america's sweet tooth obsession and its impact on oral ... america’s sweet tooth obsession...
TRANSCRIPT

Earn1 CE creditThis course was
written for dentists, dental hygienists,
and assistants.
America’s Sweet Tooth Obession and Its Impact on Oral and Systemic HealthPresented by Karen Davis, RDH, BSDH
Publication date: Jan. 2013 Expiration date: Dec. 2015
AbstractAmericans consume an average of 400 calories per day of added sugars in their diet from high-fructose corn syrup, table sugar, honey, and all other sweeteners with calories! Today’s sugar consumption has jumped 20% over the past 30 years with a correlating rise in obesity, and the domino effect continues with an increased risk for cardiovascular disease, elevated triglyceride levels, liver disease and Type II diabetes. Soft drinks which are the greatest culprit of this growing “sugar obsession” are implicated in increased risk for dental caries and tooth erosion. This program gives a review of the literature related to sugar’s impact on overall health, but also provides good news for today’s clinician seeking methods to help reduce decay, remineralize tooth structure, and motivate patients to reclaim their health!
Educational ObjectivesThe course participants at the conclusion of the course will be able to:1. The truth about “added sugars” in foods
and drinks2. What the literature says about the
consumption of sugar-sweetened drinks and the deleterious impact it has on systemic health
3. The benefits of remineralization products that can help to reverse the dental caries process
4. Tips to gain control of the sugar binge
Author ProfileKaren Davis, RDH, BSDH is founder of Cutting Edge Concepts® and a trainer with The JP Institute of San Diego, California. She is an international speaker and continues for practice dental hygiene in Dallas, Texas. Karen received her Bachelor of Science in Dental Hygiene from Midwestern State University. She has served on numerous advisory boards in the profession and has published many articles related to practicing comprehensively.
Author DisclosureKaren Davis, RDH, BSDH has no potential conflicts of interest to disclose.
This course has been made possible through an unrestricted educational grant by Phillips Oral Healthcare.This course was written for dentists, dental hygienists and assistants, from novice to skilled. Educational Methods: This course is a self-instructional journal and web activity. Provider Disclosure: PennWell does not have a leadership position or a commercial interest in any products or services discussed or shared in this educational activity nor with the commercial supporter. No manufacturer or third party has had any input into the development of course content.Requirements for Successful Completion: To obtain 1 CE credit for this educational activity you must pay the required fee, review the material, complete the course evaluation and obtain a score of at least 70%.CE Planner Disclosure: Heather Hodges, CE Coordinator does not have a leadership or commercial interest with Phillips Oral Healthcare, the commercial supporter, or with products or services discussed in this educational activity. Heather can be reached at [email protected] Disclaimer: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.Registration: The cost of this CE course is $20.00 for 1 CE credit. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing.
Supplement to PennWell Publications
PennWell designates this activity for 1 Continuing Educational Credit
Dental Board of California: Provider 4527, course registration number 01-4527-13001“This course meets the Dental Board of California’s requirements for 1 unit of continuing education.”
The PennWell Corporation is designated as an Approved PACE Program Provider by the Academy of General Dentistry. The formal continuing dental education programs of this program provider are accepted by the AGD for Fellowship, Mastership and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from (11/1/2011) to (10/31/2015) Provider ID# 320452.
Go Green, Go Online to take your course

#
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Abstract
Americans consume an average of 400 calories per day ofadded sugars in their diet from high-fructose corn syrup, tablesugar, honey, and all other sweeteners with calories! Today’ssugar consumption has jumped 20% over the past 30 yearswith a correlating rise in obesity, and the domino effectcontinues with an increased risk for cardiovascular disease,elevated triglyceride levels, liver disease and Type II diabetes.Soft drinks which are the greatest culprit of this growing “sugarobsession” are implicated in increased risk for dental caries andtooth erosion. This program gives a review of the literaturerelated to sugar’s impact on overall health, but also providesgood news for today’s clinician seeking methods to helpreduce decay, remineralize tooth structure, and motivatepatients to reclaim their health!
Effective Date: January 1, 2013
Expiration Date: December 31, 2015Educational Methods: This course is a self-instructionaljournal and web activity.
Educational Objectives
After participating in this course, the professional will havegained a better understanding of:
1. The truth about added sugars in our foods and drink.
2. The impact of sugar-sweetened drinks on both oral andsystemic health.
3. The benefits of remineralization products available tohelp reverse the caries process.
4. Tips that can help you or your patients gain control of thesugar binge for improved health.
Target Audience
This course was developed for dentists, dental hygienistsand assistants, from novice to skilled.
Author Profile
Karen Davis, RDH, BSDH, RDHMP is founder of Cutting EdgeConcepts® and a trainer with The JP Institute of San Diego,California. She is an international speaker and continues forpractice dental hygiene in Dallas, Texas. Karen received herBachelor of Science in Dental Hygiene from Midwestern StateUniversity. She has served on numerous advisory boards in theprofession and has published many articles related to practicingcomprehensively..
Karen may be reached at [email protected]
Author Disclosure
Karen Davis, RDH, BSDH has no relevant financial interestswith any products or services discussed in this presentation.
Recognition and Credits
PennWell is an ADA CERP recognized provider.
ADA CERP is a service of the American Dental Association toassist dental professionals in identifying quality providers ofcontinuing dental education. ADA CERP does not approve orendorse individual courses or instructors, nor does it implyacceptance of credit hours by boards of dentistry.
Concerns or complaints about a CE provider may be directedto the provider or to ADA CERP at www.ada.org/goto/cerp.
PennWell designates this activity for 1 Continuing EducationCredit.
Dental Board of California: Provider 4527, course registrationnumber 01-4527-12073.“This course meets the Dental Board of California’s require-ments for 1 unit of continuing education.”
The PennWell Corporation is designatedas an Approved PACE Program Providerby the Academy of General Dentistry.The formal continuing dental educationprograms of this program provider areaccepted by the AGD for Fellowship,Mastership and membership mainte-nance credit. Approval does not imply
acceptance by a state or provincial board of dentistry or AGDendorsement. The current term of approval extends from(11/1/2011) to (10/31/2015) Provider ID# 320452.
Commercial Support:
This course has been made possible through an unrestricted
educational grant by Phillips Oral Healthcare.
Requirements for Successful Completion:
To receive credit for your participation in this course you will be
required to complete the online program examination. To
complete the online examination participants must be regis-
tered and signed-in to ineedce.com and have added the
program to their user account (MyCE Archives). Once added to
your user account, a Take Exam link will be displayed from
1

#
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
within the MyCE Archives section of the website. Upon selec-
tion of the Take Exam link, participants are provided access to
the online examination form. Once completed and submitted
an immediate grade report will be displayed. All participants
scoring at least 70% on the examination will receive a Letter of
Credit (CE Verification Form) verifying 1 CE credit. Letters of
credit may be viewed and printed immediately as well as
accessed anytime in the future (24/7) from within the MyCE
Archives user records page of this website.
Not enough time to complete your online examination? No
problem, online examinations may be completed anytime
during the effective period of the program. Participants
requiring more time to complete an examination may return to
this website, sign-in and complete the online examination.
Disclosure Declaration:
Provider Disclosure: PennWell does not have a leadershipposition or a commercial interest in any products or servicesdiscussed or shared in this educational activity, No manufac-turer or third party has had any input into the development ofcourse content.
CE Planner Disclosure: Heather Hodges, CE Coordinatordoes not have a leadership or commercial interest with anycommercial supporter, or with products or services discussedin this educational activity. Heather can be reached [email protected]
Image Authenticity: No images in this educational activityhave been modified or altered.
Scientific Basis: All content has been derived from refer-ences listed and the author’s clinical experience. Researchreferences are provided in the bibliography and/or supple-mental materials.
Known Benefits and Limitations: Information presented inthis educational activity represents best practices inevidenced based dentistry with potential benefit for thepatient and clinician. No off label or experimental treatmentsare discussed.
Educational Disclaimer: Completing a single continuingeducation course does not provide enough information toresult in the participant being an expert in the field related to thecourse topic. It is a combination of many educational coursesand clinical experience that allows the participant to developskills and expertise.
Registration:
The cost of this CE course is $20.00 for 1 CE credit.
Cancellation/Refund Policy:
Any participant who is not 100% satisfied with this course canrequest a full refund by contacting PennWell in writing.
Hardware and Software Requirements
To access program materials users will need:
n A computer with an Internet connection.
n Internet Explorer 7.x or higher, Firefox 3.x or higher,Safari 3.x or higher, or any other W3C standardscompliant browser.
n Adobe Acrobat Reader or Apple Preveiw.
n Occasionally other additional software may berequired such as Adobe Flash Player and/or an HTML5 capable browser for video or audio playback.
2

3
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Welcome, I want to thank all of you for joining me in thispresentation entitled: “America’s Sweet Tooth Obsessionand Its Impact on Oral and Systemic Health.” I’d like tothank PennWell for offering me this opportunity to speakwith you about this very important topic. I’m Karen Davis.Now let’s begin.
Objectives for this program include learning the truthabout added sugars in our foods and drink; under-standing the impact of sugar-sweetened drinks on bothoral and systemic health; discovering the benefits ofremineralization products available to help reverse thecaries process; and finally, learning specific tips that canhelp you or your patients gain control of the sugar bingefor healthier living.
So, let’s begin with the basics. Sucrose, or commontable sugar, is broken down in the body to 50% fructoseand 50% glucose. At this point it is basically identical tohigh fructose corn syrup.

4
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Over the past several years high fructose corn syrup hasincreased exponentially in the processing of sugar-sweetened foods and drinks due to its lower costs, butrecently within the media you would almost think thathigh fructose corn syrup is the sole culprit for addedsugars in our diet, and all other sweeteners get a pass.
In fact, most recently some products have begun toadvertise that their products are natural sweeteners andcontain no high fructose corn syrup, implying a healthierchoice, yet labels reveal the presence of corn syrup orsome other type of sugar which is broken down in thebody much the same way as high fructose corn syrup. Inessence, whether a product is sweetened with high fruc-tose corn syrup or some other type of sweetener, it is thetotal sugar content consumers need to pay attention to.
In August of last year the American Heart Associationmodified its previous scientific statement about dietarysugars intake and cardiovascular health based uponemerging evidence in a relationship between intake ofsugars and cardiovascular health. The new recommen-dations are quite stringent. The American HeartAssociation cited worldwide pandemic of obesity andcardiovascular diseases to explain its heightenedconcerns about the adverse effects of excessive sugarconsumption. Evidence shows that increased sugarconsumption is linked with metabolic diseases, adversehealth conditions, and shortfalls of obtaining essentialnutrients in our diet. Daily consumption has increased20% over the past 35 years for Americans, and that
greatly exceeds discretionary calorie allowances based upon the updated U.S. Dietary Guidelines.

5
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
That 20% increase in added sugars for the averageAmerican translates into some alarming numbers.Consumption of added sugars equals 350 to 475 emptycalories per day, so in terms of teaspoons, that’s 22 to 34teaspoons daily, or in terms of grams, that’s between 88and 136 grams of added sugar most people thinknothing about because it has become of our dailylifestyle. Interestingly, in the American HeartAssociation’s report, 14 to 18 year olds were at thehighest ends of these ranges. If you’ve got anyteenagers as patients or living in your home, well if youdo, you probably won’t have any difficult appreciatingthat reality. The new American Heart Association recom-mendations are for slashing added sugar intake daily by
about two-thirds of the current consumption. For women, that’s only 6½ teaspoons or 26 grams of added sugar daily,and for men, it’s only 9½ teaspoons or 38 grams daily. I want you to keep those numbers in your mine; 26 grams forwomen, 38 grams for men. As you begin to read labels, you will see just how challenging it is to stay within thesestringent guidelines, based upon the habits most of us have grown accustomed to.
In order to make wise decisions about sugar consump-tion, one must almost become what I call a label detec-tive. In this sample of hot chocolate, added sugar is 19grams. Whatever is listed first in the list of ingredientstells consumers mostly what it is made of, and in thiscase obviously sugar. But reading further one can seethat in addition to sugar (which is sucrose), that is listedfirst, corn syrup is also listed twice; once as part of theadded marshmallows, and once as a separate ingre-dient. It is important also to identify the total calorieslisted. As sugar products are added to foods and drinksit directly impacts the number of calories. Based uponthe new American Heart Association recommendationsfor total added sugar consumption daily, this one 6-8
ounce cup of hot chocolate contains 19 of the recommended 26 grams for women. Wow, that would only leave 7grams of added sugar for the remainder of the day in order to meet these stringent guidelines, that remember, weregenerated out of the American Heart Association’s concern over the rise in obesity and cardiovascular diseases inthis country.

6
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
For clarity, let’s define what added sugars are. They aresimply sweeteners with calories and they are added tofoods and drinks during the processing or preparation.Added sugars are part of the total sugars listed on labels,but labels do not include any naturally occurring sugarsthat are present already in fruit, milk or vegetables. Anaverage American diet contains too many added sugarswhich ultimately squeeze out the desire for healthiernutrient-rich foods. As a result, consumption categoriesin fruits, grains and vegetables remain way below thenumber of recommended daily servings for most people.
Since added sugars on labels can be somewhatdisguised by use of other names, here is a list of someof the more commonly used names for added sugar:high fructose corn syrup; evaporated cane juice or evap-orated syrup; agave syrup; brown sugar or even rawbrown sugar; corn syrup; juice concentrate such as beetjuice, apple juice, or grape juice; maple syrup andmolasses; fructose; and of course, sucrose just to namea few.
Well, where are all these added sugars coming from?Okay, here’s a breakdown: regular soft drinks, 33%;sugars and candy, 16.1%; cakes, cookies, and pies,12.9%; fruit drinks, 9.7%; dairy desserts and milk prod-ucts, things like your ice cream or sweetened yogurt,8.6%; other grains, things like cinnamon toast andmaybe even sweetened waffles, 5.8%. When you thinkabout your or your patients eating and drinking habits,it’s easy to see why added sugars are now a hugeconcern. They are present in the majority of items weconsume on any given day.

7
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
And just so we don’t think it’s only sodas that contain all ofthe added sugars emerging onto the market over the lastseveral years, have also been sugar flavored teas, waters,and sugary energy drinks. According to the AmericanJournal of Nutrition, consumption of these beverages isincreased by 135% between 1977 and 2001.
Well, that’s not all that’s changed. Over the past 50 yearsthe proportion of soda or fountain drinks has changeddramatically. In the 1950’s, the average soda was 6.5ounces. In the 1960’s it grew to 12 ounces. By the1990’s, the average soda grew to 20 ounce servings.And by the year 2000, the 64 ounce “Big Gulp” is notuncommon.
Take a moment to look at these various drinks, their sizesin ounces, and corresponding grams of added sugarpresent. What I found surprising was even the smallestdrink, the 8.4 ounce Amp, packs 31 grams of sugar intoits can, and drinks such as Iced Teas, Green Teas, andSnapple Elements were all 50 grams or more. When youget into the energy drinks such as Mountain Dew GameFuel, we’re up to 77 grams of sugar for a 20 ounce drink.And then, I guess the winner, so-to-speak, would have tobe the 20 ounce Tropicana Twister packing at 87.5 gramsof nutrient-missing added sugar. Wow, up against that, Iguess the 12 ounce Coke and 7-up look pretty good -well, only comparatively speaking.

8
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
In a study, published in the Journal of the American DieteticAssociation, researchers analyzed the dietary habits andpurchases of nearly 1,500 students in 10 Massachusettsmiddle schools with vending machines that sold soda orother sugar-sweetened beverages. I cite this study becauseI think it’s representative of what you’ll find in most middleand high school campuses today. Sugar-sweetened bever-ages included regular soda, fruit drinks, and iced tea. Thestudents were asked about vending machine purchases inthe preceding week. Of the 646 students who reportedusing school vending machines, 71% reported buyingsugar-sweetened sodas or other beverages. Overall, sugar-sweetened drinks were purchased by almost three times asmany students than the next popular item - water.
Researchers found the number of items purchased at school vending machines was directly related to the overall sugarintake of the children. The average number of servings of sugar-sweetened drinks per day increased by 20% among those
who purchased one to three items from the vendingmachine, and 70% of those who purchased four or morevending machine items in a week, compared to childrenwho did not make any vending machine purchases at all.Even though some of the campuses have taken soda andpower drinks out of vending machines in recent years, thevast majority have not.
Now for some simple math to help all of us make betterdecisions. Food labels typically list sugars by grams, butmost recipes and some prepared foods list sugars byteaspoons. In order to convert teaspoons to grams, simplymultiply by four. So if a recipe calls for three teaspoons of
sugar, multiply that by four to equal the number of grams, which becomes an important number to watch as you andyour patients pay attention to added sugar intake. To translate how many calories are coming from teaspoons of added
sugar in a recipe, multiply it by 16. Again, if adding threeteaspoons of sugar to a large glass of iced tea, forexample, that amounts to 48 added calories.
As you can see in this slide, just adding a 12 ounce Cokeand three Pepperidge Farms Milano cookies to your dailyconsumption of added sugar would already put you overthe new American Heart Association recommendationsfor women, which remember is 26 grams and men 38grams. I think you would agree with me, the averageperson has a long way to go to meet these new guide-lines of slashing added sugar from our diets.

9
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Consumption of Sugar Alcohols rather than sucrose orother added sugars can be good options for individualsstriving to reduce sugar intake. Sugar alcohols are carbo-hydrates called “polyols” and they occur naturally inplants. One distinctive difference between added sugarsand most sugar alcohols is that they are not completelyabsorbed by the body. Meaning some of the polyolssimply pass through the system.
Sugar alcohols have a lower glycemic index thansucrose. The glycemic index describes the differenteffects carbohydrates have on our bodies by rankingthem according to how fast a food or drink will increaseglucose production in the body. Choosing low gylcemicindex carbohydrates, the ones that produce only smallfluctuations in blood glucose and insulin levels, is one ofthe secrets to long-term health, reducing the risk of heartdisease and diabetes and is key to sustainable weightloss. Sugar alcohols also have fewer calories per gramthan added sugars, and do not promote decay. In fact,sugar alcohols such as xylitol actually help to preventcaries. A word of caution about consumption of sugaralcohols however. Gradual experimentation with this
category of sweeteners is advised because for some individuals, ingestion of sugar alcohols can contribute to diges-tive distress. So, here’s what I usually recommend, start out gradually, and see how your body tolerated use of them.Individuals with conditions such as irritable bowel syndrome or Crohn’s disease should consult their physician priorto intake of sugar alcohols. On a personal note, I began cooking with xylitol crystals about two years ago, and sinceit has the same sweetness as sugar, I find it can be easily substituted in most recipes. I now recommend mymoderate and high caries risk patients consider making the same kind of substitution.
10
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
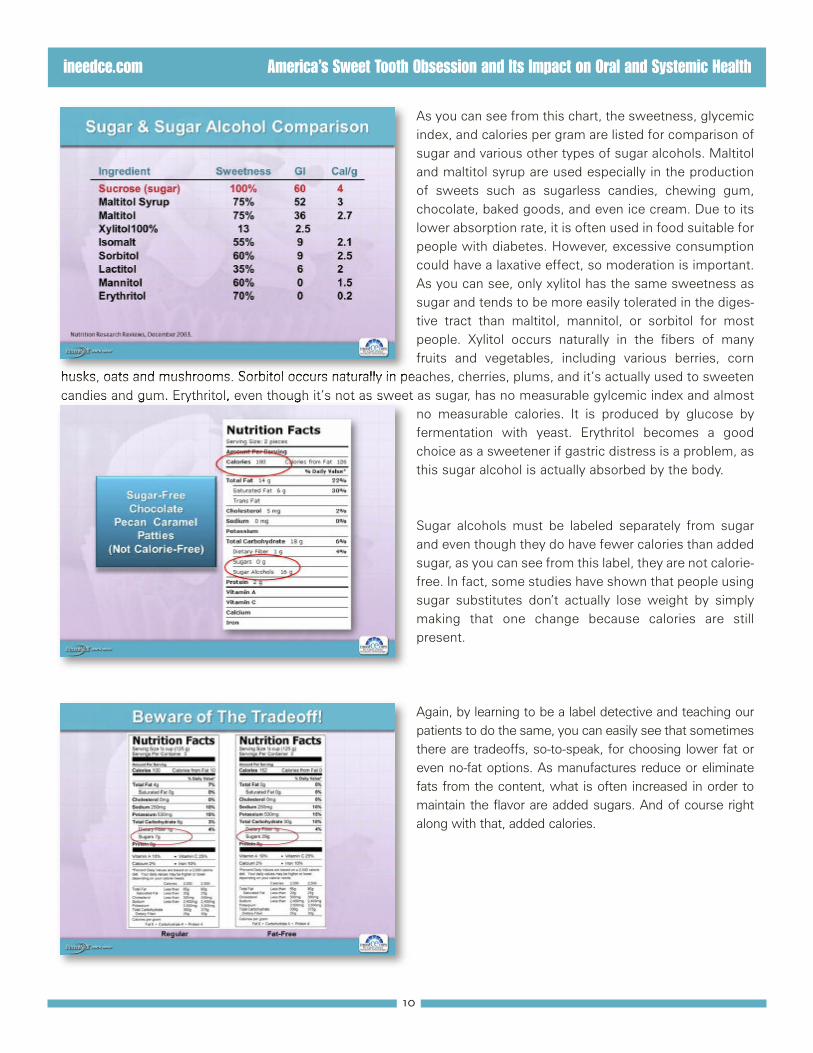
As you can see from this chart, the sweetness, glycemicindex, and calories per gram are listed for comparison ofsugar and various other types of sugar alcohols. Maltitoland maltitol syrup are used especially in the productionof sweets such as sugarless candies, chewing gum,chocolate, baked goods, and even ice cream. Due to itslower absorption rate, it is often used in food suitable forpeople with diabetes. However, excessive consumptioncould have a laxative effect, so moderation is important.As you can see, only xylitol has the same sweetness assugar and tends to be more easily tolerated in the diges-tive tract than maltitol, mannitol, or sorbitol for mostpeople. Xylitol occurs naturally in the fibers of manyfruits and vegetables, including various berries, corn
husks, oats and mushrooms. Sorbitol occurs naturally in peaches, cherries, plums, and it’s actually used to sweetencandies and gum. Erythritol, even though it’s not as sweet as sugar, has no measurable gylcemic index and almost
no measurable calories. It is produced by glucose byfermentation with yeast. Erythritol becomes a goodchoice as a sweetener if gastric distress is a problem, asthis sugar alcohol is actually absorbed by the body.
Sugar alcohols must be labeled separately from sugarand even though they do have fewer calories than addedsugar, as you can see from this label, they are not calorie-free. In fact, some studies have shown that people usingsugar substitutes don’t actually lose weight by simplymaking that one change because calories are stillpresent.
Again, by learning to be a label detective and teaching ourpatients to do the same, you can easily see that sometimesthere are tradeoffs, so-to-speak, for choosing lower fat oreven no-fat options. As manufactures reduce or eliminatefats from the content, what is often increased in order tomaintain the flavor are added sugars. And of course rightalong with that, added calories.

11
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
In addition to the American Heart Association recog-nizing the need for Americans to slash added sugarconsumption as seen from their 2009 revised statement,even before that in 2005 the U.S. Department ofAgriculture issued Dietary Guidelines for Americansbased upon calorie consumption. A new concept ofdiscretionary calories was introduced, which are basi-cally the recommended number of calories after nutrient-dense foods in each category are consumed. Theacronym SoFAAS was developed to help us rememberthe main sources of discretionary calories. They are solidfats, alcohol and added sugar. Depending upon the age,gender, and physical activity of an individual, no morethan 8% for sedentary individuals and no more than 20%
for very physically active individuals should be obtained through discretionary calories. Not surprisingly, of the morethan 6,000 individuals whose diets were analyzed to come up with these guidelines, many adults were consumingsomewhere in the range of a 30% to 42% discretionary calories. Based upon the new guidelines these percentagesfor the same individuals should have been between 13% and 17%.
The website www.mypyramid.gov has recommenda-tions of total caloric consumption and discretionary calo-ries based upon our age, gender and physical activity.The following table is a sample for individuals that partic-ipate in less than 30 minutes of moderate exercise daily,which I think sadly, applies to most of us. On the MyPyramid website, estimated calories and discretionarycalories are listed for individuals that have more than 30minutes a day of moderate activity. Let’s look together atfemales in the ages between 31 to 50 who are not veryactive. They should only have 195 calories from thediscretionary category, which remember, includes solidfats, alcohol, and added sugar. Okay, considering a 4ounce glass of red wine has 83 calories and a 4 ounce
glass of white wine 103, that doesn’t allow for very many pats of butter or sweets during the day if one chooses toend the day with a glass of wine, yet desires to stay within these healthier guidelines. I think here’s the bottom line.To increase total recommended calories and discretionary calories per day, a person must simply increase physicalactivity. Simply get moving!

12
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Okay just for fun, let’s go back to the 12 ounce Coke andthree Milano cookie sample we looked at earlier thatexceeded the new American Heart Association recom-mendations for daily added sugar. It also exceeds theU.S. Dietary Guidelines for discretionary calories forwomen aged 31 to 50 who participate in less than 30minutes of moderate activity a day. In fact, it exceeds therecommendations of 195 calories by an additional 125calories. For women of the same age that participate inmore than 30 minutes of moderate activity daily, thediscretionary calories increase, but only up to 290. Giventhe typical eating patterns of most Americans, it is notdifficult to see why obesity has become such anepidemic.
According to the World Health Organization, more than60% of the global disease burden will be attributed tochronic disorders associated with obesity by the year2020. In the United States the prevalence of obesity hasdoubled in adults and tripled in children over the pastthree decades. Fortunately, due to Michelle Obama’scampaign called, “Let’s Move,” a national goal has beenset to reduce childhood obesity to 5% or less by the year2030. Currently, the number of overweight and obeseadults surpasses that of normal weight adults as definedby a Body Mass Index of 25 for overweight and BMI of30 or more for obesity. Without factoring in the potentialimpact the nationwide campaign “Let’s Move” may havesimply based upon past trends of obesity, it is estimated
by the year 2015, 75% of adults will either be overweight or obese.
85% of children diagnosed with Type II diabetes are clas-sified as obese and actually a new term “diabesity” isused to refer to this phenomenon. According to the U.S.Surgeon General, the direct and indirect costs of obesitywere over $120 billion in the year 2000. It makes youwonder what it would be in the year 2010. The obesityepidemic is associated with various metabolic disorders,Type II diabetes, cardiovascular diseases, and had evenbeen implicated with various cancers such as colon andbreast cancer.

13
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Consumption of liquid calories from beverages hasincreased in parallel with the obesity epidemic in the U.S.population, even though the causal relationship remainsunclear. Because overweight and obesity are complexmetabolic conditions, it’s unlikely that a single food cate-gory such as simple carbohydrates, which include addedsugars, is a primary causative factor in and of itself. Yet,in a recent analysis of 88 studies exploring the relation-ship between soft drink intake and nutrition or healthoutcomes, it revealed the increased soda consumptionwas associated with higher body weight, lower intake ofnutrients, and overall worse health indices. It alsorevealed that greater weight loss was achieved as sugar-sweetened beverages were decreased.
Based upon inconsistencies in study design, the overallsystemic impact of high sugar consumption is inconclu-sive in terms of cause and effect; however studies haveshown that there is a decrease in HDL - the good choles-terol, while at the same time rising triglyceride levelsassociated with high sugar consumption which couldaccelerate atherosclerosis. In addition, it appears asthough high sugar consumption may worsen the abilityto maintain control of blood glucose levels. And, notsurprisingly, studies have revealed that as high sugarconsumption increases, compromises are made byreduced intake of necessary vitamins and minerals fromother food categories.
A study published in 2009 from the Journal of ClinicalInvestigation reported the metabolic impact of both fruc-tose and glucose, and current scientific opinion is inagreement that chronic consumption of large amountsof dietary fructose may have adverse metabolic effectssuch as; increased triglyceride levels, increased visceralfat mass in men, decreased insulin sensitivity in women,weight gain, an increase in non-alcoholic fatty liverdisease, and unfavorable effects on lipid metabolismleading to increased formation of risk factors for cardio-vascular diseases. Wow!
14
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Excess sugar consumption has been shown to increasethe risk for Type II diabetes, increase blood pressurelevels, increase the risk for heart disease and stroke, andmost recently fructose has been shown to increaseproliferation of pancreatic cancer cells. Okay, eventhough we may not have enough data to prove causeand effect for every one of these conditions, this type ofdata makes it easy to appreciate why the American HeartAssociation has made such stringent recommendationsto seriously reduce added sugars from the diet!
Just given a glimpse of the research one thing is clear,chronic overconsumption of dietary sugar is detrimentalto our health!
All of us are fully aware chronic overconsumption ofdietary sugar is also detrimental to our teeth!

15
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
The development and progression of dental caries resultsfrom the interaction of four factors in the oral environment:The plaque bacteria harbors acid-forming bacteria capableof fermenting dietary carbohydrates. The most commonbacteria implicated in dental caries is streptococcusmutans, and it tends to prefer sucrose. When sugars andstarches consumed, the pH of plaque begins to drop. At apH below 5.5, the acids can begin to demineralize enameland dissolve tooth structure. It may last for 30 minutes orlonger until the saliva neutralizes the acidic environment inthe mouth. The host factors such as exposure to fluoridesand other minerals such as calcium and phosphorus caneither increase or decrease the susceptibility to dentalcaries. The amount, the flow, and the composition of saliva
is influenced by the taste and chewing of various foods, various medications, and even salivary dysfunction. Normal sali-vary flow is protective in nature, as it buffers the plaque acids. But when it is deficient, the environment is favorable for
carries development.
High sugar intake combined with frequently low pHincreases the number of streptococci in the oral cavity.While many types of bacteria stop growing when pH levelsare low, Step Mutans tolerate acidic conditions and actuallyincrease in that environment. These gram positive bacteriaadhere easily to tooth surfaces and are actively involved inthe transportation of sugars. During high levels of sugarconsumption Strep Mutans produce lactic acid, and thisoccurs in both neutral and low pH environments. The oralcavity of newborn children does not contain Strep Mutansand are transmitted via the saliva, most frequently from the
mother to child. Streptococci Mutans trigger the process that leads to initial mineral loss and enables bacteria to penetratethe tooth structure; therefore they are regarded as the initiator of the caries process.
Another bacteria implicated in the carries process islactobacilli, and they also produce lactic acid and aretolerant of acidic environments. They are primarilyresponsible for caries progression by multiplying andspreading the bacteria throughout the oral environment.In contrast to Strep Mutans, lactobacilli do not adhere totooth surfaces, but rather they colonize in retentionniches such as pits and fissures, or margins of existingrestorations. A high lactobacilli count is an indicator ofhigh sugar intake, and lactobacilli are more resistant toantimicrobials than Step Mutans.

16
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Well due to the increases of high sugar consumption andacidic content of most sugary drinks, dental profes-sionals have also seen correlating increases in theamount of tooth demineralization present. A studypublished in 2005 revealed that the worst culprits fordissolution on enamel appear to be: non-cola sodas,energy and sports drinks, commercial lemonades, andbasically any drink that combines fructose with citricacid. As you become a label detective, you can quicklysee that includes most drinks.
In spite of the bacterial challenges and the demineraliza-tion of tooth structure that often follows high sugarconsumption, the good news is that prior to cavitationthe process of remineralization can be literally helpreverse the caries process! “Remineralization is thenatural repair process where calcium and phosphateform a new sub-surface mineral coating which is lesssoluble than the original surface, especially in the pres-ence of fluoride.” This statement is not only powerful,but offers hope for those already experiencing toothdemineralization.
The dynamics of demineralization and remineralization areprocesses ongoing in the oral environment at any givenmoment. This slide depicts the impact of what’s happeningduring the demineralization process. As the pH is lowered,calcium and phosphate minerals are lost from the toothsurface, and acids weaken tooth surfaces even further.During remineralization, the pH is higher and the conditionsare favorable for the increased uptake of calcium and phos-phate minerals in the tooth structure and saliva makesthese minerals bioavailable for absorption.

17
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
The opportunities for remineralization have increasedsubstantially as ingredients and technologies have alteredour toothpaste and rinses. Amorphous calcium phosphateused in paste have been shown to literally help fill defectspresent from demineralization, and it increases thebioavailability of fluoride to be absorbed in the tooth. Italso increases the luster and appearance of enamel as aresult of creating a smoother surface. NovaMin is a tech-nology using bioactive glass particles that bind to thetooth surface, and when the particle comes in contactwith saliva or water, it reacts to release calcium, phos-phate, silica and sodium ions. A calcium phosphate layeris formed, which then crystallizes into the hydroxylapatitecrystals, and the dentinal tubules are occluded, which also
assists in reducing sensitivity. Casein phosphopeptide, amorphous calcium phosphate, is the combined technologyusing the milk protein to form a complex called RECALDENT, which stabilizes and releases calcium and phosphate forremineralization. It has been shown to remineralize sub-surface lesions, and repeated use has the ability to removewhite spot lesions due to the demineralization process. Fluoride itself adheres to partially demineralized crystallites, itattracts calcium and phosphate, and possesses an antibacterial effect together strengthening the tooth and reducingacidic bacteria.
So, in order to educate our patients about the caries orremineralization process, let’s put this together bylooking at what conditions favor caries and what favorremineralization. When the balance tips in favor of thecaries process it is due to varying influences of patholog-ical factors such as the presence of acidic bacteria,frequent eating and drinking of sugary foods and bever-ages, reduced saliva flow or function. By altering thesepathologic factors, the balance can be tipped towardremineralization. Likewise, when remineralization doesoccur, it is due to varying influences of the followingprotective factors: Adequate saliva flow; fluoride,calcium and phosphate present in sufficient quantities inthe oral environment; and the addition of antibacterial
products such as chlorhexidine. By altering the protective factors, again, the balance can be tipped in favor ofremineralization. Caries Management by Risk Assessment or CAMBRA is an evidence-based approach for theprevention and repair of early dental caries that involves evaluating disease indicators such as white spots or restora-tions in the past three years, and then also identifying pathological factors and the presence or absence of protec-tive factors that the clinician will then use to determine the risk for the patient. Additionally, we can also use prod-ucts chair side to assess a patient’s salivary flow, and level of acidic bacteria present for an even more definitive riskassessment. Once a caries risk is identified, we must be prepared to inform patients of the potential for remineral-ization. I don’t know about you, but I find that very few patients consider much at all about what promotes decay intheir own mouth, and almost none are aware of the potential to stop or even reverse the caries process throughremineralization!
18
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
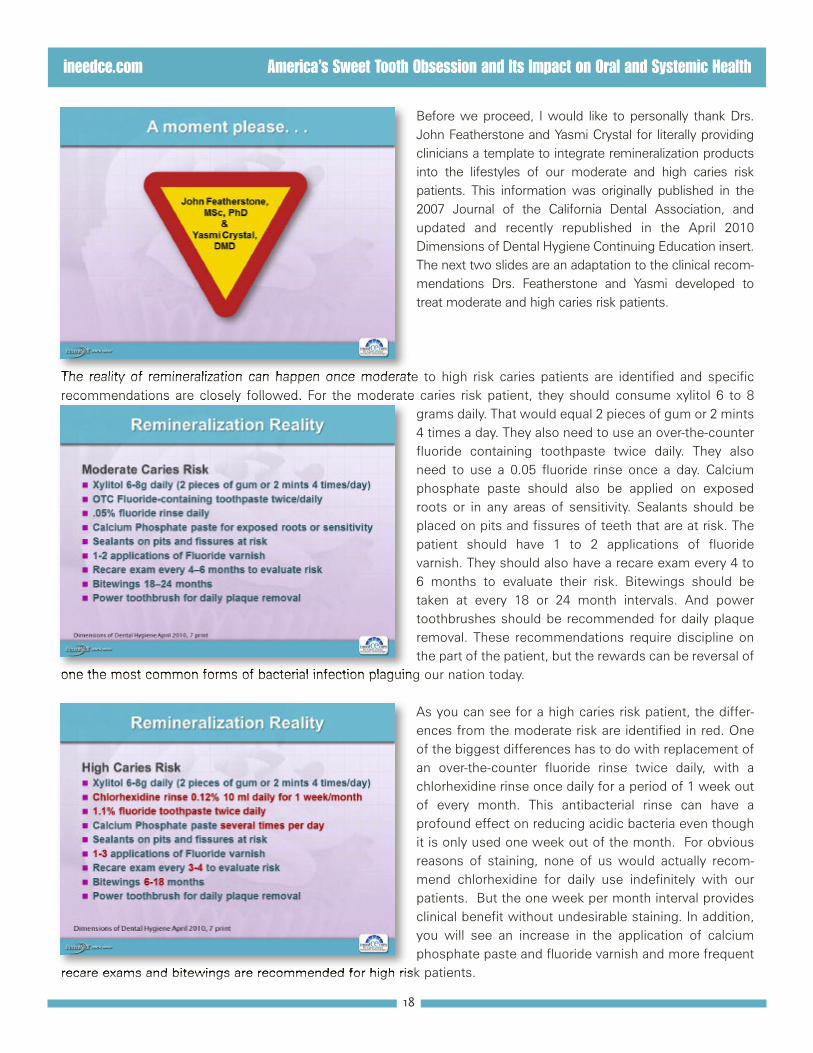
Before we proceed, I would like to personally thank Drs.John Featherstone and Yasmi Crystal for literally providingclinicians a template to integrate remineralization productsinto the lifestyles of our moderate and high caries riskpatients. This information was originally published in the2007 Journal of the California Dental Association, andupdated and recently republished in the April 2010Dimensions of Dental Hygiene Continuing Education insert.The next two slides are an adaptation to the clinical recom-mendations Drs. Featherstone and Yasmi developed totreat moderate and high caries risk patients.
The reality of remineralization can happen once moderate to high risk caries patients are identified and specificrecommendations are closely followed. For the moderate caries risk patient, they should consume xylitol 6 to 8
grams daily. That would equal 2 pieces of gum or 2 mints4 times a day. They also need to use an over-the-counterfluoride containing toothpaste twice daily. They alsoneed to use a 0.05 fluoride rinse once a day. Calciumphosphate paste should also be applied on exposedroots or in any areas of sensitivity. Sealants should beplaced on pits and fissures of teeth that are at risk. Thepatient should have 1 to 2 applications of fluoridevarnish. They should also have a recare exam every 4 to6 months to evaluate their risk. Bitewings should betaken at every 18 or 24 month intervals. And powertoothbrushes should be recommended for daily plaqueremoval. These recommendations require discipline onthe part of the patient, but the rewards can be reversal of
one the most common forms of bacterial infection plaguing our nation today.
As you can see for a high caries risk patient, the differ-ences from the moderate risk are identified in red. Oneof the biggest differences has to do with replacement ofan over-the-counter fluoride rinse twice daily, with achlorhexidine rinse once daily for a period of 1 week outof every month. This antibacterial rinse can have aprofound effect on reducing acidic bacteria even thoughit is only used one week out of the month. For obviousreasons of staining, none of us would actually recom-mend chlorhexidine for daily use indefinitely with ourpatients. But the one week per month interval providesclinical benefit without undesirable staining. In addition,you will see an increase in the application of calciumphosphate paste and fluoride varnish and more frequent
recare exams and bitewings are recommended for high risk patients.

19
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Let’s take a look at some of the products instrumental increating conditions favorable for remineralization tooccur. Xylitol is a natural sweetener derived from mainlyfrom birch trees that help restore a proper pH balance tothe mouth especially when used following consumptionof acidic foods and drinks. Studies have shown thatxylitol gum and mints can help inhibit growth of StrepMutans in the oral environment and can help arrest theprogression of caries. Chewing xylitol gum has beenshown not only to reduce decay in young children andadults, but even in children of mothers who used xylitolproducts because it reduces the transmissible bacteriabetween mother and child. Many products are availableon the market and online. Trident with xylitol is readily
found in grocery stores and pharmacies. BreathRX gum is also commercially available in some retail stores and phar-macies and is often dispensed directly in dental practices. Omni’s Theragum and Theramints are 100% xylitol sweet-ened and are dispensed in dental offices. Spry gum and mints are available online as well as the great-tastingRicochet mints and many other xylitol products. Use of your Internet search engine will provide many options forpurchasing xylitol products and making those recommendations to your patients.
While there seems to be a lot of viable toothpasteoptions that can incorporate therapeutic levels of fluo-ride, featured here is Crest Pro Health, which uses stabi-lized stannous fluoride as the active ingredient to fightdecay. And it’s also been shown to help fight gingivitis,reduce plague, fight halitosis, and whiten teeth.Sensodyne’s ProNamel uses sodium fluoride to fightdecay and strengthen the teeth. And both Crest PoHealth and ProNamel are effective in desensitizing teethalso. Colgate’s Total uses sodium fluoride as the anticavity ingredient, and the addition of Triclosan helps thefluoride adhere to the teeth to lengthen the anti cavitybenefits. ACT Fluoride Rinse uses the maximum allow-able of sodium fluoride available for an over-the-counter
rinse daily. And Peridex is one example of the many chlorhexidine products available via a prescription that is bothbactericidal, as well as bacteriostatic. And it actually is effective on both gram-negative and gram-positive bacteria.

20
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
There are many fluoride pastes available throughprescription containing 5,000 parts promoting fluoridefor patients with a high caries risk and/or sensitivity. 3M’sClinpro 5000 adds tricalcium phosphate, which is theirproprietary formula that creates a protected barrieraround the calcium, allowing it to coexist with the fluo-ride ions. When the toothpaste comes in contact withthe tooth, the saliva breaks down the barrier and fluoride,calcium, and phosphate are bioavailable for absorption.Colgate’s Prevident 5000 uses a neutral sodium fluorideto fight decay and provide desensitizing, and it comes ina paste version as well as a more liquid gel for easierflow and coverage of all tooth surfaces. Sultan’s ReNewand NUPRO NUSolutions both use neutral sodium chlo-
ride as the anti cavity agent, but also use NovaMin to assist in making the fluoride ions more bioavailable. NovaMinhas also been useful in the treating of sensitivity as well.
MI Paste and MI Paste Plus with Fluoride both containRECALDENT, the milk-derived protein which releasescalcium and phosphate ions onto the enamel duringacidic conditions enabling remineralization to take place.It can be applied in the office and followed up at homeup to 4 times per day, and should be left on the teethfollowing the application for 3 minutes prior to rinsing.Several 5% neutral sodium fluoride varnishes are avail-able to be applied in the office which can release fluoridefor up to 30 days following application. Some of theseexamples are: Discus Dental, Fluoridex varnish which isstable and easy to apply; and Waterpik’s UltraThin, justlike the name sounds in a thinner consistency than most
other fluoride varnishes and claims to have a faster uptake of the fluoride compared to many other brands, and KolorzClearShield varnish which claims to taste better than any other varnish on the market, with a money-back guarantee.
This varnish is sweetened with xylitol and is gluten-free.Then those who are interested in a longer-lasting varnishthere are products like 3M’s Vanish XT which is lightcured that can release fluoride for up to 6 months.
Pit and fissure sealants can be placed on susceptibletooth surfaces for added protection. Examples of lightcured dental sealants are: Pulpdent’s Embrace WetBondwhich can be sealed in a slightly wet environment tomake placement much easier, as well as GC’s FujiTRIAGE which is a glass-ionomer sealant that requires noetching. Both of these products release fluoride onto thetooth surface following bonding.

21
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
I think most clinicians would agree that the recommen-dation of power brushes over manual brushes forpatients needing improved plaque removal is one of thefirst considerations for behavior change related topreventing caries and gingivitis. Pictured here is theSonicare for Kids which encourages kids toward healthybrushing on their own. The built-in kid timer graduallyincreases the brushing time over a 90 day period, whichI think most of us would agree is brilliant! Anotherfeature of this power brush is that it has two powersettings both for younger and older kids. The SonicareFlexCare Plus features three brushing modes and twocleaning modes to fit the needs of different individuals.It also has the patented Sonic technology to drive fluids
between the teeth and around the gum line for effective plaque removal. The UV brush sanitizer has been shown tokill bacteria that otherwise live on the bristles. Another power brush is the Oral-B Braun SmartSeries 5000, whichfeatures five brushing modes for individual needs and a wireless SmartGuide timer to help patients visually see justhow long they’re brushing. Another feature of the Oral-B Braun is that it has a built-in pressure sensor, which stopsthe action of the brush when patients are adding too much pressure. My experience has been that unless a dentalprofessional instructs the patient on proper use of power brushes as demonstrated inside your own mouth, it’s diffi-cult for most patients to change their habits of traditional rapid brush movement all over the mouth, to simply guidinga power brush from tooth to tooth. To maximize the benefit of power brushes all patients should be instructed in thedental practice on correct technique.
Okay, Karen, good information, but what do we do if wehave a sweet tooth or we realize that’s a challenge forour patients?

22
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Well here are some tips to gain control of the sugarbinge and ultimately improve health for ourselves and forour patients. These are tips that I have applied personallyand at the same recommendations I now give mypatients. Obviously, we must read labels and teach ourpatients to be label detectives in order to make wiseeating and drinking decisions throughout the day.Ignorance in this area makes it impossible to meet thenew American Heart Association guidelines for dailyconsumption of added sugar. Next, visit themypyramid.gov website and determine what discre-tionary limits apply for calorie consumption. Part of thesuccess of meeting those goals daily includes reducingsugar-sweetened foods and drinks. Begin to prepare
foods with sugar alcohols instead of table sugar; they have fewer calories, a lower glycemic index, and they don’tpromote decay. Each person needs to experiment to find what works best for them, but fortunately there are a lotof options. Also, replace sugar with sugar alcohols in sweetened coffee, tea and other beverages. Carry a fewpackets of your preferred sweetener with you when you’re eating out. Use xylitol gum or mints 4 to 5 times a daythroughout the day to help restore proper pH. But be intentional about using xylitol following meals, it creates thesatisfaction for that desire, or maybe it’s even a habit to have just a little something sweet after meals. There are alot of great tasting xylitol products so it’s easy to have variety.
Another tip I had found helpful is to reduce cravings withsubstitution. When desiring a snack during the day,reach for a few nuts, such as almonds or walnuts ormacadamia nuts. When eating at home or eating out,select a serving of fresh fruits or berries instead ofsugary desserts. We do have choices to override thesehabits, and once you begin to make better choices, thecravings for something less healthy really does diminish.One tip that has been especially helpful in increasingsatisfaction with meals is to use fresh herbs; keepingbasil, rosemary mint, dill, and even arugula in the houseto season foods reduces the needs for salt, but surpris-ingly increases satisfaction, which again, reduces crav-ings or desire for sugary foods. I mean give yourself
permission to enjoy a great dessert in moderation, but only on occasion. Keep in mind that the third or fourth bite ofa sugary dessert doesn’t taste any better than it did the first bite, so discipline yourself to be satisfied with a fewbites rather than the whole thing. Another tip, which we can all agree benefits us in numerous ways is to be delib-erate about increasing physical activity daily. I find it interesting that when the Discretionary Calorie Guidelines weredeveloped, they did so taking into consideration how sedentary or active a person is. We need to burn the fuel weconsume to help combat obesity. Lastly, consume more water. Often we think we are feeling hungry and reach fora carb or sugar-loaded food or drink when our bodies are simply dehydrated. Drinking more water, especially fluori-dated water, has a multitude of benefits for oral health and overall health.

23
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
For those of you unaware of what this symbol is, it is thesymbol for gratitude. I hope you have found this programinformative and motivating for making changes person-ally as well as educational for your patients to gaincontrol of the sugar obsession that has been growing inthis country!
Thank you for your interest in this topic and participation.I would especially like to thank The Philips Corporationfor their sponsorship.

24
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Resources
Karen Davis, RDH, BSDH * 646 Goodwin Drive Richardson, TX 75081 * 972.669.1555 * [email protected] * www.karendavis.net
1
Karen Davis, RDH, BSDH Sucrose: 50 %Fructose / 50% Glucose High Fructose Corn Syrup: 45% Fructose / 55% Glucose American Heart Association 2009 Dietary Sugar Intake & Cardiovascular Health Scientific Statement:
Worldwide pandemic of obesity & cardiovascular disease warrants new AHA recommendations due to emerging evidence as to the relationship between sugar consumption & cardiovascular health
Sugar consumption liked with metabolic diseases, adverse health conditions, and shortfalls of obtaining essential nutrients
Daily consumption has increased 20% over past 35 years for Americans Current daily consumption greatly exceeds discretionary calorie allowances
from the US Dietary Guidelines Average consumption of Added Sugar daily = 350 470 calories Translates into 22 34 teaspoons daily or 88 136 grams daily 2009 AHA Daily Recommendations: Women 6 ½ tsps or 25 grams & for Men 8 ½ tsps or 38 grams Added Sugars By Other Names: HFCS Evaporated Cane Juice Agave Syrup Brown Sugar Corn Syrup Juice Concentrates Maple Syrup Fructose Sucrose www.ycchololate.com - Xylitol flavored chocolate bars www.dentalantioxidants.com - Clearing house for antioxidant studies www.Periosciences.com - Localized antioxidants for the oral cavity Low Fructose / Low GI Blackberry Grapefruit Lemon / Lime Nectarine Raspberry Wild Strawberry
High Fructose / High GI Ripe Banana Grapes Dates Raisins Mango Custard Apples

25
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Resources
Karen Davis, RDH, BSDH * 646 Goodwin Drive Richardson, TX 75081 * 972.669.1555 * [email protected] * www.karendavis.net
2
Sugar Alcohols:
Occur naturally in plants Not completely absorbed
Less Glycemic Index than sucrose Fewer calories per gram Do not promote decay
Sugar & Sugar Alcohol Comparison Ingredient Sweetness GI Calories / gram Sucrose (sugar) 100% 60 4 Malitol Syrup 75% 52 3 Malitol 75% 36 2.7 Xylitol 100% 7 2.5 Isomalt 55% 9 2 Sorbitol 60% 9 2.5 Lactitol 35% 6 2 Mannitol 60% 0 1.5 Erythritol 70% 0 0.2 FDA Approved Sweeteners as Additives
SACCHARIN
Sweet-n-Low ASPARTAME NutraSweet
Equal
NEOTAME SUCROLOSE Splenda
ACELSUFAME POTASSIUM
1879 1981 2002 1998 1988
sweeter sweeter 7000 13,000 sweeter sweeter sweeter
100 countries Greatest use worldwide
US, AK, UK 80+ countries 30+ countries
Bitter aftertaste high conc.
Most controversial sweetener
Cousin to Aspartame
Chemically-altered sucrose
Bitter aftertaste high conc.
Heat stable Not heat stable Heat stable Heat stable Heat stable Added to Aspartame in soft drinks
Must be avoided by those with PKT
No amino acid concern for those with PKT
Tri-chlorination process
Blended with other sweeteners
Substitute & commercial
Substitute Commercial Substitute & commercial
Mostly commercial

26
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Resources
Karen Davis, RDH, BSDH * 646 Goodwin Drive Richardson, TX 75081 * 972.669.1555 * [email protected] * www.karendavis.net
3
FDA GRAS Sweeteners (Generally Recognized As Safe) ERYTHRITOL STEVIA ISOMALT SORBITOL MALTITOL Fruits, fermented foods
Natural herb Paraguay
Beets glucose & mannitol
Stone fruits, berries
Maltose from starches
60-70% 200-sweeter
40-50% 60% 70-90%
1996 2008 1990 1963 1986 petition filed
0.2 calories/g Non-caloric 2.1 calories/g 2.5 calories/g 2.7 calories/g Heat stable Heat stable Heat stable Heat stable Heat stable < 50 g/day No daily limit < 29 g/meal <23 g/meal < 100 g/day Absorbed/not metabolized less GI distress
Bitter aftertaste high concentrations
Partially absorbed & metabolized
*Large amts. Laxative effect Caution w/ IBS
Partially absorbed & metabolized
Caution regarding prolonged use of sorbitol, isomalt, HSH found in hard candies and mints! XYLITOL Berries, oats, mushrooms, extracted from hardwood trees 100% as sweet as sucrose 1963 4 calories/g Heat stable >50 g/day / Kinder to GI than sorbitol, mannitol Ear & yeast infections, Osteoporosis, Anti-cariogenic, stimulates salivary flow Toxic to dogs www.xylitol.org - Xylitol product guide www.xlear.com - Mints, gum, xylitol crystals toothpaste & nose spray www.xywater.com - Xylitol infused water www.orahealth.com - Xylimelts www.carifree.com - products for infants & children www.3MESPE.com - mints & gum www.xylishield.com - gum, mints, toothpaste, mouth rinse 2005 & 2010 US Dietary Guidelines for Americans
Empty calories = SOFAS: Solid Fats & Added Sugars Limit SOFAS after nutrient-dense foods from each category are consumed Age, Gender & Physical Activity determine recommended ranges of 8 20%
of empty calories from total calories

27
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Resources
Karen Davis, RDH, BSDH * 646 Goodwin Drive Richardson, TX 75081 * 972.669.1555 * [email protected] * www.karendavis.net
4
Example: Females 31 50 / Less than 30 min. moderate exercise daily / 1800 calories / 160 Empty Calories Males 31 50 / Less than 30 min. moderate exercise daily / 2200 calories / 265 Empty Calories www.ChooseMyPlate.gov -
upon age, gender and physical activity Obesity by the Stats
>60% of the global disease burden will be associated with obesity by 2020 US obesity doubled in adults and tripled in children in the last 3 decades 2/3 of population overweight with BMI: 25, or obese with BMI: 30+ Direct & Indirect costs from obesity >$147 billion in 2008 Obesity associated with metabolic disorders, Type II diabetes, CVD, colon
cancer & breast cancer Current Genomics 9:239, 2008 Systemic Impact of High Sugar Consumption
Adverse effects on HDL & Triglyceride levels May worsen control of diabetes Compromises intake of dietary vitamin & mineral intake
Circulation 106:526, 2002 Systemic Impact of Fructose
Increased Triglyceride levels Increased visceral fat mass Decreased insulin sensitivity Weight gain Unfavorable lipid metabolism Non-Alcoholic Fatty Liver Disease NAFLD
Journal of Clinical Investigation 119: 1322, 2009 Excessive Sugar Consumption
Increases risk for Type II diabetes Increases blood pressure levels Increases risk for heart disease & stroke Fructose increases proliferation of pancreatic cancer cells
Journal of Cancer Research 7: 6368, 2010 Journal of American Society of Nephrology 2010 American Journal of Clinical Nutrition 89: 1037, 2009

28
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Resources
Karen Davis, RDH, BSDH * 646 Goodwin Drive Richardson, TX 75081 * 972.669.1555 * [email protected] * www.karendavis.net
5
Most aggressive dissolution on the enamel: non-cola sodas, energy / sports drinks, commercial lemonades and any drinks that combine fructose & citric acid General Dentistry 53: 28, 2005 Bacterial Testing
CRT® Bacteria by Ivoclar Vivadent www.ivoclarvivadent.us Tests for Strep Mutans & Lactobacilli to identify risk & implement
intervention before lesions appear Culture results in 2 days CariScreen Susceptibility Testing Meter by CariFree® www.carifree.com 1 minute chairside detection of Streptococci bacterial load ATP bioluminescence Assigns risk of caries between 0 9999. (1500 of lower considered healthy)
Salivary Testing
Saliva Check ® by GC America Measures salivary production Resting & chewing pH Measures buffering capacity of saliva to minimize acidic challenges
Remineralization Reality Remineralization is the natural repair process where calcium and phosphate form a new sub-surface mineral coating, which is less soluble than the original surface, especially in the presence of fluoride. Dimensions of Dental Hygiene April 2010, 4 print Remineralization Opportunities AMORPHOUS CALCIUM PHOSPATE
2 bioavailability
TRI-CALCIUM PHOSPHATE
surface & subsurface mineralization NOVAMIN

29
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Resources
Karen Davis, RDH, BSDH * 646 Goodwin Drive Richardson, TX 75081 * 972.669.1555 * [email protected] * www.karendavis.net
6
CALCIUM PHOSPHOPEPTITE & AMORPHOUS CALCIUM PHOSPHATE RECALDENT®
s sub-surface lesions
FLUORIDE
Antimicrobial effect CAMBRA www.cdafoundation.org/journal - Part I October 2011 & Part II November 2011 www.ada.org Remineralization Realtity for the MODERATE Caries Risk Patient Xylitol 6-8g daily (2 pieces of gum or 2 mints 4 times/day) OTC Fluoride-containing toothpaste twice/daily .05% fluoride rinse daily Calcium Phosphate paste for exposed roots or sensitivity Sealants on pits and fissures at risk 1-2 applications of Fluoride varnish Recare exam every 4 6 months to evaluate risk Bitewings 18 24 months Power toothbrush for daily plaque removal
Adapted from Dimensions of Dental Hygiene April 2010, 7 print Remineralization Reality for the HIGH Risk Caries Patient Xylitol 6-8g daily (2 pieces of gum or 2 mints 4 times/day) Chlorhexidine rinse 0.12% 10 ml daily for 1 week/month 1.1% fluoride toothpaste twice daily Calcium Phosphate paste several times per day Sealants on pits and fissures at risk 1-3 applications of Fluoride varnish Recare exam every 3-4 months to evaluate risk Bitewings 6 18 months Power toothbrush for daily plaque removal
Adapted from Dimensions of Dental Hygiene April 2010, 7 print

30
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Resources
Karen Davis, RDH, BSDH * 646 Goodwin Drive Richardson, TX 75081 * 972.669.1555 * [email protected] * www.karendavis.net
7
www.brushdj.com Tips for Gaining Control of the Sugar Binge for Improved Health 1. Read labels and decide wisely! 2. Set limits for empty calories daily Reduce sugar-sweetened drinks and foods 3. Substitute sugar alcohols for sugar in foods & beverages 4. Count sugar grams throughout the day 5. Use Xylitol gum or mints following meals
6. Reduce cravings with substitution Snack on almonds, walnuts & cheese & substitute fresh fruit for desserts 7. Prepare foods with fresh herbs to increase satisfaction with meals 8. Enjoy the delectable in moderation, on occasion 9. Increase physical activity 10. Drink more water!

#
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
Examination Review
This page is provided for review only. To access the online post-exam you must be “Registered” and “SignedIn.” and have completed the course selection/purchase process in its entirety. Once selected/purchased thecourse title will be added to your MyCE Archives page where a Take Exam link will be displayed directly acrossfrom the course title. A letter of credit will be issued upon successful completion of the post-exam with a scoreof 70% or higher.
Please note: Credit may not be claimed if completed after the course expiration date.
1) Why is the fact that a product is “HFCS free” not as important as the sugar content of the product?A) Because many products containing HFCS have a low glycemic indexB) Because many “HFCS free” products still contain corn syrup or other types of sugar that is broken
down in your body the same way as HFCSC) Because HFCS is not actually bad for you
2) Which of the following is not considered an added sugarA) SucroseB) High Fructose Corn SyrupC) MilkD) Juice Concentrate
3) Of the following, which is NOT a reason sugar alcohols can be better for you than added sugars:A) Sugar alcohols have a lower glycemic index than sucroseB) Sugar alcohols provide you with more energy than sucroseC) Sugar alcohols do not promote decayD) Sugar alcohols contain fewer calories per gram than sucrose
4) The acronym SoFAAS was developed to help individuals remember the main sources of discre-tionary calories: Solid Fats, Alcohol & Added Sugars.A) TrueB) False
5) Which of the following conditions are implicated in high fructose consumption?A) Weight gainB) Increased triglyceride levelsC) Decreased blood glucose levelsD) Non-alcoholic Fatty Liver DiseaseE) A, B and D
6) High sugar intake combined with frequently low pH reduces the number of lactobacilli in the oralcavity.A) TrueB) False
31

#
America’s Sweet Tooth Obsession and Its Impact on Oral and Systemic Health ineedce.com
7) Which bacteria in the oral cavity triggers the process that leads to initial mineral loss and enablesbacteria to penetrate the tooth structure?A) LactobacilliB) P GingivalisC) Streptococci Mutans
8) By altering protective factors in the oral cavity such as increased saliva flow and increased fluorideapplication, and decreasing risk factors such as consuming sugary drinks, the conditions are favor-able for remineraliation to occur.A) TrueB) False.
9) For patients with a high caries risk, rinsing with a 0.12% chlorhexidine mouth rinse is recommendedhow often?
A) Daily for one monthB) Daily every other week per monthC) Daily for one week per monthD) Indefinitely
10) Tips for gaining control of the sugar binge include:
A) Substitute sugar with sugar alcohols in food and drink preparation
B) Set discretionary limits for added sugar and calories daily
C) Snack on almonds and walnuts rather than carbohydrates
D) Prepare foods with fresh herbs to increase satisfaction
E) All of the above (correct)
32