advances in the management of skeletal related events/bone metastases in prostate cancer
DESCRIPTION
Advances in the Management of Skeletal Related Events/Bone Metastases in Prostate Cancer. Robert Dreicer, M.D., M.S., FACP, FASCO Chair Dept of Solid Tumor Oncology Taussig Cancer Institute Cleveland Clinic Professor of Medicine Cleveland Clinic Lerner College of Medicine. - PowerPoint PPT PresentationTRANSCRIPT

Advances in the Management of Skeletal Related Events/Bone Metastases in Prostate Cancer
Robert Dreicer, M.D., M.S., FACP, FASCOChair Dept of Solid Tumor OncologyTaussig Cancer InstituteCleveland ClinicProfessor of Medicine Cleveland Clinic Lerner College of Medicine

LocallyAdvancedDisease
Rising PSAHormone
Naive
Rising PSACastrate
MetastasesCastrateResistant
Asymptomatic
Metastases
CastrateResistant
Symptomatic
OrganConfined
Metastatic Disease
(De novo)
Clinical States In Prostate Cancer (circa Winter 2014)
MetastasesCastrateResistant
Post Docetaxel
MetastasesCastrateResistant
Post Cabazitaxel
Sipuleucel-T
Abiraterone
CabazitaxelDenosumab
Enzalutamide
Radium 223
Modified from Scher H, et al. Urology 2000

Bone Issues in Prostate Cancer A major bone tropic neoplasm Bone issues vary along the disease spectrum Impact of ADT
Osteoporosis Increase in osteoporotic related fx
Prevention/delay of bone metastases Castration resistant metastatic disease
SRE (SSE) prevention

Bone Events Defined
Skeletal Related Event (SRE) Radiation to bone Pathologic fracture Surgery to bone Spinal cord compression Hypercalcemia of malignancy
Symptomatic Skeletal Event (SSE) EBRT to relieve skeletal symptoms New symptomatic pathologic bone fracture Occurrence of spinal cord compression Tumor-related orthopedic surgical intervention

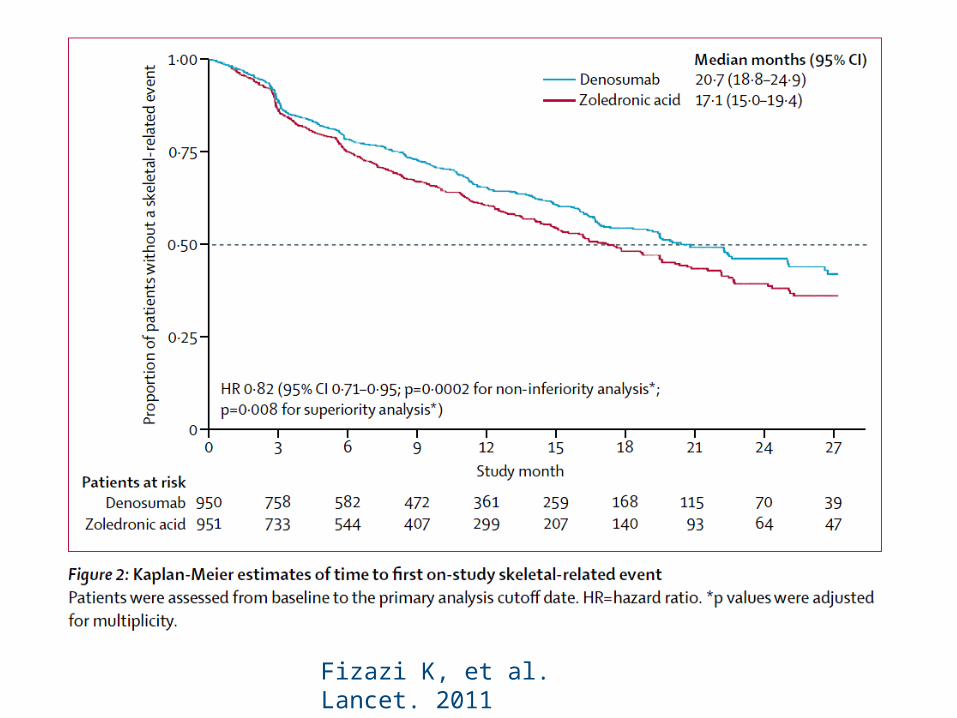
Denosumab versus zoledronic acid for treatment of bonemetastases in men with castration-resistant prostate cancer:a randomised, double-blind study 1904 men with metastatic CRPC were
randomized to receive denosumab (human monoclonal antibody against RANKL) or zolendronic acid
The primary endpoint was time to first on-study SRE (pathological fracture, radiation therapy, surgery to bone, or spinal cord compression), and was assessed for non-inferiority
The same outcome was further assessed for superiority as a secondary endpoint
Fizazi K, et al. Lancet. 2011 377:813-22
Fizazi K, et al. Lancet. 2011 377:813-22

COU-AA-301: Abiraterone Acetate Improves Overall Survival in mCRPC
HR = 0.646 (0.54-0.77) P< 0.0001
Placebo: 10.9 months (95%CI: 10.2, 12.0)
0 100 200 300 400 500 600 700
0
20
40
60
80
100
Su
rviv
al (
%)
Days from Randomization
Abiraterone acetate: 14.8 months (95%CI: 14.1, 15.4)
2 Prior Chemo OS: 1 Prior Chemo OS14.0 mos AA vs 10.3 mos placebo 15.4 mos AA vs 11.5 mos placebo
de Bono J et al: N Engl J Med 364:1995-2005, 2011

Ryan CJ, et al. N Engl J Med 2013;368:138-48
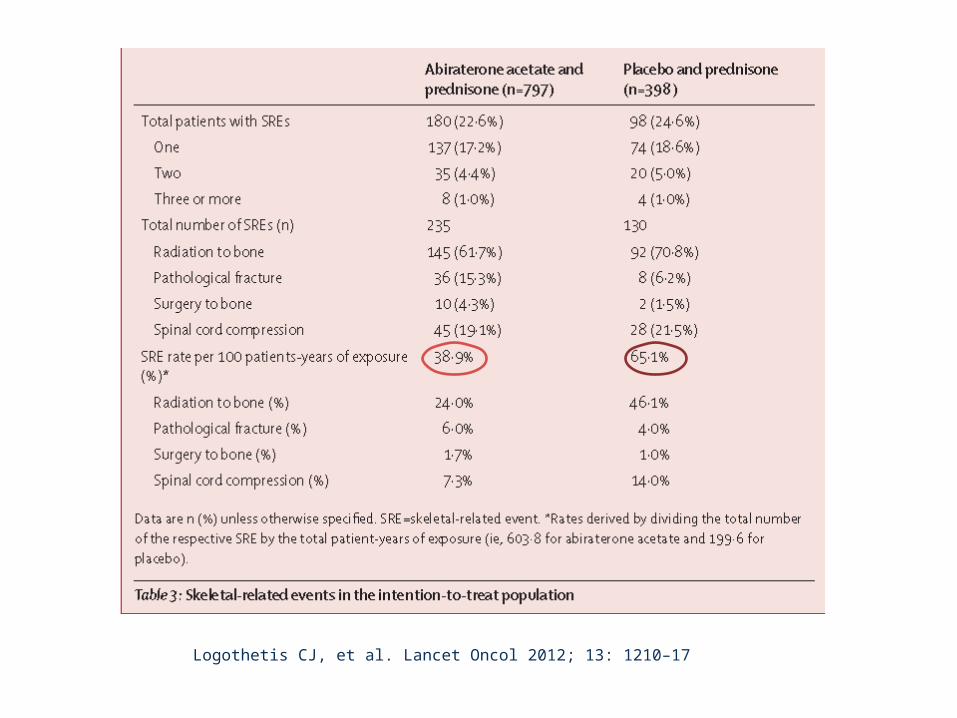
Logothetis CJ, et al. Lancet Oncol 2012; 13: 1210–17

Scher H, et al. n engl j med 367:1187 2012

Impact of Enzalutamide, an androgen receptor signaling inhibitor, on time to first skeletal related event (SRE) and pain in the phase 3 AFFIRM Study
• Median time to first SRE for enzalumatide treated patients: 16.7 months versus 13.3 months for patients receiving placebo (hazard ratio [HR] = 0.69; P = .0001) 9
• Pain palliation: as > 30% reduction in mean pain score at week 13 versus baseline without a > 30% increase in analgesic use was achieved by 45% of patients on enzalutamide compared with only 7% of patients in the placebo group (P = .0079)
Fizazi K, et al. ESMO 2012 Abstract 896O

• Confirmed symptomatic CRPC
• ≥ 2 bone metastases
• No known visceral metastases
• Post-docetaxel or unfit for docetaxel
• Confirmed symptomatic CRPC
• ≥ 2 bone metastases
• No known visceral metastases
• Post-docetaxel or unfit for docetaxel
• Total ALP: < 220 U/L vs ≥ 220 U/L• Bisphosphonate use: Yes vs No• Prior docetaxel: Yes vs No
• Total ALP: < 220 U/L vs ≥ 220 U/L• Bisphosphonate use: Yes vs No• Prior docetaxel: Yes vs No
RANDOMISED
2:1
Radium-223 (50 kBq/kg) + Best standard of careRadium-223 (50 kBq/kg) + Best standard of care
Placebo (saline) + Best standard of care
Placebo (saline) + Best standard of care
N = 922
TREATMENT
6 injections at 4-week intervals
STRATIFICATION
PATIENTS
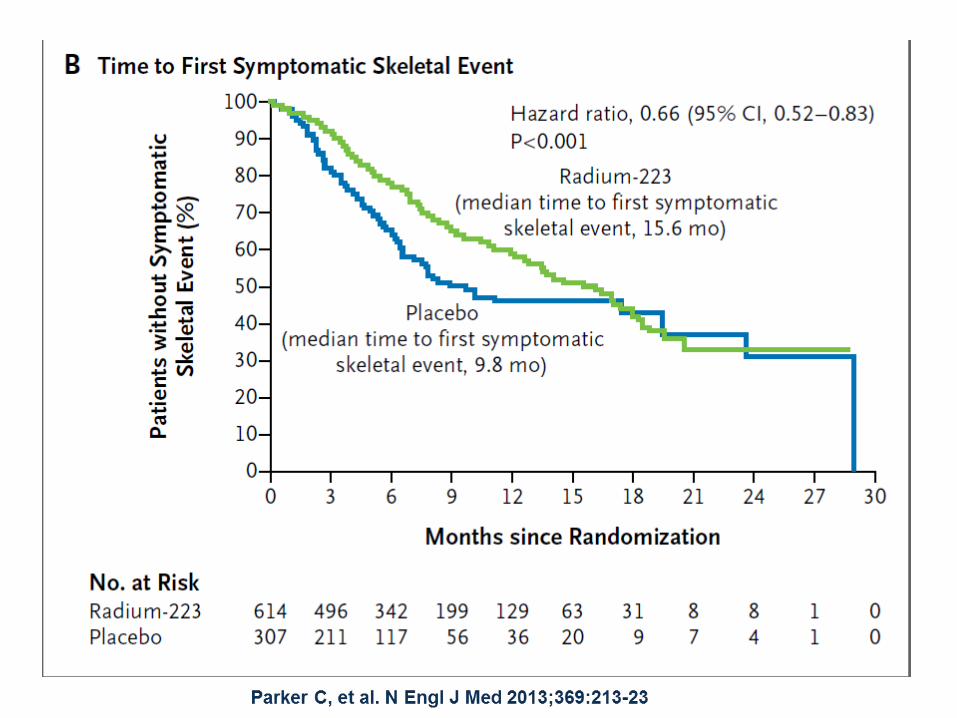
ALSYMPCA (ALpharadin in SYMptomatic Prostate CAncer) Phase III Study Design

Parker C, et al. N Engl J Med 2013;369:213-23

Questions
Does the addition of “standard” bone targeted agents to next generation therapies “add”, “synergize” or “add nothing” to more effective therapies ?
Does the introduction of more potent agents earlier mitigate the effect of older agents?
Pharmacoeconomics Bone targeted agent with drugs that already impact on
SRE?
