswas group consensus. Group consensus was unan-imous for 43/60 (72%) diagnoses and near unani-
AMNIOTIC INFECTION SYNDROME 441

Table 2. Stage and grade of infection, preliminary and final rounds, comparing expanded versuscontracted scales
Stage/grade No. of casesconsensuspositive
Individual deviations from consensusa
(% of observers)
Initial evaluation (round 1): three-tieredgrading/five-tiered staging
-2 -1 0 �1 �2
Maternal inflammatory response
Grade
1 2 — 8 67 8 17
2 2 0 8 50 42 —
3 10 3 17 80 — —
Combined 14 2 14 74 8 2
Stage
1 1 — 17 83 0 0
2 4 0 25 67 8 0
3 5 0 7 70 17 6
4 3 0 17 67 16 —
5 1 16 17 67 — —
Combined 14 1 16 68 13 2
Fetal inflammatory response
Grade
1 4 — 8 54 17 21
2 4 0 13 54 33 —
3 5 0 3 97 — —
Combined 14 0 8 68 17 7
Stage
1 4 — 8 88 4 0
2 1 0 50 50 0 0
3 2 0 0 83 17 0
4 4 3 11 83 3 —
5 1 0 0 100 — —
Combined 14 1 10 83 6 0
Overall performance (total observations) (324) 1 14 71 11 3
Maternal inflammatory response
Grade
1 5 — 3 84 13 —
2 9 0 11 89 — —
Combined 14 0 8 87 5 —
Stage
1 2 — 8 59 25 8
2 8 0 6 86 8 —
3 4 0 17 83 — —
Combined 14 0 10 81 8 1
Fetal inflammatory response
Grade
1 8 — 7 67 26 —
(continued)
442 R.W. REDLINE ET AL.

mous (5/6) for another 12%. Overall agreementbetween group prevalence and a priori prevalence(the original diagnosis of the submitting patholo-gist, R.W.R.) for the 10 lesions in the 20 cases was87%. The range of individual prevalences for eachlesion among the 20 cases was generally narrow.Group performance was evaluated in two ways.First, each individual response was classified astrue or false positive, or true or false negative,relative to the group consensus and overall sensi-tivity, specificity, and diagnostic efficiency. Overalldiagnostic efficiency was 84% or greater for alllesions studied. Sensitivity and specificity werealso high for the majority of diagnoses. Problemareas included relatively low sensitivity (� 85%)for advanced (stage 3) fetal inflammatory re-sponse, fetal vessel thrombi, decidual plasma cells,and chronic chorioamnionitis, and relatively lowspecificity (� 85%) for decidual plasma cells. Thesecond measure of individual performance was toevaluate overall agreement using the unweightedkappa (k) statistic. For this analysis, �-values wereinterpreted as follows: 0.00–0.20, poor; 0.21–0.60,fair/moderate; 0.61–1.00, substantial/near perfect[18]. By these criteria, none of the diagnoses fellinto the poor category. Reproducibility for pres-ence of any maternal inflammatory response, pres-ence of any fetal inflammatory response, severe(grade 2) maternal inflammatory response (Fig.1e), peripheral funisitis (Fig. 3a), acute villitis (Fig.3b), and acute intervillositis/intervillous abscesses(Fig. 3c) was substantial to near perfect. Reproduc-ibility for the remaining diagnoses—advanced
(stage 3) maternal inflammatory response (Fig.1d), severe (grade 2) fetal inflammatory response(Fig. 2e) advanced (stage 3) fetal inflammatory re-sponse (Fig. 2d), chronic (subacute) chorioamnio-nitis (Fig. 1f), fetal vessel thrombi (Fig. 2f), anddecidual plasma cells (Fig. 3d)—was fair to mod-erate.
DISCUSSIONPremature delivery is the major cause of perinatalmorbidity and mortality in the United States ac-counting for 70% of deaths, nearly half of cerebralpalsy, and a substantial proportion of other disor-ders including chronic lung disease, mental retar-dation, and sensorineural impairment [20]. Infec-tion of the amniotic fluid is either the initiatingevent or the final common pathway leading to de-livery in more than a third of these patients [21,22]. The term amniotic infection syndrome wasoriginally coined to encompass the circumstancesin which microorganisms enter the normally ster-ile amniotic sac, the sequence of maternal and fetalinflammatory reactions these organisms elicit, andthe adverse consequences of infection and inflam-mation for the mother and fetus [1]. Pathologistscan provide important information related to allthree components. In terms of predisposing condi-tions, pathologists contribute by recognizing bac-terial vaginosis on pap smear, detecting cervico-vaginal group B streptococci by culture, and by thediagnosis of subacute or chronic deciduitis (endo-metritis) in the delivered placenta [20, 23, 24].With respect to the sequence of maternal and fetal
Table 2. (Continued)
Stage/grade No. of casesconsensuspositive
Individual deviations from consensusa
(% of observers)
2 6 0 14 86 — —
Combined 14 0 10 76 14 —
Stage
1 4 — 17 83 0 0
2 7 0 11 79 10 —
3 3 0 28 72 — —
Combined 14 0 16 79 5 0
Overall performance (total observations) (336) 0 11 81 8 � 1
aPositive and negative numbers specify the number of stages or grades over or under the consensus score for each individual observer.
AMNIOTIC INFECTION SYNDROME 443

Tab
le3.
Fin
algr
ou
psu
rvey
resu
lts,
rou
nd
2
Les
ion
pre
vale
nce
for
the
20st
ud
yca
ses
Gro
up
con
sen
sus
Co
llec
tive
ind
ivid
ual
per
form
ance
(20
case
ssc
ore
dfo
r12
lesi
on
s)In
tero
bse
rver
rep
rod
uci
bil
ity
Pla
cen
tal
lesi
on
reac
tio
np
atte
rnA
pri
ori
Gro
up
Ind
ivid
ual
ran
ge6/
65/
64/
65S
ensi
tivi
tyS
pec
ifici
tyE
ffici
ency
Kap
pa
Mat
ern
alin
flam
mat
ory
resp
onse
An
y0.
700.
70(0
.65–
0.70
)14
00
100
9498
0.93
Gra
de
2(s
ever
e)0.
200.
45(0
.25–
0.55
)7
11
8895
920.
76
Sta
ge3
(ad
van
ced
)0.
150.
15(0
.15–
0.30
)2
10
9387
880.
49
Ch
ron
ic(s
ub
acu
te)
chor
ioam
nio
nit
is0.
100.
10(0
–0.
20)
00
275
9491
0.25
Fet
alin
flam
mat
ory
resp
onse
An
y0.
650.
70(0
.65–
0.70
)12
11
9610
098
0.90
Gra
de
2(s
ever
e)0.
300.
30(0
.25–
0.55
)4
11
9285
870.
55
Sta
ge3
(ad
van
ced
)0.
150.
10(0
–0.
20)
02
083
9493
0.52
Fet
alve
ssel
thro
mb
i0.
150.
20(0
.15–
0.35
)0
22
7587
840.
37
Oth
ersp
ecifi
cfe
atu
res
Per
iph
eral
fun
isit
is0.
100.
10(0
.10
–0.
20)
20
010
098
980.
84
Acu
tevi
llit
is0.
100.
10(0
.05–
0.10
)1
10
9210
098
0.90
Acu
tein
terv
illo
siti
s/ab
sces
ses
0.05
0.05
(0.0
5–0.
15)
10
010
097
970.
65
Dec
idu
alp
lasm
ace
lls
0.05
0.05
(0.0
5–0.
15)
00
167
7991
0.30
444 R.W. REDLINE ET AL.

inflammation, histologic chorioamnionitis has re-peatedly been shown to be both sensitive and spe-cific for infection and is considered the gold stan-dard against which other clinical predictors ofinfection should be measured [25–28]. Finally, asdescribed below, certain reaction patterns such asseverity of inflammation, associated fetal vascularthrombosis, patterns suggestive of a specific caus-ative organism, and estimation of the risk for neo-natal sepsis may identify infants at increased riskfor specific perinatal complications.
Most attempts to subclassify the inflamma-tory responses to amniotic fluid infection havebuilt upon the observations of Blanc who de-scribed what he believed to be the anatomic se-quence of events [29]. In this scheme, stage 1 wasdefined by neutrophils in the subchorionic fibrin,stage 2 by neutrophils in the chorionic plate, andstage 3 by neutrophils in the amnion. Van Hoevenand colleagues later found that amnionic necrosis(necrotizing chorioamnionitis), a late complica-tion of inflammation in the amnion, was associ-ated with an increased risk of perinatal death andpreterm delivery [9]. For this reason, they arguedthat this feature should be specified in the finalpathologic diagnosis. Mueller-Heubach and co-workers also described associations of necrotizingchorioamnionitis with preterm labor, prematurerupture of membranes, and decreased gestata-tional age in very low birthweight infants [7].
Severity of the maternal inflammatory re-sponse has been estimated in a couple of ways.keenan and colleagues in 1977 showed that sever-ity, as determined by the formation of subchori-onic microabscesses, was associated with an in-creased risk of presumed or documented fetalsepsis [4]. Muller-Heubach and colleagues pro-posed an alternative numerical system in which �
30 neutrophils in the upper half of the chorionicplate was considered severe [7]. However, severitydefined in the latter fashion has not been predictiveof clinically significant complications [10, 11, 30].This numerical definition was also poorly repro-ducible in our study (round 1). Better reproducibil-ity and the clinical significance described byKeenan et al. [4] lead us to recommend this as amore useful criterion for severity.
In Blanc’s original formulation, a fetal in-flammatory response was indicated by the pres-
ence of neutrophils in the walls of large fetal ves-sels in the chorionic plate and umbilical cord [1,29]. The presence of umbilical cord inflammationhas been shown to be a risk factor for clinicalmanifestations of the fetal inflammatory responsesyndrome including intraventricular hemorrhageand CNS echolucencies in preterm infants [6, 31].A greater association with complications in pre-term infants may relate in part to an increasedthreshold for mounting fetal inflammatory re-sponses in the less mature fetus [32]. It has gener-ally been observed that chorionic plate vesselsand/or the umbilical vein are involved prior to theumbilical arteries. Support for this sequence hasrecently been published by two recent studies dem-onstrating increased fetal cytokine levels and in-creased morbidity in patients with inflammation inone or both umbilical arteries compared to thosewith involvement of the vein alone [33, 34].Keenan et al. also demonstrated the additionalclinical significance of arterial inflammation byshowing that umbilical panvasculitis (veins plusarteries) was an independent risk factor for neona-tal sepsis [4]. In view of this data, it seems impor-tant to differentiate between involvement of theumbilical vein alone (phlebitis) and umbilical vas-culitis with arterial involvement. Use of the genericterm “funisitis” is not sufficiently specific andshould be discouraged.
Nararro and Blanc were also the first to de-scribe a later stage of fetal inflammation, subacutenecrotizing funisitis [3]. In this lesion, fetal neu-trophils migrate into the umbilical stroma (Whar-ton’s jelly), arranging themselves in a circular arearound the vessel. This pattern has been attributedto the precipitation of immune complexes formedby microbial antigens diffusing in from the amni-otic fluid and maternal antibodies diffusing outfrom the umbilical vessels [5]. Such immune com-plexes are chemotactic for fetal neutrophils. Mat-suda and coworkers later showed that infants withthis lesion are at significantly increased risk forchronic lung disease [35]. These observations de-fine three temporal stages of fetal involvement:stage 1, neutrophils in chorionic and/or umbilicalvein, stage 2, neutrophils in an umbilical artery,and stage 3, concentric arcs of degenerating neu-trophils in Wharton’s jelly.
AMNIOTIC INFECTION SYNDROME 445

Severity of fetal inflammation was found bySpong and coworkers to be a risk factor for severevariable decelerations and increased circulatingNRBC in very low birth weight infants [36]. Otherstudies by Redline et al. have shown that severefetal inflammation is a risk factor for neurologicimpairment in both very low birth weight and terminfants [11, 19]. While severity is more easily as-sessed and of better documented significance inchorionic plate vessels, umbilical vessels can alsobe assessed in cases where the chorionic plate hasnot been sampled. Much of the effect of severe fetalinflammation in the second group of studies citedabove was attributable to coexisting chorionic ves-sel thrombosis. Reproducibility for the diagnosisof fetal vessel thrombi was somewhat disappoint-ing in the present study, largely owing to ambigu-ity in cases with small foci of endothelial fibrindeposition. For diagnostic purposes, we recom-mend close adherence to the classic criteria for theidentification of true thrombi (glassy red-bluestaining, lamination, and adhesion to the vesselwall) when making this diagnosis (Fig. 2f).
Peripheral funisitis, the formation of superfi-cial umbilical cord abscesses, was a highly repro-ducible finding (kappa � 0.84). This pattern, whendiffusely distributed over the cord, is virtually pa-thognomonic for candida infection [5, 37]. Whenthe peripheral inflammatory response is focal andlocated near the placental cord insertion, the asso-ciation with candida is less specific. Our study setcontained one case of each type and both wererecognized by 100% of observers. Because of thisoverlap, a final diagnosis of candidal chorioamnio-nitis requires demonstration of fungal hyphae intissue sections.
The presence of neutrophils in the villousstroma may be found in two distinct patterns. Thefirst pattern, acute villitis with a minimal intervil-lous component, is believed to reflect overwhelm-ing fetal sepsis, often caused by gram negativebacilli such as E. coli [17]. The histologic findingsare acute capillaritis with emigration of fetal neu-trophils to villous stroma. Clusters of neutrophilsin acute villitis often accumulate between villousstroma and the villous trophoblast basement mem-brane (Fig. 3b). Bacteria are usually evident byroutine hematoxylin and eosin (H&E) stain. Thesecond pattern is acute villitis accompanied by in-
tervillositis and intervillous abscess formation(Fig. 3c). Acute villitis in these cases is less exten-sive than the intervillositis and is presumed to rep-resent secondary spread to villi. This pattern ismost commonly seen in infections caused by Lis-teria monocytogenes [38]. Campylobacter fetus anda variety of rare infections, such as coccidiomyco-sis, psittacosis, tularemia, and brucellosis, mayalso manifest some or all of these findings [39, 40].In the present study, the shared feature of acutevillitis was easily recognized and agreed upon byvirtually all observers (kappa � 0.90). The addi-tional finding of acute intervillositis/intervillousabscesses was recognized by all observers, but wasoccasionally overdiagnosed in cases of acute villitiswith occasional perivillous neutrophils leading to alower kappa value (0.65).
The final two patterns, decidual plasma cellsand chronic (subacute) chorioamnionitis, wereless reproducible and often missed in consensus-positive cases. Plasma cells in decidua, like those innonpregnant endometrium, are notoriously diffi-cult to detect. Overdiagnosis of cells lacking one ormore of the classic morphologic features can alsobe a problem. Chronic (subacute) chorioamnioni-tis requires the observer to recognize an underly-ing histiocytic infiltrate in membranes already suf-fused with neutrophils. It is possible that specialstains such as syndecan-1 for plasma cells andCD68 for histiocytes could improve reproducibil-ity. Plasma cells in particular, and B-lymphocytesin general, are always abnormal in the endometrialcavity [41]. Their presence is an indicator of inap-propriate antigenic exposure. One source of anti-gen is bacterial subacute endometritis, which maylead to recurrent acute chorioamnionitis in subse-quent pregnancies [20]. Uterine plasma cells in theabsence of acute inflammation are also associatedwith infertility, spontaneous abortion, and chronicvillitis [42–44]. We believe that the presence ofplasma cells should always be noted in the finaldiagnosis [45]. Chronic chorioamnionitis, on theother hand, is a heterogeneous entity that can ac-company either acute chorioamnionitis or chronicvillitis [46, 47]. This lesion overlaps with a veryrecently characterized lesion known as subacutechorioamnionitis [48]. In the latter report, pub-lished after completion of our study, subacute cho-rioamnionitis when combined with subacute ne-
446 R.W. REDLINE ET AL.

crotizing funisitis (our fetal Stage 3chorioamnionitis) was found to be a significantrisk factor for chronic lung disease. In view of itsevolving status and the lack of reproducibility inthe present study, we recommend that the terms“chronic” or “subacute” chorioamnionitis be usedsparingly and as descriptive adjuncts rather thanprimary diagnoses [49].
Reliability of placental diagnosis has not beenextensively examined. In one study, it was foundthat interobserver agreement between subspecialtyperinatal pathologists was better than that be-tween general surgical pathologists and perinatalsubspecialists [14]. Discrepancy rates in the lattersituation ranged from 32–59%. Some reliabilitystudies have been performed with other primarygoals, such as demonstrating that gestational agecannot be specified based on placental histologyalone and developing a working definition ofchronic deciduitis [15, 50]. Statistical measures ofreliability were not performed in these studies. Toour knowledge, only two studies have directly mea-sured reproducibility. Both were performed by ep-idemiologists for the purpose of validating the useof archived placental material in retrospectivestudies [16, 51]. Both concluded that reliability isexcellent for many placental lesions including thevarious stages of the maternal response in acutechorioamnionitis and the presence or absence of afetal response. While other diagnoses were lessreproducible, it was shown that reliability could beimproved through the use of a standardized studyprotocol. Our study is the first designed by pathol-ogists for the purpose of developing and standard-izing diagnostic criteria that included statisticalevaluation of reproducibility. Furthermore, it isthe first to comprehensively address all pathologicfindings related to a single perinatal process, inthis case amniotic fluid infection. Additional stud-ies are in progress to apply the same procedure totwo other processes—maternal vascular underper-fusion and fetal thromboocclusive disease.
In conclusion, we have proposed and vali-dated a system for describing the maternal andfetal inflammatory responses to amniotic fluid in-fection plus a number of other reaction patternsuseful for defining the etiology and clinical conse-quences of infection. We have attempted to utilizeterminology and criteria that conform as closely as
possible to previously reported schema. Westrongly advocate the use of this, or a similarlyconstructed, system to help standardize diagnosesbetween hospitals, provide useful information toclinicians, and serve as a valuable tool for conduct-ing future studies relating placental risk factors toadverse perinatal outcome.
R E F E R E N C E S1. Blanc W. Amniotic infection syndrome: pathogenesis, mor-
phology, and significance in circumnatal mortality. Clin.Obstet. Gynecol. 1959;2:705–734.
2. Naeye RL. Disorders of the Placenta, Fetus, and Neonate.Diagnosis and Clinical Significance. St. Louis: Mosby-YearBook Inc., 1992;174–179.
3. Navarro C, Blanc WA. Subacute necrotizing funisitis. Avariant of cord inflammation with a high rate of perinatalinfection. J. Pediatr. 1974;85:689–697.
4. Keenan WJ, Steichen JJ, Mahmood K, Altshuler G. Placen-tal pathology compared with clinical outcome. Am. J. Dis.Child. 1977;131:1224–1227.
5. Hood IC, DeSa DJ, Whyte RK. The inflammatory responsein candidal chorioamnionitis. Hum. Pathol. 1983;14:984–990.
6. Bejar R, Wozniak P, Allard M. Antenatal origin of neuro-logic damage in newborn infants. I. Preterm infants. Am. J.Obstet. Gynecol. 1988;159:357–363.
7. Mueller-Heubach E, Rubinstein DN, Schwarz SS. Histo-logic chorioamnionitis and preterm delivery in differentpatient populations. Obstet. Gynecol. 1990;75:622–626.
8. Gersell DJ, Phillips NJ, Beckerman K. Chronic chorioam-nionitis: a clinicopathologic study of 17 cases. Int. J. Gy-necol. Pathol. 1991;10:217–229.
9. Van Hoeven KH, Anyaegbunam A, Hochster H. Clinicalsignificance of increasing histologic severity of acute in-flammation in the fetal membranes and umbilical cord.Pediatr. Pathol. Lab. Med. 1996;16:731–744.
10. Leviton A, Paneth N, Reuss ML. Maternal infection, fetalinflammatory response, and brain damage in very low birthweight infants. Developmental Epidemiology Network In-vestigators. Pediatr. Res. 1999;46:566–575.
11. Redline RW, O’Riordan MA. Placental lesions associatedwith cerebral palsy and neurologic impairment followingterm birth. Arch. Pathol. Lab. Med. 2000;124:1785–1791.
12. Gomez B, Romero R, Ghezzi F, Yoon BH, Mazor M, BerrySM. The fetal inflammatory response syndrome. Am. J.Obstet. Gynecol. 1998;179:194–202.
13. Lockwood CJ. Recent advances in elucidating the patho-genesis of preterm delivery, the detection of patients at risk,and preventative therapies. Curr. Opin. Obstet. Gynecol.1994;6:7–18.
14. Sun CC, Revell VO, Belli AJ, Viscardi RM. Discrepancy inpathologic diagnosis of placental lesions. Arch. Pathol. Lab.Med. 2002;126:706–709.
15. Khong TY, Staples A, Bendon RW. Observer reliability inassessing placental maturity by histology. J. Clin. Pathol.1995;48:420–423.
16. Beebe LA, Cowan LD, Hyde SR, Altshuler G. Methods toimprove the reliability of histopathological diagnoses in theplacenta. Paediatr. Perinat. Epidemiol. 2000;14:172–178.
17. Langston C, Kaplan C, Macpherson T. Practice guidelinefor examination of the placenta. Arch. Pathol. Lab. Med.1997;121:449–476.
18. Landis JR, Koch GG. The measurement of observer agree-ment for categorical data. Biometrics 1977;33:159–174.
AMNIOTIC INFECTION SYNDROME 447

19. Redline RW, Wilson-Costello D, Borawski E, Fanaroff AA,Hack M. Placental lesions associated with neurologic im-pairment and cerebral palsy in very low birth weight in-fants. Arch. Pathol. Lab. Med. 1998;122:1091–1098.
20. Goldenberg R, Hauth J, Andrews W. Intrauterine infectionand preterm delivery. N. Engl. J. Med. 2000;342:1500–1507.
21. Chellam VG, Rushton DI. Chorioamnionitis and funiculitisin the placentas of 200 births weighing less than 2.5 kg.Br. J. Obstet. Gynaecol. 1985;92:808–814.
22. Romero R, Sepulveda W, Baumann P. The preterm laborsyndrome: biochemical, cytologic, immunologic, patho-logic, microbiologic, and clinical evidence that preterm la-bor is a heterogeneous disease (abstract). Am. J. Obstet.Gynecol. 1993;168:288.
23. Gibbs RS. Chorioamnionitis and bacterial vaginosis. Am. J.Obstet. Gynecol. 1993;169:460–462.
24. Locksmith GJ, Clark P, Duff P. Maternal and neonatal in-fection rates with three different protocols for prevention ofgroup B streptococcal disease. Am. J. Obstet. Gynecol.1999;180:416–422.
25. Pankuch GA, Appelbaum PC, Lorenz RP. Placental micro-biology and histology and the pathogenesis of chorioam-nionitis. Obstet. Gynecol. 1984;64:802–806.
26. Zhang JM, Kraus FT, Aquino TI. Chorioamnionitis: a com-parative histologic, bacteriologic, and clinical study. Int. J.Gynecol. Pathol. 1985;4:1–10.
27. Hillier SL, Martius J, Krohn M, Kiviat N, Holmes KK,Eschenbach DA. A case-control study of chorioamnionicinfection and histologic chorioamnionitis in prematurity.N. Engl. J. Med. 1988;319:972–980.
28. Romero R, Salafia CM, Athanassiadis AP. The relationshipbetween acute inflammatory lesions of the preterm pla-centa and amniotic fluid microbiology. Am. J. Obstet. Gy-necol. 1992;166:1382–1388.
29. Blanc W. Pathology of the placenta and cord in ascendingand hematogenous infections In: Marshall W, editors. Peri-natal Infections, CIBA Foundation Symposium 77. London:Excerpta Medica, 1980;17–38.
30. Redline RW, Wilson-Costello D, Hack M. Placental andother perinatal risk factors for chronic lung disease in verylow birth weight infants. Pediatr. Res. 2002;52:713–719.
31. DiSalvo D. The correlation between placental pathologyand intraventricular hemorrhage in the preterm infant. TheDevelopmental Epidemiology Network Investigators. Pedi-atr. Res. 1998;43:15–19.
32. Kim CJ, Yoon BH, Park SS, Kim MH, Chi JG. Acute funisi-tis of preterm but not term placentas is associated withsevere fetal inflammatory response. Hum. Pathol. 2001;32:623–629.
33. Kim CJ, Yoon BH, Romero R. Umbilical arteritis and phle-bitis mark different stages of the fetal inflammatory re-sponse. Am. J. Obstet. Gynecol. 2001;185:496–500.
34. Rogers BB, Alexander JM, Head J, McIntire D, Leveno KJ.Umbilical vein interleukin-6 levels correlate with the sever-
ity of placental inflammation and gestational age. Hum.Pathol. 2002;33:335–340.
35. Matsuda T, Nakajima T, Hattori S. Necrotizing funisitis:clinical significance and association with chronic lung dis-ease in premature infants. Am. J. Obstet. Gynecol. 1997;177:1402–1407.
36. Spong C, Salafia C, Sherer D, Ghidini A, Minior V. Severefetal heart rate decelerations are associated with umbilicalvasculitis/histologic amnionitis in preterm infants (ab-stract). Am. J. Obstet. Gynecol. 1996;174:490.
37. Qureshi F, Jacques SM, Benson RW. Candida funisitis: aclinicopathologic study of 32 cases. Pediatr. Dev. Pathol.1998;1:118–124.
38. Driscoll SG, Gorbach A, Feldman D. Congenital listeriosis:diagnosis from placental studies. Obstet. Gynecol. 1962;216–220.
39. Coid CR, Fox H. Campylobacters as placental pathogens.Placenta 1983;4:295–306.
40. Redline RW. Recurrent villitis of bacterial etiology. Pediatr.Pathol. 1996;16:995–1002.
41. Lachapelle MH, Miron P, Hemmings R. Endometrial T, B,and NK cells in patients with recurrent spontaneous abor-tion: altered profile and pregnancy outcome. J. Immunol.1996;156:4027–4034.
42. Redline RW, Zaragoza MV, Hassold T. Prevalence of devel-opmental and inflammatory lesions in non-molar first tri-mester spontaneous abortions. Hum. Pathol. 1999;30:93–100.
43. Redline RW, Abramowsky CR. Clinical and pathologic as-pects of recurrent placental villitis. Hum. Pathol. 1985;16:727–731.
44. Czernobilsky B. Endometritis and infertility. Fertil. Steril.1978;30:119–130.
45. Redline RW. Placental pathology: a neglected link betweenbasic disease mechanisms and untoward pregnancy out-come. Curr. Opin. Obstet. Gynecol. 1995;7:10–15.
46. Gersel DJ, Phillips NJ, Beckerman K. Chronic chorioam-nionitis: a clinicopathologic study of 17 cases. Int. J. Gy-necol. Pathol. 1991;10:217–229.
47. Jacques S, Qureshi F. Chronic chorioamnionitis: a clinico-pathologic and immunohistochemical study. Hum. Pathol.1998;29:1457–1461.
48. Ohyama M, Itani Y, Yamanaka M. Re-evaluation of chorio-amnionitis and funisitis with a special reference to sub-acute chorioamnionitis. Hum. Pathol. 2002;33:183–190.
49. Redline RW. Subacute chorioamnionitis with amniotic ne-crosis: a placental reaction pattern associated with neonatalchronic lung disease. Adv. Anat. Pathol. 2002;9:374.
50. Khong TY, Bendon RW, Qureshi F. Chronic deciduitis inthe placental basal plate: definition and inter-observer reli-ability. Hum. Pathol. 2000;31:292–295.
51. Grether JK, Eaton A, Redline R, Bendon R, Benirschke K,Nelson K. Reliability of placental histology using archivedspecimens. Paediatr. Perinat. Epidemiol. 1999;13:489–495.
448 R.W. REDLINE ET AL.