amir elami, md - struttura sanitaria | policlinico di monza · amir elami, md * department of...
TRANSCRIPT

Device based approach for treating Diastolic Heart Failure
Amir Elami, MD * Department of Cardiothoracic Surgery
Hebrew University – Hadassah School of Medicine
* Member of Scientific Advisory Board, CorAssist Ltd.

CHF patients
>40% EF < 0.50
SHF - “Systolic HF”
• Systolic Dysfunction
• Diastolic Dysfunction
• Dilated LV
EF > 0.50 DHF - “Diastolic HF”
• Diastolic Dysfunction
• LV not Dilated
• High LV Mass/EDV
• Hypertension

Mechanisms of Diastolic Dysfunction
Resistance to filling by:
• Impaired relaxation (early to mid-diastole) • Reduced compliance (mid- and late diastole)
Elevated diastolic pressures, limited ability to increase stroke volume through the Frank-Starling mechanism during exercise
Exertional fatigue, dyspnea and pulmonary congestion

DHF and SHF patients similar characteristics
Kitzman W et al JAMA 2002 Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure
• Reduced exercise capacity • Reduced peak oxygen consumption • Marked Neuro-endocrine activation • Reduced Quality of Life

DHF Vs SHF: Mortality and Hospitalization
• Lower short-term mortality • Similar long-term mortality • Similar hospitalization rates
Pernenkil et al. Am J Cardiol 1997 Philbin et al. Am J Med 2000

Do they need the same treatment?

• SHF • Medications
• ACE-I / ARB • β-Blocker • Aldosteron Blocker
• Devices • LVAD’s • BiV Pace (CRT)
• DHF • Medical treatment is empirical • No devices are available.
DHF Vs SHF: Treatment

Aim of CorAssist project
• Develop a mechanical solution for a mechanical problem

Diastolic Pressure Normal: 6-12mmHg DHF: 25mmHg
Systolic Pressure
120 - 140mmHg
7-8%
Pressure reduction 10 mmHg
40%
Recruiting force developed during (normal) systole and transferring it to assist (impaired) diastole

Device Concept • Facilitating LV filling, utilizing a passive,
elastic mechanical device
• The device stores energy during systole and releases it in a recoiling force during diastole

Animal Experiments Stage 1: Safety and Feasibility
• 5 healthy sheep* (35 – 45 kg)
• LV pressures were measured to evaluate whether the device restricts the heart at two extreme conditions • Accelerated heart rate
• Volume overload
* can’t decrease much the low diastolic pressures

Results (1)
• Attachment procedure was technically simple
• All animals exhibited good clinical recuperation • Ejection fraction was preserved up to 180-day
follow-up
• There were no valve motion disturbances
• Histopathology at 6 months confirms only minimal local tissue reaction around the attachment screws.
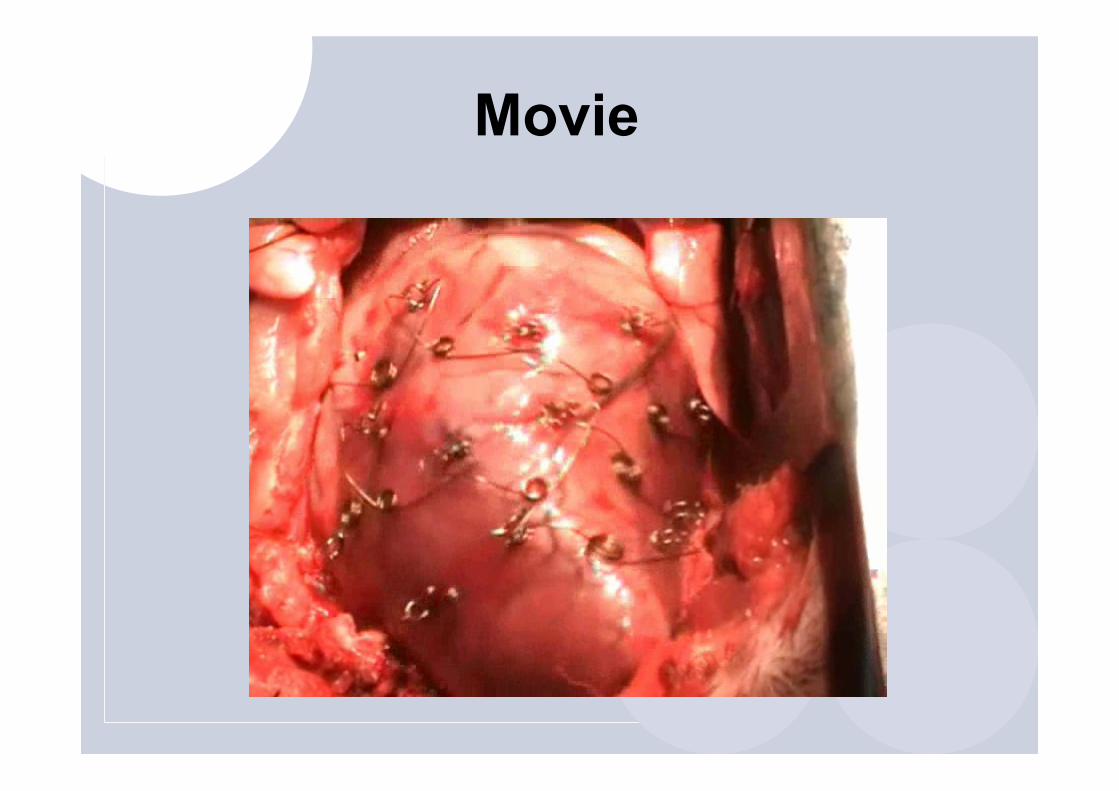
Movie
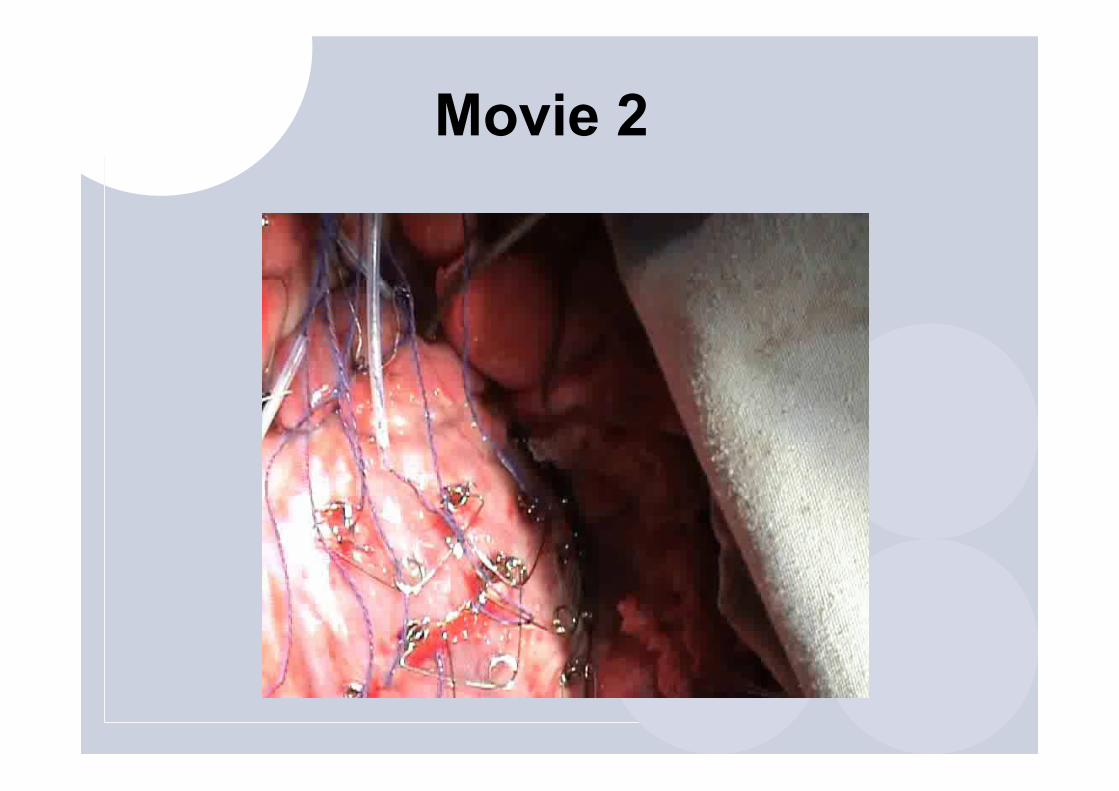
Movie 2

Results (2)
• Angiography demonstrated normal coronary flow
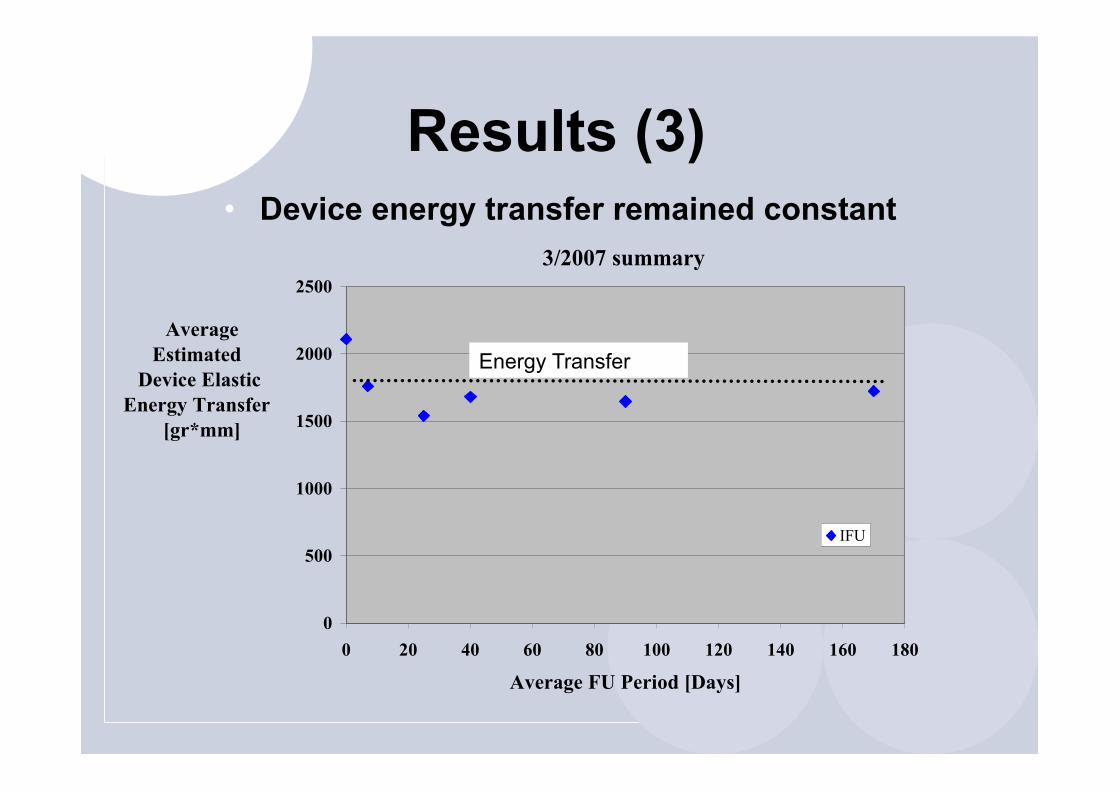
Results (3) • Device energy transfer remained constant
3/2007 summary
0
500
1000
1500
2000
2500
0 20 40 60 80 100 120 140 160 180
Average FU Period [Days]
AverageEstimated
Device Elastic Energy Transfer
[gr*mm]
IFU
Energy Transfer

Results (4) • The EDP response to extreme conditions was similar in
animals before implantation (Table 1) and animals 90 days after implantation (Table 2)
Animal ID 7369 4301 5202 LV EDP (mmHg) EF (%) HR LV EDP
(mmHg) EF (%) HR LV EDP (mmHg) EF (%) HR
Base 10.7 63 84 13 62 72 8.9 57 80 Dobutamine 10.2 83 135 13 79 120 10.2 61 130
Fluid 19.7 57 96 19.5 62 87 14.3 65 110
Animal ID 3350 5247 LV EDP (mmHg) EF
(%) HR LV EDP (mmHg) EF
(%) HR Base 5 74 82 6.7 64 95
Dobutamine 1 68 137 6.9 64 150 Fluid 15 72 82 19.1 63 100
Before
90 Days After

Conclusion
This study demonstrates for the first time that a passive mechanical device, applying outward force on the LV can be safely implanted without evidence of restriction during extreme stress conditions.

Thank You