ajcc 6 th edition staging of breast carcinoma. ajcc node staging -16 categories pnx – 1 option pn0...
TRANSCRIPT


AJCC 6TH EDITION STAGING OF
BREAST CARCINOMA.

AJCC NODE STAGING -16 CATEGORIES
pNX – 1 option pN0 – 5 options; null,(i-),(i+),(mol-),(mol+) pN1 – 4 options; mi,a,b,c pN2 -- 3 options; a,b,c pN3 – 3 options; a,b,c

5 YR SURVIVAL OF 20,547 WOMEN WITH RESPECT TO LYMPH NODE
INVOLVEMENT
Cancer 45:2917-2924, 1980.
0
10
20
30
40
50
60
70
0 2 4 6TO10
5 yr % survival

N0 N1 N2 N3
0 1-3 4-9 >10
0
10
20
30
40
50
60
70
0 2 4 6TO10
5 yr % survival
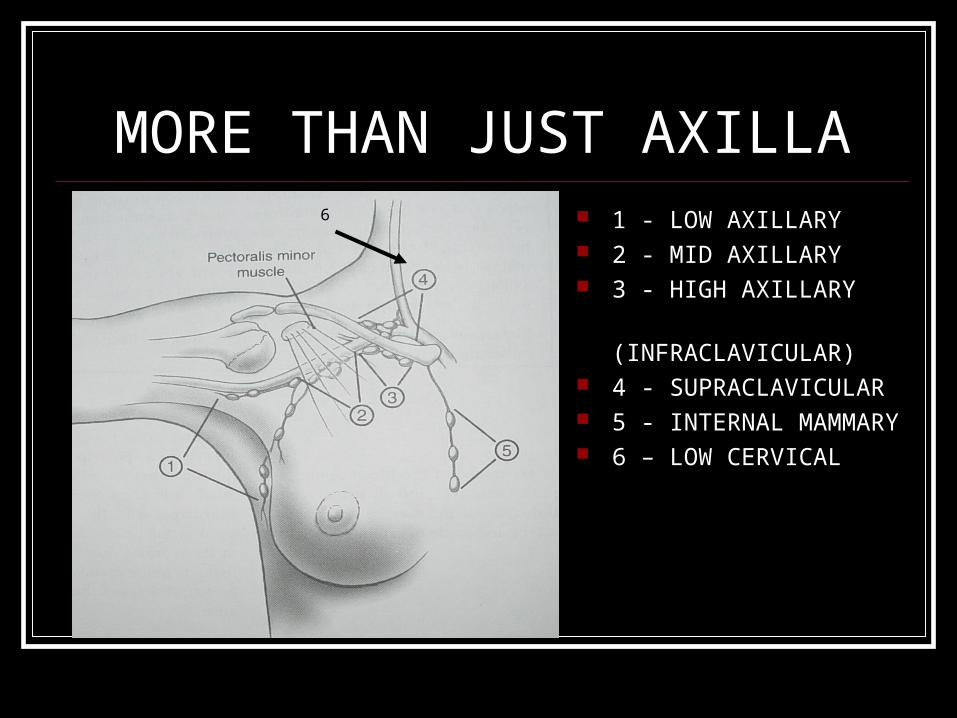
MORE THAN JUST AXILLA 1 - LOW AXILLARY 2 - MID AXILLARY 3 - HIGH AXILLARY
(INFRACLAVICULAR) 4 - SUPRACLAVICULAR 5 - INTERNAL MAMMARY 6 – LOW CERVICAL
6

NEGATIVE NODE STAGING pNX – status unknown pN0 – H&E “negative” for carcinoma pN0 (i+ or i-) – H&E “negative” and IPOX
stains ordered pN0 (mol+ or mol) – H&E “negative” and
RT-PCR ordered
“NEGATIVE” = Isolated tumor cells = pN0

DEFINITION –ISOLATED TUMOR CELLS (ITC)
Single tumor cells or small clusters of tumor cells which do not aggregate to greater than 0.2 mm and which show no evidence of “proliferation or stromal reaction”
Clinical significance unknown (i+) and (i-) (mol+) and (mol-)

ISOLATED TUMOR CELLS pN0(i+) and pN0(mol +) and pN0 (H&E
pos for ITC) are not counted as positive nodes
eg 0.8 cm tumor with 12 nodes of which 3 “positive by IPOX” onlypT1b pN0 pMX
Thus “positive” by IPOX but not by N code.

LOW NODE STAGE
pN1a1-3 nodes positive
In zones 1 and 2
DEFINITION OF CLINICALLY APPARENT
Detected by imaging studies (excluding lymphoscintigraphy)
Detected by physical exam
Note: No mention of matting of nodes though physical exam detection could represent matting.

Pathologist’s Decision Tree
H&E NEGATIVE
NO FURTHER STUDY
pN0
IPOX STUDYpN0 (i+ or i-)
RT-PCRpN0 (mol+ or mol-)

LOW NODE STAGE
pN1b
not clinically apparent but microscopically detected met

LOW NODE STAGE
pN1c
1-3 axillary nodes pos & internal mam. Nodes pos. but not clinically apparent

INTERMEDIATE NODE STAGE
pN2a
4-9 axillary nodes pos. with at least one node met > 2 mm

INTERMEDIATE NODE STAGE
pN2b
clinical apparent int. mammary node, no positive axillary nodes

HIGH STAGE NODE STAGING
pN3a
Two categories
of pN3a
- axillary only
displayed to
the left

HIGH STAGE NODE STAGING
pN3a
Infraclavicular nodes positive
-Second type of pN3a displayed to the left

HIGH STAGE NODE STAGING pN3b Category One - metastasis in
clinically apparent Int mammary node plus 1 or more
axillary nodes

HIGH STAGE NODE STAGING
pN3b Second type
- 3 or more axillary nodes + with int. mam. node positive by
microscopy only

HIGH STAGE NODE STAGING
pN3c
Ipsilateral supra-
clavicular node
met.

WHAT NODE FINDINGS NO LONGER CHANGE STAGING?
MACROSCOPIC - MATTING OF NODES MICROSCOPIC – EXTRACAPSULAR
EXTENSION OF TUMOR
Both of the above are no longer included in the MSP approved synoptic report format.

SENTINEL NODE CLASSIFICATION Sentinel node without accompanying axillary
dissection: (sn) e.g. – pN1 (sn); pN0 (i+) (sn)
Sentinel node with accompanying axillary dissection:e.g.– pN1; pN0 (i+)

AGGREGATE WITHIN A NODE? Node has no mass greater than 0.2 mm but
has multiple masses. What’s the N code?
Node has no mass > 0.2 but < 2.0 mm but has multiple masses. What’s the N code.
I don’t know the answer but it doesn’t happen very often.

AGGREGATE OR NOT TO AGGREGATE, THAT IS THE ?
Each tumor nodule is 0.15 mm.
Each is < 0.2 mm When aggregated the
sum is 0.45 cm
pN0 or pN1mic ?

INTERNAL MAMMARY NODES pN1b - IMN by sentinel node biopsy - mic +
by path but not clinically apparent pN1c – 1-3 + axillary nodes plus IMN mic +
by path pN2b – clinically apparent IMN with neg.
axillary nodes pN3b – IMN clinically apparent with any +
axillary nodes
INFRA AND SUPRACLAVICULAR LYMPH NODES
pN3a – infraclavicular node positive or >10 axillary nodes with one met > 2 mm
pN3c – ipsilateral supraclavicular node positive


GRADING OF TUMORS GX – CANNOT BE ASSESSED G1 – LOW COMBINED HISTOLOGIC
GRADE (FAVORABLE) G2 – INTERMEDIATE COMBINED
HISTOLOGIC GRADE (MODERATELY FAVORABLE)
G3 – HIGH COMBINED HISTOLOGIC GRADE (UNFAVORABLE)

GRADING SYSTEMS IN USE Scarff-Bloom-Richardson -1,2,3 Nottingham ( Elston-Ellis modification of
the Scarff-Bloom-Richardson ) – 3 to 9
- based on 1,831 pts
- prognosis correlation p < 0.0001
- can be applied to most histologic tumor
variants (e.g. - not medullary ca)

CAP AND AJCC RECOMMEDED METHOD FOR TUMOR GRADING Nottingham Combined Histologic Score
- Tubule Formation (1,2 or 3) - Nuclear Pleomorphism (1,2,or 3) - Mitotic Count (1,2, or 3)
Sum T + N + M = Combined Score Score 3-5 = grade 1
Score 6-7 = grade 2 Score 8-9 = grade 3


TUMOR STAGING 18 CATEGORIES – CLINICAL AND PATHOLOGY
STAGING THE SAMEpTX (eg – gross tumor at margin of resection)pT0 no tumor pTis (DCIS, LCIS, Paget’s)pT1 (a,b,c) 0.1 cm to 2.0 cmpT2 > 2.0 < 5.0 cmpT3 >5.0 cm pT4 (a,b,c,d) chest wall or skin spread

What about invasion < 0.1cm? Termed microinvasion. No T category reserved. Lumped under pT1 as pT1mic Number and size of microinvasive sites
should be listed by recommendation of AJCC

WHAT ABOUT COMBINED INSITU AND INVASIVE LESIONS?
The staging is by size of only the invasive component.
e.g. – 2.5 cm macroscopic tumor mass shows 60% DCIS. Staging is not pT2 (>2 cm) but pT1b or pT1c (0.5 to 2.0 cm).

WHAT ABOUT NEOADJAVANT PRESURGERY CHEMOTHERAPY?
All TNM in such case should be preceded by the prefix “y”
e.g. – ypT1a

WHAT ABOUT S/P NEEDLE CORE BIOPSIED LESIONS?
MEASURE RESIDUAL TUMOR AGGREGATE MEASUREMENT FROM
PREVIOUS CORE AND PRESENT LUMPECTOMY / MASTECTOMY
e.g. – mammatome biopsy of 0.7 cm and lumpectomy of 0.8 = 1.5 cm or pT1b
(if the mammatome biopsy is from the center of the breast mass then aggregating may not be appropriate).

WHAT ABOUT SYNCHRONOUS LESIONS?
Largest mass’ measurement provides T Smaller tumor does not get assigned a T Lesions in the same quadrant are not
considered synchronous lesions but are “satellite breast nodules” (no change in T)
Synchronous bilateral lesions are staged separately.

METASTATIC STAGING pMX - unknown pM0 – no known mets pM1 – distant mets
low cervical nodes
pectoralis muscle invasion
distant organs
malignant effusions
(supraclavicular nodes no longer > M1)

WHAT IS THE PATHOLOGIST’S RESPONSIBILITY?
Use a template that has all the required data fields.
Complete the TNM staging at the time of report signing.
Use all available resources, reports, history to accurately provide the TNM staging.
