agenda item 2.1 23 september 2014 specialist services ... · 23 september 2014: specialist services...
TRANSCRIPT
Specialist Services Quality and Safety Report Page 1 of 14 Quality Safety and Experience Committee 23 September 2014
AGENDA ITEM 2.1
23 September 2014
SPECIALIST SERVICES QUALITY AND SAFETY REPORT
Executive Lead: Nurse Director
Author: Clinical Board Nurse
Contact Details for further information: Carys Fox 029 20742266 SITUATION This report provides assurance to the Quality and Safety Committee of the progress made with implementation of Specialist Services Clinical Board Quality and Safety priorities and arrangements. The Specialist Services Clinical Board has made progress with monitoring the Quality and Safety agenda in line with Achieving excellence – The quality delivery plan for the NHS in Wales 2012-2016, UHB and Clinical Board IMTP, Infection Prevention and Control Programme and the Standards for Health Services in Wales. The report includes information and assurance on Integrated Governance and the Standards for Health Care in Wales; Infection Prevention and Control; patient experience; financial and information governance; concerns, compliments and claims; clinical audit and effectiveness; and management of clinical and non clinical risk. A patient story related to a patient with C. Difficile will start the Clinical Board’s presentation. The same patient story was presented at the last UHB IP&C Committee Meeting. Other specific issues to be brought to the Committee’s attention are the continuing challenges related to the delivery of care at Rookwood Hospital, 2 cases related to the renal transplant programme, and an update on Cardiac Surgery. The committee will recall that Specialist Services Management Team attended an extraordinary meeting of the committee and several committee meetings to provide updates on the situation. BACKGROUND The vision of the Clinical Board is:
“To deliver fast, effective and safe highly specialised care”. The Specialist Services Clinical Board consists of 7 Directorates providing a varied range of services both locally and across Wales. Detail on the services provided and the population they serve can be found in Appendix 1.

Specialist Services Quality and Safety Report Page 2 of 14 Quality Safety and Experience Committee 23 September 2014
The Clinical Board Director and the Clinical Directors have overall responsibility for all aspects of Q&S and Patient Experience. At a Clinical Board level this has been devolved to the Clinical Board Nurse and in order to ensure consistency and transparency in all Directorates Q&S and Patient Experience it is devolved to the Lead Nurse. The Clinical Board’s Quality and Safety Group is chaired by the Clinical Board Nurse; a medical lead is being identified following the stepping down of the previous lead. The Clinical Board’s Patient Safety Manager is Tara Cardew. Tara has been successful in achieving a promotion so will be leaving the Patient Safety Department in the near future. The Clinical Board would like to formally thank Tara for her dedication and support to the quality and safety agenda. All Directorates in the Clinical Board are represented by Lead Nurses and medical leads, as well as the Clinical Board Pharmacist, Lead Therapist, IP&C lead, Trade Union representative, Clinical Audit, Health and Safety, Corporate Risk Management and the Resuscitation Service. All meetings start with a patient story. Continuing on a firm foundation and an active Clinical Board Quality and Safety Group the priorities for 2014/15 include:
• Communicating patient stories across the Clinical Board as a learning exercise, to influence development of services and highlight improvements to the quality of patient care and experience.
• Coordinating response and actions required as a result of the Andrews’ report. • Improving all aspects of infection, prevention and control including hand
hygiene, reducing episodes and harm from MRSA, MSSA, C. Difficile, monitoring the Clinical Board’s Infection and Control Action Plan and seasonal flu planning.
• Ensuring statutory compliance with requirements from External Regulatory Bodies e.g. Human Tissue Authority in Haematology and Nephrology and Transplant. Following the inspections, summary reports are presented to the Clinical Board Quality and Safety Group, remedial action plans are developed where necessary and monitored.
• Circulating National Reports and guidance e.g. NICE guidance, NPSA alerts, and MDA alerts across the Clinical Board and implementing/actioning where applicable.
• Monitoring the Clinical Board’s compliance with NCEPOD reports. Particularly in 14/15, Tracheostomy Care: On The Right Trach, Subarachnoid Haemorrhage: Managing The Flow and Lower Limb Amputation due to be launched in November 2014. The Tracheostomy report has wide ranging implications throughout the UHB; the Subarachnoid report confirms the challenges within the UHB related to interventional neuroradiology and the amputation report will have implications for Artificial Limb and Appliance Service (ALAS).
• Implementing and monitoring the Standards for Health Services in Wales. • Reviewing trends relating to patient safety incidents with emphasis on
ensuring that lessons learnt and all actions to reduce the likelihood of further incidents have been identified.
• Improving concerns management performance, monitoring response times and focusing on corrective action, learning and putting things right. The
Specialist Services Quality and Safety Report Page 3 of 14 Quality Safety and Experience Committee 23 September 2014
Clinical Board Management Team (CBMT) are participating the 2nd Leading Improvements in Patient Safety (LIPS). In recognising that concerns management can always be improved this will be the focus for CBMT.
• Restructuring the Clinical Board Risk Register in line with the UHB’s 7 key objectives.
• Approving policies and protocols where appropriate and escalating those that require corporate agreement. The most recent policy agreed relates to the Rapid Access Chest Pain Protocol. Appendix 2.
• Increase compliance with staff Personal Development Reviews and mandatory training.
• Ensure that external partners are informed and kept up to date in relation to Q&S issues related to services. E.g. Welsh Health Specialised Services Committee (WHSSC).
ASSESSMENT The key Q&S issues are discussed in this section and as part of the overall governance framework these have been referenced to and linked back to the Clinical Board Risk Register. Integrated Governance and Standards for Healthcare for Wales Risk Register Reference Number SpS 13 2011 Originally, Q&S meetings were held every six weeks. CDs and Q&S leads were consulted with and it was identified that the meeting time of 2.5 hours was difficult and the 6 week gap between meetings caused a lull in awareness, actions and work stream threads. The meetings are now every 3 weeks for a shorter, more focussed meeting. E.g. the September 2014 meeting will focus on Q&S issues in the Nephrology and Transplant Directorate, October 2014 will focus on the updated Risk Register and the priorities related to the Standards for Health Services to March 2015. The new style of meetings have been evaluated and this has demonstrated that the current format has realised the anticipated benefits i.e. subject continuity is maintained, more clinicians are able to attend and there is more Directorate collaboration and learning. The March 2014 self assessment of the annual Standards for Health Services for Wales demonstrated that improvements have been made in some standards. The Standards are now managed in a dynamic, live way making them part of core Clinical Board and Directorate business. At each Q&S meeting 5 standards are reviewed ensuring that up to date evidence is gathered and the required actions are taken. Improvements made in 2013/14 include:-
• Improved Health and Safety arrangements • Improved seasonal flu vaccination rates - >53% • Improved water safety • Implementation of Clinical Board Health Care Acquired Infections subgroup.
Infection Prevention and Control Risk Register Reference Number UHB29/11 SpS 25/2011
Specialist Services Quality and Safety Report Page 4 of 14 Quality Safety and Experience Committee 23 September 2014
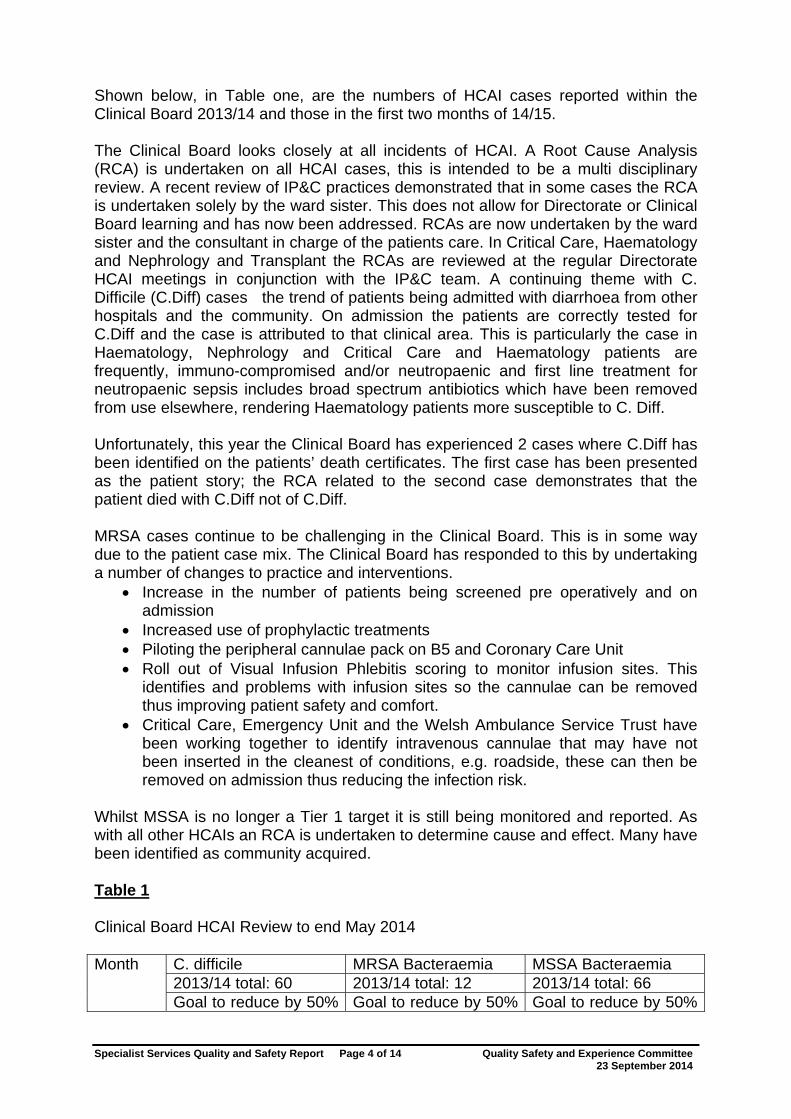
Shown below, in Table one, are the numbers of HCAI cases reported within the Clinical Board 2013/14 and those in the first two months of 14/15. The Clinical Board looks closely at all incidents of HCAI. A Root Cause Analysis (RCA) is undertaken on all HCAI cases, this is intended to be a multi disciplinary review. A recent review of IP&C practices demonstrated that in some cases the RCA is undertaken solely by the ward sister. This does not allow for Directorate or Clinical Board learning and has now been addressed. RCAs are now undertaken by the ward sister and the consultant in charge of the patients care. In Critical Care, Haematology and Nephrology and Transplant the RCAs are reviewed at the regular Directorate HCAI meetings in conjunction with the IP&C team. A continuing theme with C. Difficile (C.Diff) cases the trend of patients being admitted with diarrhoea from other hospitals and the community. On admission the patients are correctly tested for C.Diff and the case is attributed to that clinical area. This is particularly the case in Haematology, Nephrology and Critical Care and Haematology patients are frequently, immuno-compromised and/or neutropaenic and first line treatment for neutropaenic sepsis includes broad spectrum antibiotics which have been removed from use elsewhere, rendering Haematology patients more susceptible to C. Diff. Unfortunately, this year the Clinical Board has experienced 2 cases where C.Diff has been identified on the patients’ death certificates. The first case has been presented as the patient story; the RCA related to the second case demonstrates that the patient died with C.Diff not of C.Diff. MRSA cases continue to be challenging in the Clinical Board. This is in some way due to the patient case mix. The Clinical Board has responded to this by undertaking a number of changes to practice and interventions.
• Increase in the number of patients being screened pre operatively and on admission
• Increased use of prophylactic treatments • Piloting the peripheral cannulae pack on B5 and Coronary Care Unit • Roll out of Visual Infusion Phlebitis scoring to monitor infusion sites. This
identifies and problems with infusion sites so the cannulae can be removed thus improving patient safety and comfort.
• Critical Care, Emergency Unit and the Welsh Ambulance Service Trust have been working together to identify intravenous cannulae that may have not been inserted in the cleanest of conditions, e.g. roadside, these can then be removed on admission thus reducing the infection risk.
Whilst MSSA is no longer a Tier 1 target it is still being monitored and reported. As with all other HCAIs an RCA is undertaken to determine cause and effect. Many have been identified as community acquired. Table 1 Clinical Board HCAI Review to end May 2014
C. difficile MRSA Bacteraemia MSSA Bacteraemia 2013/14 total: 60 2013/14 total: 12 2013/14 total: 66
Month
Goal to reduce by 50% Goal to reduce by 50% Goal to reduce by 50%
Specialist Services Quality and Safety Report Page 5 of 14 Quality Safety and Experience Committee 23 September 2014
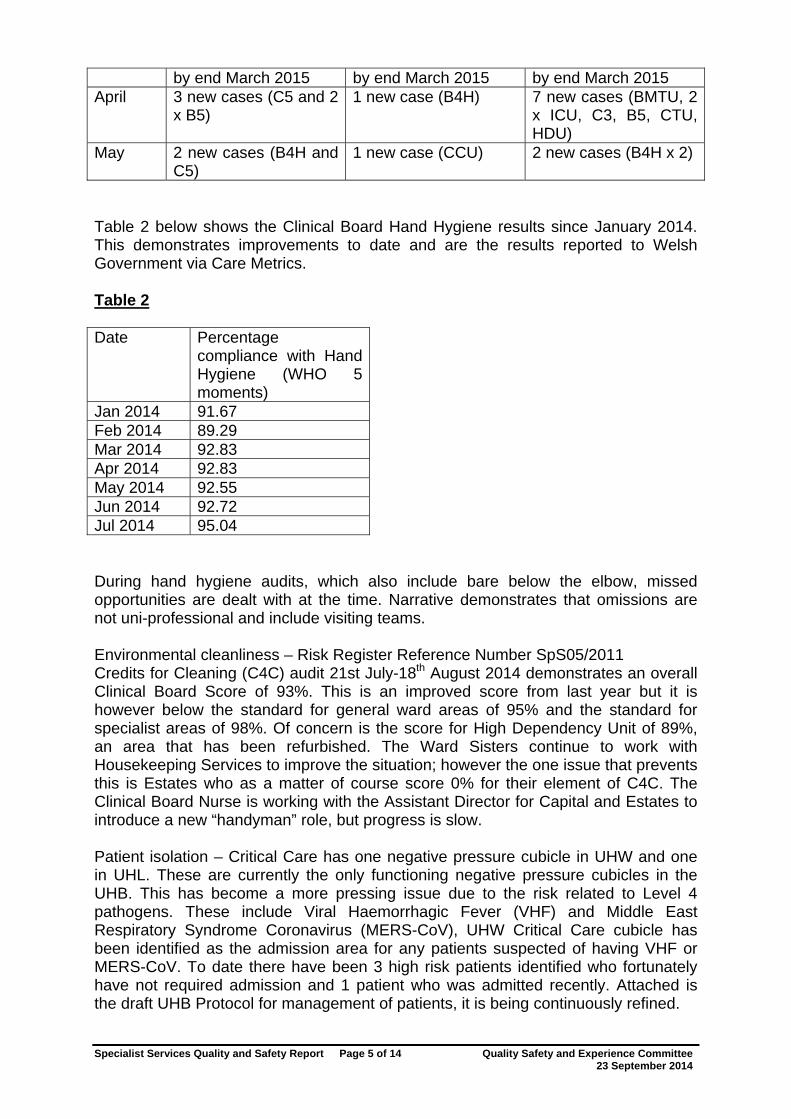
by end March 2015 by end March 2015 by end March 2015 April 3 new cases (C5 and 2
x B5) 1 new case (B4H) 7 new cases (BMTU, 2
x ICU, C3, B5, CTU, HDU)
May 2 new cases (B4H and C5)
1 new case (CCU) 2 new cases (B4H x 2)
Table 2 below shows the Clinical Board Hand Hygiene results since January 2014. This demonstrates improvements to date and are the results reported to Welsh Government via Care Metrics. Table 2 Date Percentage
compliance with Hand Hygiene (WHO 5 moments)
Jan 2014 91.67 Feb 2014 89.29 Mar 2014 92.83 Apr 2014 92.83 May 2014 92.55 Jun 2014 92.72 Jul 2014 95.04 During hand hygiene audits, which also include bare below the elbow, missed opportunities are dealt with at the time. Narrative demonstrates that omissions are not uni-professional and include visiting teams. Environmental cleanliness – Risk Register Reference Number SpS05/2011 Credits for Cleaning (C4C) audit 21st July-18th August 2014 demonstrates an overall Clinical Board Score of 93%. This is an improved score from last year but it is however below the standard for general ward areas of 95% and the standard for specialist areas of 98%. Of concern is the score for High Dependency Unit of 89%, an area that has been refurbished. The Ward Sisters continue to work with Housekeeping Services to improve the situation; however the one issue that prevents this is Estates who as a matter of course score 0% for their element of C4C. The Clinical Board Nurse is working with the Assistant Director for Capital and Estates to introduce a new “handyman” role, but progress is slow.
Patient isolation – Critical Care has one negative pressure cubicle in UHW and one in UHL. These are currently the only functioning negative pressure cubicles in the UHB. This has become a more pressing issue due to the risk related to Level 4 pathogens. These include Viral Haemorrhagic Fever (VHF) and Middle East Respiratory Syndrome Coronavirus (MERS-CoV), UHW Critical Care cubicle has been identified as the admission area for any patients suspected of having VHF or MERS-CoV. To date there have been 3 high risk patients identified who fortunately have not required admission and 1 patient who was admitted recently. Attached is the draft UHB Protocol for management of patients, it is being continuously refined.
Specialist Services Quality and Safety Report Page 6 of 14 Quality Safety and Experience Committee 23 September 2014
Appendix 3. A patient on the Spinal Injuries Rehabilitation Unit in Rookwood Hospital was diagnosed with OXA-48 carbapenemase in the last few months. Ideally this patient would be isolated but due to the requirements for rehabilitation and the importance of socialising the Director for IP&C has agreed that this is not possible. There are now 7 cases of OXA-48 carbapenemase in Rookwood but all patients are asymptomatic. Clinical and Non-Clinical Risk Management
A Prevention of Future Death Report (previously Rule 43) was issued to the UHB in relation to a fatal fall on Ward C5 Cardiac Surgery. The gentleman had been admitted due to a sternal wound infection. At the time of his fall, as he was prescribed Warfarin, his INR was raised and he was in hospital until his INR stabilised. He sustained a subdural haematoma when he fell which was not suitable for intervention and unfortunately he died of his injury. Had he been at home in familiar surroundings he may not have fallen which indicates the importance of the anticoagulation pathway into Primary Care. Serious Incidents Reported to Welsh Government
• Breach of patient confidentiality – Cardiac Surgery • Cross Infection – Nephrology – Internal Investigation • Cross Infection – Transplant. Internal Investigation and Improvement Planning • Cross Infection – Transplant. Internal Investigation. Applies to 2 English Trusts • Blood Transfusion Error – Nephrology • Hospital Acquired C.Diff – Cardiac Surgery – Patient Story • Legionella case – Haematology – Filters in use, requires new ward and water
plant • External Pacemakers – Cardiac Surgery • Death in Rookwood Hospital – Neuro rehabilitation • Death post surgery – Cardiac Surgery • IRMER – Neurosurgery • Maternal Death – Critical Care • Death due to a fall – Cardiac Surgery – Highlighted above
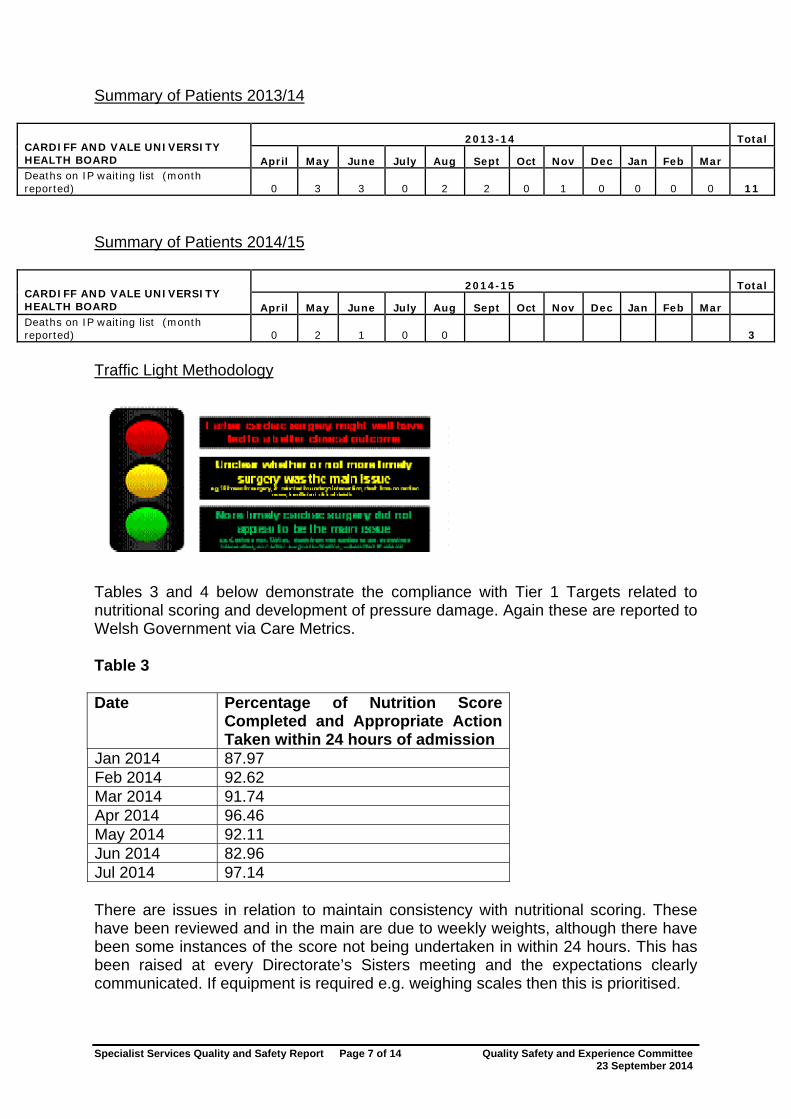
Deaths on the cardiac surgery waiting list have been a significant concern within the UHB, South East Wales and the service’s commissioners. The Clinical Board Team have attended the Corporate Q&S Committee meeting several times to provide updates and an action plan. The final figures for 13/14 and the current position for 14/15 are detailed below. Also included is the definition of the “traffic light” assessment currently being used to analyse mortality. The approach to recording and monitoring inpatient waiting list mortality is consistent across both centres in South Wales.
Specialist Services Quality and Safety Report Page 7 of 14 Quality Safety and Experience Committee 23 September 2014
Summary of Patients 2013/14
2013-14 Total CARDIFF AND VALE UNIVERSITY HEALTH BOARD April May June July Aug Sept Oct Nov Dec Jan Feb Mar Deaths on IP waiting list (month reported) 0 3 3 0 2 2 0 1 0 0 0 0 11
Summary of Patients 2014/15
2014-15 Total CARDIFF AND VALE UNIVERSITY HEALTH BOARD April May June July Aug Sept Oct Nov Dec Jan Feb Mar Deaths on IP waiting list (month reported) 0 2 1 0 0 3
Traffic Light Methodology
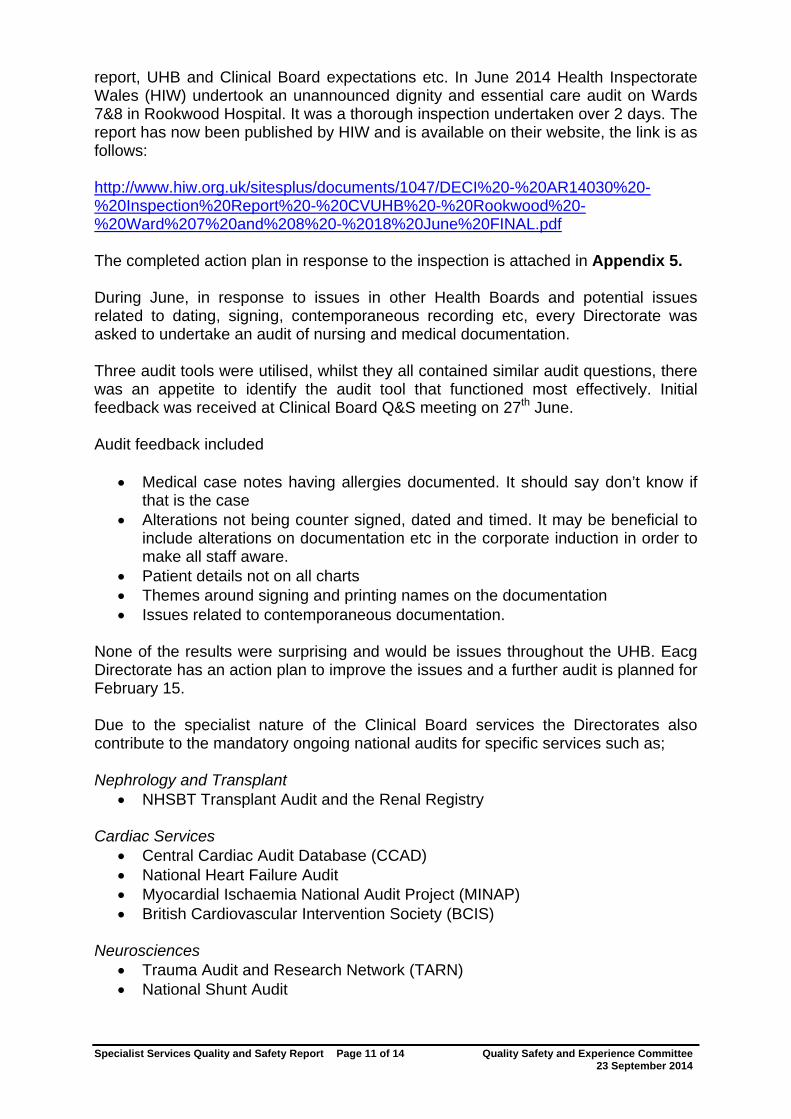
Tables 3 and 4 below demonstrate the compliance with Tier 1 Targets related to nutritional scoring and development of pressure damage. Again these are reported to Welsh Government via Care Metrics. Table 3 Date Percentage of Nutrition Score
Completed and Appropriate Action Taken within 24 hours of admission
Jan 2014 87.97 Feb 2014 92.62 Mar 2014 91.74 Apr 2014 96.46 May 2014 92.11 Jun 2014 82.96 Jul 2014 97.14 There are issues in relation to maintain consistency with nutritional scoring. These have been reviewed and in the main are due to weekly weights, although there have been some instances of the score not being undertaken in within 24 hours. This has been raised at every Directorate’s Sisters meeting and the expectations clearly communicated. If equipment is required e.g. weighing scales then this is prioritised.

Specialist Services Quality and Safety Report Page 8 of 14 Quality Safety and Experience Committee 23 September 2014
Table 4 Date Health care Acquired Pressure
Ulcers Jan 2014 13 Feb 2014 13 Mar 2014 15 Apr 2014 16 May 2014 6 Jun 2014 5 Jul 2014 8 As expected there are less Grade 3 & 4 pressure ulcers and more Grade 1 & 2. An RCA is undertaken for all Grade 3 & 4 ulcers and a report is made to Welsh Government. The significant improvements from May 2014 are related to reporting strictly within the definition of the Welsh Government. Previously all types of pressure damage were reported including moisture lesions and device related damage. It is still very important to measure and report these internally to the UHB and to take actions for improvement. Critical Care has been working with commercial companies in developing improved endotracheal tube holders, naso gastric tube fixations and repose pillows to reduce occipital damage. Table 5 below itemises the Top 10 Clinical Board Incidents by Sub category from 1st January-31st July 2014. The top 10 incidents are discussed quarterly and forms are reviewed by Senior Nurses to ensure any consequence to patients is identified. Table 5
Medication Error 97Pressure ulcer - grade 2 92Lack of suitably trained/skilled staff 77Treatment/procedure - delay/failure 49Pressure ulcer - not graded 42Documentation - misfiled 30Failure of device/equipment 26Lack/unavailability of device/equipment 22Unexpected complications 20Inappropriate/Unsafe Transfer 17
Mr Christopher Coslett, Directorate Manager for Cardiothoracic Services and Critical Care, is the new Clinical Board Health and Safety Representative. He will be providing the Q&S meeting with feedback from the Corporate H&S Committee; a robust action plan has been developed and this is monitored via the Q&S meetings. The meetings are also a conduit for staff to raise H&S issues that need to be escalated to the Corporate Committee.

Specialist Services Quality and Safety Report Page 9 of 14 Quality Safety and Experience Committee 23 September 2014
Mrs Jessica Castle, Head of Operations and Delivery attended the July UHB Committee meeting to present the H&S plan and raise issues for the Clinical Board. Particular issues raised were:
• RIDDOR Compliance – All reports complete and continuing compliance has been discussed at Clinical Board Q&S meeting.
• Rookwood Hospital – This remains in a very poor state of repair despite some refurbishment.
• Legionella incident – B4 Haematology, noted above • Environment for Bone Marrow Transplant patients – would be included in
plans to relocate B4 Haematology. Timescales awaited form Capital & Estates.
Also of concern is the ongoing leak in the roof of T4 Neurosurgery High Care Unit. There have been frequent occasions when beds have had to be closed due to rain ingress via the roof, and bodily fluids ingress from T5 Transplant Unit. Capital & Estates are planning with the contractors to undertake the repairs. Clinical Board are pressing this issue as the work needs to be undertaken before the winter. Financial and information governance The Clinical Board is forecasting a year end position of £1.6m overspent. There are some risks associated with delivery of this however, actions required to deliver this position are in place and being progressed by the Directorates. The Clinical Board has concerns about the sustainability and safety of standalone servers in the Directorates. This presents a risk to patient data and significant potential for loss of documentation. The new IT Lead for the Clinical Board is mapping all of the servers in the Clinical Board and developing a strategy for managing the risk. Critical Care and Haematology will be early adopters of the new E-Datix system. The Clinical Board’s preparedness document has been submitted and as expected does raise issues related to IT access. Workforce Issues The Clinical Board sickness target is 4%; the figure in June 2014 was 5.2% so there is obviously a challenge for the entirety of the Clinical Board. The Clinical Board Nurse and Clinical Board Head of Workforce and OD meet regularly with the Ward Sisters to review their long term and short term sickness cases, whether they are being managed appropriately which in the main they are and discuss any further actions that can be taken. Staff are aware of their responsibility in regard of the policy and sickness is being monitored by the Clinical Board Team at Directorate performance reviews. The Assistant HoWOD is taking an active role in working with the Directorates in determining the root cause of sickness and action planning for reductions. There is only one suspended member of staff in the Clinical Board which relates to a long standing issue concerning a Cardiac Surgeon. Unless there are extreme circumstances, which

Specialist Services Quality and Safety Report Page 10 of 14 Quality Safety and Experience Committee 23 September 2014
would be discussed with Chief Operating Officer, the Clinical Board does not suspend staff. If, whilst an investigation is being completed, their substantive role is not suitable then alternative work is found. Concerns and compliments Table 6 demonstrates compliance with concerns received in the Clinical Board. There is a requirement for the position to improve and this will be the focus of the Clinical Board Management Team as part of the LIPS programme. As the figures demonstrate the Clinical Board deals with as many informal concerns as it does formal. The Directorates strive to manage concerns as and when they arise which is demonstrated in the performance figures. Table 6 2014 Informal Performance
Informal 30 Days RCA Performance
30 days April 14 79% 13 62% May 10 100% 18 17% June 17 82% 23 1 48% July 20 95% 13 69% still in target August 14 79% 11 100% still in target There are 6 outstanding concerns prior to April 2014. Themes Following the retirement of a Neurosurgeon, the review of a small number of complex patients is proving problematic. The Clinical Board, Neurosciences Directorate and WHSSC are working together to provide a short term solution followed by a sustainable robust service. There has been a reduction in concerns regarding cardiac surgery waiting times but there are enquiries. It is pleasing that compliments received in the Clinical Board and in clinical services far outweigh concerns. Attached is a compliment received in Neurosciences recently. It demonstrates the care and commitment of individuals as part of the whole team. Appendix 4. Clinical Audit and Effectiveness Specialist Services wards have all undertaken Fundamentals of Care (FoC) Audits and Dignity and Respect audits have been undertaken in year. Plans are underway for the next FoC audits to take place in November 2014. Specific work has been undertaken by the Clinical Board Sisters’ forum on nursing documentation and patient dignity. Issues raised in the Andrews report have been widely discussed within the Clinical Board and every member of staff has received direct communication about the
Specialist Services Quality and Safety Report Page 11 of 14 Quality Safety and Experience Committee 23 September 2014
report, UHB and Clinical Board expectations etc. In June 2014 Health Inspectorate Wales (HIW) undertook an unannounced dignity and essential care audit on Wards 7&8 in Rookwood Hospital. It was a thorough inspection undertaken over 2 days. The report has now been published by HIW and is available on their website, the link is as follows: http://www.hiw.org.uk/sitesplus/documents/1047/DECI%20-%20AR14030%20-%20Inspection%20Report%20-%20CVUHB%20-%20Rookwood%20-%20Ward%207%20and%208%20-%2018%20June%20FINAL.pdf The completed action plan in response to the inspection is attached in Appendix 5. During June, in response to issues in other Health Boards and potential issues related to dating, signing, contemporaneous recording etc, every Directorate was asked to undertake an audit of nursing and medical documentation. Three audit tools were utilised, whilst they all contained similar audit questions, there was an appetite to identify the audit tool that functioned most effectively. Initial feedback was received at Clinical Board Q&S meeting on 27th June. Audit feedback included
• Medical case notes having allergies documented. It should say don’t know if that is the case
• Alterations not being counter signed, dated and timed. It may be beneficial to include alterations on documentation etc in the corporate induction in order to make all staff aware.
• Patient details not on all charts • Themes around signing and printing names on the documentation • Issues related to contemporaneous documentation.
None of the results were surprising and would be issues throughout the UHB. Eacg Directorate has an action plan to improve the issues and a further audit is planned for February 15. Due to the specialist nature of the Clinical Board services the Directorates also contribute to the mandatory ongoing national audits for specific services such as; Nephrology and Transplant
• NHSBT Transplant Audit and the Renal Registry Cardiac Services
• Central Cardiac Audit Database (CCAD) • National Heart Failure Audit • Myocardial Ischaemia National Audit Project (MINAP) • British Cardiovascular Intervention Society (BCIS)
Neurosciences
• Trauma Audit and Research Network (TARN) • National Shunt Audit
Specialist Services Quality and Safety Report Page 12 of 14 Quality Safety and Experience Committee 23 September 2014
Critical Care • Intensive Care National Audit and Research Centre (ICNARC)
Haematology
• British Society of Blood and Marrow Transplantation (BSBMT) • European Blood and Marrow Transplant Audit (EBMT)
The following demonstrates how staff within the Clinical Board are working in partnership with other health professional to improve patient care and effectiveness and being recognised on a worldwide basis for their constant improvements. Dietitians and nurses within the multidisciplinary team submitted patient data and information to an international nutrition survey evaluating Critical Care nutritional practices compared to published international nutritional standards. Following evaluation of the information they were eligible for consideration for the best of the best award. The organisation tied for fourth place amongst the top ten performing ICU’s in this competition. Therefore Critical Care is now recoginised as a standard by which other ICU'S in the world can strive to achieve. This work is an excellent example of the integrated and collaborative working practices established within the organisation to deliver world class nutritional care to our most vulnerable patients to maximise their treatment interventions. Appendix 6. Patient Experience All Q&S meetings commence with a patient story, this year these have included the IP&C story that will be used at corporate Q&S, a patient story related to the effectiveness of the neurology day unit opened in Neurosciences, this story was presented at the Board meeting on 9th September 2014 and the story of an incident related to small child’s wheelchair. Patient experience questionnaires are undertaken monthly and the results are discussed at Nursing Board and Q&S meetings. The results for May 2014 are attached as Appendix 7. A range of other ways of measuring patient experience are utilised within the Clinical Board and some of these are outlined below.
• Critical Care sends out questionnaires based on Fundamentals of Care to all patients discharged. Results are prominently displayed within the units and used as learning points for improvements and changes in practice.
• Nephrology & Transplant and Neurosciences have used patient stories to evaluate the provision of newly developed day services.
• Nurses in Rookwood have worked to develop a HIPO audit that is being distributed to inpatients on a monthly basis. As the patients have a long admission period, significant amounts of data will be achieved and the results will be used in the development of the new Rookwood facility in UHL.
• Critical Care undertakes patient stories, encourages relatives to keep a patient log to inform them of their experience when they recover and are in the process of commencing patient diaries which are kept by nurses for the patients.
Specialist Services Quality and Safety Report Page 13 of 14 Quality Safety and Experience Committee 23 September 2014
• Critical Care has commenced the use of patient diaries which patients have the opportunity to receive when they are well. This helps them to understand and contextualise what occurred at times when their memory was impaired due to physical or chemical issues.
• N&T have a pre dialysis support group to prepare patients and their families for the time when they will require dialysis. Patient and carer feedback demonstrates that this is a very well received service that all attendees benefit from greatly.
• Nephrology and Transplant patients and staff are on the Welsh Kidney Patients Board which has open question sessions.
• Suggestion boxes are used in Critical Care and Cardiac Services. • Cardiac Arrhythmia Nurses run two patient focus groups per year. • Heart failure services are currently undertaking a two year HIPO project. • The Clinical Board has a patient representative as part of the core Board
team. • Neurosciences have employed 6 volunteers to provide patients with extra
communication about themselves, with reading, and orientation. They are now employing volunteers in Rookwood to help patients with extra curricula activities. This is directly linked to the fact that patients identified that they are sometimes a little bored and the days are long.
One of the main concerns related to patient experience is the continued provision of care at Rookwood Hospital where the fabric of the building continues to deteriorate. The Clinical Board is working with the Director of Planning and the Chief Operating Officer to identify the most appropriate location for “new Rookwood” but it is anticipated that this will take some years. RECOMMENDATION The Quality and Safety Committee is asked to note this report. Financial Impact
Failure to manage, reduce and mitigate against risk will result in a high financial risk. Ensuring good risk management systems that reduce waste, variation and avoidable harm will result in financial efficiencies. Service developments are aimed at improving quality and safety for patients whilst achieving cost savings.
Quality, Safety and Experience
This report provides the Specialist Services Clinical Board’s Quality and Safety position
Standards for Health Services
Delivery of the Standards for Health Services is fundamental to the Clinical; Board’s Q&S Committee
Risks and Assurance
Lessons learnt from concerns action plans and service improvement plans provide assurance that appropriate standards of care minimise clinical risk.

Specialist Services Quality and Safety Report Page 14 of 14 Quality Safety and Experience Committee 23 September 2014
Compliance with the Standards for Health in Wales, effective complaints and claims investigations and demonstrating service improvements help support achievement of the UHBs aims and objectives and improve financial effectiveness. Developing an open culture of risk management and risk reduction through promoting the priorities of the quality and safety agenda help reduce the risks to organisational reputation and improve services to patients.
Equality and diversity
Ensuring compliance with the Standards for Health in Wales will help ensure the provision of safe and equitable services for all.

Appendix 1
Specialist Services Directorates Directorate Specialty Service Area
Wheelchairs South & Mid Wales Prosthetics South East Wales Orbital Prosthetics All Wales Environmental Controls All Wales War Pensioner Service South East Wales Communication Aids South & Mid Wales
ALAS
Orthotics Cardiff and Vale General Cardiology Cardiff and Vale Cardiac Rehabilitation Cardiff and Vale Diagnostic and Interventional Cardiology South East Wales
Electrophysiology and Ablation South East Wales
Complex Ablation Services South & Mid Wales Specialist Heart Failure South East Wales Thoracic Surgery South East Wales Cardiac Surgery including Cardiac Intensive Care Unit
South East Wales
Myocardial Perfusion Imaging South East Wales
Cardiothoracic Services
Cardiac Diagnostics South East Wales Specialist Device Implantation South East Wales
Adult Critical Care UHW Cardiff and Vale Critical Care
Adult Critical Care UHL Cardiff and Vale General Haematology Cardiff and Vale Malignant Haematology South East Wales Haemophilia Services (Arthur Bloom Centre) South East Wales
Sickle Cell and Thalassaemia Cardiff and Vale
Stem and Bone Marrow Transplantation South East Wales
Gene Mutation Analysis Cardiff and Vale
Clinical Haematology
Apheresis Service South East Wales Nephrology South East Wales Dialysis South East Wales Renal Surgery South East Wales
Nephrology and Transplant
Transplantation South East Wales
General Neurology Cardiff and Vale / Cwm Taff LHBs
Multiple Sclerosis Services South East Wales
Neurosciences
Epilepsy South East Wales
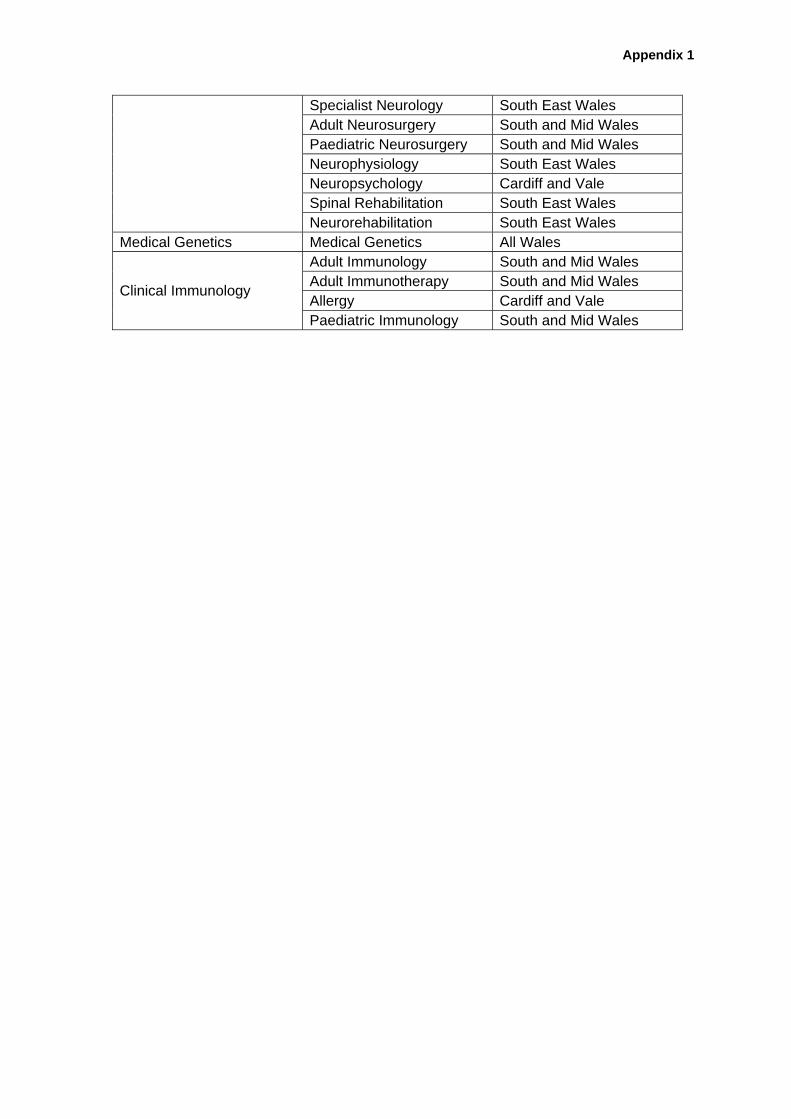
Appendix 1
Specialist Neurology South East Wales Adult Neurosurgery South and Mid Wales Paediatric Neurosurgery South and Mid Wales Neurophysiology South East Wales Neuropsychology Cardiff and Vale Spinal Rehabilitation South East Wales Neurorehabilitation South East Wales
Medical Genetics Medical Genetics All Wales Adult Immunology South and Mid Wales Adult Immunotherapy South and Mid Wales Allergy Cardiff and Vale
Clinical Immunology
Paediatric Immunology South and Mid Wales
Appendix 2
Operational Procedure for Rapid Access Chest Pain Clinic
Reference No: Issued by
Policy Manager
Version No: 2 Year: 2014
Previous Trust / LHB Ref No:
236
Documents to read alongside this Policy , Procedure etc (delete as necessary)
List titles of Policy’s, Procedures, Protocols, Guidelines, and Strategy’s etc to be read alongside this document.
Classification of document: Clinical Area for Circulation: UHB wide Author/Reviewee: Catherine Langdon ( RACPNS) Lead Clinician: Dr. N. Ossei-Gerning (Consultant Cardiologist). Group Consulted Via/ Committee: All Consultant Cardiologists,
Consultant Physicians and EU Consultants, Directorate Managers/Senior Nurses/Clinical Directors (Medicine/emergency medicine/cardiothoracic services).
Primary Care leads: Dr. Mark Smithies (Divisional Director for Primary Community & Intermediate Care Services) and Dr. Sarah Morgan (Primary Care Cardiac Lead.
Approved by: Specialist Services Quality and Safety Group(Pending) Date of Approval: Date committee approved Date of Review: To be inserted when approved – usually 3 years Date Published: We will input this when it is uploaded.
Disclaimer When using this document please ensure that the version you are using is the most up to date either by checking on the UHB database for any new
versions. If the review date has passed please contact the author.
OUT OF DATE POLICY DOCUMENTS MUST NOT BE RELIED ON

Appendix 2
Version Number
Date of Review Approved
Date Published
Summary of Amendments
1 New UHB procedure to update and replace former Trust document.
2
3

Appendix 2
Operational Procedure for the Rapid Access Chest Pain Clinic (RACPC) Contents Page 1 Introduction 4 2 Aim 4 3 Scope 4 4 Roles and Responsibility 4 5 Implementation 6 6 Assessment and Non-invasive testing (N.I.T) 7 7 Emergency Contingency Plans 7 8 Development of Management Plans 8 9 Blood Tests 8 10 Documentation 8 11 Medication 8 12 Non-attendees 9 13 Inappropriate Referrals 9 14 Unexpected Patients 9 15 Equality Impact and Assessment 9 16 Audit and Data Collection 9 17 Distribution 10 18 Review 10 19 References and Further Information 10 Appendices 1 Nurse-led Rapid Access Chest Pain Clinic Protocol. 11 2 RACPC Proforma 13 3 Three Patient letter 18 4 Patient Information Leaflet 19 5 RACPC Care Plan Form &Audit Form 21 6 GP Management Plan letter 32 7 DNA Letter 34
Appendix 2
1. INTRODUCTION The National Service Framework for Coronary Heart Disease (DoH 2000) standard 8 states that “by April 2001 there should be 50 Rapid Access Chest Pain Clinics (RACPC) to help ensure that people who develop new symptoms, that their GP thinks might be due to angina, can be assessed by a specialist within two weeks of referral. There will be 100 clinics by April 2002.” In line with these recommendations The National Assembly for Wales’ report Tackling CHD in Wales: Implementing Through Evidence (2001) standard two states that “Everyone at high risk of developing coronary heart disease and all those who have been diagnosed as having the disease should have access to a multifactorial risk assessment and be offered an appropriate treatment plan.” 2. AIM The aim of the RACPC is to provide prompt assessment and evidence-based management of patients who are experiencing new onset chest pain, suggestive of angina. The purpose of the operational procedure is to provide clarity in relation to the structure of the service. 3. SCOPE This operational procedure applies to patients referred to the Nurse-led Rapid Access Chest Pain Clinic from University Hospital of Wales General Physicians or General Practitioners within the Cardiff and the Vale area. The procedure relates to those patients seen and assessed by a chest pain clinical nurse specialist, under the clinical supervision of a Consultant Cardiologist. 4. ROLES AND RESPONSIBILITIES 4.1 The Consultant in clinic will be the primary point of contact for medical opinion; however if there is no consultant in clinic, refer to the on-call Cardiology Consultant. Should a patient require further testing or follow-up then the patient will be placed under the care of the Consultant Cardiologist on-call at the time of the clinic. 4.2 The RACPC Nurse Specialist is accountable for her/his practice under the terms of their professional body i.e. the Nursing and Midwifery Council ‘Code of Professional Standards for Conduct, Performance and Ethics’ (NMC May 2008). The Nurse-led RACPC is a role and may only be undertaken by a competent practitioner who has been assessed as competent to undertake the role by a Consultant Cardiologist and will work in accordance with the Rapid Access Chest Pain Clinic Protocol (see appendix one). The RACPC Nurse Specialist will ensure that she/he complies with all University Health Board (UHB) policies and procedures which include:

Appendix 2
• Management of Medicines • Resuscitation Policy, Procedure and Guidelines • Informed Consent to Treatment or Investigation • Risk Management • Health and Safety

Appendix 2
5. IMPLEMENTATION The RACPC is a nurse led service which will be situated in the Cardiac Outpatient Department, UHW. There will be a lead consultant and senior registrar for support if required. The RACPC will provide a service between 9am and 5pm Monday to Friday (exclusive of public holidays). The aim will be to provide six appointments per day, three in the morning and three in the afternoon initially with a view to increasing the appointment allocation once the service is established. 5.1 Referral criteria • Patients with new symptoms suggestive of exertional angina. • Patients who have previously been treated and discharged by a cardiologist and have now developed new symptoms, suggestive of exertional angina • Patients seen in the Emegency Unit (EU) with chest pain, who have negative Troponin I (less than 0.03) results at 12hrs, with or without ECG changes (as long as the changes are not suggestive of MI or ACS). Patients should not be referred if • They are suspected of having an Acute Myocardial Infarction or Acute Coronary Syndrome • They do not have a history suggestive of exertional angina • They have symptoms which appear cardiac in origin but are not suggestive of angina for example; shortness of breath, palpitations, loss of consciousness or heart failure. These patients should be referred to a Consultant Cardiologist or via EU as appropriate. N.B The RACPC should not be used to obtain an earlier appointment. 5.2 Referral process Patients can be referred to the RACPC via telephone or fax, those made by telephone must be followed up by a faxed referral form (see appendix two). Patients not felt to meet the referral criteria may be discussed with the lead Consultant Cardiologist and usually care management passed back to the General Practitioner for them to decide on the route of referral i.e. EU or Cardiology Out-patients. On receipt of an appropriate referral patients will be contacted by the RACPC Nurse Specialist and an appointment arranged. The aim will be to see patients as soon as possible (within 48hrs of referral) and that all patients should be offered an appointment within two weeks of referral to the RACPC. The date and time of the appointment will be confirmed in writing (see appendix three), and a patient information leaflet sent (see appendix four). If there is no time to send the information it will be given over the telephone.

Appendix 2
Once an appointment has been arranged medical records staff will be informed and clinic lists will be produced on a daily basis. Patient hospital numbers will be allocated as required and hospital notes located, these will accompany all patients to clinic. 6. ASSESSMENT AND NON-INVASIVE TESTING (N.I.T) The clinic co-ordinator at the reception desk will check the patients’ demographic details these will also be cross checked with the PMS clinic list to ensure that the correct notes and patient are in clinic. 6.1 Patients will have a resting ECG and set of observations including height and weight taken on arrival at the clinic. A history and physical examination will then be taken by an appropriately competent practitioner (Consultant, SpR, Specialist Nurse or Cardiac Pysiologist as deemed competent by the lead consultant); all findings will be documented in the care plan (see appendix five). 6.2 Based on all clinical findings and blood results, supplied by the referring clinicians on the referral form, the decision will then be made as to the appropriate (NIT). The Clinical Nurse Specialist, as an independent practitioner, will either be able to complete and sign the request form or will ask a medically qualified practitioner to do so as necessary. The Exercise Stress Test consent will be obtained and supervised by appropriately trained Physiologists in line with local operational policies and professional guidelines and competencies (British Cardiac Society 2003). For Myocardial Perfusion Imaging (MPI) and Dobutamine Stress Echos (DSE) a letter will be written to Dr. Wheeler for an urgent appointment. 7. EMERGENCY CONTINGENCY PLANS Patients should not be referred to the RACPC with either acute or unstable conditions. However, following initial assessment and history taking a patient may be deemed ‘unstable’ if any of the following apply: • Unpredictable symptoms occurring at rest or during sleep • Sudden increase in frequency, duration or intensity of symptoms • Limited relief from use of sub-lingual Glycerine Trinitrate (GTN) In the event of a patient being assessed as having unstable angina, the case will be discussed with the SpR/ Cardiology Consultant on call and arrangements made to admit the patient to hospital. Contact will be made with the Cardiothoracic Directorate bed management coordinator/ Bed Management Team and transfer to an appropriate environment arranged. The GP will be notified of the arrangements made. In the event of a RACPC patient having a cardiac arrest, emergency medical help must be summoned by the instigation of the UHB Cardiac Arrest Procedure. 8. DEVELOPMENT OF MANAGEMENT PLANS
Appendix 2
8.1 Following the NIT, the results will be presented to the Consultant Cardiologist/SpR in clinic and a management plan formulated. The management plan will include recommendations for drug management, further investigations, follow-up arrangements and supporting written information. A copy of the plan will be posted to the GP. 8.2 The patient will have all test results and the management plan explained. Risk factors will be revisited. British Heart Foundation education booklets will be given as appropriate. 8.3 Where the likelihood of a cardiac problem is thought to be low this will be explained to the patient and lifestyle modification plans documented. The GP will be informed of all findings and the management of the patient will be passed back to them (appendix six). 8.4 If a diagnosis of angina is reached, suggested medical therapy will be decided upon by the Cardiology Consultant or SpR for the GP to commence. Any follow-up appointments required for tests or consultations will be arranged before the patient leaves and documented in their management plan (see appendix five). The management plan and risk factors will be explained to the patient and any questions answered at this juncture. Should patients require angiography they will be placed on the waiting list on the day of the RACPC appointment. If the patient does not want to undergo angiography follow-up will be arranged in the cardiology outpatient clinic. 9. BLOOD TESTS
Blood tests are not routinely taken in the RACPC. Referring clinicians are asked to supply recent blood results on the referral form. Patients who do not have a recent cholesterol result available will be advised to have this checked by their GP. 10. DOCUMENTATION The patient notes will be located and collected prior to the appointment. The visit to the RACPC will be documented in the RACPC care plan (see appendix five), which will be filed in the patient notes. The management plan will have three copies made, one copy for the GP, one for the patient notes and one for the RACPC nurse to keep for reference. 11. MEDICATION The non-medical prescriber will be competent to commence: Aspirin, Beta-blockade, Calcium Channel blockers, Nitrates, Statins and GTN spray. Should any other medication be considered necessary a medical professional (either Consultant Cardiologist or SpR) will be consulted. Patients will be supplied with appropriate medication (if required) following their consultation. The GP will be informed of this in the management plan (see Appendix 6) 12. NON-ATTENDEES

Appendix 2
Attempts will be made to contact the patient by telephone to arrange another appointment in clinic. If the patient does not make contact with the RACPC nurse after 3 working days the GP will be informed by letter (see appendix 7). 13. INAPPROPRIATE REFERRALS If an individual clinician is found to repeatedly refer patients who do not meet the criteria for the RACPC they will be contacted and any questions answered. Dr. Sarah Morgan (Primary Care Cardiac Lead) and Dr. Mark Smithies Divisional Director for Primary Community and Intermediate Care Services) will also be informed. 14. UNEXPECTED PATIENTS Occasionally patients will turn up in the cardiology department because they feel unwell. These patients should be referred back to the EU for their own safety; the staff in EU are better equipped to decide the best course of action. Transfer will be arranged taking into account the condition of the patient and liaison with EU staff. 15. EQUALITY IMPACT AND ASSESSMENT An equality impact assessment has been undertaken to assess the relevance of this procedure to equality and potential impact on different groups, specifically in relation to the General Duty of the Race Relations (Amendment) Act 2000 and the Disability Discrimination Act 2005 and including other equality legislation. The assessment identified that the procedure presented a low risk to the UHB. Suggested is some alternative wording below which has been approved by Keithley Wilkinson the Equality Manager for the UHB. The UHB is committed to ensuring that, as far as is reasonably practicable, the way it provides services to the public and the way it treats its Employees reflects their individual needs and does not discriminate against individuals or groups. The UHB has undertaken an Equality Impact Assessment and received feedback on this Policy and Standards of Behaviour Framework and the way it operates. The UHB wanted to know of any possible or actual impact that this procedure may have on any groups in respect of gender (including maternity and pregnancy as well as marriage or civil partnership issues), race, disability, sexual orientation, Welsh language, religion or belief, transgender, age or other protected characteristics. The assessment found that there was low impact to the equality groups mentioned. Where appropriate the UHB will make plans for the necessary actions required to minimise any stated impact to ensure that it meets it’s responsibilities under the equalities and human rights legislation. 16. AUDIT AND DATA COLLECTION The RACPC nurse will maintain the RACPC audit with the insertion of each patients details onto an excel spread sheet. The information will be collated and reported on an annual basis at clinical governance and divisional quality and safety meetings. 17. DISTRIBUTION

Appendix 2
17.1 This procedure will be available via the UHB intranet and internet sites. Where staff do not have access to the intranet their line manager must ensure that they have access to a copy of this policy. 18. REVIEW This procedure will be reviewed at least every 3 years or sooner should any developments or changes in practice inform the UHB otherwise. 19. REFERENCES AND FURTHER READING British Journal of Cardiac Nursing Feb. 2006 Vol 1 No 2 pp89-94 Keenan J (2006) Rewards and Opportunities in Rapid Access Chest-Pain Clinics Kelly D et al (2011) Implementation of the new NICE guidelines for stable chest pain services in the UK. The British Journal of Cardiology. 18 (4) 185 – 188. McManus RJ et al (2002) A Systematic Review of the Evidence for Rapid Access Chest pain Clinics. International Journal of Clinical Practice 56(1):4-5 NeHL (2001) Rapid Access Chest Pain Clinic Protocol Pottle A (2005) A nurse-led rapid access chest pain clinic- experience from the first 3 years European Journal of Cardiovascular Nursing 4 (2005) 227-233
Appendix 2
Appendix 1.
Cardiff and Vale NHS Trust Nurse-led Rapid Access Chest Pain Clinic Protocol. Referral Process
• All patients referred to the RACPC will be seen within two weeks of the date that the correctly completed referral form is received.
• Referrals are received directly from GP’s or general physicians by fax. • All referral forms should be completed in their entirety including recent blood
results. • All patients will be sent an appointment letter with the date and time of
allocated clinic appointment together with a patient information leaflet. Inclusion Criteria 1) Patients with new symptoms suggestive of exertional angina. 2) Patients who have previously been treated and discharged by a Cardiologist
and have now developed new symptoms, suggestive of exertional angina. 3) Patients seen in A&E with chest pain, who have negative Troponin I (less
than 0.03) results at 12hrs, with or without ECG changes. Exclusion Criteria 1) Patients suspected of having an Acute Myocardial Infarction or Acute
Coronary Syndrome. 2) Patients who do not have a history suggestive of exertional angina. 3) Patients who have symptoms that appear cardiac in origin but are not
suggestive of exertional angina, for example shortness of breath, palpitations, loss of consciousness or heart failure.
Clinic assessment * All referrals to the RACPC are to be seen by the Nurse Specialist with oversight from a Consultant Cardiologist or (SPR). * A base line ECG, height weight and vital signs will be recorded on arrival in the clinic. * A detailed history will be taken, risk factors identified and a baseline physical examination will be performed by the Nurse Specialist. * All patients who it is deemed appropriate to perform an ETT will be asked to do so. Despite the downgrade by NICE, all patients who are deemed suitable to perform an ETT will be asked to do so. This is because of its availability, and the fact that, currently, more appropriate tests are less readily available. *Other patients will be referred for an MPI or other non-invasive investigations if available. It is hoped that in the future, when more appropriate non-invasive tests become available, that these will replace ETT in a significant proportion of patients. • Patients with unstable angina or severe resting 12-lead ECG changes
should not undergo ETT but should be admitted for appropriate treatment.
PROCEDURE IN THE EVENT OF A HIGH RISK TEST
Appendix 2
* Where the ETT is classed as high risk, the Consultant Cardiologist will be notified for a decision re; coronary angiography. * A Coronary Angiography waiting list card will be completed and taken to the appropriate Consultants secretary for actioning. * Patients who require angiography will have a full explanation of their management plan together with written information on the procedure itself. If the patient does not want to undergo angiography an outpatient appointment will be made in the clinic of the consultant for follow-up. * The GP letter will include recommendations of medications that should be considered to treat that patients stable angina e.g Beta-blocker, Aspirin, Statins and Nitrates, unless contra-indicated. *The GP letter/management plan will be sent in the post. The GP letter will also include a description of the patient’s clinical presentation, risk factors, ETT result, risk grading and plan of action/follow-up. Patients diagnosed with Stable Angina.
• All patients with a possible diagnosis of Stable Angina are to be discussed with the Consultant Cardiologist and a management plan agreed.
• An outpatient appointment will be arranged, if felt to be necessary by the Consultant Cardiologist.
• Patients will be informed of their diagnosis whilst in the clinic and will be given British Heart Foundation information leaflets.
• The GP letter will include recommendations of medications that should be considered for example Beta-blockers, Aspirin, Statins, Nitrates unless contra-indicated. Patients who are unable to tolerate Beta-blockers may be considered for rate limiting calcium channel blockers as an alternative.
• The clinic letter will be sent in the post to the GP. The letter will include a description of the patient’s clinical presentation, risk factors, ETT result, risk grading and management plan.
Follow up
• Patients who have required follow-up as part of their management plan will
have an appointment allocated based on the urgency rating expressed by the Consultant Cardiologist.
• Patients not requiring follow up will be discharged back to the care of the GP, either for further investigation of chest pain that is not thought to be cardiac, or for medical management of their chest pain using the suggested management plan.

Appendix 2
REFERRAL CRITERIA: New or recent onset of EXERTIONAL chest pain suggestive of ischaemic heart disease. Fax completed forms to: 02920743916. Incomplete Referrals will NOT be processed. Patients with UNSTABLE Cardiac Chest Pain (Acute Coronary Syndrome) should be admitted.
STEP ONE –SYMPTOMS Tick all that apply Nonanginal features:
□ Non exertional or positional pain □ Localised, lateral chest pain □ Worse during inspiration
STEP TWO – CLINICAL DIAGNOSIS Tick ONE only
□ Typical angina: score 3 of NICE criteria (above) ‐ refer to RACPS □ Atypical angina: score 2 of NICE criteria ‐ refer to RACPS □ Non‐anginal pain: score 1 of NICE criteria ‐ DO NOT refer to RACPS
Patients with Non Anginal chest pain, patients with CAD risk < 10% ‐ DO NOT REFER unless there is a strong clinical suspicion of CAD.
STEP THREE – RISK FACTORS Tick all that apply
High risk factors: Other risk factors: □ Diabetes mellitus □ Hypertension □ Hyperlipidaemia (cholesterol > 6.47) □ Family Hx of premature coronary disease □ Smoking □ History of IHD/ CABG/ PCI/ PVD/ Stroke Specify………………….
STEP FOUR – Coronary Artery Disease Risk (CAD) – see flow chart on next page CAD risk = ………% High Risk / Low Risk (circle)
STEP FIVE TREATMENT ‐ consider Aspirin, GTN, Statin, Betablocker EXCLUSION CRITERIA: (unsuitable for RACP refer to Cardiology Pool)
• AF/LBBB/Wolff‐Parkinson White syndrome.
• BP >200/100mmHg • Seen by cardiology in last 2 yrs • Re‐vascularised (last 5 years)
• Male < 40 female < 30 • Unexplained/untreated anaemia • Symptomatic arrhythmia • Cardiac murmurs/Heart failure • Unexplained syncope
University Hospital of Wales, Cardiff Rapid Access Chest Pain Clinic
Referral Form
Patient details Name:_________________________________________ Sex: Male / female (circle) DOB: __________________________________________ ID Number:____________________________________ NHS Number:_________________________________ Address: _______________________________________ _________________________________________________ Tel no.: ________________________________________ Interpreter needed YES / NO (circle) Language:______________________________________
Referring Clinician Details: Name:___________________________________________________ Practice Address_____________________________________________________________________________________________________________ Contact telephone number:___________________________ MAU/A&E referrals must state referring consultant: __________________________________________________________ Signature: ______________________________________________
Angina pain (NICE Criteria):
□ Chest discomfort radiating to neck, jaw, or arms □ Precipitated by exertion □ Relieved by rest or GTN within 5 minutes
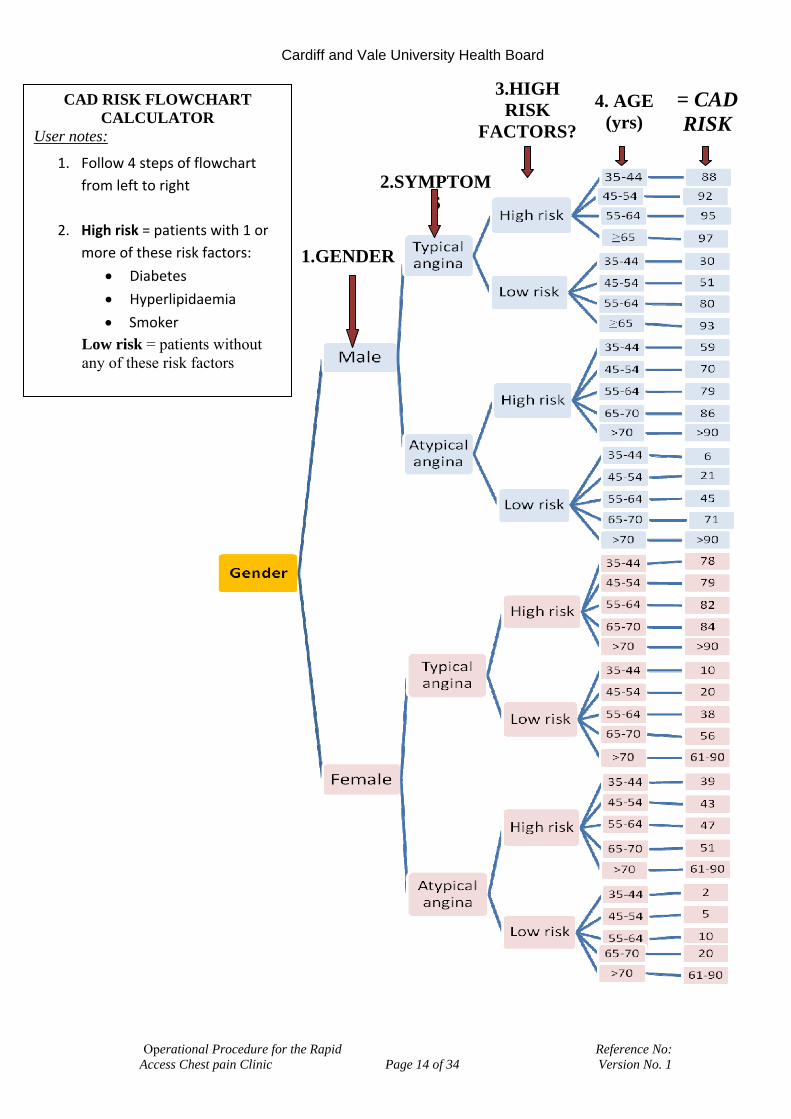
Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 14 of 34 Version No. 1
4. AGE (yrs)
= CAD RISK
3.HIGH RISK
FACTORS?
CAD RISK FLOWCHART CALCULATOR
User notes:
1. Follow 4 steps of flowchart from left to right
2. High risk = patients with 1 or more of these risk factors:
• Diabetes
• Hyperlipidaemia
• Smoker Low risk = patients without any of these risk factors
2.SYMPTOMS
1.GENDER

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 15 of 34 Version No. 1
Classical angina of recent onset +/or *known CAD with worsening angina
Symptoms suggestive of acute coronary syndrome * Chronic stable angina + Atypical chest
pain with 2 or more cardiac risk factors.
Normal Cardiology Clinic
RACPS (Consultant led: Mon, Tues, Weds and Thurs)
Dial 999
£
£ Significant comorbidities,eg, severe heart failure, significant lung disease, significant neurological deficit, and severe arthritis, please refer urgently to Cardiology Clinic.
Appendix 1a Chest Pain Referral Form
CHEST PAIN OF SUSPECTED CARDIAC ORIGIN
*Further evaluation in hospital may not be necessary if the patient is stable. +Non cardiac chest pain should not be referred.

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 16 of 34 Version No. 1
Appendix 2a Chest Pain Referral Form. ALGORHYTHM FOR MEDICAL MANAGEMENT OF CHEST PAIN ADAPTED FROM STABLE ANGINA-ESC 2006 G S
SL GTN prn ↓ Aspirin 75 mg →contraindicated→Clopidogrel 75 mg ↓ Statin (Titrate to LDL< 2)→intolerant→change statin, consider fibrate or ezetimibe ↓ ACE inhibitor in proven CVD→intolerant→use angiotensin receptor blocker
Beta- blocker (Titrate HR 50-60 bpm) Intolerant or contra-indicated ↓ ↓ Consider rate-limiting CCB or Ivabradine (target heart rate 50-60 bpm) Symptoms not controlled ↓ Add calcium channel blocker (CCB) or long acting nitrate or Ivabradine if heart rate > 70 bpm ↓ Symptom not controlled after dose optimisation ↓ Consider suitability for revascularisation Consider Ranolazine or Nicorandil
Not suitable
Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 17 of 34 Version No. 1
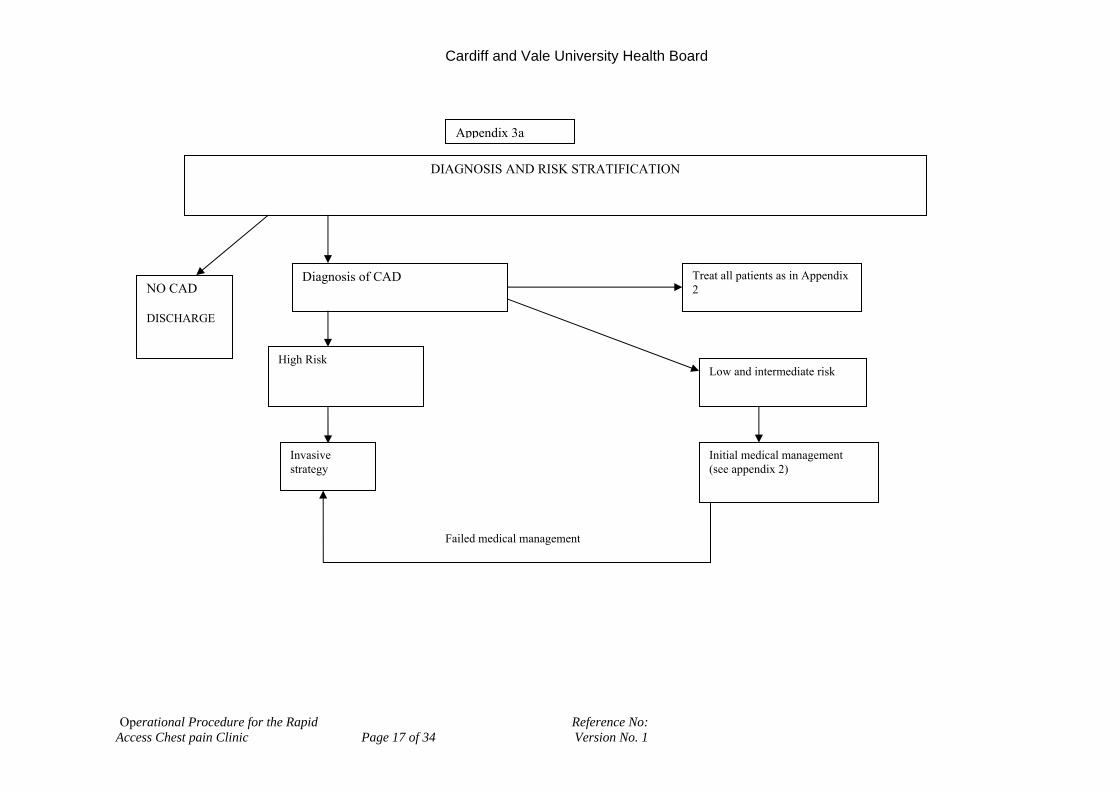
DIAGNOSIS AND RISK STRATIFICATION
NO CAD DISCHARGE
Diagnosis of CAD Treat all patients as in Appendix 2
High Risk
Invasive strategy
Low and intermediate risk
Initial medical management (see appendix 2)
Failed medical management
Appendix 3a
Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 18 of 34 Version No. 1
Appendix 3. Cardiff and Vale University Health Board University Hospital of Wales. Heath Park, Cardiff. Date:
Rapid Access Chest Pain Clinic Cardiology Out-patient Department.
Dear An appointment has been booked for you to attend the above clinic on; ………………………………………………………………………………………… At;……………………………………………………………………………………... You will need to report to the Cardiac out-patient department near B1 Ward. When you arrive please inform the receptionist that you have come for the Chest Pain Clinic. Should you need to change this appointment please telephone; Catherine Langdon on 02920745845 Bleep no. 5152 Yours sincerely, Catherine Langdon Rapid Access Chest Pain Nurse Specialist

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 19 of 34 Version No. 1
Cardiff and Vale NHS Trust. University Hospital of Wales
Patient Information leaflet
Rapid Access Chest Pain Clinic
Appendix 4.
What is the RACPC? Your General Practitioner will refer you to the Rapid Access Chest Pain Clinic to investigate the possible cause of your chest pain. Chest pain can be caused by several things and this clinic will look at whether your heart may be the cause. What is involved? At your appointment a Cardiologist (Heart doctor)or Specialist Nurse and a Cardiology physiologist will see you. We will carry out some tests to assess your chest pain and decide if you have angina. What tests may I have done?
• Blood tests • Height • Weight • Blood pressure • Electrocardiogram (ECG) This is a simple recording of your heartbeat. The
physiologist/ nurse will attach pads to your arms, legs and chest and a recording is then taken.
• Exercise ECG recording: This is a recording of your heartbeat whilst you walk on a treadmill. The treadmill begins slowly and will gradually increase. We will monitor your heart and blood pressure carefully while you perform this exercise. This test usually takes between 15-30 minutes.
• Echocardiogram (ECHO). This is a scan of the movement of the wall and valves of your heart. The technique uses ultrasound and therefore causes no pain or discomfort.
What should I wear? The exercise test is not too energetic; just wear flat shoes and comfortable clothing that you will be able to move easily in, trousers would be advisable. You will not be expected to run or exercise beyond your capabilities and the test can be stopped at any time. You may have a light meal about two hours before your appointment. Avoid heavy meals prior to exercise.

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 20 of 34 Version No. 1
What should I bring? Any tablets, medicines or inhalers that you are currently taking. A drink, as your appointment may last for two hours. What will happen after the tests? The Cardiologist or Specialist Nurse will discuss the results of your tests with you, and any further treatments or tests which are planned. If the tests show that you do have angina, you will be given some advice and information booklets about angina by the Specialist Nurse. You will be given a copy of your results and a Risk factor Management Plan. Your GP will be sent a copy of your Risk factor Management Plan within the next few days.

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 21 of 34 Version No. 1
Appendix 5
Cardiff and Vale University Health Board Ymddiriedolaeth Gi Caerdydd A’r Fro
Rapid Access Chest Pain Clinic Care Plan
GP contact details ………………………………………………. ………………………………………………. ………………………………………………. ………………………………………………. Tel.no………………………………………...
Consultant……………………………………… Date and time of appointment ………………..
Addressograph Patient’s telephone no.

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 22 of 34 Version No. 1
Insert faxed referral here
Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 23 of 34 Version No. 1
Past medical history. (Tick box if Applicable). Ischaemic heart disease Congestive cardiac failure/Left ventricular failure Hypertension Hypercholesterolaemia Rheumatic fever Transient ischaemic attacks Peripheral Vascular Disease Pulmonary embolism Epilepsy Asthma Diabetes Chronic obstructive pulmonary disease Liver disease Hyper/hypothyroidism Chronic renal failure Peptic/duodenal ulcer Aortic stenosis Murmurs Surgery (note details) Erectile dysfunction: Y/N Any other:
Presenting Complaint:

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 24 of 34 Version No. 1
Description of symptoms: Onset & chronology: Location & radiation: Quality of pain: Severity of pain: Alleviating factors: Precipitating factors: Associated symptoms: Frequency: Risk Factors: Diabetic: Y/N Smoker: Y/N Alcohol Y/N (If yes, weekly units = ) Family History ( 1st degree relative Male < 55 years; Female < 65 years): Y/N Cholesterol (Chol < 4 mmols, Trigs < 2.0 ) Y/N Hypertensive: Y/N

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 25 of 34 Version No. 1
Current Medications (Including over the counter medications). Allergies: Medication/tapes/creams/food/iodine/contrast medium.

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 26 of 34 Version No. 1
Presenting Complaint:
Description of symptoms 1) onset and chronology 2) location and radiation
3) quality of pain
4) severity of pain
5) alleviating factors
6) precipitating factors
7) associated symptoms
Resting 12 lead ECG
Obervations: Height: Weight: BMI: Blood pressure: Pulse (note if irregular) Respiratory rate: Sa02: Temperature: PHYSICAL EXAMINATION. Respiratory: Rate: Expansion: Auscultation: Percussion: Cardiovascular System: Pulse rate: bpm: Carotid Bruit: JVP: Apex beat: Heaves/thrills: Heart sounds: Pedal oedema: Varicose veins:

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 27 of 34 Version No. 1
Exercise tolerance test
Any other test results
Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 28 of 34 Version No. 1
Plan. Agreed with:
Follow up arrangements

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 29 of 34 Version No. 1
AUDIT FORM FOR RAPID ACCESS CHEST PAIN CLINIC. DATE OF CLINIC: Patient’s Name: Hospital No. Male/Female: D.O.B: Age: Source of referral: A&E Source of referral: GP If GP, note name & address: Date referred: Date received: Date of appointment: Referral Criteria: Patients with new symptoms (less than 3 months) suggestive of exertional angina Patients who have previously been treated and discharged by a cardiologist and have now developed new symptoms, suggestive of exertional angina Patients seen in A & E with chest pain who have negative Trop I (less than 0.03) results @ 12 hours, with or without ECG changes (as long as the changes are not suggestive of MI or ACS). Not met referral criteria Reason: They are suspected of having an acute Myocardial infarction or acute coronary syndrome They do not have a history suggestive of exertional angina They have symptoms which appear cardiac in origin but are not suggestive of anginal for example: Shortness of breath Palpitations Loss of consciousness Heart failure Other Length of consultation time: Nurse consultation time: Investigation time:

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 30 of 34 Version No. 1
Medical opinion time: Cardiologist: Diagnosis: Cardiac Diagnosis: Non cardiac Outcome: Angio list Angio results: Outcome: Echo on the day Echo results: Outcome: Echo referral Outcome MPI referral Results MPI: Outcome DSE referral Results DSE: Outcome ETT on the day Outcome ETT referral Results of ETT: Negative Positive Inconclusive Submaximal Patient discharged from RACPC Patient referred to cardiologist Patient admitted to hospital ECG: Normal/Twave inversion/Q waves/LBBB/RBBB (delete as appropriate) Diabetes: Y/N (Delete as appropriate)
Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 31 of 34 Version No. 1
Hypercholesterolaemia: Y/N Smoker: Y/N Hypertension: Y/N Family history Y/N History of IHD/CABG/PCI/PVD/Stoke….. (Specify) Old Medication: Statin/Aspirin/Betablocker/GTN spray/Nitrate/other New Medication: Statin/Aspirin/Betablocker/GTN spray/Nitrate/other Erectile Dysfunction: Y/N (Updated 21/03/14)
Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 32 of 34 Version No. 1
Appendix 6.
[~PAT.TRUST LOGO~]
Cardiff and Vale University Health Board
Bwrdd Iechyd Prifysgol Caerdydd a’r Fro
University Hospital of Wales Ysbyty Athrofaol Cymru
Eich cyf/Your ref: Ein cyf/Our ref: Welsh Health Telephone Network Direct Line/Llinell uniongyrchol
Heath Park, Cardiff, CF14 4XW Phone (029) 2074 7747 Fax (029) 2074 3838
Parc Y Mynydd Bychan, Caerdydd, CF14 4XW Ffôn (029) 2074 7747 Ffacs (029) 2074 3838
CARDIAC SERVICES DIRECTORATE DEPARTMENT OF CARDIOLOGY
TEL: 029 20745845 FAX: 02920 743916
EMAIL: [email protected]
MB /JP / [~PAT.CRN/U~] [~PAT.LETTER DATE~]
PRIVATE & CONFIDENTIAL. Dr [~PAT.GP FORENAME/U~] [~PAT.GP SURNAME/M~] [~PAT.SURGERY/M~] [~PAT.GP ADDR1/M~] [~PAT.GP ADDR2/M~] [~PAT.GP ADDR3/M~] [~PAT.GP ADDR4/M~] [~PAT.GP POSTCODE/U~] Dear Dr [~PAT.GP SURNAME/M~] [~PAT.PAT TITLE/M~] [~PAT.FORENAME/M~] [~PAT.SURNAME/M~] DOB [~PAT.PAT DOB~] [~PAT.PAT ADDR1/M~] [~PAT.PAT ADDR2/M~] [~PAT.PAT ADDR3/M~] [~PAT.PAT ADDR4/M~] [~PAT.PAT POSTCODE/U~] Date seen: [~PAT.SESSION DATE~] This patient who presented with chest pain has been seen and assessed. The clinical diagnosis here is: The patient has been further assessed with ETT/DSE/MPI/Coronary CT.

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 33 of 34 Version No. 1
The test was normal/abnormal. Coronary angiography has/has not been organised. Your patient has been started on : Aspiriin Beta-blocker Statin Other Follow up will be in months. This patient has been discharged. Yours sincerely Countersignature CATHERINE LANGDON DR N OSSEI-GERNING CHEST PAIN SPECIALIST NURSE CONSULTANT CARDIOLOGIST MD FRCP

Cardiff and Vale University Health Board
Operational Procedure for the Rapid Reference No: Access Chest pain Clinic Page 34 of 34 Version No. 1
Appendix 7.
University Hospital of Wales, Heath Park, Cardiff. CF14 4XW Date Dear Doctor………………… Thank you for referring……………………………......... ………………………………… ……………………………….... ………………………………… He/she failed to attend an appointment at ………….. on…………………. We have been unable to contact them by telephone since. Please do not hesitate to re-refer this patient in the future if you feel it appropriate. Yours sincerely, Catherine Langdon Rapid Access Chest Pain Nurse Specialist

Appendix 3
VHF EU protocol August 2014
1
UHW PROTOCOL FOR VIRAL HAEMORRHAGIC FEVER (VHF)
PATIENTS BOOKING IN WITH HISTORY OF TRAVEL TO/FROM INFECTED AREAS WITHIN THE LAST 21 DAYS (The incubation period for viral haemorrhagic fever virus is 21 days post exposure). Currently affected areas:
• LIBERIA
• SIERRA LEONE
• GUINEA
• IVORY COAST
• GHANA
• NIGERIA
• NB: this list is to be kept up to date by checking CDC website for up to date details on Countries involved; http://www.cdc.gov/vhf/ebola/outbreaks/guinea/index.html
RECEPTION STAFF TO BLEEP NIC AND FOLLOW RECEPTION ACTION CARD FOR VHF
PT IS TO BE DIRECTED TO WAIT BY THE YELLOW BOLLARD UNDER THE HELI PAD
NB: NO BLOODS / SPECIMENS TO BE SENT TO THE LABORATORY UNTIL AFTER RISK ASSESSMENT AND FOLLOWING DISCUSSION WITH ID / MICROBIOLOGY
IF PATIENT REQUIRES URGENT MEDICAL ATTENTION, HAS VOMITING OR DIARRHOEA OR IS BLEEDING THEN TRIAGE TENT IS TO BE ERECTED AND FURTHER ASSESSMENT CARRIED OUT USING FULL PPE
IF PATIENT IS CLINICALLY STABLE THEN PATIENT IS TO BE ADMITTED AND ASSESSED IN THE DECONTAMINATION ROOM USING APPROPRIATE PPE
FULL PPE (TO BE WORN IF PATIENT IS BLEEDING, CRITICALLY UNWELL OR HAS VOMITING OR DIARRHOEA:
• TYCHEM C OR TYVEC WATER REPELLENT OVER SUIT (BOILER SUIT). If none in the dept these can be obtained from Critical Care or the mortuary (enter mortuary, turn right, on shelf).
• WATERPROOF SURGICAL GOWN
• LONG GREEN APRON
• FFP3 MASK
Appendix 3
VHF EU protocol August 2014
2
• VISOR/GOGGLES
• DOUBLE MEDICAL GLOVES
• OVERSHOES
PPE TO BE WORN IF PATIENT CLINICALLY STABLE WITH NO HISTORY OF DIARRHOEA, VOMITING OR BLEEDING;
• WATERPROOF SURGICAL GOWN
• LONG GREEN APRON
• FFP3 MASK
• VISOR/GOGGLES
• DOUBLE MEDICAL GLOVES
• OVERSHOES
ONCE PPE WORN
NURSE AND DOCTOR TO:
• COLLECT THE PATIENT,
• TRIAGE IN THE DECONTAMINATION ROOM
• DETAILED HISTORY TO ASSESS INFECTION RISK AS PER THE VIRAL HAEMORRHAGIC FEVERS RISK ASSESSMENT ON THE HPA WEBSITE – WWW.HPA.ORG.UK ‐ FLOW CHART CARRIED BY NIC AND HELD IN TRIAGE ROOM
• YOU DO NOT HAVE TO WASH THE PATIENT AS THIS WILL NOT DECONTAMINATE THEM
• PLEASE REMEMBER THAT HOWEVER URGENT THE PATIENT/FAMILY ARE, YOU ARE TO PUT YOUR PPE ON BEFORE ANY CONTACT IS MADE IN THIS INSTANCE – DO NOT PUT YOURSELF OR PATIENTS IN THE DEPT AT RISK
WASTE:
• Orange bags and sharps disposal box to be taken into patient area • All PPE, sharps, contaminated or potentially contaminated materials to remain in
patient area until assessment complete. • Management of waste to be decided by microbiology / ID team following
completion of clinical assessment
Presentations:

Appendix 3
VHF EU protocol August 2014
3
1 Patient presents very unwell with history of diarrhoea, vomiting or bleeding.
• Full PPE to be worn at all times • ID, Microbiology and Critical care team to be informed immediately • Patient management according to clinical scenario • NB; No bloods / specimens to be sent to the laboratory prior to discussion
with Microbiology / ID team
2 Patient with a fever > 38 °C or history of fever in the previous 24 hours
• Take history whilst wearing appropriate PPE
• Ask specifically about symptoms listed below
• Contact ID team (9‐5) or Microbiology Consultant on call (out of hours) to discuss patient and further management
2 If patient presents within incubation period but does NOT have a history of fever > 38oC:
• Take history whilst wearing appropriate PPE
• Ask specifically about symptoms listed below
• Symptoms present / uncertain re risk contact ID team (9‐5) or Microbiology Consultant on call (out of hours) to discuss patient and further management
• No symptoms / alternative diagnosis made => admit to cubicle => Use basic PPE ‐ Duck mask, visors, surgical gown, green apron, 2 pairs of surgical gloves => Medical History from patient and decision made re referral etc onto Infectious Diseases team.
Specific questions to ask in history
• Did the patient travel to an area with VHF cases
• Did the patient have contact with any cases of VHF
• Does the patient have any of the following symptoms:
• Joint pains
• Muscle pains / weakness
• Sore throat and intense weakness
• Chest Pain, difficulty breathing and swallowing
• Diarrhoea and Vomiting with associated stomach pain

Appendix 3
VHF EU protocol August 2014
4
• Rash,
• Red eye
• Hiccoughs
Appropriate placement of the potentially infected patient that requires immediate admission from decontamination room:
Probable VHF:
1) Isolate in negative pressure cubicle in critical care A3
If critical care cubicle is not available discuss with ID / Microbiology re most suitable placement. Options include:
2) Remain in decontamination room / Isolation tent 3) Negative pressure cubicle A7 4) Negative pressure cubicle A&E
Possible VHF:
1) Placement depends on level of risk / clinical scenario. Discuss with Microbiology / ID.
Movement of VHF patients should be kept to a minimum. If the patient is already in the negative pressure cubicle in A&E they should be kept there until assessment has taken place unless their clinical condition dictates movement to critical care.
Admissions by Ambulance:
Identification of risk of Viral Haemorrhagic Fever
Probable VHF - Make arrangements for patient to be transferred directly to a negative pressure room on Critical Care for further management.
Possible VHF or history uncertain – admit via A&E decontamination room as per protocol above.
ESCALATION PROCEDURE FOR ALL SUSPECTED CASES OF VHF
• CONTACT SNR NURSES (in hours)
• CONTACT ID TEAM (9‐5) OR CONSULTANT MICROBIOLOGIST ON‐CALL (via switchboard)
• CONTACT IP&C TEAM (in hours)

Appendix 3
VHF EU protocol August 2014
5
• CONTACT SITE PRACTITIONER (out of hours)
ADDITIONAL INFORMATION FOR ANY PATIENTS WITH SUSPISICION OF VHF
• THESE PATIENTS ARE NOT TO ENTER THE MAIN EMERGENCY UNIT
• ADVICE MUST BE SOUGHT FROM MICROBIOLOGIST PRIOR TO ANY BLOODS BEING TAKEN / PROCESSED. THE POD SYSTEM MUST NOT BE USED. SPECIMENS MUST BE TRANSPORTED TO THE LABORATORY UNDER SPECIFIC CONDITIONS (MICROBIOLOGIST TO ADVISE).
• ALL WASTE MUST REMAIN IN THE AREA WITH THE PATIENT AND NOT BE MOVED
THE PATIENT WILL BE TRANSFERRED TO A7 OR A3 ITU. THIS IS NOT THE DECISION OF THE EU TEAM BUT WILL BE THE DECISION OF THE MICROBIOLOGIST AND INFECTIOUS DISEASES CONSULTANT.
Appendix 1:
Donning and removal of PPE:
IP&C to add Health Board version of this.



Appendix 5
Appendix A Dignity and Essential Care: Improvement Plan Hospital: Rookwood Hospital Ward/ Department: Ward 7 and 8 Neurological Rehabilitation Date of inspection: 17th and 18th June 2014
Para Ref
Finding Requirement Health Board Action Responsible Officer
Timescale
Delivery of Fundamentals of Care
5.7 During treatment, we noted an instance where curtains were not fully closed when treating a patient and another where a patient’s notes were left open on a table next to their bed and it was possible for these to be seen by others.
The Health Board must ensure patient dignity is maintained at all times and curtains are fully closed during care or treatment and notes are not left on display.
Dignity clips to be in use on all curtains, with a plan to move over to disposable curtains when the ward is refurbished.
Charge nurse will raise awareness with staff in newsletter to highlight privacy and dignity as a priority
James Bigg Immediate
September 2014
5.9 We noted that there was no fully private and comfortable room for providing sensitive information to patients and/or relatives and for breaking bad news. Staff noted that currently they may have to use the patients’ day room with a risk of interruption or to ask staff to vacate
The Health Board should ensure that appropriate facilities are available for staff to hold sensitive and private conversations with patients and relatives.
Facilities for families and a quiet room will be addressed as part of the ward refurbishment
James Bigg Commence Sept 2014

Appendix 5
their offices.
5.12 Patients reported that they would like to be provided with more mental stimulation in the form of group game activities such as Bingo. Some staff reported patients would benefit from the provision of more mental stimulation such as structured group activities to encourage routines they would be accustomed to outside of hospital.
The Health Board should consider how it could provide a stronger focus on more rounded rehabilitation which would include availability of more structured mental activities as well as physical activities.
The lead nurse will investigate the use of volunteers to work with patients to alleviate boredom and provide metal stimulation.
During the refurbishment the day room facilities will be improved
Rachel Barry
Ian Fitsall
September 2014
To commence
5.17 Staff reported that clean linen was delivered once a week, however at times the amount of linen delivered was not adequate in order to provide a consistent stock for the week and staff would have to try and obtain additional supplies of linen from other wards which was difficult.
The Health Board must ensure that the ward has an adequate stock of linen available at all times.
Discussion with Linen Services and incident forms to be encouraged to establish the extent of the problem. Senior Staff will link in with the linen services to ensure a sufficient service is provided
James Bigg Immediate
5.25 We found one of the shower rooms on ward 7 contained appropriate equipment however was small and staff reported the room was inadequate to accommodate the number of staff
The Health Board should consider the space requirements within the shower room and ensure it meets the needs of the
During the refurbishment an additional wet room is to be provided, the small shower room will be removed
Ian Fitsall Commence end September 2014
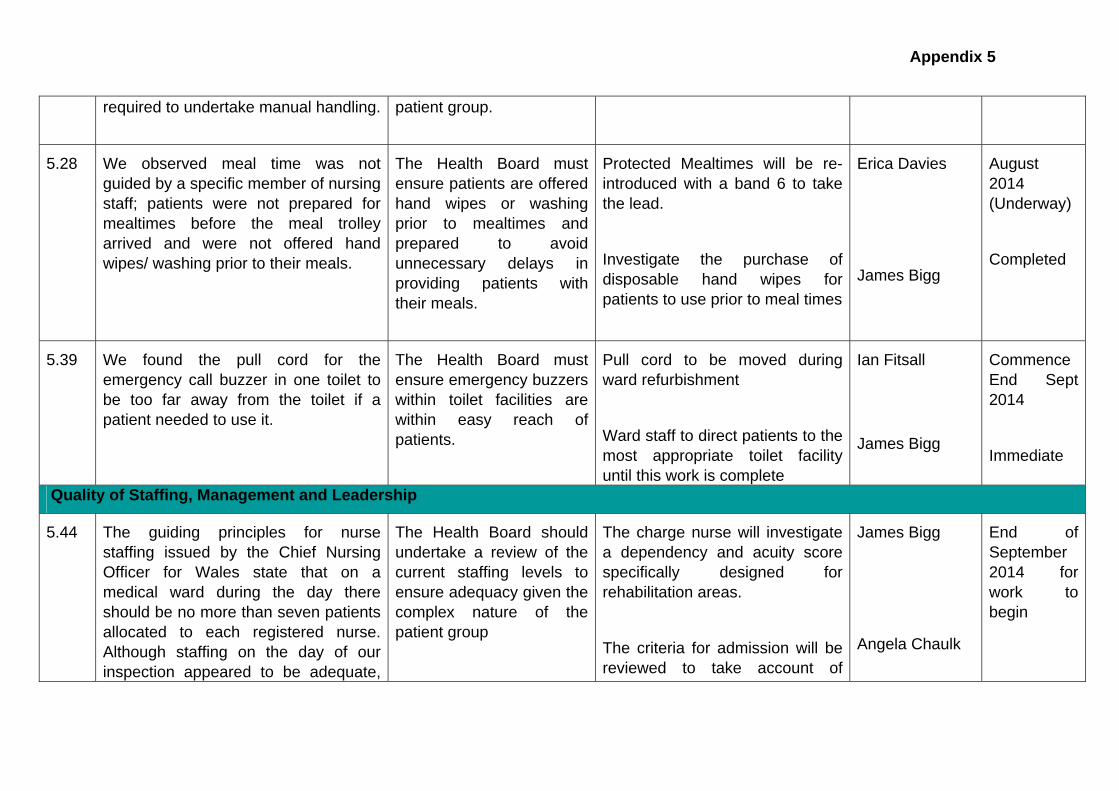
Appendix 5
required to undertake manual handling.
patient group.
5.28 We observed meal time was not guided by a specific member of nursing staff; patients were not prepared for mealtimes before the meal trolley arrived and were not offered hand wipes/ washing prior to their meals.
The Health Board must ensure patients are offered hand wipes or washing prior to mealtimes and prepared to avoid unnecessary delays in providing patients with their meals.
Protected Mealtimes will be re-introduced with a band 6 to take the lead.
Investigate the purchase of disposable hand wipes for patients to use prior to meal times
Erica Davies
James Bigg
August 2014 (Underway)
Completed
5.39 We found the pull cord for the emergency call buzzer in one toilet to be too far away from the toilet if a patient needed to use it.
The Health Board must ensure emergency buzzers within toilet facilities are within easy reach of patients.
Pull cord to be moved during ward refurbishment
Ward staff to direct patients to the most appropriate toilet facility until this work is complete
Ian Fitsall
James Bigg
Commence End Sept 2014
Immediate
Quality of Staffing, Management and Leadership
5.44 The guiding principles for nurse staffing issued by the Chief Nursing Officer for Wales state that on a medical ward during the day there should be no more than seven patients allocated to each registered nurse. Although staffing on the day of our inspection appeared to be adequate,
The Health Board should undertake a review of the current staffing levels to ensure adequacy given the complex nature of the patient group
The charge nurse will investigate a dependency and acuity score specifically designed forehabilitation areas.
r
The criteria for admission will be reviewed to take account of
James Bigg
Angela Chaulk
End of September 2014 for work to begin

Appendix 5
we observed potential for patient dependency to change due to their complex needs and staff reported they would wish to see an increased number of nurses to account for the changing acuity of patients within this specialist neurological rehabilitation ward.
patient dependency and the MDT capacity
Delivery of a Safe and Effective Service
5.51 We noted that there is a limited availability of physiotherapist time due to staff shortages in this area and staff reported they could not provide all things to all patients due to the current availability.
The Health Board should review the physiotherapy requirements of the patient group and establish if additional provision is required.
Review establishment and benchmark with other Brain Injury units to identify whether staffing levels are appropriate for the case mix. Wider review of therapies establishment has also been undertaken.
Recognising that a large part of rehabilitation involves practice within the ward environment there is a need to explore role of support workers through an integrated workforce plan.
Alun Morgan August 2014 – review of establishment completed and now in process of benchmarking.
31st October 2014

Appendix 5
5.54 The ward contained a large amount of clutter and equipment which we observed domestic and nursing staff bumping into and moving around in order to navigate their way through the ward.
The Health Board should ensure when equipment is not in use it is stored appropriately so it does not clutter the ward
Due to large deliveries storage space has been indentified as an issue. As part of the refurbishment additional storage will be available on ward 8.
Boxes will be put away at night time until the refurbishment is complete
Ian Fitsall
James Bigg
End September 2014
Complete
5.55 We found the sluices to be untidy and the ward had a number of items which had been condemned and required disposal. Some of the items had been reported to estates three months previously however had still not been removed from the ward and disposed of.
The Health Board must ensure condemned items are disposed of promptly in accordance with the All Wales Infections Prevention and Control Policy.
Charge nurse wil identify any items for disposal and contact waste management to remove them
The process for waste removal will be reminded to all staff
James Bigg Complete
5.56 We noted patient information boards were located in an area which was a main though fare for the ward and contained useful information for relatives such as the named nurse. However, the boards also contained patient sensitive information such as patient mobility which should not be visible to all relatives entering the
The Health Board must ensure the appropriate placement of patient sensitive information.
The Patient status at a glance board will be moved into the nurses office
James Bigg Complete
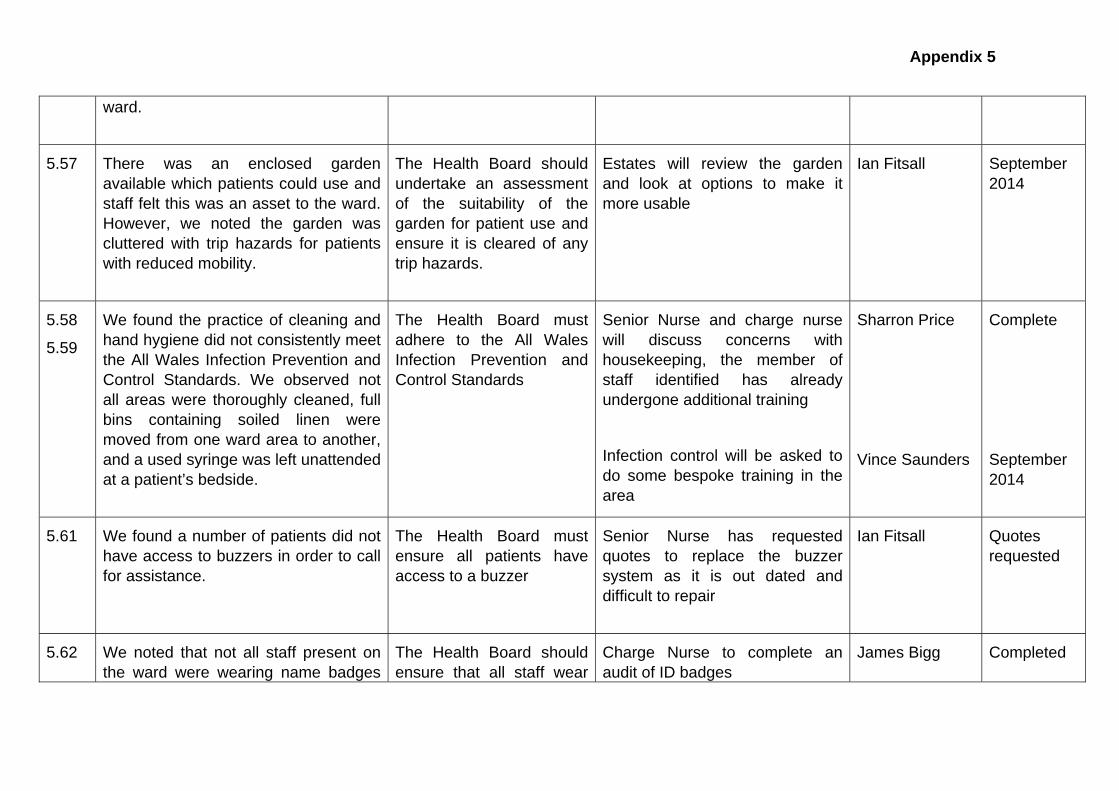
Appendix 5
ward.
5.57 There was an enclosed garden available which patients could use and staff felt this was an asset to the ward. However, we noted the garden was cluttered with trip hazards for patients with reduced mobility.
The Health Board should undertake an assessment of the suitability of the garden for patient use and ensure it is cleared of any trip hazards.
Estates will review the garden and look at options to make it more usable
Ian Fitsall September 2014
5.58
5.59
We found the practice of cleaning and hand hygiene did not consistently meet the All Wales Infection Prevention and Control Standards. We observed not all areas were thoroughly cleaned, full bins containing soiled linen were moved from one ward area to another, and a used syringe was left unattended at a patient’s bedside.
The Health Board must adhere to the All Wales Infection Prevention and Control Standards
Senior Nurse and charge nurse will discuss concerns with housekeeping, the member of staff identified has already undergone additional training
Infection control will be asked to do some bespoke training in the area
Sharron Price
Vince Saunders
Complete
September 2014
5.61 We found a number of patients did not have access to buzzers in order to call for assistance.
The Health Board must ensure all patients have access to a buzzer
Senior Nurse has requested quotes to replace the buzzer system as it is out dated and difficult to repair
Ian Fitsall Quotes requested
5.62 We noted that not all staff present on the ward were wearing name badges
The Health Board should ensure that all staff wear
Charge Nurse to complete an audit of ID badges
James Bigg Completed
Appendix 5
or other forms of official identification.
visible identification for safety purposes and are actively challenged where this is not visible.
Reminders to be put in the newsletter for all staff
Quality of Patient Experience
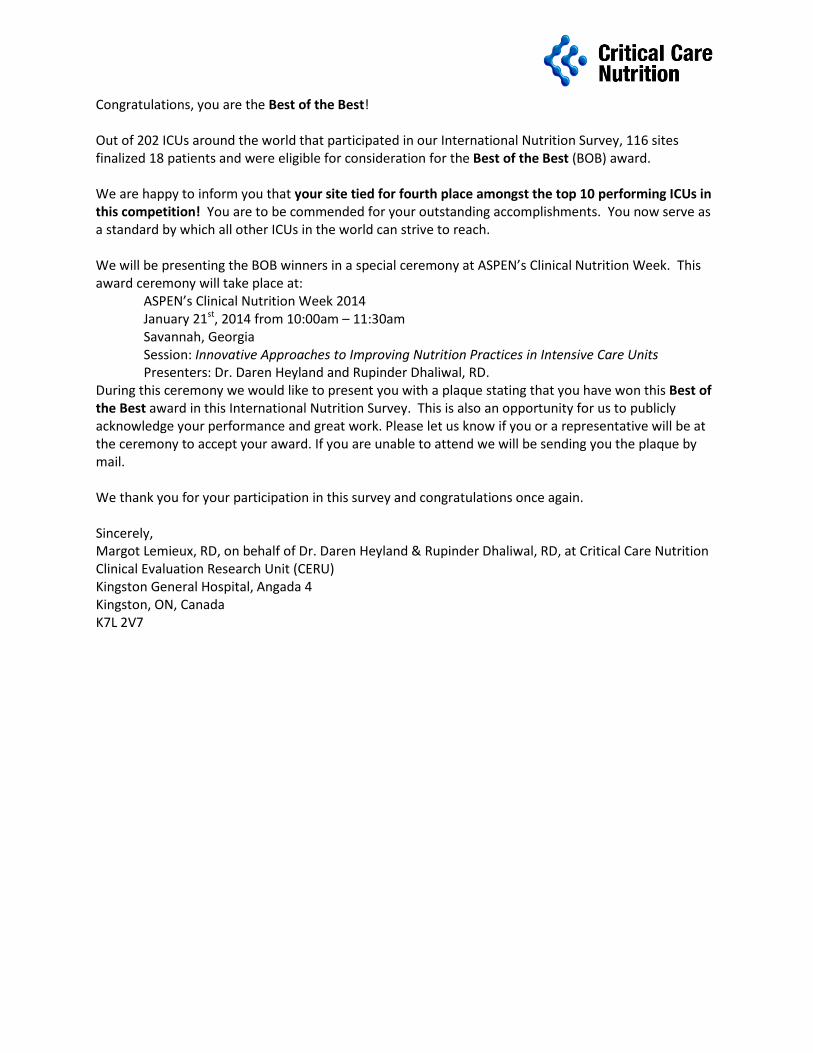
Congratulations, you are the Best of the Best! Out of 202 ICUs around the world that participated in our International Nutrition Survey, 116 sites finalized 18 patients and were eligible for consideration for the Best of the Best (BOB) award. We are happy to inform you that your site tied for fourth place amongst the top 10 performing ICUs in this competition! You are to be commended for your outstanding accomplishments. You now serve as a standard by which all other ICUs in the world can strive to reach. We will be presenting the BOB winners in a special ceremony at ASPEN’s Clinical Nutrition Week. This award ceremony will take place at: ASPEN’s Clinical Nutrition Week 2014 January 21st, 2014 from 10:00am – 11:30am Savannah, Georgia Session: Innovative Approaches to Improving Nutrition Practices in Intensive Care Units Presenters: Dr. Daren Heyland and Rupinder Dhaliwal, RD. During this ceremony we would like to present you with a plaque stating that you have won this Best of the Best award in this International Nutrition Survey. This is also an opportunity for us to publicly acknowledge your performance and great work. Please let us know if you or a representative will be at the ceremony to accept your award. If you are unable to attend we will be sending you the plaque by mail. We thank you for your participation in this survey and congratulations once again. Sincerely, Margot Lemieux, RD, on behalf of Dr. Daren Heyland & Rupinder Dhaliwal, RD, at Critical Care Nutrition Clinical Evaluation Research Unit (CERU) Kingston General Hospital, Angada 4 Kingston, ON, Canada K7L 2V7
National Survey Report
Sample:
Date:
Surveyed:
The Report
The above values relate to the patients surveyed as part of the National satisfaction survey.
Hospital:
Any further enquires please contact the project team on (029) 20336043
This report is based on information gathered from the National satisfaction survey, the
results of which are given as bar charts on pages 2-16. Each question has several possible
responses, for example ranging from 'Always' to 'Not applicable' of which the patient must
tick only one when answering. Each bar chart represents a specific question and gives the
percentage of respondents who gave the various responses.
Specialist Services Clinical Board - May 2014 returns
UHW and Rookwood
51
Returned: 51
Response rate: 100%
H I P O
For each question there are a percentage of respondents that did not answer and these have
been labelled as 'No response'.
12/08/2014
There are three sections to the report:
gives responses to the 18 'Core' questions asked in the survey.
gives responses to the 2 'Equality monitoring' questions asked in the survey.
gives responses to any 'Additional' questions asked in the survey. e.g who
completed the survey.
Section A
Section B
Section C
-
-
-

Page 2

Section A
Section A (pages 3-12) gives the responses to the 18 'Core' questions of the National
Satisfaction Survey. Questions 17 and 18 are not included in this section, as these required
handwritten responses and have been included in a separate report.
Any further enquires please contact the project team on (029) 20336043
Was there anything particularly good about your experience that you would like to tell us about ?
Question 17 -
Was there anything that we could change to improve your experience ?Question 18 -
Page 3

Do you feel that people were polite to you ?1.
Do you feel that you were listened to ?2.
78
18
40 0
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
88
12
0 0 00
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
Page 4

Do you feel that you were given all the information you needed ?3.
Do you feel you were given enough privacy ?4.
96
2 20 0
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
80
16
40 0
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
Page 5

Were you given the support you needed to help with any communication needs ?
5.
Were you able to speak in Welsh to staff if you needed to ?6.
40
24
86
4
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never Not applicable No response
Patient response
Perc
enta
ge o
f re
spondents
73
10
40
12
2
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never Not applicable No response
Patient response
Perc
enta
ge o
f re
spondents
Page 6
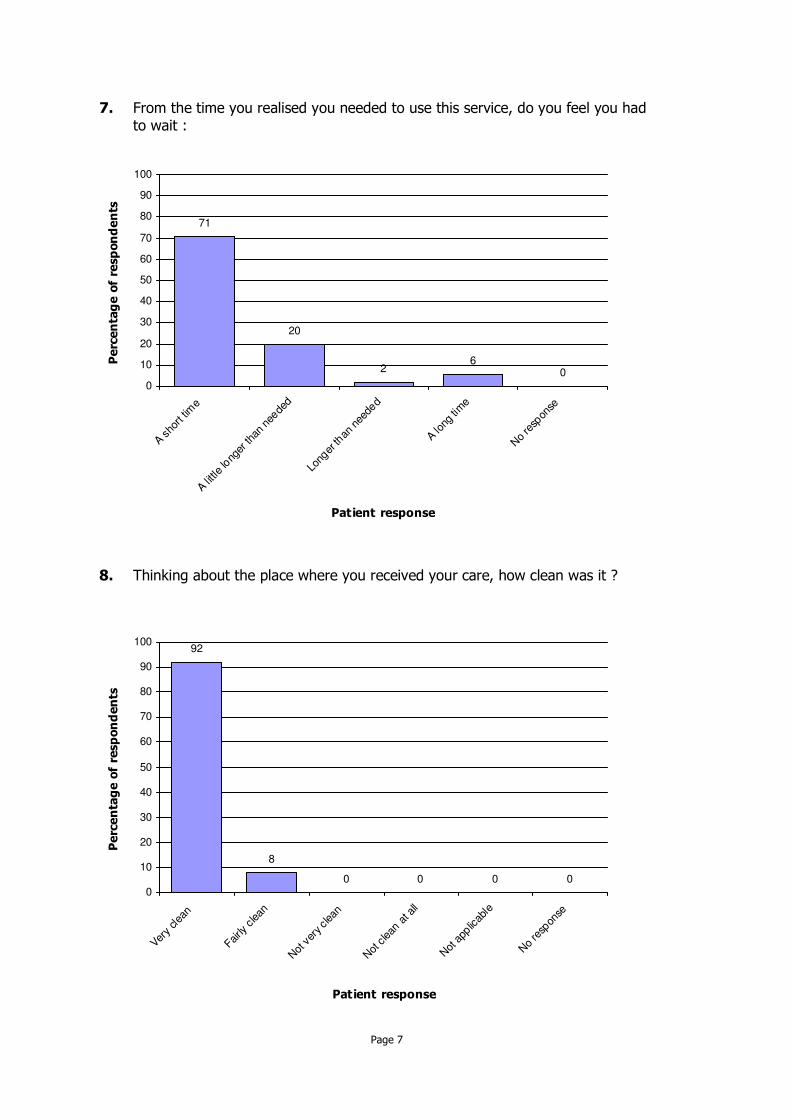
From the time you realised you needed to use this service, do you feel you had to wait :
7.
Thinking about the place where you received your care, how clean was it ?8.
92
8
0 0 0 00
10
20
30
40
50
60
70
80
90
100
Very
clea
n
Fairly
clean
Not
ver
y clea
n
Not
clean
at a
ll
Not
app
licab
le
No
resp
onse
Patient response
Perc
enta
ge o
f re
spondents
71
20
26
00
10
20
30
40
50
60
70
80
90
100
A sho
rt tim
e
A littl
e lo
nger
than
nee
ded
Long
er th
an n
eede
d
A long
tim
e
No
resp
onse
Patient response
Perc
enta
ge o
f re
spondents
Page 7

Did you see staff clean their hands before they cared for you ?9.
Did you feel that everything you needed for your care was available ?10.
82
14
40 0
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
78
20
20 0 0
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never I don't know No response
Patient response
Perc
enta
ge o
f re
spondents
Page 8

If you asked for assistance, did you get it ?11.
If you asked for assistance, did you get it when you needed it ?12.
80
16
40 0
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
90
62
0 00
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
Page 9

Were you involved as much as you wanted to be in decisions about your care ?13.
Were things explained to you in a way that you could understand ?14.
75
22
20
2
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
76
1210
02
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
Page 10

Did you feel you understood what was happening in your care ?15.
Using a scale of 0 - 10 where 0 is very bad and 10 is very good, how would you rate your overall experience ?
16.
0 0 2 0 0 0
6 812
29
41
2
0
10
20
30
40
50
60
70
80
90
100
0' 1' 2' 3' 4' 5' 6' 7' 8' 9' 10'
No
resp
onse
Patient response
Perc
enta
ge o
f re
spondents
76
20
20
2
0
10
20
30
40
50
60
70
80
90
100
Alw ays Usually Sometimes Never No response
Patient response
Perc
enta
ge o
f re
spondents
Page 11

Page 12
Section B
Section B (page 14) gives the responses to the two tick box 'Equality monitoring' questions
of the National Satisfaction Survey. Questions 3 and 4 of the Equality monitoring section are
not included here, as these required handwritten responses and have been included in a
separate report.
Any further enquires please contact the project team on (029) 20336043
If you feel that you or other people have been badly/negatively affected or discriminated against, based on the introduction to this section, then please tell us how below.
Question 3 -
Is there anything else you would like to tell us about the healthcare you have recently received ?
Question 4 -
Page 13

How old are you ?1.
What is your gender ?2.
53
41
0
6
0
10
20
30
40
50
60
70
80
90
100
Male Female Prefer not to say No response
Patient response
Perc
enta
ge o
f re
spondents
0 0
812
27
37
8
2 0
6
0
10
20
30
40
50
60
70
80
90
100
Und
er 1
8
18 -
24
25 -
39
40 -
54
55 -
64
65 -
74
75 -
84
85 a
nd ov
er
Prefe
r not
to say
No
resp
onse
Patient response
Perc
enta
ge o
f re
spondents
Page 14
Section C
Section C (page 16) gives the responses to any 'Additional' questions that may have been
included in the survey. Examples include questions on 'site visited' or 'who completed the
survey'.
Any further enquires please contact the project team on (029) 20336043
Page 15

Who completed the survey ?1.
Was the survey completed by a volunteer ?2.
65
35
00
10
20
30
40
50
60
70
80
90
100
No Yes No response
Response
Perc
enta
ge o
f re
spondents
73
27
00
10
20
30
40
50
60
70
80
90
100
Patient On behalf of patient No response
Response
Perc
enta
ge o
f re
spondents
Page 16