aesthetic treatments around the eyes
TRANSCRIPT

8/13/2019 Aesthetic Treatments Around the Eyes
http://slidepdf.com/reader/full/aesthetic-treatments-around-the-eyes 1/6
on the
www.medestheticsmagazine.com | July/August 2007
By Inga Hansen
The eyes are among the first features we notice when we meeta new person. They define a person’s face and, to our chagrin,
they love to display our age. The delicate skin around the eyes
is prone to fine lines, hyperpigmentation and skin laxity. As a re-
sult, treatments to address problems around the eyes are among
the most requested cosmetic services. To help you design the
most comprehensive treatments for the eye area, we spoke with
four Medesthetics advisory board members to discuss how they
would approach the five most common cosmetic concerns that
manifest around the eyes: dark undereye circles, fine lines, deep
lines, undereye bags and drooping upper eyelids.
P h o t o :
R a n d y B u t l e r
8/13/2019 Aesthetic Treatments Around the Eyes
http://slidepdf.com/reader/full/aesthetic-treatments-around-the-eyes 2/6
on the
DARK UNDEREYE CIRCLES
Katz: You have to determine whythe patient has the dark circles.If they are due to telangiectasiasin the eye area, we use a vas-cular pulsed dye laser. Usuallyone session will take care of it,maybe two. You do need to usehigh heat because you’re treat-ing vessels. As a result somepeople will experience swellingand bruising for a day or two af-ter the treatment.
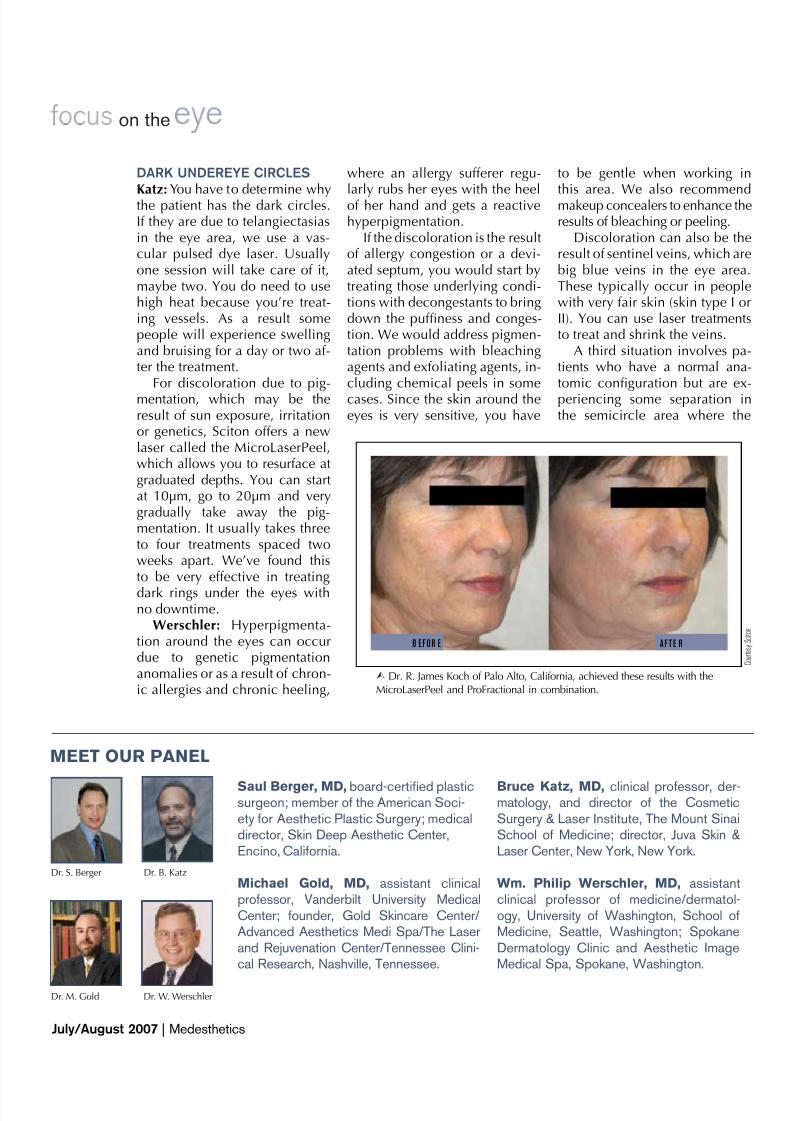
For discoloration due to pig-mentation, which may be theresult of sun exposure, irritationor genetics, Sciton offers a newlaser called the MicroLaserPeel,which allows you to resurface atgraduated depths. You can startat 10µm, go to 20µm and verygradually take away the pig-mentation. It usually takes threeto four treatments spaced twoweeks apart. We’ve found thisto be very effective in treating
dark rings under the eyes withno downtime.
Werschler: Hyperpigmenta-tion around the eyes can occurdue to genetic pigmentationanomalies or as a result of chron-ic allergies and chronic heeling,
where an allergy sufferer regu-
larly rubs her eyes with the heelof her hand and gets a reactivehyperpigmentation.
If the discoloration is the resultof allergy congestion or a devi-ated septum, you would start bytreating those underlying condi-tions with decongestants to bringdown the puffiness and conges-tion. We would address pigmen-tation problems with bleachingagents and exfoliating agents, in-cluding chemical peels in somecases. Since the skin around theeyes is very sensitive, you have
to be gentle when working in
this area. We also recommendmakeup concealers to enhance theresults of bleaching or peeling.
Discoloration can also be theresult of sentinel veins, which arebig blue veins in the eye area.These typically occur in peoplewith very fair skin (skin type I orII). You can use laser treatmentsto treat and shrink the veins.
A third situation involves pa-tients who have a normal ana-tomic configuration but are ex-periencing some separation inthe semicircle area where the
B E F O R E A F T E R
C o u r t e s y S c i t o n
Ÿ Dr. R. James Koch of Palo Alto, California, achieved these results with theMicroLaserPeel and ProFractional in combination.
Saul Berger, MD, board-certified plasticsurgeon; member of the American Soci-ety for Aesthetic Plastic Surgery; medicaldirector, Skin Deep Aesthetic Center,Encino, California.
Michael Gold, MD, assistant clinicalprofessor, Vanderbilt University MedicalCenter; founder, Gold Skincare Center/Advanced Aesthetics Medi Spa/The Laserand Rejuvenation Center/Tennessee Clini-cal Research, Nashville, Tennessee.
Bruce Katz, MD, clinical professor, der-matology, and director of the CosmeticSurgery & Laser Institute, The Mount SinaiSchool of Medicine; director, Juva Skin &Laser Center, New York, New York.
Wm. Philip Werschler, MD, assistantclinical professor of medicine/dermatol-ogy, University of Washington, School ofMedicine, Seattle, Washington; SpokaneDermatology Clinic and Aesthetic ImageMedical Spa, Spokane, Washington.
MEET OUR PANEL
Dr. S. Berger Dr. B. Katz
Dr. M. Gold Dr. W. Werschler
July/August 2007 | Medesthetics

8/13/2019 Aesthetic Treatments Around the Eyes
http://slidepdf.com/reader/full/aesthetic-treatments-around-the-eyes 3/6
on the
eye skin becomes cheek skin.
When patients come in andcomplain about their lower eye-lid being puffy, baggy and blue,most of the time it’s an age-relat-ed change. In this situation youhave two intervention options.The first is to refer the patient toa surgeon for a mid-face-lift. Oryou can use a filling substancein the lower eyelid to artificiallyrecreate thicker tissue in the areato minimize that transition line atthe arcus marginalis.
Berger: For people who havedarker pigmentation, which isoften genetic, I can offer no mag-ic bullets. A lot of these peoplerely on makeup and lighteningcreams around the lower eyelidwith mixed results.
In patients where the darkerundereye area is related to con-tour—fat protruding or a groovebetween the fat bag and the nosein the nasojugal groove—you
can get good results with wrinklefillers or fat transfer. If you’re asurgeon operating on the lowerlid, you can also take that op-portunity to release some of theindented areas and fill them, soyou have a number of options forthese patients.
FINE LINES
Katz: Botox (Allergan) is a goodway to start, and it solves theproblem pretty quickly. I mayuse the MicroLaserPeel as well.It works well for both squint linesand discoloration.
Gold: I would start with topi-cals. Clinical studies over theyears have shown that both OTCand prescription retinoids arebeneficial in reducing wrinkles,and using retinoids allows thepatient to be involved in hertreatment. Ten years ago we’dinject collagen very carefully. To-day there’s no question that Bo-tox is the treatment of choice forlines around the eye area. I thinkthere’s enough clinical evidencein the literature that says com-bining intense pulsed light andBotox improves the effect of theBotox. The Botox lasts three tofour months, and with IPL we dothree to six treatments spaced a
month apart and prescribe reti-noids for home care.
Werschler: I divide fine linesinto two categories—dynamiclines of motion or static lines.If they’re static I offer chemicalpeeling around the eyes—againyou need to be very gentle in
this area—or a hyaluronic acid
filler. Undereye wrinkle creamsthat use a large molecular weightprotein to absorb water and swellthe epidermis are also helpful.For dynamic lines, I would use alittle Botox.
Berger: Generally, fine linesaround the eyes are in either thelower lid skin or the crow’s feetarea. The most effective optionsfor these are Botox to relax themuscle activity in the area, or la-ser or light resurfacing therapies,including the Fraxel (ReliantTechnologies). Your third optionwould be to surgically removesome of the skin or muscle bulkand tighten the area.
DEEP LINES
Katz: Deep lines don’t typicallyrespond to Botox; we usually dolaser resurfacing with either theFraxel, the Affirm (Cynosure) orthe Pixel (Alma Lasers). They do
require multiple sessions but thepatient experiences very little orno downtime.
Gold: We currently have Cos-moderm and Cosmoplast (Aller-gan) that work well to fill linesaround the eyes. When RestylaneFine Lines (Medicis Aesthetics)becomes available, I think it willalso be a good option for deeplines and wrinkles in the eyearea. These very superficial fillers
can also be used to augment Bo-tox treatments, which remain thebest option for dynamic lines.
If you have very deep lines,and Botox isn’t sufficient or thepatient doesn’t want Botox, Iget into laser resurfacing. Wewould talk to the patient abouterbium peels, fractional resurfac-ing, pulsed dye laser and CO2.They all work; it just depends onhow many treatments the patient
wants and how much downtimeshe can tolerate.
B E F O R E A F T E R
C o u r t e s y R e l i a n t T e c h n o l o g i e s
Ÿ Dr. Z. Rahman used the Fraxel (Reliant Technologies) to smooth the crow’s feet forthis happy patient.
July/August 2007 | Medesthetics
8/13/2019 Aesthetic Treatments Around the Eyes
http://slidepdf.com/reader/full/aesthetic-treatments-around-the-eyes 4/6

8/13/2019 Aesthetic Treatments Around the Eyes
http://slidepdf.com/reader/full/aesthetic-treatments-around-the-eyes 5/6
on the
patients, the primary need is to
address the fat under the eye.For others, it’s more important totighten the lower eyelids beause thesupport of the lower lid is weak.
DROOPING UPPER EYELIDS
Gold: We in dermatology look atthese patients and ask what are thenonsurgical options? Botox maybe an option if you’re an expert
injector. But if we have a patient
who needs surgery to correct thedrooping, then we refer her to anocular plastic surgeon.
If a patient comes to me andsays, “I don’t want surgery,” welook at resurfacing and skin tight-ening lasers. We also have radio-frequency and pulsed light skintightening equipment. There aremultiple skin tightening devicesincluding the new Thermage foreyes and the Aluma (Lumenis),which is a bipolar radiofrequen-cy with a vacuum device. Op-tions do exist but you have to berealistic. Surgery is still the treat-ment of choice.
Werschler: For eyelid laxity,surgical intervention is the goldstandard, and we can’t forget
B E F O R E A F T E R
C o u r t e s y o f A l m a L a s e r s
Ÿ Use of the Alma Lasers Pixel achieved nice tightening of the upper eyelid in this patient.
July/August 2007 | Medesthetics

8/13/2019 Aesthetic Treatments Around the Eyes
http://slidepdf.com/reader/full/aesthetic-treatments-around-the-eyes 6/6
that. But there are patients who
don’t want surgery or can’t affordit. For those patients we offerThermage for eyelids, which isprobably better in terms of pre-dictability and the “wow” factorof results than Thermage in oth-er areas of the body. Any LLRO(laser, light, radiofrequency andoptical) tightening treatmentaround the eyes can be helpful.
With the upper lid, you eitherhave increased tissue of the up-per eyelid (blepharoptosis) oryou have a browtosis where thebrow is falling down and causingthe eyelids to droop a little bit.You need to determine what’scausing the drooping. In men it’soften browtosis; in women it’soften a combination of the two.
If it’s the brow, your choicesare referral to a surgeon for atraditional brow lift or sometightening with a laser or radio-frequency system. Thermage, IPL
or Elos (Syneron) all tend to liftthe brow nicely. Properly inject-ing Botox can also repositionthe brow.
Berger: When a patient comesin for a surgical consult, we lookat the brow, the upper eyelid andthe lower eyelid. We look at theskin, the fat and the anatomyof the area to determine whatmakes the patient appear a cer-tain way; what things are struc-
tural and what things are func-tional; what things are workingright and what is weak, loose orin need of repair.
We may find that the problemis indeed excess skin that hasstretched over time, but the prob-lem may also be that the amountof skin on the upper lid is prettynormal but the brow is too low.Doctors who don’t do a lot ofbrow surgery may not appreci-
ate the fact that a brow lift in aparticular patient is necessary,
and that can be a formula for
poor results. Once the surgeonremoves the skin from the eye-lid, that individual is trappedbecause if you lift the browat that point, the patient can’teven close her eyes. My basic
approach is to make a good as-
sessment and diagnosis and thentreat the components.
Inga Hansen is a Los Angeles-based
freelance writer and Medesthetics
contributing editor.
www.medestheticsmagazine.com | July/August 2007