ahca home health regulatory update anne menard home care unit bureau of health facility regulation...
TRANSCRIPT

AHCA Home Health Regulatory Update
Anne MenardHome Care Unit
Bureau of Health Facility RegulationAgency for Health Care Administration
July 22, 2014
2
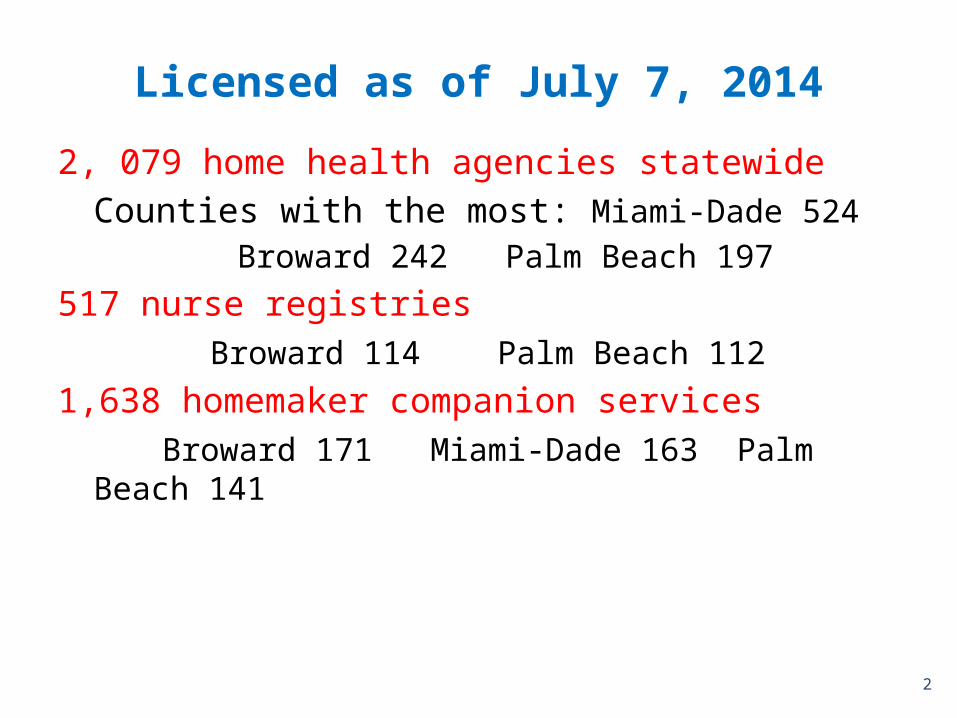
Licensed as of July 7, 2014
2, 079 home health agencies statewideCounties with the most: Miami-Dade 524
Broward 242 Palm Beach 197
517 nurse registries Broward 114 Palm Beach 112
1,638 homemaker companion services Broward 171 Miami-Dade 163 Palm
Beach 141

3
2,079 Home Health Agencies in Florida
68.5% Certified for Medicare and/or Medicaid879 Medicare only 65 Medicaid only481 Medicare & Medicaid 654 not Medicare or Medicaid (31.5%) – 92 have applied for Medicare and/or Medicaid
As of 7/7/2014

4
2014 Law ChangesHome Health Agencies
House Bill 1179 amended 400.471(2)(h), Florida Statutes to add: A home health agency that is not Medicare or Medicaid certified and does not provide skilled care is exempt from accreditation.
“Skilled care” is nursing services or therapeutic services (physical, occupational, respiratory therapy and speech language pathology) 400.462(28), Florida Statutes
“Medicaid certified” home health agencies are those that provide skilled care and meet the federal conditions of participation.
Federal regulations require that all Medicare and Medicaid certified HHAs provide nursing. 42 Code of Federal Regulations 484.14(a)
If your agency wants to change its accreditation status, fax your request to the AHCA Home Care Unit with a copy of your agency’s letter to the accrediting organization that includes the date your agency will no longer be accredited. AHCA Home Care Unit fax is (850) 922-5374.

Home Health Agency Accreditation
The state law, 400.471(2)(h), Florida Statutes, requires:
All home health agencies (HHAs) that provide skilled care that were licensed on or after July 1, 2008 must be accredited and continue to maintain accreditation.
All applicants for new HHA licenses that will provide skilled care must be accredited. This also includes changes of ownership and HHAs that fail to submit an application to renew their licenses prior to expiration and apply for new licenses.
Accreditation surveys are accepted in place of surveys by AHCA.
Complaints visits are still made by AHCA for home health agencies. For Medicare and Medicaid certified agencies that have deemed status accreditation, CMS will assign to AHCA to investigate if there is alleged non-compliance with one of more federal conditions of participation.
5

6
Is a non-skilled home health agency required to have a nurse?
Yes, for the following reasons:
1. To provide supervision of home health aides and certified nursing assistants:
“A home health agency shall arrange for supervisory visits by a registered nurse to the home of a patient receiving home health aide services in accordance with the patient’s direction, approval, and agreement to pay the charge for the visits.” 400.487(3), F.S. (Home health aide services are also provided by certified nursing assistants.)
“A registered nurse may assign selected portions of patient care to licensed practical nurses and home health aides but always retains the full responsibility for the care given and for making supervisory visits to the patient’s home.” Note: Home health agencies must obtain the patient’s verbal permission to send an RN into the home to do supervisory visits. 59A-8.0095(3)(b) and (5)(b), FAC.
Must have a supervisor available for the staff during the hours of patient service. 59A-8.003(10)(d), FAC.
2. To review patient medications if a home health aide or certified nursing assistant is to assist the patient with self-administered medications – to make sure that the caregiver is able to provide assistance in accordance with their training and the medication prescription. 59A-8.0095(5)(m), FAC and 400.488, F.S.

7
Assistance with Self-Administration of Medication
Home Health Agencies
The patient may need a registered nurse or licensed practical nurse to administer medication.
Home health aides and certified nursing assistants that are trained can only assist with medication in its previously dispensed, prescription labeled container or over-the-counter medication that has directions per state law. They cannot put pills in pill boxes or remove the pills from the pill boxes and give to the patient. Pills should be kept in the bottles that were dispensed by the pharmacy if assistance is to be provided.
Patients need to be medically stable and have routine, regularly scheduled medications that are intended to be self-administered.
Assistance with self-administration does not include:• Medications for which the time of administration, the amount, the strength of dosage, the method of
administration, or reason for administration requires judgment or discretion. • Medications to be given “as needed”, unless the order is written with specific parameters that preclude
independent judgment, and at the request of a competent patient.• Administration of medications through a tube into a body cavity, through intermittent positive pressure
breathing machine or nebulizer, or by injections.
Homemakers and companions cannot assist. They can only verbally remind the client to take medicine.
400.488, F.S. and 59A-8.0095(5)(m)-(p), FAC

Home Health Agency Quarterly Report
There were no law changes this year. The 2013 law changes reduced the fine for failure to report within the required time frame to $200 a day for each day late up to a maximum of $5,000 and provided exemptions.
Some home health agencies no longer have to report:“A home health agency is exempt from submission of the report and the imposition of the fine if it is not a Medicaid or Medicare provider or if it does not share a controlling interest with a licensee, as defined in s. 408.803, which bills the Florida Medicaid program or the Medicare program.” 400.474(7), F.S.
Call the Home Care Unit if you have questions about whether your agency should report (850) 412-4403 or send an email to [email protected].
8

2014 Nurse Registry Law Changes
HB 1179 (Chapter 2014-142, Laws of Florida) amended 400.506, F.S.
Removes any requirement for nurse registries to monitor, manage, supervise or train the RNs, LPNs, CNAs, home health aides, homemakers and companions that they refer to provide patient care.
The nurse registry shall advise the patient or person acting on behalf of the patient:
– that the caregiver referred is an independent contractor and – the nurse registry is not obligated to monitor, supervise, manage or
train the caregiver.
If there is a violation of state laws or a deficiency in the caregiver’s credentials that the nurse registry becomes aware of, the nurse registry will:
1. advise the patient to terminate the referred individual,2. provide the reason for termination, 3. cease to refer the person to other patients or facilities, and,4. if there are practice violations, notify the appropriate licensing board.
9

2014 Nurse Registry Law Changes
Nurse registries will continue to collect the records required in chapter 400, F.S., and state rules as a repository of records but has no obligation to review the records.
The Agency will be holding a rule development workshop for public input into what needs to be changed in the rules and the wording of those rules as the result of the law changes.
An email will be sent to all nurse registries on the law changes and the rule development workshop.
A notice is at the AHCA Nurse Registry web page on the law change with a link to the bill that passed. (http://ahca.myflorida.com/homecare - select “Nurse Registry”)
10
11
2014 Background Screening Law Changes
AHCA Background Screening Unit sent an email to all licensed providers on the law changes effective July 1 that affect section 408.809 and chapter 435, Florida Statutes:
1. Screenings must be initiated through the Care Provider Background Screening Clearinghouse
2. Additional crimes were added to the list of crimes which disqualify an applicant subject to background screening.
3. Permits an employee, if previously screened and qualified under the applicable statutes but has a disqualifying offense that became effective July 1, 2014, to continue to work upon rescreening if agreed to by the employer, while applying for an exemption and waiting for a determination as long as the employee is eligible to apply for an exemption and the application is received by the appropriate agency within 30 days after receipt of the rescreening results.
4. The 3 year waiting period after payment of court-ordered monetary amounts that was required to be eligible for exemption from disqualification for certain felony convictions is eliminated. However, all court ordered fees, fines or other monetary requirements must be paid in full and 3 years must have elapsed since being lawfully released from confinement, supervision, or nonmonetary condition imposed by the court as a condition of being able to apply for an exemption.
12
Background Screening Reminders
Failure to screen and re-screen employees including contract staff is a violation of state law and subject to a fine of $500 per person.
Staff required to be screened must be re-screened every 5 years through AHCA. Because of the background screening law change to level 2 several years ago, there was a phase-in time frame in state law:• If the last screening was between January 1, 2005 and December 31,
2008, must be re-screened by July 31, 2014. • If the last screening was between January 1, 2009 and July 31,2011,
must be re-screened by July 31, 2015.
When your agency re-hires staff that used to work for your agency, make sure to re-screen if there was a lapse in employment greater than 90 days.
408.809, F.S.

Initiating a Clearinghouse Screening
Screenings handled through the Clearinghouse must now be initiated and registered through the Clearinghouse prior to referring the employee or potential employee for fingerprinting. (Effective July 1, 2014 in SB 674, Chapter 2014-84 Laws of Florida) • “Initiating screening” requires the employer register the employee or potential
employee through the AHCA Background Screening website before sending the person to a Livescan Vendor for screening.
• Initiating the original screening online will provide the privacy policy required for the employee to be included in the Clearinghouse and will also supply a view of the Florida Public Rap Sheet.
• Also, initiating the screening allows the ability to track a screening through the process and email updates when an employee’s status has been changed or updated.
• To register and begin initiating screenings please visit the website at https://apps.ahca.myflorida.com/SingleSignOnPortal.
Note: Your agency can initiate a screening and have the employee schedule and pay their own LiveScan appointment. (This is not available for all LiveScan vendors. Please contact the vendor and ask.) Print the LiveScan Request form for the applicant, employee or contractor to take to the vendor.
13

Employee Roster
“Employee” means any person required by law to be screened pursuant to this chapter, including, but not limited to, persons who are contractors, licensees, or volunteers. 435.02(2), F.S. According to section 435.12(2)(c), F.S., an employer of persons subject to screening by a specified agency must register with the Clearinghouse and maintain the employment status of all employees within the Clearinghouse. Initial employment status and any changes in status must be reported within 10 business days.
• You must add an employee to your employee roster to receive arrest and criminal registration notifications. Please remember, per section 435.06(2)(b), F.S., if an employer becomes aware that an employee has been arrested for a disqualifying offense, the employer must remove the employee from contact with any vulnerable person that places the employee in a role that requires background screening.
• Even though the requirement is only for employees/contractors with a Clearinghouse screening, it is highly recommended that ALL employees/contractors are added to the employee roster. By doing so the provider will receive email notifications of employment status changes for all employees.
14

15
Current Clearinghouse Functionality
Privacy Policy:Applicants must sign a privacy policy in order for their screening to be entered into the Clearinghouse. The privacy policy is available during the ‘Initiate New Screening’ process on the website. Employers must retain a copy of the privacy policy in the employee’s personnel file.
Initiating an Agency Review:If an individual has been screened by another specified agency (i.e. Dept. of Health) and entered into the Clearinghouse, an AHCA provider must request an agency review on the Clearinghouse website. This will allow AHCA to make an eligibility determination for employment purposes without the provider having to pay for a completely new screening.

Current Clearinghouse Functionality continued
• Initiating a Resubmission:The retention of fingerprints (effective for screenings on or after January 1, 2013) provides a cost savings for applicants that are in the Clearinghouse but have had a lapse in employment greater than 90 days. If there has been a 90 day lapse in employment, these applicants would only require a new national criminal history check – a resubmission of the retained fingerprints. A new state criminal history search will also be conducted, at no additional charge. A resubmission can be requested and paid for directly through the Clearinghouse website.
• Arrest and Criminal Registration Notifications:The retention of fingerprints will allow the Florida Department of Law Enforcement (FDLE) to report any new arrest/registration information to the specified state agencies.
• Bulletin Messages: Important updates will be displayed on the Home Page of the Clearinghouse results website. Providers should regularly check the home page for notifications regarding system outages, new regulations, etc.
16

Benefits of the ClearinghouseAllows the results of criminal history checks to be shared among specified state agencies, thereby reducing duplicative screenings for individuals requiring screening across multiple state agencies.
Applicants will now have their fingerprints retained for a period of 5 years.
• The retention of fingerprints enables a provider to be notified of an arrest of their employee as soon as the information is reported to the Agency by the Florida Department of Law Enforcement (FDLE).
• The retention of fingerprints will also provide a cost savings for those employees that are in the Clearinghouse but have had a lapse in employment greater than 90 days. After a 90 day lapse in employment, these applicants would only be required to pay for a new national criminal history check (currently $16.50).
Provides a photo of the applicant taken at the time of screening.
– The provider can verify that the person who applied for the position is the same person that had their background screening done.
17

Clearinghouse Statistics• From January 1, 2013 to June 30, 2014:– 4,856 individuals were arrested AFTER they
were screened (rap backs) 1,499 individuals went from Eligible to
Not Eligible for offenses including: Grand Theft Battery and Assault Sex Offenses Exploitation of the Elderly
18
Agency for Health Care Administration Background Screening Resources
Agency for Health Care Administration Web Sitehttp://ahca.myflorida.com/backgroundscreening-- Select “Clearinghouse Website Information” at the home page.
Questions/Comments/Issues: [email protected]
19

SurveysIf you have questions about the deficiencies cited:
1. Ask the surveyor to show you the survey standard, law or regulation
2. Discuss with surveyor during the Exit Interview
3. Contact the AHCA Field Office Manager http://ahca.myflorida.com/MCHQ/Areas or
If your agency is accredited, contact your accrediting organization.
20
21
Federal Alternative Sanctions for Medicare and Medicaid Home Health Agencies – effective July
1, 2014In the past, the only sanction that CMS used for enforcement actions of HHAs that were not meeting the federal conditions of participation (CoPs) was termination within 100 days. The CoPs cited by both state agencies and accrediting organizations are:
G 100 Patient RightsG 122 Organization, services, and administrationG 151 Group of professional personnelG 156 Acceptance of patients, plan of care and medical supervisionG 310 Release of Patient Identifiable OASIS informationG 320 Reporting OASIS informationG 168 Skilled nursing servicesG 184 Therapy servicesG 194 Medical social servicesG 202 Home health aides servicesG 234 Qualifying to furnish outpatient PT/SPSG 235 Clinical recordsG 242 Evaluation of the agency’s programG 330 Comprehensive assessment of patients 42 CFR 484.10 – 484.55

Federal Alternative Sanctions for Medicare and Medicaid Home Health Agencies
New Informal dispute resolution (IDR) processOffers HHAs an informal opportunity to dispute condition level deficiencies cited by the state (AHCA) on the survey form CMS-2567 Statement of Deficiencies. Deficiencies cited at the standard level are not subject to the IDR process.
An HHA may request an IDR for:1. Condition-level deficiencies cited during a survey. 2. Condition-level deficiencies that constitute Immediate Jeopardy.3. Condition-level deficiencies identified on a subsequent survey that are new (i.e. changed facts,
new regulatory reference)
When there are one or more condition level deficiencies on a survey , the HHA will receive information with the CMS 2567 Statement of Deficiencies that an IDR may be requested and how to make the request.
22
23
Medicare/Medicaid HHA Informal Dispute Resolution continued
The IDR is generally accomplished by telephone although a meeting may be requested by the HHA. The IDR is an informal administrative process and is not a formal evidentiary hearing. If the HHA choses to have legal counsel present, counsel may not address the panel during the presentation.
The IDR telephone conference or meeting is convened by the IDR Coordinator, Kellie Caswell, Bureau of Field Operations, or designee who moderates the process. • The HHA representatives will present information on a deficiency by deficiency basis. • The field office survey staff are given the opportunity to present information
supporting the CoPs in the CMS 2567 and respond to issues presented by the HHA. • Panel members may ask questions, as may the HHA and field office staff.• Panel members may request additional information for review. The HHA will forward
this to the IDR coordinator and Field Office Manager or designee.
The IDR panel will review the information presented for each disputed condition and recommend one of more of the following outcomes:• Uphold the condition(s) as written• Delete the condition(s) • Modify the condition by: (1) Deleting extraneous or erroneous remarks from the text
and/or (2) moving an existing finding to a more appropriate regulatory citation.

24
Medicare/Medicaid HHA Informal Dispute Resolution continued
If the HHA successfully demonstrates condition-level deficiencies should not have been cited or findings should be removed or their regulatory authority modified, a revised Statement of Deficiencies (CMS 2567) will be issued. Any enforcement actions imposed solely as a result of those cited deficiencies will be adjusted accordingly.
When the condition level deficiency is deleted or modified by the IDR panel decision, any associated licensure deficiencies will be reviewed and appropriate changes made.
A report will be provided to the HHA, summarizing the conference and documenting the recommendations.
When the HHA receives a revised CMS 2567, the HHA will prepare and submit a Plan of Correction. When the plan of correction is submitted, the plan and the revised CMS 2567 will be the releasable copy of the survey report.
References: CMS State Operations Manual, Chapter 10, section 10009 – www.cms.gov/manuals; 42 CFR 488.745

25
Federal Alternative Sanctions for Medicare and Medicaid Home Health Agencies
Alternative sanctions will now allow noncompliant HHAs more time to come into compliance with the CoPs before being terminated – except when the HHA’s condition-level deficiencies immediately jeopardize the health or safety of its patients.
The alternative sanctions are: 1. Civil money penalties2. Suspension of payment for all new admissions3. Temporary management of the HHA4. Directed plan of correction5. Directed in-service training
When there is immediate jeopardy, CMS will notify the HHA of the jeopardy situation and the HHA must correct the deficiencies. If the immediate jeopardy is not removed because the HHA is unable or unwilling to correct, CMS will terminate the HHA’s provider agreement. In addition CMS may impose civil money penalties and suspension of Medicare payments.
References: 1810(e) – (f) Social Security Act and 42 CFR 488.800, 488.805, 488.810, 488.845 at http://www.gpo.gov/fdsys/; and CMS State Operations Manual, Chapter 10 at www.cms.gov/manuals

26
Federal Alternative Sanctions for Medicare and Medicaid Home Health Agencies
The state agency (AHCA) recommends alternative sanctions to the CMS regional office on which sanction(s) may be effective in prompting the HHA to return to compliance. CMS considers AHCA’s recommendations and makes a determination to agree with or impose a different sanction for the HHA.
1. Civil money penalties – imposed by CMS when one or more federal conditions of participation (CoPs) are not met. There can also be penalties per instance for a single event of condition level noncompliance. HHAs may appeal the penalties with CMS.
The amount varies based on whether there is harm to patients, the type of condition not met, whether there is repeated non-compliance and other factors as specified by CMS in federal regulation 42 CFR 488.845. The regulation specifies the amount of the penalties:
– upper range for immediate jeopardy citations, results in harm or a potential for harm ($8,500 to $10,000 per day),
– middle range for non-immediate jeopardy for direct patient care ($1,500 to $8,500),
– lower range for structure and process citations not directly related to patient care ($500 to $4,000), such as §484.26 (G 151) Group of professional personnel, 484.52 (G 242) Evaluation of the agency’s program, 484.20 Reporting OASIS information.

27
Federal Alternative Sanctions for Medicare and Medicaid Home Health Agencies – Civil Money
penalties continuedThe CMS State Operations Manual, Chapter 10, Section 1017, at www.cms.gov/manuals, includes a table that shows the amount of penalty for conditions not met in each range, including revisit surveys.
CMS may decrease the amount in increments if substantial and sustainable improvements have been made on a revisit.
CMS may increase amounts based on the HHA’s failure to correct.
Total penalties cannot exceed $10,000 for each day of noncompliance.
A written notice of intent to impose the civil money penalty is sent to the HHA including: – The amount of the penalty - per day of non-compliance or the amount per instance during a
survey – The factors that were considered in determining the amount– The date that the penalty begins to accrue – a per day penalty will accrue until substantial
compliance is achieved or until termination of the agency from participation in the program.– When the penalty is collected by CMS– Instructions for responding to the notice, including the HHA’s right to a hearing and how to
request a hearing.
For more information, see the CMS State Operations Manual, Chapter 10 at www.cms.gov/manuals

28
Federal Alternative Sanctions for Medicare and Medicaid Home Health Agencies
2. Suspension of payment for all new admissions – when a HHA is not in substantial compliance with one or more federal conditions of participation (CoPs). Suspension may be imposed alone or in combination with other sanctions. The notice from CMS includes the right to appeal.
3. Temporary management of the HHA – may be imposed in situations where the failure to comply with the CoPs is directly related to poor management or lack of management such that it is likely to impair the HHA’s ability to correct deficiencies and return the HHA to full compliance within the necessary timeframe. • A temporary manager has the authority to hire, terminate or reassign staff; alter
HHA policies and procedures and otherwise manage to correct the deficiencies. • Maximum period for use of the temporary manager is 6 months. The HHA pays the
salary.• A temporary manager may also be imposed to oversee the closing of the HHA
including the safe transfer of patients to another local HHA. • When CMS decides to impose this sanction, it considers the state agency’s
recommendation for a temporary manager whose work experience and education qualify the person to oversee correction of deficiencies.
Reference: CMS State Operations Manual, Chapter 10 at www.cms.gov/manuals

Federal Alternative Sanctions for Medicare and Medicaid Home Health Agencies
4. Directed plan of correction – May be imposed by CMS when a HHA has one or more deficiencies that warrant directing the HHA to take specific actions; or when the HHA fails to submit an acceptable plan of correction.
5. Directed in-service training – CMS may require that staff of an HHA attend in-service training programs if education is likely to correct the deficiencies. The training and trainers must be acceptable to CMS. The HHA pays for the directed in-service training of its staff.
If 4 and 5 do not result in compliance, then CMS may impose other sanctions.
References: 42 CFR 488.850 and 488.855; CMS State Operations Manual, Chapter 10 at www.cms.gov/manuals
29
30
Federal Alternative Sanctions for Medicare and Medicaid Home Health Agencies
A HHA that has deemed status accreditation loses its deemed status when a condition-level deficiency is found. The CMS regional office returns the oversight to the state agency (AHCA) until the HHA can demonstrate compliance with the conditions of participation (CoPs).
AHCA will follow the federal procedures for recommending the imposition of sanctions to CMS. CMS imposes the alternative sanctions.
Once the HHA returns to compliance with the CoPs and has not been terminated, CMS will restore its deemed status and return oversight to the accrediting organization.

Medicare Patient Confined to HomePolicy Updated
A physician must certify that the patient is confined to his or her home. State survey agencies (AHCA) are not the reviewers or enforcers of the “Face to Face” visit requirements. AHCA surveyors do check for compliance with federal survey standard G 335 and related standards. An RN must complete patient assessment and determine eligibility for the Medicare home health benefit, including homebound status. Accrediting organization surveyors must also check for compliance with federal survey standards.A patient is considered “confined to home” (homebound) if both of the following two criteria are met. 1. Criteria One:The patient must either, because of illness or injury, need the aid of supportive devices such as crutches, canes, wheelchairs, and walkers; the use of special transportation; or the assistance of another person in order to leave their place of residence. ORHave a condition such that leaving his or her home is medically contraindicated.
2. Criteria Two:There must exist a normal inability to leave home; ANDLeaving home must require a considerable and taxing effort.
Medicare Benefit Policy Manual, Chapter 7, section 30.1.1 www.cms.gov/manuals
31

32
Updated CMS Guidance to Surveyors of Home Health Agencies
Appendix B of the CMS State Operations Manual – should be at www.cms.gov/manuals web site soon. This Appendix includes all federal survey standards and interpretive guidelines used by AHCA and accrediting organizations. The revision includes:• Updated pre-survey preparation and sample selection guidance• Revised interpretive guidelines for survey standards, including
what is expected as outcomes for the survey standards.• Revises some survey processes, including explanation of Level 1
(highest priority, most related to delivering high quality patient care) and Level 2 (next highest priority) standards
• Includes guidance for citing condition level deficiencies • Electronic health records

33
Electronic Health RecordsWhile documents must be signed, electronic signatures can be used. There needs to be a process for reconstruction of the information and safeguards to prevent unauthorized access to the records. Rubber stamp signatures cannot be used.
CMS requires that the HHA:1. provide the surveyor with a tutorial on how to use its particular electronic system and 2. designate an individual who can access the system and respond to questions, and assist the surveyor as needed in accessing records.
If the HHA is unable to provide direct print capability to the surveyor, the HHA “must make available a printout of any record or part of a record upon request in a timeframe that does not impede the surveyor process. Undue delays in the production of records are unacceptable.”
The HHA should provide surveyors electronic access to records in a read-only format or other secure format.
The HHA is responsible for ensuring that all necessary back up of data and security measures are in place.
CMS State Operations Manual, Chapter 2, interpretive guidelines with clinical records, page 112: www.cms.gov/manuals

34
Statewide Medicaid Managed Care
Where can I find more information? • Visit the SMMC website at: http://ahca.myflorida.com/SMMC
• See the Frequently Asked Questions athttp://ahca.myflorida.com/Medicaid/statewide_mc/faqs.shtml
• Questions about the program can be emailed to: [email protected]
• Keep up to date by signing up to receive program updates at http://ahca.myflorida.com/SMMC. Click the red “Sign Up for Program Updates” box on the right hand side of the page.

35
Statewide Medicaid Managed Care
• View the prior webinar presentations at http://ahca.myflorida.com/medicaid/statewide_mc/materials.shtml
• Youtube.com/AHCAFlorida • Facebook.com/AHCAFlorida; • Twitter.com/AHCA_FL
Questions?
Home Care Unit (850) 412-4403