agenda - amazon s3...agenda 1996 le fevreambulance 1999 horry county fire rescue fire‐...
TRANSCRIPT


Agenda
1996 Le Fevre Ambulance1999 Horry County Fire Rescue Fire‐Fighter/Paramedic2007 Iraq2009 MEDIC ‐Paramedic FTO 2017 Safety Health Council of NC for Opiates and Meth
• Overdose: Signs and Symptoms
• Responding to an Overdose• Exposure Prevention: PPE Required• Using Naloxone

• Learn what opioids are and what they are used for
• Learn the prevalence of them in society and workplace
• Discuss workplace strategies for dealing with them
• Learn what to do in an overdose

• Opioids are a class of drugs that include the illegal drug heroin, synthetic opioids such as fentanyl, and pain relievers available legally by prescription, such as oxycodone (OxyContin®), hydrocodone (Vicodin®), codeine, morphine, and many others.
• These drugs are chemically related and interact with opioid receptors on nerve cells in the body and brain.

• Societies have coveted the euphoria and pain relief provided by opioids since Ancient Sumerians referred to opium poppies as the “joy plant” circa 3400 B.C.
OpioidsOpiates:Opiates:
Semi-SyntheticSemi-Synthetic
SyntheticSynthetic
OpiumMorphineCodeineHeroinHydrocodoneHydromorphoneOxycodoneOxymorphoneBuprenorphineFentanylMethadoneTramadolCarfentanil

• These drugs attach to one or more of the four types of opiate receptors in the brain. When receptors are stimulated, they reduce pain without eliminating its cause.
• They produce sleepiness, euphoria and respiratory depression. And they slow gut function, leading to constipation. Mu receptor.
• Peak effects generally are reached in 10 minutes if taken intravenously—30‐45 minutes with an intramuscular injection, and 90 minutes by mouth.
• Pain and pleasure rank among nature’s strongest motivators, but when mixed, the two can become irresistible.
• This is how opioids brew a potent and deadly addiction in the brain.

• According to the CDC, the transition from an initial prescription to chronic use begins very early on.
• Even a one‐day opioid prescription carried a 6 percent risk of use at one year later and a 2.9 percent risk of use at three years later.
• The sharpest increases in the likelihood of long‐term use came at five days after the initial prescription, with another spike seen at one month.

• Patients given a longer‐lasting prescription—a week or a month—at the outset were the most likely to fall into long‐term use.
• Among people given enough pills for eight days or more, 13.5 percent were still using them a year later.
• Among those given a month‐long prescription, that rate climbed to 30 percent.

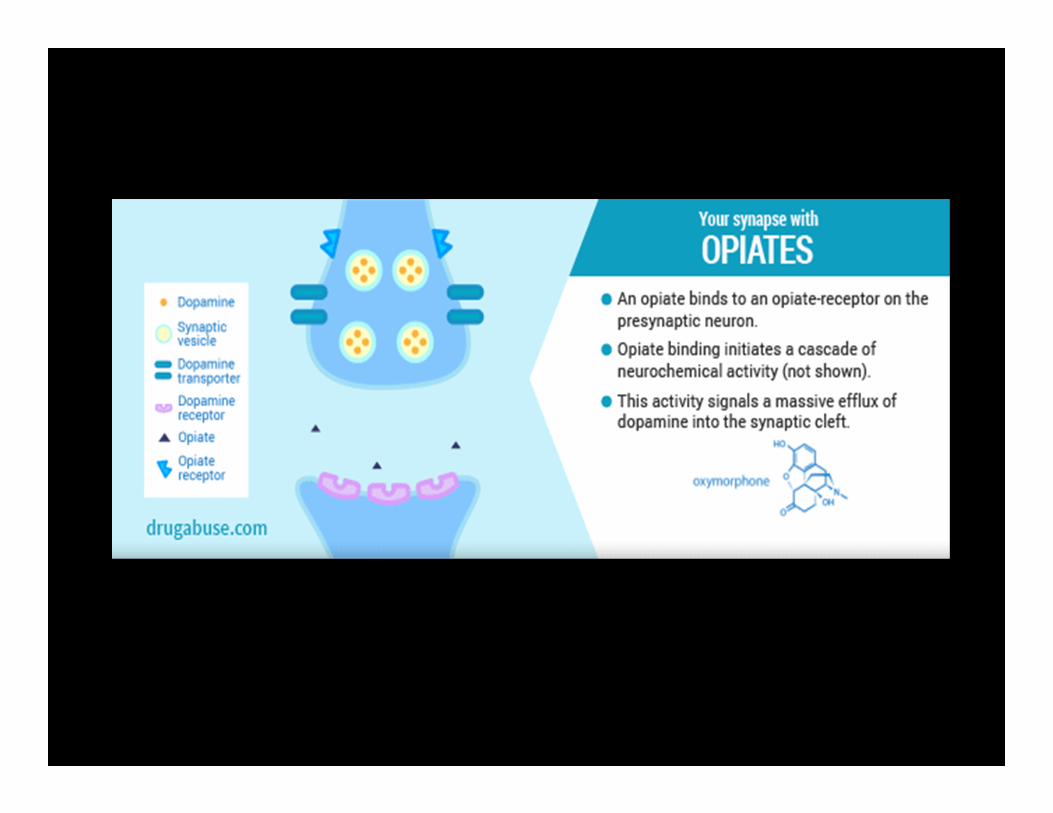
• Our brains are wired to ensure that we will repeat life‐sustaining activities by associating those activities with pleasure or reward. Whenever this reward circuit is activated, the brain notes that something important is happening that needs to be remembered, and teaches us to do it again and again, without thinking about it.
• The overstimulation of this system, which rewards our natural behaviors, produces the euphoric effects sought by people who misuse drugs and teaches them to repeat the behavior.
• Opioids target the brain's reward system by flooding the circuit with dopamine. Dopamine is a neurotransmitter present in regions of the brain that regulate movement, emotion, cognition, motivation, and feelings of pleasure.

• Respiratory depression is thechief hazard associated with opioid painkillers.
• When you take opiates, it slows thecentral nervous system, which in turns slows breathing. The more opiates you take, the more breathing can be slowed.

Ingested –pills or powder
Snorted – powdered or crushed pills
Smoked ‐ opium or heroin
Injected – powder or crystals cooked

64,000 people died from drug overdose in 2016
22% Rise over 2015 statistics
Overdose ranks as the leading cause of death in people in the United States in people under 50 years of age
95 million people reported using opioids last year
64,000 people died from drug overdose in 2016
Nearly 55,000 Americans died of car crashes at the peak of such deaths in 1972
More than 43,000 died due to HIV/AIDS during that epidemic's peak in 1995
Nearly 40,000 died of guns during the peak of those deaths in 1993


Adults aged 40 years and older are more likely to use prescription opioids than adults aged 20 – 39 years.
Women are more likely to use prescription opioids than men.
Non‐Hispanic whites are more likely to use prescription opioids than Hispanics and Non Hispanic blacks

•Federal and state officials have pushed for more treatment funding, including medication‐assisted treatment like methadone and buprenorphine.
•Some states, like Louisiana and Indiana, have taken a “tough on crime” approach that focuses on incarcerating drug traffickers.
•The incarceration approach has been around for decades — and it hasn’t stopped massive drug epidemics like the current crisis.



North Carolina loses a school bus worth of citizens every month to prescription opioid overdose.

Everyday in North Carolina
3 deaths a day in North Carolina from opioid overdose
For those three deaths there are:3 hospitalizations4 Emergency room visits
Cost: $1.3 Billion per the CDC for 2015

• Number of unintentional opioid‐related deaths 1,194 (2016, provisional)
• Total number of opioid pills dispensed 555,916,512 (2016)
• Number of EMS naloxone administrations 13,069 (2016)
•Number of community naloxone reversals 3,616 (2016)
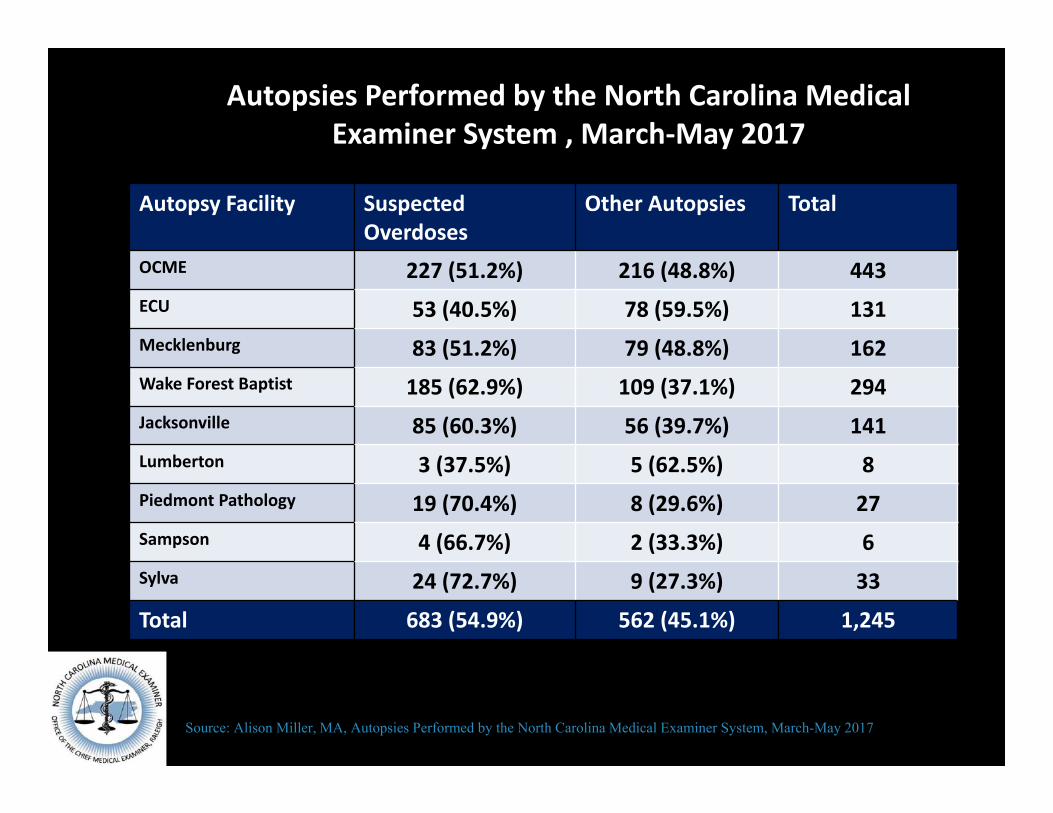
Autopsies Performed by the North Carolina Medical Examiner System , March‐May 2017
Source: Alison Miller, MA, Autopsies Performed by the North Carolina Medical Examiner System, March-May 2017
Autopsy Facility Suspected Overdoses
Other Autopsies Total
OCME 227 (51.2%) 216 (48.8%) 443ECU 53 (40.5%) 78 (59.5%) 131Mecklenburg 83 (51.2%) 79 (48.8%) 162Wake Forest Baptist 185 (62.9%) 109 (37.1%) 294Jacksonville 85 (60.3%) 56 (39.7%) 141Lumberton 3 (37.5%) 5 (62.5%) 8Piedmont Pathology 19 (70.4%) 8 (29.6%) 27Sampson 4 (66.7%) 2 (33.3%) 6Sylva 24 (72.7%) 9 (27.3%) 33
Total 683 (54.9%) 562 (45.1%) 1,245

According to American Society of Addiction Medicine (ASAM) opioidabuse costs employers approximately 10 billion dollars a year from absenteeism alone.
Half of all Americans are insured through the workplace
Opioid abusers cost employers nearly twice as much in healthcare expenses on average then non abusers. $19,450 versus $10,853
7.4% of Baby Boomers with an opioid prescription were classified as abusers versus 2.0% of Millennials.
•A recent study of more than 12,000 workers’ comp claims processed by Lansing, Mich.‐based Accident Fund Holdings found that when prescriptions for certain opioid painkillers were prescribed in workers’ comp injuries, claims were almost four times as likely to have a total cost of $100,000 or more compared with claims without any prescription.
•Although opioids are prescribed regularly when a worker is injured on the job, the Food and Drug Administration on‐labelapproved use of opioids is for cancer patients, AIDS patients and for surgery‐related pain.
•Studies have shown that for types of pain related to most workplace related injuries including musculoskeletal and soft tissue injuries, opioids are no more effective than NSAID’s or OTC pain relievers.

•Stop operating in denial
1. Create an environment where employees can disclose opioid‐related issues
Given the recent rise of opioid use, employers should consider encouraging employees to tell you when they have a problem or suspect that another employee may have an issue with prescription painkillers.
Balance the concern of being viewed as an employer who attempts to invade employees’ private home life with later dealing with an employee who quits, overdoses or creates a safety concern due to an addiction you may have ignored.The key to preventing opioid addiction is educating employees on the potential harmful impacts of abusing painkillers.

2. Reconsider zero‐tolerance drug‐testing policies
In light of the opioid epidemic, employers should consider removing any provision requiring automatic termination after the first positive drug test. Instead, amend the policy to include required counseling for employees who fail drug tests. This gives the employee a second chance to become “clean” and/or attempt to end their dependency, and it provides an opportunity to obtain much needed education and counseling on their condition.
The permitted use of prescription drug use at the worksite must also be clearly explained in the policy, and after OJI.

1: Clear written policy
• Good policy has never been more important.
• Objective measurements of impairment are difficult.
• Working in tandem with legal counsel, human resources and employee Relations is critical to ensure any policy includes protection for liability,Risk management and injury prevention.
SAMPLE POLICYProhibited BehaviorIt is a violation of our Drug‐Free Workplace Policy to use, possess, sell, trade, and/or offer for sale alcohol, illegal drugs, or intoxicants. Prescription and over‐the‐counter drugs are not prohibited when taken in standard dosage and/or according to a physician’s prescription. Any employee taking prescribed or over‐the‐counter medications will be responsible for consulting the prescribing physician and/or pharmacist to ascertain whether the medication may interfere with the safe performance of his/her job. If the use of a medication could compromise the safety of the employee, fellow employees, or the public, it is the employee’s responsibility to use appropriate personnel procedures (e.g., call in sick, use leave, request change of duty, notify supervisor, notify company doctor) to avoid unsafe workplace practices. The illegal or unauthorized use of prescription drugs is prohibited. It is a violation of our drug‐free workplace policy to intentionally misuse and/or abuse prescription medications. Appropriate disciplinary action will be taken if job performance deteriorates and/or incidents occur.
1: Informed at the point of prescription
2:Address Driving Issues
3:Discuss how opioid medication can affect work
4: Practice safety at home and work with opioids including:
Safe StorageSafe DisposalDon’t MixDon’t Share

It is in an employer’s best interest to identify opioid abuse and to supportconfidential access to treatment. Employer sponsored treatment is a costeffective solution.
While many companies have EAPs, few employees use them. Many employees don’t understand the value or may fear negative ramifications if they seek help.
Employee education on the company’s EAP services needs to clearly state whoan employee may talk to, how they can communicate with that resourceand where.
Employees also need to have details about their benefit plan coverage and aftercare

Seventy percent of all U.S. companies and 90 percent of Fortune 500 companies purchase Employee Assistance Programs (EAP) because these employers understand that EAPs improve the company’s bottom line.
Findings from 21 studies assessing the efficacy of corporatehealth and productivity programs found that EAPs have positive returns on investment.
All programs reported favorable returns ranging from $1.49 to $13.00 per dollar spent on the program. It is noteworthy that the mental health program showed one of the highest ROIs.

Treatment options• Opioid use results in profound biochemical changes in the
brain making this addiction challenging to overcome. • Recovery often requires long‐term treatment with
medications. Medication‐assisted treatment and ongoing aftercare can help people enter into and maintain recovery. However, employer support often helps.
• Research indicates that employer supported and monitored treatment yields better sustained recovery rates than treatment initiated at the request of friends and family members.
• There are three generally regarded forms of treatment:

Detox
• Detoxification from opioid addiction is accomplished in an inpatient setting or in a highly supervised outpatient setting.
• Detoxication alone is the least effective means of treatment.
• Most patients resume opioid use within six months of the detoxication process.
• A single detoxication episode should not be promoted as effective treatment.
Detox and Medication
• Detoxification followed by intensive counseling and a long‐acting injectable, naltrexone, is somewhat more effective than detoxication alone.
• Naltrexone is an opioid blocker that will negate the effects of opioids for four weeks; however, an individual may still have cravings for the opioids due to biochemical changes in the brain.

Medications• Medication replacement therapies with either methadone
or buprenorphine are very effective treatments for those who are motivated.
• Buprenorphine may cause less drowsiness or job impairment than methadone.
• Medication replacement therapy is the most effective treatment for opioid dependence and can be ofered on an outpatient basis.
• Because of serious biochemical changes that have occurred as a result of the abuse of opioids, many will often have to remain on medication for several months or a year and some for the remainder of their life.
1: Review of existing policies and updates for use of prescription opioids
2: Understanding of laws for prescription drug use at work
3: Signs of impairment and companies definition of reasonable causefor drug testing
CONTROLLED SUBSTANCE EXAMINATION REGULATION ACT: N.C. GEN. STAT. ANN. §§ 95‐230 TO 95‐239 AND 13 N.C. ADMIN. CODE 20.0101 TO 20.0602
The Controlled Substance Examination Regulation Act (CSERA) governs employment‐related drug testing in North Carolina. The CSERA does not require employers to conduct drug tests (N.C. Gen. Stat. Ann. § 95‐233). However, all North Carolina employers who perform employment‐related drug testing must follow the procedures in the CSERA (N.C. Gen. Stat. Ann. § 95‐232).
Employers may set the circumstances and conditions that trigger drug tests, for example:
•Post‐accident. •Random. •Safety‐sensitive. •Pre‐employment. •Follow‐up. •Reasonable suspicion.
(N.C. Dept. of Labor: CSERA Publication at 12.)

Florida Man Awarded $37,500 After Cops Mistake Glazed Doughnut Crumbs For Meth
•In December 2015, 64‐year‐old Daniel Rushing had just dropped off a friend at chemotherapy and was driving home an older woman from his church who worked at the 7‐Eleven and would otherwise walk the 2 miles home.
•…noticed some crystals on the floorboard of the car, and when officers used a field testing kit, the white substance tested positive for methamphetamine.
•Data from the state law enforcement lab in Florida found that 21 percent of the evidence recorded by police as methamphetamine was not in fact methamphetamine, and of that, half was not illegal drugs at all. "When we examined the department's records, they showed that officers, faced with somewhat ambiguous directions on the pouches, had simply misunderstood which colors indicated a positive result."

• Sedation, sleepiness• Slurred speech• Euphoria• Respiratory depression• Small pupils• Nausea, vomiting• Itching, flushing

• Unresponsive and unconscious
• Breathing is slow or has stopped• Muscle/Respiratory Rigidity• Overdose so quickly syringe may still be in arm (Fentanyl and Carfentanil)

•Call 911•Rescue breathing• Administer naloxone (Narcan)•Stay with person•Recovery position

911
• CALL FOR HELP (DIAL 911) • AN OPIOID OVERDOSE NEEDS IMMEDIATE MEDICAL ATTENTION. An essential step is to get someone with medical expertise to see the patient as soon as possible, so if no emergency medical services (EMS) or other trained personnel are on the scene, dial 911 immediately. All you have to say is “Someone is not breathing.” Be sure to give a clear address and/or description of your location.
CHECK FOR SIGNS OF OPIOID OVERDOSE
• Signs of OVERDOSE, which often results in death if not treated, include :
• Extreme sleepiness, inability to awaken verbally or upon sternal rub.
• Breathing problems that can range from slow to shallow breathing in a patient that cannot be awakened.
• Fingernails or lips turning blue/purple. • Extremely small “pinpoint” pupils. • Slow heartbeat and/or low blood pressure.

SUPPORT THE PERSON’S BREATHING
• Ventilatory support is an important intervention and may be lifesaving on its own. Patients should be ventilated with oxygen prior to administration of naloxone. In situations where oxygen is not available, rescue breathing can be very effective in supporting respiration. Rescue breathing for adults involves the following steps:
• Be sure the person’s airway is clear (check that nothing inside the person’s mouth or throat is blocking the airway).
• Place one hand on the person’s chin, tilt the head back and pinch the nose closed.
• Place your mouth over the person’s mouth to make a seal and give 2 slow breaths.
• The person’s chest should rise (but not the stomach). • Follow up with one breath every 5 seconds.

ADMINISTER NALOXONE• Any patient who presents with signs of opioid overdose, or
when this is suspected, should be administered naloxone. Naloxone injection is approved by the FDA and has been used for decades by EMS personnel to reverse opioid overdose and resuscitate individuals who have overdosed on opioids.
• Naloxone can be given by intranasal spray, intramuscular (into the muscle), subcutaneous (under the skin), or intravenous injection. The most rapid onset of action is achieved by intravenous administration, which is recommended in emergency situations. The dose should be titrated to the smallest effective dose that maintains spontaneous normal respiratory drive.
MONITOR THE PERSON’S RESPONSE
• All patients should be monitored for recurrence of signs and symptoms of opioid toxicity for at least 4 hours from the last dose of naloxone or discontinuation of the naloxone infusion. Patients who have overdoses on long‐acting opioids should have more prolonged monitoring.
• Most patients respond by returning to spontaneous breathing. The response generally occurs within 3 to 5 minutes of naloxone administration. (Continue rescue breathing while waiting for the naloxone to take effect.)
• Naloxone will continue to work for 30 to 90 minutes, but after that time, overdose symptoms may return.
• Therefore, it is essential to get the person to an emergency department or other source of medical care as quickly as possible, even if he or she recovers and feel better.

Naloxone (Narcan) will reverse the effects of opioids, reversing an overdose.
Simple nasal spray or injectable No effect other than blocking the opioidsNo adverse reactionsNo potential for abuse No potential for overdose
•Pharmacies in North Carolina have begun making naloxone available without a prescription.
•North Carolina is the third state in the country to issue a standing prescription order statewide for naloxone



Naloxone Formulations
Auto-injector
Kaleo Inc.
Narcan Nasal Spray
“Single‐Step”Adapt Pharma
Nasal with separate atomizer
“Multi-step”Amphastar
Pharmaceuticals
Intramuscular Injection
Various Companies

•If you are with a person who is overdosing, put them into the recovery position so they won’t choke on their own vomit.

Summary
• Opioids are major health concern to society • We need proactive forward thinking to combat this issue
• Stop acting in denial• Train everyone to understand signs and symptoms of dependency and emergent overdose
• Support recovery efforts.