airway management ii. -...
TRANSCRIPT

Airway management II.Advanced Airway Management (AAM)
UD FM DAIC
English program practice
2018

Advanced airway management (AAM)
• Invasive techniques that require specialized equipment, training
• Involves insertion of an airway securing device BELOW the vocal cords
• Allows mechanical ventilation of the patient, guards against aspiration
• Procedures− Endotracheal intubation−Conicotomy−Tracheostomy (percutaneous)

AAM devices
• Transglottic devices‒ Endotracheal tube
‒ Endobronchial tube
‒ Bronchial blockers
• Infraglottic devices‒ Tracheostomy tubes
‒ Cricothyrotomy (conicotomy) tubes / needles
• Intubation assist devices‒ Laryngoscope
‒ IntroducerStylet
Bougie
Tube exchange catheter
‒ Fiberoptic scope
‒ Magill forceps
• Devices for securing the tube
• Suctioning devices

Endotracheal tubes (ET)
• Classic ET
• Cuff-less tubes
• Spiral tube (ie. Woodbridge)
• Preformed tubes (ie. RAE)
• Tubes with supraglottic suctioning ports (ie. Teleflex ISIS HVT)

Endobronchial (double lumen) tubes
• Carlens (left)
• White (right)
• Robertshaw‒ Right selective
‒ Left selective
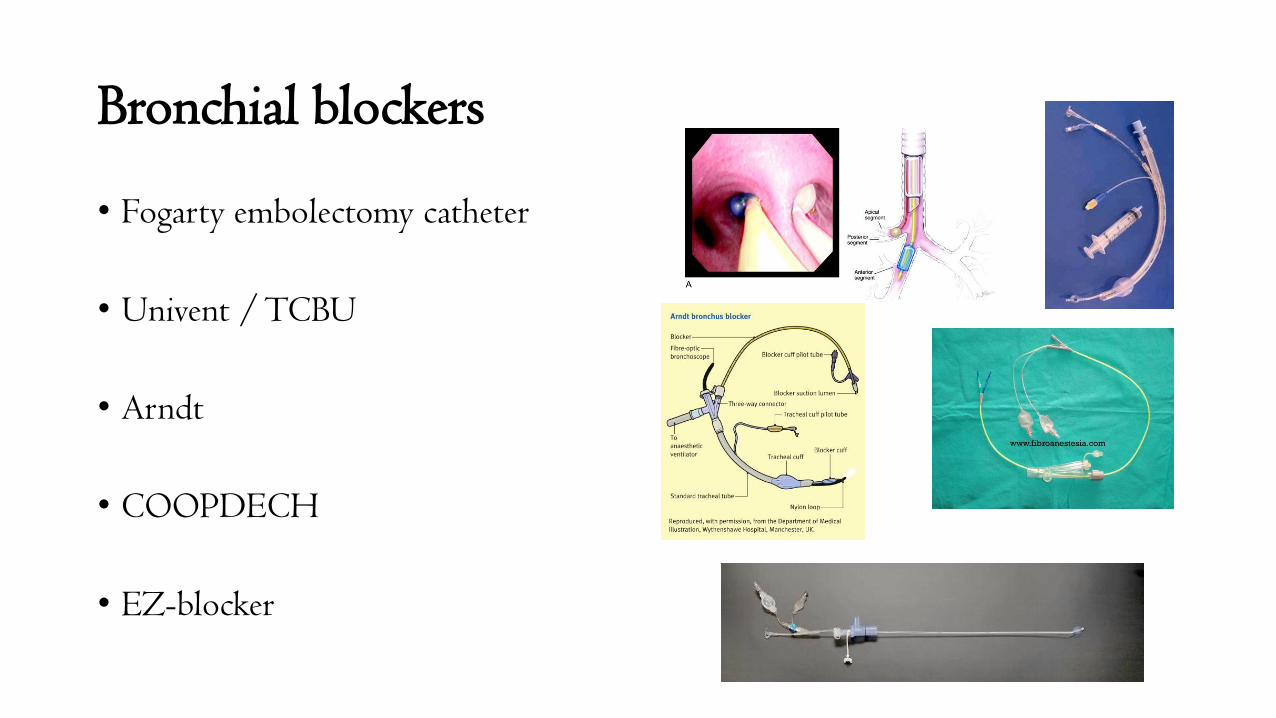
Bronchial blockers
• Fogarty embolectomy catheter
• Univent / TCBU
• Arndt
• COOPDECH
• EZ-blocker

Tracheostomy tubes
• Surgical / Percutaneous
• Transient/ permanent
• Special types:‒ Double balloon
‒ Adjustable length
‒ Flexible
‒ Supraglottic suctioning ports
‒ Fenestrated („speaking tube”)

Percutaneous dilation tracheostomy (PDT)
• Ciaglia technique
• Griggs technique
• Blue Rhino technique
• Blue Dolphin technique
• Perc Twist technique

Conicotomy (cricothyrotomy) set
Melker kit
QuickTrach
Portex kit

Needle cricothyrotomy

Laryngoscopes
• Classic‒ Parts:
Handle (with batteries)
Light source
Blade (right or left handed)• Curved (Macintosh)
• Straight (Miller)
• Flexible tip (McCoy)
• Increased angle (Polio)
• Fiberoptic (i.e. Bullard)
• Video (i.e. Glide scope)

Stylets
• Rigid
• Flexible
• Mobile (Schroeder)

Bougie

Aintree („hollow bougie”)

Tube exchenge catheter

Intubation fiberoscope
• Flexible
• Rigid

Intubating airways
• Patil-Syracuse
• Ovassapian
• Williams
• Berman
• Lee
• TIO


Magill forceps

Devices for securing the tube

Devices for verifying tube position
• TubeChek
• CO2 detector
• Capnograph

Suctioning catheters
• Open
• Closed

Suction pumps
• Manual pumps (ie. AMBU Rescuepump)
• Motorized pumps
• Wall suction

„Routine” intubation
• All required personnel and devices should be on hand. Verify operational status of all devices, structural integrity of the tube
• Monitor the patient (most important: SpO2)
• Venous access
• Turn on the suction
• Preoxygenize
• Administer iv. sedatives + opioids +/- muscle relaxants
• Verify adequate sedation depth (verbal stimulus, eyelash reflex)

„Routine” intubation II.• Direct laryngoscopy/visualization of the larynx
‒ Recline the head with your right hand‒ Open the mouth (if necessary)‒ Laryngoscope in the left hand, turned on‒ Introduce the blade from the right angle of the mouth‒ Push the tongue to the left‒ Slide the blade along the tongue until the epiglottic vallecula‒ Raise/push away with the laryngoscope, guard the teeth (never tilt!!!)‒ Direct laryngoscopy (Cormack-Lehane score?)‒ If necessary, additional patient positioning, repositioning of the blade, B.U.R.P.
maneuver (backward, upward right position – positioning of the larynx from the outside)
• Intubate (preferably with visualization of the vocal cords!)
• Inflate the cuff, bag ventilation, verify tube position.
• Secure the tube

Intubation of the patient with a full stomach:RSI – Rapid Sequence Intubation
• All required personnel and devices should be on hand. Verify operational status of all devices, structural integrity of the tube
• Monitor the patient (most important: SpO2)
• Venous access
• Turn on the suction
• Preoxygenize
• Sellick-maneuver initiated
• Patient positioning: supine, either flat, head or foot end raised
• Iv. analgo-sedation (ketamine or thiopental / propofol + fentanyl) + fast
acting NMBA (succinylcholine/rocuronium) in rapid succession
• Hold the Sellick-maneuver
• Intubation
• Inflate the cuff, bag ventilation, verify tube position.
• Release Sellick-maneuver
• Sellick maneuver:

Aspiration prophylaxis
• Fasting (if possible)‒ Solids: 6-9 hours‒ Clear fluids: 1-2 hours
• Artificial emptying of the stomach (weak evidence)‒ Nasogastric tube – only for evacuation of fluid‒ Large bore orogastric tube – for larger food particles‒ CAVE: injury
• Pharmacotherapy (little or no evidence)‒ Mucosal coaters (ie. sucralfate) – binds gastric acids and bilirubin effectively, however causes pneumonitis upon aspiration‒ Antacids (ie. Na-citrate) – quickly raises gastric pH‒ H2R-blockers (ie. apofamotidine)/PPI-s (ie. pantoprasole) – potently raise gastric pH, but require hours for full effect‒ Prokinetics (ie. metoclopramide) – facilitates gastric emptying in obstetric patients
• ETT as fast as possible – use of RSI protocol‒ Sellick maneuver’s efficiency has been questioned over the years (often performed inappropriately, anatomic variation)‒ CAVE: potential for oesophageal, laryngeal injury/laryngoscopy is more difficult during the Sellick maneuver

Treatment of aspiration
• Tracheobronchial toilette (if possible with a bronchoscope)
• Provide adequate oxygenation (SpO2 > 95%)‒ Nasal cannula, O2-mask, reservoir mask‒ Noninvasive CPAP/PS ventilation‒ Invasive ventilation
• Physiotherapy
• Pharmacotherapy‒ Mucolytics (i.e. acethylcystein)‒ Bronchodilators (i.e.. fenoterol +/- ipratropium, theophyllin)‒ Steroids (routinely not advised)‒ Antibiotics (prophylaxis is not recommended; in case of pneumonia targeted therapy as soon as
possible)
• Monitoring and further treatment according to the patients status(PACU, ICU)

Difficult airway
• Classification:‒ Difficult mask ventilation
Causes: developmental abnormality/trauma/tumors of the face and upper airways, dentures (or lack there of), airway foreign body
‒ Difficult direct laryngoscopy/tube insertionCauses: impaired mouth opening and/or
neck movements, diseases of the oral cavity, pharynx, larynx
• Protocols:‒ DAS (Difficult Airway Society)‒ ASA (American Society of
Anesthesiologists)
• Prediction‒ Inspection of the face, neck, dentition,
oral cavity, jaw and neck movements Inter-incisal distance (<3 cm) Sternomental distance (<12 cm)Mallampati score /I-IV/
‒ Direct/indirect laryngoscopy, fiberoscopyCormack-Lehane score
‒ Imaging studies (X-ray/CT, not for screening)
‒ FRONT score /0-1-2/ (F – face, R – row of teeth, O – oral cavity,
N – neck, T – trachea)

Mallampati score

Cormack-Lehane score

Planed fiberoptic intubation
• Informed consent, psychological preparation of the patient
• Preparation of devices (CAVE: ETT should be threaded onto the fiberoscope)
• Monitor, Oxygen, Venous access, Evaluate patient status
• Anaesthesia of mucous membranes (Lidocain 10%)
• Analgosedation (Propofol or Dexmedethomidine +/- opioid) ‒ (CAVE: preserve spontaneous ventilation)
• Insertion of intubating airway, if necessary
• Insertion of fiberoscope
• Insertion of ETT
• Inflate the cuff, verify tube position, secure the tube manually
• Withdraw fiberoscope
• Induction of general anaesthesia
• Secure the tube in its final position

Protocol for the unexpected difficult airway

Plan „A”
• 3 attempts (+1, with assistance)
• Every attempt should somehow be different from the previous!!!‒ Positioning
„Sniffing” position BURP
‒ Use an introducer/Bougie‒ Alternative larnygoscopy
Switch bladesVideo-laryngoscope
‒ Fiberoptic intubation CAVE: more difficult because of reduced tone in the airways – laryngoscope might help
• Continuous monitoring of oxygenation!!!
• If unsuccessful, transition to plan “B” as soon as possible!!!
Plan „B”
• If insertion of an LMA is successful:‒ Continue anaesthesia/surgery with the LMA – if the risk of aspiration is low, body
cavities are not opened (laparoscopic surgery?)
‒ Intubate through the LMA„Blind” – only attempt through iLMA (still a high risk of failure; risk of injury to the larynx and
adjacent tissues)
Fiberoptic
• Leave the LMA in position - CAVE: the diameter of the inserted tube might not be adequate
• Use Aintree catheter
• If unsuccessful, transition to plan “C” as soon as possible!!!

Plan „C”
• Goals:‒ Maintain oxygenation (and if possible CO2 elimination)
‒ Awaken the patient
• If unsuccessful: CICV („can’t intubate, can’t ventilate”) – life threatening situation!!!‒ Initiate plan „D” immediately!!!

Plan „D”
• Conicotomy with the Finger – Scalpel – Bougie – Tube method‒ Palpate the cricothyroid ligament ‒ Incision through the skin and ligament (+/- dilate the hole with
your finger/the shaft of the scalpel)‒ Insert Bougie‒ Insert ETT‒ (verify tube position)

Thanks for attention!