advanced accelerator applications - jefferies · product candidate for neuro endocrine tumours. 3....
TRANSCRIPT

Advanced Accelerator ApplicationsInvestor Presentation June 2016
Disclaimer
This presentation by Advanced Accelerator Applications S.A. (“AAA” or the “Company”) contains forward looking statements, forecasts andprojections based on discretionary and subjective expectations and estimates made at the time the statements were made and that involve anumber of risks and uncertainties, many of which are beyond our control, which could cause actual results or events to differ materially fromthose statements, forecasts and projections. Such risks and uncertainties include, but are not limited to, the uncertainties inherent inpharmaceutical research and development; risks and uncertainties related to the progress, timing, cost, and results of clinical trials and productdevelopment programs; difficulties or delays in obtaining regulatory approval for product candidates; competition from other pharmaceutical orbiotechnology companies; the ability to successfully market products; the ability to manufacture sufficient amount of our products fordevelopment and commercialization activities and to do so in a timely and cost-effective manner; the occurrence of side effects or SAEscaused by or associated with our products and product candidates; our ability to procure adequate quantities of necessary supplies and rawmaterials for Lutathera and other chemical compounds acceptable for use in our manufacturing processes from our suppliers; our ability toorganize timely and safe delivery of our products or product candidates by third parties; any problems with the manufacture, quality orperformance of our products or product candidates; the rate and degree of market acceptance and the clinical utility of Lutathera and our otherproducts or product candidates; our estimates regarding the market opportunity for Lutathera, our other product candidates and our existingproducts; our anticipation that we will generate higher sales as we diversify our products; our ability to implement our growth strategy includingexpansion in the U.S.; our ability to sustain and create additional sales, marketing and distribution capabilities; our intellectual property andlicensing position; legislation or regulation in countries where we sell our products that affect product pricing, taxation, reimbursement, accessor distribution channels; and general economic, political, demographic and business conditions in Europe, the U.S. and elsewhere.
These risks and uncertainties also include those described under the captions “Risk Factors” and “Management’s Discussion andAnalysis of Financial Condition and Results of Operations” in AAA’s Registration Statement on Form F-1 and future filings with theSecurities and Exchange Commission. Forward-looking statements speak only as of the date they are made, and AAA does notundertake any obligation to update them in light of new information or future developments or to release publicly any revisions to thesestatements in order to reflect later events or circumstances or to reflect the occurrence of unanticipated events except as required by law.All forward-looking statements are qualified in their entirety by this cautionary statement.
This presentation contains a discussion of Adjusted EBITDA. We have provided a reconciliation of this non-IFRS financial measures to themost directly comparable IFRS measure in the Appendix to these slides. Adjusted EBITDA is defined as net income (loss) calculated inaccordance with IFRS plus: (i) finance income; (ii) finance costs; (iii) income tax; and (iv) depreciation and amortization.
2
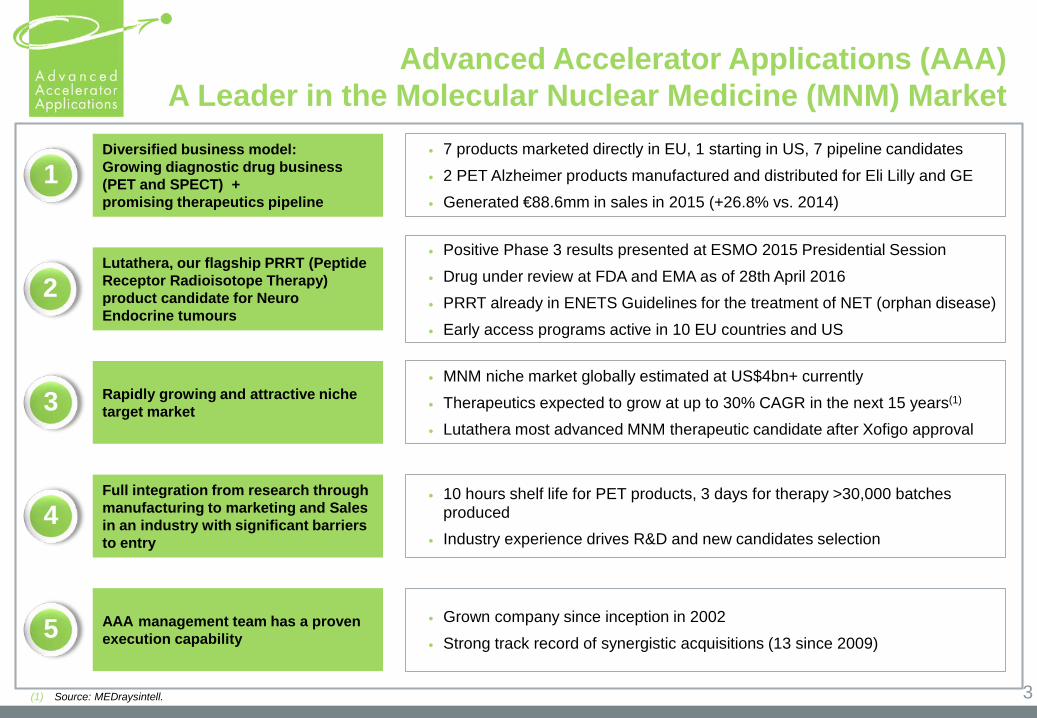
Positive Phase 3 results presented at ESMO 2015 Presidential Session Drug under review at FDA and EMA as of 28th April 2016 PRRT already in ENETS Guidelines for the treatment of NET (orphan disease) Early access programs active in 10 EU countries and US
MNM niche market globally estimated at US$4bn+ currently Therapeutics expected to grow at up to 30% CAGR in the next 15 years(1)
Lutathera most advanced MNM therapeutic candidate after Xofigo approval
10 hours shelf life for PET products, 3 days for therapy >30,000 batches produced
Industry experience drives R&D and new candidates selection
7 products marketed directly in EU, 1 starting in US, 7 pipeline candidates 2 PET Alzheimer products manufactured and distributed for Eli Lilly and GE Generated €88.6mm in sales in 2015 (+26.8% vs. 2014)
Grown company since inception in 2002 Strong track record of synergistic acquisitions (13 since 2009)
1Diversified business model:Growing diagnostic drug business (PET and SPECT) +promising therapeutics pipeline
2Lutathera, our flagship PRRT (Peptide Receptor Radioisotope Therapy) product candidate for Neuro Endocrine tumours
3 Rapidly growing and attractive niche target market
4Full integration from research through manufacturing to marketing and Sales in an industry with significant barriers to entry
5 AAA management team has a proven execution capability
Advanced Accelerator Applications (AAA)A Leader in the Molecular Nuclear Medicine (MNM) Market
3(1) Source: MEDraysintell.
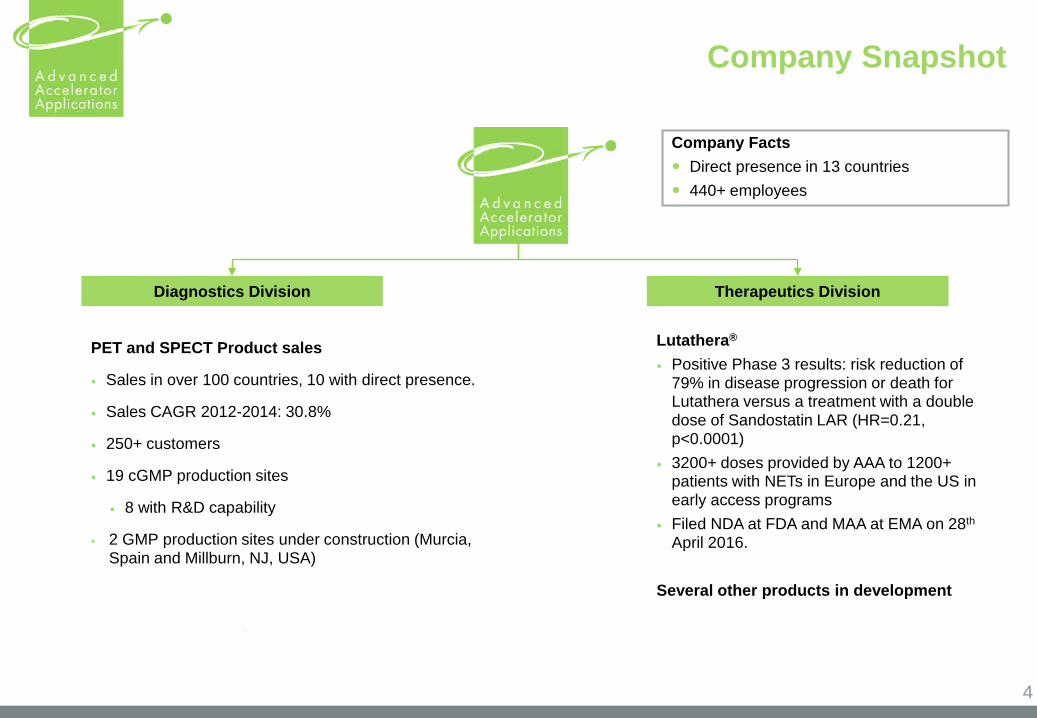
Company Snapshot
Diagnostics Division Therapeutics Division
Company Facts Direct presence in 13 countries 440+ employees
Lutathera®
Positive Phase 3 results: risk reduction of 79% in disease progression or death for Lutathera versus a treatment with a double dose of Sandostatin LAR (HR=0.21, p<0.0001)
3200+ doses provided by AAA to 1200+ patients with NETs in Europe and the US in early access programs
Filed NDA at FDA and MAA at EMA on 28th
April 2016.
Several other products in development
PET and SPECT Product sales
Sales in over 100 countries, 10 with direct presence.
Sales CAGR 2012-2014: 30.8%
250+ customers
19 cGMP production sites
8 with R&D capability
2 GMP production sites under construction (Murcia, Spain and Millburn, NJ, USA)
4
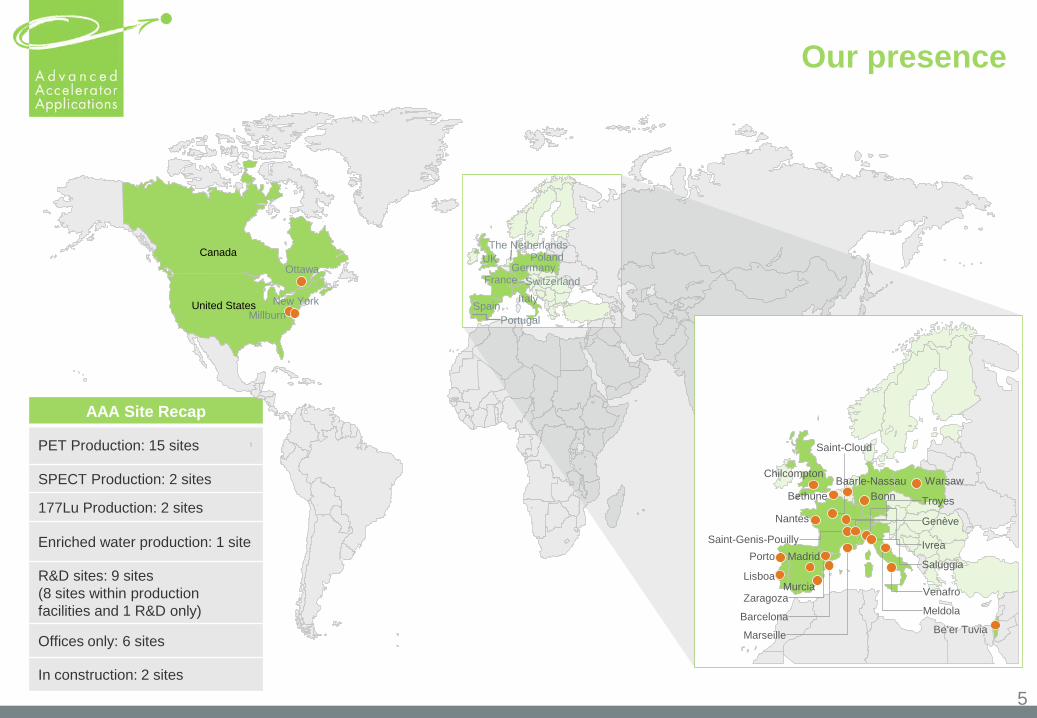
Our presence
AAA Site Recap
PET Production: 15 sites
SPECT Production: 2 sites
177Lu Production: 2 sites
Enriched water production: 1 site
R&D sites: 9 sites (8 sites within production facilities and 1 R&D only)
Offices only: 6 sites
In construction: 2 sites
Ottawa
Chilcompton
Bethune
Nantes
Porto
Zaragoza
Barcelona
Marseille
Troyes
Saint-Cloud
BonnWarsaw
Saint-Genis-PouillyGenève
Ivrea
Saluggia
Venafro
Meldola
Be’er Tuvia
New York
Canada
United States
GermanyPolandUK
France SwitzerlandItaly
SpainPortugal
5
Lisboa
Madrid
Millburn
Murcia
Baarle-Nassau
The Netherlands
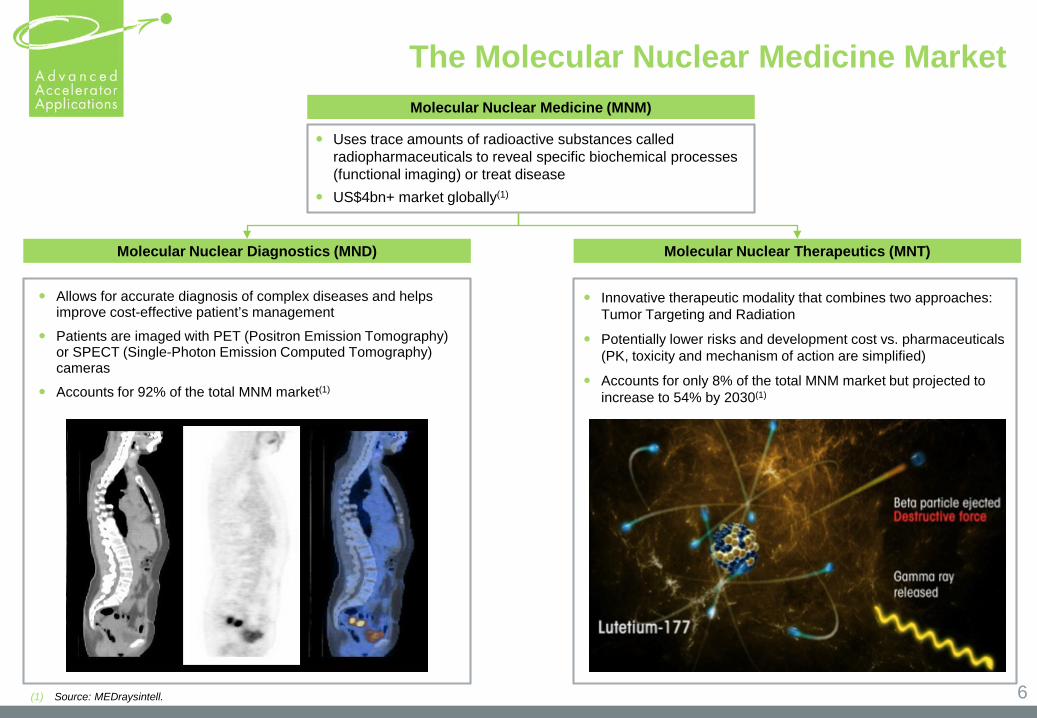
Molecular Nuclear Medicine (MNM)
Molecular Nuclear Diagnostics (MND) Molecular Nuclear Therapeutics (MNT)
Uses trace amounts of radioactive substances called radiopharmaceuticals to reveal specific biochemical processes (functional imaging) or treat disease
US$4bn+ market globally(1)
Allows for accurate diagnosis of complex diseases and helps improve cost-effective patient’s management
Patients are imaged with PET (Positron Emission Tomography) or SPECT (Single-Photon Emission Computed Tomography) cameras
Accounts for 92% of the total MNM market(1)
The Molecular Nuclear Medicine Market
Innovative therapeutic modality that combines two approaches: Tumor Targeting and Radiation
Potentially lower risks and development cost vs. pharmaceuticals (PK, toxicity and mechanism of action are simplified)
Accounts for only 8% of the total MNM market but projected to increase to 54% by 2030(1)
6(1) Source: MEDraysintell.
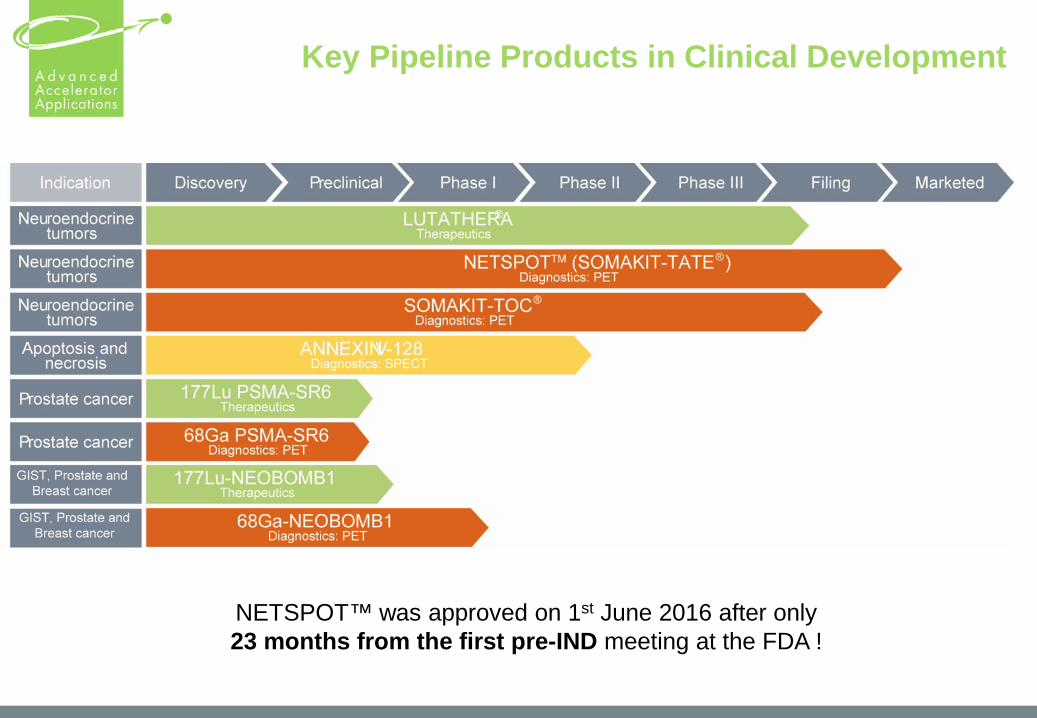
Key Pipeline Products in Clinical Development
NETSPOT™ was approved on 1st June 2016 after only 23 months from the first pre-IND meeting at the FDA !
8
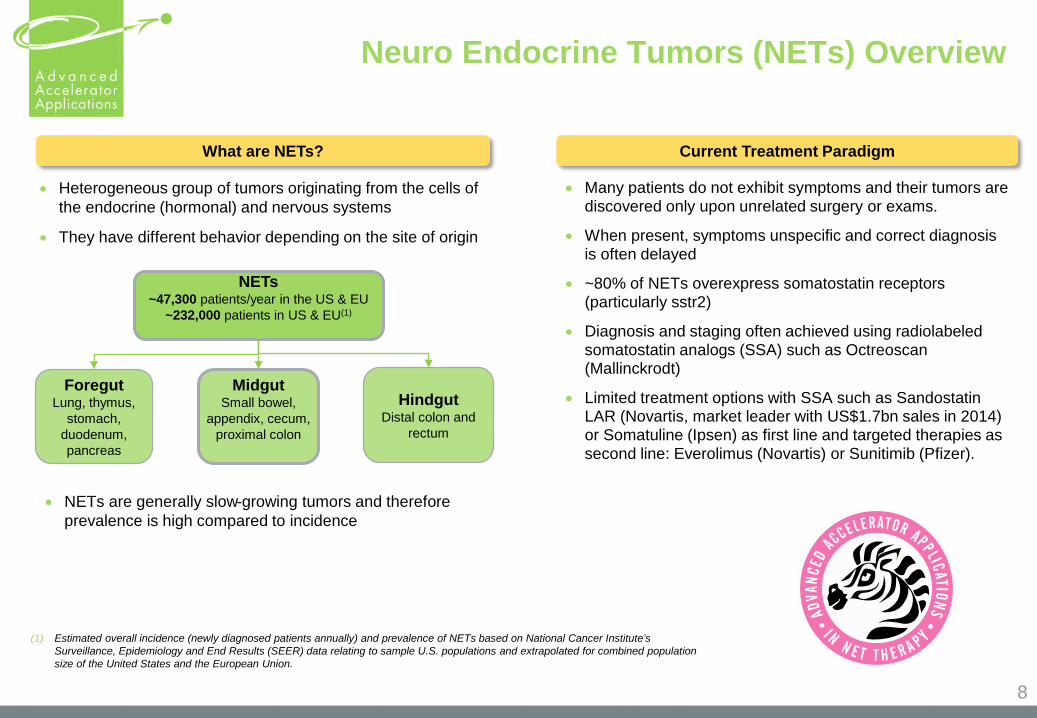
NETs~47,300 patients/year in the US & EU
~232,000 patients in US & EU(1)
MidgutSmall bowel,
appendix, cecum, proximal colon
• Heterogeneous group of tumors originating from the cells of the endocrine (hormonal) and nervous systems
• They have different behavior depending on the site of origin
What are NETs? Current Treatment Paradigm
• Many patients do not exhibit symptoms and their tumors are discovered only upon unrelated surgery or exams.
• When present, symptoms unspecific and correct diagnosis is often delayed
• ~80% of NETs overexpress somatostatin receptors (particularly sstr2)
• Diagnosis and staging often achieved using radiolabeled somatostatin analogs (SSA) such as Octreoscan(Mallinckrodt)
• Limited treatment options with SSA such as SandostatinLAR (Novartis, market leader with US$1.7bn sales in 2014) or Somatuline (Ipsen) as first line and targeted therapies as second line: Everolimus (Novartis) or Sunitimib (Pfizer).
• NETs are generally slow-growing tumors and therefore prevalence is high compared to incidence
(1) Estimated overall incidence (newly diagnosed patients annually) and prevalence of NETs based on National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER) data relating to sample U.S. populations and extrapolated for combined population size of the United States and the European Union.
ForegutLung, thymus,
stomach, duodenum, pancreas
HindgutDistal colon and
rectum
Neuro Endocrine Tumors (NETs) Overview
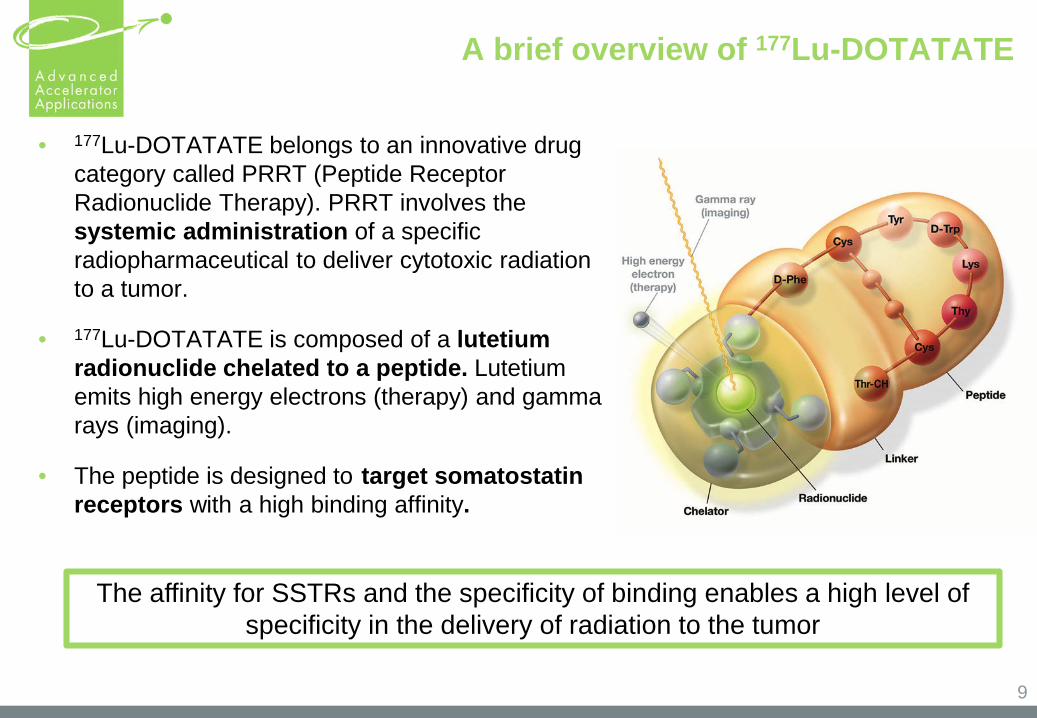
A brief overview of 177Lu-DOTATATE
• 177Lu-DOTATATE belongs to an innovative drug category called PRRT (Peptide Receptor Radionuclide Therapy). PRRT involves the systemic administration of a specific radiopharmaceutical to deliver cytotoxic radiation to a tumor.
• 177Lu-DOTATATE is composed of a lutetium radionuclide chelated to a peptide. Lutetium emits high energy electrons (therapy) and gamma rays (imaging).
• The peptide is designed to target somatostatinreceptors with a high binding affinity.
The affinity for SSTRs and the specificity of binding enables a high level of specificity in the delivery of radiation to the tumor
9
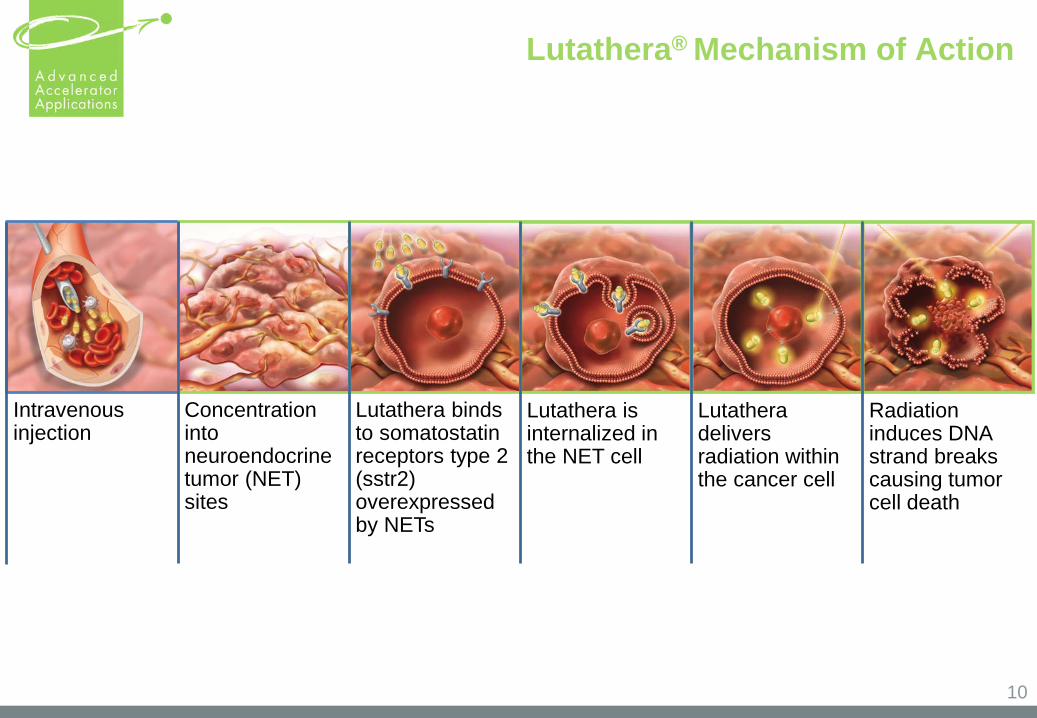
Lutathera® Mechanism of Action
10
Intravenousinjection
Concentration intoneuroendocrine tumor (NET) sites
Lutathera bindsto somatostatinreceptors type 2 (sstr2) overexpressedby NETs
Lutathera isinternalized in the NET cell
Lutatheradeliversradiation withinthe cancer cell
Radiation induces DNA strand breaks causing tumor cell death
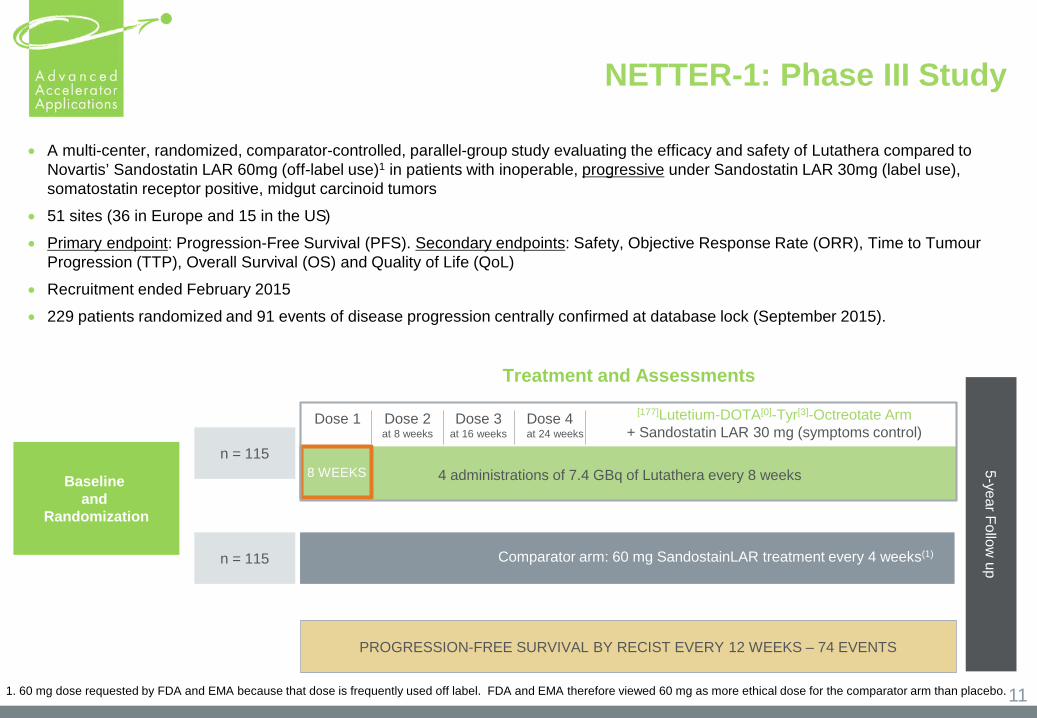
NETTER-1: Phase III Study
• A multi-center, randomized, comparator-controlled, parallel-group study evaluating the efficacy and safety of Lutathera compared to Novartis’ Sandostatin LAR 60mg (off-label use)1 in patients with inoperable, progressive under Sandostatin LAR 30mg (label use), somatostatin receptor positive, midgut carcinoid tumors
• 51 sites (36 in Europe and 15 in the US)• Primary endpoint: Progression-Free Survival (PFS). Secondary endpoints: Safety, Objective Response Rate (ORR), Time to Tumour
Progression (TTP), Overall Survival (OS) and Quality of Life (QoL)• Recruitment ended February 2015• 229 patients randomized and 91 events of disease progression centrally confirmed at database lock (September 2015).
Baseline and
Randomization
n = 115
5-year Follow up
8 WEEKS 4 administrations of 7.4 GBq of Lutathera every 8 weeks
Comparator arm: 60 mg SandostainLAR treatment every 4 weeks(1)
PROGRESSION-FREE SURVIVAL BY RECIST EVERY 12 WEEKS – 74 EVENTS
Dose 1 Dose 2at 8 weeks
Dose 3at 16 weeks
Dose 4at 24 weeks
[177]Lutetium-DOTA[0]-Tyr[3]-Octreotate Arm+ Sandostatin LAR 30 mg (symptoms control)
Treatment and Assessments
n = 115
111. 60 mg dose requested by FDA and EMA because that dose is frequently used off label. FDA and EMA therefore viewed 60 mg as more ethical dose for the comparator arm than placebo.
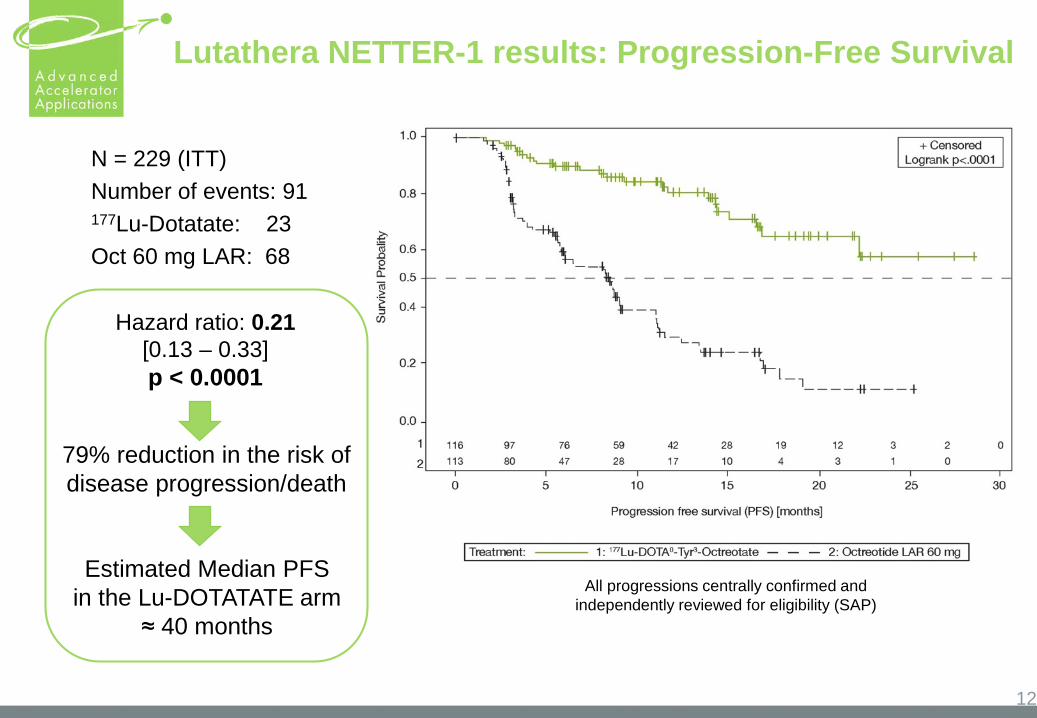
Lutathera NETTER-1 results: Progression-Free Survival
12
N = 229 (ITT)Number of events: 91 177Lu-Dotatate: 23 Oct 60 mg LAR: 68
Estimated Median PFS in the Lu-DOTATATE arm
≈ 40 months
All progressions centrally confirmed andindependently reviewed for eligibility (SAP)
Hazard ratio: 0.21[0.13 – 0.33] p < 0.0001
79% reduction in the risk ofdisease progression/death
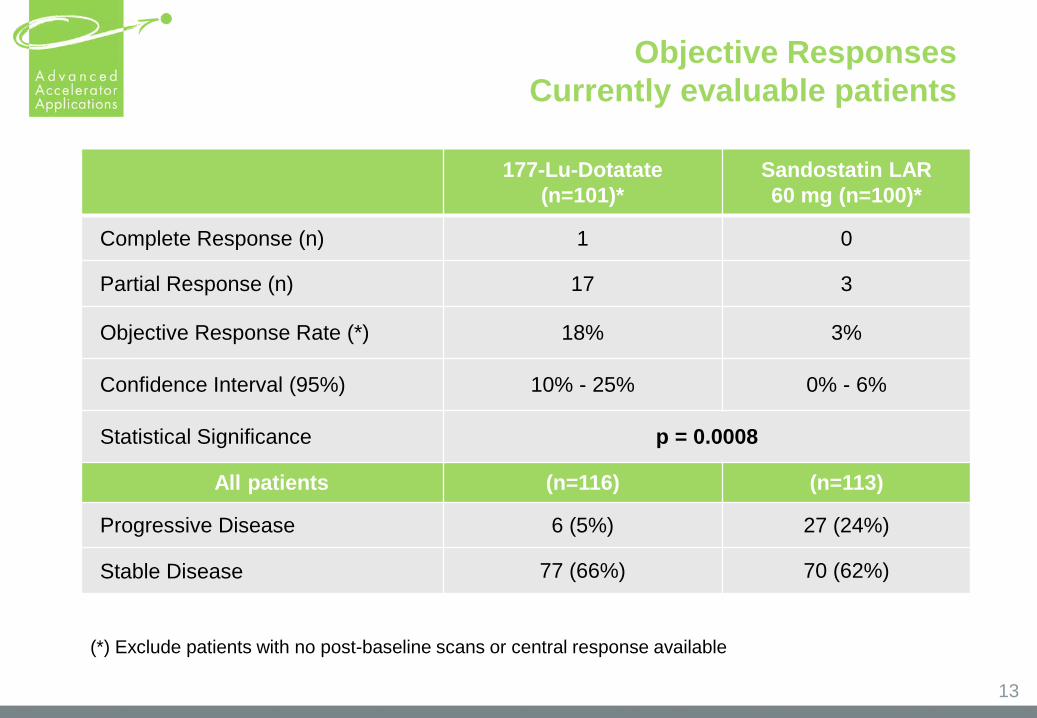
177-Lu-Dotatate(n=101)*
Sandostatin LAR 60 mg (n=100)*
Complete Response (n) 1 0
Partial Response (n) 17 3
Objective Response Rate (*) 18% 3%
Confidence Interval (95%) 10% - 25% 0% - 6%
Statistical Significance p = 0.0008
All patients (n=116) (n=113)
Progressive Disease 6 (5%) 27 (24%)
Stable Disease 77 (66%) 70 (62%)
(*) Exclude patients with no post-baseline scans or central response available
Objective ResponsesCurrently evaluable patients
13
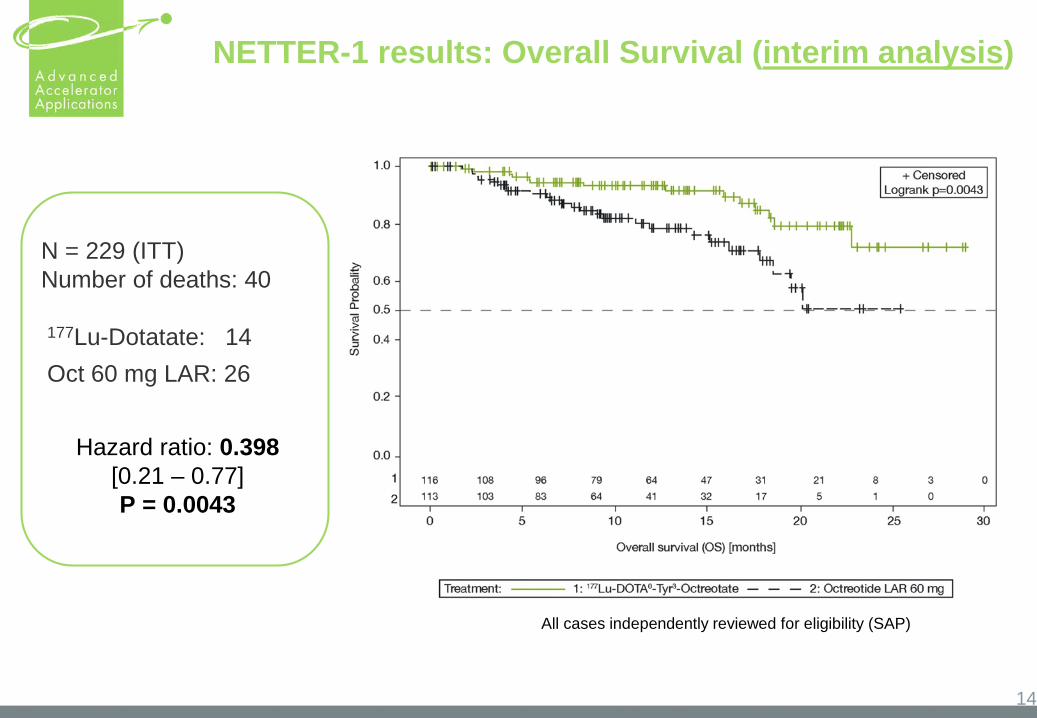
NETTER-1 results: Overall Survival (interim analysis)
14
All cases independently reviewed for eligibility (SAP)
N = 229 (ITT)Number of deaths: 40
177Lu-Dotatate: 14Oct 60 mg LAR: 26
Hazard ratio: 0.398[0.21 – 0.77]P = 0.0043
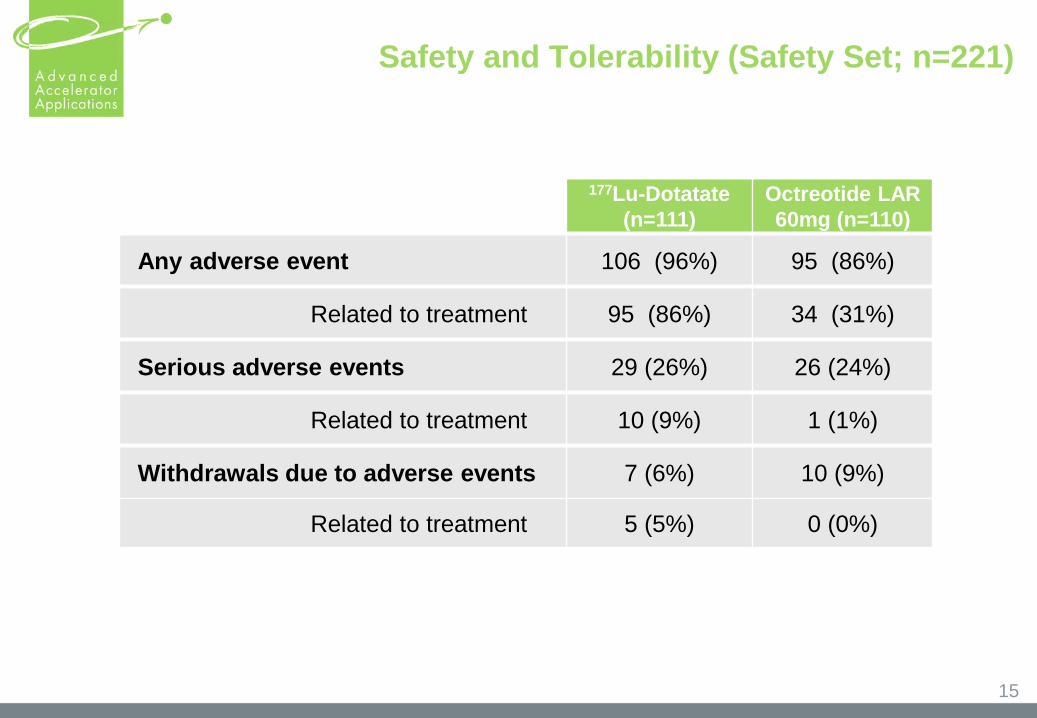
Safety and Tolerability (Safety Set; n=221)
177Lu-Dotatate(n=111)
Octreotide LAR 60mg (n=110)
Any adverse event 106 (96%) 95 (86%)
Related to treatment 95 (86%) 34 (31%)
Serious adverse events 29 (26%) 26 (24%)
Related to treatment 10 (9%) 1 (1%)
Withdrawals due to adverse events 7 (6%) 10 (9%)
Related to treatment 5 (5%) 0 (0%)
15

The preparation for the commercial launch of NETSPOT™ and Lutathera
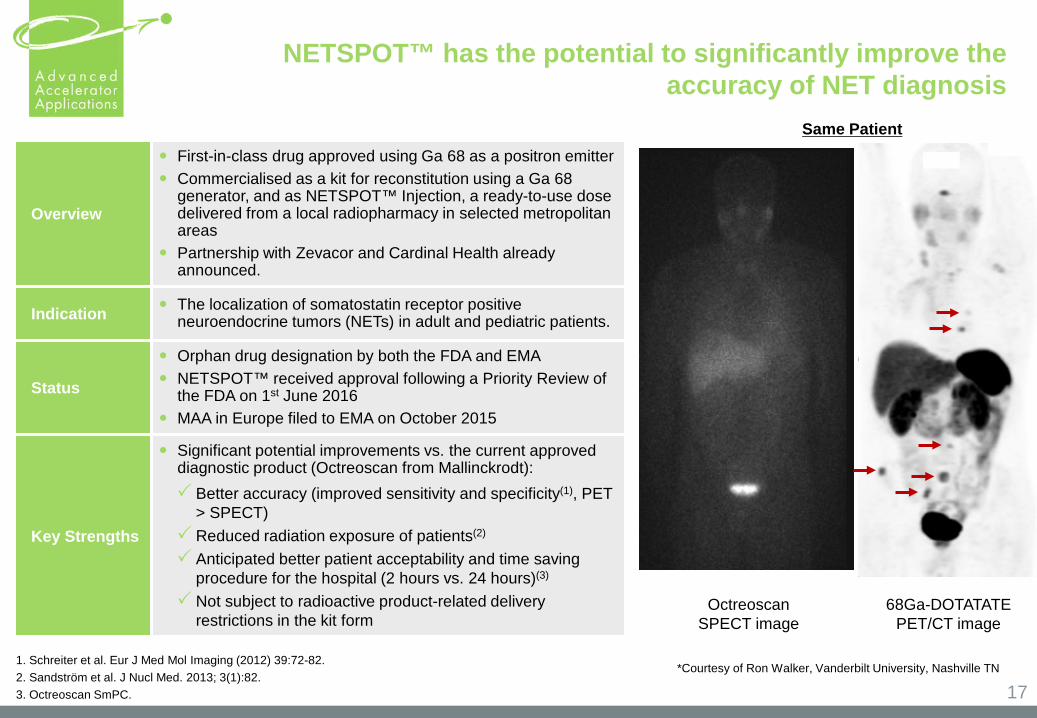
NETSPOT™ has the potential to significantly improve the accuracy of NET diagnosis
17
Overview
First-in-class drug approved using Ga 68 as a positron emitter Commercialised as a kit for reconstitution using a Ga 68
generator, and as NETSPOT™ Injection, a ready-to-use dose delivered from a local radiopharmacy in selected metropolitan areas
Partnership with Zevacor and Cardinal Health already announced.
Indication The localization of somatostatin receptor positive neuroendocrine tumors (NETs) in adult and pediatric patients.
Status
Orphan drug designation by both the FDA and EMA NETSPOT™ received approval following a Priority Review of
the FDA on 1st June 2016 MAA in Europe filed to EMA on October 2015
Key Strengths
Significant potential improvements vs. the current approved diagnostic product (Octreoscan from Mallinckrodt): Better accuracy (improved sensitivity and specificity(1), PET
> SPECT) Reduced radiation exposure of patients(2)
Anticipated better patient acceptability and time saving procedure for the hospital (2 hours vs. 24 hours)(3)
Not subject to radioactive product-related delivery restrictions in the kit form
1. Schreiter et al. Eur J Med Mol Imaging (2012) 39:72-82. 2. Sandström et al. J Nucl Med. 2013; 3(1):82.3. Octreoscan SmPC.
*Courtesy of Ron Walker, Vanderbilt University, Nashville TN
68Ga-DOTATATE PET/CT image
OctreoscanSPECT image
Same Patient
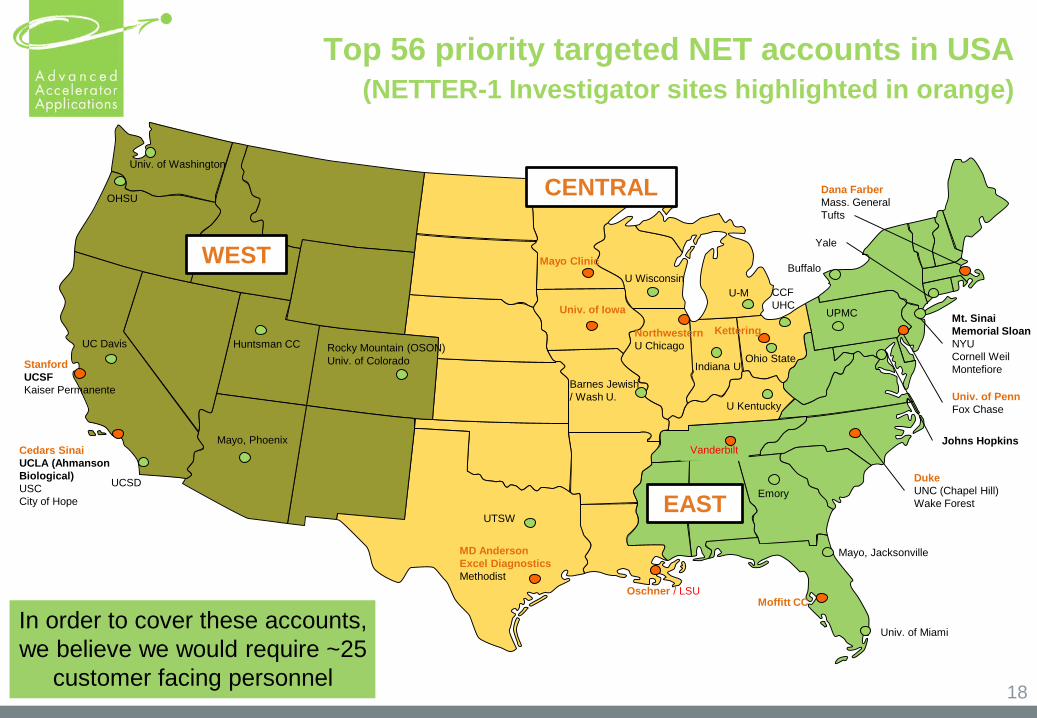
Top 56 priority targeted NET accounts in USA(NETTER-1 Investigator sites highlighted in orange)
18
StanfordUCSFKaiser Permanente
Cedars SinaiUCLA (Ahmanson Biological)USCCity of Hope
Univ. of Washington
OHSU
Mayo, Phoenix
MD AndersonExcel DiagnosticsMethodist
Univ. of Colorado
U Wisconsin
NorthwesternU Chicago
Mayo Clinic
U-MUniv. of Iowa
Barnes Jewish / Wash U.
CCFUHC
Ohio StateIndiana U
Oschner / LSU
Vanderbilt
Moffitt CC
DukeUNC (Chapel Hill)Wake Forest
Johns Hopkins
Univ. of PennFox Chase
Mt. SinaiMemorial SloanNYUCornell WeilMontefiore
U Kentucky
Dana FarberMass. GeneralTufts
Univ. of Miami
UTSW
Huntsman CC
Mayo, Jacksonville
EmoryUCSD
UPMC
UC Davis
YaleWEST
CENTRAL
EAST
Rocky Mountain (OSON)
In order to cover these accounts, we believe we would require ~25
customer facing personnel
Buffalo
Kettering
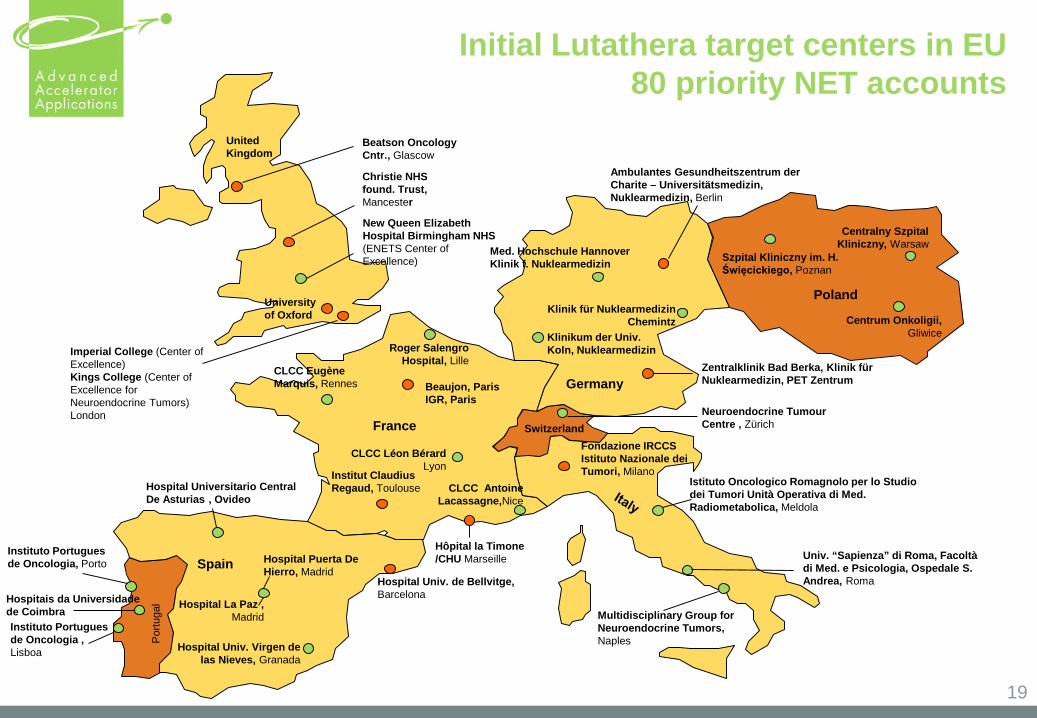
Initial Lutathera target centers in EU80 priority NET accounts
19
France
Poland
Portu
gal
UnitedKingdom
Switzerland
Imperial College (Center of Excellence)Kings College (Center of Excellence for Neuroendocrine Tumors)London
New Queen Elizabeth Hospital Birmingham NHS(ENETS Center of Excellence)
University of Oxford
Christie NHS found. Trust, Mancester
Beatson Oncology Cntr., Glascow
Roger SalengroHospital, Lille
CLCC EugèneMarquis, Rennes
CLCC Léon BérardLyon
Institut Claudius Regaud, Toulouse
Hôpital la Timone/CHU Marseille
CLCC Antoine Lacassagne,Nice
Neuroendocrine TumourCentre , Zürich
Hospital Universitario Central De Asturias , Ovideo
Hospital Puerta De Hierro, Madrid
Hospital La Paz , Madrid
Hospital Univ. de Bellvitge, Barcelona
Hospital Univ. Virgen de las Nieves, Granada
SpainInstituto Portuguesde Oncologia, Porto
Hospitais da Universidade de Coimbra Instituto Portugues de Oncologia , Lisboa
Centralny Szpital Kliniczny, Warsaw
Szpital Kliniczny im. H. Święcickiego, Poznan
Centrum Onkoligii, Gliwice
Multidisciplinary Group for Neuroendocrine Tumors, Naples
Univ. “Sapienza” di Roma, Facoltà di Med. e Psicologia, Ospedale S. Andrea, Roma
Fondazione IRCCS Istituto Nazionale dei Tumori, Milano
Istituto Oncologico Romagnolo per lo Studio dei Tumori Unità Operativa di Med. Radiometabolica, Meldola
Klinik für NuklearmedizinChemintz
Ambulantes Gesundheitszentrum der Charite – Universitätsmedizin, Nuklearmedizin, Berlin
Klinikum der Univ. Koln, Nuklearmedizin
Zentralklinik Bad Berka, Klinik für Nuklearmedizin, PET Zentrum
Med. Hochschule Hannover Klinik f. Nuklearmedizin
GermanyBeaujon, ParisIGR, Paris
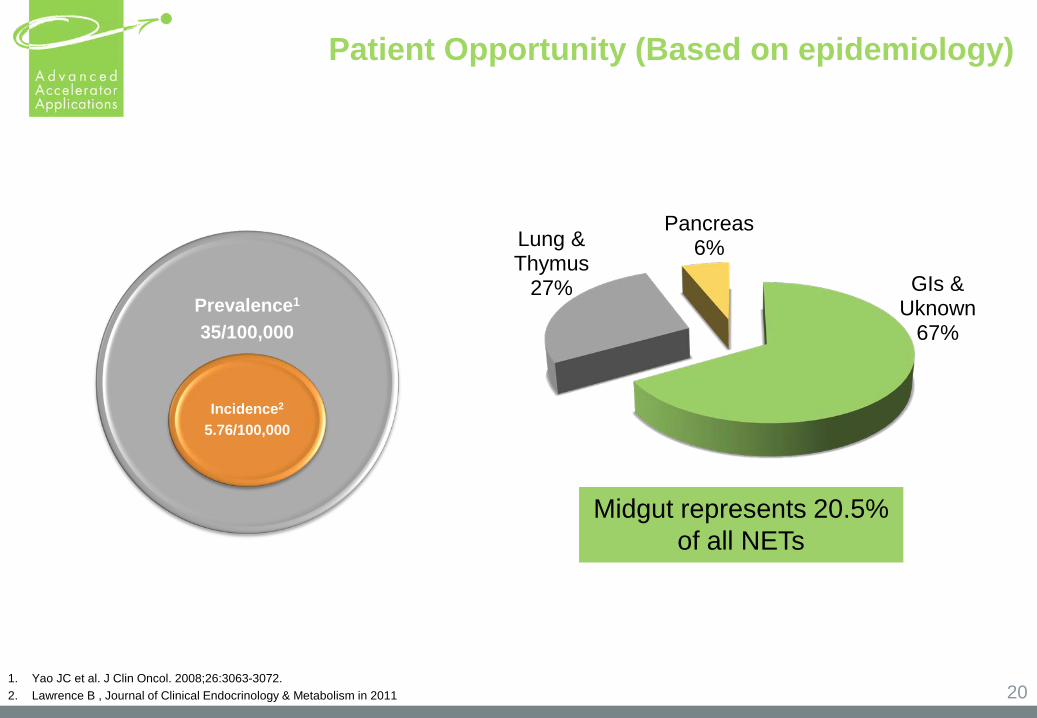
Patient Opportunity (Based on epidemiology)
20
Prevalence1
35/100,000
Incidence2
5.76/100,000
1. Yao JC et al. J Clin Oncol. 2008;26:3063-3072.2. Lawrence B , Journal of Clinical Endocrinology & Metabolism in 2011
GIs & Uknown
67%
Lung & Thymus
27%
Pancreas6%
Midgut represents 20.5% of all NETs
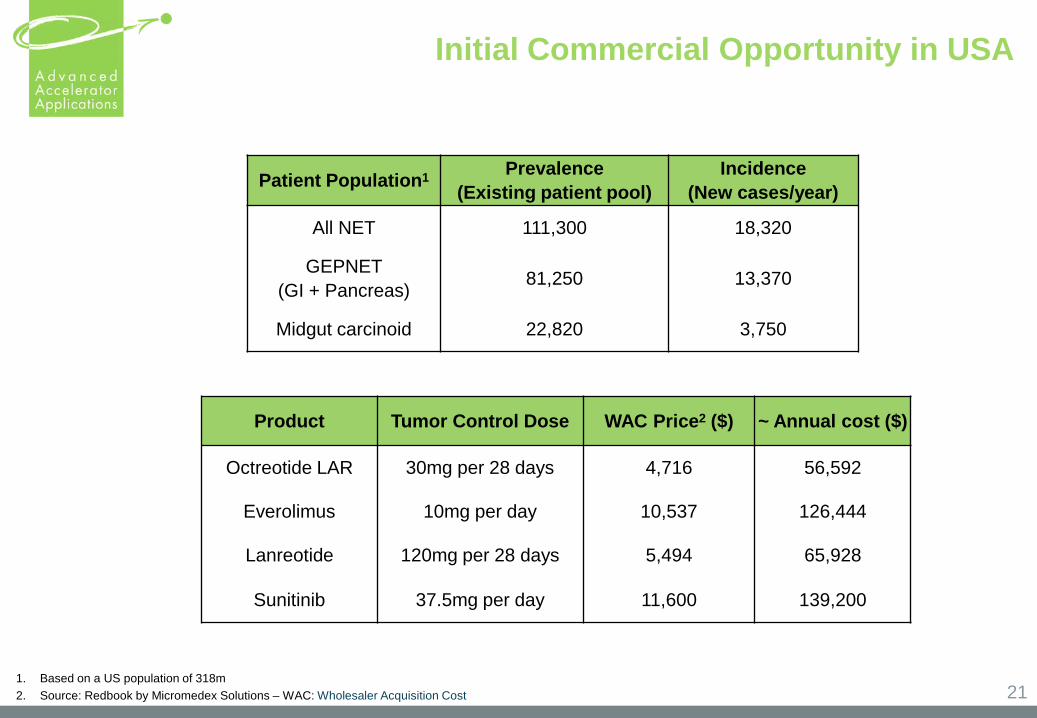
Initial Commercial Opportunity in USA
21
Product Tumor Control Dose WAC Price2 ($) ~ Annual cost ($)
Octreotide LAR 30mg per 28 days 4,716 56,592
Everolimus 10mg per day 10,537 126,444
Lanreotide 120mg per 28 days 5,494 65,928
Sunitinib 37.5mg per day 11,600 139,200
1. Based on a US population of 318m2. Source: Redbook by Micromedex Solutions – WAC: Wholesaler Acquisition Cost
Patient Population1 Prevalence (Existing patient pool)
Incidence(New cases/year)
All NET 111,300 18,320
GEPNET (GI + Pancreas) 81,250 13,370
Midgut carcinoid 22,820 3,750
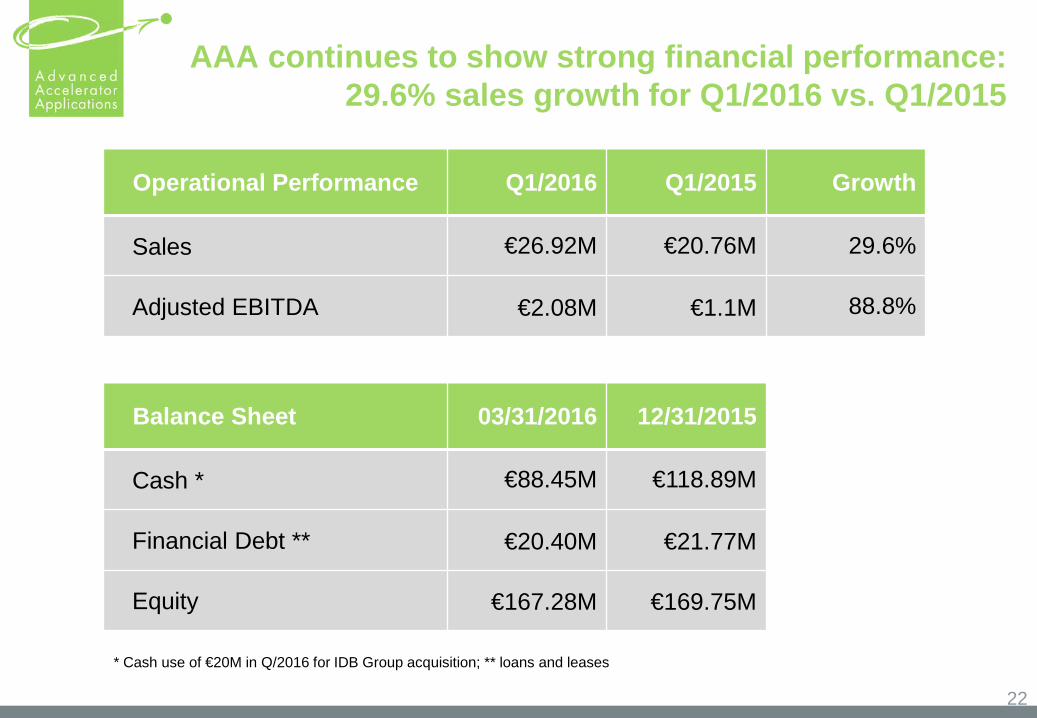
AAA continues to show strong financial performance: 29.6% sales growth for Q1/2016 vs. Q1/2015
22
Operational Performance Q1/2016 Q1/2015 Growth
Sales €26.92M €20.76M 29.6%
Adjusted EBITDA €2.08M €1.1M 88.8%
* Cash use of €20M in Q/2016 for IDB Group acquisition; ** loans and leases
Balance Sheet 03/31/2016 12/31/2015
Cash * €88.45M €118.89M
Financial Debt ** €20.40M €21.77M
Equity €167.28M €169.75M
Investment Highlights:
23
Lutathera, our flagship PRRT oncology candidate, has demonstrated favourable results in our Phase 3 study and is currently under review by FDA and EMA;
Rapidly growing and attractive target niche markets (MNM and NETs)
1
3
2
4
5
Integrated from R&D to sales in an industry with significant barriers to entry
Diversified business model: Late stage therapeutic product candidate and growing diagnostics drug business (PET and SPECT)
AAA management team has a proven execution capability and is rapidly expanding its US manufacturing and commercial presence
A Leader in the Molecular Nuclear Medicine (MNM) Market