advanced lipoprotein analysis (printer friendly)
TRANSCRIPT

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 1/16
www.medscape.org
This article is a CME certified activity. To earn credit for this activity visit:http://www.medscape.org/viewarticle/815311
CME Information
CME Released: 12/13/2013 ; Valid for credit through 12/13/2014
Target Audience
This activity was developed for practicing primary care physicians, nurse practitioners, physician assistants, andother healthcare professionals who manage patients with lipid disorders.
Goal
Lipoproteins are complex molecules containing proteins, cholesterol, and phospholipid. While standard lipid panelsprovide important clinical information, they may not fully characterize a patient's cardiovascular disease andcardiometabolic risk. In these cases, advanced lipid testing can often provide this additional information. Join us asKarol E. Watson, MD, PHD, FACC, discusses advanced lipid testing and its place in clinical practice.
Learning Objectives
Upon completion of this activity, participants should be able to:
1. Identify in their clinical practice patients who are at increased cardiometabolic risk even with adequatecholesterol lowering.
2. More confidently include advanced lipid testing in screening and treatment strategies for select patients atincreased cardiometabolic risk.
Credits Available
Physicians - maximum of 0.25 AMA PRA Category 1 Credit(s)™
All other healthcare professionals completing continuing education credit for this activity will be issued a certificate ofparticipation.
Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Accreditation Statements
For Physicians
The Omnia-Prova Education Collaborative, Inc. (TOPEC) is accredited by the Accreditation Council for ContinuingMedical Education (ACCME) to provide continuing medical education for physicians.
The Omnia-Prova Education Collaborative, Inc., designates this enduring material for a maximum of 0.25 AMA PRACategory 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 2/16
Faculty and Disclosures
Author
Karol E. Watson, MD, PHD, FACC
Professor of Medicine/Cardiology, University of California at Los Angeles, Los Angeles, California
the activity.
Contact This Provider
For questions regarding the content of this activity, contact the accredited provider for this CME/CE activity notedabove. For technical assistance, contact [email protected]
Instructions for Participation and Credit
There are no fees for participating in or receiving credit for this online educational activity. For information onapplicability and acceptance of continuing education credit for this activity, please consult your professional licensingboard.
This activity is designed to be completed within the time designated on the title page; physicians should claim onlythose credits that reflect the time actually spent in the activity. To successfully earn credit, participants mustcomplete the activity online during the valid credit period that is noted on the title page. To receive AMA PRACategory 1 Credit™, you must receive a minimum score of 75% on the post-test.
Follow these steps to earn CME/CE credit*:
1. Read the target audience, learning objectives, and author disclosures.2. Study the educational content online or printed out.3. Online, choose the best answer to each test question. To receive a certificate, you must receive a passing
score as designated at the top of the test. In addition, you must complete the Activity Evaluation to providefeedback for future programming.
You may now view or print the certificate from your CME/CE Tracker. You may print the certificate but you cannotalter it. Credits will be tallied in your CME/CE Tracker and archived for 6 years; at any point within this time periodyou can print out the tally as well as the certificates from the CME/CE Tracker.
*The credit that you receive is based on your user profile.
Hardware/Software Requirements
To access activities, users will need:
A computer with an Internet connection.Internet Explorer 7.x or higher, Firefox 4.x or higher, Safari 2.x or higher, or any other W3C standardscompliant browser.Adobe Flash Player and/or an HTML5 capable browser may be required for video or audio playback.Occasionally other additional software may be required such as PowerPoint or Adobe Acrobat Reader.

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 3/16
Disclosure: Dr. Watson is a consultant for Aegerion and on the clinical trial adjudication committee for Merck.
Reviewer
Gregory Pokrywka, MD, FACP, FNLA, NCMP
Director, Baltimore Lipid Center, Fellow, National Lipid Association, Assistant Professor, Johns Hopkins University
School of Medicine, Baltimore, Maryland
Disclosure: Dr. Pokrywka is on the commercial Interest speakers bureau for Astra Zeneca, Daichii Sankyo
International, Genentech, Health Diagnostics Labs, Kowa Pharmaceuticals America, Inc., Lilly USA, LLC, and
LipoScience.
Planners
Barry A. Fiedel, PhD
Vice President, Clinical and Scientific Affairs, The Omnia-Prova Education Collaborative, Fort Washington, PA
Disclosure: No relationship to report.
Christine Finnegan
Clinical Education Director, Prova Education, Fort Washington, PA
Disclosure: No relationship to report.
Sean T. Saunders, CCMEP
VP, CME, Outcomes and Communications, The Omnia-Prova Education Collaborative, Fort Washington, PA
Disclosure: No relationship to report.
Erica Spengler
Activity Manager, The Omnia-Prova Education Collaborative, Fort Washington, PA
Disclosure: No relationship to report.
Karol E. Watson, MD, PHD, FACC
This CME activity is based on a lecture presented by Dr. Karol Watson at Prova Education's From Guideline to
Practice: Managing Challenging Cases in Primary Care program held on October 25, 2013, in Pasadena, California.
Lipoproteins allow lipids such as cholesterol to be transported in the blood stream.
Advanced Lipoprotein Analysis CME
CME Released: 12/13/2013 ; Valid for credit through 12/13/2014
12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 4/16
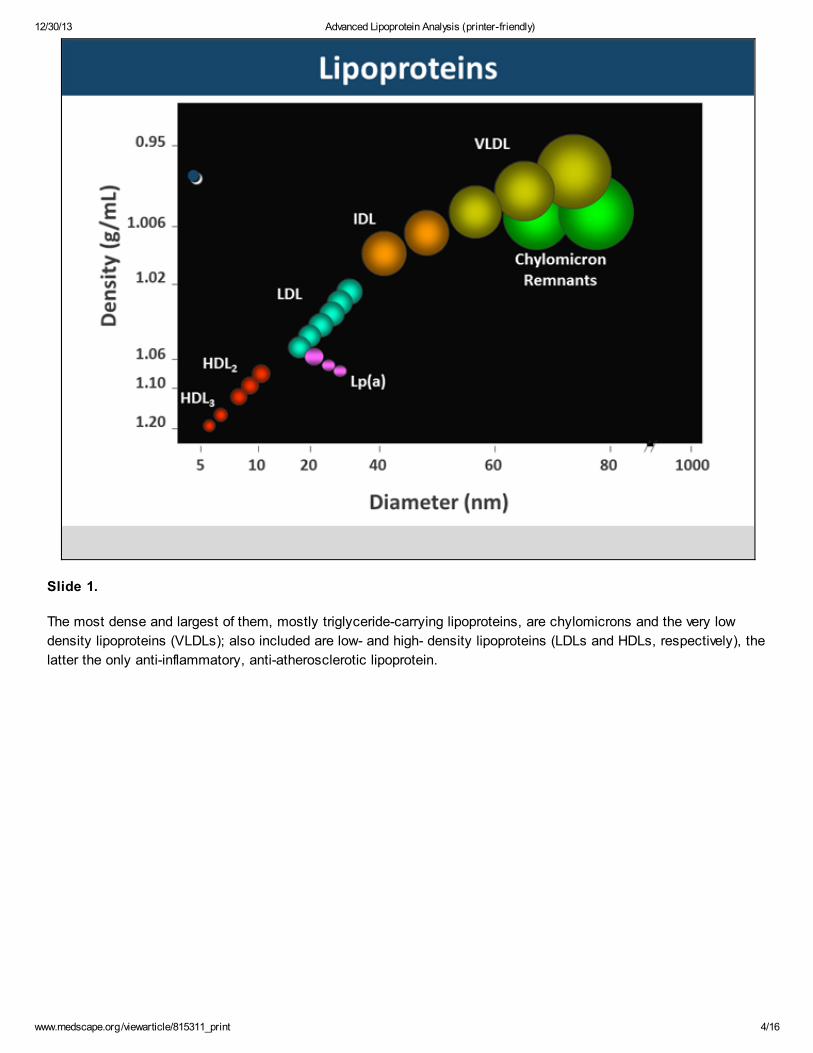
Slide 1.
The most dense and largest of them, mostly triglyceride-carrying lipoproteins, are chylomicrons and the very low
density lipoproteins (VLDLs); also included are low- and high- density lipoproteins (LDLs and HDLs, respectively), the
latter the only anti-inflammatory, anti-atherosclerotic lipoprotein.

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 5/16
Slide 2.
Cholesterol carried in LDL (LDL-C) has the most direct relationship to atherosclerosis.
Based on 2004 Guidelines, the LDL-C target for high-risk patients is <100 mg/dL; for the very high-risk patient the
target LDL-C is <70 mg/dL. Low risk is <160 mg/dL while moderately high risk falls in between at <130 mg/dL.

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 6/16
Slide 3.
What exactly are lipoproteins, how are they constructed, and what is their structural relationship with cholesterol?
Lipoproteins are physiologically complex: a non-polar lipid core surrounded with a polar surface coat, plus
(apo)proteins. For such a complicated particle, it is surprising we reduce it down to just LDL-C in our Standard Lipid
Panel.
Is the typical standard lipid panel suboptimal?

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 7/16
Slide 4.
The standard lipid panel typically provides information on total cholesterol, HDL cholesterol, triglycerides, and
sometimes VLDL. What some physicians and many patients may not realize is that the LDL-C value received in the
report is in almost all cases a calculated LDL-C, and not directly measured. It is calculated by taking total cholesterol
and then subtracting the sum of HDL plus triglycerides divided by 5. For a measured LDL-C, the actual value of
cholesterol present in LDL, a direct LDL-C measurement may need to be ordered.
Moreover, certain lipid subanalyses are often absent in the lipid profile report. One that may have import is the LDL
particle (LDL-P) number.
A recent consensus statement from the American Diabetes Association (ADA) and the American College of
Cardiology (ACC) suggests that direct LDL-C measurements are better than calculated...and ...assessment of
LDL particles (LDL-P) is actually better than measuring the LDL cholesterol, as LDL-P number is a better
predictor of cardiovascular risk than LDL-C alone.

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 8/16
Slide 5.
Another important point is that among individuals who have the exact same LDL-C level, they may have very different
LDL-P numbers. For illustration's sake, say the LDL-C is100 mg/dL. There could be a few large particles with an
average amount of cholesterol per particle, or there could be many small particles with less cholesterol per particle;
in the end, exactly the same LDL-C but the total number of LDL-P is different.
Why might this be important?
The relationship between LDL-C level and LDL-P number has been known for many years. Fredricksen and
colleagues in 1967 said:
"LDL particles are the causal agents in atherosclerosis."
"The more LDL particles a person has, the higher the risk of plaque buildup that causes heart attacks,
regardless of how much cholesterol those particles carry."
That remains basically true. The American Diabetes Association in a consensus statement relates that:
"The mean concentration of LDL cholesterol in those [patients] with type 2 diabetes is not significantly
different from that in those individuals who [do] not have diabetes. However, qualitative changes in LDL
cholesterol may be present.
"Patients with diabetes tend to have higher proportions of smaller and denser LDL-P, which is more
susceptible to oxidation and may, therefore, increase the risk of cardiovascular events in

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 9/16
atherosclerosis."
Slide 6.
Clearly, assessing more than just the cholesterol content is important. This is true for LDL, and it is also true for
HDL. These are data from the VA-HIT Study. This study evaluated individuals at risk for cardiovascular disease, using
a fibrate to help target an increase in HDL level, the primary end point being a decrement in cardiovascular risk.
The result was not fully expected.
The amount of cholesterol carried in HDL turned out to be a weak predictor of fibrate benefit and decrement in risk. A
similar result was observed with Apo-A1, though a somewhat better (though not significantly significant) predictor of
benefit.
HDL particle number was by far the best predictor of protection in this study, an outcome that was also statistically
significant. Thus, as with LDL, where LDL particle number is the best predictor of negative events, HDL particle
number is the best predictor of protection against such events.
If we are to believe that when assessing LDL-P number along with LDL-C we are potentially identifying a level of extra
CVD risk for patients, exactly how much and how significant is that extra risk?
Data gleaned from three (3) clinical trials help answer that question: 1) Framingham Heart Study; 2) the Multi-Ethnic
Study of Atherosclerosis; and 3) the VA-HIT Study.

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 10/16
Slide 7.
The Framingham Heart Study demonstrated a discordant relationship between LDL-C and LDL-P in that patients with
high LDL-C (and low LDL-P) had relatively less risk for a poor outcome (measured as Event-Free Survival) when
compared with patients with a low LDL-C but high LDL-P.

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 11/16
Slide 8.
Data from the Multi-Ethnic Study of Atherosclerosis (or MESA), which evaluated carotid atherosclerosis,
demonstrated that while carotid atherosclerosis risk was lower in individuals whose LDL-C was normal (<100 mg/dL)
when coincident with a low LDL-P number (Q1), as LDL-P numbers became progressively higher (Q2 through Q4)
carotid atherosclerosis risk continued to climb in a statistically significant trend.
12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 12/16
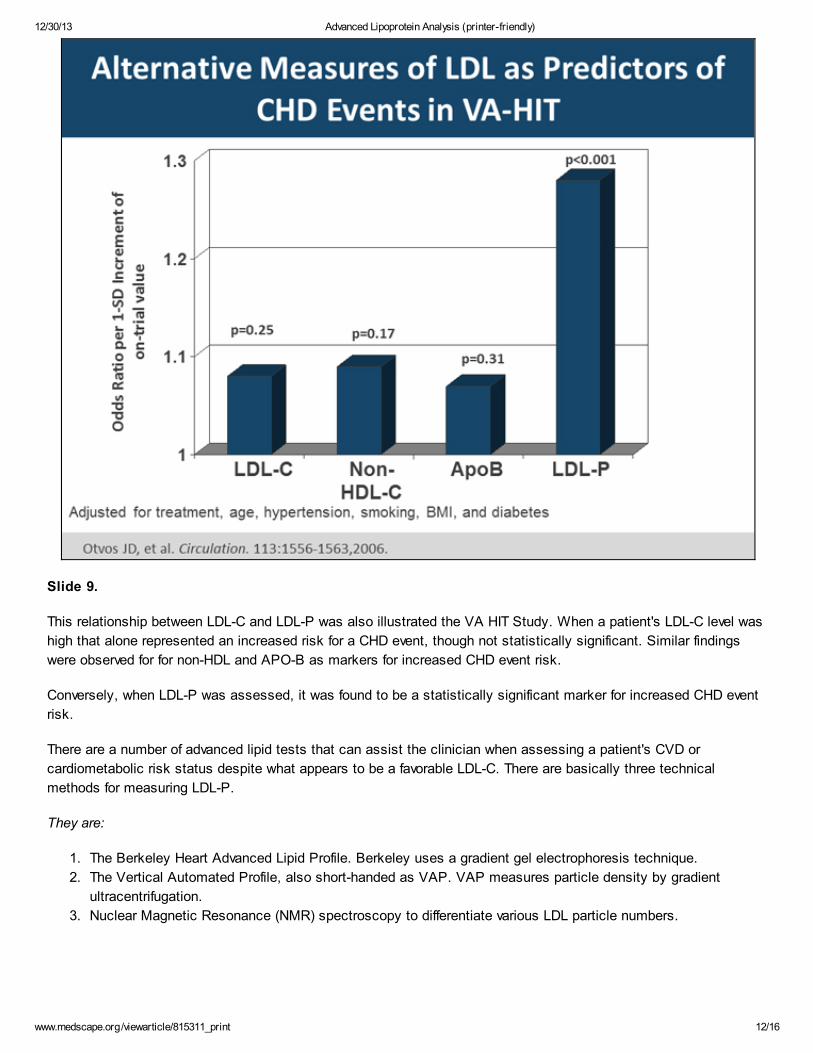
Slide 9.
This relationship between LDL-C and LDL-P was also illustrated the VA HIT Study. When a patient's LDL-C level was
high that alone represented an increased risk for a CHD event, though not statistically significant. Similar findings
were observed for for non-HDL and APO-B as markers for increased CHD event risk.
Conversely, when LDL-P was assessed, it was found to be a statistically significant marker for increased CHD event
risk.
There are a number of advanced lipid tests that can assist the clinician when assessing a patient's CVD or
cardiometabolic risk status despite what appears to be a favorable LDL-C. There are basically three technical
methods for measuring LDL-P.
They are:
1. The Berkeley Heart Advanced Lipid Profile. Berkeley uses a gradient gel electrophoresis technique.
2. The Vertical Automated Profile, also short-handed as VAP. VAP measures particle density by gradient
ultracentrifugation.
3. Nuclear Magnetic Resonance (NMR) spectroscopy to differentiate various LDL particle numbers.

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 13/16
Slide 10.
Berkeley utilizes gradient gel electrophoresis to sift/separate different lipoproteins based on their electrophoretic
characteristic sizes through a process called "mobility shifts." This technique does not give information about
cholesterol, but does offer information about size. Thus, it provides quantification of the number of particles of different
sizes and an estimate can be obtained with regard to particle number.
This is the type of profile obtained; it can provide information about LDL size, particle number, etc.

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 14/16
Slide 11.
The VAP technique employs ultracentrifugation to separate lipoprotein fractions. The technique permits resolution of
different lipoprotein subclasses based on their densities. A computerized system then provides the needed
information with regard to the different lipoprotein classes.
12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 15/16
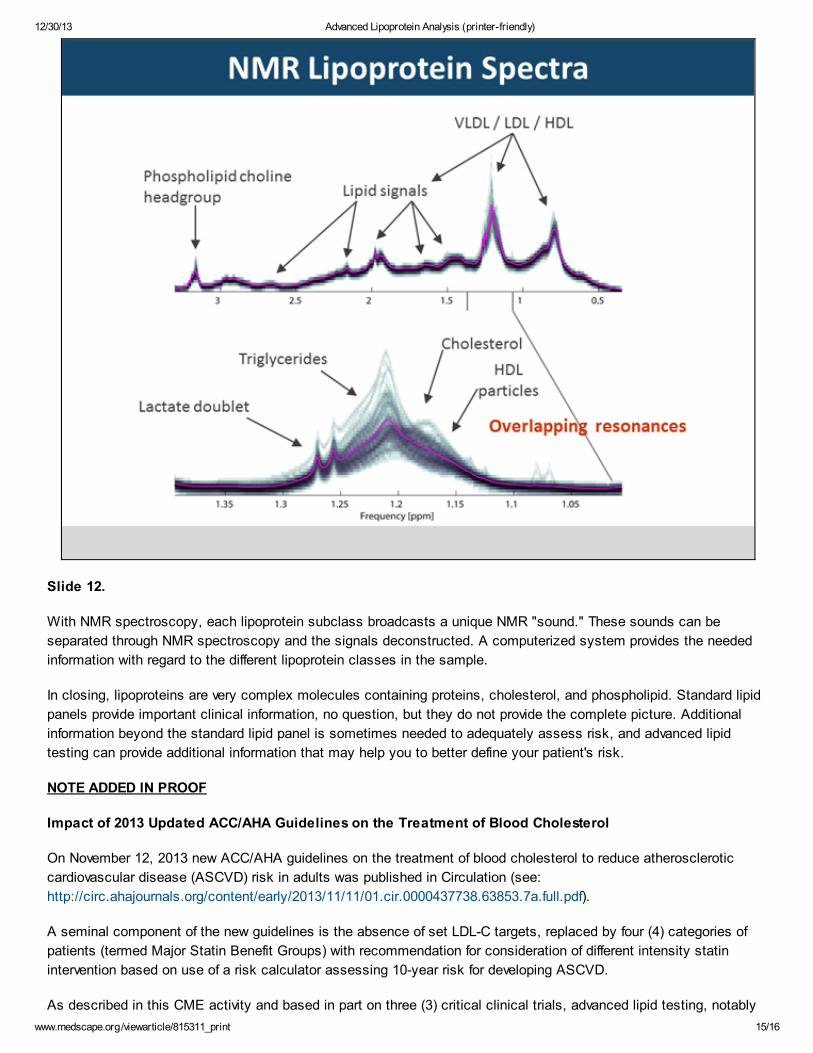
Slide 12.
With NMR spectroscopy, each lipoprotein subclass broadcasts a unique NMR "sound." These sounds can be
separated through NMR spectroscopy and the signals deconstructed. A computerized system provides the needed
information with regard to the different lipoprotein classes in the sample.
In closing, lipoproteins are very complex molecules containing proteins, cholesterol, and phospholipid. Standard lipid
panels provide important clinical information, no question, but they do not provide the complete picture. Additional
information beyond the standard lipid panel is sometimes needed to adequately assess risk, and advanced lipid
testing can provide additional information that may help you to better define your patient's risk.
NOTE ADDED IN PROOF
Impact of 2013 Updated ACC/AHA Guidelines on the Treatment of Blood Cholesterol
On November 12, 2013 new ACC/AHA guidelines on the treatment of blood cholesterol to reduce atherosclerotic
cardiovascular disease (ASCVD) risk in adults was published in Circulation (see:
http://circ.ahajournals.org/content/early/2013/11/11/01.cir.0000437738.63853.7a.full.pdf).
A seminal component of the new guidelines is the absence of set LDL-C targets, replaced by four (4) categories of
patients (termed Major Statin Benefit Groups) with recommendation for consideration of different intensity statin
intervention based on use of a risk calculator assessing 10-year risk for developing ASCVD.
As described in this CME activity and based in part on three (3) critical clinical trials, advanced lipid testing, notably

12/30/13 Advanced Lipoprotein Analysis (printer-friendly)
www.medscape.org/viewarticle/815311_print 16/16
measurement of LDL-P, has proven to be a better indicator of cardiovascular disease/cardiometabolic risk for many
patients than is LDL-C alone. The removal of set targets for LDL-C in the recently released Guidelines does not
diminish the potential benefit of advanced lipid testing within the four Major Statin Benefit Groups as part of an
ongoing assessment of therapeutic and lifestyle efficacy. As always, including advanced lipid testing is based on
physician assessment for each individual patient within their clinical practice.
This article is a CME certified activity. To earn credit for this activity visit:http://www.medscape.org/viewarticle/815311
References
1. Brunzell JD, et al. Diabetes Care. 2008;31:811-822.
2. Otvos JD, et al. Am J Cardiol. 2002;90(suppl):22i-29i.
3. Fredrickson DS, et al. NEJM. 1967;276:148-156.
4. American Diabetes Association. Diabetes Care. 2004;27:S68-S71.
5. Otvos JD, et al. Circulation. 2006;113:1556-1563.
6. Cromwell WC, et al. J Clin Lipidol. 2007;1:583–592.
7. Otvos J, et al. J Clin Lipidol. 2011;5: 105–113.
8. Otvos JD. Clin Lab. 2002;48:171-180.
9. Brunzell JD, et al. Diabetes Care. 2008;31:811-822.
Disclaimer
The educational activity presented above may involve simulated case-based scenarios. The patients depicted in thesescenarios are fictitious and no association with any actual patient is intended or should be inferred.
The material presented here does not necessarily reflect the views of Medscape, LLC, or companies that supporteducational programming on medscape.org. These materials may discuss therapeutic products that have not beenapproved by the US Food and Drug Administration and off-label uses of approved products. A qualified healthcareprofessional should be consulted before using any therapeutic product discussed. Readers should verify allinformation and data before treating patients or employing any therapies described in this educational activity.
© 2013 Prova Education, Inc. All rights reserved
This article is a CME certified activity. To earn credit for this activity visit:http://www.medscape.org/viewarticle/815311