alcoholic liver disease strategies for seamless care
TRANSCRIPT
Alcoholic Liver Disease –
Strategies for Seamless Care
or
An Clinical Approach to the
Jaundiced Alcoholic Patient
Dr Ewan Forrest
Glasgow Royal Infirmary
Liver Disease for the General Physician Royal College of Physicians July 2017
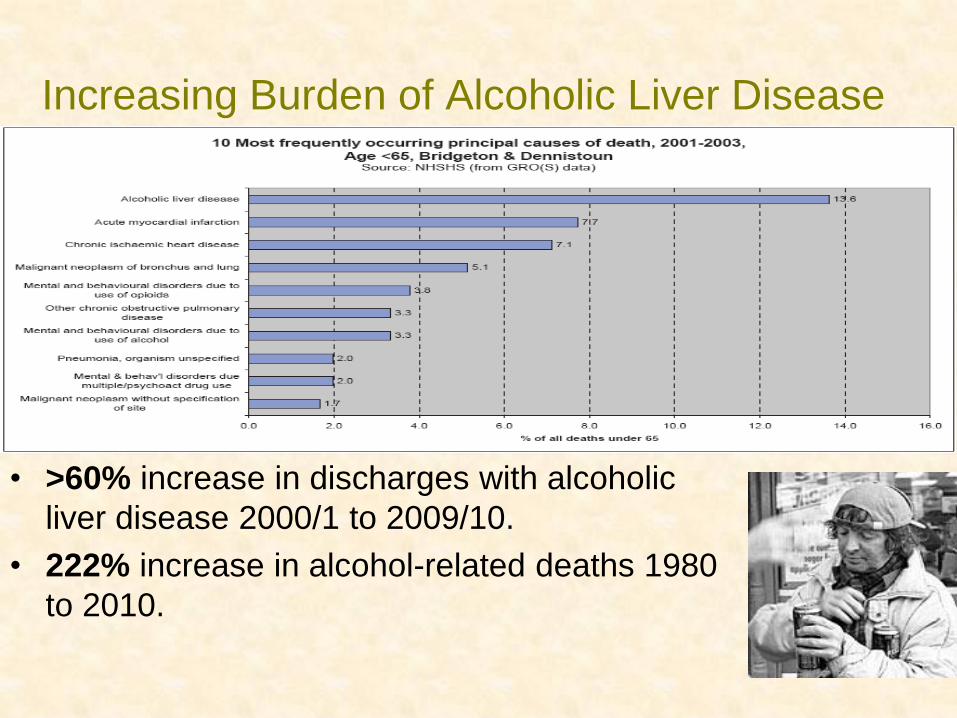
Increasing Burden of Alcoholic Liver Disease
• >60% increase in discharges with alcoholic
liver disease 2000/1 to 2009/10.
• 222% increase in alcohol-related deaths 1980
to 2010.
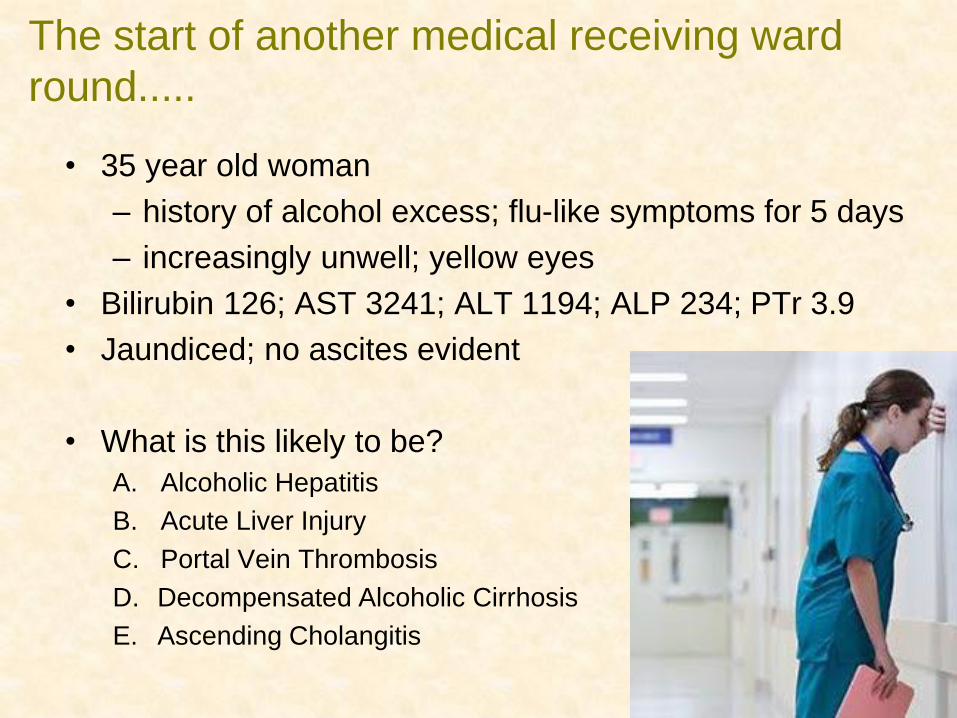
The start of another medical receiving ward
round.....
• 35 year old woman
– history of alcohol excess; flu-like symptoms for 5 days
– increasingly unwell; yellow eyes
• Bilirubin 126; AST 3241; ALT 1194; ALP 234; PTr 3.9
• Jaundiced; no ascites evident
• What is this likely to be?
A. Alcoholic Hepatitis
B. Acute Liver Injury
C. Portal Vein Thrombosis
D. Decompensated Alcoholic Cirrhosis
E. Ascending Cholangitis
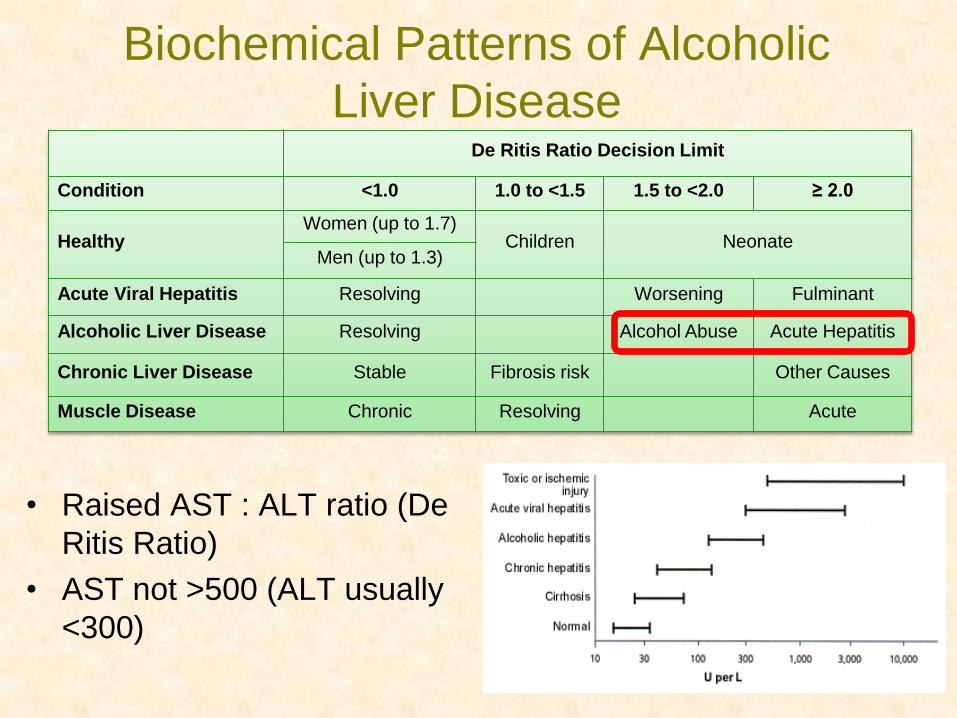
Biochemical Patterns of Alcoholic
Liver Disease
• Raised AST : ALT ratio (De
Ritis Ratio)
• AST not >500 (ALT usually
<300)
De Ritis Ratio Decision Limit
Condition <1.0 1.0 to <1.5 1.5 to <2.0 ≥ 2.0
Healthy Women (up to 1.7)
Children Neonate Men (up to 1.3)
Acute Viral Hepatitis Resolving Worsening Fulminant
Alcoholic Liver Disease Resolving Alcohol Abuse Acute Hepatitis
Chronic Liver Disease Stable Fibrosis risk Other Causes
Muscle Disease Chronic Resolving Acute
The Jaundiced Alcoholic: Scenario 1
• Acute Liver Injury
– In context of either no background fibrotic
liver disease or established cirrhosis
– Atypical biochemistry; clinical context
– Possible Causes
• Drug induced: even ‘therapeutic’
paracetamol
• Acute viral infection (HAV; HBV; HEV)
• Ischaemic/ Hypoxic hepatitis
• Co-incident primary liver disease: AIH
Another ward round in an alternate universe..... • 35 year old woman
– >80g alcohol per day; abdominal and ankle swelling
– increasingly unwell for 6 months; yellow eyes for 4 months
• Bilirubin 105; AST 93; ALT 32; ALP 234; PT 22 seconds (PTr
1.9); Urea 6.5; WCC 3.4
• Jaundiced; drowsy; moderate abdominal distension; hepatic
flap present.
• What is this likely to be?
A. Alcoholic Hepatitis
B. Acute Liver Failure
C. Acute Portal Vein Thrombosis
D. Decompensated Alcoholic Cirrhosis
E. Ascending Cholangitis
The Jaundiced Alcoholic: Scenario 2
• Chronic Decompensation of Chronic Disease
– In context of established cirrhosis
– Typical biochemistry; SIRS not florid
– Clinical Context
• Progressive deterioration over weeks/ months
• Jaundice evident >2 months
• Ascites and encephalopathy often predominant
– Represents progressive disease with continued
drinking but may herald development of
hepatoma
In the next bed, just arrived..... • 35 year old woman
– >80g alcohol per day; flu-like symptoms for 5 days
– increasingly unwell; yellow eyes for 2 weeks
• Bilirubin 326; AST 241; ALT 94; ALP 234; PT 27seconds (PTr
2.4); Urea 6.5; WCC 17.4
• Jaundiced; pyrexial; drowsy; abdominal distension
• Abdominal US showed large ascites and hepato-splenomegaly.
• What should we do next?
A. Percutaneous liver biopsy
B. MRCP
C. Transjugular liver biopsy
D. CT Head
E. Diagnostic Ascitic Aspiration
• Ascitic Fluid Analysis
– SBP diagnosed in 20% cirrhotics admitted to
hospital, and 2-3% attending for outpatient
paracentesis
– >250 neutrophils/cm3 (>500 WBC/ cm3) and
suggest spontaneous bacterial peritonitis (SBP)
– Samples to be sent in ‘blood’ culture bottles
– Early antibiotics (see local guidelines) and
Albumin (20% HAS: 1.5g/kg Day 1; 1g/kg Day 3
for high risk patients: Bilirubin >68 and/or
Urea>11)
Sepsis in Alcoholic Liver Disease
The Jaundiced Alcoholic: Scenario 3
• Acute Decompensation of Chronic Disease
– Precipitant: often GI bleeding/ Sepsis/ Portal
Vein Thrombosis
– Typical biochemistry; SIRS usually evident
– Clinical Context
• Can be difficult to differentiate from Alcoholic
Hepatitis (and may co-exist)
– Full sepsis screen: blood cultures; urinalysis and
culture; diagnostic ascitic tap; CXR
– Low threshold for antibiotics (but be wary of
gentamicin)
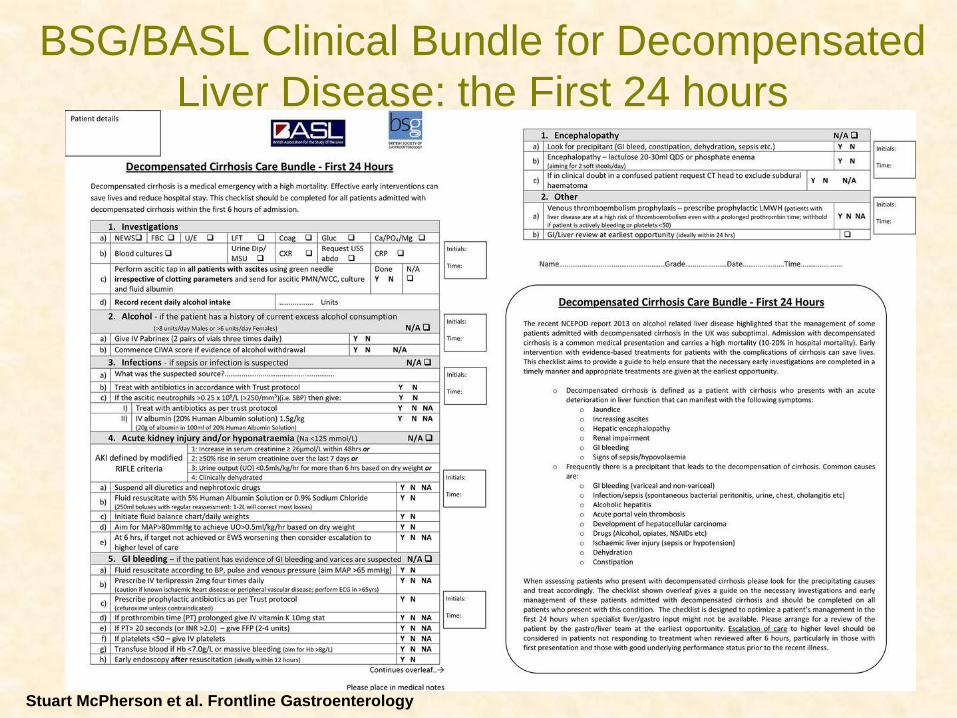
BSG/BASL Clinical Bundle for Decompensated
Liver Disease: the First 24 hours
Stuart McPherson et al. Frontline Gastroenterology
Curiously an hour later there arrives...... • 35 year old woman
• Bilirubin 326; AST 241; ALT 94; ALP 234; PT 27seconds
(PTr 2.4); Urea 6.5; WCC 17.4
• Jaundiced; pyrexial; drowsy; moderate abdominal distension
• Abdominal US showed moderate ascites and hepato-
splenomegaly.
• Sepsis screen negative
• What is this likely to be?
A. Alcoholic Hepatitis
B. Acute Liver Failure
C. Portal Vein Thrombosis
D. Decompensated Alcoholic Cirrhosis
E. Ascending Cholangitis
The Jaundiced Alcoholic: Scenario 4
• ‘Clinically relevant’ Alcoholic Hepatitis
– Essential Features
• excess alcohol within 8 weeks
• < 2 month onset of Bilirubin > 80mol/l
• Exclusion/ treatment of sepsis
• AST < 500 (AST: ALT ratio >1.5)
– Characteristic Features
• hepatomegaly fever leucocytosis hepatic bruit
NIAAA 2016: Probable Alcoholic Hepatitis Inclusion Criteria •Onset of jaundice within prior 8 weeks •Ongoing consumption of > 40 (female) or 60 (males) g alcohol/day for ≥6 months with <60 days of abstinence before the onset of jaundice •Aspartate aminotransferase > 50, aspartate aminotransferase/alanine aminotransferase > 1.5, and both values < 400 IU/L •Serum bilirubin (total) > 3.0 mg/dL (50µmol/l) •Liver biopsy confirmation in patients with confounding factors
Back to our patient...... • 35 year old woman
• Bilirubin 326; AST 241; ALT 94; ALP 234; PT 27seconds
(PTr 2.4); Urea 6.5; WCC 17.4
• Jaundiced; pyrexial; drowsy; moderate abdominal
distension
• Abdominal US showed moderate ascites and hepato-
splenomegaly.
• What is her short-term (28 day)prognosis?
A. Excellent (>95% survival)
B. Reasonable (~80% survival)
C. Moderate (~60% survival)
D. Poor (~50% survival)
E. Terrible (<40% survival)
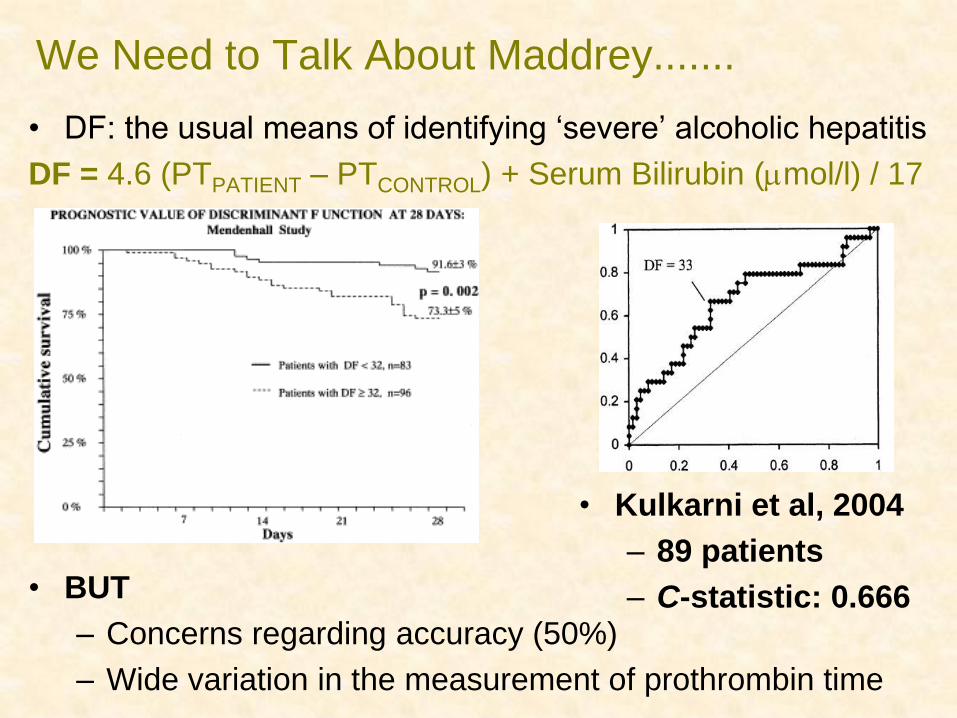
We Need to Talk About Maddrey.......
• DF: the usual means of identifying ‘severe’ alcoholic hepatitis
DF = 4.6 (PTPATIENT – PTCONTROL) + Serum Bilirubin (mol/l) / 17
• BUT
– Concerns regarding accuracy (50%)
– Wide variation in the measurement of prothrombin time
• Kulkarni et al, 2004
– 89 patients
– C-statistic: 0.666
DF
GAHS
0 20 40 60 80 100
100-Specificity
100
80
60
40
20
0
Se
nsitiv
ity
AUC:
GAHS = 0.783(0.736 – 0.825)
DF = 0.721(0.671 – 0.767)
(p=0.014)
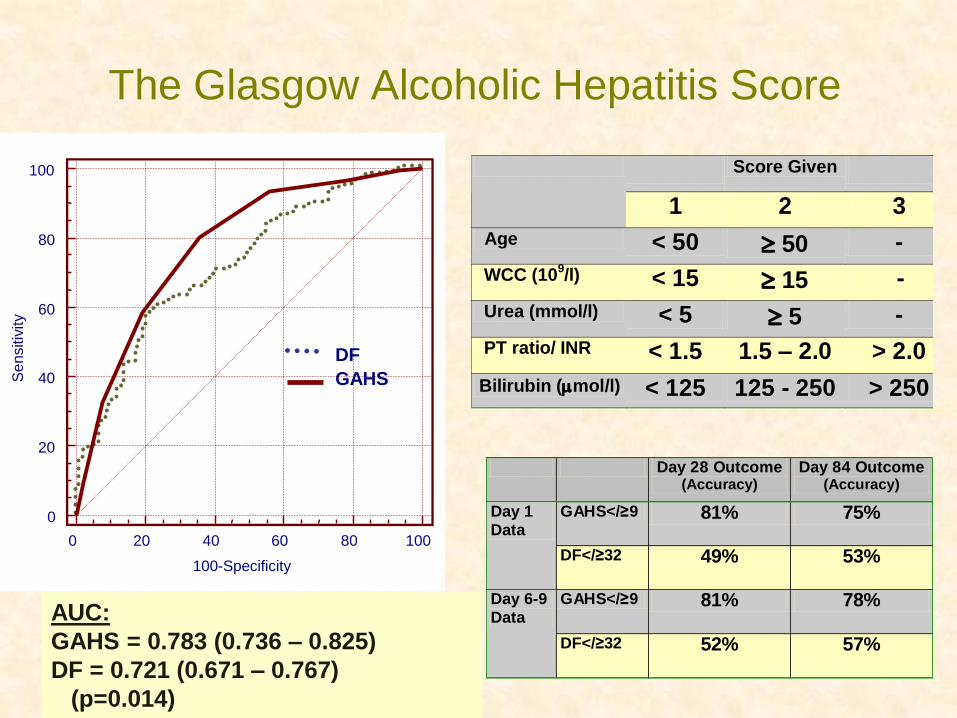
The Glasgow Alcoholic Hepatitis Score
DF
GAHS
Day 28 Outcome (Accuracy)
Day 84 Outcome (Accuracy)
GAHS</≥9 81% 75% Day 1
Data
DF</≥32 49% 53%
GAHS</≥9 81% 78% Day 6-9
Data
DF</≥32 52% 57%
Score Given
1 2 3
Age < 50 50 -
WCC (109/l) < 15 15 -
Urea (mmol/l) < 5 5 -
PT ratio/ INR < 1.5 1.5 – 2.0 > 2.0
Bilirubin (mol/l) < 125 125 - 250 > 250
AUC:
GAHS = 0.783 (0.736 – 0.825)
DF = 0.721 (0.671 – 0.767)
(p=0.014)
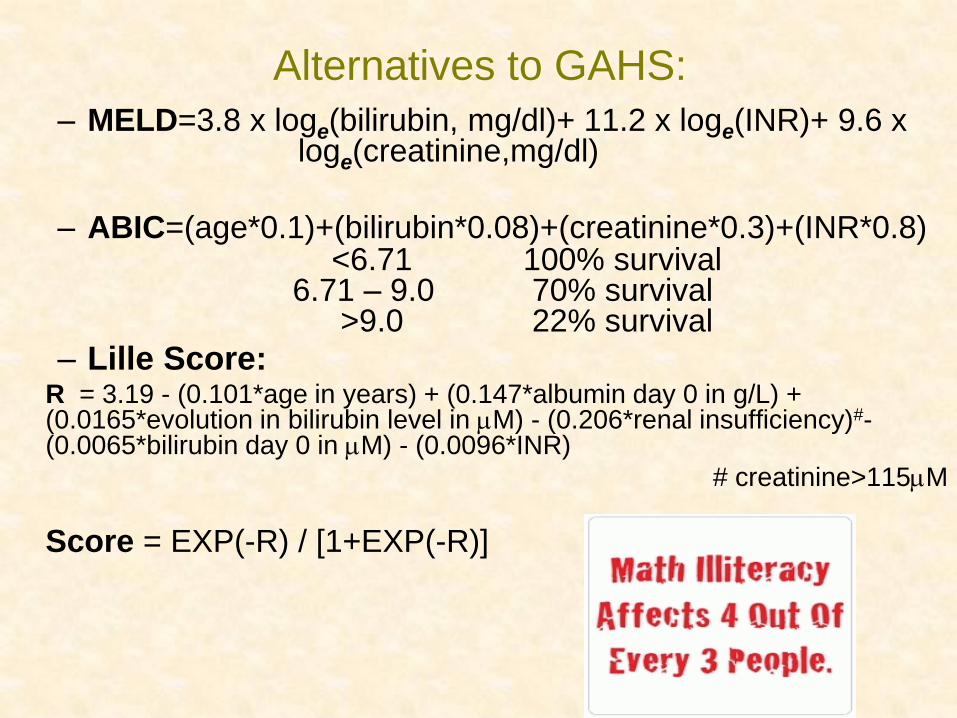
Alternatives to GAHS:
– MELD=3.8 x loge(bilirubin, mg/dl)+ 11.2 x loge(INR)+ 9.6 x loge(creatinine,mg/dl)
– ABIC=(age*0.1)+(bilirubin*0.08)+(creatinine*0.3)+(INR*0.8) <6.71 100% survival 6.71 – 9.0 70% survival >9.0 22% survival
– Lille Score: R = 3.19 - (0.101*age in years) + (0.147*albumin day 0 in g/L) +
(0.0165*evolution in bilirubin level in M) - (0.206*renal insufficiency)#- (0.0065*bilirubin day 0 in M) - (0.0096*INR)
# creatinine>115M
Score = EXP(-R) / [1+EXP(-R)]
Back to our patient...... • 35 year old woman
• Bilirubin 326; AST 241; ALT 94; ALP 234; PT 27seconds (PTr
2.4); Urea 6.5; WCC 17.4; Alb 26
• Jaundiced; pyrexial; drowsy; moderate abdominal distension
• US showed moderate ascites and hepato-splenomegaly.
• Sepsis screen negative
• What treatment should be considered?
A. Terlipressin and Albumin infusions
B. Pentoxifylline orally
C. Prednisolone orally
D. Rifaximin
E. Broad spectrum antibiotics
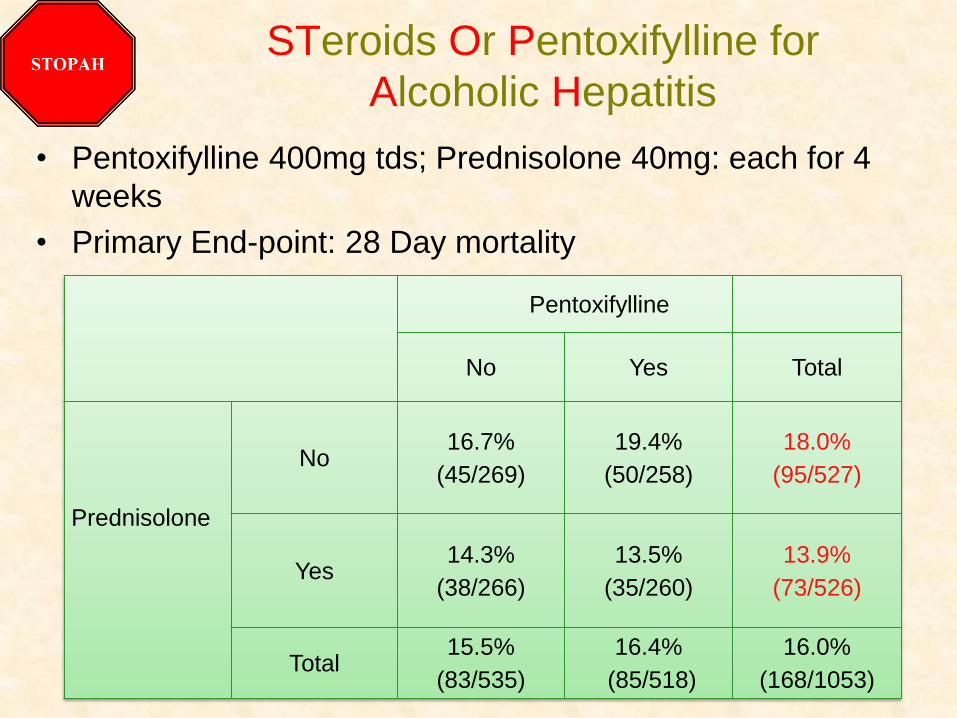
STeroids Or Pentoxifylline for
Alcoholic Hepatitis
• Pentoxifylline 400mg tds; Prednisolone 40mg: each for 4
weeks
• Primary End-point: 28 Day mortality
Pentoxifylline
No Yes Total
Prednisolone
No 16.7%
(45/269)
19.4%
(50/258)
18.0%
(95/527)
Yes 14.3%
(38/266)
13.5%
(35/260)
13.9%
(73/526)
Total 15.5%
(83/535)
16.4%
(85/518)
16.0%
(168/1053)
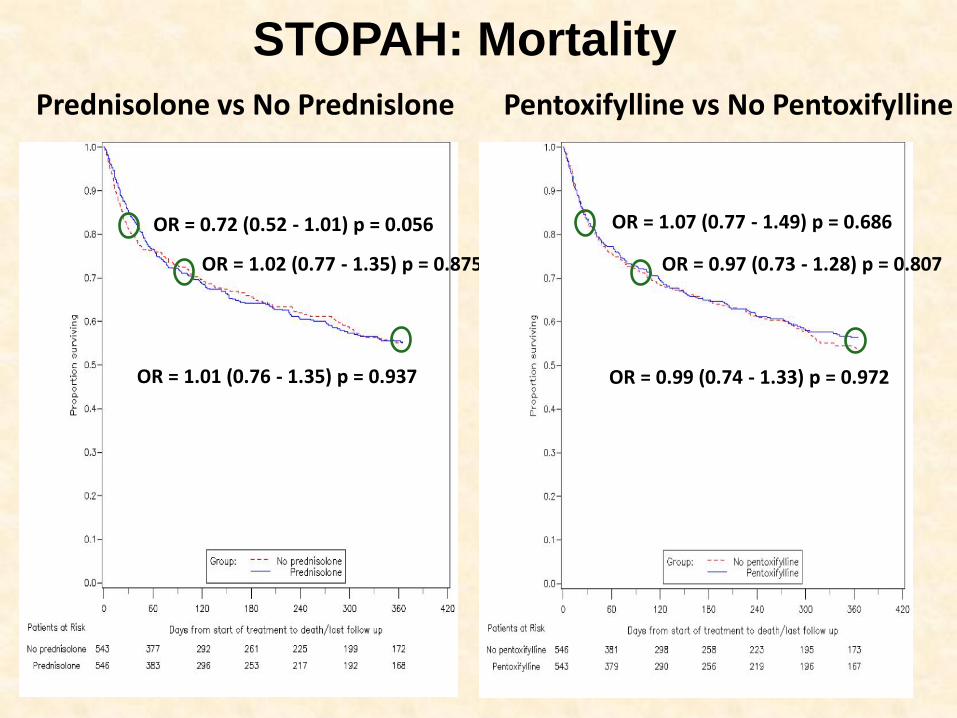
OR = 0.72 (0.52 - 1.01) p = 0.056
OR = 1.02 (0.77 - 1.35) p = 0.875
OR = 1.01 (0.76 - 1.35) p = 0.937
OR = 1.07 (0.77 - 1.49) p = 0.686
OR = 0.97 (0.73 - 1.28) p = 0.807
OR = 0.99 (0.74 - 1.33) p = 0.972
Prednisolone vs No Prednislone Pentoxifylline vs No Pentoxifylline
STOPAH: Mortality
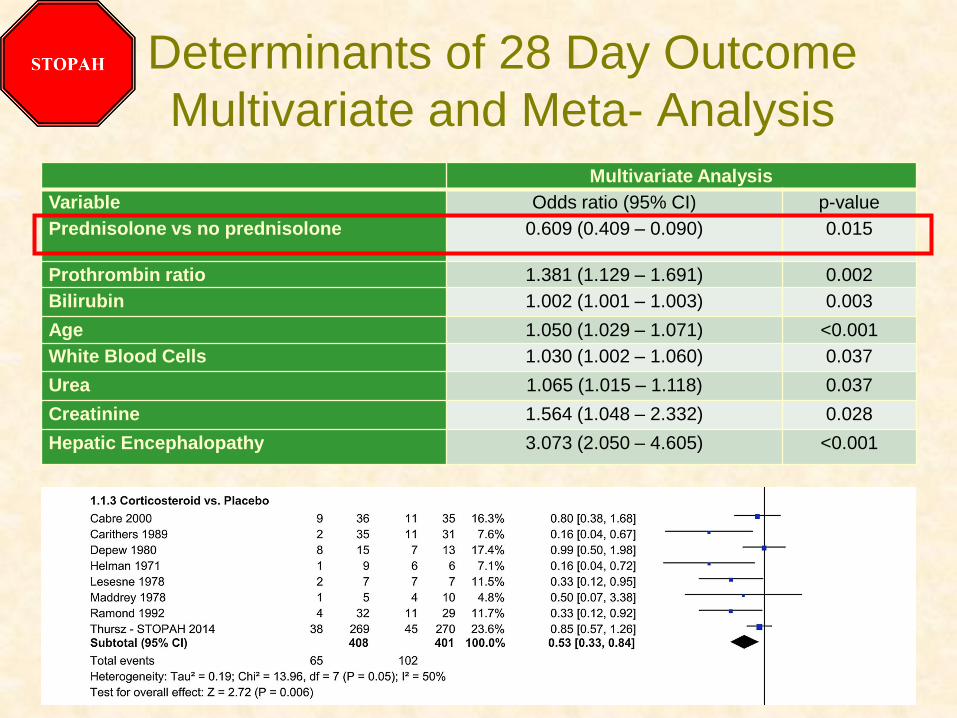
Determinants of 28 Day Outcome
Multivariate and Meta- Analysis
Multivariate Analysis
Variable Odds ratio (95% CI) p-value
Prednisolone vs no prednisolone 0.609 (0.409 – 0.090) 0.015
Prothrombin ratio 1.381 (1.129 – 1.691) 0.002
Bilirubin 1.002 (1.001 – 1.003) 0.003
Age 1.050 (1.029 – 1.071) <0.001
White Blood Cells 1.030 (1.002 – 1.060) 0.037
Urea 1.065 (1.015 – 1.118) 0.037
Creatinine 1.564 (1.048 – 2.332) 0.028
Hepatic Encephalopathy 3.073 (2.050 – 4.605) <0.001
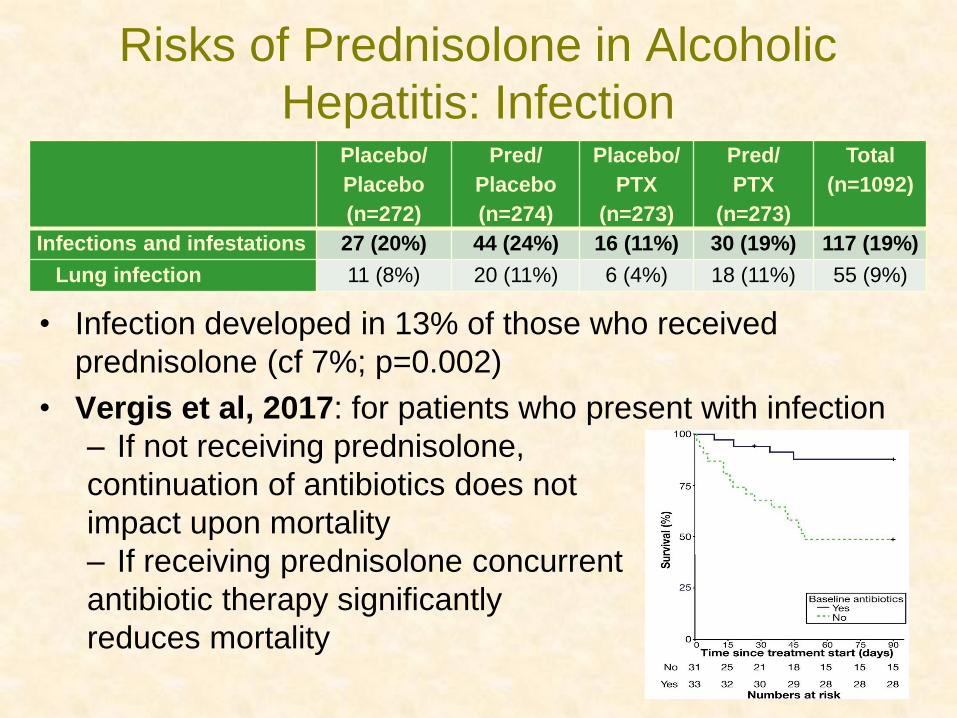
Risks of Prednisolone in Alcoholic
Hepatitis: Infection
• Infection developed in 13% of those who received
prednisolone (cf 7%; p=0.002)
• Vergis et al, 2017: for patients who present with infection
– If not receiving prednisolone,
continuation of antibiotics does not
impact upon mortality
– If receiving prednisolone concurrent
antibiotic therapy significantly
reduces mortality
Placebo/
Placebo
(n=272)
Pred/
Placebo
(n=274)
Placebo/
PTX
(n=273)
Pred/
PTX
(n=273)
Total
(n=1092)
Infections and infestations 27 (20%) 44 (24%) 16 (11%) 30 (19%) 117 (19%)
Lung infection 11 (8%) 20 (11%) 6 (4%) 18 (11%) 55 (9%)
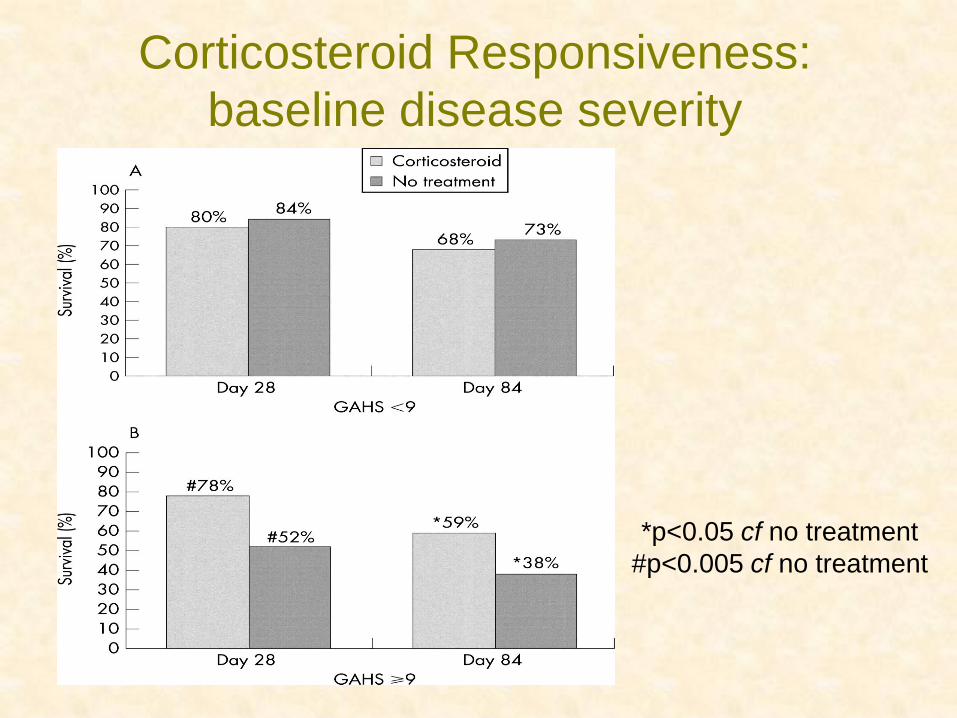
Corticosteroid Responsiveness:
baseline disease severity
*p<0.05 cf no treatment
#p<0.005 cf no treatment
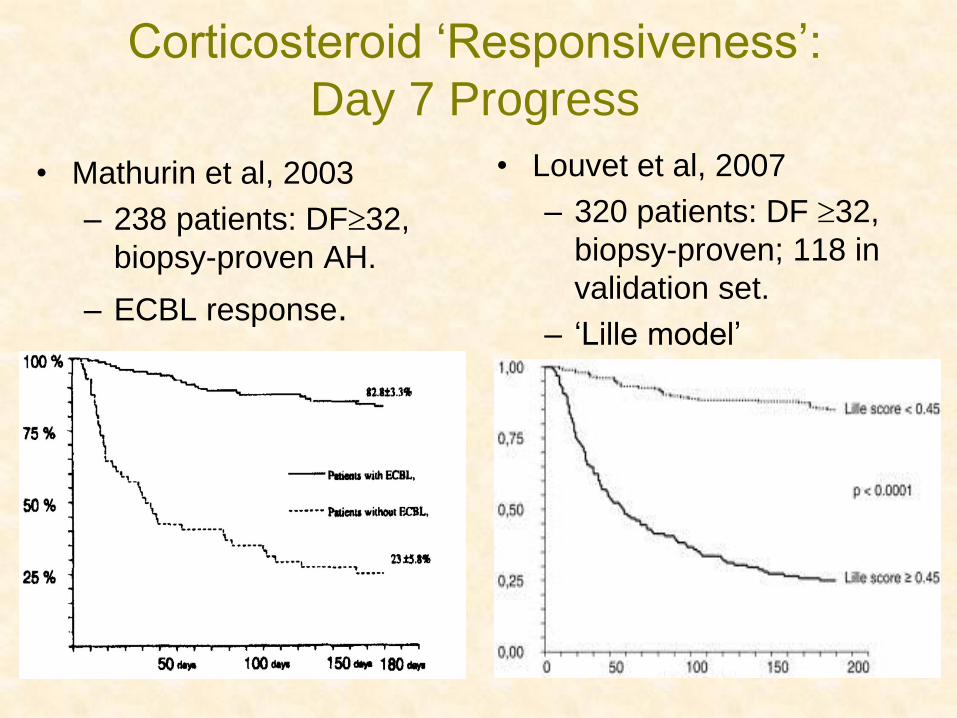
Corticosteroid ‘Responsiveness’:
Day 7 Progress
• Mathurin et al, 2003
– 238 patients: DF32,
biopsy-proven AH.
– ECBL response.
• Louvet et al, 2007
– 320 patients: DF 32,
biopsy-proven; 118 in
validation set.
– ‘Lille model’
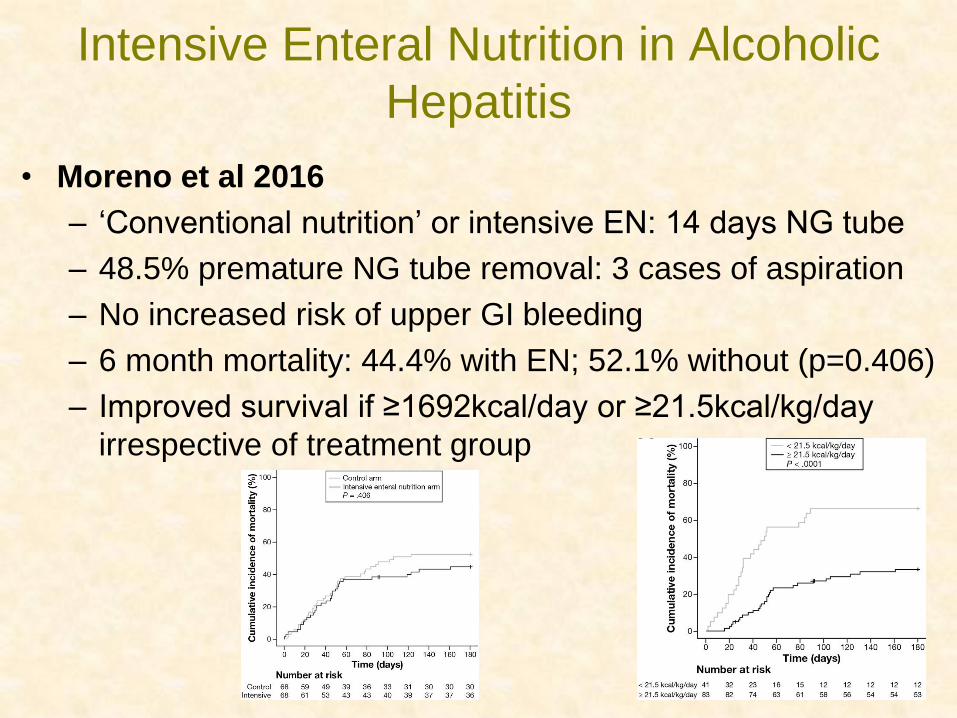
Intensive Enteral Nutrition in Alcoholic
Hepatitis
• Moreno et al 2016
– ‘Conventional nutrition’ or intensive EN: 14 days NG tube
– 48.5% premature NG tube removal: 3 cases of aspiration
– No increased risk of upper GI bleeding
– 6 month mortality: 44.4% with EN; 52.1% without (p=0.406)
– Improved survival if ≥1692kcal/day or ≥21.5kcal/kg/day
irrespective of treatment group
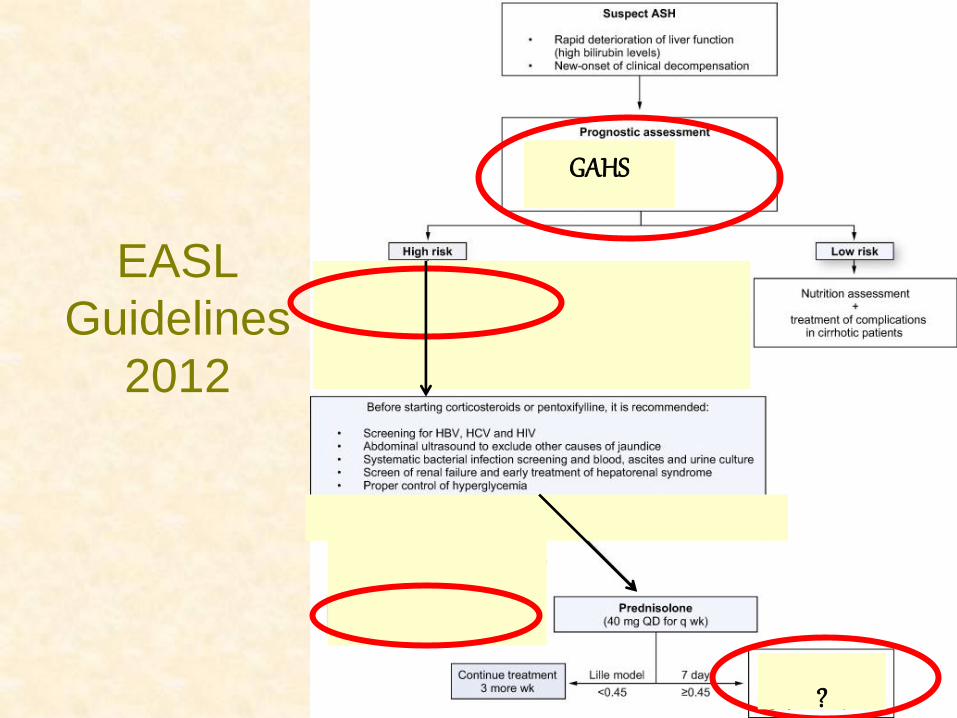
EASL
Guidelines
2012
GAHS
?
Just then in the next bed......
• Patient with known alcohol related cirrhosis
• Admitted 36 hours earlier with jaundice
• Increasing confusion with agitation
• Now shouting and threatening staff and other patients
• How should her agitation be managed?
A. Regular Diazepam
B. Symptom-triggered Diazepam
C. Symptom-triggered Lorazepam
D. Intravenous Chlormethiazole
E. 5-10mg Haloperidol

Confusion and Agitation in the Jaundiced
Alcoholic: a Broad Differential • Withdrawal State
– Alcohol; benzodiazepine; (SSRI)
• Wernicke’s Encephalopathy
– Undernourished; dextrose load; low Mg
• Hepatic Encephalopathy
– Acute; Chronic (porto-systemic)
• Brain Injury
– Traumatic: subdural (history of falls); chronic ARBD
• Seizure Disorder
– Post-ictal: unwitnessed seizure; Non-convulsive Status
• Delerium/ Metabolic
– Hyponatraemia; Possible sepsis
• Intoxication
– Prolonged effect (unknown street drugs); illicit use
• (Psychiatric)
Alcohol Withdrawal in the Liver Patient
• NICE Clinical Guidelines 100, 2010:
“In older adults and people with compromised liver function, long-acting agents are known to accumulate. In the absence of clinical evidence supporting one agent over another, the GDG agreed on consensus that a shorter-acting agent (e.g. oxazepam or lorazepam) could be offered to the elderly or if there was evidence of encephalopathy.”
• Consider Symptom Triggered Treatment (STT) rather than Fixed Dose Treatment (FDT):
– Lorazepam 1-2mg
• Haloperidol for severe agitation (note QT interval)
• Anaesthetic involvement in extreme cases
BSG 2016
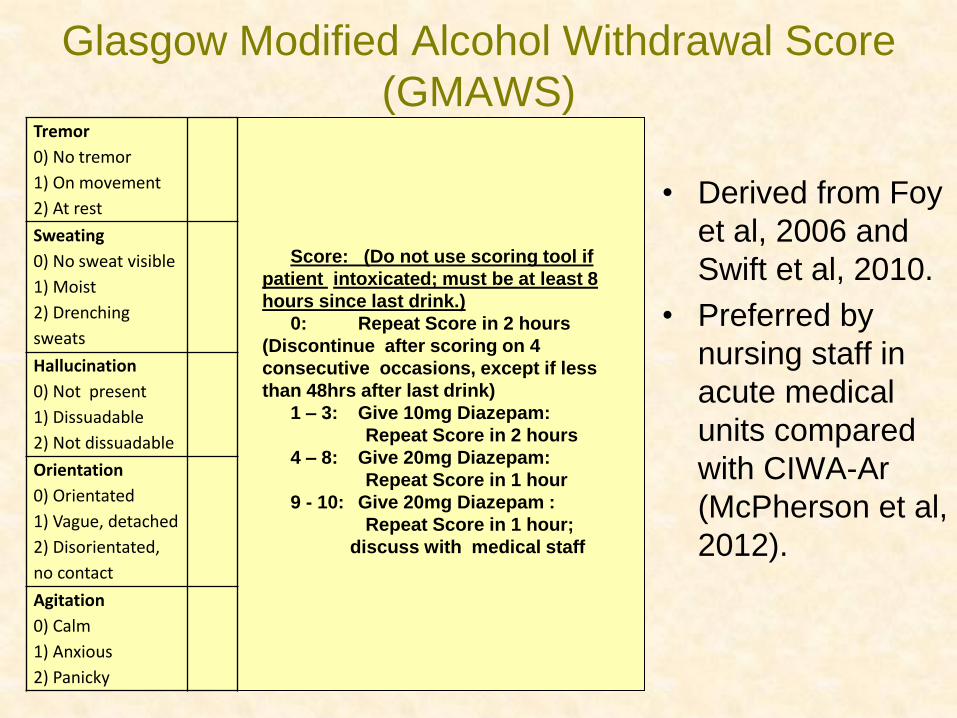
Tremor
0) No tremor
1) On movement
2) At rest
Sweating
0) No sweat visible
1) Moist
2) Drenching
sweats
Hallucination
0) Not present
1) Dissuadable
2) Not dissuadable
Orientation
0) Orientated
1) Vague, detached
2) Disorientated,
no contact
Agitation
0) Calm
1) Anxious
2) Panicky
Score: (Do not use scoring tool if
patient intoxicated; must be at least 8
hours since last drink.)
0: Repeat Score in 2 hours
(Discontinue after scoring on 4
consecutive occasions, except if less
than 48hrs after last drink)
1 – 3: Give 10mg Diazepam:
Repeat Score in 2 hours
4 – 8: Give 20mg Diazepam:
Repeat Score in 1 hour
9 - 10: Give 20mg Diazepam :
Repeat Score in 1 hour;
discuss with medical staff
Glasgow Modified Alcohol Withdrawal Score
(GMAWS)
• Derived from Foy
et al, 2006 and
Swift et al, 2010.
• Preferred by
nursing staff in
acute medical
units compared
with CIWA-Ar
(McPherson et al,
2012).
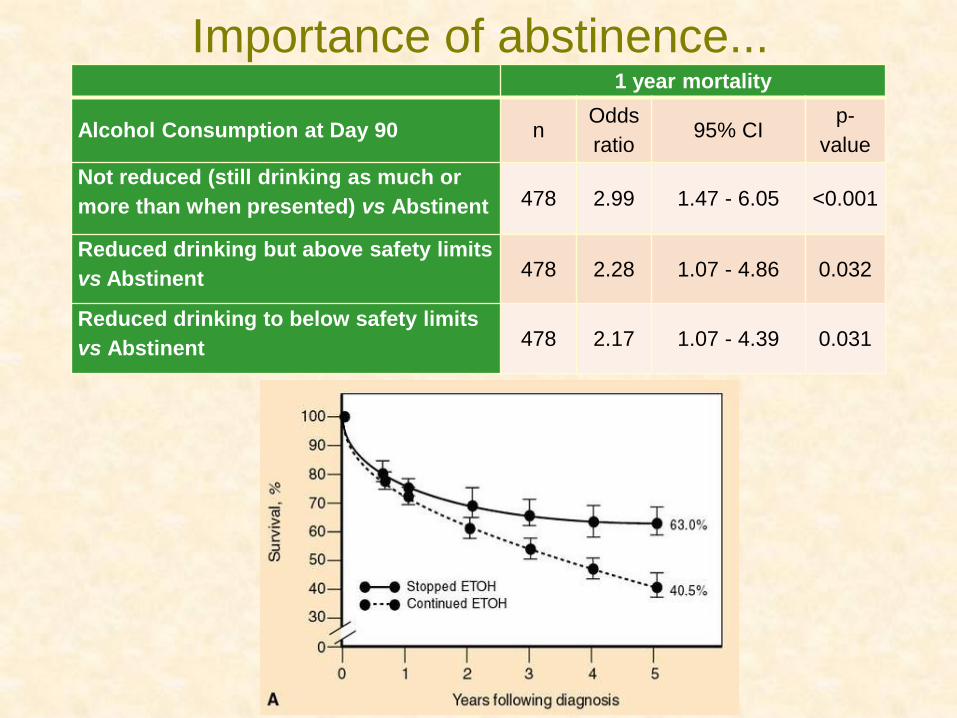
Importance of abstinence... 1 year mortality
Alcohol Consumption at Day 90 n Odds
ratio 95% CI
p-
value
Not reduced (still drinking as much or
more than when presented) vs Abstinent 478 2.99 1.47 - 6.05 <0.001
Reduced drinking but above safety limits
vs Abstinent 478 2.28 1.07 - 4.86 0.032
Reduced drinking to below safety limits
vs Abstinent 478 2.17 1.07 - 4.39 0.031
Pharmacotherapy Options in ALD
• Little evidence with significant alcohol-related liver injury.
• Acamprosate has the best safety profile.
– No hepatic metabolism and no reported hepatotoxicity.
– Acamprosate does not adversely affect neuropsychiatric status in patients with Child's Grade A and B cirrhosis.
• Naltrexone not associated with hepatotoxicity
• Disulfiram related to hepatotoxicity: 28% mortality
• Baclofen: Addolorata et al, 2007
– alcoholic cirrhosis; Baclofen 10mg tds for 12 weeks
– 71% abstinent (cf 29%): OR 6.3 (2.4, 16.1), p=0.0001
– excluded people with diabetes, encephalopathy, psychiatric comorbidity and comorbid drug misuse
The Jaundiced Alcoholic: an approach
• Is it Alcohol?
– Look for other precipitants; atypical biochemical pattern
• Is it chronic decompensation or a more acute change?
– >2 month history; relative lack of SIRS; typical biochemistry
• If acute, is there sepsis or other trigger?
– Full sepsis screen; Abdo US; early treatment
• If acute and no sepsis, likely alcoholic hepatitis
– Assess severity: Prednisolone 40mg for 4 weeks if GAHS>8
and improvement after 7 days; continue antibiotics if sepsis
• For ALL patients:
– Address general nutrition and specific deficits (Folate; B1; Mg)
– Manage AWS safely
– Engage with alcohol services