advising cancer survivors about lifestyle. a selective review of the
TRANSCRIPT

1
National Cancer Survivorship Initiative
Supported Self-Management Workstream
ADVISING CANCER SURVIVORS ABOUT
LIFESTYLE
A SELECTIVE REVIEW OF THE
EVIDENCE
Macmillan Cancer Support
July 2010
Nicola J Davies
Professor Robert Thomas
Lynn Batehup
2
Any comments or enquiries regarding this review are welcome
Nicola Davies BSc (Hons) MSc Comm PhD Researcher
Evaluation and Research Coordinator Self-Management Workstream National Cancer
Survivorship Initiative Macmillan Cancer Support
NDaviesmacmillanorguk
Robert Thomas MRCP MD FRCR
Visiting Professor Cranfield University
Consultant Oncologist Bedford Hospital amp Addenbrookelsquos Hospital Cambridge University
NHS Trusts co The Primrose Unit Bedford Hospital Bedford MK42 9DJ
Lynn Batehup BSc (Hons) MSc Nursing and Research PG Dip Health Economics
Research
Project Manager Self-Management Workstream National Cancer Survivorship Initiative
Macmillan Cancer Support Lbatehupmacmillanorguk
3
CONTENTS
Contents 3
Exectuive Summary 4
Background 8
The Purpose of this Review 12
Method and Search Strategy 14
Results 16
Part 1 Cancer Survival - Evidence for the Role of Lifestyle in Disease 17
Progression and Recurrence
Part 2 Lifestyle Evidence for Reducing and Managing Risks and Side-Effects 71
of Cancer Treatment
Cancer-Related Fatigue 72
Lymphoedema 80
Osteoporosis and Bone Health 85
Weight and Body Composition 93
Quality of Life 99
Ongoing Lifestyle Studies 110
Discussion 113
Appendix A Evidence-Based Dietary Self-Management Recommendationshelliphelliphelliphellip122
Appendix B Evidence-Based Physical Activity Recommendations 123
Referenceshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip124
4
Lifestyle Guidance for Cancer Survivors ndash Executive Summary
1 This aim of this review was to update the World Cancer Research Fund (WCRF)
report bdquoA Systematic Review of RCTs Investigating the Effect of Nutritional and
Physical Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This
has been achieved by conducting a comprehensive but pragmatic search of the
literature from 2006 onwards Where no evidence was available in the WCRF
review studies before 2006 have been included if identified in the reference lists of
acquired records To facilitate this evidence cited within the lsquoHandbook of Cancer
Survivorship‟ (Feuerstein 2006) and findings from a non-systematic review
conducted by the Cancer and Palliative Care Rehabilitation Workforce (2009) were
also utilised
2 There is now persuasive evidence that a healthy lifestyle during and after cancer is
associated with improved physical and psychological well-being reduced risks of
treatment enhanced self-esteem reduced risk of recurrence and improved survival
Clarifying the individual anti-cancer components of a healthy lifestyle will require
extensive further evaluation and even then they are likely to be multi-factorial
3 Despite gaps in the evidence for lifestyle benefits in cancer survivors there are some
key lifestyle recommendations that can be provided (Appendix A and B)
o Dietary Recommendations Reduce saturated fats increase fish intake
consume a varied diet in order to ensure adequate intakes of vitamins and
essential minerals increase consumption of green and cruciferous vegetables as
well as brightly coloured fruits and vegetables that contain carotenoids
o Physical Activity Recommendations There is substantial evidence suggesting
that the physical activity recommendations developed by the Department of
Health are sufficient for most cancer survivors - a total of at least 30-minutes a
day of moderate intensity physical activity on five or more days of the week
Additionally there is evidence of a dose-response (ie the more physical
activity the greater any benefits) Even a modest amount of exercise is
beneficial and will see gains versus doing nothing at all Body composition
changes are common in many cancer patients with the reasons varying by site
Compromised lean body mass for patients with head and neck and
gastrointestinal cancers are common and in this group exercise to build lean
muscle will be relevant However in breast cancer some treatments can lead to
significant weight gain (exacerbated if pre- diagnosis BMI is not in the healthy
range) and exerciseactivity which is more useful for controlling body weight and
losing fat will be more important
o Weight Excess weight should be avoided (ie a body mass index of 25-
29kgm or above There is also evidence that maintaining a stable healthy weight
as opposed to fluctuating between a healthy and unhealthy BMI can offer health
5
benefits for cancer survivors The evidence is strongly suggestive of weight being
implicated in breast cancer outcomes with the mechanism of benefit achieved
via physical activity or a low-fat diet most likely being due to weight loss
o Smoking Strong and consistent evidence has been presented for increased risk
of disease progression and mortality in people who continue to smoke after a
diagnosis of cancer as well as poorer outcomes in pre-diagnosis smokers
o Alcohol There is a paucity of research into the effects of alcohol pre- and post-
diagnosis on cancer progression and recurrence as well as symptom
management Evidence thus far is highly contradictory although excess alcohol
is linked to increased weight which does have negative outcomes
4 Evidence is also available for the benefits of individual lifestyle components for
specific cancer types
o A high intake of soy has been found to alter testosterone (the male sex
hormone) reducing risk of prostate cancer
o Dietary fibre might offer protection against colorectal cancer or recurrence via
increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic
mucosa (tissue that lines the colon)
o Since physical activity can alter levels of oestrogen (the female sex hormone)
evidence indicates that it might be protective against breast cancer
5 There is a wealth of evidence for physical activity during and after treatment
improving symptoms of cancer-related fatigue and increasing energy and stamina It
is also clear that a needs-based approach should be adopted ndash based on the
assessed need for improvements on low fatigue levels poor quality of life low
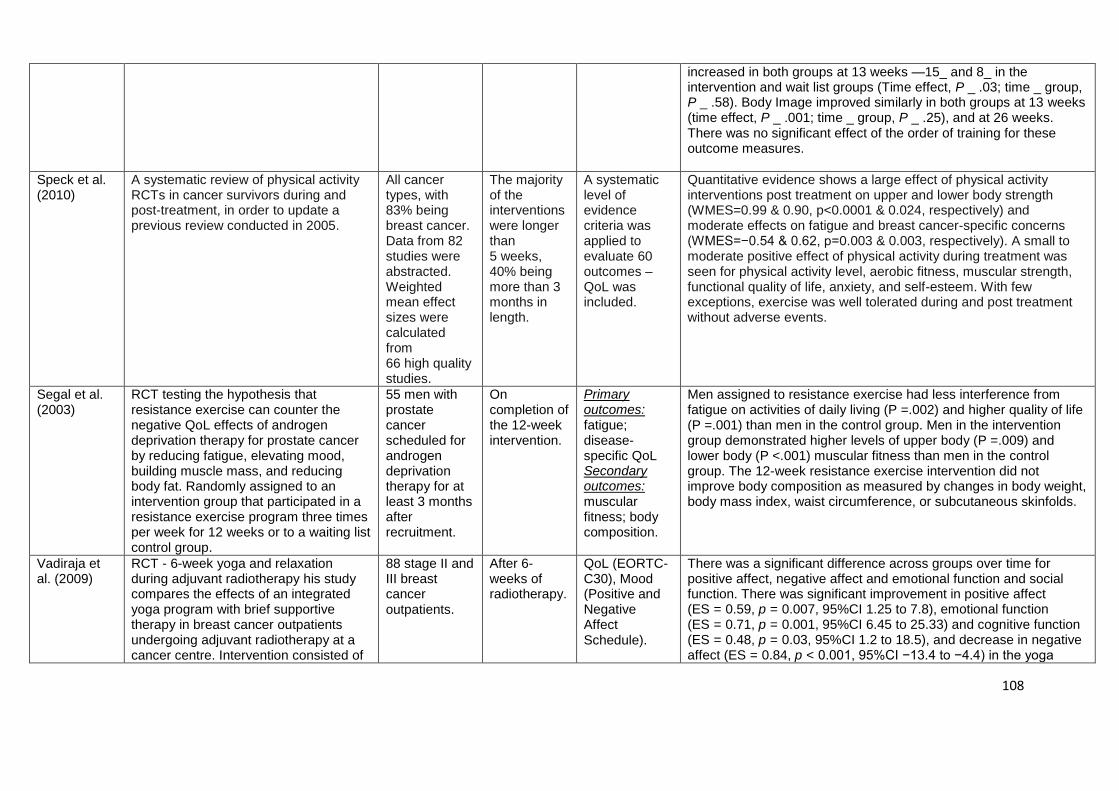
physical function (Speck et al 2009)
6 Guided progressive physical activity soon after treatment can ease the symptoms of
lymphoedema Avoidance of physical activity through fear of exacerbating symptoms
is unwarranted if physical activity is supervised and closely monitored
7 Whilst the benefits of physical activity on bone health require clarifying physical
activity can at the very least prevent loss of bone mineral density in survivors at
particular risk of developing osteoporosis
8 Even when not directly associated with overall QoL exercise has been found to
significantly improve social functioning among post-treatment survivors The benefits
of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or
group-based The evidence that physical activity can improve body image may be
one of the mechanisms through which exercise can improve quality of life
6
9 Mechanisms of benefit for diet and physical activity include the influence that these
behaviours have on hormones and insulin levels This has sparked the question of
whether pharmacological alternatives such as aromatase inhibitors and metformin
which tend to produce greater reductions in cancer risk pose competition for lifestyle
interventions This is unlikely as healthy lifestyle behaviours contribute overall to
general health and to the risk reduction for other co-morbid conditions such as
hypertension cardiac disease and diabetes Usefully the competencies framework
offered by Finders University highlights the importance of taking a holistic approach
to supported self-management whereby support is provided for a continuum of
health as opposed to a focus on one established chronic condition Based on this
model supported self-management should provide health promotion and illness
prevention not merely in terms of cancer but also for associated risks and co-
morbidities
10 The challenge remains in integrating lifestyle support into standardised models of
aftercare for cancer survivors particularly in terms of engaging both patients and
health professionals bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative identifies the need to
provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for
healthcare professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
11 The literature identifies the need for individual assessment and risk stratification for
cancer survivors so that lifestyle interventions and support can be tailored and
provided according to need Particularly high need groups are survivors who have
co-morbidities are overweight sedentary or smoke
12 Some questions that remain
o What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
o How can people most likely to benefit from lifestyle interventions be effectively
identified
o What are the various intensities of lifestyle support that can be provided based on
levels of individual need
13 Significant limitations can be found in the evidence available for lifestyle outcomes in
cancer survivors including
7
o Long-term outcomes of lifestyle choices
o Low levels of adherence to interventions
o A paucity of studies addressing external validity
o Equality across tumour groups
o Lack of cultural considerations pertaining to dietary advice
o A paucity of individualised lifestyle advice and tailored support
8
BACKGROUND SETTING THE SCENE
Lifestyle and Well-Being
In an independent report offering recommendations on enabling effective delivery of health
and well-being in England Bernstein Cosford and Williams (2010) advise that setting clear
priorities for health and well-being should start with behavioural risk factors Namely they
recommend tackling the biggest lifestyle influences on population health tobacco alcohol
physical inactivity and poor diet These four lifestyle factors are among the biggest
contributors to most preventable diseases across all social groups and in all areas of
England They are responsible for 42 of deaths from leading causes (WHO 2005) and
together they account for at least pound94 billion in annual direct costs to the NHS (DH 2009a)
expenses incurred outside the NHS would increase this figure further
An increase in longevity and the number of people living with one or more chronic conditions
for a longer period of time has led to government action aimed at making these years as
healthy as possible Interest has been particularly paid to the role of these behavioural risk
factors and the role of lifestyle in improving or maintaining health preventing illness
managing symptoms and achieving a satisfactory quality of life (QoL) (Pedersen and Saltin
2006 Taylor et al 2004)
The term lifestylelsquo refers to personal choices that might impact health such as diet physical
activity smoking and alcohol consumption The World Health Organisation (WHO 1999)
defines a healthy lifestylelsquo as
ldquoa way of living that lowers the risk of being seriously ill or dying earlyrdquo with the
emphasis that ldquohealth is not just about avoiding disease It is also about physical
mental and social well-beingrdquo (p 2)
With earlier detection and more efficacious treatments available for cancer there has been
an increase in survival as well as in the number of people living with the long-term
consequences of cancer treatment Subsequently cancer has become a chronic disease for
a number of people among the two million cancer survivors in the UK (Maddams Moller and
Devane 2008) Whilst evidence of the effects of a healthy diet and sufficient physical activity
in cancer prevention has been well-documented (Chan Gann and Giovannucci 2005
Sonn Aronson and Litwin 2005) it has become of fundamental importance to examine the
role of these lifestyle choices in cancer survivorship Furthermore the role of lifestyle in
cancer survivorship needs to be examined not only in terms of improved physical and
psychological well-being but also disease outcomes
Given the relationship between choosing a healthy lifestyle and taking an active role in the
self-management1 of the long-term effects of cancer and its treatment the self-management
workstream of the National Cancer Survivorship Initiative (NCSI) have conducted this
1 lsquoSelf-managementrsquo has been defined as ldquoawareness and active participation by the person in their recovery
recuperation and rehabilitation to minimise the consequences of treatment promote survival health and well-beingrdquo (NCSI 2009)
9
evaluation of evidence pertaining to lifestyle factors and survivorship Not only are lifestyle
choices important in terms of disease progression and recurrence but also in the effective
management of other chronic symptoms and conditions resulting from treatment such as
cancer-related fatigue lymphoedema and osteoporosis (Doyle et al 2006) Lifestyle
support and education is evidently an important component of supported self-management2
for many individuals living with or beyond cancer (Davies and Batehup 2010) Indeed as
part of a consensus meeting and evidence review self-management support and lifestyle
management were among the top ten priorities for survivorship research (Richardson et al
2009) providing further rationale for the current review
The Health of Cancer Survivors
The traditional belief has been that people with cancer should rest reduce activity and avoid
activities involving intense physical effort in other words they are passive patients of the
disease and its treatment Consequently physical activity levels do decline substantially
during and after completion of treatment for cancer and often fail to return to pre-diagnosis
levels for many people (Daley et al 2008) Fortunately it is becoming increasingly
recognised that people living with or beyond cancer do need physical activity will not be
harmed by physical effort and are active participants in the rehabilitation process
Furthermore emerging evidence is demonstrating that lifestyle factors can influence the rate
of cancer progression improve quality of life (QoL) reduce side-effects and risks during
treatment reduce the incidence of relapse and improve overall survival (Thomas Daly and
Perryman 2000) Besides the beneficial effect on recurrence a healthy diet and regular
physical activity has the potential to reduce the risk of co-morbidity such as other cancers
cardiovascular disease and diabetes etc (Jones and Demark-Wahnefried 2006)
Research suggests that although many cancer survivors report making healthy lifestyle
changes after diagnosis these changes may not be generalisable to all populations of
cancer survivors and they are often temporary (Demark-Wahnefried and Jones 2008)
Furthermore evidence suggests that the healthy lifestyle behaviours adopted by cancer
survivors tend to be directed towards clinical action such routine physical examination rather
than those health behaviours that require daily effort such as healthy eating or regular
physical activity (Findley and Sambamoorthi 2009)
A potential explanation for this difference in the uptake of clinical versus lifestyle preventive
health behaviours is that the former is easier due to the primary action being carried out by
someone else The latter on the other hand requires personal time and effort as well as
opportunity socially economically and in terms of health literacy and educational status
Behavioural and lifestyle change is notoriously difficult but even more so for people with
cancer or other chronic conditions let alone those with co-morbidities (Krein et al 2005) For
people with co-morbidities a healthy lifestyle can be even more challenging as they grapple
with the competing demands posed by the self-management of multiple conditions (Lindsay
2009)
2 lsquoSupported self-managementrsquo has been defined as ldquoWhat health and social care professionals and service
delivery organisations to do support self-managementrdquo (NCSI 2009)
10
Given the increase in survivorship the higher rates of co-morbidity within this population
and evidence that diet physical activity and other lifestyle factors affect risk for other cancers
and other chronic diseases there is a clear need for lifestyle interventions that target this
high risk group The literature suggests the need for individual risk assessment and the
provision of support with lifestyle changes in those individuals identified as high risk ndash such
as survivors who have co-morbidities are overweight sedentary or smoke (Davies and
Batehup 2010)
The Lifestyle Needs of Survivors
The National Cancer Survivorship Initiative (NCSI) highlights that people living with or
beyond cancer would like to play a more active role in their healthcare They want to know
how to look after themselves after a cancer diagnosis including information and support on
the lifestyle changes they should make so they can return to normallsquo life as much as
possible (Macmillan Cancer Support 2008) Yet the evidence suggests that this need
remains largely unaddressed In a key mapping project commissioned by the NCSI
Research workstream a number of issues pertaining to lifestyle were identified for the four
most common cancers breast colorectal lung and prostate (NCSI 2009) Each of these
four reports which were conducted by independent organisations demonstrated gaps in the
provision of lifestyle advice and support mainly during the period of aftercare In a similar
report mapping the needs of rarer cancers prolonging life through changes to lifestyle
emerged as a frequent theme by survivors asked to explore the meaning of cancer
survivorshiplsquo (Cancer52 and NCSI 2009) There was particular emphasis on the need for
diet and physical activity advice post-surgery for oesophageal cancer as well as diet advice
for mouth and throat cancers Change in bowel habits is frequently reported among post-
treatment bowel cancer survivors requiring support with dietary changes (Nikoletti et al
(2008)
In an effort to provide further insight into lifestyle advice and support for cancer survivors as
well as developing evidence-based lifestyle interventions a comprehensive review of the
evidence for lifestyle and cancer outcomes is required The perceived outcome efficacy3 of
making lifestyle changes is important in terms of whether those changes are initiated or not
as well as whether an individual possesses the confidence (self-efficacy) to maintain lifestyle
changes Outcome efficacy could be increased by the accumulation of firmly established
evidence offered alongside the opportunity for lifestyle support
Additionally this evidence needs to be evaluated in respect of current national guidelines for
diet physical activity and other lifestyle indicators such as weight and alcohol consumption
Briefly national guidance recommends a diet comprising 33 fruit and vegetables (five
portions per day) 33 starchy foods (rice bread pasta potatoes) 15 milk and dairy
foods 12 protein (meat and fish) and 8 foods and drinks high in fat andor sugar (Food
Standards Agency 2007) Adults are advised to achieve a total of at least 30-minutes daily
moderate intensity physical activity on five or more days of the week (DH 2004) Combined
with a healthy diet regular physical activity is aimed at maintaining a Body Mass Index
3 The belief that a particular outcome will result from following certain actions or behaviours
11
(BMI)4 of 185-249kgm2 25-29 is considered to be overweight and 30 or above as obese
whilst under 185 is considered underweight (National Obesity Observatory 2009)
A healthy lifestylelsquo is the same for cancer survivors as for the general population or indeed
people with other chronic conditions (Bellizzi et al 2005 Caan et al 2005 Coups and
Ostroff 2005) Cancer survivors are slightly more likely to follow physical activity guidelines
but overall their health behaviours mirror those of the general population which is marked by
inactivity and an epidemic of obesity and associated problems (Caan et al 2005) Despite
this the lifestyle advice and tailored care currently provided for specific groups of people in
the general population such as exercise prescriptions (DH 2001) is not yet integrated into
the supportive care needs of cancer survivors (Addington-Hall 2010) This is in the main
due to reluctance (usually related to knowledge and confidence) from health professionals to
discuss lifestyle factors with cancer patients due to limitations in knowledge and an
inadequacy in the available evidence on the underlying mechanisms of benefit for individual
lifestyle factors (Miles Simon and Wardle 2010) It is anticipated that this review will allay
some of this reluctance by identifying where the evidence strongly supports the efficacy of
lifestyle factors in cancer outcomes as well as where the evidence is less clear and requires
further research
4 BMI is a statistical measure which compares a persons weight and height to estimate a healthy body weight
12
The Purpose of this Review
Using the outlined national guidance on lifestyle and taking account of evidence for specific
elements or intensity of certain lifestyle factors in cancer care and self-management a
review of the literature on lifestyle and survivorship will be conducted The primary aims are
to produce evidence that can support professionals in guiding and advising cancer survivors
as well as evidence regarding resources which might support patient self-management in
relation to lifestyle factors and behaviour change The review will be comprehensive but
pragmatic drawing on a variety of sources This will commence by updating a recent review
conducted by the World Cancer Research Fund (WCRF) - bdquoA Systematic Review of RCTs
Investigating the Effect of Diet and Physical Activity Interventions on Cancer Survival‟
(Bekkering et al 2006)5
The aim of the WCRF review (Bekkering et al 2006) was to systematically locate and
review all randomised control trials (RCTs) which tested the effect of diet andor physical
activity interventions in cancer survivors their definition of a cancer survivor being
ldquoanyone who has been diagnosed with cancer from the time of diagnosis through the
rest of liferdquo (Brown et al 2003)
They conducted a systematic search of MEDLINE (from 2000 onwards) EMBASE (from
1999 onwards) AMED (from 1985 onwards) and the Cochrane Library including DARE
CDSR CENTRAL and HTA (all years) up to March 2006 scanned key texts that were
relevant to the subject field and scanned the references of relevant reviews They identified
117 trials (Table 1)
Table 1 Trials Identified in the WCRF Review (Bekkering et al 2006)
Trials Total
Diet
Food-based
Supplement-based
23
71
Physical activity
23
Total 117
5 This has been highlighted by the American Cancer Society (ACS) as being one of the most comprehensive
reviews on diet and physical activity for cancer survivors The ACS has used the review alongside other sources to produce lsquoGuidelines on Diet and Physical Activity for Cancer Preventionrsquo (Kushi et al 2006)
13
The findings will be described along with the results of the current review The overall
conclusion drawn by Bekkering et al (2006) was that there is a paucity of robust evidence
on the effects of diet and physical activity interventions in the management of cancer RCTs
were generally small and often reported inadequate details to formally assess quality While
promotion of a generic healthy diet was associated with reduced overall mortality the degree
to which lifestyle accounted for this outcome was imprecise It was concluded that given the
large investment in potential lifestyle interventions among cancer survivors large-scale trials
adequately powered to provide robust conclusions should be supported and conducted
In updating the WCRF review (Bekkering et al 2006) further scoping of the literature from
2006 to February 2010 will be conducted along with a synthesis of the evidence presented
in the lsquoHandbook of Cancer Survivorship‟ edited by Michael Feuerstein (2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (National Cancer Action Team 2009) which evaluates literature
pertaining to rehabilitation
The primary aim of the review is to guide healthcare planning and the development of
supported lifestyle self-management interventions for high risk groups In order to be able to
consider the production of useable evidence-based guidance for self-management for both
patients and professionals the following evidence will be sought
Evidence that would support professionals to be able to guide and advise
patients
Evidence regarding resources which would support patient self-management in
relation to lifestyle factors and behaviour change
It is anticipated that recent efforts to conduct research in this area will facilitate the
clarification of any key recommendations that can be made to cancer survivors by healthcare
professionals This update of the evidence will also attempt to establish where the strength
of the evidence lies and where more research is required
14
METHOD
Search Strategy
In updating the WCRF review (Bekkering et al 2006) RCTs and systematic reviews were
obtained from a systematic search of the Cochrane Library Database and Pubmed (from
March 2006 to February 2010) Where no evidence was available in the WCRF review
studies before 2006 have been included if identified in the reference lists of acquired
records this is the case with studies on smoking which were not included in the Bekkering
et al (2006) review
The selected relevant chapters were read from the bdquoHandbook of Cancer Survivorship‟
(Feuerstein 2006)6 and relevant studies referred to from the Cancer and Palliative Care
Rehabilitation Workforce (2009) non-systematic review Grey literature was also utilised
where this would provide information relevant to the review or where cancer-specific
literature was lacking as was the case with osteoporosis
All titles and abstracts of studies identified by the searches were scanned for relevance in
terms of topic and participant group For any titles or abstracts that were potentially relevant
full paper manuscripts were obtained and the relevance of each study assessed according to
the pre-specified inclusion criteria
6 Chapters include Physical Activity Potential Benefits and Guidelines DietWeight Management
Search terms cancer OR neoplasm
AND diet OR exercise OR physical
activity OR weight OR lifestyle
Cochrane systematic reviews
925 records
PubMed
4941 records
56 included 84 included
15
Inclusion Criteria
Records included within the review of the literature met the following inclusion criteria
Lifestyle-related ndashdiet physical activity weight smoking alcohol consumption
Cancer sites breast colorectal lung or prostate cancer Other tumour sites will
be included if located while searching for the primary tumour sites
Trajectory - during primary cancer treatment or post-primary treatment
Outcomes of interest ndash survival recurrenceprogression symptoms treatment-
related chronic conditions ndash fatigue lymphoedema osteoporosis weight
physical fitness quality of life rehabilitation behaviour change health and well-
being cost-effectiveness
Adult population
Type of record ndash RCTs systematic reviews prospective cohort studies
Retrospective studies will also be included since some areas of lifestyle such as
smoking have primarily been investigated via this method
16
RESULTS
A total of 140 records were included in this review not counting the review being updated
(Bekkering et al 2006) In synthesising the evidence obtained from these records and the
additional sources described in the search strategy findings are presented in two parts
1) Cancer Survival
Evidence for the role of lifestyle in disease progression and recurrence
2) The Risks and Side-Effects of Cancer Treatment
Evidence for the role of lifestyle in reducing and managing the risks and
side-effects of cancer treatment with specific focus on cancer-related
fatigue lymphoedema osteoporosis and QoL
Both sections examine five categories of evidence
Physical activity
Diet
Weight
Smoking
Alcohol
The focus is on the four most common cancers (breast colorectal lung prostate) but other
tumour sites have been included if located via the pre-defined search strategy Summary
tables for each study included within the evidence are provided at the end of relevant
sections
17
PART ONE
CANCER SURVIVAL ndash EVIDENCE FOR THE ROLE OF LIFESTYLE IN
DISEASE PROGRESSION AND RECURRENCE
Introduction
Evidence for the role of lifestyle in the development of cancer is strong and it is widely
accepted that a poor diet lack of exercise smoking and excessive alcohol consumption can
increase an individuallsquos risk of developing cancer In particular it is well established that
smoking can increase risk of lung cancer and excessive unprotected exposure to the sun
can increase risk of skin cancer More recently lifestyle after a cancer diagnosis has been
under the microscope with evidence for the role of lifestyle in cancer progression7 and
recurrence8 demonstrating that lifestyle changes post-diagnosis can influence the disease
trajectory (Thomas and Davies 2007)
The development of cancer does not mean it is too late to make lifestyle changes that can
reduce the risk of the disease progressing or recurring after remission Indeed lifestylelsquo
refers to personal choices that can impact health and well-being as well as improve an
individuallsquos chance of disease-free survival9 and overall survival10
Evidence for an interaction between lifestyle and the disease trajectory is evaluated in the
current review including cancer development progression and recurrence and
commencing with a description of three large scale multicentre trials that will be referred to
throughout (Table 3)These studies are presented in some depth because their findings have
been influential in this field of study This will be followed by a site-specific (eg breast
colorectal lung prostate) summary of the findings reported by Bekkering et al (2006) as
part of the WCRF review being updated Further evidence identified from the search criteria
will then be presented including evidence obtained from the aforementioned multicentre
trials The European Prospective Investigation into Cancer and Nutrition (EPIC) Study
The Womens Intervention Nutrition Study (WINS) and The Womens Healthy Eating
and Living (WHEL) Study
7 Defined as the cancer becoming worse or spreading within the body
8 Cancer that has returned usually after a period of time during which it could not be detected The cancer may
come back to the same place as the original (primary) tumour or to another place in the body
9 The length of time after treatment during which a person survives with no sign of the disease
10The percentage of people from the study who are alive for a certain period of time after diagnosis or treatment
(ie 5-year survival rate)
18
The European Prospective Investigation into
Cancer and Nutrition (EPIC) Study (Riboli et al
2002)
The Womens Intervention Nutrition Study (WINS)
(Chlebowski et al 2006)
The Womens Healthy Eating and Living (WHEL)
Study
(Pierce et al 1997)
The EPIC study is coordinated in the UK by Dr Elio Riboli of the Imperial College London It is an ongoing multicentre prospective cohort study designed to investigate the relationship between nutrition and cancer The study currently includes 521000 participants (aged 35ndash70 years) in 23 centres located across 10 European countries11 These participants will be followed for cancer incidence and mortality for at least 10-years At enrolment which took place between 1992 and 2000 information was collected through a lifestyle questionnaire and through a dietary questionnaire addressing usual diet Physiological measurements (eg weight) were performed and blood samples taken The main website for EPIC12 last updated in 2010 reports that 26000 cases of cancer and 16000 deaths from cancer have been identified the majority of cases being cancer of the breast (n=6218) colonrectum (n=1910) prostate (n=1547) and lung (n=1292)
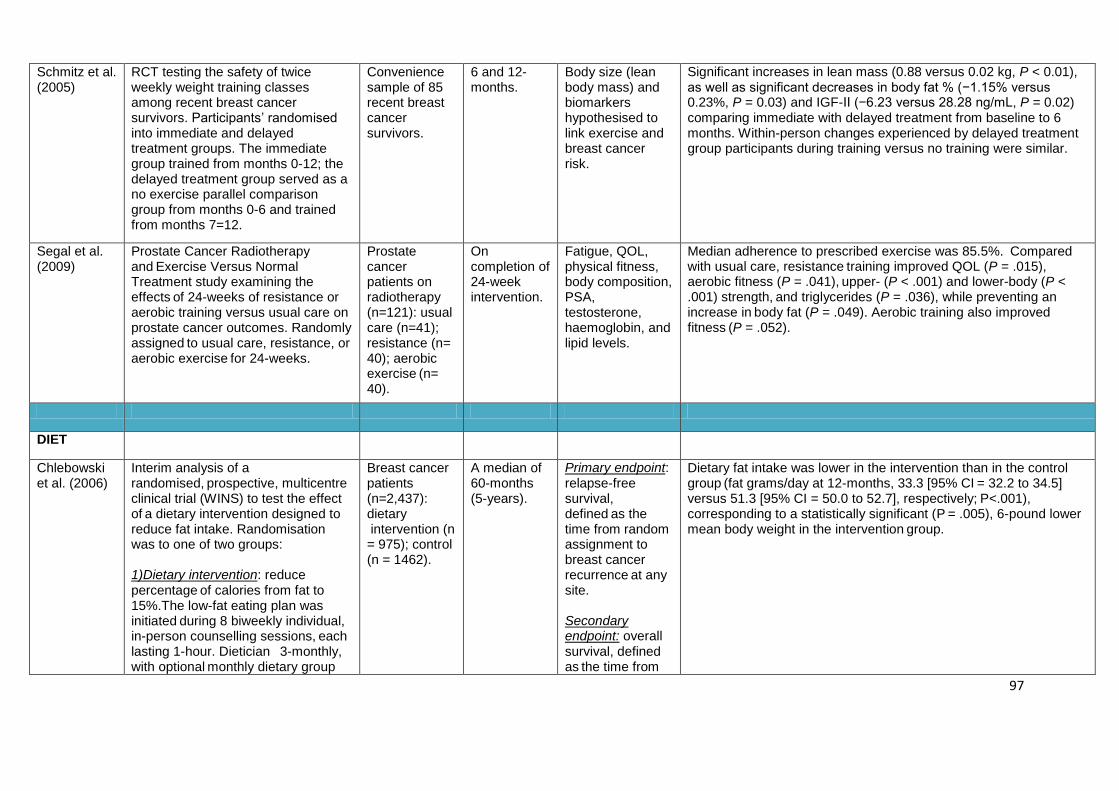
The WINS trial is a randomised multicentre study that commenced in 1994 and is now closed for recruitment It was designed to determine whether dietary fat reduction effectively prolongs disease-free and overall survival in post-menopausal women (n=2437) aged 48-78 years surgically treated for early stage breast cancer Randomisation to a reduced fat group or a control group took place between 1994 and 2001 with participants being evaluated annually via self-report and physiological measures 1) Intervention group (n=975) intensive dietary intervention for reduction of total fat intake to 15 of calories with repeated individual and group counselling sessions involving cognitive behavioural and motivational interviewing techniques 2) Control group (n=1462) US Department of Health and Human Services dietary guidelines (total fat intake between 20-35 of calories)
The WHEL study is a multicentre RCT which commenced in 1995 and also closed to recruitment aimed to determine whether a diet rich in vegetables fruit and fibre and low in fat is associated with a longer breast cancer event-free interval (ie no disease progression recurrence nor secondary cancers) Women diagnosed with stage I-III invasive breast cancer (n=3088) within the previous 4-years were randomised to a dietary intervention or control group and evaluated annually for 5-years via self-report and physiological measures 1)Intervention group (n=1540) guidelines provided for a daily dietary pattern of 5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy from fat A telephone counselling protocol focusing on goal setting self-monitoring and self-efficacy were provided as were cooking classes 2)Control group (n=1551) The US Department of Agriculture dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre and 30 energy from fat)
11
Denmark France Germany Greece Italy The Netherlands Norway Spain Sweden and the UK
12 httpepiciarcfr
Table 3 The EPIC WINS and WHEL Study (findings presented within proceeding text)
19
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in breast
cancer survival In the current review 6 studies and 2 systematic reviews were identified
These have been divided into appropriate domains according to mechanisms of benefit
hormones intensity and insulin Studies are summarised in Table 3 at the end of this
section
Hormones
Evidence exists that physical activity is associated with reduced risk of developing breast
cancer (Friedenreich and Cust 2008 Monninkhof et al 2007) One potential mechanism of
benefit is via the modification of sex hormone levels High levels of oestrogen (the
predominant sex hormone in females)13 and androgen (the predominant sex hormone in
males)14 are consistently associated with increased risk of developing breast cancer
(Eliassen et al 2006 Kaaks et al 2005) whereas high levels of sex hormone-binding
globulin (SHBG)15 are associated with a decreased risk (Key et al 2002) Regular physical
activity may alter oestrogen metabolism by shifting metabolism to favour production of 2-
hydroxyestrone (2-OHE1)16 as opposed to16α-hydroxyestrone (16α=OHE1) the former of
which has much weaker estrogenic activity Campbell et al (2007) is one of the few
researchers to examine this mechanism of benefit via a RCT In examining the effects of a
12-week aerobic exercise training programme on 2-OHE1 and 16α-OHE1 in healthylsquo pre-
menopausal women (n=17) no significant differences in oestrogen changes were found with
a control group who continued their usual level of physical activity (n=15) However a
change in lean body mass (estimated weight excluding body fat) over the 12-week
programme was found to be associated with a favourable change in 2-OHE1 to 16α-
OHE1 ratio (p lt 005)
In an effort to provide more direct evidence regarding the biological mechanisms of benefit
obtained from physical activity Friedenreich et al (2010) conducted the Alberta Physical
Activity and Breast Cancer Prevention Trial a two-centre two-arm RCT of physical
activity and cancer risk in older (50gt years) post-menopausal sedentary women from the
general population (n=320) Participants received a 1-year aerobic physical activity
programme of 225-minutes per week (n=160) or maintained their usual level of activity as
part of a control group (n=160) Significant reductions in oestrogen were found in the
intervention group compared to the control group demonstrating a protective effect
of increased physical activity in this group of high risk women (p lt 05)
13
oestrogen is suspected to activate certain oncogeneslsquo which can turn normal cells into tumour cells 14
The primary and most well-known androgen is testosterone which is also found in women to a lesser degree 15
A protein that attaches itself to oestrogen and androgen
16 Sometimes referred to as a good oestrogenlsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
20
Whilst some studies have examined the outcomes of increased physical activity others have
attempted to identify the duration and intensity required for beneficial effects Using data
from the Nursesrsquo Health Study17 (n=2987) Holmes et al (2005) found that women who
reported at least 3 MET-hours18 or more of physical activity per week were less likely
to have a recurrence or die from breast cancer compared to those who reported less
physical activity (p lt 001)
A further reduction in risk was seen with higher levels of physical activity up to 239 MET-
hours per week indicating a dose-response Interestingly the benefits of physical activity
were limited to women with hormone-receptor positive tumours (tumours that
respond to hormone treatment) as opposed to hormone-receptor negative tumours
(tumours that do not respond to hormone treatment) This provides further support for
mechanism of benefit from physical activity being hormone-related whether that be due to
the physical activity or any subsequent reductions in lean body mass that might accompany
such activity
Intensity
Expanding on evidence for the intensity of physical activity in a prospective observational
study the Health Eating Activity and Lifestyle (HEAL)19 study Irwin et al (2008) found
that of breast cancer survivors (n=933) who were sedentary pre-diagnosis women who
increased their physical activity post-diagnosis to approximately 9-MET hours per
week (eg 2-3 hours of brisk walking) had a 45 lower risk of death from cancer when
compared to those who did not increase their physical activity women who
decreased physical activity after diagnosis had a four-fold greater risk (p lt 005)
17
One of the largest and longest running investigations of factors that influence womenlsquos health comprising
information from 238000 nurse-participants
18 Metabolic equivalent (MET) values a measure of the effort required to do that activity
19 The HEAL Study is a population-based multicentre multi-ethnic prospective cohort study that has enrolled
1183 breast cancer survivors to determine whether lifestyle hormones and other exposures affect breast cancer
prognosis
METs (Ainsworth 2000) Light-intensity activities are defined as 11 MET to
29 MET Moderate-intensity activities are defined as 30 to
59 METs Vigorous-intensity activities are defined as 60 METs
or more
3 MET-hours might be using a stationary bicycle with light effort for one-hour 239 MET-hours might be running for 2-hours plus 1-hour of aerobic activity
21
Consistent with this a larger prospective observational study demonstrated that breast
cancer survivors (n=4482) who were physically active for more than 28 MET-hours per
week (eg walking at average pace of 2-29mph for 1-hour) were significantly less
likely to die from breast cancer (35-49 reduction) when compared to survivors who
did less than this (p lt 05) (Holick et al 2008) The reduced risk of mortality from cancer
was limited to total or moderate-intensity physical activity no benefit was noted for vigorous-
intensity activity
In a systematic review by Patterson et al (2010) leisure-time physical activity (ie
sportsrecreational) was associated with a 30 decreased risk of mortality from
breast cancer when compared to sedentary women In another review Saxton (2010)
identified four cohort studies demonstrating that women achieving the equivalent of 30-
minutes of moderate intensity physical activity on five or more days of the week
halved their risk of cancer-related mortality compared to those achieving less than 30-
minutes over the five days
Insulin
Evidence for the role of excess insulin in the growth of cancer cells has become more
established in recent years especially with the increase in obesity which is often
accompanied by elevated levels of insulin (Giovannucci 2005) The benefits of physical
activity on reducing insulin levels are less clear Ligibel et al (2008) conducted a RCT to test
the impact of weight training on insulin levels in overweight sedentary stage I to III breast
cancer survivors (n=101) The women were randomly assigned to one of two conditions
1) a 16-week supervised strength training and home-based cardiovascular training
protocol (two supervised 50-minute strength training sessions per week and 90-
minutes of home-based aerobic physical activity weekly)
2) a control group (routine care for 16-weeks before being offered consultation with a
physical activity trainer at the end of the control period)
Participation in the physical activity training was associated with a significant
decrease in insulin levels and hip circumference (p lt 05) Therefore the relationship
between physical activity and breast cancer recurrence may be mediated in part through
changes in insulin levels andor changes in body fat
ii DIET
Bekkering et al (2006) report on two small breast cancer studies showing a reduction in
cancer-specific mortality with healthy diet interventions (Elkort et al 1981 de Waard et al
1993) Of nine trials that included an antioxidant supplement no evidence was found for an
association between the intervention and cancer-related mortality compared with placebo or
usual treatment There was also no evidence of an effect of retinol (vitamin A - found in cod
liver oil butter liver eggs and cheese) (Meyskens et al 1994 Kucera et al 1980
Pastorino et al 1993)
22
In the current review 19 studies provide further evidence of the role of diet in breast cancer
survival many of which are part of the three multicentre studies previously described (ie
EPIC WINS WHEL p19) These studies have been divided into appropriate domains
according to dietary components dietary fat fruit and vegetables dietary fibre soy and
vitamin D
Dietary Fat
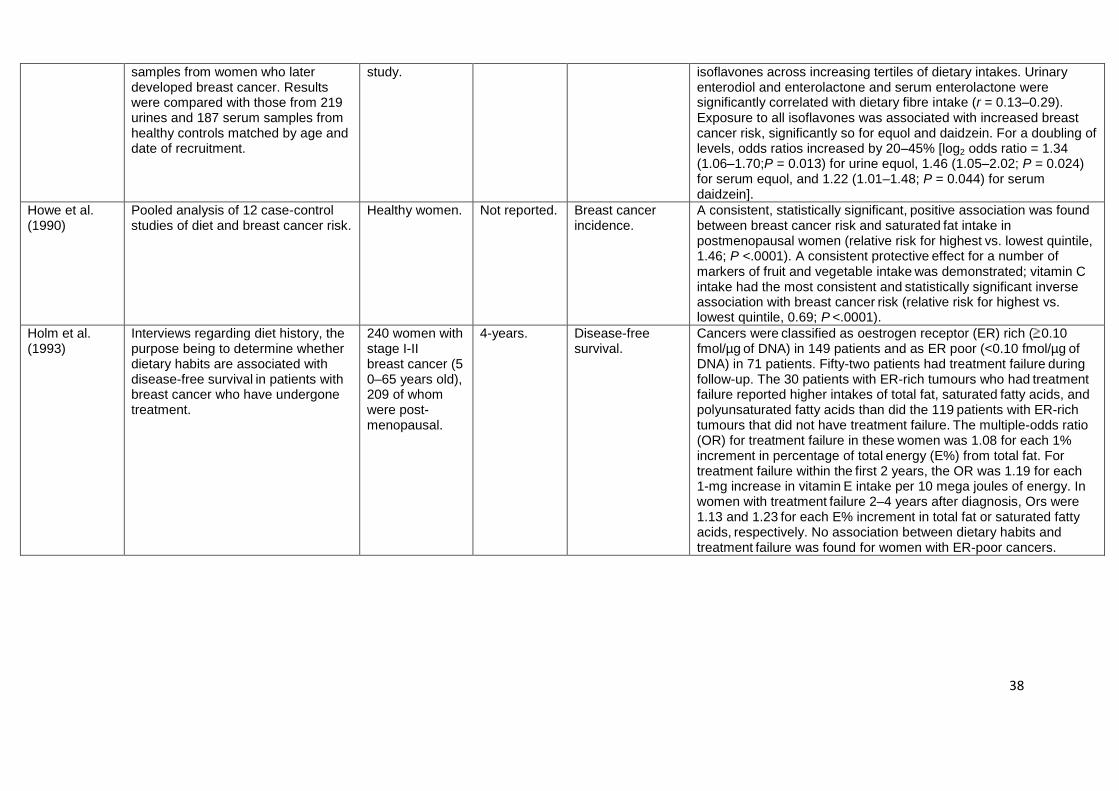
In general retrospective casendashcontrol studies have supported a positive association between
breast cancer incidence and dietary fat (Howe et al 1990) whilst many prospective cohort
studies have failed to show such an association (Kim et al 2006 Hunter et al 1996) A
meta-analysis provided evidence for a weak direct association between fat intake and breast
cancer in casendashcontrol and cohort studies combined (Boyd et al 2003) in cohort studies
that adjusted for energy intake highest versus lowest categories of total fat intake were
associated with a statistically significant 13 increased risk of developing
breast cancer (p lt 05)
Kyogoku et al (1992) utilised breast cancer patients whose dietary intake was assessed 10-
years previously in a case-control study (n= 212 patients who underwent a surgical
operation) After 10-years of follow-up 47 breast cancer deaths had occurred with no
support being provided for the hypothesis that a low fat diet influences breast cancer survival
outcomes In addition Holmes et al (1999) as part of the Nursesrsquo Health Study report
there being no evidence suggesting that lower intake of total fat or specific types of fat (eg
saturated and unsaturated fat) was associated with death from breast cancer in 2956
women who were diagnosed after 14-years of follow-up
Hebert et al (1998) studied the effect of diet on recurrence and death in women diagnosed
with early-stage breast cancer (n=472) finding that the strongest effects were observed in
pre-menopausal women Higher levels of self-reported baseline daily consumption of
butter margarine lard and beer were found to increase the risk of recurrence (p lt
01) There was also an increased risk associated with consumption of red meat liver and
bacon corresponding to about a doubling of risk for each time per day that foods in this
category were consumed (p=09)
The previously described WINS and WHEL RCTs (Table 2 p19) were anticipated to shed
light on these inconsistent findings related to dietary fat and breast cancer outcomes as
explored next in the following section
In an interim analysis of the Womens Intervention Nutrition Study (WINS) data (n=2437)
after a median follow-up of 60-months (5-years) (Chlebowski et al 2006) report that dietary
fat intake was lower in the dietary intervention than in the control group corresponding to a
significant 6-pound lower mean body weight in the intervention group (p lt 05) As a
reminder the dietary intervention group were counselled to reduce total fat intake to 15 of
calories whilst the control group were advised to keep total fat intake between 20-35 of
calories After 5-years of follow-up a total of 277 recurrences were reported in 96 of 975
23
(98) women in the dietary group and 181 of 1462 (124) women in the control group
women in the dietary intervention had a 24 lower risk of recurrence compared to the
control group (p lt 05) Exploratory analyses suggested that dietary fat reduction was most
beneficial in women diagnosed with hormone receptorndashnegative compared to hormone-
receptor positive breast cancer although this was not statistically significant
Other studies providing evidence of a differential effect of fat intake on breast cancer survival
have found such associations with hormone-receptor positive cancers (Holm et al 1993
Cho et al 2003) raising debate over the WINS findings Nevertheless in 2008 Chlebowski
et al updated survival information presented in 2006 reporting that after 7-years follow-up a
significant overall survival benefit was seen in women (n=362) with hormone-receptor
negative tumours taking part in the dietary intervention compared to the comparison
group (75 vs 181 p lt 005)
To explore the link between hormones and diet further the metabolic profiles of a subset of
WINS participants (n=53) were examined for the effect of a low-fat diet on insulin resistance
(Khaodhiar et al 2003) Insulin resistance is a physiological condition in which insulin
becomes less effective in lowering blood sugars resulting in increased blood glucose Of
those participants with initial insulin resistance after 1-year women in the dietary
intervention group had a greater decrease in their fasting insulin (insulin tested in a blood
sample collected after a 12-hour fast) than the women in the control group Although
not statistically significant these results suggest that insulin concentrations (a marker of
insulin resistance) may be influenced by dietary fat intake Alternatively since waist-to-hip
ratio is a marker for insulin weight reduction as opposed to dietary fat reductions might be
the important variable influencing disease outcomes (Borugianlsquos et al 2004)
Fruit and Vegetables
Flavonoids20 are high in fruits and vegetables and therefore might account for some of the
findings reported in WINS Dwyer et al (2008) sought to determine whether differences
existed in baseline and 12-month dietary intake of flavonoids among a random sample of
WINS participants (n=550) After 12-months of dietary intervention flavonoid intakes
remained similar in both groups demonstrating that neither total flavonoid intakes nor
intakes of subclasses of flavonoids differed between those who had dramatically decreased
their fat intake and those who had not Flavonoid intake is therefore unlikely to account for
the survival benefits reported for the WINS trial Carotenoids21 however do appear to play a
significant role in cancer survival On following 103 breast cancer survivors 27 of whom
died Ingram (1994) found that after a median of 81-months those who consumed more
beta-carotene (a carotenoid found in yellow and orange fruits such as mangoes
papayas and carrots) had significantly fewer deaths from breast cancer only one in
the group of highest beta-carotene consumers compared with 8 in the intermediate
20
Flavonoids also referred to as bioflavonoids are polyphenol antioxidants found naturally in plants ndash in other
words they are plant nutrientslsquo
21 Organic pigments that provide colour to bright fruits and vegetables including carrots apricots tomatoes and
salmon
24
group and 12 in the lowest group (p lt 0001) Overall there were 12 deaths in the lowest
total fruit consumption group compared with five in the intermediate group and 3 in the
highest (p lt 001) This benefit applied to both orangeyellow fruit (oranges melon) as well
as other fruits (apple banana berries grapes dried fruits)
Adding to this evidence is data from the aforementioned Womens Healthy Eating and
Living (WHEL) RCT (Table 2 p19) As a reminder women with breast cancer were
randomised to a dietary intervention (n=1540) comprising a daily pattern of
5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy
from fat or to a control group (n=1551) advised to follow the US Department of Agriculture
dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre
and 30 energy from fat Over a mean 73-year follow-up there was no significant
difference between groups in terms of additional breast cancer events (ie disease
progression recurrence or secondary cancer) or mortality despite statistically significant
differences in self-reported diet (low fat high fruit and vegetables) (Pierce et al 2007) On
the other hand when Rock et al (2005) examined only those participants in the control
group higher plasma total carotenoid concentration indicative of greater fruit and
vegetable consumption was significantly associated with reduced risk for a new
breast cancer event (p lt 05) This supports those findings reported by Ingram et al
(1994) and provides a potential explanation for why survival benefits were achieved in WINS
but not WHEL since both dietary interventions comprised lower dietary fat and higher levels
of carotenoids (fruit and vegetables) other factors must explain the differential survival
benefits One major difference between the two studies is that WINS participants lost weight
(mean = 6-pounds) whereas the WHEL participants did not
To follow up on these findings in terms of possible biological mechanisms of reduced risk of
recurrence Thomson et al (2007) conducted an ancillary study with post-menopausal
breast cancer survivors from the WHEL study (n=207) The aim was to test the hypothesis
that breast cancer survivors with higher levels of dietary carotenoids would show significantly
lower levels of oxidative stress (pathologic changes in response to excessive levels of cell
toxicity from the environment) than those with lower levels It was found that dietary
carotenoid levels were not significantly associated with oxidative stress indicators (measured
via urine samples)
Hot flushes post-treatment for early-stage breast cancer has been associated with an
approximately 25-30 decreased risk for additional breast cancer events (Mortimer et al
2008 Cuzick 2007) Since hot flushes are reported by women who continue to menstruate
during treatment or whose menstruation returns post-treatment this lowering of risk is
unlikely to be explained entirely by the lower oestrogen levels that sometimes accompany
hot flushes On the other hand dietary changes comprising lower energy from fat and
increased fibre can also alter oestrogen levels For example binding of fibre to estrogens in
the gut blocks reabsorption of oestrogen (Arts et al 1991) Focusing their analyses on the
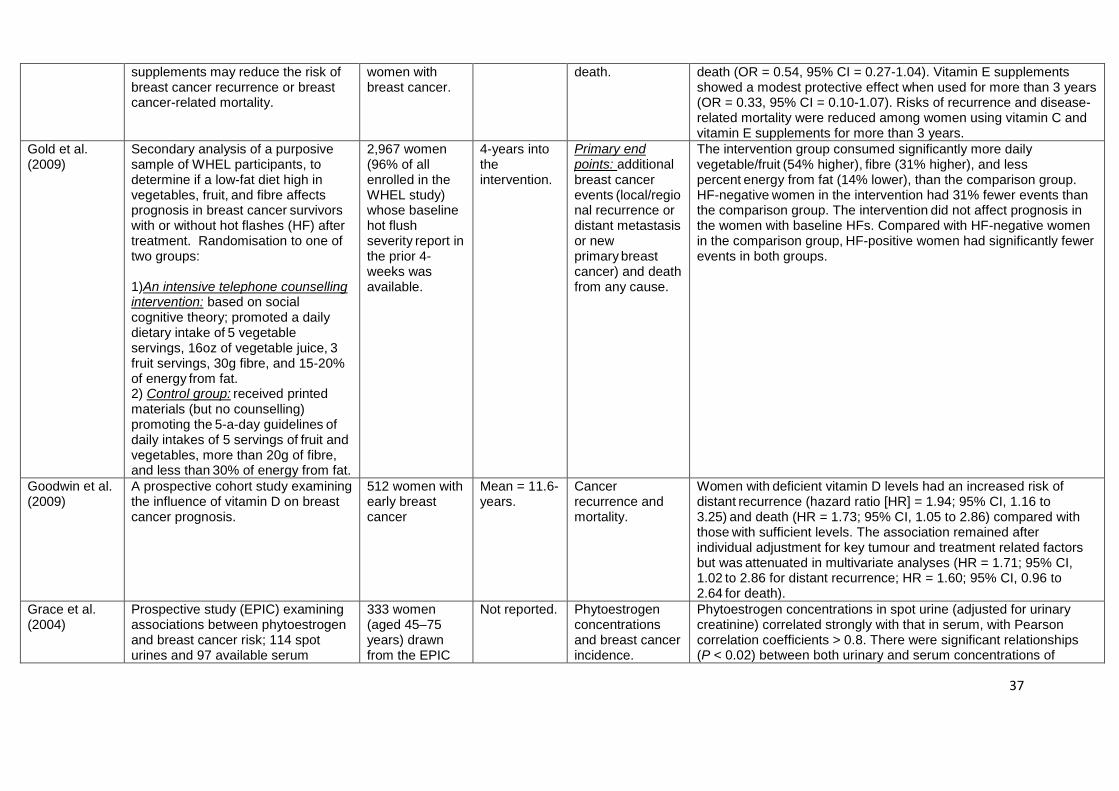
2967 of the WHEL participants who experienced baseline hot flushes Gold et al (2009)
tested the hypothesis that the increased risk of additional breast cancer events observed
among women who do not report hot flushes post-treatment can be reduced by lifestyle
interventions that lower circulating oestrogen Over a median of 73-years follow-up it was
demonstrated that the dietary intervention was associated with reduced risk of second
25
breast cancer events among women who reported no hot flushes at baseline (p lt 05)
These women had 31 fewer cancer-related events than matched-pairs in the control group
among post-menopausal women with no self-reported hot flushes at baseline the
intervention effect was even stronger with a 47 reduction in risk compared with post-
menopausal women in the control group who had no hot flushes at baseline (p lt 05)
McEligot et al (2006) conducted a retrospective investigation into the influence of diet (fat
fibre vegetable fruit folate carotenoids and vitamin C) on overall survival in post-
menopausal women with breast cancer (n= 516) Participants completed a food frequency
questionnaire for the year prior to diagnosis the analysis of which demonstrated that
women consuming the least total fat and highest total fibre and vegetables as well as
more folate vitamin C and carotenoid were significantly less likely to die from any
cause than those women consuming the opposite (p lt 05)
Dietary Fibre
Evidence linking breast cancer to the intake of dietary fibre has been conflicting although the
hypotheses remain that dietary fibre can be protective by inhibiting oestrogen (Kaaks et al
2005) as described previously in relation to physical activity or by reducing insulin-like
growth factors (Heald et al 2003) Therefore further research into these mechanisms of
benefit is clearly needed in order to provide clarity
Rohan et al (1993) examined risk of breast cancer in relation to intake of dietary fibre and
vitamins A C and E in a cohort of women (n=56837) enrolled in the Canadian National
Breast Screening Study22 After 5-years follow-up 519 incidence of breast cancer were
identified with analysis of previously completed dietary questionnaires demonstrating that
higher dietary fibre intake was associated with a small reduction in risk of developing
breast cancer Specifically there was a statistically significant decrease in risk of
developing breast cancer with increasing consumption of cereals (p lt 01) and a statistically
non-significant trend for pasta consumption (p=017) This reduced risk persisted after
adjustment for total vitamin A beta-carotene vitamin C and E
The UK Womens Cohort Study (UKWCS) (Cade et al 2007) which compares the health
outcomes of three main dietary groups (vegetarian eating fish [not meat] and meat eaters)
provides further evidence for the protective properties of fibre After a median of 75 years
follow-up analysis of self-reported dietary data of 35792 women showed that total dietary
fibre was found to be related to breast cancer incidence in women who were pre-
menopausal but not post-menopausal at baseline (p lt01) Fibre from cereals (plt
05) and fibre from fruit (p=009) was found to be protective against breast cancer
22
An RCT comprising women 40-49 years of age at study entry evaluating the efficacy of annual mammography breast physical examination and instruction on breast self-examination in reducing breast cancer mortality
26
Soy
A high intake of phytoestrogens23 particularly isoflavones (found in soy products) has been
suggested to decrease risk of developing breast cancer In one of the European
Prospective Investigation into Cancer and Nutrition (EPIC) studies a large multicentre
prospective cohort study described earlier in Table 2 the association between breast cancer
risk and isoflavones was supported in 333 women (p lt 005) (Grace et al 2004) but in
another larger EPIC study conducted in Utrecht (n=15555) no such evidence was found
(Keinan-Boker et al 2004) Analyses with pooled data sets are ongoing In the meantime
Boyapati et al (2005) provide evidence from the Shanghai Breast Cancer Study24
suggesting that after a median of 52-years follow-up soy intake pre-diagnosis is not related
to disease-free survival in women with breast cancer (n=1459)
Vitamin D
Goodwin et al (2009) measured vitamin D (usually obtained from sunlight through the skin
but also found in oily fish and eggs) levels in the stored blood of women with early breast
cancer (n=512) The mean follow-up was 116-years by which time women deficient in
vitamin D had a significantly increased risk of distant recurrence25 compared with
those who had sufficient levels (p lt 05)
Antioxidant Supplements
Despite widespread use only a few clinical or epidemiological studies have examined the
relationship between antioxidant supplements and risk of breast cancer recurrence or breast
cancer-related mortality Fleischauer et al (2003) examined recurrence and mortality
among post-menopausal women diagnosed with breast cancer (n=385) who were enrolled
into a dietary case-control study Women were contacted with a single questionnaire to
ascertain the use of nutritional supplements during 12-14 years of follow-up Antioxidant
vitamin supplement use was associated with a lower risk of breast cancer recurrence or
mortality Specifically use of vitamin C and E supplements moderately reduced risk (p lt
05) whilst vitamin E nearly halved the risk although this was not statistically
significant (p=056)
iii WEIGHT
Weight and body composition have been implicated in the development of a wide range of
cancers as well as in increased risk of recurrence or second primary cancers (Chlebowski
Aiello and McTiernan 2002) Additionally being overweight or obese can exacerbate some
23
Phytoestrogens sometimes called dietary estrogenslsquo are a group of naturally occurring plant compounds that have a similar chemical structure to estrogen they bind to estrogen receptors acting like hormone regulators
24 The Shanghai Breast Cancer Survival (SBSS) Study collected lifestyle-related factors and disease and
treatment related factors in Chinese women with breast cancer (n=2236) (Lu et al 2007) 25
The spread of cancer to parts of the body other than the place where the cancer first occurred
27
of the side-effects of cancer treatment as well as increase the risk of co-morbidities such as
diabetes and osteoporosis (Doyle et al 2006) The studies evaluated in this review thus far
further indicate weight as offering a mechanism of benefit in terms of breast cancer
outcomes Indeed the WINS and WHEL RCTs produce different outcomes when using
similar dietary interventions with weight loss in the WINS group but not the WHEL group
offering a likely explanation for improved outcomes observed in the WINS participants Since
increased adiposity (excess body fat) has been identified as a negative prognostic factor for
recurrent disease and survival after breast cancer diagnosis (Rock and Demark-Wahnefried
2002) the apparent benefit of dietary fat reduction in the intervention group could
partly result from the weight loss
Bekkering et al (2006) do not add to this evidence whilst 5 studies and one systematic
review were identified in the current review
Hebert et al (1998) studied the effect of body weight on recurrence and death in women
diagnosed with early-stage breast cancer (n=472) Body mass index (BMI) was
associated with an increased risk of recurrence at the rate of 9 for each kgm2
(equivalent to about 58-pounds for a 5 4 tall woman) For death the results were
similar but body mass index was more strongly associated increasing risk by 12
per kgm2
Additionally Lahmann et al (2004) used data from 73542 pre-menopausal and 103344
post-menopausal women taking part in the EPIC study During 47-years of follow-up 1879
cases of invasive breast cancer were identified In post-menopausal women current use
of hormone replacement therapy (HRT) modified the association between body size
and breast cancer among non-users weight body mass index and hip circumference
were positively associated with breast cancer risk (p lt 001) Obese women (BMI gt 30)
had a 31 risk compared to women with a BMI lt 25 Among pre-menopausal women hip
circumference was the only other measure significantly related to breast cancer (p lt 005)
after accounting for BMI
Enger et al (2004) conducted a retrospective follow-up study of women diagnosed with
breast cancer (n=1376) for whom complete medical records and adequate tissue
specimens existed Patients were followed for a median of 68-years after diagnosis 246 of
whom died from breast cancer Compared with women in the lowest category of weight
(lt133lb [60kg] at diagnosis) women in the highest category ( 175lb [79kg])
experienced a 25-fold increased risk of dying from breast cancer (P lt 05) Women with
hormone-receptor negative cancer experienced an approximately 2-fold higher risk of dying
from breast cancer compared with women who presented with hormone-receptor positive
cancer Women in the upper 50th percentile of weight with hormone-receptor negative cancer
had a nearly 5-fold increased risk of dying from cancer compared with women in the lower
50th percentile of weight and hormone-receptor positive cancer (p=10)
In order to determine whether weight prior to diagnosis and weight gain after diagnosis are
predictive of breast cancer survival Kroenke et al (2005) followed 5204 participants from
the Nursesrsquo Health Study diagnosed with incident invasive non-metastatic breast cancer
After a median of 9-years follow-up there were 860 total deaths 533 breast cancer deaths
28
and 681 recurrences (defined as secondary lung brain bone or liver cancer and death from
breast cancer) Weight before diagnosis and weight gain after diagnosis were related
to higher rates of breast cancer recurrence and mortality although associations were
most apparent in women who had never smoked (p lt 05) Furthermore associations
with weight were stronger in pre-menopausal than in post-menopausal women In contrast
by comparing breast cancer survivors (n=3215) with women in the comparison group of a
dietary intervention trial to prevent breast cancer recurrence Caan et al (2008) found that
neither moderate (5ndash10) nor large (gt10) weight gain post-diagnosis was associated with
an increased risk of breast cancer recurrence in the early years post-diagnosis (median time
of 737-months from diagnosis)
More recently Patterson et al (2010) reviewed published epidemiological research on
lifestyle and breast cancer outcomes reporting that the most consistent finding from
observational studies was that adiposity was associated with a 30 increased risk of
cancer-related mortality
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in breast cancer
survival Four studies were identified in the current review
In an observational study Manjer et al (2000) compared the survival of patients with breast
cancer (n=792) who had never smoked were smokers or were ex-smokers Follow-up of
breast cancer cases was through record-linkage with the Swedish Cause of Death Registry
During a mean follow-up of 121-years smokers and ex-smokers compared with those
who had never smoked had a significantly increased risk of death from cancer
Fentiman et al (2005) add to this evidence with a cohort study of breast cancer patients who
completed a lifestyle questionnaire at the time of diagnosis (n=166) They found that
smoking was the third most important predictor of breast cancer-specific and overall
survival after stage and age at diagnosis This suggests that smokers are not only more
likely to die of cancer but also of other diseases when compared with those who have never
smoked
In a much larger study Holmes et al (2007) conducted a prospective observational study
among 5056 women from the Nursesrsquo Health Study with stages I-III invasive breast
cancer Information on smoking was available for these women who were followed until
January 2002 or death whichever came first Compared with women who had never
smoked women who were current smokers had a 43 increased risk of death from
any cause with risk increasing along with more cigarettes smoked per day (p lt0001)
In contrast there was no association with current smoking and breast cancer death
Sagiv et al (2007) followed women diagnosed with a first primary breast cancer (n=1273)
for 5-6 years and found that the number of all-cause mortality (n=188) including breast
cancer-specific mortality (n=111) was slightly higher among current and former
active smokers compared with women who had never smoked No association was
found between active or passive smoking and breast cancer-specific mortality
29
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in breast cancer
survival In the current review one review and 2 studies were identified
Rock and Demark-Wahnefried (2002) reviewed the evidence from clinical and epidemiologic
studies reporting that alcohol intake was not associated with breast cancer survival in the
majority of the studies In contrast post-menopausal women (n=125) diagnosed with
invasive breast cancer who were followed through to survival demonstrated that pre-
diagnosis alcohol consumption of at least one drink per week was associated with a
27-fold increase in risk of cancer-related mortality (McDonald et al 2002) In a similar
study a larger sample of women (n=1286) diagnosed with invasive breast cancer who were
followed from diagnosis through to survival produced opposing findings compared with
non-drinkers women who consumed alcohol in the 5-years before diagnosis had a
decreased risk of cancer-related mortality (Reding et al 2009)
SUMMARY OF LIFESTYLE EVIDENCE FOR BREAST CANCER ndash MECHANISMS
OF BENEFIT
Physical Activity Physical activity is likely to prevent breast cancer via its effect on
hormones specifically by reducing levels of oestrogen in the body (Friedenreich et al 2010)
or shifting the metabolism of oestrogen to favour production of 2-hydroxyestrone (2-OHE1)26
as opposed to16α-hydroxyestrone (16α=OHE1) the former of which has much weaker
estrogenic activity This shift might also be the result of a change in lean body mass resulting
from physical exercise (Campbell et al 2007) The survival benefits of physical activity
appear to require a certain intensity or level of exertion specifically 3 MET-hours or more per
week (Holmes et al 2005 Holick et al 2008 Saxton et al 2010) this equates to moderate
intensity activity such as using a stationary bike for 1-hour However there is also evidence
of a dose-effect with greater activity (up to 239 MET-hours per week) being associated with
reduced risk of recurrence and cancer-related mortality (Holmes et al 2005) or indeed
greater levels of activity than pre-diagnosis being associated with reduced risk of recurrence
and cancer-related mortality (Irwin et al 2008 Holick et al 2008 Patterson et al 2010
Saxton et al 2010)
Diet Evidence for the role of dietary fat in breast cancer development and survival are
varied Case-control (Kyogoku et al 1992) and large prospective studies (Holmes et al
1999) do not show any significant link whilst some studies have found that dietary fat does
increase risk of recurrence or death in pre-menopausal women Indeed the large multicentre
WINS trial found a protective benefit of a reduced fat dietary intervention which was more
prominent in women diagnosed with hormone-receptor negative breast cancer (Chlebowski
et al 2006a Chlebowksi et al 2008) The differential effect of diet on hormone-receptor
positive and negative disease indicate that metabolic mechanisms involving insulin and
26
Sometimes referred to as a lsquogood estrogenrsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
30
insulin-like growth factor-1 (IGF-1)27 may be involved in the mechanisms of benefit and
although not statistically significant data has been presented suggesting that elevated
insulin concentrations (a marker of insulin resistance) may be influenced by dietary fat
reduction (Khaodhiar et al 2003 Borugian et al 2004) However this might be due to
changes in weight produced by a low fat diet rather than the lower consumption of fat itself
(Borugian et al 2004) Since low fat diets are often accompanied by high intakes of fruit
and vegetables various components of a diet comprising high levels of fruit and vegetables
have been investigated Carotenoids have received particular attention with evidence
suggesting that carotenoids play a role in survival (Ingram 1994) Other studies have found
this not to be the case (Pierce et al 2007) with the primary difference in these studies being
lack of weight loss This indicates that the mechanism of benefit produced from low fat high
fruit and vegetable (particularly carotenoids) diets is most probably through changes in body
composition Indeed the majority of studies in this review demonstrated a link between
weight and cancer-related risks (Hebert et al 1998 Enger et al 2004 Lahmann et al
2004 Patterson et al 2010)
Smoking Evidence pertaining to the smoking clearly demonstrates a link between
breast cancer survival and a history of smoking However it appears to be more likely to
increase all-cause mortality as opposed to cancer-specific mortality (Fentiman et al 2005
Holmes et al 2007 Sagiv et al 2007)
Alcohol Although the evidence is less clear pre-diagnosis alcohol consumption does
appear to be related to survival (McDonald et al 2002 Reding et al 2009) although
current drinking does not (Demark-Wahnefried 2002)
27
IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of
pathological states including cancer
31
Table 3 Breast Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Campbell et al (2007)
RCT examining the effects of 12-weeks of aerobic exercise training on 2-OHE
1 and 16α-OHE
1 in
premenopausal women Randomisation to 1) A 12-week individualised supervised moderate-to-vigorous intensity aerobic exercise training intervention (n = 17) Participants began the exercise program in the early follicular phase of the next menstrual cycle (days 1-5) The intervention was divided into three blocks (a) Weeks 1 ndash 4 ndash 3 sessions per week of base aerobic training progressing from 20-40 minutes on a stationary bike (b) Weeks 5-8 ndash 4 sessions per week Two sessions were base aerobic training sessions for 30-45 minutes (c) Weeks 9 -12 ndash 4 sessions per week with two base aerobic training sessions for 30-45 minutes and two interval sessions 2) Usual lifestyle (n = 15) Participants were asked to maintain their usual activity levels for the duration of the study Following the control cycle the first day of the next menstrual cycle was used as the reference start date for participants in the control group On completion of the 12-week post-intervention
Healthy regularly menstruating Caucasian women (n=32) 20-35 years
On completion of the 12-week intervention
Height body mass body composition by dual-energy X-ray absorptiometry and VO2max were measured at baseline and following the intervention Urine samples were collected in the luteal phase of four consecutive menstrual cycles
Participants attended an average of 40-44 (91) sessions Fourteen of 17 (82) participants completed at least 80 of the sessions The exercise group increased VO2max by 14 and had significant although modest improvements in fat and lean body mass No significant between-group differences were observed however for the changes in 2-OHE1 (P = 0944) 16α-OHE1 (P= 0411) or the ratio of 2-OHE1 to 16α-OHE1 (P = 0317) At baseline there was an inverse association between body fat and 2-OHE1 to 16α-OHE1 ratio (r = minus040 P = 0044) however it was the change in lean body mass over the intervention that was positively associated with a change in 2-OHE1 to 16α-OHE1 ratio (r = 043 P = 0015)
32
measurement participants were given guidance for starting an individualised exercise program and access to the fitness facility for 4-weeks
Friedenreich et al (2010)
A two-centre two-arm RCT examining how an aerobic exercise intervention influences
circulating
estradiol oestrone sex hormonendashbinding globulin
(SHBG)
androstenedione and testosterone levels which may
be involved in the
association between physical activity and
breast cancer risk
Randomisation to 1) A 1-year aerobic physical activity programme of 225-minutes per week (n=160) 2) Control group maintained their usual level of activity (n=160)
Older (50gt years) post-menopausal sedentary women (n=320)
On completion of the intervention
Estradiol and sex hormone-binding globulin levels Androstenedione and testosterone levels
Completion of the study was high (966) At 12-months statistically significant reductions in
estradiol (treatment effect ratio
[TER] = 093 95 CI 088 to 098) and free estradiol (TER = 091
95 CI 087 to 096) and increases in SHBG (TER = 104 95 CI
102 to 107) were observed in the exercise group compared with
the control group No significant differences in oestrone
androstenedione and testosterone levels were observed between
exercisers and controls at 12-months
Holick et al (2008)
Prospective cohort study examining the relationship between post-diagnosis recreational physical activity and risk of breast cancer death
Women with a history of previous invasive breast cancer diagnosed between the ages of 20-79 years (n=4482)
Maximum of 6-years post-diagnosis (median=56-years post-diagnosis)
Mortality from breast cancer mortality from any cause Self-reported physical activity converted to MET-hours per week
After adjusting for age at diagnosis stage of disease state of residence interval between diagnosis and physical activity assessment body mass index menopausal status hormone therapy use energy intake education family history of breast cancer and treatment modality compared with women expending lt28 MET-hwk in physical activity women who engaged in greater levels of activity had a significantly lower risk of dying from breast cancer (HR 065 95 CI 039-108 for 28-79 MET-hwk HR 059 95 CI 035-101 for 80-209 MET-hwk and HR 051 95 CI 029-089 for ge210 MET-hwk P for trend = 005) Results were similar for overall survival (HR 044 95 CI 032-060 for ge210 versus lt28 MET-hwk P for trend lt0001) and were similar regardless of a womanlsquos age stage of disease and body mass index
Holmes et al (2005)
Prospective observational study
(Nurseslsquo Health Study) to determine whether physical activity among
women with breast cancer
2987 female registered nurses
in the
Nurseslsquo Health
Women were diagnosed between 1984 and
Breast cancer mortality risk according
to
physical activity
Compared with women who engaged in less than 3 MET-hours per
week of physical activity the adjusted relative risk (RR) of death
from breast cancer was 080 (95 CI 060-106) for 3 to 89 MET-hours per week 050
(95 CI 031-082) for 9 to 149 MET-hours
33
decreases their risk of death from
breast cancer compared with
more sedentary women
Study diagnosed with stage
I II or III
breast cancer
1998 and followed until death or June 2002
category (lt3 3-89 9-149 15-239
or 24
metabolic equivalent task [MET] hours per week)
per week 056 (95 CI 038-084) for 15 to 239 MET-hours per
week and 060 (95CI 040-089) for 24 or more MET-hours per week (P for trend
= 004) Three MET-hours is equivalent to walking
at average pace of 2 to 29 mph for 1 hour The benefit of physical
activity was particularly apparent among women with hormone-
responsive tutors The RR of breast cancer death for women with hormone-responsive
tumours who engaged in 9 or more MET-hours
per week of activity compared with women with hormone-
responsive tumours who engaged in less than 9 MET-hours per
week was 050 (95 CI 034-074) Compared with women who
engaged in less than 3 MET-hours per week of activity the absolute
unadjusted mortality risk reduction was 6 at 10 years for women
who engaged in 9 or more MET-hours per week
Irwin et al (2008)
The Health Eating Activity and Lifestyle Study (HEAL) Prospective observational study investigating the association between pre- and post-diagnosis
physical activity (as well as
change in pre-diagnosis to post-diagnosis
physical activity) and
mortality among women with breast cancer
A subsample of participants from the HEAL study ndash 933 women diagnosed with local or regional breast cancer between 1995
and 1998
5 -8 years from diagnosis (median=6-years)
Primary outcomes total deaths
and breast
cancer deaths
Compared with inactive women the multivariable hazard ratios
(HRs) for total deaths for women expending at least 9 MET-
hours per week (approximately 2-3 hwk of brisk walking) were 069
(95 CI 045 to 106 P = 045) for those active in the year before
diagnosis and 033 (95 CI 015 to 073 P = 046) for those active
2-years after diagnosis Compared with women who were inactive
both before and after diagnosis women who increased physical
activity after diagnosis had a 45 lower risk of death (HR = 055
95 CI 022 to 138) and women who decreased physical activity
after diagnosis had a four-fold greater risk of death (HR = 395 95
CI 145 to 1050)
Ligibel et al (2008)
RCT examining the impact of physical activity on insulin levels Participants were randomly assigned to one of two conditions a)Physical activity intervention a 16-week supervised strength training and home-based cardiovascular training protocol (two supervised 50-minute strength training
sessions per
week and 90-minutes of home-based
aerobic physical activity
weekly) b) Control group routine care for 16-weeks before being offered consultation with an physical activity
Overweight sedentary stage
I-III breast
cancer survivors (n=101)
On completion of the 16-week intervention
Fasting insulin and glucose levels Weight body composition
and
circumference at the waist and hip
18 women withdrew consent andor did not complete the study
Baseline and 16-week measurements were available for 82 patients
Fasting insulin concentrations decreased by an average of
286 microUmL in the exercise group (P = 03) with no
significant change in the control group (decrease of 027 microUmL P
=
65) The change in insulin levels in the exercise group seemed
greater than the change in controls but the comparison
did not reach statistical significance (P = 07) There was a
trend toward improvement in insulin resistance in the exercise
group (P = 09) but no change in fasting glucose levels The
exercise group also experienced a significant decrease in hip
measurements with no change in weight or body composition
34
trainer at the end of the control
period
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer outcomes
Breast cancer Not reported Additional breast cancer events and mortality
Although observational data were not consistent physical activity appeared to be associated with a 30 decreased risk of mortality
Saxton et al (2010)
A review of studies pertaining to physical activity and cancer mortality
All cancers with more evidence obtained for breast cancer
Not reported Survival A number of prospective cohort studies have reported negative associations between physical activity and cancer mortality The most compelling observational evidence of the survival benefits to be gained from a physically active lifestyle has emerged from studies of post-diagnosis physical activity in breast and colorectal cancer survivors These studies have shown clear inverse associations between post-diagnosis activity and survival with the benefits being independent of age gender obesity and disease stage at diagnosis Three of the four cohort studies of breast cancer survivors showed that women who are achieving the equivalent of 30-miniutes of moderate intensity PA on five or more days of the week can halve their risk of mortality up to 8 years of follow-up
DIET
Borugian et al (2004)
Prospective cohort study testing the hypothesis that elevated wait-to-hip ratio is directly related to breast cancer
mortality
603 patients with incident
breast
cancer
Up to 10-years
Date of death and
primary and secondary cause of death
After adjustment for age BMI family history oestrogen
receptor (ER) status tumour stage at diagnosis and systemic
treatment (chemotherapy or tamoxifen) WHR was directly related to
breast cancer mortality in postmenopausal women (for highest
quartile vs lowest relative risk = 33 95 confidence interval
11 104) but not in premenopausal women (relative risk = 12
95 confidence interval 04 34) Stratification according to
ER
status showed that the increased mortality was restricted to ER-
positive postmenopausal women Elevated WHR was confirmed as
a predictor of breast cancer mortality with menopausal status and
ER status at diagnosis found to be important modifiers of that
relation
Boyapati et al (2005)
As part of the Shanghai Breast Cancer Cohort Study associations between soy and breast cancer survival were investigated
1459 breast cancer patients
52-years Disease-free survival
Soy intake pre-diagnosis was unrelated to disease-free breast cancer survival (adjusted hazard ratio [HR]=099 95 confidence interval [CI] 073-133 for the highest tertile compared to the lowest tertile) The association between soy protein intake and breast cancer survival did not differ according to ERPR status tumour stage age at diagnosis body mass index (BMI) waist to hip ratio (WHR) or menopausal status
Boyd et al (2003)
Meta-analysis of casendashcontrol and cohort studies published up to July 2003 which examined the
Varied Not reported Cancer incidence A total of 45 published studies containing 46 estimates of risk examined the role of dietary fat in relation to breast cancer risk by an analysis of nutrient intake Of these 31 were case control and
35
association of dietary fat or fat-containing foods with risk of breast cancer
14 were cohort in design and they contained a total of 25015 cases of breast cancer and over 580 000 control or comparison subjects The summary relative risk comparing the highest and lowest levels of intake of total fat was 113 (95 CI 103ndash125) Cohort studies (n=14) had a summary relative risk of 111 (95 CI 099ndash125) and casendashcontrol studies (N=31) had a relative risk of 114 (95 CI 099ndash132) Significant summary relative risks were also found for saturated fat (RR 119 95 CI 106ndash135) and meat intake (RR 117 95 CI 106ndash129) Combined estimates of risk for total and saturated fat intake and for meat intake all indicate an association between higher intakes and an increased risk of breast cancer Casendashcontrol and cohort studies gave similar results
Cade et al 2007)
A large UK cohort study comprising women with a wide range of different eating patterns to study the effects of different food and nutrient intakes on long-term health outcomes
35372 women (350 post- and 257 pre- menopausal women developed breast cancer)
Approx 75-years
Breast cancer incidence
In pre-menopausal but not post-menopausal women a statistically
significant inverse relationship was found between
total fibre intake and risk of breast cancer (P for trend = 001) The
top quintile of fibre intake was associated with a hazard ratio
of 048
[95 CI 024ndash096] compared with the lowest quintile Pre-
menopausal fibre from cereals was inversely associated with risk
of breast cancer (P for trend = 005) and fibre from fruit had a
borderline inverse relationship (P for trend = 009)
Chlebowski et al (2006a)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
randomisation to death from any cause
Attrition in the dietary intervention (n=44) versus control group (n=66) Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to
345] versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group A total of 277 relapse
events (local regional distant or ipsilateral breast cancer
recurrence or new contralateral breast cancer) have been reported
in 96 of 975 (98) women in the dietary group and 181 of 1462
(124) women in the control group The hazard ratio of relapse
events in the intervention group compared with the control group
was 076 (95 CI = 060 to 098 P = 077 for stratified log rank
and P = 034 for adjusted Cox model analysis)
36
dietary guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
Chlebowski et al (2008)
A protocol-mandated survival analysis update to the interim analysis of WINS (Chlebowski et al 2006a)
Breast cancer patients (n=2437)
Approximately 7-years
Overall survival Attrition in the intervention group (n=236) versus control group (n=172) Although fewer deaths were seen in the intervention group this was not statistically significant In 362 women with ER- and (progesterone receptor) PR- disease a significant overall survival benefit was seen in the intervention group (75 vs 181 cumulative mortality)
Cho et al (2003)
A prospective analysis of the relationship
between dietary fat
intake and breast cancer risk among pre-menopausal
women enrolled in
the Nurseslsquo Health Study
Pre-menopausal women (n=90655) aged between 26-46 years old when recruited in 1991
8-years after recruitment (1991-1999)
Fat intake was
assessed with a food-frequency questionnaire at baseline
in 1991
and again in 1995
During 8-years of follow-up 714 women developed incident
invasive breast cancer Relative to women in the lowest quintile of
fat intake women in the highest quintile of intake had a
slight increased risk of breast cancer (RR = 125 95 CI = 098
to 159 Ptrend = 06) The increase was associated with intake
of
animal fat but not vegetable fat RRs for the increasing quintiles of
animal fat intake were 100 (referent) 128 137 154 and 133
(95 CI = 102 to 173 Ptrend = 002) Intakes of both saturated and
monounsaturated fat were related to modestly elevated breast
cancer risk Among food groups contributing to animal fat red meat and high-fat dairy foods were each associated
with an increased
risk of breast cancer Information on oestrogen-receptor status was available for
80 (n = 570) of breast cancers and progesterone-
receptor status for 78 (n = 558) When divided according to
oestrogen and progesterone receptor status the positive
association between animal fat intake and breast cancer risk was
stronger among women with oestrogen receptor-positive or
progesterone receptor-positive cancers than among women with hormone receptor-negative cancers however the difference was not statistically significant
Dwyer et al (2008)
A sub-analysis of participants in the WINS trial (Chlebowski et al 2006a)
Breast cancer patients (n=550)
12-months of intervention
Disease-free survival
Attrition in the intervention group (n = 23 11) versus control group (n = 16 5)At baseline neither mean fat intake nor flavonoid intake differed between groups After 12-months of intervention dietary fat intake was significantly lower among those on the very low-fat diet (n =195) whilst flavonoid intake remained similar in both groups Neither total flavonoid intake nor intake of subclasses of flavonoids differed between those who had dramatically decreased their fat intake and those who had not
Fleischauer et al (2003)
Case-control study testing the hypothesis that antioxidant
385 post-menopausal
12-14-years Breast cancer recurrence or
Antioxidant supplement users compared with non-users were less likely to have a breast cancer recurrence or breast cancer-related
37
supplements may reduce the risk of breast cancer recurrence or breast cancer-related mortality
women with breast cancer
death death (OR = 054 95 CI = 027-104) Vitamin E supplements showed a modest protective effect when used for more than 3 years (OR = 033 95 CI = 010-107) Risks of recurrence and disease-related mortality were reduced among women using vitamin C and vitamin E supplements for more than 3 years
Gold et al (2009)
Secondary analysis of a purposive sample of WHEL participants to determine if a low-fat diet high in vegetables fruit
and fibre affects
prognosis in breast cancer survivors
with or without hot flashes (HF) after treatment Randomisation to one of two groups 1)An intensive telephone counselling intervention based on social cognitive theory promoted a daily dietary intake of
5 vegetable
servings 16oz of vegetable juice 3
fruit servings 30g fibre and 15-20 of energy
from fat
2) Control group received printed
materials (but no counselling) promoting the
5-a-day guidelines
of
daily intakes of 5 servings of fruit and
vegetables more than 20g of fibre and less than
30 of energy from fat
2967 women (96 of all enrolled in the WHEL study) whose baseline hot flush severity
report in
the prior 4-weeks was available
4-years into the intervention
Primary end points additional breast cancer events
(localregio
nal recurrence or distant metastasis or new primary
breast
cancer) and death from any cause
The intervention group consumed significantly more daily vegetablefruit
(54 higher)
fibre (31 higher) and less
percent energy from fat (14 lower) than the comparison group
HF-negative women in the intervention had 31 fewer events than
the comparison group The intervention did not affect prognosis in
the women with baseline HFs Compared with HF-negative women in the comparison group
HF-positive women had significantly fewer
events in both groups
Goodwin et al (2009)
A prospective cohort study examining the influence of vitamin D on breast cancer prognosis
512 women with early breast cancer
Mean = 116-years
Cancer recurrence and mortality
Women with deficient vitamin D levels had an increased risk of
distant recurrence (hazard ratio [HR] = 194 95 CI 116 to
325) and death (HR = 173 95 CI 105 to 286) compared with
those with sufficient levels The association remained after
individual adjustment for key tumour and treatment related factors but was
attenuated in multivariate analyses (HR = 171 95 CI
102 to 286 for distant recurrence HR = 160 95 CI 096 to
264 for death)
Grace et al (2004)
Prospective study (EPIC) examining associations between phytoestrogen and breast cancer risk 114 spot urines and 97 available serum
333 women (aged 45ndash75 years) drawn from the EPIC
Not reported Phytoestrogen concentrations and breast cancer incidence
Phytoestrogen concentrations in spot urine (adjusted for urinary creatinine) correlated strongly with that in serum with Pearson correlation coefficients gt 08 There were significant relationships (P lt 002) between both urinary and serum concentrations of
38
samples from women who later developed breast cancer Results were compared with those from 219 urines and 187 serum samples from healthy controls matched by age and date of recruitment
study isoflavones across increasing tertiles of dietary intakes Urinary enterodiol and enterolactone and serum enterolactone were significantly correlated with dietary fibre intake (r = 013ndash029) Exposure to all isoflavones was associated with increased breast cancer risk significantly so for equol and daidzein For a doubling of levels odds ratios increased by 20ndash45 [log2 odds ratio = 134 (106ndash170P = 0013) for urine equol 146 (105ndash202 P = 0024) for serum equol and 122 (101ndash148 P = 0044) for serum daidzein]
Howe et al (1990)
Pooled analysis of 12 case-control studies of diet and breast cancer risk
Healthy women Not reported Breast cancer incidence
A consistent statistically significant positive association was found
between breast cancer risk and saturated fat intake in
postmenopausal women (relative risk for highest vs lowest quintile
146 P lt0001) A consistent protective effect for a number of
markers of fruit and vegetable intake was demonstrated vitamin C
intake had the most consistent and statistically significant inverse
association with breast cancer risk (relative risk for highest vs
lowest quintile 069 P lt0001)
Holm et al (1993)
Interviews regarding diet history the purpose being to determine whether dietary habits are associated with disease-free survival
in patients with
breast cancer who have undergone treatment
240 women with stage I-II breast cancer (50ndash65 years old) 209 of whom were post-menopausal
4-years Disease-free survival
Cancers were classified as oestrogen receptor (ER) rich ( 010
fmolmicrog of DNA) in 149 patients and as ER poor (lt010 fmolmicrog
of
DNA) in 71 patients Fifty-two patients had treatment failure during
follow-up The 30 patients with ER-rich tumours who had treatment
failure reported higher intakes of total fat saturated fatty acids and
polyunsaturated fatty acids than did the 119 patients with ER-rich
tumours that did not have treatment failure The multiple-odds ratio
(OR) for treatment failure in these women was 108 for each 1
increment in percentage of total energy (E) from total fat For
treatment failure within the first 2 years the OR was 119 for each
1-mg increase in vitamin E intake per 10 mega joules of energy In
women with treatment failure 2ndash4 years after diagnosis Ors were
113 and 123 for each E increment in total fat or saturated fatty
acids respectively No association between dietary habits and
treatment failure was found for women with ER-poor cancers
39
Holmes et al (1999)
Cohort study (Nurseslsquo Health Study)
to determine whether intakes
of fat and fatty acids are associated
with breast cancer
88795 women free of cancer (2956 developed breast cancer)
14-years Relative risk of invasive breast
cancer for
an incremental increase of fat intake
Compared with women obtaining 301 to 35 of energy from fat women consuming 20 or less had a multivariate
RR of breast
cancer of 115 (95 CI 073-180) In multivariate models the RR
(95 CI) for a 5-of-energy increase was 097 (094-100) for total
fat 098 (096-101) for animal fat 097 (093-102) for vegetable
fat 094 (088-101) for saturated fat 091 (079-104) for
polyunsaturated fat and 094 (088-100) for monounsaturated fat
For a 1 increase in energy from trans-unsaturated fat the values
were 092 (086-098) and for a 01 increase in energy from
omega-3 fat from fish the values were 109 (103-116)
Hunter et al (1996)
Pooled analysis of 7 prospective studies in 4 countries to establish estimates of the relation of fat
intake
to the risk of breast cancer
Studies included
33781
9 women
Not reported Breast cancer incidence
Information about 4980 cases from studies including 337819
women was available When women in the highest quintile of
energy-adjusted total fat intake were compared with women in the
lowest quintile the multivariate pooled relative risk of breast cancer
was 105 (95 CI 094 to 116) Relative risks for saturated
monounsaturated and polyunsaturated fat and for cholesterol
considered individually were also close to unity There was little
overall association between the percentage of energy intake from
fat and the risk of breast cancer even among women whose energy
intake from fat was less than 20
Ingram et al (1994)
Cohort study evaluating the role of vitamins in breast cancer mortality
103 women 3-months post-operation for primary breast cancer
Mean= 81-months
Mortality from breast cancer
27 women died ndash 21 with advanced breast cancer and 6 from other causes The most important findings from the nutrient consumption assessment were associated with vitamin consumption in particular beta-carotene and vitamin C At high levels of consumption there were significantly fewer deaths from breast cancer only one in the group of highest beta-carotene consumers compared with eight in the intermediate group and 12 in the lowest group (trend P = 00012) equivalent figures for vitamin C were 3 7 and 11 deaths for the highest intermediate and lowest consumption groups respectively (trend P = 00286)
Keinan-Boker et al (2004)
An investigation of the association between phytoestrogen
intake and
breast cancer risk in a large prospective study in
a Dutch
population with a habitually low phytoestrogen intake (EPIC)
15555 women aged
49ndash70
years who constituted a Dutch cohort the EPIC study
Median = 52-years
Breast cancer incidence
A total of 280 women were newly diagnosed with breast cancer
during follow-up The median daily intakes of isoflavones and
lignans were 04 (interquartile range 03ndash05) and 07 (05ndash08)
mgd respectively Relative to the respective lowest intake
quartiles the hazard ratios for the highest intake quartiles for
isoflavones and lignans were 10 (95 CI 07 15) and 07 (05
11) respectively Tests for trend were non-significant
Khaodhiar et al (2003)
A subgroup analysis of WINS participants (Chlebowski et al
53 women from 3 clinical
sites
2-years after start of
Insulin resistance and dietary fat
Of those women with initial insulin resistance after 1-year women in
the intervention group saw their fasting insulin decrease by 18 plusmn 34
40
2006a) examining relationships between dietary intake and insulin resistance
who had serum insulin and lipid profiles evaluated at baseline
and
after 2-years
commencing intervention
intake microUmL in comparison fasting insulin of women in the control
group decreased by only 138 plusmn 47 microUmL Although not
quite
statistically significant these results predict that elevated insulin concentrations (a marker of insulin resistance)
may be influenced by
dietary fat reduction There were no significant differences between
the treatment groups over time and no time x treatment interactions
and no significant differences were seen between the insulin-
resistant and non-insulin-resistant subgroups
Kim et al (2006)
The Nurseslsquo Health Study a prospective cohort study examining the relationship between dietary fat and incidence of breast
cancer in
post-menopausal women
Cohort of 80375 US women
Followed for 20-years between 1980 and 2000 with questionnaire being mailed every 2-years
Incidence of breast cancer The Food Frequency Questionnaire
The multivariable relative risk for an increment of 5 of energy from
total dietary fat intake was 098 (95 CI 095 100) Additionally
specific types of fat were not associated with an increased risk of
breast cancer Furthermore secondary analyses indicated no
differences in breast cancer risk by oestrogen receptor or
progesterone receptor status However stratification by
waist circumference indicated a significant decrease in breast
cancer risk for participants with a waist circumference of 35
inches (889cm) or greater (p-trend = 004)
Kyogoku et al (1992)
The present study utilised breast cancer patients whose dietary intake was assessed 10-years previously in a case-control study to determine whether dietary intake is related prognosis
212 breast cancer patients post-surgery
Followed-up until 1987 (9-12 years)
Mortality A total of 47 breast cancer deaths were certified The 5- and 10-year relative survival rates were 785 and 753 respectively The investigation did not provide any support for the hypothesis that a high-fat diet is a survival determinant for breast cancer patients
McEligot et al (2006)
Retrospective study into the influence of diet (fat fibre vegetable and fruit intakes and micronutrients (folate carotenoids and vitamin C) on overall survival in women diagnosed with breast cancer
Post-menopausal breast cancer survivors (n = 516)
Mean of 80-months post-diagnosis
Death due to any cause
The hazard ratio [HR and 95 CI] of dying in the highest tertile compared to the lowest tertile of total fat fibre vegetable and fruit was 312 (95 CI = 179-544) 048 (95 CI = 027-086) 057 (95 CI = 035-094) and 063 (95 CI = 038-105) respectively (P le 005 for trend except for fruit intake) Other nutrients including folate vitamin C and carotenoid intakes were also significantly associated with reduced mortality (P le 005 for trend)
Pierce et al (2007)
The multicentre WHEL RCT (see Gold et al 2009 in table)
Breast cancer (n=3088) intervention (n=1537) comparison (n=1551)
After 7-years of intervention
Invasive breast cancer event (recurrence
or
new primary) or death from any cause
Attrition in the intervention group (n=38) versus control group (n=27) There were no additional health benefits of dramatically increasing intake of nutrient-rich plant-based foods relative to the comparison group
Thomson et al (2007)
Sub-analysis of a purposive sample of participants in the WHEL RCT (see Gold et al 2009 in table)
Breast cancer patients (n=207)
Not reported Oxidative stress A significant inverse association was found between total plasma carotenoid concentrations and oxidative stress
41
WEIGHT
Caan et al (2008)
Retrospective study examining whether weight gain after diagnosis of breast cancer affects the risk of breast cancer recurrence Weight change from 1-year pre-diagnosis to study enrolment was calculated
3215 women with early stage breast cancer
Median of 737-months post-diagnosis
Breast cancer recurrence
Neither moderate (5ndash10) nor large (gt 10) weight gain (HR 08 95 CI 06ndash11 HR 09 95 CI 07ndash12 respectively) after breast cancer diagnosis was associated with an increased risk of breast cancer recurrence in the early years post-diagnosis
Enger et al (2004)
A retrospective cohort study using patient medical
records electronic
cancer registry data and archived tissue
specimens to examine
correlates of body weight with mortality in early-stage breast cancer
Women (n=1376)
24-
81 years of age diagnosed with breast cancer
Median=68 years post-diagnosis
Body weight at the time of diagnosis
and
patient status (ie alive and free of breast cancer living
with breast
cancer dead of breast cancer or dead of other
cause) at
the time of longest follow-up
246 patients died from breast cancer Among patients with early-
stage disease (I and IIA) a dose-response relationship was
observed with increasing weight and likelihood of dying of breast
cancer Compared with women in the lowest category of weight (lt133lb [60 kg] at diagnosis) women in the highest category ( 17
lb
[79 kg]) experienced a 25-fold increased risk of dying from breast
cancer (HR ratio 254 [95 CI 108-600] trend P = 02) Women
with ER-negative cancer experienced an approximately 2-fold
higher risk of dying from breast cancer compared with women with
ER-positive cancer regardless of stage at diagnosis Women in the
upper 50th percentile of weight with early-stage
disease and with
ER-negative tumours had a nearly 5-fold increased risk of dying
(HR ratio 499 [95 CI 217-1148] P for interaction = 10)
compared with women in the lower 50th percentile of weight
and ER-
positive tumours
Hebert et al (1998)
Prospective cohort study examining the effect of diet and body weight on recurrence and death in breast cancer patients
472 women diagnosed with early-stage breast cancer in 1982ndash1984
Ranged from 8-10 years
Breast cancer recurrence and mortality
After accounting for disease stage and age reported baseline consumption (timesday) of butter margarine and lard (risk ratio (RR)=167 95 CI=117ndash239) and beer (drinksday) (RR=158 95 CI=115ndash217) increased the risk of recurrence There also appeared to be an increased risk associated with consumption of red meat liver and bacon corresponding to about a doubling of risk for each time per day that foods in this category were consumed (RR=193 95 CI=089ndash415) Relative body weight increased risk at the rate of 9 (RR=109 95 CI=102ndash117) for
each kgm2 (equivalent to about 58 pounds for a woman 5 4 tall) For death the results were similar but relative weight was more strongly associated increasing risk by 12 per kgm2 (RR=112 95 CI=103ndash122)
Kroenke et al (2005)
A prospective study of a purposive subsample of participants from the Nurseslsquo Health Study ndash to determine
5204 Nurseslsquo Health Study participants
2-26 years with a median
Incident breast cancer
Weight before diagnosis was positively associated with breast
cancer recurrence and death but this was apparent only in never
smokers Similarly among never-smoking women those who
42
whether weight prior to diagnosis and weight gain
after diagnosis are
predictive of breast cancer survival
diagnosed with
incident invasive non-metastatic breast cancer between
1976
and 2000
follow-up of
9-years Breast cancer recurrence Mortality for any cause Self-reported BMI
gained between 05 and 20 kgm2 (median gain 60 lb relative risk
[RR] 135 95 CI 093 to 195) or more than 20 kgm
2 (median
gain 170lb RR 164 95 CI 107 to 251) after diagnosis had an
elevated risk of breast cancer death during follow-up (median 9
years) compared with women who maintained their weight (test for
linear trend P = 03) Associations with weight were stronger in
premenopausal than in postmenopausal women
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer
Breast cancer Not reported Additional breast cancer events and mortality
The most consistent finding from observational studies was that adiposity was associated with a 30 increased risk of mortality
SMOKING
Holmes et al (2007)
A prospective observational study among 5056 women from the Nurseslsquo Health Study for whom data on smoking history was available
Women with Stages I-III invasive breast cancer diagnosed between 1978 and 2002
Median = 83 years
Death by any cause Cause of death was ascertained from death certificates supplemented as needed with physician review of medical records
Compared with never smokers women who were current smokers had a 43 increased adjusted relative risk (RR) 95 CI 124-165] of death from any cause A strong linear gradient was observed with the number of cigarettes per day smoked p-trend lt00001 the RR (95 CI) for 1-14 15-24 and 25 or more cigarettes per day was 127 (101-161) 130 (108-157) and 179 (147-219) In contrast there was no association with current smoking and breast cancer death the RR (95 CI) was 100 (083-119) Current and past smokers were more likely than never smokers to die from primary lung cancer chronic obstructive pulmonary disease and other lung diseases
Fentiman et al (2005)
Cohort study testing the hypothesis that smokers have a worse breast cancer prognosis
Women (n=166) with stage III invasive breast cancer
Mean = 132-months
Overall and cancer-specific disease-free survival
Smoking was the third most important predictor of distant relapse-free breast cancer-specific and overall survival after stage and age at diagnosis
Manjer et al (2000)
Cohort study examining whether smoking is associated with prognostic markers other than more advanced disease (eg hormone receptor status histopathology and tumour differentiation)
268 women with recurring breast cancer drawn from a cohort of 10902 women (35 smokers)
An average of 124-years
Hormone receptor status identified by tumour tissue
The relative risk (RR) of oestrogen receptor-negative tumours was for current smokers 221 [95 CI 123-396] and for ex-smokers 267 (95 CI 141-506) compared to never-smokers Ex-smokers had an increased risk of progesterone receptor-negative tumours (RR = 161 95 CI 107-241) but there were no other significant associations between smoking habits and oestrogen receptor-positive or progesterone receptor-positive or ndashnegative tumours The incidence of Nottingham grade III tumours was higher in ex-smokers than in never-smokers (RR = 203 95 CI 117-354)
Sagiv et al (2007)
Cohort study examining the association between active and passive cigarette smoking before
Women with invasive breast cancer
Approximately 6-years after
All-cause mortality including breast
The adjusted hazards ratios (HRs) for all-cause mortality were slightly higher among current and former active smokers compared with never smokers (HR 123 95 CI 083ndash184) and 119 (95
43
breast cancer diagnosis and survival (n=1273) participating in a population-based casendashcontrol study
diagnosis cancer-specific mortality as reported to the National Death Index
CI 085ndash166) respectively) No association was found between active or passive smoking and breast cancer-specific mortality All-cause and breast cancer-specific mortality was higher among active smokers who were postmenopausal (HR 164 95 CI 103ndash260 and HR 145 95 CI 078ndash270 respectively) or obese at diagnosis (HR 210 95 CI 103ndash427 and HR 197 95 CI 089ndash436 respectively)
ALCOHOL
McDonald et al (2002)
Prospective cohort study examining the influence of alcohol consumption on breast cancer survival in African American women
Post-menopausal African-American women with invasive breast cancer (n=125)
Followed for survival through December 1998 (median = 648 months)
Survival Pre-morbid alcohol consumption of at least one drink per week was associated with 27-fold increase in risk of death (95 CI 13ndash58)
Reding et al (2009)
Sub-analysis of participants from two case-control studies to examine the effects on prognosis of alcohol consumption after breast cancer diagnosis
1286 women diagnosed with invasive breast cancer at age le45 years from two population-based case-control studies
Followed from their diagnosis of breast cancer (between January 1983 and December 1992) through to June 2002
The primary mortality endpoint used was all-cause mortality
After adjusting for age and diagnosis year compared with non-drinkers women who consumed alcohol in the 5 years before diagnosis had a decreased risk of death [gt0 to lt3 drinks per week hazard ratio 07 95 CI 06-095 3 to lt7 drinks per week risk ratio 06 95 CI 04-087 drinks per week risk ratio 07 95 CI 05-09]
Rock and Demark-Wahnefried (2002)
A review of evidence from clinical and
epidemiologic studies examining
the relationship between nutritional
factors and breast cancer survival
Women with breast cancer
Not reported Survival Alcohol intake was not associated with survival in the majority of the
studies that examined this relationship
44
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
colorectal cancer survival In the current review 2 studies were identified Studies are
summarised in Table 4 at the end of this section
In a cohort study self-reported leisure time physical activity was assessed in 41528
Australians among whom 526 cases of colorectal cancer were identified (Haydon et al
2006) Those who reported regular physical activity (at least once per week) prior to
diagnosis had improved cancer-specific survival (73 5-year survival) compared with
those not reporting regular physical activity (61 5-year survival) Another study of
stage III colorectal cancer survivors (n=816) over a 3-year period post-surgery and
chemotherapy showed increases in disease-free survival and overall survival with
increasing volumes of physical activity (p lt 05) (Meyerhardt et al 2005)
ii DIET
Bekkering et al (2006) report on six high fibre diet interventions that showed little effect on
the risk of colorectal cancer recurrence (McKeown-Eyssen et al 1995 MacLennan et al
1999 Alberts et al 2000 Bonithon-Kopp et al 2000 Schatzkin et al 2000 Ishikawa et al
2005) On combining data from two beta-carotene trials (Greenberg et al 1994
MacLennan et al 1999) four multivitamin trials (Greenberg et al 1994 Ponz and
Roncucci 1997 Hofstad et al 1998 McKeown-Eyssen et al 1995) and one trial containing
a multivitamin arm and an N-acetylcysteine (found in high protein foods) arm (Ponz and
Roncucci 1997) there was weak evidence of a reduction in risk of colorectal polyps
(abnormal growth of tissues in the colon) Two calcium interventions showed some
evidence of a reduced risk of recurrence (Baron et al 1999 Bonithon-Kopp et al 2000)
In the current review 5 studies provided further evidence for the role of diet in colorectal
cancer survival
Dietary Fibre
The association between dietary fibre and incidence of colorectal cancer was examined in all
participants (n=519978) taking part in the EPIC study (Bingham et al 2003) After 45-years
of follow-up self-reported dietary data for 1065 reported cases of colorectal cancer were
showed that higher dietary fibre was associated with a reduced risk of developing
large bowel cancer Interestingly the protective effect was greatest for the left side of the
colon and least for the rectum No food source of fibre was significantly more protective of
cancer incidence than others Confirmation of these findings after adjustment for folate and
with a longer follow-up has been reported (Bingham et al 2004 Norat et al 2005)
45
Red and Processed Meat
The EPIC study also offers support for the hypotheses that consumption of red and
processed meat increases colorectal cancer risk while intake of fish decreases risk
(Norat et al 2005) Meyerhardt et al (2007) support this further in a study examining dietary
patterns in stage III colorectal cancer survivors (n=1009) After a median of 53-years follow-
up a significant difference was found between those who had followed a prudentlsquo diet and
those who had followed a Westernlsquo diet
A higher intake of a Western dietary pattern post-diagnosis was associated with a
significantly worse disease-free survival (colon cancer recurrences or death) (p
lt001) The Western dietary pattern was associated with a similar detriment in overall
survival (p lt001)
Vitamin D
Ng et al (2008) examined pre-diagnosis levels of vitamin D in a cohort of participants with
colorectal cancer (n=304) from the Nursesrsquo Health Study28 which demonstrated that higher
plasma vitamin D levels were associated with a significant reduction in mortality from
any cause This indicates that lifestyle pre-diagnosis can produce post-diagnosis benefits
Dietary Supplements
A double-blind randomised placebo-controlled intervention study (the FAB2 Study) was
carried out with healthy controls (n=98) and patients with colorectal polyps (n=106) to
examine the effects of folic acid (a B vitamin found in leafy vegetables such as spinach
asparagus and lettuce) and riboflavin (a B-vitamin found in lean meats eggs nuts and
dairy products) supplements on biomarkers of colorectal cancer risk (Powers et al 2007)
Participants were randomised to receive one of four treatments
1) placebo capsule daily
2) 400μg of folic acid daily
3) 1200μg of folic acid daily
4) 400μg of folic acid with 5mg of riboflavin daily
28
One of the largest and longest running investigations of factors that influence womenlsquos health
comprising information from 238000 nurse-participants
Prudent diet High intake of fruit vegetables poultry and fish
Western diet
High intake of meat fat refined
grains sweets and desserts
46
Short-term low folic acid supplements in the range of 400μg were found to elicit a
significant increase in mucosal folate concentration causing a number of physiologic
responses that may reduce the risk of cancer recurrence This adds to the evidence that
increased fibre might be protective against cancer mortality since folate and fibre are
generally found in the same foods
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in colorectal
cancer recurrence In the current review 3 studies were identified
Dignam et al (2006) explored the impact of obesity via retrospective data from patients with
confirmed Dukes B or C colorectal cancer (n=4288) and found that very obese men and
women have an increased risk of recurrence In contrast the multicentre prospective
observational CALBG 8980 trial has shown that increased BMI during and 6-months after
adjuvant chemotherapy for stage III colorectal cancer (n=1053) was not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008)
Sinicrope et al (2010) categorised stage II and III colon cancer (n=4381) patients enrolled
in seven RCTs whilst undergoing adjuvant chemotherapy according to their BMI They
found that BMI was significantly associated with both disease-free survival and overall
survival in both men and women when compared to normal-weight controls Being
overweight was associated with improved overall survival in men whilst being underweight
was associated with significantly worse overall survival in women This demonstrates that
obesity is an independent prognostic variable in colon cancer survivors as well as showing
gender-related differences that require further investigation
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in colorectal
cancer survival and no studies were identified in the current review
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in colorectal
cancer survival Preliminary EPIC results indicate that current alcohol intake is
significantly positively associated with risk of rectal but not of colon cancer (Ferrari et
al (2007)
47
SUMMARY OF LIFESTYLE EVIDENCE FOR COLORECTAL CANCER ndash
MECHANISMS OF BENEFIT
Physical Activity There is very little evidence available for the role of physical activity in
colorectal cancer outcomes however the evidence that is available looks promising
Specifically regular physical activity of at least once per week pre-diagnosis has been found
to improve 5-year survival rates (Haydon et al 2006) This highlights the importance of
physical activity being integrated into an individuallsquos way of life even before the occurrence
of illness Furthermore long-term physical activity post-surgery can further increase chances
of recurrence-free survival and there is also evidence of a dose-effect survival benefits
increase with amount of exercise (Meyerhardt et al 2005)
Diet Whilst evidence for dietary fibre has been mixed the additional evidence presented
within this review places greater weight in favour of increased dietary fibre Indeed the
conclusion of one study was that in populations with low average intake of dietary fibre an
approximate doubling of total fibre intake from foods could reduce the risk of colorectal
cancer by 40 (Bingham et al 2003) Evidence of this protective benefit for dietary fibre is
further supported by research demonstrating that short-term low folic acid (found in fibrous
foods) supplements in the range of 400μg can reduce the risk of cancer recurrence (Powers
et al 2007) There is a general consensus that mechanisms of benefit from dietary fibre
come from increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic mucosa (tissue
that lines the colon) (Kim 2000) Evidence has also been presented supporting the
hypothesis that red and processed meat increases colorectal cancer risk while fish
decreases risk (Norat et al 2004)
Weight Two large-scale studies offer contrasting findings for the role of weight
in colorectal cancer outcomes One prospective observational study demonstrates that
increased BMI during and 6-months after adjuvant chemotherapy is not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008) The other
retrospective study demonstrates that very obese men and women have an increased risk
of recurrence Drawing on 7 RCTs Sinicrope et al (2010) provides further evidence for BMI
was being significantly associated with both disease-free and overall survival Overall there
is greater evidence showing weight to be an important predictor of colorectal cancer
outcomes There is also some evidence of gender differences being overweight was
associated with improved overall survival in men whilst being underweight was associated
with significantly worse overall survival in women There is evidently a need to explore this
differential effect more closely However there is also the need to consider the impact of
body composition on the development of other chronic conditions including diabetes and
cardio-respiratory conditions
Smoking and Alcohol Further research is needed into smoking and alcohol
consumption especially in terms of colorectal cancer prognosis There is some evidence
indicating that current alcohol intake increases risk of rectal but not colon cancer a finding
that requires further investigation to ascertain underlying mechanisms of benefit (Ferrari et
al 2007) Since alcohol can reduce absorption of folate it is possible that the mechanism
48
of benefit is as with dietary fibre intake related to stool bulk and less contact time between
carcinogens and colonic mucosa
49
Table 4 Colorectal Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Haydon et al (2006)
Incident cases of colorectal cancer were identified among participants of the Melbourne Collaborative Cohort Study and examined against self-reported physical activity
526 Australians with colorectal cancer
Median = 55 years
Body fat Disease-specific survival
Exercisers had an improved disease specific survival (hazard ratio 073 (95 CI 054ndash100) The benefit of exercise was largely confined to stage IIndashIII tumours (hazard ratio 049 (95 CI 030ndash079) Increasing per cent body fat resulted in an increase in disease-specific deaths (hazard ratio 133 per 10 kg (95 CI 104ndash171) Similarly increasing waist circumference reduced disease specific survival (hazard ratio 120 per 10 cm (95 CI 105ndash137)
Meyerhardt et al (2005)
Prospective study of recreational physical activity and prognosis
among
stage III colon cancer patients enrolled in a
RCT of post-operative adjuvant
chemotherapy (bolus 5-
fluorouracilleucovorin +- irinotecan)
816 patients with stage III colon cancer
Midway through adjuvant therapy and again 6-months post-therapy (12ndash14 months after enrolment)
Physical activity levels were measured as MET-hours-per-week Disease-free survival
Levels of physical activity were associated with significantly improved
disease-free survival among patients with stage III colon cancer After
adjustment for age gender baseline performance status N stage T
stage preoperative CEA bowel obstruction and perforation level of
differentiation treatment arm and body mass index the hazard ratio
(HR) for DFS for individuals in the highest quintile (gt25 MET-
hoursweek eg Jog 3ndash4 hoursweek or brisk walk [3ndash4 mph] daily)
was 065 (95 CI 038ndash111 p for trend = 002) compared to those
in the lowest quintile of PA This relationship varied by gender with a
HR = 033 [95 CI 011ndash099] for women (p for trend = 0046) and a
HR= 089 [95 CI 044ndash178] for men (p for trend = 03)
DIET
Bingham et al (2003)
Prospective examination of the association between dietary fibre intake and incidence of colorectal cancer in individuals taking part in the EPIC study recruited from ten European countries
519978 men and women in the EPIC study (1065 cases of colorectal cancer)
45 years
Colorectal cancer incidence
Dietary fibre in foods was inversely related to incidence of large bowel cancer (adjusted relative risk 0middot75 [95 CI 0middot59ndash0middot95] for the highest versus lowest quintile of intake) the protective effect being greatest for the left side of the colon and least for the rectum After calibration with more detailed dietary data the adjusted relative risk for the highest versus lowest quintile of fibre from food intake was 0middot58 (0middot41ndash0middot85)
Meyerhardt et al (2008)
Prospective observational study to
determine the association of dietary patterns
with cancer recurrences and
mortality of colon cancer survivors
1009 patients with stage III colon cancer who were
enrolled in
a randomized
Median = 53-years
Colon cancer recurrence and mortality
A higher intake of a Western dietary pattern after cancer diagnosis
was associated with a significantly worse disease-free survival (colon
cancer recurrences or death) Compared with patients in the lowest
quintile of Western dietary pattern those in the highest quintile experienced an adjusted hazard
ratio (AHR) for disease-free survival
of 325 (95 confidence interval [CI] 204-519 P for trend lt001)
50
adjuvant chemotherapy trial (CALGB
89803)
The Western dietary pattern was associated with a similar detriment
in recurrence-free survival (AHR 285 95 CI 175-463) and overall
survival (AHR 232 95 CI 136-396]) comparing highest to
lowest quintiles (both with P for trend lt001)
Ng et al (2008)
Nurseslsquo Health Study prospective examination of the association between pre-diagnosis
25(OH)D levels and
mortality in colorectal cancer patients
304 colorectal cancer patients
Mean = 78-months for participants still alive
Colorectal cancer mortality
Higher plasma 25(OH)D levels were associated with a significant
reduction in overall mortality (P for trend = 02)
Compared with the lowest quartile participants in the highest
quartile had an adjusted HR of 052 (95 CI 029 to 094) for
overall mortality A trend toward improved colorectal cancerndash
specific mortality was also seen (HR = 061 95 CI 031 to 119)
Norat et al (2005)
The EPIC prospective study of 478040 cancer-free men and women from 10 European countries examining meat fish and colorectal cancer risk
478040 cancer-free men and women taking part in the EPIC study
Mean=48 years
Colorectal cancer incidence
Colorectal cancer risk was positively associated
with intake of red and processed meat (highest [gt160
gday] versus lowest [lt20 gday] intake HR = 135 95 CI = 096
to
188 Ptrend = 03) and inversely associated with intake of fish (gt80
gday versus lt10 gday HR = 069 95 CI = 054 to
088 Ptrendlt001) but was not related to poultry intake In this study
population the absolute risk of development of colorectal
cancer within 10-years for a study subject aged 50 years was 171
for the highest category of red and processed meat intake and 128
for the lowest category of intake and was 186 for subjects in
the lowest category of fish intake and 128 for subjects in
the highest category of fish intake
Powers et al (2007)
A double-blind RCT (the FAB2 Study) to examine effects of folic acid and riboflavin supplements on biomarkers of colorectal cancer risk Participants were randomised to receive one of the following for 6 ndash 8 weeks 1)400μg of folic acid 1200μg of folic acid or 400μg of folic acid plus 5 mg of riboflavin 2) placebo
Healthy controls (n=98) and patients with colorectal polyps (n=106)
On completion of 6-8 week intervention
Biomarkers of folate and riboflavin status
Supplementation with folic acid elicited a significant increase in mucosal 5-methyl tetrahydrofolate and a marked increase in RBC and plasma with a dose-response Measures of riboflavin status improved in response to riboflavin supplementation Riboflavin supplement enhanced the response to low-dose folate in people carrying at least one T allele and having polyps The magnitude of the response in mucosal folate was positively related to the increase in plasma 5-methyl tetrahydrofolate but was not different between the healthy group and polyp patients
WEIGHT
Dignam et al (2006)
Investigating the association between BMI and colorectal cancer outcomes in patients from cooperative group clinical trials
4288 patients with Dukes
BC
colon cancer in National
Median =112-
years Risk of recurrence second primary
Very obese patients (BMI 35 kgm2) had greater risk
of a
colon cancer event (recurrence or secondary primary tumour hazard
ratio [HR] = 138 95 confidence interval [CI] = 110 to 173) than
normal weight patients (BMI = 185ndash249 kgm
2) Mortality was
51
Surgical Adjuvant Breast and Bowel Project
RCTs
cancer and
mortality evaluated in
relation to
BMI at diagnosis
greater for very obese (HR = 128 95 CI = 104 to 157) and
underweight (BMI lt 185 kgm2) (HR
= 149 95 CI = 117 to 191)
than for normal weight patients The increased risk of mortality for
underweight patients was dominated by nonndashcolon cancer deaths
(HR of such deaths compared with normal weight patients = 223 95 CI = 150 to
331) whereas for the very obese deaths likely due
to colon cancer were increased (HR = 136 95 CI = 106 to 173)
Meyerhardt et al (2008)
A prospective observational study of patients who had stage III colon cancer and who enrolled on a RCT of adjuvant chemotherapy Results
1053 patients who had stage III colon cancer
6-months post- chemotherapy
Patients were observed for cancer recurrence or death
Increased BMI was not significantly associated with a higher risk of colon cancer recurrence or death (P trend = 54) Compared with normal-weight patients (BMI 21 to 249 kgm
2) the multivariate
hazard ratio for disease-free survival was 100 (95 CI 072 to 140) for patients with class I obesity (BMI 30 to 349 kgm
2) and 124
(95 CI 084 to 183) for those with class II to III obesity (BMI ge 35 kgm
2) after analysis was adjusted for tumour-related prognostic
factors physical activity tobacco history performance status age and sex Similarly after analysis was controlled for BMI weight change (either loss or gain) during the time period between ongoing adjuvant therapy and 6-months after completion of therapy did not significantly impact on cancer recurrence andor mortality
Sinicrope et al (2010)
BMI (kgm2) was categorised in patients
with tumour-node-metastasis stage II and III colon carcinomas enrolled in seven RCT of 5-fluorouracilndashbased adjuvant chemotherapy to determine the association of BMI with disease-free survival and overall survival
Men and women with stage II and III colon carcinomas (n = 4381) enrolled in seven RCTs of 5-fluorouracilndashbased adjuvant chemotherapy
Not reported Disease-free survival Overall survival
BMI was significantly associated with both disease-free survival (P = 0030) and overall survival (P = 00017) Men with class 23 obesity showed reduced overall survival compared with normal-weight men [hazard ratio 135 95 CI 102-179 P = 0039] Women with class I obesity had reduced overall survival [hazard ratio 124 95 CI 101-153 P = 0045] compared with normal-weight women Overweight status was associated with improved overall survival in men (P = 0006) and underweight women had significantly worse overall survival (P = 0019)
ALCOHOL
Ferrari et al (2007)
As part of the prospective EPIC study data was collected examining the relationship between lifetime and baseline alcohol consumption and colorectal cancer incidence
478732 EPIC subjects free of cancer at enrolment between 1992 and 2000
62 years Colorectal cancer incidence
Lifetime alcohol intake was significantly positively associated to CRC risk (hazard ratio HR = 108 95CI = 104-112 for 15 gday increase) with higher cancer risks observed in the rectum (HR = 112 95CI = 106-118) than distal colon (HR = 108 95CI = 101-116) and proximal colon (HR = 102 95CI = 092-112) Similar results were observed for baseline alcohol intake When assessed by alcoholic beverages at baseline the CRC risk for beer
52
(HR = 138 95CI = 108-177 for 20-399vs 01-29 gday) was higher than wine (HR = 121 95CI = 102-144) although the two risk estimates were not significantly different from each other Higher HRs for baseline alcohol were observed for low levels of folate intake (113 95CI = 106-120 for 15 gday increase) compared to high folate intake (103 95CI = 098-109)
53
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
prostate cancer survival In the current review 2 studies were identified Studies are
summarised in Table 5 at the end of this section
The underlying mechanisms for the direct anti-cancer effect of lifestyle has been indicated in
a study with men undergoing a diet and physical activity intervention comprising the majority
of calories from complex carbohydrates high in fibre combined with 1-hour of supervised
exercise (Soliman et al 2009) Serum (blood plasma) was taken from these men and added
to androgen-dependent LNCaP cells29 in the laboratory There was decreased growth and
increased apoptosis (cell death) associated with a reduction in serum Insulin-like Growth
Factor (IGF)-130 These findings indicate that diet and physical activity interventions
might slow prostate cancer progression as well as aid in its treatment during the early
stages of development
Kenfield (2010) examined the data of 2686 men from the Health Professionals Follow-Up
Study31 and found that men who engaged in 3gt MET-hours of weekly physical activity
post-diagnosis reduced their risk of death by 35 compared with men who engaged
in less weekly activity Furthermore men who walked 90-minutes per week at a normal to
brisk pace had a 51 lower risk of death due to any cause compared with men who walked
90-minutes or less at an easy pace To reduce their risk of cancer-specific death men
had to engage in vigorous activity such as jogging (6 MET-hours)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in prostate cancer
survival In the current review 7 studies were identified
Dietary Changes plus Supplements
Ornish et al (2005) conducted a diet counselling and lifestyle RCT comprising men with
early prostate cancer (n=93) The lifestyle changes in this study included a vegan diet
supplemented with soy vitamin E fish oils selenium and vitamin C together with a
moderate physical activity program and stress management techniques such as yoga
29
Human prostate cancer cells
30 IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of pathological states including cancer
31 An all-male (n=51529) study designed to complement the all-female Nurses Health Study
54
Prostate Specific Antigen (PSA)32 levels decreased by 4 at 12-months in the
intervention group but increased by 6 in the control group this was statistically
significant and strongly correlated with the degree of lifestyle change However the
intensity of this intervention and associated behavioural changes might not easily be
translated into practice (White et al 2009)
Pomegranate Juice
The potential benefits of pomegranate juice on prostate cancer outcomes frequently appear
in the media and strong evidence of its efficacy can be found within the academic literature
In a phase II open-label single-arm clinical trial men (n=46) with recurrent prostate cancer
who had rising PSA after surgery or radiotherapy were treated daily with 8oz (227g)
equivalent of pomegranate juice (Pantuck et al 2006) Mean PSA doubling time
significantly increased with treatment from 15-months to 54-months demonstrating a
good indication of a relationship between the consumption of pomegranate juice and
prostate health
Green Tea
Another beverage found to demonstrate some positive effects on prostate cancer is green
tea Bettuzzi et al (2006) in a year-long clinical trial has demonstrated that daily
consumption of green tea can produce a ten-fold decrease in the rate at which
prostate intraepithelial neoplasia (a pre-cancerous condition) progresses to prostate
cancer Support for these findings is offered by an uncontrolled open-label single-arm
phase II clinical trial testing the efficacy of Polyphenon E which contains the polyphenol
antioxidants found in green tea (McLarty et al 2009) Taking four capsules of
Polyphenon E daily (equivalent to twelve cups of green tea) for an average of 345
days leading up to radical prostatectomy the participants (n=26) experienced
significant reductions in biomarkers used to monitor likelihood of metastasis Some
patients demonstrated reductions greater than 30
Lycopene Supplements
The EPIC study has demonstrated that similar to breast cancer prostate cancer risk is not
related to fruit and vegetable consumption (Key et al 2004) However further evidence for
the role of carotenoids found in fruit and vegetables have been provided from a pilot RCT
including men with benign prostatic hyperplasia (BPH) a benign enlargement of the prostate
that can progress to cancer (Schwarz et al 2008) Men (n=20) who received 15mg od
lycopene supplementation (a carotenoid found in tomatoes and other red fruits and
32
PSA is a protein produced by the cells of the prostate gland It is present in small quantities in the serum of normal men and is often elevated in the presence of prostate cancer
55
vegetables) for 6-months had significantly decreased PSA levels compared to a
placebo group (n=20) who had no change in PSA
Salicylate
Salicylate33 intake has been implicated in the aetiology of prostate cancer but Thomas et al
(2009) have evaluated their influence on established cancer progression In a randomised
double blind phase II study involving men (n=110) with progressive prostate cancer who
were counselled to eat less saturated fat and processed food more fruit vegetables and
legumes physical activity more regularly and to stop smoking the men were then
randomised to take sodium salicylate alone or combined with vitamin C copper and
manganese gluconates34 daily Although there was no difference in outcome between those
who received sodium salicylate alone or combined the intervention as a whole (ie
including dietary counselling) slowed or stopped the rate of PSA progression in 40
patients (364) for over one-year and a further ten patients were stabilised for 10-
months This data suggests that changes in lifestyle can potentially delay PSA progression
and the need for more radical therapy highlighting an area for further research
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in prostate cancer
survival In the current review 2 studies were identified
Wright et al (2007) prospectively examined BMI and weight change in relation to prostate
cancer incidence and mortality in 287760 men enrolled in the National Institutes of
Health-AARP Diet and Health Study Higher baseline BMI was associated with
significantly reduced total prostate cancer incidence on the one hand but with
significantly increased risk of prostate cancer mortality on the other hand Adult weight
gain from age 18-years to study entry (range=50-71-years old) was positively associated
with prostate cancer staging but not with disease incidence
In a retrospective analysis exploring the interaction between obesity and surgical outcomes
in patients with prostate cancer treated by radical prostatectomy (n=437) a weak but
significant association was observed between BMI and a number of biological
biomarkers indicative of an advanced pathological stage (Gross et al 2009)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in prostate
cancer survival and no evidence was identified in the current review
33
Salicylates are chemicals that occur naturally in many plants including many fruits vegetables and herbs
Salicylates in plants act as a natural immune hormone and preservative protecting the plants against diseases
insects fungi and harmful bacteria 34
A pinkish powder soluble in water used in medicine in vitamin tablets and as a feed additive and dietary
supplement
56
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in prostate cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR PROSTATE CANCER -
MECHANISMS OF BENEFIT
Physical Activity and Diet The evidence within this review indicates that diet and physical
activity interventions might slow prostate cancer progression as well as aid in its treatment
during the early stages of development The mechanism of benefit is primarily via
decreased growth and increased apoptosis (cell death) associated with a reduction in serum
Insulin-like Growth Factor (IGF)-1 (Soliman et al 2009) Up to 3gt MET-hours of weekly
physical activity appears sufficient to increase survival with more vigorous activity of about 6
MET-hours per week for the reduction of cancer-specific mortality (Kenfield 2010) A
number of dietary steps can be taken to reduce PSA levels and thus slow down the growth
of tumours and increase survival For example a vegan diet supplemented with soy vitamin
E fish oils selenium and vitamin C together with a moderate physical activity program and
stress management techniques such as yoga have been found useful (Ornish et al 2005)
as has pomegranate juice (Pantuck et al 2006) and green tea (Betuzzi et al 2006 McLarty
et al 2009) As with breast cancer carotenoids have been found to offer protective
properties for men with benign prostatic hyperplasia which can progress to cancer (Schwarz
et al 2008) Overall the evidence for prostate cancer is suggestive of survival benefits from
combined dietary and physical activity changes In other words it appears that a healthier
diet made up of fruit and vegetables as well as drinks such as pomegranate juice or green
tea combined with 3gt MET-hours of weekly physical activity could be an effective
prescription for reducing mortality from cancer and other causes
Weight Evidence for weight was mixed whilst finding that higher baseline BMI was
associated with significantly reduced total prostate cancer incidence a significant increase in
prostate cancer severity and mortality was also observed with higher BMI levels (Wright et
al 2007a Gross et al 2009) More research is clearly needed to establish any differential
prostate cancer outcomes associated with weight
Smoking and Alcohol More research is required for smoking and alcohol in terms of
prostate cancer outcomes
57
Table 5 Prostate Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Kenfield et al (2009)
Prospective study (Health Professionals Follow-up Study) assessing the relationship between physical activity and duration and pace of walking with total and prostate cancer-specific mortality
2686 men with prostate cancer
4-years Prostate cancer mortality and total physical activity
Men who were physically active especially those engaging in 3 or more MET-hours of total activity had a 35 lower risk of death from any cause (hazard ratio 065 [95 CI 052 082]) and a modest non-significant reduction in risk of prostate cancer death (hazard ratio 088 [95 CI 052 149]) after adjustment for other risk factors for PCa mortality and pre-diagnosis physical activity While no benefit from walking was observed for PCa mortality men who walked 4 or more hours per week versus those who walked less than 20 minutes per week had a 23 lower risk of all-cause mortality (95 CI 061 097 p-trend=001) In addition compared to men who walked less than 90 minutes at an easy walking pace those who walked 90 or more minutes at a normal to very brisk pace had a 51 lower risk of all-cause mortality (95 CI 037 064) More vigorous activity and longer duration of activity was associated with significant further reductions in risk for all-cause mortality More vigorous activity was associated with a borderline-significant reduction in risk for PCa mortality
Soliman et al (2009)
Pritikin Longevity Center 3-Week
Residential Program - men were given prepared
meals with 12ndash15 fat calories
15ndash20 protein calories and the majority
of calories (65ndash70) from unrefined complex carbohydrates high in fibre (gt40 gday) The men attended daily supervised exercise classes
for 60 min
5 men in their early sixties
with no
signs of prostate cancer (PSA lt 40)
On completion of the 3-week programme
Cancer progression
The intervention slowed growth and increased apoptosis in LNCaP cells responses that were eliminated when
IGF-I was added back to
the post-intervention samples The p53 protein content was increased
and NFkB activation reduced in the post serum-stimulated LNCaP
cells Similar results were observed when the IGF-I receptor was
blocked in the pre-intervention serum In androgen-independent PC-3
cells growth was reduced while none of the other factors were
changed by the intervention
DIET
Bettuzzi et al (2006)
A proof-of-principle double-blind placebo-
controlled clinical trial assessing the safety
and efficacy of green tea catechins for the
chemoprevention of prostate cancer incidence in patients with high-grade prostate intraepithelial
neoplasia Daily
treatment consisted of three GTCs
Men with high-grade prostate intraepithelial
neoplasia who would develop cancer within
1-year
3-monthly for 1-year
Primary outcome prostate cancer incidence Secondary outcome
After 1 year only one tumour was diagnosed (incidence 3) in the
cohort receiving green tea whereas 9 cancers were found among the placebo-treated
men (incidence 30) Total PSA did not
change
significantly between the two arms but green tea-treated men showed
values constantly lower with respect to placebo-treated ones As a
secondary observation administration of green tea also reduced lower
urinary tract symptoms suggesting that these compounds might also
58
capsules 200 mg each (total 600 mgd) (n=60) PSA levels be of help for treating the symptoms of benign prostate hyperplasia
Key et al (2004)
An examination of the association between self-reported consumption of fruits and vegetables and prostate cancer risk in EPIC participants
130544 men in 7 countries recruited into EPIC
Median = 48 years
Prostate cancer incidence
There were 1104 incident cases of prostate cancer No significant associations between fruit and vegetable consumption and prostate cancer risk were observed Relative risks (95 CI) in the top fifth of the distribution of consumption compared to the bottom fifth were 106 (084 ndash134) for total fruits 100 (081ndash122) for total vegetables and 100 (079 ndash126) for total fruits and vegetables combined intake of cruciferous vegetables was not associated with risk
McLarty et al (2009)
In order to determine the effects of short-term supplementation with the active compounds in green tea on serum biomarkers in patients with prostate cancer daily doses were provided of Polyphenon E which contained a total of 13 g of tea polyphenols until time of radical prostatectomy
26 men with positive prostate biopsies scheduled for radical prostatectomy
Not reported PSA levels Biomarkers of prostate cancer decreased significantly All of the liver function tests also decreased five of them significantly total protein albumin aspartate aminotransferase alkaline phosphatase and amylase
Ornish et al (2005)
Lifestyle changes including a vegan diet supplemented with soy vitamin E fish oils selenium and vitamin C together with a moderate physical activity program and stress management techniques such as yoga
Men with early prostate cancer (n=93) Gleason scores less than 7
12-months into the intervention
PSA and serum stimulated LNCaP cell growth
PSA levels decreased by 4 at 12-months in the intervention group but increased by 6 in the control group this was statistically significant and strongly correlated with the degree of lifestyle change
Pantuck et al (2006)
A phase II two-stage clinical trial to determine the effects of pomegranate juice PSA progression in men with a rising PSA following primary therapy Patients were treated with 8 ounces of pomegranate juice daily (570mg total polyphenol gallic acid equivalents) until disease progression
46 men with rising PSA levels post-treatment (surgery or radiotherapy)
Every 3-monhs for 54-months
PSA levels Mean PSA doubling time significantly increased with treatment from a mean of 15 months at baseline to 54 months post-treatment (P lt 0001) In vitro assays comparing pre-treatment and post-treatment patient serum on the growth of LNCaP showed a 12 decrease in cell proliferation and a 17 increase in apoptosis (P = 00048 and 00004 respectively) a 23 increase in serum nitric oxide (P = 00085) and significant (P lt 002) reductions in oxidative state and sensitivity to oxidation of serum lipids after versus before pomegranate juice
Schwarz et al (2008)
15mg od lycopene supplementation for 6-months or placebo
Men with benign prostatic hyperplasia (n=40)
After 6-months of intervention
Inhibition or reduction of increased serum PSA levels
Men receiving 15mg od lycopene supplementation had significantly decreased PSA levels compared to a placebo group who had no change in PSA
Thomas et al (2009)
A randomised double blind phase II study to evaluate the influence of salicylate and lifestyle on established cancer progression Men were counselled
110 men whose PSA had risen in 3 consecutive
Not reported Prostate cancer progression (PSA levels)
Although there was no difference in outcome between the SS or CV247 (21 v 19 p=092) the intervention slowed or stopped the rate of PSA progression in 40 patients (364) for over one year A further ten patients were stabilised for ten months Patients least likely to stabilise
59
to eat less saturated fat processed food more fruit vegetables and legumes exercise more regularly and to stop smoking They were then randomised to take sodium salicylate (SS) alone or SS combined with vitamin C copper and manganese gluconates (CV247) daily without other intervention
values gt20 over the preceding 6-months
had received previous radiotherapy or had a Gleason =7 These men welcomed this addition to active surveillance
WEIGHT
Gross et al (2009)
A retrospective cohort study examining whether changes in components of the sex steroid receptor axis may contribute to the clinical aggressiveness of prostate cancer in obese patients
539 patients treated with radical prostatectomy at a single urban hospital between 1994 and 2002
Not reported Pathological stage of prostate cancer BMI
Higher BMI correlated strongly with higher pathologic stage In comparing obese versus non-obese patients there was no difference in expression of androgen or oestrogen related proteins in cancerous epithelial cells However there was a down-regulation of aromatase in the stoma of obese patients suggesting obesity may cause stromal changes in the sex steroid production and signalling pathways which may affect prostate cancer growth via intracrineparacrine mechanisms
Wright et al (2007)
A prospective examination of BMI and adult weight change in relation to prostate cancer incidence and mortality
287760 men ages 50 years to 71 years at enrolment (1995-1996) in the National Institutes of Health-AARP Diet and Health Study
6-years Prostate cancer incidence Weight gain (BMI)
Higher baseline BMI was associated with significantly reduced total prostate cancer incidence largely because of the relationship with localized tumours (for men in the highest BMI category [gtor=40 kgm (2)] vs men in the lowest BMI category [lt25 kgm (2)] RR 067 95 CI 050-089 P = 0006) Conversely a significant elevation in prostate cancer mortality was observed at higher BMI levels (BMI lt25 kgm(2) RR 10 [referent group] BMI 25-299 kgm(2) RR 125 95 CI 087-180 BMI 30-349 kgm(2) RR 146 95 CI 092-233 and BMI gtor=35 kgm(2) RR 212 95 CI 108-415 P = 02) Adult weight gain from age 18 years to baseline also was associated positively with fatal prostate cancer (P = 009) but not with incident disease
60
d) LUNG CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in lung
cancer survival and one systematic review with meta-analysis was identified in the current
review Studies are summarised in Table 6 at the end of this section
Tardon et al (2005) conducted a systematic review and meta-analysis of cohort and case-
control studies from 1966 through October 2003 evaluating the relationship between
physical activity and lung cancer incidence Nine studies were identified 6 of which
demonstrated that that higher levels of leisure-time physical activity (walking gardening
swimming) protects against lung cancer (Severson et al 1989 Thune et al 1997 Lee et
al 1999 Sellers et al 1991 Kubik et al 2002 Mao et al 2003) The estimated combined
risk for both genders was statistically significant as was a dose-response relationship (p lt
01)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in lung cancer
survival and no evidence was identified in the current review
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in lung cancer
survival and no evidence was identified in the current review
iv SMOKING
Smoking has long been accepted as an unhealthy behaviour that increases the risk of
cancer incidence and disease outcomes Yet many people continue to smoke pre- and post-
diagnosis one-third to one-half of cancer patients either continue to smoke after diagnosis or
relapse after initial quit attempts (Gritz et al 2006) Bekkering et al (2006) do not provide
any evidence for the role of smoking in lung cancer survival In the current review 5 studies
were identified that further highlight the importance of smoking cessation support for people
living with and beyond cancer
Vineis et al (2007) have estimated exposure to Environmental Tobacco Smoke (ETS) and to
air pollution in never smokers and ex-smokers in EPIC study participants (n=520000) The
proportion of lung cancers in never- and ex-smokers attributable to ETS was
estimated to be between 16 and 24 mainly due to the contribution of work-related
exposure
61
In two studies of survivors of stage I and II small cell lung cancer risk of a second cancer
was 35-44-fold higher than in the general population (Richardson et al 1993 Tucker et
al 1997) In those who continued to smoke the risk was far higher particularly in those who
also received chest irradiation and alkylating agents35 (Tucker et al 1997) highlighting the
need for risk assessment when offering smoking cessation support or advice
Another study in Japan confirmed that patients with small cell lung cancer who survive
at least 2-years greatly reduced their likelihood of a second cancer if they quit
smoking (p lt 05) (Kawahara et al 2002) Additionally smoking has been found to be
an independent risk factor in breast cancer survivors developing lung cancer (Ford et
al 2003) In support of these studies Parsons et al (2010) report that nine of ten studies
identified in a review of literature from 1966 to 2008 indicate that continuing to smoke is
associated with a significantly increased risk of all-cause mortality in early stage non-
small cell lung cancer and of all-cause mortality in limited stage small cell lung
cancer
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in lung cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR LUNG CANCER - MECHANISMS OF
BENEFIT
Smoking Evidence for the role of lifestyle factors on lung cancer progression and
recurrence has primarily examined smoking which is a strongly established risk factor for
disease progression and mortality Continuing to smoke exposes the body to high levels of
carcinogens which can cause further DNA damage to existing cancers encourage the
cancer to mutate into a more aggressive type or develop mechanisms to hide from the
bodylsquos immunological defences (Akopyan and Bonavida 2006) Indeed smoking has been
found to suppress the immune system interfering with the function of natural killer (NK) cells
- a lymphoid cell type that plays a role in the surveillance of tumour growth Patients who
have already developed one cancer are likely to be more susceptible to DNA damage from a
pre-existing genetic vulnerability or acquired damage from chemotherapy or radiotherapy
Avoiding carcinogens may therefore have a benefit in reducing the risk of developing
further cancers in patients who may be more susceptible from a pre-existing genetic
signature or damage from chemotherapy or radiotherapy The smoking cessation initiatives
currently sweeping the nation such as NHS Choices bdquoSmokefree‟ remain invaluable as
smoking continues to be an important preventable cause of morbidity and mortality
worldwide
Additional Lifestyle Factors More research is required into lifestyle factors such as diet
physical activity weight and alcohol consumption in terms of lung cancer outcomes Access
35
Cytotoxic agents used to disrupt cancer cells can damage healthy cells in the process
62
to lifestyle services such as post-treatment rehabilitation fitness planning and nutritional
support was highlighted as an important component within the disease trajectory for people
with lung cancer (NCSI Mapping Project 2009) There is evidence for the benefits of
physical activity in reducing lung cancer incidence however there is a paucity of evidence
for the survivorship period of lung cancer
63
Table 6 Lung Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Tardon et al (2004)
A meta-analysis of studies (1966-2003) evaluating the relationship between physical activity and lung cancer
Men and women in cohort and case-control studies (9 studies)
Not reported
Lung cancer incidence
The combined ORs were 087 (95 CI=079ndash095) for moderate leisure-time physical activity (LPA) and 070 (062ndash079) for high activity (p trend = 000) This inverse association occurred for both sexes although it was somewhat stronger for women No evidence of publication bias was found Several studies were able to adjust for smoking but none adjusted for possible confounding from previous malignant respiratory disease
SMOKING
Ford et al (2003)
Retrospective analysis of smoking radiation and both exposures on lung carcinoma development in women who were treated previously for breast carcinoma
Case patients (n = 280) females aged 30-89 years with breast carcinoma prior to primary lung carcinoma Control patients (n = 300) selected randomly from 37000 patients with breast carcinoma treated at The University of Texas M D Anderson Cancer Center
Not reported
Lung cancer incidence
At the time of breast carcinoma diagnosis 84 of case patients had ever smoked cigarettes compared with 37 of control patients whereas 45 of case patients and control patients received XRT for breast carcinoma Smoking increased the odds of lung carcinoma in women without XRT (odds ratio [OR] 60 95 confidence interval [95 CI] 36-101) but XRT did not increase lung carcinoma risk in non-smoking women (OR 05 95 CI 03-11) Overall the OR for both XRT and smoking compared with no XRT or smoking was 90 (95 CI 51-159)
Kawahara et al (1998)
Prospective study to investigate whether smoking cessation after successful therapy is associated with a decrease in risk for a second
980 consecutive patients with small cell lung cancer (SCLC)
Median=67 years after initiation of
Second primary tumour
Of the patients who continued to smoke 11 (33) developed a SPT Of the 31 patients who stopped smoking after therapy only three (10) had a subsequent SPT Among those who continued to smoke the risk for a SPT was significantly increased (54 times 95 CI 27-97) relative to the general
64
primary tumour being treated with combination chemotherapy with or without chest radiotherapy
therapy population In contrast those who stopped smoking showed only a 16-fold increase (95 CI 03-46) which was not significantly different from the level in the general population The relative risk for non-SCLC was significantly increased 128-fold (95 CI 34-328) in continuing smokers No second non-SCLCs have been found among those who stopped smoking The 33 patients who continued to smoke had a significantly increased risk of a SPT (43 95 CI 11-159 P=003) Relative to the risk of SPT in patients without previous radiotherapy who stopped smoking the risk is 092 in patients without radiotherapy who continued smoking 037 in patients with radiotherapy who stopped smoking and 233 in patients with radiotherapy who continued smoking The risk of current smoking in patients with previous radiotherapy is 630 relative to those with radiotherapy who stopped smoking although this interaction is not statistically significant (P = 024)
Parsons et al (2010)
A systematic review with meta-analysis of the evidence that smoking
cessation after diagnosis
of a primary lung tumour affects prognosis Databases searched CINAHL (from 1981) Embase (from 1980) Medline
(from 1966)
Web of Science (from 1966) CENTRAL (from 1977)
to
December 2008 and reference lists of included studies
RCTs or observational
st
udies measuring
the effect of quitting smoking
post-
diagnosis on lung cancer prognosis
Patients were followed for 6-months gt in 5 studies but only at time of diagnosis treatment in 4
5-year survival using death rates for continuing smokers and quitters obtained from this review
Continued smoking was associated with a significantly increased risk of all-
cause mortality (hazard ratio 294 95 CI 115 to
754) and recurrence (186
101 to 341) in early stage non-small cell lung cancer and of all-cause
mortality (186 133 to 259) development of a second primary tumour (431 109 to 1698)
and recurrence (126 106 to 150) in limited stage small
cell lung cancer No study contained data on the effect of quitting
smoking on
cancer specific mortality or on development of a second primary tumour in
non-small cell lung cancer Life table modelling on the basis of these data
estimated 33 five year survival in 65 year old patients with early stage non-
small cell lung cancer who continued to smoke compared with 70 in
those
who quit smoking In limited stage small cell lung cancer an estimated 29
of continuing smokers would survive for five years compared with 63 of
quitters on the basis of the data from this review
Richardson et al (1993)
Retrospective review to determine the incidence of second primary cancers developing in patients surviving free of cancer for 2 or more years after treatment for small-cell lung cancer and to assess the potential effect of smoking cessation
Consecutive sample of 540 patients with small-cell lung cancer
Median=61 years
Relative risk for second primary cancers and death
55 patients (10) were free of cancer 2-years after initiation of therapy 18 of these developed one or more second primary cancers including 13 who developed second primary non-small-cell lung cancer The risk for any second primary cancer compared with that in the general population was increased four times (relative risk 44 95 CI 25-72) with a relative risk of a second primary non-small-cell lung cancer of 16 (CI 84-27) Forty-three patients discontinued smoking within 6-months of starting treatment for small-cell lung cancer and 12 continued to smoke In those who stopped smoking at time of diagnosis the relative risk of a second lung cancer was 11 (CI 44 to 23) whereas in those who continued to smoke it was 32 (CI 12 to 69)
Tucker et al (1997)
A multi-institution study to investigate the risk among survivors of developing second primary
611 patients who had
been cancer
Not reported
Population-based rates of cancer
Relative to the general population the risk of all second cancers among these
patients was increased 35-fold Second lung cancer risk was increased 13-
fold among those who received chest irradiation in comparison to a sevenfold
65
cancers other than small-cell lung carcinoma
free for more than 2 years after therapy for small-cell lung cancer
incidence and mortality
increase among non-irradiated patients It was higher in those who
continued smoking with evidence of an interaction between chest irradiation and continued smoking
(relative risk = 21) Patients treated with various forms
of combination chemotherapy had comparable increases in risk (94- to 13-
fold overall) except for a 19-fold risk increase among those treated with
alkylating agents who continued smoking
Vineis et al (2007)
Prospective study to estimate exposure to Environmental Tobacco Smoke (ETS) in never smokers and ex-smokers in 10 European countries (EPIC)
Men and women in the EPIC study (n = 520000)
Not reported
Lung cancer incidence
The proportion of lung cancers in never- and ex-smokers attributable to ETS was estimated as between 16 and 24 mainly due to the contribution of work-related exposure Also 5ndash7 of lung cancers in European never smokers and ex-smokers are attributable to high levels of air pollution as expressed by NO2 or proximity to heavy traffic roads
66
e) OTHER CANCERS
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in survival
from other cancers and no evidence was identified in the current review
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in survival from other
cancers Studies identified in the current review are summarised in Table 7 at the end of this
section
Preliminary EPIC results provide some evidence that red and preserved meat increases risk
for gastric cancer (Gonzalez et al 2006) Preliminary EPIC results also indicate that fruit
reduces gastric cancer risk whilst vegetables are not associated with risk for this type of
cancer Furthermore overall consumption of fruit and vegetables is reported to be unrelated
to risk of ovarian cancer (Schultz et al 2005) There is evidence of a protective effect of a
high intake of allium vegetables (onions garlic shallots leeks and chives) on ovarian
cancer risk (Schultz et al 2005)
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in survival from
other cancers Preliminary EPIC results reported in the current review provide some
evidence that BMI is associated with endometrial cancer risk (Kaaks et al 2002
Friedenreich et al 2007)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in survival from
other cancers Preliminary EPIC results along with 4 other studies were identified in the
current review
Gonzalez et al (2003) confirm from EPIC results that smoking is associated with gastric
cancer
Similarly Yu et al (1997) evaluated 25000 heterogeneous patients who had been treated
for lung breast or colorectal cancer and found that the 15-year survival of the people
who continued to smoke was 44 compared to 55 in those who quit
In a more recent study of survivors of early stage head and neck cancer (n=264) who
retrospectively reported their tobacco histories (pre-diagnosis) and prospectively updated
67
information annually thereafter for an average of 42-years smoking history dose-
dependently increased the risk of mortality from cancer (Mayne et al 2009)
The impact of smoking on risk of secondary lung cancer has been demonstrated in survivors
of Hodgkin lymphoma (Abrahamsen et al 1993 Travis et al 2002) In the latter study risk
for subsequent lung cancer from radiation treatment and smoking was identified where
multiple effects were found for a combination of radiation and alkylating agents36 in
moderate-to-heavy smokers compared with comparison cases (Travis et al 2002)
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in survival from
other cancers One study was identified in the current review which showed that pre-
diagnosis alcohol consumption history dose-dependently increased mortality risk in
recent survivors of early stage head and neck cancer (n=264) (Mayne et al 2009)
Risks reached 49 for those who drank gt5 drinks per day an effect explained by beer and
liquor consumption Continued drinking post-diagnosis of an average of 23 drinks daily
also significantly increased risk
SUMMARY OF FINDINGS FOR OTHER CANCERS
A comprehensive evaluation of the lifestyle evidence for cancers other than the four most
common (ie breast colorectal lung prostate) was not within the scope of this review
However those studies identified whilst gathering evidence for these four cancers does
highlight the sheer importance of lifestyle in the development and progression of all types of
cancers not to forget other chronic diseases The provision of lifestyle support for cancer
survivors clearly needs to remain priority as does further research into the exact
mechanisms of benefit obtained from different lifestyle practices at different stages of the
cancer and indeed health trajectory
36
Carcinogenic agents used in chemotherapy to treat cancer
68
Table 7 Other Cancers ndash Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
DIET
Gonzalez et al (2006)
Nested case-control within the prospective EPIC study examining of
the risk of gastric cancer and
oesophageal adenocarcinoma associated
with meat consumption
521 457 men and women aged 35ndash70 years in 10 European
countrie
s (330 gastric adenocarcinoma and
65
oesophageal adenocarcinomas were diagnosed)
65-years Incidence of gastric and oesophageal cancers
Gastric noncardia cancer risk was statistically significantly associated
with intakes of total meat (calibrated HR per 100-gday increase
=
352 95 CI = 196 to 634) red meat (calibrated HR per 50-gday
increase = 173 95 CI = 103 to 288) and processed
meat (calibrated HR per 50-gday increase = 245 95 CI
= 143 to 421) The association between
the risk of gastric noncardia cancer and total meat intake was
especially large in H pylori infected subjects (odds ratio per 100-
gday increase = 532 95 CI = 210 to 134) Intakes of total red or
processed meat were not associated with
the risk of gastric cardia cancer A positive but nonndashstatistically
significant association was observed between oesophageal
adenocarcinoma cancer risk and total and processed meat intake
Schultz et al (2005)
Prospective examination of the association between consumption of fruit and vegetables and risk of ovarian cancer (EPIC)
Female participants (n = 325640) of the EPIC study
Mean=63 years
Ovarian cancer incidence
Total intake of fruit and vegetables separately or combined as well as subgroups of vegetables (fruiting root leafy vegetables cabbages) was unrelated to risk of ovarian cancer A high intake of garliconion vegetables was associated with a borderline significant reduced risk of this cancer
WEIGHT
Friedenreich et al 2007
Large prospective study (EPIC) examining the association between anthropometry and endometrial cancer particularly by menopausal status and exogenous hormone use subgroups
223008 women in the EPIC study (567 incident endometrial cancer cases)
64-years Endometrial cancer incidence
Weight BMI waist and hip circumferences and waistndashhip ratio (WHR) were strongly associated with increased risk of endometrial cancer The relative risk (RR) for obese (BMI 30ndash lt 40 kgm
2)
compared to normal weight (BMI lt 25) women was 178 95 CI = 141ndash226 and for morbidly obese women (BMI ge 40) was 302 95 CI = 166ndash552 The RR for women with a waist circumference of ge88 cm vs lt80 cm was 176 95 CI = 142ndash219 Adult weight gain of ge20 kg compared with stable weight (plusmn3 kg) increased risk independent of body weight at age 20 (RR = 175 95 CI = 111ndash277) These associations were generally stronger for postmenopausal than premenopausal women and oral contraceptives never-users than ever-users and much stronger among never-users of hormone replacement therapy compared to ever-users
Kaaks et al A review of evidence on the Endometrial Not Incidence of The authors conclude that development of ovarian hyperandrogenism
69
(2002) associations among endometrial cancer risk endogenous hormone metabolism and obesity
cancer cases reported endometrial cancer
may be a central mechanism relating to an interaction between obesity-related chronic hyperinsulinemia with genetic factors predisposing to the development of ovarian hyperandrogenism
SMOKING
Abrahamsen et al (1993)
The Norwegian Cancer Registry
identified previously untreated patients with Hodgkin lymphoma treated at NRH who had developed a secondary cancer more than 1 year after diagnosis of
Hodgkin
lymphoma
68 patients who developed secondary cancer including 9 acute non-lymphocytic leukaemialsquos (ANLLs)
8 non-
Hodgkins lymphomas (NHLs) and 51 solid tumours including 11 lung cancers
Not reported
Secondary cancer
The RR of SC and leukaemia was 186 (95 CI 14 to 24) and 243 (95 CI 111 to 462) respectively The RR of
SC was highest in
younger patients (lt 41 years RR = 38) No significant association
between splenectomy and development of ANLL was found The
influence of treatment and follow-up time on the development of SC
agrees with data from other large cancer institutions
Gonzalez et al (2003)
Assessment of the relation between tobacco use and gastric cancer incidence in the prospective EPIC study
521468 individuals recruited from 10 European countries taking part in the EPIC study 274 were eligible for the analysis
Approx 10-years
Incidence of gastric cancer
After adjustment for educational level consumption of fresh fruit vegetables and preserved meat alcohol intake and body mass index (BMI) there was a significant association between cigarette smoking and gastric cancer risk the hazard ratio (HR) for ever smokers was 145 (95 CI = 108-194) The HR of current cigarette smoking was 173 (95 CI = 106-283) in males and 187 (95 CI = 112-312) in females Hazard ratios increased with intensity and duration of cigarette smoked A significant decrease of risk was observed after 10 years of quitting smoking A preliminary analysis of 121 cases with identified anatomic site showed that current cigarette smokers had a higher HR of GC in the cardia (HR = 410) than in the distal part of the stomach (HR = 194) In this cohort 176 (95 CI = 105-295 ) of gastric cancer cases may be attributable to smoking
Mayne et al (2009)
Participants retrospectively reported their smoking histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to smoke post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Smoking history before diagnosis dose-dependently increased the risk of dying risks reached 54 [95 CI 07-401] among those with gt60 pack-years of smoking After adjusting for pre-diagnosis exposures continued smoking was associated with non-significantly higher risk (relative risk for continued smoking versus no smoking 18 95 CI 09-39)
70
Travis et al (2002)
Case-control study with a population-based cohort The cumulative amount of cytotoxic drugs the radiation dose to the specific location in the lung where cancer developed and tobacco use were compared between patients who developed lung cancer and matched control patients
1-year survivors of Hodgkins disease (n=19046) comparison between 222 patients who developed lung cancer and 444 matched controls
Not reported
Secondary cancer incidence
Tobacco use increased lung cancer risk more than 20-fold risks from smoking appeared to multiply risks from treatment
Yu et al (1997)
Retrospective study examining the effect of smoking history on survival among cancer patients
Data from Memorial Sloan-Kettering Cancer Centers tumour registry was used to identify 25436 cases of cancer (12447 male patients and 12989 female patients)
Not reported
Survival time Patients who had a history of smoking were found to have a lower rate of survival than non-smokers After controlling for age race alcohol use and histologic grade the risk ratios were 155 for males and 143 for females A dose-response relationship was found between ever-smoking and cancer patient survival The predictive effect of smoking on survival was significant for patients with oral pancreatic breast and prostate cancers but not for oesophageal stomach colon rectum laryngeal lung cervix uteri urinary bladder and kidney cancers Black patients with oral or breast cancer had a poorer prognosis associated with smoking compared with white and other non-white patients
ALCOHOL
Mayne et al (2009)
Participants retrospectively reported their alcohol consumption histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to drink post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Alcohol history before diagnosis dose-dependently increased mortality risk risks reached 49 (95 CI 15-163) for persons who drank gt5 drinksd an effect explained by beer and liquor consumption After adjusting for pre-diagnosis exposures continued drinking (average of 23 drinksd) post-diagnosis significantly increased risk (relative risk for continued drinking versus no drinking 27 95 CI 12-61)
71
PART TWO
LIFESTYLE EVIDENCE FOR REDUCING AND MANAGING THE
RISKS AND SIDE-EFFECTS OF CANCER TREATMENT
Introduction
There are a number of long-term and late effects of cancer treatment that a survivor might
be confronted with including fatigue (Bower et al 2006) psychological problems (Thewes
et al 2004) lymphoedema (Deo et al 2004) and osteoporosis (Brown et al 2006) There
might also be difficulties in terms of returning to work or withdrawal from social activities due
to disability (Taskila et al 2007) Lifestyle choices pertaining to diet physical activity
smoking and alcohol consumption for cancer survivors are not only important in terms of
disease progression and recurrence Despite there being less evidence in this area there
is accumulating data demonstrating that lifestyle can facilitate the effective management of
many of these effects of treatment some of which are chronic conditions themselves
requiring additional lifestyle modifications Research within this area has hit new heights in
order to keep up with the growing number of survivors The chronic conditions addressed
within the current review of lifestyle evidence are some of the most frequently reported
problems cited by cancer survivors they include cancer-related fatigue (CRF)
lymphoedema osteoporosis and weight gain In addition evidence for lifestyle choices and
quality of life (QoL) has been reviewed due to the QoL implications of the aforementioned
health-related problems and unhealthy behaviours (Richardson et al 2009)
Evidence for an interaction between lifestyle and these chronic conditions commences with
the findings reported by Bekkering et al (2006) as part of the WCRF review being updated
Further evidence identified from the search criteria will then be presented Evidence will be
presented by cancer site (eg breast colorectal lung prostate) where appropriate whilst
some evidence will pertain to one cancer site only (ie breast cancer related lymphoedema)
72
CANCER-RELATED FATIGUE (CRF)
Cancer-related fatigue (CRF) is defined as ldquoa distressing persistent subjective sense of
physical emotional andor cognitive tiredness or exhaustion related to cancer or cancer-
related treatment that is not proportional to recent activity and interferes with usual
functioningrdquo (NCCN 2009) It has overtaken nausea and pain as the most distressing
symptom experienced by people with cancer during and after treatment It is reported by 60-
96 of patients during chemotherapy radiotherapy or after surgery and can last for months
or even years following treatment (Wagner and Cella 2004 Thomas 2005 NCCN 2009) It
can have a profound effect on physical emotional and social well-being and can hinder
chance of remission owing to non-compliance with treatment due to the intensity of this side-
effect (Lucia Earnest and Perez 2003 Velthuis et al 2009)
The specific causes of CRF are not fully understood but there are several associated
conditions which can aggravate it These include anaemia electrolyte imbalance liver
failure and steroid withdrawal (Thomas 2005) Some conditions can also cause fatigue by
disturbing sleep patterns such as anxiety depression nocturia (a need to get up in the night
to urinate) night sweats and pruritus (itching) The self-management strategy most
extensively investigated for CRF is physical activity the evidence for which is presented
next Studies identified in the current review are summarised in Table 8 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in women with breast cancer In the current review 4 systematic reviews
three of which included a meta-analysis and 2 additional studies were identified
The first review by McNeely et al (2006) reported on 14 RCTs Despite significant
heterogeneity and relatively small samples the overall finding was that physical activity led
to statistically significant improvements in reducing symptoms of fatigue Two meta-
analyses added to this evidence The first by Cramp and Daniel (2008) evaluated 28
studies (n=2083 participants) the majority of which comprised participants with breast
cancer (n=16 studies n=1172 participants) A pooled meta-analysis of all available data
convincingly showed that physical activity was statistically more effective in reducing
CRF when compared to less active controls In the second meta-analysis Velthuis et al
(2009) reviewed 18 studies 12 of which comprised women with breast cancer Pooled
results of these 12 studies (n=674 patients) showed a small significant reduction of CRF
in favour of the physical activity group compared to the non-physical activity group
When Velthuis et al (2009) subdivided the 12 studies into two main physical activity
strategies (ie home-based versus supervised classes) home-based physical activity (n=
7 studies) led to a small non-significant reduction in CRF whereas supervised
73
aerobic physical activity (n=5 studies) showed a medium significant reduction
in CRF when compared to no intervention
Fillion et al (2008) conduced an RCT demonstrating that combining supervised walking
training with psycho-educational stress management produced significant improvements
relative to usual care for fatigue vigour anxiety and depression but not for physical
fitness This suggests a psychological benefit to physical activity which might assist in
coping with physical symptoms such as fatigue Poudevigne et al (2009)
examined adherence to 12-weeks of moderate intensity combined cardio-respiratory and
resistance training and any subsequent impact on levels of fatigue in sedentary breast
cancer survivors (n=20) 2-24 months post-treatment Not only was the training acceptable
and safe but significant decreases in fatigue (43) were also found across the12-
weeks
Danhauer et al (2009) conducted an RCT with women (n=44) who had breast cancer 34
of whom were undergoing cancer treatment in order to examine the effects of restorative
yoga between those in treatment and those not in treatment Randomisation was to a
programme of 10-weekly 75-minute yoga classes or a waiting list control group The yoga
group demonstrated a significant within-group improvement in fatigue although no
significant difference was found with the control group
In updating a previous systematic review by Schmitz et al (2005) of RCTs examining
physical activity in cancer survivors during and after treatment Speck et al (2010)
accumulated data from a further 82 studies (n=6838 participants) Of the 82 studies 66
were rated as high quality and analysed for mean effect sizes resulting from physical activity
interventions The most common diagnosis included was breast cancer (83) with 40 of
studies conducting interventions during cancer treatment and 60 post-treatment Mean
effect sizes demonstrated a large effect of physical activity interventions post-
treatment on upper and lower body strength (plt00001 and 0024 respectively) and
moderate effects on fatigue and breast cancer-specific concerns (p=0003 and 0003
respectively) The most notable progression from their previous review was that the
benefits of physical activity on fatigue moved from negative findings to the evidence
reflecting significantly reduced fatigue post-treatment in physically active survivors
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in men with prostate cancer In the current review 3 systematic reviews two
of which included a meta-analysis and 2 additional studies were identified In the current
review four studies were identified
Windsor Nichol and Potter (2004) published a study of 65 patients with prostate cancer
receiving radiotherapy who were randomly allocated to a home-based physical activity
programme or standard supportive care The home-based exercise included walking 30-
minutes three times a week with an intensity of 60-70 heart rate max for the duration of
74
radiotherapy No adverse events were reported and a non-significant reduction of CRF
was found in the physical activity group when compared to the standard care group
In the abovementioned meta-analysis conducted by Velthuis et al (2009) three RCTs in men
with prostate cancer investigated the effectiveness of supervised physical activity during
radiotherapy and androgen deprivation therapy (Segal et al 2003 Monga et al 2007
Segal et al 2009) In two studies men allocated to the intervention group participated three
times a week in a supervised physical activity programme comprising aerobic exercises with
an intensity of respectively 65 of the maximum heart frequency (HR max) adjusted for
age and 50-75 of the VO2peak (15-45 minutes) (Monga et al 2007 Segal et al 2009)
In the third study the intervention comprised resistance exercises 2-3 times a week with an
intensity of two sets of 8-12 repetitions 60-70 of the one repetition maximum (Segal et
al 2003) Pooled results from the two supervised aerobic studies showed a large non-
significant reduction in CRF in favour of the physical activity group (Monga et al
2007 Segal et al 2009) The resistance exercise study showed a small non-significant
reduction in CRF in favour of the physical activity group (Segal et al 2003) In the latter
study over 80 of the participants were reported to have completed the programme
however the programme did result in one knee injury chest pain fainting and an acute
myocardial infarction
c) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) report on one RCT comparing the impact of a 3-weeks aerobic
physical activity (stationary biking 30-minutes five times weekly) intervention versus
relaxation training (45-minutes three times per week) in post-surgery survivors (n=72) of lung
(n=27) and gastrointestinal (n=42) cancer (Dimeo et al 2004) Fatigue improved
significantly in both groups during the intervention although there was no significant
difference between groups This suggests that relaxation training can be equally as
effective as aerobic physical activity in relieving symptoms of fatigue
In the current review 3 further studies were identified
There has been one study in patients with multiple myeloma (Coleman et al 2003) which
included a home-based physical activity programme during chemotherapy and peripheral
blood stem cell transplantation The programme comprised a combination of aerobic and
resistance exercises three times a week for 20-minutes for the duration of the
chemotherapy (6-months) No adverse events were reported and a small non-significant
reduction in CRF was found in the physical activity group compared to a control
group who did not receive the intervention
Chang et al (2008) published a study involving patients with acute myelogeous leukemia
(n=22) which included allocation to the intervention group a three week supervised walking
programme during chemotherapy Participants walked five times a week for 12-minutes in
the hospital hallway The programme was completed by 69 of the participants and no
75
adverse events were reported A medium-sized non-significant reduction in CRF was
found
In a cross-sectional postal survey of ovarian cancer survivors (n=359) self-report measures
of physical activity and CRF demonstrated that those meeting physical activity guidelines of
the Centres for Disease Control and Prevention (ie minimum 25-hours of moderate
intensity aerobic activity every week plus muscle-strengthening activities on two or more
days of the week) reported significantly lower fatigue than those not meeting guidelines
(Stevinson et al 2009) There was however no evidence of a dose-response relationship
SUMMARY OF EVIDENCE FOR CANCER-RELATED FATIGUE
Evidence from 28 RCTs and 2 meta-analyses has demonstrated that physical activity
programmes can reduce the severity of CRF The studies reviewed here also show that
supervised aerobic exercise programmes were more effective in reducing CRF during breast
cancer treatment than home-based exercise advice Although more research on the optimal
timing and duration of physical activity would be useful these studies are sufficiently robust
to recommend that tailored physical activity advice be integrated into individualized care
plans
As identified in a consultation and evidence review designed to determine the priorities of
cancer survivorship research there is a modest amount of research testing physical activity
interventions for fatigue some demonstrating benefits during treatment but inconclusive
evidence for after treatment (Richardson et al 2009) Although there is clinical
heterogeneity between published RCTlsquos in terms of physical activity duration frequency and
intensity a sensible pragmatic approach based on the trials which showed most benefit is to
supervise a moderate intensity physical activity regimen of regular frequency (3-5
timesweek) for 20-30 minutes per session involving aerobic resistance or mixed physical
activity types With evidence suggesting that low intensity physical activity can also be
beneficial during cancer treatment consideration is warranted in terms of promoting physical
activity from diagnosis onwards potentially making physical activity uptake less challenging
post-treatment (Velthuis et al 2009) Further research is required to determine the optimal
type intensity and timing of physical activity interventions at different periods of the disease
trajectory and when experiencing other cancer-related symptoms or late effects
An exemplary physical activity programme available to survivors of breast colorectal and melanoma cancers is the BACSUP (Bournemouth After Cancer Survivorship Project) Active Wellness Programmelsquo developed in partnership with Royal Bournemouth Hospital NHS Bournemouth and Poole Bournemouth University and MacMillan Cancer Support (Milne et al 2010) The programme involves two initial one-to-one consultations including a holistic assessment with a trained member of staff to tailor the programme to individual needs A readiness check is done prior to referral a readiness to be physically active score of gt70 is required for participation Participants receive a telephone call at 3-weeks for the provision of support and encouragement followed by a one-to-one review at 6-weeks to assess progress and maintain motivation A one-to-one review and reassessment is also provided at 12-weeks to measure improvements Additional support options are available such as the BACSUP Active Wellness Group which provides an opportunity to meet others survivors and listen to life improvement guest speakers In a pilot study of the programme survivors who had completed primary treatment within the previous 5-years (n=180) were referred to the service 58 completed the programme 65 are currently on the programme 30 started but are on hold due to circumstances 21 were not yet ready to join the scheme
At 12-weeks 92 of participants reported reduced fatigue
76
Table 8 Cancer-Related Fatigue and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Chang et al (2008)
RCT to preliminarily examine the effects of a three-week walking exercise program (WEP) on fatigue-related experiences of acute myelogenous leukaemia (AML) patients receiving chemotherapy Eligible AML patients were randomly assigned to either an experimental group (n = 11) which received 12 minutes of WEP per day five days per week for three consecutive weeks or to a control group (n = 11) which received standard ward care
Patients with acute Myelogenous leukaemia (AML) receiving chemotherapy (n=22)
All patients were evaluated four times before treatment (baseline or Day 1) Day 7 Day 14 and Day 21
Worst and average fatigue intensities fatigue interference with patients daily life 12-minute walking distance overall symptom distress anxiety and depressive status
AML patients in the three-week WEP group had a significantly greater increase in 12-minute walking distance than the control group Patients in the WEP also had lower levels of fatigue intensity and interference symptom distress anxiety and depressive status than the control group
Coleman et al(2003)
A pilotfeasibility study with a randomized controlled design was conducted to investigate home-based exercise therapy for patients receiving high-dose chemotherapy and autologous peripheral blood stem cell transplantation as treatment for multiple myeloma
24 patients with multiple myeloma
Not reported Fatigue mood disturbance body weight
Because of the small sample size in the feasibility study the effect of exercise on lean body weight was the only end point that obtained statistical significance However the results suggest that an individualised exercise program for patients receiving aggressive treatment for multiple myeloma is feasible and may be effective for decreasing fatigue and mood disturbance and for improving sleep
Cramp and Daniel (2008)
Systematic review with meta-analysis to evaluate the effect of exercise on cancer-related fatigue both during and after cancer treatment
2083 participants from RCTs comprising cancer patients and survivors
Follow-up assessment of long-term outcomes was poor with 18 of 28 studies failing to assess outcomes beyond the end of the intervention
Cancer-related fatigue
28 studies were identified for inclusion with the majority carried out on participants with breast cancer (n = 16 studies n = 1172 participants) A meta-analysis of all fatigue data incorporating 22 comparisons provided data for 920 participants who received an exercise intervention and 742 control participants At the end of the intervention period exercise was statistically more effective than the control intervention (SMD -023 95 CIs -033 to -013)
77
period
Danhauer et al (2009)
Randomised pilot study to determine the feasibility of implementing a restorative yoga intervention for women with breast cancer and to examine group differences in self-reported emotional health-related quality of life and symptom outcomes 10 weekly 75-minute yoga classes
Women with breast cancer (n=544) 34 of whom were actively undergoing cancer treatment
Immediately post-intervention (week 10)
Emotional well-being QoL fatigue
Group differences favouring the yoga group were seen for mental health depression positive affect and spirituality (peacemeaning) Significant baselinegroup interactions were observed for negative affect and emotional well-being Women with higher negative affect and lower emotional well-being at baseline derived greater benefit from the yoga intervention compared to those with similar values at baseline in the control group The yoga group demonstrated a significant within-group improvement in fatigue no significant difference was noted for the control group
Fillion et al (2008)
RCT to verify the effectiveness of a 4-week nurse-led group intervention that combines stress management psycho-education and physical activity (ie independent variable) intervention in reducing fatigue and improving energy level quality of life (mental and physical) fitness (VO2submax) and emotional distress (ie dependent variables) in breast cancer survivors Participants were randomly assigned to either the group intervention (experimental) or the usual-care (control) condition
French-speaking women who had completed their treatments for non-metastatic breast cancer (n=87)
Post-intervention and at 3-months follow-up
Fatigue emotional distress QoL
Participants in the intervention group showed greater improvement in fatigue energy level and emotional distress at 3-month follow-up and physical quality of life at post-intervention compared with the participants in the control group
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials MEDLINE
EMBASE CINAHL Psych INFO CancerLit PEDro
and SportDiscus as well
as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
function
ing as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all
outcomes were positive even when statistical significance was not
achieved Exercise led to statistically significant improvements in
quality of life as assessed by the Functional Assessment of
Cancer TherapyndashGeneral (weighted mean difference [WMD] 458
95 CI 035 to 880) and Functional Assessment of Cancer
TherapyndashBreast (WMD 662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak
oxygen consumption and in reducing symptoms of fatigue
Poudevigne et al (2009)
Cohort study examining the effects of a 12-week cross training intervention on fatigue and mood in breast cancer survivors The training consisted of a 12-week exercise program of 3 weekly
20 sedentary breast cancer survivors between 2-24 months post-
On completion of the 12-week intervention
Fatigue and mood disturbances (Profile of Mood States) QoL
The mean (plusmnSD) attendance rate was 92 (plusmn80) No musculoskeletal injuries and problematic symptoms occurred during the cross-training Repeated measures ANOVA showed a large increase in QOL (22) and significant decrease in fatigue (43) across 12 weeks (eta squared range 491 to708 all p
78
sessions of 60 min duration supervised by a certified personal trainer and divided into resistance (30 minutes) and aerobic training (5 minutes warm-up 20 minutes training 5 minutes cool-down) The aerobic intensity was set at 60HRR and re-evaluated every three weeks
treatment Treatments ranged from lumpectomies (23) mastectomies (29) radiations (32) and chemotherapy (16)
(SF-36) and work absenteeism
valueslt05) No differences were found in work absenteeism Blood pressure was unchanged after training
Stevinson et al (2009)
A cross-sectional postal survey to investigate the associations between physical activity and health-related outcomes in ovarian cancer survivors and to examine any dose-response relationship
Ovarian cancer survivors (n=359) on and off treatment
Not reported Fatigue peripheral neuropathy sleep and psychosocial functioning
311 of participants were meeting the public health physical activity guidelines - those meeting guidelines reported significantly lower fatigue than those not meeting guidelines (mean difference 71 95 confidence interval 55-88 d = 087 Plt 0001) Meeting guidelines was also significantly inversely associated with peripheral neuropathy depression anxiety sleep latency use of sleep medication and daytime dysfunction and was positively associated with happiness sleep quality and sleep efficiency
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types were included with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) With few exceptions exercise was well tolerated during and post treatment without adverse events
Velthuis et al (2009)
Meta-analysis to evaluate the effects of different exercise prescription parameters during cancer treatment on cancer-related fatigue (CRF) A systematic search of CINAHL Cochrane Library Embase
RCTs studying the effects of exercise during cancer treatment on
Not reported Cancer-related fatigue
During breast cancer treatment home-based exercise lead to a small non-significant reduction (standardised mean difference 010 95 confidence interval minus025 to 045) whereas supervised aerobic exercise showed a medium significant reduction in CRF (standardised mean difference 030 95 confidence interval 009
79
Medline Scopus and PEDro was carried out
CRF (n=18) 12 in breast 4 in prostate and 2 in other cancer patients)
to 051) compared with no exercise A subgroup analysis of home-based (n = 65) and supervised aerobic (n = 98) and resistance exercise programmes (n = 208) in prostate cancer patients showed no significant reduction in CRF in favour of the exercise group Adherence ranged from 39 of the patients who visited at least 70 of the supervised exercise sessions to 100 completion of a home-based walking programme
Windsor Nichol and Potter (2004)
A prospective RCT to determine whether aerobic exercise would reduce the incidence of fatigue and prevent deterioration in physical functioning during radiotherapy for localised prostate carcinoma
33 men in exercise group and 33 men in control group
4-weeks post-radiotherapy
Fatigue and distance walked in a modified shuttle test before and after radiotherapy
There were no significant between group differences noted with regard to fatigue scores at baseline (P = 055) or after 4 weeks of radiotherapy (P = 018) Men in the control group had significant increases in fatigue scores from baseline to the end of radiotherapy (P = 0013) with no significant increases observed in the exercise group (P = 0203)
80
LYMPHOEDEMA
Lymphoedema is the excessive accumulation of tissue fluid (or lymph) that results from
impaired lymphatic drainage resulting in swelling of the limb The most common type of
lymphoedema in cancer survivors is most frequently the result of treatment for breast
cancer where an important prognostic indicator is the removal and evaluation of lymph
nodes (Morrell et al 2005) Removal of the lymph nodes can result in a number of side-
effects including lymphoedema (Swenson et al 2002) which manifests usually as a
swelling to the affected arm but can also occur in the hand trunk and breast The more
lymph nodes that are removed the higher the risk of developing the condition providing an
objective measure of risk that could be utilised in the provision of evidence-based
lifestyle and self-management support based on individuals needs
The condition can develop immediately or many years after treatment (Mortimer et al
1996) in either case lymphoedema is a chronic debilitating condition that can cause severe
physical and psychological morbidity as well as a reduction in QoL (Deo et al 2004)
The self-management strategy most extensively investigated for lymphoedema is physical
activity with some evidence also being available for diet Studies identified in the current
review are summarised in Table 9 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
preventing or managing lymphoedema In the current review one systematic review
(including a meta-analysis) and 3 studies were identified
In a prospective RCT testing the efficacy of two types of physiotherapy on shoulder function
and lymphatic disturbance in post-operative breast cancer survivors (n=60) participants
received one of two types of physiotherapy 48-hours post-surgery (de Rezende et al
2006)
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-
defined sequence of movements
2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely
to music
Lymphoedema is estimated to affect
about 30 of breast cancer survivors
post-treatment (Deo et al 2004)
81
Results indicated significantly better recovery of limb movement in the directed group
compared to the free group with there being no significant difference between groups in
terms of lymphatic disturbance
Ahmed et al (2006) report on a 6-month RCT examining the effects of supervised upper-
and lower-body weight training on lymphoedema incidence and symptoms in breast cancer
survivors (n = 45) 4-36 months post-treatment From baseline to 6-months three control-
group participants reported an increase in lymphoedema symptoms No participants in the
intervention group reported such symptoms suggesting that twice-a-week progressive
weight training does not increase the onset of or exacerbate lymphoedema in breast cancer
survivors (13 women had lymphoedema at baseline) The results from this study indicate
that at minimum physical activity does not exacerbate lymphoedema
Moseley and Piller (2008) reviewed the literature for evidence supporting the benefits of
physical activity for people with limb lymphoedema Their key findings from eleven studies
demonstrated that
physical activity can improve lymph clearance
physical activity can help reduce limb volume and improve subjective symptoms and
QoL
benefits from physical activity have been sustained post-physical activity regime in
some studies
physical activity is a viable option for people with lymphoedema
Moseley and Pillerlsquos (2008) conclusions were supported further in a recent RCT by Hayes
Hildegard and Turner (2009) Breast cancer survivors at least 6-months post-treatment
who had developed unilateral upper-limb lymphoedema participated in twenty supervised
group aerobic and resistance physical activity sessions over 12-weeks (n=16) or continued
habitual activities (n=16) Average attendance was more than 70 of supervised sessions
and there were no withdrawals Mean ratio and volume measures at baseline were similar
between the two groups and no changes were observed at 3-months follow-up for either
group although two women receiving supervised physical activity no longer had evidence of
lymphoedema by study completion The results from this review as with the RCT by
Ahmed et al (2006) indicate that at minimum physical activity does not exacerbate
secondary lymphoedema
In the review referred to previously by Speck et al (2010) with minor exceptions findings
indicated aerobic lifestyle and upper body resistive exercise was tolerated by breast cancer
survivors with no adverse effects on the development or exacerbation of lymphoedema
ii DIET
Bekkering et al (2006) report on one double-blind placebo-controlled RCT examining diet
and lymphoedema in breast cancer survivors (n=68) at a mean of 155-years post-treatment
For 6-months women received 500mg twice a day of dl-alpha tocopheryl acetate (a source
of vitamin E) plus pentoxifylline (a drug that improves blood circulation) 400mg twice a day
82
of dl-alpha tocopheryl acetate or placebo (Gothard et al 2004) At 6-months and 12-months
post-randomisation there was no significant difference between groups in terms of arm
volume
The current review identified one RCT
Dietary Fat
In a UK RCT Shaw Mortimer and Judd (2007) demonstrate the impact of diet and weight
loss on post-treatment arm lymphoedema in breast cancer survivors (n=51) Women were
assigned to one of three 24-week dietary groups
1) a low-fat diet (fat intake reduced to 20 of total energy intake)
2) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ)
3) a control group (continuing their usual diet)
After the end of the 24-week period of dietary intervention there was a slightly greater
reduction in excess arm volume in both dietary intervention groups compared with the
control although this was not statistically significant Furthermore despite low levels of
adherence to dietary advice weight loss was achieved in all groups demonstrating that
dietary interventions can assist in reducing excess arm volume in women with post-
treatment lymphoedema
SUMMARY OF EVIDENCE FOR LYMPHOEDEMA
The studies evaluated within this review indicate a need to re-assess the common clinical
guidelines that breast cancer survivors avoid upper body resistance activity for fear of
increasing risk of lymphoedema(Speck et al 2010) They also indicate a requirement to
develop guidelines for appropriate physical activity As concluded by Hayes Hildegard and
Turner (2009) women with secondary lymphoedema should be encouraged to be physically
active optimising their physical and psychosocial recovery Resistance exercise does not
increase the risk for or exacerbate symptoms of lymphoedema and in fact directed physical
activity 48-hours post-surgery might offer greater utility in terms of rehabilitation outcomes
Some of the studies evaluated in the review by Moseley and Piller (2008) comprised small
sample sizes and did not include control groups however when combined with other studies
presented within this review there is some support for encouraging physical activity in breast
cancer survivors Furthermore physical activity combined with changes in diet and
subsequent weight loss in survivors who are overweight might significantly reduce the
symptoms of lymphoedema although evidence for diet in reducing symptoms of
lymphoedema is limited
Weight loss across groups
9 (60) in the control group 13 (76) in the low-fat diet group 18 (95) in the weight-reduction
group
83
Table 9 Lymphoedema and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Ahmed et al (2006)
RCT comparing supervised twice weekly upper- and lower-body weight training over 6-months with control group completing no training
Breast cancer survivors (n = 45) 4-36 months post-treatment
6-months post-intervention
Incidence and symptoms of lymphoedema
From baseline to 6-months three control-group participants
reported an increase
in lymphoedema symptoms No
participants in the intervention group reported such symptoms suggesting that
twice-a-week progressive weight training does not
increase the onset of or exacerbate lymphoedema in breast
cancer
survivors
de Rezende et al (2006)
RCT examining the impact of physiotherapy on lymphoedema Participants received one of two types of physiotherapy
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-defined sequence of movements 2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely to music
48-hours post-surgery breast cancer survivors (n=60)
On completion of intervention (42-days)
Shoulder movement and lymphatic disturbance
Significantly better recovery of limb movement in the directed group compared to the free group with there being no significant difference between groups in terms of lymphatic disturbance
Hayes Hildegard and Turner (2009)
An RCT testing the impact of aerobic exercise on lymphoedema outcomes Participants randomised to 1) 20 supervised group aerobic and resistance physical activity sessions over 12-weeks (n=16) 2) continued habitual activities (n=16)
Breast cancer survivors at least 6-months post-treatment who had developed unilateral upper-limb lymphoedema
3-months post-intervention
Arm volume measurements
Mean ratio and volume measures at baseline were similar between the two groups and no changes were observed at 3-months follow-up for either group although two women receiving supervised physical activity no longer had evidence of lymphoedema by study completion
84
Moseley and Piller (2008)
Literature search of the evidence supporting the benefits of exercise for those with limb lymphoedema
Exercise studies undertaken in RCTs or cohort studies and involving secondary limb lymphoedema (with no active cancer)
Varied from post-intervention to 8-weeks follow-up
Change in limb volume and subjective symptoms
Exercise has been shown to improve lymph propulsion and clearance help reduce limb volume and improve subjective symptoms and quality of life Benefits from exercise have been sustained post-exercise regime in some studies Exercise is a viable option for those with limb lymphoedema
DIET
Gothard et al (2004)
A double-blind placebo-controlled randomised phase II trial Participants were randomised to active drugs or placebo All volunteers were given dl-alpha tocopheryl acetate 500 mg twice a day orally plus pentoxifylline 400 mg twice a day orally or corresponding placebos for 6 months
68 volunteers with a minimum 20 increase in arm volume at a median 155 years after radiotherapy (plus axillary surgery in 5168 (75) cases)
12 months post-randomisation
Volume of the ipsilateral limb measured
There was no significant difference between treatment and control groups in terms of arm volume Absolute change in arm volume at 12 months was 25 (95 CI minus040 to 53) in the treatment group compared to 12 (95 CI minus28 to 51) in the placebo group The difference in mean volume change between randomisation groups at 12 months was not statistically significant (P=06) minus13 (95 CI minus61 to 35) nor was there a significant difference in response at 6 months (P=07) where mean change in arm volume from baseline in the treatment and placebo groups was minus23 (95 CI minus79 to 34) and minus11 (95 CI minus39 to 17) respectively
Shaw Mortimer and Judd (2007)
Participants were assigned to one of three 24-week dietary groups in order to assess impact on arm volume 1)a low-fat diet (fat intake reduced to 20 of total energy intake) b) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ) c) a control group (continuing their usual diet)
Breast cancer survivors (n=51)
After 24-weeks of intervention
Arm volume There was a slightly greater reduction in excess arm volume in both dietary intervention groups compared with the control although this was not statistically significant
85
OSTEOPOROSIS AND BONE HEALTH
Osteoporosis is a condition in which the bones become less dense and more likely to
fracture which in turn can result in significant pain and disability It is known as a silent
disease because if undetected bone loss can progress for many years without symptoms
until a fracture occurs Risk factors for developing osteoporosis are often enhanced in
cancer survivors such as being post-menopausal and having had early menopause (Ada et
al 2002) Low calcium intake lack of physical activity smoking and excessive alcohol
consumption are also risk factors for osteoporosis (Guthrie et al 2000) Women who have
had breast cancer treatment may be at increased risk for osteoporosis and fracture due to
reduced levels of oestrogen whilst men who receive hormone deprivation therapy for
prostate cancer also have an increased risk of developing osteoporosis and broken bones
(National Institutes of Health Osteoporosis and Related Bone Diseases 2009)
There are no early symptoms of osteoporosis but diet physical activity and drug treatment
can prevent or reverse loss of BMD highlighting the importance of lifestyle choices in
osteoporosis outcomes Studies identified in the current review are summarised in Table 10
at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any physical activity studies examining osteoporosis
in breast cancer survivors The current review identified 3 RCTs and one cohort study
Schwartz Winters-Stone and Gallucci (2007) evaluated the impact of aerobics and
resistance training on BMD in an RCT involving women with histologically confirmed invasive
stage I-III breast cancer (n=66) beginning chemotherapy Women were randomised to one
of three groups and stratified according to menopausal status (pre-menopausal or post-
menopausal)
1) Home-based aerobic exercise - women were instructed to choose an aerobic activity
they enjoyed (eg walking jogging) and exercise for 15-30 minutes four days per
week for the duration of the study at a symptom-limited moderate intensity such that
they were breathing hard but able to talk
2) Home-based resistance exercise ndash women were instructed to exercise at home four
days per week using resistance bands and tubing
3) Usual care
It has been reported that 80 of older breast cancer survivors have osteopenia (below normal bone-mineral density [BMD]) or osteoporosis at initial diagnosis (Twiss et al 2001)
86
The average decline in BMD was -623 for usual care -492 for resistance exercise and
-076 for aerobic exercise suggesting that weight-bearing aerobic exercise attenuates
declines in BMD Pre-menopausal women demonstrated significantly greater declines in
BMD than post-menopausal women highlighting a need to provide interventions for bone
health on a risk stratification basis
Gross et al (2002) examined the intensity of physical activity (ie light moderate vigorous)
reported by a cohort of post-menopausal breast cancer survivors (n=27) and found no
relationship between activity levels and BMD However participants mainly reported light
physical activity limiting the examination of moderate and vigorous activity outcomes It is
possible that a higher intensity of physical activity is required to achieve any benefits to bone
health
Waltman et al (2009) conducted an RCT testing a 24-month self-efficacy based strength
and weight training programme on post-treatment (except tamoxifen and aromatase
inhibitors) post-menopausal breast cancer survivors (n=223) who had amenorrhea
(absence of menstruation) for at least 12-months and a bone BMD score lower than the
norm (Figure 1)
Figure 1 Bone Density Definitions
WHO Definitions of Osteoporosis
Based on Bone Density
T-Scores
BMD
Category
Examples
Range
10
05
0
-05
-10
-1 and
above Normal BMD
-15
-20
Between
-1 and -25
Low BMD
(Osteopenia)
-25
-30
-35
-40
-25 and
below Osteoporosis
Source WHO (2003)
The women were randomised to receive physical activity with medication (n=110) or
medication only (n=113) The medication taken by both groups included risedronate
(osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily) While
87
participation in strength training did not result in statistically significant improved BMD there
was a trend towards at least maintaining BMD at the total hip Participants who were 50
or greater adherent to the intervention (reasons for non-adherence included lack of
time or chronic pain due to co-morbidity) were significantly less likely than
participants on medication alone to lose BMD at the total hip and femoral neck
In a third RCT Swenson et al (2009) compared the effects of two interventions on changes
in BMD in women receiving chemotherapy for breast cancer (n=62)
1) intravenous zoledronic acid (used to prevent skeletal fractures in people with cancer)
and oral calciumvitamin D every 3-months for five treatments
2) prescribed home-based physical activity and oral calciumvitamin D
Zoledronic acid protected patients with breast cancer against bone loss during initial
treatment whereas the home-based physical activity intervention was less effective in
preventing bone loss indicating that physical activity and dietary supplements are not
always sufficient to protect done density in people with cancer However these were
patients undergoing treatment and more research is required into the effects of physical
activity on bone health in post-treatment survivors
ii DIET
Bekkering et al (2006) did not identify any diet studies examining osteoporosis in breast
cancer survivors The current review identified 3 RCTs and one cohort study
Plant Proteins and Fibres
Weikert et al (2005) performed a sub-analysis of the EPIC cohort study conducted in
Germany which included 8178 females and examined the association between protein
intake dietary calcium and bone structure It was concluded that high consumptions of
animal protein may be unfavourable whereas higher vegetable protein may be
beneficial to bone health These results support the hypothesis that high calcium intakes
combined with adequate protein intake based on a high ratio of vegetables to animal protein
may be protective against osteoporosis Indeed evidence has demonstrated the relationship
between lower incidence of osteoporosis in Asian women and vegetarian populations due to
a diet rich in vegetables and fruit (Fujii et al 2009 Merill and Aldana 2009 Thorpe et al
2008) Furthermore a large-scale dietary modification intervention of post-menopausal
women (n = 4883) showed that an increased consumption of plant proteins and fibres from
fruits vegetables and grains reduced the risk of multiple falls and slightly lowered hip BMD
although it did not change the risk of osteoporotic fractures (McTiernan et al 2009)
New et al (2003 2004) provides further evidence for the benefits of plant proteins and fibres
on bone health in two reviews where a positive link between a high consumption of fruit
and vegetables and bone health has been demonstrated In the first report it was found
that fruit and vegetables have beneficial effects on bone mass and bone metabolism in men
and women across the age ranges whilst in the second review it was concluded that
although the impact of a vegetarian diet on bone health is much more complex than merely
being related to diet vegetarians do tend to have normallsquo bone mass
88
iii WEIGHT
Bekkering et al (2006) did not identify any studies examining weight implications on
osteoporosis in breast cancer survivors The current review identified one study that found
that being underweight (BMI less than 185) was associated with lower BMD (Ryan et al
2007)
b) PROSTATE CANCER
i WEIGHT
Bekkering et al (2006) did not identify any studies examining the effect of body weight on
osteoporosis in prostate cancer survivors The current review identified one RCT Ryan et
al (2007) found a positive association between BMI and bone density of the hip in men with
prostate cancer (n=120) who were within the first 12-months of androgen-deprivation
therapy This suggests that a higher BMI can be protective of bone density loss in this
patient group
ii ALCOHOL
Bekkering et al (2006) did not identify any studies examining the effect of alcohol
consumption on osteoporosis in prostate cancer survivors The current review identified one
RCT Ryan et al (2007) also demonstrate greater bone density in prostate cancer patients
consuming seven or more weekly alcoholic beverages when compared to non-drinkers
a) OTHER CANCER
i DIET
Soya Products
Bekkering et al (2006) did not identify any studies examining the effect of diet on
osteoporosis in other cancer survivors The current review identified one RCT Marini et al
(2008) reported a randomised double-blind placebo-controlled trial of the soya derivative
genistein aglycone and its effects on bone health after 3-years in women with breast and
endometrial cancer (n=389) Bone mineral density increases were greater with
genistein for both femoral neck and lumbar spine compared to placebo the conclusion
being that after 3-years of treatment genistein exhibited a promising safety profile with
positive effects on bone formation in this cohort of osteopenic post-menopausal women
89
SUMMARY OF EVIDENCE FOR OSTEOPOROSIS AND BONE HEALTH
There is evidence that vitamin D and calcium might be associated with greater BMD
however this benefit cannot be distinguished from other potential contributors such as
physical activity and medication More research is needed into the effects of physical activity
on osteoporosis in cancer survivors The findings thus far offer different conclusions
although there is limited evidence that physical activity can at the very least prevent loss of
BMD which is a positive outcome in survivors at particular risk of bone loss Greater
adherence to physical activity interventions appeared to offer the greater benefits
highlighting the importance of designing lifestyle interventions that can be maintained as
well as providing higher intensity support for survivors with co-morbidities
Higher BMI has been found to be protective of BMD loss in men with prostate cancer
however no distinction has been made between higher BMI and a BMI that indicates excess
weight Limited evidence has been provided for the benefits of moderate alcohol
consumption but as with the evidence presented for weight much more research is needed
before any valid and reliable conclusions can be made Since the NHS advises no more than
3-4 units of alcohol per day for men more research is needed to determine the minimum
units of alcohol that offer such protective benefits It is important to deter against excessive
drinking which can have a number of serious health implications including high blood
pressure mouth and throat cancers and stroke (NHS 2010)
Men should not exceed 3-4 units of alcohol per day on a regular basis (NHS 2010) One unit is the amount of pure alcohol in a 25ml single measure of spirits (pure alcohol by volume [ABV] 40) a third of a pint of beer (ABV 5-6) or half a 175ml standardlsquo glass of red wine (ABV 12) Daily alcohol limits are provided by the NHS in order to discourage the belief that that the number of units of a weekly limit can be consumed at once (ie binge drinking) Use of daily limit
90
Table 10 Osteoporosis and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Gross et al (2002)
Descriptive correlational test of a multicomponent intervention to prevent and treat osteoporosis in breast cancer survivors
27 post-menopausal breast cancer survivorslsquo post- treatment except for tamoxifen
Not reported
Physical activity vigour vitality and BMD
More than half reported no very hard physical activity and 37 reported no hard activity The association of vigour with total metabolic equivalents for combined moderate hard and very hard activities was significant (r = 0536 p = 0007) as were the hours spent in the combined moderate to very hard activities No relationship was found between vigour vitality or any level of activity and BMD
Schwartz Winters-Stone and Gallucci (2007)
RCT testing the effects of aerobic and resistance exercise on changes in bone mineral density (BMD) in women receiving chemotherapy Participants were randomised to aerobic or resistance exercise and usual care
66 women with stage I-III breast cancer beginning adjuvant chemotherapy
6-months after starting treatment
BMD aerobic capacity and muscle strength
Aerobic exercise preserved BMD significantly better compared to usual care Premenopausal women demonstrated significantly greater declines in BMD than postmenopausal women Aerobic capacity increased by almost 25 for women in the aerobic exercise group and 4 for resistance exercise Participants in the usual care group showed a 10 decline in aerobic capacity
Swenson et al (2009)
Participants received one of two treatments a) Intravenous zoledronic acid and oral calciumvitamin D every 3-months for five treatments b) Prescribed home-based physical activity and oral calciumvitamin D
Women receiving chemotherapy for breast cancer (n=62)
On completion of 3-month intervention
Severity of lymphedema by arm circumference
BMD significantly decreased in the physical activity group but not in the zoledronic acid group Zoledronic acid protected patients with breast cancer against bone loss during initial treatment whereas the home-based physical activity intervention was less effective in preventing bone loss indicating that physical activity and dietary supplements are not always sufficient to protect done density in people with cancer
Waltman et al (2009)
A 24-month self-efficacy based strength and weight training programme Participants were randomised to receive physical activity with medication (n=110) or medication only (n=113) the medication taken by both groups including risedronate (osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily)
Post-treatment post-menopausal breast cancer survivors (n=223) with amenorrhea for at least 12-months and a BMD score lower than the norm
On completion of the 24-month intervention
Bone mineral density
While participation in strength training did not result in statistically significant improved BMD there was a trend towards at least maintaining BMD at the total hip Participants who were 50 or greater adherent to physical activities were significantly less likely than participants on medication alone to lose BMD at the total hip and femoral neck
91
DIET
Marini et al (2008)
RCT assessing the continued safety profile of genistein
aglycone on
breast and endometrium and its effects on bone after
3 years of
therapy Participants received 54mg of genistein
aglycone daily or
placebo both treatment arms
received calcium and vitamin D
Breast cancer patients ndash intervention group (n=71) and placebo (n=67)
After 3-years of treatment
BMD Bone mineral density increases were greater with genistein for both
femoral neck and lumbar spine compared to placebo Genistein also
significantly reduced pyridinoline as well as serum carboxy-terminal
cross-linking telopeptide and soluble receptor activator of NF- B
ligand while increasing bone-specific alkaline phosphatase IGF-I
and osteoprotegerin levels There were no differences in discomfort
or adverse events between groups
(McTiernan et al 2009)
RCT assessing the effect of the Womens Health Initiative
Dietary
Modification low-fat and increased fruit vegetable
and grain
intervention on incident hip total and site-specific
fractures and self-
reported falls and in a subset on bone
mineral density (BMD)
Participants were randomly assigned to
receive
a)dietary modification intervention (daily goal 20 of energy as fat 5 servings of vegetables
and fruit
and 6 servings of grains) b)comparison group
- no dietary
changes
Post-menopausal women (n=48835) intervention (40 n=19541)
versus comparison group (60 n=29294)
Mean=81-years
Incident hip total and site-specific
fractur
es and self-reported falls and in a subset on bone
mineral
density (BMD)
215 women in the intervention group and 285 women in the
comparison group (annualized rate 014 and 012 respectively)
experienced a hip fracture (hazard ratio 112 95 CI 094
134 P = 021) The intervention group (n = 5423 annualized rate
344) had a lower rate of reporting 2 falls than did the
comparison group (n = 8695 annualized rate 367) (HR 092
95 CI 089 096 P lt 001) There was a significant interaction
according to hormone therapy use those in the comparison group
receiving hormone therapy had the lowest incidence of hip fracture In a subset of 3951 women
hip BMD at years 3 6 and 9 was 04ndash
05 lower in the intervention group than in the comparison group
(P = 0003)
New et al (2004)
Literature review assessing the impact of a vegetarian diet on indices of skeletal integrity to address specifically whether vegetarians have a normal bone mass
Analysis of existing literature through a combination of observational clinical and intervention studies were assessed in relation to bone health lacto-ovo-vegetarian and
Not reported
Bone health Key findings included (i) no differences in bone health indices between lacto-ovo-vegetarians and omnivores (ii) conflicting data for protein effects on bone with high protein consumption and low protein intake (particularly with respect to vegan diets) being detrimental to the skeleton (iii) growing support for a beneficial effect of fruit and vegetable intake on bone with mechanisms of action currently remaining unclarified The impact of a vegetarian diet on bone health is a hugely complex area since 1) components of the diet (such as calcium protein alkali vitamin K phytoestrogens) may be varied 2) key lifestyle factors which are
92
vegan diets versus omnivorous consumption of animal versus vegetable protein and fruit and vegetable consumption
important to bone (such as physical activity) may be different 3) the tools available for assessing consumption of food are relatively weak However from data available vegetarians do certainly appear to have normal bone mass
Weikert et al (2005)
Prospective cohort study (EPIC) examining associations between protein intake calcium and bone structure measured by broadband ultrasound attenuation (BUA)
8178 female EPIC participants
Not reported
Bone structure
High intake of animal protein was associated with decreased BUA values ( _ = ndash003 p = 0010) whereas high vegetable protein intake was related to an increased BUA ( _ = 011 p = 0007) The effect of dietary animal protein on BUA was modified by calcium intake
WEIGHT
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and alcohol use was positively associated with the Z score
ALCOHOL
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and body mass index was positively associated with the Z score
93
WEIGHT AND BODY COMPOSITION
Weight gain during and after cancer treatment is becoming an ever-increasing significant
concern (Camoriano et al 1990 Levine et al 1991 Saquib et al 2006) Weight gain is
expected when energy intake exceeds energy expenditure a combination that is frequently
described among breast cancer patients who report exercising less during treatment and
after treatment (Schwartz 2000 Demark-Wahnefried 2001) and consuming a higher energy
diet during treatment (Mukhopadhyay and Larkin 1986) Exacerbating this is the fact that
women in general gain weight as they transition through menopause (Sammel et al 2003)
putting breast cancer patients at particular risk as treatments frequently result in a premature
menopause For individuals with bowel cancer the CALBG 8980 trial showed that 35 of
patients post-chemotherapy were overweight (BMI 250ndash299) and 34 were obese BMI
300ndash349) or very obese (BMI gt35) (Meyerhardt et al 2008) The reasons for weight gain
during and after treatment are multifactorial and the result of individual lifestyle behaviours
and the impact of certain cancer drugs Regardless of the reasons as described in part one
of this review both survival and recurrence may be adversely affected by obesity
(Chlebowski et al 2002)
The effect of obesity on survival has been evident in the majority of studies although not all
one reason for this inconsistency being the possibility that biological factors associated with
obesity and not the obesity itself are responsible for the observed effect For example
there is considerable evidence that the effects of obesity on breast cancer risk may be
mediated at least in part by the effect of obesity on insulin resistance (Friedenreich 2001
Suga et al 2001 Goodwin et al 2002)
Finding effective methods for weight loss continues to be a challenge as although some
studies have demonstrated substantial weight loss in obese individuals weight loss results
in general have been modest and new approaches are needed (Jeffery et al 2000) For
long-term reduction in body weight intensive individualised approaches toward developing
a new lifestyle may be required (Djuric et al 2002)
Studies identified in the current review are summarised in Table 11 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in breast cancer survivors The current review identified one
meta-analysis and three RCTs
In the meta-analysis Kim Kang and Park (2009) reviewed 10 studies involving 588 women
who had been treated for breast cancer examining the effectiveness of aerobic exercise
interventions on cardiopulmonary function and body composition conducted during or after
cancer treatments They concluded that regular aerobic physical activity significantly
improved cardiopulmonary function as assessed by absolute VO2 peak relative VO2
94
peak and 12-minute walk test as well as improved body composition as assessed by
percentage body fat (although body weight and lean body mass did not change
significantly)
Courneya et al (2007) conducted a multicentre RCT in which women with breast cancer on
adjuvant chemotherapy were randomly assigned to usual care (n = 82) supervised
resistance exercise (n = 82) or supervised aerobic exercise (n = 78) for the duration of their
chemotherapy (median = 17-weeks 9-24 weeks) There was 70 adherence to supervised
exercise with aerobic physical activity being superior to usual care for improving
aerobic fitness and percent body fat whilst resistance physical activity was superior
to usual care for improving muscular strength lean body mass and chemotherapy
completion rate
Schmitz et al (2005) evaluated the safety and effects of twice-weekly weight training among
85 breast cancer survivors with women being randomised into immediate or delayed
intervention groups The immediate group trained from months 0-12 the delayed group
served as a no exercise parallel comparison group from months 0-6 and trained from months
7-12 At 6-months the immediate group compared to the no exercise group showed
significantly greater increases in lean mass (p lt 01) as well as significant decreases
in percentage body fat (p lt 05) This significance remained at 12-months when
comparing the immediate group with the delayed exercise group
Mefferd et al (2006) randomised overweight or obese breast cancer survivors (n=85) to a
16-week once weekly general exercise and dietary counselling intervention or standard
care The intervention addressed a reduction in energy intake as well exercise with a goal
of an average of one-hour a day of moderate to vigorous activity Seventy six women
(894) completed the intervention demonstrating reasonable acceptability of the
intervention At 16-weeks significant group differences in favour of the intervention
were evident in weight BMI percent fat trunk fat leg fat and waist and hip
circumference
ii DIET
Bekkering et al (2006) did not identify any studies examining the effect of diet on weight loss
or maintenance in breast cancer survivors The current review identified one RCT
Chlebowski et al (2006) report an RCT conducted as part of the aforementioned WINS trial
where 2437 postmenopausal women with early breast cancer were randomised to
nutritional and lifestyle counselling (n=975) or not (n=1462) as part of routine follow-up The
dietary intervention included eight bi-weekly individual counselling sessions As a reminder
the goal of the dietary intervention was to reduce percentage of calories from fat to 15
resulting in a sustained reduction in fat intake to approximately 20 of calories Dietary fat
intake reduction was significantly greater in the dietary group compared to the control group
After 12-months of intervention dietary fat intake was lower in the intervention group
than in the control group (333g per day versus 513g per day respectively Plt001)
95
corresponding to a statistically significant 6-pound lower mean body weight in the
intervention group (P lt01) This major study also demonstrated a survival advantage in
women who lost weight as described in Part 1 of this review
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in prostate cancer survivors The current review identified
one RCT
Segal et al (2009) conducted a RCT with 121 men with prostate cancer commencing
radiotherapy with or without androgen deprivation therapy They were randomly assigned to
24-weeks of usual care resistance exercise or aerobic exercise Compared with usual
care exercise improved aerobic fitness upper- and lower-body strength while
preventing an increase in body fat Resistance exercise generated longer-term
improvements and additional benefits for strength and body fat than aerobic exercise
SUMMARY OF EVIDENCE FOR WEIGHT AND BODY COMPOSITION
Supervised physical activity programmes with or without dietary counselling are highly
effective in improving body composition or at the very least preventing increases in weight
They are also safe and have other major benefits on health including improving fitness
walking distance muscle power and reducing cholesterol More research is however
required into the most effective dietary strategies for weight loss or maintenance in cancer
survivors Thus far there is some evidence for reducing dietary fat intake
A large controlled trial has been designed to test the combined effect of physical activity and
weight control on disease-free survival and on breast cancer recurrence free survival
second primary breast cancer and total invasive plus in situ breast cancer (Ballard-Barbash
et al 2009) Goals for weight control interventions for women whose BMI is greater than
25kgm2 is to lose 10 of body weight and for women whose BMI is less than or equal to
25kgm2 to avoid weight gain The goal for the physical activity intervention would be to
achieve and maintain regular participation in a moderate intensity physical activity
programme for a total of 150-255 minutes over at least 5 days per week This study is using
evidence which is current for weight loss and physical activity and is an indicator for the
basis of advice for patients at risk in similar situations
96
Table 11 Weight and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Courneya et al (2007)
Multicentre RCT to test for factors that could counteract unfavourable changes resulting from chemotherapy (eg changes in body composition) Participants were randomly assigned to usual care (n =
82) supervised resistance exercise
(n = 82) or supervised aerobic
exercise (n = 78) for the duration of their chemotherapy
242 breast cancer
patient
s initiating adjuvant chemotherapy
Median=17-weeks
Primary Cancer-Specific QoL Secondary Fatigue psychosocial functioning physical fitness body composition chemotherapy completion rate and lymphedema
The follow-up assessment rate for our primary end point was
921 and adherence to the supervised exercise was 702
Unadjusted and adjusted mixed-model analyses indicated that
aerobic exercise was superior to usual care for improving self-
esteem (P = 015) aerobic fitness (P = 006) and percent body fat
(adjusted P = 076) Resistance exercise was superior to usual care
for improving self-esteem (P = 018) muscular strength (P lt
001)
lean body mass (P = 015) and chemotherapy completion rate (P =
033) Changes in cancer-specific QOL fatigue depression and
anxiety favoured the exercise groups but did not reach statistical
significance Exercise did not cause lymphedema or
adverse events
Kim Kang and Park (2009)
Meta-analysis to examine the effectiveness
of aerobic exercise
interventions on cardiopulmonary function
and body composition in
women with breast cancer
Of 24 relevant
studie
s reviewed 10 studies (n= 588) met the inclusion criteria
Not reported Cardiopulmonary function
and body
composition
The findings indicated that aerobic exercise significantly improved
cardiopulmonary function as assessed by absolute
VO2 peak (standardized mean difference [SMD] 916 p lt 001)
relative VO2 peak (SMD424 p lt 05) and 12-minute walk test
(SMD 502 p lt 001) Similarly aerobic exercise significantly
improved body composition as assessed by percentage body fat
(SMD mdash890 p lt001) but body weight and lean body mass did not
change significantly
Mefferd et al (2006)
RCT to test the effect of a 16-week cognitive behavioural therapy (CBT) intervention for weight loss through exercise and diet modification on risk factors for recurrence of breast cancer Participants randomly assigned to a once weekly 16-week intervention or wait-list control group
Overweight or obese breast cancer survivors (n=76)
On completion of the 16-week intervention
Weight Significant differences in weight body mass index percent fat trunk fat leg fat as well as waist and hip circumference between intervention and control groups (P le 005) Furthermore levels of triglycerides and total cholesterolhigh density lipoprotein cholesterol levels were also significantly reduced following the intervention
97
Schmitz et al (2005)
RCT testing the safety of twice weekly weight training classes among recent breast cancer survivors Participantslsquo randomised into immediate and delayed treatment groups The immediate group trained from months 0-12 the delayed treatment group served as a no exercise parallel comparison group from months 0-6 and trained from months 7=12
Convenience sample of 85 recent breast cancer survivors
6 and 12-months
Body size (lean body mass) and biomarkers hypothesised to link exercise and breast cancer risk
Significant increases in lean mass (088 versus 002 kg P lt 001) as well as significant decreases in body fat (minus115 versus 023 P = 003) and IGF-II (minus623 versus 2828 ngmL P = 002) comparing immediate with delayed treatment from baseline to 6 months Within-person changes experienced by delayed treatment group participants during training versus no training were similar
Segal et al (2009)
Prostate Cancer Radiotherapy and
Exercise Versus Normal
Treatment study examining the effects
of 24-weeks of resistance or
aerobic training versus usual care on prostate cancer outcomes Randomly assigned
to usual care resistance or
aerobic exercise for 24-weeks
Prostate cancer patients on radiotherapy (n=121) usual care (n=41) resistance (n= 40) aerobic exercise
(n=
40)
On completion of 24-week intervention
Fatigue QOL physical fitness body composition PSA testosterone haemoglobin and lipid levels
Median adherence to prescribed exercise was 855 Compared
with usual care resistance training improved QOL (P = 015)
aerobic fitness (P = 041) upper- (P lt 001) and lower-body (P lt
001) strength and triglycerides (P = 036) while preventing an
increase in body fat (P = 049) Aerobic training also improved
fitness (P = 052)
DIET
Chlebowski et al (2006)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to 345]
versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group
98
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general dietary
guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
randomisation to death from any cause
99
QUALITY OF LIFE
The advancements in diagnosis and treatment that have contributed to the rise in
survivorship are a significant achievement for healthcare science However it is important to
recognise that this has also resulted in an increase in the number of people living with the
often long-term physical and psychological consequences of cancer and its treatment
Quality of life outcomes are thus becoming just as important as hardlsquo outcomes such as
mortality (Rosenbaum Fobair and Spiegel 2006) hence an emphasis on patient-reported
outcomes (DH 2009c) Indeed there is increasing evidence that QoL can be more
predictive of cancer survival than measures of performance status (Cella et al 2009 Eton et
al 2003 Wenzel et al 2005)
A healthy lifestyle has become viewed as an important element for improved QoL (Lyon and
Langille 2000) with particular emphasis on physical activity Studies identified in the current
review are summarised in Table 12 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in breast cancer survivors In the current review one systematic review (with meta-
analysis) and 6 RCTs were identified that provide evidence for the role of physical activity in
the QoL of breast cancer survivors
McNeeley et al (2006) conducted a systematic review with meta-analysis of RCTs (n=14)
examining the effects of physical activity on outcomes in breast cancer survivors Three of
the reviewed studies involving 194 patients compared exercise with usual care
(Campbell et al 2005 Courneya et al 2003 Segal et al 2001) with pooled data
demonstrating that exercise led to significant improvements in QoL superior to the
usual care groups Four studies involving 208 patients reported physical functioning or
physical well-being components of QoL (Campbell et al 2005 Courneya et al 2003
McKenzie and Kalda 2003 Segal et al 2001) the pooled results of which showed
a statistically significant increase in this component of QoL as a result of physical
activity Two of these studies were rated as high quality by the reviewers Courneya et al
2003 Segal et al 2001
100
In addition to this meta-analysis findings by Ohira et al (2006) demonstrated that over 6-
months physical and psychological QoL significantly improved in a recent breast
cancer survivors (n=86) 4-36 months post-treatment who took part in a twice-weekly
weight-training intervention when compared to a control group Increases in upper
body strength and lean mass correlated with these improvements suggesting that twice-
weekly weight training for recent breast cancer survivors might improve QoL in part via
changes in body composition and strength
Daley et al (2007) provided evidence from an RCT comprising sedentary breast cancer
survivors who were 12-36 months post-treatment and who were randomised to one of three
conditions
1) 8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-
minute one-to-one sessions with an physical activity specialist three times per week
(n=34)
2) 8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one
sessions with an physical activity specialist three times per week (n=36)
3) usual care (n=38)
Courneya et al (2003) evaluated QoL outcomes in relation to
exercise in breast cancer survivors (n=52) who had completed
surgery radiotherapy or chemotherapy Participants trained three
times per week for 15-weeks on recumbent or upright cycle
ergometers Exercise duration began at 15-minutes for weeks 1-
3 and then systematically increased by five-minutes every 3-
weeks to 35-minutes for weeks 13-15 The exercise group completed
984 of the exercise sessions demonstrating high adherence
rates Overall QoL increased by 91 points in the exercise group
compared with 03 points in the control group (p lt 001) Change
in peak oxygen consumption correlated with change in overall QoL
demonstrating a significant relationship between exercise and
increases in QoL (p lt 01)
Segal et al (2003) compared self-directed versus supervised
exercise on QoL outcomes in women with stages I-II breast cancer
(n=123) Physical functioning in the control group decreased by 41
points whereas it increased by 57 points and 22 points in the self-
directed and supervised exercise groups respectively (p lt 05)
Post-hoc analysis showed a moderately large and clinically important
difference between the self-directed and control groups (98
points p lt 01) and a more modest difference between the
supervised and control groups (63 points P = 09) No significant
differences between groups were observed for changes in QoL
scores
101
A significant mean difference of 98 units in QoL scores favouring aerobic physical
activity therapy was found This outcome was not the result of the extra support and
attention gained from taking part in the intervention since the same findings were not elicited
for the physical activity-placebo and usual care groups
A small pilot RCT comparing QoL and functional capacity in breast cancer survivors (n=21)
provided with 12-weeks of the Chinese physical activity Tai Chi Chuan (n=11) versus
psychosocial support (n=10) was conducted by Mustian Palesh and Flecksteiner (2008)
The tai chi group demonstrated significant improvements in functional capacity and QoL the
psychosocial support group showed significant improvements only in flexibility with declines
in QoL This suggests that tai chi can enhance functional capacity and QoL among
breast cancer survivors over and above the benefits of psychosocial support
Further support for the benefits of physical activity on QoL in breast cancer survivors (n=58)
within 2-years of completing adjuvant therapy has been demonstrated in a combined aerobic
and resistance training RCT (Milne et al 2008) The women received 12-weeks immediate
supervised physical activity three times a week (n=29) or delayed physical activity
comprising the same protocol but provided 12-weeks following the immediate physical
activity group (n=29) Adherence was 613 which is relatively low However there was a
significant group by time interaction for overall QoL which increased in the
immediate physical activity group from baseline to 12-weeks by 208 points compared
to a decrease in the delayed physical activity group of 53 points
Cadmus et al (2009) report on the QoL outcomes of two 6-month RCTs designed for breast
cancer survivors and based on the national recommendation of 30-minutes of moderate to
vigorous physical activity five days per week
When combining findings from these two studies physical activity was not associated with
QoL benefits in the full sample of either study however physical activity was associated with
significantly improved social functioning (a component of QoL) among survivors who
Trial Increasing or Maintaining
Physical Activity during Cancer
Treatment (IMPACT)
Theoretical Framework Theory of
Planned Behaviour and
transtheoretical model - promoting
self-efficacy to overcome barriers to
physical activity
Sample n=45 newly diagnosed
survivors
Delivery Home-based
Trial Yale Physical activity and
Survivorship (YES)
Theoretical Framework Not
reported
Sample n=67 post-treatment
survivors
Delivery Combined supervised
training programme at a local
health club with home-based
physical activity
102
reported low social functioning at baseline which is the likely impact of greater social
interaction during the intervention This highlights the utility of risk stratification and the
provision of lifestyle support based on need survivors with low social functioning as
could be detected via the Social Difficulties Inventory (SDI Wright et al 2005b) are
likely to benefit from programmes such as the IMPACT and YES trial
Sandel et al (2005) report on a cross-over RCT testing the outcomes of a 12-week dance
and movement exercise programme in women within 5-years of treatment for breast cancer
(n=38) The study included a waiting list control (n=19) and cross-over at 13-weeks Women
attended two supervised dance sessions for six weeks and one session per week for an
additional 6-weeks for a total of eighteen sessions A total of 35 (92) women completed
the regimen with reasons for dropping out including fatigue other commitments and one
participant reported shoulder discomfort The overall finding was that breast cancerndash
specific QoL improved significantly in the intervention group compared to the waiting
list group at 13-weeks which remained unchanged
In the updated systematic review described previously Speck et al (2010) present evidence
from 66 high quality RCTs showing that physical activity during treatment has a small to
moderate positive effect on QoL (p=004) anxiety (p=002) and self-esteem (p=002)
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in colorectal cancer survivors In the current review one large cohort study was
identified Lynch et al (2008) examined physical activity and QoL data collected as part of
the Colorectal Cancer and Quality of Life Study37 Telephone interviews were conducted
at approximately 6 12 and 24-months after colorectal cancer diagnosis (n=1966) which
found that participants achieving at least 150-minutes of physical activity per week had an
18 higher QoL score than those who reported no weekly physical activity
ii DIET
Bekkering et al (2006) identified two dietary intervention studies examining impact on QoL in
colorectal cancer survivors One dietary counselling trial found a significant improvement in
health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst another reported that
an intervention aimed at a healthier dietary lifestyle had no effect on health assessment or
life satisfaction but did lead to increased health action and increased reports of feeling goodlsquo
(Corle et al 2001) No further studies were identified in the current review
37
The Colorectal Cancer and Quality of Life study in Australia examines in detail the lifestyle factors that
influence QoL in the 5-years post-diagnosis (n=2000)
103
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any dietary physical activity interventions examining
impact on QoL in prostate cancer survivors One dietary counselling trial found a significant
improvement in health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst
another reported that an intervention aimed at a healthier dietary lifestyle had no effect on
health assessment or life satisfaction but did lead to increased health action and increased
reports of feeling goodlsquo (Corle et al 2001) No further studies were identified in the current
review
Segal et al (2003) reported an RCT comparing supervised resistance exercise versus
control in men with prostate cancer (n=135) who were scheduled to receive androgen
deprivation therapy for at least 3-months Fitness levels were assessed and the men in the
intervention group met with a certified fitness consultant within 7-days of the pre-
assessment The fitness consultant provided patients with the results of their exercise
assessment and introduced a personalised resistance exercise program A significant
improvement was found in QoL outcomes in the intervention group and a significant
decline in the control group Resistance exercise improved QoL regardless of whether
men were treated with curative or palliative intent or whether androgen deprivation therapy
had been received for less than one-year or 1 year
d) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) found that out of seven physical activity trials six observed
improvements in QoL when using cancer-specific questionnaires (Burnham and Wilcox
2002 Courneya et al 2003 Segal et al 2003 Headley et al 2004 Campbell et al 2005
Sandel et al 2005) but one of these same studies found no association when using the
generic SF-36 scale (Segal et al 2001) This highlights the importance of selecting the most
appropriate outcome measures in terms of sensitivity and responsiveness to a given
intervention
In the current review three studies were identified One prospective controlled four-centre
study comprising a sample of survivors with different tumour sites was identified (Korstjens
et al 2008) QoL outcomes were compared between three groups
1) group-delivered physical training (n=71)
2) group-delivered combined physical and cognitive behavioural training (CBT) (n=76)
3) waiting-list control (n=62)
Participants in both training groups showed significant and clinically relevant improvements
in role limitations physical functioning vitality and health change Adding CBT to the
physical training did not have additional beneficial effects on QoL a finding that has been
104
observed in a number of supported self-management programmes (Davies and Batehup
2010)
Oh et al (2009) reported a RCT examining the QoL outcomes of Medical Qigong (MQ) a
mindndashbody practice that uses physical activity and meditation to harmonise the body mind
and spirit Patients (n=162) with malignancy of any stage and an expected survival length of
gt12-months were randomised to a control group or to a 10-week MQ programme comprising
two supervised 90-minute sessions per week At 10-week follow-up participants in the
MQ group reported larger improvements in QoL than those in the usual care group (p
lt 05)
Mosher et al (2009) reported a prospective cohort study examining the diet exercise and
QoL patterns of 753 breast prostate and colorectal cancer survivors who were at least 5-
years post-diagnosis Survivors underwent two 45-60 minute telephone surveys
administered by the Diet Assessment Center The data demonstrated that greater weekly
minutes of exercise were associated with better physical QoL including less pain and
better health perceptions physical functioning and vitality More exercise was also
correlated with better social functioning Diet quality had a positive association with a range
of physical QoL outcomes in analyses that were adjusted for age level of education and co-
morbidities Greater BMI was associated with worse physical QoL including greater
pain and role limitations because of physical problems and worse health perceptions
physical functioning and vitality
SUMMARY OF EVIDENCE FOR QUALITY OF LIFE
Lifestyle interventions appear to help people with a wide range of cancer types who have
received treatments ranging from surgery chemotherapy radiotherapy or hormonal
therapies although no trials have yet been published specifically addressing the newer
biological therapies Even when not directly associated with overall QoL exercise has been
found to significantly improve social functioning among post-treatment survivors The
benefits of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or group-
based A vast array of different types of exercise techniques have been tested in the studies
evaluated in this review highlighting the potential for survivors to choose activities according
to preference
Whilst some studies have recommended the uptake of physical activity during treatment
others have highlighted the benefits of introducing regular physical activity into a survivorlsquos
self-management care plan immediately after completion of treatment Overall the evidence
does suggest that immediate physical intervention provides greater QoL benefits than
delayed intervention
105
Table 12 Quality of Life and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Cadmus et al (2009)
The results of two RCTs to determine the effect of exercise on quality of life in (a) a RCT of exercise among recently diagnosed breast cancer survivors undergoing adjuvant therapy - randomised to a 6-month home-based exercise program or a usual care group (b) a similar trial among post-treatment survivors - randomised to a 6-month supervised exercise intervention or to usual care
50 newly diagnosed breast cancer survivors in the first RCT (a) 75 post-treatment survivors in the second RCT (b)
6-months Measures of happiness depressive symptoms anxiety stress self-esteem and QoL
Good adherence was observed in both studies Baseline quality of life was similar for both studies on most measures Exercise was not associated with quality of life benefits in the full sample of either study however exercise was associated with improved social functioning among post-treatment survivors who reported low social functioning at baseline (p lt005)
Courneya et al (2003)
RCT testing 15-weeks supervised aerobic and resistance training to determine the effects on cardiopulmonary
function and QoL in
post-menopausal breast cancer
survivors Randomly assigned to an exercise (n=25) or control (n=28) group The exercise group trained on cycle ergometers
three times per week for 15
weeks The control group did not train
53 post-menopausal breast cancer survivors
On completion of the 15-week intervention
Changes in peak oxygen
consu
mption and overall
Peak oxygen consumption increased by 024 Lmin in the exercise group whereas it decreased
by 005 Lmin in the control group
(mean difference 029 Lmin 95 confidence interval [CI] 018 to
040 P lt 001) Overall QOL increased by 91 points in the exercise
group compared with 03 points in the control group (mean
difference 88 points 95 CI 36 to 140 P= 001) Pearson
correlations indicated that change in peak oxygen consumption
correlated with change in overall QOL (r = 045 P lt 01)
Daley et al (2007)
RCT - Women were randomised to one of three groups a)8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-minute one-to-one sessions with an physical activity specialist three times per week (n=34) b)8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one sessions with an physical activity specialist three times
Sedentary breast cancer survivors who were 12-36 months post-treatment (n=117)
On intervention completion and at 24-weeks follow-up
QoL depression physical activity behaviour aerobic fitness
There was a significant mean difference of 98 units in QoL scores favouring aerobic physical activity therapy
106
per week (n=36) c)usual care (n=38)
Korstjens et al (2008)
RCT comparing the effects on cancer survivorslsquo QoL in a
12-week group-
based multidisciplinary self-management rehabilitation
program
combining physical training (twice weekly) and cognitive-behavioural
training (once weekly) with
those of a 12-week group-based physical
training (twice weekly) There
was also a non-intervention comparison group
All cancer types rehabilitation (n=76) physical training (n=71) comparison group (n=62)
Baseline after rehabilitation and
3-
months follow-up
QoL (SF-36) The effects of multidisciplinary rehabilitation did not outperform
those of physical training in role limitations due to emotional
problem (primary outcome) or any other domains of quality of life
(all p gt 05) Compared with no intervention participants in both
rehabilitation groups showed significant and clinically relevant
improvements in role limitations due to physical problem (primary
outcome effect size (ES) = 066) and in physical functioning (ES =
048) vitality (ES = 054) and health change (ES = 076) (all p lt
01)
Lynch et al (2008)
Colorectal Cancer and Quality of Life
Study - aimed at examining the relationships between
physical activity
and QoL after a colorectal cancer
diagnosis Participants completed telephone interviews at approximately
6
12 and 24 months after diagnosis
1966 people with colorectal
6 12 and 24-months post-diagnosis
QoL There was an overall independent association between physical
activity and QoL At a given time point
participants achieving at least 150 minutes of physical activity per
week had an 18 higher quality of life score than those who
reported no physical activity Significant associations were also
present at the interindividual level (differences between
participants) and intraindividual level (within participant changes)
Milne et al (2008)
RCT to examine the effects of a supervised exercise program on motivational variables in breast cancer survivors Participants were randomised in a cross-over design to either an immediate exercise group that exercised from baseline to week 12 or a delayed exercise group that exercised from week 12 to 24
Breast cancer survivors (n=58) within 2-years of completing adjuvant therapy
Post-intervention (12-weeks)
Quality of life There was a significant group by time interaction for overall QoL which increased in the immediate physical activity group by 208 points compared to a decrease in the delayed physical activity group of 53 points
Mosher et al (2009)
Prospective Cohort Study examining the health behaviours of older cancer survivors and the associations of those behaviours with QoL especially during the long-term post-treatment period
753 older (aged 65 years) long-term survivors ( 5 years post-diagnosis) of breast prostate and colorectal
2 telephone interviews
Exercise diet weight status and quality of life
Participants reported a median of 10 minutes of moderate-to-vigorous exercise per week and only 7 had Healthy Eating Index scores gt80 (indicative of healthful eating habits relative to national guidelines) Despite their suboptimal health behaviours survivors reported mental and physical quality of life that exceeded age-related norms Greater exercise and better diet quality were associated with better physical quality-of-life outcomes (eg better vitality and physical functioning P lt 05) whereas greater body mass index was associated with reduced physical quality of life (P lt 001)
107
cancer
Mustian Palesh and Flecksteiner (2008)
RCT testing the functional and QoL outcomes of tai chi - women who completed treatment randomised to receive tai chi or psychosocial support therapy for 12-weeks (60 minutes three times weekly)
Breast cancer survivors (n=21)
On completion of 12-week intervention
Functional capacity and quality of life
The tai chi group demonstrated significant improvements in functional capacity and QoL the psychosocial support group showed significant improvements only in flexibility with declines in QoL
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials
MEDLINE EMBASE CINAHL Psych INFO CancerLit PEDro
and
SportDiscus as well as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
functi
oning as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all outcomes
were positive even when statistical significance was not achieved
Exercise led to statistically significant improvements in quality of life
as assessed by the Functional Assessment of Cancer Therapyndash
General (weighted mean difference [WMD] 458 95 CI 035 to
880) and Functional Assessment of Cancer TherapyndashBreast (WMD
662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak oxygen consumption
and in reducing symptoms of fatigue
Oh et al (2009)
RCT comprising 10-weeks Medical Qigong (MQ) to evaluate the use of (MQ) compared with usual care in improving the QOL of cancer patients
162 patients with a range of cancers
On completion of the 10-week intervention
QOL and fatigue (FACT-GF) mood (Profile of Mood State)
Regression analysis indicated that the MQ group significantly improved overall QOL (t144thinsp=thinspminus5761 Pthinspltthinsp0001) fatigue (t153thinsp=thinspminus5621 Pthinspltthinsp0001) mood disturbance (t122 =2346 Pthinsp=thinsp0021) and inflammation (CRP) (t99thinsp=thinsp2042 Pthinspltthinsp0044) compared with usual care after controlling for baseline variables
Ohira et al (2006)
RCT to examine the effects of weight training on changes in QoL and depressive symptoms in recent breast cancer survivors Randomised to treatment or control group
Convenience sample of 86 breast cancer survivors (4-36 months post-treatment)
6-months The primary outcomes were changes in QoL (CARES-SF) and depressive symptoms (CES-D)
QoL improved in the treatment group compared with the control group (Standardized Difference = 062 P = 006) The psychosocial global score also improved significantly in the treatment group compared with the control group (Standardized Difference = 052 P = 02) There were no changes in CES-D scores Increases in upper body strength were correlated with improvements in physical global score (r = 032 P lt01) and psychosocial global score (r = 030 P lt01) Increases in lean mass were also correlated with improvements in physical global score (r = 023 P lt05) and psychosocial global score (r = 024 P lt05)
Sandel et al (2005)
RCT - 12-weeks dance and movement programme versus wait list control to determine the effect on QoL and shoulder function
35 breast cancer survivors
13 and 26-weeks
QoL (FACT-B) Shoulder range of motion (ROM) and Body Image Scale
FACT-B significantly improved in the intervention group at 13 weeks from 1020 _158 to 1167 _ 169 compared to the wait list group 1081 _ 164 to 1071 _213 (time _ group effect P _ 008) During the crossover phase the FACT-B score increased in the wait list group and was stable in the treatment group The overall effect of the training at 26 weeks was significant (time effect P _ 03) and the order of training was also significant (P _ 015) Shoulder ROM
108
increased in both groups at 13 weeks mdash15_ and 8_ in the intervention and wait list groups (Time effect P _ 03 time _ group P _ 58) Body Image improved similarly in both groups at 13 weeks (time effect P _ 001 time _ group P _ 25) and at 26 weeks There was no significant effect of the order of training for these outcome measures
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) A small to moderate positive effect of physical activity during treatment was seen for physical activity level aerobic fitness muscular strength functional quality of life anxiety and self-esteem With few exceptions exercise was well tolerated during and post treatment without adverse events
Segal et al (2003)
RCT testing the hypothesis that resistance exercise can counter the negative QoL effects of androgen deprivation therapy for prostate cancer by reducing fatigue elevating mood building muscle mass and reducing body fat Randomly assigned to an intervention group that participated in a resistance exercise program three times per week for 12 weeks or to a waiting list control group
55 men with prostate cancer scheduled for androgen deprivation therapy for at least 3 months after recruitment
On completion of the 12-week intervention
Primary outcomes fatigue disease-specific QoL Secondary outcomes muscular fitness body composition
Men assigned to resistance exercise had less interference from fatigue on activities of daily living (P =002) and higher quality of life (P =001) than men in the control group Men in the intervention group demonstrated higher levels of upper body (P =009) and lower body (P lt001) muscular fitness than men in the control group The 12-week resistance exercise intervention did not improve body composition as measured by changes in body weight body mass index waist circumference or subcutaneous skinfolds
Vadiraja et al (2009)
RCT - 6-week yoga and relaxation during adjuvant radiotherapy his study compares the effects of an integrated yoga program with brief supportive therapy in breast cancer outpatients undergoing adjuvant radiotherapy at a cancer centre Intervention consisted of
88 stage II and III breast cancer outpatients
After 6-weeks of radiotherapy
QoL (EORTC-C30) Mood (Positive and Negative Affect Schedule)
There was a significant difference across groups over time for positive affect negative affect and emotional function and social function There was significant improvement in positive affect (ES = 059 p = 0007 95CI 125 to 78) emotional function (ES = 071 p = 0001 95CI 645 to 2533) and cognitive function (ES = 048 p = 003 95CI 12 to 185) and decrease in negative affect (ES = 084 p lt 0001 95CI minus134 to minus44) in the yoga
109
yoga sessions lasting 60 minutes daily while the control group was imparted supportive therapy once in 10 days
group as compared to controls There was a significant positive correlation between positive affect with role function social function and global quality of life There was a significant negative correlation between negative affect with physical function role function emotional function and social function
110
ONGOING LIFESTYLE STUDIES
Four ongoing lifestyle studies were identified in the current review one for breast cancer and
three for colorectal cancer
a) BREAST CANCER
In the US Goodwin et al (ongoing) are trialling lsquoLifestyle Intervention Study in Adjuvant
Treatment of Early Breast Cancerrsquo (LISA) The primary objective of this trial is to evaluate
the effect of the addition of a 2-year centrally delivered individualised telephone-based
lifestyle intervention focusing on weight management to a mailed educational intervention on
disease-free survival in post-menopausal women with early stage breast cancer (hormone
receptor positive) BMI ge24-lt40 kgm2 who are receiving standard letrozole adjuvant
therapy The primary outcome is disease-free survival Secondary outcomes include overall
survival distant disease-free survival weight change QoL selected non-cancer medical
events and biologic factors (insulin) The estimated enrolment is 2150 with the study having
started in 2007 Participants will be randomised to
1) Individualised Lifestyle Intervention Experimental - Women randomised to this arm
will receive an intervention program that consists of individual weight loss diet and
physical activity goals incorporated into a 2-year standardised structured telephone
and mail-based intervention In addition to diet and physical activity the intervention
will address behavioural and motivational issues relating to weight management
including maintaining motivation overcoming obstacles to success relapse
prevention emotional distress and stress and time management The telephone
intervention will involve 19 phone calls as well as mailings and a participant manual
women will be asked to lose up to 10 of their weight by reducing their caloric and
fat intake (by 500-1000 kcalday 20 calories fat) and increasing their moderate
physical activity (to 150-200 minutesweek)
2) Mail-based Active Comparator - Participants will receive a standardised mail-based
intervention focussing on healthy living This will include mailings at study entry as
well as a 2-year subscription to health magazine
Approximately 2150 women will be enrolled follow-up will continue until target event rates
have been met (anticipated 4-6 years after completion of the intervention) This sample size
will provide 80 power (type 1 error 005 2-tailed) to detect a hazard ratio (HR) for DFS of
074-076 in the weight loss intervention arm
b) COLORECTAL CANCER
It has been suggested that interventions to improve QoL in colorectal cancer survivors are
more effective if they target symptom management psychosocial support and lifestyle
variables in a comprehensive and integrated approach to behavioural change (Steginga et
al 2009) Due to the paucity of comprehensive trials examining behavioural interventions in
this group of survivors Hawkes et al (2009) are conducting a large-scale RCT of a 6-month
telephone-delivered lifestyle coaching intervention based on Acceptance and Commitment
111
Therapy (ACT) ndash bdquoCanChange‟ The intervention aims to assist colorectal cancer survivors
(n=350) to make improvements in lifestyle including physical activity weight management
and smoking cessation Participants receive up to eleven telephone sessions over the
6-months from a qualified health professional who provides support on symptom
management and lifestyle change Outcomes will be assessed post-intervention at 6- and
12-months follow-up and will include physical activity CRF QoL and cost-effectiveness
The findings from this innovative lifestyle coaching initiative will offer insight into the intensity
of support required to achieve sustained behaviour change as well as highlight the efficacy
of various components of delivery (eg telephone-delivery coaching professionally-led
etc)
Courneya et al (2008) are leading a physical activity intervention in a collaboration between
Canada and Australia the Colon Health and Life-Long Physical activity Change
(CHALLENGE) a 3-year multicentre RCT for colon cancer survivors (n=1000) who are 2-6
months post adjuvant-treatment Any type of physical activity will be promoted the goal
being to motivate people to increase their overall activity by about 25-hours of moderate
intensity physical activity or 1-hour and 15-minutes of vigorous physical activity per week
Behavioural support counselling and supervised physical activity sessions will be used to
promote the adoption and long-term maintenance of physical activity By monitoring
participants over 10-years the trial will determine if colon cancer recurs less often in people
who increase and maintain their physical activity It will also assess whether physical activity
improves other important outcomes including QoL anxiety depression sleep and physical
function It is anticipated that this trial will provide important insight into strategies for
promoting long-term health behaviour change
Another Australian lifestyle intervention is The Colorectal Cancer and Quality of Life led
by Joanne Aitken The purpose of this project is to identify any patterns between lifestyle and
QoL over the first 5-years following a diagnosis of colorectal cancer Approximately 2000
people have been recruited to take part in this study making it the largest colorectal cancer
study of its type to be undertaken Participants complete a telephone interview and a written
Pilot testing demonstrated that
o 80 of participants (n=20) felt the intervention addressed their issues
o 100 felt more motivated to make lifestyle changes
o 100 would recommend the intervention to other survivors
From baseline to post-intervention improvements
were observed for
o Colorectal cancer symptoms o QoL o Diet o Physical activity
112
questionnaire on an annual basis over the 5-years One of the aims of the study is to
uncover how lifestyle factors particularly physical activity may improve QoL and reduce the
risk of developing other chronic diseases that cancer survivors are prone to such as heart
disease and diabetes This information will help Cancer Council Queensland properly design
and target lifestyle interventions to help improve the health and well-being of colorectal
cancer survivors (Aitken et al ongoing)
113
DISCUSSION
WHAT DO WE KNOW ABOUT LIFESTYLE AND CANCER
This aim of this review was to update the World Cancer Research Fund (WCRF) report bdquoA
Systematic Review of RCTs Investigating the Effect of Nutritional and Physical
Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This has been
achieved by conducting a comprehensive but pragmatic search of the literature from 2006
onwards Where no evidence was available in the WCRF review studies before 2006 have
been included if identified in the reference lists of acquired records To facilitate this
evidence cited within the lsquoHandbook of Cancer Survivorship‟ (Feuerstein 2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (2009) were also utilised
Before presenting a synthesis of the findings within this review there are some limitations
that first need to be addressed
Methodological Limitations
There is strong evidence from observational studies that lifestyle factors can potentially have
major influences on overall mortality risk for cancer survivors This has been most frequently
subjected to study in breast cancer survivors However it is recognised that such
associations in observational studies can be influenced by confounding and therefore that
the mechanisms of lifestyle change on all-cause mortality remains unclear (Cheblowski
2010) Therefore although the observational evidence is strong there is a need to
understand the benefits of lifestyle change ndash particularly physical activity and weight control
in the absence of confounding factors which can be achieved only within the context of a
controlled trial (Ballard-Barbash et al 2009) Such evidence in the end is most likely to
lead to promoting the wide scale adoption of lifestyle change interventions in the role of
secondary prevention of cancer
Consistent with Bekkering et al (2006) it has been found that there is a paucity of robust
evidence on the effects of lifestyle behaviours in cancer progression and recurrence as well
as in the prevention and management of the long-term health implications of cancer
treatment Studies generally comprise small sample sizes and few offer evidence of the
long-term effects of lifestyle behaviours Since lifestyle choices are generally behavioural in
nature the sustainability of these behaviours is fundamental if commissioners are to provide
funding for lifestyle interventions
There were also a large number of retrospective studies particularly for smoking This is
understandable given the challenges of research within this area however it does also raise
limitations surrounding the accuracy of findings This is especially the case when findings
rely on retrospective self-reports of health behaviours or illness experience
114
A number of methodological limitations confound the interpretation of the benefits of exercise
and diet after a diagnosis of cancer from other risks such as smoking body size
supplements and analgesic intake Nevertheless as highlighted by Doyle et al (2007) even
when the scientific evidence is incomplete reasonable conclusions can be made on issues
that can guide lifestyle choices for cancer survivors These are discussed next
THE EVIDENCE
Diet
Evidence for reducing fat intake remains unclear yet evidence for the mechanisms of benefit
of weight loss or the maintenance of a healthy weight is strong Weight control and self-
management clearly requires consideration of total fat intake highlighting the necessity to
provide cancer survivors with advice on levels of fat necessary for weight maintenance
weight loss or in some cases weight gain (Chlebowski et al 2005 Patterson et al 2010)
The same rationale applies to any inconsistencies in evidence for increased fruit and
vegetables which can also facilitate weight management Indeed where the evidence is
strongest for fruits and vegetables applies to those sources containing carotenoids The
evidence is convincing that carotenoids do provide anti-cancer properties (Rock et al 2005
Pierce et al 2007) Lycopene (found in tomatoes) is one such carotenoid found to offer
anti-cancer benefits (Schwarz et al 2008)
Fibre (found in the skins of fruit and vegetables as well as in beans and lentils) and folate
(found in broccoli brussel sprouts asparagus and peas) have in the main been found to
protect against colorectal cancer The evidence is convincing that by slowing down bowel
transit time the mechanism of benefit comes from reducing contact between potential
carcinogens
The benefits of a low fat high fruit and vegetable diet extend into the management of
treatment-related conditions such as lymphoedema In individuals carrying excess weight
the resulting weight loss achieved via a low fat high fruit and vegetable diet can ease the
symptoms of lymphoedema (Shaw Mortimer and Judd 2007)
The evidence also suggests that survivors of prostate cancer might benefit from including
pomegranate juice and green tea in their diet
In terms of other food sources vitamin D and calcium can be protective against osteoporosis
(Ryan et al 2007) although more research with a specific fouls on cancer survivors is
needed in this area
Physical Activity
In general the findings of epidemiological and large cohort studies demonstrates that the
evidence for the role of physical activity in improving breast cancer prognosis quality of life
and on the levels of several hormones associated with breast cancer is strong
115
There is substantial evidence suggesting that the physical activity recommendations
developed by the Department of Health are sufficient for cancer survivors - a total of at least
30-minutes a day of moderate intensity physical activity on five or more days of the week
This can be achieved either by doing all the daily activity in one session or through several
shorter bouts of activity of 10 minutes or more Additionally there is evidence of a dose-
response (ie the more physical activity the greater any benefits) The evidence for breast
cancer further suggest that for survival benefits to be achieved from physical activity no less
than moderate to vigorous activity is required (Gross et al 2002) However the most recent
expert advice emphasises that even a modest amount of exercise like brief walks is
beneficial and gains will be seen versus doing nothing at all38
The interpretation of physical activity evidence has been hindered by the difficulty of
distinguishing physical activity outcomes from subsequent weight loss outcomes However
again even if the main mechanism of benefit of physical activity is improved outcomes
resulting from weight loss or maintenance then this could be considered strong enough
evidence to prescribe physical activity to cancer survivors Furthermore the evidence is
encouraging in terms of its QoL-enhancing effect (McNeeley et al 2006 Daley et al 2007)
Three specific elements of physical activity interventions or advice could be addressed
(Ballard-Barbash et al 2006)
Reducing sedentary behaviours (such as watching TV)
Exercise sessions
Type and intensity of physical activity
There is sufficient evidence for supervised physical activity improving symptoms of cancer-
related fatigue (McNeely et al 2006 Cramp and Daniel 2008) and lymphoedema (Moseley
and Pillerlsquos 2008) Indeed the evidence suggests that guided progressive physical activity
soon after treatment can ease the symptoms of lymphoedema (de Rezende et al 2006)
This supports recent cautions regarding risk-averse clinical recommendations guiding
survivors to avoid the use of the affected limb which may actually lead to de-conditioning
and the very outcome women seek to avoid (Schmitz 2010) At the very least there is no
evidence of appropriate intensity physical activity causing or exacerbating either fatigue or
limb swelling The same is true for the effect of physical activity on osteoporosis Whilst the
benefits of physical activity on bone health require clarifying physical activity can at the very
least prevent loss of bone mineral density in survivors at particular risk of developing
osteoporosis (Waltman et al 2009)
A recent roundtablelsquo event by the American College of Sports Medicine has produced a
Consensus Statement detailing exercise guidelines for cancer survivors (Schmitz Courneya
and Matthews et al 2010) An expert panel reviewed the published empirical evidence and
came to the consensus regarding the safety and efficacy of exercise testing and prescription
in cancer survivors The evidence is clear that exercise during treatment (specific risk
assessment can be carried our for specific treatments and biological response) and after
38
Dr Rachel Ballard ndash Barbash in the NCI Cancer Bulletin June 29 2010
116
treatment is safe and effective Activity induced improvements can be expected on aerobic
fitness muscular strength quality of life and fatigue in breast prostate and haematological
cancers Resistance training can be performed safely by breast cancer survivors with and at
risk of lymphoedoema
Efforts are currently being made to increase the capacity and capability of exercise
professionals to address the unique needs of cancer survivors Exercise professionals need
to be able to access training which reflects the medical condition they are treating for to be
more knowledgeable about the condition and the most suitable and appropriate exercises for
them This requires the development of a national competency framework for a specialist
level 3 add on or level four qualification This would enable providers to develop national
training programmes for cancer specialist exercise professionals and lead to more
accessible referral through the exercise referral scheme (Exercise Referral Research March
2010)
Smoking
Strong and consistent evidence has been presented for increased risk of disease
progression and mortality in people who continue to smoke after a diagnosis of cancer as
well as poorer outcomes in pre-diagnosis smokers (Parsons et al 2010) This evidence
applies particularly to cancers of the lung or head and neck Further research is needed for
breast colorectal prostate and rarer cancers
Alcohol
There is a paucity of research into the effects of alcohol pre- and post-diagnosis on cancer
progression and recurrence as well as symptom management Evidence thus far is highly
contradictory with some demonstrating a protective effect some a detrimental effect and
others no effect
Weight
Substantial weight gain after diagnosis and treatment for breast cancer is adversely
associated with breast cancer prognosis Obesity appears to increase the risk of recurrence
and death among breast cancer survivors by around 30 (Patterson et al 2010) Much
more research is needed to clarify the relationship between prognosis and survival and body
weight in other tumour types
Dealing with issues of weight weight gain and weight management with patients is one of
the lifestyle behaviour change issues health care professionals feel most challenged by
Studies do confirm that health care professionals find it difficult to address these issues with
patients without appearing biased and negative It would appear that a lack of professional
training on behavioural change and motivational coaching and effective strategies for weight
117
loss combine and can lead to avoidance by health care professionals in addressing the need
for change (Puhl and Heuer 2009 Blakeman et al 2010)
Mechanisms of Benefit
Chlebowski (2010) offers some thought-provoking insight into the challenge of implementing
lifestyle change when aromatase inhibitors have been found to reduce oestrogen levels far
more than physical activity interventions One study cites approximately 90 reductions in
oestrogen levels as a result of aromatase inhibitors (Dixon et al 2008) Furthermore three
trials comparing aromatase inhibitors versus placebo anticipate 60-70 reduction in breast
cancer risk (Cuzick 2005 Goss et al 2007 Visvanathan et al 2008) Equally Chlebowski
(2010) points out that the influence of physical activity on insulin levels also has a
pharmacological competitor in the form of metformin (Goodwin et al 2008 Jiralerspong et
al 2009)
These are valid insights that are likely to complicate the successful integration of lifestyle
advice into standardised models of aftercare On the other hand if a public and community
health approach is taken to health and well-being then lifestyle change is likely to offer
health benefits beyond cancer-specific health Such an approach is recommended in the
bdquoCapabilities for Supporting Prevention and Chronic Condition Self-Management A
Resource for Educators of Primary Health Care Professionals‟ developed as part of the
Australian Better Health Initiative (Flinders University 2009) The model offered within this
capabilities framework promotes healthcare providers to view patients holistically as
opposed to focusing solely on diagnosed chronic condition The rationale for this in part
lies in the fact that chronic conditions are more often than not accompanied by co-
morbidities and therefore healthcare is not only about the established condition but also
identified risk factors for co-morbidity
MAKING LIFESTYLE RECOMMENDATIONS FOR CANCER SURVIVORS
In terms of reducing the risks of relapse evidence is strongest for breast colorectal lung
and head and neck cancers but self-management lifestyle strategies are likely to be person-
specific rather than disease or treatment specific so are likely to apply to all patients
recovering from cancer
Diet Appendix A provides evidence-based dietary recommendations that can be made in
light of the findings within this review and national health recommendations These
recommendations comprise a varied diet ensuring adequate intake of vitamins essential
minerals fibre essential fatty acids and antioxidants by eating less fat and more green and
cruciferous vegetables fruits and berries nuts and grains and healthy oils (unsaturated fats
omega)
Physical Activity In terms of physical activity based on the evidence within this report
the five a weeklsquo recommendation is just as relevant to cancer survivors as to the general
population Indeed these recommendations are also provided by the American Cancer
Society (Doyle et al 2006) as advised by a large expert panel Appendix B provides
118
suggestions for physical activity Forty-five to 60-minutes of intentional physical activity are
preferable as the benefits of physical activity do appear to be greater with increased physical
activity Even when this might seem too much survivors can be reminded that the minimum
30-minutes for 5 days a week can be tailored to individual needs and capabilities For
example graded or progressive physical activity can be utilised for those experiencing
fatigue whilst shorter physical activity sessions can be spread out across the day
Other Lifestyle Factors Body Weight In addition it is recommended that obesity (BMI
gt35 Kgm2) excessive alcohol consumption and smoking are avoided There is also
evidence that maintaining a steady healthy weight as opposed to fluctuating between a
healthy and unhealthy BMI can offer health benefits for cancer survivors (Wright et al
2007)
The evidence within this review are indicative of challenges with adherence supporting
findings from Uhley and Jen (2006) that intensive resource-heavy individualised guidance
and support is required to achieve significant long-term lifestyle change This further
emphasises the need to tailor and prescribe such interventions on a needs basis via
individualised assessment and risk stratification
Integrating Self-Management Lifestyle Strategies into Routine Care
Adopting a paternalistic approach and simply telling people is not enough If the medical
community want to help their patients embark on a road of recovery which includes dietary
change and regular exercise there has to be a comprehensive and well-funded package of
education guidance and support Attitude and culture change is imperative both to tackle the
myths and preconceptions around lifestyle factors and their influence on cancer prognosis
symptom management and a future healthy life on the part of both patients survivors and
health care professionals The bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative offers a comprehensive
framework for integrating self-management support into healthcare services (Flinders
University 2009) The emphasis is on not merely striving to change patient behaviour but
also making efforts towards organisational change
Cancer Research UK Diabetes UK and the British Heart Foundation have joined together to launch a new campaign to raise awareness of the dangers of carrying excess weight around the middle The Active Fatlsquo campaign encourages people to measure their waistlines and make positive changes to their lifestyles if they are at risk The emphasis is on educating the public that fat cells are actively working away at stimulating diseases such as cancer diabetes and heart attacks
119
The model offered within this capabilities framework promotes healthcare providers to view
patients holistically as opposed to focusing solely on the diagnosed chronic condition The
rationale for this in part lies in the fact that chronic conditions are more often than not
accompanied by co-morbidities and therefore healthcare is not only about the established
condition but also identified risk factors for co-morbidity The framework also identifies the
need to provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for healthcare
professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
Evidence based information emphasising the importance of lifestyle ideally should be
formally introduced into routine clinical practice early in the treatment pathway and re-
enforced at regular intervals thereafter This ensures patients and their relatives do not miss
the teachable moment where they are most susceptible to positive advice (Demark-
Wahnefried et al 2005) This requires close work with clinicians specialist nurses patients
and advocacy groups to enable information about new strategies to be integrated into
existing local information pathways and materials Indeed the new information prescriptions
currently being pilot tested provide ample opportunity for integrating lifestyle advice into
survivorship care plans
Information clearly has an important role to play in influencing lifestyle behaviours However
people need more than knowledge to be healthy they need the skills to change if they are to
bring about changes in often complex and habitual lifestyle behaviours (Robertson 2008)
Before investing time and money on patient information materials it is necessary to convince
the consultants other direct clinical staff and organisers of clinical services that lifestyle
advice is a priority and to re-allocate resources to enable sufficient time to discuss these
issues within routine consultations One study for example found that patients who were
encouraged by their oncologist exercised significantly more than patients who did not
(Segar et al 1998) The next step is to back up the medical consultation with further
practical verbal and written advice from specialist nurses or information officers One UK
oncology unit for example does this as part of a formal lifestyle interview together with a
bespoke lifestyle information toolbox (Thomas and Nicholson 2009) During this interview
patients can be referred to smoking cessation clinics nutritionists and physiotherapists
where necessary The specialist nurse conducting this interview provides written information
and advice to patients and just as importantly their friends and family about local support
groups dietary measures where to buy healthy foods and specific local exercise facilities
which may entice them ranging from ballroom line and salsa dance lessons aerobics yoga
and fitness classes local walking swimming and cycling groups through to gyms sport
centre tennis and badminton courts and Pilates classes giving times contact numbers and
locations to make it as easy as possible to follow the advice The rationale for these
120
interviews is that individualised lifestyle counselling is more likely to elicit a response than
generic general advice The specialist nurse then follows up the advice by telephone and
further consultations as prompting has been shown to improve update A study from North
Bedfordshire for example showed that although 52 of patients accepted referral for
exercise in a local Gym a further 23 decided to attend classes only after additional
prompting from the nurse either by telephone
Many UK Oncology Units already have instigated an exit interview system to discuss follow
up arrangements and this process could be expanded to include lifestyle counselling
provided the specialist nurses involved have received extra training This training should
include a knowledge of the evidence and importance of weight diet physical activity and
smoking after cancer as well as ways to appropriately advise home-based exercise
regimens and how to direct patients towards the myriad of council or independent exercise
activities available locally to them The courses may require additional communication and
motivational skills training to enable nurses to engage in a partnership relationship which
promotes addressing the patientlsquos agenda goals and motivation around achieving and
maintaining behaviour change Examples of a range of courses aimed to develop such skills
and competencies and which are provided by the Flinders Human Behaviour and Health
Research Unit include a Chronic Condition Self-Management workshop Communication
and Motivational Skills Workshop and a Living Well Workshop
Remaining Questions
This review has provided some clarification of the evidence pertaining to lifestyle and cancer
outcomes However in implementing this evidence into standardised practice within cancer
aftercare will require a number of questions to be explored
1) What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
At present it is unclear how soon after a cancer diagnosis an intervention should be
introduced for behaviour change(Rabin 2009) Until the teachable moment is more clearly
defined for cancer patients the advice is that professionals should repeatedly offer to assist
a patient with addressing their health behaviour risks until the patient accepts or seeks other
forms of support
The literature suggests that professional involvement in supported self-management and
lifestyle advice is required in order to maintain patient motivation by enhancing patient
engagement with health information and advice When information is supplied by healthcare
professionals and the patient is supported in using this information legitimacy is provided to
the information and advice (Protheroe et al 2008) Efficacy outcomes in terms of lifestyle
advice and behavioural change are fundamental in the initiation and maintenance of a
healthy lifestyle and the involvement of healthcare professionals strengthens outcome
efficacy whilst also motivating the patient and increasing their own self-efficacy to adapt their
lifestyle (Irwin 2008) However there is anecdotal and other evidence that on the one hand
the importance of lifestyle factors on the prognosis survival and symptom management of
121
cancer survivors is poorly understood and appreciated by significant numbers of cancer
health care professionals and on the other hand they do need specific training in the key
communication skills to be able to support effective behaviour change with their patients A
review is currently underway investigating the role of patient-professional communication in
terms of self-management
2) How can people most likely to benefit from lifestyle interventions be effectively
identified
A recent review on cancer-specific self-management programmes highlighted that patients
can be risk stratified according to needs and this according to whether they are likely to
benefit from the programme (Davies and Batehup 2010) For example people with low
levels of social support have been found to benefit most from group-delivered support As
part of the Bournemouth after Cancer Survivorship Project Active Wellness Programmelsquo
patients are assessed for the readiness to take part in physical activity (Milne et al 2010) It
is recommended that questionnaires that might facilitate such evidence-based risk
stratification be evaluated in order to provide further insight into this question A set of risk
stratification tools would be one way of ensuring cost-effectiveness
3) What are the various intensities of lifestyle support that can be provided based on
levels of individual need
As demonstrated within this review lifestyle interventions and self-management support do
generally require some level of support in order to be successful A strong
patientprofessional partnership appears to be at the essence of this intensive approach as
does longer-term follow-up and support (Davies and Batehup 2010) Addressing this
question will also in part address some of the inequalities within the current system of
cancer care with survivors identified as having low literacy being provided with extra
informational support and assistance with understanding the lifestyle recommendations
being made
122
Appendix A Evidence-Based Dietary Self-Management Recommendations
Food Advice Evidence
Reduce Saturated Fats
Unless underweight avoid processed fatty foods cakes biscuits crisps and other fatty snacks pastries cream and fried foods Cut the fat off the meat and check serum cholesterol regularly
(Ingram 1994 Hebert et al 1998 Norat et al 2004 Thomas et al 2009)
Increase all fish intake
All fresh fish but particularly the oily varieties such as mackerel and sardines Fresh water fish such as trout have the advantage of avoiding the potential heavy metal contamination of tuna amp sword fish which some suggest should not be eaten more than twice a week
(Ornish et al 2005 Meyerhardt et al 2007 Goodwin et al 2009)
Essential minerals
Vary the diet to ensure intake of adequate quantities of essential minerals consider Mixed nuts including Brazils Seafood including sardines prawns and shell fish Pulses and grains Vary carbohydrate sources such as pasta rice different brands of potatoes pulses such as lentils and quinoa
Rohan et al 1993) Powers et al 2007 McTiernan et al 2009)
Dietary Vitamins
Fresh fruit raw and calciferous vegetables grains oily fish nuts and salads Unless you have diarrhoea try to increase the amount of ripe fruit you eat each day ideally by eating the whole fruit Freshly squeezed fruit juices are recommended
(Rohan et al1993 Ingram 1994 Fleischauer et al 2003 New et al 2004 Rock et al 2005 McEligot et al 2006 Meyerhardt et al 2007 Schwarz et al 2008 Goodwin et al 2009)
Polyphenols
Onions leeks broccoli blueberries red wine tea apricots pomegranates chocolate coffee blueberries kiwis plums cherries ripe fruits parsley celery tomatoes mint citrus fruit
(Bettuzzi et al 2006 Pantuck et al 2006 Schwarz et al 2008 McLarty et al 2009)
Phytoestrogens
Soybeans and other legumes including peas lentils pinto (baked beans) and other beans and nuts (supplements not recommended)
Marini et al (2008)
Increase Carotenoids (Lycopene)
Tomatoes tomato sauce chilli carrots green vegetables and dark green salads
(Ingram 1994 Rock et al 2005 McEligot et al 2006 Pierce et al 2007 Powers et al 2007 Thomson et al 2007 Schwarz et al 2008)
123
Appendix B Evidence-Based Physical Activity Recommendations
Category Advice Evidence
Resistance Exercise
Strength training has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce fatigue and improve lean body mass and muscle strength Personalised tailored resistance exercise based on fitness assessments can improve QoL
Segal et al (2003) Poudevigne et al (2009) Courneya et al (2007) (Segal et al 2009)
Aerobic Exercise Aerobic exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of lymphoedema prevent loss of bone mineral density and reduce body fat Walking is particularly popular
Hayes Hildegard and Turner (2009) Schwartz Winters-Stone and Gallucci (2007) Courneya et al (2007) Fillion et al (2008) Kenfield et al (2009) Windsor Nichol and Potter (2004) Chang et al (2008)
Combined Resistance and Aerobic Exercise
Combined aerobic and resistance exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of fatigue and improve QoL
Coleman et al (2003) Milne et al (2008)
3gt MET-hours per week
Benefits of physical activity require 3 or more MET-hours per week (eg using a stationary bicycle for one-hour)
Holick et al (2008) Holmes et al (2005) Saxton et al (2010) Kenfield (2010)
Moderate intensity
Physical activity needs to be of at least moderate intensity in order to offer beneficial outcomes
Holick et al (2008) Patterson et al (2010) Holmes et al (2005) Saxton et al (2010) Campbell et al (2007) Poudevigne et al (2009) Tardon et al (2004)
Dose-Response Exercise can be dose-responsive thus taking part in more than 3 MET-hours per week is likely to offer greater benefits
Meyerhardt et al (2005) Kenfield (2010)
During Treatment Remaining active during treatment can help with symptoms such as fatigue as well as increase completion rates for chemotherapy
Chang et al (2008) Coleman et al (2003) Courneya et al (2007)
Home-Based
Home-based physical activity prescriptions either supervised or alone have proven effective in improving cancer outcomes including reducing fatigue and protecting bone mineral density
Ligibel et al (2008) Windsor Nichol and Potter (2004) Schwartz Winters-Stone and Gallucci (2007)
Supervised Supervised physical activity either at home in groups or during treatment have proven effective in improving cancer outcomes as well as reducing lean body mass and facilitating the completion of chemotherapy
Chang et al (2008) Coleman et al (2003) Velthuis et al (2009) Courneya et al (2007) Campbell
et al (2007) exercise (Soliman et al 2009)
124
References
Abrahamsen JF Andersen A Hannisdal E et al Second malignancies after treatment of Hodgkins disease the influence of treatment follow-up time and age J Clin Oncol 11 (2) 255-61 1993 Addington-Hall et al (2010) Older womenlsquos experience of breast cancer alongside other health conditions The EPaN study (Experiences Preferences and Needs of women aged 70 years and over) University of Southampton Funded by Macmillan Cancer Support Ahmed R L W Thomas et al (2006) Randomized Controlled Trial of Weight Training and Lymphedema in Breast Cancer Survivors J Clin Oncol 24(18) 2765-2772 Ainsworth BE et al Compendium of physical activities an update of activity codes and MET intensities Med Sci Sports Exerc 2000 Sep32(9 Suppl)S498-504 Aitken J (ongoing) Colorectal cancer and quality of life study httpwwwcancerqldorgaupageResearch_statisticsVCRCCVCRCC_research_programsLifestyle_and_Cancer [Last accessed 04062010] Akopyan and Bonavida 2006 G Akopyan and B Bonavida Understanding tobacco smoke carcinogen NNK and lung tumorigenesis Int J Oncol 29 (2006) pp 745ndash752 Alberts DS Martinez ME Roe DJ et al Lack of effect of a high-fiber cereal supplement on the recurrence of colorectal adenomas Phoenix Colon Cancer Prevention Physicians Network [Comment] New England Journal of Medicine 2000 April 20342(16)1156-62 Arts CJ Govers CA van den Berg H Wolters MG van Leeuwen P Thijssen JH In vitro binding of estrogens by dietary fiber and the in vivo apparent digestibility tested in pigs J Steroid Biochem Mol Biol 1991 May38(5)621-8 Bandura A (1977) Self-efficacy Toward a unifying theory of behavioural change Psych Rev 84 191 - 215 Barbash-Ballard R Hunsberger S Alciati MH Blaire SN Goodwin PJ McTiernan A(2009) Physical activity weight control and breast cancer risk and survival Clinical trial rationale and design considerations J Natl Cancer Inst 101630-643 Baron JA Beach M Mandel JS et al Calcium supplements and colorectal adenomas Polyp Prevention Study Group Ann N Y Acad Sci 1999889138-45
Bekkering T Beynon R Davey Smith G Davies A Harbord R Sterne J Thomas S and Wood L (2006) A systematic review of RCTs investigating the effect of dietal and physical activity interventions on cancer survival updated report World Cancer Research Fund httpwwwdietandcancerreportorg [Last accessed 150210] Bellizzi K M J H Rowland et al (2005) Health Behaviours of Cancer Survivors Examining Opportunities for Cancer Control Intervention J Clin Oncol 23(34) 8884-8893 Bernstein H Cosford P and Williams A (2010) Enabling effective delivery of health and wellbeing an independent report Department of Health February 2010
125
Bettuzzi et al 2006 S Bettuzzi M Brausi F Rizzi G Castagnetti G Peracchia and A Corti Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia a preliminary report from a one-year proof-of-principle study Cancer Research 66 (2) (2006) pp 1234ndash1240 Bingham SA Day NE Luben R Ferrari P Slimani N Norat T et al Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) an observational study Lancet 20033611496ndash501 Bingham S Riboli E Diet and cancermdashthe European Prospective Investigation into Cancer and Nutrition Nat Rev Cancer 20044206ndash15 Blakeman T Bower P Reeves D Chew-Graham C (2010) ―Bringing self management into clinical view a qualitative study of long term condition management in primary care consultations Chronic Illness 0 1-15 Blackburn G L and K A Wang (2007) Dietary fat reduction and breast cancer outcome results from the Womens Intervention Nutrition Study (WINS) Am J Clin Nutr 86(3) 878S-881 Bonithon-Kopp C Kronborg O Giacosa A Rath U Faivre J Calcium and fibre supplementation in prevention of colorectal adenoma recurrence A randomised intervention trial Lancet 2000356(9238)1300-6 Borugian MJ Sheps SB Kim-Sing C Olivotto IA Van Patten C Dunn BP Coldman AJ Potter JD Gallagher RP Hislop TG Waist-to-hip ratio and breast cancer mortality Am J Epidemiol 2003 Nov 15158(10)963-8 Boyapati SM Shue X et al (2005) Soyfood intake and breast cancer survival a follow up of the Shanghai Breast Cancer Study Breast Cancer Research and Treatment 92(1) p11-17 Boyd NF Stone J Vogt KN Connelly BS Martin LJ Minkin S Dietary fat and breast cancer risk revisited a meta-analysis of the published literature Br J Cancer 2003 Nov 389(9)1672-85 Box R Marnes T amp Robertson V Aquatic physiotherapy and breast cancer related lymphoedema 5th Australasian Lymphology Association Conference Proceedings Mar 2004 47-9 Brown J K T Byers et al (2003) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 53(5) 268-291 Cade JE Burley VJ Greenwood DC UK Womens Cohort Study Steering Group Dietary fibre and risk of breast cancer in the UK Womens Cohort Study Int J Epidemiol 2007 Apr36(2)431-8 Caan B B Sternfeld et al (2005) Life After Cancer Epidemiology (LACE) Study A cohort of early stage breast cancer survivors (United States) Cancer Causes and Control 16(5) 545-556
126
Caan BJ Kwan ML Hartzell G Castillo A Slattery ML Sternfeld B Weltzien E Pre-diagnosis body mass index post-diagnosis weight change and prognosis among women with early stage breast cancer Cancer Causes Control 2008 Dec19(10)1319-28 Cadmus L A P Salovey et al (2009) Physical activity and quality of life during and after treatment for breast cancer results of two randomized controlled trials Psycho-Oncology 18(4) 343-352 Campbell KL Westerlind KC Harber VJ Bell GJ Mackey JR Courneya KS (2007) Effects of aerobic exercise training on oestrogen metabolism in premenopausal women a randomized controlled trial Cancer Epidemiol Biomarkers Prev 16731ndash73 Cancer 52 and NCSI Research Workstream (2009) Less common cancers consultation Report June 2009 Cella D (2009) Quality of life in patients with metastatic renal cell carcinoma The importance of patient-reported outcomes Cancer treatment reviews 35(8) 733-737 Chan JM Gann PH and Giovannucci EL (2005) Role of diet in prostate cancer development and progression Journal of Clinical Oncology 23(32) p 8152-60 Chlebowski RT Aiello E McTiernan A Weight loss in breast cancer patient management Journal of Clinical Oncology 20(4) 1128-1143 2002 Chlebowski RT Blackburn GL Elashoff RE Thomson C Goodman MT Shapiro A Giuliano AE Karanja N Hoy MK Nixon DW and The WINS Investigators (2005) Dietary fat reduction in post-menopausal women with primary breast cancer Journal of Clinical Oncology (10) p 3s Chlebowski R G Blackburn et al (2006) Dietary fat reduction and breast cancer outcome interim efficacy results from the Womens Intervention Diet Study J Natl Cancer Inst 98 1767 - 1776 Chlebowski RT Blackburn GL (2007) Diet and breast cancer recurrence JAMA 2007 Nov 14298(18)2135 author reply 2135-6 Chlebowski RT (2010) Lifestyle and breast cancer risk The way forward Journal of
Clinical Oncology Vol 28 No 9 (March 20) 2010 pp 1445-1447
Cho E Spiegelman D Hunter DJ Chen WY Colditz GA Willett WC Premenopausal dietary carbohydrate glycaemic index glycaemic load and fiber in relation to risk of breast cancer Cancer Epidemiol Biomarkers Prev 2003 Coulter A and Ellins J (2006) Patient-focused Interventions A review of the evidence Picker Institute Europe (01865 208100) and Health Foundation Coups E J and J S Ostroff (2005) A population-based estimate of the prevalence of behavioural risk factors among adult cancer survivors and non-cancer controls Preventive Medicine 40(6) 702-711 Courneya K S (2003) Physical activity in Cancer Survivors An Overview of Research Medicine amp Science in Sports amp Physical activity 35(11) 1846-1852
127
Courneya K Booth CM Gill S et al (2008) The colon health and life-long physical activity change trial a randomized trial of the national institute of Canada clinical trials group Current Oncology 15(6) 271-78 Cramp F Daniel J (2008) Physical activity for the management of cancer-related fatigue in adults CochraneDatabaseSystRev 2008 Cuzick J Aromatase inhibitors for breast cancer prevention J Clin Oncol 231636-1643 2005
Cuzick J Hot flushes and the risk of recurrence Retrospective exploratory results from the ATAC trial 30th Annual San Antonio Breast Cancer Symposium San Antonio TX December 13-16 2007 (poster 2069) Daley A H Crank et al (2007) Randomized trial of physical activity therapy in women treated for breast cancer J Clin Oncol 25 1713 - 1721 Daley A S Bowden et al (2008) What advice are oncologists and surgeons in the United Kingdom giving to breast cancer patients about physical activity International Journal of Behavioural Diet and Physical Activity 5(1) 46 Danhauer S Mihalki S Russell G Campbell C Felder L Daley L et al (2009) Restorative yoga for women with breast cancer Findings from a randomized pilot study Psych oncology 18(4) 360-368 Dansinger M L J A Gleason et al (2005) Comparison of the Atkins Ornish Weight Watchers and Zone Diets for Weight Loss and Heart Disease Risk Reduction A Randomized Trial JAMA 293(1) 43-53 Davies NJ and Batehup L (2010) Self-management support for cancer survivors Guidance for developing interventions An update of the evidence National Cancer Survivorship Initiative Macmillan Cancer Support March 2010 Demark-Wahnefried W and Jones L (2008) Promoting a Healthy Lifestyle among Cancer Survivors Haematologyoncology clinics of North America 22(2) 319-342 Deo SV Ray S Rath GK et al (2004) Prevalence and risk factors for development of lymphedema following breast cancer treatment Indian J Cancer 418ndash12 Department of Health (2001) Exercise referral systems A national quality assurance framework Department of Health Report London 2001 Department of Health (2004) At least five a week Evidence on the impact of physical activity and its relationship to health Department of Health Report London 2004 Department of Health (2009a) Internal analysis unpublished Department of Health London Department of Health (2009b) Obesity general information Health survey of England 2008 Department of Health London Department of Health (2009c) Guidance on the routine collection of patient-reported outcome measures (PROMs) p 28 The Stationary Office London
128
De Rezende LF Franco RL de Rezende MF et al Two physical activity schemes in postoperative breast cancer comparison of effects on shoulder movement and lymphatic disturbance Tumori 2006 9255ndash61 de Waard F Ramlau R Mulders Y de Vries T van Waveren S A feasibility study on weight reduction in obese postmenopausal breast cancer patients Eur J Cancer Prev 1993 May 2(3)233-8 Dignam J J B N Polite et al (2006) Body Mass Index and Outcomes in Patients Who Receive Adjuvant Chemotherapy for Colon Cancer J Natl Cancer Inst 98(22) 1647-1654 Dimeo FC Thomas F Raabe-Menssen C et al Effect of aerobic exercise and relaxation training on fatigue and physical performance of cancer patients after surgery A randomised controlled trial Support Care Cancer 2004 12(11)774-9 Dixon JM Renshaw L Young O et al Letrozole suppresses plasma estradiol and oestrone sulphate more completely than anastrozole in postmenopausal women with breast cancer J Clin Oncol 261671-1675 2008
Doyle C L H Kushi et al (2006) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 56(6) 323-353 Dwyer J J Peterson et al (2008) Do Flavonoid Intakes of Postmenopausal Women With Breast Cancer Vary on Very Low Fat Diets Diet and Cancer 60(4) 450 - 460 Eakin E Hayes S and Lawler S (ongoing) Physical activity for Health Using the telephone to promote physical activity-based rehabilitation in ruralremote Australian breast cancer survivors National Breast Cancer Foundation httpwwwuqeduaucprcindexhtmlpage=60214amppid=20928 [Last accessed 300310] Eliassen AH Missmer SA Tworoger SS Spiegelman D Barbieri RL Dowsett M Hankinson SE Endogenous steroid hormone concentrations and risk of breast cancer among premenopausal women J Natl Cancer Inst 2006 Oct 4 98(19)1406-15 Elkort RJ Baker FL Vitale JJ Cordano A Long-term nutritional support as an adjunct to chemotherapy for breast cancer JPEN J Parenter Enteral Nutr 1981 Sep-Oct 5(5)385-90 Enger SM Greif JM Polikoff J Press M Body weight correlates with mortality in early-stage breast cancer Arch Surg 2004139954ndash958 discussion 58ndash60 Eton D T D L Fairclough et al (2003) Early Change in Patient-Reported Health During Lung Cancer Chemotherapy Predicts Clinical Outcomes Beyond Those Predicted by Baseline Report Results From Eastern Cooperative Oncology Group Study 5592 J Clin Oncol 21(8) 1536-1543 Fentiman IS Allen DS Hamed H (2005) Smoking and prognosis in women with breast cancer Int J Clin Pract 591051ndash1054
129
Ferrari P Jenab M Norat T et al Lifetime and baseline alcohol intake and risk of colon and rectal cancers in the European prospective investigation bettinto cancer and nutrition (EPIC) Int J Cancer 2007 121 ( 9 ) 2065 ndash 2072
Feuerstein M (2006) Handbook of Cancer Survivorship New York NY Springer 2006 Fillion L P Gagnon et al (2008) A Brief Intervention for Fatigue Management in Breast Cancer Survivors Cancer Nursing 31(2) 145-159 Findley P amp Sambamoorthi U (2009) Preventive health services and lifestyle practices in cancer survivors A population health investigation Journal of Cancer Survivorship 3 43-58 Fleischauer AT Simonsen N Arab L Antioxidant supplements and risk of breast cancer recurrence and breast cancer-related mortality among postmenopausal women Nutr Cancer 2003 46 15-22 Flinders University (2009) Capabilities for Supporting Prevention and Chronic Condition Self-Management A Resource for Educators of Primary Health Care Professionals Australian Better Health Initiative A joint Australian State and Territory government initiative
Flowers M Thompson PA 2009 t10c12 Conjugated Linoleic Acid Suppresses HER2 Protein and Enhances Apoptosis in SKBr3 Breast Cancer Cells Possible Role of COX2 PLoS ONE 4(4) e5342 doi101371journalpone0005342 Food Standards Agency (2007) FSA nutrient and food based guidelines for UK institutions httpwwwfoodgovukmultimediapdfsnutrientinstitutionpdf [Last accessed 120310] Food Standards Agency (2010) Heightweight chart httpwwweatwellgovukhealthydiethealthyweightheightweightchart [Last accessed 120310] Ford MB Sigurdson AJ Petrulis ES et al Effects of smoking and radiotherapy on lung carcinoma in breast carcinoma survivors Cancer 98 (7) 1457-64 2003 Friedenreich C Cust A Lahmann PH et al Anthropometric factors and risk of endometrial cancer the European prospective investigation into cancer and nutrition Cancer Causes Control 2007 18399-413 Friedenreich C M C G Woolcott et al (2010) Alberta Physical Activity and Breast Cancer Prevention Trial Sex Hormone Changes in a Year-Long Physical activity Intervention Among Postmenopausal Women J Clin Oncol 28(9) 1458-1466 Friedenreich CM Cust AE Physical activity and breast cancer risk impact of timing type and dose of activity and population subgroup effects Br J Sports Med 2008 Aug42(8)636-47 Giovannucci EL (2005) Obesity insulin resistance and cancer risk Cancer Prevention 5 httpwwwnypcancerpreventioncomissue5propro_featurespre_earshtml [Last accessed 03062010]
130
Gold E B J P Pierce et al (2009) Dietary Pattern Influences Breast Cancer Prognosis in Women Without Hot Flashes The Womens Healthy Eating and Living Trial J Clin Oncol 27(3) 352-359 Gonzalez CAPera GAgudo APalli DKrogh VVineis PTumino RPanico SBerglund GSiman HNyren OAgren AMartinez CDorronsoro MBarricarte ATormo MJQuiros JRAllen NBingham SDay NMiller ANagel GBoeing HOvervad KTjonneland ABueno-de-Mesquita HBBoshuizen HCPeeters PNumans MClavel-Chapelon FHelen IAgapitos ELund EFahey MSaracci RKaaks RRiboli E Smoking and the risk of gastric cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC) Int J Cancer 107 (4) 629-634 (2003) Gonzaacutelez CA Jakszyn P Pera G Agudo A Bingham S Palli D Ferrari P Boeing H del Giudice G Plebani M Carneiro F Nesi G Berrino F Sacerdote C Tumino R Panico S Berglund G Simaacuten H Nyreacuten O Hallmans G Martinez C Dorronsoro M Barricarte A Navarro C Quiroacutes JR Allen N Key TJ Day NE Linseisen J Nagel G Bergmann MM Overvad K Jensen MK Tjonneland A Olsen A Bueno-de-Mesquita HB Ocke M Peeters PH Numans ME Clavel-Chapelon F Boutron-Ruault MC Trichopoulou A Psaltopoulou T Roukos D Lund E Hemon B Kaaks R Norat T Riboli E Meat intake and risk of stomach and oesophageal adenocarcinoma within the European Prospective Investigation Into Cancer and Nutrition (EPIC) J Natl Cancer Inst 2006 Mar 198(5)345-54 Goodwin PJ Pritchard KI Ennis M et al Insulin-lowering effects of metformin in women with early breast cancer Clin Breast Cancer 8501-5052008
Goodwin PJ Ennis M Pritchard KI Koo J Hood N (2009) Prognostic Effects of 25-Hydroxyvitamin D Levels in Early Breast Cancer Journal of Clinical Oncology Vol 27 No 23 (August 10) pp 3757-3763 Goodwin PJ Lifestyle Intervention Study in Adjuvant Treatment of Early Breast Cancer (LISA) (ongoing) httpclinicaltrialsgovct2showNCT00463489 [Last accessed 04062010] Goss PE Richardson H Chlebowski RT et al National Cancer Institute of Canada Clinical Trials Group MAP 3 Trial Evaluation of exemestane to prevent breast cancer in postmenopausal women at risk Clin Breast Cancer 7895-900 2007
Gothard L Cornes P et al (2004) Double-blind placebo-controlled randomised trial of vitamin E and pentoxifylline in patients with chronic arm lymphoedema and fibrosis after surgery and radiotherapy for breast cancer Radiotherapy and oncology journal of the European Society for Therapeutic Radiology and Oncology 73(2) 133-139 Grace PB Taylor JI Low YL Luben RN Mulligan AA Botting NP Dowsett M Welch AA Khaw KT Wareham NJ Day NE Bingham SA Phytoestrogen concentrations in serum and spot urine as biomarkers for dietary phytoestrogen intake and their relation to breast cancer risk in European prospective investigation of cancer and nutrition-norfolk Cancer Epidemiol Biomarkers Prev 2004 May13(5)698-708 Greenberg ER Baron JA Tosteson TD et al A clinical trial of antioxidant vitamins to prevent colorectal adenoma Polyp Prevention Study Group[comment] New England Journal of Medicine 1994 July 21331(3)141-7 Gritz ER (1993) Cancer Smoking Epidemiology Biomarkers amp Prevention 2(3) 261-270
131
Gritz E R M C Fingeret et al (2006) Successes and failures of the teachable moment Cancer 106(1) 17-27 Gross G C Ott et al (2002) Postmenopausal Breast Cancer Survivors at Risk for Osteoporosis Physical Activity Vigour and Vitality Oncology Nursing Forum 29(9) 1295-1300 Gross M C Ramirez et al (2009) Expression of androgen and oestrogen related proteins in normal weight and obese prostate cancer patients The Prostate 69(5) 520-527 Guthrie JR Ball M Murkies A Dennerstein L Dietary phytoestrogen intake in mid-life Australian-born women relationship to health variables Climacteric 2000 3 254ndash261 Hawkes A L S Gollschewski et al (2009) A telephone-delivered lifestyle intervention for colorectal cancer survivors a pilot study Psycho-Oncology 18(4) 449-455 Haydon AM Macinnis RJ English DR Giles GG (2006) The effect of physical activity and body size on survival after diagnosis with colorectal cancer Gut 55 p 62-67 Hayes SC Spence RR Galvao DANewton RU (2009) Australian Association for Physical activity and Sport Science position stand Optimising cancer outcomes through physical activity JSciMedSport 200912428-434 Heald AH Cade JE Cruickshank JK Anderson S White A Gibson JM (2003) The influence of dietary intake on the insulin-like growth factor (IGF) system across three ethnic groups a population-based study Public Health Nutr6175ndash80 Healthy Weight Healthy Lives (2008) A Cross-Government Strategy for England Cross-Government Obesity Unit DH and Department of Children Schools and Families Hebert JR Hurley TG Ma Y (1998) The effect of dietary exposures on recurrence and mortality in early stage breast cancer Breast Cancer Res Treat 5117ndash28 Hofstad B Almendingen K Vatn M et al Growth and recurrence of colorectal polyps a double-blind 3-year intervention with calcium and antioxidants Digestion 199859(2)148-56 Holick C N P A Newcomb et al (2008) Physical Activity and Survival after Diagnosis of Invasive Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 17(2) 379-386 Holm LE Nordevang E Hjalmar ML Lidbrink E Callmer E Nilsson B (1993) Treatment failure and dietary habits in women with breast cancer J Natl Cancer Inst 8532ndash36 Holmes MD Hunter DJ Colditz GA et al Association of dietary intake of fat and fatty acids with risk of breast cancer JAMA 1999281914-920 Holmes MD Chen WY Feskanich D Kroenke CH Colditz GA (2005) Physical activity and survival after breast cancer diagnosis JAMA 293 p 2479-86
132
Holmes MD Murin S Chen WY Kroenke CH Spiegelman D Colditz GA (2007) Smoking and survival after breast cancer diagnosis Int J Cancer 1202672ndash2677
Howe GR Hirohata T Hislop TG Iscovich JM Yuan JM Katsouyanni K Lubin F Marubini E Modan B Rohan T et al Dietary factors and risk of breast cancer combined analysis of 12 case-control studies J Natl Cancer Inst 1990 Apr 482(7)561-9
Hunter DJ Spiegelman D Adami HO Beeson L van den Brandt PA Folsom ARFraser GE Goldbohm RA Graham S Howe GR et al Cohort studies of fat intake and the risk of breast cancer--a pooled analysis N Engl J Med 1996 Feb 8334(6)356-61
Ingram D Diet and subsequent survival in women with breast cancer British Journal of Cancer 1994 Mar69(3)592-5
Irwin ML Smith AW McTiernan A Ballard-Barbash R Cronin K Gilliland FD Baumgartner RN Baumgartner KB Bernstein L (2008) Influence of Pre- and Postdiagnosis Physical Activity on Mortality in Breast Cancer Survivors The Health Eating Activity and Lifestyle Study Journal of Clinical Oncology 26(24) 3958-3964
Ishikawa H Akedo I Otani T et al Randomized trial of dietary fiber and Lactobacillus casei administration for prevention of colorectal tumors Int J Cancer 2005 September 20116(5)762-7 Jiralerspong S Palla SL Giordano SH et al Metformin and pathologic complete responses to neoadjuvant chemotherapy in diabetic patients with breast cancer J Clin Oncol 273297-3302 2009
Jones LW Demark-Wahnefried W Diet physical activity and complementary therapies after primary treatment for cancer Lancet Oncol 7(12)1017-26 Nov-Dec 2006 PMID 17138223 Kaaks R A Lukanova and MA Kurzer Obesity endogenous hormones and endometrial cancer risk a synthetic review Cancer Epidemiol Biomark Prev 11 (2002) pp 1531ndash1543 Kaaks R Rinaldi S Key TJ Berrino F Peeters PH Biessy C Dossus L Lukanova A Bingham S Khaw KT Allen NE Bueno-de-Mesquita HB van Gils CH Grobbee D Boeing H Lahmann PH Nagel G Chang-Claude J Clavel-Chapelon F Fournier A Thieacutebaut A Gonzaacutelez CA Quiroacutes JR Tormo MJ Ardanaz E Amiano P Krogh V Palli D Panico S Tumino R Vineis P Trichopoulou A Kalapothaki V Trichopoulos D Ferrari P Norat T Saracci R Riboli E Postmenopausal serum androgens oestrogens and breast cancer risk the European prospective investigation into cancer and nutrition Endocr Relat Cancer 2005 Dec12(4)1071-82 Kawahara M Ushijima S Kamimori T et al Second primary tumours in more than 2-year disease-free survivors of small-cell lung cancer in Japan the role of smoking cessation Br J Cancer 78 (3) 409-12 1998 Keinan-Boker L van Der Schouw YT Grobbee DE Peeters PH Dietary phytoestrogens and breast cancer risk Am J Clin Nutr 2004 Feb79(2)282-8 Kenfield SA (2010) Physical activity and mortality in prostate cancer (In Regular Vigorous Physical Activity found to have Survival Benefits for Prostate Cancer Patients
133
AACR Frontier in Cancer Prevention Research Conference by Tuma R Oncology Times) 32(2) p 29 33 Key TJ Allen NE Hormones and breast cancer IARC Sci Publ 2002156273-6 Khaodhiar L Nixon D Chlebowski RT Elashoff R Blackburn GL Hoy MK Insulin resistance in postmenopausal women with breast cancer Proc Am Cancer Res 2003446349 (abstr) Kim EH Willett WC Colditz GA Hankinson SE Stampfer MJ Hunter DJ Rosner B Holmes MD Dietary fat and risk of postmenopausal breast cancer in a 20-year follow-up Am J Epidemiol 2006 Nov 15164(10)990-7 Korstjens I A M May et al (2008) Quality of Life After Self-Management Cancer Rehabilitation A Randomized Controlled Trial Comparing Physical and Cognitive-Behavioural Training Versus Physical Training Psychosom Med 70(4) 422-429 Krein S M Heisler J Piette F Makki and E Kerr 2005 The effect of chronic pain on diabetes patientslsquo self-management Diabetes Care 28(1)65ndash70 Kroenke CH Fung TT Hu FB Holmes MD Dietary patterns and survival after breast cancer diagnosis J Clin Oncol 2005 Dec 2023(36)9295-303 Kubik AK Zatloukal P Tomasek L Petruzelka L (2002) Lung cancer risk among Czech women a case-control study Prev Med 34(4) 436ndash444 Kucera H [Adjuvanticity of vitamin A in advanced irradiated cervical cancer (authors transl)] Wiener Klinische Wochenschrift Supplementum 19801181-20 Kushi LH Byers T Doyle C et al American Cancer Society Guidelines on Diet and Physical Activity for cancer prevention reducing the risk of cancer with healthy food choices and physical activity CA Cancer J Clin 2006 56 254ndash8 Kyogoku S Hirohata T Nomura Y Shigematsu T Takeshita S Hirohata I Diet and prognosis of breast cancer Nutr Cancer 199217(3)271-7 Lahmann PH Schulz M Hoffmann K Boeing H Tjoslashnneland A Olsen A Overvad K Key TJ Allen NE Khaw KT Bingham S Berglund G Wirfaumllt E Berrino F Krogh V Trichopoulou A Lagiou P Trichopoulos D Kaaks R Riboli E Long-term weight change and breast cancer risk the European prospective investigation into cancer and nutrition (EPIC) Br J Cancer 2005 Sep 593(5)582-9 Lee IM Sesso HD Paffenbarger RS Jr (1999) Physical activity and risk of lung cancer Int J Epidemiol 28(4) 620ndash625 Lev E L (1997) Banduras Theory of Self-Efficacy Applications to Oncology Research and Theory for Nursing Practice 11 21-37 Ligibel J A W Demark-Wahnefried et al (2009) Diet Physical activity and Supplements Guidelines for Cancer Survivors ASCO EDUCATIONAL BOOK 2009(1) 541-547 Lindsay S (2009) Prioritizing illness Lessons in self-managing multiple chronic conditions Canadian Journal of Sociology PhD Thesis ejournalslibraryualbertaca
134
Lucia A Earnest C Perez M (2003) Cancer-related fatigue can physical activity physiology assist oncologists Lancet Oncol 4616-625 Lyons R amp Langille L (2000) Healthy Lifestyle Strengthening the Effectiveness of Lifestyle Approaches to Improve Health Health Canada Ottawa Ontario Available at httpwwwhc-scgccahppbphdddocshealthy MacLennan R Macrae F Bain C et al Effect of fat fibre and beta carotene intake on colorectal adenomas further analysis of a randomized controlled dietary intervention trial after colonoscopic polypectomy Asia Pac J Clin Nutr 1999 8(suppl)S54-S58 Macmillian Cancer Support (2008) Two Million Reasons The Cancer Survivorship Agenda 2008 Maddams J Moller H and Devane C Cancer prevalence in the UK 2008 Thames Cancer Registry and Macmillan Cancer Support 2008 Manjer J Berglund G Bondesson L Garne J P Janzon L Malina J Breast cancer incidence in relation to smoking cessation Breast Cancer Res Treat 61121-129 2000 Mao Y Pan S Wen SW Johnson KC The Canadian Cancer (2003) Physical activity and the risk of lung cancer in Canada Am J Epidemiol 158(6) 564ndash575 Mayne S T B Cartmel et al (2009) Alcohol and Tobacco Use Pre-diagnosis and Postdiagnosis and Survival in a Cohort of Patients with Early Stage Cancers of the Oral Cavity Pharynx and Larynx Cancer Epidemiology Biomarkers amp Prevention 18(12) 3368-3374 McDonald P R Williams et al (2002) Breast cancer survival in African American women Is alcohol consumption a prognostic indicator Cancer Causes and Control 13(6) 543-549 McEligot AJ Largent J Ziogas A Peel D Anton-Culver H Dietary fat fiber vegetable and micronutrients are associated with overall survival in postmenopausal women diagnosed with breast cancer Nutr Cancer 200655(2)132-140 McNeely M L K L Campbell et al (2006) Effects of physical activity on breast cancer patients and survivors a systematic review and meta-analysis CMAJ 175(1) 34-41 McKenzie D C and A L Kalda (2003) Effect of Upper Extremity Physical activity on Secondary Lymphedema in Breast Cancer Patients A Pilot Study J Clin Oncol 21(3) 463-466 McKeown-Eyssen GE Bright-See E Bruce WR et al A randomized trial of a low fat high fibre diet in the recurrence of colorectal polyps Toronto Polyp Prevention Group [erratum appears in J Clin Epidemiol 1995 Feb48(2)i] Journal of Clinical Epidemiology 1994 May47(5)525-36 McLarty Jerry Bigelow Rebecca LH Smith Mylinh Elmajian Don Ankem Murali Cardelli James A (2009) Tea Polyphenols Decrease Serum Levels of Prostate-Specific Antigen Hepatocyte Growth Factor and Vascular Endothelial Growth Factor in Prostate
135
Cancer Patients and Inhibit Production of Hepatocyte Growth Factor and Vascular Endothelial Growth Factor In vitro Cancer Prev Res 1940-6207CAPR-08-0167
McTiernan A et al (2009) Low-fat increased fruit vegetable and grain dietary pattern fractures and bone mineral density the Womens Health Initiative Dietary Modification Trial Am J Clin Nutr 89 1864-1876
Meyerhardt JA Heseltine D Niedzwiecki D Hollis D Saltz LB Mayer RJ Schilsky RL and Fuchs CS (2005) The impact of physical activity on patients with stage III colon cancer Findings from Intergroup trial CALGB 89803 Proc Am Soc Clin Oncol 24 p abstract 3534 Meyerhardt J A D Niedzwiecki et al (2007) Association of Dietary Patterns With Cancer Recurrence and Survival in Patients With Stage III Colon Cancer JAMA 298(7) 754-764 Meyerhardt J A D Niedzwiecki et al (2008) Impact of Body Mass Index and Weight Change after Treatment on Cancer Recurrence and Survival in Patients With Stage III Colon Cancer Findings From Cancer and Leukemia Group B 89803 J Clin Oncol 26(25) 4109-4115 Meyskens FL Jr Kopecky KJ Appelbaum FR Balcerzak SP Samlowski W Hynes H Effects of vitamin A on survival in patients with chronic myelogenous leukemia a SWOG randomized trial Leukemia Research 1995 September 19(9)605-12 Miles A Simon A Wardle J (2010) Answering patient questions about the role lifestyle factors play in cancer onset and recurrences Journal of Health Psychology 15(2) p 291-298 Milne H K Wallman et al (2008) Impact of a Combined Resistance and Aerobic Physical activity Program on Motivational Variables in Breast Cancer Survivors A Randomized Controlled Trial Annals of Behavioral Medicine 36(2) 158-166 Milne M Hamerston L and Morrell D (2010) BACSUP adult survivorship living with and beyond cancer test community learning workshop London January 2010 Monninkhof EM Peeters PH Schuit AJ Design of the sex hormones and physical exercise (SHAPE) study BMC Public Health 2007 Sep 47232 Morrell RM Halyard MY Schild SE Ali MS Gunderson LL Pockaj BA (2005) Breast cancer-related lymphedema Mayo Clin Proc 801480ndash1484 Mortimer P S D O Bates et al (1996) The prevalence of arm oedema following treatment for breast cancer QJM 89(5) 377-380 Mortimer JE Flatt SW Parker BA et al Tamoxifen hot flashes and recurrence in breast cancer Breast Cancer Res Treat 108421-426 2008 Moseley AL Piller NB Carati CJ (2005) The effect of gentle arm physical activity and deep breathing on secondary arm lymphedemaLymphology Sep38(3)136-45 Moseley AL Piller NB (2008) Physical activity for limb Lymphoedema ndash Evidence that it is beneficial Journal of Lymphoedema vol 3(1) pp 51-56
136
Mustian KM Palesh OG Flecksteiner SA Tai Chi Chuan for breast cancer survivors Medicine and sport science 2008 52()209-17 National Cancer Action Team (2009) Cancer and palliative care rehabilitation workforce project A review of the evidence National Cancer Action Team National Comprehensive Cancer Network (2009) NCCN Clinical Practice Guidelines in Oncology Cancer-related fatigue version 1 2009 National Cancer Survivorship Initiative (NCSI) (2009) Research Work Stream Mapping Project - Summary and reports for Bowel Cancer Breast Cancer Lung Cancer Prostate cancer National Cancer Survivorship Initiative Macmillan Cancer Support National Health Service (2010) NHS advice on drinking limits NHS Choices httpwwwdrinkingnhsukquestionsrecommended-levels [Last accessed 300310] National Institutes of Health (1998) Clinical Guidelines on the Identification Evaluation and Treatment of Overweight and Obesity in Adults The Evidence Report National Heart Lung and Blood Institute in cooperation with the National Institute of Diabetes and Digestive Kidney Diseases NIH Publication No 98-4083 National Institutes of Health Osteoporosis and Related Bone Diseases (2009) Conditions and behaviours that increase osteoporosis risk National Resource Centre US Department of Health and Human Services httpwwwniamsnihgovHealth_InfoBoneOsteoporosisConditions_Behaviorsosteoporosis_breast_cancerasp [Last accessed 170210] National Obesity Observatory (2009) Body mass index as a measure of obesity Association of Public Health Observatories June 2009 Ng K J A Meyerhardt et al (2008) Circulating 25-Hydroxyvitamin D Levels and Survival in Patients With Colorectal Cancer J Clin Oncol 26(18) 2984-2991 Nikotetti S Young J Levitt M (2008) Bowel problems self-care practices and information needs of colorectal cancer survivors at 6 to 24 months after sphincter-saving surgery Cancer Nursing 31(5) p 389-398
Norat T Bingham S Ferrari P Slimani N Jenab M Mazuir M Overvad K Olsen A Tjoslashnneland A Clavel F Boutron-Ruault MC Kesse E Boeing H Bergmann MM Nieters A Linseisen J Trichopoulou A Trichopoulos D Tountas Y Berrino F Palli D Panico S Tumino R Vineis P Bueno-de-Mesquita HB Peeters PH Engeset D Lund E Skeie G Ardanaz E Gonzaacutelez C Navarro C Quiroacutes JR Sanchez MJ Berglund G Mattisson I Hallmans G Palmqvist R Day NE Khaw KT Key TJ San Joaquin M Heacutemon B Saracci R Kaaks R Riboli E Meat fish and colorectal cancer risk the European Prospective Investigation into cancer and nutrition J Natl Cancer Inst 2005 Jun 1597(12)906-16
Ornish D et al (2005) Intensive lifestyle changes may affect the progression of prostate cancer The Journal of Urology 174 p 1065-1070 Ostroff JS Jacobsen PB Moadel AB Spiro RH Shah JP Strong EW et al (1995) Prevalence and predictors of continued tobacco use after treatment of patients with head and neck cancer Cancer Jan 1575(2)569-76
137
Pantuck AJ et al (2006) Phase II study of pomegranate juice for men with rising PSA following surgery or RXT for prostate cancer Clin Cancer Res 12(13) p 4018-4026 Pantuck AJ et al Abstract presented at the American Society of Clinical Oncology 2008 Genitourinary Cancers Symposium (Abstract 40) Long Term Follow Up Of Pomegranate Juice For Men With Prostate Cancer And Rising PSA Shows Durable Improvement in PSA Doubling Time Parsons A A Daley et al Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis systematic review of observational studies with meta-analysis BMJ 340(jan21_1) Pastorino U Infante M Maioli M et al Adjuvant treatment of stage I lung cancer with high-dose vitamin A[comment] J Clin Oncol 1993 July11(7)1216-22 Patterson R E L A Cadmus et al Physical activity diet adiposity and female breast cancer prognosis A review of the epidemiologic literature Maturitas In Press Corrected Proof Pedersen BK Saltin B Evidence for prescribing physical activity as therapy in chronic disease Scand J Med Sci Sports 16 Suppl 1 3ndash63 2006Pierce J P L Natarajan et al (2007) Influence of a Diet Very High in Vegetables Fruit and Fiber and Low in Fat on Prognosis Following Treatment for Breast Cancer The Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA 298(3) 289-298 Pierce JP Faerber S Wright FA Newman V Flatt SW Kealey S Rock CL Pierce JP Natarajan L Caan BJ et al Influence of a diet very high in vegetables fruit and fiber and low in fat on prognosis following treatment for breast cancer the Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA2007298(3)289-298 Ponz dL Roncucci L Chemoprevention of colorectal tumors role of lactulose and of other agents Scandinavian Journal of Gastroenterology Supplement 199722272-5 Poudevigne M J Wojcik et al (2009) The Effects Of 12-weeks Cross Training On Fatigue And Mood In Recent Breast Cancer Survivors 2292 Board 180 May 28 200 PM - 330 PM Medicine amp Science in Sports amp Physical activity 41(5) 297-298 Powers H J M H Hill et al (2007) Responses of Biomarkers of Folate and Riboflavin Status to Folate and Riboflavin Supplementation in Healthy and Colorectal Polyp Patients (The FAB2 Study) Cancer Epidemiology Biomarkers amp Prevention 16(10) 2128-2135 Protheroe J A Rogers et al (2008) Promoting patient engagement with self-management support information a qualitative meta-synthesis of processes influencing uptake Implementation Science 3(1) 44 Provenzano E and N Johnson (2009) Overview of recommendations of HER2 testing in breast cancer Diagnostic Histopathology 15(10) 478-484 Puhl RM Heuer CA (2009) ―The stigma of obesity A Review and Update Obesity 17 (5) 941-964 Rabin C (2009) ―Promoting Lifestyle Change among Cancer Survivors When is the Teachable Moment American Journal of Lifestyle Medicine 3 (5) 369-378
138
Reding K W J R Daling et al (2008) Effect of Pre-diagnostic Alcohol Consumption on Survival after Breast Cancer in Young Women Cancer Epidemiology Biomarkers amp Prevention 17(8) 1988-1996 Riboli E Hunt KJ Slimani N Ferrari P Norat T Fahey M Charrondiegravere UR Heacutemon B Casagrande C Vignat J Overvad K Tjoslashnneland A Clavel-Chapelon F ThieacutebautA Wahrendorf J Boeing H Trichopoulos D Trichopoulou A Vineis P Palli D Bueno-De-Mesquita HB Peeters PH Lund E Engeset D Gonzaacutelez CA Barricarte A Berglund G Hallmans G Day NE Key TJ Kaaks R Saracci R (2002) European Prospective Investigation into Cancer and Nutrition (EPIC) study populations and data collection Public Health Nutr 2002 Dec5(6B)1113-24 Richardson G E M A Tucker et al (1993) Smoking Cessation after Successful Treatment of Small-Cell Lung Cancer Is Associated with Fewer Smoking-related Second Primary Cancers Annals of Internal Medicine 119(5) 383-390 Richardson A Addington-Hall J Stark D Foster C Amir Z Sharpe M (2009) Determining research priorities for cancer survivorship Consultation and evidence review Commissioned by the NCSI Robertson R (2008) Using Information to Promote Healthy Behaviours Kings Fund London Rock C L and W Demark-Wahnefried (2002) Diet and Survival After the Diagnosis of Breast Cancer A Review of the Evidence J Clin Oncol 20(15) 3302-3316 Rock C L S W Flatt et al (2005) Plasma Carotenoids and Recurrence-Free Survival in Women With a History of Breast Cancer J Clin Oncol 23(27) 6631-6638 Rohan T Howe G Friedenreich C et al (1993) Dietary fiber vitamins A C and E and risk of breast cancer a cohort study Cancer Causes and Control 4(1) p 29-37 Rosenbaum EH Fobair P Spiegel D (2006) Cancer is a Life-changing Event Cancer Supportive Care Programs httpwwwcancersupportivecarecomSurvivorsurvivehtml [Last accessed January 30 2009] Ryan CW D Huo and K Bylow et al (2007) Suppression of bone density loss and bone turnover in patients with hormone-sensitive prostate cancer and receiving zoledronic acid BJU Int 100 pp 70ndash75 Sagiv SK Gaudet MM Eng SM et al (2007) Active and passive cigarette smoke and breast cancer survival Ann Epidemiol 17385ndash393 Sandel S Judge J Landry N et al (2005) Dance and movement program improves quality-of-life measures in breast cancer survivors Cancer Nursing 28(4) 301-309 Saxton J (2010) Physical activity and cancer mortality In Physical activity and cancer Survivorship Springer New York pp 189-210 Schatzkin A Lanza E Corle D et al Lack of effect of a low-fat high-fiber diet on the recurrence of colorectal adenomas Polyp Prevention Trial Study Group [comment] New England Journal of Medicine 2000 April 20342(16)1149- 55
139
Schmitz KH Courneya KS Matthews C Demark-Wahnefried W et al (2010) ―American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors Medicine and Science in Sports and Exercise Special Communication 0195-9131104207-14090 Schmitz K Holtzman J Courneya K Masse L Duval S Kane R Controlled physical activity trials in cancer survivors A systematic review and meta-analysis Cancer Epidemiol Biomarkers Prev 2005141588ndash95
Schulz M Lahmann PH Boeing H et al Fruit and vegetable consumption and risk of epithelial ovarian cancer the European Prospective Investigation into Cancer and Nutrition Cancer Epidemiol Biomarkers Prev 2005142531ndash2535 Schwarz S U C Obermuller-Jevic et al (2008) Lycopene Inhibits Disease Progression in Patients with Benign Prostate Hyperplasia J Nutr 138(1) 49-53 Schmitz K H Balancing Lymphedema Risk Physical activity Versus Deconditioning for Breast Cancer Survivors Physical activity and Sport Sciences Reviews 38(1) 17-24 10 Segal RJ Reid RD Courneya KS et al(2003) Resistance physical activity in men receiving androgen deprivation therapy for prostate cancer JClinOncol211653-1659
Segal RJ Reid RD Courneya KS Sigal RJ Kenny GP PrudlsquoHomme DGet al Randomized Controlled Trial of Resistance or Aerobic Exercise in Men Receiving Radiation Therapy for Prostate Cancer J Clin Oncol 2009 Jan 2027344-51 Sellers TA Potter JD Folsom AR (1991) Association of incident lung cancer with family history of female reproductive cancers the Iowa Womenlsquos Health Study Genet Epidemiol 8(3) 199ndash208 Severson RK Nomura AM Grove JS Stemmermann GN A prospective analysis of physical activity and cancer Am J Epidemiol 1989 Sep130(3)522-9 Shaw C Mortimer P Judd PA Randomized controlled trial comparing a low-fat diet with a weight-reduction diet in breast cancer-related lymphedema Cancer 20071091949ndash56 Sinicrope F A N R Foster et al Obesity Is an Independent Prognostic Variable in Colon Cancer Survivors Clinical Cancer Research 16(6) 1884-1893 Siris E S P D Miller et al (2001) Identification and Fracture Outcomes of Undiagnosed Low Bone Mineral Density in Postmenopausal Women Results From the National Osteoporosis Risk Assessment JAMA 286(22) 2815-2822 Soliman S W J Aronson et al (2009) Analyzing Serum-Stimulated Prostate Cancer Cell Lines After Low-Fat High-Fiber Diet and Physical activity Intervention eCAM nep031 Sonn GA Aronson W and Litwin MS (2005) Impact of diet on prostate cancer A review Prostate cancer and prostate disease 8 p 304-310 Speck RM Courneya KS Masse L Duval S Schmitz K (2010) An update of controlled physical activity trials in cancer survivors a systematic review and meta-analysis Journal of Cancer Survivorship 4(2) p 87-100
140
Steginga S K B M Lynch et al (2009) Antecedents of domain-specific quality of life after colorectal cancer Psycho-Oncology 18(2) 216-220 Stevinson C H Steed et al (2009) Physical Activity in Ovarian Cancer Survivors Associations With Fatigue Sleep and Psychosocial Functioning International Journal of Gynecological Cancer 19(1) 73-78 Swenson KK Nissen MJ Anderson E Shapiro A Schousboe J Leach J (2009) Effects of physical activity vs bisphosphonates on bone mineral density in breast cancer patients receiving chemotherapy Support Oncol May-Jun7(3)101-7 Tardon A Lee WJ Delgado-Rodriguez M et al Leisure-time physical activity and lung cancer a meta-analysis Cancer Causes Control200516(4)389-397 Taskila T Martikainen R Hietanen P Lindbohm M Comparative study of work ability between cancer survivors and their referents Europ J of Cancer 2007 43914-920 Taylor R Brown A et al (2004) Physical activity-based rehabilitation for patients with coronary heart disease systematic review and meta-analysis of randomized controlled trials The American journal of medicine 116(10) 682-692 Taylor NFDodd KJShields NBruder A Therapeutic physical activity in physiotherapy practice is beneficial a summary of systematic reviews 2002-2005 Aust J Physiother 2007 53 7-16 Thiebaut A C M A Schatzkin et al (2006) Dietary Fat and Breast Cancer Contributions From a Survival Trial J Natl Cancer Inst 98(24) 1753-1755 Thomas R Daly M and Perryman J (2000) Forewarned is forearmed - Randomised evaluation of a preparatory information film for cancer patients European Journal of Cancer 36(2) p 52-53 Thomas R et al (2005) Dietary advice combined with a salicylate mineral and vitamin supplement (CV247) has some tumour static properties - a phase II study Diet and science 2005 35(6) p 436-451 Thomas RJ and Davies ND (2007) Lifestyle during and after cancer treatment Clinical Oncology Vol 19 Issue 8 pp 616-627 Thomas R Nicholson C (2009) Why is exercise good for us Cancer Active httpcanceractivecomcancer-active-page-linkaspxn=2600ampTitle=Why20is20exercise20good20for20us [Last accessed 230710] Thomas R Oakes R Gordon J Russell S Blades M Williams M (2009) A randomised double-blind phase II study of lifestyle counselling and salicylate compounds in patients with progressive prostate cancer Diet and Food Science 39(3) pp 295 ndash 305 Thomson C A N R Stendell-Hollis et al (2007) Plasma and Dietary Carotenoids Are Associated with Reduced Oxidative Stress in Women Previously Treated for Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 16(10) 2008-2015
141
Thune I Brenn T Lund E Gaard M Physical activity and the risk of breast cancer N Engl J Med 336 1269-1275 1997
Travis LB Gospodarowicz M Curtis RE et al Lung cancer following chemotherapy and radiotherapy for Hodgkins disease J Natl Cancer Inst 94 (3) 182-92 2002 Tucker MA Murray N Shaw EG et al Second primary cancers related to smoking and treatment of small-cell lung cancer Lung Cancer Working Cadre J Natl Cancer Inst 89 (23) 1782-8 1997 Twiss J J N Waltman et al (2001) Bone Mineral Density in Postmenopausal Breast Cancer Survivors Journal of the American Academy of Nurse Practitioners 13(6) 276-284 Uhley V and Jen C (2006) Diet and weight management in cancer survivors In Handbook of Cancer Survivorship edited by Feuerstein M New York NY Springer 2006 ISBN-13 978-0-3873-4561-1
Vadiraja HS et al (2009) Effects of yoga program on quality of life and affect in early breast cancer patients undergoing adjuvant radiotherapy A randomized controlled trial Complementary Therapies in Medicine Volume 17 Issue 5 Pages 274-280
Velthuis MJ Agasi-Idenburg SC Aufdemkampe G Wittink HM (in press) The effect of physical activity on cancer-related fatigue during cancer treatment a meta-analysis of Randomised Controlled Trials Clinical Oncology 2009 (in print) Vineis P G Hoek and M Krzyzanowski et al Lung cancers attributable to environmental tobacco smoke and air pollution in non-smokers in different European countries a prospective study Environ Health 6 (2007) pp 1ndash7 Visvanathan K Chlebowski RT Hurley P et al American Society of Clinical Oncology 2008 clinical practice guideline update on the use of pharmacologic intervention including tamoxifen raloxifene and aromatase inhibition for breast cancer risk reduction J Clin Oncol 273235-3258 2009
Wagner LI Cella D (2004) Fatigue and cancer causes prevalence and treatment approaches BrJCancer 91822-828 Waltman N J Twiss et al (2009) ―The effect of weight training on bone mineral density and bone turnover in postmenopausal breast cancer survivors with bone loss a 24-month randomized controlled trial Osteoporosis International Wenzel L H Q Huang et al (2005) Quality-of-Life Comparisons in a Randomized Trial of Interval Secondary Cytoreduction in Advanced Ovarian Carcinoma A Gynecologic Oncology Group Study J Clin Oncol 23(24) 5605-5612 Weikert C Hoffmann K Dierkes J Zyriax BC KlipsteinndashGrobusch K MB et al Homocysteine metabolismrelated dietary pattern and the risk of coronary heart disease in two independent German study populations J Nutr 2005 1351981ndash1988 White S E McAuley et al (2009) Translating Physical Activity Interventions for Breast Cancer Survivors into Practice An Evaluation of Randomized Controlled Trials Annals of Behavioural Medicine 37(1) 10-19
142
World Health Organisation (1999) What is a healthy lifestyle Health Documentation Services WHO Regional Office for Europe Copenhagen World Health Organisation (2002) The World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva WHO Scientific Group on the Prevention and Management of Osteoporosis (2000 Geneva Switzerland) (2003) Prevention and management of osteoporosis report of a WHO scientific group World Health Organisation (2005) The European health report 2005 public health action for healthier children and populations Copenhagen WHO regional office for Europe World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva Windsor P M Nichol K F Potter J A randomized controlled trial of aerobic exercise for treatment-related fatigue in men receiving radical external beam radiotherapy for localised prostate carcinoma Cancer (2004) 101 (3) 550-7 Wright M E S-C Chang et al (2007) Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality Cancer 109(4) 675-684 Wright P A Smith et al (2005) Psychosocial difficulties deprivation and cancer three questionnaire studies involving 609 cancer patients Br J Cancer 93(6) 622-626 Yu GP et al (1997) The effect of smoking after treatment for Cancer Cancer Detect Prev 21487-509

2
Any comments or enquiries regarding this review are welcome
Nicola Davies BSc (Hons) MSc Comm PhD Researcher
Evaluation and Research Coordinator Self-Management Workstream National Cancer
Survivorship Initiative Macmillan Cancer Support
NDaviesmacmillanorguk
Robert Thomas MRCP MD FRCR
Visiting Professor Cranfield University
Consultant Oncologist Bedford Hospital amp Addenbrookelsquos Hospital Cambridge University
NHS Trusts co The Primrose Unit Bedford Hospital Bedford MK42 9DJ
Lynn Batehup BSc (Hons) MSc Nursing and Research PG Dip Health Economics
Research
Project Manager Self-Management Workstream National Cancer Survivorship Initiative
Macmillan Cancer Support Lbatehupmacmillanorguk
3
CONTENTS
Contents 3
Exectuive Summary 4
Background 8
The Purpose of this Review 12
Method and Search Strategy 14
Results 16
Part 1 Cancer Survival - Evidence for the Role of Lifestyle in Disease 17
Progression and Recurrence
Part 2 Lifestyle Evidence for Reducing and Managing Risks and Side-Effects 71
of Cancer Treatment
Cancer-Related Fatigue 72
Lymphoedema 80
Osteoporosis and Bone Health 85
Weight and Body Composition 93
Quality of Life 99
Ongoing Lifestyle Studies 110
Discussion 113
Appendix A Evidence-Based Dietary Self-Management Recommendationshelliphelliphelliphellip122
Appendix B Evidence-Based Physical Activity Recommendations 123
Referenceshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip124
4
Lifestyle Guidance for Cancer Survivors ndash Executive Summary
1 This aim of this review was to update the World Cancer Research Fund (WCRF)
report bdquoA Systematic Review of RCTs Investigating the Effect of Nutritional and
Physical Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This
has been achieved by conducting a comprehensive but pragmatic search of the
literature from 2006 onwards Where no evidence was available in the WCRF
review studies before 2006 have been included if identified in the reference lists of
acquired records To facilitate this evidence cited within the lsquoHandbook of Cancer
Survivorship‟ (Feuerstein 2006) and findings from a non-systematic review
conducted by the Cancer and Palliative Care Rehabilitation Workforce (2009) were
also utilised
2 There is now persuasive evidence that a healthy lifestyle during and after cancer is
associated with improved physical and psychological well-being reduced risks of
treatment enhanced self-esteem reduced risk of recurrence and improved survival
Clarifying the individual anti-cancer components of a healthy lifestyle will require
extensive further evaluation and even then they are likely to be multi-factorial
3 Despite gaps in the evidence for lifestyle benefits in cancer survivors there are some
key lifestyle recommendations that can be provided (Appendix A and B)
o Dietary Recommendations Reduce saturated fats increase fish intake
consume a varied diet in order to ensure adequate intakes of vitamins and
essential minerals increase consumption of green and cruciferous vegetables as
well as brightly coloured fruits and vegetables that contain carotenoids
o Physical Activity Recommendations There is substantial evidence suggesting
that the physical activity recommendations developed by the Department of
Health are sufficient for most cancer survivors - a total of at least 30-minutes a
day of moderate intensity physical activity on five or more days of the week
Additionally there is evidence of a dose-response (ie the more physical
activity the greater any benefits) Even a modest amount of exercise is
beneficial and will see gains versus doing nothing at all Body composition
changes are common in many cancer patients with the reasons varying by site
Compromised lean body mass for patients with head and neck and
gastrointestinal cancers are common and in this group exercise to build lean
muscle will be relevant However in breast cancer some treatments can lead to
significant weight gain (exacerbated if pre- diagnosis BMI is not in the healthy
range) and exerciseactivity which is more useful for controlling body weight and
losing fat will be more important
o Weight Excess weight should be avoided (ie a body mass index of 25-
29kgm or above There is also evidence that maintaining a stable healthy weight
as opposed to fluctuating between a healthy and unhealthy BMI can offer health
5
benefits for cancer survivors The evidence is strongly suggestive of weight being
implicated in breast cancer outcomes with the mechanism of benefit achieved
via physical activity or a low-fat diet most likely being due to weight loss
o Smoking Strong and consistent evidence has been presented for increased risk
of disease progression and mortality in people who continue to smoke after a
diagnosis of cancer as well as poorer outcomes in pre-diagnosis smokers
o Alcohol There is a paucity of research into the effects of alcohol pre- and post-
diagnosis on cancer progression and recurrence as well as symptom
management Evidence thus far is highly contradictory although excess alcohol
is linked to increased weight which does have negative outcomes
4 Evidence is also available for the benefits of individual lifestyle components for
specific cancer types
o A high intake of soy has been found to alter testosterone (the male sex
hormone) reducing risk of prostate cancer
o Dietary fibre might offer protection against colorectal cancer or recurrence via
increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic
mucosa (tissue that lines the colon)
o Since physical activity can alter levels of oestrogen (the female sex hormone)
evidence indicates that it might be protective against breast cancer
5 There is a wealth of evidence for physical activity during and after treatment
improving symptoms of cancer-related fatigue and increasing energy and stamina It
is also clear that a needs-based approach should be adopted ndash based on the
assessed need for improvements on low fatigue levels poor quality of life low
physical function (Speck et al 2009)
6 Guided progressive physical activity soon after treatment can ease the symptoms of
lymphoedema Avoidance of physical activity through fear of exacerbating symptoms
is unwarranted if physical activity is supervised and closely monitored
7 Whilst the benefits of physical activity on bone health require clarifying physical
activity can at the very least prevent loss of bone mineral density in survivors at
particular risk of developing osteoporosis
8 Even when not directly associated with overall QoL exercise has been found to
significantly improve social functioning among post-treatment survivors The benefits
of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or
group-based The evidence that physical activity can improve body image may be
one of the mechanisms through which exercise can improve quality of life
6
9 Mechanisms of benefit for diet and physical activity include the influence that these
behaviours have on hormones and insulin levels This has sparked the question of
whether pharmacological alternatives such as aromatase inhibitors and metformin
which tend to produce greater reductions in cancer risk pose competition for lifestyle
interventions This is unlikely as healthy lifestyle behaviours contribute overall to
general health and to the risk reduction for other co-morbid conditions such as
hypertension cardiac disease and diabetes Usefully the competencies framework
offered by Finders University highlights the importance of taking a holistic approach
to supported self-management whereby support is provided for a continuum of
health as opposed to a focus on one established chronic condition Based on this
model supported self-management should provide health promotion and illness
prevention not merely in terms of cancer but also for associated risks and co-
morbidities
10 The challenge remains in integrating lifestyle support into standardised models of
aftercare for cancer survivors particularly in terms of engaging both patients and
health professionals bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative identifies the need to
provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for
healthcare professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
11 The literature identifies the need for individual assessment and risk stratification for
cancer survivors so that lifestyle interventions and support can be tailored and
provided according to need Particularly high need groups are survivors who have
co-morbidities are overweight sedentary or smoke
12 Some questions that remain
o What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
o How can people most likely to benefit from lifestyle interventions be effectively
identified
o What are the various intensities of lifestyle support that can be provided based on
levels of individual need
13 Significant limitations can be found in the evidence available for lifestyle outcomes in
cancer survivors including
7
o Long-term outcomes of lifestyle choices
o Low levels of adherence to interventions
o A paucity of studies addressing external validity
o Equality across tumour groups
o Lack of cultural considerations pertaining to dietary advice
o A paucity of individualised lifestyle advice and tailored support
8
BACKGROUND SETTING THE SCENE
Lifestyle and Well-Being
In an independent report offering recommendations on enabling effective delivery of health
and well-being in England Bernstein Cosford and Williams (2010) advise that setting clear
priorities for health and well-being should start with behavioural risk factors Namely they
recommend tackling the biggest lifestyle influences on population health tobacco alcohol
physical inactivity and poor diet These four lifestyle factors are among the biggest
contributors to most preventable diseases across all social groups and in all areas of
England They are responsible for 42 of deaths from leading causes (WHO 2005) and
together they account for at least pound94 billion in annual direct costs to the NHS (DH 2009a)
expenses incurred outside the NHS would increase this figure further
An increase in longevity and the number of people living with one or more chronic conditions
for a longer period of time has led to government action aimed at making these years as
healthy as possible Interest has been particularly paid to the role of these behavioural risk
factors and the role of lifestyle in improving or maintaining health preventing illness
managing symptoms and achieving a satisfactory quality of life (QoL) (Pedersen and Saltin
2006 Taylor et al 2004)
The term lifestylelsquo refers to personal choices that might impact health such as diet physical
activity smoking and alcohol consumption The World Health Organisation (WHO 1999)
defines a healthy lifestylelsquo as
ldquoa way of living that lowers the risk of being seriously ill or dying earlyrdquo with the
emphasis that ldquohealth is not just about avoiding disease It is also about physical
mental and social well-beingrdquo (p 2)
With earlier detection and more efficacious treatments available for cancer there has been
an increase in survival as well as in the number of people living with the long-term
consequences of cancer treatment Subsequently cancer has become a chronic disease for
a number of people among the two million cancer survivors in the UK (Maddams Moller and
Devane 2008) Whilst evidence of the effects of a healthy diet and sufficient physical activity
in cancer prevention has been well-documented (Chan Gann and Giovannucci 2005
Sonn Aronson and Litwin 2005) it has become of fundamental importance to examine the
role of these lifestyle choices in cancer survivorship Furthermore the role of lifestyle in
cancer survivorship needs to be examined not only in terms of improved physical and
psychological well-being but also disease outcomes
Given the relationship between choosing a healthy lifestyle and taking an active role in the
self-management1 of the long-term effects of cancer and its treatment the self-management
workstream of the National Cancer Survivorship Initiative (NCSI) have conducted this
1 lsquoSelf-managementrsquo has been defined as ldquoawareness and active participation by the person in their recovery
recuperation and rehabilitation to minimise the consequences of treatment promote survival health and well-beingrdquo (NCSI 2009)
9
evaluation of evidence pertaining to lifestyle factors and survivorship Not only are lifestyle
choices important in terms of disease progression and recurrence but also in the effective
management of other chronic symptoms and conditions resulting from treatment such as
cancer-related fatigue lymphoedema and osteoporosis (Doyle et al 2006) Lifestyle
support and education is evidently an important component of supported self-management2
for many individuals living with or beyond cancer (Davies and Batehup 2010) Indeed as
part of a consensus meeting and evidence review self-management support and lifestyle
management were among the top ten priorities for survivorship research (Richardson et al
2009) providing further rationale for the current review
The Health of Cancer Survivors
The traditional belief has been that people with cancer should rest reduce activity and avoid
activities involving intense physical effort in other words they are passive patients of the
disease and its treatment Consequently physical activity levels do decline substantially
during and after completion of treatment for cancer and often fail to return to pre-diagnosis
levels for many people (Daley et al 2008) Fortunately it is becoming increasingly
recognised that people living with or beyond cancer do need physical activity will not be
harmed by physical effort and are active participants in the rehabilitation process
Furthermore emerging evidence is demonstrating that lifestyle factors can influence the rate
of cancer progression improve quality of life (QoL) reduce side-effects and risks during
treatment reduce the incidence of relapse and improve overall survival (Thomas Daly and
Perryman 2000) Besides the beneficial effect on recurrence a healthy diet and regular
physical activity has the potential to reduce the risk of co-morbidity such as other cancers
cardiovascular disease and diabetes etc (Jones and Demark-Wahnefried 2006)
Research suggests that although many cancer survivors report making healthy lifestyle
changes after diagnosis these changes may not be generalisable to all populations of
cancer survivors and they are often temporary (Demark-Wahnefried and Jones 2008)
Furthermore evidence suggests that the healthy lifestyle behaviours adopted by cancer
survivors tend to be directed towards clinical action such routine physical examination rather
than those health behaviours that require daily effort such as healthy eating or regular
physical activity (Findley and Sambamoorthi 2009)
A potential explanation for this difference in the uptake of clinical versus lifestyle preventive
health behaviours is that the former is easier due to the primary action being carried out by
someone else The latter on the other hand requires personal time and effort as well as
opportunity socially economically and in terms of health literacy and educational status
Behavioural and lifestyle change is notoriously difficult but even more so for people with
cancer or other chronic conditions let alone those with co-morbidities (Krein et al 2005) For
people with co-morbidities a healthy lifestyle can be even more challenging as they grapple
with the competing demands posed by the self-management of multiple conditions (Lindsay
2009)
2 lsquoSupported self-managementrsquo has been defined as ldquoWhat health and social care professionals and service
delivery organisations to do support self-managementrdquo (NCSI 2009)
10
Given the increase in survivorship the higher rates of co-morbidity within this population
and evidence that diet physical activity and other lifestyle factors affect risk for other cancers
and other chronic diseases there is a clear need for lifestyle interventions that target this
high risk group The literature suggests the need for individual risk assessment and the
provision of support with lifestyle changes in those individuals identified as high risk ndash such
as survivors who have co-morbidities are overweight sedentary or smoke (Davies and
Batehup 2010)
The Lifestyle Needs of Survivors
The National Cancer Survivorship Initiative (NCSI) highlights that people living with or
beyond cancer would like to play a more active role in their healthcare They want to know
how to look after themselves after a cancer diagnosis including information and support on
the lifestyle changes they should make so they can return to normallsquo life as much as
possible (Macmillan Cancer Support 2008) Yet the evidence suggests that this need
remains largely unaddressed In a key mapping project commissioned by the NCSI
Research workstream a number of issues pertaining to lifestyle were identified for the four
most common cancers breast colorectal lung and prostate (NCSI 2009) Each of these
four reports which were conducted by independent organisations demonstrated gaps in the
provision of lifestyle advice and support mainly during the period of aftercare In a similar
report mapping the needs of rarer cancers prolonging life through changes to lifestyle
emerged as a frequent theme by survivors asked to explore the meaning of cancer
survivorshiplsquo (Cancer52 and NCSI 2009) There was particular emphasis on the need for
diet and physical activity advice post-surgery for oesophageal cancer as well as diet advice
for mouth and throat cancers Change in bowel habits is frequently reported among post-
treatment bowel cancer survivors requiring support with dietary changes (Nikoletti et al
(2008)
In an effort to provide further insight into lifestyle advice and support for cancer survivors as
well as developing evidence-based lifestyle interventions a comprehensive review of the
evidence for lifestyle and cancer outcomes is required The perceived outcome efficacy3 of
making lifestyle changes is important in terms of whether those changes are initiated or not
as well as whether an individual possesses the confidence (self-efficacy) to maintain lifestyle
changes Outcome efficacy could be increased by the accumulation of firmly established
evidence offered alongside the opportunity for lifestyle support
Additionally this evidence needs to be evaluated in respect of current national guidelines for
diet physical activity and other lifestyle indicators such as weight and alcohol consumption
Briefly national guidance recommends a diet comprising 33 fruit and vegetables (five
portions per day) 33 starchy foods (rice bread pasta potatoes) 15 milk and dairy
foods 12 protein (meat and fish) and 8 foods and drinks high in fat andor sugar (Food
Standards Agency 2007) Adults are advised to achieve a total of at least 30-minutes daily
moderate intensity physical activity on five or more days of the week (DH 2004) Combined
with a healthy diet regular physical activity is aimed at maintaining a Body Mass Index
3 The belief that a particular outcome will result from following certain actions or behaviours
11
(BMI)4 of 185-249kgm2 25-29 is considered to be overweight and 30 or above as obese
whilst under 185 is considered underweight (National Obesity Observatory 2009)
A healthy lifestylelsquo is the same for cancer survivors as for the general population or indeed
people with other chronic conditions (Bellizzi et al 2005 Caan et al 2005 Coups and
Ostroff 2005) Cancer survivors are slightly more likely to follow physical activity guidelines
but overall their health behaviours mirror those of the general population which is marked by
inactivity and an epidemic of obesity and associated problems (Caan et al 2005) Despite
this the lifestyle advice and tailored care currently provided for specific groups of people in
the general population such as exercise prescriptions (DH 2001) is not yet integrated into
the supportive care needs of cancer survivors (Addington-Hall 2010) This is in the main
due to reluctance (usually related to knowledge and confidence) from health professionals to
discuss lifestyle factors with cancer patients due to limitations in knowledge and an
inadequacy in the available evidence on the underlying mechanisms of benefit for individual
lifestyle factors (Miles Simon and Wardle 2010) It is anticipated that this review will allay
some of this reluctance by identifying where the evidence strongly supports the efficacy of
lifestyle factors in cancer outcomes as well as where the evidence is less clear and requires
further research
4 BMI is a statistical measure which compares a persons weight and height to estimate a healthy body weight
12
The Purpose of this Review
Using the outlined national guidance on lifestyle and taking account of evidence for specific
elements or intensity of certain lifestyle factors in cancer care and self-management a
review of the literature on lifestyle and survivorship will be conducted The primary aims are
to produce evidence that can support professionals in guiding and advising cancer survivors
as well as evidence regarding resources which might support patient self-management in
relation to lifestyle factors and behaviour change The review will be comprehensive but
pragmatic drawing on a variety of sources This will commence by updating a recent review
conducted by the World Cancer Research Fund (WCRF) - bdquoA Systematic Review of RCTs
Investigating the Effect of Diet and Physical Activity Interventions on Cancer Survival‟
(Bekkering et al 2006)5
The aim of the WCRF review (Bekkering et al 2006) was to systematically locate and
review all randomised control trials (RCTs) which tested the effect of diet andor physical
activity interventions in cancer survivors their definition of a cancer survivor being
ldquoanyone who has been diagnosed with cancer from the time of diagnosis through the
rest of liferdquo (Brown et al 2003)
They conducted a systematic search of MEDLINE (from 2000 onwards) EMBASE (from
1999 onwards) AMED (from 1985 onwards) and the Cochrane Library including DARE
CDSR CENTRAL and HTA (all years) up to March 2006 scanned key texts that were
relevant to the subject field and scanned the references of relevant reviews They identified
117 trials (Table 1)
Table 1 Trials Identified in the WCRF Review (Bekkering et al 2006)
Trials Total
Diet
Food-based
Supplement-based
23
71
Physical activity
23
Total 117
5 This has been highlighted by the American Cancer Society (ACS) as being one of the most comprehensive
reviews on diet and physical activity for cancer survivors The ACS has used the review alongside other sources to produce lsquoGuidelines on Diet and Physical Activity for Cancer Preventionrsquo (Kushi et al 2006)
13
The findings will be described along with the results of the current review The overall
conclusion drawn by Bekkering et al (2006) was that there is a paucity of robust evidence
on the effects of diet and physical activity interventions in the management of cancer RCTs
were generally small and often reported inadequate details to formally assess quality While
promotion of a generic healthy diet was associated with reduced overall mortality the degree
to which lifestyle accounted for this outcome was imprecise It was concluded that given the
large investment in potential lifestyle interventions among cancer survivors large-scale trials
adequately powered to provide robust conclusions should be supported and conducted
In updating the WCRF review (Bekkering et al 2006) further scoping of the literature from
2006 to February 2010 will be conducted along with a synthesis of the evidence presented
in the lsquoHandbook of Cancer Survivorship‟ edited by Michael Feuerstein (2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (National Cancer Action Team 2009) which evaluates literature
pertaining to rehabilitation
The primary aim of the review is to guide healthcare planning and the development of
supported lifestyle self-management interventions for high risk groups In order to be able to
consider the production of useable evidence-based guidance for self-management for both
patients and professionals the following evidence will be sought
Evidence that would support professionals to be able to guide and advise
patients
Evidence regarding resources which would support patient self-management in
relation to lifestyle factors and behaviour change
It is anticipated that recent efforts to conduct research in this area will facilitate the
clarification of any key recommendations that can be made to cancer survivors by healthcare
professionals This update of the evidence will also attempt to establish where the strength
of the evidence lies and where more research is required
14
METHOD
Search Strategy
In updating the WCRF review (Bekkering et al 2006) RCTs and systematic reviews were
obtained from a systematic search of the Cochrane Library Database and Pubmed (from
March 2006 to February 2010) Where no evidence was available in the WCRF review
studies before 2006 have been included if identified in the reference lists of acquired
records this is the case with studies on smoking which were not included in the Bekkering
et al (2006) review
The selected relevant chapters were read from the bdquoHandbook of Cancer Survivorship‟
(Feuerstein 2006)6 and relevant studies referred to from the Cancer and Palliative Care
Rehabilitation Workforce (2009) non-systematic review Grey literature was also utilised
where this would provide information relevant to the review or where cancer-specific
literature was lacking as was the case with osteoporosis
All titles and abstracts of studies identified by the searches were scanned for relevance in
terms of topic and participant group For any titles or abstracts that were potentially relevant
full paper manuscripts were obtained and the relevance of each study assessed according to
the pre-specified inclusion criteria
6 Chapters include Physical Activity Potential Benefits and Guidelines DietWeight Management
Search terms cancer OR neoplasm
AND diet OR exercise OR physical
activity OR weight OR lifestyle
Cochrane systematic reviews
925 records
PubMed
4941 records
56 included 84 included
15
Inclusion Criteria
Records included within the review of the literature met the following inclusion criteria
Lifestyle-related ndashdiet physical activity weight smoking alcohol consumption
Cancer sites breast colorectal lung or prostate cancer Other tumour sites will
be included if located while searching for the primary tumour sites
Trajectory - during primary cancer treatment or post-primary treatment
Outcomes of interest ndash survival recurrenceprogression symptoms treatment-
related chronic conditions ndash fatigue lymphoedema osteoporosis weight
physical fitness quality of life rehabilitation behaviour change health and well-
being cost-effectiveness
Adult population
Type of record ndash RCTs systematic reviews prospective cohort studies
Retrospective studies will also be included since some areas of lifestyle such as
smoking have primarily been investigated via this method
16
RESULTS
A total of 140 records were included in this review not counting the review being updated
(Bekkering et al 2006) In synthesising the evidence obtained from these records and the
additional sources described in the search strategy findings are presented in two parts
1) Cancer Survival
Evidence for the role of lifestyle in disease progression and recurrence
2) The Risks and Side-Effects of Cancer Treatment
Evidence for the role of lifestyle in reducing and managing the risks and
side-effects of cancer treatment with specific focus on cancer-related
fatigue lymphoedema osteoporosis and QoL
Both sections examine five categories of evidence
Physical activity
Diet
Weight
Smoking
Alcohol
The focus is on the four most common cancers (breast colorectal lung prostate) but other
tumour sites have been included if located via the pre-defined search strategy Summary
tables for each study included within the evidence are provided at the end of relevant
sections
17
PART ONE
CANCER SURVIVAL ndash EVIDENCE FOR THE ROLE OF LIFESTYLE IN
DISEASE PROGRESSION AND RECURRENCE
Introduction
Evidence for the role of lifestyle in the development of cancer is strong and it is widely
accepted that a poor diet lack of exercise smoking and excessive alcohol consumption can
increase an individuallsquos risk of developing cancer In particular it is well established that
smoking can increase risk of lung cancer and excessive unprotected exposure to the sun
can increase risk of skin cancer More recently lifestyle after a cancer diagnosis has been
under the microscope with evidence for the role of lifestyle in cancer progression7 and
recurrence8 demonstrating that lifestyle changes post-diagnosis can influence the disease
trajectory (Thomas and Davies 2007)
The development of cancer does not mean it is too late to make lifestyle changes that can
reduce the risk of the disease progressing or recurring after remission Indeed lifestylelsquo
refers to personal choices that can impact health and well-being as well as improve an
individuallsquos chance of disease-free survival9 and overall survival10
Evidence for an interaction between lifestyle and the disease trajectory is evaluated in the
current review including cancer development progression and recurrence and
commencing with a description of three large scale multicentre trials that will be referred to
throughout (Table 3)These studies are presented in some depth because their findings have
been influential in this field of study This will be followed by a site-specific (eg breast
colorectal lung prostate) summary of the findings reported by Bekkering et al (2006) as
part of the WCRF review being updated Further evidence identified from the search criteria
will then be presented including evidence obtained from the aforementioned multicentre
trials The European Prospective Investigation into Cancer and Nutrition (EPIC) Study
The Womens Intervention Nutrition Study (WINS) and The Womens Healthy Eating
and Living (WHEL) Study
7 Defined as the cancer becoming worse or spreading within the body
8 Cancer that has returned usually after a period of time during which it could not be detected The cancer may
come back to the same place as the original (primary) tumour or to another place in the body
9 The length of time after treatment during which a person survives with no sign of the disease
10The percentage of people from the study who are alive for a certain period of time after diagnosis or treatment
(ie 5-year survival rate)
18
The European Prospective Investigation into
Cancer and Nutrition (EPIC) Study (Riboli et al
2002)
The Womens Intervention Nutrition Study (WINS)
(Chlebowski et al 2006)
The Womens Healthy Eating and Living (WHEL)
Study
(Pierce et al 1997)
The EPIC study is coordinated in the UK by Dr Elio Riboli of the Imperial College London It is an ongoing multicentre prospective cohort study designed to investigate the relationship between nutrition and cancer The study currently includes 521000 participants (aged 35ndash70 years) in 23 centres located across 10 European countries11 These participants will be followed for cancer incidence and mortality for at least 10-years At enrolment which took place between 1992 and 2000 information was collected through a lifestyle questionnaire and through a dietary questionnaire addressing usual diet Physiological measurements (eg weight) were performed and blood samples taken The main website for EPIC12 last updated in 2010 reports that 26000 cases of cancer and 16000 deaths from cancer have been identified the majority of cases being cancer of the breast (n=6218) colonrectum (n=1910) prostate (n=1547) and lung (n=1292)
The WINS trial is a randomised multicentre study that commenced in 1994 and is now closed for recruitment It was designed to determine whether dietary fat reduction effectively prolongs disease-free and overall survival in post-menopausal women (n=2437) aged 48-78 years surgically treated for early stage breast cancer Randomisation to a reduced fat group or a control group took place between 1994 and 2001 with participants being evaluated annually via self-report and physiological measures 1) Intervention group (n=975) intensive dietary intervention for reduction of total fat intake to 15 of calories with repeated individual and group counselling sessions involving cognitive behavioural and motivational interviewing techniques 2) Control group (n=1462) US Department of Health and Human Services dietary guidelines (total fat intake between 20-35 of calories)
The WHEL study is a multicentre RCT which commenced in 1995 and also closed to recruitment aimed to determine whether a diet rich in vegetables fruit and fibre and low in fat is associated with a longer breast cancer event-free interval (ie no disease progression recurrence nor secondary cancers) Women diagnosed with stage I-III invasive breast cancer (n=3088) within the previous 4-years were randomised to a dietary intervention or control group and evaluated annually for 5-years via self-report and physiological measures 1)Intervention group (n=1540) guidelines provided for a daily dietary pattern of 5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy from fat A telephone counselling protocol focusing on goal setting self-monitoring and self-efficacy were provided as were cooking classes 2)Control group (n=1551) The US Department of Agriculture dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre and 30 energy from fat)
11
Denmark France Germany Greece Italy The Netherlands Norway Spain Sweden and the UK
12 httpepiciarcfr
Table 3 The EPIC WINS and WHEL Study (findings presented within proceeding text)
19
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in breast
cancer survival In the current review 6 studies and 2 systematic reviews were identified
These have been divided into appropriate domains according to mechanisms of benefit
hormones intensity and insulin Studies are summarised in Table 3 at the end of this
section
Hormones
Evidence exists that physical activity is associated with reduced risk of developing breast
cancer (Friedenreich and Cust 2008 Monninkhof et al 2007) One potential mechanism of
benefit is via the modification of sex hormone levels High levels of oestrogen (the
predominant sex hormone in females)13 and androgen (the predominant sex hormone in
males)14 are consistently associated with increased risk of developing breast cancer
(Eliassen et al 2006 Kaaks et al 2005) whereas high levels of sex hormone-binding
globulin (SHBG)15 are associated with a decreased risk (Key et al 2002) Regular physical
activity may alter oestrogen metabolism by shifting metabolism to favour production of 2-
hydroxyestrone (2-OHE1)16 as opposed to16α-hydroxyestrone (16α=OHE1) the former of
which has much weaker estrogenic activity Campbell et al (2007) is one of the few
researchers to examine this mechanism of benefit via a RCT In examining the effects of a
12-week aerobic exercise training programme on 2-OHE1 and 16α-OHE1 in healthylsquo pre-
menopausal women (n=17) no significant differences in oestrogen changes were found with
a control group who continued their usual level of physical activity (n=15) However a
change in lean body mass (estimated weight excluding body fat) over the 12-week
programme was found to be associated with a favourable change in 2-OHE1 to 16α-
OHE1 ratio (p lt 005)
In an effort to provide more direct evidence regarding the biological mechanisms of benefit
obtained from physical activity Friedenreich et al (2010) conducted the Alberta Physical
Activity and Breast Cancer Prevention Trial a two-centre two-arm RCT of physical
activity and cancer risk in older (50gt years) post-menopausal sedentary women from the
general population (n=320) Participants received a 1-year aerobic physical activity
programme of 225-minutes per week (n=160) or maintained their usual level of activity as
part of a control group (n=160) Significant reductions in oestrogen were found in the
intervention group compared to the control group demonstrating a protective effect
of increased physical activity in this group of high risk women (p lt 05)
13
oestrogen is suspected to activate certain oncogeneslsquo which can turn normal cells into tumour cells 14
The primary and most well-known androgen is testosterone which is also found in women to a lesser degree 15
A protein that attaches itself to oestrogen and androgen
16 Sometimes referred to as a good oestrogenlsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
20
Whilst some studies have examined the outcomes of increased physical activity others have
attempted to identify the duration and intensity required for beneficial effects Using data
from the Nursesrsquo Health Study17 (n=2987) Holmes et al (2005) found that women who
reported at least 3 MET-hours18 or more of physical activity per week were less likely
to have a recurrence or die from breast cancer compared to those who reported less
physical activity (p lt 001)
A further reduction in risk was seen with higher levels of physical activity up to 239 MET-
hours per week indicating a dose-response Interestingly the benefits of physical activity
were limited to women with hormone-receptor positive tumours (tumours that
respond to hormone treatment) as opposed to hormone-receptor negative tumours
(tumours that do not respond to hormone treatment) This provides further support for
mechanism of benefit from physical activity being hormone-related whether that be due to
the physical activity or any subsequent reductions in lean body mass that might accompany
such activity
Intensity
Expanding on evidence for the intensity of physical activity in a prospective observational
study the Health Eating Activity and Lifestyle (HEAL)19 study Irwin et al (2008) found
that of breast cancer survivors (n=933) who were sedentary pre-diagnosis women who
increased their physical activity post-diagnosis to approximately 9-MET hours per
week (eg 2-3 hours of brisk walking) had a 45 lower risk of death from cancer when
compared to those who did not increase their physical activity women who
decreased physical activity after diagnosis had a four-fold greater risk (p lt 005)
17
One of the largest and longest running investigations of factors that influence womenlsquos health comprising
information from 238000 nurse-participants
18 Metabolic equivalent (MET) values a measure of the effort required to do that activity
19 The HEAL Study is a population-based multicentre multi-ethnic prospective cohort study that has enrolled
1183 breast cancer survivors to determine whether lifestyle hormones and other exposures affect breast cancer
prognosis
METs (Ainsworth 2000) Light-intensity activities are defined as 11 MET to
29 MET Moderate-intensity activities are defined as 30 to
59 METs Vigorous-intensity activities are defined as 60 METs
or more
3 MET-hours might be using a stationary bicycle with light effort for one-hour 239 MET-hours might be running for 2-hours plus 1-hour of aerobic activity
21
Consistent with this a larger prospective observational study demonstrated that breast
cancer survivors (n=4482) who were physically active for more than 28 MET-hours per
week (eg walking at average pace of 2-29mph for 1-hour) were significantly less
likely to die from breast cancer (35-49 reduction) when compared to survivors who
did less than this (p lt 05) (Holick et al 2008) The reduced risk of mortality from cancer
was limited to total or moderate-intensity physical activity no benefit was noted for vigorous-
intensity activity
In a systematic review by Patterson et al (2010) leisure-time physical activity (ie
sportsrecreational) was associated with a 30 decreased risk of mortality from
breast cancer when compared to sedentary women In another review Saxton (2010)
identified four cohort studies demonstrating that women achieving the equivalent of 30-
minutes of moderate intensity physical activity on five or more days of the week
halved their risk of cancer-related mortality compared to those achieving less than 30-
minutes over the five days
Insulin
Evidence for the role of excess insulin in the growth of cancer cells has become more
established in recent years especially with the increase in obesity which is often
accompanied by elevated levels of insulin (Giovannucci 2005) The benefits of physical
activity on reducing insulin levels are less clear Ligibel et al (2008) conducted a RCT to test
the impact of weight training on insulin levels in overweight sedentary stage I to III breast
cancer survivors (n=101) The women were randomly assigned to one of two conditions
1) a 16-week supervised strength training and home-based cardiovascular training
protocol (two supervised 50-minute strength training sessions per week and 90-
minutes of home-based aerobic physical activity weekly)
2) a control group (routine care for 16-weeks before being offered consultation with a
physical activity trainer at the end of the control period)
Participation in the physical activity training was associated with a significant
decrease in insulin levels and hip circumference (p lt 05) Therefore the relationship
between physical activity and breast cancer recurrence may be mediated in part through
changes in insulin levels andor changes in body fat
ii DIET
Bekkering et al (2006) report on two small breast cancer studies showing a reduction in
cancer-specific mortality with healthy diet interventions (Elkort et al 1981 de Waard et al
1993) Of nine trials that included an antioxidant supplement no evidence was found for an
association between the intervention and cancer-related mortality compared with placebo or
usual treatment There was also no evidence of an effect of retinol (vitamin A - found in cod
liver oil butter liver eggs and cheese) (Meyskens et al 1994 Kucera et al 1980
Pastorino et al 1993)
22
In the current review 19 studies provide further evidence of the role of diet in breast cancer
survival many of which are part of the three multicentre studies previously described (ie
EPIC WINS WHEL p19) These studies have been divided into appropriate domains
according to dietary components dietary fat fruit and vegetables dietary fibre soy and
vitamin D
Dietary Fat
In general retrospective casendashcontrol studies have supported a positive association between
breast cancer incidence and dietary fat (Howe et al 1990) whilst many prospective cohort
studies have failed to show such an association (Kim et al 2006 Hunter et al 1996) A
meta-analysis provided evidence for a weak direct association between fat intake and breast
cancer in casendashcontrol and cohort studies combined (Boyd et al 2003) in cohort studies
that adjusted for energy intake highest versus lowest categories of total fat intake were
associated with a statistically significant 13 increased risk of developing
breast cancer (p lt 05)
Kyogoku et al (1992) utilised breast cancer patients whose dietary intake was assessed 10-
years previously in a case-control study (n= 212 patients who underwent a surgical
operation) After 10-years of follow-up 47 breast cancer deaths had occurred with no
support being provided for the hypothesis that a low fat diet influences breast cancer survival
outcomes In addition Holmes et al (1999) as part of the Nursesrsquo Health Study report
there being no evidence suggesting that lower intake of total fat or specific types of fat (eg
saturated and unsaturated fat) was associated with death from breast cancer in 2956
women who were diagnosed after 14-years of follow-up
Hebert et al (1998) studied the effect of diet on recurrence and death in women diagnosed
with early-stage breast cancer (n=472) finding that the strongest effects were observed in
pre-menopausal women Higher levels of self-reported baseline daily consumption of
butter margarine lard and beer were found to increase the risk of recurrence (p lt
01) There was also an increased risk associated with consumption of red meat liver and
bacon corresponding to about a doubling of risk for each time per day that foods in this
category were consumed (p=09)
The previously described WINS and WHEL RCTs (Table 2 p19) were anticipated to shed
light on these inconsistent findings related to dietary fat and breast cancer outcomes as
explored next in the following section
In an interim analysis of the Womens Intervention Nutrition Study (WINS) data (n=2437)
after a median follow-up of 60-months (5-years) (Chlebowski et al 2006) report that dietary
fat intake was lower in the dietary intervention than in the control group corresponding to a
significant 6-pound lower mean body weight in the intervention group (p lt 05) As a
reminder the dietary intervention group were counselled to reduce total fat intake to 15 of
calories whilst the control group were advised to keep total fat intake between 20-35 of
calories After 5-years of follow-up a total of 277 recurrences were reported in 96 of 975
23
(98) women in the dietary group and 181 of 1462 (124) women in the control group
women in the dietary intervention had a 24 lower risk of recurrence compared to the
control group (p lt 05) Exploratory analyses suggested that dietary fat reduction was most
beneficial in women diagnosed with hormone receptorndashnegative compared to hormone-
receptor positive breast cancer although this was not statistically significant
Other studies providing evidence of a differential effect of fat intake on breast cancer survival
have found such associations with hormone-receptor positive cancers (Holm et al 1993
Cho et al 2003) raising debate over the WINS findings Nevertheless in 2008 Chlebowski
et al updated survival information presented in 2006 reporting that after 7-years follow-up a
significant overall survival benefit was seen in women (n=362) with hormone-receptor
negative tumours taking part in the dietary intervention compared to the comparison
group (75 vs 181 p lt 005)
To explore the link between hormones and diet further the metabolic profiles of a subset of
WINS participants (n=53) were examined for the effect of a low-fat diet on insulin resistance
(Khaodhiar et al 2003) Insulin resistance is a physiological condition in which insulin
becomes less effective in lowering blood sugars resulting in increased blood glucose Of
those participants with initial insulin resistance after 1-year women in the dietary
intervention group had a greater decrease in their fasting insulin (insulin tested in a blood
sample collected after a 12-hour fast) than the women in the control group Although
not statistically significant these results suggest that insulin concentrations (a marker of
insulin resistance) may be influenced by dietary fat intake Alternatively since waist-to-hip
ratio is a marker for insulin weight reduction as opposed to dietary fat reductions might be
the important variable influencing disease outcomes (Borugianlsquos et al 2004)
Fruit and Vegetables
Flavonoids20 are high in fruits and vegetables and therefore might account for some of the
findings reported in WINS Dwyer et al (2008) sought to determine whether differences
existed in baseline and 12-month dietary intake of flavonoids among a random sample of
WINS participants (n=550) After 12-months of dietary intervention flavonoid intakes
remained similar in both groups demonstrating that neither total flavonoid intakes nor
intakes of subclasses of flavonoids differed between those who had dramatically decreased
their fat intake and those who had not Flavonoid intake is therefore unlikely to account for
the survival benefits reported for the WINS trial Carotenoids21 however do appear to play a
significant role in cancer survival On following 103 breast cancer survivors 27 of whom
died Ingram (1994) found that after a median of 81-months those who consumed more
beta-carotene (a carotenoid found in yellow and orange fruits such as mangoes
papayas and carrots) had significantly fewer deaths from breast cancer only one in
the group of highest beta-carotene consumers compared with 8 in the intermediate
20
Flavonoids also referred to as bioflavonoids are polyphenol antioxidants found naturally in plants ndash in other
words they are plant nutrientslsquo
21 Organic pigments that provide colour to bright fruits and vegetables including carrots apricots tomatoes and
salmon
24
group and 12 in the lowest group (p lt 0001) Overall there were 12 deaths in the lowest
total fruit consumption group compared with five in the intermediate group and 3 in the
highest (p lt 001) This benefit applied to both orangeyellow fruit (oranges melon) as well
as other fruits (apple banana berries grapes dried fruits)
Adding to this evidence is data from the aforementioned Womens Healthy Eating and
Living (WHEL) RCT (Table 2 p19) As a reminder women with breast cancer were
randomised to a dietary intervention (n=1540) comprising a daily pattern of
5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy
from fat or to a control group (n=1551) advised to follow the US Department of Agriculture
dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre
and 30 energy from fat Over a mean 73-year follow-up there was no significant
difference between groups in terms of additional breast cancer events (ie disease
progression recurrence or secondary cancer) or mortality despite statistically significant
differences in self-reported diet (low fat high fruit and vegetables) (Pierce et al 2007) On
the other hand when Rock et al (2005) examined only those participants in the control
group higher plasma total carotenoid concentration indicative of greater fruit and
vegetable consumption was significantly associated with reduced risk for a new
breast cancer event (p lt 05) This supports those findings reported by Ingram et al
(1994) and provides a potential explanation for why survival benefits were achieved in WINS
but not WHEL since both dietary interventions comprised lower dietary fat and higher levels
of carotenoids (fruit and vegetables) other factors must explain the differential survival
benefits One major difference between the two studies is that WINS participants lost weight
(mean = 6-pounds) whereas the WHEL participants did not
To follow up on these findings in terms of possible biological mechanisms of reduced risk of
recurrence Thomson et al (2007) conducted an ancillary study with post-menopausal
breast cancer survivors from the WHEL study (n=207) The aim was to test the hypothesis
that breast cancer survivors with higher levels of dietary carotenoids would show significantly
lower levels of oxidative stress (pathologic changes in response to excessive levels of cell
toxicity from the environment) than those with lower levels It was found that dietary
carotenoid levels were not significantly associated with oxidative stress indicators (measured
via urine samples)
Hot flushes post-treatment for early-stage breast cancer has been associated with an
approximately 25-30 decreased risk for additional breast cancer events (Mortimer et al
2008 Cuzick 2007) Since hot flushes are reported by women who continue to menstruate
during treatment or whose menstruation returns post-treatment this lowering of risk is
unlikely to be explained entirely by the lower oestrogen levels that sometimes accompany
hot flushes On the other hand dietary changes comprising lower energy from fat and
increased fibre can also alter oestrogen levels For example binding of fibre to estrogens in
the gut blocks reabsorption of oestrogen (Arts et al 1991) Focusing their analyses on the
2967 of the WHEL participants who experienced baseline hot flushes Gold et al (2009)
tested the hypothesis that the increased risk of additional breast cancer events observed
among women who do not report hot flushes post-treatment can be reduced by lifestyle
interventions that lower circulating oestrogen Over a median of 73-years follow-up it was
demonstrated that the dietary intervention was associated with reduced risk of second
25
breast cancer events among women who reported no hot flushes at baseline (p lt 05)
These women had 31 fewer cancer-related events than matched-pairs in the control group
among post-menopausal women with no self-reported hot flushes at baseline the
intervention effect was even stronger with a 47 reduction in risk compared with post-
menopausal women in the control group who had no hot flushes at baseline (p lt 05)
McEligot et al (2006) conducted a retrospective investigation into the influence of diet (fat
fibre vegetable fruit folate carotenoids and vitamin C) on overall survival in post-
menopausal women with breast cancer (n= 516) Participants completed a food frequency
questionnaire for the year prior to diagnosis the analysis of which demonstrated that
women consuming the least total fat and highest total fibre and vegetables as well as
more folate vitamin C and carotenoid were significantly less likely to die from any
cause than those women consuming the opposite (p lt 05)
Dietary Fibre
Evidence linking breast cancer to the intake of dietary fibre has been conflicting although the
hypotheses remain that dietary fibre can be protective by inhibiting oestrogen (Kaaks et al
2005) as described previously in relation to physical activity or by reducing insulin-like
growth factors (Heald et al 2003) Therefore further research into these mechanisms of
benefit is clearly needed in order to provide clarity
Rohan et al (1993) examined risk of breast cancer in relation to intake of dietary fibre and
vitamins A C and E in a cohort of women (n=56837) enrolled in the Canadian National
Breast Screening Study22 After 5-years follow-up 519 incidence of breast cancer were
identified with analysis of previously completed dietary questionnaires demonstrating that
higher dietary fibre intake was associated with a small reduction in risk of developing
breast cancer Specifically there was a statistically significant decrease in risk of
developing breast cancer with increasing consumption of cereals (p lt 01) and a statistically
non-significant trend for pasta consumption (p=017) This reduced risk persisted after
adjustment for total vitamin A beta-carotene vitamin C and E
The UK Womens Cohort Study (UKWCS) (Cade et al 2007) which compares the health
outcomes of three main dietary groups (vegetarian eating fish [not meat] and meat eaters)
provides further evidence for the protective properties of fibre After a median of 75 years
follow-up analysis of self-reported dietary data of 35792 women showed that total dietary
fibre was found to be related to breast cancer incidence in women who were pre-
menopausal but not post-menopausal at baseline (p lt01) Fibre from cereals (plt
05) and fibre from fruit (p=009) was found to be protective against breast cancer
22
An RCT comprising women 40-49 years of age at study entry evaluating the efficacy of annual mammography breast physical examination and instruction on breast self-examination in reducing breast cancer mortality
26
Soy
A high intake of phytoestrogens23 particularly isoflavones (found in soy products) has been
suggested to decrease risk of developing breast cancer In one of the European
Prospective Investigation into Cancer and Nutrition (EPIC) studies a large multicentre
prospective cohort study described earlier in Table 2 the association between breast cancer
risk and isoflavones was supported in 333 women (p lt 005) (Grace et al 2004) but in
another larger EPIC study conducted in Utrecht (n=15555) no such evidence was found
(Keinan-Boker et al 2004) Analyses with pooled data sets are ongoing In the meantime
Boyapati et al (2005) provide evidence from the Shanghai Breast Cancer Study24
suggesting that after a median of 52-years follow-up soy intake pre-diagnosis is not related
to disease-free survival in women with breast cancer (n=1459)
Vitamin D
Goodwin et al (2009) measured vitamin D (usually obtained from sunlight through the skin
but also found in oily fish and eggs) levels in the stored blood of women with early breast
cancer (n=512) The mean follow-up was 116-years by which time women deficient in
vitamin D had a significantly increased risk of distant recurrence25 compared with
those who had sufficient levels (p lt 05)
Antioxidant Supplements
Despite widespread use only a few clinical or epidemiological studies have examined the
relationship between antioxidant supplements and risk of breast cancer recurrence or breast
cancer-related mortality Fleischauer et al (2003) examined recurrence and mortality
among post-menopausal women diagnosed with breast cancer (n=385) who were enrolled
into a dietary case-control study Women were contacted with a single questionnaire to
ascertain the use of nutritional supplements during 12-14 years of follow-up Antioxidant
vitamin supplement use was associated with a lower risk of breast cancer recurrence or
mortality Specifically use of vitamin C and E supplements moderately reduced risk (p lt
05) whilst vitamin E nearly halved the risk although this was not statistically
significant (p=056)
iii WEIGHT
Weight and body composition have been implicated in the development of a wide range of
cancers as well as in increased risk of recurrence or second primary cancers (Chlebowski
Aiello and McTiernan 2002) Additionally being overweight or obese can exacerbate some
23
Phytoestrogens sometimes called dietary estrogenslsquo are a group of naturally occurring plant compounds that have a similar chemical structure to estrogen they bind to estrogen receptors acting like hormone regulators
24 The Shanghai Breast Cancer Survival (SBSS) Study collected lifestyle-related factors and disease and
treatment related factors in Chinese women with breast cancer (n=2236) (Lu et al 2007) 25
The spread of cancer to parts of the body other than the place where the cancer first occurred
27
of the side-effects of cancer treatment as well as increase the risk of co-morbidities such as
diabetes and osteoporosis (Doyle et al 2006) The studies evaluated in this review thus far
further indicate weight as offering a mechanism of benefit in terms of breast cancer
outcomes Indeed the WINS and WHEL RCTs produce different outcomes when using
similar dietary interventions with weight loss in the WINS group but not the WHEL group
offering a likely explanation for improved outcomes observed in the WINS participants Since
increased adiposity (excess body fat) has been identified as a negative prognostic factor for
recurrent disease and survival after breast cancer diagnosis (Rock and Demark-Wahnefried
2002) the apparent benefit of dietary fat reduction in the intervention group could
partly result from the weight loss
Bekkering et al (2006) do not add to this evidence whilst 5 studies and one systematic
review were identified in the current review
Hebert et al (1998) studied the effect of body weight on recurrence and death in women
diagnosed with early-stage breast cancer (n=472) Body mass index (BMI) was
associated with an increased risk of recurrence at the rate of 9 for each kgm2
(equivalent to about 58-pounds for a 5 4 tall woman) For death the results were
similar but body mass index was more strongly associated increasing risk by 12
per kgm2
Additionally Lahmann et al (2004) used data from 73542 pre-menopausal and 103344
post-menopausal women taking part in the EPIC study During 47-years of follow-up 1879
cases of invasive breast cancer were identified In post-menopausal women current use
of hormone replacement therapy (HRT) modified the association between body size
and breast cancer among non-users weight body mass index and hip circumference
were positively associated with breast cancer risk (p lt 001) Obese women (BMI gt 30)
had a 31 risk compared to women with a BMI lt 25 Among pre-menopausal women hip
circumference was the only other measure significantly related to breast cancer (p lt 005)
after accounting for BMI
Enger et al (2004) conducted a retrospective follow-up study of women diagnosed with
breast cancer (n=1376) for whom complete medical records and adequate tissue
specimens existed Patients were followed for a median of 68-years after diagnosis 246 of
whom died from breast cancer Compared with women in the lowest category of weight
(lt133lb [60kg] at diagnosis) women in the highest category ( 175lb [79kg])
experienced a 25-fold increased risk of dying from breast cancer (P lt 05) Women with
hormone-receptor negative cancer experienced an approximately 2-fold higher risk of dying
from breast cancer compared with women who presented with hormone-receptor positive
cancer Women in the upper 50th percentile of weight with hormone-receptor negative cancer
had a nearly 5-fold increased risk of dying from cancer compared with women in the lower
50th percentile of weight and hormone-receptor positive cancer (p=10)
In order to determine whether weight prior to diagnosis and weight gain after diagnosis are
predictive of breast cancer survival Kroenke et al (2005) followed 5204 participants from
the Nursesrsquo Health Study diagnosed with incident invasive non-metastatic breast cancer
After a median of 9-years follow-up there were 860 total deaths 533 breast cancer deaths
28
and 681 recurrences (defined as secondary lung brain bone or liver cancer and death from
breast cancer) Weight before diagnosis and weight gain after diagnosis were related
to higher rates of breast cancer recurrence and mortality although associations were
most apparent in women who had never smoked (p lt 05) Furthermore associations
with weight were stronger in pre-menopausal than in post-menopausal women In contrast
by comparing breast cancer survivors (n=3215) with women in the comparison group of a
dietary intervention trial to prevent breast cancer recurrence Caan et al (2008) found that
neither moderate (5ndash10) nor large (gt10) weight gain post-diagnosis was associated with
an increased risk of breast cancer recurrence in the early years post-diagnosis (median time
of 737-months from diagnosis)
More recently Patterson et al (2010) reviewed published epidemiological research on
lifestyle and breast cancer outcomes reporting that the most consistent finding from
observational studies was that adiposity was associated with a 30 increased risk of
cancer-related mortality
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in breast cancer
survival Four studies were identified in the current review
In an observational study Manjer et al (2000) compared the survival of patients with breast
cancer (n=792) who had never smoked were smokers or were ex-smokers Follow-up of
breast cancer cases was through record-linkage with the Swedish Cause of Death Registry
During a mean follow-up of 121-years smokers and ex-smokers compared with those
who had never smoked had a significantly increased risk of death from cancer
Fentiman et al (2005) add to this evidence with a cohort study of breast cancer patients who
completed a lifestyle questionnaire at the time of diagnosis (n=166) They found that
smoking was the third most important predictor of breast cancer-specific and overall
survival after stage and age at diagnosis This suggests that smokers are not only more
likely to die of cancer but also of other diseases when compared with those who have never
smoked
In a much larger study Holmes et al (2007) conducted a prospective observational study
among 5056 women from the Nursesrsquo Health Study with stages I-III invasive breast
cancer Information on smoking was available for these women who were followed until
January 2002 or death whichever came first Compared with women who had never
smoked women who were current smokers had a 43 increased risk of death from
any cause with risk increasing along with more cigarettes smoked per day (p lt0001)
In contrast there was no association with current smoking and breast cancer death
Sagiv et al (2007) followed women diagnosed with a first primary breast cancer (n=1273)
for 5-6 years and found that the number of all-cause mortality (n=188) including breast
cancer-specific mortality (n=111) was slightly higher among current and former
active smokers compared with women who had never smoked No association was
found between active or passive smoking and breast cancer-specific mortality
29
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in breast cancer
survival In the current review one review and 2 studies were identified
Rock and Demark-Wahnefried (2002) reviewed the evidence from clinical and epidemiologic
studies reporting that alcohol intake was not associated with breast cancer survival in the
majority of the studies In contrast post-menopausal women (n=125) diagnosed with
invasive breast cancer who were followed through to survival demonstrated that pre-
diagnosis alcohol consumption of at least one drink per week was associated with a
27-fold increase in risk of cancer-related mortality (McDonald et al 2002) In a similar
study a larger sample of women (n=1286) diagnosed with invasive breast cancer who were
followed from diagnosis through to survival produced opposing findings compared with
non-drinkers women who consumed alcohol in the 5-years before diagnosis had a
decreased risk of cancer-related mortality (Reding et al 2009)
SUMMARY OF LIFESTYLE EVIDENCE FOR BREAST CANCER ndash MECHANISMS
OF BENEFIT
Physical Activity Physical activity is likely to prevent breast cancer via its effect on
hormones specifically by reducing levels of oestrogen in the body (Friedenreich et al 2010)
or shifting the metabolism of oestrogen to favour production of 2-hydroxyestrone (2-OHE1)26
as opposed to16α-hydroxyestrone (16α=OHE1) the former of which has much weaker
estrogenic activity This shift might also be the result of a change in lean body mass resulting
from physical exercise (Campbell et al 2007) The survival benefits of physical activity
appear to require a certain intensity or level of exertion specifically 3 MET-hours or more per
week (Holmes et al 2005 Holick et al 2008 Saxton et al 2010) this equates to moderate
intensity activity such as using a stationary bike for 1-hour However there is also evidence
of a dose-effect with greater activity (up to 239 MET-hours per week) being associated with
reduced risk of recurrence and cancer-related mortality (Holmes et al 2005) or indeed
greater levels of activity than pre-diagnosis being associated with reduced risk of recurrence
and cancer-related mortality (Irwin et al 2008 Holick et al 2008 Patterson et al 2010
Saxton et al 2010)
Diet Evidence for the role of dietary fat in breast cancer development and survival are
varied Case-control (Kyogoku et al 1992) and large prospective studies (Holmes et al
1999) do not show any significant link whilst some studies have found that dietary fat does
increase risk of recurrence or death in pre-menopausal women Indeed the large multicentre
WINS trial found a protective benefit of a reduced fat dietary intervention which was more
prominent in women diagnosed with hormone-receptor negative breast cancer (Chlebowski
et al 2006a Chlebowksi et al 2008) The differential effect of diet on hormone-receptor
positive and negative disease indicate that metabolic mechanisms involving insulin and
26
Sometimes referred to as a lsquogood estrogenrsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
30
insulin-like growth factor-1 (IGF-1)27 may be involved in the mechanisms of benefit and
although not statistically significant data has been presented suggesting that elevated
insulin concentrations (a marker of insulin resistance) may be influenced by dietary fat
reduction (Khaodhiar et al 2003 Borugian et al 2004) However this might be due to
changes in weight produced by a low fat diet rather than the lower consumption of fat itself
(Borugian et al 2004) Since low fat diets are often accompanied by high intakes of fruit
and vegetables various components of a diet comprising high levels of fruit and vegetables
have been investigated Carotenoids have received particular attention with evidence
suggesting that carotenoids play a role in survival (Ingram 1994) Other studies have found
this not to be the case (Pierce et al 2007) with the primary difference in these studies being
lack of weight loss This indicates that the mechanism of benefit produced from low fat high
fruit and vegetable (particularly carotenoids) diets is most probably through changes in body
composition Indeed the majority of studies in this review demonstrated a link between
weight and cancer-related risks (Hebert et al 1998 Enger et al 2004 Lahmann et al
2004 Patterson et al 2010)
Smoking Evidence pertaining to the smoking clearly demonstrates a link between
breast cancer survival and a history of smoking However it appears to be more likely to
increase all-cause mortality as opposed to cancer-specific mortality (Fentiman et al 2005
Holmes et al 2007 Sagiv et al 2007)
Alcohol Although the evidence is less clear pre-diagnosis alcohol consumption does
appear to be related to survival (McDonald et al 2002 Reding et al 2009) although
current drinking does not (Demark-Wahnefried 2002)
27
IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of
pathological states including cancer
31
Table 3 Breast Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Campbell et al (2007)
RCT examining the effects of 12-weeks of aerobic exercise training on 2-OHE
1 and 16α-OHE
1 in
premenopausal women Randomisation to 1) A 12-week individualised supervised moderate-to-vigorous intensity aerobic exercise training intervention (n = 17) Participants began the exercise program in the early follicular phase of the next menstrual cycle (days 1-5) The intervention was divided into three blocks (a) Weeks 1 ndash 4 ndash 3 sessions per week of base aerobic training progressing from 20-40 minutes on a stationary bike (b) Weeks 5-8 ndash 4 sessions per week Two sessions were base aerobic training sessions for 30-45 minutes (c) Weeks 9 -12 ndash 4 sessions per week with two base aerobic training sessions for 30-45 minutes and two interval sessions 2) Usual lifestyle (n = 15) Participants were asked to maintain their usual activity levels for the duration of the study Following the control cycle the first day of the next menstrual cycle was used as the reference start date for participants in the control group On completion of the 12-week post-intervention
Healthy regularly menstruating Caucasian women (n=32) 20-35 years
On completion of the 12-week intervention
Height body mass body composition by dual-energy X-ray absorptiometry and VO2max were measured at baseline and following the intervention Urine samples were collected in the luteal phase of four consecutive menstrual cycles
Participants attended an average of 40-44 (91) sessions Fourteen of 17 (82) participants completed at least 80 of the sessions The exercise group increased VO2max by 14 and had significant although modest improvements in fat and lean body mass No significant between-group differences were observed however for the changes in 2-OHE1 (P = 0944) 16α-OHE1 (P= 0411) or the ratio of 2-OHE1 to 16α-OHE1 (P = 0317) At baseline there was an inverse association between body fat and 2-OHE1 to 16α-OHE1 ratio (r = minus040 P = 0044) however it was the change in lean body mass over the intervention that was positively associated with a change in 2-OHE1 to 16α-OHE1 ratio (r = 043 P = 0015)
32
measurement participants were given guidance for starting an individualised exercise program and access to the fitness facility for 4-weeks
Friedenreich et al (2010)
A two-centre two-arm RCT examining how an aerobic exercise intervention influences
circulating
estradiol oestrone sex hormonendashbinding globulin
(SHBG)
androstenedione and testosterone levels which may
be involved in the
association between physical activity and
breast cancer risk
Randomisation to 1) A 1-year aerobic physical activity programme of 225-minutes per week (n=160) 2) Control group maintained their usual level of activity (n=160)
Older (50gt years) post-menopausal sedentary women (n=320)
On completion of the intervention
Estradiol and sex hormone-binding globulin levels Androstenedione and testosterone levels
Completion of the study was high (966) At 12-months statistically significant reductions in
estradiol (treatment effect ratio
[TER] = 093 95 CI 088 to 098) and free estradiol (TER = 091
95 CI 087 to 096) and increases in SHBG (TER = 104 95 CI
102 to 107) were observed in the exercise group compared with
the control group No significant differences in oestrone
androstenedione and testosterone levels were observed between
exercisers and controls at 12-months
Holick et al (2008)
Prospective cohort study examining the relationship between post-diagnosis recreational physical activity and risk of breast cancer death
Women with a history of previous invasive breast cancer diagnosed between the ages of 20-79 years (n=4482)
Maximum of 6-years post-diagnosis (median=56-years post-diagnosis)
Mortality from breast cancer mortality from any cause Self-reported physical activity converted to MET-hours per week
After adjusting for age at diagnosis stage of disease state of residence interval between diagnosis and physical activity assessment body mass index menopausal status hormone therapy use energy intake education family history of breast cancer and treatment modality compared with women expending lt28 MET-hwk in physical activity women who engaged in greater levels of activity had a significantly lower risk of dying from breast cancer (HR 065 95 CI 039-108 for 28-79 MET-hwk HR 059 95 CI 035-101 for 80-209 MET-hwk and HR 051 95 CI 029-089 for ge210 MET-hwk P for trend = 005) Results were similar for overall survival (HR 044 95 CI 032-060 for ge210 versus lt28 MET-hwk P for trend lt0001) and were similar regardless of a womanlsquos age stage of disease and body mass index
Holmes et al (2005)
Prospective observational study
(Nurseslsquo Health Study) to determine whether physical activity among
women with breast cancer
2987 female registered nurses
in the
Nurseslsquo Health
Women were diagnosed between 1984 and
Breast cancer mortality risk according
to
physical activity
Compared with women who engaged in less than 3 MET-hours per
week of physical activity the adjusted relative risk (RR) of death
from breast cancer was 080 (95 CI 060-106) for 3 to 89 MET-hours per week 050
(95 CI 031-082) for 9 to 149 MET-hours
33
decreases their risk of death from
breast cancer compared with
more sedentary women
Study diagnosed with stage
I II or III
breast cancer
1998 and followed until death or June 2002
category (lt3 3-89 9-149 15-239
or 24
metabolic equivalent task [MET] hours per week)
per week 056 (95 CI 038-084) for 15 to 239 MET-hours per
week and 060 (95CI 040-089) for 24 or more MET-hours per week (P for trend
= 004) Three MET-hours is equivalent to walking
at average pace of 2 to 29 mph for 1 hour The benefit of physical
activity was particularly apparent among women with hormone-
responsive tutors The RR of breast cancer death for women with hormone-responsive
tumours who engaged in 9 or more MET-hours
per week of activity compared with women with hormone-
responsive tumours who engaged in less than 9 MET-hours per
week was 050 (95 CI 034-074) Compared with women who
engaged in less than 3 MET-hours per week of activity the absolute
unadjusted mortality risk reduction was 6 at 10 years for women
who engaged in 9 or more MET-hours per week
Irwin et al (2008)
The Health Eating Activity and Lifestyle Study (HEAL) Prospective observational study investigating the association between pre- and post-diagnosis
physical activity (as well as
change in pre-diagnosis to post-diagnosis
physical activity) and
mortality among women with breast cancer
A subsample of participants from the HEAL study ndash 933 women diagnosed with local or regional breast cancer between 1995
and 1998
5 -8 years from diagnosis (median=6-years)
Primary outcomes total deaths
and breast
cancer deaths
Compared with inactive women the multivariable hazard ratios
(HRs) for total deaths for women expending at least 9 MET-
hours per week (approximately 2-3 hwk of brisk walking) were 069
(95 CI 045 to 106 P = 045) for those active in the year before
diagnosis and 033 (95 CI 015 to 073 P = 046) for those active
2-years after diagnosis Compared with women who were inactive
both before and after diagnosis women who increased physical
activity after diagnosis had a 45 lower risk of death (HR = 055
95 CI 022 to 138) and women who decreased physical activity
after diagnosis had a four-fold greater risk of death (HR = 395 95
CI 145 to 1050)
Ligibel et al (2008)
RCT examining the impact of physical activity on insulin levels Participants were randomly assigned to one of two conditions a)Physical activity intervention a 16-week supervised strength training and home-based cardiovascular training protocol (two supervised 50-minute strength training
sessions per
week and 90-minutes of home-based
aerobic physical activity
weekly) b) Control group routine care for 16-weeks before being offered consultation with an physical activity
Overweight sedentary stage
I-III breast
cancer survivors (n=101)
On completion of the 16-week intervention
Fasting insulin and glucose levels Weight body composition
and
circumference at the waist and hip
18 women withdrew consent andor did not complete the study
Baseline and 16-week measurements were available for 82 patients
Fasting insulin concentrations decreased by an average of
286 microUmL in the exercise group (P = 03) with no
significant change in the control group (decrease of 027 microUmL P
=
65) The change in insulin levels in the exercise group seemed
greater than the change in controls but the comparison
did not reach statistical significance (P = 07) There was a
trend toward improvement in insulin resistance in the exercise
group (P = 09) but no change in fasting glucose levels The
exercise group also experienced a significant decrease in hip
measurements with no change in weight or body composition
34
trainer at the end of the control
period
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer outcomes
Breast cancer Not reported Additional breast cancer events and mortality
Although observational data were not consistent physical activity appeared to be associated with a 30 decreased risk of mortality
Saxton et al (2010)
A review of studies pertaining to physical activity and cancer mortality
All cancers with more evidence obtained for breast cancer
Not reported Survival A number of prospective cohort studies have reported negative associations between physical activity and cancer mortality The most compelling observational evidence of the survival benefits to be gained from a physically active lifestyle has emerged from studies of post-diagnosis physical activity in breast and colorectal cancer survivors These studies have shown clear inverse associations between post-diagnosis activity and survival with the benefits being independent of age gender obesity and disease stage at diagnosis Three of the four cohort studies of breast cancer survivors showed that women who are achieving the equivalent of 30-miniutes of moderate intensity PA on five or more days of the week can halve their risk of mortality up to 8 years of follow-up
DIET
Borugian et al (2004)
Prospective cohort study testing the hypothesis that elevated wait-to-hip ratio is directly related to breast cancer
mortality
603 patients with incident
breast
cancer
Up to 10-years
Date of death and
primary and secondary cause of death
After adjustment for age BMI family history oestrogen
receptor (ER) status tumour stage at diagnosis and systemic
treatment (chemotherapy or tamoxifen) WHR was directly related to
breast cancer mortality in postmenopausal women (for highest
quartile vs lowest relative risk = 33 95 confidence interval
11 104) but not in premenopausal women (relative risk = 12
95 confidence interval 04 34) Stratification according to
ER
status showed that the increased mortality was restricted to ER-
positive postmenopausal women Elevated WHR was confirmed as
a predictor of breast cancer mortality with menopausal status and
ER status at diagnosis found to be important modifiers of that
relation
Boyapati et al (2005)
As part of the Shanghai Breast Cancer Cohort Study associations between soy and breast cancer survival were investigated
1459 breast cancer patients
52-years Disease-free survival
Soy intake pre-diagnosis was unrelated to disease-free breast cancer survival (adjusted hazard ratio [HR]=099 95 confidence interval [CI] 073-133 for the highest tertile compared to the lowest tertile) The association between soy protein intake and breast cancer survival did not differ according to ERPR status tumour stage age at diagnosis body mass index (BMI) waist to hip ratio (WHR) or menopausal status
Boyd et al (2003)
Meta-analysis of casendashcontrol and cohort studies published up to July 2003 which examined the
Varied Not reported Cancer incidence A total of 45 published studies containing 46 estimates of risk examined the role of dietary fat in relation to breast cancer risk by an analysis of nutrient intake Of these 31 were case control and
35
association of dietary fat or fat-containing foods with risk of breast cancer
14 were cohort in design and they contained a total of 25015 cases of breast cancer and over 580 000 control or comparison subjects The summary relative risk comparing the highest and lowest levels of intake of total fat was 113 (95 CI 103ndash125) Cohort studies (n=14) had a summary relative risk of 111 (95 CI 099ndash125) and casendashcontrol studies (N=31) had a relative risk of 114 (95 CI 099ndash132) Significant summary relative risks were also found for saturated fat (RR 119 95 CI 106ndash135) and meat intake (RR 117 95 CI 106ndash129) Combined estimates of risk for total and saturated fat intake and for meat intake all indicate an association between higher intakes and an increased risk of breast cancer Casendashcontrol and cohort studies gave similar results
Cade et al 2007)
A large UK cohort study comprising women with a wide range of different eating patterns to study the effects of different food and nutrient intakes on long-term health outcomes
35372 women (350 post- and 257 pre- menopausal women developed breast cancer)
Approx 75-years
Breast cancer incidence
In pre-menopausal but not post-menopausal women a statistically
significant inverse relationship was found between
total fibre intake and risk of breast cancer (P for trend = 001) The
top quintile of fibre intake was associated with a hazard ratio
of 048
[95 CI 024ndash096] compared with the lowest quintile Pre-
menopausal fibre from cereals was inversely associated with risk
of breast cancer (P for trend = 005) and fibre from fruit had a
borderline inverse relationship (P for trend = 009)
Chlebowski et al (2006a)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
randomisation to death from any cause
Attrition in the dietary intervention (n=44) versus control group (n=66) Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to
345] versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group A total of 277 relapse
events (local regional distant or ipsilateral breast cancer
recurrence or new contralateral breast cancer) have been reported
in 96 of 975 (98) women in the dietary group and 181 of 1462
(124) women in the control group The hazard ratio of relapse
events in the intervention group compared with the control group
was 076 (95 CI = 060 to 098 P = 077 for stratified log rank
and P = 034 for adjusted Cox model analysis)
36
dietary guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
Chlebowski et al (2008)
A protocol-mandated survival analysis update to the interim analysis of WINS (Chlebowski et al 2006a)
Breast cancer patients (n=2437)
Approximately 7-years
Overall survival Attrition in the intervention group (n=236) versus control group (n=172) Although fewer deaths were seen in the intervention group this was not statistically significant In 362 women with ER- and (progesterone receptor) PR- disease a significant overall survival benefit was seen in the intervention group (75 vs 181 cumulative mortality)
Cho et al (2003)
A prospective analysis of the relationship
between dietary fat
intake and breast cancer risk among pre-menopausal
women enrolled in
the Nurseslsquo Health Study
Pre-menopausal women (n=90655) aged between 26-46 years old when recruited in 1991
8-years after recruitment (1991-1999)
Fat intake was
assessed with a food-frequency questionnaire at baseline
in 1991
and again in 1995
During 8-years of follow-up 714 women developed incident
invasive breast cancer Relative to women in the lowest quintile of
fat intake women in the highest quintile of intake had a
slight increased risk of breast cancer (RR = 125 95 CI = 098
to 159 Ptrend = 06) The increase was associated with intake
of
animal fat but not vegetable fat RRs for the increasing quintiles of
animal fat intake were 100 (referent) 128 137 154 and 133
(95 CI = 102 to 173 Ptrend = 002) Intakes of both saturated and
monounsaturated fat were related to modestly elevated breast
cancer risk Among food groups contributing to animal fat red meat and high-fat dairy foods were each associated
with an increased
risk of breast cancer Information on oestrogen-receptor status was available for
80 (n = 570) of breast cancers and progesterone-
receptor status for 78 (n = 558) When divided according to
oestrogen and progesterone receptor status the positive
association between animal fat intake and breast cancer risk was
stronger among women with oestrogen receptor-positive or
progesterone receptor-positive cancers than among women with hormone receptor-negative cancers however the difference was not statistically significant
Dwyer et al (2008)
A sub-analysis of participants in the WINS trial (Chlebowski et al 2006a)
Breast cancer patients (n=550)
12-months of intervention
Disease-free survival
Attrition in the intervention group (n = 23 11) versus control group (n = 16 5)At baseline neither mean fat intake nor flavonoid intake differed between groups After 12-months of intervention dietary fat intake was significantly lower among those on the very low-fat diet (n =195) whilst flavonoid intake remained similar in both groups Neither total flavonoid intake nor intake of subclasses of flavonoids differed between those who had dramatically decreased their fat intake and those who had not
Fleischauer et al (2003)
Case-control study testing the hypothesis that antioxidant
385 post-menopausal
12-14-years Breast cancer recurrence or
Antioxidant supplement users compared with non-users were less likely to have a breast cancer recurrence or breast cancer-related
37
supplements may reduce the risk of breast cancer recurrence or breast cancer-related mortality
women with breast cancer
death death (OR = 054 95 CI = 027-104) Vitamin E supplements showed a modest protective effect when used for more than 3 years (OR = 033 95 CI = 010-107) Risks of recurrence and disease-related mortality were reduced among women using vitamin C and vitamin E supplements for more than 3 years
Gold et al (2009)
Secondary analysis of a purposive sample of WHEL participants to determine if a low-fat diet high in vegetables fruit
and fibre affects
prognosis in breast cancer survivors
with or without hot flashes (HF) after treatment Randomisation to one of two groups 1)An intensive telephone counselling intervention based on social cognitive theory promoted a daily dietary intake of
5 vegetable
servings 16oz of vegetable juice 3
fruit servings 30g fibre and 15-20 of energy
from fat
2) Control group received printed
materials (but no counselling) promoting the
5-a-day guidelines
of
daily intakes of 5 servings of fruit and
vegetables more than 20g of fibre and less than
30 of energy from fat
2967 women (96 of all enrolled in the WHEL study) whose baseline hot flush severity
report in
the prior 4-weeks was available
4-years into the intervention
Primary end points additional breast cancer events
(localregio
nal recurrence or distant metastasis or new primary
breast
cancer) and death from any cause
The intervention group consumed significantly more daily vegetablefruit
(54 higher)
fibre (31 higher) and less
percent energy from fat (14 lower) than the comparison group
HF-negative women in the intervention had 31 fewer events than
the comparison group The intervention did not affect prognosis in
the women with baseline HFs Compared with HF-negative women in the comparison group
HF-positive women had significantly fewer
events in both groups
Goodwin et al (2009)
A prospective cohort study examining the influence of vitamin D on breast cancer prognosis
512 women with early breast cancer
Mean = 116-years
Cancer recurrence and mortality
Women with deficient vitamin D levels had an increased risk of
distant recurrence (hazard ratio [HR] = 194 95 CI 116 to
325) and death (HR = 173 95 CI 105 to 286) compared with
those with sufficient levels The association remained after
individual adjustment for key tumour and treatment related factors but was
attenuated in multivariate analyses (HR = 171 95 CI
102 to 286 for distant recurrence HR = 160 95 CI 096 to
264 for death)
Grace et al (2004)
Prospective study (EPIC) examining associations between phytoestrogen and breast cancer risk 114 spot urines and 97 available serum
333 women (aged 45ndash75 years) drawn from the EPIC
Not reported Phytoestrogen concentrations and breast cancer incidence
Phytoestrogen concentrations in spot urine (adjusted for urinary creatinine) correlated strongly with that in serum with Pearson correlation coefficients gt 08 There were significant relationships (P lt 002) between both urinary and serum concentrations of
38
samples from women who later developed breast cancer Results were compared with those from 219 urines and 187 serum samples from healthy controls matched by age and date of recruitment
study isoflavones across increasing tertiles of dietary intakes Urinary enterodiol and enterolactone and serum enterolactone were significantly correlated with dietary fibre intake (r = 013ndash029) Exposure to all isoflavones was associated with increased breast cancer risk significantly so for equol and daidzein For a doubling of levels odds ratios increased by 20ndash45 [log2 odds ratio = 134 (106ndash170P = 0013) for urine equol 146 (105ndash202 P = 0024) for serum equol and 122 (101ndash148 P = 0044) for serum daidzein]
Howe et al (1990)
Pooled analysis of 12 case-control studies of diet and breast cancer risk
Healthy women Not reported Breast cancer incidence
A consistent statistically significant positive association was found
between breast cancer risk and saturated fat intake in
postmenopausal women (relative risk for highest vs lowest quintile
146 P lt0001) A consistent protective effect for a number of
markers of fruit and vegetable intake was demonstrated vitamin C
intake had the most consistent and statistically significant inverse
association with breast cancer risk (relative risk for highest vs
lowest quintile 069 P lt0001)
Holm et al (1993)
Interviews regarding diet history the purpose being to determine whether dietary habits are associated with disease-free survival
in patients with
breast cancer who have undergone treatment
240 women with stage I-II breast cancer (50ndash65 years old) 209 of whom were post-menopausal
4-years Disease-free survival
Cancers were classified as oestrogen receptor (ER) rich ( 010
fmolmicrog of DNA) in 149 patients and as ER poor (lt010 fmolmicrog
of
DNA) in 71 patients Fifty-two patients had treatment failure during
follow-up The 30 patients with ER-rich tumours who had treatment
failure reported higher intakes of total fat saturated fatty acids and
polyunsaturated fatty acids than did the 119 patients with ER-rich
tumours that did not have treatment failure The multiple-odds ratio
(OR) for treatment failure in these women was 108 for each 1
increment in percentage of total energy (E) from total fat For
treatment failure within the first 2 years the OR was 119 for each
1-mg increase in vitamin E intake per 10 mega joules of energy In
women with treatment failure 2ndash4 years after diagnosis Ors were
113 and 123 for each E increment in total fat or saturated fatty
acids respectively No association between dietary habits and
treatment failure was found for women with ER-poor cancers
39
Holmes et al (1999)
Cohort study (Nurseslsquo Health Study)
to determine whether intakes
of fat and fatty acids are associated
with breast cancer
88795 women free of cancer (2956 developed breast cancer)
14-years Relative risk of invasive breast
cancer for
an incremental increase of fat intake
Compared with women obtaining 301 to 35 of energy from fat women consuming 20 or less had a multivariate
RR of breast
cancer of 115 (95 CI 073-180) In multivariate models the RR
(95 CI) for a 5-of-energy increase was 097 (094-100) for total
fat 098 (096-101) for animal fat 097 (093-102) for vegetable
fat 094 (088-101) for saturated fat 091 (079-104) for
polyunsaturated fat and 094 (088-100) for monounsaturated fat
For a 1 increase in energy from trans-unsaturated fat the values
were 092 (086-098) and for a 01 increase in energy from
omega-3 fat from fish the values were 109 (103-116)
Hunter et al (1996)
Pooled analysis of 7 prospective studies in 4 countries to establish estimates of the relation of fat
intake
to the risk of breast cancer
Studies included
33781
9 women
Not reported Breast cancer incidence
Information about 4980 cases from studies including 337819
women was available When women in the highest quintile of
energy-adjusted total fat intake were compared with women in the
lowest quintile the multivariate pooled relative risk of breast cancer
was 105 (95 CI 094 to 116) Relative risks for saturated
monounsaturated and polyunsaturated fat and for cholesterol
considered individually were also close to unity There was little
overall association between the percentage of energy intake from
fat and the risk of breast cancer even among women whose energy
intake from fat was less than 20
Ingram et al (1994)
Cohort study evaluating the role of vitamins in breast cancer mortality
103 women 3-months post-operation for primary breast cancer
Mean= 81-months
Mortality from breast cancer
27 women died ndash 21 with advanced breast cancer and 6 from other causes The most important findings from the nutrient consumption assessment were associated with vitamin consumption in particular beta-carotene and vitamin C At high levels of consumption there were significantly fewer deaths from breast cancer only one in the group of highest beta-carotene consumers compared with eight in the intermediate group and 12 in the lowest group (trend P = 00012) equivalent figures for vitamin C were 3 7 and 11 deaths for the highest intermediate and lowest consumption groups respectively (trend P = 00286)
Keinan-Boker et al (2004)
An investigation of the association between phytoestrogen
intake and
breast cancer risk in a large prospective study in
a Dutch
population with a habitually low phytoestrogen intake (EPIC)
15555 women aged
49ndash70
years who constituted a Dutch cohort the EPIC study
Median = 52-years
Breast cancer incidence
A total of 280 women were newly diagnosed with breast cancer
during follow-up The median daily intakes of isoflavones and
lignans were 04 (interquartile range 03ndash05) and 07 (05ndash08)
mgd respectively Relative to the respective lowest intake
quartiles the hazard ratios for the highest intake quartiles for
isoflavones and lignans were 10 (95 CI 07 15) and 07 (05
11) respectively Tests for trend were non-significant
Khaodhiar et al (2003)
A subgroup analysis of WINS participants (Chlebowski et al
53 women from 3 clinical
sites
2-years after start of
Insulin resistance and dietary fat
Of those women with initial insulin resistance after 1-year women in
the intervention group saw their fasting insulin decrease by 18 plusmn 34
40
2006a) examining relationships between dietary intake and insulin resistance
who had serum insulin and lipid profiles evaluated at baseline
and
after 2-years
commencing intervention
intake microUmL in comparison fasting insulin of women in the control
group decreased by only 138 plusmn 47 microUmL Although not
quite
statistically significant these results predict that elevated insulin concentrations (a marker of insulin resistance)
may be influenced by
dietary fat reduction There were no significant differences between
the treatment groups over time and no time x treatment interactions
and no significant differences were seen between the insulin-
resistant and non-insulin-resistant subgroups
Kim et al (2006)
The Nurseslsquo Health Study a prospective cohort study examining the relationship between dietary fat and incidence of breast
cancer in
post-menopausal women
Cohort of 80375 US women
Followed for 20-years between 1980 and 2000 with questionnaire being mailed every 2-years
Incidence of breast cancer The Food Frequency Questionnaire
The multivariable relative risk for an increment of 5 of energy from
total dietary fat intake was 098 (95 CI 095 100) Additionally
specific types of fat were not associated with an increased risk of
breast cancer Furthermore secondary analyses indicated no
differences in breast cancer risk by oestrogen receptor or
progesterone receptor status However stratification by
waist circumference indicated a significant decrease in breast
cancer risk for participants with a waist circumference of 35
inches (889cm) or greater (p-trend = 004)
Kyogoku et al (1992)
The present study utilised breast cancer patients whose dietary intake was assessed 10-years previously in a case-control study to determine whether dietary intake is related prognosis
212 breast cancer patients post-surgery
Followed-up until 1987 (9-12 years)
Mortality A total of 47 breast cancer deaths were certified The 5- and 10-year relative survival rates were 785 and 753 respectively The investigation did not provide any support for the hypothesis that a high-fat diet is a survival determinant for breast cancer patients
McEligot et al (2006)
Retrospective study into the influence of diet (fat fibre vegetable and fruit intakes and micronutrients (folate carotenoids and vitamin C) on overall survival in women diagnosed with breast cancer
Post-menopausal breast cancer survivors (n = 516)
Mean of 80-months post-diagnosis
Death due to any cause
The hazard ratio [HR and 95 CI] of dying in the highest tertile compared to the lowest tertile of total fat fibre vegetable and fruit was 312 (95 CI = 179-544) 048 (95 CI = 027-086) 057 (95 CI = 035-094) and 063 (95 CI = 038-105) respectively (P le 005 for trend except for fruit intake) Other nutrients including folate vitamin C and carotenoid intakes were also significantly associated with reduced mortality (P le 005 for trend)
Pierce et al (2007)
The multicentre WHEL RCT (see Gold et al 2009 in table)
Breast cancer (n=3088) intervention (n=1537) comparison (n=1551)
After 7-years of intervention
Invasive breast cancer event (recurrence
or
new primary) or death from any cause
Attrition in the intervention group (n=38) versus control group (n=27) There were no additional health benefits of dramatically increasing intake of nutrient-rich plant-based foods relative to the comparison group
Thomson et al (2007)
Sub-analysis of a purposive sample of participants in the WHEL RCT (see Gold et al 2009 in table)
Breast cancer patients (n=207)
Not reported Oxidative stress A significant inverse association was found between total plasma carotenoid concentrations and oxidative stress
41
WEIGHT
Caan et al (2008)
Retrospective study examining whether weight gain after diagnosis of breast cancer affects the risk of breast cancer recurrence Weight change from 1-year pre-diagnosis to study enrolment was calculated
3215 women with early stage breast cancer
Median of 737-months post-diagnosis
Breast cancer recurrence
Neither moderate (5ndash10) nor large (gt 10) weight gain (HR 08 95 CI 06ndash11 HR 09 95 CI 07ndash12 respectively) after breast cancer diagnosis was associated with an increased risk of breast cancer recurrence in the early years post-diagnosis
Enger et al (2004)
A retrospective cohort study using patient medical
records electronic
cancer registry data and archived tissue
specimens to examine
correlates of body weight with mortality in early-stage breast cancer
Women (n=1376)
24-
81 years of age diagnosed with breast cancer
Median=68 years post-diagnosis
Body weight at the time of diagnosis
and
patient status (ie alive and free of breast cancer living
with breast
cancer dead of breast cancer or dead of other
cause) at
the time of longest follow-up
246 patients died from breast cancer Among patients with early-
stage disease (I and IIA) a dose-response relationship was
observed with increasing weight and likelihood of dying of breast
cancer Compared with women in the lowest category of weight (lt133lb [60 kg] at diagnosis) women in the highest category ( 17
lb
[79 kg]) experienced a 25-fold increased risk of dying from breast
cancer (HR ratio 254 [95 CI 108-600] trend P = 02) Women
with ER-negative cancer experienced an approximately 2-fold
higher risk of dying from breast cancer compared with women with
ER-positive cancer regardless of stage at diagnosis Women in the
upper 50th percentile of weight with early-stage
disease and with
ER-negative tumours had a nearly 5-fold increased risk of dying
(HR ratio 499 [95 CI 217-1148] P for interaction = 10)
compared with women in the lower 50th percentile of weight
and ER-
positive tumours
Hebert et al (1998)
Prospective cohort study examining the effect of diet and body weight on recurrence and death in breast cancer patients
472 women diagnosed with early-stage breast cancer in 1982ndash1984
Ranged from 8-10 years
Breast cancer recurrence and mortality
After accounting for disease stage and age reported baseline consumption (timesday) of butter margarine and lard (risk ratio (RR)=167 95 CI=117ndash239) and beer (drinksday) (RR=158 95 CI=115ndash217) increased the risk of recurrence There also appeared to be an increased risk associated with consumption of red meat liver and bacon corresponding to about a doubling of risk for each time per day that foods in this category were consumed (RR=193 95 CI=089ndash415) Relative body weight increased risk at the rate of 9 (RR=109 95 CI=102ndash117) for
each kgm2 (equivalent to about 58 pounds for a woman 5 4 tall) For death the results were similar but relative weight was more strongly associated increasing risk by 12 per kgm2 (RR=112 95 CI=103ndash122)
Kroenke et al (2005)
A prospective study of a purposive subsample of participants from the Nurseslsquo Health Study ndash to determine
5204 Nurseslsquo Health Study participants
2-26 years with a median
Incident breast cancer
Weight before diagnosis was positively associated with breast
cancer recurrence and death but this was apparent only in never
smokers Similarly among never-smoking women those who
42
whether weight prior to diagnosis and weight gain
after diagnosis are
predictive of breast cancer survival
diagnosed with
incident invasive non-metastatic breast cancer between
1976
and 2000
follow-up of
9-years Breast cancer recurrence Mortality for any cause Self-reported BMI
gained between 05 and 20 kgm2 (median gain 60 lb relative risk
[RR] 135 95 CI 093 to 195) or more than 20 kgm
2 (median
gain 170lb RR 164 95 CI 107 to 251) after diagnosis had an
elevated risk of breast cancer death during follow-up (median 9
years) compared with women who maintained their weight (test for
linear trend P = 03) Associations with weight were stronger in
premenopausal than in postmenopausal women
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer
Breast cancer Not reported Additional breast cancer events and mortality
The most consistent finding from observational studies was that adiposity was associated with a 30 increased risk of mortality
SMOKING
Holmes et al (2007)
A prospective observational study among 5056 women from the Nurseslsquo Health Study for whom data on smoking history was available
Women with Stages I-III invasive breast cancer diagnosed between 1978 and 2002
Median = 83 years
Death by any cause Cause of death was ascertained from death certificates supplemented as needed with physician review of medical records
Compared with never smokers women who were current smokers had a 43 increased adjusted relative risk (RR) 95 CI 124-165] of death from any cause A strong linear gradient was observed with the number of cigarettes per day smoked p-trend lt00001 the RR (95 CI) for 1-14 15-24 and 25 or more cigarettes per day was 127 (101-161) 130 (108-157) and 179 (147-219) In contrast there was no association with current smoking and breast cancer death the RR (95 CI) was 100 (083-119) Current and past smokers were more likely than never smokers to die from primary lung cancer chronic obstructive pulmonary disease and other lung diseases
Fentiman et al (2005)
Cohort study testing the hypothesis that smokers have a worse breast cancer prognosis
Women (n=166) with stage III invasive breast cancer
Mean = 132-months
Overall and cancer-specific disease-free survival
Smoking was the third most important predictor of distant relapse-free breast cancer-specific and overall survival after stage and age at diagnosis
Manjer et al (2000)
Cohort study examining whether smoking is associated with prognostic markers other than more advanced disease (eg hormone receptor status histopathology and tumour differentiation)
268 women with recurring breast cancer drawn from a cohort of 10902 women (35 smokers)
An average of 124-years
Hormone receptor status identified by tumour tissue
The relative risk (RR) of oestrogen receptor-negative tumours was for current smokers 221 [95 CI 123-396] and for ex-smokers 267 (95 CI 141-506) compared to never-smokers Ex-smokers had an increased risk of progesterone receptor-negative tumours (RR = 161 95 CI 107-241) but there were no other significant associations between smoking habits and oestrogen receptor-positive or progesterone receptor-positive or ndashnegative tumours The incidence of Nottingham grade III tumours was higher in ex-smokers than in never-smokers (RR = 203 95 CI 117-354)
Sagiv et al (2007)
Cohort study examining the association between active and passive cigarette smoking before
Women with invasive breast cancer
Approximately 6-years after
All-cause mortality including breast
The adjusted hazards ratios (HRs) for all-cause mortality were slightly higher among current and former active smokers compared with never smokers (HR 123 95 CI 083ndash184) and 119 (95
43
breast cancer diagnosis and survival (n=1273) participating in a population-based casendashcontrol study
diagnosis cancer-specific mortality as reported to the National Death Index
CI 085ndash166) respectively) No association was found between active or passive smoking and breast cancer-specific mortality All-cause and breast cancer-specific mortality was higher among active smokers who were postmenopausal (HR 164 95 CI 103ndash260 and HR 145 95 CI 078ndash270 respectively) or obese at diagnosis (HR 210 95 CI 103ndash427 and HR 197 95 CI 089ndash436 respectively)
ALCOHOL
McDonald et al (2002)
Prospective cohort study examining the influence of alcohol consumption on breast cancer survival in African American women
Post-menopausal African-American women with invasive breast cancer (n=125)
Followed for survival through December 1998 (median = 648 months)
Survival Pre-morbid alcohol consumption of at least one drink per week was associated with 27-fold increase in risk of death (95 CI 13ndash58)
Reding et al (2009)
Sub-analysis of participants from two case-control studies to examine the effects on prognosis of alcohol consumption after breast cancer diagnosis
1286 women diagnosed with invasive breast cancer at age le45 years from two population-based case-control studies
Followed from their diagnosis of breast cancer (between January 1983 and December 1992) through to June 2002
The primary mortality endpoint used was all-cause mortality
After adjusting for age and diagnosis year compared with non-drinkers women who consumed alcohol in the 5 years before diagnosis had a decreased risk of death [gt0 to lt3 drinks per week hazard ratio 07 95 CI 06-095 3 to lt7 drinks per week risk ratio 06 95 CI 04-087 drinks per week risk ratio 07 95 CI 05-09]
Rock and Demark-Wahnefried (2002)
A review of evidence from clinical and
epidemiologic studies examining
the relationship between nutritional
factors and breast cancer survival
Women with breast cancer
Not reported Survival Alcohol intake was not associated with survival in the majority of the
studies that examined this relationship
44
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
colorectal cancer survival In the current review 2 studies were identified Studies are
summarised in Table 4 at the end of this section
In a cohort study self-reported leisure time physical activity was assessed in 41528
Australians among whom 526 cases of colorectal cancer were identified (Haydon et al
2006) Those who reported regular physical activity (at least once per week) prior to
diagnosis had improved cancer-specific survival (73 5-year survival) compared with
those not reporting regular physical activity (61 5-year survival) Another study of
stage III colorectal cancer survivors (n=816) over a 3-year period post-surgery and
chemotherapy showed increases in disease-free survival and overall survival with
increasing volumes of physical activity (p lt 05) (Meyerhardt et al 2005)
ii DIET
Bekkering et al (2006) report on six high fibre diet interventions that showed little effect on
the risk of colorectal cancer recurrence (McKeown-Eyssen et al 1995 MacLennan et al
1999 Alberts et al 2000 Bonithon-Kopp et al 2000 Schatzkin et al 2000 Ishikawa et al
2005) On combining data from two beta-carotene trials (Greenberg et al 1994
MacLennan et al 1999) four multivitamin trials (Greenberg et al 1994 Ponz and
Roncucci 1997 Hofstad et al 1998 McKeown-Eyssen et al 1995) and one trial containing
a multivitamin arm and an N-acetylcysteine (found in high protein foods) arm (Ponz and
Roncucci 1997) there was weak evidence of a reduction in risk of colorectal polyps
(abnormal growth of tissues in the colon) Two calcium interventions showed some
evidence of a reduced risk of recurrence (Baron et al 1999 Bonithon-Kopp et al 2000)
In the current review 5 studies provided further evidence for the role of diet in colorectal
cancer survival
Dietary Fibre
The association between dietary fibre and incidence of colorectal cancer was examined in all
participants (n=519978) taking part in the EPIC study (Bingham et al 2003) After 45-years
of follow-up self-reported dietary data for 1065 reported cases of colorectal cancer were
showed that higher dietary fibre was associated with a reduced risk of developing
large bowel cancer Interestingly the protective effect was greatest for the left side of the
colon and least for the rectum No food source of fibre was significantly more protective of
cancer incidence than others Confirmation of these findings after adjustment for folate and
with a longer follow-up has been reported (Bingham et al 2004 Norat et al 2005)
45
Red and Processed Meat
The EPIC study also offers support for the hypotheses that consumption of red and
processed meat increases colorectal cancer risk while intake of fish decreases risk
(Norat et al 2005) Meyerhardt et al (2007) support this further in a study examining dietary
patterns in stage III colorectal cancer survivors (n=1009) After a median of 53-years follow-
up a significant difference was found between those who had followed a prudentlsquo diet and
those who had followed a Westernlsquo diet
A higher intake of a Western dietary pattern post-diagnosis was associated with a
significantly worse disease-free survival (colon cancer recurrences or death) (p
lt001) The Western dietary pattern was associated with a similar detriment in overall
survival (p lt001)
Vitamin D
Ng et al (2008) examined pre-diagnosis levels of vitamin D in a cohort of participants with
colorectal cancer (n=304) from the Nursesrsquo Health Study28 which demonstrated that higher
plasma vitamin D levels were associated with a significant reduction in mortality from
any cause This indicates that lifestyle pre-diagnosis can produce post-diagnosis benefits
Dietary Supplements
A double-blind randomised placebo-controlled intervention study (the FAB2 Study) was
carried out with healthy controls (n=98) and patients with colorectal polyps (n=106) to
examine the effects of folic acid (a B vitamin found in leafy vegetables such as spinach
asparagus and lettuce) and riboflavin (a B-vitamin found in lean meats eggs nuts and
dairy products) supplements on biomarkers of colorectal cancer risk (Powers et al 2007)
Participants were randomised to receive one of four treatments
1) placebo capsule daily
2) 400μg of folic acid daily
3) 1200μg of folic acid daily
4) 400μg of folic acid with 5mg of riboflavin daily
28
One of the largest and longest running investigations of factors that influence womenlsquos health
comprising information from 238000 nurse-participants
Prudent diet High intake of fruit vegetables poultry and fish
Western diet
High intake of meat fat refined
grains sweets and desserts
46
Short-term low folic acid supplements in the range of 400μg were found to elicit a
significant increase in mucosal folate concentration causing a number of physiologic
responses that may reduce the risk of cancer recurrence This adds to the evidence that
increased fibre might be protective against cancer mortality since folate and fibre are
generally found in the same foods
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in colorectal
cancer recurrence In the current review 3 studies were identified
Dignam et al (2006) explored the impact of obesity via retrospective data from patients with
confirmed Dukes B or C colorectal cancer (n=4288) and found that very obese men and
women have an increased risk of recurrence In contrast the multicentre prospective
observational CALBG 8980 trial has shown that increased BMI during and 6-months after
adjuvant chemotherapy for stage III colorectal cancer (n=1053) was not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008)
Sinicrope et al (2010) categorised stage II and III colon cancer (n=4381) patients enrolled
in seven RCTs whilst undergoing adjuvant chemotherapy according to their BMI They
found that BMI was significantly associated with both disease-free survival and overall
survival in both men and women when compared to normal-weight controls Being
overweight was associated with improved overall survival in men whilst being underweight
was associated with significantly worse overall survival in women This demonstrates that
obesity is an independent prognostic variable in colon cancer survivors as well as showing
gender-related differences that require further investigation
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in colorectal
cancer survival and no studies were identified in the current review
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in colorectal
cancer survival Preliminary EPIC results indicate that current alcohol intake is
significantly positively associated with risk of rectal but not of colon cancer (Ferrari et
al (2007)
47
SUMMARY OF LIFESTYLE EVIDENCE FOR COLORECTAL CANCER ndash
MECHANISMS OF BENEFIT
Physical Activity There is very little evidence available for the role of physical activity in
colorectal cancer outcomes however the evidence that is available looks promising
Specifically regular physical activity of at least once per week pre-diagnosis has been found
to improve 5-year survival rates (Haydon et al 2006) This highlights the importance of
physical activity being integrated into an individuallsquos way of life even before the occurrence
of illness Furthermore long-term physical activity post-surgery can further increase chances
of recurrence-free survival and there is also evidence of a dose-effect survival benefits
increase with amount of exercise (Meyerhardt et al 2005)
Diet Whilst evidence for dietary fibre has been mixed the additional evidence presented
within this review places greater weight in favour of increased dietary fibre Indeed the
conclusion of one study was that in populations with low average intake of dietary fibre an
approximate doubling of total fibre intake from foods could reduce the risk of colorectal
cancer by 40 (Bingham et al 2003) Evidence of this protective benefit for dietary fibre is
further supported by research demonstrating that short-term low folic acid (found in fibrous
foods) supplements in the range of 400μg can reduce the risk of cancer recurrence (Powers
et al 2007) There is a general consensus that mechanisms of benefit from dietary fibre
come from increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic mucosa (tissue
that lines the colon) (Kim 2000) Evidence has also been presented supporting the
hypothesis that red and processed meat increases colorectal cancer risk while fish
decreases risk (Norat et al 2004)
Weight Two large-scale studies offer contrasting findings for the role of weight
in colorectal cancer outcomes One prospective observational study demonstrates that
increased BMI during and 6-months after adjuvant chemotherapy is not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008) The other
retrospective study demonstrates that very obese men and women have an increased risk
of recurrence Drawing on 7 RCTs Sinicrope et al (2010) provides further evidence for BMI
was being significantly associated with both disease-free and overall survival Overall there
is greater evidence showing weight to be an important predictor of colorectal cancer
outcomes There is also some evidence of gender differences being overweight was
associated with improved overall survival in men whilst being underweight was associated
with significantly worse overall survival in women There is evidently a need to explore this
differential effect more closely However there is also the need to consider the impact of
body composition on the development of other chronic conditions including diabetes and
cardio-respiratory conditions
Smoking and Alcohol Further research is needed into smoking and alcohol
consumption especially in terms of colorectal cancer prognosis There is some evidence
indicating that current alcohol intake increases risk of rectal but not colon cancer a finding
that requires further investigation to ascertain underlying mechanisms of benefit (Ferrari et
al 2007) Since alcohol can reduce absorption of folate it is possible that the mechanism
48
of benefit is as with dietary fibre intake related to stool bulk and less contact time between
carcinogens and colonic mucosa
49
Table 4 Colorectal Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Haydon et al (2006)
Incident cases of colorectal cancer were identified among participants of the Melbourne Collaborative Cohort Study and examined against self-reported physical activity
526 Australians with colorectal cancer
Median = 55 years
Body fat Disease-specific survival
Exercisers had an improved disease specific survival (hazard ratio 073 (95 CI 054ndash100) The benefit of exercise was largely confined to stage IIndashIII tumours (hazard ratio 049 (95 CI 030ndash079) Increasing per cent body fat resulted in an increase in disease-specific deaths (hazard ratio 133 per 10 kg (95 CI 104ndash171) Similarly increasing waist circumference reduced disease specific survival (hazard ratio 120 per 10 cm (95 CI 105ndash137)
Meyerhardt et al (2005)
Prospective study of recreational physical activity and prognosis
among
stage III colon cancer patients enrolled in a
RCT of post-operative adjuvant
chemotherapy (bolus 5-
fluorouracilleucovorin +- irinotecan)
816 patients with stage III colon cancer
Midway through adjuvant therapy and again 6-months post-therapy (12ndash14 months after enrolment)
Physical activity levels were measured as MET-hours-per-week Disease-free survival
Levels of physical activity were associated with significantly improved
disease-free survival among patients with stage III colon cancer After
adjustment for age gender baseline performance status N stage T
stage preoperative CEA bowel obstruction and perforation level of
differentiation treatment arm and body mass index the hazard ratio
(HR) for DFS for individuals in the highest quintile (gt25 MET-
hoursweek eg Jog 3ndash4 hoursweek or brisk walk [3ndash4 mph] daily)
was 065 (95 CI 038ndash111 p for trend = 002) compared to those
in the lowest quintile of PA This relationship varied by gender with a
HR = 033 [95 CI 011ndash099] for women (p for trend = 0046) and a
HR= 089 [95 CI 044ndash178] for men (p for trend = 03)
DIET
Bingham et al (2003)
Prospective examination of the association between dietary fibre intake and incidence of colorectal cancer in individuals taking part in the EPIC study recruited from ten European countries
519978 men and women in the EPIC study (1065 cases of colorectal cancer)
45 years
Colorectal cancer incidence
Dietary fibre in foods was inversely related to incidence of large bowel cancer (adjusted relative risk 0middot75 [95 CI 0middot59ndash0middot95] for the highest versus lowest quintile of intake) the protective effect being greatest for the left side of the colon and least for the rectum After calibration with more detailed dietary data the adjusted relative risk for the highest versus lowest quintile of fibre from food intake was 0middot58 (0middot41ndash0middot85)
Meyerhardt et al (2008)
Prospective observational study to
determine the association of dietary patterns
with cancer recurrences and
mortality of colon cancer survivors
1009 patients with stage III colon cancer who were
enrolled in
a randomized
Median = 53-years
Colon cancer recurrence and mortality
A higher intake of a Western dietary pattern after cancer diagnosis
was associated with a significantly worse disease-free survival (colon
cancer recurrences or death) Compared with patients in the lowest
quintile of Western dietary pattern those in the highest quintile experienced an adjusted hazard
ratio (AHR) for disease-free survival
of 325 (95 confidence interval [CI] 204-519 P for trend lt001)
50
adjuvant chemotherapy trial (CALGB
89803)
The Western dietary pattern was associated with a similar detriment
in recurrence-free survival (AHR 285 95 CI 175-463) and overall
survival (AHR 232 95 CI 136-396]) comparing highest to
lowest quintiles (both with P for trend lt001)
Ng et al (2008)
Nurseslsquo Health Study prospective examination of the association between pre-diagnosis
25(OH)D levels and
mortality in colorectal cancer patients
304 colorectal cancer patients
Mean = 78-months for participants still alive
Colorectal cancer mortality
Higher plasma 25(OH)D levels were associated with a significant
reduction in overall mortality (P for trend = 02)
Compared with the lowest quartile participants in the highest
quartile had an adjusted HR of 052 (95 CI 029 to 094) for
overall mortality A trend toward improved colorectal cancerndash
specific mortality was also seen (HR = 061 95 CI 031 to 119)
Norat et al (2005)
The EPIC prospective study of 478040 cancer-free men and women from 10 European countries examining meat fish and colorectal cancer risk
478040 cancer-free men and women taking part in the EPIC study
Mean=48 years
Colorectal cancer incidence
Colorectal cancer risk was positively associated
with intake of red and processed meat (highest [gt160
gday] versus lowest [lt20 gday] intake HR = 135 95 CI = 096
to
188 Ptrend = 03) and inversely associated with intake of fish (gt80
gday versus lt10 gday HR = 069 95 CI = 054 to
088 Ptrendlt001) but was not related to poultry intake In this study
population the absolute risk of development of colorectal
cancer within 10-years for a study subject aged 50 years was 171
for the highest category of red and processed meat intake and 128
for the lowest category of intake and was 186 for subjects in
the lowest category of fish intake and 128 for subjects in
the highest category of fish intake
Powers et al (2007)
A double-blind RCT (the FAB2 Study) to examine effects of folic acid and riboflavin supplements on biomarkers of colorectal cancer risk Participants were randomised to receive one of the following for 6 ndash 8 weeks 1)400μg of folic acid 1200μg of folic acid or 400μg of folic acid plus 5 mg of riboflavin 2) placebo
Healthy controls (n=98) and patients with colorectal polyps (n=106)
On completion of 6-8 week intervention
Biomarkers of folate and riboflavin status
Supplementation with folic acid elicited a significant increase in mucosal 5-methyl tetrahydrofolate and a marked increase in RBC and plasma with a dose-response Measures of riboflavin status improved in response to riboflavin supplementation Riboflavin supplement enhanced the response to low-dose folate in people carrying at least one T allele and having polyps The magnitude of the response in mucosal folate was positively related to the increase in plasma 5-methyl tetrahydrofolate but was not different between the healthy group and polyp patients
WEIGHT
Dignam et al (2006)
Investigating the association between BMI and colorectal cancer outcomes in patients from cooperative group clinical trials
4288 patients with Dukes
BC
colon cancer in National
Median =112-
years Risk of recurrence second primary
Very obese patients (BMI 35 kgm2) had greater risk
of a
colon cancer event (recurrence or secondary primary tumour hazard
ratio [HR] = 138 95 confidence interval [CI] = 110 to 173) than
normal weight patients (BMI = 185ndash249 kgm
2) Mortality was
51
Surgical Adjuvant Breast and Bowel Project
RCTs
cancer and
mortality evaluated in
relation to
BMI at diagnosis
greater for very obese (HR = 128 95 CI = 104 to 157) and
underweight (BMI lt 185 kgm2) (HR
= 149 95 CI = 117 to 191)
than for normal weight patients The increased risk of mortality for
underweight patients was dominated by nonndashcolon cancer deaths
(HR of such deaths compared with normal weight patients = 223 95 CI = 150 to
331) whereas for the very obese deaths likely due
to colon cancer were increased (HR = 136 95 CI = 106 to 173)
Meyerhardt et al (2008)
A prospective observational study of patients who had stage III colon cancer and who enrolled on a RCT of adjuvant chemotherapy Results
1053 patients who had stage III colon cancer
6-months post- chemotherapy
Patients were observed for cancer recurrence or death
Increased BMI was not significantly associated with a higher risk of colon cancer recurrence or death (P trend = 54) Compared with normal-weight patients (BMI 21 to 249 kgm
2) the multivariate
hazard ratio for disease-free survival was 100 (95 CI 072 to 140) for patients with class I obesity (BMI 30 to 349 kgm
2) and 124
(95 CI 084 to 183) for those with class II to III obesity (BMI ge 35 kgm
2) after analysis was adjusted for tumour-related prognostic
factors physical activity tobacco history performance status age and sex Similarly after analysis was controlled for BMI weight change (either loss or gain) during the time period between ongoing adjuvant therapy and 6-months after completion of therapy did not significantly impact on cancer recurrence andor mortality
Sinicrope et al (2010)
BMI (kgm2) was categorised in patients
with tumour-node-metastasis stage II and III colon carcinomas enrolled in seven RCT of 5-fluorouracilndashbased adjuvant chemotherapy to determine the association of BMI with disease-free survival and overall survival
Men and women with stage II and III colon carcinomas (n = 4381) enrolled in seven RCTs of 5-fluorouracilndashbased adjuvant chemotherapy
Not reported Disease-free survival Overall survival
BMI was significantly associated with both disease-free survival (P = 0030) and overall survival (P = 00017) Men with class 23 obesity showed reduced overall survival compared with normal-weight men [hazard ratio 135 95 CI 102-179 P = 0039] Women with class I obesity had reduced overall survival [hazard ratio 124 95 CI 101-153 P = 0045] compared with normal-weight women Overweight status was associated with improved overall survival in men (P = 0006) and underweight women had significantly worse overall survival (P = 0019)
ALCOHOL
Ferrari et al (2007)
As part of the prospective EPIC study data was collected examining the relationship between lifetime and baseline alcohol consumption and colorectal cancer incidence
478732 EPIC subjects free of cancer at enrolment between 1992 and 2000
62 years Colorectal cancer incidence
Lifetime alcohol intake was significantly positively associated to CRC risk (hazard ratio HR = 108 95CI = 104-112 for 15 gday increase) with higher cancer risks observed in the rectum (HR = 112 95CI = 106-118) than distal colon (HR = 108 95CI = 101-116) and proximal colon (HR = 102 95CI = 092-112) Similar results were observed for baseline alcohol intake When assessed by alcoholic beverages at baseline the CRC risk for beer
52
(HR = 138 95CI = 108-177 for 20-399vs 01-29 gday) was higher than wine (HR = 121 95CI = 102-144) although the two risk estimates were not significantly different from each other Higher HRs for baseline alcohol were observed for low levels of folate intake (113 95CI = 106-120 for 15 gday increase) compared to high folate intake (103 95CI = 098-109)
53
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
prostate cancer survival In the current review 2 studies were identified Studies are
summarised in Table 5 at the end of this section
The underlying mechanisms for the direct anti-cancer effect of lifestyle has been indicated in
a study with men undergoing a diet and physical activity intervention comprising the majority
of calories from complex carbohydrates high in fibre combined with 1-hour of supervised
exercise (Soliman et al 2009) Serum (blood plasma) was taken from these men and added
to androgen-dependent LNCaP cells29 in the laboratory There was decreased growth and
increased apoptosis (cell death) associated with a reduction in serum Insulin-like Growth
Factor (IGF)-130 These findings indicate that diet and physical activity interventions
might slow prostate cancer progression as well as aid in its treatment during the early
stages of development
Kenfield (2010) examined the data of 2686 men from the Health Professionals Follow-Up
Study31 and found that men who engaged in 3gt MET-hours of weekly physical activity
post-diagnosis reduced their risk of death by 35 compared with men who engaged
in less weekly activity Furthermore men who walked 90-minutes per week at a normal to
brisk pace had a 51 lower risk of death due to any cause compared with men who walked
90-minutes or less at an easy pace To reduce their risk of cancer-specific death men
had to engage in vigorous activity such as jogging (6 MET-hours)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in prostate cancer
survival In the current review 7 studies were identified
Dietary Changes plus Supplements
Ornish et al (2005) conducted a diet counselling and lifestyle RCT comprising men with
early prostate cancer (n=93) The lifestyle changes in this study included a vegan diet
supplemented with soy vitamin E fish oils selenium and vitamin C together with a
moderate physical activity program and stress management techniques such as yoga
29
Human prostate cancer cells
30 IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of pathological states including cancer
31 An all-male (n=51529) study designed to complement the all-female Nurses Health Study
54
Prostate Specific Antigen (PSA)32 levels decreased by 4 at 12-months in the
intervention group but increased by 6 in the control group this was statistically
significant and strongly correlated with the degree of lifestyle change However the
intensity of this intervention and associated behavioural changes might not easily be
translated into practice (White et al 2009)
Pomegranate Juice
The potential benefits of pomegranate juice on prostate cancer outcomes frequently appear
in the media and strong evidence of its efficacy can be found within the academic literature
In a phase II open-label single-arm clinical trial men (n=46) with recurrent prostate cancer
who had rising PSA after surgery or radiotherapy were treated daily with 8oz (227g)
equivalent of pomegranate juice (Pantuck et al 2006) Mean PSA doubling time
significantly increased with treatment from 15-months to 54-months demonstrating a
good indication of a relationship between the consumption of pomegranate juice and
prostate health
Green Tea
Another beverage found to demonstrate some positive effects on prostate cancer is green
tea Bettuzzi et al (2006) in a year-long clinical trial has demonstrated that daily
consumption of green tea can produce a ten-fold decrease in the rate at which
prostate intraepithelial neoplasia (a pre-cancerous condition) progresses to prostate
cancer Support for these findings is offered by an uncontrolled open-label single-arm
phase II clinical trial testing the efficacy of Polyphenon E which contains the polyphenol
antioxidants found in green tea (McLarty et al 2009) Taking four capsules of
Polyphenon E daily (equivalent to twelve cups of green tea) for an average of 345
days leading up to radical prostatectomy the participants (n=26) experienced
significant reductions in biomarkers used to monitor likelihood of metastasis Some
patients demonstrated reductions greater than 30
Lycopene Supplements
The EPIC study has demonstrated that similar to breast cancer prostate cancer risk is not
related to fruit and vegetable consumption (Key et al 2004) However further evidence for
the role of carotenoids found in fruit and vegetables have been provided from a pilot RCT
including men with benign prostatic hyperplasia (BPH) a benign enlargement of the prostate
that can progress to cancer (Schwarz et al 2008) Men (n=20) who received 15mg od
lycopene supplementation (a carotenoid found in tomatoes and other red fruits and
32
PSA is a protein produced by the cells of the prostate gland It is present in small quantities in the serum of normal men and is often elevated in the presence of prostate cancer
55
vegetables) for 6-months had significantly decreased PSA levels compared to a
placebo group (n=20) who had no change in PSA
Salicylate
Salicylate33 intake has been implicated in the aetiology of prostate cancer but Thomas et al
(2009) have evaluated their influence on established cancer progression In a randomised
double blind phase II study involving men (n=110) with progressive prostate cancer who
were counselled to eat less saturated fat and processed food more fruit vegetables and
legumes physical activity more regularly and to stop smoking the men were then
randomised to take sodium salicylate alone or combined with vitamin C copper and
manganese gluconates34 daily Although there was no difference in outcome between those
who received sodium salicylate alone or combined the intervention as a whole (ie
including dietary counselling) slowed or stopped the rate of PSA progression in 40
patients (364) for over one-year and a further ten patients were stabilised for 10-
months This data suggests that changes in lifestyle can potentially delay PSA progression
and the need for more radical therapy highlighting an area for further research
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in prostate cancer
survival In the current review 2 studies were identified
Wright et al (2007) prospectively examined BMI and weight change in relation to prostate
cancer incidence and mortality in 287760 men enrolled in the National Institutes of
Health-AARP Diet and Health Study Higher baseline BMI was associated with
significantly reduced total prostate cancer incidence on the one hand but with
significantly increased risk of prostate cancer mortality on the other hand Adult weight
gain from age 18-years to study entry (range=50-71-years old) was positively associated
with prostate cancer staging but not with disease incidence
In a retrospective analysis exploring the interaction between obesity and surgical outcomes
in patients with prostate cancer treated by radical prostatectomy (n=437) a weak but
significant association was observed between BMI and a number of biological
biomarkers indicative of an advanced pathological stage (Gross et al 2009)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in prostate
cancer survival and no evidence was identified in the current review
33
Salicylates are chemicals that occur naturally in many plants including many fruits vegetables and herbs
Salicylates in plants act as a natural immune hormone and preservative protecting the plants against diseases
insects fungi and harmful bacteria 34
A pinkish powder soluble in water used in medicine in vitamin tablets and as a feed additive and dietary
supplement
56
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in prostate cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR PROSTATE CANCER -
MECHANISMS OF BENEFIT
Physical Activity and Diet The evidence within this review indicates that diet and physical
activity interventions might slow prostate cancer progression as well as aid in its treatment
during the early stages of development The mechanism of benefit is primarily via
decreased growth and increased apoptosis (cell death) associated with a reduction in serum
Insulin-like Growth Factor (IGF)-1 (Soliman et al 2009) Up to 3gt MET-hours of weekly
physical activity appears sufficient to increase survival with more vigorous activity of about 6
MET-hours per week for the reduction of cancer-specific mortality (Kenfield 2010) A
number of dietary steps can be taken to reduce PSA levels and thus slow down the growth
of tumours and increase survival For example a vegan diet supplemented with soy vitamin
E fish oils selenium and vitamin C together with a moderate physical activity program and
stress management techniques such as yoga have been found useful (Ornish et al 2005)
as has pomegranate juice (Pantuck et al 2006) and green tea (Betuzzi et al 2006 McLarty
et al 2009) As with breast cancer carotenoids have been found to offer protective
properties for men with benign prostatic hyperplasia which can progress to cancer (Schwarz
et al 2008) Overall the evidence for prostate cancer is suggestive of survival benefits from
combined dietary and physical activity changes In other words it appears that a healthier
diet made up of fruit and vegetables as well as drinks such as pomegranate juice or green
tea combined with 3gt MET-hours of weekly physical activity could be an effective
prescription for reducing mortality from cancer and other causes
Weight Evidence for weight was mixed whilst finding that higher baseline BMI was
associated with significantly reduced total prostate cancer incidence a significant increase in
prostate cancer severity and mortality was also observed with higher BMI levels (Wright et
al 2007a Gross et al 2009) More research is clearly needed to establish any differential
prostate cancer outcomes associated with weight
Smoking and Alcohol More research is required for smoking and alcohol in terms of
prostate cancer outcomes
57
Table 5 Prostate Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Kenfield et al (2009)
Prospective study (Health Professionals Follow-up Study) assessing the relationship between physical activity and duration and pace of walking with total and prostate cancer-specific mortality
2686 men with prostate cancer
4-years Prostate cancer mortality and total physical activity
Men who were physically active especially those engaging in 3 or more MET-hours of total activity had a 35 lower risk of death from any cause (hazard ratio 065 [95 CI 052 082]) and a modest non-significant reduction in risk of prostate cancer death (hazard ratio 088 [95 CI 052 149]) after adjustment for other risk factors for PCa mortality and pre-diagnosis physical activity While no benefit from walking was observed for PCa mortality men who walked 4 or more hours per week versus those who walked less than 20 minutes per week had a 23 lower risk of all-cause mortality (95 CI 061 097 p-trend=001) In addition compared to men who walked less than 90 minutes at an easy walking pace those who walked 90 or more minutes at a normal to very brisk pace had a 51 lower risk of all-cause mortality (95 CI 037 064) More vigorous activity and longer duration of activity was associated with significant further reductions in risk for all-cause mortality More vigorous activity was associated with a borderline-significant reduction in risk for PCa mortality
Soliman et al (2009)
Pritikin Longevity Center 3-Week
Residential Program - men were given prepared
meals with 12ndash15 fat calories
15ndash20 protein calories and the majority
of calories (65ndash70) from unrefined complex carbohydrates high in fibre (gt40 gday) The men attended daily supervised exercise classes
for 60 min
5 men in their early sixties
with no
signs of prostate cancer (PSA lt 40)
On completion of the 3-week programme
Cancer progression
The intervention slowed growth and increased apoptosis in LNCaP cells responses that were eliminated when
IGF-I was added back to
the post-intervention samples The p53 protein content was increased
and NFkB activation reduced in the post serum-stimulated LNCaP
cells Similar results were observed when the IGF-I receptor was
blocked in the pre-intervention serum In androgen-independent PC-3
cells growth was reduced while none of the other factors were
changed by the intervention
DIET
Bettuzzi et al (2006)
A proof-of-principle double-blind placebo-
controlled clinical trial assessing the safety
and efficacy of green tea catechins for the
chemoprevention of prostate cancer incidence in patients with high-grade prostate intraepithelial
neoplasia Daily
treatment consisted of three GTCs
Men with high-grade prostate intraepithelial
neoplasia who would develop cancer within
1-year
3-monthly for 1-year
Primary outcome prostate cancer incidence Secondary outcome
After 1 year only one tumour was diagnosed (incidence 3) in the
cohort receiving green tea whereas 9 cancers were found among the placebo-treated
men (incidence 30) Total PSA did not
change
significantly between the two arms but green tea-treated men showed
values constantly lower with respect to placebo-treated ones As a
secondary observation administration of green tea also reduced lower
urinary tract symptoms suggesting that these compounds might also
58
capsules 200 mg each (total 600 mgd) (n=60) PSA levels be of help for treating the symptoms of benign prostate hyperplasia
Key et al (2004)
An examination of the association between self-reported consumption of fruits and vegetables and prostate cancer risk in EPIC participants
130544 men in 7 countries recruited into EPIC
Median = 48 years
Prostate cancer incidence
There were 1104 incident cases of prostate cancer No significant associations between fruit and vegetable consumption and prostate cancer risk were observed Relative risks (95 CI) in the top fifth of the distribution of consumption compared to the bottom fifth were 106 (084 ndash134) for total fruits 100 (081ndash122) for total vegetables and 100 (079 ndash126) for total fruits and vegetables combined intake of cruciferous vegetables was not associated with risk
McLarty et al (2009)
In order to determine the effects of short-term supplementation with the active compounds in green tea on serum biomarkers in patients with prostate cancer daily doses were provided of Polyphenon E which contained a total of 13 g of tea polyphenols until time of radical prostatectomy
26 men with positive prostate biopsies scheduled for radical prostatectomy
Not reported PSA levels Biomarkers of prostate cancer decreased significantly All of the liver function tests also decreased five of them significantly total protein albumin aspartate aminotransferase alkaline phosphatase and amylase
Ornish et al (2005)
Lifestyle changes including a vegan diet supplemented with soy vitamin E fish oils selenium and vitamin C together with a moderate physical activity program and stress management techniques such as yoga
Men with early prostate cancer (n=93) Gleason scores less than 7
12-months into the intervention
PSA and serum stimulated LNCaP cell growth
PSA levels decreased by 4 at 12-months in the intervention group but increased by 6 in the control group this was statistically significant and strongly correlated with the degree of lifestyle change
Pantuck et al (2006)
A phase II two-stage clinical trial to determine the effects of pomegranate juice PSA progression in men with a rising PSA following primary therapy Patients were treated with 8 ounces of pomegranate juice daily (570mg total polyphenol gallic acid equivalents) until disease progression
46 men with rising PSA levels post-treatment (surgery or radiotherapy)
Every 3-monhs for 54-months
PSA levels Mean PSA doubling time significantly increased with treatment from a mean of 15 months at baseline to 54 months post-treatment (P lt 0001) In vitro assays comparing pre-treatment and post-treatment patient serum on the growth of LNCaP showed a 12 decrease in cell proliferation and a 17 increase in apoptosis (P = 00048 and 00004 respectively) a 23 increase in serum nitric oxide (P = 00085) and significant (P lt 002) reductions in oxidative state and sensitivity to oxidation of serum lipids after versus before pomegranate juice
Schwarz et al (2008)
15mg od lycopene supplementation for 6-months or placebo
Men with benign prostatic hyperplasia (n=40)
After 6-months of intervention
Inhibition or reduction of increased serum PSA levels
Men receiving 15mg od lycopene supplementation had significantly decreased PSA levels compared to a placebo group who had no change in PSA
Thomas et al (2009)
A randomised double blind phase II study to evaluate the influence of salicylate and lifestyle on established cancer progression Men were counselled
110 men whose PSA had risen in 3 consecutive
Not reported Prostate cancer progression (PSA levels)
Although there was no difference in outcome between the SS or CV247 (21 v 19 p=092) the intervention slowed or stopped the rate of PSA progression in 40 patients (364) for over one year A further ten patients were stabilised for ten months Patients least likely to stabilise
59
to eat less saturated fat processed food more fruit vegetables and legumes exercise more regularly and to stop smoking They were then randomised to take sodium salicylate (SS) alone or SS combined with vitamin C copper and manganese gluconates (CV247) daily without other intervention
values gt20 over the preceding 6-months
had received previous radiotherapy or had a Gleason =7 These men welcomed this addition to active surveillance
WEIGHT
Gross et al (2009)
A retrospective cohort study examining whether changes in components of the sex steroid receptor axis may contribute to the clinical aggressiveness of prostate cancer in obese patients
539 patients treated with radical prostatectomy at a single urban hospital between 1994 and 2002
Not reported Pathological stage of prostate cancer BMI
Higher BMI correlated strongly with higher pathologic stage In comparing obese versus non-obese patients there was no difference in expression of androgen or oestrogen related proteins in cancerous epithelial cells However there was a down-regulation of aromatase in the stoma of obese patients suggesting obesity may cause stromal changes in the sex steroid production and signalling pathways which may affect prostate cancer growth via intracrineparacrine mechanisms
Wright et al (2007)
A prospective examination of BMI and adult weight change in relation to prostate cancer incidence and mortality
287760 men ages 50 years to 71 years at enrolment (1995-1996) in the National Institutes of Health-AARP Diet and Health Study
6-years Prostate cancer incidence Weight gain (BMI)
Higher baseline BMI was associated with significantly reduced total prostate cancer incidence largely because of the relationship with localized tumours (for men in the highest BMI category [gtor=40 kgm (2)] vs men in the lowest BMI category [lt25 kgm (2)] RR 067 95 CI 050-089 P = 0006) Conversely a significant elevation in prostate cancer mortality was observed at higher BMI levels (BMI lt25 kgm(2) RR 10 [referent group] BMI 25-299 kgm(2) RR 125 95 CI 087-180 BMI 30-349 kgm(2) RR 146 95 CI 092-233 and BMI gtor=35 kgm(2) RR 212 95 CI 108-415 P = 02) Adult weight gain from age 18 years to baseline also was associated positively with fatal prostate cancer (P = 009) but not with incident disease
60
d) LUNG CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in lung
cancer survival and one systematic review with meta-analysis was identified in the current
review Studies are summarised in Table 6 at the end of this section
Tardon et al (2005) conducted a systematic review and meta-analysis of cohort and case-
control studies from 1966 through October 2003 evaluating the relationship between
physical activity and lung cancer incidence Nine studies were identified 6 of which
demonstrated that that higher levels of leisure-time physical activity (walking gardening
swimming) protects against lung cancer (Severson et al 1989 Thune et al 1997 Lee et
al 1999 Sellers et al 1991 Kubik et al 2002 Mao et al 2003) The estimated combined
risk for both genders was statistically significant as was a dose-response relationship (p lt
01)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in lung cancer
survival and no evidence was identified in the current review
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in lung cancer
survival and no evidence was identified in the current review
iv SMOKING
Smoking has long been accepted as an unhealthy behaviour that increases the risk of
cancer incidence and disease outcomes Yet many people continue to smoke pre- and post-
diagnosis one-third to one-half of cancer patients either continue to smoke after diagnosis or
relapse after initial quit attempts (Gritz et al 2006) Bekkering et al (2006) do not provide
any evidence for the role of smoking in lung cancer survival In the current review 5 studies
were identified that further highlight the importance of smoking cessation support for people
living with and beyond cancer
Vineis et al (2007) have estimated exposure to Environmental Tobacco Smoke (ETS) and to
air pollution in never smokers and ex-smokers in EPIC study participants (n=520000) The
proportion of lung cancers in never- and ex-smokers attributable to ETS was
estimated to be between 16 and 24 mainly due to the contribution of work-related
exposure
61
In two studies of survivors of stage I and II small cell lung cancer risk of a second cancer
was 35-44-fold higher than in the general population (Richardson et al 1993 Tucker et
al 1997) In those who continued to smoke the risk was far higher particularly in those who
also received chest irradiation and alkylating agents35 (Tucker et al 1997) highlighting the
need for risk assessment when offering smoking cessation support or advice
Another study in Japan confirmed that patients with small cell lung cancer who survive
at least 2-years greatly reduced their likelihood of a second cancer if they quit
smoking (p lt 05) (Kawahara et al 2002) Additionally smoking has been found to be
an independent risk factor in breast cancer survivors developing lung cancer (Ford et
al 2003) In support of these studies Parsons et al (2010) report that nine of ten studies
identified in a review of literature from 1966 to 2008 indicate that continuing to smoke is
associated with a significantly increased risk of all-cause mortality in early stage non-
small cell lung cancer and of all-cause mortality in limited stage small cell lung
cancer
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in lung cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR LUNG CANCER - MECHANISMS OF
BENEFIT
Smoking Evidence for the role of lifestyle factors on lung cancer progression and
recurrence has primarily examined smoking which is a strongly established risk factor for
disease progression and mortality Continuing to smoke exposes the body to high levels of
carcinogens which can cause further DNA damage to existing cancers encourage the
cancer to mutate into a more aggressive type or develop mechanisms to hide from the
bodylsquos immunological defences (Akopyan and Bonavida 2006) Indeed smoking has been
found to suppress the immune system interfering with the function of natural killer (NK) cells
- a lymphoid cell type that plays a role in the surveillance of tumour growth Patients who
have already developed one cancer are likely to be more susceptible to DNA damage from a
pre-existing genetic vulnerability or acquired damage from chemotherapy or radiotherapy
Avoiding carcinogens may therefore have a benefit in reducing the risk of developing
further cancers in patients who may be more susceptible from a pre-existing genetic
signature or damage from chemotherapy or radiotherapy The smoking cessation initiatives
currently sweeping the nation such as NHS Choices bdquoSmokefree‟ remain invaluable as
smoking continues to be an important preventable cause of morbidity and mortality
worldwide
Additional Lifestyle Factors More research is required into lifestyle factors such as diet
physical activity weight and alcohol consumption in terms of lung cancer outcomes Access
35
Cytotoxic agents used to disrupt cancer cells can damage healthy cells in the process
62
to lifestyle services such as post-treatment rehabilitation fitness planning and nutritional
support was highlighted as an important component within the disease trajectory for people
with lung cancer (NCSI Mapping Project 2009) There is evidence for the benefits of
physical activity in reducing lung cancer incidence however there is a paucity of evidence
for the survivorship period of lung cancer
63
Table 6 Lung Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Tardon et al (2004)
A meta-analysis of studies (1966-2003) evaluating the relationship between physical activity and lung cancer
Men and women in cohort and case-control studies (9 studies)
Not reported
Lung cancer incidence
The combined ORs were 087 (95 CI=079ndash095) for moderate leisure-time physical activity (LPA) and 070 (062ndash079) for high activity (p trend = 000) This inverse association occurred for both sexes although it was somewhat stronger for women No evidence of publication bias was found Several studies were able to adjust for smoking but none adjusted for possible confounding from previous malignant respiratory disease
SMOKING
Ford et al (2003)
Retrospective analysis of smoking radiation and both exposures on lung carcinoma development in women who were treated previously for breast carcinoma
Case patients (n = 280) females aged 30-89 years with breast carcinoma prior to primary lung carcinoma Control patients (n = 300) selected randomly from 37000 patients with breast carcinoma treated at The University of Texas M D Anderson Cancer Center
Not reported
Lung cancer incidence
At the time of breast carcinoma diagnosis 84 of case patients had ever smoked cigarettes compared with 37 of control patients whereas 45 of case patients and control patients received XRT for breast carcinoma Smoking increased the odds of lung carcinoma in women without XRT (odds ratio [OR] 60 95 confidence interval [95 CI] 36-101) but XRT did not increase lung carcinoma risk in non-smoking women (OR 05 95 CI 03-11) Overall the OR for both XRT and smoking compared with no XRT or smoking was 90 (95 CI 51-159)
Kawahara et al (1998)
Prospective study to investigate whether smoking cessation after successful therapy is associated with a decrease in risk for a second
980 consecutive patients with small cell lung cancer (SCLC)
Median=67 years after initiation of
Second primary tumour
Of the patients who continued to smoke 11 (33) developed a SPT Of the 31 patients who stopped smoking after therapy only three (10) had a subsequent SPT Among those who continued to smoke the risk for a SPT was significantly increased (54 times 95 CI 27-97) relative to the general
64
primary tumour being treated with combination chemotherapy with or without chest radiotherapy
therapy population In contrast those who stopped smoking showed only a 16-fold increase (95 CI 03-46) which was not significantly different from the level in the general population The relative risk for non-SCLC was significantly increased 128-fold (95 CI 34-328) in continuing smokers No second non-SCLCs have been found among those who stopped smoking The 33 patients who continued to smoke had a significantly increased risk of a SPT (43 95 CI 11-159 P=003) Relative to the risk of SPT in patients without previous radiotherapy who stopped smoking the risk is 092 in patients without radiotherapy who continued smoking 037 in patients with radiotherapy who stopped smoking and 233 in patients with radiotherapy who continued smoking The risk of current smoking in patients with previous radiotherapy is 630 relative to those with radiotherapy who stopped smoking although this interaction is not statistically significant (P = 024)
Parsons et al (2010)
A systematic review with meta-analysis of the evidence that smoking
cessation after diagnosis
of a primary lung tumour affects prognosis Databases searched CINAHL (from 1981) Embase (from 1980) Medline
(from 1966)
Web of Science (from 1966) CENTRAL (from 1977)
to
December 2008 and reference lists of included studies
RCTs or observational
st
udies measuring
the effect of quitting smoking
post-
diagnosis on lung cancer prognosis
Patients were followed for 6-months gt in 5 studies but only at time of diagnosis treatment in 4
5-year survival using death rates for continuing smokers and quitters obtained from this review
Continued smoking was associated with a significantly increased risk of all-
cause mortality (hazard ratio 294 95 CI 115 to
754) and recurrence (186
101 to 341) in early stage non-small cell lung cancer and of all-cause
mortality (186 133 to 259) development of a second primary tumour (431 109 to 1698)
and recurrence (126 106 to 150) in limited stage small
cell lung cancer No study contained data on the effect of quitting
smoking on
cancer specific mortality or on development of a second primary tumour in
non-small cell lung cancer Life table modelling on the basis of these data
estimated 33 five year survival in 65 year old patients with early stage non-
small cell lung cancer who continued to smoke compared with 70 in
those
who quit smoking In limited stage small cell lung cancer an estimated 29
of continuing smokers would survive for five years compared with 63 of
quitters on the basis of the data from this review
Richardson et al (1993)
Retrospective review to determine the incidence of second primary cancers developing in patients surviving free of cancer for 2 or more years after treatment for small-cell lung cancer and to assess the potential effect of smoking cessation
Consecutive sample of 540 patients with small-cell lung cancer
Median=61 years
Relative risk for second primary cancers and death
55 patients (10) were free of cancer 2-years after initiation of therapy 18 of these developed one or more second primary cancers including 13 who developed second primary non-small-cell lung cancer The risk for any second primary cancer compared with that in the general population was increased four times (relative risk 44 95 CI 25-72) with a relative risk of a second primary non-small-cell lung cancer of 16 (CI 84-27) Forty-three patients discontinued smoking within 6-months of starting treatment for small-cell lung cancer and 12 continued to smoke In those who stopped smoking at time of diagnosis the relative risk of a second lung cancer was 11 (CI 44 to 23) whereas in those who continued to smoke it was 32 (CI 12 to 69)
Tucker et al (1997)
A multi-institution study to investigate the risk among survivors of developing second primary
611 patients who had
been cancer
Not reported
Population-based rates of cancer
Relative to the general population the risk of all second cancers among these
patients was increased 35-fold Second lung cancer risk was increased 13-
fold among those who received chest irradiation in comparison to a sevenfold
65
cancers other than small-cell lung carcinoma
free for more than 2 years after therapy for small-cell lung cancer
incidence and mortality
increase among non-irradiated patients It was higher in those who
continued smoking with evidence of an interaction between chest irradiation and continued smoking
(relative risk = 21) Patients treated with various forms
of combination chemotherapy had comparable increases in risk (94- to 13-
fold overall) except for a 19-fold risk increase among those treated with
alkylating agents who continued smoking
Vineis et al (2007)
Prospective study to estimate exposure to Environmental Tobacco Smoke (ETS) in never smokers and ex-smokers in 10 European countries (EPIC)
Men and women in the EPIC study (n = 520000)
Not reported
Lung cancer incidence
The proportion of lung cancers in never- and ex-smokers attributable to ETS was estimated as between 16 and 24 mainly due to the contribution of work-related exposure Also 5ndash7 of lung cancers in European never smokers and ex-smokers are attributable to high levels of air pollution as expressed by NO2 or proximity to heavy traffic roads
66
e) OTHER CANCERS
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in survival
from other cancers and no evidence was identified in the current review
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in survival from other
cancers Studies identified in the current review are summarised in Table 7 at the end of this
section
Preliminary EPIC results provide some evidence that red and preserved meat increases risk
for gastric cancer (Gonzalez et al 2006) Preliminary EPIC results also indicate that fruit
reduces gastric cancer risk whilst vegetables are not associated with risk for this type of
cancer Furthermore overall consumption of fruit and vegetables is reported to be unrelated
to risk of ovarian cancer (Schultz et al 2005) There is evidence of a protective effect of a
high intake of allium vegetables (onions garlic shallots leeks and chives) on ovarian
cancer risk (Schultz et al 2005)
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in survival from
other cancers Preliminary EPIC results reported in the current review provide some
evidence that BMI is associated with endometrial cancer risk (Kaaks et al 2002
Friedenreich et al 2007)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in survival from
other cancers Preliminary EPIC results along with 4 other studies were identified in the
current review
Gonzalez et al (2003) confirm from EPIC results that smoking is associated with gastric
cancer
Similarly Yu et al (1997) evaluated 25000 heterogeneous patients who had been treated
for lung breast or colorectal cancer and found that the 15-year survival of the people
who continued to smoke was 44 compared to 55 in those who quit
In a more recent study of survivors of early stage head and neck cancer (n=264) who
retrospectively reported their tobacco histories (pre-diagnosis) and prospectively updated
67
information annually thereafter for an average of 42-years smoking history dose-
dependently increased the risk of mortality from cancer (Mayne et al 2009)
The impact of smoking on risk of secondary lung cancer has been demonstrated in survivors
of Hodgkin lymphoma (Abrahamsen et al 1993 Travis et al 2002) In the latter study risk
for subsequent lung cancer from radiation treatment and smoking was identified where
multiple effects were found for a combination of radiation and alkylating agents36 in
moderate-to-heavy smokers compared with comparison cases (Travis et al 2002)
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in survival from
other cancers One study was identified in the current review which showed that pre-
diagnosis alcohol consumption history dose-dependently increased mortality risk in
recent survivors of early stage head and neck cancer (n=264) (Mayne et al 2009)
Risks reached 49 for those who drank gt5 drinks per day an effect explained by beer and
liquor consumption Continued drinking post-diagnosis of an average of 23 drinks daily
also significantly increased risk
SUMMARY OF FINDINGS FOR OTHER CANCERS
A comprehensive evaluation of the lifestyle evidence for cancers other than the four most
common (ie breast colorectal lung prostate) was not within the scope of this review
However those studies identified whilst gathering evidence for these four cancers does
highlight the sheer importance of lifestyle in the development and progression of all types of
cancers not to forget other chronic diseases The provision of lifestyle support for cancer
survivors clearly needs to remain priority as does further research into the exact
mechanisms of benefit obtained from different lifestyle practices at different stages of the
cancer and indeed health trajectory
36
Carcinogenic agents used in chemotherapy to treat cancer
68
Table 7 Other Cancers ndash Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
DIET
Gonzalez et al (2006)
Nested case-control within the prospective EPIC study examining of
the risk of gastric cancer and
oesophageal adenocarcinoma associated
with meat consumption
521 457 men and women aged 35ndash70 years in 10 European
countrie
s (330 gastric adenocarcinoma and
65
oesophageal adenocarcinomas were diagnosed)
65-years Incidence of gastric and oesophageal cancers
Gastric noncardia cancer risk was statistically significantly associated
with intakes of total meat (calibrated HR per 100-gday increase
=
352 95 CI = 196 to 634) red meat (calibrated HR per 50-gday
increase = 173 95 CI = 103 to 288) and processed
meat (calibrated HR per 50-gday increase = 245 95 CI
= 143 to 421) The association between
the risk of gastric noncardia cancer and total meat intake was
especially large in H pylori infected subjects (odds ratio per 100-
gday increase = 532 95 CI = 210 to 134) Intakes of total red or
processed meat were not associated with
the risk of gastric cardia cancer A positive but nonndashstatistically
significant association was observed between oesophageal
adenocarcinoma cancer risk and total and processed meat intake
Schultz et al (2005)
Prospective examination of the association between consumption of fruit and vegetables and risk of ovarian cancer (EPIC)
Female participants (n = 325640) of the EPIC study
Mean=63 years
Ovarian cancer incidence
Total intake of fruit and vegetables separately or combined as well as subgroups of vegetables (fruiting root leafy vegetables cabbages) was unrelated to risk of ovarian cancer A high intake of garliconion vegetables was associated with a borderline significant reduced risk of this cancer
WEIGHT
Friedenreich et al 2007
Large prospective study (EPIC) examining the association between anthropometry and endometrial cancer particularly by menopausal status and exogenous hormone use subgroups
223008 women in the EPIC study (567 incident endometrial cancer cases)
64-years Endometrial cancer incidence
Weight BMI waist and hip circumferences and waistndashhip ratio (WHR) were strongly associated with increased risk of endometrial cancer The relative risk (RR) for obese (BMI 30ndash lt 40 kgm
2)
compared to normal weight (BMI lt 25) women was 178 95 CI = 141ndash226 and for morbidly obese women (BMI ge 40) was 302 95 CI = 166ndash552 The RR for women with a waist circumference of ge88 cm vs lt80 cm was 176 95 CI = 142ndash219 Adult weight gain of ge20 kg compared with stable weight (plusmn3 kg) increased risk independent of body weight at age 20 (RR = 175 95 CI = 111ndash277) These associations were generally stronger for postmenopausal than premenopausal women and oral contraceptives never-users than ever-users and much stronger among never-users of hormone replacement therapy compared to ever-users
Kaaks et al A review of evidence on the Endometrial Not Incidence of The authors conclude that development of ovarian hyperandrogenism
69
(2002) associations among endometrial cancer risk endogenous hormone metabolism and obesity
cancer cases reported endometrial cancer
may be a central mechanism relating to an interaction between obesity-related chronic hyperinsulinemia with genetic factors predisposing to the development of ovarian hyperandrogenism
SMOKING
Abrahamsen et al (1993)
The Norwegian Cancer Registry
identified previously untreated patients with Hodgkin lymphoma treated at NRH who had developed a secondary cancer more than 1 year after diagnosis of
Hodgkin
lymphoma
68 patients who developed secondary cancer including 9 acute non-lymphocytic leukaemialsquos (ANLLs)
8 non-
Hodgkins lymphomas (NHLs) and 51 solid tumours including 11 lung cancers
Not reported
Secondary cancer
The RR of SC and leukaemia was 186 (95 CI 14 to 24) and 243 (95 CI 111 to 462) respectively The RR of
SC was highest in
younger patients (lt 41 years RR = 38) No significant association
between splenectomy and development of ANLL was found The
influence of treatment and follow-up time on the development of SC
agrees with data from other large cancer institutions
Gonzalez et al (2003)
Assessment of the relation between tobacco use and gastric cancer incidence in the prospective EPIC study
521468 individuals recruited from 10 European countries taking part in the EPIC study 274 were eligible for the analysis
Approx 10-years
Incidence of gastric cancer
After adjustment for educational level consumption of fresh fruit vegetables and preserved meat alcohol intake and body mass index (BMI) there was a significant association between cigarette smoking and gastric cancer risk the hazard ratio (HR) for ever smokers was 145 (95 CI = 108-194) The HR of current cigarette smoking was 173 (95 CI = 106-283) in males and 187 (95 CI = 112-312) in females Hazard ratios increased with intensity and duration of cigarette smoked A significant decrease of risk was observed after 10 years of quitting smoking A preliminary analysis of 121 cases with identified anatomic site showed that current cigarette smokers had a higher HR of GC in the cardia (HR = 410) than in the distal part of the stomach (HR = 194) In this cohort 176 (95 CI = 105-295 ) of gastric cancer cases may be attributable to smoking
Mayne et al (2009)
Participants retrospectively reported their smoking histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to smoke post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Smoking history before diagnosis dose-dependently increased the risk of dying risks reached 54 [95 CI 07-401] among those with gt60 pack-years of smoking After adjusting for pre-diagnosis exposures continued smoking was associated with non-significantly higher risk (relative risk for continued smoking versus no smoking 18 95 CI 09-39)
70
Travis et al (2002)
Case-control study with a population-based cohort The cumulative amount of cytotoxic drugs the radiation dose to the specific location in the lung where cancer developed and tobacco use were compared between patients who developed lung cancer and matched control patients
1-year survivors of Hodgkins disease (n=19046) comparison between 222 patients who developed lung cancer and 444 matched controls
Not reported
Secondary cancer incidence
Tobacco use increased lung cancer risk more than 20-fold risks from smoking appeared to multiply risks from treatment
Yu et al (1997)
Retrospective study examining the effect of smoking history on survival among cancer patients
Data from Memorial Sloan-Kettering Cancer Centers tumour registry was used to identify 25436 cases of cancer (12447 male patients and 12989 female patients)
Not reported
Survival time Patients who had a history of smoking were found to have a lower rate of survival than non-smokers After controlling for age race alcohol use and histologic grade the risk ratios were 155 for males and 143 for females A dose-response relationship was found between ever-smoking and cancer patient survival The predictive effect of smoking on survival was significant for patients with oral pancreatic breast and prostate cancers but not for oesophageal stomach colon rectum laryngeal lung cervix uteri urinary bladder and kidney cancers Black patients with oral or breast cancer had a poorer prognosis associated with smoking compared with white and other non-white patients
ALCOHOL
Mayne et al (2009)
Participants retrospectively reported their alcohol consumption histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to drink post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Alcohol history before diagnosis dose-dependently increased mortality risk risks reached 49 (95 CI 15-163) for persons who drank gt5 drinksd an effect explained by beer and liquor consumption After adjusting for pre-diagnosis exposures continued drinking (average of 23 drinksd) post-diagnosis significantly increased risk (relative risk for continued drinking versus no drinking 27 95 CI 12-61)
71
PART TWO
LIFESTYLE EVIDENCE FOR REDUCING AND MANAGING THE
RISKS AND SIDE-EFFECTS OF CANCER TREATMENT
Introduction
There are a number of long-term and late effects of cancer treatment that a survivor might
be confronted with including fatigue (Bower et al 2006) psychological problems (Thewes
et al 2004) lymphoedema (Deo et al 2004) and osteoporosis (Brown et al 2006) There
might also be difficulties in terms of returning to work or withdrawal from social activities due
to disability (Taskila et al 2007) Lifestyle choices pertaining to diet physical activity
smoking and alcohol consumption for cancer survivors are not only important in terms of
disease progression and recurrence Despite there being less evidence in this area there
is accumulating data demonstrating that lifestyle can facilitate the effective management of
many of these effects of treatment some of which are chronic conditions themselves
requiring additional lifestyle modifications Research within this area has hit new heights in
order to keep up with the growing number of survivors The chronic conditions addressed
within the current review of lifestyle evidence are some of the most frequently reported
problems cited by cancer survivors they include cancer-related fatigue (CRF)
lymphoedema osteoporosis and weight gain In addition evidence for lifestyle choices and
quality of life (QoL) has been reviewed due to the QoL implications of the aforementioned
health-related problems and unhealthy behaviours (Richardson et al 2009)
Evidence for an interaction between lifestyle and these chronic conditions commences with
the findings reported by Bekkering et al (2006) as part of the WCRF review being updated
Further evidence identified from the search criteria will then be presented Evidence will be
presented by cancer site (eg breast colorectal lung prostate) where appropriate whilst
some evidence will pertain to one cancer site only (ie breast cancer related lymphoedema)
72
CANCER-RELATED FATIGUE (CRF)
Cancer-related fatigue (CRF) is defined as ldquoa distressing persistent subjective sense of
physical emotional andor cognitive tiredness or exhaustion related to cancer or cancer-
related treatment that is not proportional to recent activity and interferes with usual
functioningrdquo (NCCN 2009) It has overtaken nausea and pain as the most distressing
symptom experienced by people with cancer during and after treatment It is reported by 60-
96 of patients during chemotherapy radiotherapy or after surgery and can last for months
or even years following treatment (Wagner and Cella 2004 Thomas 2005 NCCN 2009) It
can have a profound effect on physical emotional and social well-being and can hinder
chance of remission owing to non-compliance with treatment due to the intensity of this side-
effect (Lucia Earnest and Perez 2003 Velthuis et al 2009)
The specific causes of CRF are not fully understood but there are several associated
conditions which can aggravate it These include anaemia electrolyte imbalance liver
failure and steroid withdrawal (Thomas 2005) Some conditions can also cause fatigue by
disturbing sleep patterns such as anxiety depression nocturia (a need to get up in the night
to urinate) night sweats and pruritus (itching) The self-management strategy most
extensively investigated for CRF is physical activity the evidence for which is presented
next Studies identified in the current review are summarised in Table 8 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in women with breast cancer In the current review 4 systematic reviews
three of which included a meta-analysis and 2 additional studies were identified
The first review by McNeely et al (2006) reported on 14 RCTs Despite significant
heterogeneity and relatively small samples the overall finding was that physical activity led
to statistically significant improvements in reducing symptoms of fatigue Two meta-
analyses added to this evidence The first by Cramp and Daniel (2008) evaluated 28
studies (n=2083 participants) the majority of which comprised participants with breast
cancer (n=16 studies n=1172 participants) A pooled meta-analysis of all available data
convincingly showed that physical activity was statistically more effective in reducing
CRF when compared to less active controls In the second meta-analysis Velthuis et al
(2009) reviewed 18 studies 12 of which comprised women with breast cancer Pooled
results of these 12 studies (n=674 patients) showed a small significant reduction of CRF
in favour of the physical activity group compared to the non-physical activity group
When Velthuis et al (2009) subdivided the 12 studies into two main physical activity
strategies (ie home-based versus supervised classes) home-based physical activity (n=
7 studies) led to a small non-significant reduction in CRF whereas supervised
73
aerobic physical activity (n=5 studies) showed a medium significant reduction
in CRF when compared to no intervention
Fillion et al (2008) conduced an RCT demonstrating that combining supervised walking
training with psycho-educational stress management produced significant improvements
relative to usual care for fatigue vigour anxiety and depression but not for physical
fitness This suggests a psychological benefit to physical activity which might assist in
coping with physical symptoms such as fatigue Poudevigne et al (2009)
examined adherence to 12-weeks of moderate intensity combined cardio-respiratory and
resistance training and any subsequent impact on levels of fatigue in sedentary breast
cancer survivors (n=20) 2-24 months post-treatment Not only was the training acceptable
and safe but significant decreases in fatigue (43) were also found across the12-
weeks
Danhauer et al (2009) conducted an RCT with women (n=44) who had breast cancer 34
of whom were undergoing cancer treatment in order to examine the effects of restorative
yoga between those in treatment and those not in treatment Randomisation was to a
programme of 10-weekly 75-minute yoga classes or a waiting list control group The yoga
group demonstrated a significant within-group improvement in fatigue although no
significant difference was found with the control group
In updating a previous systematic review by Schmitz et al (2005) of RCTs examining
physical activity in cancer survivors during and after treatment Speck et al (2010)
accumulated data from a further 82 studies (n=6838 participants) Of the 82 studies 66
were rated as high quality and analysed for mean effect sizes resulting from physical activity
interventions The most common diagnosis included was breast cancer (83) with 40 of
studies conducting interventions during cancer treatment and 60 post-treatment Mean
effect sizes demonstrated a large effect of physical activity interventions post-
treatment on upper and lower body strength (plt00001 and 0024 respectively) and
moderate effects on fatigue and breast cancer-specific concerns (p=0003 and 0003
respectively) The most notable progression from their previous review was that the
benefits of physical activity on fatigue moved from negative findings to the evidence
reflecting significantly reduced fatigue post-treatment in physically active survivors
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in men with prostate cancer In the current review 3 systematic reviews two
of which included a meta-analysis and 2 additional studies were identified In the current
review four studies were identified
Windsor Nichol and Potter (2004) published a study of 65 patients with prostate cancer
receiving radiotherapy who were randomly allocated to a home-based physical activity
programme or standard supportive care The home-based exercise included walking 30-
minutes three times a week with an intensity of 60-70 heart rate max for the duration of
74
radiotherapy No adverse events were reported and a non-significant reduction of CRF
was found in the physical activity group when compared to the standard care group
In the abovementioned meta-analysis conducted by Velthuis et al (2009) three RCTs in men
with prostate cancer investigated the effectiveness of supervised physical activity during
radiotherapy and androgen deprivation therapy (Segal et al 2003 Monga et al 2007
Segal et al 2009) In two studies men allocated to the intervention group participated three
times a week in a supervised physical activity programme comprising aerobic exercises with
an intensity of respectively 65 of the maximum heart frequency (HR max) adjusted for
age and 50-75 of the VO2peak (15-45 minutes) (Monga et al 2007 Segal et al 2009)
In the third study the intervention comprised resistance exercises 2-3 times a week with an
intensity of two sets of 8-12 repetitions 60-70 of the one repetition maximum (Segal et
al 2003) Pooled results from the two supervised aerobic studies showed a large non-
significant reduction in CRF in favour of the physical activity group (Monga et al
2007 Segal et al 2009) The resistance exercise study showed a small non-significant
reduction in CRF in favour of the physical activity group (Segal et al 2003) In the latter
study over 80 of the participants were reported to have completed the programme
however the programme did result in one knee injury chest pain fainting and an acute
myocardial infarction
c) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) report on one RCT comparing the impact of a 3-weeks aerobic
physical activity (stationary biking 30-minutes five times weekly) intervention versus
relaxation training (45-minutes three times per week) in post-surgery survivors (n=72) of lung
(n=27) and gastrointestinal (n=42) cancer (Dimeo et al 2004) Fatigue improved
significantly in both groups during the intervention although there was no significant
difference between groups This suggests that relaxation training can be equally as
effective as aerobic physical activity in relieving symptoms of fatigue
In the current review 3 further studies were identified
There has been one study in patients with multiple myeloma (Coleman et al 2003) which
included a home-based physical activity programme during chemotherapy and peripheral
blood stem cell transplantation The programme comprised a combination of aerobic and
resistance exercises three times a week for 20-minutes for the duration of the
chemotherapy (6-months) No adverse events were reported and a small non-significant
reduction in CRF was found in the physical activity group compared to a control
group who did not receive the intervention
Chang et al (2008) published a study involving patients with acute myelogeous leukemia
(n=22) which included allocation to the intervention group a three week supervised walking
programme during chemotherapy Participants walked five times a week for 12-minutes in
the hospital hallway The programme was completed by 69 of the participants and no
75
adverse events were reported A medium-sized non-significant reduction in CRF was
found
In a cross-sectional postal survey of ovarian cancer survivors (n=359) self-report measures
of physical activity and CRF demonstrated that those meeting physical activity guidelines of
the Centres for Disease Control and Prevention (ie minimum 25-hours of moderate
intensity aerobic activity every week plus muscle-strengthening activities on two or more
days of the week) reported significantly lower fatigue than those not meeting guidelines
(Stevinson et al 2009) There was however no evidence of a dose-response relationship
SUMMARY OF EVIDENCE FOR CANCER-RELATED FATIGUE
Evidence from 28 RCTs and 2 meta-analyses has demonstrated that physical activity
programmes can reduce the severity of CRF The studies reviewed here also show that
supervised aerobic exercise programmes were more effective in reducing CRF during breast
cancer treatment than home-based exercise advice Although more research on the optimal
timing and duration of physical activity would be useful these studies are sufficiently robust
to recommend that tailored physical activity advice be integrated into individualized care
plans
As identified in a consultation and evidence review designed to determine the priorities of
cancer survivorship research there is a modest amount of research testing physical activity
interventions for fatigue some demonstrating benefits during treatment but inconclusive
evidence for after treatment (Richardson et al 2009) Although there is clinical
heterogeneity between published RCTlsquos in terms of physical activity duration frequency and
intensity a sensible pragmatic approach based on the trials which showed most benefit is to
supervise a moderate intensity physical activity regimen of regular frequency (3-5
timesweek) for 20-30 minutes per session involving aerobic resistance or mixed physical
activity types With evidence suggesting that low intensity physical activity can also be
beneficial during cancer treatment consideration is warranted in terms of promoting physical
activity from diagnosis onwards potentially making physical activity uptake less challenging
post-treatment (Velthuis et al 2009) Further research is required to determine the optimal
type intensity and timing of physical activity interventions at different periods of the disease
trajectory and when experiencing other cancer-related symptoms or late effects
An exemplary physical activity programme available to survivors of breast colorectal and melanoma cancers is the BACSUP (Bournemouth After Cancer Survivorship Project) Active Wellness Programmelsquo developed in partnership with Royal Bournemouth Hospital NHS Bournemouth and Poole Bournemouth University and MacMillan Cancer Support (Milne et al 2010) The programme involves two initial one-to-one consultations including a holistic assessment with a trained member of staff to tailor the programme to individual needs A readiness check is done prior to referral a readiness to be physically active score of gt70 is required for participation Participants receive a telephone call at 3-weeks for the provision of support and encouragement followed by a one-to-one review at 6-weeks to assess progress and maintain motivation A one-to-one review and reassessment is also provided at 12-weeks to measure improvements Additional support options are available such as the BACSUP Active Wellness Group which provides an opportunity to meet others survivors and listen to life improvement guest speakers In a pilot study of the programme survivors who had completed primary treatment within the previous 5-years (n=180) were referred to the service 58 completed the programme 65 are currently on the programme 30 started but are on hold due to circumstances 21 were not yet ready to join the scheme
At 12-weeks 92 of participants reported reduced fatigue
76
Table 8 Cancer-Related Fatigue and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Chang et al (2008)
RCT to preliminarily examine the effects of a three-week walking exercise program (WEP) on fatigue-related experiences of acute myelogenous leukaemia (AML) patients receiving chemotherapy Eligible AML patients were randomly assigned to either an experimental group (n = 11) which received 12 minutes of WEP per day five days per week for three consecutive weeks or to a control group (n = 11) which received standard ward care
Patients with acute Myelogenous leukaemia (AML) receiving chemotherapy (n=22)
All patients were evaluated four times before treatment (baseline or Day 1) Day 7 Day 14 and Day 21
Worst and average fatigue intensities fatigue interference with patients daily life 12-minute walking distance overall symptom distress anxiety and depressive status
AML patients in the three-week WEP group had a significantly greater increase in 12-minute walking distance than the control group Patients in the WEP also had lower levels of fatigue intensity and interference symptom distress anxiety and depressive status than the control group
Coleman et al(2003)
A pilotfeasibility study with a randomized controlled design was conducted to investigate home-based exercise therapy for patients receiving high-dose chemotherapy and autologous peripheral blood stem cell transplantation as treatment for multiple myeloma
24 patients with multiple myeloma
Not reported Fatigue mood disturbance body weight
Because of the small sample size in the feasibility study the effect of exercise on lean body weight was the only end point that obtained statistical significance However the results suggest that an individualised exercise program for patients receiving aggressive treatment for multiple myeloma is feasible and may be effective for decreasing fatigue and mood disturbance and for improving sleep
Cramp and Daniel (2008)
Systematic review with meta-analysis to evaluate the effect of exercise on cancer-related fatigue both during and after cancer treatment
2083 participants from RCTs comprising cancer patients and survivors
Follow-up assessment of long-term outcomes was poor with 18 of 28 studies failing to assess outcomes beyond the end of the intervention
Cancer-related fatigue
28 studies were identified for inclusion with the majority carried out on participants with breast cancer (n = 16 studies n = 1172 participants) A meta-analysis of all fatigue data incorporating 22 comparisons provided data for 920 participants who received an exercise intervention and 742 control participants At the end of the intervention period exercise was statistically more effective than the control intervention (SMD -023 95 CIs -033 to -013)
77
period
Danhauer et al (2009)
Randomised pilot study to determine the feasibility of implementing a restorative yoga intervention for women with breast cancer and to examine group differences in self-reported emotional health-related quality of life and symptom outcomes 10 weekly 75-minute yoga classes
Women with breast cancer (n=544) 34 of whom were actively undergoing cancer treatment
Immediately post-intervention (week 10)
Emotional well-being QoL fatigue
Group differences favouring the yoga group were seen for mental health depression positive affect and spirituality (peacemeaning) Significant baselinegroup interactions were observed for negative affect and emotional well-being Women with higher negative affect and lower emotional well-being at baseline derived greater benefit from the yoga intervention compared to those with similar values at baseline in the control group The yoga group demonstrated a significant within-group improvement in fatigue no significant difference was noted for the control group
Fillion et al (2008)
RCT to verify the effectiveness of a 4-week nurse-led group intervention that combines stress management psycho-education and physical activity (ie independent variable) intervention in reducing fatigue and improving energy level quality of life (mental and physical) fitness (VO2submax) and emotional distress (ie dependent variables) in breast cancer survivors Participants were randomly assigned to either the group intervention (experimental) or the usual-care (control) condition
French-speaking women who had completed their treatments for non-metastatic breast cancer (n=87)
Post-intervention and at 3-months follow-up
Fatigue emotional distress QoL
Participants in the intervention group showed greater improvement in fatigue energy level and emotional distress at 3-month follow-up and physical quality of life at post-intervention compared with the participants in the control group
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials MEDLINE
EMBASE CINAHL Psych INFO CancerLit PEDro
and SportDiscus as well
as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
function
ing as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all
outcomes were positive even when statistical significance was not
achieved Exercise led to statistically significant improvements in
quality of life as assessed by the Functional Assessment of
Cancer TherapyndashGeneral (weighted mean difference [WMD] 458
95 CI 035 to 880) and Functional Assessment of Cancer
TherapyndashBreast (WMD 662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak
oxygen consumption and in reducing symptoms of fatigue
Poudevigne et al (2009)
Cohort study examining the effects of a 12-week cross training intervention on fatigue and mood in breast cancer survivors The training consisted of a 12-week exercise program of 3 weekly
20 sedentary breast cancer survivors between 2-24 months post-
On completion of the 12-week intervention
Fatigue and mood disturbances (Profile of Mood States) QoL
The mean (plusmnSD) attendance rate was 92 (plusmn80) No musculoskeletal injuries and problematic symptoms occurred during the cross-training Repeated measures ANOVA showed a large increase in QOL (22) and significant decrease in fatigue (43) across 12 weeks (eta squared range 491 to708 all p
78
sessions of 60 min duration supervised by a certified personal trainer and divided into resistance (30 minutes) and aerobic training (5 minutes warm-up 20 minutes training 5 minutes cool-down) The aerobic intensity was set at 60HRR and re-evaluated every three weeks
treatment Treatments ranged from lumpectomies (23) mastectomies (29) radiations (32) and chemotherapy (16)
(SF-36) and work absenteeism
valueslt05) No differences were found in work absenteeism Blood pressure was unchanged after training
Stevinson et al (2009)
A cross-sectional postal survey to investigate the associations between physical activity and health-related outcomes in ovarian cancer survivors and to examine any dose-response relationship
Ovarian cancer survivors (n=359) on and off treatment
Not reported Fatigue peripheral neuropathy sleep and psychosocial functioning
311 of participants were meeting the public health physical activity guidelines - those meeting guidelines reported significantly lower fatigue than those not meeting guidelines (mean difference 71 95 confidence interval 55-88 d = 087 Plt 0001) Meeting guidelines was also significantly inversely associated with peripheral neuropathy depression anxiety sleep latency use of sleep medication and daytime dysfunction and was positively associated with happiness sleep quality and sleep efficiency
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types were included with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) With few exceptions exercise was well tolerated during and post treatment without adverse events
Velthuis et al (2009)
Meta-analysis to evaluate the effects of different exercise prescription parameters during cancer treatment on cancer-related fatigue (CRF) A systematic search of CINAHL Cochrane Library Embase
RCTs studying the effects of exercise during cancer treatment on
Not reported Cancer-related fatigue
During breast cancer treatment home-based exercise lead to a small non-significant reduction (standardised mean difference 010 95 confidence interval minus025 to 045) whereas supervised aerobic exercise showed a medium significant reduction in CRF (standardised mean difference 030 95 confidence interval 009
79
Medline Scopus and PEDro was carried out
CRF (n=18) 12 in breast 4 in prostate and 2 in other cancer patients)
to 051) compared with no exercise A subgroup analysis of home-based (n = 65) and supervised aerobic (n = 98) and resistance exercise programmes (n = 208) in prostate cancer patients showed no significant reduction in CRF in favour of the exercise group Adherence ranged from 39 of the patients who visited at least 70 of the supervised exercise sessions to 100 completion of a home-based walking programme
Windsor Nichol and Potter (2004)
A prospective RCT to determine whether aerobic exercise would reduce the incidence of fatigue and prevent deterioration in physical functioning during radiotherapy for localised prostate carcinoma
33 men in exercise group and 33 men in control group
4-weeks post-radiotherapy
Fatigue and distance walked in a modified shuttle test before and after radiotherapy
There were no significant between group differences noted with regard to fatigue scores at baseline (P = 055) or after 4 weeks of radiotherapy (P = 018) Men in the control group had significant increases in fatigue scores from baseline to the end of radiotherapy (P = 0013) with no significant increases observed in the exercise group (P = 0203)
80
LYMPHOEDEMA
Lymphoedema is the excessive accumulation of tissue fluid (or lymph) that results from
impaired lymphatic drainage resulting in swelling of the limb The most common type of
lymphoedema in cancer survivors is most frequently the result of treatment for breast
cancer where an important prognostic indicator is the removal and evaluation of lymph
nodes (Morrell et al 2005) Removal of the lymph nodes can result in a number of side-
effects including lymphoedema (Swenson et al 2002) which manifests usually as a
swelling to the affected arm but can also occur in the hand trunk and breast The more
lymph nodes that are removed the higher the risk of developing the condition providing an
objective measure of risk that could be utilised in the provision of evidence-based
lifestyle and self-management support based on individuals needs
The condition can develop immediately or many years after treatment (Mortimer et al
1996) in either case lymphoedema is a chronic debilitating condition that can cause severe
physical and psychological morbidity as well as a reduction in QoL (Deo et al 2004)
The self-management strategy most extensively investigated for lymphoedema is physical
activity with some evidence also being available for diet Studies identified in the current
review are summarised in Table 9 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
preventing or managing lymphoedema In the current review one systematic review
(including a meta-analysis) and 3 studies were identified
In a prospective RCT testing the efficacy of two types of physiotherapy on shoulder function
and lymphatic disturbance in post-operative breast cancer survivors (n=60) participants
received one of two types of physiotherapy 48-hours post-surgery (de Rezende et al
2006)
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-
defined sequence of movements
2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely
to music
Lymphoedema is estimated to affect
about 30 of breast cancer survivors
post-treatment (Deo et al 2004)
81
Results indicated significantly better recovery of limb movement in the directed group
compared to the free group with there being no significant difference between groups in
terms of lymphatic disturbance
Ahmed et al (2006) report on a 6-month RCT examining the effects of supervised upper-
and lower-body weight training on lymphoedema incidence and symptoms in breast cancer
survivors (n = 45) 4-36 months post-treatment From baseline to 6-months three control-
group participants reported an increase in lymphoedema symptoms No participants in the
intervention group reported such symptoms suggesting that twice-a-week progressive
weight training does not increase the onset of or exacerbate lymphoedema in breast cancer
survivors (13 women had lymphoedema at baseline) The results from this study indicate
that at minimum physical activity does not exacerbate lymphoedema
Moseley and Piller (2008) reviewed the literature for evidence supporting the benefits of
physical activity for people with limb lymphoedema Their key findings from eleven studies
demonstrated that
physical activity can improve lymph clearance
physical activity can help reduce limb volume and improve subjective symptoms and
QoL
benefits from physical activity have been sustained post-physical activity regime in
some studies
physical activity is a viable option for people with lymphoedema
Moseley and Pillerlsquos (2008) conclusions were supported further in a recent RCT by Hayes
Hildegard and Turner (2009) Breast cancer survivors at least 6-months post-treatment
who had developed unilateral upper-limb lymphoedema participated in twenty supervised
group aerobic and resistance physical activity sessions over 12-weeks (n=16) or continued
habitual activities (n=16) Average attendance was more than 70 of supervised sessions
and there were no withdrawals Mean ratio and volume measures at baseline were similar
between the two groups and no changes were observed at 3-months follow-up for either
group although two women receiving supervised physical activity no longer had evidence of
lymphoedema by study completion The results from this review as with the RCT by
Ahmed et al (2006) indicate that at minimum physical activity does not exacerbate
secondary lymphoedema
In the review referred to previously by Speck et al (2010) with minor exceptions findings
indicated aerobic lifestyle and upper body resistive exercise was tolerated by breast cancer
survivors with no adverse effects on the development or exacerbation of lymphoedema
ii DIET
Bekkering et al (2006) report on one double-blind placebo-controlled RCT examining diet
and lymphoedema in breast cancer survivors (n=68) at a mean of 155-years post-treatment
For 6-months women received 500mg twice a day of dl-alpha tocopheryl acetate (a source
of vitamin E) plus pentoxifylline (a drug that improves blood circulation) 400mg twice a day
82
of dl-alpha tocopheryl acetate or placebo (Gothard et al 2004) At 6-months and 12-months
post-randomisation there was no significant difference between groups in terms of arm
volume
The current review identified one RCT
Dietary Fat
In a UK RCT Shaw Mortimer and Judd (2007) demonstrate the impact of diet and weight
loss on post-treatment arm lymphoedema in breast cancer survivors (n=51) Women were
assigned to one of three 24-week dietary groups
1) a low-fat diet (fat intake reduced to 20 of total energy intake)
2) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ)
3) a control group (continuing their usual diet)
After the end of the 24-week period of dietary intervention there was a slightly greater
reduction in excess arm volume in both dietary intervention groups compared with the
control although this was not statistically significant Furthermore despite low levels of
adherence to dietary advice weight loss was achieved in all groups demonstrating that
dietary interventions can assist in reducing excess arm volume in women with post-
treatment lymphoedema
SUMMARY OF EVIDENCE FOR LYMPHOEDEMA
The studies evaluated within this review indicate a need to re-assess the common clinical
guidelines that breast cancer survivors avoid upper body resistance activity for fear of
increasing risk of lymphoedema(Speck et al 2010) They also indicate a requirement to
develop guidelines for appropriate physical activity As concluded by Hayes Hildegard and
Turner (2009) women with secondary lymphoedema should be encouraged to be physically
active optimising their physical and psychosocial recovery Resistance exercise does not
increase the risk for or exacerbate symptoms of lymphoedema and in fact directed physical
activity 48-hours post-surgery might offer greater utility in terms of rehabilitation outcomes
Some of the studies evaluated in the review by Moseley and Piller (2008) comprised small
sample sizes and did not include control groups however when combined with other studies
presented within this review there is some support for encouraging physical activity in breast
cancer survivors Furthermore physical activity combined with changes in diet and
subsequent weight loss in survivors who are overweight might significantly reduce the
symptoms of lymphoedema although evidence for diet in reducing symptoms of
lymphoedema is limited
Weight loss across groups
9 (60) in the control group 13 (76) in the low-fat diet group 18 (95) in the weight-reduction
group
83
Table 9 Lymphoedema and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Ahmed et al (2006)
RCT comparing supervised twice weekly upper- and lower-body weight training over 6-months with control group completing no training
Breast cancer survivors (n = 45) 4-36 months post-treatment
6-months post-intervention
Incidence and symptoms of lymphoedema
From baseline to 6-months three control-group participants
reported an increase
in lymphoedema symptoms No
participants in the intervention group reported such symptoms suggesting that
twice-a-week progressive weight training does not
increase the onset of or exacerbate lymphoedema in breast
cancer
survivors
de Rezende et al (2006)
RCT examining the impact of physiotherapy on lymphoedema Participants received one of two types of physiotherapy
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-defined sequence of movements 2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely to music
48-hours post-surgery breast cancer survivors (n=60)
On completion of intervention (42-days)
Shoulder movement and lymphatic disturbance
Significantly better recovery of limb movement in the directed group compared to the free group with there being no significant difference between groups in terms of lymphatic disturbance
Hayes Hildegard and Turner (2009)
An RCT testing the impact of aerobic exercise on lymphoedema outcomes Participants randomised to 1) 20 supervised group aerobic and resistance physical activity sessions over 12-weeks (n=16) 2) continued habitual activities (n=16)
Breast cancer survivors at least 6-months post-treatment who had developed unilateral upper-limb lymphoedema
3-months post-intervention
Arm volume measurements
Mean ratio and volume measures at baseline were similar between the two groups and no changes were observed at 3-months follow-up for either group although two women receiving supervised physical activity no longer had evidence of lymphoedema by study completion
84
Moseley and Piller (2008)
Literature search of the evidence supporting the benefits of exercise for those with limb lymphoedema
Exercise studies undertaken in RCTs or cohort studies and involving secondary limb lymphoedema (with no active cancer)
Varied from post-intervention to 8-weeks follow-up
Change in limb volume and subjective symptoms
Exercise has been shown to improve lymph propulsion and clearance help reduce limb volume and improve subjective symptoms and quality of life Benefits from exercise have been sustained post-exercise regime in some studies Exercise is a viable option for those with limb lymphoedema
DIET
Gothard et al (2004)
A double-blind placebo-controlled randomised phase II trial Participants were randomised to active drugs or placebo All volunteers were given dl-alpha tocopheryl acetate 500 mg twice a day orally plus pentoxifylline 400 mg twice a day orally or corresponding placebos for 6 months
68 volunteers with a minimum 20 increase in arm volume at a median 155 years after radiotherapy (plus axillary surgery in 5168 (75) cases)
12 months post-randomisation
Volume of the ipsilateral limb measured
There was no significant difference between treatment and control groups in terms of arm volume Absolute change in arm volume at 12 months was 25 (95 CI minus040 to 53) in the treatment group compared to 12 (95 CI minus28 to 51) in the placebo group The difference in mean volume change between randomisation groups at 12 months was not statistically significant (P=06) minus13 (95 CI minus61 to 35) nor was there a significant difference in response at 6 months (P=07) where mean change in arm volume from baseline in the treatment and placebo groups was minus23 (95 CI minus79 to 34) and minus11 (95 CI minus39 to 17) respectively
Shaw Mortimer and Judd (2007)
Participants were assigned to one of three 24-week dietary groups in order to assess impact on arm volume 1)a low-fat diet (fat intake reduced to 20 of total energy intake) b) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ) c) a control group (continuing their usual diet)
Breast cancer survivors (n=51)
After 24-weeks of intervention
Arm volume There was a slightly greater reduction in excess arm volume in both dietary intervention groups compared with the control although this was not statistically significant
85
OSTEOPOROSIS AND BONE HEALTH
Osteoporosis is a condition in which the bones become less dense and more likely to
fracture which in turn can result in significant pain and disability It is known as a silent
disease because if undetected bone loss can progress for many years without symptoms
until a fracture occurs Risk factors for developing osteoporosis are often enhanced in
cancer survivors such as being post-menopausal and having had early menopause (Ada et
al 2002) Low calcium intake lack of physical activity smoking and excessive alcohol
consumption are also risk factors for osteoporosis (Guthrie et al 2000) Women who have
had breast cancer treatment may be at increased risk for osteoporosis and fracture due to
reduced levels of oestrogen whilst men who receive hormone deprivation therapy for
prostate cancer also have an increased risk of developing osteoporosis and broken bones
(National Institutes of Health Osteoporosis and Related Bone Diseases 2009)
There are no early symptoms of osteoporosis but diet physical activity and drug treatment
can prevent or reverse loss of BMD highlighting the importance of lifestyle choices in
osteoporosis outcomes Studies identified in the current review are summarised in Table 10
at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any physical activity studies examining osteoporosis
in breast cancer survivors The current review identified 3 RCTs and one cohort study
Schwartz Winters-Stone and Gallucci (2007) evaluated the impact of aerobics and
resistance training on BMD in an RCT involving women with histologically confirmed invasive
stage I-III breast cancer (n=66) beginning chemotherapy Women were randomised to one
of three groups and stratified according to menopausal status (pre-menopausal or post-
menopausal)
1) Home-based aerobic exercise - women were instructed to choose an aerobic activity
they enjoyed (eg walking jogging) and exercise for 15-30 minutes four days per
week for the duration of the study at a symptom-limited moderate intensity such that
they were breathing hard but able to talk
2) Home-based resistance exercise ndash women were instructed to exercise at home four
days per week using resistance bands and tubing
3) Usual care
It has been reported that 80 of older breast cancer survivors have osteopenia (below normal bone-mineral density [BMD]) or osteoporosis at initial diagnosis (Twiss et al 2001)
86
The average decline in BMD was -623 for usual care -492 for resistance exercise and
-076 for aerobic exercise suggesting that weight-bearing aerobic exercise attenuates
declines in BMD Pre-menopausal women demonstrated significantly greater declines in
BMD than post-menopausal women highlighting a need to provide interventions for bone
health on a risk stratification basis
Gross et al (2002) examined the intensity of physical activity (ie light moderate vigorous)
reported by a cohort of post-menopausal breast cancer survivors (n=27) and found no
relationship between activity levels and BMD However participants mainly reported light
physical activity limiting the examination of moderate and vigorous activity outcomes It is
possible that a higher intensity of physical activity is required to achieve any benefits to bone
health
Waltman et al (2009) conducted an RCT testing a 24-month self-efficacy based strength
and weight training programme on post-treatment (except tamoxifen and aromatase
inhibitors) post-menopausal breast cancer survivors (n=223) who had amenorrhea
(absence of menstruation) for at least 12-months and a bone BMD score lower than the
norm (Figure 1)
Figure 1 Bone Density Definitions
WHO Definitions of Osteoporosis
Based on Bone Density
T-Scores
BMD
Category
Examples
Range
10
05
0
-05
-10
-1 and
above Normal BMD
-15
-20
Between
-1 and -25
Low BMD
(Osteopenia)
-25
-30
-35
-40
-25 and
below Osteoporosis
Source WHO (2003)
The women were randomised to receive physical activity with medication (n=110) or
medication only (n=113) The medication taken by both groups included risedronate
(osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily) While
87
participation in strength training did not result in statistically significant improved BMD there
was a trend towards at least maintaining BMD at the total hip Participants who were 50
or greater adherent to the intervention (reasons for non-adherence included lack of
time or chronic pain due to co-morbidity) were significantly less likely than
participants on medication alone to lose BMD at the total hip and femoral neck
In a third RCT Swenson et al (2009) compared the effects of two interventions on changes
in BMD in women receiving chemotherapy for breast cancer (n=62)
1) intravenous zoledronic acid (used to prevent skeletal fractures in people with cancer)
and oral calciumvitamin D every 3-months for five treatments
2) prescribed home-based physical activity and oral calciumvitamin D
Zoledronic acid protected patients with breast cancer against bone loss during initial
treatment whereas the home-based physical activity intervention was less effective in
preventing bone loss indicating that physical activity and dietary supplements are not
always sufficient to protect done density in people with cancer However these were
patients undergoing treatment and more research is required into the effects of physical
activity on bone health in post-treatment survivors
ii DIET
Bekkering et al (2006) did not identify any diet studies examining osteoporosis in breast
cancer survivors The current review identified 3 RCTs and one cohort study
Plant Proteins and Fibres
Weikert et al (2005) performed a sub-analysis of the EPIC cohort study conducted in
Germany which included 8178 females and examined the association between protein
intake dietary calcium and bone structure It was concluded that high consumptions of
animal protein may be unfavourable whereas higher vegetable protein may be
beneficial to bone health These results support the hypothesis that high calcium intakes
combined with adequate protein intake based on a high ratio of vegetables to animal protein
may be protective against osteoporosis Indeed evidence has demonstrated the relationship
between lower incidence of osteoporosis in Asian women and vegetarian populations due to
a diet rich in vegetables and fruit (Fujii et al 2009 Merill and Aldana 2009 Thorpe et al
2008) Furthermore a large-scale dietary modification intervention of post-menopausal
women (n = 4883) showed that an increased consumption of plant proteins and fibres from
fruits vegetables and grains reduced the risk of multiple falls and slightly lowered hip BMD
although it did not change the risk of osteoporotic fractures (McTiernan et al 2009)
New et al (2003 2004) provides further evidence for the benefits of plant proteins and fibres
on bone health in two reviews where a positive link between a high consumption of fruit
and vegetables and bone health has been demonstrated In the first report it was found
that fruit and vegetables have beneficial effects on bone mass and bone metabolism in men
and women across the age ranges whilst in the second review it was concluded that
although the impact of a vegetarian diet on bone health is much more complex than merely
being related to diet vegetarians do tend to have normallsquo bone mass
88
iii WEIGHT
Bekkering et al (2006) did not identify any studies examining weight implications on
osteoporosis in breast cancer survivors The current review identified one study that found
that being underweight (BMI less than 185) was associated with lower BMD (Ryan et al
2007)
b) PROSTATE CANCER
i WEIGHT
Bekkering et al (2006) did not identify any studies examining the effect of body weight on
osteoporosis in prostate cancer survivors The current review identified one RCT Ryan et
al (2007) found a positive association between BMI and bone density of the hip in men with
prostate cancer (n=120) who were within the first 12-months of androgen-deprivation
therapy This suggests that a higher BMI can be protective of bone density loss in this
patient group
ii ALCOHOL
Bekkering et al (2006) did not identify any studies examining the effect of alcohol
consumption on osteoporosis in prostate cancer survivors The current review identified one
RCT Ryan et al (2007) also demonstrate greater bone density in prostate cancer patients
consuming seven or more weekly alcoholic beverages when compared to non-drinkers
a) OTHER CANCER
i DIET
Soya Products
Bekkering et al (2006) did not identify any studies examining the effect of diet on
osteoporosis in other cancer survivors The current review identified one RCT Marini et al
(2008) reported a randomised double-blind placebo-controlled trial of the soya derivative
genistein aglycone and its effects on bone health after 3-years in women with breast and
endometrial cancer (n=389) Bone mineral density increases were greater with
genistein for both femoral neck and lumbar spine compared to placebo the conclusion
being that after 3-years of treatment genistein exhibited a promising safety profile with
positive effects on bone formation in this cohort of osteopenic post-menopausal women
89
SUMMARY OF EVIDENCE FOR OSTEOPOROSIS AND BONE HEALTH
There is evidence that vitamin D and calcium might be associated with greater BMD
however this benefit cannot be distinguished from other potential contributors such as
physical activity and medication More research is needed into the effects of physical activity
on osteoporosis in cancer survivors The findings thus far offer different conclusions
although there is limited evidence that physical activity can at the very least prevent loss of
BMD which is a positive outcome in survivors at particular risk of bone loss Greater
adherence to physical activity interventions appeared to offer the greater benefits
highlighting the importance of designing lifestyle interventions that can be maintained as
well as providing higher intensity support for survivors with co-morbidities
Higher BMI has been found to be protective of BMD loss in men with prostate cancer
however no distinction has been made between higher BMI and a BMI that indicates excess
weight Limited evidence has been provided for the benefits of moderate alcohol
consumption but as with the evidence presented for weight much more research is needed
before any valid and reliable conclusions can be made Since the NHS advises no more than
3-4 units of alcohol per day for men more research is needed to determine the minimum
units of alcohol that offer such protective benefits It is important to deter against excessive
drinking which can have a number of serious health implications including high blood
pressure mouth and throat cancers and stroke (NHS 2010)
Men should not exceed 3-4 units of alcohol per day on a regular basis (NHS 2010) One unit is the amount of pure alcohol in a 25ml single measure of spirits (pure alcohol by volume [ABV] 40) a third of a pint of beer (ABV 5-6) or half a 175ml standardlsquo glass of red wine (ABV 12) Daily alcohol limits are provided by the NHS in order to discourage the belief that that the number of units of a weekly limit can be consumed at once (ie binge drinking) Use of daily limit
90
Table 10 Osteoporosis and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Gross et al (2002)
Descriptive correlational test of a multicomponent intervention to prevent and treat osteoporosis in breast cancer survivors
27 post-menopausal breast cancer survivorslsquo post- treatment except for tamoxifen
Not reported
Physical activity vigour vitality and BMD
More than half reported no very hard physical activity and 37 reported no hard activity The association of vigour with total metabolic equivalents for combined moderate hard and very hard activities was significant (r = 0536 p = 0007) as were the hours spent in the combined moderate to very hard activities No relationship was found between vigour vitality or any level of activity and BMD
Schwartz Winters-Stone and Gallucci (2007)
RCT testing the effects of aerobic and resistance exercise on changes in bone mineral density (BMD) in women receiving chemotherapy Participants were randomised to aerobic or resistance exercise and usual care
66 women with stage I-III breast cancer beginning adjuvant chemotherapy
6-months after starting treatment
BMD aerobic capacity and muscle strength
Aerobic exercise preserved BMD significantly better compared to usual care Premenopausal women demonstrated significantly greater declines in BMD than postmenopausal women Aerobic capacity increased by almost 25 for women in the aerobic exercise group and 4 for resistance exercise Participants in the usual care group showed a 10 decline in aerobic capacity
Swenson et al (2009)
Participants received one of two treatments a) Intravenous zoledronic acid and oral calciumvitamin D every 3-months for five treatments b) Prescribed home-based physical activity and oral calciumvitamin D
Women receiving chemotherapy for breast cancer (n=62)
On completion of 3-month intervention
Severity of lymphedema by arm circumference
BMD significantly decreased in the physical activity group but not in the zoledronic acid group Zoledronic acid protected patients with breast cancer against bone loss during initial treatment whereas the home-based physical activity intervention was less effective in preventing bone loss indicating that physical activity and dietary supplements are not always sufficient to protect done density in people with cancer
Waltman et al (2009)
A 24-month self-efficacy based strength and weight training programme Participants were randomised to receive physical activity with medication (n=110) or medication only (n=113) the medication taken by both groups including risedronate (osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily)
Post-treatment post-menopausal breast cancer survivors (n=223) with amenorrhea for at least 12-months and a BMD score lower than the norm
On completion of the 24-month intervention
Bone mineral density
While participation in strength training did not result in statistically significant improved BMD there was a trend towards at least maintaining BMD at the total hip Participants who were 50 or greater adherent to physical activities were significantly less likely than participants on medication alone to lose BMD at the total hip and femoral neck
91
DIET
Marini et al (2008)
RCT assessing the continued safety profile of genistein
aglycone on
breast and endometrium and its effects on bone after
3 years of
therapy Participants received 54mg of genistein
aglycone daily or
placebo both treatment arms
received calcium and vitamin D
Breast cancer patients ndash intervention group (n=71) and placebo (n=67)
After 3-years of treatment
BMD Bone mineral density increases were greater with genistein for both
femoral neck and lumbar spine compared to placebo Genistein also
significantly reduced pyridinoline as well as serum carboxy-terminal
cross-linking telopeptide and soluble receptor activator of NF- B
ligand while increasing bone-specific alkaline phosphatase IGF-I
and osteoprotegerin levels There were no differences in discomfort
or adverse events between groups
(McTiernan et al 2009)
RCT assessing the effect of the Womens Health Initiative
Dietary
Modification low-fat and increased fruit vegetable
and grain
intervention on incident hip total and site-specific
fractures and self-
reported falls and in a subset on bone
mineral density (BMD)
Participants were randomly assigned to
receive
a)dietary modification intervention (daily goal 20 of energy as fat 5 servings of vegetables
and fruit
and 6 servings of grains) b)comparison group
- no dietary
changes
Post-menopausal women (n=48835) intervention (40 n=19541)
versus comparison group (60 n=29294)
Mean=81-years
Incident hip total and site-specific
fractur
es and self-reported falls and in a subset on bone
mineral
density (BMD)
215 women in the intervention group and 285 women in the
comparison group (annualized rate 014 and 012 respectively)
experienced a hip fracture (hazard ratio 112 95 CI 094
134 P = 021) The intervention group (n = 5423 annualized rate
344) had a lower rate of reporting 2 falls than did the
comparison group (n = 8695 annualized rate 367) (HR 092
95 CI 089 096 P lt 001) There was a significant interaction
according to hormone therapy use those in the comparison group
receiving hormone therapy had the lowest incidence of hip fracture In a subset of 3951 women
hip BMD at years 3 6 and 9 was 04ndash
05 lower in the intervention group than in the comparison group
(P = 0003)
New et al (2004)
Literature review assessing the impact of a vegetarian diet on indices of skeletal integrity to address specifically whether vegetarians have a normal bone mass
Analysis of existing literature through a combination of observational clinical and intervention studies were assessed in relation to bone health lacto-ovo-vegetarian and
Not reported
Bone health Key findings included (i) no differences in bone health indices between lacto-ovo-vegetarians and omnivores (ii) conflicting data for protein effects on bone with high protein consumption and low protein intake (particularly with respect to vegan diets) being detrimental to the skeleton (iii) growing support for a beneficial effect of fruit and vegetable intake on bone with mechanisms of action currently remaining unclarified The impact of a vegetarian diet on bone health is a hugely complex area since 1) components of the diet (such as calcium protein alkali vitamin K phytoestrogens) may be varied 2) key lifestyle factors which are
92
vegan diets versus omnivorous consumption of animal versus vegetable protein and fruit and vegetable consumption
important to bone (such as physical activity) may be different 3) the tools available for assessing consumption of food are relatively weak However from data available vegetarians do certainly appear to have normal bone mass
Weikert et al (2005)
Prospective cohort study (EPIC) examining associations between protein intake calcium and bone structure measured by broadband ultrasound attenuation (BUA)
8178 female EPIC participants
Not reported
Bone structure
High intake of animal protein was associated with decreased BUA values ( _ = ndash003 p = 0010) whereas high vegetable protein intake was related to an increased BUA ( _ = 011 p = 0007) The effect of dietary animal protein on BUA was modified by calcium intake
WEIGHT
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and alcohol use was positively associated with the Z score
ALCOHOL
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and body mass index was positively associated with the Z score
93
WEIGHT AND BODY COMPOSITION
Weight gain during and after cancer treatment is becoming an ever-increasing significant
concern (Camoriano et al 1990 Levine et al 1991 Saquib et al 2006) Weight gain is
expected when energy intake exceeds energy expenditure a combination that is frequently
described among breast cancer patients who report exercising less during treatment and
after treatment (Schwartz 2000 Demark-Wahnefried 2001) and consuming a higher energy
diet during treatment (Mukhopadhyay and Larkin 1986) Exacerbating this is the fact that
women in general gain weight as they transition through menopause (Sammel et al 2003)
putting breast cancer patients at particular risk as treatments frequently result in a premature
menopause For individuals with bowel cancer the CALBG 8980 trial showed that 35 of
patients post-chemotherapy were overweight (BMI 250ndash299) and 34 were obese BMI
300ndash349) or very obese (BMI gt35) (Meyerhardt et al 2008) The reasons for weight gain
during and after treatment are multifactorial and the result of individual lifestyle behaviours
and the impact of certain cancer drugs Regardless of the reasons as described in part one
of this review both survival and recurrence may be adversely affected by obesity
(Chlebowski et al 2002)
The effect of obesity on survival has been evident in the majority of studies although not all
one reason for this inconsistency being the possibility that biological factors associated with
obesity and not the obesity itself are responsible for the observed effect For example
there is considerable evidence that the effects of obesity on breast cancer risk may be
mediated at least in part by the effect of obesity on insulin resistance (Friedenreich 2001
Suga et al 2001 Goodwin et al 2002)
Finding effective methods for weight loss continues to be a challenge as although some
studies have demonstrated substantial weight loss in obese individuals weight loss results
in general have been modest and new approaches are needed (Jeffery et al 2000) For
long-term reduction in body weight intensive individualised approaches toward developing
a new lifestyle may be required (Djuric et al 2002)
Studies identified in the current review are summarised in Table 11 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in breast cancer survivors The current review identified one
meta-analysis and three RCTs
In the meta-analysis Kim Kang and Park (2009) reviewed 10 studies involving 588 women
who had been treated for breast cancer examining the effectiveness of aerobic exercise
interventions on cardiopulmonary function and body composition conducted during or after
cancer treatments They concluded that regular aerobic physical activity significantly
improved cardiopulmonary function as assessed by absolute VO2 peak relative VO2
94
peak and 12-minute walk test as well as improved body composition as assessed by
percentage body fat (although body weight and lean body mass did not change
significantly)
Courneya et al (2007) conducted a multicentre RCT in which women with breast cancer on
adjuvant chemotherapy were randomly assigned to usual care (n = 82) supervised
resistance exercise (n = 82) or supervised aerobic exercise (n = 78) for the duration of their
chemotherapy (median = 17-weeks 9-24 weeks) There was 70 adherence to supervised
exercise with aerobic physical activity being superior to usual care for improving
aerobic fitness and percent body fat whilst resistance physical activity was superior
to usual care for improving muscular strength lean body mass and chemotherapy
completion rate
Schmitz et al (2005) evaluated the safety and effects of twice-weekly weight training among
85 breast cancer survivors with women being randomised into immediate or delayed
intervention groups The immediate group trained from months 0-12 the delayed group
served as a no exercise parallel comparison group from months 0-6 and trained from months
7-12 At 6-months the immediate group compared to the no exercise group showed
significantly greater increases in lean mass (p lt 01) as well as significant decreases
in percentage body fat (p lt 05) This significance remained at 12-months when
comparing the immediate group with the delayed exercise group
Mefferd et al (2006) randomised overweight or obese breast cancer survivors (n=85) to a
16-week once weekly general exercise and dietary counselling intervention or standard
care The intervention addressed a reduction in energy intake as well exercise with a goal
of an average of one-hour a day of moderate to vigorous activity Seventy six women
(894) completed the intervention demonstrating reasonable acceptability of the
intervention At 16-weeks significant group differences in favour of the intervention
were evident in weight BMI percent fat trunk fat leg fat and waist and hip
circumference
ii DIET
Bekkering et al (2006) did not identify any studies examining the effect of diet on weight loss
or maintenance in breast cancer survivors The current review identified one RCT
Chlebowski et al (2006) report an RCT conducted as part of the aforementioned WINS trial
where 2437 postmenopausal women with early breast cancer were randomised to
nutritional and lifestyle counselling (n=975) or not (n=1462) as part of routine follow-up The
dietary intervention included eight bi-weekly individual counselling sessions As a reminder
the goal of the dietary intervention was to reduce percentage of calories from fat to 15
resulting in a sustained reduction in fat intake to approximately 20 of calories Dietary fat
intake reduction was significantly greater in the dietary group compared to the control group
After 12-months of intervention dietary fat intake was lower in the intervention group
than in the control group (333g per day versus 513g per day respectively Plt001)
95
corresponding to a statistically significant 6-pound lower mean body weight in the
intervention group (P lt01) This major study also demonstrated a survival advantage in
women who lost weight as described in Part 1 of this review
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in prostate cancer survivors The current review identified
one RCT
Segal et al (2009) conducted a RCT with 121 men with prostate cancer commencing
radiotherapy with or without androgen deprivation therapy They were randomly assigned to
24-weeks of usual care resistance exercise or aerobic exercise Compared with usual
care exercise improved aerobic fitness upper- and lower-body strength while
preventing an increase in body fat Resistance exercise generated longer-term
improvements and additional benefits for strength and body fat than aerobic exercise
SUMMARY OF EVIDENCE FOR WEIGHT AND BODY COMPOSITION
Supervised physical activity programmes with or without dietary counselling are highly
effective in improving body composition or at the very least preventing increases in weight
They are also safe and have other major benefits on health including improving fitness
walking distance muscle power and reducing cholesterol More research is however
required into the most effective dietary strategies for weight loss or maintenance in cancer
survivors Thus far there is some evidence for reducing dietary fat intake
A large controlled trial has been designed to test the combined effect of physical activity and
weight control on disease-free survival and on breast cancer recurrence free survival
second primary breast cancer and total invasive plus in situ breast cancer (Ballard-Barbash
et al 2009) Goals for weight control interventions for women whose BMI is greater than
25kgm2 is to lose 10 of body weight and for women whose BMI is less than or equal to
25kgm2 to avoid weight gain The goal for the physical activity intervention would be to
achieve and maintain regular participation in a moderate intensity physical activity
programme for a total of 150-255 minutes over at least 5 days per week This study is using
evidence which is current for weight loss and physical activity and is an indicator for the
basis of advice for patients at risk in similar situations
96
Table 11 Weight and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Courneya et al (2007)
Multicentre RCT to test for factors that could counteract unfavourable changes resulting from chemotherapy (eg changes in body composition) Participants were randomly assigned to usual care (n =
82) supervised resistance exercise
(n = 82) or supervised aerobic
exercise (n = 78) for the duration of their chemotherapy
242 breast cancer
patient
s initiating adjuvant chemotherapy
Median=17-weeks
Primary Cancer-Specific QoL Secondary Fatigue psychosocial functioning physical fitness body composition chemotherapy completion rate and lymphedema
The follow-up assessment rate for our primary end point was
921 and adherence to the supervised exercise was 702
Unadjusted and adjusted mixed-model analyses indicated that
aerobic exercise was superior to usual care for improving self-
esteem (P = 015) aerobic fitness (P = 006) and percent body fat
(adjusted P = 076) Resistance exercise was superior to usual care
for improving self-esteem (P = 018) muscular strength (P lt
001)
lean body mass (P = 015) and chemotherapy completion rate (P =
033) Changes in cancer-specific QOL fatigue depression and
anxiety favoured the exercise groups but did not reach statistical
significance Exercise did not cause lymphedema or
adverse events
Kim Kang and Park (2009)
Meta-analysis to examine the effectiveness
of aerobic exercise
interventions on cardiopulmonary function
and body composition in
women with breast cancer
Of 24 relevant
studie
s reviewed 10 studies (n= 588) met the inclusion criteria
Not reported Cardiopulmonary function
and body
composition
The findings indicated that aerobic exercise significantly improved
cardiopulmonary function as assessed by absolute
VO2 peak (standardized mean difference [SMD] 916 p lt 001)
relative VO2 peak (SMD424 p lt 05) and 12-minute walk test
(SMD 502 p lt 001) Similarly aerobic exercise significantly
improved body composition as assessed by percentage body fat
(SMD mdash890 p lt001) but body weight and lean body mass did not
change significantly
Mefferd et al (2006)
RCT to test the effect of a 16-week cognitive behavioural therapy (CBT) intervention for weight loss through exercise and diet modification on risk factors for recurrence of breast cancer Participants randomly assigned to a once weekly 16-week intervention or wait-list control group
Overweight or obese breast cancer survivors (n=76)
On completion of the 16-week intervention
Weight Significant differences in weight body mass index percent fat trunk fat leg fat as well as waist and hip circumference between intervention and control groups (P le 005) Furthermore levels of triglycerides and total cholesterolhigh density lipoprotein cholesterol levels were also significantly reduced following the intervention
97
Schmitz et al (2005)
RCT testing the safety of twice weekly weight training classes among recent breast cancer survivors Participantslsquo randomised into immediate and delayed treatment groups The immediate group trained from months 0-12 the delayed treatment group served as a no exercise parallel comparison group from months 0-6 and trained from months 7=12
Convenience sample of 85 recent breast cancer survivors
6 and 12-months
Body size (lean body mass) and biomarkers hypothesised to link exercise and breast cancer risk
Significant increases in lean mass (088 versus 002 kg P lt 001) as well as significant decreases in body fat (minus115 versus 023 P = 003) and IGF-II (minus623 versus 2828 ngmL P = 002) comparing immediate with delayed treatment from baseline to 6 months Within-person changes experienced by delayed treatment group participants during training versus no training were similar
Segal et al (2009)
Prostate Cancer Radiotherapy and
Exercise Versus Normal
Treatment study examining the effects
of 24-weeks of resistance or
aerobic training versus usual care on prostate cancer outcomes Randomly assigned
to usual care resistance or
aerobic exercise for 24-weeks
Prostate cancer patients on radiotherapy (n=121) usual care (n=41) resistance (n= 40) aerobic exercise
(n=
40)
On completion of 24-week intervention
Fatigue QOL physical fitness body composition PSA testosterone haemoglobin and lipid levels
Median adherence to prescribed exercise was 855 Compared
with usual care resistance training improved QOL (P = 015)
aerobic fitness (P = 041) upper- (P lt 001) and lower-body (P lt
001) strength and triglycerides (P = 036) while preventing an
increase in body fat (P = 049) Aerobic training also improved
fitness (P = 052)
DIET
Chlebowski et al (2006)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to 345]
versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group
98
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general dietary
guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
randomisation to death from any cause
99
QUALITY OF LIFE
The advancements in diagnosis and treatment that have contributed to the rise in
survivorship are a significant achievement for healthcare science However it is important to
recognise that this has also resulted in an increase in the number of people living with the
often long-term physical and psychological consequences of cancer and its treatment
Quality of life outcomes are thus becoming just as important as hardlsquo outcomes such as
mortality (Rosenbaum Fobair and Spiegel 2006) hence an emphasis on patient-reported
outcomes (DH 2009c) Indeed there is increasing evidence that QoL can be more
predictive of cancer survival than measures of performance status (Cella et al 2009 Eton et
al 2003 Wenzel et al 2005)
A healthy lifestyle has become viewed as an important element for improved QoL (Lyon and
Langille 2000) with particular emphasis on physical activity Studies identified in the current
review are summarised in Table 12 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in breast cancer survivors In the current review one systematic review (with meta-
analysis) and 6 RCTs were identified that provide evidence for the role of physical activity in
the QoL of breast cancer survivors
McNeeley et al (2006) conducted a systematic review with meta-analysis of RCTs (n=14)
examining the effects of physical activity on outcomes in breast cancer survivors Three of
the reviewed studies involving 194 patients compared exercise with usual care
(Campbell et al 2005 Courneya et al 2003 Segal et al 2001) with pooled data
demonstrating that exercise led to significant improvements in QoL superior to the
usual care groups Four studies involving 208 patients reported physical functioning or
physical well-being components of QoL (Campbell et al 2005 Courneya et al 2003
McKenzie and Kalda 2003 Segal et al 2001) the pooled results of which showed
a statistically significant increase in this component of QoL as a result of physical
activity Two of these studies were rated as high quality by the reviewers Courneya et al
2003 Segal et al 2001
100
In addition to this meta-analysis findings by Ohira et al (2006) demonstrated that over 6-
months physical and psychological QoL significantly improved in a recent breast
cancer survivors (n=86) 4-36 months post-treatment who took part in a twice-weekly
weight-training intervention when compared to a control group Increases in upper
body strength and lean mass correlated with these improvements suggesting that twice-
weekly weight training for recent breast cancer survivors might improve QoL in part via
changes in body composition and strength
Daley et al (2007) provided evidence from an RCT comprising sedentary breast cancer
survivors who were 12-36 months post-treatment and who were randomised to one of three
conditions
1) 8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-
minute one-to-one sessions with an physical activity specialist three times per week
(n=34)
2) 8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one
sessions with an physical activity specialist three times per week (n=36)
3) usual care (n=38)
Courneya et al (2003) evaluated QoL outcomes in relation to
exercise in breast cancer survivors (n=52) who had completed
surgery radiotherapy or chemotherapy Participants trained three
times per week for 15-weeks on recumbent or upright cycle
ergometers Exercise duration began at 15-minutes for weeks 1-
3 and then systematically increased by five-minutes every 3-
weeks to 35-minutes for weeks 13-15 The exercise group completed
984 of the exercise sessions demonstrating high adherence
rates Overall QoL increased by 91 points in the exercise group
compared with 03 points in the control group (p lt 001) Change
in peak oxygen consumption correlated with change in overall QoL
demonstrating a significant relationship between exercise and
increases in QoL (p lt 01)
Segal et al (2003) compared self-directed versus supervised
exercise on QoL outcomes in women with stages I-II breast cancer
(n=123) Physical functioning in the control group decreased by 41
points whereas it increased by 57 points and 22 points in the self-
directed and supervised exercise groups respectively (p lt 05)
Post-hoc analysis showed a moderately large and clinically important
difference between the self-directed and control groups (98
points p lt 01) and a more modest difference between the
supervised and control groups (63 points P = 09) No significant
differences between groups were observed for changes in QoL
scores
101
A significant mean difference of 98 units in QoL scores favouring aerobic physical
activity therapy was found This outcome was not the result of the extra support and
attention gained from taking part in the intervention since the same findings were not elicited
for the physical activity-placebo and usual care groups
A small pilot RCT comparing QoL and functional capacity in breast cancer survivors (n=21)
provided with 12-weeks of the Chinese physical activity Tai Chi Chuan (n=11) versus
psychosocial support (n=10) was conducted by Mustian Palesh and Flecksteiner (2008)
The tai chi group demonstrated significant improvements in functional capacity and QoL the
psychosocial support group showed significant improvements only in flexibility with declines
in QoL This suggests that tai chi can enhance functional capacity and QoL among
breast cancer survivors over and above the benefits of psychosocial support
Further support for the benefits of physical activity on QoL in breast cancer survivors (n=58)
within 2-years of completing adjuvant therapy has been demonstrated in a combined aerobic
and resistance training RCT (Milne et al 2008) The women received 12-weeks immediate
supervised physical activity three times a week (n=29) or delayed physical activity
comprising the same protocol but provided 12-weeks following the immediate physical
activity group (n=29) Adherence was 613 which is relatively low However there was a
significant group by time interaction for overall QoL which increased in the
immediate physical activity group from baseline to 12-weeks by 208 points compared
to a decrease in the delayed physical activity group of 53 points
Cadmus et al (2009) report on the QoL outcomes of two 6-month RCTs designed for breast
cancer survivors and based on the national recommendation of 30-minutes of moderate to
vigorous physical activity five days per week
When combining findings from these two studies physical activity was not associated with
QoL benefits in the full sample of either study however physical activity was associated with
significantly improved social functioning (a component of QoL) among survivors who
Trial Increasing or Maintaining
Physical Activity during Cancer
Treatment (IMPACT)
Theoretical Framework Theory of
Planned Behaviour and
transtheoretical model - promoting
self-efficacy to overcome barriers to
physical activity
Sample n=45 newly diagnosed
survivors
Delivery Home-based
Trial Yale Physical activity and
Survivorship (YES)
Theoretical Framework Not
reported
Sample n=67 post-treatment
survivors
Delivery Combined supervised
training programme at a local
health club with home-based
physical activity
102
reported low social functioning at baseline which is the likely impact of greater social
interaction during the intervention This highlights the utility of risk stratification and the
provision of lifestyle support based on need survivors with low social functioning as
could be detected via the Social Difficulties Inventory (SDI Wright et al 2005b) are
likely to benefit from programmes such as the IMPACT and YES trial
Sandel et al (2005) report on a cross-over RCT testing the outcomes of a 12-week dance
and movement exercise programme in women within 5-years of treatment for breast cancer
(n=38) The study included a waiting list control (n=19) and cross-over at 13-weeks Women
attended two supervised dance sessions for six weeks and one session per week for an
additional 6-weeks for a total of eighteen sessions A total of 35 (92) women completed
the regimen with reasons for dropping out including fatigue other commitments and one
participant reported shoulder discomfort The overall finding was that breast cancerndash
specific QoL improved significantly in the intervention group compared to the waiting
list group at 13-weeks which remained unchanged
In the updated systematic review described previously Speck et al (2010) present evidence
from 66 high quality RCTs showing that physical activity during treatment has a small to
moderate positive effect on QoL (p=004) anxiety (p=002) and self-esteem (p=002)
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in colorectal cancer survivors In the current review one large cohort study was
identified Lynch et al (2008) examined physical activity and QoL data collected as part of
the Colorectal Cancer and Quality of Life Study37 Telephone interviews were conducted
at approximately 6 12 and 24-months after colorectal cancer diagnosis (n=1966) which
found that participants achieving at least 150-minutes of physical activity per week had an
18 higher QoL score than those who reported no weekly physical activity
ii DIET
Bekkering et al (2006) identified two dietary intervention studies examining impact on QoL in
colorectal cancer survivors One dietary counselling trial found a significant improvement in
health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst another reported that
an intervention aimed at a healthier dietary lifestyle had no effect on health assessment or
life satisfaction but did lead to increased health action and increased reports of feeling goodlsquo
(Corle et al 2001) No further studies were identified in the current review
37
The Colorectal Cancer and Quality of Life study in Australia examines in detail the lifestyle factors that
influence QoL in the 5-years post-diagnosis (n=2000)
103
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any dietary physical activity interventions examining
impact on QoL in prostate cancer survivors One dietary counselling trial found a significant
improvement in health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst
another reported that an intervention aimed at a healthier dietary lifestyle had no effect on
health assessment or life satisfaction but did lead to increased health action and increased
reports of feeling goodlsquo (Corle et al 2001) No further studies were identified in the current
review
Segal et al (2003) reported an RCT comparing supervised resistance exercise versus
control in men with prostate cancer (n=135) who were scheduled to receive androgen
deprivation therapy for at least 3-months Fitness levels were assessed and the men in the
intervention group met with a certified fitness consultant within 7-days of the pre-
assessment The fitness consultant provided patients with the results of their exercise
assessment and introduced a personalised resistance exercise program A significant
improvement was found in QoL outcomes in the intervention group and a significant
decline in the control group Resistance exercise improved QoL regardless of whether
men were treated with curative or palliative intent or whether androgen deprivation therapy
had been received for less than one-year or 1 year
d) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) found that out of seven physical activity trials six observed
improvements in QoL when using cancer-specific questionnaires (Burnham and Wilcox
2002 Courneya et al 2003 Segal et al 2003 Headley et al 2004 Campbell et al 2005
Sandel et al 2005) but one of these same studies found no association when using the
generic SF-36 scale (Segal et al 2001) This highlights the importance of selecting the most
appropriate outcome measures in terms of sensitivity and responsiveness to a given
intervention
In the current review three studies were identified One prospective controlled four-centre
study comprising a sample of survivors with different tumour sites was identified (Korstjens
et al 2008) QoL outcomes were compared between three groups
1) group-delivered physical training (n=71)
2) group-delivered combined physical and cognitive behavioural training (CBT) (n=76)
3) waiting-list control (n=62)
Participants in both training groups showed significant and clinically relevant improvements
in role limitations physical functioning vitality and health change Adding CBT to the
physical training did not have additional beneficial effects on QoL a finding that has been
104
observed in a number of supported self-management programmes (Davies and Batehup
2010)
Oh et al (2009) reported a RCT examining the QoL outcomes of Medical Qigong (MQ) a
mindndashbody practice that uses physical activity and meditation to harmonise the body mind
and spirit Patients (n=162) with malignancy of any stage and an expected survival length of
gt12-months were randomised to a control group or to a 10-week MQ programme comprising
two supervised 90-minute sessions per week At 10-week follow-up participants in the
MQ group reported larger improvements in QoL than those in the usual care group (p
lt 05)
Mosher et al (2009) reported a prospective cohort study examining the diet exercise and
QoL patterns of 753 breast prostate and colorectal cancer survivors who were at least 5-
years post-diagnosis Survivors underwent two 45-60 minute telephone surveys
administered by the Diet Assessment Center The data demonstrated that greater weekly
minutes of exercise were associated with better physical QoL including less pain and
better health perceptions physical functioning and vitality More exercise was also
correlated with better social functioning Diet quality had a positive association with a range
of physical QoL outcomes in analyses that were adjusted for age level of education and co-
morbidities Greater BMI was associated with worse physical QoL including greater
pain and role limitations because of physical problems and worse health perceptions
physical functioning and vitality
SUMMARY OF EVIDENCE FOR QUALITY OF LIFE
Lifestyle interventions appear to help people with a wide range of cancer types who have
received treatments ranging from surgery chemotherapy radiotherapy or hormonal
therapies although no trials have yet been published specifically addressing the newer
biological therapies Even when not directly associated with overall QoL exercise has been
found to significantly improve social functioning among post-treatment survivors The
benefits of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or group-
based A vast array of different types of exercise techniques have been tested in the studies
evaluated in this review highlighting the potential for survivors to choose activities according
to preference
Whilst some studies have recommended the uptake of physical activity during treatment
others have highlighted the benefits of introducing regular physical activity into a survivorlsquos
self-management care plan immediately after completion of treatment Overall the evidence
does suggest that immediate physical intervention provides greater QoL benefits than
delayed intervention
105
Table 12 Quality of Life and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Cadmus et al (2009)
The results of two RCTs to determine the effect of exercise on quality of life in (a) a RCT of exercise among recently diagnosed breast cancer survivors undergoing adjuvant therapy - randomised to a 6-month home-based exercise program or a usual care group (b) a similar trial among post-treatment survivors - randomised to a 6-month supervised exercise intervention or to usual care
50 newly diagnosed breast cancer survivors in the first RCT (a) 75 post-treatment survivors in the second RCT (b)
6-months Measures of happiness depressive symptoms anxiety stress self-esteem and QoL
Good adherence was observed in both studies Baseline quality of life was similar for both studies on most measures Exercise was not associated with quality of life benefits in the full sample of either study however exercise was associated with improved social functioning among post-treatment survivors who reported low social functioning at baseline (p lt005)
Courneya et al (2003)
RCT testing 15-weeks supervised aerobic and resistance training to determine the effects on cardiopulmonary
function and QoL in
post-menopausal breast cancer
survivors Randomly assigned to an exercise (n=25) or control (n=28) group The exercise group trained on cycle ergometers
three times per week for 15
weeks The control group did not train
53 post-menopausal breast cancer survivors
On completion of the 15-week intervention
Changes in peak oxygen
consu
mption and overall
Peak oxygen consumption increased by 024 Lmin in the exercise group whereas it decreased
by 005 Lmin in the control group
(mean difference 029 Lmin 95 confidence interval [CI] 018 to
040 P lt 001) Overall QOL increased by 91 points in the exercise
group compared with 03 points in the control group (mean
difference 88 points 95 CI 36 to 140 P= 001) Pearson
correlations indicated that change in peak oxygen consumption
correlated with change in overall QOL (r = 045 P lt 01)
Daley et al (2007)
RCT - Women were randomised to one of three groups a)8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-minute one-to-one sessions with an physical activity specialist three times per week (n=34) b)8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one sessions with an physical activity specialist three times
Sedentary breast cancer survivors who were 12-36 months post-treatment (n=117)
On intervention completion and at 24-weeks follow-up
QoL depression physical activity behaviour aerobic fitness
There was a significant mean difference of 98 units in QoL scores favouring aerobic physical activity therapy
106
per week (n=36) c)usual care (n=38)
Korstjens et al (2008)
RCT comparing the effects on cancer survivorslsquo QoL in a
12-week group-
based multidisciplinary self-management rehabilitation
program
combining physical training (twice weekly) and cognitive-behavioural
training (once weekly) with
those of a 12-week group-based physical
training (twice weekly) There
was also a non-intervention comparison group
All cancer types rehabilitation (n=76) physical training (n=71) comparison group (n=62)
Baseline after rehabilitation and
3-
months follow-up
QoL (SF-36) The effects of multidisciplinary rehabilitation did not outperform
those of physical training in role limitations due to emotional
problem (primary outcome) or any other domains of quality of life
(all p gt 05) Compared with no intervention participants in both
rehabilitation groups showed significant and clinically relevant
improvements in role limitations due to physical problem (primary
outcome effect size (ES) = 066) and in physical functioning (ES =
048) vitality (ES = 054) and health change (ES = 076) (all p lt
01)
Lynch et al (2008)
Colorectal Cancer and Quality of Life
Study - aimed at examining the relationships between
physical activity
and QoL after a colorectal cancer
diagnosis Participants completed telephone interviews at approximately
6
12 and 24 months after diagnosis
1966 people with colorectal
6 12 and 24-months post-diagnosis
QoL There was an overall independent association between physical
activity and QoL At a given time point
participants achieving at least 150 minutes of physical activity per
week had an 18 higher quality of life score than those who
reported no physical activity Significant associations were also
present at the interindividual level (differences between
participants) and intraindividual level (within participant changes)
Milne et al (2008)
RCT to examine the effects of a supervised exercise program on motivational variables in breast cancer survivors Participants were randomised in a cross-over design to either an immediate exercise group that exercised from baseline to week 12 or a delayed exercise group that exercised from week 12 to 24
Breast cancer survivors (n=58) within 2-years of completing adjuvant therapy
Post-intervention (12-weeks)
Quality of life There was a significant group by time interaction for overall QoL which increased in the immediate physical activity group by 208 points compared to a decrease in the delayed physical activity group of 53 points
Mosher et al (2009)
Prospective Cohort Study examining the health behaviours of older cancer survivors and the associations of those behaviours with QoL especially during the long-term post-treatment period
753 older (aged 65 years) long-term survivors ( 5 years post-diagnosis) of breast prostate and colorectal
2 telephone interviews
Exercise diet weight status and quality of life
Participants reported a median of 10 minutes of moderate-to-vigorous exercise per week and only 7 had Healthy Eating Index scores gt80 (indicative of healthful eating habits relative to national guidelines) Despite their suboptimal health behaviours survivors reported mental and physical quality of life that exceeded age-related norms Greater exercise and better diet quality were associated with better physical quality-of-life outcomes (eg better vitality and physical functioning P lt 05) whereas greater body mass index was associated with reduced physical quality of life (P lt 001)
107
cancer
Mustian Palesh and Flecksteiner (2008)
RCT testing the functional and QoL outcomes of tai chi - women who completed treatment randomised to receive tai chi or psychosocial support therapy for 12-weeks (60 minutes three times weekly)
Breast cancer survivors (n=21)
On completion of 12-week intervention
Functional capacity and quality of life
The tai chi group demonstrated significant improvements in functional capacity and QoL the psychosocial support group showed significant improvements only in flexibility with declines in QoL
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials
MEDLINE EMBASE CINAHL Psych INFO CancerLit PEDro
and
SportDiscus as well as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
functi
oning as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all outcomes
were positive even when statistical significance was not achieved
Exercise led to statistically significant improvements in quality of life
as assessed by the Functional Assessment of Cancer Therapyndash
General (weighted mean difference [WMD] 458 95 CI 035 to
880) and Functional Assessment of Cancer TherapyndashBreast (WMD
662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak oxygen consumption
and in reducing symptoms of fatigue
Oh et al (2009)
RCT comprising 10-weeks Medical Qigong (MQ) to evaluate the use of (MQ) compared with usual care in improving the QOL of cancer patients
162 patients with a range of cancers
On completion of the 10-week intervention
QOL and fatigue (FACT-GF) mood (Profile of Mood State)
Regression analysis indicated that the MQ group significantly improved overall QOL (t144thinsp=thinspminus5761 Pthinspltthinsp0001) fatigue (t153thinsp=thinspminus5621 Pthinspltthinsp0001) mood disturbance (t122 =2346 Pthinsp=thinsp0021) and inflammation (CRP) (t99thinsp=thinsp2042 Pthinspltthinsp0044) compared with usual care after controlling for baseline variables
Ohira et al (2006)
RCT to examine the effects of weight training on changes in QoL and depressive symptoms in recent breast cancer survivors Randomised to treatment or control group
Convenience sample of 86 breast cancer survivors (4-36 months post-treatment)
6-months The primary outcomes were changes in QoL (CARES-SF) and depressive symptoms (CES-D)
QoL improved in the treatment group compared with the control group (Standardized Difference = 062 P = 006) The psychosocial global score also improved significantly in the treatment group compared with the control group (Standardized Difference = 052 P = 02) There were no changes in CES-D scores Increases in upper body strength were correlated with improvements in physical global score (r = 032 P lt01) and psychosocial global score (r = 030 P lt01) Increases in lean mass were also correlated with improvements in physical global score (r = 023 P lt05) and psychosocial global score (r = 024 P lt05)
Sandel et al (2005)
RCT - 12-weeks dance and movement programme versus wait list control to determine the effect on QoL and shoulder function
35 breast cancer survivors
13 and 26-weeks
QoL (FACT-B) Shoulder range of motion (ROM) and Body Image Scale
FACT-B significantly improved in the intervention group at 13 weeks from 1020 _158 to 1167 _ 169 compared to the wait list group 1081 _ 164 to 1071 _213 (time _ group effect P _ 008) During the crossover phase the FACT-B score increased in the wait list group and was stable in the treatment group The overall effect of the training at 26 weeks was significant (time effect P _ 03) and the order of training was also significant (P _ 015) Shoulder ROM
108
increased in both groups at 13 weeks mdash15_ and 8_ in the intervention and wait list groups (Time effect P _ 03 time _ group P _ 58) Body Image improved similarly in both groups at 13 weeks (time effect P _ 001 time _ group P _ 25) and at 26 weeks There was no significant effect of the order of training for these outcome measures
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) A small to moderate positive effect of physical activity during treatment was seen for physical activity level aerobic fitness muscular strength functional quality of life anxiety and self-esteem With few exceptions exercise was well tolerated during and post treatment without adverse events
Segal et al (2003)
RCT testing the hypothesis that resistance exercise can counter the negative QoL effects of androgen deprivation therapy for prostate cancer by reducing fatigue elevating mood building muscle mass and reducing body fat Randomly assigned to an intervention group that participated in a resistance exercise program three times per week for 12 weeks or to a waiting list control group
55 men with prostate cancer scheduled for androgen deprivation therapy for at least 3 months after recruitment
On completion of the 12-week intervention
Primary outcomes fatigue disease-specific QoL Secondary outcomes muscular fitness body composition
Men assigned to resistance exercise had less interference from fatigue on activities of daily living (P =002) and higher quality of life (P =001) than men in the control group Men in the intervention group demonstrated higher levels of upper body (P =009) and lower body (P lt001) muscular fitness than men in the control group The 12-week resistance exercise intervention did not improve body composition as measured by changes in body weight body mass index waist circumference or subcutaneous skinfolds
Vadiraja et al (2009)
RCT - 6-week yoga and relaxation during adjuvant radiotherapy his study compares the effects of an integrated yoga program with brief supportive therapy in breast cancer outpatients undergoing adjuvant radiotherapy at a cancer centre Intervention consisted of
88 stage II and III breast cancer outpatients
After 6-weeks of radiotherapy
QoL (EORTC-C30) Mood (Positive and Negative Affect Schedule)
There was a significant difference across groups over time for positive affect negative affect and emotional function and social function There was significant improvement in positive affect (ES = 059 p = 0007 95CI 125 to 78) emotional function (ES = 071 p = 0001 95CI 645 to 2533) and cognitive function (ES = 048 p = 003 95CI 12 to 185) and decrease in negative affect (ES = 084 p lt 0001 95CI minus134 to minus44) in the yoga
109
yoga sessions lasting 60 minutes daily while the control group was imparted supportive therapy once in 10 days
group as compared to controls There was a significant positive correlation between positive affect with role function social function and global quality of life There was a significant negative correlation between negative affect with physical function role function emotional function and social function
110
ONGOING LIFESTYLE STUDIES
Four ongoing lifestyle studies were identified in the current review one for breast cancer and
three for colorectal cancer
a) BREAST CANCER
In the US Goodwin et al (ongoing) are trialling lsquoLifestyle Intervention Study in Adjuvant
Treatment of Early Breast Cancerrsquo (LISA) The primary objective of this trial is to evaluate
the effect of the addition of a 2-year centrally delivered individualised telephone-based
lifestyle intervention focusing on weight management to a mailed educational intervention on
disease-free survival in post-menopausal women with early stage breast cancer (hormone
receptor positive) BMI ge24-lt40 kgm2 who are receiving standard letrozole adjuvant
therapy The primary outcome is disease-free survival Secondary outcomes include overall
survival distant disease-free survival weight change QoL selected non-cancer medical
events and biologic factors (insulin) The estimated enrolment is 2150 with the study having
started in 2007 Participants will be randomised to
1) Individualised Lifestyle Intervention Experimental - Women randomised to this arm
will receive an intervention program that consists of individual weight loss diet and
physical activity goals incorporated into a 2-year standardised structured telephone
and mail-based intervention In addition to diet and physical activity the intervention
will address behavioural and motivational issues relating to weight management
including maintaining motivation overcoming obstacles to success relapse
prevention emotional distress and stress and time management The telephone
intervention will involve 19 phone calls as well as mailings and a participant manual
women will be asked to lose up to 10 of their weight by reducing their caloric and
fat intake (by 500-1000 kcalday 20 calories fat) and increasing their moderate
physical activity (to 150-200 minutesweek)
2) Mail-based Active Comparator - Participants will receive a standardised mail-based
intervention focussing on healthy living This will include mailings at study entry as
well as a 2-year subscription to health magazine
Approximately 2150 women will be enrolled follow-up will continue until target event rates
have been met (anticipated 4-6 years after completion of the intervention) This sample size
will provide 80 power (type 1 error 005 2-tailed) to detect a hazard ratio (HR) for DFS of
074-076 in the weight loss intervention arm
b) COLORECTAL CANCER
It has been suggested that interventions to improve QoL in colorectal cancer survivors are
more effective if they target symptom management psychosocial support and lifestyle
variables in a comprehensive and integrated approach to behavioural change (Steginga et
al 2009) Due to the paucity of comprehensive trials examining behavioural interventions in
this group of survivors Hawkes et al (2009) are conducting a large-scale RCT of a 6-month
telephone-delivered lifestyle coaching intervention based on Acceptance and Commitment
111
Therapy (ACT) ndash bdquoCanChange‟ The intervention aims to assist colorectal cancer survivors
(n=350) to make improvements in lifestyle including physical activity weight management
and smoking cessation Participants receive up to eleven telephone sessions over the
6-months from a qualified health professional who provides support on symptom
management and lifestyle change Outcomes will be assessed post-intervention at 6- and
12-months follow-up and will include physical activity CRF QoL and cost-effectiveness
The findings from this innovative lifestyle coaching initiative will offer insight into the intensity
of support required to achieve sustained behaviour change as well as highlight the efficacy
of various components of delivery (eg telephone-delivery coaching professionally-led
etc)
Courneya et al (2008) are leading a physical activity intervention in a collaboration between
Canada and Australia the Colon Health and Life-Long Physical activity Change
(CHALLENGE) a 3-year multicentre RCT for colon cancer survivors (n=1000) who are 2-6
months post adjuvant-treatment Any type of physical activity will be promoted the goal
being to motivate people to increase their overall activity by about 25-hours of moderate
intensity physical activity or 1-hour and 15-minutes of vigorous physical activity per week
Behavioural support counselling and supervised physical activity sessions will be used to
promote the adoption and long-term maintenance of physical activity By monitoring
participants over 10-years the trial will determine if colon cancer recurs less often in people
who increase and maintain their physical activity It will also assess whether physical activity
improves other important outcomes including QoL anxiety depression sleep and physical
function It is anticipated that this trial will provide important insight into strategies for
promoting long-term health behaviour change
Another Australian lifestyle intervention is The Colorectal Cancer and Quality of Life led
by Joanne Aitken The purpose of this project is to identify any patterns between lifestyle and
QoL over the first 5-years following a diagnosis of colorectal cancer Approximately 2000
people have been recruited to take part in this study making it the largest colorectal cancer
study of its type to be undertaken Participants complete a telephone interview and a written
Pilot testing demonstrated that
o 80 of participants (n=20) felt the intervention addressed their issues
o 100 felt more motivated to make lifestyle changes
o 100 would recommend the intervention to other survivors
From baseline to post-intervention improvements
were observed for
o Colorectal cancer symptoms o QoL o Diet o Physical activity
112
questionnaire on an annual basis over the 5-years One of the aims of the study is to
uncover how lifestyle factors particularly physical activity may improve QoL and reduce the
risk of developing other chronic diseases that cancer survivors are prone to such as heart
disease and diabetes This information will help Cancer Council Queensland properly design
and target lifestyle interventions to help improve the health and well-being of colorectal
cancer survivors (Aitken et al ongoing)
113
DISCUSSION
WHAT DO WE KNOW ABOUT LIFESTYLE AND CANCER
This aim of this review was to update the World Cancer Research Fund (WCRF) report bdquoA
Systematic Review of RCTs Investigating the Effect of Nutritional and Physical
Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This has been
achieved by conducting a comprehensive but pragmatic search of the literature from 2006
onwards Where no evidence was available in the WCRF review studies before 2006 have
been included if identified in the reference lists of acquired records To facilitate this
evidence cited within the lsquoHandbook of Cancer Survivorship‟ (Feuerstein 2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (2009) were also utilised
Before presenting a synthesis of the findings within this review there are some limitations
that first need to be addressed
Methodological Limitations
There is strong evidence from observational studies that lifestyle factors can potentially have
major influences on overall mortality risk for cancer survivors This has been most frequently
subjected to study in breast cancer survivors However it is recognised that such
associations in observational studies can be influenced by confounding and therefore that
the mechanisms of lifestyle change on all-cause mortality remains unclear (Cheblowski
2010) Therefore although the observational evidence is strong there is a need to
understand the benefits of lifestyle change ndash particularly physical activity and weight control
in the absence of confounding factors which can be achieved only within the context of a
controlled trial (Ballard-Barbash et al 2009) Such evidence in the end is most likely to
lead to promoting the wide scale adoption of lifestyle change interventions in the role of
secondary prevention of cancer
Consistent with Bekkering et al (2006) it has been found that there is a paucity of robust
evidence on the effects of lifestyle behaviours in cancer progression and recurrence as well
as in the prevention and management of the long-term health implications of cancer
treatment Studies generally comprise small sample sizes and few offer evidence of the
long-term effects of lifestyle behaviours Since lifestyle choices are generally behavioural in
nature the sustainability of these behaviours is fundamental if commissioners are to provide
funding for lifestyle interventions
There were also a large number of retrospective studies particularly for smoking This is
understandable given the challenges of research within this area however it does also raise
limitations surrounding the accuracy of findings This is especially the case when findings
rely on retrospective self-reports of health behaviours or illness experience
114
A number of methodological limitations confound the interpretation of the benefits of exercise
and diet after a diagnosis of cancer from other risks such as smoking body size
supplements and analgesic intake Nevertheless as highlighted by Doyle et al (2007) even
when the scientific evidence is incomplete reasonable conclusions can be made on issues
that can guide lifestyle choices for cancer survivors These are discussed next
THE EVIDENCE
Diet
Evidence for reducing fat intake remains unclear yet evidence for the mechanisms of benefit
of weight loss or the maintenance of a healthy weight is strong Weight control and self-
management clearly requires consideration of total fat intake highlighting the necessity to
provide cancer survivors with advice on levels of fat necessary for weight maintenance
weight loss or in some cases weight gain (Chlebowski et al 2005 Patterson et al 2010)
The same rationale applies to any inconsistencies in evidence for increased fruit and
vegetables which can also facilitate weight management Indeed where the evidence is
strongest for fruits and vegetables applies to those sources containing carotenoids The
evidence is convincing that carotenoids do provide anti-cancer properties (Rock et al 2005
Pierce et al 2007) Lycopene (found in tomatoes) is one such carotenoid found to offer
anti-cancer benefits (Schwarz et al 2008)
Fibre (found in the skins of fruit and vegetables as well as in beans and lentils) and folate
(found in broccoli brussel sprouts asparagus and peas) have in the main been found to
protect against colorectal cancer The evidence is convincing that by slowing down bowel
transit time the mechanism of benefit comes from reducing contact between potential
carcinogens
The benefits of a low fat high fruit and vegetable diet extend into the management of
treatment-related conditions such as lymphoedema In individuals carrying excess weight
the resulting weight loss achieved via a low fat high fruit and vegetable diet can ease the
symptoms of lymphoedema (Shaw Mortimer and Judd 2007)
The evidence also suggests that survivors of prostate cancer might benefit from including
pomegranate juice and green tea in their diet
In terms of other food sources vitamin D and calcium can be protective against osteoporosis
(Ryan et al 2007) although more research with a specific fouls on cancer survivors is
needed in this area
Physical Activity
In general the findings of epidemiological and large cohort studies demonstrates that the
evidence for the role of physical activity in improving breast cancer prognosis quality of life
and on the levels of several hormones associated with breast cancer is strong
115
There is substantial evidence suggesting that the physical activity recommendations
developed by the Department of Health are sufficient for cancer survivors - a total of at least
30-minutes a day of moderate intensity physical activity on five or more days of the week
This can be achieved either by doing all the daily activity in one session or through several
shorter bouts of activity of 10 minutes or more Additionally there is evidence of a dose-
response (ie the more physical activity the greater any benefits) The evidence for breast
cancer further suggest that for survival benefits to be achieved from physical activity no less
than moderate to vigorous activity is required (Gross et al 2002) However the most recent
expert advice emphasises that even a modest amount of exercise like brief walks is
beneficial and gains will be seen versus doing nothing at all38
The interpretation of physical activity evidence has been hindered by the difficulty of
distinguishing physical activity outcomes from subsequent weight loss outcomes However
again even if the main mechanism of benefit of physical activity is improved outcomes
resulting from weight loss or maintenance then this could be considered strong enough
evidence to prescribe physical activity to cancer survivors Furthermore the evidence is
encouraging in terms of its QoL-enhancing effect (McNeeley et al 2006 Daley et al 2007)
Three specific elements of physical activity interventions or advice could be addressed
(Ballard-Barbash et al 2006)
Reducing sedentary behaviours (such as watching TV)
Exercise sessions
Type and intensity of physical activity
There is sufficient evidence for supervised physical activity improving symptoms of cancer-
related fatigue (McNeely et al 2006 Cramp and Daniel 2008) and lymphoedema (Moseley
and Pillerlsquos 2008) Indeed the evidence suggests that guided progressive physical activity
soon after treatment can ease the symptoms of lymphoedema (de Rezende et al 2006)
This supports recent cautions regarding risk-averse clinical recommendations guiding
survivors to avoid the use of the affected limb which may actually lead to de-conditioning
and the very outcome women seek to avoid (Schmitz 2010) At the very least there is no
evidence of appropriate intensity physical activity causing or exacerbating either fatigue or
limb swelling The same is true for the effect of physical activity on osteoporosis Whilst the
benefits of physical activity on bone health require clarifying physical activity can at the very
least prevent loss of bone mineral density in survivors at particular risk of developing
osteoporosis (Waltman et al 2009)
A recent roundtablelsquo event by the American College of Sports Medicine has produced a
Consensus Statement detailing exercise guidelines for cancer survivors (Schmitz Courneya
and Matthews et al 2010) An expert panel reviewed the published empirical evidence and
came to the consensus regarding the safety and efficacy of exercise testing and prescription
in cancer survivors The evidence is clear that exercise during treatment (specific risk
assessment can be carried our for specific treatments and biological response) and after
38
Dr Rachel Ballard ndash Barbash in the NCI Cancer Bulletin June 29 2010
116
treatment is safe and effective Activity induced improvements can be expected on aerobic
fitness muscular strength quality of life and fatigue in breast prostate and haematological
cancers Resistance training can be performed safely by breast cancer survivors with and at
risk of lymphoedoema
Efforts are currently being made to increase the capacity and capability of exercise
professionals to address the unique needs of cancer survivors Exercise professionals need
to be able to access training which reflects the medical condition they are treating for to be
more knowledgeable about the condition and the most suitable and appropriate exercises for
them This requires the development of a national competency framework for a specialist
level 3 add on or level four qualification This would enable providers to develop national
training programmes for cancer specialist exercise professionals and lead to more
accessible referral through the exercise referral scheme (Exercise Referral Research March
2010)
Smoking
Strong and consistent evidence has been presented for increased risk of disease
progression and mortality in people who continue to smoke after a diagnosis of cancer as
well as poorer outcomes in pre-diagnosis smokers (Parsons et al 2010) This evidence
applies particularly to cancers of the lung or head and neck Further research is needed for
breast colorectal prostate and rarer cancers
Alcohol
There is a paucity of research into the effects of alcohol pre- and post-diagnosis on cancer
progression and recurrence as well as symptom management Evidence thus far is highly
contradictory with some demonstrating a protective effect some a detrimental effect and
others no effect
Weight
Substantial weight gain after diagnosis and treatment for breast cancer is adversely
associated with breast cancer prognosis Obesity appears to increase the risk of recurrence
and death among breast cancer survivors by around 30 (Patterson et al 2010) Much
more research is needed to clarify the relationship between prognosis and survival and body
weight in other tumour types
Dealing with issues of weight weight gain and weight management with patients is one of
the lifestyle behaviour change issues health care professionals feel most challenged by
Studies do confirm that health care professionals find it difficult to address these issues with
patients without appearing biased and negative It would appear that a lack of professional
training on behavioural change and motivational coaching and effective strategies for weight
117
loss combine and can lead to avoidance by health care professionals in addressing the need
for change (Puhl and Heuer 2009 Blakeman et al 2010)
Mechanisms of Benefit
Chlebowski (2010) offers some thought-provoking insight into the challenge of implementing
lifestyle change when aromatase inhibitors have been found to reduce oestrogen levels far
more than physical activity interventions One study cites approximately 90 reductions in
oestrogen levels as a result of aromatase inhibitors (Dixon et al 2008) Furthermore three
trials comparing aromatase inhibitors versus placebo anticipate 60-70 reduction in breast
cancer risk (Cuzick 2005 Goss et al 2007 Visvanathan et al 2008) Equally Chlebowski
(2010) points out that the influence of physical activity on insulin levels also has a
pharmacological competitor in the form of metformin (Goodwin et al 2008 Jiralerspong et
al 2009)
These are valid insights that are likely to complicate the successful integration of lifestyle
advice into standardised models of aftercare On the other hand if a public and community
health approach is taken to health and well-being then lifestyle change is likely to offer
health benefits beyond cancer-specific health Such an approach is recommended in the
bdquoCapabilities for Supporting Prevention and Chronic Condition Self-Management A
Resource for Educators of Primary Health Care Professionals‟ developed as part of the
Australian Better Health Initiative (Flinders University 2009) The model offered within this
capabilities framework promotes healthcare providers to view patients holistically as
opposed to focusing solely on diagnosed chronic condition The rationale for this in part
lies in the fact that chronic conditions are more often than not accompanied by co-
morbidities and therefore healthcare is not only about the established condition but also
identified risk factors for co-morbidity
MAKING LIFESTYLE RECOMMENDATIONS FOR CANCER SURVIVORS
In terms of reducing the risks of relapse evidence is strongest for breast colorectal lung
and head and neck cancers but self-management lifestyle strategies are likely to be person-
specific rather than disease or treatment specific so are likely to apply to all patients
recovering from cancer
Diet Appendix A provides evidence-based dietary recommendations that can be made in
light of the findings within this review and national health recommendations These
recommendations comprise a varied diet ensuring adequate intake of vitamins essential
minerals fibre essential fatty acids and antioxidants by eating less fat and more green and
cruciferous vegetables fruits and berries nuts and grains and healthy oils (unsaturated fats
omega)
Physical Activity In terms of physical activity based on the evidence within this report
the five a weeklsquo recommendation is just as relevant to cancer survivors as to the general
population Indeed these recommendations are also provided by the American Cancer
Society (Doyle et al 2006) as advised by a large expert panel Appendix B provides
118
suggestions for physical activity Forty-five to 60-minutes of intentional physical activity are
preferable as the benefits of physical activity do appear to be greater with increased physical
activity Even when this might seem too much survivors can be reminded that the minimum
30-minutes for 5 days a week can be tailored to individual needs and capabilities For
example graded or progressive physical activity can be utilised for those experiencing
fatigue whilst shorter physical activity sessions can be spread out across the day
Other Lifestyle Factors Body Weight In addition it is recommended that obesity (BMI
gt35 Kgm2) excessive alcohol consumption and smoking are avoided There is also
evidence that maintaining a steady healthy weight as opposed to fluctuating between a
healthy and unhealthy BMI can offer health benefits for cancer survivors (Wright et al
2007)
The evidence within this review are indicative of challenges with adherence supporting
findings from Uhley and Jen (2006) that intensive resource-heavy individualised guidance
and support is required to achieve significant long-term lifestyle change This further
emphasises the need to tailor and prescribe such interventions on a needs basis via
individualised assessment and risk stratification
Integrating Self-Management Lifestyle Strategies into Routine Care
Adopting a paternalistic approach and simply telling people is not enough If the medical
community want to help their patients embark on a road of recovery which includes dietary
change and regular exercise there has to be a comprehensive and well-funded package of
education guidance and support Attitude and culture change is imperative both to tackle the
myths and preconceptions around lifestyle factors and their influence on cancer prognosis
symptom management and a future healthy life on the part of both patients survivors and
health care professionals The bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative offers a comprehensive
framework for integrating self-management support into healthcare services (Flinders
University 2009) The emphasis is on not merely striving to change patient behaviour but
also making efforts towards organisational change
Cancer Research UK Diabetes UK and the British Heart Foundation have joined together to launch a new campaign to raise awareness of the dangers of carrying excess weight around the middle The Active Fatlsquo campaign encourages people to measure their waistlines and make positive changes to their lifestyles if they are at risk The emphasis is on educating the public that fat cells are actively working away at stimulating diseases such as cancer diabetes and heart attacks
119
The model offered within this capabilities framework promotes healthcare providers to view
patients holistically as opposed to focusing solely on the diagnosed chronic condition The
rationale for this in part lies in the fact that chronic conditions are more often than not
accompanied by co-morbidities and therefore healthcare is not only about the established
condition but also identified risk factors for co-morbidity The framework also identifies the
need to provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for healthcare
professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
Evidence based information emphasising the importance of lifestyle ideally should be
formally introduced into routine clinical practice early in the treatment pathway and re-
enforced at regular intervals thereafter This ensures patients and their relatives do not miss
the teachable moment where they are most susceptible to positive advice (Demark-
Wahnefried et al 2005) This requires close work with clinicians specialist nurses patients
and advocacy groups to enable information about new strategies to be integrated into
existing local information pathways and materials Indeed the new information prescriptions
currently being pilot tested provide ample opportunity for integrating lifestyle advice into
survivorship care plans
Information clearly has an important role to play in influencing lifestyle behaviours However
people need more than knowledge to be healthy they need the skills to change if they are to
bring about changes in often complex and habitual lifestyle behaviours (Robertson 2008)
Before investing time and money on patient information materials it is necessary to convince
the consultants other direct clinical staff and organisers of clinical services that lifestyle
advice is a priority and to re-allocate resources to enable sufficient time to discuss these
issues within routine consultations One study for example found that patients who were
encouraged by their oncologist exercised significantly more than patients who did not
(Segar et al 1998) The next step is to back up the medical consultation with further
practical verbal and written advice from specialist nurses or information officers One UK
oncology unit for example does this as part of a formal lifestyle interview together with a
bespoke lifestyle information toolbox (Thomas and Nicholson 2009) During this interview
patients can be referred to smoking cessation clinics nutritionists and physiotherapists
where necessary The specialist nurse conducting this interview provides written information
and advice to patients and just as importantly their friends and family about local support
groups dietary measures where to buy healthy foods and specific local exercise facilities
which may entice them ranging from ballroom line and salsa dance lessons aerobics yoga
and fitness classes local walking swimming and cycling groups through to gyms sport
centre tennis and badminton courts and Pilates classes giving times contact numbers and
locations to make it as easy as possible to follow the advice The rationale for these
120
interviews is that individualised lifestyle counselling is more likely to elicit a response than
generic general advice The specialist nurse then follows up the advice by telephone and
further consultations as prompting has been shown to improve update A study from North
Bedfordshire for example showed that although 52 of patients accepted referral for
exercise in a local Gym a further 23 decided to attend classes only after additional
prompting from the nurse either by telephone
Many UK Oncology Units already have instigated an exit interview system to discuss follow
up arrangements and this process could be expanded to include lifestyle counselling
provided the specialist nurses involved have received extra training This training should
include a knowledge of the evidence and importance of weight diet physical activity and
smoking after cancer as well as ways to appropriately advise home-based exercise
regimens and how to direct patients towards the myriad of council or independent exercise
activities available locally to them The courses may require additional communication and
motivational skills training to enable nurses to engage in a partnership relationship which
promotes addressing the patientlsquos agenda goals and motivation around achieving and
maintaining behaviour change Examples of a range of courses aimed to develop such skills
and competencies and which are provided by the Flinders Human Behaviour and Health
Research Unit include a Chronic Condition Self-Management workshop Communication
and Motivational Skills Workshop and a Living Well Workshop
Remaining Questions
This review has provided some clarification of the evidence pertaining to lifestyle and cancer
outcomes However in implementing this evidence into standardised practice within cancer
aftercare will require a number of questions to be explored
1) What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
At present it is unclear how soon after a cancer diagnosis an intervention should be
introduced for behaviour change(Rabin 2009) Until the teachable moment is more clearly
defined for cancer patients the advice is that professionals should repeatedly offer to assist
a patient with addressing their health behaviour risks until the patient accepts or seeks other
forms of support
The literature suggests that professional involvement in supported self-management and
lifestyle advice is required in order to maintain patient motivation by enhancing patient
engagement with health information and advice When information is supplied by healthcare
professionals and the patient is supported in using this information legitimacy is provided to
the information and advice (Protheroe et al 2008) Efficacy outcomes in terms of lifestyle
advice and behavioural change are fundamental in the initiation and maintenance of a
healthy lifestyle and the involvement of healthcare professionals strengthens outcome
efficacy whilst also motivating the patient and increasing their own self-efficacy to adapt their
lifestyle (Irwin 2008) However there is anecdotal and other evidence that on the one hand
the importance of lifestyle factors on the prognosis survival and symptom management of
121
cancer survivors is poorly understood and appreciated by significant numbers of cancer
health care professionals and on the other hand they do need specific training in the key
communication skills to be able to support effective behaviour change with their patients A
review is currently underway investigating the role of patient-professional communication in
terms of self-management
2) How can people most likely to benefit from lifestyle interventions be effectively
identified
A recent review on cancer-specific self-management programmes highlighted that patients
can be risk stratified according to needs and this according to whether they are likely to
benefit from the programme (Davies and Batehup 2010) For example people with low
levels of social support have been found to benefit most from group-delivered support As
part of the Bournemouth after Cancer Survivorship Project Active Wellness Programmelsquo
patients are assessed for the readiness to take part in physical activity (Milne et al 2010) It
is recommended that questionnaires that might facilitate such evidence-based risk
stratification be evaluated in order to provide further insight into this question A set of risk
stratification tools would be one way of ensuring cost-effectiveness
3) What are the various intensities of lifestyle support that can be provided based on
levels of individual need
As demonstrated within this review lifestyle interventions and self-management support do
generally require some level of support in order to be successful A strong
patientprofessional partnership appears to be at the essence of this intensive approach as
does longer-term follow-up and support (Davies and Batehup 2010) Addressing this
question will also in part address some of the inequalities within the current system of
cancer care with survivors identified as having low literacy being provided with extra
informational support and assistance with understanding the lifestyle recommendations
being made
122
Appendix A Evidence-Based Dietary Self-Management Recommendations
Food Advice Evidence
Reduce Saturated Fats
Unless underweight avoid processed fatty foods cakes biscuits crisps and other fatty snacks pastries cream and fried foods Cut the fat off the meat and check serum cholesterol regularly
(Ingram 1994 Hebert et al 1998 Norat et al 2004 Thomas et al 2009)
Increase all fish intake
All fresh fish but particularly the oily varieties such as mackerel and sardines Fresh water fish such as trout have the advantage of avoiding the potential heavy metal contamination of tuna amp sword fish which some suggest should not be eaten more than twice a week
(Ornish et al 2005 Meyerhardt et al 2007 Goodwin et al 2009)
Essential minerals
Vary the diet to ensure intake of adequate quantities of essential minerals consider Mixed nuts including Brazils Seafood including sardines prawns and shell fish Pulses and grains Vary carbohydrate sources such as pasta rice different brands of potatoes pulses such as lentils and quinoa
Rohan et al 1993) Powers et al 2007 McTiernan et al 2009)
Dietary Vitamins
Fresh fruit raw and calciferous vegetables grains oily fish nuts and salads Unless you have diarrhoea try to increase the amount of ripe fruit you eat each day ideally by eating the whole fruit Freshly squeezed fruit juices are recommended
(Rohan et al1993 Ingram 1994 Fleischauer et al 2003 New et al 2004 Rock et al 2005 McEligot et al 2006 Meyerhardt et al 2007 Schwarz et al 2008 Goodwin et al 2009)
Polyphenols
Onions leeks broccoli blueberries red wine tea apricots pomegranates chocolate coffee blueberries kiwis plums cherries ripe fruits parsley celery tomatoes mint citrus fruit
(Bettuzzi et al 2006 Pantuck et al 2006 Schwarz et al 2008 McLarty et al 2009)
Phytoestrogens
Soybeans and other legumes including peas lentils pinto (baked beans) and other beans and nuts (supplements not recommended)
Marini et al (2008)
Increase Carotenoids (Lycopene)
Tomatoes tomato sauce chilli carrots green vegetables and dark green salads
(Ingram 1994 Rock et al 2005 McEligot et al 2006 Pierce et al 2007 Powers et al 2007 Thomson et al 2007 Schwarz et al 2008)
123
Appendix B Evidence-Based Physical Activity Recommendations
Category Advice Evidence
Resistance Exercise
Strength training has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce fatigue and improve lean body mass and muscle strength Personalised tailored resistance exercise based on fitness assessments can improve QoL
Segal et al (2003) Poudevigne et al (2009) Courneya et al (2007) (Segal et al 2009)
Aerobic Exercise Aerobic exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of lymphoedema prevent loss of bone mineral density and reduce body fat Walking is particularly popular
Hayes Hildegard and Turner (2009) Schwartz Winters-Stone and Gallucci (2007) Courneya et al (2007) Fillion et al (2008) Kenfield et al (2009) Windsor Nichol and Potter (2004) Chang et al (2008)
Combined Resistance and Aerobic Exercise
Combined aerobic and resistance exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of fatigue and improve QoL
Coleman et al (2003) Milne et al (2008)
3gt MET-hours per week
Benefits of physical activity require 3 or more MET-hours per week (eg using a stationary bicycle for one-hour)
Holick et al (2008) Holmes et al (2005) Saxton et al (2010) Kenfield (2010)
Moderate intensity
Physical activity needs to be of at least moderate intensity in order to offer beneficial outcomes
Holick et al (2008) Patterson et al (2010) Holmes et al (2005) Saxton et al (2010) Campbell et al (2007) Poudevigne et al (2009) Tardon et al (2004)
Dose-Response Exercise can be dose-responsive thus taking part in more than 3 MET-hours per week is likely to offer greater benefits
Meyerhardt et al (2005) Kenfield (2010)
During Treatment Remaining active during treatment can help with symptoms such as fatigue as well as increase completion rates for chemotherapy
Chang et al (2008) Coleman et al (2003) Courneya et al (2007)
Home-Based
Home-based physical activity prescriptions either supervised or alone have proven effective in improving cancer outcomes including reducing fatigue and protecting bone mineral density
Ligibel et al (2008) Windsor Nichol and Potter (2004) Schwartz Winters-Stone and Gallucci (2007)
Supervised Supervised physical activity either at home in groups or during treatment have proven effective in improving cancer outcomes as well as reducing lean body mass and facilitating the completion of chemotherapy
Chang et al (2008) Coleman et al (2003) Velthuis et al (2009) Courneya et al (2007) Campbell
et al (2007) exercise (Soliman et al 2009)
124
References
Abrahamsen JF Andersen A Hannisdal E et al Second malignancies after treatment of Hodgkins disease the influence of treatment follow-up time and age J Clin Oncol 11 (2) 255-61 1993 Addington-Hall et al (2010) Older womenlsquos experience of breast cancer alongside other health conditions The EPaN study (Experiences Preferences and Needs of women aged 70 years and over) University of Southampton Funded by Macmillan Cancer Support Ahmed R L W Thomas et al (2006) Randomized Controlled Trial of Weight Training and Lymphedema in Breast Cancer Survivors J Clin Oncol 24(18) 2765-2772 Ainsworth BE et al Compendium of physical activities an update of activity codes and MET intensities Med Sci Sports Exerc 2000 Sep32(9 Suppl)S498-504 Aitken J (ongoing) Colorectal cancer and quality of life study httpwwwcancerqldorgaupageResearch_statisticsVCRCCVCRCC_research_programsLifestyle_and_Cancer [Last accessed 04062010] Akopyan and Bonavida 2006 G Akopyan and B Bonavida Understanding tobacco smoke carcinogen NNK and lung tumorigenesis Int J Oncol 29 (2006) pp 745ndash752 Alberts DS Martinez ME Roe DJ et al Lack of effect of a high-fiber cereal supplement on the recurrence of colorectal adenomas Phoenix Colon Cancer Prevention Physicians Network [Comment] New England Journal of Medicine 2000 April 20342(16)1156-62 Arts CJ Govers CA van den Berg H Wolters MG van Leeuwen P Thijssen JH In vitro binding of estrogens by dietary fiber and the in vivo apparent digestibility tested in pigs J Steroid Biochem Mol Biol 1991 May38(5)621-8 Bandura A (1977) Self-efficacy Toward a unifying theory of behavioural change Psych Rev 84 191 - 215 Barbash-Ballard R Hunsberger S Alciati MH Blaire SN Goodwin PJ McTiernan A(2009) Physical activity weight control and breast cancer risk and survival Clinical trial rationale and design considerations J Natl Cancer Inst 101630-643 Baron JA Beach M Mandel JS et al Calcium supplements and colorectal adenomas Polyp Prevention Study Group Ann N Y Acad Sci 1999889138-45
Bekkering T Beynon R Davey Smith G Davies A Harbord R Sterne J Thomas S and Wood L (2006) A systematic review of RCTs investigating the effect of dietal and physical activity interventions on cancer survival updated report World Cancer Research Fund httpwwwdietandcancerreportorg [Last accessed 150210] Bellizzi K M J H Rowland et al (2005) Health Behaviours of Cancer Survivors Examining Opportunities for Cancer Control Intervention J Clin Oncol 23(34) 8884-8893 Bernstein H Cosford P and Williams A (2010) Enabling effective delivery of health and wellbeing an independent report Department of Health February 2010
125
Bettuzzi et al 2006 S Bettuzzi M Brausi F Rizzi G Castagnetti G Peracchia and A Corti Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia a preliminary report from a one-year proof-of-principle study Cancer Research 66 (2) (2006) pp 1234ndash1240 Bingham SA Day NE Luben R Ferrari P Slimani N Norat T et al Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) an observational study Lancet 20033611496ndash501 Bingham S Riboli E Diet and cancermdashthe European Prospective Investigation into Cancer and Nutrition Nat Rev Cancer 20044206ndash15 Blakeman T Bower P Reeves D Chew-Graham C (2010) ―Bringing self management into clinical view a qualitative study of long term condition management in primary care consultations Chronic Illness 0 1-15 Blackburn G L and K A Wang (2007) Dietary fat reduction and breast cancer outcome results from the Womens Intervention Nutrition Study (WINS) Am J Clin Nutr 86(3) 878S-881 Bonithon-Kopp C Kronborg O Giacosa A Rath U Faivre J Calcium and fibre supplementation in prevention of colorectal adenoma recurrence A randomised intervention trial Lancet 2000356(9238)1300-6 Borugian MJ Sheps SB Kim-Sing C Olivotto IA Van Patten C Dunn BP Coldman AJ Potter JD Gallagher RP Hislop TG Waist-to-hip ratio and breast cancer mortality Am J Epidemiol 2003 Nov 15158(10)963-8 Boyapati SM Shue X et al (2005) Soyfood intake and breast cancer survival a follow up of the Shanghai Breast Cancer Study Breast Cancer Research and Treatment 92(1) p11-17 Boyd NF Stone J Vogt KN Connelly BS Martin LJ Minkin S Dietary fat and breast cancer risk revisited a meta-analysis of the published literature Br J Cancer 2003 Nov 389(9)1672-85 Box R Marnes T amp Robertson V Aquatic physiotherapy and breast cancer related lymphoedema 5th Australasian Lymphology Association Conference Proceedings Mar 2004 47-9 Brown J K T Byers et al (2003) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 53(5) 268-291 Cade JE Burley VJ Greenwood DC UK Womens Cohort Study Steering Group Dietary fibre and risk of breast cancer in the UK Womens Cohort Study Int J Epidemiol 2007 Apr36(2)431-8 Caan B B Sternfeld et al (2005) Life After Cancer Epidemiology (LACE) Study A cohort of early stage breast cancer survivors (United States) Cancer Causes and Control 16(5) 545-556
126
Caan BJ Kwan ML Hartzell G Castillo A Slattery ML Sternfeld B Weltzien E Pre-diagnosis body mass index post-diagnosis weight change and prognosis among women with early stage breast cancer Cancer Causes Control 2008 Dec19(10)1319-28 Cadmus L A P Salovey et al (2009) Physical activity and quality of life during and after treatment for breast cancer results of two randomized controlled trials Psycho-Oncology 18(4) 343-352 Campbell KL Westerlind KC Harber VJ Bell GJ Mackey JR Courneya KS (2007) Effects of aerobic exercise training on oestrogen metabolism in premenopausal women a randomized controlled trial Cancer Epidemiol Biomarkers Prev 16731ndash73 Cancer 52 and NCSI Research Workstream (2009) Less common cancers consultation Report June 2009 Cella D (2009) Quality of life in patients with metastatic renal cell carcinoma The importance of patient-reported outcomes Cancer treatment reviews 35(8) 733-737 Chan JM Gann PH and Giovannucci EL (2005) Role of diet in prostate cancer development and progression Journal of Clinical Oncology 23(32) p 8152-60 Chlebowski RT Aiello E McTiernan A Weight loss in breast cancer patient management Journal of Clinical Oncology 20(4) 1128-1143 2002 Chlebowski RT Blackburn GL Elashoff RE Thomson C Goodman MT Shapiro A Giuliano AE Karanja N Hoy MK Nixon DW and The WINS Investigators (2005) Dietary fat reduction in post-menopausal women with primary breast cancer Journal of Clinical Oncology (10) p 3s Chlebowski R G Blackburn et al (2006) Dietary fat reduction and breast cancer outcome interim efficacy results from the Womens Intervention Diet Study J Natl Cancer Inst 98 1767 - 1776 Chlebowski RT Blackburn GL (2007) Diet and breast cancer recurrence JAMA 2007 Nov 14298(18)2135 author reply 2135-6 Chlebowski RT (2010) Lifestyle and breast cancer risk The way forward Journal of
Clinical Oncology Vol 28 No 9 (March 20) 2010 pp 1445-1447
Cho E Spiegelman D Hunter DJ Chen WY Colditz GA Willett WC Premenopausal dietary carbohydrate glycaemic index glycaemic load and fiber in relation to risk of breast cancer Cancer Epidemiol Biomarkers Prev 2003 Coulter A and Ellins J (2006) Patient-focused Interventions A review of the evidence Picker Institute Europe (01865 208100) and Health Foundation Coups E J and J S Ostroff (2005) A population-based estimate of the prevalence of behavioural risk factors among adult cancer survivors and non-cancer controls Preventive Medicine 40(6) 702-711 Courneya K S (2003) Physical activity in Cancer Survivors An Overview of Research Medicine amp Science in Sports amp Physical activity 35(11) 1846-1852
127
Courneya K Booth CM Gill S et al (2008) The colon health and life-long physical activity change trial a randomized trial of the national institute of Canada clinical trials group Current Oncology 15(6) 271-78 Cramp F Daniel J (2008) Physical activity for the management of cancer-related fatigue in adults CochraneDatabaseSystRev 2008 Cuzick J Aromatase inhibitors for breast cancer prevention J Clin Oncol 231636-1643 2005
Cuzick J Hot flushes and the risk of recurrence Retrospective exploratory results from the ATAC trial 30th Annual San Antonio Breast Cancer Symposium San Antonio TX December 13-16 2007 (poster 2069) Daley A H Crank et al (2007) Randomized trial of physical activity therapy in women treated for breast cancer J Clin Oncol 25 1713 - 1721 Daley A S Bowden et al (2008) What advice are oncologists and surgeons in the United Kingdom giving to breast cancer patients about physical activity International Journal of Behavioural Diet and Physical Activity 5(1) 46 Danhauer S Mihalki S Russell G Campbell C Felder L Daley L et al (2009) Restorative yoga for women with breast cancer Findings from a randomized pilot study Psych oncology 18(4) 360-368 Dansinger M L J A Gleason et al (2005) Comparison of the Atkins Ornish Weight Watchers and Zone Diets for Weight Loss and Heart Disease Risk Reduction A Randomized Trial JAMA 293(1) 43-53 Davies NJ and Batehup L (2010) Self-management support for cancer survivors Guidance for developing interventions An update of the evidence National Cancer Survivorship Initiative Macmillan Cancer Support March 2010 Demark-Wahnefried W and Jones L (2008) Promoting a Healthy Lifestyle among Cancer Survivors Haematologyoncology clinics of North America 22(2) 319-342 Deo SV Ray S Rath GK et al (2004) Prevalence and risk factors for development of lymphedema following breast cancer treatment Indian J Cancer 418ndash12 Department of Health (2001) Exercise referral systems A national quality assurance framework Department of Health Report London 2001 Department of Health (2004) At least five a week Evidence on the impact of physical activity and its relationship to health Department of Health Report London 2004 Department of Health (2009a) Internal analysis unpublished Department of Health London Department of Health (2009b) Obesity general information Health survey of England 2008 Department of Health London Department of Health (2009c) Guidance on the routine collection of patient-reported outcome measures (PROMs) p 28 The Stationary Office London
128
De Rezende LF Franco RL de Rezende MF et al Two physical activity schemes in postoperative breast cancer comparison of effects on shoulder movement and lymphatic disturbance Tumori 2006 9255ndash61 de Waard F Ramlau R Mulders Y de Vries T van Waveren S A feasibility study on weight reduction in obese postmenopausal breast cancer patients Eur J Cancer Prev 1993 May 2(3)233-8 Dignam J J B N Polite et al (2006) Body Mass Index and Outcomes in Patients Who Receive Adjuvant Chemotherapy for Colon Cancer J Natl Cancer Inst 98(22) 1647-1654 Dimeo FC Thomas F Raabe-Menssen C et al Effect of aerobic exercise and relaxation training on fatigue and physical performance of cancer patients after surgery A randomised controlled trial Support Care Cancer 2004 12(11)774-9 Dixon JM Renshaw L Young O et al Letrozole suppresses plasma estradiol and oestrone sulphate more completely than anastrozole in postmenopausal women with breast cancer J Clin Oncol 261671-1675 2008
Doyle C L H Kushi et al (2006) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 56(6) 323-353 Dwyer J J Peterson et al (2008) Do Flavonoid Intakes of Postmenopausal Women With Breast Cancer Vary on Very Low Fat Diets Diet and Cancer 60(4) 450 - 460 Eakin E Hayes S and Lawler S (ongoing) Physical activity for Health Using the telephone to promote physical activity-based rehabilitation in ruralremote Australian breast cancer survivors National Breast Cancer Foundation httpwwwuqeduaucprcindexhtmlpage=60214amppid=20928 [Last accessed 300310] Eliassen AH Missmer SA Tworoger SS Spiegelman D Barbieri RL Dowsett M Hankinson SE Endogenous steroid hormone concentrations and risk of breast cancer among premenopausal women J Natl Cancer Inst 2006 Oct 4 98(19)1406-15 Elkort RJ Baker FL Vitale JJ Cordano A Long-term nutritional support as an adjunct to chemotherapy for breast cancer JPEN J Parenter Enteral Nutr 1981 Sep-Oct 5(5)385-90 Enger SM Greif JM Polikoff J Press M Body weight correlates with mortality in early-stage breast cancer Arch Surg 2004139954ndash958 discussion 58ndash60 Eton D T D L Fairclough et al (2003) Early Change in Patient-Reported Health During Lung Cancer Chemotherapy Predicts Clinical Outcomes Beyond Those Predicted by Baseline Report Results From Eastern Cooperative Oncology Group Study 5592 J Clin Oncol 21(8) 1536-1543 Fentiman IS Allen DS Hamed H (2005) Smoking and prognosis in women with breast cancer Int J Clin Pract 591051ndash1054
129
Ferrari P Jenab M Norat T et al Lifetime and baseline alcohol intake and risk of colon and rectal cancers in the European prospective investigation bettinto cancer and nutrition (EPIC) Int J Cancer 2007 121 ( 9 ) 2065 ndash 2072
Feuerstein M (2006) Handbook of Cancer Survivorship New York NY Springer 2006 Fillion L P Gagnon et al (2008) A Brief Intervention for Fatigue Management in Breast Cancer Survivors Cancer Nursing 31(2) 145-159 Findley P amp Sambamoorthi U (2009) Preventive health services and lifestyle practices in cancer survivors A population health investigation Journal of Cancer Survivorship 3 43-58 Fleischauer AT Simonsen N Arab L Antioxidant supplements and risk of breast cancer recurrence and breast cancer-related mortality among postmenopausal women Nutr Cancer 2003 46 15-22 Flinders University (2009) Capabilities for Supporting Prevention and Chronic Condition Self-Management A Resource for Educators of Primary Health Care Professionals Australian Better Health Initiative A joint Australian State and Territory government initiative
Flowers M Thompson PA 2009 t10c12 Conjugated Linoleic Acid Suppresses HER2 Protein and Enhances Apoptosis in SKBr3 Breast Cancer Cells Possible Role of COX2 PLoS ONE 4(4) e5342 doi101371journalpone0005342 Food Standards Agency (2007) FSA nutrient and food based guidelines for UK institutions httpwwwfoodgovukmultimediapdfsnutrientinstitutionpdf [Last accessed 120310] Food Standards Agency (2010) Heightweight chart httpwwweatwellgovukhealthydiethealthyweightheightweightchart [Last accessed 120310] Ford MB Sigurdson AJ Petrulis ES et al Effects of smoking and radiotherapy on lung carcinoma in breast carcinoma survivors Cancer 98 (7) 1457-64 2003 Friedenreich C Cust A Lahmann PH et al Anthropometric factors and risk of endometrial cancer the European prospective investigation into cancer and nutrition Cancer Causes Control 2007 18399-413 Friedenreich C M C G Woolcott et al (2010) Alberta Physical Activity and Breast Cancer Prevention Trial Sex Hormone Changes in a Year-Long Physical activity Intervention Among Postmenopausal Women J Clin Oncol 28(9) 1458-1466 Friedenreich CM Cust AE Physical activity and breast cancer risk impact of timing type and dose of activity and population subgroup effects Br J Sports Med 2008 Aug42(8)636-47 Giovannucci EL (2005) Obesity insulin resistance and cancer risk Cancer Prevention 5 httpwwwnypcancerpreventioncomissue5propro_featurespre_earshtml [Last accessed 03062010]
130
Gold E B J P Pierce et al (2009) Dietary Pattern Influences Breast Cancer Prognosis in Women Without Hot Flashes The Womens Healthy Eating and Living Trial J Clin Oncol 27(3) 352-359 Gonzalez CAPera GAgudo APalli DKrogh VVineis PTumino RPanico SBerglund GSiman HNyren OAgren AMartinez CDorronsoro MBarricarte ATormo MJQuiros JRAllen NBingham SDay NMiller ANagel GBoeing HOvervad KTjonneland ABueno-de-Mesquita HBBoshuizen HCPeeters PNumans MClavel-Chapelon FHelen IAgapitos ELund EFahey MSaracci RKaaks RRiboli E Smoking and the risk of gastric cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC) Int J Cancer 107 (4) 629-634 (2003) Gonzaacutelez CA Jakszyn P Pera G Agudo A Bingham S Palli D Ferrari P Boeing H del Giudice G Plebani M Carneiro F Nesi G Berrino F Sacerdote C Tumino R Panico S Berglund G Simaacuten H Nyreacuten O Hallmans G Martinez C Dorronsoro M Barricarte A Navarro C Quiroacutes JR Allen N Key TJ Day NE Linseisen J Nagel G Bergmann MM Overvad K Jensen MK Tjonneland A Olsen A Bueno-de-Mesquita HB Ocke M Peeters PH Numans ME Clavel-Chapelon F Boutron-Ruault MC Trichopoulou A Psaltopoulou T Roukos D Lund E Hemon B Kaaks R Norat T Riboli E Meat intake and risk of stomach and oesophageal adenocarcinoma within the European Prospective Investigation Into Cancer and Nutrition (EPIC) J Natl Cancer Inst 2006 Mar 198(5)345-54 Goodwin PJ Pritchard KI Ennis M et al Insulin-lowering effects of metformin in women with early breast cancer Clin Breast Cancer 8501-5052008
Goodwin PJ Ennis M Pritchard KI Koo J Hood N (2009) Prognostic Effects of 25-Hydroxyvitamin D Levels in Early Breast Cancer Journal of Clinical Oncology Vol 27 No 23 (August 10) pp 3757-3763 Goodwin PJ Lifestyle Intervention Study in Adjuvant Treatment of Early Breast Cancer (LISA) (ongoing) httpclinicaltrialsgovct2showNCT00463489 [Last accessed 04062010] Goss PE Richardson H Chlebowski RT et al National Cancer Institute of Canada Clinical Trials Group MAP 3 Trial Evaluation of exemestane to prevent breast cancer in postmenopausal women at risk Clin Breast Cancer 7895-900 2007
Gothard L Cornes P et al (2004) Double-blind placebo-controlled randomised trial of vitamin E and pentoxifylline in patients with chronic arm lymphoedema and fibrosis after surgery and radiotherapy for breast cancer Radiotherapy and oncology journal of the European Society for Therapeutic Radiology and Oncology 73(2) 133-139 Grace PB Taylor JI Low YL Luben RN Mulligan AA Botting NP Dowsett M Welch AA Khaw KT Wareham NJ Day NE Bingham SA Phytoestrogen concentrations in serum and spot urine as biomarkers for dietary phytoestrogen intake and their relation to breast cancer risk in European prospective investigation of cancer and nutrition-norfolk Cancer Epidemiol Biomarkers Prev 2004 May13(5)698-708 Greenberg ER Baron JA Tosteson TD et al A clinical trial of antioxidant vitamins to prevent colorectal adenoma Polyp Prevention Study Group[comment] New England Journal of Medicine 1994 July 21331(3)141-7 Gritz ER (1993) Cancer Smoking Epidemiology Biomarkers amp Prevention 2(3) 261-270
131
Gritz E R M C Fingeret et al (2006) Successes and failures of the teachable moment Cancer 106(1) 17-27 Gross G C Ott et al (2002) Postmenopausal Breast Cancer Survivors at Risk for Osteoporosis Physical Activity Vigour and Vitality Oncology Nursing Forum 29(9) 1295-1300 Gross M C Ramirez et al (2009) Expression of androgen and oestrogen related proteins in normal weight and obese prostate cancer patients The Prostate 69(5) 520-527 Guthrie JR Ball M Murkies A Dennerstein L Dietary phytoestrogen intake in mid-life Australian-born women relationship to health variables Climacteric 2000 3 254ndash261 Hawkes A L S Gollschewski et al (2009) A telephone-delivered lifestyle intervention for colorectal cancer survivors a pilot study Psycho-Oncology 18(4) 449-455 Haydon AM Macinnis RJ English DR Giles GG (2006) The effect of physical activity and body size on survival after diagnosis with colorectal cancer Gut 55 p 62-67 Hayes SC Spence RR Galvao DANewton RU (2009) Australian Association for Physical activity and Sport Science position stand Optimising cancer outcomes through physical activity JSciMedSport 200912428-434 Heald AH Cade JE Cruickshank JK Anderson S White A Gibson JM (2003) The influence of dietary intake on the insulin-like growth factor (IGF) system across three ethnic groups a population-based study Public Health Nutr6175ndash80 Healthy Weight Healthy Lives (2008) A Cross-Government Strategy for England Cross-Government Obesity Unit DH and Department of Children Schools and Families Hebert JR Hurley TG Ma Y (1998) The effect of dietary exposures on recurrence and mortality in early stage breast cancer Breast Cancer Res Treat 5117ndash28 Hofstad B Almendingen K Vatn M et al Growth and recurrence of colorectal polyps a double-blind 3-year intervention with calcium and antioxidants Digestion 199859(2)148-56 Holick C N P A Newcomb et al (2008) Physical Activity and Survival after Diagnosis of Invasive Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 17(2) 379-386 Holm LE Nordevang E Hjalmar ML Lidbrink E Callmer E Nilsson B (1993) Treatment failure and dietary habits in women with breast cancer J Natl Cancer Inst 8532ndash36 Holmes MD Hunter DJ Colditz GA et al Association of dietary intake of fat and fatty acids with risk of breast cancer JAMA 1999281914-920 Holmes MD Chen WY Feskanich D Kroenke CH Colditz GA (2005) Physical activity and survival after breast cancer diagnosis JAMA 293 p 2479-86
132
Holmes MD Murin S Chen WY Kroenke CH Spiegelman D Colditz GA (2007) Smoking and survival after breast cancer diagnosis Int J Cancer 1202672ndash2677
Howe GR Hirohata T Hislop TG Iscovich JM Yuan JM Katsouyanni K Lubin F Marubini E Modan B Rohan T et al Dietary factors and risk of breast cancer combined analysis of 12 case-control studies J Natl Cancer Inst 1990 Apr 482(7)561-9
Hunter DJ Spiegelman D Adami HO Beeson L van den Brandt PA Folsom ARFraser GE Goldbohm RA Graham S Howe GR et al Cohort studies of fat intake and the risk of breast cancer--a pooled analysis N Engl J Med 1996 Feb 8334(6)356-61
Ingram D Diet and subsequent survival in women with breast cancer British Journal of Cancer 1994 Mar69(3)592-5
Irwin ML Smith AW McTiernan A Ballard-Barbash R Cronin K Gilliland FD Baumgartner RN Baumgartner KB Bernstein L (2008) Influence of Pre- and Postdiagnosis Physical Activity on Mortality in Breast Cancer Survivors The Health Eating Activity and Lifestyle Study Journal of Clinical Oncology 26(24) 3958-3964
Ishikawa H Akedo I Otani T et al Randomized trial of dietary fiber and Lactobacillus casei administration for prevention of colorectal tumors Int J Cancer 2005 September 20116(5)762-7 Jiralerspong S Palla SL Giordano SH et al Metformin and pathologic complete responses to neoadjuvant chemotherapy in diabetic patients with breast cancer J Clin Oncol 273297-3302 2009
Jones LW Demark-Wahnefried W Diet physical activity and complementary therapies after primary treatment for cancer Lancet Oncol 7(12)1017-26 Nov-Dec 2006 PMID 17138223 Kaaks R A Lukanova and MA Kurzer Obesity endogenous hormones and endometrial cancer risk a synthetic review Cancer Epidemiol Biomark Prev 11 (2002) pp 1531ndash1543 Kaaks R Rinaldi S Key TJ Berrino F Peeters PH Biessy C Dossus L Lukanova A Bingham S Khaw KT Allen NE Bueno-de-Mesquita HB van Gils CH Grobbee D Boeing H Lahmann PH Nagel G Chang-Claude J Clavel-Chapelon F Fournier A Thieacutebaut A Gonzaacutelez CA Quiroacutes JR Tormo MJ Ardanaz E Amiano P Krogh V Palli D Panico S Tumino R Vineis P Trichopoulou A Kalapothaki V Trichopoulos D Ferrari P Norat T Saracci R Riboli E Postmenopausal serum androgens oestrogens and breast cancer risk the European prospective investigation into cancer and nutrition Endocr Relat Cancer 2005 Dec12(4)1071-82 Kawahara M Ushijima S Kamimori T et al Second primary tumours in more than 2-year disease-free survivors of small-cell lung cancer in Japan the role of smoking cessation Br J Cancer 78 (3) 409-12 1998 Keinan-Boker L van Der Schouw YT Grobbee DE Peeters PH Dietary phytoestrogens and breast cancer risk Am J Clin Nutr 2004 Feb79(2)282-8 Kenfield SA (2010) Physical activity and mortality in prostate cancer (In Regular Vigorous Physical Activity found to have Survival Benefits for Prostate Cancer Patients
133
AACR Frontier in Cancer Prevention Research Conference by Tuma R Oncology Times) 32(2) p 29 33 Key TJ Allen NE Hormones and breast cancer IARC Sci Publ 2002156273-6 Khaodhiar L Nixon D Chlebowski RT Elashoff R Blackburn GL Hoy MK Insulin resistance in postmenopausal women with breast cancer Proc Am Cancer Res 2003446349 (abstr) Kim EH Willett WC Colditz GA Hankinson SE Stampfer MJ Hunter DJ Rosner B Holmes MD Dietary fat and risk of postmenopausal breast cancer in a 20-year follow-up Am J Epidemiol 2006 Nov 15164(10)990-7 Korstjens I A M May et al (2008) Quality of Life After Self-Management Cancer Rehabilitation A Randomized Controlled Trial Comparing Physical and Cognitive-Behavioural Training Versus Physical Training Psychosom Med 70(4) 422-429 Krein S M Heisler J Piette F Makki and E Kerr 2005 The effect of chronic pain on diabetes patientslsquo self-management Diabetes Care 28(1)65ndash70 Kroenke CH Fung TT Hu FB Holmes MD Dietary patterns and survival after breast cancer diagnosis J Clin Oncol 2005 Dec 2023(36)9295-303 Kubik AK Zatloukal P Tomasek L Petruzelka L (2002) Lung cancer risk among Czech women a case-control study Prev Med 34(4) 436ndash444 Kucera H [Adjuvanticity of vitamin A in advanced irradiated cervical cancer (authors transl)] Wiener Klinische Wochenschrift Supplementum 19801181-20 Kushi LH Byers T Doyle C et al American Cancer Society Guidelines on Diet and Physical Activity for cancer prevention reducing the risk of cancer with healthy food choices and physical activity CA Cancer J Clin 2006 56 254ndash8 Kyogoku S Hirohata T Nomura Y Shigematsu T Takeshita S Hirohata I Diet and prognosis of breast cancer Nutr Cancer 199217(3)271-7 Lahmann PH Schulz M Hoffmann K Boeing H Tjoslashnneland A Olsen A Overvad K Key TJ Allen NE Khaw KT Bingham S Berglund G Wirfaumllt E Berrino F Krogh V Trichopoulou A Lagiou P Trichopoulos D Kaaks R Riboli E Long-term weight change and breast cancer risk the European prospective investigation into cancer and nutrition (EPIC) Br J Cancer 2005 Sep 593(5)582-9 Lee IM Sesso HD Paffenbarger RS Jr (1999) Physical activity and risk of lung cancer Int J Epidemiol 28(4) 620ndash625 Lev E L (1997) Banduras Theory of Self-Efficacy Applications to Oncology Research and Theory for Nursing Practice 11 21-37 Ligibel J A W Demark-Wahnefried et al (2009) Diet Physical activity and Supplements Guidelines for Cancer Survivors ASCO EDUCATIONAL BOOK 2009(1) 541-547 Lindsay S (2009) Prioritizing illness Lessons in self-managing multiple chronic conditions Canadian Journal of Sociology PhD Thesis ejournalslibraryualbertaca
134
Lucia A Earnest C Perez M (2003) Cancer-related fatigue can physical activity physiology assist oncologists Lancet Oncol 4616-625 Lyons R amp Langille L (2000) Healthy Lifestyle Strengthening the Effectiveness of Lifestyle Approaches to Improve Health Health Canada Ottawa Ontario Available at httpwwwhc-scgccahppbphdddocshealthy MacLennan R Macrae F Bain C et al Effect of fat fibre and beta carotene intake on colorectal adenomas further analysis of a randomized controlled dietary intervention trial after colonoscopic polypectomy Asia Pac J Clin Nutr 1999 8(suppl)S54-S58 Macmillian Cancer Support (2008) Two Million Reasons The Cancer Survivorship Agenda 2008 Maddams J Moller H and Devane C Cancer prevalence in the UK 2008 Thames Cancer Registry and Macmillan Cancer Support 2008 Manjer J Berglund G Bondesson L Garne J P Janzon L Malina J Breast cancer incidence in relation to smoking cessation Breast Cancer Res Treat 61121-129 2000 Mao Y Pan S Wen SW Johnson KC The Canadian Cancer (2003) Physical activity and the risk of lung cancer in Canada Am J Epidemiol 158(6) 564ndash575 Mayne S T B Cartmel et al (2009) Alcohol and Tobacco Use Pre-diagnosis and Postdiagnosis and Survival in a Cohort of Patients with Early Stage Cancers of the Oral Cavity Pharynx and Larynx Cancer Epidemiology Biomarkers amp Prevention 18(12) 3368-3374 McDonald P R Williams et al (2002) Breast cancer survival in African American women Is alcohol consumption a prognostic indicator Cancer Causes and Control 13(6) 543-549 McEligot AJ Largent J Ziogas A Peel D Anton-Culver H Dietary fat fiber vegetable and micronutrients are associated with overall survival in postmenopausal women diagnosed with breast cancer Nutr Cancer 200655(2)132-140 McNeely M L K L Campbell et al (2006) Effects of physical activity on breast cancer patients and survivors a systematic review and meta-analysis CMAJ 175(1) 34-41 McKenzie D C and A L Kalda (2003) Effect of Upper Extremity Physical activity on Secondary Lymphedema in Breast Cancer Patients A Pilot Study J Clin Oncol 21(3) 463-466 McKeown-Eyssen GE Bright-See E Bruce WR et al A randomized trial of a low fat high fibre diet in the recurrence of colorectal polyps Toronto Polyp Prevention Group [erratum appears in J Clin Epidemiol 1995 Feb48(2)i] Journal of Clinical Epidemiology 1994 May47(5)525-36 McLarty Jerry Bigelow Rebecca LH Smith Mylinh Elmajian Don Ankem Murali Cardelli James A (2009) Tea Polyphenols Decrease Serum Levels of Prostate-Specific Antigen Hepatocyte Growth Factor and Vascular Endothelial Growth Factor in Prostate
135
Cancer Patients and Inhibit Production of Hepatocyte Growth Factor and Vascular Endothelial Growth Factor In vitro Cancer Prev Res 1940-6207CAPR-08-0167
McTiernan A et al (2009) Low-fat increased fruit vegetable and grain dietary pattern fractures and bone mineral density the Womens Health Initiative Dietary Modification Trial Am J Clin Nutr 89 1864-1876
Meyerhardt JA Heseltine D Niedzwiecki D Hollis D Saltz LB Mayer RJ Schilsky RL and Fuchs CS (2005) The impact of physical activity on patients with stage III colon cancer Findings from Intergroup trial CALGB 89803 Proc Am Soc Clin Oncol 24 p abstract 3534 Meyerhardt J A D Niedzwiecki et al (2007) Association of Dietary Patterns With Cancer Recurrence and Survival in Patients With Stage III Colon Cancer JAMA 298(7) 754-764 Meyerhardt J A D Niedzwiecki et al (2008) Impact of Body Mass Index and Weight Change after Treatment on Cancer Recurrence and Survival in Patients With Stage III Colon Cancer Findings From Cancer and Leukemia Group B 89803 J Clin Oncol 26(25) 4109-4115 Meyskens FL Jr Kopecky KJ Appelbaum FR Balcerzak SP Samlowski W Hynes H Effects of vitamin A on survival in patients with chronic myelogenous leukemia a SWOG randomized trial Leukemia Research 1995 September 19(9)605-12 Miles A Simon A Wardle J (2010) Answering patient questions about the role lifestyle factors play in cancer onset and recurrences Journal of Health Psychology 15(2) p 291-298 Milne H K Wallman et al (2008) Impact of a Combined Resistance and Aerobic Physical activity Program on Motivational Variables in Breast Cancer Survivors A Randomized Controlled Trial Annals of Behavioral Medicine 36(2) 158-166 Milne M Hamerston L and Morrell D (2010) BACSUP adult survivorship living with and beyond cancer test community learning workshop London January 2010 Monninkhof EM Peeters PH Schuit AJ Design of the sex hormones and physical exercise (SHAPE) study BMC Public Health 2007 Sep 47232 Morrell RM Halyard MY Schild SE Ali MS Gunderson LL Pockaj BA (2005) Breast cancer-related lymphedema Mayo Clin Proc 801480ndash1484 Mortimer P S D O Bates et al (1996) The prevalence of arm oedema following treatment for breast cancer QJM 89(5) 377-380 Mortimer JE Flatt SW Parker BA et al Tamoxifen hot flashes and recurrence in breast cancer Breast Cancer Res Treat 108421-426 2008 Moseley AL Piller NB Carati CJ (2005) The effect of gentle arm physical activity and deep breathing on secondary arm lymphedemaLymphology Sep38(3)136-45 Moseley AL Piller NB (2008) Physical activity for limb Lymphoedema ndash Evidence that it is beneficial Journal of Lymphoedema vol 3(1) pp 51-56
136
Mustian KM Palesh OG Flecksteiner SA Tai Chi Chuan for breast cancer survivors Medicine and sport science 2008 52()209-17 National Cancer Action Team (2009) Cancer and palliative care rehabilitation workforce project A review of the evidence National Cancer Action Team National Comprehensive Cancer Network (2009) NCCN Clinical Practice Guidelines in Oncology Cancer-related fatigue version 1 2009 National Cancer Survivorship Initiative (NCSI) (2009) Research Work Stream Mapping Project - Summary and reports for Bowel Cancer Breast Cancer Lung Cancer Prostate cancer National Cancer Survivorship Initiative Macmillan Cancer Support National Health Service (2010) NHS advice on drinking limits NHS Choices httpwwwdrinkingnhsukquestionsrecommended-levels [Last accessed 300310] National Institutes of Health (1998) Clinical Guidelines on the Identification Evaluation and Treatment of Overweight and Obesity in Adults The Evidence Report National Heart Lung and Blood Institute in cooperation with the National Institute of Diabetes and Digestive Kidney Diseases NIH Publication No 98-4083 National Institutes of Health Osteoporosis and Related Bone Diseases (2009) Conditions and behaviours that increase osteoporosis risk National Resource Centre US Department of Health and Human Services httpwwwniamsnihgovHealth_InfoBoneOsteoporosisConditions_Behaviorsosteoporosis_breast_cancerasp [Last accessed 170210] National Obesity Observatory (2009) Body mass index as a measure of obesity Association of Public Health Observatories June 2009 Ng K J A Meyerhardt et al (2008) Circulating 25-Hydroxyvitamin D Levels and Survival in Patients With Colorectal Cancer J Clin Oncol 26(18) 2984-2991 Nikotetti S Young J Levitt M (2008) Bowel problems self-care practices and information needs of colorectal cancer survivors at 6 to 24 months after sphincter-saving surgery Cancer Nursing 31(5) p 389-398
Norat T Bingham S Ferrari P Slimani N Jenab M Mazuir M Overvad K Olsen A Tjoslashnneland A Clavel F Boutron-Ruault MC Kesse E Boeing H Bergmann MM Nieters A Linseisen J Trichopoulou A Trichopoulos D Tountas Y Berrino F Palli D Panico S Tumino R Vineis P Bueno-de-Mesquita HB Peeters PH Engeset D Lund E Skeie G Ardanaz E Gonzaacutelez C Navarro C Quiroacutes JR Sanchez MJ Berglund G Mattisson I Hallmans G Palmqvist R Day NE Khaw KT Key TJ San Joaquin M Heacutemon B Saracci R Kaaks R Riboli E Meat fish and colorectal cancer risk the European Prospective Investigation into cancer and nutrition J Natl Cancer Inst 2005 Jun 1597(12)906-16
Ornish D et al (2005) Intensive lifestyle changes may affect the progression of prostate cancer The Journal of Urology 174 p 1065-1070 Ostroff JS Jacobsen PB Moadel AB Spiro RH Shah JP Strong EW et al (1995) Prevalence and predictors of continued tobacco use after treatment of patients with head and neck cancer Cancer Jan 1575(2)569-76
137
Pantuck AJ et al (2006) Phase II study of pomegranate juice for men with rising PSA following surgery or RXT for prostate cancer Clin Cancer Res 12(13) p 4018-4026 Pantuck AJ et al Abstract presented at the American Society of Clinical Oncology 2008 Genitourinary Cancers Symposium (Abstract 40) Long Term Follow Up Of Pomegranate Juice For Men With Prostate Cancer And Rising PSA Shows Durable Improvement in PSA Doubling Time Parsons A A Daley et al Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis systematic review of observational studies with meta-analysis BMJ 340(jan21_1) Pastorino U Infante M Maioli M et al Adjuvant treatment of stage I lung cancer with high-dose vitamin A[comment] J Clin Oncol 1993 July11(7)1216-22 Patterson R E L A Cadmus et al Physical activity diet adiposity and female breast cancer prognosis A review of the epidemiologic literature Maturitas In Press Corrected Proof Pedersen BK Saltin B Evidence for prescribing physical activity as therapy in chronic disease Scand J Med Sci Sports 16 Suppl 1 3ndash63 2006Pierce J P L Natarajan et al (2007) Influence of a Diet Very High in Vegetables Fruit and Fiber and Low in Fat on Prognosis Following Treatment for Breast Cancer The Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA 298(3) 289-298 Pierce JP Faerber S Wright FA Newman V Flatt SW Kealey S Rock CL Pierce JP Natarajan L Caan BJ et al Influence of a diet very high in vegetables fruit and fiber and low in fat on prognosis following treatment for breast cancer the Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA2007298(3)289-298 Ponz dL Roncucci L Chemoprevention of colorectal tumors role of lactulose and of other agents Scandinavian Journal of Gastroenterology Supplement 199722272-5 Poudevigne M J Wojcik et al (2009) The Effects Of 12-weeks Cross Training On Fatigue And Mood In Recent Breast Cancer Survivors 2292 Board 180 May 28 200 PM - 330 PM Medicine amp Science in Sports amp Physical activity 41(5) 297-298 Powers H J M H Hill et al (2007) Responses of Biomarkers of Folate and Riboflavin Status to Folate and Riboflavin Supplementation in Healthy and Colorectal Polyp Patients (The FAB2 Study) Cancer Epidemiology Biomarkers amp Prevention 16(10) 2128-2135 Protheroe J A Rogers et al (2008) Promoting patient engagement with self-management support information a qualitative meta-synthesis of processes influencing uptake Implementation Science 3(1) 44 Provenzano E and N Johnson (2009) Overview of recommendations of HER2 testing in breast cancer Diagnostic Histopathology 15(10) 478-484 Puhl RM Heuer CA (2009) ―The stigma of obesity A Review and Update Obesity 17 (5) 941-964 Rabin C (2009) ―Promoting Lifestyle Change among Cancer Survivors When is the Teachable Moment American Journal of Lifestyle Medicine 3 (5) 369-378
138
Reding K W J R Daling et al (2008) Effect of Pre-diagnostic Alcohol Consumption on Survival after Breast Cancer in Young Women Cancer Epidemiology Biomarkers amp Prevention 17(8) 1988-1996 Riboli E Hunt KJ Slimani N Ferrari P Norat T Fahey M Charrondiegravere UR Heacutemon B Casagrande C Vignat J Overvad K Tjoslashnneland A Clavel-Chapelon F ThieacutebautA Wahrendorf J Boeing H Trichopoulos D Trichopoulou A Vineis P Palli D Bueno-De-Mesquita HB Peeters PH Lund E Engeset D Gonzaacutelez CA Barricarte A Berglund G Hallmans G Day NE Key TJ Kaaks R Saracci R (2002) European Prospective Investigation into Cancer and Nutrition (EPIC) study populations and data collection Public Health Nutr 2002 Dec5(6B)1113-24 Richardson G E M A Tucker et al (1993) Smoking Cessation after Successful Treatment of Small-Cell Lung Cancer Is Associated with Fewer Smoking-related Second Primary Cancers Annals of Internal Medicine 119(5) 383-390 Richardson A Addington-Hall J Stark D Foster C Amir Z Sharpe M (2009) Determining research priorities for cancer survivorship Consultation and evidence review Commissioned by the NCSI Robertson R (2008) Using Information to Promote Healthy Behaviours Kings Fund London Rock C L and W Demark-Wahnefried (2002) Diet and Survival After the Diagnosis of Breast Cancer A Review of the Evidence J Clin Oncol 20(15) 3302-3316 Rock C L S W Flatt et al (2005) Plasma Carotenoids and Recurrence-Free Survival in Women With a History of Breast Cancer J Clin Oncol 23(27) 6631-6638 Rohan T Howe G Friedenreich C et al (1993) Dietary fiber vitamins A C and E and risk of breast cancer a cohort study Cancer Causes and Control 4(1) p 29-37 Rosenbaum EH Fobair P Spiegel D (2006) Cancer is a Life-changing Event Cancer Supportive Care Programs httpwwwcancersupportivecarecomSurvivorsurvivehtml [Last accessed January 30 2009] Ryan CW D Huo and K Bylow et al (2007) Suppression of bone density loss and bone turnover in patients with hormone-sensitive prostate cancer and receiving zoledronic acid BJU Int 100 pp 70ndash75 Sagiv SK Gaudet MM Eng SM et al (2007) Active and passive cigarette smoke and breast cancer survival Ann Epidemiol 17385ndash393 Sandel S Judge J Landry N et al (2005) Dance and movement program improves quality-of-life measures in breast cancer survivors Cancer Nursing 28(4) 301-309 Saxton J (2010) Physical activity and cancer mortality In Physical activity and cancer Survivorship Springer New York pp 189-210 Schatzkin A Lanza E Corle D et al Lack of effect of a low-fat high-fiber diet on the recurrence of colorectal adenomas Polyp Prevention Trial Study Group [comment] New England Journal of Medicine 2000 April 20342(16)1149- 55
139
Schmitz KH Courneya KS Matthews C Demark-Wahnefried W et al (2010) ―American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors Medicine and Science in Sports and Exercise Special Communication 0195-9131104207-14090 Schmitz K Holtzman J Courneya K Masse L Duval S Kane R Controlled physical activity trials in cancer survivors A systematic review and meta-analysis Cancer Epidemiol Biomarkers Prev 2005141588ndash95
Schulz M Lahmann PH Boeing H et al Fruit and vegetable consumption and risk of epithelial ovarian cancer the European Prospective Investigation into Cancer and Nutrition Cancer Epidemiol Biomarkers Prev 2005142531ndash2535 Schwarz S U C Obermuller-Jevic et al (2008) Lycopene Inhibits Disease Progression in Patients with Benign Prostate Hyperplasia J Nutr 138(1) 49-53 Schmitz K H Balancing Lymphedema Risk Physical activity Versus Deconditioning for Breast Cancer Survivors Physical activity and Sport Sciences Reviews 38(1) 17-24 10 Segal RJ Reid RD Courneya KS et al(2003) Resistance physical activity in men receiving androgen deprivation therapy for prostate cancer JClinOncol211653-1659
Segal RJ Reid RD Courneya KS Sigal RJ Kenny GP PrudlsquoHomme DGet al Randomized Controlled Trial of Resistance or Aerobic Exercise in Men Receiving Radiation Therapy for Prostate Cancer J Clin Oncol 2009 Jan 2027344-51 Sellers TA Potter JD Folsom AR (1991) Association of incident lung cancer with family history of female reproductive cancers the Iowa Womenlsquos Health Study Genet Epidemiol 8(3) 199ndash208 Severson RK Nomura AM Grove JS Stemmermann GN A prospective analysis of physical activity and cancer Am J Epidemiol 1989 Sep130(3)522-9 Shaw C Mortimer P Judd PA Randomized controlled trial comparing a low-fat diet with a weight-reduction diet in breast cancer-related lymphedema Cancer 20071091949ndash56 Sinicrope F A N R Foster et al Obesity Is an Independent Prognostic Variable in Colon Cancer Survivors Clinical Cancer Research 16(6) 1884-1893 Siris E S P D Miller et al (2001) Identification and Fracture Outcomes of Undiagnosed Low Bone Mineral Density in Postmenopausal Women Results From the National Osteoporosis Risk Assessment JAMA 286(22) 2815-2822 Soliman S W J Aronson et al (2009) Analyzing Serum-Stimulated Prostate Cancer Cell Lines After Low-Fat High-Fiber Diet and Physical activity Intervention eCAM nep031 Sonn GA Aronson W and Litwin MS (2005) Impact of diet on prostate cancer A review Prostate cancer and prostate disease 8 p 304-310 Speck RM Courneya KS Masse L Duval S Schmitz K (2010) An update of controlled physical activity trials in cancer survivors a systematic review and meta-analysis Journal of Cancer Survivorship 4(2) p 87-100
140
Steginga S K B M Lynch et al (2009) Antecedents of domain-specific quality of life after colorectal cancer Psycho-Oncology 18(2) 216-220 Stevinson C H Steed et al (2009) Physical Activity in Ovarian Cancer Survivors Associations With Fatigue Sleep and Psychosocial Functioning International Journal of Gynecological Cancer 19(1) 73-78 Swenson KK Nissen MJ Anderson E Shapiro A Schousboe J Leach J (2009) Effects of physical activity vs bisphosphonates on bone mineral density in breast cancer patients receiving chemotherapy Support Oncol May-Jun7(3)101-7 Tardon A Lee WJ Delgado-Rodriguez M et al Leisure-time physical activity and lung cancer a meta-analysis Cancer Causes Control200516(4)389-397 Taskila T Martikainen R Hietanen P Lindbohm M Comparative study of work ability between cancer survivors and their referents Europ J of Cancer 2007 43914-920 Taylor R Brown A et al (2004) Physical activity-based rehabilitation for patients with coronary heart disease systematic review and meta-analysis of randomized controlled trials The American journal of medicine 116(10) 682-692 Taylor NFDodd KJShields NBruder A Therapeutic physical activity in physiotherapy practice is beneficial a summary of systematic reviews 2002-2005 Aust J Physiother 2007 53 7-16 Thiebaut A C M A Schatzkin et al (2006) Dietary Fat and Breast Cancer Contributions From a Survival Trial J Natl Cancer Inst 98(24) 1753-1755 Thomas R Daly M and Perryman J (2000) Forewarned is forearmed - Randomised evaluation of a preparatory information film for cancer patients European Journal of Cancer 36(2) p 52-53 Thomas R et al (2005) Dietary advice combined with a salicylate mineral and vitamin supplement (CV247) has some tumour static properties - a phase II study Diet and science 2005 35(6) p 436-451 Thomas RJ and Davies ND (2007) Lifestyle during and after cancer treatment Clinical Oncology Vol 19 Issue 8 pp 616-627 Thomas R Nicholson C (2009) Why is exercise good for us Cancer Active httpcanceractivecomcancer-active-page-linkaspxn=2600ampTitle=Why20is20exercise20good20for20us [Last accessed 230710] Thomas R Oakes R Gordon J Russell S Blades M Williams M (2009) A randomised double-blind phase II study of lifestyle counselling and salicylate compounds in patients with progressive prostate cancer Diet and Food Science 39(3) pp 295 ndash 305 Thomson C A N R Stendell-Hollis et al (2007) Plasma and Dietary Carotenoids Are Associated with Reduced Oxidative Stress in Women Previously Treated for Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 16(10) 2008-2015
141
Thune I Brenn T Lund E Gaard M Physical activity and the risk of breast cancer N Engl J Med 336 1269-1275 1997
Travis LB Gospodarowicz M Curtis RE et al Lung cancer following chemotherapy and radiotherapy for Hodgkins disease J Natl Cancer Inst 94 (3) 182-92 2002 Tucker MA Murray N Shaw EG et al Second primary cancers related to smoking and treatment of small-cell lung cancer Lung Cancer Working Cadre J Natl Cancer Inst 89 (23) 1782-8 1997 Twiss J J N Waltman et al (2001) Bone Mineral Density in Postmenopausal Breast Cancer Survivors Journal of the American Academy of Nurse Practitioners 13(6) 276-284 Uhley V and Jen C (2006) Diet and weight management in cancer survivors In Handbook of Cancer Survivorship edited by Feuerstein M New York NY Springer 2006 ISBN-13 978-0-3873-4561-1
Vadiraja HS et al (2009) Effects of yoga program on quality of life and affect in early breast cancer patients undergoing adjuvant radiotherapy A randomized controlled trial Complementary Therapies in Medicine Volume 17 Issue 5 Pages 274-280
Velthuis MJ Agasi-Idenburg SC Aufdemkampe G Wittink HM (in press) The effect of physical activity on cancer-related fatigue during cancer treatment a meta-analysis of Randomised Controlled Trials Clinical Oncology 2009 (in print) Vineis P G Hoek and M Krzyzanowski et al Lung cancers attributable to environmental tobacco smoke and air pollution in non-smokers in different European countries a prospective study Environ Health 6 (2007) pp 1ndash7 Visvanathan K Chlebowski RT Hurley P et al American Society of Clinical Oncology 2008 clinical practice guideline update on the use of pharmacologic intervention including tamoxifen raloxifene and aromatase inhibition for breast cancer risk reduction J Clin Oncol 273235-3258 2009
Wagner LI Cella D (2004) Fatigue and cancer causes prevalence and treatment approaches BrJCancer 91822-828 Waltman N J Twiss et al (2009) ―The effect of weight training on bone mineral density and bone turnover in postmenopausal breast cancer survivors with bone loss a 24-month randomized controlled trial Osteoporosis International Wenzel L H Q Huang et al (2005) Quality-of-Life Comparisons in a Randomized Trial of Interval Secondary Cytoreduction in Advanced Ovarian Carcinoma A Gynecologic Oncology Group Study J Clin Oncol 23(24) 5605-5612 Weikert C Hoffmann K Dierkes J Zyriax BC KlipsteinndashGrobusch K MB et al Homocysteine metabolismrelated dietary pattern and the risk of coronary heart disease in two independent German study populations J Nutr 2005 1351981ndash1988 White S E McAuley et al (2009) Translating Physical Activity Interventions for Breast Cancer Survivors into Practice An Evaluation of Randomized Controlled Trials Annals of Behavioural Medicine 37(1) 10-19
142
World Health Organisation (1999) What is a healthy lifestyle Health Documentation Services WHO Regional Office for Europe Copenhagen World Health Organisation (2002) The World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva WHO Scientific Group on the Prevention and Management of Osteoporosis (2000 Geneva Switzerland) (2003) Prevention and management of osteoporosis report of a WHO scientific group World Health Organisation (2005) The European health report 2005 public health action for healthier children and populations Copenhagen WHO regional office for Europe World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva Windsor P M Nichol K F Potter J A randomized controlled trial of aerobic exercise for treatment-related fatigue in men receiving radical external beam radiotherapy for localised prostate carcinoma Cancer (2004) 101 (3) 550-7 Wright M E S-C Chang et al (2007) Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality Cancer 109(4) 675-684 Wright P A Smith et al (2005) Psychosocial difficulties deprivation and cancer three questionnaire studies involving 609 cancer patients Br J Cancer 93(6) 622-626 Yu GP et al (1997) The effect of smoking after treatment for Cancer Cancer Detect Prev 21487-509

3
CONTENTS
Contents 3
Exectuive Summary 4
Background 8
The Purpose of this Review 12
Method and Search Strategy 14
Results 16
Part 1 Cancer Survival - Evidence for the Role of Lifestyle in Disease 17
Progression and Recurrence
Part 2 Lifestyle Evidence for Reducing and Managing Risks and Side-Effects 71
of Cancer Treatment
Cancer-Related Fatigue 72
Lymphoedema 80
Osteoporosis and Bone Health 85
Weight and Body Composition 93
Quality of Life 99
Ongoing Lifestyle Studies 110
Discussion 113
Appendix A Evidence-Based Dietary Self-Management Recommendationshelliphelliphelliphellip122
Appendix B Evidence-Based Physical Activity Recommendations 123
Referenceshelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphelliphellip124
4
Lifestyle Guidance for Cancer Survivors ndash Executive Summary
1 This aim of this review was to update the World Cancer Research Fund (WCRF)
report bdquoA Systematic Review of RCTs Investigating the Effect of Nutritional and
Physical Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This
has been achieved by conducting a comprehensive but pragmatic search of the
literature from 2006 onwards Where no evidence was available in the WCRF
review studies before 2006 have been included if identified in the reference lists of
acquired records To facilitate this evidence cited within the lsquoHandbook of Cancer
Survivorship‟ (Feuerstein 2006) and findings from a non-systematic review
conducted by the Cancer and Palliative Care Rehabilitation Workforce (2009) were
also utilised
2 There is now persuasive evidence that a healthy lifestyle during and after cancer is
associated with improved physical and psychological well-being reduced risks of
treatment enhanced self-esteem reduced risk of recurrence and improved survival
Clarifying the individual anti-cancer components of a healthy lifestyle will require
extensive further evaluation and even then they are likely to be multi-factorial
3 Despite gaps in the evidence for lifestyle benefits in cancer survivors there are some
key lifestyle recommendations that can be provided (Appendix A and B)
o Dietary Recommendations Reduce saturated fats increase fish intake
consume a varied diet in order to ensure adequate intakes of vitamins and
essential minerals increase consumption of green and cruciferous vegetables as
well as brightly coloured fruits and vegetables that contain carotenoids
o Physical Activity Recommendations There is substantial evidence suggesting
that the physical activity recommendations developed by the Department of
Health are sufficient for most cancer survivors - a total of at least 30-minutes a
day of moderate intensity physical activity on five or more days of the week
Additionally there is evidence of a dose-response (ie the more physical
activity the greater any benefits) Even a modest amount of exercise is
beneficial and will see gains versus doing nothing at all Body composition
changes are common in many cancer patients with the reasons varying by site
Compromised lean body mass for patients with head and neck and
gastrointestinal cancers are common and in this group exercise to build lean
muscle will be relevant However in breast cancer some treatments can lead to
significant weight gain (exacerbated if pre- diagnosis BMI is not in the healthy
range) and exerciseactivity which is more useful for controlling body weight and
losing fat will be more important
o Weight Excess weight should be avoided (ie a body mass index of 25-
29kgm or above There is also evidence that maintaining a stable healthy weight
as opposed to fluctuating between a healthy and unhealthy BMI can offer health
5
benefits for cancer survivors The evidence is strongly suggestive of weight being
implicated in breast cancer outcomes with the mechanism of benefit achieved
via physical activity or a low-fat diet most likely being due to weight loss
o Smoking Strong and consistent evidence has been presented for increased risk
of disease progression and mortality in people who continue to smoke after a
diagnosis of cancer as well as poorer outcomes in pre-diagnosis smokers
o Alcohol There is a paucity of research into the effects of alcohol pre- and post-
diagnosis on cancer progression and recurrence as well as symptom
management Evidence thus far is highly contradictory although excess alcohol
is linked to increased weight which does have negative outcomes
4 Evidence is also available for the benefits of individual lifestyle components for
specific cancer types
o A high intake of soy has been found to alter testosterone (the male sex
hormone) reducing risk of prostate cancer
o Dietary fibre might offer protection against colorectal cancer or recurrence via
increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic
mucosa (tissue that lines the colon)
o Since physical activity can alter levels of oestrogen (the female sex hormone)
evidence indicates that it might be protective against breast cancer
5 There is a wealth of evidence for physical activity during and after treatment
improving symptoms of cancer-related fatigue and increasing energy and stamina It
is also clear that a needs-based approach should be adopted ndash based on the
assessed need for improvements on low fatigue levels poor quality of life low
physical function (Speck et al 2009)
6 Guided progressive physical activity soon after treatment can ease the symptoms of
lymphoedema Avoidance of physical activity through fear of exacerbating symptoms
is unwarranted if physical activity is supervised and closely monitored
7 Whilst the benefits of physical activity on bone health require clarifying physical
activity can at the very least prevent loss of bone mineral density in survivors at
particular risk of developing osteoporosis
8 Even when not directly associated with overall QoL exercise has been found to
significantly improve social functioning among post-treatment survivors The benefits
of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or
group-based The evidence that physical activity can improve body image may be
one of the mechanisms through which exercise can improve quality of life
6
9 Mechanisms of benefit for diet and physical activity include the influence that these
behaviours have on hormones and insulin levels This has sparked the question of
whether pharmacological alternatives such as aromatase inhibitors and metformin
which tend to produce greater reductions in cancer risk pose competition for lifestyle
interventions This is unlikely as healthy lifestyle behaviours contribute overall to
general health and to the risk reduction for other co-morbid conditions such as
hypertension cardiac disease and diabetes Usefully the competencies framework
offered by Finders University highlights the importance of taking a holistic approach
to supported self-management whereby support is provided for a continuum of
health as opposed to a focus on one established chronic condition Based on this
model supported self-management should provide health promotion and illness
prevention not merely in terms of cancer but also for associated risks and co-
morbidities
10 The challenge remains in integrating lifestyle support into standardised models of
aftercare for cancer survivors particularly in terms of engaging both patients and
health professionals bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative identifies the need to
provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for
healthcare professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
11 The literature identifies the need for individual assessment and risk stratification for
cancer survivors so that lifestyle interventions and support can be tailored and
provided according to need Particularly high need groups are survivors who have
co-morbidities are overweight sedentary or smoke
12 Some questions that remain
o What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
o How can people most likely to benefit from lifestyle interventions be effectively
identified
o What are the various intensities of lifestyle support that can be provided based on
levels of individual need
13 Significant limitations can be found in the evidence available for lifestyle outcomes in
cancer survivors including
7
o Long-term outcomes of lifestyle choices
o Low levels of adherence to interventions
o A paucity of studies addressing external validity
o Equality across tumour groups
o Lack of cultural considerations pertaining to dietary advice
o A paucity of individualised lifestyle advice and tailored support
8
BACKGROUND SETTING THE SCENE
Lifestyle and Well-Being
In an independent report offering recommendations on enabling effective delivery of health
and well-being in England Bernstein Cosford and Williams (2010) advise that setting clear
priorities for health and well-being should start with behavioural risk factors Namely they
recommend tackling the biggest lifestyle influences on population health tobacco alcohol
physical inactivity and poor diet These four lifestyle factors are among the biggest
contributors to most preventable diseases across all social groups and in all areas of
England They are responsible for 42 of deaths from leading causes (WHO 2005) and
together they account for at least pound94 billion in annual direct costs to the NHS (DH 2009a)
expenses incurred outside the NHS would increase this figure further
An increase in longevity and the number of people living with one or more chronic conditions
for a longer period of time has led to government action aimed at making these years as
healthy as possible Interest has been particularly paid to the role of these behavioural risk
factors and the role of lifestyle in improving or maintaining health preventing illness
managing symptoms and achieving a satisfactory quality of life (QoL) (Pedersen and Saltin
2006 Taylor et al 2004)
The term lifestylelsquo refers to personal choices that might impact health such as diet physical
activity smoking and alcohol consumption The World Health Organisation (WHO 1999)
defines a healthy lifestylelsquo as
ldquoa way of living that lowers the risk of being seriously ill or dying earlyrdquo with the
emphasis that ldquohealth is not just about avoiding disease It is also about physical
mental and social well-beingrdquo (p 2)
With earlier detection and more efficacious treatments available for cancer there has been
an increase in survival as well as in the number of people living with the long-term
consequences of cancer treatment Subsequently cancer has become a chronic disease for
a number of people among the two million cancer survivors in the UK (Maddams Moller and
Devane 2008) Whilst evidence of the effects of a healthy diet and sufficient physical activity
in cancer prevention has been well-documented (Chan Gann and Giovannucci 2005
Sonn Aronson and Litwin 2005) it has become of fundamental importance to examine the
role of these lifestyle choices in cancer survivorship Furthermore the role of lifestyle in
cancer survivorship needs to be examined not only in terms of improved physical and
psychological well-being but also disease outcomes
Given the relationship between choosing a healthy lifestyle and taking an active role in the
self-management1 of the long-term effects of cancer and its treatment the self-management
workstream of the National Cancer Survivorship Initiative (NCSI) have conducted this
1 lsquoSelf-managementrsquo has been defined as ldquoawareness and active participation by the person in their recovery
recuperation and rehabilitation to minimise the consequences of treatment promote survival health and well-beingrdquo (NCSI 2009)
9
evaluation of evidence pertaining to lifestyle factors and survivorship Not only are lifestyle
choices important in terms of disease progression and recurrence but also in the effective
management of other chronic symptoms and conditions resulting from treatment such as
cancer-related fatigue lymphoedema and osteoporosis (Doyle et al 2006) Lifestyle
support and education is evidently an important component of supported self-management2
for many individuals living with or beyond cancer (Davies and Batehup 2010) Indeed as
part of a consensus meeting and evidence review self-management support and lifestyle
management were among the top ten priorities for survivorship research (Richardson et al
2009) providing further rationale for the current review
The Health of Cancer Survivors
The traditional belief has been that people with cancer should rest reduce activity and avoid
activities involving intense physical effort in other words they are passive patients of the
disease and its treatment Consequently physical activity levels do decline substantially
during and after completion of treatment for cancer and often fail to return to pre-diagnosis
levels for many people (Daley et al 2008) Fortunately it is becoming increasingly
recognised that people living with or beyond cancer do need physical activity will not be
harmed by physical effort and are active participants in the rehabilitation process
Furthermore emerging evidence is demonstrating that lifestyle factors can influence the rate
of cancer progression improve quality of life (QoL) reduce side-effects and risks during
treatment reduce the incidence of relapse and improve overall survival (Thomas Daly and
Perryman 2000) Besides the beneficial effect on recurrence a healthy diet and regular
physical activity has the potential to reduce the risk of co-morbidity such as other cancers
cardiovascular disease and diabetes etc (Jones and Demark-Wahnefried 2006)
Research suggests that although many cancer survivors report making healthy lifestyle
changes after diagnosis these changes may not be generalisable to all populations of
cancer survivors and they are often temporary (Demark-Wahnefried and Jones 2008)
Furthermore evidence suggests that the healthy lifestyle behaviours adopted by cancer
survivors tend to be directed towards clinical action such routine physical examination rather
than those health behaviours that require daily effort such as healthy eating or regular
physical activity (Findley and Sambamoorthi 2009)
A potential explanation for this difference in the uptake of clinical versus lifestyle preventive
health behaviours is that the former is easier due to the primary action being carried out by
someone else The latter on the other hand requires personal time and effort as well as
opportunity socially economically and in terms of health literacy and educational status
Behavioural and lifestyle change is notoriously difficult but even more so for people with
cancer or other chronic conditions let alone those with co-morbidities (Krein et al 2005) For
people with co-morbidities a healthy lifestyle can be even more challenging as they grapple
with the competing demands posed by the self-management of multiple conditions (Lindsay
2009)
2 lsquoSupported self-managementrsquo has been defined as ldquoWhat health and social care professionals and service
delivery organisations to do support self-managementrdquo (NCSI 2009)
10
Given the increase in survivorship the higher rates of co-morbidity within this population
and evidence that diet physical activity and other lifestyle factors affect risk for other cancers
and other chronic diseases there is a clear need for lifestyle interventions that target this
high risk group The literature suggests the need for individual risk assessment and the
provision of support with lifestyle changes in those individuals identified as high risk ndash such
as survivors who have co-morbidities are overweight sedentary or smoke (Davies and
Batehup 2010)
The Lifestyle Needs of Survivors
The National Cancer Survivorship Initiative (NCSI) highlights that people living with or
beyond cancer would like to play a more active role in their healthcare They want to know
how to look after themselves after a cancer diagnosis including information and support on
the lifestyle changes they should make so they can return to normallsquo life as much as
possible (Macmillan Cancer Support 2008) Yet the evidence suggests that this need
remains largely unaddressed In a key mapping project commissioned by the NCSI
Research workstream a number of issues pertaining to lifestyle were identified for the four
most common cancers breast colorectal lung and prostate (NCSI 2009) Each of these
four reports which were conducted by independent organisations demonstrated gaps in the
provision of lifestyle advice and support mainly during the period of aftercare In a similar
report mapping the needs of rarer cancers prolonging life through changes to lifestyle
emerged as a frequent theme by survivors asked to explore the meaning of cancer
survivorshiplsquo (Cancer52 and NCSI 2009) There was particular emphasis on the need for
diet and physical activity advice post-surgery for oesophageal cancer as well as diet advice
for mouth and throat cancers Change in bowel habits is frequently reported among post-
treatment bowel cancer survivors requiring support with dietary changes (Nikoletti et al
(2008)
In an effort to provide further insight into lifestyle advice and support for cancer survivors as
well as developing evidence-based lifestyle interventions a comprehensive review of the
evidence for lifestyle and cancer outcomes is required The perceived outcome efficacy3 of
making lifestyle changes is important in terms of whether those changes are initiated or not
as well as whether an individual possesses the confidence (self-efficacy) to maintain lifestyle
changes Outcome efficacy could be increased by the accumulation of firmly established
evidence offered alongside the opportunity for lifestyle support
Additionally this evidence needs to be evaluated in respect of current national guidelines for
diet physical activity and other lifestyle indicators such as weight and alcohol consumption
Briefly national guidance recommends a diet comprising 33 fruit and vegetables (five
portions per day) 33 starchy foods (rice bread pasta potatoes) 15 milk and dairy
foods 12 protein (meat and fish) and 8 foods and drinks high in fat andor sugar (Food
Standards Agency 2007) Adults are advised to achieve a total of at least 30-minutes daily
moderate intensity physical activity on five or more days of the week (DH 2004) Combined
with a healthy diet regular physical activity is aimed at maintaining a Body Mass Index
3 The belief that a particular outcome will result from following certain actions or behaviours
11
(BMI)4 of 185-249kgm2 25-29 is considered to be overweight and 30 or above as obese
whilst under 185 is considered underweight (National Obesity Observatory 2009)
A healthy lifestylelsquo is the same for cancer survivors as for the general population or indeed
people with other chronic conditions (Bellizzi et al 2005 Caan et al 2005 Coups and
Ostroff 2005) Cancer survivors are slightly more likely to follow physical activity guidelines
but overall their health behaviours mirror those of the general population which is marked by
inactivity and an epidemic of obesity and associated problems (Caan et al 2005) Despite
this the lifestyle advice and tailored care currently provided for specific groups of people in
the general population such as exercise prescriptions (DH 2001) is not yet integrated into
the supportive care needs of cancer survivors (Addington-Hall 2010) This is in the main
due to reluctance (usually related to knowledge and confidence) from health professionals to
discuss lifestyle factors with cancer patients due to limitations in knowledge and an
inadequacy in the available evidence on the underlying mechanisms of benefit for individual
lifestyle factors (Miles Simon and Wardle 2010) It is anticipated that this review will allay
some of this reluctance by identifying where the evidence strongly supports the efficacy of
lifestyle factors in cancer outcomes as well as where the evidence is less clear and requires
further research
4 BMI is a statistical measure which compares a persons weight and height to estimate a healthy body weight
12
The Purpose of this Review
Using the outlined national guidance on lifestyle and taking account of evidence for specific
elements or intensity of certain lifestyle factors in cancer care and self-management a
review of the literature on lifestyle and survivorship will be conducted The primary aims are
to produce evidence that can support professionals in guiding and advising cancer survivors
as well as evidence regarding resources which might support patient self-management in
relation to lifestyle factors and behaviour change The review will be comprehensive but
pragmatic drawing on a variety of sources This will commence by updating a recent review
conducted by the World Cancer Research Fund (WCRF) - bdquoA Systematic Review of RCTs
Investigating the Effect of Diet and Physical Activity Interventions on Cancer Survival‟
(Bekkering et al 2006)5
The aim of the WCRF review (Bekkering et al 2006) was to systematically locate and
review all randomised control trials (RCTs) which tested the effect of diet andor physical
activity interventions in cancer survivors their definition of a cancer survivor being
ldquoanyone who has been diagnosed with cancer from the time of diagnosis through the
rest of liferdquo (Brown et al 2003)
They conducted a systematic search of MEDLINE (from 2000 onwards) EMBASE (from
1999 onwards) AMED (from 1985 onwards) and the Cochrane Library including DARE
CDSR CENTRAL and HTA (all years) up to March 2006 scanned key texts that were
relevant to the subject field and scanned the references of relevant reviews They identified
117 trials (Table 1)
Table 1 Trials Identified in the WCRF Review (Bekkering et al 2006)
Trials Total
Diet
Food-based
Supplement-based
23
71
Physical activity
23
Total 117
5 This has been highlighted by the American Cancer Society (ACS) as being one of the most comprehensive
reviews on diet and physical activity for cancer survivors The ACS has used the review alongside other sources to produce lsquoGuidelines on Diet and Physical Activity for Cancer Preventionrsquo (Kushi et al 2006)
13
The findings will be described along with the results of the current review The overall
conclusion drawn by Bekkering et al (2006) was that there is a paucity of robust evidence
on the effects of diet and physical activity interventions in the management of cancer RCTs
were generally small and often reported inadequate details to formally assess quality While
promotion of a generic healthy diet was associated with reduced overall mortality the degree
to which lifestyle accounted for this outcome was imprecise It was concluded that given the
large investment in potential lifestyle interventions among cancer survivors large-scale trials
adequately powered to provide robust conclusions should be supported and conducted
In updating the WCRF review (Bekkering et al 2006) further scoping of the literature from
2006 to February 2010 will be conducted along with a synthesis of the evidence presented
in the lsquoHandbook of Cancer Survivorship‟ edited by Michael Feuerstein (2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (National Cancer Action Team 2009) which evaluates literature
pertaining to rehabilitation
The primary aim of the review is to guide healthcare planning and the development of
supported lifestyle self-management interventions for high risk groups In order to be able to
consider the production of useable evidence-based guidance for self-management for both
patients and professionals the following evidence will be sought
Evidence that would support professionals to be able to guide and advise
patients
Evidence regarding resources which would support patient self-management in
relation to lifestyle factors and behaviour change
It is anticipated that recent efforts to conduct research in this area will facilitate the
clarification of any key recommendations that can be made to cancer survivors by healthcare
professionals This update of the evidence will also attempt to establish where the strength
of the evidence lies and where more research is required
14
METHOD
Search Strategy
In updating the WCRF review (Bekkering et al 2006) RCTs and systematic reviews were
obtained from a systematic search of the Cochrane Library Database and Pubmed (from
March 2006 to February 2010) Where no evidence was available in the WCRF review
studies before 2006 have been included if identified in the reference lists of acquired
records this is the case with studies on smoking which were not included in the Bekkering
et al (2006) review
The selected relevant chapters were read from the bdquoHandbook of Cancer Survivorship‟
(Feuerstein 2006)6 and relevant studies referred to from the Cancer and Palliative Care
Rehabilitation Workforce (2009) non-systematic review Grey literature was also utilised
where this would provide information relevant to the review or where cancer-specific
literature was lacking as was the case with osteoporosis
All titles and abstracts of studies identified by the searches were scanned for relevance in
terms of topic and participant group For any titles or abstracts that were potentially relevant
full paper manuscripts were obtained and the relevance of each study assessed according to
the pre-specified inclusion criteria
6 Chapters include Physical Activity Potential Benefits and Guidelines DietWeight Management
Search terms cancer OR neoplasm
AND diet OR exercise OR physical
activity OR weight OR lifestyle
Cochrane systematic reviews
925 records
PubMed
4941 records
56 included 84 included
15
Inclusion Criteria
Records included within the review of the literature met the following inclusion criteria
Lifestyle-related ndashdiet physical activity weight smoking alcohol consumption
Cancer sites breast colorectal lung or prostate cancer Other tumour sites will
be included if located while searching for the primary tumour sites
Trajectory - during primary cancer treatment or post-primary treatment
Outcomes of interest ndash survival recurrenceprogression symptoms treatment-
related chronic conditions ndash fatigue lymphoedema osteoporosis weight
physical fitness quality of life rehabilitation behaviour change health and well-
being cost-effectiveness
Adult population
Type of record ndash RCTs systematic reviews prospective cohort studies
Retrospective studies will also be included since some areas of lifestyle such as
smoking have primarily been investigated via this method
16
RESULTS
A total of 140 records were included in this review not counting the review being updated
(Bekkering et al 2006) In synthesising the evidence obtained from these records and the
additional sources described in the search strategy findings are presented in two parts
1) Cancer Survival
Evidence for the role of lifestyle in disease progression and recurrence
2) The Risks and Side-Effects of Cancer Treatment
Evidence for the role of lifestyle in reducing and managing the risks and
side-effects of cancer treatment with specific focus on cancer-related
fatigue lymphoedema osteoporosis and QoL
Both sections examine five categories of evidence
Physical activity
Diet
Weight
Smoking
Alcohol
The focus is on the four most common cancers (breast colorectal lung prostate) but other
tumour sites have been included if located via the pre-defined search strategy Summary
tables for each study included within the evidence are provided at the end of relevant
sections
17
PART ONE
CANCER SURVIVAL ndash EVIDENCE FOR THE ROLE OF LIFESTYLE IN
DISEASE PROGRESSION AND RECURRENCE
Introduction
Evidence for the role of lifestyle in the development of cancer is strong and it is widely
accepted that a poor diet lack of exercise smoking and excessive alcohol consumption can
increase an individuallsquos risk of developing cancer In particular it is well established that
smoking can increase risk of lung cancer and excessive unprotected exposure to the sun
can increase risk of skin cancer More recently lifestyle after a cancer diagnosis has been
under the microscope with evidence for the role of lifestyle in cancer progression7 and
recurrence8 demonstrating that lifestyle changes post-diagnosis can influence the disease
trajectory (Thomas and Davies 2007)
The development of cancer does not mean it is too late to make lifestyle changes that can
reduce the risk of the disease progressing or recurring after remission Indeed lifestylelsquo
refers to personal choices that can impact health and well-being as well as improve an
individuallsquos chance of disease-free survival9 and overall survival10
Evidence for an interaction between lifestyle and the disease trajectory is evaluated in the
current review including cancer development progression and recurrence and
commencing with a description of three large scale multicentre trials that will be referred to
throughout (Table 3)These studies are presented in some depth because their findings have
been influential in this field of study This will be followed by a site-specific (eg breast
colorectal lung prostate) summary of the findings reported by Bekkering et al (2006) as
part of the WCRF review being updated Further evidence identified from the search criteria
will then be presented including evidence obtained from the aforementioned multicentre
trials The European Prospective Investigation into Cancer and Nutrition (EPIC) Study
The Womens Intervention Nutrition Study (WINS) and The Womens Healthy Eating
and Living (WHEL) Study
7 Defined as the cancer becoming worse or spreading within the body
8 Cancer that has returned usually after a period of time during which it could not be detected The cancer may
come back to the same place as the original (primary) tumour or to another place in the body
9 The length of time after treatment during which a person survives with no sign of the disease
10The percentage of people from the study who are alive for a certain period of time after diagnosis or treatment
(ie 5-year survival rate)
18
The European Prospective Investigation into
Cancer and Nutrition (EPIC) Study (Riboli et al
2002)
The Womens Intervention Nutrition Study (WINS)
(Chlebowski et al 2006)
The Womens Healthy Eating and Living (WHEL)
Study
(Pierce et al 1997)
The EPIC study is coordinated in the UK by Dr Elio Riboli of the Imperial College London It is an ongoing multicentre prospective cohort study designed to investigate the relationship between nutrition and cancer The study currently includes 521000 participants (aged 35ndash70 years) in 23 centres located across 10 European countries11 These participants will be followed for cancer incidence and mortality for at least 10-years At enrolment which took place between 1992 and 2000 information was collected through a lifestyle questionnaire and through a dietary questionnaire addressing usual diet Physiological measurements (eg weight) were performed and blood samples taken The main website for EPIC12 last updated in 2010 reports that 26000 cases of cancer and 16000 deaths from cancer have been identified the majority of cases being cancer of the breast (n=6218) colonrectum (n=1910) prostate (n=1547) and lung (n=1292)
The WINS trial is a randomised multicentre study that commenced in 1994 and is now closed for recruitment It was designed to determine whether dietary fat reduction effectively prolongs disease-free and overall survival in post-menopausal women (n=2437) aged 48-78 years surgically treated for early stage breast cancer Randomisation to a reduced fat group or a control group took place between 1994 and 2001 with participants being evaluated annually via self-report and physiological measures 1) Intervention group (n=975) intensive dietary intervention for reduction of total fat intake to 15 of calories with repeated individual and group counselling sessions involving cognitive behavioural and motivational interviewing techniques 2) Control group (n=1462) US Department of Health and Human Services dietary guidelines (total fat intake between 20-35 of calories)
The WHEL study is a multicentre RCT which commenced in 1995 and also closed to recruitment aimed to determine whether a diet rich in vegetables fruit and fibre and low in fat is associated with a longer breast cancer event-free interval (ie no disease progression recurrence nor secondary cancers) Women diagnosed with stage I-III invasive breast cancer (n=3088) within the previous 4-years were randomised to a dietary intervention or control group and evaluated annually for 5-years via self-report and physiological measures 1)Intervention group (n=1540) guidelines provided for a daily dietary pattern of 5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy from fat A telephone counselling protocol focusing on goal setting self-monitoring and self-efficacy were provided as were cooking classes 2)Control group (n=1551) The US Department of Agriculture dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre and 30 energy from fat)
11
Denmark France Germany Greece Italy The Netherlands Norway Spain Sweden and the UK
12 httpepiciarcfr
Table 3 The EPIC WINS and WHEL Study (findings presented within proceeding text)
19
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in breast
cancer survival In the current review 6 studies and 2 systematic reviews were identified
These have been divided into appropriate domains according to mechanisms of benefit
hormones intensity and insulin Studies are summarised in Table 3 at the end of this
section
Hormones
Evidence exists that physical activity is associated with reduced risk of developing breast
cancer (Friedenreich and Cust 2008 Monninkhof et al 2007) One potential mechanism of
benefit is via the modification of sex hormone levels High levels of oestrogen (the
predominant sex hormone in females)13 and androgen (the predominant sex hormone in
males)14 are consistently associated with increased risk of developing breast cancer
(Eliassen et al 2006 Kaaks et al 2005) whereas high levels of sex hormone-binding
globulin (SHBG)15 are associated with a decreased risk (Key et al 2002) Regular physical
activity may alter oestrogen metabolism by shifting metabolism to favour production of 2-
hydroxyestrone (2-OHE1)16 as opposed to16α-hydroxyestrone (16α=OHE1) the former of
which has much weaker estrogenic activity Campbell et al (2007) is one of the few
researchers to examine this mechanism of benefit via a RCT In examining the effects of a
12-week aerobic exercise training programme on 2-OHE1 and 16α-OHE1 in healthylsquo pre-
menopausal women (n=17) no significant differences in oestrogen changes were found with
a control group who continued their usual level of physical activity (n=15) However a
change in lean body mass (estimated weight excluding body fat) over the 12-week
programme was found to be associated with a favourable change in 2-OHE1 to 16α-
OHE1 ratio (p lt 005)
In an effort to provide more direct evidence regarding the biological mechanisms of benefit
obtained from physical activity Friedenreich et al (2010) conducted the Alberta Physical
Activity and Breast Cancer Prevention Trial a two-centre two-arm RCT of physical
activity and cancer risk in older (50gt years) post-menopausal sedentary women from the
general population (n=320) Participants received a 1-year aerobic physical activity
programme of 225-minutes per week (n=160) or maintained their usual level of activity as
part of a control group (n=160) Significant reductions in oestrogen were found in the
intervention group compared to the control group demonstrating a protective effect
of increased physical activity in this group of high risk women (p lt 05)
13
oestrogen is suspected to activate certain oncogeneslsquo which can turn normal cells into tumour cells 14
The primary and most well-known androgen is testosterone which is also found in women to a lesser degree 15
A protein that attaches itself to oestrogen and androgen
16 Sometimes referred to as a good oestrogenlsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
20
Whilst some studies have examined the outcomes of increased physical activity others have
attempted to identify the duration and intensity required for beneficial effects Using data
from the Nursesrsquo Health Study17 (n=2987) Holmes et al (2005) found that women who
reported at least 3 MET-hours18 or more of physical activity per week were less likely
to have a recurrence or die from breast cancer compared to those who reported less
physical activity (p lt 001)
A further reduction in risk was seen with higher levels of physical activity up to 239 MET-
hours per week indicating a dose-response Interestingly the benefits of physical activity
were limited to women with hormone-receptor positive tumours (tumours that
respond to hormone treatment) as opposed to hormone-receptor negative tumours
(tumours that do not respond to hormone treatment) This provides further support for
mechanism of benefit from physical activity being hormone-related whether that be due to
the physical activity or any subsequent reductions in lean body mass that might accompany
such activity
Intensity
Expanding on evidence for the intensity of physical activity in a prospective observational
study the Health Eating Activity and Lifestyle (HEAL)19 study Irwin et al (2008) found
that of breast cancer survivors (n=933) who were sedentary pre-diagnosis women who
increased their physical activity post-diagnosis to approximately 9-MET hours per
week (eg 2-3 hours of brisk walking) had a 45 lower risk of death from cancer when
compared to those who did not increase their physical activity women who
decreased physical activity after diagnosis had a four-fold greater risk (p lt 005)
17
One of the largest and longest running investigations of factors that influence womenlsquos health comprising
information from 238000 nurse-participants
18 Metabolic equivalent (MET) values a measure of the effort required to do that activity
19 The HEAL Study is a population-based multicentre multi-ethnic prospective cohort study that has enrolled
1183 breast cancer survivors to determine whether lifestyle hormones and other exposures affect breast cancer
prognosis
METs (Ainsworth 2000) Light-intensity activities are defined as 11 MET to
29 MET Moderate-intensity activities are defined as 30 to
59 METs Vigorous-intensity activities are defined as 60 METs
or more
3 MET-hours might be using a stationary bicycle with light effort for one-hour 239 MET-hours might be running for 2-hours plus 1-hour of aerobic activity
21
Consistent with this a larger prospective observational study demonstrated that breast
cancer survivors (n=4482) who were physically active for more than 28 MET-hours per
week (eg walking at average pace of 2-29mph for 1-hour) were significantly less
likely to die from breast cancer (35-49 reduction) when compared to survivors who
did less than this (p lt 05) (Holick et al 2008) The reduced risk of mortality from cancer
was limited to total or moderate-intensity physical activity no benefit was noted for vigorous-
intensity activity
In a systematic review by Patterson et al (2010) leisure-time physical activity (ie
sportsrecreational) was associated with a 30 decreased risk of mortality from
breast cancer when compared to sedentary women In another review Saxton (2010)
identified four cohort studies demonstrating that women achieving the equivalent of 30-
minutes of moderate intensity physical activity on five or more days of the week
halved their risk of cancer-related mortality compared to those achieving less than 30-
minutes over the five days
Insulin
Evidence for the role of excess insulin in the growth of cancer cells has become more
established in recent years especially with the increase in obesity which is often
accompanied by elevated levels of insulin (Giovannucci 2005) The benefits of physical
activity on reducing insulin levels are less clear Ligibel et al (2008) conducted a RCT to test
the impact of weight training on insulin levels in overweight sedentary stage I to III breast
cancer survivors (n=101) The women were randomly assigned to one of two conditions
1) a 16-week supervised strength training and home-based cardiovascular training
protocol (two supervised 50-minute strength training sessions per week and 90-
minutes of home-based aerobic physical activity weekly)
2) a control group (routine care for 16-weeks before being offered consultation with a
physical activity trainer at the end of the control period)
Participation in the physical activity training was associated with a significant
decrease in insulin levels and hip circumference (p lt 05) Therefore the relationship
between physical activity and breast cancer recurrence may be mediated in part through
changes in insulin levels andor changes in body fat
ii DIET
Bekkering et al (2006) report on two small breast cancer studies showing a reduction in
cancer-specific mortality with healthy diet interventions (Elkort et al 1981 de Waard et al
1993) Of nine trials that included an antioxidant supplement no evidence was found for an
association between the intervention and cancer-related mortality compared with placebo or
usual treatment There was also no evidence of an effect of retinol (vitamin A - found in cod
liver oil butter liver eggs and cheese) (Meyskens et al 1994 Kucera et al 1980
Pastorino et al 1993)
22
In the current review 19 studies provide further evidence of the role of diet in breast cancer
survival many of which are part of the three multicentre studies previously described (ie
EPIC WINS WHEL p19) These studies have been divided into appropriate domains
according to dietary components dietary fat fruit and vegetables dietary fibre soy and
vitamin D
Dietary Fat
In general retrospective casendashcontrol studies have supported a positive association between
breast cancer incidence and dietary fat (Howe et al 1990) whilst many prospective cohort
studies have failed to show such an association (Kim et al 2006 Hunter et al 1996) A
meta-analysis provided evidence for a weak direct association between fat intake and breast
cancer in casendashcontrol and cohort studies combined (Boyd et al 2003) in cohort studies
that adjusted for energy intake highest versus lowest categories of total fat intake were
associated with a statistically significant 13 increased risk of developing
breast cancer (p lt 05)
Kyogoku et al (1992) utilised breast cancer patients whose dietary intake was assessed 10-
years previously in a case-control study (n= 212 patients who underwent a surgical
operation) After 10-years of follow-up 47 breast cancer deaths had occurred with no
support being provided for the hypothesis that a low fat diet influences breast cancer survival
outcomes In addition Holmes et al (1999) as part of the Nursesrsquo Health Study report
there being no evidence suggesting that lower intake of total fat or specific types of fat (eg
saturated and unsaturated fat) was associated with death from breast cancer in 2956
women who were diagnosed after 14-years of follow-up
Hebert et al (1998) studied the effect of diet on recurrence and death in women diagnosed
with early-stage breast cancer (n=472) finding that the strongest effects were observed in
pre-menopausal women Higher levels of self-reported baseline daily consumption of
butter margarine lard and beer were found to increase the risk of recurrence (p lt
01) There was also an increased risk associated with consumption of red meat liver and
bacon corresponding to about a doubling of risk for each time per day that foods in this
category were consumed (p=09)
The previously described WINS and WHEL RCTs (Table 2 p19) were anticipated to shed
light on these inconsistent findings related to dietary fat and breast cancer outcomes as
explored next in the following section
In an interim analysis of the Womens Intervention Nutrition Study (WINS) data (n=2437)
after a median follow-up of 60-months (5-years) (Chlebowski et al 2006) report that dietary
fat intake was lower in the dietary intervention than in the control group corresponding to a
significant 6-pound lower mean body weight in the intervention group (p lt 05) As a
reminder the dietary intervention group were counselled to reduce total fat intake to 15 of
calories whilst the control group were advised to keep total fat intake between 20-35 of
calories After 5-years of follow-up a total of 277 recurrences were reported in 96 of 975
23
(98) women in the dietary group and 181 of 1462 (124) women in the control group
women in the dietary intervention had a 24 lower risk of recurrence compared to the
control group (p lt 05) Exploratory analyses suggested that dietary fat reduction was most
beneficial in women diagnosed with hormone receptorndashnegative compared to hormone-
receptor positive breast cancer although this was not statistically significant
Other studies providing evidence of a differential effect of fat intake on breast cancer survival
have found such associations with hormone-receptor positive cancers (Holm et al 1993
Cho et al 2003) raising debate over the WINS findings Nevertheless in 2008 Chlebowski
et al updated survival information presented in 2006 reporting that after 7-years follow-up a
significant overall survival benefit was seen in women (n=362) with hormone-receptor
negative tumours taking part in the dietary intervention compared to the comparison
group (75 vs 181 p lt 005)
To explore the link between hormones and diet further the metabolic profiles of a subset of
WINS participants (n=53) were examined for the effect of a low-fat diet on insulin resistance
(Khaodhiar et al 2003) Insulin resistance is a physiological condition in which insulin
becomes less effective in lowering blood sugars resulting in increased blood glucose Of
those participants with initial insulin resistance after 1-year women in the dietary
intervention group had a greater decrease in their fasting insulin (insulin tested in a blood
sample collected after a 12-hour fast) than the women in the control group Although
not statistically significant these results suggest that insulin concentrations (a marker of
insulin resistance) may be influenced by dietary fat intake Alternatively since waist-to-hip
ratio is a marker for insulin weight reduction as opposed to dietary fat reductions might be
the important variable influencing disease outcomes (Borugianlsquos et al 2004)
Fruit and Vegetables
Flavonoids20 are high in fruits and vegetables and therefore might account for some of the
findings reported in WINS Dwyer et al (2008) sought to determine whether differences
existed in baseline and 12-month dietary intake of flavonoids among a random sample of
WINS participants (n=550) After 12-months of dietary intervention flavonoid intakes
remained similar in both groups demonstrating that neither total flavonoid intakes nor
intakes of subclasses of flavonoids differed between those who had dramatically decreased
their fat intake and those who had not Flavonoid intake is therefore unlikely to account for
the survival benefits reported for the WINS trial Carotenoids21 however do appear to play a
significant role in cancer survival On following 103 breast cancer survivors 27 of whom
died Ingram (1994) found that after a median of 81-months those who consumed more
beta-carotene (a carotenoid found in yellow and orange fruits such as mangoes
papayas and carrots) had significantly fewer deaths from breast cancer only one in
the group of highest beta-carotene consumers compared with 8 in the intermediate
20
Flavonoids also referred to as bioflavonoids are polyphenol antioxidants found naturally in plants ndash in other
words they are plant nutrientslsquo
21 Organic pigments that provide colour to bright fruits and vegetables including carrots apricots tomatoes and
salmon
24
group and 12 in the lowest group (p lt 0001) Overall there were 12 deaths in the lowest
total fruit consumption group compared with five in the intermediate group and 3 in the
highest (p lt 001) This benefit applied to both orangeyellow fruit (oranges melon) as well
as other fruits (apple banana berries grapes dried fruits)
Adding to this evidence is data from the aforementioned Womens Healthy Eating and
Living (WHEL) RCT (Table 2 p19) As a reminder women with breast cancer were
randomised to a dietary intervention (n=1540) comprising a daily pattern of
5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy
from fat or to a control group (n=1551) advised to follow the US Department of Agriculture
dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre
and 30 energy from fat Over a mean 73-year follow-up there was no significant
difference between groups in terms of additional breast cancer events (ie disease
progression recurrence or secondary cancer) or mortality despite statistically significant
differences in self-reported diet (low fat high fruit and vegetables) (Pierce et al 2007) On
the other hand when Rock et al (2005) examined only those participants in the control
group higher plasma total carotenoid concentration indicative of greater fruit and
vegetable consumption was significantly associated with reduced risk for a new
breast cancer event (p lt 05) This supports those findings reported by Ingram et al
(1994) and provides a potential explanation for why survival benefits were achieved in WINS
but not WHEL since both dietary interventions comprised lower dietary fat and higher levels
of carotenoids (fruit and vegetables) other factors must explain the differential survival
benefits One major difference between the two studies is that WINS participants lost weight
(mean = 6-pounds) whereas the WHEL participants did not
To follow up on these findings in terms of possible biological mechanisms of reduced risk of
recurrence Thomson et al (2007) conducted an ancillary study with post-menopausal
breast cancer survivors from the WHEL study (n=207) The aim was to test the hypothesis
that breast cancer survivors with higher levels of dietary carotenoids would show significantly
lower levels of oxidative stress (pathologic changes in response to excessive levels of cell
toxicity from the environment) than those with lower levels It was found that dietary
carotenoid levels were not significantly associated with oxidative stress indicators (measured
via urine samples)
Hot flushes post-treatment for early-stage breast cancer has been associated with an
approximately 25-30 decreased risk for additional breast cancer events (Mortimer et al
2008 Cuzick 2007) Since hot flushes are reported by women who continue to menstruate
during treatment or whose menstruation returns post-treatment this lowering of risk is
unlikely to be explained entirely by the lower oestrogen levels that sometimes accompany
hot flushes On the other hand dietary changes comprising lower energy from fat and
increased fibre can also alter oestrogen levels For example binding of fibre to estrogens in
the gut blocks reabsorption of oestrogen (Arts et al 1991) Focusing their analyses on the
2967 of the WHEL participants who experienced baseline hot flushes Gold et al (2009)
tested the hypothesis that the increased risk of additional breast cancer events observed
among women who do not report hot flushes post-treatment can be reduced by lifestyle
interventions that lower circulating oestrogen Over a median of 73-years follow-up it was
demonstrated that the dietary intervention was associated with reduced risk of second
25
breast cancer events among women who reported no hot flushes at baseline (p lt 05)
These women had 31 fewer cancer-related events than matched-pairs in the control group
among post-menopausal women with no self-reported hot flushes at baseline the
intervention effect was even stronger with a 47 reduction in risk compared with post-
menopausal women in the control group who had no hot flushes at baseline (p lt 05)
McEligot et al (2006) conducted a retrospective investigation into the influence of diet (fat
fibre vegetable fruit folate carotenoids and vitamin C) on overall survival in post-
menopausal women with breast cancer (n= 516) Participants completed a food frequency
questionnaire for the year prior to diagnosis the analysis of which demonstrated that
women consuming the least total fat and highest total fibre and vegetables as well as
more folate vitamin C and carotenoid were significantly less likely to die from any
cause than those women consuming the opposite (p lt 05)
Dietary Fibre
Evidence linking breast cancer to the intake of dietary fibre has been conflicting although the
hypotheses remain that dietary fibre can be protective by inhibiting oestrogen (Kaaks et al
2005) as described previously in relation to physical activity or by reducing insulin-like
growth factors (Heald et al 2003) Therefore further research into these mechanisms of
benefit is clearly needed in order to provide clarity
Rohan et al (1993) examined risk of breast cancer in relation to intake of dietary fibre and
vitamins A C and E in a cohort of women (n=56837) enrolled in the Canadian National
Breast Screening Study22 After 5-years follow-up 519 incidence of breast cancer were
identified with analysis of previously completed dietary questionnaires demonstrating that
higher dietary fibre intake was associated with a small reduction in risk of developing
breast cancer Specifically there was a statistically significant decrease in risk of
developing breast cancer with increasing consumption of cereals (p lt 01) and a statistically
non-significant trend for pasta consumption (p=017) This reduced risk persisted after
adjustment for total vitamin A beta-carotene vitamin C and E
The UK Womens Cohort Study (UKWCS) (Cade et al 2007) which compares the health
outcomes of three main dietary groups (vegetarian eating fish [not meat] and meat eaters)
provides further evidence for the protective properties of fibre After a median of 75 years
follow-up analysis of self-reported dietary data of 35792 women showed that total dietary
fibre was found to be related to breast cancer incidence in women who were pre-
menopausal but not post-menopausal at baseline (p lt01) Fibre from cereals (plt
05) and fibre from fruit (p=009) was found to be protective against breast cancer
22
An RCT comprising women 40-49 years of age at study entry evaluating the efficacy of annual mammography breast physical examination and instruction on breast self-examination in reducing breast cancer mortality
26
Soy
A high intake of phytoestrogens23 particularly isoflavones (found in soy products) has been
suggested to decrease risk of developing breast cancer In one of the European
Prospective Investigation into Cancer and Nutrition (EPIC) studies a large multicentre
prospective cohort study described earlier in Table 2 the association between breast cancer
risk and isoflavones was supported in 333 women (p lt 005) (Grace et al 2004) but in
another larger EPIC study conducted in Utrecht (n=15555) no such evidence was found
(Keinan-Boker et al 2004) Analyses with pooled data sets are ongoing In the meantime
Boyapati et al (2005) provide evidence from the Shanghai Breast Cancer Study24
suggesting that after a median of 52-years follow-up soy intake pre-diagnosis is not related
to disease-free survival in women with breast cancer (n=1459)
Vitamin D
Goodwin et al (2009) measured vitamin D (usually obtained from sunlight through the skin
but also found in oily fish and eggs) levels in the stored blood of women with early breast
cancer (n=512) The mean follow-up was 116-years by which time women deficient in
vitamin D had a significantly increased risk of distant recurrence25 compared with
those who had sufficient levels (p lt 05)
Antioxidant Supplements
Despite widespread use only a few clinical or epidemiological studies have examined the
relationship between antioxidant supplements and risk of breast cancer recurrence or breast
cancer-related mortality Fleischauer et al (2003) examined recurrence and mortality
among post-menopausal women diagnosed with breast cancer (n=385) who were enrolled
into a dietary case-control study Women were contacted with a single questionnaire to
ascertain the use of nutritional supplements during 12-14 years of follow-up Antioxidant
vitamin supplement use was associated with a lower risk of breast cancer recurrence or
mortality Specifically use of vitamin C and E supplements moderately reduced risk (p lt
05) whilst vitamin E nearly halved the risk although this was not statistically
significant (p=056)
iii WEIGHT
Weight and body composition have been implicated in the development of a wide range of
cancers as well as in increased risk of recurrence or second primary cancers (Chlebowski
Aiello and McTiernan 2002) Additionally being overweight or obese can exacerbate some
23
Phytoestrogens sometimes called dietary estrogenslsquo are a group of naturally occurring plant compounds that have a similar chemical structure to estrogen they bind to estrogen receptors acting like hormone regulators
24 The Shanghai Breast Cancer Survival (SBSS) Study collected lifestyle-related factors and disease and
treatment related factors in Chinese women with breast cancer (n=2236) (Lu et al 2007) 25
The spread of cancer to parts of the body other than the place where the cancer first occurred
27
of the side-effects of cancer treatment as well as increase the risk of co-morbidities such as
diabetes and osteoporosis (Doyle et al 2006) The studies evaluated in this review thus far
further indicate weight as offering a mechanism of benefit in terms of breast cancer
outcomes Indeed the WINS and WHEL RCTs produce different outcomes when using
similar dietary interventions with weight loss in the WINS group but not the WHEL group
offering a likely explanation for improved outcomes observed in the WINS participants Since
increased adiposity (excess body fat) has been identified as a negative prognostic factor for
recurrent disease and survival after breast cancer diagnosis (Rock and Demark-Wahnefried
2002) the apparent benefit of dietary fat reduction in the intervention group could
partly result from the weight loss
Bekkering et al (2006) do not add to this evidence whilst 5 studies and one systematic
review were identified in the current review
Hebert et al (1998) studied the effect of body weight on recurrence and death in women
diagnosed with early-stage breast cancer (n=472) Body mass index (BMI) was
associated with an increased risk of recurrence at the rate of 9 for each kgm2
(equivalent to about 58-pounds for a 5 4 tall woman) For death the results were
similar but body mass index was more strongly associated increasing risk by 12
per kgm2
Additionally Lahmann et al (2004) used data from 73542 pre-menopausal and 103344
post-menopausal women taking part in the EPIC study During 47-years of follow-up 1879
cases of invasive breast cancer were identified In post-menopausal women current use
of hormone replacement therapy (HRT) modified the association between body size
and breast cancer among non-users weight body mass index and hip circumference
were positively associated with breast cancer risk (p lt 001) Obese women (BMI gt 30)
had a 31 risk compared to women with a BMI lt 25 Among pre-menopausal women hip
circumference was the only other measure significantly related to breast cancer (p lt 005)
after accounting for BMI
Enger et al (2004) conducted a retrospective follow-up study of women diagnosed with
breast cancer (n=1376) for whom complete medical records and adequate tissue
specimens existed Patients were followed for a median of 68-years after diagnosis 246 of
whom died from breast cancer Compared with women in the lowest category of weight
(lt133lb [60kg] at diagnosis) women in the highest category ( 175lb [79kg])
experienced a 25-fold increased risk of dying from breast cancer (P lt 05) Women with
hormone-receptor negative cancer experienced an approximately 2-fold higher risk of dying
from breast cancer compared with women who presented with hormone-receptor positive
cancer Women in the upper 50th percentile of weight with hormone-receptor negative cancer
had a nearly 5-fold increased risk of dying from cancer compared with women in the lower
50th percentile of weight and hormone-receptor positive cancer (p=10)
In order to determine whether weight prior to diagnosis and weight gain after diagnosis are
predictive of breast cancer survival Kroenke et al (2005) followed 5204 participants from
the Nursesrsquo Health Study diagnosed with incident invasive non-metastatic breast cancer
After a median of 9-years follow-up there were 860 total deaths 533 breast cancer deaths
28
and 681 recurrences (defined as secondary lung brain bone or liver cancer and death from
breast cancer) Weight before diagnosis and weight gain after diagnosis were related
to higher rates of breast cancer recurrence and mortality although associations were
most apparent in women who had never smoked (p lt 05) Furthermore associations
with weight were stronger in pre-menopausal than in post-menopausal women In contrast
by comparing breast cancer survivors (n=3215) with women in the comparison group of a
dietary intervention trial to prevent breast cancer recurrence Caan et al (2008) found that
neither moderate (5ndash10) nor large (gt10) weight gain post-diagnosis was associated with
an increased risk of breast cancer recurrence in the early years post-diagnosis (median time
of 737-months from diagnosis)
More recently Patterson et al (2010) reviewed published epidemiological research on
lifestyle and breast cancer outcomes reporting that the most consistent finding from
observational studies was that adiposity was associated with a 30 increased risk of
cancer-related mortality
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in breast cancer
survival Four studies were identified in the current review
In an observational study Manjer et al (2000) compared the survival of patients with breast
cancer (n=792) who had never smoked were smokers or were ex-smokers Follow-up of
breast cancer cases was through record-linkage with the Swedish Cause of Death Registry
During a mean follow-up of 121-years smokers and ex-smokers compared with those
who had never smoked had a significantly increased risk of death from cancer
Fentiman et al (2005) add to this evidence with a cohort study of breast cancer patients who
completed a lifestyle questionnaire at the time of diagnosis (n=166) They found that
smoking was the third most important predictor of breast cancer-specific and overall
survival after stage and age at diagnosis This suggests that smokers are not only more
likely to die of cancer but also of other diseases when compared with those who have never
smoked
In a much larger study Holmes et al (2007) conducted a prospective observational study
among 5056 women from the Nursesrsquo Health Study with stages I-III invasive breast
cancer Information on smoking was available for these women who were followed until
January 2002 or death whichever came first Compared with women who had never
smoked women who were current smokers had a 43 increased risk of death from
any cause with risk increasing along with more cigarettes smoked per day (p lt0001)
In contrast there was no association with current smoking and breast cancer death
Sagiv et al (2007) followed women diagnosed with a first primary breast cancer (n=1273)
for 5-6 years and found that the number of all-cause mortality (n=188) including breast
cancer-specific mortality (n=111) was slightly higher among current and former
active smokers compared with women who had never smoked No association was
found between active or passive smoking and breast cancer-specific mortality
29
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in breast cancer
survival In the current review one review and 2 studies were identified
Rock and Demark-Wahnefried (2002) reviewed the evidence from clinical and epidemiologic
studies reporting that alcohol intake was not associated with breast cancer survival in the
majority of the studies In contrast post-menopausal women (n=125) diagnosed with
invasive breast cancer who were followed through to survival demonstrated that pre-
diagnosis alcohol consumption of at least one drink per week was associated with a
27-fold increase in risk of cancer-related mortality (McDonald et al 2002) In a similar
study a larger sample of women (n=1286) diagnosed with invasive breast cancer who were
followed from diagnosis through to survival produced opposing findings compared with
non-drinkers women who consumed alcohol in the 5-years before diagnosis had a
decreased risk of cancer-related mortality (Reding et al 2009)
SUMMARY OF LIFESTYLE EVIDENCE FOR BREAST CANCER ndash MECHANISMS
OF BENEFIT
Physical Activity Physical activity is likely to prevent breast cancer via its effect on
hormones specifically by reducing levels of oestrogen in the body (Friedenreich et al 2010)
or shifting the metabolism of oestrogen to favour production of 2-hydroxyestrone (2-OHE1)26
as opposed to16α-hydroxyestrone (16α=OHE1) the former of which has much weaker
estrogenic activity This shift might also be the result of a change in lean body mass resulting
from physical exercise (Campbell et al 2007) The survival benefits of physical activity
appear to require a certain intensity or level of exertion specifically 3 MET-hours or more per
week (Holmes et al 2005 Holick et al 2008 Saxton et al 2010) this equates to moderate
intensity activity such as using a stationary bike for 1-hour However there is also evidence
of a dose-effect with greater activity (up to 239 MET-hours per week) being associated with
reduced risk of recurrence and cancer-related mortality (Holmes et al 2005) or indeed
greater levels of activity than pre-diagnosis being associated with reduced risk of recurrence
and cancer-related mortality (Irwin et al 2008 Holick et al 2008 Patterson et al 2010
Saxton et al 2010)
Diet Evidence for the role of dietary fat in breast cancer development and survival are
varied Case-control (Kyogoku et al 1992) and large prospective studies (Holmes et al
1999) do not show any significant link whilst some studies have found that dietary fat does
increase risk of recurrence or death in pre-menopausal women Indeed the large multicentre
WINS trial found a protective benefit of a reduced fat dietary intervention which was more
prominent in women diagnosed with hormone-receptor negative breast cancer (Chlebowski
et al 2006a Chlebowksi et al 2008) The differential effect of diet on hormone-receptor
positive and negative disease indicate that metabolic mechanisms involving insulin and
26
Sometimes referred to as a lsquogood estrogenrsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
30
insulin-like growth factor-1 (IGF-1)27 may be involved in the mechanisms of benefit and
although not statistically significant data has been presented suggesting that elevated
insulin concentrations (a marker of insulin resistance) may be influenced by dietary fat
reduction (Khaodhiar et al 2003 Borugian et al 2004) However this might be due to
changes in weight produced by a low fat diet rather than the lower consumption of fat itself
(Borugian et al 2004) Since low fat diets are often accompanied by high intakes of fruit
and vegetables various components of a diet comprising high levels of fruit and vegetables
have been investigated Carotenoids have received particular attention with evidence
suggesting that carotenoids play a role in survival (Ingram 1994) Other studies have found
this not to be the case (Pierce et al 2007) with the primary difference in these studies being
lack of weight loss This indicates that the mechanism of benefit produced from low fat high
fruit and vegetable (particularly carotenoids) diets is most probably through changes in body
composition Indeed the majority of studies in this review demonstrated a link between
weight and cancer-related risks (Hebert et al 1998 Enger et al 2004 Lahmann et al
2004 Patterson et al 2010)
Smoking Evidence pertaining to the smoking clearly demonstrates a link between
breast cancer survival and a history of smoking However it appears to be more likely to
increase all-cause mortality as opposed to cancer-specific mortality (Fentiman et al 2005
Holmes et al 2007 Sagiv et al 2007)
Alcohol Although the evidence is less clear pre-diagnosis alcohol consumption does
appear to be related to survival (McDonald et al 2002 Reding et al 2009) although
current drinking does not (Demark-Wahnefried 2002)
27
IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of
pathological states including cancer
31
Table 3 Breast Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Campbell et al (2007)
RCT examining the effects of 12-weeks of aerobic exercise training on 2-OHE
1 and 16α-OHE
1 in
premenopausal women Randomisation to 1) A 12-week individualised supervised moderate-to-vigorous intensity aerobic exercise training intervention (n = 17) Participants began the exercise program in the early follicular phase of the next menstrual cycle (days 1-5) The intervention was divided into three blocks (a) Weeks 1 ndash 4 ndash 3 sessions per week of base aerobic training progressing from 20-40 minutes on a stationary bike (b) Weeks 5-8 ndash 4 sessions per week Two sessions were base aerobic training sessions for 30-45 minutes (c) Weeks 9 -12 ndash 4 sessions per week with two base aerobic training sessions for 30-45 minutes and two interval sessions 2) Usual lifestyle (n = 15) Participants were asked to maintain their usual activity levels for the duration of the study Following the control cycle the first day of the next menstrual cycle was used as the reference start date for participants in the control group On completion of the 12-week post-intervention
Healthy regularly menstruating Caucasian women (n=32) 20-35 years
On completion of the 12-week intervention
Height body mass body composition by dual-energy X-ray absorptiometry and VO2max were measured at baseline and following the intervention Urine samples were collected in the luteal phase of four consecutive menstrual cycles
Participants attended an average of 40-44 (91) sessions Fourteen of 17 (82) participants completed at least 80 of the sessions The exercise group increased VO2max by 14 and had significant although modest improvements in fat and lean body mass No significant between-group differences were observed however for the changes in 2-OHE1 (P = 0944) 16α-OHE1 (P= 0411) or the ratio of 2-OHE1 to 16α-OHE1 (P = 0317) At baseline there was an inverse association between body fat and 2-OHE1 to 16α-OHE1 ratio (r = minus040 P = 0044) however it was the change in lean body mass over the intervention that was positively associated with a change in 2-OHE1 to 16α-OHE1 ratio (r = 043 P = 0015)
32
measurement participants were given guidance for starting an individualised exercise program and access to the fitness facility for 4-weeks
Friedenreich et al (2010)
A two-centre two-arm RCT examining how an aerobic exercise intervention influences
circulating
estradiol oestrone sex hormonendashbinding globulin
(SHBG)
androstenedione and testosterone levels which may
be involved in the
association between physical activity and
breast cancer risk
Randomisation to 1) A 1-year aerobic physical activity programme of 225-minutes per week (n=160) 2) Control group maintained their usual level of activity (n=160)
Older (50gt years) post-menopausal sedentary women (n=320)
On completion of the intervention
Estradiol and sex hormone-binding globulin levels Androstenedione and testosterone levels
Completion of the study was high (966) At 12-months statistically significant reductions in
estradiol (treatment effect ratio
[TER] = 093 95 CI 088 to 098) and free estradiol (TER = 091
95 CI 087 to 096) and increases in SHBG (TER = 104 95 CI
102 to 107) were observed in the exercise group compared with
the control group No significant differences in oestrone
androstenedione and testosterone levels were observed between
exercisers and controls at 12-months
Holick et al (2008)
Prospective cohort study examining the relationship between post-diagnosis recreational physical activity and risk of breast cancer death
Women with a history of previous invasive breast cancer diagnosed between the ages of 20-79 years (n=4482)
Maximum of 6-years post-diagnosis (median=56-years post-diagnosis)
Mortality from breast cancer mortality from any cause Self-reported physical activity converted to MET-hours per week
After adjusting for age at diagnosis stage of disease state of residence interval between diagnosis and physical activity assessment body mass index menopausal status hormone therapy use energy intake education family history of breast cancer and treatment modality compared with women expending lt28 MET-hwk in physical activity women who engaged in greater levels of activity had a significantly lower risk of dying from breast cancer (HR 065 95 CI 039-108 for 28-79 MET-hwk HR 059 95 CI 035-101 for 80-209 MET-hwk and HR 051 95 CI 029-089 for ge210 MET-hwk P for trend = 005) Results were similar for overall survival (HR 044 95 CI 032-060 for ge210 versus lt28 MET-hwk P for trend lt0001) and were similar regardless of a womanlsquos age stage of disease and body mass index
Holmes et al (2005)
Prospective observational study
(Nurseslsquo Health Study) to determine whether physical activity among
women with breast cancer
2987 female registered nurses
in the
Nurseslsquo Health
Women were diagnosed between 1984 and
Breast cancer mortality risk according
to
physical activity
Compared with women who engaged in less than 3 MET-hours per
week of physical activity the adjusted relative risk (RR) of death
from breast cancer was 080 (95 CI 060-106) for 3 to 89 MET-hours per week 050
(95 CI 031-082) for 9 to 149 MET-hours
33
decreases their risk of death from
breast cancer compared with
more sedentary women
Study diagnosed with stage
I II or III
breast cancer
1998 and followed until death or June 2002
category (lt3 3-89 9-149 15-239
or 24
metabolic equivalent task [MET] hours per week)
per week 056 (95 CI 038-084) for 15 to 239 MET-hours per
week and 060 (95CI 040-089) for 24 or more MET-hours per week (P for trend
= 004) Three MET-hours is equivalent to walking
at average pace of 2 to 29 mph for 1 hour The benefit of physical
activity was particularly apparent among women with hormone-
responsive tutors The RR of breast cancer death for women with hormone-responsive
tumours who engaged in 9 or more MET-hours
per week of activity compared with women with hormone-
responsive tumours who engaged in less than 9 MET-hours per
week was 050 (95 CI 034-074) Compared with women who
engaged in less than 3 MET-hours per week of activity the absolute
unadjusted mortality risk reduction was 6 at 10 years for women
who engaged in 9 or more MET-hours per week
Irwin et al (2008)
The Health Eating Activity and Lifestyle Study (HEAL) Prospective observational study investigating the association between pre- and post-diagnosis
physical activity (as well as
change in pre-diagnosis to post-diagnosis
physical activity) and
mortality among women with breast cancer
A subsample of participants from the HEAL study ndash 933 women diagnosed with local or regional breast cancer between 1995
and 1998
5 -8 years from diagnosis (median=6-years)
Primary outcomes total deaths
and breast
cancer deaths
Compared with inactive women the multivariable hazard ratios
(HRs) for total deaths for women expending at least 9 MET-
hours per week (approximately 2-3 hwk of brisk walking) were 069
(95 CI 045 to 106 P = 045) for those active in the year before
diagnosis and 033 (95 CI 015 to 073 P = 046) for those active
2-years after diagnosis Compared with women who were inactive
both before and after diagnosis women who increased physical
activity after diagnosis had a 45 lower risk of death (HR = 055
95 CI 022 to 138) and women who decreased physical activity
after diagnosis had a four-fold greater risk of death (HR = 395 95
CI 145 to 1050)
Ligibel et al (2008)
RCT examining the impact of physical activity on insulin levels Participants were randomly assigned to one of two conditions a)Physical activity intervention a 16-week supervised strength training and home-based cardiovascular training protocol (two supervised 50-minute strength training
sessions per
week and 90-minutes of home-based
aerobic physical activity
weekly) b) Control group routine care for 16-weeks before being offered consultation with an physical activity
Overweight sedentary stage
I-III breast
cancer survivors (n=101)
On completion of the 16-week intervention
Fasting insulin and glucose levels Weight body composition
and
circumference at the waist and hip
18 women withdrew consent andor did not complete the study
Baseline and 16-week measurements were available for 82 patients
Fasting insulin concentrations decreased by an average of
286 microUmL in the exercise group (P = 03) with no
significant change in the control group (decrease of 027 microUmL P
=
65) The change in insulin levels in the exercise group seemed
greater than the change in controls but the comparison
did not reach statistical significance (P = 07) There was a
trend toward improvement in insulin resistance in the exercise
group (P = 09) but no change in fasting glucose levels The
exercise group also experienced a significant decrease in hip
measurements with no change in weight or body composition
34
trainer at the end of the control
period
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer outcomes
Breast cancer Not reported Additional breast cancer events and mortality
Although observational data were not consistent physical activity appeared to be associated with a 30 decreased risk of mortality
Saxton et al (2010)
A review of studies pertaining to physical activity and cancer mortality
All cancers with more evidence obtained for breast cancer
Not reported Survival A number of prospective cohort studies have reported negative associations between physical activity and cancer mortality The most compelling observational evidence of the survival benefits to be gained from a physically active lifestyle has emerged from studies of post-diagnosis physical activity in breast and colorectal cancer survivors These studies have shown clear inverse associations between post-diagnosis activity and survival with the benefits being independent of age gender obesity and disease stage at diagnosis Three of the four cohort studies of breast cancer survivors showed that women who are achieving the equivalent of 30-miniutes of moderate intensity PA on five or more days of the week can halve their risk of mortality up to 8 years of follow-up
DIET
Borugian et al (2004)
Prospective cohort study testing the hypothesis that elevated wait-to-hip ratio is directly related to breast cancer
mortality
603 patients with incident
breast
cancer
Up to 10-years
Date of death and
primary and secondary cause of death
After adjustment for age BMI family history oestrogen
receptor (ER) status tumour stage at diagnosis and systemic
treatment (chemotherapy or tamoxifen) WHR was directly related to
breast cancer mortality in postmenopausal women (for highest
quartile vs lowest relative risk = 33 95 confidence interval
11 104) but not in premenopausal women (relative risk = 12
95 confidence interval 04 34) Stratification according to
ER
status showed that the increased mortality was restricted to ER-
positive postmenopausal women Elevated WHR was confirmed as
a predictor of breast cancer mortality with menopausal status and
ER status at diagnosis found to be important modifiers of that
relation
Boyapati et al (2005)
As part of the Shanghai Breast Cancer Cohort Study associations between soy and breast cancer survival were investigated
1459 breast cancer patients
52-years Disease-free survival
Soy intake pre-diagnosis was unrelated to disease-free breast cancer survival (adjusted hazard ratio [HR]=099 95 confidence interval [CI] 073-133 for the highest tertile compared to the lowest tertile) The association between soy protein intake and breast cancer survival did not differ according to ERPR status tumour stage age at diagnosis body mass index (BMI) waist to hip ratio (WHR) or menopausal status
Boyd et al (2003)
Meta-analysis of casendashcontrol and cohort studies published up to July 2003 which examined the
Varied Not reported Cancer incidence A total of 45 published studies containing 46 estimates of risk examined the role of dietary fat in relation to breast cancer risk by an analysis of nutrient intake Of these 31 were case control and
35
association of dietary fat or fat-containing foods with risk of breast cancer
14 were cohort in design and they contained a total of 25015 cases of breast cancer and over 580 000 control or comparison subjects The summary relative risk comparing the highest and lowest levels of intake of total fat was 113 (95 CI 103ndash125) Cohort studies (n=14) had a summary relative risk of 111 (95 CI 099ndash125) and casendashcontrol studies (N=31) had a relative risk of 114 (95 CI 099ndash132) Significant summary relative risks were also found for saturated fat (RR 119 95 CI 106ndash135) and meat intake (RR 117 95 CI 106ndash129) Combined estimates of risk for total and saturated fat intake and for meat intake all indicate an association between higher intakes and an increased risk of breast cancer Casendashcontrol and cohort studies gave similar results
Cade et al 2007)
A large UK cohort study comprising women with a wide range of different eating patterns to study the effects of different food and nutrient intakes on long-term health outcomes
35372 women (350 post- and 257 pre- menopausal women developed breast cancer)
Approx 75-years
Breast cancer incidence
In pre-menopausal but not post-menopausal women a statistically
significant inverse relationship was found between
total fibre intake and risk of breast cancer (P for trend = 001) The
top quintile of fibre intake was associated with a hazard ratio
of 048
[95 CI 024ndash096] compared with the lowest quintile Pre-
menopausal fibre from cereals was inversely associated with risk
of breast cancer (P for trend = 005) and fibre from fruit had a
borderline inverse relationship (P for trend = 009)
Chlebowski et al (2006a)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
randomisation to death from any cause
Attrition in the dietary intervention (n=44) versus control group (n=66) Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to
345] versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group A total of 277 relapse
events (local regional distant or ipsilateral breast cancer
recurrence or new contralateral breast cancer) have been reported
in 96 of 975 (98) women in the dietary group and 181 of 1462
(124) women in the control group The hazard ratio of relapse
events in the intervention group compared with the control group
was 076 (95 CI = 060 to 098 P = 077 for stratified log rank
and P = 034 for adjusted Cox model analysis)
36
dietary guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
Chlebowski et al (2008)
A protocol-mandated survival analysis update to the interim analysis of WINS (Chlebowski et al 2006a)
Breast cancer patients (n=2437)
Approximately 7-years
Overall survival Attrition in the intervention group (n=236) versus control group (n=172) Although fewer deaths were seen in the intervention group this was not statistically significant In 362 women with ER- and (progesterone receptor) PR- disease a significant overall survival benefit was seen in the intervention group (75 vs 181 cumulative mortality)
Cho et al (2003)
A prospective analysis of the relationship
between dietary fat
intake and breast cancer risk among pre-menopausal
women enrolled in
the Nurseslsquo Health Study
Pre-menopausal women (n=90655) aged between 26-46 years old when recruited in 1991
8-years after recruitment (1991-1999)
Fat intake was
assessed with a food-frequency questionnaire at baseline
in 1991
and again in 1995
During 8-years of follow-up 714 women developed incident
invasive breast cancer Relative to women in the lowest quintile of
fat intake women in the highest quintile of intake had a
slight increased risk of breast cancer (RR = 125 95 CI = 098
to 159 Ptrend = 06) The increase was associated with intake
of
animal fat but not vegetable fat RRs for the increasing quintiles of
animal fat intake were 100 (referent) 128 137 154 and 133
(95 CI = 102 to 173 Ptrend = 002) Intakes of both saturated and
monounsaturated fat were related to modestly elevated breast
cancer risk Among food groups contributing to animal fat red meat and high-fat dairy foods were each associated
with an increased
risk of breast cancer Information on oestrogen-receptor status was available for
80 (n = 570) of breast cancers and progesterone-
receptor status for 78 (n = 558) When divided according to
oestrogen and progesterone receptor status the positive
association between animal fat intake and breast cancer risk was
stronger among women with oestrogen receptor-positive or
progesterone receptor-positive cancers than among women with hormone receptor-negative cancers however the difference was not statistically significant
Dwyer et al (2008)
A sub-analysis of participants in the WINS trial (Chlebowski et al 2006a)
Breast cancer patients (n=550)
12-months of intervention
Disease-free survival
Attrition in the intervention group (n = 23 11) versus control group (n = 16 5)At baseline neither mean fat intake nor flavonoid intake differed between groups After 12-months of intervention dietary fat intake was significantly lower among those on the very low-fat diet (n =195) whilst flavonoid intake remained similar in both groups Neither total flavonoid intake nor intake of subclasses of flavonoids differed between those who had dramatically decreased their fat intake and those who had not
Fleischauer et al (2003)
Case-control study testing the hypothesis that antioxidant
385 post-menopausal
12-14-years Breast cancer recurrence or
Antioxidant supplement users compared with non-users were less likely to have a breast cancer recurrence or breast cancer-related
37
supplements may reduce the risk of breast cancer recurrence or breast cancer-related mortality
women with breast cancer
death death (OR = 054 95 CI = 027-104) Vitamin E supplements showed a modest protective effect when used for more than 3 years (OR = 033 95 CI = 010-107) Risks of recurrence and disease-related mortality were reduced among women using vitamin C and vitamin E supplements for more than 3 years
Gold et al (2009)
Secondary analysis of a purposive sample of WHEL participants to determine if a low-fat diet high in vegetables fruit
and fibre affects
prognosis in breast cancer survivors
with or without hot flashes (HF) after treatment Randomisation to one of two groups 1)An intensive telephone counselling intervention based on social cognitive theory promoted a daily dietary intake of
5 vegetable
servings 16oz of vegetable juice 3
fruit servings 30g fibre and 15-20 of energy
from fat
2) Control group received printed
materials (but no counselling) promoting the
5-a-day guidelines
of
daily intakes of 5 servings of fruit and
vegetables more than 20g of fibre and less than
30 of energy from fat
2967 women (96 of all enrolled in the WHEL study) whose baseline hot flush severity
report in
the prior 4-weeks was available
4-years into the intervention
Primary end points additional breast cancer events
(localregio
nal recurrence or distant metastasis or new primary
breast
cancer) and death from any cause
The intervention group consumed significantly more daily vegetablefruit
(54 higher)
fibre (31 higher) and less
percent energy from fat (14 lower) than the comparison group
HF-negative women in the intervention had 31 fewer events than
the comparison group The intervention did not affect prognosis in
the women with baseline HFs Compared with HF-negative women in the comparison group
HF-positive women had significantly fewer
events in both groups
Goodwin et al (2009)
A prospective cohort study examining the influence of vitamin D on breast cancer prognosis
512 women with early breast cancer
Mean = 116-years
Cancer recurrence and mortality
Women with deficient vitamin D levels had an increased risk of
distant recurrence (hazard ratio [HR] = 194 95 CI 116 to
325) and death (HR = 173 95 CI 105 to 286) compared with
those with sufficient levels The association remained after
individual adjustment for key tumour and treatment related factors but was
attenuated in multivariate analyses (HR = 171 95 CI
102 to 286 for distant recurrence HR = 160 95 CI 096 to
264 for death)
Grace et al (2004)
Prospective study (EPIC) examining associations between phytoestrogen and breast cancer risk 114 spot urines and 97 available serum
333 women (aged 45ndash75 years) drawn from the EPIC
Not reported Phytoestrogen concentrations and breast cancer incidence
Phytoestrogen concentrations in spot urine (adjusted for urinary creatinine) correlated strongly with that in serum with Pearson correlation coefficients gt 08 There were significant relationships (P lt 002) between both urinary and serum concentrations of
38
samples from women who later developed breast cancer Results were compared with those from 219 urines and 187 serum samples from healthy controls matched by age and date of recruitment
study isoflavones across increasing tertiles of dietary intakes Urinary enterodiol and enterolactone and serum enterolactone were significantly correlated with dietary fibre intake (r = 013ndash029) Exposure to all isoflavones was associated with increased breast cancer risk significantly so for equol and daidzein For a doubling of levels odds ratios increased by 20ndash45 [log2 odds ratio = 134 (106ndash170P = 0013) for urine equol 146 (105ndash202 P = 0024) for serum equol and 122 (101ndash148 P = 0044) for serum daidzein]
Howe et al (1990)
Pooled analysis of 12 case-control studies of diet and breast cancer risk
Healthy women Not reported Breast cancer incidence
A consistent statistically significant positive association was found
between breast cancer risk and saturated fat intake in
postmenopausal women (relative risk for highest vs lowest quintile
146 P lt0001) A consistent protective effect for a number of
markers of fruit and vegetable intake was demonstrated vitamin C
intake had the most consistent and statistically significant inverse
association with breast cancer risk (relative risk for highest vs
lowest quintile 069 P lt0001)
Holm et al (1993)
Interviews regarding diet history the purpose being to determine whether dietary habits are associated with disease-free survival
in patients with
breast cancer who have undergone treatment
240 women with stage I-II breast cancer (50ndash65 years old) 209 of whom were post-menopausal
4-years Disease-free survival
Cancers were classified as oestrogen receptor (ER) rich ( 010
fmolmicrog of DNA) in 149 patients and as ER poor (lt010 fmolmicrog
of
DNA) in 71 patients Fifty-two patients had treatment failure during
follow-up The 30 patients with ER-rich tumours who had treatment
failure reported higher intakes of total fat saturated fatty acids and
polyunsaturated fatty acids than did the 119 patients with ER-rich
tumours that did not have treatment failure The multiple-odds ratio
(OR) for treatment failure in these women was 108 for each 1
increment in percentage of total energy (E) from total fat For
treatment failure within the first 2 years the OR was 119 for each
1-mg increase in vitamin E intake per 10 mega joules of energy In
women with treatment failure 2ndash4 years after diagnosis Ors were
113 and 123 for each E increment in total fat or saturated fatty
acids respectively No association between dietary habits and
treatment failure was found for women with ER-poor cancers
39
Holmes et al (1999)
Cohort study (Nurseslsquo Health Study)
to determine whether intakes
of fat and fatty acids are associated
with breast cancer
88795 women free of cancer (2956 developed breast cancer)
14-years Relative risk of invasive breast
cancer for
an incremental increase of fat intake
Compared with women obtaining 301 to 35 of energy from fat women consuming 20 or less had a multivariate
RR of breast
cancer of 115 (95 CI 073-180) In multivariate models the RR
(95 CI) for a 5-of-energy increase was 097 (094-100) for total
fat 098 (096-101) for animal fat 097 (093-102) for vegetable
fat 094 (088-101) for saturated fat 091 (079-104) for
polyunsaturated fat and 094 (088-100) for monounsaturated fat
For a 1 increase in energy from trans-unsaturated fat the values
were 092 (086-098) and for a 01 increase in energy from
omega-3 fat from fish the values were 109 (103-116)
Hunter et al (1996)
Pooled analysis of 7 prospective studies in 4 countries to establish estimates of the relation of fat
intake
to the risk of breast cancer
Studies included
33781
9 women
Not reported Breast cancer incidence
Information about 4980 cases from studies including 337819
women was available When women in the highest quintile of
energy-adjusted total fat intake were compared with women in the
lowest quintile the multivariate pooled relative risk of breast cancer
was 105 (95 CI 094 to 116) Relative risks for saturated
monounsaturated and polyunsaturated fat and for cholesterol
considered individually were also close to unity There was little
overall association between the percentage of energy intake from
fat and the risk of breast cancer even among women whose energy
intake from fat was less than 20
Ingram et al (1994)
Cohort study evaluating the role of vitamins in breast cancer mortality
103 women 3-months post-operation for primary breast cancer
Mean= 81-months
Mortality from breast cancer
27 women died ndash 21 with advanced breast cancer and 6 from other causes The most important findings from the nutrient consumption assessment were associated with vitamin consumption in particular beta-carotene and vitamin C At high levels of consumption there were significantly fewer deaths from breast cancer only one in the group of highest beta-carotene consumers compared with eight in the intermediate group and 12 in the lowest group (trend P = 00012) equivalent figures for vitamin C were 3 7 and 11 deaths for the highest intermediate and lowest consumption groups respectively (trend P = 00286)
Keinan-Boker et al (2004)
An investigation of the association between phytoestrogen
intake and
breast cancer risk in a large prospective study in
a Dutch
population with a habitually low phytoestrogen intake (EPIC)
15555 women aged
49ndash70
years who constituted a Dutch cohort the EPIC study
Median = 52-years
Breast cancer incidence
A total of 280 women were newly diagnosed with breast cancer
during follow-up The median daily intakes of isoflavones and
lignans were 04 (interquartile range 03ndash05) and 07 (05ndash08)
mgd respectively Relative to the respective lowest intake
quartiles the hazard ratios for the highest intake quartiles for
isoflavones and lignans were 10 (95 CI 07 15) and 07 (05
11) respectively Tests for trend were non-significant
Khaodhiar et al (2003)
A subgroup analysis of WINS participants (Chlebowski et al
53 women from 3 clinical
sites
2-years after start of
Insulin resistance and dietary fat
Of those women with initial insulin resistance after 1-year women in
the intervention group saw their fasting insulin decrease by 18 plusmn 34
40
2006a) examining relationships between dietary intake and insulin resistance
who had serum insulin and lipid profiles evaluated at baseline
and
after 2-years
commencing intervention
intake microUmL in comparison fasting insulin of women in the control
group decreased by only 138 plusmn 47 microUmL Although not
quite
statistically significant these results predict that elevated insulin concentrations (a marker of insulin resistance)
may be influenced by
dietary fat reduction There were no significant differences between
the treatment groups over time and no time x treatment interactions
and no significant differences were seen between the insulin-
resistant and non-insulin-resistant subgroups
Kim et al (2006)
The Nurseslsquo Health Study a prospective cohort study examining the relationship between dietary fat and incidence of breast
cancer in
post-menopausal women
Cohort of 80375 US women
Followed for 20-years between 1980 and 2000 with questionnaire being mailed every 2-years
Incidence of breast cancer The Food Frequency Questionnaire
The multivariable relative risk for an increment of 5 of energy from
total dietary fat intake was 098 (95 CI 095 100) Additionally
specific types of fat were not associated with an increased risk of
breast cancer Furthermore secondary analyses indicated no
differences in breast cancer risk by oestrogen receptor or
progesterone receptor status However stratification by
waist circumference indicated a significant decrease in breast
cancer risk for participants with a waist circumference of 35
inches (889cm) or greater (p-trend = 004)
Kyogoku et al (1992)
The present study utilised breast cancer patients whose dietary intake was assessed 10-years previously in a case-control study to determine whether dietary intake is related prognosis
212 breast cancer patients post-surgery
Followed-up until 1987 (9-12 years)
Mortality A total of 47 breast cancer deaths were certified The 5- and 10-year relative survival rates were 785 and 753 respectively The investigation did not provide any support for the hypothesis that a high-fat diet is a survival determinant for breast cancer patients
McEligot et al (2006)
Retrospective study into the influence of diet (fat fibre vegetable and fruit intakes and micronutrients (folate carotenoids and vitamin C) on overall survival in women diagnosed with breast cancer
Post-menopausal breast cancer survivors (n = 516)
Mean of 80-months post-diagnosis
Death due to any cause
The hazard ratio [HR and 95 CI] of dying in the highest tertile compared to the lowest tertile of total fat fibre vegetable and fruit was 312 (95 CI = 179-544) 048 (95 CI = 027-086) 057 (95 CI = 035-094) and 063 (95 CI = 038-105) respectively (P le 005 for trend except for fruit intake) Other nutrients including folate vitamin C and carotenoid intakes were also significantly associated with reduced mortality (P le 005 for trend)
Pierce et al (2007)
The multicentre WHEL RCT (see Gold et al 2009 in table)
Breast cancer (n=3088) intervention (n=1537) comparison (n=1551)
After 7-years of intervention
Invasive breast cancer event (recurrence
or
new primary) or death from any cause
Attrition in the intervention group (n=38) versus control group (n=27) There were no additional health benefits of dramatically increasing intake of nutrient-rich plant-based foods relative to the comparison group
Thomson et al (2007)
Sub-analysis of a purposive sample of participants in the WHEL RCT (see Gold et al 2009 in table)
Breast cancer patients (n=207)
Not reported Oxidative stress A significant inverse association was found between total plasma carotenoid concentrations and oxidative stress
41
WEIGHT
Caan et al (2008)
Retrospective study examining whether weight gain after diagnosis of breast cancer affects the risk of breast cancer recurrence Weight change from 1-year pre-diagnosis to study enrolment was calculated
3215 women with early stage breast cancer
Median of 737-months post-diagnosis
Breast cancer recurrence
Neither moderate (5ndash10) nor large (gt 10) weight gain (HR 08 95 CI 06ndash11 HR 09 95 CI 07ndash12 respectively) after breast cancer diagnosis was associated with an increased risk of breast cancer recurrence in the early years post-diagnosis
Enger et al (2004)
A retrospective cohort study using patient medical
records electronic
cancer registry data and archived tissue
specimens to examine
correlates of body weight with mortality in early-stage breast cancer
Women (n=1376)
24-
81 years of age diagnosed with breast cancer
Median=68 years post-diagnosis
Body weight at the time of diagnosis
and
patient status (ie alive and free of breast cancer living
with breast
cancer dead of breast cancer or dead of other
cause) at
the time of longest follow-up
246 patients died from breast cancer Among patients with early-
stage disease (I and IIA) a dose-response relationship was
observed with increasing weight and likelihood of dying of breast
cancer Compared with women in the lowest category of weight (lt133lb [60 kg] at diagnosis) women in the highest category ( 17
lb
[79 kg]) experienced a 25-fold increased risk of dying from breast
cancer (HR ratio 254 [95 CI 108-600] trend P = 02) Women
with ER-negative cancer experienced an approximately 2-fold
higher risk of dying from breast cancer compared with women with
ER-positive cancer regardless of stage at diagnosis Women in the
upper 50th percentile of weight with early-stage
disease and with
ER-negative tumours had a nearly 5-fold increased risk of dying
(HR ratio 499 [95 CI 217-1148] P for interaction = 10)
compared with women in the lower 50th percentile of weight
and ER-
positive tumours
Hebert et al (1998)
Prospective cohort study examining the effect of diet and body weight on recurrence and death in breast cancer patients
472 women diagnosed with early-stage breast cancer in 1982ndash1984
Ranged from 8-10 years
Breast cancer recurrence and mortality
After accounting for disease stage and age reported baseline consumption (timesday) of butter margarine and lard (risk ratio (RR)=167 95 CI=117ndash239) and beer (drinksday) (RR=158 95 CI=115ndash217) increased the risk of recurrence There also appeared to be an increased risk associated with consumption of red meat liver and bacon corresponding to about a doubling of risk for each time per day that foods in this category were consumed (RR=193 95 CI=089ndash415) Relative body weight increased risk at the rate of 9 (RR=109 95 CI=102ndash117) for
each kgm2 (equivalent to about 58 pounds for a woman 5 4 tall) For death the results were similar but relative weight was more strongly associated increasing risk by 12 per kgm2 (RR=112 95 CI=103ndash122)
Kroenke et al (2005)
A prospective study of a purposive subsample of participants from the Nurseslsquo Health Study ndash to determine
5204 Nurseslsquo Health Study participants
2-26 years with a median
Incident breast cancer
Weight before diagnosis was positively associated with breast
cancer recurrence and death but this was apparent only in never
smokers Similarly among never-smoking women those who
42
whether weight prior to diagnosis and weight gain
after diagnosis are
predictive of breast cancer survival
diagnosed with
incident invasive non-metastatic breast cancer between
1976
and 2000
follow-up of
9-years Breast cancer recurrence Mortality for any cause Self-reported BMI
gained between 05 and 20 kgm2 (median gain 60 lb relative risk
[RR] 135 95 CI 093 to 195) or more than 20 kgm
2 (median
gain 170lb RR 164 95 CI 107 to 251) after diagnosis had an
elevated risk of breast cancer death during follow-up (median 9
years) compared with women who maintained their weight (test for
linear trend P = 03) Associations with weight were stronger in
premenopausal than in postmenopausal women
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer
Breast cancer Not reported Additional breast cancer events and mortality
The most consistent finding from observational studies was that adiposity was associated with a 30 increased risk of mortality
SMOKING
Holmes et al (2007)
A prospective observational study among 5056 women from the Nurseslsquo Health Study for whom data on smoking history was available
Women with Stages I-III invasive breast cancer diagnosed between 1978 and 2002
Median = 83 years
Death by any cause Cause of death was ascertained from death certificates supplemented as needed with physician review of medical records
Compared with never smokers women who were current smokers had a 43 increased adjusted relative risk (RR) 95 CI 124-165] of death from any cause A strong linear gradient was observed with the number of cigarettes per day smoked p-trend lt00001 the RR (95 CI) for 1-14 15-24 and 25 or more cigarettes per day was 127 (101-161) 130 (108-157) and 179 (147-219) In contrast there was no association with current smoking and breast cancer death the RR (95 CI) was 100 (083-119) Current and past smokers were more likely than never smokers to die from primary lung cancer chronic obstructive pulmonary disease and other lung diseases
Fentiman et al (2005)
Cohort study testing the hypothesis that smokers have a worse breast cancer prognosis
Women (n=166) with stage III invasive breast cancer
Mean = 132-months
Overall and cancer-specific disease-free survival
Smoking was the third most important predictor of distant relapse-free breast cancer-specific and overall survival after stage and age at diagnosis
Manjer et al (2000)
Cohort study examining whether smoking is associated with prognostic markers other than more advanced disease (eg hormone receptor status histopathology and tumour differentiation)
268 women with recurring breast cancer drawn from a cohort of 10902 women (35 smokers)
An average of 124-years
Hormone receptor status identified by tumour tissue
The relative risk (RR) of oestrogen receptor-negative tumours was for current smokers 221 [95 CI 123-396] and for ex-smokers 267 (95 CI 141-506) compared to never-smokers Ex-smokers had an increased risk of progesterone receptor-negative tumours (RR = 161 95 CI 107-241) but there were no other significant associations between smoking habits and oestrogen receptor-positive or progesterone receptor-positive or ndashnegative tumours The incidence of Nottingham grade III tumours was higher in ex-smokers than in never-smokers (RR = 203 95 CI 117-354)
Sagiv et al (2007)
Cohort study examining the association between active and passive cigarette smoking before
Women with invasive breast cancer
Approximately 6-years after
All-cause mortality including breast
The adjusted hazards ratios (HRs) for all-cause mortality were slightly higher among current and former active smokers compared with never smokers (HR 123 95 CI 083ndash184) and 119 (95
43
breast cancer diagnosis and survival (n=1273) participating in a population-based casendashcontrol study
diagnosis cancer-specific mortality as reported to the National Death Index
CI 085ndash166) respectively) No association was found between active or passive smoking and breast cancer-specific mortality All-cause and breast cancer-specific mortality was higher among active smokers who were postmenopausal (HR 164 95 CI 103ndash260 and HR 145 95 CI 078ndash270 respectively) or obese at diagnosis (HR 210 95 CI 103ndash427 and HR 197 95 CI 089ndash436 respectively)
ALCOHOL
McDonald et al (2002)
Prospective cohort study examining the influence of alcohol consumption on breast cancer survival in African American women
Post-menopausal African-American women with invasive breast cancer (n=125)
Followed for survival through December 1998 (median = 648 months)
Survival Pre-morbid alcohol consumption of at least one drink per week was associated with 27-fold increase in risk of death (95 CI 13ndash58)
Reding et al (2009)
Sub-analysis of participants from two case-control studies to examine the effects on prognosis of alcohol consumption after breast cancer diagnosis
1286 women diagnosed with invasive breast cancer at age le45 years from two population-based case-control studies
Followed from their diagnosis of breast cancer (between January 1983 and December 1992) through to June 2002
The primary mortality endpoint used was all-cause mortality
After adjusting for age and diagnosis year compared with non-drinkers women who consumed alcohol in the 5 years before diagnosis had a decreased risk of death [gt0 to lt3 drinks per week hazard ratio 07 95 CI 06-095 3 to lt7 drinks per week risk ratio 06 95 CI 04-087 drinks per week risk ratio 07 95 CI 05-09]
Rock and Demark-Wahnefried (2002)
A review of evidence from clinical and
epidemiologic studies examining
the relationship between nutritional
factors and breast cancer survival
Women with breast cancer
Not reported Survival Alcohol intake was not associated with survival in the majority of the
studies that examined this relationship
44
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
colorectal cancer survival In the current review 2 studies were identified Studies are
summarised in Table 4 at the end of this section
In a cohort study self-reported leisure time physical activity was assessed in 41528
Australians among whom 526 cases of colorectal cancer were identified (Haydon et al
2006) Those who reported regular physical activity (at least once per week) prior to
diagnosis had improved cancer-specific survival (73 5-year survival) compared with
those not reporting regular physical activity (61 5-year survival) Another study of
stage III colorectal cancer survivors (n=816) over a 3-year period post-surgery and
chemotherapy showed increases in disease-free survival and overall survival with
increasing volumes of physical activity (p lt 05) (Meyerhardt et al 2005)
ii DIET
Bekkering et al (2006) report on six high fibre diet interventions that showed little effect on
the risk of colorectal cancer recurrence (McKeown-Eyssen et al 1995 MacLennan et al
1999 Alberts et al 2000 Bonithon-Kopp et al 2000 Schatzkin et al 2000 Ishikawa et al
2005) On combining data from two beta-carotene trials (Greenberg et al 1994
MacLennan et al 1999) four multivitamin trials (Greenberg et al 1994 Ponz and
Roncucci 1997 Hofstad et al 1998 McKeown-Eyssen et al 1995) and one trial containing
a multivitamin arm and an N-acetylcysteine (found in high protein foods) arm (Ponz and
Roncucci 1997) there was weak evidence of a reduction in risk of colorectal polyps
(abnormal growth of tissues in the colon) Two calcium interventions showed some
evidence of a reduced risk of recurrence (Baron et al 1999 Bonithon-Kopp et al 2000)
In the current review 5 studies provided further evidence for the role of diet in colorectal
cancer survival
Dietary Fibre
The association between dietary fibre and incidence of colorectal cancer was examined in all
participants (n=519978) taking part in the EPIC study (Bingham et al 2003) After 45-years
of follow-up self-reported dietary data for 1065 reported cases of colorectal cancer were
showed that higher dietary fibre was associated with a reduced risk of developing
large bowel cancer Interestingly the protective effect was greatest for the left side of the
colon and least for the rectum No food source of fibre was significantly more protective of
cancer incidence than others Confirmation of these findings after adjustment for folate and
with a longer follow-up has been reported (Bingham et al 2004 Norat et al 2005)
45
Red and Processed Meat
The EPIC study also offers support for the hypotheses that consumption of red and
processed meat increases colorectal cancer risk while intake of fish decreases risk
(Norat et al 2005) Meyerhardt et al (2007) support this further in a study examining dietary
patterns in stage III colorectal cancer survivors (n=1009) After a median of 53-years follow-
up a significant difference was found between those who had followed a prudentlsquo diet and
those who had followed a Westernlsquo diet
A higher intake of a Western dietary pattern post-diagnosis was associated with a
significantly worse disease-free survival (colon cancer recurrences or death) (p
lt001) The Western dietary pattern was associated with a similar detriment in overall
survival (p lt001)
Vitamin D
Ng et al (2008) examined pre-diagnosis levels of vitamin D in a cohort of participants with
colorectal cancer (n=304) from the Nursesrsquo Health Study28 which demonstrated that higher
plasma vitamin D levels were associated with a significant reduction in mortality from
any cause This indicates that lifestyle pre-diagnosis can produce post-diagnosis benefits
Dietary Supplements
A double-blind randomised placebo-controlled intervention study (the FAB2 Study) was
carried out with healthy controls (n=98) and patients with colorectal polyps (n=106) to
examine the effects of folic acid (a B vitamin found in leafy vegetables such as spinach
asparagus and lettuce) and riboflavin (a B-vitamin found in lean meats eggs nuts and
dairy products) supplements on biomarkers of colorectal cancer risk (Powers et al 2007)
Participants were randomised to receive one of four treatments
1) placebo capsule daily
2) 400μg of folic acid daily
3) 1200μg of folic acid daily
4) 400μg of folic acid with 5mg of riboflavin daily
28
One of the largest and longest running investigations of factors that influence womenlsquos health
comprising information from 238000 nurse-participants
Prudent diet High intake of fruit vegetables poultry and fish
Western diet
High intake of meat fat refined
grains sweets and desserts
46
Short-term low folic acid supplements in the range of 400μg were found to elicit a
significant increase in mucosal folate concentration causing a number of physiologic
responses that may reduce the risk of cancer recurrence This adds to the evidence that
increased fibre might be protective against cancer mortality since folate and fibre are
generally found in the same foods
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in colorectal
cancer recurrence In the current review 3 studies were identified
Dignam et al (2006) explored the impact of obesity via retrospective data from patients with
confirmed Dukes B or C colorectal cancer (n=4288) and found that very obese men and
women have an increased risk of recurrence In contrast the multicentre prospective
observational CALBG 8980 trial has shown that increased BMI during and 6-months after
adjuvant chemotherapy for stage III colorectal cancer (n=1053) was not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008)
Sinicrope et al (2010) categorised stage II and III colon cancer (n=4381) patients enrolled
in seven RCTs whilst undergoing adjuvant chemotherapy according to their BMI They
found that BMI was significantly associated with both disease-free survival and overall
survival in both men and women when compared to normal-weight controls Being
overweight was associated with improved overall survival in men whilst being underweight
was associated with significantly worse overall survival in women This demonstrates that
obesity is an independent prognostic variable in colon cancer survivors as well as showing
gender-related differences that require further investigation
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in colorectal
cancer survival and no studies were identified in the current review
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in colorectal
cancer survival Preliminary EPIC results indicate that current alcohol intake is
significantly positively associated with risk of rectal but not of colon cancer (Ferrari et
al (2007)
47
SUMMARY OF LIFESTYLE EVIDENCE FOR COLORECTAL CANCER ndash
MECHANISMS OF BENEFIT
Physical Activity There is very little evidence available for the role of physical activity in
colorectal cancer outcomes however the evidence that is available looks promising
Specifically regular physical activity of at least once per week pre-diagnosis has been found
to improve 5-year survival rates (Haydon et al 2006) This highlights the importance of
physical activity being integrated into an individuallsquos way of life even before the occurrence
of illness Furthermore long-term physical activity post-surgery can further increase chances
of recurrence-free survival and there is also evidence of a dose-effect survival benefits
increase with amount of exercise (Meyerhardt et al 2005)
Diet Whilst evidence for dietary fibre has been mixed the additional evidence presented
within this review places greater weight in favour of increased dietary fibre Indeed the
conclusion of one study was that in populations with low average intake of dietary fibre an
approximate doubling of total fibre intake from foods could reduce the risk of colorectal
cancer by 40 (Bingham et al 2003) Evidence of this protective benefit for dietary fibre is
further supported by research demonstrating that short-term low folic acid (found in fibrous
foods) supplements in the range of 400μg can reduce the risk of cancer recurrence (Powers
et al 2007) There is a general consensus that mechanisms of benefit from dietary fibre
come from increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic mucosa (tissue
that lines the colon) (Kim 2000) Evidence has also been presented supporting the
hypothesis that red and processed meat increases colorectal cancer risk while fish
decreases risk (Norat et al 2004)
Weight Two large-scale studies offer contrasting findings for the role of weight
in colorectal cancer outcomes One prospective observational study demonstrates that
increased BMI during and 6-months after adjuvant chemotherapy is not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008) The other
retrospective study demonstrates that very obese men and women have an increased risk
of recurrence Drawing on 7 RCTs Sinicrope et al (2010) provides further evidence for BMI
was being significantly associated with both disease-free and overall survival Overall there
is greater evidence showing weight to be an important predictor of colorectal cancer
outcomes There is also some evidence of gender differences being overweight was
associated with improved overall survival in men whilst being underweight was associated
with significantly worse overall survival in women There is evidently a need to explore this
differential effect more closely However there is also the need to consider the impact of
body composition on the development of other chronic conditions including diabetes and
cardio-respiratory conditions
Smoking and Alcohol Further research is needed into smoking and alcohol
consumption especially in terms of colorectal cancer prognosis There is some evidence
indicating that current alcohol intake increases risk of rectal but not colon cancer a finding
that requires further investigation to ascertain underlying mechanisms of benefit (Ferrari et
al 2007) Since alcohol can reduce absorption of folate it is possible that the mechanism
48
of benefit is as with dietary fibre intake related to stool bulk and less contact time between
carcinogens and colonic mucosa
49
Table 4 Colorectal Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Haydon et al (2006)
Incident cases of colorectal cancer were identified among participants of the Melbourne Collaborative Cohort Study and examined against self-reported physical activity
526 Australians with colorectal cancer
Median = 55 years
Body fat Disease-specific survival
Exercisers had an improved disease specific survival (hazard ratio 073 (95 CI 054ndash100) The benefit of exercise was largely confined to stage IIndashIII tumours (hazard ratio 049 (95 CI 030ndash079) Increasing per cent body fat resulted in an increase in disease-specific deaths (hazard ratio 133 per 10 kg (95 CI 104ndash171) Similarly increasing waist circumference reduced disease specific survival (hazard ratio 120 per 10 cm (95 CI 105ndash137)
Meyerhardt et al (2005)
Prospective study of recreational physical activity and prognosis
among
stage III colon cancer patients enrolled in a
RCT of post-operative adjuvant
chemotherapy (bolus 5-
fluorouracilleucovorin +- irinotecan)
816 patients with stage III colon cancer
Midway through adjuvant therapy and again 6-months post-therapy (12ndash14 months after enrolment)
Physical activity levels were measured as MET-hours-per-week Disease-free survival
Levels of physical activity were associated with significantly improved
disease-free survival among patients with stage III colon cancer After
adjustment for age gender baseline performance status N stage T
stage preoperative CEA bowel obstruction and perforation level of
differentiation treatment arm and body mass index the hazard ratio
(HR) for DFS for individuals in the highest quintile (gt25 MET-
hoursweek eg Jog 3ndash4 hoursweek or brisk walk [3ndash4 mph] daily)
was 065 (95 CI 038ndash111 p for trend = 002) compared to those
in the lowest quintile of PA This relationship varied by gender with a
HR = 033 [95 CI 011ndash099] for women (p for trend = 0046) and a
HR= 089 [95 CI 044ndash178] for men (p for trend = 03)
DIET
Bingham et al (2003)
Prospective examination of the association between dietary fibre intake and incidence of colorectal cancer in individuals taking part in the EPIC study recruited from ten European countries
519978 men and women in the EPIC study (1065 cases of colorectal cancer)
45 years
Colorectal cancer incidence
Dietary fibre in foods was inversely related to incidence of large bowel cancer (adjusted relative risk 0middot75 [95 CI 0middot59ndash0middot95] for the highest versus lowest quintile of intake) the protective effect being greatest for the left side of the colon and least for the rectum After calibration with more detailed dietary data the adjusted relative risk for the highest versus lowest quintile of fibre from food intake was 0middot58 (0middot41ndash0middot85)
Meyerhardt et al (2008)
Prospective observational study to
determine the association of dietary patterns
with cancer recurrences and
mortality of colon cancer survivors
1009 patients with stage III colon cancer who were
enrolled in
a randomized
Median = 53-years
Colon cancer recurrence and mortality
A higher intake of a Western dietary pattern after cancer diagnosis
was associated with a significantly worse disease-free survival (colon
cancer recurrences or death) Compared with patients in the lowest
quintile of Western dietary pattern those in the highest quintile experienced an adjusted hazard
ratio (AHR) for disease-free survival
of 325 (95 confidence interval [CI] 204-519 P for trend lt001)
50
adjuvant chemotherapy trial (CALGB
89803)
The Western dietary pattern was associated with a similar detriment
in recurrence-free survival (AHR 285 95 CI 175-463) and overall
survival (AHR 232 95 CI 136-396]) comparing highest to
lowest quintiles (both with P for trend lt001)
Ng et al (2008)
Nurseslsquo Health Study prospective examination of the association between pre-diagnosis
25(OH)D levels and
mortality in colorectal cancer patients
304 colorectal cancer patients
Mean = 78-months for participants still alive
Colorectal cancer mortality
Higher plasma 25(OH)D levels were associated with a significant
reduction in overall mortality (P for trend = 02)
Compared with the lowest quartile participants in the highest
quartile had an adjusted HR of 052 (95 CI 029 to 094) for
overall mortality A trend toward improved colorectal cancerndash
specific mortality was also seen (HR = 061 95 CI 031 to 119)
Norat et al (2005)
The EPIC prospective study of 478040 cancer-free men and women from 10 European countries examining meat fish and colorectal cancer risk
478040 cancer-free men and women taking part in the EPIC study
Mean=48 years
Colorectal cancer incidence
Colorectal cancer risk was positively associated
with intake of red and processed meat (highest [gt160
gday] versus lowest [lt20 gday] intake HR = 135 95 CI = 096
to
188 Ptrend = 03) and inversely associated with intake of fish (gt80
gday versus lt10 gday HR = 069 95 CI = 054 to
088 Ptrendlt001) but was not related to poultry intake In this study
population the absolute risk of development of colorectal
cancer within 10-years for a study subject aged 50 years was 171
for the highest category of red and processed meat intake and 128
for the lowest category of intake and was 186 for subjects in
the lowest category of fish intake and 128 for subjects in
the highest category of fish intake
Powers et al (2007)
A double-blind RCT (the FAB2 Study) to examine effects of folic acid and riboflavin supplements on biomarkers of colorectal cancer risk Participants were randomised to receive one of the following for 6 ndash 8 weeks 1)400μg of folic acid 1200μg of folic acid or 400μg of folic acid plus 5 mg of riboflavin 2) placebo
Healthy controls (n=98) and patients with colorectal polyps (n=106)
On completion of 6-8 week intervention
Biomarkers of folate and riboflavin status
Supplementation with folic acid elicited a significant increase in mucosal 5-methyl tetrahydrofolate and a marked increase in RBC and plasma with a dose-response Measures of riboflavin status improved in response to riboflavin supplementation Riboflavin supplement enhanced the response to low-dose folate in people carrying at least one T allele and having polyps The magnitude of the response in mucosal folate was positively related to the increase in plasma 5-methyl tetrahydrofolate but was not different between the healthy group and polyp patients
WEIGHT
Dignam et al (2006)
Investigating the association between BMI and colorectal cancer outcomes in patients from cooperative group clinical trials
4288 patients with Dukes
BC
colon cancer in National
Median =112-
years Risk of recurrence second primary
Very obese patients (BMI 35 kgm2) had greater risk
of a
colon cancer event (recurrence or secondary primary tumour hazard
ratio [HR] = 138 95 confidence interval [CI] = 110 to 173) than
normal weight patients (BMI = 185ndash249 kgm
2) Mortality was
51
Surgical Adjuvant Breast and Bowel Project
RCTs
cancer and
mortality evaluated in
relation to
BMI at diagnosis
greater for very obese (HR = 128 95 CI = 104 to 157) and
underweight (BMI lt 185 kgm2) (HR
= 149 95 CI = 117 to 191)
than for normal weight patients The increased risk of mortality for
underweight patients was dominated by nonndashcolon cancer deaths
(HR of such deaths compared with normal weight patients = 223 95 CI = 150 to
331) whereas for the very obese deaths likely due
to colon cancer were increased (HR = 136 95 CI = 106 to 173)
Meyerhardt et al (2008)
A prospective observational study of patients who had stage III colon cancer and who enrolled on a RCT of adjuvant chemotherapy Results
1053 patients who had stage III colon cancer
6-months post- chemotherapy
Patients were observed for cancer recurrence or death
Increased BMI was not significantly associated with a higher risk of colon cancer recurrence or death (P trend = 54) Compared with normal-weight patients (BMI 21 to 249 kgm
2) the multivariate
hazard ratio for disease-free survival was 100 (95 CI 072 to 140) for patients with class I obesity (BMI 30 to 349 kgm
2) and 124
(95 CI 084 to 183) for those with class II to III obesity (BMI ge 35 kgm
2) after analysis was adjusted for tumour-related prognostic
factors physical activity tobacco history performance status age and sex Similarly after analysis was controlled for BMI weight change (either loss or gain) during the time period between ongoing adjuvant therapy and 6-months after completion of therapy did not significantly impact on cancer recurrence andor mortality
Sinicrope et al (2010)
BMI (kgm2) was categorised in patients
with tumour-node-metastasis stage II and III colon carcinomas enrolled in seven RCT of 5-fluorouracilndashbased adjuvant chemotherapy to determine the association of BMI with disease-free survival and overall survival
Men and women with stage II and III colon carcinomas (n = 4381) enrolled in seven RCTs of 5-fluorouracilndashbased adjuvant chemotherapy
Not reported Disease-free survival Overall survival
BMI was significantly associated with both disease-free survival (P = 0030) and overall survival (P = 00017) Men with class 23 obesity showed reduced overall survival compared with normal-weight men [hazard ratio 135 95 CI 102-179 P = 0039] Women with class I obesity had reduced overall survival [hazard ratio 124 95 CI 101-153 P = 0045] compared with normal-weight women Overweight status was associated with improved overall survival in men (P = 0006) and underweight women had significantly worse overall survival (P = 0019)
ALCOHOL
Ferrari et al (2007)
As part of the prospective EPIC study data was collected examining the relationship between lifetime and baseline alcohol consumption and colorectal cancer incidence
478732 EPIC subjects free of cancer at enrolment between 1992 and 2000
62 years Colorectal cancer incidence
Lifetime alcohol intake was significantly positively associated to CRC risk (hazard ratio HR = 108 95CI = 104-112 for 15 gday increase) with higher cancer risks observed in the rectum (HR = 112 95CI = 106-118) than distal colon (HR = 108 95CI = 101-116) and proximal colon (HR = 102 95CI = 092-112) Similar results were observed for baseline alcohol intake When assessed by alcoholic beverages at baseline the CRC risk for beer
52
(HR = 138 95CI = 108-177 for 20-399vs 01-29 gday) was higher than wine (HR = 121 95CI = 102-144) although the two risk estimates were not significantly different from each other Higher HRs for baseline alcohol were observed for low levels of folate intake (113 95CI = 106-120 for 15 gday increase) compared to high folate intake (103 95CI = 098-109)
53
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
prostate cancer survival In the current review 2 studies were identified Studies are
summarised in Table 5 at the end of this section
The underlying mechanisms for the direct anti-cancer effect of lifestyle has been indicated in
a study with men undergoing a diet and physical activity intervention comprising the majority
of calories from complex carbohydrates high in fibre combined with 1-hour of supervised
exercise (Soliman et al 2009) Serum (blood plasma) was taken from these men and added
to androgen-dependent LNCaP cells29 in the laboratory There was decreased growth and
increased apoptosis (cell death) associated with a reduction in serum Insulin-like Growth
Factor (IGF)-130 These findings indicate that diet and physical activity interventions
might slow prostate cancer progression as well as aid in its treatment during the early
stages of development
Kenfield (2010) examined the data of 2686 men from the Health Professionals Follow-Up
Study31 and found that men who engaged in 3gt MET-hours of weekly physical activity
post-diagnosis reduced their risk of death by 35 compared with men who engaged
in less weekly activity Furthermore men who walked 90-minutes per week at a normal to
brisk pace had a 51 lower risk of death due to any cause compared with men who walked
90-minutes or less at an easy pace To reduce their risk of cancer-specific death men
had to engage in vigorous activity such as jogging (6 MET-hours)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in prostate cancer
survival In the current review 7 studies were identified
Dietary Changes plus Supplements
Ornish et al (2005) conducted a diet counselling and lifestyle RCT comprising men with
early prostate cancer (n=93) The lifestyle changes in this study included a vegan diet
supplemented with soy vitamin E fish oils selenium and vitamin C together with a
moderate physical activity program and stress management techniques such as yoga
29
Human prostate cancer cells
30 IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of pathological states including cancer
31 An all-male (n=51529) study designed to complement the all-female Nurses Health Study
54
Prostate Specific Antigen (PSA)32 levels decreased by 4 at 12-months in the
intervention group but increased by 6 in the control group this was statistically
significant and strongly correlated with the degree of lifestyle change However the
intensity of this intervention and associated behavioural changes might not easily be
translated into practice (White et al 2009)
Pomegranate Juice
The potential benefits of pomegranate juice on prostate cancer outcomes frequently appear
in the media and strong evidence of its efficacy can be found within the academic literature
In a phase II open-label single-arm clinical trial men (n=46) with recurrent prostate cancer
who had rising PSA after surgery or radiotherapy were treated daily with 8oz (227g)
equivalent of pomegranate juice (Pantuck et al 2006) Mean PSA doubling time
significantly increased with treatment from 15-months to 54-months demonstrating a
good indication of a relationship between the consumption of pomegranate juice and
prostate health
Green Tea
Another beverage found to demonstrate some positive effects on prostate cancer is green
tea Bettuzzi et al (2006) in a year-long clinical trial has demonstrated that daily
consumption of green tea can produce a ten-fold decrease in the rate at which
prostate intraepithelial neoplasia (a pre-cancerous condition) progresses to prostate
cancer Support for these findings is offered by an uncontrolled open-label single-arm
phase II clinical trial testing the efficacy of Polyphenon E which contains the polyphenol
antioxidants found in green tea (McLarty et al 2009) Taking four capsules of
Polyphenon E daily (equivalent to twelve cups of green tea) for an average of 345
days leading up to radical prostatectomy the participants (n=26) experienced
significant reductions in biomarkers used to monitor likelihood of metastasis Some
patients demonstrated reductions greater than 30
Lycopene Supplements
The EPIC study has demonstrated that similar to breast cancer prostate cancer risk is not
related to fruit and vegetable consumption (Key et al 2004) However further evidence for
the role of carotenoids found in fruit and vegetables have been provided from a pilot RCT
including men with benign prostatic hyperplasia (BPH) a benign enlargement of the prostate
that can progress to cancer (Schwarz et al 2008) Men (n=20) who received 15mg od
lycopene supplementation (a carotenoid found in tomatoes and other red fruits and
32
PSA is a protein produced by the cells of the prostate gland It is present in small quantities in the serum of normal men and is often elevated in the presence of prostate cancer
55
vegetables) for 6-months had significantly decreased PSA levels compared to a
placebo group (n=20) who had no change in PSA
Salicylate
Salicylate33 intake has been implicated in the aetiology of prostate cancer but Thomas et al
(2009) have evaluated their influence on established cancer progression In a randomised
double blind phase II study involving men (n=110) with progressive prostate cancer who
were counselled to eat less saturated fat and processed food more fruit vegetables and
legumes physical activity more regularly and to stop smoking the men were then
randomised to take sodium salicylate alone or combined with vitamin C copper and
manganese gluconates34 daily Although there was no difference in outcome between those
who received sodium salicylate alone or combined the intervention as a whole (ie
including dietary counselling) slowed or stopped the rate of PSA progression in 40
patients (364) for over one-year and a further ten patients were stabilised for 10-
months This data suggests that changes in lifestyle can potentially delay PSA progression
and the need for more radical therapy highlighting an area for further research
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in prostate cancer
survival In the current review 2 studies were identified
Wright et al (2007) prospectively examined BMI and weight change in relation to prostate
cancer incidence and mortality in 287760 men enrolled in the National Institutes of
Health-AARP Diet and Health Study Higher baseline BMI was associated with
significantly reduced total prostate cancer incidence on the one hand but with
significantly increased risk of prostate cancer mortality on the other hand Adult weight
gain from age 18-years to study entry (range=50-71-years old) was positively associated
with prostate cancer staging but not with disease incidence
In a retrospective analysis exploring the interaction between obesity and surgical outcomes
in patients with prostate cancer treated by radical prostatectomy (n=437) a weak but
significant association was observed between BMI and a number of biological
biomarkers indicative of an advanced pathological stage (Gross et al 2009)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in prostate
cancer survival and no evidence was identified in the current review
33
Salicylates are chemicals that occur naturally in many plants including many fruits vegetables and herbs
Salicylates in plants act as a natural immune hormone and preservative protecting the plants against diseases
insects fungi and harmful bacteria 34
A pinkish powder soluble in water used in medicine in vitamin tablets and as a feed additive and dietary
supplement
56
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in prostate cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR PROSTATE CANCER -
MECHANISMS OF BENEFIT
Physical Activity and Diet The evidence within this review indicates that diet and physical
activity interventions might slow prostate cancer progression as well as aid in its treatment
during the early stages of development The mechanism of benefit is primarily via
decreased growth and increased apoptosis (cell death) associated with a reduction in serum
Insulin-like Growth Factor (IGF)-1 (Soliman et al 2009) Up to 3gt MET-hours of weekly
physical activity appears sufficient to increase survival with more vigorous activity of about 6
MET-hours per week for the reduction of cancer-specific mortality (Kenfield 2010) A
number of dietary steps can be taken to reduce PSA levels and thus slow down the growth
of tumours and increase survival For example a vegan diet supplemented with soy vitamin
E fish oils selenium and vitamin C together with a moderate physical activity program and
stress management techniques such as yoga have been found useful (Ornish et al 2005)
as has pomegranate juice (Pantuck et al 2006) and green tea (Betuzzi et al 2006 McLarty
et al 2009) As with breast cancer carotenoids have been found to offer protective
properties for men with benign prostatic hyperplasia which can progress to cancer (Schwarz
et al 2008) Overall the evidence for prostate cancer is suggestive of survival benefits from
combined dietary and physical activity changes In other words it appears that a healthier
diet made up of fruit and vegetables as well as drinks such as pomegranate juice or green
tea combined with 3gt MET-hours of weekly physical activity could be an effective
prescription for reducing mortality from cancer and other causes
Weight Evidence for weight was mixed whilst finding that higher baseline BMI was
associated with significantly reduced total prostate cancer incidence a significant increase in
prostate cancer severity and mortality was also observed with higher BMI levels (Wright et
al 2007a Gross et al 2009) More research is clearly needed to establish any differential
prostate cancer outcomes associated with weight
Smoking and Alcohol More research is required for smoking and alcohol in terms of
prostate cancer outcomes
57
Table 5 Prostate Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Kenfield et al (2009)
Prospective study (Health Professionals Follow-up Study) assessing the relationship between physical activity and duration and pace of walking with total and prostate cancer-specific mortality
2686 men with prostate cancer
4-years Prostate cancer mortality and total physical activity
Men who were physically active especially those engaging in 3 or more MET-hours of total activity had a 35 lower risk of death from any cause (hazard ratio 065 [95 CI 052 082]) and a modest non-significant reduction in risk of prostate cancer death (hazard ratio 088 [95 CI 052 149]) after adjustment for other risk factors for PCa mortality and pre-diagnosis physical activity While no benefit from walking was observed for PCa mortality men who walked 4 or more hours per week versus those who walked less than 20 minutes per week had a 23 lower risk of all-cause mortality (95 CI 061 097 p-trend=001) In addition compared to men who walked less than 90 minutes at an easy walking pace those who walked 90 or more minutes at a normal to very brisk pace had a 51 lower risk of all-cause mortality (95 CI 037 064) More vigorous activity and longer duration of activity was associated with significant further reductions in risk for all-cause mortality More vigorous activity was associated with a borderline-significant reduction in risk for PCa mortality
Soliman et al (2009)
Pritikin Longevity Center 3-Week
Residential Program - men were given prepared
meals with 12ndash15 fat calories
15ndash20 protein calories and the majority
of calories (65ndash70) from unrefined complex carbohydrates high in fibre (gt40 gday) The men attended daily supervised exercise classes
for 60 min
5 men in their early sixties
with no
signs of prostate cancer (PSA lt 40)
On completion of the 3-week programme
Cancer progression
The intervention slowed growth and increased apoptosis in LNCaP cells responses that were eliminated when
IGF-I was added back to
the post-intervention samples The p53 protein content was increased
and NFkB activation reduced in the post serum-stimulated LNCaP
cells Similar results were observed when the IGF-I receptor was
blocked in the pre-intervention serum In androgen-independent PC-3
cells growth was reduced while none of the other factors were
changed by the intervention
DIET
Bettuzzi et al (2006)
A proof-of-principle double-blind placebo-
controlled clinical trial assessing the safety
and efficacy of green tea catechins for the
chemoprevention of prostate cancer incidence in patients with high-grade prostate intraepithelial
neoplasia Daily
treatment consisted of three GTCs
Men with high-grade prostate intraepithelial
neoplasia who would develop cancer within
1-year
3-monthly for 1-year
Primary outcome prostate cancer incidence Secondary outcome
After 1 year only one tumour was diagnosed (incidence 3) in the
cohort receiving green tea whereas 9 cancers were found among the placebo-treated
men (incidence 30) Total PSA did not
change
significantly between the two arms but green tea-treated men showed
values constantly lower with respect to placebo-treated ones As a
secondary observation administration of green tea also reduced lower
urinary tract symptoms suggesting that these compounds might also
58
capsules 200 mg each (total 600 mgd) (n=60) PSA levels be of help for treating the symptoms of benign prostate hyperplasia
Key et al (2004)
An examination of the association between self-reported consumption of fruits and vegetables and prostate cancer risk in EPIC participants
130544 men in 7 countries recruited into EPIC
Median = 48 years
Prostate cancer incidence
There were 1104 incident cases of prostate cancer No significant associations between fruit and vegetable consumption and prostate cancer risk were observed Relative risks (95 CI) in the top fifth of the distribution of consumption compared to the bottom fifth were 106 (084 ndash134) for total fruits 100 (081ndash122) for total vegetables and 100 (079 ndash126) for total fruits and vegetables combined intake of cruciferous vegetables was not associated with risk
McLarty et al (2009)
In order to determine the effects of short-term supplementation with the active compounds in green tea on serum biomarkers in patients with prostate cancer daily doses were provided of Polyphenon E which contained a total of 13 g of tea polyphenols until time of radical prostatectomy
26 men with positive prostate biopsies scheduled for radical prostatectomy
Not reported PSA levels Biomarkers of prostate cancer decreased significantly All of the liver function tests also decreased five of them significantly total protein albumin aspartate aminotransferase alkaline phosphatase and amylase
Ornish et al (2005)
Lifestyle changes including a vegan diet supplemented with soy vitamin E fish oils selenium and vitamin C together with a moderate physical activity program and stress management techniques such as yoga
Men with early prostate cancer (n=93) Gleason scores less than 7
12-months into the intervention
PSA and serum stimulated LNCaP cell growth
PSA levels decreased by 4 at 12-months in the intervention group but increased by 6 in the control group this was statistically significant and strongly correlated with the degree of lifestyle change
Pantuck et al (2006)
A phase II two-stage clinical trial to determine the effects of pomegranate juice PSA progression in men with a rising PSA following primary therapy Patients were treated with 8 ounces of pomegranate juice daily (570mg total polyphenol gallic acid equivalents) until disease progression
46 men with rising PSA levels post-treatment (surgery or radiotherapy)
Every 3-monhs for 54-months
PSA levels Mean PSA doubling time significantly increased with treatment from a mean of 15 months at baseline to 54 months post-treatment (P lt 0001) In vitro assays comparing pre-treatment and post-treatment patient serum on the growth of LNCaP showed a 12 decrease in cell proliferation and a 17 increase in apoptosis (P = 00048 and 00004 respectively) a 23 increase in serum nitric oxide (P = 00085) and significant (P lt 002) reductions in oxidative state and sensitivity to oxidation of serum lipids after versus before pomegranate juice
Schwarz et al (2008)
15mg od lycopene supplementation for 6-months or placebo
Men with benign prostatic hyperplasia (n=40)
After 6-months of intervention
Inhibition or reduction of increased serum PSA levels
Men receiving 15mg od lycopene supplementation had significantly decreased PSA levels compared to a placebo group who had no change in PSA
Thomas et al (2009)
A randomised double blind phase II study to evaluate the influence of salicylate and lifestyle on established cancer progression Men were counselled
110 men whose PSA had risen in 3 consecutive
Not reported Prostate cancer progression (PSA levels)
Although there was no difference in outcome between the SS or CV247 (21 v 19 p=092) the intervention slowed or stopped the rate of PSA progression in 40 patients (364) for over one year A further ten patients were stabilised for ten months Patients least likely to stabilise
59
to eat less saturated fat processed food more fruit vegetables and legumes exercise more regularly and to stop smoking They were then randomised to take sodium salicylate (SS) alone or SS combined with vitamin C copper and manganese gluconates (CV247) daily without other intervention
values gt20 over the preceding 6-months
had received previous radiotherapy or had a Gleason =7 These men welcomed this addition to active surveillance
WEIGHT
Gross et al (2009)
A retrospective cohort study examining whether changes in components of the sex steroid receptor axis may contribute to the clinical aggressiveness of prostate cancer in obese patients
539 patients treated with radical prostatectomy at a single urban hospital between 1994 and 2002
Not reported Pathological stage of prostate cancer BMI
Higher BMI correlated strongly with higher pathologic stage In comparing obese versus non-obese patients there was no difference in expression of androgen or oestrogen related proteins in cancerous epithelial cells However there was a down-regulation of aromatase in the stoma of obese patients suggesting obesity may cause stromal changes in the sex steroid production and signalling pathways which may affect prostate cancer growth via intracrineparacrine mechanisms
Wright et al (2007)
A prospective examination of BMI and adult weight change in relation to prostate cancer incidence and mortality
287760 men ages 50 years to 71 years at enrolment (1995-1996) in the National Institutes of Health-AARP Diet and Health Study
6-years Prostate cancer incidence Weight gain (BMI)
Higher baseline BMI was associated with significantly reduced total prostate cancer incidence largely because of the relationship with localized tumours (for men in the highest BMI category [gtor=40 kgm (2)] vs men in the lowest BMI category [lt25 kgm (2)] RR 067 95 CI 050-089 P = 0006) Conversely a significant elevation in prostate cancer mortality was observed at higher BMI levels (BMI lt25 kgm(2) RR 10 [referent group] BMI 25-299 kgm(2) RR 125 95 CI 087-180 BMI 30-349 kgm(2) RR 146 95 CI 092-233 and BMI gtor=35 kgm(2) RR 212 95 CI 108-415 P = 02) Adult weight gain from age 18 years to baseline also was associated positively with fatal prostate cancer (P = 009) but not with incident disease
60
d) LUNG CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in lung
cancer survival and one systematic review with meta-analysis was identified in the current
review Studies are summarised in Table 6 at the end of this section
Tardon et al (2005) conducted a systematic review and meta-analysis of cohort and case-
control studies from 1966 through October 2003 evaluating the relationship between
physical activity and lung cancer incidence Nine studies were identified 6 of which
demonstrated that that higher levels of leisure-time physical activity (walking gardening
swimming) protects against lung cancer (Severson et al 1989 Thune et al 1997 Lee et
al 1999 Sellers et al 1991 Kubik et al 2002 Mao et al 2003) The estimated combined
risk for both genders was statistically significant as was a dose-response relationship (p lt
01)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in lung cancer
survival and no evidence was identified in the current review
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in lung cancer
survival and no evidence was identified in the current review
iv SMOKING
Smoking has long been accepted as an unhealthy behaviour that increases the risk of
cancer incidence and disease outcomes Yet many people continue to smoke pre- and post-
diagnosis one-third to one-half of cancer patients either continue to smoke after diagnosis or
relapse after initial quit attempts (Gritz et al 2006) Bekkering et al (2006) do not provide
any evidence for the role of smoking in lung cancer survival In the current review 5 studies
were identified that further highlight the importance of smoking cessation support for people
living with and beyond cancer
Vineis et al (2007) have estimated exposure to Environmental Tobacco Smoke (ETS) and to
air pollution in never smokers and ex-smokers in EPIC study participants (n=520000) The
proportion of lung cancers in never- and ex-smokers attributable to ETS was
estimated to be between 16 and 24 mainly due to the contribution of work-related
exposure
61
In two studies of survivors of stage I and II small cell lung cancer risk of a second cancer
was 35-44-fold higher than in the general population (Richardson et al 1993 Tucker et
al 1997) In those who continued to smoke the risk was far higher particularly in those who
also received chest irradiation and alkylating agents35 (Tucker et al 1997) highlighting the
need for risk assessment when offering smoking cessation support or advice
Another study in Japan confirmed that patients with small cell lung cancer who survive
at least 2-years greatly reduced their likelihood of a second cancer if they quit
smoking (p lt 05) (Kawahara et al 2002) Additionally smoking has been found to be
an independent risk factor in breast cancer survivors developing lung cancer (Ford et
al 2003) In support of these studies Parsons et al (2010) report that nine of ten studies
identified in a review of literature from 1966 to 2008 indicate that continuing to smoke is
associated with a significantly increased risk of all-cause mortality in early stage non-
small cell lung cancer and of all-cause mortality in limited stage small cell lung
cancer
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in lung cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR LUNG CANCER - MECHANISMS OF
BENEFIT
Smoking Evidence for the role of lifestyle factors on lung cancer progression and
recurrence has primarily examined smoking which is a strongly established risk factor for
disease progression and mortality Continuing to smoke exposes the body to high levels of
carcinogens which can cause further DNA damage to existing cancers encourage the
cancer to mutate into a more aggressive type or develop mechanisms to hide from the
bodylsquos immunological defences (Akopyan and Bonavida 2006) Indeed smoking has been
found to suppress the immune system interfering with the function of natural killer (NK) cells
- a lymphoid cell type that plays a role in the surveillance of tumour growth Patients who
have already developed one cancer are likely to be more susceptible to DNA damage from a
pre-existing genetic vulnerability or acquired damage from chemotherapy or radiotherapy
Avoiding carcinogens may therefore have a benefit in reducing the risk of developing
further cancers in patients who may be more susceptible from a pre-existing genetic
signature or damage from chemotherapy or radiotherapy The smoking cessation initiatives
currently sweeping the nation such as NHS Choices bdquoSmokefree‟ remain invaluable as
smoking continues to be an important preventable cause of morbidity and mortality
worldwide
Additional Lifestyle Factors More research is required into lifestyle factors such as diet
physical activity weight and alcohol consumption in terms of lung cancer outcomes Access
35
Cytotoxic agents used to disrupt cancer cells can damage healthy cells in the process
62
to lifestyle services such as post-treatment rehabilitation fitness planning and nutritional
support was highlighted as an important component within the disease trajectory for people
with lung cancer (NCSI Mapping Project 2009) There is evidence for the benefits of
physical activity in reducing lung cancer incidence however there is a paucity of evidence
for the survivorship period of lung cancer
63
Table 6 Lung Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Tardon et al (2004)
A meta-analysis of studies (1966-2003) evaluating the relationship between physical activity and lung cancer
Men and women in cohort and case-control studies (9 studies)
Not reported
Lung cancer incidence
The combined ORs were 087 (95 CI=079ndash095) for moderate leisure-time physical activity (LPA) and 070 (062ndash079) for high activity (p trend = 000) This inverse association occurred for both sexes although it was somewhat stronger for women No evidence of publication bias was found Several studies were able to adjust for smoking but none adjusted for possible confounding from previous malignant respiratory disease
SMOKING
Ford et al (2003)
Retrospective analysis of smoking radiation and both exposures on lung carcinoma development in women who were treated previously for breast carcinoma
Case patients (n = 280) females aged 30-89 years with breast carcinoma prior to primary lung carcinoma Control patients (n = 300) selected randomly from 37000 patients with breast carcinoma treated at The University of Texas M D Anderson Cancer Center
Not reported
Lung cancer incidence
At the time of breast carcinoma diagnosis 84 of case patients had ever smoked cigarettes compared with 37 of control patients whereas 45 of case patients and control patients received XRT for breast carcinoma Smoking increased the odds of lung carcinoma in women without XRT (odds ratio [OR] 60 95 confidence interval [95 CI] 36-101) but XRT did not increase lung carcinoma risk in non-smoking women (OR 05 95 CI 03-11) Overall the OR for both XRT and smoking compared with no XRT or smoking was 90 (95 CI 51-159)
Kawahara et al (1998)
Prospective study to investigate whether smoking cessation after successful therapy is associated with a decrease in risk for a second
980 consecutive patients with small cell lung cancer (SCLC)
Median=67 years after initiation of
Second primary tumour
Of the patients who continued to smoke 11 (33) developed a SPT Of the 31 patients who stopped smoking after therapy only three (10) had a subsequent SPT Among those who continued to smoke the risk for a SPT was significantly increased (54 times 95 CI 27-97) relative to the general
64
primary tumour being treated with combination chemotherapy with or without chest radiotherapy
therapy population In contrast those who stopped smoking showed only a 16-fold increase (95 CI 03-46) which was not significantly different from the level in the general population The relative risk for non-SCLC was significantly increased 128-fold (95 CI 34-328) in continuing smokers No second non-SCLCs have been found among those who stopped smoking The 33 patients who continued to smoke had a significantly increased risk of a SPT (43 95 CI 11-159 P=003) Relative to the risk of SPT in patients without previous radiotherapy who stopped smoking the risk is 092 in patients without radiotherapy who continued smoking 037 in patients with radiotherapy who stopped smoking and 233 in patients with radiotherapy who continued smoking The risk of current smoking in patients with previous radiotherapy is 630 relative to those with radiotherapy who stopped smoking although this interaction is not statistically significant (P = 024)
Parsons et al (2010)
A systematic review with meta-analysis of the evidence that smoking
cessation after diagnosis
of a primary lung tumour affects prognosis Databases searched CINAHL (from 1981) Embase (from 1980) Medline
(from 1966)
Web of Science (from 1966) CENTRAL (from 1977)
to
December 2008 and reference lists of included studies
RCTs or observational
st
udies measuring
the effect of quitting smoking
post-
diagnosis on lung cancer prognosis
Patients were followed for 6-months gt in 5 studies but only at time of diagnosis treatment in 4
5-year survival using death rates for continuing smokers and quitters obtained from this review
Continued smoking was associated with a significantly increased risk of all-
cause mortality (hazard ratio 294 95 CI 115 to
754) and recurrence (186
101 to 341) in early stage non-small cell lung cancer and of all-cause
mortality (186 133 to 259) development of a second primary tumour (431 109 to 1698)
and recurrence (126 106 to 150) in limited stage small
cell lung cancer No study contained data on the effect of quitting
smoking on
cancer specific mortality or on development of a second primary tumour in
non-small cell lung cancer Life table modelling on the basis of these data
estimated 33 five year survival in 65 year old patients with early stage non-
small cell lung cancer who continued to smoke compared with 70 in
those
who quit smoking In limited stage small cell lung cancer an estimated 29
of continuing smokers would survive for five years compared with 63 of
quitters on the basis of the data from this review
Richardson et al (1993)
Retrospective review to determine the incidence of second primary cancers developing in patients surviving free of cancer for 2 or more years after treatment for small-cell lung cancer and to assess the potential effect of smoking cessation
Consecutive sample of 540 patients with small-cell lung cancer
Median=61 years
Relative risk for second primary cancers and death
55 patients (10) were free of cancer 2-years after initiation of therapy 18 of these developed one or more second primary cancers including 13 who developed second primary non-small-cell lung cancer The risk for any second primary cancer compared with that in the general population was increased four times (relative risk 44 95 CI 25-72) with a relative risk of a second primary non-small-cell lung cancer of 16 (CI 84-27) Forty-three patients discontinued smoking within 6-months of starting treatment for small-cell lung cancer and 12 continued to smoke In those who stopped smoking at time of diagnosis the relative risk of a second lung cancer was 11 (CI 44 to 23) whereas in those who continued to smoke it was 32 (CI 12 to 69)
Tucker et al (1997)
A multi-institution study to investigate the risk among survivors of developing second primary
611 patients who had
been cancer
Not reported
Population-based rates of cancer
Relative to the general population the risk of all second cancers among these
patients was increased 35-fold Second lung cancer risk was increased 13-
fold among those who received chest irradiation in comparison to a sevenfold
65
cancers other than small-cell lung carcinoma
free for more than 2 years after therapy for small-cell lung cancer
incidence and mortality
increase among non-irradiated patients It was higher in those who
continued smoking with evidence of an interaction between chest irradiation and continued smoking
(relative risk = 21) Patients treated with various forms
of combination chemotherapy had comparable increases in risk (94- to 13-
fold overall) except for a 19-fold risk increase among those treated with
alkylating agents who continued smoking
Vineis et al (2007)
Prospective study to estimate exposure to Environmental Tobacco Smoke (ETS) in never smokers and ex-smokers in 10 European countries (EPIC)
Men and women in the EPIC study (n = 520000)
Not reported
Lung cancer incidence
The proportion of lung cancers in never- and ex-smokers attributable to ETS was estimated as between 16 and 24 mainly due to the contribution of work-related exposure Also 5ndash7 of lung cancers in European never smokers and ex-smokers are attributable to high levels of air pollution as expressed by NO2 or proximity to heavy traffic roads
66
e) OTHER CANCERS
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in survival
from other cancers and no evidence was identified in the current review
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in survival from other
cancers Studies identified in the current review are summarised in Table 7 at the end of this
section
Preliminary EPIC results provide some evidence that red and preserved meat increases risk
for gastric cancer (Gonzalez et al 2006) Preliminary EPIC results also indicate that fruit
reduces gastric cancer risk whilst vegetables are not associated with risk for this type of
cancer Furthermore overall consumption of fruit and vegetables is reported to be unrelated
to risk of ovarian cancer (Schultz et al 2005) There is evidence of a protective effect of a
high intake of allium vegetables (onions garlic shallots leeks and chives) on ovarian
cancer risk (Schultz et al 2005)
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in survival from
other cancers Preliminary EPIC results reported in the current review provide some
evidence that BMI is associated with endometrial cancer risk (Kaaks et al 2002
Friedenreich et al 2007)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in survival from
other cancers Preliminary EPIC results along with 4 other studies were identified in the
current review
Gonzalez et al (2003) confirm from EPIC results that smoking is associated with gastric
cancer
Similarly Yu et al (1997) evaluated 25000 heterogeneous patients who had been treated
for lung breast or colorectal cancer and found that the 15-year survival of the people
who continued to smoke was 44 compared to 55 in those who quit
In a more recent study of survivors of early stage head and neck cancer (n=264) who
retrospectively reported their tobacco histories (pre-diagnosis) and prospectively updated
67
information annually thereafter for an average of 42-years smoking history dose-
dependently increased the risk of mortality from cancer (Mayne et al 2009)
The impact of smoking on risk of secondary lung cancer has been demonstrated in survivors
of Hodgkin lymphoma (Abrahamsen et al 1993 Travis et al 2002) In the latter study risk
for subsequent lung cancer from radiation treatment and smoking was identified where
multiple effects were found for a combination of radiation and alkylating agents36 in
moderate-to-heavy smokers compared with comparison cases (Travis et al 2002)
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in survival from
other cancers One study was identified in the current review which showed that pre-
diagnosis alcohol consumption history dose-dependently increased mortality risk in
recent survivors of early stage head and neck cancer (n=264) (Mayne et al 2009)
Risks reached 49 for those who drank gt5 drinks per day an effect explained by beer and
liquor consumption Continued drinking post-diagnosis of an average of 23 drinks daily
also significantly increased risk
SUMMARY OF FINDINGS FOR OTHER CANCERS
A comprehensive evaluation of the lifestyle evidence for cancers other than the four most
common (ie breast colorectal lung prostate) was not within the scope of this review
However those studies identified whilst gathering evidence for these four cancers does
highlight the sheer importance of lifestyle in the development and progression of all types of
cancers not to forget other chronic diseases The provision of lifestyle support for cancer
survivors clearly needs to remain priority as does further research into the exact
mechanisms of benefit obtained from different lifestyle practices at different stages of the
cancer and indeed health trajectory
36
Carcinogenic agents used in chemotherapy to treat cancer
68
Table 7 Other Cancers ndash Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
DIET
Gonzalez et al (2006)
Nested case-control within the prospective EPIC study examining of
the risk of gastric cancer and
oesophageal adenocarcinoma associated
with meat consumption
521 457 men and women aged 35ndash70 years in 10 European
countrie
s (330 gastric adenocarcinoma and
65
oesophageal adenocarcinomas were diagnosed)
65-years Incidence of gastric and oesophageal cancers
Gastric noncardia cancer risk was statistically significantly associated
with intakes of total meat (calibrated HR per 100-gday increase
=
352 95 CI = 196 to 634) red meat (calibrated HR per 50-gday
increase = 173 95 CI = 103 to 288) and processed
meat (calibrated HR per 50-gday increase = 245 95 CI
= 143 to 421) The association between
the risk of gastric noncardia cancer and total meat intake was
especially large in H pylori infected subjects (odds ratio per 100-
gday increase = 532 95 CI = 210 to 134) Intakes of total red or
processed meat were not associated with
the risk of gastric cardia cancer A positive but nonndashstatistically
significant association was observed between oesophageal
adenocarcinoma cancer risk and total and processed meat intake
Schultz et al (2005)
Prospective examination of the association between consumption of fruit and vegetables and risk of ovarian cancer (EPIC)
Female participants (n = 325640) of the EPIC study
Mean=63 years
Ovarian cancer incidence
Total intake of fruit and vegetables separately or combined as well as subgroups of vegetables (fruiting root leafy vegetables cabbages) was unrelated to risk of ovarian cancer A high intake of garliconion vegetables was associated with a borderline significant reduced risk of this cancer
WEIGHT
Friedenreich et al 2007
Large prospective study (EPIC) examining the association between anthropometry and endometrial cancer particularly by menopausal status and exogenous hormone use subgroups
223008 women in the EPIC study (567 incident endometrial cancer cases)
64-years Endometrial cancer incidence
Weight BMI waist and hip circumferences and waistndashhip ratio (WHR) were strongly associated with increased risk of endometrial cancer The relative risk (RR) for obese (BMI 30ndash lt 40 kgm
2)
compared to normal weight (BMI lt 25) women was 178 95 CI = 141ndash226 and for morbidly obese women (BMI ge 40) was 302 95 CI = 166ndash552 The RR for women with a waist circumference of ge88 cm vs lt80 cm was 176 95 CI = 142ndash219 Adult weight gain of ge20 kg compared with stable weight (plusmn3 kg) increased risk independent of body weight at age 20 (RR = 175 95 CI = 111ndash277) These associations were generally stronger for postmenopausal than premenopausal women and oral contraceptives never-users than ever-users and much stronger among never-users of hormone replacement therapy compared to ever-users
Kaaks et al A review of evidence on the Endometrial Not Incidence of The authors conclude that development of ovarian hyperandrogenism
69
(2002) associations among endometrial cancer risk endogenous hormone metabolism and obesity
cancer cases reported endometrial cancer
may be a central mechanism relating to an interaction between obesity-related chronic hyperinsulinemia with genetic factors predisposing to the development of ovarian hyperandrogenism
SMOKING
Abrahamsen et al (1993)
The Norwegian Cancer Registry
identified previously untreated patients with Hodgkin lymphoma treated at NRH who had developed a secondary cancer more than 1 year after diagnosis of
Hodgkin
lymphoma
68 patients who developed secondary cancer including 9 acute non-lymphocytic leukaemialsquos (ANLLs)
8 non-
Hodgkins lymphomas (NHLs) and 51 solid tumours including 11 lung cancers
Not reported
Secondary cancer
The RR of SC and leukaemia was 186 (95 CI 14 to 24) and 243 (95 CI 111 to 462) respectively The RR of
SC was highest in
younger patients (lt 41 years RR = 38) No significant association
between splenectomy and development of ANLL was found The
influence of treatment and follow-up time on the development of SC
agrees with data from other large cancer institutions
Gonzalez et al (2003)
Assessment of the relation between tobacco use and gastric cancer incidence in the prospective EPIC study
521468 individuals recruited from 10 European countries taking part in the EPIC study 274 were eligible for the analysis
Approx 10-years
Incidence of gastric cancer
After adjustment for educational level consumption of fresh fruit vegetables and preserved meat alcohol intake and body mass index (BMI) there was a significant association between cigarette smoking and gastric cancer risk the hazard ratio (HR) for ever smokers was 145 (95 CI = 108-194) The HR of current cigarette smoking was 173 (95 CI = 106-283) in males and 187 (95 CI = 112-312) in females Hazard ratios increased with intensity and duration of cigarette smoked A significant decrease of risk was observed after 10 years of quitting smoking A preliminary analysis of 121 cases with identified anatomic site showed that current cigarette smokers had a higher HR of GC in the cardia (HR = 410) than in the distal part of the stomach (HR = 194) In this cohort 176 (95 CI = 105-295 ) of gastric cancer cases may be attributable to smoking
Mayne et al (2009)
Participants retrospectively reported their smoking histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to smoke post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Smoking history before diagnosis dose-dependently increased the risk of dying risks reached 54 [95 CI 07-401] among those with gt60 pack-years of smoking After adjusting for pre-diagnosis exposures continued smoking was associated with non-significantly higher risk (relative risk for continued smoking versus no smoking 18 95 CI 09-39)
70
Travis et al (2002)
Case-control study with a population-based cohort The cumulative amount of cytotoxic drugs the radiation dose to the specific location in the lung where cancer developed and tobacco use were compared between patients who developed lung cancer and matched control patients
1-year survivors of Hodgkins disease (n=19046) comparison between 222 patients who developed lung cancer and 444 matched controls
Not reported
Secondary cancer incidence
Tobacco use increased lung cancer risk more than 20-fold risks from smoking appeared to multiply risks from treatment
Yu et al (1997)
Retrospective study examining the effect of smoking history on survival among cancer patients
Data from Memorial Sloan-Kettering Cancer Centers tumour registry was used to identify 25436 cases of cancer (12447 male patients and 12989 female patients)
Not reported
Survival time Patients who had a history of smoking were found to have a lower rate of survival than non-smokers After controlling for age race alcohol use and histologic grade the risk ratios were 155 for males and 143 for females A dose-response relationship was found between ever-smoking and cancer patient survival The predictive effect of smoking on survival was significant for patients with oral pancreatic breast and prostate cancers but not for oesophageal stomach colon rectum laryngeal lung cervix uteri urinary bladder and kidney cancers Black patients with oral or breast cancer had a poorer prognosis associated with smoking compared with white and other non-white patients
ALCOHOL
Mayne et al (2009)
Participants retrospectively reported their alcohol consumption histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to drink post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Alcohol history before diagnosis dose-dependently increased mortality risk risks reached 49 (95 CI 15-163) for persons who drank gt5 drinksd an effect explained by beer and liquor consumption After adjusting for pre-diagnosis exposures continued drinking (average of 23 drinksd) post-diagnosis significantly increased risk (relative risk for continued drinking versus no drinking 27 95 CI 12-61)
71
PART TWO
LIFESTYLE EVIDENCE FOR REDUCING AND MANAGING THE
RISKS AND SIDE-EFFECTS OF CANCER TREATMENT
Introduction
There are a number of long-term and late effects of cancer treatment that a survivor might
be confronted with including fatigue (Bower et al 2006) psychological problems (Thewes
et al 2004) lymphoedema (Deo et al 2004) and osteoporosis (Brown et al 2006) There
might also be difficulties in terms of returning to work or withdrawal from social activities due
to disability (Taskila et al 2007) Lifestyle choices pertaining to diet physical activity
smoking and alcohol consumption for cancer survivors are not only important in terms of
disease progression and recurrence Despite there being less evidence in this area there
is accumulating data demonstrating that lifestyle can facilitate the effective management of
many of these effects of treatment some of which are chronic conditions themselves
requiring additional lifestyle modifications Research within this area has hit new heights in
order to keep up with the growing number of survivors The chronic conditions addressed
within the current review of lifestyle evidence are some of the most frequently reported
problems cited by cancer survivors they include cancer-related fatigue (CRF)
lymphoedema osteoporosis and weight gain In addition evidence for lifestyle choices and
quality of life (QoL) has been reviewed due to the QoL implications of the aforementioned
health-related problems and unhealthy behaviours (Richardson et al 2009)
Evidence for an interaction between lifestyle and these chronic conditions commences with
the findings reported by Bekkering et al (2006) as part of the WCRF review being updated
Further evidence identified from the search criteria will then be presented Evidence will be
presented by cancer site (eg breast colorectal lung prostate) where appropriate whilst
some evidence will pertain to one cancer site only (ie breast cancer related lymphoedema)
72
CANCER-RELATED FATIGUE (CRF)
Cancer-related fatigue (CRF) is defined as ldquoa distressing persistent subjective sense of
physical emotional andor cognitive tiredness or exhaustion related to cancer or cancer-
related treatment that is not proportional to recent activity and interferes with usual
functioningrdquo (NCCN 2009) It has overtaken nausea and pain as the most distressing
symptom experienced by people with cancer during and after treatment It is reported by 60-
96 of patients during chemotherapy radiotherapy or after surgery and can last for months
or even years following treatment (Wagner and Cella 2004 Thomas 2005 NCCN 2009) It
can have a profound effect on physical emotional and social well-being and can hinder
chance of remission owing to non-compliance with treatment due to the intensity of this side-
effect (Lucia Earnest and Perez 2003 Velthuis et al 2009)
The specific causes of CRF are not fully understood but there are several associated
conditions which can aggravate it These include anaemia electrolyte imbalance liver
failure and steroid withdrawal (Thomas 2005) Some conditions can also cause fatigue by
disturbing sleep patterns such as anxiety depression nocturia (a need to get up in the night
to urinate) night sweats and pruritus (itching) The self-management strategy most
extensively investigated for CRF is physical activity the evidence for which is presented
next Studies identified in the current review are summarised in Table 8 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in women with breast cancer In the current review 4 systematic reviews
three of which included a meta-analysis and 2 additional studies were identified
The first review by McNeely et al (2006) reported on 14 RCTs Despite significant
heterogeneity and relatively small samples the overall finding was that physical activity led
to statistically significant improvements in reducing symptoms of fatigue Two meta-
analyses added to this evidence The first by Cramp and Daniel (2008) evaluated 28
studies (n=2083 participants) the majority of which comprised participants with breast
cancer (n=16 studies n=1172 participants) A pooled meta-analysis of all available data
convincingly showed that physical activity was statistically more effective in reducing
CRF when compared to less active controls In the second meta-analysis Velthuis et al
(2009) reviewed 18 studies 12 of which comprised women with breast cancer Pooled
results of these 12 studies (n=674 patients) showed a small significant reduction of CRF
in favour of the physical activity group compared to the non-physical activity group
When Velthuis et al (2009) subdivided the 12 studies into two main physical activity
strategies (ie home-based versus supervised classes) home-based physical activity (n=
7 studies) led to a small non-significant reduction in CRF whereas supervised
73
aerobic physical activity (n=5 studies) showed a medium significant reduction
in CRF when compared to no intervention
Fillion et al (2008) conduced an RCT demonstrating that combining supervised walking
training with psycho-educational stress management produced significant improvements
relative to usual care for fatigue vigour anxiety and depression but not for physical
fitness This suggests a psychological benefit to physical activity which might assist in
coping with physical symptoms such as fatigue Poudevigne et al (2009)
examined adherence to 12-weeks of moderate intensity combined cardio-respiratory and
resistance training and any subsequent impact on levels of fatigue in sedentary breast
cancer survivors (n=20) 2-24 months post-treatment Not only was the training acceptable
and safe but significant decreases in fatigue (43) were also found across the12-
weeks
Danhauer et al (2009) conducted an RCT with women (n=44) who had breast cancer 34
of whom were undergoing cancer treatment in order to examine the effects of restorative
yoga between those in treatment and those not in treatment Randomisation was to a
programme of 10-weekly 75-minute yoga classes or a waiting list control group The yoga
group demonstrated a significant within-group improvement in fatigue although no
significant difference was found with the control group
In updating a previous systematic review by Schmitz et al (2005) of RCTs examining
physical activity in cancer survivors during and after treatment Speck et al (2010)
accumulated data from a further 82 studies (n=6838 participants) Of the 82 studies 66
were rated as high quality and analysed for mean effect sizes resulting from physical activity
interventions The most common diagnosis included was breast cancer (83) with 40 of
studies conducting interventions during cancer treatment and 60 post-treatment Mean
effect sizes demonstrated a large effect of physical activity interventions post-
treatment on upper and lower body strength (plt00001 and 0024 respectively) and
moderate effects on fatigue and breast cancer-specific concerns (p=0003 and 0003
respectively) The most notable progression from their previous review was that the
benefits of physical activity on fatigue moved from negative findings to the evidence
reflecting significantly reduced fatigue post-treatment in physically active survivors
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in men with prostate cancer In the current review 3 systematic reviews two
of which included a meta-analysis and 2 additional studies were identified In the current
review four studies were identified
Windsor Nichol and Potter (2004) published a study of 65 patients with prostate cancer
receiving radiotherapy who were randomly allocated to a home-based physical activity
programme or standard supportive care The home-based exercise included walking 30-
minutes three times a week with an intensity of 60-70 heart rate max for the duration of
74
radiotherapy No adverse events were reported and a non-significant reduction of CRF
was found in the physical activity group when compared to the standard care group
In the abovementioned meta-analysis conducted by Velthuis et al (2009) three RCTs in men
with prostate cancer investigated the effectiveness of supervised physical activity during
radiotherapy and androgen deprivation therapy (Segal et al 2003 Monga et al 2007
Segal et al 2009) In two studies men allocated to the intervention group participated three
times a week in a supervised physical activity programme comprising aerobic exercises with
an intensity of respectively 65 of the maximum heart frequency (HR max) adjusted for
age and 50-75 of the VO2peak (15-45 minutes) (Monga et al 2007 Segal et al 2009)
In the third study the intervention comprised resistance exercises 2-3 times a week with an
intensity of two sets of 8-12 repetitions 60-70 of the one repetition maximum (Segal et
al 2003) Pooled results from the two supervised aerobic studies showed a large non-
significant reduction in CRF in favour of the physical activity group (Monga et al
2007 Segal et al 2009) The resistance exercise study showed a small non-significant
reduction in CRF in favour of the physical activity group (Segal et al 2003) In the latter
study over 80 of the participants were reported to have completed the programme
however the programme did result in one knee injury chest pain fainting and an acute
myocardial infarction
c) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) report on one RCT comparing the impact of a 3-weeks aerobic
physical activity (stationary biking 30-minutes five times weekly) intervention versus
relaxation training (45-minutes three times per week) in post-surgery survivors (n=72) of lung
(n=27) and gastrointestinal (n=42) cancer (Dimeo et al 2004) Fatigue improved
significantly in both groups during the intervention although there was no significant
difference between groups This suggests that relaxation training can be equally as
effective as aerobic physical activity in relieving symptoms of fatigue
In the current review 3 further studies were identified
There has been one study in patients with multiple myeloma (Coleman et al 2003) which
included a home-based physical activity programme during chemotherapy and peripheral
blood stem cell transplantation The programme comprised a combination of aerobic and
resistance exercises three times a week for 20-minutes for the duration of the
chemotherapy (6-months) No adverse events were reported and a small non-significant
reduction in CRF was found in the physical activity group compared to a control
group who did not receive the intervention
Chang et al (2008) published a study involving patients with acute myelogeous leukemia
(n=22) which included allocation to the intervention group a three week supervised walking
programme during chemotherapy Participants walked five times a week for 12-minutes in
the hospital hallway The programme was completed by 69 of the participants and no
75
adverse events were reported A medium-sized non-significant reduction in CRF was
found
In a cross-sectional postal survey of ovarian cancer survivors (n=359) self-report measures
of physical activity and CRF demonstrated that those meeting physical activity guidelines of
the Centres for Disease Control and Prevention (ie minimum 25-hours of moderate
intensity aerobic activity every week plus muscle-strengthening activities on two or more
days of the week) reported significantly lower fatigue than those not meeting guidelines
(Stevinson et al 2009) There was however no evidence of a dose-response relationship
SUMMARY OF EVIDENCE FOR CANCER-RELATED FATIGUE
Evidence from 28 RCTs and 2 meta-analyses has demonstrated that physical activity
programmes can reduce the severity of CRF The studies reviewed here also show that
supervised aerobic exercise programmes were more effective in reducing CRF during breast
cancer treatment than home-based exercise advice Although more research on the optimal
timing and duration of physical activity would be useful these studies are sufficiently robust
to recommend that tailored physical activity advice be integrated into individualized care
plans
As identified in a consultation and evidence review designed to determine the priorities of
cancer survivorship research there is a modest amount of research testing physical activity
interventions for fatigue some demonstrating benefits during treatment but inconclusive
evidence for after treatment (Richardson et al 2009) Although there is clinical
heterogeneity between published RCTlsquos in terms of physical activity duration frequency and
intensity a sensible pragmatic approach based on the trials which showed most benefit is to
supervise a moderate intensity physical activity regimen of regular frequency (3-5
timesweek) for 20-30 minutes per session involving aerobic resistance or mixed physical
activity types With evidence suggesting that low intensity physical activity can also be
beneficial during cancer treatment consideration is warranted in terms of promoting physical
activity from diagnosis onwards potentially making physical activity uptake less challenging
post-treatment (Velthuis et al 2009) Further research is required to determine the optimal
type intensity and timing of physical activity interventions at different periods of the disease
trajectory and when experiencing other cancer-related symptoms or late effects
An exemplary physical activity programme available to survivors of breast colorectal and melanoma cancers is the BACSUP (Bournemouth After Cancer Survivorship Project) Active Wellness Programmelsquo developed in partnership with Royal Bournemouth Hospital NHS Bournemouth and Poole Bournemouth University and MacMillan Cancer Support (Milne et al 2010) The programme involves two initial one-to-one consultations including a holistic assessment with a trained member of staff to tailor the programme to individual needs A readiness check is done prior to referral a readiness to be physically active score of gt70 is required for participation Participants receive a telephone call at 3-weeks for the provision of support and encouragement followed by a one-to-one review at 6-weeks to assess progress and maintain motivation A one-to-one review and reassessment is also provided at 12-weeks to measure improvements Additional support options are available such as the BACSUP Active Wellness Group which provides an opportunity to meet others survivors and listen to life improvement guest speakers In a pilot study of the programme survivors who had completed primary treatment within the previous 5-years (n=180) were referred to the service 58 completed the programme 65 are currently on the programme 30 started but are on hold due to circumstances 21 were not yet ready to join the scheme
At 12-weeks 92 of participants reported reduced fatigue
76
Table 8 Cancer-Related Fatigue and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Chang et al (2008)
RCT to preliminarily examine the effects of a three-week walking exercise program (WEP) on fatigue-related experiences of acute myelogenous leukaemia (AML) patients receiving chemotherapy Eligible AML patients were randomly assigned to either an experimental group (n = 11) which received 12 minutes of WEP per day five days per week for three consecutive weeks or to a control group (n = 11) which received standard ward care
Patients with acute Myelogenous leukaemia (AML) receiving chemotherapy (n=22)
All patients were evaluated four times before treatment (baseline or Day 1) Day 7 Day 14 and Day 21
Worst and average fatigue intensities fatigue interference with patients daily life 12-minute walking distance overall symptom distress anxiety and depressive status
AML patients in the three-week WEP group had a significantly greater increase in 12-minute walking distance than the control group Patients in the WEP also had lower levels of fatigue intensity and interference symptom distress anxiety and depressive status than the control group
Coleman et al(2003)
A pilotfeasibility study with a randomized controlled design was conducted to investigate home-based exercise therapy for patients receiving high-dose chemotherapy and autologous peripheral blood stem cell transplantation as treatment for multiple myeloma
24 patients with multiple myeloma
Not reported Fatigue mood disturbance body weight
Because of the small sample size in the feasibility study the effect of exercise on lean body weight was the only end point that obtained statistical significance However the results suggest that an individualised exercise program for patients receiving aggressive treatment for multiple myeloma is feasible and may be effective for decreasing fatigue and mood disturbance and for improving sleep
Cramp and Daniel (2008)
Systematic review with meta-analysis to evaluate the effect of exercise on cancer-related fatigue both during and after cancer treatment
2083 participants from RCTs comprising cancer patients and survivors
Follow-up assessment of long-term outcomes was poor with 18 of 28 studies failing to assess outcomes beyond the end of the intervention
Cancer-related fatigue
28 studies were identified for inclusion with the majority carried out on participants with breast cancer (n = 16 studies n = 1172 participants) A meta-analysis of all fatigue data incorporating 22 comparisons provided data for 920 participants who received an exercise intervention and 742 control participants At the end of the intervention period exercise was statistically more effective than the control intervention (SMD -023 95 CIs -033 to -013)
77
period
Danhauer et al (2009)
Randomised pilot study to determine the feasibility of implementing a restorative yoga intervention for women with breast cancer and to examine group differences in self-reported emotional health-related quality of life and symptom outcomes 10 weekly 75-minute yoga classes
Women with breast cancer (n=544) 34 of whom were actively undergoing cancer treatment
Immediately post-intervention (week 10)
Emotional well-being QoL fatigue
Group differences favouring the yoga group were seen for mental health depression positive affect and spirituality (peacemeaning) Significant baselinegroup interactions were observed for negative affect and emotional well-being Women with higher negative affect and lower emotional well-being at baseline derived greater benefit from the yoga intervention compared to those with similar values at baseline in the control group The yoga group demonstrated a significant within-group improvement in fatigue no significant difference was noted for the control group
Fillion et al (2008)
RCT to verify the effectiveness of a 4-week nurse-led group intervention that combines stress management psycho-education and physical activity (ie independent variable) intervention in reducing fatigue and improving energy level quality of life (mental and physical) fitness (VO2submax) and emotional distress (ie dependent variables) in breast cancer survivors Participants were randomly assigned to either the group intervention (experimental) or the usual-care (control) condition
French-speaking women who had completed their treatments for non-metastatic breast cancer (n=87)
Post-intervention and at 3-months follow-up
Fatigue emotional distress QoL
Participants in the intervention group showed greater improvement in fatigue energy level and emotional distress at 3-month follow-up and physical quality of life at post-intervention compared with the participants in the control group
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials MEDLINE
EMBASE CINAHL Psych INFO CancerLit PEDro
and SportDiscus as well
as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
function
ing as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all
outcomes were positive even when statistical significance was not
achieved Exercise led to statistically significant improvements in
quality of life as assessed by the Functional Assessment of
Cancer TherapyndashGeneral (weighted mean difference [WMD] 458
95 CI 035 to 880) and Functional Assessment of Cancer
TherapyndashBreast (WMD 662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak
oxygen consumption and in reducing symptoms of fatigue
Poudevigne et al (2009)
Cohort study examining the effects of a 12-week cross training intervention on fatigue and mood in breast cancer survivors The training consisted of a 12-week exercise program of 3 weekly
20 sedentary breast cancer survivors between 2-24 months post-
On completion of the 12-week intervention
Fatigue and mood disturbances (Profile of Mood States) QoL
The mean (plusmnSD) attendance rate was 92 (plusmn80) No musculoskeletal injuries and problematic symptoms occurred during the cross-training Repeated measures ANOVA showed a large increase in QOL (22) and significant decrease in fatigue (43) across 12 weeks (eta squared range 491 to708 all p
78
sessions of 60 min duration supervised by a certified personal trainer and divided into resistance (30 minutes) and aerobic training (5 minutes warm-up 20 minutes training 5 minutes cool-down) The aerobic intensity was set at 60HRR and re-evaluated every three weeks
treatment Treatments ranged from lumpectomies (23) mastectomies (29) radiations (32) and chemotherapy (16)
(SF-36) and work absenteeism
valueslt05) No differences were found in work absenteeism Blood pressure was unchanged after training
Stevinson et al (2009)
A cross-sectional postal survey to investigate the associations between physical activity and health-related outcomes in ovarian cancer survivors and to examine any dose-response relationship
Ovarian cancer survivors (n=359) on and off treatment
Not reported Fatigue peripheral neuropathy sleep and psychosocial functioning
311 of participants were meeting the public health physical activity guidelines - those meeting guidelines reported significantly lower fatigue than those not meeting guidelines (mean difference 71 95 confidence interval 55-88 d = 087 Plt 0001) Meeting guidelines was also significantly inversely associated with peripheral neuropathy depression anxiety sleep latency use of sleep medication and daytime dysfunction and was positively associated with happiness sleep quality and sleep efficiency
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types were included with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) With few exceptions exercise was well tolerated during and post treatment without adverse events
Velthuis et al (2009)
Meta-analysis to evaluate the effects of different exercise prescription parameters during cancer treatment on cancer-related fatigue (CRF) A systematic search of CINAHL Cochrane Library Embase
RCTs studying the effects of exercise during cancer treatment on
Not reported Cancer-related fatigue
During breast cancer treatment home-based exercise lead to a small non-significant reduction (standardised mean difference 010 95 confidence interval minus025 to 045) whereas supervised aerobic exercise showed a medium significant reduction in CRF (standardised mean difference 030 95 confidence interval 009
79
Medline Scopus and PEDro was carried out
CRF (n=18) 12 in breast 4 in prostate and 2 in other cancer patients)
to 051) compared with no exercise A subgroup analysis of home-based (n = 65) and supervised aerobic (n = 98) and resistance exercise programmes (n = 208) in prostate cancer patients showed no significant reduction in CRF in favour of the exercise group Adherence ranged from 39 of the patients who visited at least 70 of the supervised exercise sessions to 100 completion of a home-based walking programme
Windsor Nichol and Potter (2004)
A prospective RCT to determine whether aerobic exercise would reduce the incidence of fatigue and prevent deterioration in physical functioning during radiotherapy for localised prostate carcinoma
33 men in exercise group and 33 men in control group
4-weeks post-radiotherapy
Fatigue and distance walked in a modified shuttle test before and after radiotherapy
There were no significant between group differences noted with regard to fatigue scores at baseline (P = 055) or after 4 weeks of radiotherapy (P = 018) Men in the control group had significant increases in fatigue scores from baseline to the end of radiotherapy (P = 0013) with no significant increases observed in the exercise group (P = 0203)
80
LYMPHOEDEMA
Lymphoedema is the excessive accumulation of tissue fluid (or lymph) that results from
impaired lymphatic drainage resulting in swelling of the limb The most common type of
lymphoedema in cancer survivors is most frequently the result of treatment for breast
cancer where an important prognostic indicator is the removal and evaluation of lymph
nodes (Morrell et al 2005) Removal of the lymph nodes can result in a number of side-
effects including lymphoedema (Swenson et al 2002) which manifests usually as a
swelling to the affected arm but can also occur in the hand trunk and breast The more
lymph nodes that are removed the higher the risk of developing the condition providing an
objective measure of risk that could be utilised in the provision of evidence-based
lifestyle and self-management support based on individuals needs
The condition can develop immediately or many years after treatment (Mortimer et al
1996) in either case lymphoedema is a chronic debilitating condition that can cause severe
physical and psychological morbidity as well as a reduction in QoL (Deo et al 2004)
The self-management strategy most extensively investigated for lymphoedema is physical
activity with some evidence also being available for diet Studies identified in the current
review are summarised in Table 9 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
preventing or managing lymphoedema In the current review one systematic review
(including a meta-analysis) and 3 studies were identified
In a prospective RCT testing the efficacy of two types of physiotherapy on shoulder function
and lymphatic disturbance in post-operative breast cancer survivors (n=60) participants
received one of two types of physiotherapy 48-hours post-surgery (de Rezende et al
2006)
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-
defined sequence of movements
2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely
to music
Lymphoedema is estimated to affect
about 30 of breast cancer survivors
post-treatment (Deo et al 2004)
81
Results indicated significantly better recovery of limb movement in the directed group
compared to the free group with there being no significant difference between groups in
terms of lymphatic disturbance
Ahmed et al (2006) report on a 6-month RCT examining the effects of supervised upper-
and lower-body weight training on lymphoedema incidence and symptoms in breast cancer
survivors (n = 45) 4-36 months post-treatment From baseline to 6-months three control-
group participants reported an increase in lymphoedema symptoms No participants in the
intervention group reported such symptoms suggesting that twice-a-week progressive
weight training does not increase the onset of or exacerbate lymphoedema in breast cancer
survivors (13 women had lymphoedema at baseline) The results from this study indicate
that at minimum physical activity does not exacerbate lymphoedema
Moseley and Piller (2008) reviewed the literature for evidence supporting the benefits of
physical activity for people with limb lymphoedema Their key findings from eleven studies
demonstrated that
physical activity can improve lymph clearance
physical activity can help reduce limb volume and improve subjective symptoms and
QoL
benefits from physical activity have been sustained post-physical activity regime in
some studies
physical activity is a viable option for people with lymphoedema
Moseley and Pillerlsquos (2008) conclusions were supported further in a recent RCT by Hayes
Hildegard and Turner (2009) Breast cancer survivors at least 6-months post-treatment
who had developed unilateral upper-limb lymphoedema participated in twenty supervised
group aerobic and resistance physical activity sessions over 12-weeks (n=16) or continued
habitual activities (n=16) Average attendance was more than 70 of supervised sessions
and there were no withdrawals Mean ratio and volume measures at baseline were similar
between the two groups and no changes were observed at 3-months follow-up for either
group although two women receiving supervised physical activity no longer had evidence of
lymphoedema by study completion The results from this review as with the RCT by
Ahmed et al (2006) indicate that at minimum physical activity does not exacerbate
secondary lymphoedema
In the review referred to previously by Speck et al (2010) with minor exceptions findings
indicated aerobic lifestyle and upper body resistive exercise was tolerated by breast cancer
survivors with no adverse effects on the development or exacerbation of lymphoedema
ii DIET
Bekkering et al (2006) report on one double-blind placebo-controlled RCT examining diet
and lymphoedema in breast cancer survivors (n=68) at a mean of 155-years post-treatment
For 6-months women received 500mg twice a day of dl-alpha tocopheryl acetate (a source
of vitamin E) plus pentoxifylline (a drug that improves blood circulation) 400mg twice a day
82
of dl-alpha tocopheryl acetate or placebo (Gothard et al 2004) At 6-months and 12-months
post-randomisation there was no significant difference between groups in terms of arm
volume
The current review identified one RCT
Dietary Fat
In a UK RCT Shaw Mortimer and Judd (2007) demonstrate the impact of diet and weight
loss on post-treatment arm lymphoedema in breast cancer survivors (n=51) Women were
assigned to one of three 24-week dietary groups
1) a low-fat diet (fat intake reduced to 20 of total energy intake)
2) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ)
3) a control group (continuing their usual diet)
After the end of the 24-week period of dietary intervention there was a slightly greater
reduction in excess arm volume in both dietary intervention groups compared with the
control although this was not statistically significant Furthermore despite low levels of
adherence to dietary advice weight loss was achieved in all groups demonstrating that
dietary interventions can assist in reducing excess arm volume in women with post-
treatment lymphoedema
SUMMARY OF EVIDENCE FOR LYMPHOEDEMA
The studies evaluated within this review indicate a need to re-assess the common clinical
guidelines that breast cancer survivors avoid upper body resistance activity for fear of
increasing risk of lymphoedema(Speck et al 2010) They also indicate a requirement to
develop guidelines for appropriate physical activity As concluded by Hayes Hildegard and
Turner (2009) women with secondary lymphoedema should be encouraged to be physically
active optimising their physical and psychosocial recovery Resistance exercise does not
increase the risk for or exacerbate symptoms of lymphoedema and in fact directed physical
activity 48-hours post-surgery might offer greater utility in terms of rehabilitation outcomes
Some of the studies evaluated in the review by Moseley and Piller (2008) comprised small
sample sizes and did not include control groups however when combined with other studies
presented within this review there is some support for encouraging physical activity in breast
cancer survivors Furthermore physical activity combined with changes in diet and
subsequent weight loss in survivors who are overweight might significantly reduce the
symptoms of lymphoedema although evidence for diet in reducing symptoms of
lymphoedema is limited
Weight loss across groups
9 (60) in the control group 13 (76) in the low-fat diet group 18 (95) in the weight-reduction
group
83
Table 9 Lymphoedema and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Ahmed et al (2006)
RCT comparing supervised twice weekly upper- and lower-body weight training over 6-months with control group completing no training
Breast cancer survivors (n = 45) 4-36 months post-treatment
6-months post-intervention
Incidence and symptoms of lymphoedema
From baseline to 6-months three control-group participants
reported an increase
in lymphoedema symptoms No
participants in the intervention group reported such symptoms suggesting that
twice-a-week progressive weight training does not
increase the onset of or exacerbate lymphoedema in breast
cancer
survivors
de Rezende et al (2006)
RCT examining the impact of physiotherapy on lymphoedema Participants received one of two types of physiotherapy
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-defined sequence of movements 2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely to music
48-hours post-surgery breast cancer survivors (n=60)
On completion of intervention (42-days)
Shoulder movement and lymphatic disturbance
Significantly better recovery of limb movement in the directed group compared to the free group with there being no significant difference between groups in terms of lymphatic disturbance
Hayes Hildegard and Turner (2009)
An RCT testing the impact of aerobic exercise on lymphoedema outcomes Participants randomised to 1) 20 supervised group aerobic and resistance physical activity sessions over 12-weeks (n=16) 2) continued habitual activities (n=16)
Breast cancer survivors at least 6-months post-treatment who had developed unilateral upper-limb lymphoedema
3-months post-intervention
Arm volume measurements
Mean ratio and volume measures at baseline were similar between the two groups and no changes were observed at 3-months follow-up for either group although two women receiving supervised physical activity no longer had evidence of lymphoedema by study completion
84
Moseley and Piller (2008)
Literature search of the evidence supporting the benefits of exercise for those with limb lymphoedema
Exercise studies undertaken in RCTs or cohort studies and involving secondary limb lymphoedema (with no active cancer)
Varied from post-intervention to 8-weeks follow-up
Change in limb volume and subjective symptoms
Exercise has been shown to improve lymph propulsion and clearance help reduce limb volume and improve subjective symptoms and quality of life Benefits from exercise have been sustained post-exercise regime in some studies Exercise is a viable option for those with limb lymphoedema
DIET
Gothard et al (2004)
A double-blind placebo-controlled randomised phase II trial Participants were randomised to active drugs or placebo All volunteers were given dl-alpha tocopheryl acetate 500 mg twice a day orally plus pentoxifylline 400 mg twice a day orally or corresponding placebos for 6 months
68 volunteers with a minimum 20 increase in arm volume at a median 155 years after radiotherapy (plus axillary surgery in 5168 (75) cases)
12 months post-randomisation
Volume of the ipsilateral limb measured
There was no significant difference between treatment and control groups in terms of arm volume Absolute change in arm volume at 12 months was 25 (95 CI minus040 to 53) in the treatment group compared to 12 (95 CI minus28 to 51) in the placebo group The difference in mean volume change between randomisation groups at 12 months was not statistically significant (P=06) minus13 (95 CI minus61 to 35) nor was there a significant difference in response at 6 months (P=07) where mean change in arm volume from baseline in the treatment and placebo groups was minus23 (95 CI minus79 to 34) and minus11 (95 CI minus39 to 17) respectively
Shaw Mortimer and Judd (2007)
Participants were assigned to one of three 24-week dietary groups in order to assess impact on arm volume 1)a low-fat diet (fat intake reduced to 20 of total energy intake) b) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ) c) a control group (continuing their usual diet)
Breast cancer survivors (n=51)
After 24-weeks of intervention
Arm volume There was a slightly greater reduction in excess arm volume in both dietary intervention groups compared with the control although this was not statistically significant
85
OSTEOPOROSIS AND BONE HEALTH
Osteoporosis is a condition in which the bones become less dense and more likely to
fracture which in turn can result in significant pain and disability It is known as a silent
disease because if undetected bone loss can progress for many years without symptoms
until a fracture occurs Risk factors for developing osteoporosis are often enhanced in
cancer survivors such as being post-menopausal and having had early menopause (Ada et
al 2002) Low calcium intake lack of physical activity smoking and excessive alcohol
consumption are also risk factors for osteoporosis (Guthrie et al 2000) Women who have
had breast cancer treatment may be at increased risk for osteoporosis and fracture due to
reduced levels of oestrogen whilst men who receive hormone deprivation therapy for
prostate cancer also have an increased risk of developing osteoporosis and broken bones
(National Institutes of Health Osteoporosis and Related Bone Diseases 2009)
There are no early symptoms of osteoporosis but diet physical activity and drug treatment
can prevent or reverse loss of BMD highlighting the importance of lifestyle choices in
osteoporosis outcomes Studies identified in the current review are summarised in Table 10
at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any physical activity studies examining osteoporosis
in breast cancer survivors The current review identified 3 RCTs and one cohort study
Schwartz Winters-Stone and Gallucci (2007) evaluated the impact of aerobics and
resistance training on BMD in an RCT involving women with histologically confirmed invasive
stage I-III breast cancer (n=66) beginning chemotherapy Women were randomised to one
of three groups and stratified according to menopausal status (pre-menopausal or post-
menopausal)
1) Home-based aerobic exercise - women were instructed to choose an aerobic activity
they enjoyed (eg walking jogging) and exercise for 15-30 minutes four days per
week for the duration of the study at a symptom-limited moderate intensity such that
they were breathing hard but able to talk
2) Home-based resistance exercise ndash women were instructed to exercise at home four
days per week using resistance bands and tubing
3) Usual care
It has been reported that 80 of older breast cancer survivors have osteopenia (below normal bone-mineral density [BMD]) or osteoporosis at initial diagnosis (Twiss et al 2001)
86
The average decline in BMD was -623 for usual care -492 for resistance exercise and
-076 for aerobic exercise suggesting that weight-bearing aerobic exercise attenuates
declines in BMD Pre-menopausal women demonstrated significantly greater declines in
BMD than post-menopausal women highlighting a need to provide interventions for bone
health on a risk stratification basis
Gross et al (2002) examined the intensity of physical activity (ie light moderate vigorous)
reported by a cohort of post-menopausal breast cancer survivors (n=27) and found no
relationship between activity levels and BMD However participants mainly reported light
physical activity limiting the examination of moderate and vigorous activity outcomes It is
possible that a higher intensity of physical activity is required to achieve any benefits to bone
health
Waltman et al (2009) conducted an RCT testing a 24-month self-efficacy based strength
and weight training programme on post-treatment (except tamoxifen and aromatase
inhibitors) post-menopausal breast cancer survivors (n=223) who had amenorrhea
(absence of menstruation) for at least 12-months and a bone BMD score lower than the
norm (Figure 1)
Figure 1 Bone Density Definitions
WHO Definitions of Osteoporosis
Based on Bone Density
T-Scores
BMD
Category
Examples
Range
10
05
0
-05
-10
-1 and
above Normal BMD
-15
-20
Between
-1 and -25
Low BMD
(Osteopenia)
-25
-30
-35
-40
-25 and
below Osteoporosis
Source WHO (2003)
The women were randomised to receive physical activity with medication (n=110) or
medication only (n=113) The medication taken by both groups included risedronate
(osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily) While
87
participation in strength training did not result in statistically significant improved BMD there
was a trend towards at least maintaining BMD at the total hip Participants who were 50
or greater adherent to the intervention (reasons for non-adherence included lack of
time or chronic pain due to co-morbidity) were significantly less likely than
participants on medication alone to lose BMD at the total hip and femoral neck
In a third RCT Swenson et al (2009) compared the effects of two interventions on changes
in BMD in women receiving chemotherapy for breast cancer (n=62)
1) intravenous zoledronic acid (used to prevent skeletal fractures in people with cancer)
and oral calciumvitamin D every 3-months for five treatments
2) prescribed home-based physical activity and oral calciumvitamin D
Zoledronic acid protected patients with breast cancer against bone loss during initial
treatment whereas the home-based physical activity intervention was less effective in
preventing bone loss indicating that physical activity and dietary supplements are not
always sufficient to protect done density in people with cancer However these were
patients undergoing treatment and more research is required into the effects of physical
activity on bone health in post-treatment survivors
ii DIET
Bekkering et al (2006) did not identify any diet studies examining osteoporosis in breast
cancer survivors The current review identified 3 RCTs and one cohort study
Plant Proteins and Fibres
Weikert et al (2005) performed a sub-analysis of the EPIC cohort study conducted in
Germany which included 8178 females and examined the association between protein
intake dietary calcium and bone structure It was concluded that high consumptions of
animal protein may be unfavourable whereas higher vegetable protein may be
beneficial to bone health These results support the hypothesis that high calcium intakes
combined with adequate protein intake based on a high ratio of vegetables to animal protein
may be protective against osteoporosis Indeed evidence has demonstrated the relationship
between lower incidence of osteoporosis in Asian women and vegetarian populations due to
a diet rich in vegetables and fruit (Fujii et al 2009 Merill and Aldana 2009 Thorpe et al
2008) Furthermore a large-scale dietary modification intervention of post-menopausal
women (n = 4883) showed that an increased consumption of plant proteins and fibres from
fruits vegetables and grains reduced the risk of multiple falls and slightly lowered hip BMD
although it did not change the risk of osteoporotic fractures (McTiernan et al 2009)
New et al (2003 2004) provides further evidence for the benefits of plant proteins and fibres
on bone health in two reviews where a positive link between a high consumption of fruit
and vegetables and bone health has been demonstrated In the first report it was found
that fruit and vegetables have beneficial effects on bone mass and bone metabolism in men
and women across the age ranges whilst in the second review it was concluded that
although the impact of a vegetarian diet on bone health is much more complex than merely
being related to diet vegetarians do tend to have normallsquo bone mass
88
iii WEIGHT
Bekkering et al (2006) did not identify any studies examining weight implications on
osteoporosis in breast cancer survivors The current review identified one study that found
that being underweight (BMI less than 185) was associated with lower BMD (Ryan et al
2007)
b) PROSTATE CANCER
i WEIGHT
Bekkering et al (2006) did not identify any studies examining the effect of body weight on
osteoporosis in prostate cancer survivors The current review identified one RCT Ryan et
al (2007) found a positive association between BMI and bone density of the hip in men with
prostate cancer (n=120) who were within the first 12-months of androgen-deprivation
therapy This suggests that a higher BMI can be protective of bone density loss in this
patient group
ii ALCOHOL
Bekkering et al (2006) did not identify any studies examining the effect of alcohol
consumption on osteoporosis in prostate cancer survivors The current review identified one
RCT Ryan et al (2007) also demonstrate greater bone density in prostate cancer patients
consuming seven or more weekly alcoholic beverages when compared to non-drinkers
a) OTHER CANCER
i DIET
Soya Products
Bekkering et al (2006) did not identify any studies examining the effect of diet on
osteoporosis in other cancer survivors The current review identified one RCT Marini et al
(2008) reported a randomised double-blind placebo-controlled trial of the soya derivative
genistein aglycone and its effects on bone health after 3-years in women with breast and
endometrial cancer (n=389) Bone mineral density increases were greater with
genistein for both femoral neck and lumbar spine compared to placebo the conclusion
being that after 3-years of treatment genistein exhibited a promising safety profile with
positive effects on bone formation in this cohort of osteopenic post-menopausal women
89
SUMMARY OF EVIDENCE FOR OSTEOPOROSIS AND BONE HEALTH
There is evidence that vitamin D and calcium might be associated with greater BMD
however this benefit cannot be distinguished from other potential contributors such as
physical activity and medication More research is needed into the effects of physical activity
on osteoporosis in cancer survivors The findings thus far offer different conclusions
although there is limited evidence that physical activity can at the very least prevent loss of
BMD which is a positive outcome in survivors at particular risk of bone loss Greater
adherence to physical activity interventions appeared to offer the greater benefits
highlighting the importance of designing lifestyle interventions that can be maintained as
well as providing higher intensity support for survivors with co-morbidities
Higher BMI has been found to be protective of BMD loss in men with prostate cancer
however no distinction has been made between higher BMI and a BMI that indicates excess
weight Limited evidence has been provided for the benefits of moderate alcohol
consumption but as with the evidence presented for weight much more research is needed
before any valid and reliable conclusions can be made Since the NHS advises no more than
3-4 units of alcohol per day for men more research is needed to determine the minimum
units of alcohol that offer such protective benefits It is important to deter against excessive
drinking which can have a number of serious health implications including high blood
pressure mouth and throat cancers and stroke (NHS 2010)
Men should not exceed 3-4 units of alcohol per day on a regular basis (NHS 2010) One unit is the amount of pure alcohol in a 25ml single measure of spirits (pure alcohol by volume [ABV] 40) a third of a pint of beer (ABV 5-6) or half a 175ml standardlsquo glass of red wine (ABV 12) Daily alcohol limits are provided by the NHS in order to discourage the belief that that the number of units of a weekly limit can be consumed at once (ie binge drinking) Use of daily limit
90
Table 10 Osteoporosis and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Gross et al (2002)
Descriptive correlational test of a multicomponent intervention to prevent and treat osteoporosis in breast cancer survivors
27 post-menopausal breast cancer survivorslsquo post- treatment except for tamoxifen
Not reported
Physical activity vigour vitality and BMD
More than half reported no very hard physical activity and 37 reported no hard activity The association of vigour with total metabolic equivalents for combined moderate hard and very hard activities was significant (r = 0536 p = 0007) as were the hours spent in the combined moderate to very hard activities No relationship was found between vigour vitality or any level of activity and BMD
Schwartz Winters-Stone and Gallucci (2007)
RCT testing the effects of aerobic and resistance exercise on changes in bone mineral density (BMD) in women receiving chemotherapy Participants were randomised to aerobic or resistance exercise and usual care
66 women with stage I-III breast cancer beginning adjuvant chemotherapy
6-months after starting treatment
BMD aerobic capacity and muscle strength
Aerobic exercise preserved BMD significantly better compared to usual care Premenopausal women demonstrated significantly greater declines in BMD than postmenopausal women Aerobic capacity increased by almost 25 for women in the aerobic exercise group and 4 for resistance exercise Participants in the usual care group showed a 10 decline in aerobic capacity
Swenson et al (2009)
Participants received one of two treatments a) Intravenous zoledronic acid and oral calciumvitamin D every 3-months for five treatments b) Prescribed home-based physical activity and oral calciumvitamin D
Women receiving chemotherapy for breast cancer (n=62)
On completion of 3-month intervention
Severity of lymphedema by arm circumference
BMD significantly decreased in the physical activity group but not in the zoledronic acid group Zoledronic acid protected patients with breast cancer against bone loss during initial treatment whereas the home-based physical activity intervention was less effective in preventing bone loss indicating that physical activity and dietary supplements are not always sufficient to protect done density in people with cancer
Waltman et al (2009)
A 24-month self-efficacy based strength and weight training programme Participants were randomised to receive physical activity with medication (n=110) or medication only (n=113) the medication taken by both groups including risedronate (osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily)
Post-treatment post-menopausal breast cancer survivors (n=223) with amenorrhea for at least 12-months and a BMD score lower than the norm
On completion of the 24-month intervention
Bone mineral density
While participation in strength training did not result in statistically significant improved BMD there was a trend towards at least maintaining BMD at the total hip Participants who were 50 or greater adherent to physical activities were significantly less likely than participants on medication alone to lose BMD at the total hip and femoral neck
91
DIET
Marini et al (2008)
RCT assessing the continued safety profile of genistein
aglycone on
breast and endometrium and its effects on bone after
3 years of
therapy Participants received 54mg of genistein
aglycone daily or
placebo both treatment arms
received calcium and vitamin D
Breast cancer patients ndash intervention group (n=71) and placebo (n=67)
After 3-years of treatment
BMD Bone mineral density increases were greater with genistein for both
femoral neck and lumbar spine compared to placebo Genistein also
significantly reduced pyridinoline as well as serum carboxy-terminal
cross-linking telopeptide and soluble receptor activator of NF- B
ligand while increasing bone-specific alkaline phosphatase IGF-I
and osteoprotegerin levels There were no differences in discomfort
or adverse events between groups
(McTiernan et al 2009)
RCT assessing the effect of the Womens Health Initiative
Dietary
Modification low-fat and increased fruit vegetable
and grain
intervention on incident hip total and site-specific
fractures and self-
reported falls and in a subset on bone
mineral density (BMD)
Participants were randomly assigned to
receive
a)dietary modification intervention (daily goal 20 of energy as fat 5 servings of vegetables
and fruit
and 6 servings of grains) b)comparison group
- no dietary
changes
Post-menopausal women (n=48835) intervention (40 n=19541)
versus comparison group (60 n=29294)
Mean=81-years
Incident hip total and site-specific
fractur
es and self-reported falls and in a subset on bone
mineral
density (BMD)
215 women in the intervention group and 285 women in the
comparison group (annualized rate 014 and 012 respectively)
experienced a hip fracture (hazard ratio 112 95 CI 094
134 P = 021) The intervention group (n = 5423 annualized rate
344) had a lower rate of reporting 2 falls than did the
comparison group (n = 8695 annualized rate 367) (HR 092
95 CI 089 096 P lt 001) There was a significant interaction
according to hormone therapy use those in the comparison group
receiving hormone therapy had the lowest incidence of hip fracture In a subset of 3951 women
hip BMD at years 3 6 and 9 was 04ndash
05 lower in the intervention group than in the comparison group
(P = 0003)
New et al (2004)
Literature review assessing the impact of a vegetarian diet on indices of skeletal integrity to address specifically whether vegetarians have a normal bone mass
Analysis of existing literature through a combination of observational clinical and intervention studies were assessed in relation to bone health lacto-ovo-vegetarian and
Not reported
Bone health Key findings included (i) no differences in bone health indices between lacto-ovo-vegetarians and omnivores (ii) conflicting data for protein effects on bone with high protein consumption and low protein intake (particularly with respect to vegan diets) being detrimental to the skeleton (iii) growing support for a beneficial effect of fruit and vegetable intake on bone with mechanisms of action currently remaining unclarified The impact of a vegetarian diet on bone health is a hugely complex area since 1) components of the diet (such as calcium protein alkali vitamin K phytoestrogens) may be varied 2) key lifestyle factors which are
92
vegan diets versus omnivorous consumption of animal versus vegetable protein and fruit and vegetable consumption
important to bone (such as physical activity) may be different 3) the tools available for assessing consumption of food are relatively weak However from data available vegetarians do certainly appear to have normal bone mass
Weikert et al (2005)
Prospective cohort study (EPIC) examining associations between protein intake calcium and bone structure measured by broadband ultrasound attenuation (BUA)
8178 female EPIC participants
Not reported
Bone structure
High intake of animal protein was associated with decreased BUA values ( _ = ndash003 p = 0010) whereas high vegetable protein intake was related to an increased BUA ( _ = 011 p = 0007) The effect of dietary animal protein on BUA was modified by calcium intake
WEIGHT
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and alcohol use was positively associated with the Z score
ALCOHOL
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and body mass index was positively associated with the Z score
93
WEIGHT AND BODY COMPOSITION
Weight gain during and after cancer treatment is becoming an ever-increasing significant
concern (Camoriano et al 1990 Levine et al 1991 Saquib et al 2006) Weight gain is
expected when energy intake exceeds energy expenditure a combination that is frequently
described among breast cancer patients who report exercising less during treatment and
after treatment (Schwartz 2000 Demark-Wahnefried 2001) and consuming a higher energy
diet during treatment (Mukhopadhyay and Larkin 1986) Exacerbating this is the fact that
women in general gain weight as they transition through menopause (Sammel et al 2003)
putting breast cancer patients at particular risk as treatments frequently result in a premature
menopause For individuals with bowel cancer the CALBG 8980 trial showed that 35 of
patients post-chemotherapy were overweight (BMI 250ndash299) and 34 were obese BMI
300ndash349) or very obese (BMI gt35) (Meyerhardt et al 2008) The reasons for weight gain
during and after treatment are multifactorial and the result of individual lifestyle behaviours
and the impact of certain cancer drugs Regardless of the reasons as described in part one
of this review both survival and recurrence may be adversely affected by obesity
(Chlebowski et al 2002)
The effect of obesity on survival has been evident in the majority of studies although not all
one reason for this inconsistency being the possibility that biological factors associated with
obesity and not the obesity itself are responsible for the observed effect For example
there is considerable evidence that the effects of obesity on breast cancer risk may be
mediated at least in part by the effect of obesity on insulin resistance (Friedenreich 2001
Suga et al 2001 Goodwin et al 2002)
Finding effective methods for weight loss continues to be a challenge as although some
studies have demonstrated substantial weight loss in obese individuals weight loss results
in general have been modest and new approaches are needed (Jeffery et al 2000) For
long-term reduction in body weight intensive individualised approaches toward developing
a new lifestyle may be required (Djuric et al 2002)
Studies identified in the current review are summarised in Table 11 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in breast cancer survivors The current review identified one
meta-analysis and three RCTs
In the meta-analysis Kim Kang and Park (2009) reviewed 10 studies involving 588 women
who had been treated for breast cancer examining the effectiveness of aerobic exercise
interventions on cardiopulmonary function and body composition conducted during or after
cancer treatments They concluded that regular aerobic physical activity significantly
improved cardiopulmonary function as assessed by absolute VO2 peak relative VO2
94
peak and 12-minute walk test as well as improved body composition as assessed by
percentage body fat (although body weight and lean body mass did not change
significantly)
Courneya et al (2007) conducted a multicentre RCT in which women with breast cancer on
adjuvant chemotherapy were randomly assigned to usual care (n = 82) supervised
resistance exercise (n = 82) or supervised aerobic exercise (n = 78) for the duration of their
chemotherapy (median = 17-weeks 9-24 weeks) There was 70 adherence to supervised
exercise with aerobic physical activity being superior to usual care for improving
aerobic fitness and percent body fat whilst resistance physical activity was superior
to usual care for improving muscular strength lean body mass and chemotherapy
completion rate
Schmitz et al (2005) evaluated the safety and effects of twice-weekly weight training among
85 breast cancer survivors with women being randomised into immediate or delayed
intervention groups The immediate group trained from months 0-12 the delayed group
served as a no exercise parallel comparison group from months 0-6 and trained from months
7-12 At 6-months the immediate group compared to the no exercise group showed
significantly greater increases in lean mass (p lt 01) as well as significant decreases
in percentage body fat (p lt 05) This significance remained at 12-months when
comparing the immediate group with the delayed exercise group
Mefferd et al (2006) randomised overweight or obese breast cancer survivors (n=85) to a
16-week once weekly general exercise and dietary counselling intervention or standard
care The intervention addressed a reduction in energy intake as well exercise with a goal
of an average of one-hour a day of moderate to vigorous activity Seventy six women
(894) completed the intervention demonstrating reasonable acceptability of the
intervention At 16-weeks significant group differences in favour of the intervention
were evident in weight BMI percent fat trunk fat leg fat and waist and hip
circumference
ii DIET
Bekkering et al (2006) did not identify any studies examining the effect of diet on weight loss
or maintenance in breast cancer survivors The current review identified one RCT
Chlebowski et al (2006) report an RCT conducted as part of the aforementioned WINS trial
where 2437 postmenopausal women with early breast cancer were randomised to
nutritional and lifestyle counselling (n=975) or not (n=1462) as part of routine follow-up The
dietary intervention included eight bi-weekly individual counselling sessions As a reminder
the goal of the dietary intervention was to reduce percentage of calories from fat to 15
resulting in a sustained reduction in fat intake to approximately 20 of calories Dietary fat
intake reduction was significantly greater in the dietary group compared to the control group
After 12-months of intervention dietary fat intake was lower in the intervention group
than in the control group (333g per day versus 513g per day respectively Plt001)
95
corresponding to a statistically significant 6-pound lower mean body weight in the
intervention group (P lt01) This major study also demonstrated a survival advantage in
women who lost weight as described in Part 1 of this review
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in prostate cancer survivors The current review identified
one RCT
Segal et al (2009) conducted a RCT with 121 men with prostate cancer commencing
radiotherapy with or without androgen deprivation therapy They were randomly assigned to
24-weeks of usual care resistance exercise or aerobic exercise Compared with usual
care exercise improved aerobic fitness upper- and lower-body strength while
preventing an increase in body fat Resistance exercise generated longer-term
improvements and additional benefits for strength and body fat than aerobic exercise
SUMMARY OF EVIDENCE FOR WEIGHT AND BODY COMPOSITION
Supervised physical activity programmes with or without dietary counselling are highly
effective in improving body composition or at the very least preventing increases in weight
They are also safe and have other major benefits on health including improving fitness
walking distance muscle power and reducing cholesterol More research is however
required into the most effective dietary strategies for weight loss or maintenance in cancer
survivors Thus far there is some evidence for reducing dietary fat intake
A large controlled trial has been designed to test the combined effect of physical activity and
weight control on disease-free survival and on breast cancer recurrence free survival
second primary breast cancer and total invasive plus in situ breast cancer (Ballard-Barbash
et al 2009) Goals for weight control interventions for women whose BMI is greater than
25kgm2 is to lose 10 of body weight and for women whose BMI is less than or equal to
25kgm2 to avoid weight gain The goal for the physical activity intervention would be to
achieve and maintain regular participation in a moderate intensity physical activity
programme for a total of 150-255 minutes over at least 5 days per week This study is using
evidence which is current for weight loss and physical activity and is an indicator for the
basis of advice for patients at risk in similar situations
96
Table 11 Weight and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Courneya et al (2007)
Multicentre RCT to test for factors that could counteract unfavourable changes resulting from chemotherapy (eg changes in body composition) Participants were randomly assigned to usual care (n =
82) supervised resistance exercise
(n = 82) or supervised aerobic
exercise (n = 78) for the duration of their chemotherapy
242 breast cancer
patient
s initiating adjuvant chemotherapy
Median=17-weeks
Primary Cancer-Specific QoL Secondary Fatigue psychosocial functioning physical fitness body composition chemotherapy completion rate and lymphedema
The follow-up assessment rate for our primary end point was
921 and adherence to the supervised exercise was 702
Unadjusted and adjusted mixed-model analyses indicated that
aerobic exercise was superior to usual care for improving self-
esteem (P = 015) aerobic fitness (P = 006) and percent body fat
(adjusted P = 076) Resistance exercise was superior to usual care
for improving self-esteem (P = 018) muscular strength (P lt
001)
lean body mass (P = 015) and chemotherapy completion rate (P =
033) Changes in cancer-specific QOL fatigue depression and
anxiety favoured the exercise groups but did not reach statistical
significance Exercise did not cause lymphedema or
adverse events
Kim Kang and Park (2009)
Meta-analysis to examine the effectiveness
of aerobic exercise
interventions on cardiopulmonary function
and body composition in
women with breast cancer
Of 24 relevant
studie
s reviewed 10 studies (n= 588) met the inclusion criteria
Not reported Cardiopulmonary function
and body
composition
The findings indicated that aerobic exercise significantly improved
cardiopulmonary function as assessed by absolute
VO2 peak (standardized mean difference [SMD] 916 p lt 001)
relative VO2 peak (SMD424 p lt 05) and 12-minute walk test
(SMD 502 p lt 001) Similarly aerobic exercise significantly
improved body composition as assessed by percentage body fat
(SMD mdash890 p lt001) but body weight and lean body mass did not
change significantly
Mefferd et al (2006)
RCT to test the effect of a 16-week cognitive behavioural therapy (CBT) intervention for weight loss through exercise and diet modification on risk factors for recurrence of breast cancer Participants randomly assigned to a once weekly 16-week intervention or wait-list control group
Overweight or obese breast cancer survivors (n=76)
On completion of the 16-week intervention
Weight Significant differences in weight body mass index percent fat trunk fat leg fat as well as waist and hip circumference between intervention and control groups (P le 005) Furthermore levels of triglycerides and total cholesterolhigh density lipoprotein cholesterol levels were also significantly reduced following the intervention
97
Schmitz et al (2005)
RCT testing the safety of twice weekly weight training classes among recent breast cancer survivors Participantslsquo randomised into immediate and delayed treatment groups The immediate group trained from months 0-12 the delayed treatment group served as a no exercise parallel comparison group from months 0-6 and trained from months 7=12
Convenience sample of 85 recent breast cancer survivors
6 and 12-months
Body size (lean body mass) and biomarkers hypothesised to link exercise and breast cancer risk
Significant increases in lean mass (088 versus 002 kg P lt 001) as well as significant decreases in body fat (minus115 versus 023 P = 003) and IGF-II (minus623 versus 2828 ngmL P = 002) comparing immediate with delayed treatment from baseline to 6 months Within-person changes experienced by delayed treatment group participants during training versus no training were similar
Segal et al (2009)
Prostate Cancer Radiotherapy and
Exercise Versus Normal
Treatment study examining the effects
of 24-weeks of resistance or
aerobic training versus usual care on prostate cancer outcomes Randomly assigned
to usual care resistance or
aerobic exercise for 24-weeks
Prostate cancer patients on radiotherapy (n=121) usual care (n=41) resistance (n= 40) aerobic exercise
(n=
40)
On completion of 24-week intervention
Fatigue QOL physical fitness body composition PSA testosterone haemoglobin and lipid levels
Median adherence to prescribed exercise was 855 Compared
with usual care resistance training improved QOL (P = 015)
aerobic fitness (P = 041) upper- (P lt 001) and lower-body (P lt
001) strength and triglycerides (P = 036) while preventing an
increase in body fat (P = 049) Aerobic training also improved
fitness (P = 052)
DIET
Chlebowski et al (2006)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to 345]
versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group
98
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general dietary
guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
randomisation to death from any cause
99
QUALITY OF LIFE
The advancements in diagnosis and treatment that have contributed to the rise in
survivorship are a significant achievement for healthcare science However it is important to
recognise that this has also resulted in an increase in the number of people living with the
often long-term physical and psychological consequences of cancer and its treatment
Quality of life outcomes are thus becoming just as important as hardlsquo outcomes such as
mortality (Rosenbaum Fobair and Spiegel 2006) hence an emphasis on patient-reported
outcomes (DH 2009c) Indeed there is increasing evidence that QoL can be more
predictive of cancer survival than measures of performance status (Cella et al 2009 Eton et
al 2003 Wenzel et al 2005)
A healthy lifestyle has become viewed as an important element for improved QoL (Lyon and
Langille 2000) with particular emphasis on physical activity Studies identified in the current
review are summarised in Table 12 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in breast cancer survivors In the current review one systematic review (with meta-
analysis) and 6 RCTs were identified that provide evidence for the role of physical activity in
the QoL of breast cancer survivors
McNeeley et al (2006) conducted a systematic review with meta-analysis of RCTs (n=14)
examining the effects of physical activity on outcomes in breast cancer survivors Three of
the reviewed studies involving 194 patients compared exercise with usual care
(Campbell et al 2005 Courneya et al 2003 Segal et al 2001) with pooled data
demonstrating that exercise led to significant improvements in QoL superior to the
usual care groups Four studies involving 208 patients reported physical functioning or
physical well-being components of QoL (Campbell et al 2005 Courneya et al 2003
McKenzie and Kalda 2003 Segal et al 2001) the pooled results of which showed
a statistically significant increase in this component of QoL as a result of physical
activity Two of these studies were rated as high quality by the reviewers Courneya et al
2003 Segal et al 2001
100
In addition to this meta-analysis findings by Ohira et al (2006) demonstrated that over 6-
months physical and psychological QoL significantly improved in a recent breast
cancer survivors (n=86) 4-36 months post-treatment who took part in a twice-weekly
weight-training intervention when compared to a control group Increases in upper
body strength and lean mass correlated with these improvements suggesting that twice-
weekly weight training for recent breast cancer survivors might improve QoL in part via
changes in body composition and strength
Daley et al (2007) provided evidence from an RCT comprising sedentary breast cancer
survivors who were 12-36 months post-treatment and who were randomised to one of three
conditions
1) 8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-
minute one-to-one sessions with an physical activity specialist three times per week
(n=34)
2) 8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one
sessions with an physical activity specialist three times per week (n=36)
3) usual care (n=38)
Courneya et al (2003) evaluated QoL outcomes in relation to
exercise in breast cancer survivors (n=52) who had completed
surgery radiotherapy or chemotherapy Participants trained three
times per week for 15-weeks on recumbent or upright cycle
ergometers Exercise duration began at 15-minutes for weeks 1-
3 and then systematically increased by five-minutes every 3-
weeks to 35-minutes for weeks 13-15 The exercise group completed
984 of the exercise sessions demonstrating high adherence
rates Overall QoL increased by 91 points in the exercise group
compared with 03 points in the control group (p lt 001) Change
in peak oxygen consumption correlated with change in overall QoL
demonstrating a significant relationship between exercise and
increases in QoL (p lt 01)
Segal et al (2003) compared self-directed versus supervised
exercise on QoL outcomes in women with stages I-II breast cancer
(n=123) Physical functioning in the control group decreased by 41
points whereas it increased by 57 points and 22 points in the self-
directed and supervised exercise groups respectively (p lt 05)
Post-hoc analysis showed a moderately large and clinically important
difference between the self-directed and control groups (98
points p lt 01) and a more modest difference between the
supervised and control groups (63 points P = 09) No significant
differences between groups were observed for changes in QoL
scores
101
A significant mean difference of 98 units in QoL scores favouring aerobic physical
activity therapy was found This outcome was not the result of the extra support and
attention gained from taking part in the intervention since the same findings were not elicited
for the physical activity-placebo and usual care groups
A small pilot RCT comparing QoL and functional capacity in breast cancer survivors (n=21)
provided with 12-weeks of the Chinese physical activity Tai Chi Chuan (n=11) versus
psychosocial support (n=10) was conducted by Mustian Palesh and Flecksteiner (2008)
The tai chi group demonstrated significant improvements in functional capacity and QoL the
psychosocial support group showed significant improvements only in flexibility with declines
in QoL This suggests that tai chi can enhance functional capacity and QoL among
breast cancer survivors over and above the benefits of psychosocial support
Further support for the benefits of physical activity on QoL in breast cancer survivors (n=58)
within 2-years of completing adjuvant therapy has been demonstrated in a combined aerobic
and resistance training RCT (Milne et al 2008) The women received 12-weeks immediate
supervised physical activity three times a week (n=29) or delayed physical activity
comprising the same protocol but provided 12-weeks following the immediate physical
activity group (n=29) Adherence was 613 which is relatively low However there was a
significant group by time interaction for overall QoL which increased in the
immediate physical activity group from baseline to 12-weeks by 208 points compared
to a decrease in the delayed physical activity group of 53 points
Cadmus et al (2009) report on the QoL outcomes of two 6-month RCTs designed for breast
cancer survivors and based on the national recommendation of 30-minutes of moderate to
vigorous physical activity five days per week
When combining findings from these two studies physical activity was not associated with
QoL benefits in the full sample of either study however physical activity was associated with
significantly improved social functioning (a component of QoL) among survivors who
Trial Increasing or Maintaining
Physical Activity during Cancer
Treatment (IMPACT)
Theoretical Framework Theory of
Planned Behaviour and
transtheoretical model - promoting
self-efficacy to overcome barriers to
physical activity
Sample n=45 newly diagnosed
survivors
Delivery Home-based
Trial Yale Physical activity and
Survivorship (YES)
Theoretical Framework Not
reported
Sample n=67 post-treatment
survivors
Delivery Combined supervised
training programme at a local
health club with home-based
physical activity
102
reported low social functioning at baseline which is the likely impact of greater social
interaction during the intervention This highlights the utility of risk stratification and the
provision of lifestyle support based on need survivors with low social functioning as
could be detected via the Social Difficulties Inventory (SDI Wright et al 2005b) are
likely to benefit from programmes such as the IMPACT and YES trial
Sandel et al (2005) report on a cross-over RCT testing the outcomes of a 12-week dance
and movement exercise programme in women within 5-years of treatment for breast cancer
(n=38) The study included a waiting list control (n=19) and cross-over at 13-weeks Women
attended two supervised dance sessions for six weeks and one session per week for an
additional 6-weeks for a total of eighteen sessions A total of 35 (92) women completed
the regimen with reasons for dropping out including fatigue other commitments and one
participant reported shoulder discomfort The overall finding was that breast cancerndash
specific QoL improved significantly in the intervention group compared to the waiting
list group at 13-weeks which remained unchanged
In the updated systematic review described previously Speck et al (2010) present evidence
from 66 high quality RCTs showing that physical activity during treatment has a small to
moderate positive effect on QoL (p=004) anxiety (p=002) and self-esteem (p=002)
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in colorectal cancer survivors In the current review one large cohort study was
identified Lynch et al (2008) examined physical activity and QoL data collected as part of
the Colorectal Cancer and Quality of Life Study37 Telephone interviews were conducted
at approximately 6 12 and 24-months after colorectal cancer diagnosis (n=1966) which
found that participants achieving at least 150-minutes of physical activity per week had an
18 higher QoL score than those who reported no weekly physical activity
ii DIET
Bekkering et al (2006) identified two dietary intervention studies examining impact on QoL in
colorectal cancer survivors One dietary counselling trial found a significant improvement in
health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst another reported that
an intervention aimed at a healthier dietary lifestyle had no effect on health assessment or
life satisfaction but did lead to increased health action and increased reports of feeling goodlsquo
(Corle et al 2001) No further studies were identified in the current review
37
The Colorectal Cancer and Quality of Life study in Australia examines in detail the lifestyle factors that
influence QoL in the 5-years post-diagnosis (n=2000)
103
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any dietary physical activity interventions examining
impact on QoL in prostate cancer survivors One dietary counselling trial found a significant
improvement in health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst
another reported that an intervention aimed at a healthier dietary lifestyle had no effect on
health assessment or life satisfaction but did lead to increased health action and increased
reports of feeling goodlsquo (Corle et al 2001) No further studies were identified in the current
review
Segal et al (2003) reported an RCT comparing supervised resistance exercise versus
control in men with prostate cancer (n=135) who were scheduled to receive androgen
deprivation therapy for at least 3-months Fitness levels were assessed and the men in the
intervention group met with a certified fitness consultant within 7-days of the pre-
assessment The fitness consultant provided patients with the results of their exercise
assessment and introduced a personalised resistance exercise program A significant
improvement was found in QoL outcomes in the intervention group and a significant
decline in the control group Resistance exercise improved QoL regardless of whether
men were treated with curative or palliative intent or whether androgen deprivation therapy
had been received for less than one-year or 1 year
d) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) found that out of seven physical activity trials six observed
improvements in QoL when using cancer-specific questionnaires (Burnham and Wilcox
2002 Courneya et al 2003 Segal et al 2003 Headley et al 2004 Campbell et al 2005
Sandel et al 2005) but one of these same studies found no association when using the
generic SF-36 scale (Segal et al 2001) This highlights the importance of selecting the most
appropriate outcome measures in terms of sensitivity and responsiveness to a given
intervention
In the current review three studies were identified One prospective controlled four-centre
study comprising a sample of survivors with different tumour sites was identified (Korstjens
et al 2008) QoL outcomes were compared between three groups
1) group-delivered physical training (n=71)
2) group-delivered combined physical and cognitive behavioural training (CBT) (n=76)
3) waiting-list control (n=62)
Participants in both training groups showed significant and clinically relevant improvements
in role limitations physical functioning vitality and health change Adding CBT to the
physical training did not have additional beneficial effects on QoL a finding that has been
104
observed in a number of supported self-management programmes (Davies and Batehup
2010)
Oh et al (2009) reported a RCT examining the QoL outcomes of Medical Qigong (MQ) a
mindndashbody practice that uses physical activity and meditation to harmonise the body mind
and spirit Patients (n=162) with malignancy of any stage and an expected survival length of
gt12-months were randomised to a control group or to a 10-week MQ programme comprising
two supervised 90-minute sessions per week At 10-week follow-up participants in the
MQ group reported larger improvements in QoL than those in the usual care group (p
lt 05)
Mosher et al (2009) reported a prospective cohort study examining the diet exercise and
QoL patterns of 753 breast prostate and colorectal cancer survivors who were at least 5-
years post-diagnosis Survivors underwent two 45-60 minute telephone surveys
administered by the Diet Assessment Center The data demonstrated that greater weekly
minutes of exercise were associated with better physical QoL including less pain and
better health perceptions physical functioning and vitality More exercise was also
correlated with better social functioning Diet quality had a positive association with a range
of physical QoL outcomes in analyses that were adjusted for age level of education and co-
morbidities Greater BMI was associated with worse physical QoL including greater
pain and role limitations because of physical problems and worse health perceptions
physical functioning and vitality
SUMMARY OF EVIDENCE FOR QUALITY OF LIFE
Lifestyle interventions appear to help people with a wide range of cancer types who have
received treatments ranging from surgery chemotherapy radiotherapy or hormonal
therapies although no trials have yet been published specifically addressing the newer
biological therapies Even when not directly associated with overall QoL exercise has been
found to significantly improve social functioning among post-treatment survivors The
benefits of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or group-
based A vast array of different types of exercise techniques have been tested in the studies
evaluated in this review highlighting the potential for survivors to choose activities according
to preference
Whilst some studies have recommended the uptake of physical activity during treatment
others have highlighted the benefits of introducing regular physical activity into a survivorlsquos
self-management care plan immediately after completion of treatment Overall the evidence
does suggest that immediate physical intervention provides greater QoL benefits than
delayed intervention
105
Table 12 Quality of Life and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Cadmus et al (2009)
The results of two RCTs to determine the effect of exercise on quality of life in (a) a RCT of exercise among recently diagnosed breast cancer survivors undergoing adjuvant therapy - randomised to a 6-month home-based exercise program or a usual care group (b) a similar trial among post-treatment survivors - randomised to a 6-month supervised exercise intervention or to usual care
50 newly diagnosed breast cancer survivors in the first RCT (a) 75 post-treatment survivors in the second RCT (b)
6-months Measures of happiness depressive symptoms anxiety stress self-esteem and QoL
Good adherence was observed in both studies Baseline quality of life was similar for both studies on most measures Exercise was not associated with quality of life benefits in the full sample of either study however exercise was associated with improved social functioning among post-treatment survivors who reported low social functioning at baseline (p lt005)
Courneya et al (2003)
RCT testing 15-weeks supervised aerobic and resistance training to determine the effects on cardiopulmonary
function and QoL in
post-menopausal breast cancer
survivors Randomly assigned to an exercise (n=25) or control (n=28) group The exercise group trained on cycle ergometers
three times per week for 15
weeks The control group did not train
53 post-menopausal breast cancer survivors
On completion of the 15-week intervention
Changes in peak oxygen
consu
mption and overall
Peak oxygen consumption increased by 024 Lmin in the exercise group whereas it decreased
by 005 Lmin in the control group
(mean difference 029 Lmin 95 confidence interval [CI] 018 to
040 P lt 001) Overall QOL increased by 91 points in the exercise
group compared with 03 points in the control group (mean
difference 88 points 95 CI 36 to 140 P= 001) Pearson
correlations indicated that change in peak oxygen consumption
correlated with change in overall QOL (r = 045 P lt 01)
Daley et al (2007)
RCT - Women were randomised to one of three groups a)8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-minute one-to-one sessions with an physical activity specialist three times per week (n=34) b)8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one sessions with an physical activity specialist three times
Sedentary breast cancer survivors who were 12-36 months post-treatment (n=117)
On intervention completion and at 24-weeks follow-up
QoL depression physical activity behaviour aerobic fitness
There was a significant mean difference of 98 units in QoL scores favouring aerobic physical activity therapy
106
per week (n=36) c)usual care (n=38)
Korstjens et al (2008)
RCT comparing the effects on cancer survivorslsquo QoL in a
12-week group-
based multidisciplinary self-management rehabilitation
program
combining physical training (twice weekly) and cognitive-behavioural
training (once weekly) with
those of a 12-week group-based physical
training (twice weekly) There
was also a non-intervention comparison group
All cancer types rehabilitation (n=76) physical training (n=71) comparison group (n=62)
Baseline after rehabilitation and
3-
months follow-up
QoL (SF-36) The effects of multidisciplinary rehabilitation did not outperform
those of physical training in role limitations due to emotional
problem (primary outcome) or any other domains of quality of life
(all p gt 05) Compared with no intervention participants in both
rehabilitation groups showed significant and clinically relevant
improvements in role limitations due to physical problem (primary
outcome effect size (ES) = 066) and in physical functioning (ES =
048) vitality (ES = 054) and health change (ES = 076) (all p lt
01)
Lynch et al (2008)
Colorectal Cancer and Quality of Life
Study - aimed at examining the relationships between
physical activity
and QoL after a colorectal cancer
diagnosis Participants completed telephone interviews at approximately
6
12 and 24 months after diagnosis
1966 people with colorectal
6 12 and 24-months post-diagnosis
QoL There was an overall independent association between physical
activity and QoL At a given time point
participants achieving at least 150 minutes of physical activity per
week had an 18 higher quality of life score than those who
reported no physical activity Significant associations were also
present at the interindividual level (differences between
participants) and intraindividual level (within participant changes)
Milne et al (2008)
RCT to examine the effects of a supervised exercise program on motivational variables in breast cancer survivors Participants were randomised in a cross-over design to either an immediate exercise group that exercised from baseline to week 12 or a delayed exercise group that exercised from week 12 to 24
Breast cancer survivors (n=58) within 2-years of completing adjuvant therapy
Post-intervention (12-weeks)
Quality of life There was a significant group by time interaction for overall QoL which increased in the immediate physical activity group by 208 points compared to a decrease in the delayed physical activity group of 53 points
Mosher et al (2009)
Prospective Cohort Study examining the health behaviours of older cancer survivors and the associations of those behaviours with QoL especially during the long-term post-treatment period
753 older (aged 65 years) long-term survivors ( 5 years post-diagnosis) of breast prostate and colorectal
2 telephone interviews
Exercise diet weight status and quality of life
Participants reported a median of 10 minutes of moderate-to-vigorous exercise per week and only 7 had Healthy Eating Index scores gt80 (indicative of healthful eating habits relative to national guidelines) Despite their suboptimal health behaviours survivors reported mental and physical quality of life that exceeded age-related norms Greater exercise and better diet quality were associated with better physical quality-of-life outcomes (eg better vitality and physical functioning P lt 05) whereas greater body mass index was associated with reduced physical quality of life (P lt 001)
107
cancer
Mustian Palesh and Flecksteiner (2008)
RCT testing the functional and QoL outcomes of tai chi - women who completed treatment randomised to receive tai chi or psychosocial support therapy for 12-weeks (60 minutes three times weekly)
Breast cancer survivors (n=21)
On completion of 12-week intervention
Functional capacity and quality of life
The tai chi group demonstrated significant improvements in functional capacity and QoL the psychosocial support group showed significant improvements only in flexibility with declines in QoL
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials
MEDLINE EMBASE CINAHL Psych INFO CancerLit PEDro
and
SportDiscus as well as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
functi
oning as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all outcomes
were positive even when statistical significance was not achieved
Exercise led to statistically significant improvements in quality of life
as assessed by the Functional Assessment of Cancer Therapyndash
General (weighted mean difference [WMD] 458 95 CI 035 to
880) and Functional Assessment of Cancer TherapyndashBreast (WMD
662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak oxygen consumption
and in reducing symptoms of fatigue
Oh et al (2009)
RCT comprising 10-weeks Medical Qigong (MQ) to evaluate the use of (MQ) compared with usual care in improving the QOL of cancer patients
162 patients with a range of cancers
On completion of the 10-week intervention
QOL and fatigue (FACT-GF) mood (Profile of Mood State)
Regression analysis indicated that the MQ group significantly improved overall QOL (t144thinsp=thinspminus5761 Pthinspltthinsp0001) fatigue (t153thinsp=thinspminus5621 Pthinspltthinsp0001) mood disturbance (t122 =2346 Pthinsp=thinsp0021) and inflammation (CRP) (t99thinsp=thinsp2042 Pthinspltthinsp0044) compared with usual care after controlling for baseline variables
Ohira et al (2006)
RCT to examine the effects of weight training on changes in QoL and depressive symptoms in recent breast cancer survivors Randomised to treatment or control group
Convenience sample of 86 breast cancer survivors (4-36 months post-treatment)
6-months The primary outcomes were changes in QoL (CARES-SF) and depressive symptoms (CES-D)
QoL improved in the treatment group compared with the control group (Standardized Difference = 062 P = 006) The psychosocial global score also improved significantly in the treatment group compared with the control group (Standardized Difference = 052 P = 02) There were no changes in CES-D scores Increases in upper body strength were correlated with improvements in physical global score (r = 032 P lt01) and psychosocial global score (r = 030 P lt01) Increases in lean mass were also correlated with improvements in physical global score (r = 023 P lt05) and psychosocial global score (r = 024 P lt05)
Sandel et al (2005)
RCT - 12-weeks dance and movement programme versus wait list control to determine the effect on QoL and shoulder function
35 breast cancer survivors
13 and 26-weeks
QoL (FACT-B) Shoulder range of motion (ROM) and Body Image Scale
FACT-B significantly improved in the intervention group at 13 weeks from 1020 _158 to 1167 _ 169 compared to the wait list group 1081 _ 164 to 1071 _213 (time _ group effect P _ 008) During the crossover phase the FACT-B score increased in the wait list group and was stable in the treatment group The overall effect of the training at 26 weeks was significant (time effect P _ 03) and the order of training was also significant (P _ 015) Shoulder ROM
108
increased in both groups at 13 weeks mdash15_ and 8_ in the intervention and wait list groups (Time effect P _ 03 time _ group P _ 58) Body Image improved similarly in both groups at 13 weeks (time effect P _ 001 time _ group P _ 25) and at 26 weeks There was no significant effect of the order of training for these outcome measures
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) A small to moderate positive effect of physical activity during treatment was seen for physical activity level aerobic fitness muscular strength functional quality of life anxiety and self-esteem With few exceptions exercise was well tolerated during and post treatment without adverse events
Segal et al (2003)
RCT testing the hypothesis that resistance exercise can counter the negative QoL effects of androgen deprivation therapy for prostate cancer by reducing fatigue elevating mood building muscle mass and reducing body fat Randomly assigned to an intervention group that participated in a resistance exercise program three times per week for 12 weeks or to a waiting list control group
55 men with prostate cancer scheduled for androgen deprivation therapy for at least 3 months after recruitment
On completion of the 12-week intervention
Primary outcomes fatigue disease-specific QoL Secondary outcomes muscular fitness body composition
Men assigned to resistance exercise had less interference from fatigue on activities of daily living (P =002) and higher quality of life (P =001) than men in the control group Men in the intervention group demonstrated higher levels of upper body (P =009) and lower body (P lt001) muscular fitness than men in the control group The 12-week resistance exercise intervention did not improve body composition as measured by changes in body weight body mass index waist circumference or subcutaneous skinfolds
Vadiraja et al (2009)
RCT - 6-week yoga and relaxation during adjuvant radiotherapy his study compares the effects of an integrated yoga program with brief supportive therapy in breast cancer outpatients undergoing adjuvant radiotherapy at a cancer centre Intervention consisted of
88 stage II and III breast cancer outpatients
After 6-weeks of radiotherapy
QoL (EORTC-C30) Mood (Positive and Negative Affect Schedule)
There was a significant difference across groups over time for positive affect negative affect and emotional function and social function There was significant improvement in positive affect (ES = 059 p = 0007 95CI 125 to 78) emotional function (ES = 071 p = 0001 95CI 645 to 2533) and cognitive function (ES = 048 p = 003 95CI 12 to 185) and decrease in negative affect (ES = 084 p lt 0001 95CI minus134 to minus44) in the yoga
109
yoga sessions lasting 60 minutes daily while the control group was imparted supportive therapy once in 10 days
group as compared to controls There was a significant positive correlation between positive affect with role function social function and global quality of life There was a significant negative correlation between negative affect with physical function role function emotional function and social function
110
ONGOING LIFESTYLE STUDIES
Four ongoing lifestyle studies were identified in the current review one for breast cancer and
three for colorectal cancer
a) BREAST CANCER
In the US Goodwin et al (ongoing) are trialling lsquoLifestyle Intervention Study in Adjuvant
Treatment of Early Breast Cancerrsquo (LISA) The primary objective of this trial is to evaluate
the effect of the addition of a 2-year centrally delivered individualised telephone-based
lifestyle intervention focusing on weight management to a mailed educational intervention on
disease-free survival in post-menopausal women with early stage breast cancer (hormone
receptor positive) BMI ge24-lt40 kgm2 who are receiving standard letrozole adjuvant
therapy The primary outcome is disease-free survival Secondary outcomes include overall
survival distant disease-free survival weight change QoL selected non-cancer medical
events and biologic factors (insulin) The estimated enrolment is 2150 with the study having
started in 2007 Participants will be randomised to
1) Individualised Lifestyle Intervention Experimental - Women randomised to this arm
will receive an intervention program that consists of individual weight loss diet and
physical activity goals incorporated into a 2-year standardised structured telephone
and mail-based intervention In addition to diet and physical activity the intervention
will address behavioural and motivational issues relating to weight management
including maintaining motivation overcoming obstacles to success relapse
prevention emotional distress and stress and time management The telephone
intervention will involve 19 phone calls as well as mailings and a participant manual
women will be asked to lose up to 10 of their weight by reducing their caloric and
fat intake (by 500-1000 kcalday 20 calories fat) and increasing their moderate
physical activity (to 150-200 minutesweek)
2) Mail-based Active Comparator - Participants will receive a standardised mail-based
intervention focussing on healthy living This will include mailings at study entry as
well as a 2-year subscription to health magazine
Approximately 2150 women will be enrolled follow-up will continue until target event rates
have been met (anticipated 4-6 years after completion of the intervention) This sample size
will provide 80 power (type 1 error 005 2-tailed) to detect a hazard ratio (HR) for DFS of
074-076 in the weight loss intervention arm
b) COLORECTAL CANCER
It has been suggested that interventions to improve QoL in colorectal cancer survivors are
more effective if they target symptom management psychosocial support and lifestyle
variables in a comprehensive and integrated approach to behavioural change (Steginga et
al 2009) Due to the paucity of comprehensive trials examining behavioural interventions in
this group of survivors Hawkes et al (2009) are conducting a large-scale RCT of a 6-month
telephone-delivered lifestyle coaching intervention based on Acceptance and Commitment
111
Therapy (ACT) ndash bdquoCanChange‟ The intervention aims to assist colorectal cancer survivors
(n=350) to make improvements in lifestyle including physical activity weight management
and smoking cessation Participants receive up to eleven telephone sessions over the
6-months from a qualified health professional who provides support on symptom
management and lifestyle change Outcomes will be assessed post-intervention at 6- and
12-months follow-up and will include physical activity CRF QoL and cost-effectiveness
The findings from this innovative lifestyle coaching initiative will offer insight into the intensity
of support required to achieve sustained behaviour change as well as highlight the efficacy
of various components of delivery (eg telephone-delivery coaching professionally-led
etc)
Courneya et al (2008) are leading a physical activity intervention in a collaboration between
Canada and Australia the Colon Health and Life-Long Physical activity Change
(CHALLENGE) a 3-year multicentre RCT for colon cancer survivors (n=1000) who are 2-6
months post adjuvant-treatment Any type of physical activity will be promoted the goal
being to motivate people to increase their overall activity by about 25-hours of moderate
intensity physical activity or 1-hour and 15-minutes of vigorous physical activity per week
Behavioural support counselling and supervised physical activity sessions will be used to
promote the adoption and long-term maintenance of physical activity By monitoring
participants over 10-years the trial will determine if colon cancer recurs less often in people
who increase and maintain their physical activity It will also assess whether physical activity
improves other important outcomes including QoL anxiety depression sleep and physical
function It is anticipated that this trial will provide important insight into strategies for
promoting long-term health behaviour change
Another Australian lifestyle intervention is The Colorectal Cancer and Quality of Life led
by Joanne Aitken The purpose of this project is to identify any patterns between lifestyle and
QoL over the first 5-years following a diagnosis of colorectal cancer Approximately 2000
people have been recruited to take part in this study making it the largest colorectal cancer
study of its type to be undertaken Participants complete a telephone interview and a written
Pilot testing demonstrated that
o 80 of participants (n=20) felt the intervention addressed their issues
o 100 felt more motivated to make lifestyle changes
o 100 would recommend the intervention to other survivors
From baseline to post-intervention improvements
were observed for
o Colorectal cancer symptoms o QoL o Diet o Physical activity
112
questionnaire on an annual basis over the 5-years One of the aims of the study is to
uncover how lifestyle factors particularly physical activity may improve QoL and reduce the
risk of developing other chronic diseases that cancer survivors are prone to such as heart
disease and diabetes This information will help Cancer Council Queensland properly design
and target lifestyle interventions to help improve the health and well-being of colorectal
cancer survivors (Aitken et al ongoing)
113
DISCUSSION
WHAT DO WE KNOW ABOUT LIFESTYLE AND CANCER
This aim of this review was to update the World Cancer Research Fund (WCRF) report bdquoA
Systematic Review of RCTs Investigating the Effect of Nutritional and Physical
Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This has been
achieved by conducting a comprehensive but pragmatic search of the literature from 2006
onwards Where no evidence was available in the WCRF review studies before 2006 have
been included if identified in the reference lists of acquired records To facilitate this
evidence cited within the lsquoHandbook of Cancer Survivorship‟ (Feuerstein 2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (2009) were also utilised
Before presenting a synthesis of the findings within this review there are some limitations
that first need to be addressed
Methodological Limitations
There is strong evidence from observational studies that lifestyle factors can potentially have
major influences on overall mortality risk for cancer survivors This has been most frequently
subjected to study in breast cancer survivors However it is recognised that such
associations in observational studies can be influenced by confounding and therefore that
the mechanisms of lifestyle change on all-cause mortality remains unclear (Cheblowski
2010) Therefore although the observational evidence is strong there is a need to
understand the benefits of lifestyle change ndash particularly physical activity and weight control
in the absence of confounding factors which can be achieved only within the context of a
controlled trial (Ballard-Barbash et al 2009) Such evidence in the end is most likely to
lead to promoting the wide scale adoption of lifestyle change interventions in the role of
secondary prevention of cancer
Consistent with Bekkering et al (2006) it has been found that there is a paucity of robust
evidence on the effects of lifestyle behaviours in cancer progression and recurrence as well
as in the prevention and management of the long-term health implications of cancer
treatment Studies generally comprise small sample sizes and few offer evidence of the
long-term effects of lifestyle behaviours Since lifestyle choices are generally behavioural in
nature the sustainability of these behaviours is fundamental if commissioners are to provide
funding for lifestyle interventions
There were also a large number of retrospective studies particularly for smoking This is
understandable given the challenges of research within this area however it does also raise
limitations surrounding the accuracy of findings This is especially the case when findings
rely on retrospective self-reports of health behaviours or illness experience
114
A number of methodological limitations confound the interpretation of the benefits of exercise
and diet after a diagnosis of cancer from other risks such as smoking body size
supplements and analgesic intake Nevertheless as highlighted by Doyle et al (2007) even
when the scientific evidence is incomplete reasonable conclusions can be made on issues
that can guide lifestyle choices for cancer survivors These are discussed next
THE EVIDENCE
Diet
Evidence for reducing fat intake remains unclear yet evidence for the mechanisms of benefit
of weight loss or the maintenance of a healthy weight is strong Weight control and self-
management clearly requires consideration of total fat intake highlighting the necessity to
provide cancer survivors with advice on levels of fat necessary for weight maintenance
weight loss or in some cases weight gain (Chlebowski et al 2005 Patterson et al 2010)
The same rationale applies to any inconsistencies in evidence for increased fruit and
vegetables which can also facilitate weight management Indeed where the evidence is
strongest for fruits and vegetables applies to those sources containing carotenoids The
evidence is convincing that carotenoids do provide anti-cancer properties (Rock et al 2005
Pierce et al 2007) Lycopene (found in tomatoes) is one such carotenoid found to offer
anti-cancer benefits (Schwarz et al 2008)
Fibre (found in the skins of fruit and vegetables as well as in beans and lentils) and folate
(found in broccoli brussel sprouts asparagus and peas) have in the main been found to
protect against colorectal cancer The evidence is convincing that by slowing down bowel
transit time the mechanism of benefit comes from reducing contact between potential
carcinogens
The benefits of a low fat high fruit and vegetable diet extend into the management of
treatment-related conditions such as lymphoedema In individuals carrying excess weight
the resulting weight loss achieved via a low fat high fruit and vegetable diet can ease the
symptoms of lymphoedema (Shaw Mortimer and Judd 2007)
The evidence also suggests that survivors of prostate cancer might benefit from including
pomegranate juice and green tea in their diet
In terms of other food sources vitamin D and calcium can be protective against osteoporosis
(Ryan et al 2007) although more research with a specific fouls on cancer survivors is
needed in this area
Physical Activity
In general the findings of epidemiological and large cohort studies demonstrates that the
evidence for the role of physical activity in improving breast cancer prognosis quality of life
and on the levels of several hormones associated with breast cancer is strong
115
There is substantial evidence suggesting that the physical activity recommendations
developed by the Department of Health are sufficient for cancer survivors - a total of at least
30-minutes a day of moderate intensity physical activity on five or more days of the week
This can be achieved either by doing all the daily activity in one session or through several
shorter bouts of activity of 10 minutes or more Additionally there is evidence of a dose-
response (ie the more physical activity the greater any benefits) The evidence for breast
cancer further suggest that for survival benefits to be achieved from physical activity no less
than moderate to vigorous activity is required (Gross et al 2002) However the most recent
expert advice emphasises that even a modest amount of exercise like brief walks is
beneficial and gains will be seen versus doing nothing at all38
The interpretation of physical activity evidence has been hindered by the difficulty of
distinguishing physical activity outcomes from subsequent weight loss outcomes However
again even if the main mechanism of benefit of physical activity is improved outcomes
resulting from weight loss or maintenance then this could be considered strong enough
evidence to prescribe physical activity to cancer survivors Furthermore the evidence is
encouraging in terms of its QoL-enhancing effect (McNeeley et al 2006 Daley et al 2007)
Three specific elements of physical activity interventions or advice could be addressed
(Ballard-Barbash et al 2006)
Reducing sedentary behaviours (such as watching TV)
Exercise sessions
Type and intensity of physical activity
There is sufficient evidence for supervised physical activity improving symptoms of cancer-
related fatigue (McNeely et al 2006 Cramp and Daniel 2008) and lymphoedema (Moseley
and Pillerlsquos 2008) Indeed the evidence suggests that guided progressive physical activity
soon after treatment can ease the symptoms of lymphoedema (de Rezende et al 2006)
This supports recent cautions regarding risk-averse clinical recommendations guiding
survivors to avoid the use of the affected limb which may actually lead to de-conditioning
and the very outcome women seek to avoid (Schmitz 2010) At the very least there is no
evidence of appropriate intensity physical activity causing or exacerbating either fatigue or
limb swelling The same is true for the effect of physical activity on osteoporosis Whilst the
benefits of physical activity on bone health require clarifying physical activity can at the very
least prevent loss of bone mineral density in survivors at particular risk of developing
osteoporosis (Waltman et al 2009)
A recent roundtablelsquo event by the American College of Sports Medicine has produced a
Consensus Statement detailing exercise guidelines for cancer survivors (Schmitz Courneya
and Matthews et al 2010) An expert panel reviewed the published empirical evidence and
came to the consensus regarding the safety and efficacy of exercise testing and prescription
in cancer survivors The evidence is clear that exercise during treatment (specific risk
assessment can be carried our for specific treatments and biological response) and after
38
Dr Rachel Ballard ndash Barbash in the NCI Cancer Bulletin June 29 2010
116
treatment is safe and effective Activity induced improvements can be expected on aerobic
fitness muscular strength quality of life and fatigue in breast prostate and haematological
cancers Resistance training can be performed safely by breast cancer survivors with and at
risk of lymphoedoema
Efforts are currently being made to increase the capacity and capability of exercise
professionals to address the unique needs of cancer survivors Exercise professionals need
to be able to access training which reflects the medical condition they are treating for to be
more knowledgeable about the condition and the most suitable and appropriate exercises for
them This requires the development of a national competency framework for a specialist
level 3 add on or level four qualification This would enable providers to develop national
training programmes for cancer specialist exercise professionals and lead to more
accessible referral through the exercise referral scheme (Exercise Referral Research March
2010)
Smoking
Strong and consistent evidence has been presented for increased risk of disease
progression and mortality in people who continue to smoke after a diagnosis of cancer as
well as poorer outcomes in pre-diagnosis smokers (Parsons et al 2010) This evidence
applies particularly to cancers of the lung or head and neck Further research is needed for
breast colorectal prostate and rarer cancers
Alcohol
There is a paucity of research into the effects of alcohol pre- and post-diagnosis on cancer
progression and recurrence as well as symptom management Evidence thus far is highly
contradictory with some demonstrating a protective effect some a detrimental effect and
others no effect
Weight
Substantial weight gain after diagnosis and treatment for breast cancer is adversely
associated with breast cancer prognosis Obesity appears to increase the risk of recurrence
and death among breast cancer survivors by around 30 (Patterson et al 2010) Much
more research is needed to clarify the relationship between prognosis and survival and body
weight in other tumour types
Dealing with issues of weight weight gain and weight management with patients is one of
the lifestyle behaviour change issues health care professionals feel most challenged by
Studies do confirm that health care professionals find it difficult to address these issues with
patients without appearing biased and negative It would appear that a lack of professional
training on behavioural change and motivational coaching and effective strategies for weight
117
loss combine and can lead to avoidance by health care professionals in addressing the need
for change (Puhl and Heuer 2009 Blakeman et al 2010)
Mechanisms of Benefit
Chlebowski (2010) offers some thought-provoking insight into the challenge of implementing
lifestyle change when aromatase inhibitors have been found to reduce oestrogen levels far
more than physical activity interventions One study cites approximately 90 reductions in
oestrogen levels as a result of aromatase inhibitors (Dixon et al 2008) Furthermore three
trials comparing aromatase inhibitors versus placebo anticipate 60-70 reduction in breast
cancer risk (Cuzick 2005 Goss et al 2007 Visvanathan et al 2008) Equally Chlebowski
(2010) points out that the influence of physical activity on insulin levels also has a
pharmacological competitor in the form of metformin (Goodwin et al 2008 Jiralerspong et
al 2009)
These are valid insights that are likely to complicate the successful integration of lifestyle
advice into standardised models of aftercare On the other hand if a public and community
health approach is taken to health and well-being then lifestyle change is likely to offer
health benefits beyond cancer-specific health Such an approach is recommended in the
bdquoCapabilities for Supporting Prevention and Chronic Condition Self-Management A
Resource for Educators of Primary Health Care Professionals‟ developed as part of the
Australian Better Health Initiative (Flinders University 2009) The model offered within this
capabilities framework promotes healthcare providers to view patients holistically as
opposed to focusing solely on diagnosed chronic condition The rationale for this in part
lies in the fact that chronic conditions are more often than not accompanied by co-
morbidities and therefore healthcare is not only about the established condition but also
identified risk factors for co-morbidity
MAKING LIFESTYLE RECOMMENDATIONS FOR CANCER SURVIVORS
In terms of reducing the risks of relapse evidence is strongest for breast colorectal lung
and head and neck cancers but self-management lifestyle strategies are likely to be person-
specific rather than disease or treatment specific so are likely to apply to all patients
recovering from cancer
Diet Appendix A provides evidence-based dietary recommendations that can be made in
light of the findings within this review and national health recommendations These
recommendations comprise a varied diet ensuring adequate intake of vitamins essential
minerals fibre essential fatty acids and antioxidants by eating less fat and more green and
cruciferous vegetables fruits and berries nuts and grains and healthy oils (unsaturated fats
omega)
Physical Activity In terms of physical activity based on the evidence within this report
the five a weeklsquo recommendation is just as relevant to cancer survivors as to the general
population Indeed these recommendations are also provided by the American Cancer
Society (Doyle et al 2006) as advised by a large expert panel Appendix B provides
118
suggestions for physical activity Forty-five to 60-minutes of intentional physical activity are
preferable as the benefits of physical activity do appear to be greater with increased physical
activity Even when this might seem too much survivors can be reminded that the minimum
30-minutes for 5 days a week can be tailored to individual needs and capabilities For
example graded or progressive physical activity can be utilised for those experiencing
fatigue whilst shorter physical activity sessions can be spread out across the day
Other Lifestyle Factors Body Weight In addition it is recommended that obesity (BMI
gt35 Kgm2) excessive alcohol consumption and smoking are avoided There is also
evidence that maintaining a steady healthy weight as opposed to fluctuating between a
healthy and unhealthy BMI can offer health benefits for cancer survivors (Wright et al
2007)
The evidence within this review are indicative of challenges with adherence supporting
findings from Uhley and Jen (2006) that intensive resource-heavy individualised guidance
and support is required to achieve significant long-term lifestyle change This further
emphasises the need to tailor and prescribe such interventions on a needs basis via
individualised assessment and risk stratification
Integrating Self-Management Lifestyle Strategies into Routine Care
Adopting a paternalistic approach and simply telling people is not enough If the medical
community want to help their patients embark on a road of recovery which includes dietary
change and regular exercise there has to be a comprehensive and well-funded package of
education guidance and support Attitude and culture change is imperative both to tackle the
myths and preconceptions around lifestyle factors and their influence on cancer prognosis
symptom management and a future healthy life on the part of both patients survivors and
health care professionals The bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative offers a comprehensive
framework for integrating self-management support into healthcare services (Flinders
University 2009) The emphasis is on not merely striving to change patient behaviour but
also making efforts towards organisational change
Cancer Research UK Diabetes UK and the British Heart Foundation have joined together to launch a new campaign to raise awareness of the dangers of carrying excess weight around the middle The Active Fatlsquo campaign encourages people to measure their waistlines and make positive changes to their lifestyles if they are at risk The emphasis is on educating the public that fat cells are actively working away at stimulating diseases such as cancer diabetes and heart attacks
119
The model offered within this capabilities framework promotes healthcare providers to view
patients holistically as opposed to focusing solely on the diagnosed chronic condition The
rationale for this in part lies in the fact that chronic conditions are more often than not
accompanied by co-morbidities and therefore healthcare is not only about the established
condition but also identified risk factors for co-morbidity The framework also identifies the
need to provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for healthcare
professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
Evidence based information emphasising the importance of lifestyle ideally should be
formally introduced into routine clinical practice early in the treatment pathway and re-
enforced at regular intervals thereafter This ensures patients and their relatives do not miss
the teachable moment where they are most susceptible to positive advice (Demark-
Wahnefried et al 2005) This requires close work with clinicians specialist nurses patients
and advocacy groups to enable information about new strategies to be integrated into
existing local information pathways and materials Indeed the new information prescriptions
currently being pilot tested provide ample opportunity for integrating lifestyle advice into
survivorship care plans
Information clearly has an important role to play in influencing lifestyle behaviours However
people need more than knowledge to be healthy they need the skills to change if they are to
bring about changes in often complex and habitual lifestyle behaviours (Robertson 2008)
Before investing time and money on patient information materials it is necessary to convince
the consultants other direct clinical staff and organisers of clinical services that lifestyle
advice is a priority and to re-allocate resources to enable sufficient time to discuss these
issues within routine consultations One study for example found that patients who were
encouraged by their oncologist exercised significantly more than patients who did not
(Segar et al 1998) The next step is to back up the medical consultation with further
practical verbal and written advice from specialist nurses or information officers One UK
oncology unit for example does this as part of a formal lifestyle interview together with a
bespoke lifestyle information toolbox (Thomas and Nicholson 2009) During this interview
patients can be referred to smoking cessation clinics nutritionists and physiotherapists
where necessary The specialist nurse conducting this interview provides written information
and advice to patients and just as importantly their friends and family about local support
groups dietary measures where to buy healthy foods and specific local exercise facilities
which may entice them ranging from ballroom line and salsa dance lessons aerobics yoga
and fitness classes local walking swimming and cycling groups through to gyms sport
centre tennis and badminton courts and Pilates classes giving times contact numbers and
locations to make it as easy as possible to follow the advice The rationale for these
120
interviews is that individualised lifestyle counselling is more likely to elicit a response than
generic general advice The specialist nurse then follows up the advice by telephone and
further consultations as prompting has been shown to improve update A study from North
Bedfordshire for example showed that although 52 of patients accepted referral for
exercise in a local Gym a further 23 decided to attend classes only after additional
prompting from the nurse either by telephone
Many UK Oncology Units already have instigated an exit interview system to discuss follow
up arrangements and this process could be expanded to include lifestyle counselling
provided the specialist nurses involved have received extra training This training should
include a knowledge of the evidence and importance of weight diet physical activity and
smoking after cancer as well as ways to appropriately advise home-based exercise
regimens and how to direct patients towards the myriad of council or independent exercise
activities available locally to them The courses may require additional communication and
motivational skills training to enable nurses to engage in a partnership relationship which
promotes addressing the patientlsquos agenda goals and motivation around achieving and
maintaining behaviour change Examples of a range of courses aimed to develop such skills
and competencies and which are provided by the Flinders Human Behaviour and Health
Research Unit include a Chronic Condition Self-Management workshop Communication
and Motivational Skills Workshop and a Living Well Workshop
Remaining Questions
This review has provided some clarification of the evidence pertaining to lifestyle and cancer
outcomes However in implementing this evidence into standardised practice within cancer
aftercare will require a number of questions to be explored
1) What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
At present it is unclear how soon after a cancer diagnosis an intervention should be
introduced for behaviour change(Rabin 2009) Until the teachable moment is more clearly
defined for cancer patients the advice is that professionals should repeatedly offer to assist
a patient with addressing their health behaviour risks until the patient accepts or seeks other
forms of support
The literature suggests that professional involvement in supported self-management and
lifestyle advice is required in order to maintain patient motivation by enhancing patient
engagement with health information and advice When information is supplied by healthcare
professionals and the patient is supported in using this information legitimacy is provided to
the information and advice (Protheroe et al 2008) Efficacy outcomes in terms of lifestyle
advice and behavioural change are fundamental in the initiation and maintenance of a
healthy lifestyle and the involvement of healthcare professionals strengthens outcome
efficacy whilst also motivating the patient and increasing their own self-efficacy to adapt their
lifestyle (Irwin 2008) However there is anecdotal and other evidence that on the one hand
the importance of lifestyle factors on the prognosis survival and symptom management of
121
cancer survivors is poorly understood and appreciated by significant numbers of cancer
health care professionals and on the other hand they do need specific training in the key
communication skills to be able to support effective behaviour change with their patients A
review is currently underway investigating the role of patient-professional communication in
terms of self-management
2) How can people most likely to benefit from lifestyle interventions be effectively
identified
A recent review on cancer-specific self-management programmes highlighted that patients
can be risk stratified according to needs and this according to whether they are likely to
benefit from the programme (Davies and Batehup 2010) For example people with low
levels of social support have been found to benefit most from group-delivered support As
part of the Bournemouth after Cancer Survivorship Project Active Wellness Programmelsquo
patients are assessed for the readiness to take part in physical activity (Milne et al 2010) It
is recommended that questionnaires that might facilitate such evidence-based risk
stratification be evaluated in order to provide further insight into this question A set of risk
stratification tools would be one way of ensuring cost-effectiveness
3) What are the various intensities of lifestyle support that can be provided based on
levels of individual need
As demonstrated within this review lifestyle interventions and self-management support do
generally require some level of support in order to be successful A strong
patientprofessional partnership appears to be at the essence of this intensive approach as
does longer-term follow-up and support (Davies and Batehup 2010) Addressing this
question will also in part address some of the inequalities within the current system of
cancer care with survivors identified as having low literacy being provided with extra
informational support and assistance with understanding the lifestyle recommendations
being made
122
Appendix A Evidence-Based Dietary Self-Management Recommendations
Food Advice Evidence
Reduce Saturated Fats
Unless underweight avoid processed fatty foods cakes biscuits crisps and other fatty snacks pastries cream and fried foods Cut the fat off the meat and check serum cholesterol regularly
(Ingram 1994 Hebert et al 1998 Norat et al 2004 Thomas et al 2009)
Increase all fish intake
All fresh fish but particularly the oily varieties such as mackerel and sardines Fresh water fish such as trout have the advantage of avoiding the potential heavy metal contamination of tuna amp sword fish which some suggest should not be eaten more than twice a week
(Ornish et al 2005 Meyerhardt et al 2007 Goodwin et al 2009)
Essential minerals
Vary the diet to ensure intake of adequate quantities of essential minerals consider Mixed nuts including Brazils Seafood including sardines prawns and shell fish Pulses and grains Vary carbohydrate sources such as pasta rice different brands of potatoes pulses such as lentils and quinoa
Rohan et al 1993) Powers et al 2007 McTiernan et al 2009)
Dietary Vitamins
Fresh fruit raw and calciferous vegetables grains oily fish nuts and salads Unless you have diarrhoea try to increase the amount of ripe fruit you eat each day ideally by eating the whole fruit Freshly squeezed fruit juices are recommended
(Rohan et al1993 Ingram 1994 Fleischauer et al 2003 New et al 2004 Rock et al 2005 McEligot et al 2006 Meyerhardt et al 2007 Schwarz et al 2008 Goodwin et al 2009)
Polyphenols
Onions leeks broccoli blueberries red wine tea apricots pomegranates chocolate coffee blueberries kiwis plums cherries ripe fruits parsley celery tomatoes mint citrus fruit
(Bettuzzi et al 2006 Pantuck et al 2006 Schwarz et al 2008 McLarty et al 2009)
Phytoestrogens
Soybeans and other legumes including peas lentils pinto (baked beans) and other beans and nuts (supplements not recommended)
Marini et al (2008)
Increase Carotenoids (Lycopene)
Tomatoes tomato sauce chilli carrots green vegetables and dark green salads
(Ingram 1994 Rock et al 2005 McEligot et al 2006 Pierce et al 2007 Powers et al 2007 Thomson et al 2007 Schwarz et al 2008)
123
Appendix B Evidence-Based Physical Activity Recommendations
Category Advice Evidence
Resistance Exercise
Strength training has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce fatigue and improve lean body mass and muscle strength Personalised tailored resistance exercise based on fitness assessments can improve QoL
Segal et al (2003) Poudevigne et al (2009) Courneya et al (2007) (Segal et al 2009)
Aerobic Exercise Aerobic exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of lymphoedema prevent loss of bone mineral density and reduce body fat Walking is particularly popular
Hayes Hildegard and Turner (2009) Schwartz Winters-Stone and Gallucci (2007) Courneya et al (2007) Fillion et al (2008) Kenfield et al (2009) Windsor Nichol and Potter (2004) Chang et al (2008)
Combined Resistance and Aerobic Exercise
Combined aerobic and resistance exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of fatigue and improve QoL
Coleman et al (2003) Milne et al (2008)
3gt MET-hours per week
Benefits of physical activity require 3 or more MET-hours per week (eg using a stationary bicycle for one-hour)
Holick et al (2008) Holmes et al (2005) Saxton et al (2010) Kenfield (2010)
Moderate intensity
Physical activity needs to be of at least moderate intensity in order to offer beneficial outcomes
Holick et al (2008) Patterson et al (2010) Holmes et al (2005) Saxton et al (2010) Campbell et al (2007) Poudevigne et al (2009) Tardon et al (2004)
Dose-Response Exercise can be dose-responsive thus taking part in more than 3 MET-hours per week is likely to offer greater benefits
Meyerhardt et al (2005) Kenfield (2010)
During Treatment Remaining active during treatment can help with symptoms such as fatigue as well as increase completion rates for chemotherapy
Chang et al (2008) Coleman et al (2003) Courneya et al (2007)
Home-Based
Home-based physical activity prescriptions either supervised or alone have proven effective in improving cancer outcomes including reducing fatigue and protecting bone mineral density
Ligibel et al (2008) Windsor Nichol and Potter (2004) Schwartz Winters-Stone and Gallucci (2007)
Supervised Supervised physical activity either at home in groups or during treatment have proven effective in improving cancer outcomes as well as reducing lean body mass and facilitating the completion of chemotherapy
Chang et al (2008) Coleman et al (2003) Velthuis et al (2009) Courneya et al (2007) Campbell
et al (2007) exercise (Soliman et al 2009)
124
References
Abrahamsen JF Andersen A Hannisdal E et al Second malignancies after treatment of Hodgkins disease the influence of treatment follow-up time and age J Clin Oncol 11 (2) 255-61 1993 Addington-Hall et al (2010) Older womenlsquos experience of breast cancer alongside other health conditions The EPaN study (Experiences Preferences and Needs of women aged 70 years and over) University of Southampton Funded by Macmillan Cancer Support Ahmed R L W Thomas et al (2006) Randomized Controlled Trial of Weight Training and Lymphedema in Breast Cancer Survivors J Clin Oncol 24(18) 2765-2772 Ainsworth BE et al Compendium of physical activities an update of activity codes and MET intensities Med Sci Sports Exerc 2000 Sep32(9 Suppl)S498-504 Aitken J (ongoing) Colorectal cancer and quality of life study httpwwwcancerqldorgaupageResearch_statisticsVCRCCVCRCC_research_programsLifestyle_and_Cancer [Last accessed 04062010] Akopyan and Bonavida 2006 G Akopyan and B Bonavida Understanding tobacco smoke carcinogen NNK and lung tumorigenesis Int J Oncol 29 (2006) pp 745ndash752 Alberts DS Martinez ME Roe DJ et al Lack of effect of a high-fiber cereal supplement on the recurrence of colorectal adenomas Phoenix Colon Cancer Prevention Physicians Network [Comment] New England Journal of Medicine 2000 April 20342(16)1156-62 Arts CJ Govers CA van den Berg H Wolters MG van Leeuwen P Thijssen JH In vitro binding of estrogens by dietary fiber and the in vivo apparent digestibility tested in pigs J Steroid Biochem Mol Biol 1991 May38(5)621-8 Bandura A (1977) Self-efficacy Toward a unifying theory of behavioural change Psych Rev 84 191 - 215 Barbash-Ballard R Hunsberger S Alciati MH Blaire SN Goodwin PJ McTiernan A(2009) Physical activity weight control and breast cancer risk and survival Clinical trial rationale and design considerations J Natl Cancer Inst 101630-643 Baron JA Beach M Mandel JS et al Calcium supplements and colorectal adenomas Polyp Prevention Study Group Ann N Y Acad Sci 1999889138-45
Bekkering T Beynon R Davey Smith G Davies A Harbord R Sterne J Thomas S and Wood L (2006) A systematic review of RCTs investigating the effect of dietal and physical activity interventions on cancer survival updated report World Cancer Research Fund httpwwwdietandcancerreportorg [Last accessed 150210] Bellizzi K M J H Rowland et al (2005) Health Behaviours of Cancer Survivors Examining Opportunities for Cancer Control Intervention J Clin Oncol 23(34) 8884-8893 Bernstein H Cosford P and Williams A (2010) Enabling effective delivery of health and wellbeing an independent report Department of Health February 2010
125
Bettuzzi et al 2006 S Bettuzzi M Brausi F Rizzi G Castagnetti G Peracchia and A Corti Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia a preliminary report from a one-year proof-of-principle study Cancer Research 66 (2) (2006) pp 1234ndash1240 Bingham SA Day NE Luben R Ferrari P Slimani N Norat T et al Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) an observational study Lancet 20033611496ndash501 Bingham S Riboli E Diet and cancermdashthe European Prospective Investigation into Cancer and Nutrition Nat Rev Cancer 20044206ndash15 Blakeman T Bower P Reeves D Chew-Graham C (2010) ―Bringing self management into clinical view a qualitative study of long term condition management in primary care consultations Chronic Illness 0 1-15 Blackburn G L and K A Wang (2007) Dietary fat reduction and breast cancer outcome results from the Womens Intervention Nutrition Study (WINS) Am J Clin Nutr 86(3) 878S-881 Bonithon-Kopp C Kronborg O Giacosa A Rath U Faivre J Calcium and fibre supplementation in prevention of colorectal adenoma recurrence A randomised intervention trial Lancet 2000356(9238)1300-6 Borugian MJ Sheps SB Kim-Sing C Olivotto IA Van Patten C Dunn BP Coldman AJ Potter JD Gallagher RP Hislop TG Waist-to-hip ratio and breast cancer mortality Am J Epidemiol 2003 Nov 15158(10)963-8 Boyapati SM Shue X et al (2005) Soyfood intake and breast cancer survival a follow up of the Shanghai Breast Cancer Study Breast Cancer Research and Treatment 92(1) p11-17 Boyd NF Stone J Vogt KN Connelly BS Martin LJ Minkin S Dietary fat and breast cancer risk revisited a meta-analysis of the published literature Br J Cancer 2003 Nov 389(9)1672-85 Box R Marnes T amp Robertson V Aquatic physiotherapy and breast cancer related lymphoedema 5th Australasian Lymphology Association Conference Proceedings Mar 2004 47-9 Brown J K T Byers et al (2003) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 53(5) 268-291 Cade JE Burley VJ Greenwood DC UK Womens Cohort Study Steering Group Dietary fibre and risk of breast cancer in the UK Womens Cohort Study Int J Epidemiol 2007 Apr36(2)431-8 Caan B B Sternfeld et al (2005) Life After Cancer Epidemiology (LACE) Study A cohort of early stage breast cancer survivors (United States) Cancer Causes and Control 16(5) 545-556
126
Caan BJ Kwan ML Hartzell G Castillo A Slattery ML Sternfeld B Weltzien E Pre-diagnosis body mass index post-diagnosis weight change and prognosis among women with early stage breast cancer Cancer Causes Control 2008 Dec19(10)1319-28 Cadmus L A P Salovey et al (2009) Physical activity and quality of life during and after treatment for breast cancer results of two randomized controlled trials Psycho-Oncology 18(4) 343-352 Campbell KL Westerlind KC Harber VJ Bell GJ Mackey JR Courneya KS (2007) Effects of aerobic exercise training on oestrogen metabolism in premenopausal women a randomized controlled trial Cancer Epidemiol Biomarkers Prev 16731ndash73 Cancer 52 and NCSI Research Workstream (2009) Less common cancers consultation Report June 2009 Cella D (2009) Quality of life in patients with metastatic renal cell carcinoma The importance of patient-reported outcomes Cancer treatment reviews 35(8) 733-737 Chan JM Gann PH and Giovannucci EL (2005) Role of diet in prostate cancer development and progression Journal of Clinical Oncology 23(32) p 8152-60 Chlebowski RT Aiello E McTiernan A Weight loss in breast cancer patient management Journal of Clinical Oncology 20(4) 1128-1143 2002 Chlebowski RT Blackburn GL Elashoff RE Thomson C Goodman MT Shapiro A Giuliano AE Karanja N Hoy MK Nixon DW and The WINS Investigators (2005) Dietary fat reduction in post-menopausal women with primary breast cancer Journal of Clinical Oncology (10) p 3s Chlebowski R G Blackburn et al (2006) Dietary fat reduction and breast cancer outcome interim efficacy results from the Womens Intervention Diet Study J Natl Cancer Inst 98 1767 - 1776 Chlebowski RT Blackburn GL (2007) Diet and breast cancer recurrence JAMA 2007 Nov 14298(18)2135 author reply 2135-6 Chlebowski RT (2010) Lifestyle and breast cancer risk The way forward Journal of
Clinical Oncology Vol 28 No 9 (March 20) 2010 pp 1445-1447
Cho E Spiegelman D Hunter DJ Chen WY Colditz GA Willett WC Premenopausal dietary carbohydrate glycaemic index glycaemic load and fiber in relation to risk of breast cancer Cancer Epidemiol Biomarkers Prev 2003 Coulter A and Ellins J (2006) Patient-focused Interventions A review of the evidence Picker Institute Europe (01865 208100) and Health Foundation Coups E J and J S Ostroff (2005) A population-based estimate of the prevalence of behavioural risk factors among adult cancer survivors and non-cancer controls Preventive Medicine 40(6) 702-711 Courneya K S (2003) Physical activity in Cancer Survivors An Overview of Research Medicine amp Science in Sports amp Physical activity 35(11) 1846-1852
127
Courneya K Booth CM Gill S et al (2008) The colon health and life-long physical activity change trial a randomized trial of the national institute of Canada clinical trials group Current Oncology 15(6) 271-78 Cramp F Daniel J (2008) Physical activity for the management of cancer-related fatigue in adults CochraneDatabaseSystRev 2008 Cuzick J Aromatase inhibitors for breast cancer prevention J Clin Oncol 231636-1643 2005
Cuzick J Hot flushes and the risk of recurrence Retrospective exploratory results from the ATAC trial 30th Annual San Antonio Breast Cancer Symposium San Antonio TX December 13-16 2007 (poster 2069) Daley A H Crank et al (2007) Randomized trial of physical activity therapy in women treated for breast cancer J Clin Oncol 25 1713 - 1721 Daley A S Bowden et al (2008) What advice are oncologists and surgeons in the United Kingdom giving to breast cancer patients about physical activity International Journal of Behavioural Diet and Physical Activity 5(1) 46 Danhauer S Mihalki S Russell G Campbell C Felder L Daley L et al (2009) Restorative yoga for women with breast cancer Findings from a randomized pilot study Psych oncology 18(4) 360-368 Dansinger M L J A Gleason et al (2005) Comparison of the Atkins Ornish Weight Watchers and Zone Diets for Weight Loss and Heart Disease Risk Reduction A Randomized Trial JAMA 293(1) 43-53 Davies NJ and Batehup L (2010) Self-management support for cancer survivors Guidance for developing interventions An update of the evidence National Cancer Survivorship Initiative Macmillan Cancer Support March 2010 Demark-Wahnefried W and Jones L (2008) Promoting a Healthy Lifestyle among Cancer Survivors Haematologyoncology clinics of North America 22(2) 319-342 Deo SV Ray S Rath GK et al (2004) Prevalence and risk factors for development of lymphedema following breast cancer treatment Indian J Cancer 418ndash12 Department of Health (2001) Exercise referral systems A national quality assurance framework Department of Health Report London 2001 Department of Health (2004) At least five a week Evidence on the impact of physical activity and its relationship to health Department of Health Report London 2004 Department of Health (2009a) Internal analysis unpublished Department of Health London Department of Health (2009b) Obesity general information Health survey of England 2008 Department of Health London Department of Health (2009c) Guidance on the routine collection of patient-reported outcome measures (PROMs) p 28 The Stationary Office London
128
De Rezende LF Franco RL de Rezende MF et al Two physical activity schemes in postoperative breast cancer comparison of effects on shoulder movement and lymphatic disturbance Tumori 2006 9255ndash61 de Waard F Ramlau R Mulders Y de Vries T van Waveren S A feasibility study on weight reduction in obese postmenopausal breast cancer patients Eur J Cancer Prev 1993 May 2(3)233-8 Dignam J J B N Polite et al (2006) Body Mass Index and Outcomes in Patients Who Receive Adjuvant Chemotherapy for Colon Cancer J Natl Cancer Inst 98(22) 1647-1654 Dimeo FC Thomas F Raabe-Menssen C et al Effect of aerobic exercise and relaxation training on fatigue and physical performance of cancer patients after surgery A randomised controlled trial Support Care Cancer 2004 12(11)774-9 Dixon JM Renshaw L Young O et al Letrozole suppresses plasma estradiol and oestrone sulphate more completely than anastrozole in postmenopausal women with breast cancer J Clin Oncol 261671-1675 2008
Doyle C L H Kushi et al (2006) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 56(6) 323-353 Dwyer J J Peterson et al (2008) Do Flavonoid Intakes of Postmenopausal Women With Breast Cancer Vary on Very Low Fat Diets Diet and Cancer 60(4) 450 - 460 Eakin E Hayes S and Lawler S (ongoing) Physical activity for Health Using the telephone to promote physical activity-based rehabilitation in ruralremote Australian breast cancer survivors National Breast Cancer Foundation httpwwwuqeduaucprcindexhtmlpage=60214amppid=20928 [Last accessed 300310] Eliassen AH Missmer SA Tworoger SS Spiegelman D Barbieri RL Dowsett M Hankinson SE Endogenous steroid hormone concentrations and risk of breast cancer among premenopausal women J Natl Cancer Inst 2006 Oct 4 98(19)1406-15 Elkort RJ Baker FL Vitale JJ Cordano A Long-term nutritional support as an adjunct to chemotherapy for breast cancer JPEN J Parenter Enteral Nutr 1981 Sep-Oct 5(5)385-90 Enger SM Greif JM Polikoff J Press M Body weight correlates with mortality in early-stage breast cancer Arch Surg 2004139954ndash958 discussion 58ndash60 Eton D T D L Fairclough et al (2003) Early Change in Patient-Reported Health During Lung Cancer Chemotherapy Predicts Clinical Outcomes Beyond Those Predicted by Baseline Report Results From Eastern Cooperative Oncology Group Study 5592 J Clin Oncol 21(8) 1536-1543 Fentiman IS Allen DS Hamed H (2005) Smoking and prognosis in women with breast cancer Int J Clin Pract 591051ndash1054
129
Ferrari P Jenab M Norat T et al Lifetime and baseline alcohol intake and risk of colon and rectal cancers in the European prospective investigation bettinto cancer and nutrition (EPIC) Int J Cancer 2007 121 ( 9 ) 2065 ndash 2072
Feuerstein M (2006) Handbook of Cancer Survivorship New York NY Springer 2006 Fillion L P Gagnon et al (2008) A Brief Intervention for Fatigue Management in Breast Cancer Survivors Cancer Nursing 31(2) 145-159 Findley P amp Sambamoorthi U (2009) Preventive health services and lifestyle practices in cancer survivors A population health investigation Journal of Cancer Survivorship 3 43-58 Fleischauer AT Simonsen N Arab L Antioxidant supplements and risk of breast cancer recurrence and breast cancer-related mortality among postmenopausal women Nutr Cancer 2003 46 15-22 Flinders University (2009) Capabilities for Supporting Prevention and Chronic Condition Self-Management A Resource for Educators of Primary Health Care Professionals Australian Better Health Initiative A joint Australian State and Territory government initiative
Flowers M Thompson PA 2009 t10c12 Conjugated Linoleic Acid Suppresses HER2 Protein and Enhances Apoptosis in SKBr3 Breast Cancer Cells Possible Role of COX2 PLoS ONE 4(4) e5342 doi101371journalpone0005342 Food Standards Agency (2007) FSA nutrient and food based guidelines for UK institutions httpwwwfoodgovukmultimediapdfsnutrientinstitutionpdf [Last accessed 120310] Food Standards Agency (2010) Heightweight chart httpwwweatwellgovukhealthydiethealthyweightheightweightchart [Last accessed 120310] Ford MB Sigurdson AJ Petrulis ES et al Effects of smoking and radiotherapy on lung carcinoma in breast carcinoma survivors Cancer 98 (7) 1457-64 2003 Friedenreich C Cust A Lahmann PH et al Anthropometric factors and risk of endometrial cancer the European prospective investigation into cancer and nutrition Cancer Causes Control 2007 18399-413 Friedenreich C M C G Woolcott et al (2010) Alberta Physical Activity and Breast Cancer Prevention Trial Sex Hormone Changes in a Year-Long Physical activity Intervention Among Postmenopausal Women J Clin Oncol 28(9) 1458-1466 Friedenreich CM Cust AE Physical activity and breast cancer risk impact of timing type and dose of activity and population subgroup effects Br J Sports Med 2008 Aug42(8)636-47 Giovannucci EL (2005) Obesity insulin resistance and cancer risk Cancer Prevention 5 httpwwwnypcancerpreventioncomissue5propro_featurespre_earshtml [Last accessed 03062010]
130
Gold E B J P Pierce et al (2009) Dietary Pattern Influences Breast Cancer Prognosis in Women Without Hot Flashes The Womens Healthy Eating and Living Trial J Clin Oncol 27(3) 352-359 Gonzalez CAPera GAgudo APalli DKrogh VVineis PTumino RPanico SBerglund GSiman HNyren OAgren AMartinez CDorronsoro MBarricarte ATormo MJQuiros JRAllen NBingham SDay NMiller ANagel GBoeing HOvervad KTjonneland ABueno-de-Mesquita HBBoshuizen HCPeeters PNumans MClavel-Chapelon FHelen IAgapitos ELund EFahey MSaracci RKaaks RRiboli E Smoking and the risk of gastric cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC) Int J Cancer 107 (4) 629-634 (2003) Gonzaacutelez CA Jakszyn P Pera G Agudo A Bingham S Palli D Ferrari P Boeing H del Giudice G Plebani M Carneiro F Nesi G Berrino F Sacerdote C Tumino R Panico S Berglund G Simaacuten H Nyreacuten O Hallmans G Martinez C Dorronsoro M Barricarte A Navarro C Quiroacutes JR Allen N Key TJ Day NE Linseisen J Nagel G Bergmann MM Overvad K Jensen MK Tjonneland A Olsen A Bueno-de-Mesquita HB Ocke M Peeters PH Numans ME Clavel-Chapelon F Boutron-Ruault MC Trichopoulou A Psaltopoulou T Roukos D Lund E Hemon B Kaaks R Norat T Riboli E Meat intake and risk of stomach and oesophageal adenocarcinoma within the European Prospective Investigation Into Cancer and Nutrition (EPIC) J Natl Cancer Inst 2006 Mar 198(5)345-54 Goodwin PJ Pritchard KI Ennis M et al Insulin-lowering effects of metformin in women with early breast cancer Clin Breast Cancer 8501-5052008
Goodwin PJ Ennis M Pritchard KI Koo J Hood N (2009) Prognostic Effects of 25-Hydroxyvitamin D Levels in Early Breast Cancer Journal of Clinical Oncology Vol 27 No 23 (August 10) pp 3757-3763 Goodwin PJ Lifestyle Intervention Study in Adjuvant Treatment of Early Breast Cancer (LISA) (ongoing) httpclinicaltrialsgovct2showNCT00463489 [Last accessed 04062010] Goss PE Richardson H Chlebowski RT et al National Cancer Institute of Canada Clinical Trials Group MAP 3 Trial Evaluation of exemestane to prevent breast cancer in postmenopausal women at risk Clin Breast Cancer 7895-900 2007
Gothard L Cornes P et al (2004) Double-blind placebo-controlled randomised trial of vitamin E and pentoxifylline in patients with chronic arm lymphoedema and fibrosis after surgery and radiotherapy for breast cancer Radiotherapy and oncology journal of the European Society for Therapeutic Radiology and Oncology 73(2) 133-139 Grace PB Taylor JI Low YL Luben RN Mulligan AA Botting NP Dowsett M Welch AA Khaw KT Wareham NJ Day NE Bingham SA Phytoestrogen concentrations in serum and spot urine as biomarkers for dietary phytoestrogen intake and their relation to breast cancer risk in European prospective investigation of cancer and nutrition-norfolk Cancer Epidemiol Biomarkers Prev 2004 May13(5)698-708 Greenberg ER Baron JA Tosteson TD et al A clinical trial of antioxidant vitamins to prevent colorectal adenoma Polyp Prevention Study Group[comment] New England Journal of Medicine 1994 July 21331(3)141-7 Gritz ER (1993) Cancer Smoking Epidemiology Biomarkers amp Prevention 2(3) 261-270
131
Gritz E R M C Fingeret et al (2006) Successes and failures of the teachable moment Cancer 106(1) 17-27 Gross G C Ott et al (2002) Postmenopausal Breast Cancer Survivors at Risk for Osteoporosis Physical Activity Vigour and Vitality Oncology Nursing Forum 29(9) 1295-1300 Gross M C Ramirez et al (2009) Expression of androgen and oestrogen related proteins in normal weight and obese prostate cancer patients The Prostate 69(5) 520-527 Guthrie JR Ball M Murkies A Dennerstein L Dietary phytoestrogen intake in mid-life Australian-born women relationship to health variables Climacteric 2000 3 254ndash261 Hawkes A L S Gollschewski et al (2009) A telephone-delivered lifestyle intervention for colorectal cancer survivors a pilot study Psycho-Oncology 18(4) 449-455 Haydon AM Macinnis RJ English DR Giles GG (2006) The effect of physical activity and body size on survival after diagnosis with colorectal cancer Gut 55 p 62-67 Hayes SC Spence RR Galvao DANewton RU (2009) Australian Association for Physical activity and Sport Science position stand Optimising cancer outcomes through physical activity JSciMedSport 200912428-434 Heald AH Cade JE Cruickshank JK Anderson S White A Gibson JM (2003) The influence of dietary intake on the insulin-like growth factor (IGF) system across three ethnic groups a population-based study Public Health Nutr6175ndash80 Healthy Weight Healthy Lives (2008) A Cross-Government Strategy for England Cross-Government Obesity Unit DH and Department of Children Schools and Families Hebert JR Hurley TG Ma Y (1998) The effect of dietary exposures on recurrence and mortality in early stage breast cancer Breast Cancer Res Treat 5117ndash28 Hofstad B Almendingen K Vatn M et al Growth and recurrence of colorectal polyps a double-blind 3-year intervention with calcium and antioxidants Digestion 199859(2)148-56 Holick C N P A Newcomb et al (2008) Physical Activity and Survival after Diagnosis of Invasive Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 17(2) 379-386 Holm LE Nordevang E Hjalmar ML Lidbrink E Callmer E Nilsson B (1993) Treatment failure and dietary habits in women with breast cancer J Natl Cancer Inst 8532ndash36 Holmes MD Hunter DJ Colditz GA et al Association of dietary intake of fat and fatty acids with risk of breast cancer JAMA 1999281914-920 Holmes MD Chen WY Feskanich D Kroenke CH Colditz GA (2005) Physical activity and survival after breast cancer diagnosis JAMA 293 p 2479-86
132
Holmes MD Murin S Chen WY Kroenke CH Spiegelman D Colditz GA (2007) Smoking and survival after breast cancer diagnosis Int J Cancer 1202672ndash2677
Howe GR Hirohata T Hislop TG Iscovich JM Yuan JM Katsouyanni K Lubin F Marubini E Modan B Rohan T et al Dietary factors and risk of breast cancer combined analysis of 12 case-control studies J Natl Cancer Inst 1990 Apr 482(7)561-9
Hunter DJ Spiegelman D Adami HO Beeson L van den Brandt PA Folsom ARFraser GE Goldbohm RA Graham S Howe GR et al Cohort studies of fat intake and the risk of breast cancer--a pooled analysis N Engl J Med 1996 Feb 8334(6)356-61
Ingram D Diet and subsequent survival in women with breast cancer British Journal of Cancer 1994 Mar69(3)592-5
Irwin ML Smith AW McTiernan A Ballard-Barbash R Cronin K Gilliland FD Baumgartner RN Baumgartner KB Bernstein L (2008) Influence of Pre- and Postdiagnosis Physical Activity on Mortality in Breast Cancer Survivors The Health Eating Activity and Lifestyle Study Journal of Clinical Oncology 26(24) 3958-3964
Ishikawa H Akedo I Otani T et al Randomized trial of dietary fiber and Lactobacillus casei administration for prevention of colorectal tumors Int J Cancer 2005 September 20116(5)762-7 Jiralerspong S Palla SL Giordano SH et al Metformin and pathologic complete responses to neoadjuvant chemotherapy in diabetic patients with breast cancer J Clin Oncol 273297-3302 2009
Jones LW Demark-Wahnefried W Diet physical activity and complementary therapies after primary treatment for cancer Lancet Oncol 7(12)1017-26 Nov-Dec 2006 PMID 17138223 Kaaks R A Lukanova and MA Kurzer Obesity endogenous hormones and endometrial cancer risk a synthetic review Cancer Epidemiol Biomark Prev 11 (2002) pp 1531ndash1543 Kaaks R Rinaldi S Key TJ Berrino F Peeters PH Biessy C Dossus L Lukanova A Bingham S Khaw KT Allen NE Bueno-de-Mesquita HB van Gils CH Grobbee D Boeing H Lahmann PH Nagel G Chang-Claude J Clavel-Chapelon F Fournier A Thieacutebaut A Gonzaacutelez CA Quiroacutes JR Tormo MJ Ardanaz E Amiano P Krogh V Palli D Panico S Tumino R Vineis P Trichopoulou A Kalapothaki V Trichopoulos D Ferrari P Norat T Saracci R Riboli E Postmenopausal serum androgens oestrogens and breast cancer risk the European prospective investigation into cancer and nutrition Endocr Relat Cancer 2005 Dec12(4)1071-82 Kawahara M Ushijima S Kamimori T et al Second primary tumours in more than 2-year disease-free survivors of small-cell lung cancer in Japan the role of smoking cessation Br J Cancer 78 (3) 409-12 1998 Keinan-Boker L van Der Schouw YT Grobbee DE Peeters PH Dietary phytoestrogens and breast cancer risk Am J Clin Nutr 2004 Feb79(2)282-8 Kenfield SA (2010) Physical activity and mortality in prostate cancer (In Regular Vigorous Physical Activity found to have Survival Benefits for Prostate Cancer Patients
133
AACR Frontier in Cancer Prevention Research Conference by Tuma R Oncology Times) 32(2) p 29 33 Key TJ Allen NE Hormones and breast cancer IARC Sci Publ 2002156273-6 Khaodhiar L Nixon D Chlebowski RT Elashoff R Blackburn GL Hoy MK Insulin resistance in postmenopausal women with breast cancer Proc Am Cancer Res 2003446349 (abstr) Kim EH Willett WC Colditz GA Hankinson SE Stampfer MJ Hunter DJ Rosner B Holmes MD Dietary fat and risk of postmenopausal breast cancer in a 20-year follow-up Am J Epidemiol 2006 Nov 15164(10)990-7 Korstjens I A M May et al (2008) Quality of Life After Self-Management Cancer Rehabilitation A Randomized Controlled Trial Comparing Physical and Cognitive-Behavioural Training Versus Physical Training Psychosom Med 70(4) 422-429 Krein S M Heisler J Piette F Makki and E Kerr 2005 The effect of chronic pain on diabetes patientslsquo self-management Diabetes Care 28(1)65ndash70 Kroenke CH Fung TT Hu FB Holmes MD Dietary patterns and survival after breast cancer diagnosis J Clin Oncol 2005 Dec 2023(36)9295-303 Kubik AK Zatloukal P Tomasek L Petruzelka L (2002) Lung cancer risk among Czech women a case-control study Prev Med 34(4) 436ndash444 Kucera H [Adjuvanticity of vitamin A in advanced irradiated cervical cancer (authors transl)] Wiener Klinische Wochenschrift Supplementum 19801181-20 Kushi LH Byers T Doyle C et al American Cancer Society Guidelines on Diet and Physical Activity for cancer prevention reducing the risk of cancer with healthy food choices and physical activity CA Cancer J Clin 2006 56 254ndash8 Kyogoku S Hirohata T Nomura Y Shigematsu T Takeshita S Hirohata I Diet and prognosis of breast cancer Nutr Cancer 199217(3)271-7 Lahmann PH Schulz M Hoffmann K Boeing H Tjoslashnneland A Olsen A Overvad K Key TJ Allen NE Khaw KT Bingham S Berglund G Wirfaumllt E Berrino F Krogh V Trichopoulou A Lagiou P Trichopoulos D Kaaks R Riboli E Long-term weight change and breast cancer risk the European prospective investigation into cancer and nutrition (EPIC) Br J Cancer 2005 Sep 593(5)582-9 Lee IM Sesso HD Paffenbarger RS Jr (1999) Physical activity and risk of lung cancer Int J Epidemiol 28(4) 620ndash625 Lev E L (1997) Banduras Theory of Self-Efficacy Applications to Oncology Research and Theory for Nursing Practice 11 21-37 Ligibel J A W Demark-Wahnefried et al (2009) Diet Physical activity and Supplements Guidelines for Cancer Survivors ASCO EDUCATIONAL BOOK 2009(1) 541-547 Lindsay S (2009) Prioritizing illness Lessons in self-managing multiple chronic conditions Canadian Journal of Sociology PhD Thesis ejournalslibraryualbertaca
134
Lucia A Earnest C Perez M (2003) Cancer-related fatigue can physical activity physiology assist oncologists Lancet Oncol 4616-625 Lyons R amp Langille L (2000) Healthy Lifestyle Strengthening the Effectiveness of Lifestyle Approaches to Improve Health Health Canada Ottawa Ontario Available at httpwwwhc-scgccahppbphdddocshealthy MacLennan R Macrae F Bain C et al Effect of fat fibre and beta carotene intake on colorectal adenomas further analysis of a randomized controlled dietary intervention trial after colonoscopic polypectomy Asia Pac J Clin Nutr 1999 8(suppl)S54-S58 Macmillian Cancer Support (2008) Two Million Reasons The Cancer Survivorship Agenda 2008 Maddams J Moller H and Devane C Cancer prevalence in the UK 2008 Thames Cancer Registry and Macmillan Cancer Support 2008 Manjer J Berglund G Bondesson L Garne J P Janzon L Malina J Breast cancer incidence in relation to smoking cessation Breast Cancer Res Treat 61121-129 2000 Mao Y Pan S Wen SW Johnson KC The Canadian Cancer (2003) Physical activity and the risk of lung cancer in Canada Am J Epidemiol 158(6) 564ndash575 Mayne S T B Cartmel et al (2009) Alcohol and Tobacco Use Pre-diagnosis and Postdiagnosis and Survival in a Cohort of Patients with Early Stage Cancers of the Oral Cavity Pharynx and Larynx Cancer Epidemiology Biomarkers amp Prevention 18(12) 3368-3374 McDonald P R Williams et al (2002) Breast cancer survival in African American women Is alcohol consumption a prognostic indicator Cancer Causes and Control 13(6) 543-549 McEligot AJ Largent J Ziogas A Peel D Anton-Culver H Dietary fat fiber vegetable and micronutrients are associated with overall survival in postmenopausal women diagnosed with breast cancer Nutr Cancer 200655(2)132-140 McNeely M L K L Campbell et al (2006) Effects of physical activity on breast cancer patients and survivors a systematic review and meta-analysis CMAJ 175(1) 34-41 McKenzie D C and A L Kalda (2003) Effect of Upper Extremity Physical activity on Secondary Lymphedema in Breast Cancer Patients A Pilot Study J Clin Oncol 21(3) 463-466 McKeown-Eyssen GE Bright-See E Bruce WR et al A randomized trial of a low fat high fibre diet in the recurrence of colorectal polyps Toronto Polyp Prevention Group [erratum appears in J Clin Epidemiol 1995 Feb48(2)i] Journal of Clinical Epidemiology 1994 May47(5)525-36 McLarty Jerry Bigelow Rebecca LH Smith Mylinh Elmajian Don Ankem Murali Cardelli James A (2009) Tea Polyphenols Decrease Serum Levels of Prostate-Specific Antigen Hepatocyte Growth Factor and Vascular Endothelial Growth Factor in Prostate
135
Cancer Patients and Inhibit Production of Hepatocyte Growth Factor and Vascular Endothelial Growth Factor In vitro Cancer Prev Res 1940-6207CAPR-08-0167
McTiernan A et al (2009) Low-fat increased fruit vegetable and grain dietary pattern fractures and bone mineral density the Womens Health Initiative Dietary Modification Trial Am J Clin Nutr 89 1864-1876
Meyerhardt JA Heseltine D Niedzwiecki D Hollis D Saltz LB Mayer RJ Schilsky RL and Fuchs CS (2005) The impact of physical activity on patients with stage III colon cancer Findings from Intergroup trial CALGB 89803 Proc Am Soc Clin Oncol 24 p abstract 3534 Meyerhardt J A D Niedzwiecki et al (2007) Association of Dietary Patterns With Cancer Recurrence and Survival in Patients With Stage III Colon Cancer JAMA 298(7) 754-764 Meyerhardt J A D Niedzwiecki et al (2008) Impact of Body Mass Index and Weight Change after Treatment on Cancer Recurrence and Survival in Patients With Stage III Colon Cancer Findings From Cancer and Leukemia Group B 89803 J Clin Oncol 26(25) 4109-4115 Meyskens FL Jr Kopecky KJ Appelbaum FR Balcerzak SP Samlowski W Hynes H Effects of vitamin A on survival in patients with chronic myelogenous leukemia a SWOG randomized trial Leukemia Research 1995 September 19(9)605-12 Miles A Simon A Wardle J (2010) Answering patient questions about the role lifestyle factors play in cancer onset and recurrences Journal of Health Psychology 15(2) p 291-298 Milne H K Wallman et al (2008) Impact of a Combined Resistance and Aerobic Physical activity Program on Motivational Variables in Breast Cancer Survivors A Randomized Controlled Trial Annals of Behavioral Medicine 36(2) 158-166 Milne M Hamerston L and Morrell D (2010) BACSUP adult survivorship living with and beyond cancer test community learning workshop London January 2010 Monninkhof EM Peeters PH Schuit AJ Design of the sex hormones and physical exercise (SHAPE) study BMC Public Health 2007 Sep 47232 Morrell RM Halyard MY Schild SE Ali MS Gunderson LL Pockaj BA (2005) Breast cancer-related lymphedema Mayo Clin Proc 801480ndash1484 Mortimer P S D O Bates et al (1996) The prevalence of arm oedema following treatment for breast cancer QJM 89(5) 377-380 Mortimer JE Flatt SW Parker BA et al Tamoxifen hot flashes and recurrence in breast cancer Breast Cancer Res Treat 108421-426 2008 Moseley AL Piller NB Carati CJ (2005) The effect of gentle arm physical activity and deep breathing on secondary arm lymphedemaLymphology Sep38(3)136-45 Moseley AL Piller NB (2008) Physical activity for limb Lymphoedema ndash Evidence that it is beneficial Journal of Lymphoedema vol 3(1) pp 51-56
136
Mustian KM Palesh OG Flecksteiner SA Tai Chi Chuan for breast cancer survivors Medicine and sport science 2008 52()209-17 National Cancer Action Team (2009) Cancer and palliative care rehabilitation workforce project A review of the evidence National Cancer Action Team National Comprehensive Cancer Network (2009) NCCN Clinical Practice Guidelines in Oncology Cancer-related fatigue version 1 2009 National Cancer Survivorship Initiative (NCSI) (2009) Research Work Stream Mapping Project - Summary and reports for Bowel Cancer Breast Cancer Lung Cancer Prostate cancer National Cancer Survivorship Initiative Macmillan Cancer Support National Health Service (2010) NHS advice on drinking limits NHS Choices httpwwwdrinkingnhsukquestionsrecommended-levels [Last accessed 300310] National Institutes of Health (1998) Clinical Guidelines on the Identification Evaluation and Treatment of Overweight and Obesity in Adults The Evidence Report National Heart Lung and Blood Institute in cooperation with the National Institute of Diabetes and Digestive Kidney Diseases NIH Publication No 98-4083 National Institutes of Health Osteoporosis and Related Bone Diseases (2009) Conditions and behaviours that increase osteoporosis risk National Resource Centre US Department of Health and Human Services httpwwwniamsnihgovHealth_InfoBoneOsteoporosisConditions_Behaviorsosteoporosis_breast_cancerasp [Last accessed 170210] National Obesity Observatory (2009) Body mass index as a measure of obesity Association of Public Health Observatories June 2009 Ng K J A Meyerhardt et al (2008) Circulating 25-Hydroxyvitamin D Levels and Survival in Patients With Colorectal Cancer J Clin Oncol 26(18) 2984-2991 Nikotetti S Young J Levitt M (2008) Bowel problems self-care practices and information needs of colorectal cancer survivors at 6 to 24 months after sphincter-saving surgery Cancer Nursing 31(5) p 389-398
Norat T Bingham S Ferrari P Slimani N Jenab M Mazuir M Overvad K Olsen A Tjoslashnneland A Clavel F Boutron-Ruault MC Kesse E Boeing H Bergmann MM Nieters A Linseisen J Trichopoulou A Trichopoulos D Tountas Y Berrino F Palli D Panico S Tumino R Vineis P Bueno-de-Mesquita HB Peeters PH Engeset D Lund E Skeie G Ardanaz E Gonzaacutelez C Navarro C Quiroacutes JR Sanchez MJ Berglund G Mattisson I Hallmans G Palmqvist R Day NE Khaw KT Key TJ San Joaquin M Heacutemon B Saracci R Kaaks R Riboli E Meat fish and colorectal cancer risk the European Prospective Investigation into cancer and nutrition J Natl Cancer Inst 2005 Jun 1597(12)906-16
Ornish D et al (2005) Intensive lifestyle changes may affect the progression of prostate cancer The Journal of Urology 174 p 1065-1070 Ostroff JS Jacobsen PB Moadel AB Spiro RH Shah JP Strong EW et al (1995) Prevalence and predictors of continued tobacco use after treatment of patients with head and neck cancer Cancer Jan 1575(2)569-76
137
Pantuck AJ et al (2006) Phase II study of pomegranate juice for men with rising PSA following surgery or RXT for prostate cancer Clin Cancer Res 12(13) p 4018-4026 Pantuck AJ et al Abstract presented at the American Society of Clinical Oncology 2008 Genitourinary Cancers Symposium (Abstract 40) Long Term Follow Up Of Pomegranate Juice For Men With Prostate Cancer And Rising PSA Shows Durable Improvement in PSA Doubling Time Parsons A A Daley et al Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis systematic review of observational studies with meta-analysis BMJ 340(jan21_1) Pastorino U Infante M Maioli M et al Adjuvant treatment of stage I lung cancer with high-dose vitamin A[comment] J Clin Oncol 1993 July11(7)1216-22 Patterson R E L A Cadmus et al Physical activity diet adiposity and female breast cancer prognosis A review of the epidemiologic literature Maturitas In Press Corrected Proof Pedersen BK Saltin B Evidence for prescribing physical activity as therapy in chronic disease Scand J Med Sci Sports 16 Suppl 1 3ndash63 2006Pierce J P L Natarajan et al (2007) Influence of a Diet Very High in Vegetables Fruit and Fiber and Low in Fat on Prognosis Following Treatment for Breast Cancer The Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA 298(3) 289-298 Pierce JP Faerber S Wright FA Newman V Flatt SW Kealey S Rock CL Pierce JP Natarajan L Caan BJ et al Influence of a diet very high in vegetables fruit and fiber and low in fat on prognosis following treatment for breast cancer the Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA2007298(3)289-298 Ponz dL Roncucci L Chemoprevention of colorectal tumors role of lactulose and of other agents Scandinavian Journal of Gastroenterology Supplement 199722272-5 Poudevigne M J Wojcik et al (2009) The Effects Of 12-weeks Cross Training On Fatigue And Mood In Recent Breast Cancer Survivors 2292 Board 180 May 28 200 PM - 330 PM Medicine amp Science in Sports amp Physical activity 41(5) 297-298 Powers H J M H Hill et al (2007) Responses of Biomarkers of Folate and Riboflavin Status to Folate and Riboflavin Supplementation in Healthy and Colorectal Polyp Patients (The FAB2 Study) Cancer Epidemiology Biomarkers amp Prevention 16(10) 2128-2135 Protheroe J A Rogers et al (2008) Promoting patient engagement with self-management support information a qualitative meta-synthesis of processes influencing uptake Implementation Science 3(1) 44 Provenzano E and N Johnson (2009) Overview of recommendations of HER2 testing in breast cancer Diagnostic Histopathology 15(10) 478-484 Puhl RM Heuer CA (2009) ―The stigma of obesity A Review and Update Obesity 17 (5) 941-964 Rabin C (2009) ―Promoting Lifestyle Change among Cancer Survivors When is the Teachable Moment American Journal of Lifestyle Medicine 3 (5) 369-378
138
Reding K W J R Daling et al (2008) Effect of Pre-diagnostic Alcohol Consumption on Survival after Breast Cancer in Young Women Cancer Epidemiology Biomarkers amp Prevention 17(8) 1988-1996 Riboli E Hunt KJ Slimani N Ferrari P Norat T Fahey M Charrondiegravere UR Heacutemon B Casagrande C Vignat J Overvad K Tjoslashnneland A Clavel-Chapelon F ThieacutebautA Wahrendorf J Boeing H Trichopoulos D Trichopoulou A Vineis P Palli D Bueno-De-Mesquita HB Peeters PH Lund E Engeset D Gonzaacutelez CA Barricarte A Berglund G Hallmans G Day NE Key TJ Kaaks R Saracci R (2002) European Prospective Investigation into Cancer and Nutrition (EPIC) study populations and data collection Public Health Nutr 2002 Dec5(6B)1113-24 Richardson G E M A Tucker et al (1993) Smoking Cessation after Successful Treatment of Small-Cell Lung Cancer Is Associated with Fewer Smoking-related Second Primary Cancers Annals of Internal Medicine 119(5) 383-390 Richardson A Addington-Hall J Stark D Foster C Amir Z Sharpe M (2009) Determining research priorities for cancer survivorship Consultation and evidence review Commissioned by the NCSI Robertson R (2008) Using Information to Promote Healthy Behaviours Kings Fund London Rock C L and W Demark-Wahnefried (2002) Diet and Survival After the Diagnosis of Breast Cancer A Review of the Evidence J Clin Oncol 20(15) 3302-3316 Rock C L S W Flatt et al (2005) Plasma Carotenoids and Recurrence-Free Survival in Women With a History of Breast Cancer J Clin Oncol 23(27) 6631-6638 Rohan T Howe G Friedenreich C et al (1993) Dietary fiber vitamins A C and E and risk of breast cancer a cohort study Cancer Causes and Control 4(1) p 29-37 Rosenbaum EH Fobair P Spiegel D (2006) Cancer is a Life-changing Event Cancer Supportive Care Programs httpwwwcancersupportivecarecomSurvivorsurvivehtml [Last accessed January 30 2009] Ryan CW D Huo and K Bylow et al (2007) Suppression of bone density loss and bone turnover in patients with hormone-sensitive prostate cancer and receiving zoledronic acid BJU Int 100 pp 70ndash75 Sagiv SK Gaudet MM Eng SM et al (2007) Active and passive cigarette smoke and breast cancer survival Ann Epidemiol 17385ndash393 Sandel S Judge J Landry N et al (2005) Dance and movement program improves quality-of-life measures in breast cancer survivors Cancer Nursing 28(4) 301-309 Saxton J (2010) Physical activity and cancer mortality In Physical activity and cancer Survivorship Springer New York pp 189-210 Schatzkin A Lanza E Corle D et al Lack of effect of a low-fat high-fiber diet on the recurrence of colorectal adenomas Polyp Prevention Trial Study Group [comment] New England Journal of Medicine 2000 April 20342(16)1149- 55
139
Schmitz KH Courneya KS Matthews C Demark-Wahnefried W et al (2010) ―American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors Medicine and Science in Sports and Exercise Special Communication 0195-9131104207-14090 Schmitz K Holtzman J Courneya K Masse L Duval S Kane R Controlled physical activity trials in cancer survivors A systematic review and meta-analysis Cancer Epidemiol Biomarkers Prev 2005141588ndash95
Schulz M Lahmann PH Boeing H et al Fruit and vegetable consumption and risk of epithelial ovarian cancer the European Prospective Investigation into Cancer and Nutrition Cancer Epidemiol Biomarkers Prev 2005142531ndash2535 Schwarz S U C Obermuller-Jevic et al (2008) Lycopene Inhibits Disease Progression in Patients with Benign Prostate Hyperplasia J Nutr 138(1) 49-53 Schmitz K H Balancing Lymphedema Risk Physical activity Versus Deconditioning for Breast Cancer Survivors Physical activity and Sport Sciences Reviews 38(1) 17-24 10 Segal RJ Reid RD Courneya KS et al(2003) Resistance physical activity in men receiving androgen deprivation therapy for prostate cancer JClinOncol211653-1659
Segal RJ Reid RD Courneya KS Sigal RJ Kenny GP PrudlsquoHomme DGet al Randomized Controlled Trial of Resistance or Aerobic Exercise in Men Receiving Radiation Therapy for Prostate Cancer J Clin Oncol 2009 Jan 2027344-51 Sellers TA Potter JD Folsom AR (1991) Association of incident lung cancer with family history of female reproductive cancers the Iowa Womenlsquos Health Study Genet Epidemiol 8(3) 199ndash208 Severson RK Nomura AM Grove JS Stemmermann GN A prospective analysis of physical activity and cancer Am J Epidemiol 1989 Sep130(3)522-9 Shaw C Mortimer P Judd PA Randomized controlled trial comparing a low-fat diet with a weight-reduction diet in breast cancer-related lymphedema Cancer 20071091949ndash56 Sinicrope F A N R Foster et al Obesity Is an Independent Prognostic Variable in Colon Cancer Survivors Clinical Cancer Research 16(6) 1884-1893 Siris E S P D Miller et al (2001) Identification and Fracture Outcomes of Undiagnosed Low Bone Mineral Density in Postmenopausal Women Results From the National Osteoporosis Risk Assessment JAMA 286(22) 2815-2822 Soliman S W J Aronson et al (2009) Analyzing Serum-Stimulated Prostate Cancer Cell Lines After Low-Fat High-Fiber Diet and Physical activity Intervention eCAM nep031 Sonn GA Aronson W and Litwin MS (2005) Impact of diet on prostate cancer A review Prostate cancer and prostate disease 8 p 304-310 Speck RM Courneya KS Masse L Duval S Schmitz K (2010) An update of controlled physical activity trials in cancer survivors a systematic review and meta-analysis Journal of Cancer Survivorship 4(2) p 87-100
140
Steginga S K B M Lynch et al (2009) Antecedents of domain-specific quality of life after colorectal cancer Psycho-Oncology 18(2) 216-220 Stevinson C H Steed et al (2009) Physical Activity in Ovarian Cancer Survivors Associations With Fatigue Sleep and Psychosocial Functioning International Journal of Gynecological Cancer 19(1) 73-78 Swenson KK Nissen MJ Anderson E Shapiro A Schousboe J Leach J (2009) Effects of physical activity vs bisphosphonates on bone mineral density in breast cancer patients receiving chemotherapy Support Oncol May-Jun7(3)101-7 Tardon A Lee WJ Delgado-Rodriguez M et al Leisure-time physical activity and lung cancer a meta-analysis Cancer Causes Control200516(4)389-397 Taskila T Martikainen R Hietanen P Lindbohm M Comparative study of work ability between cancer survivors and their referents Europ J of Cancer 2007 43914-920 Taylor R Brown A et al (2004) Physical activity-based rehabilitation for patients with coronary heart disease systematic review and meta-analysis of randomized controlled trials The American journal of medicine 116(10) 682-692 Taylor NFDodd KJShields NBruder A Therapeutic physical activity in physiotherapy practice is beneficial a summary of systematic reviews 2002-2005 Aust J Physiother 2007 53 7-16 Thiebaut A C M A Schatzkin et al (2006) Dietary Fat and Breast Cancer Contributions From a Survival Trial J Natl Cancer Inst 98(24) 1753-1755 Thomas R Daly M and Perryman J (2000) Forewarned is forearmed - Randomised evaluation of a preparatory information film for cancer patients European Journal of Cancer 36(2) p 52-53 Thomas R et al (2005) Dietary advice combined with a salicylate mineral and vitamin supplement (CV247) has some tumour static properties - a phase II study Diet and science 2005 35(6) p 436-451 Thomas RJ and Davies ND (2007) Lifestyle during and after cancer treatment Clinical Oncology Vol 19 Issue 8 pp 616-627 Thomas R Nicholson C (2009) Why is exercise good for us Cancer Active httpcanceractivecomcancer-active-page-linkaspxn=2600ampTitle=Why20is20exercise20good20for20us [Last accessed 230710] Thomas R Oakes R Gordon J Russell S Blades M Williams M (2009) A randomised double-blind phase II study of lifestyle counselling and salicylate compounds in patients with progressive prostate cancer Diet and Food Science 39(3) pp 295 ndash 305 Thomson C A N R Stendell-Hollis et al (2007) Plasma and Dietary Carotenoids Are Associated with Reduced Oxidative Stress in Women Previously Treated for Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 16(10) 2008-2015
141
Thune I Brenn T Lund E Gaard M Physical activity and the risk of breast cancer N Engl J Med 336 1269-1275 1997
Travis LB Gospodarowicz M Curtis RE et al Lung cancer following chemotherapy and radiotherapy for Hodgkins disease J Natl Cancer Inst 94 (3) 182-92 2002 Tucker MA Murray N Shaw EG et al Second primary cancers related to smoking and treatment of small-cell lung cancer Lung Cancer Working Cadre J Natl Cancer Inst 89 (23) 1782-8 1997 Twiss J J N Waltman et al (2001) Bone Mineral Density in Postmenopausal Breast Cancer Survivors Journal of the American Academy of Nurse Practitioners 13(6) 276-284 Uhley V and Jen C (2006) Diet and weight management in cancer survivors In Handbook of Cancer Survivorship edited by Feuerstein M New York NY Springer 2006 ISBN-13 978-0-3873-4561-1
Vadiraja HS et al (2009) Effects of yoga program on quality of life and affect in early breast cancer patients undergoing adjuvant radiotherapy A randomized controlled trial Complementary Therapies in Medicine Volume 17 Issue 5 Pages 274-280
Velthuis MJ Agasi-Idenburg SC Aufdemkampe G Wittink HM (in press) The effect of physical activity on cancer-related fatigue during cancer treatment a meta-analysis of Randomised Controlled Trials Clinical Oncology 2009 (in print) Vineis P G Hoek and M Krzyzanowski et al Lung cancers attributable to environmental tobacco smoke and air pollution in non-smokers in different European countries a prospective study Environ Health 6 (2007) pp 1ndash7 Visvanathan K Chlebowski RT Hurley P et al American Society of Clinical Oncology 2008 clinical practice guideline update on the use of pharmacologic intervention including tamoxifen raloxifene and aromatase inhibition for breast cancer risk reduction J Clin Oncol 273235-3258 2009
Wagner LI Cella D (2004) Fatigue and cancer causes prevalence and treatment approaches BrJCancer 91822-828 Waltman N J Twiss et al (2009) ―The effect of weight training on bone mineral density and bone turnover in postmenopausal breast cancer survivors with bone loss a 24-month randomized controlled trial Osteoporosis International Wenzel L H Q Huang et al (2005) Quality-of-Life Comparisons in a Randomized Trial of Interval Secondary Cytoreduction in Advanced Ovarian Carcinoma A Gynecologic Oncology Group Study J Clin Oncol 23(24) 5605-5612 Weikert C Hoffmann K Dierkes J Zyriax BC KlipsteinndashGrobusch K MB et al Homocysteine metabolismrelated dietary pattern and the risk of coronary heart disease in two independent German study populations J Nutr 2005 1351981ndash1988 White S E McAuley et al (2009) Translating Physical Activity Interventions for Breast Cancer Survivors into Practice An Evaluation of Randomized Controlled Trials Annals of Behavioural Medicine 37(1) 10-19
142
World Health Organisation (1999) What is a healthy lifestyle Health Documentation Services WHO Regional Office for Europe Copenhagen World Health Organisation (2002) The World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva WHO Scientific Group on the Prevention and Management of Osteoporosis (2000 Geneva Switzerland) (2003) Prevention and management of osteoporosis report of a WHO scientific group World Health Organisation (2005) The European health report 2005 public health action for healthier children and populations Copenhagen WHO regional office for Europe World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva Windsor P M Nichol K F Potter J A randomized controlled trial of aerobic exercise for treatment-related fatigue in men receiving radical external beam radiotherapy for localised prostate carcinoma Cancer (2004) 101 (3) 550-7 Wright M E S-C Chang et al (2007) Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality Cancer 109(4) 675-684 Wright P A Smith et al (2005) Psychosocial difficulties deprivation and cancer three questionnaire studies involving 609 cancer patients Br J Cancer 93(6) 622-626 Yu GP et al (1997) The effect of smoking after treatment for Cancer Cancer Detect Prev 21487-509

4
Lifestyle Guidance for Cancer Survivors ndash Executive Summary
1 This aim of this review was to update the World Cancer Research Fund (WCRF)
report bdquoA Systematic Review of RCTs Investigating the Effect of Nutritional and
Physical Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This
has been achieved by conducting a comprehensive but pragmatic search of the
literature from 2006 onwards Where no evidence was available in the WCRF
review studies before 2006 have been included if identified in the reference lists of
acquired records To facilitate this evidence cited within the lsquoHandbook of Cancer
Survivorship‟ (Feuerstein 2006) and findings from a non-systematic review
conducted by the Cancer and Palliative Care Rehabilitation Workforce (2009) were
also utilised
2 There is now persuasive evidence that a healthy lifestyle during and after cancer is
associated with improved physical and psychological well-being reduced risks of
treatment enhanced self-esteem reduced risk of recurrence and improved survival
Clarifying the individual anti-cancer components of a healthy lifestyle will require
extensive further evaluation and even then they are likely to be multi-factorial
3 Despite gaps in the evidence for lifestyle benefits in cancer survivors there are some
key lifestyle recommendations that can be provided (Appendix A and B)
o Dietary Recommendations Reduce saturated fats increase fish intake
consume a varied diet in order to ensure adequate intakes of vitamins and
essential minerals increase consumption of green and cruciferous vegetables as
well as brightly coloured fruits and vegetables that contain carotenoids
o Physical Activity Recommendations There is substantial evidence suggesting
that the physical activity recommendations developed by the Department of
Health are sufficient for most cancer survivors - a total of at least 30-minutes a
day of moderate intensity physical activity on five or more days of the week
Additionally there is evidence of a dose-response (ie the more physical
activity the greater any benefits) Even a modest amount of exercise is
beneficial and will see gains versus doing nothing at all Body composition
changes are common in many cancer patients with the reasons varying by site
Compromised lean body mass for patients with head and neck and
gastrointestinal cancers are common and in this group exercise to build lean
muscle will be relevant However in breast cancer some treatments can lead to
significant weight gain (exacerbated if pre- diagnosis BMI is not in the healthy
range) and exerciseactivity which is more useful for controlling body weight and
losing fat will be more important
o Weight Excess weight should be avoided (ie a body mass index of 25-
29kgm or above There is also evidence that maintaining a stable healthy weight
as opposed to fluctuating between a healthy and unhealthy BMI can offer health
5
benefits for cancer survivors The evidence is strongly suggestive of weight being
implicated in breast cancer outcomes with the mechanism of benefit achieved
via physical activity or a low-fat diet most likely being due to weight loss
o Smoking Strong and consistent evidence has been presented for increased risk
of disease progression and mortality in people who continue to smoke after a
diagnosis of cancer as well as poorer outcomes in pre-diagnosis smokers
o Alcohol There is a paucity of research into the effects of alcohol pre- and post-
diagnosis on cancer progression and recurrence as well as symptom
management Evidence thus far is highly contradictory although excess alcohol
is linked to increased weight which does have negative outcomes
4 Evidence is also available for the benefits of individual lifestyle components for
specific cancer types
o A high intake of soy has been found to alter testosterone (the male sex
hormone) reducing risk of prostate cancer
o Dietary fibre might offer protection against colorectal cancer or recurrence via
increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic
mucosa (tissue that lines the colon)
o Since physical activity can alter levels of oestrogen (the female sex hormone)
evidence indicates that it might be protective against breast cancer
5 There is a wealth of evidence for physical activity during and after treatment
improving symptoms of cancer-related fatigue and increasing energy and stamina It
is also clear that a needs-based approach should be adopted ndash based on the
assessed need for improvements on low fatigue levels poor quality of life low
physical function (Speck et al 2009)
6 Guided progressive physical activity soon after treatment can ease the symptoms of
lymphoedema Avoidance of physical activity through fear of exacerbating symptoms
is unwarranted if physical activity is supervised and closely monitored
7 Whilst the benefits of physical activity on bone health require clarifying physical
activity can at the very least prevent loss of bone mineral density in survivors at
particular risk of developing osteoporosis
8 Even when not directly associated with overall QoL exercise has been found to
significantly improve social functioning among post-treatment survivors The benefits
of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or
group-based The evidence that physical activity can improve body image may be
one of the mechanisms through which exercise can improve quality of life
6
9 Mechanisms of benefit for diet and physical activity include the influence that these
behaviours have on hormones and insulin levels This has sparked the question of
whether pharmacological alternatives such as aromatase inhibitors and metformin
which tend to produce greater reductions in cancer risk pose competition for lifestyle
interventions This is unlikely as healthy lifestyle behaviours contribute overall to
general health and to the risk reduction for other co-morbid conditions such as
hypertension cardiac disease and diabetes Usefully the competencies framework
offered by Finders University highlights the importance of taking a holistic approach
to supported self-management whereby support is provided for a continuum of
health as opposed to a focus on one established chronic condition Based on this
model supported self-management should provide health promotion and illness
prevention not merely in terms of cancer but also for associated risks and co-
morbidities
10 The challenge remains in integrating lifestyle support into standardised models of
aftercare for cancer survivors particularly in terms of engaging both patients and
health professionals bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative identifies the need to
provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for
healthcare professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
11 The literature identifies the need for individual assessment and risk stratification for
cancer survivors so that lifestyle interventions and support can be tailored and
provided according to need Particularly high need groups are survivors who have
co-morbidities are overweight sedentary or smoke
12 Some questions that remain
o What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
o How can people most likely to benefit from lifestyle interventions be effectively
identified
o What are the various intensities of lifestyle support that can be provided based on
levels of individual need
13 Significant limitations can be found in the evidence available for lifestyle outcomes in
cancer survivors including
7
o Long-term outcomes of lifestyle choices
o Low levels of adherence to interventions
o A paucity of studies addressing external validity
o Equality across tumour groups
o Lack of cultural considerations pertaining to dietary advice
o A paucity of individualised lifestyle advice and tailored support
8
BACKGROUND SETTING THE SCENE
Lifestyle and Well-Being
In an independent report offering recommendations on enabling effective delivery of health
and well-being in England Bernstein Cosford and Williams (2010) advise that setting clear
priorities for health and well-being should start with behavioural risk factors Namely they
recommend tackling the biggest lifestyle influences on population health tobacco alcohol
physical inactivity and poor diet These four lifestyle factors are among the biggest
contributors to most preventable diseases across all social groups and in all areas of
England They are responsible for 42 of deaths from leading causes (WHO 2005) and
together they account for at least pound94 billion in annual direct costs to the NHS (DH 2009a)
expenses incurred outside the NHS would increase this figure further
An increase in longevity and the number of people living with one or more chronic conditions
for a longer period of time has led to government action aimed at making these years as
healthy as possible Interest has been particularly paid to the role of these behavioural risk
factors and the role of lifestyle in improving or maintaining health preventing illness
managing symptoms and achieving a satisfactory quality of life (QoL) (Pedersen and Saltin
2006 Taylor et al 2004)
The term lifestylelsquo refers to personal choices that might impact health such as diet physical
activity smoking and alcohol consumption The World Health Organisation (WHO 1999)
defines a healthy lifestylelsquo as
ldquoa way of living that lowers the risk of being seriously ill or dying earlyrdquo with the
emphasis that ldquohealth is not just about avoiding disease It is also about physical
mental and social well-beingrdquo (p 2)
With earlier detection and more efficacious treatments available for cancer there has been
an increase in survival as well as in the number of people living with the long-term
consequences of cancer treatment Subsequently cancer has become a chronic disease for
a number of people among the two million cancer survivors in the UK (Maddams Moller and
Devane 2008) Whilst evidence of the effects of a healthy diet and sufficient physical activity
in cancer prevention has been well-documented (Chan Gann and Giovannucci 2005
Sonn Aronson and Litwin 2005) it has become of fundamental importance to examine the
role of these lifestyle choices in cancer survivorship Furthermore the role of lifestyle in
cancer survivorship needs to be examined not only in terms of improved physical and
psychological well-being but also disease outcomes
Given the relationship between choosing a healthy lifestyle and taking an active role in the
self-management1 of the long-term effects of cancer and its treatment the self-management
workstream of the National Cancer Survivorship Initiative (NCSI) have conducted this
1 lsquoSelf-managementrsquo has been defined as ldquoawareness and active participation by the person in their recovery
recuperation and rehabilitation to minimise the consequences of treatment promote survival health and well-beingrdquo (NCSI 2009)
9
evaluation of evidence pertaining to lifestyle factors and survivorship Not only are lifestyle
choices important in terms of disease progression and recurrence but also in the effective
management of other chronic symptoms and conditions resulting from treatment such as
cancer-related fatigue lymphoedema and osteoporosis (Doyle et al 2006) Lifestyle
support and education is evidently an important component of supported self-management2
for many individuals living with or beyond cancer (Davies and Batehup 2010) Indeed as
part of a consensus meeting and evidence review self-management support and lifestyle
management were among the top ten priorities for survivorship research (Richardson et al
2009) providing further rationale for the current review
The Health of Cancer Survivors
The traditional belief has been that people with cancer should rest reduce activity and avoid
activities involving intense physical effort in other words they are passive patients of the
disease and its treatment Consequently physical activity levels do decline substantially
during and after completion of treatment for cancer and often fail to return to pre-diagnosis
levels for many people (Daley et al 2008) Fortunately it is becoming increasingly
recognised that people living with or beyond cancer do need physical activity will not be
harmed by physical effort and are active participants in the rehabilitation process
Furthermore emerging evidence is demonstrating that lifestyle factors can influence the rate
of cancer progression improve quality of life (QoL) reduce side-effects and risks during
treatment reduce the incidence of relapse and improve overall survival (Thomas Daly and
Perryman 2000) Besides the beneficial effect on recurrence a healthy diet and regular
physical activity has the potential to reduce the risk of co-morbidity such as other cancers
cardiovascular disease and diabetes etc (Jones and Demark-Wahnefried 2006)
Research suggests that although many cancer survivors report making healthy lifestyle
changes after diagnosis these changes may not be generalisable to all populations of
cancer survivors and they are often temporary (Demark-Wahnefried and Jones 2008)
Furthermore evidence suggests that the healthy lifestyle behaviours adopted by cancer
survivors tend to be directed towards clinical action such routine physical examination rather
than those health behaviours that require daily effort such as healthy eating or regular
physical activity (Findley and Sambamoorthi 2009)
A potential explanation for this difference in the uptake of clinical versus lifestyle preventive
health behaviours is that the former is easier due to the primary action being carried out by
someone else The latter on the other hand requires personal time and effort as well as
opportunity socially economically and in terms of health literacy and educational status
Behavioural and lifestyle change is notoriously difficult but even more so for people with
cancer or other chronic conditions let alone those with co-morbidities (Krein et al 2005) For
people with co-morbidities a healthy lifestyle can be even more challenging as they grapple
with the competing demands posed by the self-management of multiple conditions (Lindsay
2009)
2 lsquoSupported self-managementrsquo has been defined as ldquoWhat health and social care professionals and service
delivery organisations to do support self-managementrdquo (NCSI 2009)
10
Given the increase in survivorship the higher rates of co-morbidity within this population
and evidence that diet physical activity and other lifestyle factors affect risk for other cancers
and other chronic diseases there is a clear need for lifestyle interventions that target this
high risk group The literature suggests the need for individual risk assessment and the
provision of support with lifestyle changes in those individuals identified as high risk ndash such
as survivors who have co-morbidities are overweight sedentary or smoke (Davies and
Batehup 2010)
The Lifestyle Needs of Survivors
The National Cancer Survivorship Initiative (NCSI) highlights that people living with or
beyond cancer would like to play a more active role in their healthcare They want to know
how to look after themselves after a cancer diagnosis including information and support on
the lifestyle changes they should make so they can return to normallsquo life as much as
possible (Macmillan Cancer Support 2008) Yet the evidence suggests that this need
remains largely unaddressed In a key mapping project commissioned by the NCSI
Research workstream a number of issues pertaining to lifestyle were identified for the four
most common cancers breast colorectal lung and prostate (NCSI 2009) Each of these
four reports which were conducted by independent organisations demonstrated gaps in the
provision of lifestyle advice and support mainly during the period of aftercare In a similar
report mapping the needs of rarer cancers prolonging life through changes to lifestyle
emerged as a frequent theme by survivors asked to explore the meaning of cancer
survivorshiplsquo (Cancer52 and NCSI 2009) There was particular emphasis on the need for
diet and physical activity advice post-surgery for oesophageal cancer as well as diet advice
for mouth and throat cancers Change in bowel habits is frequently reported among post-
treatment bowel cancer survivors requiring support with dietary changes (Nikoletti et al
(2008)
In an effort to provide further insight into lifestyle advice and support for cancer survivors as
well as developing evidence-based lifestyle interventions a comprehensive review of the
evidence for lifestyle and cancer outcomes is required The perceived outcome efficacy3 of
making lifestyle changes is important in terms of whether those changes are initiated or not
as well as whether an individual possesses the confidence (self-efficacy) to maintain lifestyle
changes Outcome efficacy could be increased by the accumulation of firmly established
evidence offered alongside the opportunity for lifestyle support
Additionally this evidence needs to be evaluated in respect of current national guidelines for
diet physical activity and other lifestyle indicators such as weight and alcohol consumption
Briefly national guidance recommends a diet comprising 33 fruit and vegetables (five
portions per day) 33 starchy foods (rice bread pasta potatoes) 15 milk and dairy
foods 12 protein (meat and fish) and 8 foods and drinks high in fat andor sugar (Food
Standards Agency 2007) Adults are advised to achieve a total of at least 30-minutes daily
moderate intensity physical activity on five or more days of the week (DH 2004) Combined
with a healthy diet regular physical activity is aimed at maintaining a Body Mass Index
3 The belief that a particular outcome will result from following certain actions or behaviours
11
(BMI)4 of 185-249kgm2 25-29 is considered to be overweight and 30 or above as obese
whilst under 185 is considered underweight (National Obesity Observatory 2009)
A healthy lifestylelsquo is the same for cancer survivors as for the general population or indeed
people with other chronic conditions (Bellizzi et al 2005 Caan et al 2005 Coups and
Ostroff 2005) Cancer survivors are slightly more likely to follow physical activity guidelines
but overall their health behaviours mirror those of the general population which is marked by
inactivity and an epidemic of obesity and associated problems (Caan et al 2005) Despite
this the lifestyle advice and tailored care currently provided for specific groups of people in
the general population such as exercise prescriptions (DH 2001) is not yet integrated into
the supportive care needs of cancer survivors (Addington-Hall 2010) This is in the main
due to reluctance (usually related to knowledge and confidence) from health professionals to
discuss lifestyle factors with cancer patients due to limitations in knowledge and an
inadequacy in the available evidence on the underlying mechanisms of benefit for individual
lifestyle factors (Miles Simon and Wardle 2010) It is anticipated that this review will allay
some of this reluctance by identifying where the evidence strongly supports the efficacy of
lifestyle factors in cancer outcomes as well as where the evidence is less clear and requires
further research
4 BMI is a statistical measure which compares a persons weight and height to estimate a healthy body weight
12
The Purpose of this Review
Using the outlined national guidance on lifestyle and taking account of evidence for specific
elements or intensity of certain lifestyle factors in cancer care and self-management a
review of the literature on lifestyle and survivorship will be conducted The primary aims are
to produce evidence that can support professionals in guiding and advising cancer survivors
as well as evidence regarding resources which might support patient self-management in
relation to lifestyle factors and behaviour change The review will be comprehensive but
pragmatic drawing on a variety of sources This will commence by updating a recent review
conducted by the World Cancer Research Fund (WCRF) - bdquoA Systematic Review of RCTs
Investigating the Effect of Diet and Physical Activity Interventions on Cancer Survival‟
(Bekkering et al 2006)5
The aim of the WCRF review (Bekkering et al 2006) was to systematically locate and
review all randomised control trials (RCTs) which tested the effect of diet andor physical
activity interventions in cancer survivors their definition of a cancer survivor being
ldquoanyone who has been diagnosed with cancer from the time of diagnosis through the
rest of liferdquo (Brown et al 2003)
They conducted a systematic search of MEDLINE (from 2000 onwards) EMBASE (from
1999 onwards) AMED (from 1985 onwards) and the Cochrane Library including DARE
CDSR CENTRAL and HTA (all years) up to March 2006 scanned key texts that were
relevant to the subject field and scanned the references of relevant reviews They identified
117 trials (Table 1)
Table 1 Trials Identified in the WCRF Review (Bekkering et al 2006)
Trials Total
Diet
Food-based
Supplement-based
23
71
Physical activity
23
Total 117
5 This has been highlighted by the American Cancer Society (ACS) as being one of the most comprehensive
reviews on diet and physical activity for cancer survivors The ACS has used the review alongside other sources to produce lsquoGuidelines on Diet and Physical Activity for Cancer Preventionrsquo (Kushi et al 2006)
13
The findings will be described along with the results of the current review The overall
conclusion drawn by Bekkering et al (2006) was that there is a paucity of robust evidence
on the effects of diet and physical activity interventions in the management of cancer RCTs
were generally small and often reported inadequate details to formally assess quality While
promotion of a generic healthy diet was associated with reduced overall mortality the degree
to which lifestyle accounted for this outcome was imprecise It was concluded that given the
large investment in potential lifestyle interventions among cancer survivors large-scale trials
adequately powered to provide robust conclusions should be supported and conducted
In updating the WCRF review (Bekkering et al 2006) further scoping of the literature from
2006 to February 2010 will be conducted along with a synthesis of the evidence presented
in the lsquoHandbook of Cancer Survivorship‟ edited by Michael Feuerstein (2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (National Cancer Action Team 2009) which evaluates literature
pertaining to rehabilitation
The primary aim of the review is to guide healthcare planning and the development of
supported lifestyle self-management interventions for high risk groups In order to be able to
consider the production of useable evidence-based guidance for self-management for both
patients and professionals the following evidence will be sought
Evidence that would support professionals to be able to guide and advise
patients
Evidence regarding resources which would support patient self-management in
relation to lifestyle factors and behaviour change
It is anticipated that recent efforts to conduct research in this area will facilitate the
clarification of any key recommendations that can be made to cancer survivors by healthcare
professionals This update of the evidence will also attempt to establish where the strength
of the evidence lies and where more research is required
14
METHOD
Search Strategy
In updating the WCRF review (Bekkering et al 2006) RCTs and systematic reviews were
obtained from a systematic search of the Cochrane Library Database and Pubmed (from
March 2006 to February 2010) Where no evidence was available in the WCRF review
studies before 2006 have been included if identified in the reference lists of acquired
records this is the case with studies on smoking which were not included in the Bekkering
et al (2006) review
The selected relevant chapters were read from the bdquoHandbook of Cancer Survivorship‟
(Feuerstein 2006)6 and relevant studies referred to from the Cancer and Palliative Care
Rehabilitation Workforce (2009) non-systematic review Grey literature was also utilised
where this would provide information relevant to the review or where cancer-specific
literature was lacking as was the case with osteoporosis
All titles and abstracts of studies identified by the searches were scanned for relevance in
terms of topic and participant group For any titles or abstracts that were potentially relevant
full paper manuscripts were obtained and the relevance of each study assessed according to
the pre-specified inclusion criteria
6 Chapters include Physical Activity Potential Benefits and Guidelines DietWeight Management
Search terms cancer OR neoplasm
AND diet OR exercise OR physical
activity OR weight OR lifestyle
Cochrane systematic reviews
925 records
PubMed
4941 records
56 included 84 included
15
Inclusion Criteria
Records included within the review of the literature met the following inclusion criteria
Lifestyle-related ndashdiet physical activity weight smoking alcohol consumption
Cancer sites breast colorectal lung or prostate cancer Other tumour sites will
be included if located while searching for the primary tumour sites
Trajectory - during primary cancer treatment or post-primary treatment
Outcomes of interest ndash survival recurrenceprogression symptoms treatment-
related chronic conditions ndash fatigue lymphoedema osteoporosis weight
physical fitness quality of life rehabilitation behaviour change health and well-
being cost-effectiveness
Adult population
Type of record ndash RCTs systematic reviews prospective cohort studies
Retrospective studies will also be included since some areas of lifestyle such as
smoking have primarily been investigated via this method
16
RESULTS
A total of 140 records were included in this review not counting the review being updated
(Bekkering et al 2006) In synthesising the evidence obtained from these records and the
additional sources described in the search strategy findings are presented in two parts
1) Cancer Survival
Evidence for the role of lifestyle in disease progression and recurrence
2) The Risks and Side-Effects of Cancer Treatment
Evidence for the role of lifestyle in reducing and managing the risks and
side-effects of cancer treatment with specific focus on cancer-related
fatigue lymphoedema osteoporosis and QoL
Both sections examine five categories of evidence
Physical activity
Diet
Weight
Smoking
Alcohol
The focus is on the four most common cancers (breast colorectal lung prostate) but other
tumour sites have been included if located via the pre-defined search strategy Summary
tables for each study included within the evidence are provided at the end of relevant
sections
17
PART ONE
CANCER SURVIVAL ndash EVIDENCE FOR THE ROLE OF LIFESTYLE IN
DISEASE PROGRESSION AND RECURRENCE
Introduction
Evidence for the role of lifestyle in the development of cancer is strong and it is widely
accepted that a poor diet lack of exercise smoking and excessive alcohol consumption can
increase an individuallsquos risk of developing cancer In particular it is well established that
smoking can increase risk of lung cancer and excessive unprotected exposure to the sun
can increase risk of skin cancer More recently lifestyle after a cancer diagnosis has been
under the microscope with evidence for the role of lifestyle in cancer progression7 and
recurrence8 demonstrating that lifestyle changes post-diagnosis can influence the disease
trajectory (Thomas and Davies 2007)
The development of cancer does not mean it is too late to make lifestyle changes that can
reduce the risk of the disease progressing or recurring after remission Indeed lifestylelsquo
refers to personal choices that can impact health and well-being as well as improve an
individuallsquos chance of disease-free survival9 and overall survival10
Evidence for an interaction between lifestyle and the disease trajectory is evaluated in the
current review including cancer development progression and recurrence and
commencing with a description of three large scale multicentre trials that will be referred to
throughout (Table 3)These studies are presented in some depth because their findings have
been influential in this field of study This will be followed by a site-specific (eg breast
colorectal lung prostate) summary of the findings reported by Bekkering et al (2006) as
part of the WCRF review being updated Further evidence identified from the search criteria
will then be presented including evidence obtained from the aforementioned multicentre
trials The European Prospective Investigation into Cancer and Nutrition (EPIC) Study
The Womens Intervention Nutrition Study (WINS) and The Womens Healthy Eating
and Living (WHEL) Study
7 Defined as the cancer becoming worse or spreading within the body
8 Cancer that has returned usually after a period of time during which it could not be detected The cancer may
come back to the same place as the original (primary) tumour or to another place in the body
9 The length of time after treatment during which a person survives with no sign of the disease
10The percentage of people from the study who are alive for a certain period of time after diagnosis or treatment
(ie 5-year survival rate)
18
The European Prospective Investigation into
Cancer and Nutrition (EPIC) Study (Riboli et al
2002)
The Womens Intervention Nutrition Study (WINS)
(Chlebowski et al 2006)
The Womens Healthy Eating and Living (WHEL)
Study
(Pierce et al 1997)
The EPIC study is coordinated in the UK by Dr Elio Riboli of the Imperial College London It is an ongoing multicentre prospective cohort study designed to investigate the relationship between nutrition and cancer The study currently includes 521000 participants (aged 35ndash70 years) in 23 centres located across 10 European countries11 These participants will be followed for cancer incidence and mortality for at least 10-years At enrolment which took place between 1992 and 2000 information was collected through a lifestyle questionnaire and through a dietary questionnaire addressing usual diet Physiological measurements (eg weight) were performed and blood samples taken The main website for EPIC12 last updated in 2010 reports that 26000 cases of cancer and 16000 deaths from cancer have been identified the majority of cases being cancer of the breast (n=6218) colonrectum (n=1910) prostate (n=1547) and lung (n=1292)
The WINS trial is a randomised multicentre study that commenced in 1994 and is now closed for recruitment It was designed to determine whether dietary fat reduction effectively prolongs disease-free and overall survival in post-menopausal women (n=2437) aged 48-78 years surgically treated for early stage breast cancer Randomisation to a reduced fat group or a control group took place between 1994 and 2001 with participants being evaluated annually via self-report and physiological measures 1) Intervention group (n=975) intensive dietary intervention for reduction of total fat intake to 15 of calories with repeated individual and group counselling sessions involving cognitive behavioural and motivational interviewing techniques 2) Control group (n=1462) US Department of Health and Human Services dietary guidelines (total fat intake between 20-35 of calories)
The WHEL study is a multicentre RCT which commenced in 1995 and also closed to recruitment aimed to determine whether a diet rich in vegetables fruit and fibre and low in fat is associated with a longer breast cancer event-free interval (ie no disease progression recurrence nor secondary cancers) Women diagnosed with stage I-III invasive breast cancer (n=3088) within the previous 4-years were randomised to a dietary intervention or control group and evaluated annually for 5-years via self-report and physiological measures 1)Intervention group (n=1540) guidelines provided for a daily dietary pattern of 5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy from fat A telephone counselling protocol focusing on goal setting self-monitoring and self-efficacy were provided as were cooking classes 2)Control group (n=1551) The US Department of Agriculture dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre and 30 energy from fat)
11
Denmark France Germany Greece Italy The Netherlands Norway Spain Sweden and the UK
12 httpepiciarcfr
Table 3 The EPIC WINS and WHEL Study (findings presented within proceeding text)
19
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in breast
cancer survival In the current review 6 studies and 2 systematic reviews were identified
These have been divided into appropriate domains according to mechanisms of benefit
hormones intensity and insulin Studies are summarised in Table 3 at the end of this
section
Hormones
Evidence exists that physical activity is associated with reduced risk of developing breast
cancer (Friedenreich and Cust 2008 Monninkhof et al 2007) One potential mechanism of
benefit is via the modification of sex hormone levels High levels of oestrogen (the
predominant sex hormone in females)13 and androgen (the predominant sex hormone in
males)14 are consistently associated with increased risk of developing breast cancer
(Eliassen et al 2006 Kaaks et al 2005) whereas high levels of sex hormone-binding
globulin (SHBG)15 are associated with a decreased risk (Key et al 2002) Regular physical
activity may alter oestrogen metabolism by shifting metabolism to favour production of 2-
hydroxyestrone (2-OHE1)16 as opposed to16α-hydroxyestrone (16α=OHE1) the former of
which has much weaker estrogenic activity Campbell et al (2007) is one of the few
researchers to examine this mechanism of benefit via a RCT In examining the effects of a
12-week aerobic exercise training programme on 2-OHE1 and 16α-OHE1 in healthylsquo pre-
menopausal women (n=17) no significant differences in oestrogen changes were found with
a control group who continued their usual level of physical activity (n=15) However a
change in lean body mass (estimated weight excluding body fat) over the 12-week
programme was found to be associated with a favourable change in 2-OHE1 to 16α-
OHE1 ratio (p lt 005)
In an effort to provide more direct evidence regarding the biological mechanisms of benefit
obtained from physical activity Friedenreich et al (2010) conducted the Alberta Physical
Activity and Breast Cancer Prevention Trial a two-centre two-arm RCT of physical
activity and cancer risk in older (50gt years) post-menopausal sedentary women from the
general population (n=320) Participants received a 1-year aerobic physical activity
programme of 225-minutes per week (n=160) or maintained their usual level of activity as
part of a control group (n=160) Significant reductions in oestrogen were found in the
intervention group compared to the control group demonstrating a protective effect
of increased physical activity in this group of high risk women (p lt 05)
13
oestrogen is suspected to activate certain oncogeneslsquo which can turn normal cells into tumour cells 14
The primary and most well-known androgen is testosterone which is also found in women to a lesser degree 15
A protein that attaches itself to oestrogen and androgen
16 Sometimes referred to as a good oestrogenlsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
20
Whilst some studies have examined the outcomes of increased physical activity others have
attempted to identify the duration and intensity required for beneficial effects Using data
from the Nursesrsquo Health Study17 (n=2987) Holmes et al (2005) found that women who
reported at least 3 MET-hours18 or more of physical activity per week were less likely
to have a recurrence or die from breast cancer compared to those who reported less
physical activity (p lt 001)
A further reduction in risk was seen with higher levels of physical activity up to 239 MET-
hours per week indicating a dose-response Interestingly the benefits of physical activity
were limited to women with hormone-receptor positive tumours (tumours that
respond to hormone treatment) as opposed to hormone-receptor negative tumours
(tumours that do not respond to hormone treatment) This provides further support for
mechanism of benefit from physical activity being hormone-related whether that be due to
the physical activity or any subsequent reductions in lean body mass that might accompany
such activity
Intensity
Expanding on evidence for the intensity of physical activity in a prospective observational
study the Health Eating Activity and Lifestyle (HEAL)19 study Irwin et al (2008) found
that of breast cancer survivors (n=933) who were sedentary pre-diagnosis women who
increased their physical activity post-diagnosis to approximately 9-MET hours per
week (eg 2-3 hours of brisk walking) had a 45 lower risk of death from cancer when
compared to those who did not increase their physical activity women who
decreased physical activity after diagnosis had a four-fold greater risk (p lt 005)
17
One of the largest and longest running investigations of factors that influence womenlsquos health comprising
information from 238000 nurse-participants
18 Metabolic equivalent (MET) values a measure of the effort required to do that activity
19 The HEAL Study is a population-based multicentre multi-ethnic prospective cohort study that has enrolled
1183 breast cancer survivors to determine whether lifestyle hormones and other exposures affect breast cancer
prognosis
METs (Ainsworth 2000) Light-intensity activities are defined as 11 MET to
29 MET Moderate-intensity activities are defined as 30 to
59 METs Vigorous-intensity activities are defined as 60 METs
or more
3 MET-hours might be using a stationary bicycle with light effort for one-hour 239 MET-hours might be running for 2-hours plus 1-hour of aerobic activity
21
Consistent with this a larger prospective observational study demonstrated that breast
cancer survivors (n=4482) who were physically active for more than 28 MET-hours per
week (eg walking at average pace of 2-29mph for 1-hour) were significantly less
likely to die from breast cancer (35-49 reduction) when compared to survivors who
did less than this (p lt 05) (Holick et al 2008) The reduced risk of mortality from cancer
was limited to total or moderate-intensity physical activity no benefit was noted for vigorous-
intensity activity
In a systematic review by Patterson et al (2010) leisure-time physical activity (ie
sportsrecreational) was associated with a 30 decreased risk of mortality from
breast cancer when compared to sedentary women In another review Saxton (2010)
identified four cohort studies demonstrating that women achieving the equivalent of 30-
minutes of moderate intensity physical activity on five or more days of the week
halved their risk of cancer-related mortality compared to those achieving less than 30-
minutes over the five days
Insulin
Evidence for the role of excess insulin in the growth of cancer cells has become more
established in recent years especially with the increase in obesity which is often
accompanied by elevated levels of insulin (Giovannucci 2005) The benefits of physical
activity on reducing insulin levels are less clear Ligibel et al (2008) conducted a RCT to test
the impact of weight training on insulin levels in overweight sedentary stage I to III breast
cancer survivors (n=101) The women were randomly assigned to one of two conditions
1) a 16-week supervised strength training and home-based cardiovascular training
protocol (two supervised 50-minute strength training sessions per week and 90-
minutes of home-based aerobic physical activity weekly)
2) a control group (routine care for 16-weeks before being offered consultation with a
physical activity trainer at the end of the control period)
Participation in the physical activity training was associated with a significant
decrease in insulin levels and hip circumference (p lt 05) Therefore the relationship
between physical activity and breast cancer recurrence may be mediated in part through
changes in insulin levels andor changes in body fat
ii DIET
Bekkering et al (2006) report on two small breast cancer studies showing a reduction in
cancer-specific mortality with healthy diet interventions (Elkort et al 1981 de Waard et al
1993) Of nine trials that included an antioxidant supplement no evidence was found for an
association between the intervention and cancer-related mortality compared with placebo or
usual treatment There was also no evidence of an effect of retinol (vitamin A - found in cod
liver oil butter liver eggs and cheese) (Meyskens et al 1994 Kucera et al 1980
Pastorino et al 1993)
22
In the current review 19 studies provide further evidence of the role of diet in breast cancer
survival many of which are part of the three multicentre studies previously described (ie
EPIC WINS WHEL p19) These studies have been divided into appropriate domains
according to dietary components dietary fat fruit and vegetables dietary fibre soy and
vitamin D
Dietary Fat
In general retrospective casendashcontrol studies have supported a positive association between
breast cancer incidence and dietary fat (Howe et al 1990) whilst many prospective cohort
studies have failed to show such an association (Kim et al 2006 Hunter et al 1996) A
meta-analysis provided evidence for a weak direct association between fat intake and breast
cancer in casendashcontrol and cohort studies combined (Boyd et al 2003) in cohort studies
that adjusted for energy intake highest versus lowest categories of total fat intake were
associated with a statistically significant 13 increased risk of developing
breast cancer (p lt 05)
Kyogoku et al (1992) utilised breast cancer patients whose dietary intake was assessed 10-
years previously in a case-control study (n= 212 patients who underwent a surgical
operation) After 10-years of follow-up 47 breast cancer deaths had occurred with no
support being provided for the hypothesis that a low fat diet influences breast cancer survival
outcomes In addition Holmes et al (1999) as part of the Nursesrsquo Health Study report
there being no evidence suggesting that lower intake of total fat or specific types of fat (eg
saturated and unsaturated fat) was associated with death from breast cancer in 2956
women who were diagnosed after 14-years of follow-up
Hebert et al (1998) studied the effect of diet on recurrence and death in women diagnosed
with early-stage breast cancer (n=472) finding that the strongest effects were observed in
pre-menopausal women Higher levels of self-reported baseline daily consumption of
butter margarine lard and beer were found to increase the risk of recurrence (p lt
01) There was also an increased risk associated with consumption of red meat liver and
bacon corresponding to about a doubling of risk for each time per day that foods in this
category were consumed (p=09)
The previously described WINS and WHEL RCTs (Table 2 p19) were anticipated to shed
light on these inconsistent findings related to dietary fat and breast cancer outcomes as
explored next in the following section
In an interim analysis of the Womens Intervention Nutrition Study (WINS) data (n=2437)
after a median follow-up of 60-months (5-years) (Chlebowski et al 2006) report that dietary
fat intake was lower in the dietary intervention than in the control group corresponding to a
significant 6-pound lower mean body weight in the intervention group (p lt 05) As a
reminder the dietary intervention group were counselled to reduce total fat intake to 15 of
calories whilst the control group were advised to keep total fat intake between 20-35 of
calories After 5-years of follow-up a total of 277 recurrences were reported in 96 of 975
23
(98) women in the dietary group and 181 of 1462 (124) women in the control group
women in the dietary intervention had a 24 lower risk of recurrence compared to the
control group (p lt 05) Exploratory analyses suggested that dietary fat reduction was most
beneficial in women diagnosed with hormone receptorndashnegative compared to hormone-
receptor positive breast cancer although this was not statistically significant
Other studies providing evidence of a differential effect of fat intake on breast cancer survival
have found such associations with hormone-receptor positive cancers (Holm et al 1993
Cho et al 2003) raising debate over the WINS findings Nevertheless in 2008 Chlebowski
et al updated survival information presented in 2006 reporting that after 7-years follow-up a
significant overall survival benefit was seen in women (n=362) with hormone-receptor
negative tumours taking part in the dietary intervention compared to the comparison
group (75 vs 181 p lt 005)
To explore the link between hormones and diet further the metabolic profiles of a subset of
WINS participants (n=53) were examined for the effect of a low-fat diet on insulin resistance
(Khaodhiar et al 2003) Insulin resistance is a physiological condition in which insulin
becomes less effective in lowering blood sugars resulting in increased blood glucose Of
those participants with initial insulin resistance after 1-year women in the dietary
intervention group had a greater decrease in their fasting insulin (insulin tested in a blood
sample collected after a 12-hour fast) than the women in the control group Although
not statistically significant these results suggest that insulin concentrations (a marker of
insulin resistance) may be influenced by dietary fat intake Alternatively since waist-to-hip
ratio is a marker for insulin weight reduction as opposed to dietary fat reductions might be
the important variable influencing disease outcomes (Borugianlsquos et al 2004)
Fruit and Vegetables
Flavonoids20 are high in fruits and vegetables and therefore might account for some of the
findings reported in WINS Dwyer et al (2008) sought to determine whether differences
existed in baseline and 12-month dietary intake of flavonoids among a random sample of
WINS participants (n=550) After 12-months of dietary intervention flavonoid intakes
remained similar in both groups demonstrating that neither total flavonoid intakes nor
intakes of subclasses of flavonoids differed between those who had dramatically decreased
their fat intake and those who had not Flavonoid intake is therefore unlikely to account for
the survival benefits reported for the WINS trial Carotenoids21 however do appear to play a
significant role in cancer survival On following 103 breast cancer survivors 27 of whom
died Ingram (1994) found that after a median of 81-months those who consumed more
beta-carotene (a carotenoid found in yellow and orange fruits such as mangoes
papayas and carrots) had significantly fewer deaths from breast cancer only one in
the group of highest beta-carotene consumers compared with 8 in the intermediate
20
Flavonoids also referred to as bioflavonoids are polyphenol antioxidants found naturally in plants ndash in other
words they are plant nutrientslsquo
21 Organic pigments that provide colour to bright fruits and vegetables including carrots apricots tomatoes and
salmon
24
group and 12 in the lowest group (p lt 0001) Overall there were 12 deaths in the lowest
total fruit consumption group compared with five in the intermediate group and 3 in the
highest (p lt 001) This benefit applied to both orangeyellow fruit (oranges melon) as well
as other fruits (apple banana berries grapes dried fruits)
Adding to this evidence is data from the aforementioned Womens Healthy Eating and
Living (WHEL) RCT (Table 2 p19) As a reminder women with breast cancer were
randomised to a dietary intervention (n=1540) comprising a daily pattern of
5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy
from fat or to a control group (n=1551) advised to follow the US Department of Agriculture
dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre
and 30 energy from fat Over a mean 73-year follow-up there was no significant
difference between groups in terms of additional breast cancer events (ie disease
progression recurrence or secondary cancer) or mortality despite statistically significant
differences in self-reported diet (low fat high fruit and vegetables) (Pierce et al 2007) On
the other hand when Rock et al (2005) examined only those participants in the control
group higher plasma total carotenoid concentration indicative of greater fruit and
vegetable consumption was significantly associated with reduced risk for a new
breast cancer event (p lt 05) This supports those findings reported by Ingram et al
(1994) and provides a potential explanation for why survival benefits were achieved in WINS
but not WHEL since both dietary interventions comprised lower dietary fat and higher levels
of carotenoids (fruit and vegetables) other factors must explain the differential survival
benefits One major difference between the two studies is that WINS participants lost weight
(mean = 6-pounds) whereas the WHEL participants did not
To follow up on these findings in terms of possible biological mechanisms of reduced risk of
recurrence Thomson et al (2007) conducted an ancillary study with post-menopausal
breast cancer survivors from the WHEL study (n=207) The aim was to test the hypothesis
that breast cancer survivors with higher levels of dietary carotenoids would show significantly
lower levels of oxidative stress (pathologic changes in response to excessive levels of cell
toxicity from the environment) than those with lower levels It was found that dietary
carotenoid levels were not significantly associated with oxidative stress indicators (measured
via urine samples)
Hot flushes post-treatment for early-stage breast cancer has been associated with an
approximately 25-30 decreased risk for additional breast cancer events (Mortimer et al
2008 Cuzick 2007) Since hot flushes are reported by women who continue to menstruate
during treatment or whose menstruation returns post-treatment this lowering of risk is
unlikely to be explained entirely by the lower oestrogen levels that sometimes accompany
hot flushes On the other hand dietary changes comprising lower energy from fat and
increased fibre can also alter oestrogen levels For example binding of fibre to estrogens in
the gut blocks reabsorption of oestrogen (Arts et al 1991) Focusing their analyses on the
2967 of the WHEL participants who experienced baseline hot flushes Gold et al (2009)
tested the hypothesis that the increased risk of additional breast cancer events observed
among women who do not report hot flushes post-treatment can be reduced by lifestyle
interventions that lower circulating oestrogen Over a median of 73-years follow-up it was
demonstrated that the dietary intervention was associated with reduced risk of second
25
breast cancer events among women who reported no hot flushes at baseline (p lt 05)
These women had 31 fewer cancer-related events than matched-pairs in the control group
among post-menopausal women with no self-reported hot flushes at baseline the
intervention effect was even stronger with a 47 reduction in risk compared with post-
menopausal women in the control group who had no hot flushes at baseline (p lt 05)
McEligot et al (2006) conducted a retrospective investigation into the influence of diet (fat
fibre vegetable fruit folate carotenoids and vitamin C) on overall survival in post-
menopausal women with breast cancer (n= 516) Participants completed a food frequency
questionnaire for the year prior to diagnosis the analysis of which demonstrated that
women consuming the least total fat and highest total fibre and vegetables as well as
more folate vitamin C and carotenoid were significantly less likely to die from any
cause than those women consuming the opposite (p lt 05)
Dietary Fibre
Evidence linking breast cancer to the intake of dietary fibre has been conflicting although the
hypotheses remain that dietary fibre can be protective by inhibiting oestrogen (Kaaks et al
2005) as described previously in relation to physical activity or by reducing insulin-like
growth factors (Heald et al 2003) Therefore further research into these mechanisms of
benefit is clearly needed in order to provide clarity
Rohan et al (1993) examined risk of breast cancer in relation to intake of dietary fibre and
vitamins A C and E in a cohort of women (n=56837) enrolled in the Canadian National
Breast Screening Study22 After 5-years follow-up 519 incidence of breast cancer were
identified with analysis of previously completed dietary questionnaires demonstrating that
higher dietary fibre intake was associated with a small reduction in risk of developing
breast cancer Specifically there was a statistically significant decrease in risk of
developing breast cancer with increasing consumption of cereals (p lt 01) and a statistically
non-significant trend for pasta consumption (p=017) This reduced risk persisted after
adjustment for total vitamin A beta-carotene vitamin C and E
The UK Womens Cohort Study (UKWCS) (Cade et al 2007) which compares the health
outcomes of three main dietary groups (vegetarian eating fish [not meat] and meat eaters)
provides further evidence for the protective properties of fibre After a median of 75 years
follow-up analysis of self-reported dietary data of 35792 women showed that total dietary
fibre was found to be related to breast cancer incidence in women who were pre-
menopausal but not post-menopausal at baseline (p lt01) Fibre from cereals (plt
05) and fibre from fruit (p=009) was found to be protective against breast cancer
22
An RCT comprising women 40-49 years of age at study entry evaluating the efficacy of annual mammography breast physical examination and instruction on breast self-examination in reducing breast cancer mortality
26
Soy
A high intake of phytoestrogens23 particularly isoflavones (found in soy products) has been
suggested to decrease risk of developing breast cancer In one of the European
Prospective Investigation into Cancer and Nutrition (EPIC) studies a large multicentre
prospective cohort study described earlier in Table 2 the association between breast cancer
risk and isoflavones was supported in 333 women (p lt 005) (Grace et al 2004) but in
another larger EPIC study conducted in Utrecht (n=15555) no such evidence was found
(Keinan-Boker et al 2004) Analyses with pooled data sets are ongoing In the meantime
Boyapati et al (2005) provide evidence from the Shanghai Breast Cancer Study24
suggesting that after a median of 52-years follow-up soy intake pre-diagnosis is not related
to disease-free survival in women with breast cancer (n=1459)
Vitamin D
Goodwin et al (2009) measured vitamin D (usually obtained from sunlight through the skin
but also found in oily fish and eggs) levels in the stored blood of women with early breast
cancer (n=512) The mean follow-up was 116-years by which time women deficient in
vitamin D had a significantly increased risk of distant recurrence25 compared with
those who had sufficient levels (p lt 05)
Antioxidant Supplements
Despite widespread use only a few clinical or epidemiological studies have examined the
relationship between antioxidant supplements and risk of breast cancer recurrence or breast
cancer-related mortality Fleischauer et al (2003) examined recurrence and mortality
among post-menopausal women diagnosed with breast cancer (n=385) who were enrolled
into a dietary case-control study Women were contacted with a single questionnaire to
ascertain the use of nutritional supplements during 12-14 years of follow-up Antioxidant
vitamin supplement use was associated with a lower risk of breast cancer recurrence or
mortality Specifically use of vitamin C and E supplements moderately reduced risk (p lt
05) whilst vitamin E nearly halved the risk although this was not statistically
significant (p=056)
iii WEIGHT
Weight and body composition have been implicated in the development of a wide range of
cancers as well as in increased risk of recurrence or second primary cancers (Chlebowski
Aiello and McTiernan 2002) Additionally being overweight or obese can exacerbate some
23
Phytoestrogens sometimes called dietary estrogenslsquo are a group of naturally occurring plant compounds that have a similar chemical structure to estrogen they bind to estrogen receptors acting like hormone regulators
24 The Shanghai Breast Cancer Survival (SBSS) Study collected lifestyle-related factors and disease and
treatment related factors in Chinese women with breast cancer (n=2236) (Lu et al 2007) 25
The spread of cancer to parts of the body other than the place where the cancer first occurred
27
of the side-effects of cancer treatment as well as increase the risk of co-morbidities such as
diabetes and osteoporosis (Doyle et al 2006) The studies evaluated in this review thus far
further indicate weight as offering a mechanism of benefit in terms of breast cancer
outcomes Indeed the WINS and WHEL RCTs produce different outcomes when using
similar dietary interventions with weight loss in the WINS group but not the WHEL group
offering a likely explanation for improved outcomes observed in the WINS participants Since
increased adiposity (excess body fat) has been identified as a negative prognostic factor for
recurrent disease and survival after breast cancer diagnosis (Rock and Demark-Wahnefried
2002) the apparent benefit of dietary fat reduction in the intervention group could
partly result from the weight loss
Bekkering et al (2006) do not add to this evidence whilst 5 studies and one systematic
review were identified in the current review
Hebert et al (1998) studied the effect of body weight on recurrence and death in women
diagnosed with early-stage breast cancer (n=472) Body mass index (BMI) was
associated with an increased risk of recurrence at the rate of 9 for each kgm2
(equivalent to about 58-pounds for a 5 4 tall woman) For death the results were
similar but body mass index was more strongly associated increasing risk by 12
per kgm2
Additionally Lahmann et al (2004) used data from 73542 pre-menopausal and 103344
post-menopausal women taking part in the EPIC study During 47-years of follow-up 1879
cases of invasive breast cancer were identified In post-menopausal women current use
of hormone replacement therapy (HRT) modified the association between body size
and breast cancer among non-users weight body mass index and hip circumference
were positively associated with breast cancer risk (p lt 001) Obese women (BMI gt 30)
had a 31 risk compared to women with a BMI lt 25 Among pre-menopausal women hip
circumference was the only other measure significantly related to breast cancer (p lt 005)
after accounting for BMI
Enger et al (2004) conducted a retrospective follow-up study of women diagnosed with
breast cancer (n=1376) for whom complete medical records and adequate tissue
specimens existed Patients were followed for a median of 68-years after diagnosis 246 of
whom died from breast cancer Compared with women in the lowest category of weight
(lt133lb [60kg] at diagnosis) women in the highest category ( 175lb [79kg])
experienced a 25-fold increased risk of dying from breast cancer (P lt 05) Women with
hormone-receptor negative cancer experienced an approximately 2-fold higher risk of dying
from breast cancer compared with women who presented with hormone-receptor positive
cancer Women in the upper 50th percentile of weight with hormone-receptor negative cancer
had a nearly 5-fold increased risk of dying from cancer compared with women in the lower
50th percentile of weight and hormone-receptor positive cancer (p=10)
In order to determine whether weight prior to diagnosis and weight gain after diagnosis are
predictive of breast cancer survival Kroenke et al (2005) followed 5204 participants from
the Nursesrsquo Health Study diagnosed with incident invasive non-metastatic breast cancer
After a median of 9-years follow-up there were 860 total deaths 533 breast cancer deaths
28
and 681 recurrences (defined as secondary lung brain bone or liver cancer and death from
breast cancer) Weight before diagnosis and weight gain after diagnosis were related
to higher rates of breast cancer recurrence and mortality although associations were
most apparent in women who had never smoked (p lt 05) Furthermore associations
with weight were stronger in pre-menopausal than in post-menopausal women In contrast
by comparing breast cancer survivors (n=3215) with women in the comparison group of a
dietary intervention trial to prevent breast cancer recurrence Caan et al (2008) found that
neither moderate (5ndash10) nor large (gt10) weight gain post-diagnosis was associated with
an increased risk of breast cancer recurrence in the early years post-diagnosis (median time
of 737-months from diagnosis)
More recently Patterson et al (2010) reviewed published epidemiological research on
lifestyle and breast cancer outcomes reporting that the most consistent finding from
observational studies was that adiposity was associated with a 30 increased risk of
cancer-related mortality
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in breast cancer
survival Four studies were identified in the current review
In an observational study Manjer et al (2000) compared the survival of patients with breast
cancer (n=792) who had never smoked were smokers or were ex-smokers Follow-up of
breast cancer cases was through record-linkage with the Swedish Cause of Death Registry
During a mean follow-up of 121-years smokers and ex-smokers compared with those
who had never smoked had a significantly increased risk of death from cancer
Fentiman et al (2005) add to this evidence with a cohort study of breast cancer patients who
completed a lifestyle questionnaire at the time of diagnosis (n=166) They found that
smoking was the third most important predictor of breast cancer-specific and overall
survival after stage and age at diagnosis This suggests that smokers are not only more
likely to die of cancer but also of other diseases when compared with those who have never
smoked
In a much larger study Holmes et al (2007) conducted a prospective observational study
among 5056 women from the Nursesrsquo Health Study with stages I-III invasive breast
cancer Information on smoking was available for these women who were followed until
January 2002 or death whichever came first Compared with women who had never
smoked women who were current smokers had a 43 increased risk of death from
any cause with risk increasing along with more cigarettes smoked per day (p lt0001)
In contrast there was no association with current smoking and breast cancer death
Sagiv et al (2007) followed women diagnosed with a first primary breast cancer (n=1273)
for 5-6 years and found that the number of all-cause mortality (n=188) including breast
cancer-specific mortality (n=111) was slightly higher among current and former
active smokers compared with women who had never smoked No association was
found between active or passive smoking and breast cancer-specific mortality
29
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in breast cancer
survival In the current review one review and 2 studies were identified
Rock and Demark-Wahnefried (2002) reviewed the evidence from clinical and epidemiologic
studies reporting that alcohol intake was not associated with breast cancer survival in the
majority of the studies In contrast post-menopausal women (n=125) diagnosed with
invasive breast cancer who were followed through to survival demonstrated that pre-
diagnosis alcohol consumption of at least one drink per week was associated with a
27-fold increase in risk of cancer-related mortality (McDonald et al 2002) In a similar
study a larger sample of women (n=1286) diagnosed with invasive breast cancer who were
followed from diagnosis through to survival produced opposing findings compared with
non-drinkers women who consumed alcohol in the 5-years before diagnosis had a
decreased risk of cancer-related mortality (Reding et al 2009)
SUMMARY OF LIFESTYLE EVIDENCE FOR BREAST CANCER ndash MECHANISMS
OF BENEFIT
Physical Activity Physical activity is likely to prevent breast cancer via its effect on
hormones specifically by reducing levels of oestrogen in the body (Friedenreich et al 2010)
or shifting the metabolism of oestrogen to favour production of 2-hydroxyestrone (2-OHE1)26
as opposed to16α-hydroxyestrone (16α=OHE1) the former of which has much weaker
estrogenic activity This shift might also be the result of a change in lean body mass resulting
from physical exercise (Campbell et al 2007) The survival benefits of physical activity
appear to require a certain intensity or level of exertion specifically 3 MET-hours or more per
week (Holmes et al 2005 Holick et al 2008 Saxton et al 2010) this equates to moderate
intensity activity such as using a stationary bike for 1-hour However there is also evidence
of a dose-effect with greater activity (up to 239 MET-hours per week) being associated with
reduced risk of recurrence and cancer-related mortality (Holmes et al 2005) or indeed
greater levels of activity than pre-diagnosis being associated with reduced risk of recurrence
and cancer-related mortality (Irwin et al 2008 Holick et al 2008 Patterson et al 2010
Saxton et al 2010)
Diet Evidence for the role of dietary fat in breast cancer development and survival are
varied Case-control (Kyogoku et al 1992) and large prospective studies (Holmes et al
1999) do not show any significant link whilst some studies have found that dietary fat does
increase risk of recurrence or death in pre-menopausal women Indeed the large multicentre
WINS trial found a protective benefit of a reduced fat dietary intervention which was more
prominent in women diagnosed with hormone-receptor negative breast cancer (Chlebowski
et al 2006a Chlebowksi et al 2008) The differential effect of diet on hormone-receptor
positive and negative disease indicate that metabolic mechanisms involving insulin and
26
Sometimes referred to as a lsquogood estrogenrsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
30
insulin-like growth factor-1 (IGF-1)27 may be involved in the mechanisms of benefit and
although not statistically significant data has been presented suggesting that elevated
insulin concentrations (a marker of insulin resistance) may be influenced by dietary fat
reduction (Khaodhiar et al 2003 Borugian et al 2004) However this might be due to
changes in weight produced by a low fat diet rather than the lower consumption of fat itself
(Borugian et al 2004) Since low fat diets are often accompanied by high intakes of fruit
and vegetables various components of a diet comprising high levels of fruit and vegetables
have been investigated Carotenoids have received particular attention with evidence
suggesting that carotenoids play a role in survival (Ingram 1994) Other studies have found
this not to be the case (Pierce et al 2007) with the primary difference in these studies being
lack of weight loss This indicates that the mechanism of benefit produced from low fat high
fruit and vegetable (particularly carotenoids) diets is most probably through changes in body
composition Indeed the majority of studies in this review demonstrated a link between
weight and cancer-related risks (Hebert et al 1998 Enger et al 2004 Lahmann et al
2004 Patterson et al 2010)
Smoking Evidence pertaining to the smoking clearly demonstrates a link between
breast cancer survival and a history of smoking However it appears to be more likely to
increase all-cause mortality as opposed to cancer-specific mortality (Fentiman et al 2005
Holmes et al 2007 Sagiv et al 2007)
Alcohol Although the evidence is less clear pre-diagnosis alcohol consumption does
appear to be related to survival (McDonald et al 2002 Reding et al 2009) although
current drinking does not (Demark-Wahnefried 2002)
27
IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of
pathological states including cancer
31
Table 3 Breast Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Campbell et al (2007)
RCT examining the effects of 12-weeks of aerobic exercise training on 2-OHE
1 and 16α-OHE
1 in
premenopausal women Randomisation to 1) A 12-week individualised supervised moderate-to-vigorous intensity aerobic exercise training intervention (n = 17) Participants began the exercise program in the early follicular phase of the next menstrual cycle (days 1-5) The intervention was divided into three blocks (a) Weeks 1 ndash 4 ndash 3 sessions per week of base aerobic training progressing from 20-40 minutes on a stationary bike (b) Weeks 5-8 ndash 4 sessions per week Two sessions were base aerobic training sessions for 30-45 minutes (c) Weeks 9 -12 ndash 4 sessions per week with two base aerobic training sessions for 30-45 minutes and two interval sessions 2) Usual lifestyle (n = 15) Participants were asked to maintain their usual activity levels for the duration of the study Following the control cycle the first day of the next menstrual cycle was used as the reference start date for participants in the control group On completion of the 12-week post-intervention
Healthy regularly menstruating Caucasian women (n=32) 20-35 years
On completion of the 12-week intervention
Height body mass body composition by dual-energy X-ray absorptiometry and VO2max were measured at baseline and following the intervention Urine samples were collected in the luteal phase of four consecutive menstrual cycles
Participants attended an average of 40-44 (91) sessions Fourteen of 17 (82) participants completed at least 80 of the sessions The exercise group increased VO2max by 14 and had significant although modest improvements in fat and lean body mass No significant between-group differences were observed however for the changes in 2-OHE1 (P = 0944) 16α-OHE1 (P= 0411) or the ratio of 2-OHE1 to 16α-OHE1 (P = 0317) At baseline there was an inverse association between body fat and 2-OHE1 to 16α-OHE1 ratio (r = minus040 P = 0044) however it was the change in lean body mass over the intervention that was positively associated with a change in 2-OHE1 to 16α-OHE1 ratio (r = 043 P = 0015)
32
measurement participants were given guidance for starting an individualised exercise program and access to the fitness facility for 4-weeks
Friedenreich et al (2010)
A two-centre two-arm RCT examining how an aerobic exercise intervention influences
circulating
estradiol oestrone sex hormonendashbinding globulin
(SHBG)
androstenedione and testosterone levels which may
be involved in the
association between physical activity and
breast cancer risk
Randomisation to 1) A 1-year aerobic physical activity programme of 225-minutes per week (n=160) 2) Control group maintained their usual level of activity (n=160)
Older (50gt years) post-menopausal sedentary women (n=320)
On completion of the intervention
Estradiol and sex hormone-binding globulin levels Androstenedione and testosterone levels
Completion of the study was high (966) At 12-months statistically significant reductions in
estradiol (treatment effect ratio
[TER] = 093 95 CI 088 to 098) and free estradiol (TER = 091
95 CI 087 to 096) and increases in SHBG (TER = 104 95 CI
102 to 107) were observed in the exercise group compared with
the control group No significant differences in oestrone
androstenedione and testosterone levels were observed between
exercisers and controls at 12-months
Holick et al (2008)
Prospective cohort study examining the relationship between post-diagnosis recreational physical activity and risk of breast cancer death
Women with a history of previous invasive breast cancer diagnosed between the ages of 20-79 years (n=4482)
Maximum of 6-years post-diagnosis (median=56-years post-diagnosis)
Mortality from breast cancer mortality from any cause Self-reported physical activity converted to MET-hours per week
After adjusting for age at diagnosis stage of disease state of residence interval between diagnosis and physical activity assessment body mass index menopausal status hormone therapy use energy intake education family history of breast cancer and treatment modality compared with women expending lt28 MET-hwk in physical activity women who engaged in greater levels of activity had a significantly lower risk of dying from breast cancer (HR 065 95 CI 039-108 for 28-79 MET-hwk HR 059 95 CI 035-101 for 80-209 MET-hwk and HR 051 95 CI 029-089 for ge210 MET-hwk P for trend = 005) Results were similar for overall survival (HR 044 95 CI 032-060 for ge210 versus lt28 MET-hwk P for trend lt0001) and were similar regardless of a womanlsquos age stage of disease and body mass index
Holmes et al (2005)
Prospective observational study
(Nurseslsquo Health Study) to determine whether physical activity among
women with breast cancer
2987 female registered nurses
in the
Nurseslsquo Health
Women were diagnosed between 1984 and
Breast cancer mortality risk according
to
physical activity
Compared with women who engaged in less than 3 MET-hours per
week of physical activity the adjusted relative risk (RR) of death
from breast cancer was 080 (95 CI 060-106) for 3 to 89 MET-hours per week 050
(95 CI 031-082) for 9 to 149 MET-hours
33
decreases their risk of death from
breast cancer compared with
more sedentary women
Study diagnosed with stage
I II or III
breast cancer
1998 and followed until death or June 2002
category (lt3 3-89 9-149 15-239
or 24
metabolic equivalent task [MET] hours per week)
per week 056 (95 CI 038-084) for 15 to 239 MET-hours per
week and 060 (95CI 040-089) for 24 or more MET-hours per week (P for trend
= 004) Three MET-hours is equivalent to walking
at average pace of 2 to 29 mph for 1 hour The benefit of physical
activity was particularly apparent among women with hormone-
responsive tutors The RR of breast cancer death for women with hormone-responsive
tumours who engaged in 9 or more MET-hours
per week of activity compared with women with hormone-
responsive tumours who engaged in less than 9 MET-hours per
week was 050 (95 CI 034-074) Compared with women who
engaged in less than 3 MET-hours per week of activity the absolute
unadjusted mortality risk reduction was 6 at 10 years for women
who engaged in 9 or more MET-hours per week
Irwin et al (2008)
The Health Eating Activity and Lifestyle Study (HEAL) Prospective observational study investigating the association between pre- and post-diagnosis
physical activity (as well as
change in pre-diagnosis to post-diagnosis
physical activity) and
mortality among women with breast cancer
A subsample of participants from the HEAL study ndash 933 women diagnosed with local or regional breast cancer between 1995
and 1998
5 -8 years from diagnosis (median=6-years)
Primary outcomes total deaths
and breast
cancer deaths
Compared with inactive women the multivariable hazard ratios
(HRs) for total deaths for women expending at least 9 MET-
hours per week (approximately 2-3 hwk of brisk walking) were 069
(95 CI 045 to 106 P = 045) for those active in the year before
diagnosis and 033 (95 CI 015 to 073 P = 046) for those active
2-years after diagnosis Compared with women who were inactive
both before and after diagnosis women who increased physical
activity after diagnosis had a 45 lower risk of death (HR = 055
95 CI 022 to 138) and women who decreased physical activity
after diagnosis had a four-fold greater risk of death (HR = 395 95
CI 145 to 1050)
Ligibel et al (2008)
RCT examining the impact of physical activity on insulin levels Participants were randomly assigned to one of two conditions a)Physical activity intervention a 16-week supervised strength training and home-based cardiovascular training protocol (two supervised 50-minute strength training
sessions per
week and 90-minutes of home-based
aerobic physical activity
weekly) b) Control group routine care for 16-weeks before being offered consultation with an physical activity
Overweight sedentary stage
I-III breast
cancer survivors (n=101)
On completion of the 16-week intervention
Fasting insulin and glucose levels Weight body composition
and
circumference at the waist and hip
18 women withdrew consent andor did not complete the study
Baseline and 16-week measurements were available for 82 patients
Fasting insulin concentrations decreased by an average of
286 microUmL in the exercise group (P = 03) with no
significant change in the control group (decrease of 027 microUmL P
=
65) The change in insulin levels in the exercise group seemed
greater than the change in controls but the comparison
did not reach statistical significance (P = 07) There was a
trend toward improvement in insulin resistance in the exercise
group (P = 09) but no change in fasting glucose levels The
exercise group also experienced a significant decrease in hip
measurements with no change in weight or body composition
34
trainer at the end of the control
period
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer outcomes
Breast cancer Not reported Additional breast cancer events and mortality
Although observational data were not consistent physical activity appeared to be associated with a 30 decreased risk of mortality
Saxton et al (2010)
A review of studies pertaining to physical activity and cancer mortality
All cancers with more evidence obtained for breast cancer
Not reported Survival A number of prospective cohort studies have reported negative associations between physical activity and cancer mortality The most compelling observational evidence of the survival benefits to be gained from a physically active lifestyle has emerged from studies of post-diagnosis physical activity in breast and colorectal cancer survivors These studies have shown clear inverse associations between post-diagnosis activity and survival with the benefits being independent of age gender obesity and disease stage at diagnosis Three of the four cohort studies of breast cancer survivors showed that women who are achieving the equivalent of 30-miniutes of moderate intensity PA on five or more days of the week can halve their risk of mortality up to 8 years of follow-up
DIET
Borugian et al (2004)
Prospective cohort study testing the hypothesis that elevated wait-to-hip ratio is directly related to breast cancer
mortality
603 patients with incident
breast
cancer
Up to 10-years
Date of death and
primary and secondary cause of death
After adjustment for age BMI family history oestrogen
receptor (ER) status tumour stage at diagnosis and systemic
treatment (chemotherapy or tamoxifen) WHR was directly related to
breast cancer mortality in postmenopausal women (for highest
quartile vs lowest relative risk = 33 95 confidence interval
11 104) but not in premenopausal women (relative risk = 12
95 confidence interval 04 34) Stratification according to
ER
status showed that the increased mortality was restricted to ER-
positive postmenopausal women Elevated WHR was confirmed as
a predictor of breast cancer mortality with menopausal status and
ER status at diagnosis found to be important modifiers of that
relation
Boyapati et al (2005)
As part of the Shanghai Breast Cancer Cohort Study associations between soy and breast cancer survival were investigated
1459 breast cancer patients
52-years Disease-free survival
Soy intake pre-diagnosis was unrelated to disease-free breast cancer survival (adjusted hazard ratio [HR]=099 95 confidence interval [CI] 073-133 for the highest tertile compared to the lowest tertile) The association between soy protein intake and breast cancer survival did not differ according to ERPR status tumour stage age at diagnosis body mass index (BMI) waist to hip ratio (WHR) or menopausal status
Boyd et al (2003)
Meta-analysis of casendashcontrol and cohort studies published up to July 2003 which examined the
Varied Not reported Cancer incidence A total of 45 published studies containing 46 estimates of risk examined the role of dietary fat in relation to breast cancer risk by an analysis of nutrient intake Of these 31 were case control and
35
association of dietary fat or fat-containing foods with risk of breast cancer
14 were cohort in design and they contained a total of 25015 cases of breast cancer and over 580 000 control or comparison subjects The summary relative risk comparing the highest and lowest levels of intake of total fat was 113 (95 CI 103ndash125) Cohort studies (n=14) had a summary relative risk of 111 (95 CI 099ndash125) and casendashcontrol studies (N=31) had a relative risk of 114 (95 CI 099ndash132) Significant summary relative risks were also found for saturated fat (RR 119 95 CI 106ndash135) and meat intake (RR 117 95 CI 106ndash129) Combined estimates of risk for total and saturated fat intake and for meat intake all indicate an association between higher intakes and an increased risk of breast cancer Casendashcontrol and cohort studies gave similar results
Cade et al 2007)
A large UK cohort study comprising women with a wide range of different eating patterns to study the effects of different food and nutrient intakes on long-term health outcomes
35372 women (350 post- and 257 pre- menopausal women developed breast cancer)
Approx 75-years
Breast cancer incidence
In pre-menopausal but not post-menopausal women a statistically
significant inverse relationship was found between
total fibre intake and risk of breast cancer (P for trend = 001) The
top quintile of fibre intake was associated with a hazard ratio
of 048
[95 CI 024ndash096] compared with the lowest quintile Pre-
menopausal fibre from cereals was inversely associated with risk
of breast cancer (P for trend = 005) and fibre from fruit had a
borderline inverse relationship (P for trend = 009)
Chlebowski et al (2006a)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
randomisation to death from any cause
Attrition in the dietary intervention (n=44) versus control group (n=66) Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to
345] versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group A total of 277 relapse
events (local regional distant or ipsilateral breast cancer
recurrence or new contralateral breast cancer) have been reported
in 96 of 975 (98) women in the dietary group and 181 of 1462
(124) women in the control group The hazard ratio of relapse
events in the intervention group compared with the control group
was 076 (95 CI = 060 to 098 P = 077 for stratified log rank
and P = 034 for adjusted Cox model analysis)
36
dietary guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
Chlebowski et al (2008)
A protocol-mandated survival analysis update to the interim analysis of WINS (Chlebowski et al 2006a)
Breast cancer patients (n=2437)
Approximately 7-years
Overall survival Attrition in the intervention group (n=236) versus control group (n=172) Although fewer deaths were seen in the intervention group this was not statistically significant In 362 women with ER- and (progesterone receptor) PR- disease a significant overall survival benefit was seen in the intervention group (75 vs 181 cumulative mortality)
Cho et al (2003)
A prospective analysis of the relationship
between dietary fat
intake and breast cancer risk among pre-menopausal
women enrolled in
the Nurseslsquo Health Study
Pre-menopausal women (n=90655) aged between 26-46 years old when recruited in 1991
8-years after recruitment (1991-1999)
Fat intake was
assessed with a food-frequency questionnaire at baseline
in 1991
and again in 1995
During 8-years of follow-up 714 women developed incident
invasive breast cancer Relative to women in the lowest quintile of
fat intake women in the highest quintile of intake had a
slight increased risk of breast cancer (RR = 125 95 CI = 098
to 159 Ptrend = 06) The increase was associated with intake
of
animal fat but not vegetable fat RRs for the increasing quintiles of
animal fat intake were 100 (referent) 128 137 154 and 133
(95 CI = 102 to 173 Ptrend = 002) Intakes of both saturated and
monounsaturated fat were related to modestly elevated breast
cancer risk Among food groups contributing to animal fat red meat and high-fat dairy foods were each associated
with an increased
risk of breast cancer Information on oestrogen-receptor status was available for
80 (n = 570) of breast cancers and progesterone-
receptor status for 78 (n = 558) When divided according to
oestrogen and progesterone receptor status the positive
association between animal fat intake and breast cancer risk was
stronger among women with oestrogen receptor-positive or
progesterone receptor-positive cancers than among women with hormone receptor-negative cancers however the difference was not statistically significant
Dwyer et al (2008)
A sub-analysis of participants in the WINS trial (Chlebowski et al 2006a)
Breast cancer patients (n=550)
12-months of intervention
Disease-free survival
Attrition in the intervention group (n = 23 11) versus control group (n = 16 5)At baseline neither mean fat intake nor flavonoid intake differed between groups After 12-months of intervention dietary fat intake was significantly lower among those on the very low-fat diet (n =195) whilst flavonoid intake remained similar in both groups Neither total flavonoid intake nor intake of subclasses of flavonoids differed between those who had dramatically decreased their fat intake and those who had not
Fleischauer et al (2003)
Case-control study testing the hypothesis that antioxidant
385 post-menopausal
12-14-years Breast cancer recurrence or
Antioxidant supplement users compared with non-users were less likely to have a breast cancer recurrence or breast cancer-related
37
supplements may reduce the risk of breast cancer recurrence or breast cancer-related mortality
women with breast cancer
death death (OR = 054 95 CI = 027-104) Vitamin E supplements showed a modest protective effect when used for more than 3 years (OR = 033 95 CI = 010-107) Risks of recurrence and disease-related mortality were reduced among women using vitamin C and vitamin E supplements for more than 3 years
Gold et al (2009)
Secondary analysis of a purposive sample of WHEL participants to determine if a low-fat diet high in vegetables fruit
and fibre affects
prognosis in breast cancer survivors
with or without hot flashes (HF) after treatment Randomisation to one of two groups 1)An intensive telephone counselling intervention based on social cognitive theory promoted a daily dietary intake of
5 vegetable
servings 16oz of vegetable juice 3
fruit servings 30g fibre and 15-20 of energy
from fat
2) Control group received printed
materials (but no counselling) promoting the
5-a-day guidelines
of
daily intakes of 5 servings of fruit and
vegetables more than 20g of fibre and less than
30 of energy from fat
2967 women (96 of all enrolled in the WHEL study) whose baseline hot flush severity
report in
the prior 4-weeks was available
4-years into the intervention
Primary end points additional breast cancer events
(localregio
nal recurrence or distant metastasis or new primary
breast
cancer) and death from any cause
The intervention group consumed significantly more daily vegetablefruit
(54 higher)
fibre (31 higher) and less
percent energy from fat (14 lower) than the comparison group
HF-negative women in the intervention had 31 fewer events than
the comparison group The intervention did not affect prognosis in
the women with baseline HFs Compared with HF-negative women in the comparison group
HF-positive women had significantly fewer
events in both groups
Goodwin et al (2009)
A prospective cohort study examining the influence of vitamin D on breast cancer prognosis
512 women with early breast cancer
Mean = 116-years
Cancer recurrence and mortality
Women with deficient vitamin D levels had an increased risk of
distant recurrence (hazard ratio [HR] = 194 95 CI 116 to
325) and death (HR = 173 95 CI 105 to 286) compared with
those with sufficient levels The association remained after
individual adjustment for key tumour and treatment related factors but was
attenuated in multivariate analyses (HR = 171 95 CI
102 to 286 for distant recurrence HR = 160 95 CI 096 to
264 for death)
Grace et al (2004)
Prospective study (EPIC) examining associations between phytoestrogen and breast cancer risk 114 spot urines and 97 available serum
333 women (aged 45ndash75 years) drawn from the EPIC
Not reported Phytoestrogen concentrations and breast cancer incidence
Phytoestrogen concentrations in spot urine (adjusted for urinary creatinine) correlated strongly with that in serum with Pearson correlation coefficients gt 08 There were significant relationships (P lt 002) between both urinary and serum concentrations of
38
samples from women who later developed breast cancer Results were compared with those from 219 urines and 187 serum samples from healthy controls matched by age and date of recruitment
study isoflavones across increasing tertiles of dietary intakes Urinary enterodiol and enterolactone and serum enterolactone were significantly correlated with dietary fibre intake (r = 013ndash029) Exposure to all isoflavones was associated with increased breast cancer risk significantly so for equol and daidzein For a doubling of levels odds ratios increased by 20ndash45 [log2 odds ratio = 134 (106ndash170P = 0013) for urine equol 146 (105ndash202 P = 0024) for serum equol and 122 (101ndash148 P = 0044) for serum daidzein]
Howe et al (1990)
Pooled analysis of 12 case-control studies of diet and breast cancer risk
Healthy women Not reported Breast cancer incidence
A consistent statistically significant positive association was found
between breast cancer risk and saturated fat intake in
postmenopausal women (relative risk for highest vs lowest quintile
146 P lt0001) A consistent protective effect for a number of
markers of fruit and vegetable intake was demonstrated vitamin C
intake had the most consistent and statistically significant inverse
association with breast cancer risk (relative risk for highest vs
lowest quintile 069 P lt0001)
Holm et al (1993)
Interviews regarding diet history the purpose being to determine whether dietary habits are associated with disease-free survival
in patients with
breast cancer who have undergone treatment
240 women with stage I-II breast cancer (50ndash65 years old) 209 of whom were post-menopausal
4-years Disease-free survival
Cancers were classified as oestrogen receptor (ER) rich ( 010
fmolmicrog of DNA) in 149 patients and as ER poor (lt010 fmolmicrog
of
DNA) in 71 patients Fifty-two patients had treatment failure during
follow-up The 30 patients with ER-rich tumours who had treatment
failure reported higher intakes of total fat saturated fatty acids and
polyunsaturated fatty acids than did the 119 patients with ER-rich
tumours that did not have treatment failure The multiple-odds ratio
(OR) for treatment failure in these women was 108 for each 1
increment in percentage of total energy (E) from total fat For
treatment failure within the first 2 years the OR was 119 for each
1-mg increase in vitamin E intake per 10 mega joules of energy In
women with treatment failure 2ndash4 years after diagnosis Ors were
113 and 123 for each E increment in total fat or saturated fatty
acids respectively No association between dietary habits and
treatment failure was found for women with ER-poor cancers
39
Holmes et al (1999)
Cohort study (Nurseslsquo Health Study)
to determine whether intakes
of fat and fatty acids are associated
with breast cancer
88795 women free of cancer (2956 developed breast cancer)
14-years Relative risk of invasive breast
cancer for
an incremental increase of fat intake
Compared with women obtaining 301 to 35 of energy from fat women consuming 20 or less had a multivariate
RR of breast
cancer of 115 (95 CI 073-180) In multivariate models the RR
(95 CI) for a 5-of-energy increase was 097 (094-100) for total
fat 098 (096-101) for animal fat 097 (093-102) for vegetable
fat 094 (088-101) for saturated fat 091 (079-104) for
polyunsaturated fat and 094 (088-100) for monounsaturated fat
For a 1 increase in energy from trans-unsaturated fat the values
were 092 (086-098) and for a 01 increase in energy from
omega-3 fat from fish the values were 109 (103-116)
Hunter et al (1996)
Pooled analysis of 7 prospective studies in 4 countries to establish estimates of the relation of fat
intake
to the risk of breast cancer
Studies included
33781
9 women
Not reported Breast cancer incidence
Information about 4980 cases from studies including 337819
women was available When women in the highest quintile of
energy-adjusted total fat intake were compared with women in the
lowest quintile the multivariate pooled relative risk of breast cancer
was 105 (95 CI 094 to 116) Relative risks for saturated
monounsaturated and polyunsaturated fat and for cholesterol
considered individually were also close to unity There was little
overall association between the percentage of energy intake from
fat and the risk of breast cancer even among women whose energy
intake from fat was less than 20
Ingram et al (1994)
Cohort study evaluating the role of vitamins in breast cancer mortality
103 women 3-months post-operation for primary breast cancer
Mean= 81-months
Mortality from breast cancer
27 women died ndash 21 with advanced breast cancer and 6 from other causes The most important findings from the nutrient consumption assessment were associated with vitamin consumption in particular beta-carotene and vitamin C At high levels of consumption there were significantly fewer deaths from breast cancer only one in the group of highest beta-carotene consumers compared with eight in the intermediate group and 12 in the lowest group (trend P = 00012) equivalent figures for vitamin C were 3 7 and 11 deaths for the highest intermediate and lowest consumption groups respectively (trend P = 00286)
Keinan-Boker et al (2004)
An investigation of the association between phytoestrogen
intake and
breast cancer risk in a large prospective study in
a Dutch
population with a habitually low phytoestrogen intake (EPIC)
15555 women aged
49ndash70
years who constituted a Dutch cohort the EPIC study
Median = 52-years
Breast cancer incidence
A total of 280 women were newly diagnosed with breast cancer
during follow-up The median daily intakes of isoflavones and
lignans were 04 (interquartile range 03ndash05) and 07 (05ndash08)
mgd respectively Relative to the respective lowest intake
quartiles the hazard ratios for the highest intake quartiles for
isoflavones and lignans were 10 (95 CI 07 15) and 07 (05
11) respectively Tests for trend were non-significant
Khaodhiar et al (2003)
A subgroup analysis of WINS participants (Chlebowski et al
53 women from 3 clinical
sites
2-years after start of
Insulin resistance and dietary fat
Of those women with initial insulin resistance after 1-year women in
the intervention group saw their fasting insulin decrease by 18 plusmn 34
40
2006a) examining relationships between dietary intake and insulin resistance
who had serum insulin and lipid profiles evaluated at baseline
and
after 2-years
commencing intervention
intake microUmL in comparison fasting insulin of women in the control
group decreased by only 138 plusmn 47 microUmL Although not
quite
statistically significant these results predict that elevated insulin concentrations (a marker of insulin resistance)
may be influenced by
dietary fat reduction There were no significant differences between
the treatment groups over time and no time x treatment interactions
and no significant differences were seen between the insulin-
resistant and non-insulin-resistant subgroups
Kim et al (2006)
The Nurseslsquo Health Study a prospective cohort study examining the relationship between dietary fat and incidence of breast
cancer in
post-menopausal women
Cohort of 80375 US women
Followed for 20-years between 1980 and 2000 with questionnaire being mailed every 2-years
Incidence of breast cancer The Food Frequency Questionnaire
The multivariable relative risk for an increment of 5 of energy from
total dietary fat intake was 098 (95 CI 095 100) Additionally
specific types of fat were not associated with an increased risk of
breast cancer Furthermore secondary analyses indicated no
differences in breast cancer risk by oestrogen receptor or
progesterone receptor status However stratification by
waist circumference indicated a significant decrease in breast
cancer risk for participants with a waist circumference of 35
inches (889cm) or greater (p-trend = 004)
Kyogoku et al (1992)
The present study utilised breast cancer patients whose dietary intake was assessed 10-years previously in a case-control study to determine whether dietary intake is related prognosis
212 breast cancer patients post-surgery
Followed-up until 1987 (9-12 years)
Mortality A total of 47 breast cancer deaths were certified The 5- and 10-year relative survival rates were 785 and 753 respectively The investigation did not provide any support for the hypothesis that a high-fat diet is a survival determinant for breast cancer patients
McEligot et al (2006)
Retrospective study into the influence of diet (fat fibre vegetable and fruit intakes and micronutrients (folate carotenoids and vitamin C) on overall survival in women diagnosed with breast cancer
Post-menopausal breast cancer survivors (n = 516)
Mean of 80-months post-diagnosis
Death due to any cause
The hazard ratio [HR and 95 CI] of dying in the highest tertile compared to the lowest tertile of total fat fibre vegetable and fruit was 312 (95 CI = 179-544) 048 (95 CI = 027-086) 057 (95 CI = 035-094) and 063 (95 CI = 038-105) respectively (P le 005 for trend except for fruit intake) Other nutrients including folate vitamin C and carotenoid intakes were also significantly associated with reduced mortality (P le 005 for trend)
Pierce et al (2007)
The multicentre WHEL RCT (see Gold et al 2009 in table)
Breast cancer (n=3088) intervention (n=1537) comparison (n=1551)
After 7-years of intervention
Invasive breast cancer event (recurrence
or
new primary) or death from any cause
Attrition in the intervention group (n=38) versus control group (n=27) There were no additional health benefits of dramatically increasing intake of nutrient-rich plant-based foods relative to the comparison group
Thomson et al (2007)
Sub-analysis of a purposive sample of participants in the WHEL RCT (see Gold et al 2009 in table)
Breast cancer patients (n=207)
Not reported Oxidative stress A significant inverse association was found between total plasma carotenoid concentrations and oxidative stress
41
WEIGHT
Caan et al (2008)
Retrospective study examining whether weight gain after diagnosis of breast cancer affects the risk of breast cancer recurrence Weight change from 1-year pre-diagnosis to study enrolment was calculated
3215 women with early stage breast cancer
Median of 737-months post-diagnosis
Breast cancer recurrence
Neither moderate (5ndash10) nor large (gt 10) weight gain (HR 08 95 CI 06ndash11 HR 09 95 CI 07ndash12 respectively) after breast cancer diagnosis was associated with an increased risk of breast cancer recurrence in the early years post-diagnosis
Enger et al (2004)
A retrospective cohort study using patient medical
records electronic
cancer registry data and archived tissue
specimens to examine
correlates of body weight with mortality in early-stage breast cancer
Women (n=1376)
24-
81 years of age diagnosed with breast cancer
Median=68 years post-diagnosis
Body weight at the time of diagnosis
and
patient status (ie alive and free of breast cancer living
with breast
cancer dead of breast cancer or dead of other
cause) at
the time of longest follow-up
246 patients died from breast cancer Among patients with early-
stage disease (I and IIA) a dose-response relationship was
observed with increasing weight and likelihood of dying of breast
cancer Compared with women in the lowest category of weight (lt133lb [60 kg] at diagnosis) women in the highest category ( 17
lb
[79 kg]) experienced a 25-fold increased risk of dying from breast
cancer (HR ratio 254 [95 CI 108-600] trend P = 02) Women
with ER-negative cancer experienced an approximately 2-fold
higher risk of dying from breast cancer compared with women with
ER-positive cancer regardless of stage at diagnosis Women in the
upper 50th percentile of weight with early-stage
disease and with
ER-negative tumours had a nearly 5-fold increased risk of dying
(HR ratio 499 [95 CI 217-1148] P for interaction = 10)
compared with women in the lower 50th percentile of weight
and ER-
positive tumours
Hebert et al (1998)
Prospective cohort study examining the effect of diet and body weight on recurrence and death in breast cancer patients
472 women diagnosed with early-stage breast cancer in 1982ndash1984
Ranged from 8-10 years
Breast cancer recurrence and mortality
After accounting for disease stage and age reported baseline consumption (timesday) of butter margarine and lard (risk ratio (RR)=167 95 CI=117ndash239) and beer (drinksday) (RR=158 95 CI=115ndash217) increased the risk of recurrence There also appeared to be an increased risk associated with consumption of red meat liver and bacon corresponding to about a doubling of risk for each time per day that foods in this category were consumed (RR=193 95 CI=089ndash415) Relative body weight increased risk at the rate of 9 (RR=109 95 CI=102ndash117) for
each kgm2 (equivalent to about 58 pounds for a woman 5 4 tall) For death the results were similar but relative weight was more strongly associated increasing risk by 12 per kgm2 (RR=112 95 CI=103ndash122)
Kroenke et al (2005)
A prospective study of a purposive subsample of participants from the Nurseslsquo Health Study ndash to determine
5204 Nurseslsquo Health Study participants
2-26 years with a median
Incident breast cancer
Weight before diagnosis was positively associated with breast
cancer recurrence and death but this was apparent only in never
smokers Similarly among never-smoking women those who
42
whether weight prior to diagnosis and weight gain
after diagnosis are
predictive of breast cancer survival
diagnosed with
incident invasive non-metastatic breast cancer between
1976
and 2000
follow-up of
9-years Breast cancer recurrence Mortality for any cause Self-reported BMI
gained between 05 and 20 kgm2 (median gain 60 lb relative risk
[RR] 135 95 CI 093 to 195) or more than 20 kgm
2 (median
gain 170lb RR 164 95 CI 107 to 251) after diagnosis had an
elevated risk of breast cancer death during follow-up (median 9
years) compared with women who maintained their weight (test for
linear trend P = 03) Associations with weight were stronger in
premenopausal than in postmenopausal women
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer
Breast cancer Not reported Additional breast cancer events and mortality
The most consistent finding from observational studies was that adiposity was associated with a 30 increased risk of mortality
SMOKING
Holmes et al (2007)
A prospective observational study among 5056 women from the Nurseslsquo Health Study for whom data on smoking history was available
Women with Stages I-III invasive breast cancer diagnosed between 1978 and 2002
Median = 83 years
Death by any cause Cause of death was ascertained from death certificates supplemented as needed with physician review of medical records
Compared with never smokers women who were current smokers had a 43 increased adjusted relative risk (RR) 95 CI 124-165] of death from any cause A strong linear gradient was observed with the number of cigarettes per day smoked p-trend lt00001 the RR (95 CI) for 1-14 15-24 and 25 or more cigarettes per day was 127 (101-161) 130 (108-157) and 179 (147-219) In contrast there was no association with current smoking and breast cancer death the RR (95 CI) was 100 (083-119) Current and past smokers were more likely than never smokers to die from primary lung cancer chronic obstructive pulmonary disease and other lung diseases
Fentiman et al (2005)
Cohort study testing the hypothesis that smokers have a worse breast cancer prognosis
Women (n=166) with stage III invasive breast cancer
Mean = 132-months
Overall and cancer-specific disease-free survival
Smoking was the third most important predictor of distant relapse-free breast cancer-specific and overall survival after stage and age at diagnosis
Manjer et al (2000)
Cohort study examining whether smoking is associated with prognostic markers other than more advanced disease (eg hormone receptor status histopathology and tumour differentiation)
268 women with recurring breast cancer drawn from a cohort of 10902 women (35 smokers)
An average of 124-years
Hormone receptor status identified by tumour tissue
The relative risk (RR) of oestrogen receptor-negative tumours was for current smokers 221 [95 CI 123-396] and for ex-smokers 267 (95 CI 141-506) compared to never-smokers Ex-smokers had an increased risk of progesterone receptor-negative tumours (RR = 161 95 CI 107-241) but there were no other significant associations between smoking habits and oestrogen receptor-positive or progesterone receptor-positive or ndashnegative tumours The incidence of Nottingham grade III tumours was higher in ex-smokers than in never-smokers (RR = 203 95 CI 117-354)
Sagiv et al (2007)
Cohort study examining the association between active and passive cigarette smoking before
Women with invasive breast cancer
Approximately 6-years after
All-cause mortality including breast
The adjusted hazards ratios (HRs) for all-cause mortality were slightly higher among current and former active smokers compared with never smokers (HR 123 95 CI 083ndash184) and 119 (95
43
breast cancer diagnosis and survival (n=1273) participating in a population-based casendashcontrol study
diagnosis cancer-specific mortality as reported to the National Death Index
CI 085ndash166) respectively) No association was found between active or passive smoking and breast cancer-specific mortality All-cause and breast cancer-specific mortality was higher among active smokers who were postmenopausal (HR 164 95 CI 103ndash260 and HR 145 95 CI 078ndash270 respectively) or obese at diagnosis (HR 210 95 CI 103ndash427 and HR 197 95 CI 089ndash436 respectively)
ALCOHOL
McDonald et al (2002)
Prospective cohort study examining the influence of alcohol consumption on breast cancer survival in African American women
Post-menopausal African-American women with invasive breast cancer (n=125)
Followed for survival through December 1998 (median = 648 months)
Survival Pre-morbid alcohol consumption of at least one drink per week was associated with 27-fold increase in risk of death (95 CI 13ndash58)
Reding et al (2009)
Sub-analysis of participants from two case-control studies to examine the effects on prognosis of alcohol consumption after breast cancer diagnosis
1286 women diagnosed with invasive breast cancer at age le45 years from two population-based case-control studies
Followed from their diagnosis of breast cancer (between January 1983 and December 1992) through to June 2002
The primary mortality endpoint used was all-cause mortality
After adjusting for age and diagnosis year compared with non-drinkers women who consumed alcohol in the 5 years before diagnosis had a decreased risk of death [gt0 to lt3 drinks per week hazard ratio 07 95 CI 06-095 3 to lt7 drinks per week risk ratio 06 95 CI 04-087 drinks per week risk ratio 07 95 CI 05-09]
Rock and Demark-Wahnefried (2002)
A review of evidence from clinical and
epidemiologic studies examining
the relationship between nutritional
factors and breast cancer survival
Women with breast cancer
Not reported Survival Alcohol intake was not associated with survival in the majority of the
studies that examined this relationship
44
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
colorectal cancer survival In the current review 2 studies were identified Studies are
summarised in Table 4 at the end of this section
In a cohort study self-reported leisure time physical activity was assessed in 41528
Australians among whom 526 cases of colorectal cancer were identified (Haydon et al
2006) Those who reported regular physical activity (at least once per week) prior to
diagnosis had improved cancer-specific survival (73 5-year survival) compared with
those not reporting regular physical activity (61 5-year survival) Another study of
stage III colorectal cancer survivors (n=816) over a 3-year period post-surgery and
chemotherapy showed increases in disease-free survival and overall survival with
increasing volumes of physical activity (p lt 05) (Meyerhardt et al 2005)
ii DIET
Bekkering et al (2006) report on six high fibre diet interventions that showed little effect on
the risk of colorectal cancer recurrence (McKeown-Eyssen et al 1995 MacLennan et al
1999 Alberts et al 2000 Bonithon-Kopp et al 2000 Schatzkin et al 2000 Ishikawa et al
2005) On combining data from two beta-carotene trials (Greenberg et al 1994
MacLennan et al 1999) four multivitamin trials (Greenberg et al 1994 Ponz and
Roncucci 1997 Hofstad et al 1998 McKeown-Eyssen et al 1995) and one trial containing
a multivitamin arm and an N-acetylcysteine (found in high protein foods) arm (Ponz and
Roncucci 1997) there was weak evidence of a reduction in risk of colorectal polyps
(abnormal growth of tissues in the colon) Two calcium interventions showed some
evidence of a reduced risk of recurrence (Baron et al 1999 Bonithon-Kopp et al 2000)
In the current review 5 studies provided further evidence for the role of diet in colorectal
cancer survival
Dietary Fibre
The association between dietary fibre and incidence of colorectal cancer was examined in all
participants (n=519978) taking part in the EPIC study (Bingham et al 2003) After 45-years
of follow-up self-reported dietary data for 1065 reported cases of colorectal cancer were
showed that higher dietary fibre was associated with a reduced risk of developing
large bowel cancer Interestingly the protective effect was greatest for the left side of the
colon and least for the rectum No food source of fibre was significantly more protective of
cancer incidence than others Confirmation of these findings after adjustment for folate and
with a longer follow-up has been reported (Bingham et al 2004 Norat et al 2005)
45
Red and Processed Meat
The EPIC study also offers support for the hypotheses that consumption of red and
processed meat increases colorectal cancer risk while intake of fish decreases risk
(Norat et al 2005) Meyerhardt et al (2007) support this further in a study examining dietary
patterns in stage III colorectal cancer survivors (n=1009) After a median of 53-years follow-
up a significant difference was found between those who had followed a prudentlsquo diet and
those who had followed a Westernlsquo diet
A higher intake of a Western dietary pattern post-diagnosis was associated with a
significantly worse disease-free survival (colon cancer recurrences or death) (p
lt001) The Western dietary pattern was associated with a similar detriment in overall
survival (p lt001)
Vitamin D
Ng et al (2008) examined pre-diagnosis levels of vitamin D in a cohort of participants with
colorectal cancer (n=304) from the Nursesrsquo Health Study28 which demonstrated that higher
plasma vitamin D levels were associated with a significant reduction in mortality from
any cause This indicates that lifestyle pre-diagnosis can produce post-diagnosis benefits
Dietary Supplements
A double-blind randomised placebo-controlled intervention study (the FAB2 Study) was
carried out with healthy controls (n=98) and patients with colorectal polyps (n=106) to
examine the effects of folic acid (a B vitamin found in leafy vegetables such as spinach
asparagus and lettuce) and riboflavin (a B-vitamin found in lean meats eggs nuts and
dairy products) supplements on biomarkers of colorectal cancer risk (Powers et al 2007)
Participants were randomised to receive one of four treatments
1) placebo capsule daily
2) 400μg of folic acid daily
3) 1200μg of folic acid daily
4) 400μg of folic acid with 5mg of riboflavin daily
28
One of the largest and longest running investigations of factors that influence womenlsquos health
comprising information from 238000 nurse-participants
Prudent diet High intake of fruit vegetables poultry and fish
Western diet
High intake of meat fat refined
grains sweets and desserts
46
Short-term low folic acid supplements in the range of 400μg were found to elicit a
significant increase in mucosal folate concentration causing a number of physiologic
responses that may reduce the risk of cancer recurrence This adds to the evidence that
increased fibre might be protective against cancer mortality since folate and fibre are
generally found in the same foods
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in colorectal
cancer recurrence In the current review 3 studies were identified
Dignam et al (2006) explored the impact of obesity via retrospective data from patients with
confirmed Dukes B or C colorectal cancer (n=4288) and found that very obese men and
women have an increased risk of recurrence In contrast the multicentre prospective
observational CALBG 8980 trial has shown that increased BMI during and 6-months after
adjuvant chemotherapy for stage III colorectal cancer (n=1053) was not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008)
Sinicrope et al (2010) categorised stage II and III colon cancer (n=4381) patients enrolled
in seven RCTs whilst undergoing adjuvant chemotherapy according to their BMI They
found that BMI was significantly associated with both disease-free survival and overall
survival in both men and women when compared to normal-weight controls Being
overweight was associated with improved overall survival in men whilst being underweight
was associated with significantly worse overall survival in women This demonstrates that
obesity is an independent prognostic variable in colon cancer survivors as well as showing
gender-related differences that require further investigation
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in colorectal
cancer survival and no studies were identified in the current review
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in colorectal
cancer survival Preliminary EPIC results indicate that current alcohol intake is
significantly positively associated with risk of rectal but not of colon cancer (Ferrari et
al (2007)
47
SUMMARY OF LIFESTYLE EVIDENCE FOR COLORECTAL CANCER ndash
MECHANISMS OF BENEFIT
Physical Activity There is very little evidence available for the role of physical activity in
colorectal cancer outcomes however the evidence that is available looks promising
Specifically regular physical activity of at least once per week pre-diagnosis has been found
to improve 5-year survival rates (Haydon et al 2006) This highlights the importance of
physical activity being integrated into an individuallsquos way of life even before the occurrence
of illness Furthermore long-term physical activity post-surgery can further increase chances
of recurrence-free survival and there is also evidence of a dose-effect survival benefits
increase with amount of exercise (Meyerhardt et al 2005)
Diet Whilst evidence for dietary fibre has been mixed the additional evidence presented
within this review places greater weight in favour of increased dietary fibre Indeed the
conclusion of one study was that in populations with low average intake of dietary fibre an
approximate doubling of total fibre intake from foods could reduce the risk of colorectal
cancer by 40 (Bingham et al 2003) Evidence of this protective benefit for dietary fibre is
further supported by research demonstrating that short-term low folic acid (found in fibrous
foods) supplements in the range of 400μg can reduce the risk of cancer recurrence (Powers
et al 2007) There is a general consensus that mechanisms of benefit from dietary fibre
come from increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic mucosa (tissue
that lines the colon) (Kim 2000) Evidence has also been presented supporting the
hypothesis that red and processed meat increases colorectal cancer risk while fish
decreases risk (Norat et al 2004)
Weight Two large-scale studies offer contrasting findings for the role of weight
in colorectal cancer outcomes One prospective observational study demonstrates that
increased BMI during and 6-months after adjuvant chemotherapy is not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008) The other
retrospective study demonstrates that very obese men and women have an increased risk
of recurrence Drawing on 7 RCTs Sinicrope et al (2010) provides further evidence for BMI
was being significantly associated with both disease-free and overall survival Overall there
is greater evidence showing weight to be an important predictor of colorectal cancer
outcomes There is also some evidence of gender differences being overweight was
associated with improved overall survival in men whilst being underweight was associated
with significantly worse overall survival in women There is evidently a need to explore this
differential effect more closely However there is also the need to consider the impact of
body composition on the development of other chronic conditions including diabetes and
cardio-respiratory conditions
Smoking and Alcohol Further research is needed into smoking and alcohol
consumption especially in terms of colorectal cancer prognosis There is some evidence
indicating that current alcohol intake increases risk of rectal but not colon cancer a finding
that requires further investigation to ascertain underlying mechanisms of benefit (Ferrari et
al 2007) Since alcohol can reduce absorption of folate it is possible that the mechanism
48
of benefit is as with dietary fibre intake related to stool bulk and less contact time between
carcinogens and colonic mucosa
49
Table 4 Colorectal Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Haydon et al (2006)
Incident cases of colorectal cancer were identified among participants of the Melbourne Collaborative Cohort Study and examined against self-reported physical activity
526 Australians with colorectal cancer
Median = 55 years
Body fat Disease-specific survival
Exercisers had an improved disease specific survival (hazard ratio 073 (95 CI 054ndash100) The benefit of exercise was largely confined to stage IIndashIII tumours (hazard ratio 049 (95 CI 030ndash079) Increasing per cent body fat resulted in an increase in disease-specific deaths (hazard ratio 133 per 10 kg (95 CI 104ndash171) Similarly increasing waist circumference reduced disease specific survival (hazard ratio 120 per 10 cm (95 CI 105ndash137)
Meyerhardt et al (2005)
Prospective study of recreational physical activity and prognosis
among
stage III colon cancer patients enrolled in a
RCT of post-operative adjuvant
chemotherapy (bolus 5-
fluorouracilleucovorin +- irinotecan)
816 patients with stage III colon cancer
Midway through adjuvant therapy and again 6-months post-therapy (12ndash14 months after enrolment)
Physical activity levels were measured as MET-hours-per-week Disease-free survival
Levels of physical activity were associated with significantly improved
disease-free survival among patients with stage III colon cancer After
adjustment for age gender baseline performance status N stage T
stage preoperative CEA bowel obstruction and perforation level of
differentiation treatment arm and body mass index the hazard ratio
(HR) for DFS for individuals in the highest quintile (gt25 MET-
hoursweek eg Jog 3ndash4 hoursweek or brisk walk [3ndash4 mph] daily)
was 065 (95 CI 038ndash111 p for trend = 002) compared to those
in the lowest quintile of PA This relationship varied by gender with a
HR = 033 [95 CI 011ndash099] for women (p for trend = 0046) and a
HR= 089 [95 CI 044ndash178] for men (p for trend = 03)
DIET
Bingham et al (2003)
Prospective examination of the association between dietary fibre intake and incidence of colorectal cancer in individuals taking part in the EPIC study recruited from ten European countries
519978 men and women in the EPIC study (1065 cases of colorectal cancer)
45 years
Colorectal cancer incidence
Dietary fibre in foods was inversely related to incidence of large bowel cancer (adjusted relative risk 0middot75 [95 CI 0middot59ndash0middot95] for the highest versus lowest quintile of intake) the protective effect being greatest for the left side of the colon and least for the rectum After calibration with more detailed dietary data the adjusted relative risk for the highest versus lowest quintile of fibre from food intake was 0middot58 (0middot41ndash0middot85)
Meyerhardt et al (2008)
Prospective observational study to
determine the association of dietary patterns
with cancer recurrences and
mortality of colon cancer survivors
1009 patients with stage III colon cancer who were
enrolled in
a randomized
Median = 53-years
Colon cancer recurrence and mortality
A higher intake of a Western dietary pattern after cancer diagnosis
was associated with a significantly worse disease-free survival (colon
cancer recurrences or death) Compared with patients in the lowest
quintile of Western dietary pattern those in the highest quintile experienced an adjusted hazard
ratio (AHR) for disease-free survival
of 325 (95 confidence interval [CI] 204-519 P for trend lt001)
50
adjuvant chemotherapy trial (CALGB
89803)
The Western dietary pattern was associated with a similar detriment
in recurrence-free survival (AHR 285 95 CI 175-463) and overall
survival (AHR 232 95 CI 136-396]) comparing highest to
lowest quintiles (both with P for trend lt001)
Ng et al (2008)
Nurseslsquo Health Study prospective examination of the association between pre-diagnosis
25(OH)D levels and
mortality in colorectal cancer patients
304 colorectal cancer patients
Mean = 78-months for participants still alive
Colorectal cancer mortality
Higher plasma 25(OH)D levels were associated with a significant
reduction in overall mortality (P for trend = 02)
Compared with the lowest quartile participants in the highest
quartile had an adjusted HR of 052 (95 CI 029 to 094) for
overall mortality A trend toward improved colorectal cancerndash
specific mortality was also seen (HR = 061 95 CI 031 to 119)
Norat et al (2005)
The EPIC prospective study of 478040 cancer-free men and women from 10 European countries examining meat fish and colorectal cancer risk
478040 cancer-free men and women taking part in the EPIC study
Mean=48 years
Colorectal cancer incidence
Colorectal cancer risk was positively associated
with intake of red and processed meat (highest [gt160
gday] versus lowest [lt20 gday] intake HR = 135 95 CI = 096
to
188 Ptrend = 03) and inversely associated with intake of fish (gt80
gday versus lt10 gday HR = 069 95 CI = 054 to
088 Ptrendlt001) but was not related to poultry intake In this study
population the absolute risk of development of colorectal
cancer within 10-years for a study subject aged 50 years was 171
for the highest category of red and processed meat intake and 128
for the lowest category of intake and was 186 for subjects in
the lowest category of fish intake and 128 for subjects in
the highest category of fish intake
Powers et al (2007)
A double-blind RCT (the FAB2 Study) to examine effects of folic acid and riboflavin supplements on biomarkers of colorectal cancer risk Participants were randomised to receive one of the following for 6 ndash 8 weeks 1)400μg of folic acid 1200μg of folic acid or 400μg of folic acid plus 5 mg of riboflavin 2) placebo
Healthy controls (n=98) and patients with colorectal polyps (n=106)
On completion of 6-8 week intervention
Biomarkers of folate and riboflavin status
Supplementation with folic acid elicited a significant increase in mucosal 5-methyl tetrahydrofolate and a marked increase in RBC and plasma with a dose-response Measures of riboflavin status improved in response to riboflavin supplementation Riboflavin supplement enhanced the response to low-dose folate in people carrying at least one T allele and having polyps The magnitude of the response in mucosal folate was positively related to the increase in plasma 5-methyl tetrahydrofolate but was not different between the healthy group and polyp patients
WEIGHT
Dignam et al (2006)
Investigating the association between BMI and colorectal cancer outcomes in patients from cooperative group clinical trials
4288 patients with Dukes
BC
colon cancer in National
Median =112-
years Risk of recurrence second primary
Very obese patients (BMI 35 kgm2) had greater risk
of a
colon cancer event (recurrence or secondary primary tumour hazard
ratio [HR] = 138 95 confidence interval [CI] = 110 to 173) than
normal weight patients (BMI = 185ndash249 kgm
2) Mortality was
51
Surgical Adjuvant Breast and Bowel Project
RCTs
cancer and
mortality evaluated in
relation to
BMI at diagnosis
greater for very obese (HR = 128 95 CI = 104 to 157) and
underweight (BMI lt 185 kgm2) (HR
= 149 95 CI = 117 to 191)
than for normal weight patients The increased risk of mortality for
underweight patients was dominated by nonndashcolon cancer deaths
(HR of such deaths compared with normal weight patients = 223 95 CI = 150 to
331) whereas for the very obese deaths likely due
to colon cancer were increased (HR = 136 95 CI = 106 to 173)
Meyerhardt et al (2008)
A prospective observational study of patients who had stage III colon cancer and who enrolled on a RCT of adjuvant chemotherapy Results
1053 patients who had stage III colon cancer
6-months post- chemotherapy
Patients were observed for cancer recurrence or death
Increased BMI was not significantly associated with a higher risk of colon cancer recurrence or death (P trend = 54) Compared with normal-weight patients (BMI 21 to 249 kgm
2) the multivariate
hazard ratio for disease-free survival was 100 (95 CI 072 to 140) for patients with class I obesity (BMI 30 to 349 kgm
2) and 124
(95 CI 084 to 183) for those with class II to III obesity (BMI ge 35 kgm
2) after analysis was adjusted for tumour-related prognostic
factors physical activity tobacco history performance status age and sex Similarly after analysis was controlled for BMI weight change (either loss or gain) during the time period between ongoing adjuvant therapy and 6-months after completion of therapy did not significantly impact on cancer recurrence andor mortality
Sinicrope et al (2010)
BMI (kgm2) was categorised in patients
with tumour-node-metastasis stage II and III colon carcinomas enrolled in seven RCT of 5-fluorouracilndashbased adjuvant chemotherapy to determine the association of BMI with disease-free survival and overall survival
Men and women with stage II and III colon carcinomas (n = 4381) enrolled in seven RCTs of 5-fluorouracilndashbased adjuvant chemotherapy
Not reported Disease-free survival Overall survival
BMI was significantly associated with both disease-free survival (P = 0030) and overall survival (P = 00017) Men with class 23 obesity showed reduced overall survival compared with normal-weight men [hazard ratio 135 95 CI 102-179 P = 0039] Women with class I obesity had reduced overall survival [hazard ratio 124 95 CI 101-153 P = 0045] compared with normal-weight women Overweight status was associated with improved overall survival in men (P = 0006) and underweight women had significantly worse overall survival (P = 0019)
ALCOHOL
Ferrari et al (2007)
As part of the prospective EPIC study data was collected examining the relationship between lifetime and baseline alcohol consumption and colorectal cancer incidence
478732 EPIC subjects free of cancer at enrolment between 1992 and 2000
62 years Colorectal cancer incidence
Lifetime alcohol intake was significantly positively associated to CRC risk (hazard ratio HR = 108 95CI = 104-112 for 15 gday increase) with higher cancer risks observed in the rectum (HR = 112 95CI = 106-118) than distal colon (HR = 108 95CI = 101-116) and proximal colon (HR = 102 95CI = 092-112) Similar results were observed for baseline alcohol intake When assessed by alcoholic beverages at baseline the CRC risk for beer
52
(HR = 138 95CI = 108-177 for 20-399vs 01-29 gday) was higher than wine (HR = 121 95CI = 102-144) although the two risk estimates were not significantly different from each other Higher HRs for baseline alcohol were observed for low levels of folate intake (113 95CI = 106-120 for 15 gday increase) compared to high folate intake (103 95CI = 098-109)
53
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
prostate cancer survival In the current review 2 studies were identified Studies are
summarised in Table 5 at the end of this section
The underlying mechanisms for the direct anti-cancer effect of lifestyle has been indicated in
a study with men undergoing a diet and physical activity intervention comprising the majority
of calories from complex carbohydrates high in fibre combined with 1-hour of supervised
exercise (Soliman et al 2009) Serum (blood plasma) was taken from these men and added
to androgen-dependent LNCaP cells29 in the laboratory There was decreased growth and
increased apoptosis (cell death) associated with a reduction in serum Insulin-like Growth
Factor (IGF)-130 These findings indicate that diet and physical activity interventions
might slow prostate cancer progression as well as aid in its treatment during the early
stages of development
Kenfield (2010) examined the data of 2686 men from the Health Professionals Follow-Up
Study31 and found that men who engaged in 3gt MET-hours of weekly physical activity
post-diagnosis reduced their risk of death by 35 compared with men who engaged
in less weekly activity Furthermore men who walked 90-minutes per week at a normal to
brisk pace had a 51 lower risk of death due to any cause compared with men who walked
90-minutes or less at an easy pace To reduce their risk of cancer-specific death men
had to engage in vigorous activity such as jogging (6 MET-hours)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in prostate cancer
survival In the current review 7 studies were identified
Dietary Changes plus Supplements
Ornish et al (2005) conducted a diet counselling and lifestyle RCT comprising men with
early prostate cancer (n=93) The lifestyle changes in this study included a vegan diet
supplemented with soy vitamin E fish oils selenium and vitamin C together with a
moderate physical activity program and stress management techniques such as yoga
29
Human prostate cancer cells
30 IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of pathological states including cancer
31 An all-male (n=51529) study designed to complement the all-female Nurses Health Study
54
Prostate Specific Antigen (PSA)32 levels decreased by 4 at 12-months in the
intervention group but increased by 6 in the control group this was statistically
significant and strongly correlated with the degree of lifestyle change However the
intensity of this intervention and associated behavioural changes might not easily be
translated into practice (White et al 2009)
Pomegranate Juice
The potential benefits of pomegranate juice on prostate cancer outcomes frequently appear
in the media and strong evidence of its efficacy can be found within the academic literature
In a phase II open-label single-arm clinical trial men (n=46) with recurrent prostate cancer
who had rising PSA after surgery or radiotherapy were treated daily with 8oz (227g)
equivalent of pomegranate juice (Pantuck et al 2006) Mean PSA doubling time
significantly increased with treatment from 15-months to 54-months demonstrating a
good indication of a relationship between the consumption of pomegranate juice and
prostate health
Green Tea
Another beverage found to demonstrate some positive effects on prostate cancer is green
tea Bettuzzi et al (2006) in a year-long clinical trial has demonstrated that daily
consumption of green tea can produce a ten-fold decrease in the rate at which
prostate intraepithelial neoplasia (a pre-cancerous condition) progresses to prostate
cancer Support for these findings is offered by an uncontrolled open-label single-arm
phase II clinical trial testing the efficacy of Polyphenon E which contains the polyphenol
antioxidants found in green tea (McLarty et al 2009) Taking four capsules of
Polyphenon E daily (equivalent to twelve cups of green tea) for an average of 345
days leading up to radical prostatectomy the participants (n=26) experienced
significant reductions in biomarkers used to monitor likelihood of metastasis Some
patients demonstrated reductions greater than 30
Lycopene Supplements
The EPIC study has demonstrated that similar to breast cancer prostate cancer risk is not
related to fruit and vegetable consumption (Key et al 2004) However further evidence for
the role of carotenoids found in fruit and vegetables have been provided from a pilot RCT
including men with benign prostatic hyperplasia (BPH) a benign enlargement of the prostate
that can progress to cancer (Schwarz et al 2008) Men (n=20) who received 15mg od
lycopene supplementation (a carotenoid found in tomatoes and other red fruits and
32
PSA is a protein produced by the cells of the prostate gland It is present in small quantities in the serum of normal men and is often elevated in the presence of prostate cancer
55
vegetables) for 6-months had significantly decreased PSA levels compared to a
placebo group (n=20) who had no change in PSA
Salicylate
Salicylate33 intake has been implicated in the aetiology of prostate cancer but Thomas et al
(2009) have evaluated their influence on established cancer progression In a randomised
double blind phase II study involving men (n=110) with progressive prostate cancer who
were counselled to eat less saturated fat and processed food more fruit vegetables and
legumes physical activity more regularly and to stop smoking the men were then
randomised to take sodium salicylate alone or combined with vitamin C copper and
manganese gluconates34 daily Although there was no difference in outcome between those
who received sodium salicylate alone or combined the intervention as a whole (ie
including dietary counselling) slowed or stopped the rate of PSA progression in 40
patients (364) for over one-year and a further ten patients were stabilised for 10-
months This data suggests that changes in lifestyle can potentially delay PSA progression
and the need for more radical therapy highlighting an area for further research
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in prostate cancer
survival In the current review 2 studies were identified
Wright et al (2007) prospectively examined BMI and weight change in relation to prostate
cancer incidence and mortality in 287760 men enrolled in the National Institutes of
Health-AARP Diet and Health Study Higher baseline BMI was associated with
significantly reduced total prostate cancer incidence on the one hand but with
significantly increased risk of prostate cancer mortality on the other hand Adult weight
gain from age 18-years to study entry (range=50-71-years old) was positively associated
with prostate cancer staging but not with disease incidence
In a retrospective analysis exploring the interaction between obesity and surgical outcomes
in patients with prostate cancer treated by radical prostatectomy (n=437) a weak but
significant association was observed between BMI and a number of biological
biomarkers indicative of an advanced pathological stage (Gross et al 2009)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in prostate
cancer survival and no evidence was identified in the current review
33
Salicylates are chemicals that occur naturally in many plants including many fruits vegetables and herbs
Salicylates in plants act as a natural immune hormone and preservative protecting the plants against diseases
insects fungi and harmful bacteria 34
A pinkish powder soluble in water used in medicine in vitamin tablets and as a feed additive and dietary
supplement
56
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in prostate cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR PROSTATE CANCER -
MECHANISMS OF BENEFIT
Physical Activity and Diet The evidence within this review indicates that diet and physical
activity interventions might slow prostate cancer progression as well as aid in its treatment
during the early stages of development The mechanism of benefit is primarily via
decreased growth and increased apoptosis (cell death) associated with a reduction in serum
Insulin-like Growth Factor (IGF)-1 (Soliman et al 2009) Up to 3gt MET-hours of weekly
physical activity appears sufficient to increase survival with more vigorous activity of about 6
MET-hours per week for the reduction of cancer-specific mortality (Kenfield 2010) A
number of dietary steps can be taken to reduce PSA levels and thus slow down the growth
of tumours and increase survival For example a vegan diet supplemented with soy vitamin
E fish oils selenium and vitamin C together with a moderate physical activity program and
stress management techniques such as yoga have been found useful (Ornish et al 2005)
as has pomegranate juice (Pantuck et al 2006) and green tea (Betuzzi et al 2006 McLarty
et al 2009) As with breast cancer carotenoids have been found to offer protective
properties for men with benign prostatic hyperplasia which can progress to cancer (Schwarz
et al 2008) Overall the evidence for prostate cancer is suggestive of survival benefits from
combined dietary and physical activity changes In other words it appears that a healthier
diet made up of fruit and vegetables as well as drinks such as pomegranate juice or green
tea combined with 3gt MET-hours of weekly physical activity could be an effective
prescription for reducing mortality from cancer and other causes
Weight Evidence for weight was mixed whilst finding that higher baseline BMI was
associated with significantly reduced total prostate cancer incidence a significant increase in
prostate cancer severity and mortality was also observed with higher BMI levels (Wright et
al 2007a Gross et al 2009) More research is clearly needed to establish any differential
prostate cancer outcomes associated with weight
Smoking and Alcohol More research is required for smoking and alcohol in terms of
prostate cancer outcomes
57
Table 5 Prostate Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Kenfield et al (2009)
Prospective study (Health Professionals Follow-up Study) assessing the relationship between physical activity and duration and pace of walking with total and prostate cancer-specific mortality
2686 men with prostate cancer
4-years Prostate cancer mortality and total physical activity
Men who were physically active especially those engaging in 3 or more MET-hours of total activity had a 35 lower risk of death from any cause (hazard ratio 065 [95 CI 052 082]) and a modest non-significant reduction in risk of prostate cancer death (hazard ratio 088 [95 CI 052 149]) after adjustment for other risk factors for PCa mortality and pre-diagnosis physical activity While no benefit from walking was observed for PCa mortality men who walked 4 or more hours per week versus those who walked less than 20 minutes per week had a 23 lower risk of all-cause mortality (95 CI 061 097 p-trend=001) In addition compared to men who walked less than 90 minutes at an easy walking pace those who walked 90 or more minutes at a normal to very brisk pace had a 51 lower risk of all-cause mortality (95 CI 037 064) More vigorous activity and longer duration of activity was associated with significant further reductions in risk for all-cause mortality More vigorous activity was associated with a borderline-significant reduction in risk for PCa mortality
Soliman et al (2009)
Pritikin Longevity Center 3-Week
Residential Program - men were given prepared
meals with 12ndash15 fat calories
15ndash20 protein calories and the majority
of calories (65ndash70) from unrefined complex carbohydrates high in fibre (gt40 gday) The men attended daily supervised exercise classes
for 60 min
5 men in their early sixties
with no
signs of prostate cancer (PSA lt 40)
On completion of the 3-week programme
Cancer progression
The intervention slowed growth and increased apoptosis in LNCaP cells responses that were eliminated when
IGF-I was added back to
the post-intervention samples The p53 protein content was increased
and NFkB activation reduced in the post serum-stimulated LNCaP
cells Similar results were observed when the IGF-I receptor was
blocked in the pre-intervention serum In androgen-independent PC-3
cells growth was reduced while none of the other factors were
changed by the intervention
DIET
Bettuzzi et al (2006)
A proof-of-principle double-blind placebo-
controlled clinical trial assessing the safety
and efficacy of green tea catechins for the
chemoprevention of prostate cancer incidence in patients with high-grade prostate intraepithelial
neoplasia Daily
treatment consisted of three GTCs
Men with high-grade prostate intraepithelial
neoplasia who would develop cancer within
1-year
3-monthly for 1-year
Primary outcome prostate cancer incidence Secondary outcome
After 1 year only one tumour was diagnosed (incidence 3) in the
cohort receiving green tea whereas 9 cancers were found among the placebo-treated
men (incidence 30) Total PSA did not
change
significantly between the two arms but green tea-treated men showed
values constantly lower with respect to placebo-treated ones As a
secondary observation administration of green tea also reduced lower
urinary tract symptoms suggesting that these compounds might also
58
capsules 200 mg each (total 600 mgd) (n=60) PSA levels be of help for treating the symptoms of benign prostate hyperplasia
Key et al (2004)
An examination of the association between self-reported consumption of fruits and vegetables and prostate cancer risk in EPIC participants
130544 men in 7 countries recruited into EPIC
Median = 48 years
Prostate cancer incidence
There were 1104 incident cases of prostate cancer No significant associations between fruit and vegetable consumption and prostate cancer risk were observed Relative risks (95 CI) in the top fifth of the distribution of consumption compared to the bottom fifth were 106 (084 ndash134) for total fruits 100 (081ndash122) for total vegetables and 100 (079 ndash126) for total fruits and vegetables combined intake of cruciferous vegetables was not associated with risk
McLarty et al (2009)
In order to determine the effects of short-term supplementation with the active compounds in green tea on serum biomarkers in patients with prostate cancer daily doses were provided of Polyphenon E which contained a total of 13 g of tea polyphenols until time of radical prostatectomy
26 men with positive prostate biopsies scheduled for radical prostatectomy
Not reported PSA levels Biomarkers of prostate cancer decreased significantly All of the liver function tests also decreased five of them significantly total protein albumin aspartate aminotransferase alkaline phosphatase and amylase
Ornish et al (2005)
Lifestyle changes including a vegan diet supplemented with soy vitamin E fish oils selenium and vitamin C together with a moderate physical activity program and stress management techniques such as yoga
Men with early prostate cancer (n=93) Gleason scores less than 7
12-months into the intervention
PSA and serum stimulated LNCaP cell growth
PSA levels decreased by 4 at 12-months in the intervention group but increased by 6 in the control group this was statistically significant and strongly correlated with the degree of lifestyle change
Pantuck et al (2006)
A phase II two-stage clinical trial to determine the effects of pomegranate juice PSA progression in men with a rising PSA following primary therapy Patients were treated with 8 ounces of pomegranate juice daily (570mg total polyphenol gallic acid equivalents) until disease progression
46 men with rising PSA levels post-treatment (surgery or radiotherapy)
Every 3-monhs for 54-months
PSA levels Mean PSA doubling time significantly increased with treatment from a mean of 15 months at baseline to 54 months post-treatment (P lt 0001) In vitro assays comparing pre-treatment and post-treatment patient serum on the growth of LNCaP showed a 12 decrease in cell proliferation and a 17 increase in apoptosis (P = 00048 and 00004 respectively) a 23 increase in serum nitric oxide (P = 00085) and significant (P lt 002) reductions in oxidative state and sensitivity to oxidation of serum lipids after versus before pomegranate juice
Schwarz et al (2008)
15mg od lycopene supplementation for 6-months or placebo
Men with benign prostatic hyperplasia (n=40)
After 6-months of intervention
Inhibition or reduction of increased serum PSA levels
Men receiving 15mg od lycopene supplementation had significantly decreased PSA levels compared to a placebo group who had no change in PSA
Thomas et al (2009)
A randomised double blind phase II study to evaluate the influence of salicylate and lifestyle on established cancer progression Men were counselled
110 men whose PSA had risen in 3 consecutive
Not reported Prostate cancer progression (PSA levels)
Although there was no difference in outcome between the SS or CV247 (21 v 19 p=092) the intervention slowed or stopped the rate of PSA progression in 40 patients (364) for over one year A further ten patients were stabilised for ten months Patients least likely to stabilise
59
to eat less saturated fat processed food more fruit vegetables and legumes exercise more regularly and to stop smoking They were then randomised to take sodium salicylate (SS) alone or SS combined with vitamin C copper and manganese gluconates (CV247) daily without other intervention
values gt20 over the preceding 6-months
had received previous radiotherapy or had a Gleason =7 These men welcomed this addition to active surveillance
WEIGHT
Gross et al (2009)
A retrospective cohort study examining whether changes in components of the sex steroid receptor axis may contribute to the clinical aggressiveness of prostate cancer in obese patients
539 patients treated with radical prostatectomy at a single urban hospital between 1994 and 2002
Not reported Pathological stage of prostate cancer BMI
Higher BMI correlated strongly with higher pathologic stage In comparing obese versus non-obese patients there was no difference in expression of androgen or oestrogen related proteins in cancerous epithelial cells However there was a down-regulation of aromatase in the stoma of obese patients suggesting obesity may cause stromal changes in the sex steroid production and signalling pathways which may affect prostate cancer growth via intracrineparacrine mechanisms
Wright et al (2007)
A prospective examination of BMI and adult weight change in relation to prostate cancer incidence and mortality
287760 men ages 50 years to 71 years at enrolment (1995-1996) in the National Institutes of Health-AARP Diet and Health Study
6-years Prostate cancer incidence Weight gain (BMI)
Higher baseline BMI was associated with significantly reduced total prostate cancer incidence largely because of the relationship with localized tumours (for men in the highest BMI category [gtor=40 kgm (2)] vs men in the lowest BMI category [lt25 kgm (2)] RR 067 95 CI 050-089 P = 0006) Conversely a significant elevation in prostate cancer mortality was observed at higher BMI levels (BMI lt25 kgm(2) RR 10 [referent group] BMI 25-299 kgm(2) RR 125 95 CI 087-180 BMI 30-349 kgm(2) RR 146 95 CI 092-233 and BMI gtor=35 kgm(2) RR 212 95 CI 108-415 P = 02) Adult weight gain from age 18 years to baseline also was associated positively with fatal prostate cancer (P = 009) but not with incident disease
60
d) LUNG CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in lung
cancer survival and one systematic review with meta-analysis was identified in the current
review Studies are summarised in Table 6 at the end of this section
Tardon et al (2005) conducted a systematic review and meta-analysis of cohort and case-
control studies from 1966 through October 2003 evaluating the relationship between
physical activity and lung cancer incidence Nine studies were identified 6 of which
demonstrated that that higher levels of leisure-time physical activity (walking gardening
swimming) protects against lung cancer (Severson et al 1989 Thune et al 1997 Lee et
al 1999 Sellers et al 1991 Kubik et al 2002 Mao et al 2003) The estimated combined
risk for both genders was statistically significant as was a dose-response relationship (p lt
01)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in lung cancer
survival and no evidence was identified in the current review
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in lung cancer
survival and no evidence was identified in the current review
iv SMOKING
Smoking has long been accepted as an unhealthy behaviour that increases the risk of
cancer incidence and disease outcomes Yet many people continue to smoke pre- and post-
diagnosis one-third to one-half of cancer patients either continue to smoke after diagnosis or
relapse after initial quit attempts (Gritz et al 2006) Bekkering et al (2006) do not provide
any evidence for the role of smoking in lung cancer survival In the current review 5 studies
were identified that further highlight the importance of smoking cessation support for people
living with and beyond cancer
Vineis et al (2007) have estimated exposure to Environmental Tobacco Smoke (ETS) and to
air pollution in never smokers and ex-smokers in EPIC study participants (n=520000) The
proportion of lung cancers in never- and ex-smokers attributable to ETS was
estimated to be between 16 and 24 mainly due to the contribution of work-related
exposure
61
In two studies of survivors of stage I and II small cell lung cancer risk of a second cancer
was 35-44-fold higher than in the general population (Richardson et al 1993 Tucker et
al 1997) In those who continued to smoke the risk was far higher particularly in those who
also received chest irradiation and alkylating agents35 (Tucker et al 1997) highlighting the
need for risk assessment when offering smoking cessation support or advice
Another study in Japan confirmed that patients with small cell lung cancer who survive
at least 2-years greatly reduced their likelihood of a second cancer if they quit
smoking (p lt 05) (Kawahara et al 2002) Additionally smoking has been found to be
an independent risk factor in breast cancer survivors developing lung cancer (Ford et
al 2003) In support of these studies Parsons et al (2010) report that nine of ten studies
identified in a review of literature from 1966 to 2008 indicate that continuing to smoke is
associated with a significantly increased risk of all-cause mortality in early stage non-
small cell lung cancer and of all-cause mortality in limited stage small cell lung
cancer
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in lung cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR LUNG CANCER - MECHANISMS OF
BENEFIT
Smoking Evidence for the role of lifestyle factors on lung cancer progression and
recurrence has primarily examined smoking which is a strongly established risk factor for
disease progression and mortality Continuing to smoke exposes the body to high levels of
carcinogens which can cause further DNA damage to existing cancers encourage the
cancer to mutate into a more aggressive type or develop mechanisms to hide from the
bodylsquos immunological defences (Akopyan and Bonavida 2006) Indeed smoking has been
found to suppress the immune system interfering with the function of natural killer (NK) cells
- a lymphoid cell type that plays a role in the surveillance of tumour growth Patients who
have already developed one cancer are likely to be more susceptible to DNA damage from a
pre-existing genetic vulnerability or acquired damage from chemotherapy or radiotherapy
Avoiding carcinogens may therefore have a benefit in reducing the risk of developing
further cancers in patients who may be more susceptible from a pre-existing genetic
signature or damage from chemotherapy or radiotherapy The smoking cessation initiatives
currently sweeping the nation such as NHS Choices bdquoSmokefree‟ remain invaluable as
smoking continues to be an important preventable cause of morbidity and mortality
worldwide
Additional Lifestyle Factors More research is required into lifestyle factors such as diet
physical activity weight and alcohol consumption in terms of lung cancer outcomes Access
35
Cytotoxic agents used to disrupt cancer cells can damage healthy cells in the process
62
to lifestyle services such as post-treatment rehabilitation fitness planning and nutritional
support was highlighted as an important component within the disease trajectory for people
with lung cancer (NCSI Mapping Project 2009) There is evidence for the benefits of
physical activity in reducing lung cancer incidence however there is a paucity of evidence
for the survivorship period of lung cancer
63
Table 6 Lung Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Tardon et al (2004)
A meta-analysis of studies (1966-2003) evaluating the relationship between physical activity and lung cancer
Men and women in cohort and case-control studies (9 studies)
Not reported
Lung cancer incidence
The combined ORs were 087 (95 CI=079ndash095) for moderate leisure-time physical activity (LPA) and 070 (062ndash079) for high activity (p trend = 000) This inverse association occurred for both sexes although it was somewhat stronger for women No evidence of publication bias was found Several studies were able to adjust for smoking but none adjusted for possible confounding from previous malignant respiratory disease
SMOKING
Ford et al (2003)
Retrospective analysis of smoking radiation and both exposures on lung carcinoma development in women who were treated previously for breast carcinoma
Case patients (n = 280) females aged 30-89 years with breast carcinoma prior to primary lung carcinoma Control patients (n = 300) selected randomly from 37000 patients with breast carcinoma treated at The University of Texas M D Anderson Cancer Center
Not reported
Lung cancer incidence
At the time of breast carcinoma diagnosis 84 of case patients had ever smoked cigarettes compared with 37 of control patients whereas 45 of case patients and control patients received XRT for breast carcinoma Smoking increased the odds of lung carcinoma in women without XRT (odds ratio [OR] 60 95 confidence interval [95 CI] 36-101) but XRT did not increase lung carcinoma risk in non-smoking women (OR 05 95 CI 03-11) Overall the OR for both XRT and smoking compared with no XRT or smoking was 90 (95 CI 51-159)
Kawahara et al (1998)
Prospective study to investigate whether smoking cessation after successful therapy is associated with a decrease in risk for a second
980 consecutive patients with small cell lung cancer (SCLC)
Median=67 years after initiation of
Second primary tumour
Of the patients who continued to smoke 11 (33) developed a SPT Of the 31 patients who stopped smoking after therapy only three (10) had a subsequent SPT Among those who continued to smoke the risk for a SPT was significantly increased (54 times 95 CI 27-97) relative to the general
64
primary tumour being treated with combination chemotherapy with or without chest radiotherapy
therapy population In contrast those who stopped smoking showed only a 16-fold increase (95 CI 03-46) which was not significantly different from the level in the general population The relative risk for non-SCLC was significantly increased 128-fold (95 CI 34-328) in continuing smokers No second non-SCLCs have been found among those who stopped smoking The 33 patients who continued to smoke had a significantly increased risk of a SPT (43 95 CI 11-159 P=003) Relative to the risk of SPT in patients without previous radiotherapy who stopped smoking the risk is 092 in patients without radiotherapy who continued smoking 037 in patients with radiotherapy who stopped smoking and 233 in patients with radiotherapy who continued smoking The risk of current smoking in patients with previous radiotherapy is 630 relative to those with radiotherapy who stopped smoking although this interaction is not statistically significant (P = 024)
Parsons et al (2010)
A systematic review with meta-analysis of the evidence that smoking
cessation after diagnosis
of a primary lung tumour affects prognosis Databases searched CINAHL (from 1981) Embase (from 1980) Medline
(from 1966)
Web of Science (from 1966) CENTRAL (from 1977)
to
December 2008 and reference lists of included studies
RCTs or observational
st
udies measuring
the effect of quitting smoking
post-
diagnosis on lung cancer prognosis
Patients were followed for 6-months gt in 5 studies but only at time of diagnosis treatment in 4
5-year survival using death rates for continuing smokers and quitters obtained from this review
Continued smoking was associated with a significantly increased risk of all-
cause mortality (hazard ratio 294 95 CI 115 to
754) and recurrence (186
101 to 341) in early stage non-small cell lung cancer and of all-cause
mortality (186 133 to 259) development of a second primary tumour (431 109 to 1698)
and recurrence (126 106 to 150) in limited stage small
cell lung cancer No study contained data on the effect of quitting
smoking on
cancer specific mortality or on development of a second primary tumour in
non-small cell lung cancer Life table modelling on the basis of these data
estimated 33 five year survival in 65 year old patients with early stage non-
small cell lung cancer who continued to smoke compared with 70 in
those
who quit smoking In limited stage small cell lung cancer an estimated 29
of continuing smokers would survive for five years compared with 63 of
quitters on the basis of the data from this review
Richardson et al (1993)
Retrospective review to determine the incidence of second primary cancers developing in patients surviving free of cancer for 2 or more years after treatment for small-cell lung cancer and to assess the potential effect of smoking cessation
Consecutive sample of 540 patients with small-cell lung cancer
Median=61 years
Relative risk for second primary cancers and death
55 patients (10) were free of cancer 2-years after initiation of therapy 18 of these developed one or more second primary cancers including 13 who developed second primary non-small-cell lung cancer The risk for any second primary cancer compared with that in the general population was increased four times (relative risk 44 95 CI 25-72) with a relative risk of a second primary non-small-cell lung cancer of 16 (CI 84-27) Forty-three patients discontinued smoking within 6-months of starting treatment for small-cell lung cancer and 12 continued to smoke In those who stopped smoking at time of diagnosis the relative risk of a second lung cancer was 11 (CI 44 to 23) whereas in those who continued to smoke it was 32 (CI 12 to 69)
Tucker et al (1997)
A multi-institution study to investigate the risk among survivors of developing second primary
611 patients who had
been cancer
Not reported
Population-based rates of cancer
Relative to the general population the risk of all second cancers among these
patients was increased 35-fold Second lung cancer risk was increased 13-
fold among those who received chest irradiation in comparison to a sevenfold
65
cancers other than small-cell lung carcinoma
free for more than 2 years after therapy for small-cell lung cancer
incidence and mortality
increase among non-irradiated patients It was higher in those who
continued smoking with evidence of an interaction between chest irradiation and continued smoking
(relative risk = 21) Patients treated with various forms
of combination chemotherapy had comparable increases in risk (94- to 13-
fold overall) except for a 19-fold risk increase among those treated with
alkylating agents who continued smoking
Vineis et al (2007)
Prospective study to estimate exposure to Environmental Tobacco Smoke (ETS) in never smokers and ex-smokers in 10 European countries (EPIC)
Men and women in the EPIC study (n = 520000)
Not reported
Lung cancer incidence
The proportion of lung cancers in never- and ex-smokers attributable to ETS was estimated as between 16 and 24 mainly due to the contribution of work-related exposure Also 5ndash7 of lung cancers in European never smokers and ex-smokers are attributable to high levels of air pollution as expressed by NO2 or proximity to heavy traffic roads
66
e) OTHER CANCERS
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in survival
from other cancers and no evidence was identified in the current review
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in survival from other
cancers Studies identified in the current review are summarised in Table 7 at the end of this
section
Preliminary EPIC results provide some evidence that red and preserved meat increases risk
for gastric cancer (Gonzalez et al 2006) Preliminary EPIC results also indicate that fruit
reduces gastric cancer risk whilst vegetables are not associated with risk for this type of
cancer Furthermore overall consumption of fruit and vegetables is reported to be unrelated
to risk of ovarian cancer (Schultz et al 2005) There is evidence of a protective effect of a
high intake of allium vegetables (onions garlic shallots leeks and chives) on ovarian
cancer risk (Schultz et al 2005)
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in survival from
other cancers Preliminary EPIC results reported in the current review provide some
evidence that BMI is associated with endometrial cancer risk (Kaaks et al 2002
Friedenreich et al 2007)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in survival from
other cancers Preliminary EPIC results along with 4 other studies were identified in the
current review
Gonzalez et al (2003) confirm from EPIC results that smoking is associated with gastric
cancer
Similarly Yu et al (1997) evaluated 25000 heterogeneous patients who had been treated
for lung breast or colorectal cancer and found that the 15-year survival of the people
who continued to smoke was 44 compared to 55 in those who quit
In a more recent study of survivors of early stage head and neck cancer (n=264) who
retrospectively reported their tobacco histories (pre-diagnosis) and prospectively updated
67
information annually thereafter for an average of 42-years smoking history dose-
dependently increased the risk of mortality from cancer (Mayne et al 2009)
The impact of smoking on risk of secondary lung cancer has been demonstrated in survivors
of Hodgkin lymphoma (Abrahamsen et al 1993 Travis et al 2002) In the latter study risk
for subsequent lung cancer from radiation treatment and smoking was identified where
multiple effects were found for a combination of radiation and alkylating agents36 in
moderate-to-heavy smokers compared with comparison cases (Travis et al 2002)
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in survival from
other cancers One study was identified in the current review which showed that pre-
diagnosis alcohol consumption history dose-dependently increased mortality risk in
recent survivors of early stage head and neck cancer (n=264) (Mayne et al 2009)
Risks reached 49 for those who drank gt5 drinks per day an effect explained by beer and
liquor consumption Continued drinking post-diagnosis of an average of 23 drinks daily
also significantly increased risk
SUMMARY OF FINDINGS FOR OTHER CANCERS
A comprehensive evaluation of the lifestyle evidence for cancers other than the four most
common (ie breast colorectal lung prostate) was not within the scope of this review
However those studies identified whilst gathering evidence for these four cancers does
highlight the sheer importance of lifestyle in the development and progression of all types of
cancers not to forget other chronic diseases The provision of lifestyle support for cancer
survivors clearly needs to remain priority as does further research into the exact
mechanisms of benefit obtained from different lifestyle practices at different stages of the
cancer and indeed health trajectory
36
Carcinogenic agents used in chemotherapy to treat cancer
68
Table 7 Other Cancers ndash Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
DIET
Gonzalez et al (2006)
Nested case-control within the prospective EPIC study examining of
the risk of gastric cancer and
oesophageal adenocarcinoma associated
with meat consumption
521 457 men and women aged 35ndash70 years in 10 European
countrie
s (330 gastric adenocarcinoma and
65
oesophageal adenocarcinomas were diagnosed)
65-years Incidence of gastric and oesophageal cancers
Gastric noncardia cancer risk was statistically significantly associated
with intakes of total meat (calibrated HR per 100-gday increase
=
352 95 CI = 196 to 634) red meat (calibrated HR per 50-gday
increase = 173 95 CI = 103 to 288) and processed
meat (calibrated HR per 50-gday increase = 245 95 CI
= 143 to 421) The association between
the risk of gastric noncardia cancer and total meat intake was
especially large in H pylori infected subjects (odds ratio per 100-
gday increase = 532 95 CI = 210 to 134) Intakes of total red or
processed meat were not associated with
the risk of gastric cardia cancer A positive but nonndashstatistically
significant association was observed between oesophageal
adenocarcinoma cancer risk and total and processed meat intake
Schultz et al (2005)
Prospective examination of the association between consumption of fruit and vegetables and risk of ovarian cancer (EPIC)
Female participants (n = 325640) of the EPIC study
Mean=63 years
Ovarian cancer incidence
Total intake of fruit and vegetables separately or combined as well as subgroups of vegetables (fruiting root leafy vegetables cabbages) was unrelated to risk of ovarian cancer A high intake of garliconion vegetables was associated with a borderline significant reduced risk of this cancer
WEIGHT
Friedenreich et al 2007
Large prospective study (EPIC) examining the association between anthropometry and endometrial cancer particularly by menopausal status and exogenous hormone use subgroups
223008 women in the EPIC study (567 incident endometrial cancer cases)
64-years Endometrial cancer incidence
Weight BMI waist and hip circumferences and waistndashhip ratio (WHR) were strongly associated with increased risk of endometrial cancer The relative risk (RR) for obese (BMI 30ndash lt 40 kgm
2)
compared to normal weight (BMI lt 25) women was 178 95 CI = 141ndash226 and for morbidly obese women (BMI ge 40) was 302 95 CI = 166ndash552 The RR for women with a waist circumference of ge88 cm vs lt80 cm was 176 95 CI = 142ndash219 Adult weight gain of ge20 kg compared with stable weight (plusmn3 kg) increased risk independent of body weight at age 20 (RR = 175 95 CI = 111ndash277) These associations were generally stronger for postmenopausal than premenopausal women and oral contraceptives never-users than ever-users and much stronger among never-users of hormone replacement therapy compared to ever-users
Kaaks et al A review of evidence on the Endometrial Not Incidence of The authors conclude that development of ovarian hyperandrogenism
69
(2002) associations among endometrial cancer risk endogenous hormone metabolism and obesity
cancer cases reported endometrial cancer
may be a central mechanism relating to an interaction between obesity-related chronic hyperinsulinemia with genetic factors predisposing to the development of ovarian hyperandrogenism
SMOKING
Abrahamsen et al (1993)
The Norwegian Cancer Registry
identified previously untreated patients with Hodgkin lymphoma treated at NRH who had developed a secondary cancer more than 1 year after diagnosis of
Hodgkin
lymphoma
68 patients who developed secondary cancer including 9 acute non-lymphocytic leukaemialsquos (ANLLs)
8 non-
Hodgkins lymphomas (NHLs) and 51 solid tumours including 11 lung cancers
Not reported
Secondary cancer
The RR of SC and leukaemia was 186 (95 CI 14 to 24) and 243 (95 CI 111 to 462) respectively The RR of
SC was highest in
younger patients (lt 41 years RR = 38) No significant association
between splenectomy and development of ANLL was found The
influence of treatment and follow-up time on the development of SC
agrees with data from other large cancer institutions
Gonzalez et al (2003)
Assessment of the relation between tobacco use and gastric cancer incidence in the prospective EPIC study
521468 individuals recruited from 10 European countries taking part in the EPIC study 274 were eligible for the analysis
Approx 10-years
Incidence of gastric cancer
After adjustment for educational level consumption of fresh fruit vegetables and preserved meat alcohol intake and body mass index (BMI) there was a significant association between cigarette smoking and gastric cancer risk the hazard ratio (HR) for ever smokers was 145 (95 CI = 108-194) The HR of current cigarette smoking was 173 (95 CI = 106-283) in males and 187 (95 CI = 112-312) in females Hazard ratios increased with intensity and duration of cigarette smoked A significant decrease of risk was observed after 10 years of quitting smoking A preliminary analysis of 121 cases with identified anatomic site showed that current cigarette smokers had a higher HR of GC in the cardia (HR = 410) than in the distal part of the stomach (HR = 194) In this cohort 176 (95 CI = 105-295 ) of gastric cancer cases may be attributable to smoking
Mayne et al (2009)
Participants retrospectively reported their smoking histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to smoke post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Smoking history before diagnosis dose-dependently increased the risk of dying risks reached 54 [95 CI 07-401] among those with gt60 pack-years of smoking After adjusting for pre-diagnosis exposures continued smoking was associated with non-significantly higher risk (relative risk for continued smoking versus no smoking 18 95 CI 09-39)
70
Travis et al (2002)
Case-control study with a population-based cohort The cumulative amount of cytotoxic drugs the radiation dose to the specific location in the lung where cancer developed and tobacco use were compared between patients who developed lung cancer and matched control patients
1-year survivors of Hodgkins disease (n=19046) comparison between 222 patients who developed lung cancer and 444 matched controls
Not reported
Secondary cancer incidence
Tobacco use increased lung cancer risk more than 20-fold risks from smoking appeared to multiply risks from treatment
Yu et al (1997)
Retrospective study examining the effect of smoking history on survival among cancer patients
Data from Memorial Sloan-Kettering Cancer Centers tumour registry was used to identify 25436 cases of cancer (12447 male patients and 12989 female patients)
Not reported
Survival time Patients who had a history of smoking were found to have a lower rate of survival than non-smokers After controlling for age race alcohol use and histologic grade the risk ratios were 155 for males and 143 for females A dose-response relationship was found between ever-smoking and cancer patient survival The predictive effect of smoking on survival was significant for patients with oral pancreatic breast and prostate cancers but not for oesophageal stomach colon rectum laryngeal lung cervix uteri urinary bladder and kidney cancers Black patients with oral or breast cancer had a poorer prognosis associated with smoking compared with white and other non-white patients
ALCOHOL
Mayne et al (2009)
Participants retrospectively reported their alcohol consumption histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to drink post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Alcohol history before diagnosis dose-dependently increased mortality risk risks reached 49 (95 CI 15-163) for persons who drank gt5 drinksd an effect explained by beer and liquor consumption After adjusting for pre-diagnosis exposures continued drinking (average of 23 drinksd) post-diagnosis significantly increased risk (relative risk for continued drinking versus no drinking 27 95 CI 12-61)
71
PART TWO
LIFESTYLE EVIDENCE FOR REDUCING AND MANAGING THE
RISKS AND SIDE-EFFECTS OF CANCER TREATMENT
Introduction
There are a number of long-term and late effects of cancer treatment that a survivor might
be confronted with including fatigue (Bower et al 2006) psychological problems (Thewes
et al 2004) lymphoedema (Deo et al 2004) and osteoporosis (Brown et al 2006) There
might also be difficulties in terms of returning to work or withdrawal from social activities due
to disability (Taskila et al 2007) Lifestyle choices pertaining to diet physical activity
smoking and alcohol consumption for cancer survivors are not only important in terms of
disease progression and recurrence Despite there being less evidence in this area there
is accumulating data demonstrating that lifestyle can facilitate the effective management of
many of these effects of treatment some of which are chronic conditions themselves
requiring additional lifestyle modifications Research within this area has hit new heights in
order to keep up with the growing number of survivors The chronic conditions addressed
within the current review of lifestyle evidence are some of the most frequently reported
problems cited by cancer survivors they include cancer-related fatigue (CRF)
lymphoedema osteoporosis and weight gain In addition evidence for lifestyle choices and
quality of life (QoL) has been reviewed due to the QoL implications of the aforementioned
health-related problems and unhealthy behaviours (Richardson et al 2009)
Evidence for an interaction between lifestyle and these chronic conditions commences with
the findings reported by Bekkering et al (2006) as part of the WCRF review being updated
Further evidence identified from the search criteria will then be presented Evidence will be
presented by cancer site (eg breast colorectal lung prostate) where appropriate whilst
some evidence will pertain to one cancer site only (ie breast cancer related lymphoedema)
72
CANCER-RELATED FATIGUE (CRF)
Cancer-related fatigue (CRF) is defined as ldquoa distressing persistent subjective sense of
physical emotional andor cognitive tiredness or exhaustion related to cancer or cancer-
related treatment that is not proportional to recent activity and interferes with usual
functioningrdquo (NCCN 2009) It has overtaken nausea and pain as the most distressing
symptom experienced by people with cancer during and after treatment It is reported by 60-
96 of patients during chemotherapy radiotherapy or after surgery and can last for months
or even years following treatment (Wagner and Cella 2004 Thomas 2005 NCCN 2009) It
can have a profound effect on physical emotional and social well-being and can hinder
chance of remission owing to non-compliance with treatment due to the intensity of this side-
effect (Lucia Earnest and Perez 2003 Velthuis et al 2009)
The specific causes of CRF are not fully understood but there are several associated
conditions which can aggravate it These include anaemia electrolyte imbalance liver
failure and steroid withdrawal (Thomas 2005) Some conditions can also cause fatigue by
disturbing sleep patterns such as anxiety depression nocturia (a need to get up in the night
to urinate) night sweats and pruritus (itching) The self-management strategy most
extensively investigated for CRF is physical activity the evidence for which is presented
next Studies identified in the current review are summarised in Table 8 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in women with breast cancer In the current review 4 systematic reviews
three of which included a meta-analysis and 2 additional studies were identified
The first review by McNeely et al (2006) reported on 14 RCTs Despite significant
heterogeneity and relatively small samples the overall finding was that physical activity led
to statistically significant improvements in reducing symptoms of fatigue Two meta-
analyses added to this evidence The first by Cramp and Daniel (2008) evaluated 28
studies (n=2083 participants) the majority of which comprised participants with breast
cancer (n=16 studies n=1172 participants) A pooled meta-analysis of all available data
convincingly showed that physical activity was statistically more effective in reducing
CRF when compared to less active controls In the second meta-analysis Velthuis et al
(2009) reviewed 18 studies 12 of which comprised women with breast cancer Pooled
results of these 12 studies (n=674 patients) showed a small significant reduction of CRF
in favour of the physical activity group compared to the non-physical activity group
When Velthuis et al (2009) subdivided the 12 studies into two main physical activity
strategies (ie home-based versus supervised classes) home-based physical activity (n=
7 studies) led to a small non-significant reduction in CRF whereas supervised
73
aerobic physical activity (n=5 studies) showed a medium significant reduction
in CRF when compared to no intervention
Fillion et al (2008) conduced an RCT demonstrating that combining supervised walking
training with psycho-educational stress management produced significant improvements
relative to usual care for fatigue vigour anxiety and depression but not for physical
fitness This suggests a psychological benefit to physical activity which might assist in
coping with physical symptoms such as fatigue Poudevigne et al (2009)
examined adherence to 12-weeks of moderate intensity combined cardio-respiratory and
resistance training and any subsequent impact on levels of fatigue in sedentary breast
cancer survivors (n=20) 2-24 months post-treatment Not only was the training acceptable
and safe but significant decreases in fatigue (43) were also found across the12-
weeks
Danhauer et al (2009) conducted an RCT with women (n=44) who had breast cancer 34
of whom were undergoing cancer treatment in order to examine the effects of restorative
yoga between those in treatment and those not in treatment Randomisation was to a
programme of 10-weekly 75-minute yoga classes or a waiting list control group The yoga
group demonstrated a significant within-group improvement in fatigue although no
significant difference was found with the control group
In updating a previous systematic review by Schmitz et al (2005) of RCTs examining
physical activity in cancer survivors during and after treatment Speck et al (2010)
accumulated data from a further 82 studies (n=6838 participants) Of the 82 studies 66
were rated as high quality and analysed for mean effect sizes resulting from physical activity
interventions The most common diagnosis included was breast cancer (83) with 40 of
studies conducting interventions during cancer treatment and 60 post-treatment Mean
effect sizes demonstrated a large effect of physical activity interventions post-
treatment on upper and lower body strength (plt00001 and 0024 respectively) and
moderate effects on fatigue and breast cancer-specific concerns (p=0003 and 0003
respectively) The most notable progression from their previous review was that the
benefits of physical activity on fatigue moved from negative findings to the evidence
reflecting significantly reduced fatigue post-treatment in physically active survivors
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in men with prostate cancer In the current review 3 systematic reviews two
of which included a meta-analysis and 2 additional studies were identified In the current
review four studies were identified
Windsor Nichol and Potter (2004) published a study of 65 patients with prostate cancer
receiving radiotherapy who were randomly allocated to a home-based physical activity
programme or standard supportive care The home-based exercise included walking 30-
minutes three times a week with an intensity of 60-70 heart rate max for the duration of
74
radiotherapy No adverse events were reported and a non-significant reduction of CRF
was found in the physical activity group when compared to the standard care group
In the abovementioned meta-analysis conducted by Velthuis et al (2009) three RCTs in men
with prostate cancer investigated the effectiveness of supervised physical activity during
radiotherapy and androgen deprivation therapy (Segal et al 2003 Monga et al 2007
Segal et al 2009) In two studies men allocated to the intervention group participated three
times a week in a supervised physical activity programme comprising aerobic exercises with
an intensity of respectively 65 of the maximum heart frequency (HR max) adjusted for
age and 50-75 of the VO2peak (15-45 minutes) (Monga et al 2007 Segal et al 2009)
In the third study the intervention comprised resistance exercises 2-3 times a week with an
intensity of two sets of 8-12 repetitions 60-70 of the one repetition maximum (Segal et
al 2003) Pooled results from the two supervised aerobic studies showed a large non-
significant reduction in CRF in favour of the physical activity group (Monga et al
2007 Segal et al 2009) The resistance exercise study showed a small non-significant
reduction in CRF in favour of the physical activity group (Segal et al 2003) In the latter
study over 80 of the participants were reported to have completed the programme
however the programme did result in one knee injury chest pain fainting and an acute
myocardial infarction
c) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) report on one RCT comparing the impact of a 3-weeks aerobic
physical activity (stationary biking 30-minutes five times weekly) intervention versus
relaxation training (45-minutes three times per week) in post-surgery survivors (n=72) of lung
(n=27) and gastrointestinal (n=42) cancer (Dimeo et al 2004) Fatigue improved
significantly in both groups during the intervention although there was no significant
difference between groups This suggests that relaxation training can be equally as
effective as aerobic physical activity in relieving symptoms of fatigue
In the current review 3 further studies were identified
There has been one study in patients with multiple myeloma (Coleman et al 2003) which
included a home-based physical activity programme during chemotherapy and peripheral
blood stem cell transplantation The programme comprised a combination of aerobic and
resistance exercises three times a week for 20-minutes for the duration of the
chemotherapy (6-months) No adverse events were reported and a small non-significant
reduction in CRF was found in the physical activity group compared to a control
group who did not receive the intervention
Chang et al (2008) published a study involving patients with acute myelogeous leukemia
(n=22) which included allocation to the intervention group a three week supervised walking
programme during chemotherapy Participants walked five times a week for 12-minutes in
the hospital hallway The programme was completed by 69 of the participants and no
75
adverse events were reported A medium-sized non-significant reduction in CRF was
found
In a cross-sectional postal survey of ovarian cancer survivors (n=359) self-report measures
of physical activity and CRF demonstrated that those meeting physical activity guidelines of
the Centres for Disease Control and Prevention (ie minimum 25-hours of moderate
intensity aerobic activity every week plus muscle-strengthening activities on two or more
days of the week) reported significantly lower fatigue than those not meeting guidelines
(Stevinson et al 2009) There was however no evidence of a dose-response relationship
SUMMARY OF EVIDENCE FOR CANCER-RELATED FATIGUE
Evidence from 28 RCTs and 2 meta-analyses has demonstrated that physical activity
programmes can reduce the severity of CRF The studies reviewed here also show that
supervised aerobic exercise programmes were more effective in reducing CRF during breast
cancer treatment than home-based exercise advice Although more research on the optimal
timing and duration of physical activity would be useful these studies are sufficiently robust
to recommend that tailored physical activity advice be integrated into individualized care
plans
As identified in a consultation and evidence review designed to determine the priorities of
cancer survivorship research there is a modest amount of research testing physical activity
interventions for fatigue some demonstrating benefits during treatment but inconclusive
evidence for after treatment (Richardson et al 2009) Although there is clinical
heterogeneity between published RCTlsquos in terms of physical activity duration frequency and
intensity a sensible pragmatic approach based on the trials which showed most benefit is to
supervise a moderate intensity physical activity regimen of regular frequency (3-5
timesweek) for 20-30 minutes per session involving aerobic resistance or mixed physical
activity types With evidence suggesting that low intensity physical activity can also be
beneficial during cancer treatment consideration is warranted in terms of promoting physical
activity from diagnosis onwards potentially making physical activity uptake less challenging
post-treatment (Velthuis et al 2009) Further research is required to determine the optimal
type intensity and timing of physical activity interventions at different periods of the disease
trajectory and when experiencing other cancer-related symptoms or late effects
An exemplary physical activity programme available to survivors of breast colorectal and melanoma cancers is the BACSUP (Bournemouth After Cancer Survivorship Project) Active Wellness Programmelsquo developed in partnership with Royal Bournemouth Hospital NHS Bournemouth and Poole Bournemouth University and MacMillan Cancer Support (Milne et al 2010) The programme involves two initial one-to-one consultations including a holistic assessment with a trained member of staff to tailor the programme to individual needs A readiness check is done prior to referral a readiness to be physically active score of gt70 is required for participation Participants receive a telephone call at 3-weeks for the provision of support and encouragement followed by a one-to-one review at 6-weeks to assess progress and maintain motivation A one-to-one review and reassessment is also provided at 12-weeks to measure improvements Additional support options are available such as the BACSUP Active Wellness Group which provides an opportunity to meet others survivors and listen to life improvement guest speakers In a pilot study of the programme survivors who had completed primary treatment within the previous 5-years (n=180) were referred to the service 58 completed the programme 65 are currently on the programme 30 started but are on hold due to circumstances 21 were not yet ready to join the scheme
At 12-weeks 92 of participants reported reduced fatigue
76
Table 8 Cancer-Related Fatigue and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Chang et al (2008)
RCT to preliminarily examine the effects of a three-week walking exercise program (WEP) on fatigue-related experiences of acute myelogenous leukaemia (AML) patients receiving chemotherapy Eligible AML patients were randomly assigned to either an experimental group (n = 11) which received 12 minutes of WEP per day five days per week for three consecutive weeks or to a control group (n = 11) which received standard ward care
Patients with acute Myelogenous leukaemia (AML) receiving chemotherapy (n=22)
All patients were evaluated four times before treatment (baseline or Day 1) Day 7 Day 14 and Day 21
Worst and average fatigue intensities fatigue interference with patients daily life 12-minute walking distance overall symptom distress anxiety and depressive status
AML patients in the three-week WEP group had a significantly greater increase in 12-minute walking distance than the control group Patients in the WEP also had lower levels of fatigue intensity and interference symptom distress anxiety and depressive status than the control group
Coleman et al(2003)
A pilotfeasibility study with a randomized controlled design was conducted to investigate home-based exercise therapy for patients receiving high-dose chemotherapy and autologous peripheral blood stem cell transplantation as treatment for multiple myeloma
24 patients with multiple myeloma
Not reported Fatigue mood disturbance body weight
Because of the small sample size in the feasibility study the effect of exercise on lean body weight was the only end point that obtained statistical significance However the results suggest that an individualised exercise program for patients receiving aggressive treatment for multiple myeloma is feasible and may be effective for decreasing fatigue and mood disturbance and for improving sleep
Cramp and Daniel (2008)
Systematic review with meta-analysis to evaluate the effect of exercise on cancer-related fatigue both during and after cancer treatment
2083 participants from RCTs comprising cancer patients and survivors
Follow-up assessment of long-term outcomes was poor with 18 of 28 studies failing to assess outcomes beyond the end of the intervention
Cancer-related fatigue
28 studies were identified for inclusion with the majority carried out on participants with breast cancer (n = 16 studies n = 1172 participants) A meta-analysis of all fatigue data incorporating 22 comparisons provided data for 920 participants who received an exercise intervention and 742 control participants At the end of the intervention period exercise was statistically more effective than the control intervention (SMD -023 95 CIs -033 to -013)
77
period
Danhauer et al (2009)
Randomised pilot study to determine the feasibility of implementing a restorative yoga intervention for women with breast cancer and to examine group differences in self-reported emotional health-related quality of life and symptom outcomes 10 weekly 75-minute yoga classes
Women with breast cancer (n=544) 34 of whom were actively undergoing cancer treatment
Immediately post-intervention (week 10)
Emotional well-being QoL fatigue
Group differences favouring the yoga group were seen for mental health depression positive affect and spirituality (peacemeaning) Significant baselinegroup interactions were observed for negative affect and emotional well-being Women with higher negative affect and lower emotional well-being at baseline derived greater benefit from the yoga intervention compared to those with similar values at baseline in the control group The yoga group demonstrated a significant within-group improvement in fatigue no significant difference was noted for the control group
Fillion et al (2008)
RCT to verify the effectiveness of a 4-week nurse-led group intervention that combines stress management psycho-education and physical activity (ie independent variable) intervention in reducing fatigue and improving energy level quality of life (mental and physical) fitness (VO2submax) and emotional distress (ie dependent variables) in breast cancer survivors Participants were randomly assigned to either the group intervention (experimental) or the usual-care (control) condition
French-speaking women who had completed their treatments for non-metastatic breast cancer (n=87)
Post-intervention and at 3-months follow-up
Fatigue emotional distress QoL
Participants in the intervention group showed greater improvement in fatigue energy level and emotional distress at 3-month follow-up and physical quality of life at post-intervention compared with the participants in the control group
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials MEDLINE
EMBASE CINAHL Psych INFO CancerLit PEDro
and SportDiscus as well
as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
function
ing as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all
outcomes were positive even when statistical significance was not
achieved Exercise led to statistically significant improvements in
quality of life as assessed by the Functional Assessment of
Cancer TherapyndashGeneral (weighted mean difference [WMD] 458
95 CI 035 to 880) and Functional Assessment of Cancer
TherapyndashBreast (WMD 662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak
oxygen consumption and in reducing symptoms of fatigue
Poudevigne et al (2009)
Cohort study examining the effects of a 12-week cross training intervention on fatigue and mood in breast cancer survivors The training consisted of a 12-week exercise program of 3 weekly
20 sedentary breast cancer survivors between 2-24 months post-
On completion of the 12-week intervention
Fatigue and mood disturbances (Profile of Mood States) QoL
The mean (plusmnSD) attendance rate was 92 (plusmn80) No musculoskeletal injuries and problematic symptoms occurred during the cross-training Repeated measures ANOVA showed a large increase in QOL (22) and significant decrease in fatigue (43) across 12 weeks (eta squared range 491 to708 all p
78
sessions of 60 min duration supervised by a certified personal trainer and divided into resistance (30 minutes) and aerobic training (5 minutes warm-up 20 minutes training 5 minutes cool-down) The aerobic intensity was set at 60HRR and re-evaluated every three weeks
treatment Treatments ranged from lumpectomies (23) mastectomies (29) radiations (32) and chemotherapy (16)
(SF-36) and work absenteeism
valueslt05) No differences were found in work absenteeism Blood pressure was unchanged after training
Stevinson et al (2009)
A cross-sectional postal survey to investigate the associations between physical activity and health-related outcomes in ovarian cancer survivors and to examine any dose-response relationship
Ovarian cancer survivors (n=359) on and off treatment
Not reported Fatigue peripheral neuropathy sleep and psychosocial functioning
311 of participants were meeting the public health physical activity guidelines - those meeting guidelines reported significantly lower fatigue than those not meeting guidelines (mean difference 71 95 confidence interval 55-88 d = 087 Plt 0001) Meeting guidelines was also significantly inversely associated with peripheral neuropathy depression anxiety sleep latency use of sleep medication and daytime dysfunction and was positively associated with happiness sleep quality and sleep efficiency
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types were included with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) With few exceptions exercise was well tolerated during and post treatment without adverse events
Velthuis et al (2009)
Meta-analysis to evaluate the effects of different exercise prescription parameters during cancer treatment on cancer-related fatigue (CRF) A systematic search of CINAHL Cochrane Library Embase
RCTs studying the effects of exercise during cancer treatment on
Not reported Cancer-related fatigue
During breast cancer treatment home-based exercise lead to a small non-significant reduction (standardised mean difference 010 95 confidence interval minus025 to 045) whereas supervised aerobic exercise showed a medium significant reduction in CRF (standardised mean difference 030 95 confidence interval 009
79
Medline Scopus and PEDro was carried out
CRF (n=18) 12 in breast 4 in prostate and 2 in other cancer patients)
to 051) compared with no exercise A subgroup analysis of home-based (n = 65) and supervised aerobic (n = 98) and resistance exercise programmes (n = 208) in prostate cancer patients showed no significant reduction in CRF in favour of the exercise group Adherence ranged from 39 of the patients who visited at least 70 of the supervised exercise sessions to 100 completion of a home-based walking programme
Windsor Nichol and Potter (2004)
A prospective RCT to determine whether aerobic exercise would reduce the incidence of fatigue and prevent deterioration in physical functioning during radiotherapy for localised prostate carcinoma
33 men in exercise group and 33 men in control group
4-weeks post-radiotherapy
Fatigue and distance walked in a modified shuttle test before and after radiotherapy
There were no significant between group differences noted with regard to fatigue scores at baseline (P = 055) or after 4 weeks of radiotherapy (P = 018) Men in the control group had significant increases in fatigue scores from baseline to the end of radiotherapy (P = 0013) with no significant increases observed in the exercise group (P = 0203)
80
LYMPHOEDEMA
Lymphoedema is the excessive accumulation of tissue fluid (or lymph) that results from
impaired lymphatic drainage resulting in swelling of the limb The most common type of
lymphoedema in cancer survivors is most frequently the result of treatment for breast
cancer where an important prognostic indicator is the removal and evaluation of lymph
nodes (Morrell et al 2005) Removal of the lymph nodes can result in a number of side-
effects including lymphoedema (Swenson et al 2002) which manifests usually as a
swelling to the affected arm but can also occur in the hand trunk and breast The more
lymph nodes that are removed the higher the risk of developing the condition providing an
objective measure of risk that could be utilised in the provision of evidence-based
lifestyle and self-management support based on individuals needs
The condition can develop immediately or many years after treatment (Mortimer et al
1996) in either case lymphoedema is a chronic debilitating condition that can cause severe
physical and psychological morbidity as well as a reduction in QoL (Deo et al 2004)
The self-management strategy most extensively investigated for lymphoedema is physical
activity with some evidence also being available for diet Studies identified in the current
review are summarised in Table 9 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
preventing or managing lymphoedema In the current review one systematic review
(including a meta-analysis) and 3 studies were identified
In a prospective RCT testing the efficacy of two types of physiotherapy on shoulder function
and lymphatic disturbance in post-operative breast cancer survivors (n=60) participants
received one of two types of physiotherapy 48-hours post-surgery (de Rezende et al
2006)
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-
defined sequence of movements
2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely
to music
Lymphoedema is estimated to affect
about 30 of breast cancer survivors
post-treatment (Deo et al 2004)
81
Results indicated significantly better recovery of limb movement in the directed group
compared to the free group with there being no significant difference between groups in
terms of lymphatic disturbance
Ahmed et al (2006) report on a 6-month RCT examining the effects of supervised upper-
and lower-body weight training on lymphoedema incidence and symptoms in breast cancer
survivors (n = 45) 4-36 months post-treatment From baseline to 6-months three control-
group participants reported an increase in lymphoedema symptoms No participants in the
intervention group reported such symptoms suggesting that twice-a-week progressive
weight training does not increase the onset of or exacerbate lymphoedema in breast cancer
survivors (13 women had lymphoedema at baseline) The results from this study indicate
that at minimum physical activity does not exacerbate lymphoedema
Moseley and Piller (2008) reviewed the literature for evidence supporting the benefits of
physical activity for people with limb lymphoedema Their key findings from eleven studies
demonstrated that
physical activity can improve lymph clearance
physical activity can help reduce limb volume and improve subjective symptoms and
QoL
benefits from physical activity have been sustained post-physical activity regime in
some studies
physical activity is a viable option for people with lymphoedema
Moseley and Pillerlsquos (2008) conclusions were supported further in a recent RCT by Hayes
Hildegard and Turner (2009) Breast cancer survivors at least 6-months post-treatment
who had developed unilateral upper-limb lymphoedema participated in twenty supervised
group aerobic and resistance physical activity sessions over 12-weeks (n=16) or continued
habitual activities (n=16) Average attendance was more than 70 of supervised sessions
and there were no withdrawals Mean ratio and volume measures at baseline were similar
between the two groups and no changes were observed at 3-months follow-up for either
group although two women receiving supervised physical activity no longer had evidence of
lymphoedema by study completion The results from this review as with the RCT by
Ahmed et al (2006) indicate that at minimum physical activity does not exacerbate
secondary lymphoedema
In the review referred to previously by Speck et al (2010) with minor exceptions findings
indicated aerobic lifestyle and upper body resistive exercise was tolerated by breast cancer
survivors with no adverse effects on the development or exacerbation of lymphoedema
ii DIET
Bekkering et al (2006) report on one double-blind placebo-controlled RCT examining diet
and lymphoedema in breast cancer survivors (n=68) at a mean of 155-years post-treatment
For 6-months women received 500mg twice a day of dl-alpha tocopheryl acetate (a source
of vitamin E) plus pentoxifylline (a drug that improves blood circulation) 400mg twice a day
82
of dl-alpha tocopheryl acetate or placebo (Gothard et al 2004) At 6-months and 12-months
post-randomisation there was no significant difference between groups in terms of arm
volume
The current review identified one RCT
Dietary Fat
In a UK RCT Shaw Mortimer and Judd (2007) demonstrate the impact of diet and weight
loss on post-treatment arm lymphoedema in breast cancer survivors (n=51) Women were
assigned to one of three 24-week dietary groups
1) a low-fat diet (fat intake reduced to 20 of total energy intake)
2) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ)
3) a control group (continuing their usual diet)
After the end of the 24-week period of dietary intervention there was a slightly greater
reduction in excess arm volume in both dietary intervention groups compared with the
control although this was not statistically significant Furthermore despite low levels of
adherence to dietary advice weight loss was achieved in all groups demonstrating that
dietary interventions can assist in reducing excess arm volume in women with post-
treatment lymphoedema
SUMMARY OF EVIDENCE FOR LYMPHOEDEMA
The studies evaluated within this review indicate a need to re-assess the common clinical
guidelines that breast cancer survivors avoid upper body resistance activity for fear of
increasing risk of lymphoedema(Speck et al 2010) They also indicate a requirement to
develop guidelines for appropriate physical activity As concluded by Hayes Hildegard and
Turner (2009) women with secondary lymphoedema should be encouraged to be physically
active optimising their physical and psychosocial recovery Resistance exercise does not
increase the risk for or exacerbate symptoms of lymphoedema and in fact directed physical
activity 48-hours post-surgery might offer greater utility in terms of rehabilitation outcomes
Some of the studies evaluated in the review by Moseley and Piller (2008) comprised small
sample sizes and did not include control groups however when combined with other studies
presented within this review there is some support for encouraging physical activity in breast
cancer survivors Furthermore physical activity combined with changes in diet and
subsequent weight loss in survivors who are overweight might significantly reduce the
symptoms of lymphoedema although evidence for diet in reducing symptoms of
lymphoedema is limited
Weight loss across groups
9 (60) in the control group 13 (76) in the low-fat diet group 18 (95) in the weight-reduction
group
83
Table 9 Lymphoedema and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Ahmed et al (2006)
RCT comparing supervised twice weekly upper- and lower-body weight training over 6-months with control group completing no training
Breast cancer survivors (n = 45) 4-36 months post-treatment
6-months post-intervention
Incidence and symptoms of lymphoedema
From baseline to 6-months three control-group participants
reported an increase
in lymphoedema symptoms No
participants in the intervention group reported such symptoms suggesting that
twice-a-week progressive weight training does not
increase the onset of or exacerbate lymphoedema in breast
cancer
survivors
de Rezende et al (2006)
RCT examining the impact of physiotherapy on lymphoedema Participants received one of two types of physiotherapy
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-defined sequence of movements 2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely to music
48-hours post-surgery breast cancer survivors (n=60)
On completion of intervention (42-days)
Shoulder movement and lymphatic disturbance
Significantly better recovery of limb movement in the directed group compared to the free group with there being no significant difference between groups in terms of lymphatic disturbance
Hayes Hildegard and Turner (2009)
An RCT testing the impact of aerobic exercise on lymphoedema outcomes Participants randomised to 1) 20 supervised group aerobic and resistance physical activity sessions over 12-weeks (n=16) 2) continued habitual activities (n=16)
Breast cancer survivors at least 6-months post-treatment who had developed unilateral upper-limb lymphoedema
3-months post-intervention
Arm volume measurements
Mean ratio and volume measures at baseline were similar between the two groups and no changes were observed at 3-months follow-up for either group although two women receiving supervised physical activity no longer had evidence of lymphoedema by study completion
84
Moseley and Piller (2008)
Literature search of the evidence supporting the benefits of exercise for those with limb lymphoedema
Exercise studies undertaken in RCTs or cohort studies and involving secondary limb lymphoedema (with no active cancer)
Varied from post-intervention to 8-weeks follow-up
Change in limb volume and subjective symptoms
Exercise has been shown to improve lymph propulsion and clearance help reduce limb volume and improve subjective symptoms and quality of life Benefits from exercise have been sustained post-exercise regime in some studies Exercise is a viable option for those with limb lymphoedema
DIET
Gothard et al (2004)
A double-blind placebo-controlled randomised phase II trial Participants were randomised to active drugs or placebo All volunteers were given dl-alpha tocopheryl acetate 500 mg twice a day orally plus pentoxifylline 400 mg twice a day orally or corresponding placebos for 6 months
68 volunteers with a minimum 20 increase in arm volume at a median 155 years after radiotherapy (plus axillary surgery in 5168 (75) cases)
12 months post-randomisation
Volume of the ipsilateral limb measured
There was no significant difference between treatment and control groups in terms of arm volume Absolute change in arm volume at 12 months was 25 (95 CI minus040 to 53) in the treatment group compared to 12 (95 CI minus28 to 51) in the placebo group The difference in mean volume change between randomisation groups at 12 months was not statistically significant (P=06) minus13 (95 CI minus61 to 35) nor was there a significant difference in response at 6 months (P=07) where mean change in arm volume from baseline in the treatment and placebo groups was minus23 (95 CI minus79 to 34) and minus11 (95 CI minus39 to 17) respectively
Shaw Mortimer and Judd (2007)
Participants were assigned to one of three 24-week dietary groups in order to assess impact on arm volume 1)a low-fat diet (fat intake reduced to 20 of total energy intake) b) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ) c) a control group (continuing their usual diet)
Breast cancer survivors (n=51)
After 24-weeks of intervention
Arm volume There was a slightly greater reduction in excess arm volume in both dietary intervention groups compared with the control although this was not statistically significant
85
OSTEOPOROSIS AND BONE HEALTH
Osteoporosis is a condition in which the bones become less dense and more likely to
fracture which in turn can result in significant pain and disability It is known as a silent
disease because if undetected bone loss can progress for many years without symptoms
until a fracture occurs Risk factors for developing osteoporosis are often enhanced in
cancer survivors such as being post-menopausal and having had early menopause (Ada et
al 2002) Low calcium intake lack of physical activity smoking and excessive alcohol
consumption are also risk factors for osteoporosis (Guthrie et al 2000) Women who have
had breast cancer treatment may be at increased risk for osteoporosis and fracture due to
reduced levels of oestrogen whilst men who receive hormone deprivation therapy for
prostate cancer also have an increased risk of developing osteoporosis and broken bones
(National Institutes of Health Osteoporosis and Related Bone Diseases 2009)
There are no early symptoms of osteoporosis but diet physical activity and drug treatment
can prevent or reverse loss of BMD highlighting the importance of lifestyle choices in
osteoporosis outcomes Studies identified in the current review are summarised in Table 10
at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any physical activity studies examining osteoporosis
in breast cancer survivors The current review identified 3 RCTs and one cohort study
Schwartz Winters-Stone and Gallucci (2007) evaluated the impact of aerobics and
resistance training on BMD in an RCT involving women with histologically confirmed invasive
stage I-III breast cancer (n=66) beginning chemotherapy Women were randomised to one
of three groups and stratified according to menopausal status (pre-menopausal or post-
menopausal)
1) Home-based aerobic exercise - women were instructed to choose an aerobic activity
they enjoyed (eg walking jogging) and exercise for 15-30 minutes four days per
week for the duration of the study at a symptom-limited moderate intensity such that
they were breathing hard but able to talk
2) Home-based resistance exercise ndash women were instructed to exercise at home four
days per week using resistance bands and tubing
3) Usual care
It has been reported that 80 of older breast cancer survivors have osteopenia (below normal bone-mineral density [BMD]) or osteoporosis at initial diagnosis (Twiss et al 2001)
86
The average decline in BMD was -623 for usual care -492 for resistance exercise and
-076 for aerobic exercise suggesting that weight-bearing aerobic exercise attenuates
declines in BMD Pre-menopausal women demonstrated significantly greater declines in
BMD than post-menopausal women highlighting a need to provide interventions for bone
health on a risk stratification basis
Gross et al (2002) examined the intensity of physical activity (ie light moderate vigorous)
reported by a cohort of post-menopausal breast cancer survivors (n=27) and found no
relationship between activity levels and BMD However participants mainly reported light
physical activity limiting the examination of moderate and vigorous activity outcomes It is
possible that a higher intensity of physical activity is required to achieve any benefits to bone
health
Waltman et al (2009) conducted an RCT testing a 24-month self-efficacy based strength
and weight training programme on post-treatment (except tamoxifen and aromatase
inhibitors) post-menopausal breast cancer survivors (n=223) who had amenorrhea
(absence of menstruation) for at least 12-months and a bone BMD score lower than the
norm (Figure 1)
Figure 1 Bone Density Definitions
WHO Definitions of Osteoporosis
Based on Bone Density
T-Scores
BMD
Category
Examples
Range
10
05
0
-05
-10
-1 and
above Normal BMD
-15
-20
Between
-1 and -25
Low BMD
(Osteopenia)
-25
-30
-35
-40
-25 and
below Osteoporosis
Source WHO (2003)
The women were randomised to receive physical activity with medication (n=110) or
medication only (n=113) The medication taken by both groups included risedronate
(osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily) While
87
participation in strength training did not result in statistically significant improved BMD there
was a trend towards at least maintaining BMD at the total hip Participants who were 50
or greater adherent to the intervention (reasons for non-adherence included lack of
time or chronic pain due to co-morbidity) were significantly less likely than
participants on medication alone to lose BMD at the total hip and femoral neck
In a third RCT Swenson et al (2009) compared the effects of two interventions on changes
in BMD in women receiving chemotherapy for breast cancer (n=62)
1) intravenous zoledronic acid (used to prevent skeletal fractures in people with cancer)
and oral calciumvitamin D every 3-months for five treatments
2) prescribed home-based physical activity and oral calciumvitamin D
Zoledronic acid protected patients with breast cancer against bone loss during initial
treatment whereas the home-based physical activity intervention was less effective in
preventing bone loss indicating that physical activity and dietary supplements are not
always sufficient to protect done density in people with cancer However these were
patients undergoing treatment and more research is required into the effects of physical
activity on bone health in post-treatment survivors
ii DIET
Bekkering et al (2006) did not identify any diet studies examining osteoporosis in breast
cancer survivors The current review identified 3 RCTs and one cohort study
Plant Proteins and Fibres
Weikert et al (2005) performed a sub-analysis of the EPIC cohort study conducted in
Germany which included 8178 females and examined the association between protein
intake dietary calcium and bone structure It was concluded that high consumptions of
animal protein may be unfavourable whereas higher vegetable protein may be
beneficial to bone health These results support the hypothesis that high calcium intakes
combined with adequate protein intake based on a high ratio of vegetables to animal protein
may be protective against osteoporosis Indeed evidence has demonstrated the relationship
between lower incidence of osteoporosis in Asian women and vegetarian populations due to
a diet rich in vegetables and fruit (Fujii et al 2009 Merill and Aldana 2009 Thorpe et al
2008) Furthermore a large-scale dietary modification intervention of post-menopausal
women (n = 4883) showed that an increased consumption of plant proteins and fibres from
fruits vegetables and grains reduced the risk of multiple falls and slightly lowered hip BMD
although it did not change the risk of osteoporotic fractures (McTiernan et al 2009)
New et al (2003 2004) provides further evidence for the benefits of plant proteins and fibres
on bone health in two reviews where a positive link between a high consumption of fruit
and vegetables and bone health has been demonstrated In the first report it was found
that fruit and vegetables have beneficial effects on bone mass and bone metabolism in men
and women across the age ranges whilst in the second review it was concluded that
although the impact of a vegetarian diet on bone health is much more complex than merely
being related to diet vegetarians do tend to have normallsquo bone mass
88
iii WEIGHT
Bekkering et al (2006) did not identify any studies examining weight implications on
osteoporosis in breast cancer survivors The current review identified one study that found
that being underweight (BMI less than 185) was associated with lower BMD (Ryan et al
2007)
b) PROSTATE CANCER
i WEIGHT
Bekkering et al (2006) did not identify any studies examining the effect of body weight on
osteoporosis in prostate cancer survivors The current review identified one RCT Ryan et
al (2007) found a positive association between BMI and bone density of the hip in men with
prostate cancer (n=120) who were within the first 12-months of androgen-deprivation
therapy This suggests that a higher BMI can be protective of bone density loss in this
patient group
ii ALCOHOL
Bekkering et al (2006) did not identify any studies examining the effect of alcohol
consumption on osteoporosis in prostate cancer survivors The current review identified one
RCT Ryan et al (2007) also demonstrate greater bone density in prostate cancer patients
consuming seven or more weekly alcoholic beverages when compared to non-drinkers
a) OTHER CANCER
i DIET
Soya Products
Bekkering et al (2006) did not identify any studies examining the effect of diet on
osteoporosis in other cancer survivors The current review identified one RCT Marini et al
(2008) reported a randomised double-blind placebo-controlled trial of the soya derivative
genistein aglycone and its effects on bone health after 3-years in women with breast and
endometrial cancer (n=389) Bone mineral density increases were greater with
genistein for both femoral neck and lumbar spine compared to placebo the conclusion
being that after 3-years of treatment genistein exhibited a promising safety profile with
positive effects on bone formation in this cohort of osteopenic post-menopausal women
89
SUMMARY OF EVIDENCE FOR OSTEOPOROSIS AND BONE HEALTH
There is evidence that vitamin D and calcium might be associated with greater BMD
however this benefit cannot be distinguished from other potential contributors such as
physical activity and medication More research is needed into the effects of physical activity
on osteoporosis in cancer survivors The findings thus far offer different conclusions
although there is limited evidence that physical activity can at the very least prevent loss of
BMD which is a positive outcome in survivors at particular risk of bone loss Greater
adherence to physical activity interventions appeared to offer the greater benefits
highlighting the importance of designing lifestyle interventions that can be maintained as
well as providing higher intensity support for survivors with co-morbidities
Higher BMI has been found to be protective of BMD loss in men with prostate cancer
however no distinction has been made between higher BMI and a BMI that indicates excess
weight Limited evidence has been provided for the benefits of moderate alcohol
consumption but as with the evidence presented for weight much more research is needed
before any valid and reliable conclusions can be made Since the NHS advises no more than
3-4 units of alcohol per day for men more research is needed to determine the minimum
units of alcohol that offer such protective benefits It is important to deter against excessive
drinking which can have a number of serious health implications including high blood
pressure mouth and throat cancers and stroke (NHS 2010)
Men should not exceed 3-4 units of alcohol per day on a regular basis (NHS 2010) One unit is the amount of pure alcohol in a 25ml single measure of spirits (pure alcohol by volume [ABV] 40) a third of a pint of beer (ABV 5-6) or half a 175ml standardlsquo glass of red wine (ABV 12) Daily alcohol limits are provided by the NHS in order to discourage the belief that that the number of units of a weekly limit can be consumed at once (ie binge drinking) Use of daily limit
90
Table 10 Osteoporosis and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Gross et al (2002)
Descriptive correlational test of a multicomponent intervention to prevent and treat osteoporosis in breast cancer survivors
27 post-menopausal breast cancer survivorslsquo post- treatment except for tamoxifen
Not reported
Physical activity vigour vitality and BMD
More than half reported no very hard physical activity and 37 reported no hard activity The association of vigour with total metabolic equivalents for combined moderate hard and very hard activities was significant (r = 0536 p = 0007) as were the hours spent in the combined moderate to very hard activities No relationship was found between vigour vitality or any level of activity and BMD
Schwartz Winters-Stone and Gallucci (2007)
RCT testing the effects of aerobic and resistance exercise on changes in bone mineral density (BMD) in women receiving chemotherapy Participants were randomised to aerobic or resistance exercise and usual care
66 women with stage I-III breast cancer beginning adjuvant chemotherapy
6-months after starting treatment
BMD aerobic capacity and muscle strength
Aerobic exercise preserved BMD significantly better compared to usual care Premenopausal women demonstrated significantly greater declines in BMD than postmenopausal women Aerobic capacity increased by almost 25 for women in the aerobic exercise group and 4 for resistance exercise Participants in the usual care group showed a 10 decline in aerobic capacity
Swenson et al (2009)
Participants received one of two treatments a) Intravenous zoledronic acid and oral calciumvitamin D every 3-months for five treatments b) Prescribed home-based physical activity and oral calciumvitamin D
Women receiving chemotherapy for breast cancer (n=62)
On completion of 3-month intervention
Severity of lymphedema by arm circumference
BMD significantly decreased in the physical activity group but not in the zoledronic acid group Zoledronic acid protected patients with breast cancer against bone loss during initial treatment whereas the home-based physical activity intervention was less effective in preventing bone loss indicating that physical activity and dietary supplements are not always sufficient to protect done density in people with cancer
Waltman et al (2009)
A 24-month self-efficacy based strength and weight training programme Participants were randomised to receive physical activity with medication (n=110) or medication only (n=113) the medication taken by both groups including risedronate (osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily)
Post-treatment post-menopausal breast cancer survivors (n=223) with amenorrhea for at least 12-months and a BMD score lower than the norm
On completion of the 24-month intervention
Bone mineral density
While participation in strength training did not result in statistically significant improved BMD there was a trend towards at least maintaining BMD at the total hip Participants who were 50 or greater adherent to physical activities were significantly less likely than participants on medication alone to lose BMD at the total hip and femoral neck
91
DIET
Marini et al (2008)
RCT assessing the continued safety profile of genistein
aglycone on
breast and endometrium and its effects on bone after
3 years of
therapy Participants received 54mg of genistein
aglycone daily or
placebo both treatment arms
received calcium and vitamin D
Breast cancer patients ndash intervention group (n=71) and placebo (n=67)
After 3-years of treatment
BMD Bone mineral density increases were greater with genistein for both
femoral neck and lumbar spine compared to placebo Genistein also
significantly reduced pyridinoline as well as serum carboxy-terminal
cross-linking telopeptide and soluble receptor activator of NF- B
ligand while increasing bone-specific alkaline phosphatase IGF-I
and osteoprotegerin levels There were no differences in discomfort
or adverse events between groups
(McTiernan et al 2009)
RCT assessing the effect of the Womens Health Initiative
Dietary
Modification low-fat and increased fruit vegetable
and grain
intervention on incident hip total and site-specific
fractures and self-
reported falls and in a subset on bone
mineral density (BMD)
Participants were randomly assigned to
receive
a)dietary modification intervention (daily goal 20 of energy as fat 5 servings of vegetables
and fruit
and 6 servings of grains) b)comparison group
- no dietary
changes
Post-menopausal women (n=48835) intervention (40 n=19541)
versus comparison group (60 n=29294)
Mean=81-years
Incident hip total and site-specific
fractur
es and self-reported falls and in a subset on bone
mineral
density (BMD)
215 women in the intervention group and 285 women in the
comparison group (annualized rate 014 and 012 respectively)
experienced a hip fracture (hazard ratio 112 95 CI 094
134 P = 021) The intervention group (n = 5423 annualized rate
344) had a lower rate of reporting 2 falls than did the
comparison group (n = 8695 annualized rate 367) (HR 092
95 CI 089 096 P lt 001) There was a significant interaction
according to hormone therapy use those in the comparison group
receiving hormone therapy had the lowest incidence of hip fracture In a subset of 3951 women
hip BMD at years 3 6 and 9 was 04ndash
05 lower in the intervention group than in the comparison group
(P = 0003)
New et al (2004)
Literature review assessing the impact of a vegetarian diet on indices of skeletal integrity to address specifically whether vegetarians have a normal bone mass
Analysis of existing literature through a combination of observational clinical and intervention studies were assessed in relation to bone health lacto-ovo-vegetarian and
Not reported
Bone health Key findings included (i) no differences in bone health indices between lacto-ovo-vegetarians and omnivores (ii) conflicting data for protein effects on bone with high protein consumption and low protein intake (particularly with respect to vegan diets) being detrimental to the skeleton (iii) growing support for a beneficial effect of fruit and vegetable intake on bone with mechanisms of action currently remaining unclarified The impact of a vegetarian diet on bone health is a hugely complex area since 1) components of the diet (such as calcium protein alkali vitamin K phytoestrogens) may be varied 2) key lifestyle factors which are
92
vegan diets versus omnivorous consumption of animal versus vegetable protein and fruit and vegetable consumption
important to bone (such as physical activity) may be different 3) the tools available for assessing consumption of food are relatively weak However from data available vegetarians do certainly appear to have normal bone mass
Weikert et al (2005)
Prospective cohort study (EPIC) examining associations between protein intake calcium and bone structure measured by broadband ultrasound attenuation (BUA)
8178 female EPIC participants
Not reported
Bone structure
High intake of animal protein was associated with decreased BUA values ( _ = ndash003 p = 0010) whereas high vegetable protein intake was related to an increased BUA ( _ = 011 p = 0007) The effect of dietary animal protein on BUA was modified by calcium intake
WEIGHT
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and alcohol use was positively associated with the Z score
ALCOHOL
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and body mass index was positively associated with the Z score
93
WEIGHT AND BODY COMPOSITION
Weight gain during and after cancer treatment is becoming an ever-increasing significant
concern (Camoriano et al 1990 Levine et al 1991 Saquib et al 2006) Weight gain is
expected when energy intake exceeds energy expenditure a combination that is frequently
described among breast cancer patients who report exercising less during treatment and
after treatment (Schwartz 2000 Demark-Wahnefried 2001) and consuming a higher energy
diet during treatment (Mukhopadhyay and Larkin 1986) Exacerbating this is the fact that
women in general gain weight as they transition through menopause (Sammel et al 2003)
putting breast cancer patients at particular risk as treatments frequently result in a premature
menopause For individuals with bowel cancer the CALBG 8980 trial showed that 35 of
patients post-chemotherapy were overweight (BMI 250ndash299) and 34 were obese BMI
300ndash349) or very obese (BMI gt35) (Meyerhardt et al 2008) The reasons for weight gain
during and after treatment are multifactorial and the result of individual lifestyle behaviours
and the impact of certain cancer drugs Regardless of the reasons as described in part one
of this review both survival and recurrence may be adversely affected by obesity
(Chlebowski et al 2002)
The effect of obesity on survival has been evident in the majority of studies although not all
one reason for this inconsistency being the possibility that biological factors associated with
obesity and not the obesity itself are responsible for the observed effect For example
there is considerable evidence that the effects of obesity on breast cancer risk may be
mediated at least in part by the effect of obesity on insulin resistance (Friedenreich 2001
Suga et al 2001 Goodwin et al 2002)
Finding effective methods for weight loss continues to be a challenge as although some
studies have demonstrated substantial weight loss in obese individuals weight loss results
in general have been modest and new approaches are needed (Jeffery et al 2000) For
long-term reduction in body weight intensive individualised approaches toward developing
a new lifestyle may be required (Djuric et al 2002)
Studies identified in the current review are summarised in Table 11 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in breast cancer survivors The current review identified one
meta-analysis and three RCTs
In the meta-analysis Kim Kang and Park (2009) reviewed 10 studies involving 588 women
who had been treated for breast cancer examining the effectiveness of aerobic exercise
interventions on cardiopulmonary function and body composition conducted during or after
cancer treatments They concluded that regular aerobic physical activity significantly
improved cardiopulmonary function as assessed by absolute VO2 peak relative VO2
94
peak and 12-minute walk test as well as improved body composition as assessed by
percentage body fat (although body weight and lean body mass did not change
significantly)
Courneya et al (2007) conducted a multicentre RCT in which women with breast cancer on
adjuvant chemotherapy were randomly assigned to usual care (n = 82) supervised
resistance exercise (n = 82) or supervised aerobic exercise (n = 78) for the duration of their
chemotherapy (median = 17-weeks 9-24 weeks) There was 70 adherence to supervised
exercise with aerobic physical activity being superior to usual care for improving
aerobic fitness and percent body fat whilst resistance physical activity was superior
to usual care for improving muscular strength lean body mass and chemotherapy
completion rate
Schmitz et al (2005) evaluated the safety and effects of twice-weekly weight training among
85 breast cancer survivors with women being randomised into immediate or delayed
intervention groups The immediate group trained from months 0-12 the delayed group
served as a no exercise parallel comparison group from months 0-6 and trained from months
7-12 At 6-months the immediate group compared to the no exercise group showed
significantly greater increases in lean mass (p lt 01) as well as significant decreases
in percentage body fat (p lt 05) This significance remained at 12-months when
comparing the immediate group with the delayed exercise group
Mefferd et al (2006) randomised overweight or obese breast cancer survivors (n=85) to a
16-week once weekly general exercise and dietary counselling intervention or standard
care The intervention addressed a reduction in energy intake as well exercise with a goal
of an average of one-hour a day of moderate to vigorous activity Seventy six women
(894) completed the intervention demonstrating reasonable acceptability of the
intervention At 16-weeks significant group differences in favour of the intervention
were evident in weight BMI percent fat trunk fat leg fat and waist and hip
circumference
ii DIET
Bekkering et al (2006) did not identify any studies examining the effect of diet on weight loss
or maintenance in breast cancer survivors The current review identified one RCT
Chlebowski et al (2006) report an RCT conducted as part of the aforementioned WINS trial
where 2437 postmenopausal women with early breast cancer were randomised to
nutritional and lifestyle counselling (n=975) or not (n=1462) as part of routine follow-up The
dietary intervention included eight bi-weekly individual counselling sessions As a reminder
the goal of the dietary intervention was to reduce percentage of calories from fat to 15
resulting in a sustained reduction in fat intake to approximately 20 of calories Dietary fat
intake reduction was significantly greater in the dietary group compared to the control group
After 12-months of intervention dietary fat intake was lower in the intervention group
than in the control group (333g per day versus 513g per day respectively Plt001)
95
corresponding to a statistically significant 6-pound lower mean body weight in the
intervention group (P lt01) This major study also demonstrated a survival advantage in
women who lost weight as described in Part 1 of this review
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in prostate cancer survivors The current review identified
one RCT
Segal et al (2009) conducted a RCT with 121 men with prostate cancer commencing
radiotherapy with or without androgen deprivation therapy They were randomly assigned to
24-weeks of usual care resistance exercise or aerobic exercise Compared with usual
care exercise improved aerobic fitness upper- and lower-body strength while
preventing an increase in body fat Resistance exercise generated longer-term
improvements and additional benefits for strength and body fat than aerobic exercise
SUMMARY OF EVIDENCE FOR WEIGHT AND BODY COMPOSITION
Supervised physical activity programmes with or without dietary counselling are highly
effective in improving body composition or at the very least preventing increases in weight
They are also safe and have other major benefits on health including improving fitness
walking distance muscle power and reducing cholesterol More research is however
required into the most effective dietary strategies for weight loss or maintenance in cancer
survivors Thus far there is some evidence for reducing dietary fat intake
A large controlled trial has been designed to test the combined effect of physical activity and
weight control on disease-free survival and on breast cancer recurrence free survival
second primary breast cancer and total invasive plus in situ breast cancer (Ballard-Barbash
et al 2009) Goals for weight control interventions for women whose BMI is greater than
25kgm2 is to lose 10 of body weight and for women whose BMI is less than or equal to
25kgm2 to avoid weight gain The goal for the physical activity intervention would be to
achieve and maintain regular participation in a moderate intensity physical activity
programme for a total of 150-255 minutes over at least 5 days per week This study is using
evidence which is current for weight loss and physical activity and is an indicator for the
basis of advice for patients at risk in similar situations
96
Table 11 Weight and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Courneya et al (2007)
Multicentre RCT to test for factors that could counteract unfavourable changes resulting from chemotherapy (eg changes in body composition) Participants were randomly assigned to usual care (n =
82) supervised resistance exercise
(n = 82) or supervised aerobic
exercise (n = 78) for the duration of their chemotherapy
242 breast cancer
patient
s initiating adjuvant chemotherapy
Median=17-weeks
Primary Cancer-Specific QoL Secondary Fatigue psychosocial functioning physical fitness body composition chemotherapy completion rate and lymphedema
The follow-up assessment rate for our primary end point was
921 and adherence to the supervised exercise was 702
Unadjusted and adjusted mixed-model analyses indicated that
aerobic exercise was superior to usual care for improving self-
esteem (P = 015) aerobic fitness (P = 006) and percent body fat
(adjusted P = 076) Resistance exercise was superior to usual care
for improving self-esteem (P = 018) muscular strength (P lt
001)
lean body mass (P = 015) and chemotherapy completion rate (P =
033) Changes in cancer-specific QOL fatigue depression and
anxiety favoured the exercise groups but did not reach statistical
significance Exercise did not cause lymphedema or
adverse events
Kim Kang and Park (2009)
Meta-analysis to examine the effectiveness
of aerobic exercise
interventions on cardiopulmonary function
and body composition in
women with breast cancer
Of 24 relevant
studie
s reviewed 10 studies (n= 588) met the inclusion criteria
Not reported Cardiopulmonary function
and body
composition
The findings indicated that aerobic exercise significantly improved
cardiopulmonary function as assessed by absolute
VO2 peak (standardized mean difference [SMD] 916 p lt 001)
relative VO2 peak (SMD424 p lt 05) and 12-minute walk test
(SMD 502 p lt 001) Similarly aerobic exercise significantly
improved body composition as assessed by percentage body fat
(SMD mdash890 p lt001) but body weight and lean body mass did not
change significantly
Mefferd et al (2006)
RCT to test the effect of a 16-week cognitive behavioural therapy (CBT) intervention for weight loss through exercise and diet modification on risk factors for recurrence of breast cancer Participants randomly assigned to a once weekly 16-week intervention or wait-list control group
Overweight or obese breast cancer survivors (n=76)
On completion of the 16-week intervention
Weight Significant differences in weight body mass index percent fat trunk fat leg fat as well as waist and hip circumference between intervention and control groups (P le 005) Furthermore levels of triglycerides and total cholesterolhigh density lipoprotein cholesterol levels were also significantly reduced following the intervention
97
Schmitz et al (2005)
RCT testing the safety of twice weekly weight training classes among recent breast cancer survivors Participantslsquo randomised into immediate and delayed treatment groups The immediate group trained from months 0-12 the delayed treatment group served as a no exercise parallel comparison group from months 0-6 and trained from months 7=12
Convenience sample of 85 recent breast cancer survivors
6 and 12-months
Body size (lean body mass) and biomarkers hypothesised to link exercise and breast cancer risk
Significant increases in lean mass (088 versus 002 kg P lt 001) as well as significant decreases in body fat (minus115 versus 023 P = 003) and IGF-II (minus623 versus 2828 ngmL P = 002) comparing immediate with delayed treatment from baseline to 6 months Within-person changes experienced by delayed treatment group participants during training versus no training were similar
Segal et al (2009)
Prostate Cancer Radiotherapy and
Exercise Versus Normal
Treatment study examining the effects
of 24-weeks of resistance or
aerobic training versus usual care on prostate cancer outcomes Randomly assigned
to usual care resistance or
aerobic exercise for 24-weeks
Prostate cancer patients on radiotherapy (n=121) usual care (n=41) resistance (n= 40) aerobic exercise
(n=
40)
On completion of 24-week intervention
Fatigue QOL physical fitness body composition PSA testosterone haemoglobin and lipid levels
Median adherence to prescribed exercise was 855 Compared
with usual care resistance training improved QOL (P = 015)
aerobic fitness (P = 041) upper- (P lt 001) and lower-body (P lt
001) strength and triglycerides (P = 036) while preventing an
increase in body fat (P = 049) Aerobic training also improved
fitness (P = 052)
DIET
Chlebowski et al (2006)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to 345]
versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group
98
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general dietary
guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
randomisation to death from any cause
99
QUALITY OF LIFE
The advancements in diagnosis and treatment that have contributed to the rise in
survivorship are a significant achievement for healthcare science However it is important to
recognise that this has also resulted in an increase in the number of people living with the
often long-term physical and psychological consequences of cancer and its treatment
Quality of life outcomes are thus becoming just as important as hardlsquo outcomes such as
mortality (Rosenbaum Fobair and Spiegel 2006) hence an emphasis on patient-reported
outcomes (DH 2009c) Indeed there is increasing evidence that QoL can be more
predictive of cancer survival than measures of performance status (Cella et al 2009 Eton et
al 2003 Wenzel et al 2005)
A healthy lifestyle has become viewed as an important element for improved QoL (Lyon and
Langille 2000) with particular emphasis on physical activity Studies identified in the current
review are summarised in Table 12 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in breast cancer survivors In the current review one systematic review (with meta-
analysis) and 6 RCTs were identified that provide evidence for the role of physical activity in
the QoL of breast cancer survivors
McNeeley et al (2006) conducted a systematic review with meta-analysis of RCTs (n=14)
examining the effects of physical activity on outcomes in breast cancer survivors Three of
the reviewed studies involving 194 patients compared exercise with usual care
(Campbell et al 2005 Courneya et al 2003 Segal et al 2001) with pooled data
demonstrating that exercise led to significant improvements in QoL superior to the
usual care groups Four studies involving 208 patients reported physical functioning or
physical well-being components of QoL (Campbell et al 2005 Courneya et al 2003
McKenzie and Kalda 2003 Segal et al 2001) the pooled results of which showed
a statistically significant increase in this component of QoL as a result of physical
activity Two of these studies were rated as high quality by the reviewers Courneya et al
2003 Segal et al 2001
100
In addition to this meta-analysis findings by Ohira et al (2006) demonstrated that over 6-
months physical and psychological QoL significantly improved in a recent breast
cancer survivors (n=86) 4-36 months post-treatment who took part in a twice-weekly
weight-training intervention when compared to a control group Increases in upper
body strength and lean mass correlated with these improvements suggesting that twice-
weekly weight training for recent breast cancer survivors might improve QoL in part via
changes in body composition and strength
Daley et al (2007) provided evidence from an RCT comprising sedentary breast cancer
survivors who were 12-36 months post-treatment and who were randomised to one of three
conditions
1) 8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-
minute one-to-one sessions with an physical activity specialist three times per week
(n=34)
2) 8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one
sessions with an physical activity specialist three times per week (n=36)
3) usual care (n=38)
Courneya et al (2003) evaluated QoL outcomes in relation to
exercise in breast cancer survivors (n=52) who had completed
surgery radiotherapy or chemotherapy Participants trained three
times per week for 15-weeks on recumbent or upright cycle
ergometers Exercise duration began at 15-minutes for weeks 1-
3 and then systematically increased by five-minutes every 3-
weeks to 35-minutes for weeks 13-15 The exercise group completed
984 of the exercise sessions demonstrating high adherence
rates Overall QoL increased by 91 points in the exercise group
compared with 03 points in the control group (p lt 001) Change
in peak oxygen consumption correlated with change in overall QoL
demonstrating a significant relationship between exercise and
increases in QoL (p lt 01)
Segal et al (2003) compared self-directed versus supervised
exercise on QoL outcomes in women with stages I-II breast cancer
(n=123) Physical functioning in the control group decreased by 41
points whereas it increased by 57 points and 22 points in the self-
directed and supervised exercise groups respectively (p lt 05)
Post-hoc analysis showed a moderately large and clinically important
difference between the self-directed and control groups (98
points p lt 01) and a more modest difference between the
supervised and control groups (63 points P = 09) No significant
differences between groups were observed for changes in QoL
scores
101
A significant mean difference of 98 units in QoL scores favouring aerobic physical
activity therapy was found This outcome was not the result of the extra support and
attention gained from taking part in the intervention since the same findings were not elicited
for the physical activity-placebo and usual care groups
A small pilot RCT comparing QoL and functional capacity in breast cancer survivors (n=21)
provided with 12-weeks of the Chinese physical activity Tai Chi Chuan (n=11) versus
psychosocial support (n=10) was conducted by Mustian Palesh and Flecksteiner (2008)
The tai chi group demonstrated significant improvements in functional capacity and QoL the
psychosocial support group showed significant improvements only in flexibility with declines
in QoL This suggests that tai chi can enhance functional capacity and QoL among
breast cancer survivors over and above the benefits of psychosocial support
Further support for the benefits of physical activity on QoL in breast cancer survivors (n=58)
within 2-years of completing adjuvant therapy has been demonstrated in a combined aerobic
and resistance training RCT (Milne et al 2008) The women received 12-weeks immediate
supervised physical activity three times a week (n=29) or delayed physical activity
comprising the same protocol but provided 12-weeks following the immediate physical
activity group (n=29) Adherence was 613 which is relatively low However there was a
significant group by time interaction for overall QoL which increased in the
immediate physical activity group from baseline to 12-weeks by 208 points compared
to a decrease in the delayed physical activity group of 53 points
Cadmus et al (2009) report on the QoL outcomes of two 6-month RCTs designed for breast
cancer survivors and based on the national recommendation of 30-minutes of moderate to
vigorous physical activity five days per week
When combining findings from these two studies physical activity was not associated with
QoL benefits in the full sample of either study however physical activity was associated with
significantly improved social functioning (a component of QoL) among survivors who
Trial Increasing or Maintaining
Physical Activity during Cancer
Treatment (IMPACT)
Theoretical Framework Theory of
Planned Behaviour and
transtheoretical model - promoting
self-efficacy to overcome barriers to
physical activity
Sample n=45 newly diagnosed
survivors
Delivery Home-based
Trial Yale Physical activity and
Survivorship (YES)
Theoretical Framework Not
reported
Sample n=67 post-treatment
survivors
Delivery Combined supervised
training programme at a local
health club with home-based
physical activity
102
reported low social functioning at baseline which is the likely impact of greater social
interaction during the intervention This highlights the utility of risk stratification and the
provision of lifestyle support based on need survivors with low social functioning as
could be detected via the Social Difficulties Inventory (SDI Wright et al 2005b) are
likely to benefit from programmes such as the IMPACT and YES trial
Sandel et al (2005) report on a cross-over RCT testing the outcomes of a 12-week dance
and movement exercise programme in women within 5-years of treatment for breast cancer
(n=38) The study included a waiting list control (n=19) and cross-over at 13-weeks Women
attended two supervised dance sessions for six weeks and one session per week for an
additional 6-weeks for a total of eighteen sessions A total of 35 (92) women completed
the regimen with reasons for dropping out including fatigue other commitments and one
participant reported shoulder discomfort The overall finding was that breast cancerndash
specific QoL improved significantly in the intervention group compared to the waiting
list group at 13-weeks which remained unchanged
In the updated systematic review described previously Speck et al (2010) present evidence
from 66 high quality RCTs showing that physical activity during treatment has a small to
moderate positive effect on QoL (p=004) anxiety (p=002) and self-esteem (p=002)
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in colorectal cancer survivors In the current review one large cohort study was
identified Lynch et al (2008) examined physical activity and QoL data collected as part of
the Colorectal Cancer and Quality of Life Study37 Telephone interviews were conducted
at approximately 6 12 and 24-months after colorectal cancer diagnosis (n=1966) which
found that participants achieving at least 150-minutes of physical activity per week had an
18 higher QoL score than those who reported no weekly physical activity
ii DIET
Bekkering et al (2006) identified two dietary intervention studies examining impact on QoL in
colorectal cancer survivors One dietary counselling trial found a significant improvement in
health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst another reported that
an intervention aimed at a healthier dietary lifestyle had no effect on health assessment or
life satisfaction but did lead to increased health action and increased reports of feeling goodlsquo
(Corle et al 2001) No further studies were identified in the current review
37
The Colorectal Cancer and Quality of Life study in Australia examines in detail the lifestyle factors that
influence QoL in the 5-years post-diagnosis (n=2000)
103
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any dietary physical activity interventions examining
impact on QoL in prostate cancer survivors One dietary counselling trial found a significant
improvement in health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst
another reported that an intervention aimed at a healthier dietary lifestyle had no effect on
health assessment or life satisfaction but did lead to increased health action and increased
reports of feeling goodlsquo (Corle et al 2001) No further studies were identified in the current
review
Segal et al (2003) reported an RCT comparing supervised resistance exercise versus
control in men with prostate cancer (n=135) who were scheduled to receive androgen
deprivation therapy for at least 3-months Fitness levels were assessed and the men in the
intervention group met with a certified fitness consultant within 7-days of the pre-
assessment The fitness consultant provided patients with the results of their exercise
assessment and introduced a personalised resistance exercise program A significant
improvement was found in QoL outcomes in the intervention group and a significant
decline in the control group Resistance exercise improved QoL regardless of whether
men were treated with curative or palliative intent or whether androgen deprivation therapy
had been received for less than one-year or 1 year
d) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) found that out of seven physical activity trials six observed
improvements in QoL when using cancer-specific questionnaires (Burnham and Wilcox
2002 Courneya et al 2003 Segal et al 2003 Headley et al 2004 Campbell et al 2005
Sandel et al 2005) but one of these same studies found no association when using the
generic SF-36 scale (Segal et al 2001) This highlights the importance of selecting the most
appropriate outcome measures in terms of sensitivity and responsiveness to a given
intervention
In the current review three studies were identified One prospective controlled four-centre
study comprising a sample of survivors with different tumour sites was identified (Korstjens
et al 2008) QoL outcomes were compared between three groups
1) group-delivered physical training (n=71)
2) group-delivered combined physical and cognitive behavioural training (CBT) (n=76)
3) waiting-list control (n=62)
Participants in both training groups showed significant and clinically relevant improvements
in role limitations physical functioning vitality and health change Adding CBT to the
physical training did not have additional beneficial effects on QoL a finding that has been
104
observed in a number of supported self-management programmes (Davies and Batehup
2010)
Oh et al (2009) reported a RCT examining the QoL outcomes of Medical Qigong (MQ) a
mindndashbody practice that uses physical activity and meditation to harmonise the body mind
and spirit Patients (n=162) with malignancy of any stage and an expected survival length of
gt12-months were randomised to a control group or to a 10-week MQ programme comprising
two supervised 90-minute sessions per week At 10-week follow-up participants in the
MQ group reported larger improvements in QoL than those in the usual care group (p
lt 05)
Mosher et al (2009) reported a prospective cohort study examining the diet exercise and
QoL patterns of 753 breast prostate and colorectal cancer survivors who were at least 5-
years post-diagnosis Survivors underwent two 45-60 minute telephone surveys
administered by the Diet Assessment Center The data demonstrated that greater weekly
minutes of exercise were associated with better physical QoL including less pain and
better health perceptions physical functioning and vitality More exercise was also
correlated with better social functioning Diet quality had a positive association with a range
of physical QoL outcomes in analyses that were adjusted for age level of education and co-
morbidities Greater BMI was associated with worse physical QoL including greater
pain and role limitations because of physical problems and worse health perceptions
physical functioning and vitality
SUMMARY OF EVIDENCE FOR QUALITY OF LIFE
Lifestyle interventions appear to help people with a wide range of cancer types who have
received treatments ranging from surgery chemotherapy radiotherapy or hormonal
therapies although no trials have yet been published specifically addressing the newer
biological therapies Even when not directly associated with overall QoL exercise has been
found to significantly improve social functioning among post-treatment survivors The
benefits of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or group-
based A vast array of different types of exercise techniques have been tested in the studies
evaluated in this review highlighting the potential for survivors to choose activities according
to preference
Whilst some studies have recommended the uptake of physical activity during treatment
others have highlighted the benefits of introducing regular physical activity into a survivorlsquos
self-management care plan immediately after completion of treatment Overall the evidence
does suggest that immediate physical intervention provides greater QoL benefits than
delayed intervention
105
Table 12 Quality of Life and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Cadmus et al (2009)
The results of two RCTs to determine the effect of exercise on quality of life in (a) a RCT of exercise among recently diagnosed breast cancer survivors undergoing adjuvant therapy - randomised to a 6-month home-based exercise program or a usual care group (b) a similar trial among post-treatment survivors - randomised to a 6-month supervised exercise intervention or to usual care
50 newly diagnosed breast cancer survivors in the first RCT (a) 75 post-treatment survivors in the second RCT (b)
6-months Measures of happiness depressive symptoms anxiety stress self-esteem and QoL
Good adherence was observed in both studies Baseline quality of life was similar for both studies on most measures Exercise was not associated with quality of life benefits in the full sample of either study however exercise was associated with improved social functioning among post-treatment survivors who reported low social functioning at baseline (p lt005)
Courneya et al (2003)
RCT testing 15-weeks supervised aerobic and resistance training to determine the effects on cardiopulmonary
function and QoL in
post-menopausal breast cancer
survivors Randomly assigned to an exercise (n=25) or control (n=28) group The exercise group trained on cycle ergometers
three times per week for 15
weeks The control group did not train
53 post-menopausal breast cancer survivors
On completion of the 15-week intervention
Changes in peak oxygen
consu
mption and overall
Peak oxygen consumption increased by 024 Lmin in the exercise group whereas it decreased
by 005 Lmin in the control group
(mean difference 029 Lmin 95 confidence interval [CI] 018 to
040 P lt 001) Overall QOL increased by 91 points in the exercise
group compared with 03 points in the control group (mean
difference 88 points 95 CI 36 to 140 P= 001) Pearson
correlations indicated that change in peak oxygen consumption
correlated with change in overall QOL (r = 045 P lt 01)
Daley et al (2007)
RCT - Women were randomised to one of three groups a)8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-minute one-to-one sessions with an physical activity specialist three times per week (n=34) b)8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one sessions with an physical activity specialist three times
Sedentary breast cancer survivors who were 12-36 months post-treatment (n=117)
On intervention completion and at 24-weeks follow-up
QoL depression physical activity behaviour aerobic fitness
There was a significant mean difference of 98 units in QoL scores favouring aerobic physical activity therapy
106
per week (n=36) c)usual care (n=38)
Korstjens et al (2008)
RCT comparing the effects on cancer survivorslsquo QoL in a
12-week group-
based multidisciplinary self-management rehabilitation
program
combining physical training (twice weekly) and cognitive-behavioural
training (once weekly) with
those of a 12-week group-based physical
training (twice weekly) There
was also a non-intervention comparison group
All cancer types rehabilitation (n=76) physical training (n=71) comparison group (n=62)
Baseline after rehabilitation and
3-
months follow-up
QoL (SF-36) The effects of multidisciplinary rehabilitation did not outperform
those of physical training in role limitations due to emotional
problem (primary outcome) or any other domains of quality of life
(all p gt 05) Compared with no intervention participants in both
rehabilitation groups showed significant and clinically relevant
improvements in role limitations due to physical problem (primary
outcome effect size (ES) = 066) and in physical functioning (ES =
048) vitality (ES = 054) and health change (ES = 076) (all p lt
01)
Lynch et al (2008)
Colorectal Cancer and Quality of Life
Study - aimed at examining the relationships between
physical activity
and QoL after a colorectal cancer
diagnosis Participants completed telephone interviews at approximately
6
12 and 24 months after diagnosis
1966 people with colorectal
6 12 and 24-months post-diagnosis
QoL There was an overall independent association between physical
activity and QoL At a given time point
participants achieving at least 150 minutes of physical activity per
week had an 18 higher quality of life score than those who
reported no physical activity Significant associations were also
present at the interindividual level (differences between
participants) and intraindividual level (within participant changes)
Milne et al (2008)
RCT to examine the effects of a supervised exercise program on motivational variables in breast cancer survivors Participants were randomised in a cross-over design to either an immediate exercise group that exercised from baseline to week 12 or a delayed exercise group that exercised from week 12 to 24
Breast cancer survivors (n=58) within 2-years of completing adjuvant therapy
Post-intervention (12-weeks)
Quality of life There was a significant group by time interaction for overall QoL which increased in the immediate physical activity group by 208 points compared to a decrease in the delayed physical activity group of 53 points
Mosher et al (2009)
Prospective Cohort Study examining the health behaviours of older cancer survivors and the associations of those behaviours with QoL especially during the long-term post-treatment period
753 older (aged 65 years) long-term survivors ( 5 years post-diagnosis) of breast prostate and colorectal
2 telephone interviews
Exercise diet weight status and quality of life
Participants reported a median of 10 minutes of moderate-to-vigorous exercise per week and only 7 had Healthy Eating Index scores gt80 (indicative of healthful eating habits relative to national guidelines) Despite their suboptimal health behaviours survivors reported mental and physical quality of life that exceeded age-related norms Greater exercise and better diet quality were associated with better physical quality-of-life outcomes (eg better vitality and physical functioning P lt 05) whereas greater body mass index was associated with reduced physical quality of life (P lt 001)
107
cancer
Mustian Palesh and Flecksteiner (2008)
RCT testing the functional and QoL outcomes of tai chi - women who completed treatment randomised to receive tai chi or psychosocial support therapy for 12-weeks (60 minutes three times weekly)
Breast cancer survivors (n=21)
On completion of 12-week intervention
Functional capacity and quality of life
The tai chi group demonstrated significant improvements in functional capacity and QoL the psychosocial support group showed significant improvements only in flexibility with declines in QoL
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials
MEDLINE EMBASE CINAHL Psych INFO CancerLit PEDro
and
SportDiscus as well as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
functi
oning as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all outcomes
were positive even when statistical significance was not achieved
Exercise led to statistically significant improvements in quality of life
as assessed by the Functional Assessment of Cancer Therapyndash
General (weighted mean difference [WMD] 458 95 CI 035 to
880) and Functional Assessment of Cancer TherapyndashBreast (WMD
662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak oxygen consumption
and in reducing symptoms of fatigue
Oh et al (2009)
RCT comprising 10-weeks Medical Qigong (MQ) to evaluate the use of (MQ) compared with usual care in improving the QOL of cancer patients
162 patients with a range of cancers
On completion of the 10-week intervention
QOL and fatigue (FACT-GF) mood (Profile of Mood State)
Regression analysis indicated that the MQ group significantly improved overall QOL (t144thinsp=thinspminus5761 Pthinspltthinsp0001) fatigue (t153thinsp=thinspminus5621 Pthinspltthinsp0001) mood disturbance (t122 =2346 Pthinsp=thinsp0021) and inflammation (CRP) (t99thinsp=thinsp2042 Pthinspltthinsp0044) compared with usual care after controlling for baseline variables
Ohira et al (2006)
RCT to examine the effects of weight training on changes in QoL and depressive symptoms in recent breast cancer survivors Randomised to treatment or control group
Convenience sample of 86 breast cancer survivors (4-36 months post-treatment)
6-months The primary outcomes were changes in QoL (CARES-SF) and depressive symptoms (CES-D)
QoL improved in the treatment group compared with the control group (Standardized Difference = 062 P = 006) The psychosocial global score also improved significantly in the treatment group compared with the control group (Standardized Difference = 052 P = 02) There were no changes in CES-D scores Increases in upper body strength were correlated with improvements in physical global score (r = 032 P lt01) and psychosocial global score (r = 030 P lt01) Increases in lean mass were also correlated with improvements in physical global score (r = 023 P lt05) and psychosocial global score (r = 024 P lt05)
Sandel et al (2005)
RCT - 12-weeks dance and movement programme versus wait list control to determine the effect on QoL and shoulder function
35 breast cancer survivors
13 and 26-weeks
QoL (FACT-B) Shoulder range of motion (ROM) and Body Image Scale
FACT-B significantly improved in the intervention group at 13 weeks from 1020 _158 to 1167 _ 169 compared to the wait list group 1081 _ 164 to 1071 _213 (time _ group effect P _ 008) During the crossover phase the FACT-B score increased in the wait list group and was stable in the treatment group The overall effect of the training at 26 weeks was significant (time effect P _ 03) and the order of training was also significant (P _ 015) Shoulder ROM
108
increased in both groups at 13 weeks mdash15_ and 8_ in the intervention and wait list groups (Time effect P _ 03 time _ group P _ 58) Body Image improved similarly in both groups at 13 weeks (time effect P _ 001 time _ group P _ 25) and at 26 weeks There was no significant effect of the order of training for these outcome measures
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) A small to moderate positive effect of physical activity during treatment was seen for physical activity level aerobic fitness muscular strength functional quality of life anxiety and self-esteem With few exceptions exercise was well tolerated during and post treatment without adverse events
Segal et al (2003)
RCT testing the hypothesis that resistance exercise can counter the negative QoL effects of androgen deprivation therapy for prostate cancer by reducing fatigue elevating mood building muscle mass and reducing body fat Randomly assigned to an intervention group that participated in a resistance exercise program three times per week for 12 weeks or to a waiting list control group
55 men with prostate cancer scheduled for androgen deprivation therapy for at least 3 months after recruitment
On completion of the 12-week intervention
Primary outcomes fatigue disease-specific QoL Secondary outcomes muscular fitness body composition
Men assigned to resistance exercise had less interference from fatigue on activities of daily living (P =002) and higher quality of life (P =001) than men in the control group Men in the intervention group demonstrated higher levels of upper body (P =009) and lower body (P lt001) muscular fitness than men in the control group The 12-week resistance exercise intervention did not improve body composition as measured by changes in body weight body mass index waist circumference or subcutaneous skinfolds
Vadiraja et al (2009)
RCT - 6-week yoga and relaxation during adjuvant radiotherapy his study compares the effects of an integrated yoga program with brief supportive therapy in breast cancer outpatients undergoing adjuvant radiotherapy at a cancer centre Intervention consisted of
88 stage II and III breast cancer outpatients
After 6-weeks of radiotherapy
QoL (EORTC-C30) Mood (Positive and Negative Affect Schedule)
There was a significant difference across groups over time for positive affect negative affect and emotional function and social function There was significant improvement in positive affect (ES = 059 p = 0007 95CI 125 to 78) emotional function (ES = 071 p = 0001 95CI 645 to 2533) and cognitive function (ES = 048 p = 003 95CI 12 to 185) and decrease in negative affect (ES = 084 p lt 0001 95CI minus134 to minus44) in the yoga
109
yoga sessions lasting 60 minutes daily while the control group was imparted supportive therapy once in 10 days
group as compared to controls There was a significant positive correlation between positive affect with role function social function and global quality of life There was a significant negative correlation between negative affect with physical function role function emotional function and social function
110
ONGOING LIFESTYLE STUDIES
Four ongoing lifestyle studies were identified in the current review one for breast cancer and
three for colorectal cancer
a) BREAST CANCER
In the US Goodwin et al (ongoing) are trialling lsquoLifestyle Intervention Study in Adjuvant
Treatment of Early Breast Cancerrsquo (LISA) The primary objective of this trial is to evaluate
the effect of the addition of a 2-year centrally delivered individualised telephone-based
lifestyle intervention focusing on weight management to a mailed educational intervention on
disease-free survival in post-menopausal women with early stage breast cancer (hormone
receptor positive) BMI ge24-lt40 kgm2 who are receiving standard letrozole adjuvant
therapy The primary outcome is disease-free survival Secondary outcomes include overall
survival distant disease-free survival weight change QoL selected non-cancer medical
events and biologic factors (insulin) The estimated enrolment is 2150 with the study having
started in 2007 Participants will be randomised to
1) Individualised Lifestyle Intervention Experimental - Women randomised to this arm
will receive an intervention program that consists of individual weight loss diet and
physical activity goals incorporated into a 2-year standardised structured telephone
and mail-based intervention In addition to diet and physical activity the intervention
will address behavioural and motivational issues relating to weight management
including maintaining motivation overcoming obstacles to success relapse
prevention emotional distress and stress and time management The telephone
intervention will involve 19 phone calls as well as mailings and a participant manual
women will be asked to lose up to 10 of their weight by reducing their caloric and
fat intake (by 500-1000 kcalday 20 calories fat) and increasing their moderate
physical activity (to 150-200 minutesweek)
2) Mail-based Active Comparator - Participants will receive a standardised mail-based
intervention focussing on healthy living This will include mailings at study entry as
well as a 2-year subscription to health magazine
Approximately 2150 women will be enrolled follow-up will continue until target event rates
have been met (anticipated 4-6 years after completion of the intervention) This sample size
will provide 80 power (type 1 error 005 2-tailed) to detect a hazard ratio (HR) for DFS of
074-076 in the weight loss intervention arm
b) COLORECTAL CANCER
It has been suggested that interventions to improve QoL in colorectal cancer survivors are
more effective if they target symptom management psychosocial support and lifestyle
variables in a comprehensive and integrated approach to behavioural change (Steginga et
al 2009) Due to the paucity of comprehensive trials examining behavioural interventions in
this group of survivors Hawkes et al (2009) are conducting a large-scale RCT of a 6-month
telephone-delivered lifestyle coaching intervention based on Acceptance and Commitment
111
Therapy (ACT) ndash bdquoCanChange‟ The intervention aims to assist colorectal cancer survivors
(n=350) to make improvements in lifestyle including physical activity weight management
and smoking cessation Participants receive up to eleven telephone sessions over the
6-months from a qualified health professional who provides support on symptom
management and lifestyle change Outcomes will be assessed post-intervention at 6- and
12-months follow-up and will include physical activity CRF QoL and cost-effectiveness
The findings from this innovative lifestyle coaching initiative will offer insight into the intensity
of support required to achieve sustained behaviour change as well as highlight the efficacy
of various components of delivery (eg telephone-delivery coaching professionally-led
etc)
Courneya et al (2008) are leading a physical activity intervention in a collaboration between
Canada and Australia the Colon Health and Life-Long Physical activity Change
(CHALLENGE) a 3-year multicentre RCT for colon cancer survivors (n=1000) who are 2-6
months post adjuvant-treatment Any type of physical activity will be promoted the goal
being to motivate people to increase their overall activity by about 25-hours of moderate
intensity physical activity or 1-hour and 15-minutes of vigorous physical activity per week
Behavioural support counselling and supervised physical activity sessions will be used to
promote the adoption and long-term maintenance of physical activity By monitoring
participants over 10-years the trial will determine if colon cancer recurs less often in people
who increase and maintain their physical activity It will also assess whether physical activity
improves other important outcomes including QoL anxiety depression sleep and physical
function It is anticipated that this trial will provide important insight into strategies for
promoting long-term health behaviour change
Another Australian lifestyle intervention is The Colorectal Cancer and Quality of Life led
by Joanne Aitken The purpose of this project is to identify any patterns between lifestyle and
QoL over the first 5-years following a diagnosis of colorectal cancer Approximately 2000
people have been recruited to take part in this study making it the largest colorectal cancer
study of its type to be undertaken Participants complete a telephone interview and a written
Pilot testing demonstrated that
o 80 of participants (n=20) felt the intervention addressed their issues
o 100 felt more motivated to make lifestyle changes
o 100 would recommend the intervention to other survivors
From baseline to post-intervention improvements
were observed for
o Colorectal cancer symptoms o QoL o Diet o Physical activity
112
questionnaire on an annual basis over the 5-years One of the aims of the study is to
uncover how lifestyle factors particularly physical activity may improve QoL and reduce the
risk of developing other chronic diseases that cancer survivors are prone to such as heart
disease and diabetes This information will help Cancer Council Queensland properly design
and target lifestyle interventions to help improve the health and well-being of colorectal
cancer survivors (Aitken et al ongoing)
113
DISCUSSION
WHAT DO WE KNOW ABOUT LIFESTYLE AND CANCER
This aim of this review was to update the World Cancer Research Fund (WCRF) report bdquoA
Systematic Review of RCTs Investigating the Effect of Nutritional and Physical
Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This has been
achieved by conducting a comprehensive but pragmatic search of the literature from 2006
onwards Where no evidence was available in the WCRF review studies before 2006 have
been included if identified in the reference lists of acquired records To facilitate this
evidence cited within the lsquoHandbook of Cancer Survivorship‟ (Feuerstein 2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (2009) were also utilised
Before presenting a synthesis of the findings within this review there are some limitations
that first need to be addressed
Methodological Limitations
There is strong evidence from observational studies that lifestyle factors can potentially have
major influences on overall mortality risk for cancer survivors This has been most frequently
subjected to study in breast cancer survivors However it is recognised that such
associations in observational studies can be influenced by confounding and therefore that
the mechanisms of lifestyle change on all-cause mortality remains unclear (Cheblowski
2010) Therefore although the observational evidence is strong there is a need to
understand the benefits of lifestyle change ndash particularly physical activity and weight control
in the absence of confounding factors which can be achieved only within the context of a
controlled trial (Ballard-Barbash et al 2009) Such evidence in the end is most likely to
lead to promoting the wide scale adoption of lifestyle change interventions in the role of
secondary prevention of cancer
Consistent with Bekkering et al (2006) it has been found that there is a paucity of robust
evidence on the effects of lifestyle behaviours in cancer progression and recurrence as well
as in the prevention and management of the long-term health implications of cancer
treatment Studies generally comprise small sample sizes and few offer evidence of the
long-term effects of lifestyle behaviours Since lifestyle choices are generally behavioural in
nature the sustainability of these behaviours is fundamental if commissioners are to provide
funding for lifestyle interventions
There were also a large number of retrospective studies particularly for smoking This is
understandable given the challenges of research within this area however it does also raise
limitations surrounding the accuracy of findings This is especially the case when findings
rely on retrospective self-reports of health behaviours or illness experience
114
A number of methodological limitations confound the interpretation of the benefits of exercise
and diet after a diagnosis of cancer from other risks such as smoking body size
supplements and analgesic intake Nevertheless as highlighted by Doyle et al (2007) even
when the scientific evidence is incomplete reasonable conclusions can be made on issues
that can guide lifestyle choices for cancer survivors These are discussed next
THE EVIDENCE
Diet
Evidence for reducing fat intake remains unclear yet evidence for the mechanisms of benefit
of weight loss or the maintenance of a healthy weight is strong Weight control and self-
management clearly requires consideration of total fat intake highlighting the necessity to
provide cancer survivors with advice on levels of fat necessary for weight maintenance
weight loss or in some cases weight gain (Chlebowski et al 2005 Patterson et al 2010)
The same rationale applies to any inconsistencies in evidence for increased fruit and
vegetables which can also facilitate weight management Indeed where the evidence is
strongest for fruits and vegetables applies to those sources containing carotenoids The
evidence is convincing that carotenoids do provide anti-cancer properties (Rock et al 2005
Pierce et al 2007) Lycopene (found in tomatoes) is one such carotenoid found to offer
anti-cancer benefits (Schwarz et al 2008)
Fibre (found in the skins of fruit and vegetables as well as in beans and lentils) and folate
(found in broccoli brussel sprouts asparagus and peas) have in the main been found to
protect against colorectal cancer The evidence is convincing that by slowing down bowel
transit time the mechanism of benefit comes from reducing contact between potential
carcinogens
The benefits of a low fat high fruit and vegetable diet extend into the management of
treatment-related conditions such as lymphoedema In individuals carrying excess weight
the resulting weight loss achieved via a low fat high fruit and vegetable diet can ease the
symptoms of lymphoedema (Shaw Mortimer and Judd 2007)
The evidence also suggests that survivors of prostate cancer might benefit from including
pomegranate juice and green tea in their diet
In terms of other food sources vitamin D and calcium can be protective against osteoporosis
(Ryan et al 2007) although more research with a specific fouls on cancer survivors is
needed in this area
Physical Activity
In general the findings of epidemiological and large cohort studies demonstrates that the
evidence for the role of physical activity in improving breast cancer prognosis quality of life
and on the levels of several hormones associated with breast cancer is strong
115
There is substantial evidence suggesting that the physical activity recommendations
developed by the Department of Health are sufficient for cancer survivors - a total of at least
30-minutes a day of moderate intensity physical activity on five or more days of the week
This can be achieved either by doing all the daily activity in one session or through several
shorter bouts of activity of 10 minutes or more Additionally there is evidence of a dose-
response (ie the more physical activity the greater any benefits) The evidence for breast
cancer further suggest that for survival benefits to be achieved from physical activity no less
than moderate to vigorous activity is required (Gross et al 2002) However the most recent
expert advice emphasises that even a modest amount of exercise like brief walks is
beneficial and gains will be seen versus doing nothing at all38
The interpretation of physical activity evidence has been hindered by the difficulty of
distinguishing physical activity outcomes from subsequent weight loss outcomes However
again even if the main mechanism of benefit of physical activity is improved outcomes
resulting from weight loss or maintenance then this could be considered strong enough
evidence to prescribe physical activity to cancer survivors Furthermore the evidence is
encouraging in terms of its QoL-enhancing effect (McNeeley et al 2006 Daley et al 2007)
Three specific elements of physical activity interventions or advice could be addressed
(Ballard-Barbash et al 2006)
Reducing sedentary behaviours (such as watching TV)
Exercise sessions
Type and intensity of physical activity
There is sufficient evidence for supervised physical activity improving symptoms of cancer-
related fatigue (McNeely et al 2006 Cramp and Daniel 2008) and lymphoedema (Moseley
and Pillerlsquos 2008) Indeed the evidence suggests that guided progressive physical activity
soon after treatment can ease the symptoms of lymphoedema (de Rezende et al 2006)
This supports recent cautions regarding risk-averse clinical recommendations guiding
survivors to avoid the use of the affected limb which may actually lead to de-conditioning
and the very outcome women seek to avoid (Schmitz 2010) At the very least there is no
evidence of appropriate intensity physical activity causing or exacerbating either fatigue or
limb swelling The same is true for the effect of physical activity on osteoporosis Whilst the
benefits of physical activity on bone health require clarifying physical activity can at the very
least prevent loss of bone mineral density in survivors at particular risk of developing
osteoporosis (Waltman et al 2009)
A recent roundtablelsquo event by the American College of Sports Medicine has produced a
Consensus Statement detailing exercise guidelines for cancer survivors (Schmitz Courneya
and Matthews et al 2010) An expert panel reviewed the published empirical evidence and
came to the consensus regarding the safety and efficacy of exercise testing and prescription
in cancer survivors The evidence is clear that exercise during treatment (specific risk
assessment can be carried our for specific treatments and biological response) and after
38
Dr Rachel Ballard ndash Barbash in the NCI Cancer Bulletin June 29 2010
116
treatment is safe and effective Activity induced improvements can be expected on aerobic
fitness muscular strength quality of life and fatigue in breast prostate and haematological
cancers Resistance training can be performed safely by breast cancer survivors with and at
risk of lymphoedoema
Efforts are currently being made to increase the capacity and capability of exercise
professionals to address the unique needs of cancer survivors Exercise professionals need
to be able to access training which reflects the medical condition they are treating for to be
more knowledgeable about the condition and the most suitable and appropriate exercises for
them This requires the development of a national competency framework for a specialist
level 3 add on or level four qualification This would enable providers to develop national
training programmes for cancer specialist exercise professionals and lead to more
accessible referral through the exercise referral scheme (Exercise Referral Research March
2010)
Smoking
Strong and consistent evidence has been presented for increased risk of disease
progression and mortality in people who continue to smoke after a diagnosis of cancer as
well as poorer outcomes in pre-diagnosis smokers (Parsons et al 2010) This evidence
applies particularly to cancers of the lung or head and neck Further research is needed for
breast colorectal prostate and rarer cancers
Alcohol
There is a paucity of research into the effects of alcohol pre- and post-diagnosis on cancer
progression and recurrence as well as symptom management Evidence thus far is highly
contradictory with some demonstrating a protective effect some a detrimental effect and
others no effect
Weight
Substantial weight gain after diagnosis and treatment for breast cancer is adversely
associated with breast cancer prognosis Obesity appears to increase the risk of recurrence
and death among breast cancer survivors by around 30 (Patterson et al 2010) Much
more research is needed to clarify the relationship between prognosis and survival and body
weight in other tumour types
Dealing with issues of weight weight gain and weight management with patients is one of
the lifestyle behaviour change issues health care professionals feel most challenged by
Studies do confirm that health care professionals find it difficult to address these issues with
patients without appearing biased and negative It would appear that a lack of professional
training on behavioural change and motivational coaching and effective strategies for weight
117
loss combine and can lead to avoidance by health care professionals in addressing the need
for change (Puhl and Heuer 2009 Blakeman et al 2010)
Mechanisms of Benefit
Chlebowski (2010) offers some thought-provoking insight into the challenge of implementing
lifestyle change when aromatase inhibitors have been found to reduce oestrogen levels far
more than physical activity interventions One study cites approximately 90 reductions in
oestrogen levels as a result of aromatase inhibitors (Dixon et al 2008) Furthermore three
trials comparing aromatase inhibitors versus placebo anticipate 60-70 reduction in breast
cancer risk (Cuzick 2005 Goss et al 2007 Visvanathan et al 2008) Equally Chlebowski
(2010) points out that the influence of physical activity on insulin levels also has a
pharmacological competitor in the form of metformin (Goodwin et al 2008 Jiralerspong et
al 2009)
These are valid insights that are likely to complicate the successful integration of lifestyle
advice into standardised models of aftercare On the other hand if a public and community
health approach is taken to health and well-being then lifestyle change is likely to offer
health benefits beyond cancer-specific health Such an approach is recommended in the
bdquoCapabilities for Supporting Prevention and Chronic Condition Self-Management A
Resource for Educators of Primary Health Care Professionals‟ developed as part of the
Australian Better Health Initiative (Flinders University 2009) The model offered within this
capabilities framework promotes healthcare providers to view patients holistically as
opposed to focusing solely on diagnosed chronic condition The rationale for this in part
lies in the fact that chronic conditions are more often than not accompanied by co-
morbidities and therefore healthcare is not only about the established condition but also
identified risk factors for co-morbidity
MAKING LIFESTYLE RECOMMENDATIONS FOR CANCER SURVIVORS
In terms of reducing the risks of relapse evidence is strongest for breast colorectal lung
and head and neck cancers but self-management lifestyle strategies are likely to be person-
specific rather than disease or treatment specific so are likely to apply to all patients
recovering from cancer
Diet Appendix A provides evidence-based dietary recommendations that can be made in
light of the findings within this review and national health recommendations These
recommendations comprise a varied diet ensuring adequate intake of vitamins essential
minerals fibre essential fatty acids and antioxidants by eating less fat and more green and
cruciferous vegetables fruits and berries nuts and grains and healthy oils (unsaturated fats
omega)
Physical Activity In terms of physical activity based on the evidence within this report
the five a weeklsquo recommendation is just as relevant to cancer survivors as to the general
population Indeed these recommendations are also provided by the American Cancer
Society (Doyle et al 2006) as advised by a large expert panel Appendix B provides
118
suggestions for physical activity Forty-five to 60-minutes of intentional physical activity are
preferable as the benefits of physical activity do appear to be greater with increased physical
activity Even when this might seem too much survivors can be reminded that the minimum
30-minutes for 5 days a week can be tailored to individual needs and capabilities For
example graded or progressive physical activity can be utilised for those experiencing
fatigue whilst shorter physical activity sessions can be spread out across the day
Other Lifestyle Factors Body Weight In addition it is recommended that obesity (BMI
gt35 Kgm2) excessive alcohol consumption and smoking are avoided There is also
evidence that maintaining a steady healthy weight as opposed to fluctuating between a
healthy and unhealthy BMI can offer health benefits for cancer survivors (Wright et al
2007)
The evidence within this review are indicative of challenges with adherence supporting
findings from Uhley and Jen (2006) that intensive resource-heavy individualised guidance
and support is required to achieve significant long-term lifestyle change This further
emphasises the need to tailor and prescribe such interventions on a needs basis via
individualised assessment and risk stratification
Integrating Self-Management Lifestyle Strategies into Routine Care
Adopting a paternalistic approach and simply telling people is not enough If the medical
community want to help their patients embark on a road of recovery which includes dietary
change and regular exercise there has to be a comprehensive and well-funded package of
education guidance and support Attitude and culture change is imperative both to tackle the
myths and preconceptions around lifestyle factors and their influence on cancer prognosis
symptom management and a future healthy life on the part of both patients survivors and
health care professionals The bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative offers a comprehensive
framework for integrating self-management support into healthcare services (Flinders
University 2009) The emphasis is on not merely striving to change patient behaviour but
also making efforts towards organisational change
Cancer Research UK Diabetes UK and the British Heart Foundation have joined together to launch a new campaign to raise awareness of the dangers of carrying excess weight around the middle The Active Fatlsquo campaign encourages people to measure their waistlines and make positive changes to their lifestyles if they are at risk The emphasis is on educating the public that fat cells are actively working away at stimulating diseases such as cancer diabetes and heart attacks
119
The model offered within this capabilities framework promotes healthcare providers to view
patients holistically as opposed to focusing solely on the diagnosed chronic condition The
rationale for this in part lies in the fact that chronic conditions are more often than not
accompanied by co-morbidities and therefore healthcare is not only about the established
condition but also identified risk factors for co-morbidity The framework also identifies the
need to provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for healthcare
professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
Evidence based information emphasising the importance of lifestyle ideally should be
formally introduced into routine clinical practice early in the treatment pathway and re-
enforced at regular intervals thereafter This ensures patients and their relatives do not miss
the teachable moment where they are most susceptible to positive advice (Demark-
Wahnefried et al 2005) This requires close work with clinicians specialist nurses patients
and advocacy groups to enable information about new strategies to be integrated into
existing local information pathways and materials Indeed the new information prescriptions
currently being pilot tested provide ample opportunity for integrating lifestyle advice into
survivorship care plans
Information clearly has an important role to play in influencing lifestyle behaviours However
people need more than knowledge to be healthy they need the skills to change if they are to
bring about changes in often complex and habitual lifestyle behaviours (Robertson 2008)
Before investing time and money on patient information materials it is necessary to convince
the consultants other direct clinical staff and organisers of clinical services that lifestyle
advice is a priority and to re-allocate resources to enable sufficient time to discuss these
issues within routine consultations One study for example found that patients who were
encouraged by their oncologist exercised significantly more than patients who did not
(Segar et al 1998) The next step is to back up the medical consultation with further
practical verbal and written advice from specialist nurses or information officers One UK
oncology unit for example does this as part of a formal lifestyle interview together with a
bespoke lifestyle information toolbox (Thomas and Nicholson 2009) During this interview
patients can be referred to smoking cessation clinics nutritionists and physiotherapists
where necessary The specialist nurse conducting this interview provides written information
and advice to patients and just as importantly their friends and family about local support
groups dietary measures where to buy healthy foods and specific local exercise facilities
which may entice them ranging from ballroom line and salsa dance lessons aerobics yoga
and fitness classes local walking swimming and cycling groups through to gyms sport
centre tennis and badminton courts and Pilates classes giving times contact numbers and
locations to make it as easy as possible to follow the advice The rationale for these
120
interviews is that individualised lifestyle counselling is more likely to elicit a response than
generic general advice The specialist nurse then follows up the advice by telephone and
further consultations as prompting has been shown to improve update A study from North
Bedfordshire for example showed that although 52 of patients accepted referral for
exercise in a local Gym a further 23 decided to attend classes only after additional
prompting from the nurse either by telephone
Many UK Oncology Units already have instigated an exit interview system to discuss follow
up arrangements and this process could be expanded to include lifestyle counselling
provided the specialist nurses involved have received extra training This training should
include a knowledge of the evidence and importance of weight diet physical activity and
smoking after cancer as well as ways to appropriately advise home-based exercise
regimens and how to direct patients towards the myriad of council or independent exercise
activities available locally to them The courses may require additional communication and
motivational skills training to enable nurses to engage in a partnership relationship which
promotes addressing the patientlsquos agenda goals and motivation around achieving and
maintaining behaviour change Examples of a range of courses aimed to develop such skills
and competencies and which are provided by the Flinders Human Behaviour and Health
Research Unit include a Chronic Condition Self-Management workshop Communication
and Motivational Skills Workshop and a Living Well Workshop
Remaining Questions
This review has provided some clarification of the evidence pertaining to lifestyle and cancer
outcomes However in implementing this evidence into standardised practice within cancer
aftercare will require a number of questions to be explored
1) What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
At present it is unclear how soon after a cancer diagnosis an intervention should be
introduced for behaviour change(Rabin 2009) Until the teachable moment is more clearly
defined for cancer patients the advice is that professionals should repeatedly offer to assist
a patient with addressing their health behaviour risks until the patient accepts or seeks other
forms of support
The literature suggests that professional involvement in supported self-management and
lifestyle advice is required in order to maintain patient motivation by enhancing patient
engagement with health information and advice When information is supplied by healthcare
professionals and the patient is supported in using this information legitimacy is provided to
the information and advice (Protheroe et al 2008) Efficacy outcomes in terms of lifestyle
advice and behavioural change are fundamental in the initiation and maintenance of a
healthy lifestyle and the involvement of healthcare professionals strengthens outcome
efficacy whilst also motivating the patient and increasing their own self-efficacy to adapt their
lifestyle (Irwin 2008) However there is anecdotal and other evidence that on the one hand
the importance of lifestyle factors on the prognosis survival and symptom management of
121
cancer survivors is poorly understood and appreciated by significant numbers of cancer
health care professionals and on the other hand they do need specific training in the key
communication skills to be able to support effective behaviour change with their patients A
review is currently underway investigating the role of patient-professional communication in
terms of self-management
2) How can people most likely to benefit from lifestyle interventions be effectively
identified
A recent review on cancer-specific self-management programmes highlighted that patients
can be risk stratified according to needs and this according to whether they are likely to
benefit from the programme (Davies and Batehup 2010) For example people with low
levels of social support have been found to benefit most from group-delivered support As
part of the Bournemouth after Cancer Survivorship Project Active Wellness Programmelsquo
patients are assessed for the readiness to take part in physical activity (Milne et al 2010) It
is recommended that questionnaires that might facilitate such evidence-based risk
stratification be evaluated in order to provide further insight into this question A set of risk
stratification tools would be one way of ensuring cost-effectiveness
3) What are the various intensities of lifestyle support that can be provided based on
levels of individual need
As demonstrated within this review lifestyle interventions and self-management support do
generally require some level of support in order to be successful A strong
patientprofessional partnership appears to be at the essence of this intensive approach as
does longer-term follow-up and support (Davies and Batehup 2010) Addressing this
question will also in part address some of the inequalities within the current system of
cancer care with survivors identified as having low literacy being provided with extra
informational support and assistance with understanding the lifestyle recommendations
being made
122
Appendix A Evidence-Based Dietary Self-Management Recommendations
Food Advice Evidence
Reduce Saturated Fats
Unless underweight avoid processed fatty foods cakes biscuits crisps and other fatty snacks pastries cream and fried foods Cut the fat off the meat and check serum cholesterol regularly
(Ingram 1994 Hebert et al 1998 Norat et al 2004 Thomas et al 2009)
Increase all fish intake
All fresh fish but particularly the oily varieties such as mackerel and sardines Fresh water fish such as trout have the advantage of avoiding the potential heavy metal contamination of tuna amp sword fish which some suggest should not be eaten more than twice a week
(Ornish et al 2005 Meyerhardt et al 2007 Goodwin et al 2009)
Essential minerals
Vary the diet to ensure intake of adequate quantities of essential minerals consider Mixed nuts including Brazils Seafood including sardines prawns and shell fish Pulses and grains Vary carbohydrate sources such as pasta rice different brands of potatoes pulses such as lentils and quinoa
Rohan et al 1993) Powers et al 2007 McTiernan et al 2009)
Dietary Vitamins
Fresh fruit raw and calciferous vegetables grains oily fish nuts and salads Unless you have diarrhoea try to increase the amount of ripe fruit you eat each day ideally by eating the whole fruit Freshly squeezed fruit juices are recommended
(Rohan et al1993 Ingram 1994 Fleischauer et al 2003 New et al 2004 Rock et al 2005 McEligot et al 2006 Meyerhardt et al 2007 Schwarz et al 2008 Goodwin et al 2009)
Polyphenols
Onions leeks broccoli blueberries red wine tea apricots pomegranates chocolate coffee blueberries kiwis plums cherries ripe fruits parsley celery tomatoes mint citrus fruit
(Bettuzzi et al 2006 Pantuck et al 2006 Schwarz et al 2008 McLarty et al 2009)
Phytoestrogens
Soybeans and other legumes including peas lentils pinto (baked beans) and other beans and nuts (supplements not recommended)
Marini et al (2008)
Increase Carotenoids (Lycopene)
Tomatoes tomato sauce chilli carrots green vegetables and dark green salads
(Ingram 1994 Rock et al 2005 McEligot et al 2006 Pierce et al 2007 Powers et al 2007 Thomson et al 2007 Schwarz et al 2008)
123
Appendix B Evidence-Based Physical Activity Recommendations
Category Advice Evidence
Resistance Exercise
Strength training has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce fatigue and improve lean body mass and muscle strength Personalised tailored resistance exercise based on fitness assessments can improve QoL
Segal et al (2003) Poudevigne et al (2009) Courneya et al (2007) (Segal et al 2009)
Aerobic Exercise Aerobic exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of lymphoedema prevent loss of bone mineral density and reduce body fat Walking is particularly popular
Hayes Hildegard and Turner (2009) Schwartz Winters-Stone and Gallucci (2007) Courneya et al (2007) Fillion et al (2008) Kenfield et al (2009) Windsor Nichol and Potter (2004) Chang et al (2008)
Combined Resistance and Aerobic Exercise
Combined aerobic and resistance exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of fatigue and improve QoL
Coleman et al (2003) Milne et al (2008)
3gt MET-hours per week
Benefits of physical activity require 3 or more MET-hours per week (eg using a stationary bicycle for one-hour)
Holick et al (2008) Holmes et al (2005) Saxton et al (2010) Kenfield (2010)
Moderate intensity
Physical activity needs to be of at least moderate intensity in order to offer beneficial outcomes
Holick et al (2008) Patterson et al (2010) Holmes et al (2005) Saxton et al (2010) Campbell et al (2007) Poudevigne et al (2009) Tardon et al (2004)
Dose-Response Exercise can be dose-responsive thus taking part in more than 3 MET-hours per week is likely to offer greater benefits
Meyerhardt et al (2005) Kenfield (2010)
During Treatment Remaining active during treatment can help with symptoms such as fatigue as well as increase completion rates for chemotherapy
Chang et al (2008) Coleman et al (2003) Courneya et al (2007)
Home-Based
Home-based physical activity prescriptions either supervised or alone have proven effective in improving cancer outcomes including reducing fatigue and protecting bone mineral density
Ligibel et al (2008) Windsor Nichol and Potter (2004) Schwartz Winters-Stone and Gallucci (2007)
Supervised Supervised physical activity either at home in groups or during treatment have proven effective in improving cancer outcomes as well as reducing lean body mass and facilitating the completion of chemotherapy
Chang et al (2008) Coleman et al (2003) Velthuis et al (2009) Courneya et al (2007) Campbell
et al (2007) exercise (Soliman et al 2009)
124
References
Abrahamsen JF Andersen A Hannisdal E et al Second malignancies after treatment of Hodgkins disease the influence of treatment follow-up time and age J Clin Oncol 11 (2) 255-61 1993 Addington-Hall et al (2010) Older womenlsquos experience of breast cancer alongside other health conditions The EPaN study (Experiences Preferences and Needs of women aged 70 years and over) University of Southampton Funded by Macmillan Cancer Support Ahmed R L W Thomas et al (2006) Randomized Controlled Trial of Weight Training and Lymphedema in Breast Cancer Survivors J Clin Oncol 24(18) 2765-2772 Ainsworth BE et al Compendium of physical activities an update of activity codes and MET intensities Med Sci Sports Exerc 2000 Sep32(9 Suppl)S498-504 Aitken J (ongoing) Colorectal cancer and quality of life study httpwwwcancerqldorgaupageResearch_statisticsVCRCCVCRCC_research_programsLifestyle_and_Cancer [Last accessed 04062010] Akopyan and Bonavida 2006 G Akopyan and B Bonavida Understanding tobacco smoke carcinogen NNK and lung tumorigenesis Int J Oncol 29 (2006) pp 745ndash752 Alberts DS Martinez ME Roe DJ et al Lack of effect of a high-fiber cereal supplement on the recurrence of colorectal adenomas Phoenix Colon Cancer Prevention Physicians Network [Comment] New England Journal of Medicine 2000 April 20342(16)1156-62 Arts CJ Govers CA van den Berg H Wolters MG van Leeuwen P Thijssen JH In vitro binding of estrogens by dietary fiber and the in vivo apparent digestibility tested in pigs J Steroid Biochem Mol Biol 1991 May38(5)621-8 Bandura A (1977) Self-efficacy Toward a unifying theory of behavioural change Psych Rev 84 191 - 215 Barbash-Ballard R Hunsberger S Alciati MH Blaire SN Goodwin PJ McTiernan A(2009) Physical activity weight control and breast cancer risk and survival Clinical trial rationale and design considerations J Natl Cancer Inst 101630-643 Baron JA Beach M Mandel JS et al Calcium supplements and colorectal adenomas Polyp Prevention Study Group Ann N Y Acad Sci 1999889138-45
Bekkering T Beynon R Davey Smith G Davies A Harbord R Sterne J Thomas S and Wood L (2006) A systematic review of RCTs investigating the effect of dietal and physical activity interventions on cancer survival updated report World Cancer Research Fund httpwwwdietandcancerreportorg [Last accessed 150210] Bellizzi K M J H Rowland et al (2005) Health Behaviours of Cancer Survivors Examining Opportunities for Cancer Control Intervention J Clin Oncol 23(34) 8884-8893 Bernstein H Cosford P and Williams A (2010) Enabling effective delivery of health and wellbeing an independent report Department of Health February 2010
125
Bettuzzi et al 2006 S Bettuzzi M Brausi F Rizzi G Castagnetti G Peracchia and A Corti Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia a preliminary report from a one-year proof-of-principle study Cancer Research 66 (2) (2006) pp 1234ndash1240 Bingham SA Day NE Luben R Ferrari P Slimani N Norat T et al Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) an observational study Lancet 20033611496ndash501 Bingham S Riboli E Diet and cancermdashthe European Prospective Investigation into Cancer and Nutrition Nat Rev Cancer 20044206ndash15 Blakeman T Bower P Reeves D Chew-Graham C (2010) ―Bringing self management into clinical view a qualitative study of long term condition management in primary care consultations Chronic Illness 0 1-15 Blackburn G L and K A Wang (2007) Dietary fat reduction and breast cancer outcome results from the Womens Intervention Nutrition Study (WINS) Am J Clin Nutr 86(3) 878S-881 Bonithon-Kopp C Kronborg O Giacosa A Rath U Faivre J Calcium and fibre supplementation in prevention of colorectal adenoma recurrence A randomised intervention trial Lancet 2000356(9238)1300-6 Borugian MJ Sheps SB Kim-Sing C Olivotto IA Van Patten C Dunn BP Coldman AJ Potter JD Gallagher RP Hislop TG Waist-to-hip ratio and breast cancer mortality Am J Epidemiol 2003 Nov 15158(10)963-8 Boyapati SM Shue X et al (2005) Soyfood intake and breast cancer survival a follow up of the Shanghai Breast Cancer Study Breast Cancer Research and Treatment 92(1) p11-17 Boyd NF Stone J Vogt KN Connelly BS Martin LJ Minkin S Dietary fat and breast cancer risk revisited a meta-analysis of the published literature Br J Cancer 2003 Nov 389(9)1672-85 Box R Marnes T amp Robertson V Aquatic physiotherapy and breast cancer related lymphoedema 5th Australasian Lymphology Association Conference Proceedings Mar 2004 47-9 Brown J K T Byers et al (2003) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 53(5) 268-291 Cade JE Burley VJ Greenwood DC UK Womens Cohort Study Steering Group Dietary fibre and risk of breast cancer in the UK Womens Cohort Study Int J Epidemiol 2007 Apr36(2)431-8 Caan B B Sternfeld et al (2005) Life After Cancer Epidemiology (LACE) Study A cohort of early stage breast cancer survivors (United States) Cancer Causes and Control 16(5) 545-556
126
Caan BJ Kwan ML Hartzell G Castillo A Slattery ML Sternfeld B Weltzien E Pre-diagnosis body mass index post-diagnosis weight change and prognosis among women with early stage breast cancer Cancer Causes Control 2008 Dec19(10)1319-28 Cadmus L A P Salovey et al (2009) Physical activity and quality of life during and after treatment for breast cancer results of two randomized controlled trials Psycho-Oncology 18(4) 343-352 Campbell KL Westerlind KC Harber VJ Bell GJ Mackey JR Courneya KS (2007) Effects of aerobic exercise training on oestrogen metabolism in premenopausal women a randomized controlled trial Cancer Epidemiol Biomarkers Prev 16731ndash73 Cancer 52 and NCSI Research Workstream (2009) Less common cancers consultation Report June 2009 Cella D (2009) Quality of life in patients with metastatic renal cell carcinoma The importance of patient-reported outcomes Cancer treatment reviews 35(8) 733-737 Chan JM Gann PH and Giovannucci EL (2005) Role of diet in prostate cancer development and progression Journal of Clinical Oncology 23(32) p 8152-60 Chlebowski RT Aiello E McTiernan A Weight loss in breast cancer patient management Journal of Clinical Oncology 20(4) 1128-1143 2002 Chlebowski RT Blackburn GL Elashoff RE Thomson C Goodman MT Shapiro A Giuliano AE Karanja N Hoy MK Nixon DW and The WINS Investigators (2005) Dietary fat reduction in post-menopausal women with primary breast cancer Journal of Clinical Oncology (10) p 3s Chlebowski R G Blackburn et al (2006) Dietary fat reduction and breast cancer outcome interim efficacy results from the Womens Intervention Diet Study J Natl Cancer Inst 98 1767 - 1776 Chlebowski RT Blackburn GL (2007) Diet and breast cancer recurrence JAMA 2007 Nov 14298(18)2135 author reply 2135-6 Chlebowski RT (2010) Lifestyle and breast cancer risk The way forward Journal of
Clinical Oncology Vol 28 No 9 (March 20) 2010 pp 1445-1447
Cho E Spiegelman D Hunter DJ Chen WY Colditz GA Willett WC Premenopausal dietary carbohydrate glycaemic index glycaemic load and fiber in relation to risk of breast cancer Cancer Epidemiol Biomarkers Prev 2003 Coulter A and Ellins J (2006) Patient-focused Interventions A review of the evidence Picker Institute Europe (01865 208100) and Health Foundation Coups E J and J S Ostroff (2005) A population-based estimate of the prevalence of behavioural risk factors among adult cancer survivors and non-cancer controls Preventive Medicine 40(6) 702-711 Courneya K S (2003) Physical activity in Cancer Survivors An Overview of Research Medicine amp Science in Sports amp Physical activity 35(11) 1846-1852
127
Courneya K Booth CM Gill S et al (2008) The colon health and life-long physical activity change trial a randomized trial of the national institute of Canada clinical trials group Current Oncology 15(6) 271-78 Cramp F Daniel J (2008) Physical activity for the management of cancer-related fatigue in adults CochraneDatabaseSystRev 2008 Cuzick J Aromatase inhibitors for breast cancer prevention J Clin Oncol 231636-1643 2005
Cuzick J Hot flushes and the risk of recurrence Retrospective exploratory results from the ATAC trial 30th Annual San Antonio Breast Cancer Symposium San Antonio TX December 13-16 2007 (poster 2069) Daley A H Crank et al (2007) Randomized trial of physical activity therapy in women treated for breast cancer J Clin Oncol 25 1713 - 1721 Daley A S Bowden et al (2008) What advice are oncologists and surgeons in the United Kingdom giving to breast cancer patients about physical activity International Journal of Behavioural Diet and Physical Activity 5(1) 46 Danhauer S Mihalki S Russell G Campbell C Felder L Daley L et al (2009) Restorative yoga for women with breast cancer Findings from a randomized pilot study Psych oncology 18(4) 360-368 Dansinger M L J A Gleason et al (2005) Comparison of the Atkins Ornish Weight Watchers and Zone Diets for Weight Loss and Heart Disease Risk Reduction A Randomized Trial JAMA 293(1) 43-53 Davies NJ and Batehup L (2010) Self-management support for cancer survivors Guidance for developing interventions An update of the evidence National Cancer Survivorship Initiative Macmillan Cancer Support March 2010 Demark-Wahnefried W and Jones L (2008) Promoting a Healthy Lifestyle among Cancer Survivors Haematologyoncology clinics of North America 22(2) 319-342 Deo SV Ray S Rath GK et al (2004) Prevalence and risk factors for development of lymphedema following breast cancer treatment Indian J Cancer 418ndash12 Department of Health (2001) Exercise referral systems A national quality assurance framework Department of Health Report London 2001 Department of Health (2004) At least five a week Evidence on the impact of physical activity and its relationship to health Department of Health Report London 2004 Department of Health (2009a) Internal analysis unpublished Department of Health London Department of Health (2009b) Obesity general information Health survey of England 2008 Department of Health London Department of Health (2009c) Guidance on the routine collection of patient-reported outcome measures (PROMs) p 28 The Stationary Office London
128
De Rezende LF Franco RL de Rezende MF et al Two physical activity schemes in postoperative breast cancer comparison of effects on shoulder movement and lymphatic disturbance Tumori 2006 9255ndash61 de Waard F Ramlau R Mulders Y de Vries T van Waveren S A feasibility study on weight reduction in obese postmenopausal breast cancer patients Eur J Cancer Prev 1993 May 2(3)233-8 Dignam J J B N Polite et al (2006) Body Mass Index and Outcomes in Patients Who Receive Adjuvant Chemotherapy for Colon Cancer J Natl Cancer Inst 98(22) 1647-1654 Dimeo FC Thomas F Raabe-Menssen C et al Effect of aerobic exercise and relaxation training on fatigue and physical performance of cancer patients after surgery A randomised controlled trial Support Care Cancer 2004 12(11)774-9 Dixon JM Renshaw L Young O et al Letrozole suppresses plasma estradiol and oestrone sulphate more completely than anastrozole in postmenopausal women with breast cancer J Clin Oncol 261671-1675 2008
Doyle C L H Kushi et al (2006) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 56(6) 323-353 Dwyer J J Peterson et al (2008) Do Flavonoid Intakes of Postmenopausal Women With Breast Cancer Vary on Very Low Fat Diets Diet and Cancer 60(4) 450 - 460 Eakin E Hayes S and Lawler S (ongoing) Physical activity for Health Using the telephone to promote physical activity-based rehabilitation in ruralremote Australian breast cancer survivors National Breast Cancer Foundation httpwwwuqeduaucprcindexhtmlpage=60214amppid=20928 [Last accessed 300310] Eliassen AH Missmer SA Tworoger SS Spiegelman D Barbieri RL Dowsett M Hankinson SE Endogenous steroid hormone concentrations and risk of breast cancer among premenopausal women J Natl Cancer Inst 2006 Oct 4 98(19)1406-15 Elkort RJ Baker FL Vitale JJ Cordano A Long-term nutritional support as an adjunct to chemotherapy for breast cancer JPEN J Parenter Enteral Nutr 1981 Sep-Oct 5(5)385-90 Enger SM Greif JM Polikoff J Press M Body weight correlates with mortality in early-stage breast cancer Arch Surg 2004139954ndash958 discussion 58ndash60 Eton D T D L Fairclough et al (2003) Early Change in Patient-Reported Health During Lung Cancer Chemotherapy Predicts Clinical Outcomes Beyond Those Predicted by Baseline Report Results From Eastern Cooperative Oncology Group Study 5592 J Clin Oncol 21(8) 1536-1543 Fentiman IS Allen DS Hamed H (2005) Smoking and prognosis in women with breast cancer Int J Clin Pract 591051ndash1054
129
Ferrari P Jenab M Norat T et al Lifetime and baseline alcohol intake and risk of colon and rectal cancers in the European prospective investigation bettinto cancer and nutrition (EPIC) Int J Cancer 2007 121 ( 9 ) 2065 ndash 2072
Feuerstein M (2006) Handbook of Cancer Survivorship New York NY Springer 2006 Fillion L P Gagnon et al (2008) A Brief Intervention for Fatigue Management in Breast Cancer Survivors Cancer Nursing 31(2) 145-159 Findley P amp Sambamoorthi U (2009) Preventive health services and lifestyle practices in cancer survivors A population health investigation Journal of Cancer Survivorship 3 43-58 Fleischauer AT Simonsen N Arab L Antioxidant supplements and risk of breast cancer recurrence and breast cancer-related mortality among postmenopausal women Nutr Cancer 2003 46 15-22 Flinders University (2009) Capabilities for Supporting Prevention and Chronic Condition Self-Management A Resource for Educators of Primary Health Care Professionals Australian Better Health Initiative A joint Australian State and Territory government initiative
Flowers M Thompson PA 2009 t10c12 Conjugated Linoleic Acid Suppresses HER2 Protein and Enhances Apoptosis in SKBr3 Breast Cancer Cells Possible Role of COX2 PLoS ONE 4(4) e5342 doi101371journalpone0005342 Food Standards Agency (2007) FSA nutrient and food based guidelines for UK institutions httpwwwfoodgovukmultimediapdfsnutrientinstitutionpdf [Last accessed 120310] Food Standards Agency (2010) Heightweight chart httpwwweatwellgovukhealthydiethealthyweightheightweightchart [Last accessed 120310] Ford MB Sigurdson AJ Petrulis ES et al Effects of smoking and radiotherapy on lung carcinoma in breast carcinoma survivors Cancer 98 (7) 1457-64 2003 Friedenreich C Cust A Lahmann PH et al Anthropometric factors and risk of endometrial cancer the European prospective investigation into cancer and nutrition Cancer Causes Control 2007 18399-413 Friedenreich C M C G Woolcott et al (2010) Alberta Physical Activity and Breast Cancer Prevention Trial Sex Hormone Changes in a Year-Long Physical activity Intervention Among Postmenopausal Women J Clin Oncol 28(9) 1458-1466 Friedenreich CM Cust AE Physical activity and breast cancer risk impact of timing type and dose of activity and population subgroup effects Br J Sports Med 2008 Aug42(8)636-47 Giovannucci EL (2005) Obesity insulin resistance and cancer risk Cancer Prevention 5 httpwwwnypcancerpreventioncomissue5propro_featurespre_earshtml [Last accessed 03062010]
130
Gold E B J P Pierce et al (2009) Dietary Pattern Influences Breast Cancer Prognosis in Women Without Hot Flashes The Womens Healthy Eating and Living Trial J Clin Oncol 27(3) 352-359 Gonzalez CAPera GAgudo APalli DKrogh VVineis PTumino RPanico SBerglund GSiman HNyren OAgren AMartinez CDorronsoro MBarricarte ATormo MJQuiros JRAllen NBingham SDay NMiller ANagel GBoeing HOvervad KTjonneland ABueno-de-Mesquita HBBoshuizen HCPeeters PNumans MClavel-Chapelon FHelen IAgapitos ELund EFahey MSaracci RKaaks RRiboli E Smoking and the risk of gastric cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC) Int J Cancer 107 (4) 629-634 (2003) Gonzaacutelez CA Jakszyn P Pera G Agudo A Bingham S Palli D Ferrari P Boeing H del Giudice G Plebani M Carneiro F Nesi G Berrino F Sacerdote C Tumino R Panico S Berglund G Simaacuten H Nyreacuten O Hallmans G Martinez C Dorronsoro M Barricarte A Navarro C Quiroacutes JR Allen N Key TJ Day NE Linseisen J Nagel G Bergmann MM Overvad K Jensen MK Tjonneland A Olsen A Bueno-de-Mesquita HB Ocke M Peeters PH Numans ME Clavel-Chapelon F Boutron-Ruault MC Trichopoulou A Psaltopoulou T Roukos D Lund E Hemon B Kaaks R Norat T Riboli E Meat intake and risk of stomach and oesophageal adenocarcinoma within the European Prospective Investigation Into Cancer and Nutrition (EPIC) J Natl Cancer Inst 2006 Mar 198(5)345-54 Goodwin PJ Pritchard KI Ennis M et al Insulin-lowering effects of metformin in women with early breast cancer Clin Breast Cancer 8501-5052008
Goodwin PJ Ennis M Pritchard KI Koo J Hood N (2009) Prognostic Effects of 25-Hydroxyvitamin D Levels in Early Breast Cancer Journal of Clinical Oncology Vol 27 No 23 (August 10) pp 3757-3763 Goodwin PJ Lifestyle Intervention Study in Adjuvant Treatment of Early Breast Cancer (LISA) (ongoing) httpclinicaltrialsgovct2showNCT00463489 [Last accessed 04062010] Goss PE Richardson H Chlebowski RT et al National Cancer Institute of Canada Clinical Trials Group MAP 3 Trial Evaluation of exemestane to prevent breast cancer in postmenopausal women at risk Clin Breast Cancer 7895-900 2007
Gothard L Cornes P et al (2004) Double-blind placebo-controlled randomised trial of vitamin E and pentoxifylline in patients with chronic arm lymphoedema and fibrosis after surgery and radiotherapy for breast cancer Radiotherapy and oncology journal of the European Society for Therapeutic Radiology and Oncology 73(2) 133-139 Grace PB Taylor JI Low YL Luben RN Mulligan AA Botting NP Dowsett M Welch AA Khaw KT Wareham NJ Day NE Bingham SA Phytoestrogen concentrations in serum and spot urine as biomarkers for dietary phytoestrogen intake and their relation to breast cancer risk in European prospective investigation of cancer and nutrition-norfolk Cancer Epidemiol Biomarkers Prev 2004 May13(5)698-708 Greenberg ER Baron JA Tosteson TD et al A clinical trial of antioxidant vitamins to prevent colorectal adenoma Polyp Prevention Study Group[comment] New England Journal of Medicine 1994 July 21331(3)141-7 Gritz ER (1993) Cancer Smoking Epidemiology Biomarkers amp Prevention 2(3) 261-270
131
Gritz E R M C Fingeret et al (2006) Successes and failures of the teachable moment Cancer 106(1) 17-27 Gross G C Ott et al (2002) Postmenopausal Breast Cancer Survivors at Risk for Osteoporosis Physical Activity Vigour and Vitality Oncology Nursing Forum 29(9) 1295-1300 Gross M C Ramirez et al (2009) Expression of androgen and oestrogen related proteins in normal weight and obese prostate cancer patients The Prostate 69(5) 520-527 Guthrie JR Ball M Murkies A Dennerstein L Dietary phytoestrogen intake in mid-life Australian-born women relationship to health variables Climacteric 2000 3 254ndash261 Hawkes A L S Gollschewski et al (2009) A telephone-delivered lifestyle intervention for colorectal cancer survivors a pilot study Psycho-Oncology 18(4) 449-455 Haydon AM Macinnis RJ English DR Giles GG (2006) The effect of physical activity and body size on survival after diagnosis with colorectal cancer Gut 55 p 62-67 Hayes SC Spence RR Galvao DANewton RU (2009) Australian Association for Physical activity and Sport Science position stand Optimising cancer outcomes through physical activity JSciMedSport 200912428-434 Heald AH Cade JE Cruickshank JK Anderson S White A Gibson JM (2003) The influence of dietary intake on the insulin-like growth factor (IGF) system across three ethnic groups a population-based study Public Health Nutr6175ndash80 Healthy Weight Healthy Lives (2008) A Cross-Government Strategy for England Cross-Government Obesity Unit DH and Department of Children Schools and Families Hebert JR Hurley TG Ma Y (1998) The effect of dietary exposures on recurrence and mortality in early stage breast cancer Breast Cancer Res Treat 5117ndash28 Hofstad B Almendingen K Vatn M et al Growth and recurrence of colorectal polyps a double-blind 3-year intervention with calcium and antioxidants Digestion 199859(2)148-56 Holick C N P A Newcomb et al (2008) Physical Activity and Survival after Diagnosis of Invasive Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 17(2) 379-386 Holm LE Nordevang E Hjalmar ML Lidbrink E Callmer E Nilsson B (1993) Treatment failure and dietary habits in women with breast cancer J Natl Cancer Inst 8532ndash36 Holmes MD Hunter DJ Colditz GA et al Association of dietary intake of fat and fatty acids with risk of breast cancer JAMA 1999281914-920 Holmes MD Chen WY Feskanich D Kroenke CH Colditz GA (2005) Physical activity and survival after breast cancer diagnosis JAMA 293 p 2479-86
132
Holmes MD Murin S Chen WY Kroenke CH Spiegelman D Colditz GA (2007) Smoking and survival after breast cancer diagnosis Int J Cancer 1202672ndash2677
Howe GR Hirohata T Hislop TG Iscovich JM Yuan JM Katsouyanni K Lubin F Marubini E Modan B Rohan T et al Dietary factors and risk of breast cancer combined analysis of 12 case-control studies J Natl Cancer Inst 1990 Apr 482(7)561-9
Hunter DJ Spiegelman D Adami HO Beeson L van den Brandt PA Folsom ARFraser GE Goldbohm RA Graham S Howe GR et al Cohort studies of fat intake and the risk of breast cancer--a pooled analysis N Engl J Med 1996 Feb 8334(6)356-61
Ingram D Diet and subsequent survival in women with breast cancer British Journal of Cancer 1994 Mar69(3)592-5
Irwin ML Smith AW McTiernan A Ballard-Barbash R Cronin K Gilliland FD Baumgartner RN Baumgartner KB Bernstein L (2008) Influence of Pre- and Postdiagnosis Physical Activity on Mortality in Breast Cancer Survivors The Health Eating Activity and Lifestyle Study Journal of Clinical Oncology 26(24) 3958-3964
Ishikawa H Akedo I Otani T et al Randomized trial of dietary fiber and Lactobacillus casei administration for prevention of colorectal tumors Int J Cancer 2005 September 20116(5)762-7 Jiralerspong S Palla SL Giordano SH et al Metformin and pathologic complete responses to neoadjuvant chemotherapy in diabetic patients with breast cancer J Clin Oncol 273297-3302 2009
Jones LW Demark-Wahnefried W Diet physical activity and complementary therapies after primary treatment for cancer Lancet Oncol 7(12)1017-26 Nov-Dec 2006 PMID 17138223 Kaaks R A Lukanova and MA Kurzer Obesity endogenous hormones and endometrial cancer risk a synthetic review Cancer Epidemiol Biomark Prev 11 (2002) pp 1531ndash1543 Kaaks R Rinaldi S Key TJ Berrino F Peeters PH Biessy C Dossus L Lukanova A Bingham S Khaw KT Allen NE Bueno-de-Mesquita HB van Gils CH Grobbee D Boeing H Lahmann PH Nagel G Chang-Claude J Clavel-Chapelon F Fournier A Thieacutebaut A Gonzaacutelez CA Quiroacutes JR Tormo MJ Ardanaz E Amiano P Krogh V Palli D Panico S Tumino R Vineis P Trichopoulou A Kalapothaki V Trichopoulos D Ferrari P Norat T Saracci R Riboli E Postmenopausal serum androgens oestrogens and breast cancer risk the European prospective investigation into cancer and nutrition Endocr Relat Cancer 2005 Dec12(4)1071-82 Kawahara M Ushijima S Kamimori T et al Second primary tumours in more than 2-year disease-free survivors of small-cell lung cancer in Japan the role of smoking cessation Br J Cancer 78 (3) 409-12 1998 Keinan-Boker L van Der Schouw YT Grobbee DE Peeters PH Dietary phytoestrogens and breast cancer risk Am J Clin Nutr 2004 Feb79(2)282-8 Kenfield SA (2010) Physical activity and mortality in prostate cancer (In Regular Vigorous Physical Activity found to have Survival Benefits for Prostate Cancer Patients
133
AACR Frontier in Cancer Prevention Research Conference by Tuma R Oncology Times) 32(2) p 29 33 Key TJ Allen NE Hormones and breast cancer IARC Sci Publ 2002156273-6 Khaodhiar L Nixon D Chlebowski RT Elashoff R Blackburn GL Hoy MK Insulin resistance in postmenopausal women with breast cancer Proc Am Cancer Res 2003446349 (abstr) Kim EH Willett WC Colditz GA Hankinson SE Stampfer MJ Hunter DJ Rosner B Holmes MD Dietary fat and risk of postmenopausal breast cancer in a 20-year follow-up Am J Epidemiol 2006 Nov 15164(10)990-7 Korstjens I A M May et al (2008) Quality of Life After Self-Management Cancer Rehabilitation A Randomized Controlled Trial Comparing Physical and Cognitive-Behavioural Training Versus Physical Training Psychosom Med 70(4) 422-429 Krein S M Heisler J Piette F Makki and E Kerr 2005 The effect of chronic pain on diabetes patientslsquo self-management Diabetes Care 28(1)65ndash70 Kroenke CH Fung TT Hu FB Holmes MD Dietary patterns and survival after breast cancer diagnosis J Clin Oncol 2005 Dec 2023(36)9295-303 Kubik AK Zatloukal P Tomasek L Petruzelka L (2002) Lung cancer risk among Czech women a case-control study Prev Med 34(4) 436ndash444 Kucera H [Adjuvanticity of vitamin A in advanced irradiated cervical cancer (authors transl)] Wiener Klinische Wochenschrift Supplementum 19801181-20 Kushi LH Byers T Doyle C et al American Cancer Society Guidelines on Diet and Physical Activity for cancer prevention reducing the risk of cancer with healthy food choices and physical activity CA Cancer J Clin 2006 56 254ndash8 Kyogoku S Hirohata T Nomura Y Shigematsu T Takeshita S Hirohata I Diet and prognosis of breast cancer Nutr Cancer 199217(3)271-7 Lahmann PH Schulz M Hoffmann K Boeing H Tjoslashnneland A Olsen A Overvad K Key TJ Allen NE Khaw KT Bingham S Berglund G Wirfaumllt E Berrino F Krogh V Trichopoulou A Lagiou P Trichopoulos D Kaaks R Riboli E Long-term weight change and breast cancer risk the European prospective investigation into cancer and nutrition (EPIC) Br J Cancer 2005 Sep 593(5)582-9 Lee IM Sesso HD Paffenbarger RS Jr (1999) Physical activity and risk of lung cancer Int J Epidemiol 28(4) 620ndash625 Lev E L (1997) Banduras Theory of Self-Efficacy Applications to Oncology Research and Theory for Nursing Practice 11 21-37 Ligibel J A W Demark-Wahnefried et al (2009) Diet Physical activity and Supplements Guidelines for Cancer Survivors ASCO EDUCATIONAL BOOK 2009(1) 541-547 Lindsay S (2009) Prioritizing illness Lessons in self-managing multiple chronic conditions Canadian Journal of Sociology PhD Thesis ejournalslibraryualbertaca
134
Lucia A Earnest C Perez M (2003) Cancer-related fatigue can physical activity physiology assist oncologists Lancet Oncol 4616-625 Lyons R amp Langille L (2000) Healthy Lifestyle Strengthening the Effectiveness of Lifestyle Approaches to Improve Health Health Canada Ottawa Ontario Available at httpwwwhc-scgccahppbphdddocshealthy MacLennan R Macrae F Bain C et al Effect of fat fibre and beta carotene intake on colorectal adenomas further analysis of a randomized controlled dietary intervention trial after colonoscopic polypectomy Asia Pac J Clin Nutr 1999 8(suppl)S54-S58 Macmillian Cancer Support (2008) Two Million Reasons The Cancer Survivorship Agenda 2008 Maddams J Moller H and Devane C Cancer prevalence in the UK 2008 Thames Cancer Registry and Macmillan Cancer Support 2008 Manjer J Berglund G Bondesson L Garne J P Janzon L Malina J Breast cancer incidence in relation to smoking cessation Breast Cancer Res Treat 61121-129 2000 Mao Y Pan S Wen SW Johnson KC The Canadian Cancer (2003) Physical activity and the risk of lung cancer in Canada Am J Epidemiol 158(6) 564ndash575 Mayne S T B Cartmel et al (2009) Alcohol and Tobacco Use Pre-diagnosis and Postdiagnosis and Survival in a Cohort of Patients with Early Stage Cancers of the Oral Cavity Pharynx and Larynx Cancer Epidemiology Biomarkers amp Prevention 18(12) 3368-3374 McDonald P R Williams et al (2002) Breast cancer survival in African American women Is alcohol consumption a prognostic indicator Cancer Causes and Control 13(6) 543-549 McEligot AJ Largent J Ziogas A Peel D Anton-Culver H Dietary fat fiber vegetable and micronutrients are associated with overall survival in postmenopausal women diagnosed with breast cancer Nutr Cancer 200655(2)132-140 McNeely M L K L Campbell et al (2006) Effects of physical activity on breast cancer patients and survivors a systematic review and meta-analysis CMAJ 175(1) 34-41 McKenzie D C and A L Kalda (2003) Effect of Upper Extremity Physical activity on Secondary Lymphedema in Breast Cancer Patients A Pilot Study J Clin Oncol 21(3) 463-466 McKeown-Eyssen GE Bright-See E Bruce WR et al A randomized trial of a low fat high fibre diet in the recurrence of colorectal polyps Toronto Polyp Prevention Group [erratum appears in J Clin Epidemiol 1995 Feb48(2)i] Journal of Clinical Epidemiology 1994 May47(5)525-36 McLarty Jerry Bigelow Rebecca LH Smith Mylinh Elmajian Don Ankem Murali Cardelli James A (2009) Tea Polyphenols Decrease Serum Levels of Prostate-Specific Antigen Hepatocyte Growth Factor and Vascular Endothelial Growth Factor in Prostate
135
Cancer Patients and Inhibit Production of Hepatocyte Growth Factor and Vascular Endothelial Growth Factor In vitro Cancer Prev Res 1940-6207CAPR-08-0167
McTiernan A et al (2009) Low-fat increased fruit vegetable and grain dietary pattern fractures and bone mineral density the Womens Health Initiative Dietary Modification Trial Am J Clin Nutr 89 1864-1876
Meyerhardt JA Heseltine D Niedzwiecki D Hollis D Saltz LB Mayer RJ Schilsky RL and Fuchs CS (2005) The impact of physical activity on patients with stage III colon cancer Findings from Intergroup trial CALGB 89803 Proc Am Soc Clin Oncol 24 p abstract 3534 Meyerhardt J A D Niedzwiecki et al (2007) Association of Dietary Patterns With Cancer Recurrence and Survival in Patients With Stage III Colon Cancer JAMA 298(7) 754-764 Meyerhardt J A D Niedzwiecki et al (2008) Impact of Body Mass Index and Weight Change after Treatment on Cancer Recurrence and Survival in Patients With Stage III Colon Cancer Findings From Cancer and Leukemia Group B 89803 J Clin Oncol 26(25) 4109-4115 Meyskens FL Jr Kopecky KJ Appelbaum FR Balcerzak SP Samlowski W Hynes H Effects of vitamin A on survival in patients with chronic myelogenous leukemia a SWOG randomized trial Leukemia Research 1995 September 19(9)605-12 Miles A Simon A Wardle J (2010) Answering patient questions about the role lifestyle factors play in cancer onset and recurrences Journal of Health Psychology 15(2) p 291-298 Milne H K Wallman et al (2008) Impact of a Combined Resistance and Aerobic Physical activity Program on Motivational Variables in Breast Cancer Survivors A Randomized Controlled Trial Annals of Behavioral Medicine 36(2) 158-166 Milne M Hamerston L and Morrell D (2010) BACSUP adult survivorship living with and beyond cancer test community learning workshop London January 2010 Monninkhof EM Peeters PH Schuit AJ Design of the sex hormones and physical exercise (SHAPE) study BMC Public Health 2007 Sep 47232 Morrell RM Halyard MY Schild SE Ali MS Gunderson LL Pockaj BA (2005) Breast cancer-related lymphedema Mayo Clin Proc 801480ndash1484 Mortimer P S D O Bates et al (1996) The prevalence of arm oedema following treatment for breast cancer QJM 89(5) 377-380 Mortimer JE Flatt SW Parker BA et al Tamoxifen hot flashes and recurrence in breast cancer Breast Cancer Res Treat 108421-426 2008 Moseley AL Piller NB Carati CJ (2005) The effect of gentle arm physical activity and deep breathing on secondary arm lymphedemaLymphology Sep38(3)136-45 Moseley AL Piller NB (2008) Physical activity for limb Lymphoedema ndash Evidence that it is beneficial Journal of Lymphoedema vol 3(1) pp 51-56
136
Mustian KM Palesh OG Flecksteiner SA Tai Chi Chuan for breast cancer survivors Medicine and sport science 2008 52()209-17 National Cancer Action Team (2009) Cancer and palliative care rehabilitation workforce project A review of the evidence National Cancer Action Team National Comprehensive Cancer Network (2009) NCCN Clinical Practice Guidelines in Oncology Cancer-related fatigue version 1 2009 National Cancer Survivorship Initiative (NCSI) (2009) Research Work Stream Mapping Project - Summary and reports for Bowel Cancer Breast Cancer Lung Cancer Prostate cancer National Cancer Survivorship Initiative Macmillan Cancer Support National Health Service (2010) NHS advice on drinking limits NHS Choices httpwwwdrinkingnhsukquestionsrecommended-levels [Last accessed 300310] National Institutes of Health (1998) Clinical Guidelines on the Identification Evaluation and Treatment of Overweight and Obesity in Adults The Evidence Report National Heart Lung and Blood Institute in cooperation with the National Institute of Diabetes and Digestive Kidney Diseases NIH Publication No 98-4083 National Institutes of Health Osteoporosis and Related Bone Diseases (2009) Conditions and behaviours that increase osteoporosis risk National Resource Centre US Department of Health and Human Services httpwwwniamsnihgovHealth_InfoBoneOsteoporosisConditions_Behaviorsosteoporosis_breast_cancerasp [Last accessed 170210] National Obesity Observatory (2009) Body mass index as a measure of obesity Association of Public Health Observatories June 2009 Ng K J A Meyerhardt et al (2008) Circulating 25-Hydroxyvitamin D Levels and Survival in Patients With Colorectal Cancer J Clin Oncol 26(18) 2984-2991 Nikotetti S Young J Levitt M (2008) Bowel problems self-care practices and information needs of colorectal cancer survivors at 6 to 24 months after sphincter-saving surgery Cancer Nursing 31(5) p 389-398
Norat T Bingham S Ferrari P Slimani N Jenab M Mazuir M Overvad K Olsen A Tjoslashnneland A Clavel F Boutron-Ruault MC Kesse E Boeing H Bergmann MM Nieters A Linseisen J Trichopoulou A Trichopoulos D Tountas Y Berrino F Palli D Panico S Tumino R Vineis P Bueno-de-Mesquita HB Peeters PH Engeset D Lund E Skeie G Ardanaz E Gonzaacutelez C Navarro C Quiroacutes JR Sanchez MJ Berglund G Mattisson I Hallmans G Palmqvist R Day NE Khaw KT Key TJ San Joaquin M Heacutemon B Saracci R Kaaks R Riboli E Meat fish and colorectal cancer risk the European Prospective Investigation into cancer and nutrition J Natl Cancer Inst 2005 Jun 1597(12)906-16
Ornish D et al (2005) Intensive lifestyle changes may affect the progression of prostate cancer The Journal of Urology 174 p 1065-1070 Ostroff JS Jacobsen PB Moadel AB Spiro RH Shah JP Strong EW et al (1995) Prevalence and predictors of continued tobacco use after treatment of patients with head and neck cancer Cancer Jan 1575(2)569-76
137
Pantuck AJ et al (2006) Phase II study of pomegranate juice for men with rising PSA following surgery or RXT for prostate cancer Clin Cancer Res 12(13) p 4018-4026 Pantuck AJ et al Abstract presented at the American Society of Clinical Oncology 2008 Genitourinary Cancers Symposium (Abstract 40) Long Term Follow Up Of Pomegranate Juice For Men With Prostate Cancer And Rising PSA Shows Durable Improvement in PSA Doubling Time Parsons A A Daley et al Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis systematic review of observational studies with meta-analysis BMJ 340(jan21_1) Pastorino U Infante M Maioli M et al Adjuvant treatment of stage I lung cancer with high-dose vitamin A[comment] J Clin Oncol 1993 July11(7)1216-22 Patterson R E L A Cadmus et al Physical activity diet adiposity and female breast cancer prognosis A review of the epidemiologic literature Maturitas In Press Corrected Proof Pedersen BK Saltin B Evidence for prescribing physical activity as therapy in chronic disease Scand J Med Sci Sports 16 Suppl 1 3ndash63 2006Pierce J P L Natarajan et al (2007) Influence of a Diet Very High in Vegetables Fruit and Fiber and Low in Fat on Prognosis Following Treatment for Breast Cancer The Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA 298(3) 289-298 Pierce JP Faerber S Wright FA Newman V Flatt SW Kealey S Rock CL Pierce JP Natarajan L Caan BJ et al Influence of a diet very high in vegetables fruit and fiber and low in fat on prognosis following treatment for breast cancer the Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA2007298(3)289-298 Ponz dL Roncucci L Chemoprevention of colorectal tumors role of lactulose and of other agents Scandinavian Journal of Gastroenterology Supplement 199722272-5 Poudevigne M J Wojcik et al (2009) The Effects Of 12-weeks Cross Training On Fatigue And Mood In Recent Breast Cancer Survivors 2292 Board 180 May 28 200 PM - 330 PM Medicine amp Science in Sports amp Physical activity 41(5) 297-298 Powers H J M H Hill et al (2007) Responses of Biomarkers of Folate and Riboflavin Status to Folate and Riboflavin Supplementation in Healthy and Colorectal Polyp Patients (The FAB2 Study) Cancer Epidemiology Biomarkers amp Prevention 16(10) 2128-2135 Protheroe J A Rogers et al (2008) Promoting patient engagement with self-management support information a qualitative meta-synthesis of processes influencing uptake Implementation Science 3(1) 44 Provenzano E and N Johnson (2009) Overview of recommendations of HER2 testing in breast cancer Diagnostic Histopathology 15(10) 478-484 Puhl RM Heuer CA (2009) ―The stigma of obesity A Review and Update Obesity 17 (5) 941-964 Rabin C (2009) ―Promoting Lifestyle Change among Cancer Survivors When is the Teachable Moment American Journal of Lifestyle Medicine 3 (5) 369-378
138
Reding K W J R Daling et al (2008) Effect of Pre-diagnostic Alcohol Consumption on Survival after Breast Cancer in Young Women Cancer Epidemiology Biomarkers amp Prevention 17(8) 1988-1996 Riboli E Hunt KJ Slimani N Ferrari P Norat T Fahey M Charrondiegravere UR Heacutemon B Casagrande C Vignat J Overvad K Tjoslashnneland A Clavel-Chapelon F ThieacutebautA Wahrendorf J Boeing H Trichopoulos D Trichopoulou A Vineis P Palli D Bueno-De-Mesquita HB Peeters PH Lund E Engeset D Gonzaacutelez CA Barricarte A Berglund G Hallmans G Day NE Key TJ Kaaks R Saracci R (2002) European Prospective Investigation into Cancer and Nutrition (EPIC) study populations and data collection Public Health Nutr 2002 Dec5(6B)1113-24 Richardson G E M A Tucker et al (1993) Smoking Cessation after Successful Treatment of Small-Cell Lung Cancer Is Associated with Fewer Smoking-related Second Primary Cancers Annals of Internal Medicine 119(5) 383-390 Richardson A Addington-Hall J Stark D Foster C Amir Z Sharpe M (2009) Determining research priorities for cancer survivorship Consultation and evidence review Commissioned by the NCSI Robertson R (2008) Using Information to Promote Healthy Behaviours Kings Fund London Rock C L and W Demark-Wahnefried (2002) Diet and Survival After the Diagnosis of Breast Cancer A Review of the Evidence J Clin Oncol 20(15) 3302-3316 Rock C L S W Flatt et al (2005) Plasma Carotenoids and Recurrence-Free Survival in Women With a History of Breast Cancer J Clin Oncol 23(27) 6631-6638 Rohan T Howe G Friedenreich C et al (1993) Dietary fiber vitamins A C and E and risk of breast cancer a cohort study Cancer Causes and Control 4(1) p 29-37 Rosenbaum EH Fobair P Spiegel D (2006) Cancer is a Life-changing Event Cancer Supportive Care Programs httpwwwcancersupportivecarecomSurvivorsurvivehtml [Last accessed January 30 2009] Ryan CW D Huo and K Bylow et al (2007) Suppression of bone density loss and bone turnover in patients with hormone-sensitive prostate cancer and receiving zoledronic acid BJU Int 100 pp 70ndash75 Sagiv SK Gaudet MM Eng SM et al (2007) Active and passive cigarette smoke and breast cancer survival Ann Epidemiol 17385ndash393 Sandel S Judge J Landry N et al (2005) Dance and movement program improves quality-of-life measures in breast cancer survivors Cancer Nursing 28(4) 301-309 Saxton J (2010) Physical activity and cancer mortality In Physical activity and cancer Survivorship Springer New York pp 189-210 Schatzkin A Lanza E Corle D et al Lack of effect of a low-fat high-fiber diet on the recurrence of colorectal adenomas Polyp Prevention Trial Study Group [comment] New England Journal of Medicine 2000 April 20342(16)1149- 55
139
Schmitz KH Courneya KS Matthews C Demark-Wahnefried W et al (2010) ―American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors Medicine and Science in Sports and Exercise Special Communication 0195-9131104207-14090 Schmitz K Holtzman J Courneya K Masse L Duval S Kane R Controlled physical activity trials in cancer survivors A systematic review and meta-analysis Cancer Epidemiol Biomarkers Prev 2005141588ndash95
Schulz M Lahmann PH Boeing H et al Fruit and vegetable consumption and risk of epithelial ovarian cancer the European Prospective Investigation into Cancer and Nutrition Cancer Epidemiol Biomarkers Prev 2005142531ndash2535 Schwarz S U C Obermuller-Jevic et al (2008) Lycopene Inhibits Disease Progression in Patients with Benign Prostate Hyperplasia J Nutr 138(1) 49-53 Schmitz K H Balancing Lymphedema Risk Physical activity Versus Deconditioning for Breast Cancer Survivors Physical activity and Sport Sciences Reviews 38(1) 17-24 10 Segal RJ Reid RD Courneya KS et al(2003) Resistance physical activity in men receiving androgen deprivation therapy for prostate cancer JClinOncol211653-1659
Segal RJ Reid RD Courneya KS Sigal RJ Kenny GP PrudlsquoHomme DGet al Randomized Controlled Trial of Resistance or Aerobic Exercise in Men Receiving Radiation Therapy for Prostate Cancer J Clin Oncol 2009 Jan 2027344-51 Sellers TA Potter JD Folsom AR (1991) Association of incident lung cancer with family history of female reproductive cancers the Iowa Womenlsquos Health Study Genet Epidemiol 8(3) 199ndash208 Severson RK Nomura AM Grove JS Stemmermann GN A prospective analysis of physical activity and cancer Am J Epidemiol 1989 Sep130(3)522-9 Shaw C Mortimer P Judd PA Randomized controlled trial comparing a low-fat diet with a weight-reduction diet in breast cancer-related lymphedema Cancer 20071091949ndash56 Sinicrope F A N R Foster et al Obesity Is an Independent Prognostic Variable in Colon Cancer Survivors Clinical Cancer Research 16(6) 1884-1893 Siris E S P D Miller et al (2001) Identification and Fracture Outcomes of Undiagnosed Low Bone Mineral Density in Postmenopausal Women Results From the National Osteoporosis Risk Assessment JAMA 286(22) 2815-2822 Soliman S W J Aronson et al (2009) Analyzing Serum-Stimulated Prostate Cancer Cell Lines After Low-Fat High-Fiber Diet and Physical activity Intervention eCAM nep031 Sonn GA Aronson W and Litwin MS (2005) Impact of diet on prostate cancer A review Prostate cancer and prostate disease 8 p 304-310 Speck RM Courneya KS Masse L Duval S Schmitz K (2010) An update of controlled physical activity trials in cancer survivors a systematic review and meta-analysis Journal of Cancer Survivorship 4(2) p 87-100
140
Steginga S K B M Lynch et al (2009) Antecedents of domain-specific quality of life after colorectal cancer Psycho-Oncology 18(2) 216-220 Stevinson C H Steed et al (2009) Physical Activity in Ovarian Cancer Survivors Associations With Fatigue Sleep and Psychosocial Functioning International Journal of Gynecological Cancer 19(1) 73-78 Swenson KK Nissen MJ Anderson E Shapiro A Schousboe J Leach J (2009) Effects of physical activity vs bisphosphonates on bone mineral density in breast cancer patients receiving chemotherapy Support Oncol May-Jun7(3)101-7 Tardon A Lee WJ Delgado-Rodriguez M et al Leisure-time physical activity and lung cancer a meta-analysis Cancer Causes Control200516(4)389-397 Taskila T Martikainen R Hietanen P Lindbohm M Comparative study of work ability between cancer survivors and their referents Europ J of Cancer 2007 43914-920 Taylor R Brown A et al (2004) Physical activity-based rehabilitation for patients with coronary heart disease systematic review and meta-analysis of randomized controlled trials The American journal of medicine 116(10) 682-692 Taylor NFDodd KJShields NBruder A Therapeutic physical activity in physiotherapy practice is beneficial a summary of systematic reviews 2002-2005 Aust J Physiother 2007 53 7-16 Thiebaut A C M A Schatzkin et al (2006) Dietary Fat and Breast Cancer Contributions From a Survival Trial J Natl Cancer Inst 98(24) 1753-1755 Thomas R Daly M and Perryman J (2000) Forewarned is forearmed - Randomised evaluation of a preparatory information film for cancer patients European Journal of Cancer 36(2) p 52-53 Thomas R et al (2005) Dietary advice combined with a salicylate mineral and vitamin supplement (CV247) has some tumour static properties - a phase II study Diet and science 2005 35(6) p 436-451 Thomas RJ and Davies ND (2007) Lifestyle during and after cancer treatment Clinical Oncology Vol 19 Issue 8 pp 616-627 Thomas R Nicholson C (2009) Why is exercise good for us Cancer Active httpcanceractivecomcancer-active-page-linkaspxn=2600ampTitle=Why20is20exercise20good20for20us [Last accessed 230710] Thomas R Oakes R Gordon J Russell S Blades M Williams M (2009) A randomised double-blind phase II study of lifestyle counselling and salicylate compounds in patients with progressive prostate cancer Diet and Food Science 39(3) pp 295 ndash 305 Thomson C A N R Stendell-Hollis et al (2007) Plasma and Dietary Carotenoids Are Associated with Reduced Oxidative Stress in Women Previously Treated for Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 16(10) 2008-2015
141
Thune I Brenn T Lund E Gaard M Physical activity and the risk of breast cancer N Engl J Med 336 1269-1275 1997
Travis LB Gospodarowicz M Curtis RE et al Lung cancer following chemotherapy and radiotherapy for Hodgkins disease J Natl Cancer Inst 94 (3) 182-92 2002 Tucker MA Murray N Shaw EG et al Second primary cancers related to smoking and treatment of small-cell lung cancer Lung Cancer Working Cadre J Natl Cancer Inst 89 (23) 1782-8 1997 Twiss J J N Waltman et al (2001) Bone Mineral Density in Postmenopausal Breast Cancer Survivors Journal of the American Academy of Nurse Practitioners 13(6) 276-284 Uhley V and Jen C (2006) Diet and weight management in cancer survivors In Handbook of Cancer Survivorship edited by Feuerstein M New York NY Springer 2006 ISBN-13 978-0-3873-4561-1
Vadiraja HS et al (2009) Effects of yoga program on quality of life and affect in early breast cancer patients undergoing adjuvant radiotherapy A randomized controlled trial Complementary Therapies in Medicine Volume 17 Issue 5 Pages 274-280
Velthuis MJ Agasi-Idenburg SC Aufdemkampe G Wittink HM (in press) The effect of physical activity on cancer-related fatigue during cancer treatment a meta-analysis of Randomised Controlled Trials Clinical Oncology 2009 (in print) Vineis P G Hoek and M Krzyzanowski et al Lung cancers attributable to environmental tobacco smoke and air pollution in non-smokers in different European countries a prospective study Environ Health 6 (2007) pp 1ndash7 Visvanathan K Chlebowski RT Hurley P et al American Society of Clinical Oncology 2008 clinical practice guideline update on the use of pharmacologic intervention including tamoxifen raloxifene and aromatase inhibition for breast cancer risk reduction J Clin Oncol 273235-3258 2009
Wagner LI Cella D (2004) Fatigue and cancer causes prevalence and treatment approaches BrJCancer 91822-828 Waltman N J Twiss et al (2009) ―The effect of weight training on bone mineral density and bone turnover in postmenopausal breast cancer survivors with bone loss a 24-month randomized controlled trial Osteoporosis International Wenzel L H Q Huang et al (2005) Quality-of-Life Comparisons in a Randomized Trial of Interval Secondary Cytoreduction in Advanced Ovarian Carcinoma A Gynecologic Oncology Group Study J Clin Oncol 23(24) 5605-5612 Weikert C Hoffmann K Dierkes J Zyriax BC KlipsteinndashGrobusch K MB et al Homocysteine metabolismrelated dietary pattern and the risk of coronary heart disease in two independent German study populations J Nutr 2005 1351981ndash1988 White S E McAuley et al (2009) Translating Physical Activity Interventions for Breast Cancer Survivors into Practice An Evaluation of Randomized Controlled Trials Annals of Behavioural Medicine 37(1) 10-19
142
World Health Organisation (1999) What is a healthy lifestyle Health Documentation Services WHO Regional Office for Europe Copenhagen World Health Organisation (2002) The World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva WHO Scientific Group on the Prevention and Management of Osteoporosis (2000 Geneva Switzerland) (2003) Prevention and management of osteoporosis report of a WHO scientific group World Health Organisation (2005) The European health report 2005 public health action for healthier children and populations Copenhagen WHO regional office for Europe World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva Windsor P M Nichol K F Potter J A randomized controlled trial of aerobic exercise for treatment-related fatigue in men receiving radical external beam radiotherapy for localised prostate carcinoma Cancer (2004) 101 (3) 550-7 Wright M E S-C Chang et al (2007) Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality Cancer 109(4) 675-684 Wright P A Smith et al (2005) Psychosocial difficulties deprivation and cancer three questionnaire studies involving 609 cancer patients Br J Cancer 93(6) 622-626 Yu GP et al (1997) The effect of smoking after treatment for Cancer Cancer Detect Prev 21487-509

5
benefits for cancer survivors The evidence is strongly suggestive of weight being
implicated in breast cancer outcomes with the mechanism of benefit achieved
via physical activity or a low-fat diet most likely being due to weight loss
o Smoking Strong and consistent evidence has been presented for increased risk
of disease progression and mortality in people who continue to smoke after a
diagnosis of cancer as well as poorer outcomes in pre-diagnosis smokers
o Alcohol There is a paucity of research into the effects of alcohol pre- and post-
diagnosis on cancer progression and recurrence as well as symptom
management Evidence thus far is highly contradictory although excess alcohol
is linked to increased weight which does have negative outcomes
4 Evidence is also available for the benefits of individual lifestyle components for
specific cancer types
o A high intake of soy has been found to alter testosterone (the male sex
hormone) reducing risk of prostate cancer
o Dietary fibre might offer protection against colorectal cancer or recurrence via
increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic
mucosa (tissue that lines the colon)
o Since physical activity can alter levels of oestrogen (the female sex hormone)
evidence indicates that it might be protective against breast cancer
5 There is a wealth of evidence for physical activity during and after treatment
improving symptoms of cancer-related fatigue and increasing energy and stamina It
is also clear that a needs-based approach should be adopted ndash based on the
assessed need for improvements on low fatigue levels poor quality of life low
physical function (Speck et al 2009)
6 Guided progressive physical activity soon after treatment can ease the symptoms of
lymphoedema Avoidance of physical activity through fear of exacerbating symptoms
is unwarranted if physical activity is supervised and closely monitored
7 Whilst the benefits of physical activity on bone health require clarifying physical
activity can at the very least prevent loss of bone mineral density in survivors at
particular risk of developing osteoporosis
8 Even when not directly associated with overall QoL exercise has been found to
significantly improve social functioning among post-treatment survivors The benefits
of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or
group-based The evidence that physical activity can improve body image may be
one of the mechanisms through which exercise can improve quality of life
6
9 Mechanisms of benefit for diet and physical activity include the influence that these
behaviours have on hormones and insulin levels This has sparked the question of
whether pharmacological alternatives such as aromatase inhibitors and metformin
which tend to produce greater reductions in cancer risk pose competition for lifestyle
interventions This is unlikely as healthy lifestyle behaviours contribute overall to
general health and to the risk reduction for other co-morbid conditions such as
hypertension cardiac disease and diabetes Usefully the competencies framework
offered by Finders University highlights the importance of taking a holistic approach
to supported self-management whereby support is provided for a continuum of
health as opposed to a focus on one established chronic condition Based on this
model supported self-management should provide health promotion and illness
prevention not merely in terms of cancer but also for associated risks and co-
morbidities
10 The challenge remains in integrating lifestyle support into standardised models of
aftercare for cancer survivors particularly in terms of engaging both patients and
health professionals bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative identifies the need to
provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for
healthcare professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
11 The literature identifies the need for individual assessment and risk stratification for
cancer survivors so that lifestyle interventions and support can be tailored and
provided according to need Particularly high need groups are survivors who have
co-morbidities are overweight sedentary or smoke
12 Some questions that remain
o What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
o How can people most likely to benefit from lifestyle interventions be effectively
identified
o What are the various intensities of lifestyle support that can be provided based on
levels of individual need
13 Significant limitations can be found in the evidence available for lifestyle outcomes in
cancer survivors including
7
o Long-term outcomes of lifestyle choices
o Low levels of adherence to interventions
o A paucity of studies addressing external validity
o Equality across tumour groups
o Lack of cultural considerations pertaining to dietary advice
o A paucity of individualised lifestyle advice and tailored support
8
BACKGROUND SETTING THE SCENE
Lifestyle and Well-Being
In an independent report offering recommendations on enabling effective delivery of health
and well-being in England Bernstein Cosford and Williams (2010) advise that setting clear
priorities for health and well-being should start with behavioural risk factors Namely they
recommend tackling the biggest lifestyle influences on population health tobacco alcohol
physical inactivity and poor diet These four lifestyle factors are among the biggest
contributors to most preventable diseases across all social groups and in all areas of
England They are responsible for 42 of deaths from leading causes (WHO 2005) and
together they account for at least pound94 billion in annual direct costs to the NHS (DH 2009a)
expenses incurred outside the NHS would increase this figure further
An increase in longevity and the number of people living with one or more chronic conditions
for a longer period of time has led to government action aimed at making these years as
healthy as possible Interest has been particularly paid to the role of these behavioural risk
factors and the role of lifestyle in improving or maintaining health preventing illness
managing symptoms and achieving a satisfactory quality of life (QoL) (Pedersen and Saltin
2006 Taylor et al 2004)
The term lifestylelsquo refers to personal choices that might impact health such as diet physical
activity smoking and alcohol consumption The World Health Organisation (WHO 1999)
defines a healthy lifestylelsquo as
ldquoa way of living that lowers the risk of being seriously ill or dying earlyrdquo with the
emphasis that ldquohealth is not just about avoiding disease It is also about physical
mental and social well-beingrdquo (p 2)
With earlier detection and more efficacious treatments available for cancer there has been
an increase in survival as well as in the number of people living with the long-term
consequences of cancer treatment Subsequently cancer has become a chronic disease for
a number of people among the two million cancer survivors in the UK (Maddams Moller and
Devane 2008) Whilst evidence of the effects of a healthy diet and sufficient physical activity
in cancer prevention has been well-documented (Chan Gann and Giovannucci 2005
Sonn Aronson and Litwin 2005) it has become of fundamental importance to examine the
role of these lifestyle choices in cancer survivorship Furthermore the role of lifestyle in
cancer survivorship needs to be examined not only in terms of improved physical and
psychological well-being but also disease outcomes
Given the relationship between choosing a healthy lifestyle and taking an active role in the
self-management1 of the long-term effects of cancer and its treatment the self-management
workstream of the National Cancer Survivorship Initiative (NCSI) have conducted this
1 lsquoSelf-managementrsquo has been defined as ldquoawareness and active participation by the person in their recovery
recuperation and rehabilitation to minimise the consequences of treatment promote survival health and well-beingrdquo (NCSI 2009)
9
evaluation of evidence pertaining to lifestyle factors and survivorship Not only are lifestyle
choices important in terms of disease progression and recurrence but also in the effective
management of other chronic symptoms and conditions resulting from treatment such as
cancer-related fatigue lymphoedema and osteoporosis (Doyle et al 2006) Lifestyle
support and education is evidently an important component of supported self-management2
for many individuals living with or beyond cancer (Davies and Batehup 2010) Indeed as
part of a consensus meeting and evidence review self-management support and lifestyle
management were among the top ten priorities for survivorship research (Richardson et al
2009) providing further rationale for the current review
The Health of Cancer Survivors
The traditional belief has been that people with cancer should rest reduce activity and avoid
activities involving intense physical effort in other words they are passive patients of the
disease and its treatment Consequently physical activity levels do decline substantially
during and after completion of treatment for cancer and often fail to return to pre-diagnosis
levels for many people (Daley et al 2008) Fortunately it is becoming increasingly
recognised that people living with or beyond cancer do need physical activity will not be
harmed by physical effort and are active participants in the rehabilitation process
Furthermore emerging evidence is demonstrating that lifestyle factors can influence the rate
of cancer progression improve quality of life (QoL) reduce side-effects and risks during
treatment reduce the incidence of relapse and improve overall survival (Thomas Daly and
Perryman 2000) Besides the beneficial effect on recurrence a healthy diet and regular
physical activity has the potential to reduce the risk of co-morbidity such as other cancers
cardiovascular disease and diabetes etc (Jones and Demark-Wahnefried 2006)
Research suggests that although many cancer survivors report making healthy lifestyle
changes after diagnosis these changes may not be generalisable to all populations of
cancer survivors and they are often temporary (Demark-Wahnefried and Jones 2008)
Furthermore evidence suggests that the healthy lifestyle behaviours adopted by cancer
survivors tend to be directed towards clinical action such routine physical examination rather
than those health behaviours that require daily effort such as healthy eating or regular
physical activity (Findley and Sambamoorthi 2009)
A potential explanation for this difference in the uptake of clinical versus lifestyle preventive
health behaviours is that the former is easier due to the primary action being carried out by
someone else The latter on the other hand requires personal time and effort as well as
opportunity socially economically and in terms of health literacy and educational status
Behavioural and lifestyle change is notoriously difficult but even more so for people with
cancer or other chronic conditions let alone those with co-morbidities (Krein et al 2005) For
people with co-morbidities a healthy lifestyle can be even more challenging as they grapple
with the competing demands posed by the self-management of multiple conditions (Lindsay
2009)
2 lsquoSupported self-managementrsquo has been defined as ldquoWhat health and social care professionals and service
delivery organisations to do support self-managementrdquo (NCSI 2009)
10
Given the increase in survivorship the higher rates of co-morbidity within this population
and evidence that diet physical activity and other lifestyle factors affect risk for other cancers
and other chronic diseases there is a clear need for lifestyle interventions that target this
high risk group The literature suggests the need for individual risk assessment and the
provision of support with lifestyle changes in those individuals identified as high risk ndash such
as survivors who have co-morbidities are overweight sedentary or smoke (Davies and
Batehup 2010)
The Lifestyle Needs of Survivors
The National Cancer Survivorship Initiative (NCSI) highlights that people living with or
beyond cancer would like to play a more active role in their healthcare They want to know
how to look after themselves after a cancer diagnosis including information and support on
the lifestyle changes they should make so they can return to normallsquo life as much as
possible (Macmillan Cancer Support 2008) Yet the evidence suggests that this need
remains largely unaddressed In a key mapping project commissioned by the NCSI
Research workstream a number of issues pertaining to lifestyle were identified for the four
most common cancers breast colorectal lung and prostate (NCSI 2009) Each of these
four reports which were conducted by independent organisations demonstrated gaps in the
provision of lifestyle advice and support mainly during the period of aftercare In a similar
report mapping the needs of rarer cancers prolonging life through changes to lifestyle
emerged as a frequent theme by survivors asked to explore the meaning of cancer
survivorshiplsquo (Cancer52 and NCSI 2009) There was particular emphasis on the need for
diet and physical activity advice post-surgery for oesophageal cancer as well as diet advice
for mouth and throat cancers Change in bowel habits is frequently reported among post-
treatment bowel cancer survivors requiring support with dietary changes (Nikoletti et al
(2008)
In an effort to provide further insight into lifestyle advice and support for cancer survivors as
well as developing evidence-based lifestyle interventions a comprehensive review of the
evidence for lifestyle and cancer outcomes is required The perceived outcome efficacy3 of
making lifestyle changes is important in terms of whether those changes are initiated or not
as well as whether an individual possesses the confidence (self-efficacy) to maintain lifestyle
changes Outcome efficacy could be increased by the accumulation of firmly established
evidence offered alongside the opportunity for lifestyle support
Additionally this evidence needs to be evaluated in respect of current national guidelines for
diet physical activity and other lifestyle indicators such as weight and alcohol consumption
Briefly national guidance recommends a diet comprising 33 fruit and vegetables (five
portions per day) 33 starchy foods (rice bread pasta potatoes) 15 milk and dairy
foods 12 protein (meat and fish) and 8 foods and drinks high in fat andor sugar (Food
Standards Agency 2007) Adults are advised to achieve a total of at least 30-minutes daily
moderate intensity physical activity on five or more days of the week (DH 2004) Combined
with a healthy diet regular physical activity is aimed at maintaining a Body Mass Index
3 The belief that a particular outcome will result from following certain actions or behaviours
11
(BMI)4 of 185-249kgm2 25-29 is considered to be overweight and 30 or above as obese
whilst under 185 is considered underweight (National Obesity Observatory 2009)
A healthy lifestylelsquo is the same for cancer survivors as for the general population or indeed
people with other chronic conditions (Bellizzi et al 2005 Caan et al 2005 Coups and
Ostroff 2005) Cancer survivors are slightly more likely to follow physical activity guidelines
but overall their health behaviours mirror those of the general population which is marked by
inactivity and an epidemic of obesity and associated problems (Caan et al 2005) Despite
this the lifestyle advice and tailored care currently provided for specific groups of people in
the general population such as exercise prescriptions (DH 2001) is not yet integrated into
the supportive care needs of cancer survivors (Addington-Hall 2010) This is in the main
due to reluctance (usually related to knowledge and confidence) from health professionals to
discuss lifestyle factors with cancer patients due to limitations in knowledge and an
inadequacy in the available evidence on the underlying mechanisms of benefit for individual
lifestyle factors (Miles Simon and Wardle 2010) It is anticipated that this review will allay
some of this reluctance by identifying where the evidence strongly supports the efficacy of
lifestyle factors in cancer outcomes as well as where the evidence is less clear and requires
further research
4 BMI is a statistical measure which compares a persons weight and height to estimate a healthy body weight
12
The Purpose of this Review
Using the outlined national guidance on lifestyle and taking account of evidence for specific
elements or intensity of certain lifestyle factors in cancer care and self-management a
review of the literature on lifestyle and survivorship will be conducted The primary aims are
to produce evidence that can support professionals in guiding and advising cancer survivors
as well as evidence regarding resources which might support patient self-management in
relation to lifestyle factors and behaviour change The review will be comprehensive but
pragmatic drawing on a variety of sources This will commence by updating a recent review
conducted by the World Cancer Research Fund (WCRF) - bdquoA Systematic Review of RCTs
Investigating the Effect of Diet and Physical Activity Interventions on Cancer Survival‟
(Bekkering et al 2006)5
The aim of the WCRF review (Bekkering et al 2006) was to systematically locate and
review all randomised control trials (RCTs) which tested the effect of diet andor physical
activity interventions in cancer survivors their definition of a cancer survivor being
ldquoanyone who has been diagnosed with cancer from the time of diagnosis through the
rest of liferdquo (Brown et al 2003)
They conducted a systematic search of MEDLINE (from 2000 onwards) EMBASE (from
1999 onwards) AMED (from 1985 onwards) and the Cochrane Library including DARE
CDSR CENTRAL and HTA (all years) up to March 2006 scanned key texts that were
relevant to the subject field and scanned the references of relevant reviews They identified
117 trials (Table 1)
Table 1 Trials Identified in the WCRF Review (Bekkering et al 2006)
Trials Total
Diet
Food-based
Supplement-based
23
71
Physical activity
23
Total 117
5 This has been highlighted by the American Cancer Society (ACS) as being one of the most comprehensive
reviews on diet and physical activity for cancer survivors The ACS has used the review alongside other sources to produce lsquoGuidelines on Diet and Physical Activity for Cancer Preventionrsquo (Kushi et al 2006)
13
The findings will be described along with the results of the current review The overall
conclusion drawn by Bekkering et al (2006) was that there is a paucity of robust evidence
on the effects of diet and physical activity interventions in the management of cancer RCTs
were generally small and often reported inadequate details to formally assess quality While
promotion of a generic healthy diet was associated with reduced overall mortality the degree
to which lifestyle accounted for this outcome was imprecise It was concluded that given the
large investment in potential lifestyle interventions among cancer survivors large-scale trials
adequately powered to provide robust conclusions should be supported and conducted
In updating the WCRF review (Bekkering et al 2006) further scoping of the literature from
2006 to February 2010 will be conducted along with a synthesis of the evidence presented
in the lsquoHandbook of Cancer Survivorship‟ edited by Michael Feuerstein (2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (National Cancer Action Team 2009) which evaluates literature
pertaining to rehabilitation
The primary aim of the review is to guide healthcare planning and the development of
supported lifestyle self-management interventions for high risk groups In order to be able to
consider the production of useable evidence-based guidance for self-management for both
patients and professionals the following evidence will be sought
Evidence that would support professionals to be able to guide and advise
patients
Evidence regarding resources which would support patient self-management in
relation to lifestyle factors and behaviour change
It is anticipated that recent efforts to conduct research in this area will facilitate the
clarification of any key recommendations that can be made to cancer survivors by healthcare
professionals This update of the evidence will also attempt to establish where the strength
of the evidence lies and where more research is required
14
METHOD
Search Strategy
In updating the WCRF review (Bekkering et al 2006) RCTs and systematic reviews were
obtained from a systematic search of the Cochrane Library Database and Pubmed (from
March 2006 to February 2010) Where no evidence was available in the WCRF review
studies before 2006 have been included if identified in the reference lists of acquired
records this is the case with studies on smoking which were not included in the Bekkering
et al (2006) review
The selected relevant chapters were read from the bdquoHandbook of Cancer Survivorship‟
(Feuerstein 2006)6 and relevant studies referred to from the Cancer and Palliative Care
Rehabilitation Workforce (2009) non-systematic review Grey literature was also utilised
where this would provide information relevant to the review or where cancer-specific
literature was lacking as was the case with osteoporosis
All titles and abstracts of studies identified by the searches were scanned for relevance in
terms of topic and participant group For any titles or abstracts that were potentially relevant
full paper manuscripts were obtained and the relevance of each study assessed according to
the pre-specified inclusion criteria
6 Chapters include Physical Activity Potential Benefits and Guidelines DietWeight Management
Search terms cancer OR neoplasm
AND diet OR exercise OR physical
activity OR weight OR lifestyle
Cochrane systematic reviews
925 records
PubMed
4941 records
56 included 84 included
15
Inclusion Criteria
Records included within the review of the literature met the following inclusion criteria
Lifestyle-related ndashdiet physical activity weight smoking alcohol consumption
Cancer sites breast colorectal lung or prostate cancer Other tumour sites will
be included if located while searching for the primary tumour sites
Trajectory - during primary cancer treatment or post-primary treatment
Outcomes of interest ndash survival recurrenceprogression symptoms treatment-
related chronic conditions ndash fatigue lymphoedema osteoporosis weight
physical fitness quality of life rehabilitation behaviour change health and well-
being cost-effectiveness
Adult population
Type of record ndash RCTs systematic reviews prospective cohort studies
Retrospective studies will also be included since some areas of lifestyle such as
smoking have primarily been investigated via this method
16
RESULTS
A total of 140 records were included in this review not counting the review being updated
(Bekkering et al 2006) In synthesising the evidence obtained from these records and the
additional sources described in the search strategy findings are presented in two parts
1) Cancer Survival
Evidence for the role of lifestyle in disease progression and recurrence
2) The Risks and Side-Effects of Cancer Treatment
Evidence for the role of lifestyle in reducing and managing the risks and
side-effects of cancer treatment with specific focus on cancer-related
fatigue lymphoedema osteoporosis and QoL
Both sections examine five categories of evidence
Physical activity
Diet
Weight
Smoking
Alcohol
The focus is on the four most common cancers (breast colorectal lung prostate) but other
tumour sites have been included if located via the pre-defined search strategy Summary
tables for each study included within the evidence are provided at the end of relevant
sections
17
PART ONE
CANCER SURVIVAL ndash EVIDENCE FOR THE ROLE OF LIFESTYLE IN
DISEASE PROGRESSION AND RECURRENCE
Introduction
Evidence for the role of lifestyle in the development of cancer is strong and it is widely
accepted that a poor diet lack of exercise smoking and excessive alcohol consumption can
increase an individuallsquos risk of developing cancer In particular it is well established that
smoking can increase risk of lung cancer and excessive unprotected exposure to the sun
can increase risk of skin cancer More recently lifestyle after a cancer diagnosis has been
under the microscope with evidence for the role of lifestyle in cancer progression7 and
recurrence8 demonstrating that lifestyle changes post-diagnosis can influence the disease
trajectory (Thomas and Davies 2007)
The development of cancer does not mean it is too late to make lifestyle changes that can
reduce the risk of the disease progressing or recurring after remission Indeed lifestylelsquo
refers to personal choices that can impact health and well-being as well as improve an
individuallsquos chance of disease-free survival9 and overall survival10
Evidence for an interaction between lifestyle and the disease trajectory is evaluated in the
current review including cancer development progression and recurrence and
commencing with a description of three large scale multicentre trials that will be referred to
throughout (Table 3)These studies are presented in some depth because their findings have
been influential in this field of study This will be followed by a site-specific (eg breast
colorectal lung prostate) summary of the findings reported by Bekkering et al (2006) as
part of the WCRF review being updated Further evidence identified from the search criteria
will then be presented including evidence obtained from the aforementioned multicentre
trials The European Prospective Investigation into Cancer and Nutrition (EPIC) Study
The Womens Intervention Nutrition Study (WINS) and The Womens Healthy Eating
and Living (WHEL) Study
7 Defined as the cancer becoming worse or spreading within the body
8 Cancer that has returned usually after a period of time during which it could not be detected The cancer may
come back to the same place as the original (primary) tumour or to another place in the body
9 The length of time after treatment during which a person survives with no sign of the disease
10The percentage of people from the study who are alive for a certain period of time after diagnosis or treatment
(ie 5-year survival rate)
18
The European Prospective Investigation into
Cancer and Nutrition (EPIC) Study (Riboli et al
2002)
The Womens Intervention Nutrition Study (WINS)
(Chlebowski et al 2006)
The Womens Healthy Eating and Living (WHEL)
Study
(Pierce et al 1997)
The EPIC study is coordinated in the UK by Dr Elio Riboli of the Imperial College London It is an ongoing multicentre prospective cohort study designed to investigate the relationship between nutrition and cancer The study currently includes 521000 participants (aged 35ndash70 years) in 23 centres located across 10 European countries11 These participants will be followed for cancer incidence and mortality for at least 10-years At enrolment which took place between 1992 and 2000 information was collected through a lifestyle questionnaire and through a dietary questionnaire addressing usual diet Physiological measurements (eg weight) were performed and blood samples taken The main website for EPIC12 last updated in 2010 reports that 26000 cases of cancer and 16000 deaths from cancer have been identified the majority of cases being cancer of the breast (n=6218) colonrectum (n=1910) prostate (n=1547) and lung (n=1292)
The WINS trial is a randomised multicentre study that commenced in 1994 and is now closed for recruitment It was designed to determine whether dietary fat reduction effectively prolongs disease-free and overall survival in post-menopausal women (n=2437) aged 48-78 years surgically treated for early stage breast cancer Randomisation to a reduced fat group or a control group took place between 1994 and 2001 with participants being evaluated annually via self-report and physiological measures 1) Intervention group (n=975) intensive dietary intervention for reduction of total fat intake to 15 of calories with repeated individual and group counselling sessions involving cognitive behavioural and motivational interviewing techniques 2) Control group (n=1462) US Department of Health and Human Services dietary guidelines (total fat intake between 20-35 of calories)
The WHEL study is a multicentre RCT which commenced in 1995 and also closed to recruitment aimed to determine whether a diet rich in vegetables fruit and fibre and low in fat is associated with a longer breast cancer event-free interval (ie no disease progression recurrence nor secondary cancers) Women diagnosed with stage I-III invasive breast cancer (n=3088) within the previous 4-years were randomised to a dietary intervention or control group and evaluated annually for 5-years via self-report and physiological measures 1)Intervention group (n=1540) guidelines provided for a daily dietary pattern of 5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy from fat A telephone counselling protocol focusing on goal setting self-monitoring and self-efficacy were provided as were cooking classes 2)Control group (n=1551) The US Department of Agriculture dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre and 30 energy from fat)
11
Denmark France Germany Greece Italy The Netherlands Norway Spain Sweden and the UK
12 httpepiciarcfr
Table 3 The EPIC WINS and WHEL Study (findings presented within proceeding text)
19
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in breast
cancer survival In the current review 6 studies and 2 systematic reviews were identified
These have been divided into appropriate domains according to mechanisms of benefit
hormones intensity and insulin Studies are summarised in Table 3 at the end of this
section
Hormones
Evidence exists that physical activity is associated with reduced risk of developing breast
cancer (Friedenreich and Cust 2008 Monninkhof et al 2007) One potential mechanism of
benefit is via the modification of sex hormone levels High levels of oestrogen (the
predominant sex hormone in females)13 and androgen (the predominant sex hormone in
males)14 are consistently associated with increased risk of developing breast cancer
(Eliassen et al 2006 Kaaks et al 2005) whereas high levels of sex hormone-binding
globulin (SHBG)15 are associated with a decreased risk (Key et al 2002) Regular physical
activity may alter oestrogen metabolism by shifting metabolism to favour production of 2-
hydroxyestrone (2-OHE1)16 as opposed to16α-hydroxyestrone (16α=OHE1) the former of
which has much weaker estrogenic activity Campbell et al (2007) is one of the few
researchers to examine this mechanism of benefit via a RCT In examining the effects of a
12-week aerobic exercise training programme on 2-OHE1 and 16α-OHE1 in healthylsquo pre-
menopausal women (n=17) no significant differences in oestrogen changes were found with
a control group who continued their usual level of physical activity (n=15) However a
change in lean body mass (estimated weight excluding body fat) over the 12-week
programme was found to be associated with a favourable change in 2-OHE1 to 16α-
OHE1 ratio (p lt 005)
In an effort to provide more direct evidence regarding the biological mechanisms of benefit
obtained from physical activity Friedenreich et al (2010) conducted the Alberta Physical
Activity and Breast Cancer Prevention Trial a two-centre two-arm RCT of physical
activity and cancer risk in older (50gt years) post-menopausal sedentary women from the
general population (n=320) Participants received a 1-year aerobic physical activity
programme of 225-minutes per week (n=160) or maintained their usual level of activity as
part of a control group (n=160) Significant reductions in oestrogen were found in the
intervention group compared to the control group demonstrating a protective effect
of increased physical activity in this group of high risk women (p lt 05)
13
oestrogen is suspected to activate certain oncogeneslsquo which can turn normal cells into tumour cells 14
The primary and most well-known androgen is testosterone which is also found in women to a lesser degree 15
A protein that attaches itself to oestrogen and androgen
16 Sometimes referred to as a good oestrogenlsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
20
Whilst some studies have examined the outcomes of increased physical activity others have
attempted to identify the duration and intensity required for beneficial effects Using data
from the Nursesrsquo Health Study17 (n=2987) Holmes et al (2005) found that women who
reported at least 3 MET-hours18 or more of physical activity per week were less likely
to have a recurrence or die from breast cancer compared to those who reported less
physical activity (p lt 001)
A further reduction in risk was seen with higher levels of physical activity up to 239 MET-
hours per week indicating a dose-response Interestingly the benefits of physical activity
were limited to women with hormone-receptor positive tumours (tumours that
respond to hormone treatment) as opposed to hormone-receptor negative tumours
(tumours that do not respond to hormone treatment) This provides further support for
mechanism of benefit from physical activity being hormone-related whether that be due to
the physical activity or any subsequent reductions in lean body mass that might accompany
such activity
Intensity
Expanding on evidence for the intensity of physical activity in a prospective observational
study the Health Eating Activity and Lifestyle (HEAL)19 study Irwin et al (2008) found
that of breast cancer survivors (n=933) who were sedentary pre-diagnosis women who
increased their physical activity post-diagnosis to approximately 9-MET hours per
week (eg 2-3 hours of brisk walking) had a 45 lower risk of death from cancer when
compared to those who did not increase their physical activity women who
decreased physical activity after diagnosis had a four-fold greater risk (p lt 005)
17
One of the largest and longest running investigations of factors that influence womenlsquos health comprising
information from 238000 nurse-participants
18 Metabolic equivalent (MET) values a measure of the effort required to do that activity
19 The HEAL Study is a population-based multicentre multi-ethnic prospective cohort study that has enrolled
1183 breast cancer survivors to determine whether lifestyle hormones and other exposures affect breast cancer
prognosis
METs (Ainsworth 2000) Light-intensity activities are defined as 11 MET to
29 MET Moderate-intensity activities are defined as 30 to
59 METs Vigorous-intensity activities are defined as 60 METs
or more
3 MET-hours might be using a stationary bicycle with light effort for one-hour 239 MET-hours might be running for 2-hours plus 1-hour of aerobic activity
21
Consistent with this a larger prospective observational study demonstrated that breast
cancer survivors (n=4482) who were physically active for more than 28 MET-hours per
week (eg walking at average pace of 2-29mph for 1-hour) were significantly less
likely to die from breast cancer (35-49 reduction) when compared to survivors who
did less than this (p lt 05) (Holick et al 2008) The reduced risk of mortality from cancer
was limited to total or moderate-intensity physical activity no benefit was noted for vigorous-
intensity activity
In a systematic review by Patterson et al (2010) leisure-time physical activity (ie
sportsrecreational) was associated with a 30 decreased risk of mortality from
breast cancer when compared to sedentary women In another review Saxton (2010)
identified four cohort studies demonstrating that women achieving the equivalent of 30-
minutes of moderate intensity physical activity on five or more days of the week
halved their risk of cancer-related mortality compared to those achieving less than 30-
minutes over the five days
Insulin
Evidence for the role of excess insulin in the growth of cancer cells has become more
established in recent years especially with the increase in obesity which is often
accompanied by elevated levels of insulin (Giovannucci 2005) The benefits of physical
activity on reducing insulin levels are less clear Ligibel et al (2008) conducted a RCT to test
the impact of weight training on insulin levels in overweight sedentary stage I to III breast
cancer survivors (n=101) The women were randomly assigned to one of two conditions
1) a 16-week supervised strength training and home-based cardiovascular training
protocol (two supervised 50-minute strength training sessions per week and 90-
minutes of home-based aerobic physical activity weekly)
2) a control group (routine care for 16-weeks before being offered consultation with a
physical activity trainer at the end of the control period)
Participation in the physical activity training was associated with a significant
decrease in insulin levels and hip circumference (p lt 05) Therefore the relationship
between physical activity and breast cancer recurrence may be mediated in part through
changes in insulin levels andor changes in body fat
ii DIET
Bekkering et al (2006) report on two small breast cancer studies showing a reduction in
cancer-specific mortality with healthy diet interventions (Elkort et al 1981 de Waard et al
1993) Of nine trials that included an antioxidant supplement no evidence was found for an
association between the intervention and cancer-related mortality compared with placebo or
usual treatment There was also no evidence of an effect of retinol (vitamin A - found in cod
liver oil butter liver eggs and cheese) (Meyskens et al 1994 Kucera et al 1980
Pastorino et al 1993)
22
In the current review 19 studies provide further evidence of the role of diet in breast cancer
survival many of which are part of the three multicentre studies previously described (ie
EPIC WINS WHEL p19) These studies have been divided into appropriate domains
according to dietary components dietary fat fruit and vegetables dietary fibre soy and
vitamin D
Dietary Fat
In general retrospective casendashcontrol studies have supported a positive association between
breast cancer incidence and dietary fat (Howe et al 1990) whilst many prospective cohort
studies have failed to show such an association (Kim et al 2006 Hunter et al 1996) A
meta-analysis provided evidence for a weak direct association between fat intake and breast
cancer in casendashcontrol and cohort studies combined (Boyd et al 2003) in cohort studies
that adjusted for energy intake highest versus lowest categories of total fat intake were
associated with a statistically significant 13 increased risk of developing
breast cancer (p lt 05)
Kyogoku et al (1992) utilised breast cancer patients whose dietary intake was assessed 10-
years previously in a case-control study (n= 212 patients who underwent a surgical
operation) After 10-years of follow-up 47 breast cancer deaths had occurred with no
support being provided for the hypothesis that a low fat diet influences breast cancer survival
outcomes In addition Holmes et al (1999) as part of the Nursesrsquo Health Study report
there being no evidence suggesting that lower intake of total fat or specific types of fat (eg
saturated and unsaturated fat) was associated with death from breast cancer in 2956
women who were diagnosed after 14-years of follow-up
Hebert et al (1998) studied the effect of diet on recurrence and death in women diagnosed
with early-stage breast cancer (n=472) finding that the strongest effects were observed in
pre-menopausal women Higher levels of self-reported baseline daily consumption of
butter margarine lard and beer were found to increase the risk of recurrence (p lt
01) There was also an increased risk associated with consumption of red meat liver and
bacon corresponding to about a doubling of risk for each time per day that foods in this
category were consumed (p=09)
The previously described WINS and WHEL RCTs (Table 2 p19) were anticipated to shed
light on these inconsistent findings related to dietary fat and breast cancer outcomes as
explored next in the following section
In an interim analysis of the Womens Intervention Nutrition Study (WINS) data (n=2437)
after a median follow-up of 60-months (5-years) (Chlebowski et al 2006) report that dietary
fat intake was lower in the dietary intervention than in the control group corresponding to a
significant 6-pound lower mean body weight in the intervention group (p lt 05) As a
reminder the dietary intervention group were counselled to reduce total fat intake to 15 of
calories whilst the control group were advised to keep total fat intake between 20-35 of
calories After 5-years of follow-up a total of 277 recurrences were reported in 96 of 975
23
(98) women in the dietary group and 181 of 1462 (124) women in the control group
women in the dietary intervention had a 24 lower risk of recurrence compared to the
control group (p lt 05) Exploratory analyses suggested that dietary fat reduction was most
beneficial in women diagnosed with hormone receptorndashnegative compared to hormone-
receptor positive breast cancer although this was not statistically significant
Other studies providing evidence of a differential effect of fat intake on breast cancer survival
have found such associations with hormone-receptor positive cancers (Holm et al 1993
Cho et al 2003) raising debate over the WINS findings Nevertheless in 2008 Chlebowski
et al updated survival information presented in 2006 reporting that after 7-years follow-up a
significant overall survival benefit was seen in women (n=362) with hormone-receptor
negative tumours taking part in the dietary intervention compared to the comparison
group (75 vs 181 p lt 005)
To explore the link between hormones and diet further the metabolic profiles of a subset of
WINS participants (n=53) were examined for the effect of a low-fat diet on insulin resistance
(Khaodhiar et al 2003) Insulin resistance is a physiological condition in which insulin
becomes less effective in lowering blood sugars resulting in increased blood glucose Of
those participants with initial insulin resistance after 1-year women in the dietary
intervention group had a greater decrease in their fasting insulin (insulin tested in a blood
sample collected after a 12-hour fast) than the women in the control group Although
not statistically significant these results suggest that insulin concentrations (a marker of
insulin resistance) may be influenced by dietary fat intake Alternatively since waist-to-hip
ratio is a marker for insulin weight reduction as opposed to dietary fat reductions might be
the important variable influencing disease outcomes (Borugianlsquos et al 2004)
Fruit and Vegetables
Flavonoids20 are high in fruits and vegetables and therefore might account for some of the
findings reported in WINS Dwyer et al (2008) sought to determine whether differences
existed in baseline and 12-month dietary intake of flavonoids among a random sample of
WINS participants (n=550) After 12-months of dietary intervention flavonoid intakes
remained similar in both groups demonstrating that neither total flavonoid intakes nor
intakes of subclasses of flavonoids differed between those who had dramatically decreased
their fat intake and those who had not Flavonoid intake is therefore unlikely to account for
the survival benefits reported for the WINS trial Carotenoids21 however do appear to play a
significant role in cancer survival On following 103 breast cancer survivors 27 of whom
died Ingram (1994) found that after a median of 81-months those who consumed more
beta-carotene (a carotenoid found in yellow and orange fruits such as mangoes
papayas and carrots) had significantly fewer deaths from breast cancer only one in
the group of highest beta-carotene consumers compared with 8 in the intermediate
20
Flavonoids also referred to as bioflavonoids are polyphenol antioxidants found naturally in plants ndash in other
words they are plant nutrientslsquo
21 Organic pigments that provide colour to bright fruits and vegetables including carrots apricots tomatoes and
salmon
24
group and 12 in the lowest group (p lt 0001) Overall there were 12 deaths in the lowest
total fruit consumption group compared with five in the intermediate group and 3 in the
highest (p lt 001) This benefit applied to both orangeyellow fruit (oranges melon) as well
as other fruits (apple banana berries grapes dried fruits)
Adding to this evidence is data from the aforementioned Womens Healthy Eating and
Living (WHEL) RCT (Table 2 p19) As a reminder women with breast cancer were
randomised to a dietary intervention (n=1540) comprising a daily pattern of
5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy
from fat or to a control group (n=1551) advised to follow the US Department of Agriculture
dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre
and 30 energy from fat Over a mean 73-year follow-up there was no significant
difference between groups in terms of additional breast cancer events (ie disease
progression recurrence or secondary cancer) or mortality despite statistically significant
differences in self-reported diet (low fat high fruit and vegetables) (Pierce et al 2007) On
the other hand when Rock et al (2005) examined only those participants in the control
group higher plasma total carotenoid concentration indicative of greater fruit and
vegetable consumption was significantly associated with reduced risk for a new
breast cancer event (p lt 05) This supports those findings reported by Ingram et al
(1994) and provides a potential explanation for why survival benefits were achieved in WINS
but not WHEL since both dietary interventions comprised lower dietary fat and higher levels
of carotenoids (fruit and vegetables) other factors must explain the differential survival
benefits One major difference between the two studies is that WINS participants lost weight
(mean = 6-pounds) whereas the WHEL participants did not
To follow up on these findings in terms of possible biological mechanisms of reduced risk of
recurrence Thomson et al (2007) conducted an ancillary study with post-menopausal
breast cancer survivors from the WHEL study (n=207) The aim was to test the hypothesis
that breast cancer survivors with higher levels of dietary carotenoids would show significantly
lower levels of oxidative stress (pathologic changes in response to excessive levels of cell
toxicity from the environment) than those with lower levels It was found that dietary
carotenoid levels were not significantly associated with oxidative stress indicators (measured
via urine samples)
Hot flushes post-treatment for early-stage breast cancer has been associated with an
approximately 25-30 decreased risk for additional breast cancer events (Mortimer et al
2008 Cuzick 2007) Since hot flushes are reported by women who continue to menstruate
during treatment or whose menstruation returns post-treatment this lowering of risk is
unlikely to be explained entirely by the lower oestrogen levels that sometimes accompany
hot flushes On the other hand dietary changes comprising lower energy from fat and
increased fibre can also alter oestrogen levels For example binding of fibre to estrogens in
the gut blocks reabsorption of oestrogen (Arts et al 1991) Focusing their analyses on the
2967 of the WHEL participants who experienced baseline hot flushes Gold et al (2009)
tested the hypothesis that the increased risk of additional breast cancer events observed
among women who do not report hot flushes post-treatment can be reduced by lifestyle
interventions that lower circulating oestrogen Over a median of 73-years follow-up it was
demonstrated that the dietary intervention was associated with reduced risk of second
25
breast cancer events among women who reported no hot flushes at baseline (p lt 05)
These women had 31 fewer cancer-related events than matched-pairs in the control group
among post-menopausal women with no self-reported hot flushes at baseline the
intervention effect was even stronger with a 47 reduction in risk compared with post-
menopausal women in the control group who had no hot flushes at baseline (p lt 05)
McEligot et al (2006) conducted a retrospective investigation into the influence of diet (fat
fibre vegetable fruit folate carotenoids and vitamin C) on overall survival in post-
menopausal women with breast cancer (n= 516) Participants completed a food frequency
questionnaire for the year prior to diagnosis the analysis of which demonstrated that
women consuming the least total fat and highest total fibre and vegetables as well as
more folate vitamin C and carotenoid were significantly less likely to die from any
cause than those women consuming the opposite (p lt 05)
Dietary Fibre
Evidence linking breast cancer to the intake of dietary fibre has been conflicting although the
hypotheses remain that dietary fibre can be protective by inhibiting oestrogen (Kaaks et al
2005) as described previously in relation to physical activity or by reducing insulin-like
growth factors (Heald et al 2003) Therefore further research into these mechanisms of
benefit is clearly needed in order to provide clarity
Rohan et al (1993) examined risk of breast cancer in relation to intake of dietary fibre and
vitamins A C and E in a cohort of women (n=56837) enrolled in the Canadian National
Breast Screening Study22 After 5-years follow-up 519 incidence of breast cancer were
identified with analysis of previously completed dietary questionnaires demonstrating that
higher dietary fibre intake was associated with a small reduction in risk of developing
breast cancer Specifically there was a statistically significant decrease in risk of
developing breast cancer with increasing consumption of cereals (p lt 01) and a statistically
non-significant trend for pasta consumption (p=017) This reduced risk persisted after
adjustment for total vitamin A beta-carotene vitamin C and E
The UK Womens Cohort Study (UKWCS) (Cade et al 2007) which compares the health
outcomes of three main dietary groups (vegetarian eating fish [not meat] and meat eaters)
provides further evidence for the protective properties of fibre After a median of 75 years
follow-up analysis of self-reported dietary data of 35792 women showed that total dietary
fibre was found to be related to breast cancer incidence in women who were pre-
menopausal but not post-menopausal at baseline (p lt01) Fibre from cereals (plt
05) and fibre from fruit (p=009) was found to be protective against breast cancer
22
An RCT comprising women 40-49 years of age at study entry evaluating the efficacy of annual mammography breast physical examination and instruction on breast self-examination in reducing breast cancer mortality
26
Soy
A high intake of phytoestrogens23 particularly isoflavones (found in soy products) has been
suggested to decrease risk of developing breast cancer In one of the European
Prospective Investigation into Cancer and Nutrition (EPIC) studies a large multicentre
prospective cohort study described earlier in Table 2 the association between breast cancer
risk and isoflavones was supported in 333 women (p lt 005) (Grace et al 2004) but in
another larger EPIC study conducted in Utrecht (n=15555) no such evidence was found
(Keinan-Boker et al 2004) Analyses with pooled data sets are ongoing In the meantime
Boyapati et al (2005) provide evidence from the Shanghai Breast Cancer Study24
suggesting that after a median of 52-years follow-up soy intake pre-diagnosis is not related
to disease-free survival in women with breast cancer (n=1459)
Vitamin D
Goodwin et al (2009) measured vitamin D (usually obtained from sunlight through the skin
but also found in oily fish and eggs) levels in the stored blood of women with early breast
cancer (n=512) The mean follow-up was 116-years by which time women deficient in
vitamin D had a significantly increased risk of distant recurrence25 compared with
those who had sufficient levels (p lt 05)
Antioxidant Supplements
Despite widespread use only a few clinical or epidemiological studies have examined the
relationship between antioxidant supplements and risk of breast cancer recurrence or breast
cancer-related mortality Fleischauer et al (2003) examined recurrence and mortality
among post-menopausal women diagnosed with breast cancer (n=385) who were enrolled
into a dietary case-control study Women were contacted with a single questionnaire to
ascertain the use of nutritional supplements during 12-14 years of follow-up Antioxidant
vitamin supplement use was associated with a lower risk of breast cancer recurrence or
mortality Specifically use of vitamin C and E supplements moderately reduced risk (p lt
05) whilst vitamin E nearly halved the risk although this was not statistically
significant (p=056)
iii WEIGHT
Weight and body composition have been implicated in the development of a wide range of
cancers as well as in increased risk of recurrence or second primary cancers (Chlebowski
Aiello and McTiernan 2002) Additionally being overweight or obese can exacerbate some
23
Phytoestrogens sometimes called dietary estrogenslsquo are a group of naturally occurring plant compounds that have a similar chemical structure to estrogen they bind to estrogen receptors acting like hormone regulators
24 The Shanghai Breast Cancer Survival (SBSS) Study collected lifestyle-related factors and disease and
treatment related factors in Chinese women with breast cancer (n=2236) (Lu et al 2007) 25
The spread of cancer to parts of the body other than the place where the cancer first occurred
27
of the side-effects of cancer treatment as well as increase the risk of co-morbidities such as
diabetes and osteoporosis (Doyle et al 2006) The studies evaluated in this review thus far
further indicate weight as offering a mechanism of benefit in terms of breast cancer
outcomes Indeed the WINS and WHEL RCTs produce different outcomes when using
similar dietary interventions with weight loss in the WINS group but not the WHEL group
offering a likely explanation for improved outcomes observed in the WINS participants Since
increased adiposity (excess body fat) has been identified as a negative prognostic factor for
recurrent disease and survival after breast cancer diagnosis (Rock and Demark-Wahnefried
2002) the apparent benefit of dietary fat reduction in the intervention group could
partly result from the weight loss
Bekkering et al (2006) do not add to this evidence whilst 5 studies and one systematic
review were identified in the current review
Hebert et al (1998) studied the effect of body weight on recurrence and death in women
diagnosed with early-stage breast cancer (n=472) Body mass index (BMI) was
associated with an increased risk of recurrence at the rate of 9 for each kgm2
(equivalent to about 58-pounds for a 5 4 tall woman) For death the results were
similar but body mass index was more strongly associated increasing risk by 12
per kgm2
Additionally Lahmann et al (2004) used data from 73542 pre-menopausal and 103344
post-menopausal women taking part in the EPIC study During 47-years of follow-up 1879
cases of invasive breast cancer were identified In post-menopausal women current use
of hormone replacement therapy (HRT) modified the association between body size
and breast cancer among non-users weight body mass index and hip circumference
were positively associated with breast cancer risk (p lt 001) Obese women (BMI gt 30)
had a 31 risk compared to women with a BMI lt 25 Among pre-menopausal women hip
circumference was the only other measure significantly related to breast cancer (p lt 005)
after accounting for BMI
Enger et al (2004) conducted a retrospective follow-up study of women diagnosed with
breast cancer (n=1376) for whom complete medical records and adequate tissue
specimens existed Patients were followed for a median of 68-years after diagnosis 246 of
whom died from breast cancer Compared with women in the lowest category of weight
(lt133lb [60kg] at diagnosis) women in the highest category ( 175lb [79kg])
experienced a 25-fold increased risk of dying from breast cancer (P lt 05) Women with
hormone-receptor negative cancer experienced an approximately 2-fold higher risk of dying
from breast cancer compared with women who presented with hormone-receptor positive
cancer Women in the upper 50th percentile of weight with hormone-receptor negative cancer
had a nearly 5-fold increased risk of dying from cancer compared with women in the lower
50th percentile of weight and hormone-receptor positive cancer (p=10)
In order to determine whether weight prior to diagnosis and weight gain after diagnosis are
predictive of breast cancer survival Kroenke et al (2005) followed 5204 participants from
the Nursesrsquo Health Study diagnosed with incident invasive non-metastatic breast cancer
After a median of 9-years follow-up there were 860 total deaths 533 breast cancer deaths
28
and 681 recurrences (defined as secondary lung brain bone or liver cancer and death from
breast cancer) Weight before diagnosis and weight gain after diagnosis were related
to higher rates of breast cancer recurrence and mortality although associations were
most apparent in women who had never smoked (p lt 05) Furthermore associations
with weight were stronger in pre-menopausal than in post-menopausal women In contrast
by comparing breast cancer survivors (n=3215) with women in the comparison group of a
dietary intervention trial to prevent breast cancer recurrence Caan et al (2008) found that
neither moderate (5ndash10) nor large (gt10) weight gain post-diagnosis was associated with
an increased risk of breast cancer recurrence in the early years post-diagnosis (median time
of 737-months from diagnosis)
More recently Patterson et al (2010) reviewed published epidemiological research on
lifestyle and breast cancer outcomes reporting that the most consistent finding from
observational studies was that adiposity was associated with a 30 increased risk of
cancer-related mortality
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in breast cancer
survival Four studies were identified in the current review
In an observational study Manjer et al (2000) compared the survival of patients with breast
cancer (n=792) who had never smoked were smokers or were ex-smokers Follow-up of
breast cancer cases was through record-linkage with the Swedish Cause of Death Registry
During a mean follow-up of 121-years smokers and ex-smokers compared with those
who had never smoked had a significantly increased risk of death from cancer
Fentiman et al (2005) add to this evidence with a cohort study of breast cancer patients who
completed a lifestyle questionnaire at the time of diagnosis (n=166) They found that
smoking was the third most important predictor of breast cancer-specific and overall
survival after stage and age at diagnosis This suggests that smokers are not only more
likely to die of cancer but also of other diseases when compared with those who have never
smoked
In a much larger study Holmes et al (2007) conducted a prospective observational study
among 5056 women from the Nursesrsquo Health Study with stages I-III invasive breast
cancer Information on smoking was available for these women who were followed until
January 2002 or death whichever came first Compared with women who had never
smoked women who were current smokers had a 43 increased risk of death from
any cause with risk increasing along with more cigarettes smoked per day (p lt0001)
In contrast there was no association with current smoking and breast cancer death
Sagiv et al (2007) followed women diagnosed with a first primary breast cancer (n=1273)
for 5-6 years and found that the number of all-cause mortality (n=188) including breast
cancer-specific mortality (n=111) was slightly higher among current and former
active smokers compared with women who had never smoked No association was
found between active or passive smoking and breast cancer-specific mortality
29
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in breast cancer
survival In the current review one review and 2 studies were identified
Rock and Demark-Wahnefried (2002) reviewed the evidence from clinical and epidemiologic
studies reporting that alcohol intake was not associated with breast cancer survival in the
majority of the studies In contrast post-menopausal women (n=125) diagnosed with
invasive breast cancer who were followed through to survival demonstrated that pre-
diagnosis alcohol consumption of at least one drink per week was associated with a
27-fold increase in risk of cancer-related mortality (McDonald et al 2002) In a similar
study a larger sample of women (n=1286) diagnosed with invasive breast cancer who were
followed from diagnosis through to survival produced opposing findings compared with
non-drinkers women who consumed alcohol in the 5-years before diagnosis had a
decreased risk of cancer-related mortality (Reding et al 2009)
SUMMARY OF LIFESTYLE EVIDENCE FOR BREAST CANCER ndash MECHANISMS
OF BENEFIT
Physical Activity Physical activity is likely to prevent breast cancer via its effect on
hormones specifically by reducing levels of oestrogen in the body (Friedenreich et al 2010)
or shifting the metabolism of oestrogen to favour production of 2-hydroxyestrone (2-OHE1)26
as opposed to16α-hydroxyestrone (16α=OHE1) the former of which has much weaker
estrogenic activity This shift might also be the result of a change in lean body mass resulting
from physical exercise (Campbell et al 2007) The survival benefits of physical activity
appear to require a certain intensity or level of exertion specifically 3 MET-hours or more per
week (Holmes et al 2005 Holick et al 2008 Saxton et al 2010) this equates to moderate
intensity activity such as using a stationary bike for 1-hour However there is also evidence
of a dose-effect with greater activity (up to 239 MET-hours per week) being associated with
reduced risk of recurrence and cancer-related mortality (Holmes et al 2005) or indeed
greater levels of activity than pre-diagnosis being associated with reduced risk of recurrence
and cancer-related mortality (Irwin et al 2008 Holick et al 2008 Patterson et al 2010
Saxton et al 2010)
Diet Evidence for the role of dietary fat in breast cancer development and survival are
varied Case-control (Kyogoku et al 1992) and large prospective studies (Holmes et al
1999) do not show any significant link whilst some studies have found that dietary fat does
increase risk of recurrence or death in pre-menopausal women Indeed the large multicentre
WINS trial found a protective benefit of a reduced fat dietary intervention which was more
prominent in women diagnosed with hormone-receptor negative breast cancer (Chlebowski
et al 2006a Chlebowksi et al 2008) The differential effect of diet on hormone-receptor
positive and negative disease indicate that metabolic mechanisms involving insulin and
26
Sometimes referred to as a lsquogood estrogenrsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
30
insulin-like growth factor-1 (IGF-1)27 may be involved in the mechanisms of benefit and
although not statistically significant data has been presented suggesting that elevated
insulin concentrations (a marker of insulin resistance) may be influenced by dietary fat
reduction (Khaodhiar et al 2003 Borugian et al 2004) However this might be due to
changes in weight produced by a low fat diet rather than the lower consumption of fat itself
(Borugian et al 2004) Since low fat diets are often accompanied by high intakes of fruit
and vegetables various components of a diet comprising high levels of fruit and vegetables
have been investigated Carotenoids have received particular attention with evidence
suggesting that carotenoids play a role in survival (Ingram 1994) Other studies have found
this not to be the case (Pierce et al 2007) with the primary difference in these studies being
lack of weight loss This indicates that the mechanism of benefit produced from low fat high
fruit and vegetable (particularly carotenoids) diets is most probably through changes in body
composition Indeed the majority of studies in this review demonstrated a link between
weight and cancer-related risks (Hebert et al 1998 Enger et al 2004 Lahmann et al
2004 Patterson et al 2010)
Smoking Evidence pertaining to the smoking clearly demonstrates a link between
breast cancer survival and a history of smoking However it appears to be more likely to
increase all-cause mortality as opposed to cancer-specific mortality (Fentiman et al 2005
Holmes et al 2007 Sagiv et al 2007)
Alcohol Although the evidence is less clear pre-diagnosis alcohol consumption does
appear to be related to survival (McDonald et al 2002 Reding et al 2009) although
current drinking does not (Demark-Wahnefried 2002)
27
IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of
pathological states including cancer
31
Table 3 Breast Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Campbell et al (2007)
RCT examining the effects of 12-weeks of aerobic exercise training on 2-OHE
1 and 16α-OHE
1 in
premenopausal women Randomisation to 1) A 12-week individualised supervised moderate-to-vigorous intensity aerobic exercise training intervention (n = 17) Participants began the exercise program in the early follicular phase of the next menstrual cycle (days 1-5) The intervention was divided into three blocks (a) Weeks 1 ndash 4 ndash 3 sessions per week of base aerobic training progressing from 20-40 minutes on a stationary bike (b) Weeks 5-8 ndash 4 sessions per week Two sessions were base aerobic training sessions for 30-45 minutes (c) Weeks 9 -12 ndash 4 sessions per week with two base aerobic training sessions for 30-45 minutes and two interval sessions 2) Usual lifestyle (n = 15) Participants were asked to maintain their usual activity levels for the duration of the study Following the control cycle the first day of the next menstrual cycle was used as the reference start date for participants in the control group On completion of the 12-week post-intervention
Healthy regularly menstruating Caucasian women (n=32) 20-35 years
On completion of the 12-week intervention
Height body mass body composition by dual-energy X-ray absorptiometry and VO2max were measured at baseline and following the intervention Urine samples were collected in the luteal phase of four consecutive menstrual cycles
Participants attended an average of 40-44 (91) sessions Fourteen of 17 (82) participants completed at least 80 of the sessions The exercise group increased VO2max by 14 and had significant although modest improvements in fat and lean body mass No significant between-group differences were observed however for the changes in 2-OHE1 (P = 0944) 16α-OHE1 (P= 0411) or the ratio of 2-OHE1 to 16α-OHE1 (P = 0317) At baseline there was an inverse association between body fat and 2-OHE1 to 16α-OHE1 ratio (r = minus040 P = 0044) however it was the change in lean body mass over the intervention that was positively associated with a change in 2-OHE1 to 16α-OHE1 ratio (r = 043 P = 0015)
32
measurement participants were given guidance for starting an individualised exercise program and access to the fitness facility for 4-weeks
Friedenreich et al (2010)
A two-centre two-arm RCT examining how an aerobic exercise intervention influences
circulating
estradiol oestrone sex hormonendashbinding globulin
(SHBG)
androstenedione and testosterone levels which may
be involved in the
association between physical activity and
breast cancer risk
Randomisation to 1) A 1-year aerobic physical activity programme of 225-minutes per week (n=160) 2) Control group maintained their usual level of activity (n=160)
Older (50gt years) post-menopausal sedentary women (n=320)
On completion of the intervention
Estradiol and sex hormone-binding globulin levels Androstenedione and testosterone levels
Completion of the study was high (966) At 12-months statistically significant reductions in
estradiol (treatment effect ratio
[TER] = 093 95 CI 088 to 098) and free estradiol (TER = 091
95 CI 087 to 096) and increases in SHBG (TER = 104 95 CI
102 to 107) were observed in the exercise group compared with
the control group No significant differences in oestrone
androstenedione and testosterone levels were observed between
exercisers and controls at 12-months
Holick et al (2008)
Prospective cohort study examining the relationship between post-diagnosis recreational physical activity and risk of breast cancer death
Women with a history of previous invasive breast cancer diagnosed between the ages of 20-79 years (n=4482)
Maximum of 6-years post-diagnosis (median=56-years post-diagnosis)
Mortality from breast cancer mortality from any cause Self-reported physical activity converted to MET-hours per week
After adjusting for age at diagnosis stage of disease state of residence interval between diagnosis and physical activity assessment body mass index menopausal status hormone therapy use energy intake education family history of breast cancer and treatment modality compared with women expending lt28 MET-hwk in physical activity women who engaged in greater levels of activity had a significantly lower risk of dying from breast cancer (HR 065 95 CI 039-108 for 28-79 MET-hwk HR 059 95 CI 035-101 for 80-209 MET-hwk and HR 051 95 CI 029-089 for ge210 MET-hwk P for trend = 005) Results were similar for overall survival (HR 044 95 CI 032-060 for ge210 versus lt28 MET-hwk P for trend lt0001) and were similar regardless of a womanlsquos age stage of disease and body mass index
Holmes et al (2005)
Prospective observational study
(Nurseslsquo Health Study) to determine whether physical activity among
women with breast cancer
2987 female registered nurses
in the
Nurseslsquo Health
Women were diagnosed between 1984 and
Breast cancer mortality risk according
to
physical activity
Compared with women who engaged in less than 3 MET-hours per
week of physical activity the adjusted relative risk (RR) of death
from breast cancer was 080 (95 CI 060-106) for 3 to 89 MET-hours per week 050
(95 CI 031-082) for 9 to 149 MET-hours
33
decreases their risk of death from
breast cancer compared with
more sedentary women
Study diagnosed with stage
I II or III
breast cancer
1998 and followed until death or June 2002
category (lt3 3-89 9-149 15-239
or 24
metabolic equivalent task [MET] hours per week)
per week 056 (95 CI 038-084) for 15 to 239 MET-hours per
week and 060 (95CI 040-089) for 24 or more MET-hours per week (P for trend
= 004) Three MET-hours is equivalent to walking
at average pace of 2 to 29 mph for 1 hour The benefit of physical
activity was particularly apparent among women with hormone-
responsive tutors The RR of breast cancer death for women with hormone-responsive
tumours who engaged in 9 or more MET-hours
per week of activity compared with women with hormone-
responsive tumours who engaged in less than 9 MET-hours per
week was 050 (95 CI 034-074) Compared with women who
engaged in less than 3 MET-hours per week of activity the absolute
unadjusted mortality risk reduction was 6 at 10 years for women
who engaged in 9 or more MET-hours per week
Irwin et al (2008)
The Health Eating Activity and Lifestyle Study (HEAL) Prospective observational study investigating the association between pre- and post-diagnosis
physical activity (as well as
change in pre-diagnosis to post-diagnosis
physical activity) and
mortality among women with breast cancer
A subsample of participants from the HEAL study ndash 933 women diagnosed with local or regional breast cancer between 1995
and 1998
5 -8 years from diagnosis (median=6-years)
Primary outcomes total deaths
and breast
cancer deaths
Compared with inactive women the multivariable hazard ratios
(HRs) for total deaths for women expending at least 9 MET-
hours per week (approximately 2-3 hwk of brisk walking) were 069
(95 CI 045 to 106 P = 045) for those active in the year before
diagnosis and 033 (95 CI 015 to 073 P = 046) for those active
2-years after diagnosis Compared with women who were inactive
both before and after diagnosis women who increased physical
activity after diagnosis had a 45 lower risk of death (HR = 055
95 CI 022 to 138) and women who decreased physical activity
after diagnosis had a four-fold greater risk of death (HR = 395 95
CI 145 to 1050)
Ligibel et al (2008)
RCT examining the impact of physical activity on insulin levels Participants were randomly assigned to one of two conditions a)Physical activity intervention a 16-week supervised strength training and home-based cardiovascular training protocol (two supervised 50-minute strength training
sessions per
week and 90-minutes of home-based
aerobic physical activity
weekly) b) Control group routine care for 16-weeks before being offered consultation with an physical activity
Overweight sedentary stage
I-III breast
cancer survivors (n=101)
On completion of the 16-week intervention
Fasting insulin and glucose levels Weight body composition
and
circumference at the waist and hip
18 women withdrew consent andor did not complete the study
Baseline and 16-week measurements were available for 82 patients
Fasting insulin concentrations decreased by an average of
286 microUmL in the exercise group (P = 03) with no
significant change in the control group (decrease of 027 microUmL P
=
65) The change in insulin levels in the exercise group seemed
greater than the change in controls but the comparison
did not reach statistical significance (P = 07) There was a
trend toward improvement in insulin resistance in the exercise
group (P = 09) but no change in fasting glucose levels The
exercise group also experienced a significant decrease in hip
measurements with no change in weight or body composition
34
trainer at the end of the control
period
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer outcomes
Breast cancer Not reported Additional breast cancer events and mortality
Although observational data were not consistent physical activity appeared to be associated with a 30 decreased risk of mortality
Saxton et al (2010)
A review of studies pertaining to physical activity and cancer mortality
All cancers with more evidence obtained for breast cancer
Not reported Survival A number of prospective cohort studies have reported negative associations between physical activity and cancer mortality The most compelling observational evidence of the survival benefits to be gained from a physically active lifestyle has emerged from studies of post-diagnosis physical activity in breast and colorectal cancer survivors These studies have shown clear inverse associations between post-diagnosis activity and survival with the benefits being independent of age gender obesity and disease stage at diagnosis Three of the four cohort studies of breast cancer survivors showed that women who are achieving the equivalent of 30-miniutes of moderate intensity PA on five or more days of the week can halve their risk of mortality up to 8 years of follow-up
DIET
Borugian et al (2004)
Prospective cohort study testing the hypothesis that elevated wait-to-hip ratio is directly related to breast cancer
mortality
603 patients with incident
breast
cancer
Up to 10-years
Date of death and
primary and secondary cause of death
After adjustment for age BMI family history oestrogen
receptor (ER) status tumour stage at diagnosis and systemic
treatment (chemotherapy or tamoxifen) WHR was directly related to
breast cancer mortality in postmenopausal women (for highest
quartile vs lowest relative risk = 33 95 confidence interval
11 104) but not in premenopausal women (relative risk = 12
95 confidence interval 04 34) Stratification according to
ER
status showed that the increased mortality was restricted to ER-
positive postmenopausal women Elevated WHR was confirmed as
a predictor of breast cancer mortality with menopausal status and
ER status at diagnosis found to be important modifiers of that
relation
Boyapati et al (2005)
As part of the Shanghai Breast Cancer Cohort Study associations between soy and breast cancer survival were investigated
1459 breast cancer patients
52-years Disease-free survival
Soy intake pre-diagnosis was unrelated to disease-free breast cancer survival (adjusted hazard ratio [HR]=099 95 confidence interval [CI] 073-133 for the highest tertile compared to the lowest tertile) The association between soy protein intake and breast cancer survival did not differ according to ERPR status tumour stage age at diagnosis body mass index (BMI) waist to hip ratio (WHR) or menopausal status
Boyd et al (2003)
Meta-analysis of casendashcontrol and cohort studies published up to July 2003 which examined the
Varied Not reported Cancer incidence A total of 45 published studies containing 46 estimates of risk examined the role of dietary fat in relation to breast cancer risk by an analysis of nutrient intake Of these 31 were case control and
35
association of dietary fat or fat-containing foods with risk of breast cancer
14 were cohort in design and they contained a total of 25015 cases of breast cancer and over 580 000 control or comparison subjects The summary relative risk comparing the highest and lowest levels of intake of total fat was 113 (95 CI 103ndash125) Cohort studies (n=14) had a summary relative risk of 111 (95 CI 099ndash125) and casendashcontrol studies (N=31) had a relative risk of 114 (95 CI 099ndash132) Significant summary relative risks were also found for saturated fat (RR 119 95 CI 106ndash135) and meat intake (RR 117 95 CI 106ndash129) Combined estimates of risk for total and saturated fat intake and for meat intake all indicate an association between higher intakes and an increased risk of breast cancer Casendashcontrol and cohort studies gave similar results
Cade et al 2007)
A large UK cohort study comprising women with a wide range of different eating patterns to study the effects of different food and nutrient intakes on long-term health outcomes
35372 women (350 post- and 257 pre- menopausal women developed breast cancer)
Approx 75-years
Breast cancer incidence
In pre-menopausal but not post-menopausal women a statistically
significant inverse relationship was found between
total fibre intake and risk of breast cancer (P for trend = 001) The
top quintile of fibre intake was associated with a hazard ratio
of 048
[95 CI 024ndash096] compared with the lowest quintile Pre-
menopausal fibre from cereals was inversely associated with risk
of breast cancer (P for trend = 005) and fibre from fruit had a
borderline inverse relationship (P for trend = 009)
Chlebowski et al (2006a)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
randomisation to death from any cause
Attrition in the dietary intervention (n=44) versus control group (n=66) Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to
345] versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group A total of 277 relapse
events (local regional distant or ipsilateral breast cancer
recurrence or new contralateral breast cancer) have been reported
in 96 of 975 (98) women in the dietary group and 181 of 1462
(124) women in the control group The hazard ratio of relapse
events in the intervention group compared with the control group
was 076 (95 CI = 060 to 098 P = 077 for stratified log rank
and P = 034 for adjusted Cox model analysis)
36
dietary guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
Chlebowski et al (2008)
A protocol-mandated survival analysis update to the interim analysis of WINS (Chlebowski et al 2006a)
Breast cancer patients (n=2437)
Approximately 7-years
Overall survival Attrition in the intervention group (n=236) versus control group (n=172) Although fewer deaths were seen in the intervention group this was not statistically significant In 362 women with ER- and (progesterone receptor) PR- disease a significant overall survival benefit was seen in the intervention group (75 vs 181 cumulative mortality)
Cho et al (2003)
A prospective analysis of the relationship
between dietary fat
intake and breast cancer risk among pre-menopausal
women enrolled in
the Nurseslsquo Health Study
Pre-menopausal women (n=90655) aged between 26-46 years old when recruited in 1991
8-years after recruitment (1991-1999)
Fat intake was
assessed with a food-frequency questionnaire at baseline
in 1991
and again in 1995
During 8-years of follow-up 714 women developed incident
invasive breast cancer Relative to women in the lowest quintile of
fat intake women in the highest quintile of intake had a
slight increased risk of breast cancer (RR = 125 95 CI = 098
to 159 Ptrend = 06) The increase was associated with intake
of
animal fat but not vegetable fat RRs for the increasing quintiles of
animal fat intake were 100 (referent) 128 137 154 and 133
(95 CI = 102 to 173 Ptrend = 002) Intakes of both saturated and
monounsaturated fat were related to modestly elevated breast
cancer risk Among food groups contributing to animal fat red meat and high-fat dairy foods were each associated
with an increased
risk of breast cancer Information on oestrogen-receptor status was available for
80 (n = 570) of breast cancers and progesterone-
receptor status for 78 (n = 558) When divided according to
oestrogen and progesterone receptor status the positive
association between animal fat intake and breast cancer risk was
stronger among women with oestrogen receptor-positive or
progesterone receptor-positive cancers than among women with hormone receptor-negative cancers however the difference was not statistically significant
Dwyer et al (2008)
A sub-analysis of participants in the WINS trial (Chlebowski et al 2006a)
Breast cancer patients (n=550)
12-months of intervention
Disease-free survival
Attrition in the intervention group (n = 23 11) versus control group (n = 16 5)At baseline neither mean fat intake nor flavonoid intake differed between groups After 12-months of intervention dietary fat intake was significantly lower among those on the very low-fat diet (n =195) whilst flavonoid intake remained similar in both groups Neither total flavonoid intake nor intake of subclasses of flavonoids differed between those who had dramatically decreased their fat intake and those who had not
Fleischauer et al (2003)
Case-control study testing the hypothesis that antioxidant
385 post-menopausal
12-14-years Breast cancer recurrence or
Antioxidant supplement users compared with non-users were less likely to have a breast cancer recurrence or breast cancer-related
37
supplements may reduce the risk of breast cancer recurrence or breast cancer-related mortality
women with breast cancer
death death (OR = 054 95 CI = 027-104) Vitamin E supplements showed a modest protective effect when used for more than 3 years (OR = 033 95 CI = 010-107) Risks of recurrence and disease-related mortality were reduced among women using vitamin C and vitamin E supplements for more than 3 years
Gold et al (2009)
Secondary analysis of a purposive sample of WHEL participants to determine if a low-fat diet high in vegetables fruit
and fibre affects
prognosis in breast cancer survivors
with or without hot flashes (HF) after treatment Randomisation to one of two groups 1)An intensive telephone counselling intervention based on social cognitive theory promoted a daily dietary intake of
5 vegetable
servings 16oz of vegetable juice 3
fruit servings 30g fibre and 15-20 of energy
from fat
2) Control group received printed
materials (but no counselling) promoting the
5-a-day guidelines
of
daily intakes of 5 servings of fruit and
vegetables more than 20g of fibre and less than
30 of energy from fat
2967 women (96 of all enrolled in the WHEL study) whose baseline hot flush severity
report in
the prior 4-weeks was available
4-years into the intervention
Primary end points additional breast cancer events
(localregio
nal recurrence or distant metastasis or new primary
breast
cancer) and death from any cause
The intervention group consumed significantly more daily vegetablefruit
(54 higher)
fibre (31 higher) and less
percent energy from fat (14 lower) than the comparison group
HF-negative women in the intervention had 31 fewer events than
the comparison group The intervention did not affect prognosis in
the women with baseline HFs Compared with HF-negative women in the comparison group
HF-positive women had significantly fewer
events in both groups
Goodwin et al (2009)
A prospective cohort study examining the influence of vitamin D on breast cancer prognosis
512 women with early breast cancer
Mean = 116-years
Cancer recurrence and mortality
Women with deficient vitamin D levels had an increased risk of
distant recurrence (hazard ratio [HR] = 194 95 CI 116 to
325) and death (HR = 173 95 CI 105 to 286) compared with
those with sufficient levels The association remained after
individual adjustment for key tumour and treatment related factors but was
attenuated in multivariate analyses (HR = 171 95 CI
102 to 286 for distant recurrence HR = 160 95 CI 096 to
264 for death)
Grace et al (2004)
Prospective study (EPIC) examining associations between phytoestrogen and breast cancer risk 114 spot urines and 97 available serum
333 women (aged 45ndash75 years) drawn from the EPIC
Not reported Phytoestrogen concentrations and breast cancer incidence
Phytoestrogen concentrations in spot urine (adjusted for urinary creatinine) correlated strongly with that in serum with Pearson correlation coefficients gt 08 There were significant relationships (P lt 002) between both urinary and serum concentrations of
38
samples from women who later developed breast cancer Results were compared with those from 219 urines and 187 serum samples from healthy controls matched by age and date of recruitment
study isoflavones across increasing tertiles of dietary intakes Urinary enterodiol and enterolactone and serum enterolactone were significantly correlated with dietary fibre intake (r = 013ndash029) Exposure to all isoflavones was associated with increased breast cancer risk significantly so for equol and daidzein For a doubling of levels odds ratios increased by 20ndash45 [log2 odds ratio = 134 (106ndash170P = 0013) for urine equol 146 (105ndash202 P = 0024) for serum equol and 122 (101ndash148 P = 0044) for serum daidzein]
Howe et al (1990)
Pooled analysis of 12 case-control studies of diet and breast cancer risk
Healthy women Not reported Breast cancer incidence
A consistent statistically significant positive association was found
between breast cancer risk and saturated fat intake in
postmenopausal women (relative risk for highest vs lowest quintile
146 P lt0001) A consistent protective effect for a number of
markers of fruit and vegetable intake was demonstrated vitamin C
intake had the most consistent and statistically significant inverse
association with breast cancer risk (relative risk for highest vs
lowest quintile 069 P lt0001)
Holm et al (1993)
Interviews regarding diet history the purpose being to determine whether dietary habits are associated with disease-free survival
in patients with
breast cancer who have undergone treatment
240 women with stage I-II breast cancer (50ndash65 years old) 209 of whom were post-menopausal
4-years Disease-free survival
Cancers were classified as oestrogen receptor (ER) rich ( 010
fmolmicrog of DNA) in 149 patients and as ER poor (lt010 fmolmicrog
of
DNA) in 71 patients Fifty-two patients had treatment failure during
follow-up The 30 patients with ER-rich tumours who had treatment
failure reported higher intakes of total fat saturated fatty acids and
polyunsaturated fatty acids than did the 119 patients with ER-rich
tumours that did not have treatment failure The multiple-odds ratio
(OR) for treatment failure in these women was 108 for each 1
increment in percentage of total energy (E) from total fat For
treatment failure within the first 2 years the OR was 119 for each
1-mg increase in vitamin E intake per 10 mega joules of energy In
women with treatment failure 2ndash4 years after diagnosis Ors were
113 and 123 for each E increment in total fat or saturated fatty
acids respectively No association between dietary habits and
treatment failure was found for women with ER-poor cancers
39
Holmes et al (1999)
Cohort study (Nurseslsquo Health Study)
to determine whether intakes
of fat and fatty acids are associated
with breast cancer
88795 women free of cancer (2956 developed breast cancer)
14-years Relative risk of invasive breast
cancer for
an incremental increase of fat intake
Compared with women obtaining 301 to 35 of energy from fat women consuming 20 or less had a multivariate
RR of breast
cancer of 115 (95 CI 073-180) In multivariate models the RR
(95 CI) for a 5-of-energy increase was 097 (094-100) for total
fat 098 (096-101) for animal fat 097 (093-102) for vegetable
fat 094 (088-101) for saturated fat 091 (079-104) for
polyunsaturated fat and 094 (088-100) for monounsaturated fat
For a 1 increase in energy from trans-unsaturated fat the values
were 092 (086-098) and for a 01 increase in energy from
omega-3 fat from fish the values were 109 (103-116)
Hunter et al (1996)
Pooled analysis of 7 prospective studies in 4 countries to establish estimates of the relation of fat
intake
to the risk of breast cancer
Studies included
33781
9 women
Not reported Breast cancer incidence
Information about 4980 cases from studies including 337819
women was available When women in the highest quintile of
energy-adjusted total fat intake were compared with women in the
lowest quintile the multivariate pooled relative risk of breast cancer
was 105 (95 CI 094 to 116) Relative risks for saturated
monounsaturated and polyunsaturated fat and for cholesterol
considered individually were also close to unity There was little
overall association between the percentage of energy intake from
fat and the risk of breast cancer even among women whose energy
intake from fat was less than 20
Ingram et al (1994)
Cohort study evaluating the role of vitamins in breast cancer mortality
103 women 3-months post-operation for primary breast cancer
Mean= 81-months
Mortality from breast cancer
27 women died ndash 21 with advanced breast cancer and 6 from other causes The most important findings from the nutrient consumption assessment were associated with vitamin consumption in particular beta-carotene and vitamin C At high levels of consumption there were significantly fewer deaths from breast cancer only one in the group of highest beta-carotene consumers compared with eight in the intermediate group and 12 in the lowest group (trend P = 00012) equivalent figures for vitamin C were 3 7 and 11 deaths for the highest intermediate and lowest consumption groups respectively (trend P = 00286)
Keinan-Boker et al (2004)
An investigation of the association between phytoestrogen
intake and
breast cancer risk in a large prospective study in
a Dutch
population with a habitually low phytoestrogen intake (EPIC)
15555 women aged
49ndash70
years who constituted a Dutch cohort the EPIC study
Median = 52-years
Breast cancer incidence
A total of 280 women were newly diagnosed with breast cancer
during follow-up The median daily intakes of isoflavones and
lignans were 04 (interquartile range 03ndash05) and 07 (05ndash08)
mgd respectively Relative to the respective lowest intake
quartiles the hazard ratios for the highest intake quartiles for
isoflavones and lignans were 10 (95 CI 07 15) and 07 (05
11) respectively Tests for trend were non-significant
Khaodhiar et al (2003)
A subgroup analysis of WINS participants (Chlebowski et al
53 women from 3 clinical
sites
2-years after start of
Insulin resistance and dietary fat
Of those women with initial insulin resistance after 1-year women in
the intervention group saw their fasting insulin decrease by 18 plusmn 34
40
2006a) examining relationships between dietary intake and insulin resistance
who had serum insulin and lipid profiles evaluated at baseline
and
after 2-years
commencing intervention
intake microUmL in comparison fasting insulin of women in the control
group decreased by only 138 plusmn 47 microUmL Although not
quite
statistically significant these results predict that elevated insulin concentrations (a marker of insulin resistance)
may be influenced by
dietary fat reduction There were no significant differences between
the treatment groups over time and no time x treatment interactions
and no significant differences were seen between the insulin-
resistant and non-insulin-resistant subgroups
Kim et al (2006)
The Nurseslsquo Health Study a prospective cohort study examining the relationship between dietary fat and incidence of breast
cancer in
post-menopausal women
Cohort of 80375 US women
Followed for 20-years between 1980 and 2000 with questionnaire being mailed every 2-years
Incidence of breast cancer The Food Frequency Questionnaire
The multivariable relative risk for an increment of 5 of energy from
total dietary fat intake was 098 (95 CI 095 100) Additionally
specific types of fat were not associated with an increased risk of
breast cancer Furthermore secondary analyses indicated no
differences in breast cancer risk by oestrogen receptor or
progesterone receptor status However stratification by
waist circumference indicated a significant decrease in breast
cancer risk for participants with a waist circumference of 35
inches (889cm) or greater (p-trend = 004)
Kyogoku et al (1992)
The present study utilised breast cancer patients whose dietary intake was assessed 10-years previously in a case-control study to determine whether dietary intake is related prognosis
212 breast cancer patients post-surgery
Followed-up until 1987 (9-12 years)
Mortality A total of 47 breast cancer deaths were certified The 5- and 10-year relative survival rates were 785 and 753 respectively The investigation did not provide any support for the hypothesis that a high-fat diet is a survival determinant for breast cancer patients
McEligot et al (2006)
Retrospective study into the influence of diet (fat fibre vegetable and fruit intakes and micronutrients (folate carotenoids and vitamin C) on overall survival in women diagnosed with breast cancer
Post-menopausal breast cancer survivors (n = 516)
Mean of 80-months post-diagnosis
Death due to any cause
The hazard ratio [HR and 95 CI] of dying in the highest tertile compared to the lowest tertile of total fat fibre vegetable and fruit was 312 (95 CI = 179-544) 048 (95 CI = 027-086) 057 (95 CI = 035-094) and 063 (95 CI = 038-105) respectively (P le 005 for trend except for fruit intake) Other nutrients including folate vitamin C and carotenoid intakes were also significantly associated with reduced mortality (P le 005 for trend)
Pierce et al (2007)
The multicentre WHEL RCT (see Gold et al 2009 in table)
Breast cancer (n=3088) intervention (n=1537) comparison (n=1551)
After 7-years of intervention
Invasive breast cancer event (recurrence
or
new primary) or death from any cause
Attrition in the intervention group (n=38) versus control group (n=27) There were no additional health benefits of dramatically increasing intake of nutrient-rich plant-based foods relative to the comparison group
Thomson et al (2007)
Sub-analysis of a purposive sample of participants in the WHEL RCT (see Gold et al 2009 in table)
Breast cancer patients (n=207)
Not reported Oxidative stress A significant inverse association was found between total plasma carotenoid concentrations and oxidative stress
41
WEIGHT
Caan et al (2008)
Retrospective study examining whether weight gain after diagnosis of breast cancer affects the risk of breast cancer recurrence Weight change from 1-year pre-diagnosis to study enrolment was calculated
3215 women with early stage breast cancer
Median of 737-months post-diagnosis
Breast cancer recurrence
Neither moderate (5ndash10) nor large (gt 10) weight gain (HR 08 95 CI 06ndash11 HR 09 95 CI 07ndash12 respectively) after breast cancer diagnosis was associated with an increased risk of breast cancer recurrence in the early years post-diagnosis
Enger et al (2004)
A retrospective cohort study using patient medical
records electronic
cancer registry data and archived tissue
specimens to examine
correlates of body weight with mortality in early-stage breast cancer
Women (n=1376)
24-
81 years of age diagnosed with breast cancer
Median=68 years post-diagnosis
Body weight at the time of diagnosis
and
patient status (ie alive and free of breast cancer living
with breast
cancer dead of breast cancer or dead of other
cause) at
the time of longest follow-up
246 patients died from breast cancer Among patients with early-
stage disease (I and IIA) a dose-response relationship was
observed with increasing weight and likelihood of dying of breast
cancer Compared with women in the lowest category of weight (lt133lb [60 kg] at diagnosis) women in the highest category ( 17
lb
[79 kg]) experienced a 25-fold increased risk of dying from breast
cancer (HR ratio 254 [95 CI 108-600] trend P = 02) Women
with ER-negative cancer experienced an approximately 2-fold
higher risk of dying from breast cancer compared with women with
ER-positive cancer regardless of stage at diagnosis Women in the
upper 50th percentile of weight with early-stage
disease and with
ER-negative tumours had a nearly 5-fold increased risk of dying
(HR ratio 499 [95 CI 217-1148] P for interaction = 10)
compared with women in the lower 50th percentile of weight
and ER-
positive tumours
Hebert et al (1998)
Prospective cohort study examining the effect of diet and body weight on recurrence and death in breast cancer patients
472 women diagnosed with early-stage breast cancer in 1982ndash1984
Ranged from 8-10 years
Breast cancer recurrence and mortality
After accounting for disease stage and age reported baseline consumption (timesday) of butter margarine and lard (risk ratio (RR)=167 95 CI=117ndash239) and beer (drinksday) (RR=158 95 CI=115ndash217) increased the risk of recurrence There also appeared to be an increased risk associated with consumption of red meat liver and bacon corresponding to about a doubling of risk for each time per day that foods in this category were consumed (RR=193 95 CI=089ndash415) Relative body weight increased risk at the rate of 9 (RR=109 95 CI=102ndash117) for
each kgm2 (equivalent to about 58 pounds for a woman 5 4 tall) For death the results were similar but relative weight was more strongly associated increasing risk by 12 per kgm2 (RR=112 95 CI=103ndash122)
Kroenke et al (2005)
A prospective study of a purposive subsample of participants from the Nurseslsquo Health Study ndash to determine
5204 Nurseslsquo Health Study participants
2-26 years with a median
Incident breast cancer
Weight before diagnosis was positively associated with breast
cancer recurrence and death but this was apparent only in never
smokers Similarly among never-smoking women those who
42
whether weight prior to diagnosis and weight gain
after diagnosis are
predictive of breast cancer survival
diagnosed with
incident invasive non-metastatic breast cancer between
1976
and 2000
follow-up of
9-years Breast cancer recurrence Mortality for any cause Self-reported BMI
gained between 05 and 20 kgm2 (median gain 60 lb relative risk
[RR] 135 95 CI 093 to 195) or more than 20 kgm
2 (median
gain 170lb RR 164 95 CI 107 to 251) after diagnosis had an
elevated risk of breast cancer death during follow-up (median 9
years) compared with women who maintained their weight (test for
linear trend P = 03) Associations with weight were stronger in
premenopausal than in postmenopausal women
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer
Breast cancer Not reported Additional breast cancer events and mortality
The most consistent finding from observational studies was that adiposity was associated with a 30 increased risk of mortality
SMOKING
Holmes et al (2007)
A prospective observational study among 5056 women from the Nurseslsquo Health Study for whom data on smoking history was available
Women with Stages I-III invasive breast cancer diagnosed between 1978 and 2002
Median = 83 years
Death by any cause Cause of death was ascertained from death certificates supplemented as needed with physician review of medical records
Compared with never smokers women who were current smokers had a 43 increased adjusted relative risk (RR) 95 CI 124-165] of death from any cause A strong linear gradient was observed with the number of cigarettes per day smoked p-trend lt00001 the RR (95 CI) for 1-14 15-24 and 25 or more cigarettes per day was 127 (101-161) 130 (108-157) and 179 (147-219) In contrast there was no association with current smoking and breast cancer death the RR (95 CI) was 100 (083-119) Current and past smokers were more likely than never smokers to die from primary lung cancer chronic obstructive pulmonary disease and other lung diseases
Fentiman et al (2005)
Cohort study testing the hypothesis that smokers have a worse breast cancer prognosis
Women (n=166) with stage III invasive breast cancer
Mean = 132-months
Overall and cancer-specific disease-free survival
Smoking was the third most important predictor of distant relapse-free breast cancer-specific and overall survival after stage and age at diagnosis
Manjer et al (2000)
Cohort study examining whether smoking is associated with prognostic markers other than more advanced disease (eg hormone receptor status histopathology and tumour differentiation)
268 women with recurring breast cancer drawn from a cohort of 10902 women (35 smokers)
An average of 124-years
Hormone receptor status identified by tumour tissue
The relative risk (RR) of oestrogen receptor-negative tumours was for current smokers 221 [95 CI 123-396] and for ex-smokers 267 (95 CI 141-506) compared to never-smokers Ex-smokers had an increased risk of progesterone receptor-negative tumours (RR = 161 95 CI 107-241) but there were no other significant associations between smoking habits and oestrogen receptor-positive or progesterone receptor-positive or ndashnegative tumours The incidence of Nottingham grade III tumours was higher in ex-smokers than in never-smokers (RR = 203 95 CI 117-354)
Sagiv et al (2007)
Cohort study examining the association between active and passive cigarette smoking before
Women with invasive breast cancer
Approximately 6-years after
All-cause mortality including breast
The adjusted hazards ratios (HRs) for all-cause mortality were slightly higher among current and former active smokers compared with never smokers (HR 123 95 CI 083ndash184) and 119 (95
43
breast cancer diagnosis and survival (n=1273) participating in a population-based casendashcontrol study
diagnosis cancer-specific mortality as reported to the National Death Index
CI 085ndash166) respectively) No association was found between active or passive smoking and breast cancer-specific mortality All-cause and breast cancer-specific mortality was higher among active smokers who were postmenopausal (HR 164 95 CI 103ndash260 and HR 145 95 CI 078ndash270 respectively) or obese at diagnosis (HR 210 95 CI 103ndash427 and HR 197 95 CI 089ndash436 respectively)
ALCOHOL
McDonald et al (2002)
Prospective cohort study examining the influence of alcohol consumption on breast cancer survival in African American women
Post-menopausal African-American women with invasive breast cancer (n=125)
Followed for survival through December 1998 (median = 648 months)
Survival Pre-morbid alcohol consumption of at least one drink per week was associated with 27-fold increase in risk of death (95 CI 13ndash58)
Reding et al (2009)
Sub-analysis of participants from two case-control studies to examine the effects on prognosis of alcohol consumption after breast cancer diagnosis
1286 women diagnosed with invasive breast cancer at age le45 years from two population-based case-control studies
Followed from their diagnosis of breast cancer (between January 1983 and December 1992) through to June 2002
The primary mortality endpoint used was all-cause mortality
After adjusting for age and diagnosis year compared with non-drinkers women who consumed alcohol in the 5 years before diagnosis had a decreased risk of death [gt0 to lt3 drinks per week hazard ratio 07 95 CI 06-095 3 to lt7 drinks per week risk ratio 06 95 CI 04-087 drinks per week risk ratio 07 95 CI 05-09]
Rock and Demark-Wahnefried (2002)
A review of evidence from clinical and
epidemiologic studies examining
the relationship between nutritional
factors and breast cancer survival
Women with breast cancer
Not reported Survival Alcohol intake was not associated with survival in the majority of the
studies that examined this relationship
44
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
colorectal cancer survival In the current review 2 studies were identified Studies are
summarised in Table 4 at the end of this section
In a cohort study self-reported leisure time physical activity was assessed in 41528
Australians among whom 526 cases of colorectal cancer were identified (Haydon et al
2006) Those who reported regular physical activity (at least once per week) prior to
diagnosis had improved cancer-specific survival (73 5-year survival) compared with
those not reporting regular physical activity (61 5-year survival) Another study of
stage III colorectal cancer survivors (n=816) over a 3-year period post-surgery and
chemotherapy showed increases in disease-free survival and overall survival with
increasing volumes of physical activity (p lt 05) (Meyerhardt et al 2005)
ii DIET
Bekkering et al (2006) report on six high fibre diet interventions that showed little effect on
the risk of colorectal cancer recurrence (McKeown-Eyssen et al 1995 MacLennan et al
1999 Alberts et al 2000 Bonithon-Kopp et al 2000 Schatzkin et al 2000 Ishikawa et al
2005) On combining data from two beta-carotene trials (Greenberg et al 1994
MacLennan et al 1999) four multivitamin trials (Greenberg et al 1994 Ponz and
Roncucci 1997 Hofstad et al 1998 McKeown-Eyssen et al 1995) and one trial containing
a multivitamin arm and an N-acetylcysteine (found in high protein foods) arm (Ponz and
Roncucci 1997) there was weak evidence of a reduction in risk of colorectal polyps
(abnormal growth of tissues in the colon) Two calcium interventions showed some
evidence of a reduced risk of recurrence (Baron et al 1999 Bonithon-Kopp et al 2000)
In the current review 5 studies provided further evidence for the role of diet in colorectal
cancer survival
Dietary Fibre
The association between dietary fibre and incidence of colorectal cancer was examined in all
participants (n=519978) taking part in the EPIC study (Bingham et al 2003) After 45-years
of follow-up self-reported dietary data for 1065 reported cases of colorectal cancer were
showed that higher dietary fibre was associated with a reduced risk of developing
large bowel cancer Interestingly the protective effect was greatest for the left side of the
colon and least for the rectum No food source of fibre was significantly more protective of
cancer incidence than others Confirmation of these findings after adjustment for folate and
with a longer follow-up has been reported (Bingham et al 2004 Norat et al 2005)
45
Red and Processed Meat
The EPIC study also offers support for the hypotheses that consumption of red and
processed meat increases colorectal cancer risk while intake of fish decreases risk
(Norat et al 2005) Meyerhardt et al (2007) support this further in a study examining dietary
patterns in stage III colorectal cancer survivors (n=1009) After a median of 53-years follow-
up a significant difference was found between those who had followed a prudentlsquo diet and
those who had followed a Westernlsquo diet
A higher intake of a Western dietary pattern post-diagnosis was associated with a
significantly worse disease-free survival (colon cancer recurrences or death) (p
lt001) The Western dietary pattern was associated with a similar detriment in overall
survival (p lt001)
Vitamin D
Ng et al (2008) examined pre-diagnosis levels of vitamin D in a cohort of participants with
colorectal cancer (n=304) from the Nursesrsquo Health Study28 which demonstrated that higher
plasma vitamin D levels were associated with a significant reduction in mortality from
any cause This indicates that lifestyle pre-diagnosis can produce post-diagnosis benefits
Dietary Supplements
A double-blind randomised placebo-controlled intervention study (the FAB2 Study) was
carried out with healthy controls (n=98) and patients with colorectal polyps (n=106) to
examine the effects of folic acid (a B vitamin found in leafy vegetables such as spinach
asparagus and lettuce) and riboflavin (a B-vitamin found in lean meats eggs nuts and
dairy products) supplements on biomarkers of colorectal cancer risk (Powers et al 2007)
Participants were randomised to receive one of four treatments
1) placebo capsule daily
2) 400μg of folic acid daily
3) 1200μg of folic acid daily
4) 400μg of folic acid with 5mg of riboflavin daily
28
One of the largest and longest running investigations of factors that influence womenlsquos health
comprising information from 238000 nurse-participants
Prudent diet High intake of fruit vegetables poultry and fish
Western diet
High intake of meat fat refined
grains sweets and desserts
46
Short-term low folic acid supplements in the range of 400μg were found to elicit a
significant increase in mucosal folate concentration causing a number of physiologic
responses that may reduce the risk of cancer recurrence This adds to the evidence that
increased fibre might be protective against cancer mortality since folate and fibre are
generally found in the same foods
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in colorectal
cancer recurrence In the current review 3 studies were identified
Dignam et al (2006) explored the impact of obesity via retrospective data from patients with
confirmed Dukes B or C colorectal cancer (n=4288) and found that very obese men and
women have an increased risk of recurrence In contrast the multicentre prospective
observational CALBG 8980 trial has shown that increased BMI during and 6-months after
adjuvant chemotherapy for stage III colorectal cancer (n=1053) was not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008)
Sinicrope et al (2010) categorised stage II and III colon cancer (n=4381) patients enrolled
in seven RCTs whilst undergoing adjuvant chemotherapy according to their BMI They
found that BMI was significantly associated with both disease-free survival and overall
survival in both men and women when compared to normal-weight controls Being
overweight was associated with improved overall survival in men whilst being underweight
was associated with significantly worse overall survival in women This demonstrates that
obesity is an independent prognostic variable in colon cancer survivors as well as showing
gender-related differences that require further investigation
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in colorectal
cancer survival and no studies were identified in the current review
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in colorectal
cancer survival Preliminary EPIC results indicate that current alcohol intake is
significantly positively associated with risk of rectal but not of colon cancer (Ferrari et
al (2007)
47
SUMMARY OF LIFESTYLE EVIDENCE FOR COLORECTAL CANCER ndash
MECHANISMS OF BENEFIT
Physical Activity There is very little evidence available for the role of physical activity in
colorectal cancer outcomes however the evidence that is available looks promising
Specifically regular physical activity of at least once per week pre-diagnosis has been found
to improve 5-year survival rates (Haydon et al 2006) This highlights the importance of
physical activity being integrated into an individuallsquos way of life even before the occurrence
of illness Furthermore long-term physical activity post-surgery can further increase chances
of recurrence-free survival and there is also evidence of a dose-effect survival benefits
increase with amount of exercise (Meyerhardt et al 2005)
Diet Whilst evidence for dietary fibre has been mixed the additional evidence presented
within this review places greater weight in favour of increased dietary fibre Indeed the
conclusion of one study was that in populations with low average intake of dietary fibre an
approximate doubling of total fibre intake from foods could reduce the risk of colorectal
cancer by 40 (Bingham et al 2003) Evidence of this protective benefit for dietary fibre is
further supported by research demonstrating that short-term low folic acid (found in fibrous
foods) supplements in the range of 400μg can reduce the risk of cancer recurrence (Powers
et al 2007) There is a general consensus that mechanisms of benefit from dietary fibre
come from increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic mucosa (tissue
that lines the colon) (Kim 2000) Evidence has also been presented supporting the
hypothesis that red and processed meat increases colorectal cancer risk while fish
decreases risk (Norat et al 2004)
Weight Two large-scale studies offer contrasting findings for the role of weight
in colorectal cancer outcomes One prospective observational study demonstrates that
increased BMI during and 6-months after adjuvant chemotherapy is not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008) The other
retrospective study demonstrates that very obese men and women have an increased risk
of recurrence Drawing on 7 RCTs Sinicrope et al (2010) provides further evidence for BMI
was being significantly associated with both disease-free and overall survival Overall there
is greater evidence showing weight to be an important predictor of colorectal cancer
outcomes There is also some evidence of gender differences being overweight was
associated with improved overall survival in men whilst being underweight was associated
with significantly worse overall survival in women There is evidently a need to explore this
differential effect more closely However there is also the need to consider the impact of
body composition on the development of other chronic conditions including diabetes and
cardio-respiratory conditions
Smoking and Alcohol Further research is needed into smoking and alcohol
consumption especially in terms of colorectal cancer prognosis There is some evidence
indicating that current alcohol intake increases risk of rectal but not colon cancer a finding
that requires further investigation to ascertain underlying mechanisms of benefit (Ferrari et
al 2007) Since alcohol can reduce absorption of folate it is possible that the mechanism
48
of benefit is as with dietary fibre intake related to stool bulk and less contact time between
carcinogens and colonic mucosa
49
Table 4 Colorectal Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Haydon et al (2006)
Incident cases of colorectal cancer were identified among participants of the Melbourne Collaborative Cohort Study and examined against self-reported physical activity
526 Australians with colorectal cancer
Median = 55 years
Body fat Disease-specific survival
Exercisers had an improved disease specific survival (hazard ratio 073 (95 CI 054ndash100) The benefit of exercise was largely confined to stage IIndashIII tumours (hazard ratio 049 (95 CI 030ndash079) Increasing per cent body fat resulted in an increase in disease-specific deaths (hazard ratio 133 per 10 kg (95 CI 104ndash171) Similarly increasing waist circumference reduced disease specific survival (hazard ratio 120 per 10 cm (95 CI 105ndash137)
Meyerhardt et al (2005)
Prospective study of recreational physical activity and prognosis
among
stage III colon cancer patients enrolled in a
RCT of post-operative adjuvant
chemotherapy (bolus 5-
fluorouracilleucovorin +- irinotecan)
816 patients with stage III colon cancer
Midway through adjuvant therapy and again 6-months post-therapy (12ndash14 months after enrolment)
Physical activity levels were measured as MET-hours-per-week Disease-free survival
Levels of physical activity were associated with significantly improved
disease-free survival among patients with stage III colon cancer After
adjustment for age gender baseline performance status N stage T
stage preoperative CEA bowel obstruction and perforation level of
differentiation treatment arm and body mass index the hazard ratio
(HR) for DFS for individuals in the highest quintile (gt25 MET-
hoursweek eg Jog 3ndash4 hoursweek or brisk walk [3ndash4 mph] daily)
was 065 (95 CI 038ndash111 p for trend = 002) compared to those
in the lowest quintile of PA This relationship varied by gender with a
HR = 033 [95 CI 011ndash099] for women (p for trend = 0046) and a
HR= 089 [95 CI 044ndash178] for men (p for trend = 03)
DIET
Bingham et al (2003)
Prospective examination of the association between dietary fibre intake and incidence of colorectal cancer in individuals taking part in the EPIC study recruited from ten European countries
519978 men and women in the EPIC study (1065 cases of colorectal cancer)
45 years
Colorectal cancer incidence
Dietary fibre in foods was inversely related to incidence of large bowel cancer (adjusted relative risk 0middot75 [95 CI 0middot59ndash0middot95] for the highest versus lowest quintile of intake) the protective effect being greatest for the left side of the colon and least for the rectum After calibration with more detailed dietary data the adjusted relative risk for the highest versus lowest quintile of fibre from food intake was 0middot58 (0middot41ndash0middot85)
Meyerhardt et al (2008)
Prospective observational study to
determine the association of dietary patterns
with cancer recurrences and
mortality of colon cancer survivors
1009 patients with stage III colon cancer who were
enrolled in
a randomized
Median = 53-years
Colon cancer recurrence and mortality
A higher intake of a Western dietary pattern after cancer diagnosis
was associated with a significantly worse disease-free survival (colon
cancer recurrences or death) Compared with patients in the lowest
quintile of Western dietary pattern those in the highest quintile experienced an adjusted hazard
ratio (AHR) for disease-free survival
of 325 (95 confidence interval [CI] 204-519 P for trend lt001)
50
adjuvant chemotherapy trial (CALGB
89803)
The Western dietary pattern was associated with a similar detriment
in recurrence-free survival (AHR 285 95 CI 175-463) and overall
survival (AHR 232 95 CI 136-396]) comparing highest to
lowest quintiles (both with P for trend lt001)
Ng et al (2008)
Nurseslsquo Health Study prospective examination of the association between pre-diagnosis
25(OH)D levels and
mortality in colorectal cancer patients
304 colorectal cancer patients
Mean = 78-months for participants still alive
Colorectal cancer mortality
Higher plasma 25(OH)D levels were associated with a significant
reduction in overall mortality (P for trend = 02)
Compared with the lowest quartile participants in the highest
quartile had an adjusted HR of 052 (95 CI 029 to 094) for
overall mortality A trend toward improved colorectal cancerndash
specific mortality was also seen (HR = 061 95 CI 031 to 119)
Norat et al (2005)
The EPIC prospective study of 478040 cancer-free men and women from 10 European countries examining meat fish and colorectal cancer risk
478040 cancer-free men and women taking part in the EPIC study
Mean=48 years
Colorectal cancer incidence
Colorectal cancer risk was positively associated
with intake of red and processed meat (highest [gt160
gday] versus lowest [lt20 gday] intake HR = 135 95 CI = 096
to
188 Ptrend = 03) and inversely associated with intake of fish (gt80
gday versus lt10 gday HR = 069 95 CI = 054 to
088 Ptrendlt001) but was not related to poultry intake In this study
population the absolute risk of development of colorectal
cancer within 10-years for a study subject aged 50 years was 171
for the highest category of red and processed meat intake and 128
for the lowest category of intake and was 186 for subjects in
the lowest category of fish intake and 128 for subjects in
the highest category of fish intake
Powers et al (2007)
A double-blind RCT (the FAB2 Study) to examine effects of folic acid and riboflavin supplements on biomarkers of colorectal cancer risk Participants were randomised to receive one of the following for 6 ndash 8 weeks 1)400μg of folic acid 1200μg of folic acid or 400μg of folic acid plus 5 mg of riboflavin 2) placebo
Healthy controls (n=98) and patients with colorectal polyps (n=106)
On completion of 6-8 week intervention
Biomarkers of folate and riboflavin status
Supplementation with folic acid elicited a significant increase in mucosal 5-methyl tetrahydrofolate and a marked increase in RBC and plasma with a dose-response Measures of riboflavin status improved in response to riboflavin supplementation Riboflavin supplement enhanced the response to low-dose folate in people carrying at least one T allele and having polyps The magnitude of the response in mucosal folate was positively related to the increase in plasma 5-methyl tetrahydrofolate but was not different between the healthy group and polyp patients
WEIGHT
Dignam et al (2006)
Investigating the association between BMI and colorectal cancer outcomes in patients from cooperative group clinical trials
4288 patients with Dukes
BC
colon cancer in National
Median =112-
years Risk of recurrence second primary
Very obese patients (BMI 35 kgm2) had greater risk
of a
colon cancer event (recurrence or secondary primary tumour hazard
ratio [HR] = 138 95 confidence interval [CI] = 110 to 173) than
normal weight patients (BMI = 185ndash249 kgm
2) Mortality was
51
Surgical Adjuvant Breast and Bowel Project
RCTs
cancer and
mortality evaluated in
relation to
BMI at diagnosis
greater for very obese (HR = 128 95 CI = 104 to 157) and
underweight (BMI lt 185 kgm2) (HR
= 149 95 CI = 117 to 191)
than for normal weight patients The increased risk of mortality for
underweight patients was dominated by nonndashcolon cancer deaths
(HR of such deaths compared with normal weight patients = 223 95 CI = 150 to
331) whereas for the very obese deaths likely due
to colon cancer were increased (HR = 136 95 CI = 106 to 173)
Meyerhardt et al (2008)
A prospective observational study of patients who had stage III colon cancer and who enrolled on a RCT of adjuvant chemotherapy Results
1053 patients who had stage III colon cancer
6-months post- chemotherapy
Patients were observed for cancer recurrence or death
Increased BMI was not significantly associated with a higher risk of colon cancer recurrence or death (P trend = 54) Compared with normal-weight patients (BMI 21 to 249 kgm
2) the multivariate
hazard ratio for disease-free survival was 100 (95 CI 072 to 140) for patients with class I obesity (BMI 30 to 349 kgm
2) and 124
(95 CI 084 to 183) for those with class II to III obesity (BMI ge 35 kgm
2) after analysis was adjusted for tumour-related prognostic
factors physical activity tobacco history performance status age and sex Similarly after analysis was controlled for BMI weight change (either loss or gain) during the time period between ongoing adjuvant therapy and 6-months after completion of therapy did not significantly impact on cancer recurrence andor mortality
Sinicrope et al (2010)
BMI (kgm2) was categorised in patients
with tumour-node-metastasis stage II and III colon carcinomas enrolled in seven RCT of 5-fluorouracilndashbased adjuvant chemotherapy to determine the association of BMI with disease-free survival and overall survival
Men and women with stage II and III colon carcinomas (n = 4381) enrolled in seven RCTs of 5-fluorouracilndashbased adjuvant chemotherapy
Not reported Disease-free survival Overall survival
BMI was significantly associated with both disease-free survival (P = 0030) and overall survival (P = 00017) Men with class 23 obesity showed reduced overall survival compared with normal-weight men [hazard ratio 135 95 CI 102-179 P = 0039] Women with class I obesity had reduced overall survival [hazard ratio 124 95 CI 101-153 P = 0045] compared with normal-weight women Overweight status was associated with improved overall survival in men (P = 0006) and underweight women had significantly worse overall survival (P = 0019)
ALCOHOL
Ferrari et al (2007)
As part of the prospective EPIC study data was collected examining the relationship between lifetime and baseline alcohol consumption and colorectal cancer incidence
478732 EPIC subjects free of cancer at enrolment between 1992 and 2000
62 years Colorectal cancer incidence
Lifetime alcohol intake was significantly positively associated to CRC risk (hazard ratio HR = 108 95CI = 104-112 for 15 gday increase) with higher cancer risks observed in the rectum (HR = 112 95CI = 106-118) than distal colon (HR = 108 95CI = 101-116) and proximal colon (HR = 102 95CI = 092-112) Similar results were observed for baseline alcohol intake When assessed by alcoholic beverages at baseline the CRC risk for beer
52
(HR = 138 95CI = 108-177 for 20-399vs 01-29 gday) was higher than wine (HR = 121 95CI = 102-144) although the two risk estimates were not significantly different from each other Higher HRs for baseline alcohol were observed for low levels of folate intake (113 95CI = 106-120 for 15 gday increase) compared to high folate intake (103 95CI = 098-109)
53
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
prostate cancer survival In the current review 2 studies were identified Studies are
summarised in Table 5 at the end of this section
The underlying mechanisms for the direct anti-cancer effect of lifestyle has been indicated in
a study with men undergoing a diet and physical activity intervention comprising the majority
of calories from complex carbohydrates high in fibre combined with 1-hour of supervised
exercise (Soliman et al 2009) Serum (blood plasma) was taken from these men and added
to androgen-dependent LNCaP cells29 in the laboratory There was decreased growth and
increased apoptosis (cell death) associated with a reduction in serum Insulin-like Growth
Factor (IGF)-130 These findings indicate that diet and physical activity interventions
might slow prostate cancer progression as well as aid in its treatment during the early
stages of development
Kenfield (2010) examined the data of 2686 men from the Health Professionals Follow-Up
Study31 and found that men who engaged in 3gt MET-hours of weekly physical activity
post-diagnosis reduced their risk of death by 35 compared with men who engaged
in less weekly activity Furthermore men who walked 90-minutes per week at a normal to
brisk pace had a 51 lower risk of death due to any cause compared with men who walked
90-minutes or less at an easy pace To reduce their risk of cancer-specific death men
had to engage in vigorous activity such as jogging (6 MET-hours)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in prostate cancer
survival In the current review 7 studies were identified
Dietary Changes plus Supplements
Ornish et al (2005) conducted a diet counselling and lifestyle RCT comprising men with
early prostate cancer (n=93) The lifestyle changes in this study included a vegan diet
supplemented with soy vitamin E fish oils selenium and vitamin C together with a
moderate physical activity program and stress management techniques such as yoga
29
Human prostate cancer cells
30 IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of pathological states including cancer
31 An all-male (n=51529) study designed to complement the all-female Nurses Health Study
54
Prostate Specific Antigen (PSA)32 levels decreased by 4 at 12-months in the
intervention group but increased by 6 in the control group this was statistically
significant and strongly correlated with the degree of lifestyle change However the
intensity of this intervention and associated behavioural changes might not easily be
translated into practice (White et al 2009)
Pomegranate Juice
The potential benefits of pomegranate juice on prostate cancer outcomes frequently appear
in the media and strong evidence of its efficacy can be found within the academic literature
In a phase II open-label single-arm clinical trial men (n=46) with recurrent prostate cancer
who had rising PSA after surgery or radiotherapy were treated daily with 8oz (227g)
equivalent of pomegranate juice (Pantuck et al 2006) Mean PSA doubling time
significantly increased with treatment from 15-months to 54-months demonstrating a
good indication of a relationship between the consumption of pomegranate juice and
prostate health
Green Tea
Another beverage found to demonstrate some positive effects on prostate cancer is green
tea Bettuzzi et al (2006) in a year-long clinical trial has demonstrated that daily
consumption of green tea can produce a ten-fold decrease in the rate at which
prostate intraepithelial neoplasia (a pre-cancerous condition) progresses to prostate
cancer Support for these findings is offered by an uncontrolled open-label single-arm
phase II clinical trial testing the efficacy of Polyphenon E which contains the polyphenol
antioxidants found in green tea (McLarty et al 2009) Taking four capsules of
Polyphenon E daily (equivalent to twelve cups of green tea) for an average of 345
days leading up to radical prostatectomy the participants (n=26) experienced
significant reductions in biomarkers used to monitor likelihood of metastasis Some
patients demonstrated reductions greater than 30
Lycopene Supplements
The EPIC study has demonstrated that similar to breast cancer prostate cancer risk is not
related to fruit and vegetable consumption (Key et al 2004) However further evidence for
the role of carotenoids found in fruit and vegetables have been provided from a pilot RCT
including men with benign prostatic hyperplasia (BPH) a benign enlargement of the prostate
that can progress to cancer (Schwarz et al 2008) Men (n=20) who received 15mg od
lycopene supplementation (a carotenoid found in tomatoes and other red fruits and
32
PSA is a protein produced by the cells of the prostate gland It is present in small quantities in the serum of normal men and is often elevated in the presence of prostate cancer
55
vegetables) for 6-months had significantly decreased PSA levels compared to a
placebo group (n=20) who had no change in PSA
Salicylate
Salicylate33 intake has been implicated in the aetiology of prostate cancer but Thomas et al
(2009) have evaluated their influence on established cancer progression In a randomised
double blind phase II study involving men (n=110) with progressive prostate cancer who
were counselled to eat less saturated fat and processed food more fruit vegetables and
legumes physical activity more regularly and to stop smoking the men were then
randomised to take sodium salicylate alone or combined with vitamin C copper and
manganese gluconates34 daily Although there was no difference in outcome between those
who received sodium salicylate alone or combined the intervention as a whole (ie
including dietary counselling) slowed or stopped the rate of PSA progression in 40
patients (364) for over one-year and a further ten patients were stabilised for 10-
months This data suggests that changes in lifestyle can potentially delay PSA progression
and the need for more radical therapy highlighting an area for further research
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in prostate cancer
survival In the current review 2 studies were identified
Wright et al (2007) prospectively examined BMI and weight change in relation to prostate
cancer incidence and mortality in 287760 men enrolled in the National Institutes of
Health-AARP Diet and Health Study Higher baseline BMI was associated with
significantly reduced total prostate cancer incidence on the one hand but with
significantly increased risk of prostate cancer mortality on the other hand Adult weight
gain from age 18-years to study entry (range=50-71-years old) was positively associated
with prostate cancer staging but not with disease incidence
In a retrospective analysis exploring the interaction between obesity and surgical outcomes
in patients with prostate cancer treated by radical prostatectomy (n=437) a weak but
significant association was observed between BMI and a number of biological
biomarkers indicative of an advanced pathological stage (Gross et al 2009)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in prostate
cancer survival and no evidence was identified in the current review
33
Salicylates are chemicals that occur naturally in many plants including many fruits vegetables and herbs
Salicylates in plants act as a natural immune hormone and preservative protecting the plants against diseases
insects fungi and harmful bacteria 34
A pinkish powder soluble in water used in medicine in vitamin tablets and as a feed additive and dietary
supplement
56
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in prostate cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR PROSTATE CANCER -
MECHANISMS OF BENEFIT
Physical Activity and Diet The evidence within this review indicates that diet and physical
activity interventions might slow prostate cancer progression as well as aid in its treatment
during the early stages of development The mechanism of benefit is primarily via
decreased growth and increased apoptosis (cell death) associated with a reduction in serum
Insulin-like Growth Factor (IGF)-1 (Soliman et al 2009) Up to 3gt MET-hours of weekly
physical activity appears sufficient to increase survival with more vigorous activity of about 6
MET-hours per week for the reduction of cancer-specific mortality (Kenfield 2010) A
number of dietary steps can be taken to reduce PSA levels and thus slow down the growth
of tumours and increase survival For example a vegan diet supplemented with soy vitamin
E fish oils selenium and vitamin C together with a moderate physical activity program and
stress management techniques such as yoga have been found useful (Ornish et al 2005)
as has pomegranate juice (Pantuck et al 2006) and green tea (Betuzzi et al 2006 McLarty
et al 2009) As with breast cancer carotenoids have been found to offer protective
properties for men with benign prostatic hyperplasia which can progress to cancer (Schwarz
et al 2008) Overall the evidence for prostate cancer is suggestive of survival benefits from
combined dietary and physical activity changes In other words it appears that a healthier
diet made up of fruit and vegetables as well as drinks such as pomegranate juice or green
tea combined with 3gt MET-hours of weekly physical activity could be an effective
prescription for reducing mortality from cancer and other causes
Weight Evidence for weight was mixed whilst finding that higher baseline BMI was
associated with significantly reduced total prostate cancer incidence a significant increase in
prostate cancer severity and mortality was also observed with higher BMI levels (Wright et
al 2007a Gross et al 2009) More research is clearly needed to establish any differential
prostate cancer outcomes associated with weight
Smoking and Alcohol More research is required for smoking and alcohol in terms of
prostate cancer outcomes
57
Table 5 Prostate Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Kenfield et al (2009)
Prospective study (Health Professionals Follow-up Study) assessing the relationship between physical activity and duration and pace of walking with total and prostate cancer-specific mortality
2686 men with prostate cancer
4-years Prostate cancer mortality and total physical activity
Men who were physically active especially those engaging in 3 or more MET-hours of total activity had a 35 lower risk of death from any cause (hazard ratio 065 [95 CI 052 082]) and a modest non-significant reduction in risk of prostate cancer death (hazard ratio 088 [95 CI 052 149]) after adjustment for other risk factors for PCa mortality and pre-diagnosis physical activity While no benefit from walking was observed for PCa mortality men who walked 4 or more hours per week versus those who walked less than 20 minutes per week had a 23 lower risk of all-cause mortality (95 CI 061 097 p-trend=001) In addition compared to men who walked less than 90 minutes at an easy walking pace those who walked 90 or more minutes at a normal to very brisk pace had a 51 lower risk of all-cause mortality (95 CI 037 064) More vigorous activity and longer duration of activity was associated with significant further reductions in risk for all-cause mortality More vigorous activity was associated with a borderline-significant reduction in risk for PCa mortality
Soliman et al (2009)
Pritikin Longevity Center 3-Week
Residential Program - men were given prepared
meals with 12ndash15 fat calories
15ndash20 protein calories and the majority
of calories (65ndash70) from unrefined complex carbohydrates high in fibre (gt40 gday) The men attended daily supervised exercise classes
for 60 min
5 men in their early sixties
with no
signs of prostate cancer (PSA lt 40)
On completion of the 3-week programme
Cancer progression
The intervention slowed growth and increased apoptosis in LNCaP cells responses that were eliminated when
IGF-I was added back to
the post-intervention samples The p53 protein content was increased
and NFkB activation reduced in the post serum-stimulated LNCaP
cells Similar results were observed when the IGF-I receptor was
blocked in the pre-intervention serum In androgen-independent PC-3
cells growth was reduced while none of the other factors were
changed by the intervention
DIET
Bettuzzi et al (2006)
A proof-of-principle double-blind placebo-
controlled clinical trial assessing the safety
and efficacy of green tea catechins for the
chemoprevention of prostate cancer incidence in patients with high-grade prostate intraepithelial
neoplasia Daily
treatment consisted of three GTCs
Men with high-grade prostate intraepithelial
neoplasia who would develop cancer within
1-year
3-monthly for 1-year
Primary outcome prostate cancer incidence Secondary outcome
After 1 year only one tumour was diagnosed (incidence 3) in the
cohort receiving green tea whereas 9 cancers were found among the placebo-treated
men (incidence 30) Total PSA did not
change
significantly between the two arms but green tea-treated men showed
values constantly lower with respect to placebo-treated ones As a
secondary observation administration of green tea also reduced lower
urinary tract symptoms suggesting that these compounds might also
58
capsules 200 mg each (total 600 mgd) (n=60) PSA levels be of help for treating the symptoms of benign prostate hyperplasia
Key et al (2004)
An examination of the association between self-reported consumption of fruits and vegetables and prostate cancer risk in EPIC participants
130544 men in 7 countries recruited into EPIC
Median = 48 years
Prostate cancer incidence
There were 1104 incident cases of prostate cancer No significant associations between fruit and vegetable consumption and prostate cancer risk were observed Relative risks (95 CI) in the top fifth of the distribution of consumption compared to the bottom fifth were 106 (084 ndash134) for total fruits 100 (081ndash122) for total vegetables and 100 (079 ndash126) for total fruits and vegetables combined intake of cruciferous vegetables was not associated with risk
McLarty et al (2009)
In order to determine the effects of short-term supplementation with the active compounds in green tea on serum biomarkers in patients with prostate cancer daily doses were provided of Polyphenon E which contained a total of 13 g of tea polyphenols until time of radical prostatectomy
26 men with positive prostate biopsies scheduled for radical prostatectomy
Not reported PSA levels Biomarkers of prostate cancer decreased significantly All of the liver function tests also decreased five of them significantly total protein albumin aspartate aminotransferase alkaline phosphatase and amylase
Ornish et al (2005)
Lifestyle changes including a vegan diet supplemented with soy vitamin E fish oils selenium and vitamin C together with a moderate physical activity program and stress management techniques such as yoga
Men with early prostate cancer (n=93) Gleason scores less than 7
12-months into the intervention
PSA and serum stimulated LNCaP cell growth
PSA levels decreased by 4 at 12-months in the intervention group but increased by 6 in the control group this was statistically significant and strongly correlated with the degree of lifestyle change
Pantuck et al (2006)
A phase II two-stage clinical trial to determine the effects of pomegranate juice PSA progression in men with a rising PSA following primary therapy Patients were treated with 8 ounces of pomegranate juice daily (570mg total polyphenol gallic acid equivalents) until disease progression
46 men with rising PSA levels post-treatment (surgery or radiotherapy)
Every 3-monhs for 54-months
PSA levels Mean PSA doubling time significantly increased with treatment from a mean of 15 months at baseline to 54 months post-treatment (P lt 0001) In vitro assays comparing pre-treatment and post-treatment patient serum on the growth of LNCaP showed a 12 decrease in cell proliferation and a 17 increase in apoptosis (P = 00048 and 00004 respectively) a 23 increase in serum nitric oxide (P = 00085) and significant (P lt 002) reductions in oxidative state and sensitivity to oxidation of serum lipids after versus before pomegranate juice
Schwarz et al (2008)
15mg od lycopene supplementation for 6-months or placebo
Men with benign prostatic hyperplasia (n=40)
After 6-months of intervention
Inhibition or reduction of increased serum PSA levels
Men receiving 15mg od lycopene supplementation had significantly decreased PSA levels compared to a placebo group who had no change in PSA
Thomas et al (2009)
A randomised double blind phase II study to evaluate the influence of salicylate and lifestyle on established cancer progression Men were counselled
110 men whose PSA had risen in 3 consecutive
Not reported Prostate cancer progression (PSA levels)
Although there was no difference in outcome between the SS or CV247 (21 v 19 p=092) the intervention slowed or stopped the rate of PSA progression in 40 patients (364) for over one year A further ten patients were stabilised for ten months Patients least likely to stabilise
59
to eat less saturated fat processed food more fruit vegetables and legumes exercise more regularly and to stop smoking They were then randomised to take sodium salicylate (SS) alone or SS combined with vitamin C copper and manganese gluconates (CV247) daily without other intervention
values gt20 over the preceding 6-months
had received previous radiotherapy or had a Gleason =7 These men welcomed this addition to active surveillance
WEIGHT
Gross et al (2009)
A retrospective cohort study examining whether changes in components of the sex steroid receptor axis may contribute to the clinical aggressiveness of prostate cancer in obese patients
539 patients treated with radical prostatectomy at a single urban hospital between 1994 and 2002
Not reported Pathological stage of prostate cancer BMI
Higher BMI correlated strongly with higher pathologic stage In comparing obese versus non-obese patients there was no difference in expression of androgen or oestrogen related proteins in cancerous epithelial cells However there was a down-regulation of aromatase in the stoma of obese patients suggesting obesity may cause stromal changes in the sex steroid production and signalling pathways which may affect prostate cancer growth via intracrineparacrine mechanisms
Wright et al (2007)
A prospective examination of BMI and adult weight change in relation to prostate cancer incidence and mortality
287760 men ages 50 years to 71 years at enrolment (1995-1996) in the National Institutes of Health-AARP Diet and Health Study
6-years Prostate cancer incidence Weight gain (BMI)
Higher baseline BMI was associated with significantly reduced total prostate cancer incidence largely because of the relationship with localized tumours (for men in the highest BMI category [gtor=40 kgm (2)] vs men in the lowest BMI category [lt25 kgm (2)] RR 067 95 CI 050-089 P = 0006) Conversely a significant elevation in prostate cancer mortality was observed at higher BMI levels (BMI lt25 kgm(2) RR 10 [referent group] BMI 25-299 kgm(2) RR 125 95 CI 087-180 BMI 30-349 kgm(2) RR 146 95 CI 092-233 and BMI gtor=35 kgm(2) RR 212 95 CI 108-415 P = 02) Adult weight gain from age 18 years to baseline also was associated positively with fatal prostate cancer (P = 009) but not with incident disease
60
d) LUNG CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in lung
cancer survival and one systematic review with meta-analysis was identified in the current
review Studies are summarised in Table 6 at the end of this section
Tardon et al (2005) conducted a systematic review and meta-analysis of cohort and case-
control studies from 1966 through October 2003 evaluating the relationship between
physical activity and lung cancer incidence Nine studies were identified 6 of which
demonstrated that that higher levels of leisure-time physical activity (walking gardening
swimming) protects against lung cancer (Severson et al 1989 Thune et al 1997 Lee et
al 1999 Sellers et al 1991 Kubik et al 2002 Mao et al 2003) The estimated combined
risk for both genders was statistically significant as was a dose-response relationship (p lt
01)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in lung cancer
survival and no evidence was identified in the current review
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in lung cancer
survival and no evidence was identified in the current review
iv SMOKING
Smoking has long been accepted as an unhealthy behaviour that increases the risk of
cancer incidence and disease outcomes Yet many people continue to smoke pre- and post-
diagnosis one-third to one-half of cancer patients either continue to smoke after diagnosis or
relapse after initial quit attempts (Gritz et al 2006) Bekkering et al (2006) do not provide
any evidence for the role of smoking in lung cancer survival In the current review 5 studies
were identified that further highlight the importance of smoking cessation support for people
living with and beyond cancer
Vineis et al (2007) have estimated exposure to Environmental Tobacco Smoke (ETS) and to
air pollution in never smokers and ex-smokers in EPIC study participants (n=520000) The
proportion of lung cancers in never- and ex-smokers attributable to ETS was
estimated to be between 16 and 24 mainly due to the contribution of work-related
exposure
61
In two studies of survivors of stage I and II small cell lung cancer risk of a second cancer
was 35-44-fold higher than in the general population (Richardson et al 1993 Tucker et
al 1997) In those who continued to smoke the risk was far higher particularly in those who
also received chest irradiation and alkylating agents35 (Tucker et al 1997) highlighting the
need for risk assessment when offering smoking cessation support or advice
Another study in Japan confirmed that patients with small cell lung cancer who survive
at least 2-years greatly reduced their likelihood of a second cancer if they quit
smoking (p lt 05) (Kawahara et al 2002) Additionally smoking has been found to be
an independent risk factor in breast cancer survivors developing lung cancer (Ford et
al 2003) In support of these studies Parsons et al (2010) report that nine of ten studies
identified in a review of literature from 1966 to 2008 indicate that continuing to smoke is
associated with a significantly increased risk of all-cause mortality in early stage non-
small cell lung cancer and of all-cause mortality in limited stage small cell lung
cancer
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in lung cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR LUNG CANCER - MECHANISMS OF
BENEFIT
Smoking Evidence for the role of lifestyle factors on lung cancer progression and
recurrence has primarily examined smoking which is a strongly established risk factor for
disease progression and mortality Continuing to smoke exposes the body to high levels of
carcinogens which can cause further DNA damage to existing cancers encourage the
cancer to mutate into a more aggressive type or develop mechanisms to hide from the
bodylsquos immunological defences (Akopyan and Bonavida 2006) Indeed smoking has been
found to suppress the immune system interfering with the function of natural killer (NK) cells
- a lymphoid cell type that plays a role in the surveillance of tumour growth Patients who
have already developed one cancer are likely to be more susceptible to DNA damage from a
pre-existing genetic vulnerability or acquired damage from chemotherapy or radiotherapy
Avoiding carcinogens may therefore have a benefit in reducing the risk of developing
further cancers in patients who may be more susceptible from a pre-existing genetic
signature or damage from chemotherapy or radiotherapy The smoking cessation initiatives
currently sweeping the nation such as NHS Choices bdquoSmokefree‟ remain invaluable as
smoking continues to be an important preventable cause of morbidity and mortality
worldwide
Additional Lifestyle Factors More research is required into lifestyle factors such as diet
physical activity weight and alcohol consumption in terms of lung cancer outcomes Access
35
Cytotoxic agents used to disrupt cancer cells can damage healthy cells in the process
62
to lifestyle services such as post-treatment rehabilitation fitness planning and nutritional
support was highlighted as an important component within the disease trajectory for people
with lung cancer (NCSI Mapping Project 2009) There is evidence for the benefits of
physical activity in reducing lung cancer incidence however there is a paucity of evidence
for the survivorship period of lung cancer
63
Table 6 Lung Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Tardon et al (2004)
A meta-analysis of studies (1966-2003) evaluating the relationship between physical activity and lung cancer
Men and women in cohort and case-control studies (9 studies)
Not reported
Lung cancer incidence
The combined ORs were 087 (95 CI=079ndash095) for moderate leisure-time physical activity (LPA) and 070 (062ndash079) for high activity (p trend = 000) This inverse association occurred for both sexes although it was somewhat stronger for women No evidence of publication bias was found Several studies were able to adjust for smoking but none adjusted for possible confounding from previous malignant respiratory disease
SMOKING
Ford et al (2003)
Retrospective analysis of smoking radiation and both exposures on lung carcinoma development in women who were treated previously for breast carcinoma
Case patients (n = 280) females aged 30-89 years with breast carcinoma prior to primary lung carcinoma Control patients (n = 300) selected randomly from 37000 patients with breast carcinoma treated at The University of Texas M D Anderson Cancer Center
Not reported
Lung cancer incidence
At the time of breast carcinoma diagnosis 84 of case patients had ever smoked cigarettes compared with 37 of control patients whereas 45 of case patients and control patients received XRT for breast carcinoma Smoking increased the odds of lung carcinoma in women without XRT (odds ratio [OR] 60 95 confidence interval [95 CI] 36-101) but XRT did not increase lung carcinoma risk in non-smoking women (OR 05 95 CI 03-11) Overall the OR for both XRT and smoking compared with no XRT or smoking was 90 (95 CI 51-159)
Kawahara et al (1998)
Prospective study to investigate whether smoking cessation after successful therapy is associated with a decrease in risk for a second
980 consecutive patients with small cell lung cancer (SCLC)
Median=67 years after initiation of
Second primary tumour
Of the patients who continued to smoke 11 (33) developed a SPT Of the 31 patients who stopped smoking after therapy only three (10) had a subsequent SPT Among those who continued to smoke the risk for a SPT was significantly increased (54 times 95 CI 27-97) relative to the general
64
primary tumour being treated with combination chemotherapy with or without chest radiotherapy
therapy population In contrast those who stopped smoking showed only a 16-fold increase (95 CI 03-46) which was not significantly different from the level in the general population The relative risk for non-SCLC was significantly increased 128-fold (95 CI 34-328) in continuing smokers No second non-SCLCs have been found among those who stopped smoking The 33 patients who continued to smoke had a significantly increased risk of a SPT (43 95 CI 11-159 P=003) Relative to the risk of SPT in patients without previous radiotherapy who stopped smoking the risk is 092 in patients without radiotherapy who continued smoking 037 in patients with radiotherapy who stopped smoking and 233 in patients with radiotherapy who continued smoking The risk of current smoking in patients with previous radiotherapy is 630 relative to those with radiotherapy who stopped smoking although this interaction is not statistically significant (P = 024)
Parsons et al (2010)
A systematic review with meta-analysis of the evidence that smoking
cessation after diagnosis
of a primary lung tumour affects prognosis Databases searched CINAHL (from 1981) Embase (from 1980) Medline
(from 1966)
Web of Science (from 1966) CENTRAL (from 1977)
to
December 2008 and reference lists of included studies
RCTs or observational
st
udies measuring
the effect of quitting smoking
post-
diagnosis on lung cancer prognosis
Patients were followed for 6-months gt in 5 studies but only at time of diagnosis treatment in 4
5-year survival using death rates for continuing smokers and quitters obtained from this review
Continued smoking was associated with a significantly increased risk of all-
cause mortality (hazard ratio 294 95 CI 115 to
754) and recurrence (186
101 to 341) in early stage non-small cell lung cancer and of all-cause
mortality (186 133 to 259) development of a second primary tumour (431 109 to 1698)
and recurrence (126 106 to 150) in limited stage small
cell lung cancer No study contained data on the effect of quitting
smoking on
cancer specific mortality or on development of a second primary tumour in
non-small cell lung cancer Life table modelling on the basis of these data
estimated 33 five year survival in 65 year old patients with early stage non-
small cell lung cancer who continued to smoke compared with 70 in
those
who quit smoking In limited stage small cell lung cancer an estimated 29
of continuing smokers would survive for five years compared with 63 of
quitters on the basis of the data from this review
Richardson et al (1993)
Retrospective review to determine the incidence of second primary cancers developing in patients surviving free of cancer for 2 or more years after treatment for small-cell lung cancer and to assess the potential effect of smoking cessation
Consecutive sample of 540 patients with small-cell lung cancer
Median=61 years
Relative risk for second primary cancers and death
55 patients (10) were free of cancer 2-years after initiation of therapy 18 of these developed one or more second primary cancers including 13 who developed second primary non-small-cell lung cancer The risk for any second primary cancer compared with that in the general population was increased four times (relative risk 44 95 CI 25-72) with a relative risk of a second primary non-small-cell lung cancer of 16 (CI 84-27) Forty-three patients discontinued smoking within 6-months of starting treatment for small-cell lung cancer and 12 continued to smoke In those who stopped smoking at time of diagnosis the relative risk of a second lung cancer was 11 (CI 44 to 23) whereas in those who continued to smoke it was 32 (CI 12 to 69)
Tucker et al (1997)
A multi-institution study to investigate the risk among survivors of developing second primary
611 patients who had
been cancer
Not reported
Population-based rates of cancer
Relative to the general population the risk of all second cancers among these
patients was increased 35-fold Second lung cancer risk was increased 13-
fold among those who received chest irradiation in comparison to a sevenfold
65
cancers other than small-cell lung carcinoma
free for more than 2 years after therapy for small-cell lung cancer
incidence and mortality
increase among non-irradiated patients It was higher in those who
continued smoking with evidence of an interaction between chest irradiation and continued smoking
(relative risk = 21) Patients treated with various forms
of combination chemotherapy had comparable increases in risk (94- to 13-
fold overall) except for a 19-fold risk increase among those treated with
alkylating agents who continued smoking
Vineis et al (2007)
Prospective study to estimate exposure to Environmental Tobacco Smoke (ETS) in never smokers and ex-smokers in 10 European countries (EPIC)
Men and women in the EPIC study (n = 520000)
Not reported
Lung cancer incidence
The proportion of lung cancers in never- and ex-smokers attributable to ETS was estimated as between 16 and 24 mainly due to the contribution of work-related exposure Also 5ndash7 of lung cancers in European never smokers and ex-smokers are attributable to high levels of air pollution as expressed by NO2 or proximity to heavy traffic roads
66
e) OTHER CANCERS
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in survival
from other cancers and no evidence was identified in the current review
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in survival from other
cancers Studies identified in the current review are summarised in Table 7 at the end of this
section
Preliminary EPIC results provide some evidence that red and preserved meat increases risk
for gastric cancer (Gonzalez et al 2006) Preliminary EPIC results also indicate that fruit
reduces gastric cancer risk whilst vegetables are not associated with risk for this type of
cancer Furthermore overall consumption of fruit and vegetables is reported to be unrelated
to risk of ovarian cancer (Schultz et al 2005) There is evidence of a protective effect of a
high intake of allium vegetables (onions garlic shallots leeks and chives) on ovarian
cancer risk (Schultz et al 2005)
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in survival from
other cancers Preliminary EPIC results reported in the current review provide some
evidence that BMI is associated with endometrial cancer risk (Kaaks et al 2002
Friedenreich et al 2007)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in survival from
other cancers Preliminary EPIC results along with 4 other studies were identified in the
current review
Gonzalez et al (2003) confirm from EPIC results that smoking is associated with gastric
cancer
Similarly Yu et al (1997) evaluated 25000 heterogeneous patients who had been treated
for lung breast or colorectal cancer and found that the 15-year survival of the people
who continued to smoke was 44 compared to 55 in those who quit
In a more recent study of survivors of early stage head and neck cancer (n=264) who
retrospectively reported their tobacco histories (pre-diagnosis) and prospectively updated
67
information annually thereafter for an average of 42-years smoking history dose-
dependently increased the risk of mortality from cancer (Mayne et al 2009)
The impact of smoking on risk of secondary lung cancer has been demonstrated in survivors
of Hodgkin lymphoma (Abrahamsen et al 1993 Travis et al 2002) In the latter study risk
for subsequent lung cancer from radiation treatment and smoking was identified where
multiple effects were found for a combination of radiation and alkylating agents36 in
moderate-to-heavy smokers compared with comparison cases (Travis et al 2002)
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in survival from
other cancers One study was identified in the current review which showed that pre-
diagnosis alcohol consumption history dose-dependently increased mortality risk in
recent survivors of early stage head and neck cancer (n=264) (Mayne et al 2009)
Risks reached 49 for those who drank gt5 drinks per day an effect explained by beer and
liquor consumption Continued drinking post-diagnosis of an average of 23 drinks daily
also significantly increased risk
SUMMARY OF FINDINGS FOR OTHER CANCERS
A comprehensive evaluation of the lifestyle evidence for cancers other than the four most
common (ie breast colorectal lung prostate) was not within the scope of this review
However those studies identified whilst gathering evidence for these four cancers does
highlight the sheer importance of lifestyle in the development and progression of all types of
cancers not to forget other chronic diseases The provision of lifestyle support for cancer
survivors clearly needs to remain priority as does further research into the exact
mechanisms of benefit obtained from different lifestyle practices at different stages of the
cancer and indeed health trajectory
36
Carcinogenic agents used in chemotherapy to treat cancer
68
Table 7 Other Cancers ndash Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
DIET
Gonzalez et al (2006)
Nested case-control within the prospective EPIC study examining of
the risk of gastric cancer and
oesophageal adenocarcinoma associated
with meat consumption
521 457 men and women aged 35ndash70 years in 10 European
countrie
s (330 gastric adenocarcinoma and
65
oesophageal adenocarcinomas were diagnosed)
65-years Incidence of gastric and oesophageal cancers
Gastric noncardia cancer risk was statistically significantly associated
with intakes of total meat (calibrated HR per 100-gday increase
=
352 95 CI = 196 to 634) red meat (calibrated HR per 50-gday
increase = 173 95 CI = 103 to 288) and processed
meat (calibrated HR per 50-gday increase = 245 95 CI
= 143 to 421) The association between
the risk of gastric noncardia cancer and total meat intake was
especially large in H pylori infected subjects (odds ratio per 100-
gday increase = 532 95 CI = 210 to 134) Intakes of total red or
processed meat were not associated with
the risk of gastric cardia cancer A positive but nonndashstatistically
significant association was observed between oesophageal
adenocarcinoma cancer risk and total and processed meat intake
Schultz et al (2005)
Prospective examination of the association between consumption of fruit and vegetables and risk of ovarian cancer (EPIC)
Female participants (n = 325640) of the EPIC study
Mean=63 years
Ovarian cancer incidence
Total intake of fruit and vegetables separately or combined as well as subgroups of vegetables (fruiting root leafy vegetables cabbages) was unrelated to risk of ovarian cancer A high intake of garliconion vegetables was associated with a borderline significant reduced risk of this cancer
WEIGHT
Friedenreich et al 2007
Large prospective study (EPIC) examining the association between anthropometry and endometrial cancer particularly by menopausal status and exogenous hormone use subgroups
223008 women in the EPIC study (567 incident endometrial cancer cases)
64-years Endometrial cancer incidence
Weight BMI waist and hip circumferences and waistndashhip ratio (WHR) were strongly associated with increased risk of endometrial cancer The relative risk (RR) for obese (BMI 30ndash lt 40 kgm
2)
compared to normal weight (BMI lt 25) women was 178 95 CI = 141ndash226 and for morbidly obese women (BMI ge 40) was 302 95 CI = 166ndash552 The RR for women with a waist circumference of ge88 cm vs lt80 cm was 176 95 CI = 142ndash219 Adult weight gain of ge20 kg compared with stable weight (plusmn3 kg) increased risk independent of body weight at age 20 (RR = 175 95 CI = 111ndash277) These associations were generally stronger for postmenopausal than premenopausal women and oral contraceptives never-users than ever-users and much stronger among never-users of hormone replacement therapy compared to ever-users
Kaaks et al A review of evidence on the Endometrial Not Incidence of The authors conclude that development of ovarian hyperandrogenism
69
(2002) associations among endometrial cancer risk endogenous hormone metabolism and obesity
cancer cases reported endometrial cancer
may be a central mechanism relating to an interaction between obesity-related chronic hyperinsulinemia with genetic factors predisposing to the development of ovarian hyperandrogenism
SMOKING
Abrahamsen et al (1993)
The Norwegian Cancer Registry
identified previously untreated patients with Hodgkin lymphoma treated at NRH who had developed a secondary cancer more than 1 year after diagnosis of
Hodgkin
lymphoma
68 patients who developed secondary cancer including 9 acute non-lymphocytic leukaemialsquos (ANLLs)
8 non-
Hodgkins lymphomas (NHLs) and 51 solid tumours including 11 lung cancers
Not reported
Secondary cancer
The RR of SC and leukaemia was 186 (95 CI 14 to 24) and 243 (95 CI 111 to 462) respectively The RR of
SC was highest in
younger patients (lt 41 years RR = 38) No significant association
between splenectomy and development of ANLL was found The
influence of treatment and follow-up time on the development of SC
agrees with data from other large cancer institutions
Gonzalez et al (2003)
Assessment of the relation between tobacco use and gastric cancer incidence in the prospective EPIC study
521468 individuals recruited from 10 European countries taking part in the EPIC study 274 were eligible for the analysis
Approx 10-years
Incidence of gastric cancer
After adjustment for educational level consumption of fresh fruit vegetables and preserved meat alcohol intake and body mass index (BMI) there was a significant association between cigarette smoking and gastric cancer risk the hazard ratio (HR) for ever smokers was 145 (95 CI = 108-194) The HR of current cigarette smoking was 173 (95 CI = 106-283) in males and 187 (95 CI = 112-312) in females Hazard ratios increased with intensity and duration of cigarette smoked A significant decrease of risk was observed after 10 years of quitting smoking A preliminary analysis of 121 cases with identified anatomic site showed that current cigarette smokers had a higher HR of GC in the cardia (HR = 410) than in the distal part of the stomach (HR = 194) In this cohort 176 (95 CI = 105-295 ) of gastric cancer cases may be attributable to smoking
Mayne et al (2009)
Participants retrospectively reported their smoking histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to smoke post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Smoking history before diagnosis dose-dependently increased the risk of dying risks reached 54 [95 CI 07-401] among those with gt60 pack-years of smoking After adjusting for pre-diagnosis exposures continued smoking was associated with non-significantly higher risk (relative risk for continued smoking versus no smoking 18 95 CI 09-39)
70
Travis et al (2002)
Case-control study with a population-based cohort The cumulative amount of cytotoxic drugs the radiation dose to the specific location in the lung where cancer developed and tobacco use were compared between patients who developed lung cancer and matched control patients
1-year survivors of Hodgkins disease (n=19046) comparison between 222 patients who developed lung cancer and 444 matched controls
Not reported
Secondary cancer incidence
Tobacco use increased lung cancer risk more than 20-fold risks from smoking appeared to multiply risks from treatment
Yu et al (1997)
Retrospective study examining the effect of smoking history on survival among cancer patients
Data from Memorial Sloan-Kettering Cancer Centers tumour registry was used to identify 25436 cases of cancer (12447 male patients and 12989 female patients)
Not reported
Survival time Patients who had a history of smoking were found to have a lower rate of survival than non-smokers After controlling for age race alcohol use and histologic grade the risk ratios were 155 for males and 143 for females A dose-response relationship was found between ever-smoking and cancer patient survival The predictive effect of smoking on survival was significant for patients with oral pancreatic breast and prostate cancers but not for oesophageal stomach colon rectum laryngeal lung cervix uteri urinary bladder and kidney cancers Black patients with oral or breast cancer had a poorer prognosis associated with smoking compared with white and other non-white patients
ALCOHOL
Mayne et al (2009)
Participants retrospectively reported their alcohol consumption histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to drink post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Alcohol history before diagnosis dose-dependently increased mortality risk risks reached 49 (95 CI 15-163) for persons who drank gt5 drinksd an effect explained by beer and liquor consumption After adjusting for pre-diagnosis exposures continued drinking (average of 23 drinksd) post-diagnosis significantly increased risk (relative risk for continued drinking versus no drinking 27 95 CI 12-61)
71
PART TWO
LIFESTYLE EVIDENCE FOR REDUCING AND MANAGING THE
RISKS AND SIDE-EFFECTS OF CANCER TREATMENT
Introduction
There are a number of long-term and late effects of cancer treatment that a survivor might
be confronted with including fatigue (Bower et al 2006) psychological problems (Thewes
et al 2004) lymphoedema (Deo et al 2004) and osteoporosis (Brown et al 2006) There
might also be difficulties in terms of returning to work or withdrawal from social activities due
to disability (Taskila et al 2007) Lifestyle choices pertaining to diet physical activity
smoking and alcohol consumption for cancer survivors are not only important in terms of
disease progression and recurrence Despite there being less evidence in this area there
is accumulating data demonstrating that lifestyle can facilitate the effective management of
many of these effects of treatment some of which are chronic conditions themselves
requiring additional lifestyle modifications Research within this area has hit new heights in
order to keep up with the growing number of survivors The chronic conditions addressed
within the current review of lifestyle evidence are some of the most frequently reported
problems cited by cancer survivors they include cancer-related fatigue (CRF)
lymphoedema osteoporosis and weight gain In addition evidence for lifestyle choices and
quality of life (QoL) has been reviewed due to the QoL implications of the aforementioned
health-related problems and unhealthy behaviours (Richardson et al 2009)
Evidence for an interaction between lifestyle and these chronic conditions commences with
the findings reported by Bekkering et al (2006) as part of the WCRF review being updated
Further evidence identified from the search criteria will then be presented Evidence will be
presented by cancer site (eg breast colorectal lung prostate) where appropriate whilst
some evidence will pertain to one cancer site only (ie breast cancer related lymphoedema)
72
CANCER-RELATED FATIGUE (CRF)
Cancer-related fatigue (CRF) is defined as ldquoa distressing persistent subjective sense of
physical emotional andor cognitive tiredness or exhaustion related to cancer or cancer-
related treatment that is not proportional to recent activity and interferes with usual
functioningrdquo (NCCN 2009) It has overtaken nausea and pain as the most distressing
symptom experienced by people with cancer during and after treatment It is reported by 60-
96 of patients during chemotherapy radiotherapy or after surgery and can last for months
or even years following treatment (Wagner and Cella 2004 Thomas 2005 NCCN 2009) It
can have a profound effect on physical emotional and social well-being and can hinder
chance of remission owing to non-compliance with treatment due to the intensity of this side-
effect (Lucia Earnest and Perez 2003 Velthuis et al 2009)
The specific causes of CRF are not fully understood but there are several associated
conditions which can aggravate it These include anaemia electrolyte imbalance liver
failure and steroid withdrawal (Thomas 2005) Some conditions can also cause fatigue by
disturbing sleep patterns such as anxiety depression nocturia (a need to get up in the night
to urinate) night sweats and pruritus (itching) The self-management strategy most
extensively investigated for CRF is physical activity the evidence for which is presented
next Studies identified in the current review are summarised in Table 8 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in women with breast cancer In the current review 4 systematic reviews
three of which included a meta-analysis and 2 additional studies were identified
The first review by McNeely et al (2006) reported on 14 RCTs Despite significant
heterogeneity and relatively small samples the overall finding was that physical activity led
to statistically significant improvements in reducing symptoms of fatigue Two meta-
analyses added to this evidence The first by Cramp and Daniel (2008) evaluated 28
studies (n=2083 participants) the majority of which comprised participants with breast
cancer (n=16 studies n=1172 participants) A pooled meta-analysis of all available data
convincingly showed that physical activity was statistically more effective in reducing
CRF when compared to less active controls In the second meta-analysis Velthuis et al
(2009) reviewed 18 studies 12 of which comprised women with breast cancer Pooled
results of these 12 studies (n=674 patients) showed a small significant reduction of CRF
in favour of the physical activity group compared to the non-physical activity group
When Velthuis et al (2009) subdivided the 12 studies into two main physical activity
strategies (ie home-based versus supervised classes) home-based physical activity (n=
7 studies) led to a small non-significant reduction in CRF whereas supervised
73
aerobic physical activity (n=5 studies) showed a medium significant reduction
in CRF when compared to no intervention
Fillion et al (2008) conduced an RCT demonstrating that combining supervised walking
training with psycho-educational stress management produced significant improvements
relative to usual care for fatigue vigour anxiety and depression but not for physical
fitness This suggests a psychological benefit to physical activity which might assist in
coping with physical symptoms such as fatigue Poudevigne et al (2009)
examined adherence to 12-weeks of moderate intensity combined cardio-respiratory and
resistance training and any subsequent impact on levels of fatigue in sedentary breast
cancer survivors (n=20) 2-24 months post-treatment Not only was the training acceptable
and safe but significant decreases in fatigue (43) were also found across the12-
weeks
Danhauer et al (2009) conducted an RCT with women (n=44) who had breast cancer 34
of whom were undergoing cancer treatment in order to examine the effects of restorative
yoga between those in treatment and those not in treatment Randomisation was to a
programme of 10-weekly 75-minute yoga classes or a waiting list control group The yoga
group demonstrated a significant within-group improvement in fatigue although no
significant difference was found with the control group
In updating a previous systematic review by Schmitz et al (2005) of RCTs examining
physical activity in cancer survivors during and after treatment Speck et al (2010)
accumulated data from a further 82 studies (n=6838 participants) Of the 82 studies 66
were rated as high quality and analysed for mean effect sizes resulting from physical activity
interventions The most common diagnosis included was breast cancer (83) with 40 of
studies conducting interventions during cancer treatment and 60 post-treatment Mean
effect sizes demonstrated a large effect of physical activity interventions post-
treatment on upper and lower body strength (plt00001 and 0024 respectively) and
moderate effects on fatigue and breast cancer-specific concerns (p=0003 and 0003
respectively) The most notable progression from their previous review was that the
benefits of physical activity on fatigue moved from negative findings to the evidence
reflecting significantly reduced fatigue post-treatment in physically active survivors
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in men with prostate cancer In the current review 3 systematic reviews two
of which included a meta-analysis and 2 additional studies were identified In the current
review four studies were identified
Windsor Nichol and Potter (2004) published a study of 65 patients with prostate cancer
receiving radiotherapy who were randomly allocated to a home-based physical activity
programme or standard supportive care The home-based exercise included walking 30-
minutes three times a week with an intensity of 60-70 heart rate max for the duration of
74
radiotherapy No adverse events were reported and a non-significant reduction of CRF
was found in the physical activity group when compared to the standard care group
In the abovementioned meta-analysis conducted by Velthuis et al (2009) three RCTs in men
with prostate cancer investigated the effectiveness of supervised physical activity during
radiotherapy and androgen deprivation therapy (Segal et al 2003 Monga et al 2007
Segal et al 2009) In two studies men allocated to the intervention group participated three
times a week in a supervised physical activity programme comprising aerobic exercises with
an intensity of respectively 65 of the maximum heart frequency (HR max) adjusted for
age and 50-75 of the VO2peak (15-45 minutes) (Monga et al 2007 Segal et al 2009)
In the third study the intervention comprised resistance exercises 2-3 times a week with an
intensity of two sets of 8-12 repetitions 60-70 of the one repetition maximum (Segal et
al 2003) Pooled results from the two supervised aerobic studies showed a large non-
significant reduction in CRF in favour of the physical activity group (Monga et al
2007 Segal et al 2009) The resistance exercise study showed a small non-significant
reduction in CRF in favour of the physical activity group (Segal et al 2003) In the latter
study over 80 of the participants were reported to have completed the programme
however the programme did result in one knee injury chest pain fainting and an acute
myocardial infarction
c) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) report on one RCT comparing the impact of a 3-weeks aerobic
physical activity (stationary biking 30-minutes five times weekly) intervention versus
relaxation training (45-minutes three times per week) in post-surgery survivors (n=72) of lung
(n=27) and gastrointestinal (n=42) cancer (Dimeo et al 2004) Fatigue improved
significantly in both groups during the intervention although there was no significant
difference between groups This suggests that relaxation training can be equally as
effective as aerobic physical activity in relieving symptoms of fatigue
In the current review 3 further studies were identified
There has been one study in patients with multiple myeloma (Coleman et al 2003) which
included a home-based physical activity programme during chemotherapy and peripheral
blood stem cell transplantation The programme comprised a combination of aerobic and
resistance exercises three times a week for 20-minutes for the duration of the
chemotherapy (6-months) No adverse events were reported and a small non-significant
reduction in CRF was found in the physical activity group compared to a control
group who did not receive the intervention
Chang et al (2008) published a study involving patients with acute myelogeous leukemia
(n=22) which included allocation to the intervention group a three week supervised walking
programme during chemotherapy Participants walked five times a week for 12-minutes in
the hospital hallway The programme was completed by 69 of the participants and no
75
adverse events were reported A medium-sized non-significant reduction in CRF was
found
In a cross-sectional postal survey of ovarian cancer survivors (n=359) self-report measures
of physical activity and CRF demonstrated that those meeting physical activity guidelines of
the Centres for Disease Control and Prevention (ie minimum 25-hours of moderate
intensity aerobic activity every week plus muscle-strengthening activities on two or more
days of the week) reported significantly lower fatigue than those not meeting guidelines
(Stevinson et al 2009) There was however no evidence of a dose-response relationship
SUMMARY OF EVIDENCE FOR CANCER-RELATED FATIGUE
Evidence from 28 RCTs and 2 meta-analyses has demonstrated that physical activity
programmes can reduce the severity of CRF The studies reviewed here also show that
supervised aerobic exercise programmes were more effective in reducing CRF during breast
cancer treatment than home-based exercise advice Although more research on the optimal
timing and duration of physical activity would be useful these studies are sufficiently robust
to recommend that tailored physical activity advice be integrated into individualized care
plans
As identified in a consultation and evidence review designed to determine the priorities of
cancer survivorship research there is a modest amount of research testing physical activity
interventions for fatigue some demonstrating benefits during treatment but inconclusive
evidence for after treatment (Richardson et al 2009) Although there is clinical
heterogeneity between published RCTlsquos in terms of physical activity duration frequency and
intensity a sensible pragmatic approach based on the trials which showed most benefit is to
supervise a moderate intensity physical activity regimen of regular frequency (3-5
timesweek) for 20-30 minutes per session involving aerobic resistance or mixed physical
activity types With evidence suggesting that low intensity physical activity can also be
beneficial during cancer treatment consideration is warranted in terms of promoting physical
activity from diagnosis onwards potentially making physical activity uptake less challenging
post-treatment (Velthuis et al 2009) Further research is required to determine the optimal
type intensity and timing of physical activity interventions at different periods of the disease
trajectory and when experiencing other cancer-related symptoms or late effects
An exemplary physical activity programme available to survivors of breast colorectal and melanoma cancers is the BACSUP (Bournemouth After Cancer Survivorship Project) Active Wellness Programmelsquo developed in partnership with Royal Bournemouth Hospital NHS Bournemouth and Poole Bournemouth University and MacMillan Cancer Support (Milne et al 2010) The programme involves two initial one-to-one consultations including a holistic assessment with a trained member of staff to tailor the programme to individual needs A readiness check is done prior to referral a readiness to be physically active score of gt70 is required for participation Participants receive a telephone call at 3-weeks for the provision of support and encouragement followed by a one-to-one review at 6-weeks to assess progress and maintain motivation A one-to-one review and reassessment is also provided at 12-weeks to measure improvements Additional support options are available such as the BACSUP Active Wellness Group which provides an opportunity to meet others survivors and listen to life improvement guest speakers In a pilot study of the programme survivors who had completed primary treatment within the previous 5-years (n=180) were referred to the service 58 completed the programme 65 are currently on the programme 30 started but are on hold due to circumstances 21 were not yet ready to join the scheme
At 12-weeks 92 of participants reported reduced fatigue
76
Table 8 Cancer-Related Fatigue and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Chang et al (2008)
RCT to preliminarily examine the effects of a three-week walking exercise program (WEP) on fatigue-related experiences of acute myelogenous leukaemia (AML) patients receiving chemotherapy Eligible AML patients were randomly assigned to either an experimental group (n = 11) which received 12 minutes of WEP per day five days per week for three consecutive weeks or to a control group (n = 11) which received standard ward care
Patients with acute Myelogenous leukaemia (AML) receiving chemotherapy (n=22)
All patients were evaluated four times before treatment (baseline or Day 1) Day 7 Day 14 and Day 21
Worst and average fatigue intensities fatigue interference with patients daily life 12-minute walking distance overall symptom distress anxiety and depressive status
AML patients in the three-week WEP group had a significantly greater increase in 12-minute walking distance than the control group Patients in the WEP also had lower levels of fatigue intensity and interference symptom distress anxiety and depressive status than the control group
Coleman et al(2003)
A pilotfeasibility study with a randomized controlled design was conducted to investigate home-based exercise therapy for patients receiving high-dose chemotherapy and autologous peripheral blood stem cell transplantation as treatment for multiple myeloma
24 patients with multiple myeloma
Not reported Fatigue mood disturbance body weight
Because of the small sample size in the feasibility study the effect of exercise on lean body weight was the only end point that obtained statistical significance However the results suggest that an individualised exercise program for patients receiving aggressive treatment for multiple myeloma is feasible and may be effective for decreasing fatigue and mood disturbance and for improving sleep
Cramp and Daniel (2008)
Systematic review with meta-analysis to evaluate the effect of exercise on cancer-related fatigue both during and after cancer treatment
2083 participants from RCTs comprising cancer patients and survivors
Follow-up assessment of long-term outcomes was poor with 18 of 28 studies failing to assess outcomes beyond the end of the intervention
Cancer-related fatigue
28 studies were identified for inclusion with the majority carried out on participants with breast cancer (n = 16 studies n = 1172 participants) A meta-analysis of all fatigue data incorporating 22 comparisons provided data for 920 participants who received an exercise intervention and 742 control participants At the end of the intervention period exercise was statistically more effective than the control intervention (SMD -023 95 CIs -033 to -013)
77
period
Danhauer et al (2009)
Randomised pilot study to determine the feasibility of implementing a restorative yoga intervention for women with breast cancer and to examine group differences in self-reported emotional health-related quality of life and symptom outcomes 10 weekly 75-minute yoga classes
Women with breast cancer (n=544) 34 of whom were actively undergoing cancer treatment
Immediately post-intervention (week 10)
Emotional well-being QoL fatigue
Group differences favouring the yoga group were seen for mental health depression positive affect and spirituality (peacemeaning) Significant baselinegroup interactions were observed for negative affect and emotional well-being Women with higher negative affect and lower emotional well-being at baseline derived greater benefit from the yoga intervention compared to those with similar values at baseline in the control group The yoga group demonstrated a significant within-group improvement in fatigue no significant difference was noted for the control group
Fillion et al (2008)
RCT to verify the effectiveness of a 4-week nurse-led group intervention that combines stress management psycho-education and physical activity (ie independent variable) intervention in reducing fatigue and improving energy level quality of life (mental and physical) fitness (VO2submax) and emotional distress (ie dependent variables) in breast cancer survivors Participants were randomly assigned to either the group intervention (experimental) or the usual-care (control) condition
French-speaking women who had completed their treatments for non-metastatic breast cancer (n=87)
Post-intervention and at 3-months follow-up
Fatigue emotional distress QoL
Participants in the intervention group showed greater improvement in fatigue energy level and emotional distress at 3-month follow-up and physical quality of life at post-intervention compared with the participants in the control group
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials MEDLINE
EMBASE CINAHL Psych INFO CancerLit PEDro
and SportDiscus as well
as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
function
ing as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all
outcomes were positive even when statistical significance was not
achieved Exercise led to statistically significant improvements in
quality of life as assessed by the Functional Assessment of
Cancer TherapyndashGeneral (weighted mean difference [WMD] 458
95 CI 035 to 880) and Functional Assessment of Cancer
TherapyndashBreast (WMD 662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak
oxygen consumption and in reducing symptoms of fatigue
Poudevigne et al (2009)
Cohort study examining the effects of a 12-week cross training intervention on fatigue and mood in breast cancer survivors The training consisted of a 12-week exercise program of 3 weekly
20 sedentary breast cancer survivors between 2-24 months post-
On completion of the 12-week intervention
Fatigue and mood disturbances (Profile of Mood States) QoL
The mean (plusmnSD) attendance rate was 92 (plusmn80) No musculoskeletal injuries and problematic symptoms occurred during the cross-training Repeated measures ANOVA showed a large increase in QOL (22) and significant decrease in fatigue (43) across 12 weeks (eta squared range 491 to708 all p
78
sessions of 60 min duration supervised by a certified personal trainer and divided into resistance (30 minutes) and aerobic training (5 minutes warm-up 20 minutes training 5 minutes cool-down) The aerobic intensity was set at 60HRR and re-evaluated every three weeks
treatment Treatments ranged from lumpectomies (23) mastectomies (29) radiations (32) and chemotherapy (16)
(SF-36) and work absenteeism
valueslt05) No differences were found in work absenteeism Blood pressure was unchanged after training
Stevinson et al (2009)
A cross-sectional postal survey to investigate the associations between physical activity and health-related outcomes in ovarian cancer survivors and to examine any dose-response relationship
Ovarian cancer survivors (n=359) on and off treatment
Not reported Fatigue peripheral neuropathy sleep and psychosocial functioning
311 of participants were meeting the public health physical activity guidelines - those meeting guidelines reported significantly lower fatigue than those not meeting guidelines (mean difference 71 95 confidence interval 55-88 d = 087 Plt 0001) Meeting guidelines was also significantly inversely associated with peripheral neuropathy depression anxiety sleep latency use of sleep medication and daytime dysfunction and was positively associated with happiness sleep quality and sleep efficiency
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types were included with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) With few exceptions exercise was well tolerated during and post treatment without adverse events
Velthuis et al (2009)
Meta-analysis to evaluate the effects of different exercise prescription parameters during cancer treatment on cancer-related fatigue (CRF) A systematic search of CINAHL Cochrane Library Embase
RCTs studying the effects of exercise during cancer treatment on
Not reported Cancer-related fatigue
During breast cancer treatment home-based exercise lead to a small non-significant reduction (standardised mean difference 010 95 confidence interval minus025 to 045) whereas supervised aerobic exercise showed a medium significant reduction in CRF (standardised mean difference 030 95 confidence interval 009
79
Medline Scopus and PEDro was carried out
CRF (n=18) 12 in breast 4 in prostate and 2 in other cancer patients)
to 051) compared with no exercise A subgroup analysis of home-based (n = 65) and supervised aerobic (n = 98) and resistance exercise programmes (n = 208) in prostate cancer patients showed no significant reduction in CRF in favour of the exercise group Adherence ranged from 39 of the patients who visited at least 70 of the supervised exercise sessions to 100 completion of a home-based walking programme
Windsor Nichol and Potter (2004)
A prospective RCT to determine whether aerobic exercise would reduce the incidence of fatigue and prevent deterioration in physical functioning during radiotherapy for localised prostate carcinoma
33 men in exercise group and 33 men in control group
4-weeks post-radiotherapy
Fatigue and distance walked in a modified shuttle test before and after radiotherapy
There were no significant between group differences noted with regard to fatigue scores at baseline (P = 055) or after 4 weeks of radiotherapy (P = 018) Men in the control group had significant increases in fatigue scores from baseline to the end of radiotherapy (P = 0013) with no significant increases observed in the exercise group (P = 0203)
80
LYMPHOEDEMA
Lymphoedema is the excessive accumulation of tissue fluid (or lymph) that results from
impaired lymphatic drainage resulting in swelling of the limb The most common type of
lymphoedema in cancer survivors is most frequently the result of treatment for breast
cancer where an important prognostic indicator is the removal and evaluation of lymph
nodes (Morrell et al 2005) Removal of the lymph nodes can result in a number of side-
effects including lymphoedema (Swenson et al 2002) which manifests usually as a
swelling to the affected arm but can also occur in the hand trunk and breast The more
lymph nodes that are removed the higher the risk of developing the condition providing an
objective measure of risk that could be utilised in the provision of evidence-based
lifestyle and self-management support based on individuals needs
The condition can develop immediately or many years after treatment (Mortimer et al
1996) in either case lymphoedema is a chronic debilitating condition that can cause severe
physical and psychological morbidity as well as a reduction in QoL (Deo et al 2004)
The self-management strategy most extensively investigated for lymphoedema is physical
activity with some evidence also being available for diet Studies identified in the current
review are summarised in Table 9 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
preventing or managing lymphoedema In the current review one systematic review
(including a meta-analysis) and 3 studies were identified
In a prospective RCT testing the efficacy of two types of physiotherapy on shoulder function
and lymphatic disturbance in post-operative breast cancer survivors (n=60) participants
received one of two types of physiotherapy 48-hours post-surgery (de Rezende et al
2006)
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-
defined sequence of movements
2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely
to music
Lymphoedema is estimated to affect
about 30 of breast cancer survivors
post-treatment (Deo et al 2004)
81
Results indicated significantly better recovery of limb movement in the directed group
compared to the free group with there being no significant difference between groups in
terms of lymphatic disturbance
Ahmed et al (2006) report on a 6-month RCT examining the effects of supervised upper-
and lower-body weight training on lymphoedema incidence and symptoms in breast cancer
survivors (n = 45) 4-36 months post-treatment From baseline to 6-months three control-
group participants reported an increase in lymphoedema symptoms No participants in the
intervention group reported such symptoms suggesting that twice-a-week progressive
weight training does not increase the onset of or exacerbate lymphoedema in breast cancer
survivors (13 women had lymphoedema at baseline) The results from this study indicate
that at minimum physical activity does not exacerbate lymphoedema
Moseley and Piller (2008) reviewed the literature for evidence supporting the benefits of
physical activity for people with limb lymphoedema Their key findings from eleven studies
demonstrated that
physical activity can improve lymph clearance
physical activity can help reduce limb volume and improve subjective symptoms and
QoL
benefits from physical activity have been sustained post-physical activity regime in
some studies
physical activity is a viable option for people with lymphoedema
Moseley and Pillerlsquos (2008) conclusions were supported further in a recent RCT by Hayes
Hildegard and Turner (2009) Breast cancer survivors at least 6-months post-treatment
who had developed unilateral upper-limb lymphoedema participated in twenty supervised
group aerobic and resistance physical activity sessions over 12-weeks (n=16) or continued
habitual activities (n=16) Average attendance was more than 70 of supervised sessions
and there were no withdrawals Mean ratio and volume measures at baseline were similar
between the two groups and no changes were observed at 3-months follow-up for either
group although two women receiving supervised physical activity no longer had evidence of
lymphoedema by study completion The results from this review as with the RCT by
Ahmed et al (2006) indicate that at minimum physical activity does not exacerbate
secondary lymphoedema
In the review referred to previously by Speck et al (2010) with minor exceptions findings
indicated aerobic lifestyle and upper body resistive exercise was tolerated by breast cancer
survivors with no adverse effects on the development or exacerbation of lymphoedema
ii DIET
Bekkering et al (2006) report on one double-blind placebo-controlled RCT examining diet
and lymphoedema in breast cancer survivors (n=68) at a mean of 155-years post-treatment
For 6-months women received 500mg twice a day of dl-alpha tocopheryl acetate (a source
of vitamin E) plus pentoxifylline (a drug that improves blood circulation) 400mg twice a day
82
of dl-alpha tocopheryl acetate or placebo (Gothard et al 2004) At 6-months and 12-months
post-randomisation there was no significant difference between groups in terms of arm
volume
The current review identified one RCT
Dietary Fat
In a UK RCT Shaw Mortimer and Judd (2007) demonstrate the impact of diet and weight
loss on post-treatment arm lymphoedema in breast cancer survivors (n=51) Women were
assigned to one of three 24-week dietary groups
1) a low-fat diet (fat intake reduced to 20 of total energy intake)
2) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ)
3) a control group (continuing their usual diet)
After the end of the 24-week period of dietary intervention there was a slightly greater
reduction in excess arm volume in both dietary intervention groups compared with the
control although this was not statistically significant Furthermore despite low levels of
adherence to dietary advice weight loss was achieved in all groups demonstrating that
dietary interventions can assist in reducing excess arm volume in women with post-
treatment lymphoedema
SUMMARY OF EVIDENCE FOR LYMPHOEDEMA
The studies evaluated within this review indicate a need to re-assess the common clinical
guidelines that breast cancer survivors avoid upper body resistance activity for fear of
increasing risk of lymphoedema(Speck et al 2010) They also indicate a requirement to
develop guidelines for appropriate physical activity As concluded by Hayes Hildegard and
Turner (2009) women with secondary lymphoedema should be encouraged to be physically
active optimising their physical and psychosocial recovery Resistance exercise does not
increase the risk for or exacerbate symptoms of lymphoedema and in fact directed physical
activity 48-hours post-surgery might offer greater utility in terms of rehabilitation outcomes
Some of the studies evaluated in the review by Moseley and Piller (2008) comprised small
sample sizes and did not include control groups however when combined with other studies
presented within this review there is some support for encouraging physical activity in breast
cancer survivors Furthermore physical activity combined with changes in diet and
subsequent weight loss in survivors who are overweight might significantly reduce the
symptoms of lymphoedema although evidence for diet in reducing symptoms of
lymphoedema is limited
Weight loss across groups
9 (60) in the control group 13 (76) in the low-fat diet group 18 (95) in the weight-reduction
group
83
Table 9 Lymphoedema and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Ahmed et al (2006)
RCT comparing supervised twice weekly upper- and lower-body weight training over 6-months with control group completing no training
Breast cancer survivors (n = 45) 4-36 months post-treatment
6-months post-intervention
Incidence and symptoms of lymphoedema
From baseline to 6-months three control-group participants
reported an increase
in lymphoedema symptoms No
participants in the intervention group reported such symptoms suggesting that
twice-a-week progressive weight training does not
increase the onset of or exacerbate lymphoedema in breast
cancer
survivors
de Rezende et al (2006)
RCT examining the impact of physiotherapy on lymphoedema Participants received one of two types of physiotherapy
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-defined sequence of movements 2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely to music
48-hours post-surgery breast cancer survivors (n=60)
On completion of intervention (42-days)
Shoulder movement and lymphatic disturbance
Significantly better recovery of limb movement in the directed group compared to the free group with there being no significant difference between groups in terms of lymphatic disturbance
Hayes Hildegard and Turner (2009)
An RCT testing the impact of aerobic exercise on lymphoedema outcomes Participants randomised to 1) 20 supervised group aerobic and resistance physical activity sessions over 12-weeks (n=16) 2) continued habitual activities (n=16)
Breast cancer survivors at least 6-months post-treatment who had developed unilateral upper-limb lymphoedema
3-months post-intervention
Arm volume measurements
Mean ratio and volume measures at baseline were similar between the two groups and no changes were observed at 3-months follow-up for either group although two women receiving supervised physical activity no longer had evidence of lymphoedema by study completion
84
Moseley and Piller (2008)
Literature search of the evidence supporting the benefits of exercise for those with limb lymphoedema
Exercise studies undertaken in RCTs or cohort studies and involving secondary limb lymphoedema (with no active cancer)
Varied from post-intervention to 8-weeks follow-up
Change in limb volume and subjective symptoms
Exercise has been shown to improve lymph propulsion and clearance help reduce limb volume and improve subjective symptoms and quality of life Benefits from exercise have been sustained post-exercise regime in some studies Exercise is a viable option for those with limb lymphoedema
DIET
Gothard et al (2004)
A double-blind placebo-controlled randomised phase II trial Participants were randomised to active drugs or placebo All volunteers were given dl-alpha tocopheryl acetate 500 mg twice a day orally plus pentoxifylline 400 mg twice a day orally or corresponding placebos for 6 months
68 volunteers with a minimum 20 increase in arm volume at a median 155 years after radiotherapy (plus axillary surgery in 5168 (75) cases)
12 months post-randomisation
Volume of the ipsilateral limb measured
There was no significant difference between treatment and control groups in terms of arm volume Absolute change in arm volume at 12 months was 25 (95 CI minus040 to 53) in the treatment group compared to 12 (95 CI minus28 to 51) in the placebo group The difference in mean volume change between randomisation groups at 12 months was not statistically significant (P=06) minus13 (95 CI minus61 to 35) nor was there a significant difference in response at 6 months (P=07) where mean change in arm volume from baseline in the treatment and placebo groups was minus23 (95 CI minus79 to 34) and minus11 (95 CI minus39 to 17) respectively
Shaw Mortimer and Judd (2007)
Participants were assigned to one of three 24-week dietary groups in order to assess impact on arm volume 1)a low-fat diet (fat intake reduced to 20 of total energy intake) b) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ) c) a control group (continuing their usual diet)
Breast cancer survivors (n=51)
After 24-weeks of intervention
Arm volume There was a slightly greater reduction in excess arm volume in both dietary intervention groups compared with the control although this was not statistically significant
85
OSTEOPOROSIS AND BONE HEALTH
Osteoporosis is a condition in which the bones become less dense and more likely to
fracture which in turn can result in significant pain and disability It is known as a silent
disease because if undetected bone loss can progress for many years without symptoms
until a fracture occurs Risk factors for developing osteoporosis are often enhanced in
cancer survivors such as being post-menopausal and having had early menopause (Ada et
al 2002) Low calcium intake lack of physical activity smoking and excessive alcohol
consumption are also risk factors for osteoporosis (Guthrie et al 2000) Women who have
had breast cancer treatment may be at increased risk for osteoporosis and fracture due to
reduced levels of oestrogen whilst men who receive hormone deprivation therapy for
prostate cancer also have an increased risk of developing osteoporosis and broken bones
(National Institutes of Health Osteoporosis and Related Bone Diseases 2009)
There are no early symptoms of osteoporosis but diet physical activity and drug treatment
can prevent or reverse loss of BMD highlighting the importance of lifestyle choices in
osteoporosis outcomes Studies identified in the current review are summarised in Table 10
at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any physical activity studies examining osteoporosis
in breast cancer survivors The current review identified 3 RCTs and one cohort study
Schwartz Winters-Stone and Gallucci (2007) evaluated the impact of aerobics and
resistance training on BMD in an RCT involving women with histologically confirmed invasive
stage I-III breast cancer (n=66) beginning chemotherapy Women were randomised to one
of three groups and stratified according to menopausal status (pre-menopausal or post-
menopausal)
1) Home-based aerobic exercise - women were instructed to choose an aerobic activity
they enjoyed (eg walking jogging) and exercise for 15-30 minutes four days per
week for the duration of the study at a symptom-limited moderate intensity such that
they were breathing hard but able to talk
2) Home-based resistance exercise ndash women were instructed to exercise at home four
days per week using resistance bands and tubing
3) Usual care
It has been reported that 80 of older breast cancer survivors have osteopenia (below normal bone-mineral density [BMD]) or osteoporosis at initial diagnosis (Twiss et al 2001)
86
The average decline in BMD was -623 for usual care -492 for resistance exercise and
-076 for aerobic exercise suggesting that weight-bearing aerobic exercise attenuates
declines in BMD Pre-menopausal women demonstrated significantly greater declines in
BMD than post-menopausal women highlighting a need to provide interventions for bone
health on a risk stratification basis
Gross et al (2002) examined the intensity of physical activity (ie light moderate vigorous)
reported by a cohort of post-menopausal breast cancer survivors (n=27) and found no
relationship between activity levels and BMD However participants mainly reported light
physical activity limiting the examination of moderate and vigorous activity outcomes It is
possible that a higher intensity of physical activity is required to achieve any benefits to bone
health
Waltman et al (2009) conducted an RCT testing a 24-month self-efficacy based strength
and weight training programme on post-treatment (except tamoxifen and aromatase
inhibitors) post-menopausal breast cancer survivors (n=223) who had amenorrhea
(absence of menstruation) for at least 12-months and a bone BMD score lower than the
norm (Figure 1)
Figure 1 Bone Density Definitions
WHO Definitions of Osteoporosis
Based on Bone Density
T-Scores
BMD
Category
Examples
Range
10
05
0
-05
-10
-1 and
above Normal BMD
-15
-20
Between
-1 and -25
Low BMD
(Osteopenia)
-25
-30
-35
-40
-25 and
below Osteoporosis
Source WHO (2003)
The women were randomised to receive physical activity with medication (n=110) or
medication only (n=113) The medication taken by both groups included risedronate
(osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily) While
87
participation in strength training did not result in statistically significant improved BMD there
was a trend towards at least maintaining BMD at the total hip Participants who were 50
or greater adherent to the intervention (reasons for non-adherence included lack of
time or chronic pain due to co-morbidity) were significantly less likely than
participants on medication alone to lose BMD at the total hip and femoral neck
In a third RCT Swenson et al (2009) compared the effects of two interventions on changes
in BMD in women receiving chemotherapy for breast cancer (n=62)
1) intravenous zoledronic acid (used to prevent skeletal fractures in people with cancer)
and oral calciumvitamin D every 3-months for five treatments
2) prescribed home-based physical activity and oral calciumvitamin D
Zoledronic acid protected patients with breast cancer against bone loss during initial
treatment whereas the home-based physical activity intervention was less effective in
preventing bone loss indicating that physical activity and dietary supplements are not
always sufficient to protect done density in people with cancer However these were
patients undergoing treatment and more research is required into the effects of physical
activity on bone health in post-treatment survivors
ii DIET
Bekkering et al (2006) did not identify any diet studies examining osteoporosis in breast
cancer survivors The current review identified 3 RCTs and one cohort study
Plant Proteins and Fibres
Weikert et al (2005) performed a sub-analysis of the EPIC cohort study conducted in
Germany which included 8178 females and examined the association between protein
intake dietary calcium and bone structure It was concluded that high consumptions of
animal protein may be unfavourable whereas higher vegetable protein may be
beneficial to bone health These results support the hypothesis that high calcium intakes
combined with adequate protein intake based on a high ratio of vegetables to animal protein
may be protective against osteoporosis Indeed evidence has demonstrated the relationship
between lower incidence of osteoporosis in Asian women and vegetarian populations due to
a diet rich in vegetables and fruit (Fujii et al 2009 Merill and Aldana 2009 Thorpe et al
2008) Furthermore a large-scale dietary modification intervention of post-menopausal
women (n = 4883) showed that an increased consumption of plant proteins and fibres from
fruits vegetables and grains reduced the risk of multiple falls and slightly lowered hip BMD
although it did not change the risk of osteoporotic fractures (McTiernan et al 2009)
New et al (2003 2004) provides further evidence for the benefits of plant proteins and fibres
on bone health in two reviews where a positive link between a high consumption of fruit
and vegetables and bone health has been demonstrated In the first report it was found
that fruit and vegetables have beneficial effects on bone mass and bone metabolism in men
and women across the age ranges whilst in the second review it was concluded that
although the impact of a vegetarian diet on bone health is much more complex than merely
being related to diet vegetarians do tend to have normallsquo bone mass
88
iii WEIGHT
Bekkering et al (2006) did not identify any studies examining weight implications on
osteoporosis in breast cancer survivors The current review identified one study that found
that being underweight (BMI less than 185) was associated with lower BMD (Ryan et al
2007)
b) PROSTATE CANCER
i WEIGHT
Bekkering et al (2006) did not identify any studies examining the effect of body weight on
osteoporosis in prostate cancer survivors The current review identified one RCT Ryan et
al (2007) found a positive association between BMI and bone density of the hip in men with
prostate cancer (n=120) who were within the first 12-months of androgen-deprivation
therapy This suggests that a higher BMI can be protective of bone density loss in this
patient group
ii ALCOHOL
Bekkering et al (2006) did not identify any studies examining the effect of alcohol
consumption on osteoporosis in prostate cancer survivors The current review identified one
RCT Ryan et al (2007) also demonstrate greater bone density in prostate cancer patients
consuming seven or more weekly alcoholic beverages when compared to non-drinkers
a) OTHER CANCER
i DIET
Soya Products
Bekkering et al (2006) did not identify any studies examining the effect of diet on
osteoporosis in other cancer survivors The current review identified one RCT Marini et al
(2008) reported a randomised double-blind placebo-controlled trial of the soya derivative
genistein aglycone and its effects on bone health after 3-years in women with breast and
endometrial cancer (n=389) Bone mineral density increases were greater with
genistein for both femoral neck and lumbar spine compared to placebo the conclusion
being that after 3-years of treatment genistein exhibited a promising safety profile with
positive effects on bone formation in this cohort of osteopenic post-menopausal women
89
SUMMARY OF EVIDENCE FOR OSTEOPOROSIS AND BONE HEALTH
There is evidence that vitamin D and calcium might be associated with greater BMD
however this benefit cannot be distinguished from other potential contributors such as
physical activity and medication More research is needed into the effects of physical activity
on osteoporosis in cancer survivors The findings thus far offer different conclusions
although there is limited evidence that physical activity can at the very least prevent loss of
BMD which is a positive outcome in survivors at particular risk of bone loss Greater
adherence to physical activity interventions appeared to offer the greater benefits
highlighting the importance of designing lifestyle interventions that can be maintained as
well as providing higher intensity support for survivors with co-morbidities
Higher BMI has been found to be protective of BMD loss in men with prostate cancer
however no distinction has been made between higher BMI and a BMI that indicates excess
weight Limited evidence has been provided for the benefits of moderate alcohol
consumption but as with the evidence presented for weight much more research is needed
before any valid and reliable conclusions can be made Since the NHS advises no more than
3-4 units of alcohol per day for men more research is needed to determine the minimum
units of alcohol that offer such protective benefits It is important to deter against excessive
drinking which can have a number of serious health implications including high blood
pressure mouth and throat cancers and stroke (NHS 2010)
Men should not exceed 3-4 units of alcohol per day on a regular basis (NHS 2010) One unit is the amount of pure alcohol in a 25ml single measure of spirits (pure alcohol by volume [ABV] 40) a third of a pint of beer (ABV 5-6) or half a 175ml standardlsquo glass of red wine (ABV 12) Daily alcohol limits are provided by the NHS in order to discourage the belief that that the number of units of a weekly limit can be consumed at once (ie binge drinking) Use of daily limit
90
Table 10 Osteoporosis and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Gross et al (2002)
Descriptive correlational test of a multicomponent intervention to prevent and treat osteoporosis in breast cancer survivors
27 post-menopausal breast cancer survivorslsquo post- treatment except for tamoxifen
Not reported
Physical activity vigour vitality and BMD
More than half reported no very hard physical activity and 37 reported no hard activity The association of vigour with total metabolic equivalents for combined moderate hard and very hard activities was significant (r = 0536 p = 0007) as were the hours spent in the combined moderate to very hard activities No relationship was found between vigour vitality or any level of activity and BMD
Schwartz Winters-Stone and Gallucci (2007)
RCT testing the effects of aerobic and resistance exercise on changes in bone mineral density (BMD) in women receiving chemotherapy Participants were randomised to aerobic or resistance exercise and usual care
66 women with stage I-III breast cancer beginning adjuvant chemotherapy
6-months after starting treatment
BMD aerobic capacity and muscle strength
Aerobic exercise preserved BMD significantly better compared to usual care Premenopausal women demonstrated significantly greater declines in BMD than postmenopausal women Aerobic capacity increased by almost 25 for women in the aerobic exercise group and 4 for resistance exercise Participants in the usual care group showed a 10 decline in aerobic capacity
Swenson et al (2009)
Participants received one of two treatments a) Intravenous zoledronic acid and oral calciumvitamin D every 3-months for five treatments b) Prescribed home-based physical activity and oral calciumvitamin D
Women receiving chemotherapy for breast cancer (n=62)
On completion of 3-month intervention
Severity of lymphedema by arm circumference
BMD significantly decreased in the physical activity group but not in the zoledronic acid group Zoledronic acid protected patients with breast cancer against bone loss during initial treatment whereas the home-based physical activity intervention was less effective in preventing bone loss indicating that physical activity and dietary supplements are not always sufficient to protect done density in people with cancer
Waltman et al (2009)
A 24-month self-efficacy based strength and weight training programme Participants were randomised to receive physical activity with medication (n=110) or medication only (n=113) the medication taken by both groups including risedronate (osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily)
Post-treatment post-menopausal breast cancer survivors (n=223) with amenorrhea for at least 12-months and a BMD score lower than the norm
On completion of the 24-month intervention
Bone mineral density
While participation in strength training did not result in statistically significant improved BMD there was a trend towards at least maintaining BMD at the total hip Participants who were 50 or greater adherent to physical activities were significantly less likely than participants on medication alone to lose BMD at the total hip and femoral neck
91
DIET
Marini et al (2008)
RCT assessing the continued safety profile of genistein
aglycone on
breast and endometrium and its effects on bone after
3 years of
therapy Participants received 54mg of genistein
aglycone daily or
placebo both treatment arms
received calcium and vitamin D
Breast cancer patients ndash intervention group (n=71) and placebo (n=67)
After 3-years of treatment
BMD Bone mineral density increases were greater with genistein for both
femoral neck and lumbar spine compared to placebo Genistein also
significantly reduced pyridinoline as well as serum carboxy-terminal
cross-linking telopeptide and soluble receptor activator of NF- B
ligand while increasing bone-specific alkaline phosphatase IGF-I
and osteoprotegerin levels There were no differences in discomfort
or adverse events between groups
(McTiernan et al 2009)
RCT assessing the effect of the Womens Health Initiative
Dietary
Modification low-fat and increased fruit vegetable
and grain
intervention on incident hip total and site-specific
fractures and self-
reported falls and in a subset on bone
mineral density (BMD)
Participants were randomly assigned to
receive
a)dietary modification intervention (daily goal 20 of energy as fat 5 servings of vegetables
and fruit
and 6 servings of grains) b)comparison group
- no dietary
changes
Post-menopausal women (n=48835) intervention (40 n=19541)
versus comparison group (60 n=29294)
Mean=81-years
Incident hip total and site-specific
fractur
es and self-reported falls and in a subset on bone
mineral
density (BMD)
215 women in the intervention group and 285 women in the
comparison group (annualized rate 014 and 012 respectively)
experienced a hip fracture (hazard ratio 112 95 CI 094
134 P = 021) The intervention group (n = 5423 annualized rate
344) had a lower rate of reporting 2 falls than did the
comparison group (n = 8695 annualized rate 367) (HR 092
95 CI 089 096 P lt 001) There was a significant interaction
according to hormone therapy use those in the comparison group
receiving hormone therapy had the lowest incidence of hip fracture In a subset of 3951 women
hip BMD at years 3 6 and 9 was 04ndash
05 lower in the intervention group than in the comparison group
(P = 0003)
New et al (2004)
Literature review assessing the impact of a vegetarian diet on indices of skeletal integrity to address specifically whether vegetarians have a normal bone mass
Analysis of existing literature through a combination of observational clinical and intervention studies were assessed in relation to bone health lacto-ovo-vegetarian and
Not reported
Bone health Key findings included (i) no differences in bone health indices between lacto-ovo-vegetarians and omnivores (ii) conflicting data for protein effects on bone with high protein consumption and low protein intake (particularly with respect to vegan diets) being detrimental to the skeleton (iii) growing support for a beneficial effect of fruit and vegetable intake on bone with mechanisms of action currently remaining unclarified The impact of a vegetarian diet on bone health is a hugely complex area since 1) components of the diet (such as calcium protein alkali vitamin K phytoestrogens) may be varied 2) key lifestyle factors which are
92
vegan diets versus omnivorous consumption of animal versus vegetable protein and fruit and vegetable consumption
important to bone (such as physical activity) may be different 3) the tools available for assessing consumption of food are relatively weak However from data available vegetarians do certainly appear to have normal bone mass
Weikert et al (2005)
Prospective cohort study (EPIC) examining associations between protein intake calcium and bone structure measured by broadband ultrasound attenuation (BUA)
8178 female EPIC participants
Not reported
Bone structure
High intake of animal protein was associated with decreased BUA values ( _ = ndash003 p = 0010) whereas high vegetable protein intake was related to an increased BUA ( _ = 011 p = 0007) The effect of dietary animal protein on BUA was modified by calcium intake
WEIGHT
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and alcohol use was positively associated with the Z score
ALCOHOL
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and body mass index was positively associated with the Z score
93
WEIGHT AND BODY COMPOSITION
Weight gain during and after cancer treatment is becoming an ever-increasing significant
concern (Camoriano et al 1990 Levine et al 1991 Saquib et al 2006) Weight gain is
expected when energy intake exceeds energy expenditure a combination that is frequently
described among breast cancer patients who report exercising less during treatment and
after treatment (Schwartz 2000 Demark-Wahnefried 2001) and consuming a higher energy
diet during treatment (Mukhopadhyay and Larkin 1986) Exacerbating this is the fact that
women in general gain weight as they transition through menopause (Sammel et al 2003)
putting breast cancer patients at particular risk as treatments frequently result in a premature
menopause For individuals with bowel cancer the CALBG 8980 trial showed that 35 of
patients post-chemotherapy were overweight (BMI 250ndash299) and 34 were obese BMI
300ndash349) or very obese (BMI gt35) (Meyerhardt et al 2008) The reasons for weight gain
during and after treatment are multifactorial and the result of individual lifestyle behaviours
and the impact of certain cancer drugs Regardless of the reasons as described in part one
of this review both survival and recurrence may be adversely affected by obesity
(Chlebowski et al 2002)
The effect of obesity on survival has been evident in the majority of studies although not all
one reason for this inconsistency being the possibility that biological factors associated with
obesity and not the obesity itself are responsible for the observed effect For example
there is considerable evidence that the effects of obesity on breast cancer risk may be
mediated at least in part by the effect of obesity on insulin resistance (Friedenreich 2001
Suga et al 2001 Goodwin et al 2002)
Finding effective methods for weight loss continues to be a challenge as although some
studies have demonstrated substantial weight loss in obese individuals weight loss results
in general have been modest and new approaches are needed (Jeffery et al 2000) For
long-term reduction in body weight intensive individualised approaches toward developing
a new lifestyle may be required (Djuric et al 2002)
Studies identified in the current review are summarised in Table 11 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in breast cancer survivors The current review identified one
meta-analysis and three RCTs
In the meta-analysis Kim Kang and Park (2009) reviewed 10 studies involving 588 women
who had been treated for breast cancer examining the effectiveness of aerobic exercise
interventions on cardiopulmonary function and body composition conducted during or after
cancer treatments They concluded that regular aerobic physical activity significantly
improved cardiopulmonary function as assessed by absolute VO2 peak relative VO2
94
peak and 12-minute walk test as well as improved body composition as assessed by
percentage body fat (although body weight and lean body mass did not change
significantly)
Courneya et al (2007) conducted a multicentre RCT in which women with breast cancer on
adjuvant chemotherapy were randomly assigned to usual care (n = 82) supervised
resistance exercise (n = 82) or supervised aerobic exercise (n = 78) for the duration of their
chemotherapy (median = 17-weeks 9-24 weeks) There was 70 adherence to supervised
exercise with aerobic physical activity being superior to usual care for improving
aerobic fitness and percent body fat whilst resistance physical activity was superior
to usual care for improving muscular strength lean body mass and chemotherapy
completion rate
Schmitz et al (2005) evaluated the safety and effects of twice-weekly weight training among
85 breast cancer survivors with women being randomised into immediate or delayed
intervention groups The immediate group trained from months 0-12 the delayed group
served as a no exercise parallel comparison group from months 0-6 and trained from months
7-12 At 6-months the immediate group compared to the no exercise group showed
significantly greater increases in lean mass (p lt 01) as well as significant decreases
in percentage body fat (p lt 05) This significance remained at 12-months when
comparing the immediate group with the delayed exercise group
Mefferd et al (2006) randomised overweight or obese breast cancer survivors (n=85) to a
16-week once weekly general exercise and dietary counselling intervention or standard
care The intervention addressed a reduction in energy intake as well exercise with a goal
of an average of one-hour a day of moderate to vigorous activity Seventy six women
(894) completed the intervention demonstrating reasonable acceptability of the
intervention At 16-weeks significant group differences in favour of the intervention
were evident in weight BMI percent fat trunk fat leg fat and waist and hip
circumference
ii DIET
Bekkering et al (2006) did not identify any studies examining the effect of diet on weight loss
or maintenance in breast cancer survivors The current review identified one RCT
Chlebowski et al (2006) report an RCT conducted as part of the aforementioned WINS trial
where 2437 postmenopausal women with early breast cancer were randomised to
nutritional and lifestyle counselling (n=975) or not (n=1462) as part of routine follow-up The
dietary intervention included eight bi-weekly individual counselling sessions As a reminder
the goal of the dietary intervention was to reduce percentage of calories from fat to 15
resulting in a sustained reduction in fat intake to approximately 20 of calories Dietary fat
intake reduction was significantly greater in the dietary group compared to the control group
After 12-months of intervention dietary fat intake was lower in the intervention group
than in the control group (333g per day versus 513g per day respectively Plt001)
95
corresponding to a statistically significant 6-pound lower mean body weight in the
intervention group (P lt01) This major study also demonstrated a survival advantage in
women who lost weight as described in Part 1 of this review
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in prostate cancer survivors The current review identified
one RCT
Segal et al (2009) conducted a RCT with 121 men with prostate cancer commencing
radiotherapy with or without androgen deprivation therapy They were randomly assigned to
24-weeks of usual care resistance exercise or aerobic exercise Compared with usual
care exercise improved aerobic fitness upper- and lower-body strength while
preventing an increase in body fat Resistance exercise generated longer-term
improvements and additional benefits for strength and body fat than aerobic exercise
SUMMARY OF EVIDENCE FOR WEIGHT AND BODY COMPOSITION
Supervised physical activity programmes with or without dietary counselling are highly
effective in improving body composition or at the very least preventing increases in weight
They are also safe and have other major benefits on health including improving fitness
walking distance muscle power and reducing cholesterol More research is however
required into the most effective dietary strategies for weight loss or maintenance in cancer
survivors Thus far there is some evidence for reducing dietary fat intake
A large controlled trial has been designed to test the combined effect of physical activity and
weight control on disease-free survival and on breast cancer recurrence free survival
second primary breast cancer and total invasive plus in situ breast cancer (Ballard-Barbash
et al 2009) Goals for weight control interventions for women whose BMI is greater than
25kgm2 is to lose 10 of body weight and for women whose BMI is less than or equal to
25kgm2 to avoid weight gain The goal for the physical activity intervention would be to
achieve and maintain regular participation in a moderate intensity physical activity
programme for a total of 150-255 minutes over at least 5 days per week This study is using
evidence which is current for weight loss and physical activity and is an indicator for the
basis of advice for patients at risk in similar situations
96
Table 11 Weight and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Courneya et al (2007)
Multicentre RCT to test for factors that could counteract unfavourable changes resulting from chemotherapy (eg changes in body composition) Participants were randomly assigned to usual care (n =
82) supervised resistance exercise
(n = 82) or supervised aerobic
exercise (n = 78) for the duration of their chemotherapy
242 breast cancer
patient
s initiating adjuvant chemotherapy
Median=17-weeks
Primary Cancer-Specific QoL Secondary Fatigue psychosocial functioning physical fitness body composition chemotherapy completion rate and lymphedema
The follow-up assessment rate for our primary end point was
921 and adherence to the supervised exercise was 702
Unadjusted and adjusted mixed-model analyses indicated that
aerobic exercise was superior to usual care for improving self-
esteem (P = 015) aerobic fitness (P = 006) and percent body fat
(adjusted P = 076) Resistance exercise was superior to usual care
for improving self-esteem (P = 018) muscular strength (P lt
001)
lean body mass (P = 015) and chemotherapy completion rate (P =
033) Changes in cancer-specific QOL fatigue depression and
anxiety favoured the exercise groups but did not reach statistical
significance Exercise did not cause lymphedema or
adverse events
Kim Kang and Park (2009)
Meta-analysis to examine the effectiveness
of aerobic exercise
interventions on cardiopulmonary function
and body composition in
women with breast cancer
Of 24 relevant
studie
s reviewed 10 studies (n= 588) met the inclusion criteria
Not reported Cardiopulmonary function
and body
composition
The findings indicated that aerobic exercise significantly improved
cardiopulmonary function as assessed by absolute
VO2 peak (standardized mean difference [SMD] 916 p lt 001)
relative VO2 peak (SMD424 p lt 05) and 12-minute walk test
(SMD 502 p lt 001) Similarly aerobic exercise significantly
improved body composition as assessed by percentage body fat
(SMD mdash890 p lt001) but body weight and lean body mass did not
change significantly
Mefferd et al (2006)
RCT to test the effect of a 16-week cognitive behavioural therapy (CBT) intervention for weight loss through exercise and diet modification on risk factors for recurrence of breast cancer Participants randomly assigned to a once weekly 16-week intervention or wait-list control group
Overweight or obese breast cancer survivors (n=76)
On completion of the 16-week intervention
Weight Significant differences in weight body mass index percent fat trunk fat leg fat as well as waist and hip circumference between intervention and control groups (P le 005) Furthermore levels of triglycerides and total cholesterolhigh density lipoprotein cholesterol levels were also significantly reduced following the intervention
97
Schmitz et al (2005)
RCT testing the safety of twice weekly weight training classes among recent breast cancer survivors Participantslsquo randomised into immediate and delayed treatment groups The immediate group trained from months 0-12 the delayed treatment group served as a no exercise parallel comparison group from months 0-6 and trained from months 7=12
Convenience sample of 85 recent breast cancer survivors
6 and 12-months
Body size (lean body mass) and biomarkers hypothesised to link exercise and breast cancer risk
Significant increases in lean mass (088 versus 002 kg P lt 001) as well as significant decreases in body fat (minus115 versus 023 P = 003) and IGF-II (minus623 versus 2828 ngmL P = 002) comparing immediate with delayed treatment from baseline to 6 months Within-person changes experienced by delayed treatment group participants during training versus no training were similar
Segal et al (2009)
Prostate Cancer Radiotherapy and
Exercise Versus Normal
Treatment study examining the effects
of 24-weeks of resistance or
aerobic training versus usual care on prostate cancer outcomes Randomly assigned
to usual care resistance or
aerobic exercise for 24-weeks
Prostate cancer patients on radiotherapy (n=121) usual care (n=41) resistance (n= 40) aerobic exercise
(n=
40)
On completion of 24-week intervention
Fatigue QOL physical fitness body composition PSA testosterone haemoglobin and lipid levels
Median adherence to prescribed exercise was 855 Compared
with usual care resistance training improved QOL (P = 015)
aerobic fitness (P = 041) upper- (P lt 001) and lower-body (P lt
001) strength and triglycerides (P = 036) while preventing an
increase in body fat (P = 049) Aerobic training also improved
fitness (P = 052)
DIET
Chlebowski et al (2006)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to 345]
versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group
98
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general dietary
guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
randomisation to death from any cause
99
QUALITY OF LIFE
The advancements in diagnosis and treatment that have contributed to the rise in
survivorship are a significant achievement for healthcare science However it is important to
recognise that this has also resulted in an increase in the number of people living with the
often long-term physical and psychological consequences of cancer and its treatment
Quality of life outcomes are thus becoming just as important as hardlsquo outcomes such as
mortality (Rosenbaum Fobair and Spiegel 2006) hence an emphasis on patient-reported
outcomes (DH 2009c) Indeed there is increasing evidence that QoL can be more
predictive of cancer survival than measures of performance status (Cella et al 2009 Eton et
al 2003 Wenzel et al 2005)
A healthy lifestyle has become viewed as an important element for improved QoL (Lyon and
Langille 2000) with particular emphasis on physical activity Studies identified in the current
review are summarised in Table 12 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in breast cancer survivors In the current review one systematic review (with meta-
analysis) and 6 RCTs were identified that provide evidence for the role of physical activity in
the QoL of breast cancer survivors
McNeeley et al (2006) conducted a systematic review with meta-analysis of RCTs (n=14)
examining the effects of physical activity on outcomes in breast cancer survivors Three of
the reviewed studies involving 194 patients compared exercise with usual care
(Campbell et al 2005 Courneya et al 2003 Segal et al 2001) with pooled data
demonstrating that exercise led to significant improvements in QoL superior to the
usual care groups Four studies involving 208 patients reported physical functioning or
physical well-being components of QoL (Campbell et al 2005 Courneya et al 2003
McKenzie and Kalda 2003 Segal et al 2001) the pooled results of which showed
a statistically significant increase in this component of QoL as a result of physical
activity Two of these studies were rated as high quality by the reviewers Courneya et al
2003 Segal et al 2001
100
In addition to this meta-analysis findings by Ohira et al (2006) demonstrated that over 6-
months physical and psychological QoL significantly improved in a recent breast
cancer survivors (n=86) 4-36 months post-treatment who took part in a twice-weekly
weight-training intervention when compared to a control group Increases in upper
body strength and lean mass correlated with these improvements suggesting that twice-
weekly weight training for recent breast cancer survivors might improve QoL in part via
changes in body composition and strength
Daley et al (2007) provided evidence from an RCT comprising sedentary breast cancer
survivors who were 12-36 months post-treatment and who were randomised to one of three
conditions
1) 8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-
minute one-to-one sessions with an physical activity specialist three times per week
(n=34)
2) 8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one
sessions with an physical activity specialist three times per week (n=36)
3) usual care (n=38)
Courneya et al (2003) evaluated QoL outcomes in relation to
exercise in breast cancer survivors (n=52) who had completed
surgery radiotherapy or chemotherapy Participants trained three
times per week for 15-weeks on recumbent or upright cycle
ergometers Exercise duration began at 15-minutes for weeks 1-
3 and then systematically increased by five-minutes every 3-
weeks to 35-minutes for weeks 13-15 The exercise group completed
984 of the exercise sessions demonstrating high adherence
rates Overall QoL increased by 91 points in the exercise group
compared with 03 points in the control group (p lt 001) Change
in peak oxygen consumption correlated with change in overall QoL
demonstrating a significant relationship between exercise and
increases in QoL (p lt 01)
Segal et al (2003) compared self-directed versus supervised
exercise on QoL outcomes in women with stages I-II breast cancer
(n=123) Physical functioning in the control group decreased by 41
points whereas it increased by 57 points and 22 points in the self-
directed and supervised exercise groups respectively (p lt 05)
Post-hoc analysis showed a moderately large and clinically important
difference between the self-directed and control groups (98
points p lt 01) and a more modest difference between the
supervised and control groups (63 points P = 09) No significant
differences between groups were observed for changes in QoL
scores
101
A significant mean difference of 98 units in QoL scores favouring aerobic physical
activity therapy was found This outcome was not the result of the extra support and
attention gained from taking part in the intervention since the same findings were not elicited
for the physical activity-placebo and usual care groups
A small pilot RCT comparing QoL and functional capacity in breast cancer survivors (n=21)
provided with 12-weeks of the Chinese physical activity Tai Chi Chuan (n=11) versus
psychosocial support (n=10) was conducted by Mustian Palesh and Flecksteiner (2008)
The tai chi group demonstrated significant improvements in functional capacity and QoL the
psychosocial support group showed significant improvements only in flexibility with declines
in QoL This suggests that tai chi can enhance functional capacity and QoL among
breast cancer survivors over and above the benefits of psychosocial support
Further support for the benefits of physical activity on QoL in breast cancer survivors (n=58)
within 2-years of completing adjuvant therapy has been demonstrated in a combined aerobic
and resistance training RCT (Milne et al 2008) The women received 12-weeks immediate
supervised physical activity three times a week (n=29) or delayed physical activity
comprising the same protocol but provided 12-weeks following the immediate physical
activity group (n=29) Adherence was 613 which is relatively low However there was a
significant group by time interaction for overall QoL which increased in the
immediate physical activity group from baseline to 12-weeks by 208 points compared
to a decrease in the delayed physical activity group of 53 points
Cadmus et al (2009) report on the QoL outcomes of two 6-month RCTs designed for breast
cancer survivors and based on the national recommendation of 30-minutes of moderate to
vigorous physical activity five days per week
When combining findings from these two studies physical activity was not associated with
QoL benefits in the full sample of either study however physical activity was associated with
significantly improved social functioning (a component of QoL) among survivors who
Trial Increasing or Maintaining
Physical Activity during Cancer
Treatment (IMPACT)
Theoretical Framework Theory of
Planned Behaviour and
transtheoretical model - promoting
self-efficacy to overcome barriers to
physical activity
Sample n=45 newly diagnosed
survivors
Delivery Home-based
Trial Yale Physical activity and
Survivorship (YES)
Theoretical Framework Not
reported
Sample n=67 post-treatment
survivors
Delivery Combined supervised
training programme at a local
health club with home-based
physical activity
102
reported low social functioning at baseline which is the likely impact of greater social
interaction during the intervention This highlights the utility of risk stratification and the
provision of lifestyle support based on need survivors with low social functioning as
could be detected via the Social Difficulties Inventory (SDI Wright et al 2005b) are
likely to benefit from programmes such as the IMPACT and YES trial
Sandel et al (2005) report on a cross-over RCT testing the outcomes of a 12-week dance
and movement exercise programme in women within 5-years of treatment for breast cancer
(n=38) The study included a waiting list control (n=19) and cross-over at 13-weeks Women
attended two supervised dance sessions for six weeks and one session per week for an
additional 6-weeks for a total of eighteen sessions A total of 35 (92) women completed
the regimen with reasons for dropping out including fatigue other commitments and one
participant reported shoulder discomfort The overall finding was that breast cancerndash
specific QoL improved significantly in the intervention group compared to the waiting
list group at 13-weeks which remained unchanged
In the updated systematic review described previously Speck et al (2010) present evidence
from 66 high quality RCTs showing that physical activity during treatment has a small to
moderate positive effect on QoL (p=004) anxiety (p=002) and self-esteem (p=002)
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in colorectal cancer survivors In the current review one large cohort study was
identified Lynch et al (2008) examined physical activity and QoL data collected as part of
the Colorectal Cancer and Quality of Life Study37 Telephone interviews were conducted
at approximately 6 12 and 24-months after colorectal cancer diagnosis (n=1966) which
found that participants achieving at least 150-minutes of physical activity per week had an
18 higher QoL score than those who reported no weekly physical activity
ii DIET
Bekkering et al (2006) identified two dietary intervention studies examining impact on QoL in
colorectal cancer survivors One dietary counselling trial found a significant improvement in
health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst another reported that
an intervention aimed at a healthier dietary lifestyle had no effect on health assessment or
life satisfaction but did lead to increased health action and increased reports of feeling goodlsquo
(Corle et al 2001) No further studies were identified in the current review
37
The Colorectal Cancer and Quality of Life study in Australia examines in detail the lifestyle factors that
influence QoL in the 5-years post-diagnosis (n=2000)
103
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any dietary physical activity interventions examining
impact on QoL in prostate cancer survivors One dietary counselling trial found a significant
improvement in health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst
another reported that an intervention aimed at a healthier dietary lifestyle had no effect on
health assessment or life satisfaction but did lead to increased health action and increased
reports of feeling goodlsquo (Corle et al 2001) No further studies were identified in the current
review
Segal et al (2003) reported an RCT comparing supervised resistance exercise versus
control in men with prostate cancer (n=135) who were scheduled to receive androgen
deprivation therapy for at least 3-months Fitness levels were assessed and the men in the
intervention group met with a certified fitness consultant within 7-days of the pre-
assessment The fitness consultant provided patients with the results of their exercise
assessment and introduced a personalised resistance exercise program A significant
improvement was found in QoL outcomes in the intervention group and a significant
decline in the control group Resistance exercise improved QoL regardless of whether
men were treated with curative or palliative intent or whether androgen deprivation therapy
had been received for less than one-year or 1 year
d) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) found that out of seven physical activity trials six observed
improvements in QoL when using cancer-specific questionnaires (Burnham and Wilcox
2002 Courneya et al 2003 Segal et al 2003 Headley et al 2004 Campbell et al 2005
Sandel et al 2005) but one of these same studies found no association when using the
generic SF-36 scale (Segal et al 2001) This highlights the importance of selecting the most
appropriate outcome measures in terms of sensitivity and responsiveness to a given
intervention
In the current review three studies were identified One prospective controlled four-centre
study comprising a sample of survivors with different tumour sites was identified (Korstjens
et al 2008) QoL outcomes were compared between three groups
1) group-delivered physical training (n=71)
2) group-delivered combined physical and cognitive behavioural training (CBT) (n=76)
3) waiting-list control (n=62)
Participants in both training groups showed significant and clinically relevant improvements
in role limitations physical functioning vitality and health change Adding CBT to the
physical training did not have additional beneficial effects on QoL a finding that has been
104
observed in a number of supported self-management programmes (Davies and Batehup
2010)
Oh et al (2009) reported a RCT examining the QoL outcomes of Medical Qigong (MQ) a
mindndashbody practice that uses physical activity and meditation to harmonise the body mind
and spirit Patients (n=162) with malignancy of any stage and an expected survival length of
gt12-months were randomised to a control group or to a 10-week MQ programme comprising
two supervised 90-minute sessions per week At 10-week follow-up participants in the
MQ group reported larger improvements in QoL than those in the usual care group (p
lt 05)
Mosher et al (2009) reported a prospective cohort study examining the diet exercise and
QoL patterns of 753 breast prostate and colorectal cancer survivors who were at least 5-
years post-diagnosis Survivors underwent two 45-60 minute telephone surveys
administered by the Diet Assessment Center The data demonstrated that greater weekly
minutes of exercise were associated with better physical QoL including less pain and
better health perceptions physical functioning and vitality More exercise was also
correlated with better social functioning Diet quality had a positive association with a range
of physical QoL outcomes in analyses that were adjusted for age level of education and co-
morbidities Greater BMI was associated with worse physical QoL including greater
pain and role limitations because of physical problems and worse health perceptions
physical functioning and vitality
SUMMARY OF EVIDENCE FOR QUALITY OF LIFE
Lifestyle interventions appear to help people with a wide range of cancer types who have
received treatments ranging from surgery chemotherapy radiotherapy or hormonal
therapies although no trials have yet been published specifically addressing the newer
biological therapies Even when not directly associated with overall QoL exercise has been
found to significantly improve social functioning among post-treatment survivors The
benefits of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or group-
based A vast array of different types of exercise techniques have been tested in the studies
evaluated in this review highlighting the potential for survivors to choose activities according
to preference
Whilst some studies have recommended the uptake of physical activity during treatment
others have highlighted the benefits of introducing regular physical activity into a survivorlsquos
self-management care plan immediately after completion of treatment Overall the evidence
does suggest that immediate physical intervention provides greater QoL benefits than
delayed intervention
105
Table 12 Quality of Life and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Cadmus et al (2009)
The results of two RCTs to determine the effect of exercise on quality of life in (a) a RCT of exercise among recently diagnosed breast cancer survivors undergoing adjuvant therapy - randomised to a 6-month home-based exercise program or a usual care group (b) a similar trial among post-treatment survivors - randomised to a 6-month supervised exercise intervention or to usual care
50 newly diagnosed breast cancer survivors in the first RCT (a) 75 post-treatment survivors in the second RCT (b)
6-months Measures of happiness depressive symptoms anxiety stress self-esteem and QoL
Good adherence was observed in both studies Baseline quality of life was similar for both studies on most measures Exercise was not associated with quality of life benefits in the full sample of either study however exercise was associated with improved social functioning among post-treatment survivors who reported low social functioning at baseline (p lt005)
Courneya et al (2003)
RCT testing 15-weeks supervised aerobic and resistance training to determine the effects on cardiopulmonary
function and QoL in
post-menopausal breast cancer
survivors Randomly assigned to an exercise (n=25) or control (n=28) group The exercise group trained on cycle ergometers
three times per week for 15
weeks The control group did not train
53 post-menopausal breast cancer survivors
On completion of the 15-week intervention
Changes in peak oxygen
consu
mption and overall
Peak oxygen consumption increased by 024 Lmin in the exercise group whereas it decreased
by 005 Lmin in the control group
(mean difference 029 Lmin 95 confidence interval [CI] 018 to
040 P lt 001) Overall QOL increased by 91 points in the exercise
group compared with 03 points in the control group (mean
difference 88 points 95 CI 36 to 140 P= 001) Pearson
correlations indicated that change in peak oxygen consumption
correlated with change in overall QOL (r = 045 P lt 01)
Daley et al (2007)
RCT - Women were randomised to one of three groups a)8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-minute one-to-one sessions with an physical activity specialist three times per week (n=34) b)8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one sessions with an physical activity specialist three times
Sedentary breast cancer survivors who were 12-36 months post-treatment (n=117)
On intervention completion and at 24-weeks follow-up
QoL depression physical activity behaviour aerobic fitness
There was a significant mean difference of 98 units in QoL scores favouring aerobic physical activity therapy
106
per week (n=36) c)usual care (n=38)
Korstjens et al (2008)
RCT comparing the effects on cancer survivorslsquo QoL in a
12-week group-
based multidisciplinary self-management rehabilitation
program
combining physical training (twice weekly) and cognitive-behavioural
training (once weekly) with
those of a 12-week group-based physical
training (twice weekly) There
was also a non-intervention comparison group
All cancer types rehabilitation (n=76) physical training (n=71) comparison group (n=62)
Baseline after rehabilitation and
3-
months follow-up
QoL (SF-36) The effects of multidisciplinary rehabilitation did not outperform
those of physical training in role limitations due to emotional
problem (primary outcome) or any other domains of quality of life
(all p gt 05) Compared with no intervention participants in both
rehabilitation groups showed significant and clinically relevant
improvements in role limitations due to physical problem (primary
outcome effect size (ES) = 066) and in physical functioning (ES =
048) vitality (ES = 054) and health change (ES = 076) (all p lt
01)
Lynch et al (2008)
Colorectal Cancer and Quality of Life
Study - aimed at examining the relationships between
physical activity
and QoL after a colorectal cancer
diagnosis Participants completed telephone interviews at approximately
6
12 and 24 months after diagnosis
1966 people with colorectal
6 12 and 24-months post-diagnosis
QoL There was an overall independent association between physical
activity and QoL At a given time point
participants achieving at least 150 minutes of physical activity per
week had an 18 higher quality of life score than those who
reported no physical activity Significant associations were also
present at the interindividual level (differences between
participants) and intraindividual level (within participant changes)
Milne et al (2008)
RCT to examine the effects of a supervised exercise program on motivational variables in breast cancer survivors Participants were randomised in a cross-over design to either an immediate exercise group that exercised from baseline to week 12 or a delayed exercise group that exercised from week 12 to 24
Breast cancer survivors (n=58) within 2-years of completing adjuvant therapy
Post-intervention (12-weeks)
Quality of life There was a significant group by time interaction for overall QoL which increased in the immediate physical activity group by 208 points compared to a decrease in the delayed physical activity group of 53 points
Mosher et al (2009)
Prospective Cohort Study examining the health behaviours of older cancer survivors and the associations of those behaviours with QoL especially during the long-term post-treatment period
753 older (aged 65 years) long-term survivors ( 5 years post-diagnosis) of breast prostate and colorectal
2 telephone interviews
Exercise diet weight status and quality of life
Participants reported a median of 10 minutes of moderate-to-vigorous exercise per week and only 7 had Healthy Eating Index scores gt80 (indicative of healthful eating habits relative to national guidelines) Despite their suboptimal health behaviours survivors reported mental and physical quality of life that exceeded age-related norms Greater exercise and better diet quality were associated with better physical quality-of-life outcomes (eg better vitality and physical functioning P lt 05) whereas greater body mass index was associated with reduced physical quality of life (P lt 001)
107
cancer
Mustian Palesh and Flecksteiner (2008)
RCT testing the functional and QoL outcomes of tai chi - women who completed treatment randomised to receive tai chi or psychosocial support therapy for 12-weeks (60 minutes three times weekly)
Breast cancer survivors (n=21)
On completion of 12-week intervention
Functional capacity and quality of life
The tai chi group demonstrated significant improvements in functional capacity and QoL the psychosocial support group showed significant improvements only in flexibility with declines in QoL
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials
MEDLINE EMBASE CINAHL Psych INFO CancerLit PEDro
and
SportDiscus as well as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
functi
oning as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all outcomes
were positive even when statistical significance was not achieved
Exercise led to statistically significant improvements in quality of life
as assessed by the Functional Assessment of Cancer Therapyndash
General (weighted mean difference [WMD] 458 95 CI 035 to
880) and Functional Assessment of Cancer TherapyndashBreast (WMD
662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak oxygen consumption
and in reducing symptoms of fatigue
Oh et al (2009)
RCT comprising 10-weeks Medical Qigong (MQ) to evaluate the use of (MQ) compared with usual care in improving the QOL of cancer patients
162 patients with a range of cancers
On completion of the 10-week intervention
QOL and fatigue (FACT-GF) mood (Profile of Mood State)
Regression analysis indicated that the MQ group significantly improved overall QOL (t144thinsp=thinspminus5761 Pthinspltthinsp0001) fatigue (t153thinsp=thinspminus5621 Pthinspltthinsp0001) mood disturbance (t122 =2346 Pthinsp=thinsp0021) and inflammation (CRP) (t99thinsp=thinsp2042 Pthinspltthinsp0044) compared with usual care after controlling for baseline variables
Ohira et al (2006)
RCT to examine the effects of weight training on changes in QoL and depressive symptoms in recent breast cancer survivors Randomised to treatment or control group
Convenience sample of 86 breast cancer survivors (4-36 months post-treatment)
6-months The primary outcomes were changes in QoL (CARES-SF) and depressive symptoms (CES-D)
QoL improved in the treatment group compared with the control group (Standardized Difference = 062 P = 006) The psychosocial global score also improved significantly in the treatment group compared with the control group (Standardized Difference = 052 P = 02) There were no changes in CES-D scores Increases in upper body strength were correlated with improvements in physical global score (r = 032 P lt01) and psychosocial global score (r = 030 P lt01) Increases in lean mass were also correlated with improvements in physical global score (r = 023 P lt05) and psychosocial global score (r = 024 P lt05)
Sandel et al (2005)
RCT - 12-weeks dance and movement programme versus wait list control to determine the effect on QoL and shoulder function
35 breast cancer survivors
13 and 26-weeks
QoL (FACT-B) Shoulder range of motion (ROM) and Body Image Scale
FACT-B significantly improved in the intervention group at 13 weeks from 1020 _158 to 1167 _ 169 compared to the wait list group 1081 _ 164 to 1071 _213 (time _ group effect P _ 008) During the crossover phase the FACT-B score increased in the wait list group and was stable in the treatment group The overall effect of the training at 26 weeks was significant (time effect P _ 03) and the order of training was also significant (P _ 015) Shoulder ROM
108
increased in both groups at 13 weeks mdash15_ and 8_ in the intervention and wait list groups (Time effect P _ 03 time _ group P _ 58) Body Image improved similarly in both groups at 13 weeks (time effect P _ 001 time _ group P _ 25) and at 26 weeks There was no significant effect of the order of training for these outcome measures
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) A small to moderate positive effect of physical activity during treatment was seen for physical activity level aerobic fitness muscular strength functional quality of life anxiety and self-esteem With few exceptions exercise was well tolerated during and post treatment without adverse events
Segal et al (2003)
RCT testing the hypothesis that resistance exercise can counter the negative QoL effects of androgen deprivation therapy for prostate cancer by reducing fatigue elevating mood building muscle mass and reducing body fat Randomly assigned to an intervention group that participated in a resistance exercise program three times per week for 12 weeks or to a waiting list control group
55 men with prostate cancer scheduled for androgen deprivation therapy for at least 3 months after recruitment
On completion of the 12-week intervention
Primary outcomes fatigue disease-specific QoL Secondary outcomes muscular fitness body composition
Men assigned to resistance exercise had less interference from fatigue on activities of daily living (P =002) and higher quality of life (P =001) than men in the control group Men in the intervention group demonstrated higher levels of upper body (P =009) and lower body (P lt001) muscular fitness than men in the control group The 12-week resistance exercise intervention did not improve body composition as measured by changes in body weight body mass index waist circumference or subcutaneous skinfolds
Vadiraja et al (2009)
RCT - 6-week yoga and relaxation during adjuvant radiotherapy his study compares the effects of an integrated yoga program with brief supportive therapy in breast cancer outpatients undergoing adjuvant radiotherapy at a cancer centre Intervention consisted of
88 stage II and III breast cancer outpatients
After 6-weeks of radiotherapy
QoL (EORTC-C30) Mood (Positive and Negative Affect Schedule)
There was a significant difference across groups over time for positive affect negative affect and emotional function and social function There was significant improvement in positive affect (ES = 059 p = 0007 95CI 125 to 78) emotional function (ES = 071 p = 0001 95CI 645 to 2533) and cognitive function (ES = 048 p = 003 95CI 12 to 185) and decrease in negative affect (ES = 084 p lt 0001 95CI minus134 to minus44) in the yoga
109
yoga sessions lasting 60 minutes daily while the control group was imparted supportive therapy once in 10 days
group as compared to controls There was a significant positive correlation between positive affect with role function social function and global quality of life There was a significant negative correlation between negative affect with physical function role function emotional function and social function
110
ONGOING LIFESTYLE STUDIES
Four ongoing lifestyle studies were identified in the current review one for breast cancer and
three for colorectal cancer
a) BREAST CANCER
In the US Goodwin et al (ongoing) are trialling lsquoLifestyle Intervention Study in Adjuvant
Treatment of Early Breast Cancerrsquo (LISA) The primary objective of this trial is to evaluate
the effect of the addition of a 2-year centrally delivered individualised telephone-based
lifestyle intervention focusing on weight management to a mailed educational intervention on
disease-free survival in post-menopausal women with early stage breast cancer (hormone
receptor positive) BMI ge24-lt40 kgm2 who are receiving standard letrozole adjuvant
therapy The primary outcome is disease-free survival Secondary outcomes include overall
survival distant disease-free survival weight change QoL selected non-cancer medical
events and biologic factors (insulin) The estimated enrolment is 2150 with the study having
started in 2007 Participants will be randomised to
1) Individualised Lifestyle Intervention Experimental - Women randomised to this arm
will receive an intervention program that consists of individual weight loss diet and
physical activity goals incorporated into a 2-year standardised structured telephone
and mail-based intervention In addition to diet and physical activity the intervention
will address behavioural and motivational issues relating to weight management
including maintaining motivation overcoming obstacles to success relapse
prevention emotional distress and stress and time management The telephone
intervention will involve 19 phone calls as well as mailings and a participant manual
women will be asked to lose up to 10 of their weight by reducing their caloric and
fat intake (by 500-1000 kcalday 20 calories fat) and increasing their moderate
physical activity (to 150-200 minutesweek)
2) Mail-based Active Comparator - Participants will receive a standardised mail-based
intervention focussing on healthy living This will include mailings at study entry as
well as a 2-year subscription to health magazine
Approximately 2150 women will be enrolled follow-up will continue until target event rates
have been met (anticipated 4-6 years after completion of the intervention) This sample size
will provide 80 power (type 1 error 005 2-tailed) to detect a hazard ratio (HR) for DFS of
074-076 in the weight loss intervention arm
b) COLORECTAL CANCER
It has been suggested that interventions to improve QoL in colorectal cancer survivors are
more effective if they target symptom management psychosocial support and lifestyle
variables in a comprehensive and integrated approach to behavioural change (Steginga et
al 2009) Due to the paucity of comprehensive trials examining behavioural interventions in
this group of survivors Hawkes et al (2009) are conducting a large-scale RCT of a 6-month
telephone-delivered lifestyle coaching intervention based on Acceptance and Commitment
111
Therapy (ACT) ndash bdquoCanChange‟ The intervention aims to assist colorectal cancer survivors
(n=350) to make improvements in lifestyle including physical activity weight management
and smoking cessation Participants receive up to eleven telephone sessions over the
6-months from a qualified health professional who provides support on symptom
management and lifestyle change Outcomes will be assessed post-intervention at 6- and
12-months follow-up and will include physical activity CRF QoL and cost-effectiveness
The findings from this innovative lifestyle coaching initiative will offer insight into the intensity
of support required to achieve sustained behaviour change as well as highlight the efficacy
of various components of delivery (eg telephone-delivery coaching professionally-led
etc)
Courneya et al (2008) are leading a physical activity intervention in a collaboration between
Canada and Australia the Colon Health and Life-Long Physical activity Change
(CHALLENGE) a 3-year multicentre RCT for colon cancer survivors (n=1000) who are 2-6
months post adjuvant-treatment Any type of physical activity will be promoted the goal
being to motivate people to increase their overall activity by about 25-hours of moderate
intensity physical activity or 1-hour and 15-minutes of vigorous physical activity per week
Behavioural support counselling and supervised physical activity sessions will be used to
promote the adoption and long-term maintenance of physical activity By monitoring
participants over 10-years the trial will determine if colon cancer recurs less often in people
who increase and maintain their physical activity It will also assess whether physical activity
improves other important outcomes including QoL anxiety depression sleep and physical
function It is anticipated that this trial will provide important insight into strategies for
promoting long-term health behaviour change
Another Australian lifestyle intervention is The Colorectal Cancer and Quality of Life led
by Joanne Aitken The purpose of this project is to identify any patterns between lifestyle and
QoL over the first 5-years following a diagnosis of colorectal cancer Approximately 2000
people have been recruited to take part in this study making it the largest colorectal cancer
study of its type to be undertaken Participants complete a telephone interview and a written
Pilot testing demonstrated that
o 80 of participants (n=20) felt the intervention addressed their issues
o 100 felt more motivated to make lifestyle changes
o 100 would recommend the intervention to other survivors
From baseline to post-intervention improvements
were observed for
o Colorectal cancer symptoms o QoL o Diet o Physical activity
112
questionnaire on an annual basis over the 5-years One of the aims of the study is to
uncover how lifestyle factors particularly physical activity may improve QoL and reduce the
risk of developing other chronic diseases that cancer survivors are prone to such as heart
disease and diabetes This information will help Cancer Council Queensland properly design
and target lifestyle interventions to help improve the health and well-being of colorectal
cancer survivors (Aitken et al ongoing)
113
DISCUSSION
WHAT DO WE KNOW ABOUT LIFESTYLE AND CANCER
This aim of this review was to update the World Cancer Research Fund (WCRF) report bdquoA
Systematic Review of RCTs Investigating the Effect of Nutritional and Physical
Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This has been
achieved by conducting a comprehensive but pragmatic search of the literature from 2006
onwards Where no evidence was available in the WCRF review studies before 2006 have
been included if identified in the reference lists of acquired records To facilitate this
evidence cited within the lsquoHandbook of Cancer Survivorship‟ (Feuerstein 2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (2009) were also utilised
Before presenting a synthesis of the findings within this review there are some limitations
that first need to be addressed
Methodological Limitations
There is strong evidence from observational studies that lifestyle factors can potentially have
major influences on overall mortality risk for cancer survivors This has been most frequently
subjected to study in breast cancer survivors However it is recognised that such
associations in observational studies can be influenced by confounding and therefore that
the mechanisms of lifestyle change on all-cause mortality remains unclear (Cheblowski
2010) Therefore although the observational evidence is strong there is a need to
understand the benefits of lifestyle change ndash particularly physical activity and weight control
in the absence of confounding factors which can be achieved only within the context of a
controlled trial (Ballard-Barbash et al 2009) Such evidence in the end is most likely to
lead to promoting the wide scale adoption of lifestyle change interventions in the role of
secondary prevention of cancer
Consistent with Bekkering et al (2006) it has been found that there is a paucity of robust
evidence on the effects of lifestyle behaviours in cancer progression and recurrence as well
as in the prevention and management of the long-term health implications of cancer
treatment Studies generally comprise small sample sizes and few offer evidence of the
long-term effects of lifestyle behaviours Since lifestyle choices are generally behavioural in
nature the sustainability of these behaviours is fundamental if commissioners are to provide
funding for lifestyle interventions
There were also a large number of retrospective studies particularly for smoking This is
understandable given the challenges of research within this area however it does also raise
limitations surrounding the accuracy of findings This is especially the case when findings
rely on retrospective self-reports of health behaviours or illness experience
114
A number of methodological limitations confound the interpretation of the benefits of exercise
and diet after a diagnosis of cancer from other risks such as smoking body size
supplements and analgesic intake Nevertheless as highlighted by Doyle et al (2007) even
when the scientific evidence is incomplete reasonable conclusions can be made on issues
that can guide lifestyle choices for cancer survivors These are discussed next
THE EVIDENCE
Diet
Evidence for reducing fat intake remains unclear yet evidence for the mechanisms of benefit
of weight loss or the maintenance of a healthy weight is strong Weight control and self-
management clearly requires consideration of total fat intake highlighting the necessity to
provide cancer survivors with advice on levels of fat necessary for weight maintenance
weight loss or in some cases weight gain (Chlebowski et al 2005 Patterson et al 2010)
The same rationale applies to any inconsistencies in evidence for increased fruit and
vegetables which can also facilitate weight management Indeed where the evidence is
strongest for fruits and vegetables applies to those sources containing carotenoids The
evidence is convincing that carotenoids do provide anti-cancer properties (Rock et al 2005
Pierce et al 2007) Lycopene (found in tomatoes) is one such carotenoid found to offer
anti-cancer benefits (Schwarz et al 2008)
Fibre (found in the skins of fruit and vegetables as well as in beans and lentils) and folate
(found in broccoli brussel sprouts asparagus and peas) have in the main been found to
protect against colorectal cancer The evidence is convincing that by slowing down bowel
transit time the mechanism of benefit comes from reducing contact between potential
carcinogens
The benefits of a low fat high fruit and vegetable diet extend into the management of
treatment-related conditions such as lymphoedema In individuals carrying excess weight
the resulting weight loss achieved via a low fat high fruit and vegetable diet can ease the
symptoms of lymphoedema (Shaw Mortimer and Judd 2007)
The evidence also suggests that survivors of prostate cancer might benefit from including
pomegranate juice and green tea in their diet
In terms of other food sources vitamin D and calcium can be protective against osteoporosis
(Ryan et al 2007) although more research with a specific fouls on cancer survivors is
needed in this area
Physical Activity
In general the findings of epidemiological and large cohort studies demonstrates that the
evidence for the role of physical activity in improving breast cancer prognosis quality of life
and on the levels of several hormones associated with breast cancer is strong
115
There is substantial evidence suggesting that the physical activity recommendations
developed by the Department of Health are sufficient for cancer survivors - a total of at least
30-minutes a day of moderate intensity physical activity on five or more days of the week
This can be achieved either by doing all the daily activity in one session or through several
shorter bouts of activity of 10 minutes or more Additionally there is evidence of a dose-
response (ie the more physical activity the greater any benefits) The evidence for breast
cancer further suggest that for survival benefits to be achieved from physical activity no less
than moderate to vigorous activity is required (Gross et al 2002) However the most recent
expert advice emphasises that even a modest amount of exercise like brief walks is
beneficial and gains will be seen versus doing nothing at all38
The interpretation of physical activity evidence has been hindered by the difficulty of
distinguishing physical activity outcomes from subsequent weight loss outcomes However
again even if the main mechanism of benefit of physical activity is improved outcomes
resulting from weight loss or maintenance then this could be considered strong enough
evidence to prescribe physical activity to cancer survivors Furthermore the evidence is
encouraging in terms of its QoL-enhancing effect (McNeeley et al 2006 Daley et al 2007)
Three specific elements of physical activity interventions or advice could be addressed
(Ballard-Barbash et al 2006)
Reducing sedentary behaviours (such as watching TV)
Exercise sessions
Type and intensity of physical activity
There is sufficient evidence for supervised physical activity improving symptoms of cancer-
related fatigue (McNeely et al 2006 Cramp and Daniel 2008) and lymphoedema (Moseley
and Pillerlsquos 2008) Indeed the evidence suggests that guided progressive physical activity
soon after treatment can ease the symptoms of lymphoedema (de Rezende et al 2006)
This supports recent cautions regarding risk-averse clinical recommendations guiding
survivors to avoid the use of the affected limb which may actually lead to de-conditioning
and the very outcome women seek to avoid (Schmitz 2010) At the very least there is no
evidence of appropriate intensity physical activity causing or exacerbating either fatigue or
limb swelling The same is true for the effect of physical activity on osteoporosis Whilst the
benefits of physical activity on bone health require clarifying physical activity can at the very
least prevent loss of bone mineral density in survivors at particular risk of developing
osteoporosis (Waltman et al 2009)
A recent roundtablelsquo event by the American College of Sports Medicine has produced a
Consensus Statement detailing exercise guidelines for cancer survivors (Schmitz Courneya
and Matthews et al 2010) An expert panel reviewed the published empirical evidence and
came to the consensus regarding the safety and efficacy of exercise testing and prescription
in cancer survivors The evidence is clear that exercise during treatment (specific risk
assessment can be carried our for specific treatments and biological response) and after
38
Dr Rachel Ballard ndash Barbash in the NCI Cancer Bulletin June 29 2010
116
treatment is safe and effective Activity induced improvements can be expected on aerobic
fitness muscular strength quality of life and fatigue in breast prostate and haematological
cancers Resistance training can be performed safely by breast cancer survivors with and at
risk of lymphoedoema
Efforts are currently being made to increase the capacity and capability of exercise
professionals to address the unique needs of cancer survivors Exercise professionals need
to be able to access training which reflects the medical condition they are treating for to be
more knowledgeable about the condition and the most suitable and appropriate exercises for
them This requires the development of a national competency framework for a specialist
level 3 add on or level four qualification This would enable providers to develop national
training programmes for cancer specialist exercise professionals and lead to more
accessible referral through the exercise referral scheme (Exercise Referral Research March
2010)
Smoking
Strong and consistent evidence has been presented for increased risk of disease
progression and mortality in people who continue to smoke after a diagnosis of cancer as
well as poorer outcomes in pre-diagnosis smokers (Parsons et al 2010) This evidence
applies particularly to cancers of the lung or head and neck Further research is needed for
breast colorectal prostate and rarer cancers
Alcohol
There is a paucity of research into the effects of alcohol pre- and post-diagnosis on cancer
progression and recurrence as well as symptom management Evidence thus far is highly
contradictory with some demonstrating a protective effect some a detrimental effect and
others no effect
Weight
Substantial weight gain after diagnosis and treatment for breast cancer is adversely
associated with breast cancer prognosis Obesity appears to increase the risk of recurrence
and death among breast cancer survivors by around 30 (Patterson et al 2010) Much
more research is needed to clarify the relationship between prognosis and survival and body
weight in other tumour types
Dealing with issues of weight weight gain and weight management with patients is one of
the lifestyle behaviour change issues health care professionals feel most challenged by
Studies do confirm that health care professionals find it difficult to address these issues with
patients without appearing biased and negative It would appear that a lack of professional
training on behavioural change and motivational coaching and effective strategies for weight
117
loss combine and can lead to avoidance by health care professionals in addressing the need
for change (Puhl and Heuer 2009 Blakeman et al 2010)
Mechanisms of Benefit
Chlebowski (2010) offers some thought-provoking insight into the challenge of implementing
lifestyle change when aromatase inhibitors have been found to reduce oestrogen levels far
more than physical activity interventions One study cites approximately 90 reductions in
oestrogen levels as a result of aromatase inhibitors (Dixon et al 2008) Furthermore three
trials comparing aromatase inhibitors versus placebo anticipate 60-70 reduction in breast
cancer risk (Cuzick 2005 Goss et al 2007 Visvanathan et al 2008) Equally Chlebowski
(2010) points out that the influence of physical activity on insulin levels also has a
pharmacological competitor in the form of metformin (Goodwin et al 2008 Jiralerspong et
al 2009)
These are valid insights that are likely to complicate the successful integration of lifestyle
advice into standardised models of aftercare On the other hand if a public and community
health approach is taken to health and well-being then lifestyle change is likely to offer
health benefits beyond cancer-specific health Such an approach is recommended in the
bdquoCapabilities for Supporting Prevention and Chronic Condition Self-Management A
Resource for Educators of Primary Health Care Professionals‟ developed as part of the
Australian Better Health Initiative (Flinders University 2009) The model offered within this
capabilities framework promotes healthcare providers to view patients holistically as
opposed to focusing solely on diagnosed chronic condition The rationale for this in part
lies in the fact that chronic conditions are more often than not accompanied by co-
morbidities and therefore healthcare is not only about the established condition but also
identified risk factors for co-morbidity
MAKING LIFESTYLE RECOMMENDATIONS FOR CANCER SURVIVORS
In terms of reducing the risks of relapse evidence is strongest for breast colorectal lung
and head and neck cancers but self-management lifestyle strategies are likely to be person-
specific rather than disease or treatment specific so are likely to apply to all patients
recovering from cancer
Diet Appendix A provides evidence-based dietary recommendations that can be made in
light of the findings within this review and national health recommendations These
recommendations comprise a varied diet ensuring adequate intake of vitamins essential
minerals fibre essential fatty acids and antioxidants by eating less fat and more green and
cruciferous vegetables fruits and berries nuts and grains and healthy oils (unsaturated fats
omega)
Physical Activity In terms of physical activity based on the evidence within this report
the five a weeklsquo recommendation is just as relevant to cancer survivors as to the general
population Indeed these recommendations are also provided by the American Cancer
Society (Doyle et al 2006) as advised by a large expert panel Appendix B provides
118
suggestions for physical activity Forty-five to 60-minutes of intentional physical activity are
preferable as the benefits of physical activity do appear to be greater with increased physical
activity Even when this might seem too much survivors can be reminded that the minimum
30-minutes for 5 days a week can be tailored to individual needs and capabilities For
example graded or progressive physical activity can be utilised for those experiencing
fatigue whilst shorter physical activity sessions can be spread out across the day
Other Lifestyle Factors Body Weight In addition it is recommended that obesity (BMI
gt35 Kgm2) excessive alcohol consumption and smoking are avoided There is also
evidence that maintaining a steady healthy weight as opposed to fluctuating between a
healthy and unhealthy BMI can offer health benefits for cancer survivors (Wright et al
2007)
The evidence within this review are indicative of challenges with adherence supporting
findings from Uhley and Jen (2006) that intensive resource-heavy individualised guidance
and support is required to achieve significant long-term lifestyle change This further
emphasises the need to tailor and prescribe such interventions on a needs basis via
individualised assessment and risk stratification
Integrating Self-Management Lifestyle Strategies into Routine Care
Adopting a paternalistic approach and simply telling people is not enough If the medical
community want to help their patients embark on a road of recovery which includes dietary
change and regular exercise there has to be a comprehensive and well-funded package of
education guidance and support Attitude and culture change is imperative both to tackle the
myths and preconceptions around lifestyle factors and their influence on cancer prognosis
symptom management and a future healthy life on the part of both patients survivors and
health care professionals The bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative offers a comprehensive
framework for integrating self-management support into healthcare services (Flinders
University 2009) The emphasis is on not merely striving to change patient behaviour but
also making efforts towards organisational change
Cancer Research UK Diabetes UK and the British Heart Foundation have joined together to launch a new campaign to raise awareness of the dangers of carrying excess weight around the middle The Active Fatlsquo campaign encourages people to measure their waistlines and make positive changes to their lifestyles if they are at risk The emphasis is on educating the public that fat cells are actively working away at stimulating diseases such as cancer diabetes and heart attacks
119
The model offered within this capabilities framework promotes healthcare providers to view
patients holistically as opposed to focusing solely on the diagnosed chronic condition The
rationale for this in part lies in the fact that chronic conditions are more often than not
accompanied by co-morbidities and therefore healthcare is not only about the established
condition but also identified risk factors for co-morbidity The framework also identifies the
need to provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for healthcare
professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
Evidence based information emphasising the importance of lifestyle ideally should be
formally introduced into routine clinical practice early in the treatment pathway and re-
enforced at regular intervals thereafter This ensures patients and their relatives do not miss
the teachable moment where they are most susceptible to positive advice (Demark-
Wahnefried et al 2005) This requires close work with clinicians specialist nurses patients
and advocacy groups to enable information about new strategies to be integrated into
existing local information pathways and materials Indeed the new information prescriptions
currently being pilot tested provide ample opportunity for integrating lifestyle advice into
survivorship care plans
Information clearly has an important role to play in influencing lifestyle behaviours However
people need more than knowledge to be healthy they need the skills to change if they are to
bring about changes in often complex and habitual lifestyle behaviours (Robertson 2008)
Before investing time and money on patient information materials it is necessary to convince
the consultants other direct clinical staff and organisers of clinical services that lifestyle
advice is a priority and to re-allocate resources to enable sufficient time to discuss these
issues within routine consultations One study for example found that patients who were
encouraged by their oncologist exercised significantly more than patients who did not
(Segar et al 1998) The next step is to back up the medical consultation with further
practical verbal and written advice from specialist nurses or information officers One UK
oncology unit for example does this as part of a formal lifestyle interview together with a
bespoke lifestyle information toolbox (Thomas and Nicholson 2009) During this interview
patients can be referred to smoking cessation clinics nutritionists and physiotherapists
where necessary The specialist nurse conducting this interview provides written information
and advice to patients and just as importantly their friends and family about local support
groups dietary measures where to buy healthy foods and specific local exercise facilities
which may entice them ranging from ballroom line and salsa dance lessons aerobics yoga
and fitness classes local walking swimming and cycling groups through to gyms sport
centre tennis and badminton courts and Pilates classes giving times contact numbers and
locations to make it as easy as possible to follow the advice The rationale for these
120
interviews is that individualised lifestyle counselling is more likely to elicit a response than
generic general advice The specialist nurse then follows up the advice by telephone and
further consultations as prompting has been shown to improve update A study from North
Bedfordshire for example showed that although 52 of patients accepted referral for
exercise in a local Gym a further 23 decided to attend classes only after additional
prompting from the nurse either by telephone
Many UK Oncology Units already have instigated an exit interview system to discuss follow
up arrangements and this process could be expanded to include lifestyle counselling
provided the specialist nurses involved have received extra training This training should
include a knowledge of the evidence and importance of weight diet physical activity and
smoking after cancer as well as ways to appropriately advise home-based exercise
regimens and how to direct patients towards the myriad of council or independent exercise
activities available locally to them The courses may require additional communication and
motivational skills training to enable nurses to engage in a partnership relationship which
promotes addressing the patientlsquos agenda goals and motivation around achieving and
maintaining behaviour change Examples of a range of courses aimed to develop such skills
and competencies and which are provided by the Flinders Human Behaviour and Health
Research Unit include a Chronic Condition Self-Management workshop Communication
and Motivational Skills Workshop and a Living Well Workshop
Remaining Questions
This review has provided some clarification of the evidence pertaining to lifestyle and cancer
outcomes However in implementing this evidence into standardised practice within cancer
aftercare will require a number of questions to be explored
1) What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
At present it is unclear how soon after a cancer diagnosis an intervention should be
introduced for behaviour change(Rabin 2009) Until the teachable moment is more clearly
defined for cancer patients the advice is that professionals should repeatedly offer to assist
a patient with addressing their health behaviour risks until the patient accepts or seeks other
forms of support
The literature suggests that professional involvement in supported self-management and
lifestyle advice is required in order to maintain patient motivation by enhancing patient
engagement with health information and advice When information is supplied by healthcare
professionals and the patient is supported in using this information legitimacy is provided to
the information and advice (Protheroe et al 2008) Efficacy outcomes in terms of lifestyle
advice and behavioural change are fundamental in the initiation and maintenance of a
healthy lifestyle and the involvement of healthcare professionals strengthens outcome
efficacy whilst also motivating the patient and increasing their own self-efficacy to adapt their
lifestyle (Irwin 2008) However there is anecdotal and other evidence that on the one hand
the importance of lifestyle factors on the prognosis survival and symptom management of
121
cancer survivors is poorly understood and appreciated by significant numbers of cancer
health care professionals and on the other hand they do need specific training in the key
communication skills to be able to support effective behaviour change with their patients A
review is currently underway investigating the role of patient-professional communication in
terms of self-management
2) How can people most likely to benefit from lifestyle interventions be effectively
identified
A recent review on cancer-specific self-management programmes highlighted that patients
can be risk stratified according to needs and this according to whether they are likely to
benefit from the programme (Davies and Batehup 2010) For example people with low
levels of social support have been found to benefit most from group-delivered support As
part of the Bournemouth after Cancer Survivorship Project Active Wellness Programmelsquo
patients are assessed for the readiness to take part in physical activity (Milne et al 2010) It
is recommended that questionnaires that might facilitate such evidence-based risk
stratification be evaluated in order to provide further insight into this question A set of risk
stratification tools would be one way of ensuring cost-effectiveness
3) What are the various intensities of lifestyle support that can be provided based on
levels of individual need
As demonstrated within this review lifestyle interventions and self-management support do
generally require some level of support in order to be successful A strong
patientprofessional partnership appears to be at the essence of this intensive approach as
does longer-term follow-up and support (Davies and Batehup 2010) Addressing this
question will also in part address some of the inequalities within the current system of
cancer care with survivors identified as having low literacy being provided with extra
informational support and assistance with understanding the lifestyle recommendations
being made
122
Appendix A Evidence-Based Dietary Self-Management Recommendations
Food Advice Evidence
Reduce Saturated Fats
Unless underweight avoid processed fatty foods cakes biscuits crisps and other fatty snacks pastries cream and fried foods Cut the fat off the meat and check serum cholesterol regularly
(Ingram 1994 Hebert et al 1998 Norat et al 2004 Thomas et al 2009)
Increase all fish intake
All fresh fish but particularly the oily varieties such as mackerel and sardines Fresh water fish such as trout have the advantage of avoiding the potential heavy metal contamination of tuna amp sword fish which some suggest should not be eaten more than twice a week
(Ornish et al 2005 Meyerhardt et al 2007 Goodwin et al 2009)
Essential minerals
Vary the diet to ensure intake of adequate quantities of essential minerals consider Mixed nuts including Brazils Seafood including sardines prawns and shell fish Pulses and grains Vary carbohydrate sources such as pasta rice different brands of potatoes pulses such as lentils and quinoa
Rohan et al 1993) Powers et al 2007 McTiernan et al 2009)
Dietary Vitamins
Fresh fruit raw and calciferous vegetables grains oily fish nuts and salads Unless you have diarrhoea try to increase the amount of ripe fruit you eat each day ideally by eating the whole fruit Freshly squeezed fruit juices are recommended
(Rohan et al1993 Ingram 1994 Fleischauer et al 2003 New et al 2004 Rock et al 2005 McEligot et al 2006 Meyerhardt et al 2007 Schwarz et al 2008 Goodwin et al 2009)
Polyphenols
Onions leeks broccoli blueberries red wine tea apricots pomegranates chocolate coffee blueberries kiwis plums cherries ripe fruits parsley celery tomatoes mint citrus fruit
(Bettuzzi et al 2006 Pantuck et al 2006 Schwarz et al 2008 McLarty et al 2009)
Phytoestrogens
Soybeans and other legumes including peas lentils pinto (baked beans) and other beans and nuts (supplements not recommended)
Marini et al (2008)
Increase Carotenoids (Lycopene)
Tomatoes tomato sauce chilli carrots green vegetables and dark green salads
(Ingram 1994 Rock et al 2005 McEligot et al 2006 Pierce et al 2007 Powers et al 2007 Thomson et al 2007 Schwarz et al 2008)
123
Appendix B Evidence-Based Physical Activity Recommendations
Category Advice Evidence
Resistance Exercise
Strength training has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce fatigue and improve lean body mass and muscle strength Personalised tailored resistance exercise based on fitness assessments can improve QoL
Segal et al (2003) Poudevigne et al (2009) Courneya et al (2007) (Segal et al 2009)
Aerobic Exercise Aerobic exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of lymphoedema prevent loss of bone mineral density and reduce body fat Walking is particularly popular
Hayes Hildegard and Turner (2009) Schwartz Winters-Stone and Gallucci (2007) Courneya et al (2007) Fillion et al (2008) Kenfield et al (2009) Windsor Nichol and Potter (2004) Chang et al (2008)
Combined Resistance and Aerobic Exercise
Combined aerobic and resistance exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of fatigue and improve QoL
Coleman et al (2003) Milne et al (2008)
3gt MET-hours per week
Benefits of physical activity require 3 or more MET-hours per week (eg using a stationary bicycle for one-hour)
Holick et al (2008) Holmes et al (2005) Saxton et al (2010) Kenfield (2010)
Moderate intensity
Physical activity needs to be of at least moderate intensity in order to offer beneficial outcomes
Holick et al (2008) Patterson et al (2010) Holmes et al (2005) Saxton et al (2010) Campbell et al (2007) Poudevigne et al (2009) Tardon et al (2004)
Dose-Response Exercise can be dose-responsive thus taking part in more than 3 MET-hours per week is likely to offer greater benefits
Meyerhardt et al (2005) Kenfield (2010)
During Treatment Remaining active during treatment can help with symptoms such as fatigue as well as increase completion rates for chemotherapy
Chang et al (2008) Coleman et al (2003) Courneya et al (2007)
Home-Based
Home-based physical activity prescriptions either supervised or alone have proven effective in improving cancer outcomes including reducing fatigue and protecting bone mineral density
Ligibel et al (2008) Windsor Nichol and Potter (2004) Schwartz Winters-Stone and Gallucci (2007)
Supervised Supervised physical activity either at home in groups or during treatment have proven effective in improving cancer outcomes as well as reducing lean body mass and facilitating the completion of chemotherapy
Chang et al (2008) Coleman et al (2003) Velthuis et al (2009) Courneya et al (2007) Campbell
et al (2007) exercise (Soliman et al 2009)
124
References
Abrahamsen JF Andersen A Hannisdal E et al Second malignancies after treatment of Hodgkins disease the influence of treatment follow-up time and age J Clin Oncol 11 (2) 255-61 1993 Addington-Hall et al (2010) Older womenlsquos experience of breast cancer alongside other health conditions The EPaN study (Experiences Preferences and Needs of women aged 70 years and over) University of Southampton Funded by Macmillan Cancer Support Ahmed R L W Thomas et al (2006) Randomized Controlled Trial of Weight Training and Lymphedema in Breast Cancer Survivors J Clin Oncol 24(18) 2765-2772 Ainsworth BE et al Compendium of physical activities an update of activity codes and MET intensities Med Sci Sports Exerc 2000 Sep32(9 Suppl)S498-504 Aitken J (ongoing) Colorectal cancer and quality of life study httpwwwcancerqldorgaupageResearch_statisticsVCRCCVCRCC_research_programsLifestyle_and_Cancer [Last accessed 04062010] Akopyan and Bonavida 2006 G Akopyan and B Bonavida Understanding tobacco smoke carcinogen NNK and lung tumorigenesis Int J Oncol 29 (2006) pp 745ndash752 Alberts DS Martinez ME Roe DJ et al Lack of effect of a high-fiber cereal supplement on the recurrence of colorectal adenomas Phoenix Colon Cancer Prevention Physicians Network [Comment] New England Journal of Medicine 2000 April 20342(16)1156-62 Arts CJ Govers CA van den Berg H Wolters MG van Leeuwen P Thijssen JH In vitro binding of estrogens by dietary fiber and the in vivo apparent digestibility tested in pigs J Steroid Biochem Mol Biol 1991 May38(5)621-8 Bandura A (1977) Self-efficacy Toward a unifying theory of behavioural change Psych Rev 84 191 - 215 Barbash-Ballard R Hunsberger S Alciati MH Blaire SN Goodwin PJ McTiernan A(2009) Physical activity weight control and breast cancer risk and survival Clinical trial rationale and design considerations J Natl Cancer Inst 101630-643 Baron JA Beach M Mandel JS et al Calcium supplements and colorectal adenomas Polyp Prevention Study Group Ann N Y Acad Sci 1999889138-45
Bekkering T Beynon R Davey Smith G Davies A Harbord R Sterne J Thomas S and Wood L (2006) A systematic review of RCTs investigating the effect of dietal and physical activity interventions on cancer survival updated report World Cancer Research Fund httpwwwdietandcancerreportorg [Last accessed 150210] Bellizzi K M J H Rowland et al (2005) Health Behaviours of Cancer Survivors Examining Opportunities for Cancer Control Intervention J Clin Oncol 23(34) 8884-8893 Bernstein H Cosford P and Williams A (2010) Enabling effective delivery of health and wellbeing an independent report Department of Health February 2010
125
Bettuzzi et al 2006 S Bettuzzi M Brausi F Rizzi G Castagnetti G Peracchia and A Corti Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia a preliminary report from a one-year proof-of-principle study Cancer Research 66 (2) (2006) pp 1234ndash1240 Bingham SA Day NE Luben R Ferrari P Slimani N Norat T et al Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) an observational study Lancet 20033611496ndash501 Bingham S Riboli E Diet and cancermdashthe European Prospective Investigation into Cancer and Nutrition Nat Rev Cancer 20044206ndash15 Blakeman T Bower P Reeves D Chew-Graham C (2010) ―Bringing self management into clinical view a qualitative study of long term condition management in primary care consultations Chronic Illness 0 1-15 Blackburn G L and K A Wang (2007) Dietary fat reduction and breast cancer outcome results from the Womens Intervention Nutrition Study (WINS) Am J Clin Nutr 86(3) 878S-881 Bonithon-Kopp C Kronborg O Giacosa A Rath U Faivre J Calcium and fibre supplementation in prevention of colorectal adenoma recurrence A randomised intervention trial Lancet 2000356(9238)1300-6 Borugian MJ Sheps SB Kim-Sing C Olivotto IA Van Patten C Dunn BP Coldman AJ Potter JD Gallagher RP Hislop TG Waist-to-hip ratio and breast cancer mortality Am J Epidemiol 2003 Nov 15158(10)963-8 Boyapati SM Shue X et al (2005) Soyfood intake and breast cancer survival a follow up of the Shanghai Breast Cancer Study Breast Cancer Research and Treatment 92(1) p11-17 Boyd NF Stone J Vogt KN Connelly BS Martin LJ Minkin S Dietary fat and breast cancer risk revisited a meta-analysis of the published literature Br J Cancer 2003 Nov 389(9)1672-85 Box R Marnes T amp Robertson V Aquatic physiotherapy and breast cancer related lymphoedema 5th Australasian Lymphology Association Conference Proceedings Mar 2004 47-9 Brown J K T Byers et al (2003) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 53(5) 268-291 Cade JE Burley VJ Greenwood DC UK Womens Cohort Study Steering Group Dietary fibre and risk of breast cancer in the UK Womens Cohort Study Int J Epidemiol 2007 Apr36(2)431-8 Caan B B Sternfeld et al (2005) Life After Cancer Epidemiology (LACE) Study A cohort of early stage breast cancer survivors (United States) Cancer Causes and Control 16(5) 545-556
126
Caan BJ Kwan ML Hartzell G Castillo A Slattery ML Sternfeld B Weltzien E Pre-diagnosis body mass index post-diagnosis weight change and prognosis among women with early stage breast cancer Cancer Causes Control 2008 Dec19(10)1319-28 Cadmus L A P Salovey et al (2009) Physical activity and quality of life during and after treatment for breast cancer results of two randomized controlled trials Psycho-Oncology 18(4) 343-352 Campbell KL Westerlind KC Harber VJ Bell GJ Mackey JR Courneya KS (2007) Effects of aerobic exercise training on oestrogen metabolism in premenopausal women a randomized controlled trial Cancer Epidemiol Biomarkers Prev 16731ndash73 Cancer 52 and NCSI Research Workstream (2009) Less common cancers consultation Report June 2009 Cella D (2009) Quality of life in patients with metastatic renal cell carcinoma The importance of patient-reported outcomes Cancer treatment reviews 35(8) 733-737 Chan JM Gann PH and Giovannucci EL (2005) Role of diet in prostate cancer development and progression Journal of Clinical Oncology 23(32) p 8152-60 Chlebowski RT Aiello E McTiernan A Weight loss in breast cancer patient management Journal of Clinical Oncology 20(4) 1128-1143 2002 Chlebowski RT Blackburn GL Elashoff RE Thomson C Goodman MT Shapiro A Giuliano AE Karanja N Hoy MK Nixon DW and The WINS Investigators (2005) Dietary fat reduction in post-menopausal women with primary breast cancer Journal of Clinical Oncology (10) p 3s Chlebowski R G Blackburn et al (2006) Dietary fat reduction and breast cancer outcome interim efficacy results from the Womens Intervention Diet Study J Natl Cancer Inst 98 1767 - 1776 Chlebowski RT Blackburn GL (2007) Diet and breast cancer recurrence JAMA 2007 Nov 14298(18)2135 author reply 2135-6 Chlebowski RT (2010) Lifestyle and breast cancer risk The way forward Journal of
Clinical Oncology Vol 28 No 9 (March 20) 2010 pp 1445-1447
Cho E Spiegelman D Hunter DJ Chen WY Colditz GA Willett WC Premenopausal dietary carbohydrate glycaemic index glycaemic load and fiber in relation to risk of breast cancer Cancer Epidemiol Biomarkers Prev 2003 Coulter A and Ellins J (2006) Patient-focused Interventions A review of the evidence Picker Institute Europe (01865 208100) and Health Foundation Coups E J and J S Ostroff (2005) A population-based estimate of the prevalence of behavioural risk factors among adult cancer survivors and non-cancer controls Preventive Medicine 40(6) 702-711 Courneya K S (2003) Physical activity in Cancer Survivors An Overview of Research Medicine amp Science in Sports amp Physical activity 35(11) 1846-1852
127
Courneya K Booth CM Gill S et al (2008) The colon health and life-long physical activity change trial a randomized trial of the national institute of Canada clinical trials group Current Oncology 15(6) 271-78 Cramp F Daniel J (2008) Physical activity for the management of cancer-related fatigue in adults CochraneDatabaseSystRev 2008 Cuzick J Aromatase inhibitors for breast cancer prevention J Clin Oncol 231636-1643 2005
Cuzick J Hot flushes and the risk of recurrence Retrospective exploratory results from the ATAC trial 30th Annual San Antonio Breast Cancer Symposium San Antonio TX December 13-16 2007 (poster 2069) Daley A H Crank et al (2007) Randomized trial of physical activity therapy in women treated for breast cancer J Clin Oncol 25 1713 - 1721 Daley A S Bowden et al (2008) What advice are oncologists and surgeons in the United Kingdom giving to breast cancer patients about physical activity International Journal of Behavioural Diet and Physical Activity 5(1) 46 Danhauer S Mihalki S Russell G Campbell C Felder L Daley L et al (2009) Restorative yoga for women with breast cancer Findings from a randomized pilot study Psych oncology 18(4) 360-368 Dansinger M L J A Gleason et al (2005) Comparison of the Atkins Ornish Weight Watchers and Zone Diets for Weight Loss and Heart Disease Risk Reduction A Randomized Trial JAMA 293(1) 43-53 Davies NJ and Batehup L (2010) Self-management support for cancer survivors Guidance for developing interventions An update of the evidence National Cancer Survivorship Initiative Macmillan Cancer Support March 2010 Demark-Wahnefried W and Jones L (2008) Promoting a Healthy Lifestyle among Cancer Survivors Haematologyoncology clinics of North America 22(2) 319-342 Deo SV Ray S Rath GK et al (2004) Prevalence and risk factors for development of lymphedema following breast cancer treatment Indian J Cancer 418ndash12 Department of Health (2001) Exercise referral systems A national quality assurance framework Department of Health Report London 2001 Department of Health (2004) At least five a week Evidence on the impact of physical activity and its relationship to health Department of Health Report London 2004 Department of Health (2009a) Internal analysis unpublished Department of Health London Department of Health (2009b) Obesity general information Health survey of England 2008 Department of Health London Department of Health (2009c) Guidance on the routine collection of patient-reported outcome measures (PROMs) p 28 The Stationary Office London
128
De Rezende LF Franco RL de Rezende MF et al Two physical activity schemes in postoperative breast cancer comparison of effects on shoulder movement and lymphatic disturbance Tumori 2006 9255ndash61 de Waard F Ramlau R Mulders Y de Vries T van Waveren S A feasibility study on weight reduction in obese postmenopausal breast cancer patients Eur J Cancer Prev 1993 May 2(3)233-8 Dignam J J B N Polite et al (2006) Body Mass Index and Outcomes in Patients Who Receive Adjuvant Chemotherapy for Colon Cancer J Natl Cancer Inst 98(22) 1647-1654 Dimeo FC Thomas F Raabe-Menssen C et al Effect of aerobic exercise and relaxation training on fatigue and physical performance of cancer patients after surgery A randomised controlled trial Support Care Cancer 2004 12(11)774-9 Dixon JM Renshaw L Young O et al Letrozole suppresses plasma estradiol and oestrone sulphate more completely than anastrozole in postmenopausal women with breast cancer J Clin Oncol 261671-1675 2008
Doyle C L H Kushi et al (2006) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 56(6) 323-353 Dwyer J J Peterson et al (2008) Do Flavonoid Intakes of Postmenopausal Women With Breast Cancer Vary on Very Low Fat Diets Diet and Cancer 60(4) 450 - 460 Eakin E Hayes S and Lawler S (ongoing) Physical activity for Health Using the telephone to promote physical activity-based rehabilitation in ruralremote Australian breast cancer survivors National Breast Cancer Foundation httpwwwuqeduaucprcindexhtmlpage=60214amppid=20928 [Last accessed 300310] Eliassen AH Missmer SA Tworoger SS Spiegelman D Barbieri RL Dowsett M Hankinson SE Endogenous steroid hormone concentrations and risk of breast cancer among premenopausal women J Natl Cancer Inst 2006 Oct 4 98(19)1406-15 Elkort RJ Baker FL Vitale JJ Cordano A Long-term nutritional support as an adjunct to chemotherapy for breast cancer JPEN J Parenter Enteral Nutr 1981 Sep-Oct 5(5)385-90 Enger SM Greif JM Polikoff J Press M Body weight correlates with mortality in early-stage breast cancer Arch Surg 2004139954ndash958 discussion 58ndash60 Eton D T D L Fairclough et al (2003) Early Change in Patient-Reported Health During Lung Cancer Chemotherapy Predicts Clinical Outcomes Beyond Those Predicted by Baseline Report Results From Eastern Cooperative Oncology Group Study 5592 J Clin Oncol 21(8) 1536-1543 Fentiman IS Allen DS Hamed H (2005) Smoking and prognosis in women with breast cancer Int J Clin Pract 591051ndash1054
129
Ferrari P Jenab M Norat T et al Lifetime and baseline alcohol intake and risk of colon and rectal cancers in the European prospective investigation bettinto cancer and nutrition (EPIC) Int J Cancer 2007 121 ( 9 ) 2065 ndash 2072
Feuerstein M (2006) Handbook of Cancer Survivorship New York NY Springer 2006 Fillion L P Gagnon et al (2008) A Brief Intervention for Fatigue Management in Breast Cancer Survivors Cancer Nursing 31(2) 145-159 Findley P amp Sambamoorthi U (2009) Preventive health services and lifestyle practices in cancer survivors A population health investigation Journal of Cancer Survivorship 3 43-58 Fleischauer AT Simonsen N Arab L Antioxidant supplements and risk of breast cancer recurrence and breast cancer-related mortality among postmenopausal women Nutr Cancer 2003 46 15-22 Flinders University (2009) Capabilities for Supporting Prevention and Chronic Condition Self-Management A Resource for Educators of Primary Health Care Professionals Australian Better Health Initiative A joint Australian State and Territory government initiative
Flowers M Thompson PA 2009 t10c12 Conjugated Linoleic Acid Suppresses HER2 Protein and Enhances Apoptosis in SKBr3 Breast Cancer Cells Possible Role of COX2 PLoS ONE 4(4) e5342 doi101371journalpone0005342 Food Standards Agency (2007) FSA nutrient and food based guidelines for UK institutions httpwwwfoodgovukmultimediapdfsnutrientinstitutionpdf [Last accessed 120310] Food Standards Agency (2010) Heightweight chart httpwwweatwellgovukhealthydiethealthyweightheightweightchart [Last accessed 120310] Ford MB Sigurdson AJ Petrulis ES et al Effects of smoking and radiotherapy on lung carcinoma in breast carcinoma survivors Cancer 98 (7) 1457-64 2003 Friedenreich C Cust A Lahmann PH et al Anthropometric factors and risk of endometrial cancer the European prospective investigation into cancer and nutrition Cancer Causes Control 2007 18399-413 Friedenreich C M C G Woolcott et al (2010) Alberta Physical Activity and Breast Cancer Prevention Trial Sex Hormone Changes in a Year-Long Physical activity Intervention Among Postmenopausal Women J Clin Oncol 28(9) 1458-1466 Friedenreich CM Cust AE Physical activity and breast cancer risk impact of timing type and dose of activity and population subgroup effects Br J Sports Med 2008 Aug42(8)636-47 Giovannucci EL (2005) Obesity insulin resistance and cancer risk Cancer Prevention 5 httpwwwnypcancerpreventioncomissue5propro_featurespre_earshtml [Last accessed 03062010]
130
Gold E B J P Pierce et al (2009) Dietary Pattern Influences Breast Cancer Prognosis in Women Without Hot Flashes The Womens Healthy Eating and Living Trial J Clin Oncol 27(3) 352-359 Gonzalez CAPera GAgudo APalli DKrogh VVineis PTumino RPanico SBerglund GSiman HNyren OAgren AMartinez CDorronsoro MBarricarte ATormo MJQuiros JRAllen NBingham SDay NMiller ANagel GBoeing HOvervad KTjonneland ABueno-de-Mesquita HBBoshuizen HCPeeters PNumans MClavel-Chapelon FHelen IAgapitos ELund EFahey MSaracci RKaaks RRiboli E Smoking and the risk of gastric cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC) Int J Cancer 107 (4) 629-634 (2003) Gonzaacutelez CA Jakszyn P Pera G Agudo A Bingham S Palli D Ferrari P Boeing H del Giudice G Plebani M Carneiro F Nesi G Berrino F Sacerdote C Tumino R Panico S Berglund G Simaacuten H Nyreacuten O Hallmans G Martinez C Dorronsoro M Barricarte A Navarro C Quiroacutes JR Allen N Key TJ Day NE Linseisen J Nagel G Bergmann MM Overvad K Jensen MK Tjonneland A Olsen A Bueno-de-Mesquita HB Ocke M Peeters PH Numans ME Clavel-Chapelon F Boutron-Ruault MC Trichopoulou A Psaltopoulou T Roukos D Lund E Hemon B Kaaks R Norat T Riboli E Meat intake and risk of stomach and oesophageal adenocarcinoma within the European Prospective Investigation Into Cancer and Nutrition (EPIC) J Natl Cancer Inst 2006 Mar 198(5)345-54 Goodwin PJ Pritchard KI Ennis M et al Insulin-lowering effects of metformin in women with early breast cancer Clin Breast Cancer 8501-5052008
Goodwin PJ Ennis M Pritchard KI Koo J Hood N (2009) Prognostic Effects of 25-Hydroxyvitamin D Levels in Early Breast Cancer Journal of Clinical Oncology Vol 27 No 23 (August 10) pp 3757-3763 Goodwin PJ Lifestyle Intervention Study in Adjuvant Treatment of Early Breast Cancer (LISA) (ongoing) httpclinicaltrialsgovct2showNCT00463489 [Last accessed 04062010] Goss PE Richardson H Chlebowski RT et al National Cancer Institute of Canada Clinical Trials Group MAP 3 Trial Evaluation of exemestane to prevent breast cancer in postmenopausal women at risk Clin Breast Cancer 7895-900 2007
Gothard L Cornes P et al (2004) Double-blind placebo-controlled randomised trial of vitamin E and pentoxifylline in patients with chronic arm lymphoedema and fibrosis after surgery and radiotherapy for breast cancer Radiotherapy and oncology journal of the European Society for Therapeutic Radiology and Oncology 73(2) 133-139 Grace PB Taylor JI Low YL Luben RN Mulligan AA Botting NP Dowsett M Welch AA Khaw KT Wareham NJ Day NE Bingham SA Phytoestrogen concentrations in serum and spot urine as biomarkers for dietary phytoestrogen intake and their relation to breast cancer risk in European prospective investigation of cancer and nutrition-norfolk Cancer Epidemiol Biomarkers Prev 2004 May13(5)698-708 Greenberg ER Baron JA Tosteson TD et al A clinical trial of antioxidant vitamins to prevent colorectal adenoma Polyp Prevention Study Group[comment] New England Journal of Medicine 1994 July 21331(3)141-7 Gritz ER (1993) Cancer Smoking Epidemiology Biomarkers amp Prevention 2(3) 261-270
131
Gritz E R M C Fingeret et al (2006) Successes and failures of the teachable moment Cancer 106(1) 17-27 Gross G C Ott et al (2002) Postmenopausal Breast Cancer Survivors at Risk for Osteoporosis Physical Activity Vigour and Vitality Oncology Nursing Forum 29(9) 1295-1300 Gross M C Ramirez et al (2009) Expression of androgen and oestrogen related proteins in normal weight and obese prostate cancer patients The Prostate 69(5) 520-527 Guthrie JR Ball M Murkies A Dennerstein L Dietary phytoestrogen intake in mid-life Australian-born women relationship to health variables Climacteric 2000 3 254ndash261 Hawkes A L S Gollschewski et al (2009) A telephone-delivered lifestyle intervention for colorectal cancer survivors a pilot study Psycho-Oncology 18(4) 449-455 Haydon AM Macinnis RJ English DR Giles GG (2006) The effect of physical activity and body size on survival after diagnosis with colorectal cancer Gut 55 p 62-67 Hayes SC Spence RR Galvao DANewton RU (2009) Australian Association for Physical activity and Sport Science position stand Optimising cancer outcomes through physical activity JSciMedSport 200912428-434 Heald AH Cade JE Cruickshank JK Anderson S White A Gibson JM (2003) The influence of dietary intake on the insulin-like growth factor (IGF) system across three ethnic groups a population-based study Public Health Nutr6175ndash80 Healthy Weight Healthy Lives (2008) A Cross-Government Strategy for England Cross-Government Obesity Unit DH and Department of Children Schools and Families Hebert JR Hurley TG Ma Y (1998) The effect of dietary exposures on recurrence and mortality in early stage breast cancer Breast Cancer Res Treat 5117ndash28 Hofstad B Almendingen K Vatn M et al Growth and recurrence of colorectal polyps a double-blind 3-year intervention with calcium and antioxidants Digestion 199859(2)148-56 Holick C N P A Newcomb et al (2008) Physical Activity and Survival after Diagnosis of Invasive Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 17(2) 379-386 Holm LE Nordevang E Hjalmar ML Lidbrink E Callmer E Nilsson B (1993) Treatment failure and dietary habits in women with breast cancer J Natl Cancer Inst 8532ndash36 Holmes MD Hunter DJ Colditz GA et al Association of dietary intake of fat and fatty acids with risk of breast cancer JAMA 1999281914-920 Holmes MD Chen WY Feskanich D Kroenke CH Colditz GA (2005) Physical activity and survival after breast cancer diagnosis JAMA 293 p 2479-86
132
Holmes MD Murin S Chen WY Kroenke CH Spiegelman D Colditz GA (2007) Smoking and survival after breast cancer diagnosis Int J Cancer 1202672ndash2677
Howe GR Hirohata T Hislop TG Iscovich JM Yuan JM Katsouyanni K Lubin F Marubini E Modan B Rohan T et al Dietary factors and risk of breast cancer combined analysis of 12 case-control studies J Natl Cancer Inst 1990 Apr 482(7)561-9
Hunter DJ Spiegelman D Adami HO Beeson L van den Brandt PA Folsom ARFraser GE Goldbohm RA Graham S Howe GR et al Cohort studies of fat intake and the risk of breast cancer--a pooled analysis N Engl J Med 1996 Feb 8334(6)356-61
Ingram D Diet and subsequent survival in women with breast cancer British Journal of Cancer 1994 Mar69(3)592-5
Irwin ML Smith AW McTiernan A Ballard-Barbash R Cronin K Gilliland FD Baumgartner RN Baumgartner KB Bernstein L (2008) Influence of Pre- and Postdiagnosis Physical Activity on Mortality in Breast Cancer Survivors The Health Eating Activity and Lifestyle Study Journal of Clinical Oncology 26(24) 3958-3964
Ishikawa H Akedo I Otani T et al Randomized trial of dietary fiber and Lactobacillus casei administration for prevention of colorectal tumors Int J Cancer 2005 September 20116(5)762-7 Jiralerspong S Palla SL Giordano SH et al Metformin and pathologic complete responses to neoadjuvant chemotherapy in diabetic patients with breast cancer J Clin Oncol 273297-3302 2009
Jones LW Demark-Wahnefried W Diet physical activity and complementary therapies after primary treatment for cancer Lancet Oncol 7(12)1017-26 Nov-Dec 2006 PMID 17138223 Kaaks R A Lukanova and MA Kurzer Obesity endogenous hormones and endometrial cancer risk a synthetic review Cancer Epidemiol Biomark Prev 11 (2002) pp 1531ndash1543 Kaaks R Rinaldi S Key TJ Berrino F Peeters PH Biessy C Dossus L Lukanova A Bingham S Khaw KT Allen NE Bueno-de-Mesquita HB van Gils CH Grobbee D Boeing H Lahmann PH Nagel G Chang-Claude J Clavel-Chapelon F Fournier A Thieacutebaut A Gonzaacutelez CA Quiroacutes JR Tormo MJ Ardanaz E Amiano P Krogh V Palli D Panico S Tumino R Vineis P Trichopoulou A Kalapothaki V Trichopoulos D Ferrari P Norat T Saracci R Riboli E Postmenopausal serum androgens oestrogens and breast cancer risk the European prospective investigation into cancer and nutrition Endocr Relat Cancer 2005 Dec12(4)1071-82 Kawahara M Ushijima S Kamimori T et al Second primary tumours in more than 2-year disease-free survivors of small-cell lung cancer in Japan the role of smoking cessation Br J Cancer 78 (3) 409-12 1998 Keinan-Boker L van Der Schouw YT Grobbee DE Peeters PH Dietary phytoestrogens and breast cancer risk Am J Clin Nutr 2004 Feb79(2)282-8 Kenfield SA (2010) Physical activity and mortality in prostate cancer (In Regular Vigorous Physical Activity found to have Survival Benefits for Prostate Cancer Patients
133
AACR Frontier in Cancer Prevention Research Conference by Tuma R Oncology Times) 32(2) p 29 33 Key TJ Allen NE Hormones and breast cancer IARC Sci Publ 2002156273-6 Khaodhiar L Nixon D Chlebowski RT Elashoff R Blackburn GL Hoy MK Insulin resistance in postmenopausal women with breast cancer Proc Am Cancer Res 2003446349 (abstr) Kim EH Willett WC Colditz GA Hankinson SE Stampfer MJ Hunter DJ Rosner B Holmes MD Dietary fat and risk of postmenopausal breast cancer in a 20-year follow-up Am J Epidemiol 2006 Nov 15164(10)990-7 Korstjens I A M May et al (2008) Quality of Life After Self-Management Cancer Rehabilitation A Randomized Controlled Trial Comparing Physical and Cognitive-Behavioural Training Versus Physical Training Psychosom Med 70(4) 422-429 Krein S M Heisler J Piette F Makki and E Kerr 2005 The effect of chronic pain on diabetes patientslsquo self-management Diabetes Care 28(1)65ndash70 Kroenke CH Fung TT Hu FB Holmes MD Dietary patterns and survival after breast cancer diagnosis J Clin Oncol 2005 Dec 2023(36)9295-303 Kubik AK Zatloukal P Tomasek L Petruzelka L (2002) Lung cancer risk among Czech women a case-control study Prev Med 34(4) 436ndash444 Kucera H [Adjuvanticity of vitamin A in advanced irradiated cervical cancer (authors transl)] Wiener Klinische Wochenschrift Supplementum 19801181-20 Kushi LH Byers T Doyle C et al American Cancer Society Guidelines on Diet and Physical Activity for cancer prevention reducing the risk of cancer with healthy food choices and physical activity CA Cancer J Clin 2006 56 254ndash8 Kyogoku S Hirohata T Nomura Y Shigematsu T Takeshita S Hirohata I Diet and prognosis of breast cancer Nutr Cancer 199217(3)271-7 Lahmann PH Schulz M Hoffmann K Boeing H Tjoslashnneland A Olsen A Overvad K Key TJ Allen NE Khaw KT Bingham S Berglund G Wirfaumllt E Berrino F Krogh V Trichopoulou A Lagiou P Trichopoulos D Kaaks R Riboli E Long-term weight change and breast cancer risk the European prospective investigation into cancer and nutrition (EPIC) Br J Cancer 2005 Sep 593(5)582-9 Lee IM Sesso HD Paffenbarger RS Jr (1999) Physical activity and risk of lung cancer Int J Epidemiol 28(4) 620ndash625 Lev E L (1997) Banduras Theory of Self-Efficacy Applications to Oncology Research and Theory for Nursing Practice 11 21-37 Ligibel J A W Demark-Wahnefried et al (2009) Diet Physical activity and Supplements Guidelines for Cancer Survivors ASCO EDUCATIONAL BOOK 2009(1) 541-547 Lindsay S (2009) Prioritizing illness Lessons in self-managing multiple chronic conditions Canadian Journal of Sociology PhD Thesis ejournalslibraryualbertaca
134
Lucia A Earnest C Perez M (2003) Cancer-related fatigue can physical activity physiology assist oncologists Lancet Oncol 4616-625 Lyons R amp Langille L (2000) Healthy Lifestyle Strengthening the Effectiveness of Lifestyle Approaches to Improve Health Health Canada Ottawa Ontario Available at httpwwwhc-scgccahppbphdddocshealthy MacLennan R Macrae F Bain C et al Effect of fat fibre and beta carotene intake on colorectal adenomas further analysis of a randomized controlled dietary intervention trial after colonoscopic polypectomy Asia Pac J Clin Nutr 1999 8(suppl)S54-S58 Macmillian Cancer Support (2008) Two Million Reasons The Cancer Survivorship Agenda 2008 Maddams J Moller H and Devane C Cancer prevalence in the UK 2008 Thames Cancer Registry and Macmillan Cancer Support 2008 Manjer J Berglund G Bondesson L Garne J P Janzon L Malina J Breast cancer incidence in relation to smoking cessation Breast Cancer Res Treat 61121-129 2000 Mao Y Pan S Wen SW Johnson KC The Canadian Cancer (2003) Physical activity and the risk of lung cancer in Canada Am J Epidemiol 158(6) 564ndash575 Mayne S T B Cartmel et al (2009) Alcohol and Tobacco Use Pre-diagnosis and Postdiagnosis and Survival in a Cohort of Patients with Early Stage Cancers of the Oral Cavity Pharynx and Larynx Cancer Epidemiology Biomarkers amp Prevention 18(12) 3368-3374 McDonald P R Williams et al (2002) Breast cancer survival in African American women Is alcohol consumption a prognostic indicator Cancer Causes and Control 13(6) 543-549 McEligot AJ Largent J Ziogas A Peel D Anton-Culver H Dietary fat fiber vegetable and micronutrients are associated with overall survival in postmenopausal women diagnosed with breast cancer Nutr Cancer 200655(2)132-140 McNeely M L K L Campbell et al (2006) Effects of physical activity on breast cancer patients and survivors a systematic review and meta-analysis CMAJ 175(1) 34-41 McKenzie D C and A L Kalda (2003) Effect of Upper Extremity Physical activity on Secondary Lymphedema in Breast Cancer Patients A Pilot Study J Clin Oncol 21(3) 463-466 McKeown-Eyssen GE Bright-See E Bruce WR et al A randomized trial of a low fat high fibre diet in the recurrence of colorectal polyps Toronto Polyp Prevention Group [erratum appears in J Clin Epidemiol 1995 Feb48(2)i] Journal of Clinical Epidemiology 1994 May47(5)525-36 McLarty Jerry Bigelow Rebecca LH Smith Mylinh Elmajian Don Ankem Murali Cardelli James A (2009) Tea Polyphenols Decrease Serum Levels of Prostate-Specific Antigen Hepatocyte Growth Factor and Vascular Endothelial Growth Factor in Prostate
135
Cancer Patients and Inhibit Production of Hepatocyte Growth Factor and Vascular Endothelial Growth Factor In vitro Cancer Prev Res 1940-6207CAPR-08-0167
McTiernan A et al (2009) Low-fat increased fruit vegetable and grain dietary pattern fractures and bone mineral density the Womens Health Initiative Dietary Modification Trial Am J Clin Nutr 89 1864-1876
Meyerhardt JA Heseltine D Niedzwiecki D Hollis D Saltz LB Mayer RJ Schilsky RL and Fuchs CS (2005) The impact of physical activity on patients with stage III colon cancer Findings from Intergroup trial CALGB 89803 Proc Am Soc Clin Oncol 24 p abstract 3534 Meyerhardt J A D Niedzwiecki et al (2007) Association of Dietary Patterns With Cancer Recurrence and Survival in Patients With Stage III Colon Cancer JAMA 298(7) 754-764 Meyerhardt J A D Niedzwiecki et al (2008) Impact of Body Mass Index and Weight Change after Treatment on Cancer Recurrence and Survival in Patients With Stage III Colon Cancer Findings From Cancer and Leukemia Group B 89803 J Clin Oncol 26(25) 4109-4115 Meyskens FL Jr Kopecky KJ Appelbaum FR Balcerzak SP Samlowski W Hynes H Effects of vitamin A on survival in patients with chronic myelogenous leukemia a SWOG randomized trial Leukemia Research 1995 September 19(9)605-12 Miles A Simon A Wardle J (2010) Answering patient questions about the role lifestyle factors play in cancer onset and recurrences Journal of Health Psychology 15(2) p 291-298 Milne H K Wallman et al (2008) Impact of a Combined Resistance and Aerobic Physical activity Program on Motivational Variables in Breast Cancer Survivors A Randomized Controlled Trial Annals of Behavioral Medicine 36(2) 158-166 Milne M Hamerston L and Morrell D (2010) BACSUP adult survivorship living with and beyond cancer test community learning workshop London January 2010 Monninkhof EM Peeters PH Schuit AJ Design of the sex hormones and physical exercise (SHAPE) study BMC Public Health 2007 Sep 47232 Morrell RM Halyard MY Schild SE Ali MS Gunderson LL Pockaj BA (2005) Breast cancer-related lymphedema Mayo Clin Proc 801480ndash1484 Mortimer P S D O Bates et al (1996) The prevalence of arm oedema following treatment for breast cancer QJM 89(5) 377-380 Mortimer JE Flatt SW Parker BA et al Tamoxifen hot flashes and recurrence in breast cancer Breast Cancer Res Treat 108421-426 2008 Moseley AL Piller NB Carati CJ (2005) The effect of gentle arm physical activity and deep breathing on secondary arm lymphedemaLymphology Sep38(3)136-45 Moseley AL Piller NB (2008) Physical activity for limb Lymphoedema ndash Evidence that it is beneficial Journal of Lymphoedema vol 3(1) pp 51-56
136
Mustian KM Palesh OG Flecksteiner SA Tai Chi Chuan for breast cancer survivors Medicine and sport science 2008 52()209-17 National Cancer Action Team (2009) Cancer and palliative care rehabilitation workforce project A review of the evidence National Cancer Action Team National Comprehensive Cancer Network (2009) NCCN Clinical Practice Guidelines in Oncology Cancer-related fatigue version 1 2009 National Cancer Survivorship Initiative (NCSI) (2009) Research Work Stream Mapping Project - Summary and reports for Bowel Cancer Breast Cancer Lung Cancer Prostate cancer National Cancer Survivorship Initiative Macmillan Cancer Support National Health Service (2010) NHS advice on drinking limits NHS Choices httpwwwdrinkingnhsukquestionsrecommended-levels [Last accessed 300310] National Institutes of Health (1998) Clinical Guidelines on the Identification Evaluation and Treatment of Overweight and Obesity in Adults The Evidence Report National Heart Lung and Blood Institute in cooperation with the National Institute of Diabetes and Digestive Kidney Diseases NIH Publication No 98-4083 National Institutes of Health Osteoporosis and Related Bone Diseases (2009) Conditions and behaviours that increase osteoporosis risk National Resource Centre US Department of Health and Human Services httpwwwniamsnihgovHealth_InfoBoneOsteoporosisConditions_Behaviorsosteoporosis_breast_cancerasp [Last accessed 170210] National Obesity Observatory (2009) Body mass index as a measure of obesity Association of Public Health Observatories June 2009 Ng K J A Meyerhardt et al (2008) Circulating 25-Hydroxyvitamin D Levels and Survival in Patients With Colorectal Cancer J Clin Oncol 26(18) 2984-2991 Nikotetti S Young J Levitt M (2008) Bowel problems self-care practices and information needs of colorectal cancer survivors at 6 to 24 months after sphincter-saving surgery Cancer Nursing 31(5) p 389-398
Norat T Bingham S Ferrari P Slimani N Jenab M Mazuir M Overvad K Olsen A Tjoslashnneland A Clavel F Boutron-Ruault MC Kesse E Boeing H Bergmann MM Nieters A Linseisen J Trichopoulou A Trichopoulos D Tountas Y Berrino F Palli D Panico S Tumino R Vineis P Bueno-de-Mesquita HB Peeters PH Engeset D Lund E Skeie G Ardanaz E Gonzaacutelez C Navarro C Quiroacutes JR Sanchez MJ Berglund G Mattisson I Hallmans G Palmqvist R Day NE Khaw KT Key TJ San Joaquin M Heacutemon B Saracci R Kaaks R Riboli E Meat fish and colorectal cancer risk the European Prospective Investigation into cancer and nutrition J Natl Cancer Inst 2005 Jun 1597(12)906-16
Ornish D et al (2005) Intensive lifestyle changes may affect the progression of prostate cancer The Journal of Urology 174 p 1065-1070 Ostroff JS Jacobsen PB Moadel AB Spiro RH Shah JP Strong EW et al (1995) Prevalence and predictors of continued tobacco use after treatment of patients with head and neck cancer Cancer Jan 1575(2)569-76
137
Pantuck AJ et al (2006) Phase II study of pomegranate juice for men with rising PSA following surgery or RXT for prostate cancer Clin Cancer Res 12(13) p 4018-4026 Pantuck AJ et al Abstract presented at the American Society of Clinical Oncology 2008 Genitourinary Cancers Symposium (Abstract 40) Long Term Follow Up Of Pomegranate Juice For Men With Prostate Cancer And Rising PSA Shows Durable Improvement in PSA Doubling Time Parsons A A Daley et al Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis systematic review of observational studies with meta-analysis BMJ 340(jan21_1) Pastorino U Infante M Maioli M et al Adjuvant treatment of stage I lung cancer with high-dose vitamin A[comment] J Clin Oncol 1993 July11(7)1216-22 Patterson R E L A Cadmus et al Physical activity diet adiposity and female breast cancer prognosis A review of the epidemiologic literature Maturitas In Press Corrected Proof Pedersen BK Saltin B Evidence for prescribing physical activity as therapy in chronic disease Scand J Med Sci Sports 16 Suppl 1 3ndash63 2006Pierce J P L Natarajan et al (2007) Influence of a Diet Very High in Vegetables Fruit and Fiber and Low in Fat on Prognosis Following Treatment for Breast Cancer The Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA 298(3) 289-298 Pierce JP Faerber S Wright FA Newman V Flatt SW Kealey S Rock CL Pierce JP Natarajan L Caan BJ et al Influence of a diet very high in vegetables fruit and fiber and low in fat on prognosis following treatment for breast cancer the Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA2007298(3)289-298 Ponz dL Roncucci L Chemoprevention of colorectal tumors role of lactulose and of other agents Scandinavian Journal of Gastroenterology Supplement 199722272-5 Poudevigne M J Wojcik et al (2009) The Effects Of 12-weeks Cross Training On Fatigue And Mood In Recent Breast Cancer Survivors 2292 Board 180 May 28 200 PM - 330 PM Medicine amp Science in Sports amp Physical activity 41(5) 297-298 Powers H J M H Hill et al (2007) Responses of Biomarkers of Folate and Riboflavin Status to Folate and Riboflavin Supplementation in Healthy and Colorectal Polyp Patients (The FAB2 Study) Cancer Epidemiology Biomarkers amp Prevention 16(10) 2128-2135 Protheroe J A Rogers et al (2008) Promoting patient engagement with self-management support information a qualitative meta-synthesis of processes influencing uptake Implementation Science 3(1) 44 Provenzano E and N Johnson (2009) Overview of recommendations of HER2 testing in breast cancer Diagnostic Histopathology 15(10) 478-484 Puhl RM Heuer CA (2009) ―The stigma of obesity A Review and Update Obesity 17 (5) 941-964 Rabin C (2009) ―Promoting Lifestyle Change among Cancer Survivors When is the Teachable Moment American Journal of Lifestyle Medicine 3 (5) 369-378
138
Reding K W J R Daling et al (2008) Effect of Pre-diagnostic Alcohol Consumption on Survival after Breast Cancer in Young Women Cancer Epidemiology Biomarkers amp Prevention 17(8) 1988-1996 Riboli E Hunt KJ Slimani N Ferrari P Norat T Fahey M Charrondiegravere UR Heacutemon B Casagrande C Vignat J Overvad K Tjoslashnneland A Clavel-Chapelon F ThieacutebautA Wahrendorf J Boeing H Trichopoulos D Trichopoulou A Vineis P Palli D Bueno-De-Mesquita HB Peeters PH Lund E Engeset D Gonzaacutelez CA Barricarte A Berglund G Hallmans G Day NE Key TJ Kaaks R Saracci R (2002) European Prospective Investigation into Cancer and Nutrition (EPIC) study populations and data collection Public Health Nutr 2002 Dec5(6B)1113-24 Richardson G E M A Tucker et al (1993) Smoking Cessation after Successful Treatment of Small-Cell Lung Cancer Is Associated with Fewer Smoking-related Second Primary Cancers Annals of Internal Medicine 119(5) 383-390 Richardson A Addington-Hall J Stark D Foster C Amir Z Sharpe M (2009) Determining research priorities for cancer survivorship Consultation and evidence review Commissioned by the NCSI Robertson R (2008) Using Information to Promote Healthy Behaviours Kings Fund London Rock C L and W Demark-Wahnefried (2002) Diet and Survival After the Diagnosis of Breast Cancer A Review of the Evidence J Clin Oncol 20(15) 3302-3316 Rock C L S W Flatt et al (2005) Plasma Carotenoids and Recurrence-Free Survival in Women With a History of Breast Cancer J Clin Oncol 23(27) 6631-6638 Rohan T Howe G Friedenreich C et al (1993) Dietary fiber vitamins A C and E and risk of breast cancer a cohort study Cancer Causes and Control 4(1) p 29-37 Rosenbaum EH Fobair P Spiegel D (2006) Cancer is a Life-changing Event Cancer Supportive Care Programs httpwwwcancersupportivecarecomSurvivorsurvivehtml [Last accessed January 30 2009] Ryan CW D Huo and K Bylow et al (2007) Suppression of bone density loss and bone turnover in patients with hormone-sensitive prostate cancer and receiving zoledronic acid BJU Int 100 pp 70ndash75 Sagiv SK Gaudet MM Eng SM et al (2007) Active and passive cigarette smoke and breast cancer survival Ann Epidemiol 17385ndash393 Sandel S Judge J Landry N et al (2005) Dance and movement program improves quality-of-life measures in breast cancer survivors Cancer Nursing 28(4) 301-309 Saxton J (2010) Physical activity and cancer mortality In Physical activity and cancer Survivorship Springer New York pp 189-210 Schatzkin A Lanza E Corle D et al Lack of effect of a low-fat high-fiber diet on the recurrence of colorectal adenomas Polyp Prevention Trial Study Group [comment] New England Journal of Medicine 2000 April 20342(16)1149- 55
139
Schmitz KH Courneya KS Matthews C Demark-Wahnefried W et al (2010) ―American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors Medicine and Science in Sports and Exercise Special Communication 0195-9131104207-14090 Schmitz K Holtzman J Courneya K Masse L Duval S Kane R Controlled physical activity trials in cancer survivors A systematic review and meta-analysis Cancer Epidemiol Biomarkers Prev 2005141588ndash95
Schulz M Lahmann PH Boeing H et al Fruit and vegetable consumption and risk of epithelial ovarian cancer the European Prospective Investigation into Cancer and Nutrition Cancer Epidemiol Biomarkers Prev 2005142531ndash2535 Schwarz S U C Obermuller-Jevic et al (2008) Lycopene Inhibits Disease Progression in Patients with Benign Prostate Hyperplasia J Nutr 138(1) 49-53 Schmitz K H Balancing Lymphedema Risk Physical activity Versus Deconditioning for Breast Cancer Survivors Physical activity and Sport Sciences Reviews 38(1) 17-24 10 Segal RJ Reid RD Courneya KS et al(2003) Resistance physical activity in men receiving androgen deprivation therapy for prostate cancer JClinOncol211653-1659
Segal RJ Reid RD Courneya KS Sigal RJ Kenny GP PrudlsquoHomme DGet al Randomized Controlled Trial of Resistance or Aerobic Exercise in Men Receiving Radiation Therapy for Prostate Cancer J Clin Oncol 2009 Jan 2027344-51 Sellers TA Potter JD Folsom AR (1991) Association of incident lung cancer with family history of female reproductive cancers the Iowa Womenlsquos Health Study Genet Epidemiol 8(3) 199ndash208 Severson RK Nomura AM Grove JS Stemmermann GN A prospective analysis of physical activity and cancer Am J Epidemiol 1989 Sep130(3)522-9 Shaw C Mortimer P Judd PA Randomized controlled trial comparing a low-fat diet with a weight-reduction diet in breast cancer-related lymphedema Cancer 20071091949ndash56 Sinicrope F A N R Foster et al Obesity Is an Independent Prognostic Variable in Colon Cancer Survivors Clinical Cancer Research 16(6) 1884-1893 Siris E S P D Miller et al (2001) Identification and Fracture Outcomes of Undiagnosed Low Bone Mineral Density in Postmenopausal Women Results From the National Osteoporosis Risk Assessment JAMA 286(22) 2815-2822 Soliman S W J Aronson et al (2009) Analyzing Serum-Stimulated Prostate Cancer Cell Lines After Low-Fat High-Fiber Diet and Physical activity Intervention eCAM nep031 Sonn GA Aronson W and Litwin MS (2005) Impact of diet on prostate cancer A review Prostate cancer and prostate disease 8 p 304-310 Speck RM Courneya KS Masse L Duval S Schmitz K (2010) An update of controlled physical activity trials in cancer survivors a systematic review and meta-analysis Journal of Cancer Survivorship 4(2) p 87-100
140
Steginga S K B M Lynch et al (2009) Antecedents of domain-specific quality of life after colorectal cancer Psycho-Oncology 18(2) 216-220 Stevinson C H Steed et al (2009) Physical Activity in Ovarian Cancer Survivors Associations With Fatigue Sleep and Psychosocial Functioning International Journal of Gynecological Cancer 19(1) 73-78 Swenson KK Nissen MJ Anderson E Shapiro A Schousboe J Leach J (2009) Effects of physical activity vs bisphosphonates on bone mineral density in breast cancer patients receiving chemotherapy Support Oncol May-Jun7(3)101-7 Tardon A Lee WJ Delgado-Rodriguez M et al Leisure-time physical activity and lung cancer a meta-analysis Cancer Causes Control200516(4)389-397 Taskila T Martikainen R Hietanen P Lindbohm M Comparative study of work ability between cancer survivors and their referents Europ J of Cancer 2007 43914-920 Taylor R Brown A et al (2004) Physical activity-based rehabilitation for patients with coronary heart disease systematic review and meta-analysis of randomized controlled trials The American journal of medicine 116(10) 682-692 Taylor NFDodd KJShields NBruder A Therapeutic physical activity in physiotherapy practice is beneficial a summary of systematic reviews 2002-2005 Aust J Physiother 2007 53 7-16 Thiebaut A C M A Schatzkin et al (2006) Dietary Fat and Breast Cancer Contributions From a Survival Trial J Natl Cancer Inst 98(24) 1753-1755 Thomas R Daly M and Perryman J (2000) Forewarned is forearmed - Randomised evaluation of a preparatory information film for cancer patients European Journal of Cancer 36(2) p 52-53 Thomas R et al (2005) Dietary advice combined with a salicylate mineral and vitamin supplement (CV247) has some tumour static properties - a phase II study Diet and science 2005 35(6) p 436-451 Thomas RJ and Davies ND (2007) Lifestyle during and after cancer treatment Clinical Oncology Vol 19 Issue 8 pp 616-627 Thomas R Nicholson C (2009) Why is exercise good for us Cancer Active httpcanceractivecomcancer-active-page-linkaspxn=2600ampTitle=Why20is20exercise20good20for20us [Last accessed 230710] Thomas R Oakes R Gordon J Russell S Blades M Williams M (2009) A randomised double-blind phase II study of lifestyle counselling and salicylate compounds in patients with progressive prostate cancer Diet and Food Science 39(3) pp 295 ndash 305 Thomson C A N R Stendell-Hollis et al (2007) Plasma and Dietary Carotenoids Are Associated with Reduced Oxidative Stress in Women Previously Treated for Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 16(10) 2008-2015
141
Thune I Brenn T Lund E Gaard M Physical activity and the risk of breast cancer N Engl J Med 336 1269-1275 1997
Travis LB Gospodarowicz M Curtis RE et al Lung cancer following chemotherapy and radiotherapy for Hodgkins disease J Natl Cancer Inst 94 (3) 182-92 2002 Tucker MA Murray N Shaw EG et al Second primary cancers related to smoking and treatment of small-cell lung cancer Lung Cancer Working Cadre J Natl Cancer Inst 89 (23) 1782-8 1997 Twiss J J N Waltman et al (2001) Bone Mineral Density in Postmenopausal Breast Cancer Survivors Journal of the American Academy of Nurse Practitioners 13(6) 276-284 Uhley V and Jen C (2006) Diet and weight management in cancer survivors In Handbook of Cancer Survivorship edited by Feuerstein M New York NY Springer 2006 ISBN-13 978-0-3873-4561-1
Vadiraja HS et al (2009) Effects of yoga program on quality of life and affect in early breast cancer patients undergoing adjuvant radiotherapy A randomized controlled trial Complementary Therapies in Medicine Volume 17 Issue 5 Pages 274-280
Velthuis MJ Agasi-Idenburg SC Aufdemkampe G Wittink HM (in press) The effect of physical activity on cancer-related fatigue during cancer treatment a meta-analysis of Randomised Controlled Trials Clinical Oncology 2009 (in print) Vineis P G Hoek and M Krzyzanowski et al Lung cancers attributable to environmental tobacco smoke and air pollution in non-smokers in different European countries a prospective study Environ Health 6 (2007) pp 1ndash7 Visvanathan K Chlebowski RT Hurley P et al American Society of Clinical Oncology 2008 clinical practice guideline update on the use of pharmacologic intervention including tamoxifen raloxifene and aromatase inhibition for breast cancer risk reduction J Clin Oncol 273235-3258 2009
Wagner LI Cella D (2004) Fatigue and cancer causes prevalence and treatment approaches BrJCancer 91822-828 Waltman N J Twiss et al (2009) ―The effect of weight training on bone mineral density and bone turnover in postmenopausal breast cancer survivors with bone loss a 24-month randomized controlled trial Osteoporosis International Wenzel L H Q Huang et al (2005) Quality-of-Life Comparisons in a Randomized Trial of Interval Secondary Cytoreduction in Advanced Ovarian Carcinoma A Gynecologic Oncology Group Study J Clin Oncol 23(24) 5605-5612 Weikert C Hoffmann K Dierkes J Zyriax BC KlipsteinndashGrobusch K MB et al Homocysteine metabolismrelated dietary pattern and the risk of coronary heart disease in two independent German study populations J Nutr 2005 1351981ndash1988 White S E McAuley et al (2009) Translating Physical Activity Interventions for Breast Cancer Survivors into Practice An Evaluation of Randomized Controlled Trials Annals of Behavioural Medicine 37(1) 10-19
142
World Health Organisation (1999) What is a healthy lifestyle Health Documentation Services WHO Regional Office for Europe Copenhagen World Health Organisation (2002) The World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva WHO Scientific Group on the Prevention and Management of Osteoporosis (2000 Geneva Switzerland) (2003) Prevention and management of osteoporosis report of a WHO scientific group World Health Organisation (2005) The European health report 2005 public health action for healthier children and populations Copenhagen WHO regional office for Europe World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva Windsor P M Nichol K F Potter J A randomized controlled trial of aerobic exercise for treatment-related fatigue in men receiving radical external beam radiotherapy for localised prostate carcinoma Cancer (2004) 101 (3) 550-7 Wright M E S-C Chang et al (2007) Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality Cancer 109(4) 675-684 Wright P A Smith et al (2005) Psychosocial difficulties deprivation and cancer three questionnaire studies involving 609 cancer patients Br J Cancer 93(6) 622-626 Yu GP et al (1997) The effect of smoking after treatment for Cancer Cancer Detect Prev 21487-509

6
9 Mechanisms of benefit for diet and physical activity include the influence that these
behaviours have on hormones and insulin levels This has sparked the question of
whether pharmacological alternatives such as aromatase inhibitors and metformin
which tend to produce greater reductions in cancer risk pose competition for lifestyle
interventions This is unlikely as healthy lifestyle behaviours contribute overall to
general health and to the risk reduction for other co-morbid conditions such as
hypertension cardiac disease and diabetes Usefully the competencies framework
offered by Finders University highlights the importance of taking a holistic approach
to supported self-management whereby support is provided for a continuum of
health as opposed to a focus on one established chronic condition Based on this
model supported self-management should provide health promotion and illness
prevention not merely in terms of cancer but also for associated risks and co-
morbidities
10 The challenge remains in integrating lifestyle support into standardised models of
aftercare for cancer survivors particularly in terms of engaging both patients and
health professionals bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative identifies the need to
provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for
healthcare professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
11 The literature identifies the need for individual assessment and risk stratification for
cancer survivors so that lifestyle interventions and support can be tailored and
provided according to need Particularly high need groups are survivors who have
co-morbidities are overweight sedentary or smoke
12 Some questions that remain
o What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
o How can people most likely to benefit from lifestyle interventions be effectively
identified
o What are the various intensities of lifestyle support that can be provided based on
levels of individual need
13 Significant limitations can be found in the evidence available for lifestyle outcomes in
cancer survivors including
7
o Long-term outcomes of lifestyle choices
o Low levels of adherence to interventions
o A paucity of studies addressing external validity
o Equality across tumour groups
o Lack of cultural considerations pertaining to dietary advice
o A paucity of individualised lifestyle advice and tailored support
8
BACKGROUND SETTING THE SCENE
Lifestyle and Well-Being
In an independent report offering recommendations on enabling effective delivery of health
and well-being in England Bernstein Cosford and Williams (2010) advise that setting clear
priorities for health and well-being should start with behavioural risk factors Namely they
recommend tackling the biggest lifestyle influences on population health tobacco alcohol
physical inactivity and poor diet These four lifestyle factors are among the biggest
contributors to most preventable diseases across all social groups and in all areas of
England They are responsible for 42 of deaths from leading causes (WHO 2005) and
together they account for at least pound94 billion in annual direct costs to the NHS (DH 2009a)
expenses incurred outside the NHS would increase this figure further
An increase in longevity and the number of people living with one or more chronic conditions
for a longer period of time has led to government action aimed at making these years as
healthy as possible Interest has been particularly paid to the role of these behavioural risk
factors and the role of lifestyle in improving or maintaining health preventing illness
managing symptoms and achieving a satisfactory quality of life (QoL) (Pedersen and Saltin
2006 Taylor et al 2004)
The term lifestylelsquo refers to personal choices that might impact health such as diet physical
activity smoking and alcohol consumption The World Health Organisation (WHO 1999)
defines a healthy lifestylelsquo as
ldquoa way of living that lowers the risk of being seriously ill or dying earlyrdquo with the
emphasis that ldquohealth is not just about avoiding disease It is also about physical
mental and social well-beingrdquo (p 2)
With earlier detection and more efficacious treatments available for cancer there has been
an increase in survival as well as in the number of people living with the long-term
consequences of cancer treatment Subsequently cancer has become a chronic disease for
a number of people among the two million cancer survivors in the UK (Maddams Moller and
Devane 2008) Whilst evidence of the effects of a healthy diet and sufficient physical activity
in cancer prevention has been well-documented (Chan Gann and Giovannucci 2005
Sonn Aronson and Litwin 2005) it has become of fundamental importance to examine the
role of these lifestyle choices in cancer survivorship Furthermore the role of lifestyle in
cancer survivorship needs to be examined not only in terms of improved physical and
psychological well-being but also disease outcomes
Given the relationship between choosing a healthy lifestyle and taking an active role in the
self-management1 of the long-term effects of cancer and its treatment the self-management
workstream of the National Cancer Survivorship Initiative (NCSI) have conducted this
1 lsquoSelf-managementrsquo has been defined as ldquoawareness and active participation by the person in their recovery
recuperation and rehabilitation to minimise the consequences of treatment promote survival health and well-beingrdquo (NCSI 2009)
9
evaluation of evidence pertaining to lifestyle factors and survivorship Not only are lifestyle
choices important in terms of disease progression and recurrence but also in the effective
management of other chronic symptoms and conditions resulting from treatment such as
cancer-related fatigue lymphoedema and osteoporosis (Doyle et al 2006) Lifestyle
support and education is evidently an important component of supported self-management2
for many individuals living with or beyond cancer (Davies and Batehup 2010) Indeed as
part of a consensus meeting and evidence review self-management support and lifestyle
management were among the top ten priorities for survivorship research (Richardson et al
2009) providing further rationale for the current review
The Health of Cancer Survivors
The traditional belief has been that people with cancer should rest reduce activity and avoid
activities involving intense physical effort in other words they are passive patients of the
disease and its treatment Consequently physical activity levels do decline substantially
during and after completion of treatment for cancer and often fail to return to pre-diagnosis
levels for many people (Daley et al 2008) Fortunately it is becoming increasingly
recognised that people living with or beyond cancer do need physical activity will not be
harmed by physical effort and are active participants in the rehabilitation process
Furthermore emerging evidence is demonstrating that lifestyle factors can influence the rate
of cancer progression improve quality of life (QoL) reduce side-effects and risks during
treatment reduce the incidence of relapse and improve overall survival (Thomas Daly and
Perryman 2000) Besides the beneficial effect on recurrence a healthy diet and regular
physical activity has the potential to reduce the risk of co-morbidity such as other cancers
cardiovascular disease and diabetes etc (Jones and Demark-Wahnefried 2006)
Research suggests that although many cancer survivors report making healthy lifestyle
changes after diagnosis these changes may not be generalisable to all populations of
cancer survivors and they are often temporary (Demark-Wahnefried and Jones 2008)
Furthermore evidence suggests that the healthy lifestyle behaviours adopted by cancer
survivors tend to be directed towards clinical action such routine physical examination rather
than those health behaviours that require daily effort such as healthy eating or regular
physical activity (Findley and Sambamoorthi 2009)
A potential explanation for this difference in the uptake of clinical versus lifestyle preventive
health behaviours is that the former is easier due to the primary action being carried out by
someone else The latter on the other hand requires personal time and effort as well as
opportunity socially economically and in terms of health literacy and educational status
Behavioural and lifestyle change is notoriously difficult but even more so for people with
cancer or other chronic conditions let alone those with co-morbidities (Krein et al 2005) For
people with co-morbidities a healthy lifestyle can be even more challenging as they grapple
with the competing demands posed by the self-management of multiple conditions (Lindsay
2009)
2 lsquoSupported self-managementrsquo has been defined as ldquoWhat health and social care professionals and service
delivery organisations to do support self-managementrdquo (NCSI 2009)
10
Given the increase in survivorship the higher rates of co-morbidity within this population
and evidence that diet physical activity and other lifestyle factors affect risk for other cancers
and other chronic diseases there is a clear need for lifestyle interventions that target this
high risk group The literature suggests the need for individual risk assessment and the
provision of support with lifestyle changes in those individuals identified as high risk ndash such
as survivors who have co-morbidities are overweight sedentary or smoke (Davies and
Batehup 2010)
The Lifestyle Needs of Survivors
The National Cancer Survivorship Initiative (NCSI) highlights that people living with or
beyond cancer would like to play a more active role in their healthcare They want to know
how to look after themselves after a cancer diagnosis including information and support on
the lifestyle changes they should make so they can return to normallsquo life as much as
possible (Macmillan Cancer Support 2008) Yet the evidence suggests that this need
remains largely unaddressed In a key mapping project commissioned by the NCSI
Research workstream a number of issues pertaining to lifestyle were identified for the four
most common cancers breast colorectal lung and prostate (NCSI 2009) Each of these
four reports which were conducted by independent organisations demonstrated gaps in the
provision of lifestyle advice and support mainly during the period of aftercare In a similar
report mapping the needs of rarer cancers prolonging life through changes to lifestyle
emerged as a frequent theme by survivors asked to explore the meaning of cancer
survivorshiplsquo (Cancer52 and NCSI 2009) There was particular emphasis on the need for
diet and physical activity advice post-surgery for oesophageal cancer as well as diet advice
for mouth and throat cancers Change in bowel habits is frequently reported among post-
treatment bowel cancer survivors requiring support with dietary changes (Nikoletti et al
(2008)
In an effort to provide further insight into lifestyle advice and support for cancer survivors as
well as developing evidence-based lifestyle interventions a comprehensive review of the
evidence for lifestyle and cancer outcomes is required The perceived outcome efficacy3 of
making lifestyle changes is important in terms of whether those changes are initiated or not
as well as whether an individual possesses the confidence (self-efficacy) to maintain lifestyle
changes Outcome efficacy could be increased by the accumulation of firmly established
evidence offered alongside the opportunity for lifestyle support
Additionally this evidence needs to be evaluated in respect of current national guidelines for
diet physical activity and other lifestyle indicators such as weight and alcohol consumption
Briefly national guidance recommends a diet comprising 33 fruit and vegetables (five
portions per day) 33 starchy foods (rice bread pasta potatoes) 15 milk and dairy
foods 12 protein (meat and fish) and 8 foods and drinks high in fat andor sugar (Food
Standards Agency 2007) Adults are advised to achieve a total of at least 30-minutes daily
moderate intensity physical activity on five or more days of the week (DH 2004) Combined
with a healthy diet regular physical activity is aimed at maintaining a Body Mass Index
3 The belief that a particular outcome will result from following certain actions or behaviours
11
(BMI)4 of 185-249kgm2 25-29 is considered to be overweight and 30 or above as obese
whilst under 185 is considered underweight (National Obesity Observatory 2009)
A healthy lifestylelsquo is the same for cancer survivors as for the general population or indeed
people with other chronic conditions (Bellizzi et al 2005 Caan et al 2005 Coups and
Ostroff 2005) Cancer survivors are slightly more likely to follow physical activity guidelines
but overall their health behaviours mirror those of the general population which is marked by
inactivity and an epidemic of obesity and associated problems (Caan et al 2005) Despite
this the lifestyle advice and tailored care currently provided for specific groups of people in
the general population such as exercise prescriptions (DH 2001) is not yet integrated into
the supportive care needs of cancer survivors (Addington-Hall 2010) This is in the main
due to reluctance (usually related to knowledge and confidence) from health professionals to
discuss lifestyle factors with cancer patients due to limitations in knowledge and an
inadequacy in the available evidence on the underlying mechanisms of benefit for individual
lifestyle factors (Miles Simon and Wardle 2010) It is anticipated that this review will allay
some of this reluctance by identifying where the evidence strongly supports the efficacy of
lifestyle factors in cancer outcomes as well as where the evidence is less clear and requires
further research
4 BMI is a statistical measure which compares a persons weight and height to estimate a healthy body weight
12
The Purpose of this Review
Using the outlined national guidance on lifestyle and taking account of evidence for specific
elements or intensity of certain lifestyle factors in cancer care and self-management a
review of the literature on lifestyle and survivorship will be conducted The primary aims are
to produce evidence that can support professionals in guiding and advising cancer survivors
as well as evidence regarding resources which might support patient self-management in
relation to lifestyle factors and behaviour change The review will be comprehensive but
pragmatic drawing on a variety of sources This will commence by updating a recent review
conducted by the World Cancer Research Fund (WCRF) - bdquoA Systematic Review of RCTs
Investigating the Effect of Diet and Physical Activity Interventions on Cancer Survival‟
(Bekkering et al 2006)5
The aim of the WCRF review (Bekkering et al 2006) was to systematically locate and
review all randomised control trials (RCTs) which tested the effect of diet andor physical
activity interventions in cancer survivors their definition of a cancer survivor being
ldquoanyone who has been diagnosed with cancer from the time of diagnosis through the
rest of liferdquo (Brown et al 2003)
They conducted a systematic search of MEDLINE (from 2000 onwards) EMBASE (from
1999 onwards) AMED (from 1985 onwards) and the Cochrane Library including DARE
CDSR CENTRAL and HTA (all years) up to March 2006 scanned key texts that were
relevant to the subject field and scanned the references of relevant reviews They identified
117 trials (Table 1)
Table 1 Trials Identified in the WCRF Review (Bekkering et al 2006)
Trials Total
Diet
Food-based
Supplement-based
23
71
Physical activity
23
Total 117
5 This has been highlighted by the American Cancer Society (ACS) as being one of the most comprehensive
reviews on diet and physical activity for cancer survivors The ACS has used the review alongside other sources to produce lsquoGuidelines on Diet and Physical Activity for Cancer Preventionrsquo (Kushi et al 2006)
13
The findings will be described along with the results of the current review The overall
conclusion drawn by Bekkering et al (2006) was that there is a paucity of robust evidence
on the effects of diet and physical activity interventions in the management of cancer RCTs
were generally small and often reported inadequate details to formally assess quality While
promotion of a generic healthy diet was associated with reduced overall mortality the degree
to which lifestyle accounted for this outcome was imprecise It was concluded that given the
large investment in potential lifestyle interventions among cancer survivors large-scale trials
adequately powered to provide robust conclusions should be supported and conducted
In updating the WCRF review (Bekkering et al 2006) further scoping of the literature from
2006 to February 2010 will be conducted along with a synthesis of the evidence presented
in the lsquoHandbook of Cancer Survivorship‟ edited by Michael Feuerstein (2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (National Cancer Action Team 2009) which evaluates literature
pertaining to rehabilitation
The primary aim of the review is to guide healthcare planning and the development of
supported lifestyle self-management interventions for high risk groups In order to be able to
consider the production of useable evidence-based guidance for self-management for both
patients and professionals the following evidence will be sought
Evidence that would support professionals to be able to guide and advise
patients
Evidence regarding resources which would support patient self-management in
relation to lifestyle factors and behaviour change
It is anticipated that recent efforts to conduct research in this area will facilitate the
clarification of any key recommendations that can be made to cancer survivors by healthcare
professionals This update of the evidence will also attempt to establish where the strength
of the evidence lies and where more research is required
14
METHOD
Search Strategy
In updating the WCRF review (Bekkering et al 2006) RCTs and systematic reviews were
obtained from a systematic search of the Cochrane Library Database and Pubmed (from
March 2006 to February 2010) Where no evidence was available in the WCRF review
studies before 2006 have been included if identified in the reference lists of acquired
records this is the case with studies on smoking which were not included in the Bekkering
et al (2006) review
The selected relevant chapters were read from the bdquoHandbook of Cancer Survivorship‟
(Feuerstein 2006)6 and relevant studies referred to from the Cancer and Palliative Care
Rehabilitation Workforce (2009) non-systematic review Grey literature was also utilised
where this would provide information relevant to the review or where cancer-specific
literature was lacking as was the case with osteoporosis
All titles and abstracts of studies identified by the searches were scanned for relevance in
terms of topic and participant group For any titles or abstracts that were potentially relevant
full paper manuscripts were obtained and the relevance of each study assessed according to
the pre-specified inclusion criteria
6 Chapters include Physical Activity Potential Benefits and Guidelines DietWeight Management
Search terms cancer OR neoplasm
AND diet OR exercise OR physical
activity OR weight OR lifestyle
Cochrane systematic reviews
925 records
PubMed
4941 records
56 included 84 included
15
Inclusion Criteria
Records included within the review of the literature met the following inclusion criteria
Lifestyle-related ndashdiet physical activity weight smoking alcohol consumption
Cancer sites breast colorectal lung or prostate cancer Other tumour sites will
be included if located while searching for the primary tumour sites
Trajectory - during primary cancer treatment or post-primary treatment
Outcomes of interest ndash survival recurrenceprogression symptoms treatment-
related chronic conditions ndash fatigue lymphoedema osteoporosis weight
physical fitness quality of life rehabilitation behaviour change health and well-
being cost-effectiveness
Adult population
Type of record ndash RCTs systematic reviews prospective cohort studies
Retrospective studies will also be included since some areas of lifestyle such as
smoking have primarily been investigated via this method
16
RESULTS
A total of 140 records were included in this review not counting the review being updated
(Bekkering et al 2006) In synthesising the evidence obtained from these records and the
additional sources described in the search strategy findings are presented in two parts
1) Cancer Survival
Evidence for the role of lifestyle in disease progression and recurrence
2) The Risks and Side-Effects of Cancer Treatment
Evidence for the role of lifestyle in reducing and managing the risks and
side-effects of cancer treatment with specific focus on cancer-related
fatigue lymphoedema osteoporosis and QoL
Both sections examine five categories of evidence
Physical activity
Diet
Weight
Smoking
Alcohol
The focus is on the four most common cancers (breast colorectal lung prostate) but other
tumour sites have been included if located via the pre-defined search strategy Summary
tables for each study included within the evidence are provided at the end of relevant
sections
17
PART ONE
CANCER SURVIVAL ndash EVIDENCE FOR THE ROLE OF LIFESTYLE IN
DISEASE PROGRESSION AND RECURRENCE
Introduction
Evidence for the role of lifestyle in the development of cancer is strong and it is widely
accepted that a poor diet lack of exercise smoking and excessive alcohol consumption can
increase an individuallsquos risk of developing cancer In particular it is well established that
smoking can increase risk of lung cancer and excessive unprotected exposure to the sun
can increase risk of skin cancer More recently lifestyle after a cancer diagnosis has been
under the microscope with evidence for the role of lifestyle in cancer progression7 and
recurrence8 demonstrating that lifestyle changes post-diagnosis can influence the disease
trajectory (Thomas and Davies 2007)
The development of cancer does not mean it is too late to make lifestyle changes that can
reduce the risk of the disease progressing or recurring after remission Indeed lifestylelsquo
refers to personal choices that can impact health and well-being as well as improve an
individuallsquos chance of disease-free survival9 and overall survival10
Evidence for an interaction between lifestyle and the disease trajectory is evaluated in the
current review including cancer development progression and recurrence and
commencing with a description of three large scale multicentre trials that will be referred to
throughout (Table 3)These studies are presented in some depth because their findings have
been influential in this field of study This will be followed by a site-specific (eg breast
colorectal lung prostate) summary of the findings reported by Bekkering et al (2006) as
part of the WCRF review being updated Further evidence identified from the search criteria
will then be presented including evidence obtained from the aforementioned multicentre
trials The European Prospective Investigation into Cancer and Nutrition (EPIC) Study
The Womens Intervention Nutrition Study (WINS) and The Womens Healthy Eating
and Living (WHEL) Study
7 Defined as the cancer becoming worse or spreading within the body
8 Cancer that has returned usually after a period of time during which it could not be detected The cancer may
come back to the same place as the original (primary) tumour or to another place in the body
9 The length of time after treatment during which a person survives with no sign of the disease
10The percentage of people from the study who are alive for a certain period of time after diagnosis or treatment
(ie 5-year survival rate)
18
The European Prospective Investigation into
Cancer and Nutrition (EPIC) Study (Riboli et al
2002)
The Womens Intervention Nutrition Study (WINS)
(Chlebowski et al 2006)
The Womens Healthy Eating and Living (WHEL)
Study
(Pierce et al 1997)
The EPIC study is coordinated in the UK by Dr Elio Riboli of the Imperial College London It is an ongoing multicentre prospective cohort study designed to investigate the relationship between nutrition and cancer The study currently includes 521000 participants (aged 35ndash70 years) in 23 centres located across 10 European countries11 These participants will be followed for cancer incidence and mortality for at least 10-years At enrolment which took place between 1992 and 2000 information was collected through a lifestyle questionnaire and through a dietary questionnaire addressing usual diet Physiological measurements (eg weight) were performed and blood samples taken The main website for EPIC12 last updated in 2010 reports that 26000 cases of cancer and 16000 deaths from cancer have been identified the majority of cases being cancer of the breast (n=6218) colonrectum (n=1910) prostate (n=1547) and lung (n=1292)
The WINS trial is a randomised multicentre study that commenced in 1994 and is now closed for recruitment It was designed to determine whether dietary fat reduction effectively prolongs disease-free and overall survival in post-menopausal women (n=2437) aged 48-78 years surgically treated for early stage breast cancer Randomisation to a reduced fat group or a control group took place between 1994 and 2001 with participants being evaluated annually via self-report and physiological measures 1) Intervention group (n=975) intensive dietary intervention for reduction of total fat intake to 15 of calories with repeated individual and group counselling sessions involving cognitive behavioural and motivational interviewing techniques 2) Control group (n=1462) US Department of Health and Human Services dietary guidelines (total fat intake between 20-35 of calories)
The WHEL study is a multicentre RCT which commenced in 1995 and also closed to recruitment aimed to determine whether a diet rich in vegetables fruit and fibre and low in fat is associated with a longer breast cancer event-free interval (ie no disease progression recurrence nor secondary cancers) Women diagnosed with stage I-III invasive breast cancer (n=3088) within the previous 4-years were randomised to a dietary intervention or control group and evaluated annually for 5-years via self-report and physiological measures 1)Intervention group (n=1540) guidelines provided for a daily dietary pattern of 5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy from fat A telephone counselling protocol focusing on goal setting self-monitoring and self-efficacy were provided as were cooking classes 2)Control group (n=1551) The US Department of Agriculture dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre and 30 energy from fat)
11
Denmark France Germany Greece Italy The Netherlands Norway Spain Sweden and the UK
12 httpepiciarcfr
Table 3 The EPIC WINS and WHEL Study (findings presented within proceeding text)
19
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in breast
cancer survival In the current review 6 studies and 2 systematic reviews were identified
These have been divided into appropriate domains according to mechanisms of benefit
hormones intensity and insulin Studies are summarised in Table 3 at the end of this
section
Hormones
Evidence exists that physical activity is associated with reduced risk of developing breast
cancer (Friedenreich and Cust 2008 Monninkhof et al 2007) One potential mechanism of
benefit is via the modification of sex hormone levels High levels of oestrogen (the
predominant sex hormone in females)13 and androgen (the predominant sex hormone in
males)14 are consistently associated with increased risk of developing breast cancer
(Eliassen et al 2006 Kaaks et al 2005) whereas high levels of sex hormone-binding
globulin (SHBG)15 are associated with a decreased risk (Key et al 2002) Regular physical
activity may alter oestrogen metabolism by shifting metabolism to favour production of 2-
hydroxyestrone (2-OHE1)16 as opposed to16α-hydroxyestrone (16α=OHE1) the former of
which has much weaker estrogenic activity Campbell et al (2007) is one of the few
researchers to examine this mechanism of benefit via a RCT In examining the effects of a
12-week aerobic exercise training programme on 2-OHE1 and 16α-OHE1 in healthylsquo pre-
menopausal women (n=17) no significant differences in oestrogen changes were found with
a control group who continued their usual level of physical activity (n=15) However a
change in lean body mass (estimated weight excluding body fat) over the 12-week
programme was found to be associated with a favourable change in 2-OHE1 to 16α-
OHE1 ratio (p lt 005)
In an effort to provide more direct evidence regarding the biological mechanisms of benefit
obtained from physical activity Friedenreich et al (2010) conducted the Alberta Physical
Activity and Breast Cancer Prevention Trial a two-centre two-arm RCT of physical
activity and cancer risk in older (50gt years) post-menopausal sedentary women from the
general population (n=320) Participants received a 1-year aerobic physical activity
programme of 225-minutes per week (n=160) or maintained their usual level of activity as
part of a control group (n=160) Significant reductions in oestrogen were found in the
intervention group compared to the control group demonstrating a protective effect
of increased physical activity in this group of high risk women (p lt 05)
13
oestrogen is suspected to activate certain oncogeneslsquo which can turn normal cells into tumour cells 14
The primary and most well-known androgen is testosterone which is also found in women to a lesser degree 15
A protein that attaches itself to oestrogen and androgen
16 Sometimes referred to as a good oestrogenlsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
20
Whilst some studies have examined the outcomes of increased physical activity others have
attempted to identify the duration and intensity required for beneficial effects Using data
from the Nursesrsquo Health Study17 (n=2987) Holmes et al (2005) found that women who
reported at least 3 MET-hours18 or more of physical activity per week were less likely
to have a recurrence or die from breast cancer compared to those who reported less
physical activity (p lt 001)
A further reduction in risk was seen with higher levels of physical activity up to 239 MET-
hours per week indicating a dose-response Interestingly the benefits of physical activity
were limited to women with hormone-receptor positive tumours (tumours that
respond to hormone treatment) as opposed to hormone-receptor negative tumours
(tumours that do not respond to hormone treatment) This provides further support for
mechanism of benefit from physical activity being hormone-related whether that be due to
the physical activity or any subsequent reductions in lean body mass that might accompany
such activity
Intensity
Expanding on evidence for the intensity of physical activity in a prospective observational
study the Health Eating Activity and Lifestyle (HEAL)19 study Irwin et al (2008) found
that of breast cancer survivors (n=933) who were sedentary pre-diagnosis women who
increased their physical activity post-diagnosis to approximately 9-MET hours per
week (eg 2-3 hours of brisk walking) had a 45 lower risk of death from cancer when
compared to those who did not increase their physical activity women who
decreased physical activity after diagnosis had a four-fold greater risk (p lt 005)
17
One of the largest and longest running investigations of factors that influence womenlsquos health comprising
information from 238000 nurse-participants
18 Metabolic equivalent (MET) values a measure of the effort required to do that activity
19 The HEAL Study is a population-based multicentre multi-ethnic prospective cohort study that has enrolled
1183 breast cancer survivors to determine whether lifestyle hormones and other exposures affect breast cancer
prognosis
METs (Ainsworth 2000) Light-intensity activities are defined as 11 MET to
29 MET Moderate-intensity activities are defined as 30 to
59 METs Vigorous-intensity activities are defined as 60 METs
or more
3 MET-hours might be using a stationary bicycle with light effort for one-hour 239 MET-hours might be running for 2-hours plus 1-hour of aerobic activity
21
Consistent with this a larger prospective observational study demonstrated that breast
cancer survivors (n=4482) who were physically active for more than 28 MET-hours per
week (eg walking at average pace of 2-29mph for 1-hour) were significantly less
likely to die from breast cancer (35-49 reduction) when compared to survivors who
did less than this (p lt 05) (Holick et al 2008) The reduced risk of mortality from cancer
was limited to total or moderate-intensity physical activity no benefit was noted for vigorous-
intensity activity
In a systematic review by Patterson et al (2010) leisure-time physical activity (ie
sportsrecreational) was associated with a 30 decreased risk of mortality from
breast cancer when compared to sedentary women In another review Saxton (2010)
identified four cohort studies demonstrating that women achieving the equivalent of 30-
minutes of moderate intensity physical activity on five or more days of the week
halved their risk of cancer-related mortality compared to those achieving less than 30-
minutes over the five days
Insulin
Evidence for the role of excess insulin in the growth of cancer cells has become more
established in recent years especially with the increase in obesity which is often
accompanied by elevated levels of insulin (Giovannucci 2005) The benefits of physical
activity on reducing insulin levels are less clear Ligibel et al (2008) conducted a RCT to test
the impact of weight training on insulin levels in overweight sedentary stage I to III breast
cancer survivors (n=101) The women were randomly assigned to one of two conditions
1) a 16-week supervised strength training and home-based cardiovascular training
protocol (two supervised 50-minute strength training sessions per week and 90-
minutes of home-based aerobic physical activity weekly)
2) a control group (routine care for 16-weeks before being offered consultation with a
physical activity trainer at the end of the control period)
Participation in the physical activity training was associated with a significant
decrease in insulin levels and hip circumference (p lt 05) Therefore the relationship
between physical activity and breast cancer recurrence may be mediated in part through
changes in insulin levels andor changes in body fat
ii DIET
Bekkering et al (2006) report on two small breast cancer studies showing a reduction in
cancer-specific mortality with healthy diet interventions (Elkort et al 1981 de Waard et al
1993) Of nine trials that included an antioxidant supplement no evidence was found for an
association between the intervention and cancer-related mortality compared with placebo or
usual treatment There was also no evidence of an effect of retinol (vitamin A - found in cod
liver oil butter liver eggs and cheese) (Meyskens et al 1994 Kucera et al 1980
Pastorino et al 1993)
22
In the current review 19 studies provide further evidence of the role of diet in breast cancer
survival many of which are part of the three multicentre studies previously described (ie
EPIC WINS WHEL p19) These studies have been divided into appropriate domains
according to dietary components dietary fat fruit and vegetables dietary fibre soy and
vitamin D
Dietary Fat
In general retrospective casendashcontrol studies have supported a positive association between
breast cancer incidence and dietary fat (Howe et al 1990) whilst many prospective cohort
studies have failed to show such an association (Kim et al 2006 Hunter et al 1996) A
meta-analysis provided evidence for a weak direct association between fat intake and breast
cancer in casendashcontrol and cohort studies combined (Boyd et al 2003) in cohort studies
that adjusted for energy intake highest versus lowest categories of total fat intake were
associated with a statistically significant 13 increased risk of developing
breast cancer (p lt 05)
Kyogoku et al (1992) utilised breast cancer patients whose dietary intake was assessed 10-
years previously in a case-control study (n= 212 patients who underwent a surgical
operation) After 10-years of follow-up 47 breast cancer deaths had occurred with no
support being provided for the hypothesis that a low fat diet influences breast cancer survival
outcomes In addition Holmes et al (1999) as part of the Nursesrsquo Health Study report
there being no evidence suggesting that lower intake of total fat or specific types of fat (eg
saturated and unsaturated fat) was associated with death from breast cancer in 2956
women who were diagnosed after 14-years of follow-up
Hebert et al (1998) studied the effect of diet on recurrence and death in women diagnosed
with early-stage breast cancer (n=472) finding that the strongest effects were observed in
pre-menopausal women Higher levels of self-reported baseline daily consumption of
butter margarine lard and beer were found to increase the risk of recurrence (p lt
01) There was also an increased risk associated with consumption of red meat liver and
bacon corresponding to about a doubling of risk for each time per day that foods in this
category were consumed (p=09)
The previously described WINS and WHEL RCTs (Table 2 p19) were anticipated to shed
light on these inconsistent findings related to dietary fat and breast cancer outcomes as
explored next in the following section
In an interim analysis of the Womens Intervention Nutrition Study (WINS) data (n=2437)
after a median follow-up of 60-months (5-years) (Chlebowski et al 2006) report that dietary
fat intake was lower in the dietary intervention than in the control group corresponding to a
significant 6-pound lower mean body weight in the intervention group (p lt 05) As a
reminder the dietary intervention group were counselled to reduce total fat intake to 15 of
calories whilst the control group were advised to keep total fat intake between 20-35 of
calories After 5-years of follow-up a total of 277 recurrences were reported in 96 of 975
23
(98) women in the dietary group and 181 of 1462 (124) women in the control group
women in the dietary intervention had a 24 lower risk of recurrence compared to the
control group (p lt 05) Exploratory analyses suggested that dietary fat reduction was most
beneficial in women diagnosed with hormone receptorndashnegative compared to hormone-
receptor positive breast cancer although this was not statistically significant
Other studies providing evidence of a differential effect of fat intake on breast cancer survival
have found such associations with hormone-receptor positive cancers (Holm et al 1993
Cho et al 2003) raising debate over the WINS findings Nevertheless in 2008 Chlebowski
et al updated survival information presented in 2006 reporting that after 7-years follow-up a
significant overall survival benefit was seen in women (n=362) with hormone-receptor
negative tumours taking part in the dietary intervention compared to the comparison
group (75 vs 181 p lt 005)
To explore the link between hormones and diet further the metabolic profiles of a subset of
WINS participants (n=53) were examined for the effect of a low-fat diet on insulin resistance
(Khaodhiar et al 2003) Insulin resistance is a physiological condition in which insulin
becomes less effective in lowering blood sugars resulting in increased blood glucose Of
those participants with initial insulin resistance after 1-year women in the dietary
intervention group had a greater decrease in their fasting insulin (insulin tested in a blood
sample collected after a 12-hour fast) than the women in the control group Although
not statistically significant these results suggest that insulin concentrations (a marker of
insulin resistance) may be influenced by dietary fat intake Alternatively since waist-to-hip
ratio is a marker for insulin weight reduction as opposed to dietary fat reductions might be
the important variable influencing disease outcomes (Borugianlsquos et al 2004)
Fruit and Vegetables
Flavonoids20 are high in fruits and vegetables and therefore might account for some of the
findings reported in WINS Dwyer et al (2008) sought to determine whether differences
existed in baseline and 12-month dietary intake of flavonoids among a random sample of
WINS participants (n=550) After 12-months of dietary intervention flavonoid intakes
remained similar in both groups demonstrating that neither total flavonoid intakes nor
intakes of subclasses of flavonoids differed between those who had dramatically decreased
their fat intake and those who had not Flavonoid intake is therefore unlikely to account for
the survival benefits reported for the WINS trial Carotenoids21 however do appear to play a
significant role in cancer survival On following 103 breast cancer survivors 27 of whom
died Ingram (1994) found that after a median of 81-months those who consumed more
beta-carotene (a carotenoid found in yellow and orange fruits such as mangoes
papayas and carrots) had significantly fewer deaths from breast cancer only one in
the group of highest beta-carotene consumers compared with 8 in the intermediate
20
Flavonoids also referred to as bioflavonoids are polyphenol antioxidants found naturally in plants ndash in other
words they are plant nutrientslsquo
21 Organic pigments that provide colour to bright fruits and vegetables including carrots apricots tomatoes and
salmon
24
group and 12 in the lowest group (p lt 0001) Overall there were 12 deaths in the lowest
total fruit consumption group compared with five in the intermediate group and 3 in the
highest (p lt 001) This benefit applied to both orangeyellow fruit (oranges melon) as well
as other fruits (apple banana berries grapes dried fruits)
Adding to this evidence is data from the aforementioned Womens Healthy Eating and
Living (WHEL) RCT (Table 2 p19) As a reminder women with breast cancer were
randomised to a dietary intervention (n=1540) comprising a daily pattern of
5 vegetable servings 16oz of vegetable juice 3 fruit servings 30g fibre and 15ndash20 energy
from fat or to a control group (n=1551) advised to follow the US Department of Agriculture
dietary guidelines for a daily consumption of 5 servings of vegetables and fruits 20g fibre
and 30 energy from fat Over a mean 73-year follow-up there was no significant
difference between groups in terms of additional breast cancer events (ie disease
progression recurrence or secondary cancer) or mortality despite statistically significant
differences in self-reported diet (low fat high fruit and vegetables) (Pierce et al 2007) On
the other hand when Rock et al (2005) examined only those participants in the control
group higher plasma total carotenoid concentration indicative of greater fruit and
vegetable consumption was significantly associated with reduced risk for a new
breast cancer event (p lt 05) This supports those findings reported by Ingram et al
(1994) and provides a potential explanation for why survival benefits were achieved in WINS
but not WHEL since both dietary interventions comprised lower dietary fat and higher levels
of carotenoids (fruit and vegetables) other factors must explain the differential survival
benefits One major difference between the two studies is that WINS participants lost weight
(mean = 6-pounds) whereas the WHEL participants did not
To follow up on these findings in terms of possible biological mechanisms of reduced risk of
recurrence Thomson et al (2007) conducted an ancillary study with post-menopausal
breast cancer survivors from the WHEL study (n=207) The aim was to test the hypothesis
that breast cancer survivors with higher levels of dietary carotenoids would show significantly
lower levels of oxidative stress (pathologic changes in response to excessive levels of cell
toxicity from the environment) than those with lower levels It was found that dietary
carotenoid levels were not significantly associated with oxidative stress indicators (measured
via urine samples)
Hot flushes post-treatment for early-stage breast cancer has been associated with an
approximately 25-30 decreased risk for additional breast cancer events (Mortimer et al
2008 Cuzick 2007) Since hot flushes are reported by women who continue to menstruate
during treatment or whose menstruation returns post-treatment this lowering of risk is
unlikely to be explained entirely by the lower oestrogen levels that sometimes accompany
hot flushes On the other hand dietary changes comprising lower energy from fat and
increased fibre can also alter oestrogen levels For example binding of fibre to estrogens in
the gut blocks reabsorption of oestrogen (Arts et al 1991) Focusing their analyses on the
2967 of the WHEL participants who experienced baseline hot flushes Gold et al (2009)
tested the hypothesis that the increased risk of additional breast cancer events observed
among women who do not report hot flushes post-treatment can be reduced by lifestyle
interventions that lower circulating oestrogen Over a median of 73-years follow-up it was
demonstrated that the dietary intervention was associated with reduced risk of second
25
breast cancer events among women who reported no hot flushes at baseline (p lt 05)
These women had 31 fewer cancer-related events than matched-pairs in the control group
among post-menopausal women with no self-reported hot flushes at baseline the
intervention effect was even stronger with a 47 reduction in risk compared with post-
menopausal women in the control group who had no hot flushes at baseline (p lt 05)
McEligot et al (2006) conducted a retrospective investigation into the influence of diet (fat
fibre vegetable fruit folate carotenoids and vitamin C) on overall survival in post-
menopausal women with breast cancer (n= 516) Participants completed a food frequency
questionnaire for the year prior to diagnosis the analysis of which demonstrated that
women consuming the least total fat and highest total fibre and vegetables as well as
more folate vitamin C and carotenoid were significantly less likely to die from any
cause than those women consuming the opposite (p lt 05)
Dietary Fibre
Evidence linking breast cancer to the intake of dietary fibre has been conflicting although the
hypotheses remain that dietary fibre can be protective by inhibiting oestrogen (Kaaks et al
2005) as described previously in relation to physical activity or by reducing insulin-like
growth factors (Heald et al 2003) Therefore further research into these mechanisms of
benefit is clearly needed in order to provide clarity
Rohan et al (1993) examined risk of breast cancer in relation to intake of dietary fibre and
vitamins A C and E in a cohort of women (n=56837) enrolled in the Canadian National
Breast Screening Study22 After 5-years follow-up 519 incidence of breast cancer were
identified with analysis of previously completed dietary questionnaires demonstrating that
higher dietary fibre intake was associated with a small reduction in risk of developing
breast cancer Specifically there was a statistically significant decrease in risk of
developing breast cancer with increasing consumption of cereals (p lt 01) and a statistically
non-significant trend for pasta consumption (p=017) This reduced risk persisted after
adjustment for total vitamin A beta-carotene vitamin C and E
The UK Womens Cohort Study (UKWCS) (Cade et al 2007) which compares the health
outcomes of three main dietary groups (vegetarian eating fish [not meat] and meat eaters)
provides further evidence for the protective properties of fibre After a median of 75 years
follow-up analysis of self-reported dietary data of 35792 women showed that total dietary
fibre was found to be related to breast cancer incidence in women who were pre-
menopausal but not post-menopausal at baseline (p lt01) Fibre from cereals (plt
05) and fibre from fruit (p=009) was found to be protective against breast cancer
22
An RCT comprising women 40-49 years of age at study entry evaluating the efficacy of annual mammography breast physical examination and instruction on breast self-examination in reducing breast cancer mortality
26
Soy
A high intake of phytoestrogens23 particularly isoflavones (found in soy products) has been
suggested to decrease risk of developing breast cancer In one of the European
Prospective Investigation into Cancer and Nutrition (EPIC) studies a large multicentre
prospective cohort study described earlier in Table 2 the association between breast cancer
risk and isoflavones was supported in 333 women (p lt 005) (Grace et al 2004) but in
another larger EPIC study conducted in Utrecht (n=15555) no such evidence was found
(Keinan-Boker et al 2004) Analyses with pooled data sets are ongoing In the meantime
Boyapati et al (2005) provide evidence from the Shanghai Breast Cancer Study24
suggesting that after a median of 52-years follow-up soy intake pre-diagnosis is not related
to disease-free survival in women with breast cancer (n=1459)
Vitamin D
Goodwin et al (2009) measured vitamin D (usually obtained from sunlight through the skin
but also found in oily fish and eggs) levels in the stored blood of women with early breast
cancer (n=512) The mean follow-up was 116-years by which time women deficient in
vitamin D had a significantly increased risk of distant recurrence25 compared with
those who had sufficient levels (p lt 05)
Antioxidant Supplements
Despite widespread use only a few clinical or epidemiological studies have examined the
relationship between antioxidant supplements and risk of breast cancer recurrence or breast
cancer-related mortality Fleischauer et al (2003) examined recurrence and mortality
among post-menopausal women diagnosed with breast cancer (n=385) who were enrolled
into a dietary case-control study Women were contacted with a single questionnaire to
ascertain the use of nutritional supplements during 12-14 years of follow-up Antioxidant
vitamin supplement use was associated with a lower risk of breast cancer recurrence or
mortality Specifically use of vitamin C and E supplements moderately reduced risk (p lt
05) whilst vitamin E nearly halved the risk although this was not statistically
significant (p=056)
iii WEIGHT
Weight and body composition have been implicated in the development of a wide range of
cancers as well as in increased risk of recurrence or second primary cancers (Chlebowski
Aiello and McTiernan 2002) Additionally being overweight or obese can exacerbate some
23
Phytoestrogens sometimes called dietary estrogenslsquo are a group of naturally occurring plant compounds that have a similar chemical structure to estrogen they bind to estrogen receptors acting like hormone regulators
24 The Shanghai Breast Cancer Survival (SBSS) Study collected lifestyle-related factors and disease and
treatment related factors in Chinese women with breast cancer (n=2236) (Lu et al 2007) 25
The spread of cancer to parts of the body other than the place where the cancer first occurred
27
of the side-effects of cancer treatment as well as increase the risk of co-morbidities such as
diabetes and osteoporosis (Doyle et al 2006) The studies evaluated in this review thus far
further indicate weight as offering a mechanism of benefit in terms of breast cancer
outcomes Indeed the WINS and WHEL RCTs produce different outcomes when using
similar dietary interventions with weight loss in the WINS group but not the WHEL group
offering a likely explanation for improved outcomes observed in the WINS participants Since
increased adiposity (excess body fat) has been identified as a negative prognostic factor for
recurrent disease and survival after breast cancer diagnosis (Rock and Demark-Wahnefried
2002) the apparent benefit of dietary fat reduction in the intervention group could
partly result from the weight loss
Bekkering et al (2006) do not add to this evidence whilst 5 studies and one systematic
review were identified in the current review
Hebert et al (1998) studied the effect of body weight on recurrence and death in women
diagnosed with early-stage breast cancer (n=472) Body mass index (BMI) was
associated with an increased risk of recurrence at the rate of 9 for each kgm2
(equivalent to about 58-pounds for a 5 4 tall woman) For death the results were
similar but body mass index was more strongly associated increasing risk by 12
per kgm2
Additionally Lahmann et al (2004) used data from 73542 pre-menopausal and 103344
post-menopausal women taking part in the EPIC study During 47-years of follow-up 1879
cases of invasive breast cancer were identified In post-menopausal women current use
of hormone replacement therapy (HRT) modified the association between body size
and breast cancer among non-users weight body mass index and hip circumference
were positively associated with breast cancer risk (p lt 001) Obese women (BMI gt 30)
had a 31 risk compared to women with a BMI lt 25 Among pre-menopausal women hip
circumference was the only other measure significantly related to breast cancer (p lt 005)
after accounting for BMI
Enger et al (2004) conducted a retrospective follow-up study of women diagnosed with
breast cancer (n=1376) for whom complete medical records and adequate tissue
specimens existed Patients were followed for a median of 68-years after diagnosis 246 of
whom died from breast cancer Compared with women in the lowest category of weight
(lt133lb [60kg] at diagnosis) women in the highest category ( 175lb [79kg])
experienced a 25-fold increased risk of dying from breast cancer (P lt 05) Women with
hormone-receptor negative cancer experienced an approximately 2-fold higher risk of dying
from breast cancer compared with women who presented with hormone-receptor positive
cancer Women in the upper 50th percentile of weight with hormone-receptor negative cancer
had a nearly 5-fold increased risk of dying from cancer compared with women in the lower
50th percentile of weight and hormone-receptor positive cancer (p=10)
In order to determine whether weight prior to diagnosis and weight gain after diagnosis are
predictive of breast cancer survival Kroenke et al (2005) followed 5204 participants from
the Nursesrsquo Health Study diagnosed with incident invasive non-metastatic breast cancer
After a median of 9-years follow-up there were 860 total deaths 533 breast cancer deaths
28
and 681 recurrences (defined as secondary lung brain bone or liver cancer and death from
breast cancer) Weight before diagnosis and weight gain after diagnosis were related
to higher rates of breast cancer recurrence and mortality although associations were
most apparent in women who had never smoked (p lt 05) Furthermore associations
with weight were stronger in pre-menopausal than in post-menopausal women In contrast
by comparing breast cancer survivors (n=3215) with women in the comparison group of a
dietary intervention trial to prevent breast cancer recurrence Caan et al (2008) found that
neither moderate (5ndash10) nor large (gt10) weight gain post-diagnosis was associated with
an increased risk of breast cancer recurrence in the early years post-diagnosis (median time
of 737-months from diagnosis)
More recently Patterson et al (2010) reviewed published epidemiological research on
lifestyle and breast cancer outcomes reporting that the most consistent finding from
observational studies was that adiposity was associated with a 30 increased risk of
cancer-related mortality
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in breast cancer
survival Four studies were identified in the current review
In an observational study Manjer et al (2000) compared the survival of patients with breast
cancer (n=792) who had never smoked were smokers or were ex-smokers Follow-up of
breast cancer cases was through record-linkage with the Swedish Cause of Death Registry
During a mean follow-up of 121-years smokers and ex-smokers compared with those
who had never smoked had a significantly increased risk of death from cancer
Fentiman et al (2005) add to this evidence with a cohort study of breast cancer patients who
completed a lifestyle questionnaire at the time of diagnosis (n=166) They found that
smoking was the third most important predictor of breast cancer-specific and overall
survival after stage and age at diagnosis This suggests that smokers are not only more
likely to die of cancer but also of other diseases when compared with those who have never
smoked
In a much larger study Holmes et al (2007) conducted a prospective observational study
among 5056 women from the Nursesrsquo Health Study with stages I-III invasive breast
cancer Information on smoking was available for these women who were followed until
January 2002 or death whichever came first Compared with women who had never
smoked women who were current smokers had a 43 increased risk of death from
any cause with risk increasing along with more cigarettes smoked per day (p lt0001)
In contrast there was no association with current smoking and breast cancer death
Sagiv et al (2007) followed women diagnosed with a first primary breast cancer (n=1273)
for 5-6 years and found that the number of all-cause mortality (n=188) including breast
cancer-specific mortality (n=111) was slightly higher among current and former
active smokers compared with women who had never smoked No association was
found between active or passive smoking and breast cancer-specific mortality
29
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in breast cancer
survival In the current review one review and 2 studies were identified
Rock and Demark-Wahnefried (2002) reviewed the evidence from clinical and epidemiologic
studies reporting that alcohol intake was not associated with breast cancer survival in the
majority of the studies In contrast post-menopausal women (n=125) diagnosed with
invasive breast cancer who were followed through to survival demonstrated that pre-
diagnosis alcohol consumption of at least one drink per week was associated with a
27-fold increase in risk of cancer-related mortality (McDonald et al 2002) In a similar
study a larger sample of women (n=1286) diagnosed with invasive breast cancer who were
followed from diagnosis through to survival produced opposing findings compared with
non-drinkers women who consumed alcohol in the 5-years before diagnosis had a
decreased risk of cancer-related mortality (Reding et al 2009)
SUMMARY OF LIFESTYLE EVIDENCE FOR BREAST CANCER ndash MECHANISMS
OF BENEFIT
Physical Activity Physical activity is likely to prevent breast cancer via its effect on
hormones specifically by reducing levels of oestrogen in the body (Friedenreich et al 2010)
or shifting the metabolism of oestrogen to favour production of 2-hydroxyestrone (2-OHE1)26
as opposed to16α-hydroxyestrone (16α=OHE1) the former of which has much weaker
estrogenic activity This shift might also be the result of a change in lean body mass resulting
from physical exercise (Campbell et al 2007) The survival benefits of physical activity
appear to require a certain intensity or level of exertion specifically 3 MET-hours or more per
week (Holmes et al 2005 Holick et al 2008 Saxton et al 2010) this equates to moderate
intensity activity such as using a stationary bike for 1-hour However there is also evidence
of a dose-effect with greater activity (up to 239 MET-hours per week) being associated with
reduced risk of recurrence and cancer-related mortality (Holmes et al 2005) or indeed
greater levels of activity than pre-diagnosis being associated with reduced risk of recurrence
and cancer-related mortality (Irwin et al 2008 Holick et al 2008 Patterson et al 2010
Saxton et al 2010)
Diet Evidence for the role of dietary fat in breast cancer development and survival are
varied Case-control (Kyogoku et al 1992) and large prospective studies (Holmes et al
1999) do not show any significant link whilst some studies have found that dietary fat does
increase risk of recurrence or death in pre-menopausal women Indeed the large multicentre
WINS trial found a protective benefit of a reduced fat dietary intervention which was more
prominent in women diagnosed with hormone-receptor negative breast cancer (Chlebowski
et al 2006a Chlebowksi et al 2008) The differential effect of diet on hormone-receptor
positive and negative disease indicate that metabolic mechanisms involving insulin and
26
Sometimes referred to as a lsquogood estrogenrsquo due to its weak estrogenic activity in contrast to its alternative
16α-hydroxyestrone (16α=OHE1)
30
insulin-like growth factor-1 (IGF-1)27 may be involved in the mechanisms of benefit and
although not statistically significant data has been presented suggesting that elevated
insulin concentrations (a marker of insulin resistance) may be influenced by dietary fat
reduction (Khaodhiar et al 2003 Borugian et al 2004) However this might be due to
changes in weight produced by a low fat diet rather than the lower consumption of fat itself
(Borugian et al 2004) Since low fat diets are often accompanied by high intakes of fruit
and vegetables various components of a diet comprising high levels of fruit and vegetables
have been investigated Carotenoids have received particular attention with evidence
suggesting that carotenoids play a role in survival (Ingram 1994) Other studies have found
this not to be the case (Pierce et al 2007) with the primary difference in these studies being
lack of weight loss This indicates that the mechanism of benefit produced from low fat high
fruit and vegetable (particularly carotenoids) diets is most probably through changes in body
composition Indeed the majority of studies in this review demonstrated a link between
weight and cancer-related risks (Hebert et al 1998 Enger et al 2004 Lahmann et al
2004 Patterson et al 2010)
Smoking Evidence pertaining to the smoking clearly demonstrates a link between
breast cancer survival and a history of smoking However it appears to be more likely to
increase all-cause mortality as opposed to cancer-specific mortality (Fentiman et al 2005
Holmes et al 2007 Sagiv et al 2007)
Alcohol Although the evidence is less clear pre-diagnosis alcohol consumption does
appear to be related to survival (McDonald et al 2002 Reding et al 2009) although
current drinking does not (Demark-Wahnefried 2002)
27
IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of
pathological states including cancer
31
Table 3 Breast Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Campbell et al (2007)
RCT examining the effects of 12-weeks of aerobic exercise training on 2-OHE
1 and 16α-OHE
1 in
premenopausal women Randomisation to 1) A 12-week individualised supervised moderate-to-vigorous intensity aerobic exercise training intervention (n = 17) Participants began the exercise program in the early follicular phase of the next menstrual cycle (days 1-5) The intervention was divided into three blocks (a) Weeks 1 ndash 4 ndash 3 sessions per week of base aerobic training progressing from 20-40 minutes on a stationary bike (b) Weeks 5-8 ndash 4 sessions per week Two sessions were base aerobic training sessions for 30-45 minutes (c) Weeks 9 -12 ndash 4 sessions per week with two base aerobic training sessions for 30-45 minutes and two interval sessions 2) Usual lifestyle (n = 15) Participants were asked to maintain their usual activity levels for the duration of the study Following the control cycle the first day of the next menstrual cycle was used as the reference start date for participants in the control group On completion of the 12-week post-intervention
Healthy regularly menstruating Caucasian women (n=32) 20-35 years
On completion of the 12-week intervention
Height body mass body composition by dual-energy X-ray absorptiometry and VO2max were measured at baseline and following the intervention Urine samples were collected in the luteal phase of four consecutive menstrual cycles
Participants attended an average of 40-44 (91) sessions Fourteen of 17 (82) participants completed at least 80 of the sessions The exercise group increased VO2max by 14 and had significant although modest improvements in fat and lean body mass No significant between-group differences were observed however for the changes in 2-OHE1 (P = 0944) 16α-OHE1 (P= 0411) or the ratio of 2-OHE1 to 16α-OHE1 (P = 0317) At baseline there was an inverse association between body fat and 2-OHE1 to 16α-OHE1 ratio (r = minus040 P = 0044) however it was the change in lean body mass over the intervention that was positively associated with a change in 2-OHE1 to 16α-OHE1 ratio (r = 043 P = 0015)
32
measurement participants were given guidance for starting an individualised exercise program and access to the fitness facility for 4-weeks
Friedenreich et al (2010)
A two-centre two-arm RCT examining how an aerobic exercise intervention influences
circulating
estradiol oestrone sex hormonendashbinding globulin
(SHBG)
androstenedione and testosterone levels which may
be involved in the
association between physical activity and
breast cancer risk
Randomisation to 1) A 1-year aerobic physical activity programme of 225-minutes per week (n=160) 2) Control group maintained their usual level of activity (n=160)
Older (50gt years) post-menopausal sedentary women (n=320)
On completion of the intervention
Estradiol and sex hormone-binding globulin levels Androstenedione and testosterone levels
Completion of the study was high (966) At 12-months statistically significant reductions in
estradiol (treatment effect ratio
[TER] = 093 95 CI 088 to 098) and free estradiol (TER = 091
95 CI 087 to 096) and increases in SHBG (TER = 104 95 CI
102 to 107) were observed in the exercise group compared with
the control group No significant differences in oestrone
androstenedione and testosterone levels were observed between
exercisers and controls at 12-months
Holick et al (2008)
Prospective cohort study examining the relationship between post-diagnosis recreational physical activity and risk of breast cancer death
Women with a history of previous invasive breast cancer diagnosed between the ages of 20-79 years (n=4482)
Maximum of 6-years post-diagnosis (median=56-years post-diagnosis)
Mortality from breast cancer mortality from any cause Self-reported physical activity converted to MET-hours per week
After adjusting for age at diagnosis stage of disease state of residence interval between diagnosis and physical activity assessment body mass index menopausal status hormone therapy use energy intake education family history of breast cancer and treatment modality compared with women expending lt28 MET-hwk in physical activity women who engaged in greater levels of activity had a significantly lower risk of dying from breast cancer (HR 065 95 CI 039-108 for 28-79 MET-hwk HR 059 95 CI 035-101 for 80-209 MET-hwk and HR 051 95 CI 029-089 for ge210 MET-hwk P for trend = 005) Results were similar for overall survival (HR 044 95 CI 032-060 for ge210 versus lt28 MET-hwk P for trend lt0001) and were similar regardless of a womanlsquos age stage of disease and body mass index
Holmes et al (2005)
Prospective observational study
(Nurseslsquo Health Study) to determine whether physical activity among
women with breast cancer
2987 female registered nurses
in the
Nurseslsquo Health
Women were diagnosed between 1984 and
Breast cancer mortality risk according
to
physical activity
Compared with women who engaged in less than 3 MET-hours per
week of physical activity the adjusted relative risk (RR) of death
from breast cancer was 080 (95 CI 060-106) for 3 to 89 MET-hours per week 050
(95 CI 031-082) for 9 to 149 MET-hours
33
decreases their risk of death from
breast cancer compared with
more sedentary women
Study diagnosed with stage
I II or III
breast cancer
1998 and followed until death or June 2002
category (lt3 3-89 9-149 15-239
or 24
metabolic equivalent task [MET] hours per week)
per week 056 (95 CI 038-084) for 15 to 239 MET-hours per
week and 060 (95CI 040-089) for 24 or more MET-hours per week (P for trend
= 004) Three MET-hours is equivalent to walking
at average pace of 2 to 29 mph for 1 hour The benefit of physical
activity was particularly apparent among women with hormone-
responsive tutors The RR of breast cancer death for women with hormone-responsive
tumours who engaged in 9 or more MET-hours
per week of activity compared with women with hormone-
responsive tumours who engaged in less than 9 MET-hours per
week was 050 (95 CI 034-074) Compared with women who
engaged in less than 3 MET-hours per week of activity the absolute
unadjusted mortality risk reduction was 6 at 10 years for women
who engaged in 9 or more MET-hours per week
Irwin et al (2008)
The Health Eating Activity and Lifestyle Study (HEAL) Prospective observational study investigating the association between pre- and post-diagnosis
physical activity (as well as
change in pre-diagnosis to post-diagnosis
physical activity) and
mortality among women with breast cancer
A subsample of participants from the HEAL study ndash 933 women diagnosed with local or regional breast cancer between 1995
and 1998
5 -8 years from diagnosis (median=6-years)
Primary outcomes total deaths
and breast
cancer deaths
Compared with inactive women the multivariable hazard ratios
(HRs) for total deaths for women expending at least 9 MET-
hours per week (approximately 2-3 hwk of brisk walking) were 069
(95 CI 045 to 106 P = 045) for those active in the year before
diagnosis and 033 (95 CI 015 to 073 P = 046) for those active
2-years after diagnosis Compared with women who were inactive
both before and after diagnosis women who increased physical
activity after diagnosis had a 45 lower risk of death (HR = 055
95 CI 022 to 138) and women who decreased physical activity
after diagnosis had a four-fold greater risk of death (HR = 395 95
CI 145 to 1050)
Ligibel et al (2008)
RCT examining the impact of physical activity on insulin levels Participants were randomly assigned to one of two conditions a)Physical activity intervention a 16-week supervised strength training and home-based cardiovascular training protocol (two supervised 50-minute strength training
sessions per
week and 90-minutes of home-based
aerobic physical activity
weekly) b) Control group routine care for 16-weeks before being offered consultation with an physical activity
Overweight sedentary stage
I-III breast
cancer survivors (n=101)
On completion of the 16-week intervention
Fasting insulin and glucose levels Weight body composition
and
circumference at the waist and hip
18 women withdrew consent andor did not complete the study
Baseline and 16-week measurements were available for 82 patients
Fasting insulin concentrations decreased by an average of
286 microUmL in the exercise group (P = 03) with no
significant change in the control group (decrease of 027 microUmL P
=
65) The change in insulin levels in the exercise group seemed
greater than the change in controls but the comparison
did not reach statistical significance (P = 07) There was a
trend toward improvement in insulin resistance in the exercise
group (P = 09) but no change in fasting glucose levels The
exercise group also experienced a significant decrease in hip
measurements with no change in weight or body composition
34
trainer at the end of the control
period
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer outcomes
Breast cancer Not reported Additional breast cancer events and mortality
Although observational data were not consistent physical activity appeared to be associated with a 30 decreased risk of mortality
Saxton et al (2010)
A review of studies pertaining to physical activity and cancer mortality
All cancers with more evidence obtained for breast cancer
Not reported Survival A number of prospective cohort studies have reported negative associations between physical activity and cancer mortality The most compelling observational evidence of the survival benefits to be gained from a physically active lifestyle has emerged from studies of post-diagnosis physical activity in breast and colorectal cancer survivors These studies have shown clear inverse associations between post-diagnosis activity and survival with the benefits being independent of age gender obesity and disease stage at diagnosis Three of the four cohort studies of breast cancer survivors showed that women who are achieving the equivalent of 30-miniutes of moderate intensity PA on five or more days of the week can halve their risk of mortality up to 8 years of follow-up
DIET
Borugian et al (2004)
Prospective cohort study testing the hypothesis that elevated wait-to-hip ratio is directly related to breast cancer
mortality
603 patients with incident
breast
cancer
Up to 10-years
Date of death and
primary and secondary cause of death
After adjustment for age BMI family history oestrogen
receptor (ER) status tumour stage at diagnosis and systemic
treatment (chemotherapy or tamoxifen) WHR was directly related to
breast cancer mortality in postmenopausal women (for highest
quartile vs lowest relative risk = 33 95 confidence interval
11 104) but not in premenopausal women (relative risk = 12
95 confidence interval 04 34) Stratification according to
ER
status showed that the increased mortality was restricted to ER-
positive postmenopausal women Elevated WHR was confirmed as
a predictor of breast cancer mortality with menopausal status and
ER status at diagnosis found to be important modifiers of that
relation
Boyapati et al (2005)
As part of the Shanghai Breast Cancer Cohort Study associations between soy and breast cancer survival were investigated
1459 breast cancer patients
52-years Disease-free survival
Soy intake pre-diagnosis was unrelated to disease-free breast cancer survival (adjusted hazard ratio [HR]=099 95 confidence interval [CI] 073-133 for the highest tertile compared to the lowest tertile) The association between soy protein intake and breast cancer survival did not differ according to ERPR status tumour stage age at diagnosis body mass index (BMI) waist to hip ratio (WHR) or menopausal status
Boyd et al (2003)
Meta-analysis of casendashcontrol and cohort studies published up to July 2003 which examined the
Varied Not reported Cancer incidence A total of 45 published studies containing 46 estimates of risk examined the role of dietary fat in relation to breast cancer risk by an analysis of nutrient intake Of these 31 were case control and
35
association of dietary fat or fat-containing foods with risk of breast cancer
14 were cohort in design and they contained a total of 25015 cases of breast cancer and over 580 000 control or comparison subjects The summary relative risk comparing the highest and lowest levels of intake of total fat was 113 (95 CI 103ndash125) Cohort studies (n=14) had a summary relative risk of 111 (95 CI 099ndash125) and casendashcontrol studies (N=31) had a relative risk of 114 (95 CI 099ndash132) Significant summary relative risks were also found for saturated fat (RR 119 95 CI 106ndash135) and meat intake (RR 117 95 CI 106ndash129) Combined estimates of risk for total and saturated fat intake and for meat intake all indicate an association between higher intakes and an increased risk of breast cancer Casendashcontrol and cohort studies gave similar results
Cade et al 2007)
A large UK cohort study comprising women with a wide range of different eating patterns to study the effects of different food and nutrient intakes on long-term health outcomes
35372 women (350 post- and 257 pre- menopausal women developed breast cancer)
Approx 75-years
Breast cancer incidence
In pre-menopausal but not post-menopausal women a statistically
significant inverse relationship was found between
total fibre intake and risk of breast cancer (P for trend = 001) The
top quintile of fibre intake was associated with a hazard ratio
of 048
[95 CI 024ndash096] compared with the lowest quintile Pre-
menopausal fibre from cereals was inversely associated with risk
of breast cancer (P for trend = 005) and fibre from fruit had a
borderline inverse relationship (P for trend = 009)
Chlebowski et al (2006a)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
randomisation to death from any cause
Attrition in the dietary intervention (n=44) versus control group (n=66) Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to
345] versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group A total of 277 relapse
events (local regional distant or ipsilateral breast cancer
recurrence or new contralateral breast cancer) have been reported
in 96 of 975 (98) women in the dietary group and 181 of 1462
(124) women in the control group The hazard ratio of relapse
events in the intervention group compared with the control group
was 076 (95 CI = 060 to 098 P = 077 for stratified log rank
and P = 034 for adjusted Cox model analysis)
36
dietary guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
Chlebowski et al (2008)
A protocol-mandated survival analysis update to the interim analysis of WINS (Chlebowski et al 2006a)
Breast cancer patients (n=2437)
Approximately 7-years
Overall survival Attrition in the intervention group (n=236) versus control group (n=172) Although fewer deaths were seen in the intervention group this was not statistically significant In 362 women with ER- and (progesterone receptor) PR- disease a significant overall survival benefit was seen in the intervention group (75 vs 181 cumulative mortality)
Cho et al (2003)
A prospective analysis of the relationship
between dietary fat
intake and breast cancer risk among pre-menopausal
women enrolled in
the Nurseslsquo Health Study
Pre-menopausal women (n=90655) aged between 26-46 years old when recruited in 1991
8-years after recruitment (1991-1999)
Fat intake was
assessed with a food-frequency questionnaire at baseline
in 1991
and again in 1995
During 8-years of follow-up 714 women developed incident
invasive breast cancer Relative to women in the lowest quintile of
fat intake women in the highest quintile of intake had a
slight increased risk of breast cancer (RR = 125 95 CI = 098
to 159 Ptrend = 06) The increase was associated with intake
of
animal fat but not vegetable fat RRs for the increasing quintiles of
animal fat intake were 100 (referent) 128 137 154 and 133
(95 CI = 102 to 173 Ptrend = 002) Intakes of both saturated and
monounsaturated fat were related to modestly elevated breast
cancer risk Among food groups contributing to animal fat red meat and high-fat dairy foods were each associated
with an increased
risk of breast cancer Information on oestrogen-receptor status was available for
80 (n = 570) of breast cancers and progesterone-
receptor status for 78 (n = 558) When divided according to
oestrogen and progesterone receptor status the positive
association between animal fat intake and breast cancer risk was
stronger among women with oestrogen receptor-positive or
progesterone receptor-positive cancers than among women with hormone receptor-negative cancers however the difference was not statistically significant
Dwyer et al (2008)
A sub-analysis of participants in the WINS trial (Chlebowski et al 2006a)
Breast cancer patients (n=550)
12-months of intervention
Disease-free survival
Attrition in the intervention group (n = 23 11) versus control group (n = 16 5)At baseline neither mean fat intake nor flavonoid intake differed between groups After 12-months of intervention dietary fat intake was significantly lower among those on the very low-fat diet (n =195) whilst flavonoid intake remained similar in both groups Neither total flavonoid intake nor intake of subclasses of flavonoids differed between those who had dramatically decreased their fat intake and those who had not
Fleischauer et al (2003)
Case-control study testing the hypothesis that antioxidant
385 post-menopausal
12-14-years Breast cancer recurrence or
Antioxidant supplement users compared with non-users were less likely to have a breast cancer recurrence or breast cancer-related
37
supplements may reduce the risk of breast cancer recurrence or breast cancer-related mortality
women with breast cancer
death death (OR = 054 95 CI = 027-104) Vitamin E supplements showed a modest protective effect when used for more than 3 years (OR = 033 95 CI = 010-107) Risks of recurrence and disease-related mortality were reduced among women using vitamin C and vitamin E supplements for more than 3 years
Gold et al (2009)
Secondary analysis of a purposive sample of WHEL participants to determine if a low-fat diet high in vegetables fruit
and fibre affects
prognosis in breast cancer survivors
with or without hot flashes (HF) after treatment Randomisation to one of two groups 1)An intensive telephone counselling intervention based on social cognitive theory promoted a daily dietary intake of
5 vegetable
servings 16oz of vegetable juice 3
fruit servings 30g fibre and 15-20 of energy
from fat
2) Control group received printed
materials (but no counselling) promoting the
5-a-day guidelines
of
daily intakes of 5 servings of fruit and
vegetables more than 20g of fibre and less than
30 of energy from fat
2967 women (96 of all enrolled in the WHEL study) whose baseline hot flush severity
report in
the prior 4-weeks was available
4-years into the intervention
Primary end points additional breast cancer events
(localregio
nal recurrence or distant metastasis or new primary
breast
cancer) and death from any cause
The intervention group consumed significantly more daily vegetablefruit
(54 higher)
fibre (31 higher) and less
percent energy from fat (14 lower) than the comparison group
HF-negative women in the intervention had 31 fewer events than
the comparison group The intervention did not affect prognosis in
the women with baseline HFs Compared with HF-negative women in the comparison group
HF-positive women had significantly fewer
events in both groups
Goodwin et al (2009)
A prospective cohort study examining the influence of vitamin D on breast cancer prognosis
512 women with early breast cancer
Mean = 116-years
Cancer recurrence and mortality
Women with deficient vitamin D levels had an increased risk of
distant recurrence (hazard ratio [HR] = 194 95 CI 116 to
325) and death (HR = 173 95 CI 105 to 286) compared with
those with sufficient levels The association remained after
individual adjustment for key tumour and treatment related factors but was
attenuated in multivariate analyses (HR = 171 95 CI
102 to 286 for distant recurrence HR = 160 95 CI 096 to
264 for death)
Grace et al (2004)
Prospective study (EPIC) examining associations between phytoestrogen and breast cancer risk 114 spot urines and 97 available serum
333 women (aged 45ndash75 years) drawn from the EPIC
Not reported Phytoestrogen concentrations and breast cancer incidence
Phytoestrogen concentrations in spot urine (adjusted for urinary creatinine) correlated strongly with that in serum with Pearson correlation coefficients gt 08 There were significant relationships (P lt 002) between both urinary and serum concentrations of
38
samples from women who later developed breast cancer Results were compared with those from 219 urines and 187 serum samples from healthy controls matched by age and date of recruitment
study isoflavones across increasing tertiles of dietary intakes Urinary enterodiol and enterolactone and serum enterolactone were significantly correlated with dietary fibre intake (r = 013ndash029) Exposure to all isoflavones was associated with increased breast cancer risk significantly so for equol and daidzein For a doubling of levels odds ratios increased by 20ndash45 [log2 odds ratio = 134 (106ndash170P = 0013) for urine equol 146 (105ndash202 P = 0024) for serum equol and 122 (101ndash148 P = 0044) for serum daidzein]
Howe et al (1990)
Pooled analysis of 12 case-control studies of diet and breast cancer risk
Healthy women Not reported Breast cancer incidence
A consistent statistically significant positive association was found
between breast cancer risk and saturated fat intake in
postmenopausal women (relative risk for highest vs lowest quintile
146 P lt0001) A consistent protective effect for a number of
markers of fruit and vegetable intake was demonstrated vitamin C
intake had the most consistent and statistically significant inverse
association with breast cancer risk (relative risk for highest vs
lowest quintile 069 P lt0001)
Holm et al (1993)
Interviews regarding diet history the purpose being to determine whether dietary habits are associated with disease-free survival
in patients with
breast cancer who have undergone treatment
240 women with stage I-II breast cancer (50ndash65 years old) 209 of whom were post-menopausal
4-years Disease-free survival
Cancers were classified as oestrogen receptor (ER) rich ( 010
fmolmicrog of DNA) in 149 patients and as ER poor (lt010 fmolmicrog
of
DNA) in 71 patients Fifty-two patients had treatment failure during
follow-up The 30 patients with ER-rich tumours who had treatment
failure reported higher intakes of total fat saturated fatty acids and
polyunsaturated fatty acids than did the 119 patients with ER-rich
tumours that did not have treatment failure The multiple-odds ratio
(OR) for treatment failure in these women was 108 for each 1
increment in percentage of total energy (E) from total fat For
treatment failure within the first 2 years the OR was 119 for each
1-mg increase in vitamin E intake per 10 mega joules of energy In
women with treatment failure 2ndash4 years after diagnosis Ors were
113 and 123 for each E increment in total fat or saturated fatty
acids respectively No association between dietary habits and
treatment failure was found for women with ER-poor cancers
39
Holmes et al (1999)
Cohort study (Nurseslsquo Health Study)
to determine whether intakes
of fat and fatty acids are associated
with breast cancer
88795 women free of cancer (2956 developed breast cancer)
14-years Relative risk of invasive breast
cancer for
an incremental increase of fat intake
Compared with women obtaining 301 to 35 of energy from fat women consuming 20 or less had a multivariate
RR of breast
cancer of 115 (95 CI 073-180) In multivariate models the RR
(95 CI) for a 5-of-energy increase was 097 (094-100) for total
fat 098 (096-101) for animal fat 097 (093-102) for vegetable
fat 094 (088-101) for saturated fat 091 (079-104) for
polyunsaturated fat and 094 (088-100) for monounsaturated fat
For a 1 increase in energy from trans-unsaturated fat the values
were 092 (086-098) and for a 01 increase in energy from
omega-3 fat from fish the values were 109 (103-116)
Hunter et al (1996)
Pooled analysis of 7 prospective studies in 4 countries to establish estimates of the relation of fat
intake
to the risk of breast cancer
Studies included
33781
9 women
Not reported Breast cancer incidence
Information about 4980 cases from studies including 337819
women was available When women in the highest quintile of
energy-adjusted total fat intake were compared with women in the
lowest quintile the multivariate pooled relative risk of breast cancer
was 105 (95 CI 094 to 116) Relative risks for saturated
monounsaturated and polyunsaturated fat and for cholesterol
considered individually were also close to unity There was little
overall association between the percentage of energy intake from
fat and the risk of breast cancer even among women whose energy
intake from fat was less than 20
Ingram et al (1994)
Cohort study evaluating the role of vitamins in breast cancer mortality
103 women 3-months post-operation for primary breast cancer
Mean= 81-months
Mortality from breast cancer
27 women died ndash 21 with advanced breast cancer and 6 from other causes The most important findings from the nutrient consumption assessment were associated with vitamin consumption in particular beta-carotene and vitamin C At high levels of consumption there were significantly fewer deaths from breast cancer only one in the group of highest beta-carotene consumers compared with eight in the intermediate group and 12 in the lowest group (trend P = 00012) equivalent figures for vitamin C were 3 7 and 11 deaths for the highest intermediate and lowest consumption groups respectively (trend P = 00286)
Keinan-Boker et al (2004)
An investigation of the association between phytoestrogen
intake and
breast cancer risk in a large prospective study in
a Dutch
population with a habitually low phytoestrogen intake (EPIC)
15555 women aged
49ndash70
years who constituted a Dutch cohort the EPIC study
Median = 52-years
Breast cancer incidence
A total of 280 women were newly diagnosed with breast cancer
during follow-up The median daily intakes of isoflavones and
lignans were 04 (interquartile range 03ndash05) and 07 (05ndash08)
mgd respectively Relative to the respective lowest intake
quartiles the hazard ratios for the highest intake quartiles for
isoflavones and lignans were 10 (95 CI 07 15) and 07 (05
11) respectively Tests for trend were non-significant
Khaodhiar et al (2003)
A subgroup analysis of WINS participants (Chlebowski et al
53 women from 3 clinical
sites
2-years after start of
Insulin resistance and dietary fat
Of those women with initial insulin resistance after 1-year women in
the intervention group saw their fasting insulin decrease by 18 plusmn 34
40
2006a) examining relationships between dietary intake and insulin resistance
who had serum insulin and lipid profiles evaluated at baseline
and
after 2-years
commencing intervention
intake microUmL in comparison fasting insulin of women in the control
group decreased by only 138 plusmn 47 microUmL Although not
quite
statistically significant these results predict that elevated insulin concentrations (a marker of insulin resistance)
may be influenced by
dietary fat reduction There were no significant differences between
the treatment groups over time and no time x treatment interactions
and no significant differences were seen between the insulin-
resistant and non-insulin-resistant subgroups
Kim et al (2006)
The Nurseslsquo Health Study a prospective cohort study examining the relationship between dietary fat and incidence of breast
cancer in
post-menopausal women
Cohort of 80375 US women
Followed for 20-years between 1980 and 2000 with questionnaire being mailed every 2-years
Incidence of breast cancer The Food Frequency Questionnaire
The multivariable relative risk for an increment of 5 of energy from
total dietary fat intake was 098 (95 CI 095 100) Additionally
specific types of fat were not associated with an increased risk of
breast cancer Furthermore secondary analyses indicated no
differences in breast cancer risk by oestrogen receptor or
progesterone receptor status However stratification by
waist circumference indicated a significant decrease in breast
cancer risk for participants with a waist circumference of 35
inches (889cm) or greater (p-trend = 004)
Kyogoku et al (1992)
The present study utilised breast cancer patients whose dietary intake was assessed 10-years previously in a case-control study to determine whether dietary intake is related prognosis
212 breast cancer patients post-surgery
Followed-up until 1987 (9-12 years)
Mortality A total of 47 breast cancer deaths were certified The 5- and 10-year relative survival rates were 785 and 753 respectively The investigation did not provide any support for the hypothesis that a high-fat diet is a survival determinant for breast cancer patients
McEligot et al (2006)
Retrospective study into the influence of diet (fat fibre vegetable and fruit intakes and micronutrients (folate carotenoids and vitamin C) on overall survival in women diagnosed with breast cancer
Post-menopausal breast cancer survivors (n = 516)
Mean of 80-months post-diagnosis
Death due to any cause
The hazard ratio [HR and 95 CI] of dying in the highest tertile compared to the lowest tertile of total fat fibre vegetable and fruit was 312 (95 CI = 179-544) 048 (95 CI = 027-086) 057 (95 CI = 035-094) and 063 (95 CI = 038-105) respectively (P le 005 for trend except for fruit intake) Other nutrients including folate vitamin C and carotenoid intakes were also significantly associated with reduced mortality (P le 005 for trend)
Pierce et al (2007)
The multicentre WHEL RCT (see Gold et al 2009 in table)
Breast cancer (n=3088) intervention (n=1537) comparison (n=1551)
After 7-years of intervention
Invasive breast cancer event (recurrence
or
new primary) or death from any cause
Attrition in the intervention group (n=38) versus control group (n=27) There were no additional health benefits of dramatically increasing intake of nutrient-rich plant-based foods relative to the comparison group
Thomson et al (2007)
Sub-analysis of a purposive sample of participants in the WHEL RCT (see Gold et al 2009 in table)
Breast cancer patients (n=207)
Not reported Oxidative stress A significant inverse association was found between total plasma carotenoid concentrations and oxidative stress
41
WEIGHT
Caan et al (2008)
Retrospective study examining whether weight gain after diagnosis of breast cancer affects the risk of breast cancer recurrence Weight change from 1-year pre-diagnosis to study enrolment was calculated
3215 women with early stage breast cancer
Median of 737-months post-diagnosis
Breast cancer recurrence
Neither moderate (5ndash10) nor large (gt 10) weight gain (HR 08 95 CI 06ndash11 HR 09 95 CI 07ndash12 respectively) after breast cancer diagnosis was associated with an increased risk of breast cancer recurrence in the early years post-diagnosis
Enger et al (2004)
A retrospective cohort study using patient medical
records electronic
cancer registry data and archived tissue
specimens to examine
correlates of body weight with mortality in early-stage breast cancer
Women (n=1376)
24-
81 years of age diagnosed with breast cancer
Median=68 years post-diagnosis
Body weight at the time of diagnosis
and
patient status (ie alive and free of breast cancer living
with breast
cancer dead of breast cancer or dead of other
cause) at
the time of longest follow-up
246 patients died from breast cancer Among patients with early-
stage disease (I and IIA) a dose-response relationship was
observed with increasing weight and likelihood of dying of breast
cancer Compared with women in the lowest category of weight (lt133lb [60 kg] at diagnosis) women in the highest category ( 17
lb
[79 kg]) experienced a 25-fold increased risk of dying from breast
cancer (HR ratio 254 [95 CI 108-600] trend P = 02) Women
with ER-negative cancer experienced an approximately 2-fold
higher risk of dying from breast cancer compared with women with
ER-positive cancer regardless of stage at diagnosis Women in the
upper 50th percentile of weight with early-stage
disease and with
ER-negative tumours had a nearly 5-fold increased risk of dying
(HR ratio 499 [95 CI 217-1148] P for interaction = 10)
compared with women in the lower 50th percentile of weight
and ER-
positive tumours
Hebert et al (1998)
Prospective cohort study examining the effect of diet and body weight on recurrence and death in breast cancer patients
472 women diagnosed with early-stage breast cancer in 1982ndash1984
Ranged from 8-10 years
Breast cancer recurrence and mortality
After accounting for disease stage and age reported baseline consumption (timesday) of butter margarine and lard (risk ratio (RR)=167 95 CI=117ndash239) and beer (drinksday) (RR=158 95 CI=115ndash217) increased the risk of recurrence There also appeared to be an increased risk associated with consumption of red meat liver and bacon corresponding to about a doubling of risk for each time per day that foods in this category were consumed (RR=193 95 CI=089ndash415) Relative body weight increased risk at the rate of 9 (RR=109 95 CI=102ndash117) for
each kgm2 (equivalent to about 58 pounds for a woman 5 4 tall) For death the results were similar but relative weight was more strongly associated increasing risk by 12 per kgm2 (RR=112 95 CI=103ndash122)
Kroenke et al (2005)
A prospective study of a purposive subsample of participants from the Nurseslsquo Health Study ndash to determine
5204 Nurseslsquo Health Study participants
2-26 years with a median
Incident breast cancer
Weight before diagnosis was positively associated with breast
cancer recurrence and death but this was apparent only in never
smokers Similarly among never-smoking women those who
42
whether weight prior to diagnosis and weight gain
after diagnosis are
predictive of breast cancer survival
diagnosed with
incident invasive non-metastatic breast cancer between
1976
and 2000
follow-up of
9-years Breast cancer recurrence Mortality for any cause Self-reported BMI
gained between 05 and 20 kgm2 (median gain 60 lb relative risk
[RR] 135 95 CI 093 to 195) or more than 20 kgm
2 (median
gain 170lb RR 164 95 CI 107 to 251) after diagnosis had an
elevated risk of breast cancer death during follow-up (median 9
years) compared with women who maintained their weight (test for
linear trend P = 03) Associations with weight were stronger in
premenopausal than in postmenopausal women
Patterson et al (2010)
A review of the published epidemiologic research on lifestyle and breast cancer
Breast cancer Not reported Additional breast cancer events and mortality
The most consistent finding from observational studies was that adiposity was associated with a 30 increased risk of mortality
SMOKING
Holmes et al (2007)
A prospective observational study among 5056 women from the Nurseslsquo Health Study for whom data on smoking history was available
Women with Stages I-III invasive breast cancer diagnosed between 1978 and 2002
Median = 83 years
Death by any cause Cause of death was ascertained from death certificates supplemented as needed with physician review of medical records
Compared with never smokers women who were current smokers had a 43 increased adjusted relative risk (RR) 95 CI 124-165] of death from any cause A strong linear gradient was observed with the number of cigarettes per day smoked p-trend lt00001 the RR (95 CI) for 1-14 15-24 and 25 or more cigarettes per day was 127 (101-161) 130 (108-157) and 179 (147-219) In contrast there was no association with current smoking and breast cancer death the RR (95 CI) was 100 (083-119) Current and past smokers were more likely than never smokers to die from primary lung cancer chronic obstructive pulmonary disease and other lung diseases
Fentiman et al (2005)
Cohort study testing the hypothesis that smokers have a worse breast cancer prognosis
Women (n=166) with stage III invasive breast cancer
Mean = 132-months
Overall and cancer-specific disease-free survival
Smoking was the third most important predictor of distant relapse-free breast cancer-specific and overall survival after stage and age at diagnosis
Manjer et al (2000)
Cohort study examining whether smoking is associated with prognostic markers other than more advanced disease (eg hormone receptor status histopathology and tumour differentiation)
268 women with recurring breast cancer drawn from a cohort of 10902 women (35 smokers)
An average of 124-years
Hormone receptor status identified by tumour tissue
The relative risk (RR) of oestrogen receptor-negative tumours was for current smokers 221 [95 CI 123-396] and for ex-smokers 267 (95 CI 141-506) compared to never-smokers Ex-smokers had an increased risk of progesterone receptor-negative tumours (RR = 161 95 CI 107-241) but there were no other significant associations between smoking habits and oestrogen receptor-positive or progesterone receptor-positive or ndashnegative tumours The incidence of Nottingham grade III tumours was higher in ex-smokers than in never-smokers (RR = 203 95 CI 117-354)
Sagiv et al (2007)
Cohort study examining the association between active and passive cigarette smoking before
Women with invasive breast cancer
Approximately 6-years after
All-cause mortality including breast
The adjusted hazards ratios (HRs) for all-cause mortality were slightly higher among current and former active smokers compared with never smokers (HR 123 95 CI 083ndash184) and 119 (95
43
breast cancer diagnosis and survival (n=1273) participating in a population-based casendashcontrol study
diagnosis cancer-specific mortality as reported to the National Death Index
CI 085ndash166) respectively) No association was found between active or passive smoking and breast cancer-specific mortality All-cause and breast cancer-specific mortality was higher among active smokers who were postmenopausal (HR 164 95 CI 103ndash260 and HR 145 95 CI 078ndash270 respectively) or obese at diagnosis (HR 210 95 CI 103ndash427 and HR 197 95 CI 089ndash436 respectively)
ALCOHOL
McDonald et al (2002)
Prospective cohort study examining the influence of alcohol consumption on breast cancer survival in African American women
Post-menopausal African-American women with invasive breast cancer (n=125)
Followed for survival through December 1998 (median = 648 months)
Survival Pre-morbid alcohol consumption of at least one drink per week was associated with 27-fold increase in risk of death (95 CI 13ndash58)
Reding et al (2009)
Sub-analysis of participants from two case-control studies to examine the effects on prognosis of alcohol consumption after breast cancer diagnosis
1286 women diagnosed with invasive breast cancer at age le45 years from two population-based case-control studies
Followed from their diagnosis of breast cancer (between January 1983 and December 1992) through to June 2002
The primary mortality endpoint used was all-cause mortality
After adjusting for age and diagnosis year compared with non-drinkers women who consumed alcohol in the 5 years before diagnosis had a decreased risk of death [gt0 to lt3 drinks per week hazard ratio 07 95 CI 06-095 3 to lt7 drinks per week risk ratio 06 95 CI 04-087 drinks per week risk ratio 07 95 CI 05-09]
Rock and Demark-Wahnefried (2002)
A review of evidence from clinical and
epidemiologic studies examining
the relationship between nutritional
factors and breast cancer survival
Women with breast cancer
Not reported Survival Alcohol intake was not associated with survival in the majority of the
studies that examined this relationship
44
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
colorectal cancer survival In the current review 2 studies were identified Studies are
summarised in Table 4 at the end of this section
In a cohort study self-reported leisure time physical activity was assessed in 41528
Australians among whom 526 cases of colorectal cancer were identified (Haydon et al
2006) Those who reported regular physical activity (at least once per week) prior to
diagnosis had improved cancer-specific survival (73 5-year survival) compared with
those not reporting regular physical activity (61 5-year survival) Another study of
stage III colorectal cancer survivors (n=816) over a 3-year period post-surgery and
chemotherapy showed increases in disease-free survival and overall survival with
increasing volumes of physical activity (p lt 05) (Meyerhardt et al 2005)
ii DIET
Bekkering et al (2006) report on six high fibre diet interventions that showed little effect on
the risk of colorectal cancer recurrence (McKeown-Eyssen et al 1995 MacLennan et al
1999 Alberts et al 2000 Bonithon-Kopp et al 2000 Schatzkin et al 2000 Ishikawa et al
2005) On combining data from two beta-carotene trials (Greenberg et al 1994
MacLennan et al 1999) four multivitamin trials (Greenberg et al 1994 Ponz and
Roncucci 1997 Hofstad et al 1998 McKeown-Eyssen et al 1995) and one trial containing
a multivitamin arm and an N-acetylcysteine (found in high protein foods) arm (Ponz and
Roncucci 1997) there was weak evidence of a reduction in risk of colorectal polyps
(abnormal growth of tissues in the colon) Two calcium interventions showed some
evidence of a reduced risk of recurrence (Baron et al 1999 Bonithon-Kopp et al 2000)
In the current review 5 studies provided further evidence for the role of diet in colorectal
cancer survival
Dietary Fibre
The association between dietary fibre and incidence of colorectal cancer was examined in all
participants (n=519978) taking part in the EPIC study (Bingham et al 2003) After 45-years
of follow-up self-reported dietary data for 1065 reported cases of colorectal cancer were
showed that higher dietary fibre was associated with a reduced risk of developing
large bowel cancer Interestingly the protective effect was greatest for the left side of the
colon and least for the rectum No food source of fibre was significantly more protective of
cancer incidence than others Confirmation of these findings after adjustment for folate and
with a longer follow-up has been reported (Bingham et al 2004 Norat et al 2005)
45
Red and Processed Meat
The EPIC study also offers support for the hypotheses that consumption of red and
processed meat increases colorectal cancer risk while intake of fish decreases risk
(Norat et al 2005) Meyerhardt et al (2007) support this further in a study examining dietary
patterns in stage III colorectal cancer survivors (n=1009) After a median of 53-years follow-
up a significant difference was found between those who had followed a prudentlsquo diet and
those who had followed a Westernlsquo diet
A higher intake of a Western dietary pattern post-diagnosis was associated with a
significantly worse disease-free survival (colon cancer recurrences or death) (p
lt001) The Western dietary pattern was associated with a similar detriment in overall
survival (p lt001)
Vitamin D
Ng et al (2008) examined pre-diagnosis levels of vitamin D in a cohort of participants with
colorectal cancer (n=304) from the Nursesrsquo Health Study28 which demonstrated that higher
plasma vitamin D levels were associated with a significant reduction in mortality from
any cause This indicates that lifestyle pre-diagnosis can produce post-diagnosis benefits
Dietary Supplements
A double-blind randomised placebo-controlled intervention study (the FAB2 Study) was
carried out with healthy controls (n=98) and patients with colorectal polyps (n=106) to
examine the effects of folic acid (a B vitamin found in leafy vegetables such as spinach
asparagus and lettuce) and riboflavin (a B-vitamin found in lean meats eggs nuts and
dairy products) supplements on biomarkers of colorectal cancer risk (Powers et al 2007)
Participants were randomised to receive one of four treatments
1) placebo capsule daily
2) 400μg of folic acid daily
3) 1200μg of folic acid daily
4) 400μg of folic acid with 5mg of riboflavin daily
28
One of the largest and longest running investigations of factors that influence womenlsquos health
comprising information from 238000 nurse-participants
Prudent diet High intake of fruit vegetables poultry and fish
Western diet
High intake of meat fat refined
grains sweets and desserts
46
Short-term low folic acid supplements in the range of 400μg were found to elicit a
significant increase in mucosal folate concentration causing a number of physiologic
responses that may reduce the risk of cancer recurrence This adds to the evidence that
increased fibre might be protective against cancer mortality since folate and fibre are
generally found in the same foods
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in colorectal
cancer recurrence In the current review 3 studies were identified
Dignam et al (2006) explored the impact of obesity via retrospective data from patients with
confirmed Dukes B or C colorectal cancer (n=4288) and found that very obese men and
women have an increased risk of recurrence In contrast the multicentre prospective
observational CALBG 8980 trial has shown that increased BMI during and 6-months after
adjuvant chemotherapy for stage III colorectal cancer (n=1053) was not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008)
Sinicrope et al (2010) categorised stage II and III colon cancer (n=4381) patients enrolled
in seven RCTs whilst undergoing adjuvant chemotherapy according to their BMI They
found that BMI was significantly associated with both disease-free survival and overall
survival in both men and women when compared to normal-weight controls Being
overweight was associated with improved overall survival in men whilst being underweight
was associated with significantly worse overall survival in women This demonstrates that
obesity is an independent prognostic variable in colon cancer survivors as well as showing
gender-related differences that require further investigation
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in colorectal
cancer survival and no studies were identified in the current review
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in colorectal
cancer survival Preliminary EPIC results indicate that current alcohol intake is
significantly positively associated with risk of rectal but not of colon cancer (Ferrari et
al (2007)
47
SUMMARY OF LIFESTYLE EVIDENCE FOR COLORECTAL CANCER ndash
MECHANISMS OF BENEFIT
Physical Activity There is very little evidence available for the role of physical activity in
colorectal cancer outcomes however the evidence that is available looks promising
Specifically regular physical activity of at least once per week pre-diagnosis has been found
to improve 5-year survival rates (Haydon et al 2006) This highlights the importance of
physical activity being integrated into an individuallsquos way of life even before the occurrence
of illness Furthermore long-term physical activity post-surgery can further increase chances
of recurrence-free survival and there is also evidence of a dose-effect survival benefits
increase with amount of exercise (Meyerhardt et al 2005)
Diet Whilst evidence for dietary fibre has been mixed the additional evidence presented
within this review places greater weight in favour of increased dietary fibre Indeed the
conclusion of one study was that in populations with low average intake of dietary fibre an
approximate doubling of total fibre intake from foods could reduce the risk of colorectal
cancer by 40 (Bingham et al 2003) Evidence of this protective benefit for dietary fibre is
further supported by research demonstrating that short-term low folic acid (found in fibrous
foods) supplements in the range of 400μg can reduce the risk of cancer recurrence (Powers
et al 2007) There is a general consensus that mechanisms of benefit from dietary fibre
come from increases in stool bulk which decreases transit time and reduces contact time
between potential carcinogens (agents that exacerbate cancer) and colonic mucosa (tissue
that lines the colon) (Kim 2000) Evidence has also been presented supporting the
hypothesis that red and processed meat increases colorectal cancer risk while fish
decreases risk (Norat et al 2004)
Weight Two large-scale studies offer contrasting findings for the role of weight
in colorectal cancer outcomes One prospective observational study demonstrates that
increased BMI during and 6-months after adjuvant chemotherapy is not significantly
associated with a higher risk of recurrence or mortality (Meyerhardt et al 2008) The other
retrospective study demonstrates that very obese men and women have an increased risk
of recurrence Drawing on 7 RCTs Sinicrope et al (2010) provides further evidence for BMI
was being significantly associated with both disease-free and overall survival Overall there
is greater evidence showing weight to be an important predictor of colorectal cancer
outcomes There is also some evidence of gender differences being overweight was
associated with improved overall survival in men whilst being underweight was associated
with significantly worse overall survival in women There is evidently a need to explore this
differential effect more closely However there is also the need to consider the impact of
body composition on the development of other chronic conditions including diabetes and
cardio-respiratory conditions
Smoking and Alcohol Further research is needed into smoking and alcohol
consumption especially in terms of colorectal cancer prognosis There is some evidence
indicating that current alcohol intake increases risk of rectal but not colon cancer a finding
that requires further investigation to ascertain underlying mechanisms of benefit (Ferrari et
al 2007) Since alcohol can reduce absorption of folate it is possible that the mechanism
48
of benefit is as with dietary fibre intake related to stool bulk and less contact time between
carcinogens and colonic mucosa
49
Table 4 Colorectal Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Haydon et al (2006)
Incident cases of colorectal cancer were identified among participants of the Melbourne Collaborative Cohort Study and examined against self-reported physical activity
526 Australians with colorectal cancer
Median = 55 years
Body fat Disease-specific survival
Exercisers had an improved disease specific survival (hazard ratio 073 (95 CI 054ndash100) The benefit of exercise was largely confined to stage IIndashIII tumours (hazard ratio 049 (95 CI 030ndash079) Increasing per cent body fat resulted in an increase in disease-specific deaths (hazard ratio 133 per 10 kg (95 CI 104ndash171) Similarly increasing waist circumference reduced disease specific survival (hazard ratio 120 per 10 cm (95 CI 105ndash137)
Meyerhardt et al (2005)
Prospective study of recreational physical activity and prognosis
among
stage III colon cancer patients enrolled in a
RCT of post-operative adjuvant
chemotherapy (bolus 5-
fluorouracilleucovorin +- irinotecan)
816 patients with stage III colon cancer
Midway through adjuvant therapy and again 6-months post-therapy (12ndash14 months after enrolment)
Physical activity levels were measured as MET-hours-per-week Disease-free survival
Levels of physical activity were associated with significantly improved
disease-free survival among patients with stage III colon cancer After
adjustment for age gender baseline performance status N stage T
stage preoperative CEA bowel obstruction and perforation level of
differentiation treatment arm and body mass index the hazard ratio
(HR) for DFS for individuals in the highest quintile (gt25 MET-
hoursweek eg Jog 3ndash4 hoursweek or brisk walk [3ndash4 mph] daily)
was 065 (95 CI 038ndash111 p for trend = 002) compared to those
in the lowest quintile of PA This relationship varied by gender with a
HR = 033 [95 CI 011ndash099] for women (p for trend = 0046) and a
HR= 089 [95 CI 044ndash178] for men (p for trend = 03)
DIET
Bingham et al (2003)
Prospective examination of the association between dietary fibre intake and incidence of colorectal cancer in individuals taking part in the EPIC study recruited from ten European countries
519978 men and women in the EPIC study (1065 cases of colorectal cancer)
45 years
Colorectal cancer incidence
Dietary fibre in foods was inversely related to incidence of large bowel cancer (adjusted relative risk 0middot75 [95 CI 0middot59ndash0middot95] for the highest versus lowest quintile of intake) the protective effect being greatest for the left side of the colon and least for the rectum After calibration with more detailed dietary data the adjusted relative risk for the highest versus lowest quintile of fibre from food intake was 0middot58 (0middot41ndash0middot85)
Meyerhardt et al (2008)
Prospective observational study to
determine the association of dietary patterns
with cancer recurrences and
mortality of colon cancer survivors
1009 patients with stage III colon cancer who were
enrolled in
a randomized
Median = 53-years
Colon cancer recurrence and mortality
A higher intake of a Western dietary pattern after cancer diagnosis
was associated with a significantly worse disease-free survival (colon
cancer recurrences or death) Compared with patients in the lowest
quintile of Western dietary pattern those in the highest quintile experienced an adjusted hazard
ratio (AHR) for disease-free survival
of 325 (95 confidence interval [CI] 204-519 P for trend lt001)
50
adjuvant chemotherapy trial (CALGB
89803)
The Western dietary pattern was associated with a similar detriment
in recurrence-free survival (AHR 285 95 CI 175-463) and overall
survival (AHR 232 95 CI 136-396]) comparing highest to
lowest quintiles (both with P for trend lt001)
Ng et al (2008)
Nurseslsquo Health Study prospective examination of the association between pre-diagnosis
25(OH)D levels and
mortality in colorectal cancer patients
304 colorectal cancer patients
Mean = 78-months for participants still alive
Colorectal cancer mortality
Higher plasma 25(OH)D levels were associated with a significant
reduction in overall mortality (P for trend = 02)
Compared with the lowest quartile participants in the highest
quartile had an adjusted HR of 052 (95 CI 029 to 094) for
overall mortality A trend toward improved colorectal cancerndash
specific mortality was also seen (HR = 061 95 CI 031 to 119)
Norat et al (2005)
The EPIC prospective study of 478040 cancer-free men and women from 10 European countries examining meat fish and colorectal cancer risk
478040 cancer-free men and women taking part in the EPIC study
Mean=48 years
Colorectal cancer incidence
Colorectal cancer risk was positively associated
with intake of red and processed meat (highest [gt160
gday] versus lowest [lt20 gday] intake HR = 135 95 CI = 096
to
188 Ptrend = 03) and inversely associated with intake of fish (gt80
gday versus lt10 gday HR = 069 95 CI = 054 to
088 Ptrendlt001) but was not related to poultry intake In this study
population the absolute risk of development of colorectal
cancer within 10-years for a study subject aged 50 years was 171
for the highest category of red and processed meat intake and 128
for the lowest category of intake and was 186 for subjects in
the lowest category of fish intake and 128 for subjects in
the highest category of fish intake
Powers et al (2007)
A double-blind RCT (the FAB2 Study) to examine effects of folic acid and riboflavin supplements on biomarkers of colorectal cancer risk Participants were randomised to receive one of the following for 6 ndash 8 weeks 1)400μg of folic acid 1200μg of folic acid or 400μg of folic acid plus 5 mg of riboflavin 2) placebo
Healthy controls (n=98) and patients with colorectal polyps (n=106)
On completion of 6-8 week intervention
Biomarkers of folate and riboflavin status
Supplementation with folic acid elicited a significant increase in mucosal 5-methyl tetrahydrofolate and a marked increase in RBC and plasma with a dose-response Measures of riboflavin status improved in response to riboflavin supplementation Riboflavin supplement enhanced the response to low-dose folate in people carrying at least one T allele and having polyps The magnitude of the response in mucosal folate was positively related to the increase in plasma 5-methyl tetrahydrofolate but was not different between the healthy group and polyp patients
WEIGHT
Dignam et al (2006)
Investigating the association between BMI and colorectal cancer outcomes in patients from cooperative group clinical trials
4288 patients with Dukes
BC
colon cancer in National
Median =112-
years Risk of recurrence second primary
Very obese patients (BMI 35 kgm2) had greater risk
of a
colon cancer event (recurrence or secondary primary tumour hazard
ratio [HR] = 138 95 confidence interval [CI] = 110 to 173) than
normal weight patients (BMI = 185ndash249 kgm
2) Mortality was
51
Surgical Adjuvant Breast and Bowel Project
RCTs
cancer and
mortality evaluated in
relation to
BMI at diagnosis
greater for very obese (HR = 128 95 CI = 104 to 157) and
underweight (BMI lt 185 kgm2) (HR
= 149 95 CI = 117 to 191)
than for normal weight patients The increased risk of mortality for
underweight patients was dominated by nonndashcolon cancer deaths
(HR of such deaths compared with normal weight patients = 223 95 CI = 150 to
331) whereas for the very obese deaths likely due
to colon cancer were increased (HR = 136 95 CI = 106 to 173)
Meyerhardt et al (2008)
A prospective observational study of patients who had stage III colon cancer and who enrolled on a RCT of adjuvant chemotherapy Results
1053 patients who had stage III colon cancer
6-months post- chemotherapy
Patients were observed for cancer recurrence or death
Increased BMI was not significantly associated with a higher risk of colon cancer recurrence or death (P trend = 54) Compared with normal-weight patients (BMI 21 to 249 kgm
2) the multivariate
hazard ratio for disease-free survival was 100 (95 CI 072 to 140) for patients with class I obesity (BMI 30 to 349 kgm
2) and 124
(95 CI 084 to 183) for those with class II to III obesity (BMI ge 35 kgm
2) after analysis was adjusted for tumour-related prognostic
factors physical activity tobacco history performance status age and sex Similarly after analysis was controlled for BMI weight change (either loss or gain) during the time period between ongoing adjuvant therapy and 6-months after completion of therapy did not significantly impact on cancer recurrence andor mortality
Sinicrope et al (2010)
BMI (kgm2) was categorised in patients
with tumour-node-metastasis stage II and III colon carcinomas enrolled in seven RCT of 5-fluorouracilndashbased adjuvant chemotherapy to determine the association of BMI with disease-free survival and overall survival
Men and women with stage II and III colon carcinomas (n = 4381) enrolled in seven RCTs of 5-fluorouracilndashbased adjuvant chemotherapy
Not reported Disease-free survival Overall survival
BMI was significantly associated with both disease-free survival (P = 0030) and overall survival (P = 00017) Men with class 23 obesity showed reduced overall survival compared with normal-weight men [hazard ratio 135 95 CI 102-179 P = 0039] Women with class I obesity had reduced overall survival [hazard ratio 124 95 CI 101-153 P = 0045] compared with normal-weight women Overweight status was associated with improved overall survival in men (P = 0006) and underweight women had significantly worse overall survival (P = 0019)
ALCOHOL
Ferrari et al (2007)
As part of the prospective EPIC study data was collected examining the relationship between lifetime and baseline alcohol consumption and colorectal cancer incidence
478732 EPIC subjects free of cancer at enrolment between 1992 and 2000
62 years Colorectal cancer incidence
Lifetime alcohol intake was significantly positively associated to CRC risk (hazard ratio HR = 108 95CI = 104-112 for 15 gday increase) with higher cancer risks observed in the rectum (HR = 112 95CI = 106-118) than distal colon (HR = 108 95CI = 101-116) and proximal colon (HR = 102 95CI = 092-112) Similar results were observed for baseline alcohol intake When assessed by alcoholic beverages at baseline the CRC risk for beer
52
(HR = 138 95CI = 108-177 for 20-399vs 01-29 gday) was higher than wine (HR = 121 95CI = 102-144) although the two risk estimates were not significantly different from each other Higher HRs for baseline alcohol were observed for low levels of folate intake (113 95CI = 106-120 for 15 gday increase) compared to high folate intake (103 95CI = 098-109)
53
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
prostate cancer survival In the current review 2 studies were identified Studies are
summarised in Table 5 at the end of this section
The underlying mechanisms for the direct anti-cancer effect of lifestyle has been indicated in
a study with men undergoing a diet and physical activity intervention comprising the majority
of calories from complex carbohydrates high in fibre combined with 1-hour of supervised
exercise (Soliman et al 2009) Serum (blood plasma) was taken from these men and added
to androgen-dependent LNCaP cells29 in the laboratory There was decreased growth and
increased apoptosis (cell death) associated with a reduction in serum Insulin-like Growth
Factor (IGF)-130 These findings indicate that diet and physical activity interventions
might slow prostate cancer progression as well as aid in its treatment during the early
stages of development
Kenfield (2010) examined the data of 2686 men from the Health Professionals Follow-Up
Study31 and found that men who engaged in 3gt MET-hours of weekly physical activity
post-diagnosis reduced their risk of death by 35 compared with men who engaged
in less weekly activity Furthermore men who walked 90-minutes per week at a normal to
brisk pace had a 51 lower risk of death due to any cause compared with men who walked
90-minutes or less at an easy pace To reduce their risk of cancer-specific death men
had to engage in vigorous activity such as jogging (6 MET-hours)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in prostate cancer
survival In the current review 7 studies were identified
Dietary Changes plus Supplements
Ornish et al (2005) conducted a diet counselling and lifestyle RCT comprising men with
early prostate cancer (n=93) The lifestyle changes in this study included a vegan diet
supplemented with soy vitamin E fish oils selenium and vitamin C together with a
moderate physical activity program and stress management techniques such as yoga
29
Human prostate cancer cells
30 IGF-1 is an amino acid with high sequence similarity to insulin mainly secreted by the liver as a result of
stimulation by growth hormone It is important for the regulation of normal physiology as well as a number of pathological states including cancer
31 An all-male (n=51529) study designed to complement the all-female Nurses Health Study
54
Prostate Specific Antigen (PSA)32 levels decreased by 4 at 12-months in the
intervention group but increased by 6 in the control group this was statistically
significant and strongly correlated with the degree of lifestyle change However the
intensity of this intervention and associated behavioural changes might not easily be
translated into practice (White et al 2009)
Pomegranate Juice
The potential benefits of pomegranate juice on prostate cancer outcomes frequently appear
in the media and strong evidence of its efficacy can be found within the academic literature
In a phase II open-label single-arm clinical trial men (n=46) with recurrent prostate cancer
who had rising PSA after surgery or radiotherapy were treated daily with 8oz (227g)
equivalent of pomegranate juice (Pantuck et al 2006) Mean PSA doubling time
significantly increased with treatment from 15-months to 54-months demonstrating a
good indication of a relationship between the consumption of pomegranate juice and
prostate health
Green Tea
Another beverage found to demonstrate some positive effects on prostate cancer is green
tea Bettuzzi et al (2006) in a year-long clinical trial has demonstrated that daily
consumption of green tea can produce a ten-fold decrease in the rate at which
prostate intraepithelial neoplasia (a pre-cancerous condition) progresses to prostate
cancer Support for these findings is offered by an uncontrolled open-label single-arm
phase II clinical trial testing the efficacy of Polyphenon E which contains the polyphenol
antioxidants found in green tea (McLarty et al 2009) Taking four capsules of
Polyphenon E daily (equivalent to twelve cups of green tea) for an average of 345
days leading up to radical prostatectomy the participants (n=26) experienced
significant reductions in biomarkers used to monitor likelihood of metastasis Some
patients demonstrated reductions greater than 30
Lycopene Supplements
The EPIC study has demonstrated that similar to breast cancer prostate cancer risk is not
related to fruit and vegetable consumption (Key et al 2004) However further evidence for
the role of carotenoids found in fruit and vegetables have been provided from a pilot RCT
including men with benign prostatic hyperplasia (BPH) a benign enlargement of the prostate
that can progress to cancer (Schwarz et al 2008) Men (n=20) who received 15mg od
lycopene supplementation (a carotenoid found in tomatoes and other red fruits and
32
PSA is a protein produced by the cells of the prostate gland It is present in small quantities in the serum of normal men and is often elevated in the presence of prostate cancer
55
vegetables) for 6-months had significantly decreased PSA levels compared to a
placebo group (n=20) who had no change in PSA
Salicylate
Salicylate33 intake has been implicated in the aetiology of prostate cancer but Thomas et al
(2009) have evaluated their influence on established cancer progression In a randomised
double blind phase II study involving men (n=110) with progressive prostate cancer who
were counselled to eat less saturated fat and processed food more fruit vegetables and
legumes physical activity more regularly and to stop smoking the men were then
randomised to take sodium salicylate alone or combined with vitamin C copper and
manganese gluconates34 daily Although there was no difference in outcome between those
who received sodium salicylate alone or combined the intervention as a whole (ie
including dietary counselling) slowed or stopped the rate of PSA progression in 40
patients (364) for over one-year and a further ten patients were stabilised for 10-
months This data suggests that changes in lifestyle can potentially delay PSA progression
and the need for more radical therapy highlighting an area for further research
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in prostate cancer
survival In the current review 2 studies were identified
Wright et al (2007) prospectively examined BMI and weight change in relation to prostate
cancer incidence and mortality in 287760 men enrolled in the National Institutes of
Health-AARP Diet and Health Study Higher baseline BMI was associated with
significantly reduced total prostate cancer incidence on the one hand but with
significantly increased risk of prostate cancer mortality on the other hand Adult weight
gain from age 18-years to study entry (range=50-71-years old) was positively associated
with prostate cancer staging but not with disease incidence
In a retrospective analysis exploring the interaction between obesity and surgical outcomes
in patients with prostate cancer treated by radical prostatectomy (n=437) a weak but
significant association was observed between BMI and a number of biological
biomarkers indicative of an advanced pathological stage (Gross et al 2009)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in prostate
cancer survival and no evidence was identified in the current review
33
Salicylates are chemicals that occur naturally in many plants including many fruits vegetables and herbs
Salicylates in plants act as a natural immune hormone and preservative protecting the plants against diseases
insects fungi and harmful bacteria 34
A pinkish powder soluble in water used in medicine in vitamin tablets and as a feed additive and dietary
supplement
56
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in prostate cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR PROSTATE CANCER -
MECHANISMS OF BENEFIT
Physical Activity and Diet The evidence within this review indicates that diet and physical
activity interventions might slow prostate cancer progression as well as aid in its treatment
during the early stages of development The mechanism of benefit is primarily via
decreased growth and increased apoptosis (cell death) associated with a reduction in serum
Insulin-like Growth Factor (IGF)-1 (Soliman et al 2009) Up to 3gt MET-hours of weekly
physical activity appears sufficient to increase survival with more vigorous activity of about 6
MET-hours per week for the reduction of cancer-specific mortality (Kenfield 2010) A
number of dietary steps can be taken to reduce PSA levels and thus slow down the growth
of tumours and increase survival For example a vegan diet supplemented with soy vitamin
E fish oils selenium and vitamin C together with a moderate physical activity program and
stress management techniques such as yoga have been found useful (Ornish et al 2005)
as has pomegranate juice (Pantuck et al 2006) and green tea (Betuzzi et al 2006 McLarty
et al 2009) As with breast cancer carotenoids have been found to offer protective
properties for men with benign prostatic hyperplasia which can progress to cancer (Schwarz
et al 2008) Overall the evidence for prostate cancer is suggestive of survival benefits from
combined dietary and physical activity changes In other words it appears that a healthier
diet made up of fruit and vegetables as well as drinks such as pomegranate juice or green
tea combined with 3gt MET-hours of weekly physical activity could be an effective
prescription for reducing mortality from cancer and other causes
Weight Evidence for weight was mixed whilst finding that higher baseline BMI was
associated with significantly reduced total prostate cancer incidence a significant increase in
prostate cancer severity and mortality was also observed with higher BMI levels (Wright et
al 2007a Gross et al 2009) More research is clearly needed to establish any differential
prostate cancer outcomes associated with weight
Smoking and Alcohol More research is required for smoking and alcohol in terms of
prostate cancer outcomes
57
Table 5 Prostate Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Kenfield et al (2009)
Prospective study (Health Professionals Follow-up Study) assessing the relationship between physical activity and duration and pace of walking with total and prostate cancer-specific mortality
2686 men with prostate cancer
4-years Prostate cancer mortality and total physical activity
Men who were physically active especially those engaging in 3 or more MET-hours of total activity had a 35 lower risk of death from any cause (hazard ratio 065 [95 CI 052 082]) and a modest non-significant reduction in risk of prostate cancer death (hazard ratio 088 [95 CI 052 149]) after adjustment for other risk factors for PCa mortality and pre-diagnosis physical activity While no benefit from walking was observed for PCa mortality men who walked 4 or more hours per week versus those who walked less than 20 minutes per week had a 23 lower risk of all-cause mortality (95 CI 061 097 p-trend=001) In addition compared to men who walked less than 90 minutes at an easy walking pace those who walked 90 or more minutes at a normal to very brisk pace had a 51 lower risk of all-cause mortality (95 CI 037 064) More vigorous activity and longer duration of activity was associated with significant further reductions in risk for all-cause mortality More vigorous activity was associated with a borderline-significant reduction in risk for PCa mortality
Soliman et al (2009)
Pritikin Longevity Center 3-Week
Residential Program - men were given prepared
meals with 12ndash15 fat calories
15ndash20 protein calories and the majority
of calories (65ndash70) from unrefined complex carbohydrates high in fibre (gt40 gday) The men attended daily supervised exercise classes
for 60 min
5 men in their early sixties
with no
signs of prostate cancer (PSA lt 40)
On completion of the 3-week programme
Cancer progression
The intervention slowed growth and increased apoptosis in LNCaP cells responses that were eliminated when
IGF-I was added back to
the post-intervention samples The p53 protein content was increased
and NFkB activation reduced in the post serum-stimulated LNCaP
cells Similar results were observed when the IGF-I receptor was
blocked in the pre-intervention serum In androgen-independent PC-3
cells growth was reduced while none of the other factors were
changed by the intervention
DIET
Bettuzzi et al (2006)
A proof-of-principle double-blind placebo-
controlled clinical trial assessing the safety
and efficacy of green tea catechins for the
chemoprevention of prostate cancer incidence in patients with high-grade prostate intraepithelial
neoplasia Daily
treatment consisted of three GTCs
Men with high-grade prostate intraepithelial
neoplasia who would develop cancer within
1-year
3-monthly for 1-year
Primary outcome prostate cancer incidence Secondary outcome
After 1 year only one tumour was diagnosed (incidence 3) in the
cohort receiving green tea whereas 9 cancers were found among the placebo-treated
men (incidence 30) Total PSA did not
change
significantly between the two arms but green tea-treated men showed
values constantly lower with respect to placebo-treated ones As a
secondary observation administration of green tea also reduced lower
urinary tract symptoms suggesting that these compounds might also
58
capsules 200 mg each (total 600 mgd) (n=60) PSA levels be of help for treating the symptoms of benign prostate hyperplasia
Key et al (2004)
An examination of the association between self-reported consumption of fruits and vegetables and prostate cancer risk in EPIC participants
130544 men in 7 countries recruited into EPIC
Median = 48 years
Prostate cancer incidence
There were 1104 incident cases of prostate cancer No significant associations between fruit and vegetable consumption and prostate cancer risk were observed Relative risks (95 CI) in the top fifth of the distribution of consumption compared to the bottom fifth were 106 (084 ndash134) for total fruits 100 (081ndash122) for total vegetables and 100 (079 ndash126) for total fruits and vegetables combined intake of cruciferous vegetables was not associated with risk
McLarty et al (2009)
In order to determine the effects of short-term supplementation with the active compounds in green tea on serum biomarkers in patients with prostate cancer daily doses were provided of Polyphenon E which contained a total of 13 g of tea polyphenols until time of radical prostatectomy
26 men with positive prostate biopsies scheduled for radical prostatectomy
Not reported PSA levels Biomarkers of prostate cancer decreased significantly All of the liver function tests also decreased five of them significantly total protein albumin aspartate aminotransferase alkaline phosphatase and amylase
Ornish et al (2005)
Lifestyle changes including a vegan diet supplemented with soy vitamin E fish oils selenium and vitamin C together with a moderate physical activity program and stress management techniques such as yoga
Men with early prostate cancer (n=93) Gleason scores less than 7
12-months into the intervention
PSA and serum stimulated LNCaP cell growth
PSA levels decreased by 4 at 12-months in the intervention group but increased by 6 in the control group this was statistically significant and strongly correlated with the degree of lifestyle change
Pantuck et al (2006)
A phase II two-stage clinical trial to determine the effects of pomegranate juice PSA progression in men with a rising PSA following primary therapy Patients were treated with 8 ounces of pomegranate juice daily (570mg total polyphenol gallic acid equivalents) until disease progression
46 men with rising PSA levels post-treatment (surgery or radiotherapy)
Every 3-monhs for 54-months
PSA levels Mean PSA doubling time significantly increased with treatment from a mean of 15 months at baseline to 54 months post-treatment (P lt 0001) In vitro assays comparing pre-treatment and post-treatment patient serum on the growth of LNCaP showed a 12 decrease in cell proliferation and a 17 increase in apoptosis (P = 00048 and 00004 respectively) a 23 increase in serum nitric oxide (P = 00085) and significant (P lt 002) reductions in oxidative state and sensitivity to oxidation of serum lipids after versus before pomegranate juice
Schwarz et al (2008)
15mg od lycopene supplementation for 6-months or placebo
Men with benign prostatic hyperplasia (n=40)
After 6-months of intervention
Inhibition or reduction of increased serum PSA levels
Men receiving 15mg od lycopene supplementation had significantly decreased PSA levels compared to a placebo group who had no change in PSA
Thomas et al (2009)
A randomised double blind phase II study to evaluate the influence of salicylate and lifestyle on established cancer progression Men were counselled
110 men whose PSA had risen in 3 consecutive
Not reported Prostate cancer progression (PSA levels)
Although there was no difference in outcome between the SS or CV247 (21 v 19 p=092) the intervention slowed or stopped the rate of PSA progression in 40 patients (364) for over one year A further ten patients were stabilised for ten months Patients least likely to stabilise
59
to eat less saturated fat processed food more fruit vegetables and legumes exercise more regularly and to stop smoking They were then randomised to take sodium salicylate (SS) alone or SS combined with vitamin C copper and manganese gluconates (CV247) daily without other intervention
values gt20 over the preceding 6-months
had received previous radiotherapy or had a Gleason =7 These men welcomed this addition to active surveillance
WEIGHT
Gross et al (2009)
A retrospective cohort study examining whether changes in components of the sex steroid receptor axis may contribute to the clinical aggressiveness of prostate cancer in obese patients
539 patients treated with radical prostatectomy at a single urban hospital between 1994 and 2002
Not reported Pathological stage of prostate cancer BMI
Higher BMI correlated strongly with higher pathologic stage In comparing obese versus non-obese patients there was no difference in expression of androgen or oestrogen related proteins in cancerous epithelial cells However there was a down-regulation of aromatase in the stoma of obese patients suggesting obesity may cause stromal changes in the sex steroid production and signalling pathways which may affect prostate cancer growth via intracrineparacrine mechanisms
Wright et al (2007)
A prospective examination of BMI and adult weight change in relation to prostate cancer incidence and mortality
287760 men ages 50 years to 71 years at enrolment (1995-1996) in the National Institutes of Health-AARP Diet and Health Study
6-years Prostate cancer incidence Weight gain (BMI)
Higher baseline BMI was associated with significantly reduced total prostate cancer incidence largely because of the relationship with localized tumours (for men in the highest BMI category [gtor=40 kgm (2)] vs men in the lowest BMI category [lt25 kgm (2)] RR 067 95 CI 050-089 P = 0006) Conversely a significant elevation in prostate cancer mortality was observed at higher BMI levels (BMI lt25 kgm(2) RR 10 [referent group] BMI 25-299 kgm(2) RR 125 95 CI 087-180 BMI 30-349 kgm(2) RR 146 95 CI 092-233 and BMI gtor=35 kgm(2) RR 212 95 CI 108-415 P = 02) Adult weight gain from age 18 years to baseline also was associated positively with fatal prostate cancer (P = 009) but not with incident disease
60
d) LUNG CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in lung
cancer survival and one systematic review with meta-analysis was identified in the current
review Studies are summarised in Table 6 at the end of this section
Tardon et al (2005) conducted a systematic review and meta-analysis of cohort and case-
control studies from 1966 through October 2003 evaluating the relationship between
physical activity and lung cancer incidence Nine studies were identified 6 of which
demonstrated that that higher levels of leisure-time physical activity (walking gardening
swimming) protects against lung cancer (Severson et al 1989 Thune et al 1997 Lee et
al 1999 Sellers et al 1991 Kubik et al 2002 Mao et al 2003) The estimated combined
risk for both genders was statistically significant as was a dose-response relationship (p lt
01)
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in lung cancer
survival and no evidence was identified in the current review
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in lung cancer
survival and no evidence was identified in the current review
iv SMOKING
Smoking has long been accepted as an unhealthy behaviour that increases the risk of
cancer incidence and disease outcomes Yet many people continue to smoke pre- and post-
diagnosis one-third to one-half of cancer patients either continue to smoke after diagnosis or
relapse after initial quit attempts (Gritz et al 2006) Bekkering et al (2006) do not provide
any evidence for the role of smoking in lung cancer survival In the current review 5 studies
were identified that further highlight the importance of smoking cessation support for people
living with and beyond cancer
Vineis et al (2007) have estimated exposure to Environmental Tobacco Smoke (ETS) and to
air pollution in never smokers and ex-smokers in EPIC study participants (n=520000) The
proportion of lung cancers in never- and ex-smokers attributable to ETS was
estimated to be between 16 and 24 mainly due to the contribution of work-related
exposure
61
In two studies of survivors of stage I and II small cell lung cancer risk of a second cancer
was 35-44-fold higher than in the general population (Richardson et al 1993 Tucker et
al 1997) In those who continued to smoke the risk was far higher particularly in those who
also received chest irradiation and alkylating agents35 (Tucker et al 1997) highlighting the
need for risk assessment when offering smoking cessation support or advice
Another study in Japan confirmed that patients with small cell lung cancer who survive
at least 2-years greatly reduced their likelihood of a second cancer if they quit
smoking (p lt 05) (Kawahara et al 2002) Additionally smoking has been found to be
an independent risk factor in breast cancer survivors developing lung cancer (Ford et
al 2003) In support of these studies Parsons et al (2010) report that nine of ten studies
identified in a review of literature from 1966 to 2008 indicate that continuing to smoke is
associated with a significantly increased risk of all-cause mortality in early stage non-
small cell lung cancer and of all-cause mortality in limited stage small cell lung
cancer
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in lung cancer
survival and no evidence was identified in the current review
SUMMARY OF LIFESTYLE EVIDENCE FOR LUNG CANCER - MECHANISMS OF
BENEFIT
Smoking Evidence for the role of lifestyle factors on lung cancer progression and
recurrence has primarily examined smoking which is a strongly established risk factor for
disease progression and mortality Continuing to smoke exposes the body to high levels of
carcinogens which can cause further DNA damage to existing cancers encourage the
cancer to mutate into a more aggressive type or develop mechanisms to hide from the
bodylsquos immunological defences (Akopyan and Bonavida 2006) Indeed smoking has been
found to suppress the immune system interfering with the function of natural killer (NK) cells
- a lymphoid cell type that plays a role in the surveillance of tumour growth Patients who
have already developed one cancer are likely to be more susceptible to DNA damage from a
pre-existing genetic vulnerability or acquired damage from chemotherapy or radiotherapy
Avoiding carcinogens may therefore have a benefit in reducing the risk of developing
further cancers in patients who may be more susceptible from a pre-existing genetic
signature or damage from chemotherapy or radiotherapy The smoking cessation initiatives
currently sweeping the nation such as NHS Choices bdquoSmokefree‟ remain invaluable as
smoking continues to be an important preventable cause of morbidity and mortality
worldwide
Additional Lifestyle Factors More research is required into lifestyle factors such as diet
physical activity weight and alcohol consumption in terms of lung cancer outcomes Access
35
Cytotoxic agents used to disrupt cancer cells can damage healthy cells in the process
62
to lifestyle services such as post-treatment rehabilitation fitness planning and nutritional
support was highlighted as an important component within the disease trajectory for people
with lung cancer (NCSI Mapping Project 2009) There is evidence for the benefits of
physical activity in reducing lung cancer incidence however there is a paucity of evidence
for the survivorship period of lung cancer
63
Table 6 Lung Cancer Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Tardon et al (2004)
A meta-analysis of studies (1966-2003) evaluating the relationship between physical activity and lung cancer
Men and women in cohort and case-control studies (9 studies)
Not reported
Lung cancer incidence
The combined ORs were 087 (95 CI=079ndash095) for moderate leisure-time physical activity (LPA) and 070 (062ndash079) for high activity (p trend = 000) This inverse association occurred for both sexes although it was somewhat stronger for women No evidence of publication bias was found Several studies were able to adjust for smoking but none adjusted for possible confounding from previous malignant respiratory disease
SMOKING
Ford et al (2003)
Retrospective analysis of smoking radiation and both exposures on lung carcinoma development in women who were treated previously for breast carcinoma
Case patients (n = 280) females aged 30-89 years with breast carcinoma prior to primary lung carcinoma Control patients (n = 300) selected randomly from 37000 patients with breast carcinoma treated at The University of Texas M D Anderson Cancer Center
Not reported
Lung cancer incidence
At the time of breast carcinoma diagnosis 84 of case patients had ever smoked cigarettes compared with 37 of control patients whereas 45 of case patients and control patients received XRT for breast carcinoma Smoking increased the odds of lung carcinoma in women without XRT (odds ratio [OR] 60 95 confidence interval [95 CI] 36-101) but XRT did not increase lung carcinoma risk in non-smoking women (OR 05 95 CI 03-11) Overall the OR for both XRT and smoking compared with no XRT or smoking was 90 (95 CI 51-159)
Kawahara et al (1998)
Prospective study to investigate whether smoking cessation after successful therapy is associated with a decrease in risk for a second
980 consecutive patients with small cell lung cancer (SCLC)
Median=67 years after initiation of
Second primary tumour
Of the patients who continued to smoke 11 (33) developed a SPT Of the 31 patients who stopped smoking after therapy only three (10) had a subsequent SPT Among those who continued to smoke the risk for a SPT was significantly increased (54 times 95 CI 27-97) relative to the general
64
primary tumour being treated with combination chemotherapy with or without chest radiotherapy
therapy population In contrast those who stopped smoking showed only a 16-fold increase (95 CI 03-46) which was not significantly different from the level in the general population The relative risk for non-SCLC was significantly increased 128-fold (95 CI 34-328) in continuing smokers No second non-SCLCs have been found among those who stopped smoking The 33 patients who continued to smoke had a significantly increased risk of a SPT (43 95 CI 11-159 P=003) Relative to the risk of SPT in patients without previous radiotherapy who stopped smoking the risk is 092 in patients without radiotherapy who continued smoking 037 in patients with radiotherapy who stopped smoking and 233 in patients with radiotherapy who continued smoking The risk of current smoking in patients with previous radiotherapy is 630 relative to those with radiotherapy who stopped smoking although this interaction is not statistically significant (P = 024)
Parsons et al (2010)
A systematic review with meta-analysis of the evidence that smoking
cessation after diagnosis
of a primary lung tumour affects prognosis Databases searched CINAHL (from 1981) Embase (from 1980) Medline
(from 1966)
Web of Science (from 1966) CENTRAL (from 1977)
to
December 2008 and reference lists of included studies
RCTs or observational
st
udies measuring
the effect of quitting smoking
post-
diagnosis on lung cancer prognosis
Patients were followed for 6-months gt in 5 studies but only at time of diagnosis treatment in 4
5-year survival using death rates for continuing smokers and quitters obtained from this review
Continued smoking was associated with a significantly increased risk of all-
cause mortality (hazard ratio 294 95 CI 115 to
754) and recurrence (186
101 to 341) in early stage non-small cell lung cancer and of all-cause
mortality (186 133 to 259) development of a second primary tumour (431 109 to 1698)
and recurrence (126 106 to 150) in limited stage small
cell lung cancer No study contained data on the effect of quitting
smoking on
cancer specific mortality or on development of a second primary tumour in
non-small cell lung cancer Life table modelling on the basis of these data
estimated 33 five year survival in 65 year old patients with early stage non-
small cell lung cancer who continued to smoke compared with 70 in
those
who quit smoking In limited stage small cell lung cancer an estimated 29
of continuing smokers would survive for five years compared with 63 of
quitters on the basis of the data from this review
Richardson et al (1993)
Retrospective review to determine the incidence of second primary cancers developing in patients surviving free of cancer for 2 or more years after treatment for small-cell lung cancer and to assess the potential effect of smoking cessation
Consecutive sample of 540 patients with small-cell lung cancer
Median=61 years
Relative risk for second primary cancers and death
55 patients (10) were free of cancer 2-years after initiation of therapy 18 of these developed one or more second primary cancers including 13 who developed second primary non-small-cell lung cancer The risk for any second primary cancer compared with that in the general population was increased four times (relative risk 44 95 CI 25-72) with a relative risk of a second primary non-small-cell lung cancer of 16 (CI 84-27) Forty-three patients discontinued smoking within 6-months of starting treatment for small-cell lung cancer and 12 continued to smoke In those who stopped smoking at time of diagnosis the relative risk of a second lung cancer was 11 (CI 44 to 23) whereas in those who continued to smoke it was 32 (CI 12 to 69)
Tucker et al (1997)
A multi-institution study to investigate the risk among survivors of developing second primary
611 patients who had
been cancer
Not reported
Population-based rates of cancer
Relative to the general population the risk of all second cancers among these
patients was increased 35-fold Second lung cancer risk was increased 13-
fold among those who received chest irradiation in comparison to a sevenfold
65
cancers other than small-cell lung carcinoma
free for more than 2 years after therapy for small-cell lung cancer
incidence and mortality
increase among non-irradiated patients It was higher in those who
continued smoking with evidence of an interaction between chest irradiation and continued smoking
(relative risk = 21) Patients treated with various forms
of combination chemotherapy had comparable increases in risk (94- to 13-
fold overall) except for a 19-fold risk increase among those treated with
alkylating agents who continued smoking
Vineis et al (2007)
Prospective study to estimate exposure to Environmental Tobacco Smoke (ETS) in never smokers and ex-smokers in 10 European countries (EPIC)
Men and women in the EPIC study (n = 520000)
Not reported
Lung cancer incidence
The proportion of lung cancers in never- and ex-smokers attributable to ETS was estimated as between 16 and 24 mainly due to the contribution of work-related exposure Also 5ndash7 of lung cancers in European never smokers and ex-smokers are attributable to high levels of air pollution as expressed by NO2 or proximity to heavy traffic roads
66
e) OTHER CANCERS
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in survival
from other cancers and no evidence was identified in the current review
ii DIET
Bekkering et al (2006) do not provide any evidence for the role of diet in survival from other
cancers Studies identified in the current review are summarised in Table 7 at the end of this
section
Preliminary EPIC results provide some evidence that red and preserved meat increases risk
for gastric cancer (Gonzalez et al 2006) Preliminary EPIC results also indicate that fruit
reduces gastric cancer risk whilst vegetables are not associated with risk for this type of
cancer Furthermore overall consumption of fruit and vegetables is reported to be unrelated
to risk of ovarian cancer (Schultz et al 2005) There is evidence of a protective effect of a
high intake of allium vegetables (onions garlic shallots leeks and chives) on ovarian
cancer risk (Schultz et al 2005)
iii WEIGHT
Bekkering et al (2006) do not provide any evidence for the role of weight in survival from
other cancers Preliminary EPIC results reported in the current review provide some
evidence that BMI is associated with endometrial cancer risk (Kaaks et al 2002
Friedenreich et al 2007)
iv SMOKING
Bekkering et al (2006) do not provide any evidence for the role of smoking in survival from
other cancers Preliminary EPIC results along with 4 other studies were identified in the
current review
Gonzalez et al (2003) confirm from EPIC results that smoking is associated with gastric
cancer
Similarly Yu et al (1997) evaluated 25000 heterogeneous patients who had been treated
for lung breast or colorectal cancer and found that the 15-year survival of the people
who continued to smoke was 44 compared to 55 in those who quit
In a more recent study of survivors of early stage head and neck cancer (n=264) who
retrospectively reported their tobacco histories (pre-diagnosis) and prospectively updated
67
information annually thereafter for an average of 42-years smoking history dose-
dependently increased the risk of mortality from cancer (Mayne et al 2009)
The impact of smoking on risk of secondary lung cancer has been demonstrated in survivors
of Hodgkin lymphoma (Abrahamsen et al 1993 Travis et al 2002) In the latter study risk
for subsequent lung cancer from radiation treatment and smoking was identified where
multiple effects were found for a combination of radiation and alkylating agents36 in
moderate-to-heavy smokers compared with comparison cases (Travis et al 2002)
v ALCOHOL
Bekkering et al (2006) do not provide any evidence for the role of alcohol in survival from
other cancers One study was identified in the current review which showed that pre-
diagnosis alcohol consumption history dose-dependently increased mortality risk in
recent survivors of early stage head and neck cancer (n=264) (Mayne et al 2009)
Risks reached 49 for those who drank gt5 drinks per day an effect explained by beer and
liquor consumption Continued drinking post-diagnosis of an average of 23 drinks daily
also significantly increased risk
SUMMARY OF FINDINGS FOR OTHER CANCERS
A comprehensive evaluation of the lifestyle evidence for cancers other than the four most
common (ie breast colorectal lung prostate) was not within the scope of this review
However those studies identified whilst gathering evidence for these four cancers does
highlight the sheer importance of lifestyle in the development and progression of all types of
cancers not to forget other chronic diseases The provision of lifestyle support for cancer
survivors clearly needs to remain priority as does further research into the exact
mechanisms of benefit obtained from different lifestyle practices at different stages of the
cancer and indeed health trajectory
36
Carcinogenic agents used in chemotherapy to treat cancer
68
Table 7 Other Cancers ndash Survival and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
DIET
Gonzalez et al (2006)
Nested case-control within the prospective EPIC study examining of
the risk of gastric cancer and
oesophageal adenocarcinoma associated
with meat consumption
521 457 men and women aged 35ndash70 years in 10 European
countrie
s (330 gastric adenocarcinoma and
65
oesophageal adenocarcinomas were diagnosed)
65-years Incidence of gastric and oesophageal cancers
Gastric noncardia cancer risk was statistically significantly associated
with intakes of total meat (calibrated HR per 100-gday increase
=
352 95 CI = 196 to 634) red meat (calibrated HR per 50-gday
increase = 173 95 CI = 103 to 288) and processed
meat (calibrated HR per 50-gday increase = 245 95 CI
= 143 to 421) The association between
the risk of gastric noncardia cancer and total meat intake was
especially large in H pylori infected subjects (odds ratio per 100-
gday increase = 532 95 CI = 210 to 134) Intakes of total red or
processed meat were not associated with
the risk of gastric cardia cancer A positive but nonndashstatistically
significant association was observed between oesophageal
adenocarcinoma cancer risk and total and processed meat intake
Schultz et al (2005)
Prospective examination of the association between consumption of fruit and vegetables and risk of ovarian cancer (EPIC)
Female participants (n = 325640) of the EPIC study
Mean=63 years
Ovarian cancer incidence
Total intake of fruit and vegetables separately or combined as well as subgroups of vegetables (fruiting root leafy vegetables cabbages) was unrelated to risk of ovarian cancer A high intake of garliconion vegetables was associated with a borderline significant reduced risk of this cancer
WEIGHT
Friedenreich et al 2007
Large prospective study (EPIC) examining the association between anthropometry and endometrial cancer particularly by menopausal status and exogenous hormone use subgroups
223008 women in the EPIC study (567 incident endometrial cancer cases)
64-years Endometrial cancer incidence
Weight BMI waist and hip circumferences and waistndashhip ratio (WHR) were strongly associated with increased risk of endometrial cancer The relative risk (RR) for obese (BMI 30ndash lt 40 kgm
2)
compared to normal weight (BMI lt 25) women was 178 95 CI = 141ndash226 and for morbidly obese women (BMI ge 40) was 302 95 CI = 166ndash552 The RR for women with a waist circumference of ge88 cm vs lt80 cm was 176 95 CI = 142ndash219 Adult weight gain of ge20 kg compared with stable weight (plusmn3 kg) increased risk independent of body weight at age 20 (RR = 175 95 CI = 111ndash277) These associations were generally stronger for postmenopausal than premenopausal women and oral contraceptives never-users than ever-users and much stronger among never-users of hormone replacement therapy compared to ever-users
Kaaks et al A review of evidence on the Endometrial Not Incidence of The authors conclude that development of ovarian hyperandrogenism
69
(2002) associations among endometrial cancer risk endogenous hormone metabolism and obesity
cancer cases reported endometrial cancer
may be a central mechanism relating to an interaction between obesity-related chronic hyperinsulinemia with genetic factors predisposing to the development of ovarian hyperandrogenism
SMOKING
Abrahamsen et al (1993)
The Norwegian Cancer Registry
identified previously untreated patients with Hodgkin lymphoma treated at NRH who had developed a secondary cancer more than 1 year after diagnosis of
Hodgkin
lymphoma
68 patients who developed secondary cancer including 9 acute non-lymphocytic leukaemialsquos (ANLLs)
8 non-
Hodgkins lymphomas (NHLs) and 51 solid tumours including 11 lung cancers
Not reported
Secondary cancer
The RR of SC and leukaemia was 186 (95 CI 14 to 24) and 243 (95 CI 111 to 462) respectively The RR of
SC was highest in
younger patients (lt 41 years RR = 38) No significant association
between splenectomy and development of ANLL was found The
influence of treatment and follow-up time on the development of SC
agrees with data from other large cancer institutions
Gonzalez et al (2003)
Assessment of the relation between tobacco use and gastric cancer incidence in the prospective EPIC study
521468 individuals recruited from 10 European countries taking part in the EPIC study 274 were eligible for the analysis
Approx 10-years
Incidence of gastric cancer
After adjustment for educational level consumption of fresh fruit vegetables and preserved meat alcohol intake and body mass index (BMI) there was a significant association between cigarette smoking and gastric cancer risk the hazard ratio (HR) for ever smokers was 145 (95 CI = 108-194) The HR of current cigarette smoking was 173 (95 CI = 106-283) in males and 187 (95 CI = 112-312) in females Hazard ratios increased with intensity and duration of cigarette smoked A significant decrease of risk was observed after 10 years of quitting smoking A preliminary analysis of 121 cases with identified anatomic site showed that current cigarette smokers had a higher HR of GC in the cardia (HR = 410) than in the distal part of the stomach (HR = 194) In this cohort 176 (95 CI = 105-295 ) of gastric cancer cases may be attributable to smoking
Mayne et al (2009)
Participants retrospectively reported their smoking histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to smoke post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Smoking history before diagnosis dose-dependently increased the risk of dying risks reached 54 [95 CI 07-401] among those with gt60 pack-years of smoking After adjusting for pre-diagnosis exposures continued smoking was associated with non-significantly higher risk (relative risk for continued smoking versus no smoking 18 95 CI 09-39)
70
Travis et al (2002)
Case-control study with a population-based cohort The cumulative amount of cytotoxic drugs the radiation dose to the specific location in the lung where cancer developed and tobacco use were compared between patients who developed lung cancer and matched control patients
1-year survivors of Hodgkins disease (n=19046) comparison between 222 patients who developed lung cancer and 444 matched controls
Not reported
Secondary cancer incidence
Tobacco use increased lung cancer risk more than 20-fold risks from smoking appeared to multiply risks from treatment
Yu et al (1997)
Retrospective study examining the effect of smoking history on survival among cancer patients
Data from Memorial Sloan-Kettering Cancer Centers tumour registry was used to identify 25436 cases of cancer (12447 male patients and 12989 female patients)
Not reported
Survival time Patients who had a history of smoking were found to have a lower rate of survival than non-smokers After controlling for age race alcohol use and histologic grade the risk ratios were 155 for males and 143 for females A dose-response relationship was found between ever-smoking and cancer patient survival The predictive effect of smoking on survival was significant for patients with oral pancreatic breast and prostate cancers but not for oesophageal stomach colon rectum laryngeal lung cervix uteri urinary bladder and kidney cancers Black patients with oral or breast cancer had a poorer prognosis associated with smoking compared with white and other non-white patients
ALCOHOL
Mayne et al (2009)
Participants retrospectively reported their alcohol consumption histories (before diagnosis) with information prospectively updated annually thereafter to assess the role of continuing to drink post-diagnosis on mortality
Patients (n = 264) who were recent survivors of early stage head and neck cancer
Mean=42-years
Mortality Alcohol history before diagnosis dose-dependently increased mortality risk risks reached 49 (95 CI 15-163) for persons who drank gt5 drinksd an effect explained by beer and liquor consumption After adjusting for pre-diagnosis exposures continued drinking (average of 23 drinksd) post-diagnosis significantly increased risk (relative risk for continued drinking versus no drinking 27 95 CI 12-61)
71
PART TWO
LIFESTYLE EVIDENCE FOR REDUCING AND MANAGING THE
RISKS AND SIDE-EFFECTS OF CANCER TREATMENT
Introduction
There are a number of long-term and late effects of cancer treatment that a survivor might
be confronted with including fatigue (Bower et al 2006) psychological problems (Thewes
et al 2004) lymphoedema (Deo et al 2004) and osteoporosis (Brown et al 2006) There
might also be difficulties in terms of returning to work or withdrawal from social activities due
to disability (Taskila et al 2007) Lifestyle choices pertaining to diet physical activity
smoking and alcohol consumption for cancer survivors are not only important in terms of
disease progression and recurrence Despite there being less evidence in this area there
is accumulating data demonstrating that lifestyle can facilitate the effective management of
many of these effects of treatment some of which are chronic conditions themselves
requiring additional lifestyle modifications Research within this area has hit new heights in
order to keep up with the growing number of survivors The chronic conditions addressed
within the current review of lifestyle evidence are some of the most frequently reported
problems cited by cancer survivors they include cancer-related fatigue (CRF)
lymphoedema osteoporosis and weight gain In addition evidence for lifestyle choices and
quality of life (QoL) has been reviewed due to the QoL implications of the aforementioned
health-related problems and unhealthy behaviours (Richardson et al 2009)
Evidence for an interaction between lifestyle and these chronic conditions commences with
the findings reported by Bekkering et al (2006) as part of the WCRF review being updated
Further evidence identified from the search criteria will then be presented Evidence will be
presented by cancer site (eg breast colorectal lung prostate) where appropriate whilst
some evidence will pertain to one cancer site only (ie breast cancer related lymphoedema)
72
CANCER-RELATED FATIGUE (CRF)
Cancer-related fatigue (CRF) is defined as ldquoa distressing persistent subjective sense of
physical emotional andor cognitive tiredness or exhaustion related to cancer or cancer-
related treatment that is not proportional to recent activity and interferes with usual
functioningrdquo (NCCN 2009) It has overtaken nausea and pain as the most distressing
symptom experienced by people with cancer during and after treatment It is reported by 60-
96 of patients during chemotherapy radiotherapy or after surgery and can last for months
or even years following treatment (Wagner and Cella 2004 Thomas 2005 NCCN 2009) It
can have a profound effect on physical emotional and social well-being and can hinder
chance of remission owing to non-compliance with treatment due to the intensity of this side-
effect (Lucia Earnest and Perez 2003 Velthuis et al 2009)
The specific causes of CRF are not fully understood but there are several associated
conditions which can aggravate it These include anaemia electrolyte imbalance liver
failure and steroid withdrawal (Thomas 2005) Some conditions can also cause fatigue by
disturbing sleep patterns such as anxiety depression nocturia (a need to get up in the night
to urinate) night sweats and pruritus (itching) The self-management strategy most
extensively investigated for CRF is physical activity the evidence for which is presented
next Studies identified in the current review are summarised in Table 8 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in women with breast cancer In the current review 4 systematic reviews
three of which included a meta-analysis and 2 additional studies were identified
The first review by McNeely et al (2006) reported on 14 RCTs Despite significant
heterogeneity and relatively small samples the overall finding was that physical activity led
to statistically significant improvements in reducing symptoms of fatigue Two meta-
analyses added to this evidence The first by Cramp and Daniel (2008) evaluated 28
studies (n=2083 participants) the majority of which comprised participants with breast
cancer (n=16 studies n=1172 participants) A pooled meta-analysis of all available data
convincingly showed that physical activity was statistically more effective in reducing
CRF when compared to less active controls In the second meta-analysis Velthuis et al
(2009) reviewed 18 studies 12 of which comprised women with breast cancer Pooled
results of these 12 studies (n=674 patients) showed a small significant reduction of CRF
in favour of the physical activity group compared to the non-physical activity group
When Velthuis et al (2009) subdivided the 12 studies into two main physical activity
strategies (ie home-based versus supervised classes) home-based physical activity (n=
7 studies) led to a small non-significant reduction in CRF whereas supervised
73
aerobic physical activity (n=5 studies) showed a medium significant reduction
in CRF when compared to no intervention
Fillion et al (2008) conduced an RCT demonstrating that combining supervised walking
training with psycho-educational stress management produced significant improvements
relative to usual care for fatigue vigour anxiety and depression but not for physical
fitness This suggests a psychological benefit to physical activity which might assist in
coping with physical symptoms such as fatigue Poudevigne et al (2009)
examined adherence to 12-weeks of moderate intensity combined cardio-respiratory and
resistance training and any subsequent impact on levels of fatigue in sedentary breast
cancer survivors (n=20) 2-24 months post-treatment Not only was the training acceptable
and safe but significant decreases in fatigue (43) were also found across the12-
weeks
Danhauer et al (2009) conducted an RCT with women (n=44) who had breast cancer 34
of whom were undergoing cancer treatment in order to examine the effects of restorative
yoga between those in treatment and those not in treatment Randomisation was to a
programme of 10-weekly 75-minute yoga classes or a waiting list control group The yoga
group demonstrated a significant within-group improvement in fatigue although no
significant difference was found with the control group
In updating a previous systematic review by Schmitz et al (2005) of RCTs examining
physical activity in cancer survivors during and after treatment Speck et al (2010)
accumulated data from a further 82 studies (n=6838 participants) Of the 82 studies 66
were rated as high quality and analysed for mean effect sizes resulting from physical activity
interventions The most common diagnosis included was breast cancer (83) with 40 of
studies conducting interventions during cancer treatment and 60 post-treatment Mean
effect sizes demonstrated a large effect of physical activity interventions post-
treatment on upper and lower body strength (plt00001 and 0024 respectively) and
moderate effects on fatigue and breast cancer-specific concerns (p=0003 and 0003
respectively) The most notable progression from their previous review was that the
benefits of physical activity on fatigue moved from negative findings to the evidence
reflecting significantly reduced fatigue post-treatment in physically active survivors
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
managing CRF in men with prostate cancer In the current review 3 systematic reviews two
of which included a meta-analysis and 2 additional studies were identified In the current
review four studies were identified
Windsor Nichol and Potter (2004) published a study of 65 patients with prostate cancer
receiving radiotherapy who were randomly allocated to a home-based physical activity
programme or standard supportive care The home-based exercise included walking 30-
minutes three times a week with an intensity of 60-70 heart rate max for the duration of
74
radiotherapy No adverse events were reported and a non-significant reduction of CRF
was found in the physical activity group when compared to the standard care group
In the abovementioned meta-analysis conducted by Velthuis et al (2009) three RCTs in men
with prostate cancer investigated the effectiveness of supervised physical activity during
radiotherapy and androgen deprivation therapy (Segal et al 2003 Monga et al 2007
Segal et al 2009) In two studies men allocated to the intervention group participated three
times a week in a supervised physical activity programme comprising aerobic exercises with
an intensity of respectively 65 of the maximum heart frequency (HR max) adjusted for
age and 50-75 of the VO2peak (15-45 minutes) (Monga et al 2007 Segal et al 2009)
In the third study the intervention comprised resistance exercises 2-3 times a week with an
intensity of two sets of 8-12 repetitions 60-70 of the one repetition maximum (Segal et
al 2003) Pooled results from the two supervised aerobic studies showed a large non-
significant reduction in CRF in favour of the physical activity group (Monga et al
2007 Segal et al 2009) The resistance exercise study showed a small non-significant
reduction in CRF in favour of the physical activity group (Segal et al 2003) In the latter
study over 80 of the participants were reported to have completed the programme
however the programme did result in one knee injury chest pain fainting and an acute
myocardial infarction
c) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) report on one RCT comparing the impact of a 3-weeks aerobic
physical activity (stationary biking 30-minutes five times weekly) intervention versus
relaxation training (45-minutes three times per week) in post-surgery survivors (n=72) of lung
(n=27) and gastrointestinal (n=42) cancer (Dimeo et al 2004) Fatigue improved
significantly in both groups during the intervention although there was no significant
difference between groups This suggests that relaxation training can be equally as
effective as aerobic physical activity in relieving symptoms of fatigue
In the current review 3 further studies were identified
There has been one study in patients with multiple myeloma (Coleman et al 2003) which
included a home-based physical activity programme during chemotherapy and peripheral
blood stem cell transplantation The programme comprised a combination of aerobic and
resistance exercises three times a week for 20-minutes for the duration of the
chemotherapy (6-months) No adverse events were reported and a small non-significant
reduction in CRF was found in the physical activity group compared to a control
group who did not receive the intervention
Chang et al (2008) published a study involving patients with acute myelogeous leukemia
(n=22) which included allocation to the intervention group a three week supervised walking
programme during chemotherapy Participants walked five times a week for 12-minutes in
the hospital hallway The programme was completed by 69 of the participants and no
75
adverse events were reported A medium-sized non-significant reduction in CRF was
found
In a cross-sectional postal survey of ovarian cancer survivors (n=359) self-report measures
of physical activity and CRF demonstrated that those meeting physical activity guidelines of
the Centres for Disease Control and Prevention (ie minimum 25-hours of moderate
intensity aerobic activity every week plus muscle-strengthening activities on two or more
days of the week) reported significantly lower fatigue than those not meeting guidelines
(Stevinson et al 2009) There was however no evidence of a dose-response relationship
SUMMARY OF EVIDENCE FOR CANCER-RELATED FATIGUE
Evidence from 28 RCTs and 2 meta-analyses has demonstrated that physical activity
programmes can reduce the severity of CRF The studies reviewed here also show that
supervised aerobic exercise programmes were more effective in reducing CRF during breast
cancer treatment than home-based exercise advice Although more research on the optimal
timing and duration of physical activity would be useful these studies are sufficiently robust
to recommend that tailored physical activity advice be integrated into individualized care
plans
As identified in a consultation and evidence review designed to determine the priorities of
cancer survivorship research there is a modest amount of research testing physical activity
interventions for fatigue some demonstrating benefits during treatment but inconclusive
evidence for after treatment (Richardson et al 2009) Although there is clinical
heterogeneity between published RCTlsquos in terms of physical activity duration frequency and
intensity a sensible pragmatic approach based on the trials which showed most benefit is to
supervise a moderate intensity physical activity regimen of regular frequency (3-5
timesweek) for 20-30 minutes per session involving aerobic resistance or mixed physical
activity types With evidence suggesting that low intensity physical activity can also be
beneficial during cancer treatment consideration is warranted in terms of promoting physical
activity from diagnosis onwards potentially making physical activity uptake less challenging
post-treatment (Velthuis et al 2009) Further research is required to determine the optimal
type intensity and timing of physical activity interventions at different periods of the disease
trajectory and when experiencing other cancer-related symptoms or late effects
An exemplary physical activity programme available to survivors of breast colorectal and melanoma cancers is the BACSUP (Bournemouth After Cancer Survivorship Project) Active Wellness Programmelsquo developed in partnership with Royal Bournemouth Hospital NHS Bournemouth and Poole Bournemouth University and MacMillan Cancer Support (Milne et al 2010) The programme involves two initial one-to-one consultations including a holistic assessment with a trained member of staff to tailor the programme to individual needs A readiness check is done prior to referral a readiness to be physically active score of gt70 is required for participation Participants receive a telephone call at 3-weeks for the provision of support and encouragement followed by a one-to-one review at 6-weeks to assess progress and maintain motivation A one-to-one review and reassessment is also provided at 12-weeks to measure improvements Additional support options are available such as the BACSUP Active Wellness Group which provides an opportunity to meet others survivors and listen to life improvement guest speakers In a pilot study of the programme survivors who had completed primary treatment within the previous 5-years (n=180) were referred to the service 58 completed the programme 65 are currently on the programme 30 started but are on hold due to circumstances 21 were not yet ready to join the scheme
At 12-weeks 92 of participants reported reduced fatigue
76
Table 8 Cancer-Related Fatigue and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Chang et al (2008)
RCT to preliminarily examine the effects of a three-week walking exercise program (WEP) on fatigue-related experiences of acute myelogenous leukaemia (AML) patients receiving chemotherapy Eligible AML patients were randomly assigned to either an experimental group (n = 11) which received 12 minutes of WEP per day five days per week for three consecutive weeks or to a control group (n = 11) which received standard ward care
Patients with acute Myelogenous leukaemia (AML) receiving chemotherapy (n=22)
All patients were evaluated four times before treatment (baseline or Day 1) Day 7 Day 14 and Day 21
Worst and average fatigue intensities fatigue interference with patients daily life 12-minute walking distance overall symptom distress anxiety and depressive status
AML patients in the three-week WEP group had a significantly greater increase in 12-minute walking distance than the control group Patients in the WEP also had lower levels of fatigue intensity and interference symptom distress anxiety and depressive status than the control group
Coleman et al(2003)
A pilotfeasibility study with a randomized controlled design was conducted to investigate home-based exercise therapy for patients receiving high-dose chemotherapy and autologous peripheral blood stem cell transplantation as treatment for multiple myeloma
24 patients with multiple myeloma
Not reported Fatigue mood disturbance body weight
Because of the small sample size in the feasibility study the effect of exercise on lean body weight was the only end point that obtained statistical significance However the results suggest that an individualised exercise program for patients receiving aggressive treatment for multiple myeloma is feasible and may be effective for decreasing fatigue and mood disturbance and for improving sleep
Cramp and Daniel (2008)
Systematic review with meta-analysis to evaluate the effect of exercise on cancer-related fatigue both during and after cancer treatment
2083 participants from RCTs comprising cancer patients and survivors
Follow-up assessment of long-term outcomes was poor with 18 of 28 studies failing to assess outcomes beyond the end of the intervention
Cancer-related fatigue
28 studies were identified for inclusion with the majority carried out on participants with breast cancer (n = 16 studies n = 1172 participants) A meta-analysis of all fatigue data incorporating 22 comparisons provided data for 920 participants who received an exercise intervention and 742 control participants At the end of the intervention period exercise was statistically more effective than the control intervention (SMD -023 95 CIs -033 to -013)
77
period
Danhauer et al (2009)
Randomised pilot study to determine the feasibility of implementing a restorative yoga intervention for women with breast cancer and to examine group differences in self-reported emotional health-related quality of life and symptom outcomes 10 weekly 75-minute yoga classes
Women with breast cancer (n=544) 34 of whom were actively undergoing cancer treatment
Immediately post-intervention (week 10)
Emotional well-being QoL fatigue
Group differences favouring the yoga group were seen for mental health depression positive affect and spirituality (peacemeaning) Significant baselinegroup interactions were observed for negative affect and emotional well-being Women with higher negative affect and lower emotional well-being at baseline derived greater benefit from the yoga intervention compared to those with similar values at baseline in the control group The yoga group demonstrated a significant within-group improvement in fatigue no significant difference was noted for the control group
Fillion et al (2008)
RCT to verify the effectiveness of a 4-week nurse-led group intervention that combines stress management psycho-education and physical activity (ie independent variable) intervention in reducing fatigue and improving energy level quality of life (mental and physical) fitness (VO2submax) and emotional distress (ie dependent variables) in breast cancer survivors Participants were randomly assigned to either the group intervention (experimental) or the usual-care (control) condition
French-speaking women who had completed their treatments for non-metastatic breast cancer (n=87)
Post-intervention and at 3-months follow-up
Fatigue emotional distress QoL
Participants in the intervention group showed greater improvement in fatigue energy level and emotional distress at 3-month follow-up and physical quality of life at post-intervention compared with the participants in the control group
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials MEDLINE
EMBASE CINAHL Psych INFO CancerLit PEDro
and SportDiscus as well
as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
function
ing as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all
outcomes were positive even when statistical significance was not
achieved Exercise led to statistically significant improvements in
quality of life as assessed by the Functional Assessment of
Cancer TherapyndashGeneral (weighted mean difference [WMD] 458
95 CI 035 to 880) and Functional Assessment of Cancer
TherapyndashBreast (WMD 662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak
oxygen consumption and in reducing symptoms of fatigue
Poudevigne et al (2009)
Cohort study examining the effects of a 12-week cross training intervention on fatigue and mood in breast cancer survivors The training consisted of a 12-week exercise program of 3 weekly
20 sedentary breast cancer survivors between 2-24 months post-
On completion of the 12-week intervention
Fatigue and mood disturbances (Profile of Mood States) QoL
The mean (plusmnSD) attendance rate was 92 (plusmn80) No musculoskeletal injuries and problematic symptoms occurred during the cross-training Repeated measures ANOVA showed a large increase in QOL (22) and significant decrease in fatigue (43) across 12 weeks (eta squared range 491 to708 all p
78
sessions of 60 min duration supervised by a certified personal trainer and divided into resistance (30 minutes) and aerobic training (5 minutes warm-up 20 minutes training 5 minutes cool-down) The aerobic intensity was set at 60HRR and re-evaluated every three weeks
treatment Treatments ranged from lumpectomies (23) mastectomies (29) radiations (32) and chemotherapy (16)
(SF-36) and work absenteeism
valueslt05) No differences were found in work absenteeism Blood pressure was unchanged after training
Stevinson et al (2009)
A cross-sectional postal survey to investigate the associations between physical activity and health-related outcomes in ovarian cancer survivors and to examine any dose-response relationship
Ovarian cancer survivors (n=359) on and off treatment
Not reported Fatigue peripheral neuropathy sleep and psychosocial functioning
311 of participants were meeting the public health physical activity guidelines - those meeting guidelines reported significantly lower fatigue than those not meeting guidelines (mean difference 71 95 confidence interval 55-88 d = 087 Plt 0001) Meeting guidelines was also significantly inversely associated with peripheral neuropathy depression anxiety sleep latency use of sleep medication and daytime dysfunction and was positively associated with happiness sleep quality and sleep efficiency
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types were included with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) With few exceptions exercise was well tolerated during and post treatment without adverse events
Velthuis et al (2009)
Meta-analysis to evaluate the effects of different exercise prescription parameters during cancer treatment on cancer-related fatigue (CRF) A systematic search of CINAHL Cochrane Library Embase
RCTs studying the effects of exercise during cancer treatment on
Not reported Cancer-related fatigue
During breast cancer treatment home-based exercise lead to a small non-significant reduction (standardised mean difference 010 95 confidence interval minus025 to 045) whereas supervised aerobic exercise showed a medium significant reduction in CRF (standardised mean difference 030 95 confidence interval 009
79
Medline Scopus and PEDro was carried out
CRF (n=18) 12 in breast 4 in prostate and 2 in other cancer patients)
to 051) compared with no exercise A subgroup analysis of home-based (n = 65) and supervised aerobic (n = 98) and resistance exercise programmes (n = 208) in prostate cancer patients showed no significant reduction in CRF in favour of the exercise group Adherence ranged from 39 of the patients who visited at least 70 of the supervised exercise sessions to 100 completion of a home-based walking programme
Windsor Nichol and Potter (2004)
A prospective RCT to determine whether aerobic exercise would reduce the incidence of fatigue and prevent deterioration in physical functioning during radiotherapy for localised prostate carcinoma
33 men in exercise group and 33 men in control group
4-weeks post-radiotherapy
Fatigue and distance walked in a modified shuttle test before and after radiotherapy
There were no significant between group differences noted with regard to fatigue scores at baseline (P = 055) or after 4 weeks of radiotherapy (P = 018) Men in the control group had significant increases in fatigue scores from baseline to the end of radiotherapy (P = 0013) with no significant increases observed in the exercise group (P = 0203)
80
LYMPHOEDEMA
Lymphoedema is the excessive accumulation of tissue fluid (or lymph) that results from
impaired lymphatic drainage resulting in swelling of the limb The most common type of
lymphoedema in cancer survivors is most frequently the result of treatment for breast
cancer where an important prognostic indicator is the removal and evaluation of lymph
nodes (Morrell et al 2005) Removal of the lymph nodes can result in a number of side-
effects including lymphoedema (Swenson et al 2002) which manifests usually as a
swelling to the affected arm but can also occur in the hand trunk and breast The more
lymph nodes that are removed the higher the risk of developing the condition providing an
objective measure of risk that could be utilised in the provision of evidence-based
lifestyle and self-management support based on individuals needs
The condition can develop immediately or many years after treatment (Mortimer et al
1996) in either case lymphoedema is a chronic debilitating condition that can cause severe
physical and psychological morbidity as well as a reduction in QoL (Deo et al 2004)
The self-management strategy most extensively investigated for lymphoedema is physical
activity with some evidence also being available for diet Studies identified in the current
review are summarised in Table 9 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) do not provide any evidence for the role of physical activity in
preventing or managing lymphoedema In the current review one systematic review
(including a meta-analysis) and 3 studies were identified
In a prospective RCT testing the efficacy of two types of physiotherapy on shoulder function
and lymphatic disturbance in post-operative breast cancer survivors (n=60) participants
received one of two types of physiotherapy 48-hours post-surgery (de Rezende et al
2006)
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-
defined sequence of movements
2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely
to music
Lymphoedema is estimated to affect
about 30 of breast cancer survivors
post-treatment (Deo et al 2004)
81
Results indicated significantly better recovery of limb movement in the directed group
compared to the free group with there being no significant difference between groups in
terms of lymphatic disturbance
Ahmed et al (2006) report on a 6-month RCT examining the effects of supervised upper-
and lower-body weight training on lymphoedema incidence and symptoms in breast cancer
survivors (n = 45) 4-36 months post-treatment From baseline to 6-months three control-
group participants reported an increase in lymphoedema symptoms No participants in the
intervention group reported such symptoms suggesting that twice-a-week progressive
weight training does not increase the onset of or exacerbate lymphoedema in breast cancer
survivors (13 women had lymphoedema at baseline) The results from this study indicate
that at minimum physical activity does not exacerbate lymphoedema
Moseley and Piller (2008) reviewed the literature for evidence supporting the benefits of
physical activity for people with limb lymphoedema Their key findings from eleven studies
demonstrated that
physical activity can improve lymph clearance
physical activity can help reduce limb volume and improve subjective symptoms and
QoL
benefits from physical activity have been sustained post-physical activity regime in
some studies
physical activity is a viable option for people with lymphoedema
Moseley and Pillerlsquos (2008) conclusions were supported further in a recent RCT by Hayes
Hildegard and Turner (2009) Breast cancer survivors at least 6-months post-treatment
who had developed unilateral upper-limb lymphoedema participated in twenty supervised
group aerobic and resistance physical activity sessions over 12-weeks (n=16) or continued
habitual activities (n=16) Average attendance was more than 70 of supervised sessions
and there were no withdrawals Mean ratio and volume measures at baseline were similar
between the two groups and no changes were observed at 3-months follow-up for either
group although two women receiving supervised physical activity no longer had evidence of
lymphoedema by study completion The results from this review as with the RCT by
Ahmed et al (2006) indicate that at minimum physical activity does not exacerbate
secondary lymphoedema
In the review referred to previously by Speck et al (2010) with minor exceptions findings
indicated aerobic lifestyle and upper body resistive exercise was tolerated by breast cancer
survivors with no adverse effects on the development or exacerbation of lymphoedema
ii DIET
Bekkering et al (2006) report on one double-blind placebo-controlled RCT examining diet
and lymphoedema in breast cancer survivors (n=68) at a mean of 155-years post-treatment
For 6-months women received 500mg twice a day of dl-alpha tocopheryl acetate (a source
of vitamin E) plus pentoxifylline (a drug that improves blood circulation) 400mg twice a day
82
of dl-alpha tocopheryl acetate or placebo (Gothard et al 2004) At 6-months and 12-months
post-randomisation there was no significant difference between groups in terms of arm
volume
The current review identified one RCT
Dietary Fat
In a UK RCT Shaw Mortimer and Judd (2007) demonstrate the impact of diet and weight
loss on post-treatment arm lymphoedema in breast cancer survivors (n=51) Women were
assigned to one of three 24-week dietary groups
1) a low-fat diet (fat intake reduced to 20 of total energy intake)
2) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ)
3) a control group (continuing their usual diet)
After the end of the 24-week period of dietary intervention there was a slightly greater
reduction in excess arm volume in both dietary intervention groups compared with the
control although this was not statistically significant Furthermore despite low levels of
adherence to dietary advice weight loss was achieved in all groups demonstrating that
dietary interventions can assist in reducing excess arm volume in women with post-
treatment lymphoedema
SUMMARY OF EVIDENCE FOR LYMPHOEDEMA
The studies evaluated within this review indicate a need to re-assess the common clinical
guidelines that breast cancer survivors avoid upper body resistance activity for fear of
increasing risk of lymphoedema(Speck et al 2010) They also indicate a requirement to
develop guidelines for appropriate physical activity As concluded by Hayes Hildegard and
Turner (2009) women with secondary lymphoedema should be encouraged to be physically
active optimising their physical and psychosocial recovery Resistance exercise does not
increase the risk for or exacerbate symptoms of lymphoedema and in fact directed physical
activity 48-hours post-surgery might offer greater utility in terms of rehabilitation outcomes
Some of the studies evaluated in the review by Moseley and Piller (2008) comprised small
sample sizes and did not include control groups however when combined with other studies
presented within this review there is some support for encouraging physical activity in breast
cancer survivors Furthermore physical activity combined with changes in diet and
subsequent weight loss in survivors who are overweight might significantly reduce the
symptoms of lymphoedema although evidence for diet in reducing symptoms of
lymphoedema is limited
Weight loss across groups
9 (60) in the control group 13 (76) in the low-fat diet group 18 (95) in the weight-reduction
group
83
Table 9 Lymphoedema and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Ahmed et al (2006)
RCT comparing supervised twice weekly upper- and lower-body weight training over 6-months with control group completing no training
Breast cancer survivors (n = 45) 4-36 months post-treatment
6-months post-intervention
Incidence and symptoms of lymphoedema
From baseline to 6-months three control-group participants
reported an increase
in lymphoedema symptoms No
participants in the intervention group reported such symptoms suggesting that
twice-a-week progressive weight training does not
increase the onset of or exacerbate lymphoedema in breast
cancer
survivors
de Rezende et al (2006)
RCT examining the impact of physiotherapy on lymphoedema Participants received one of two types of physiotherapy
1) 40-minutes directed physiotherapy three times a week for 42-days following a pre-defined sequence of movements 2) 40-minutes free-moving physiotherapy three times a week for 42-days moving freely to music
48-hours post-surgery breast cancer survivors (n=60)
On completion of intervention (42-days)
Shoulder movement and lymphatic disturbance
Significantly better recovery of limb movement in the directed group compared to the free group with there being no significant difference between groups in terms of lymphatic disturbance
Hayes Hildegard and Turner (2009)
An RCT testing the impact of aerobic exercise on lymphoedema outcomes Participants randomised to 1) 20 supervised group aerobic and resistance physical activity sessions over 12-weeks (n=16) 2) continued habitual activities (n=16)
Breast cancer survivors at least 6-months post-treatment who had developed unilateral upper-limb lymphoedema
3-months post-intervention
Arm volume measurements
Mean ratio and volume measures at baseline were similar between the two groups and no changes were observed at 3-months follow-up for either group although two women receiving supervised physical activity no longer had evidence of lymphoedema by study completion
84
Moseley and Piller (2008)
Literature search of the evidence supporting the benefits of exercise for those with limb lymphoedema
Exercise studies undertaken in RCTs or cohort studies and involving secondary limb lymphoedema (with no active cancer)
Varied from post-intervention to 8-weeks follow-up
Change in limb volume and subjective symptoms
Exercise has been shown to improve lymph propulsion and clearance help reduce limb volume and improve subjective symptoms and quality of life Benefits from exercise have been sustained post-exercise regime in some studies Exercise is a viable option for those with limb lymphoedema
DIET
Gothard et al (2004)
A double-blind placebo-controlled randomised phase II trial Participants were randomised to active drugs or placebo All volunteers were given dl-alpha tocopheryl acetate 500 mg twice a day orally plus pentoxifylline 400 mg twice a day orally or corresponding placebos for 6 months
68 volunteers with a minimum 20 increase in arm volume at a median 155 years after radiotherapy (plus axillary surgery in 5168 (75) cases)
12 months post-randomisation
Volume of the ipsilateral limb measured
There was no significant difference between treatment and control groups in terms of arm volume Absolute change in arm volume at 12 months was 25 (95 CI minus040 to 53) in the treatment group compared to 12 (95 CI minus28 to 51) in the placebo group The difference in mean volume change between randomisation groups at 12 months was not statistically significant (P=06) minus13 (95 CI minus61 to 35) nor was there a significant difference in response at 6 months (P=07) where mean change in arm volume from baseline in the treatment and placebo groups was minus23 (95 CI minus79 to 34) and minus11 (95 CI minus39 to 17) respectively
Shaw Mortimer and Judd (2007)
Participants were assigned to one of three 24-week dietary groups in order to assess impact on arm volume 1)a low-fat diet (fat intake reduced to 20 of total energy intake) b) a weight reduction diet (daily energy intake reduced to 1000-1200kcal 42-50MJ) c) a control group (continuing their usual diet)
Breast cancer survivors (n=51)
After 24-weeks of intervention
Arm volume There was a slightly greater reduction in excess arm volume in both dietary intervention groups compared with the control although this was not statistically significant
85
OSTEOPOROSIS AND BONE HEALTH
Osteoporosis is a condition in which the bones become less dense and more likely to
fracture which in turn can result in significant pain and disability It is known as a silent
disease because if undetected bone loss can progress for many years without symptoms
until a fracture occurs Risk factors for developing osteoporosis are often enhanced in
cancer survivors such as being post-menopausal and having had early menopause (Ada et
al 2002) Low calcium intake lack of physical activity smoking and excessive alcohol
consumption are also risk factors for osteoporosis (Guthrie et al 2000) Women who have
had breast cancer treatment may be at increased risk for osteoporosis and fracture due to
reduced levels of oestrogen whilst men who receive hormone deprivation therapy for
prostate cancer also have an increased risk of developing osteoporosis and broken bones
(National Institutes of Health Osteoporosis and Related Bone Diseases 2009)
There are no early symptoms of osteoporosis but diet physical activity and drug treatment
can prevent or reverse loss of BMD highlighting the importance of lifestyle choices in
osteoporosis outcomes Studies identified in the current review are summarised in Table 10
at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any physical activity studies examining osteoporosis
in breast cancer survivors The current review identified 3 RCTs and one cohort study
Schwartz Winters-Stone and Gallucci (2007) evaluated the impact of aerobics and
resistance training on BMD in an RCT involving women with histologically confirmed invasive
stage I-III breast cancer (n=66) beginning chemotherapy Women were randomised to one
of three groups and stratified according to menopausal status (pre-menopausal or post-
menopausal)
1) Home-based aerobic exercise - women were instructed to choose an aerobic activity
they enjoyed (eg walking jogging) and exercise for 15-30 minutes four days per
week for the duration of the study at a symptom-limited moderate intensity such that
they were breathing hard but able to talk
2) Home-based resistance exercise ndash women were instructed to exercise at home four
days per week using resistance bands and tubing
3) Usual care
It has been reported that 80 of older breast cancer survivors have osteopenia (below normal bone-mineral density [BMD]) or osteoporosis at initial diagnosis (Twiss et al 2001)
86
The average decline in BMD was -623 for usual care -492 for resistance exercise and
-076 for aerobic exercise suggesting that weight-bearing aerobic exercise attenuates
declines in BMD Pre-menopausal women demonstrated significantly greater declines in
BMD than post-menopausal women highlighting a need to provide interventions for bone
health on a risk stratification basis
Gross et al (2002) examined the intensity of physical activity (ie light moderate vigorous)
reported by a cohort of post-menopausal breast cancer survivors (n=27) and found no
relationship between activity levels and BMD However participants mainly reported light
physical activity limiting the examination of moderate and vigorous activity outcomes It is
possible that a higher intensity of physical activity is required to achieve any benefits to bone
health
Waltman et al (2009) conducted an RCT testing a 24-month self-efficacy based strength
and weight training programme on post-treatment (except tamoxifen and aromatase
inhibitors) post-menopausal breast cancer survivors (n=223) who had amenorrhea
(absence of menstruation) for at least 12-months and a bone BMD score lower than the
norm (Figure 1)
Figure 1 Bone Density Definitions
WHO Definitions of Osteoporosis
Based on Bone Density
T-Scores
BMD
Category
Examples
Range
10
05
0
-05
-10
-1 and
above Normal BMD
-15
-20
Between
-1 and -25
Low BMD
(Osteopenia)
-25
-30
-35
-40
-25 and
below Osteoporosis
Source WHO (2003)
The women were randomised to receive physical activity with medication (n=110) or
medication only (n=113) The medication taken by both groups included risedronate
(osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily) While
87
participation in strength training did not result in statistically significant improved BMD there
was a trend towards at least maintaining BMD at the total hip Participants who were 50
or greater adherent to the intervention (reasons for non-adherence included lack of
time or chronic pain due to co-morbidity) were significantly less likely than
participants on medication alone to lose BMD at the total hip and femoral neck
In a third RCT Swenson et al (2009) compared the effects of two interventions on changes
in BMD in women receiving chemotherapy for breast cancer (n=62)
1) intravenous zoledronic acid (used to prevent skeletal fractures in people with cancer)
and oral calciumvitamin D every 3-months for five treatments
2) prescribed home-based physical activity and oral calciumvitamin D
Zoledronic acid protected patients with breast cancer against bone loss during initial
treatment whereas the home-based physical activity intervention was less effective in
preventing bone loss indicating that physical activity and dietary supplements are not
always sufficient to protect done density in people with cancer However these were
patients undergoing treatment and more research is required into the effects of physical
activity on bone health in post-treatment survivors
ii DIET
Bekkering et al (2006) did not identify any diet studies examining osteoporosis in breast
cancer survivors The current review identified 3 RCTs and one cohort study
Plant Proteins and Fibres
Weikert et al (2005) performed a sub-analysis of the EPIC cohort study conducted in
Germany which included 8178 females and examined the association between protein
intake dietary calcium and bone structure It was concluded that high consumptions of
animal protein may be unfavourable whereas higher vegetable protein may be
beneficial to bone health These results support the hypothesis that high calcium intakes
combined with adequate protein intake based on a high ratio of vegetables to animal protein
may be protective against osteoporosis Indeed evidence has demonstrated the relationship
between lower incidence of osteoporosis in Asian women and vegetarian populations due to
a diet rich in vegetables and fruit (Fujii et al 2009 Merill and Aldana 2009 Thorpe et al
2008) Furthermore a large-scale dietary modification intervention of post-menopausal
women (n = 4883) showed that an increased consumption of plant proteins and fibres from
fruits vegetables and grains reduced the risk of multiple falls and slightly lowered hip BMD
although it did not change the risk of osteoporotic fractures (McTiernan et al 2009)
New et al (2003 2004) provides further evidence for the benefits of plant proteins and fibres
on bone health in two reviews where a positive link between a high consumption of fruit
and vegetables and bone health has been demonstrated In the first report it was found
that fruit and vegetables have beneficial effects on bone mass and bone metabolism in men
and women across the age ranges whilst in the second review it was concluded that
although the impact of a vegetarian diet on bone health is much more complex than merely
being related to diet vegetarians do tend to have normallsquo bone mass
88
iii WEIGHT
Bekkering et al (2006) did not identify any studies examining weight implications on
osteoporosis in breast cancer survivors The current review identified one study that found
that being underweight (BMI less than 185) was associated with lower BMD (Ryan et al
2007)
b) PROSTATE CANCER
i WEIGHT
Bekkering et al (2006) did not identify any studies examining the effect of body weight on
osteoporosis in prostate cancer survivors The current review identified one RCT Ryan et
al (2007) found a positive association between BMI and bone density of the hip in men with
prostate cancer (n=120) who were within the first 12-months of androgen-deprivation
therapy This suggests that a higher BMI can be protective of bone density loss in this
patient group
ii ALCOHOL
Bekkering et al (2006) did not identify any studies examining the effect of alcohol
consumption on osteoporosis in prostate cancer survivors The current review identified one
RCT Ryan et al (2007) also demonstrate greater bone density in prostate cancer patients
consuming seven or more weekly alcoholic beverages when compared to non-drinkers
a) OTHER CANCER
i DIET
Soya Products
Bekkering et al (2006) did not identify any studies examining the effect of diet on
osteoporosis in other cancer survivors The current review identified one RCT Marini et al
(2008) reported a randomised double-blind placebo-controlled trial of the soya derivative
genistein aglycone and its effects on bone health after 3-years in women with breast and
endometrial cancer (n=389) Bone mineral density increases were greater with
genistein for both femoral neck and lumbar spine compared to placebo the conclusion
being that after 3-years of treatment genistein exhibited a promising safety profile with
positive effects on bone formation in this cohort of osteopenic post-menopausal women
89
SUMMARY OF EVIDENCE FOR OSTEOPOROSIS AND BONE HEALTH
There is evidence that vitamin D and calcium might be associated with greater BMD
however this benefit cannot be distinguished from other potential contributors such as
physical activity and medication More research is needed into the effects of physical activity
on osteoporosis in cancer survivors The findings thus far offer different conclusions
although there is limited evidence that physical activity can at the very least prevent loss of
BMD which is a positive outcome in survivors at particular risk of bone loss Greater
adherence to physical activity interventions appeared to offer the greater benefits
highlighting the importance of designing lifestyle interventions that can be maintained as
well as providing higher intensity support for survivors with co-morbidities
Higher BMI has been found to be protective of BMD loss in men with prostate cancer
however no distinction has been made between higher BMI and a BMI that indicates excess
weight Limited evidence has been provided for the benefits of moderate alcohol
consumption but as with the evidence presented for weight much more research is needed
before any valid and reliable conclusions can be made Since the NHS advises no more than
3-4 units of alcohol per day for men more research is needed to determine the minimum
units of alcohol that offer such protective benefits It is important to deter against excessive
drinking which can have a number of serious health implications including high blood
pressure mouth and throat cancers and stroke (NHS 2010)
Men should not exceed 3-4 units of alcohol per day on a regular basis (NHS 2010) One unit is the amount of pure alcohol in a 25ml single measure of spirits (pure alcohol by volume [ABV] 40) a third of a pint of beer (ABV 5-6) or half a 175ml standardlsquo glass of red wine (ABV 12) Daily alcohol limits are provided by the NHS in order to discourage the belief that that the number of units of a weekly limit can be consumed at once (ie binge drinking) Use of daily limit
90
Table 10 Osteoporosis and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Gross et al (2002)
Descriptive correlational test of a multicomponent intervention to prevent and treat osteoporosis in breast cancer survivors
27 post-menopausal breast cancer survivorslsquo post- treatment except for tamoxifen
Not reported
Physical activity vigour vitality and BMD
More than half reported no very hard physical activity and 37 reported no hard activity The association of vigour with total metabolic equivalents for combined moderate hard and very hard activities was significant (r = 0536 p = 0007) as were the hours spent in the combined moderate to very hard activities No relationship was found between vigour vitality or any level of activity and BMD
Schwartz Winters-Stone and Gallucci (2007)
RCT testing the effects of aerobic and resistance exercise on changes in bone mineral density (BMD) in women receiving chemotherapy Participants were randomised to aerobic or resistance exercise and usual care
66 women with stage I-III breast cancer beginning adjuvant chemotherapy
6-months after starting treatment
BMD aerobic capacity and muscle strength
Aerobic exercise preserved BMD significantly better compared to usual care Premenopausal women demonstrated significantly greater declines in BMD than postmenopausal women Aerobic capacity increased by almost 25 for women in the aerobic exercise group and 4 for resistance exercise Participants in the usual care group showed a 10 decline in aerobic capacity
Swenson et al (2009)
Participants received one of two treatments a) Intravenous zoledronic acid and oral calciumvitamin D every 3-months for five treatments b) Prescribed home-based physical activity and oral calciumvitamin D
Women receiving chemotherapy for breast cancer (n=62)
On completion of 3-month intervention
Severity of lymphedema by arm circumference
BMD significantly decreased in the physical activity group but not in the zoledronic acid group Zoledronic acid protected patients with breast cancer against bone loss during initial treatment whereas the home-based physical activity intervention was less effective in preventing bone loss indicating that physical activity and dietary supplements are not always sufficient to protect done density in people with cancer
Waltman et al (2009)
A 24-month self-efficacy based strength and weight training programme Participants were randomised to receive physical activity with medication (n=110) or medication only (n=113) the medication taken by both groups including risedronate (osteoporosis medication) calcium (1500mg daily) and vitamin D (400IU daily)
Post-treatment post-menopausal breast cancer survivors (n=223) with amenorrhea for at least 12-months and a BMD score lower than the norm
On completion of the 24-month intervention
Bone mineral density
While participation in strength training did not result in statistically significant improved BMD there was a trend towards at least maintaining BMD at the total hip Participants who were 50 or greater adherent to physical activities were significantly less likely than participants on medication alone to lose BMD at the total hip and femoral neck
91
DIET
Marini et al (2008)
RCT assessing the continued safety profile of genistein
aglycone on
breast and endometrium and its effects on bone after
3 years of
therapy Participants received 54mg of genistein
aglycone daily or
placebo both treatment arms
received calcium and vitamin D
Breast cancer patients ndash intervention group (n=71) and placebo (n=67)
After 3-years of treatment
BMD Bone mineral density increases were greater with genistein for both
femoral neck and lumbar spine compared to placebo Genistein also
significantly reduced pyridinoline as well as serum carboxy-terminal
cross-linking telopeptide and soluble receptor activator of NF- B
ligand while increasing bone-specific alkaline phosphatase IGF-I
and osteoprotegerin levels There were no differences in discomfort
or adverse events between groups
(McTiernan et al 2009)
RCT assessing the effect of the Womens Health Initiative
Dietary
Modification low-fat and increased fruit vegetable
and grain
intervention on incident hip total and site-specific
fractures and self-
reported falls and in a subset on bone
mineral density (BMD)
Participants were randomly assigned to
receive
a)dietary modification intervention (daily goal 20 of energy as fat 5 servings of vegetables
and fruit
and 6 servings of grains) b)comparison group
- no dietary
changes
Post-menopausal women (n=48835) intervention (40 n=19541)
versus comparison group (60 n=29294)
Mean=81-years
Incident hip total and site-specific
fractur
es and self-reported falls and in a subset on bone
mineral
density (BMD)
215 women in the intervention group and 285 women in the
comparison group (annualized rate 014 and 012 respectively)
experienced a hip fracture (hazard ratio 112 95 CI 094
134 P = 021) The intervention group (n = 5423 annualized rate
344) had a lower rate of reporting 2 falls than did the
comparison group (n = 8695 annualized rate 367) (HR 092
95 CI 089 096 P lt 001) There was a significant interaction
according to hormone therapy use those in the comparison group
receiving hormone therapy had the lowest incidence of hip fracture In a subset of 3951 women
hip BMD at years 3 6 and 9 was 04ndash
05 lower in the intervention group than in the comparison group
(P = 0003)
New et al (2004)
Literature review assessing the impact of a vegetarian diet on indices of skeletal integrity to address specifically whether vegetarians have a normal bone mass
Analysis of existing literature through a combination of observational clinical and intervention studies were assessed in relation to bone health lacto-ovo-vegetarian and
Not reported
Bone health Key findings included (i) no differences in bone health indices between lacto-ovo-vegetarians and omnivores (ii) conflicting data for protein effects on bone with high protein consumption and low protein intake (particularly with respect to vegan diets) being detrimental to the skeleton (iii) growing support for a beneficial effect of fruit and vegetable intake on bone with mechanisms of action currently remaining unclarified The impact of a vegetarian diet on bone health is a hugely complex area since 1) components of the diet (such as calcium protein alkali vitamin K phytoestrogens) may be varied 2) key lifestyle factors which are
92
vegan diets versus omnivorous consumption of animal versus vegetable protein and fruit and vegetable consumption
important to bone (such as physical activity) may be different 3) the tools available for assessing consumption of food are relatively weak However from data available vegetarians do certainly appear to have normal bone mass
Weikert et al (2005)
Prospective cohort study (EPIC) examining associations between protein intake calcium and bone structure measured by broadband ultrasound attenuation (BUA)
8178 female EPIC participants
Not reported
Bone structure
High intake of animal protein was associated with decreased BUA values ( _ = ndash003 p = 0010) whereas high vegetable protein intake was related to an increased BUA ( _ = 011 p = 0007) The effect of dietary animal protein on BUA was modified by calcium intake
WEIGHT
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and alcohol use was positively associated with the Z score
ALCOHOL
Ryan et al (2007)
Cohort study examining the impact of androgen deprivation therapy (ADT) on loss of bone mineral density (BMD) and fracture risk in men with prostate cancer
120 patients with prostate cancer and without bone metastases who had been treated with ADT for less than 12-months
Not reported
BMD Osteopenia or osteoporosis (T score of less than minus1) was detected in two thirds of the subjects at one or more measured sites The mean baseline BMD Z scores were femoral neck minus0091 plusmn 0959 total hip 0122 plusmn 1005 and lumbar spine 0657 plusmn 1789 On multiple linear regression analysis the duration of ADT was negatively associated with the Z score at all three sites and body mass index was positively associated with the Z score
93
WEIGHT AND BODY COMPOSITION
Weight gain during and after cancer treatment is becoming an ever-increasing significant
concern (Camoriano et al 1990 Levine et al 1991 Saquib et al 2006) Weight gain is
expected when energy intake exceeds energy expenditure a combination that is frequently
described among breast cancer patients who report exercising less during treatment and
after treatment (Schwartz 2000 Demark-Wahnefried 2001) and consuming a higher energy
diet during treatment (Mukhopadhyay and Larkin 1986) Exacerbating this is the fact that
women in general gain weight as they transition through menopause (Sammel et al 2003)
putting breast cancer patients at particular risk as treatments frequently result in a premature
menopause For individuals with bowel cancer the CALBG 8980 trial showed that 35 of
patients post-chemotherapy were overweight (BMI 250ndash299) and 34 were obese BMI
300ndash349) or very obese (BMI gt35) (Meyerhardt et al 2008) The reasons for weight gain
during and after treatment are multifactorial and the result of individual lifestyle behaviours
and the impact of certain cancer drugs Regardless of the reasons as described in part one
of this review both survival and recurrence may be adversely affected by obesity
(Chlebowski et al 2002)
The effect of obesity on survival has been evident in the majority of studies although not all
one reason for this inconsistency being the possibility that biological factors associated with
obesity and not the obesity itself are responsible for the observed effect For example
there is considerable evidence that the effects of obesity on breast cancer risk may be
mediated at least in part by the effect of obesity on insulin resistance (Friedenreich 2001
Suga et al 2001 Goodwin et al 2002)
Finding effective methods for weight loss continues to be a challenge as although some
studies have demonstrated substantial weight loss in obese individuals weight loss results
in general have been modest and new approaches are needed (Jeffery et al 2000) For
long-term reduction in body weight intensive individualised approaches toward developing
a new lifestyle may be required (Djuric et al 2002)
Studies identified in the current review are summarised in Table 11 at the end of this
section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in breast cancer survivors The current review identified one
meta-analysis and three RCTs
In the meta-analysis Kim Kang and Park (2009) reviewed 10 studies involving 588 women
who had been treated for breast cancer examining the effectiveness of aerobic exercise
interventions on cardiopulmonary function and body composition conducted during or after
cancer treatments They concluded that regular aerobic physical activity significantly
improved cardiopulmonary function as assessed by absolute VO2 peak relative VO2
94
peak and 12-minute walk test as well as improved body composition as assessed by
percentage body fat (although body weight and lean body mass did not change
significantly)
Courneya et al (2007) conducted a multicentre RCT in which women with breast cancer on
adjuvant chemotherapy were randomly assigned to usual care (n = 82) supervised
resistance exercise (n = 82) or supervised aerobic exercise (n = 78) for the duration of their
chemotherapy (median = 17-weeks 9-24 weeks) There was 70 adherence to supervised
exercise with aerobic physical activity being superior to usual care for improving
aerobic fitness and percent body fat whilst resistance physical activity was superior
to usual care for improving muscular strength lean body mass and chemotherapy
completion rate
Schmitz et al (2005) evaluated the safety and effects of twice-weekly weight training among
85 breast cancer survivors with women being randomised into immediate or delayed
intervention groups The immediate group trained from months 0-12 the delayed group
served as a no exercise parallel comparison group from months 0-6 and trained from months
7-12 At 6-months the immediate group compared to the no exercise group showed
significantly greater increases in lean mass (p lt 01) as well as significant decreases
in percentage body fat (p lt 05) This significance remained at 12-months when
comparing the immediate group with the delayed exercise group
Mefferd et al (2006) randomised overweight or obese breast cancer survivors (n=85) to a
16-week once weekly general exercise and dietary counselling intervention or standard
care The intervention addressed a reduction in energy intake as well exercise with a goal
of an average of one-hour a day of moderate to vigorous activity Seventy six women
(894) completed the intervention demonstrating reasonable acceptability of the
intervention At 16-weeks significant group differences in favour of the intervention
were evident in weight BMI percent fat trunk fat leg fat and waist and hip
circumference
ii DIET
Bekkering et al (2006) did not identify any studies examining the effect of diet on weight loss
or maintenance in breast cancer survivors The current review identified one RCT
Chlebowski et al (2006) report an RCT conducted as part of the aforementioned WINS trial
where 2437 postmenopausal women with early breast cancer were randomised to
nutritional and lifestyle counselling (n=975) or not (n=1462) as part of routine follow-up The
dietary intervention included eight bi-weekly individual counselling sessions As a reminder
the goal of the dietary intervention was to reduce percentage of calories from fat to 15
resulting in a sustained reduction in fat intake to approximately 20 of calories Dietary fat
intake reduction was significantly greater in the dietary group compared to the control group
After 12-months of intervention dietary fat intake was lower in the intervention group
than in the control group (333g per day versus 513g per day respectively Plt001)
95
corresponding to a statistically significant 6-pound lower mean body weight in the
intervention group (P lt01) This major study also demonstrated a survival advantage in
women who lost weight as described in Part 1 of this review
b) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on weight loss or maintenance in prostate cancer survivors The current review identified
one RCT
Segal et al (2009) conducted a RCT with 121 men with prostate cancer commencing
radiotherapy with or without androgen deprivation therapy They were randomly assigned to
24-weeks of usual care resistance exercise or aerobic exercise Compared with usual
care exercise improved aerobic fitness upper- and lower-body strength while
preventing an increase in body fat Resistance exercise generated longer-term
improvements and additional benefits for strength and body fat than aerobic exercise
SUMMARY OF EVIDENCE FOR WEIGHT AND BODY COMPOSITION
Supervised physical activity programmes with or without dietary counselling are highly
effective in improving body composition or at the very least preventing increases in weight
They are also safe and have other major benefits on health including improving fitness
walking distance muscle power and reducing cholesterol More research is however
required into the most effective dietary strategies for weight loss or maintenance in cancer
survivors Thus far there is some evidence for reducing dietary fat intake
A large controlled trial has been designed to test the combined effect of physical activity and
weight control on disease-free survival and on breast cancer recurrence free survival
second primary breast cancer and total invasive plus in situ breast cancer (Ballard-Barbash
et al 2009) Goals for weight control interventions for women whose BMI is greater than
25kgm2 is to lose 10 of body weight and for women whose BMI is less than or equal to
25kgm2 to avoid weight gain The goal for the physical activity intervention would be to
achieve and maintain regular participation in a moderate intensity physical activity
programme for a total of 150-255 minutes over at least 5 days per week This study is using
evidence which is current for weight loss and physical activity and is an indicator for the
basis of advice for patients at risk in similar situations
96
Table 11 Weight and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Courneya et al (2007)
Multicentre RCT to test for factors that could counteract unfavourable changes resulting from chemotherapy (eg changes in body composition) Participants were randomly assigned to usual care (n =
82) supervised resistance exercise
(n = 82) or supervised aerobic
exercise (n = 78) for the duration of their chemotherapy
242 breast cancer
patient
s initiating adjuvant chemotherapy
Median=17-weeks
Primary Cancer-Specific QoL Secondary Fatigue psychosocial functioning physical fitness body composition chemotherapy completion rate and lymphedema
The follow-up assessment rate for our primary end point was
921 and adherence to the supervised exercise was 702
Unadjusted and adjusted mixed-model analyses indicated that
aerobic exercise was superior to usual care for improving self-
esteem (P = 015) aerobic fitness (P = 006) and percent body fat
(adjusted P = 076) Resistance exercise was superior to usual care
for improving self-esteem (P = 018) muscular strength (P lt
001)
lean body mass (P = 015) and chemotherapy completion rate (P =
033) Changes in cancer-specific QOL fatigue depression and
anxiety favoured the exercise groups but did not reach statistical
significance Exercise did not cause lymphedema or
adverse events
Kim Kang and Park (2009)
Meta-analysis to examine the effectiveness
of aerobic exercise
interventions on cardiopulmonary function
and body composition in
women with breast cancer
Of 24 relevant
studie
s reviewed 10 studies (n= 588) met the inclusion criteria
Not reported Cardiopulmonary function
and body
composition
The findings indicated that aerobic exercise significantly improved
cardiopulmonary function as assessed by absolute
VO2 peak (standardized mean difference [SMD] 916 p lt 001)
relative VO2 peak (SMD424 p lt 05) and 12-minute walk test
(SMD 502 p lt 001) Similarly aerobic exercise significantly
improved body composition as assessed by percentage body fat
(SMD mdash890 p lt001) but body weight and lean body mass did not
change significantly
Mefferd et al (2006)
RCT to test the effect of a 16-week cognitive behavioural therapy (CBT) intervention for weight loss through exercise and diet modification on risk factors for recurrence of breast cancer Participants randomly assigned to a once weekly 16-week intervention or wait-list control group
Overweight or obese breast cancer survivors (n=76)
On completion of the 16-week intervention
Weight Significant differences in weight body mass index percent fat trunk fat leg fat as well as waist and hip circumference between intervention and control groups (P le 005) Furthermore levels of triglycerides and total cholesterolhigh density lipoprotein cholesterol levels were also significantly reduced following the intervention
97
Schmitz et al (2005)
RCT testing the safety of twice weekly weight training classes among recent breast cancer survivors Participantslsquo randomised into immediate and delayed treatment groups The immediate group trained from months 0-12 the delayed treatment group served as a no exercise parallel comparison group from months 0-6 and trained from months 7=12
Convenience sample of 85 recent breast cancer survivors
6 and 12-months
Body size (lean body mass) and biomarkers hypothesised to link exercise and breast cancer risk
Significant increases in lean mass (088 versus 002 kg P lt 001) as well as significant decreases in body fat (minus115 versus 023 P = 003) and IGF-II (minus623 versus 2828 ngmL P = 002) comparing immediate with delayed treatment from baseline to 6 months Within-person changes experienced by delayed treatment group participants during training versus no training were similar
Segal et al (2009)
Prostate Cancer Radiotherapy and
Exercise Versus Normal
Treatment study examining the effects
of 24-weeks of resistance or
aerobic training versus usual care on prostate cancer outcomes Randomly assigned
to usual care resistance or
aerobic exercise for 24-weeks
Prostate cancer patients on radiotherapy (n=121) usual care (n=41) resistance (n= 40) aerobic exercise
(n=
40)
On completion of 24-week intervention
Fatigue QOL physical fitness body composition PSA testosterone haemoglobin and lipid levels
Median adherence to prescribed exercise was 855 Compared
with usual care resistance training improved QOL (P = 015)
aerobic fitness (P = 041) upper- (P lt 001) and lower-body (P lt
001) strength and triglycerides (P = 036) while preventing an
increase in body fat (P = 049) Aerobic training also improved
fitness (P = 052)
DIET
Chlebowski et al (2006)
Interim analysis of a randomised
prospective multicentre
clinical trial (WINS) to test the effect of
a dietary intervention designed to
reduce fat intake Randomisation was to one of two groups 1)Dietary intervention reduce percentage
of calories from fat to
15The low-fat eating plan was initiated
during 8 biweekly individual
in-person counselling sessions each
lasting 1-hour Dietician 3-monthly
with optional monthly dietary group
Breast cancer patients (n=2437) dietary intervention (n = 975) control (n = 1462)
A median of 60-months (5-years)
Primary endpoint relapse-free survival defined
as the
time from random assignment to breast cancer recurrence
at any
site Secondary endpoint overall survival defined as
the time from
Dietary fat intake was lower in the intervention than in the control group
(fat gramsday at 12-months 333 [95 CI
= 322 to 345]
versus 513 [95 CI = 500 to 527] respectively Plt001)
corresponding to a statistically significant (P = 005) 6-pound lower
mean body weight in the intervention group
98
sessions 2) Control group one baseline
dietician visit and contacts
every 3-months thereafter Written
information provided on general dietary
guidelines and counselling on
nutritional adequacy for vitamin and
mineral intake only
randomisation to death from any cause
99
QUALITY OF LIFE
The advancements in diagnosis and treatment that have contributed to the rise in
survivorship are a significant achievement for healthcare science However it is important to
recognise that this has also resulted in an increase in the number of people living with the
often long-term physical and psychological consequences of cancer and its treatment
Quality of life outcomes are thus becoming just as important as hardlsquo outcomes such as
mortality (Rosenbaum Fobair and Spiegel 2006) hence an emphasis on patient-reported
outcomes (DH 2009c) Indeed there is increasing evidence that QoL can be more
predictive of cancer survival than measures of performance status (Cella et al 2009 Eton et
al 2003 Wenzel et al 2005)
A healthy lifestyle has become viewed as an important element for improved QoL (Lyon and
Langille 2000) with particular emphasis on physical activity Studies identified in the current
review are summarised in Table 12 at the end of this section
a) BREAST CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in breast cancer survivors In the current review one systematic review (with meta-
analysis) and 6 RCTs were identified that provide evidence for the role of physical activity in
the QoL of breast cancer survivors
McNeeley et al (2006) conducted a systematic review with meta-analysis of RCTs (n=14)
examining the effects of physical activity on outcomes in breast cancer survivors Three of
the reviewed studies involving 194 patients compared exercise with usual care
(Campbell et al 2005 Courneya et al 2003 Segal et al 2001) with pooled data
demonstrating that exercise led to significant improvements in QoL superior to the
usual care groups Four studies involving 208 patients reported physical functioning or
physical well-being components of QoL (Campbell et al 2005 Courneya et al 2003
McKenzie and Kalda 2003 Segal et al 2001) the pooled results of which showed
a statistically significant increase in this component of QoL as a result of physical
activity Two of these studies were rated as high quality by the reviewers Courneya et al
2003 Segal et al 2001
100
In addition to this meta-analysis findings by Ohira et al (2006) demonstrated that over 6-
months physical and psychological QoL significantly improved in a recent breast
cancer survivors (n=86) 4-36 months post-treatment who took part in a twice-weekly
weight-training intervention when compared to a control group Increases in upper
body strength and lean mass correlated with these improvements suggesting that twice-
weekly weight training for recent breast cancer survivors might improve QoL in part via
changes in body composition and strength
Daley et al (2007) provided evidence from an RCT comprising sedentary breast cancer
survivors who were 12-36 months post-treatment and who were randomised to one of three
conditions
1) 8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-
minute one-to-one sessions with an physical activity specialist three times per week
(n=34)
2) 8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one
sessions with an physical activity specialist three times per week (n=36)
3) usual care (n=38)
Courneya et al (2003) evaluated QoL outcomes in relation to
exercise in breast cancer survivors (n=52) who had completed
surgery radiotherapy or chemotherapy Participants trained three
times per week for 15-weeks on recumbent or upright cycle
ergometers Exercise duration began at 15-minutes for weeks 1-
3 and then systematically increased by five-minutes every 3-
weeks to 35-minutes for weeks 13-15 The exercise group completed
984 of the exercise sessions demonstrating high adherence
rates Overall QoL increased by 91 points in the exercise group
compared with 03 points in the control group (p lt 001) Change
in peak oxygen consumption correlated with change in overall QoL
demonstrating a significant relationship between exercise and
increases in QoL (p lt 01)
Segal et al (2003) compared self-directed versus supervised
exercise on QoL outcomes in women with stages I-II breast cancer
(n=123) Physical functioning in the control group decreased by 41
points whereas it increased by 57 points and 22 points in the self-
directed and supervised exercise groups respectively (p lt 05)
Post-hoc analysis showed a moderately large and clinically important
difference between the self-directed and control groups (98
points p lt 01) and a more modest difference between the
supervised and control groups (63 points P = 09) No significant
differences between groups were observed for changes in QoL
scores
101
A significant mean difference of 98 units in QoL scores favouring aerobic physical
activity therapy was found This outcome was not the result of the extra support and
attention gained from taking part in the intervention since the same findings were not elicited
for the physical activity-placebo and usual care groups
A small pilot RCT comparing QoL and functional capacity in breast cancer survivors (n=21)
provided with 12-weeks of the Chinese physical activity Tai Chi Chuan (n=11) versus
psychosocial support (n=10) was conducted by Mustian Palesh and Flecksteiner (2008)
The tai chi group demonstrated significant improvements in functional capacity and QoL the
psychosocial support group showed significant improvements only in flexibility with declines
in QoL This suggests that tai chi can enhance functional capacity and QoL among
breast cancer survivors over and above the benefits of psychosocial support
Further support for the benefits of physical activity on QoL in breast cancer survivors (n=58)
within 2-years of completing adjuvant therapy has been demonstrated in a combined aerobic
and resistance training RCT (Milne et al 2008) The women received 12-weeks immediate
supervised physical activity three times a week (n=29) or delayed physical activity
comprising the same protocol but provided 12-weeks following the immediate physical
activity group (n=29) Adherence was 613 which is relatively low However there was a
significant group by time interaction for overall QoL which increased in the
immediate physical activity group from baseline to 12-weeks by 208 points compared
to a decrease in the delayed physical activity group of 53 points
Cadmus et al (2009) report on the QoL outcomes of two 6-month RCTs designed for breast
cancer survivors and based on the national recommendation of 30-minutes of moderate to
vigorous physical activity five days per week
When combining findings from these two studies physical activity was not associated with
QoL benefits in the full sample of either study however physical activity was associated with
significantly improved social functioning (a component of QoL) among survivors who
Trial Increasing or Maintaining
Physical Activity during Cancer
Treatment (IMPACT)
Theoretical Framework Theory of
Planned Behaviour and
transtheoretical model - promoting
self-efficacy to overcome barriers to
physical activity
Sample n=45 newly diagnosed
survivors
Delivery Home-based
Trial Yale Physical activity and
Survivorship (YES)
Theoretical Framework Not
reported
Sample n=67 post-treatment
survivors
Delivery Combined supervised
training programme at a local
health club with home-based
physical activity
102
reported low social functioning at baseline which is the likely impact of greater social
interaction during the intervention This highlights the utility of risk stratification and the
provision of lifestyle support based on need survivors with low social functioning as
could be detected via the Social Difficulties Inventory (SDI Wright et al 2005b) are
likely to benefit from programmes such as the IMPACT and YES trial
Sandel et al (2005) report on a cross-over RCT testing the outcomes of a 12-week dance
and movement exercise programme in women within 5-years of treatment for breast cancer
(n=38) The study included a waiting list control (n=19) and cross-over at 13-weeks Women
attended two supervised dance sessions for six weeks and one session per week for an
additional 6-weeks for a total of eighteen sessions A total of 35 (92) women completed
the regimen with reasons for dropping out including fatigue other commitments and one
participant reported shoulder discomfort The overall finding was that breast cancerndash
specific QoL improved significantly in the intervention group compared to the waiting
list group at 13-weeks which remained unchanged
In the updated systematic review described previously Speck et al (2010) present evidence
from 66 high quality RCTs showing that physical activity during treatment has a small to
moderate positive effect on QoL (p=004) anxiety (p=002) and self-esteem (p=002)
b) COLORECTAL CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any studies examining the effect of physical activity
on QoL in colorectal cancer survivors In the current review one large cohort study was
identified Lynch et al (2008) examined physical activity and QoL data collected as part of
the Colorectal Cancer and Quality of Life Study37 Telephone interviews were conducted
at approximately 6 12 and 24-months after colorectal cancer diagnosis (n=1966) which
found that participants achieving at least 150-minutes of physical activity per week had an
18 higher QoL score than those who reported no weekly physical activity
ii DIET
Bekkering et al (2006) identified two dietary intervention studies examining impact on QoL in
colorectal cancer survivors One dietary counselling trial found a significant improvement in
health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst another reported that
an intervention aimed at a healthier dietary lifestyle had no effect on health assessment or
life satisfaction but did lead to increased health action and increased reports of feeling goodlsquo
(Corle et al 2001) No further studies were identified in the current review
37
The Colorectal Cancer and Quality of Life study in Australia examines in detail the lifestyle factors that
influence QoL in the 5-years post-diagnosis (n=2000)
103
c) PROSTATE CANCER
i PHYSICAL ACTIVITY
Bekkering et al (2006) did not identify any dietary physical activity interventions examining
impact on QoL in prostate cancer survivors One dietary counselling trial found a significant
improvement in health actionlsquo in colorectal cancer survivors (Pakiz et al 2005) whilst
another reported that an intervention aimed at a healthier dietary lifestyle had no effect on
health assessment or life satisfaction but did lead to increased health action and increased
reports of feeling goodlsquo (Corle et al 2001) No further studies were identified in the current
review
Segal et al (2003) reported an RCT comparing supervised resistance exercise versus
control in men with prostate cancer (n=135) who were scheduled to receive androgen
deprivation therapy for at least 3-months Fitness levels were assessed and the men in the
intervention group met with a certified fitness consultant within 7-days of the pre-
assessment The fitness consultant provided patients with the results of their exercise
assessment and introduced a personalised resistance exercise program A significant
improvement was found in QoL outcomes in the intervention group and a significant
decline in the control group Resistance exercise improved QoL regardless of whether
men were treated with curative or palliative intent or whether androgen deprivation therapy
had been received for less than one-year or 1 year
d) OTHER CANCERS AND NON-SITE SPECIFIC STUDIES
i PHYSICAL ACTIVITY
Bekkering et al (2006) found that out of seven physical activity trials six observed
improvements in QoL when using cancer-specific questionnaires (Burnham and Wilcox
2002 Courneya et al 2003 Segal et al 2003 Headley et al 2004 Campbell et al 2005
Sandel et al 2005) but one of these same studies found no association when using the
generic SF-36 scale (Segal et al 2001) This highlights the importance of selecting the most
appropriate outcome measures in terms of sensitivity and responsiveness to a given
intervention
In the current review three studies were identified One prospective controlled four-centre
study comprising a sample of survivors with different tumour sites was identified (Korstjens
et al 2008) QoL outcomes were compared between three groups
1) group-delivered physical training (n=71)
2) group-delivered combined physical and cognitive behavioural training (CBT) (n=76)
3) waiting-list control (n=62)
Participants in both training groups showed significant and clinically relevant improvements
in role limitations physical functioning vitality and health change Adding CBT to the
physical training did not have additional beneficial effects on QoL a finding that has been
104
observed in a number of supported self-management programmes (Davies and Batehup
2010)
Oh et al (2009) reported a RCT examining the QoL outcomes of Medical Qigong (MQ) a
mindndashbody practice that uses physical activity and meditation to harmonise the body mind
and spirit Patients (n=162) with malignancy of any stage and an expected survival length of
gt12-months were randomised to a control group or to a 10-week MQ programme comprising
two supervised 90-minute sessions per week At 10-week follow-up participants in the
MQ group reported larger improvements in QoL than those in the usual care group (p
lt 05)
Mosher et al (2009) reported a prospective cohort study examining the diet exercise and
QoL patterns of 753 breast prostate and colorectal cancer survivors who were at least 5-
years post-diagnosis Survivors underwent two 45-60 minute telephone surveys
administered by the Diet Assessment Center The data demonstrated that greater weekly
minutes of exercise were associated with better physical QoL including less pain and
better health perceptions physical functioning and vitality More exercise was also
correlated with better social functioning Diet quality had a positive association with a range
of physical QoL outcomes in analyses that were adjusted for age level of education and co-
morbidities Greater BMI was associated with worse physical QoL including greater
pain and role limitations because of physical problems and worse health perceptions
physical functioning and vitality
SUMMARY OF EVIDENCE FOR QUALITY OF LIFE
Lifestyle interventions appear to help people with a wide range of cancer types who have
received treatments ranging from surgery chemotherapy radiotherapy or hormonal
therapies although no trials have yet been published specifically addressing the newer
biological therapies Even when not directly associated with overall QoL exercise has been
found to significantly improve social functioning among post-treatment survivors The
benefits of physical activity on holistic QoL appear to be present under a number of
conditions be the physical activity supervised or home-based individualised or group-
based A vast array of different types of exercise techniques have been tested in the studies
evaluated in this review highlighting the potential for survivors to choose activities according
to preference
Whilst some studies have recommended the uptake of physical activity during treatment
others have highlighted the benefits of introducing regular physical activity into a survivorlsquos
self-management care plan immediately after completion of treatment Overall the evidence
does suggest that immediate physical intervention provides greater QoL benefits than
delayed intervention
105
Table 12 Quality of Life and Lifestyle Summary of Evidence
Author Study DesignIntervention Sample Inclusion
Follow-up Period
Outcomes Results
PHYSICAL ACTIVITY
Cadmus et al (2009)
The results of two RCTs to determine the effect of exercise on quality of life in (a) a RCT of exercise among recently diagnosed breast cancer survivors undergoing adjuvant therapy - randomised to a 6-month home-based exercise program or a usual care group (b) a similar trial among post-treatment survivors - randomised to a 6-month supervised exercise intervention or to usual care
50 newly diagnosed breast cancer survivors in the first RCT (a) 75 post-treatment survivors in the second RCT (b)
6-months Measures of happiness depressive symptoms anxiety stress self-esteem and QoL
Good adherence was observed in both studies Baseline quality of life was similar for both studies on most measures Exercise was not associated with quality of life benefits in the full sample of either study however exercise was associated with improved social functioning among post-treatment survivors who reported low social functioning at baseline (p lt005)
Courneya et al (2003)
RCT testing 15-weeks supervised aerobic and resistance training to determine the effects on cardiopulmonary
function and QoL in
post-menopausal breast cancer
survivors Randomly assigned to an exercise (n=25) or control (n=28) group The exercise group trained on cycle ergometers
three times per week for 15
weeks The control group did not train
53 post-menopausal breast cancer survivors
On completion of the 15-week intervention
Changes in peak oxygen
consu
mption and overall
Peak oxygen consumption increased by 024 Lmin in the exercise group whereas it decreased
by 005 Lmin in the control group
(mean difference 029 Lmin 95 confidence interval [CI] 018 to
040 P lt 001) Overall QOL increased by 91 points in the exercise
group compared with 03 points in the control group (mean
difference 88 points 95 CI 36 to 140 P= 001) Pearson
correlations indicated that change in peak oxygen consumption
correlated with change in overall QOL (r = 045 P lt 01)
Daley et al (2007)
RCT - Women were randomised to one of three groups a)8-weeks of moderate-intensity aerobics physical activity therapy comprising 50-minute one-to-one sessions with an physical activity specialist three times per week (n=34) b)8-weeks light-intensity body conditioning-placebo comprising 50-minute one-to-one sessions with an physical activity specialist three times
Sedentary breast cancer survivors who were 12-36 months post-treatment (n=117)
On intervention completion and at 24-weeks follow-up
QoL depression physical activity behaviour aerobic fitness
There was a significant mean difference of 98 units in QoL scores favouring aerobic physical activity therapy
106
per week (n=36) c)usual care (n=38)
Korstjens et al (2008)
RCT comparing the effects on cancer survivorslsquo QoL in a
12-week group-
based multidisciplinary self-management rehabilitation
program
combining physical training (twice weekly) and cognitive-behavioural
training (once weekly) with
those of a 12-week group-based physical
training (twice weekly) There
was also a non-intervention comparison group
All cancer types rehabilitation (n=76) physical training (n=71) comparison group (n=62)
Baseline after rehabilitation and
3-
months follow-up
QoL (SF-36) The effects of multidisciplinary rehabilitation did not outperform
those of physical training in role limitations due to emotional
problem (primary outcome) or any other domains of quality of life
(all p gt 05) Compared with no intervention participants in both
rehabilitation groups showed significant and clinically relevant
improvements in role limitations due to physical problem (primary
outcome effect size (ES) = 066) and in physical functioning (ES =
048) vitality (ES = 054) and health change (ES = 076) (all p lt
01)
Lynch et al (2008)
Colorectal Cancer and Quality of Life
Study - aimed at examining the relationships between
physical activity
and QoL after a colorectal cancer
diagnosis Participants completed telephone interviews at approximately
6
12 and 24 months after diagnosis
1966 people with colorectal
6 12 and 24-months post-diagnosis
QoL There was an overall independent association between physical
activity and QoL At a given time point
participants achieving at least 150 minutes of physical activity per
week had an 18 higher quality of life score than those who
reported no physical activity Significant associations were also
present at the interindividual level (differences between
participants) and intraindividual level (within participant changes)
Milne et al (2008)
RCT to examine the effects of a supervised exercise program on motivational variables in breast cancer survivors Participants were randomised in a cross-over design to either an immediate exercise group that exercised from baseline to week 12 or a delayed exercise group that exercised from week 12 to 24
Breast cancer survivors (n=58) within 2-years of completing adjuvant therapy
Post-intervention (12-weeks)
Quality of life There was a significant group by time interaction for overall QoL which increased in the immediate physical activity group by 208 points compared to a decrease in the delayed physical activity group of 53 points
Mosher et al (2009)
Prospective Cohort Study examining the health behaviours of older cancer survivors and the associations of those behaviours with QoL especially during the long-term post-treatment period
753 older (aged 65 years) long-term survivors ( 5 years post-diagnosis) of breast prostate and colorectal
2 telephone interviews
Exercise diet weight status and quality of life
Participants reported a median of 10 minutes of moderate-to-vigorous exercise per week and only 7 had Healthy Eating Index scores gt80 (indicative of healthful eating habits relative to national guidelines) Despite their suboptimal health behaviours survivors reported mental and physical quality of life that exceeded age-related norms Greater exercise and better diet quality were associated with better physical quality-of-life outcomes (eg better vitality and physical functioning P lt 05) whereas greater body mass index was associated with reduced physical quality of life (P lt 001)
107
cancer
Mustian Palesh and Flecksteiner (2008)
RCT testing the functional and QoL outcomes of tai chi - women who completed treatment randomised to receive tai chi or psychosocial support therapy for 12-weeks (60 minutes three times weekly)
Breast cancer survivors (n=21)
On completion of 12-week intervention
Functional capacity and quality of life
The tai chi group demonstrated significant improvements in functional capacity and QoL the psychosocial support group showed significant improvements only in flexibility with declines in QoL
McNeely et al (2006)
Systematic review with meta-analysis summarising the available evidence concerning
the effects of exercise on
breast cancer patients and survivors Searches took place of Cochrane Central Register of Controlled
Trials
MEDLINE EMBASE CINAHL Psych INFO CancerLit PEDro
and
SportDiscus as well as conference proceedings
Included in the review were RCTs (n=14) that examined
exercise interventions for breast cancer patients or survivors
Not reported Quality of life cardio fitness or physical
functi
oning as primary outcomes
Despite significant heterogeneity and relatively small samples the
point estimates in terms of the benefits of exercise for all outcomes
were positive even when statistical significance was not achieved
Exercise led to statistically significant improvements in quality of life
as assessed by the Functional Assessment of Cancer Therapyndash
General (weighted mean difference [WMD] 458 95 CI 035 to
880) and Functional Assessment of Cancer TherapyndashBreast (WMD
662 95 CI121 to 1203) Exercise also led to significant improvements
in physical functioning and peak oxygen consumption
and in reducing symptoms of fatigue
Oh et al (2009)
RCT comprising 10-weeks Medical Qigong (MQ) to evaluate the use of (MQ) compared with usual care in improving the QOL of cancer patients
162 patients with a range of cancers
On completion of the 10-week intervention
QOL and fatigue (FACT-GF) mood (Profile of Mood State)
Regression analysis indicated that the MQ group significantly improved overall QOL (t144thinsp=thinspminus5761 Pthinspltthinsp0001) fatigue (t153thinsp=thinspminus5621 Pthinspltthinsp0001) mood disturbance (t122 =2346 Pthinsp=thinsp0021) and inflammation (CRP) (t99thinsp=thinsp2042 Pthinspltthinsp0044) compared with usual care after controlling for baseline variables
Ohira et al (2006)
RCT to examine the effects of weight training on changes in QoL and depressive symptoms in recent breast cancer survivors Randomised to treatment or control group
Convenience sample of 86 breast cancer survivors (4-36 months post-treatment)
6-months The primary outcomes were changes in QoL (CARES-SF) and depressive symptoms (CES-D)
QoL improved in the treatment group compared with the control group (Standardized Difference = 062 P = 006) The psychosocial global score also improved significantly in the treatment group compared with the control group (Standardized Difference = 052 P = 02) There were no changes in CES-D scores Increases in upper body strength were correlated with improvements in physical global score (r = 032 P lt01) and psychosocial global score (r = 030 P lt01) Increases in lean mass were also correlated with improvements in physical global score (r = 023 P lt05) and psychosocial global score (r = 024 P lt05)
Sandel et al (2005)
RCT - 12-weeks dance and movement programme versus wait list control to determine the effect on QoL and shoulder function
35 breast cancer survivors
13 and 26-weeks
QoL (FACT-B) Shoulder range of motion (ROM) and Body Image Scale
FACT-B significantly improved in the intervention group at 13 weeks from 1020 _158 to 1167 _ 169 compared to the wait list group 1081 _ 164 to 1071 _213 (time _ group effect P _ 008) During the crossover phase the FACT-B score increased in the wait list group and was stable in the treatment group The overall effect of the training at 26 weeks was significant (time effect P _ 03) and the order of training was also significant (P _ 015) Shoulder ROM
108
increased in both groups at 13 weeks mdash15_ and 8_ in the intervention and wait list groups (Time effect P _ 03 time _ group P _ 58) Body Image improved similarly in both groups at 13 weeks (time effect P _ 001 time _ group P _ 25) and at 26 weeks There was no significant effect of the order of training for these outcome measures
Speck et al (2010)
A systematic review of physical activity RCTs in cancer survivors during and post-treatment in order to update a previous review conducted in 2005
All cancer types with 83 being breast cancer Data from 82 studies were abstracted Weighted mean effect sizes were calculated from 66 high quality studies
The majority of the interventions were longer than 5 weeks 40 being more than 3 months in length
A systematic level of evidence criteria was applied to evaluate 60 outcomes ndash QoL was included
Quantitative evidence shows a large effect of physical activity interventions post treatment on upper and lower body strength (WMES=099 amp 090 plt00001 amp 0024 respectively) and moderate effects on fatigue and breast cancer-specific concerns (WMES=minus054 amp 062 p=0003 amp 0003 respectively) A small to moderate positive effect of physical activity during treatment was seen for physical activity level aerobic fitness muscular strength functional quality of life anxiety and self-esteem With few exceptions exercise was well tolerated during and post treatment without adverse events
Segal et al (2003)
RCT testing the hypothesis that resistance exercise can counter the negative QoL effects of androgen deprivation therapy for prostate cancer by reducing fatigue elevating mood building muscle mass and reducing body fat Randomly assigned to an intervention group that participated in a resistance exercise program three times per week for 12 weeks or to a waiting list control group
55 men with prostate cancer scheduled for androgen deprivation therapy for at least 3 months after recruitment
On completion of the 12-week intervention
Primary outcomes fatigue disease-specific QoL Secondary outcomes muscular fitness body composition
Men assigned to resistance exercise had less interference from fatigue on activities of daily living (P =002) and higher quality of life (P =001) than men in the control group Men in the intervention group demonstrated higher levels of upper body (P =009) and lower body (P lt001) muscular fitness than men in the control group The 12-week resistance exercise intervention did not improve body composition as measured by changes in body weight body mass index waist circumference or subcutaneous skinfolds
Vadiraja et al (2009)
RCT - 6-week yoga and relaxation during adjuvant radiotherapy his study compares the effects of an integrated yoga program with brief supportive therapy in breast cancer outpatients undergoing adjuvant radiotherapy at a cancer centre Intervention consisted of
88 stage II and III breast cancer outpatients
After 6-weeks of radiotherapy
QoL (EORTC-C30) Mood (Positive and Negative Affect Schedule)
There was a significant difference across groups over time for positive affect negative affect and emotional function and social function There was significant improvement in positive affect (ES = 059 p = 0007 95CI 125 to 78) emotional function (ES = 071 p = 0001 95CI 645 to 2533) and cognitive function (ES = 048 p = 003 95CI 12 to 185) and decrease in negative affect (ES = 084 p lt 0001 95CI minus134 to minus44) in the yoga
109
yoga sessions lasting 60 minutes daily while the control group was imparted supportive therapy once in 10 days
group as compared to controls There was a significant positive correlation between positive affect with role function social function and global quality of life There was a significant negative correlation between negative affect with physical function role function emotional function and social function
110
ONGOING LIFESTYLE STUDIES
Four ongoing lifestyle studies were identified in the current review one for breast cancer and
three for colorectal cancer
a) BREAST CANCER
In the US Goodwin et al (ongoing) are trialling lsquoLifestyle Intervention Study in Adjuvant
Treatment of Early Breast Cancerrsquo (LISA) The primary objective of this trial is to evaluate
the effect of the addition of a 2-year centrally delivered individualised telephone-based
lifestyle intervention focusing on weight management to a mailed educational intervention on
disease-free survival in post-menopausal women with early stage breast cancer (hormone
receptor positive) BMI ge24-lt40 kgm2 who are receiving standard letrozole adjuvant
therapy The primary outcome is disease-free survival Secondary outcomes include overall
survival distant disease-free survival weight change QoL selected non-cancer medical
events and biologic factors (insulin) The estimated enrolment is 2150 with the study having
started in 2007 Participants will be randomised to
1) Individualised Lifestyle Intervention Experimental - Women randomised to this arm
will receive an intervention program that consists of individual weight loss diet and
physical activity goals incorporated into a 2-year standardised structured telephone
and mail-based intervention In addition to diet and physical activity the intervention
will address behavioural and motivational issues relating to weight management
including maintaining motivation overcoming obstacles to success relapse
prevention emotional distress and stress and time management The telephone
intervention will involve 19 phone calls as well as mailings and a participant manual
women will be asked to lose up to 10 of their weight by reducing their caloric and
fat intake (by 500-1000 kcalday 20 calories fat) and increasing their moderate
physical activity (to 150-200 minutesweek)
2) Mail-based Active Comparator - Participants will receive a standardised mail-based
intervention focussing on healthy living This will include mailings at study entry as
well as a 2-year subscription to health magazine
Approximately 2150 women will be enrolled follow-up will continue until target event rates
have been met (anticipated 4-6 years after completion of the intervention) This sample size
will provide 80 power (type 1 error 005 2-tailed) to detect a hazard ratio (HR) for DFS of
074-076 in the weight loss intervention arm
b) COLORECTAL CANCER
It has been suggested that interventions to improve QoL in colorectal cancer survivors are
more effective if they target symptom management psychosocial support and lifestyle
variables in a comprehensive and integrated approach to behavioural change (Steginga et
al 2009) Due to the paucity of comprehensive trials examining behavioural interventions in
this group of survivors Hawkes et al (2009) are conducting a large-scale RCT of a 6-month
telephone-delivered lifestyle coaching intervention based on Acceptance and Commitment
111
Therapy (ACT) ndash bdquoCanChange‟ The intervention aims to assist colorectal cancer survivors
(n=350) to make improvements in lifestyle including physical activity weight management
and smoking cessation Participants receive up to eleven telephone sessions over the
6-months from a qualified health professional who provides support on symptom
management and lifestyle change Outcomes will be assessed post-intervention at 6- and
12-months follow-up and will include physical activity CRF QoL and cost-effectiveness
The findings from this innovative lifestyle coaching initiative will offer insight into the intensity
of support required to achieve sustained behaviour change as well as highlight the efficacy
of various components of delivery (eg telephone-delivery coaching professionally-led
etc)
Courneya et al (2008) are leading a physical activity intervention in a collaboration between
Canada and Australia the Colon Health and Life-Long Physical activity Change
(CHALLENGE) a 3-year multicentre RCT for colon cancer survivors (n=1000) who are 2-6
months post adjuvant-treatment Any type of physical activity will be promoted the goal
being to motivate people to increase their overall activity by about 25-hours of moderate
intensity physical activity or 1-hour and 15-minutes of vigorous physical activity per week
Behavioural support counselling and supervised physical activity sessions will be used to
promote the adoption and long-term maintenance of physical activity By monitoring
participants over 10-years the trial will determine if colon cancer recurs less often in people
who increase and maintain their physical activity It will also assess whether physical activity
improves other important outcomes including QoL anxiety depression sleep and physical
function It is anticipated that this trial will provide important insight into strategies for
promoting long-term health behaviour change
Another Australian lifestyle intervention is The Colorectal Cancer and Quality of Life led
by Joanne Aitken The purpose of this project is to identify any patterns between lifestyle and
QoL over the first 5-years following a diagnosis of colorectal cancer Approximately 2000
people have been recruited to take part in this study making it the largest colorectal cancer
study of its type to be undertaken Participants complete a telephone interview and a written
Pilot testing demonstrated that
o 80 of participants (n=20) felt the intervention addressed their issues
o 100 felt more motivated to make lifestyle changes
o 100 would recommend the intervention to other survivors
From baseline to post-intervention improvements
were observed for
o Colorectal cancer symptoms o QoL o Diet o Physical activity
112
questionnaire on an annual basis over the 5-years One of the aims of the study is to
uncover how lifestyle factors particularly physical activity may improve QoL and reduce the
risk of developing other chronic diseases that cancer survivors are prone to such as heart
disease and diabetes This information will help Cancer Council Queensland properly design
and target lifestyle interventions to help improve the health and well-being of colorectal
cancer survivors (Aitken et al ongoing)
113
DISCUSSION
WHAT DO WE KNOW ABOUT LIFESTYLE AND CANCER
This aim of this review was to update the World Cancer Research Fund (WCRF) report bdquoA
Systematic Review of RCTs Investigating the Effect of Nutritional and Physical
Activity Interventions on Cancer Survival‟ (Bekkering et al 2006) This has been
achieved by conducting a comprehensive but pragmatic search of the literature from 2006
onwards Where no evidence was available in the WCRF review studies before 2006 have
been included if identified in the reference lists of acquired records To facilitate this
evidence cited within the lsquoHandbook of Cancer Survivorship‟ (Feuerstein 2006) and
findings from a non-systematic review conducted by the Cancer and Palliative Care
Rehabilitation Workforce (2009) were also utilised
Before presenting a synthesis of the findings within this review there are some limitations
that first need to be addressed
Methodological Limitations
There is strong evidence from observational studies that lifestyle factors can potentially have
major influences on overall mortality risk for cancer survivors This has been most frequently
subjected to study in breast cancer survivors However it is recognised that such
associations in observational studies can be influenced by confounding and therefore that
the mechanisms of lifestyle change on all-cause mortality remains unclear (Cheblowski
2010) Therefore although the observational evidence is strong there is a need to
understand the benefits of lifestyle change ndash particularly physical activity and weight control
in the absence of confounding factors which can be achieved only within the context of a
controlled trial (Ballard-Barbash et al 2009) Such evidence in the end is most likely to
lead to promoting the wide scale adoption of lifestyle change interventions in the role of
secondary prevention of cancer
Consistent with Bekkering et al (2006) it has been found that there is a paucity of robust
evidence on the effects of lifestyle behaviours in cancer progression and recurrence as well
as in the prevention and management of the long-term health implications of cancer
treatment Studies generally comprise small sample sizes and few offer evidence of the
long-term effects of lifestyle behaviours Since lifestyle choices are generally behavioural in
nature the sustainability of these behaviours is fundamental if commissioners are to provide
funding for lifestyle interventions
There were also a large number of retrospective studies particularly for smoking This is
understandable given the challenges of research within this area however it does also raise
limitations surrounding the accuracy of findings This is especially the case when findings
rely on retrospective self-reports of health behaviours or illness experience
114
A number of methodological limitations confound the interpretation of the benefits of exercise
and diet after a diagnosis of cancer from other risks such as smoking body size
supplements and analgesic intake Nevertheless as highlighted by Doyle et al (2007) even
when the scientific evidence is incomplete reasonable conclusions can be made on issues
that can guide lifestyle choices for cancer survivors These are discussed next
THE EVIDENCE
Diet
Evidence for reducing fat intake remains unclear yet evidence for the mechanisms of benefit
of weight loss or the maintenance of a healthy weight is strong Weight control and self-
management clearly requires consideration of total fat intake highlighting the necessity to
provide cancer survivors with advice on levels of fat necessary for weight maintenance
weight loss or in some cases weight gain (Chlebowski et al 2005 Patterson et al 2010)
The same rationale applies to any inconsistencies in evidence for increased fruit and
vegetables which can also facilitate weight management Indeed where the evidence is
strongest for fruits and vegetables applies to those sources containing carotenoids The
evidence is convincing that carotenoids do provide anti-cancer properties (Rock et al 2005
Pierce et al 2007) Lycopene (found in tomatoes) is one such carotenoid found to offer
anti-cancer benefits (Schwarz et al 2008)
Fibre (found in the skins of fruit and vegetables as well as in beans and lentils) and folate
(found in broccoli brussel sprouts asparagus and peas) have in the main been found to
protect against colorectal cancer The evidence is convincing that by slowing down bowel
transit time the mechanism of benefit comes from reducing contact between potential
carcinogens
The benefits of a low fat high fruit and vegetable diet extend into the management of
treatment-related conditions such as lymphoedema In individuals carrying excess weight
the resulting weight loss achieved via a low fat high fruit and vegetable diet can ease the
symptoms of lymphoedema (Shaw Mortimer and Judd 2007)
The evidence also suggests that survivors of prostate cancer might benefit from including
pomegranate juice and green tea in their diet
In terms of other food sources vitamin D and calcium can be protective against osteoporosis
(Ryan et al 2007) although more research with a specific fouls on cancer survivors is
needed in this area
Physical Activity
In general the findings of epidemiological and large cohort studies demonstrates that the
evidence for the role of physical activity in improving breast cancer prognosis quality of life
and on the levels of several hormones associated with breast cancer is strong
115
There is substantial evidence suggesting that the physical activity recommendations
developed by the Department of Health are sufficient for cancer survivors - a total of at least
30-minutes a day of moderate intensity physical activity on five or more days of the week
This can be achieved either by doing all the daily activity in one session or through several
shorter bouts of activity of 10 minutes or more Additionally there is evidence of a dose-
response (ie the more physical activity the greater any benefits) The evidence for breast
cancer further suggest that for survival benefits to be achieved from physical activity no less
than moderate to vigorous activity is required (Gross et al 2002) However the most recent
expert advice emphasises that even a modest amount of exercise like brief walks is
beneficial and gains will be seen versus doing nothing at all38
The interpretation of physical activity evidence has been hindered by the difficulty of
distinguishing physical activity outcomes from subsequent weight loss outcomes However
again even if the main mechanism of benefit of physical activity is improved outcomes
resulting from weight loss or maintenance then this could be considered strong enough
evidence to prescribe physical activity to cancer survivors Furthermore the evidence is
encouraging in terms of its QoL-enhancing effect (McNeeley et al 2006 Daley et al 2007)
Three specific elements of physical activity interventions or advice could be addressed
(Ballard-Barbash et al 2006)
Reducing sedentary behaviours (such as watching TV)
Exercise sessions
Type and intensity of physical activity
There is sufficient evidence for supervised physical activity improving symptoms of cancer-
related fatigue (McNeely et al 2006 Cramp and Daniel 2008) and lymphoedema (Moseley
and Pillerlsquos 2008) Indeed the evidence suggests that guided progressive physical activity
soon after treatment can ease the symptoms of lymphoedema (de Rezende et al 2006)
This supports recent cautions regarding risk-averse clinical recommendations guiding
survivors to avoid the use of the affected limb which may actually lead to de-conditioning
and the very outcome women seek to avoid (Schmitz 2010) At the very least there is no
evidence of appropriate intensity physical activity causing or exacerbating either fatigue or
limb swelling The same is true for the effect of physical activity on osteoporosis Whilst the
benefits of physical activity on bone health require clarifying physical activity can at the very
least prevent loss of bone mineral density in survivors at particular risk of developing
osteoporosis (Waltman et al 2009)
A recent roundtablelsquo event by the American College of Sports Medicine has produced a
Consensus Statement detailing exercise guidelines for cancer survivors (Schmitz Courneya
and Matthews et al 2010) An expert panel reviewed the published empirical evidence and
came to the consensus regarding the safety and efficacy of exercise testing and prescription
in cancer survivors The evidence is clear that exercise during treatment (specific risk
assessment can be carried our for specific treatments and biological response) and after
38
Dr Rachel Ballard ndash Barbash in the NCI Cancer Bulletin June 29 2010
116
treatment is safe and effective Activity induced improvements can be expected on aerobic
fitness muscular strength quality of life and fatigue in breast prostate and haematological
cancers Resistance training can be performed safely by breast cancer survivors with and at
risk of lymphoedoema
Efforts are currently being made to increase the capacity and capability of exercise
professionals to address the unique needs of cancer survivors Exercise professionals need
to be able to access training which reflects the medical condition they are treating for to be
more knowledgeable about the condition and the most suitable and appropriate exercises for
them This requires the development of a national competency framework for a specialist
level 3 add on or level four qualification This would enable providers to develop national
training programmes for cancer specialist exercise professionals and lead to more
accessible referral through the exercise referral scheme (Exercise Referral Research March
2010)
Smoking
Strong and consistent evidence has been presented for increased risk of disease
progression and mortality in people who continue to smoke after a diagnosis of cancer as
well as poorer outcomes in pre-diagnosis smokers (Parsons et al 2010) This evidence
applies particularly to cancers of the lung or head and neck Further research is needed for
breast colorectal prostate and rarer cancers
Alcohol
There is a paucity of research into the effects of alcohol pre- and post-diagnosis on cancer
progression and recurrence as well as symptom management Evidence thus far is highly
contradictory with some demonstrating a protective effect some a detrimental effect and
others no effect
Weight
Substantial weight gain after diagnosis and treatment for breast cancer is adversely
associated with breast cancer prognosis Obesity appears to increase the risk of recurrence
and death among breast cancer survivors by around 30 (Patterson et al 2010) Much
more research is needed to clarify the relationship between prognosis and survival and body
weight in other tumour types
Dealing with issues of weight weight gain and weight management with patients is one of
the lifestyle behaviour change issues health care professionals feel most challenged by
Studies do confirm that health care professionals find it difficult to address these issues with
patients without appearing biased and negative It would appear that a lack of professional
training on behavioural change and motivational coaching and effective strategies for weight
117
loss combine and can lead to avoidance by health care professionals in addressing the need
for change (Puhl and Heuer 2009 Blakeman et al 2010)
Mechanisms of Benefit
Chlebowski (2010) offers some thought-provoking insight into the challenge of implementing
lifestyle change when aromatase inhibitors have been found to reduce oestrogen levels far
more than physical activity interventions One study cites approximately 90 reductions in
oestrogen levels as a result of aromatase inhibitors (Dixon et al 2008) Furthermore three
trials comparing aromatase inhibitors versus placebo anticipate 60-70 reduction in breast
cancer risk (Cuzick 2005 Goss et al 2007 Visvanathan et al 2008) Equally Chlebowski
(2010) points out that the influence of physical activity on insulin levels also has a
pharmacological competitor in the form of metformin (Goodwin et al 2008 Jiralerspong et
al 2009)
These are valid insights that are likely to complicate the successful integration of lifestyle
advice into standardised models of aftercare On the other hand if a public and community
health approach is taken to health and well-being then lifestyle change is likely to offer
health benefits beyond cancer-specific health Such an approach is recommended in the
bdquoCapabilities for Supporting Prevention and Chronic Condition Self-Management A
Resource for Educators of Primary Health Care Professionals‟ developed as part of the
Australian Better Health Initiative (Flinders University 2009) The model offered within this
capabilities framework promotes healthcare providers to view patients holistically as
opposed to focusing solely on diagnosed chronic condition The rationale for this in part
lies in the fact that chronic conditions are more often than not accompanied by co-
morbidities and therefore healthcare is not only about the established condition but also
identified risk factors for co-morbidity
MAKING LIFESTYLE RECOMMENDATIONS FOR CANCER SURVIVORS
In terms of reducing the risks of relapse evidence is strongest for breast colorectal lung
and head and neck cancers but self-management lifestyle strategies are likely to be person-
specific rather than disease or treatment specific so are likely to apply to all patients
recovering from cancer
Diet Appendix A provides evidence-based dietary recommendations that can be made in
light of the findings within this review and national health recommendations These
recommendations comprise a varied diet ensuring adequate intake of vitamins essential
minerals fibre essential fatty acids and antioxidants by eating less fat and more green and
cruciferous vegetables fruits and berries nuts and grains and healthy oils (unsaturated fats
omega)
Physical Activity In terms of physical activity based on the evidence within this report
the five a weeklsquo recommendation is just as relevant to cancer survivors as to the general
population Indeed these recommendations are also provided by the American Cancer
Society (Doyle et al 2006) as advised by a large expert panel Appendix B provides
118
suggestions for physical activity Forty-five to 60-minutes of intentional physical activity are
preferable as the benefits of physical activity do appear to be greater with increased physical
activity Even when this might seem too much survivors can be reminded that the minimum
30-minutes for 5 days a week can be tailored to individual needs and capabilities For
example graded or progressive physical activity can be utilised for those experiencing
fatigue whilst shorter physical activity sessions can be spread out across the day
Other Lifestyle Factors Body Weight In addition it is recommended that obesity (BMI
gt35 Kgm2) excessive alcohol consumption and smoking are avoided There is also
evidence that maintaining a steady healthy weight as opposed to fluctuating between a
healthy and unhealthy BMI can offer health benefits for cancer survivors (Wright et al
2007)
The evidence within this review are indicative of challenges with adherence supporting
findings from Uhley and Jen (2006) that intensive resource-heavy individualised guidance
and support is required to achieve significant long-term lifestyle change This further
emphasises the need to tailor and prescribe such interventions on a needs basis via
individualised assessment and risk stratification
Integrating Self-Management Lifestyle Strategies into Routine Care
Adopting a paternalistic approach and simply telling people is not enough If the medical
community want to help their patients embark on a road of recovery which includes dietary
change and regular exercise there has to be a comprehensive and well-funded package of
education guidance and support Attitude and culture change is imperative both to tackle the
myths and preconceptions around lifestyle factors and their influence on cancer prognosis
symptom management and a future healthy life on the part of both patients survivors and
health care professionals The bdquoCapabilities for Supporting Prevention and Chronic Condition
Self-Management A Resource for Educators of Primary Health Care Professionals‟
developed as part of the Australian Better Health Initiative offers a comprehensive
framework for integrating self-management support into healthcare services (Flinders
University 2009) The emphasis is on not merely striving to change patient behaviour but
also making efforts towards organisational change
Cancer Research UK Diabetes UK and the British Heart Foundation have joined together to launch a new campaign to raise awareness of the dangers of carrying excess weight around the middle The Active Fatlsquo campaign encourages people to measure their waistlines and make positive changes to their lifestyles if they are at risk The emphasis is on educating the public that fat cells are actively working away at stimulating diseases such as cancer diabetes and heart attacks
119
The model offered within this capabilities framework promotes healthcare providers to view
patients holistically as opposed to focusing solely on the diagnosed chronic condition The
rationale for this in part lies in the fact that chronic conditions are more often than not
accompanied by co-morbidities and therefore healthcare is not only about the established
condition but also identified risk factors for co-morbidity The framework also identifies the
need to provide education and training to healthcare professionals in how to most effectively
empower patients to self-manage (Flinders University 2009) Core skills for healthcare
professionals include
o Patient-centred focus (ie communication skills risk assessment care
planning)
o Behaviour change capabilities (ie motivational interviewing goal setting
problem solving)
o Organisational change (ie evidence-based healthcare multidisciplinary
working)
Evidence based information emphasising the importance of lifestyle ideally should be
formally introduced into routine clinical practice early in the treatment pathway and re-
enforced at regular intervals thereafter This ensures patients and their relatives do not miss
the teachable moment where they are most susceptible to positive advice (Demark-
Wahnefried et al 2005) This requires close work with clinicians specialist nurses patients
and advocacy groups to enable information about new strategies to be integrated into
existing local information pathways and materials Indeed the new information prescriptions
currently being pilot tested provide ample opportunity for integrating lifestyle advice into
survivorship care plans
Information clearly has an important role to play in influencing lifestyle behaviours However
people need more than knowledge to be healthy they need the skills to change if they are to
bring about changes in often complex and habitual lifestyle behaviours (Robertson 2008)
Before investing time and money on patient information materials it is necessary to convince
the consultants other direct clinical staff and organisers of clinical services that lifestyle
advice is a priority and to re-allocate resources to enable sufficient time to discuss these
issues within routine consultations One study for example found that patients who were
encouraged by their oncologist exercised significantly more than patients who did not
(Segar et al 1998) The next step is to back up the medical consultation with further
practical verbal and written advice from specialist nurses or information officers One UK
oncology unit for example does this as part of a formal lifestyle interview together with a
bespoke lifestyle information toolbox (Thomas and Nicholson 2009) During this interview
patients can be referred to smoking cessation clinics nutritionists and physiotherapists
where necessary The specialist nurse conducting this interview provides written information
and advice to patients and just as importantly their friends and family about local support
groups dietary measures where to buy healthy foods and specific local exercise facilities
which may entice them ranging from ballroom line and salsa dance lessons aerobics yoga
and fitness classes local walking swimming and cycling groups through to gyms sport
centre tennis and badminton courts and Pilates classes giving times contact numbers and
locations to make it as easy as possible to follow the advice The rationale for these
120
interviews is that individualised lifestyle counselling is more likely to elicit a response than
generic general advice The specialist nurse then follows up the advice by telephone and
further consultations as prompting has been shown to improve update A study from North
Bedfordshire for example showed that although 52 of patients accepted referral for
exercise in a local Gym a further 23 decided to attend classes only after additional
prompting from the nurse either by telephone
Many UK Oncology Units already have instigated an exit interview system to discuss follow
up arrangements and this process could be expanded to include lifestyle counselling
provided the specialist nurses involved have received extra training This training should
include a knowledge of the evidence and importance of weight diet physical activity and
smoking after cancer as well as ways to appropriately advise home-based exercise
regimens and how to direct patients towards the myriad of council or independent exercise
activities available locally to them The courses may require additional communication and
motivational skills training to enable nurses to engage in a partnership relationship which
promotes addressing the patientlsquos agenda goals and motivation around achieving and
maintaining behaviour change Examples of a range of courses aimed to develop such skills
and competencies and which are provided by the Flinders Human Behaviour and Health
Research Unit include a Chronic Condition Self-Management workshop Communication
and Motivational Skills Workshop and a Living Well Workshop
Remaining Questions
This review has provided some clarification of the evidence pertaining to lifestyle and cancer
outcomes However in implementing this evidence into standardised practice within cancer
aftercare will require a number of questions to be explored
1) What motivates cancer survivors to change unhealthy behaviours and maintain a
healthy lifestyle
At present it is unclear how soon after a cancer diagnosis an intervention should be
introduced for behaviour change(Rabin 2009) Until the teachable moment is more clearly
defined for cancer patients the advice is that professionals should repeatedly offer to assist
a patient with addressing their health behaviour risks until the patient accepts or seeks other
forms of support
The literature suggests that professional involvement in supported self-management and
lifestyle advice is required in order to maintain patient motivation by enhancing patient
engagement with health information and advice When information is supplied by healthcare
professionals and the patient is supported in using this information legitimacy is provided to
the information and advice (Protheroe et al 2008) Efficacy outcomes in terms of lifestyle
advice and behavioural change are fundamental in the initiation and maintenance of a
healthy lifestyle and the involvement of healthcare professionals strengthens outcome
efficacy whilst also motivating the patient and increasing their own self-efficacy to adapt their
lifestyle (Irwin 2008) However there is anecdotal and other evidence that on the one hand
the importance of lifestyle factors on the prognosis survival and symptom management of
121
cancer survivors is poorly understood and appreciated by significant numbers of cancer
health care professionals and on the other hand they do need specific training in the key
communication skills to be able to support effective behaviour change with their patients A
review is currently underway investigating the role of patient-professional communication in
terms of self-management
2) How can people most likely to benefit from lifestyle interventions be effectively
identified
A recent review on cancer-specific self-management programmes highlighted that patients
can be risk stratified according to needs and this according to whether they are likely to
benefit from the programme (Davies and Batehup 2010) For example people with low
levels of social support have been found to benefit most from group-delivered support As
part of the Bournemouth after Cancer Survivorship Project Active Wellness Programmelsquo
patients are assessed for the readiness to take part in physical activity (Milne et al 2010) It
is recommended that questionnaires that might facilitate such evidence-based risk
stratification be evaluated in order to provide further insight into this question A set of risk
stratification tools would be one way of ensuring cost-effectiveness
3) What are the various intensities of lifestyle support that can be provided based on
levels of individual need
As demonstrated within this review lifestyle interventions and self-management support do
generally require some level of support in order to be successful A strong
patientprofessional partnership appears to be at the essence of this intensive approach as
does longer-term follow-up and support (Davies and Batehup 2010) Addressing this
question will also in part address some of the inequalities within the current system of
cancer care with survivors identified as having low literacy being provided with extra
informational support and assistance with understanding the lifestyle recommendations
being made
122
Appendix A Evidence-Based Dietary Self-Management Recommendations
Food Advice Evidence
Reduce Saturated Fats
Unless underweight avoid processed fatty foods cakes biscuits crisps and other fatty snacks pastries cream and fried foods Cut the fat off the meat and check serum cholesterol regularly
(Ingram 1994 Hebert et al 1998 Norat et al 2004 Thomas et al 2009)
Increase all fish intake
All fresh fish but particularly the oily varieties such as mackerel and sardines Fresh water fish such as trout have the advantage of avoiding the potential heavy metal contamination of tuna amp sword fish which some suggest should not be eaten more than twice a week
(Ornish et al 2005 Meyerhardt et al 2007 Goodwin et al 2009)
Essential minerals
Vary the diet to ensure intake of adequate quantities of essential minerals consider Mixed nuts including Brazils Seafood including sardines prawns and shell fish Pulses and grains Vary carbohydrate sources such as pasta rice different brands of potatoes pulses such as lentils and quinoa
Rohan et al 1993) Powers et al 2007 McTiernan et al 2009)
Dietary Vitamins
Fresh fruit raw and calciferous vegetables grains oily fish nuts and salads Unless you have diarrhoea try to increase the amount of ripe fruit you eat each day ideally by eating the whole fruit Freshly squeezed fruit juices are recommended
(Rohan et al1993 Ingram 1994 Fleischauer et al 2003 New et al 2004 Rock et al 2005 McEligot et al 2006 Meyerhardt et al 2007 Schwarz et al 2008 Goodwin et al 2009)
Polyphenols
Onions leeks broccoli blueberries red wine tea apricots pomegranates chocolate coffee blueberries kiwis plums cherries ripe fruits parsley celery tomatoes mint citrus fruit
(Bettuzzi et al 2006 Pantuck et al 2006 Schwarz et al 2008 McLarty et al 2009)
Phytoestrogens
Soybeans and other legumes including peas lentils pinto (baked beans) and other beans and nuts (supplements not recommended)
Marini et al (2008)
Increase Carotenoids (Lycopene)
Tomatoes tomato sauce chilli carrots green vegetables and dark green salads
(Ingram 1994 Rock et al 2005 McEligot et al 2006 Pierce et al 2007 Powers et al 2007 Thomson et al 2007 Schwarz et al 2008)
123
Appendix B Evidence-Based Physical Activity Recommendations
Category Advice Evidence
Resistance Exercise
Strength training has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce fatigue and improve lean body mass and muscle strength Personalised tailored resistance exercise based on fitness assessments can improve QoL
Segal et al (2003) Poudevigne et al (2009) Courneya et al (2007) (Segal et al 2009)
Aerobic Exercise Aerobic exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of lymphoedema prevent loss of bone mineral density and reduce body fat Walking is particularly popular
Hayes Hildegard and Turner (2009) Schwartz Winters-Stone and Gallucci (2007) Courneya et al (2007) Fillion et al (2008) Kenfield et al (2009) Windsor Nichol and Potter (2004) Chang et al (2008)
Combined Resistance and Aerobic Exercise
Combined aerobic and resistance exercise has been found to reduce risk of cancer reoccurrence and mortality as well as to reduce symptoms of fatigue and improve QoL
Coleman et al (2003) Milne et al (2008)
3gt MET-hours per week
Benefits of physical activity require 3 or more MET-hours per week (eg using a stationary bicycle for one-hour)
Holick et al (2008) Holmes et al (2005) Saxton et al (2010) Kenfield (2010)
Moderate intensity
Physical activity needs to be of at least moderate intensity in order to offer beneficial outcomes
Holick et al (2008) Patterson et al (2010) Holmes et al (2005) Saxton et al (2010) Campbell et al (2007) Poudevigne et al (2009) Tardon et al (2004)
Dose-Response Exercise can be dose-responsive thus taking part in more than 3 MET-hours per week is likely to offer greater benefits
Meyerhardt et al (2005) Kenfield (2010)
During Treatment Remaining active during treatment can help with symptoms such as fatigue as well as increase completion rates for chemotherapy
Chang et al (2008) Coleman et al (2003) Courneya et al (2007)
Home-Based
Home-based physical activity prescriptions either supervised or alone have proven effective in improving cancer outcomes including reducing fatigue and protecting bone mineral density
Ligibel et al (2008) Windsor Nichol and Potter (2004) Schwartz Winters-Stone and Gallucci (2007)
Supervised Supervised physical activity either at home in groups or during treatment have proven effective in improving cancer outcomes as well as reducing lean body mass and facilitating the completion of chemotherapy
Chang et al (2008) Coleman et al (2003) Velthuis et al (2009) Courneya et al (2007) Campbell
et al (2007) exercise (Soliman et al 2009)
124
References
Abrahamsen JF Andersen A Hannisdal E et al Second malignancies after treatment of Hodgkins disease the influence of treatment follow-up time and age J Clin Oncol 11 (2) 255-61 1993 Addington-Hall et al (2010) Older womenlsquos experience of breast cancer alongside other health conditions The EPaN study (Experiences Preferences and Needs of women aged 70 years and over) University of Southampton Funded by Macmillan Cancer Support Ahmed R L W Thomas et al (2006) Randomized Controlled Trial of Weight Training and Lymphedema in Breast Cancer Survivors J Clin Oncol 24(18) 2765-2772 Ainsworth BE et al Compendium of physical activities an update of activity codes and MET intensities Med Sci Sports Exerc 2000 Sep32(9 Suppl)S498-504 Aitken J (ongoing) Colorectal cancer and quality of life study httpwwwcancerqldorgaupageResearch_statisticsVCRCCVCRCC_research_programsLifestyle_and_Cancer [Last accessed 04062010] Akopyan and Bonavida 2006 G Akopyan and B Bonavida Understanding tobacco smoke carcinogen NNK and lung tumorigenesis Int J Oncol 29 (2006) pp 745ndash752 Alberts DS Martinez ME Roe DJ et al Lack of effect of a high-fiber cereal supplement on the recurrence of colorectal adenomas Phoenix Colon Cancer Prevention Physicians Network [Comment] New England Journal of Medicine 2000 April 20342(16)1156-62 Arts CJ Govers CA van den Berg H Wolters MG van Leeuwen P Thijssen JH In vitro binding of estrogens by dietary fiber and the in vivo apparent digestibility tested in pigs J Steroid Biochem Mol Biol 1991 May38(5)621-8 Bandura A (1977) Self-efficacy Toward a unifying theory of behavioural change Psych Rev 84 191 - 215 Barbash-Ballard R Hunsberger S Alciati MH Blaire SN Goodwin PJ McTiernan A(2009) Physical activity weight control and breast cancer risk and survival Clinical trial rationale and design considerations J Natl Cancer Inst 101630-643 Baron JA Beach M Mandel JS et al Calcium supplements and colorectal adenomas Polyp Prevention Study Group Ann N Y Acad Sci 1999889138-45
Bekkering T Beynon R Davey Smith G Davies A Harbord R Sterne J Thomas S and Wood L (2006) A systematic review of RCTs investigating the effect of dietal and physical activity interventions on cancer survival updated report World Cancer Research Fund httpwwwdietandcancerreportorg [Last accessed 150210] Bellizzi K M J H Rowland et al (2005) Health Behaviours of Cancer Survivors Examining Opportunities for Cancer Control Intervention J Clin Oncol 23(34) 8884-8893 Bernstein H Cosford P and Williams A (2010) Enabling effective delivery of health and wellbeing an independent report Department of Health February 2010
125
Bettuzzi et al 2006 S Bettuzzi M Brausi F Rizzi G Castagnetti G Peracchia and A Corti Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia a preliminary report from a one-year proof-of-principle study Cancer Research 66 (2) (2006) pp 1234ndash1240 Bingham SA Day NE Luben R Ferrari P Slimani N Norat T et al Dietary fibre in food and protection against colorectal cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC) an observational study Lancet 20033611496ndash501 Bingham S Riboli E Diet and cancermdashthe European Prospective Investigation into Cancer and Nutrition Nat Rev Cancer 20044206ndash15 Blakeman T Bower P Reeves D Chew-Graham C (2010) ―Bringing self management into clinical view a qualitative study of long term condition management in primary care consultations Chronic Illness 0 1-15 Blackburn G L and K A Wang (2007) Dietary fat reduction and breast cancer outcome results from the Womens Intervention Nutrition Study (WINS) Am J Clin Nutr 86(3) 878S-881 Bonithon-Kopp C Kronborg O Giacosa A Rath U Faivre J Calcium and fibre supplementation in prevention of colorectal adenoma recurrence A randomised intervention trial Lancet 2000356(9238)1300-6 Borugian MJ Sheps SB Kim-Sing C Olivotto IA Van Patten C Dunn BP Coldman AJ Potter JD Gallagher RP Hislop TG Waist-to-hip ratio and breast cancer mortality Am J Epidemiol 2003 Nov 15158(10)963-8 Boyapati SM Shue X et al (2005) Soyfood intake and breast cancer survival a follow up of the Shanghai Breast Cancer Study Breast Cancer Research and Treatment 92(1) p11-17 Boyd NF Stone J Vogt KN Connelly BS Martin LJ Minkin S Dietary fat and breast cancer risk revisited a meta-analysis of the published literature Br J Cancer 2003 Nov 389(9)1672-85 Box R Marnes T amp Robertson V Aquatic physiotherapy and breast cancer related lymphoedema 5th Australasian Lymphology Association Conference Proceedings Mar 2004 47-9 Brown J K T Byers et al (2003) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 53(5) 268-291 Cade JE Burley VJ Greenwood DC UK Womens Cohort Study Steering Group Dietary fibre and risk of breast cancer in the UK Womens Cohort Study Int J Epidemiol 2007 Apr36(2)431-8 Caan B B Sternfeld et al (2005) Life After Cancer Epidemiology (LACE) Study A cohort of early stage breast cancer survivors (United States) Cancer Causes and Control 16(5) 545-556
126
Caan BJ Kwan ML Hartzell G Castillo A Slattery ML Sternfeld B Weltzien E Pre-diagnosis body mass index post-diagnosis weight change and prognosis among women with early stage breast cancer Cancer Causes Control 2008 Dec19(10)1319-28 Cadmus L A P Salovey et al (2009) Physical activity and quality of life during and after treatment for breast cancer results of two randomized controlled trials Psycho-Oncology 18(4) 343-352 Campbell KL Westerlind KC Harber VJ Bell GJ Mackey JR Courneya KS (2007) Effects of aerobic exercise training on oestrogen metabolism in premenopausal women a randomized controlled trial Cancer Epidemiol Biomarkers Prev 16731ndash73 Cancer 52 and NCSI Research Workstream (2009) Less common cancers consultation Report June 2009 Cella D (2009) Quality of life in patients with metastatic renal cell carcinoma The importance of patient-reported outcomes Cancer treatment reviews 35(8) 733-737 Chan JM Gann PH and Giovannucci EL (2005) Role of diet in prostate cancer development and progression Journal of Clinical Oncology 23(32) p 8152-60 Chlebowski RT Aiello E McTiernan A Weight loss in breast cancer patient management Journal of Clinical Oncology 20(4) 1128-1143 2002 Chlebowski RT Blackburn GL Elashoff RE Thomson C Goodman MT Shapiro A Giuliano AE Karanja N Hoy MK Nixon DW and The WINS Investigators (2005) Dietary fat reduction in post-menopausal women with primary breast cancer Journal of Clinical Oncology (10) p 3s Chlebowski R G Blackburn et al (2006) Dietary fat reduction and breast cancer outcome interim efficacy results from the Womens Intervention Diet Study J Natl Cancer Inst 98 1767 - 1776 Chlebowski RT Blackburn GL (2007) Diet and breast cancer recurrence JAMA 2007 Nov 14298(18)2135 author reply 2135-6 Chlebowski RT (2010) Lifestyle and breast cancer risk The way forward Journal of
Clinical Oncology Vol 28 No 9 (March 20) 2010 pp 1445-1447
Cho E Spiegelman D Hunter DJ Chen WY Colditz GA Willett WC Premenopausal dietary carbohydrate glycaemic index glycaemic load and fiber in relation to risk of breast cancer Cancer Epidemiol Biomarkers Prev 2003 Coulter A and Ellins J (2006) Patient-focused Interventions A review of the evidence Picker Institute Europe (01865 208100) and Health Foundation Coups E J and J S Ostroff (2005) A population-based estimate of the prevalence of behavioural risk factors among adult cancer survivors and non-cancer controls Preventive Medicine 40(6) 702-711 Courneya K S (2003) Physical activity in Cancer Survivors An Overview of Research Medicine amp Science in Sports amp Physical activity 35(11) 1846-1852
127
Courneya K Booth CM Gill S et al (2008) The colon health and life-long physical activity change trial a randomized trial of the national institute of Canada clinical trials group Current Oncology 15(6) 271-78 Cramp F Daniel J (2008) Physical activity for the management of cancer-related fatigue in adults CochraneDatabaseSystRev 2008 Cuzick J Aromatase inhibitors for breast cancer prevention J Clin Oncol 231636-1643 2005
Cuzick J Hot flushes and the risk of recurrence Retrospective exploratory results from the ATAC trial 30th Annual San Antonio Breast Cancer Symposium San Antonio TX December 13-16 2007 (poster 2069) Daley A H Crank et al (2007) Randomized trial of physical activity therapy in women treated for breast cancer J Clin Oncol 25 1713 - 1721 Daley A S Bowden et al (2008) What advice are oncologists and surgeons in the United Kingdom giving to breast cancer patients about physical activity International Journal of Behavioural Diet and Physical Activity 5(1) 46 Danhauer S Mihalki S Russell G Campbell C Felder L Daley L et al (2009) Restorative yoga for women with breast cancer Findings from a randomized pilot study Psych oncology 18(4) 360-368 Dansinger M L J A Gleason et al (2005) Comparison of the Atkins Ornish Weight Watchers and Zone Diets for Weight Loss and Heart Disease Risk Reduction A Randomized Trial JAMA 293(1) 43-53 Davies NJ and Batehup L (2010) Self-management support for cancer survivors Guidance for developing interventions An update of the evidence National Cancer Survivorship Initiative Macmillan Cancer Support March 2010 Demark-Wahnefried W and Jones L (2008) Promoting a Healthy Lifestyle among Cancer Survivors Haematologyoncology clinics of North America 22(2) 319-342 Deo SV Ray S Rath GK et al (2004) Prevalence and risk factors for development of lymphedema following breast cancer treatment Indian J Cancer 418ndash12 Department of Health (2001) Exercise referral systems A national quality assurance framework Department of Health Report London 2001 Department of Health (2004) At least five a week Evidence on the impact of physical activity and its relationship to health Department of Health Report London 2004 Department of Health (2009a) Internal analysis unpublished Department of Health London Department of Health (2009b) Obesity general information Health survey of England 2008 Department of Health London Department of Health (2009c) Guidance on the routine collection of patient-reported outcome measures (PROMs) p 28 The Stationary Office London
128
De Rezende LF Franco RL de Rezende MF et al Two physical activity schemes in postoperative breast cancer comparison of effects on shoulder movement and lymphatic disturbance Tumori 2006 9255ndash61 de Waard F Ramlau R Mulders Y de Vries T van Waveren S A feasibility study on weight reduction in obese postmenopausal breast cancer patients Eur J Cancer Prev 1993 May 2(3)233-8 Dignam J J B N Polite et al (2006) Body Mass Index and Outcomes in Patients Who Receive Adjuvant Chemotherapy for Colon Cancer J Natl Cancer Inst 98(22) 1647-1654 Dimeo FC Thomas F Raabe-Menssen C et al Effect of aerobic exercise and relaxation training on fatigue and physical performance of cancer patients after surgery A randomised controlled trial Support Care Cancer 2004 12(11)774-9 Dixon JM Renshaw L Young O et al Letrozole suppresses plasma estradiol and oestrone sulphate more completely than anastrozole in postmenopausal women with breast cancer J Clin Oncol 261671-1675 2008
Doyle C L H Kushi et al (2006) Diet and Physical Activity During and After Cancer Treatment An American Cancer Society Guide for Informed Choices CA Cancer J Clin 56(6) 323-353 Dwyer J J Peterson et al (2008) Do Flavonoid Intakes of Postmenopausal Women With Breast Cancer Vary on Very Low Fat Diets Diet and Cancer 60(4) 450 - 460 Eakin E Hayes S and Lawler S (ongoing) Physical activity for Health Using the telephone to promote physical activity-based rehabilitation in ruralremote Australian breast cancer survivors National Breast Cancer Foundation httpwwwuqeduaucprcindexhtmlpage=60214amppid=20928 [Last accessed 300310] Eliassen AH Missmer SA Tworoger SS Spiegelman D Barbieri RL Dowsett M Hankinson SE Endogenous steroid hormone concentrations and risk of breast cancer among premenopausal women J Natl Cancer Inst 2006 Oct 4 98(19)1406-15 Elkort RJ Baker FL Vitale JJ Cordano A Long-term nutritional support as an adjunct to chemotherapy for breast cancer JPEN J Parenter Enteral Nutr 1981 Sep-Oct 5(5)385-90 Enger SM Greif JM Polikoff J Press M Body weight correlates with mortality in early-stage breast cancer Arch Surg 2004139954ndash958 discussion 58ndash60 Eton D T D L Fairclough et al (2003) Early Change in Patient-Reported Health During Lung Cancer Chemotherapy Predicts Clinical Outcomes Beyond Those Predicted by Baseline Report Results From Eastern Cooperative Oncology Group Study 5592 J Clin Oncol 21(8) 1536-1543 Fentiman IS Allen DS Hamed H (2005) Smoking and prognosis in women with breast cancer Int J Clin Pract 591051ndash1054
129
Ferrari P Jenab M Norat T et al Lifetime and baseline alcohol intake and risk of colon and rectal cancers in the European prospective investigation bettinto cancer and nutrition (EPIC) Int J Cancer 2007 121 ( 9 ) 2065 ndash 2072
Feuerstein M (2006) Handbook of Cancer Survivorship New York NY Springer 2006 Fillion L P Gagnon et al (2008) A Brief Intervention for Fatigue Management in Breast Cancer Survivors Cancer Nursing 31(2) 145-159 Findley P amp Sambamoorthi U (2009) Preventive health services and lifestyle practices in cancer survivors A population health investigation Journal of Cancer Survivorship 3 43-58 Fleischauer AT Simonsen N Arab L Antioxidant supplements and risk of breast cancer recurrence and breast cancer-related mortality among postmenopausal women Nutr Cancer 2003 46 15-22 Flinders University (2009) Capabilities for Supporting Prevention and Chronic Condition Self-Management A Resource for Educators of Primary Health Care Professionals Australian Better Health Initiative A joint Australian State and Territory government initiative
Flowers M Thompson PA 2009 t10c12 Conjugated Linoleic Acid Suppresses HER2 Protein and Enhances Apoptosis in SKBr3 Breast Cancer Cells Possible Role of COX2 PLoS ONE 4(4) e5342 doi101371journalpone0005342 Food Standards Agency (2007) FSA nutrient and food based guidelines for UK institutions httpwwwfoodgovukmultimediapdfsnutrientinstitutionpdf [Last accessed 120310] Food Standards Agency (2010) Heightweight chart httpwwweatwellgovukhealthydiethealthyweightheightweightchart [Last accessed 120310] Ford MB Sigurdson AJ Petrulis ES et al Effects of smoking and radiotherapy on lung carcinoma in breast carcinoma survivors Cancer 98 (7) 1457-64 2003 Friedenreich C Cust A Lahmann PH et al Anthropometric factors and risk of endometrial cancer the European prospective investigation into cancer and nutrition Cancer Causes Control 2007 18399-413 Friedenreich C M C G Woolcott et al (2010) Alberta Physical Activity and Breast Cancer Prevention Trial Sex Hormone Changes in a Year-Long Physical activity Intervention Among Postmenopausal Women J Clin Oncol 28(9) 1458-1466 Friedenreich CM Cust AE Physical activity and breast cancer risk impact of timing type and dose of activity and population subgroup effects Br J Sports Med 2008 Aug42(8)636-47 Giovannucci EL (2005) Obesity insulin resistance and cancer risk Cancer Prevention 5 httpwwwnypcancerpreventioncomissue5propro_featurespre_earshtml [Last accessed 03062010]
130
Gold E B J P Pierce et al (2009) Dietary Pattern Influences Breast Cancer Prognosis in Women Without Hot Flashes The Womens Healthy Eating and Living Trial J Clin Oncol 27(3) 352-359 Gonzalez CAPera GAgudo APalli DKrogh VVineis PTumino RPanico SBerglund GSiman HNyren OAgren AMartinez CDorronsoro MBarricarte ATormo MJQuiros JRAllen NBingham SDay NMiller ANagel GBoeing HOvervad KTjonneland ABueno-de-Mesquita HBBoshuizen HCPeeters PNumans MClavel-Chapelon FHelen IAgapitos ELund EFahey MSaracci RKaaks RRiboli E Smoking and the risk of gastric cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC) Int J Cancer 107 (4) 629-634 (2003) Gonzaacutelez CA Jakszyn P Pera G Agudo A Bingham S Palli D Ferrari P Boeing H del Giudice G Plebani M Carneiro F Nesi G Berrino F Sacerdote C Tumino R Panico S Berglund G Simaacuten H Nyreacuten O Hallmans G Martinez C Dorronsoro M Barricarte A Navarro C Quiroacutes JR Allen N Key TJ Day NE Linseisen J Nagel G Bergmann MM Overvad K Jensen MK Tjonneland A Olsen A Bueno-de-Mesquita HB Ocke M Peeters PH Numans ME Clavel-Chapelon F Boutron-Ruault MC Trichopoulou A Psaltopoulou T Roukos D Lund E Hemon B Kaaks R Norat T Riboli E Meat intake and risk of stomach and oesophageal adenocarcinoma within the European Prospective Investigation Into Cancer and Nutrition (EPIC) J Natl Cancer Inst 2006 Mar 198(5)345-54 Goodwin PJ Pritchard KI Ennis M et al Insulin-lowering effects of metformin in women with early breast cancer Clin Breast Cancer 8501-5052008
Goodwin PJ Ennis M Pritchard KI Koo J Hood N (2009) Prognostic Effects of 25-Hydroxyvitamin D Levels in Early Breast Cancer Journal of Clinical Oncology Vol 27 No 23 (August 10) pp 3757-3763 Goodwin PJ Lifestyle Intervention Study in Adjuvant Treatment of Early Breast Cancer (LISA) (ongoing) httpclinicaltrialsgovct2showNCT00463489 [Last accessed 04062010] Goss PE Richardson H Chlebowski RT et al National Cancer Institute of Canada Clinical Trials Group MAP 3 Trial Evaluation of exemestane to prevent breast cancer in postmenopausal women at risk Clin Breast Cancer 7895-900 2007
Gothard L Cornes P et al (2004) Double-blind placebo-controlled randomised trial of vitamin E and pentoxifylline in patients with chronic arm lymphoedema and fibrosis after surgery and radiotherapy for breast cancer Radiotherapy and oncology journal of the European Society for Therapeutic Radiology and Oncology 73(2) 133-139 Grace PB Taylor JI Low YL Luben RN Mulligan AA Botting NP Dowsett M Welch AA Khaw KT Wareham NJ Day NE Bingham SA Phytoestrogen concentrations in serum and spot urine as biomarkers for dietary phytoestrogen intake and their relation to breast cancer risk in European prospective investigation of cancer and nutrition-norfolk Cancer Epidemiol Biomarkers Prev 2004 May13(5)698-708 Greenberg ER Baron JA Tosteson TD et al A clinical trial of antioxidant vitamins to prevent colorectal adenoma Polyp Prevention Study Group[comment] New England Journal of Medicine 1994 July 21331(3)141-7 Gritz ER (1993) Cancer Smoking Epidemiology Biomarkers amp Prevention 2(3) 261-270
131
Gritz E R M C Fingeret et al (2006) Successes and failures of the teachable moment Cancer 106(1) 17-27 Gross G C Ott et al (2002) Postmenopausal Breast Cancer Survivors at Risk for Osteoporosis Physical Activity Vigour and Vitality Oncology Nursing Forum 29(9) 1295-1300 Gross M C Ramirez et al (2009) Expression of androgen and oestrogen related proteins in normal weight and obese prostate cancer patients The Prostate 69(5) 520-527 Guthrie JR Ball M Murkies A Dennerstein L Dietary phytoestrogen intake in mid-life Australian-born women relationship to health variables Climacteric 2000 3 254ndash261 Hawkes A L S Gollschewski et al (2009) A telephone-delivered lifestyle intervention for colorectal cancer survivors a pilot study Psycho-Oncology 18(4) 449-455 Haydon AM Macinnis RJ English DR Giles GG (2006) The effect of physical activity and body size on survival after diagnosis with colorectal cancer Gut 55 p 62-67 Hayes SC Spence RR Galvao DANewton RU (2009) Australian Association for Physical activity and Sport Science position stand Optimising cancer outcomes through physical activity JSciMedSport 200912428-434 Heald AH Cade JE Cruickshank JK Anderson S White A Gibson JM (2003) The influence of dietary intake on the insulin-like growth factor (IGF) system across three ethnic groups a population-based study Public Health Nutr6175ndash80 Healthy Weight Healthy Lives (2008) A Cross-Government Strategy for England Cross-Government Obesity Unit DH and Department of Children Schools and Families Hebert JR Hurley TG Ma Y (1998) The effect of dietary exposures on recurrence and mortality in early stage breast cancer Breast Cancer Res Treat 5117ndash28 Hofstad B Almendingen K Vatn M et al Growth and recurrence of colorectal polyps a double-blind 3-year intervention with calcium and antioxidants Digestion 199859(2)148-56 Holick C N P A Newcomb et al (2008) Physical Activity and Survival after Diagnosis of Invasive Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 17(2) 379-386 Holm LE Nordevang E Hjalmar ML Lidbrink E Callmer E Nilsson B (1993) Treatment failure and dietary habits in women with breast cancer J Natl Cancer Inst 8532ndash36 Holmes MD Hunter DJ Colditz GA et al Association of dietary intake of fat and fatty acids with risk of breast cancer JAMA 1999281914-920 Holmes MD Chen WY Feskanich D Kroenke CH Colditz GA (2005) Physical activity and survival after breast cancer diagnosis JAMA 293 p 2479-86
132
Holmes MD Murin S Chen WY Kroenke CH Spiegelman D Colditz GA (2007) Smoking and survival after breast cancer diagnosis Int J Cancer 1202672ndash2677
Howe GR Hirohata T Hislop TG Iscovich JM Yuan JM Katsouyanni K Lubin F Marubini E Modan B Rohan T et al Dietary factors and risk of breast cancer combined analysis of 12 case-control studies J Natl Cancer Inst 1990 Apr 482(7)561-9
Hunter DJ Spiegelman D Adami HO Beeson L van den Brandt PA Folsom ARFraser GE Goldbohm RA Graham S Howe GR et al Cohort studies of fat intake and the risk of breast cancer--a pooled analysis N Engl J Med 1996 Feb 8334(6)356-61
Ingram D Diet and subsequent survival in women with breast cancer British Journal of Cancer 1994 Mar69(3)592-5
Irwin ML Smith AW McTiernan A Ballard-Barbash R Cronin K Gilliland FD Baumgartner RN Baumgartner KB Bernstein L (2008) Influence of Pre- and Postdiagnosis Physical Activity on Mortality in Breast Cancer Survivors The Health Eating Activity and Lifestyle Study Journal of Clinical Oncology 26(24) 3958-3964
Ishikawa H Akedo I Otani T et al Randomized trial of dietary fiber and Lactobacillus casei administration for prevention of colorectal tumors Int J Cancer 2005 September 20116(5)762-7 Jiralerspong S Palla SL Giordano SH et al Metformin and pathologic complete responses to neoadjuvant chemotherapy in diabetic patients with breast cancer J Clin Oncol 273297-3302 2009
Jones LW Demark-Wahnefried W Diet physical activity and complementary therapies after primary treatment for cancer Lancet Oncol 7(12)1017-26 Nov-Dec 2006 PMID 17138223 Kaaks R A Lukanova and MA Kurzer Obesity endogenous hormones and endometrial cancer risk a synthetic review Cancer Epidemiol Biomark Prev 11 (2002) pp 1531ndash1543 Kaaks R Rinaldi S Key TJ Berrino F Peeters PH Biessy C Dossus L Lukanova A Bingham S Khaw KT Allen NE Bueno-de-Mesquita HB van Gils CH Grobbee D Boeing H Lahmann PH Nagel G Chang-Claude J Clavel-Chapelon F Fournier A Thieacutebaut A Gonzaacutelez CA Quiroacutes JR Tormo MJ Ardanaz E Amiano P Krogh V Palli D Panico S Tumino R Vineis P Trichopoulou A Kalapothaki V Trichopoulos D Ferrari P Norat T Saracci R Riboli E Postmenopausal serum androgens oestrogens and breast cancer risk the European prospective investigation into cancer and nutrition Endocr Relat Cancer 2005 Dec12(4)1071-82 Kawahara M Ushijima S Kamimori T et al Second primary tumours in more than 2-year disease-free survivors of small-cell lung cancer in Japan the role of smoking cessation Br J Cancer 78 (3) 409-12 1998 Keinan-Boker L van Der Schouw YT Grobbee DE Peeters PH Dietary phytoestrogens and breast cancer risk Am J Clin Nutr 2004 Feb79(2)282-8 Kenfield SA (2010) Physical activity and mortality in prostate cancer (In Regular Vigorous Physical Activity found to have Survival Benefits for Prostate Cancer Patients
133
AACR Frontier in Cancer Prevention Research Conference by Tuma R Oncology Times) 32(2) p 29 33 Key TJ Allen NE Hormones and breast cancer IARC Sci Publ 2002156273-6 Khaodhiar L Nixon D Chlebowski RT Elashoff R Blackburn GL Hoy MK Insulin resistance in postmenopausal women with breast cancer Proc Am Cancer Res 2003446349 (abstr) Kim EH Willett WC Colditz GA Hankinson SE Stampfer MJ Hunter DJ Rosner B Holmes MD Dietary fat and risk of postmenopausal breast cancer in a 20-year follow-up Am J Epidemiol 2006 Nov 15164(10)990-7 Korstjens I A M May et al (2008) Quality of Life After Self-Management Cancer Rehabilitation A Randomized Controlled Trial Comparing Physical and Cognitive-Behavioural Training Versus Physical Training Psychosom Med 70(4) 422-429 Krein S M Heisler J Piette F Makki and E Kerr 2005 The effect of chronic pain on diabetes patientslsquo self-management Diabetes Care 28(1)65ndash70 Kroenke CH Fung TT Hu FB Holmes MD Dietary patterns and survival after breast cancer diagnosis J Clin Oncol 2005 Dec 2023(36)9295-303 Kubik AK Zatloukal P Tomasek L Petruzelka L (2002) Lung cancer risk among Czech women a case-control study Prev Med 34(4) 436ndash444 Kucera H [Adjuvanticity of vitamin A in advanced irradiated cervical cancer (authors transl)] Wiener Klinische Wochenschrift Supplementum 19801181-20 Kushi LH Byers T Doyle C et al American Cancer Society Guidelines on Diet and Physical Activity for cancer prevention reducing the risk of cancer with healthy food choices and physical activity CA Cancer J Clin 2006 56 254ndash8 Kyogoku S Hirohata T Nomura Y Shigematsu T Takeshita S Hirohata I Diet and prognosis of breast cancer Nutr Cancer 199217(3)271-7 Lahmann PH Schulz M Hoffmann K Boeing H Tjoslashnneland A Olsen A Overvad K Key TJ Allen NE Khaw KT Bingham S Berglund G Wirfaumllt E Berrino F Krogh V Trichopoulou A Lagiou P Trichopoulos D Kaaks R Riboli E Long-term weight change and breast cancer risk the European prospective investigation into cancer and nutrition (EPIC) Br J Cancer 2005 Sep 593(5)582-9 Lee IM Sesso HD Paffenbarger RS Jr (1999) Physical activity and risk of lung cancer Int J Epidemiol 28(4) 620ndash625 Lev E L (1997) Banduras Theory of Self-Efficacy Applications to Oncology Research and Theory for Nursing Practice 11 21-37 Ligibel J A W Demark-Wahnefried et al (2009) Diet Physical activity and Supplements Guidelines for Cancer Survivors ASCO EDUCATIONAL BOOK 2009(1) 541-547 Lindsay S (2009) Prioritizing illness Lessons in self-managing multiple chronic conditions Canadian Journal of Sociology PhD Thesis ejournalslibraryualbertaca
134
Lucia A Earnest C Perez M (2003) Cancer-related fatigue can physical activity physiology assist oncologists Lancet Oncol 4616-625 Lyons R amp Langille L (2000) Healthy Lifestyle Strengthening the Effectiveness of Lifestyle Approaches to Improve Health Health Canada Ottawa Ontario Available at httpwwwhc-scgccahppbphdddocshealthy MacLennan R Macrae F Bain C et al Effect of fat fibre and beta carotene intake on colorectal adenomas further analysis of a randomized controlled dietary intervention trial after colonoscopic polypectomy Asia Pac J Clin Nutr 1999 8(suppl)S54-S58 Macmillian Cancer Support (2008) Two Million Reasons The Cancer Survivorship Agenda 2008 Maddams J Moller H and Devane C Cancer prevalence in the UK 2008 Thames Cancer Registry and Macmillan Cancer Support 2008 Manjer J Berglund G Bondesson L Garne J P Janzon L Malina J Breast cancer incidence in relation to smoking cessation Breast Cancer Res Treat 61121-129 2000 Mao Y Pan S Wen SW Johnson KC The Canadian Cancer (2003) Physical activity and the risk of lung cancer in Canada Am J Epidemiol 158(6) 564ndash575 Mayne S T B Cartmel et al (2009) Alcohol and Tobacco Use Pre-diagnosis and Postdiagnosis and Survival in a Cohort of Patients with Early Stage Cancers of the Oral Cavity Pharynx and Larynx Cancer Epidemiology Biomarkers amp Prevention 18(12) 3368-3374 McDonald P R Williams et al (2002) Breast cancer survival in African American women Is alcohol consumption a prognostic indicator Cancer Causes and Control 13(6) 543-549 McEligot AJ Largent J Ziogas A Peel D Anton-Culver H Dietary fat fiber vegetable and micronutrients are associated with overall survival in postmenopausal women diagnosed with breast cancer Nutr Cancer 200655(2)132-140 McNeely M L K L Campbell et al (2006) Effects of physical activity on breast cancer patients and survivors a systematic review and meta-analysis CMAJ 175(1) 34-41 McKenzie D C and A L Kalda (2003) Effect of Upper Extremity Physical activity on Secondary Lymphedema in Breast Cancer Patients A Pilot Study J Clin Oncol 21(3) 463-466 McKeown-Eyssen GE Bright-See E Bruce WR et al A randomized trial of a low fat high fibre diet in the recurrence of colorectal polyps Toronto Polyp Prevention Group [erratum appears in J Clin Epidemiol 1995 Feb48(2)i] Journal of Clinical Epidemiology 1994 May47(5)525-36 McLarty Jerry Bigelow Rebecca LH Smith Mylinh Elmajian Don Ankem Murali Cardelli James A (2009) Tea Polyphenols Decrease Serum Levels of Prostate-Specific Antigen Hepatocyte Growth Factor and Vascular Endothelial Growth Factor in Prostate
135
Cancer Patients and Inhibit Production of Hepatocyte Growth Factor and Vascular Endothelial Growth Factor In vitro Cancer Prev Res 1940-6207CAPR-08-0167
McTiernan A et al (2009) Low-fat increased fruit vegetable and grain dietary pattern fractures and bone mineral density the Womens Health Initiative Dietary Modification Trial Am J Clin Nutr 89 1864-1876
Meyerhardt JA Heseltine D Niedzwiecki D Hollis D Saltz LB Mayer RJ Schilsky RL and Fuchs CS (2005) The impact of physical activity on patients with stage III colon cancer Findings from Intergroup trial CALGB 89803 Proc Am Soc Clin Oncol 24 p abstract 3534 Meyerhardt J A D Niedzwiecki et al (2007) Association of Dietary Patterns With Cancer Recurrence and Survival in Patients With Stage III Colon Cancer JAMA 298(7) 754-764 Meyerhardt J A D Niedzwiecki et al (2008) Impact of Body Mass Index and Weight Change after Treatment on Cancer Recurrence and Survival in Patients With Stage III Colon Cancer Findings From Cancer and Leukemia Group B 89803 J Clin Oncol 26(25) 4109-4115 Meyskens FL Jr Kopecky KJ Appelbaum FR Balcerzak SP Samlowski W Hynes H Effects of vitamin A on survival in patients with chronic myelogenous leukemia a SWOG randomized trial Leukemia Research 1995 September 19(9)605-12 Miles A Simon A Wardle J (2010) Answering patient questions about the role lifestyle factors play in cancer onset and recurrences Journal of Health Psychology 15(2) p 291-298 Milne H K Wallman et al (2008) Impact of a Combined Resistance and Aerobic Physical activity Program on Motivational Variables in Breast Cancer Survivors A Randomized Controlled Trial Annals of Behavioral Medicine 36(2) 158-166 Milne M Hamerston L and Morrell D (2010) BACSUP adult survivorship living with and beyond cancer test community learning workshop London January 2010 Monninkhof EM Peeters PH Schuit AJ Design of the sex hormones and physical exercise (SHAPE) study BMC Public Health 2007 Sep 47232 Morrell RM Halyard MY Schild SE Ali MS Gunderson LL Pockaj BA (2005) Breast cancer-related lymphedema Mayo Clin Proc 801480ndash1484 Mortimer P S D O Bates et al (1996) The prevalence of arm oedema following treatment for breast cancer QJM 89(5) 377-380 Mortimer JE Flatt SW Parker BA et al Tamoxifen hot flashes and recurrence in breast cancer Breast Cancer Res Treat 108421-426 2008 Moseley AL Piller NB Carati CJ (2005) The effect of gentle arm physical activity and deep breathing on secondary arm lymphedemaLymphology Sep38(3)136-45 Moseley AL Piller NB (2008) Physical activity for limb Lymphoedema ndash Evidence that it is beneficial Journal of Lymphoedema vol 3(1) pp 51-56
136
Mustian KM Palesh OG Flecksteiner SA Tai Chi Chuan for breast cancer survivors Medicine and sport science 2008 52()209-17 National Cancer Action Team (2009) Cancer and palliative care rehabilitation workforce project A review of the evidence National Cancer Action Team National Comprehensive Cancer Network (2009) NCCN Clinical Practice Guidelines in Oncology Cancer-related fatigue version 1 2009 National Cancer Survivorship Initiative (NCSI) (2009) Research Work Stream Mapping Project - Summary and reports for Bowel Cancer Breast Cancer Lung Cancer Prostate cancer National Cancer Survivorship Initiative Macmillan Cancer Support National Health Service (2010) NHS advice on drinking limits NHS Choices httpwwwdrinkingnhsukquestionsrecommended-levels [Last accessed 300310] National Institutes of Health (1998) Clinical Guidelines on the Identification Evaluation and Treatment of Overweight and Obesity in Adults The Evidence Report National Heart Lung and Blood Institute in cooperation with the National Institute of Diabetes and Digestive Kidney Diseases NIH Publication No 98-4083 National Institutes of Health Osteoporosis and Related Bone Diseases (2009) Conditions and behaviours that increase osteoporosis risk National Resource Centre US Department of Health and Human Services httpwwwniamsnihgovHealth_InfoBoneOsteoporosisConditions_Behaviorsosteoporosis_breast_cancerasp [Last accessed 170210] National Obesity Observatory (2009) Body mass index as a measure of obesity Association of Public Health Observatories June 2009 Ng K J A Meyerhardt et al (2008) Circulating 25-Hydroxyvitamin D Levels and Survival in Patients With Colorectal Cancer J Clin Oncol 26(18) 2984-2991 Nikotetti S Young J Levitt M (2008) Bowel problems self-care practices and information needs of colorectal cancer survivors at 6 to 24 months after sphincter-saving surgery Cancer Nursing 31(5) p 389-398
Norat T Bingham S Ferrari P Slimani N Jenab M Mazuir M Overvad K Olsen A Tjoslashnneland A Clavel F Boutron-Ruault MC Kesse E Boeing H Bergmann MM Nieters A Linseisen J Trichopoulou A Trichopoulos D Tountas Y Berrino F Palli D Panico S Tumino R Vineis P Bueno-de-Mesquita HB Peeters PH Engeset D Lund E Skeie G Ardanaz E Gonzaacutelez C Navarro C Quiroacutes JR Sanchez MJ Berglund G Mattisson I Hallmans G Palmqvist R Day NE Khaw KT Key TJ San Joaquin M Heacutemon B Saracci R Kaaks R Riboli E Meat fish and colorectal cancer risk the European Prospective Investigation into cancer and nutrition J Natl Cancer Inst 2005 Jun 1597(12)906-16
Ornish D et al (2005) Intensive lifestyle changes may affect the progression of prostate cancer The Journal of Urology 174 p 1065-1070 Ostroff JS Jacobsen PB Moadel AB Spiro RH Shah JP Strong EW et al (1995) Prevalence and predictors of continued tobacco use after treatment of patients with head and neck cancer Cancer Jan 1575(2)569-76
137
Pantuck AJ et al (2006) Phase II study of pomegranate juice for men with rising PSA following surgery or RXT for prostate cancer Clin Cancer Res 12(13) p 4018-4026 Pantuck AJ et al Abstract presented at the American Society of Clinical Oncology 2008 Genitourinary Cancers Symposium (Abstract 40) Long Term Follow Up Of Pomegranate Juice For Men With Prostate Cancer And Rising PSA Shows Durable Improvement in PSA Doubling Time Parsons A A Daley et al Influence of smoking cessation after diagnosis of early stage lung cancer on prognosis systematic review of observational studies with meta-analysis BMJ 340(jan21_1) Pastorino U Infante M Maioli M et al Adjuvant treatment of stage I lung cancer with high-dose vitamin A[comment] J Clin Oncol 1993 July11(7)1216-22 Patterson R E L A Cadmus et al Physical activity diet adiposity and female breast cancer prognosis A review of the epidemiologic literature Maturitas In Press Corrected Proof Pedersen BK Saltin B Evidence for prescribing physical activity as therapy in chronic disease Scand J Med Sci Sports 16 Suppl 1 3ndash63 2006Pierce J P L Natarajan et al (2007) Influence of a Diet Very High in Vegetables Fruit and Fiber and Low in Fat on Prognosis Following Treatment for Breast Cancer The Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA 298(3) 289-298 Pierce JP Faerber S Wright FA Newman V Flatt SW Kealey S Rock CL Pierce JP Natarajan L Caan BJ et al Influence of a diet very high in vegetables fruit and fiber and low in fat on prognosis following treatment for breast cancer the Womens Healthy Eating and Living (WHEL) Randomized Trial JAMA2007298(3)289-298 Ponz dL Roncucci L Chemoprevention of colorectal tumors role of lactulose and of other agents Scandinavian Journal of Gastroenterology Supplement 199722272-5 Poudevigne M J Wojcik et al (2009) The Effects Of 12-weeks Cross Training On Fatigue And Mood In Recent Breast Cancer Survivors 2292 Board 180 May 28 200 PM - 330 PM Medicine amp Science in Sports amp Physical activity 41(5) 297-298 Powers H J M H Hill et al (2007) Responses of Biomarkers of Folate and Riboflavin Status to Folate and Riboflavin Supplementation in Healthy and Colorectal Polyp Patients (The FAB2 Study) Cancer Epidemiology Biomarkers amp Prevention 16(10) 2128-2135 Protheroe J A Rogers et al (2008) Promoting patient engagement with self-management support information a qualitative meta-synthesis of processes influencing uptake Implementation Science 3(1) 44 Provenzano E and N Johnson (2009) Overview of recommendations of HER2 testing in breast cancer Diagnostic Histopathology 15(10) 478-484 Puhl RM Heuer CA (2009) ―The stigma of obesity A Review and Update Obesity 17 (5) 941-964 Rabin C (2009) ―Promoting Lifestyle Change among Cancer Survivors When is the Teachable Moment American Journal of Lifestyle Medicine 3 (5) 369-378
138
Reding K W J R Daling et al (2008) Effect of Pre-diagnostic Alcohol Consumption on Survival after Breast Cancer in Young Women Cancer Epidemiology Biomarkers amp Prevention 17(8) 1988-1996 Riboli E Hunt KJ Slimani N Ferrari P Norat T Fahey M Charrondiegravere UR Heacutemon B Casagrande C Vignat J Overvad K Tjoslashnneland A Clavel-Chapelon F ThieacutebautA Wahrendorf J Boeing H Trichopoulos D Trichopoulou A Vineis P Palli D Bueno-De-Mesquita HB Peeters PH Lund E Engeset D Gonzaacutelez CA Barricarte A Berglund G Hallmans G Day NE Key TJ Kaaks R Saracci R (2002) European Prospective Investigation into Cancer and Nutrition (EPIC) study populations and data collection Public Health Nutr 2002 Dec5(6B)1113-24 Richardson G E M A Tucker et al (1993) Smoking Cessation after Successful Treatment of Small-Cell Lung Cancer Is Associated with Fewer Smoking-related Second Primary Cancers Annals of Internal Medicine 119(5) 383-390 Richardson A Addington-Hall J Stark D Foster C Amir Z Sharpe M (2009) Determining research priorities for cancer survivorship Consultation and evidence review Commissioned by the NCSI Robertson R (2008) Using Information to Promote Healthy Behaviours Kings Fund London Rock C L and W Demark-Wahnefried (2002) Diet and Survival After the Diagnosis of Breast Cancer A Review of the Evidence J Clin Oncol 20(15) 3302-3316 Rock C L S W Flatt et al (2005) Plasma Carotenoids and Recurrence-Free Survival in Women With a History of Breast Cancer J Clin Oncol 23(27) 6631-6638 Rohan T Howe G Friedenreich C et al (1993) Dietary fiber vitamins A C and E and risk of breast cancer a cohort study Cancer Causes and Control 4(1) p 29-37 Rosenbaum EH Fobair P Spiegel D (2006) Cancer is a Life-changing Event Cancer Supportive Care Programs httpwwwcancersupportivecarecomSurvivorsurvivehtml [Last accessed January 30 2009] Ryan CW D Huo and K Bylow et al (2007) Suppression of bone density loss and bone turnover in patients with hormone-sensitive prostate cancer and receiving zoledronic acid BJU Int 100 pp 70ndash75 Sagiv SK Gaudet MM Eng SM et al (2007) Active and passive cigarette smoke and breast cancer survival Ann Epidemiol 17385ndash393 Sandel S Judge J Landry N et al (2005) Dance and movement program improves quality-of-life measures in breast cancer survivors Cancer Nursing 28(4) 301-309 Saxton J (2010) Physical activity and cancer mortality In Physical activity and cancer Survivorship Springer New York pp 189-210 Schatzkin A Lanza E Corle D et al Lack of effect of a low-fat high-fiber diet on the recurrence of colorectal adenomas Polyp Prevention Trial Study Group [comment] New England Journal of Medicine 2000 April 20342(16)1149- 55
139
Schmitz KH Courneya KS Matthews C Demark-Wahnefried W et al (2010) ―American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors Medicine and Science in Sports and Exercise Special Communication 0195-9131104207-14090 Schmitz K Holtzman J Courneya K Masse L Duval S Kane R Controlled physical activity trials in cancer survivors A systematic review and meta-analysis Cancer Epidemiol Biomarkers Prev 2005141588ndash95
Schulz M Lahmann PH Boeing H et al Fruit and vegetable consumption and risk of epithelial ovarian cancer the European Prospective Investigation into Cancer and Nutrition Cancer Epidemiol Biomarkers Prev 2005142531ndash2535 Schwarz S U C Obermuller-Jevic et al (2008) Lycopene Inhibits Disease Progression in Patients with Benign Prostate Hyperplasia J Nutr 138(1) 49-53 Schmitz K H Balancing Lymphedema Risk Physical activity Versus Deconditioning for Breast Cancer Survivors Physical activity and Sport Sciences Reviews 38(1) 17-24 10 Segal RJ Reid RD Courneya KS et al(2003) Resistance physical activity in men receiving androgen deprivation therapy for prostate cancer JClinOncol211653-1659
Segal RJ Reid RD Courneya KS Sigal RJ Kenny GP PrudlsquoHomme DGet al Randomized Controlled Trial of Resistance or Aerobic Exercise in Men Receiving Radiation Therapy for Prostate Cancer J Clin Oncol 2009 Jan 2027344-51 Sellers TA Potter JD Folsom AR (1991) Association of incident lung cancer with family history of female reproductive cancers the Iowa Womenlsquos Health Study Genet Epidemiol 8(3) 199ndash208 Severson RK Nomura AM Grove JS Stemmermann GN A prospective analysis of physical activity and cancer Am J Epidemiol 1989 Sep130(3)522-9 Shaw C Mortimer P Judd PA Randomized controlled trial comparing a low-fat diet with a weight-reduction diet in breast cancer-related lymphedema Cancer 20071091949ndash56 Sinicrope F A N R Foster et al Obesity Is an Independent Prognostic Variable in Colon Cancer Survivors Clinical Cancer Research 16(6) 1884-1893 Siris E S P D Miller et al (2001) Identification and Fracture Outcomes of Undiagnosed Low Bone Mineral Density in Postmenopausal Women Results From the National Osteoporosis Risk Assessment JAMA 286(22) 2815-2822 Soliman S W J Aronson et al (2009) Analyzing Serum-Stimulated Prostate Cancer Cell Lines After Low-Fat High-Fiber Diet and Physical activity Intervention eCAM nep031 Sonn GA Aronson W and Litwin MS (2005) Impact of diet on prostate cancer A review Prostate cancer and prostate disease 8 p 304-310 Speck RM Courneya KS Masse L Duval S Schmitz K (2010) An update of controlled physical activity trials in cancer survivors a systematic review and meta-analysis Journal of Cancer Survivorship 4(2) p 87-100
140
Steginga S K B M Lynch et al (2009) Antecedents of domain-specific quality of life after colorectal cancer Psycho-Oncology 18(2) 216-220 Stevinson C H Steed et al (2009) Physical Activity in Ovarian Cancer Survivors Associations With Fatigue Sleep and Psychosocial Functioning International Journal of Gynecological Cancer 19(1) 73-78 Swenson KK Nissen MJ Anderson E Shapiro A Schousboe J Leach J (2009) Effects of physical activity vs bisphosphonates on bone mineral density in breast cancer patients receiving chemotherapy Support Oncol May-Jun7(3)101-7 Tardon A Lee WJ Delgado-Rodriguez M et al Leisure-time physical activity and lung cancer a meta-analysis Cancer Causes Control200516(4)389-397 Taskila T Martikainen R Hietanen P Lindbohm M Comparative study of work ability between cancer survivors and their referents Europ J of Cancer 2007 43914-920 Taylor R Brown A et al (2004) Physical activity-based rehabilitation for patients with coronary heart disease systematic review and meta-analysis of randomized controlled trials The American journal of medicine 116(10) 682-692 Taylor NFDodd KJShields NBruder A Therapeutic physical activity in physiotherapy practice is beneficial a summary of systematic reviews 2002-2005 Aust J Physiother 2007 53 7-16 Thiebaut A C M A Schatzkin et al (2006) Dietary Fat and Breast Cancer Contributions From a Survival Trial J Natl Cancer Inst 98(24) 1753-1755 Thomas R Daly M and Perryman J (2000) Forewarned is forearmed - Randomised evaluation of a preparatory information film for cancer patients European Journal of Cancer 36(2) p 52-53 Thomas R et al (2005) Dietary advice combined with a salicylate mineral and vitamin supplement (CV247) has some tumour static properties - a phase II study Diet and science 2005 35(6) p 436-451 Thomas RJ and Davies ND (2007) Lifestyle during and after cancer treatment Clinical Oncology Vol 19 Issue 8 pp 616-627 Thomas R Nicholson C (2009) Why is exercise good for us Cancer Active httpcanceractivecomcancer-active-page-linkaspxn=2600ampTitle=Why20is20exercise20good20for20us [Last accessed 230710] Thomas R Oakes R Gordon J Russell S Blades M Williams M (2009) A randomised double-blind phase II study of lifestyle counselling and salicylate compounds in patients with progressive prostate cancer Diet and Food Science 39(3) pp 295 ndash 305 Thomson C A N R Stendell-Hollis et al (2007) Plasma and Dietary Carotenoids Are Associated with Reduced Oxidative Stress in Women Previously Treated for Breast Cancer Cancer Epidemiology Biomarkers amp Prevention 16(10) 2008-2015
141
Thune I Brenn T Lund E Gaard M Physical activity and the risk of breast cancer N Engl J Med 336 1269-1275 1997
Travis LB Gospodarowicz M Curtis RE et al Lung cancer following chemotherapy and radiotherapy for Hodgkins disease J Natl Cancer Inst 94 (3) 182-92 2002 Tucker MA Murray N Shaw EG et al Second primary cancers related to smoking and treatment of small-cell lung cancer Lung Cancer Working Cadre J Natl Cancer Inst 89 (23) 1782-8 1997 Twiss J J N Waltman et al (2001) Bone Mineral Density in Postmenopausal Breast Cancer Survivors Journal of the American Academy of Nurse Practitioners 13(6) 276-284 Uhley V and Jen C (2006) Diet and weight management in cancer survivors In Handbook of Cancer Survivorship edited by Feuerstein M New York NY Springer 2006 ISBN-13 978-0-3873-4561-1
Vadiraja HS et al (2009) Effects of yoga program on quality of life and affect in early breast cancer patients undergoing adjuvant radiotherapy A randomized controlled trial Complementary Therapies in Medicine Volume 17 Issue 5 Pages 274-280
Velthuis MJ Agasi-Idenburg SC Aufdemkampe G Wittink HM (in press) The effect of physical activity on cancer-related fatigue during cancer treatment a meta-analysis of Randomised Controlled Trials Clinical Oncology 2009 (in print) Vineis P G Hoek and M Krzyzanowski et al Lung cancers attributable to environmental tobacco smoke and air pollution in non-smokers in different European countries a prospective study Environ Health 6 (2007) pp 1ndash7 Visvanathan K Chlebowski RT Hurley P et al American Society of Clinical Oncology 2008 clinical practice guideline update on the use of pharmacologic intervention including tamoxifen raloxifene and aromatase inhibition for breast cancer risk reduction J Clin Oncol 273235-3258 2009
Wagner LI Cella D (2004) Fatigue and cancer causes prevalence and treatment approaches BrJCancer 91822-828 Waltman N J Twiss et al (2009) ―The effect of weight training on bone mineral density and bone turnover in postmenopausal breast cancer survivors with bone loss a 24-month randomized controlled trial Osteoporosis International Wenzel L H Q Huang et al (2005) Quality-of-Life Comparisons in a Randomized Trial of Interval Secondary Cytoreduction in Advanced Ovarian Carcinoma A Gynecologic Oncology Group Study J Clin Oncol 23(24) 5605-5612 Weikert C Hoffmann K Dierkes J Zyriax BC KlipsteinndashGrobusch K MB et al Homocysteine metabolismrelated dietary pattern and the risk of coronary heart disease in two independent German study populations J Nutr 2005 1351981ndash1988 White S E McAuley et al (2009) Translating Physical Activity Interventions for Breast Cancer Survivors into Practice An Evaluation of Randomized Controlled Trials Annals of Behavioural Medicine 37(1) 10-19
142
World Health Organisation (1999) What is a healthy lifestyle Health Documentation Services WHO Regional Office for Europe Copenhagen World Health Organisation (2002) The World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva WHO Scientific Group on the Prevention and Management of Osteoporosis (2000 Geneva Switzerland) (2003) Prevention and management of osteoporosis report of a WHO scientific group World Health Organisation (2005) The European health report 2005 public health action for healthier children and populations Copenhagen WHO regional office for Europe World Health Report 2002 ndash Reducing Risks Promoting Healthy Life World Health Organisation Geneva Windsor P M Nichol K F Potter J A randomized controlled trial of aerobic exercise for treatment-related fatigue in men receiving radical external beam radiotherapy for localised prostate carcinoma Cancer (2004) 101 (3) 550-7 Wright M E S-C Chang et al (2007) Prospective study of adiposity and weight change in relation to prostate cancer incidence and mortality Cancer 109(4) 675-684 Wright P A Smith et al (2005) Psychosocial difficulties deprivation and cancer three questionnaire studies involving 609 cancer patients Br J Cancer 93(6) 622-626 Yu GP et al (1997) The effect of smoking after treatment for Cancer Cancer Detect Prev 21487-509